Please see the Transcriber’s Notes at the end of this text.
The cover image has been created for this text and is placed in the public domain.
BY
ROSWELL PARK, A.M., M.D., LL.D. (Yale)
PROFESSOR OF THE PRINCIPLES AND PRACTICE OF
SURGERY AND OF CLINICAL SURGERY IN THE MEDICAL
DEPARTMENT OF THE UNIVERSITY OF BUFFALO, BUFFALO, NEW YORK; MEMBER OF THE
GERMAN, ITALIAN AND FRENCH SURGICAL SOCIETIES; EX-PRESIDENT OF THE
AMERICAN SURGICAL ASSOCIATION AND OF THE MEDICAL SOCIETY OF
THE STATE OF NEW YORK; SURGEON TO THE BUFFALO
GENERAL HOSPITAL, ETC.
WITH 722 ENGRAVINGS AND 60 FULL-PAGE PLATES IN COLORS
AND MONOCHROME

LEA BROTHERS & CO.
PHILADELPHIA AND NEW YORK
1907
Entered
according to Act of Congress, in the year 1907, by
LEA BROTHERS & CO.
in the Office of the Librarian of Congress. All rights reserved.
[iii]
A new work on Surgery enters a field of literature already rich in excellent books differing widely in plan and viewpoint. Fortunately nothing else is possible in representing so vast a subject, for it is obviously advantageous that the reader should have the benefit of the personal equation of his author as reflected in his knowledge, experience, and assimilation from the writings of others. When Surgery can be represented by a conventional and well-settled type of book it will have ceased to advance. There is still room for many a serious effort to place the subject before students and practitioners in a way to instruct from the beginning through to the operative and postoperative treatment. This has been the object of the present volume, upon which the author has brought to bear the experience of many years as a teacher and surgeon, and into which he has also endeavored to infuse the most advanced knowledge gleaned from the surgical literature of America and Europe.
To the extent of the author’s ability the work therefore represents the net Surgery of to-day, obsolete and obsolescent material having been excluded, and the pages being devoted to sound principles and practice, stated as clearly and succinctly as possible. The author has been free to employ illustrations wherever a point could be so explained to the eye. In the pictorial department utility and effectiveness have been considered of more importance than extreme and unusual cases. Simple drawings and even diagrams are often most instructive, and such have been accordingly liberally used.
With every effort at conciseness it has not been practicable to cover the subject in less than the equivalent of about fifteen hundred ordinary octavo pages. By adopting a larger form the publishers have presented this material in a convenient volume. In justification of the size of the work it should be borne in mind that its scope is very extensive, for it aims to cover the Principles as well as the Practice of Surgery, thus supplying the needs of students and general practitioners, and, the author hopes, also interesting his surgical confrères.
He takes this opportunity to extend his warmest acknowledgments to his fellow-collaborators of the Treatise on Surgery by American Authors, who on the exhaustion of the third edition most kindly consented to allow it to be succeeded by this individual work, placing their material and illustrations freely at his command. He also wishes to acknowledge the kindness of Dr. H. R. Gaylord, who has contributed certain material utilized in the chapter on Tumors, the assistance of Dr. E. R. McGuire, who has helped in many ways during the preparation of the book, and that of other colleagues who have furnished illustrations that are duly credited in their proper places.
R. P.
Buffalo, N. Y.
1907.
[iv]
[v]
| PAGE | |
|---|---|
| INTRODUCTION | 17 |
| PART I. | |
| SURGICAL PATHOLOGY. | |
| CHAPTER I. | |
| HYPEREMIA: ITS CONSEQUENCES AND TREATMENT | 19 |
| CHAPTER II. | |
| SURGICAL PATHOLOGY OF THE BLOOD | 28 |
| CHAPTER III. | |
| INFLAMMATION | 43 |
| CHAPTER IV. | |
| ULCER AND ULCERATION | 65 |
| CHAPTER V. | |
| GANGRENE | 73 |
| PART II. | |
| SURGICAL DISEASES. | |
| CHAPTER VI. | |
| AUTO-INFECTION, ESPECIALLY IN SURGICAL PATIENTS | 79 |
| CHAPTER VII. | |
| THE SURGICAL FEVERS AND SEPTIC INFECTIONS | 85 |
| CHAPTER VIII. | |
| SURGICAL DISEASES COMMON TO MAN AND DOMESTIC ANIMALS | 97 |
| CHAPTER IX.[vi] | |
| SURGICAL DISEASES COMMON TO MAN AND DOMESTIC ANIMALS (Continued) | 111 |
| CHAPTER X. | |
| SYPHILIS. | 122 |
| CHAPTER XI. | |
| CHANCROID OR VENEREAL ULCER | 144 |
| CHAPTER XII. | |
| GONORRHEA | 146 |
| CHAPTER XIII. | |
| SCURVY AND RICKETS | 160 |
| CHAPTER XIV. | |
| THE STATUS LYMPHATICUS | 163 |
| CHAPTER XV. | |
| SURGICAL ASPECTS AND SEQUELS OF OTHER INFECTIONS AND DISEASES | 166 |
| CHAPTER XVI. | |
| POISONING BY ANIMALS AND PLANTS | 171 |
| CHAPTER XVII. | |
| ACUTE INTOXICATIONS, INCLUDING DELIRIUM TREMENS | 174 |
| PART III. | |
| SURGICAL PRINCIPLES, METHODS AND MINOR PROCEDURES. | |
| CHAPTER XVIII. | |
| DISTURBANCES OF BLOOD-PRESSURE; SHOCK AND COLLAPSE | 177 |
| CHAPTER XIX. | |
| ABSTRACTION OF BLOOD; COUNTERIRRITATION; PARACENTESIS; TRANSFUSION; CATHETERIZATION; SKIN GRAFTING; BANDAGING | 182 |
| CHAPTER XX. | |
| ANESTHESIA AND ANESTHETICS, GENERAL AND LOCAL | 192 |
| PART IV.[vii] | |
| INJURY AND REPAIR. | |
| CHAPTER XXI. | |
| WOUNDS AND THEIR REPAIR | 211 |
| CHAPTER XXII. | |
| GUNSHOT WOUNDS | 220 |
| CHAPTER XXIII. | |
| PREVENTION AND CONTROL OF HEMORRHAGES; SUTURES; KNOTS | 234 |
| CHAPTER XXIV. | |
| ASEPSIS AND ANTISEPSIS; TREATMENT OF WOUNDS | 243 |
| CHAPTER XXV. | |
| PREPARATION OF PATIENTS FOR OPERATION AND THEIR AFTER-TREATMENT | 250 |
| PART V. | |
| SURGICAL AFFECTIONS OF THE TISSUES AND TISSUE SYSTEMS. | |
| CHAPTER XXVI. | |
| CYSTS AND TUMORS | 255 |
| CHAPTER XXVII. | |
| THE SKIN | 299 |
| CHAPTER XXVIII. | |
| SURGICAL DISEASES OF THE FASCIÆ; APONEUROSES; TENDONS AND TENDON SHEATHS; MUSCLES AND BURSÆ | 319 |
| CHAPTER XXIX. | |
| SURGICAL DISEASES OF THE HEART AND VASCULAR SYSTEM | 334 |
| CHAPTER XXX. | |
| INJURIES AND DISEASES OF THE LYMPH VESSELS AND NODES | 368 |
| CHAPTER XXXI. | |
| SURGICAL DISEASES OF THE JOINTS AND JOINT STRUCTURES | 379 |
| CHAPTER XXXII.[viii] | |
| SURGICAL DISEASES OF THE OSSEOUS SYSTEM | 416 |
| CHAPTER XXXIII. | |
| DEFORMITIES DUE TO CONGENITAL DEFECTS OR ACQUIRED DISEASES OF THE LOCOMOTOR APPARATUS; ORTHOPEDICS | 444 |
| CHAPTER XXXIV. | |
| FRACTURES | 479 |
| CHAPTER XXXV. | |
| DISLOCATIONS | 524 |
| PART VI. | |
| SPECIAL OR REGIONAL SURGERY. | |
| CHAPTER XXXVI. | |
| INJURIES AND SURGICAL DISEASES OF THE HEAD | 545 |
| CHAPTER XXXVII. | |
| THE ORBIT AND ITS ADNEXA; THE EXTERNAL AUDITORY APPARATUS; THE ACCESSORY SINUSES; THE CRANIAL AND CERVICAL NERVES; THE ORBITAL CONTENTS AND ADNEXA | 592 |
| CHAPTER XXXVIII. | |
| THE SPINE, THE SPINAL CORD AND THE PERIPHERAL NERVES | 621 |
| CHAPTER XXXIX. | |
| THE FACE AND EXTERIOR OF THE NOSE AND MOUTH | 638 |
| CHAPTER XL. | |
| THE MOUTH, THE TONGUE, THE TEETH AND THE JAWS | 652 |
| CHAPTER XLI. | |
| THE RESPIRATORY PASSAGES PROPER | 671 |
| CHAPTER XLII. | |
| THE NECK | 698 |
| CHAPTER XLIII. | |
| THE THORAX AND ITS CONTENTS | 718 |
| CHAPTER XLIV.[ix] | |
| THE BREAST | 755 |
| CHAPTER XLV. | |
| THE ABDOMEN AND ABDOMINAL VISCERA | 767 |
| CHAPTER XLVI. | |
| THE PERITONEUM AND ITS DISEASES | 785 |
| CHAPTER XLVII. | |
| INJURIES AND SURGICAL DISEASES OF THE STOMACH | 793 |
| CHAPTER XLVIII. | |
| THE SMALL INTESTINES | 822 |
| CHAPTER XLIX. | |
| THE APPENDIX AND ITS DISEASES | 851 |
| CHAPTER L. | |
| THE LARGE INTESTINES AND THE RECTUM | 869 |
| CHAPTER LI. | |
| HERNIA | 890 |
| CHAPTER LII. | |
| THE LIVER | 910 |
| CHAPTER LIII. | |
| THE OMENTUM, THE MESENTERY, THE SPLEEN AND THE PANCREAS | 934 |
| CHAPTER LIV. | |
| THE KIDNEYS | 955 |
| CHAPTER LV. | |
| THE BLADDER AND PROSTATE | 977 |
| CHAPTER LVI. | |
| THE MALE GENITAL ORGANS | 1004 |
| CHAPTER LVII. | |
| AMPUTATIONS | 1023 |
[17]
An ultimate analysis of the primary causes of disease, excluding traumatisms, will permit their reduction to one or the other of the following categories: nutritional (functional) and parasitic. These may co-exist, in which case each tends to modify the other more or less, usually unpleasantly, or either may precede and perhaps pave the way for the other. In general, it may be said that parasitism perverts nutrition, locally or generally, and, per contra, that perverted nutrition often prepares the way for parasitic infection, so that even between these primary causes there may occur all possible combinations.
With traumatisms surgery alone is mainly concerned, but its conceded scope is now widened to include an ever-increasing number of morbid conditions, which, in time past, were treated medicinally—or not at all. Thus it has come to pass that it is no longer possible to make an abrupt distinction between medicine and surgery, nor even briefly to define the words “surgery” and “surgeon,” nor yet to ascribe to either the physician or the surgeon his exact functions as such. In centuries past physicians were exceedingly jealous of their vested rights, and with propriety, when the only surgeons were uneducated barbers. But about one hundred years ago conditions were materially altered for the better, and surgery, liberated from its medieval environment, and from the restrictions imposed by the clergy, rapidly developed into both a science and an art, while the surgeon came to take that position in society to which his increasing attainments entitled him. During the past thirty years surgery, thanks to earnest workers in the surgical laboratories of the world, has made progress scarcely equalled by the science of electricity, and the impossibilities of yesterday have become the routine of today.
Thus has come about the earlier separation, and now, in some respects at least, the closer appreciation of the respective scope and functions of the physician and the surgeon. Between them lies yet what has been felicitously called the “borderland,” where they meet on common ground, too often as rivals and not often enough as co-workers. Nowhere do comprehensive knowledge, wide experience, and trained judgment appear to better advantage, nor lead to better results, than when exhibited where co-operation in these respects is most hearty. Someone has most happily said that “the surgeon is a physician who knows how to use his hands,” yet to regard a course in surgery as one in manual training would be a most lamentable conception of its purposes. Rather is it to be regarded as a superstructure, to be built upon a thorough familiarity with anatomy, physiology, pathology, and therapeutics. In fact, the better general practitioner a man is, the better surgeon may he thereby become, providing he possess the other necessary attributes. John Hunter took this view, but too many since his day have forgotten or never realized it.
In the pages which follow it has been impossible to do more than epitomize our present-day knowledge of surgery, an early disavowal which is intended to save too frequent repetition of the advice to consult, as needed, other larger and more specialized works. The attempt here has been rather to build up a framework upon which the student and the investigator may build with such other material as they may later select from the quarries which are accessible to them. Hence it has been impossible to describe or even mention all the operations which have been devised to meet various indications.[18] Preference has therefore been given to those which have best served the author in his personal experience.
Because of the numerous interrelations between surgery and internal medicine, so called, I have not hesitated to insert paragraphs and even whole chapters on subjects hitherto omitted from the later works on surgery. To teach a student how to recognize nasopharyngeal adenoids, to appreciate the widespread harm they may cause and how to cope with them, and at the same time to leave him quite unfamiliar with their too frequent relation to the status lymphaticus and its dangers, and to omit in such a work all reference to the latter, is to put knowledge and instruments into his possession without teaching him how rightly to employ them. A case of exophthalmic goitre affords another equally apt illustration, as being one in which the physician and the surgeon should heartily co-operate.
The surgeon and the physician have drifted too far apart. It is time that they met again in the presence of the pathologist. Such a group, when properly constituted, forms an almost invincible triumvirate.
It has been said that “the resources of surgery are rarely successful when practised on the dying.” Throughout these pages the attempt has been made to impress the fact that delay, in many of the borderland cases, is dangerous, and, often fatal, and that it is not just to charge to surgery the blame for such a result due to the physician’s dilatoriness.
It may lead to a better understanding of the teaching contained in the following pages if it is here made clear just what is understood by the suffix “itis” in medical terminology. The old tendency was to regard all morbid conditions as expressions of inflammation in some of its protean manifestations. The attempt has been made in this work to distinguish as clearly as possible between inflammation, as an expression of infection, and the vascular, nutritional, and other changes which may be brought about by perverted nutrition without necessary participation of parasites. To describe “ostitis,” for example, as “inflammation of bone,” is to revert to an obsolete definition. Let us, then, always translate the termination “itis” as implying an affection, not necessarily an inflammation, of the structure named in the word to which it is affixed. With this conception of the word or the term there can be no contradiction in its use under various conditions, and one does not necessarily commit himself, by using it, to any definite view concerning the pathology of the affection which is thereby implied.
With regard to one other feature there has been also a departure from previous nomenclature. The term “lymph glands” or “lymphatic glands” has always seemed objectionable, because, although they belong to the lymphatic system, they are in no sense glands, having no ducts, and no distinct secretion to be discharged through passageways. Whether in any sense they are to be regarded as furnishing an “internal secretion” is not the question here, their most obvious function being to act as filters. Throughout the work, then, the term “lymph gland” has been carefully excluded and the more accurate and far preferable term “lymph node” has been substituted. This seems to be a suitable place to explain the substitution and the reason therefor.
[19]
The reactionary results of injury to various tissues and the first local appearances due to the surgical infectious diseases are indicated by certain appearances, which, for a few hours at least, are in large measure common to both. Their beginnings being pathologically similar, their results depend not alone on the violence or intensity of the process, but also, and in predominating measure, upon the primary influences at work. The consequences of mere mechanical injury—such as strain, laceration, etc.—are in healthy individuals promptly repaired by processes which will be taken into consideration in the ensuing chapters. They are throughout conservative and reparative, and are directed toward restoring, as far as possible, the original condition. The consequences, on the other hand, of the surgical infections are more or less disastrous from the outset, although the extent of the disaster may be localized within a very small area, as after a trifling furuncle, or they may be so widespread as to disable a limb or an organ, or they may even be fatal. It is of the greatest importance, not alone for scientific reasons, but also because treatment must in large measure depend upon the underlying conditions, to differentiate between these two general classes of disturbance, which we speak of as—
A. Those produced by external or extrinsic disturbances, i. e., traumatisms, sprains, lacerations, etc.; and
B. Those produced by internal and intrinsic causes, which, for the main part, are the now well-known microörganisms, such as cause the various surgical diseases.
These latter disturbances may be imitated or simulated in the presence of certain irritants within the tissues, such as the poisons of various insects and plants; the irritation produced by foreign bodies, minute or large; and possibly the presence within the system of certain poisons whose nature is not yet known, such as that of syphilis, or certain others whose chemistry is fairly well understood, but whose presence cannot be easily explained, as uric acid, etc.
Clinically, all these disturbances are manifested by certain phenomena common to each, which may present themselves at one time more prominently, at another less so. These significant appearances have been recognized from time immemorial as the calor, rubor, dolor, tumor, et functio lesa of our ancestors, or as the heat, redness, pain, swelling, and loss of function of our common experience. When one or more of these are present, the surgeon cannot afford to disregard the fact, while he should, moreover, be able to account for each on general principles which should to him be well known.
To their more exact study we must, however, make some preface in the way of general remarks concerning a phenomenon everywhere easily recognized, but as yet incompletely understood. This phenomenon has reference to an undue supply of blood to a part, and is commonly known under two terms which are practically synonymous,[20] namely, congestion and hyperemia. To begin with these, then, we must note, first of all, that congestion and hyperemia may be—
They may also be spoken of as—
Considering first the two latter distinctions, it will be found that the acute hyperemias are met with most often in consequence of sharp mechanical disturbances. The chronic hyperemias, on the contrary, are conditions which in many individuals are more or less permanent. Note accurately here the proper significance of certain terms. Hyperemia means, in effect, an oversupply of blood to the given part; the term should have only a local significance. When the entire body seems to be too well supplied with blood, the condition is known as plethora, the counterpart of which term is usually anemia. The direct counterpart of the term hyperemia should perhaps be ischemia, meaning a perverted blood supply in reduced amount. With plethora and anemia as terms implying general conditions, with hyperemia and ischemia implying local conditions, there should be little room for confusion in phraseology.
The active form of hyperemia used to be called “fluxion,” a term now rarely used. Active hyperemia means an increased supply of arterial blood. In passive hyperemia the oversupply is rather of venous blood. In the former case the condition seems due to overactivity of the heart, with such local tissue changes as permit it to occur. In passive hyperemia the blood current is slower—there is a tendency toward, and sometimes an actual, stagnation; all of which is usually due to obstruction of the return of blood to the heart. The conditions permitting these two results may be widely variant.
—Active hyperemia may be produced by purely nervous influences, even those of emotional origin. The flushing of the face which is known as “blushing” is, perhaps, the most common illustration of this fact. It is well known also that this is, in some degree at least, the result of division of certain nerves which have to do with the regulation of the blood supply. The cervical sympathetic is the best known and most often studied of these, and the consequences of division of this nerve in the neck are stated in all the text-books on physiology. So also by electrical stimulation of certain nerves the parts supplied by them can be made to show a very active hyperemia, which will subside shortly after discontinuance of stimulation, providing this has not been kept up too long. In active hyperemia there is absolute increase of intra-arterial tension, and under these circumstances pulsation may be noted in those small vessels in which commonly it is not seen nor felt. This is the explanation of the throbbing pain complained of under many actively hyperemic conditions. This hyperemia affords the explanation of the clinical signs to which attention has already been called. The increased heat of the part is the result of greater access of blood, which prevents cooling by radiation and evaporation; the peculiar redness is due to the greater filling of the capillaries with the blood, which gives the peculiar hue to the skin and visible textures; while to the increased pressure upon sensory nerves is also due the pain. The minuter changes occurring within the congested part call for more accurate description. Whether or not there is actual dilatation of capillaries under these circumstances is a matter still under dispute, but of the dilatation of the larger vessels there can be no possible question.
As hyperemia is to such a great extent brought about by action of the nervous system, it is well to divide it more accurately into the hyperemia of paralysis, or neuroparalytic congestion, which is the result of a paralysis of the constrictor fibers of the vasomotor system, and into the hyperemia of irritation, or neurotonic congestion, which is due to the irritation of the dilators (Recklinghausen). Physiologists are fairly well agreed that as between the dilating and the constricting apparatus of the vasomotor system there is ordinarily preserved a certain degree of equilibrium; to which fact is probably due that normal condition of affairs inaugurated after temporary disturbance, since overaction in one direction succeeds reaction in the other. As Warren has illustrated this, our common treatment of frostbite by cold applications is a concession to this fact, since by the cold applications we endeavor to limit the reaction which would otherwise follow after thawing out the frozen part.
[21]
The best examples of the hyperemia of paralysis are perhaps to be met with after certain injuries to nerves, as, for instance, flushing of the face and hypersecretion of nasal mucus, tears, etc., after injury to the cervical sympathetic. Such, too, in its essentials is that form of shock known as brain concussion, which is often followed by nutritive disturbances among the brain cells, with consequent perversion of brain function.
Waller’s experiment of placing a freezing mixture over the ulnar nerve at the back of the elbow is also significant, the result being congestion and elevation of surface temperature of the fingers supplied by this nerve. Congestion and swelling have also been observed after fracture of the internal condyle of the humerus, by which this nerve was pressed upon; and similar phenomena may be noted in fingers or toes as the result of injuries of other nerves.
Hyperemia due to paralysis of the perivascular ganglia is observed sometimes in transplanted flaps, in the suffusion of a limb after removal of the Esmarch bandage, in the congestion of certain sac walls after tapping, in the hyperemia of, perhaps even hemorrhage from, the bladder wall after too quickly relieving its overdistention, and in the swelling of the extremities when they begin to be first used after having been put at rest because of injury.
The hyperemias of dilatation are more acute in course and manifestation. Along with them go sharp pain, hypersecretion of glands, edema, and sometimes desquamation of superficial parts. The facial blush due to effusion; the temporary flushing due to indulgence in alcohol; the suffusion of the conjunctiva, perhaps the face, with hyperlacrymation, accompanying facial neuralgia or hemicrania; and the hyperemia consequent upon herpes zoster, urticaria, etc., are illustrative examples of this form. The erythema due to nerve irritation or injury, the swelling of the joints which appears after similar lesions, and that condition described by Mitchell as erythromelalgia, probably also belong here. In fact, almost all the reflex hyperemias are hyperemias of dilatation.
The forms of hyperemia considered above belong mainly to the designation of active.
—Passive hyperemia is most often a mechanical consequence of obstruction of the return of blood, which can be imitated at will, and which is not infrequently the result of carelessness, as when an injured limb is bandaged too tightly. Experiment shows that when such mechanical obstruction has taken place there is temporary increase of intravenous pressure, which soon returns to the normal standard, such readjustment meaning that blood has found its way back by collateral circulation. Only when such rearrangement is possible do we have anything like permanent passive hyperemia. In organs with a single vein, such as the kidneys, the question of obstruction may assume a very important aspect. Under these circumstances the appearance of the involved part, when visible, is spoken of as cyanotic, while its surface, instead of being abnormally warm, is the reverse, due to impeded access of warm blood and more rapid surface cooling. The blood under such conditions is often darker than natural, because, remaining longer in the part, it absorbs more carbonic dioxide, or at least gives up more of its oxygen. As long as actual gangrene is not threatened, the blood column has a communicated pulsation, at least in the large veins. Escape of corpuscular elements may occur after the phenomena above noted have been present for some time; but the corpuscles rarely, if ever, escape until there has been more or less copious transudation of the fluid portion of the blood—i. e., the serum. When anatomical changes can be grossly, yet carefully, observed, as in the fundus of the eye, it is seen that under these circumstances the arteries become smaller, although whether this is a primary or secondary change is not to be determined. Discoloration of the integument is the frequent result of leakage of blood corpuscles and their pigmentary substance into the tissues, and is consequently a frequent accompaniment of chronic passive edema. It is seen often in connection with varicose veins of the legs.
Another form of passive congestion or hyperemia is that due to enfeeblement of the heart’s action by serious injury or wasting disease. When under these circumstances the lung has become more or less infiltrated with fluid, with hemorrhagic extravasation, the condition is known as hypostatic pneumonia—a misnomer, nevertheless indicating a condition which is only too frequent in the aged and feeble.
[22]
These may be—
—The speedy subsidence of hyperemic phenomena is known as resolution—a term which has also been applied to the retrograde phenomena after a genuine inflammation. For present purposes it implies, first, the subsidence into inactivity of the exciting cause or its complete removal. This may include the passing of an emotion, the removal of an irritant, the loosening of a bandage, the resort to certain applications or to constringing or astringing measures by which the effect is counteracted. A particle of dust in the conjunctiva may within a few moments produce an active congestion of the conjunctival vessels, which, ordinarily scarcely visible, becomes prominent and easily noted. The removal of the offending substance permits a return to their original size in perhaps a half-hour. This is an example of the speedy subsidence of the hyperemia of dilatation after removal of the cause. Should the hyperemia not subside promptly, it is well to use cold applications, or in this instance an astringent collyrium, or some agent whose physiological effect it is to produce vascular contraction, as cocaine, adrenal extract, etc.
—When the effusion above referred to takes place into loose connective tissues the condition is spoken of technically as edema, while when it occurs into a previously existing cavity, such as that of a joint, it is known as an effusion. The amount of blood thus effused will be influenced by the anatomical and mechanical conditions existing about the part. It may be presumed, as a general rule, that when the extra vascular pressure equals the intravascular pressure little or no more fluid may escape. As a matter of fact, it is seldom that the former rises to the degree of the latter. Conversely, one method of treating such edemas and effusions is by some device which shall make the extravascular pressure exceed the intravascular, when the fluid is, as it were, forced back into the vessels, and is made to resume its proper place within the same. This is often done by taking advantage of elastic compression, as when a rubber bandage is applied about the part. In certain parts of the body it may be done by pressure brought about by some other device. Pressure may be used for two purposes:
A. To so increase extravascular pressure as to limit the possible amount of an effusion, as when it is put on early after an injury; or,
B. When it is used as a later resort for the purpose of reducing swelling which has already occurred.
—This is something more than the swelling alluded to under Acute Swelling. Chronic swelling implies either a continuous passive hyperemia, or, what is more common, a positive increase in tissue elements as the result of an oversupply of nutrition brought by the blood, which itself was furnished to the part in a degree far in excess of its needs. The result is a more rapid reproduction of cell elements, with result in the shape of tissue thickenings or tissue enlargements, known as hypertrophy, or, more properly speaking, hyperplasia, of a part, and to the laity as “overgrowth.” This chronic swelling or chronic enlargement is in some degree also connected with the phenomena of escape of white corpuscles from the bloodvessels and mitotic division of certain tissue cells, which have up to this time been usually regarded as a feature of the true inflammatory process.
—This may be the result of hyperemia—for the most part the passive forms—though most instances of gangrene due to intrinsic causes are inseparable from the presence of infectious microörganisms. The gangrene which is spoken of here includes that due to the pressure of tumors, tight dressings, or any natural or intrinsic agency, and that due to pressure from without when not so pronounced as to produce immediate and total loss of circulation in a part. It includes the formation of many bed-sores and so-called pressure-sores, which may be due to an enfeebled heart, to an obstructed pulmonary circulation, or to external pressure in conjunction[23] with cardiac debility. While insisting, then, that gangrene should be recognized as a possible result of hyperemia, it may be added that it is in effect a tissue death, and that dead tissue is always and everywhere practically the same thing, no matter by what causes brought about. Consequently, the subject of gangrene will be considered under a separate heading.
will be considered later.
The consequence of persistent hyperemia is transudation—i. e., escape of blood plasm from the vessels into body cavities and tissue interspaces. This leads to consideration under a distinct heading of—
Exudation may occur in vascular and non-vascular, in firm and soft tissues, in, under, and upon membranes. With respect to location, exudates are described as free, when found upon free surfaces or within natural cavities; interstitial, when found between the tissues or parts of tissues; and parenchymatous, when they are situated within the tissues themselves, particularly in epithelial and glandular cells of any kind.
Exudates are serous, mucous, fibrinous, or mixed, the mixed forms including the so-called seropurulent, the mucopurulent, the croupous, and the diphtheritic.
When any exudate contains red globules in sufficient quantity to stain it, it is called hemorrhagic.
Serous transudates from free surfaces are sometimes spoken of as serous catarrhs; when into cavities, as dropsies; when into tissues, as edema; when occurring beneath the epidermis they form serous vesicles or blebs or bullæ.
Fibrinous exudation refers to the fluid which coagulates soon after its exit from the vessels within those spaces into which it has oozed. When flocculi of coagula float in serous fluid it is known as a serofibrinous exudate. Pure fibrinous exudate occurs rarely, save in and upon mucous membranes. The extent to which exposure to the air is responsible for the firm coagulation of the fibrin previously held in solution is uncertain. The most potent factors in producing such coagulation are bacteria, but it is not yet disproved that coagulation may occur without their aid. When such coagulation occurs upon the surface of a mucous membrane it has been spoken of as croupous. When the epithelial covering as well as the basement membrane, and often the submucous tissues, are involved, so that the membrane cannot be stripped off without tearing across minute bloodvessels, the exudate has been known as diphtheritic. These terms may possibly be still retained in an adjective sense as implying the exact location of a surface exudate, but are scarcely to be used in any other significance.
The following table illustrates significant differences whose full importance cannot be impressed before a study of inflammation has been carefully entered upon:
| Hyperemic Transudates. | Inflammatory Exudates. |
|---|---|
| Poor in albumin. | Rich in albumin. |
| Rarely coagulate in the tissues. | Usually coagulate in the tissues. |
| Contain few cells. | Contain numerous cells. |
| Low specific gravity. | High specific gravity. |
| Contain no peptone. | Contain peptone (product of cell disintegration). |
These disturbances are to be combated, first of all, by insisting upon physiological rest. This, perhaps, is the most important measure of all. The profession is indebted to Hilton for the decided advance which he made in the treatment of congestive and inflammatory affections by insisting upon this principle in his celebrated work on Rest and Pain, which every young practitioner should read. Aside from this first and underlying principle, the treatment must, in some measure at least, be based upon the time at which we are called upon to treat the case. If seen at once, before exudation[24] has been excessive or the other disturbances marked, we may carry out a certain line of treatment for the purpose of limiting all these unpleasant features. On the other hand, if seen late, when exudation has been copious and when pain and other disturbances are due to its presence, a distinctly different course will be adopted.
Toward the end first mentioned—namely, the limitation of hyperemia—we may adopt local and general measures. Local measures include graduated pressure, providing this is not intolerable to the patient, so equalized that outside of the vessels it shall equal that inside. This may be done by careful bandaging, extreme care being taken that the pressure be applied from the very extremity of the limb; otherwise, passive exudation might be augmented and gangrene be precipitated. Elevation of a limb will often accomplish the same purpose. Cold, which is in effect an astringent and which tends to contract bloodvessels, is another measure in the same direction, and if applied early will do much to limit the degree of the attack. This may be applied as dry or moist cold, and should be gradually mitigated as the congestion subsides. It acts through the vasomotor system, and is a measure to be resorted to with caution. An efficient way of applying dry cold can be extemporized by a few yards of rubber tubing, held in place by wire or sewed in place to a piece of cloth, through which a stream of cold water is permitted to pass.
Heat is another efficient means, acting, however, in a rather different way. Heat is a measure to be employed to hasten the disappearance of exudation—in other words to quicken resorption, which it does by equalizing blood pressure, dilating the capillaries, stimulating the lymphatic current, and in every way helping to clear the tissues of that which has left the bloodvessels.
It is necessary also, at least in extreme cases, to employ some detergent or derivative measures, including bloodletting, to which we do not resort sufficiently often. When used for this purpose, depletion should be applied at the area involved, if possible. This may be done either as venesection, by leeching, either with the natural or the artificial leech, or by a series of minute punctures or incisions, which give relief to tension, permit the rapid escape of fluid exudate, and often save tissues from the disastrous effects of strangulation. In some cases of deep-seated congestions these measures are inapplicable, and venesection at the point of election—say the cephalic vein in the arm—may be followed by great benefit. Another method of depletion is by administration of cathartics, such intestinal activity being stimulated as shall lead to copious watery evacuations. The salines rank high as measures directed to this end, but in emergency much stronger and more drastic drugs may be administered, such as jalap, calomel, elaterium, etc. Diaphoretics and diuretics help to reduce temperature and in some degree to deplete, but their action is usually slow. When exudation is considerable in amount and confined to some one of the body cavities, it is often best combated, if at all obstinate, by the method of aspiration. This includes any suitable suction apparatus by which the fluid may be withdrawn through a small needle or cannula, the operation being trifling in difficulty, but one to be performed under strictest aseptic precautions, lest infection of an exudate already at hand be permitted.
Certain individuals, especially the neurotic, will need more or less anodyne, particularly when local applications fail to give relief. Sometimes a small dose of morphine administered hypodermically will act magically in making efficient those measures which would otherwise be inefficient. In little children some anodyne or hypnotic will be of great service. Under all circumstances it is well to keep the lower bowel empty, and certain elderly individuals with weak and enfeebled hearts will need the stimulation to be afforded by digitalis, quinine, and alcohol, or preferably strychnine administered subcutaneously.
In cases of chronic hyperemia and its consequent hyperplasias (induration, thickening, etc.) there is no one measure so generally applicable and effective as the continued use of cold-water dressings. These are generally spoken of as “cold wet packs,” and may be continued—constantly or intermittently—for many days.
Massage is also an invaluable agent in the reduction of swelling and tissue overproduction. It promotes absorption, even of acute effusions, by equalizing the blood and hastening the lymph circulation, and under its scientific application it is surprising how firm exudates and old adhesions seem to disappear.
[25]
As a consequence of increase of nutrition we have a condition known commonly as hypertrophy, more accurately as hyperplasia. Hypertrophy literally means overgrowth, whereas hyperplasia more accurately describes that which constitutes hypertrophy—namely, numerical increase of constituent cells. Common usage has made the more inaccurate name “hypertrophy” cover nearly all these conditions. Hypertrophy, or hyperplasia, means enlargement of a part or of an organ beyond its usual limits, and as the result of increased function or increased nutrition. It is to be distinguished from gigantism, which means inordinate enlargement as the result of a congenital tendency or condition. Hypertrophy is—
| A. | Physiological | - | 1. | Compensatory; | |
| 2. | From deficient use. | ||||
| B. | Pathological | - | 3. | Local; | |
| 4. | General; | ||||
| 5. | Senile; | ||||
| 6. | Congenital. | ||||
Fig. 1
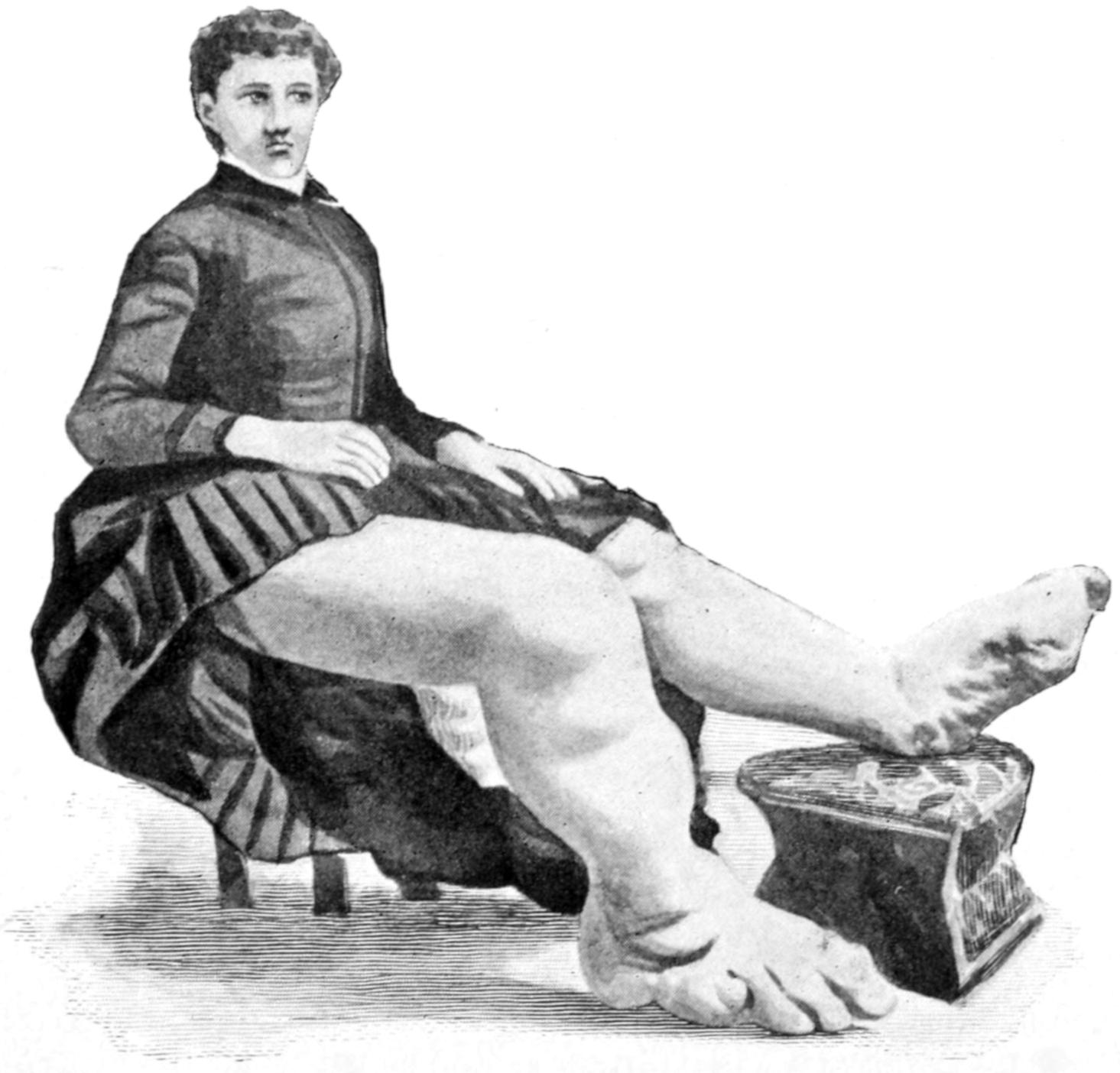
Congenital hypertrophy: gigantism of both lower extremities. (Case of Dr. Graefe [Sandusky].)
—1. This includes many of the compensatory enlargements of an organ or a part when extra work is put upon it, owing to deficiency of some other organ or part. This is spoken of as compensatory enlargement. Illustrative examples may be seen in the heart, which becomes larger and stronger when the bloodvessel walls are diseased and their lumen narrowed, or when other obstructions to circulation are brought about; again, in enlargement of one kidney after extirpation of the other, or of the wall of the stomach when the pylorus is constricted or obstructed; again, of the fibula after weakening or more or less destruction of the tibia, or of the shaft of any bone when it has been weakened at some point by not too acute disease; or, again, of the walls of bursæ after constant friction.
2. The best examples of physiological hypertrophy owing to deficient use are perhaps seen in some of the lower animals; as, for instance, in the teeth of such rodents as beavers when kept in captivity and prevented from natural use.
[26]
—3, 4. Instances of this are everywhere and every day are met in the results of so-called chronic inflammation, a term which is a complete misnomer and should be expunged from text-book use. So-called chronic inflammation simply means increase of nutrition owing to a certain degree of hyperemia, which may have been produced in the first place as the result of traumatism, which may have come from chemical irritants circulating in the fluids of the part—as, for example, uric acid, etc.—or which is brought about as the result of perverted trophic-nerve influence. Instances of local pathological hypertrophy may be seen in the thickened periosteum after injury, in the enlargement of a phalanx known as the “baseball finger,” and in numerous other places; or they may be general, in which case they are brought about mainly by some irritating material in the general circulation. The unknown poison of syphilis generally provokes such nutritive disturbances.
5. Senile hypertrophy is connected with nutritional disturbances characteristic of old age, as to whose remote causes we are still uncertain. Instances of senile hypertrophy, however, are common, particularly in the prostates of elderly men, which are liable to undergo extensive enlargement.
6. Of congenital hypertrophy and that of unknown origin we see, for instance, examples in certain rare cases of hypertrophy of the breast, in leontiasis, perhaps even in acromegaly, etc.; and these are to be distinguished from gigantism, because in most instances of the former type the hypertrophic tendency is not manifested until youth or adult life, whereas gigantism is a condition in which the tendency was apparent even before the birth of the individual.
Atrophy implies impaired nutrition, and means diminution in the size of an organ or part, and is the converse of hypertrophy. It is necessary to make plain that in atrophy nutrition is only impaired and not arrested, since complete arrest of nutrition means necrosis—i. e., gangrene or disappearance of parts. It may be—
| A. | Physiological | - | 1. | From disuse without disease; | |
| 2. | Biological or developmental; | ||||
| 3. | Senile. | ||||
| B. | Pathological | - | 4. | Result of acute tissue losses; | |
| 5. | Result of phagocytic activity; | ||||
| 6. | Result of continuous pressure; | ||||
| 7. | Specific. | ||||
—1. This is always the result of disuse or impaired function from any cause. Its evidences are generally seen in the fatty structures and muscles—i. e., in the soft parts. It is true, however, even of the bones, or, of greater interest, even in the brain cells. We see evidences of it also in minute organs; as, for example, in the digestive glands in certain cases where diet is restricted. Again, we see it in the diminution of the size of the heart after hip amputation, less being required of that organ, and also in the entire structure of the rectum after colostomy.
2. Examples of the developmental type are best seen in the natural disappearance of the hypogastric arteries, the ductus arteriosus, the vitelline duct, the Wolffian bodies, and in the various generative ducts (Gärtner’s, etc.) shortly after the birth of the human individual. We sometimes see it also in the prostate after orchidectomy. Equally illustrative is the disappearance of the tail and gills of the tadpole, the eyes of animals living in caverns, and, in a general way, of organs which become useless owing to a different environment.
3. Senile atrophy is seen equally well in the hair follicles, the teeth, the bones, and the sexual organs of elderly people—in fact, in all their tissues, even in the brain.
—4. Acute atrophy of surrounding tissues is the necessary accompaniment of destruction by suppurative or other disturbances; that is, parts disappear by absorption which have not been interfered with by pyogenic organisms. So complete may atrophy occur under these circumstances as to cause disablement of an organ or part. This kind of senile disappearance is merely an expression of phagocytic activity, although not now a question of bacteria.
[27]
5. The same is true of that variety spoken of above as biological or developmental, since phagocytes are the active agents in producing the disappearance of the tadpole’s tail.
6. A more slow form of pathological atrophy is seen in the gradual disappearance of tissues in the neighborhood of advancing tumors, enlarging cysts, etc. This is perhaps but another expression of atrophy from continuous pressure. But a still better illustration is the atrophy which comes from immobilization of a part without pressure. This is usually the case when splints or orthopedic apparatus have to be kept in place for some time.
7. Specific forms of pathological atrophy are largely connected with disturbances in the central nervous system. They are often referred to as trophoneurotic. Their exact mechanism is not yet understood, and cases may be confused under this head whose remote causes are widely different. Here should be included, for instance, the atrophy of a deep bone which occurs after extensive burn of the surface; also that peculiar form of atrophy of tissues in the stump which produces the so-called conical stump. These cases are of a more complicated character, for if pressure is removed from the bone end, especially in young people, the bone tends to grow faster than it should, while the soft parts disappear, partly as the result of mere disuse or loss of function. In this way conicity is produced, which sometimes calls for subsequent re-amputation. Under this head might also be included the so-called “trophic inflammation” (misnomer) of some writers, such, for example, as ulceration of the cornea after division of the trigeminus. The general subject of atrophic elongation also belongs here, referring to the fact that as a result of disuse, or sometimes of active disease, the bones, while showing atrophic changes in other respects, actually increase in length. Should such increase occur in one bone of those portions of the limbs which are supplied with two, the result would be posture deformity and displacement of the terminal portion.
[28]
The part played by the constituent elements of the blood in inflammation, suppuration, and other still more disastrous conditions is so great and so important that, before proceeding to discussion of these lesions, it seems necessary to set forth a resume of facts illustrating the importance of accurate knowledge concerning this most important fluid.
The total amount of blood in the human body has been variously estimated at from one-eleventh to one-twenty-fifth of the body weight, the average being about one-sixteenth. The amount which the body may lose and still retain vitality is very vague and differs not only with individuals, but very greatly under various conditions. Severe loss of blood is one to be atoned for as quickly as possible, and is to be prevented as far as it can be after accidents or during operation. For this reason the so-called bloodless method of operating upon limbs, by the use of the rubber bandage, constituted a great advance in surgery. For the same reason the use of hemostatic forceps is of equal value in operating upon other parts of the body; other things being equal the quickest and most satisfactory recoveries follow the bloodless operations, and it is an advantage to conserve this vital fluid as far as possible.
It has been roughly estimated that the blood is divided about as follows, between the different parts of the body: the heart, lungs, and large vessels holding one-fourth, the skeletal muscles one-fourth, the liver one-fourth, the remaining quarter being distributed over the balance of the body.
The blood varies within wide limits in its coagulability, and this variation occurs apparently even within conditions of health. In some patients the blood may be seen to coagulate almost as rapidly as it collects upon the surface, while in others the exposed parts continue to ooze, and the checking of hemorrhage is a difficult, sometimes almost impossible, matter. There are certain diseases in which the blood is known to have reduced power in this direction; for example, in the toxemias, especially those connected with biliary obstruction and jaundice. There were not a few of these cases of slow bleeding to death in days gone by, simply because the capillary hemorrhage could not be controlled. Recently, it has been shown that calcium chloride administered internally has a marked effect in favoring coagulation, and when opportunity is afforded it should be given for several days previous to operating and as part of the necessary preparation. It may be administered in doses of from 1 to 2 Gm., and should be given three or four times, at least, in twenty-four hours.
A test of the coagulation time, normally three to five minutes, but lengthened under circumstances like those mentioned above, even to an hour, will often prove of great value.
There are certain albumoses whose effect on coagulation of the blood is very suggestive and very mysterious. A very minute dose of cobra poison, for instance, will make the blood of an experimental animal remain fluid for days, unless this animal has been previously immunized against it, in which case coagulation takes place even more rapidly than normally. A trace of serum from an immunized rabbit is enough to prevent the fluidifying effect of the cobra poison, but quite insufficient to neutralize its toxic effects. The surgeon practically never desires to reduce coagulability of the blood, but frequently to increase it. When it is increased by natural conditions or those not easily controlled, then it may lead to thrombosis and produce trouble in that way.
—Increase of fibrin, hyperinosis, accompanies the leukocytosis of inflammation and suppuration. It may be approximately estimated on the cover-glass by noting the closeness of the network resulting after fifteen minutes’ exposure. The inflammatory indication of leukocytosis may, therefore, be inferred from its determination, while the leukocytosis of malignant disease will not be so accompanied. Hyperinosis is most marked in pyogenic processes, pneumonia and rheumatism. Its opposite, hypinosis, is met with in pernicious anemia. There is no change in the percentage of[29] fibrin in the ordinary anemias or chlorosis. In hemophilia and purpura hemorrhagica the coagulation time is greatly increased.
—The specialized elements of the blood which are of particular interest to the surgeon are the red and the white corpuscles. These may both vary in relative size within certain physiological limits. The red cells especially are not of uniform size and vary from 6 to 9 microns in diameter. There are also present in normal blood a small number of red cells having a diameter of only 6 microns, which are known as microcytes. In infancy there are present also so-called giant corpuscles, or megalocytes, with a diameter of 10 microns or more. Considerable variation occurs in disease, especially in the severe anemias. Red corpuscles ordinarily stain with acid dyes, which facilitate their examination and a computation of the number present. When present in unusually large number the condition is spoken of as a polycythemia; when in reduced number as oligocythemia. In several of the anemias variations in size, shape, and color occur, and in certain of them many of the red corpuscles are found to be nucleated. Red cells which are nucleated are known as erythroblasts, and according to their size are spoken of as microblasts, normoblasts, and megaloblasts. Again, under certain diseased conditions the ordinary discoid form of the cells becomes irregular and crenated, and to those which are thus altered is given the name of poikilocytes.
There is another form of degeneration which consists in death or necrobiosis of the cell, whereby it loses its capacity for staining, or, at all events, stains irregularly and abnormally. This is seen also in cases of severe anemia and in conditions where the blood has been altered by the addition of toxic material, such as chloroform, etc. Occasionally also the red cells show a tendency to a granular change, which is probably entirely degenerative.
The red corpuscles have a certain degree of elasticity which helps them to pass through capillaries which are smaller even than their own diameter; after escaping from these the corpuscles regain their original form. In the presence of carbon dioxide they lose this elasticity and become distorted or crenate. The influence of high altitudes in increasing the number of corpuscles is known, but unexplained. For instance, a residence of less than a month in the mountains will cause an increase of from 2,000,000 to 3,000,000 corpuscles per cubic millimeter. It has been surmised that under the influence of oxygen red corpuscle formation is stimulated to greater activity; in other words, that the red marrow becomes more active in the production of the hematoblasts.
In general terms it may be said that the blood of a normal adult male contains 5,000,000 red corpuscles per cubic millimeter, and that of an adult female 4,500,000. These figures are, of course, approximate and variable. When the number is reduced to 3,000,000 by common consent the case will be regarded as oligocythemia, and when increased to 6,000,000 as one of polycythemia.
The latter condition is most evident in cases of newly born infants. The excess rapidly diminishes during the first week of extrauterine life. It is to be explained by the loss of fluid suffered by the infant upon the establishment of respiration. The proportion of red cells also varies according to the nutrition of the individual, the season of the year, the altitude (as above), and climate, and varies during menstruation, pregnancy, lactation, and at the climacteric. With the loss of red cells the number is reduced in proportion to the hemoglobin, although the change in one respect is not exactly proportionate to that in the other.
That the colorless corpuscles, or leukocytes, are not all of one kind has been recognized for nearly sixty years, and long ago they were divided into granular and nucleated cells. A vast impetus to the study of hemocytology was given by Ehrlich, in 1878, when he introduced the use of aniline dyes. The reader must be reminded that some of these, like eosin, are acid in reaction, and others, like methyl blue, are basic; while a third group has been supposed to be neutral in reaction, like a mixture of methyl blue and acid fuchsin; but it has been found that the so-called neutral dyes have really a slightly acid reaction. We may, therefore, divide the cells according to the reaction of the dyes with which they usually are distinguished into the acid and basic, or, more technically, into oxyphile, which includes neutrophile, and basophile.
This is not the place in which to go into any minute discussion of this subject nor further than should be of practical interest to the surgeon; nevertheless an examination of the blood by some common and routine procedure is so necessary in many surgical[30] conditions that it is impossible to entirely avoid the subject in a work like this. I have accordingly condensed it and put the salient facts about leukocytes into the following table:
Classification of Leukocytes.
| Granular. | Non-granular. | ||||||
|---|---|---|---|---|---|---|---|
| Normal. | - | Oxyphile. | A. | With fine granules | C. | Hyaline. Transitional (large | |
| Neutrophile. The so-called | (polynuclear) 60-70 per cent. | mononuclear) 4-8 per cent. | |||||
| neutral stain being | B. | With coarse granules | D. | Lymphocytes (small | |||
| slightly acid. | (eosinophiles) 2-5 per cent. | mononuclear) 20-30 per cent. | |||||
| Pathological. | - | Basophile. | E. | Fine and coarse granules | G. | Atypical hyaline | |
| (basophiles, mast-cells, etc.). | (myelocytes). | ||||||
| Oxyphile. | F. | Atypical (myelocytes). | |||||
In normal blood by far the greater part of the leukocytes consists of A and D. Lymphocytosis means a relatively high percentage of C and D. Eosinophilia means an increase in the proportion of B. Basophile cells are not absolutely pathological, for they may be present in very small numbers in normal blood.
The number of leukocytes in normal blood will average about 7000 to 10,000 per cubic millimeter, the percentage of each variety being given in the above table. Leukocytes are sometimes diminished in number; under diseased conditions they are often increased, and these are then included under the term leukocytosis. Variations occur daily and almost hourly under normal conditions. Increase naturally occurs after digestion, when the number of leukocytes may be almost doubled, the same being due principally to lymphocytes which are washed into the blood system from the lymph nodes by the flow of lymph or chyle. In starvation, however, the number may be remarkably reduced and in the case of the fasting man, Succi, the leukocytes were reduced at the end of the first week to 860 per cubic millimeter. The rather unusual condition of reduction of the number of corpuscles is called leukopenia.
Leukocytosis is usually the rule in carcinoma, with increase in A and F; the more rapid the growth, the greater this increase. In sarcoma this is even more pronounced; when occurring without hyperinosis the probability of malignancy is greater. Non-malignant tumors produce no such changes.
The blood platelets or plaques first described by Bizzozero, in 1882, have no small interest for physiologists and pathologists, but little for the practising surgeon. They number perhaps 5,000,000 per cubic millimeter and sustain a fairly constant ratio to the red cells. Their surgical interest is limited to the role which they may play in the formation of thrombus.
The term phagocytosis has to do in a general way with those leukocytes which act as scavengers by removing from the blood its noxious elements, presumably by a process of ingestion and digestion (see Chapter III).
Examination and estimation of the various formed elements of the blood are very valuable to the surgeon in the study of the anemias, of acute inflammation when the presence of pus is suspected, in the presence of suspected cancer, and in the presence of such conditions as Hodgkin’s disease, the various disorders of the spleen, etc. The so-called primary anemias include only the pernicious anemias and chlorosis; all others are designated as secondary. This distinction is not for convenience only, but serves a useful purpose.
Pernicious anemias produce a reduction both of the red corpuscles and the hemoglobin, the former usually in a greater degree than the latter, so that the color index (see below) is usually plus. Many of the cells become nucleated and, in general, their size is increased. In chlorosis the reduction of the hemoglobin is relatively large and the color index is extremely low. In the secondary anemias the red cells and hemoglobin are reduced disproportionately, so that the color index is minus. There may or may not be a relative increase of leukocytes and of the nucleated red cells, but these latter are not so likely to be as large as those seen in primary anemias. The color index is obtained by dividing the percentage of the hemoglobin present by the percentage of the red cells.
Leukocytosis becomes pathological in conditions of acute inflammation where the neutrophiles (A) show the greatest relative increase. The degree of leukocytosis depends on two different factors: the intensity or the virulence of the infection, and the vitality or resisting power of the individual. These vary within such wide limits that it is hard to predicate anything definite in a given case. In general the increase is supposed[31] to be proportionate to the severity of the infection, though the greater the reactionary ability of the patient the larger the number of white cells. Where vitality is very low leukocytosis is less pronounced. It is possible to have toxemia to such a degree that the activity of the leukocytes seems to be destroyed. The following summary from Cabot puts things in very distinct form.
Infection mild, vital reaction good—small leukocytosis.
Infection less mild, vital reaction less good—moderate leukocytosis.
Infection severe, vital reaction good—very marked leukocytosis.
Infection severe, vital reaction poor—no leukocytosis.
From this it will appear that the absence of leukocytosis in cases where it naturally would be expected is a serious indication and justifies an unfavorable prognosis; or else it may be interpreted in evidently favorable cases as indicating infection of very mild grade.
There are but few diseases in which leukocytosis by itself (or for that matter any other indication which the ordinary examination or blood count may give) is wholly sufficient for diagnostic purposes. But a blood count and estimate of the amount of hemoglobin present will often be of such advantage to the surgeon that he may well afford to wait in order to secure them. This is rarely necessary in acute cases, but in chronic cases, and especially the anemias, he may gain great benefit by such investigation. In trichinosis, for example, eosinophilia is most pronounced, B forming even as high as 70 per cent. of the leukocytes present.
The anemias which are of particular interest to the surgeon may be classified as follows:
1. A. Anemias due to hemorrhage may assume one of two forms, that resulting from sudden and extensive loss of blood or that resulting from constant oozing. Example of the former is seen in hemorrhages of the stomach or intestines after perforating ulcer, etc. Examples of the latter are met with in hemophilia and in uterine hemorrhages, or in excessive menstruation where the loss of blood extends over a considerable length of time. It is known, moreover, that certain entozoa in the intestines will produce a chronic anemia. Thus the red corpuscles may be reduced to even less than 1,000,000 per cubic millimeter. Immediately after acute hemorrhage the hemoglobin percentage is still normal, but after a short time it becomes reduced. If such cases do not speedily end fatally, nucleated red corpuscles appear in the blood and the observer will recognize both normoblasts and megaloblasts. At the same time the bone-marrow, which is normally yellow, becomes red, vascular, and richly cellular, and seems to furnish these cells just mentioned. Certain drugs, like potassium chlorate and glycerin, affect also the number of red corpuscles, but such poisons as these cause not only disintegration of the red cells, but produce also jaundice and hemoglobinuria. Pernicious anemia sometimes interferes with or fatally complicates surgical treatment. It is characterized by the extreme changes already mentioned, with which it marches steadily to a fatal termination. Quincke has reported an instance in which their number was reduced to 43,000 per cubic millimeter, while the hemoglobin was reduced to 20 or 25 per cent. of the normal amount.
1. B. The best example of anemia which depends upon diminution of the hemoglobin content of the red cells is that known as chlorosis. In this there are few recognizable signs of destruction of corpuscles, even under chemical microscopic examination; consequently the blood picture is very simple. The color index is very low, yet similar conditions may also be seen in syphilis, tuberculosis, and cancer. The underlying feature of all of these cases is malnutrition.
Within a few years a peculiar form of intense anemia has been described by Banti and others, and is often spoken of as splenic anemia or Banti’s disease. It is characterized by three stages: first, of splenic enlargement and anemia; second, a transitional stage; third, a stage of ascites which increases up to death. It is quite closely allied to Hanot’s hypertrophic cirrhosis of the liver. It is quite generally regarded as an example[32] of an infection by some as yet unknown organism. It is of interest to the surgeon because if the spleen is removed early there are fair prospects of recovery.
2. A. Anemias with marked leukocytosis include especially those first spoken of by Virchow as leukemia. Originally he applied the term to a particular alteration of the blood, but it is now made to cover a group of diseases, all of which are characterized by peculiar and more or less similar increase of white corpuscles. Sometimes these are increased to such an extent as to make the blood grossly resemble a mixture of blood and pus. This resemblance led some of the earlier observers to speak of the condition as “suppuration of the blood.” The number of leukocytes is sometimes enormously increased; 1 to 10 of the red cells is quite common and 1 to 5 not exceedingly rare. Cases have been known in which the white cells outnumbered the red. In well-marked cases of leukemia, the red cells will be somewhat diminished, while the white will number from 100,000 to 500,000 per cubic millimeter. Accompanying this change in the blood there are alterations in the spleen, the lymph nodes, and the bone-marrow, sometimes one predominating, sometimes another. It has been customary in fact to speak of splenic, lymphatic, and medullary leukemia, but these forms are not sharply differentiated and a pure type of either form is rare. In this country we speak mainly of lymphatic and splenomedullary forms, the latter being much more common. The latter is accompanied by enlargement of the spleen, while in the lymphatic form the lymph nodes are involved and may become as large as walnuts. In the lymphatic form over 90 per cent. belong to C and D; in the splenomedullary or splenomyelogenous form the increase of F and G is most marked, while A will be reduced to 50 per cent. and D to about 10 per cent. The red corpuscles are decreased in number, but not necessarily in an inverse ratio; their number may be reduced even to 2,000,000 in extreme cases.
In these cases, besides the change in number and form of the leukocytes already described, there are frequently found in the blood very minute crystals first described by Charcot. These are small, often adherent to the leukocytes, and most frequently found when eosinophile cells predominate; their exact significance is not known. The pathology of leukemia is too remote from the purpose of this work to receive consideration here. Without asserting its germ character one may say that it is under suspicion, and that various observers have described appearances supposed to indicate a specific cause, probably a protozoön.
2. B. Pseudoleukemia.—This has, in time past, gone under many different names, of which the most common is Hodgkin’s disease (q. v.). Many speak of it as malignant lymphoma. This is doubtless a disease with a specific cause, as yet unrecognized, which produces very significant changes in the blood, especially in the white corpuscles. The spleen and lymph nodes are both involved, mainly the latter. The general blood changes are quite variable and one may find many types. As a rule, these comprise not so much an increase in the number of leukocytes as a decrease in the number of red cells by which an apparent leukocytosis is brought about; hence the expression pseudoleukemia. Many cases, however, will present a certain degree of actual leukocytosis, the proportion of the whites to the reds being about 40 to 50.
What interpretation in general is to be given to leukocytosis? A condition deserving this name is, first of all, essentially temporary. In acute infectious diseases it shows itself during the febrile stage and the principal increase is in the finely granular oxyphile cells. In such diseases as erysipelas, as well as pneumonia, it lasts but a short time after the crisis has been reached and the temperature has fallen. In diseases like acute appendicitis and acute peritonitis from any cause a marked leukocytosis may be regarded as indicating the presence of pus; it should be emphasized, however, that pus may be present without this indication, and it has been previously stated that such a fact is to be interpreted either as an example of a mild degree of infection or an exceedingly reduced vitality.
—It seems to be now quite clearly demonstrated that the mere establishment of a certain degree of leukocytosis does not furnish the surgeon a reliable guide for determining the presence of pus, it being an index of reaction rather than of actual severity of any particular kind of infection. A much more reliable guide is found in the proportion of polynuclear cells to the total number of leukocytes counted, i. e., by what may be called a differential count. In order to make this reliable, the normal ratio should first be determined. This is put at a point between 68 and 80 per cent. by various writers. As Gibson (Annals of Surgery, April, 1906) says, 75 per cent. may be considered the best working average. This average should be maintained as the total number of leukocytes increases, or else there is a disproportion which becomes significant. With a moderate leukocytosis there is a notable increase in polynuclear cells, and it may be estimated that there is either a severe form of lesion or less resistance to absorption, or both.
PLATE I
Fig. I.

Fig. II.
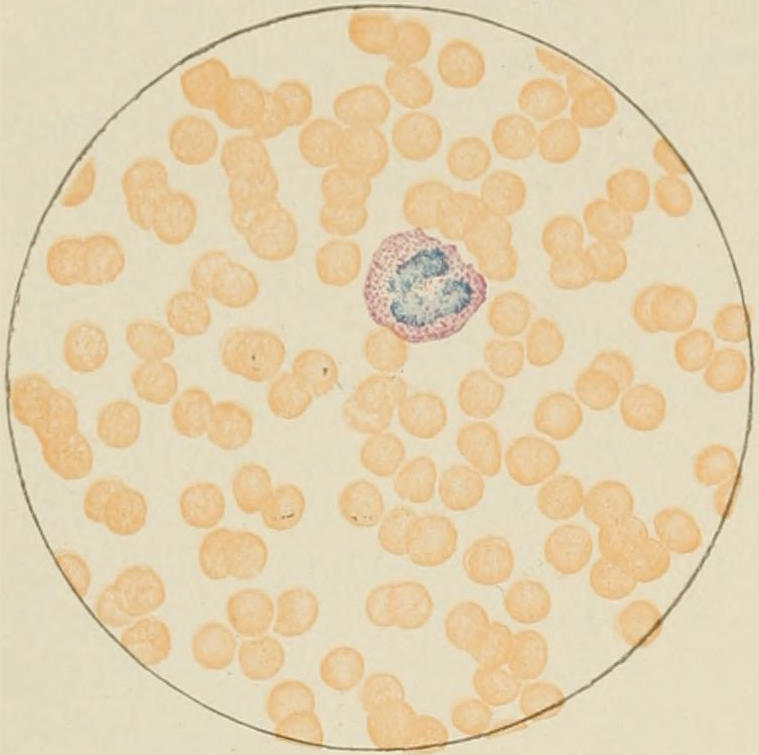
Fig. III.
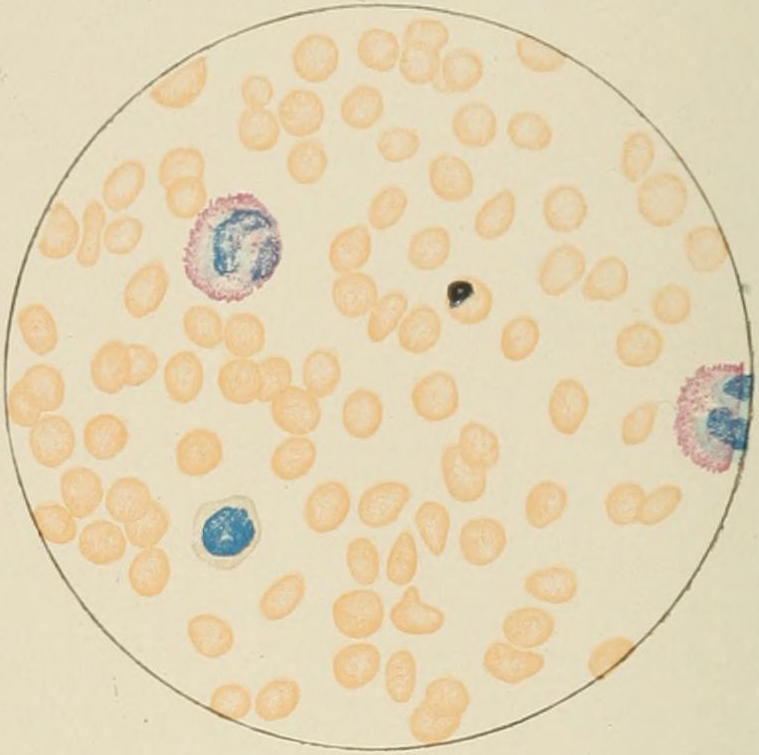
Fig. IV.
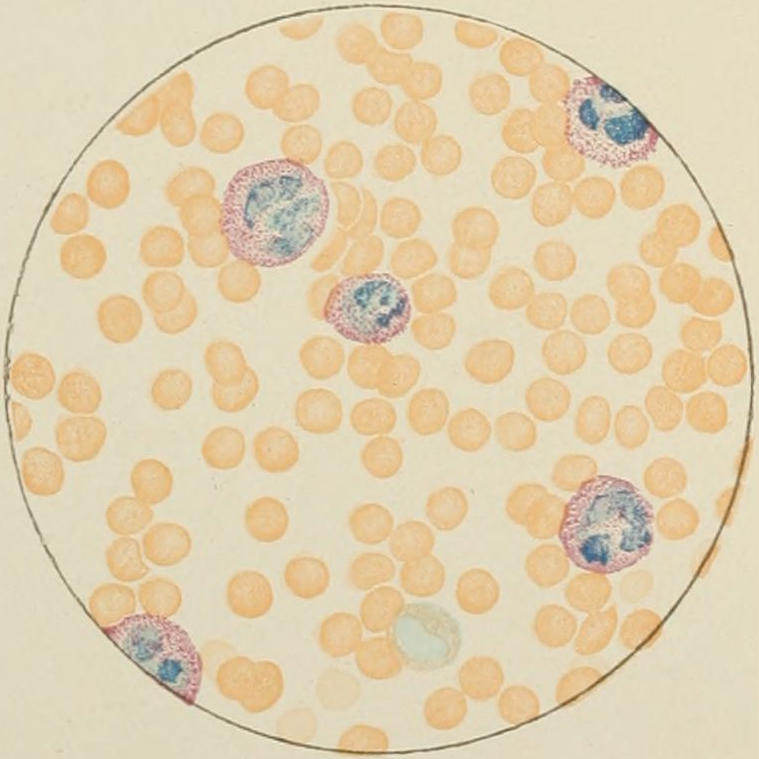
Fig. V.
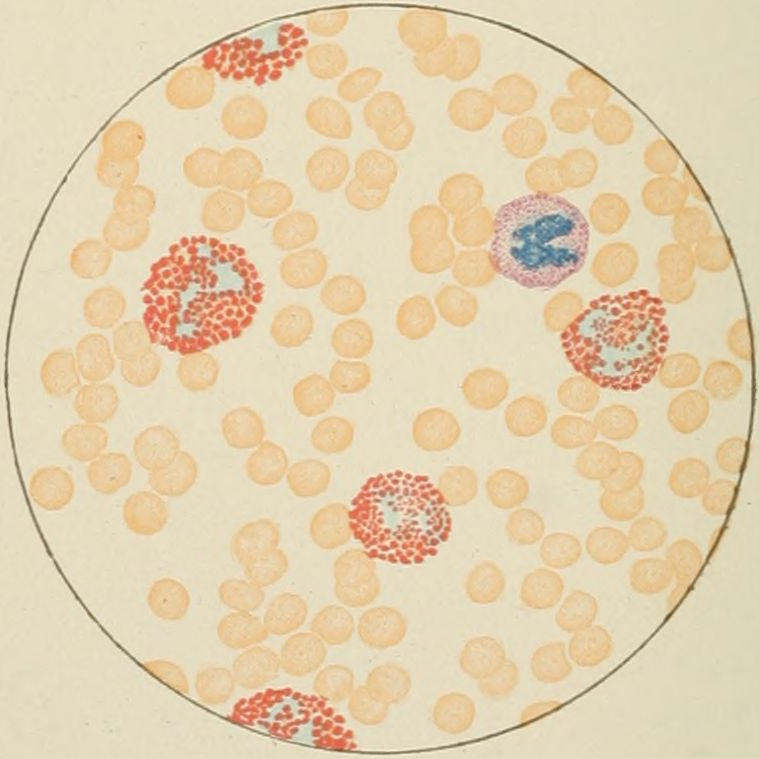
Fig. VI.
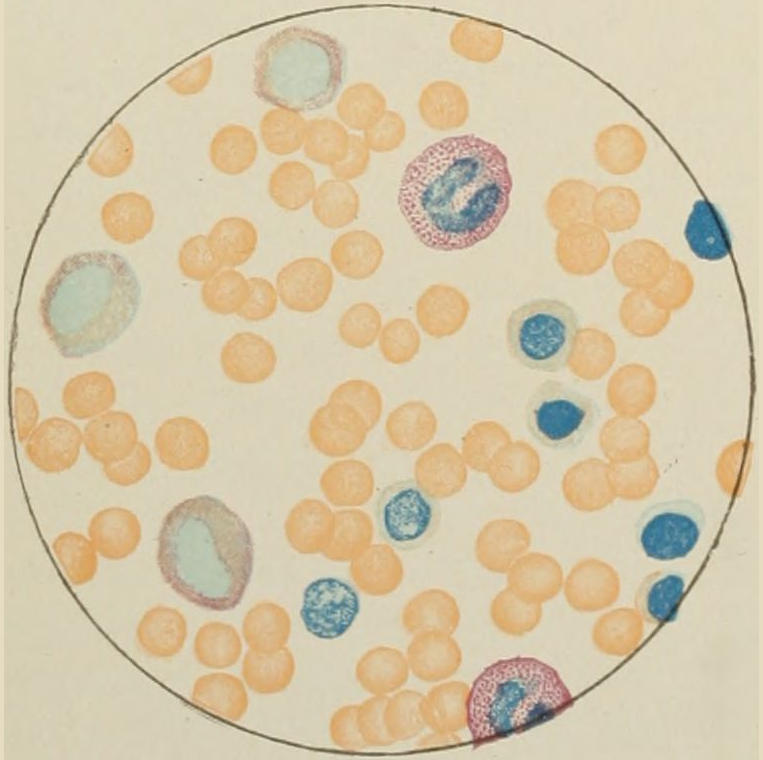
Fig. VII.
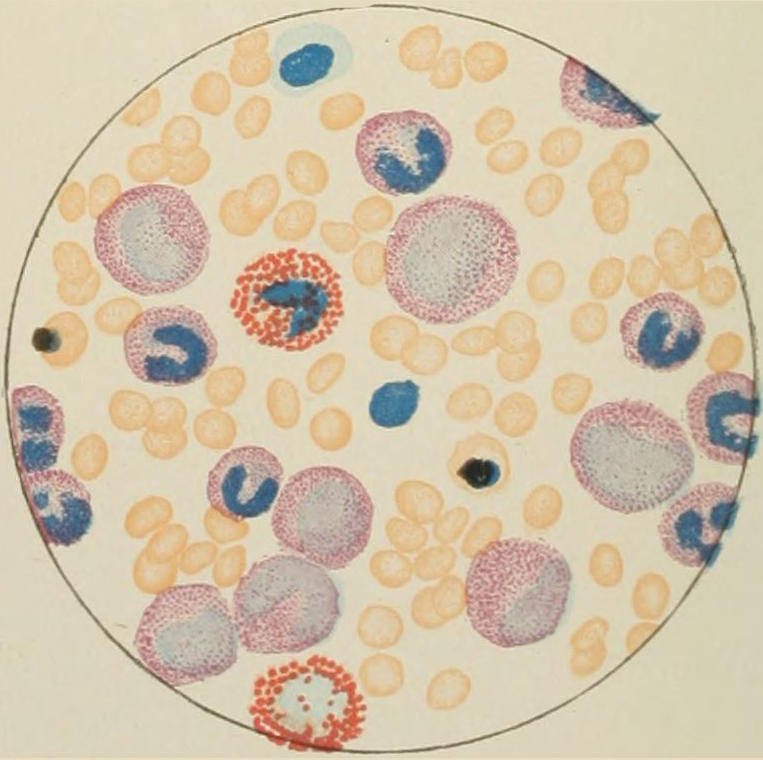
Fig. VIII.

DRAWN BY J. N. Z. CHASE
PLATE I.
BLOOD.
(Ehrlich triple stain.)
(Prepared by Dr. I. P. Lyon.)
Fig. I. TYPES OF LEUCOCYTES.
a. Polymorphonuclear Neutrophile. b. Polymorphonuclear Eosinophile. c. Myelocyte (Neutrophilic). d. Eosinophilic Myelocyte. e. Large Lymphocyte (large Mononuclear). f. Small Lymphocyte (small Mononuclear).
Fig. II. NORMAL BLOOD.
Field contains one neutrophile. Reds are normal.
Fig. III. ANÆMIA, POST-OPERATIVE (secondary).
The reds are fewer than normal, and are deficient in hæmoglobin and somewhat irregular in form. One normoblast is seen in the field, and two neutrophiles and one small lymphocyte, showing a marked post-hæmorrhagic anæmia, with leucocytosis.
Fig. IV. LEUCOCYTOSIS, INFLAMMATORY.
The reds are normal. A marked leucocytosis is shown, with five neutrophiles and one small lymphocyte. This illustration may also serve the purpose of showing the leucocytosis of malignant tumor.
Fig. V. TRICHINOSIS.
A marked leucocytosis is shown, consisting of an eosinophilia.
Fig. VI. LYMPHATIC LEUKÆMIA.
Slight anæmia. A large relative and absolute increase of the lymphocytes (chiefly the small lymphocytes) is shown.
Fig. VII. SPLENO-MYELOGENOUS LEUKÆMIA.
The reds show a secondary anæmia. Two normoblasts are shown. The leucocytosis is massive. Twenty leucocytes are shown, consisting of nine neutrophiles, seven myelocytes, two small lymphocytes, one eosinophile (polymorphonuclear) and one eosinophilic myelocyte. Note the polymorphous condition of the leucocytes, i. e., their variations from the typical in size and form.
Fig. VIII. VARIETIES OF RED CORPUSCLES.
a. Normal Red Corpuscle (normocyte). b, c. Anæmic Red Corpuscles. d-g. Poikilocytes. h. Microcyte. i. Megalocyte. j-n. Nucleated Red Corpuscles. j, k. Normoblasts. l. Microblast. m, n. Megaloblasts.
[33]
Gibson has suggested the formation of a chart where the number 10,000 of leukocytes shall appear upon the same line with 75 per cent. as the average normal proportion of polynuclears. Then drawing a parallel line, which shall indicate on one side each 1000 in increase of the former and each advance of one in the percentage, it will be seen that 15,000 leukocytes will correspond to 80 per cent. of polynuclears, 20,000 to 85 per cent., etc. When upon this chart there is drawn a line between that dot which represents the total leukocytosis on one side and that on the other which indicates the percentage of polynuclears, then the more horizontal this line the less the disproportion, while the more marked the angle it makes with the base line the greater the disproportion appears. It furnishes an admirable graphic record which the eye appreciates at once.
It would appear, then, that a differential blood count made in this way, and thus recorded, affords the most valuable diagnostic and prognostic aid in acute surgical diseases, indicating especially the presence of suppuration or of gangrene.
—Glycogen occurs in the blood especially in three classes of cases: those where there is marked respiratory disturbance in certain of the anemias, and, what is of especial interest to the surgeon, toxemias, either of chemical or bacterial origin. It is usually present in the secondary and pernicious anemias as well as in acute and late leukemias. It is considered by some that in these cases it really indicates the occurrence of some bacterial infection. Especially is glycogen present in cases of suppuration and surgical sepsis, i. e., in those cases where leukocytosis is usually, but not invariably, present; indeed, it would seem to be a most significant indication. While the iodine test is more easily carried out than is a blood count, the latter affords more information. The reaction is reliable and its relative intensity gives an idea of the intensity of the inflammatory process. In many cases with obscure symptoms and without leukocytosis its presence will afford much aid in diagnosis. It is of great assistance also in distinguishing between a deep-seated pneumonia and serous pleurisy, since in the latter there is no reaction, or in distinguishing between pleurisy with effusion and empyema; again, in distinguishing gonorrheal arthritis from true rheumatism. In a case of strangulated hernia the presence of the iodine reaction would indicate that pressure had produced gangrene, whereas its absence would indicate a relatively lesser degree of destruction. It has been aptly said that the presence of iodine reaction indicates that the patient is seriously sick.
It is easily obtained by staining a cover-glass with a blood smear in a gummy solution of iodine and potassium iodide. When the blood is normal all the cells take on a uniform, bright-yellow color, while the white cells stain more lightly than does their protoplasm. When the glycogen reaction is present, brown granules are seen in the protoplasm of the polynuclear leukocytes, which may often take on a different brown tint. Frequently brown particles are to be seen outside of the corpuscles, while occasionally the other forms of leukocytes show also the reaction.
The value of a careful blood examination is well illustrated by Plate I, prepared by Dr. Irving P. Lyon, in which are displayed the alterations of greatest interest to the surgeon.
The principal interest of the red blood corpuscles for the surgeon, aside from their relative number and shape, inheres in their relation to hemoglobin, and hemoglobin is of particular interest here because much can be learned by estimating the proportion in which it is present. Hemoglobin has, furthermore, an interest which reaches beyond the mere blood appearance, since it is considered to be the apparent source from which both the urinary and biliary pigments are produced. That the amount contained in the blood varies within wide limits under different conditions has long been known. When notably reduced in amount the condition is referred to as oligochromemia. The ideal normal standard is present in but a small proportion of cases, even in strong young men in the[34] third decade of life. The average is considerably lower and can scarcely be placed above 90 per cent. Females show a smaller amount than males—3 or 4 per cent. less. In anemia its reduction is not usually proportionate to that in the number of red cells. After hemoglobin loss, as after surgical operations, much can be gained in the matter of prognosis by estimating the speed of its regeneration. With regard to how much actual hemoglobin loss a patient can bear, it seems to be more important to determine how much still remains in the body. The minimum is apparently 20 per cent. In three cases dying of collapse after operation, Mikulicz found only 15 per cent. remaining. The rapidity of regeneration is a fairly accurate indication of improvement in every other respect. Regeneration is interfered with by constitutional syphilis, and, on the other hand, is often apparently favored in cases of tuberculosis. In malignant tumors the average of hemoglobin is reduced to about 60 per cent., and in these cases also complete regeneration is materially retarded. Incomplete removal or recurrence of cancer prevents typical regeneration or restoration, while, after successful or radical removal, complete restoration to the previous standard, often with positive gain, is obtained. Thus, a woman who had gained thirty pounds after resection of a cancerous pylorus, showed, after three months, hemoglobin repair to the amount of 65 per cent. A prognostic significance often attaches to the accurate estimation of hemoglobin at intervals after removal of malignant tumors.
A very convenient method for the ready estimation of hemoglobin is afforded by the Tallquist color scale. It can be practised at the bedside and is sufficiently accurate for the surgeon’s general purposes.
Thrombosis is a term applied to the formation of a thrombus—i. e., a clot within the cavity of the heart or one of the bloodvessels—the term being limited to coagulation of blood within these natural cavities, and without specifying the exciting cause of the same. A clot so formed is called a thrombus. To be accurate, a distinction should be made between a thrombus, which is caused always before death—or, rather, during life—and the clot, which is essentially a postmortem affair. Our application, then, of the terms “thrombosis” and “thrombus” refers solely to that which takes place during life. In order to appreciate the conditions which lead to thrombosis it is necessary to fully appreciate the reciprocal conditions which must normally be maintained between the circulating blood and the walls of the vessels in which it flows. Fluidity of blood depends always upon integrity of the vessel wall. As long as its lining membrane is absolutely undisturbed and normal, moving blood will never coagulate within it, and the only thrombi that may be met within it are those which are propagated from a distance. Coagulation of blood is, for the main part, associated with the peculiar properties of fibrin.
Fibrin is produced from fibrinogen, a globulin which is held in solution under ordinary circumstances, which has certain peculiarities of its own. When the change occurs it is entirely consumed and none remains in the blood serum. Fibrinogen is split up by a peculiar ferment called thrombin into what we ordinarily speak of as fibrin and a small amount of a soluble globulin, which remains in solution in the serum. Thrombin is not a normal constituent of the blood, but is formed when it escapes, as the result of the reaction between certain calcium salts and a nucleoproteid, which has been called prothrombin. The latter arises from the disintegration of the leukocytes, especially the polynuclear, and the blood plaques, after the blood leaves the bloodvessels. Calcium salts seem absolutely necessary for coagulation; hence the value of the administration of calcium chloride in certain cases previous to operation. Another essential feature seems to be the absolute integrity of the endothelial lining of the bloodvessels, although for this fact there is no satisfactory explanation. If a portion of a vein is removed from the body after double ligation its contained blood will not coagulate for a long time. Blood which is kept circulating through the lungs and heart alone soon loses its coagulability; hence the liver seems to be concerned in some way in maintaining it. Certain other substances also seem to retard coagulation, such as the albumoses of snake venom, and certain synthetic, colloid, proteid-like substances, which can be introduced very gradually. If, however, they are introduced rapidly, or in large quantities, thrombosis occurs promptly. We have much to learn about the coagulation of the blood, but the above facts are at least suggestive to the surgeon.
PLATE II
FIG. 1
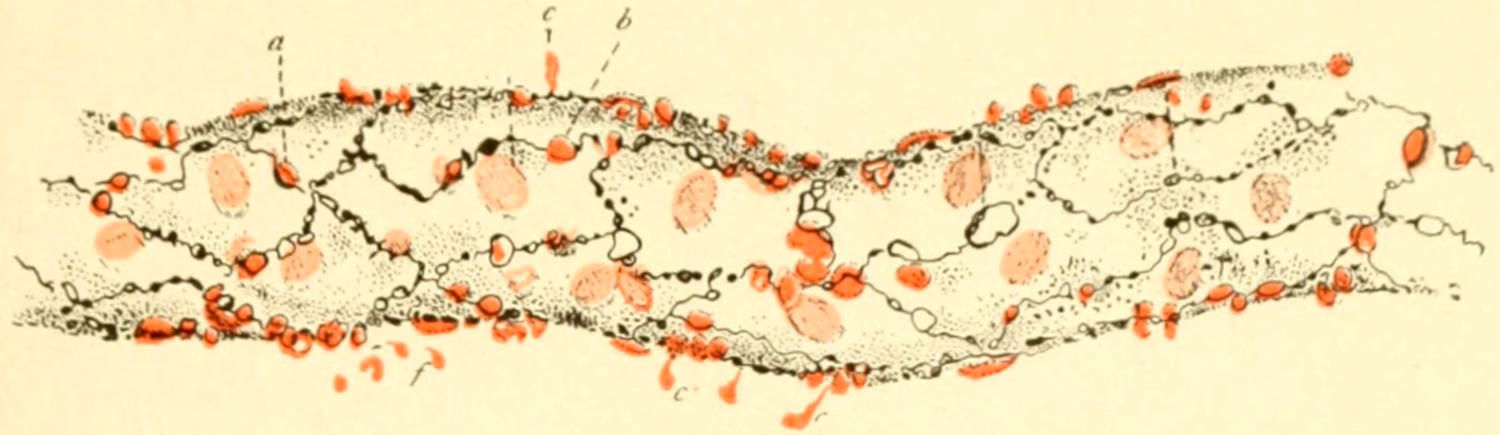
Small Vein showing Diapedesis of Leukocytes. (Engelmann.)
a, leukocyte escaping between endothelial cells; b, c, leukocytes escaped; f, leukocytes migrating toward centre of attraction.
FIG. 2
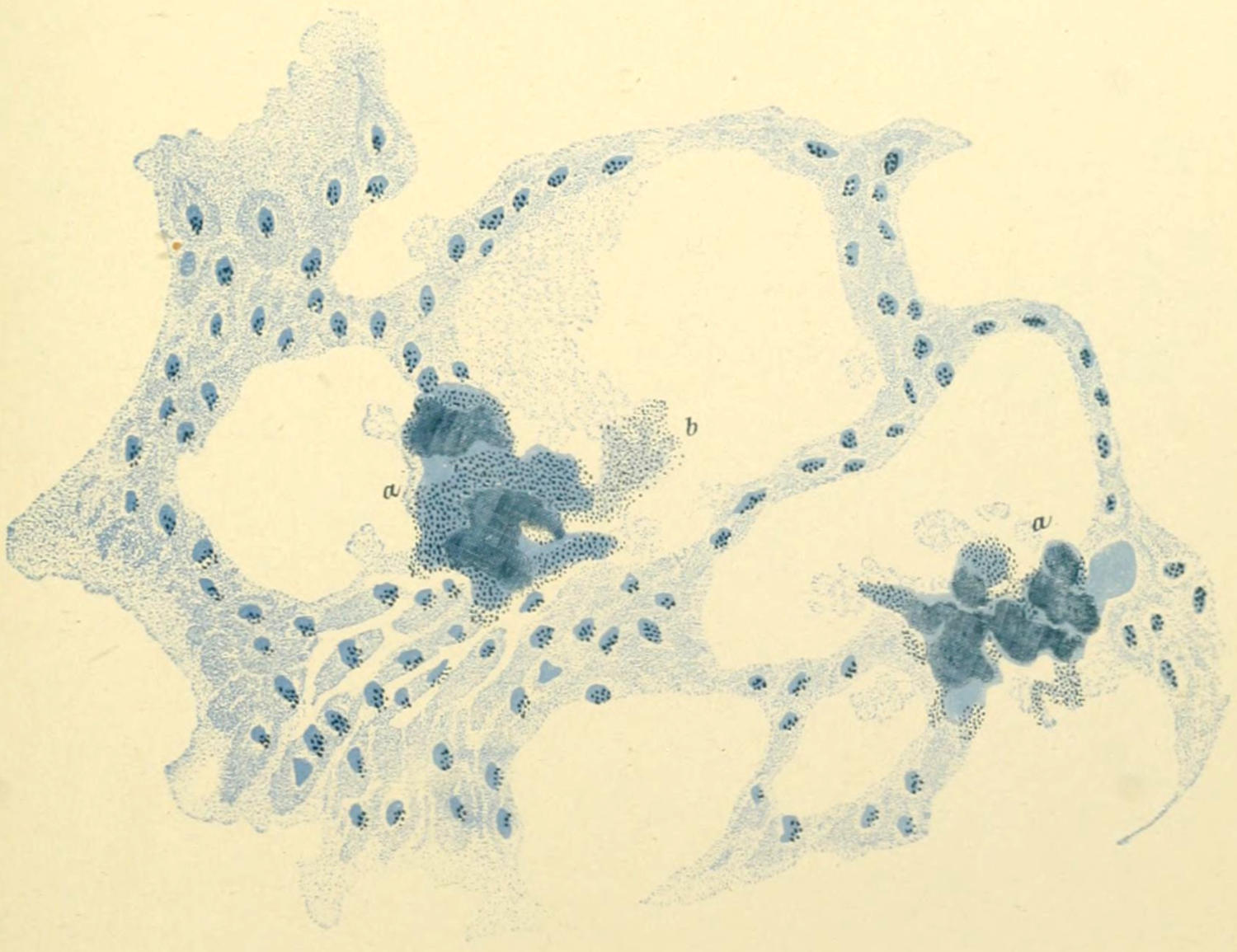
Septic Thrombosis of Pulmonary Capillaries after Puerperal Septicemia, showing Rapidly Increasing Colonies of Streptococci. (Klebs.)
[35]
—The underlying cause of all thrombi is, then, alteration of the endothelium. In consequence, when it is desirable to produce coagulation artificially, advantage may be taken of this fact, and mechanical injury to the vessel walls may be quickly followed by the desired results. Advantage is also taken of this fact in surgery, especially in certain methods of treating aneurysm, by rude handling, by needling, by the introduction of horsehairs, fine wire, etc. A venous thrombosis is certainly favored by the thinness of the venous walls, by which poorer protection is afforded to their lining endothelium, and infection more easily occurs. Arterial thrombosis is favored when cardiac vigor is impaired and vessel walls are thickened so as to obstruct the blood current. This occurs particularly in syphilitic endarteritis, where the intima suffers most, and final occlusion is due to the thrombus thus formed. Arteriosclerosis does not, by itself, often produce this trouble; it comes rather with atheromatous and calcareous degenerations. The local ischemia which is occasioned by ergotism, by pellagra (due to use of certain kinds of maize), by the vasomotor spasm of Raynaud’s disease (see under Gangrene), by too long-continued constriction, or by frostbite, causes results comparable to those produced experimentally in parts supplied by a terminal artery, e. g., in the kidney after temporary occlusion of its artery. All the tissues involved undergo profound alterations, in which thrombosis figures very largely and may lead to gangrene.
While such endothelial lesions are essential, there are, nevertheless, numerous other accessory causes which should be mentioned. These comprise:
A. The presence of foreign bodies, as, for example, needles, hooklets of echinococci, parasites, particles of tumors, fragments from the heart valves, and, most of all, that which is essentially a foreign body, a clot which has come from some other point. Around such foreign particles will quickly group themselves a relatively large number of leukocytes, thus affording another example of phagocytosis, soon to be described. Mere slowing of blood stream without some such mechanical irritation is not sufficient to produce coagulation. If, for instance, a section of vein is isolated between two ligatures, the ligation being aseptically done and the surroundings of the vein wall disturbed as little as possible, the blood thus shut up within the vein remains fluid indefinitely. If, however, the vessel wall is separated from its surroundings, so that its nourishment is compromised, the contained fluid quickly coagulates.
B. Necrosis, gangrene, etc., lead to quick involvement of the endothelium of the vessels contained within the involved part, and consequently to quick coagulation of the blood which they contain.
C. Temperature has also an influence in the same direction, and extremes in either direction, or drying of vessels which may happen to be exposed to the air for some time, lead to the same results.
D. Inflammatory and degenerative processes occurring in and about the vessel walls tend always to produce coagulation. This is well seen in the influence exerted by the so-called atheromatous ulcers—i. e., the degeneration of certain areas in the walls of large vessels.
E. Microörganisms and their products are perhaps the most frequently effective of all the accessory causes of thrombosis. In other words, in all the surgical infectious diseases we may expect to find more or less, sometimes extensive, thrombosis in the vessels of the affected part. This may so far shut off circulation as to produce temporary or permanent edema, or it may lead to gangrene, which may be local or may terminate the life of the patient.
Thrombi are classified as:
The primary thrombus is one which has originated at the spot where it has been first produced, and is usually co-extensive with its cause. The propagated thrombus may be one which has been carried to a considerable distance, and is met with at a point widely different from that where it originated, or one which has extended along the vascular channel in which it was first formed, but far beyond the limits of its prime cause. When a thrombus attaches itself to a part of the vessel wall it is called parietal or valvular, because it does not completely occlude the vessel; when it involves the entire circumference of the vessel, but does not completely occlude it, it is spoken of as annular.[36] The obstructive thrombus is that which completely fills a given vessel and shuts off all circulation through it.
The propagated thrombus extends usually in both directions, and always much farther in veins than in arteries. Thus, thrombi may be met with extending from the ankles even into the inferior vena cava. The venous valves may on one hand excite coagulation, or on the other tend to fix the coagula more firmly in their place. In arteries thrombi usually extend only to the first collateral channel on the cardiac side, but occasionally they spread farther. The cause of a primary thrombus is to be sought at the site of its lodgement; the cause of propagated thrombi is often observed at a wide distance from the effect.
Thrombosis is, again, to be spoken of as—
a. The marasmic forms are due to essential alterations in the constituents of the blood, which are due mainly to starvation or wasting disease. Marasmic thrombi seldom give rise to serious disturbance during life until the condition is so complex and grave that the patient is at death’s door. Postmortem evidences of marasmic thrombi, however, are often found, and yet have but little surgical significance. They are seen perhaps as often in the cranial sinuses as anywhere.
b. Thrombi of mechanical or traumatic origin are those, for instance, which are due to the presence of foreign bodies, to stagnation of blood as the result of ischemia or local anemia, to compression by tumors, etc.
c. Infective thrombi are those distinctly due to the injurious effects of micro-organisms, and are those mainly concerned in the various manifestations of sepsis which are of interest to surgeons.
While the ordinary evidences of thrombosis are most often looked for in the veins of the extremities, in the lungs, and in the cranial sinuses, it must not be forgotten that thrombosis may occur equally easily in the portal system of vessels; in which case we find the most marked expressions in this system and in the liver. In cases also of pyemia proceeding from lesions in the rectum or in the bowels there are evidences of infection, abscess, etc., in the liver, but not in the lungs, to which point infective thrombi from other sources are promptly carried.
The ultimate fate of a thrombus depends entirely upon the presence or absence of bacteria. If septic, it invariably breaks down. If aseptic, it may undergo one or more of the following metamorphoses:
A. Decolorization.—This is noted particularly in the red thrombi, and is due to disintegration of the red corpuscles, their coloring matter being diffused and resorbed or transformed into hematoidin. It would be a mistake, however, to suppose that all light-colored thrombi are those which, originally red, have been decolorized. The possibility of white thrombi must always be remembered.
B. Organization.—This is the result of time, and means a metamorphosis into solid vascular connective tissue. Newly formed, minute, vascular loops project from the vasa vasorum into the thrombus, and it becomes thus vascularized, while the completion of the organization is due, in the main, to spindle-cell connective tissue, which is formed by wandering cells that penetrate into the thrombus from without. This gives the organized thrombus a certain resemblance to a sponge, and makes the original vein resemble a cranial sinus, since its interior is spanned by bands of connective tissue. Typical illustrations of this kind are seen, for instance, where the iliac veins join to form the inferior cava, by which a certain amount of obstruction to venous return is produced without its being total. The length of time required for these changes is indefinite. They begin, however, within a short time after ligature of a vein, and proceed with a rapidity varying according to circumstances.
C. Calcification.—Calcium salts are occasionally deposited in thrombi, usually not until they have undergone considerable contraction and alteration; as the result of which we have formation of small masses, essentially minute calculi, to which the name of phleboliths has been given. These phleboliths are not infrequently found in more or less occluded and much distended varicose veins of the extremities, and they prohibit the occurrence of softening.
[37]
D. Softening.—This is the most serious termination of the thrombotic accident, and is usually due to the agency of infecting organisms. A non-infectious form is, however, recognized, by which there is a metamorphosis of original clot into an oily or pulpy fluid, usually dark colored, but in the white thrombi often yellowish white, reminding one crudely of pus. The discovery of such material under these circumstances has led in time past to the supposition that pus, as such, was found floating in the blood—a condition that does not exist except under extraordinary circumstances. It is with infection of thrombi and consequent softening, however, that surgeons have most to deal, and the paramount importance to them of such disturbances is emphasized in the article under Pyemia.
A closely allied topic to that above considered is the subject of thrombophlebitis. This means, in effect, inflammation of one or more veins, which is directly due to the presence therein of thrombi. Such a condition is, in its strict sense, an inflammation, since it is always an infectious process. If in the veins of a non-infected region simple thrombi form, they may be occluded by organization of the included masses, but such a process never extends beyond the immediate area involved. On the other hand, if the process is essentially an infectious one, either from without or from within, then both vessel and its contained thrombi succumb completely to the infectious process, which is also essentially a spreading one; and this is limited only by mechanical barriers, by conservative suppuration, or often only by the life of the individual. Excellent examples of thrombophlebitis are seen in the involved uterine sinuses in cases of puerperal septicemia, and in the cranial sinuses after infected compound fractures, or particularly after disease originating in the middle ear has extended to them.
Thrombosis is, at times, a distinctly surgical condition, and often a surgical complication of febrile and other diseases, especially typhoid, in which it constitutes a serious complication and prolongs convalescence for a period of several months. If foreseen it can scarcely be prevented, and when present calls for treatment varying with the location of the lesion and the exciting causes. In the earlier stage anything like rude manipulation or massage is very unfortunate, since soft clots might thus be broken up and distributed to other parts of the body. Absolute physiological rest combined with the application of silver ointment, of ichthyol-mercurial ointment, which should be covered with some non-absorbent material, will probably give the best results. If the lower limbs are affected it may be well to elevate the feet so as to favor return of blood through vessels not yet obstructed. After a certain length of time the thrombi may be regarded as at least adherent if not organized, and massage will prove an important remedy, since by it the lymphatics will be better enabled to take up the fluids which have leaked from the bloodvessels and produced the edema which always characterizes these cases. Sluggishness of circulation is nearly always followed by more or less laxness of tissue, or actual hypertrophy, and a limb thus involved may never regain its original size or flexibility. Veins once compromised, if not occluded, frequently become varicose, or varicosities develop in adjoining veins and still further complicate the case. For such difficulty the measures discussed in the chapter on the Veins may be later required.
In every fresh case of thrombosis or thrombophlebitis great care should be taken in order that by no means shall the clots be disengaged and float away. The dangers correspond to those existing in variocele and nevi, often treated by the older methods of injection of coagulating material. In one instance reported, a child died within half an hour after the injection of an iron salt into a small nevus of the face. Coagulation was excited to a point far beyond the limits intended.
Thrombophlebitis is essentially a surgical condition, occasionally terminating favorably by suppuration and spontaneous evacuation, but calling for surgical intervention whenever it can be recognized and the parts are accessible. The principles of treatment of these conditions are positive and unmistakable. They comprise evacuation of the infective material and disinfection of the involved cavities and tissues. Thus, in sinus phlebitis—i. e., thrombophlebitis of the lateral sinus—it has been made practicable not only to open the sinus in the mastoid region, but to expose the jugular vein in the neck, to ligate it, and to wash through from one opening to the other, effectually getting rid in this way of a long mass of infected thrombi. Only by such bold and radical measures in many of these instances may life be saved.
[38]
Embolism means the transportation of any material by which a bloodvessel can be occluded or plugged from one part of the vascular system to some other. The underlying idea is that of transportation or carriage. An embolus is anything so transported, without implying its exact character. The name is even applied to so unsubstantial an affair as a minute bubble of air, which, however, in a tube containing a circulating fluid is a possible source of considerable disturbance. A single bubble thus carried would, by itself, be a trifling affair, but when numerous bubbles are thus transported the result is such local disturbance as may lead to loss of function. Thus, air embolism, so called, may provoke profound, even fatal, disturbances, as, when, with the returning blood stream through the cranial sinuses or one of the large veins in the neck, when opened by accident or operation, air is sucked in, it is carried to the right side of the heart, whose action is perhaps completely perverted because of the new and strange substance which thus enters it, so different from that for which its lining membrane is prepared and to which it reacts. The entrance of air into veins, which constitutes in effect air embolism, has been in time past a bugbear to surgeons, but nevertheless is a source of probable danger when large venous trunks in proximity to the heart are thus exposed. Air embolism is certainly a rarity. On the other hand, those substances which figure most often as emboli are vegetations from the valves of the heart; drops of fat; fragments of tumors; pieces of softened and disintegrated thrombi; foreign bodies, as hooklets of echinococcus cysts; and, perhaps most often of all, the microorganisms clinging to some minute fragment of thrombus which has been dislodged. Embolism is also produced experimentally by the artificial introduction into the circulating blood of cinnabar or small particles of pith or other material. Emboli differ in number and size from the smallest appreciable up to the largest, which may be met with in the larger venous trunks. They are dislodged from their primary site sometimes by accident, as by rude manipulation, injury, etc.; sometimes by undue cardiac activity, as when detached from a valve wall; sometimes by the process of softening of thrombus and a subsequent introduction into the blood stream as a result of some trifling motion; or even by spontaneous processes. Emboli also differ in numbers according to the nature of the primary lesion. In cases of so-called fat embolism fluidified fat is taken into the returning blood stream, carried to the heart, churned up with the contained blood, and distributed to the lungs in such a way that myriads of minute fat masses are distributed throughout the capillaries of the lungs, and free circulation of blood through them is thereby impeded.
It will thus be seen that the relations between thrombosis and embolism are most intimate, but that either one may occur without the occurrence of the other.
Among the viscera, with the exception possibly of the brain, the disastrous consequences of such processes as those just described are more apparent and indicative than in thrombosis and embolism of the mesenteric bloodvessels—a condition not so rare as journal articles would imply, yet, nevertheless, one seldom recognized either during life or after death. Its principal symptoms consist of intense abdominal pain, bloody diarrhea, subnormal temperature, sometimes with vomiting, perhaps in the latter stages vomiting of blood. Shock is usually also extremely marked. The consequence of this condition is almost inevitably gangrene of the intestine supplied by that particular portion of the mesenteric vessels. The pain comes on within a short time after the occurrence, and under the peculiar circumstances gangrene may be practically determined within a few hours. Some two hundred and fifty cases of this kind are now on record, and the condition is one well worth the prompt attention of the surgeon, because only by surgical intervention—i. e., by resection of the necrotic mass of intestine—can life possibly be saved. That when a limited portion of the intestine is involved the gangrenous part may be successfully removed has been proved by several operators. (See Chapter LII.)
It will thus be seen that embolism constitutes often a distinctly surgical condition for which unfortunately only radical measures are suitable. Many cases of gangrene of the toes and feet, extending to the legs, are produced by embolism of the femoral and popliteal arteries, similar conditions being noted less often in the upper extremities. Amputation offers the only resource in such instances, at the same time affording no guarantee against any similar embolic disturbance elsewhere. In only most exceptional[39] instances is it possible, by resorting to moist heat, position, etc., to encourage circulation to such an extent as to obviate the necessity of amputation. (See Chapter V.)
—Fat embolism as a distinct, sometimes fatal, surgical condition has received of late so much study as to be entitled to consideration by itself. By this term is meant a plugging of small arteries by minute drops of fat, which, having been set free somewhere about the periphery, are carried into the venous circulation and thence distributed to various parts of the system. Inasmuch as the capillaries of the lungs are often their first lodging place, fat embolism here is most often met with, and consequently recognized and studied. But it may occur in the brain, the choroid, the kidneys, or other parts, provided only that there has been sufficient ris a tergo on the part of the heart to force the fat globules through the pulmonary capillaries and into the systemic circulation.
Fig. 2
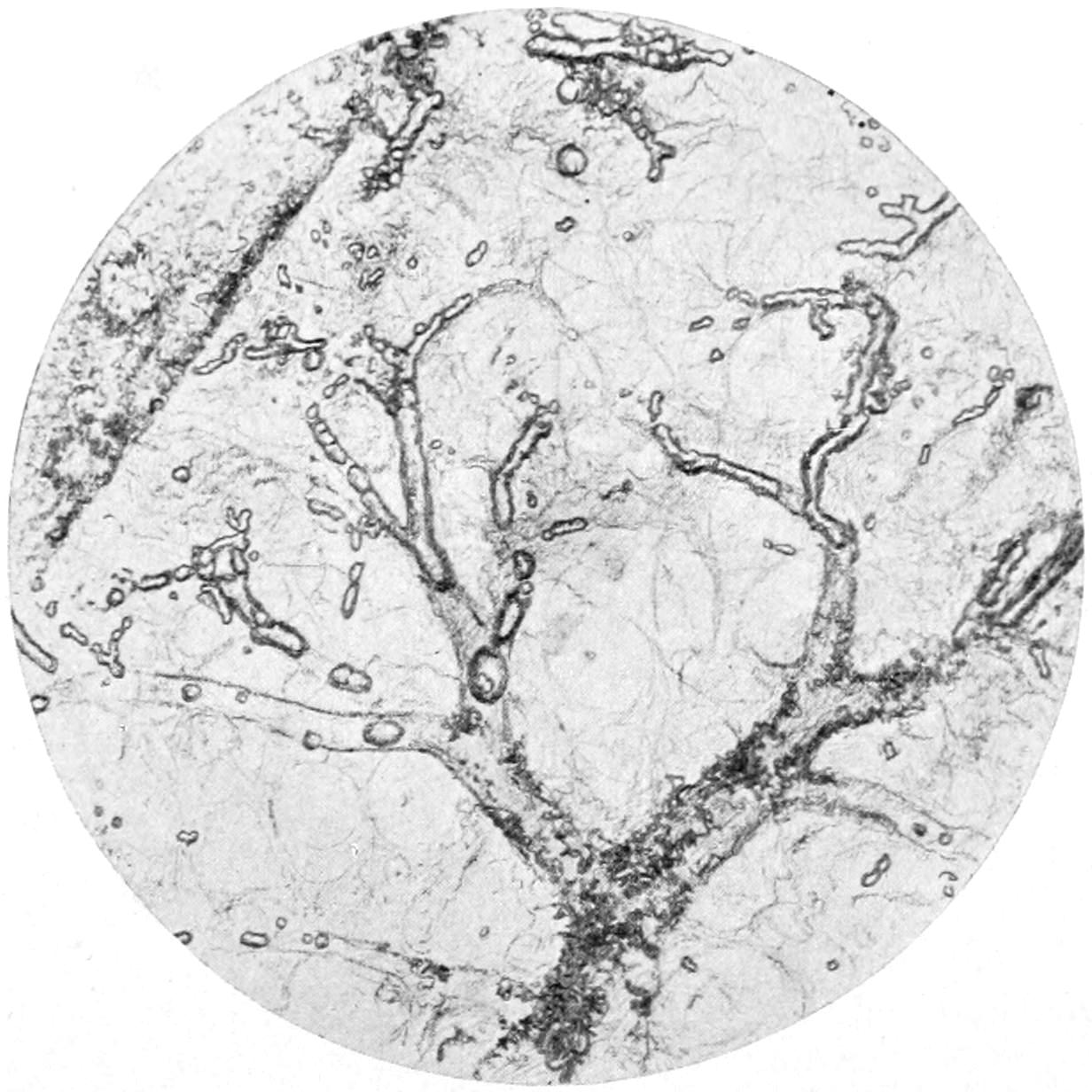
Fat embolism of lungs. Large branching pulmonary artery filled with spherical, oval, cylindrical, and branching masses of fat. Fresh mashed preparation in potassium hydrate. (Kaiserling.)
Fat embolism occurs frequently, and to a slight extent in nearly every case of fracture and laceration. So common is it, and so closely allied are some of its most prominent symptoms to those of shock, that as a matter of fact many cases heretofore considered shock are to be regarded as instances of this condition. Indeed, even in a miscellaneous series of 260 dead bodies fat embolism was found in 10 per cent. The injuries most likely to be followed by it are simple, and particularly compound fractures of bones; laceration of soft parts, especially of adipose tissues; certain surgical operations; acute infections of bone and periosteum; rupture of fatty liver; and certain pathological conditions where the phenomena are not so easily explained, e. g., icterus gravis, diabetes, etc.
Drops of fat may be seen floating on fluid or semifluid blood after many operations and compound injuries, and the possibility of escape of fat—or, more accurately, its suction into the vessels from which this blood has escaped—is easily appreciable. But it has also been shown that absorption of fat is possible even from serous surfaces, and that fat embolism may occur when fluid fat has been passed into the heart through the thoracic duct, although more slowly. Oil drops are also found in the interior of the tissues, while in a piece of lung spread out in water in the visible vessels highly refracting fatty material may be noted. Fatty infarction, particularly in the lower lobes, is sometimes plainly visible to the naked eye. Under a low objective, especially with osmic-acid staining, the presence of fat is easily demonstrated.
The essential danger in case of fat embolism is of so clogging the pulmonary capillaries that oxygenation shall become so imperfect as to lead to absolute asphyxiation[40] from carbonic dioxide poisoning. When this fact is understood, the cyanosis, the rapid breathing, the overaction of the heart, etc., are easily and correctly interpreted.
Fat embolism by itself cannot cause inflammation nor infection, nor sepsis in any sense. It may, however, lead to ecchymoses in conjunction with fatty infarcts in the organs most affected. The minute hemorrhages are easily explained by the bursting of the capillaries in the attempt to force blood through them. Fatty emboli, however, take the same course as do septic—are carried first to the right side of the heart and distributed over the lungs; are, if the patient lives, forced through the lungs into the systemic circulation, and are then carried to the brain, kidneys, etc. The first symptoms are referable to the plugging of the pulmonary capillaries; the secondary symptoms to the systemic disturbance.
—Pallor of countenance with facial expression of anxiety and distress, followed by cyanosis and contracted pupils, are seen. Patients are usually first excited, sometimes more or less disturbed, then become somnolent, and, finally, comatose in the fatal cases. The respiration rate increases from normal up to 50 or 60, and breathing is sometimes stertorous. Dyspnea, increasing in intensity until it becomes agonizing, sometimes marks these cases. Occasionally foam, possibly blood, proceeds from the mouth, as in edema of the lungs. Sometimes hemoptysis occurs. The pulse becomes weak, frequent, and irregular, while toward the close it is fluttering. Temperature is not notably disturbed, at least not typically.
These symptoms set in usually within thirty-six to seventy-two hours after the lesion which has caused them. I have, however, known death to occur in one or more cases within eighteen hours after reception of injury.
After fat has been forced through the lungs and carried to the kidneys it will be eliminated with the urine, and may be found floating upon it in the shape of oil-like drops. Discovery of this condition is positive evidence of fat embolism. It is to be distinguished from shock in that by the time the symptoms of embolic disturbance are at their height, all or nearly all symptoms of pure shock have subsided. Furthermore, cyanosis and embarrassment of respiration are not indicative of shock; and, finally, the discovery of fat in the urine will be corroborative.
A mild degree of fat embolism may be noted, if looked for, after almost all serious fractures. It will give rise to slight embarrassment of respiration and cyanosis and to the elimination of fat by the kidneys.
—Prognosis varies according to the extent of the injury and the proximity of the lesion to the heart and lungs; also to the possibility of continuous entrance of fat, i. e., from its continual absorption. Prognosis really depends upon whether the heart can be given sufficient vigor and endurance to continue pumping blood with its burden of fat through the pulmonary circulation. A secondary danger may come from the circulation of this fat-ladened blood through the capillaries of the brain. Should the source of motive power thus become paralyzed with resulting general enfeeblement, death may ensue. When well-marked evidences of fat embolism are present, but are followed by recovery, the worst of the trouble is usually over within forty-eight hours after it begins.
—Obviously treatment is mainly directed toward the heart, so that we may stimulate it to carry its load of fat through from the venous into the arterial system. If it can do this, the fat is disposed of by oxidation or is saponified by the alkalies in the blood. Physiological rest of the injured part is the first indication, however, and if this occurs in a patient, say with delirium tremens, powerful mechanical restraint may be necessary. The most effective cardiac stimulants are called for—alcohol, adrenalin, strychnine. In other respects treatment is largely symptomatic. Next to giving the heart vigor in this way, inhalations of oxygen give the most promise, because of the crying need of the system during this ordeal for this life-giving gas.[1]
[1] See paper by the author. New York Medical Journal, August 16, 1884.
—All leukocytes have the power of shifting their location. The lymphocytes, so called, being the youngest of the white corpuscles, show it less than the older forms. The eosinophile cells are less able to manifest the peculiar activities of[41] the other forms. It is particularly the mononuclear and polynuclear corpuscles which are endowed with most pronounced activity. These have the power, like the ameba among the lowest forms of life, to not only spread themselves around inert bodies, like granules of carmine or other particles used for experiment, or the particles of coal-dust found in certain conditions in the human body, but they also have the power to englobe many living organisms, for the main part vegetable (bacteria). Under the microscope it is possible to see living bacilli, performing active movements, although enclosed in the nutritive vacuoles of the leukocytes, in some of the lower animals. This ameboid power possessed by these cells of thus attacking and disposing of foreign bodies or irritants has been demonstrated and proved, especially by Metchnikoff, and has been called by him phagocytosis. His views were for a long time disputed, and are perhaps not yet absolutely and generally accepted. Nevertheless, they fulfil every demand made upon them for explanation, and are susceptible of such demonstration under the microscope that we now have practically a new and apparently a correct theory of the inflammatory process. (See Chapter III.) Any cell which has this property is known as a phagocyte. It is shared by some of the leukocytes with certain other cells to be spoken of later (wandering tissue cells). Cells which possess this power do not attract all microbes indiscriminately, and it is often the case that the leukocytes of an animal peculiarly susceptible to a certain kind of bacteria do not attract them at all, even though they are directly in contact. It is plausible that an explanation of the peculiar susceptibility of certain animals to certain diseases is furnished by this fact (Fig. 3).
Fig. 3
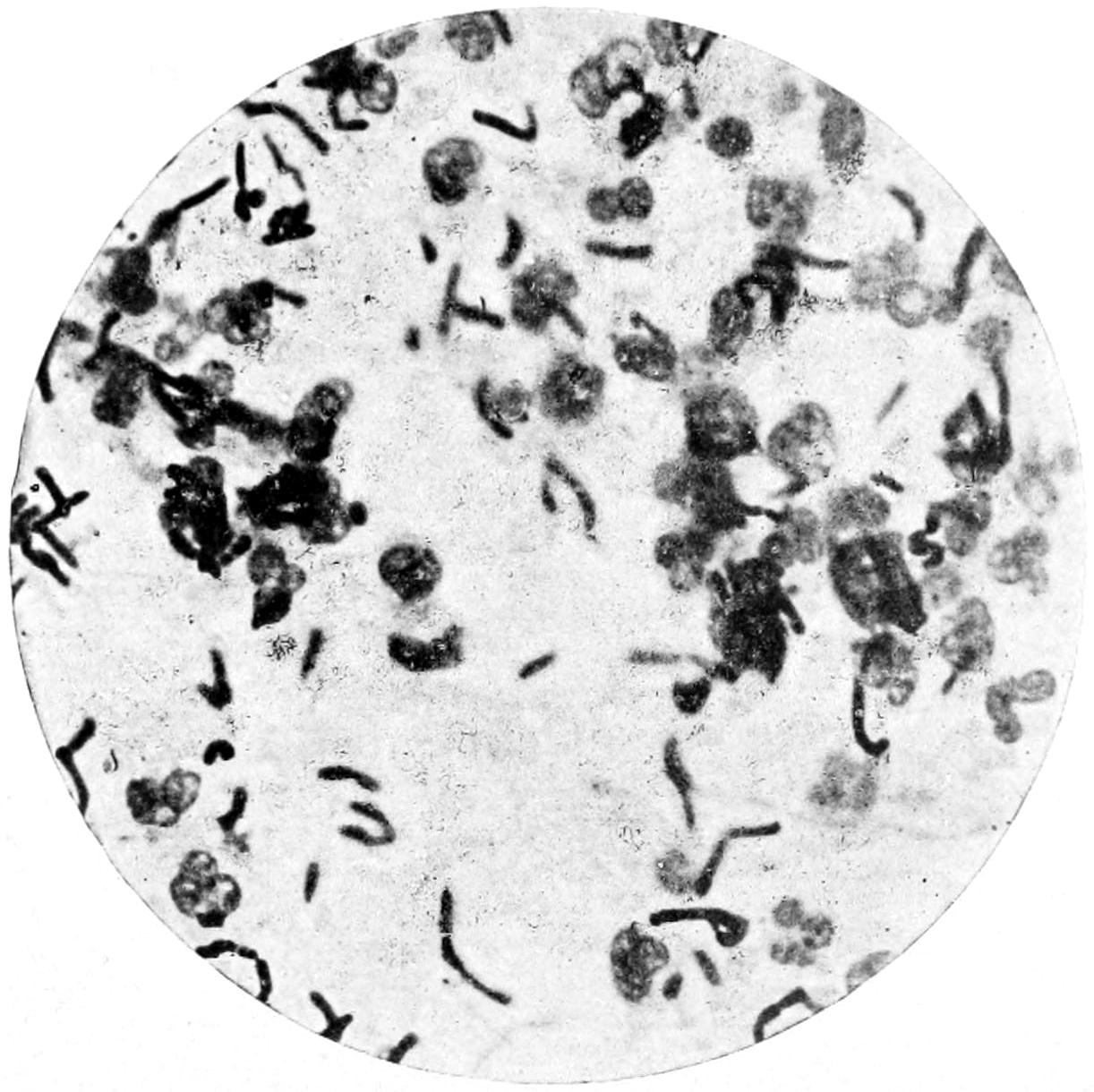
Phagocytosis in anthrax pustule. (Gaylord.)
On the other hand, leukocytes may and do englobe virulent microbes. In man the mononuclear forms do not take up either the streptococcus of erysipelas or the gonococcus; whereas these two organisms are readily attracted by the polynuclear neutrophile cells. The bacillus of leprosy, on the other hand, is never attacked by the polynuclear forms, but is speedily devoured by the mononuclear cells. This shows that the various leukocytes may exercise a marked selective ability. This inclusion of minute bodies within ameboid cells seems to be an evidence of a peculiar tactile sensibility upon the part of the latter. In fact, this is clearly established, and seems to be inseparable from the peculiar attraction between leukocyte and bacterium, to which the name chemotaxis has been given, and which is described in an ensuing chapter. If the included organism is, as is usually the case, killed, it is disposed of by a true process of intracellular digestion in a neutral or alkaline protoplasmic medium, and its inert portions are again extruded. On the other hand, if the leukocyte is poisoned[42] or die in this phagocytic attempt, it presents usually as a so-called pus cell or corpuscle, and the solid part of pus is made up in large measure of cells which have perished in this way. (See Inflammation and Suppuration.)
To regard phagocytosis as an affair mostly of certain tissue cells and invading bacteria would be altogether too narrow a view to take of it. It is really a process of the greatest importance and of constant performance in our systems. By virtue of it disintegrated muscle fibers and other tissue cells are disposed of, sloughs are separated, certain absorbable foreign bodies (catgut, etc.) taken away—i. e., absorbed—cellular tissue reduced in numerical strength (progressive atrophy), and a great variety of changes, either normal, as those pertaining to health and advancing years, or abnormal, like those incident to many diseases, are actually the product of this kind of phagocytic activity. The protective power, then, which the phagocytes exert as against bacteria is only one part of their normal functions, by virtue of which they become, in effect, perhaps the most important cells within our bodies. Their powers are limited, however, as will be seen when describing pus, for the so-called pus corpuscle is nothing but a phagocyte which has perished in its self-assumed task. It is known also that in certain instances phagocytes, which are incapable of defence as against the mature bacterial organism, are nevertheless capable of englobing its spores and preventing their development. This is true, for instance, in case of anthrax in animals ordinarily immune, as, for instance, the frog and fowl. If, however, in these very animals the vitality of the phagocytes be affected—as by cooling in fowls or heating in frogs—phagocytosis is so far interfered with that the spores germinate within the enfeebled leukocytes and the entire organism is infected.
[43]
Inflammation is an expression of the effort made by a given organism to rid itself of or render inert noxious irritants, arising from within or introduced from without (Sutton, modified).
After having duly considered hyperemia as a phenomenon having an identity and termination of its own, we are prepared to study the more complex processes included under the term inflammation, the first of which is the hyperemia already considered. The characteristic of the truly inflammatory process is that it does not stop with mere congestion nor with any of its previously mentioned terminations, but goes on to something more complex. It must be understood, therefore, in this consideration that hyperemia is the first act of the vessels, resulting from peculiar stimuli which will shortly be considered. Even the hyperemia seems to be now more distinct than under other circumstances, and, along with the dilatation of vessels and the stagnation of blood current, the capillary vessels seem crowded with blood corpuscles to an abnormal degree, the rapidity of their motion is checked, and there occurs accumulation of blood cells along the walls of the small veins, to which they seem to adhere as if by some new cohesive property. The result is that before long the vessel wall appears to have received a new coating of white corpuscles, this being more marked in the veins than in the arterioles, while in the latter the red are more numerously mingled with the white than in the veins, in which the distinction between the two classes of cells is better maintained.
Next comes the phenomenon whose clear recognition and description is inseparably connected with Cohnheim’s name. This is known under different names as migration or diapedesis of the leukocytes. The program is about as follows: A little protrusion of the vascular wall, a marked alteration in the shape of a leukocyte, which yet adheres to this point of its lumen, and then the curious fact so often seen under the microscope—the gradual passage of this cell through the vascular wall, from its inner to its outer side, by what is generally known as its ameboid movement. This migration of the leukocyte is not confined to its mere escape from the restriction of the vessel lumen, but goes on to an indeterminate extent after it has detached itself from the outer surface of the vessel. This seems to occur by virtue of the same ameboid characteristic which it exhibited in passing through between the cells of the vessel itself. If this occurs at one point, it occurs at innumerable points, in consequence of which a large number of leukocytes escape into the tissues of the part involved. This diapedesis occurs most markedly from the smaller veins, to a less extent from the capillaries. The cells which escape from the latter are usually accompanied by red cells, the consequence being that the exudate which necessarily occurs at the same time is more or less tinged with the coloring matter of the blood, and is known as a hemorrhagic exudate.
The above phenomenon, described in so few words, is in its minutiæ a really complex one, depending on a variety of causes not easily appreciated; but it is at least positive and well known, because it can be observed at will in the mesentery or web or tongue of certain animals which can be confined upon the stage of the microscope. The phenomena of inflammation, therefore, comprise, first, hyperemia, and then escape from the bloodvessels of the corpuscular and fluid elements of the blood. The former may be due, as already seen, to various irritations of a non-specific character; while, as we shall learn, the latter practically never take place save when the irritation has been, as pathologists say, specific or infectious.
The phenomena of true inflammation comprise practically the roles played by the three elements which conspire to produce those changes—namely, the tissues, the blood, and the specific irritants which are the primary cause of the entire lesion. Each of these should be considered separately.
[44]
All observers agree that in actively inflamed tissues the number of cells is very greatly increased. A certain increase may be accounted for by that which has already been described—namely, the escape into the tissues of the wandering cells from the bloodvessels. But neither this alone nor the products of their rapid proliferation are sufficient to account for all the cells found in the truly inflammatory condition. It is now well established that in connective tissue there are two varieties of cells—the fixed and the wandering—the former concealed in the trabeculæ of the intercellular substance, while the latter are small, ordinarily round in shape, much resembling the white corpuscles, possessed of ameboid characteristics, and having the power of changing position. These are known as the wandering cells, which meander through the lymph spaces of the tissues or back and forth into and out of the blood-vascular system, their migration being regulated by causes not yet known. Under natural conditions their number is relatively small. Once given a true inflammatory disturbance they are reproduced with amazing rapidity; and their numbers, added to those produced by diapedesis of leukocytes, with the combined proliferative activity of both forms, serve to account for the new cells whose presence characterizes phlegmonous and other similar disturbances. That these wandering connective-tissue cells have much to do with these changes is shown by the unmistakable evidences of excessive activity known as karyokinesis (i. e., nuclear activity).
Karyokinesis is common not only in inflammatory disturbances, but in new-growths of rapid formation, especially sarcomas, which are formed from mesoblastic cells, the same which have to do with connective tissue. Endothelial cells also undergo the same changes.
The peculiar characteristics of the leukocytes have already been described at considerable length in the preceding chapter. It must suffice, then, here to say that during the inflammatory attack the leukocytes are increased in number, i. e., there is a temporary leukocytosis which is the usual accompaniment of suppuration. For instance, this is regularly present in purulent, but not in catarrhal, forms of appendicitis. The recognition of this fact may be of great value in diagnosis. For instance, leukocytosis is rarely present in tuberculous disease unless suppuration complicates the case. It is met with in suppurative osteomyelitis and in all cases of pocketing of pus. Moreover, when leukocytosis is present coagulability of the blood is increased. Of the various leukocytes, it is the mononuclear and polynuclear forms (see Chapter II) which are endowed with the most pronounced activity and which play the principal role among the blood cells or phagocytes. That phagocytosis plays a most important part in the inflammatory process is a matter to be emphasized in more than one way and in more than one place. The account of the process already given should suffice for descriptive purposes; the importance of the act, however, should be made most prominent in considering inflammation and suppuration. That the phagocytic properties of these cells are limited will be remembered when we recall that in certain instances phagocytes, which are incapable of defence as against the mature bacterial organism, are yet capable of englobing the spores and preventing their development. Nevertheless, the activities of even the most lively phagocytes are capable of being influenced and repressed by extremes of heat and cold to which patients may be exposed, either locally or generally.
Having considered briefly the cells which take prominent part in the inflammatory process, and the escape along with them of the fluid portions of the blood, whether these coagulate or not, it is necessary before referring to specific factors to discuss that which induces the above cells to act in this way. That there is a peculiar, even a mysterious, attraction which brings specific irritant and phagocyte together has been for some time recognized, but it remained for Pfeffer to study it carefully and to give it the name by which it now passes, i. e., chemotaxis, while others have widened our knowledge of it, especially by a recognition of the opsonins or material which “prepares food,” i. e., prepare microbes for ingestion by the phagocytes.
Chemotaxis is a term implying a peculiar property of attraction and repulsion between cells, both animal and vegetable. It mainly pertains to vegetable cells alone, and has been offered as the explanation of the sporulation of ferns, for example; but as it[45] interests us most in this place it is manifested between the animal cells of the human body and the bacteria, which are vegetable cells. As a result the former, i. e., the phagocytes, having power of migration, are drawn toward the latter. To be more accurate, this mutual or peculiar attraction is known as positive chemotaxis, it being also known that exactly the reverse prevails under certain circumstances, and that mobile cells will move away as rapidly as possible from certain organisms or substances for which they seem to have a repugnance, this being known as negative chemotaxis.
These are essentially living organisms, bacteria, fungi, and the protozoa, the first named being by far the most frequent. Before a lesion can assume the type of inflammation as here understood some one or more of these organisms must have secured an entrance into the tissues, the circumstances determining such invasion being considered a little farther on. It is these living organisms which, having once invaded the tissues, determine that most active congregation and proliferation of certain cells which we have just described under the head of Phagocytosis. When once the irritants are present there begins that very active conflict which Virchow has so graphically alluded to as the battle of the cells. Now the mysterious chemotactic properties of the component substances manifest themselves, and now phagocyte is drawn toward bacterium, or the reverse, while the tiny war goes on with sometimes varying results, it being a question which can prove victor in the conquest. This is no fiction of the imagination, but is a contest which may be seen under the microscope in certain of the lower animals, while its results may be seen in the examination of pus from any human source. In another place I have also likened this conflict to that in which certain of the enemy resort to poisoned weapons, because modern biological chemistry has now shown very evidently that it is a part of the life history of many of these microörganisms to produce, probably as excretory products, albuminoid or other substances having sometimes extremely toxic properties. And so it comes about that in many of the surgical infections, while the local destruction is produced by the actual death of tissues which have been invaded by microörganisms, the general or systemic symptoms, generally referred to as the toxic symptoms, are literally due to poisons generated in the infected area, dispersed throughout the system, and often proving fatal.
The local effect of these specific irritants, when they are not promptly attacked, devoured, and removed by phagocytes, is pus, which means cellular death, or gangrene, which is death of masses of cells which have not had time to separate from each other. Pus, then, is the ordinary consequence of the contest above alluded to, and each pus cell represents the dead body of a phagocyte which has perished in the attempt to protect the parent organism from harm. That it has died valiantly can almost invariably be determined, because within its dead body may be seen one or more of the minute invaders which it has attacked. This, then, is the light in which inflammation and infection should be viewed.
In other words, we may have escape of fluid portions of the blood, which may or may not coagulate; we may even have some escape of corpuscular elements with some activity in the extravascular cells, which shall lead to temporary or even permanent enlargement of a part; all of which may be provoked by injury or by the presence of certain chemical irritants within the blood or tissues; for example, alcohol, uric acid, etc. But the factors which provoke the greatest activity on the part of intravascular and extravascular cells, and which determine the richness in albumin of fluid exudates, or their prompt coagulation as soon as blood serum has escaped from the vessels, and which particularly determine the furious rush of phagocytes and that kind of intercellular conflict which leads many of the contestants on both sides to death, are living organisms which are introduced from without, whose presence at the point of inflammation is abnormal and injurious, which are offending substances in every respect, while the whole phenomenon of inflammation is an expression of an effort to rid the system thereof. Taking this view of the subject, there is an important distinction between hyperemia and its consequences, which is absolutely a non-infectious condition, and[46] inflammation with its consequences, which is always an infection and is always followed by more or less death of cells, the same being often extruded in a semifluid mass known as pus.
—There is the widest difference between various forms of microörganisms in the matter of virulence; and it is true that there are very great differences between the same species under different circumstances, these differences depending on conditions as yet absolutely unknown. With certain organisms it is enough to infect an animal with one alone in order to bring about a fatal result, this meaning that the organism itself is extremely virulent and the animal extremely susceptible.
In a guinea-pig, for instance, a single virulent anthrax bacillus will produce death, whereas in a more resistant animal many are required, and in still others there is absolute immunity against the disease. Man is much more susceptible to the pyogenic organisms than most of the lower animals, which is one reason why wrong deductions have been drawn from many experiments, and why veterinary surgeons, who are so careless of all antiseptic precautions, as a rule have good results in work which, done after the same fashion on the human being, would be inevitably fatal. It is one reason also why one may draw false inferences from experimental work, for instance, upon dogs, which survive many an operation which can scarcely be successfully repeated upon a human being. The influences which affect the vitality and virulence of microörganisms are most numerous and widespread. Temperature, sunlight, moisture or dryness, association with other bacteria, are but a few of the conditions known to be more or less operative. Inoculation with a small number of certain bacteria may be harmless; up to a certain number it may produce only a local disturbance, like abscess, while a still larger dosage may produce fatal results. This is not the case with all, however, but only with some organisms. Bacteria which have been repeatedly passed through the animal body become more virulent than those cultivated for many generations in test-tubes in the laboratory. This variable virulence is especially characteristic of the colon bacillus, the anthrax bacillus, and the micrococcus of erysipelas. Nor does it always follow that the most virulent organism is necessarily cultivated from the most toxic or serous manifestation of its activity.
—Bacteria are seldom found in pure cultures under natural conditions. By mutual association remarkable changes are produced, sometimes in the direction of enhanced virulence, sometimes in the direction of attenuation of effect. Certain organisms, extremely dangerous alone, lose their power when combined with others, while still others have their virulence increased to a rapidly fatal degree. In fact, these effects are so strange and so contradictory that no law governing them has yet been formulated, it being necessary to establish each case by experimental investigation. The virulence of the anthrax bacillus under ordinary circumstances is well known, as is also that of the streptococcus of erysipelas in man. Yet, when these two organisms are introduced simultaneously, the mixture is apparently wellnigh harmless. On the other hand, the simultaneous inoculation of certain other species greatly increases the danger from either alone. The diplococcus pneumoniæ when combined with the anthrax bacillus seems to have a greatly augmented power.
—The fact that immunity against certain infections and susceptibility to other conditions are transmitted from parent to offspring is one which admits of no dispute. The explanation, however, is almost as remote from us today as it ever was. But the recognition of the fact is of the greatest importance to all practising surgeons. That bacteria frequently enter through wounds and bruises is self-evident, but we all know that such wounds are more likely to suppurate in some than in others, and the causes of infection in some are, to a certain extent, connected with the hereditary habit of tissues. The same causes influence not merely liability to infection, but its severity and character. There are undoubtedly also local as well as general variations, and it is very certain that among these the results of bruising or contusion are by far the most prominent. There is also undoubted experimental evidence that under certain circumstances bacteria produce only local lesions, whereas under others they produce general and even fatal infection.
[47]
—Local predisposition is a factor of almost equal importance. Once given a distinct infection, and hyperemia is sometimes a contributing cause of inflammation. Per contra, anemia of tissues seems to be also a favoring condition. In parts involved in chronic congestion the blood flows more slowly, while the vessels are dilated and apparently susceptibility is increased. Infection here produces a type of disease mentioned as hypostatic inflammation. Conspicuous exception as to the occasional value of an artificial passive hyperemia is seen, however, in the so-called congestion treatment (Bier’s) of tuberculous joints, where the more or less constant flooding of the tissues with venous blood seems to render them uninhabitable for living bacilli, which apparently die and disappear (by phagocytosis), thus permitting a slow return to the normal condition. General anemia, again, is a predisposing cause, while toxemias, including diabetes, etc., are still more so. The liability of diabetic patients to suppurative and even gangrenous infection is proverbial. The presence of foreign bodies has much to do also, and, infection once having occurred along with its introduction, the presence of a foreign body will nearly always excite suppuration; otherwise it will ordinarily remain inert. The withdrawal of trophic nerve influences also apparently permits infection, as is instanced by the ease with which bed-sores form in paralytic patients. Obstruction to the circulation or to escape of secretions more easily permits infection; for example, in the appendix, in the kidney, in the gall-bladder, the salivary glands, etc. Furthermore, one may formulate a quite comprehensive statement and say that all such lesions as solutions of continuity, hemorrhages, degenerations, vascular stasis produced by strangulation, etc., and all perforations, increase more or less the liability to infection.
—Here are reckoned, first, previous and long existent toxemias, e. g., syphilis, diabetes, scurvy, etc. Other conditions, like lithemia, cholemia, acetonemia, and the various conditions represented by oxaluria, or in which acetone, peptone, and excess of uric acid are found in the urine, also come under this head. One need never be surprised to find suppuration occurring in those cases in spite of due observance of all ordinary precautions, since by their existence immunity is destroyed and vulnerability increased. (See chapter on Auto-infections.)
Recent toxemias also have important bearing in this same respect. For instance, after typhoid fever and other acute wasting diseases, including the exanthemas, surgical operations are sometimes followed by failure, and should always be postponed until complete recovery, except in cases of emergency. The condition to be hereafter described as enterosepsis, and which has previously been known under many different names, as fecal anemia, stercoremia, etc., is one which makes the performance of all operations dangerous, and which certainly predisposes to septic disturbances of all kinds. The postpuerperal state is also one in which operations are to be avoided if possible.
Certain anatomical changes peculiar to the various ages also belong in this category. Old age, with its accompanying arterial sclerosis, its cardiac debility, and other well-known tissue alterations, favors sluggishness of wound repair and leads not infrequently to sloughing or to bed-sores. Amyloid changes betoken impaired vitality. Children are much more liable to acute osteomyelitis than adults. Nursing infants are apparently exempt from many of the infectious diseases, but possess relatively small power of vital resistance to surgical operations. General anemia and impaired nutrition of the body predispose to most infections and to acute starvation.
—Diet has much to do with tissue resistance. Rats fed on bread are more susceptible to anthrax than those fed on meat. Hunger makes pigeons highly susceptible to the same disease, and artificial immunity induced in various animals is quickly destroyed by starvation. Prolonged thirst seems to have the same result. Excessive fatigue generally reduces immunity, as already mentioned. The various drugs which destroy red corpuscles impair immunity, and even by injection of water into the circulation the bactericidal power of the blood is reduced. White mice fed with phloridzin, which produces artificial diabetes, become highly susceptible to glanders, from which they are ordinarily exempt. In this connection may also be mentioned the various toxemias alluded to under the previous heading, which may proceed from the intestine, from the genito-urinary tract, and probably also from other sources. Climate has more or less to do, as also extremes of weather, with power to resist infection or to survive serious operations. Dark habitations,[48] poorly ventilated, constitute surroundings which manifestly predispose to infection of all kinds. Rabbits inoculated with tuberculosis and confined within a dark cell, badly ventilated, become rapidly diseased, while others similarly inoculated, but allowed to roam at large, present but slight evidences of the affection. Certain occupations predispose to certain diseases. This is pre-eminently the case, for example, with workers in mother-of-pearl, who are exceedingly liable to a particular form of osteomyelitis; and with those who make phosphorus matches, who are prone to suffer from a peculiar necrosis of the lower jaw. Prolonged suppuration may produce such changes in the blood and tissues that vital processes of repair, cell resistance, and chemotaxis may be so far interfered with as to facilitate subsequent infection.
Finally, the influence of local injury to tissues, particularly of contusions which cause tissues to lose their vitality, is strenuously insisted upon by all, and is spoken of repeatedly in other places in this work. Many tissues will succumb to inoculation after bruising, ligature en masse, etc., which before such injury are not in the least disturbed.
—It is only in a very limited class of cases that infection can be transmitted from mother to fetus, but there are instances of this kind in which the surgeon is deeply concerned. As Welch has stated, syphilis is the only infection capable of direct transmission through the ovum or spermatozoön; but intra-uterine infection may occur in many ways, and many diseases may be thus transmitted. The placenta is usually regarded as a perfect filter; nevertheless, it is occasionally passable to microörganisms. These may be caused by preëxisting lesions in the placenta or by the virulence and activity of bacteria. It is known that in animals the bacilli of chicken cholera (inoculated into the mammalia), of symptomatic anthrax, and the pyogenic cocci, frequently traverse this barrier. In mankind infection in utero has been observed in smallpox, measles, scarlatina, relapsing fever, syphilis, tuberculosis, croupous pneumonia, typhoid fever, anthrax, and surgical sepsis.
That the effects of bacterial invasion may be anticipated and guarded against most effectually it is necessary that the practitioner should be thoroughly familiar with the sources from which they come, and the localities in and about the body which they most commonly inhabit or where they are met with in largest numbers.
—Of all possible sources of infection, the skin itself is probably the most fertile. It is exposed to contamination by air and by everything which may come in contact with the body, and there is perhaps no organism met with in disease which may not be found upon its surface or within its recesses. In fact, these recesses, such as the crevices beneath the nails, the spaces between the toes, and the various pockets like the tonsils, the axillæ, etc., are those most commonly inhabited by microörganisms.
Bacteria may penetrate the skin by means of three different routes, namely, the sweat glands, the hair follicles, and the sebaceous glands, by means of their regular openings. The hairy appendages of the skin are even greater sources of danger than the skin itself, since a direct path of infection into the depths of the skin is afforded by their follicles. Experimentally it has been shown that when bacteria are rubbed into the skin where there are no follicles, there is freedom from infection, whereas the reverse is equally true, and it is clinically generally recognized that furuncles and carbuncles form almost exclusively in those parts provided with hair and sebaceous glands.
The mucous membranes are in constant contact with microörganisms and furnish conditions in many respects favorable for their rapid development. Nevertheless, the latter is interfered with and often inhibited by certain mechanical and chemical influences which afford protection. The conjunctiva is an extremely exposed membrane, which harbors, however, but a relatively small number of bacteria under ordinary circumstances. The tears before escaping from the conjunctival sac are sterile, and are probably saline enough to act as an antiseptic bath for the cornea. Moreover, by free escape of secretion through the nasal duct the conjunctival sac is kept constantly irrigated, to which is mainly due its ordinary healthy condition, as it is well known how commonly lesions follow obstruction to the lacrymal duct. The horrible results of Egyptian ophthalmia, i. e., the pyogenic form of conjunctivitis, are familiar to travellers in Egypt. Howe and others have shown that this disturbance is due to flies, which are carriers of infection, and are attracted toward the eyes of infants, while the superstitious notions of the parents restrain their children from instinctive protection of the eyes when thus irritated. There is probably no greater common carrier of pyogenic infection than the common house-fly, and nowhere is this agency more demonstrated than in the hot climates of the Orient.
PLATE III
FIG. 1
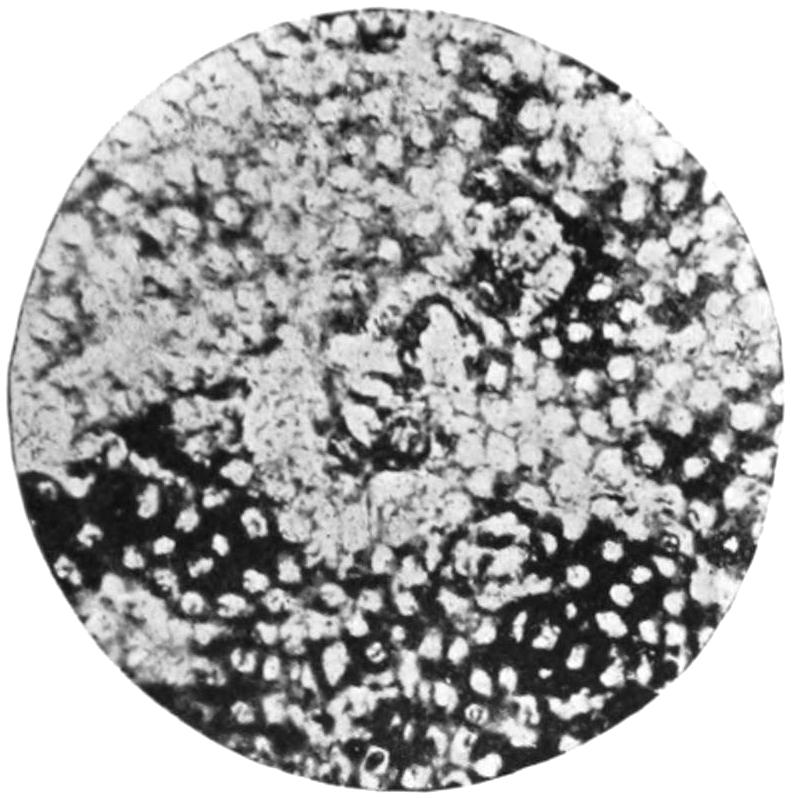
Artificial Dental Caries in Cross-section. Tubules Filled with Bacteria. (Miller.)
FIG. 2
Putrid Tooth Pulp. Infection of Dental Tissue. × 1000. (Miller.)
FIG. 3
Dental Caries. Disappearance of Dental Tissues as Result of Presence of Bacteria. (Miller.)
FIG. 4
Dental Caries. Tubule Filled with Cocci. (Miller.)
FIG. 5

Dental Caries. × 500. (Miller.)
FIG. 6
Dental Caries. Tubules Plugged with Cocci. × 500. (Miller.)
[49]
—The oral cavity and pharynx are seldom free from bacteria. Miller has studied over one hundred species that he has found under various circumstances in the human mouth. Some of these are pathogenic; others are apparently absolutely innocent. Many of the forms which grow in saliva will not grow in ordinary media. (See Plate III, illustrating infection of the teeth.) Miller has also shown that many forms of dental caries are but expressions of bacterial invasion even of those apparently most solid structures, the teeth; and of late we have been taught more fully that such invasion may extend far beyond the confines of the teeth alone, and may spread to various, even to distant parts, and produce possibly fatal mischief. Abscesses in the brain and extensive septic infections have been traced to invasion along the line of the dental tubules. One of the most virulent of all the common inhabitants of the mouth is the pneumococcus of Fränkel, known also as the micrococcus lanceolatus of Stebernrg. In virulence it is a variable organism, but it is present in a virulent state in only 12 or 15 per cent. of cases of infection due to it. This is the organism which is the cause of lobar pneumonia, and frequently of bronchopneumonia, as well as of numerous phlegmons and other inflammations of the throat, and which, getting into the general circulation through the tonsils or other possible ports of entry about the mouth, causes serious septic and inflammatory disturbances in widely distant regions. Aside from dental caries, a widely opened port of entry is often afforded by those ulcerations around the margins of the gums which are produced by accumulations of tartar. Disease in the antrum of Highmore, for instance, and many other local destructions, are frequently caused in this way.
The next most common port of entry is the tonsils, faucial, lingual, and pharyngeal, which contain a variety of crypts which are often filled with secretions or retentions loaded with bacteria. One of the most common sources of an involvement of the cervical lymph nodes in tuberculous disease is an infection springing first from the tonsils or the teeth.
In spite of the fact that myriads of bacteria are swept into the nasal cavities with the air we breathe, few are seen in the nose. A peculiar capsule bacillus, closely allied to that described by Friedländer, has been found in a number of cases of ozena, while the pneumococcus of Fränkel is also often found there, and is known to produce abscesses of the brain. One specific organism—namely, that of rhinoscleroma—concerns the nose almost solely, its first ravages being met with in this location.
—Probably more microörganisms enter the alimentary canal than gain access in any other way, these coming both from food and drink as well as air. Once within its confines, few of them are capable of prolonged existence. Welch states that the meconium of newborn infants is sterile, but that within twenty-four hours it usually contains abundant bacteria. That bacterial infection through this passage-way is a fertile source of non-surgical lesions is well known. The possibility of surgical infections being produced in the same way is both more remote and less demonstrable. Naturally, anaërobic organisms find here more favorable conditions, and even extremely acid or extremely alkaline conditions do not serve to destroy all such life. Pyogenic cocci are often present and are frequently found in peritoneal exudates. In the intestines of herbivorous animals the tetanus bacilli and those of malignant edema are regularly found. The fungus of actinomycosis also finds its way into the bowel along with ingested food. Under ordinary conditions the bile in its natural reservoirs is free from bacteria, but the colon bacilli and pyogenic cocci often invade these precincts.
—Even the healthy urethra may contain bacteria. While these may wander upward to an indefinite extent, it is believed that the urine contained within the bladder in a condition of perfect health is free from bacteria, and that if such gain entrance they do not long remain. The same is true of the female bladder and urethra. The vagina contains organisms of many species, some of which do not grow[50] on ordinary culture media, but are to be recognized by the microscope. While it is generally acknowledged that the vaginal secretion is, as a rule, possessed of bactericidal properties, there is as yet no satisfactory nor comprehensive explanation of this fact, its normal acidity not being sufficient to account for the fact.
—In a condition of perfect health milk secreted from the ideal mammary gland is sterile, but may easily become contaminated upon its exit from the nipple. Conversely, under many favoring conditions organisms may travel into the lacteal ducts from the skin without, and thus contaminate the milk. In all probability the breast corresponds in behavior to other glands whose ducts open upon the surface, and, while such openings invite entrance of bacteria, their migrations do not extend far from the surface unless some of the other conditions already mentioned predispose to further infection or extension.
In summarizing the general topic of possible sources and paths of infection bacteria may enter and exert deleterious action:
A. From within they may enter the tissues either through the inspired air, through food and drink, i. e., ingesta, or by means of more direct inoculation, e. g., by foreign bodies or by venereal contact. The danger through infection by inspired air is very small, and concerns probably a limited number of organisms, of which the tubercle bacillus is the most important. Foul air and air which emanates from sewers, cesspools, etc., while most unpleasant to breathe and deleterious in many other ways, do not necessarily contain any microörganisms which can be injurious. This fact, in opposition to general belief, is, nevertheless, proved by recent investigations. The ingesta furnish the most fertile source of contagion from within, but the diseases thereby produced fall for the most part into the domain of medicine rather than that of surgery.
B. Infection from without the body may come by actual contact with previous skin or mucous lesions, and particularly from noxious insects and certain parasites. Among surgeons the principal sources of contact infection to be enumerated and guarded against are:
While insisting here upon the recognition of these sources of danger, the precautions to be taken against them are to be considered under another heading, to which the reader is referred.
One of the greatest sources of possible infection has of late been shown to be the presence of flies and other noxious insects, which act as carriers of infection. The Egyptian ophthalmia, which ruins the sight of 30 per cent. of the inhabitants of Egypt, has been shown by Howe and others to be due to infection by this mechanism; and a simple bacteriological experiment will suffice to show that the foot-tracks of a single fly across a wound furnish abundant opportunities for infection with organisms which are presumably virulent. In fact, the danger of carriage of infection by this means is greater than from almost all other sources, except the use of improper materials during surgical operations.
We speak of infections as primary, secondary, and mixed; and it is necessary, for purposes of accuracy at least, to make a reasonably clear distinction between them.
—By primary infection is meant infection with a single form of organism whose effects are prompt and speedy. Of this, erysipelas or syphilis may serve as illustrations. Most of the acute infections belong to the primary type.
[51]
—Secondary infection means that after certain disturbances due to a primary infection, i. e., one of a given type, there occurs at some later period and from a distinct source another infection whose results may be more or less disastrous, and cause the case, at least for the time being, to assume a different aspect. We have an illustration of this in the case, for example, of primary tuberculosis with distinct infection of a number of lymph nodes, which, acting as filters, have caught in their tissue net a large number of tubercle bacilli that, lodging there, have produced the usual well-known results and have practically converted the infected nodes into granulomata. In these infected masses well-known changes, such as those which follow tuberculous infection—atrophy, caseation, calcification, etc.—may be occurring, when suddenly there comes infection of a pyogenic type from another source, and suppuration of the granuloma is the result. It is possible even to have a tertiary infection, of which the following may be a hypothetical instance: Primary infection with scarlatina or measles, by which vital susceptibility is in some instances lowered; as the result of this, secondary tuberculous infection in an individual previously resistant; and, third, a suppurative infection, as above described.
In contradistinction to these distinct events, separated by an appreciable, sometimes a considerable, length of time, we recognize a mixed infection, where two or more organisms are implanted at or about the same time. An illustration of this is seen in most cases of gonorrhea in which there is a synchronous attack made by the gonococcus, which is a specific microörganism, accompanied by staphylococci or streptococci, whose effect will complicate the case and make it assume a less particulate type of infection. Mixed infections may often occur in other ways, as syphilis and chancroid, chancroid and gonorrhea, etc. Most cases of mixed infection belong rather to surgery than to general medicine, and constitute an apparent violation of the rule to which physicians often point—that two distinct infectious diseases are seldom communicated or acquired at the same time. Nevertheless, the facts remain as above.
—Terminal infections constitute an apparent paradox, perhaps oftener in medical than in surgical cases. Few people, as Osler has shown, die of the diseases from which they suffer. The final exitus is due to a more or less rapid infection which terminates life. These terminal infections are mainly due to a few well-known microbes, such as the streptococcus, staphylococcus aureus, pneumococcus, bacillus proteus, gonococcus, bacillus pyocyaneus, and the gas bacillus. In surgery such infections are, perhaps, most often seen in malignant lymphoma, diabetes, tuberculosis, syphilis, cancer, and in the so-called surgical kidney.
Bacteria which act as agents in the formation of pus are collectively known as pyogenic organisms. These are divided into two groups:
Obligate pyogenic organisms are those whose activity is manifested in the direction of pus formation, which seem to produce it if they produce any unpleasant action whatever. On the other hand, the facultative organisms are those which are known occasionally to be active in this direction, and yet which are not always nor necessarily so. The members of group A are fairly well known and catalogued, and are not numerous. On the other hand, there is reason to believe that many organisms may have the occasional effect of producing pus, as it were, by accident or at least in a way not absolutely natural or peculiar to themselves, but still are frequently found when there is no pus present. A suitable list of the facultative organisms, therefore, can hardly be made, and will not be here attempted, the effort being only to mention the more common organisms which play this facultative role. It may be mentioned also that even the adjectives “obligate” and “facultative” are to be accepted with some mental reservation, since staphylococci, for instance, may be met with even in the absence of pus, although nearly all that we know about these organisms implies that pus would be the result of their presence. Furthermore, there are certain other organisms, not, strictly speaking, bacteria, which also have the power of producing either pus or pyoid material. These also will be mentioned in their place. Some of them belong not only to the vegetable, but also to the animal kingdom.
[52]
—One of the characteristics of the staphylococci as a group is the powerful peptonizing action which they exert. Moreover, the chemical products of their life changes seem to be more potent in a local than a general way, leading to greater destruction of tissue in their immediate vicinity, with greater inhibition of the chemotactic powers of the leukocytes; that is, with more interference with phagocytosis, by which their progress would be interfered with. Their presence is recognized by a peculiar odor, as of sour paste, which should lead to a prompt change of dressings and disinfection of the wound (by irrigation, spraying with hydrogen dioxide, etc.).
—These two organisms do not differ in morphology nor characteristics, and, while for some time considered as distinct from each other, are now by most observers regarded as identical. The streptococci grow in chains of variable length, and individual cocci vary in size. They grow with and without oxygen, in all media, at ordinary temperatures, do not liquefy gelatin, stain readily, sometimes but not invariably coagulate milk, and vary in longevity. They differ extraordinarily in virulence according to their sources.
Fig. 4
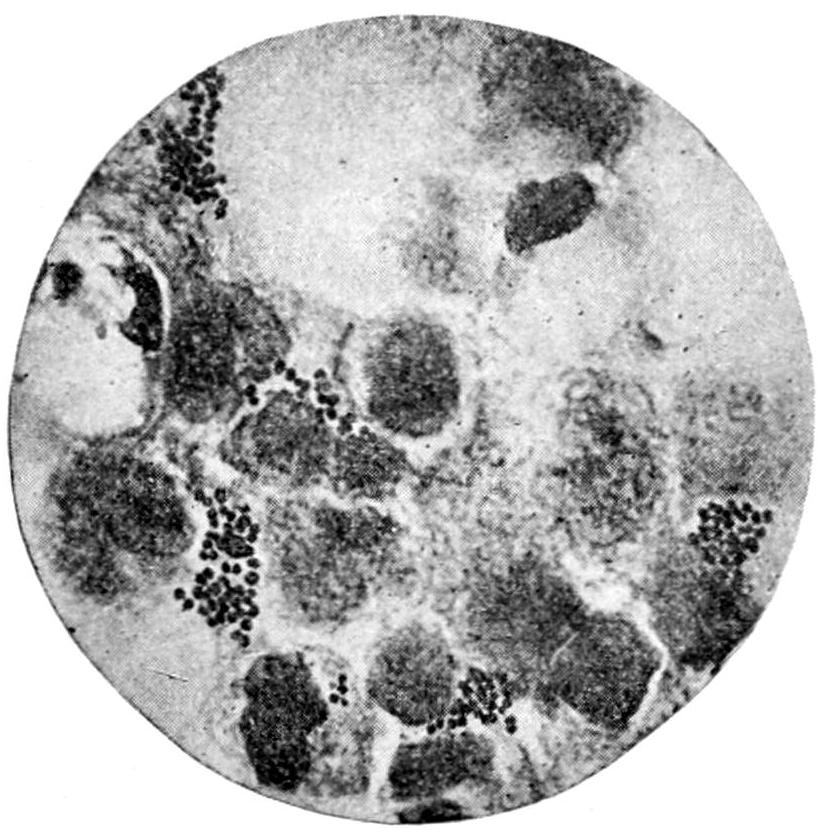
Staphylococci in pus. × 1000. (Fränkel and Pfeiffer.)
Fig. 5
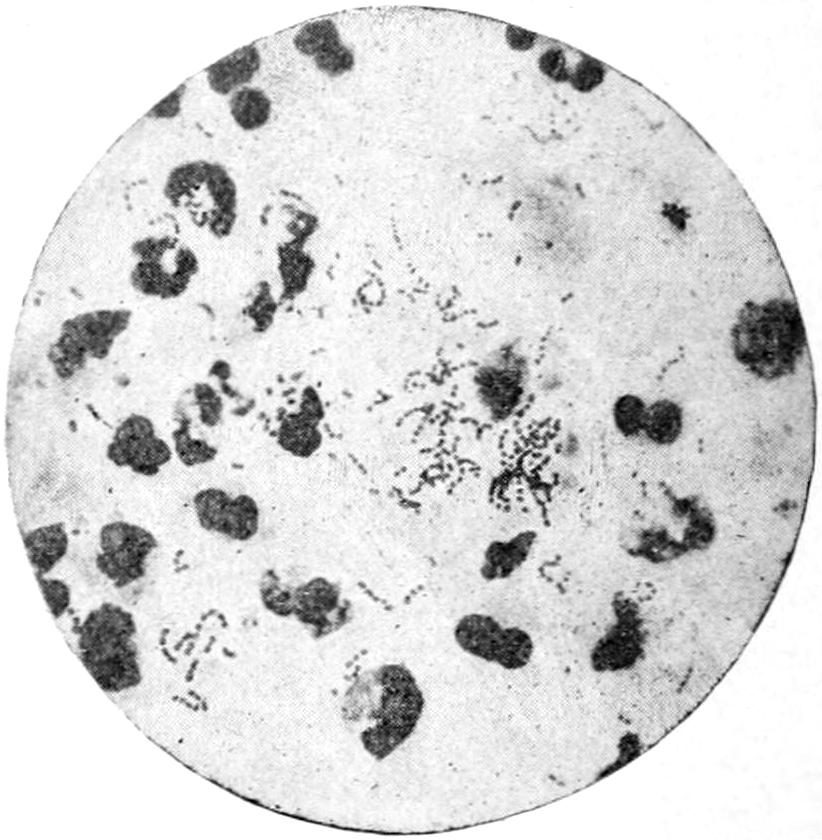
Streptococci in pus. × 1000. (Fränkel and Pfeiffer.)
There are many streptococci not included under the above head which are indistinguishable morphologically and in other respects, and yet which are partly or entirely free from pathogenic activity in man. A biological study reveals remarkable and unexplainable transformation between the different members of this species, a part of which may be referable to conditions pertaining to the organisms infected, but part of which apparently pertains to the bacteria. It is held by some that scarlatina is an invasion by certain organisms of this class; this, however, is not yet definitely established. When found in the stools of children with summer diarrheas they are regarded as indicating ulceration of the intestinal mucosa.
In contradistinction to the staphylococci, the streptococci manifest a predilection for lymph vessels and lymph spaces, along which they extend with great rapidity. They have less peptonizing power than the staphylococci (except in the absence of oxygen); hence streptococcus infection assumes usually the type of widespread infiltration rather than of circumscribed and distinct edema. One sees remarkable instances of this in cases of phlegmonous erysipelas. It is suggested also that the peculiar manner of growth of the streptococci, in long chains which may coil up and entangle blood corpuscles, has much to do with the formation of fat emboli and with pyemic disturbances.
Both these bacterial forms have the power of producing lactic fermentation in milk; and lactic-acid formation sometimes takes place with suppuration in the human tissues, causing acidity of discharge, sour odor, and watery pus. It appears also that these two pyogenic forms have less power of ptomain or toxin formation than many others, and, consequently, that the pyrexia attending suppuration or purulent infiltration is not always to be ascribed to this cause alone, for fever may in some measure be due to[53] tissue metabolism attending their growth, the metabolic products being pyretic. This is in a measure substantiated by the fever attending trichinosis, where the question of ptomain poisoning has not yet been raised.
—Micrococcus lanceolatus is also known as the diplococcus pneumoniæ or the pneumococcus of Fränkel and Weichselbaum, and as the micrococcus of sputum septicemia of Pasteur and of Sternberg. It is of interest to surgeons because it causes many localized inflammations and is a frequent factor in causing septicemia; it is often present in the mouths of healthy individuals. It may produce the various forms of exudates as the result of congestion set up by its presence; also otitis media, meningitis, osteomyelitis, and suppurative disturbance in the periosteum, the salivary glands, the thyroid, the kidney, the endocardium, etc.
Fig. 6
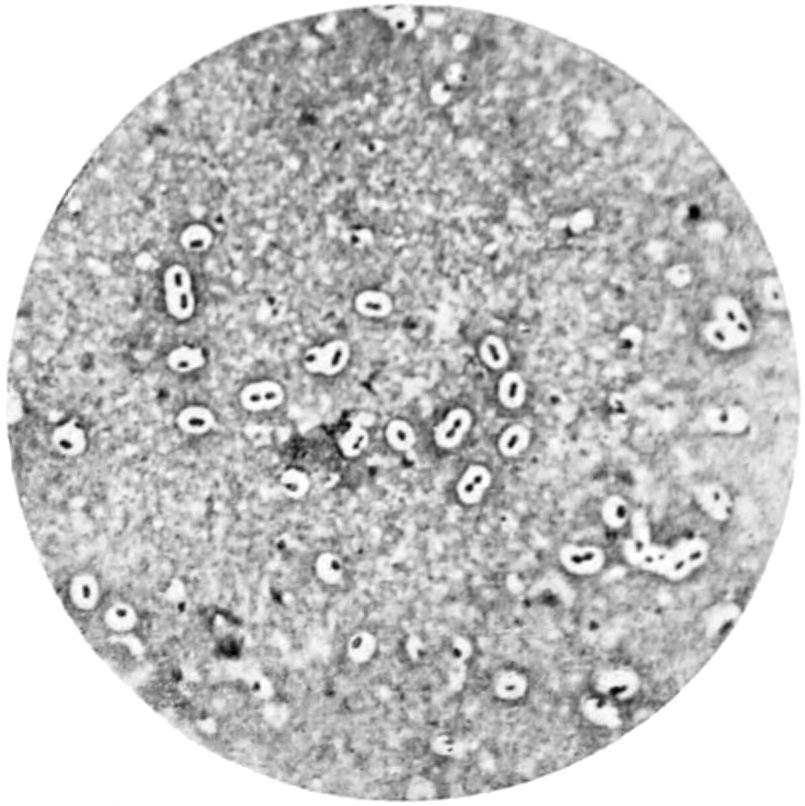
Diplococcus pneumoniæ of Fränkel. (Karg and Schmorl.)
—Suppurations produced by these organisms are prolonged, mild in character, not painful, but accompanied by much brawny induration of tissues.
—The micrococcus gonorrhœæ, or gonococcus, is found constantly in the pus of true gonorrhea, in many cases the pus being a pure culture of this organism. These cocci are generally seen in pairs (biscuit-shaped), while their inclusion within the leukocytes or their attachment in or to epithelial cells is characteristic. Unlike other pyogenic cocci, they do not stain by Gram’s method, being decolorized by iodine, by which fact they may be distinguished. They are cultivated with difficulty, and are known rather by their clinical effects than by their laboratory characteristics; are human parasites, other animals, so far as known, being practically immune. The gonococcus may also produce abscesses, and may be carried to distant parts of the body, where its effects are commonly noted as pyarthrosis, although endocarditis, pericarditis, pleurisy, etc., are known to be due to it, and fatal pyemia has been produced in consequence. In some way it is probably the explanation of the post gonorrheal arthritis, wrongly spoken of as gonorrheal rheumatism.
—This is an inhabitant of the intestinal canal; varies extremely in virulence and somewhat in morphological appearances; coagulates milk; is often associated with other organisms; migrates easily both along the alimentary canal and from it into the surrounding tissues or channels. It is a disturbing element in the production of kidney and hepatic disease, also in the production of appendicitis and peritonitis. Ordinarily its pyogenic properties are not virulent; occasionally, however, it becomes extremely virulent.
—The bacillus pyocyaneus, a widely distributed organism, often observed in the skin and outside of the body; a motile, liquefying bacillus, growing at ordinary temperatures, seldom seen alone, but occasionally producing pus without association with other organisms; it stains the discharges and dressings a bluish-green and imparts sometimes an offensive odor. Suppuration caused by this bacillus is usually prolonged, but characterized by little constitutional disturbance.
—i. e., those which have the power of provoking suppuration, but which have other and more distinct pathogenic activities as well.
—This is found in many pus foci, developing during or after typhoid fever. It is occasionally met with alone, though most of these abscesses are really mixed infections. It is generally found in the bone or beneath the periosteum. Such abscesses are frequently seen in the ribs, and may not be noticed until months after convalescence from the fever. The pus contained within them is not always typical in appearance, but may be unduly thin or unduly thick.
—Under this name are included three distinct forms, which were originally described by Hauser as distinct species, but which are now regarded as pleomorphic forms of the same organism. It is a motile bacillus, met with in decomposing[54] animal and vegetable material, and occasionally found in the alimentary canal. It has been known to produce pus, especially in the peritoneal cavity and about the appendix. It may even cause general infection and peritonitis.
—A non-motile bacillus, varying considerably in size and shape, changing the reaction in sweet bouillon from acid to alkaline; produces a dangerous infective inflammation of exposed surfaces, with tenacious exudate amounting to a distinct membrane. As a part of its life history it also produces a toxalbumin, which is one of the most powerful cell poisons known, the disintegration of the cell constituents due to its action being rapid and pronounced. This accounts for the heart failures which are often reported in connection with the disease.
—More will be said about this organism when considering tetanus, and to that subject the reader is referred. The tetanus bacillus is occasionally found in pus which comes from the area through which the original infection was produced. But these bacilli do not travel to any distance in the human body, and are seldom found away from the area involved. Under most circumstances the pus is the product of a mixed infection.
—This organism will be more fully considered under a different heading. (See Malignant Edema.) It is a long, anaërobic bacillus, widely distributed in the soil and the feces of animals. It is believed that this, like the tetanus bacillus, may occasionally lead to formation of pus.
—This organism likewise will receive fuller description in an ensuing chapter. (See Tuberculosis.) The pus of old cold abscesses in which the more obligate pyogenic organisms have long since died usually contains this organism in mildly virulent form. On the other hand, fresh suppurations occurring in connection with tuberculous disease are mixed infections. There is reason to believe, however, that this organism is capable of producing pus even when none of these are present; for example, in that form of acute miliary tuberculosis which is occasionally met with as bone abscess it may be found.
—This is one of the most malignant and resistant organisms known, being in the highest degree poisonous for the smaller animals, man being less susceptible. One of its characteristic lesions in the human body is a form of pustule commonly known as malignant pustule, the pus in which is usually a pure culture of this organism. (See Anthrax.)
—This is the organism which produces glanders in the lower animals and in man. That form of the disease known as farcy, in which the infected nodules rapidly break down, is likely to contain pus which will be more or less a pure culture of this organism.
—This is the microörganism which produces leprosy, closely resembling the tubercle bacillus. It is constantly and exclusively present in the lesions of leprosy, which are often of the suppurative type, the bacilli being enclosed within pus cells; it is also found in the fluid surrounding them. Although suppuration in these cases may be in a large measure due to secondary infection, it is positive that the leprous bacilli deserve to be grouped in this place.
—The bacillus pneumoniæ of Friedländer was at one time regarded as the cause of croupous pneumonia, which is now known to be due to the micrococcus lanceolatus. The Friedländer bacillus, however, is capable of producing bronchopneumonia, and is occasionally met with in empyema, suppurative meningitis, and inflammations about the nasopharyngeal cavity, of which it is known to be an occasional inhabitant.
—A distinctive organism has been described for this disease and given this name. It has such wide morphological differences, however, that it is possible that it is only the bacillus of Friedländer above mentioned. At all events, an organism of this general character is constantly found in this disease in the thickened tissues from the nose (Fig. 8).
—This was recently discovered by Kitasato, and, in view of the recent ravages of the disease in the Orient, has assumed considerable importance. It grows upon most media, and is found in the blood, in buboes, and in all internal organs of patients suffering from this disease. The smaller animals are susceptible upon inoculation. Animals fed with inoculated foods die also, showing the possibility of infection through the intestine. When exposed to direct sunlight[55] for a few hours the bacillus dies. The general symptoms of the disease are those of hemorrhagic septicemia and its consequences.
—This is seldom, if ever, seen in this country. It is known in England as “the black-leg” or “quarter-evil.” It is an anaërobic organism, frequently met with in cattle, which causes a peculiar emphysema of subcutaneous tissue, spreads deeply, and is followed by a copious exudate of dark serum with gas formation. The smaller animals are not ordinarily inoculable; but if to the culture material there is added 20 per cent. of lactic acid, their insusceptibility is overcome and they succumb to the disease. So, also, as in the case of the tetanus bacillus, by addition of the bacillus prodigiosus or of proteus vulgaris the disease may be produced in otherwise insusceptible animals.
—The bacillus aërogenes capsulatus seems capable sometimes of causing pyogenic and even fatal infection. Its presence is associated with gas formation. It grows as an anaërobe.
—The bacillus of chancroid identified by Ducrey, and briefly described in the chapter on that subject.
Fig. 7
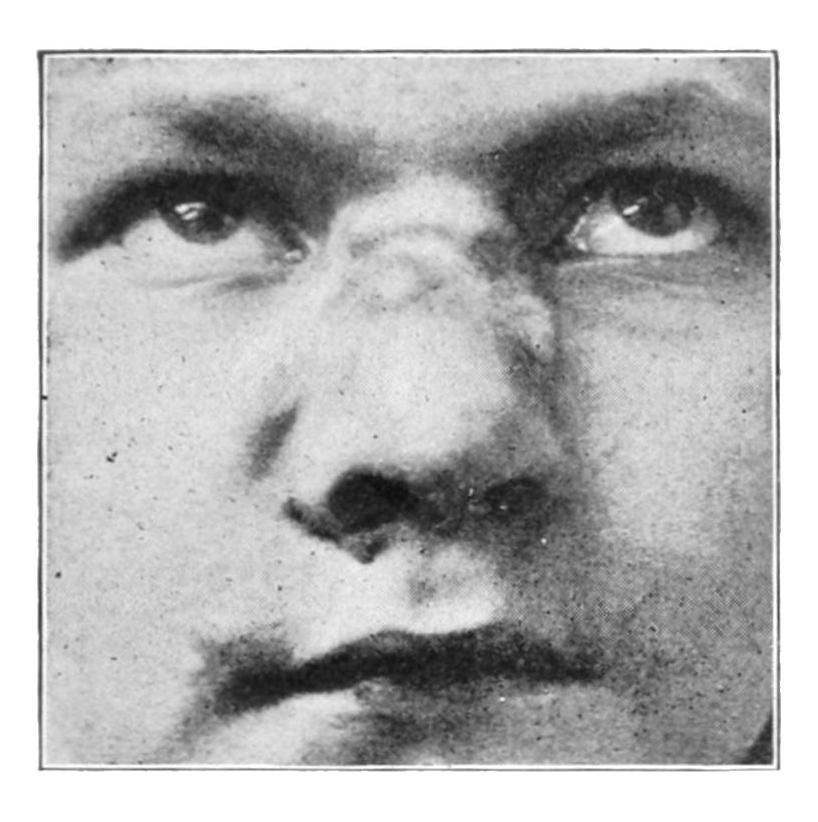
Rhinoscleroma: infiltration of tissues about the nose. (Case reported by Dr. Wende, Buffalo.)
Fig. 8
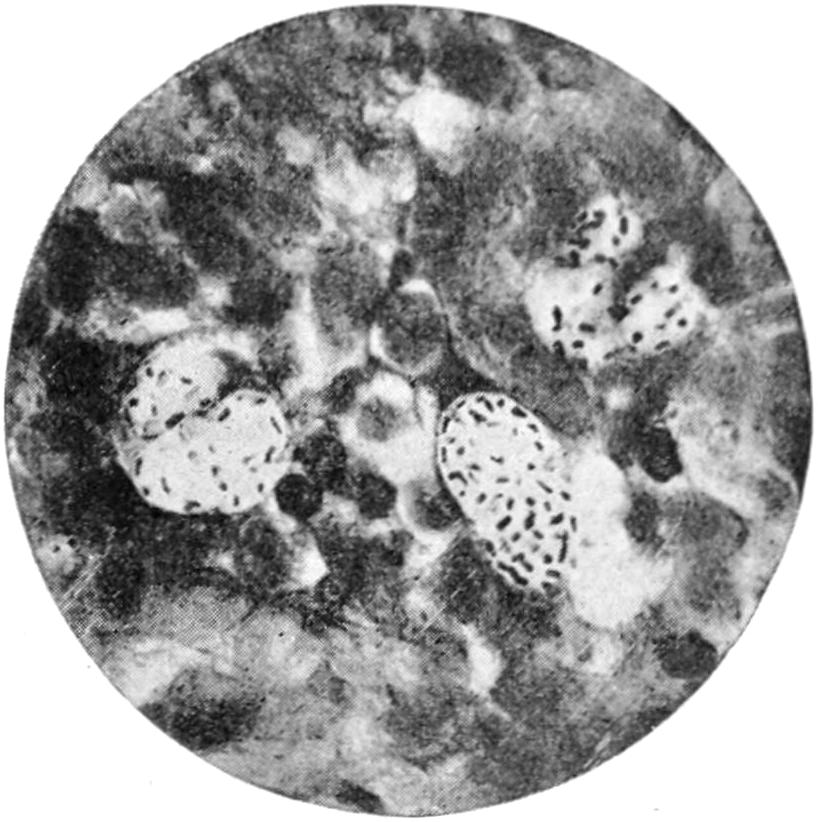
Bacilli of rhinoscleroma. × 1000. (Fränkel and Pfeiffer.)
Busse was the first to call attention of clinicians and pathologists to the role played by yeasts in certain infections. Since the original observations of Busse in a case in which the organism produced a general infection, the lesions of which were a combination of tumor and abscess formation, various observers have noted the presence of pathogenic yeasts, usually in skin lesions. Gilchrist and Stokes were the first in this country to determine the nature of these organisms, and their observations have been followed by the detection of a large number of similar cases. In the skin lesions the organisms are found in minute abscesses; in the subcutaneous tissue and in the infections similar to those of Busse large abscesses surrounded by extensive masses of granulation tissue characterize the infection. The organisms can be detected in the pus by means of an examination of the fresh unstained fluid (Fig. 9).
Besides the micro-organisms everywhere grouped as bacteria, there are other minute organisms which have also the power of engendering pus. One of these is the ray fungus, known as the actinomycis, which causes the disease known as lumpy jaw or actinomycosis. Suppuration is always a concomitant of the advanced lesions of this disease, and, while it may be in many instances a mixed infection, it is not necessarily[56] so. Moreover, the pus produced under these circumstances contains minute calcareous particles which are pathognomonic, by which a diagnosis can sometimes be made off-hand.
Besides these fungi, others, belonging rather to the class of vegetable molds, which are yet pathogenic for human beings, may be occasionally met with under these circumstances—e. g., the fungus of Madura foot, the leptothrix, and other molds from the mouth, while the different varieties of aspergillus may be found in pus about the ear or even in that from the brain.
The protozoa have the power of producing, if not absolute ideal pus, something so nearly resembling it that we may include them among the facultative pyogenic organisms. The best known of these protozoa are the amebæ, which are met with in the intestinal canal in some countries, occasionally in the United States, especially as the exciting causes of a peculiar type of dysentery often accompanied by abscess of the liver. In these abscesses the amebæ are found, and no other organisms. Another group of the protozoa, known to biologists as the coccidia, are also capable of causing pus formation, more particularly in some of the lower animals. Numerous other parasites, belonging higher in the animal kingdom, are undoubted exciters of pus formation, though it is not necessary to lengthen the list beyond those already mentioned.
Fig. 9
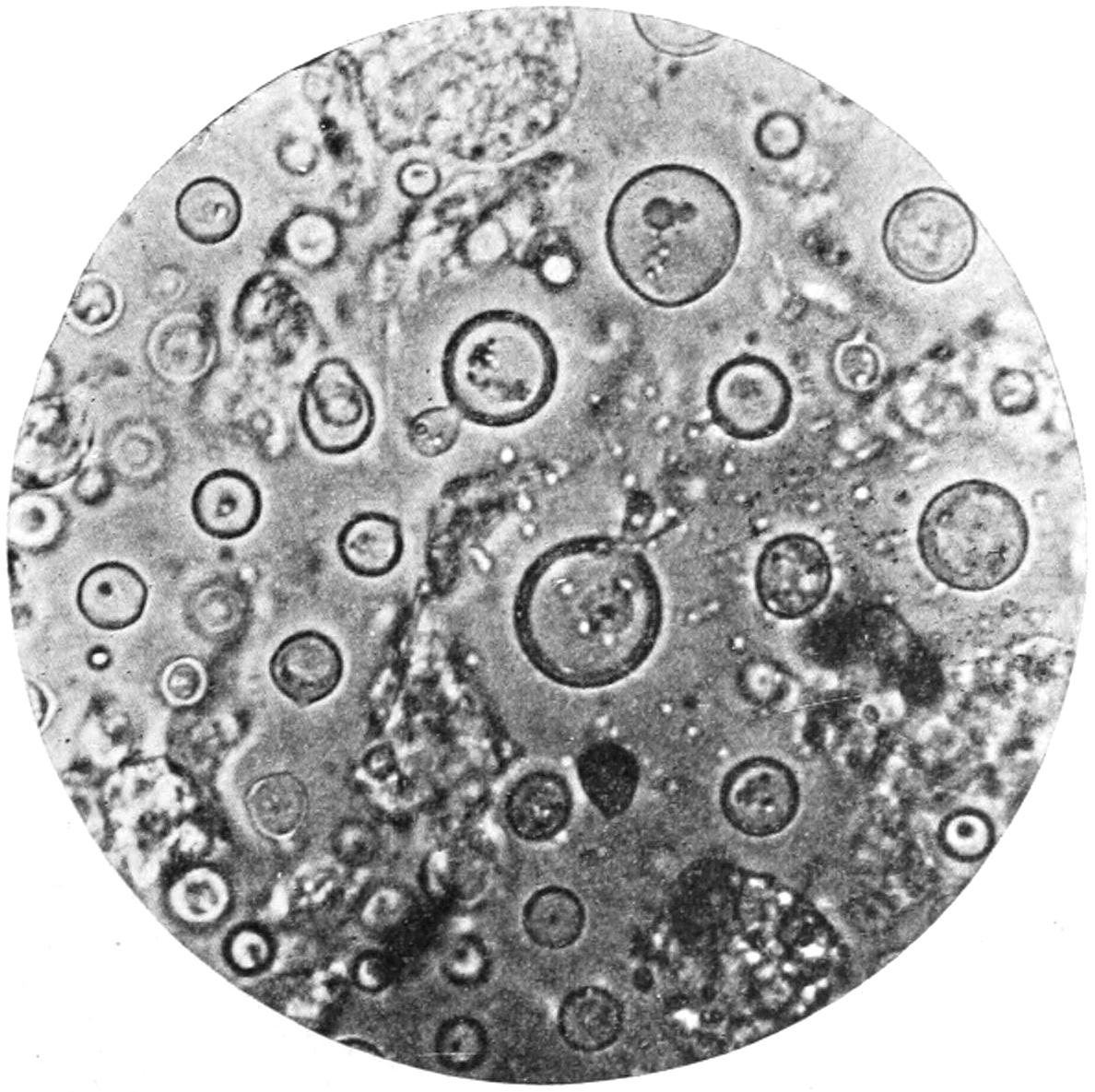
Blastomycetic pus (fresh). × 1000. (Gaylord.)
Protozoa have recently been established as the active agents in the production of smallpox and probably also of scarlatina. They have been seen so generally in and around cancer cells as to make it extremely probable that cancer is a protozoan infection. In syphilis also they are found as the spirochetæ, now regarded as its cause.
Protozoa are as ubiquitous as bacteria, but their recognition is as yet more difficult, as but little is known of them. The numerous stages through which they pass in completing their life cycles only complicate the subject, while the difficulties encountered in cultivating them are still to be overcome. As we become more familiar with them we shall more frequently find them to be pathogenic organisms.
[57]
Staphylococcus.—Dirty white, moderately thick, with sour-paste odor.
Streptococcus.—Thin, white, often with shreds of tissue.
Colon Bacillus.—Thick, brownish, with fetid odor, or thin, dirty white, with thicker masses.
Micrococcus Lanceolatus.—Thin, watery, greenish, often copious.
Bacillus Pyocyaneus.—Distinctly green or blue in tint.
Bacillus Tuberculosis.—Thick, curdy, white paste, or thin, greenish, with small, cheesy lumps or even with bone spicules.
Actinomycis.—Thick, brownish white, with small, firm, gritty or chalky nodules of yellow color.
Ameba Coli.—Thick, brownish red.
There is a practical side of great importance pertaining to the recognition of the nature of the infectious organism in many cases of suppuration and abscess. For instance, pus which is due to streptococcus invasion indicates a collection which should be freely evacuated and carefully drained. This is also true in essential respects of staphylococcus pus, particularly that due to the streptococcus aureus. Putrid pus from any source requires disinfection and free drainage, the former preferably perhaps by hydrogen dioxide. Pus which is due to the colon bacillus is not often extremely virulent, which accounts for so many cases of appendicitis recovering with or without operation. A collection of this pus needs little more than mere drainage and opportunity for escape. Pus from a recognizable tuberculous source may still contain living tubercle bacilli. This means either that the cavity whence it came should be completely destroyed and eradicated, or else that the margins of the incision or opening through which it has escaped should be so cauterized that infection of a fresh surface is impossible. The same is true of abscesses due to glanders bacilli and to certain cases of suppurating bubo following chancroid, where the whole course of events shows the virulent character of the organisms at fault.
Although it may be possible to produce in certain laboratory experiments metamorphosed material which very closely simulates pus, or, in fact, by injection of chemical irritants, to sometimes imitate the suppurative processes, nevertheless, the student should be brought face to face with the statement, to which for surgical purposes there is no practical exception, that suppuration, i. e., formation of pus, is due to the presence in the tissues of the specific irritants already catalogued and described, and of the peculiar peptonizing or other biochemical changes which bacteria exert upon living animal cells.
—Coagulation necrosis is the term applied to the characteristic changes occurring in the tissue cells when thus attacked, which may be summarized as a fading away of cell outlines, diminution in reaction to reagents, and a merging of cells and intercellular substance. Coagulation necrosis is not the only result of bacterial activity, but may be produced by other causes. Nevertheless, pyogenic bacteria do not exert their deleterious action upon the tissues without occasioning changes included under this term. In an area thus infected, as already described, leukocytes, i. e., phagocytes, are present in increased number for purposes already mentioned. As we approach the centre of activity phagocytes are more numerous than cells, and intercellular barriers completely break down. When bacteria are found in greatest number, there also occurs the greatest phagocytic activity, and there also will be found the evidence of suppuration, i. e., pus. As already indicated, the polynuclear leukocytes are most active in the process of defence. Where coagulation necrosis is most marked there has been the greatest activity of conflict with the greatest death of cells. Around these areas bacteria and cells are found in indiscriminate arrangement. Tissue vitality is impaired by intoxication of the cells by the excretory products of the bacteria,[58] i. e., the so-called ptomains, toxins, etc., and their power of resistance is thus weakened. From the mechanical results of pressure tension around the centre of activity is increased, by which tension vitality is still more impaired and more rapid tissue death occurs. Thus there occurs migration or burrowing of pus; or, to state it more clearly, the tissues break down in front of the advancing destruction, and in the direction of least resistance. This is known as the pointing of pus, which brings it many times to the surface, and often in other and less desirable directions.
—An abscess is a circumscribed collection of pus. The term is used in contradistinction to purulent infiltration, in which the collection is not circumscribed, but is exceedingly diffuse and extends itself in various directions, the amount at any spot being almost inappreciable. Purulent infiltration is regarded as the more serious of the two conditions, as it is more difficult for pus to escape under these circumstances than when it can be evacuated through a single opening. The term phlegmon is one now generally used to indicate a suppurative process, usually of the general character of purulent infiltration rather than of abrupt abscess, but generally employed to include both conditions. The adjective phlegmonous is coupled with the names of other surgical infectious diseases to indicate that it is complicated by suppuration, e. g., phlegmonous erysipelas. Pus is a product of bacterial activity usually formed rapidly rather than otherwise, and abscess formation or phlegmonous activity of any kind is a question of but a few days. Empyema means a collection of pus in a preëxisting cavity.
The significance of this condition is well described in the story of inflammation and suppuration, to paraphrase Sutton, read zoölogically, as though it were the story of a battle: The leukocytes (phagocytes) are the defending army, the vessels its lines of communication, the leukocytes being, in effect, the standing army maintained by every composite organism. When this body is invaded by bacteria or other irritants, information of the invasion is telegraphed by means of the vasomotor nerves, and leukocytes are pushed to the front, reinforcements being rapidly furnished, so that the standing army of white corpuscles may be increased to thirty or forty times the normal standard. In this conflict cells die, and often are eaten by their companions. Frequently the slaughter is so great that the tissues become burdened by the dead bodies of the soldiers in the form of pus, the activity of the cells being proved by the fact that their protoplasm often contains bacilli in various stages of destruction. These dead cells, like the corpses of soldiers who fall in battle, later become hurtful to the organism which, during their lives, it was their duty to protect, for they are fertile sources of septicemia and pyemia. This illustration may seem romantic, but is warranted by the facts.
Around the margin of the site of an acute abscess a barrier is formed by condensation and cell infiltration of the surrounding tissues. This is not a distinct wall nor membrane, yet, nevertheless, serves as a sanitary cordon to confine the mimic conflict within reasonable bounds. This is the zone of real inflammation; within it there are tissue destruction and coagulation necrosis. By virtue of the peptonizing power of the pyogenic organisms the parts involved in this necrosis gradually liquefy the intercellular substance dissolving first. It is this which in the main forms the fluid portion of the pus. Various tissues show widely differing resistance to this softening process. In true glands the interlobular septa seem to break down first, and in this way suppuration extends around the acini or gland lobules, and thus pus may contain masses of easily recognizable size. These masses are ordinarily known as sloughs.
It is by virtue of the so-called lymphoid cells, which are those principally involved in producing the barrier or boundary of the acute abscess as above described, that granulation tissue is formed, which takes up the effort of repair as soon as pus is evacuated. This boundary has no sharp limit, but shades off into healthy surrounding tissues.
Under the term “abscess” is meant that which is described as acute abscess. Under certain circumstances, especially when they are produced by the facultative pyogenic organisms rather than the obligate, abscesses form more slowly, and may be spoken of as subacute. These are terms used in contradistinction to the so-called cold abscesses, which, although clinically bearing a certain resemblance to the acute, are in almost every pathological respect different from it. Cold abscesses will be considered under the head of Tuberculosis. It is possible to have an acute pyogenic infection of a cold abscess; in such case we have acute manifestations. Gravitation abscesses are those where pus forming in one part tends to migrate, usually in the direction in which gravity would take it, extending into portions deeper or lower. Perhaps the best illustration of this is[59] the pointing of a psoas abscess below Poupart’s ligament. Metastatic abscesses are those which are formed as the result of embolic processes, each one being in miniature a repetition of a lesion which has occurred at some other part of the body. The underlying fact concerning metastatic abscesses is that the primary process has occurred in some other portion of the body, whence it has been distributed as above. These will be considered in the chapter treating of Pyemia.
The product of all acute suppurative lesions is pus. This is an opaque fluid of creamy consistence and whitish or grayish appearance, varying in density, met with in amounts from a minute drop to half a gallon or more. Under ordinary circumstances it is odorless, and its reaction, either acid or alkaline, is very faint. It is, like the blood, composed of a fluid and a solid portion. The solid portion consists of so-called pus corpuscles and other debris of tissue, which vary with the site of the disease and the parts involved. The source of the pus corpuscles has been cited and the statement made that they are in effect the bodies of phagocytes which have perished in the biochemical fight for existence of the parent organism. Cocci or bacilli are found in pus corpuscles and also in the surrounding fluid.
Pus should be without odor, but under certain circumstances it possesses an odor which will vary in character according to the source of the pus or the nature of its principal bacterial excitant. Pus from the upper end of the alimentary canal frequently has the sour smell of gastric contents; that from the neighborhood of the lower end, the fetid odor which is for the most part due to the action of the colon bacillus. Inasmuch as colon bacilli are found in widely distant parts of the body, they may also give an unpleasant odor to pus even from a brain abscess. When the pus has become contaminated with the ordinary saprophytic organisms, it may smell like any other decomposing material. The older writers called it ichorous pus, while sanious pus was supposed to be that more or less mixed with blood, undergoing ammoniacal decomposition or else strongly acid. Pus sometimes has a well-marked blue or bluish-green tint. This is due to the presence of the bacillus pyocyaneus, already described. An orange tint is sometimes given by the presence of hematoidin crystals, due to the original hemorrhagic character of the infected exudate. The former appearance indicates usually a slow course to the suppurative lesion, while the latter has been regarded by some as affording an unfavorable prognosis. Distinctly red pus, whose tint is due to the presence of a bacillus giving bright-red cultures on blood serum, has been noted in other instances. This can readily be distinguished from blood, because upon dressings it does not change color.
Pus may form superficially, when it is called subcutaneous suppuration, in which case there is a minimum of pain, because tension is not great and the distance to the surface is short. Collections which form beneath the fasciæ, especially the deeper fasciæ of the limbs and trunk, give rise to much more extensive disturbance, both locally and generally, and frequently do not point for many days; or, instead of pointing, burrow deeply and find their outlet at some undesirable point. These are known as subfascial collections. Subperiosteal abscesses give rise to still more pain, because of the unyielding character of their limiting structures, and the symptoms caused by them are acute and distressing.
An illustration of the pain which may follow deep suppuration may also be seen in the ordinary panaritium, or bone felon, where the path of infection is from without, but the destructive lesion is confined within absolutely unyielding tissues, at least at first. Along certain tissues infection spreads with rapidity. This is particularly true of the delicate areolar tissue seen between tendons and tendon sheaths, and the infectious process may follow this tissue wherever it shall lead, even along complex courses.
The question often arises, Can pus be resorbed? There is no question but that small amounts of pus are disposed of by phagocytic activity, and the disappearance of purulent infiltration, under the influence of favoring remedies, or even when let alone, is not infrequently noted. True pus resorption is a question of phagocytic possibilities, and can occur only in very limited degree, as a result upon which it is not safe to count, and which is capable of encouragement only up to a certain point.
One inevitable law seems to govern collections of pus, that when they advance or migrate in any direction it is in that of least resistance. This causes them to take peculiar and sometimes disastrous courses, but it is a law which is never violated. It leads to the bursting of abscesses into the brain, into the pleural cavity, into the peritoneal cavity, the bowel, and elsewhere; it leads to a condition where pus may travel along a path even[60] a foot or more in length, rather than come to the surface, a distance of perhaps an inch, and affords one of the best reasons for early operative interference so that the disastrous effects of burrowing may be obviated. When the pus is limited to a drop or fraction thereof the abscess is called a furuncle, especially when in the skin. The average “boil” of the layman is a subcutaneous or subfascial abscess. When the infiltration is pronounced, and when there has been more or less extensive destruction of tissue, with perhaps formation of numerous outlets for the escape of pus and detritus, it is known as a carbuncle. (See Chapter XXVI.) In certain conditions small superficial furuncles or boils form, sometimes in great number and almost synchronously, or, as it were, in crops. This condition is known as general furunculosis.
—The appearances by which pus may be suspected or detected are those of congestion and hyperemia, more or less abruptly circumscribed and markedly accentuated. Along with these there is more or less edema or edematous infiltration of the skin and overlying tissue, which permits of that peculiar appearance known as “pitting on pressure.” Often, too, there is a distinctly edematous swelling of the parts, especially around the margin, with brawny infiltration of the centre of the infected area. Numerous vesicles occasionally are noted upon the skin, which may be filled with reddish serum. When softening and pus formation occur, there is a condition which to the palpating fingers gives the characteristic sensation known as fluctuation. Fluctuation simply points out the presence of fluid beneath; but when in an area marked as thus described fluctuation is noted, it means the presence of pus. It is detected by manipulating in a direction parallel to and concentric with the axis of the limb or part. The pain is also in most instances significant; patients speak of it as having an intense and throbbing character. With these local signs occur symptoms indicating some degree of septic intoxication, i. e., pyrexia, chills, malaise, sweats, etc., which are corroborative indications, their intensity being a reasonably correct index of the severity and gravity of the local infection.
When a deep-seated abscess is suspected a careful blood count will often permit a diagnosis to be made. This is conspicuously true of cases of appendicitis. If leukocytosis is established there should be immediate operation. (See Chapter II.)
It is seldom that a superficial collection of pus can be mistaken for anything else. In small and superficial abscesses (boils, furuncles) as pus approaches the superficial layer (epidermis) of the skin it may be discovered through its thin covering. In deep lesions there is often a doubt, even on the part of the most experienced. The measure now usually resorted to for purposes of diagnosis and exact recognition is the exploring or aspirating needle. The old exploring needle was one of good size, having a groove along which, after introduction, pus might pass. Since the almost universal use of the hypodermic syringe, a small aspirating needle attached to the ordinary syringe is the measure commonly adopted. Such a needle may be introduced into the brain, into the liver, or into almost any and every soft tissue without danger, and if properly manipulated is almost sure to facilitate detection of pus. Exploration done with either of these means and for this purpose should always be conducted as an aseptic, even if a minor operation, in order that no extra infection may be added from without. The skin should be carefully washed, the needle sterilized, etc.
It is good surgery to resort to the knife either for the above purpose or in order that by a longer incision or by opening the cavity deep exploration may be made. Such explorations are of benefit even though a circumscribed collection of pus is not found, since by relief of tension and local abstraction of blood they act in a revulsive way and do much good. Acting upon the same principle the trephine or the bone chisel may be used for the purpose of opening the cranium and exploring for pus, or of opening into the medullary canal of the long bones and hunting there for that which is suspected.
—As soon as suppuration threatens speedy measures should be adopted, either for the purpose of bringing about resorption, or of favoring and hastening suppuration. In theory antiseptic applications are demanded; in practice they are sometimes of benefit. These may consist of mere soothing applications, as a lead and opium wash, or some other wet or dry astringent applied upon the surface; or they may consist of cold applications, which by their astringent action will limit the amount of exudate and prevent its further infection. Or advantage may be taken of the properties of moist heat, and the application of hot poultices or fomentations may encourage exudation,[61] but particularly quicken superficial breaking down, and thus hasten the time when the phlegmon shall point, or come sufficiently close to the surface to show that its contents are pus and permit of evacuation. Such local applications, therefore, give relief from pain and hasten favorably the suppurative process. In cases of phlegmonous infiltration, the application of an ointment composed of resorcin 5, ichthyol 10, mercurial ointment 35, and lanolin 50 parts, or else the Credé silver ointment, is beneficial. Under the influence of these antiseptic and sorbefacient preparations, and of moist heat, many phlegmonous infiltrations assume a kindlier type, and may secure the actual resorption of pus.
Finally in almost every case pus must be evacuated. Here the universal rule may be applied, to which there are practically no exceptions, and which should be stamped on the mind of every student and young practitioner. It is—that pus left to itself will do more harm than will the knife of the surgeon if judiciously used for its evacuation. Action taken in accordance with this rule may be considered wise and timely. The operation of evacuation may at one time be a mere puncture, or possibly the aspirating needle alone will be enough; at other times it requires extensive and careful dissection and entails no little responsibility. This is particularly true in such deep-seated suppurations as those around the appendix and in the brain, while in the deep-seated bone lesions of this character the use of the bone chisel or the cutting forceps may be of use. But the rule holds good, no matter where the pus may be, and as long as good judgment is shown in the operative procedure nothing but good can come from recognition of this law. After the evacuation of pus the cavity should be cleansed and disinfected with hydrogen dioxide, perhaps even with caustic pyrozone, or, if these are not at hand, with other suitable antiseptic solutions.
Ordinary judgment should be exercised in evacuating every abscess, in order that opening be made at that point which in the common position of the body shall be most favorable to drainage by mere gravity alone. If circumstances compel opening when advantage cannot be taken of gravity, then one or more counteropenings should be made at points selected where drainage may be best effected, and where anatomical conditions do not make it injudicious to incise. Drainage should be favored by the introduction of a drainage tube or of other aids, such as gauze, strands of catgut, bundles of horse-hair, etc. Finally, a dressing should be applied which is both protective and absorbent, and in quantity sufficient to make compression of the walls of the abscess cavity—not sufficient to obstruct drainage, but enough to favor prompt adhesion of surfaces, which by speedy granulation shall ensure prompt healing.
Abscesses are found in proximity to large vessels or dangerous anatomical regions, when care must be exercised in opening them. Here careful dissection should be made under an anesthetic. This is true of abscesses in the neck and of those around the appendix, for example, where the general peritoneal cavity is shut off only by more or less delicate adhesions, and where the surgeon must literally feel his way with great precaution lest adhesions be torn and the previously protected cavity infected. At other times, especially in abdominal abscesses, it is necessary to pack sponges or absorbent gauze in and about the parts, so that any fluid which may escape may be absorbed by these dressings.
—The disturbance of function which accompanies all congestion and exudation, whether provoked by specific irritants or not, has been alluded to; but in cases of surgical infections, especially those which produce local suppuration, disturbance of function is much greater, while there are other disturbances which sometimes constitute the worst feature of these cases. The presence of pus is often indicated, especially when deeply seated, by one or more chills, and the occurrence of a chill is always marked to varying degree by pyrexia. It is conceded that the chill is an expression of a general septic disturbance; but it is necessary also not to forget that general septic disturbance is a frequent accompaniment of pus which is not evacuated as soon as formed. Moreover in certain cases suppuration and septic infection seem to occur synchronously, one being local, the other general.
Pus may also be suspected beneath a surface which is red, tender, swollen, edematous, and pitting on pressure. When fluctuation is added to these indications any element of doubt is thereby dissipated.
Other indications of the presence of pus are a well-marked leukocytosis, coupled with the iodine reaction indicating the existence of glycogen in the blood, the presence of[62] indican in the urine, and the positive results frequently obtained by making cultures from the blood. When pyogenic bacteria are found in the blood the inference is very plain, and both treatment and prognosis are influenced. In such a case the introduction into the blood of an antiseptic such as Credé’s soluble metallic silver or of the antistreptococcus serum, is plainly indicated. The absence of bacteria from the blood, under these circumstances, does not disprove the presence of pus, but their presence gives a very serious character to the disease, and should lead to a most guarded prognosis. Invasion of the blood by staphylococci is nearly twice as serious as when streptococci gain entrance. Suppuration of the bones and of the tendon sheaths is liable to produce such invasion.
The other disturbance with which suppuration is so often complicated is septic infection. In fact it may be questioned whether pyrexia is not an expression of this condition. Any collection of pus, no matter how small, may show signs of septic infection; and, on the other hand, large collections may be formed without serious septic symptoms—in other words, suppuration and expressions of septic infection may be blended in almost every conceivable way. Sepsis as a distinct condition will be described in another chapter.
It is important to summarize what may become of pus when once it has formed and is not promptly evacuated. Pus when long present may be—
A. The possibility of the absorption of pus, or, what is equivalent to it, its spontaneous disappearance, has been mentioned. While it does not usually take this course, it may thus disappear; as, for instance, in the anterior chamber of the eye in cases of hypopyon, or in various other localities, particularly when present only in small amounts. The absorption of pus is purely a matter, as far as we know, of phagocytic activity plus the power of the tissues to take up various fluids.
B. Encapsulation.—This occurs only when pus has been present for some time and when the virulence of the pyogenic organisms is not intense. We may get encapsulation of pus in any part of the body, the most typical illustration naturally being within the bones. Around the purulent focus, as around any other irritating foreign body, the capsule is formed by condensation of surrounding tissue. This is the way in which most cold abscesses with their limiting membranes are produced, those produced by tubercle bacilli having slight irritating properties. Inasmuch, then, as the biological activity in such a focus is small, there is time for such encapsulation; while by the membrane thus formed, or the sanitary cordon, already referred to, protection is afforded to the surrounding tissues. In such a collection fresh infection may incite acute disturbances again, and many abscesses which thus lie latent for a considerable length of time are fanned, as it were, into a conflagration, when a new and acute inflammation is produced.
C. Of the various metamorphoses and chemical changes that occur in that which was originally pus, the caseous and the calcific are the most common. These also are connected largely with the tuberculous process, although calcareous particles are found in the pus of actinomycosis. Under their respective heads these degenerations will be more particularly described.
Certain names have been given to collections of pus in different localities or under peculiar circumstances. A collection of pus in the anterior chamber of the eye is known as hypopyon; when in any preëxisting cavity, it is known as empyema of that cavity, the distinction between empyema and abscess being that “abscess” means a circumscribed collection where previously there was no cavity, while “empyema” implies a normal cavity, without respect to size or location, filled with this abnormal fluid. The term empyema, when not used in connection with some particular cavity, is understood to refer to a collection of pus in the pleural cavity. Other names also are used which are particulate and distinctive; in these the prefix pyo is used while the suffix indicates the part involved; thus we have pyothorax, pyopericardium, pyarthrosis, etc.
[63]
These are terms applied to more or less tubular channels abnormally connecting various parts of the body, or connecting some cavity with the surface of the body in a way anatomically quite abnormal. Or they may be regarded as tubular ulcers, or ulcerated tunnels, connecting as above. A more exact distinction between the two terms would imply that a sinus connects the surface with some deeper portion where a cavity is not normally present—i. e., with a focus of disease—whereas a fistula properly refers to a tubular passage connecting natural or preëxisting cavities in an abnormal manner. Thus we speak of buccal, rectal, vesicovaginal fistulas, etc., whereas a passage leading down to an old abscess or to a focus of disease in bone, for instance, is properly referred to as a sinus. It is possible for the margins of a fistula to become more or less cicatrized and cease to be ulcerous, whereas the entire track of a sinus is practically a continuous ulcer, only tubular in arrangement.
—There are numerous points about the body where, as the result of arrest of development or failure to grow, fistulous passages which are comprised within the normal fetal arrangements, but which should close later, either before or at birth, fail to do so. Thus we have congenital fistulas of the neck, persistent urachus, persistent omphalomesenteric duct, etc. These are in no sense primarily connected with diseased conditions, but may become so secondarily.
—e. g., rectal, fecal, and other fistulas and sinuses which connect with tuberculous foci in any part of the body.
—e. g., vesicovaginal fistulas due to tissue death from pressure, buccal fistulas from gangrene of the cheek, as in noma.
—bullets, ligatures, etc.—which prove irritating or infectious enough to prevent absolute healing. More or less tortuous sinuses will generally be found leading down to the irritating material.
—e. g., a sequestrum in bone, which is usually evidenced by the presence of one or more sinuses.
—If the determining cause is still acting, the treatment is to remove the cause. Consequently, when the sinus leads down to diseased bone or other dead or dying tissue, the complete evacuation of the cavity is necessary before the sinus may heal. If the cause is a foreign body, its removal should be at once insisted upon.
An excellent suggestion is to stain all fistulous tracks with methylene-blue; the blue trail after doing this may be followed, no matter how irregular its course (Fergusson). If the color is mixed with a little hydrogen dioxide, and this forced into a sinus mouth or a fistulous opening, it will carry the dye to all parts of the cavity. This may be used even in dealing with fecal fistulas or those extending deeply into the interior of the body or among the viscera.
Fistulas of congenital origin and those which connect two normal cavities of the human body are usually due to a cause which has ceased to act. Consequently we should endeavor solely to atone for the result. The direction and the course of a sinus may be learned by the use of a probe curved to suit and manipulated by a gentle hand, force never being required. Or sometimes, when the silver instrument fails to pass, a flexible bougie or catheter may be introduced. The character of the passage can be judged for the most part by the appearance of the discharges. With sinuses of recent origin leading down to recent suppurative foci it may be sufficient to enlarge the opening and to wash the cavity thoroughly. If a particle of gauze, tube, or sponge has been left therein, its removal is necessary to secure prompt healing. In cases of long standing antiseptic and stimulating substances should be injected or the interior should be cauterized with strong solutions of zinc chloride or silver nitrate, or with these melted upon the end of a probe. The chronic sinus, as well as the chronic rectal fistula, is usually an expression of local tuberculous disease. Accordingly these passages may be found lined with the same dense, fungating membrane which lines a cold abscess cavity—the membrane, protective in its purpose, to which I have given the name pyophylactic. Whenever such tissue and such membrane are met with they should both be extirpated thoroughly, since in this way only can absolute eradication of the tuberculous infection be relied upon. After such complete excision—which means usually laying open the[64] entire sinus—the parts may be brought together with sutures (this, at least, is usually possible about the rectum) to secure primary union; otherwise, the whole sinus, as well as the cavity to which it has led, must heal by the granulating process, both being kept packed with gauze or some other desirable foreign body acting as an irritant, thereby provoking more rapid formation of granulation tissue. When it is necessary thus to pack a cavity, or when it is desired to keep its upper exit open lest it heal before the lower part, ordinary white beeswax, as suggested by Gunn, makes a serviceable material. This can be molded in hot water to fit the cavity; can be tunnelled or bored for drainage; can be diminished in size as the cavity heals, and is absolutely non-absorbent.
Finally there are numerous plastic methods which have been resorted to in various parts of the body, most of which are made to comprise, first, the absolute eradication of the diseased tract, and, later, the closure of the wound thus made by transplantation or sliding of flaps, or any other plastic expedient which may be considered best. These, as well as the special treatment made necessary for particular forms of sinus and fistula, will be dealt with under their proper headings.
[65]
The term ulcer pertains to surfaces, and should be defined as a surface which is or ought to be granulating, i. e., healing.
While an ulcer may be the result of ulceration, it is not necessarily so, the term ulceration being one of very loose significance and applied to many different processes. The idea underlying ulceration is infection, and, when limited to its proper significance, the term should never be used for a process in which infection and consequent breaking down of tissue do not virtually comprise the whole process. Therefore, it is to be distinguished from certain disappearances of tissue alluded to under the head of Atrophy or Interstitial Absorption. It is not correct to say that the sternum ulcerates away, making room for a growing aortic aneurysm, the question of infection here not being raised. These distinctions should be accurately maintained and constantly borne in mind.
The causes of ulcers may be—
—This includes all surfaces which are granulating and healing more or less rapidly, or are displaying a disposition toward healing, and which may have been produced by wounds, burns, frostbites, etc. These include also ulcers due to pressure, as from splints, bandages, orthopedic apparatus, or from external friction. Ulcers which form around foreign bodies may also be included under this head, their essential cause being traumatic. It should include also destruction of the surface by various chemical agencies, such as strong caustics, and the consequences of intense heat or cold, including burns and frostbites.
—1. Among local causes may be mentioned local infections, with tissue death in consequence, such as occur in tuberculous, cancerous, leprous, syphilitic, and other specific manifestations where surfaces are involved.
2. Tumors, either benign or malignant, whose blood supply is cut off and whose surface is thereby predisposed to infection.
3. Perverted surface nutrition, for example, in connection with varicose veins of the extremities, where, aside from any perverted trophoneurotic influence, there is stagnation of blood, saturation of tissues with serum, and final leakage of the same, even to the surface. Varicose veins of the leg which lie near or underlie ulcerating surfaces become thrombosed and obliterated, so that such ulcers rarely bleed. On the other hand, a passive hyperemia here leads to edema, perversion of nutrition, failure to repair trifling surface injury, and a surface is left which of itself rarely, if ever, heals.
4. So-called pressure sores or bed-sores, which in some cases may be regarded as having a traumatic origin, but which, nevertheless, would not occur from purely traumatic influences without predisposing tissue changes. The bed-sore is probably the best illustration of this. Simple ulcer is known as bed-sore, while a sloughing ulcer of this kind is frequently alluded to as decubitus. Such ulcers are usually found over those regions of the body made most prominent by bony projections, upon which undue pressure is made when debilitated patients have lain for a long time in bed.
5. Ulcer is the frequent result of numerous skin diseases, into whose etiology as yet bacteria have not been introduced—e. g., pemphigus, eczema, etc.
6. Ulcer is the occasional result of embolic or other disturbance of the principal artery of the part, by which nutrition is cut off and tissue death results.
[66]
7. Bites of insects or other parasites or of noxious animals frequently lead to ulceration.
8. Certain more specific forms of ulcer are described by some writers, apparently with more or less reason, among them being chancroid, perforating ulcer of the foot, etc. (Chancroid is described in Chapter X.) Trophic ulcers of the fingers or hand are also seen, particularly after injury to or division of nerve trunks in the arm or forearm. Perforating ulcer of the foot is a circumscribed circular ulcer with thickened edges, often nearly concealed by overhanging skin. It may be found in any part of the sole of the foot, but is most common near the first joint of the great toe. The borders of the ulcer are usually anesthetic. It is frequently seen in diabetics. By some it is associated with trophic nerve disturbance; by others it is regarded as having a specific etiology of its own. The probability, however, is that it is simply a subvariety of pressure sore.
9. Since the introduction of the Röntgen or x-rays into surgical therapeutics a new local cause of painful and intractable ulcers should be enumerated. A too prolonged or injudicious exposure of a part to this peculiar influence induces first a dermatitis, which is not always immediate, but may be tardy in appearance, and which may be followed by desquamation or exfoliation that may proceed to absolute surface destruction and sloughing. These lesions are popularly spoken of as x-ray burns. The superficial ulcers thus produced may be extensive and are nearly always excessively sensitive and painful. The very structure of the surface vessels is affected and they undergo a species of sclerosis. A strong preparation of radium has been known to produce a similar effect.
—1. Ulcers are frequently met with in certain constitutional conditions which are characterized by tendency to local manifestation at points of least resistance. Among these may be mentioned scurvy.
2. There are ulcers of apparently distinctive trophoneurotic origin, of which that mentioned above as B, 8—perforating ulcer of the foot—may possibly be one. These accompany certain nervous disorders of central origin, prominent among which are locomotor ataxia and tabetic disease of all forms.
3. Ulcers are produced sometimes as the result of specific or selective action of certain drugs, among them mercury and phosphorus being the most prominent. These manifestations are usually perceived in the mouth, and may be regarded as infections at points of least resistance. Nevertheless, they are commonly associated with the tendency of these drugs.
4. There are many constitutional conditions in which vitality is so lowered that a special liability to ulcer—i. e., infection and production of ulcer at many points—is noted. It is well, however, to mention that the common diseases in which this tendency is most often noted are typhoid, diphtheria, diabetes, and syphilis.
With this summary of the common causes of ulcer it is again stated that ulcers may be due to direct consequence of traumatic loss of substance or to the process of ulceration—i. e., as a consequence of previous infection, or as permitted by trophoneurotic disturbance and ischemia. Ulceration is a process of molecular death, in which cells die successively and more slowly, as distinguished from gangrene, in which there is simultaneous death of large aggregations of cells, by which a slough or its equivalent is produced.
Ulcers are referred to as healthy when the process of granulation is proceeding with average rapidity; indolent, when the reverse prevails; sloughing, when there is actual visible tissue death in connection with the ulcerative process; phagedenic, when the gangrenous tendency is well marked and the process exceedingly rapid; irritable or erethistic, when the surface is exquisitely sensitive; hemorrhagic, when bleeding easily; fungous or fungoid, when the granulations have risen above the surface and are increasing at too rapid a rate. There is a peculiar form of ulcer, seen mostly upon the face, to which the name rodent ulcer (also lupus exedens) has been given. This is now known to be a slowly growing form of epithelioma, and is described in Chapter XXV.
The best examples of the indolent ulcer are seen in connection with varicose veins of the extremities; of the phagedenic ulcer, in certain cases of chancroid; of the irritable ulcer, in ulceration of the cornea, when the pain and photophobia are intense; or in fissured ulcer of the anus, where the pain and sphincter spasm are sometimes agonizing.
Ulcers are described according to their shape as regular or irregular; as fissured, when they extend more or less deeply and abruptly into the surface involved; as fistulous[67] when they have a tubular arrangement; as rodent, when they spare nothing in their course.
The borders of ulcers are described as healthy, indurated, tumid, edematous, undermined, livid, inflamed, etc., these adjectives explaining themselves.
The surfaces of ulcers are described as healthy when they have normal color and appearance, inflamed, excavated, covered with sloughs, callous, etc. The callous ulcer is one which exhibits little change from month to month; its surface is dirty, and its secretion thin and mucopurulent. It is usually sunk considerably below the surrounding level, while its border is firm and nodular. The best examples of this form are those accompanying varicose veins.
In size or area ulcers may vary from the slightest local destruction of tissue to an area covering an entire limb or a large part of the trunk. In depth they vary within lesser limits; while an external ulcer may connect with some deep lesion by means of a tubular passage or sinus. It thus appears that the term ulcer may be applied to the result of a natural effort to repair loss of substance without introducing the element of disease, or that it may be the consequence of local infection with local tissue disaster.
The character of the material discharged from an ulcer will vary according to the category in which it belongs. The healthy, healing, or granulating surface, often spoken of as ulcer, discharges a material in gross appearance much resembling pus from an acute abscess; in consistency, color, and other appearances it is the same. Nevertheless, its origin is essentially distinct. This material represents simply the waste of reparative material, sent up to the surface for the purpose of hurrying the process. Its fluid, like that of pus, comes from the serum of the blood; its corpuscular elements, like those of pus, are leukocytes or wandering tissue cells, which have been furnished in great numbers—in fact, in excess. As it comes to the surface—or as, rather, it is rejected from the surface, being superfluous in amount—it is likely to become contaminated with bacteria by contact infection, and consequently may be seen under the microscope to contain various microörganisms. This contamination, however, has been final, accidental, and irrelevant. This material is not pus; has no infectious properties, except those which may accidentally be conveyed to it; represents no warfare of cells, only excess of supply or overdemand; and should be spoken of as pyoid or puruloid material, and never confused with pus. In amount it will vary according to the activity of the reparative endeavor, and somewhat according to the amount of irritation of the surface by dressings which may be applied. If a granulating surface is absolutely protected from possibility of contact infection, it will never contain microörganisms; while this pyoid, if allowed to remain too long, especially when infection is permitted, may decompose and become irritating, and is a material to be gently dislodged by a spray or an irrigating stream with each dressing, which dressing should be made once in twenty-four to sixty hours.
An ulcer having been defined as a surface which is or ought to be granulating, it becomes necessary to define the granulation process and to show how healing is thereby achieved. Granulation tissue is a name applied to a new and temporary tissue of embryonic type, which acts as a scaffolding or temporary structure, permitting the construction of more permanent tissue. It is produced entirely by the activity of cells, which are the mononuclear and polynuclear leukocytes and the wandering cells already mentioned. They are frequently known as embryonal cells when performing this function; sometimes as formative cells. They have a distinct nucleus, which stains readily, and, having this resemblance to epithelial cells, they are often referred to as epithelioid cells—sometimes as fibroblasts, because they may later assume the dignity of connective-tissue cells. They assume a multitude of shapes. Between these cells as they are drawn toward the point at which they are most needed, perhaps by chemotactic activity, there is an intercellular substance which later becomes fibrillated. As these fibers develop the remaining cells become entangled between them, and in this way a new connective tissue is formed of cells of originally mesoblastic origin. Of such tissue the solid part of granulation tissue is built. This tissue is essentially different from the epithelium which it is expected will subsequently cover it. If a normal granulating surface is scanned with a magnifying glass of small magnifying power, it will be seen to consist[68] of numerous minute projections, each of which is known as a granulation, consisting of the tissue above described, formed as a minute eminence around a budding capillary bloodvessel, from which a projection has arisen upon the exposed surface. This capillary bud is the result of karyokinetic activity on the part of the endothelium—namely, the hypoblastic cells of which it is essentially composed. In each of these cells, under certain circumstances, the karyokinetic threads already mentioned develop and become loosely coiled, while the chromatin in the nucleus increases in amount and the nucleolus disappears. The chromatin threads become thicker, arrange themselves equatorially around the poles of the nucleus, and gradually turn so as to point toward it, while a new membrane forms around each separate coil, and two nuclei are thus made out of one. While this is taking place within the nucleus the cell protoplasm undergoes active rotary motion, is finally segmented, and by the time the nucleus is divided is nearly ready for complete division of the cell. While nuclear division is usually bipolar, it may be multipolar; if a rearrangement of the protoplasm is delayed, the result becomes a multinuclear cell, known as a giant cell.
The consequence of this endothelial activity is new cell formation and the construction of a projection from the capillary which soon attains the dignity of its parent vessel, and, as connective-tissue cells form around it, soon becomes a granulation by itself, each granulation being marked by a capillary loop of its own. Healing by granulation or the granulation process, no matter how set up or caused, is essentially the formation of hundreds or thousands of these tiny structures, a new one being formed on top of those which precede it, while those first formed and deeper down undergo condensation and metamorphosis of tissues, by which they are converted into something higher in the tissue scale. Under ideal conditions true granulation building proceeds pari passu with epithelial reproduction around the margin of the granulating surface, so that by the time granulation tissue has completely filled the defect, no matter how caused, epithelial covering has been completely constructed and the healing process thus completed. These two processes, however, do not necessarily keep pace with each other. Should surface repair take place relatively early, we may have a depressed scar; while, on the other hand, should it not proceed rapidly enough, or, to state it in another way, should the granulating process be too rapid, we have such excess of granulations as shall rise considerably above the surrounding level, and may, under certain circumstances, become so exuberant that nutritive material cannot be formed rapidly enough, and those granulations farthest away from the centre of supply may die. Such exuberant granulation is often spoken of as fungoid, and constitutes that great bugbear in the eyes of the laity which is termed by them proud flesh. It has no further significance than that the supply has exceeded the demand and that the granulating process has been overdone. Such luxuriant granulations may be cut away with scissors or knife, may be burned away with caustic agents or the actual cautery, or may be disposed of in any other manner without harm and only with benefit; in fact, it is often necessary to suppress this exuberant tendency by caustics and pressure, in order that the desired epithelial covering may be properly formed.
Epithelium, being an epiblastic structure and capable of no other origin save from its kind, can only be supplied from those regions where it has preëxisted. Consequently, ulcers involving the external surface of the body demand a lively epithelial reproduction in order that they may have a normal covering. Epithelial activity sometimes becomes retarded, and is much slower toward the termination of the healing process than at the beginning. The epithelial covering of a healing ulcer is always marked by a delicate whitish or pinkish film, which proceeds from the periphery as well as from any little island of original epithelial structure left. It is well known that after a certain amount of this repair the process sometimes comes to a complete halt, and the various expedients for stimulating and promoting it, as sponge grafting and the different methods of skin grafting, have been devised solely to atone for such sluggishness or inability.
Ulcers of small size, which are more or less exposed to the air in healthy individuals, while also exposed to possibility of infection, nevertheless seem to escape it, owing to the defensive power of the blood serum and the active cells. Such discharge as naturally comes from them, when not excessive, undergoes evaporation until a point is reached where a dry crust or scab is formed. Under this scab granulation proceeds to a point where the pressure of the scab itself, presumably on the level of the surrounding parts, checks its activity, while at the same time epithelial reproduction goes on until it has[69] been completed. Then the scab, being no longer of use, drops off or is detached by slight friction.
Such is granulation tissue: at first a mere trelliswork of temporary and delicate cell structure, traced in a certain amount of intercellular, homogeneous substance, into which the budding vessels project, the whole mounting, nearer and nearer to the surface, day by day, with variable rapidity, diminishing in this regard as the days go by, so that frequently the granulation process comes to an apparent halt before enough new tissue has been formed. While the superficial granulations preserve the characteristics above noted, those deeper down undergo firmer and more complete organization, and the delicate embryonic structures show the same tendency which they do in the growing embryo, by virtue of what Virchow has called metaplasia, to become converted into something higher and more dignified in the tissue scale. These cells do not specialize themselves to the extent of permitting complete repair of organs of special sense. Thus, while a wound in the cornea or retina may be completely healed, it heals by cicatricial tissue, and not by repair of the special structures involved. On the other hand, tissues of more common connective type—fibrous, bone, cartilage, etc.—are capable of regeneration; and it seems to be a part of the privilege of these new granulations to merge themselves into that kind of tissue necessary for filling the gap. Nevertheless the most common result of granulation is its metablastic conversion into fibrous tissue, which has the special characteristic of contractility without elasticity. As a result the scars contract, in consequence of which disfiguring results are sometimes the almost inevitable consequence of healing of extensive losses of substance. In certain instances it is possible by constant effort to overcome the unpleasant effect of this cicatricial contraction. For example, after extensive burn of the anterior part of the arm, the forearm will be gradually and permanently flexed upon the arm by virtue of contraction of the scar in front of the elbow unless some forcible means is practised for maintaining extension of the limb for at least a part of the time. So with many other injuries and the various mechanical or other expedients required to prevent the untoward result. Nowhere are the after-effects more disfiguring or serious than about the face, where the eyelids are drawn out of shape, the contour of the mouth altered, and where, sometimes, there are other extensive manifestations (Figs. 10 and 11).
Fig. 10
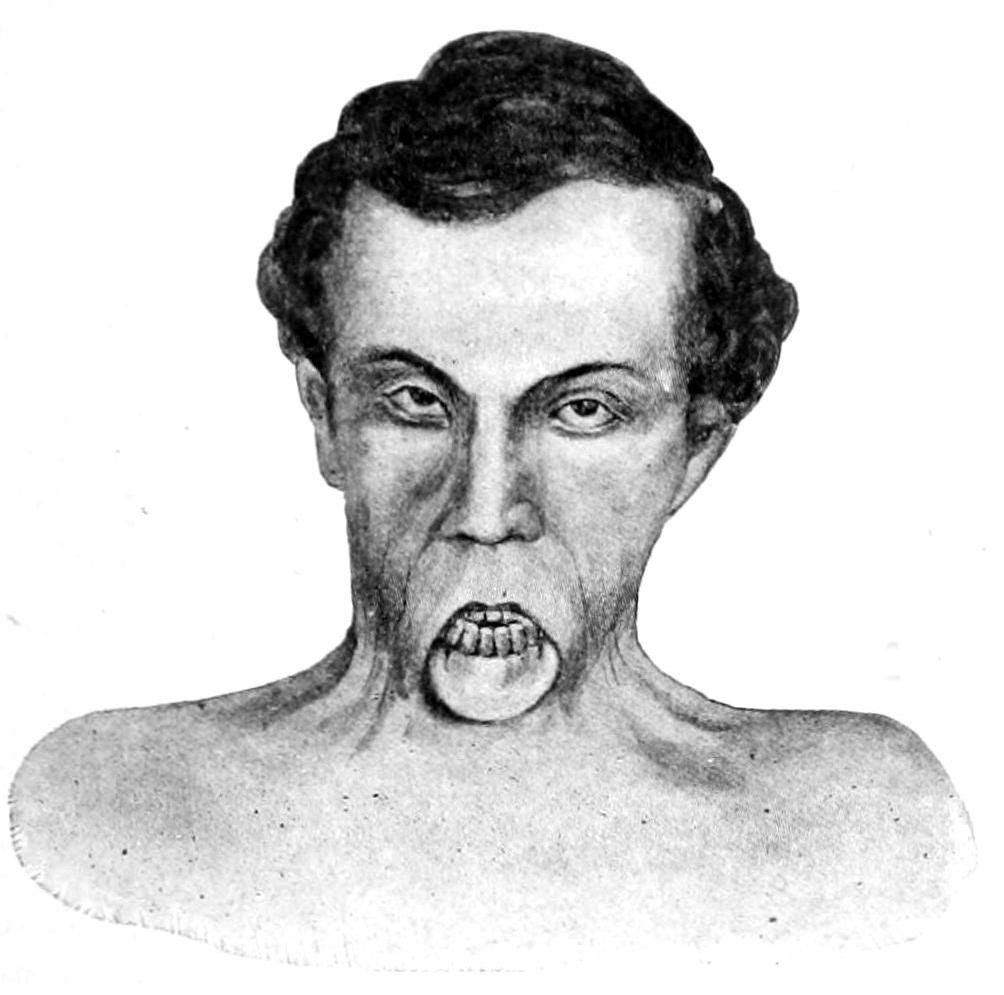
Cicatricial deformity following burn. (Original.)
Fig. 11
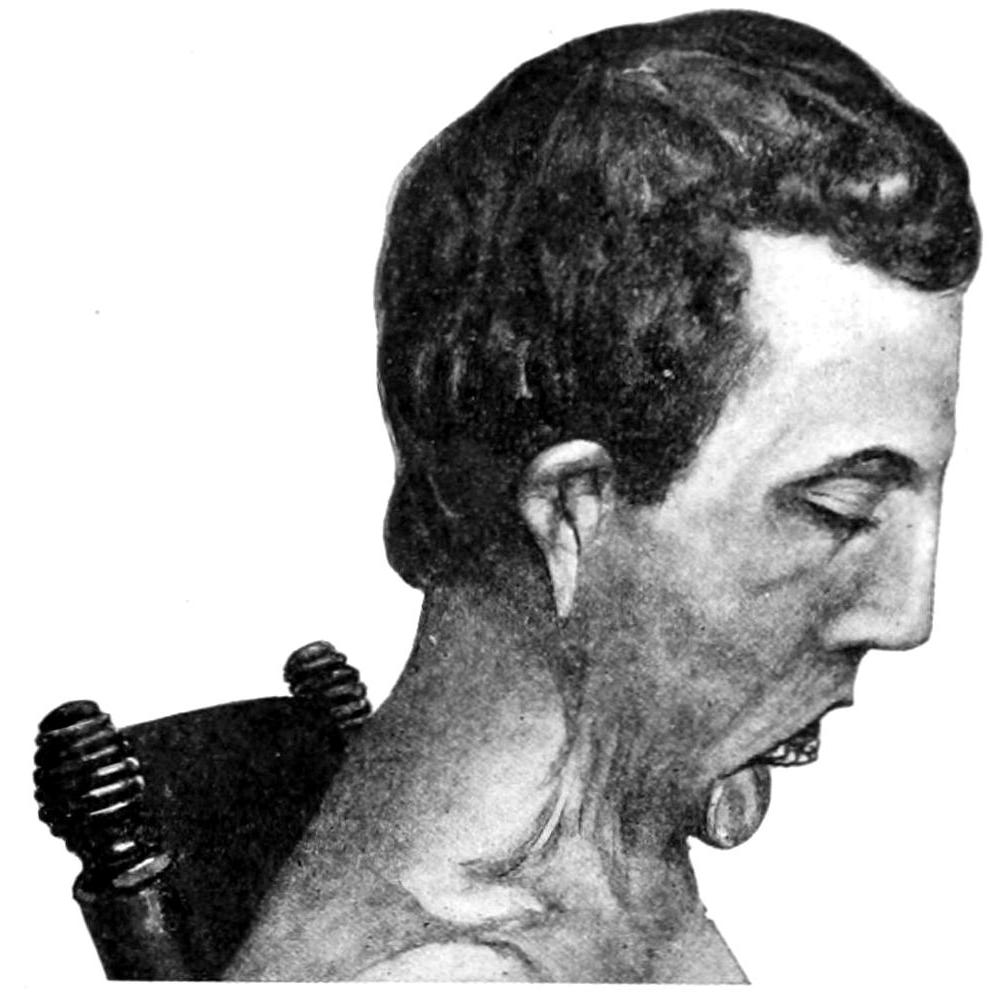
Cicatricial deformity following burn: side view of same case.
Fig. 12

Epitheliomatous degeneration of chronic ulcer, necessitating amputation. (Original.)
As a result of healing of the granulating surface there is what is known as a cicatrix or scar. This is composed of fibrous tissue, probably more or less distorted by virtue of its contractility, and of epithelial covering furnished from the margin of the original ulcer, constituting a thin, glistening membrane, applied closely to the scar tissue beneath, without intervening fat or tissue which permits of the play of the one upon the other. When this epithelial surface is abraded it is repaired with difficulty, and a raw or ulcerating[70] scar is difficult to heal. Manifestation of perverted epithelial outgrowth is frequently provoked at these points by the action of continuous irritation. In consequence there is what is generally recognized as the transformation of a chronic ulcer, or the site of one, into an epithelioma, or possibly, by similar irritation of the connective-tissue elements, into a sarcoma. This is the so-called cancerous degeneration of previous ulcers, and is noted occasionally. The lesion is one which often requires disfiguring, or even mutilating operations in order to get rid of the malignant disease (Fig. 12.) All the scars thus resulting are liable to undergo a fibrous and degenerative change to which is given the name cicatricial keloid. It is marked by increase in size and density, by reddening which denotes increased vascularity, and extension into surrounding previously healthy tissue. By these changes a given scar is made much more prominent and disfiguring. It cannot be prevented by any ordinary treatment, and is often the bête noir of surgeons. (See also under Fibroma, and chapter on Diseases of the Skin.)
The surface of a superficial scar while thus covered with epithelium shows a complete lack of all the other skin elements. No hair grows upon such a surface, because the original hair follicles are destroyed; neither is it moistened by perspiration nor anointed by sebaceous material, because the secretory glands have also disappeared. It is a surface which often needs more or less protection, especially when in exposed situations.
—Here, as in all other instances, the first effort of the surgeon should be to remove the cause. This may be done by local, or may require constitutional measures. If a definite local cause can be established, its removal may be a slight or may entail a more or less serious surgical operation. Aside from this disposal of the exciting agent, treatment should be divided into the general and the local. General treatment is scarcely called for when dealing with healthy ulcers; but in all those instances where the constitutional condition of the patient is below par, or where there is a general poisoning or infection underlying the ulcer itself, prompt and energetic constitutional treatment should be at once instituted. In scurvy, for instance, the diet and hygienic surroundings of the patient should be rectified immediately. In syphilis no lasting nor deep impression can be made on local manifestations without general constitutional treatment. In tuberculosis and the other surgical infections much will be accomplished by internal medication, by proper hygiene, as well as by local applications or operation. The importance of these general measures is likely to be underestimated, and many fail to realize the advantage of combining suitable internal and external therapeutic measures.
—First of all may be mentioned the insistence upon repose which induces physiological rest. The ulcer may then show a tendency to heal. This may necessitate wearing a splint or restraining apparatus, or confinement in bed, depending upon the location of the ulcer. Physiological rest will be enforced sometimes by stretching a sphincter in order to temporarily paralyze it in cases of irritable rectal ulcer, where the principal pain is produced by the reflex spasm of its fibers. Again, the eye with irritable ulcer of the cornea is sometimes kept so tightly closed by the same kind of spasm there that it may be necessary to divide the lids, or the orbicularis muscle at the angle of the lids, in order to make access to the part. This is carrying out the principle of physiological rest, because it permits proper exposure and treatment.
The healthy and healing ulcer needs no treatment except protection. Epithelial covering will probably keep pace with filling of the depression by granulations, and[71] all that is necessary to do is to prevent external irritation. Should there be excess of discharge, the simplest absorbent dressing, with enough antiseptic material to prevent putrefaction by contamination with the bacteria of the surrounding air, should be employed. The ulcer which is becoming tardy in its repair may be stimulated by silver nitrate, zinc chloride, or other caustic applications, which act as a spur to the sluggish granulations, destroying those with which it comes in contact, but stimulating those below to do their duty more promptly.
The conventional applications to ulcers fall usually under two categories—the watery solutions and the unguents.
Fig. 13

Cicatricial deformity following specific ulcer. (Original.)
Investigations in the laboratory have led to the employment of peptonized preparations, among which are peptonized cod-liver oil and some of the partially or predigested foods, such as bovinine, etc. These appear to have the power of digesting sloughs and of causing a speedy separation or disposal of everything necessary in the endeavor to secure a healthy condition of the ulcerating surface and give most satisfactory results. When sloughs are present it is an advantage to dust over them papoid, caroid, etc., which have the power of catalytic disposition of decomposing material without reference to the action of bacteria. Under their use there seems to be a solution and disposition of these dead products. With a foul ulcer—one from which the discharge is more or less offensive, due usually to decomposition of sloughing masses, not yet separated—the method of continuous immersion in hot water, when it can be performed, is always valuable. But nothing seems to equal brewers’ yeast for this purpose. It may be applied on absorbent cotton (which should be soaked in it) and covered with oiled silk. Its curative property may be ascribed to the nuclein which it contains in a nascent state. It will, when fresh, clean off a sloughing surface better than anything I ever used.
Many ulcers are surrounded with such firm, indurated borders that it seems impossible that any active regenerative process can arise from such source. Hence, incisions have been practised for centuries. These have been made radially from the centre or have been made parallel to the margin of the ulcer, or sometimes the firm, dense tissues have been minced or chopped by a series of cross-cut stabs or incisions; as the result of which renewed activity has arisen, and an impetus given to the healing process. These methods, however, have yielded to that alluded to above. The ulcer in which granulation has come to a standstill is often treated with the sharp spoon or curette. The result of this has been to provoke again a speedy renewal of granulation efforts, and treatment by curetting is standard and often useful. Actual cauterization of the ulcer with a view to such complete destruction of its covering and border as shall lead to their separation by the sloughing process is occasionally practised. This is perhaps best performed with the actual cautery. It lacks, however, the valuable features of the operative method, to be described below. Modern methods have made it plain that it is often an absolute waste of valuable time to resort to the older expedients of stimulation, incising the edges, etc., and that one can accomplish by an operation in perhaps three weeks what ten times that length of time would fail to do by older methods. The most effective method, therefore, in dealing with old and chronic ulcers is to anesthetize the patient, to excise the entire affected area—i. e., the surface which ought to be granulating and the firm border and tissue in its neighborhood—and then to cover the surface either with skin grafts, pared off with a razor according to the Thiersch method, or with a strip of skin whose full thickness is raised, which is taken from surrounding parts by some autoplastic or heteroplastic method. This line of treatment is so far preferable to all others that, except in case of refusal of the patient to submit to it, it is the one which must hereafter commend itself. It may afford opportunity for extensive plastic operations or for the exercise of the best discretion and knowledge of experienced men; yet cases are rare in which it cannot be successfully performed. These methods of skin grafting have so far supplanted the older method of sponge grafting that the latter is now seldom practised. It may possibly have a sphere of usefulness in certain ulcerated cavities, but under all other circumstances it must take a position far below the plastic methods in practical value.
[72]
Finally, ulcers of specific type—syphilitic, tuberculous, leprous, glanderous, etc.—need methods in which the first effort should be not so much to arrange for healing as to dispose of infectious material. The knife, the scissors, the sharp spoon come first into use here, the surgeon bearing in mind that almost all this material is more or less infectious, and that inoculation of his own hands is possible as the result of carelessness. After taking away with instruments all the granulation tissue, with its surroundings, which seems to expose to danger, it is well to cauterize the part with the actual cautery, nitric acid, bromine, or zinc chloride.
The markedly hemorrhagic ulcer, whose surface bleeds on the slightest contact or disturbance, is often a cancerous ulcer, though not necessarily so. This ready bleeding is usually the effect of the fragility of the walls of the new-formed bloodvessels. In many instances it is sufficient to scrape until harder or more resisting tissue is encountered. Hemorrhage may be profuse for the moment, but it is easily controlled. Caustics may then be applied or not, according to the judgment of the surgeon.
Another method is to treat such a surface with the actual cautery. Another is to operate, even in the presence of incurable disease, in order to check a tendency to fatal hemorrhage before the disease has expended itself. In a general way, in regard to small, ulcerating, cancerous surfaces, it may be said that if they bleed excessively or are unduly irritable, it is preferable to attack them by operative measures in spite of the impossibility of effecting a cure.
There are other methods of treating ulcers, but they have mainly been abandoned for those mentioned.
[73]
Gangrene is known also as necrosis, although this term is usually limited to gangrene of bone. It is known also as mortification, and to the older writers, especially when soft parts die and separate in sloughs, as sphacelus. Gangrene means death of tissue in visible and more or less circumscribed masses. It is distinguished from ulceration not on account of molecular disintegration, particle by particle, but because of death in toto and synchronously of a large, perhaps innumerable, number of cells. Gangrene is described as due to causes which may be:
, including the so-called thermal causes as essentially mechanical injuries. Under this head are included cases where injury is the primary cause, whether this injury is the crushing of a limb, the separation or occlusion of its main bloodvessels, the division of its main nerves, or the crushing or pulpefying of its entire structure by machinery or accident; also those so-called thermal cases which are due to intense heat or intense cold. To these might be added the chemical causes, comprising injuries by powerful caustics, alkalies, or acids, which are known to cause speedy death of every living tissue with which they come in contact.
Gangrene from frostbite is often of the moist type. There is scarcely a limit to its extent, either in area or depth. It is due primarily to thrombosis, which is followed by a purplish color of the skin, by loss of local warmth, and numbness. Naturally it involves the ears, nose, fingers, and toes. But after alcoholism and exposure one or more entire limbs may be involved. With moist gangrene there is danger of septic infection (q. v.). After formation of a line of demarcation the line of amputation may be made to follow it closely, but the best results are obtained by higher division, at points of election, where tissues are less sensitive and less infiltrated.
—These are largely connected with ischemia. Gangrene from edema—itself the result of passive hyperemia and exudation—is not infrequent, the most common expression of this condition being seen perhaps in the external genitals of the male. Embolism due to valvular heart disease, thrombosis due usually to a preceding phlebitis, but possibly to marasmic origin, especially met with after confinement, with disturbance in the uterine sinuses, shutting off the circulation by endarteritis, which thus assumes the form obliterans, are some of the local causes which concern the bloodvessels alone. In fact, the majority of cases of spontaneous gangrene are probably due to changes in the vessels, endarteritis being the cause of a condition known as atheroma of vessels, in which fungoid outgrowths, or, rather, ingrowths into the vessel lumen, are common. Any one of these, if detached, may serve as an embolus. The degenerative excavations in the thickened walls of the bloodvessels, which discharge more or less cholesterin and other debris, and which have been known as atheromatous abscesses (misnomer), are frequently the precursors of the disease under consideration. As the result of these changes alone, without reference to formation of emboli, vessels may become completely occluded, especially when slightly injured.[2]
[2] Intermittent claudication, when recognized, may be regarded as a precursor of that arteriosclerosis which may proceed to gangrene. The term implies temporary anemia of one or more of the extremities, with numbness, burning, or prickling sensations in the skin, occasional cramps in the muscles, with loss of power, tenderness of the nerve trunks, weakening or loss of pulse in the affected part. When these symptoms occur in the feet they are not infrequently followed by terminal gangrene or other evidences of angioneurotic necrosis, including even those forms known as erythromelalgia and Raynaud’s disease. Its treatment, of course, is relaxation of vasomotor spasm, best accomplished by the use of the nitrites, among which nitroglycerin is perhaps most valuable.
Extravasation of blood is another cause connected with the bloodvessels, this coming usually from traumatic rupture, possibly from idiopathic causes. At any rate, the tension in the part may threaten its life because of the pressure which overcomes the circulation of blood. Ligation of the main trunk of an artery is sometimes followed by gangrene, no matter how carefully done, collateral circulation being insufficient to[74] sustain the nourishment of the part. In certain fractures, simple as well as compound, the blood supply of a part is rudely broken off by injury to a bloodvessel in such a way as to cause local or general death, either of a bone or of the entire limb. Flaps made for plastic purposes, arranged without sufficient regard to their proper blood supply, or so dressed after operation as to sustain undue pressure, are often so shut off from the heart as to die for want of blood. Finally, gangrene may be the result of pressure either from splints, bandages, etc., or from tumors increasing in size, or possibly, as in certain pressure sores, etc., from the mere weight of the body. Here, too, chemical agents must be mentioned, referring now to the peculiar action of certain foods or drugs, particularly ergot. Thus antiseptic solutions, particularly carbolic acid, may be made strong enough to destroy the vitality of certain tissues. Carbolic gangrene (Warren) is a possibility not to be forgotten.
Extravasation of urine, unless promptly recognized and appropriately treated, or especially as occurring when the urine is peculiarly toxic (ammoniacal) and the patient’s vitality reduced, as in confirmed alcoholics, is almost sure to produce gangrene which may easily terminate fatally.
Fig. 14
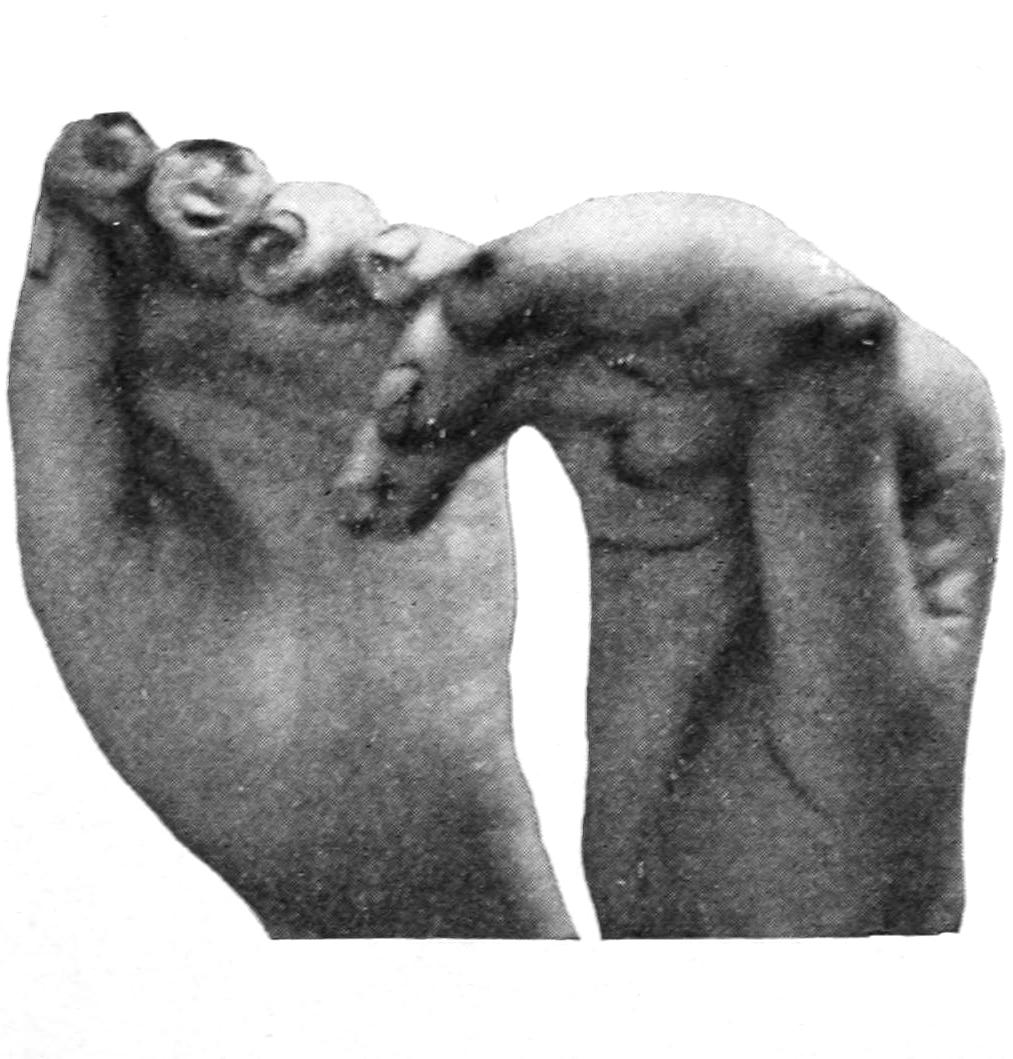
Raynaud’s disease: digiti mortui. (Original.)
Fig. 15
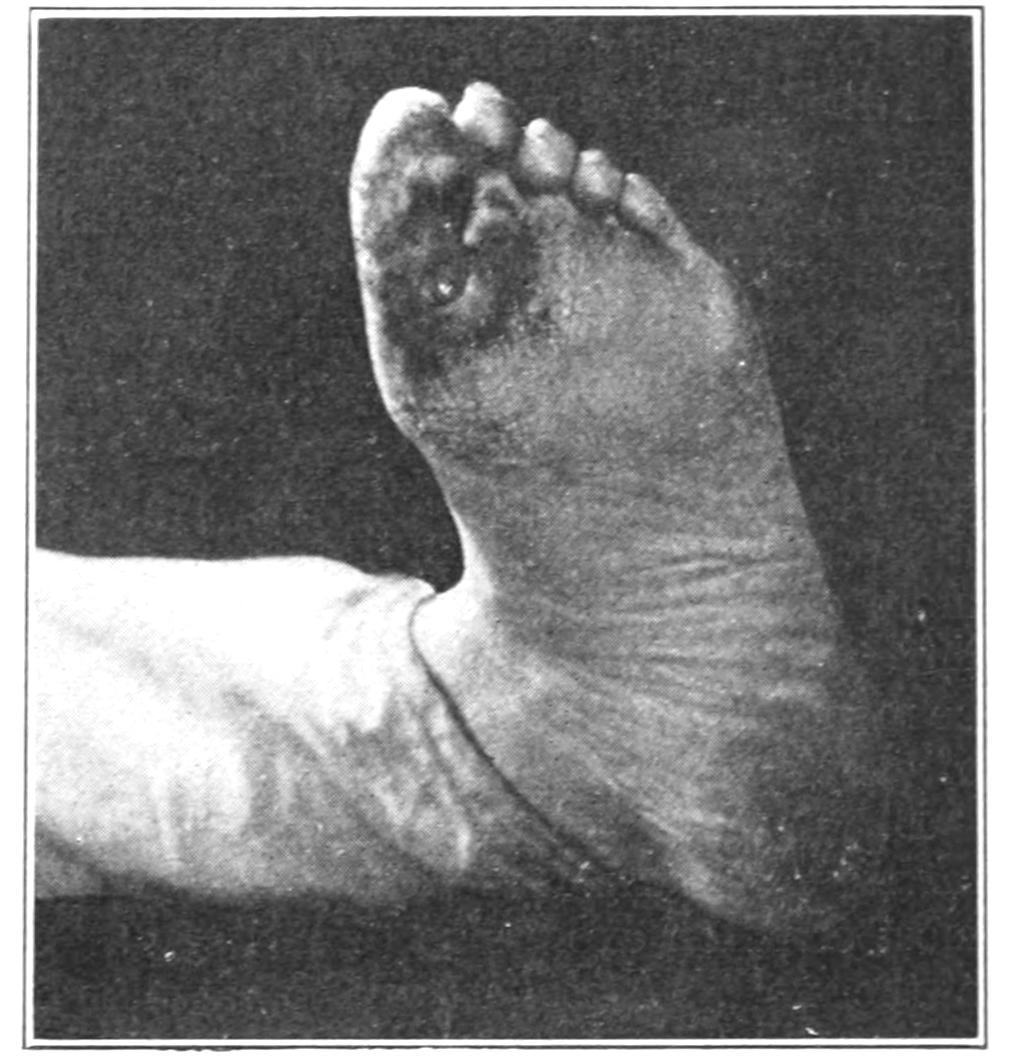
Raynaud’s disease: perforating ulcer of foot. (Original.)
—Among these are to be mentioned particularly that symptom-complex ordinarily known as diabetes or glycosuria. This means a depraved condition of the system in which gangrene is threatened or permitted under circumstances which otherwise would have little or no disastrous effect. Thus diabetic gangrene has come to be one of the recognized manifestations of the general disease. That the trophic nerves have a more or less pronounced effect in determining gangrene in certain cases seems to be now quite well established. It is well known how quickly bed-sores form after injuries to the spine, while in certain nervous affections a minimum of friction of the skin may determine its death, particularly about the labia or scrotum. It is said that the insane, when made to sleep by chloral, may develop decubitus from pressure in a single night. There is also a well-known form of symmetrical gangrene, known sometimes as Raynaud’s disease, which is characterized by symmetry of lesions and absence of definite pathological changes (Figs. 14 and 15). The so-called digiti mortui, or dead fingers, and erythromelalgia are examples of this character. A condition almost leading up to gangrene, but perhaps not absolutely terminating in such a way, has been known as local asphyxia, which seems to be a condition of arterial spasm with venous congestion and slight edema. While the aged will often recover from a legitimate surgical operation without disturbance, it is, nevertheless, true that senile gangrene commencing in the toes has for its cause some very trifling injury or lesion, such, e. g., as paring of a corn, or the like. This shows a weakened local and general resistance, as well as the wisdom of redoubling aseptic precautions in operations upon such patients.
[75]
As constitutional causes also should be included the deleterious effects of certain drugs, particularly ergot, mercury, and phosphorus.
—In the instances already mentioned reference to the infectious microörganisms has been avoided. There remain to be considered types of gangrene due to the activity of certain microörganisms—hospital gangrene, phlegmonous erysipelas, malignant edema, gangrenous emphysema, noma, ainhum, etc.
Gangrene as the result of infectious processes is seen in phlegmonous erysipelas, where death of tissue seems to be due to the combined influence of the invading organisms and of mechanical agencies—i. e., tension produced by stasis and exudation, with such stretching of tissues or overcrowding with inflammatory products as to virtually strangle them, in consequence of all of which they die. Gangrene of an entire hand may thus result, or, more commonly, the gangrene is limited in extent to the more superficial parts, so that sloughs separate. A specific form of gangrenous inflammation known as malignant edema, due to a peculiar anaërobic bacillus, will be treated of separately under a distinct heading. Quite like it in several respects is the gangrenous emphysema of certain writers, known also as the fulminating form, or, as the French call it, the “gangrène foudroyante.” More or less emphysematous condition may accompany malignant edema; yet that we do have gaseous forms of gangrene without the specific bacillus of malignant edema is established. At least sixteen cases of so-called gaseous gangrene due to infection by the bacillus aërogenes capsulatus are on record, of which twelve were fatal. Most of them followed surgical injuries—e. g., compound fracture.
Fig. 16
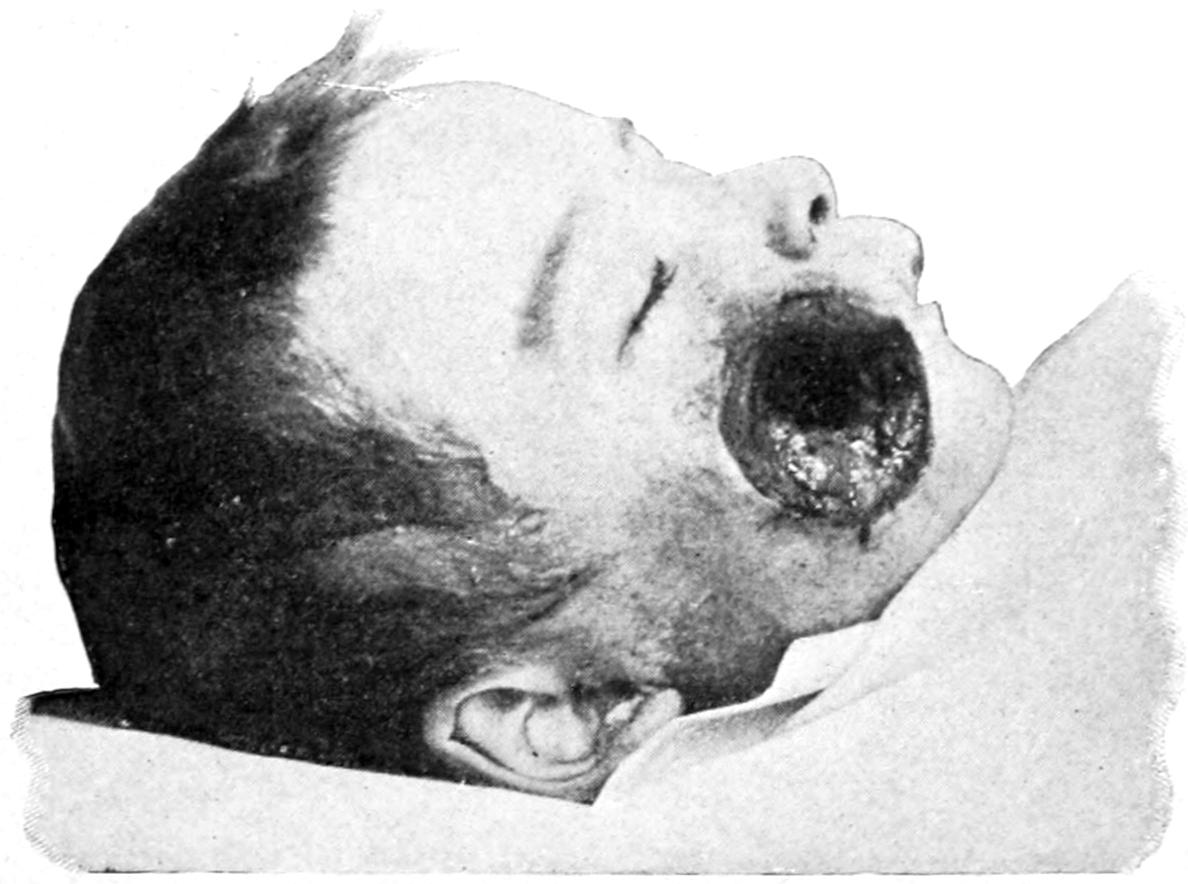
Noma. (Original.)
Hospital gangrene, so called, has been in years past the terror of military surgeons and camp hospitals. As a type it has almost completely disappeared from observation, and, in its old manifestations at least, is now practically never seen.
Noma, known also as gangrenous stomatitis, cancrum oris, and gangræna oris, is a term applied to a form of tissue necrosis affecting the cheeks or parts about the face of young children, occurring frequently as a complication of the exanthemata. A similar condition occasionally involves the external genitals. From the fact that it seldom passes across the middle line, it has been regarded by some as of neurotic origin. Naturally bacteria are always found in the decomposing tissues; but whether there as cause or as result is not yet established. The probability is, however, that we have to deal with a specific form of infection. The loss of substance is usually so great as to determine complete perforation of the cheek, so that the jaw bones may be laid bare. The gums and alveolar processes also frequently share in the process, and the teeth occasionally drop out. Death of tissue is rapid, and septic infection may accompany it to such an extent as to cause the death of the patient in a few days. While most vigorous measures are necessary for combating it, the patients are often so reduced as to preclude the possibility of doing much, and death is the termination of noma. Free incision, even complete excision, is called for, perhaps with combined resort to the actual cautery or such remedies as bromine (strong or diluted). Antistreptococcic serum has also been[76] used with success. Obviously it must be used early if success is expected. Should patients recover, there is extensive deformity as the result of cicatricial contraction.
Along the coast of Africa and in the West Indies there occurs among the negroes a peculiar gangrenous affection of the toes known as ainhum. This may assume either the moist or the dry type of gangrene, but the result is gradual separation of the part, usually by the dry process, as if it had been strangulated by a ligature. The disease is slow and may extend over ten years. The cause is unknown.
Finally, gangrene is the termination of the infectious process in several other zymotic diseases, among the best illustrations being that afforded by diphtheria. The formation of diphtheritic ulcers in the mouth and the vulva, about the eyes and elsewhere, as the result of separation of sloughs, is too frequent to pass unnoticed, yet at the same time does not essentially differ from the separation of sloughs due to any other specific cause. All these acute zymotic diseases, therefore, need to be regarded as among the possible causes of gangrene by infection of tissues.
The symmetrical gangrene, often paroxysmal, affecting the fingers and toes, described by Raynaud and often called by his name, is due to vasomotor spasm, and is accompanied by neuralgia and sensory disturbances, with coldness of the part and discoloration suggestive of impending gangrene. (See above.)
Billroth and others have also described a spontaneous or angioneurotic gangrene of the extremities, occurring during youth, in abrupt distinction to senile gangrene, whose course is tedious and painful, which will usually necessitate amputation. The cause of this condition has been found to be a well-marked arteriosclerosis and thrombosis, both in the arteries and veins. This form of gangrene occurs most often in the frigid zone—e. g., in Northern Russia.
There are also forms of visceral gangrene, traumatic and non-traumatic, which often constitute fatal maladies. The latter are mainly due to thrombotic or embolic lesions, for example, the gangrene of the mesentery, already alluded to when discussing thrombosis (q. v.), clinically described under Surgical Diseases of the Mesentery.
—In a general way tissue death, known as gangrene, assumes two opposite types—the moist and the dry. In moist gangrene, aside from those appearances which indicate commencing putrefaction of tissues, and the loss of heat due to stoppage of the blood supply, one of the most characteristic features is the formation of a so-called line of demarcation, i. e., a line which separates the dead from the living tissues. While this is usually plainly indicated by a red line which abruptly separates the discolored, usually dark, dead portion from the bright red, congested appearance of the living tissues, it is noted that this area of redness shades out into a more and more natural appearance as we pass upward, while below the line is seen a surface, usually covered with blisters, from which exudes a foul-smelling, altered serum, while the gangrenous portion assumes a dark, finally an almost black appearance, retaining only the crude outlines of its original shape. Along with this the objective evidences of putrefaction are unmistakable, appearances and odor being characteristic. With all there are more or less constitutional disturbances, and a recognizable, often a profound, condition of septic infection, due to the fact that along the line of demarcation absorbents are still active and that the poisonous products of putrefaction are being absorbed into the general system. Consequently collapse, profuse perspiration, septic diarrhea, etc., are noted. In gangrene from frostbite the process is slower than in the traumatic forms. In gangrene from extravasation of urine the separation of sloughs is extensive, and sloughing of the scrotum with exposure of the testicles is a frequent result. In decubitus, or bed-sore, the process is still more slow, but always of the moist type. After a variable length of time there is separation of slough and a resulting large, often foul, ulcer.
Dry or senile gangrene presents a very distinct contrast to the moist type. It occurs generally in patients over fifty, often as the result of causes which are slow of action. As a result of the shrinking and corrugation of the tissues, with the dryness of the same by evaporation, there is a peculiar appearance known as mummification, the foot, for instance—the feet are usually first involved—resembling the foot of a person who has been embalmed, except that it is discolored. It is possible sometimes to have a combination of moist and senile gangrene, especially when there has been infection by which putrefaction is permitted. When from the outset putrefactive processes are prevented, the gangrene of this type is almost invariably dry. In practically all of the[77] cases of this character there will be found evidences of vascular disease, usually in the femoral artery and its branches. Gangrene of the foot alone is most commonly due to endarteritis, while gangrene of the foot and leg together are usually due to embolism or thrombosis.
While disease of the vessel walls is usually of the type either of endarteritis or arterial sclerosis, peculiar to the closing years of life, and commonly affecting the lower extremities, gangrene due to embolism of arteries or thrombosis, or both, may occur in the young, and in the upper extremities as well, in the latter case the emboli being detached from the heart, while thrombosis may be caused by a tight splint or bandage, or even the use of crutches. I have repeatedly amputated the arm as well as the leg for gangrene of this type.
—The appearance and the odor of a part will indicate impending or actual traumatic gangrene. The pallor, the coldness, the dryness of senile gangrene are also characteristic. In the latter form constitutional symptoms are not indicative nor essentially of septic type. As soon, however, as a process of spontaneous separation begins putrefaction is inevitable and sepsis unavoidable. In moist gangrene there is seldom acute pain. This is one of the predominating subjective features of the senile form. Hemorrhages occur, sometimes terminating fatally, in the moist forms when large vessels are eroded. This is particularly true of the phagedenic or hospital form. A recognition of their possibility may enable us to avoid sudden death from this source.
—Threatening gangrene should be attacked and the cause removed. Threatening bed-sores may be avoided by equalizing surface pressure, which can be done with the water-bed; by protecting the skin or by stimulating and toughening it with alcoholic and astringent lotions; by frequent changes of position; by attention to the heart, which should be stimulated to a point that may make it capable of forcing or distributing blood equally over the entire body. So, too, with limbs which are enveloped in dressings or splints; it is well to leave exposed the tips of the toes or fingers in order that discoloration of the same may be recognized and the threatening disasters averted. Local gangrene as the result of pressure by tumors, aneurysms, etc., cannot always be averted.
For gangrene there is but one relief, the removal of the dead and dying tissue. The method and location of the operation must be determined by the general character of the cause. For a case of acute traumatic gangrene amputation at the nearest point of election above the injury will often suffice. In case of gangrene from frostbite the tissues in the neighborhood of the line of demarcation are so affected or their vitality so compromised that to separate the tissues along the lines at which nature is endeavoring to remove them is not enough, and to go an inch or so above this line is to operate in tissues which bleed readily and heal badly. Consequently it is often advisable to select a point at some distance above. It is especially in diabetic and senile gangrene that surgeons have laid down the rule that if amputation is done at all it must be high. For gangrene of the toe, as the result of disease of the vessels, it is best to amputate above the ankle; whereas if any greater portion of the foot is threatened, amputation should take place above the knee. The tibial arteries have been found so brittle as to snap under a ligature, and the femorals so disorganized as to require handling and ligating with the greatest caution. These high amputations are therefore necessitated by the condition of the vessel walls. While amputation for traumatic and acute cases is, in the majority of instances, if not too long delayed, successful in saving life, in the senile and particularly in the diabetic forms it is, in the majority of cases, a disappointment.
One of the greatest advances made in pathology has been the establishment of the fact that a great many of the morbid conditions from which the human race suffer are those due to causes arising entirely from within their own systems and in consequence of deficiencies of elimination or of perverted physiological processes which, in large degree, are themselves the result of errors and indiscretions in diet, in manner of life, in habits, etc. That these general facts have been recognized for centuries is perhaps a credit to the powers of observation of practitioners of past generations. Exact knowledge, however, has come only with exact laboratory methods of research and most painstaking study of the secretions and excretions, both under normal and morbid conditions. The subject of auto-intoxication has been too commonly relegated to the domain of internal medicine, and has been supposed to be one in which the surgeon need take only passing interest.
The alkaloids are by no means the only poisonous products which the human body may produce and retain. That most important excrementitious material of all—i. e., carbon dioxide—could not be retained in the organism for more than a few moments without death as the inevitable consequence. The various soluble ferments elaborated by certain glands may exert deleterious influence, both local and general; and in the saliva are also found products which are not ferments. The biliary acids also, if they do not find free escape, may produce fatal poisoning. So also leucin, tyrosin, and all the excrementitious products which arise from insufficient liver activity, are capable of producing forms of intoxication—such, for example, as eclampsia, etc. The character of the solvent has much to do with toxicity. Thus aqueous extract of putrid matter is more poisonous than that of fecal matter, while alcoholic extract of fecal material is more toxic than that of putrid. All the alkaloids produced within the body are not poisonous. Some are found in the normal tissues, and they are, perhaps, only one of the results of the disassimilation of animal cells. Nor are all these poisons of bacterial origin, although many are formed only in the presence of microbes.
From these constantly menacing sources of intoxication man escapes by virtue of his intestinal, cutaneous, pulmonary, and renal emunctories. For instance, the usefulness of the perspiration is shown by the odor which it assumes under the influence of certain disorders. Among hypochondriacs and the inactive fatty acids are eliminated by the skin. Hence the odors of hospital wards, asylums, prisons, etc. So, too, in the case of many who suffer from deep-seated, indolent ulcers, the odor of the skin is suggestive of the presence of pus. During twenty-four hours there is eliminated from the lungs 1100 grams of carbon dioxide, water, etc., which sometimes contain ammonia and various volatile fatty acids; all of which will explain fetor of breath when it is the result of incomplete nutrition and destruction of food. Of the organs of elimination, the most important is the kidney, which does not reabsorb a part of its own products, as does the intestine. The kidneys eliminate fluids and solids, not gases. The most important of the toxic principles contained in the urine are:
[80]
1. Urea, which plays an important and useful role in the economy, since it possesses the property of forcing the renal barrier and removing along with itself the water in which it is dissolved and other toxic matters. Urea is toxic, but only in the sense that any other substance, even water, may be—i. e., it is toxic only in large doses, less than sugar, and no more than the most inoffensive salts. This is contrary to generally received views, but is established by the researches of Bouchard.
2. A narcotic substance, and
3. A sialagogue substance, whose composition is unknown;
4, 5. Two substances having the property of causing convulsions, one having the power of contracting the pupils. The composition of both is unknown.
6. A substance which produces heat by diminishing heat production—possibly a coloring matter. That coloring matters are absorbed by charcoal and that urine thus decolorized is rendered less toxic are no proof that the coloring matters themselves are responsible for this toxic action. There is no doubt that numerous alkaloidal bodies possessing a high molecular weight are precipitated by means of carbon or charcoal, and to these bodies may be attributed a portion of that toxic action previously considered as due to coloring matters.
7. Potassium salts, which are really convulsing agencies, are the most toxic perhaps of any of the poisons contained in the urine. Chloride of potassium, for instance, is toxic at 18 Gm. for every kilo of animal.
Salivation and myosis, as well as diarrhea, are often noticed in so-called uremia. In that form known as hepatic uremia, when the liver no longer forms urea, the kidneys scarcely act. In other words, if urea is no longer present in the body, the kidneys are deprived of their principal stimulation to physiological activity. Consequently urea, for so long a time the bugbear of physicians, is shown to be most dangerous when absent. When urea is deficient, blood serum or water in which the other toxic substances are dissolved should be withdrawn. This is best done by venesection, whose value in so-called uremia experience amply corroborates. When kidney activity ceases, intoxication is likely to be produced by potassium salts. Ptomains, amido bases, etc., are proved to be present in normal urine and are known to produce toxic effect. These ptomains increase enormously in pathological urines, and to this increase, rather than to that of potassium and coloring matters (which remain fairly constant), may be attributed the higher toxicity of pathological urine. In certain cases, however, as in that of jaundice, the toxicity of the urine is partly due to decomposition of tissue cells, whereby potassium salts and organic decomposition products are liberated and excreted in the urine. The toxicity of the urine also increases with the increase of indican, which is indirectly a product of intestinal fermentation.
The osmotic pressure of the blood has much to do with the general subject of auto-intoxication, since it surrounds and permeates all the organs of the body, which are necessarily in equilibrium with it. Their individual cells functionate, then, in accordance with it, and variations in such pressure must affect their activities. It is a special function of the kidneys to eliminate enough of the accumulated metabolic products in the blood to keep this osmotic pressure at its normal. Should investigation or symptoms of disease show a wide divergence from this standard, the inference is plain, i. e., that there is renal insufficiency from impairment.
This test may be made with a small amount of blood by cryoscopy (determination of freezing point). So, too, a determination of electrical conductivity may, in a similar way and for a similar purpose, be made of clinical value. Unfortunately, these investigations are not exactly simple in character, and are not available outside of well-equipped hospitals.
Correct performance of hepatic function is also necessary that surgical cases may progress without disturbance. Bile escapes direct absorption by the blood, but not all contact with it, since in the intestine it is in contact with mesenteric capillaries, but must pass again through the liver, which takes it up again and pours it once more into the intestine.
Bile in the blood is always dangerous, although its toxicity is much smaller than has been supposed. Of all the bile thrown out into the duodenum, we are only able to account for about one-half. Its coloring matter and biliary salts are metamorphosed. Yet in certain morbid conditions bile, as such, may be reabsorbed in the liver along the margin of the hepatic cells. In these cases, if the kidneys remain permeable, auto-intoxication[81] is simply threatened; if they have ceased to be permeable, actual auto-intoxication is the result.
Putrefaction of intestinal contents affords another source of auto-intoxication. This comes both from imperfect metamorphosis of food and from bacterial infection. Here the conditions are most favorable. Nitrogenous substances become peptonized, and peptones form the best culture media for microbes. Water is present in sufficient quantities, and a constant temperature of 37° C. is maintained. The digestive tube is always open, and invaded at frequent intervals. By such mechanism are formed those products whose effects are revealed in the so-called putrid fever of Gaspard. Brieger has shown that alkaloids are developed during the act of peptonization. Fecal matter contains also excretin, whose toxicity has been amply proved, and several other alkaloidal substances, soluble in various media, varying in toxicity. The potassium and ammonium salts contribute largely to the toxicity of feces; bile also, but in lesser degree. It has been shown that the aqueous extract of putrid matter is very toxic, while that of fecal matter is otherwise.
The most serious features of the conditions grouped under the heading of Bright’s disease are their so-called uremic features. These happen at the period when retention of toxic products is peculiarly harmful. As long as the urine is ample in amount and density—i. e., containing enough toxic materials in solution—there is no danger of intoxication. But when it no longer eliminates in twenty-four hours what it should, then we see the chronic and paroxysmal nervous accidents, the edemas, fluctuations of temperature, etc. Oliguria with urine of increasing density and general edema of the tissues may be noticed, although the other secretions continue natural and the tongue moist. As long as the normal amount of solids is eliminated, this form of “uremia” may be due to mere accumulation of water and may not be serious. Ordinarily, uremic patients are those whose urine has lost its toxicity. Usually on the day in which so-called uremic accidents happen the urine quite ceases to be toxic and is scarcely more so than distilled water. Urea alone is not to be held guilty for this condition. In order to kill a man with urea it would require the quantity which he makes in sixteen days. Nevertheless, it may become harmful after undergoing transformation into ammonium carbonate or other substances.
Among the most poisonous substances in the urine are the extractive and coloring materials. Normal urine loses one-half of its toxicity by decoloration; bile acts in the same way. Urea alone represents about one-eighth of the total toxicity of urine. Ammonia is toxic, but present in small amounts. The coloring matters of the urine cause two-thirds of its toxicity, the remainder of which is to be ascribed to its mineral salts, which it contains in the following proportion: A liter of urine ordinarily contains 44 Gm. of solid matter, of which 32 are organic, 12 mineral. Of the latter, potassium salts constitute 3 Gm., sodium salts 7.5 Gm., and other earthy salts constitute the remainder.
In these conditions physicians have relied largely upon purgatives, hoping thereby to remove urea from the blood. But intestinal elimination has no elective affinity for it, and removes it only in its normal proportion with the balance of the blood. Purgatives, however, help, first, by dehydrating the tissues—i. e., removing water with toxic material in solution. But they should be followed by restoring to the tissues pure water. By bleeding more extractives are removed than by any other channel, except by the kidneys. A bleeding of 32 Gm. removes from the body as much toxic matter as would 280 Gm. of a liquid diarrhea or 100 liters of perspiration. This much may be removed by two leeches. It is especially in the subacute nephritis of scarlatina, etc., that bleeding finds its greatest indication. If the kidneys are chronically diseased, the utility of bleeding is doubtful. Between the arterial capillaries of the bowels, however, and the liver is found a mass of blood accumulated in the portal vessels. This may be regarded as a reserve which can be thrown into the general circulation when needed, in order that thereby arterial tension may be augmented and the function of the kidney increased. Cold injections into the bowels will often accomplish this, and serious anuria frequently disappears after their use. It is advisable, also, to make use of urea by subcutaneous administration, as the most powerful diuretic known, surface friction, caffeine, digitalis, etc., being far behind it in efficiency. In the form of intoxication noted in the eclampsia of puerperal patients inhalations of chloroform are valuable. Potassium salts should, under these circumstances, never be employed. An exposure of urine in compressed air will diminish its toxicity, on account of contact with the oxygen; the[82] most toxic bacteria are those which grow without oxygen. Consequently patients inhaling this gas may overcome this kind of auto-intoxication.
The value of an active liver is not appreciated by most surgeons to the full extent. The blood of the portal vein is so much more toxic than that of the hepatic vein that it is evident that the function of the liver is to purify and remove the toxic material from the blood that comes from the intestines. This has been called by Flint and others the depurative action of the liver. The activity of the liver also may be proved by grinding up a freshly removed liver with alkaloids, whereby the latter are chemically changed.
That the facts above stated, or others related thereto, have not been lost sight of by surgeons is shown by such expressions as septic enteritis, enterosepsis, etc., which are used by various writers. In previous publications the writer has made a separate topic of so-called intestinal toxemia, which he has preferred to introduce here as one of the many possible auto-intoxications. It is a condition not always permitting of exact definition, nor, still less, can the exact toxic agency be indicated in a given case. Nevertheless, it has been made plain that there is perhaps no condition which so predisposes to sapremia, septicemia, or even pyemia as this vague condition of intestinal toxemia, which, notwithstanding, is so often present. Many surgical patients present forms of blood poisoning in which the poison has not proceeded from the wound, for which the surgeon is not responsible, except that he may have neglected to avail himself of certain precautions.
The auto-intoxications, then, which have peculiar interest for the surgeon may be conveniently classified as follows:
1. Those caused by failure in the function of particular organs; e. g., myxedema, cretinism, and cachexia strumipriva from thyroidal failure; pancreatic diabetes, where the islands of Langerhans are invaded (interstitial pancreatitis, q. v.); Addison’s disease from adrenal failure (this being at present the prevailing belief).
2. Those caused by general disturbance of metabolism, where its incomplete or abnormal products reach the general circulation, e. g., oxaluria, gout, diabetes. (See Diabetic Gangrene.)
3. Those caused by retention in particular organs or tissues of disturbed metabolic products, e. g., the toxemias following serious burns and many septic conditions.
4. Those due to excessive formation of more or less normal products, e. g.:
(a) Hydrothionemia, i. e., the presence of hydrogen sulphide in the blood. This results from one form of gastro-intestinal putrefaction and causes violent symptoms with evidences of hydrogen sulphide poisoning. It is seen in some cases of gastric dilatation, especially those caused by pyloric obstruction (q. v.).
(b) Acetonuria and Acetonemia.—The former sometimes follows chloroform anesthesia, and occurs especially in diabetes (particularly after removal of the pancreas in experimental animals). Acetone per se is nearly or quite harmless, but its congeners, diacetic and beta-oxybutyric acids, are very toxic. The danger in so-called acetonuria is from acid intoxication by these acids, which has been described as “excessive acidosis,” and its co-existence with glycosuria makes diabetes certain, while prognosis is grave in proportion to its presence. Prominent among the symptoms produced by it are delirium and coma.
When either or all of these three substances are present in the blood its alkalinity is reduced and its ability to absorb carbon dioxide impaired; hence, acetonemia is evidenced by carbon dioxide poisoning. To the brain symptoms above noted is added a peculiar odor in the breath—sweetish or ethereal. This has been noted in pyemia. This condition may set in after various operations, but whether due to disease, the traumatism itself, or to chloroform may not always be determined.[3]
[3] See paper by Brewer, Annals of Surgery, 1902, vol. xxxvi, No. 4, p. 481.
(c) Cystinuria.
(d) Coma of cancerous cachexia (coma carcinomatosum).
(e) Exophthalmic goitre, from excess of thyroidal activity (thyroidism).
Besides the above there is auto-intoxication proceeding especially from the gastro-intestinal and hepatic systems. Of the former, the best surgical examples are seen in the tetany which occasionally takes its rise from a dilated stomach, and which may be cured by a pyloroplasty or a gastro-enterostomy; in the nephritis which follows stercoremia of intestinal obstruction; and in oxaluria, with its painful, serious, and often[83] deforming or crippling joint affections. Of the latter we have examples in the cholemia of acute atrophy or of biliary obstruction, and in the uremia of hepatic origin which occasionally terminates a surgical case.
In addition to the above there should also be mentioned the auto-intoxications of pregnancy, with the consequent salivation, peripheral neuritis, pigmentations of the skin, icterus, and pruritus, which are mainly attributed to perverted action of the liver or kidneys.
The practice of preparing patients for operation by a course of purgatives, emetics, etc., is based upon the recognition of certain principles. The general symptoms included under the name enterosepsis, stercoremia, copremia, are due to the activity of the colon bacillus, which seems to be made more virulent by certain conditions of diet or retained fecal excretions, and to such an extent that it wanders widely from its normal habitat and may be found in distant parts of the body. Enterosepsis may be mistaken for surgical fever, and is to be distinguished from it, perhaps, only by the study of the excretions of a case and establishing the fact that they are free, and that consequently pyrexia, etc., cannot be due to diminished elimination. Aside from the migrations of the colon bacillus, it is also possible for auto-intoxication to occur. Thus that which is stercoremia one day may later become a genuine septicemia, vital resistance being so lowered as to permit of local infection. The various conditions are so often merged that it is difficult to separate and identify them. Nevertheless, enterosepsis differs from sapremia in that in the one instance the putrefying material is contained within a normal cavity, whereas in sapremia it is contained within an abnormal cavity, in either case corresponding to a septic suppository, varying, however, in the place of insertion, also in the nature of the surrounding tissues, which in the latter case are more capable of absorption and of becoming infected than in the former.
A determination of indol and indican is often of the greatest value, both in determining the extent of infection and the presence of pus. Indol is set free under the following circumstances: (a) Suppuration in a closed cavity. (b) Continued suppuration in a cavity with an outlet. (c) Ulceration or necrosis of tissue. The degree of indicanuria will depend on the length of time pus has been present, the possibility of absorption from the tissues surrounding it, and its degree. When pus is fully formed in a serous sac the indican reaction becomes intense according to the length of time pus has been present. This is particularly true in the empyemas of childhood. In continued suppuration with a free outlet the production of indol will be great; but the amount finally eliminated will depend upon the character of the surrounding tissue. When solid tissue, like bone, becomes affected, the elimination of indol is intense. Rapid biogenic degeneration of tissue causes an increased amount of indol to be deposited in the liver, and it is possible at postmortem, by simple extraction with absolute alcohol, to take from the liver this excess deposit in the shape of its oxidation product, indigo blue. Lardaceous degeneration is characterized by marked and persistent elimination of indol, which seems to be a product of tyrosin. It occurs frequently in the liver, in which indol is notably deposited. Its primary factor is deposited by the blood, in which latter indol circulates and is oxidized. Lardaceous material gives a red or blue color with oxidizing agents, which latter yield with indol an indigo red or blue.
The practical outcome of such a chapter as this is, then, to insist as strongly as possible on the preparation of patients, whenever this is feasible, for an ordeal which comprises the combined effect of anesthesia and consequent disturbance of secretion and elimination, with loss of blood and of strength, and subsequent confinement in bed, with, moreover, all that this entails in further impairment of activities of important organs. It is not always possible, practically rarely so in emergency cases, to adopt these precautions; in which cases they must be atoned for, as far as possible, by extra attention in the same directions after the emergency is passed or has been met. In the former case, however, the functions of the skin, the kidneys, and the abdominal viscera should be regulated, the first by hot-air baths; the second by this same measure in conjunction with copious draughts of pure water, the correction of hyperacidity of the urine, and the administration of whatever drugs may be of benefit as diuretics, etc.; and the third by a course, perhaps covering several days, of gentle or active purgation, by which the alimentary canal will be entirely emptied of all that may serve to act as a source of poisoning. In addition to this, in certain cases careful massage will dislodge from the muscles and other tissues material which they ought not to retain, and which[84] will be washed away, as it were, by the extra amount of fluid which this preparation, necessitates. Again, the activity of the heart should be stimulated, perhaps by digitalis, but preferably by that best of all tonics, strychnine, which is to be administered hypodermically in average doses of a thirtieth or twenty-fifth of a grain, morning and night. When these precautions are taken, patients will successfully pass through trying ordeals without anything which may give rise to alarm. When they are not possible, the risk of operating, even in a small way, is materially enhanced. So, too, after operations when these precautions have not been taken, it is necessary to give careful attention to atoning for their lack by such active purgation as a now reduced patient may bear—by hot-air baths, if feasible, and by the administration of such intestinal antiseptics as charcoal, naphthalin, corrosive sublimate, bismuth salicylate, salol, etc., for the purpose of reducing to the lowest possible minimum the opportunity for formation of poisons which will disturb the proper repair of injury.
[85]
Formerly the surgical fevers were all grouped together, and a certain amount of febrile disturbance was looked for after any injury. But with the introduction of antiseptic methods and the healing of wounds by primary union, with absence of all septic phenomena, and the use of the clinical thermometer, it is noted that there is a certain rise of temperature more or less quickly after an operation or reception of a wound, with fever of mild grade, persisting for several hours or two or three days, and with other accompaniments. This phenomenon has been carefully studied, and so separated from the septic fevers as to deserve a distinct recognition under the names above given, of which the most common in this country is surgical fever.
As long as this fever is free from indications of septic character it is without significance and needs only symptomatic treatment. It begins usually within the first twenty-four or thirty-six hours, after which the temperature may rise, progressively or with a morning remission, to a height of 102° or possibly 103°. In children we are more likely to get extremes in this regard than in healthy adults. It will be followed by some disturbance of alimentary function, glazing or drying of the tongue, deficiency in urinary secretion, and subside generally spontaneously—invariably so if cathartics, diuretics, cool sponge baths, etc., are used. It is usually due to the retention of blood clot, ligatures, etc., or tissues which have been ligated and whose stumps remain; in all instances there is some foreign material to be removed. This means unusual phagocytic activity, perhaps temporary leukocytosis, with active metamorphosis of clot and other material, of all of which the elevated temperature is an accompaniment and expression. It is not unlikely that the antiseptic materials used may sometimes occasion this pyrexia.
Iodoform and carbolic acid are among the drugs in common use which are known to be irritating and capable of producing toxic symptoms. Often after the use of the latter the urine will be discolored and will furnish the clue to the fever. In young children particularly, and not infrequently in adults, mental disturbance, even active delirium, may characterize the case. This is not always to be explained by cerebral anemia due to loss of blood during the operation or accident, but is probably due to drug toxemia or to intoxication from materials furnished by the altered tissues.
Surgical fever of strict type may merge into a more or less continuous fever as the result of intestinal toxemia permitted by failure to evacuate the bowels, and this intestinal toxemia may be a predisposing cause of genuine septic infection. Consequently a surgical fever which does not disappear within two days is to be viewed with suspicion, especially if it does not subside after the administration of cathartics.
Some surgical fevers are accompanied by eruptions, a number of which may be due to drugs and some to intrinsic poisons. Thus carbolic acid and iodoform give rise occasionally to erythematous eruptions, and the concomitant administration of drugs like potassium iodide, quinine, antipyrine, and copaiba may produce urticarial or other manifestations. Again, it is known that certain toxins—produced, e. g., by the bacillus pyocyaneus—are capable of causing dilatation of the superficial vessels and various flushes or eruptions. To one of these, which dilates the capillaries, Bouchard has given the name of ectasine. Consequently it by no means follows that every eruption or rash following operations or injuries is of a specific character. On the other hand it seems to be established by numerous observers—among whom Paget is perhaps the most prominent—that surgical patients, particularly the young, are particularly liable to infection by scarlatina; and in the experience of Thomas Smith, of forty-three children whom he cut for stone, ten had scarlet fever. Therefore, in spite[86] of the fact that a certain number of cases of eruption may have been mistaken for scarlet fever, it is undoubtedly true that in surgical and puerperal cases patients are more than usually liable to this invasion. The use of antitoxins or serums is also occasionally followed by intense urticaria.
The subject of surgical fever may then be epitomized as consisting of elevation of temperature with certain accompanying disturbances, which appear to be essentially due to the results of tissue metabolism, including also metabolism of blood clot, ligatures, etc. It is not a necessary nor conspicuous accompaniment of all surgical cases, and in some individuals, even after grave operations, it will scarcely be noted. It is more likely to be extreme in children than in adults. As a result of excessive loss of blood it may be postponed. It may be complicated and prolonged by any one of the auto-infections, particularly that already mentioned in the preceding chapter as intestinal toxemia, as a result of which septic infection may ensue, and that which was at first a legitimate surgical fever may thus become merged into a septic condition. In the absence of auto-infection, and with appropriate treatment, surgical fever should quickly subside until it becomes indistinguishable about the second or third day.
Proceeding then in the order of pathological complexities, the first of the surgical infectious fevers to be considered is sapremia.
The term sapremia will be used here as indicating a condition which is often likened to an intoxication produced by a supposititious septic suppository. The term was first used by Duncan, and was largely confined to puerperal cases. Some of the most ideal cases of sapremia are those of puerperal origin.
In each of the three conditions comprised under the general term of septic infection it is not now a question of particular organisms, but of intoxication by products which are more or less common to at least several of them. In a general way, they are mainly due to the activity of the organisms already grouped as pyogenic. Those which produce pus are capable of causing septic infection. In addition to these, it is probable that certain of the saprophytes or ordinary putrefactive organisms may produce the same effect.
—In sapremia the symptoms begin promptly, depend for their intensity upon the dosage of poison, and recede quickly as soon as the source of poisoning is removed or its activity subdued. An instance of the possible causes of sapremia will perhaps best illustrate its pathology. Take, for example, the act of delivery of the full-term fetus. At the completion of this operation there is left a fresh, bleeding wound of large area which is more or less exposed to putrefactive agencies. This is reduced with the contraction of the uterine walls to a comparatively small cavity containing more or less freshly coagulated blood. As long as this clot does not putrefy it is disintegrated inoffensively, to be discharged in large part with the lochia. If germs of putrefaction enter, either during the act of labor or afterward, and linger, putrefactive processes are set up in the clot with the prompt production of certain toxins and ptomains. There is here then a septic suppository with conditions favorable for absorption by the containing tissues. How quickly the poisoning may show itself, and how soon it may subside after removal of the putrefying clot, daily experience may tell.
Sapremia then is intoxication produced by absorption of the results of putrefaction of a contained material within a more or less closed cavity, whose walls are capable of absorption of noxious products as they form. As long as putrefaction is essentially limited to the contained mass, and does not spread to and involve the containing or surrounding tissues the case is one of sapremia. As soon as the process spreads from the containing tissues the case merges from one of sapremia into one of septicemia. That this may occur in any case without prompt intervention will be readily understood. Sometimes patients may die of sapremia, though rarely, and in such case ordinarily as the result of gross neglect. Once the septicemic process is begun, however, its spread cannot always be checked, and the case which one day is sapremic and redeemable may later become septicemic and practically lost.
The symptoms of sapremia are not essentially different from those common to septic infection, save that ordinarily they are, at least at first, milder. There are flushing of[87] the face, dry tongue, mental disturbance, pyrexia, while usually all the symptoms are ushered in by a chill, which may have been preceded only by slight malaise. These are followed by nausea and vomiting, with headache, and often, later, by diarrhea or active purging. Later delirium may occur, possibly even fatal coma. On postmortem examination there are few changes revealed; alterations in the blood, a failure to coagulate, and some softening of the spleen and liver would probably be the only ones.
—The treatment should be prompt and the cause removed. In puerperal sapremia the uterus should be emptied, antiseptic douches given, irrigating as often as necessary to prevent offensive odor to the discharge, and combating general signs of poisoning by plainly indicated measures. Heart depression should be overcome by diffusible stimulants and hypodermic injections of strychnine in doses of ¹⁄₂₅ grain or more. The bowels should be unloaded by a mercurial followed by a saline cathartic; suppression of urine treated by venesection and hot-air baths or sweats; diuretics should also be prescribed, and fluids administered copiously. If the patient is restless, an opiate should be given; if delirious, necessary restraint should be resorted to.
Essentially the same measures should be pursued in a surgical wound or in a case of compound fracture, or any injury where retained material may be undergoing changes already alluded to. General measures should be the same. Purgatives are advisable in these cases.
—Chronic sapremia is a better name for what used to be known as hectic fever. It is characterized by rapid, feeble pulse, a temperature but little elevated in the morning and rising to 102° or 103° in the latter part of the day, with profuse perspiration, or sometimes colliquative sweats that leave patients exhausted. There is usually a distinctive flushing of the cheeks. Emaciation is a marked feature in most instances. Hectic means simply habitual fever. It is met with particularly in tuberculous cases, whether of lungs or bones or joints, in empyema, psoas abscess, and most all chronic pyogenic infections. It is frequently followed by or associated with amyloid or waxy degeneration of the liver, kidneys, and spleen. This process commences in the walls of the bloodvessels and by its spread to the surrounding connective tissue leads to notable enlargement of these organs, with albuminuria, edema, ascites, and the usual associated phenomena.
—Treatment, in addition to that already indicated above, should be addressed to removal of the cause. In all instances it should comprise attention to elimination, digestion, nutrition, and fresh air. By such measures even distinct amyloid changes may be arrested, or possibly improved.
—Cryptogenetic or spontaneous septicemia is a term applied to those cases in which the port of entry of the germs is no longer visible—e. g., a hypodermic puncture—or cannot be positively determined. On careful study this may be found to consist of a small focus where pus is forming within narrow confines and under great pressure. Under these circumstances, as Kocher has shown, toxic virulence is rapidly augmented. This is doubtless one reason why the septic features of many cases of osteomyelitis and appendicitis are so pronounced.
According to the views thus enunciated, the difference between sapremia and septicemia is not one of character as much as of location. In septicemia the putrefactive action is no longer confined to material enclosed by (yet not of) the tissues themselves, but has spread from this to the surrounding living cells, which are being attacked by bacterial enemies; in other words, we deal with infection of living tissues rather than with mere intoxication. This is a progressive invasion of tissues by continuity, with a constantly proceeding systemic intoxication by poisons produced in larger quantities. So rapid may this action be—as may be seen in malignant diphtheria—that the individual speedily succumbs before evidences of abscess or local gangrene appear. On the other hand, providing that the toxic action is less pronounced or the patient’s vitality more enduring,—i. e., his tissues more resistant—abscess, phlegmon, or local gangrene may result in the destruction of tissue being limited to the environs of the parts first involved. Bacteria are also found in the blood.
While septicemia then may be a direct continuance of an original sapremia, it is not[88] intended to intimate that it may not originate de novo; that is, many cases may begin as a pronounced septicemia from a local infection. This is the case, for instance, with the majority of dissecting wounds, etc.
—In septicemia there is a period of incubation, usually two or three days, often longer. If this follows an operation, the mild fever which would indicate the slumbering fire is usually regarded as surgical fever. But when this rises and is followed by prostration, with alimentary disturbance, loss of appetite, headache, etc., followed by typhoidal symptoms, the alarm is sounded and should be quickly heeded. Usually, but not always, there is a preliminary or premonitory chill, after which prostration will be more marked than before. The severity of the symptoms cannot be foretold from the size, location, or character of the wound. The character of the fever is essentially continued, usually with morning remissions. Gussenbauer has called attention to a class of cases in which subnormal temperature is caused by the absorption of ammonia compounds. To these he has given the name ammoniemia. This condition may be seen in connection with gangrenous hernia, and has even been mistaken for shock (Warren). (See also acetonemia, in previous chapter.)
In septicemia from infection of a visible portion of the body there are usually seen evidences of lymphangitis and perilymphangitis of septic character. These will be evidenced by tender and purplish lines, extending subcutaneously along the course of the known lymphatics or in connection with the more prominent subcutaneous veins. The lymph nodes, into which these visible vessels as well as the deeper ones empty, become enlarged and tender; the whole lymphatic system participates; the spleen in aggravated cases becomes notably enlarged, and even the bone-marrow more or less involved. Diarrhea is commonly an early but controllable symptom. A hematogenous icterus of mild degree is another frequent accompaniment. The conjunctiva becomes discolored and the skin slightly so. Should the blood be examined marked leukocytosis will be noted, and should cultures be made from it, in many instances at least, the organisms at fault can be detected and recovered from it. The vigor of the heart muscle is seriously impaired; the pulse becomes rapid and weak. In scarcely any form of septic infection is this more prominent than in diphtheria; and microscopic examination shows the rapid disintegration of the cells of the heart muscle, as well as those of other parts of the body, even to the almost complete molecular disintegration of the nuclei. Erythematoid, pustular, and even hemorrhagic eruptions are met with upon the skin, some of which are probably to be explained by thrombosis of the dermal capillaries. Certain complications are not infrequent, among which inflammations of the pericardium and endocardium—e. g., ulcerative endocarditis—are frequent. As the case becomes aggravated the temperature rises irregularly; the hot, dry skin becomes cold and clammy; prostration and indifference more marked; diarrhea more colliquative; icterus more pronounced; urine more reduced in quantity or suppressed; and these symptoms are succeeded by indifference, mental apathy, stupor or delirium, and finally death, the patients being comatose and collapsed.
While these are the general indications of septicemia, the wound or site of injury has undergone changes which are also characteristic. They comprise the edema and redness of wound margins, which may be seen even in sapremia, followed by increasing tumefaction, escape of foul-smelling discharge, and finally by sloughing and gangrene of the parts involved. On microscopic examination the capillaries are filled with infective thrombi and vessel walls infiltrated with microörganisms, which abound also in the lymph spaces. Bacterial infection can be traced in microscopic sections from the infected area, from the point in the neighborhood of the wound where microbes infest the tissues to points remote from it, where they are sparsely found, if at all. The same evidences of infection may be traced along the lymphatic vessels, and often the veins.
—The postmortem evidences of septicemia are indicative on first sight: the blood is of the consistency of tar and does not coagulate; evidences of putrefaction are plain to sight and smell; the serous membranes, particularly the pia mater, are often extravasated; the muscles are discolored and of a darker hue than natural, edema of the lung is frequent; the intestines reveal a gastro-intestinal catarrh, the duodenum and rectum showing punctate hemorrhages; the spleen is darkened, enlarged, and softened; the liver shows similar signs, less marked, and at times an emphysematous condition due to putrefactive gases. Cultures can be made from the fluids and tissues[89] of organs thus affected. It is also of importance to emphasize that such material is powerfully and often fatally infectious; some of the worst forms of dissecting wounds and instances of fatal infection have come from carelessness in making these postmortem examinations.
So far as concerns the character of the wound, which is most likely to be followed by septicemia, there is but little to be said. Wounds made by infected tools, the butcher’s knife, the anatomist’s scalpel, etc., are the most dangerous. All forms of phlegmonous erysipelas, many cases of gangrene following frostbite, nearly all instances of traumatic gangrene, most cases of carbuncle, and, in fact, all similar lesions, are likely to be followed by septicemia. The so-called spontaneous cases have an equally infectious origin, though one which is concealed. In unrecognized instances of appendicitis, for instance, and in many other conditions, although the path of infection may not be easily traced, it is, nevertheless, always present, and can be found if diligent search is made. The nasal cavity, the tonsils, the teeth, the middle ear, the deep urethra, and the rectum are often overlooked as offering possibilities for septic infection which may follow this general type.
—This should be both local and general. Local treatment should consist in complete and absolute removal of the active cause. This comprises the reopening of wounds, evacuation of clot, cutting or scraping away of sloughs and gangrenous tissue, with cauterization of the exposed living tissue, in order that absorption may be prevented, and will often include amputation or extirpation of a part. For tissues which are not too completely riddled by disease, and lost beyond possibility of redemption, continuous immersion in hot water offers the best possible prospect. By it putrefaction seems checked, the separation of dead from living tissues is accelerated, relief of pain or discomfort is afforded, and disinfection of material which is foul and infectious is guaranteed. An excellent local application is the mixture of resorcin 5 parts, ichthyol 10 parts, ung. hydrarg. 40 parts, and lanolin 45 parts, already mentioned in Chapter IV, or the application of brewers’ yeast. (See chapter on Ulcers.) Of great value also will be found the silver ointment of Credé (Unguentum Credé). This permits of absorption of silver through the unbroken skin (as in the case of ung. hydrarg.), and the dissemination throughout the system of the antiseptic virtues of the silver itself. To ensure its greatest efficiency this ointment should be thoroughly rubbed in, especially over parts which are not too tender. Many cases of septic infection promptly yield under the influence of the argentine preparations which Credé has lately introduced.
In suitable cases also the subcutaneous injections of antistreptococcic serum will be followed by beneficial effects. The earlier the injection is given the better the prospect of benefit. Evidence is strongly in favor of this serum as a prophylactic measure, especially before operations, when septic pneumonia or other septic accidents are feared.
Another measure of great utility in selected cases is the intravenous infusion of a solution of Credé’s soluble silver, made with 1 gram of silver in 1000 Cc. of sterilized water at a temperature of 105° to 110°. In cases of profound toxemia a small amount of blood may be withdrawn (50 to 400 Cc.), for reasons stated in Chapter VI. No hesitation need be felt in introducing 500 Cc. or even 1000 Cc. of this solution. It is the ideal way of bringing a powerful non-toxic antiseptic into immediate contact with pathogenic microbes.
There have been recent suggestions as to the intravenous injection of very dilute formalin solution, in order to take advantage of its remarkable germicidal activity; it has been employed in a few cases, especially of puerperal sepsis, with success, 1 Cc. of standard formalin solution is mixed with 800 Cc. of sterilized salt solution. It has been shown that if 50 Cc. of this is thrown into the veins of an average adult it will form with the 5000 Cc. of blood a mixture of 1 to 200,000, in which strength it may be expected to prove an efficient bactericidal agent. Indeed, a smaller amount or a weaker preparation would probably suffice. Barrows has reported success following two infusions, two days apart, of first 500 Cc., then 750 Cc. of a 1 to 5000 formalin solution. Still, these injections may be followed by cramps in the arms, cardiac discomfort or distress, and blood (or blood cells) in the urine. It would probably be well to limit this use of formalin to those cases at least in which the presence of cocci in the blood can be demonstrated by culture or other method.
An excellent method in the local treatment of parts which admit of it (hands and feet) is their exposure to dry hot air in the Kelly heater or some similar apparatus. Hot[90] air will be borne at a temperature of 210° to 220°, which may be destructive to germs while still tolerable for a short time by the tissues. Clinton, of Buffalo, with whom this method is original, reports that the temperature within the tissues thus treated is raised to about 107°, which is above the thermal death point of the ordinary pyogenic organisms, and that this method gives better results than any other of treatment of septic infection of those parts which can be subjected to it.
The general treatment of septicemia is, in the main, stimulant and tonic. Fever is not to be treated with arterial sedatives nor often with antipyretics. It is a symptom of poisoning, and its too prompt suppression prevents both the recognition of the intoxication and the measure of its degree. Pyrexia then is best combated with cool sponge baths and stimulant measures of a general character. The principal reliance must be upon nutrition and stimulants. Assimilation may be impaired when gastro-intestinal catarrh is as prominent a feature as it is in many of these cases. Consequently the simplest and most assimilable food, often that which is predigested, should be administered. Milk, eggs, beef peptonoids, and fruits are among the most appropriate. The best stimulants and tonics are alcohol and strychnine. Strychnine is preferably administered hypodermically in doses of ¹⁄₂₅ grain from two to four times a day. Heart depression is best combated by this measure, or by quinine in large doses, while digitalis and atropine may be added. For internal use alcohol is, par excellence, the remedy. This is administered in doses only to be measured by their effect. In fact, the administration of alcohol in these cases is a matter of effect, and not of dosage. Aside from these measures the intestinal antiseptics should be administered, among these being corrosive sublimate, ¹⁄₁₀₀ grain, every three or four hours, salol in large doses, bismuth salicylate, or naphthalin—any or all of these in connection with powdered charcoal. Intestinal pain and frequency of stool can be more or less controlled by opium, while disinfection of the alimentary canal is only to be accomplished by the above remedies, in connection with flushing of the colon with saturated boric acid solution or something of that kind. Pain is to be controlled by morphine administered subcutaneously.
No special attention need be given to the so-called septicopyemia. It represents a mixed condition of septic intoxication, local infection, and destruction, with metastatic abscess, and is a term appropriately applied to cases which combine the significant features of each type.
The derivation of the term pyemia, which came into general use in 1828, is misleading. Although septic fever always accompanies suppuration, it is not certain that pus as such circulates in the blood, as the term pyemia implies, the error having arisen originally from mistaking the contents of breaking-down thrombi for pus from ordinary sources. While a recognition of the etiology of the disease is new, the disease itself has been recognized for many centuries.
Pyemia is only met with in connection with suppuration, as far as known, never without it. In those cases which appear to be free from suppuration pus will be found. Pyemia may be described as septicemia plus thrombotic and embolic accidents, which lead to distribution of infectious material to all parts of the body. This distribution is made by the bloodvessels, although to some extent the lymphatics undoubtedly participate. When pyogenic organisms reach bloodvessel walls they tend to set up a mycotic phlebitis, which, by virtue of the coagulating blood, becomes soon what is known as thrombophlebitis. Infection proceeding through the vessel walls, the endothelial lining is loosened, while to these rotting spots leukocytes adhere and coalesce into a more or less homogeneous mass. This so-called white thrombus becomes also infected with bacteria; portions of it, loosened and dislodged, are carried by the returning blood stream to the right side of the heart, whence they are distributed through the lungs. Dislodgement may be made by mere force of the blood stream, or may be assisted by movements of the part or handling of the same. These particles of thrombi are loaded with the infectious organisms which began the disease, and wherever one settles a reproduction of the original thrombophlebitis is rapidly produced. In this way numerous infected thrombi are formed within the vessels of the lungs, which, again, loosen, and are now swept into the left side of the heart, whence they are distributed with arterial blood in all directions. While it is true that they are equably distributed, it is also positive that[91] certain tissues seem more capable of lodging and being attacked by the contained organisms than are others. When it is once appreciated that each particle of infected clot is capable of setting up, either in the lungs or in the other tissues, upon the second distribution, other abscess formations analogous in etiology to that from which came the first disturbance, then the fundamental idea of metastatic abscess is fully impressed. The term metastasis may be regarded as synonymous with transportation, and metastatic abscesses are those produced by transportation of infected particles from one part of the body to another. Wherever they lodge similar trouble will result. Contiguous minute metastatic abscesses quickly coalesce, and in this way large collections of pus are formed. The blood also contains organisms not attached to thrombi, and from the blood of the pyemic patient cultures can at almost any time be made. Until this is done it will be virtually impossible to incriminate any particular organism as the one at fault. Thrombo-arteritis is the equivalent in the arteries of thrombophlebitis in the veins, and is accompanied by the same detachment of endothelium, adhesion of leukocytes, etc. Whenever such a lesion occurs in artery or vein, coagulation necrosis takes place and suppuration occurs around it. The metastatic abscess is thus the result of breaking down of this affected tissue, and is often called miliary abscess. Particles of infective thrombi cling also to the valves of the heart and a septic endocarditis may result.
The possibility of so-called spontaneous or idiopathic pyemia is occasionally discussed. This means a pyemia whose cause is concealed. The explanation will be found sometimes in an acute infectious osteomyelitis, sometimes in ulcerative endocarditis, or inflamed appendix or other portion of the peritoneal cavity. Again, it may proceed from middle-ear disease, in which there is so little discharge as scarcely to attract attention. Thus causes which predispose to suppuration (see Chapter III) come into play here, and the influence of exposure, fatigue, starvation, etc., is not to be ignored in furnishing an explanation for the so-called idiopathic cases.
In the majority of instances, however, pyemia follows surgical operations and injuries, among which are compound fractures, deep injuries with small superficial evidence thereof, compound injuries of the skull, and injuries by which veins are exposed. Inasmuch as the typical pyemic manifestations require a certain length of time for their development, the onset of this disease is more delayed than in the case of septicemia. While the case may be manifestly one of septic infection of unrecognizable type, the characteristic indications of pyemia seldom appear in less than ten days, and frequently not for several days longer.
—The symptoms of pyemia do not essentially differ from those of other septic infections. The principal difference is in the frequency of chill and range of temperature. Chills are more common at the inception of the condition, and more frequent throughout its continuance than in other septic conditions. The chill may be slight or assume the proportions of a rigor, and each chill is followed by colliquative sweat and exhaustion. In other words, chills which are infrequent in septicemia are common in pyemia. There is reason to believe that with each fresh distribution of emboli we have one or more chills as the objective evidence thereof. Distinctive also of pyemia is the temperature curve, which much resembles that of intermittent fever, without the regularity of change characteristic of malarial fevers. It is without regular remissions, and has been referred to as irregularly intermittent. The first rise is abrupt and usually excessive, while with each fresh chill or series of chills similar abrupt alterations will be noted. These occur so frequently and fluctuate so irregularly that in order to note them accurately the temperature should be taken at least every two hours. The temperature seldom drops to normal.
As the lungs fill with the first crop of infected emboli, and the first series of metastatic abscesses form there, there is more or less dyspnea and sense of oppression; there may be also pulmonary complications—pleurisy, bronchitis, etc., even pulmonary edema. Frequently there is expectoration of frothy and discolored sputum; occasionally there is blood in the sputum. A peculiar sweetish odor of the breath has been noted by many observers in this disease, and is supposed to be idiopathic and characteristic. (See acetonemia in previous chapter.) With the dispersion of the second crop of emboli from the lungs there is apt to be icterus, with evidence of metastatic abscess in the liver, and collection of pus as the result of coalescence of small abscesses. The sensorium is not so affected in pyemia as in septicemia, and in the former disease patients are more[92] likely to be alert and active in mind. General hyperesthesia and restlessness are common. Colliquative sweats are also a feature of pyemia. There is the same liability to eruptions, etc., which may mislead or complicate the diagnosis. A dermatitis is seen sometimes in pyemia, the lesions assuming a papular or pustular form, due to local infections of the skin. Purpuric spots are also seen, and vesication is not infrequent. Within the mouth sordes collect upon the teeth or gums; the tongue becomes dry and brown and heavily coated. Diarrhea is less common in pyemia. The urine is usually scanty and high colored, containing solids in excess; albumin is sometimes found therein, as well as peptone. The presence of peptone in the urine is probably an indication of the breaking down of pus corpuscles in various parts of the tissues.
A significant objective evidence of pyemia is met with in the metastatic collections of pus within the joints, which occur relatively early, and which, if multiple, may lead to a correct diagnosis. One of the earliest joints to be involved is the sternoclavicular, although none of the joints are free from the possibility of invasion. The articular serous membranes seem to have the property of carrying and holding the infective thrombi better than any other tissue in the body. The pyarthrosis of pyemia is for the most part painless, yet implies loss of function of the affected joints. The distention of these is usually evident to the eye, the fluctuation pronounced, tenderness not extreme, but the swollen part merges into tissues which are edematous and reddened. When pain in the limb is extreme, it is usually because of metastatic abscess within the bone-marrow cavity. In other words, we now have a metastatic osteomyelitis.
In all cases of pyemia prostration is marked, yet the pulse is seldom weak, at least until toward the close of life. As cases progress from bad to worse subsultus tendinum is often noted.
The appearance of the wound or site of operation does not differ essentially from that already described under Septicemia. There is usually, however, less discharge, granulations are smoother and dryer, and if tissues are gangrenous they are not as wet and nauseous as in the other case. Evidences of thrombophlebitis and lymphangitis will proceed from the wound toward the body, as in other instances of septic infection.
—Prognosis is usually bad. While recovery may follow where metastatic infiltration has not been too general, the ordinary case of pyemia will die within twelve to fourteen days after diagnosis. Sometimes the entire process is much slower, and isolated cases occur which can be designated as so-called chronic pyemia, which differs but little from the acute form. A case of pyemia should not fail of recognition because there is no evidence of infection from without. A fatal case of pyemia has been known to occur from a suppurating soft corn which was not discovered during life; also from peridental abscess, etc., which had been overlooked. Death is the result of tissue destruction and septic intoxication.
—In the vessels these consist essentially of thrombosis, examples of which may be seen, for instance, in the cranial sinuses and in the large veins. Aside from these, with the enlargement and softening of the spleen, the liver, and lymphatic structures, already described under Septicemia, the principal objective evidences consist in the discovery of metastatic abscesses in many or all parts of the body. As stated above, there is no tissue or organ in which they may not be found. The mechanism of their production has been already described. Infarcts may also be met with, in the kidneys especially, the liver and spleen as well, and indicate areas already cut off from blood supply by thrombo-arteritis, in which abscess formation would have occurred had time been given. In the liver large abscesses may be found; joint cavities may be filled with pus; the lungs are usually the site of innumerable small abscesses. The other postmortem changes commonly noted are not difficult of explanation, but are not so characteristic or pathognomonic as to call for further mention. In a joint which has become filled with pus there usually has been loosening of the cartilage and more or less disorganization of all the joint structures, which appear to have undergone rapid ulcerative destruction and putrefaction.
—Treatment of pyemia is in large degree unsatisfactory. That which used to be the terror of surgeons in the pre-antiseptic era is now, thanks to Lister and others, almost abolished. Pyemia is a rare disease in modern surgical practice. Its possibility should be borne constantly in mind, however, and the necessity for careful antiseptic or for a rigid aseptic technique is in large degree based upon fear of pyemic consequences.
[93]
When once established, the disease is to be treated on lines nearly similar to those laid down for septicemia, including resort to the ichthyol or silver ointments, and to intravenous infusion of silver solution. (See p. 89.) Amputation or extirpation of the part from which infection has first proceeded may be of avail. Among the most successful measures for surgical treatment of this disease is to expose the infected area, open the involved veins, and either excise them or scrape them out and disinfect them. This treatment has been successful in cases of cranial infection following middle-ear disease, etc. (See chapter on Cranial Surgery.)
Disinfection of the infected area and immersion in hot water should be practised. Metastatic abscesses should be opened and drained, and every accessible collection of pus evacuated, either by the knife or aspirator needle—e. g., in the liver.
The medicinal treatment is practically the same as in septicemia, while the surgeon’s mainstays are alcohol and strychnine. These, with cathartics and intestinal antiseptics, will practically sum up the drug treatment, the surgeon meantime not neglecting the matter of nutrition, crowding it in every assimilable form.
Erysipelas is an acute infectious disease characterized by its tendency to involve the skin and cellular structures, to extend along the lymphatic vessels, to involve wounds and injuries under certain conditions, accompanied by more or less fever of septic type, leading frequently to septic disturbances of profoundest character, yet tending in the majority of instances to spontaneous recovery. It has been observed probably from prehistoric times, but has not found a proper description nor appreciation until perhaps within the past century. It occurs in so-called traumatic and idiopathic form—which latter means that the site of infection is not discovered—and also in a virulent and contagious type, which leads to the appearance of a number of cases over a large territory; it often appears in the epidemic form. On account of the reddening of the skin it goes by the name of the rose among the German laity. It may assume the type of an infectious dermatitis, subsiding without suppuration, or a similar lesion of exposed mucous membrane may be noted, or, occasionally, its virulence seeming greater, its lesions are met with in more deeply seated parts, accompanied by suppuration or even gangrene, and it is then called phlegmonous. In a small proportion of cases the infectious organism appears to be transported from one part of the body to another, and thus we have metastatic expressions of this disease. The most common examples of this are seen in erysipelatous meningitis after erysipelas of the face or scalp, and erysipelatous peritonitis after the disease has manifested itself on the truncal surface. It is of a type which makes itself almost interchangeable with puerperal fever; and when epidemics of erysipelas have involved certain states or areas, it has been noted also that nearly every obstetrical case developed puerperal septicemia.
—There is more than passing interest connected with this last statement. It is now definitely established that the infectious organism is a streptococcus which is allied to, if not identical with, the streptococcus pyogenes, the ordinary pyogenic organism of this form. This specific organism has been separated, studied, and its role assigned by Fehleisen, and the organism is frequently called Fehleisen’s coccus. Preserving always its morphological characteristics, it acts, as do many other pathogenic organisms, within wide limits in virulence. Cultivated from some cases, it scarcely seems infectious, while from others it is fatal.
—The disease manifests a tendency to travel via lymphatic routes. As long as it is confined to the skin and superficial tissues it has the appearance of an acute dermatitis. When it migrates deeper it generally leads to suppuration, another reason for believing that the streptococci of erysipelas and of pus production are the same. In the affected and infected area the minute lymphatics will be found crowded with the cocci, which are seen much less often in the small bloodvessels; also in the tissues beyond the apparently infected area they may be found dispersed less freely. The bacterial activity seems most active along the advancing border of the superficial lesion. Here the phenomena of hyperemia and phagocytosis are most active. Even in the vesicles that are characteristic of the disease the organisms may be found.
The discharges from this region are infectious, and caution should be observed[94] in dressing such cases. A finger pricked by a pin from a dressing may subject the individual to loss of life. The dressings containing the discharges should be burned immediately.
The path of infection is usually through a wound, and as soon as discovered a case of erysipelas should be separated from all surgical cases, or if the erysipelatous patient cannot be isolated, he should be removed from proximity of other wounded individuals.
Erysipelas which follows injury, however slight, is termed traumatic. The terms “idiopathic” or “spontaneous” should be restricted to those cases in which the path of infection is not discovered.
—With the exception of the local appearances, they are essentially the same in both of the above-mentioned forms. The characteristic feature of the disease is a dermatitis with its peculiar roseate hue, which it is impossible to describe in words. In tint it differs slightly from that noted in certain cases of erythema. It is, however, accompanied by an infiltration of the structures of the skin, so that the area which is reddened is at the same time elevated above the surrounding surface. Its edges are often irregular. As exudate takes the place of blood in the tissues, the red tint merges into a yellow. At this time there is more induration of the skin and tendency to pit on pressure. Vesication of this involved area is now frequent, the vesicles often coalescing and forming large blebs and bullæ, which fill with serum that may become discolored or purulent. When exposed to the air, unless the tissues become gangrenous, this serum usually evaporates and forms scabs. This disturbance of the skin is always followed after a number of days by desquamation. This infectious dermatitis shows a constant tendency to spread in all directions. Its most characteristic appearances are limited to the margin of the enlarging zone, while in its centre there may be evidences of recession of the disease. If it commences in the vicinity of a wound it will probably spread in all directions from it. Beginning in the face, it usually spreads upward; in the trunk, in all directions; if on the extremities it tends to migrate toward the trunk. Wandering erysipelas is a term often applied to these phenomena. The metastatic expressions of the disease have been described.
When this affection attacks a recent wound the local appearances are not essentially distinct from those mentioned under Septicemia. The wound margins separate to a greater or less extent, the surfaces slough, and a characteristic seropurulent discharge occurs. Granulating surfaces usually become glazed—often covered with a membrane resembling that of diphtheria; deep sloughs may occur, undermining of wound edges, even hemorrhages from destruction of vessel walls. In rare instances, however, under the influence of the microbic stimulation granulations proceed faster than normal.
Whether the disease proceeds from an injury or not, the constitutional symptoms vary but little. There is usually a period of malaise with nausea, followed by alimentary disturbance, coating of the tongue, elevation of temperature, sometimes with occurrence of chill. Complaint of pain or unpleasant sensation will lead to examination of the area involved, when the above symptoms will be noted, with evidences of lymphangitis and enlargement of lymph nodes. When chill occurs it is followed by pyrexia. Temperature fluctuates, with a tendency to assume the remittent type. When the disease subsides spontaneously it is by a gradual process of betterment and subsidence of temperature. In other instances the constitutional symptoms assume more or less of the septicemic or typhoid type, and it is seen that the patient’s condition is practically one of mild septicemia, which often proves fatal.
When the disease assumes the phlegmonous type the constitutional symptoms become more and more typhoidal and the septicemia becomes most pronounced. Locally exudation goes on to the point of threatening, even of actual, gangrene, unless tension is relieved by incisions. Pain is usually intense, partly because of confined exudates beneath resisting structures. More or less rapidly the local and constitutional signs of pus formation are noted, and unless these are observed and acted upon early there will not only be suppuration, but more or less actual gangrene, so that not only pus, but sloughs of tissue will be discharged through the incision, or will, when this is delayed, make their escape by death of overlying textures.
In all phlegmonous cases there is practically coincidence of septicemia, already described, and of the local appearances above noted. In proportion to the extent of the lesion in these phlegmonous cases, and failure to afford relief, will be the opportunity for septic intoxication.
[95]
The mucous membrane does not always escape, and even in the nose, the pharynx, the vagina, and the rectum a distinctive erysipelatous lesion may be found. The disease may travel from the pharynx through the nose and involve the face, or through the Eustachian tube to the ear and thence to the scalp, or vice versa. Erysipelatous laryngitis is to be feared on account of edema of the glottis, which would soon be fatal unless overcome by intubation or tracheotomy. An infectious exudation into the lungs is also known to follow erysipelas, and has been considered an erysipelatous pneumonia. The cellular tissue of the orbits may also be involved, when abscesses will occur, which should be opened early; the parotid and other salivary glands may become involved, usually in suppuration.
Many cases are accompanied by much gastric irritation, which it is difficult to explain. Ulcers are sometimes found in the intestines, as after burns. These usually give rise to bloody diarrhea. The cerebral symptoms may be simply those of delirium from irritation or of meningitis from infection. Strange phenomena have followed the disease in certain instances—cessation of neuralgic and of vague, unexplainable pain, improvement in deranged mental condition, spontaneous disappearance of tumors, etc. Advantage has been taken of this last in the treatment of these cases. (See Cancer.)
It is quite likely that some of the worst forms of phlegmonous erysipelas are due to mixed infection. To inject the bacillus prodigiosus together with the streptococcus of erysipelas will greatly enhance the virulence of the latter, so that reaction may proceed even to gangrene.
—These are not distinctive, but are a combination of local evidences of suppuration and gangrene, with the deterioration of the blood, the softening of the spleen, etc., which are characteristic of septic poisoning. Only in the skin, and then under microscopic examination, can any pathognomonic appearance be discovered. This will consist in the crowding of the lymphatic vessels and connective-tissue spaces with cocci, in the evidences of rapid cell proliferation, in the quantity of exudate, in vesication, sloughs, etc.
—Diagnosis of erysipelas should be made mainly from various forms of erythema, from certain drug eruptions, and from other forms of septic infection which do not assume the clinical type of erysipelas. The gastric symptoms of this disease are sometimes produced by certain poisonous foods or the distress which is produced by medicines, such as quinine, antipyrine, etc.
—The majority of instances of idiopathic erysipelas run a certain limited course, although the eruption may spread to almost any distance upon the body. When the disease attacks surgical cases, and especially when it involves wound areas, the prognosis is not so good. When the disease assumes an epidemic type and involves cases of all kinds, it will be found to have a virulence that may make it a most serious affair. In proportion to the extent to which it assumes the phlegmonous type it will be found locally, if not generally, destructive. The ordinary case of facial erysipelas will recover with almost any treatment. Nevertheless meningitis may develop, and even a mild case is to be treated with care and caution.
—Danger comes from two sources—septic intoxication and local phlegmons or gangrenous destruction. Each is therefore to be combated. Treatment should consist of isolation. There is no specific internal treatment for this disease. Tincture of iron, which was long vaunted as such, has proved unsatisfactory, and is of benefit only as a supporting measure in a limited class of cases. Constitutional measures should be employed: First, for the purpose of maintaining free excretion by bowels and kidneys; second, for the purpose of supporting and maintaining strength; third, for tonic and stimulant measures in prostrated and debilitated patients; and, fourth, for the purpose of combating intestinal sepsis or intoxication from any other source. The robust patients with this disease need no particular tonic. The aged, the enfeebled, the dissipated, the prostrated individuals, and the confirmed alcoholics are those who need vigorous stimulation, partly by alcohol and quinine, and partly by strychnine, preferably given hypodermically, and by the other diffusible stimulants by which they may be kept alive. Pilocarpine, given subcutaneously and pushed to the physiological limit, has been praised by some. If along with prostration there occur restlessness and delirium, then anodynes and hypnotics are serviceable, and should be administered to meet the indication—morphine hypodermically and any of the agents which produce sleep are now most beneficial. Finally, if there is any drug which[96] can be administered in doses sufficient to saturate the system with an antiseptic which shall at the same time not prove fatal because of toxicity, this is the ideal medicament for constitutional use only. Such a drug is not known, but it will be well to give some near approach to it internally, as by administering corrosive sublimate, salol, naphthalin, or something else of this character in doses as large as can be tolerated.
Should patients become violent it may be necessary to resort to mechanical restraint—a strait-jacket, a restraining sheet, a camisole, etc.
Nourishment must be kept up by the administration of the easily assimilable and predigested foods.
Locally the number of remedies that have been resorted to is legion. In a mild case of spontaneous erysipelas—i. e., where no infection can be traced—it will sometimes be sufficient to put on a soothing application, like a lead-and-opium wash. It often gives relief to have the part protected from air contact, which may be done by a soothing ointment or by dusting the part with a powder, such as bismuth oleate or subnitrate, zinc oxide, etc., these being rubbed up with powdered starch; or by a film of rubber tissue or of oiled silk. Brewers’ yeast applied on compresses and covered with oiled silk is efficacious.
Even before the bacterial origin of the disease was accepted it had been suggested to use antiseptic applications, either in watery solution or combined with oil or some unguent; this is now the ideal method of local treatment, the difficulty being only to find that which shall be efficacious as an antiseptic, yet not injurious in other ways. Compresses wrung in solutions of various antiseptics are often serviceable. The following preparation has given satisfaction: Resorcin (or naphthalin) 5, ichthyol 5, mercurial ointment 40, lanolin 50. The proportions of these ingredients may be varied, and the amount of ichthyol sometimes increased, especially when the skin is not too tender. The affected parts are anointed with this, and then covered with oiled silk or other impermeable material, simply to prevent its absorption by the dressings; the parts are then enveloped in a light dressing and bandaged. Credé’s silver ointment has also proved useful. As the disease becomes mitigated the ointment may be reduced with simple lard, and discontinued when local signs have disappeared. Absorption of any of these preparations may be hastened by scratches over the affected area with the sharp point of a knife.
Treatment of threatening phlegmon, or phlegmonous erysipelas, must be more radical, and consists of free incision down to the depth of the deepest tissues involved. In treating dissecting and other septic wounds of the fingers incision should be made to the tendon sheaths, even to the bone. It is only by such radical measures that worse disaster may be avoided. Some aggravated local cases are treated by a series of deep incisions with the use of the curette, the surface after careful clearing being kept buried under an antiseptic solution (silver lactate 1 to 500) or ointment.
In connection with erysipelas and the role of the lymphatics, it is advisable to consider the relation and behavior of the lymph nodes and granulation tissue to infecting agents. Depending on the virulence of the infectious material, the site of infection, and the variety of the microbe will be its arrival in these protective filters. Then follows a series of cycles of maximum and minimum activity in the nodes, during the former the bacteria almost disappearing. The more pathogenic the microörganism the more certain the destruction of the lymph node, or perhaps of the individual. The well-known enlargement of the nodes is due almost solely to an increase in their lymphoid elements. Halban, who demonstrated these cyclic variations in the contents of the lymph nodes, is inclined to insist on an intimate relation between them and the temperature variations noted in cases of septic infection.
When granulations are present the lymph sacs are closed, as by a sanitary cordon. Unless this tissue is broken they are proof against ordinary infection. It is well known that erysipelas will appear about an old wound or sinus that has been rudely probed. Even virulent organisms spread upon healthy granulating surfaces fail to infect. Strong carbolic and other toxic agents can be used in and about such granulating cavities with an exemption from poisoning that otherwise would produce dangerous effects.
[97]
Synonyms: Trismus, Lockjaw.
Tetanus is an acute infectious disease, of relatively infrequent occurrence, invariably of microbic origin, characterized by more or less tonic muscle spasm with clonic exacerbations, which, for the most part, occurs first in the muscles of the jaw and neck, involving progressively, in fatal cases, nearly the entire musculature of the body. Certain races of people seem predisposed, and in certain climates and geographical areas the disease is exceedingly prevalent. Negroes, Hindoos, and many of the South Sea Islanders show a peculiar racial predisposition, and, in a general way, inhabitants of warm countries are less resistant. This is shown partly by the fact that in various European wars the Italians and French have suffered more than the soldiers of more northern climes. Tetanus is by no means confined to adult life, since infants are far from exempt, and in the tropics the trismus of the newborn is the cause of a high mortality rate. In Jamaica one-fourth of the newborn negroes succumb within eight days after birth, and in various other hot countries the proportion is at times equally great. One plantation owner states that fully three-fourths of the colored children born upon his plantation succumbed to the disease. The peculiar reason for this infection will appear later when speaking of tetanus neonatorum. Men seem more commonly affected than women, probably because of their occupations, by which they are more exposed. Military surgeons have had to contend with the disease in its most virulent form, and it has been noted that soldiers when worn out by fatigue or suffering from the disaster of defeat seemed more liable to the disease. In 1813 the English soldiers in Spain suffered from tetanus in the proportion of 1 case to 80 wounded men. In the East Indies, in 1782, this proportion was doubled. Quick variations of heat and cold, such as warm days and cold nights, coupled with the other exposures incidental to military life, seem to exert a great effect. Curiously enough, the wounded in many campaigns who have been cared for in churches have suffered more from the disease than those cared for in any other way. Tetanus, however, is by no means necessarily confined to any one clime or race, but may be met with anywhere, at any time, providing only that infection has occurred. A celebrated Belgian surgeon lost by tetanus ten cases of major operations before he discovered that the source of the infection was his hemostatic forceps. As soon as these were thoroughly sterilized by heat he had no further undesirable complications. If the disease can be conveyed by the instruments of a careful surgeon, how much more so by the dirty scissors of a careless midwife, etc.
It is true, also, that the popular notions of the laity concerning the liability to tetanus after certain forms of injury are not ill-founded. Small, ragged wounds of the hands and feet are those which ordinarily receive little or no attention, and are among those most likely to be followed by this disease. The toy pistol, which, a few years ago, was such a prevalent and widely sold children’s toy, was the cause of many a small laceration of the hand, due to careless handling and the peculiar injury produced by the explosion of a small charge of fulminating powder in a paper or other cap. It was not the character of the laceration or injury thereby produced, but the fact that such injuries occurred in the dirty hands of dirty children, which were most likely to become infected, that has caused the so-called toy-pistol tetanus to be raised almost to the dignity of a special form of this disease. During the month of July, 1881, in Chicago alone, there were over 60 deaths from tetanus among children who had been injured in this way by these little toys. This led to their sale being suppressed by law.
—Two theories have had strong advocates, one being that which would account for the disease by irritation of nerves; while the second, the humoral, would[98] explain the disease by alterations in the blood. Each has had its most ardent defenders, but both have now completely yielded to the investigations of a few observers, among whom Kitasato and Nicolaier are the most prominent. These ardent workers were, in 1885, able to clearly establish the parasitic nature of this disease, and to isolate and investigate the organisms by which it is produced.
Fig. 17
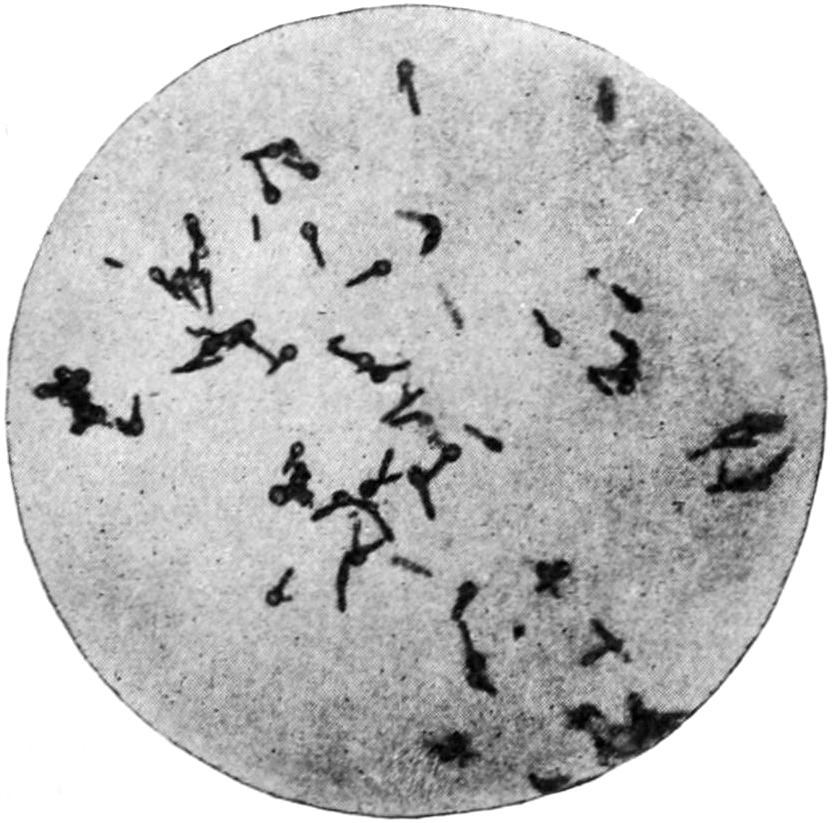
Tetanus bacilli, showing spore formation. (Kitasato.)
The bacillus of tetanus is a somewhat slender, rod-shaped organism, with a peculiar tendency to spore formation at one end, which gives it a drumstick appearance. It is essentially an anaërobic organism, and can never be cultivated in contact with the air. In laboratory experiments it is grown in the depths of a solid culture medium or else in fluids and on surfaces in an atmosphere of hydrogen gas. It is one of the apparent contradictions of bacteriology that this organism, which can only be grown as an anaërobe, nevertheless abounds in earth, particularly the rich, black loam which best supports luxuriant vegetable life, and that it practically inhabits the upper layers of the soil, which accounts for the fact that so many contaminations and infections have occurred from stepping upon planks or boards with nails projecting, or from introduction of splinters, or from lacerations of the hands and feet which are so often followed by contact with such materials. There is nothing about a rusty nail wound which, by itself, predisposes to tetanus, but the rusty nail upon which a person steps is either itself infected or leaves a rent or wound which may become infected within the next few moments, and which is not likely to receive the careful attention which it should. Verneuil has of late laid stress upon the fact that in localities where horses are kept tetanus is more prevalent, and that the infectious organism abounds in and upon stable floors, about barn-yards, and wherever the excretions of a horse may be found. Bacteriologists are aware that in the intestines of herbivorous animals the bacilli (anaërobic) of tetanus and malignant edema are often found. Verneuil has further shown that almost the only instances of tetanus which occur on shipboard are upon those ships which are used for transportation of horses and cattle. His statements are at least interesting, if not absolutely well-founded. At all events, tetanus is certainly of telluric origin.
A French veterinary surgeon of twenty-five years’ experience had not seen a single case of tetanus until 1884, when he “removed a tumefied testicle from a horse, with the ecraseur, and it died of tetanus; in the following six months he castrated five, and all died; another castrated fifteen in one day, and all died but one; another in ten days castrated six bulls and operated on three fillies for umbilical hernia, when five of the bulls and one of the fillies died.” This will illustrate how the infectious agent may be conveyed by instruments, etc.
The tetanus bacillus manifests other peculiar properties, for some of which it is most difficult to account. Upon susceptible animals it is violently infectious, but is rarely found at any distance from the tissues in which it has first lodged. In laboratory investigations the period of incubation is seldom longer than forty-eight hours. Another peculiarity of the organism is that it generates certain poisons of active properties which may be separated from pure cultures, by whose injection the peculiar spasms of the disease itself may be reproduced. These have been isolated, especially by Brieger, who has given to them the names of tetanin, tetanotoxin, spasmotoxin, etc. It has been estimated that about ¹⁄₃₀₀ Gm. of the pure toxin of tetanus would be a fatal dose for a man. This toxin seems to have a specific affinity for the ganglion cells of the anterior horn of the spinal cord, with which it unites with great force. Herein lies the secret of its disturbing power.
It is peculiar that some time may elapse after its injection before the appearance of the first symptoms. Diphtheria toxins appear to be prompt in their action, and thus display quite opposite characteristics. Experiment would seem to show, moreover, that the tetanus toxins do not reach the cord through the blood stream, but appear to[99] slowly pass along the axis cylinders. Sensory nerves do not transport the toxins to the cord. The toxin enters the nerve termination, first of all, at the site of the infection, where it is most concentrated, which will explain why the spasms most frequently begin in the vicinity of the infection, or are the most marked there. Most of the toxin is taken up by the blood and lymph and distributed all over the body, and then passing along the motor fibers it enters the cord and leads to general convulsion. When the toxin is injected directly into the cord the symptoms begin at once. Therefore, for protective purposes, much may be expected from the administration of the antitoxin in cases of suspicious injury or those where experiment has shown there is reason to fear the development of tetanus. There does not appear to be on record a single instance in which a person who had been given antitoxin soon after receiving such a wound has developed tetanus, nor does the antitoxin by itself seem to have done any harm. Obviously, then, the earlier antitoxin is used in the case the better. It may be recalled that there are no diagnostic symptoms of tetanus until the first spasm develops, usually after the expiration of from five to twelve days. By this time the nerve cells are thoroughly saturated with the poison and considerable time may elapse before the antitoxin can reach these cells by a more indirect route.
—Tetanus neonatorum, or tetanus of the newborn, a condition already alluded to, is a remarkably fatal affection, very prevalent among the negro race, especially in hot climates. It nowise differs from traumatic tetanus, but is such in effect, since the infection in these instances always follows the division of the umbilical cord, which is usually effected with dirty scissors in the hands of a dirty midwife, while the thread with which the cord is tied is itself a possible source of infection, as well as the rags which are used to cover the umbilicus in the first dressing. It is generally fatal, because of the weakness and lack of resistance of these little patients. It occurs usually within a week after birth, if at all.
—Tetanus cephalicus, called also tetanus hydrophobicus and head tetanus, is only a peculiar manifestation of this same affection, confined mainly to the head and usually following injuries to this region. The muscle spasms are mostly confined to the facial, pharyngeal, and cervical muscles, sometimes extending to the abdominal. These manifestations may be reproduced in animals by inoculating them on the head rather than upon the extremities. It is the least fatal form of the disease.
—There is always a period of incubation, usually three or four days, occasionally a week in length, but rarely longer.
It is generally held that the longer the period of incubation the more hopeful the prognosis. While for the great part the disease assumes an acute type, a chronic tetanus is described and occasionally seen. The first warning of the disease usually comes as more or less stiffness of the cervical and maxillary muscles, which is likely to be referred to by the patient as a “sore throat,” because of the consequent difficulty in deglutition. A complaint to this effect should be regarded as a warning, especially if on inspection no visible reason for it can be detected in the pharynx. This complaint is usually made in the morning after an ordinary night’s rest. This muscle stiffness will be followed by increasing tonic spasm in the muscles of the jaw, making it difficult to open the mouth, while the head and neck gradually become stiffened and fixed by spasm of the cervical muscles. These muscles may now be felt more or less rigidly contracted, as if by voluntary effort, and the condition, which is at first not painful, becomes after some hours a source of discomfort, perhaps of actual pain, to the patient. If the disease pursues the usual course, the other muscles of the body become gradually affected, usually in the order of their proximity, but not necessarily so. The abdominal muscles are firm and board-like, and the dorsal muscles more or less contracted, sometimes to an extent which causes arching of the spine. Should the original wound or port of entry for infectious germs have been in the hand or foot, the muscles of this limb become contracted, more or less rigidly, holding it in a position which is not easily changed, even by efforts of the attendant. Sensation is also often more or less perverted. In this condition of tonic rigidity the muscles remain, to relax usually only with death.
The most characteristic features of the disease, however, are the peculiar clonic exacerbations, which convert spastic rigidity into violent and convulsive muscle activity, so that the limbs and even the frame of the patient are more or less contorted, the muscle exertion being sometimes painful to witness. Notable effects are thus produced;[100] the mouth is peculiarly puckered, and its corners drawn upward and backward by the risorius muscles, giving to the face that peculiar expression known as the “sardonic grin.” When the abdominal and flexor muscles of the thighs are involved, and the body is more or less curved forward, this condition is known as emprosthotonos; when the muscles of the back especially are involved, with the extensor muscles of the thighs, as opisthotonos; and when the body is bent to one side or to the other it is called pleurosthotonos. It is said that opisthotonic convulsions occur to such an extent in some instances that the heels touch the head. At all events, the patient’s body is frequently raised from the bed, so that he rests upon the head and feet.
Another characteristic feature of the disease is the reflex irritability, or hyperesthesia, by which these convulsive attacks apparently are produced. Into this condition the patient falls more or less rapidly within the first day after the inception of the disease, and to such a height may it be augmented that the slightest movement in the room, jarring of the bed, or displacement of clothing, even noise or a flash of light, may immediately bring on a convulsion. Rupture of muscles has been reported during some of these violent convulsions.
Fig. 18
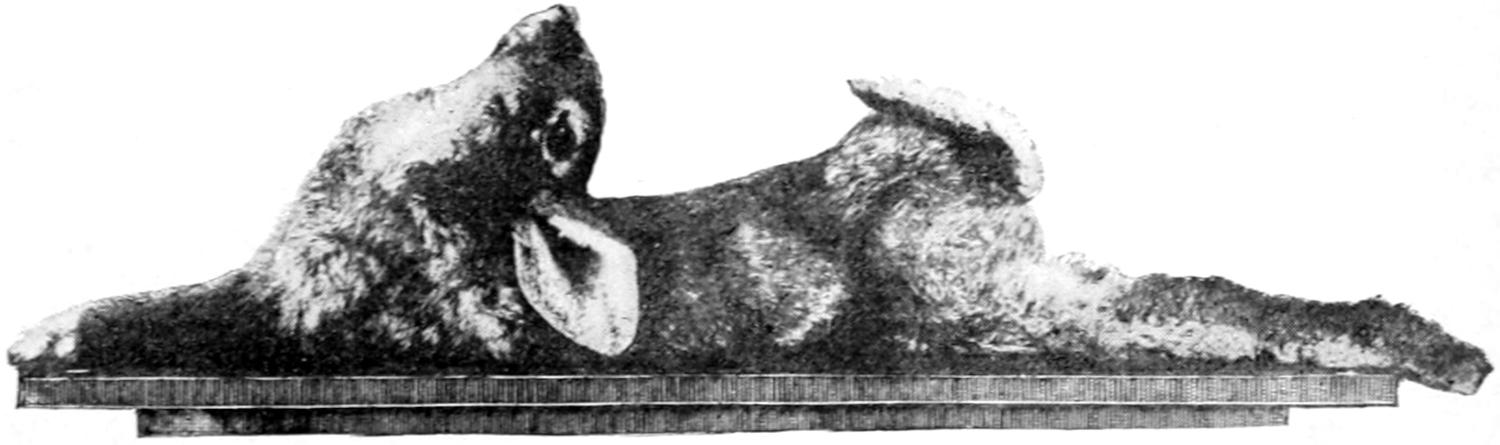
Characteristic tetanic spasm in a rabbit twenty-six hours after inoculation with pure culture of tetanus bacilli. (Tizzoni and Cattani.)
During the course of this disease the jaws are so fixed that patients speak with extreme difficulty and the tongue cannot be protruded. The mind is clear until the end. The pain is rather the acute soreness due to intense muscle strain. There is spasm of the sphincters, by which urine and feces are often retained. There is nothing characteristic about the temperature, which is seldom much augmented. Attempts to swallow give pain, and are resisted because of the renewed muscle spasm which is likely to follow the irritation inseparable from the act itself. As the result of spasm of the glottis peculiar respiratory sounds may be noted.
Until the last only the voluntary muscles are involved. Finally, however, there are spasms of the accessory respiratory muscles and of the diaphragm. Death is usually produced by involvement of these muscles analogous to those of the others, and results usually from apnea or suffocation. During the last hour or two perspiration may be copious and the temperature may rise.
Chronic tetanus is characterized throughout by a milder and much more prolonged series of symptoms. The period of incubation is much longer, and, while the general program of the acute form is adhered to, it is of less severe degree and is spread over a longer time; in fact, cases covering two months or more are reported. In chronic tetanus the prognosis is much more hopeful than in the acute form.
The wound is but slightly, if at all, affected. In some cases it will be found to have healed before the onset of the disease. If suppurating or open, its evidences of repair will be found unsatisfactory and some indications of septic infection may be noted. Pricking or needle sensations may be subjective phenomena.
—Prognosis is almost invariably bad; if patients live more than five or six days it is thereby improved.
—These are rarely distinctive. In most instances there are evidences at least of hyperemia, if not of more active changes, in the upper portions of the cord. Less often slight changes have been noted in the brain, consisting, in some measure, of disintegration and softening. Evidences of ascending neuritis in the nerve trunks leading to the injured area have been claimed in some instances. Few if any distinctive postmortem changes can be described as due to this disease.
[101]
—The diagnosis should be made as between strychnine poisoning, hysteria, hydrophobia, tetany, and, in the beginning, from pharyngitis, tonsillitis, etc. When the disease is fully developed it is not likely to be mistaken for anything else.
Tetanus may be simulated by hysteria, but in this event the phenomena will be so uncertain, and the evidences of organic disease so essentially lacking, that it is not likely that mistake can occur.
—If any case can be imagined in which efficient treatment is most urgently demanded it is one of tetanus. In scarcely any disease, however, is drug treatment so unsatisfactory. In the rare instances in which patients have recovered it is questionable whether it is not due to individual resistance rather than to medication. Treatment may be subdivided into local, constitutional, and specific. If there is still an open suppurating or discharging wound, it is, of course, essential to cleanse this out, basing this advice in some measure upon general principles—largely upon the fact, already stated, that ordinarily only the immediate surroundings of such a wound are found infected by the bacilli themselves. Consequently thorough scraping, excising, and cauterization, either with powerful caustics or the actual cautery, are indicated. Since the specific germ is an anaërobe, hydrogen dioxide may be used locally with great advantage, mainly because it oxidizes the albuminous material upon which the bacilli thrive. If it is in a finger or toe, amputation may be the simplest method of eradicating the local lesions.
Constitutional treatment may be divided into nutrition and medication. The tendency too often in these cases is to be careless or indefinite with regard to the excretions and the nutrition of the patient. If, for instance, each attempt at catheterization throws him into convulsions, the bladder may become overdistended and burst. So, too, there is apprehension usually in regard to fecal evacuations. At the same time these patients are allowed to almost starve because of the difficulty of feeding them. It is advisable to resort to chloroform to permit the introduction of the stomach tube—through the nostrils, if necessary—by which nutrition may be introduced into the stomach without causing the violent convulsions that would occur without an anesthetic. At the same time the catheter may be used.
In the way of active medication there is no agent so efficacious for controlling the tetanic spasms as chloroform, which may be administered occasionally, or more or less continuously, according to the wishes of the attendant. By its use the severest spasms can be kept in abeyance, and the horrible character of the disease somewhat mitigated. Of the other medicaments used, most of them are of the nature of nerve sedatives, such as chloral, the bromides, Calabar bean, cannabis indica, opium, etc. Hot-air baths or diaphoretics, by which copious perspiration may be induced, have yielded good results.
Specific treatment means in these instances taking advantage of the well-known properties which the blood serum of an animal artificially immunized against the disease possesses. This is in accordance with experimental labors with a number of different diseases, of which tetanus is one. It is, in effect, similar to the serum therapy of diphtheria.
The most hopeful of remedies is antitoxin. More lives can be saved by this preparation, if used early and freely, than by any other known remedy. Moschcowitz, in 1900, collected 338 cases, with a mortality of 40 per cent. In many of these cases it was not used early. It is of importance, however, to use it at the very outset, and to repeat its use as soon or as often as may be indicated by any exacerbation of symptoms. In one instance under my observation twenty-three phials of antitoxin were used before muscle rigidity subsided; in another case double this amount was used. Without quoting figures it is safe to say that the former great mortality rate of tetanus has been reduced at least 50 per cent. by its use, and that further reduction can be effected by its early and prolonged use.
The use of antitoxin nowise takes away the necessity for proper physical care of the laceration or the wound. Every particle of affected tissue should be cut away, all the principles of physical cleanliness adhered to, and proper antiseptics used.
When the antitoxin is used in the presence of the disease it should be injected into the spinal canal, as it is known that the cerebrospinal fluid may contain a considerable amount of the toxin and is of itself highly poisonous. Therefore after inserting the needle into the canal it is well to withdraw a considerable amount of the fluid before injecting the antitoxin. If this method is pursued the material is brought into more[102] immediate contact with the anterior horns of the cord than could be effected in any other way. After withdrawing all the fluid that will run through the needle without applying the syringe—probably 150 to 200 Gm.—10 to 15 Cc. of the antitoxin may be slowly injected, the process consuming from three to five minutes. Then a further injection should be made along some of the large nerve trunks, preferably those leading to the part involved. This injection should be made with a finer needle, such as that with which cocaine solution is injected during anesthesia for the prevention of shock. This is a more effective and less serious matter than trephining the skull for the injection of fluid upon the surface of the brain. This may be done while the patient is under the influence of the anesthetic administered for the purpose of giving proper attention to the wound. The antitoxin should be injected into the nerve trunks after their exposure. At the same time it is well to make intravenous saline injections at more than one point. After from twelve to fifteen hours the injection of antitoxin and perhaps of saline solution should be repeated, if necessary, under such light anesthesia as can be produced by ethyl chloride. Recently a substitute for antitoxin has been suggested in an emulsion of brain tissue which has been shown to have a specific affinity for the tetanus toxin. It has been seen that when these two substances have been thoroughly shaken together the toxin is removed from the fluid and confined in harmless form within the brain-tissue cells.
In injecting the antitoxin into the spinal canal no harm will ensue if a little blood flow through the needle, showing that the cord itself has been touched.
When there is need to employ this material the brain of a freshly killed small animal should be removed under antiseptic precautions. 10 Gm. or 15 Gm. should be emulsified in about 30 Cc. of sterile salt solution, which should then be strained through a sterile cloth under light pressure. This is then injected as near the wound as possible and the procedure repeated every day as long as indicated. This method can only be expected to neutralize toxin that has not yet entered the nerve cells. Nevertheless, Russian observers have reported thirteen recoveries out of sixteen instances in which the method was practised.
When no other means are at hand a 1 per cent. carbolic acid solution may be injected after the same fashion, using such an amount that about five grains are administered during twenty-four hours to an adult. This is the method especially favored by the Italians, and is due especially to Baccelli.
Matthews has devised a method which seems quite effective in experimental animals. It consists of the use of a solution of the following: Sodium chloride 4 Gm., sodium sulphate 10 Gm., sodium nitrate 3 Gm., calcium chloride 14 Cgm., water 1000 Cc. This is intended for intravenous injection, and must be introduced very slowly. The performance should be repeated twice during the first twenty-four hours and once each succeeding twenty-four hours. It produces profound diuresis, i. e., a washing out of tissue cells, as he calls it.
Hydrophobia is an acute specific or infectious disease, as far as known never originating in man, but transmitted to him, usually through the bite or by inoculation from the saliva of a rabid animal—in this country usually the dog, although the wolf, the cat, the skunk, and even certain of the domestic poultry, are capable of conveying the disease. Chickens are said to be immune save when their vital resistance is lowered by starvation. Chicken blood injected into other animals seems to antidote the virulence of the virus. It can also be inoculated in other animals, like rabbits. The virus is ordinarily conveyed in the saliva of the rabid animal. This may be wiped off as the teeth of the animal pass through the clothing of the injured individual; consequently, infection does not certainly follow such bites. But those upon exposed portions of the body, where animals generally bite, are almost invariably followed by infection. Hydrophobia is frequently spoken of as rabies, sometimes as lyssa. While rare in this country, it is by no means uncommon in Central Europe, especially perhaps in Russia, where bites from infuriated wolves are common. In the United States infection comes almost invariably from the rabid dog, in which this disease presents two types.
The so-called furious form is that which is marked by frenzy and canine madness, the objective symptoms being more pronounced and alarming, though not less dangerous[103] than the other variety. After the period of incubation, which varies considerably, these animals show depression and uneasiness, and even thus early their saliva is infectious. Their sense of hunger becomes perverted; they exhibit unusual tastes, secrete saliva abundantly, which becomes very tenacious and even frothy, exhibit a dry and edematous condition of the faucial mucous membranes; the character of the bark is altered, while they are usually infuriated at the sight of other dogs. In this stage there is usually insensibility to pain. Finally, come more or less paralysis of deglutition, quickened respiration, dilated pupils, and frenzy and madness of manner, by which they attack indiscriminately men and other animals. To this stage of furious excitation succeeds one of paralysis, and death follows from exhaustion. These manifestations usually last about a week.
Dumb hydrophobia is the more common form. Here paralysis appears much earlier and involves especially the lower jaw; the tongue falls out of the mouth; and the posterior extremities are quickly paralyzed. This form is much more quickly fatal than the other.
Animals thought to have hydrophobia should be kept by themselves in a secure enclosure and carefully watched, especially those known to have bitten men or other animals. If a suspected dog have been killed before the suspicion has been confirmed, the head and upper part of the neck should be removed for examination. Veterinarians claim that what they call the plexiform ganglion permits an almost certain diagnosis to be made. The presence of foreign bodies in the stomach of the animal is a corroborative feature. Diagnosis by subdural inoculation requires two or three weeks, and in at least one case a human patient died while waiting for diagnosis to be thus established.
Hydrophobia in man is rare in this country, yet is occasionally observed. Its etiology is as yet obscure. That a contagion vivum is present is positive, but its nature is uncertain. Negri, of Pavia, has recently described certain bodies observed in the nervous system of animals dead of hydrophobia which may offer the solution of the problem that has so long been sought. They are found in the protoplasm of nerve cells, but not in their nuclei. They are round or oval in shape, vary in size from 25 microns down to those which can be barely seen with the highest powers. They take ordinary stains.
Negri maintains that these bodies are parasites and he has invariably failed to find them in animals which did not have rabies. His work has been confirmed by a number of his colleagues, and bids fair to furnish a reliable and rapid means of diagnosis. The fact that the virus of hydrophobia will pass through a porcelain filter nowise contradicts the view that these bodies may be parasitic, for it is quite possible that they undergo different stages of development, in some of which they are small enough to pass even barriers of porcelain.
In fact it seems to have been positively demonstrated that these bodies described by Negri, in 1903, are diagnostic for rabies. They are most likely to be found in the horns of Ammon or the cerebellum. When found here, careful examination must be made of the Gasserian ganglion, where may be found the lesions first described by Van Gehuchten and Nelis, which consist of a proliferation of the endothelial cells to such an extent that the ganglion cells are first invaded and then destroyed, their places being taken by the new cells.
The Negri bodies have been generally regarded as protozoa and the specific cause of the disease. At all events, it seems possible always to successfully reproduce the disease in rabbits or guinea-pigs by inoculation with these bodies.
If examination shows neither the Negri bodies nor the lesions in the ganglion the presence of the disease can scarcely be suspected, and could only be proved by animal inoculations, which, however, would be advisable in doubtful cases where human beings have been bitten.
—The period of incubation in man is variable, ten weeks being perhaps the average. It is shorter in children, as also when the bites are numerous. It is even stated that it may be as long as a year or more, during which time the poison seems to lie latent. When the active symptoms supervene there are, locally, discomfort about the wound, itching, heat, and peculiar unpleasant sensations. It is said also that vesicles may make their appearance in the neighborhood of the original lesion. As in animals, so in man, the disease may assume either the furious or the paralytic type. These cases are nearly all marked by mental depression and apathy, with complete loss of courage. The earlier symptoms are connected perhaps with the respiration,[104] which is infrequent, while inspiration is halting and speech is interfered with. The facial appearance is often changed to one of anxiety, even despair. The muscles of deglutition are next involved in a combination of spasm and paralysis, and the act of swallowing is interfered with, sometimes made almost impossible. Although patients can swallow their own saliva, they find it difficult to swallow any foreign substances, such as water, etc. This is not due to the fear of water, as the term “hydrophobia” would imply—this being an absolute misnomer—but is due to reflex spasm excited by the attempt. It is accompanied by more or less sense of suffocation and palpitation of the heart. Indeed, a paroxysm of this kind may be precipitated by the attempt to swallow, so that the patient instinctively refuses water or any other fluid. Reflex excitability is also very great, and a breath of air or a trifling disturbance may precipitate a paroxysm, almost as in extreme cases of tetanus. As the case progresses the saliva becomes more tenacious and viscid, faucial irritation more marked, and the attempts to expel the secretion, along with the disturbed respiratory efforts, have given rise to the foolish lay notion that these patients bark like dogs. The paroxysms, as the case progresses, become more marked, the patient more restless, until, later, furious mania or muttering delirium is present, to be followed by prostration and paralytic phenomena, muscle tremor, etc., and death.
The paralytic form in man, as in dogs, is marked by the much earlier paretic phenomena, anesthesia, and, finally, respiratory paralysis which terminates the case. Curtis and others have insisted that the hydrophobic paroxysms are not convulsions in the ordinary sense of the term, but are due to temporary inhibitions of the most important respiratory and cardiac centres as the result of peripheral impressions. He likens them to the shock of a shower bath.
—Postmortem changes are indistinct and only suggestive. They consist for the greater part of a sort of vacuolous degeneration of the ganglion cells of the nerve centres—most prominently in the medulla, next in the hemispheres, and then in the spinal cord. There is hyperemia, with minute ecchymoses, with infiltration of the adventitia of the vessels and perivascular extravasation. The changes met with in the other viscera bear no constant relation to symptoms. Nevertheless, Gowers holds that because of the location of the lesions and their intensity in the neighborhood of certain nerve nuclei we have here a distinguishing anatomical character of the disease.
The toxin (as we may call it for the lack of a better term) seems to be transmitted much as is that of tetanus (q. v.), along the afferent nerves to the cells of the anterior horns of the cord.
—As between hydrophobia and tetanus diagnosis is not difficult, as already described. In certain hysterical individuals nervous paroxysms, largely due to fright, may be precipitated by dog-bites and other incidents or accidents. In these cases there is rarely such a period of incubation, and in a true hysterical case there will be no such mimicry of this awful disease. A condition known as lyssophobia (fear of hydrophobia) has been described. It is seen in hysterical subjects. It is said to have even been fatal, but this must have been from other complications.
—There is no authenticated case on record of recovery after medication by drugs. It is probable that recovery has never followed anything but the modern inoculation treatment.
The only successful treatment for this disease has been elaborated as the result of the labors of that indefatigable French savant, Pasteur, and is among the glorious triumphs of laboratory research, against which it is so often charged that it is not practical in its results. It is in some respects a curious commentary on the study of infectious disease that we can secure and work with the peculiar virus of hydrophobia, and at the same time be utterly unacquainted with its true character. To this fact is due the modern cure. It is based upon the fact that the virus is not only in the saliva, but also in the nervous system of animals suffering from this disease, and that its effects are intensified and hastened by inoculation directly into the cerebral substance. Accordingly, when a diagnosis of hydrophobia can be reasonably well established, no time should be lost in sending the patient to one of the “Pasteur Institutes,” to be found now in most of the great centres, there to undergo a regular course of treatment. It was reported that in the Institute in Paris, between the years 1886 to 1894, there were treated a total of 13,817 cases, and that the mortality was 0.05 per cent. Of course but a small proportion of these really had or would have developed the disease.
[105]
Virus obtained from the brain or cord and inoculated into the dura of another animal quickly precipitates the disease. It is, moreover, modified in virulence as it passes through successive animals of certain species—for example, monkeys. It is increased by passage through rabbits, and the period of incubation thereby shortened. The weakest virus can by proper handling and manipulation in this way be so intensified as to produce disease within seven days after inoculation. Desiccation reduces the virulence, and preparations from the cord of an infected animal may be attenuated to almost any desired extent by drying. By inoculating a dog or a rabbit with virus prepared from this weakened source, and daily making injections from stronger and stronger preparations, it is in the course of a couple of weeks rendered practically immune to the disease. Animals thus made immune are trephined and the virus injected beneath the dura, by which more certain results are obtained. The treatment consists in using a section of a rabbit’s spinal cord, 0.5 Cm. in length, rubbed up in 6 Cc. of sterile salt solution. Half of this amount is injected each day into the flank of the patient. The cord first used is one that is thirteen or fourteen days old, which has been kept suspended in a sterile flask, over caustic potash, in order to assist in its desiccation. The next day a cord one day younger is used, and so on until by the twelfth day of treatment the cord is one only two days old, and at the end of two weeks a fresh cord can be used which would convey the disease had it been used first. If this course of treatment can be carried through before the first symptoms of the disease appear, the antidote has gained complete mastery over the infecting agent and the patient is saved.
Glanders as it is known in man is a specific infectious disease, transmitted usually from the horse, characterized by rapid formation of specific granulomas, particularly in the skin and mucous membranes, which quickly break down into ulcers, and by the general toxemia characteristic of any acute infection. In German it is known as Rotz, in French as morve, while its old Latin name was “malleus” (hence we speak of the bacillus mallei). It was also known in former days as equinia. In horses the disease has also been known as farcy, because of the peculiar subcutaneous nodules which farriers and hostlers, almost from time immemorial, have called “farcy buds.” The disease, while capable of transmission from man to man, is generally produced by contagion from some of the domestic animals, most commonly the horse, although sheep and goats are known to occasionally have it, and dogs are susceptible, though seldom showing manifestations of it.
Like some of the other infectious diseases glanders appears to be variable in its manifestations. While infection occurs probably through some superficial abrasion, it is almost certain that it may also occur through the unbroken mucous membrane of the respiratory organs. It is said to be also capable of transmission from mother to fetus in utero. So far as known in man, infection occurs practically invariably through some slight abrasion, either of the skin or the mucous membrane of the nose, the eye, or the mouth. The discharges from the nostrils of affected animals are extremely virulent, and infection comes usually from this source. It is said to have been communicated from one patient to another by eating from the same dish or by drinking from a pail used by a diseased horse.
Glanders is due to the specific bacillus known as the bacillus mallei. It is shorter and plumper than the tubercle bacillus, in length about one-third the diameter of a red corpuscle. It is a non-motile organism, occasionally spore-bearing, not very resistant, belonging to the facultative anaërobic forms, growing best at blood temperature, taking stains easily, and losing them in the same way.
—Glanders is seen usually in workers and hangers-on in stables. The acute—the common—form has a period of incubation of from three to seven or eight days, after which both local and general symptoms supervene. About the infected region a form of cellulitis appears, assuming often a more or less phlegmonous type, with implication of the adjacent lymphatic nodes and evidences of periphlebitis and perilymphangitis. Over the affected area vesicles appear, which become hemorrhagic and later suppurate. A wound which has healed may reopen. Almost always there are accompanying constitutional disturbances of septic type, occasionally chills, pyrexia, etc. It is rather characteristic of glanders to have severe pain in the muscles and extremities,[106] with epistaxis and formation of metastatic tumors and edematous swellings in various parts of the body. Frequently, later in the disease, appears a somewhat distinctive eruption, papular in character, merging into pustular. Hemorrhagic bullæ are also often seen. Pustulation and edema of the face change its appearance. There are also edema of the eyelids and mucopurulent discharge from the conjunctivæ and the nose. This latter discharge is often ozenous in character. Upon inspection of the nasopharynx and oropharynx a similar condition will be noted. In connection with these local signs more or less general furunculosis also will be observed. Obviously, as these local conditions intensify and multiply, septic disturbance will be increased, and the patient dying of acute glanders dies generally of septicemia or intoxication and exhaustion combined.
A chronic form is known, distinguished mainly by slowness or tardiness of lesions, though the local changes are not particularly different in character. There is perhaps more tendency to suppuration and less to lymphatic complications. The nodule which breaks down will leave a foul ulcer, the discharge from these lesions being extremely infectious.
—This is not always easy, but may be based in suspicious cases to some extent upon the occupation of the patient. The presence of multiple lymphatic lesions and subcutaneous nodes, especially when breaking down as above described, and accompanied by ozenous discharge from the nose, should at least be suggestive, and will serve to distinguish between this disease and, for instance, typhoid fever. The chronic type of glanders might be mistaken for syphilis, and here is where the real difficulty of diagnosis will probably occur. In doubtful cases the crucial tests are the microscopic examination of discharges, after staining for bacilli, and the cultivation test.
—A generalized attack of glanders is a matter of gravest import, especially when acute. Scarcely more than 10 or 15 per cent. of such cases recover. In the more chronic manifestations the prognosis is more favorable, half of the patients making a final recovery.
—All infected animals should be isolated and destroyed, their carcasses being burned. If possible, the infected wound or abrasion should be induced to bleed freely, and then cauterized with an active caustic. By prompt interference with the first manifestations it may be possible to cut short the disease. This would necessarily be done by excision, cauterization, packing, etc. Bayard Holmes has reported a case in which, during two and a half years of chronic manifestations of this disease, he anesthetized the patient twenty times for the purpose of opening new foci or scraping out old ones, finally obtaining a permanent cure. There is no specific treatment, but the septic symptoms should be combated as indicated in the chapter on Septicemia.
By making a glycerin extract from the filtered and evaporated culture of the glanders bacillus it is possible to prepare a toxalbumin analogous to tuberculin, which reacts in a similar way. By it animals may be fortified against inoculation, and by its use a peculiar reaction is produced in those affected by the disease. It is known as mallein, and by it are tested all horses used for the preparation of the diphtheria antitoxin, in order that all possibility of glanders may be eliminated. It is probable that it might be made of therapeutic value in treating the disease when actively present in man.
Anthrax is more commonly known as splenic fever, malignant pustule, or woolsorters’ disease; in Germany as Milzbrand, and in France as charbon. It is an infectious disease of cattle, which has devastated many parts of Central Europe, and has been frequently met with on the Continent among men, though but rarely in the United States. All the domestic and nearly all the experimental animals are subject to it. Gronin has stated that in the district of Novgorod, in Russia, during four years more than 56,000 cattle and 528 men perished from anthrax. Poultry and dogs are not strictly immune, but possess a low susceptibility to the disease. It generally prevails in low districts and in marshy grounds.
The disease is the result of the invasion of the bacillus anthracis, which is a relatively large-sized bacillus, varying in breadth from 1 to 1¹⁄₂ and in length from 5 to 20 microns. It is easily cultivated outside the body, and multiplies with great rapidity in the bodies of susceptible animals; it is the type of spore-bearing bacilli, and is so readily recognized and worked with that it is commonly used in laboratory investigations. The demonstration of its specificity we owe to Davaine, in 1873, although he had described it in 1850.
PLATE IV
FIG. 1
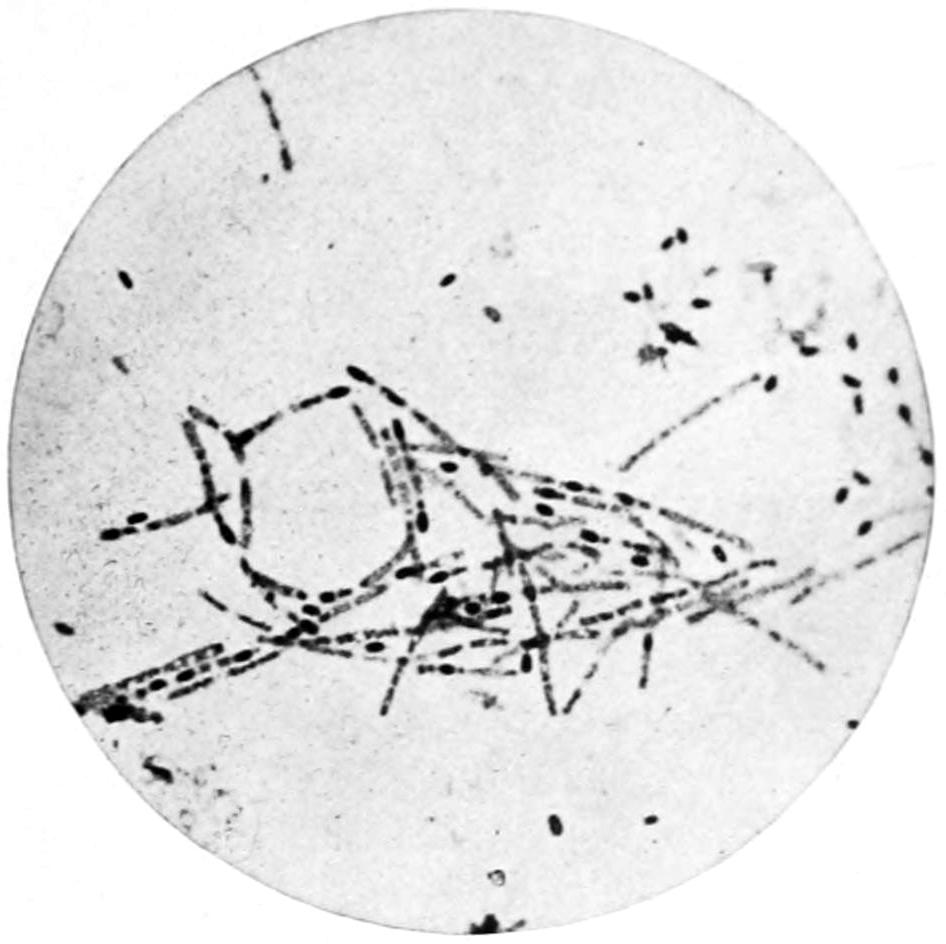
Anthrax Bacilli. Spore Formation. (Karg and Schmorl.)
From an agar culture twenty-four hours old. About the margin of the photograph are a number of free spores, × 600.
FIG. 2
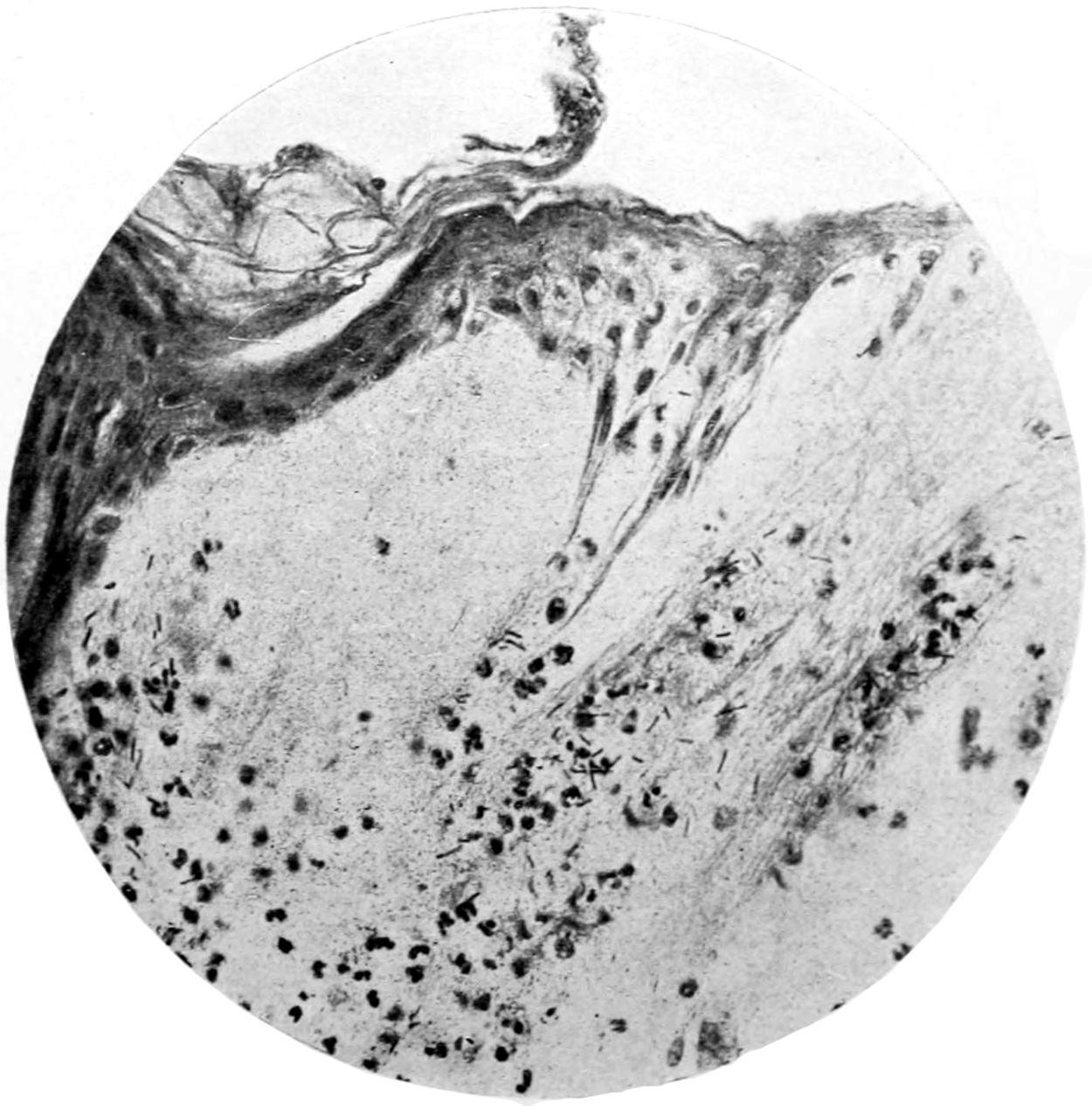
Anthrax Pustule. Removed from Arm of Man. (Karg and Schmorl.)
Marked edema of the skin, causing elevation and separation of the papillæ. In the edematous exudate a large number of anthrax bacilli and leukocytes. × 50.
[107]
Anthrax bacilli may enter the body through the respiratory organs, through any abraded surface, and possibly even through the alimentary canal. They may also pass through the placenta and affect the fetus in utero. They are too large to pass through the walls of the capillaries of ordinary size; consequently they plug them and produce a mechanical stasis which is rapidly followed by gangrene. From the kidney structures and capillaries, however, they may escape, as bacilli are found in the urine in certain cases of anthrax. (See Plate IV.)
In man the disease occurs usually as the so-called malignant pustule, or woolsorters’ disease, the latter name being given because of the liability of those individuals who come in contact with the carcasses and hides of diseased animals or their immediate products. The period of incubation is brief—on the average two or three days. The first lesion appears usually on the face, hands, or arms, and is characterized by local discomfort with formation of a small papule, which rapidly becomes a vesicle with an areola of cellulitis about it. This is rapidly followed by induration and infiltration, and these by local gangrene, the result being the separation of a core-like mass, similar to that of carbuncle. The affected area is usually discolored, often quite black. The process is not usually accompanied by suppuration, nor is there the pain of true carbuncle. The lesions tend to spread peripherally, but there is more or less vesication of the surrounding skin. On account of the local ischemia there will always be edema of the affected region, and sometimes the swelling and local disturbance become extreme. These peculiar lesions have given rise to the common name malignant pustule, which is well deserved. At last a line of demarcation becomes manifest, and if the disease progresses favorably the included area is sloughed out, leaving a surface which it is hoped will soon become covered with reasonably healthy granulations.
Absence of pain, and usually of pus, are significant features of anthrax. Should mixed infection occur, however, we are likely to see pus formation. When the disease partakes less of the characteristics of malignant pustule and more of a general infection, the local symptoms may not predominate, but, on the contrary, septic indications may become serious and even fatal. The evidence of more or less toxemia is usually at hand, however, and the toxin of anthrax is almost as destructive of muscle cell integrity as is that of diphtheria.
The local lesions may be single or multiple, but will be met with almost always upon exposed areas of the body.
—These will depend upon the clinical course of the disease. In the sloughing tissues the bacilli are very numerous, while around the margin more than one bacterial form will probably be met—i. e., mixed infection. Should saprophytic organisms complicate the case, they may have replaced the anthrax bacilli by the time the examination is made. The latter abound, however, in the blood, and may usually be found occluding the capillaries of the liver, spleen, kidney, etc. In intestinal infection, particularly in animals, the mesenteric nodes are involved. Inasmuch as septic features accompany all fatal cases, putrefaction will be found to begin early, and the changes in the blood and the gross changes in the other organs will resemble sepsis rather than anthrax.
—Prognosis for man is not usually unfavorable, the majority of cases recovering with more or less local destruction of tissue. Should, however, infection become generalized, the case will probably terminate fatally. Cases assuming the type of splenic fever are of much more serious character, and their prognosis graver.
—This should be both local and constitutional. The former should consist of the most radical possible attack and include complete excision of the infected area, with the use of active caustics or the actual cautery. In fact, the latter instrument offers a most valuable means for combating the destructive tendency of the disease. Sloughing and separation of the cauterized mass may be hastened by warm antiseptic poultices. Subcutaneous injections of 5 per cent. carbolic solution have been given, with apparent benefit, in a number of cases, but should only be relied upon in the treatment of the milder manifestations.
Benefit will accrue from the use of the ichthyol-mercurial ointment whose formula was given under treatment of Erysipelas. It has been suggested to treat these cases by[108] the employment of the bacillus pyocyaneus, since it is known that this organism when injected with the anthrax bacillus materially attenuates its effect.
—Prophylaxis is most important. The bodies of all infected animals should be burned, not buried, since the resistant bacilli are often brought to the surface of the soil by earth-worms. Every discoverable source or medium of infection should be destroyed or sterilized.
This disease has been recognized for some time, mainly by French and Continental clinicians, and under such names as gangrène foudroyante, gangrène gazeuse, gangrenous septicemia, and gangrenous emphysema. The name malignant edema was given by Koch, who identified the infecting organism. It is one of the most dangerous forms of gangrenous inflammation, and occurs sometimes after serious injuries, and, again, after most trifling lesions, such as those inflicted by the dirty pointed implements of the gardener, etc., or even the stings of insects. Two cases are on record where the disease followed a puncture of the hypodermic needle for the administration of morphine. In one of these the organism was found in the solution; in the other it probably had been deposited upon the skin.
Malignant edema is essentially a specific form of gangrene (see Chapter V), and is mentioned here rather because of its specific character. It is characterized by rapidity of spread and the specific nature of the exudate, as well as by the speedy destruction of the tissue involved, and by more or less gas formation. It is not the same as the gaseous phlegmons described by some German surgeons, yet partakes of their general character. Gas phlegmons have been rarely noted, their peculiarity being formation not only of pus, but of more or less offensive gases, which escape when the phlegmon is incised. The gases are mainly due to the presence of bacillus aërogenes capsulatus, and gas phlegmons, as such, are to be regarded as instances of mixed or rarely pure infection.
Malignant edema is known by the brownish discoloration of the overlying skin, which is streaked with blue where the overfilled veins show through it, while the underlying tissues are sodden with fluid and more or less inflated by the gaseous products of decomposition, so that the finger detects a firm crepitus, as is common in subcutaneous emphysema. From the wound, if there is one, flows a thin, foul-smelling secretion, which may also be expressed from the deeper layers. That the neighboring lymph spaces and nodes are actively involved is evident from the enormous swelling of the latter, as well as from the general condition of the patient. The rapid elevation of temperature with but trifling remissions remains constant until shortly before death. The tongue early becomes dry and cleaves to the palate, its surface being covered with a thick, foul fur. Patients early become apathetic, complaining only of pain and burning thirst. Delirium and coma usually precede death, which may occur in fifteen to thirty hours. After death the cadaver bloats quickly and putrefaction goes on with amazing rapidity.
—At the seat of the lesion even muscles and tendons will be found macerated, bone denuded and surrounded by a putrid fluid, the entire region presenting a notable swelling and infiltration of soft parts with reddish fluids and stinking gases. The overlying skin will be stretched, and superficial blisters may deepen the intensity of the process. The veins are clogged with decomposed blood and broken-down thrombi, and in the heart and large vessels will be found putrid liquid as well as gas, to whose presence early and sudden death is probably due.
—This is unsatisfactory, especially when the bacillus of malignant edema is alone at fault. Patients may escape with their lives, but always at the expense of more or less tissue destruction.
—This should consist of extensive incision to permit escape of fluids and gases and relieve tension; of such antiseptic applications as can be made available; of immersion of the affected part in a hot antiseptic bath; and of such vigorous stimulation by the most powerful measures—strychnine, alcohol, etc.—in order to support the patient through the period of profound depression characteristic of the disease.
PLATE V
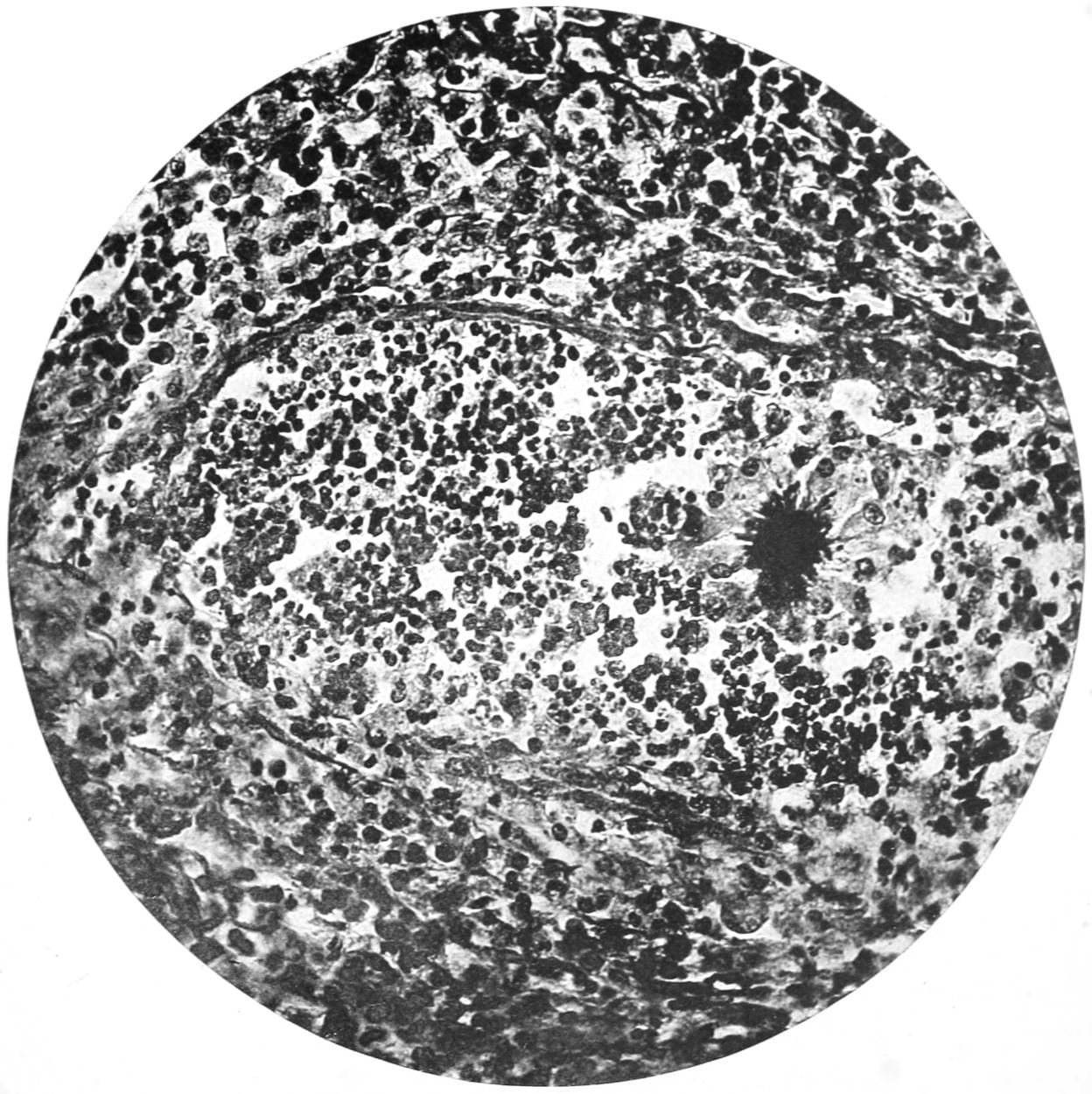
Actinomycosis. Ray Fungus in Man. (Gaylord.)
[109]
This also is a subacute but always destructive infection by a specific microörganism, though not a bacterium. Known always as actinomycosis in man, the disease, which is most common in cattle, is called lumpy jaw or swelled head, and years ago was usually regarded as cancer or as a malignant affection.
Many museum specimens labelled as cancer of the tongue, jaw, etc., have been shown to be instances of actinomycosis of these parts. It is occasionally met with in man, so that there are at least four hundred cases on record in this country and in Europe. The organism was recognized a half-century ago by Langenbeck and Lebert, but was not scientifically described until many years later. The names of Bollinger, Israel, and Ponfick will always be connected with these researches.
The organism belongs among the ray fungi, is known as the actinomycis, and occupies an uncertain place in classification. It is large enough, when entire, to be perceived by the naked eye, has ordinarily a yellowish tint, a tallowy consistence, and may be seen under the microscope to consist of a cluster of branching prolongations, club-shaped at the end, radiating from a common centre. They give it a sunflower appearance. It is stained with difficulty, the best stain being a combination of picrocarmine and an aniline dye. In tissue sections the Gram stain is the best. It is cultivated with difficulty, but can be grown upon solid media and may be inoculated. (See Plate V.)
As met with in tissue or in pus these fungi constitute small granulations, giving usually a gritty sensation to the finger, which is due to the presence of calcium salts. The recognition of this calcareous material is of importance, since it may enable a diagnosis to be made offhand, in a case which otherwise might puzzle one.
The disease is very common among cattle in certain regions, and causes the condemnation of many animals in every large stockyard establishment where inspection is careful and scientific. It occurs oftener in young than in old animals, and most frequently in those which come from valley regions and marshes. In animals infection occurs almost invariably through the mouth, which is easily explained by the fact that, in grazing, the lips, tongue, and gums are likely to be irritated and infected at any time from soil containing these fungi along with growing grain. The path of infection is usually by the mouth, while accident seems to determine whether the infection shall manifest itself mainly in the intestinal canal or the respiratory tract. In animals there is less tendency to suppuration than in man, the infection in man being usually a mixed one. The name lumpy jaw, so generally given to the affection, is indicative of the most conspicuous lesion in cattle, for the organism, having once invaded the gum, for instance, passes quickly to the bone, or, having involved the tongue, is not slow to infect the lymphatics of that region. In consequence we have tumors, often of inordinate size, which may involve the bones or the soft parts and cause great disfigurement, along with necrosis, leading eventually to the death of the animal. These tumors are essentially granulation tumors due to the presence of a specific irritant—the actinomycis—which acts here as do the tubercle bacillus, the lepra bacillus, etc., in other infectious granulomata.
In man the disease is generally accompanied by abscess formation, the pus containing the distinctive yellow gritty particles which are found in no other disease. The strong resemblance between the lymphoid cells of this form of granuloma and the embryonal cells of sarcoma has permitted the perpetuation of confusion between these two neoplasms.
Fig. 19
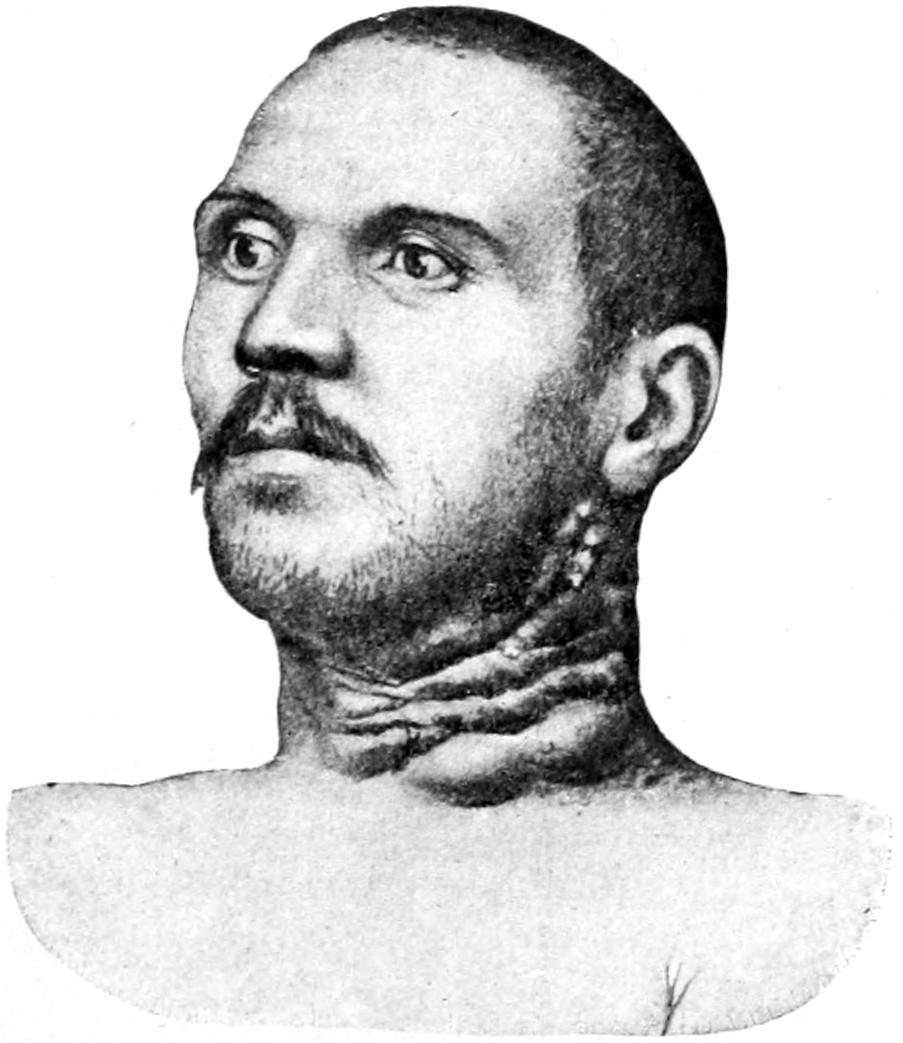
Actinomycosis in man. (Lexer.)
Large abscesses form as the result of the coalescence of small ones, and by the time the disease is recognized extensive destruction and loss of substance may have taken place. In man it is not alone about the mouth that the disease is noted, although primary lesion here is by no means infrequent. It leads to affections similar to that already spoken of in cattle, with a progressive infiltration and breaking down, including actual necrosis of bone, etc. The pus will escape at various points, and may give to the surface an appearance as of many craters with a central cause. When the disease has involved the lung, either directly or indirectly, the fungi and the calcareous particles may be found in the sputum. Should there be suspicion of this involvement, the sputum should always be examined. Even in the heart substance tumors of this same character have been found. The first case noted in man had undergone extensive vertebral caries. Intestinal infection is possible, in which case multiple lesions will form in the intestinal walls, which may contract adhesions to the abdominal parietes and discharge externally[110] through them. The appendix has been found involved in such lesions. Infection of the skin has also been described, though this occurs more rarely.
—Actinomycotic lesions have been mistaken for cancer, sarcoma, tuberculosis, syphilis, etc. In man it will always be characterized by more or less suppuration, and in the purulent discharge from the infected focus the yellow calcareous particles should enable recognition of this disease at once.
—As long as the focus is accessible it is a purely local matter, and prognosis is as favorable as in local tuberculosis; but, inasmuch as in many cases infection has proceeded to a point where the surgeon cannot safely follow it, prognosis must be guarded. Actinomycosis is free from acute manifestations, for the main part free from pain, pursues a chronic course, and is characterized, as are the other slow infections, by progressive emaciation, prostration, etc. As it is essentially a chronic condition, time is afforded for careful study in doubtful cases, for microscopic examination, etc.
—This must consist of extirpation of all infected tissues and areas. If this can be done thoroughly there is a prospect of positive cure. Free incision, wide dissection, the use of the actual cautery, etc., are always called for in these cases. If it involves the tongue alone, there is an excellent prospect; if but a portion of the jaw is involved, a complete excision of one-half or more may be followed by excellent results. If, however, the lung, liver, vertebrae, or other vital and inaccessible parts are involved, surgical measures may afford amelioration, but can hardly be expected to cure.
Iodine, alone or in combination, has been found efficacious in the therapy of actinomycosis. In diluted solutions used locally, or as potassium iodide given internally or injected into tumors, it doubtless has a beneficial effect during the period of its administration. Recent reports and experiences show that great value attaches to the use, as suggested by Bevan, of copper sulphate in the treatment of actinomycosis, its use having been suggested by the fact that copper is used to destroy rusts (fungi) on grain. One-half grain (3 Cg.) may be given internally three times a day, while the sinuses are irrigated with a 1 per cent. solution. I have seen apparently complete cure of an aggravated case follow its use. Incidentally it may be stated that Bevan advises its use also in cases of blastomycosis.
While madura foot is not a disease from which domestic animals suffer, its general characteristics make it a proper subject for brief consideration. It is essentially a disease of the tropics and subtropics, and is often seen in some of our new possessions.
It commences as a painless swelling upon either aspect of the foot, in which hard nodules form, which later soften, ulcerate, and discharge puruloid material containing granules in which the microscope reveals mycelia of the peculiar fungus that produces the disease. In some cases these particles are black, in others colorless. The disease is of slow progress, and the lower limbs become weak, atrophied, and finally useless Death results from exhaustion or some terminal infection.
The principal lesion is the slowly growing gumma or granuloma, whose presence is unmistakable. This is due to the presence of a fungus, called by Vincent the streptothrix maduræ. Thus in its pathology the disease much resembles actinomycosis. The habitually bare feet of most of the inhabitants of the tropics and the habitat of the fungus explain the site of the primary lesion.
—The only treatment is extirpation of the growth—i. e., amputation.
PLATE VI
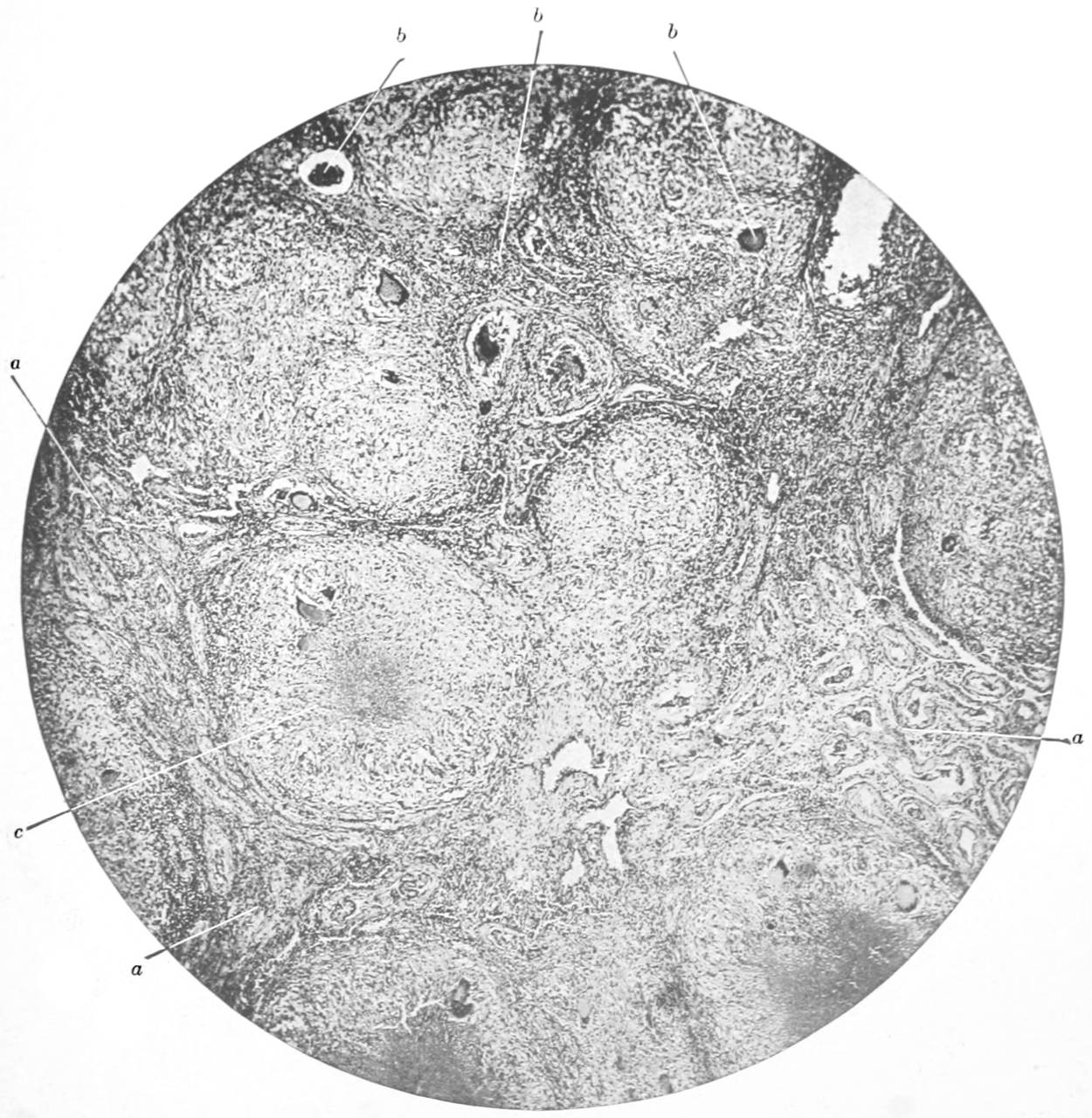
Tuberculosis of Testicle.
Miliary Tubercle with Caseation and Giant Cells. (Gaylord and Aschoff.)
a, seminal tubules; b, giant cells; c, caseated tubercles.
[111]
The most important and frequent of the infectious diseases common to animals and man is tuberculosis. This appears usually as a subacute or chronic affection, although in a small proportion of cases it assumes an acuteness of type which may make it fatal within as short a time as fourteen or fifteen days, or even less, from the first recognizable symptom. Tuberculosis is more prevalent than any other form of disease, and is the cause of death of a proportion variously estimated at from 20 to 30 per cent. of mankind. It is a disease which perhaps concerns the surgeon more than the physician, inasmuch as it is also the most common of the so-called surgical diseases. Its frequency varies in different parts of the country. In the average surgical clinic of the United States probably 20 to 25 per cent. of cases are manifestations of this affection.
Surgical tuberculosis covers the entire range of diseases formerly described as scrofula. The term scrofula is now expurgated from medical terminology. All of the active manifestations formerly regarded as scrofulous are known to be due to tuberculosis.
To the presence of tubercle bacilli in the tissues is due that distinctive aggregation of cells which constitutes the so-called miliary tubercle. Its presence and arrangement are apparently the direct outcome of the irritation produced by these minute foreign bodies, and its method of grouping is so characteristic that it may be everywhere and usually easily recognized. Its centre is composed of one, possibly several, giant cells, whose nuclei are generally arranged around its margin, with perhaps degenerative changes going on in the interior of the cell itself. In this giant cell, as well as outside of it, may be seen one or several tubercle bacilli. Around this centre are clustered a number of large cells known as epithelioid, which may also contain bacilli. These cells are probably derived from epithelium when at hand, or from the endothelium of the vessel walls, or from the fixed tissue cells. Outside of these are other, usually spindle-shaped, cells, contained in a connective-tissue network and regarded mostly as lymphoid cells. When tubercle is experimentally produced the bacilli seem more numerous than they do in instances of spontaneous disease. This little aggregation of cells constitutes a mass which may be recognized by the naked eye—a minute, usually white point or nodule, which is known as a miliary tubercle. It is subject to any one of several changes to be presently considered, and it is usually found in large numbers. The punctate appearance of miliary tuberculosis is perhaps best seen upon the cerebral membranes or the peritoneum in cases of acute miliary tuberculosis. By coalescence of a number of these nodules larger tubercles are formed, and by combination of coalescence and caseous degeneration are produced the large cheesy masses which were formerly called yellow tubercle. (See Plate VI.)
The epithelioid cells are by some regarded as modified leukocytes; by others as the product of division of the fixed cells. The giant cell is probably the result of irritation in one of these cells, the stimulus being sufficient to provoke division of the nucleus, but not of the entire cell. As the principal cellular activity occurs in the interior of this nodule the result is a condensation about the periphery which furnishes eventually a sort of capsule, the tissues being hardened and condensed as if for this special purpose. The effect of this is to interfere with vascular supply and finally to shut it off completely. As long as no pyogenic infection occurs, the original tubercle may gradually shrivel down and disappear or caseous degeneration may occur, and it may persist as a cheesy nodule for an indefinite time. As such a tubercle grows old the cells lose their identity, refuse to take stains, and a slow or quiet coagulation necrosis results. In this nest sometimes[112] calcium salts are precipitated, the result being a calcareous nodule. On the other hand, during the active stage of this tubercle formation cell resistance may be lowered, either from general or constitutional causes; the original focus disintegrates; tubercle bacilli are liberated, and are now carried hither and thither, metastatic tubercles being the result of their dissemination.
Spontaneous healing of tubercle is possible, and may be due to three different causes:
Looked at from another point of view, the possible fates awaiting the miliary tubercle are the following:
—Absorption of tubercle undoubtedly is possible under favorable circumstances, but just what constitute these favoring circumstances no one knows, since they occur in cases which do not terminate fatally. To be able to describe them would be to detail minutely the changes which permit of recovery after non-traumatic tuberculous infection, which clinical fact is amply demonstrated by the experience of the profession. Absorption is probably largely a matter of phagocytosis.
—Encapsulation has already been spoken of, the capsule being formed by the condensation of the original cells of the tuberculous agglomeration, the infectious organisms being thereby imprisoned as long that they are practically starved and finally die. The tubercle bacilli, however, may long lie latent in such a cellular prison, and should anything occur to break the prison wall they may escape and still prove actively infectious. In this way are to be accounted for the fresh eruptions from old miliary or other deposits.
—Caseation comprises a series of changes in the chemical constitution of the cells by which an albuminoid mass much resembling casein in composition and appearance is produced. The English equivalent cheesy well describes many of these masses, which both cut and appear very much like domestic cheese. They have a yellowish color, and are met with in masses in size from a pin’s head up to a robin’s egg. These are the yellow tubercles of the older writers, and such a cheesy tumor has been called tyroma.
—Calcification refers to a peculiar deposition of calcium salts within the interior of these nodules, the first precipitation occurring usually in the centre of the giant cell, which is itself the topographical centre of the miliary tubercle. It may spread from this until a mass easily recognizable by the naked eye and detectable by the finger is produced. Such calcareous particles are frequently found in sputa, and are always an index of the tuberculous character of the case. They differ markedly from the yellow calcareous nodules found in the pus of actinomycosis, the circumstances under which they are likely to be confused being met in pulmonary disease.
Suppuration, as indicated, is the result of a mixed or secondary infection with pyogenic organisms. In the previous chapter tubercle bacilli were grouped as among the facultative pyogenic bacteria, yet pus is not formed in this disease except in consequence of coincident activity of other bacterial organisms. Suppuration of tuberculous foci is of importance to the surgeon, because thereby is produced a distinct class of so-called abscesses—namely, the cold or congestion abscesses. These are of the chronic type, and are generally free from the ordinary signs of abscess formation. They are invariably the result of local infection, sometimes perhaps by the tubercle bacilli alone, but frequently by the combined action of these with pyogenic forms. For their formation a previous tuberculous lesion is essential. Wherever old tuberculous lesions are encountered cold abscesses also may form. No tissue or organ is exempt: they are found in the brain, in the bones, viscera, joints, skin—in fact, in all parts of the body.
[113]
Cold abscesses have not only a significance of their own, but for the most part an identity. Their distinguishing feature is a limiting membrane, which forms whenever sufficient time has elapsed. Much has been written about it, and much error has been perpetuated with regard to it. This is the membrane formerly considered and called pyogenic, under the misapprehension that by it the pus or contents of the abscess were produced. I desire to emphasize in every possible way that this is a mistake. This membrane does not act to produce pus, but is rather the result of condensation of cells around the margin of the tuberculous lesion, forming, as it were, a sanitary cordon, for the absolute and definite purpose of protection against further ravages. I would suggest that the term pyogenic membrane be abolished, there being no such membrane under any circumstances, and that, this be known as that which in effect it is—namely, a pyophylactic membrane. It is a protection against pus, and were it not for its presence there would be no limit to the spread of tuberculous invasion. A lesion thus surrounded is shut off from most possibilities of harm, rarely encroaches, except by the most gradual processes, and, on the contrary, often contracts and reduces its dimensions, the watery portion of its contents being gradually absorbed and the more solid and cellular portions becoming condensed into matter which undergoes caseous degeneration, so that eventually recovery may ensue as the consequence of a metamorphosis of an original cold abscess into a caseous nodule surrounded by the old pyophylactic membrane, which is now serving as a capsule.
The contents of the cold abscess are, in some instances at least, of acute origin, and consequently may have been originally pus or its near ally. On the other hand, in cases which have occurred very slowly this material is not real pus, but is a semifluid debris having certain properties which remind one of pus. It has been my effort hitherto to devise for this material a name which should distinguish it from pus and indicate what it really is. Inasmuch as most of it has been of a puruloid character, at least at one time, I have suggested that it be called archepyon (i. e., originally pus or puruloid). As this flows from such a cold abscess, it is more or less watery and contains caseous, sometimes calcareous, nodules in masses of considerable size, and not infrequently sloughs of tissue and old shreds of white fibrous tissue which resist decomposition for a long time. This material has been thus imprisoned, sometimes for months or even years, and consequently has lost most of its resemblance to what it was originally. The organisms which first produced it have long since died, and it is practically sterile. If any organisms survive, they are the tubercle bacilli, which are more resistant and tenacious of life than the ordinary pyogenic organisms. This is why most culture experiments fail, and why even inoculation with the contents of an old cold abscess is often without effect even on most susceptible animals. Nevertheless the bacilli which the semifluid contents do not contain may yet linger in the meshes of the pyophylactic membrane; and here lurks the greatest danger in dealing with these lesions.
In old cases the pyophylactic membrane is very tough and very adherent by its outer surface. It can sometimes be peeled off in strips of considerable extent, at other times cannot even be separated, or sometimes is so placed as to render it impossible to follow it to its termination. There must be complete extirpation of this membrane, or at least destruction; and when its removal is impracticable, failure to remove it should be atoned for by some powerful caustic, such as zinc chloride, nitric acid, caustic pyrozone or the actual cautery, which should be made to follow it to its ultimate ramification. The membrane and the tissues underlying, when thus cauterized, will separate as sloughs, and these will be replaced by presumably healthy granulations, which should be encouraged until the original cavity is filled or the surface healed.
Acute abscesses, as indicated in the previous chapter, have no real limiting membrane, although there is more or less condensation of tissues about the focus of infection. A typical membrane is distinctive of tuberculous abscesses, and is to be regarded always as their natural protection and a barrier against their further encroachment—a membrane whose inner surface may harbor active organisms which cannot escape through its outer texture. Consequently, to simply incise it or inefficiently scrape it is to do a worse than useless thing; and one should never attack it unless he is prepared to extirpate it or destroy its integrity, and in this way dispose of it.
Cold abscesses when near the surface cause a bluish or dusky discoloration of the overlying skin, while the superficial and subcutaneous veins of this region are usually enlarged. Fluctuation is also a prominent phenomena in connection with them when[114] they can be palpated. Deep collections of this kind may be mistaken for cysts or tumors, in which case the aspirator needle may be used to facilitate diagnosis. They vary in size from the smallest possible collection of fluid to abscesses which may contain a gallon or more of puruloid material or archepyon. They are known often as gravitation abscesses, because by the weight of the contained fluid they tend to elongate or spread themselves in the direction in which gravity would naturally carry a collection of fluid. Thus cold abscesses originating from tuberculous disease of the lower spine frequently work their way along the psoas muscle and present below Poupart’s ligament as psoas abscesses, or elsewhere about the thigh, while those which come from similar disease of the uppermost cervical vertebrae may present behind the pharynx, as the so-called retropharyngeal abscesses, and those from the dorsal spine present not infrequently as lumbar abscesses. These are but two or three familiar examples of what may occur in any part of the body.
—Aside from the treatment of cold abscesses, already indicated by radical measures, other means have been suggested, and particularly for the treatment of those in which such extreme measures are impracticable or impossible. It is sometimes efficacious to simply tap or remove by aspiration the contents of such a cavity. It may never refill, or but slowly, and after repeated tapping alone a very small percentage of such cases will subside into inactivity and the lesion be subdued, if not absolutely cured. Treatment by injection of emulsions of iodoform has found favor with many surgeons. I have never been able to secure the good results reported by others, and consequently have abandoned it; yet it deserves mention here because of the repute it has enjoyed.
This is based upon the alleged specific properties of iodoform as being peculiarly fatal to tubercle bacilli, presumably by liberation of free iodine. A cavity to be thus treated should be first emptied as completely as possible, after which may be thrown into it a glycerin emulsion or an ethereal solution, or a suspension in sterilized oil of 5 to 10 per cent. of iodoform. From 25 to 200 Cc. of some such preparation is introduced, while the walls of the abscess are more or less manipulated in the endeavor to completely disseminate the mixture. The cannula through which it has been introduced is then withdrawn; and this can usually be done with but little unpleasant iodoform effect. This is due to the pyophylactic membrane, which limits the activity of the drug as it has done that of the previous contents of the abscess. Such cavities have also been treated by washing out through a trocar with an injection of various antiseptic or stimulating solutions, among which may be mentioned hydrogen peroxide, weak iodine solutions, etc. My own advice is to treat all tuberculous lesions radically when such measures are not contra-indicated by their multiplicity or by too great depression of the patient, and so long as lesions are accessible to ordinary operative procedures. This same advice pertains also to those which have already spontaneously evacuated themselves, or where the overlying skin is threatening to break and permit escape of contents. Almost any case where this is imminent is one in which the surgeon, as such, ought to interfere. On the other hand, in deep collections and in debilitated individuals the treatment by injection may be tried.
The best way to treat accessible tuberculous lesions is by extirpation, as this hastens convalescence and leads to more permanent results.
The other and essential characteristic of tuberculous disease is the infectious granuloma to which it gives rise. This is a term first applied by Virchow to new formations of granulation tissue which are the result of the presence of invading and specific irritants. This tissue varies little in type from that already described under Ulcers, and is common to the neoplasms which are found in tuberculosis, syphilis, leprosy, glanders, and other local infections. So little does the tissue type vary in these different instances that it is difficult to distinguish by microscopic sections of the unstained tissues, or at least those unstained for bacteria, to which class of lesions they belong.
PLATE VII
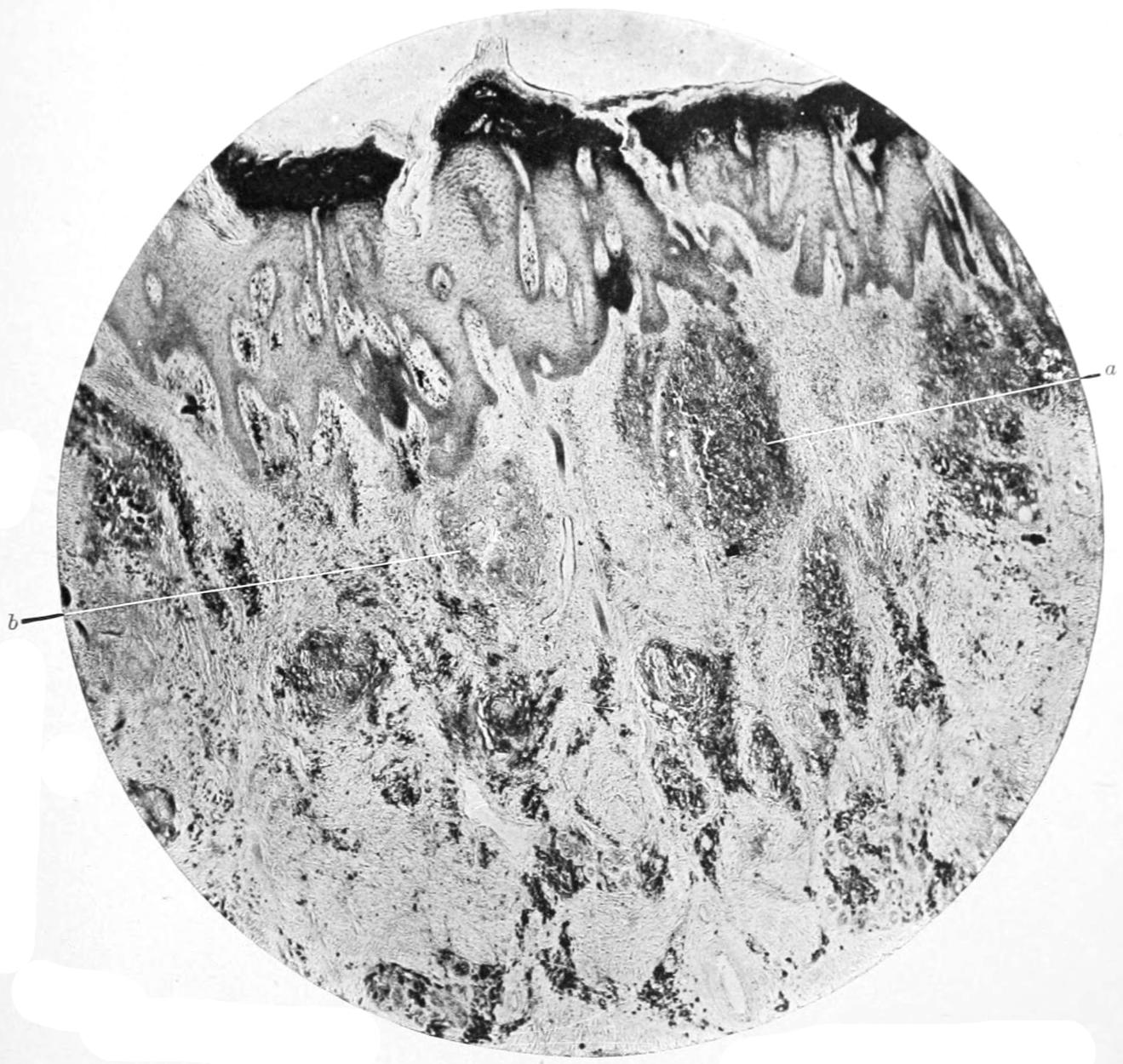
Lupus of Skin. (Gaylord.)
a, fresh tubercles containing numerous
plasma cells; b, mature tubercle with giant cells. Below
are accumulations of plasma cells about the vessels. Low power.
Unna’s polychrome methylene blue.
[115]
This tissue may be met with in any of the tissues of the body, but is less seen upon the serous membranes of the cranial and peritoneal cavities, whereas in the joint cavities it is common. It is provoked, as just stated, by the presence of tubercle, and has the power of penetration into and substitution for almost all the other tissues of the body. Thus in a primary tuberculous focus within the bone a granuloma will form and extend its limits, while the surrounding bony tissue melts away before it; and it is by the growth of this tissue in a particular direction that tuberculous products from within the bone cavity are finally carried to the surface. When this material has escaped from bone, or from tissues without the bone, toward the surface its presence is marked by induration, by livid discoloration of a limited area of skin, with elevation of the surface, which finally breaks down and shows discolored, bleeding, and pouting granulations, which in the absence of restraint now proliferate more rapidly, and often to the point where they loose their former blood supply, and consequently necrose upon the surface. This is the fungous granulation tissue, especially of the German writers, and may be met with upon the surface, or is frequently seen in opening into joint cavities and other tissues infected by tubercle. The appearances of this fungous tissue are modified somewhat by environment and pressure: in joints flat and radiating masses of it will be found, extending along the synovial surfaces and into the articular crevices. This fungous tissue may grow in any direction, but apparently advances in the direction of least resistance. It leads to complete perforations of the flat bones, like those of the skull, while tuberculous masses from the dura may cause multiple perforations, the granulation tissue finally escaping through the overlying skin. In tuberculosis of synovial sheaths and bursæ it extends along and may completely fill and even distend them. It will separate tissues which were united together, and it may lead to disintegration and disorganization of the firmest textures in the body. So long as it is not exposed to the air nor to pyogenic infection, it will preserve its characteristics for a considerable length of time. Immediately upon exposure it is likely to break down, and infection will travel speedily along it into the deeper cavity whence it has sprung. A mass of this tissue contained within the normal tissues, condensed more or less by pressure, uninfected, and not freely supplied with blood, is entitled to the name of tuberculous gumma, whose tendency, however, is too often to break down and suppurate. Such gummas may be found in any part of the body, and differ only in unessential respects from the diffuse and more or less infiltrated masses of granulation tissue which occupy serous cavities or which extend in various directions.
The lesions of surgical tuberculosis, except those already spoken of as constituting cold abscess, are so essentially connected with the presence of granulation tissue, just described, or of this form of the infectious granulomas, that no student can appreciate the subject until he is familiar with this tissue in its various phases and in various locations. Of such great importance is it that this be realized that some of the local manifestations of this new tissue must here be considered, although they may be rehearsed in other form in succeeding chapters.
In the skin and subcutaneous tissues and in and under mucous membranes this granulation tissue may be studied at places where it is free from most mechanical restraints to growth, and where, in other respects, its appearances are typical. The most characteristic manifestations in the skin occur as lupus, a disease considered cancerous or of uncertain etiology. Lupus is always a cutaneous manifestation of this protean disease. (See Plate VII.)
In its incipient stages lupus consists of multiple minute nodules of granulation tissue just beneath the surface, containing all the elements of true miliary tubercle, with infiltration of the surrounding skin, even into the subcutaneous fat. The most common location of these lesions is on exposed surfaces. Bacilli are not numerous in them, yet may be demonstrated. The tendency is more or less rapidly to break down, the result being a tuberculous ulcer, which, as it extends, manifests usually a disposition to cicatrize in the centre while enlarging around its periphery. The dermatologists describe several different forms of lupus under the names hypertrophicus, vulgaris, maculosus, etc., all of which are essentially the same in character, the differences being largely constituted by the rapidity or slowness with which the granuloma of the skin breaks down. From the surface these growths may extend and involve parts at considerable depth, even the periosteum. This name should also include the lesions described as scrofuloderma or scrofulous ulcers of the skin, they being all of the same character.
A variety known as anatomical tubercle has been described by some writers, found especially upon the hands of those who frequent dissecting-rooms or handle dead[116] bodies, and is supposed to be the result of local inoculation. It appears usually as a warty growth, which ulcerates and becomes covered with a scab—is usually indolent in character, but is followed by lymphatic involvement, and in rare instances by death from tuberculous disease.
Fig. 20
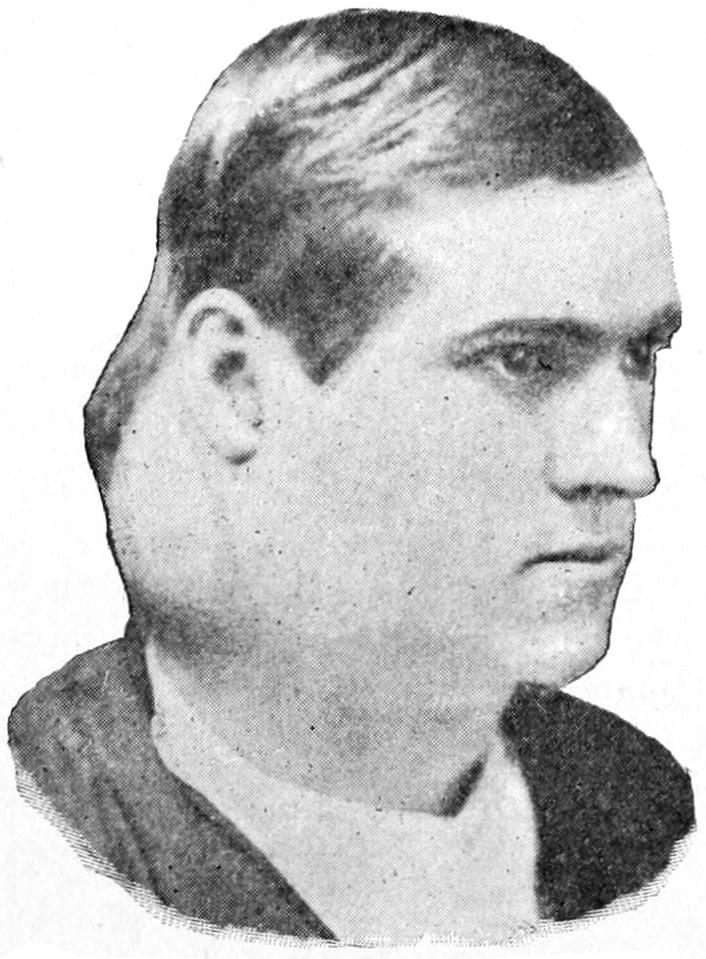
Tuberculosis of cervical lymph nodes.
In the lymphatic structures and lymph nodes tuberculosis is a most frequent affection. In these localities it may occasionally be primary, but is almost always a secondary lesion. It is in separating from the lymph stream the tubercle bacilli, which would otherwise be passed into the general circulation, that the lymph nodes, acting as filters, render us the greatest possible service. These filters themselves, however, almost always become infected, and, enlarging, they assume the appearances known to the laity as scrofula, which have been generally referred to as scrofulous glands. These lesions abound rather about the axilla and the cervical and bronchial nodes than about the lower extremities. Nevertheless, the retroperitoneal, mesenteric, and inguinal nodes are occasionally infected. In these nodes will be found giant cells surrounded with epithelioid cells, containing bacilli and undergoing cheesy degeneration or suppuration. Infection often proceeds from centre to periphery, and then to the surrounding tissues, the filter, as such, having become so choked that nothing seems to pass it. By virtue of this surrounding infiltration (which used to be known as peri-adenitis, when lymph nodes were spoken of as lymph glands) generalized infection is in some measure prevented, while the natural barriers are altered and natural distinctions between tissues are lost. This makes complete extirpation of these tuberculous foci often very difficult, while the adhesions which they contract, for instance in the neck, are often to the large vessels and nerve sheaths, by all of which their operative treatment is naturally complicated. When infection from the superficial nodes extends toward the surface it is easily recognized by the dusky hue of the overlying skin, the hardness, infiltration, and, later, the fixation, of these masses, accompanied usually by evidences of suppuration.
In and on the serous membranes we find tuberculous lesions, either primary or metastatic, usually miliary in type. In the pleural cavity they produce effusion (hydrothorax), which may necessitate repeated paracentesis, or by a mixed or secondary infection may cause empyema, for which much more radical and even extensive operations are demanded. (See Thoracoplasty.)
In the case of the peritoneum we find (a) miliary tuberculosis, (b) a slower non-exudative form with firm, sometimes pigmented nodules, and (c) a form characterized by small gummas which become caseous, coalesce, and ulcerate, binding together intestinal coils and producing extensive and irregular adhesions, with seropurulent exudation, often enclosed in walled-off sacs. In all of these cases surgical intervention should be considered, while in the more acute miliary forms abdominal section, with flushing, has in many instances afforded relief.
Tuberculous meningitis, cerebral or spinal, is in surgical cases practically always of miliary type, accompanied by the inevitable increase of fluid, and, in the cerebrospinal canal, of consequent tension. Inasmuch as the latter constitutes the most formidable feature of these cases, its possible relief by puncture may be considered. And so lumbar puncture (q. v.) may be practised, and even tapping the cerebral ventricles after making the small trephine opening has been done a few times, though not with encouraging success. (See Hydrocephalus.) Too often tuberculous meningitis is the terminal infection which ends many a case of local tuberculous disease in other parts of the body.
In general the more acute and miliary the lesions presented in tuberculous disease of serous membranes the greater the tendency to profuse watery (serous) exudate, whose volume may demand operative measures for relief.
In the bones we often find indications of tuberculous disease. It is not much more than sixty years since Nélaton called attention to the frequency of these intra-osseous[117] lesions, and demonstrated the essentially tuberculous character of much that had hitherto been overlooked or considered under that vague term scrofula. All those forms of bone disease comprehended under the names Pott’s disease, spina ventosa, tumor albus, etc., are now known to be distinctly tuberculous lesions. In many instances these follow the slight circulatory disturbances brought about by contusions sprains, etc. This is especially the case in those who are predisposed to this disease.
Fig. 21
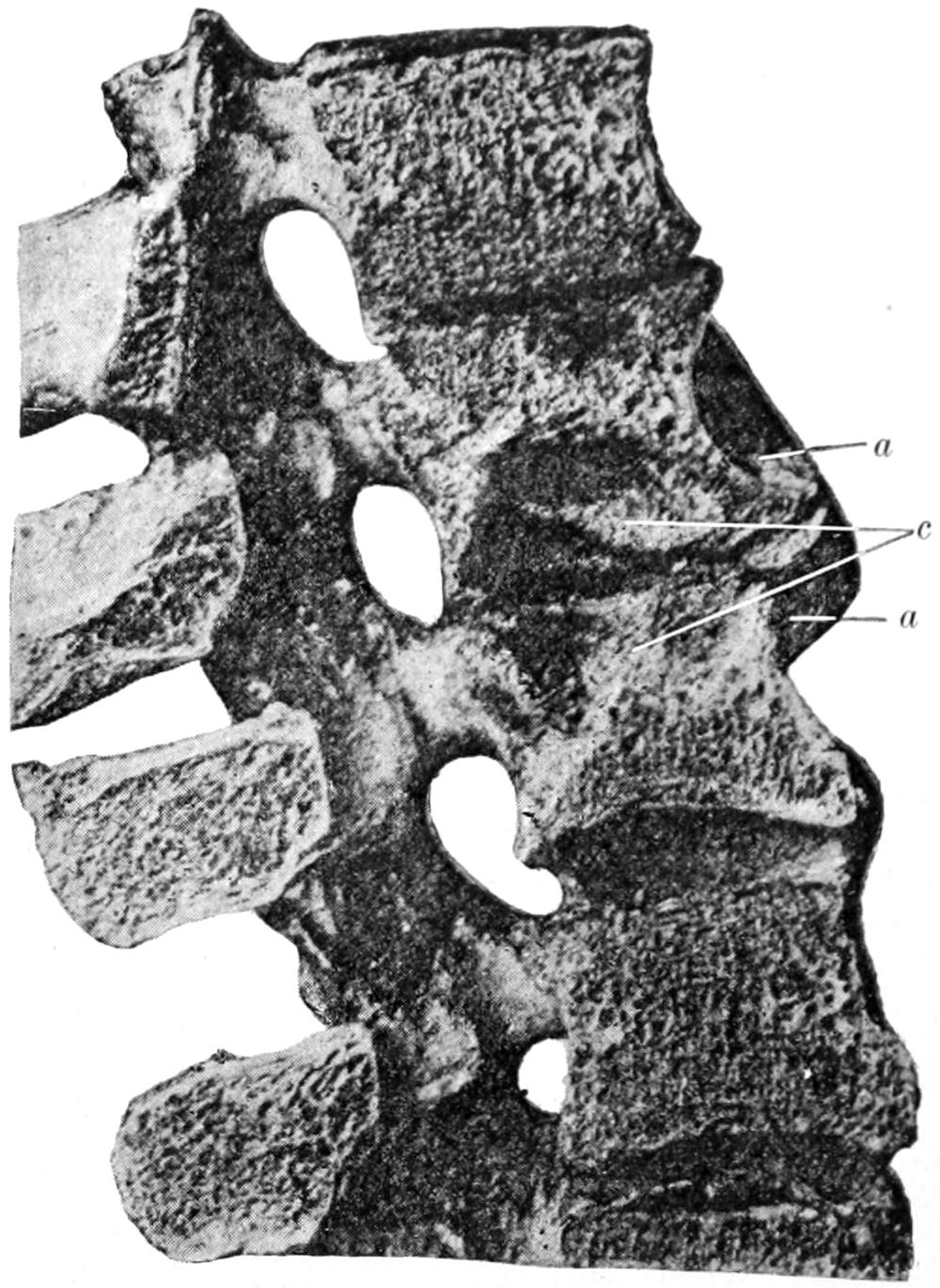
Tuberculous spondylitis (caries): a, osteogenesis and osteosclerosis; c, cavity formed by degeneration of tuberculous focus. (Krause.)
Tuberculosis of bone always assumes the phase of miliary lesions, followed by the formation of a granuloma, which may gradually encroach upon surrounding tissues or may assume a more fulminating type and spread rapidly. Apparently because of the circulatory conditions these lesions generally occur near the epiphyseal lines of the long bones, apparently seeking the ends of the bones, as pulmonary lesions seek the terminations of the lungs. These lesions may be solitary or multiple. Beginning always minutely, they spread so as to produce foci perhaps two inches in diameter. As the result of the formation of granulation tissue, the surrounding bone melts away and disappears, the result being a great weakening of its structure and expansion of its dimensions in order to make room for the growing mass within. The tendency of this granulation tissue thus imprisoned is always to escape in the direction of least resistance. This carries it sometimes into the joint, sometimes out through epiphyseal junctions, and sometimes through channels in the bone made by its own pressure, with external escape and appearance of the dusky distinctive tissue, felt beneath and then upon the skin. Where bone is so weakened in one direction it is usually strengthened by compensatory deposition of calcium salts at other points, and the result frequently is a striking combination of osteoporosis in the immediate presence of the disease, with osteosclerosis, sometimes to a remarkable degree, even to eburnation, of an adjoining portion. When this mass undergoes caseous degeneration the progress of the disease is much slower and the pain less. When it undergoes suppuration there are more evidences of inflammation, with more pain and systemic disturbance, as well as local swelling, tenderness, etc. The surrounding musculature is rarely involved, although the periosteum is nearly always so. In fact, it is stated that in an inflamed and suppurating bone lesion, if the muscles are extensively invaded, it may be regarded as of syphilitic rather than of tuberculous origin. The pyophylactic membrane already alluded to is seen in almost every instance of tuberculous disease. The spina ventosa of some writers refers to the expansion of the shaft and medullary cavity of a long bone whose interior is occupied by a mass of tuberculous gumma, which is perforated at one point, and through which opening it escapes as does lava from a crater, to involve the structures on the outer side. The appearance of this granulation tissue in joints as fungous tissue has already been mentioned. In a general way it preserves its fungoid characteristics until attacked by pyogenic or saprogenic organisms, when it quickly breaks down, forming an ulcer if upon the surface, or a cold abscess if not externally open. Tuberculous disease of the bone is most common in the young, and in them the majority of tuberculous joints are those whose bony structures have been first involved. In other words, the majority of cases of tuberculous pyarthrosis are due to primary bone disease. As the result of the tuberculous infection the bones become distorted, which is best illustrated in Pott’s disease of the[118] spine; while, as the result of the constant irritation, joint ends become displaced by chronic muscle spasm, and joint contours entirely altered by expansion of the affected bone and thickening and infiltration of the overlying soft parts.
I have often, for the sake of illustration to medical students, drawn a certain analogy (following Savory) of the gross resemblances between lungs and bones in their behavior when involved in tuberculous disease. In either case the structure is in a measure spongy and contains cavities and networks of tissue; in each case the structures are invested by a resisting membrane—in the one instance pleura, in the other periosteum. Again, each is closely related to a serous cavity—the lungs to the pleural cavity, the bones to the serous cavities of the joints. Tuberculous disease manifests a predilection for the extremities of both organs. Perforation into the adjoining serous cavity is frequent, and previous to perforation collections of serous fluid are frequently noted—in one instance pleurisy, in the other hydrarthrosis. Moreover, these fluids may frequently become contaminated, and then become purulent, constituting empyema or pyarthrosis as the condition may be. One sees, too, in each place the same striking combinations of weakening of tissue and strengthening in order to atone for the undermining of the disease. These are not all of the similarities that might be adduced, but are perhaps sufficient for the purpose of showing that tuberculous disease is essentially one and the same thing, no matter what tissue is invaded.
In the tendon sheaths and bursæ we frequently find manifestations of tuberculosis. When seen early these are always in the direction either of miliary affection, or, most commonly, of tuberculous gumma, while when seen late the disease has usually advanced to the point of suppuration, and we now have cold abscess of the affected part.
In many joints and tendon sheaths, particularly the latter, we find certain detached, usually colorless, firmly resistant masses, of smooth and polished surface, lying in a collection of fluid, in size from a minute particle up to that of a melon-seed. These have been known at various times as rice grains, melon-seed bodies, corpora oryzoidea, etc., and for a long time their explanation was a mystery. It is now well established that in the majority of instances these are the result of fungous granulations which have become detached in small pieces, which then, in the absence of infection, have shrunken and become rounded and polished by attrition. The bursal enlargement and distention with fluid in which they are usually found is commonly spoken of as hygroma of that particular bursa. Tuberculosis of these bursæ, however, does not always result so harmlessly as the formation of these bodies, but, on the contrary, tuberculous infiltration may extend beyond the serous limits to the surrounding soft parts, with a tendency finally to external escape, just as in the case of bone lesions. These constitute affections of the soft parts which are more or less destructive, and are difficult, often impossible, to deal with, because of the mutilation which a thorough extirpation of the disease would necessitate.
In the testicles and ovaries, particularly in the former, tuberculous disease is frequently met with. In the testicles it begins usually in the epididymis, forming a somewhat dense nodule and a distinct tumor, easily observed from the outside, although its minute character may be still concealed. The tendency here is almost invariably to progressive infiltration and breaking down, either into a caseous mass or, more commonly, into puruloid material, while sometimes acute infection supervenes.
It is not always easy to distinguish between syphilis and tuberculosis of the testicle, though the latter is usually characterized by the same tendency to effusion into the adjoining serous cavity, i. e., that of the tunica vaginalis, as is manifested in disease of the lungs or bones. When the disease is extensive the overlying skin is involved, and frequently the surgeon is called to deal with cases of perforation and escape of fungoid tissue on the outside.
In the kidneys, in the ureters, as also in the bladder, tuberculous lesions are noted, the miliary form being particularly frequent in the former. Tuberculous disease of the kidney leads sooner or later to caseation and a condition of pyonephrosis or its equivalent, which calls practically always for extirpation of the affected organ. Tubercle bacilli are sometimes recognized in the urine, but only when the lesion has an opportunity of discharging into one of the urinary passages.
In the peritoneum tubercle appears usually in the miliary form, leading sometimes to such extensive involvement of and interference with visceral functions as to produce anasarca or more general disturbance prior to death. Acute miliary disease here is as[119] rapid and as essentially fatal as the same affection of the dura or pia, while the more chronic forms are followed by degenerations that may involve the intestines either in agglutinated masses or in ulcerations and possible perforations. The indication in all tuberculous lesions of serous membranes is for exposure by operation, disinfection of the surface, and evacuation of retained fluids. Recovery from tuberculous peritonitis, even of acute type, after abdominal section, is now definitely established as a possibility. The same would probably be true of tuberculous meningitis were we permitted to expose the membranes and attack them or drain them in the same way.
Although a few distinct organs or tissues have here been specifically considered in their relations to tuberculous disease, there is no organ or tissue in the body which is exempt from its ravages and in which evidences of tuberculous disease may not be found. Even the mammary gland occasionally presents tumors composed of tuberculous granuloma which more or less simulate malignant disease, while calling for the same radical treatment (Fig. 22).
Fig. 22
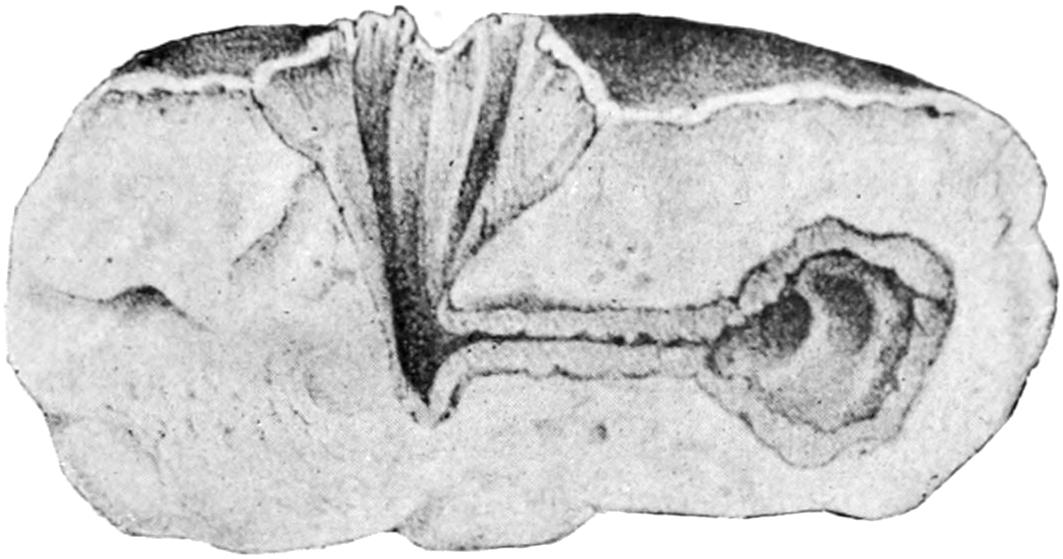
Gross appearance in tuberculosis of the mamma. (Dubar.)
—The tuberculous virus may enter the body through various channels. Probably in the majority of instances it gains entrance through the respiratory tract, less often by the alimentary canal, and occasionally by air contact of open wounds or direct infection by local agencies. It is now well established that tuberculous disease is easily inherited, although a predisposition to its ravages is transmitted from parent to children.
In what this predisposition consists is not always easy to say. As the tubercle bacillus grows in the tissues, it is by preference an anaërobe, and it seems to be lowered in activity or banished by access of oxygen. It has been shown that in those individuals in whose pallid skin, long bones, flabby muscles, and pale conjunctivæ we recognize a predisposition to this disease, the heart is disproportionately small as compared with the weight and size of the lungs. This means a relatively feeble pumping power, and is perhaps the best explanation for what is accepted as a fact. The mucous membranes of the nose and throat are usually the first lodging places for germs carried by the air, they finding here the warmth and moisture necessary for their detention, development, and growth. As long as these membranes are unbroken and healthy, infection is rarely possible; but let tubercle bacilli become caught in the crypts of the tonsils or in adenoid tissue in the nasopharynx, and the other disturbance, set up by irritant organisms of various species, will usually bring about conditions favoring their growth and incorporation into the living tissues. This lymphadenoid tissue is often the port of entry for these organisms. The explanation for local and surgical tuberculosis in bones and other accessible tissues probably is connected with causes determining at these points an area of least resistance, in which the germs find tissues more susceptible than elsewhere, and in which they may live and thrive.
Not the least interesting and important of the considerations regarding tuberculous disease is the possibility of an acute outbreak of tuberculosis after long latent or chronic manifestations of the disease. This means, in effect, the onset of general miliary tuberculosis which soon terminates fatally, and death is not the infrequent result of such extremely rapid outbreaks from tuberculous disease of joints, bones, ovaries, etc. For the disease when it has assumed this extremely rapid type there is, so far as known, no relief.
[120]
—So far as the general recognition of tuberculous disease is concerned, it is not often difficult. It is accompanied usually by more or less marked cachexia (at least this is the case when infection is serious and widespread), one of whose principal characteristics is the so-called hectic (habitual) fever of old writers. This was a fever of a remittent type, accompanied also by more or less colliquative night sweats, with dryness of the skin during the daytime, and flushing of the face. Hectic fever, as a matter of fact, often accompanies tuberculous disease, but is seldom encountered until pyogenic infection has occurred and suppuration is taking or has taken place. There is now much reason to consider hectic fever as an auto-intoxication from absorption of morbid products. In advanced cases we may find evidence of amyloid changes, although these are seldom recognized prior to autopsy. It is seldom difficult to recognize tuberculous disease except when at a considerable depth. Here, as long as there is no suppuration, there is little tendency to leukocytosis, by which diagnosis as between sarcoma and tuberculous infection may perhaps be made. Sometimes when in doubt the exploring trocar or an exploratory incision may be resorted to, it being always best to be prepared at the same time to proceed with whatever further operative procedure the findings may indicate.
—It is well to emphasize, first of all, that tuberculous disease when circumscribed and accessible is a distinctly curable affection. If this is accepted, it puts a much more hopeful aspect upon the condition than it formerly bore. It moreover justifies operations of a more radical nature than were formerly practised. Treatment should be divided into the hygienic and constitutional and the local and operative.
Of all the natural remedies, oxygen undoubtedly ranks first. This means the best of ventilation, an outdoor life if possible, and preferably in localities and at altitudes free from dust and well supplied with ozone. When this is impossible inhalations of dilute oxygen are capable of doing much good. The two canons of successful treatment of pulmonary tuberculosis are equally of value in surgical tuberculosis, viz., abundance of oxygen and hypernutrition. The diet should be rich and nutritious, at the same time capable of complete digestion. The emunctories should be stimulated and elimination favored in every possible way. Undoubtedly the old standard remedies—cod-liver oil, compound syrup of hypophosphites, etc.—are beneficial, and much good may be accomplished by their proper use.
Certain remedies have been at various times supposed to be endowed with specific properties, and for many years clinicians have endeavored to find that substance with which the system could be safely saturated and prove inimical to the parasite causing this disease. Such agent has not yet been discovered; nevertheless, much has been done in this direction. Of the remedies highly spoken of for this purpose, creosote and guaiacol are considered the best. These are somewhat difficult of administration, but if the latter is given in the form of the carbonate, generally known as benzosol, it comes the nearest to the ideal for which we are striving. Benzosol should be given to the adult in doses of at least a gram a day, perhaps more. It is better tolerated and less offensive than the guaiacol from which it is made. I have never seen anything but benefit result from its use, and yet would not extol it as a positive cure. Nevertheless in conjunction with other local and constitutional measures its administration may be followed by complete recovery.
Of the various local measures, physiological rest should be placed first, and can be achieved in some places better than in others. The various forms of apparatus resorted to by orthopedists are simply mechanical measures in furtherance of this purpose. Some surgeons have faith in iodoform, used locally in solution or suspension in some menstruum like glycerin, oil, etc. The benefit which has been claimed in some cases is not duplicated in the experience of all surgeons; nevertheless, it has undoubtedly been of service. A recent and most promising method of treating tuberculous disease of the extremities has been suggested by Bier, and consists in the establishment of a permanent hyperemia by the application of a rubber tourniquet on the proximal side of the lesion. (See chapter on the Joints.)
It would appear that the access of more blood which is thus permitted is inimical, presumably by the presence of the oxygen which it brings, to the development of the disease germ. The method depends for its rationale upon the fact that the congested lung does not become tuberculous. Lannelongue has suggested what he calls the sclerogenic treatment of tuberculous lesions, by injection of a very dilute solution of zinc[121] chloride, which serves as an irritant and produces a tissue sclerosis that serves the purpose of a prophylactic membrane, while at the same time the solution is fatal to those germs with which it comes in contact. This treatment is painful and has not proved acceptable.
The astute surgeon, who gains the confidence of his patients and retains it, will not hesitate to remove by a suitable operation the tuberculous focus which he feels confident that he can reach and extirpate. The resulting tissue defects may be in many instances atoned for by plastic operations. At other times this procedure means excision of some joint, which leaves usually a much better functionating member than would the disease if permitted to go on to spontaneous recovery—i. e., ankylosis—and at the same time removes a focus of disease which is a menace if left to the future welfare of the patient. It may mean at other times amputation, but the artificial limbmaker now supplies a member vastly more useful than a natural one crippled by this infectious disease. In a general way, then, time may be saved and recovery ensured by early and judicious operation, while later in the course of this protean malady it may be absolutely necessitated in the endeavor to save life.
After operations where clean extirpation and reunion of the parts with primary healing is impossible a local dressing of balsam of Peru containing 10 per cent. of guaiacol is recommended. Gauze saturated with this dressing and packed into the cavity best accomplishes the purposes of a surgical dressing for such cases.
The superficial and ulcerative (skin) lesions due to tuberculosis often yield very readily to exposure to the Röntgen rays and the ultraviolet rays. Recrudescences appear not infrequently, and the treatment should be administered at intervals long after the apparent subsidence of the lesion.
Deep pain of tuberculous lesions, especially in bone, is often relieved by ignipuncture, meaning thereby a perforation into the depth even of the bone-marrow by the actual cautery (Paquelin’s), which may be thrust directly through the skin or which may be used after exposing the bone by incision. The use of the actual cautery is indicated in eradicating and destroying tuberculous tissue when a neat dissection or extirpation is impossible.
—Finally the treatment of tuberculosis cannot be dismissed without a reference to the glycerin extract made from a filtered culture of the tubercle bacillus, containing the peculiar toxalbumin first prepared by Koch, forever associated with his name, and first given to the world in 1890, when its announcement created a furore and aroused hopes that have never been completely realized. Yet in spite of disappointments which have often followed its use, it is a remedy of great value when judiciously used in selected cases. The diagnostic value of the material should also not be forgotten, as by its use one may possibly decide in doubtful cases as between tuberculous or some other disease. The best preparation for use today is that made by Koch’s new process, by which the possibility of the presence of microörganisms is eliminated. It contains those constituents of the bacilli which are insoluble in glycerin, and which have distinct immunizing power. On the market it is known as tuberculin rest, indicated simply as T. R. The initial dose is ¹⁄₅₀₀ Mg., to be increased with each injection. Its effect, e. g., on lupus, is very marked.
[122]
The younger generation, when studying the subject of syphilis, should be referred back one hundred years or more to the time when the opinions held by John Hunter generally prevailed—when venereal diseases were grouped under one heading, and considered to be but three manifestations of the same morbid condition. It took years for the profession to break away from this mistaken teaching, and a generation had passed before gonorrhea was separated from the others. This left chancroid and syphilis still more or less confused in the minds of many, and until the middle of the previous century they were considered as different types of the same disease by some of the most experienced observers. Thus it happened that those who made a special study of this subject were grouped into two classes, the unicists and the dualists, according as they held to the unity or duality of syphilis and chancroid. It was a question of importance, and differences of opinions led to bitter antagonisms. Its importance inhered in this: either all venereal sores were to be subjected to constitutional treatment, or else differences in treatment were to be made according to the local or constitutional nature of the malady. Men sacrificed their own health, even their own lives, in their willingness to make experiments upon themselves, and auto-inoculability was proved by one observer through some 1700 inoculations produced upon his own body. Such devotion to medical science has been rarely eclipsed. In the latter half of the eighteenth century came clearer distinctions, and toward its close there were none who ranked as authorities who held to the old view of the unity of these diseases.
Syphilis is a disease of ancient if not of respectable origin. We read much of the possibility of so-called pre-Columbian syphilis, implying by that term that the Spaniards who came over to this country found it here and carried it with them back to Europe. This is probably the case, and yet the disease antedates the Christian era, as may be established by familiarity with ancient literature, whether Arabian, Egyptian, or Hebraic. No one can read the Psalms of David, for instance, without finding therein intrinsic evidence that the writer thereof, whoever he may have been, suffered from this disease. Of its antiquity, however, as well as of its universal distribution, we need not speak. History has shown that whenever it has appeared in a community previously unaffected by it, it has assumed malignant and epidemic features, and has spread rapidly while claiming many victims; on the other hand, in those communities where it has long been domesticated, it assumes usually a milder type, as though a racial immunity were being gradually established.
Syphilis is an infectious chronic disease, acquired either by inheritance or by contagion, mediate or immediate, with a certain period of incubation, characterized by an initial lesion at the site of infection, which is followed in time by a series of systemic disturbances, usually quite characteristic, in a commonly determinate order. A large proportion of these consist of neoplastic lesions of the general type of the infectious granulomas. In the majority of instances it is of distinctly venereal origin, although not always. It is known among the common people as pox, while a frequent synonym for it in foreign literature is lues venerea, or often lues alone, the adjective being luetic.
Syphilis is always transmitted as such and is not interchangeable with leprosy, tuberculosis, or anything else, although it is not unfrequently complicated with them as well as with cancer. It has certain resemblances to the exanthemas in its periods of incubation, and in the fact that one attack is supposed to confer immunity, as well as that many of the typical symptoms of syphilis pertain to the skin and mucous membrane; further resemblances may also be found in each case.
Within certain limits the specific infection of syphilis, or, as it is frequently spoken of, the specific disease, passes through a somewhat regular program in which periods of activity and latency seem to alternate. The first visible lesion is at the point of entrance of the virus, in acquired cases, after a certain period of incubation, and is known always[123] as the chancre. Of course, in inherited syphilis no chancre or primary sore is found. Then occurs a second period of incubation, during which there is a still more widespread general infection of the body, in which at first the lymphatic system seems to suffer most. This is characterized by a certain degree of fever, progressive anemia, malaise, tenderness and pain in bones and joints, all of which indicate a progressive toxemia.
—The manner of contagion in acquired cases is naturally most often that of the sexual act, although contagion may come from many sources, including unclean utensils, pipes, etc., as well as the instruments of the dentist or the surgeon. Some abrasion of the infected surface is almost invariably presupposed, since it is not established that the virus of syphilis will enter an unbroken surface, though it may lurk thereon; but the abrasion may be trifling and occur in such situation, especially on the female genitalia, as to be undiscoverable or unnoticed. It is then possible that patients may speak truthfully when denying the existence in the past of any venereal sores. The transmission of infection from parent to offspring in the uterus will be discussed later.
—That syphilis is a disease of parasitic character, i. e., contagious, there can, of course, be no question. The nature of the contagium vivum which produces these changes, long unknown, is now believed to be revealed in the spirochæta pallida recently described by Schaudinn and others; an organism 4 to 10 μ in length, ¹⁄₂ μ in width, possessing several curves like those of a corkscrew, with sharpened poles, mobile, its motions consisting of rotations and bendings. It has been demonstrated that primary lesions contain the organism, either constantly or in the majority of cases, while in skin and nearly all other lesions it can be also shown (Fig. 23).
Fig. 23
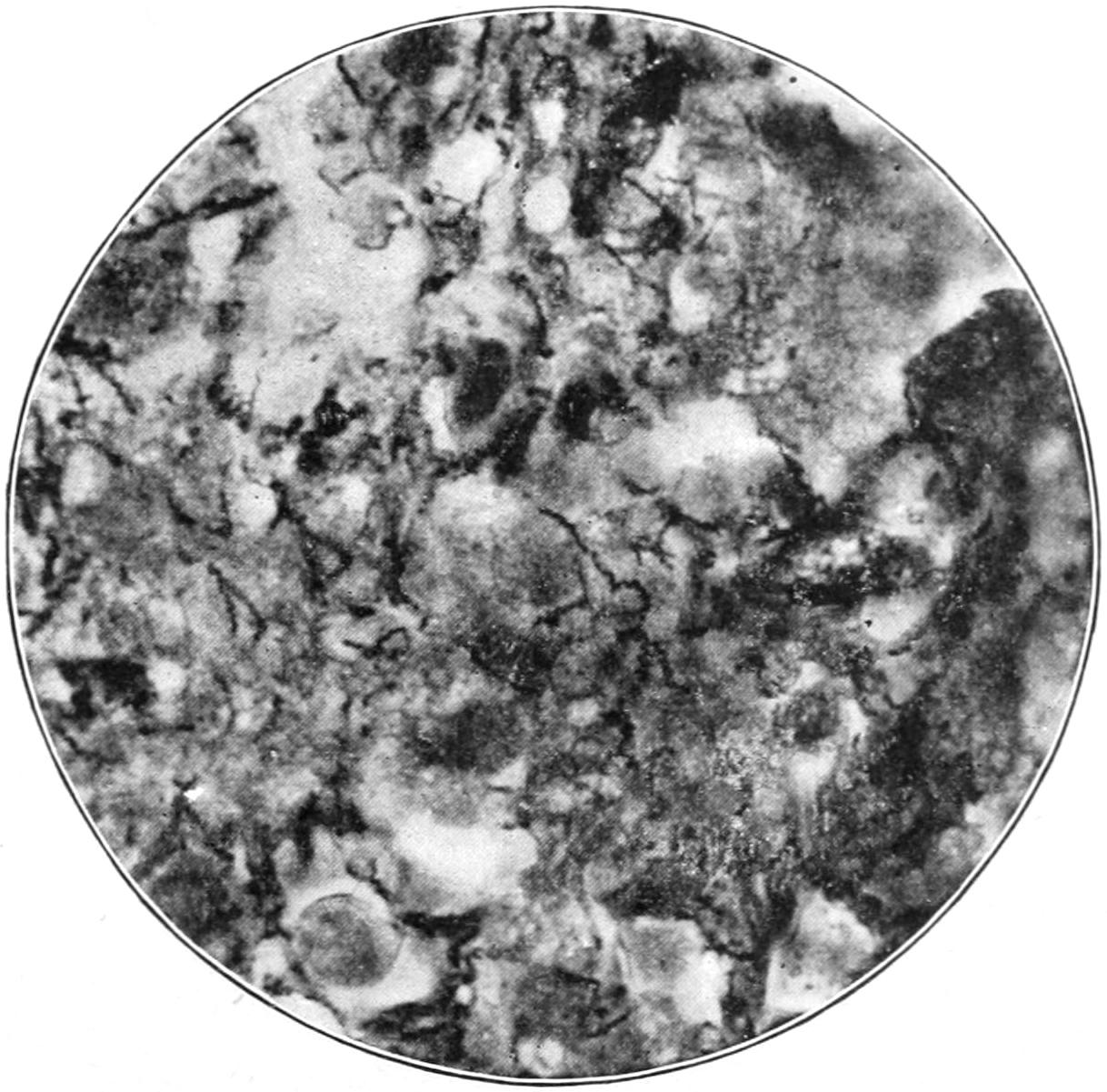
Spirochæta pallida (syphilis) in adrenal of child with congenital syphilis. (Gaylord.)
—Ever since the days of Ricord’s writings on the subject it has been customary to group the manifestations of syphilis into three groups or stages: the primary, the secondary, and the tertiary. Less stress is laid upon these stages than previously, yet it is convenient to retain them for descriptive purposes. It should be emphasized, however, that between them there are no arbitrary limits of time or tissue. Primary syphilis under this classification includes the first period of incubation and the symptoms and appearances of the initial lesions. Secondary syphilis may be made to include the earlier constitutional symptoms which involve or at least become apparent upon the more superficial portions of the body, i. e., skin, mucous membrane, lymphatics, etc. Later comes the so-called tertiary period, in which the body surfaces are not necessarily spared, but in which also deep lesions of the viscera, the bones, the brain, etc., are noted. Between the first and the second stages comes the so-called second period of[124] incubation. The second and third stages are characterized by frequent neoplastic formations, which assume the type of the infectious granulomas and are commonly spoken of as gummas; these lesions are destructive in their tendency, and will so prove unless dissipated or aborted by suitable treatment.
In the first and second stages of the disease it can be conveyed by inheritance and inoculation; in the later stage such an occurrence is exceptional.
That syphilis is, per se, an infection is proved by the constitutional symptoms which accompany its earlier manifestations; the fever, usually mild, though sometimes well marked, which comes early in the course of the disease, the general lymphatic involvement, the malaise and depression, all indicate the systemic disturbances of a true toxemia.
The periods of quiescence between successive outbreaks of the disease are, moreover, characteristic, although they sometimes lull the patient and his physician into an inactive state, during which medication is too often suspended, so that when fresh disturbance arises vigorous treatment must be renewed.
The infection of syphilis occurs on the instant of inoculation, as in the case of tetanus. This is important, as upon it depends the question of early local treatment. While excision of the primary sore, or even of an area which might have become infected during exposure, and before the actual formation of the chancre, has been often practised and urged by some, experience has shown that it has little to commend it, since the general experience is that it does not prevent the development of the disease.
In its tendency syphilis is constantly progressive and destructive, although it often behaves in a capricious manner, sometimes when under efficient treatment and generally when treatment is inefficient. It is usually more virulent in the dissipated and those who are weakened by inheritance or poor constitutions, or by other disease. One reads in literature on the subject about the malignancy of some cases and the benignancy of others. Some cases seem to have a malignant aspect, while others run an unusually mild course, so much so as to raise the question whether the patient had syphilis. As far as the nature of the parasitic cause is understood, this would depend on differences in the make-up of the individual rather than in the actual virulence of the germ. In the extremes of life individuals are more susceptible. When implanted upon a tuberculous constitution it sometimes renders the tuberculous lesions more active; whether it acts as a mixed infection is not definitely known. Tuberculous lymph nodes frequently break down during the course of secondary syphilis, and consumptive patients grow rapidly worse. Syphilis, like alcohol, tends to play havoc with the bloodvessel walls, and their combined effects in this direction are greatly to be deprecated and should be prevented.
—As far as acquired syphilis is concerned absolute contact is necessary between the infecting material and the infected area, while upon the latter must exist some abrasion of the surface. Chancres and the early eruptions or mixed lesions have been proved to be absolutely virulent. The genitalia of both sexes are frequently the site of wart-like lesions referred to as condylomas, which are usually kept more or less moistened by the secretion of the parts, and are fruitful sources of contagion. The discharging lesion of those suffering from syphilitic disease should be regarded as capable of transmitting it, while during the primary and secondary stages the blood and lymph should be regarded as probable sources of danger.
Inoculation with the blood of patients during these stages has been known to be successful. How long the blood retains its power of infection is uncertain; it is usually regarded as free from it when the disease is latent.
The natural and physiological secretions of various organs, e. g., saliva, milk, perspiration, tears, and urine, are not generally believed to be capable of transmitting the disease. The semen of syphilitic men may reproduce the disease by heredity but not by direct inoculation. It is possible under these circumstances for the father to transmit the disease to the ovum without previously infecting the mother; such infection of the ovum by diseased spermatozoa is quite different from the infection of the ovum by the mother who has acquired the disease, the father having escaped it.
In a general way it may be held that secretions of organs, or even of lesions, which are non-specific, are not contagious except as they happen to be mixed with blood or with disintegrated portions of actual syphilitic lesions; thus, for instance, vaccinal lymph might be safely taken from a syphilitic subject if there were absolutely no admixture of blood.[125] But the difficulty of securing pure lymph is such as to make its use inadvisable because of its danger.
Suppuration frequently complicates syphilitic lesions. This is to be regarded as in the nature of a secondary and pyogenic infection. It has not been established that the germ of syphilis is by itself a pyogenic organism.
Gonorrhea or chancroid is often simultaneously contracted with syphilis, with resulting clinical complications that are perplexing as well as difficult to treat. The contagion of chancroid acts promptly, as will be stated in the chapter on Chancroid; and so it may happen that the sore which begins as a chancroid is gradually converted into a true chancre, the change taking place so gradually that it is difficult to state when it begins or is completed. In this way result the so-called mixed sores, which may give rise to so much doubt that the surgeon feels it wise to wait for some secondary manifestations before deciding that syphilis has been acquired. Confusion is often created by preliminary treatment which the local lesion has received previous to its examination by the surgeon. Patients, especially in the lower walks of life, frequently go to a druggist or to someone who will cauterize the sore and thus mask its characteristics to a degree which makes prompt diagnosis impossible. Again, patients are often uncertain regarding the matter of time, which is of great importance; thus the sore which appears within a few days after exposure may be chancroidal, while one which comes on twenty or thirty days afterward may be syphilitic. These periods, however, afford little help when there have been repeated exposures, by which confusion may be caused; but an accurate and complete personal history will be helpful toward a correct diagnosis.
—Owing to the greater delicacy of the mucous membranes they are more frequently the site of primary lesions than the skin: 85 to 90 per cent. of all primary sores occur about the genitalia; in men, especially on the inner side of the prepuce, the glands, and the sulcus behind it; externally, chancre may occur upon any part of the surrounding skin; in women, the tissues about the vulva are most frequently its seat. Occasionally it is found within the vagina, but rarely upon the os. The so-called extragenital chancres are met with anywhere, especially on the most exposed parts, as the lips, tongue, tonsils, eyelids, and nipples. Syphilis is occasionally conveyed to a wet-nurse by the infected mouth of an infant suffering from hereditary disease; even multiple chancres sometimes occurring. Conversely, children have been infected by wet-nurses with syphilitic lesions about the nipple. The disease has been conveyed by bites, as upon the face and fingers. Surgeons and obstetricians are peculiarly exposed, as are also nurses, to this disease, especially occurring upon the fingers and hands. Infants have been known to be inoculated during parturition. These are all examples of direct or immediate contagion. On the other hand, the disease may be positively conveyed by utensils in common use between different individuals, as table-ware or tobacco-pipes; by tools of trade which are passed from one person to another, as, for instance, the blowpipe in glass factories; and by cigars as they are made in some places, the wrapper being moistened from the mouth of the cigarmaker. These are examples of its indirect transmission. Physicians are familiar as well with instances where the disease has been conveyed by instruments, either surgical or those of the dentist. So possible is this last form of contagion that dentists are trained to sterilize their instruments as carefully as does the surgeon.
Possibility of conveying syphilis by vaccinal lymph has been alluded to as occurring only in those instances where the blood of the syphilitic patient is mingled with the lymph. The production of vaccinal virus is now, however, so well regulated that it is rare that the surgeon employs humanized lymph. Some cases considered vaccinal have been due to the use of infected instruments; hence the necessity for extreme caution in this regard. When the disease is acquired in a non-venereal manner it is called syphilis insontium, or syphilis of the innocent; this, however, is an unfortunate expression, as it tends to cast reflections upon other cases which may be, in effect, just as innocent.
—In all probability the initial sore and the ensuing lymphatic involvement are due to the parasite and to its toxic products. These latter are quickly taken into the general circulation and are held to confer the immunity which syphilitics enjoy before the outbreak of the general eruption. Anemia, malaise, and other like symptoms are evidences of a progressive intoxication or toxemia, while the earlier eruptions, which tend to evince the contagious element in a rather virulent form, may be due[126] to the germs alone, or combined with their toxins. On this hypothesis can be explained the partial or complete immunity evinced by mothers who bear syphilitic children, the infection coming from the father.
From the first evidence of infection the whole syphilitic process gives evidence of its infectious character. The bloodvessel walls undergo a thickening of their coats and more or less obliteration of their lumen, and this, of course, causes a disturbance in the nutrition of the parts supplied by them. This vascular change can be recognized even in the minute vessels of the initial lesion, and thereafter pertains to most if not all specific manifestations of the disease.
Our knowledge of the nature of this disease would be more complete were it possible to convey it to animals, but these are practically exempt from it, for the few and rare instances where, it is said, the disease has been inoculated upon the higher quadrumana furnish insufficient data. In this respect the disease is like the exanthemas, of whose parasitic origin there can be no question.
The First Period of Incubation and the Chancre.—The time which elapses between the exposure and the first appearance of the initial lesion is known as the first period of incubation. This varies, within wide limits, from ten days to forty or fifty; some writers have made it even seventy days. The average period varies from three to four weeks. There is often uncertainty as to when the induration began, and patients, women especially, may easily make a mistake of several days in fixing this date.
Every case of acquired syphilis begins with an initial sore, though this may be so located or so complicated with some other lesion as to be overlooked. The character of the induration varies somewhat with the location, i. e., whether upon the skin or mucous membrane. The amount of moisture or maceration to which it is exposed will also influence its appearance. It may be minute, so as to almost elude observation even on visible parts, or it may spread and involve an area 1 Cm. in diameter. The lesion is usually solitary, but when several abraded spots are infected at the same time there may be multiple sores. When a surgeon sees a lesion of this character it has usually changed its original appearance—perhaps by some previous treatment, perhaps by maceration. There is one invariable feature upon varying expressions of which diagnosis is based, and that is induration. The instances in which this fails are very rare; on the other hand, it is possible that it may be the result of treatment already undergone, and for this reason the recent history of the case should be obtained; in other words, the typical chancroid is always indurated, but an indurated sore does not of itself necessarily indicate syphilis if it can be satisfactorily accounted for in other ways. The presence of an active primary lesion seems to confer immunity to subsequent infection for a period co-equal with the active manifestations of the disease, although even in this respect exceptions are occasionally to be noted.
The induration of syphilis develops beyond and beneath the limits of the superficial lesion, and gives the sensation, when grasped between the fingers, of a piece of firm material embedded in the skin or membrane. It is firm, slightly elastic, with usually well-defined boundaries, which accounts for the expression, parchment induration. Ordinarily no pain or other sensations accompany its formation or attract attention; hence the frequency with which it escapes observation for some time and the uncertainty which the patient feels regarding the dates. The surface of the induration usually becomes moist or abraded and frequently ulcerated; but these surface lesions tend eventually to heal, even if let alone, except in those parts, e. g., the lips, where they are constantly bathed by discharge.
The characteristic induration disappears slowly in a few weeks or months, leaving ordinarily no trace of its existence, although sometimes a small scar, occasionally pigmented, is left to mark its site.
There are two or three classical varieties of chancre which deserve more minute description. As ordinarily seen upon the genitalia, a chancre may assume the following types:
—The dry papule commences as a small rounded area of redness, becoming infiltrated and rising above the surface, gradually developing into a nodule the size of a pea or larger, over which the superficial skin seems to be thickened. Should[127] the summit of this nodule become abraded there will escape a serous fluid, which dries and forms a thin scab. This papule may disappear more slowly than it came, or may become more infiltrated, while its surface breaks down into an ulcer, whose area will be dropped a little below that of the surrounding tissue. In this case the induration is produced almost entirely by new round-cell infiltration, as in the other varieties; when it ulcerates these cells are the ones mainly to suffer, so that there is not much destruction of the original elements, and but little scar remains.
—The superficial erosion is the most common of the primitive sores, but is not often seen so early as to have its first appearance noted. It begins as a well-defined, dark-red area, which loses its epithelium and exposes a raw surface, with a trifling depression whose edges are usually on a level with the surrounding skin, while in the previous case the edges are generally characterized by an elevated margin. The base of this sore is also indurated, and partakes usually of the parchment-like character already described.
—The Hunterian chancre, so named after John Hunter’s description of it, is the most distinct and typical of these primary lesions. It begins as a papule, with some erosion, increasing slowly in size, sharply outlined, with a somewhat flat top. As it grows larger it increases in firmness until its base is extremely dense. In color it is greenish or bluish red, and this color appearance is more distinctive than in the other forms. In from one to three weeks its surface epithelium is usually loosened by maceration, and serous discharge is the consequence, or else it becomes covered with a grayish exudate, which, by its location, is rarely allowed to form a scab. The centre of the ulcer becomes deeper, its edges more elevated, and in typical cases a minute crater is formed by a characteristic destructive process. While the Hunterian chancre tends in ordinary cases to slowly disappear of itself, this involution can be materially hastened by local and constitutional treatment, and usually heals, when properly treated, with but slight local evidence of its previous existence.
—Chancroid will now be described, and its consideration will include the statement that it may be followed by true syphilitic chancre. Such a lesion is known as mixed chancre or mixed sore, and indicates a simultaneous infection by two distinct infecting agencies; it may easily cause confusion, for if seen early it will lack the characteristic induration of syphilis. This latter will only appear about the time that the chancroidal ulcers should be healed, if promptly and properly treated. Supposing this treatment to consist at least in part of caustics, the surgeon may be in doubt as to whether the induration is due to this agency or to developing syphilis. It seems justifiable to imagine causes of this kind while awaiting the further developments of the case, and to postpone vigorous antisyphilitic remedies until the diagnosis is established. It is a serious thing to condemn to a long course of mercurials a patient who perhaps does not need such drastic drugs. Instances arise where the situation is to be carefully considered in view of these possibilities. Should the healing and apparently healthy ulcer, however, take on an indurated base and develop the typical scleroses of chancre, it may be supposed that all doubt has been removed. The possibility of syphilitic infection being implanted upon a chancroidal base by subsequent exposure should also be taken into consideration. This will require an accurate history and a faithful narration of the same by the patient.
There are, also, the extragenital chancres, which may be met with upon the hands, upon the breasts, in the oropharynx, as well as about the eyelids. Chancres on those surfaces of the body where tissues are loose may attain considerable size and ulcerate early, the discharge drying into scabs or crusts, which mask the underlying ulcer. Around the margins of the nails these lesions show but slight induration. Sometimes suppuration and granulation are profuse. When appearing upon the tonsils there is nearly always ulceration, with considerable swelling and often a false membrane. A patient with this lesion will complain of sore throat, and involvement of the surrounding lymphatics is usually extensive.
When chancre appears upon the lips there is usually extensive induration; the lesion attains considerable size, with protrusion, unless recognized and treated, and ulceration takes place early and deeply. It may be confused here with epithelioma. The latter occurs during the later period of life, is slower in its evolution, and its involvement of the neighboring lymph nodes. The local changes which often precede cancer, e. g., hyperkeratosis and papilloma, will be lacking in chancre of the lip.
[128]
Sometimes at the site of the original chancre, which may have healed, there will be found one of the later lesions of the disease, which may be mistaken for another primary sore occupying the site of the first one. It may be distinguished by its central ulceration, its tendency to extend, and by the absence of the lymphatic involvement which is met with in the early stages of the disease.
—The chancre should be regarded as the first neoplastic evidence of a disease which is throughout characterized by its tendency toward new-cell formation. In the developed chancre there is a well-defined cell proliferation in the skin or mucous membrane, whose bloodvessels show the same character of change already mentioned, since in the walls, both of the minute arteries and veins, are found many new cells, some of which were originally leukocytes, but most of which are products of cell division, as shown by their numerous mitoses. All the coats of the vessels are involved and even the perivascular spaces are involved and obliterated. Essentially, then, the chancre consists of a local infiltration of the superficial tissues by cells, most of which are of the round type; the whole constitutes what may be spoken of as the initial sclerosis, which remains or disappears as such unless infected secondarily. This sclerosis should be carefully sought in every suspected region when the patient is first examined. It may range in bulk from a millet-seed to that of a good-sized grape; it is usually movable upon the tissues beneath; it may ulcerate deeply, and, should it persist for a long time, it may seem unusually active just before the outbreak of the so-called secondary symptoms.
But little can be predicted with regard to the future course of the disease from the size, number, or appearance of the primary sores. The nature of the tissues upon which the virus has been implanted is a more important feature in the evolution of the disease than anything pertaining to its primary lesions, so far as appearances go. In patients of depraved habits or vitiated constitutions the chancre may often become gangrenous or phagedenic.
—Soon after the appearance of the primary sore, or coincident with it, the enlargement of the adjoining lymphvessels and nodes begins. This is noted first in those which are in closest communication with the site of the chancre, usually in the groin. Occasionally thickened lymphvessels may be felt as cords extending along the dorsum of the penis. There may be enough involvement of the perivascular spaces to produce this appearance and sensation even around the bloodvessels. This lymphatic involvement is exceedingly significant, and yet may be found to some degree after chancroid and even after herpes of the genitals. It is, of course, an expression of a travelling infection—in the first case produced by the syphilitic virus; in the second, by the chancroidal virus; and in the third, by ordinary pyogenic organisms which enter through the pathway afforded by the herpes.
The involved lymph nodes of syphilis suppurate much less often than do those of chancroid, and suppurating bubo is, therefore, not common in syphilis. The term bubo generally means an involvement of the lymphatics in the groin, although, strictly speaking, it implies a similar condition in any part of the body. Syphilitic bubo, therefore, is to be distinguished from chancroidal as well as from non-specific bubo. These lymphatic lesions are sometimes spoken of as constituting the characteristic adenopathy of the disease, but this is an unfortunate expression, as it implies glandular involvement, and the term lymph gland should never be used, since the structures are not glandular in any respect. The enlargement and persistence of these lymph nodes constitute peculiar features of the disease, and may be noted long after the subsidence of active manifestations.
—With the earliest possible recognition of a syphilitic chancre or sore there is need for active and prolonged constitutional treatment, in addition to whatever may be required locally. If the diagnosis can be made, constitutional treatment should commence at once; only in cases of doubt is it advisable to wait. The local treatment is a matter of ordinarily small importance; the sores tend to heal spontaneously and quickly when the system is brought under the influence of mercurials. There are few authorities who recommend excision of the primary lesion or believe it is possible to abort syphilis by anything that can be done to the chancre. It is advisable to make mild antiseptic applications only. A chancre, however, in a location which makes it difficult to keep the parts clean, should be exposed to treatment by a minor operation, as an incision of the prepuce, circumcision, or a dilatation or incision of the hymen. Aside[129] from such operation the indication is for surgical cleanliness; soap and water followed by hydrogen peroxide, which may be continued as an application, or dusting with calomel, will usually prove sufficient. Various antiseptic solutions may be used. Dry applications, however, are the most convenient and usually the most serviceable; iodoform should be avoided on account of its penetrating odor; and pure, dry calomel will sometimes prove a mild caustic, and is best reduced with one to three parts by weight of bismuth subnitrate. The stronger applications, especially caustic, are only employed when there is unhealthy ulceration. If the sore is gangrenous it should be cocainized, then the surface thoroughly treated with some powerful caustic like nitric acid, and thereafter kept moist with aqueous antiseptic solutions. When the surface is practically healthy, dry preparations or unguents may be employed, preferably the mercurial ointments. There is greater difficulty in preserving cleanliness about the female genitalia, and here the use of antiseptic cotton or gauze will probably be necessary in addition to the other precautions. Surfaces should be kept apart by their aid, and it is well to use frequent antiseptic douches or occasionally to insert a suppository containing an antiseptic drug. Of the various preparations used those containing mercury in some form are doubly serviceable. The inguinal lymphatics should be kept anointed with a mercurial ointment, which should be thoroughly rubbed in, and the parts afterward protected with oiled silk.
While these local measures are being employed vigorous general treatment should be promptly instituted. This will be discussed when dealing with treatment of the constitutional features of the disease.
There are locations in which chancre gives rise to considerable distress, as, for instance, upon the lip and tonsils. Great improvement and relief of pain in these lesions is afforded by proper use of auxiliary drugs.
In regard to local precautions, the patient should be impressed with the virulent and infectious character of the discharge from every primary lesion, and given minute and cautious directions so that its transmission to others can be prevented. This will mean the use of separate utensils, as well as soap, towels, etc., possibly the temporary isolation of the patient.
Between the time of appearance of the primary sore and the development of widespread constitutional symptoms there intervenes a period of latency, the second period of incubation. This is more variable in duration than the first. The shortest time on record is about two weeks, and the longest about two hundred days, the average time being six or seven weeks. The secondary symptoms indicate complete generalization of the syphilitic poison, and follow the early manifestations in almost every case; nevertheless, there are instances in which they are either wanting or are so trifling as to escape observation. A careful examination during the second period will usually show, however, that the lymph nodes throughout the body are gradually becoming enlarged, especially those in the neck, along the border of the sternomastoid, the occipital nodes, those in the axilla and groin, and particularly one or two small ones above the inner condyle of the humerus, known as the supracondyloid or epitrochlear nodes. When these latter become involved without evident and local cause, syphilis is always to be suspected or even diagnosticated. This node is to be found by bending the patient’s elbow and feeling for it on the inner side, above the condyle, in the interval between the biceps and the triceps. The other lymph nodes of the body might also be found involved if they could be as easily palpated. This lymphatic involvement is quite independent of skin or other lesions, and does not yield as readily to mercurial treatment. The enlargements are usually movable, distinct in outline, and never suppurate unless locally and secondarily infected. In tuberculous patients, however, they may break down. This generalized involvement of the lymphatics is also of importance in diagnosticating old syphilitic infections.
During the second period of incubation there is generally a certain degree of malaise and progressive anemia. Examination of the blood will show diminution of hemoglobin, and a relative if not actual leukocytosis, due to reduction in the number of the red corpuscles. Occasionally the anemic features become pronounced; the patient may complain of weakness, lassitude, sleeplessness, failure of appetite, and of pain and[130] discomfort in the bones and joints, more pronounced at night, and often regarded by patients as “rheumatic.” The painful joints may also show a slight swelling due to increase of the joint serum.
Sometimes intermittent fever accompanies these cases, especially during the early eruptive period. The rise of temperature is noted mainly in the evening, when it may reach 104° or even 105° F. It does not last long, and often precedes the appearance of a well-marked and characteristic eruption. It is a peculiar feature of the syphilitic poison that it seems to attack points of least resistance in each patient, as is the case with that of influenza. In one patient fibrous tissues will suffer most; in another, joints; in others there will be headache or expressions of perverted nerve activity, as vertigo, convulsions, disturbances of sensation, temporary paralysis; again there occur disturbances like mild pleurisy, splenic enlargement, or jaundice. Occasionally there will be a typhoidal condition, during which the kidneys are seriously compromised. Morbid conditions are intensified by an attack of syphilis. During rheumatism and the various forms of neuritis, and during almost all affections of the central nervous system, symptoms are, under these circumstances, frequently aggravated. In malarial countries it is said that latent syphilis sometimes becomes active when malaria is present. Lesions of the bones and joints are occasionally influenced, while some claim that fractures occur more readily in syphilitic subjects, and it is generally conceded that delayed union of fractures is often due to this cause. I have seen fracture, apparently spontaneous, of both tibiæ, one after the other, in a patient with syphilitic disease of the cord and bones. I have also seen exuberant callus form around a fracture in a syphilitic subject, as it never does under ordinary circumstances. Injury seems sometimes to localize the manifestations of the disease; thus chronic irritation at the site of old syphilitic lesions frequently becomes a point of development for epithelioma, or some other expression of malignant growth. This is seen particularly in cancer of the tongue, which sometimes follows the change in the epithelium known as leukoplakia.
The influence of an attack of erysipelas upon certain specific lesions is remarkable. In many instances eruptions and ulcerations have been known to subside, and gummas and exostoses to disappear, after an attack of erysipelas involving their site, but these lesions are likely to reappear after the disappearance of the acute infectious process. The temporary effect of the toxins of erysipelas upon syphilitic lesions is similar to their influence upon some malignant growths.
—Passing now to the lesions of early constitutional syphilis as manifested in particular regions or organs of the body, we take, first, the skin. When syphilis seems to have ended its existence during the primary stage (Fordyce) no further disturbances are expected, and only by waiting can the termination of the disease be determined.
The malignancy of the disease may be estimated by noting the rapidity with which the destructive lesions appear; thus gummas which appear early in the skin or mucous membranes, or elsewhere, indicate a serious type of the disease. So also does profound cachexia, including in this term more than mere anemia. The devastations of the disease in Europe during the fifteenth century show that it presented at that time a severe type.
The eruptions of syphilis have been grouped under distinctive terms, and are usually referred to as syphilides or syphilodermas. It has been already stated that among the new formations of syphilis are those known as syphilodermas; any of the former which are distinctly due to syphilis may be syphilomas. Thus, we may have syphiloma in the skin, in the bones, in the viscera, etc. It has been customary to speak of the syphilides as simulating the non-specific eruptions and identify them by placing before them the adjective syphilitic. Thus writers formerly described syphilitic psoriasis, syphilitic erythema, etc.; but these terms have been abandoned, because it is recognized that the skin lesions of syphilis while imitating most of the features of the non-specific diseases are yet distinctly different from them. We speak, therefore, now of a macular, vesicular, papular, squamous syphilide, etc., implying thereby that it is vesicular, scaly, or otherwise, as the case may be, and at the same time that it is a cutaneous expression of syphilis.
PLATE VIII
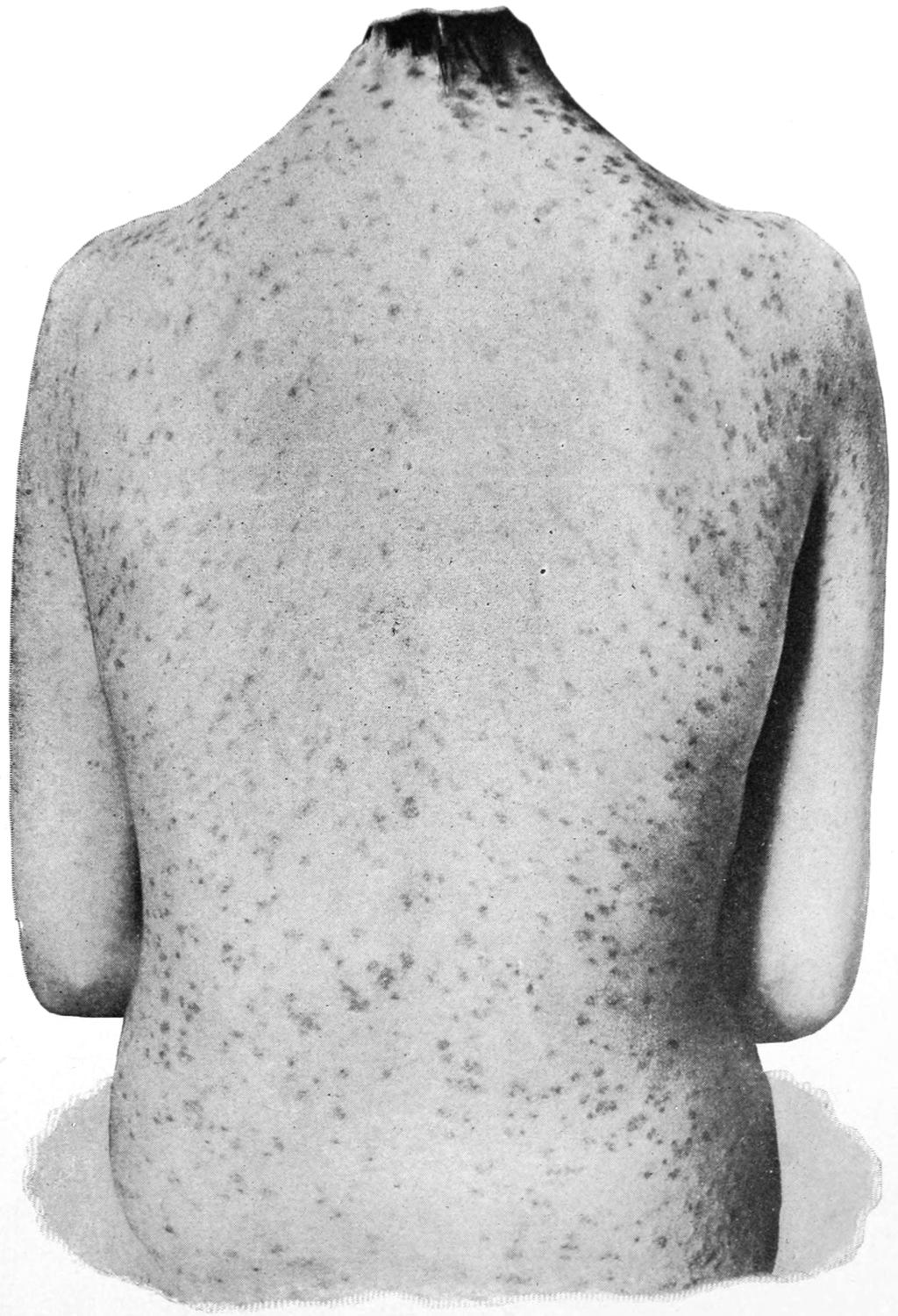
Grouped Miliary Papular Syphilide.
PLATE IX
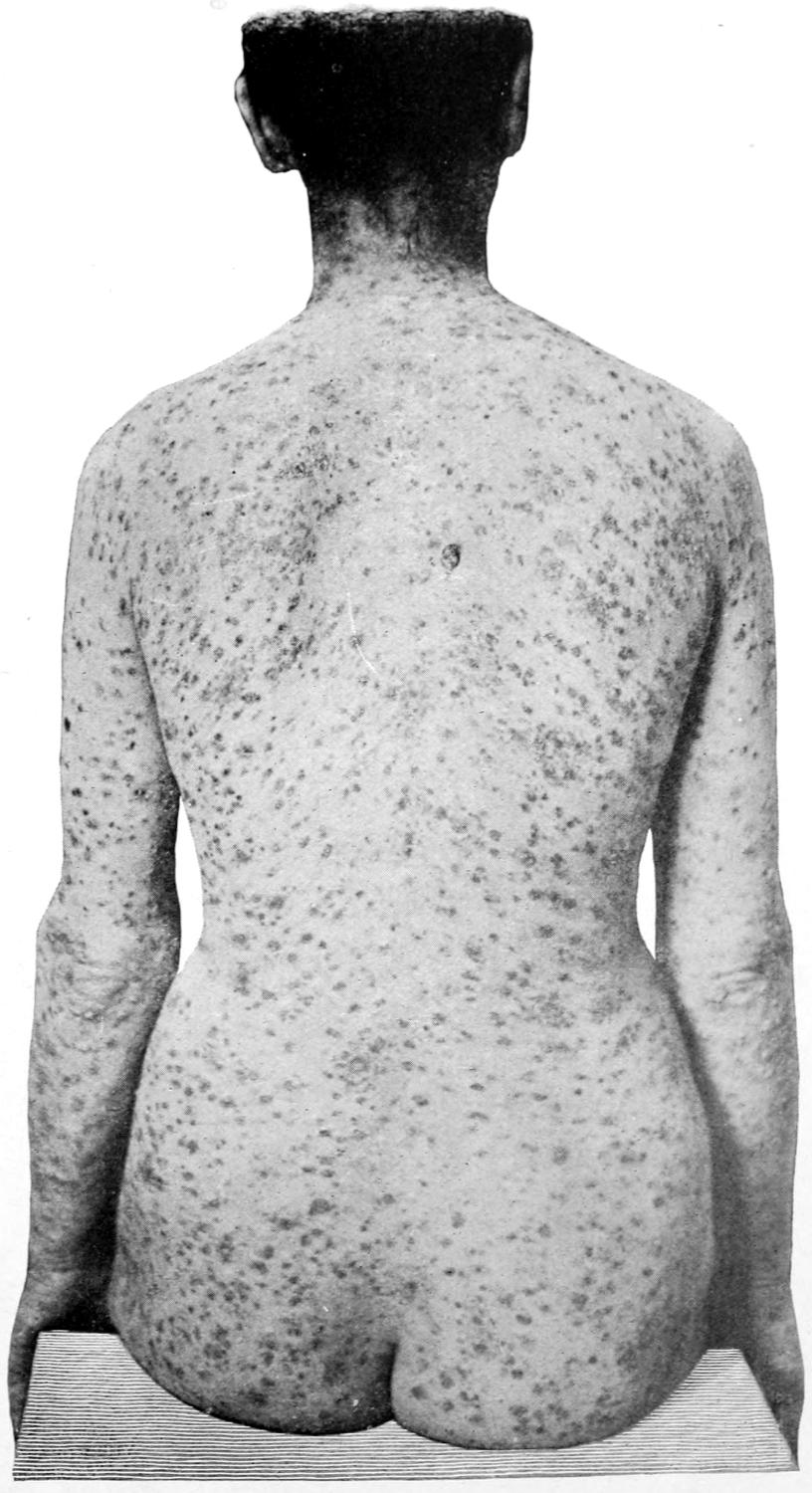
Mixed Papular and Papulopustular Syphilide.
PLATE X

Tuberculous Ulcerating Syphilide, showing Lesions in Different Stages.
[131]
The syphilodermas have certain peculiarities which are striking and distinctive; they are symmetrically distributed; their color is characteristic, and is due to the disease of the bloodvessel walls, which has been referred to, by which stasis is favored and exudation encouraged. The pigmentation is often striking, and, whatever it may be at first, it assumes a tint described by the terms “raw ham” or “coppery.” Dark pigmentation may take the place of the lighter colored, as the sole evidence of the existence of the previous lesion. Occasionally, however, the normal pigment of the skin disappears and a bleached-out area marks the site of the previous lesion. This is often irregular in shape and considerable in size. Such a spot is spoken of as leukoderma. Again, the syphilodermas are generally polymorphous, and seem to be capable of imitating almost every known non-specific skin affection; so close is the resemblance that it often requires careful study of the case to permit of diagnosis. The absence of itching is also a feature of most of these cases.
The early syphilides are superficial, distributed generally and symmetrically, and disappear spontaneously.
When skin lesions are clustered, as in the macular and papular forms, they usually group themselves symmetrically and in more or less circular outline. When, however, they are too regularly arranged, it may be taken as evidence of their older and more relapsing character.
The later skin lesions of syphilis differ in several respects from the earlier. They are less regularly grouped; they involve a greater depth of tissue; they tend to ulcerate and to leave permanent scars; and they have around them a more infiltrated area, probably because they are deeper. They are, however, not so infectious as the earlier lesions, and it is rare that they are of serious menace to others. (See Plates VIII, IX, X.)
Fordyce and others have pointed out that the prompt and specific influence of mercury and even of iodine upon these eruptions is an instance of the selective action of certain drugs, and nothing could be more conspicuous in demonstrating it.
Certain types of syphilide are common in the earlier stages and others in the later; there may be a well-defined limit between the two, since in not a few instances all types seem to be combined.
The first eruption of so-called secondary syphilis assumes the erythematous or macular type, and has been referred to as roseola syphilitica. It appears as a generalized eruption, in spots varying from 0.5 to 1 Cm. in size, which are of a vivid color and scarcely elevated above the surface. It commences usually upon the abdomen, proceeds to the chest, and then to the extremities. It does not often appear upon the face. Two or three weeks may be consumed in its generalization over the entire body. If let alone it has a duration of a few days to several weeks, and may then fade away, leaving nothing to indicate its presence save a slight pigmentation.
Of more pronounced character is the papular eruption, which commences as a small papule, and is described as lenticulopapular and miliary papular. At first these are generalized, then become circumscribed, and exhibit transition forms from the early to the later type of lesions. The papules vary in size from that of a millet-seed to that of a split pea; even this type may disappear without ulceration or suppuration.
Lichen planus may be mistaken for papular syphilide, but may be distinguished from it by intense itching and by lack of the pigment changes which characterize the syphilide.
The squamous syphilide is sometimes a continuance of the papular, and sometimes it begins as such. It is characterized by a variety of scaly macules and papules, which strikingly resemble the lesions of psoriasis. The latter are seldom seen on the palms and soles, while the squamous syphilide is very frequently seen in these locations. Moreover, along with the squamous lesions are frequently associated other skin lesions, which give the case a complex type, resembling at one point one of the non-specific affections, and others at other points. Such changes are mainly expressions of various stages in the involution or degeneration of the papule, but they may give the case a variegated appearance, in which pigmentation may be prominent.
Some years ago Biett described a form of syphilide which he claimed was unmistakable and indicative. Since he described the lesion it has been known as Biett’s collarette. It appears in from ten to twenty weeks after the secondary symptoms are fully declared, is superficial, usually situated upon the trunk and extremities, but never upon the palms or soles. It consists of a flat papule almost level with the skin, 1 to 2 Cm. in diameter, rounded in contour, while around it there is seen a zone of white epidermal scales pretty sharply defined and giving it the name of collarette. The area within is dry and painless, and the ring itself narrow. There is little or no itching. It may be followed by some other skin lesion. The lesion is often so mild as to pass unnoticed.
[132]
At other times pustulocrustaceous syphilides will appear above the level of the skin, surrounded by a series of narrow concentric rings, not scaly, but composed of a number of small pustules, the first ring being perhaps an inch from the centre of the inner lesion. This is seen more often in males than in females, and it seems as though the smaller pustules were the result of an auto-infection of ordinary pyogenic character. In the presence of either of these lesions a positive diagnosis of syphilis can be made.
The pustular syphilide may give rise to large or small pustules, which soon become superficial ulcers, often irregular in shape, with an unhealthy floor which may be livid or gangrenous, or may resemble a diphtheritic lesion, while from its surface exudes a mixture of blood, debris, and pus, which dries into dark-colored crusts and constitutes the lesion known as ecthyma. These lesions are often deceptive, since while scabbing seems to be occurring over the surface the ulceration may be extending beneath. This is an intermediate or earlier tertiary rather than a secondary lesion.
Another type of pustular syphilide is that known as rupia, where the ulcers are larger and are covered with concentric layers of crust resembling an oyster-shell. These lesions begin as papules and undergo changes which make them bullæ or pustules and then open ulcers. The peculiar scabs are somewhat conical in shape when not disturbed, and are greenish or brownish in color. If they are dislodged, irregular, indolent, and often sensitive ulcerated areas will be found beneath them. Even when these ulcers heal they are irregular in outline and show a white scar often surrounded by an areola of pigment. This rupia is the most visible lesion of syphilis, as no other skin disease assumes any such type.
In the last-described and ulcerative forms of syphilide there is a possibility of septic infection, or at least of septic intoxication by absorption; hence the need for care in this direction. In fact, into the treatment of every pustular indication of syphilis the elements of local protection and local antisepsis should enter.
—Here the manifestations of syphilis are of great importance because of their extreme infectiousness. The earlier manifestations are seen mainly about the mouth. When an eruption appears upon the skin a condition corresponding to it may often be recognized in the pharynx and upon the uvula and soft palate. This will be accompanied by discomfort, and the patient complains of “soreness of the throat.” These throat lesions are chronic, liable to recur, and disappear slowly, unless the patient is vigorously treated; they sometimes cause dryness of the fauces, followed by a free flow of mucus. The dusky discoloration of the rash is quite distinctive.
The congested areas have a dusky hue on the skin and are spoken of as “coppery” or “raw-ham” in tint. They are usually well outlined; should the disease progress they become eroded. “Syphilitic sore throat,” as this condition is often called, may be aggravated by the use of tobacco and by unclean mouths. The involvement of the cervical lymphatics will be proportionate to the vividness of the lesion.
There is no distinctive time limit between the so-called secondary and the tertiary symptoms of syphilis. Generally the lesions disappear with but little treatment; in many instances they will fade away without any. In most cases, however, the patient, even under poor management, takes enough medicine to disperse the lesions more quickly than they would spontaneously subside. If he discontinues medicine for several weeks, sometimes many months will elapse before there are any active manifestations of the disease. During this period, however, the lymphatic enlargements will not decrease perceptibly, and there may be evidence of advance in this direction. The so-called tertiary symptoms appear usually without fever or other symptoms, and not often in less than five or six months after the commencement of the disease. On the other hand, their advent may be delayed for years, even when the early treatment of the case has been but partially effective.
No organ or tissue in the body is exempt from the ravages of tertiary syphilis. Even the finger-nails and the hair may suffer, while the teeth are affected in the hereditary manifestations. Affections of the skin occur, according to Haslund, in about 12 per cent. of the cases.
The mucous membranes are liable to exhibit those lesions above described, known[133] as mucous patches, usually regarded as late secondary symptoms. The description applies equally well to the tertiary lesions. They occur about the oropharynx, upon the tongue, the lips, the nostrils, and the eyelids. They are frequently found also about the rectum, anus, and genitalia of either sex. In general they present about the same appearance. They commence usually with a slight elevation of the surface and at several points, sometimes simultaneously and successively. These surfaces ulcerate superficially, and thus are produced irregular but rounded patches, with uneven edges, of grayish-yellow surface, which ordinarily are not sensitive, but occasionally extremely so. They may disappear under local treatment, but in that case tend to recur at frequent intervals. If unnoticed or not properly cared for the ulcers may become deeper and assume an unhealthy appearance. In the mucus-lined cavities affected the condition of these ulcers will depend upon the personal habits of the patient. In mouths where tartar has accumulated upon the teeth, or where the toothbrush is seldom used, the patches may become large and foul.
These lesions are extremely infectious and the disease may be conveyed by kissing, by the common use of small domestic utensils, by the pipe, by dentists’ instruments, etc. Patches occurring at the junction of the skin and mucous membrane may extend over onto the latter and become deep, specific ulcers. Lesions of this character need judicious local as well as constitutional treatment. They will often disappear under the latter alone, but it should be combined with local measures. These consist in cleanliness and the use of various antiseptic solutions or applications. An antiseptic mouth wash, as diluted hydrogen dioxide, or of water given a mahogany color by tincture of iodine, should be frequently used. There should be an application of a 5 per cent. solution of silver nitrate, or some other astringent, stimulating, or mild caustic.
Fig. 24

Grouped papulopustular syphilide and numerous pigmented spots from former lesions. (Fordyce.)
—The late syphilides of syphilis belong to the gummatous or tuberculous types (i. e., tuberculous in the anatomical sense, or nodular). The latter may occupy the entire thickness of the skin or lie even deeper. Such lesions may begin as papules and develop into distinct and circumscribed nodules, while these may coalesce into considerable masses. These tend to break down and leave scars after they have disappeared. There is little difference, microscopically, between the nodule and the gumma. Clinically, the tuberculous lesions spread usually in a serpiginous manner, producing a more or less curvilinear outline. (See Figs. 24 to 27.) These ulcerations undermine the tissues to a greater or less extent, and pus and debris will be formed in consequence. In this way they imitate considerably the lesions of lupus, and it may require a careful study of the case and of its history to make a diagnosis. Some of these lesions are extremely slow in their course and long in duration. When scars form they are usually white and smooth, with irregular borders, but sometimes are surrounded by pigment that makes them characteristic. The extent of the scar is no criterion as to the size of the originating lesion, the former being always smaller than the latter.
Fig. 25

Ulcers resulting from deep ecthymatous syphilide. (Fordyce.)
—This is as characteristic of late syphilis as is the condyloma of the earlier stage. By this term is meant a new formation which may vary in size from a millet-seed to a large mass. Sometimes it is diffuse, or it may be circumscribed. It seems to originate from connective tissue, and may be met in all parts of the body. Microscopically it consists of a delicate stroma filled with small, round cells, the mass being furnished usually with bloodvessels, also of new formation. Such a gumma may pass[134] through various stages of integration and disintegration. The cells sometimes undergo fatty changes by which the entire mass is softened, and its interior contains a puruloid material resembling pus. The gumma, as it increases, will replace other tissues and cause them to disappear, and thus it happens that when it disappears the region previously occupied by it seems to have diminished in size. Sometimes, however, cicatricial tissue takes its place and not only distorts an organ or part but impairs its function. Thus softening and melting may occur at one time and a dense scar or mass at another.
The degree of infectiousness of gummatous and other late syphilitic ulcerations is uncertain. The later they occur, the less infectious. It would be safe, however, to assume that they are all dangerous.
—This begins, as a rule, as a subcutaneous gumma which quickly proceeds to and involves the skin. At first it appears as an induration, developing into a distinct tumor, becoming more indurated and firmly implanted as it grows, the overlying skin becoming reddened and swollen. After a time there occurs softening in the interior of the mass, and upon incision there will escape not pus but viscid, puruloid fluid, yellowish gray in color, which may contain corpuscles resembling those of pus. It is the content of such a tumor as this which has given it its peculiar name, gumma. Should proper treatment be rapidly pushed, it is possible for a softened gumma to disappear by absorption, but if ulceration or evacuation has taken place, there remains usually a permanent disfigurement at the site of the mass; like tuberculous gummas these growths may undergo caseous or even calcareous degeneration.
A gumma of the skin will open at one or several points, and, becoming thus secondarily infected, may give exit to sloughing tissue and foul discharge. If the skin directly overlies the bone, then the tumor may involve the latter as well; and when it ulcerates, the bone will be exposed. In the healing process, however brought about, deformity from cicatricial contraction may cause much disfigurement. When a gumma appears beneath the true skin and then disappears it may leave areas of depression, with more or less adherent, bleached-out scars, perhaps with a pigmented margin. The appearance of such scars is suggestive of the disease even without a definite history.
The gummas form the most important features of syphilis, at least from a surgical standpoint, since they frequently appear in the depths as well as on the surface of the body, without any other symptoms, and they often cause no little perplexity in diagnosis. Syphilomas, tuberculous gummas, phlegmons, innocent and benign tumors, as occurring especially in and upon the bone, in the muscles, tongue, the breast, the testicle, and elsewhere, may be difficult of diagnosis. Of course, a history of syphilis is a great help. Doubt frequently arises when such a history cannot be obtained. Scarcely any other disease will produce multiple lesions such as are seen in syphilis, and when multiple[135] they are usually distributed, with some appearance of symmetry. Ulcers formed by their breaking down are often extremely sensitive, but do not bleed easily, nor show a tendency to exuberant granulation. In cases of doubt the most successful test is perhaps the therapeutic, and consists in giving mercurial or mixed treatment to the point of toleration and noting its effect.
Fig. 26
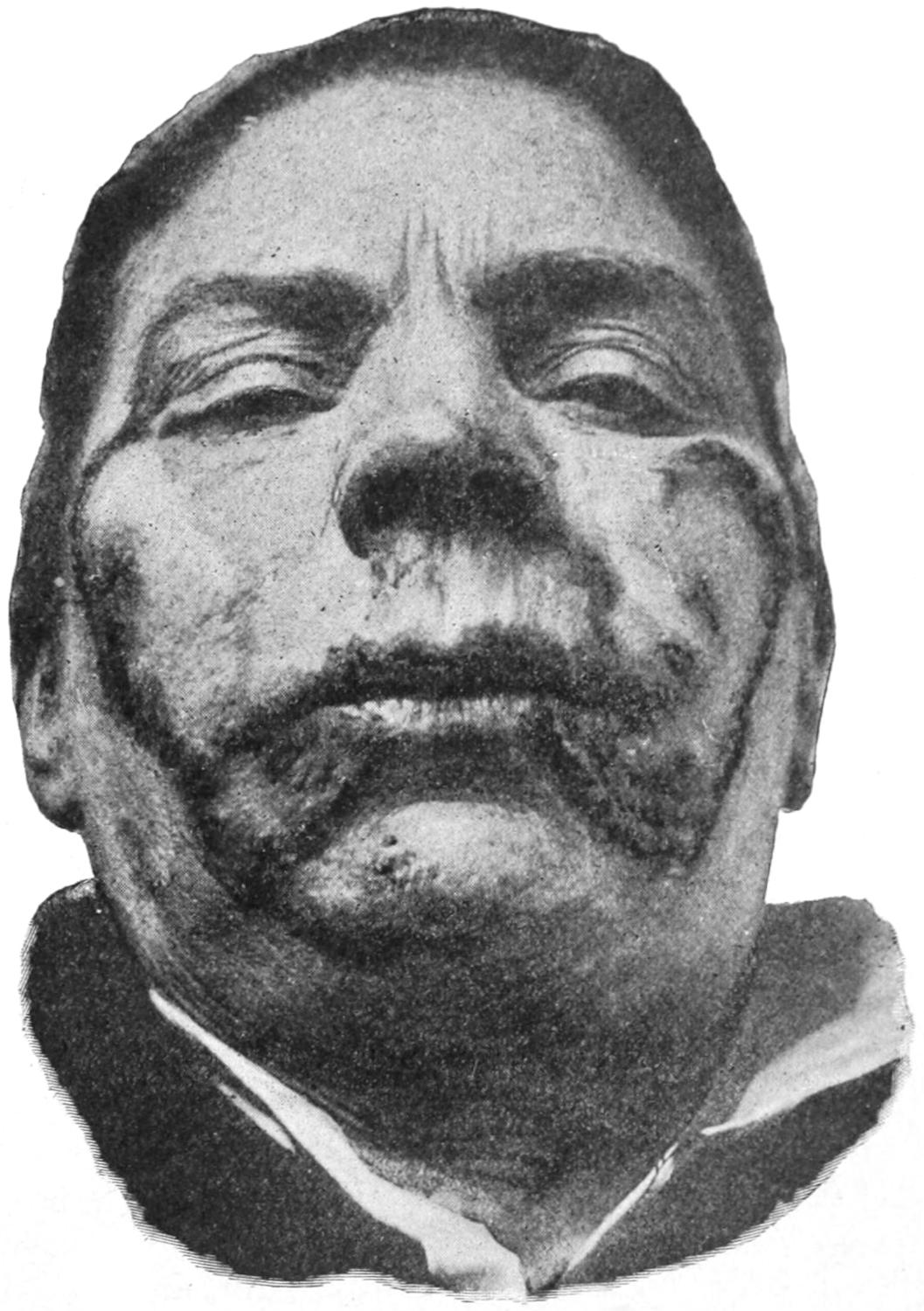
Tuberculous serpiginous syphilide resembling lupus vulgaris. (Fordyce.)
Fig. 27
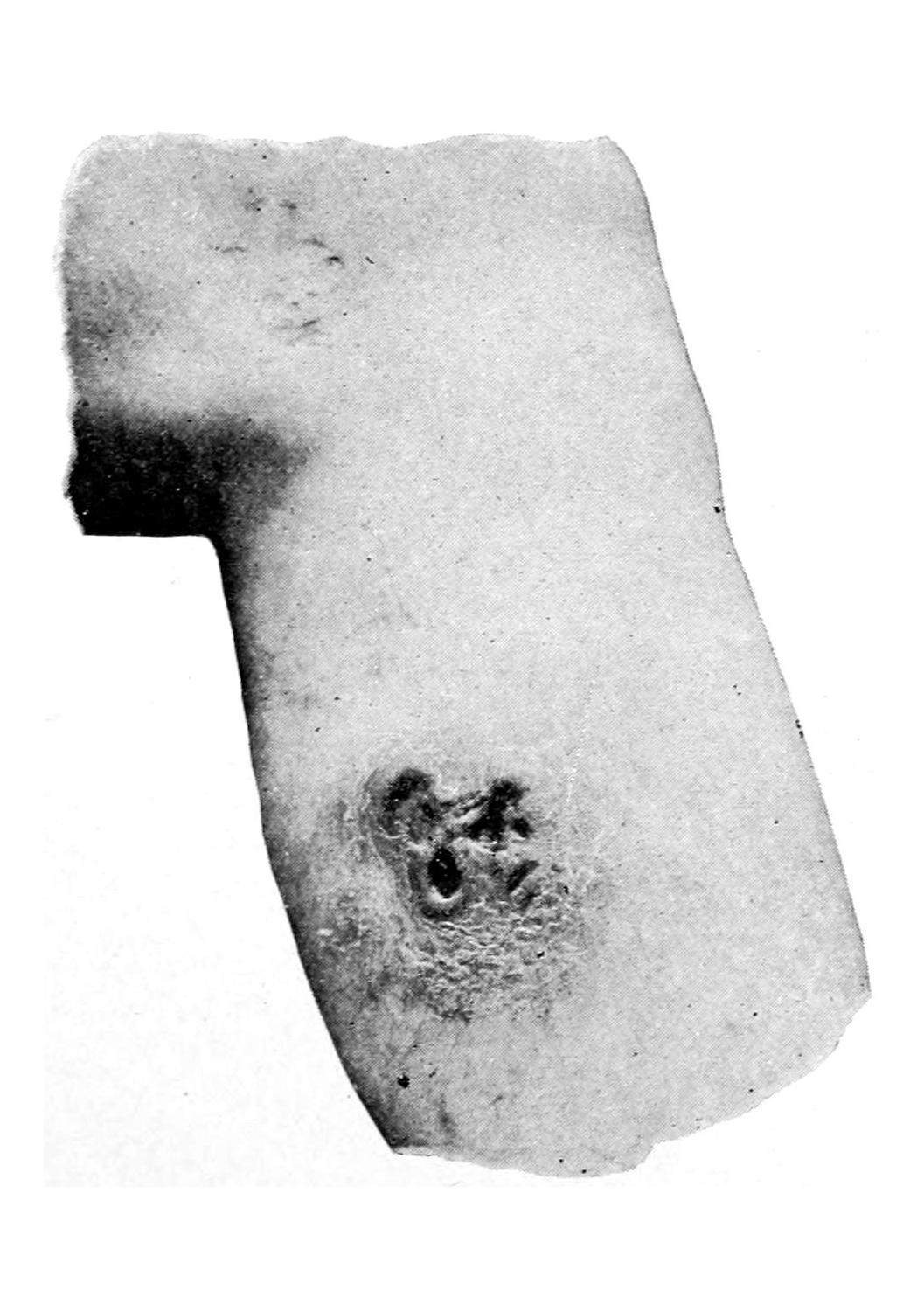
An ulcerating gumma of the leg. (Fordyce.)
In many patients, especially of the hospital class, scars, which are strongly suggestive, will be visible upon the legs. It does not follow, however, that an old scar upon the legs, even if surrounded by a pigmented area, is necessarily of syphilitic origin. Old ulcers of the limbs are frequently seen in connection with varicose veins, and may show exceedingly chronic tendencies; moreover, it is possible for chronic and non-specific ulcers to occur in old syphilitic subjects when the course of the local lesions may be influenced by the old affection, although they are not specific ulcers. Benefit, however, will in such cases accrue by the reasonable administration of antispecific treatment, but it should be combined with suitable local measures.
—The lesions which are encountered in the bloodvessel walls in chancre and early syphilis have been described. The heart and vessels are liable to suffer, as they contain connective tissue. Gummas have been noted in the heart, while the poison also may produce thickening of the valves, and disease of the coronary arteries, the endocardium and the myocardial structure.
The arteries often suffer from arteriosclerosis, which is either diffuse or nodular. Endarteritis is a common manifestation of syphilis and leads frequently to the formation of aneurysm. Sometimes this appears as a single and large lesion; at other times hundreds of small aneurysms will form in the arterial system of the brain, so that the arteries are studded with them. The explanation of aneurysm under these circumstances is that the arterial walls, being weakened, dilate under the influence of blood pressure. Thus the arteries, from the largest to the smallest, also may suffer. The veins likewise are subject to syphilitic phlebitis, which is frequent in the superficial veins of the extremities.
—Syphilitic manifestations in bones are frequent, but are not so common in the joints. While early syphilitic periostitis is not infrequent the actual lesions of the bone are mostly expressions of late syphilis. Nearly all of them are painful. The pain is worse at night, and is called the osteocopic pain of syphilis. At first these bone lesions are hyperplastic, because of the connective tissue in the bone. Periostitis is a common manifestation, and here, again, the neoplastic tendency of the disease is manifested, in that the periosteum is thickened as well as the bone beneath, and swellings called nodes are thus formed. Nodes are met with more often on the tibia and the sternum than elsewhere, but are frequent upon the skull and clavicles. No bone is exempt from these lesions. They often form at points where there has been previous injury. These swellings are ill-defined, and usually quite tender, while the skin[136] over them is easily movable unless secondary infection has occurred and suppuration is present. The nocturnal pains in these lesions, of which patients often complain, are sometimes excruciating. Should suppuration occur, with subsequent formation of ulcer, there may be necrosis of the exposed bone. Another bone lesion of syphilis assumes the type of ostitis. Physiologically this consists essentially of gummatous involvement of the connective tissue, which may be either localized or diffuse. When this undergoes retrocession there occurs a rarefaction of the bone, by which it is weakened and easily broken, so easily in fact that we have to deal sometimes with what is referred to as spontaneous fracture. There is frequently a thickening and condensation of the entire bone, with some distortion, so that the actual weight of the bone may be nearly doubled. Dactylitis is the name given to syphilitic ostitis of the phalanges, which increase in size and become tender and useless, while the skin becomes glazed. Occasionally the disturbance appears to involve the extra-osseous tissues rather than the bones themselves. Bones which are spongy are liable to this disease. Some of the bones in the face are peculiarly susceptible; hence the loss of the bridge of the nose, or of a portion of the hard palate, by the ulcerative processes so common in this disease.
The joints are subject to changes somewhat similar to those occurring in tuberculous disease. There may be either a gummatous synovitis or an arthritis, or else destruction of articular surfaces. These joint lesions of syphilis are all slow in their course, and sometimes difficult of distinction from tuberculous and other lesions. They have so much in common with the joint expressions of tabes that some writers believe that tabes is necessarily an expression of syphilis of the cord.
As long as no active destruction has occurred within a bone or joint these cases are usually amenable to treatment, but for the actual destructions caused here or elsewhere by syphilis there is no repair possible, and the harm once done cannot be undone. Plastic operations and injections of paraffin may have to be practised for cosmetic purposes and relief of disfigurement.
—It is the connective tissue of muscles which suffers most in the luetic affection of these structures. It may be met with as a diffuse process or as a gumma. In the former cases the muscle becomes irregular in shape and size, and in the latter distinct tumors are formed. As such growths advance and contract adhesions to surrounding structures, there is interference with muscle play.
Syphilitic myositis causes little pain, and patients with gummas in muscles are often not seen until ulceration has begun.
The dense fibrous structure of tendons and aponeuroses is frequently involved in late syphilis, causing pain and disability. Little is discovered on physical examination, but considerable loss of function may result. Points of tenderness sometimes are noted along junctions with the adjoining periosteum. Such a tendoperiostitis may be painful, and even crippling.
—Bursæ are prone to be involved in syphilis, especially those in front of the patella. A gumma frequently develops at this point, where it constitutes a painless, somewhat tender enlargement, which may be dense or elastic. After it has become adherent to the skin it is usually infected, and a chronic ulcer results at this point, which may often manifest gangrenous tendencies. This constitutes one form of so-called housemaid’s knee.
—Of the manifestations of syphilis in particular organs the eye sometimes suffers severely. Iritis is the most common and serious manifestations of constitutional[137] syphilis. It has been estimated that nearly 60 per cent. of all cases of iritis are due to this cause. It may occur in two months after the primary sore; it is usually acute, and rarely begins in both eyes at the same time, but may involve one after the other. The ciliary body is frequently associated in the lesion, and iridocyclitis occurs. It commences with congestion of the conjunctiva, photophobia, and lacrymation. The pain is not always severe. Inspection of the iris will show beads of lymph, a small pupil, with loss of contractility, or the dull iris may appear infiltrated and inflexible. The pain in some cases is extreme. Where treatment has been only partially effective relapses are common. The greatest danger to be feared is formation of adhesions between the anterior surface of the lens and the margin of the pupil, i. e., anterior synechiæ. These are detrimental, and serve as the cause of many irritations.
The treatment of these affections is constitutional; locally solutions of atropine of sufficient strength to ensure dilatation of the pupil should be used, not only to relieve the pain, but to carry the margin of the pupil from the central portion of the lens and prevent adhesions. The patients should be kept in the dark because of their photophobia. Atropine may be substituted by duboisine if the former tends to produce congestion. Leeches applied to the temples will also give relief from pain.
The cornea is often affected by a deposit on its posterior surface of particles of debris, which give it a punctate appearance known as keratitis punctata. It also becomes the seat of opacities which materially interfere with vision, and prove only partially amenable to treatment. Lesions of the cornea are frequent in hereditary syphilis.
Retinitis and choroiditis, of either acute or chronic type, are the most common syphilitic lesions of the fundus. They are usually associated and involve both eyes. They come on so insidiously that they are often far advanced when first discovered. The lesions consist of patches of exudation and areas of atrophy, accompanied by some haziness in the vitreous. Vision is affected in proportion to the area involved.
The movements of the eyes are interfered with by lesions which pertain, however, rather to the brain and the ocular nerves than to the eye itself. The sixth nerve, lying on the floor of the skull, is affected by syphilitic disease at the base of the bone. As a result of these nerve lesions paralysis is often seen, or at least disturbances of motility from which diplopia results. Ptosis occurs from affection of the third nerve. In lesions situated below the aqueduct of Sylvius, the paralytic condition which Hutchinson has spoken of as ophthalmoplegia is likely to appear. Optic neuritis is also a late manifestation of syphilis, and may be either chronic and mild, with a small disturbance of vision, or acute, with rapid loss of eyesight.
—The ear may suffer in various ways. The external ear may participate in affections of the adjoining skin. The middle ear may be affected as a result of extension of trouble from the nasopharynx, while in the late stages of the disease patients may suffer from labyrinthine disease, with partial or almost total deafness.
—The lesions of syphilis in the nose are numerous and offensive. Ulceration is frequent and followed by perforation through the septum or into the mouth. When the vomer is involved the bridge of the nose falls in. In neglected cases the whole substance of the nose may be involved and subsequently lost. The bone is often exfoliated. These ulcerations of the mucous membrane and periosteum give rise to a characteristic condition known as ozena, with its characteristic discharge.
—The tongue may be the site of intermediate and late syphilitic lesions. Men suffer more than women, apparently because of their use of tobacco. Mucous patches, deep ulcers, and even gummas, single or multiple, are seen here. Gummas in the tongue are inclined to undergo superficial ulcerative infection and become abscesses. In these lesions there will be notable involvement of the adjoining lymphatics. The appearance of smooth, bluish-gray patches upon the mucous membrane of the tongue and cheeks is known as leukoplakia or leukokeratosis. These lesions do not respond readily to treatment; they give rise to little or no complaint, and are often followed by malignant disease.
It is difficult to distinguish between gumma of the tongue and epithelioma. Usually the latter is a single lesion; the former often multiple. In epithelioma the ulcer is superficially painful, with more elevated and indurated edges, while the pain is sometimes intense and radiates toward the ears.
[138]
Interstitial glossitis is a late manifestation of a sclerosis beginning in the connective tissue and involving the muscle fibers, leading to enlargement of the tongue and later to atrophy and inflexibility.
—Syphilis of the larynx appears either as one or more ulcers, as gumma, or as chondritis or perichondritis, often with necrosis of cartilage. When ulcers form they are deep and destructive, involving even the intrinsic muscles of the larynx, and causing harshness or loss of voice, with dyspnea. Subsequently they lead to cicatrization, often leaving a stricture which may call for tracheotomy. The epiglottis is also liable to ulceration and gummatous lesions.
In these cases, aside from the general treatment, there is need also for local applications of combined antiseptic and anodyne character. Cocaine or one of its less toxic substitutes may be used in spray or by insufflation, in connection with an antiseptic powder, morphine or heroine. Edema of the glottis may be subdued by the local use of adrenalin.
—Between the mouth and the rectum the intestinal canal is rarely involved in syphilitic disease. In the rectum, however, ulcers, as well as gummatous infiltrations, are frequently encountered. If the ulcers are low, within two inches of the anus, they will cause great pain. Higher up the rectum is not so well supplied with sensory nerves. Ulceration may involve the entire circumference of the anus.
In the rectum chronic ulcers are liable to be followed by stricture, which will call for surgical relief. (See chapter on the Rectum.)
In the colon chronic ulcers have been so serious as to lead to dysentery, followed by stricture formation. It has been suggested to make an artificial anus at the cecum and allow the large intestine to rest, treating it at the same time with irrigation through the opening.
—Of the solid viscera the liver is more commonly affected than the spleen or kidneys. Chronic interstitial hepatitis may lead to cirrhosis, the new tissue being less distinctly distributed than when due to alcohol, the liver consequently becoming irregular, with a deep separation between its lobes. The pain is sometimes intense.
On the other hand isolated gummas, or confluent masses of smaller gummas, may be found beneath the capsule or in the substance of the liver. From one or both of these cases combined this viscus may attain an enormous size, with acute pain. Under these conditions there may occur albuminuria and evidences of amyloid disease.
Likewise in the spleen there may be diffuse or localized trouble. Here the lesions cause but slight distress.
The mercurials are of greater importance than the iodides in treatment of these lesions. The kidneys suffer less often than the spleen. Syphilitic patients do not lose their liability to renal disorders, but there seems to be but small, direct connection between syphilis and the common changes in these organs.
—In both sexes the genitalia are subject to gummatous involvement during the later stages; in the male more frequently in the corpora cavernosa and testicle. In the latter a chronic induration, with some enlargement of the epididymis, is one of the manifestations of constitutional disease. Most of the enlargements of the testicle are slow and painless, and occasionally some fluid will collect. The prostate and the seminal vesicles are rarely involved in syphilis, but frequently in a tuberculous process. This is an important diagnostic point.
In the ovaries there may occur a diffuse cirrhotic process.
—Here the manifestations of syphilis are often serious and widespread. They are produced by the same new tissue to which we have so often alluded, with its tendency at first to degeneration and later to sclerosis. They are always insidious. Gummatous thickening may occur at any point, springing often from the pia of the brain and cord. The arterial walls are frequently so affected, and at many points, that multiple minute aneurysms are produced, any one of which may give way and produce the fatal results of a cerebral hemorrhage. In diffuse gumma of the membranes or cortex the process is slow, and likely to involve areas which may be recognized by cerebral localization. Many cases presenting the features of brain tumor will yield to antisyphilitic treatment, and thus show themselves to be syphilomas.
In the spinal canal implication of the membranes is more likely to occur than in the vessels. In the cord these sclerotic changes are also quite common and produce symptoms[139] strongly suggestive of tabes; in fact, there are those who hold that tabes is of specific origin.
In the motor and sensory nerves much connective tissue is present, and consequently these nerves are not exempt from sclerotic changes with pressure symptoms, which will give the clinical picture of a neuritis.
Syphilis appears in young children under the following circumstances:
A. The disease may have been transmitted from the father to the ovum, at the time of conception, by infected spermatozoa.
B. From the mother, who may have acquired it before impregnation or during the early part of her pregnancy. In the latter case the infecting influence is transmitted through the placental circulation.
C. From the mother at the time of its birth, from a recently infected puerperal tract.
D. From some possible extrinsic source, a short time after its birth, as, e. g., through the umbilicus.
The later the mother acquires the disease after conception, the less likelihood that the child will be infected. If infection takes place from the placenta, then it also will be found to be diseased.
—Profeta first made the statement that the child of an infected mother who acquired the disease late in her pregnancy may not only be born healthy, but may be immune to subsequent infection, as are other healthy children of syphilitic parents. But, on the other hand, such a child may be anemic, puny, with small resisting power, or it may develop a late hereditary syphilis. When the ovum is infected by the father the healthy mother may escape, or she may acquire the disease through the placenta in her own uterus, or she may suffer from a mitigated form of syphilis whose principal features will appear as late manifestations of the disease.
—Colles, in 1837, made the statement that such a mother may remain healthy with an acquired immunity to subsequent infection. The statements above made have often been alluded to as Profeta’s and Colles’ “laws.” These should, however, be regarded simply as statements of what usually occurs, and too much dependence should not be placed upon them. In fact, the immunity which the mother or the child may enjoy under conditions mentioned above is not likely to be permanent, though it may last for a varying period of time. There is no limit to the time when a parent may transmit syphilis to the child. The five-year limit given for the father is often overstepped, and the longer the man waits before marrying after acquiring the disease, and the more thoroughly he submits to judicious treatment, the less likely he is to convey it to offspring. This is the strongest kind of argument that can be used to delay marriage of syphilitics.
The indication of syphilis on the part of the mother is, in addition to those already given above, a tendency to miscarriage or abortion. The earlier she acquires the disease the earlier will the mishap occur. Should she escape the child may go on to full term, or it may die and be expelled as a dead fetus two or three months before the expiration of term. Should a child be born alive with hereditary syphilis, the evidences may appear at birth or within three months. Should a child apparently escape for six months it may grow up to be puny or develop some form of late hereditary disease, or it may possibly remain well. These children usually show developmental defect in some direction, and manifest a much weakened resisting power to other diseases; moreover, the spleen will usually be found enlarged.
Among the changes which may occur are the following: The skin becomes loose and resembles that of an old person. This is partly because it grows even faster than the tissues beneath it, so pronounced is the emaciation. Snuffles, or nasal catarrh, is one of the earliest features. This is due to specific swelling of portions of the Schneiderian membrane. Snuffles may occur in children without syphilis, but syphilis will nearly always produce snuffles, which may last for some time, and cause a widening at the root of the nose which will persist through life. Following the snuffles there usually appears a rash over the trunk and thighs and about the anus, accompanied by mucous patches. This will have the same bright, coppery tint as roseola syphilitica, already[140] mentioned, which it much resembles. Sometimes it assumes the mixed type of eruption, while upon the palms and soles appears the so-called pemphigus syphiliticus. Should the child live nodular or gummatous syphilides may develop.
In the bone and cartilage characteristic changes are met at the lower end of the femur and at the costochondral junctions. This consists of an osteochondritis syphilitica. At the affected points enlargements take place, which may disappear under treatment or may go on to ulceration and necrosis. In the fingers and toes there are manifestations already described as syphilitic dactylitis.
The bones of the skull are likely to be involved in thickenings, especially about the anterior fontanelle, where they form the so-called Parrot’s nodes. These may disappear, with or without treatment, and the affected bone may undergo atrophy or may entirely disappear.
Among the viscera the spleen generally becomes affected first and then the liver. Syphilitic iritis may occur early, but is rather rare; ocular changes occur more often in the choroid. In the brain distinctive lesions may occur to such an extent as to lead to considerable thickening of the dura, with or without hydrocephalus, and subsequent imbecility or idiocy.
Deafness is not infrequent in hereditary syphilis. It may begin suddenly and at any age, even during infancy. It is produced by deep lesions which do not yield readily to treatment, and sometimes leads to deaf-mutism, especially when it occurs before the child has learned to talk.
Among the later manifestations of hereditary syphilis are opacities of the cornea from interstitial keratitis. This may occur in children who are apparently in good health and free from other signs of hereditary disease. The condition is rather obstinate, but it can be made to disappear under suitable treatment. Retinitis occurs frequently in young women, and is likely to lead to atrophy or detachment.
—The permanent teeth often show peculiar changes that are distinctive, especially in those who have shown signs of corneal involvement, which, having been first described by Hutchinson, are frequently alluded to as Hutchinson’s teeth. When they first appear they are smaller than natural and irregular. Later they become notched. The crescentic notches show best upon the incisor teeth. Sometimes the canines are also affected, being narrow, rounded, and peg-like, with jagged edges. These teeth are usually so formed that they do not meet properly, and so small that they scarcely touch each other. The most characteristic changes are met with in the upper incisors, which may be affected when all the others are fairly normal. In such cases they will be found narrow and short, with a single broad notch at the edge, with perhaps a furrow passing from it upward and on both anterior and posterior aspects. Notching is usually symmetrical. No conclusions can be drawn from the teeth if they are normal, as they may be, but when they present the above-described features they prove a very important indication.
The relations between syphilis and rickets have attracted much attention, and there is little doubt but that rachitic changes are prone to occur in subjects with inherited syphilis. The two conditions are sometimes blended in various degrees and ways, and yet it is not safe to say that rickets is always an expression of inherited syphilis.
There is no question but that some of the above-described lesions constitute as disgusting and repelling diseased conditions as the physician or surgeon is ever called upon to treat. In spite of these circumstances, however, it is generally believed that syphilis is a most satisfactory disease to treat. This is because of the almost mathematical certainty with which results can be predicted and estimated. There is nothing more satisfactory in therapeutics than the rapidity with which many pronounced and serious manifestations of syphilis will disappear under the influence of proper treatment. These statements, however, should be modified to make room for exceptional cases, where the disease assumes a malignant type, owing probably to some defect in the patient’s constitution, or where patients show peculiar idiosyncrasies and susceptibilities to the influence of mercury and iodine. Such cases happen occasionally and prove difficult of solution, while they sorely try the surgeon’s ingenuity and resources.
[141]
In the majority of instances syphilis is a curable disease. A patient should be first impressed with the necessity of faithfully following the directions of his physician, and continuing under treatment for a period of at least three years after the disappearance of the last manifestation of the disease. The disease is curable, but only by the judicious combination of two principal remedies, i. e., mercury and iodine. Those rare instances in which cure seems to have followed lines of treatment which do not include the use of these two drugs are so exceptional and misleading that they should not be considered criteria. Mercury and iodine are powerful remedies, needing to be administered with caution and judgment. Unfortunately there is no arbitrary limit of time for any given case. The time stated above is that usually considered requisite. While syphilis may be curable in some cases in less than the stated time, it is better to give it longer treatment than is absolutely required rather than the reverse. The treatment entails no unpleasant consequences. Warnings as to the approach of toxic symptoms from the drugs can be easily recognized.
Of the two drugs the preparations of mercury are the more important. The surgeon may adopt as his motto, mercury, more mercury, and again mercury, and if he begins with this measure early in the disease he may be able to conduct it to a successful termination with but little resort to iodine. Iodine is effective rather in those cases where treatment has been begun relatively late, and where it seems necessary to make a double impression upon the disease.
When the nature of the primary lesion is positive treatment should begin with the first visit of the patient to the surgeon. When there is uncertainty regarding the character of the venereal sore, treatment may be postponed until the appearance of the first eruption. As soon as this has appeared the treatment should be hastened. It is necessary to begin with mercury. The patient’s mouth should be examined by a dentist and all tartar removed from the teeth, especially from the gingival borders, at which lines the gums are likely to become sore when mercury is too freely used. All diseased teeth should be extracted or filled, and the mouth and its contents should be put in normal condition. The dentist should be informed as to the reason for the visit. Smoking should be discontinued, especially when there are mucous patches, since it is apt to irritate and make subsequent lesions of the mucous membrane more likely to occur. The habits of the patient should be regulated as to alcohol and other indulgences, and he should be warned as to the infectious nature of the disease, in order that others may be protected. In many instances tonic, even roborant treatment may be advantageously combined with the antispecific. It will be found that the anemia so characteristic of well-marked secondary syphilis will improve materially under the influence of mercury alone.
Should the disease occur in a married person, or develop after marriage, caution should be given as to the danger to offspring, and to the other associate in the marriage relation, which might follow the occurrence of pregnancy.
Mercury may be given by the mouth, by inunction, by hypodermic injection, or by fumigation. The intent should be to get the patient under its influence as rapidly as is consistent with safety. The most effective of these methods to which patients will ordinarily submit is that by inunction. This consists essentially in the use of mercurial ointment (blue ointment), of which 15 Gm. may be used daily or nightly, which should be thoroughly rubbed into some area of the body; the areas selected being changed at perhaps three-day intervals, in order that irritation, which its prolonged use produces, may be avoided. It takes considerable effort to so completely rub this in as to make most of it disappear, and it can be done more easily upon those parts of the body which are free from hair. It can be best done by employing someone for the purpose, but patients can be easily taught to use it themselves. There are upon the market, ointments containing mercury made with other excipients than lard, which are less uncomfortable to the skin and seem to be absorbed better; among these is a preparation made with a petroleum compound called vasogen, which may be procured in different strengths; that containing 33 per cent. or 50 per cent. is the best.
Inunction should be practised at least once every twenty-four hours, until either the gums become tender or swollen, with an offensive odor of the breath, or until the skin is irritated. The mouth should be protected by use of an astringent antiseptic mouth-wash, such as the following: Carbolic acid 10 parts, oil of wintergreen 1 part, tincture of myrrh 50 parts. A little of this solution in a tablespoonful or more of water makes[142] a serviceable wash, which should be used several times a day. There are sanitaria and springs, or health resorts, in this country where a specialty is made of this manner of treatment. At these resorts inunction is practised freely and thoroughly, but the benefit which is obtained comes rather from the attention which patients give to the treatment, and their abstention from business or dissipation, than from any inherent medicinal features either in the mineral water or climate.
Under the influence of mercurial ointment alone, if a patient is willing to persist in its use, many cases of syphilis may be conducted to a successful termination; but its use is disagreeable to some people, and it may be impossible to resort to it for any great length of time. It has its inconveniences and disadvantages, but it should be applied in at least the first stages of the disease.
When mercurial ointment is seen to have made a distinctive impression upon the constitution of the patient it may be discarded and the treatment changed to the internal administration of the drug.
Mercurials may be given internally in any one of several different preparations. Hutchinson has recommended gray powder, in doses of ¹⁄₄ to ¹⁄₃ Gm. three or four times a day. Corrosive sublimate is a reliable form in which to administer mercury in doses which can be tolerated, from 1 to 2 Mg., three or four times a day. The red iodide may be given in similar doses, or the green iodide may be administered in doses of 0.15 to 2 Cg. These preparations sometimes irritate the intestinal tract and produce a certain amount of colic or looseness of the bowel. For the latter some astringent may be combined with the mercury, while intestinal pain may be checked by the use of extract of conium.
The hypodermic use of mercury can be made effective, but there are but few preparations which can be used that do not cause pain and subsequent irritation. Perhaps that which gives least pain is the sozoiodolate of mercury. This is sparingly soluble in water, dissolving in about 500 parts by weight. As the dose is 9 or 10 Cg., the amount of water necessary for this solution is so bulky that the dose should be injected into the gluteal region. Corrosive sublimate is also used in 1 per cent. solution, made up in common salt solution of the usual strength of 9 to 1000. Of this 10 minims represent a suitable dose to commence with, which may be increased to 30 or 40 minims when necessary. This should be given in the same region, the needle being driven in its full length perpendicularly to the surface. When this is done an injection is made into the muscle, where it seems to be more effective than in the subcutaneous fat. When the dose is increased to more than 20 minims a 2 per cent. solution may be used and the amount of fluid correspondingly reduced.
Fumigation is a method now not often adopted, calomel being used for the purpose, an ordinary cabinet hot-air bath confining the vapor about the patient. One treatment a day by either of these methods is usually sufficient.
About the initial sore dry calomel, pure or reduced with bismuth subnitrate, may be used. The condylomas met with about the perineum will often shrink and disappear under the influence of this application. Mucous patches should be treated with absolute cleanliness; in the mouth a wash of diluted hydrogen dioxide may be used, and the patches touched with a strong nitrate of silver solution, pure carbolic acid, or camphophenol. This will not prevent contagion from such a source, but will reduce it to a minimum beneficial in every respect.
The various eruptions of syphilis will disappear gradually under the influence of a local application of one of the mercurial preparations, either the ordinary mercurial ointment or ammoniated mercury.
In cases of inherited syphilis, especially in young children, a reduced mercurial ointment, or the use of gray powder (mercury with chalk) will give the best results. The dose should be regulated by the age of the patient; for instance, of the latter 1 to 2 Cg. for an infant. The iodides have also proved successful.
Iodine and its preparations have by many authorities been held to be useful in the later and especially in the gummatous lesions of syphilis. There are patients who cannot take iodine to any extent without suffering from such disturbance of mucous membranes, especially in the nose and intestines, as to make it an exceedingly unpleasant remedy.
The iodides have not proved as successful as the mercurials; nevertheless, the combination is a popular one and sometimes of peculiar value. The potassium salt is the[143] one generally used, as it is cheaper than the sodium compound. The latter, however, is less irritating and often more available. The lithium compound is ideal in some respects, but very expensive. The iodides may be given in large doses, to the extent of 30 Gm. or more (an ounce or more) in twenty-four hours. Large doses are sometimes necessary in the treatment of late syphilis of the nervous system. When it is necessary to put the patient rapidly under the influence of antispecific medication the combined use of these two drugs, as for example by mercurial inunction and the use of one of the iodides internally, will most speedily bring about the desired result. This result may be overreached, and sore mouth or other toxic manifestations may appear suddenly and unexpectedly.
The mercuric salts are soluble in solutions of the iodides, and what is known as mixed treatment is often employed. The salts may be combined in any desired preparation. Donovan’s solution is exceedingly valuable, the arsenic which it contains seeming to reinforce both the mercury and the iodine.
The iodides produce eruptions or rashes which strongly simulate both syphilitic and non-syphilitic skin diseases, and confusion may arise from their use. In those who are sensitive to the iodides, and in whom catarrh of the mucous membranes is easily produced, it is best to begin with small doses, increasing them as circumstances may warrant. Some patients cannot take iodine in any form. When iodides irritate the stomach they should be given in essence of pepsin.
Of the various vegetable remedies some are unreliable and of little value. Certain combinations can, however, be effected in some cases by which the value of the effective agents may be enhanced. Zittmann’s decoction or McDade’s formula will occasionally prove of service. In aggravated cases the former is believed to be the most effective of all methods of administering mercury. Tonics or any other medicines which may be called for in particular cases should be given judiciously. There is nothing in antisyphilitic treatment which precludes other treatment when needed.
[144]
Since the time of John Hunter and his pupils, who confused the three totally different and so-called venereal diseases, pathologists have drawn a distinct line between chancre, which is simply the initial sore of syphilis, and chancroid or venereal ulcer, which is a distinctly local lesion, often destructive, but never followed by constitutional disease, except of septicemic or pyemic type. It is usually found upon the genitals, about the foreskin, glans, and vulva, but may be met anywhere upon the body where infection has occurred. It is distinctly auto-inoculable, in which respect it differs from chancre.
Varying views have been held as to the minute agency concerned in the production of this lesion. The bacillus discovered and studied by Ducrey, in 1889, is now accepted as the exciting cause. This is 1.5 μ long and 1 μ thick, with rounded deep-staining ends and fainter-staining central portion, occurring with great constancy in chancroidal pus, less often in buboes than in ulcers, in and outside of the cells, and in chains. It is cultivated with difficulty, grows best on human blood, takes basic aniline stains, but is easily decolorized by alcohol or by Gram’s method. Characteristic ulcers can be produced by inoculating it, even in monkeys.
Chancroid begins, in twenty-four hours, as a red point or papule, which is quickly converted into a pustule and then into an ulcer. The borders of this ulcer enlarge, its depth increases, until after a few days it forms a more or less deep, often undermined excavation, irregular in contour, discharging grayish purulent material. In this respect it differs also from chancre, whose natural discharge is more like serum. In other words, chancroid is essentially destructive, chancre constructive, since the latter forms a new-growth which ordinarily has little or no discharge. When the necrosis of chancroid becomes extensive and tends to spread rapidly the ulcer is spoken of as phagedenic. This tendency to rapid local gangrene is the combined result, probably, of virulence of virus and lowered local or constitutional tissue resistance. It is consequently most often seen in alcoholics and prostitutes. In rare instances a surface larger than the hand may be rapidly destroyed, every particle of material sloughed being infectious.
In chancroids of the mild variety the discharge may dry upon their surfaces and scabs or crusts result, beneath which, when detached, the characteristic ulcer is present.
Under proper treatment this foul ulcer is soon converted into an ordinary granulating surface, which heals by cicatrization.
Infection, by propagation along the lymphatics, of the inguinal nodes is frequent, and, since the infection is almost always a mixed one, suppuration is frequent.
The pus of a suppurating chancroidal bubo is as infectious as the discharge from the original sore; hence the need of great caution. The edges of the local incision should be promptly cauterized so that they may not become linear chancroids. Phagedena shows itself here as well as about the genitals proper, and differs only in that it makes the case more serious. A chancroidal bubo may, however, subside without abscess formation. The signs of suppuration are those incident to pus formation anywhere near the surface. When pus is present its early evacuation is demanded.
—Chancroid is likely to be confounded with chancre and herpes preputialis. It has no period of incubation. Destruction commences after infection, so that within twenty-four hours macroscopic evidence may be observed, and within two or three days the sore has attained distinct size and shape.
[145]
| Chancroid. | Chancre. | Herpes. |
|---|---|---|
| Local ulcer. | First local sign of a constitutional disease. | Local neurosis. |
| A distinctly venereal infection. | Usually a venereal infection. | May be non-venereal, from friction, irritation, uncleanliness, etc. |
| No incubation; lesion noticed within a few days. | Incubation from ten to seventy days before first lymphatic induration. | No incubation. |
| Commences and remains as an ulcer. | Commences as a papule, or occasionally as an erosion. This may ulcerate later. | Commences as a crop of vesicles. |
| Usually multiple. | Usually single. | Multiple and occurring in crops or series. |
| Secretion purulent and abundant. | Secretion slight and serous or bloody. | Little or no secretion. |
| May occur again and again. | As a rule, it only occurs once in the same patient. | Patients who once have it are frequently subject to it. |
| Auto-inoculable. | Not auto-inoculable. | Not inoculable. |
| Phagedena frequent. | Phagedenic action very rare. | Never. |
| Buboes in about 65 per cent. of cases. | Bubonic enlargement nearly always. | Lymphatics rarely involved. |
| Buboes usually suppurate. | Buboes as a rule do not suppurate. |
—Except in the most debilitated and dissipated, in whom phagedena may prove fatal, recovery always occurs, but often with the loss of tissue and disfiguring scars.
—In mild cases—i. e., those showing but little destructive tendency—cleanliness and the use of hydrogen peroxide, followed by local use of any of the ordinary antiseptic powders, or even of calomel, will usually prove sufficient. Sodium sozoiodolate makes an excellent application. It is odorless and non-toxic. At first its use may be preceded by morphine or cocaine, but after a few days it will prove a painless application. If the ulcer manifest any tendency to spread, it should be cleansed, cocainized, and then cauterized with nitric acid or the actual cautery, after which it should be so treated as to encourage granulation. This plan should be followed in phagedenic cases, which may call for general anesthesia, with the use of scissors and a sharp spoon, followed by cauterization of every particle of raw or diseased surface.
Widespread phagedena is more rare now than formerly. Cases which are extensive do best when submitted to continuous immersion of the hips in a sitz-bath as hot as can be tolerated. All aggravated cases call for invigorating and tonic measures, laxatives, improved nutrition, and stimulants.
Suppurating buboes should be incised, usually curetted, and thoroughly swabbed with pure carbolic acid, followed by pure alcohol to neutralize the acid, then packed lightly with antiseptic gauze, and allowed to close by granulation. Virulent cases will be accompanied by sloughing of so much tissue that it is best to remove all sloughs with scissors. Here even stronger caustics will be called for. Phimosis often complicates chancroid, and will necessitate circumcision or incision along the dorsum of the prepuce, with such attention to the parts thus exposed as their condition may require.
—Mixed chancre, or the combination of the two lesions, has been already discussed.
—Extragenital chancroid may occur upon any portion of the body, but is more rare than extragenital chancre. It is characterized by the same peculiarities as pertain to the venereal sores already described, and is amenable to similar treatment.
[146]
Gonorrhea is an acute infectious process, involving especially the mucous membranes of the genito-urinary organs, but met with elsewhere about the body, in both superficial and deep tissues. The name itself is a misnomer, since it implies a flow of semen, whereas the discharge which issues from the male urethra is simply mucopus, and is the product of a severe inflammation of the mucous membrane. A less inaccurate name for it is blennorrhea, although this is usually limited rather to a discharge from the vagina, and indicates a whitish and copious fluid exudate, mingled with pus corpuscles and bacteria. It is stated that probably 80 per cent. of men have at some time contracted this disease. Neisser claims that it is a more common affection than measles.
True gonorrhea is the result of an infection by a specific organism universally recognized as the gonococcus of Neisser, though the discharge, when studied in the clinical laboratory, may give evidence of being the product of a mixed infection and contain the ordinary pyogenic or other organisms. The common name for the disease is clap.
The gonococcus is a diplococcus which seems to be injurious only to the tissues of the human being, as inoculations in animals have produced no definite or reliable result. Like syphilis, it is spread by direct or indirect contagion, and usually in the same way. It is generally found in the genito-urinary mucosa of both sexes, but it has been accidentally and even innocently conveyed by immediate and mediate transfer to the mucous membranes of the eye, the rectum, and even to the mouth, although here, as in the nose, the mucous membrane is but little susceptible to its activity. It is generally stated that 20 per cent. of the blindness occurring in the young is due to gonorrheal conjunctivitis. Those membranes covered with cylindrical epithelium are more liable to succumb to infection by this parasite than are those covered with squamous epithelium. The more the epithelial cells conform to the former type, the more difficult it is to get rid of the infection; hence the disease lingers in the cervical canal longer than in the vagina.
The disease always commences as a contagious catarrhal discharge from the mucous membrane. It may spread much farther than this, invading deeper tissues by continuity, or tissues at a distance by the lymph stream, or producing even metastatic expressions of infection in distant tissues and organs. Under these circumstances the serous membranes are likely to suffer, and the peritoneum, the endocardium, the pericardium, the pleuræ, the meninges, and particularly the serous linings of some of the joints, as the elbow and knee, show unmistakable evidences of infection; while through the medium of the venous and then the arterial systems typical representations of pyemia following gonorrhea may occur.
The disease as it usually appears is seriously and often obstinately complicated by the structure of the membranes which it involves. The mucous membranes throughout the body are more than mere mucous surfaces; they are dotted with openings for the escape of glandular secretions, and nowhere is this more conspicuous than in the urethra, where many minute follicles, so called, empty tiny drops of secretion into the mucous canal. Infection may easily travel along these routes and lurk within such minute recesses long after it has apparently disappeared from the surface; and so it often happens that in the male not only the urethral follicles but the ducts leading to Cowper’s glands and prostate become involved, while in the female the follicles around the meatus, the urethra, and the vulva rarely escape. The clinical importance of this statement is of interest, as by it may be explained many of those cases where an old infection seems to have been lighted up, or where the contagion has been conveyed to another after an attack which was supposed to have been entirely cured. Nothing seems to favor outbreaks of this kind as do alcoholic and sexual excesses.
The gonococcus may be scarcely regarded as an obligate pyogenic organism by itself, but the parts most often involved in this disease may be regarded as never free from the[147] presence of other germs of greater or less activity, and by association, if not by actual symbiosis, such an intense reaction is provoked that the resulting products do not differ from true pus, save by the added presence of the specific organism most at fault. Under these circumstances abscesses may form in any tissue infected. Another expression of this fact would be the establishment of a pyarthrosis after involvement of one or more joints. Gonococci may be found in almost every abscess of truly gonorrheal origin; on the other hand, in some of the serous cavities it is possible, at least for a time, that gonococci may be present in the serous fluid without producing in it more than a disturbing effect, the fluid now appearing turbid rather than puruloid.
The amount of toxemia which may be produced by gonococci without reference to formation of pus has not yet been established. It is, moreover, a difficult thing to estimate in cases of mixed infection. Occasionally there are cases of metastasis and gonorrheal invasion which are free from evidences of suppuration, and yet there may be anemia and cachexia of profound type; these can only be explained on the theory of an intoxication.
Besides the serous tissues of the body the fibrous structures may suffer seriously, not only in an acute manner, but also in a chronic and obstinate form.
It has been the custom to speak of urethritis as a synonym for gonorrhea, and to divide it into the specific and non-specific forms, including under the former expression cases where the gonococcus can be demonstrated, and under the latter term those which do not seem to show it. There is no doubt but that urethritis may be set up by the introduction of a foreign body, such as a sound or catheter, as well as by some irritating discharge from the vagina, and also as the result of excess of uric acid in the system, perhaps even of alcohol. These, if occurring in a previously uninfected urethra, may be regarded as distinctly non-specific lesions. It is also supposed that under certain circumstances inflammation may be set up by other organisms than the gonococcus; nevertheless almost all cases of so-called clap are positively gonococcus infections, simple or mixed, and have but one origin.
—Diagnosis can be made positive only with the microscope. A recognition of the gonococci by staining them and then watching the effect of iodine in their decolorization will be of great importance and reliable. The affinity of these germs for basic aniline dyes, and the fact that they do not take the iodine stain of Gram, will serve to differentiate them from the numerous other organisms with which they may be found mixed. By staining a cover-glass preparation first with methyl blue or other basic color, then placing it in Gram’s solution, and finally in a solution of Bismarck brown, the true gonococci which have been made visible by the methyl blue will have disappeared under the influence of the iodine, while other bacteria will be stained by it. It has been mentioned that the germ is a diplococcus of rather ovoid form, met in clusters but not in chains, and in groups of four or multiples of four; it may be attached to epithelium and pus corpuscles, or found within them, and is rarely found free in fluid except when present in large numbers. These organisms are capable of cultivation, growing best upon a mixture of human serum and neutral agar, at a temperature of 36° C.
The urethra may be infected from without and from within, and this infection may be either of a truly specific type (gonococcus) or of the pyogenic type; as between these forms information may be gained by the history and the clinical course, but the minute diagnosis is only to be made with the microscope. This is of more than theoretical value, inasmuch as it substitutes a certainty for a working hypothesis. It is, moreover, sometimes of great value, as when the question of infection of one of the opposite sex comes up, or it may have at times even an important medicolegal value, as in cases of rape.
Infection from without, so far as the male urethra is concerned, is a question of the venereal origin of the disease. Infection from within, in the specific form, is a matter of recrudescence of a formerly active lesion supposed to have disappeared. Infection of non-specific type from without affects the introduction of germs either by venereal contact or by the medium of an unclean catheter, sound, or some other instrument, or from within by the extension forward of an inflammation higher up in the genito-urinary tract, such as may be due to stone in the bladder, cystitis, enlarged prostate, or uric acid or oxalic acid crystals. Urethritis, usually of mild type, is not infrequent in old men from either of these causes. It may also be produced by the infection of a too strong or irritant injection, whether used either for prophylaxis or for ordinary treatment.
[148]
Classifying them we may then have urethritis of the following four types:
A. The period of incubation is short, usually two to six days, and the resulting inflammation is severe; the consequences are often remote and sometimes disastrous. Gonococci will be found in the pus and epithelial debris.
B. This has been described as “bastard clap.” It is really an auto-infection, with an incubation period of a few hours, and is practically the reawakening of a quiescent stage of A. It is characterized by abundant purulent discharge; this latter is thin and mucilaginous, more like that of so-called gleet, with an abundance of pus threads, or “clap threads,” in the urine. In this form gonococci are also found, but less frequently.
C. Much like A in its clinical course, but less violent, and with less widespread reaction. Its period of incubation is rarely over thirty-six hours. This type is most common after alcoholic and sexual excesses; the latter especially with one already suffering from vaginal discharge, particularly so when near the time of menstruation. Here the microscope will show few if any true gonococci, but a profusion of pyogenic organisms.
D. This form of disease is of non-venereal origin, and is susceptible of easy explanation and of satisfactory treatment if the cause be properly treated. No case of urethral discharge which does not seem to fall easily into one of the above categories should be treated without a search of the anterior urethra, especially the fossa navicularis, for possible chancre or chancroid, as well as for stricture.
Among the laity the idea is prevalent that gonorrhea is a disease of more or less trifling import, while many of the profession regard it as rarely worthy of serious consideration. This is an unfortunate notion regarding this disease, and those who have had largest experience unite in expressing the opinion that gonorrhea reckons more victims in the death list than does syphilis—not because it is more common, but because of its complications and the ravages, especially in the kidneys, resulting therefrom. It has been shown that the specific organism producing it may linger for years in the follicles of the urethra, whence it may issue forth, unexpectedly, to produce vaginitis, perhaps in the most innocent of women, and thus bring on a train of pelvic disorders which may involve the ovaries, the tubes, and the peritoneum. Doubtless gonorrhea has made in this indirect way many more victims than syphilis.
Regarding gonorrhea thus seriously, it is well to treat it cautiously and to inculcate vigilance in the daily life and habits of the patient. There are no arbitrary limits during which danger exists and then passes; peril lurks about such a case for an almost indefinite time. There is danger not alone to the individual, but to all with whom he may have sexual or even other relations. This advice pertains not alone to the urethral discharge and the care of the urethra, but especially to the avoidance of all possible contamination of the conjunctiva. One of the saddest spectacles in the domain of medicine is to see one or both eyes of an innocent victim injured or ruined by gonorrheal infection.
There is no denying the clinical fact that individuals vary considerably in their susceptibility to this disease; moreover, individual susceptibility varies at different times. Alcoholic and sexual indulgence seem to materially lower this susceptibility. Thus from the same individual, and within twenty-four hours, one may acquire the disease while others escape. In some instances immunity seems to be afforded by repeated attacks; in other individuals repeated attacks seem only to enhance the liability to the disease. The gonococcus grows best in alkaline media. Prolonged sexual excitement diminishes the acidity of the urethral fluids, and this favors the growth and development of the germ. No credence should be given to popular notions concerning the possible avoidance of infection after exposure. Even a careful toilet is usually inefficient for this purpose, while the use of prophylactic injections is to be reprehended. They do more harm than good. If strong enough to be bactericidal, they should be extremely irritant; if weak enough to be tolerated, they will prove useless. The patient should also be warned concerning possible transfer of the disease without sexual contact, and all toilet utensils, towels, etc., should be kept by themselves, and all syringes and instruments used in the treatment of the case should be carefully sterilized.
[149]
—The period of incubation generally varies within wide limits, as mentioned above under classification of the various types; it may be as short as a few hours or may extend to ten days, or possibly even longer. Usually it is from two to five days. The early symptoms consist of discomfort along the course of the urethra, chemosis or edema, and swelling of the meatus. Within a short time after these symptoms the characteristic discharge appears. It may at first be viscid, but soon becomes purulent, and then more or less profuse, while urination gives rise to great discomfort. By the end of the first week the discharge is usually grayish in color, thick, continuous, and so profuse as to equal in volume 20 to 50 Cc. in twenty-four hours. The lesion is not confined to the urethra, and soon spreads to the peri-urethral tissues and thence to the lymphatics. A peri-urethritis with venous engorgement is added to the urethritis, and there is such an obstruction of the return circulation as to produce swelling and edema of the prepuce; this not only makes access to the urethra difficult, but conceals any excoriation and ulceration which may be going on beneath it. Sometimes this tumefaction proceeds to a degree where gangrene results.
All these local disturbances will be accompanied by more or less lymphatic involvement in the groins and in the perineum, with great soreness and tenderness throughout the entire genital tract. Chordee (painful erection) is a common and painful complication of this stage of the disease. Finally a well-marked degree of auto-intoxication, with its ordinary febrile and septic manifestations, may ensue. As the disease spreads farther back into the deep urethra there is irritability of the bladder, while in severe cases the frequent attempts at urination thus excited, with the accompanying pain during the act of expelling a few drops of urine, are distressing features of the disease. The pains are not limited to the organs involved, but are often referred to the back, to the perineum, and down the thighs. The symptoms above referred to belong to a well-marked case of acute specific type. There may be milder manifestations of each kind, and occasionally a case will run its course with but a minimum of the difficulties and discomforts above mentioned. Sometimes by the end of the third week, usually before, the disease will show a tendency to subside, even if inadequately treated. The inflammatory symptoms become less marked, the discharge thinner and less voluminous, until perhaps by the end of the seventh week there is noticed only a small amount when the patient rises in the morning. With all this apparent and spontaneous improvement there may be present, nevertheless, a serious and distressing amount of peri-urethral infiltration, which will soon be followed by cicatricial contraction and the formation of a stricture, the most frequent sequel of gonorrhea.
—Complications may occur along any portion of the genito-urinary tract. These will be considered in their anatomical order.
—Balanitis signifies an inflammation of the mucosa covering the glans. When the mucous surface of the prepuce is also involved, as it usually is when the orifice is contracted, then the condition is known as balanoposthitis. In the absence of ordinary cleanliness of the parts this may go on to erosion or extensive ulceration. It is sometimes complicated with chancroid or chancre. When such a condition exists, and the glans cannot be sufficiently exposed for purposes of cleanliness, the dorsum of the prepuce should be slit up sufficiently to permit of complete exposure, while in some cases the edema and the infiltration will be such as to justify circumcision. When needed these operations should be practised even if raw surfaces are thereby left exposed to infection. Such possibility may be usually obviated by cauterizing a fresh surface, as soon as exposed, with pure carbolic acid or one of the stronger caustics, or operation may be made with the thermocautery.
—Folliculitis implies the extension of the infection to the follicles and lacunæ which abound within the urethral canal. As long as their orifices do not become occluded they easily discharge their contents into the urethra, but when so swollen as to become occluded they lead to the formation of abscesses, which, beginning in a minute way, may sometimes give relatively extensive disturbance. These discharge internally; sometimes they so present that they may be opened externally, as they should be under these circumstances. They form a communication between the urethra and the exterior, and in this manner the majority of the ordinary urinary fistulæ are produced. These often occur in the perineum, but sometimes even in the pendulous portion.
—Inflammation frequently extends beyond the anatomical confines of the urethra, and produces a degree of infiltration which is often well marked and[150] disastrous. The site of such a lesion is marked by a nodule, more or less tender, which may subsequently break down into an abscess. The pus from these abscesses will usually escape into the urethra. Sometimes it burrows into the tissues of the corpus spongiosum, or travels even farther, and produces locally extensive destruction of tissue, with its possibility of urinary infiltration as a sequel, and all the septic disturbances which can be imagined as resulting therefrom. Thus fistulas often follow abscess formation, and these may be succeeded by phlebitis of the peri-urethral and prostatic plexuses, extensive destruction or multiple abscesses, or even gangrene and pyemia. Peri-urethritis is the essential factor in the production of strictures of the urethra, which constitute an exceedingly common condition.
While urethral stricture is a common result of gonorrhea it constitutes by itself a special lesion. (See chapter on the Genito-urinary Tract.) These peri-urethral infiltrations may occur in irregular patches, so variously placed as to encroach upon the urethra at different points without completely surrounding it, or they may form tubular lesions by which very serious annular constriction is produced. The degree of infiltration is, to some extent, a measure of the violence of the inflammation and of the virulence of the infection. This is true, however, only up to a certain point. One object of properly directed treatment should be to guard against the deep extension of a gonorrheal infection, in order to limit the tendency to the formation of stricture.
Between the folds of the triangular ligament are situated two racemose follicles known as Cowper’s glands. These occasionally become infected in the same way as the anterior follicles of the urethra and give rise to a painful swelling in the perineum, which gives most discomfort to the patient in the sitting posture. This condition is known as Cowperitis. It may proceed to abscess formation, in which case incision in the perineum should be made for its relief.
—The prostate consists of a collection of follicles embedded in a mass of involuntary muscle fiber. The largest of these follicles is known as the utricle, or, under the old anatomical name, uterus masculinus. These are liable to invasion when the infection has reached the deep urethra. The reaction which follows in this tissue after such invasion gives rise to prostatitis and causes much pain and general reaction. The prostate, being embedded within a fibrous capsule, cannot expand easily when it becomes inflamed, and the pressure thus made not only causes intense pain, but will also obstruct the urethra and occasion great difficulty in urination, sometimes retention of urine. In proportion to the other disturbance will be the general reaction, and fever may run high, with early expressions of septic intoxication or of septicemia. The prostate becomes tender, and pain is felt not only in the pelvic region, but in the back and in the thighs, as well as along the urethra. Prostatic abscess is a frequent sequel to this condition; it sometimes evacuates spontaneously into the urethra, or bursts through the capsule and burrows along the structures in the perineum and lower pelvis; occasionally it empties into the rectum. Intensity of symptoms should give rise to a suspicion of prostatic abscess, and a perineal incision should be made early and the abscess evacuated. Occasionally these abscesses present toward the rectum, when they should be tapped or incised through the bowel.
From the prostatic urethra inflammation may extend on one side or both along the vas deferens to the seminal vesicles. The production in this way of a vesiculitis is made known by the reference of pain to the rectum and by the appearance of blood, sometimes with pus, in the seminal discharge. By a digital examination of the rectum the enlarged and tender vesicles can be recognized above the prostate.
When the deep urethra has become seriously involved the condition of the patient is unpromising. Belfield calls attention to the triple function of the deep urethra, in that the impulse to urinate originates therein, that it is a sphincter for the bladder, and that it is intimately concerned with the sexual act. When it is disturbed by gonorrheal infection all of these functions are disturbed, the most serious symptoms being increased desire to urinate, amounting to almost constant vesical tenesmus; marked difficulty in expulsion of urine, which may increase to complete retention, and frequent bloody emissions, with chordee. The pain, the heat, and the sense of tension in the perineum and in the parts around it are distressing, as well as pain during and after urination, which is usually referred to the end of the urethra. The last few drops of urine will often be bloody.
[151]
—Cystitis is the not infrequent result of the further migration of the infectious process from the deep urethra to the bladder. The process is usually acute and serves to further complicate the case and to harass the patient. Except in the nature of the exciting causes cystitis differs but little from the other varieties to be considered in their appropriate place (q. v.). Cystitis of gonorrheal origin is likely to travel along the ureters and lead to involvement of the kidneys. Ascending infection is most commonly of gonorrheal origin. In proportion to the extent and rapidity with which the disease travels upward the case is marked by expressions of septic intoxication and infection, such as chills, fever, pain in the loins, along the ureters, and in the testicles. The kidneys may become enlarged. A more minute appreciation of the condition of affairs can be obtained by microscopic examination of the urine. In proportion as the kidney is involved, there is a preponderance of albumin, i. e., more than pus alone would produce. One of the numerous ways in which gonorrhea kills its victims is by the production of a pyelonephritis of the type known as “surgical kidney.”
—No such invasion of mucous membrane by septic organisms can take place without active participation of the lymphatics in the region involved. In cases of gonorrheal or even non-gonorrheal urethritis, not merely enlargement of the lymph nodes in the groin may occur, but an active lymphangitis, manifested as a tender, sensitive cord beneath the skin, especially along the dorsum of the penis. The lymph nodes thus become involved and sometimes suppurate, and these abscesses are referred to as suppurating gonorrheal buboes. The suppurative feature is probably caused by contamination with the ordinary pyogenic organisms.
—Gonorrheal infection seems often to extend along the vas and thus invades the epididymis, where evidences of activity are more frequent than in the vas itself. Epididymitis complicates cases of clap usually after the second week. It is characterized by pain, tenderness, and swelling of the epididymis, which occupies the same position relative to the testis proper that the heel does to the rest of the foot when a person stands in the ordinary military position, i. e., to the rear and inner side. The swelling becomes pronounced, and it is not unusual for a certain degree of swelling to be manifested in the testis proper, with the accumulation of a small amount of fluid in the sac of the tunica vaginalis, thus constituting a mild degree of acute hydrocele. While the inflammation is confined to the epididymis the pain is not intense, but of a dull, heavy character; but when the testis proper is involved there is a true orchitis, the inflammation being confined within the inelastic sclerotic tunic, and the pain then may be severe. Considerable fever accompanies many of these cases, with occasionally some edema of the scrotum and congestion of the testicular coverings. The weight of such a “swelled testicle,” as this condition is called by the laity, is irksome, and occasionally causes extreme discomfort. Under these circumstances physiological rest, i. e., in bed, and the use of a suitable suspensory apparatus are essential.
While resolution of this swelling ordinarily begins early and proceeds satisfactorily, the latter portion of the process is often slow and tedious, and the epididymis thus once involved will for months contain nodules and irregularities of contour. Usually the affection is limited to one side; but both testicles may be involved. If the infection be violent and the treatment inefficient abscesses may result.
This condition calls for early and effective treatment. If seen at the very outset, progress of the lesion may be checked by embedding the affected part in cold, wet compresses, and keeping them cold with ice. Relief later is more likely to be afforded by hot applications, and a hot poultice containing a small amount of fine-cut tobacco has been popular as a local application—the tobacco apparently being anodyne in its effect, although perhaps no more so than belladonna leaves. This may be regarded as a good emergency dressing when it affords the only means of treatment. The greatest relief will be obtained by the application of guaiacol, diluted with three volumes of olive oil or castor oil, well applied over the scrotum, and covered with oiled silk or rubber tissue. This application should be made twice a day. Later, in the more chronic and less painful stages, a reduced mercurial ointment containing a little guaiacol or ichthyol may be used to advantage, resolution being thereby assisted. In quite tedious cases the flying application of the actual cautery is serviceable. Internally tincture of pulsatilla has proved beneficial. It should be given in 1 Cc. doses every two hours. While the benefits accruing from its use are questionable, it has helped to allay fever and subdue pain.
[152]
Much has been said about the sterility which results from epididymitis, especially when both sides have been involved. It is easy to understand how the vas may become occluded in many cases, either temporarily or permanently, and yet within my own observation men have suffered from the double lesion and yet begotten children.
—Considering the extent of the mucous tract involved, the open port of entry for germs, and the virulence of these organisms in many cases, it is remarkable that there are not more conspicuous illustrations of septic absorption in cases of gonorrheal urethritis. That these do occur and have a widespread, sometimes disastrous, effect has long been recognized. The severe forms are usually the more acute, and if they assume the septicemic type, go on to abscess formation, and in parts which are not always accessible. In rare instances septic disturbance assumes the pyemic type. The writer believes that he was the first to report a case of typical pyemia following gonorrhea, and to recognize it as such.
Aside from these acute manifestations, more chronic and mild affections, especially of the serous membranes, are well known. The most common of these exhibitions occur in the joints, mostly in the knee. A gonococcus peritonitis, pericarditis, or endocarditis are, however, well known. Because of the similarity of the discomfort and the disability resulting from the joint complications of clap to the ordinary joint manifestations of rheumatism, these lesions have long been popularly called gonorrheal rheumatism. The name, however, should be discarded as being incorrect, and for it the best substitute would be postgonorrheal arthritis.
These lesions may be sudden in their onset or may come slowly. They may occur at any time during the acute stage or after its apparent subsidence. The first manifestations involve the serous membranes proper; the fibrous tissues participate sooner or later, and the infiltration resulting from the inflammation thus set up will often permanently compromise their integrity and cause an impairment of their function for the rest of the patient’s life. They are usually confined to one of the larger joints, but may involve several, either simultaneously or consecutively. In acute cases the swelling is somewhat pronounced and the pain and soreness intense. The local symptoms simulate those of acute articular rheumatism. In the fluid drawn from these joints the gonococcus can be occasionally demonstrated. The course of the disease is usually slow, and convalescence may be protracted. Nor is the disability acute only and temporary, but it is often made permanent by the formation of adhesions resulting from the condensation of exudates. Partial or complete ankylosis may result, with considerable deformity. The muscle spasm provoked by the acute joint inflammation will occasion the same distortions and subluxations as are produced by tuberculous and other forms of arthritis, and operations varying in severity from forced motion to joint exsection may later be necessary. (See pp. 392 and 393.)
The writer has seen cases of postgonorrheal toxemia of extremely chronic and even fatal type, where the joints were conspicuously involved and where they did not constitute the most serious features of the disease. These cases proved most intractable to treatment and illustrate the possible complications of gonorrhea.
In addition to the joints various bursæ and tendon sheaths may suffer in the same way as do the joint membranes. Such lesions are seen about the hands and feet, especially about the tendo Achillis, and are also seen in the muscles of the neck and of the orbit.
The treatment of these gonorrheal complications should be effected largely by improving elimination and getting rid of the general toxemia; thus hot-air baths, diuretics, and cathartics are advisable. These eliminants, with free massage, are useful in dislodging the toxic products.
—The treatment of gonorrhea is directed not alone toward the mere alleviation of symptoms, but to the destruction of the invading germs. The patient should abstain from much exercise, and in cases of severity should be kept in bed, avoid alcohol and tobacco, and eat sparingly of meats and of richly seasoned foods. He should wear a “gonorrhea bag,” or large condom, and there should be no obstruction to the outflow of pus. His hands should be washed immediately after contact with the parts involved, and all dressings and linen which may have been contaminated should be promptly burned.
The actual treatment of gonorrhea should be both internal and local. Internal treatment should consist (1) of the administration of laxatives; (2) of such amount of[153] alkali as may be necessary to overcome hyperacidity of the urine and mitigate the distress caused during its passage; (3) of remedies which, being eliminated by the kidneys, serve to medicate the urine and give it the effect of a retrojection; (4) of such anodynes and sedatives as may be necessary to give comfort, allay distress, and produce sleep or relieve and prevent chordee.
Of the drugs which are supposed to be eliminated by the kidneys, the balsams have sustained a high reputation. Among these is cubebs, of which 2 or 3 Gm. may be taken every two or three hours, as this remedy favorably influences the amount of discharge, though sometimes disturbing the stomach. Of the oleoresin of copaiba a ¹⁄₂ Gm. capsule, taken several times a day, is more pleasantly borne by the stomach, and with nearly as good effect as cubebs. Copaiba is known to produce a vivid scarlatiniform rash. The oil of sandal-wood, or santal oil, is the most efficient of these remedies, and may be given in the same dose as copaiba. That these drugs are eliminated by the kidneys is shown by the odor which they impart to the urine. It must be said, however, that these remedies are of but trifling benefit until the bladder is involved; when this occurs, they may prove of great value.
The urine should be diluted that it may be less irritating, and also to overcome its acidity. Fluids should be administered in profusion and alkaline diuretics in considerable doses. Hyperacidity is readily controlled by the administration of liquor potassæ, or the common sodium bicarbonate.
Sedatives may be necessary even from the first. The stronger anodynes are rarely needed during the first day or two, but by the end of the first week vesical tenesmus and chordee may be so marked that remedies such as cannabis indica, lactucarium, chloral, and the bromides may prove insufficient, and an opiate should then be administered. When required, morphine or heroine subcutaneously and in doses sufficient to promptly bring about the effect desired are preferable.
The local treatment of urethritis is directed to the alleviation of discomfort and distress and the cure of the local disease. Much has been said about abortive treatment. There is no such thing as aborting the disease. Much may, however, be done in the way of mitigating and shortening its course, and mild cases, especially of the non-specific form, may be considerably relieved within a few days.
The local treatment is carried out by injections into the urethra, which must be made with a syringe, preferably of hard rubber, with a blunt tip and without a nozzle, or by a douche bag connected with a soft catheter, all of which should be kept constantly sterilized. During the first days of an attack, when only the anterior part of the urethra is affected, treatment can be made more readily and effectively with a small “P” syringe, and at this time only 15 to 20 Cc. of fluid will be required, which should be held in the urethra for some time. When irrigation is decided upon a douche should be employed. Accurate directions should be given the patient as to how to make the injections, and he should be cautioned to first empty the bladder before using the syringe. The patient’s comfort may be increased by injections of water up to a temperature of 115° F. Antiseptics, i. e., potassium permanganate, boric acid, or one of the new preparations of the silver salts, may be added to the water. The parts may be advantageously immersed in hot water at intervals during the day, and for fifteen or twenty minutes at a time. There are many ways of conducting local treatment in these cases. Those mentioned below have given the best results in the practice of the writer.
A very satisfactory method would be to commence the local treatment with the use of hot water, as above, every two to six hours, and to follow it with a small injection of an emulsion of bismuth subnitrate, with sufficient cocaine and a little morphine to blunt sensibility and diminish tenderness and pain. The following formula, which may be varied, will accomplish this purpose: Morphine sulphate 0.3, cocaine muriate 2, bismuth subnitrate 20, cherry-laurel water 150, mucilage of acacia 50.
The injection should be retained for a few moments and no effort made to expel it. The bismuth salt is not only antiseptic, but is soothing, slightly astringent, and non-irritating.
Belfield has recommended the use of the yellow hydrastia muriate in connection with protargol. His formula is as follows: Yellow hydrastia muriate 2.50, protargol 1.50, glycerin 15, water 500. After using this for a few days the proportion of protargol may be doubled. Of this preparation 15 to 20 Cc. should be injected several times a day. The silver salts are the least irritating of all the stronger and more reliable[154] antiseptics, and drug manufacturers are putting upon the market at frequent intervals new preparations for which much is claimed. Among the latest of these is argyrol, a combination of silver with albumen (vitellin), in such form as to make it antiseptic and non-irritating. In solution it is of a dark mahogany color and stains whatever it comes in contact with; these stains, however, are readily washed out. Argyrol in solutions of 2 to 5 per cent. strength has proved reliable, and if such a solution be retained in the urethra for five minutes at a time a pronounced effect may be made upon the disease. It is my custom to alternate the use of the bismuth formula with a solution of argyrol as above, and in this way give the greatest relief in the shortest time. It has been demonstrated that under the influence of this preparation all gonococci which are reached by it are destroyed; therefore the earlier it is employed the better. Before using either of these formulas the anterior urethra should be washed with hot water or with hot normal salt solution. No harm need be feared should either of the above injections reach the deep urethra, and the effort should be to make them reach at least as deeply as the disease has gone.
When the discharge has reached what Finger has called “the mucous terminal stage,” then the argyrol may be used two or three times a day only, and one of the following solutions substituted for it part of the time: Zinc sulphate 0.75, bismuth subnitrate 8, colorless liquor hydrastis 15, cherry-laurel water 60. Of this solution 10 Cc. may be used three or four times a day.
Belfield strongly recommends the use at this time of a solution of muriate of berberine, in strength of ¹⁄₂ to 1 per cent., or the yellow hydrastia muriate in about the same strength. He also recommends zinc chloride 0.25, zinc iodide 0.50, water 500. Either of the above salts may be added to this.
When nothing remains of the discharge but the so-called “morning” or “military drop,” and the urine is almost clear, argyrol solution at night and one of the above formulas once or twice through the day will be sufficient. This, in brief, is a description of how a case of urethritis may be satisfactorily treated.
The systematic use of potassium permanganate solutions was introduced by Janet, and has been enthusiastically described and prescribed by Valentine. The treatment is more complicated and less satisfactory than that advised above.
With deep extension of the disease and its added symptoms of tenesmus, pain local and referred, etc., the limit of the injection should be extended and the entire urethra should now be treated. The bladder being empty, the patient should make a strong effort to empty it again at the moment when fluid is being injected into the urethra; the compressor muscle being thus relaxed, the fluid passes into the deep urethra. It will take a little practice to enable him to do this, but when once learned the procedure is simple, and those who cannot accomplish it in the standing position will succeed if they lie down before making the attempt. In this way the entire urethra may be traversed.
In the treatment of deep urethritis it is not necessary to change the formulas or drugs above advised.
Under this line of treatment it may be possible to cure the majority of cases of gonorrhea in from two to five or six weeks. This by no means indicates that the lesion is actually cured, for trifling evidences, such as adhesion of the lips of the meatus, with the retention of a drop or so of mucopus, and the presence in the urine of the so-called “clap threads,” i. e., threads of flocculent material that consist of mucus and epithelial debris loaded with bacteria, will for a long time be noted. These appearances indicate that there are still areas along the urinary tract which are infected, and are sources of possible danger.
The vesiculitis which often follows deep urethritis, as shown by the enlargement of the vesicles, detected by rectal examination, requires physiological rest, hot sitz baths, hot enemas, and opiates, the latter usually by suppository. After a short time the vesicles should be “milked” with a finger in the rectum, gentle pressure being made toward the prostate in the direction of their outlet. This will frequently cause an outflow into the urethra of pus and debris and give great relief. Should the infection persist and the above manipulation prove insufficient, the vesicles may be opened through the rectum, washed out, and packed with gauze.
[155]
Gleet is the name given to gonorrhea which persists, being only partly influenced by treatment, and which has extended over an arbitrary period placed usually at six weeks to two months. Strictly speaking the term gleet should be restricted to cases where there is a mucopurulent discharge from the meatus, often complicated by formation of strictures in the anterior urethra; on the other hand, a chronic gonorrhea may for a long time persist in the deep urethra and the glands and ducts adjoining, whence will issue a discharge which appears anteriorly, but, nevertheless, comes from the depths of the genito-urinary tract.
It is possible to have a chronic gonorrhea with little or no true gleet, the infection being latent, but nevertheless persisting. In gleet the discharge varies from a thin watery flow to one which is profuse and purulent, most noticeable in the morning on rising, when the meatus may be occluded by adhesion of the surfaces and there appears the so-called “morning drop.” Careful investigation of the urethra will generally disclose at least some constriction, with tender areas along the anterior urethra. To successfully treat the disease these areas and constrictions should be determined and suitably medicated. For this purpose two instruments especially are necessary—the bulbous bougie, for which a sound of the same size is an unsatisfactory substitute, and the endoscope, through which the lesions may be not only viewed but suitably treated.
The peculiar discharge comes from a lesion of one of the following varieties—either from isolated areas of inflamed mucous membrane with underlying exudate, from follicles and vesicles which fail to completely empty themselves, or from preëxisting strictures. The endoscope will easily reveal the first and second of these; the bulbous bougie the first and third, while further examination by the rectum may be necessary to decide in regard to the seminal vesicles.
Fig. 28

Bulbous sound.
The bulbous bougie is an instrument of great importance in urethral work. It should be carefully sterilized before introduction, and the urethra should be cleansed before its use. The instrument should be gently passed into the urethra; its course will be obstructed by any constriction which will give rise to stricture of smaller caliber than the bougie itself, while the discomfort or pain which it will excite as it passes over a tender or ulcerated area will be significant. The urethra is most distensible at its bulbous portion, while its caliber varies in different individuals, ranging ordinarily from 30 to 35 of the French scale, while the urethral diameter is about four-tenths of the circumference of the penis. We owe more to the studies of Otis in this matter than to any other investigator. He also showed that the size of the meatal opening is not a criterion as to the size of the urethra; that the contracted meatus often produced a certain degree of reflex and spasmodic stricture behind it, and that when the meatus is too small to permit the introduction of such an instrument as the urethra should take it should be enlarged, the operation for its enlargement being known as meatotomy, which may be easily effected with a blunt bistoury under the local use of cocaine. The meatus having been enlarged to suitable size, any consistent and organic constriction which then prevents the passage of the bougie should be considered a stricture and treated accordingly. Such a constriction may be of recent origin, when it will be found easily dilatable, or it may be old, resillient, and tough. Otis also devised an instrument known as the urethrometer, which is of value in the accurate estimation but not necessary in the treatment of many cases.
Fig. 29

Urethrometer.
[156]
These instruments may be passed down to the bulbous portion of the urethra; beyond this further investigation should be made with the ordinary sounds. By their use much may be determined in regard to prostatic tenderness, and the combined use of the sound in the deep urethra with the finger in the rectum will give more accurate information regarding the size of the prostate than can easily be obtained in any other way. Much reaction, however, may occur from the use of the sounds in this way, and it is a good rule never to introduce an instrument into the deep urethra without having ample reason therefor, and then doing it under antiseptic precautions; while, as a formal measure after it, the patient should be placed at absolute rest. This serious reaction, which occasionally follows instrumentation of the deep urethral passage, is commonly known as urethral fever. It is characterized by chills, elevation of temperature, and often by local indications, the constitutional features being sometimes pronounced, and in rare cases terminating fatally. Such serious symptoms are difficult to explain. Doubtless the use of the instrument opens up paths of fresh infection, and absorption rapidly follows, which may be limited to the surrounding tissues or cause widespread trouble. This may ensue after every precaution has been adopted, although doubtless many of these cases have been the result of carelessness and failure in antisepsis. Much may be done in the way of prevention when this condition is feared, for these cases are rarely so urgent but that the urine can be medicated and its quality improved, while a part of the procedure may consist in having the patient empty the bladder and then carefully washing it, or filling it with an antiseptic solution, which may be expelled before any instrument is used except the catheter, through which it may be necessary to introduce the bladder wash. The administration of 2 or 3 Gm. doses of urotropin, with or without quinine, previous to the exploration, may also be of great service. The surgeon perhaps does not always take these precautions, but he should when the history of the case shows that patients have already suffered in this way. In the presence of such a history the urethra should be explored with great caution.
When the rectal examination is made the intent should be to discover any enlargement, irregularity, or undue sensitiveness of the prostate, and then to pass the finger still farther and ascertain if there is involvement of the seminal vesicles. At the same time a species of manipulation described as “milking” may be conducted, by which the contents of the vesicles as well as of the prostatic utricle may be incited by gentle pressure, directed from above downward, to empty into the deep urethra, whence they may be promptly expelled or may be carried out by the urinary stream, or removed through the endoscope. The discharge of pus or catarrhal debris in any visible amount is suggestive, and indicates that these passages have participated in the infectious process. This act may be repeated at three or four day intervals; it should be so gently done as not to cause much pain, and will be found of great value in cases calling for it.
—The treatment of gleet is essentially treatment of the causes which produce it, and these should be carefully determined. In the urethra, as in all other tubular channels of the body, an abnormal constriction is accompanied by an area of excitement behind it, from which will issue more than the normal mucous discharge. We see this in stricture of the esophagus, intestine, or any of the ducts. This discharge is not to be subdued by mere applications nor by astringent and antiseptic injections, but the stricture itself, being the most important factor, must be suitably managed. In recent cases its gradual distention by the use of conical sounds will usually suffice.
In long-existing strictures more radical measures should be adopted, and they should be divided with one of the numerous urethrotomes in general use. Mere division, however, is not sufficient, but the patient should be impressed with the fact that cicatricial tissue tends invariably to contract, and that persistent dilatation is to be practised lest the stricture recur. The old saying used to be, “Once a stricture, always a stricture.” If this is to be disproved, it can only be by the frequent and long-continued use of sounds. Ignorance or indifference impel many a patient to return for further treatment, sometimes in a condition worse than at first, while occasionally the penalty paid for carelessness is life itself.
No routine in the treatment of gleet will give satisfactory results beyond this fact, that patients should be instructed to regulate their lives by absolute rules as regards indulgence of every description, and avoidance of intestinal inactivity and constipation. The[157] urine will be found concentrated and irritating in many of these cases, and this should be overcome by the free use of water and diluent drinks. Hyperacidity should be corrected by suitable alkaline medication, and remedies administered, already mentioned, which are supposed to medicate the urine. Capsules may be procured containing salol, oleoresin of cubebs, balsam of copaiba, and pepsin, and except in cases where there is already great irritation of the urinary tract, these serve their purpose admirably.
When the anterior urethra alone seems to be involved, one of the milder injections already mentioned in describing the treatment of acute cases may be employed. When the deep urethra appears to be the site of continued irritation, it should then be treated extensively with deep irrigations and injections of suitable medicaments. The deep irrigations can be practised with or without the use of a catheter. The deep urethra may be flushed through a smaller catheter than the urethra will comfortably take, allowing the fluid to return through the urethral channel outside of the catheter itself. When this practice is adopted, hot water which has been made antiseptic should be used, preferably with one of the silver salts. The nitrate may be used in proportion of 1 to 500, and the citrate or lactate in strength of 1 to 300 or 1 to 400. Protargol is effective in 1 per cent. solution, or argyrol in 1 to 3 per cent. strength.
In the employment of irrigation in these cases a shield should be used, by which the end of the penis may be covered and all danger of spattering avoided. The simplest expedient for this purpose is one-half of an old atomizer bulb, which may be punctured and slipped over the catheter or irrigator tube.
Apart from mere irrigation it is well to deposit within the depths of the urethra, in the membranous portion, by means of a deep urethral syringe, a drop or two of a fresh solution of silver nitrate in distilled water, in strength of ¹⁄₂ to 1 per cent. This should be deposited behind the “cut-off” muscle, where it will cause a burning sensation for a short time. The strength of the solution is to be regulated by this complaint, as no benefit is derived from using it too strong.
Of all the medication that has been suggested, nothing gives better results for this purpose than this silver nitrate.
For ordinary urethral injections, besides those already mentioned, formalin may be used, but in weak solution (1 to 2000, or stronger if the patient can tolerate it); while picric acid has been recommended by Belfield and others in strength of 1 to 1000 or 1 to 2000.
Some surgeons believe that patients can learn to flush the deep urethra, or even the bladder itself, without the use of the catheter or internal tubing of any kind. The procedure may have to be learned in the sitz bath, the pelvis being immersed in warm water; the nozzle of the irrigator tube is inserted into the urethra and the patient is told to make an effort as if to void his urine. This will so relax the “cut-off” muscle as to permit the passage of fluid into the bladder, and this, which is most desirable in many cases of cystitis, where the bladder washing is an essential feature of the case, is to be avoided when the gonorrheal infection has travelled backward beyond the prostate; no attempt should be made to pass the solution into the bladder, but simply to wash out the urethra. The better plan is to teach the patient the proper use of a small soft catheter, which may also be used in the sitz bath, inserted to the proper extent.
Recent strictures should be treated by sounds after the urethra has been thoroughly cleansed. For this purpose a conical cylindrical sound should be selected, whose urethral end will comfortably enter the stricture. Gentle force should then be brought to bear to pass it beyond the stricture. If gradual dilatation be aimed at, it is well not to go beyond the point of drawing a drop or two of blood; even this may be avoided. On the other hand, should it be decided to use sufficient force, the dilatation should be done thoroughly and at one sitting, in order to avoid repetition of the irritation. The instrument generally in use in this country for this purpose is the Otis dilating urethrotome, by which the degree of dilatation and the size of the cicatricial ring can be estimated and the extent of the division and the effect gained also regulated. (See Operative Surgery of the Urethral Canal.)
The divulsion of strictures, formerly in vogue, is now abandoned for the more accurate division performed by this instrument. The strictures having been thus divided, sounds should be passed at intervals of from three to five days, by which the urethra is distended to its full caliber and the divided surfaces not allowed to contract. This is an important part of the treatment, and gives opportunity for widest discretion in their employment.[158] Ordinarily they should not be carried farther back than the lesion calls for, as the deep urethra is best let alone. On the other hand, there are many cases where the stimulus of the cold metal passing the entire length of the urethra and the effect which it seems to have in expressing from the various follicles any retained contents seem beneficial. It has been stated that instrumentation sometimes leads to epididymitis or “swelled testicle;” should this take place in a case undergoing treatment for gleet it may necessitate a temporary cessation of the mechanical treatment. It is not good surgery to introduce any instrument into the urethra when one or both testicles present this complication.
In the local treatment of these lesions, cocaine or one of its substitutes should be employed. It is questionable whether the full benefit of applications is obtained when the surfaces are so anesthetized; on the other hand, the treatment can be made more endurable by its use.
This is true, also, of the use of the endoscope, and applications which may be made through it to inflamed or hypersensitive patches. When these are recognized or exposed, they are best treated by a probang moistened with silver nitrate solution, in 5 to 10 per cent. strength, or by the solid stick or crystal of copper sulphate, pure or mitigated, as used by the oculists.
One of the most important features in the consideration of gonorrhea is to determine, if possible, when a given case has ceased to be dangerous to others. In theory the danger passes with the disappearance of the gonococci, but it is so difficult to determine when this has occurred that it is almost impossible to fix a time limit in any given case. An excellent method of determining the matter in a reasonably accurate way is by having the patient void urine in two different glasses; a small quantity in the first, which will contain, then, the washings of the urethra. In this glass will be found those chains of gonococci clustering around masses of epithelial cells or debris which have been especially described as “clap threads” (tripper-faden of the Germans), upon which, by careful examination, gonococci can often be recognized. As long as these threads are in evidence it may be held that the infection still persists, and might be either brought into activity again by excitement or convey the disease in the sexual act.
Gonococci have been found in clap threads years after the last known infection, and this will illustrate why they are such a source of danger, and how an innocent woman has been made to suffer when it was supposed that all danger of infection had passed away.
This naturally assumes the type of a specific vaginitis, usually with active participation of the mucous membrane of the vulva and of the vulvovaginal glands, the urethra and bladder being sometimes secondarily involved, while the role of the lymphatics is about as described in the male. In the young, especially in young girls upon whom rape has been attempted, the mucosa is extremely susceptible. In adults, particularly in those who have borne children, the vaginal walls offer more resistance. The nature of the parts permits of more violent chemosis of the mucous membrane, while in serious cases there will be well-marked edema of the labia. The urethral orifice is usually inflamed and chemotic, even though the infection travel no farther in this direction.
It has been stated that 80 per cent. of deaths from pelvic disease in women are due directly or indirectly to gonorrhea, as well as one-half of the cases of involuntary sterility.
As in the male, there may be different types of so-called gonorrheal infection of the vagina, varying from the pure gonococcus type to that in which the preponderating bacteria are of the ordinary pyogenic varieties. The detection of gonococci in the discharges sometimes assumes medicolegal importance, and upon it has depended the guilt or innocence of more than one individual.
The intensity of the vaginitis will vary with that of the infection. In the worst cases the discharge is profuse and acrid. It may amount to 50 Cc. or even 100 Cc. in twenty-four hours. The burning pain will be extreme, while backache and pelvic soreness will be bitterly complained of. In mild cases the disease assumes the clinical form of a low-grade vaginitis with abnormal discharge, such as may be characterized as a severe case of “whites.”
[159]
In these cases of either type the question is, whether infection has already travelled upward beyond the vagina into the uterine cavity or through it into the tubes.
Gonorrhea is the most common, and some believe almost the sole, cause of pyosalpinx with its attendant complications and dangers. Even when not severe, vaginitis may permit of such extension, and so not only induce sterility, but compromise the physical welfare of the patient; while in acute cases the activity is so great that it occasionally terminates in peritonitis, primarily of gonorrheal origin. When both tubes have become involved, the patient is almost invariably sterile.
In nearly all of these cases strings of mucopus will be found hanging out, or beads of it presenting at the external os, and when examined this exudation will afford a fair test as to the character and degree of the infection. Here, as in the male, there are so many follicles difficult of access, and so many recesses in which germs may lurk, that a complete disinfection of the parts is almost impossible. For this reason, then, latent gonorrhea is a frequent outcome of the disease when once it has existed, and a possible and more or less constant source of danger to others.
—A case of acute gonorrheal vaginitis with its accompaniments will present a difficult problem. The discharge is so great that the danger to others, and especially to the eyes, is pronounced, while the exquisite tenderness of the parts makes radical treatment difficult. The treatment should consist of antiseptic douches, which in serious cases should be made as nearly continuous as possible. The water used for the purpose should be as warm as the patient can tolerate, and contain an antiseptic, of which corrosive sublimate, in strength of 1 to 2000, silver nitrate in the same strength, or formalin in double this strength, are the most serviceable. The irrigating tube should be carried to the upper end of the vagina and the stream made to flow outward. In milder cases a douche at intervals through the day may suffice. The vaginal surface should later be exposed through a speculum and the entire mucous surface treated with nitrate of silver solution in from 6 to 10 per cent. strength. Should the surface be tender, this will be painful, and might justify the use of an anesthetic, especially of nitrous oxide.
If the disease extend upward and there is an endometritis or a salpingitis, external applications of ice may be used to lull the pain; but probably hot poultices or some application of external heat might afford greater comfort to the patient. Byford has used succinic dioxide in the treatment of specific vaginitis with great satisfaction. It is sold in the open market under the trade name “Alphozone.”
The edema of the vulva will subside with the general improvement of the case. Abscesses in the vulvovaginal glands are not uncommon. These are easily recognized, are often painful, and should be incised early or as soon as recognized, cleaned out thoroughly, the interior of the cavity cauterized to prevent the result of fresh infection, and then packed and left to heal by granulation.
Urethritis and cystitis may be treated as when they occur in the male. There is the same liability in women as in men to lymphatic involvement, with the consequent bubo, which may perhaps suppurate. They are less liable to the widespread manifestations of postgonorrheal infections of the joints, etc., although they are even more liable to infection of the endocardium, and, as will be readily understood, more so to infection of the peritoneum. It will then be seen that the treatment of the disease is essentially the same in either sex, certain differences in method rather than in principle having to be made in accordance with anatomical requirements.
As to the rectal mucous membrane participating in gonorrheal infection, under ordinary circumstances it would escape. In the treatment of any of these cases by the sitz bath, the question might arise whether there would be danger of extending the contagion in this direction. It does not appear that much fear need be felt, for two reasons: the grasp of the sphincter is usually sufficient to prevent entrance of fluid, and, furthermore, the rectal mucosa is itself extremely resistant to the gonococcus. Gonorrheal proctitis is an exceedingly uncommon infection, and one rarely seen, except in extreme cases of sexual perversion. It should be treated in about the same manner as gonorrheal vaginitis, i. e., by continuous irrigation with hot water, and stretching the sphincter in order to overcome the spasm into which it would be thrown by reflex activity.
Gonorrheal urethritis in women is best treated with local applications of argyrol or one of the other silver compounds. These can be made with a syringe or with a small swab. Cystitis is to be treated in the same manner as when it occurs in the male.
[160]
Scurvy is placed among the so-called surgical diseases, since it manifests many distinctly surgical features and is possibly of parasitic character, although this feature of its existence has not been incontrovertibly established. It is a starvation disease, its principal characteristic being that of malassimilation, accompanied by profound anemia. Well-marked cases are seen during long sieges, like that of Paris, in 1871, or during long imprisonment, as in Andersonville prison. It has certain points of resemblance to that condition of multiple neuritis met with in warm climates, and known usually as beriberi. The former is apparently due to the absence of a vegetable regimen, while beriberi is largely due to the absence of an animal regimen, nature having intended that man’s diet should be mixed, and having ordained that suffering and disease always follow confinement to one or the other.
—The pathology of scurvy is obscure. It has been shown that gastric digestion is seriously at fault, that there is much intestinal putrefaction, that the urine shows great absorption of toxins, that the hematopoietic function is incomplete: that scurvy is a toxemic or chronic ptomain poisoning, which may in part or at times be due to the use of tainted food. Morphological changes are, however, neither distinct nor pathognomonic. It has been described as a disease of diet and occupation rather than of race, age, sex, or season. The ease with which hemorrhagic effusions occur, the degeneration of muscles and other tissues, the frequent detachment of cartilages, can be accounted for by conditions thus summarized, for which, however, we have no minute explanation. Scurvy may so complicate various other diseases, and usually does when occurring in large bodies of men—as in armies, prisons, among convicts, etc.—that it is hard to dissociate morbid phenomena and assign to each its proper place.
—The disease begins by a condition of generalized prostration, with an icteric tint of the skin, malaise, mental torpor, loss of appetite, insomnia, etc. The first recognizable or distinctive local appearances occur about the margins of the gums. Here, in the intervals between the teeth, the gums become livid, friable, and bleed easily, while the breath assumes a characteristic fetid odor. The skin becomes dry and brittle, and covered with minute prominences, which give it the popular name “goose-flesh.” These appearances are followed by local pains, diversified and sometimes excessive, and extravasations of blood in the skin and under the visible mucous membranes, causing small ecchymoses, which by themselves would be considered as simple purpura hæmorrhagica. These pass through the usual phases of extravasations, while it is made evident by pain, nodular masses, etc., and by postmortem examination, that similar hæmorrhages occur in the deeper tissues, especially in the muscles, even in the bones and epiphyses. So easily do hemorrhages occur in advanced stages that there is often external bleeding, particularly from the gums and mucous membranes, while from points thus involved pyogenic infection may proceed internally. Near the close the victim presents a picture apparently of an animated corpse, with surface discolored and mottled, often appearing bruised, with ulcerations where extravasations have failed to resolve, and where infection has occurred, possibly with epiphyses loosened, and necrosis of the bones of the extremities. In such cases death results from marasmus and sepsis.
—As long as the patient is not in the desperate condition just described the prognosis and outlook for treatment are promising, as all the milder manifestations of scurvy can be dispersed by suitable feeding and medication. Loss of teeth and cicatrices of ulcers leave permanent traces, but function can be restored. The purpura is but one expression of the scorbutic condition. Nearly all cases of scurvy will present purpuric manifestations, but all cases of purpura are not necessarily scorbutic. The course of treatment may be summed up in proper diet and in the administration of certain drugs. Proper diet should be prescribed at once, but administered, especially in severe cases, with extreme caution. The food selected should be given in small quantities, but frequently. It should consist in large measure of fresh fruits and vegetables, while cranberries and lime-juice figure largely among the former. Buttermilk is excellent, and cider may be allowed; also lemonade, with but little sugar.
PLATE XI
FIG. 1
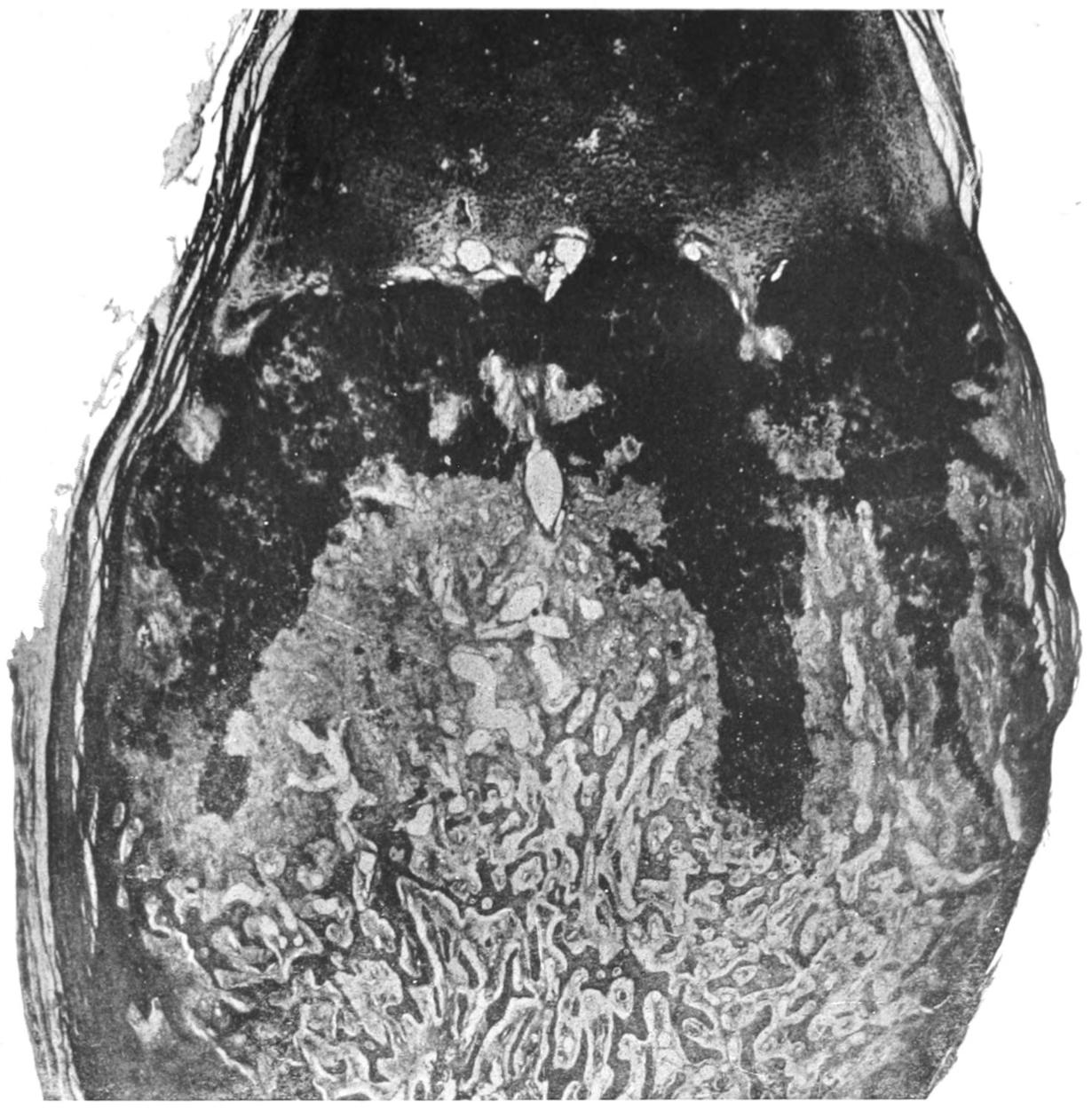
Rickets. Rib. Very low power. (Gaylord and Aschoff.)
FIG. 2
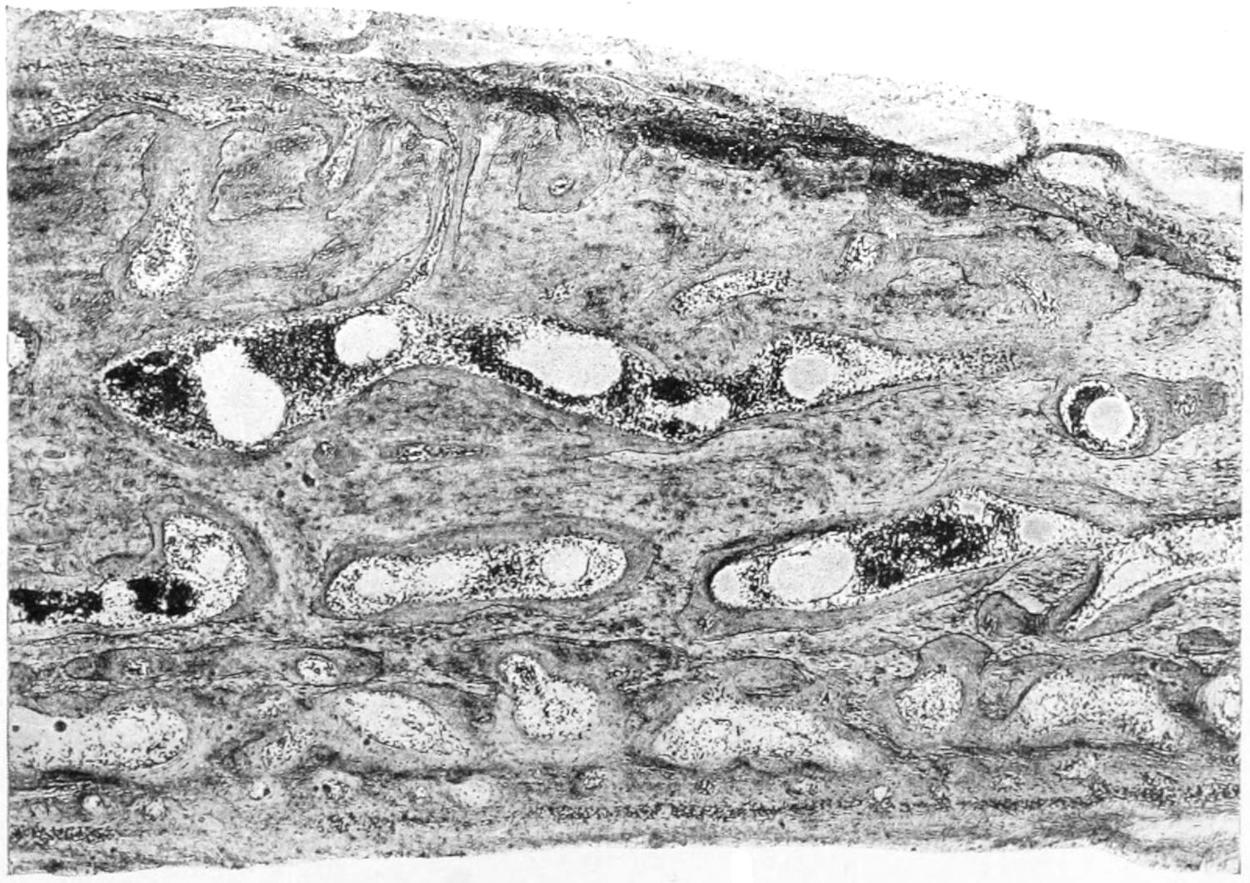
Rickets. Flat Bone of Skull (Craniotabes). (Karg and Schmorl.)
[161]
For the local condition in the mouth an antiseptic mouth-wash containing a fair proportion of hydrogen dioxide is advisable. Alcoholic stimulants are called for, at least up to a certain point. Strychnine and cinchona preparations will give force to the heart’s action, and the horizontal position, for a time at least, will prevent sudden heart failure. Compound syrup of the hypophosphites, with meat preparations, will supply lacking material, while the hemorrhagic manifestations are best controlled by the fluid extract of ergot and aromatic sulphuric acid, separately or combined. Particular attention should be given to cleanliness and fresh air.
—Infantile scorbutus sometimes furnishes the surgeon with very young patients who are brought to him especially for disability of the limbs, with pain and fretfulness, leading to immobility, followed by enlargement of the lower ends of the femurs (due to subperiosteal hemorrhages) with fixation by muscle spasm; this may be followed by “spontaneous” fractures. The gums will show the same changes as are seen in adults, while subcutaneous hemorrhages and infiltrated muscles, with foul breath, ashen pallor, listlessness and apathy, and perhaps several swollen joints, will complete an unmistakable picture.
Fresh milk with orange-juice in small amounts between feedings, combined with more strictly surgical measures if needed, will secure good results in these little patients.
Rickets, or rachitis, is another of the diathetic conditions, in this instance not yet considered of parasitic origin, most commonly occurring in infancy and early childhood, although its resulting lesions may persist throughout life. It is characterized by nutritional disturbances and organic irregularities.
—Rickets is generally referred to as “fetal” or “congenital,” according to whether the infant presents characteristic markings at birth or whether they develop later. The most marked constitutional defect seems to be in the supply of calcium salts, which leads apparently to formation of bone which has not sufficient compact tissue to make it strong. Especially along the line of junction between bone and cartilage do we see the most marked expressions of rachitic lesions. Here the cartilage is evidently actively growing, while the bone formation proceeds with difficulty, and the proportion of vascular tissue is excessive. The result is prolongations of soft vascular into the cartilaginous tissue, by which the latter becomes more or less absorbed, and this essentially interferes with ossification. In severe cases it may be lacking. At epiphyseal lines one may see a layer of osteoid tissue which is not cartilage and will not become bone. Because of its yielding nature it warps under the mechanical strain to which the bones of the extremities in young children are constantly subjected.
The obscure but unmistakable relations existing between rickets and the status lymphaticus will be referred to in Chapter XIV.
The osseous lesions of rickets differ from those seen in osteomalacia, since in the latter the softened tissue is practically decalcified bone, while in the former case most of the affected tissue has never gone so far as genuine bone formation, but is arrested in its perverted state.
The result of rickety changes in the skeleton is a thickening of the shafts of the long bones, of the outer table of flat ones, of the epiphyseal extremities of shafts, and frequently a stunting of their development, so that they do not attain their normal length. The periosteum is also affected in rickets, with the result that when the changes occur, mostly subperiosteally, there are warpings and curvings of the bone shafts, while so long as the disturbance is epiphyseal more or less abrupt curvatures and angular deformities will be produced as the result of muscle action. So marked are the changes in some instances that it has been stated that bones may even lose three-fourths of their calcium salts. When rachitic bones are so soft as to be easily cut with a knife, marked deformities occur as the result of muscular activity. (See Plate XI.)
[162]
In the extremities we see bow-legs, knock-knees, clubbing of the ends of the long bones, bending of the neck of the femur, flat-foot, club-foot, etc.; while the clubbing of the bone ends also may be well marked in the bones of the upper extremity, where, however, marked deformity is less common, because the upper extremity does not bear the weight of the growing body. In the skull the bones remain soft and yielding to pressure, with a tendency to return to their original membranous condition, and this is the condition comprised under the term craniotabes rachitica. The fontanelles always remain open for an undue time; the sutures are broad and membranous. The bones of the face grow less rapidly, giving to the face a disproportionately small size; dentition is delayed and the teeth decay easily. The upper incisors often project far over the lower.
In the thorax there are enlargements of the sternal ends of the ribs, causing a row of nodules referred to as the rachitic rosary. The ribs tend to sink in, the sternum to be protruded forward, and the deformity known as pigeon-breast becomes often pronounced. Curvatures of the spinal column, especially kyphosis, are common, and distinct degrees of lateral curvature are frequently begun as rachitic deformities, to be magnified by perverted muscle action as the child grows older. In the pelvis the innominate bones approach each other, causing the pelvic cavity to become contracted, or the sacral promontory projects too far, or in various other ways the normal pelvic diameters are so far compromised that rachitic deformities of the pelvis constitute the most common and serious obstacles to normal labor in adult women, and are frequently the cause of major obstetric operations.
While the rachitic changes in the osseous system are the most distinctive and easily recognized, numerous other organs and tissues of the body are more or less seriously compromised. Ventricular dilatation, leading to chronic hydrocephalus, is one of the common results of rachitis of the skull, which may be followed by convulsions and terminate fatally. Porencephalon and cerebral sclerosis may also ensue. Disturbances of digestion are common in rickety children—the liver may decrease in size or become much enlarged; the spleen often enlarges, sometimes to enormous dimensions. In various other parts of the body there are the same expressions of malnutrition as are met with in tuberculous disease. Rickety children perspire easily, particularly at night, when the head will often be found bathed in perspiration. They are fretful and irritable, as a rule, and difficult to control. A child with protuberant belly, due to enlargement of liver and spleen, as well as to crowding of pelvic organs, with relaxation of abdominal walls, and a contracted and distorted thorax, the skull flattened on the top, clubbed bone ends, a history of resting badly at night and sweating profusely, constitute a clinical picture of rachitis so marked that it can be recognized at a glance. Between this picture in its worst forms and the slightest deviation from the ideal type there may be met all degrees in manifestations of rickets in the children of the rich or the poor, while in adults may often be seen evidences of that which prevailed during early childhood. In order that all these features may be made out the child should be stripped and examined from head to foot.
Laryngismus stridulus is a frequent accompaniment. It may be followed by general convulsions and tetany. (See Chapter XIV.) While rickets may be a very acute disease, it is as a rule chronic, and children dying essentially from this disease die rather from cerebral or other manifestations which may be regarded as in some degree accidental. Scurvy and other nutritive disturbances may be associated with rickets.
—The treatment for the condition consists mainly in proper nutrition. Mothers’ milk is certainly preferable to any other, and should be demanded. If feeding must be artificial, it should be in accordance with the best precepts of modern therapeutics. Cod-liver-oil emulsions are of advantage; compound syrup of the hypophosphites is a remedy of great virtue. Minute doses of phosphorus seem to be of value—1 Mg. pro die. It is a mistake to let rickety children begin to walk or even to creep too early. They should be kept upon the back in their cribs.
The modern opotherapy of rickets includes the employment of thyroid and pituitary extracts. The dose should be graduated to the age of the patient, based upon 30 Cg. for an adult, and given thrice daily. This will not preclude the necessity for a careful regulation of diet, etc., but will constitute a valuable adjunct in treatment.
The deformities due to rickets are so numerous as to constitute a large part of those to which special or orthopedic surgery is addressed. The mechanical and operative treatment of these cases will be referred to in their appropriate place.
[163]
Under the term status lymphaticus has been described a condition which is of interest to the surgeon, as it includes not only minor complications, and even those which are serious, which follow surgical procedure, but it also has reference to the cases of sudden death during or after operation, some of which have been attributed to the anesthetic, while others have been considered absolutely unexplainable. The condition is so easily described or defined that it should be recognized during life, but it has often been discovered only after sudden death.
The essential feature of the condition is enlargement of the lymphatic tissue and apparatus, perhaps throughout the entire body, more frequently through its internal portions. It usually occurs in children. It is accompanied by much lowering of the power of resistance, and results in sudden death from cardiac failure, as the result of causes which seem disproportionately trivial; as, for instance, such deaths as occur not merely during anesthesia, but during bathing, convalescence from the exanthemas, etc. It stands in close relation to diphtheria, perhaps because of its peculiarly depressing toxins, and probably accounts for cases of sudden demise in that disease, even when mild.
The status lymphaticus is also designated by other names, as lymphatism, lymphatic constitution, and status thymicus, the latter because of the active participation of the thymus. Enlargement of this body has been noted at autopsy, but its relation to the other features of status lymphaticus were unknown until Rokitansky, in 1842, first recognized the condition in its entirety, but confused it with the tuberculosis of the lymphatics formerly called scrofula.
The death of a son of a German professor, a few years ago, shortly after an injection of antitoxin to protect him from diphtheria, and the subsequent discovery that the boy was the victim of this condition, caused a widespread interest in and a most careful study of the problems involved. They occur in the thymus more frequently than in any other organ of the body. Normally the thymus begins its involution within a few months after birth, and this process should be completed at puberty. In the status lymphaticus this involution does not occur, but enlargement persists or increases even into adult life, varying in different cases, the weight of the thymus varying from 20 to 135 grams.
While the thymus may for some purposes be grouped among the lymphatic tissues of the body, little is known as to its function. Its juice contains leukocytes, which find their way into the general circulation, and it is supposed to have an internal secretion correlated with that of other ductless glands.
Injections into dogs of thymus extract produce a fall in the blood pressure, with acceleration of the heart, and, in fatal doses, dyspnea and collapse. While enlargement of the thymus may cause death by pressure on important structures other than the trachea, it produces a type of asthma known as thymic asthma, in which death sometimes occurs unexpectedly and rapidly by strangulation.
An examination of the thymus rarely shows anything more abnormal than the enlargement of its natural structure, with perhaps acute hyperemia, while occasionally the cut surfaces will exude a milky fluid; there will be found, in addition to these changes in the thymus, a general hyperplasia of the lymphatic system, with enlargement of the superficial and deep nodes, especially the cervical and axillary, the inguinal and those in the abdomen. The spleen enlarges and the Malpighian bodies seem to be packed with lymphoid cells. There may be enlargement of the heart and increase in the thickness of the arterial walls. This is so marked that Virchow suggested the name lymphatic chlorotic constitution. It has been suggested that the narrowing of the aortic valve in these cases is due to this lymphoid infiltration.
The relations between rickets and the status lymphaticus are so frequent and so conspicuous as to make one suspect a more than casual connection between them. Nearly[164] all cases of lymphatism show the ordinary clinical evidences of rickets. By some such relation may be explained the benefit which accrues in rickets from the administration of the extract of thymus, as well as of the thyroid and the pituitary body.
Enlargement of the lymphoid tissue in the wall of the alimentary canal also occurs, and in those rings of adenoid tissue which mark the site of the embryonic canals. This tissue may be seen around the origin of the appendix, while its most conspicuous illustrations are seen about the pharynx, where not only the faucial, but the lingual and the pharyngeal tonsils are enlarged. In many of these cases there are the so-called “adenoids” of the throat specialists, while, of still greater interest to the surgeon, the deaths that have occurred from the status lymphaticus have happened repeatedly in operations for these growths within the nasopharynx. Furthermore, the yellow marrow of the bones seems to be replaced by red marrow, but whether this is due to the anemia which always accompanies the condition is not known.
Kaposi some years ago described under the name lymphodermia perniciosa a rare condition characterized by a scaly and itching skin, exuding fluid, with later a diffuse and doughy condition of the affected parts, and then by nodules which sometimes ulcerate, lymph nodes and spleen being also enlarged, and the general health impaired. While some have held that this is a variety of mycosis fungoides, it is supposed that it is only another expression of lymphatism.
Another variety of this condition occurs in young people, in which coma comes on suddenly, followed by death in twelve to eighteen hours. Vomiting may occur during the coma, but it is convulsions and spasm of the glottis that cause the death of the patient.
Thymic asthma has been called laryngismus stridulus. Whether the latter can ever occur without the former is not definitely known, but doubtless the asthma is very frequently the cause of the obstruction and the difficulty in breathing.
Medicolegal questions arise in this connection which are of interest. Death occurs, except under anesthesia, after a series of convulsions, yet it may happen almost instantly. Some claim that death may take place as the result of pressure of an enlarged thymus upon the vessels, and especially upon the nerves, while others claim it to be due to a sudden arrest of heart action by reflex activity.
Convulsions of any character in adolescent individuals and young children should raise a suspicion of this condition, and, of greater importance for the surgeon, all possibility of existence of the condition should be eliminated before operation is undertaken. Deaths occurring during anesthesia are often attributable to the anesthetist; nevertheless there are instances where he is absolutely blameless, and where death may occur as by a flash of lightning.
It does not follow that chloroform is the agent at fault in these cases, and opinion seems to trend in the direction of ascribing the censure to the status itself rather than to the anesthetic used. Deaths may occur at any stage of anesthesia, or some minutes after the anesthetic has been stopped. It is significant that the most conspicuous illustrations of the relations between the condition and sudden death have occurred during operations upon the throat and nose. This seems to show the role played by the adenoid tissue.
Another interesting question is why individuals with well-marked status lymphaticus should live, apparently comfortable for years, and then suddenly succumb from apparently trifling causes.
The relations between the thymus and the thyroid are unmistakable, yet obscure. In perhaps one-half of the cases where the thymus is enlarged the thyroid is also increased in size. When one is removed the other seems to undergo more or less compensatory enlargement. This would seem to indicate a species of interchangeable function. Much less has been ascertained between the relations of either of these bodies and the pituitary, while nothing has as yet appeared concerning any sympathetic involvement of the coccygeal body or Luschka’s gland.
—Recognition of the status lymphaticus during life is somewhat difficult, nevertheless there are certain suggestive features which should arouse suspicion. Of these the close relation between the status lymphaticus and rickets, already alluded to, furnishes a hint, and, when recognized, a positive warning. Widespread enlargement of the lymph nodes may furnish another. Adenoid growths in the nasopharynx accompanied by enlargement of the spleen should be regarded as a suspicious combination; and when an area of dulness is discovered over the thymus, or when it can be detected[165] by palpation, the diagnosis may be regarded as established. Moreover, children who are subject to this condition usually have a pasty complexion and an anxious facies. Besides showing evidences of rickets they are anemic, with liability to spasm of the glottis. The thyroid is often enlarged. In young adults the condition may simulate cretinism, in that they are retarded in growth and infantile in appearance, while sexual development is incomplete.
—In well-marked instances of status lymphaticus there should be ordinarily no operative intervention; yet when the nose and pharynx are obstructed it is advisable to give free channels for breathing purposes.
Assuming that the result of experimental injection of thymic juice shows it to have a depressing and pressure-lowering effect, an effort should be made to ward off danger by the use of adrenalin, which should be given previous to the commencement of the anesthesia. These are cases where it is best to treat the surfaces to be operated with a spray of mild cocaine solution, in order to deaden liability to those impressions which may produce secondary and reflex cardiac disturbances if conveyed to the brain. When operation is necessary for glottic spasm or laryngismus stridulus it may be commenced with a tracheotomy, with the use of a long trachea tube. When operation is required for the relief of thymic enlargement, a preliminary tracheotomy should be made, with the use of a long tube. The improvement which results after the completion of the surgical treatment, for instance after removing adenoids from the nasopharynx, is gratifying.
The most reliable measures have proved to be adrenalin and artificial respiration, used as described in the chapters on Blood Pressure and Shock and Anesthetics.
[166]
As a result of the conditions which two centuries ago and more so distinctly separated the barber surgeon from the practitioner of medicine, there has been evolved an artificial separation of surgery from so-called internal medicine. The consequence has been a more or less deep-rooted feeling that medical cases were to be treated exclusively by non-operative measures, and that surgical cases could scarcely be expected to present any perplexities that were not to be solved by an operating surgeon. It has been no small part of the benefit resulting from modern teachings that these imaginary boundaries and limitations have been swept away; and one of the lessons which this text-book is intended to inculcate is that broad principles underlie disease conditions, and that their bearings must be appreciated thoroughly in order to practise either medicine or surgery successfully. In order better to inculcate this teaching a chapter with the above general heading has been inserted, in order to impress the statement that any of the so-called internal diseases may present at almost any time indications for distinctly surgical intervention.
Some of the surgical sequels of the exanthematous and continued fevers are well known and commonly recognized: for example, orchitis following mumps, suppurative inflammation of the middle ear after scarlatina, and bed-sores after typhus and typhoid. These are easily recognized. Moreover, scarlatiniform eruptions occasionally follow various operations and give rise to great perplexity.[4]
[4] Medical News, February 20, 1897, p. 234.
Joint complications in this disease have been recognized from the earliest times. One hundred and fifty years ago Strack expressed himself thus: “If the dysenteric poison affect only the chest, it causes asthma; if the limbs, it produces arthritis; if both, abscess.”
Joint pains and swellings, with other suppurations, have been noted in several of the epidemics of this disease which have ravaged various parts of the world at different times. Postdysenteric arthritis may assume noticeable and even pyemic aspects, and is occasionally fatal. The bones and joints may become involved in painful and even suppurative swellings, not alone during the active stage of the disease, but during the period of convalescence; while mildness of the primary attack does not necessarily provide immunity from later complications. Here thrombosis of large veins or thrombophlebitis are also observed. When the joints are involved it is usually in irregular order and not simultaneously. Joint lesion does not necessarily proceed to suppuration, but perhaps only to the point of edema and fluid exudation or hydrops. In the Cuban and South African campaigns, during which dysentery prevailed, joint complications were noted.
Cholera is usually too rapid and too violent in its course to be followed by secondary infections. Nevertheless, Poulet reports from Val-de-Grace several instances of articular and osseous lesions, some of these characterized by effusion of fluid which was sometimes very thick and resembled balsam, while at other times pus was present.
[167]
Pneumonia having now taken its place as a distinct germ disease, and the micrococcus of Fränkel and the capsule coccus of Friedländer being well established as the active agents in the two principal forms of this disease, pus may be found in other parts of the body. The most common surgical sequels of pneumonia occur as postpneumonic pyarthrosis, which has been wrongly considered a rheumatic affection. These lesions are of embolic or of metastatic origin.
This disease has assumed prominence in medical literature, and not a few instances have been reported of surgical sequels—abscesses, purulent ear disease, pyarthrosis, bone lesions, etc. Even necrosis has been repeatedly observed.
The infectious agent in these affections is not yet recognized and their surgical sequels should be regarded as due to secondary pyogenic infections.
Surgical tuberculosis appears often as a sequel of the exanthemas. In the lymphatics, periosteum, bones, and joint cavities, and in and about the eye and ear, manifestations of suppurative disease are often found. It is believed that these sequels are likely to appear when the eruption has been incomplete. Hyperplastic thickening of periosteum and neuralgic pains of the affected parts occur without suppuration, hence the rheumatic character which Bonnet and others have wrongly ascribed to these manifestations.
While the absence of pus takes these out of the category of pyogenic infections, it nevertheless leaves them still as surgical complications which have often to be dealt with by mechanical measures, such as orthopedic apparatus, etc.; while more or less formidable operations, as for relief of ankylosis, have to be performed. Postscarlatinal arthralgia may be explained as a local ischemia; so may acute swelling or chronic thickening. But pus is an expression of infection, and cannot be otherwise regarded. Retropharyngeal abscesses and a peculiar necrosis of the alveolar process of the jaws, described by Salter, are among the various serious surgical complications of scarlatina. Epiphyseal separations and purulent destruction of ribs have also been noted.
Although in elaborate treatises, as by Liebermeister and Murchison, there is no mention of bone and joint complications as sequels of typhoid, they have, nevertheless, been recognized by surgeons. Post-typhoid hip dislocations have been reported by several German surgeons. Boyer observed spontaneous dislocation of both thighs after what he called “essential fever,” and the general topic of spontaneous luxations subsequent to typhoid has been frequently discussed.
Those affections of joints formerly considered rheumatic occur much less often after typhoid than after dysentery. Nevertheless, post-typhoidal arthralgia and myodynia have been recognized by several French writers. Some with affected joints, supposed to be rheumatic, have later been discovered to be suffering from genuine typhoid fever, and it has been afterward recognized that the joint lesion was a bizarre expression of the typhoid poisoning. The works on general practice call attention to the frequent complications of the pleural and pericardial serous membranes in this disease. They say little, however, about the implications of the articular serous membranes, though one is as easy to explain as the other. Post-typhoidal polyarticular serous arthritis has been described by more than one writer. Multiple joint abscesses have been rarely seen. Pus has been known to collect not only in the joints, but also in the tendon sheaths and bursæ. The lymph nodes are also frequently affected, and cervical, axillary, and[168] inguinal abscesses are not rare. Post-typhoidal pyarthrosis, as leading to spontaneous luxation, has had a medicolegal interest, for luxation has been known to occur while raising or lifting a patient, the question of violence being subsequently brought into court. When the joint disease assumes the mono-articular form it is likely to terminate in suppuration; when polyarticular, pyarthrosis is less common. In the pus from many of these abscesses typhoid bacilli may be recognized, but by no means in all. The writer has found them in a case of abscess in the abdominal wall occurring during convalescence from typhoid in a young woman. A non-suppurative but painful form of periostitis is occasionally observed. I have never seen more exquisite tenderness nor expressions of suffering than I met in a case of this kind in a boy in whom the bones of both lower extremities, of the pelvis, and the lower spine were involved. The slightest jar upon the floor would make him exclaim with pain, and to minister to his ordinary wants was a distressing task. He eventually recovered without any pus formation. Deep suppuration in bones occasionally occurs, and even necrosis with separation of sequestra.
Thrombosis and thrombophlebitis are also well-known sequels of typhoid, which may lead to unpleasant complications. Typhoid fever appears to bear a peculiar relation to the growth of bones, as it has been noticed that during its course, or during convalescence, they show an extraordinarily rapid growth in length, even to the extent of 1 Mm. a day. This is probably caused by the irritation of the typhoid toxin upon the osteogenic tissue, since hyperemic areas have been found in the bone-marrow of those dying of the disease, and bone pains are a frequent accompaniment of the disease. Typhoid bacilli have the power of remaining latent in the tissues for a long time after cessation of active symptoms, and have been found alive and capable of active growth seven months after cessation of the fever. Remembering the multiple ulcers of the lymphoid tissue which characterize the intestinal lesions of typhoid, it is difficult to explain pyogenic or other septic infection by absorption through these open ports of entry; and the typhoid bacilli themselves, entering the circulation through these paths, may be carried to all parts of the body, and have been found in the pia.
A large amount of interest has attached to the so-called “surgery of typhoid fever,” which, however, has been permitted to include only abdominal section for perforation of intestinal ulcers. The mortality due to this accident is nearly 70 per cent.—i. e., is formidable. It occurs generally during the third week. It is usually preceded by leukocytosis, and is followed by profound shock. Operation offers almost the only hope. It has been successful in about one out of five cases. (See Surgery of the Intestines.)
Post-typhoidal infections of the biliary and pancreatic ducts, with their resulting complications, play a conspicuous part in the etiology of biliary obstruction. They are regarded as among the most common causes of acute and chronic or latent disease in these passages.
This also belongs to the diseases frequently complicated by lesions, aside from those of laryngeal obstruction calling for surgical relief. Abscess occurs so frequently as to scarcely call for comment. Here, as in the cases of scarlatina, the location of the throat lesions and the absorbing powers of the lymphadenoid tissue so completely involved will readily account for all septic or pyogenic manifestations at a distance. Multiple abscesses have been found in the liver, the spleen, and lungs, in and around bones, betokening thereby a pyemic manifestation. Infectious nephritis is also common.
Mann, of Denver, has communicated to me personally cases of embolus of the femoral artery with resulting gangrene as sequels of diphtheria, as well as instances of true diphtheria of the penis, established by bacteriological diagnosis.
The infectious character of this disease is not questioned, although not definitely established. Orchitis, ovaritis, stomatitis, enlargement of the tonsils and spleen, and albuminuria are frequent accompaniments of the disease, while articular and peri-articular[169] complications have been noted. Bursal abscesses and pyarthroses have also been reported. These surgical complications have been regarded as rheumatoid or rheumatic, their essential significance not being recognized until recently.
The writers of the earlier part of this century allude frequently to the rheumatoid complications of smallpox, among which pyarthrosis seemed the most common and most serious. The various arthropathies are the most interesting of the surgical complications of this disease. The joints become swollen, red, and painful, one joint after another being involved.
The individuality of this condition has been recognized only within the last thirty years. That it deserves the characterization of “malignant” often given to it is well known. It is an infectious disease with a special localization in the heart, the term cardiac typhus being very expressive. Although so apparently spontaneous, it is usually a secondary lesion, sometimes a primary infection. The arthritic manifestations often assume a pyemic character, and even at the beginning of the affection, as Trousseau pointed out, there are frequently severe joint pains.
Nearly one hundred species of microörganisms from the mouth have been studied and identified by W. D. Miller, who has clearly established that dental caries is due to the specific action of some of these parasites, which, gaining entrance into the dental tubules, determine fermentation and acid production, with erosion of the dental structure of the teeth and an increase in softening and destruction. In this way the teeth, as already indicated in Chapter IV, become paths of infection for germs which may travel but a short distance, causing only local disturbance, or which may be carried to other points about the head, producing disturbance in the antrum, in the neighboring bones, in the middle ear, and not infrequently in the brain. Abscess in the brain has been distinctly traced to caries of the teeth. Tuberculous infection is also common through this channel, and its most common expression is probably the invasion of the cervical lymphatics, superficial and deep, constituting those lymphatic tumors of the neck, formerly known as scrofulous, with their disastrous train of adhesions, suppuration, erosion, etc.
These are surgical affections whose secondary complications in the way of abscesses, infarcts, tumors, etc., have been dealt with in other parts of this work. It will be well to group all of these infections with anthrax, glanders, etc., into a class of infections which may be followed by tardy or late surgical sequels that may call for more or less radical operation. In the case of gonorrhea this is best seen, perhaps, in the so-called pus tubes of the female pelvis, which often require removal years after the date of the primary invasion.
Endocarditis and pyemia are occasionally of solely gonorrheal origin, as well as peritonitis by extension from infected pelvic viscera.
This is seldom followed by surgical sequels, save in the instance of mechanical lacerations demanding plastic repair, or of septic infections, which, when life is saved, sometimes lead to disastrous consequences. Puerperal septicemia is in no respect different, pathologically speaking, from septicemia due to any other presumably streptococcus[170] invasion; and the predilection which streptococci manifest for serous membranes, and especially joints, is well known. Consequently after puerperal fever one may meet with articular or peri-articular abscesses, affections of tendon sheaths, lymphatics, etc., or the complication may assume a different type, the veins and their contents being mainly involved, with thrombosis, infarct, etc., for its immediate results.
There is probably no disease of known or suspected germ origin which may not be followed by disastrous or unexpected surgical complications, while even degenerative changes, for which as yet no theory of parasitism has been invoked, are followed by conditions which may call for serious surgical measures. In other words, the surgical complications of any so-called non-surgical disease may loom up at any moment in any case.
[171]
Certain poisons or deleterious substances are introduced in various ways into the human system from without, some of which produce only symptoms of moderate intensity, while others are fatal. It is authentically stated that in India many thousands of individuals lose their lives every year as the result of the bites of poisonous snakes. In 1903 there were officially reported 23,164 deaths from this cause. Nothing approaching such injuries in frequency or intensity can be found in any other part of the world. Animal poisons may be introduced by animals of many species. The poison of hydrophobia has been described. The bites of the mammalia may be serious and may be followed by septic symptoms, but are not ordinarily regarded as due to any special toxin secreted by the animal. A number of reptiles, however, possess special poison glands which are connected, in most of them, with a tooth on either side of the upper jaw which is canaliculated, and serves as a duct through which the poison is injected when the animal inflicts its bite.
The principal poisonous serpents in North America are the rattlesnakes—of which there are several species, usually placed at eighteen—the copperheads, the moccasins, and the vipers. Some of these have movable poison fangs, some fixed. In other parts of the world others equally or even more poisonous are known.
The poison gland is analogous to the parotid in location and structure. The duct which runs through it is so dilated as to contain a small amount of the peculiar poison. The amount of poison contained in these reservoirs varies from eight to twelve minims, and is secreted somewhat slowly. It seems to be, in some cases at least, a glucoside; in others, a toxalbumin. It is capable of being preserved either dry or in alcohol or in glycerin. The active poisonous principle seems to pertain to a globulin or to a peptone. Almost all of these venoms are innocuous if swallowed, and like septic infections seem inoculable only through the tissues and the circulating fluids. According to Mitchell, the venom of the rattlesnake renders the blood incoagulable, paralyzes the walls of the capillaries, and facilitates escape of leukocytes into the tissues, thus making actual hemorrhagic swelling occur; while the red corpuscles rapidly lose shape and fuse into irregular masses and their hemoglobin is dissolved or disappears. This poison seems to paralyze both the respiratory centre and the heart. Cobra poison, not containing globulin, at least to a great extent, does not produce the rapid changes of rattlesnake poison.
—A snake bite is like a hypodermic injection of a deadly poison, and symptoms set in promptly. These are both local and general. There is more or less local pain, with swelling and discoloration, which are due to effusion of blood. They increase in intensity, and are followed by vesication and necrosis of tissues—that is, gangrene—if the patient survive for some time. Constitutional symptoms are not long delayed, and are characterized by severe prostration, including cold, clammy sweat; feeble and rapid pulse, irregular respiration, etc. When patients succumb they usually die in collapse. The pathological changes are not well-marked or characteristic.
—Treatment of snake bite must be prompt if it is to be successful. It should consist of incision and drainage of blood from the part, in order to prevent diffusion into the rest of the body by means of the returning blood and lymph. Bleeding should be facilitated by cups or by sucking the wound. An elastic tourniquet should be applied around the limb near the trunk, the site of the wound freely incised, and the blood worked both ways toward the wound by “stripping” the member. If there be any known antidote to snake poison it consists of potassium permanganate or calcium hypochlorite (chloride of lime), applied locally in solution, the former sufficiently[172] strong to have a marked color and capable of producing local irritation (1 per cent.). With these local measures, constitutional stimulation should be indulged by means of volatile and other stimulants. There is a popular fallacy in favor of inducing alcoholic intoxication. To do this is a mistake. Nevertheless, alcohol may be given freely, dosage being limited not by amount but by effect. Strychnine, digitalis, atropine, etc., will often prove serviceable. The tourniquet should be gradually released after being in use for two or three hours, and an assistant ready to antidote the poison which may then enter the system with the necessary doses of stimulants above mentioned. One-half grain of strychnine may be administered in divided doses, it apparently being an antidote to the snake venom. There is much reason from recent experimentation to expect benefit from serum therapy—i. e., by injection of serum from immunized animals who have been fortified by increasing doses of the snake poison. Calmette advises the use of 20 Cc. of serum from a horse which has been immunized by cobra poison. He believes the active poison of all venomous serpents to be essentially identical. Good results have been reported even after an interval of an hour. In this country, however, such treatment will be called for so seldom that there is not the hopeful outlook for the serum therapy of snake bite that there is in India.
A large lizard found in the southwestern part of this country and in Northern Mexico, known as the Gila Monster (Heloderma suspectum), is credited with being a poisonous animal. The probability is that the bite is fatal to some of the lower animals and may produce more or less serious disturbances in man. Nevertheless there is little real evidence that this is to be considered in the same category with the venomous serpents above mentioned.
Certain species of spiders are venomous, the tarantula being the best known. Certain scorpions also inflict poisonous stings, and centipedes and other animals occasion at least serious local disturbance by bites or stings. These insects and animals seldom attack unless irritated or disturbed. Tarantula bites are occasionally inflicted in the Northern States by spiders which have concealed themselves in shipments of fruit, bunches of bananas being especially likely to be their hiding places. The injuries inflicted by these animal organisms cause local pain, considerable swelling, with remote effects on the nervous system, prostration, restlessness, etc. They are seldom fatal, but may cause annoyance and serious disturbance. These cases are to be treated in the same way as bites of poisonous serpents, adapting the measures and the energy of the treatment to the severity of the symptoms.
Wasps, hornets, and bees are capable of inflicting severe stings; domestic insects, like mosquitoes, bed-bugs, etc., inflict minute wounds which sometimes occasion excessive annoyance. Their sting is followed by pain, burning sensation, sometimes intense itching, and more or less swelling. Enough poison is deposited to produce local vasomotor paralysis, as the result of which wheals resembling those of urticaria, or more extensive swellings, quickly result. If the sting of an insect has been broken off in the flesh it may remain and intensify the disturbance. Two or three injuries of this kind create local disturbance, but there are some instances on record where men and animals have been stung to death when attacked by swarms of these insects, death apparently being due to intensification of effect owing to increased dosage of poison. If a sting occur upon loose tissues, like the eyelid, or upon the tongue or lips, swelling and suffering may be extreme. If symptoms of depression present, they should be combated by[173] stimulants, diffusible or other, and by hypodermic medication pro re nata. Local discomfort may be alleviated by ice, by menthol, by chloral camphor, etc.[5]
[5] Oil of lavender is a pleasant means of local protection against mosquitoes, etc. Oil of tar is also in common use. A mixture of equal parts of camphor and chloral, with menthol dissolved in the mixture (camphor and chloral when mixed without other ingredients quickly form a dense fluid like glycerin), gives great local relief from the itching and pain of insect bites.
Many of the lower forms of marine animals are capable of inflicting stings by their rays, or minute injuries in other ways, which give rise to great temporary annoyance. The stinging nettle, etc., is an instance of this kind. The lesions produced in this way partake of the nature of a more or less acute dermatitis.
The arrow poison of various Indian and savage tribes is a composition of variable and usually unknown nature. It is compounded, for the most part, from vegetable substances, and, if one may judge from the specimens of curare sold by importing houses, their strength is unreliable.
While some of these preparations are made by the natives from a species of Strychnos growing in the northern part of South America, this tree is not in universal use for this purpose: in the East Indies they are made from a species of Upas (the deadly Upas of song and story). Some of the poisoned arrows are dipped in putrefying blood. A wound made by these is not necessarily promptly fatal, but would tend to kill by setting up septic disturbance. The vegetable poisons have the property of paralyzing the motor nerves and the circulation to such an extent that death may occur within a few moments after injury. All of these poisons are innocuous when swallowed, and game killed by their agency may be eaten without fear of ill results. Arrow poison of the vegetable variety which is not fatal within a few hours may be recovered from if stimulation be vigorous. Artificial respiration is a factor in keeping such patients alive.
In the vegetable kingdom there is one kind of plant, the so-called poison ivy (Rhus toxicodendron), which is capable of producing intense dermatitis. All persons are not susceptible to this poison—least so those of thick skin and dark hair. It is generally those of blonde type and thin skin who seem most liable to its irritation.
The active agent is toxicodendric acid, and it is capable of setting up an intense irritation of the eczematous type, with a large amount of hyperemia and edema, especially of soft tissues. When the face is involved the eyelids become puffed so as to make it almost impossible to separate them for purposes of vision. Ivy poisoning is usually contracted by contact with the plant. Symptoms supervene generally within twenty-four hours, and in well-marked cases do not subside for three or four days. The itching is intolerable, and is best combated by strong alkaline solutions or brine. A dilute bromine solution sometimes proves beneficial. Salt and soda in strong solution and vigorous catharsis are also useful. Hypodermic injections may be necessary to induce sleep.
Certain species of sumach, particularly the genus Cypripedium, may produce similar symptoms, usually less severe.
[174]
Delirium tremens as an expression of acute or subacute alcoholic poisoning is in no essential degree a surgical condition. This form of toxic delirium may occur while the individual is still drinking inordinately, or not until several days have elapsed after active drinking has ceased. It is precipitated in many cases, where otherwise it would simply remain imminent, by surgical injuries and operations. In one in whom it is feared, the surgeon should become apprehensive in proportion as the muscular system becomes unsteady and tremulous, the mind disturbed, and the individual sleepless.
Patients in a well-marked condition of delirium tremens may become so uncontrollable and so lost to sensation of pain that it may be practically impossible to enforce the physiological rest which their surgical condition demands. The restraining sheet will answer for general purposes, but the strait-jacket and even the most carefully applied plaster splint or mechanical restraint will not always be sufficient to carry out the indication.
Ingenuity may be taxed beyond its limit to enforce the needed rest, for patients will tear off bandages and injure themselves in various ways.
—The local indications are in the direction of physiological rest. Constitutionally the indications are in two directions: First, to keep up nutrition and excretion; secondly, to properly medicate. Nutrition is difficult unless excretion is maintained. Hot-air baths, laxative enemas, preferably of cold water, when necessary, and administration of a fluid and easily assimilable diet are measures of the utmost importance. Should the case present features of an acute alcoholic gastritis, stomach feeding may be abandoned and the rectum utilized for this purpose. Medication should consist mostly of stimulants, with such sedatives, laxatives, diuretics, etc., as may be necessary. In surgical cases it is not wise to abruptly deprive these patients of the alcohol which they have so abused. Consequently in many instances a mild degree of alcoholic stimulation, at least for a time, should be continued. Two stimulants rank higher than all others as substitutes for alcohol, and in some degree antidotes to its effect. These are strychnine and digitalis. The former should be given preferably subcutaneously; the latter by the stomach if tolerated, otherwise by the rectum or beneath the skin. My own preference for the use of digitalis is in the direction of large and few doses. I have not hesitated in many instances to give 15 Cc. of ordinary tincture, repeated once or twice at intervals of a few hours, and then to discontinue it. The effect is to brace up the heart and to equalize the circulation, while at the same time it acts as an efficient diuretic. Adrenalin may be necessary, but should be used with discrimination.
Of the sedatives, bromides, chloral, and remedies of that class are those most often resorted to, and should be given in doses sufficient to meet the symptoms. They are all more or less depressant, and stimulation by strychnine, etc., is necessary even while they are being administered, in spite of the apparent physiological antagonism between them. Opium is the remedy of choice, and is best given in the form of morphine introduced beneath the skin.
The first indication is in the direction of ensuring rest and sleep, even at the expense of inconvenience or misfortune in other directions. I write this with a realizing sense of its significance, yet with positive conviction as to its truth.
Upon the assumption that this form of delirium is a toxemia of complicated type, only benefit can accrue, in aggravated cases, from a free venesection, followed by intravenous infusion of a pint or more of saline solution, at a temperature of 105° F.
[175]
It is difficult to distinguish this form of mania from that known as puerperal mania, the two conditions being essentially similar. This, too, is to be regarded as a complicated toxemia, in which products of defective metabolism, of insufficient elimination, and of phagocytic activity mingle in a blood whose corpuscular elements are already much disturbed by injury or hemorrhage. Regarding these cases from a surgeon’s standpoint, and carefully avoiding any attempt at minute explanation of the phenomena, such cases are met with in the practice of operating surgeons, as in the experience of obstetricians, presenting themselves either as mild forms of harmless mental aberration, or assuming almost any of the types of insanity as made out and classified by experts in that subject. From the mildest mental alienation up to intense and even homicidal or suicidal mania, one may meet with all degrees of departure from the normal standard. Bowel washing, hot-air baths, hepatic stimulants, and carefully regulated nutrition will usually restore to the brain its natural food supply, and hence its normal function. I have repeatedly seen much good result from the exhibition of small doses (0.30 to 0.50) of potassium iodide.
As stated above, it is generally recognized that in people of peculiar idiosyncrasies the administration of certain drugs ordinarily considered harmless is followed by more or less toxic symptoms. Obviously if this were universally the case, or true in the majority of instances, the use of these drugs would speedily be abandoned. As it is, it is well to have in mind the consequences which are occasionally known to ensue, and perhaps to weigh in every case the chances as to whether it is worth while to use a given substance of known occasional toxic power as against another which is not known to possess it.
Of the less active antiseptic agents, boric acid is considered absolutely innocuous, yet is known sometimes to cause intestinal disturbance, while in one instance serious toxic effects followed its use. Naphthalin will sometimes produce vertigo or vasomotor symptoms, especially when administered internally. Many of the antiseptic materials used are more or less irritating to the skin, and such local expressions as eczema, etc., provoke little comment.
Iodine is a drug whose activity should be borne in mind. Applied upon the surface, it tans the skin and does no good. Injected in solutions of varying strength into serous cavities (for example, hydroceles, etc.) it gives rise to symptoms which may be alarming. Fatal poisoning following its injection into an ovarian cyst has been reported, and alarming symptoms have been produced by injection of the ordinary solution into a hydrocele sac. Much of the virtue ascribed to iodoform is credited to the liberation of free iodine by its decomposition. Whether or not this be true, iodoform is one of the most frequently toxic of the antiseptic agents in ordinary use. In mild cases it produces headache, restlessness, wakefulness, and often a distinct taste of iodoform in the mouth. In more pronounced degrees of poisoning there is fever, often with mental derangement which may amount to delirium or even to acute mania, and may cause well-founded suspicion of meningitis. Death after its use has repeatedly occurred from syncope or in coma.
Carbolic acid produces unpleasant effects, both upon patient and operator, or with whoever it may come in contact. Aside from its local effect upon the skin, which is most unpleasant, but which usually passes away within a few hours, it seems to affect especially the kidneys, causing often temporary albuminuria with discolored urine, deranged secretion, and sometimes more acute forms of disturbance, similar to those met with after its internal use. Carbolic poisoning was observed most frequently during the era when Lister’s original directions were scrupulously followed, and at a time before it was learned that it is much better to remove dirt than to try to antagonize its action. Eminent surgeons were compelled to discontinue its use because of its unpleasant effect upon themselves as well as upon their patients.
Among the powerful antiseptic agents in common use are the soluble preparations of mercury, ordinarily corrosive sublimate, in solutions of varying strength, which are used for irrigation, douching, etc., and for preparation of dressings. An intense eczema[176] may follow its local use, and symptoms of mercurial poisoning may appear in individuals of peculiar susceptibility to this drug. Salivation, intestinal irritation, and other phenomena of mercurial poisoning have been produced, with the result that the solutions and preparations of corrosive sublimate are much weaker than those which were used at first. The drug eczema produced by corrosive sublimate interferes with one of the essentials of ideal wound healing—i. e., physiological rest. The area involved should be protected with a sterilized powder or by anointing it with sterilized ointment.
[177]
The maintenance of the normal pressure of the blood is a material factor in the welfare of surgical cases. Deviations in the direction of lowered pressure constitute the most important features of shock and collapse. Prevention of loss of blood is but one of several complex indications in prophylaxis and after-treatment.
Blood pressure is maintained in large part by the vasomotor system of nerves, whose prime centre is in the gray matter of the fourth ventricle, with subsidiary centres in the spinal cord and great ganglia. Stimulation of these centres causes contraction of the peripheral arterioles and increases intravascular pressure. If, however, it be long-continued or excessive, these centres become exhausted, vasomotor paralysis results, the arterioles dilate, and pressure is lowered.
Three factors coöperate to maintain this pressure:
Departure from the normal in any one of these factors causes perceptible disturbance, but when in all three of them it may prove fatal. Whether this be caused by emotion, accidental injury, or deliberate operation is of slight concern, as the effect is essentially the same.
The pulse will usually tell its own story to the experienced observer, but scientific accuracy in measuring blood pressure can only be obtained by certain instruments of precision, such as the tonometer or the sphygmomanometer, consisting of an air-containing armlet which encircles the arm, a bulb by which the pressure of air can be regulated, and the whole connected with a manometric gauge and mercury tube. These instruments can be procured of the dealers, and their employment during an operation gives the operator a continuous record of the blood pressure, by which he may judge at any moment of the degree of shock.
The normal blood pressure in healthy adults is 130 to 140 Mm. of mercury in the tube. In children it ranges from 90 to 110 Mm. Females have an average lower pressure of 10 Mm.
Excitement or slight stimuli will send the pressure up thirty or forty points. It is also higher than the above average in arteriosclerosis. In uremia it is always high. In cases of intracranial tension it is also high, as the brain alone of all the organs of the body has no complete vasomotor apparatus of its own; when it needs more blood this has to be contributed from the general supply. When pressed upon by a clot, depressed bone, or foreign body it becomes anemic, and on effort to furnish the needed blood from other parts the vascular tonus is increased. Cushing has shown the value of these estimations in cases of head injury, for the rise of blood pressure may be regarded as an indication for operation. In typhoid fever a sudden rise of pressure is associated[178] with perforation, or perhaps with the peritonitis which is its immediate result. On the other hand, in this disease a sudden fall of pressure is an indication of hemorrhage.
The course of events in surgical shock is about as follows: Injury to afferent sensory nerves acts as a vasomotor stimulus after it reaches the centre in the fourth ventricle; a reflex impulse is then sent out which produces arterial contraction and raises the blood pressure. When the abdomen is concerned the opening and handling of its contents produce the same result through the splanchnic centres. If, however, the stimulus is excessive, too often repeated, or too prolonged the vasomotor grip is lost, the arterioles dilate, and the blood pressure is reduced. A severe injury to any part of the body may produce this effect without the preliminary rise. The popular impression that a patient “bleeds to death into his own veins” has this to justify itself, that the arterial tonus is lost and the blood is pumped through the arterioles to accumulate in the capillaries and veins, especially the abdominal, thus overloading the right side of the heart and giving it a disproportionate amount of work.
Accompanying these circulatory disturbances are others, secondary and unavoidable, as of respiration, which becomes rapid and enfeebled in proportion to the degree of shock.
Any factor which tends to weaken the heart’s force favors both phenomena. So important is the respiratory action that patients die from cessation of respiration rather than from impairment of the circulation. This shows the importance of maintaining artificial respiration in cases of severe shock.
Cushing and Crile have studied the subject exhaustively in animals. They have shown that certain injuries are likely to be followed by well-marked reduction of blood pressure; for example, those of the brain, the interior of the larynx, the abdomen and testicle, are often followed by a marked reduction of pressure without any preliminary rise. In other words, vasomotor paralysis is sometimes an almost instantaneous effect of certain injuries. When most of the blood is collected in the venous system and the central nervous system fails, because of lack of blood supply, to respond to those normal stimuli which are essential to heart action and respiration, the heart weakness or heart failure is due, not alone to failure of its innervation, but to its reduced output and its diminished content of blood on the left side.
Crile has shown that the more abundant the blood supply to a given part the more it contributes to production of shock; hence, the value of cocainizing the interior of the larynx and the nerve trunks.
Aside from emotional causes—which are sometimes inseparable from even surgical cases—the principal agencies in the production of surgical shock and collapse are those which make a sudden and deep impression through the medium of the sensory nerves upon the central nervous system or the large sympathetic ganglia; ultimately upon the latter in all serious cases. Loss of blood, then, need not play a very important role.
Weakened, anemic, or neurotic patients are predisposed by virtue of these conditions, and also the young and aged. Fright combined with injury increases the degree of the effect. Crile has shown that trifling lesions of the interior of the larynx will cause symptoms which do not occur in animals if the superior laryngeal nerves be divided or if the parts be cocainized.
The upper portions of the abdomen are more sensitive in this respect than are the lower, testicles particularly. The skin is more impressible than the muscles or tissues beneath, save the nerve trunks, which are very sensitive; the bones and large joints slightly so. After shock has been once produced further injury causes a disproportionate lowering of blood pressure.
So-called “concussion of the brain” is essentially a condition of shock following injury to this particular part of the body. (See Head Injuries.)
Shock and hemorrhage are often closely associated, and loss of blood is doubtless a powerful factor in the production of the former, especially in those already reduced or whose blood contains a lowered percentage of hemoglobin. There are, therefore, great advantages in entrusting an assistant with the duty of watching blood pressure during serious operations.
The terms shock and collapse are nearly interchangeable, but, by common consent, the latter is usually the name given to conditions that are more sudden and overwhelming. Shock may be of all degrees—from temporary faintness, from which the patient recovers within a few moments, up to a condition of vital depression which terminates fatally, there being no reaction in spite of all efforts to produce it.
[179]
—These vary to a considerable extent according as the patient is or is not under a general anesthetic. The description of types and symptoms includes an expressionless face, pallor of the skin and mucous membranes, with corresponding coldness of the same, i. e., reduction of surface circulation and heat; dilated pupils, reacting slowly to light; irregularity of the heart’s action, with a weak, irregular, thready, or almost imperceptible pulse; irregular respiration, i. e., irregular both in rate and depth; mental inactivity and apathy; loss of voluntary muscle movement; impairment of superficial sensibility; reduction of body temperature; and nausea or actual vomiting. These at least constitute the symptoms and form the apathetic or torpid type of shock.
In the so-called erethistic type (Travers) the patients are restless and excited, uncontrollable, with irregular pulse and breathing, often with dilated pupils.
In a third type, described by Travers as the delayed, the symptoms are as above detailed, but do not appear until some hours after the cause which has produced them, which may be a concealed (internal) hemorrhage. The delayed type is also seen in those who escape serious accident with a minimum of physical harm.
As shock becomes more pronounced, mental depression deepens into coma, or mental excitement subsides into it; the surface becomes colder and bathed with perspiration, and death follows. These symptoms are those generally noted, whether following injury to the head and denoting so-called concussion of the brain, loss of blood, wound of the abdomen with injury to the viscera, blows upon the testicles, gunshot wounds or other accidents which are causes of shock. They follow also after perforation of the bowel, as in typhoid fever or appendicitis; depression following the receipt of bad news, or fright, etc.; in other words, the physical condition is practically the same no matter what the exciting cause.
—Shock is mainly to be diagnosticated from fat embolism; concealed hemorrhage as well as pulmonary edema and suppression of urine are to be suspected. It is unquestionable that many patients have died of fat embolism in whom the actual cause of death has not been ascertained, yet has been ascribed to shock. (See Fat Embolism, Chapter II.)
—The treatment of shock consists essentially in measures directed toward raising the lowered blood pressure. At the outset reaction should not be established too quickly, lest it be succeeded by overaction, with attendant disasters in the shape of secondary hemorrhage, etc. Patients should not be expected to swallow nor act as they would under other circumstances. They should not drink strong liquors, for the irritating fluid may escape into the larynx and induce coughing, which might prove fatal. The same is true of inhalations of strong volatile stimulants, like ammonia. These measures, therefore, should all be resorted to with great care and discretion. Warm, stimulating drinks, if they can be swallowed, are useful; and whisky, brandy, etc., should be given dilute and warm rather than strong and cold. External heat is advisable, and can be supplied by immersing the patient in a bath-tub of warm water, care being taken to keep the face out of the water. When this is not at hand, bottles and other receptacles for warm water may be used, but with caution, since too much heat has been the cause of serious burns.
Numerous drugs have been recommended in the treatment of shock. There are but two or three which are worthy of confidence. Crile, of Cleveland, subjected a large number of animals to tests in regard to the effect of various drugs in influencing blood pressure. He found, for example, that alcohol apparently produces more depression, and in deep shock is dangerous. Nitroglycerin and amyl nitrite seem to increase shock and lower pressure. Digitalis may produce a temporary rise in pressure, but in considerable doses impairs or arrests respiration, and it seemed to him that cases of severe shock treated with it did not live as long as the control animals. Strychnine has been one of the main reliances in these conditions. Crile found that if enough were given to cause increased excitability of the spinal cord it raised the blood pressure, while small doses had little or no effect. Pressure was raised by doses large enough to produce convulsions; repeated smaller doses had little effect, tending rather to increase shock.
These were the experimental results in the treatment of shock, and are to be distinguished from what may be done with the same drugs in the way of fortification and preparation as against shock. Thus strychnine always exalts susceptibility of the cord of the medulla and digitalis may temporarily supplement its use; together they may help[180] to sustain pressure or to fortify as against depressing agencies. They are like whip or spur to a jaded horse.
Morphine alone, or in combination with ether as a general anesthetic, reduces susceptibility to shock, and appears to be an equalizer of pressure and a tranquillizer of an excited heart. Nitroglycerin and the nitrites usually fail to raise or even sustain pressure. Saline infusion and adrenalin are the reliable and efficient means to be used in combating shock and collapse; they always raise blood pressure, and the latter is the most powerful of all known vasomotor constrictors. Adrenalin always produces rise of blood pressure, even after cocainization of the medulla and cord or destruction of the medulla, division of the splanchnics, or arrest of the heart by powerful electrical currents (2300 volts, alternating). Even after death by decapitation and an interval of fifteen minutes, adrenalin salt solution thrown into the veins causes a rise of blood pressure. If this be combined with artificial respiration and rhythmic pressure over the heart, resuscitation is possible in most extreme cases. In one case, reported by Crile, a human heart which had stopped beating for nine minutes was made to resume its pulsation for thirty-two minutes. From all this it will appear that the heart stimulants, so called, have a very limited applicability.
Crile further experimented by raising the atmospheric pressure surrounding the animal, and found that blood pressure was somewhat exalted. The reverse was also found to be true. When he so arranged his experiment that an animal inhaled air under increased pressure he found the tendency was rather to impairment of heart action, blocking the circulation and reducing pressure. Changing the experiment and causing the animal to breathe air at normal pressure while the body was under increased atmospheric pressure, blood pressure was notably raised, but respiration became labored and the heart’s action impaired. After death the heart and the pulmonary vessels were found engorged.
This has its practical interest because it concerns not alone the general treatment of shock, but the management of those cases where the thorax must be opened, as in the surgery of the heart, the lungs, the esophagus, etc., and the mechanical devices recently suggested for maintaining differences of atmospheric pressure, and preventing a traumatic collapse of the lungs.
These experiments also suggested the so-called “pneumatic suit” devised by Dr. Crile, which is in effect a double-layered garment of rubber cloth. The patient is enveloped in the suit, which can be inflated with an ordinary bicycle pump, so that pressure is made upon the surface of the body, and at the same time evenly distributed. By such pressure accumulation of blood in the venous reservoirs is prevented, and the emptying of the arteries, especially those in the brain, is prevented. This is a more perfect and ideal application of the idea underlying the practice of bandaging the extremities or raising them, in extreme conditions of shock; the former requires an elaborate and expensive outfit, while for the latter purpose cotton bandages or rubber may suffice. The latter, however, must be used with great caution lest pressure be overdone. When the bandages are removed they should be taken off slowly, and from one limb at a time, lest the change be too abrupt.
Two other expedients are of the greatest value in conditions of this kind; the first is artificial respiration. This cannot be carried out, as is done on experimental animals, in a well-furnished laboratory, by opening the trachea and making connection with a pump; it must be effected by the usual methods, coupled with the aid afforded by the improved Fell apparatus. If oxygen can be administered at the same time it will enhance the effect.
The second expedient is rhythmic pressure made over the lower part of the thorax, or beneath the ribs, by which is produced a stimulus to contraction of the heart. This may be made slowly at first, but may approximate a rate corresponding to a slow pulse.
The temptation is to use the adrenalin solution too strong or in too large doses. It may be administered in doses of 4 or 5 minims in a small syringeful of salt solution, but when the symptoms are profound and the case urgent, 300 to 500 Cc. of sterilized salt solution, containing the same amount, should be injected beneath the skin into the subcutaneous cellular tissue about the shoulder-blade, the buttock, behind the breast, or into a convenient vein. Much larger amounts, even up to 1000 Cc., may be used, but the adrenalin should never be mixed until just before using it, as it is quickly oxidized and changed, and should be used in the freshest possible condition. With salt solution[181] containing 1 to 50,000 of adrenalin and continuously administered, Crile has kept a decapitated dog alive for over ten hours—that is, the heart continued its action. One may agree with him, then, in the statement that “control of blood pressure is the control of life itself.”
Mathews, after a careful study of the osmotic behavior of blood plasma and saline solutions, has shown that the ordinary salt solution, which has been usually made in proportion of 6 to 1000, is not the best which can be used for purposes of saline infusion. Many observers have added potassium and calcium salts to such a mixture, the latter, especially, because of its property of increasing the coagulability of the blood.
The following mixture meets the indications for what may be called the “balanced” physiological solution: Sodium chloride 0.9, potassium chloride 0.03, calcium chloride 0.02, water 100.[6]
[6] To the fluid for hypodermoclysis (salt solution) there may be added a proportion of grape sugar, by which much is gained of true nutritive value, which may be enhanced by the addition of pure pepsin peptone free from albumose. Thus if every four hours there be injected beneath the skin 100 Cc. of water containing 2 grams each of grape sugar and table salt to 4 grams of pepsin peptone, the necessity for further nourishment may be almost obviated, at least for a period of two or three days at a time; as for instance when intense nausea of severe peritonitis prevents the ingestion of anything possessing food value. Credé recommends for the same purpose a preparation containing soluble albumin in the strength of 95 per cent., with traces of iron and salt. This preparation is called by him kalodol, and much resembles blood albumin, which is why it is so easily assimilated. According to Credé, four injections of kalodol a day will suffice for ordinary needs.
It must not be forgotten that indiscriminate resort to intravenous infusion may do great harm. It is a minor procedure which requires skill. When the lungs are congested from the irritating effect of ether, and the right heart is embarrassed, a too sudden flushing with saline solution may further embarrass it or even check its activity. So with a patient in the Trendelenburg posture, the intestines are crowded up against the diaphragm and its natural downward play impeded, though the brain is better supplied with blood in this than in any other position.
Much may be done in the way of prevention when shock can be foreseen. This includes the general fortification of the patient by overcoming any auto-intoxication which may have been previously noticed, by improving elimination, and by stimulating the heart’s action with strychnine, digitalis, cactus, etc. Atropine is especially a stimulant to the respiratory centres.
Once the operation is begun, and remembering that the depressing influences which tend to reduce blood pressure are transmitted through the afferent nerves, we may take advantage of Crile’s suggestions and temporarily paralyze them, by exposing them and injecting directly into the nerve trunks two or three drops of 1 per cent. cocaine solution. This should be done before division of the main trunks and at a point above the line of section. It is possible during an amputation, by taking a little extra time and pains, to “block off,” as it is called, the nerves in this way and prevent their conveying any depressing sensation. At other times, as in operations on the mouth, and especially the larynx, cocaine solution may be used locally, as by the spray, and the same effect produced. Cocaine seems to be a protoplasmatic poison which inhibits nerve action.
In the description of the treatment of shock there has been little reference made to the result of loss of blood as such. In cases where this has already occurred, or cannot be prevented, it should be atoned for by the infusion of saline solution, either by intravenous introduction or by hypodermoclysis, i. e., its injection into the loose connective tissues in various parts of the body. While a special apparatus has been devised for this purpose, a sterile fountain syringe with an ordinary aspirator needle will be found to be sufficient for nearly all purposes.
The erethistic, or extremely restless type of shock, may be profitably treated by small doses of morphine given subcutaneously.
The question of immediate operation or delay should be carefully considered. Shock is often alleviated by prompt removal of mutilated limbs or parts whose fragments, while still connected with the trunk, seem rather to perpetuate the condition, especially if the principal nerve trunks are cocainized. In serious cases intravenous infusion should be practised.
After commencing with the anesthetic, while scrubbing and cleansing the field of operation it is advisable to scrub an arm where it may be necessary to expose a vein, or the skin at several points, where a needle may be entered, so that there may be no delay for this purpose should infusion or hypodermoclysis be suddenly required.
[182]
Abstraction of blood, usually of venous blood, known as venesection, was a practice frequently indulged in years ago. At one time in the history of medicine it seemed to be the measure regarded as a panacea for all ills. The reaction from the period of excessive bloodletting came during the previous century, and was so strong that the practice was for a generation or so almost abandoned. The eminent surgeon S. D. Gross wrote a paper entitled “Bleeding as a Lost Art.” Bloodletting is an expedient of great value in a somewhat restricted class of cases, but is capable of affording such relief in certain emergencies that practitioners should be ready to resort to it at any moment when it may be required.
After removal of a certain amount of fluid blood pressure is naturally reduced and at the same time equalized, while when the right side of the heart is overburdened with its task it is thus made to beat more easily and regularly; thus indirectly there may be brought about a subsidence of violent heart effort, a reduction of the respiration rate, a lowering of temperature, and sometimes a diminution in the activity of morbid processes which may be beneficial, and even life-saving. Even after moderate bleeding, say a half-pint, the amount of urine is increased and the proportion of solids raised. More air is taken into the lungs, and oxygenation is thereby much improved.
The indications for venesection are:
There may be added later the introduction of balanced physiological salt solution as recommended in the treatment of shock, and of some of the acute toxemias, e. g., delirium tremens.
The effect on an embarrassed and overfilled right heart of the abstraction of blood is prompt. Nowhere is this more conspicuous than in the early stages of pneumonia, and in some cases of heart failure during administration of an anesthetic where a dilated heart seems to become so overfilled as to be unable to empty itself. In profound uremia, especially in puerperal eclampsia, the relief afforded by it is usually immediate and permanent.
The question of the amount of blood to be withdrawn must be settled at the time and for each individual case. The pulse is watched, as well as the patient’s face; the best indications when to cease being noted in this way. From 500 to 1000 Cc. may be removed according to the condition of the patient and the degree of emergency. While the operation is a trifling one, it should, nevertheless, be performed with strict aseptic precautions. One of the veins at the bend of the elbow, usually in the left arm, is commonly chosen, although in rare instances, when there is intense cerebral venous congestion, the external jugular may be selected. At the elbow the median basilic vein crosses the brachial artery, being separated from it only by a thin prolongation of the biceps tendon. It was especially in opening this vein at this point with the old-fashioned lancet, which was plunged perpendicularly to the surface and directly into the vein, that injury to the artery occasionally occurred, thus leading to varicose aneurysms and aneurysmal varices.
The skin should be thoroughly cleansed; a reasonably tight constriction is made about the middle of the arm by a bandage, not so tight as to completely occlude the radial[183] pulse; the arm is allowed to hang downward and the patient encouraged to grip some object in order to better fill the vein. This soon becomes prominent, after which an oblique incision is made through the skin above it, so that the vessel itself is exposed. Then with a sharp bistoury the external surface of the vein is pricked with the point, and a cut made outward. The opening in the skin should be free; the skin may be frozen, or in very sensitive patients local anesthesia may be first produced with cocaine. By tightening and releasing the grasp, that is by closing and opening the hand, the flow of blood may be hastened. When it is time to cease, the bandage should be removed and an aseptic pad be applied over the site of the wound, suitable pressure being made, and the arm kept at rest for two or three days.
When the jugular or some other vein is selected the procedure is essentially the same.
—Arteriotomy, or the opening of an artery for bloodletting purposes, is resorted to only in rare instances, and in an emergency. The temporal artery is the one usually selected because of its accessibility and the ease with which its outflow can be controlled. Its position is determined by its pulsation; it should then be exposed by incision through the skin, and opened exactly as is a vein, not cut through, lest it retract and furnish an insufficient amount of blood. It should, however, be divided and tied before application of the dressings.
—By the application of “cups,” blood is drawn to the surface, but ordinarily not abstracted, unless the surfaces have been previously scarified or incised. Dry cupping has the effect of attracting blood to one portion of the body, thus drawing it from another and congested part. It has the temporary effect of a venesection. Cupping glasses are small tumblers which are rinsed in alcohol; their edges are wiped and the remaining film within the glass is ignited from a candle or flame. The glass is then instantly applied to the affected area. The oxygen within the contained air is sufficiently consumed to create a slight vacuum and the skin quickly becomes congested, being sucked upward into the glass. These cups may be allowed to remain for a few moments, or until they drop off. Care should be exercised with alcohol and a lighted lamp around a patient who may be unconscious or excitable, as serious burns have followed carelessness in this regard. Small vacuum pumps, like the Allen surgical pump, have been provided for this purpose, and give very satisfactory results.
There was formerly employed for the purpose of wet cupping a small spring instrument, containing several sharp knives, by which a series of incisions were made in order that blood might be drawn. This instrument cannot be kept clean and is not used at present. When wet cupping is desired the part should be scarified with a sharp knife and the cup applied as above.
—Leeches figure largely in literature of the past, but are not often used, although they may be made effective, especially when applied behind the ears in cases of cerebral congestion. The American leech can be relied on only to abstract about a teaspoonful of blood, while the Swedish will draw three or four times that amount. The region to which they are applied must be washed, and, if necessary, shaved. The part should then be smeared with milk, blood, or sugar-water. The leeches should be put in a basin of fresh water, after which they are placed upon a dry towel for two or three minutes. Each one is then taken up in a small glass or test-tube and inverted over the spot chosen. As soon as the animal fastens itself upon the skin the glass may be removed. Leeches are often capricious and will sometimes wait considerable time before attaching themselves. When full of blood they usually relax and drop. If it be desired to remove them a little salt will make them relax. Leeches should never be applied over loose cellular tissue nor over superficial vessels or nerves. If used in the interior of a cavity they should be prevented from passing too far.
Counterirritation is a valuable means of accomplishing that which is sometimes induced by leeches—namely, attracting blood to the surface for the relief of deep congestion. In fact it comprises more than this, since there is some deep influence exerted through the medium of the nervous system; it not only equalizes the circulation, but tranquillizes a disturbed innervation. The milder and more domestic means include the use of the so-called rubefacients—hot water, mustard, and turpentine. These are[184] of little use in surgical conditions which call for counterirritation; their use should be controlled with caution lest mere counterirritation be converted into actual burning.
By the use of vesicants a blister is produced, i. e., an effusion of serum and lymph beneath the superficial and outside of the deeper layer of the skin. Mustard and cantharis are the principal vesicants in common use. The former may be used in full strength, in which case it is active, or it may be reduced with wheat flour or linseed meal. To bring out the full strength of mustard, hot water should not be used in its preparation, as it renders it almost valueless. A mustard paste or plaster should be watched at intervals, and it should be removed when the desired effect has been obtained—at all events, when the surface to which it has been applied is covered with vesicles.
Cantharis, or Spanish fly, is used either in the form of the cantharidal cerate or mixed with collodion, the latter being the neatest and most pleasant preparation. Several layers are painted on the surface where its effect is desired. This is then protected, and vesication will be found to have been produced within an hour or two, except where the skin is most resistant. The stronger chemicals, like ammonia, chloroform, strong iodine, and nitrate of silver solutions, will be found to be active blistering agents, but should be used with caution.
Two other methods of irritation were at one time in favor—namely, the seton and the issue. The former consisted of a bundle of threads or a wick, drawn into a large needle with a lancet-shaped point; the skin was picked up into a fold, the needle made to traverse it, and the wick was thus drawn through and cut off, so as to be left in place. The issue was made by drawing a blister with a powerful agent, and then preventing it from healing by the use of an irritating foreign body. These procedures have been abandoned by the medical profession, but are still in vogue among veterinary surgeons.
—In some one of its improved forms the Paquelin cautery has replaced all the old cruder methods of cauterization. When properly employed its counterirritant effect can be made most serviceable for the relief of pain, or for any desired form or degree of counterirritation. Applied over the upper abdomen, with the lightest possible touch, in such a way as to deserve the term “flying cautery,” it will sometimes afford great relief in nausea and vomiting, especially when these symptoms are purely reflex.
Used over the course of the larger nerves it does much to relieve the pain of neuritis; while over swollen joints and swollen testicles it affords great relief from the pain of chronic arthritis and chronic or acute epididymitis. In deep-seated congestions and inflammations ignipuncture may be made with a small cautery point, by plunging it through the skin into the underlying tissues, and into bone. The relief of tension as well as the counterirritation will give great relief. When practised in this manner local or general anesthesia may be used. Except when thus used it will rarely be necessary to do more with it than to disturb the exterior of the skin. When skilfully used this can be done with the production of very little pain.
Paracentesis is the technical name given to the act of tapping, or the withdrawal of fluid from any of the closed cavities of the body. It includes aspiration, tapping, and incision.
—By aspiration is meant the removal of fluid without the admission of air; it comprises the use of a suction apparatus, usually known as an aspirator, which may be had in various forms and sizes. A small so-called exploring syringe will answer for small cavities, while for large collections of fluid, such as may be met with in the thorax, more elaborate apparatus is used, consisting of a suction pump connected by tubing with a bottle in which the vacuum is produced. By another tube this bottle is connected with a hollow needle used for the withdrawal of the fluid. Absolute asepsis should be observed, even in this minor procedure. The skin should be cleansed, and the needle, instrument, and hands should be sterilized. The pain of puncture may be prevented by use of the freezing spray, of cocaine injected locally, or by touching the skin with a drop of pure carbolic acid. The vacuum is commonly resorted to in the removal of fluid from the thorax, the spinal and the cranial cavities, and from joints; also in small collections of pus in any part of the body.
[185]
—Tapping means a somewhat similar procedure with a larger instrument known as a trocar and a surrounding cannula, without the aid of the vacuum. Precaution should be taken in every regard that the instruments and the parts should be sterilized.
The trocar, inserted in the cannula, should be plunged quickly into the cavity at the site selected. Considerable resistance will be offered by the skin. If the trocar be small it is enough to anesthetize the skin; if large, a small incision will permit of its better use. The instrument makers have provided cannulas of various descriptions, to which tubing may be attached, so that the fluid may be conducted into a suitable receptacle, and wetting the patient avoided. It is well to draw the skin aside and not to make the instrument pass directly into the cavity to be tapped unless it contain pus and it be desired to keep it open. If this precaution is taken the skin will cover the deep opening after it slips back into its position, and will act as a valve to prevent leakage. In this way infection may be avoided.
When fluid has ceased to be serous and has become purulent, as in empyema, it is often so thick that it will not flow through any hollow instrument. In such an event free incision should be made. When the thorax is involved incision is made between the ribs, and in order to maintain drainage a good-sized drainage tube should be inserted. This at times may be so compressed between the ribs that an inch or more of one rib should be exsected to provide against this possibility.
Though much has been said concerning the indications for these procedures no explicit directions have been given. While they are often emergency measures they are, nevertheless, frequently practised. In well-regulated institutions the conveniences are always at hand for instant resort when needed; but it would be well for every general practitioner to have ready at all times the few things that are required, for at least hypodermoclysis. In country practice, however, a clean fountain syringe, a suitable aspirator needle (both carefully sterilized), some boiled water, table salt (when nothing else is at hand), and soap and water for sterilization of the operator’s hands and the patient’s skin are all that are necessary. In every outfit there should be a needle which may be used for this purpose. It may be carried in a glass tube, always sterilized, and ready for use. No fountain syringe should be used which has not been freshly boiled, except in an emergency. Tablets containing common salt in definite amount, so that a solution of given strength can be made by adding them to a definite amount of water, can be procured. With such a needle, a few tablets, and a fountain syringe the surgeon is prepared for any emergency.
For intravenous infusion for which no pressure is required, an ordinary funnel, with rubber tubing attached, will be sufficient without the use of a rubber bag.
The use of salt solution has supplanted the transfusion of blood. This requires a source of blood which is not always at hand and an amount of attention which can rarely be given in emergencies; moreover, it has been shown that the injection even of defibrinated blood is a dangerous procedure, because of liberation of hemoglobin and destruction of white corpuscles, with the liability to coagulation of the blood from increase of fibrin ferment, and the possible death of the patient. Direct transfusion from another person into the veins of the patient is also difficult, and has rarely been of service.
As already stated in the chapter on Shock, the best solution for infusion is composed of calcium chloride 2 parts, potassium chloride 3 parts, sodium chloride 9 parts, sterile water, 1000 parts. The addition of one part of sodium bicarbonate will sometimes prove of advantage, while in diabetic cases this may be increased to three parts to a thousand. It has also been suggested to add a small proportion of sugar, even up to thirty parts, to this solution, in order to increase osmotic action and better preserve the red corpuscles from injury. It is supposed also to give a certain nutritive value.
When the fluid is injected into the venous system all that is desired is that it barely enter; consequently the receptacle containing the fluid should be held but a few inches above the level of the opening. When hypodermoclysis is practised more pressure will be needed and a greater difference of level should be maintained. In the veins the amount injected should not exceed 100 Cc. each minute. From 500 to 1500 Cc. may[186] be used altogether. There need be no hesitation in introducing it at a temperature considerably above the body normal, and in cases of shock it may be introduced even at 115° F. The character of the pulse will afford the indication as to the amount of fluid to be used as well as the wisdom of repeating the measure after an interval.
For intravenous infusion a vein in the arm is usually exposed and the needle point carefully inserted. It is an advantage to have for this purpose a special needle, made with a blunted extremity, enlarged a little, so that by the use of a temporary ligature the vein may be held tightly around the cannula, for such it really is, and the escape of fluid be prevented. After withdrawal of the needle a double ligature should be placed for purposes of security. The limb should also be kept at rest for a few days.
For hypodermoclysis from 500 to 1000 Cc. may be employed; the anterior abdominal wall, the flank, the thigh, and the retromammary tissues are the best regions in which to inject the solution. Absorption will be assisted by gentle massage. Local anesthesia by the freezing spray, or by cocaine, will rob the procedure of its discomfort. Adrenalin may be added to the solution, whose formula is given above, in emergency cases where it seems to be especially needed. In instances where infusion is practised for the purpose of washing out the blood, i. e., in the acute toxemia of uremia, alcoholism, etc., nothing of the kind will be required; but in conditions of lowered blood pressure, i. e., shock, it will prove of great value, as already indicated.
Catheters, as such, are intended for the withdrawal of urine from the urinary bladder, or for the introduction and withdrawal of cleansing fluids. They are made of metal, glass, gum, and silk, or other similar material, in various sizes, while some are specially formed or bent in order to pass more easily over the obstruction offered by a median prostatic enlargement. Various forms are sold in the surgical depots, from which the purchaser may make a choice. Next to the simple tubular forms the elbowed or Coudé catheters are of the greatest value.
Catheters should be sterilized before use. Those used occasionally should be cleaned after use and dried, while those in daily use may be kept in an antiseptic solution after cleansing. The cleansing of a catheter should include not only attention to the exterior, but also removal from its bore of all clots, debris, etc. Some pressure behind the fluid used for this purpose is advisable. A clean metal or glass catheter may be sterilized in a flame just before use. All flexible catheters should be boiled just prior to their insertion, or they should be taken out of an air-tight receptacle in which they have been kept in contact with some antiseptic, or in an antiseptic vapor. For the latter purpose paraform offers an excellent material, as there is given off from it formaldehyde vapor, which is a powerful bactericide. It comes in crystals and in tablets. Rubber catheters should be boiled in a 5 to 10 per cent. solution of ammonium sulphate.
The urethra should also be cleansed, especially the meatus, in either sex. Cases of cystitis may be directly traced to infection introduced by a catheter, the result being the same whether the germs be not removed from the instrument or are carried in by it from the anterior urethra. This is particularly true in paralytics who have no power of expelling the urine, and in prostatics who need regular catheterization.
The technique of using the metal catheter in the male is the same as that of introducing a sound. A lubricant is necessary for the easy introduction of the instrument, and a sterilized ointment or oil will serve the purpose. Olive oil, mixed with iodoform, as often used, is not sterile. The hands of the operator should also be clean, and no part of a clean instrument should be allowed to come into contact with any portion of the patient’s surface. On this account the parts exposed should be covered with sterile towels.
The catheter being intended to afford relief with the least amount of discomfort, a smaller instrument may be used than would be inserted were it meant for the dilatation of a stricture. Occasionally, and in a sensitive patient or hyperesthetic urethra, a little cocaine solution may be used to advantage, especially if force or pressure need be made in order to overcome spasm of the cut-off muscle. The metal instrument is too rigid in some cases, while the gum catheter is too flexible. Under these circumstances, the silk instrument may be used.
If the tip of the instrument be kept close to the floor of the urethra it will rarely catch[187] in any fossa or lacuna, particularly if the size has been correctly chosen. When apparent obstruction occurs at the triangular ligament the instrument should be withdrawn a little, tilted differently, or lifted a little so that it is made to hug the roof of the urethra rather than to press upon its floor. By a little manipulation of the end of the instrument any obstruction at the neck of the bladder may also be overcome. A sudden depression of the outer end as the catheter reaches this part, or a little pressure by the finger of the disengaged hand in the perineum, will give much help. It is well, occasionally, to introduce one finger into the rectum in order that by it the instrument may be better guided along its course. Only in cases where there has been previous disease or where unsuccessful attempts have already been made to pass an instrument will much real difficulty be found; that is, only in those already suffering from stricture, or from enlarged prostate with the difficulties which it affords, will one have to resort to manipulation requiring more than ordinary dexterity. In some of these cases even the expert is likely to meet with difficulty, rarely with absolute disappointment. Should it be impossible to empty a distended bladder with a catheter suprapubic puncture with the aspirator needle should be made.
When difficulty is experienced it is enhanced by spasm of the deep muscles, as a reflex from the soreness produced by repeated efforts and by hemorrhage.
Hemorrhage from this source is rarely of serious character and quickly ceases. In certain instances where it is aggravated much can be accomplished by leaving the catheter in situ for a few hours, or even for two or three days.
False passages will occur sometimes in spite of at least ordinary care, and are always serious in their nature. Extravasation of urine may result, with more or less disastrous consequences, or speedy septic infection may quickly terminate the life of the individual. They are to be avoided, as far as possible, by the use of instruments of large rather than of small size, with blunt tips, and by delicacy of manipulation. For this purpose it is well to avoid the use of catheters which require a wire stylet for the maintenance of their proper curve, lest during manipulation the point of the wire may work injury. The various accidents due to or connected with catheterization will be dealt with in their proper places in connection with the surgery of the urethra and bladder.
There are certain constitutional complications, however, which deserve mention. One of these is known as urethral fever, which comes on usually with a chill, followed by more or less rise in temperature, and with general disturbance of the system. It is to be regarded as a manifestation of septic intoxication, the hope being that the disturbance may not go beyond this degree. In cases that have once suffered from this intoxication precautions should be doubled. The deep urethra should be irrigated before and after the withdrawal of the urine, the patient should be kept in bed, and urotropin and quinine may be administered before and after the discharge of urine. Much may be done in the prevention of this as of other unpleasant occurrences, such as pain, excitement, suppression of urine, syncope, etc., by the previous use of cocaine and by due regard for gentleness. Should a septic process be set up in the deep urethra it may lead to sapremia of urethral origin, and to septicemia and pyemia. Septic complications accompanied by any local indications, such as swelling, should make the surgeon watchful for the time when an incision must be made for relief of tension or escape of pus.
Postoperative suppression of urine, which may occur even after catheterization, may be treated by giving 0.08 to 0.15 Cg. of sulphate of sparteine every three or four hours (McGuire).
The whole method of skin grafting is based on the fact that if epithelium be removed from any portion of the body and planted on favorable soil elsewhere it will take root and grow, reproducing only itself and no other kind of tissue. It is closely analogous to sewing seed upon a favorable soil, or even to sodding. Furthermore it is not necessary that epithelium be furnished from the individual upon whom it is to be implanted; it may come from another of the same species or even from a different species. Thus the skin of the frog has been used for grafting upon human beings, and even the lining membrane of the egg. Nor is it necessary that the epithelial cells should be apparently alive when thus employed. Very thin shavings of human skin which have been dried,[188] or have been kept from decomposing by some antiseptic, have been successfully used; nevertheless the ideal method consists in taking what is needed from the individual who needs it.
The term skin grafting is now applied to the employment of very thin layers of the epidermis, i. e., as thin as can be shaved off with a sharp razor, and it does not apply to the autoplastic methods of skin transplantation.
Hamilton, of Buffalo, and Reverdin, of Geneva, a number of years ago independently discovered that minute particles of healthy skin might be implanted upon healthy granulations and that from such minute grafts epithelium would be produced and a fresh epidermal covering be afforded. This method was in use for years and was a great advance on what had previously been done. Then Hamilton, of Edinburgh, suggested the use of thin slices of clean sponge, in order that thereby a trellis might be offered for the growing and climbing granulation tissue; this served a good purpose in many cavities. But the greatest advance came when Thiersch demonstrated that large areas might be covered with skin shavings, and that thus in a few days there would be accomplished that which took weeks or months by older methods. His original plan comprehended only the use of these grafts upon granulation tissue; later it was found that they might be applied to fresh raw tissue, even to denuded bone. Thus originated the so-called Thiersch method of skin grafting.
The surface to which these grafts are applied must be thoroughly cleansed as well as the surface from which they are removed. If an ulcerated surface is to be prepared for grafting it should be scraped thoroughly with a sharp spoon; all sloughing or suspicious tissue should be carefully removed, and all oozing allowed to subside. Not until the surface is prepared is it advisable to remove the grafts. These are best removed by putting upon the stretch the skin of the selected area, so as to render it taut and as nearly flat as possible. The razor used for the purpose should be sterilized and sharp. Salt solution may be allowed to drip upon the razor while the surgeon is using it. It is rarely practicable to remove a strip over 5 Cm. wide or 25 Cm. long. The endeavor should be to remove only the superficial layer of the skin, and when properly done this removal should be followed by but a trifling oozing of blood. If bleeding be profuse the layer removed has been too thick. Grafts of sufficient number and size are removed to nearly cover the desired area. The more completely it is covered the more acceptable will be the final appearance of the surface. If the grafts adhere, we may confidently rely upon their furnishing enough fresh epithelium to fill in the irregular defects between the edges. The grafts when cut should be raised with a razor and a spatula and gently spread out upon the prepared surface, and so pressed and treated that no air bubbles are retained beneath them. If the surface be dry enough they will adhere to the very thin coagulum of blood which glazes it, and after a few moments it will take friction to disturb them.
Should the margin of the surface to be grafted be old and indurated it is best to trim off any depression that exists, so that the new skin may not be let in below the surface of the surrounding skin.
The dressing should consist of a layer of sterilized oiled silk, gutta-percha tissue, or green protective, laid on in strips, in order that excessive fluid may escape between them. A little antiseptic powder may be dusted upon the grafts, if such be the choice of the surgeon, but if the operation has been properly managed this will hardly be necessary. Careful regulated pressure should be made outside of the protective, by cotton and a suitable dressing, and then the part, if a limb, may be bound upon a splint in order to ensure physiological rest. Silver, tin, or aluminum foil also make a good protective, and, on theoretical principles, are even better than the textile materials.
Some surgeons leave these dressings for several days. I have found it an advantage to remove them within thirty-six hours, as sometimes the grafts appear to be macerated in the fluids and to lose their first cohesion to the prepared surface. The main thing about the dressing is that it should be non-adhesive and restful. After three or four days, when the grafts have completely adhered, any ointment dressing may be used. It may happen that only a portion of the entire number of grafts serve their purpose, and that others fail to do their work. Even when the failure has been apparently considerable it will often be seen that individual epithelial cells have adhered and later will grow. The unhealed portions of such a surface now fall within the definition given earlier of an ulcer, and should be subjected to the same treatment.
[189]
Grafting may be repeated as often as seems to be necessary. The best surfaces from which to take the grafts are usually the outer aspects of the arms and thighs. The places from which they are removed need only the simplest antiseptic dressings. If the grafts have been of sufficient thinness the scars left by their removal are scarcely permanent and rarely disfiguring.
Wight, of Brooklyn, has suggested that advantage be taken of the properties of high-frequency discharges from a suitable apparatus to secure their hemostatic and coagulant effect. He has shown that such electrical discharge will clot blood and coagulate albumin, this effect being partly due to the formation of nitric acid from the air. In this way it is theoretically possible to so seal the surfaces as to fix grafts firmly in place. The apparatus calls for a pointed electrode, passed at a distance of about 1 Cm. above the entire surface, until the clot is firm and reasonably dry, all serum that is expressed in the process being removed with sponges. Where the apparatus can be employed this affords an effective way of fixing the grafts and preventing their displacement.
Surface epithelium from an animal source may be used when necessary—as from a young pig after it has left the packing-house, a young calf, or some smaller animal. All that is required is epithelium. That from a negro will reproduce only pigmented cells like the original. At the time when amputating a limb about which there is still left healthy unbroken skin, shavings may be removed from it and preserved for a week or two between dry sterilized towels or in a weak antiseptic solution; these may then be utilized for skin grafting during the ensuing few days.
Fig. 30
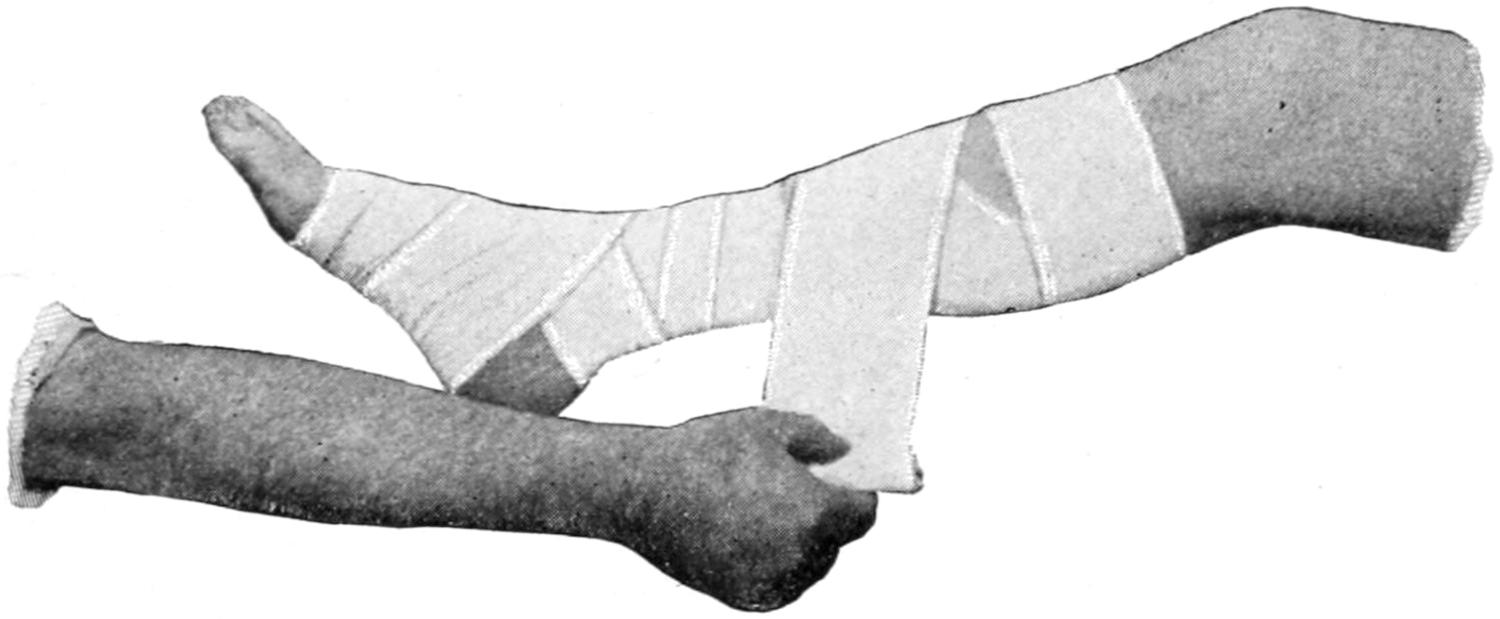
Figure-of-8 bandage of leg.
Fig. 31
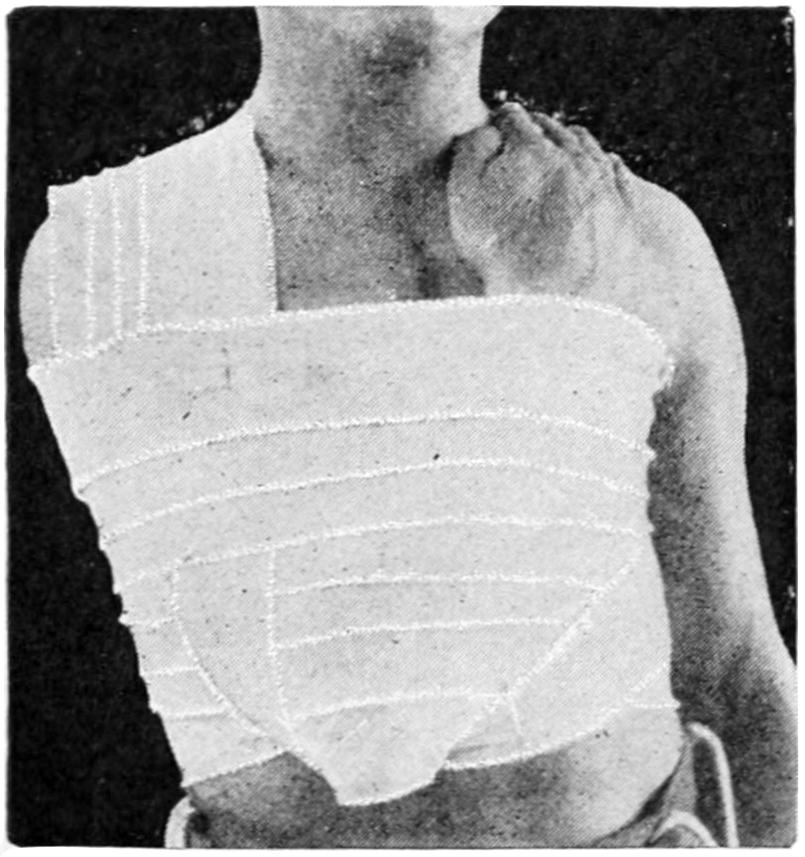
Velpeau’s bandage.
Fig. 32
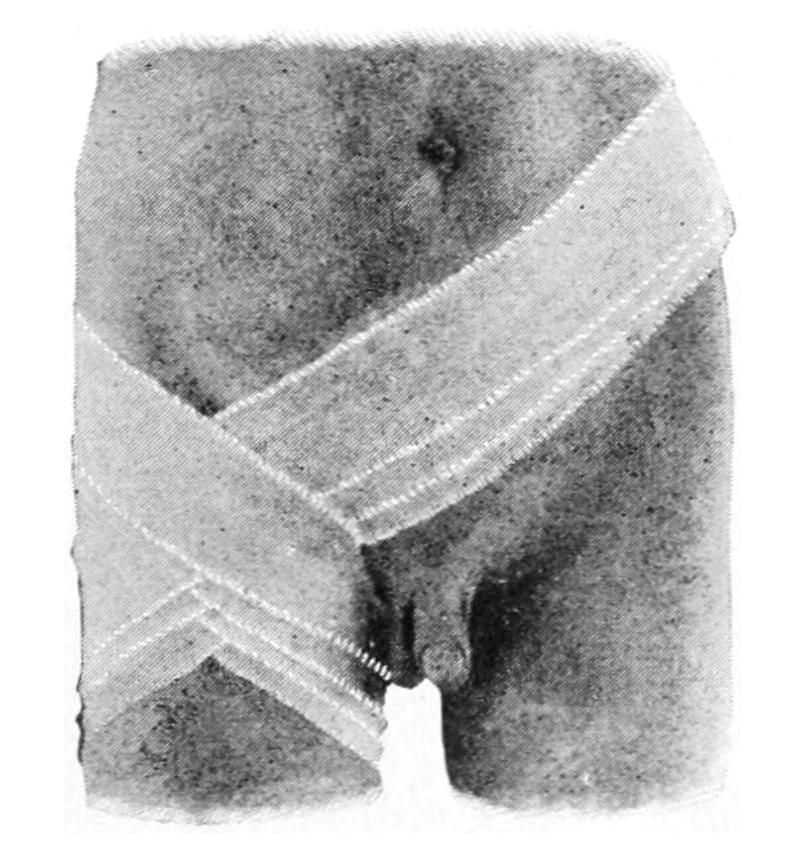
Ascending spica bandage of the groin.
Bandaging is a subject now taught so generally by actual demonstration, and so simplified, that it scarcely seems necessary to more than present a few illustrations showing how simple bandages can be applied in the most effective manner.
[190]
The purposes of a bandage are either to afford means of retaining splints and dressings, to exert pressure, or to afford physiological rest. After every operation of importance it is necessary to apply and retain an occlusive and aseptic dressing, under which the wound may heal or into which wound discharges may be received; but the ideal dressing affords more than this—it furnishes support and rest.
Fig. 33
Fig. 34
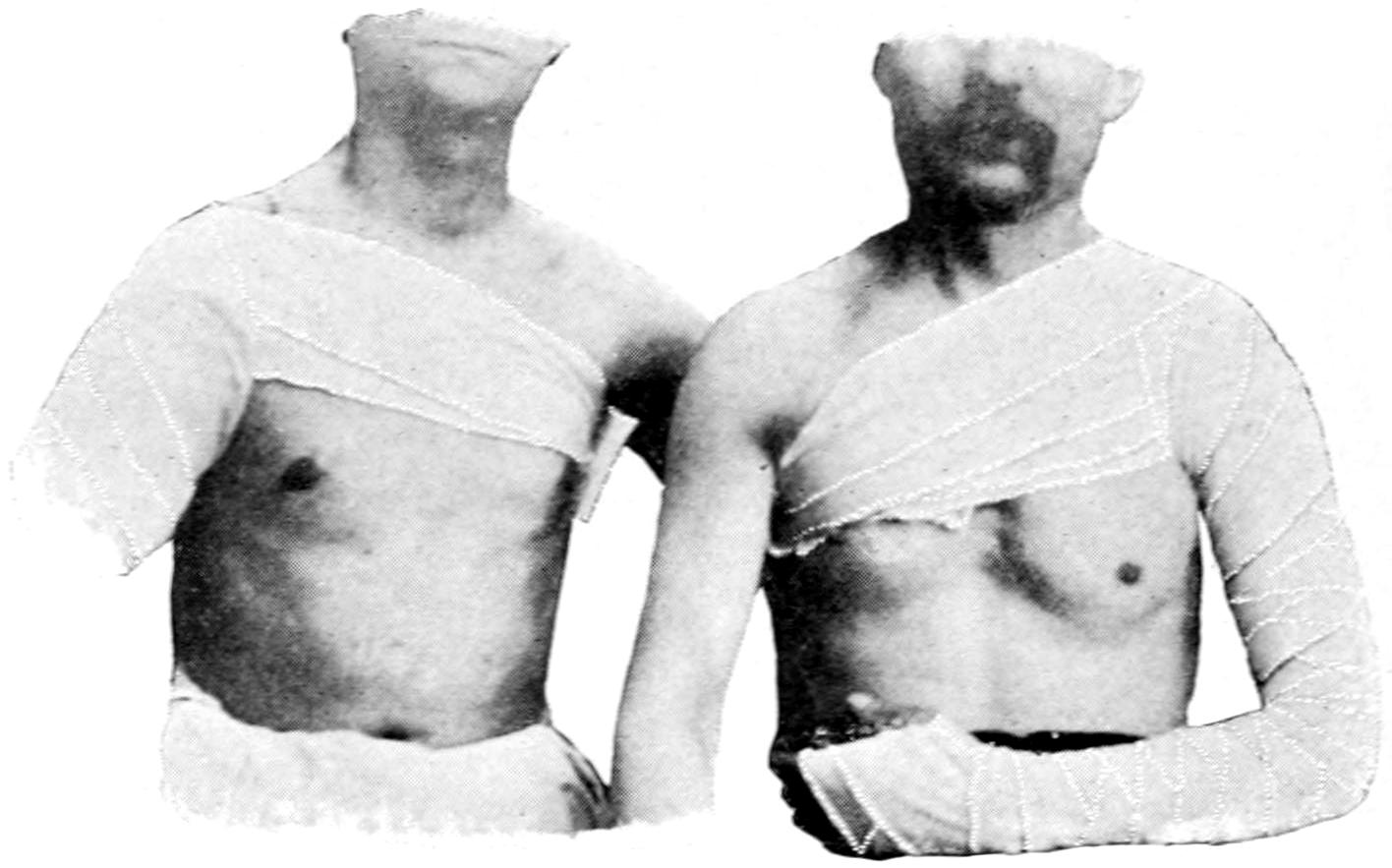
Spica bandage of shoulder.
Fig. 35
Fig. 36
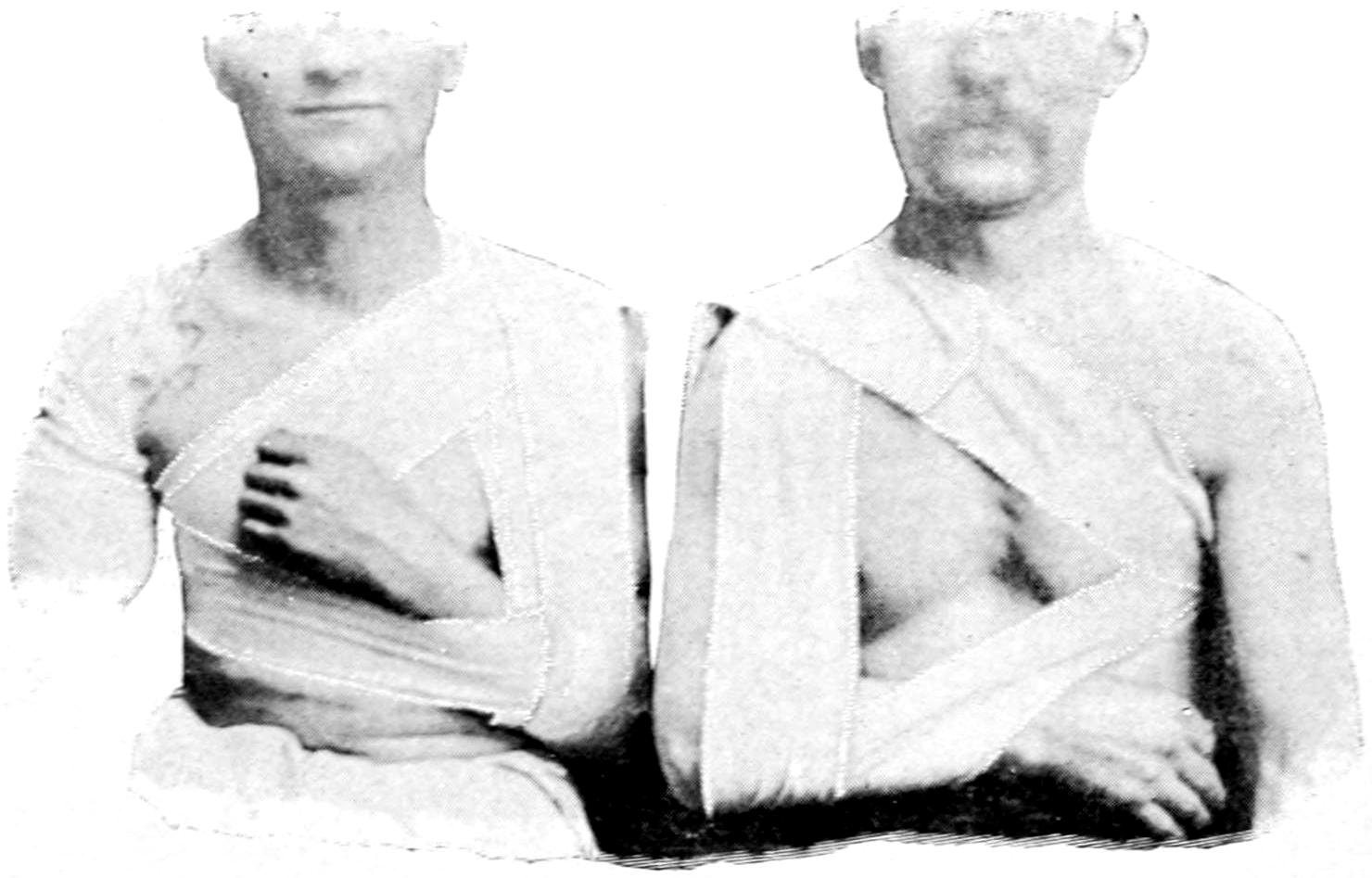
Third roller of Desault’s bandage.
There is danger in the injudicious use of any bandage, as by the exertion of undue pressure it may interfere with wound healing, or may even lead to gangrene. If applied loosely at the extremity and too tightly above it will lead to venous obstruction and possibly secondary hemorrhage. Moreover a bandage which seems properly arranged may become so tight as to be painful and even unbearable after swelling has occurred. There is but one safe rule, and that is to take note of the appearance of the part as well as of the sensations of the patient. An abdominal bandage may have been placed with a proper degree of snugness at the conclusion of an operation, and yet be altogether too tight when the abdomen becomes distended with a little gas. There is then always room for discretion and good judgment in the matter of bandaging. It may be necessary to apply a bandage quite firmly at first in order to repress hemorrhage, with the intention to relax it after a few hours.
[191]
A splint may be a necessary feature in a surgical dressing; after amputating at the lower part of the leg it is advisable to bind the limb upon a splint in order that the necessary physiological rest may be thus afforded. The first requisite of a bandage is not its appearance but its effectiveness; a due regard for the esthetic in surgery will, however, dictate that it be made as presentable as possible.
Fig. 37
Fig. 38
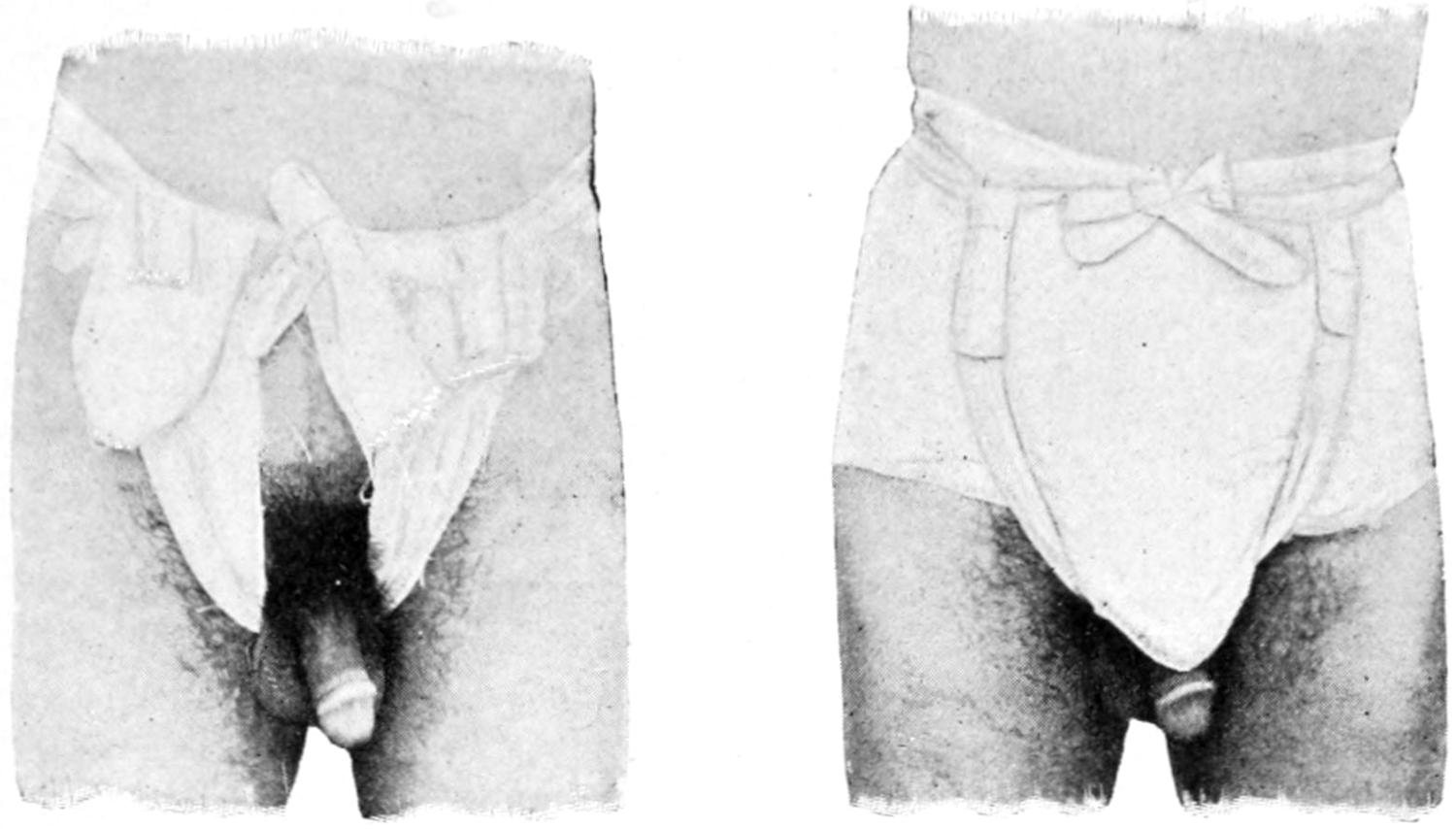
T-bandage.
Kelly’s bandage with perineal straps.
For the roller bandages of cotton cloth, universally in use twenty-five years ago, there have been substituted bandages of thin gauze or crinoline, which have scarcely body enough to be applied, as was the roller, or else of flannel, made wider and necessarily thicker, which are more flexible, comfortable, and applicable.
Fig. 39

Barton’s head bandage as employed for suspension in applying plaster-of-Paris bandage.
Crinoline impregnated with starch is also in general use and makes a serviceable bandage for head injuries. When prepared with plaster of Paris it is capable of affording absolute support and even rigidity.
[192]
To Oliver Wendell Holmes we owe the term anesthesia, as generally employed and made to mean insensibility to pain, no matter how produced. A more strict definition would limit the term to conditions comprising not only insensibility to pain but loss of consciousness. For mere loss of sensation we should, strictly speaking, use the word analgesia. This is a distinction with a difference. Thus I have on rare occasions seen a patient under chloroform absolutely oblivious to pain but perfectly conscious, and chatting intelligently throughout the operation. This is a rare phenomenon, but has been noted by various observers. So after intraspinal cocaine injections we secure complete analgesia of the lower portion of the body, but not complete anesthesia, the former being what we are most anxious to produce.
The discovery of anesthesia is essentially to America’s credit. Long, of Georgia, had produced anesthesia by ether as early as 1842; Jackson, of Boston, also claims credit for the discovery; but to Morton, a dentist of Boston, is undoubtedly due the honor of having introduced it for surgical purposes. The first public demonstration of its properties was made by Morton and Warren, October 16, 1846, in the Massachusetts General Hospital. Chloroform seems to have been exploited independently by Guthrie, of Sackett’s Harbor, N. Y., and Simpson, of Edinburgh, in 1847. It is a curious historical fact that the patient to whom Simpson meant first to administer chloroform in his clinic did not receive it because of some failure to have it on hand; she took ether instead and died, presumably of the anesthetic. Had she died under the influence of chloroform it would have been a serious setback to any general appreciation of its merits. Nitrous oxide is also an anesthetic for which America may take the credit. These are the three drugs in common use today, although there are others which are coming into general favor.
It can be stated as an axiom that when a surgeon tries to abolish human sensibility, or pass an instrument through the human skin, he introduces elements of danger which can never be certainly and completely controlled—that is to say, the administration of an anesthetic is never to be undertaken as a trifling matter, but should be entered upon as carefully for a minor procedure as for a dangerous and prolonged operation.
Anesthetics are sources of danger, not only for the moment while they are in use, but because of the disturbances which may follow in their train. These drugs should never be administered carelessly nor thoughtlessly, nor by inexperienced individuals, but entrusted to the wisest and the most discreet. More is expected of the anesthetizer than that he shall barely keep the patient alive; he should be so expert as to keep the patient safely on the side of complete anesthesia and muscle relaxation. Nor should he be willing to yield to the importunities of an impatient operator who may be continually appealing to him to crowd the anesthetic. When thus given, and by an expert, such postanesthetic distress as nausea, vomiting, coughing, etc., may be avoided. So generally are these facts now realized and appreciated, that in many of the large hospitals a regular anesthetizer is employed, whose sole duty it is to administer the anesthetic for the attending surgeons. The management of an anesthetic has much to do with the allied subjects of the preparation of the patient, the management of shock or reduced blood pressure, and the status lymphaticus, which have already been considered.
Fatal accidents from anesthetics are the appalling ones which have generally occurred in cases where it has been assumed that the patient is in good condition, and where neither preliminary examination nor preparation has been made. In the presence of unmistakable cardiac disease, or of great arterial tension, the surgeon may, by foreseeing the possibility of trouble, do much to prevent it; but when an apparently healthy individual is placed upon the operating table without attention to these matters it may happen that his heart will stop as suddenly and unexpectedly as though it had been transfixed. In other words, the accidents of anesthesia usually occur when least[193] expected; on the other hand, accidents will be few and far between when all cases are handled as though promising to be severe ones.
The odor of most anesthetics is so distasteful to patients that they inhale at first with difficulty and with signs of irritation. Much of this can be guarded against by spraying the nasopharynx with a 1 or 2 per cent. solution of cocaine. This expedient will make anesthesia much easier for them. The mouth should be examined; all false teeth or foreign bodies, such as pins, chewing-gum, etc., should be removed. Unpleasant burning of the sensitive mucosa of the nose and lips may be avoided by anointing these parts with cold cream. Attention should be given to the avoidance of irritation of the eyes or the careless escape of an anesthetic into the conjunctival sac; with a struggling patient, or a careless administrator, this may easily happen.
Circumstances which would justify the administration of an anesthetic without the consent of the patient, or the friends or parents, occur but rarely; still in an emergency case, with a patient incompetent to decide for himself, the surgeon must assume the responsibility, in which in all probability the law will sustain him.
The anesthetizer should always be accompanied by an assistant; preferably in the case of a female patient, by a female nurse, who may not only be of assistance to him at the time, but an actual protection should the patient experience any erotic delusions during or after her period of anesthesia. This applies equally well to dentists giving nitrous oxide for the extraction of teeth, or physicians attending cases of accident, convulsions, and the like.
The anesthetics in general use are ether and chloroform. If statistics alone are appealed to it can be easily shown that ether is the safer of the two by a large ratio. But the recovery of consciousness by no means indicates the conclusion of the period of danger. The harm which chloroform does is largely done promptly, whereas the unpleasant effect of ether lasts through a much greater period, and the statistics which give ether an advantage are in many respects fallacious. Chloroform is doubtless the stronger and the more subtle agent of the two, and in careless hands would, in all probability, become the more dangerous. But no anesthetic should be given carelessly, and no one should give it who cannot give it properly. There may be emergency cases, especially in the rural districts, in which the surgeon may have to act in the capacity of anesthetizer and operator as well, and where he may have to transfer the inhaler to some lay assistant who knows nothing of the action of these drugs. If this happen it would be safer to use ether.
When administered by a thoroughly competent person chloroform is the safer anesthetic of the two, and is usually to be preferred. So largely does the personal equation figure in this consideration that it seems unnecessary to reproduce here statistical tables in regard to its efficiency.
The writer’s intention is to confine his views on anesthesia to the practical application of certain drugs whose chemistry, materia medica, and ordinary therapeutic properties are appropriately treated of in other works.
Ether anesthesia has by some been considered to be simply one form of carbon dioxide poisoning; that it may be all of this, in certain cases, may be granted; but it is certainly something more, as is shown, among other things, by the peculiar odor which persists in the breath of the patient for hours or even for days after its use. Various ways of administering it have been recommended. Some give it well diluted with air, and some give it as strong as a patient can possibly bear it, and from the outset. Some keep mixing air with the vapor, while others have devised inhalers, by which the same ether-ladened air is breathed over and over again. These latter produce a certain degree of the carbon dioxide poisoning above alluded to, and are not ideal even if effective.
Even when well diluted with air the vapor of ether causes irritation of the air passages, in both the nose and throat, and leads quickly to a sensation at first of oppression and then almost of suffocation, which is trying to the self-control of intelligent patients and disturbing to those having little or none. An inhaler saturated with ether should not be pressed tightly over the patient’s face, as it is likely to produce struggling to such an extent that weakened bloodvessels may give way and by their rupture produce serious disturbance.
[194]
The first momentary period of irritation having subsided, there will likely follow a few deep inspirations, and then perhaps a fixation and immobility of the chest, so that for half a minute or a minute it would seem as though the patient had forgotten to breathe (Hare). But deep respiration is quickly reëstablished, or may be stimulated by slapping the chest, by a few movements at artificial respiration, or at least by compressing the thorax. Then follows the period of “primary anesthesia,” so called, or a period of excitement, during which the patient may rave or become quite disturbed, and in a manner sometimes quite at variance with his ordinary temperament. As this period subsides the state of complete anesthesia begins, and when muscular relaxation is complete, or even before, the surgeon may commence his work. The respiration under complete anesthesia is usually deeper and sometimes more rapid than in health, while as the muscles become more relaxed a positively stertorous breathing is noted, along with an increase in flow of saliva, due to the irritation of the ether vapor. As anesthesia passes into complete narcosis, and this into asphyxia, the color of the surface, especially of the face, changes to a cyanotic hue, the skin becomes moist and clammy, and the pulse, which had been accelerated, fails. The blood also becomes exceedingly dark from lack of oxygen. Under these circumstances the heart may continue to beat feebly for a short time after respiration has ceased. As Hare puts it: “In producing its effects ether first attacks the perceptive and intellectual cerebral centres, next the sensory side of the spinal cord, next the motor side of the cord, then the medulla, and with this last depression death ensues.”
Ether is more pungent and less agreeable to breathe than chloroform, but the chief advantage usually connected with its use is its supposed factor of safety.
On the other hand, the accidents which are due to ether are in a large measure those common to the use of any anesthetic agent. Among the most prominent is arrest of respiration, which may be caused either by mucus or some foreign body in the air passages, or by the tongue dropping back in the pharynx, and the impediment to respiration thereby offered. When the cause of the difficulty is ascertained it is usually easily removed. Should great pallor accompany these symptoms, then, it is usually because the heart as well is at fault, and vigorous stimulation of this organ should be promptly instituted.
Another disadvantage pertaining to ether results from the irritation which its vapor produces in the bronchi and lungs, or in the kidneys during its elimination. From the former may result bronchitis, congestion, or even pneumonia; the latter more often of the catarrhal type than of the croupous. As the result of renal irritation there may be temporary albuminuria, or the congestion resulting may assume so serious a type as to produce absolute suppression (anuria), which is practically always fatal. Ether is said to be particularly undesirable in cases of diabetes, because of the resulting acetonuria. Patients have even been known to pass from anesthesia into diabetic coma.
It has been found that complications are more common in males than in females, but more severe in the latter. Vomiting following the use of ether is a frequent and most unpleasant sequel. It is to be prevented by previous lavage, as well as by the same measure at the conclusion of the operation. It will rarely subside when present until the ether vapor has been eliminated. So far as it is possible to suppress it with drugs probably 2 Gm. doses of chloral and one of the bromides, with a little laudanum, given by the rectum in salt solution or a little starch-water, will give the best results.
As already stated, it was formerly held that anesthesia was carbon dioxide poisoning, plus something else which was vaguely described by different authorities; much clearer notions now prevail regarding the mechanism of anesthesia. A few years ago Meyer and Overton concluded that anesthesia is produced by solution of the fatty constituents of the cells by the anesthetic absorbed, this being true at least with chloroform and ether, both of which are solvents of fat. The absorbability of the anesthetic varies with the blood temperature, this varying widely between the cold-blooded and warm-blooded animals. They estimate that 1 part of ether to 400 parts of serum is necessary for complete anesthesia in man, while one part in 4500 to 6000 parts is a sufficient proportion of chloroform. According to these views the dissolved fat is not removed from the cells, and no satisfactory explanation yet accompanies this theory, even assuming its accuracy.
Of no small importance are the experiences of Snel, who found that anesthetics decrease the bactericidal properties both of the blood and of the tissues, but that this power is[195] quickly recovered after the elimination of the anesthetic. He furnishes reason for the theory that the thus lowered resistance of the lungs is an important factor in the production of the pneumonia which occasionally follows operations.
There is a belief that ether is more irritating to the kidneys than chloroform. This, however, does not seem to be justified by evidence, neither is the prejudice against the use of ether during the existence of albuminuria or in the presence of casts. In the presence of a high degree of albuminuria any anesthetic is dangerous, and here ether would be the less desirable of the two. Nevertheless in ordinary mild albuminuria one need not fear to give ether.
About twenty years ago it was suggested that ether anesthesia could be induced by passing its vapor into the colon through an ordinary rectal tube. There are many obvious reasons why it would be of great advantage if anesthesia could be safely practised in this way, not only in operations about the face and head, but because of the avoidance of pulmonary and gastric irritation.
The method was to thoroughly empty the colon and then connect a rectal tube with a receptacle containing ether, which was placed in warm water and the vapor passed into the intestine. It was found that patients could be readily anesthetized in this manner, but unfortunately it was also found that a considerable degree of intestinal irritation was produced.
The writer recalls one case in which this method was practised, which terminated fatally within twenty-four hours after the operation, where the autopsy disclosed a violent degree of acute colitis.[7]
[7] Ether Narcosis by the Rectum.—Cunningham and Lahey have revived the almost abandoned method of rectal ether narcosis, after improving the technique. The rectal tube is introduced for ten to fifteen inches and ether vapor is then forced in until considerable gas is pressed around the rectal tube, keeping the forefinger in the rectum opposite the tube until it causes pain and hastens the expulsion of the rectal gases. It is essential that the rectum be distended to the point of keeping closed around the tube, since unless the gas normally in the bowel be first removed the patient absorbs the ether much more slowly, presumably because of its dilution. At the first introduction of the ether vapor the patient may feel a natural discomfort and desire to defecate, but in a short time this sensation disappears; the breath becomes ether-ladened in from one to five minutes, he becomes drowsy, the breathing stertorous, and he passes into complete surgical narcosis without any excitement.
The apparatus used consists of a bottle seven inches in height, of which five inches are used for ether space and the balance for vapor. The afferent tube which leads to the bottom of the ether ends in a bulb, with small perforations, so that the air escapes in several bubbles. This bottle is placed in a water-bath at a temperature between 80° and 90°. By keeping the ether warm, without boiling, the air forced through it is more easily saturated.
The same care must be given to see that the tongue does not fall over the larynx as when ether is given by the mouth. Should narcosis be too pronounced the tube should be disconnected and ether gas forced out of the bowel by abdominal massage. Oxygen may be given through the same tube if desired, while artificial respiration and stimulation are practised as usual when needed. After completion of the operation the ether vapor should be completely expelled by pressure.
The advantages of the method are that but a small amount of ether is used, there is no stage of excitement, vomiting is rare, bronchial secretion is prevented, and recovery is rapid. It has been shown that six volumes per cent. of ether are required in the blood for the production of complete anesthesia. The rapidity with which the latter can be produced depends upon the rapid production of this percentage. This result is attained more readily by the rectum than by the lungs. For the production of narcosis by this method the rectum should be previously and thoroughly emptied.
It is important that pure chloroform should be secured for anesthetic purposes. It should be kept in dark bottles, and in the dark, as it is liable to undergo decomposition in the presence of sunlight. It is less volatile than ether, and mixtures of the two drugs are not stabile, since the ether is likely to evaporate first. In its anesthetic effects it resembles ether, acting first upon the perceptive and last upon the motor centres.
The British Chloroform Committee estimate that from 1 to 2 per cent. of chloroform in the inspired air is sufficient for anesthetic purposes, and may be safely used; that 5 per cent. is more than adequate, and that anything stronger than 2.5 per cent. is dangerous.
The effect of chloroform upon the heart is to quicken and then slacken it. The former action is due to a depression of the vagus centre, while subsequent slowing is due partly to vagus stimulation and partly to direct weakening of the heart muscle. While chloroform does not materially affect the excitability either of the vagus or accelerator nerves[196] its main effect is on the strength of the heart action, and is less marked on the auricles than on the ventricles. Ether has a more marked tendency to raise blood pressure than chloroform, while the latter is likely to be more responsible for sudden falls in blood pressure even after its administration has ceased.
The question of the relative dangers of the two drugs has engaged the attention of investigators the world over, and one of the side questions to be discussed is whether chloroform kills by arresting the circulation or the respiration. Chloroform produces a fall in blood pressure (see Chapter XVII) but as long as the blood pressure within the brain, and especially the medulla, is maintained this effect is of secondary importance; but when the respiratory centres lack their natural stimulus, and respiration becomes irregular, then, as it were, the patient “bleeds into his own vessels.” It is under these circumstances that adrenalin produces its most marked and prompt effect.
The first effect of chloroform inhalations is to raise blood pressure, but this is soon followed by lowered tension. The pupils may dilate slightly at first, but usually contract and remain contracted during anesthesia. When they dilate suddenly means should be adopted to avert the danger threatened, as the relaxation of the iris is the first visible relaxation of death. While the pupils react to light there is little danger.[8]
[8] Lehmann believes it is a bad sign when a patient who is taking an anesthetic keeps the eyes partially or completely open, or frequently reopens them after being under the influence of the drug. He holds it to be a premonitory symptom of more or less serious complications.
Death from chloroform usually occurs when it is assumed that no accident is likely to happen, as when it is given to an athlete, or to drunkards who are supposed to be secure from any reflex influences. Patients with weak hearts can be conducted safely through a prolonged anesthesia if there be time to prepare them. (See chapter on the Preparation of Patients.)
The after-dangers of chloroform are smaller than those of ether, due in part to the fact that a much smaller amount of the drug suffices; in other words—that it is the stronger.
After anesthesia has been produced and the patient is unconscious it requires but small additional amounts to maintain unconsciousness, as it is necessary to add only as much as may be required to replace what is lost by evaporation and exhalation. It is sometimes advantageous to commence with nitrous oxide gas, for there are fewer unpleasant reflexes, less salivation, and less disturbance of every kind. Shallow breathing may be improved at almost any time with a few drops of ether.
Many anesthetizers have a habit of testing the degree of anesthesia by touching the cornea with their fingers. A piece of sterile gauze will prove equally effective and less irritating.
When the mask upon which chloroform or ether is given is held over the face free salivation will frequently be excited, and the patient will be tempted to swallow as well as inhale. In this way the vapor of the anesthetic is taken into the stomach as well as into the air passages, and when the stomach is empty this comes into direct contact with the gastric mucosa. This may produce not only irritation, but, in extreme cases, gastritis. It has been suggested that to allow the patient to drink a quantity of water at intervals before taking the anesthetic, and especially a half-pint or more immediately before beginning it, will be to permit of absorption and dilution of the anesthetic vapor without their causing this irritation.
Fig. 40
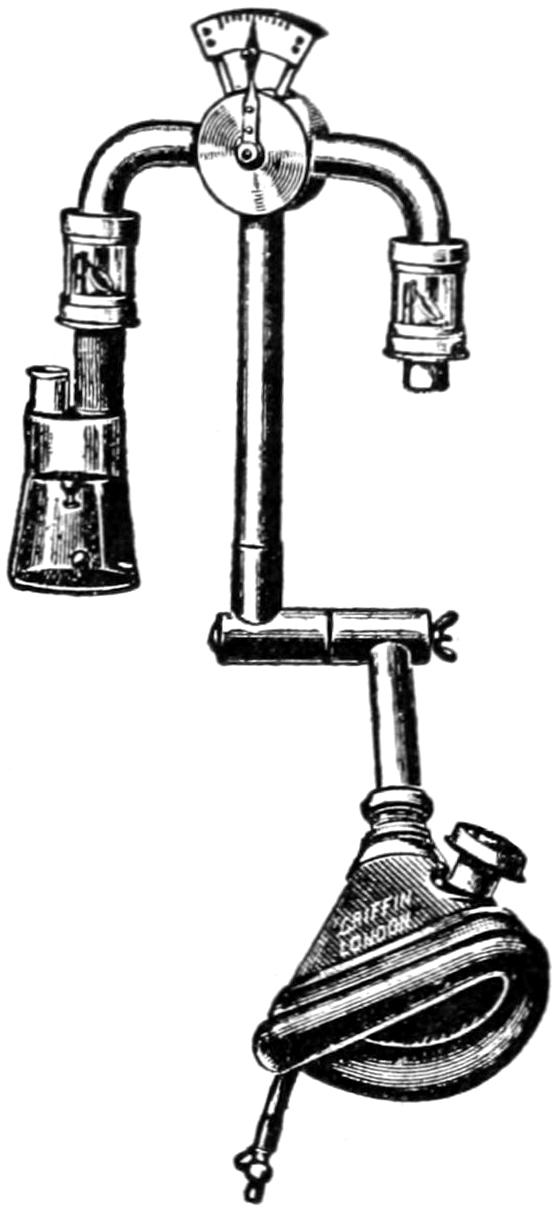
Harcourt inhaler.
The simplest method of administering chloroform is upon an ordinary mask, the covering of which should be thin in order to permit of easy play of air. By this method a patient can always be anesthetized, but with a waste of the anesthetic and with absolute uncertainty as to the proportion of chloroform vapor in the inspired air. A variety of expedients have been suggested in time past, and chloroform inhalers of various patterns are constantly upon the market. The Junker inhaler, introduced some twenty-five years ago, was a great improvement upon its predecessors, but only recently has a really scientific measuring inhaler been placed before the profession. This is the one devised for and introduced by a committee of the British Medical Association, and is the result of the study and ingenuity of Prof. Vernon Harcourt. It has already been stated that more than 2 per cent. of chloroform vapor in the inhaled air is dangerous. The Harcourt apparatus consists of a two-necked bottle, nearly filled with chloroform, into which are dropped two colored glass beads, which serve to indicate when the temperature is between 55° and 59° F. If the temperature be below 55° F., both beads will float;[197] if it be above 50° F. both will sink. If the former, the proportion of chloroform will be below that indicated by the pointer; if the latter, it will be greater. Inasmuch as during inhalation the chloroform is cooled by evaporation, it is necessary to occasionally place the warm hand over the bottle until the blue bead has sunk and the red bead is beginning to sink, indicating that the temperature is again approaching 59° F. A stopcock is so constructed that when the pointer is at one end of the arc the maximum amount of chloroform which may be taken up is 2 per cent.; when the pointer is at the opposite end, the patient breathes only pure air. There are valves which prevent the entrance of expired air into the apparatus, and which show whether the stopcock is working. They also show the character of the respiration. Administration is begun with the pointer at 0.2, and while it may require 2 per cent. of vapor to produce narcosis; i. e., the complete and final stage of anesthesia, it will take scarcely more than 1 per cent. to maintain it. The mouth-piece has an expiratory valve, and the apparatus can be held in any position, but should be kept nearly vertical. The mask is fitted with an air cushion, which can be molded in hot water so as to fit the patient’s face. Buxton, who is the leading authority on anesthetics in London, has abandoned all other apparatus for this. While he is a most skilled expert, he has shown that by means of this apparatus chloroform can be given with almost absolute safety.
Aside from the danger and discomfort pertaining to the use of chloroform in apartments lighted or heated with natural gas, there is another similar danger in connection with ordinary city illuminating gas. In the presence of a flame produced by the latter the vapor of chloroform is broken up not only into chlorine and hydrochloric acid, but into a carbon oxychloride, known also as phosgene, which is toxic and produces a sense of suffocation by producing decomposition within the blood. A fatal occurrence of this kind led to experiments on animals by an Italian observer, which showed that the substance produced rapid disintegration of hemoglobin, which fell rapidly to 40 per cent., and that accompanying this there was suppression of urine with convulsions.
Unless chloroform be given by one familiar with its use, it is best given from a dropping bottle. If this be so arranged that it will discharge but one drop at a time, and the anesthetizer so administer it as to allow perhaps one drop to fall each second, the patient will at no time get an overdose, nor will there be struggling or choking. Irregularity of breathing is usually the result of insufficient air, and the mask should be at once removed, so that the patient may take one or two deep inspirations. When the cornea is insensitive the patient will stand almost any manipulation except, perhaps, stretching of the sphincters. When the sphincter can be stretched without provoking any effect except a prolonged inspiration, then the patient is, in all probability, completely relaxed and ready for any procedure. When the breath becomes stertorous the mask should be removed even though the cornea be sensitive. It will quickly lose its sensitiveness again within a few seconds. Proper breathing must be maintained. Free supply of air is important above all other things, and it is better that the surgeon should wait rather than the anesthetizer.
Additional safety in the use of chloroform may be afforded by the simultaneous use of oxygen gas, by which cyanosis is usually avoided and vomiting often prevented. It may be safely used with chloroform, but not with ether. If ozonized air be conducted into anhydrous ether it forms a thick liquid, probably ethyl peroxide, which explodes if heated (Hare). It is a mistake to so manage the administration of chloroform with oxygen that the patient receives no pure air. Oxygen is of great value, but it is not physiologically breathed in its pure state. When the gas is allowed to bubble through a bottle of chloroform, carrying with it the vapor, no idea can be formed as to relative percentages. A better way is to administer the chloroform upon a mask, and the oxygen by a tube from a wash-bottle filled with water and passed into the nostril under the edge of the inhaler (Hare).
[198]
Gwathmey has introduced a modification of the well-known standard Junker inhaler, by which oxygen and chloroform, or nitrous oxide and ether, may be given together, or by which any desired combination can be effected. Its special advantage is the same as the Harcourt apparatus, that the percentage of chloroform or ether vapor can be estimated or controlled. So far as the administration of chloroform with oxygen is concerned, Roth has shown that oxygen does not decompose the chloroform, but diminishes the danger of its administration.
Gwathmey refers to the advantage of keeping an open airway by turning the head a little to one side and pressing the jaw well forward; he also advises that when the anesthetic is removed from the face it is well to replace its odor by some other perfume, such as cologne or smelling salts, as it is presumed that the olfactory nerve is responsible for the initial symptoms of nausea and gastric distress.
In some States natural gas is used as fuel, usually in open fireplaces or stoves. When chloroform is administered in a room thus heated, or even lighted by natural gas, formaldehyde gas is the result of a mutual decomposition, and this is exceedingly pungent and irritating, and will soon produce violent coughing in all who are present in the room. It may be impossible to avoid this, but natural gas flames should be extinguished and some other source of illumination should be depended upon when practicable.
Under this term are known various mixtures of alcohol, chloroform, and ether, the intent being to counteract the depressing influence of chloroform by alcohol and ether. It may be said of every mixture of anesthetics that it is no less dangerous than its strongest constituent. Thus a mixture of chloroform and ether should be given with as much precaution as pure chloroform.
Mixtures of this kind should be made fresh for each administration, as the most volatile ingredient may evaporate in unknown amount and thus change the proportions. This is true of the mixture even after it is poured upon the inhaler, and the patient will thus be subjected to a chloroform mixture of varying strength.
The administration of ether for a few seconds during chloroform anesthesia will often prove beneficial in regulating or deepening inspiration, but it would be best to have the two drugs separate, and use the ether as it may seem called for, rather than to rely upon any such mixture. Moreover the vapor of alcohol is of itself irritating and undesirable.
For operations of but short duration ethyl bromide offers some advantages, in that its effects quickly pass away and that there are few unpleasant sequels. Indeed, patients may take it for a few minutes with almost as little disturbance as is produced by nitrous oxide; nevertheless it cannot be regarded as being as free from danger as was originally claimed. Only a pure preparation should be used. When given as ether is usually given, upon a cone or mask, complete anesthesia may often be produced within one minute. It can hardly be relied upon to produce muscular relaxation and it frequently causes great congestion of the face and head, consequently it is not as convenient for short operations on the nasopharynx as its other good qualities might render it. It is not unpleasant to take, and ordinary ether anesthesia may well be begun with it.
For a number of years this anesthetic agent was in favor, especially in Great Britain, where it was warmly advocated by Spencer Wells. Its odor is agreeable, its action rapid, and recovery from its effects is usually prompt. But it proved to be unsafe, since it was found that the substance commonly used under this name was really chloroform diluted with one-fifth of methyl alcohol, while the genuine methylene bichloride was found by experiment to be a dangerous substance, and its use has been discarded.
[199]
This, like every other drug used for the purpose, should be used in perfectly pure form. While this can be obtained from manufacturers in this country, there seems to be a tendency to rely upon the imported preparation sold here under the name of Kelene. For certain short operations, such as those upon the eye, nose, and throat, and for children, it has many advantages and appears to be a reasonably safe drug for the purpose. Consciousness is quickly recovered after its use, and the after-effects are slight. It is in general use preparatory to one of the stronger anesthetics, like ether or chloroform, and affords a means of putting patients under the relaxing effect of either of these drugs. It should be administered upon a cone or mask, from which evaporation should not occur too easily, because it is extremely volatile. In the hands of one accustomed to its use, operations of considerable magnitude and duration may be successfully maintained. A special valveless mask has been devised for its use, consisting of a rubber mouth-piece which can be snugly fitted to the face, and a movable tube over which two or three layers of gauze may be stretched, upon which the ethyl chloride is allowed to drop or is ejected from the tube in which it is sold. Sometimes the expired air will freeze upon this gauze. This is of no disadvantage.
—On account of its extreme volatility, chloride of ethyl affords a ready means of producing local anesthesia. It boils at 50° F., and when the tube containing it is held in the hands and its capillary tip is opened it issues in the form of a fine spray, which being directed upon the part to be desensitized first chills and then freezes it. Whether this part be skin or mucous membrane the effect is the same. As soon as the desired area is covered with a thin layer of small frozen crystals, looking like hoar-frost, the surface is anesthetized and the necessary instruments may be used. Blowing on the part to be anesthetized will favor evaporation and shorten the time necessary for the purpose.
The purposes to which this drug may thus be used are numerous and obvious. For instance, in dentistry it will do much to allay the pain of tooth extraction; in genito-urinary surgery such operations as incision of the prepuce, the cauterization of venereal ulcers, and circumcision may be done with little or no pain. The small operations required in various skin diseases, the incision of small abscesses, the use of caustics wherever they may be needed, may all be made easy under its effect; while in cases of neuralgia, stings, bites, etc., it will often alleviate the symptoms. The skin may also be anesthetized in this way before the introduction of the needle through which antitoxins are injected or hypodermoclysis practised. Before venesection or before exploratory puncture it may also be used.
—This agent, composed of ethyl bromide 5 parts methyl chloride 35 parts, and ethyl chloride 60 parts, was introduced by Rowland, of Bordeaux, as a convenient means of producing an analgesic condition, i. e., something between complete anesthesia and conscious sensibility. The dose is about 5 Cc., to be sprayed upon a tightly fitting mask. The patient should be told to breathe and swallow as naturally as possible, and the effect is obtained within a few seconds. The agent is so speedy in producing its effects that it is sometimes difficult to tell when the proper degree of unconsciousness has been secured. A patient may be directed to hold up an arm in order that when it drops the surgeon may proceed. There is neither cyanosis nor corneal reflex, and nausea does not usually occur. The essential point of administration is the exclusion of air. Twenty seconds of administration will give from one to two minutes of anesthetic effect, during which various brief operations can be performed. By proper management this period can be lengthened many times.
—Petroleum ether was introduced by Schleich for the purpose of diluting chloroform. By itself it has a weak anesthetic power, and seems to possess some dangers of its own in the way of depressing the heart’s action and producing convulsions.
Schleich was among the first to demonstrate that the retention of an anesthetic within the body depends upon its boiling point. W. Meyer carried Schleich’s views still farther and showed the at least theoretical value of an anesthetic mixture whose[200] boiling point was that of the normal blood temperature. If the evaporating point be much higher than the blood it is volatilized too easily, while if it be lower it reduces body temperature as it evaporates. After considerable experimentation Meyer recommended a mixture by volume of chloroform 3 parts, ether 2 parts, and ethyl chloride 1 part, and introduced this mixture under the name of anesthol. This composition does not seem to have met with great favor as yet, although it has theoretically much to commend it, as it seems slower in action and but little more satisfactory in other respects.
This is by all means the most rapid general anesthetic in use. Patients can be placed under its influence in from twenty-five to sixty seconds. For a long time its employment was confined to dental practice, but it is now in general use by surgeons, as a preliminary to the use of ether or as the sole anesthetic agent. When managed properly patients can be kept for a half-hour or even an hour under its influence. Two disadvantages attend its administration: (1) It is difficult to completely relax the muscles and so maintain them that no difficulties are placed in the operator’s way, e. g., in certain operations upon the abdomen where muscle rigidity delays and makes difficult the operation. (2) The use of nitrous oxide alone so far impairs proper oxygenation of the blood that this fluid becomes dark or almost black and frequently obscures the field of operation. These difficulties, especially the latter, can be overcome by the skilful simultaneous use of oxygen gas, by which the blood is kept well oxygenated, and by which the deep stupor of nitrous oxide poisoning can be made so safe that it can be prolonged to the degree necessary to afford relaxation.
Nitrous oxide anesthesia is thus proved to be something more than mere asphyxia, or it would be completely counteracted by oxygen. Suitable apparatus can now be procured by which both gases can be blended together as desired; considerable experience, however, is necessary for their successful use. It is generally stated that nitrous oxide alone should not be given to persons with fatty hearts or atheromatous vessels. From a brief period of nitrous oxide anesthesia patients usually recover within a few minutes and without after-effects; still, relaxation of the sphincters may occur. After its prolonged use there may be considerable headache and vertigo.
This will depend upon who is to be the anesthetizer as well as upon the actual condition of the patient. If an inexperienced person is to administer the anesthetic, ether is safer than chloroform, though slower. On the other hand, when given by an expert, and after due preparation of the patient, chloroform is ordinarily preferable. The latter is especially indicated in the young and aged, as well as in those who have bronchitis or chronic cough, and those who have advanced renal diseases or atheroma, because it is not likely to produce such high arterial tension.
Ether should never be given near an unprotected flame, and lamps or gas-jets should be held above the level of the operating table, as the vapor of ether is heavier than air and will tend to sink. The disadvantages of chloroform where natural gas is in use have already been mentioned.
Efforts should be made to prevent struggling, as in the violence of this unconscious act an overtaxed heart might yield, or at least undergo dilatation. Chloroform is notably less likely to be followed by nausea and vomiting than ether, and yet nausea cannot always be prevented. There can be no doubt that morphine, alone or with atropine, may be given with advantage to most patients before administration of a general anesthetic. The treatment of postanesthetic nausea has been referred to in the chapter on the Preparation and After-care of Patients. By general consent, chloroform is the anesthetic of choice during labor.
[201]
The principal dangers from any of the volatile anesthetics come from interference with circulation and with respiration. The heart may give rise to alarm by gradual failure in strength, while the pulse becomes more rapid and irregular, or by sudden and apparently complete cessation of activity. When the pupils suddenly dilate and do not react to light danger is close at hand, if it have not already manifested itself, and then is the time to discontinue the anesthetic and resort to vigorous methods, which may include artificial respiration, but must include attention to the heart. It is customary to use injections of strychnine, which are often too weak or too small to be of service, nothing less than ¹⁄₂₀ Gr., which may be repeated in a few moments, will be of any service. If ¹⁄₁₅₀ to ¹⁄₁₀₀ Gr. of atropine be given with the strychnine it will prove a much more effective stimulus. It is right and proper to administer these drugs in this emergency, but still more reliable measures are at hand.
Sudden stoppage of the heart, being the most disastrous accident during or after anesthesia, has attracted no small amount of attention on the part of experimenters. An active massage of the heart seems to furnish the basis for all the newer methods of treating it, all of which are accompanied by artificial respiration. Some of Crile’s work in this connection was alluded to in the chapter on Blood Pressure and Shock.
Fig. 41

Showing how proper traction on the tongue pulls on the epiglottis. (Hare.)
Numerous investigators have revived the hearts of experimental animals by massage and saline injections, and Crile has shown the advantage of adding adrenalin to the latter. It is better to begin the efforts while the heart is still feebly beating than to wait until it has ceased. Ordinarily this massage should be made through the intact thorax, but the time is coming when it will be esteemed life-saving either to open the abdomen and massage the heart through the diaphragm, or to open the thorax and do it directly. The former can be done during almost any abdominal operation. The greatest obstacle to success has been the formation of clots in the cardiac cavities. These are formed within a few moments after the heart has ceased to act.
Massage of the heart, coupled with the use of adrenalin, will prove of service.
Approaching cardiac weakness is always indicated by failure of capillary circulation, which may be easily and instantly estimated by making pressure upon the finger-nails. The rapidity with which the blood will return to give them a natural appearance, after such pressure is made, will be the index as to whether or no stimulation is necessary. Tardiness in return of color, or absence, is a better indication of the approach of shock than is coldness of the nose or moisture of the skin. It often precedes acceleration of the pulse.
[202]
Respiration may be interfered with by a variety of causes. Not infrequently the tongue is allowed to drop backward into the pharynx as the patient lies upon his back, which, by its pressure, causes the epiglottis to fall backward upon and close the glottis. The indication here is to lift the tongue forward and carry the epiglottis upward so as to restore the air channel. Extension of the head and neck will accomplish much in this direction, as well as holding the lower jaw forward and upward by well-regulated pressure exerted behind the angle and at the same time by upward and forward traction upon the hyoid bone. But when it is necessary in cases of emergency to carry out this maneuver forcibly and extensively, then the tongue should be drawn upward and forward in the direction indicated in Figs. 41 and 42.
Tongue forceps are often resorted to for this purpose, and can be procured in various forms and shapes. To the writer their employment has always seemed far more barbarous than the much simpler expedient of passing a curved needle, armed with silk, through the tongue in either direction, 3 to 5 Cm. back of its tip. The suture thus drawn through is knotted and made into a loop, and may be employed through a long operation to make all the traction that will be required. This really makes the tongue less sore and produces less swelling and after-discomfort than does the use of forceps.
Fig. 42
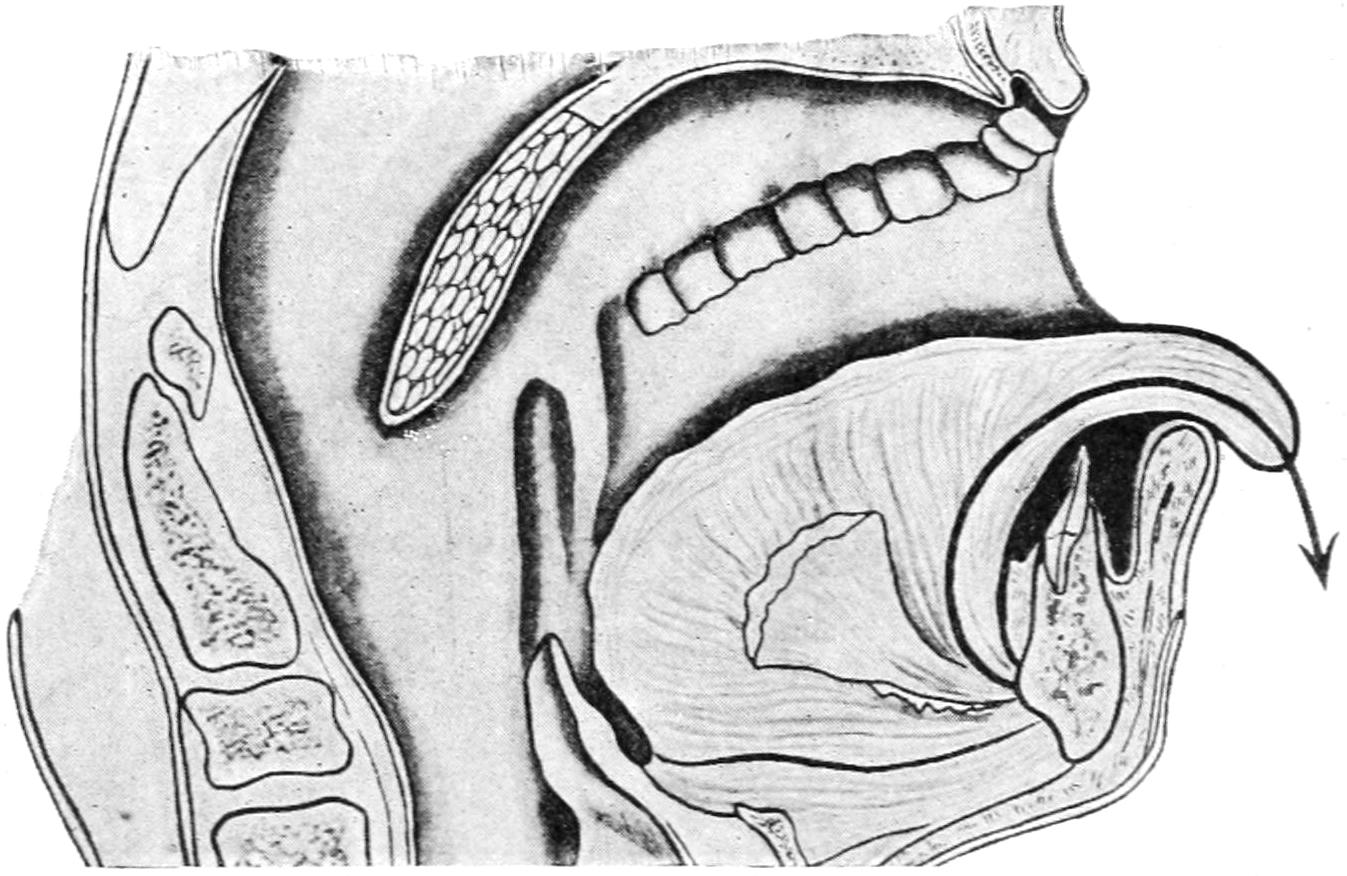
Showing how dragging the tongue over the teeth fails to pull on the epiglottis. (Hare.)
Respiration may also be impeded or suddenly checked by the presence of a foreign body. This may possibly be a plate which the anesthetizer has failed to require the patient to remove, or it may be material ejected from the stomach; this latter is especially likely to happen when emergency has required anesthesia without due preparation. When this happens the fingers should be passed behind the epiglottis and the obstructing body removed. In rare instances some portion of food may have been so impacted in the glottis as to completely obstruct it. If such an emergency arise the trachea should be opened and relief thus afforded. Only in this way can life be saved. Embarrassment of respiration is caused at other times by the patient apparently “forgetting to breathe” or by his taking such shallow inspirations that nothing is accomplished. This may be combated in several ways. In the former instance the use of ether or injections of atropine will frequently afford the necessary stimulus to the respiratory centres. In the latter class of cases especially the most valuable expedient is the dilatation of the sphincter ani, which may be stretched with a speculum, or with the fingers. Long-drawn, even gasping inspirations may follow this expedient.
Finally in certain cases artificial respiration will be required, combined with rhythmical traction upon the tongue. The tongue should be grasped, or controlled by a suture, and retracted from the mouth at the rate of at least sixteen times a minute, while the chest is compressed at the same rate, the traction being made at the moment of relaxation of chest pressure. Tongue traction alone will sometimes renew respiratory movements in extreme cases.[9] Figs. 43 and 44 from Hare, show the combined manipulation of[203] inverting the patient in order that the brain may not lack for blood supply, and carrying out artificial respiration.
[9] Freudenthal has called attention to the extreme irritability of both surfaces of the epiglottis, and advises to pass the index finger down upon it, irritating it by friction. This causes a powerful reflex effect, as the glossopharyngeal supplies its anterior surface and the inner branch of the superior laryngeal its posterior surface.
While these measures are to be regarded as emergency expedients, they will often need to be supplemented by others, the use of adrenalin and of salt solution, either beneath the skin or in the veins, and the use of the Crile pneumatic rubber suit described in the chapter on Shock.
Fig. 43
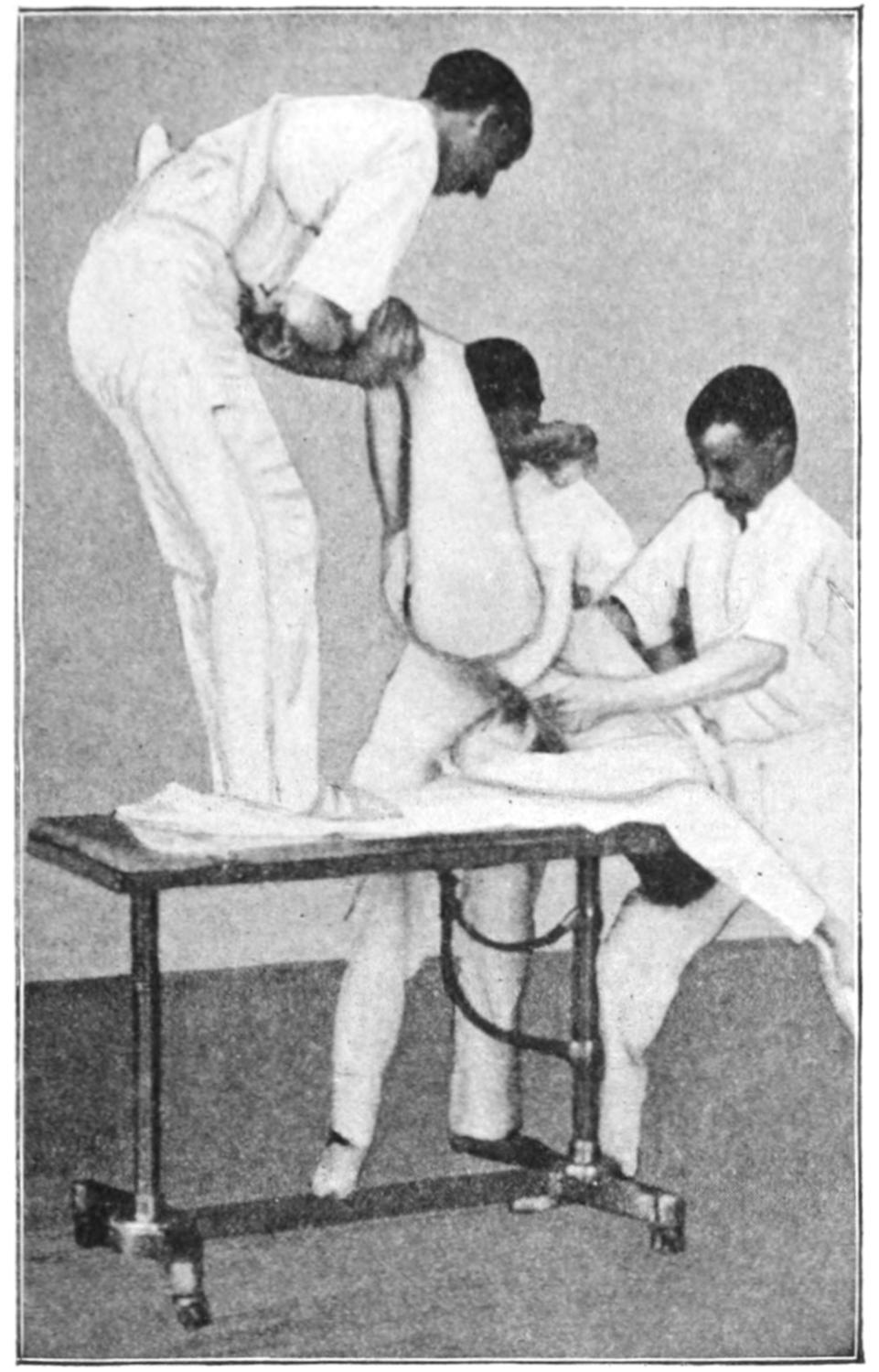
Showing inversion of patient and method of performing artificial respiration simultaneously. (Hare.)
Fig. 44
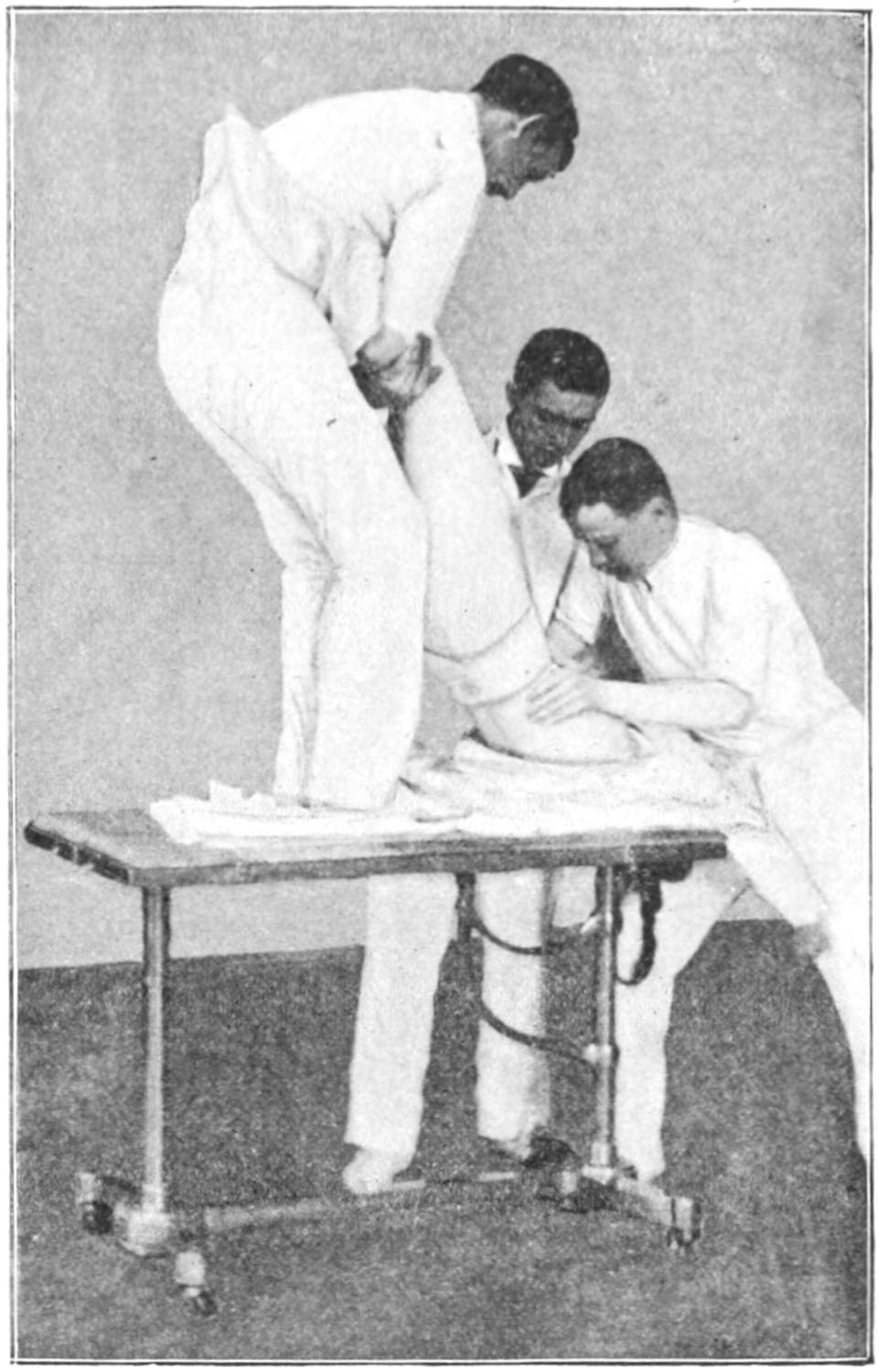
Same as Fig. 43.
There is a delay in the management of the patient after the conclusion of an operation which is too often neglected—namely, prevention of such exposure as shall produce a sudden checking of perspiration. The patient should be wrapped in several thicknesses of blanket, leaving only the face exposed; and only when fully conscious should he be uncovered gradually and well dried with a bath towel. Such procedure takes away much of the danger of congestion of the lungs, or of the kidneys, which may cause serious disturbance should they occur.[10]
[10] The following is quoted from a recent journal article by an unknown writer:
Acid Intoxication after Anesthetics.—Occasionally some surgeon reports a case of peculiar rapid fatal toxemia after a prolonged operation, the cause of which is obscure. We have also heard of this trouble after parturition, during which chloroform was given for a prolonged period, and the ultimate cause of the violent symptoms has been unknown. Now we are beginning to believe that anesthetics, especially chloroform, can produce a destructive effect on the liver and kidney cells very similar to phosphorus poisoning. In many cases a peculiar idiosyncrasy seems necessary to explain the toxic effect, but certain predisposing causes have been noted, e. g., hemorrhage. The symptom-complex makes its appearance from a few hours to a few days after the anesthesia, and consists of vomiting, restlessness, delirium, convulsions, coma, irregular breathing, cyanosis, and icterus in varying degree. The disease as described by Bevan and Favill is a hepatic toxemia, resulting from acute fatty degeneration of the liver, and seems to be a clinical entity. It is characterized by an acid intoxication, acetone, diacetic acid, and beta-oxybutyric acid being found in the blood and urine. Several clinical varieties must receive renewed interest in the light of this investigation. First is acute yellow atrophy of the liver, many cases of which occur after chloroform anesthesia. Next, the rapid death after abdominal operations, which have hitherto been attributed to intestinal toxemia; and lastly, certain fatal cases of nephritis after operation need a more careful study.
[204]
All foreign bodies should be removed from the mouth and pharynx. If the patient have been in water he should be suspended head downward, in order that the water may escape by gravity from the lungs. In all of these methods rhythmical traction upon the tongue will be found a valuable aid in the procedure.
Sylvester’s method utilizes the arms as levers by which to expand the thorax, by means of the muscles which pass between them and the chest. The patient is laid on his back, the shoulders somewhat elevated and the head thrown backward. The forearms are seized just below the elbows and carried upward over his head, by which movement the chest is expanded; here they are held about two seconds, and then brought down to the side of the chest and actual compression of the thorax made with them, for the same period of time. When the chest is compressed, an assistant may also press the liver upward and thus help to empty the lungs. The intent is to make from sixteen to eighteen of these movements in a minute. In children the movements are made more rapidly, and in infants considerably more. It is usually necessary that traction be made upon the feet to prevent pulling the body upward when the arms are moved to expand the thorax. If the manipulations can be carried out upon a table whose feet can be somewhat elevated this will also help, as the blood is thereby induced to enter the cranium.
Marshall Hall’s method is to roll the patient from his back on to his side, the uppermost arm being utilized to make pressure upon the side of the thorax in order to expel air. Then the body is rolled over on to the back, by which movement the chest is expanded. This method is not nearly as efficient as that mentioned above.
Fig. 45
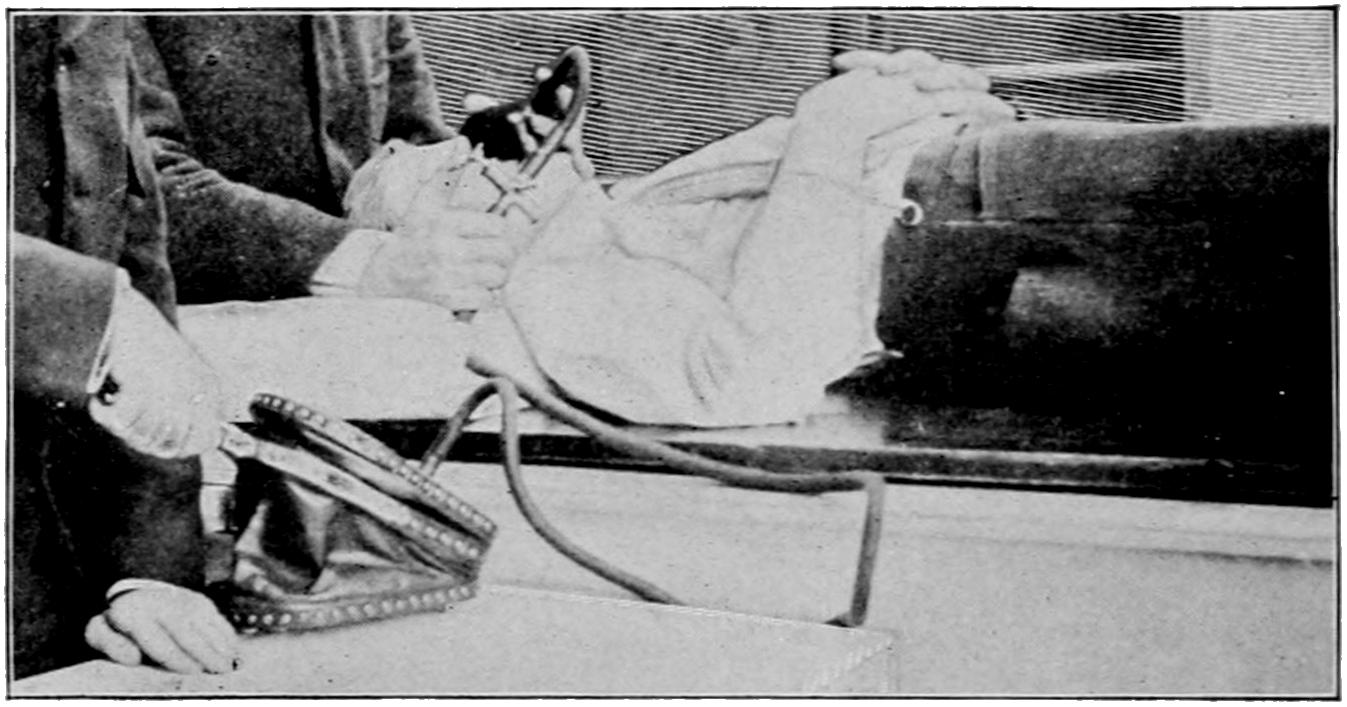
Fell’s apparatus for forced or artificial respiration.
In case of drowning Howard’s method is quite applicable. The maneuvers are as follows:
1. Turning the patient upon the face, with a large firm roll under the stomach and chest, and protecting his mouth from the surface upon which he is lying, press with full weight two or three times, for four or five seconds, each time upon his back, so that the water is expelled from his lungs and stomach.
2. Then quickly turn him face upward with the roll beneath his back, with his head hanging downward and his hands above his head. The operator then kneels astride over the patient, with the hips between his knees, and grasps the lower part of the patient’s chest firmly, bracing his own hands with his elbows firmly against his own hips. With his full weight he then makes pressure upon the patient’s chest, compressing it laterally for two or three seconds, gradually leaning forward while doing this, and then with a sudden jerk pushing himself backward. The intent here is to imitate the ordinary respiration rate as above, or perhaps a little less often. This may be continued for a half-hour or even for an hour, sometimes with eventual success.
There should be also massage of the heart, in addition to traction upon the tongue. Artificial assistance should not be discontinued until the patient is breathing regularly and sufficiently without help. In Fig. 45 is represented the Fell apparatus for making[205] forced artificial respiration, this being a great improvement on the so-called mouth-to-mouth inflation. The essential feature of it is a bellows, by which the air is forced into the lungs, through a mouth-piece made to fit tightly over the face, or through a tracheotomy tube. In accident cases other measures, such as artificial warmth, etc., should be employed.
Morphine offers no little aid in the production of anesthesia in many cases. Those patients who are terrified by the thought of operation, and who are in a semihysterical state when anesthesia is begun, may be greatly tranquillized by a hypodermic injection of 0.01 to 0.015 of morphine, fifteen or twenty minutes previously. Given in this way it acts as a heart tonic and general equalizer to the circulation. If a small dose of atropine be added the effect upon the respiratory centres is much enhanced. Again, in those cases where anesthesia is begun without it, and patients prove very rebellious, it will have the same happy effect. The only objection to its use is the nausea which may thereby be produced. There is no way by which to dissociate this from the nausea due to the anesthetic, elsewhere considered under the heading of the After-care of Patients.
Patients can rarely be so completely put under the influence of morphine as to justify its use alone.
—The Germans sell under this name an alkaloid made from the Solanaceæ, which seems to be identical with the hyoscyamine of the U.S. Pharmacopœia. Schneiderlin, in 1900, published a method of producing anesthesia with little discomfort by using it combined with morphine. The mixture seems more effective than either alkaloid alone, but is rather slow in action. On the day preceding the operation a trial dose of 0.02 of morphine and 0.008 to 0.01 of scopolamine may be given. This will demonstrate the susceptibility of the patient to the mixture. One hour and a half before the operation this dose, or a larger one, should be administered, and, if necessary, another one of smaller size fifteen minutes before the time of operation.
According to this method an interval of sixty to eighty minutes should elapse between the first dose and the operation itself. When anesthesia is thus produced it lasts from three to several hours. Others have advised to divide the dose into three injections, giving the first about two and one-half hours, the second one and one-half hours, and the third one-half hour before operating. In some cases this has produced complete and satisfactory anesthesia; in some it has not been complete, while in others serious symptoms have been produced. The statement that each alkaloid counteracts the dangerous effects of the other is not substantiated; it is probable that the combined effect is greater than would be that of either used alone. This mixture should rarely be used, save in those cases where general anesthesia is inadvisable, and where there are difficulties, even about the employment of local anesthetics.
The use of ethyl chloride, as the most volatile of the ordinary drugs, by which chilling or freezing of the skin may be produced, has been already mentioned. Other agents which chill or freeze may be used, e. g., a spray of common ether or of rhigolene, or the local application of ice and salt.
—Liquid air, when available, affords an excellent means of benumbing sensibility, since one or two very light applications, two or three minutes apart, admirably serve the purpose. It is, however, rarely available and should be used with great caution.
—Of the local anesthetics cocaine, or some of its compounds or substitutes, will give the best results; although it is said that injections of pure water, if sufficiently bulky, will also answer the purpose of a local anesthetic. Cocaine has marvellous properties upon mucous surfaces or in the tissues, but none upon the unbroken skin. Where the parts to be operated are covered with skin it is necessary to inject the drug with a hypodermic syringe, as in the case of all deeper tissues. About the eye, the drug is used in from 1 to 4 per cent. strength; in the nasopharynx, from 2 to 4 for ordinary purposes; about the genitals, 2 to 5 per cent.; beneath the skin, ordinarily in strength of[206] 1 to 2 per cent. In operations upon the nasopharynx and larynx it is often advisable to make a local application of a small amount of an almost saturated solution, by which a more complete effect is gained.
Cocaine is not without dangerous toxic properties, to which some persons are peculiarly susceptible. It will seriously disturb heart action in some; in others produce vertigo and mild delirium, and in still others peculiar erotic symptoms. Warm solutions are more quickly absorbed than cold ones. The use of more than 0.06 (1 grain) should be avoided.
When the skin alone is to be anesthetized the injection should be made into and not beneath. The nearer the cocaine solution is deposited to the principal nerve trunk or branches the more promising will be its effect.
The use of cocaine in operations, under general anesthesia, for the prevention of those depressing influences which cause lowered blood pressure and shock, has been alluded to in the chapter on Shock. For instance, it is well to spray the larynx after opening it and before making further operation upon it; while in all major operations in which large nerve trunks are exposed or divided, e. g., amputations, etc., the injection into the nerve trunks of a few drops of 2 or 3 per cent. cocaine solution prevents this kind of disturbance.
For small and localized operations the direct injection of cocaine into and around the area involved will prove sufficient. It is rarely necessary to use for this purpose a solution stronger than 1 or 2 per cent., especially if it is deposited drop by drop around the entire margin of the area and if the part have been previously made bloodless by pressure, as by the Esmarch rubber bandage. But when extensive operations are to be undertaken the method of “blocking,” so called, should be carried out. This consists in cocainizing the principal nerve trunks which supply the part, for which purpose an accurate knowledge of regional neural anatomy is necessary, with the intent to inject into or closely around the nerve trunks a few drops of a 1 or 2 per cent. solution. Working in this way by combination of injection, then of incision, by which the nerve trunks are better exposed and more fully protected in order to be more completely injected, and then proceeding farther with the operative part, extensive operations have been and may be done; such for instance as amputations, not alone of the limbs but even of the shoulder girdle, removal of large tumors, etc. In this way, for example, Kocher now removes most of the goitres which he attacks. The essential feature of this work is to first get the cocaine inside of the nerve sheaths. In this way a minimum of the drug is used with a maximum of effect. Nevertheless when a large nerve trunk is thus to be paralyzed temporarily it is best to inject the solution directly into it as well as around it inside the sheath. Cocaine is a temporary protoplasmic poison, and for the time being shuts off the afferent power of the nerve. One advantage of this method is the avoidance of shock as well as of pain. Another method, devised by Schleich, is to be preferred. He uses three different solutions, of which the second is commonly used. Tablets for making these solutions can now be obtained. In order to secure the best effect with them the parts should be made bloodless. The solution is deposited subcutaneously in a series of drops around the margin of the area, and then massage may be made to distribute the fluid more uniformly in the tissues. When the tissue to be operated upon is inflamed the injections should be made first into the healthy area on the proximal side.
Schleich’s formulas are as follows:
| No. 1. | ||
| Cocainæ hydrochloridi | .200 | (gr. iij). |
| Morphinæ hydrochloridi | .025 | (gr. ²⁄₅). |
| Sodii chloridi | .200 | (gr. iij). |
| Aquæ destillatæ | ad 100.000 | (f ℥ iiiss). |
| No. 2. | ||
| Cocainæ hydrochloridi | .100 | (gr. iss). |
| Morphinæ hydrochloridi | .025 | (gr. ²⁄₅). |
| Sodii chloridi | .200 | (gr. iij). |
| Aquæ destillatæ | ad 100.000 | (f ℥ iiiss). |
| No. 3. | ||
| Cocainæ hydrochloridi | .010 | (gr. ¹⁄₆). |
| Morphinæ hydrochloridi | .005 | (gr. ²⁄₅). |
| Sodii chloridi | .200 | (gr. iij). |
| Aquæ destillatæ | ad 100.000 | (f ℥ iiiss). |
[207]
Various substitutes for cocaine are now on the market. Some of these are soluble and some insoluble. Eucaine is most commonly used, especially in form known as eucaine B., or beta-eucaine. It is weaker than cocaine, especially so in toxic properties, and solutions of twice the strength can be used, often with satisfaction, and almost always without danger. For urethral and eye work, e. g., it answers the purpose; nevertheless, it will sometimes prove disappointing. Orthoform is a crystalline, sparingly soluble artificial product, which is too light and too coherent to be generally serviceable. It often gives satisfaction mixed with other powders or in ointments, and it is usually free from toxic properties. Nervanin is another laboratory product, not equal in activity to cocaine, but almost free from unpleasant properties. Anesthesin is another similar product, which is practically free from physiological properties save that it acts as a local anesthetic. The latter may be employed for infiltration anesthesia in the following proportion, recommended by Dunbar:
| Anesthesin hydrochloride | 0.250 | |
| Sodium chloride | 0.150 | |
| Morphine hydrochloride | 0.005 | to 0.015 |
| Water | 100.000 | Cc. |
Stovaine and alypin are among the latest synthetic substitutes for cocaine. The latter seems to offer promise of usefulness.
Adrenalin may be added to any of these solutions in proportion of 1 per cent. of a 1 to 1000 solution, and will have a beneficial effect in all cases.
The intraspinal injection of remedies was first suggested by Corning, of New York, in 1885; it remained, however, for Bier to perfect the technique in 1899, and to make it so popular that the same maneuver has been practised for various other purposes; as, for instance, for withdrawal of cerebrospinal fluid in cases of hydrocephalus, etc., or the injection of tetanus antitoxin. (See chapter on Tetanus.)
The intent in this use of cocaine is to spread the solution over the surface of the cord and beneath the arachnoid. For this purpose a needle about 4 inches in length, with a point not too sharp, preferably gold or platinum plated, is used; with this also a syringe which will hold 2 to 4 Cc., which can be firmly, yet easily, attached to the needle. The accompanying illustration (Fig. 46) will give an idea of the technique. The patient should be seated leaning forward so as to curve the back and open the intervertebral spaces. A sterilized towel is stretched tightly across the back from one iliac crest to the other; its upper edge should then pass just over the spinous process of the fourth lumbar vertebra. The injection is usually practised between the second and third lumbar spines, or between the third and fourth; the latter having been identified, the former are easily made out. The needle is entered about 1 Cm. to the right of the middle line and passed forward, inward, and upward, to a depth of 7 or 8 Cm. in the ordinary adult, until the resistance offered by the tissues is felt to have been passed and the point to have entered a cavity. If the needle has been passed alone the escape of a drop or two of cerebrospinal fluid will indicate that the spinal canal has been entered; if the syringe is attached to the needle the piston should be withdrawn in order to show the same result. It is possible to practise this operation with a patient in the recumbent position, but it is done more easily as above outlined. The skin may be frozen by the freezing spray, or may be anesthetized by the local injection of cocaine solution with the ordinary hypodermic syringe.
It is astonishing what beneficial effects can be gained from the use of a small amount of cocaine. It is rarely necessary to use more than 0.03 (¹⁄₂ grain) of pure cocaine in order to procure analgesia of the entire lower part of the body.
Beta-cocaine or tropacocaine may be used for the same purpose, in double this amount, but they do not give as reliable results. Morton, of San Francisco, has suggested that ¹⁄₂ Gr. powders of cocaine be wrapped in such a way that they can be repeatedly sterilized by a heat of 200° F., and that one of these be dropped into the syringe barrel, that this be attached to the needle, and the cocaine itself be dissolved in the cerebrospinal fluid withdrawn through the latter, and then thrown back again. This is probably[208] the neatest and most serviceable method yet devised, and its originator has assured the writer that with 1 Gr. of tropacocaine used in this way, thrown into the spinal canal with considerable force, i. e., in such a way as to more completely distribute it, he has been able to practise operations even upon the tongue with little or no pain to the patient. The solution used for this purpose should be sterilized, also the needle, the syringe, the patient’s skin, and the operator’s hands. The water with which the cocaine solution is made should be first pure, then measured, and the solution made in such strength that not more than the amount indicated above will be used. This should then be again heated, but not quite to the boiling point, since cocaine solutions are impaired by too much heat.
Fig. 46
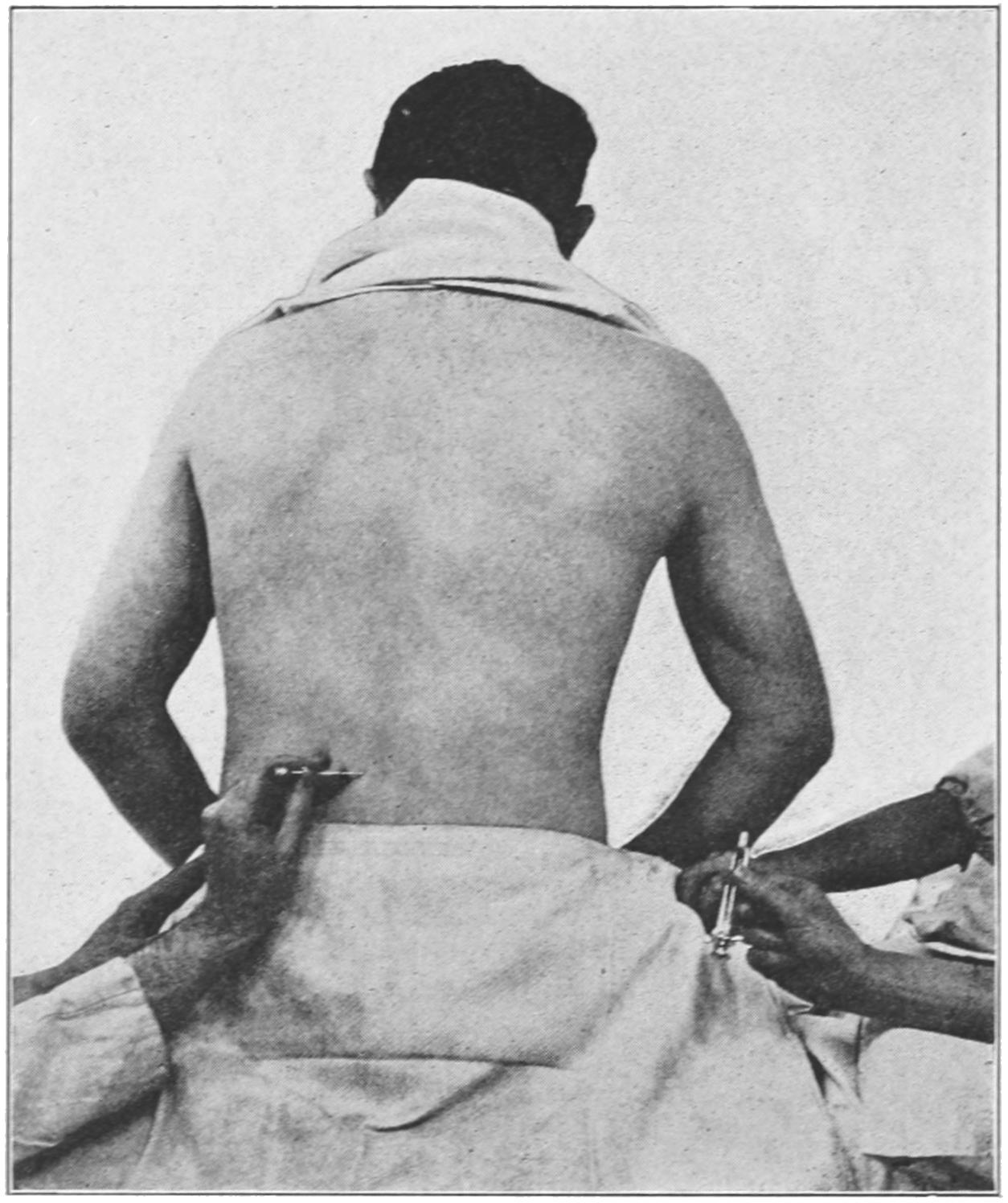
Technique of intraspinal injection.
The advantages of intraspinal anesthesia are many and obvious, and were it not for disadvantages this method would have supplanted all others for certain work. It is, however, by no means free from danger, both from the maneuver and from the drug itself. Carelessness in its introduction may lead to septic meningitis, while the drug itself may produce considerable and even serious or fatal disturbance, though these cases are rare. It has been claimed that 2 per cent. of the cases in which this method has been employed have, in consequence, terminated fatally. The immediate effects are largely confined to the stomach and the nervous system, and include nausea, intense headache, and profound depression. The remote effects are less positive, but have been stated to include serious changes in the cord itself. It is often a disadvantage to have the patient mentally conscious of what is going on, even though oblivious to pain. Inasmuch as cocaine produces analgesia rather than anesthesia, nervous patients will be likely to mistake the general sensation of lifting a limb, or manipulating it, for actual pain. There are not a few cases where chloroform and ether are so plainly contra-indicated that if it were possible to use any other agent with safety this would offer a valuable substitute.
The effect desired is not produced immediately, but comes on slowly, after the expiration of ten to twelve minutes. As ordinarily used, anesthesia of the surface will be produced up to the height of about the waist. Should it be desired, however, to increase[209] or enhance the effect the solution might be injected between some of the dorsal vertebræ, although at this point it will require more skill to introduce the needle, and the operator should be cautious not to injure the cord. Below the second lumbar vertebra the cord breaks up into its segments and the patient would be almost exempt from this danger. It is occasionally necessary to tranquillize the patient’s fear by using morphine subcutaneously at the same time. It is a question whether this can be safely combined with cocaine for the subarachnoid injection. Failing in this it may be necessary to supplement the use of cocaine with ether or chloroform.
The intraspinal injection of normal saline solution, or even of pure water, has been shown by Eden to be almost as effective in some cases as the cocaine solutions. Bier has largely modified his statements about the value of intraspinal cocaine injections, and speaks of them as more dangerous than he had first appreciated.[11]
[11] Magnesium Salts as Local Anesthetics.—Six years ago Meltzer discovered that magnesium salts have the property of inhibiting functional activity in nerve tissue, and in December, 1899, he announced that the intracerebral injection of magnesium sulphate in a rabbit caused paralysis without previous convulsions. He has recently announced the local anesthetic effect of small doses of a 25 per cent. solution of magnesium sulphate, an effect which lasts from one to two hours. It is the magnesium “ion” which possesses the anesthetic property, since the chloride and the bromides give the same effects.
These salts have this advantage over other local anesthetics that there is no primary period of excitation. Moreover, applied locally to nerve trunks they have the effect of “blocking” them; and when applied to the sciatic, pneumogastric, and other nerves, temporarily abolish their power of conducting influences, either motor or sensory. This effect is apparently due to the fact that the magnesium normally present in the tissues constantly exercises an inhibitory power over them, and that when thus applied from without they merely exaggerate the condition already present; thus, if this be true, affording an ideal anesthetic.
In December, 1905, Meltzer read a paper before the New York Academy of Medicine, announcing success with intraspinal injection of magnesium sulphate in 25 per cent. strength. Blake, of New York, promptly made use of the suggestion in a child with tetanus. Two injections of antitoxin had been made into the cervical cord on successive days, with apparently no effect. He then made lumbar puncture and a subdural injection of magnesium sulphate, giving 1 Cc. of 25 per cent. solution for every twenty-five pounds of body weight, administering it every thirty-six hours, employing four doses. The effect was marked, in immediate control of convulsions, which, however, was not permanent; hence the repetition of the doses. How much influence the previous antitoxin had produced does not appear.
Meltzer suggests that the best time for an operation is three or four hours after a spinal injection. He reports four cases thus operated, in one of which, after the operation, the patient passed into a period of deep general anesthesia, in which he remained for five hours, the pulse keeping up, the respirations falling to ten per minute. In this case another spinal puncture was made, some of the spinal fluid let out, and the spinal cavity treated by repeated irrigations with sterile salt solution.
Meltzer’s few but important experiences indicate that at least three or four hours should be allowed to elapse after the introduction of the magnesium solution. He advises 1 Cc. for every twenty-five pounds of body weight, for intraspinal injection, which causes not only analgesia but temporary paralysis of the legs, sensation and motion returning in from eight to fourteen hours, with possible retention of urine for a day or two, requiring the use of the catheter.
Doses a little larger than the above, he thinks, would permit the performance of extensive operations in the abdominal cavity, or even higher up, without the aid of a general anesthesia. He is inclined to think that it would be preferable not to wait four hours, but to operate within about two hours after injection, with the aid of a small amount of chloroform, the operation to be followed by another puncture, with the removal of at least as much fluid as was introduced, and irrigation with sterile salt solution, finally leaving some of it within the canal.
The old classification of wounds divides them into contused, lacerated, punctured, and incised. For descriptive purposes these adjectives are self-sufficient; they can be criticised only in case the injuries differ in character. The adjectives thus employed allude to the character of the injury as well as to its cause, but no meaning should be conveyed by any of them other than to indicate a severance of continuity in tissues. In either case cells are rudely torn apart. But whether the injury be subcutaneous and the tearing make a ragged surface; or whether the wound be an open one, with the possibility of introduction of germ-laden air and grosser impurities, even though the surfaces separated present an even plane, as in an incised wound; or a channel or tunnel, as when made by a pointed instrument or a gunshot missile, the principle is the same, and the same processes of repair are brought to work to undo the harm. There is but one natural method of repair, and that includes the exudate, or the utilization of the fluid portion of the blood already poured out, and the activity of cells, those which lie in the vicinity and those which are furnished from a distance, i. e., leukocytes and wandering corpuscles. It is of advantage to have the injury subcutaneous and protected from contact with the air, yet extensive injuries of this kind are often much longer in healing than those inflicted by the surgeon’s knife, when the parts can be brought into complete apposition with each other by sutures.
It is the writer’s intent to simplify the description of the healing processes and to insist that it is always the same, not modified in character but in duration and extent, according to the nature of the injury.
The term contusion implies a subcutaneous injury of varied extent, in which laceration cannot be left out of consideration. Even in the mildest contusion mechanical harm has been done, permitting a dilatation of the vessels and the escape of fluid. Should this occur in linear form, as by a whip-lash, there may be what is called a wheal. In loose tissues swelling occurs more easily, as in the eyelid, the scrotum, etc. Injuries of severity will produce laceration, at least of capillaries if not of arterioles, and the result is the escape of an amount of blood which will infiltrate the surrounding tissues and discolor them and produce an extravasation or ecchymosis. The blood barely escapes and coagulates before its absorption begins. The fluid portion disappears before the solid, and the pigment is usually the last. There results a black and blue spot; the color when near the surface is at first indigo or purple, and fades out through bluish and greenish tints into a yellow, which may not disappear for two or three weeks. Should blood collect in a cavity or in large amount the mass is called a hematoma; this is especially common in the pelvis and in the cranial cavity. Should a vessel wall give way from weakness caused by disease instead of by accident the result is the same.
[212]
Contused wounds of the surface often cover excessive and even fatal injuries within, as when a heavy object falls upon or injures the abdomen or a limb. The skin is resistant, and the writer has seen a limb pulpified by being run over by a heavy car, the skin being but slightly torn. In such accidents exploratory incisions are imperative. Better results will follow opening the abdomen in cases of severe contusion, for the purpose of exploring the viscera, than will follow the “let-alone” policy of waiting for something serious to appear.
An outpour of blood should be expected in every contusion, save the most trifling, while clot formation may ensue. Whether the clot will be absorbed or require the aid of the surgeon will depend upon its size, its location, and its liability to infection. Clot in some locations, e. g., pressing upon the brain or spinal cord, may justify extensive operation for its removal.
Pain produced by contusion is variable. When nerve trunks of considerable size have been injured pain is frequently aggravated. In general it is proportionate to the amount of swelling, i. e., to the density or laxity of the injured tissue. When exudate occurs beneath unyielding membranes, for instance the periosteum and the capsules of certain organs, the pain may be severe. The appearance of discoloration is proportionate to the depth of the injury and the amount of hemorrhage. The time of its appearance will depend upon the distance from the surface; after fracture of the neck of the femur it may not be observed for several days. The general condition of the patient will depend greatly upon his temperament. When there has been considerable extravasation the release of the fibrin ferment may produce a mild rise in temperature.
—So long as air or other infection can be excluded the treatment of contusions is simple. Cleanliness of the injured parts should be enjoined; also physiological rest, by their confinement within dressings or splints, or by placing the patient in bed. An antiseptic application, dry, watery, or in ointment form, should be applied upon a surface which has been abraded. Differences of opinion exist as to the respective values of heat and cold. When the case is seen early, before much swelling has occurred, the exudate may be limited by the application of cold dressings; whereas if seen after the swelling is at its height the use of moist heat may favor a more speedy re-absorption. The effect of extremes, either of heat or cold, is sedative, although hot applications afford more relief than do those of ice. Of domestic remedies in use among the laity it may be said that those which have any value owe it to the alcohol which they contain. Elastic constriction will reduce the amount of exudate and assist in the absorption of that already present. It is a measure, however, to be used with great caution lest venous return be interfered with and edema or gangrene be the consequence. A joint tensely distended with fluid as a result of combined contusion and laceration, called a sprain, may be emptied by aspiration, but this should be used only under antiseptic precautions. Finally any collection of blood which fails to disappear may be incised and cleaned, its cavity mopped out with compresses, and its surface made to come in contact by pressure. In hematomas and large extravasations of blood, sometimes in joints, but rarely in the pleural or peritoneal cavities, this method may also be used.
Lacerated wounds differ from contused in the character of the tears in the tissues affected and in the exposure to infection by contact. They vary in extent and severity. Not infrequently tissues or organs of the greatest importance are lacerated, e. g., the globe of the eye, the liver, the intestines. The term laceration itself implies such open injury that part of it may be exposed to infection. The first danger is from hemorrhage. This may subside spontaneously, or may have been checked by some first aid, or may prove nearly fatal by the time the patient is seen by the surgeon. The first measure will be hemostasis by the readiest and most effective measures at hand. This may mean the application of compresses or of a tourniquet, or even of manual pressure, until surgical procedures can be instituted. Shock should be treated by lowering the head and raising the extremities, or bandaging the latter, and the subcutaneous administration of morphine or atropine. Emergency treatment of these cases should include removal of foreign bodies, and such cleanliness and attention to antisepsis as may be possible at the time. Support of the injured part should be effected temporarily until dressings[213] can be scientifically applied. If cane sugar will keep fruit and meat from decomposition it will have the same effect in human tissues, and a laceration with or without compound fracture of bone may be filled with granulated sugar until a suitable dressing can be applied.
The surgical treatment of laceration should include the following measures: Hemostasis; the removal of foreign bodies, as well as of tissue which is so injured as to make repair impossible or even questionable; a careful study of nerve supply, in order to be sure that no nerve suture should be made; a similar study of muscles and tendons, in order that tendon suture may be promptly made; careful antisepsis throughout, asepsis being impossible; closure of the wound by buried and superficial sutures, and such drainage tubes or outlets as may permit free escape of whatever products of inflammation or disintegration may result. There should also be provision for physiological rest of the injured parts as well as of the patient’s mind and body.
When large areas of skin or deep tissues are destroyed or torn away, as in scalp wounds, avulsion of limbs or parts of limbs, it may be necessary to retain that which can be saved and to remove that which would slough if left to itself, thereby providing for flaps of skin by which the wound may subsequently be covered, or leaving them in case removal of a part must be made.
Everything which has vitality should be spared; on the other hand, that which has lost its vitality should be removed at once. Thus amputations may be sometimes called for because of extensive lacerations with destruction of vascular and nerve supply, even though the bones be uninjured.
In cases where the question of viability of tissues cannot be promptly decided it is best to keep the injured part immersed in water as warm as can be borne. In hospitals the entire body may be kept immersed for days. By the use of warm water parts which have been seriously injured may be restored. Ulcerations which are seen after the sloughing process has begun can be best treated by immersion or by the application of brewers’ yeast upon compresses or cotton. No other substance, perhaps, will so quickly clear up an indolent or foul surface as this; it hastens the time of separation of all that is dead or dying and restores healthful activity to the surrounding tissues.
Extensive lacerations leave frequent opportunity for operations by which function may be restored or improvement affected.
The essential features of punctured wounds are sufficiently indicated by the descriptive name; but harm may be done through a small external opening. An important subvariety of punctured wounds is inflicted by gunshot missiles, which will receive consideration by themselves. Injury to important vessels may lead to serious hemorrhage; while injuries to nerve trunks may be followed by paralysis of sensation and motion, or, as in the case of a sympathetic trunk, by the well-known consequences of division of vasomotor nerves, e. g., in the neck. When the punctured wound bleeds freely and externally it may be assumed that some large vessel has been injured. When it bleeds into one of the cavities of the body delay in recognition may occur. This is true of a puncture of the skull by which the middle meningeal artery or one of the sinuses is wounded, when the symptoms of brain pressure may tardily or rapidly appear. In the chest the intercostal or internal mammary artery may be so injured as to bleed into the pleural cavity and cause death. A puncture of the heart frequently leads to fatal hemorrhage into the pericardial cavity, and in the abdomen puncture of the various viscera has led to consequences beyond help save when prompt relief could be afforded.
The dangers attending punctures pertain to the introduction of infectious material which may produce sepsis or may slowly produce tetanus. No ordinary weapon or tool is clean in a surgical sense, while a rusty nail is even less so. It will be seen, therefore, that the danger inherent in such a case is not to be measured by either the size or the depth of the wound.
In dealing with these cases the first attention is to be given to hemorrhage. Obviously punctures in certain regions are much more likely to be followed by hemorrhage, and any puncture in the vicinity of one of the large vessels should be managed with caution,[214] especially if the surgeon ascertain that it had bled profusely when first inflicted. Such a puncture, when seen a few hours later, may have become occluded by clot, or a considerable hematoma may have formed beneath the skin. It is safe to presume that there is more danger of septic infection than can accrue from later attention, and it would be advisable in such cases to anesthetize the patient and lay open the parts freely under full aseptic precautions, in order that the clot be turned out and any bleeding vessel secured. A brief study of such a case will decide the question of injury to the principal nerve trunks. A principal nerve which has been injured or divided should be carefully sought for and its ends freshened and sutured. This is true also of any tendon whose function is evidently lost. If the thorax have been punctured and the physical signs indicate the presence of fluid, i. e., blood in the pleural cavity, it should be incised and the blood withdrawn. This method should also be applied to punctures of the heart. These measures will be more completely dealt with in treating of the surgery of the chest and its contents.
Punctured wounds of the abdomen may give rise to great anxiety. If none of the viscera have been injured they may be let alone, but if doubt exists as to the safety or injury of any of them the abdomen should be opened. (See Surgery of the Abdomen.)
—For emergency purposes antiseptic occlusion is the best procedure, and all punctures inflicted by ragged and infectious materials, as rusty nails, should be treated by free incision, with thorough cleansing and packing with antiseptic material, that the wounds may heal by granulation.
Incised wounds are those inflicted by a sharp object which divides the tissues abruptly and with a minimum amount of disruption. They invariably bleed, sometimes seriously, even to a fatal degree, the hemorrhage in such cases being due to severance of large vascular trunks. Like contused wounds they vary as infinitely in extent as in locality. According to their locality and dimensions important structures may be severed, e. g., the trachea, the large nerve trunks of the body, the tendons, etc., while visceral and joint cavities may be more or less widely opened. When death occurs soon after injury it is generally from hemorrhage. They are attended by the same dangers of septic infection as are punctures, especially when there is neglect in the emergency dressing. Should the pleural cavity be opened there may be collapse of the lung.
Hemostasis is the paramount indication in all incised wounds which bleed seriously. Hemorrhage is to be controlled temporarily by any expedient, later by ligation or suture, or both. The remarks above in relation to possible injury to vessels and nerves are of equal force in this consideration. Every divided nerve trunk, as well as every severed tendon, should be reunited by suture. If a joint have been opened it should be cleansed and drained, even though the incision be closed. Should there be injury to any of the viscera, the wound may be enlarged in order that exploration may be made and suitable remedies applied. This is true of every punctured or incised wound. No hesitation need be felt about enlarging it so as to permit of investigation. Hemorrhage having been checked and all required attention having been given, the closure of an incised wound may be made partial or complete according to its condition. If fresh and clean it may be almost completely reunited, using deep and buried sutures in order to bring into contact its deeper portions, while superficial sutures will suffice for the skin. Drainage may be by tubes or gauze or by loose suturing of the surface; but no incised wound whose surfaces have become contaminated should be completely closed by primary suture until all such surfaces have been freely cut away and appear healthy and uninfected. An old infected and gaping incised wound may be cleaned by the application of brewers’ yeast, and when granulating it may be closed secondarily with sutures, by which granulating surfaces are brought into close contact.
Of wounds in general it may be said that there are mixed types as well as illustrative examples. Thus a wound made by a hatchet or axe may partake of the nature of contusion and of incision. In instances where personal violence has been applied multiple wounds of varied character may complicate the case. The statements made above pertain to their conventional and common characteristics. Treatment which would be proper in one case may be impossible in another. There is always room for discretion[215] and good judgment, though there are fundamental rules which apply to all cases, and include exact hemostasis, surgical cleanliness, repair of severed nerves and tendons, removal of foreign bodies and involved tissue, and the enforcement of physiological rest.
The process of repair is essentially the same, being modified only by the needs of the wound and the tissues involved, and by their environment. Whether soft tissues or bones are being repaired the differences are apparent rather than real, as bony tissue is temporarily decalcified, and then, as soon as the process permits, is once more stiffened by deposition of calcium salts.
The process of repair should be begun immediately after the cessation of the disturbance which has produced the wound, and as soon as the bleeding is checked. It may be materially influenced and retarded by the presence of bacteria or other foreign bodies, but its character remains unchanged. Healing has been described as occurring by primary union, or by “the first intention,” and by granulation, or the “second intention.”
Wounds which have been permitted to remain clean, with their edges brought together so that the surfaces are in contact, are healed with a minimum of waste of reparative material, the process being as follows: The small vessels are occluded with thrombi up to the first collateral branches; the leukocytes begin to penetrate the film of blood, which, having coagulated, serves as a cement to help hold the surfaces together. By their proliferation and more complete organization the gap between the surfaces is bridged with both fibrous and capillary bloodvessels, and within sixty or seventy hours the clot has become largely replaced by organized cells. Meantime from the endothelial cells of the vessels and vascular spaces, as well as from the fixed cells of the connective tissue, the so-called fibroblasts are formed, which are later converted into connective tissue. Many of the cells which have wandered to the scene of activity, or have been there reproduced in unnecessary numbers, disappear again, either into the circulation or they serve as food for the fibroblasts. Branching cells attach themselves more intimately, and thus the original clot is completely converted into fibrous and connective tissue, and this becomes a scar, which extends as deeply as did the original injury. New capillaries are rapidly formed by a budding process, and supply the pabulum required for nourishment of the new cells. By fusion or amalgamation of neighboring vascular buds complete new vessels are formed, extending through the new tissue from one side to the other, while around them the fibroblasts or connective-tissue elements arrange themselves. From this it will appear that the coagulum which forms within a wound is desirable as a scaffolding upon which the process of repair may be begun. But it is desirable that this coagulum should be small in amount, in order that these processes may not be too long delayed; hence the advisability of removing all clots within a wound when closing it, and preventing the formation or leaving of dead spaces in the tissues in which blood clots may collect.
The process of granulation is not dissimilar to that described above, save only in its gross appearances. Granulations consist of vascular buds surrounded by leukocytes and lightly covered by them, while around the base of each bud epithelioid and spindle cells arrange themselves, these fixed cells organizing themselves more and more, as the wound fills up, with the more superficial layers of granulations. In time they are converted into a dense fibrous tissue which forms later what is known as the scar. As before, also, the spaces between the young capillary loops are filled with large nucleated cells derived from the fixed cells of the tissue, and from the endothelial lining of the newly formed vessels. Thus fibroblasts are produced in each case, and are often more or less mingled with giant cells, especially if some foreign body, such as a silk ligature, be embodied in the tissues. The particular function of the leukocytes seems to be the removal of red corpuscles and fibrin from the original clot.
The granulation tissue thus constituted by capillary loops and proliferating cells constitutes the basis of all wound repair. Later this tissue assumes more of the fibrous and less of the cellular character, while the fibroblasts arrange themselves in accordance with the mechanical requirements of the tissues and the stress or strain placed upon them. This tissue is at first vascular, but as it condenses its capillaries become less numerous and smaller, and the final white fibrous scar is usually almost bloodless.
[216]
When there has been loss of skin, or when skin edges are not brought together, the deeper process of granulation needs an epithelial covering, which cannot be afforded by mesoblastic or endothelial cells. The formation of an epithelial or epidermal covering is a process peculiar to epithelial tissue alone, and takes place mainly from the cells of the rete Malpighii.
Epithelial elements of the skin will afford a large amount of covering, and yet even their activity sometimes is insufficient and has to be atoned for by skin grafting. Should the granulating surface be small, and so situated that the fluid upon its surface may dry by evaporation, there will result a crust or scab, which, while it conceals from observation what is going on beneath, serves as an admirable protection, beneath which proliferation of epithelium takes place. A spontaneous detachment of the scab may take place when this process is complete, and with the loosening of the crust it is apparent that repair has become complete. This is known as healing under a scab or under a crust.
Two clean and healthy granulating surfaces may be so placed in contact with each other as to blend together by exactly the same process as that by which granulations are first formed. This is called secondary adhesion, or by the older writers the “third intention.” Advantage is taken of this possibility in the application of what are called secondary sutures, which may be placed some days before they are utilized, with the intent to bring together surfaces so soon as they shall present granulations.
One of the most interesting of all healing processes is that by which severed tissues, when promptly replaced, often reëstablish vascular communication and grow again in a satisfactory manner. Thus a severed ear, nose, or finger-tip may be replaced, and, if carefully held in situ, the parts being kept at rest, will prevent disfigurement and the loss of important tissues. In these cases the severed tissue remains passive several days until it has become vascularized. Meantime its nutrition seems to be maintained through the medium of the living tissues to which it has been affixed, probably by absorption of their blood plasma.
Two human tissues are essentially non-vascular, the cornea and cartilage. The former appears to be nourished by cellular interspaces which may admit leukocytes from the surrounding tissues, and through these proliferation and vascularization occur; while a scar in the cornea remains permanent, and the new tissue by which repair is brought about never becomes transparent like the cells composing the cornea proper. In cartilage scar tissue is produced, as in other tissues, by a similar process, in spite of the extent of the cartilaginous layer and its non-vascularity. In general the more specialized a tissue the less completely does it heal, and the specialized tissues, like the retina, etc., seem to be incapable of reproducing themselves. Low down in the animal scale some parts can be more or less reproduced. In the ascending forms there is less tendency in this direction; in man there is little reproduction of an original tissue, scar tissue taking the place of most of that which has been lost. An apparent exception to this is seen in the osseous system, where a large amount of bone may often be reproduced. Epithelium, also, whether on the external or internal surfaces of the body, can regenerate itself in large degree and amount. From every small island or mass of epithelial cells which can be retained new cells may thus be reproduced; hence accrues the advantage of leaving such epithelial collections whenever possible, and wherever they may be beneficial. If upon a burnt area it happens that epithelium has not been completely destroyed, new skin may be confidently looked for from each clump of epidermal cells. It should be remembered, however, that with the epidermization of a surface under these circumstances merely an epithelial covering is secured. The distinctively dermal appendages, such as hair, sweat glands, and sebaceous glands, are not reproduced. If the highest ideal results are to be secured in any case the parts must be put in the most favorable condition, which means early surgical attention to every wound.
Bloodvessels are subject to contusion, to laceration, and to incision. They may be contused by superficial blows, compressed against underlying bone, torn in the replacement of old dislocations, or punctured or incised by accidental or homicidal injuries. A vessel which is not abruptly divided but is seriously injured will usually sustain a separation of its internal and middle coats, which curl up within the external coat,[217] occlude the channel, and lead to thrombosis. A vessel thus occluded may tend to gangrene of the parts supplied by it or to a temporary ischemia, with numbness and pallor if an artery, or to passive edema if a vein. In cases of such injury it is always hoped that the blood supply will be provided through the collateral circulation. If a vessel be torn or cut across there may result a hematoma which may lead to immediate prostration, from hemorrhage, and to gangrene by stopping the blood supply. Such blood tumor rarely pulsates, but may cause extreme pain. The character and the size of the swelling will depend upon the tissues which surround the injured vessel. Cessation of the pulse on the distal side of an injury nearly always implies temporary occlusion. Traumatic aneurysm may be produced by lateral injury to an arterial trunk, by which its continuity as such is yet not completely disrupted.
If a large outpour of blood has occurred it will be safer to incise and turn out the clot and secure the injured vessel. In milder cases the surgeon should do all that he can by rest and by position to favor restoration of blood circulation. After the subsidence of acute symptoms massage and gentle motion will serve to promote absorption of the escaped blood. Cases will occasionally occur in which the principal arterial trunk of a limb should be tied, hoping thereby to save the member. Amputation may be the last resort when gangrene is impending.
Injury to the veins is of a less serious nature in so far as immediate consequences are concerned; nevertheless a punctured wound or a large vein is always a serious matter. The pressure of the blood may produce gangrene, or cause so large a hematoma that it should be incised.
Fine silk sutures may be applied to wounded vessels, arteries or veins, when they have been partially severed.
The healing process in all these cases is essentially the same. It may mean the formation of a clot in or around a vessel, followed by absorption of its principal portion and organization of what remains. A vessel itself which has once been occluded by thrombus will usually remain closed, a cord of fibrous tissue taking its place. Only in rare instances is continuity of the blood channel preserved or regained. In such cases the collateral circulation affords the life-saving feature. The granulations which intrude themselves into the clot gradually substitute tissue for coagulum, the conversion beginning promptly, but often occupying weeks for its completion.
Lymph vessels may be lacerated in almost any injuries and more or less lymph escape with the blood. When the skin is torn from the underlying parts lymph collects in the cavity thus made, while its wall may undergo more or less organization, and formation of a lymph cyst results. Should one of these connect with a good-sized lymph duct, as, for instance, in the neck the thoracic duct, then lymph cysts of considerable size might form. Should these rupture or be opened lymph fistulæ might result.
By small hemorrhages into a nerve sheath nerve function may be either temporarily or permanently disturbed. A compression too long-continued may lead to degeneration within the nerve fibers. Providing this do not occur there may be complete restoration of function, or there may result chronic neuritis, with pain and irritation. A later consequence of all nerve injuries is more or less serious disturbance of sensation, while still later parts supplied by the affected nerves may undergo more or less atrophy as well as spastic contraction, by which loss of function and deformity are produced.
There is a form of nerve injury which is due to the temporary pressure of the elastic tourniquet, frequently applied around limbs previous to operations, or to pressure which is made by crutch handles upon the axillary plexus, and called crutch paralysis. Limbs carelessly allowed to hang over the edge of the operating table during prolonged operations also have suffered in the same way. Such lesions are of the character of a contusion, but are often followed by paresis, paralysis, and by various sensory disturbances.
Injury to a nerve trunk having been recognized by a study of the local features of a given case requires special treatment in case laceration or more localized division can be assumed. The nerve known to be lacerated and torn across should have its ends freshened and be reunited by fine catgut sutures; also a nerve trunk known to be punctured or divided. Such injury is not necessarily inflicted from without, as it may be[218] produced by a fragment of bone; in this case the operation should be directed toward the bone as well as toward the nerve trunk itself. A divided nerve trunk, if neatly sutured, heals by the organization of blood clot, as in other instances, actual nerve communication being made across the intervening clot by a process of regeneration or reduplication of the true nerve elements, the peripheral neurilemma playing an important part. Autogenetic power decreases with the age of the individual. By careful nerve suturing disability may be prevented.
Even months after injury much can be accomplished by nerve suture properly performed. Symptoms similar to those of division may occur when a nerve trunk is surrounded and compressed by bone callus after fracture, as when the ulnar nerve is thus caught. If too long a time have intervened it may be necessary to exsect the injured portion and then bring the ends into apposition by sutures. Other methods of atoning for these nerve injuries by nerve grafting, etc., will be described in the chapter on Surgery of the Peripheral Nerves.
Neuritis may be overcome by counterirritation, preferably with the actual cautery, i. e., the “flying cautery,” by massage, and by galvanization. The pain in many of these cases can be mitigated, if not completely relieved, by the x-rays, or by the high-frequency current. In some cases nerve elongation may be brought to bear and a tender and irritable nerve be thus brought under subjection.
Lacerations or divisions of muscles are usually repaired at first by fibrous tissue, the result of organization of a clot. Later a true muscle regeneration takes place and muscle scar finally disappears. Atrophy of a muscle is not a sign of injury directly to itself, but often results from injury to the nerve which supplies it; for example, the circumflex nerve may be injured in shoulder dislocations, while the deltoid muscle, which is supplied by it, speedily undergoes atrophy.
Muscle fibers may be torn by violent exertion. Such an accident may be followed by pain and loss of function. An interval can often be felt, even from the outside, between the torn muscle ends. The injury will produce considerable hemorrhage. The amount of function regained in a muscle will depend to some degree on the extent of its injury. If it have been injured by an incised wound it will depend upon the way in which it is brought together after an open incision. The origin and insertion of such a muscle should be approximated by proper position, and so maintained by the dressings, in order that perfect rest may be more easily maintained. When a portion of the fascia or aponeurosis is torn the muscle fiber may protrude and form a hernia of muscle.
Tendons often suffer from contusion, in consequence of which they may become adherent within their tendon sheaths; this leads to stiffness of the part and more or less loss of function. Sometimes they calcify, as does the adductor magnus tendon in the formation of the so-called rider’s bone. The tendon most frequently injured is that of the quadriceps, near the knee.
If it can be decided that a tendon has been divided or torn across its prompt reunion by suture should be always practised. Also a divided muscle, if exposed, should be drawn together with sutures, chromic or hardened, so as to make them more reliable. Tears of aponeuroses and fasciæ should also be sutured. Tendon suturing is nearly always successful, especially if it can be done in a cleanly manner; while tendon grafting is a measure which may be reserved to overcome the consequences of injuries to muscles and tendons not disposed to repair.
Aside from simple and compound fractures, which are essentially bone wounds, there may be seen hemorrhages beneath the periosteum or in the immediate vicinity of bones, which are usually small in amount, yet may cause considerable disturbance. The traumatic hematoma of the scalp which often follows delivery is an illustration of an injury of this class, the periosteum itself being sometimes separated. Collections of blood under these circumstances which fail to disappear by absorption may be incised and the contained clot turned out.
PLATE XII
FIG. 1
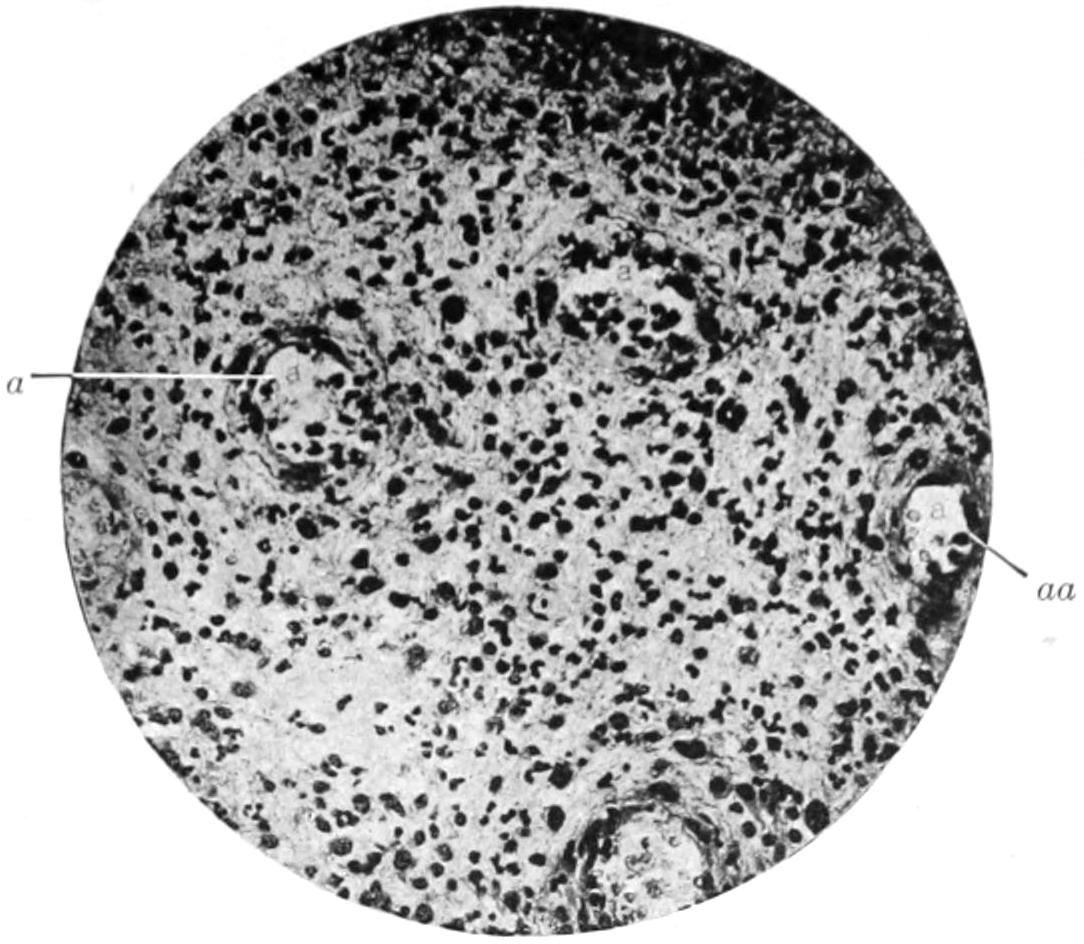
Young Granulation Tissue Following Bur., a, aa, thin-walled capillaries. Large nuclei, fibroblasts horseshoe nuclei, leukocytes. × 250.
FIG. 2
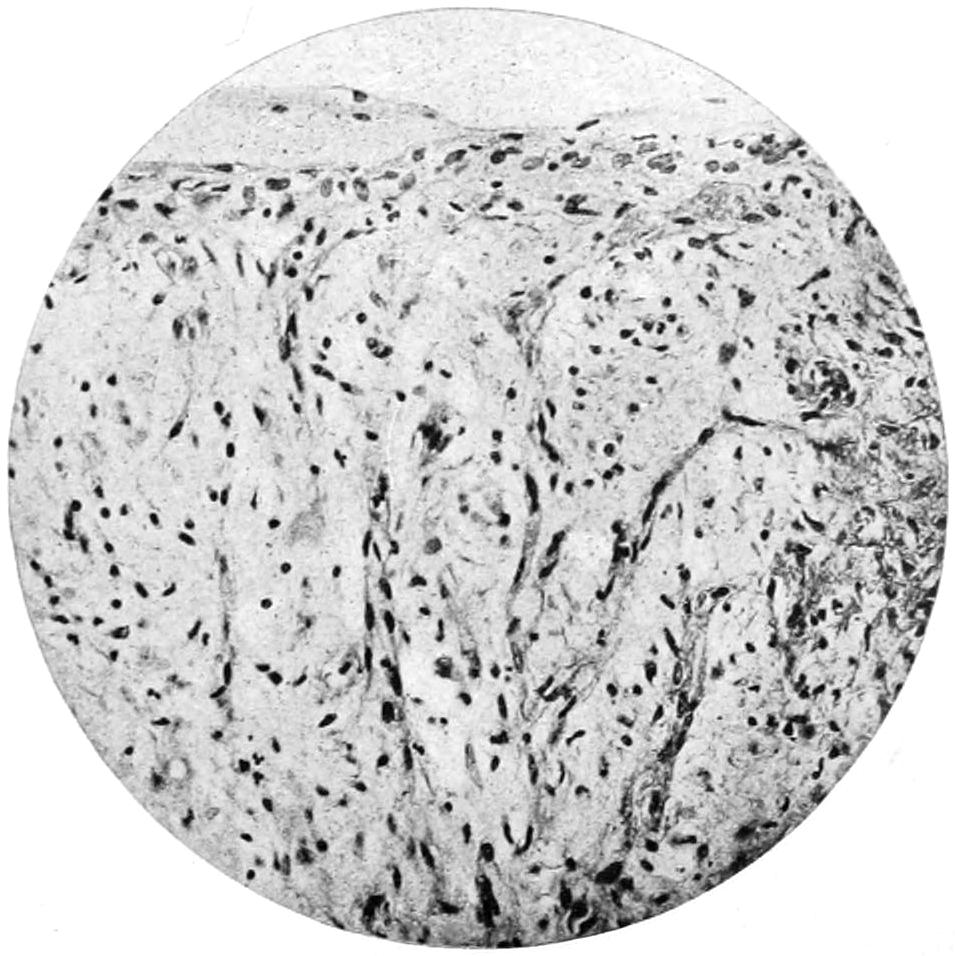
Young Scar. Numerous capillaries perpendicular to surface. Spindle elements, fibroblasts considerably smaller than in Fig. 1. × 250.
FIG. 3
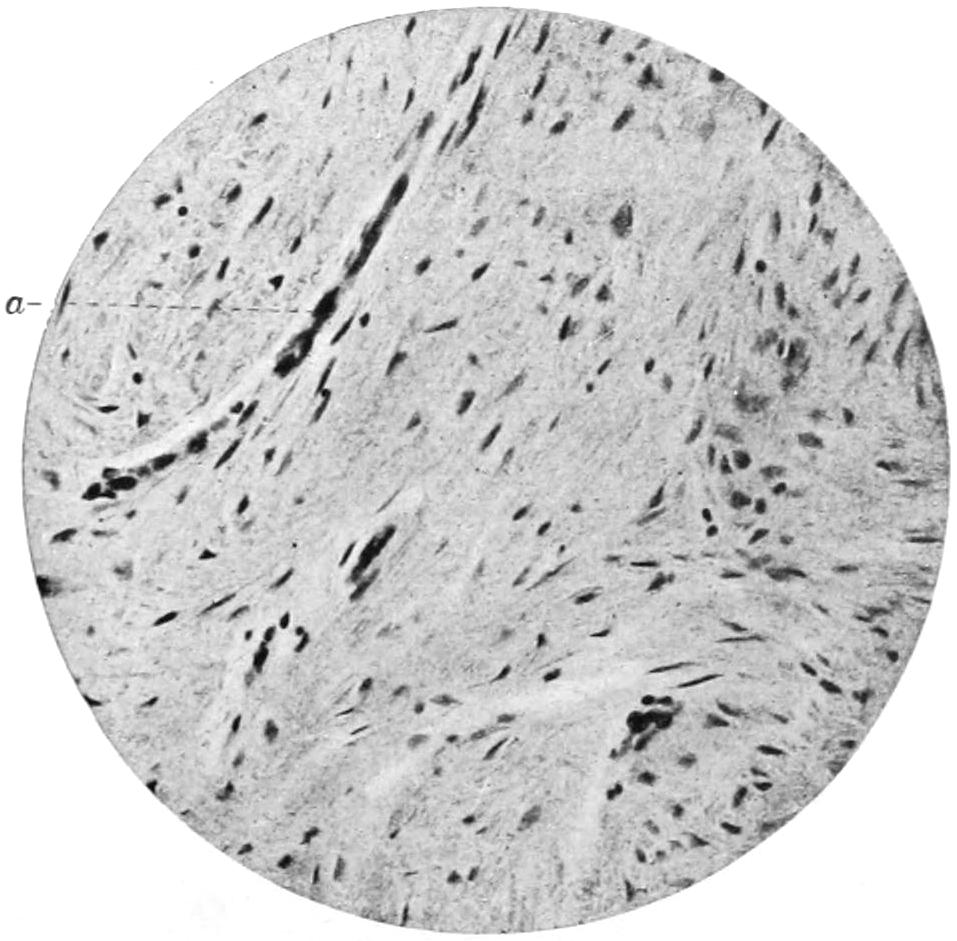
Mature Scar. Dense fibrous connective tissue with a few fibroblasts. At a, a small bloodvessel. × 250.
Granulation Tissue organizing into Cicatricial Tissue. (Karg and Schmorl.)
Illustrating statements made on several of the foregoing pages.
[219]
Contusions of the viscera may be followed by many and disastrous consequences. They compromise such lesions as rupture of the liver, kidney, spleen, laceration of the bowel, bladder, or gall-bladder, and may occur by blows which do not break the surface; or any of the viscera may be lacerated, punctured, or gashed by gunshot, punctured, or incised wounds. These will be more completely considered in Chapter XLV.
[220]
Gunshot wounds are usually considered with the special subject of military surgery. Military surgery as such, however, consists in the application of general surgical principles. Nevertheless a gunshot wound is essentially the same whether it be received upon the battle-field or in civil life, and the injury inflicted by a piece of flying shell is in no sense different from that which may be received in a blasting accident.
A gunshot wound is always contused and lacerated, and often punctured. According to its size and shape, its location, the nature and velocity of the missile, the distance at which the weapon was discharged will depend its severity and prognosis.
Shot vary in size from those which weigh but a fraction of a grain to buckshot which weigh nearly one-third of an ounce. Revolver and pistol bullets vary in diameter from 0.22″ to 0.45″, and in weight from twenty-five grains to ten times that amount, and nearly always of conical form. They are usually made of compressed lead, sometimes hardened by the addition of tin or antimony.
The old military weapons, such as the Springfield rifle, have been entirely abandoned, and for them have been substituted rifles of smaller bore, projecting bullets of from 0.25″ to 0.31″, varying in weight from one-fourth to one-half ounce and attaining a muzzle velocity of nearly 2500 feet per second. They have, therefore, a much increased range and may kill at two miles. Their trajectory is flatter and the character of the wound caused by these modern weapons is different from those inflicted, for instance, during the Civil War. The bullets now in use in the armies and navies of the world are nearly all encased in a thin covering of steel, copper, etc., which is known as the jacket or mantle. They are from 3.5″ to 4″ in length, possessing a much greater range than a shell bullet, while the rifling of the weapon is so made as to give them a more rapid rotation. In active service, moreover, these are usually fired with smokeless powder. The so-called “dangerous zone,” i. e., that where mounted men or infantry can be injured, is much wider than formerly.
In India the practice has been introduced of leaving the point of the bullet uncovered by the mantle, so that when it strikes it would “mushroom”—especially in the bone. These “Dumdum bullets,” as they are called, from the place of manufacture, inflict much more serious injuries than do the relatively smooth perforations made by the others, and have been considered so cruel that they are excluded from use in civilized warfare.
During the Russo-Japanese war, in which nearly all previous records were broken, the deaths from gunshot wounds constituted but a small proportion of the entire loss in camp and warfare, a larger number of soldiers dying from disease and exposure. Statistics also show that out of every 100 cases of gunshot wounds 12 per cent. have been produced by bullets, the remaining portion being caused by shell, etc. De Nancrède has epitomized some interesting figures which may be here quoted: In the United States army during the Spanish war 4750 casualties were accurately studied; of these wounds of the lower extremities constituted nearly 33 per cent., those of the upper extremities nearly 30 per cent., those of the trunk a little over 22 per cent., and those of the head and neck a little over 15 per cent. During the South African campaign the mortality among the wounded was 5.7 per cent., essentially the same as that during our Cuban and Filipino campaigns, and in marked contrast to the 14 per cent. mortality of the Civil War. Considering that with our Mauser weapons the trajectory is practically flat up to 500 yards, and they may kill up to a distance of two miles, it will be seen that this difference in figures is important. The British discovered in their campaign against the Afghans, who were using antiquated weapons, that their own Lee-Metford bullets would pass through their enemies without disabling them, while the British soldiers who were once struck by the large, soft-lead bullets of their antagonists were far more seriously injured or absolutely disabled.
[221]
As one explanation of the injury inflicted by modern projectiles there has been advanced the theory that a bullet with a high-muzzle velocity, striking an object while it still retains most of its original speed, compresses and forces ahead of it into the wounded tissues a small column of air, which, exercising an expansive force, produces more or less explosive effect, that may be seen along the bullet track or at the point of exit. These explosive effects are proportionate to the size of the bullet, its bluntness, and its velocity. This theory was more tenable in the days of large and blunt projectiles than today, for in time past experiments have shown that when a bullet is dropped into water from a height there is forced into the water along with it a certain amount of air, estimated by Longmore at twenty times the actual volume of the bullet itself. It may be doubted, however, whether the rifle projectiles of today can produce sufficient air pressure to cause the destructive effects thus attributed to it.
Fig. 47
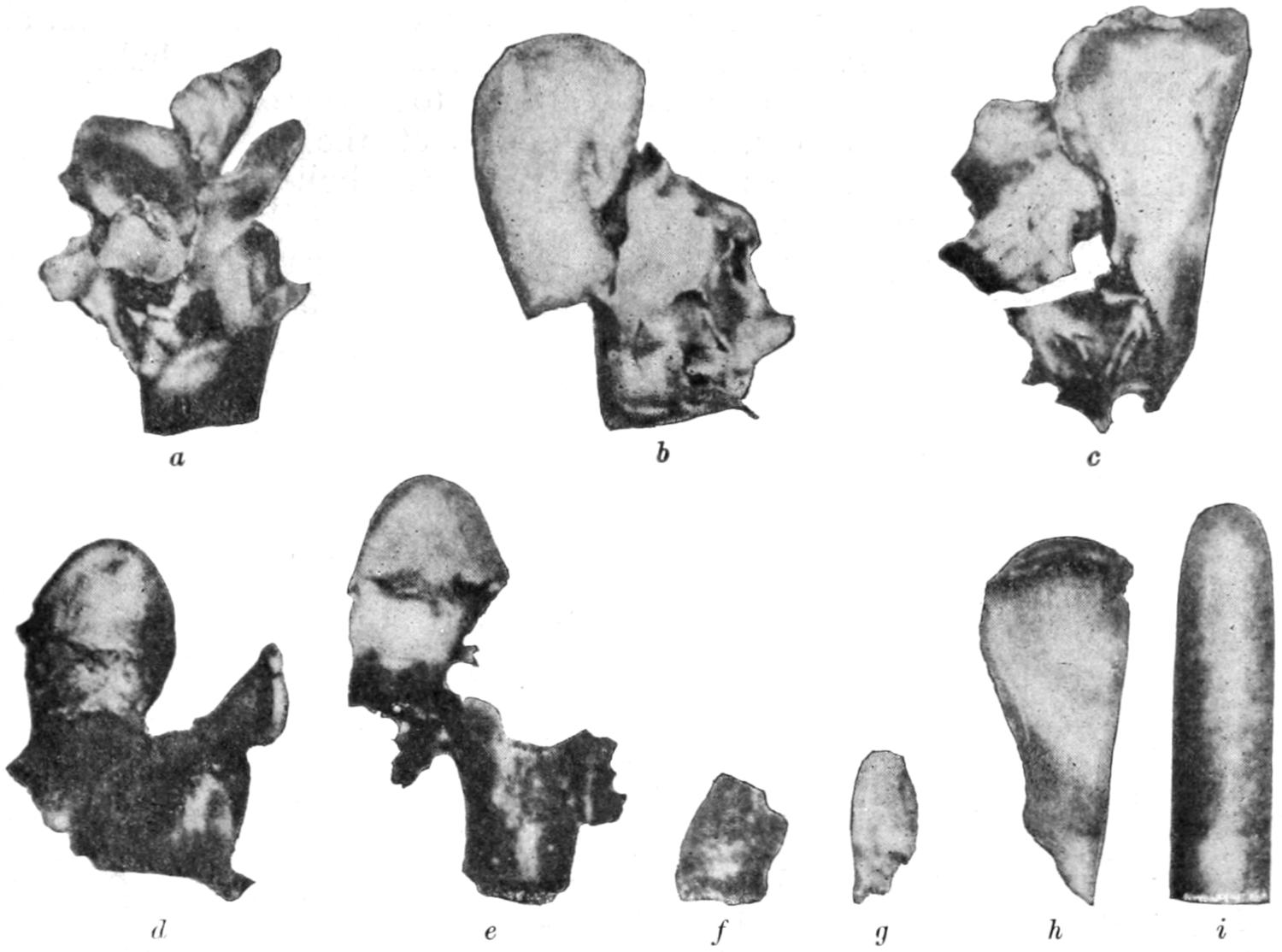
a, completely shattered after perforating a horse’s thigh-bone at 220 yards; steel mantle stripped; b, ball with mantle torn off and rolled up, core deformed, after shattering human tibia at 60 yards; c, wholly disorganized ball, which destroyed middle metatarsal bone of horse at 660 yards, steel-mantled; d, ball which shattered a human femur at about 750 yards, steel-mantled; e, remains of steel mantle and part of core lodged in human femur, wound inflicted at about 1100 yards; f, g, fragments of mantle found near the orifice of the wound of exit at about 1100 yards’ range, steel-mantled; h, piece of steel mantle split off by striking a dried horse’s metatarsal at over 1300 yards; i, steel-mantled ball which perforated the internal femoral condyle and lodged beneath the skin at nearly 2200 yards. (Recent foreign report.) (De Nancrède.)
Another method of accounting for shattering effects noted in many of these wounds is hydrodynamic pressure, depending upon the incompressibility of fluid and of tissue containing it, and the narrowing of the space occupied by fluid as a result of the transfer of pressure in all directions. Other things being equal, the most marked effects would be manifest in organs containing the most fluid, the effect increasing with the amount of fluid, the speed of the bullet, its size, and any alteration of shape which it has undergone in transit. It has been shown that the hydrodynamic pressure of steel-jacketed modern bullets varies from six to eight atmospheres. This theory accounts for the peculiar destructive effects seen in the brain, the heart, the stomach, and intestines when struck at short range.
Another method of accounting for the results of a bullet wound takes account of the peculiar effect due to the rapid rotation of the bullet, the movement given it by the rifling of the barrel from which it is fired. It appears that a bullet travelling at the rate of 620 meters per second will average about four rotations per meter. Even in passing through[222] a human body this would scarcely give it but two rotations in transit, while in passing through any given bone the force would be too slight to be appreciable.
While the theories mentioned above, the hydraulic and hydrodynamic, are attractive, yet they are unsatisfactory; we can do little more than sum up the damage done by a rifle ball as due to arrest and divergence of its energy, penetration depending upon its remaining velocity, its preservation of its original shape, and the resistance offered by the part injured. If the latter be great, and its shape be but slightly changed, there are pronounced explosive effects. Moreover, one end of the bullet is a little heavier than the other, and this will tend to produce a certain amount of tilting, by which a key-hole wound may be also produced. Fig. 47, from De Nancrède, shows the many alterations in shape which may be produced under various circumstances. Again, hard-metal jackets or mantles may be stripped off bullets before the latter reach the body, or in passing through it, as has been shown.
Bruns has shown that with the ordinary small arms the size of the wounds of entrance and exit diminishes with the decrease in velocity or increase of the distance, although allowance should be made for the manner and angle at which the bullet strikes the surface, the wound being circular or oval according to these conditions. The wound of exit will depend upon the direction of the axis of the bullet at the instant it leaves it; thus it may be oval or irregular. When the bullet in transit shatters or comminutes a bone the wound of exit may be made much larger and more ragged than otherwise. In a general way Bruns makes the statement that, other things being equal, the damage inflicted by the escape of a projectile from the body varies according to distance from the weapon. Thus up to fifty meters a considerable amount of destruction of muscle, etc., may be produced. The area is small and the track of the bullet is smooth and little larger than the caliber of the projectile. Between 100 and 300 meters there is little destruction of muscle, and the wound of exit is smooth and may contain some bone debris. Thus Bruns would make it appear that the distinguishable characteristics of near and distant shots appear in the variations to be noted between the wounds of entrance and exit.
After a careful study of the alterations in the shape of the bullets themselves, Coler and Schjerning reported at the Twelfth International Medical Congress that only in 4.5 per cent. of all hits does deforming of the bullet occur; if hits in the bones only are considered, the percentage would be much greater. In wounds of the other parts alone there is rarely any deforming effect upon the projectile. They also show that careful distinction must be made between the deformity of the bullet caused by the body and that resulting from impact upon some object before reaching the body. Thus if a bullet have first struck a branch of a tree, or some object upon the ground, it may have become so altered in shape as to correspond almost to a Dumdum bullet. The harm done by such a ricochet shot depends upon its unexpended energy and its altered shape, but will always be greater than if it had struck in the direction of its long axis.
The question of the heat imparted to a projectile in its course and the possibility of its being sterilized by such heating are questions which have been carefully investigated. The heat of a bullet produced by penetration into a hard material will depend upon the striking distance and the density of the material. In the human tissues the heat attained by a bullet, even when penetrating a bone at short range, is rarely 100°C., while at long range it will scarcely amount to half of that. There is no accurate measure of the heat that may be engendered in its passage through the atmosphere, but the question is one of interest, in that it brings up the possible sterilization of the bullet and its capacity for destroying such septic material as it may carry in with it. A series of experiments made in Baltimore and elsewhere permit the following conclusions to be drawn:
1. The majority of cartridges in their original packages are free from septic germs, this freedom being due to the precautions observed during their manufacture.
2. As a result of this cleanliness the majority of gunshot wounds are not septic.
3. Such resistant germs as those of anthrax, when applied to the small bullet of a hand weapon, are rarely completely destroyed by the act of firing, and it is possible to infect an experimental animal with such a projectile.
4. The ordinary germs of suppuration are not always destroyed, and may also cause infection.
These conclusions may be epitomized in these two statements: that bullets from[223] small hand weapons are not necessarily sterilized by the act of firing, and that they also may infect.
The principal features to be noted in a case of gunshot wound are the following:
—Hemorrhage may be internal or external. When internal it is rarely so accessible as to permit of the saving of life, yet the effort should be made to ascertain the source of the hemorrhage, as only in this way can life be saved. For example: A patient may bleed to death from injury to an intercostal artery, an epigastric, etc., while in either case a very simple expedient would tend to save life. External hemorrhage is generally due to injury of main vessels, and may end fatally unless first help be instantly rendered. Since the introduction into the army of a trained hospital corps, and a widespread diffusion of a knowledge of “first-aid dressings,” this is much less likely to occur than in the days previous to the use of the emergency packet. Recent military experiences have been that hemorrhages from limb vessels are much more likely to subside spontaneously than those of the viscera.
—Shock is present in a large proportion of gunshot injuries, especially those of the viscera and the region of the spine. Experienced army surgeons speak of the peculiar facial expression in those cases of shock which demand immediate attention.
—The symptom of pain is exceedingly variable. It is rarely complained of at the time of infliction, especially when the individual is laboring under stress of excitement. The pain of a wound will be increased by every movement of the body. When momentary pain is followed by local anesthesia, and especially if the latter be permanent, it will indicate the division of a nerve trunk, which will justify an operation for exposure of the site of the injury and nerve suture.
—Powder burn is met with only as one of the complications of a short range and injury of an exposed part. Its degree is modified by the distance of the injured part from the muzzle, by the character of the powder, and the dimensions of the barrel. Fish has shown that in a pistol wound at short range the burning or scorching effects, which he calls the “brand,” are always found on the hammer side of the weapon which inflicted the wound, i. e., if the hammer were held up the brand would be above the entrance wound. The bullet wound in such a case shows the direction of the aim, but the recoil will so far change the direction of the barrel as to divert the stream of gases of combustion, so that they follow the new direction of the barrel, which is always toward the side of the hammer. This is a point in medical jurisprudence which has been testified to in the courts. The use of smokeless powder minimizes any effect of this kind. It has been claimed that a homicide has been recognized in the dark by the flash of the old-fashioned gunpowder used in the weapon, but the use of smokeless powder would obviate this possibility. The most distinctive part of a powder burn is the appearance of the tattooing caused by the lodgement under the skin of grains of unconsumed powder. Such grains, when accidentally or purposely contaminated with germs, are not purified by the act of firing. This is less true of certain brands of smokeless powder. Nevertheless the opinion prevails that gunpowder may serve for conveyance of infection. The so-called smokeless powders are of secret composition, although it is known that in a general way they are composed of gun-cotton, dynamite (i. e., nitroglycerin), or picric acid. Melinite is composed of picric acid and collodium—i. e., gun-cotton. There are many of the modern explosives which depend for their final effect upon the combination of two or more substances. In the smokeless powers there is usually enough nitroglycerin to have a very noticeable effect should they be touched to the tongue, while even the fumes might be disagreeable or disabling.
—The greater the distance and the smaller the velocity the more likely is a bullet to lodge within some[224] portion of the body instead of passing through it. In the Cuban campaign the proportion of cases of lodgement was less than 10 per cent. of the entire number of bullet wounds. A bullet which rests within the body either will or will not produce disturbances which may be more or less lasting. In a large proportion of cases the latter will prevail. The number of pensioned soldiers who are carrying unremoved bullets in some portions of their body is by no means small. A rifle bullet may remain in certain portions of the cranium without producing much disturbance. Bullets which cause no trouble are best left undisturbed. Those which produce serious symptoms should be removed. To Esmarch is attributed the dictum that the harm produced by a bullet is usually done during its passage, and after it has found lodgement it ceases to be a source of trouble. While not invariably true, this is so generally the case that acceptance of this statement has revolutionized the previously prevailing view, i. e., that a bullet should be always removed if it be possible to locate and extract it. In some instances it may be located by a study of the symptoms; as, for instance, in certain areas of the brain, or when lying in close proximity to joint surfaces it interferes with their function; although a bullet embedded in bone often does not seriously interfere with the use of the affected part. The bullet which divides a nerve trunk rarely lodges in such position as to be considered when the repair of the nerve injury is undertaken; such wounds will generally be found to be perforating.
Fig. 48

Multiple shot wounds of arms and back. The ulcer over the spine was produced by pressure, not by the ball (case in Cincinnati Hospital, 1884). (Conner, Dennis’ System of Surgery.)
—The same bullet may sometimes inflict multiple wounds, and, with modern projectiles, these are now more common, as many as six wounds having been made by one missile in its passage, e. g., wounds of the arm and body. Thus multiplicity of wounds may not indicate that the patient has really been shot more than once. In cases of perforation, for each wound of entrance there should be found one of exit, and at the first examination of the patient the discovery and consideration of each of these injuries should be part of the routine. If on examination but one wound be discovered, then the inference is natural and unavoidable that the bullet is still within the patient’s body (Fig. 48).
—The entrance of fragments of cloth or other extraneous matter is now less frequent, for bullets of tremendous velocity rarely carry[225] in any perceptible material, their diameter being small and their surfaces polished. A ricochet bullet may carry tetanus or other spores from the earth, and lockjaw may be the result. In other words, gunshot wounds now are less likely to become infected wounds than they were years ago.
—The shattering and explosive effects of the impact of bullets upon certain of the viscera are sometimes disastrous, and yet not easily seen from the outside. This is especially true in the brain, heart, liver, spleen, kidneys, and bones. Almost complete pulpification of the semisolid viscera may occur as the result of perforation by a small missile, and the general condition of the patient should be relied upon to indicate this fact.
usually implies perforation of at least a portion of their contained viscera. Thus if a man be shot through the chest it may be assumed that perforation of the lung has occurred, while in a case of bullet wound of the abdomen it will rarely be found that the viscera, especially the intestines, have escaped perforation. Still, remarkable cases are occasionally recorded. Thus I have seen a man who had been shot through the abdomen from front to back, the bullet entering just above the pubis and escaping near the lumbar spine, who never seemed to have suffered seriously from his injury, although the bullet was a large soft one from the old Springfield musket.
—More or less characteristic appearances pertain to most wounds of entrance and of exit, which render them reasonably distinct and recognizable, even though no history be obtained. Nevertheless much depends upon distance, velocity, and any deformation of the bullet due to its impact upon some other substance previous to its entering the body. An elongated wound may suggest that the direction of the bullet was at an angle with the surface struck. Such wounds are known as “key-hole” wounds. A bullet already deformed may inflict a wound that will baffle speculation. The wound of exit is usually a little larger than that of entrance. When much larger a bone lesion should be expected. Trifling punctures, perhaps made by particles of the bullet, may be found around the principal wound or in the bone which it has shattered.
Diagnosis may include a recognition not merely of the general character of the injury, but whether it was inflicted by one or more bullets; whether these bullets have escaped; and if not, in what part they are probably lodged. In the preantiseptic days much of this information was gathered by the use of the probe, and the porcelain-tipped probe devised by Nélaton was relied on for much more than it could possibly safely tell. In those days probing was indiscriminately practised, and accomplished more harm than good. Now the probe is rarely used, at least at first, and when used, it is connected with some electrical device by which results are attained with a minimum of handling. For this purpose the telephone probe of Girdner was formerly a popular and ingenious device, which has been more recently supplanted by a simpler mechanism by which, when the end of the probe comes in contact with metal, a little bell, or buzzer, is rung. No probe or other instrument should be introduced into a gunshot wound, for diagnostic or other purposes, without observing aseptic precautions.
The most valuable expedient for the detection and location of bullets, as of other foreign bodies, is the Röntgen ray. With a suitable apparatus of this kind the surgeon can not only decide as to the location of the missile, but whether it is best to attempt an operation for its removal.
—In gunshot wounds not speedily fatal the prognosis depends upon the part injured, the size and shape of the missile, its velocity, the distance from the weapon, the amount of blood lost before attention was given, the character of the attention first received, and the absence of such complications as exposure, rough handling, etc. The dictum that the fate of a wounded man is in the hands of the surgeon who first attends him made its author, Esmarch, famous. The patient having escaped the dangers of hemorrhage and shock is to be carefully guarded from sepsis, and if thus guarded can be protected against most of the other visible dangers save those due to perforations of large cavities. If, therefore, a gunshot wound can be promptly provided with a primary aseptic or antiseptic dressing, and in other respects be let alone, the outlook for the patient will be encouraging. The prognosis often depends upon how completely the patient is let alone after the application of occlusive dressing.
—Hemorrhage is the first consideration, and should be the first care of the surgeon. Digital pressure may be resorted to, which may suffice until a temporary[226] expedient has been supplied. Next in importance is disinfection of the area surrounding the wound and the application of a sterilized absorbent dressing, with pressure to prevent loss of blood. The use of the probe, or any attempt to at once ascertain the location of the bullet, is not advisable. The question is not, “Where is the bullet?” but, “How much harm has it already done?” And the first attention should be addressed to atoning for any harm that may have been done. Even though the intestines have been perforated, or the heart wounded, there is no need in doing anything more than meeting the immediate emergency. If shock be extreme it may be atoned for in some measure by lowering the head and bandaging the extremities; while in extreme cases hypodermoclysis or venous infusion of saline solution, often with the addition of a little adrenalin, will be of service.
Again, physiological rest of the part injured, i. e., immobilization, as well as absolute rest of the patient’s body and mind, must not be neglected.
Primary laparotomy has been done upon the battle-field, and is of itself a testimony to the intrepidity and zeal of those who have done it; yet, as a practice, it is to be condemned. All operations upon gunshot wounds should be done in a well-equipped hospital.
Fig. 49
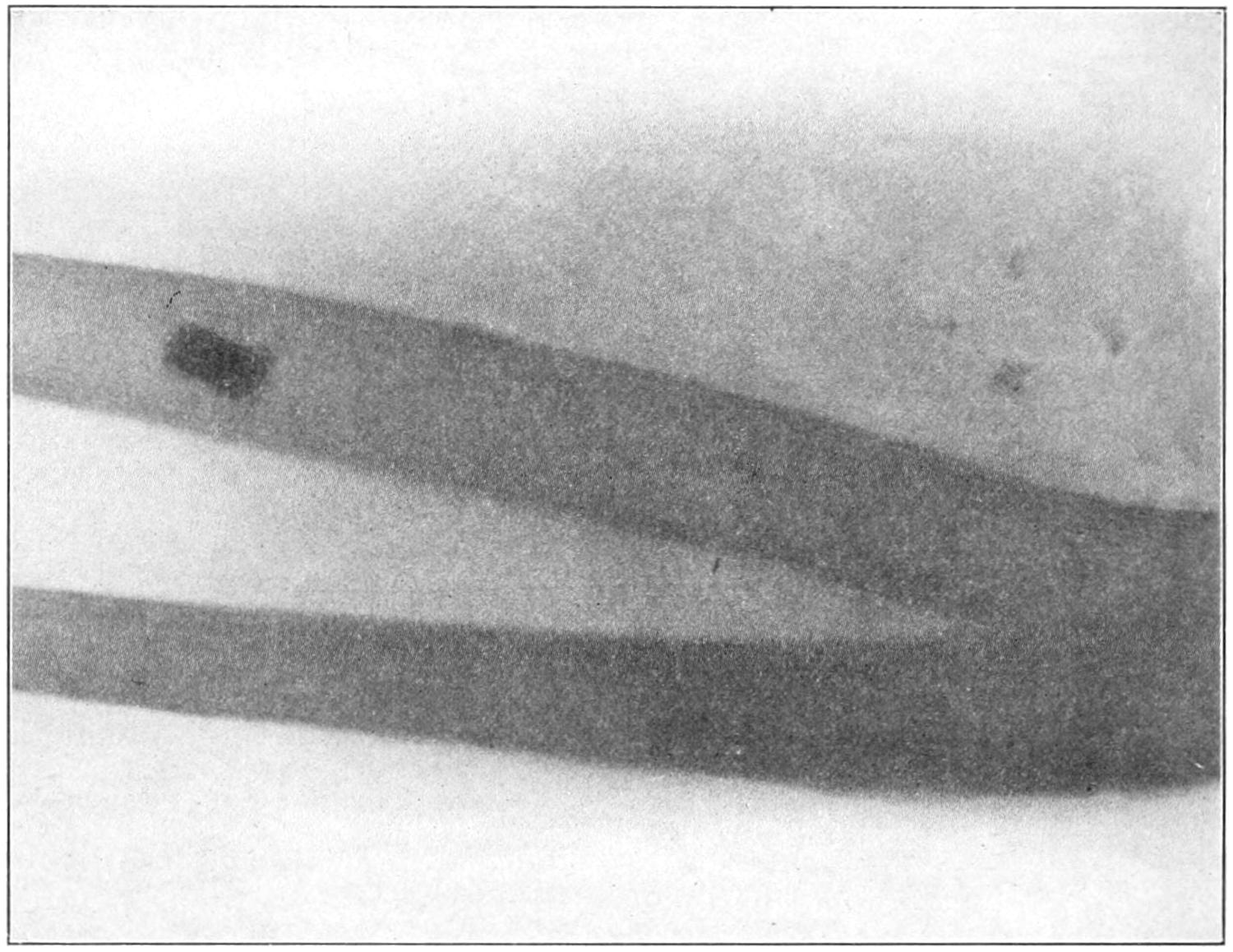
Gunshot wound of forearm. Bullet in situ in bone.
The probing of bullet wounds is so unwise that it may be well to state the reasons for its general condemnation:
1. As it used to be practised, neither probe nor skin nor the operator’s hands were sterilized.
2. Even when carefully done it is often absolutely disappointing, the probe failing to reveal the presence of the bullet.
3. By the time the probe is introduced the wound will be usually more or less filled with blood clot. To stir this with a probe is to invite a secondary hemorrhage or annoying oozing.
4. Even when properly used the probe may carry in infectious material from the surface.
5. Most wounds made by modern bullets, even pistol bullets, are of such a character that it is difficult to follow their track without using force.
6. I have known a wound on the anterior surface of the body to be probed for a bullet that had escaped, as shown by an examination of the other side of the body, which the attendants had failed to search.
[227]
7. If there be good reason for exploration of a wound let it be postponed until the surgeon is prepared to follow a bullet and extract it. When it does not call for extraction, it does not call for probing.
8. The best probe is the surgeon’s finger, and for its use the patient generally requires an anesthetic and free incision.
When muscle is torn and needs suturing, or when tendons or nerves are divided and need the same resource; when bones are shattered and fragments need to be removed; when the skull has been fractured and portions of bone driven into or upon the brain; when the intestines have been perforated; when even the heart has been wounded and the pericardium is filling with blood so that the heart’s action is becoming impeded; in any or all of these emergencies the patient needs surgical relief. But this should be of a kind that, save in an emergency, should be postponed until suitable preparation can be afforded.
Fig. 50
Fig. 51
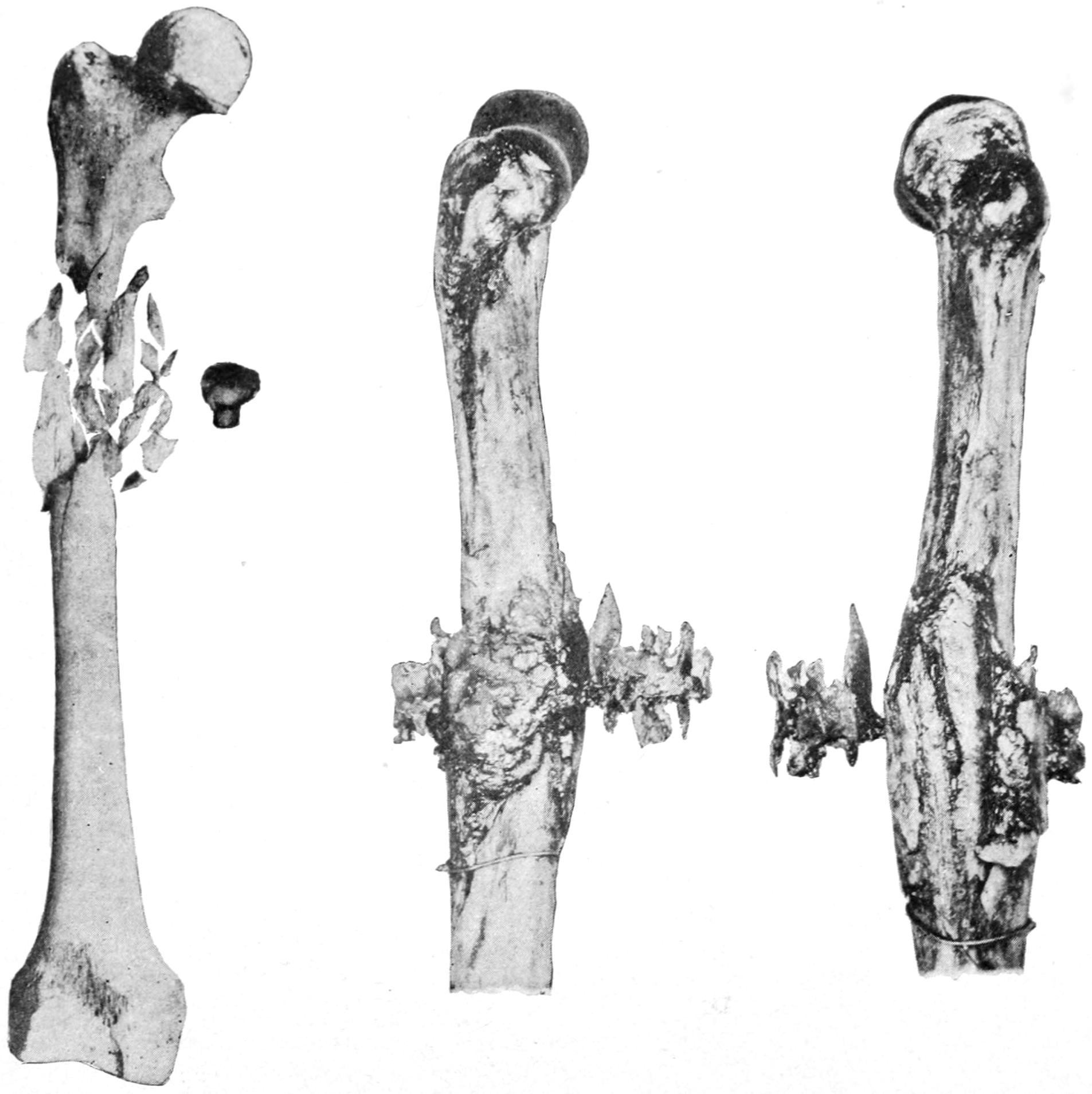
Wound inflicted at 1300 yards by steel-mantled ball (from a recent foreign report). (De Nancrède.)
Shattering of humerus at long range with modern projectile; fusible metal cast showing extent and character of laceration of soft parts (from a recent foreign report).
In regard to regional indications in the treatment of gunshot wounds it will only be possible here to give some brief general hints, the reader being referred to the chapters on Regional Surgery for more specific instructions. Nearly all gunshot wounds of bones are compound fractures, and are comminuted as well. The best treatment is primary aseptic occlusion and immobilization, without effort in the direction of exploration. In an open wound the vessels should be secured, loose pieces of bone removed, and jagged bone ends trimmed; while in some instances a wire suture or other[228] mechanical expedient may be resorted to with advantage. Provision should also be made for drainage.
In the regions of the large joints the same general principles are applicable. Under the old regime a gunshot wound of the knee would condemn a person to amputation in the middle of the thigh. Now, if such a limb be promptly provided with suitable antiseptic dressing, and placed at rest, the patient may save not only the limb, but the use of the joint. Extensive comminution may call for excision. Amputation is seldom necessary, except when important bloodvessels have been divided.
Fig. 52
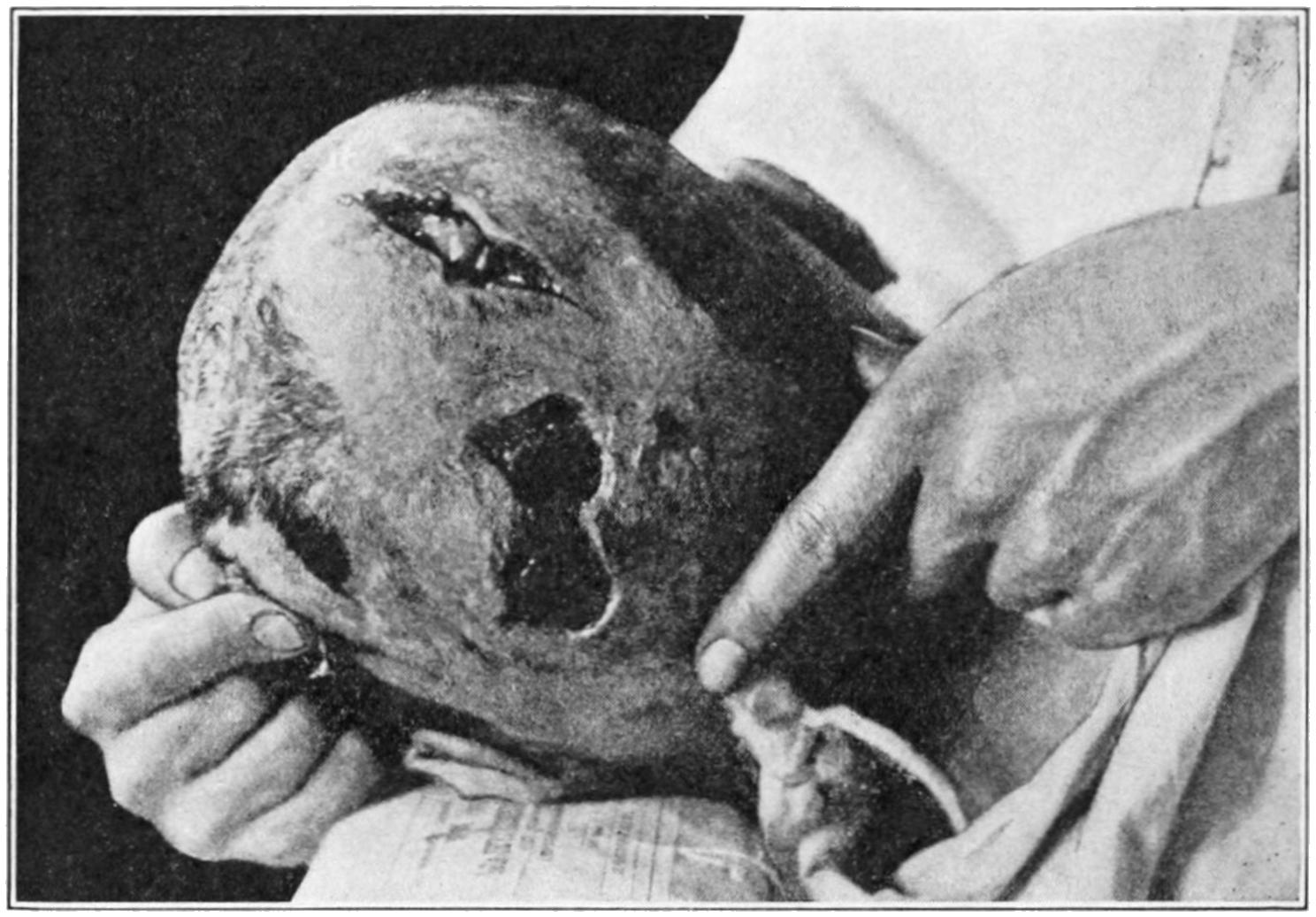
Perforating bullet wound of head, wound of exit showing brain protrusion. Sloughing pressure-sore of scalp. Complete paralysis of motion and loss of speech. Battle of Mukden. (Major Charles Lynch.)
Fig. 53
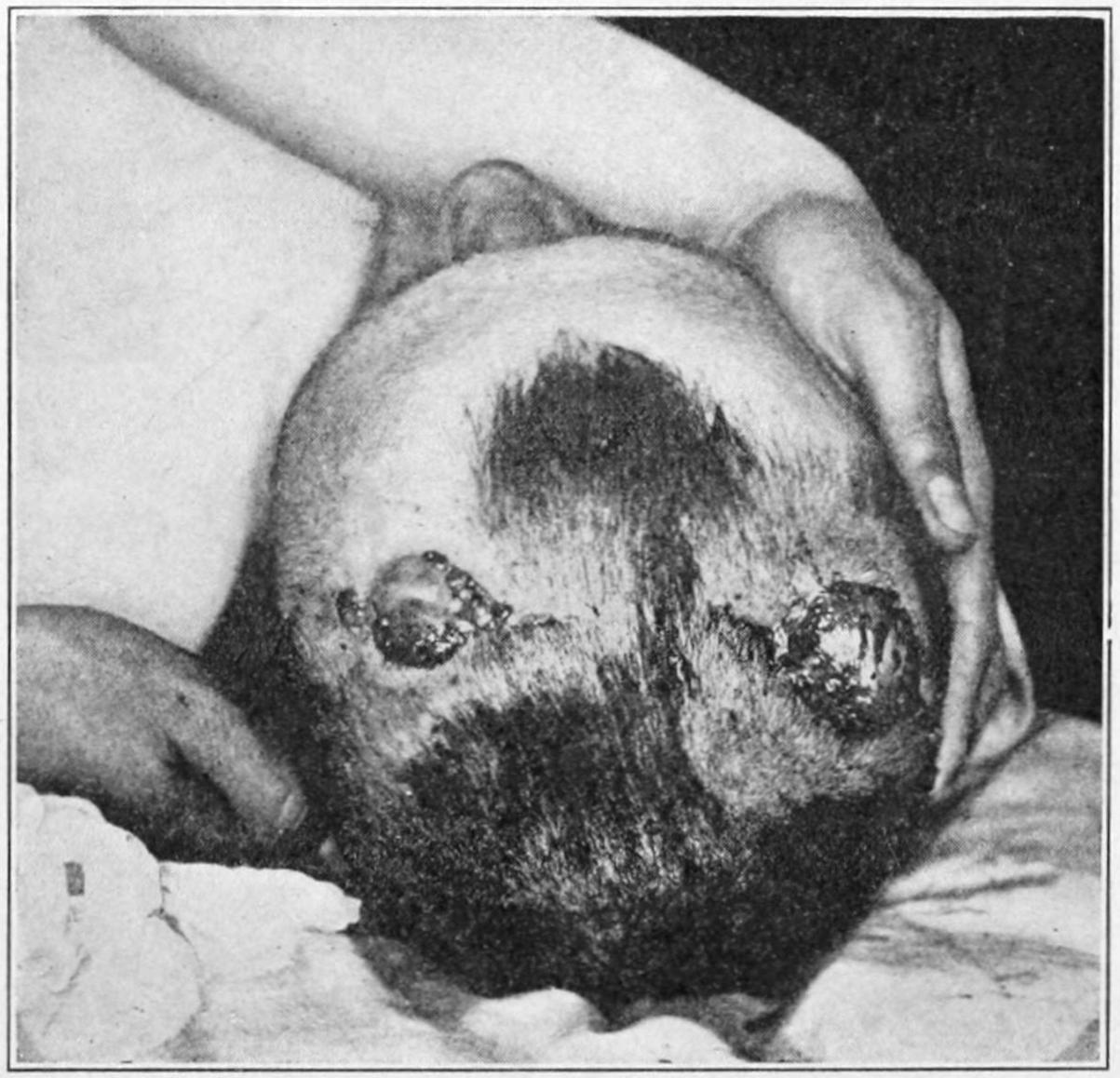
Perforating bullet wound of head, with prolapse of brain at wound of entrance. Operation done in Russian Red Cross Hospital at Mukden. Left hemiplegia; mind clear. (Major Charles Lynch.)
PLATE XIII
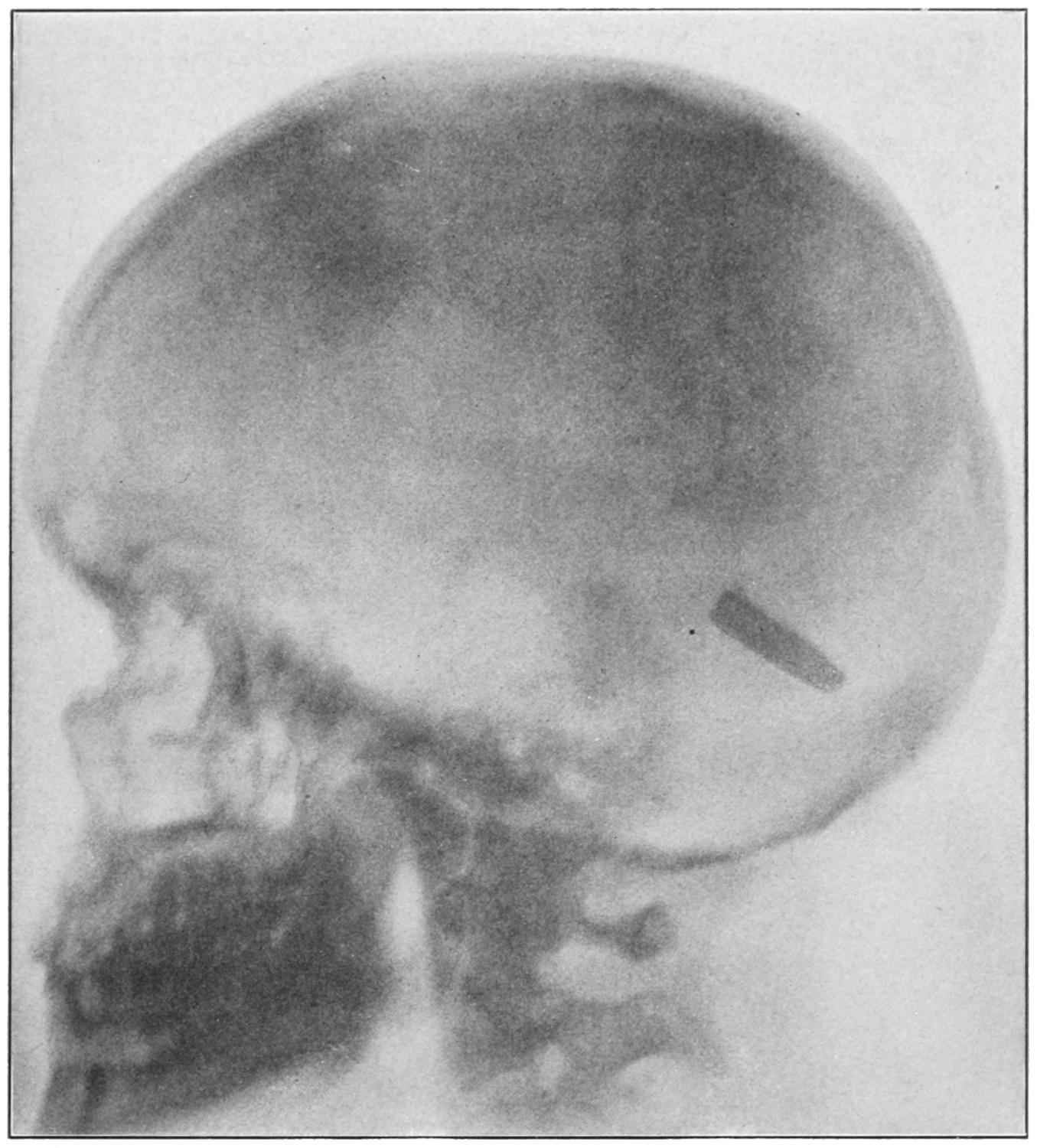
Radiograph of Head viewed from the Left Side, showing Mauser Bullet Lodged in Brain. (Surgeon-General’s Report on Use of Röntgen Ray, 1900.)
[229]
Fig. 54
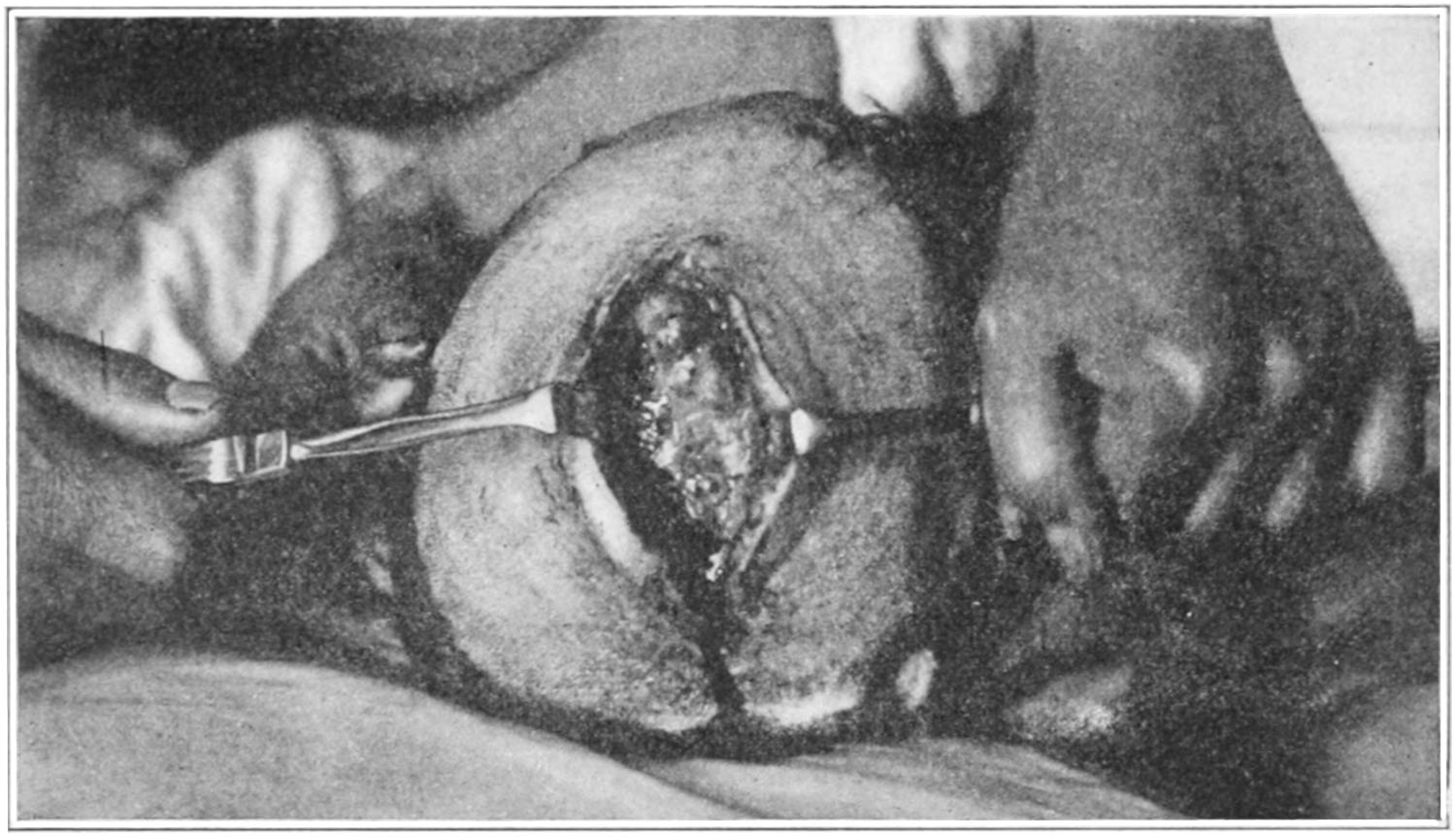
Perforating gunshot wound of head; two wounds converted into one by removal of comminuted bone. From Russian Red Cross Hospital, Mukden. (Major Charles Lynch.)
Fig. 55
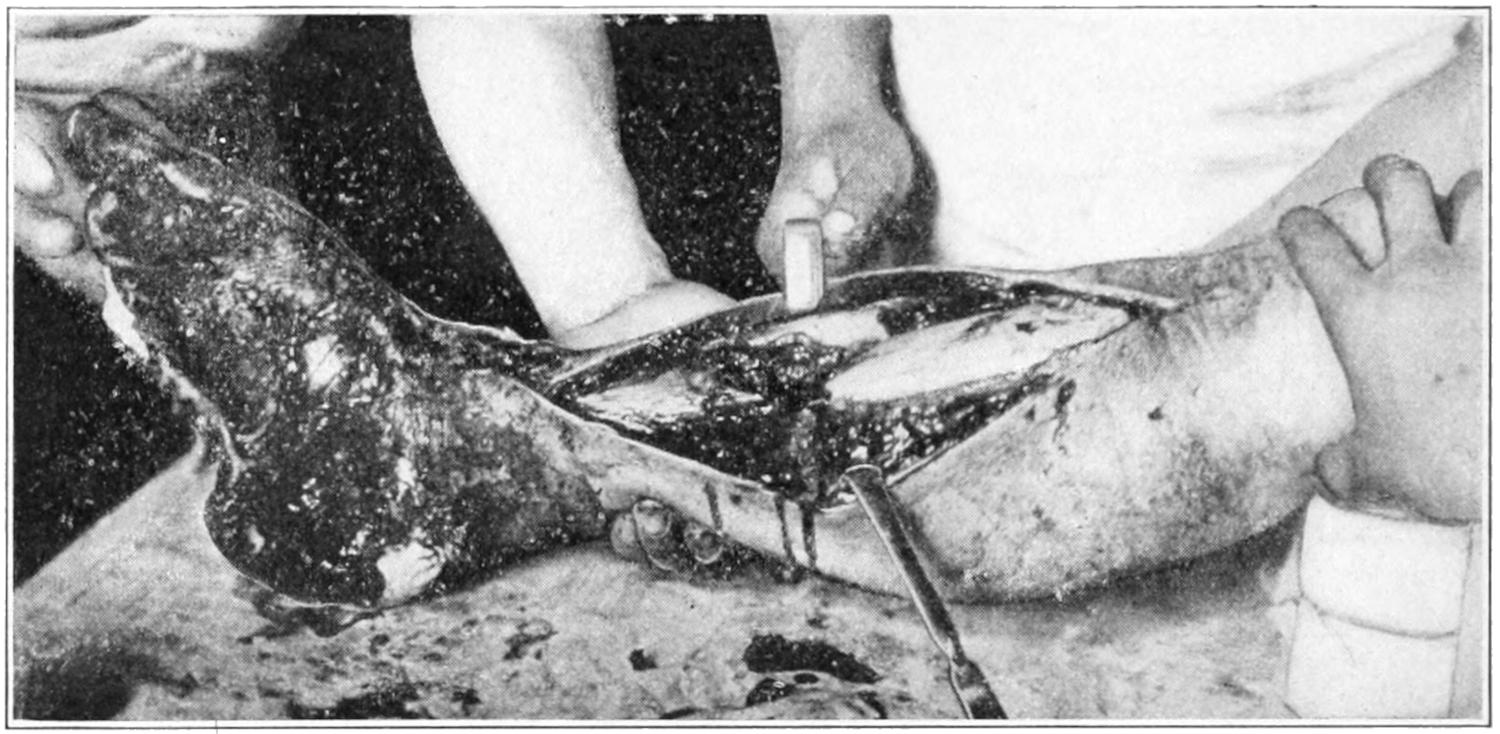
Result of accidental explosion of hand grenade, in a Chinese coolie with Fourth Division of Japanese Army, near Mukden. (Major Lynch.)
Fig. 56
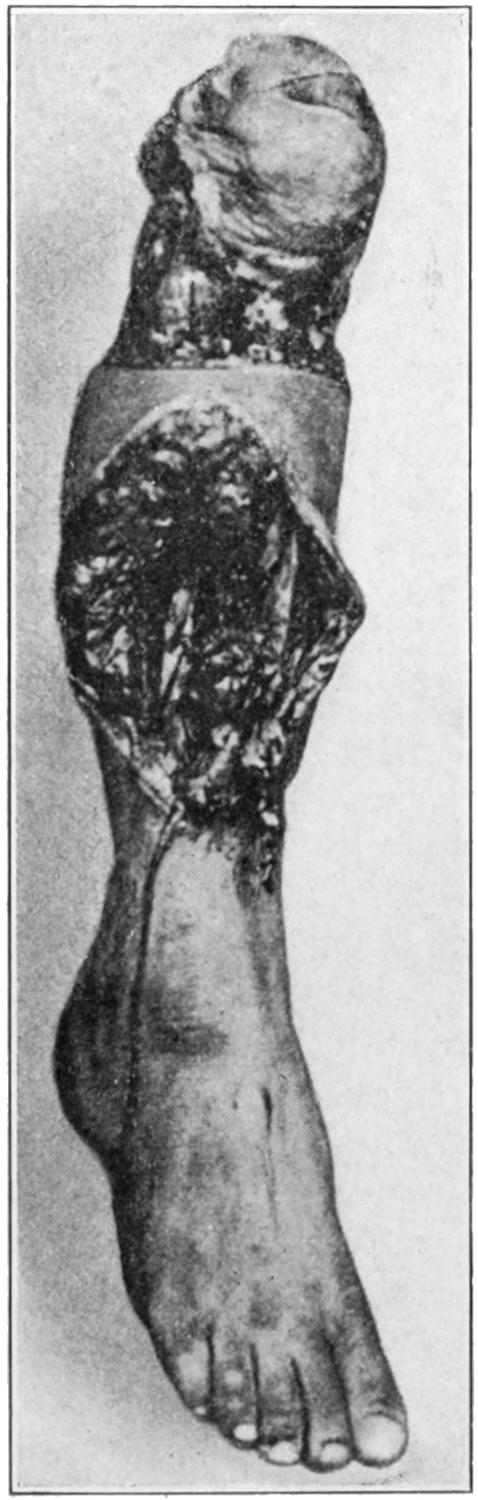
Shrapnel wound of leg necessitating amputation. Japanese soldier at battle of Mukden. (Major Lynch.)
About the head may be seen all varieties of gunshot wounds and their complications. The bullets from small weapons may not penetrate, but those from larger ones usually penetrate and sometimes perforate. Infection is not an uncommon sequel to all of these injuries, even if involving the skin alone; the skull, especially the diploë; the membranes, or the brain itself. (See Chapter XXXVI.) Septic complications are more likely to occur in proportion to disregard of antiseptic precautions in the first treatment. Usually the most serious head injuries are those connected with penetrating bullets. Sometimes the skull undergoes extensive shattering, and occasionally the base is fractured. Instantaneous death, such as occurs when a soldier is beheaded by a cannon ball, sometimes causes a peculiar cataleptic rigidity, which is a species of immediate postmortem rigidity, by which a body may be maintained in the position it occupied when struck. Obviously, lesions at the base are still more serious than those of the vertex, and wounds of the cerebrum are nearly always fatal. I have seen a number of men who had been shot entirely through the head—by Mauser or smaller bullets—who, nevertheless, recovered more or less completely. In one soldier, I recall, the bullet traversed an orbit in such a way as to divide the optic nerve. He was blinded, but recovered most of his other functions; he remained well for some years, and then developed symptoms of insanity. Epilepsy and other psychical disturbances are all more or less frequent after head injuries. Plate XIII illustrates how a bullet may be, apparently, harmlessly embedded in the interior of the cranium. Sometimes years after such injuries active symptoms make their first appearance. There can be no question as to the value of the information usually afforded in such cases by the aid of the x-rays.
The same necessity exists here as elsewhere for primary antiseptic occlusion, including careful shaving and cleansing of the scalp. Inasmuch as nearly every gunshot wound of the skull calls for subsequent operation—just as does almost every compound fracture—the parts should be prepared for it early, and everything else should be left until the time when the surgeon is ready to make a complete operation and meet all the indications. In such a case hemorrhage may be temporarily checked by tampon. The surgeon should not omit to take advantage of all the information which a study of cerebral localization may afford him, since localizing symptoms may reveal not only the course of a bullet, but something regarding its location.
Penetrating wounds of the face are less serious than those of the cranium proper. Occasionally a bullet striking a tooth will displace it and drive it in some other portion of the face, e. g., the tongue. Bullets and loose pieces of bone should be removed in wounds of the face. Hemorrhage can usually be controlled by tampons. Interdental splints may often be used to advantage, and in every case where the mouth has been injured antiseptic mouth-washes should be frequently used; in the case of the nose, an antiseptic spray should be employed.
The neck is often penetrated, but if the spine and the important vessels and nerve trunks escape, little apparent damage may be done. If infection occur and suppuration take place resulting abscesses should be opened promptly, as they might migrate into[230] the thorax or axilla. Even in the neck bullets which are producing no disturbance need not be disturbed; but if positive irritation or paralysis be caused by them they should be removed. Wounds of the larynx or trachea, by involving the parts in subsequent stricture, may call for tracheotomy.
Gunshot wounds of the spinal column below the neck are often complicated by perforations of the thorax or of the abdomen. So far as the spine is concerned the principal question is regarding the injury to the cord itself. In rare instances cerebrospinal fluid escapes from the wound; hemorrhage, or even the possibility of air entering the canal, is a more common possibility. I have seen perforation of the spinal canal, in connection with penetration of the thorax and lung, so that, after the operation of laminectomy, air escaped through the bullet wound in the spine with each inspiration and expiration. Infection in spinal injuries is always to be feared and caution should be observed regarding the maintenance of asepsis. The indications for laminectomy scarcely differ from those in other injuries to the cord. (See chapter on the Spine.)
Wounds of the thorax are more likely to be penetrating than formerly, owing to the conical shape and greater velocity of even small-arm bullets. Emphysema does not necessarily imply perforation of the lung, as air may enter through the external wound with each respiratory effort. When an imaginary line connecting the wounds of entrance and exit would naturally pass through the lung, it may be assumed that this viscus has been perforated. Signs indicating such lung injuries are peculiar pain, disorder of the respiration, more or less cough, usually with raising of blood; when the pleural cavity is more or less filled with blood there will be signs of pressure on the lung from presence of fluid. In other words a bullet wound of the lung will usually lead to a more or less complete picture of traumatic hydropneumothorax. Sometimes external hemorrhage is severe, even though it come from an intercostal or internal mammary vessel; usually the blood from these vessels escapes within the thorax. I have known an intercostal artery to[231] be divided by a small pistol bullet which scarcely penetrated the thorax of a man, who died in consequence, when the insertion of a small tampon would have checked the hemorrhage and saved his life. Lung tissue rarely bleeds seriously. When hemorrhage is from the lung it comes from a divided vessel of some size. A collection of blood in the chest is subject to the danger of infection, and empyema is a frequent but somewhat delayed consequence of gunshot wounds of the chest; while abscesses in the lung or mediastinum occasionally result.
To the primary occlusion, which should be the first attention given to every bullet wound of the thorax, there may be added complete immobilization of the chest. Fluid already present, unless it be clotted blood, may be withdrawn by aspiration. Traumatic, not to say septic pneumonia, is a serious complication. Should any operation be called for, like removal of fragments of rib or the checking of hemorrhage, it is best to make a free opening and a liberal removal of all particles or fragments, with ample provision for drainage. Hernia of any of the viscera through such wounds occasionally occurs.
[12] Figs. 57, 58 and 59, as well as the others preceding credited to Major Lynch, are due to the courtesy of Major Charles Lynch, now of the United States Army General Staff, who was attached to the Russian Army as our Military Attaché, and who took them himself.
Fig. 58
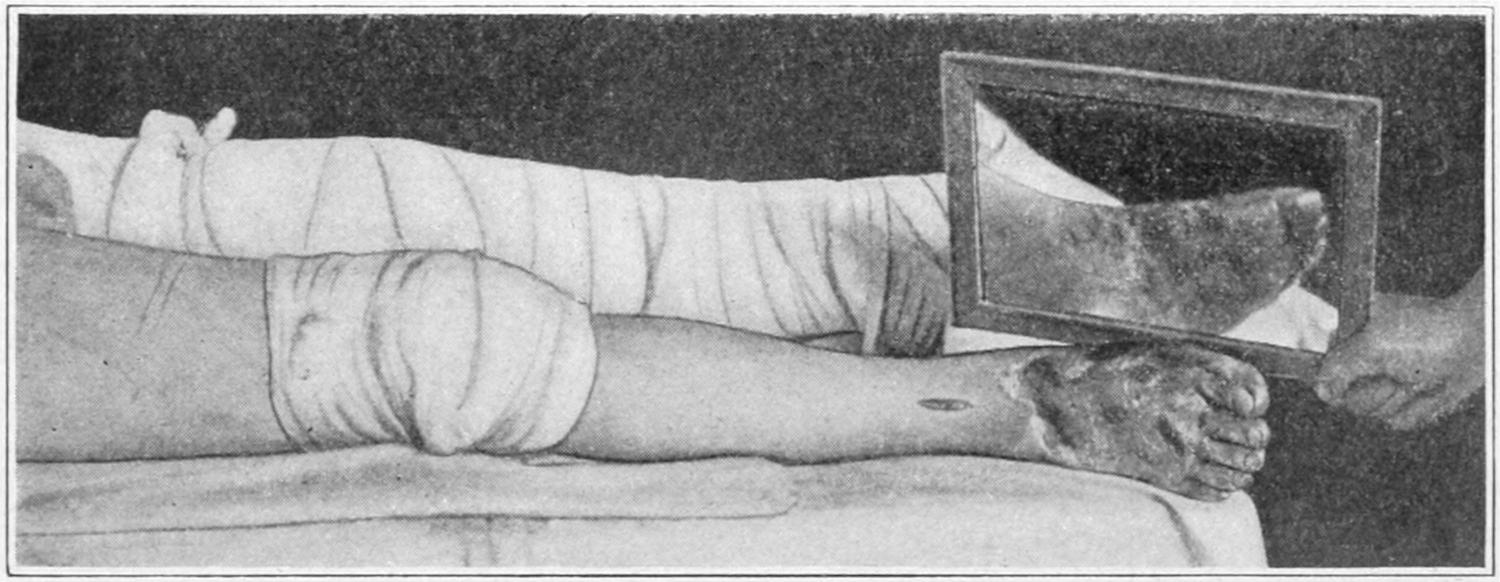
Result of frostbite after two days and nights of exposure. After battle of Mukden. (Major Lynch.)
The subject of injuries to the heart will be dealt with in the chapter devoted to the surgery of that organ. Not every perforation of the heart substance is fatal, and there are enough successful cases on record of radical intervention by resection of the thoracic wall, and of exposure of the pericardium, even of the heart itself, to justify this method of attack in any case which will permit of it. Not the least of the dangers pertaining to heart injuries is the impediment to heart action caused by a collection of blood in the[232] pericardial sac. Should anything further be called for it would be warrantable at any time to explore this sac and withdraw fluid through the aspirating needle, through a trocar, or even by incision and drainage.
In the abdomen all conceivable forms of injury may be met with, from contusions produced possibly by a spent cannon ball, to lacerations from fragments of a bursting shell and multiple perforations produced by one or more bullets. A first requisite in all such injuries is immediate antiseptic occlusion. This will not prevent such prompt and further study of the case as may indicate suitable treatment. When shock is extreme, indicating the possible result of contusions or laceration, or when perforation of the stomach, intestines, or bladder is probable, laparotomy should be performed at once. According to De Nancrède the order of probable frequency of these injuries of the abdomen is small intestine, large intestine, liver, stomach, kidney, spleen, and pancreas. Multiple lesions are also common. The immediate dangers are those from shock and hemorrhage, to be supplemented later by imminent danger of septic peritonitis.
Fig. 59
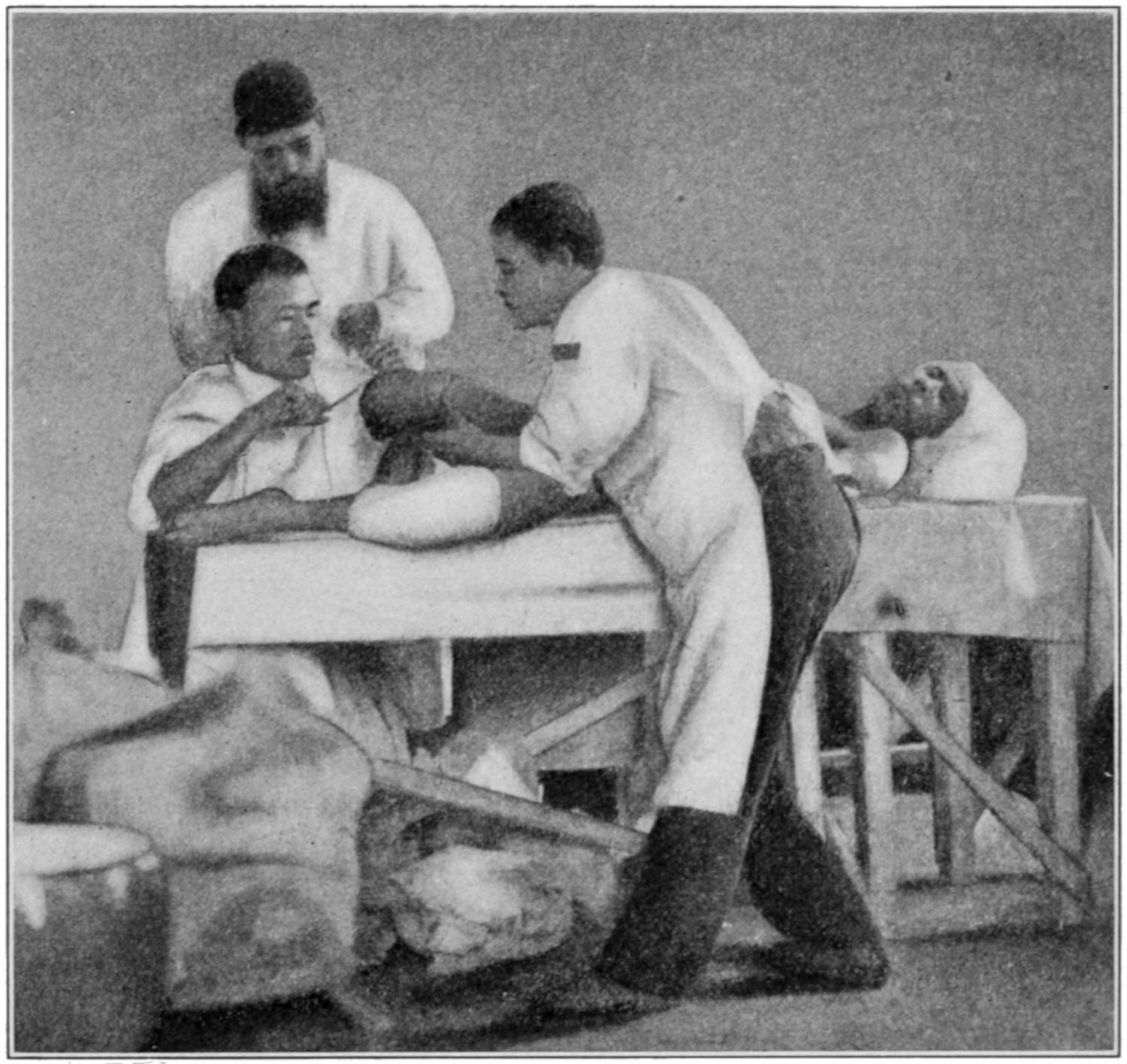
Scene in operating room in Second Field Hospital of Fifth Division of Japanese Army, at Mukden Railway Station. (Major Lynch.)
The modern small bullet causes few surface indications as to the amount of damage done within, as in the thorax. A careful consideration of the location of the wounds of entrance and exit will indicate the probability of perforation, especially of the hollow viscera. The appearance of blood, either in the mouth or from the rectum or urethra, the recognition of a rapidly accumulating amount of fluid, the presence of gas in the abdomen, are all significant indications of perforating injury. Several years ago Senn advised the insufflation of hydrogen gas into the colon, on the theory that its escape from the intestine into the abdominal cavity and thence out of one of the abdominal wounds, where it could be lighted as it passed through a small tube, would afford a certain and unmistakable test as to perforation of the bowel, and such is undoubtedly the case. Nevertheless, it is not one which is always easy or even possible of application, and no time should be wasted in waiting for a supply of hydrogen for this purpose.
[233]
The safest course and the most life-saving one is exploration when there is any doubt as to the nature of the injury. This means an operator possessed of good judgment, a suitable environment, rigid antiseptic precautions, and a small incision to begin with, with the finger as the best of all probes. The escape of bloody fluid, bloody urine, or fecal matter will immediately justify a much more extended incision through which complete orientation may be obtained. The first incision may be best made as an enlargement of the bullet wound, but any extensive operation within the abdominal cavity can be made through a sufficiently long median incision. Only in this way can the source of hemorrhage be ascertained. Thus the intestines may be systematically gone over inch by inch. When perforations are found they may be either dealt with as they appear—each opening being closed transversely—or the entire intestinal canal may be exposed. Contused spots will eventually slough, and should be treated as if they were perforations. Injuries, therefore, of short portions of the intestines might justify the removal of several inches. Instead of making multiple resections, it would be better to remove en masse the involved portion of the bowel, and then make lateral anastomosis or an end-to-end suture. Perforations of the mesentery as well as tears in the omentum should be carefully closed. Everything which is not vitally necessary and which has been injured should be removed. The posterior surface of the stomach, the lesser cavity of the omentum, the region of the gall-bladder and pancreas, the kidneys and ureters, and the bladder should be examined, in order that injury may be detected. After operations of this kind the abdominal cavity may be flushed with sterile salt solution; while the question of drainage should be decided upon the individual merits and indications of each case, as it is safer to drain the contaminated peritoneal cavity than to rely upon mere cleansing and drying.
If the spleen or kidney be injured, it is safer to make a primary removal of them; if they are not removed, posterior drainage should be made.
In uncertain cases of abdominal wounds the back as well as the abdomen should be scrubbed in order that if posterior drainage be necessary it can be made without delay.
The after-treatment of such patients does not differ from that of non-traumatic cases. Abstention from stomach feeding, the judicious use of salines, dependence upon hypodermoclysis and rectal nourishment, and the use of opiates are all matters of importance.
When the bladder has been injured there is usually more or less injury of some of the other pelvic organs. An empty bladder will escape more often than one which is full; while the latter will nearly always leak into the peritoneal cavity or along the bullet track, thus infecting one or both. The appearance of blood in the urine is one of the indications of bladder injury, and sometimes the bladder will fill with blood clot, which will produce the phenomenon of retention. Such a case may rapidly succumb to infection if relief be not promptly afforded, and this may come through abdominal section or a combination of it with exploration through the perineum. Particles of clothing and bone and even the bullet itself have been removed from the cavity of the bladder. It is advisable to open the bladder from below and insert a self-retaining drainage tube, by which, especially when combined with the method of drainage by siphonage, as described in the chapter on Surgery of the Bladder, a satisfactory and continuous emptying of the organ may be maintained.
[234]
The first requisite after the infliction of a wound is to arrest and control the hemorrhage. In many operations upon the extremities precautions are taken to avoid its occurrence, and the so-called bloodless method of operating, which is effected by the use of an elastic bandage of pure rubber, is frequently employed and generally gives satisfactory results. The pure-gum bandage was first introduced into surgery by Martin, of Massachusetts, and its combined use both as an elastic bandage and tourniquet was so promoted by Esmarch that it is generally known as Esmarch’s bandage, and Martin has failed to receive the credit due him.
The elastic bandage used for this purpose should be about three inches in width and five or six yards in length, and made of pure rubber. The operator begins by applying this to the tip of the extremity which is to be made bloodless. It is wound around the limb in spiral turns, with sufficient force to press out the blood from the tissues and to empty the vessels into those of the trunk. It is continued above the site of the operation, and then the limb is either constricted with a tourniquet of the old type or with one of the rubber appliances used for this purpose. A few turns of the rubber bandage may be passed more tightly about the limb at this point and secured with forceps. The rest of the bandage is then unwrapped from the limb, which will be found pale and bloodless. Operation may then be practised without the loss of more than a few drops of blood. All divided vessels should be secured before the constriction is removed and the wound closed.
In septic, tuberculous, and malignant conditions no such pressure should be made, as harmful elements might be forced into the circulation. In such cases the elastic tourniquet is applied high up and no attempt is made to force the blood out of the limb. The limb should be elevated so that its veins may empty before the bandage is applied, and a certain amount of blood will thus be saved.
Care should be taken in graduating the tightness of the constricting band, as well as its narrowness, and in preventing undue pressure upon nerve trunks. Cases are on record of temporary and even permanent paralysis, due to too vigorous application of the tourniquet, and except upon large and stout limbs it is not often necessary to apply it as tightly as is often done. Moreover even a wide rubber bandage when stretched taut becomes little better than a rubber cord or rubber tube and sinks into the tissues. A sterile towel should be folded into a strip and wound around the limb, and then a tourniquet should be applied over it so that pressure may be more equably distributed and danger of paralysis reduced.
Exigencies may require the application of the elastic tourniquet as high as it can be possibly used, either upon the shoulder or the hip. This necessity is usually observed in amputations at those joints, and the special methods required will be more fully dealt with when speaking of these procedures. (See Chapter LVII.)
The elastic bandage should have been unrolled and sterilized with the rest of the surgical equipment required, and even when so protected it would be well to cover the limb with wet sterile towels before applying the bandage, which is usually done at the last in order to avoid contamination. When this is not done the final scrubbing should not be effected until the bandage has been placed, the tourniquet applied, and the bandage again removed.
Fig. 60
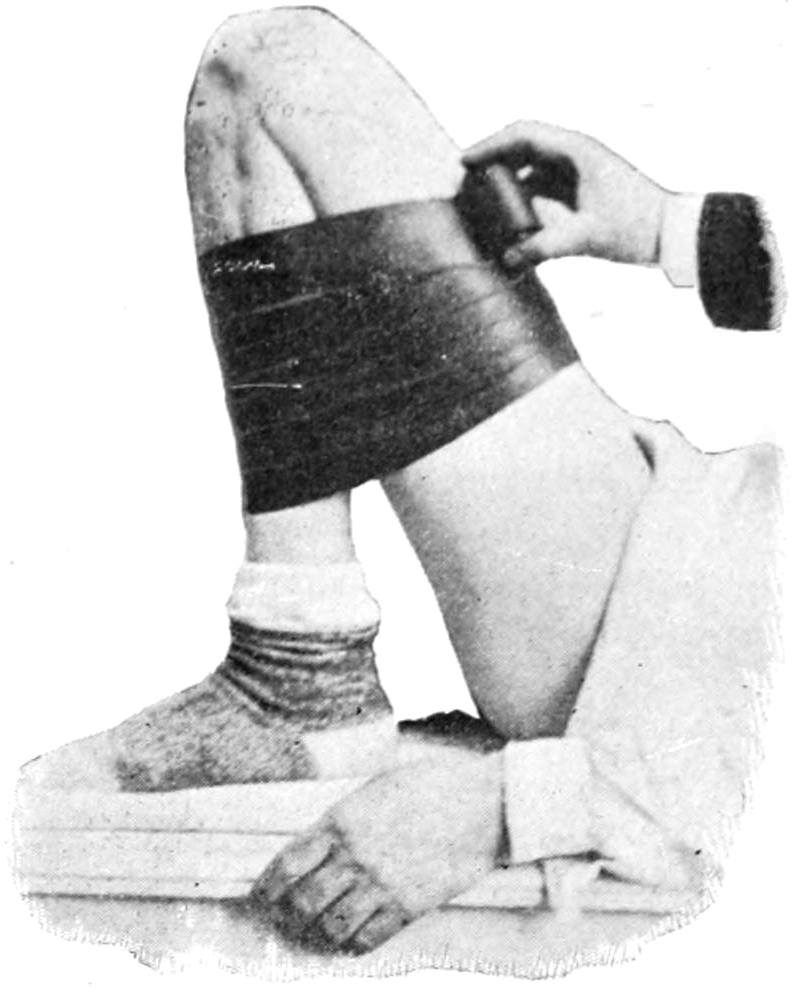
Illustrating forced flexion for control of hemorrhage.
The first measure, then, in the treatment of a wound is to prevent loss of blood. This may be done in various ways, and the method should depend upon the circumstances of the case. In emergency cases it may be accomplished either by direct pressure, by constriction of the limb above the injury, or in some instances by mere position. If it be possible to make direct pressure through the medium of some clean—preferably sterile—dressing[235] or material, this of course would be desirable. In all civilized armies soldiers are now equipped with a package of sterile dressing by which an emergency pad for this purpose can be promptly applied. Railroads and steamers are now providing emergency outfits. In injury of the arm or leg advantage may be taken of position, i. e., forced flexion, which is maintained by any measure or material which can be made available for this purpose (Fig. 60). Digital compression over a main vessel may also serve a good purpose. Mere elevation of the part, as, for example, the head, when not otherwise contra-indicated, or a hand or foot, will do much to check venous or arterial flow. Moreover, in these positions reflex contraction of arteries occurs, even in those of the head when the arms are elevated. For this reason in cases of serious nose-bleed it is often advisable to keep the arms raised high above the head.
Of other means resorted to may be mentioned:
—Water at a temperature of 130° to 160° F. is a powerful hemostatic. It stimulates contraction of the muscular coats of the vessels and produces coagulation of the albuminous portions of the blood upon the surface to which it is applied, and in this way plugs the capillaries and small arteries and so prevents oozing. Heat with pressure will be serviceable in many instances. Cold may be employed by means of ice or iced water and may be made serviceable in cavities like the mouth, the vagina, or the rectum, after patients have recovered from the anesthetic and at a time when hot water could not be borne. Cold has more of a constringing effect but less coagulating property.
—This may be made with a tampon in some cavity, or by a graduated absorbent dressing whose effect may be regulated by pressure of a bandage or an elastic bandage. Care should be always given that pressure be not too long nor too firmly made, and it should be released as soon as there appears edema of the part below or any evidence of insufficient circulation.
—There are many substances which contract vessels and cause more or less coagulation of blood, and at one time there were many of these in general use, but they have been supplemented by other products, i. e., cocaine, antipyrine, and adrenalin. The effect of cocaine is temporary, but sometimes is sufficient in the urethra or the nasal cavity. Antipyrine, in 5 to 10 per cent. solution, alone or with cocaine, has a similar effect, but is more lasting. Some years ago the writer stated that by mixing 10 per cent. solutions of antipyrine and tannin there was precipitated a gum-like material of extraordinary tenacity. This will check oozing from any part to which it may be applied, but it may adhere so tightly as to make it difficult to later remove the tampon. Of the hemostatic drugs, adrenalin has the most marvellous properties. It can be procured in solutions of 1 to 1000. A solution of this strength, somewhat diluted, may be spread or applied upon an oozing surface with almost instantaneous effect.
The use of gelatin in checking hemorrhage has given some satisfaction upon the Continent, but has not found much favor in this country. It consists of a solution of 2 parts of pure gelatin to 100 parts of normal salt solution, which should be thoroughly sterilized. It is injected subcutaneously to increase the coagulability of the blood, and has also been injected directly into an aneurysmal sac or its immediate vicinity to induce coagulation. It is likely that if the surgeon have a patient with the hemorrhagic diathesis the combined use of gelatin in this way and of calcium chloride internally would give satisfactory results.
A styptic has recently been introduced by Freund under the name “stypticin.” It is a product of the oxidation of narcotin, one of the opium alkaloids, and is a yellowish powder of bitter taste. Chemically it is cotarnin hydrochloride. It has been used[236] especially in the treatment of uterine hemorrhage, with a certain degree of success, regardless of the cause of the hemorrhage. It may also be given in cases of too profuse menstruation. The average dose is 2 to 3 Gr. (0.15 to 0.20) at intervals of two or three hours. When a speedy result is desired twice the above amount in 10 per cent. solution may be given subcutaneously.
may include the use of the sharp spoon, chemical caustics, or the actual cautery. The curette is usually employed for removal of surfaces which have attained a spongy or easily bleeding condition, as the interior of the uterus, bleeding ulcers in other cavities, etc. When fungoid tissue is scraped to a base of healthy tissue there is usually a cessation of further hemorrhage. Occasionally there are cases of fungating cancer which bleed upon the slightest touch. The most radical way in which to deal with these for temporary purposes is to destroy the spongy tissue which bleeds so frequently. The gross part may be done with the sharp spoon and the cautery may be made to finish the work. Bleeding piles, when it is not permissible to treat them more radically, should be touched with the actual cautery, with stretching of the sphincter. The cautery knife should not be made too hot, as it may act similar to a sharp blade instead of merely searing by its heat.
—When vessels of considerable size or masses of tissue containing them can be made accessible, the best means of control of hemorrhage are those which can be applied directly to the vessels. When this is not possible they should be tied en masse. A method formerly in use was acupressure. To effect this a needle was passed through the overlying skin beneath the vessel and out again, and around this a suture was tied to make pressure. Since the introduction of absorbable materials this method has been supplanted by the use of catgut sutures, which may be tied, cut short, and left to absorb.
Under the term “forcipressure” is included the method of seizing vessels before, or as they bleed, in small forceps, which are variously shaped and constructed, and grouped under the name of hemostats. Small vessels seized between the blades of such an instrument will have their walls so crushed that blood clot is so quickly entangled that the forceps can be removed in a few moments with little or no danger of subsequent bleeding. Larger vessels should be ligated.
Torsion is a substitute for ligature, especially with the smaller vessels, and denotes a twisting of the vessel end after its seizure, breaking up its inner coat, and effectually sealing its lumen. Some surgeons rely on torsion for the large vessels.
Angiotribe is the name applied to strong crushing forceps, by which a pressure of several hundred pounds can be made through a lever mechanism. In this a mass of tissue, as the broad ligament, can be secured and such tremendous pressure brought to bear that its vessels are crushed and destroyed beyond possibility of bleeding. Downes has improved upon this mechanism by adapting to it an electrocautery arrangement, by which not only pressure but also heat is brought to bear. His instrument is called an electrothermic clamp. To all of these instruments there are at least theoretical objections, in that they are more or less clumsy or unwieldy and require special equipment. They devitalize a considerable amount of tissue, all of which has subsequently to be removed either by a process of sloughing or by active phagocytosis; but they serve perhaps a useful purpose in the crushing treatment of hemorrhoidal tumors. They have been used only by a few, and have not found wide acceptance.
—These are also mechanical means of controlling hemorrhage, but deserve to be grouped by themselves. Ligation of vessels may be preliminary or may be performed as needed during an operation.
By a preliminary ligature is meant taking such precaution as tying the carotid before operations on the face, the brain, or the femoral artery before amputation at the hip. There is also the method of temporary ligation of vessels by the application of a ligature which should not be drawn too tightly, but simply serve the purpose of gentle constriction for the half-hour or so during which it may be needed, after which the vessel is promptly released. If this ligature has not been too tightly applied the vessel walls will not have been injured and circulation is restored. Crile has effected the same purpose with the carotids by a small clamp whose pressure may be regulated by a thumb-screw.
Ligation of large trunks is made for the purpose of influencing nutrition by diminishing[237] blood supply, as when the femoral is tied for elephantiasis of the leg, or the carotid is tied or excised, as suggested by Dawbarn, to cut off the blood supply from cancer of the face or neck.
Ligatures are usually made of absorbable material, such as catgut, chromicized or not, as may be desired, or of silk, which disappears after a time, but which is not regarded as absorbable. For special purposes other material has been used at times, such as strips of ox aorta. The surgeon has his choice of these, whether he intends to ligate the end of an artery or tie a vessel in its continuity. For the latter purpose the ligature is threaded into an artery needle, or a specially devised curved forceps known as the “Cleveland” needle. When tying the exposed end of a bleeding vessel it is desirable to tie near the cut end, so as not to leave tissue which should be absorbed, and for the same reason to not include unnecessary tissue. One of the forms of knot similar to the “reef” knot, which will not slip, should be used. Silk has the advantage over catgut in that a knot tied with it will rarely become loose, whereas catgut knots, unless carefully tied, will occasionally slip. The ligature knots should be left as short as is consistent with protection against slipping.
—Silk or celluloid thread are the most unabsorbable of ligature materials ordinarily used. Even these usually disappear after the lapse of time. Absorbable ligatures of catgut disappear after a few days or weeks, according to the method of their preparation. Absorption is practically a matter of phagocytosis, the end of the vessel or tissue beyond the ligature disappearing with the latter by the process of tissue digestion.
When vessels of large size are ligated the blood supply is taken up by the collateral circulation. On the possibility or practicability of the latter will depend the success of such operations as ligation of large trunks for the cure of aneurysm. Should the collateral supply prove insufficient, gangrene, beginning at the tip of an extremity, is an assured fact.
The effects of the ligature on the vessel wall will depend upon the security with which it is tied. The damage done to the inner and middle coats by a ligature tied for permanent purposes is usually sufficient to rupture them, after which they roll up inside the outer coat, while the blood contained in that part of the vessel coagulates, the clot extending to the first vessels above and below. This quickly organizes, becomes infiltrated with cells, and brings about the complete obliteration of that part of the vessel and its transformation into a fibrous cord. This can only occur, however, when asepsis has prevailed. Should the ligature prove septic the patient is exposed to two dangers: that of secondary hemorrhage by ulceration and breaking down of the clot instead of organization, and the ordinary dangers of septic infection.
There are circumstances under which it may be well to modify the ordinary methods of ligation and not to tie knots too tightly—i. e., when the vessels are greatly weakened by extensive disease, or so stiffened by calcareous degeneration as to cause them to snap under rough handling. It has been suggested to use pieces of ox aorta to prevent these accidents.
The dangers of secondary hemorrhage pertain mostly to septic conditions. In an absolutely aseptic wound, properly cared for, secondary hemorrhage is almost impossible, but as soon as germ activity begins lymph barriers are broken down, tissues softened, and weakened vascular walls may give way.
Secondary hemorrhage may call for ligation of a main trunk not previously attacked, but in a majority of cases will demand reopening of the wound and further search for bleeding points. Should the patient’s condition be materially weakened the effects of position and of pressure may be tried in suitable cases. But the pressure which may be effective to check the hemorrhage may be sufficient to completely shut off circulation from parts beyond, and such pressure should, therefore, be judiciously practised and its effects carefully watched. The signs of secondary hemorrhage will vary with the location of its source. Occurring on or near the surface it will usually stain the dressing; occurring deeply, as in the pelvic or abdominal cavities, it will produce prompt symptoms of shock, i. e., lowered blood pressure, whose degree will indicate the extent of the blood loss. In these cases, unless the patient’s condition contra-indicate the measure, the wound should be opened under anesthesia, and the source of the bleeding sought out and mastered. The surgeon should never overlook the fact that after the gradual[238] restoration of the force of the heart’s action, as the patient recovers from anesthesia and becomes uncontrollably restless, vessels may bleed which upon the operating table scarcely emitted a drop of blood. Experiences of this kind teach the value of hemostasis during operation, and even of absolute rest induced by an opiate, immediately after.
There are certain conditions in which the surgeon is led by experience to anticipate liability to unusual hemorrhage; such as cases of hemophilia, or anything that savors of it or of scurvy. In patients who claim to be “bleeders,” the surgeon should be extremely chary and careful during his operative work. There are, furthermore, certain toxemias, especially that of cholemia, during which the blood is slow in coagulation. When the time for preparation is afforded no cholemic patient should be operated without a few days’ previous preparation by four or five daily doses of calcium chloride, 20 to 30 grains given in plenty of water. This is known to greatly increase blood coagulability, and thereby to measurably protect the patient against the danger of an oozing of blood difficult to control.
The other measures needful in the treatment of secondary hemorrhage are those described in Chapter XVIII.
The general consideration of wounds in the previous chapters necessarily included many suggestions concerning their treatment. The first essential in the treatment of open wounds is exact hemostasis; the next is the removal of dirt and foreign material of all kinds, i. e., visible and invisible. Accidental wounds are practically never received upon surgically clean surfaces, and it may be always assumed that the possibility of infection is present. It becomes then a question to what extent the surgeon should go in removing or avoiding danger. Obviously all visible foreign material should be carefully removed and all dirt should be scrupulously washed away. Emergency treatment of a bleeding injury in a well-regulated hospital is one thing, and the exigency of a railroad accident or casualty away from civilization is quite another. The canons of antisepsis and asepsis have been elsewhere sufficiently well laid down to indicate what should be done at the time when it can be done.
The protective vitality of the human tissues permits them to bear frightful injuries or resist infection in a surprising way. But occasional escapes from severe accidents by no means justify carelessness when caution can be taken, and cannot be held as excusing the surgeon for any neglect in antisepsis.
A bruise or contusion accompanied by a slight abrasion may seem a trifling injury, and yet by virtue of the injury the resisting powers of the tissues may be rendered insufficient to protect them from infection through a break of the surface. No relatively small lesions of this kind can be safely neglected, but should be cleaned and covered with an antiseptic compress, either wet with some suitable solution or smeared with a protective ointment, or used dry with a suitable antiseptic powder, as, for example, bismuth subiodide. Injuries followed by considerable swelling should be treated according to the time which has elapsed since their reception. If, for instance, a bruise or sprain be seen early and before much swelling has occurred, ice-cold applications can be made in the hope that, by limiting the flow of blood, the outpour of fluids may be prevented. This effort should be seconded by position, and perhaps by gentle pressure. Conversely when a case is seen late, after the tissues have become waterlogged with fluids, heat should be applied in order that by stimulating the circulation reabsorption may more speedily take place. In this case, also, suitable pressure may be of service.
When there is actual hematoma, and the exuded fluid fails to disappear, an incision properly made and in the right place may permit the clot to be turned out, and then speedy recovery secured by coaptation with sutures and pressure.
Poultices are nauseous applications to make to the human body. By their indiscriminate use much harm has been done and suppuration encouraged or brought about, which but for them would not have occurred. There are occasions when a hot flaxseed poultice may be of use, but they are very few and far between. With regard to such remedies as arnica, witch-hazel, etc., the best that can be said of them is that they may be of some use by virtue of the alcohol which they contain; they serve the purpose, then, of a diluted alcohol and nothing else.
[239]
There is virtue in the use of a cold wet pack, or compress, especially in the treatment of chronic affections of the joints, and their value can be perceptibly enhanced by using solutions of sodium, or preferably ammonium chloride, and the addition of a little alcohol. Absorbent material wet in such a solution, wrapped around the part, covered with oiled silk or some impervious material, while the part is kept at rest, will render valuable service in conditions of this kind.
In regard to the relative worth of heat and cold for relief of pain, the alleviating effect of heat is more promptly manifested, but that of cold is more permanent, and especially is this true of chronic affections of the joints and bones.
In the treatment of open wounds, bleeding having been first controlled, all the surrounding parts, as well as the wound itself, should be sterilized. In a scalp wound the scalp should be shaved as well as scrubbed. All particles of visible dirt should be carefully picked out, and every particle of tissue whose vitality is so compromised that it apparently cannot live should be excised. The wound may then be irrigated or washed out with hydrogen peroxide, and not until all this is done should the operator consider how he may best close it, as well as whether he needs to provide for drainage. A ragged line of tearing will leave a jagged and more unsightly scar, especially on the face; therefore the margins of such a lacerated wound should be trimmed before coapting them.
The method of closure will depend on the degree of tension necessary for the purpose. Parts that come together easily may require but slight suturing, and with fine catgut which will loosen of itself within two or three days; the intent in such cases always being to assist the sutures by proper support of the external dressings.
Buried sutures will serve a useful purpose in many instances, and upon the face or exposed parts of the body a subcutaneous suture of fine silk or horse-hair may be so applied as to be easily removed by a single pull and leave but trifling disfigurement. Female patients will be doubly grateful if the surgeon can leave but a minimum of unsightly scar. Fasciæ will sometimes retract widely. They should be brought together by distinct separate catgut sutures. Before closure of a wound it is important to determine that no such structures as nerves or tendons have been divided, or, if such injuries have occurred, to reunite their ends by fine silk or catgut sutures. The writer prefers silk for most of these purposes, although in a nerve a fine formalin catgut suture would perhaps be the most ideal.
There are occasions when it seems impossible with the means at hand to tie or secure in any way a deep bleeding vessel which has already been seized with a hemostat. In such case the forceps may be left in situ for thirty-six to forty-eight hours. This may be done, for instance, in the groin, in the axilla, in the depths of the neck, and about the cranial sinuses. Life may be occasionally saved by this procedure which would be lost from hemorrhage without it. At other times a firm tampon of gauze may be forced into the depths of a wound for the same purpose, and maintained there by position, or by the pressure of secondary sutures, which serve the same purpose and require removal in two or three days. These measures refer rather to wounds of veins than of arteries.
If one can be absolutely sure of his asepsis, he may close even an extensive wound with little or no provision for drainage; but unless he is certain regarding it he should provide at least for escape of fluid by omitting a suture occasionally, or by drainage with a tube or a cigarette drain. In compound fractures not only must such provision be made, but the treatment of the wound may also include the introduction of wire sutures through bone ends or the use of other mechanical expedients.
The further and equally important treatment of wounds consists largely in maintaining physiological rest of the injured part, as well as the general welfare of the patient. Pain which becomes unendurable causes the patient to lose self-control and to disturb not only the dressings but apposition of wound surfaces. Pain, therefore, should be controlled by the mildest expedient that may suffice to master it. Elimination must be maintained, because the circumstances attending the injury may act to disturb it. A patient who shows no irregularity of pulse, temperature, elimination, or general comfort may be assumed to be doing as well as could be expected, and the dressings need not perhaps be changed for several days. On the other hand, with rise of temperature or pulse, increase of restlessness, swelling of the parts, or discomfort in the vicinity of the wound, the dressings should be promptly changed. It may be necessary to make such change at the end of forty-eight hours in order to permit the removal of the drain. The second[240] dressing may then often remain a week, but any dressing which becomes saturated, even with blood, may dry and adhere to the skin, and should be removed.
It would be best to inspect the wound in all cases when the temperature and pulse are rising or when there is any disturbance in the wound. The accumulation of blood in an aseptic wound may cause much discomfort, and by its presence interfere with primary union. Should, therefore, a wound be found pouting or its edges reddened and swollen it may be safely assumed that there is something wrong, and as many sutures should be removed as may be necessary to reveal its condition and permit of its treatment.
Wounds which are foul or septic when they come under surgical observation should be treated differently. Here the first attempt should be at antisepsis. In some cases continuous immersion in warm water will give the best results. I have never found anything so prompt, however, in cleaning up a sloughing area as brewers’ yeast. When this can be obtained it should be used in sufficient abundance to get the diseased surface thoroughly wet with it. In sloughing cases moist dressings are usually preferable, and the best are the two above mentioned. This is true of those cases where part of the wound is granulating satisfactorily, while part is acting badly. Dressings in all of these cases require to be frequently changed, that they may be kept effective.
I have elsewhere called attention to the value of granulated sugar as an emergency antiseptic material of great value.
—There are many varieties of sutures which have found favor. Until the surgeon becomes expert by long practice he should confine himself to few sutures and knots. Primary sutures include continuous, interrupted, plate or modified plate, quill or modified quill, chain, and transfixion sutures, and also certain forms of suture used in intestinal surgery. The above forms are illustrated in Figs. 61 to 66. Several of them may be used in making what are known as buried sutures, i. e., those which are tied deeply, whose ends are cut off below the surface and left either permanently or for later absorption.
The purpose of a suture is to bring the parts into accurate apposition and so maintain them. It is a mistake to employ a superficial suture alone, which may leave a “dead space” beneath it. If but one suture is used, as in closing an abdominal wound, it should pass through the tissue layers of the abdomen and bring each layer into contact with the corresponding layer on the other side. Unless this can be done a series of sutures should be used uniting the tissues layer by layer. If these be made of formalin or chromic gut they will remain in situ for a length of time sufficient to serve their purpose. Some prefer silk for this purpose, but it may work out later; if sterile and freshly boiled just before using it will rarely cause this trouble. In closing a thick and fat abdominal wall four or five tiers of buried sutures may be used and their effect may be reinforced by the addition of a modified plate or quill suture, as shown in Figs. 63 and 64.
Fine wire is preferred by some operators, and horse-hair by others. Success pertains rather to the perfection of the method than to the material used. The primary feature of all wound sutures should be prevention of tension and protection against it. Further support in the same direction can be made by the use of adhesive plaster after fastening the dressing upon the wound, thus taking off strain.
Certain expedients have been resorted to in superficial wounds, some of which include the affixion of a strip of plaster on either side of the wound and then the application of the suture material through the plaster rather than through the skin. Plasters with small hooks have also been applied, and then a shoelace suture applied over the hooks, thus lacing the wound margins together. Such measures are convenient for certain cases, although they make the maintenance of strict asepsis difficult or impossible. Fine-wire clips have also been introduced, by which skin margins may be held together for three or four days, or until they have had time to unite with some firmness, after which they may be removed. These little implements can be sterilized and repeatedly used.
[241]
Fig. 61
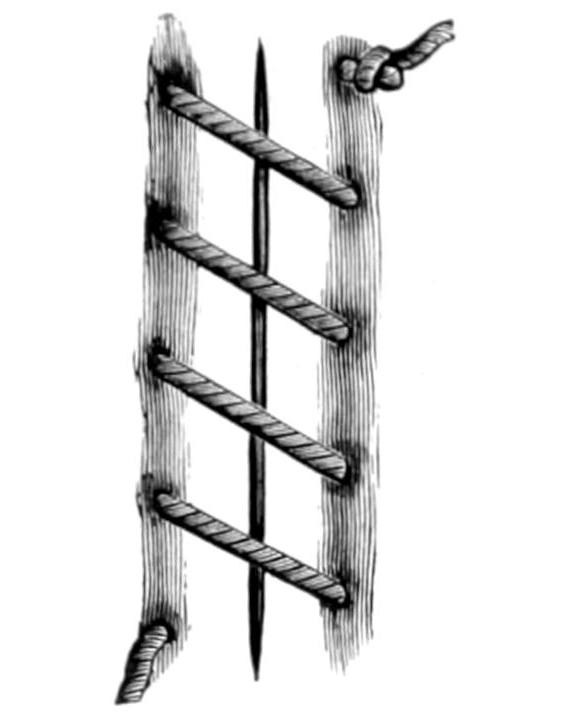
Continuous suture.
Fig. 62
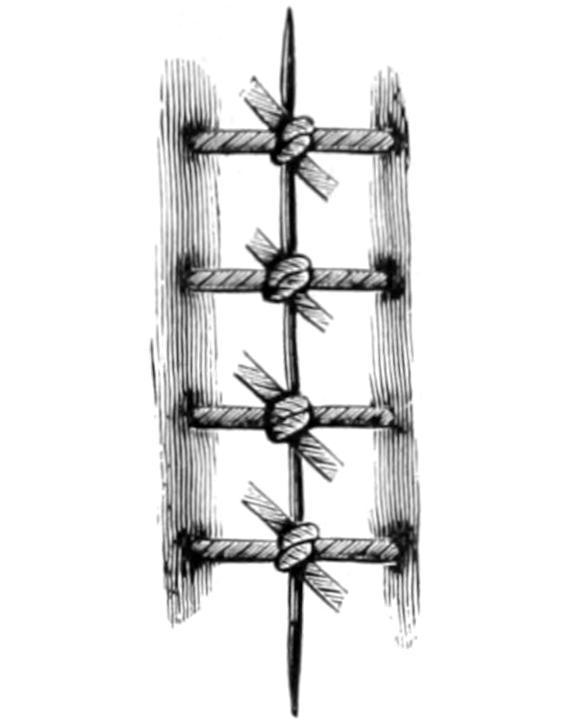
Interrupted suture.
Fig. 63
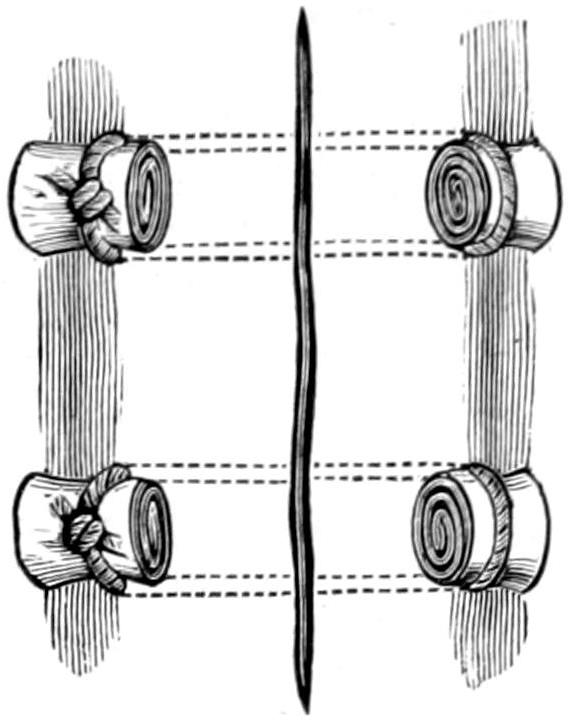
Modified plate suture, using gauze instead.
Fig. 64
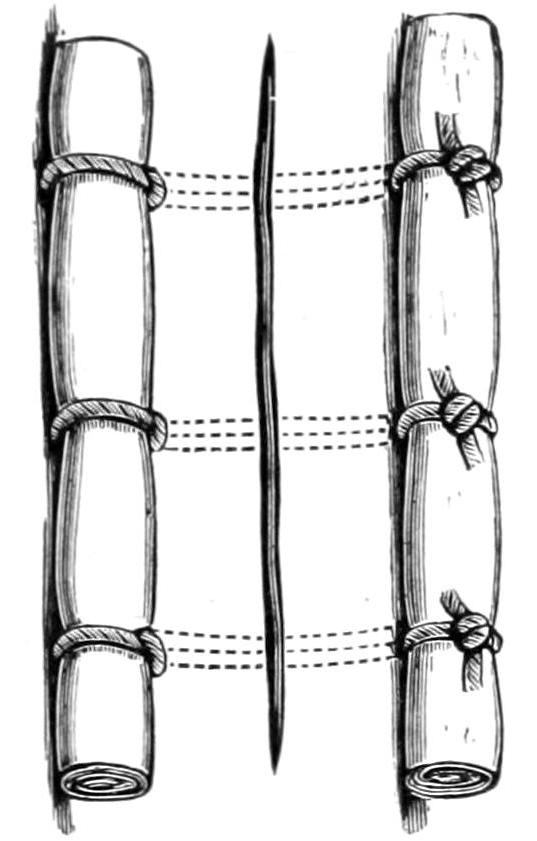
Modified quill suture, using gauze.
Fig. 65
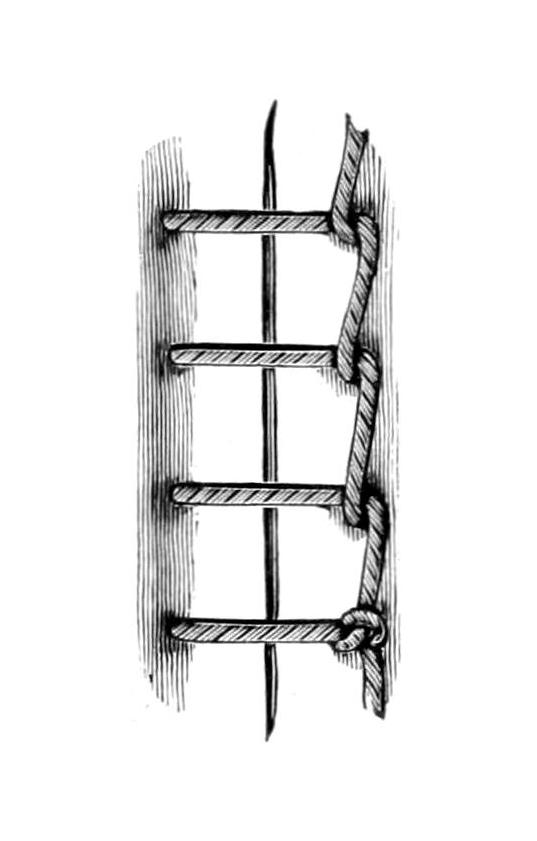
Billroth’s chain-stitch.
Fig. 66
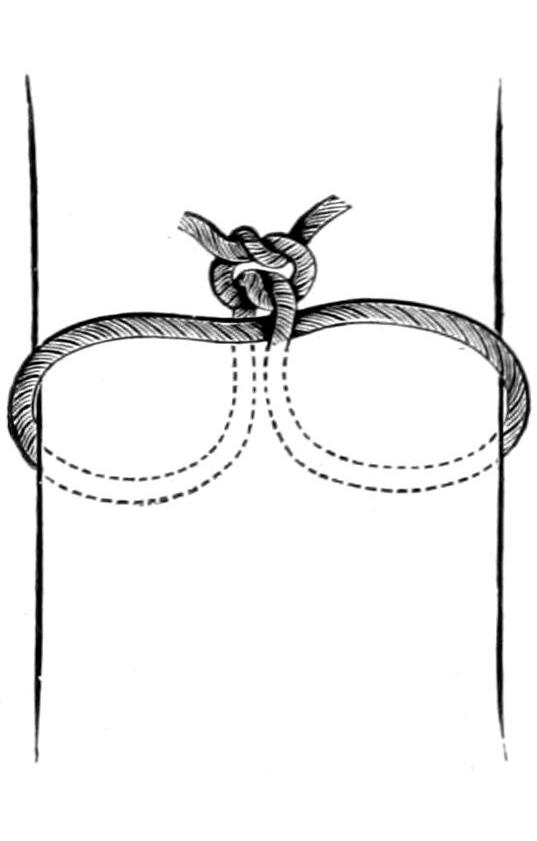
Transfixion suture.
Fig. 67

Reef knot.
Fig. 68
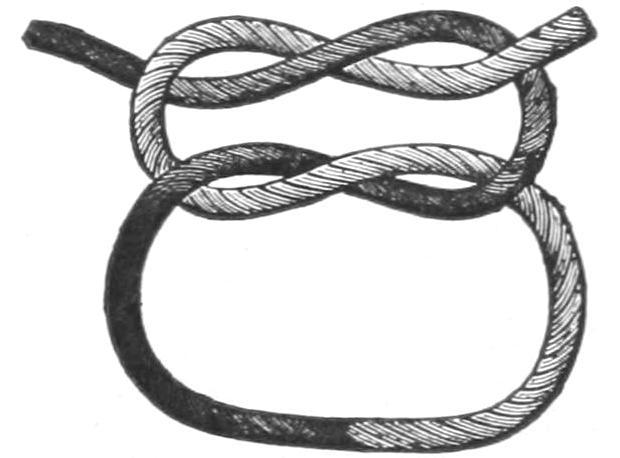
Granny knot.
Fig. 69
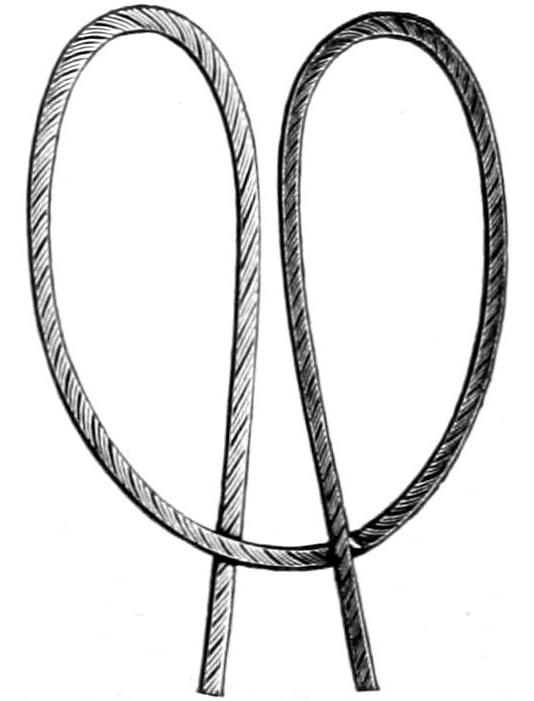
Fig. 70
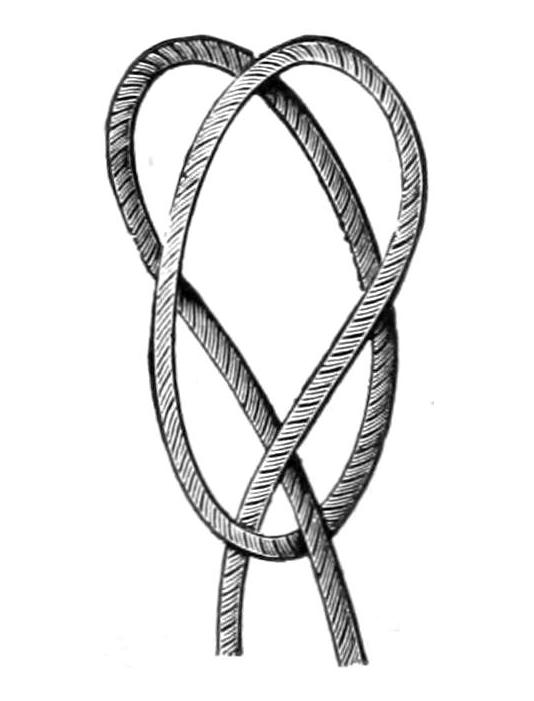
Clove hitch.
Fig. 71
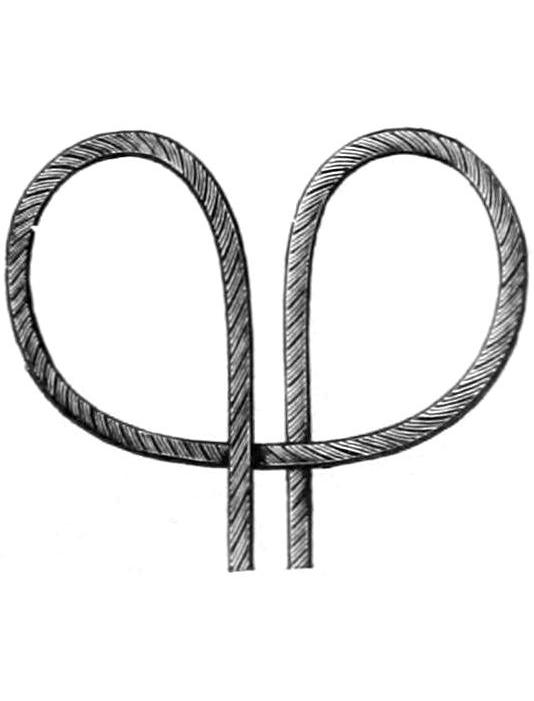
Staffordshire knot.
[242]
When an absorbable suture will serve the purpose it is desirable to use it, since the necessity of subsequent removal is thereby avoided. Inasmuch as every point through which a suture is passed will show its own minute scar, it is desirable for cosmetic purposes to use a subcutaneous suture, which may be made of chromic gut, silk, or fine wire. If of catgut it may be left to disappear spontaneously; but a silk or wire suture should be left with ends protruding from the wound so that after a few days it may be withdrawn by steady traction in the proper direction.
Secondary sutures are those which are placed at the time of the operation, but either not drawn so as to unite the wound edges, or are tied with a bow-knot, so that they may be untied and utilized later. They are useful when either hemorrhage or suppuration is anticipated, and when it is compulsory to pack a cavity with gauze.
Every suture which has failed of its purpose or ceased to be effective should be removed. Ordinarily they are left in place from four to ten days. They should be removed by dividing upon one side of the knot, which should be seized with forceps and pulled upward and to the other side. The suture should be cut at a point where it is moist, so that only its flexible portion may be drawn through the parts which it has held. Moreover the buried portion is more likely to be sterile. Secondary sutures are usually made of silkworm-gut, celluloid thread, or wire. So soon as they are found unserviceable they also should be removed.
—The purpose of a knot is not achieved if it slips, and the “surgeon’s knot” is best for the purpose, since in the first formation one end is carried twice around the other before being tied in the opposite direction. It requires more force in making it taut, but it is safer than the ordinary reef knot (Fig. 67).
Figs. 69 and 70 illustrate the clove-hitch, which becomes firmer the tighter it is pulled. It is rarely used in ordinary sutures or ligatures, but may be made exceedingly valuable. The Staffordshire knot (Fig. 71) serves especially for securing pedicles, which are first transfixed with a double thread, the loop thus formed being slipped over the stump and secured between the two loose ends of the ligature, one end being placed over and the other under it; each is pulled tightly and secured by an ordinary knot. When properly applied it is effective. When knots are improperly applied none of them should be trusted.
When wire sutures are used it is sufficient to twist the ends, unless very fine wire is used, when it may be tied.
[243]
The medical student of the present generation has no conception of the contrast between the results of today and those of a generation ago, or before the introduction of antiseptic technique and its later perfection, asepsis. Under the term “antiseptic” should be included those measures intended to combat sepsis, or surgical infection, from without. The term asepsis is of later date, and was introduced when it was found that the prevention of infection was better than measures calculated to overcome it, or atone for its presence. A perusal of former surgical horrors will afford but an insufficient comparison as to the incalculable benefits for which we are indebted to a small group of men, of whom Lister is the most important; although the names of Pasteur and of Ogston should ever be held memorable in this connection. The two great nineteenth century achievements in surgery were anesthesia and antisepsis, both of Anglo-Saxon origin, one American, the other British.
It was the recognition of the parasitic, i. e., the germ nature of surgical infections, which led to Lister’s first attempts to exclude and combat the infecting agents. And while the original technique which he introduced has been changed in nearly every particular, the correctness of the views upon which it was based has been ever broadened and strengthened. We have learned that simple measures may be as effective as those more complicated, and the principal changes which have been made in three decades have tended toward simplicity and prevention. Thus heat has been made to take the place formerly occupied by carbolic acid. And we have learned that parts made clean need little antiseptic protection. We have learned that healthy tissues are endowed with large powers of self-protection, and also that this self-protection is interfered with by causes over which the surgeon has sometimes but little control. A wound in a body loaded with toxic products is by no means protected against infectious agents by mere external agencies. The appearance of pus in a wound is a reflection upon the surgeon. The ideal aseptic technique will include many days of local and constitutional protection, as has been stated in the sections on Auto-intoxication and on the Preparation of the Patient.
The methods of either antiseptic or aseptic technique include as a fundamental basis the necessity for perfect sterilization of everything which may come in contact with the wound, so far as the surgeon can control it. The atmosphere contains in suspension bacteria, but their contact is no longer dreaded, because of reliance upon the germicidal powers of the fluids and tissues of the body. It is known, however, that in accumulation of fluids there is danger as well to the tissues, either from rude handling, application of large pressure forceps, the insertion of too many stitches, or whatever else may lacerate or impair the circulation.
There are parts of the body where no precautions can afford complete freedom from germ activity, as in the mouth, the vagina, the rectum. Here the surgeon must be cleanly in his work, assuring himself that he introduces nothing new from without. Furthermore, after operation upon these parts he must ensure his precautions by the use of mouth-washes, douches, etc. On the other hand, ample opportunity should be afforded for sterilization of the field of operation, of the hands of the operator and his assistants, the instruments, ligatures, and dressings—everything which may come in contact with the raw surface.
Heat, moist or dry, is the simplest of all sterilizing methods. It is used in dry and in moist form. The most resistant spores are those of anthrax, which is supposed to be a laboratory germ, one not seen in practice. Most of the imported catgut is made from the intestines of sheep, and sheep die frequently (on the Continent) of anthrax; it will thus be seen that the danger of an anthrax infection is not so remote as might first appear, and that no precautions are sufficient which do not include a degree of heat and length[244] of exposure sufficient to kill these germs. In the operating-room, as in the laboratory, has been introduced the method of “fractional,” i. e., repeated sterilization. Most of the materials thus exposed may be left in superheated steam under pressure from thirty to sixty minutes. They are then exposed once or twice more to the same heat at intervals of twenty-four hours. In order to make heat thoroughly useful its effects should permeate everything which it is expected to so sterilize; hence the addition of steam under pressure, especially when dressings, towels, etc., are folded. It is well to have a form of sterilizer that permits steam to be turned off and drying to be accomplished slowly by the aid of dry heat.
Next to steam thus utilized is boiling water, in which nearly everything can be sterilized. Silk sutures and silkworm-gut may also be sterilized in this way; animal suture does not permit of it unless previously hardened. The effectiveness of boiling water is increased by adding to it 1 per cent. of sodium bicarbonate, by which its boiling point is raised.
Dry heat is employed in an oven, or its equivalent, preferably in some apparatus by which temperature can not only be measured but maintained. In such a mechanism it is well to have the temperature raised to 300° F. for at least half an hour, and then let its contents cool slowly.
Another method of sterilization is by using volatile or easily volatilized chemicals, such as formalin in its fluid form, or its equivalent called paraform, which comes in crystals or may be had in tablets ready for use. Formalin is a powerful bactericidal agent, and if used in such form as to be sure of its penetration, good results may be expected. Some materials and instruments which are injured by steam or dry heat may be kept in an atmosphere of paraform, or sterilized by exposure to formalin vapor, being then subsequently protected against exposure in a sealed package. Catheters which have been boiled or cleansed can be thus exposed, as Hutchings has shown, and can be regarded as safe for use. They can, moreover, be resterilized in the same way. Naphthalene has similar properties, but is not quite so strong. The writer is accustomed to use one or the other of these in jars or receptacles containing dry dressings, catheters, and rubber gloves.
If aseptic methods are practised there will be but little use for the employment of any antiseptic, either in solution or in any other form.
Boiled water and sterile salt solution should be available for all purposes. It is customary, however, to have a solution of mercuric chloride on hand, which is colored in order that it may not be mistaken for any other, in which to rinse the hands, especially after they have been in alkaline solution.
The first thing to be sterilized should be that part of the body upon which operation is to be made. In some cases, as about the feet, the mouth, etc., this preparation should be begun two or three days beforehand; in other cases twelve to twenty-four hours will suffice. Preparation should be begun with soap, nail-brush, and razor, the parts being thoroughly cleansed and shaved. It is then customary with most operators to keep a moist and antiseptic dressing applied upon surfaces thus cleansed, which should be protected from drying by a covering of oiled silk or rubber tissue. Green soap is usually employed, which may have added to it a small percentage of carbolic acid or lysol. The mercurial preparations are too irritating to the skin. Carbolic acid has the reputation of being absorbed rapidly. On tender skins and in certain parts of the body it is impossible to make such applications, especially of soap poultices. Under these circumstances repeated washings and some protection should be practised. Feet upon which operations are to be made should be soaked repeatedly and scrubbed. Twenty-four hours previously to operating on the head the scalp should be shaved—preferably forty-eight hours—and prepared as above. For operations in the mouth the tooth-brush and antiseptic mouth-washes should be frequently used. For those in the vagina, douches, etc., should be frequently administered.
The preparation of the field of operation includes a final scrubbing, with a washing of alcohol or alcohol and ether. The hands and external clothing of the surgeon and his assistants should be sterilized, also the towels, suture materials, instruments, and dressings.
Lawson Tait was the first to teach the great value of absolute and mere cleanliness. This applies in large degree to the hands of the chief operator and of the assistants. With a large amount of scrubbing and cleansing of the hands it is not possible to put[245] them into a condition of ideal sterilization. This is perhaps more true of the hands of some than those of others. A realization of this fact has led to the introduction of gloves, either thin rubber or cheap cotton. The former may be used repeatedly. The latter are sterilized by repeated boiling and may then be used again. Rubber gloves may be sterilized by steam or boiling water, and may be cleansed with soap and water or one of the stronger antiseptic solutions. The introduction of rubber gloves has brought great improvement in results. The gloves, however, constitute an impediment to some of the finer work and the easy recognition of tissue. Not the least important of the advantages of rubber gloves is the protection they afford to the surgeon’s hands and to other patients. Many accidental infections may be saved the operator if his hands can be kept out of pus, while the use of gloves permits the operator to pass from a pus case to a clean one without exciting fear. A snugly fitting glove is best drawn upon the dry hand by the aid of sterilized talcum. But the hand which it encloses should have been previously thoroughly sterilized so that it will not be a source of danger should the glove be pricked or torn. The operator can keep his hands in more favorable condition by using gloves dry in this way than by macerating his hands inside of wet ones.
The question of hand sterilization is an important one, whether the gloves are to be worn by some or all of the operating staff. There are occasions when it is important to make the hands absolutely clean because no gloves can be procured. Even the hands encased in gloves should be thoroughly prepared, as there is no knowing when the glove may tear and the surgeon’s bare hand come into contact with the patient’s tissues. Running water is preferable to a basin filled with it, for while it runs it carries away such material as may be detached by soap or nail-brush. If it be not possible thus to wash the hands, then repeated basins of sterilized water should be used, and all the crockery or metal ware used in the process should be sterilized, so that the hands will not be contaminated by handling unsterilized material. Nail cleaners are essential agents, to be vigorously used, and nail-brushes should be sterilized after each using, and there should be a separate brush for each operator. The common soaps and even the officinal green soap are not sterile. The former should be relied on only for the first cleaning, and the latter should be sterilized before use. A dirty hand should not be thrust into a receptacle containing freshly sterilized green soap. The outside coating of dirt should first be removed by an ordinary soap. Vegetable fiber has been recommended by many, but it is not as good as ordinary corn-meal, which should be sterilized before using. It is not as gritty nor as keen as sand, and yet it is sufficiently rough to serve admirably the purposes of a curry-comb. A first scrubbing with common soap and a nail-brush, followed by green soap with corn-meal, and this by a thorough use of the nail cleaner and a clean nail-brush, will ordinarily serve to put the hands in a reliable condition. It is the practice of some to add antiseptics to the soap, e. g., lysol and thymol. A number of years ago I introduced ordinary mustard flour for this purpose, basing its use upon the fact that the essential oil of mustard is one of the most potent of the vegetable antiseptics, in addition to its power as a deodorizer. (Parenthetically it may be said that when unpleasant odor attaches to the unprotected hands after making a postmortem examination, or opening an offensive collection of pus, the use of mustard will quickly remove the taint.) Even mustard is not absolutely reliable, nor is anything else which can be tolerated by the human skin. A method much in vogue a few years ago was to wash the hands in a solution of potassium permanganate, and then to decolorize the skin in another strong solution of oxalic solution. This method was at one time regarded as an effective one, but it is severe upon the skin. Another method in use at present combines commercial chloride of lime with saleratus; here free chlorine is supposed to be the active agent.
The bacteriological side of this subject has been investigated by numerous observers, particularly Dr. E. R. McGuire, attached to the Buffalo Surgical Clinic, who reached the following conclusions: Absolute sterility of the hands is unattainable, but as toward this result nothing takes the place of long and vigorous mechanical scrubbing under aseptic precautions; the use of antiseptics on the skin is of questionable value and often distinctly harmful; the operator whose hands perspire freely should wear gloves in every case; the use of rubber gloves is not ideal, but gives the nearest approach to it.
No material should be used which is so harsh that it will injure or destroy the epithelial cells either upon the operator’s hands or upon the patient’s skin.
[246]
Solutions of gutta-percha in its different solvents, or of collodion in acetone, have been suggested as forming a covering for the hands by quickly drying upon the skin. The merit of these preparations is questionable, and the length of time required to dissolve the coating makes them impracticable. They have found little favor among surgeons.
Next to the sterilization of the parts to be operated, and the hands, may be considered treatment of septic tissues or fluids and protection against further infection. Clean and uninfected tissues need no other precautions than those already described, plus extra care in hemostasis, in order that there be no clot left in which germs may find a nidus, and the careful closure of the wound in such a way that no cavities or “dead spaces” may be left in which blood may later collect. Surgeons generally agree that the less clean tissues are handled and the less contact they undergo with foreign materials the more readily they heal. The ideal fluids with which to cleanse parts or to wash away blood clot are sterile salt solution and boiled water. Antiseptic solutions should not be used upon healthy tissue; but when abscess cavities have been opened and when pus or other infectious material have come in contact with fresh raw surfaces, every effort should be made to overcome its effects. It is customary in abdominal operations to “wall off” the site of a pus focus so that contamination of adjoining surfaces may be avoided, by placing gauze packing around it. Other expedients, e. g., the use of a rubber dam in any of its modifications, which will aid in this purpose, should be adopted. Upon brain surfaces, as upon the ruptured perineum, and in vaginal, rectal, and numerous other operations, a continuous fine stream of salt solution may be directed with great benefit.
An abscess of any kind, no matter where located, should be thoroughly cleansed, its cavity disinfected, and easy access made to the outer wound. The interior of such cavities should be scraped with a sharp spoon. After curetting, a thorough washing or swabbing, often with the use of hydrogen dioxide, will often prove serviceable. Even a treatment of this kind does not afford as complete disinfection as may be secured by free application of pure carbolic acid or of a strong solution of zinc chloride (50 per cent.). The effect of this is not only to more completely sterilize, but to so sear the cauterized surfaces as to make them incapable of absorption. Excess of the caustic should be wiped away, or antidoted, in the case of carbolic acid by further swabbing with alcohol, or in the case of zinc chloride by merely washing out. Such a surface should heal naturally after sloughing, yet it is rarely safe to completely close such a cavity. A light packing of clean gauze, or, as the writer is fond of using it, of gauze sopped in balsam of Peru, will permit such a cavity to quickly close by the granulation process without further disturbance. Bone cavities, especially, are well treated with zinc chloride, it being difficult to so thoroughly disinfect such a focus that it may be safely closed without drainage; or they may be filled with bone chips or paraffin.
Visible tissue which is sure to slough should be removed with scissors or the sharp spoon, in order to save valuable time. Sometimes the actual cautery may be used to great advantage, as in chancroidal buboes, where every particle of raw surface will be infected by the pus which flows over it, and where it is advisable to cauterize not merely the suppurative focus, but everything which may come in contact with its pus.
—Instruments are now all made of metal, usually nickel-plated, which will stand at least a certain amount of exposure to heat. It is not sufficient, however, to sterilize instruments alone, but basins, irrigator nozzles, and everything else which may be wanted during the course of an operation should be equally prepared for it. Inasmuch as hard rubber does not well stand even boiling water, instruments should be made, so far as possible, of metal or of glass. Boiling water, or “live” steam, are universally employed for this purpose; while to the water is often added 1 per cent. of ordinary washing soda, which enhances its serviceability. Fifteen to twenty minutes’ actual boiling, or its equivalent, will be sufficient for ordinary purposes. All instruments, such as knives and scissors, deteriorate after repeated use in this way and need to be frequently sharpened. Catheters also may be sterilized by boiling and should be constantly kept exposed to some volatile antiseptic, such as formalin (see above). Sterile material should be used upon the inhalers, and the metal parts of these, as well as mouth-gags, hypodermic syringes, and the like, should all be boiled.
[247]
—Not only the dressings which are to be employed after an operation, but the gauze, the cotton, or the sea-sponges which may be used during the same should have been twice sterilized either by dry heat or steam, in order to ensure security. No absorbent material should be packed tightly if it is to be subjected to steam, as it is not easily penetrated, even under pressure. Moreover, not only these materials but the sheets, gowns, aprons, towels, splints, and everything which may come into near approach or actual contact with the wound should be prepared in the same way. After sterilization all these materials should be enclosed in germ-proof, sterile wrappers of some kind or in sterile jars or boxes.
As a postoperative precaution, all materials which can be destroyed after use in a septic case should be burned. If this be not practicable, they should be soaked for twenty-four hours in a strong solution of corrosive sublimate, say 1 to 500. At the conclusion of operation there should be no opportunity left for dissemination of infection.
—In place of sponges, gauze or absorbent cotton wrapped in gauze are now generally in use, prepared as above. There are some purposes for which sea-sponges are very convenient if they can be made reliable. Those which are received fresh from the dealer should be freed from sand by beating in a mortar, placed in a solution of 1 to 500 of potassium permanganate, and then transferred to a solution of sodium sulphite containing 5 per cent. by volume of pure hydrochloric acid; in this they remain until they are bleached out, which will take but a few minutes. They are then thoroughly washed in sterile water and stored in 5 per cent. carbolic solution.
—Wire, silkworm-gut, horse-hair, and silk or linen thread may be sterilized, if not rolled too tightly, by twice boiling for a half-hour, and then being allowed to dry, or preserved in 5 per cent. carbolic solution or in sterile alcohol. Disappointment often comes from rolling these materials so tightly upon spools that sterilization of the deeper layers is not complete. This is true of catgut as well as of the other animal sutures.
—Catgut, so called, is usually made from the intestine of the sheep, and must be freed from anthrax germs or spores. It should be rolled loosely on spools or rods, each layer separated from that beneath by a piece of gauze. The writer prefers to free it from animal fat by a preliminary soaking in ether or benzene. After this it may be sterilized by boiling in alcohol, preferably absolute, which must be in a container not tightly closed. This is placed in water, raised gradually to boiling, and should boil for two hours. This process should be repeated at least once after the expiration of twenty-four hours. This is the simplest of all procedures and generally proves reliable. Other methods are those of exposure, for instance, to cumol, a volatile paraffin oil, in which it is boiled under pressure in a special apparatus, the temperature being raised considerably above the boiling point of water (300° F.). When the receptacle is opened the cumol is drawn off or evaporates and the catgut is left dry and sterile. It should be either kept dry in a sterile jar or in alcohol. Some prefer to add to the latter a small amount of oil of juniper, which has a little hardening effect upon the animal material.
Catgut should be tested repeatedly to be assured of its sterility. Special methods of preparing catgut are as follows:
is prepared by placing the gut, wound as mentioned, in a 3 per cent. formalin solution for three hours. If the sterility of that which is used be not assured, then this preparation should be boiled in water for fifteen minutes. Catgut of large size should be immersed in a solution stronger than the above. It will probably be sufficient to give this a final boiling at the time of operation. This is almost as lasting as chromicized gut.
—Gut to be thus prepared should be wound in single layers on spools and immersed in a solution of potassium bichromate 1.5 to 2.5, carbolic acid and glycerin each 10, and water 1000 parts. It is allowed to remain in this solution for twenty-four hours, then dried and boiled in water, or in alcohol under pressure, in which it is subsequently stored. According to the length of exposure and the strength of the solution, this gut will resist absorption from ten to thirty days.
is growing in favor with some surgeons. It is prepared by immersing catgut in a 10 per cent. solution of iodine, in which it is kept for a week. After removal it is allowed to dry and is stored dry, but should be kept protected from exposure.
[248]
may be boiled in a 2 per cent. lysol solution for one hour, which makes it pliable. Sometimes it is convenient to have it stained black in order that the sutures may be better distinguished when removed. In this case it is allowed to stand in a 1 per cent. silver nitrate solution for from twelve to twenty-four hours. This gives it an almost black stain, but tends to make it more brittle. It may be kept in alcohol, or dry in a sterile receptacle.
—Silk should be spooled loosely, boiled in a similar solution for one-half hour, and again in plain water just before using. It may be stored dry or in alcohol. It may be also stained black.
—This should be washed and scrubbed in green soap and hot water, after which it is spooled, and then boiled for thirty minutes. It may be stored dry or in alcohol. This is a linen thread covered with a film of celluloid.
are prepared essentially as is catgut, but if boiled in alcohol they must be kept covered with the fluid, as they tend to disintegrate.
of rubber should be boiled in soda solution for fifteen minutes, and may then be stored either in 1 per cent. formalin solution, or dry in a suitable tube.
are first prepared by washing in 1 to 500 sublimate solution, then dried, and exposed in an air-tight jar to the vapor of formalin or paraform.
The above are the methods usually in vogue in the writer’s clinic, and may be relied upon. These materials should be frequently tested by dropping fragments into culture tubes and watching the result, but only after taking the precaution to precipitate or neutralize the antiseptic previously used in their preparation.
—In well-regulated clinics sterile salt solution is always at hand. As has been stated the old six per mille solution may be improved by adding 1 part of potassium chloride and 2 parts calcium chloride. For emergency purposes tablets are now prepared which will permit the rapid preparation of these, of any desired strength. To this a little corrosive sublimate may be added without producing decomposition. When sublimate is used alone, or in other combinations, a little vegetable or mineral acid, such as tartaric or hydrochloric, should be added, as most of the water used contains lime.
When a maximum of bactericidal effect is desired with a minimum of irritation, the silver salts, either the lactate or the citrate, will probably afford the best results. The former may be used as strong as 1 to 300, the latter 1 to 500. The writer has frequently used these solutions for washing out the peritoneal cavity, in cases of tuberculous peritonitis, where they serve their purpose admirably. For washing out tuberculous joints and many other abscess cavities, solutions of silver nitrate of 1 to 1000 to 1 to 2000 are most serviceable; or, for the same purposes, boiled water, to which has been added sufficient tincture of iodine to give it a mahogany color. In caring for such cases it is good practice to alternate the solutions, using them on alternate days.
Antiseptic powders or applications in dry form are useful for many purposes. At one time iodoform was very popular; it was supposed to act by virtue of the iodine set free in the presence of decomposing organic material. It is now seldom used, partly because of its tell-tale odor, and partly because of the disappointment which its use often brings. It is, moreover, an active toxic agent of itself, and has many times given rise to symptoms of intoxication, such as mental depression, delirium, nausea, and anorexia. Under all these circumstances free iodine can be detected in the urine.
There are numerous substitutes for iodoform, many of which are superior to it in antiseptic properties, while most of them are free from odor and toxic qualities. Two substances, however, are used extensively—naphthalene and bismuth subiodide or red iodide. The former has a marked odor and is more or less volatile, which makes it particularly valuable. The latter is odorless, non-toxic, and of much greater value as an antiseptic than most of the others, because it will give off free iodine under favorable circumstances. A good plan is to use it in the preparation of gauze and dressings, as well as for a dusting powder upon the skin.
The absolute value of these local applications is questionable, because a wound will sometimes heal under the protection of a piece of foil or gutta-percha tissue as well as when dressed in any other way. This is true only of wounds in part surgically clean.
—Drainage has been resorted to, more or less intermittently, since earliest historical times. It is provided for the removal of deleterious fluids or of superfluous[249] exudates or transudates. It is a recognition sometimes of a necessity, at other times a confession of fear which may or may not be justified. It is bad practice to cover a focus of previous gangrene or suppuration in such a way that the infected cavity is closed to the escape of accumulating fluid. This may be prevented by the use of a suitable drain. At times a clean operation may be made, and yet in such loose tissue, or to such an extent, that it is preferable to provide for the escape of blood rather than let it occur and force apart surfaces which should be in close contact. A drainage tube may serve as a vent through which blood may escape that has oozed after closure of the wound. After pelvic operations provision should be made for the withdrawal of accumulating fluid which might serve as a culture medium for germs. Drainage is therefore necessary in many instances.
It will suffice sometimes to suture loosely a part or the whole of a wound, so that should tension occur from retention there may be spontaneous escape. This may be termed indirect drainage, and sometimes has to be made still more complete by leaving out some sutures, or by placing secondary sutures, which are only utilized some days later, when previously infected surfaces have become healthy and are granulating, so that they can be brought together.
By direct drainage secretions and fluids are guided toward the dressings, which should be absorbent or so arranged as to provide for their accommodation; thus in drainage of the gall-bladder or of the urinary bladder the tube may be connected with a suitable receptacle by siphonage. Capillary drains may be made of a few strands of silkworm-gut, which is non-absorbable, or of catgut, which is absorbable, and to which, perhaps, no further attention need be paid. This will answer for conducting away small amounts of fluid which exude. Gauze, or its equivalent in the shape of some form of wicking, affords an excellent material for removing fluid by osmosis. The thinner the fluid the more perfectly it serves this purpose. The gauze must be changed frequently, as these lesions may become filled with coagulated material, in which case it would act merely as a plug. The so-called cigarette drain consists of folds of gauze, or a small roll of it, surrounded by sterilized oiled silk or gutta-percha tissue, in which are cut numerous holes. The same purpose may be achieved, but often not so well, by a piece of rubber tubing split down one side. The gauze drains by osmosis, and the rubber prevents any adhesion to the wound margins and any pain in the removal of the drain; while a certain amount of fluid may escape around and outside the smoother surface.
When the fluids to be removed are more dense—e. g., pus—tubular drains should be provided. These vary in size from that of a lead-pencil to that of the finger. A tube which is too small becomes easily plugged. They are perforated with numerous openings for the ready entrance of fluid save in those cases, like the gall-bladder or the pelvis, where it is desirable to drain only the depths of a cavity. These tubes are usually made of rubber, the purer forms of gum being preferable. For some purposes, especially in the pelvis, tubes of glass or aluminum are used; these are non-collapsible. They may be emptied by a capillary drain, or by the frequent use of a small syringe with a long nozzle, by which they are pumped out at regular intervals. Metal and glass tubes can be resterilized and used again. All other drainage material should be burned as soon as removed. There are occasions when it is well to use a dressed drain—i. e., a tube surrounded by absorbent gauze, and this again by rubber tissue or oiled silk. In many instances it is well to prevent the loss of a drainage tube by passing through its outer end a safety pin, or by stitching it to the margin of the skin wound. Tubes have been lost, especially within the thoracic cavity after operating for empyema, more often than is perhaps generally known, and for a lack of precaution in this respect.
Tubes of decalcified chicken bone have been used and are occasionally serviceable. They are made by cleaning the cooked bones of the fowl, soaking them in 20 per cent. hydrochloric acid solution until decalcified, trimming the ends, cleaning the interior, and are then sterilized by boiling in a saturated solution of ammonium sulphate. They are then washed in sterile water and preserved in alcohol. They correspond to catgut, and will ordinarily last in the tissues for about eight days. They may be chromicized, as is catgut, in which case they endure considerably longer.
[250]
At the risk of some repetition it is proposed to epitomize here a few directions on a subject of great importance, to which, as well in theory as in practice, too little attention is often paid. For present purposes patients may be divided into two classes: those who have sustained accidents or sudden surgical diseases, where no time is afforded for preparation; and those who, having chronic conditions, are subjected to surgical measures which are, however, sometimes made abrupt by sudden decision. In the former case the surgeon is compelled to work hastily; for the latter, time for preparation should be always afforded. Experience teaches that a few days, sometimes even a few weeks, may be well spent in preparing a patient for a surgical operation.
In emergency cases, aside from the usual scrubbing and shaving, there may be several matters to which it is well to give attention. The stomach should be washed out just before the administration of the anesthetic, or soon afterward. If there be time the rectum should be emptied, and the bladder always; too much care cannot be given to these performances. The degree of shock should be estimated and appropriate treatment given, according to principles stated in the chapter on Shock.
Foresight will often dictate the preparation of some part of the body not directly involved in the field of injury; for example, in any gunshot or stab wound of the abdomen or in a case of acute pancreatitis the back should be scrubbed and cleansed and the patient laid upon sterilized material, so that should posterior drainage be required it may be promptly made without waste of time required for preparation. In head injuries, if the scalp or cortex of the skull be involved, the entire head should be shaved. In preparation of patients for operation upon the mouth, tonsils, or stomach an antiseptic mouth-wash should be used in order to avoid, so far as possible, contamination from these germ-laden regions. It Is especially in cases undertaken for the chronic pathological conditions that time can be afforded for careful preparation. It may be assumed that every patient suffering from a chronic surgical malady has been so disabled, in at least some function, that elimination has been interfered with. The emunctories of the body comprise essentially the skin, the lungs, the intestines, and the kidneys. Every one of these should be made to perform its work more fully.
The skin should be stimulated by hot-air baths, for which purpose patients may be sent daily to the Turkish baths, while others should take their sweats in cabinets or in bed. If it be possible after the skin has been made to perspire profusely the patient should be put into a hot bath and the skin thoroughly scrubbed.
The lungs may be stimulated partly by improving the heart’s action, partly by certain exercises, and by getting the patient out into the open. The intestines should be made to perform their work, preferably by the mildest measures that may prove effective. Mercurials are agents of great value, as they not only stimulate secretions but are antiseptic in their effects. Sodium phosphate is useful when something stronger is not required.
Many patients who are found in this class will have impaired digestion, for which a regulated diet should be supplied; and such cases may call for lavage, as well as for a careful examination of stomach contents, in order that appropriate aids to digestion may be given. Most patients suffer from intestinal torpor, especially of the large intestine, and the daily administration of a high-up colon wash, with the patient in the knee-chest position, will give gratifying results.
It has been suggested that in all operations upon the upper alimentary canal it would be of great advantage to feed the patient during the previous forty-eight hours upon sterilized food.
[251]
A careful study of the urine should be made, both quantitative and qualitative. The gross measurement of the amount excreted in twenty-four hours is of importance. It is necessary to know what amount of solids is being daily excreted, as well as the amount of fluid. Renal insufficiency is one of the difficulties with which the surgeon has often to deal, and caution should be used when operating upon a patient suffering from this condition. Extra work is thereby imposed upon other emunctories. A depraved blood circulation through the brain will often impair its function and lead to delirium in mild or serious form. The heart’s action will be impaired and septic infection is made more possible, in spite of every precaution included in antiseptic technique. In the chapter on Infection it was stated that certain cases of surgical sepsis commence as infections from within, due to failure in unloading the body of its content of disease germs.
Hyperacidity should be also corrected. In order that this may be properly done, the urine should be tested by a more accurate method than by litmus paper. The restlessness and consequent wound disturbances which may ensue after operation may be due to failure in the elimination of uric acid and the oxalates; alkaline diuretics, therefore, are an important feature in the preparation of many surgical patients.
The blood and circulation should not be neglected in these cases. These patients are frequently anemic. A high degree of anemia is recognized by methods described in the chapter on the Blood. Much may be done, even in a short time, to improve the quantity and the quality of the blood, by attention to nutrition and elimination. By these same measures the heart’s action will be also greatly strengthened, but much can be accomplished in this direction by the use of digitalis, cactus, or other of the heart stimulants, and by the administration, preferably subcutaneously, of strychnine. This is usually given in too small doses. Two hypodermic injections of ¹⁄₃₀ Gr. (0.002) a day will have a pronounced effect. While the heart is thus fortified as against shock before the ordeal, adrenalin will prove the most effective agent during it and after it is passed.
Intestinal fermentation or decomposition is a prominent feature of many of these cases. If it be possible to select a drug which has antiseptic properties that may be effective in the intestine and in the kidneys, it will come near to being the ideal in this respect. The attendant has here to choose from many remedies, and his choice will depend largely on his personal experience. It is better to use a few remedies and use them well than to be indiscriminate.
Salol, benzosol, betanaphthol, sodium sulphocarbolate, and the salts of mercury and arsenic will furnish sufficient compounds from which to select. When the urine is alkaline, as it often is in certain kidney and bladder diseases, urotropin may be advantageously combined with one of the others.
In the way of general preparation of those patients who have to undergo operations upon the mouth, the nasopharynx, the esophagus, trachea or larynx, and upper alimentary canal, they should be sent to the dentist in order that their teeth may be put in good condition and accumulations of tartar removed, and then use an antiseptic mouth-wash, or, when necessary, a nasal spray, in order that there may be avoidance of infection from the bacteria which abound in these parts. Patients often have diseased and carious teeth, and, in hospital patients especially, the mouth is often in a dirty condition. So long as any wound surface is so situated as to be in danger of contamination from these sources, this should be minimized as far as possible.
—Experiments have been made by Mikulicz with regard to the value of nuclein in producing an artificial and protective leukocytosis before abdominal operations, hoping thereby to accomplish more or less in the way of prevention of peritonitis. The procedure is based upon the well-known property of nucleinic acid, or nuclein, to produce a prompt but transitory increase in the number of leukocytes. To take advantage of this, 3 to 5 Cc. of nuclein solution is administered beneath the skin, say twelve hours and again six hours previous to the operation. Should any septic agent be introduced or liberated during its performance, the leukocytes will be present in additional numbers to act as phagocytes and exert their active protective powers.
[252]
The care of patients after operation is a factor in a surgeon’s success and calls for discrimination and judgment. The fact that the odor of chloroform or ether persists about the patient and in his breath for hours after their administration shows to what extent they have been dissolved and are circulating in the blood. If elimination have already been attended to, and so far improved as to permit the emunctories of the body to do work up to their capacity, these anesthetics may be promptly eliminated. The longer they circulate in the blood the greater the disturbance to other functions and the more difficult it is to get normal function equalized.
The things especially to be guarded against, so far as one may prevent them, are nausea, vomiting, extreme restlessness, pain, inactivity of the bowels, insufficiency of the kidneys, and the toxic action of any antiseptics or drugs which may have been used, e. g., iodoform.
Nausea and vomiting after operations are due not so much to mere reflex activity as to the elimination of the anesthetic by the stomach and its irritant action. No matter how produced, such vomiting is of itself most depressing, mentally and physiologically, and is injurious in a large proportion of cases, and efforts should be made to prevent it. So long as it was regarded simply as a reflex act drugs were theoretically sufficient for its treatment, but with the appreciation of its actual causation it will be seen that the irritating material should be removed. This may be done with the minimum of discomfort and the maximum of advantage by means of the stomach tube. Lavage, therefore, constitutes the most rational and effective treatment in cases of postoperative vomiting.
That the anesthetic reaches the stomach by way of the circulation and is excreted by the gastric mucosa has been proved by the studies of Türck. He showed that the same is also true of morphine. He showed, moreover, that the stronger anesthetics disturb the metabolism of the cells and that toxic products are thereby produced which, being reabsorbed, cause an auto-intoxication reducing vital resistance of the blood serum and the tissues. Thus during anesthesia there occurs an atony of the stomach walls with the escape of the anesthetic into the stomach, which, acting as an irritant, leads to an increased amount of toxin production. The discoloration of the gastric mucosa and the capillary hemorrhage which take place, as shown postmortem in cases where persistent vomiting is a feature, illustrate the disturbing effect of the stronger anesthetics upon the stomach itself. This furnishes, then, the reason for washing out the stomach immediately after stopping the anesthetic and before the patient leaves the operating table. It cannot be said that by this measure postoperative vomiting will be abolished, but its frequency will be materially lessened.
Lavage may also be practised to great advantage not merely immediately after the operation, but during the ensuing twenty-four hours, or later should vomiting recur or come on late. On the other hand, where time has not been afforded in which to suitably prepare a patient for operation, it is advantageous to wash out the stomach before administering the anesthetic as well as after. This is recommended as a general measure, and without special reference to those cases where operation is directed to the stomach itself or to the intestinal tract, where it has become an established part of the preparation to carefully cleanse these viscera.
Several points in the performance of lavage will be of great service to patient and operator. It should be performed quickly in order to reduce the length of the discomfort, and the water used should be warm, at least 110° F. If the throat be previously sprayed with weak cocaine solution (2 per cent.), or if a cocaine lozenge be dissolved in the mouth, the tube can be introduced with less gagging and difficulty. The lubricant should be flavored with wintergreen or some other aromatic.
Where vomiting continues in spite of lavage it is advantageous to give a full dose of chloral with a little starch-water in the rectum; 2 or 3 Gm. of chloral, with as much sodium bromide, to which, in case of severe pain, a little opiate may be added, may be profitably used in cases where the patient is restless and where sleep is fitful or perhaps impossible. This will be more beneficial than drugs administered by the mouth. It is seldom rejected, and is very soothing.
[253]
Extreme restlessness is undesirable from every point of view. In some cases when it comes on early it is an evidence of insufficient oxygenation and may be combated by the administration of oxygen gas. It frequently accompanies shock and constitutes one of its most disturbing features. It may be combated by a subcutaneous dose of morphine or heroine, or chloral in doses of 2 Gm., with as much sodium bromide, thrown into the rectum with salt solution. The effect may not be as prompt, but it is often much better. Restlessness is not always a symptom of pain, but is occasionally an uncontrollable reflex nervous phenomenon.
After operations physiological rest of the operated part is necessary for the process of prompt repair. After abdominal operations, especially when restlessness and vomiting are combined, much harm may be done if the patient cannot keep the parts quiet.
Pain will often accompany restlessness, and frequently accentuate it, especially when patients have not yet fully returned to consciousness. It may be relieved by warm or cold applications. In some cases an ice-bag may be used as soon as the patient is placed in bed—for example, after breaking up an ankylosis. In mild cases the use of chloral in the rectum, as above, with an opiate added, may be sufficient. When pain is severe hypodermics of morphine or heroine should be given. Secretion should not be disturbed by such drugs as these, yet as between them or permitting patients to suffer intensely, my opinion is that opium should be given judiciously, providing it prove sufficient. In extreme cases morphine seems to be the only medicament upon which complete reliance can be placed. When the opiates seem to produce nausea the difficulties are heightened. It may be decided in some cases to push the opiate to the point of narcotism, preferring to keep the patient in this semistupefied condition for two or three days and until the series of early dangers have been passed. Opiates should be given with great discretion lest the opium habit be encouraged if not formed.
Lately there has come into use a remedy which has little or no unpleasant after-effects, and upon which a good deal of reliance can be placed, namely, aspirin, which may be given in 1 Gm. doses, repeated as necessary. If it be combined with phenacetin, in doses of half that amount, the combination will be more effective than either alone. This will often prove a serviceable substitute for opiates in any form.
After operation upon the lower bowel, or in any part of the pelvis, patients may complain of pain, sometimes severe, referred to the rectum. Relief may be obtained by throwing into the rectum, through a flexible tube, one-half to one pint of warm linseed oil. This will often take the place of an anodyne or a suppository.
The next question is one of catharsis. If the alimentary canal have been properly emptied, as it should have been before the operation, the bowels may be allowed to rest for the ensuing forty-eight hours. At the expiration of that time the lower bowel should be emptied. Whether this be done with laxatives administered by the mouth or by enema will depend on the character of the case and the reliability of the stomach. When vomiting is distressing little can be accomplished from above. In most cases the first effort is to be made by the administration of a thorough colon wash, or by the use of an enema, which may perhaps best consist of ox-gall, glycerin, and a saturated solution of Epsom salt. If this be thrown up high, and retained a while, it will in all probability be effective. Should the operation have been one upon the rectum extra care will be needed for the patient’s comfort, and just preceding the stool a small amount olive oil should be administered through a tube. Many patients will complain of gaseous distention or other discomfort, due apparently to fermentation, and partly perhaps to the air which they have swallowed during the act of vomiting, or because of nausea. No matter how produced it will afford relief to get rid of this gas, and while this may be partly accomplished by an enema, it will be more thoroughly effected by a mercurial, given by the mouth, to be followed by a saline laxative. In order that flatus may escape without effort, a rectal tube may be inserted, which later may be utilized for the administration of an enema. Save in rare instances it is a mistake to allow accumulation of fecal matter, as the stercoremia thus favored may easily lead into a more profound form of poisoning by its interference with elimination and vital resistance.
Attention should be also given to the bladder and to the urine. Renal insufficiency is one of the great dangers pertaining to the use of anesthetics. This may be combated by 2 Gr. doses of sparteine sulphate every three hours (McGuire).
[254]
Many patients are unable to void urine after operations, particularly after those upon the female genitalia, and the use of a catheter is often necessary. This should be used with antiseptic precautions, both as to the patient, the instrument, and the operator’s hands. Much of this difficulty can be avoided by injecting 20 Cc. of a 2 per cent. sterilized boroglycerin solution through a catheter in the evening after the operation. Its action is usually prompt, and in five to ten minutes the patient spontaneously empties the bladder without unpleasant after-effects.
After abdominal and pelvic operations the patient should not be allowed to urinate, but should be systematically catheterized. The bladder should never be allowed to become distended. The amount and character of urine passed should be carefully noted. In serious cases the amount of solids eliminated should be estimated, in order that it may be kept up to the necessary standard. In fact, efficient and sufficient elimination is more necessary after the prolonged administration of an anesthetic than after almost any other event. When sufficient fluid to keep up the standard cannot be administered by the stomach, it should be introduced into the rectum or given beneath the skin. Two or three enemas of salt solution should be administered each day, and in urgent cases the normal solution should be thrown beneath the skin, and this should be repeated as often and as long as may be necessary. When the patient begins to show evidence of what is vaguely described as uremia, i. e., the toxemia of renal insufficiency, not only should warm water be used in these ways, but hot-air bed baths should be given twice a day if necessary, in order that some of the work of the kidneys may be assumed by the skin. Hot-air baths stimulate the kidneys as well, and these measures will prove more effective than most of the diuretics, although digitalis and pilocarpine by the skin may be of assistance.
Patients frequently complain of excessive dryness in the mouth. This may be relieved by occasionally dropping beneath the tongue one-half of an ordinary hypodermic tablet of ¹⁄₁₀ Gr. pilocarpine; also by mouth-washes which contain a little glycerin, and by keeping the lips moistened with glycerin. Excessive sweating can sometimes be relieved by giving a hot-air bed bath or a hot mustard foot bath, as the extra action of the skin thus induced checks the spontaneous drain.
Delirium and acute mania occasionally supervene after operations. It should first be made clear that these are not due to any antiseptic or drug. Iodoform is less frequently used than formerly. Children and aged people become delirious with less provocation than do those in middle life. Such delirium is generally an expression of a toxemia, and, in addition to such other measures as may be necessary, calls for control and restraint and more active elimination, as in so-called uremia. In proportion to the degree of mania must be the restraint prescribed. A restraining sheet or a strait-jacket may be sometimes needed. When these conditions arise in surgical patients more harm will come from the violation of the principle of physiological rest than from the drugs which may be needed to secure it. The milder measures should be first used, abstaining as far as possible from opiates, which are probably the least desirable of all, but which may be occasionally demanded. Chloral, the bromides, cannabis indica, alone or in combination, may be made to render more valuable service. Hyoscine, in doses of ¹⁄₁₀₀ to ¹⁄₅₀ Gr. beneath the skin, will often control when other remedies fail; it may prove invaluable. When delirium tremens complicates a case it may be treated as suggested in the chapter on Various Intoxications.
[255]
A tumor is a new formation, not of inflammatory origin, characterized by more or less histological conformity to the tissue in which it has originated, and having no physiological function.
By the above definition it is intended to separate the new-growths from a distinctive class of neoplasms which are of inflammatory (i. e., of infectious) origin, to which the generic term of infectious granulomas has been given. (See Part II.)
Exceedingly vague notions have prevailed concerning the nature and origin of tumors, and, while the clinical observations of writers in the past will never lose their value, the ideas which have prevailed concerning their pathology constitute interesting reading in a historical sense, but are now of small value. Accurate notions scarcely prevailed until Virchow demonstrated that tumor cells nowise differ from cell types which are met either in embryonic or in adult tissues. Tumors, like all other parts of the body, are built up of cells, and the points concerning which we need most light regard the influences which determine cell overproduction in these characteristic forms. Concerning the views that have prevailed, this is scarcely the place in which to offer an epitome. I shall therefore take up but few of the explanations which have been offered to account for tumor growth, and will emphasize that, according to our present light, there is no explanation sufficient to cover all cases, but that it is now one cause and now another which may determine this peculiar form of cell activity.
—The effort is often made to explain the presence of tumors upon the hypothesis or the known fact of some previous injury. Frequently tumors appear in sites where there have been previous traumatisms, but this sequence of events by no means proves a definite relation of cause and effect. On the other hand, there are forms of irritation which are often followed by tumor formations. Probably no woman escapes without one or more bumps or bruises upon the breast, yet they do not produce tumors in more than a trifling proportion of cases. Per contra, upon the lower lip of inveterate clay-pipe smokers and the scrotum of chimney-sweepers there develop certain forms of malignant ulcer (epithelioma) which so often and so significantly follow upon the irritation thus produced that it is impossible to avoid conviction that one is the cause of the other. Should events prove the parasitic nature of any of these growths they will also prove that the irritation causes surface lesions through which infection easily occurs. In regard to the relative frequency with which cancer in some form follows trauma we should not forget the well-known fact that traumatism usually diminishes tissue resistance. If cancer be an expression of infection, as many (including the writer) believe, the possible relation between trauma and malignant disease may be better appreciated.
[256]
—This refers to inflammation in the sense in which it has been used in the past, implying a variable condition, sometimes including and sometimes excluding infection, the term covering a confused mixture of irritation, hyperemia, and infection. In so far as it concerns inflammation as considered in the present work it should not be here included, since inflammation (i. e., infection) produces neoplasms of a class considered in Part II and is distinctly ruled out from present consideration (i. e., the infectious granulomas).
If inflammation in the former sense be more than hyperemia it may be regarded as predisposing to cell activity, but not necessarily to tumor formation as distinguished from hypertrophy of a given part or tissue. If it refer to irritation, this has been acknowledged as a factor in the etiology of tumors, but as an uncertain one. Cancer of the gall-bladder or liver, which occasionally results from the irritation of a gallstone, or the cancer of the breast that follows eczema of the nipple, may be regarded in this light as additional illustrations if it is preferred to interpret them in this way. If by inflammation be meant the infectious granulomas, they have already been considered. As the term “inflammation” can scarcely mean anything except hyperemia, irritation, or infection, we seem to have completely ruled it out from consideration as by itself an active cause leading to tumor formation.
—This in its ingenuity and in its applicability is a fascinating explanation, which is undoubtedly sufficient for at least a certain number of instances. According to Cohnheim, only one causal factor for tumors exists—i. e., anomalous embryonic arrangement. He regards them as entirely of embryonal origin, no matter how late in life they may develop and appear. Briefly summarizing his views, they are to the effect that in the early stages of embryonal development there are produced more cells than are necessary for the construction of a certain part, so that a number of them remain superfluous. While these may remain very small, they possess, on account of their embryonal nature, a potent proliferating power. This superfluous cell material may be distributed uniformly, in which case it will develop whole system arrangements, like supernumerary fingers, etc., or it may remain by itself in one place, and will then develop a tumor. In the latter case the tumor may appear early or not until late in life, according to the time at which the cell collection receives the necessary stimulus, or because of its suppression by resistance of surrounding structures. It may be an irritation or an injury, such as above alluded to, which shall give it this stimulus; as, for example, it is reasonable to think that certain nevi and other congenital conditions which develop later into cancers do so in accordance with this view. Surgeons generally find little fault with Cohnheim’s hypothesis, except that as yet they decline to see in it an explanation for all cases. Nevertheless for dermoid and teratomatous, and for all heteroblastic tumors, it seems to afford the only tenable explanation. Thus chondromas of the parotid and of the testicle are most easily explained in this way, and that cartilaginous islands occur in the shafts of adult bones is well known.
—In regard to heredity being a factor in the etiology of neoplasms there is reason to believe that a favorable tissue disposition may be inherited, but there is nothing to show that it permits the actual transmission of the disease.
—The parasitic theory of tumor formation has only within a few years taken definite form and shape, as a result of evolution from vague suggestions and scattered observations. It implies that tumors, and they are mainly of the malignant type, are due to irritation produced by extrinsic agencies, parasites of some kind, which, introduced from without, act as do bacteria in the now well-known infectious granulomas. While this theory, perhaps, does not afford an absolutely satisfactory explanation of all the phenomena of malignancy, it nevertheless comes nearer to it than does any other hypothesis now before the profession, the arguments in favor of it being scientific and positive, and those against consisting mainly of mere negations. Summed up these arguments may be stated as follows:
—The argument from comparative pathology begins with the lower forms of life. Tumors in trees and plants are well known to vegetable pathologists and botanists as of frequent occurrence. They vary in size from the most trifling galls to those large woody masses known as xylomas, which are essentially tree cancers, since they tend to the destruction of the tree. These are known to be invariably due to extrinsic agencies, such as insects, fungi, etc. As water freezing in the bark of a tree may crack it open and thus leave opportunity for subsequent infection, so may injuries upon the body surface make trifling lesions which predispose to subsequent infection and cancer in man and animals. Exclude parasites from such traumatic lesions on plants and there will be no xylomas.
PLATE XIV
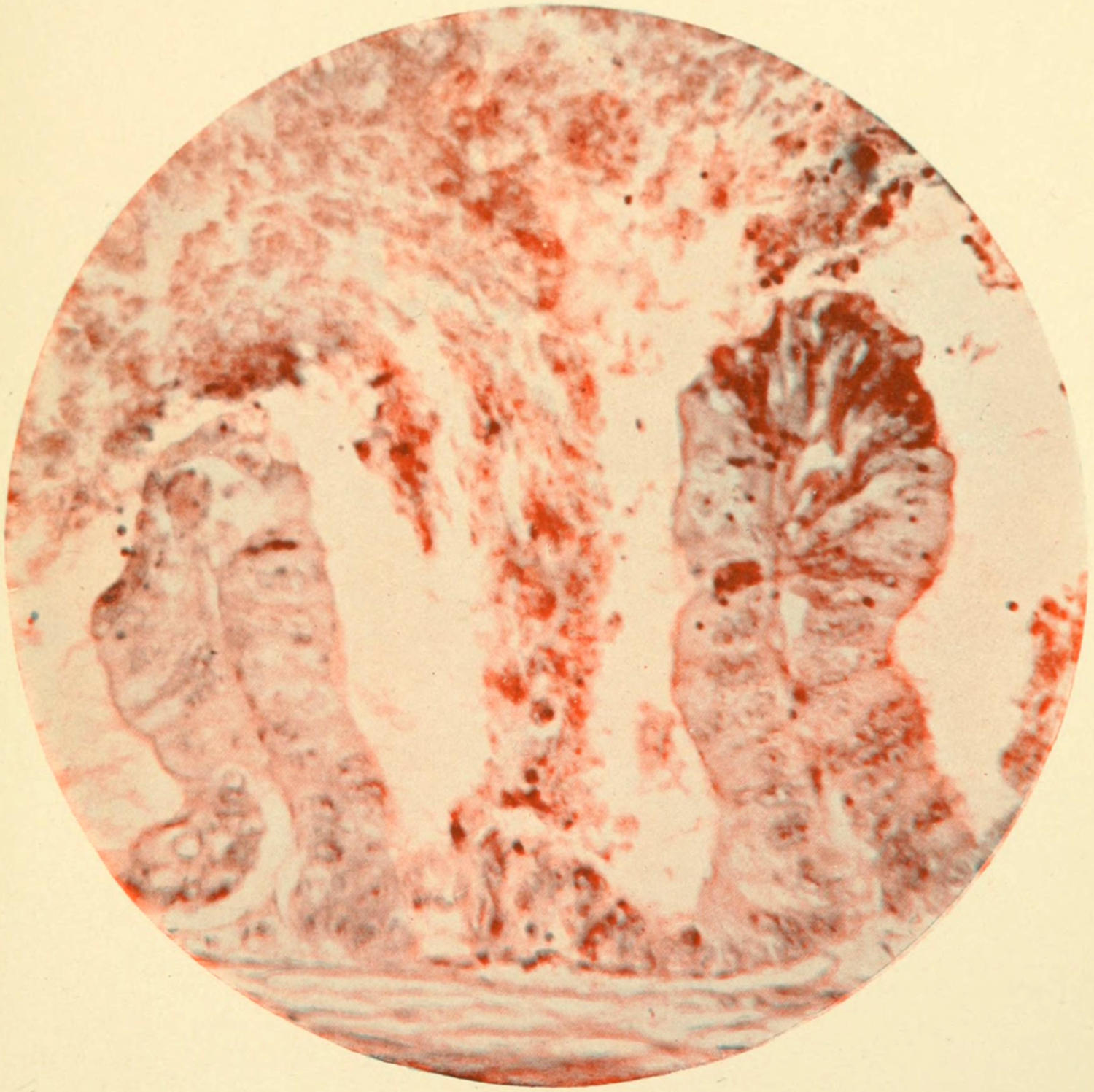
Adenocarcinoma with Young Parasites. (Parasites blue. Plimmer’s method.)
This plate is introduced to illustrate the presence of parasites, whose minute and actual character is not yet positively determined, but whose existence is undeniable.
From Gaylord’s paper in the Third Annual Report of the New York State Pathological Laboratory of the University of Buffalo.
PLATE XV
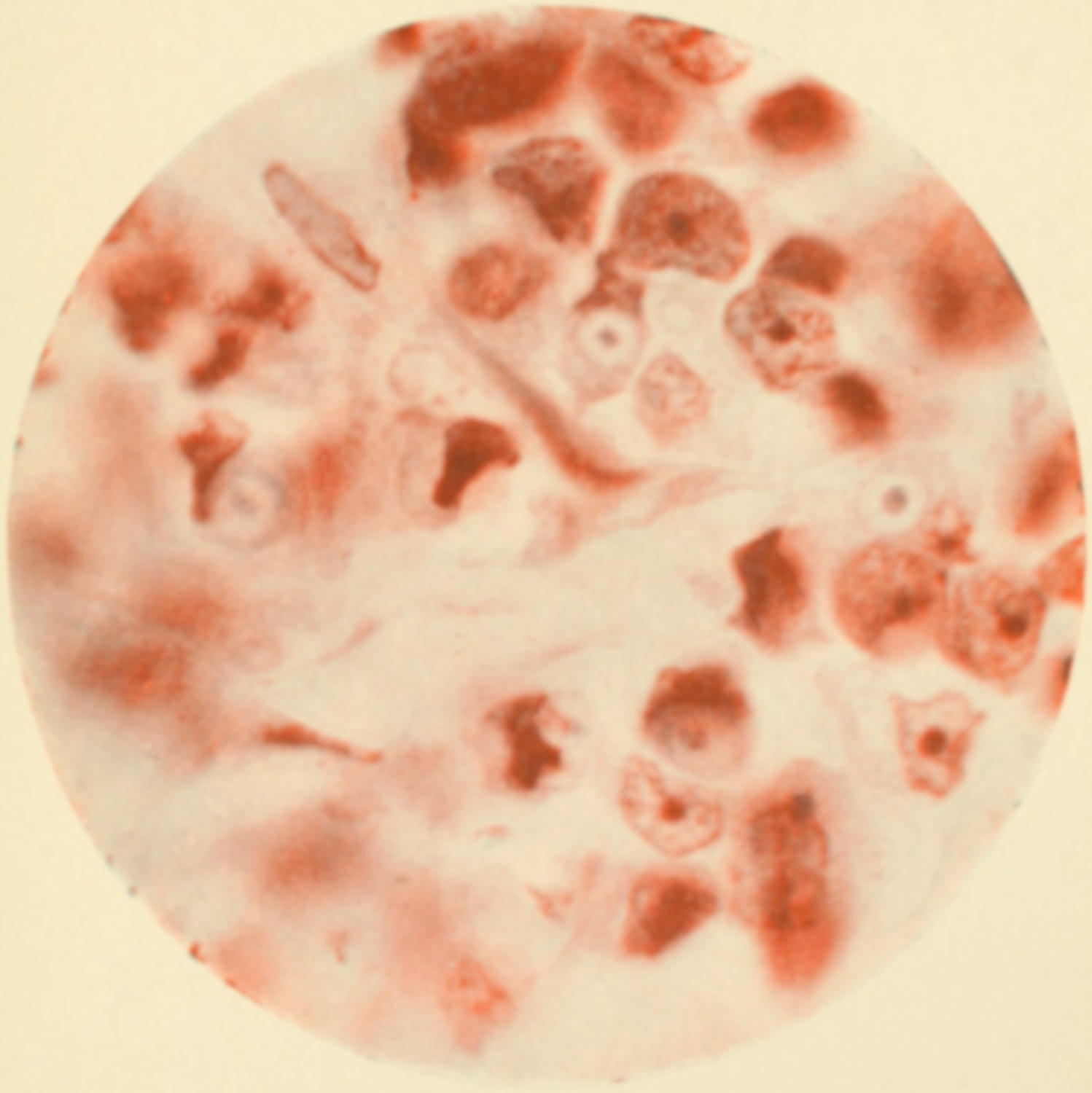
Rapidly Growing Carcinoma of Breast.
The parasites herein demonstrated are still subjects of careful and minute study. It would therefore seem premature to make detailed statements concerning their exact nature.
From Gaylord’s paper in the Third Annual Report of the New York State Pathological Laboratory of the University of Buffalo.
PLATE XVI
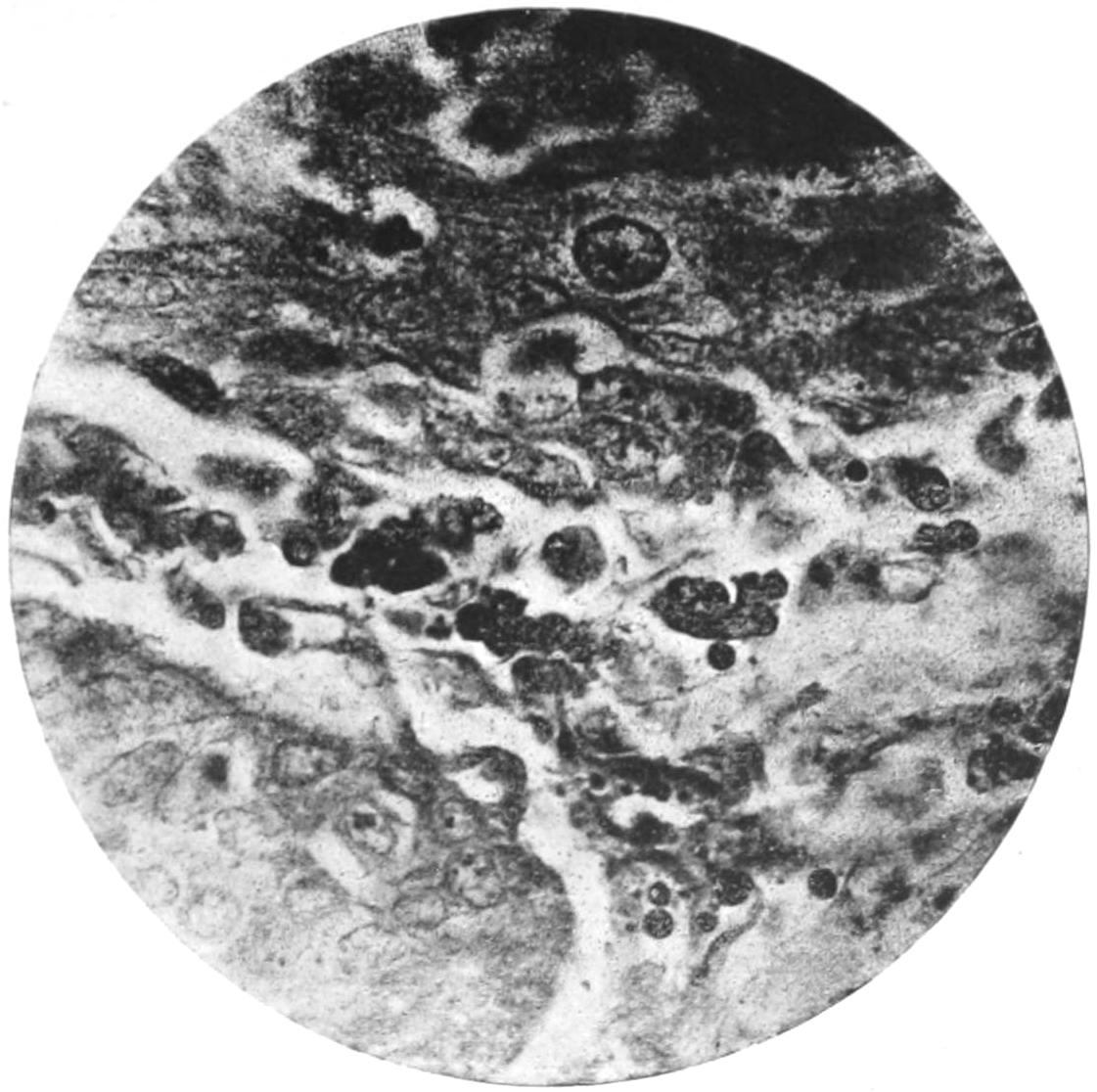
Fig. 1. Parasites, at one time called Russell’s Bodies, at Periphery of Epithelioma of Tonsil. (Oil immersion.)
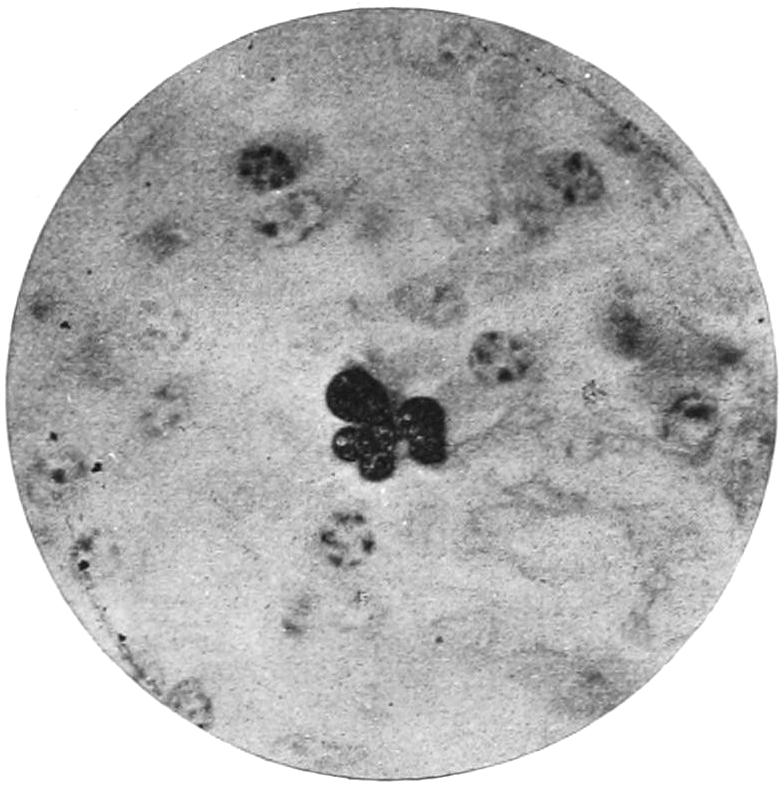
Fig. 2. Same in Lymph Node before Epithelial Invasion. (From N. Y. State Path. Lab. Rep.)
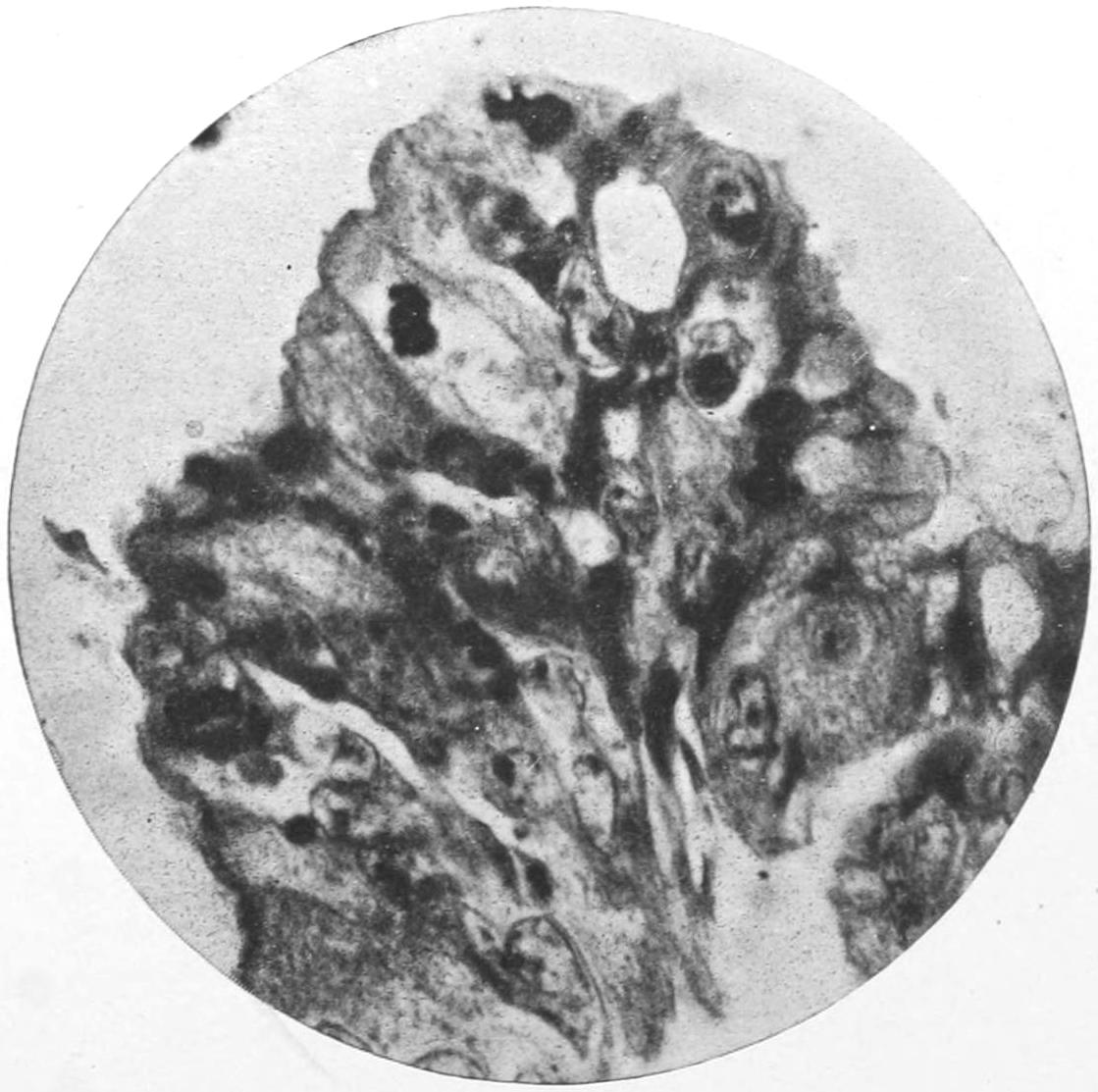
Fig. 3. Papillary Adenocarcinoma of Ovary, showing Intracellular Ameboid Forms of Parasites. (From N. Y. State Path. Lab. Rep.)
[257]
—These are universally conceded to be of parasitic origin, while their clinical course and behavior in every respect make many of them almost as malignant as the true cancers become.
—This is in every other disease considered to be one of the most significant expressions of infection, yet until recently few of those who have willingly accorded to metastasis its now common interpretation in tuberculosis have been willing to give it the same dignity as a factor in the spread of cancer and an important explanation of its nature. Why should every other disease characterized by metastasis be everywhere viewed as parasitic, and cancer, in which occur some of its most positive expressions, be denied? Metastasis has the force and significance of an inoculation experiment performed under favorable circumstances.
—The involvement of a part which has lain in contact with a cancerous lesion, as about the mouth or the vulva, and in many other ways and places of which medical literature is now full, and the instances of cancer following the knife wound, especially following the track of the trocar used for tapping a case of cancerous ascites, stamp the disease as having an infectivity which cannot be explained on any inherent property of its own.
—While it is true that but few observers have been able to agree upon a definite cancer parasite, it is also true that many of the best observers have seen, described, and figured bodies that do not belong in the cells of a cancerous growth except they are there in the roll of active agents, and the appearances which have been described by Pfeiffer, Plimmer, Gaylord, Calkins, and others are not to be explained away as mere artefacts, but must be given a place in our estimation which they would attain of themselves, as exciting suspicion, were there no other facts corroborating the views that they are in some way actively connected with the production of the disease. (See Plates XIV, XV, XVI.)
—No feasible plan has been devised for practising inoculation experiments upon human beings. It is known, however, that the disease may be transmitted in some cases among animals of the same species, and the transfer has been made in a few instances from man to the lower animals. In the Gratwick Laboratory (Buffalo) the disease has been thus transmitted through hundreds of mice, and has thus afforded the best means of studying it in its varied phases, albeit in small animals, ever yet enjoyed. But cancer does occur in animals and has proved to be capable of inoculation, and, therefore, has responded to one of the severest tests of the value of the theory. Moreover the facts cited above (under 4) are essentially successful auto-inoculation.
—Add to the features already mentioned above those impressions which come from accurate observation and correlation of the phenomena attending many cases of cancer, and a plausibility is thus lent to the parasitic theory which it can never gain from study in the dead-house or through the microscope. The resemblance between it and other known infections, the local and general alterations of tissues and fluids, the chemical changes by which the cachexia of the disease is brought about—these with other features all conspire to give the keen observer of cases of cancer an impression of parasitism or infectiousness which nothing can efface. Add to these its endemic, sometimes almost epidemic occurrence, its apparent transmission by contact, and the fact that it is but little influenced either by nutrition or drugs, and the argument is still strengthened. As against these arguments little has been advanced save denials or negations.
In thus upholding the parasitic theory, the writer would not wish to be understood as claiming either that the parasite has yet been discovered or its nature positively made out, nor that it is a question of one organism alone; rather, on the contrary, he feels that it is probably a question of several agents, probably of protozoan character, perhaps too small to be recognized with the lenses of today, perhaps belonging to some as yet unstudied class of organisms, making themselves known, however, as do the hypothetical[258] parasites of syphilis and scarlatina, by their effects. To accept the parasitic view is to reconcile many discrepancies of earlier times and to give an entity to the disease by which, and until something better be found, we may be more safely guided in its management.
The parasitic theory lends plausibility to the statement which the writer wishes to emphasize, that cancer, like many of the other infectious diseases, is at first a local condition, that it is not transmitted by inheritance, and that there is a time in the history of every cancer when, if it could be recognized sufficiently early, and if it were also accessible and thoroughly removed, it could be cured.
—The nomenclature of tumors has been much confused, and if some new terms are introduced it is perhaps better than to cling to some which have prevailed in the past. Various systems have been followed of naming them according to their supposed nature or their evident tendency, or according to some purely arbitrary classification; thus there is the distinction into homologous and heterologous or heteroplastic, according as they are similar to or variant from that tissue in which they seem to originate; or they have been referred to as benign and malignant according to the disposition which they evince; and these terms are in sufficiently frequent use to demand acceptance. The distinction between benign and malignant is convenient and in some respects accurate, implying little in regard to histological structure, but much in regard to their effect upon the individual.
So far as method of classification goes, the anatomical (i. e., the histological) has proved far the most satisfactory, and is that which is now generally adopted. It is the basis for the classification followed in the ensuing pages. But even here it is impossible to maintain abrupt or always accurate distinctions, because tumors are frequently of mixed type, and it is required, if desired to express their composition by their names, to sometimes combine words in an awkward fashion.
By common consent that tissue which predominates furnishes the concluding portion of the compound term, while by prefixing other terms we endeavor to imply the composite character of the neoplasm.
Thus we have osteochondroma, fibromyoma, myofibroma, etc., and it is necessary often to reduplicate terms in order to be accurate in description. While this complicates phraseology, it nevertheless furnishes to the reader a reliable clue as to the general character of such a growth; and if one reads, for instance, of a myxochondrosarcoma, he promptly infers therefrom that thereby is meant a tumor essentially a sarcoma, in which both myxomatous degeneration and cartilaginous formation have taken place.
In the same way the prefix cysto is frequently used to imply a combination of originally solid tumor which had undergone cystic changes in whole or in part.
The old term cele is frequently used as a suffix, implying neoplastic changes in an organ, or at least the formation there of a tumor. Thus we have bronchocele, hydrocele, and cystocele. Again, certain terms are used in a different sense from that originally intended. Thus the term sarcoma has a definite significance, whereas originally it had little meaning and was applied inadequately and indiscriminately. Old terms also, like fungus hematodes, are now used rather in a descriptive sense, because for any such tumor we can find, on accurate examination, a proper term taken from descriptive pathology. Therefore the student of today should read the works of the older writers, especially concerning neoplasms, with a certain amount of intelligence, as well as of apology for the inaccuracy and misnomers of the past.
The results of treatment of tumors leave much still to be desired, particularly when dealing with those of malignant nature. So far as purely internal treatment is concerned, we have not yet discovered drugs which with any certainty influence cell growth to the extent of making them reliable or effective. In the past, and even at present, numerous remedies have been advocated as having more or less power in this direction. Of them all it is probable that arsenic in some form is more efficacious than any other. This is true in the case of the disease elsewhere spoken of as malignant lymphoma, or[259] Hodgkin’s disease, which partakes much of the character of some of the other neoplasms. But to say that arsenic alone or any other known remedy can be relied upon at all times is making a bold assertion.
—The treatment of operable tumors is essentially surgical (i. e., operative), although to a large extent results are based upon the essential character of individual cases. But it can be stated that to be successful in the removal of any tumor its complete extirpation is imperative. Even the most benign growths will return if only partially removed. This is true even of innocent cysts, which will be often reformed if a portion of the cyst wall be allowed to remain. Complete extirpation is ordinarily a simple measure when tumors are encapsulated, as are often many of the innocent tumors. On the other hand, the performance of some of these operations is made difficult and hazardous by the location of the tumor, as in many large uterine fibroids, tumors of the thyroid, etc. But when dealing with malignant tumors the secret of success is to extirpate them, sacrificing everything which may appear to be involved unless, like a large bloodvessel or important organ, it be essential to the life of the part or of the individual. These statements are made when speaking of tumors in a general way. More specific directions will be given when dealing with particular forms or in the chapters on Special and Regional Surgery.
Following custom in large degree, yet being guided by undeniable facts concerning histological structure, tumors will be classified and considered as follows:
A cyst may be defined as a tumor containing one or more cavities filled with fluid or semifluid contents. This specifies nothing with regard to the location nor the character of the cyst wall nor the nature of the fluid contents. Following Sutton, I divide cysts into four groups:
—These imply a previously existing cavity whose outlet is obstructed and whose contents consequently accumulate, often to such a degree that the original character of both containing wall and contained fluid is entirely altered. When this occurs in glands or gland ducts there is usually complete atrophy of gland tissue, providing sufficient time have elapsed. Such cysts are due either to permanent or temporary arrest of flow. In hydronephrosis, for example, there is obstruction of the renal outlet and dilatation of its pelvis, with partial or complete atrophy of the kidney structure, until a cyst of enormous size may be present. When a similar condition obtains in the uterus, as by obstruction of the cervix, perhaps due to injury done during labor, we have a condition known as hydrometra, seen occasionally in women, often in the lower animals, and particularly in those having a bicornate uterus, causing a condition often mistaken for an enormously dilated Fallopian tube. Similarly, when the common bile-duct is obstructed, which may be due to impacted gallstones, to inflammatory lesions or tumors, there may be such backing up of bile in the gall-bladder as to produce the condition known as hydrocholecyst.
Under any of these circumstances pyogenic bacteria may produce infection which will be more or less promptly followed by suppuration; and then, instead of hydronephrosis,[260] ydrometra, hydrosalpinx, etc., we have pyonephrosis, pyometra, and pyosalpinx.
—These are cystic dilatations of certain functionless ducts and obsolete canals which no longer serve a useful purpose. They comprise:
1. Cysts of the Vitello-intestinal Duct.
—Cysts originating from this functionless duct occupy the umbilical region, sometimes projecting externally, sometimes internally. They are usually lined with mucous membrane furnished with villi and columnar epithelium. Such a cyst may be confounded with an umbilical hernia. These cysts occasionally open at the umbilicus and discharge irritating material, sometimes fecal matter. Cystic dilatation of the portion of the duct originally connected with the ileum is also sometimes seen.
2. Allantoic Cysts.
—These are connected with the urachus, which should ordinarily be found as a fibrous cord, but which occasionally persists in a pervious condition, in whole or in part. At birth it is often traversed by a narrow canal lined with epithelium continuous with that of the bladder. The urachus lies outside the peritoneum, and may be dilated at any point between its two extremities. When the entire urachus is pervious urine is discharged from the navel.
3. Cysts Connected with Remains of the Wolffian Body.
—The Wolffian body, or the mesonephros, is intimately related with the development of the kidney, the ovary, and the testis. In the two latter locations glandular elements may be met, persisting in adult life.
In the male the tubules persist as excretory ducts from the testis, but in the female they persist, in a vestigial condition, as the parovarium and Gärtner’s ducts. The ovary proper consists of the oöphoron and the paroöphoron, the former being the egg-bearing portion, the latter receiving the tubules from the adjoining structure known as the parovarium. The paroöphoron gives rise to cysts which burrow deeply between the layers of the broad ligament, make their way alongside the uterus, and raise the peritoneum. It is a peculiarity of these cysts that their inner walls often become papillomatous, and may even develop such a crop of warty outgrowths that these make their way through the cyst wall and protrude into the abdominal cavity, where they sometimes become detached and are dropped as loose bodies into the peritoneal sac. The condition is also often accompanied by warty growths upon the peritoneal surfaces. These need give rise to no alarm, because they usually disappear spontaneously with removal of the tumor. Paroöphoritic cysts are to be distinguished from parovarian cysts, which develop from the parovarium, this latter consisting of a number of tubules situated between the layers of the mesosalpinx, composed of an outer series known as Kobelt’s, an inner set, about a dozen in number, known as the vertical tubules, with a straight tube, running at right angles to these through the broad ligament to the vagina, known as Gärtner’s duct, which is homologous with the vas deferens in the male. Cystic dilatation of Kobelt’s tubes is often seen, these cysts being very small and having no clinical importance. Cysts arising from the vertical tubules are usually transparent until they attain considerable size, when their walls thicken. Their contained fluid is not harmful, and after rupture of such cysts internally the fluid is absorbed. Such cysts may rupture and refill several times. As between the paroöphorous and parovarian cysts the latter are easily enucleated, carry the ovary upon one side, and have the Fallopian tube stretched over them without communication.
The internal sections of Gärtner’s duct are more often involved in animals than in women, but excellent illustrations of cystic dilatation of its various portions have been observed, usually in the walls of the vagina.
Corresponding to the above-mentioned conditions in the female there are in the male, as the result of changes in the Wolffian body, two conditions—encysted hydrocele of the testicle, and general cystic degeneration of the same. Like the ovary, the testicle is a complex organ with remnants of the mesonephros persisting among its ducts, while only a few of the Wolffian tubules remain. True encysted hydroceles arise sometimes in the efferent tubes of the testis and sometimes in Kobelt’s tubes (the same structures which in the female give rise to parovarian cysts), the two conditions, therefore, being analogous and homologous. These cysts, though closely associated with the testis, lie outside its tunica vaginalis. Their contained fluid is usually clear or of a milky whiteness, due to fat globules. Sometimes it contains spermatozoa. Another variety[261] is cystic dilatation of one or more of Kobelt’s tubules, which is often described as involving the hydatid of Morgagni.
General cystic disease of the testis, known also as adenomatous degeneration, was formerly referred to as hydatid disease of the same organ. The multiple cysts appear to originate in the remnant of the mesonephros still persisting, known as the paradidymis. The cavities are lined with epithelium, and papillomatous intracystic formation is not uncommon. These tumors have been called by a number of improper names, such as “cystic sarcoma,” etc.
—The term hydrocele has covered numerous conditions. At present, when no other locality is designated, hydrocele of the tunica vaginalis is understood. (The term implies a collection of watery fluid in a previously existing serous cavity.) This is the most common form.
Possibility of its formation depends upon the prolongation of the peritoneal cavity which takes place in advance of or along with the descending testicle, and which in many of the lower animals remains connected with the general cavity throughout life. In men only is it expected to close, even before birth. When the portion which extends along the spermatic cord is not completely obliterated there is encysted hydrocele of the cord, or funicular hydrocele, which is not common. The common form of hydrocele is constituted by serous effusion into the tunica vaginalis, and occurs usually without recognizable exciting cause. It will be treated more fully in its appropriate place.
The corresponding process of peritoneum in the female is known as the canal of Nuck; and, when persistent, this also becomes distended with fluid and forms a cyst known as hydrocele of the canal of Nuck, occupying the inguinal canal.
In many of the lower animals the ovaries are contained within a serous sac derived from the peritoneum, which is so connected with the opening of the Fallopian tubes that when the ova escape from the ovary they enter these tubes and pass to the uterus without entering the general peritoneal cavity. This ovarian sac is subject to serous distention, and constitutes a condition called by Sutton an ovarian hydrocele. An homologous condition occurs sometimes in the human female, by pathological adhesion, and such cysts may attain large size. They project from, and are intimately connected with, the posterior layer of the broad ligament.
Hydroceles of the Neck.
—Hydroceles of the neck, so called, are cystic collections of congenital origin found in the cervical region, due to dilatation of ducts or clefts which should have disappeared at or before birth. The forms of cyst to which the name “hydrocele of the neck” are usually limited are recognizable at or soon after birth, and constitute fluctuating tumors, often extending beneath the clavicle into the axilla or down upon the thorax. They may occupy the entire lateral region of the neck, and may be unilateral or bilateral—may be single or multilocular, and may even intercommunicate.
They originate always beneath the deep fascia. Some of these cysts are undoubtedly due to dilatation of lymph spaces. This is particularly true of the multilocular forms. There is noted in many of them a tendency toward spontaneous recovery, but many again require operative measures for their eradication. Occasionally their walls are extremely vascular, even to the degree meriting the term nevoid.
Some of these cysts are considered by Sutton to be essentially examples of the laryngeal saccules which are met with as diverticula from the laryngeal mucous membrane, which undermine the deep cervical fasciæ of certain monkeys. These air chambers, which are normal in the monkey, communicate with the larynx through the thyrohyoid membrane, and occasionally run down beneath the upper border of the thorax. Many of the cysts having this resemblance are closely related to the hyoid bone and to the larynx, and there is much to substantiate the view thus quoted.
—Ranula is an altogether too comprehensive term which has long been used in surgery, alluding to cysts in the floor of the mouth, and not indicating minutely their character nor their exact location. At present this term should either be restricted in signification or be eliminated. If used, it should be confined to retention cysts due to obstruction of the submaxillary or sublingual ducts. Such obstruction is often caused by salivary calculi impacted in the duct orifices. In other instances it is due to cohesion of the margins of the outlet. A similar condition in the parotid duct is known, but is less common. Aside from this, certain other cysts originate from minute beginnings in and about the floor of the mouth, being due to dilatation of the[262] mucous glands, particularly one near the tip of the tongue, sometimes known as Nuhn’s gland. Dermoid cysts in this locality are not uncommon. Formerly cysts of the floor of the mouth were described as ranula.
Pancreatic cysts correspond in large degree to salivary cysts, the pancreatic duct becoming dilated by retention when its orifice is obscured; and, indeed, the condition has been referred to as pancreatic ranula. Sometimes the canal is dilated in distinct portions, so that the condition resembles a string of cysts; at other times it is the terminal portion which is most enlarged. Such cysts attain large size and contain mainly mucoid material. Examples have been reported showing that they have attained a capacity of two gallons.
In the mesentery there sometimes develop cysts which are known as chyle cysts, whose sacs appear to be formed of separate mesenteric layers, their cavity being occupied by fluid identical with chyle. Such tumors also sometimes attain great size.
In the eyelids one occasionally meets with cystic dilatations of the lacrymal ducts. These are known as dacryopic cysts or dacryops. Fistulas result when they are opened through the skin, and if meddled with at all they should be radically extirpated.[13]
[13] In the treatment of cysts, as of many abscesses (e. g., those of the gland of Bartholin), it will be of advantage to empty the cavity through a small trocar or needle and then to fill it with melted paraffin, as suggested by Pozzi. When it has thus been distended it can be dissected out with much more deliberation and more easily than would be otherwise possible.
—In his elaborate work on tumors Sutton has made a distinct classification of pseudocysts, which lack some of the characteristics of genuine cysts, yet, nevertheless, are entitled to consideration in this place. Among these are included intestinal diverticula and vesical diverticula, in either of which instances hernial protrusions of the mucous membrane through the outer coating of the bowel or of the bladder occur, thus forming pouches. These are common in the bowel, rare in the bladder; especially in the former locality they are often multiple. This condition is often referred to as sacculation, and sacculation of the bladder may even be confounded with true urachus cyst. They are of little consequence so long as foreign materials, such as feces, urinary calculi, etc., do not lodge in them. But they occasionally cause serious trouble. Diverticula have been mistaken for appendices, while diverticula from the bladder have been encountered in hernia operations.
Pharyngeal diverticula give rise to rare but most interesting tumors. It is well known that the branchial clefts, which in early fetal life connect with the pharynx, are sometimes not completely closed, and that a portion of one may persist abnormally, giving rise to a condition known as the pouch of Rathke. There may also occur sacculation of the pharyngeal wall where it joins the esophagus, or hernial protrusions, especially in Rosenmüller’s fossa.
Cystic dilatation of Rathke’s pouch occurs near the upper part of the pharynx, and may attain the size of a marble. Hernial pouches are seldom mistaken for cysts, and are of importance mainly because of the fact that food or other foreign material gathers and lodges in them. Most of the other cystic abnormalities of the pharynx pertain to dermoids, and will be considered shortly. In a general way, these pharyngeal tumors have been grouped as pharyngoceles.
Similarly in the esophagus and trachea hernial protrusions occur, and lesions closely resembling retention cysts may be seen.
Synovial cysts (i. e., those containing synovial fluid) may arise (1) by protrusion of synovial sheaths, (2) by distention of bursæ in the vicinity of joints, or (3) by hernial protrusions of joint membranes. They are often met with in connection with the larger joints, more particularly about the knee. In this way tumors as large as goose-eggs may be formed, while their location may be so shifted that they present themselves in perplexing ways. To that form produced by hernial protrusion of the lining of a tendon sheath has been given the name ganglion.
The simple ganglion is frequently seen on the back of the wrist, and, while it is always connected with the tendon sheath, it undoubtedly often connects with the synovial membrane of the carpal joints. The compound ganglion, so called, is a much more serious and extensive affair, being one which has prolongations in two or more directions, and containing peculiar bodies, known as melon-seed bodies, which appear to be fibrinous concretions worn round and smooth by attrition. These are present sometimes in enormous numbers. (See Tuberculosis of Synovial Structures, Chapter IX.)
[263]
Bursæ are normal in many well-known situations in the body, but may undergo cystic dilatation and become annoying tumors. In many other places, under the influence of friction or mechanical irritation, there develop bursæ which are known as adventitious. These are sometimes subtendinous, and may communicate alike with joint sheaths and tendon sheaths. These are true cysts of new formation not developed from a pre-existing cavity.
They are largely the effect of peculiar occupation, as in housemaids and carpet-layers there are formed frequently prepatellar bursæ, while miners get them upon the elbow, porters upon the shoulder, plasterers upon the forearm, etc. In the same way, by the pressure of ill-fitting boots, an adventitious bursa is developed over the expanded head of the first metacarpal bone, thus forming a condition known as bunion.
—This term has been applied by Sutton to pseudocystic dilatation of certain cavities found in the brain and central nervous system. Hydrocephalus is in one sense a pseudocyst of this variety. Corresponding to it in fetal life is hydramnios. Hydrocele or cystic dilatation of the fourth ventricle is well known. Cranial meningoceles, which are hernial protrusions of brain membranes, are also pseudocysts, to be included in this category. They will be considered in Chapter XXXVI. Cephalhematoma may be also included in the same way. Spina bifida, a condition which will be described in Chapter XXXVIII, is, nevertheless, practically a cyst of congenital origin involving the spinal meninges. One form of spina bifida is constituted by cystic dilatation of the central canal of the spinal cord, and produces syringomyelocele. These conditions will be treated more fully in their appropriate places.
Sutton has rendered a great service by showing that the brain and spinal cord are evolved from a segment of the primary intestines, and that the intestinal canal and the neural canal communicate in fetal life at their lower terminations; while it has been shown by several that in the earlier forms of mammalian life they were also connected by their anterior terminations. It is in this way that certain complex tumors of the sacral and coccygeal region are to be explained. So also is the collection of lymphoid tissue in the vault of the pharynx, known as Luschka’s tonsil, and in the coccygeal region, known as Luschka’s gland, it being a curious and instructive fact that lymphoid tissue of this character is always met with in the neighborhood of obsolete canals.
—These cysts are the indirect product of the eggs of the Tænia echinococcus, a form of tape-worm which infests the alimentary canal of dogs. The eggs reach in some direct or indirect way the food or water taken into the human stomach and are there hatched; the young animals migrate through vessel walls and are deposited in some tissue or organ where the cyst later develops. These cysts have a thick, elastic wall, with a lining containing cells, involuntary muscle fibers, and a water-vascular system. After such a cyst has attained the size of an inch or more, small vesicles, or “brood capsules,” begin to develop, which present at one point a retractable head, with scolices so arranged in crown form as to produce sucking disks. According to the date at which the cyst is opened appearances will differ. Sometimes a large cavity will be filled with multiple “daughter cysts,” and sometimes these will have disappeared, so that the cyst fluid contains nothing distinctive. After having ceased to develop, hydatids frequently undergo atrophy and even become calcified; the characteristic hooklets are the last of the distinctive features to disappear.
These growths may be rapid, even to the point of producing necrosis and rupture, or may be very slow and persist almost unchanged for years. The disease is uncommon among the native-born population of the United States, and most of its examples are seen in emigrants. It is exceedingly prevalent in Iceland and in New Zealand. It occurs most often in the liver, but is frequently met with in these countries in the lungs, the brain and spinal canal, and the bones, but may be encountered in any part of the body. When located near the intestinal tract or the air tract the cysts are more liable to penetration by ordinary germs of sepsis, and then may suppurate. It is not infrequent to have conversion of an hydatid cyst into an abscess. Before or after such change it may undergo rupture, spontaneous or traumatic, and this, according to the nature and amount of its contents, and the location of the opening, will promptly produce more or less grave symptoms. While spontaneous recovery has, in rare instances, followed rupture, it has perhaps more often led to fatal result. At all events, it will produce serious and perhaps distressing symptoms.
The only radical treatment for hydatid cysts is extirpation. When this is not possible[264] the cyst may be opened and the margins of the opening attached to those of the skin wound. After being evacuated it should be packed and drained, and then may be expected to slowly contract, perhaps even to the point of obliteration. The contents of such a cyst should not be allowed to escape into any of the body cavities, since their sterility can not be always relied upon.
—Hematocele is an expression meaning a tumor composed originally of effused blood which has undergone chemical and other changes, which consist of lamination and thickening of its exterior portion and fluidification of the interior, until in course of time such an internal blood clot may be converted into a distinct and plainly walled cyst. This condition may be seen in two locations—namely, in the pelvis and between the cranium and the brain, or in the brain. The hemoglobin gradually disappears, and the contents of these cysts are translucent or even watery in appearance. Hematoceles may form where there has been internal hemorrhage in certain locations which has failed to absorb, and where no pyogenic infection has occurred.
Pseudocystic changes occur in other tumors and in other parts of the body as the result of mucoid and colloid liquefactions. In the midst even of apparently dense and entirely defined tumor masses changes of this kind occur, and lead to formation of cavities containing fluid of variable consistence, causing the tumor when divided to present the appearance of the geodes or quartz rocks, containing cavities lined with quartz crystals. The occurrence of such cystic changes is indicated, in naming such a tumor, by prefixing the term cysto-, as cystosarcoma, cystofibroma, etc.
Dermoids are cysts or tumors containing tissues and appendages which are developed from the epiblast, and which occur when skin and mucous membrane are not normally found. The simplest form of dermoid is a cyst whose interior is lined with modified skin, containing sebaceous glands and hair follicles, from which often numerous long hairs are produced. Even sweat glands may be present. Its cavity is occupied by mixed material, pultaceous in character, made up of sebum, cholesterine, and growing hairs which are often rolled into balls. The sebum is the product of the glands contained in the cyst wall.
A complex form of so-called dermoid cyst is met with in which there are unstriped muscle fiber, teeth, mammary glands, etc. These belong rather to the class of teratomas, as they contain more or less tissue not of epiblastic origin.
A dermoid tumor is one lacking cystic characteristics, made up of tissue largely developed from the epiblast, with more or less tissue of mesoblastic origin. Such a tumor may contain much connective tissue, fat, fetal hyaline cartilage, and nerve tissue, while from its exterior long hair may grow, and teeth project from its surface or be embedded within its substance. Such tumors are generally found in the pharynx and about the rectum.
The explanation of dermoids and teratomas may be gleaned from embryology, and rests upon the arrangement of the different blastodermic layers of the developing ovum, and upon the facts already alluded to in explaining Cohnheim’s hypothesis of the origin of tumors. Strictly speaking, a dermoid should contain only that which may be developed from the epiblastic layer. It is well known that teeth and hair, as well as sebaceous material, are epiblastic products. Consequently such material may be found within a dermoid and needs no further explanation than an epiblastic inclusion, according to Cohnheim’s views. But so soon as such a tumor contains bone, muscle, etc. (i. e., tissues of mesoblastic origin), we should drop the term dermoid and consider it a teratoma. Such is the distinction between these two terms. According to Wilm’s researches, any tumor of this sort which contains epithelial products as teeth or hair is sure to contain also mesoblastic elements, and thus to belong to the latter. The term epidermoids has been applied to the former.
The most prominent characteristics of dermoid cysts are: (1) Skin, which may be thick or thin, lined with papillæ, containing more or less pigment, its deeper layers possessing a quantity of fat. (2) Hair, which next to skin is the most constant structure found in dermoids; this may be present in trifling amount or in long coils or balls. It is of interest that in dermoids found in animals covered with wool we find the same[265] character of hairy structure, while in birds dermoids contain feathers rather than hairs. (3) Sebaceous glands and their peculiar secretion are invariably found. These may be of large size, and sebaceous retention cysts may be seen in the walls of dermoids. Sometimes horny matter or tissue is found in these, indicating the same relation between horn and sebaceous structures, as we see upon the external skin in other instances. So, too, material resembling the texture of finger-nails is occasionally found projecting into the cavity.
The fluid or semifluid contents of these cysts consist usually of sebaceous material, cholesterin, epithelial debris, etc. Sometimes it is thick, sometimes thin—and occasionally consists almost entirely of mucus.
It is not uncommon to find structures in ovarian dermoids closely analogous to, or actually resembling, mammary glands. These may be mere nipple-like processes of skin, or completely developed mammæ, well formed, but without ducts or gland tissue, may occupy such a cyst. These really are pseudomammæ, because they have no ducts. Nevertheless, glandular tissue is not always absent. This resemblance proceeds even farther, in that in some of these ovarian mammæ changes occur analogous to those which take place in normal breasts.
The epiblast seems to have the power of developing mammary glands or supernumerary mammæ in many locations—in fact, upon any part of the body surface. About the thorax they are common; upon the abdomen they are rarely observed; and they have been found even upon the labia.
Sweat glands are infrequent in dermoids. Teeth are quite common. These may vary in number from two or three up to several hundred—may be embedded in definite sockets or simply sprout from the cyst wall. Occasionally bone material, lodging such teeth and crudely resembling a jaw, will be found.
Dermoids containing mucous membrane are found, especially in connection with the ovary and with the postanal gut (i. e., the original communication between the spinal and alimentary canals).
It is curious that under these circumstances mucous membrane is sometimes furnished with hair, as it normally is in the stomach or other cavities of some of the lower animals. Mucous glands and retention cysts of these glands are also found in ovarian dermoids. This will be more readily understood if the mutability of skin and mucous membrane be not forgotten. The transition from one to the other is not difficult, and we find all intermediate stages between the two extremes—if not in man, at least in animals. This will account for the fact that skin-covered dermoid tumors are found in certain parts of the alimentary canal, and particularly in the pharynx. These tumors grow also from the mucous membrane of the bowel, of the rectum, or even of the small intestine.
Sutton has made a division of dermoids into three classes:
—Sequestration dermoids occur chiefly in situations where during embryonic life coalescence takes place between two surfaces possessing an epiblastic covering, although sometimes this coalescence practically occurs late in life and by implantation.
Dermoids of the trunk occur particularly where opposite halves of the body wall coalesce—that is, in the midline of the trunk and head. Dermoid cysts are rarely found in connection with spina bifida, and certain tumors spoken of as spina bifida undoubtedly are dermoids. Anteriorly dermoids occur frequently in the scrotum, and occasionally in the testicle. At the umbilicus they are rarely found—usually as pedunculated tumors projecting externally. In the midline of the thorax and neck they are most common opposite the manubrium, dropping down behind it to invade the anterior mediastinum. Near the hyoid bone they occur relatively frequently; about the head they are met with most commonly at the angles of the orbits—more so at the outer than at the inner angle. Dermoid cysts are known to oculists as growing upon the iris or springing from the conjunctiva. About the ear they are not infrequent; in the roof of the mouth, especially if this be incomplete, we frequently find cysts of epiblastic origin.
Sequestration dermoid cysts are also undoubtedly found in connection with the[266] dura mater, in the scalp, most commonly at the anterior fontanelle, at the root of the nose, and at the external occipital protuberance, where they may be confounded with sebaceous cysts or with meningoceles. In order that a dermoid of the dura may communicate with the skin there must of course be osseous defect.
Sequestration dermoids upon the limbs have been mostly reported as sebaceous cysts. They are rare, and usually associated with antecedent injury, by which epiblastic structures are driven in and implanted in such a way that as they develop they give rise to these peculiar tumors. These are what Sutton calls implantation dermoids. They are found upon the fingers and elsewhere.
—These are largely connected with obsolete canals and ducts. It is a great service which Sutton has rendered in proving, apparently beyond the possibility of doubt, that the central canal of the nervous system is really of intestinal origin, and may be regarded as a disused segment of the primary alimentary canal. He has also shown how it behaves occasionally as do other functionless ducts, and that cysts and dermoids in connection with it are to be thus explained. He and others have also shown the anterior as well as the posterior communication of these canals, and the pituitary body are to be regarded in this light as the same formation of lymphoid tissue around an obsolete canal which we see in Luschka’s tonsil close by, and in Luschka’s gland at the other extreme of the canal.
Fig. 72
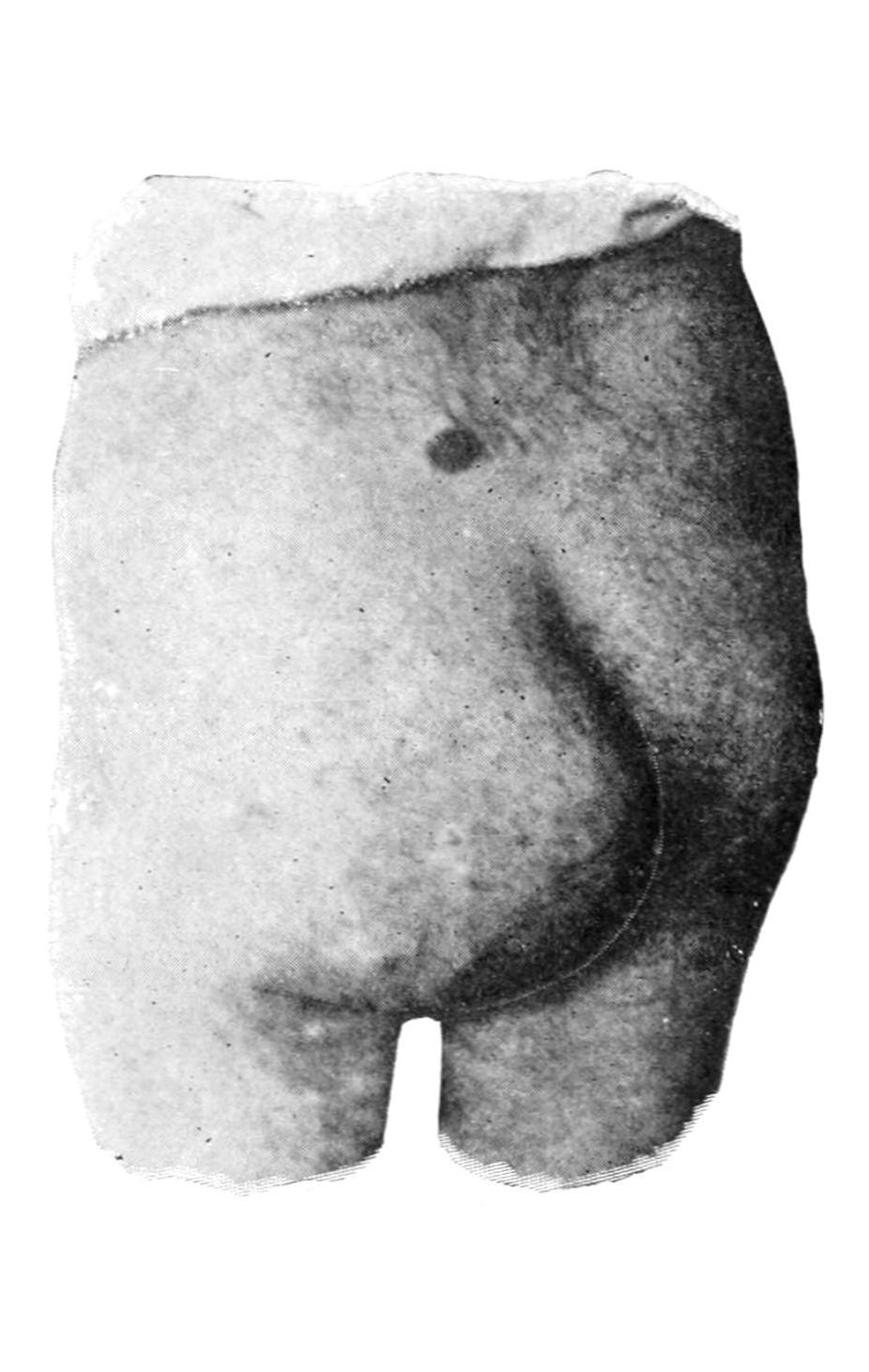
Solid dermoid escaping from pelvis. (Original.)
Fig. 73
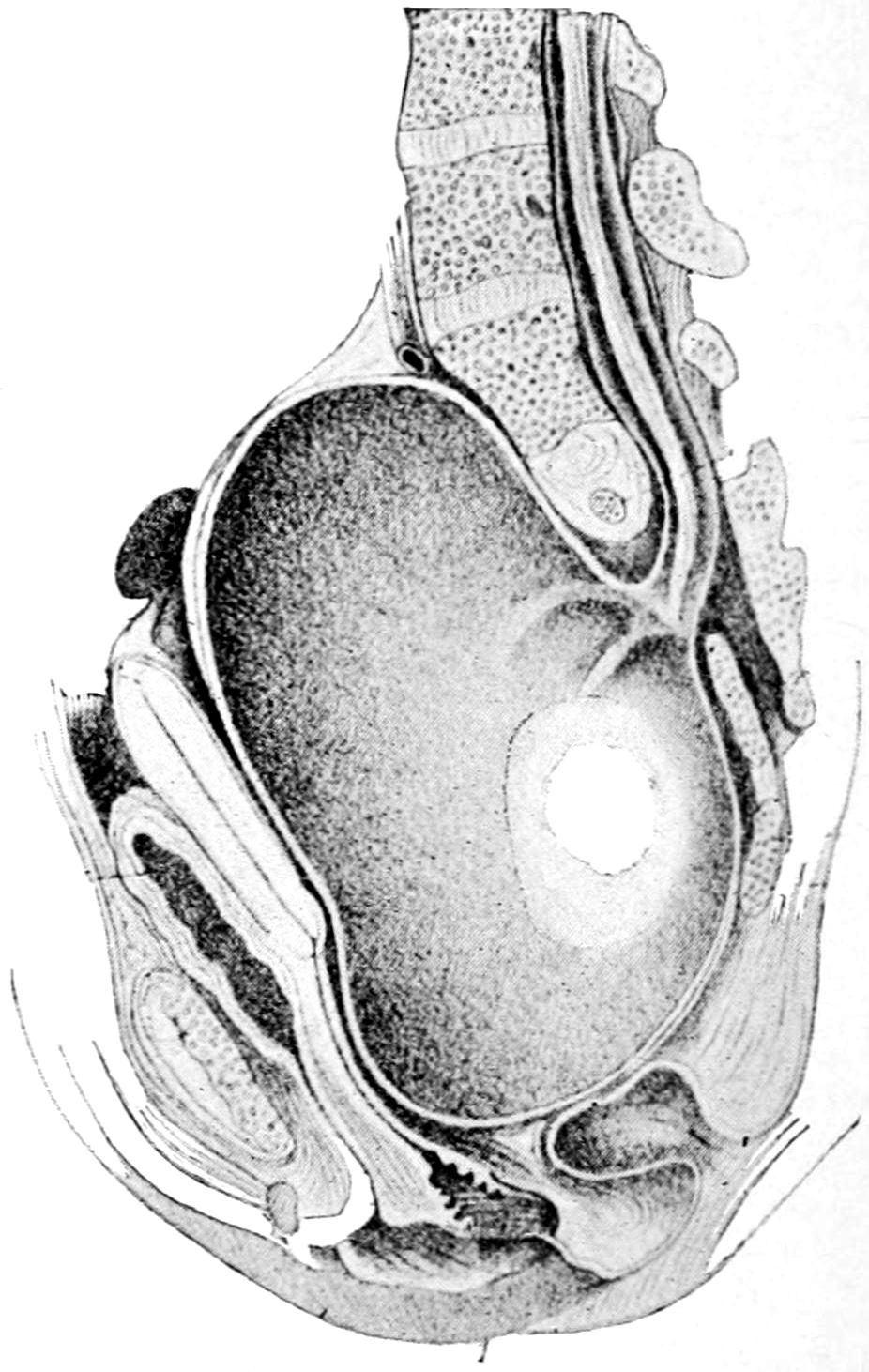
Congenital dermoid cyst of pelvis. (Ahlfeld.)
The primary alimentary canal was a continuous tube lined with a continuous layer of columnar epithelium. That portion connected with the yolk sac develops into the intestine, the balance into the central nervous canal. Portions of this canal are in postnatal life absolutely obsolete; others persist in a rudimentary condition. Dermoid cysts and dermoid tumors develop in connection with each of these. In some there is a large central cavity; others are almost absolutely solid. Thus we find dermoids in the coccygeal region, which have been variously regarded as sarcomas, adenomas, etc., which are really of origin as stated above and should be considered simply as dermoid tumors. Most of these project outwardly; some of them arise and develop within the pelvis. Dermoid cysts and tumors are also met with in connection with the rectum—sometimes[267] between the rectum and the bladder, and between the rectum and the spine. Dermoid tumors are also found in connection with the pituitary body. These sometimes develop within the cranium, or, again, protrude perhaps into the orbit, perhaps into the pharynx.
Thyroid dermoids are tumors of great interest. They develop sometimes about the craniopharyngeal canal, which may be detected as a small canal in the macerated sphenoid bone of a fetus, and which before birth is filled with fibrous tissue. It connects with a recess in the middle line and at the base of the skull, presenting in the pharynx, which is often referred to as the bursa pharyngea. It is around this recess that the lymphoid tissue known as the “pharyngeal tonsil” develops. It may be thus expected that the roof of the pharynx should be the occasional site of dermoids. It is from the pharynx or the floor of the mouth that in vertebrates the thyroid body arises. In higher forms it becomes dissociated from the pharynx and shifts its position. The thyroid body is developed around the thyroid duct, which first appears as the thyrohyoid duct, which later becomes divided, that portion in relation with the tongue becoming the thyrolingual duct, the remaining portion persisting as the thyroid duct. These are present about once in every ten subjects, according to Sutton, the canal when persistent being lined with epithelium. When the extremities of these ducts become occluded retention cysts may form. In the same way dermoids of the tongue are formed, similar to those occurring on the scalp. These are frequently mistaken for sebaceous cysts. They may be unilateral, central, or even bilateral. The lingual duct is also of interest, because it would appear that certain cases of epithelioma of the tongue arise along this duct, and perforating malignant ulcer of the tongue is thus produced. Dermoid tumors of the lingual or thyroid ducts resemble in structure the thyroid body. The thyroid duct may also be detected in many adults running from the isthmus of the thyroid body to the posterior aspect of the hyoid bone, and surrounded by muscle tissue. Sometimes the space usually occupied by this duct is represented by a series of detached bodies known as accessory thyroids. These are not infrequently the seat of cysts, sometimes of considerable size. (The accessory thyroids often enlarge when the main thyroid has been extirpated for disease.) Thus cysts in close relation to the hyoid bone are common. Some of them grow slowly, while others grow rapidly and contain much fluid. Many of them are unilateral, and are often mistaken for enlargements of one lobe of the thyroid. Cysts growing from accessory thyroids are often filled with papillomatous masses, and are occasionally the seat of malignant degeneration.
In the omphalomesenteric duct or its remains, especially in relation with the umbilicus, we often meet with small cysts or tumors in infants and young children. When the duct is persistent it presents normal intestinal structure, and, like the appendix, possesses much adenoid or lymphoid tissue.
Another and very important form of tubulodermoids develops in connection with the branchial clefts of the neck. Congenital fistulas of the neck have been long known, but only comparatively recently understood. Of the branchial clefts it is well known that the first alone should persist, as the Eustachian tube. Occasionally, however, they fail to become obliterated, and then we have congenital tumors or cysts, which may, perhaps, not develop to appreciable size until somewhat late in life; or there may be fistulous passages opening either into the pharynx or externally, forming canals varying in length from half an inch to two inches, secreting a little fluid because lined with epithelium. When these become inflamed an abscess results. When they open externally the opening is often marked by a little tag of skin containing a fragment of yellow cartilage. These are often referred to as cervical auricles. They open along the line of the sternomastoid muscle. The internal openings of these fistulas frequently form diverticula from the pharynx or esophagus. Thus it will be seen that dermoid cysts about the neck are principally relics of openings or ducts, which are normal in embryonic life, but which should have been obliterated at or long before birth. Congenital fistulas, however, may be met with in the middle line of the neck, which are not to be confounded with branchial fistulas, but rather with the ducts previously described.
—These may be unilocular or multilocular cysts, usually the latter. They are lined with epithelium, and contain mostly mucoid fluid, the inner coat being practically identical with mucous membrane. Occasionally, however, the skin is furnished with hair, sebaceous glands, teeth, and even nipples. The multilocular cysts are practically an aggregation of those just described.[268] They are surrounded by dense capsules, often attain great dimensions, and are made up of primary cysts resembling large cavities in a honeycomb-like mass, which itself is occupied by secondary cysts, and belong rather to the class of mucous retention cysts, these being occupied by still smaller ones, which are histologically indistinguishable from distended ovarian follicles. In these large tumors we find in some cases hair, in others teeth, and in others sebaceous glands, etc., the dermoid constituents being scattered throughout. As Wilms has shown, in almost every tumor of this character a projection may be found whose summit is covered with epiblastic elements, which when cut in serial transverse sections will show in its deeper portion other epithelial collections representing a feeble attempt to develop a nervous system, or lung tissue, while mesoblastic elements, like connective tissue, cartilage, and bone, appear scattered throughout, as though a very crude effort had been made to reproduce an atypical embryo.
So far the endeavor has been to limit the term dermoid to tumors which are essentially of epiblastic formation, their location being explained on the inclusion theory of Cohnheim. There is also a still more complicated type of tumor, composed of tissues of both epiblastic and mesoblastic origin, perhaps even hypoblastic. Their consideration belongs to that department of pathology known as teratology, which is supposed to deal especially with monsters. Strictly speaking a teratoma refers to an irregular tumor or mass containing tissues and fragments of viscera of a suppressed fetus which is attached to an otherwise normal individual. Nevertheless the term is often applied to growths which are the result of luxuriant mesoblastic development in which neither form nor member of a suppressed fetus is present.
The presence of supernumerary members is largely connected with what is called dichotomy, alluding thereby to cleavage either at the anterior or posterior end of the developing embryo. When the whole embryonic axis divides twins may be produced, but should cleavage be partial we may have a monster with two heads if it be anterior, or one with three or more limbs if it be posterior. Children born with these deformities are usually called monsters, and the study of such cases belongs entirely to teratology. But in certain tumors small portions of a suppressed fetus may develop, as, for instance, from the posterior portion of the sacrum, or within the abdomen or thorax, or upon the neck or face, which on dissection may contain a few vertebrae or processes resembling fingers associated perhaps with a structure resembling intestine or liver. This should be called a teratoma. Such tumors possess for the pathologist the greatest value. In surgery, however, they are rare, and there are scarcely two cases alike. The question of operation will often arise, as it does with supernumerary limbs, and each case should be studied upon its own merits. Sometimes they are amenable to extirpation.
—Embryonal adenosarcoma is a term given to certain teratomatous tumors peculiar to renal and adrenal structure, which present peculiar characteristics in the mixture of elements which enter into their composition. At various times these tumors have been called adenoma, sarcoma, rhabdomyoma, congenital cystic kidney, etc. They have been also likened to the thyroid. They comprise a group of neoplasms, always congenital in origin, which usually appear early in life, but occasionally occur in advanced adult life. One of the most marked specimens of this kind the writer removed from a man over fifty years of age. Most of the specimens, however, described in literature pertain to the young. On minute examination they often present a strange, mixed picture of voluntary muscle elements intermingled with epithelium arranged to imitate acinous glands, with cystic dilatations of the true kidney tissue. They often attain enormous size, and undergo such proliferation of mesoblastic elements as to resemble sarcoma. Their occurrence is to be explained only on the principles of Cohnheim’s hypothesis. When the original Wolffian body is being differentiated from the elements about it a confusion of the same with the excretory tubular beginnings, which are to empty into the Wolffian duct, occurs. Thus we have the commencement of a mixed mass which presents itself as a more or less rapidly growing tumor, in which even cartilage or other mesoblastic structures may be met with. It is scarcely possible that any two specimens should yield exactly the same[269] microscopic picture, much depending on whether one element or the other prevail. In a few of them there may occur also a mixture of adrenal elements. Sometimes the renal structure itself is more or less distinct, and rides, as it were, upon the surface of the tumor; at other times it is entirely mixed up with it. While the condition is usually limited to one side it may be a double affection, so that the second kidney becomes useless and the patient succumbs. The only treatment is extirpation.
Teratomatous tumors are sometimes found hanging in the pharynx, attached by a small pedicle, where they may be confounded with dermoids unless carefully examined after removal. Many instances of this type of tumor are found in animals. Here no false sentiment will prevent complete examination and preservation of the specimen. They are also encountered in the sacral and coccygeal regions.
—Lipomas, or tumors composed of fat, are the most common of the neoplasms. Their normal type is the ordinary adipose tissue of the body, and may be divided into the encapsulated and the diffuse, the former of which are surrounded by fibrous tissue. The diffuse lipomas are those which have no capsule, and where the pathological collection of fat merges into that normally present—in other words, they are not circumscribed.
Subcutaneous Lipomas.
—Subcutaneous lipomas are perhaps the most common of all, and are usually irregularly lobulated and encapsulated, adherent rather to the skin than to the deeper tissues. Usually but one is found in an individual, though instances of multiple lipomas are not rare. They develop sometimes to enormous size, cases being on record where the tumor has even weighed one hundred pounds. They may be met with at any point on the surface of the body. The lobules often burrow between the muscles, and those found in the palm of the hand penetrate even beneath the palmar fasciæ. They are sometimes markedly pedunculated, and often hang by a small stem. The diffuse subcutaneous lipoma is most common about the neck, in the groin, and in the axilla.
Subserous Lipomas.
—Subserous lipomas are mostly retroperitoneal, and large tumors of this character, mistaken for ovarian, have been successfully removed by operation. They also occur in the hernial canals and spaces. They develop beneath the peritoneum covering the intestines, and in this location give rise occasionally to intussusception. Here in their pathological development they have the general form and significance of appendices epiploicæ.
Subsynovial Lipomas.
—Subsynovial lipomas occur about various joints and tendon sheaths; within the knee they assume a distinctive type which has been called lipoma arborescens, where they take on a dendritic appearance and arrangement. Submucous lipomas are rare. Intermuscular fatty tumors are occasionally met with, an interesting variety being that which develops between the masseter and buccinator muscles. Intramuscular forms rarely occur, as well as a variety known as parosteal, which arises in connection with the periosteum. Fatty tumors also occur within the spinal dura, as well as outside of it within the spinal canal, and more or less lipomatous alterations are common in connection with spina bifida.
Lipomas are ordinarily easy of recognition, save when deeply located. The subcutaneous forms are intimately related with the overlying skin, and have a dough-like consistence which is usually pathognomonic. Tumors, suspected to be fatty, in the middle line of the back or cranium are always to be viewed with suspicion, as they are often connected with congenital meningeal protrusions.
An encapsulated lipoma when thoroughly removed will not return.
Mixed forms of fibrous and fatty neoplasm are occasionally seen, and are referred to as lipoma fibromatosum or fibroma lipomatosum, according as one or the other tissue predominates. These growths are innocent in their character, but call for thorough extirpation. They frequently give rise to considerable discomfort or pain, and are called lipoma dolorosa.
—Fibromas are tumors composed of fibrous tissue, which, when of pure type, are found to be not so common as was formerly supposed, the majority of tumors hitherto roughly grouped as fibromas containing either muscle tissue or sarcomatous[270] elements, which takes them out of the category of pure fibroma. A typical fibroma is ordinarily dense, and is composed of wavy bundles of fibrous tissue whose cells are long and slender and closely packed together, the mass being permeated by distinct bloodvessels.
Fibroma occurs most commonly in the ovary, the uterus, the intestine, the gum (epulis), in nerve sheaths, and in the skin in the form of so-called painful subcutaneous tubercles and molluscum fibrosum. There is also a fibrous tumor of the skin, known as keloid, sustaining to fibroma the same relation that exists between exostosis and osteoma.
Painful subcutaneous tubercle is a sample of pure fibroma in the shape of a small, flattened, pea-like tumor which never attains great size. It is situated loosely in the subcutaneous structure and may form a visible prominence. Insignificant as it would thus appear, it becomes the seat of exasperating pain, particularly when touched or handled, which may radiate to considerable distances. The etiology of these growths is unknown.
In the ovary, the uterus, the intestine, and the larynx true fibrous tumors are pathological curiosities rather than common lesions.
Fig. 74
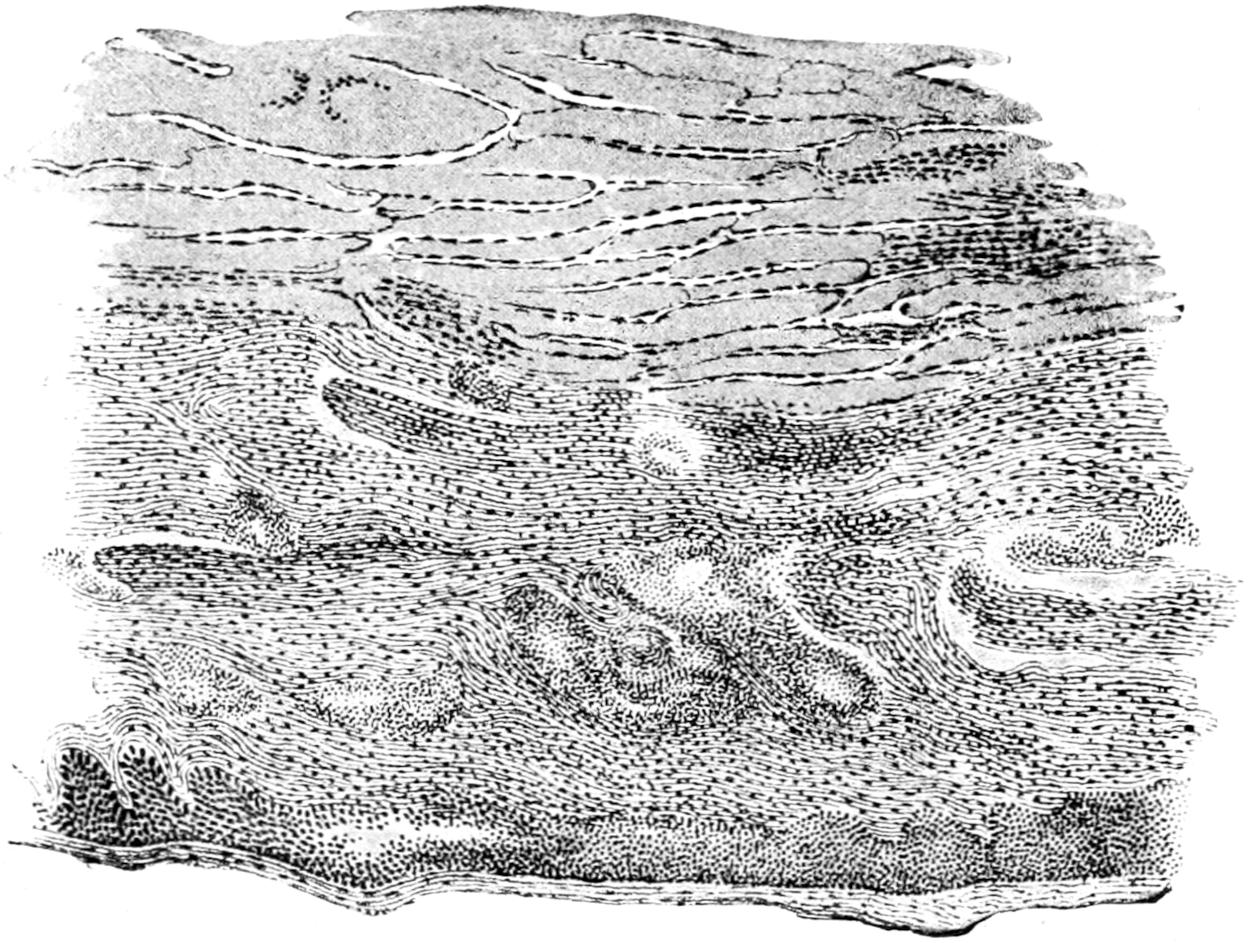
Keloid of external ear: a, dense tissue of skin; b, fibrous connective tissue; c, epidermis. (Klebs.)
Epulis.
—Epulis means any tumor growing upon the gum. The term was formerly applied in an indistinct and too comprehensive way, although it is still retained in literature. But pure fibromas do spring from the fibroösseous structure of the gum and alveolar process. They are covered with the gingival mucous membrane and seem to spring from the periodontal membrane. They seldom attain large size, and then only by neglect. By the pressure of such tumors teeth may be separated and distortion of the mouth produced. They should be promptly extirpated.
Keloid.
—Keloid is a fibrous neoplasm arising mainly in cicatricial tissue, which is essentially fibroid in structure. It is a neoplasm which often follows the general outline of the scar in which it grows, consists in elevation of the surface, ordinarily quite smooth, sometimes of a delicate pink from the dilated vessels which it contains. Keloid is the bête noir of surgeons, as it frequently complicates and disfigures scars which have at first been satisfactory, and since it indicates a condition which it is discouraging to deal with, because when it is removed there is usually recurrence of growth within a few months after cicatrization. It often occurs in stitch-hole scars and upon the site of extensive burns, and may be observed after puncture of the ears for ear-rings, and has also been observed in scars left by smallpox, acne, etc. It is more prevalent in the colored race than in the white. In negroes multiple keloid tumors are often seen, occasionally in large numbers. Their explanation is[271] unknown, and it may be that some trifling injury has preceded each individual tumor (Fig. 74).
The treatment of keloid will be considered in the chapter on the Surgical Diseases of the Skin.
Desmoids.
—This term has been applied to tumors of a certain clinical type which arise from the fibrous structures, usually of the abdominal wall, and produce neoplasms like the fibromas of other parts of the body. The use of the term should be restricted to those tumors which proceed primarily only from muscles, tendons, and aponeuroses, or perhaps from ligamentous and periosteal tissues. These tumors are usually single, attain sometimes considerable size, grow slowly, rarely involve other structures, and not infrequently develop to such an extent as to encroach upon either pelvis or the abdomen, or both. They have been known to attain to the weight even of ten pounds or more. They are usually more or less encapsulated, and are firm and dense in structure. Under the microscope they have the general appearance of cellular fibroma. Sarcomatous elements may be met, while they occasionally undergo cystic degeneration. Their occurrence may be explained, at least in some instances, on the embryological theory of Cohnheim.
Fig. 75

Multiple enchondromas.
The treatment of desmoids consists in their complete extirpation. They should not be allowed to attain large size because their removal may entail a serious weakening of the abdominal wall. There should be such plastic rearrangement of abdominal protecting membranes as to reduce the resulting weakening to a minimum.
Psammoma.
—Psammoma is a term applied to a form of hard fibroma met with in the dura mater, in which there has occurred a petrefaction of some of the cells—i. e., a deposition of calcareous salts, which gives it a gritty or sandy appearance.
—The true chondroma is a tumor composed of hyaline cartilage. It occurs in the long bones, usually in relation with epiphyseal cartilages, and is often noted during the earlier years of life. While it is usually a solitary tumor, multiple chondromas are often seen, especially upon the hands. These tumors are often encapsulated and form deep hollows, in which they rest. Unless pressing upon nerve trunks they are painless and slow of growth. They are exceedingly dense and hard, and ordinarily immovable. Mucoid softening (i. e., cystic degeneration) is common, and the softened areas may give rise to fluctuation. There may be coincident calcification or ossification in any of these growths. It is noted as a curious circumstance by Sutton that their tissue resembles histologically the bluish, translucent, epiphyseal cartilage seen in progressive rickets.
To the small local hypertrophies of cartilage which are seen especially about joints,[272] about the laryngeal cartilages, and the triangular cartilage of the nose, are given the term ecchondroses. They are most common in the knee in connection with rheumatoid arthritis, and occur as prominences along the margins of the joint cartilage. They may project to such an extent as to be detached by accident, after which they become movable and floating bodies in the joints. Many of the floating cartilages or bodies found in joints are detached ecchondroses, which may be smoothed off by attrition, and may be found singly or multiple, even several hundred existing in one joint.
Chondromatous changes as occurring in sarcomatous tumors have been alluded to. It seems to be easy for connective tissue to form hyaline cartilage, and mixed tumors may thus be seen in connection either with sarcoma, fibroma, or other forms.
Treatment.
—The treatment of chondroma is solely operative. Unless the integrity of a member or a limb be compromised, such a tumor can usually be shelled out from its location, but requires that the matrix be completely extirpated; all of which may call for the use of powerful bone instruments. At other times amputation is the only measure which may relieve from deformity, pain, and disability. The ecchondroses occurring within joints necessitate incision and evacuation, with the most rigid aseptic precautions, with or without drainage. When practised according to modern technique this is almost invariably successful. In former times many lives were lost because of septic infection.
—Under the head of nomenclature I have already endeavored to distinguish as between exostosis, or irregular bone outgrowth, and osteoma, as a distinct tumor which is composed of bone tissue, with the subvariety odontoma, or tumors of dental origin and structure. Osteoma is regarded by some as ossifying chondroma, for it is nearly always found near epiphyseal lines, and is always covered by hyaline cartilage when thus found. Nevertheless it is not invariably such. We speak of compact or ivory osteoma and of a cancellous form. The former is identical with the compact tissue of the shafts of long bones, and may occur anywhere, but is most common about the cranium, at the frontal sinus, the external meatus, and the mastoid process. Osteomas growing into the frontal sinus of oxen form large, lobulated, bony masses, sometimes weighing several pounds, and as dense as ivory. Some of these tumors growing into the cranial cavity have been regarded as ossified brains. Osteomas in connection with the external auditory meatus may partially obscure this channel and cause deafness. They constitute ivory-like growths, which sometimes defy the finest steel instruments with which the surgeon can supply himself.
Fig. 76
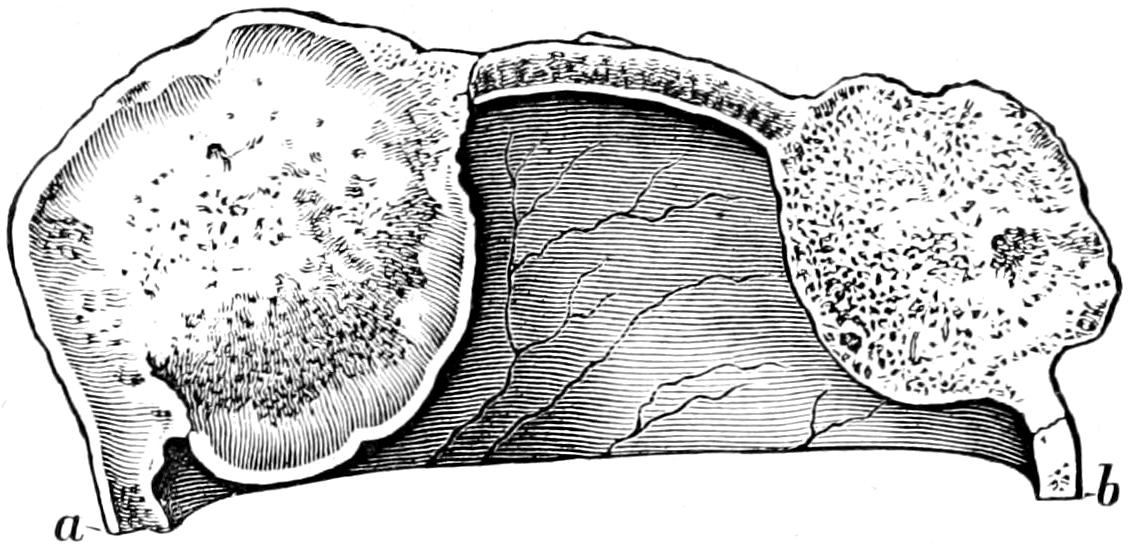
Double osteoma of the skull. (Musée Dupuytren.)
Cancellous osteomas grow in the cranium as well as in the long bones, and, like the compact forms, only occasion pain by pressure upon nerve trunks.
—Exostoses are classed by Sutton as—
1. Those formed by ossification of tendons and their attachments. There should be excluded from this group such natural or evolutionary processes as the supracondyloid process, the third trochanter of the femur, etc. Over or around such exostoses bursæ will form to mitigate as much as possible the effect of friction. Such an outgrowth is known as an exostosis bursa; it is most frequently seen on the inside of the femur immediately above the knee.
2. Subungual exostoses, occurring usually beneath the nail of the big toe.
3. Exostoses due to calcification of inflammatory exudations, including the rare condition known as myositis ossificans.
PLATE XVII
FIG. 1

Round-cell Sarcoma. (Low power.)
FIG. 2
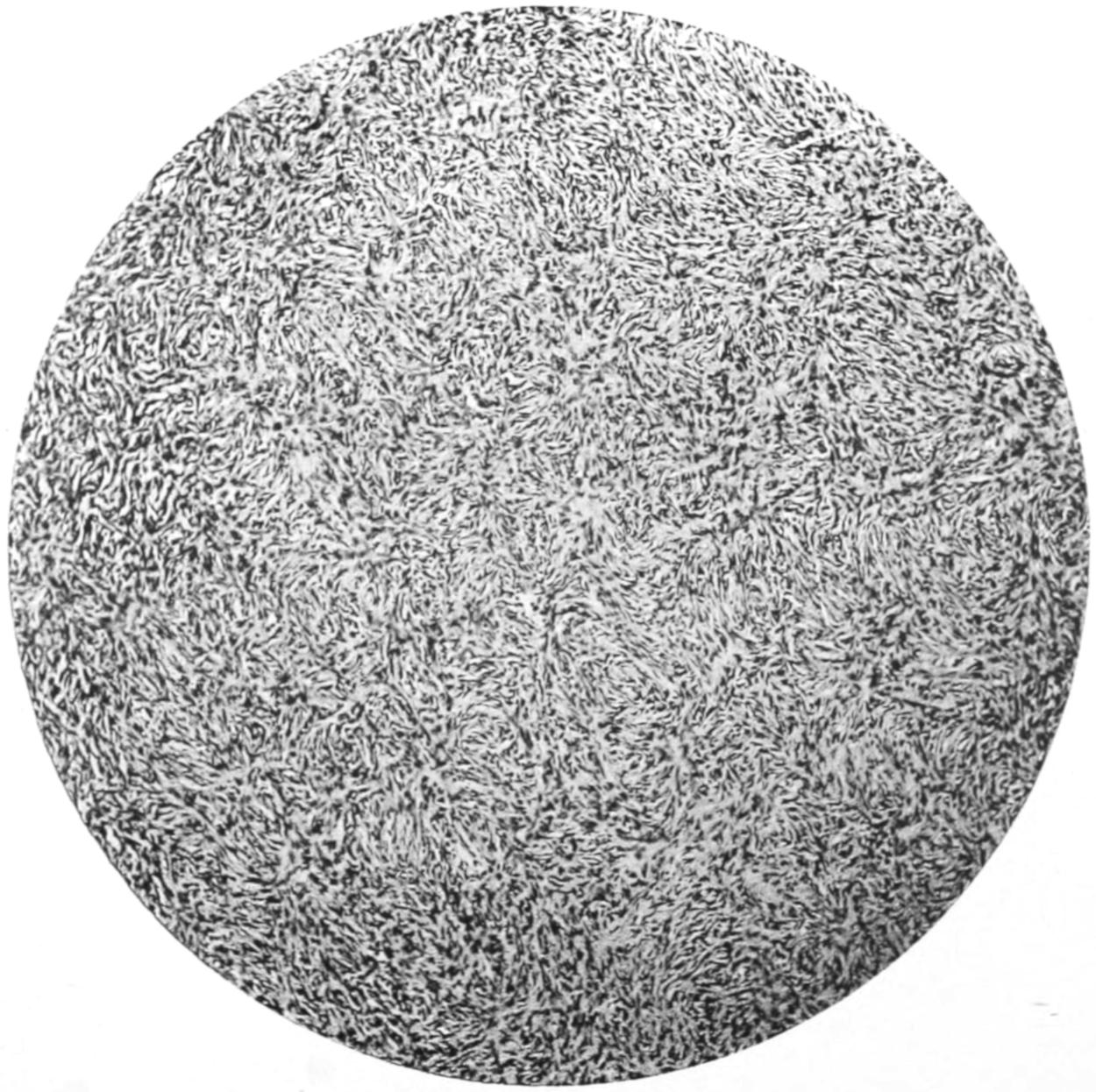
Spindle-cell Sarcoma. (Low power.)
[273]
When a true osteoma is once thoroughly removed there is no tendency to recurrence. Thorough removal, however, calls sometimes for serious and often mutilating operations, which may become dangerous when the growth involves the curve of a rib or a large portion of the skull. At other times amputation is rendered necessary. Special forms require special treatment.
—Formerly this name implied a fleshy tumor, and was made to cover many different conditions. Now sarcoma means a tumor composed of immature mesoblastic or embryonic tissue in which cells predominate over intercellular material. Sarcomas are sometimes encapsulated; they merge into and infiltrate the surrounding tissue and disseminate widely, and have usually these propensities and characteristics to such a degree as to constitute malignancy. For the laity sarcomas and carcinomas are together included in the comprehensive term of cancer; for the surgeon they constitute but one form of cancer. Sarcomas are classified, according to the shape of their cells and their disposition, into—
To these are added other varieties mentioned below.
Fig. 77

Osteoma of frontal sinus. (Neisser.)
Fig. 78
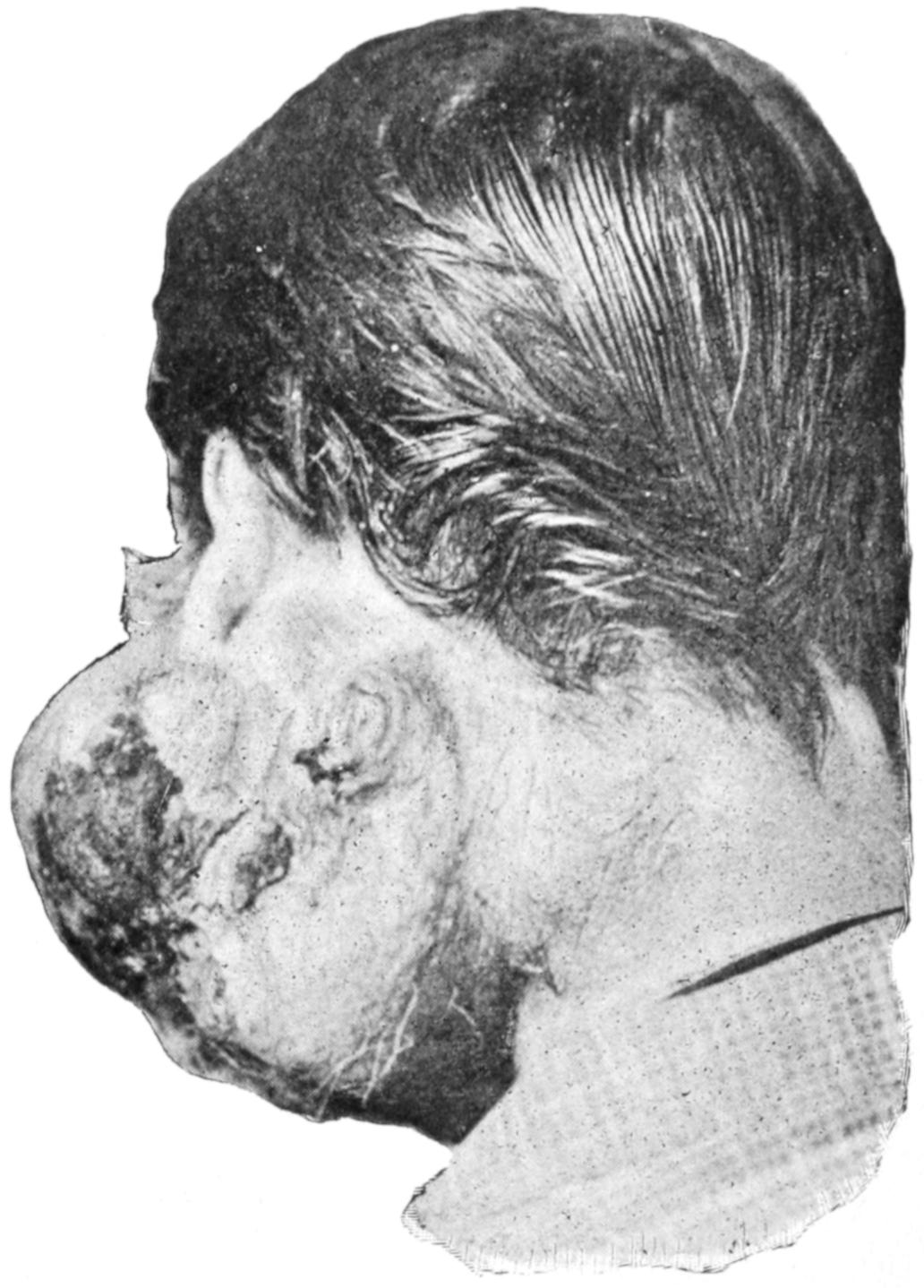
Recurring sarcoma of parotid. (Original.)
A. Round-cell Sarcoma.
—This is simple in construction, and consists of round cells containing very little intercellular substance. The nuclei of the tumor cells stain easily, the cells themselves varying in size in different cases. Bloodvessels lead up to the tumor, but in the interior appear rather as channels. These tumors have no lymphatics: they grow rapidly, infiltrate easily, recur quickly, and give rise to numerous metastatic or secondary deposits. They may affect any part of the human body. The size of the cells is supposed to be in some measure an index of their malignancy—the smaller the cell the more malignant the tumor. They appear at all periods of life. They are perhaps the most commonly seen of malignant tumors in animals. (See Plate XVII.)
Lymphosarcoma.
—This tumor is composed of cells similar to the previous form, but enclosed in a delicate meshwork resembling that of lymph nodes, hence the term lymphosarcoma. Lymphosarcomas are not to be confounded with enlargements nor with the specific granulomas involving these lymphatic structures.
[274]
B. Spindle-cell Sarcoma.
—In this form the cells have a spindle shape and run in all directions, so that sections will show them in various shapes and sizes. In some cases the cells are small and slender, in others large. The size of the cell is a measure of the malignancy of the tumor. (See Plate XVII.)
The largest of these spindle cells are frequently striated transversely like voluntary muscle fiber, and tumors composed of this form have been considered as tumors of striped muscle tissue, and are generally called rhabdomyoma. There is no tumor of striped muscle fiber, and the rhabdomyomas of writers generally should be considered as spindle-cell sarcoma, or may be dignified by the name myosarcoma. (See Rhabdomyoma, under Myoma.)
Alveolar Sarcoma.
—This is a rare form, in which the cells, contrary to the general rule of sarcomas, assume an alveolar arrangement strongly imitating that of epithelial cells in carcinoma. Almost invariably, however, on close examination it will be possible to distinguish a delicate reticulum between individual cells, which is never met with in cancer.
C. Myeloid, or Giant-cell Sarcoma.
—In this form the tissue resembles histologically the red marrow of young and growing bone, containing large numbers of multinuclear cells embedded in a matrix of spindle or round cells. These tumors usually occur in the long bones, and when freshly cut look like a piece of liver. They constitute most of the epulides or cases of epulis—i. e., spongy tumors springing from the gums. (See Plate XVIII., Fig. 2.)
Fig. 79
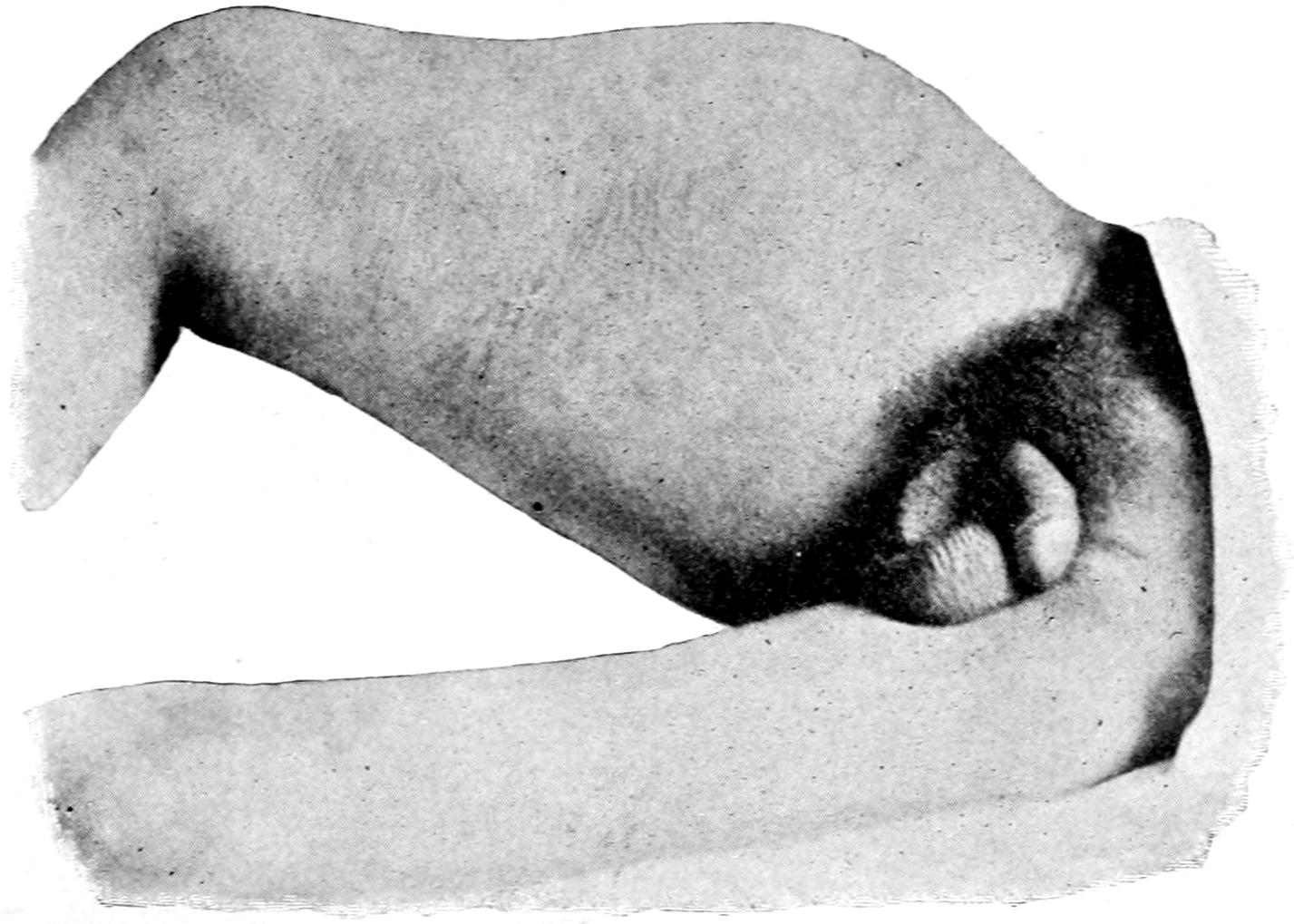
Sarcoma of femur following fracture—i. e., developing in callus. (Original.)
Giant or multinuclear cells should be present in considerable numbers to entitle a tumor to classification in this group. When round cells, spindle cells, or giant cells mingle in nearly equal proportion the tumor should be called a mixed-cell sarcoma.
D. Osteosarcoma.
—Osteosarcoma is something more than sarcoma of bone, which latter may spring from the fibrous or medullary elements. It is sarcoma of the specific bone-forming connective tissue, including the osteoblasts and osteoclasts; in other words, of the stroma of the bone. Under these circumstances real bone develops throughout the tumor, and it is essentially a bony neoplasm. In like manner there may be true osteofibroma. These tumors are to be distinguished, even clinically, from the medullary sarcomas, which develop within the bone and expand it, even to enormous proportions, the bony covering then being a mere shell.
E. Chondrosarcoma.
—Chondrosarcoma resembles osteosarcoma in that it is sarcoma of the stroma of cartilage, or of the specific tissue which produces cartilage. In it true cartilage (white fibrous) also is found throughout the tumor. Chondrofibroma is also possible. (See Plate XIX.)
F. Endothelioma.
—Endothelioma has been called various names, and its true character has been only lately determined. It is composed particularly of the endothelial cells which line the lymph spaces, and which have no peculiar secretion. It is met with most often in the skin (especially of the face), in the parotid region, in the genital glands, the bones, the lymph nodes, and dura.
PLATE XVIII
FIG. 1
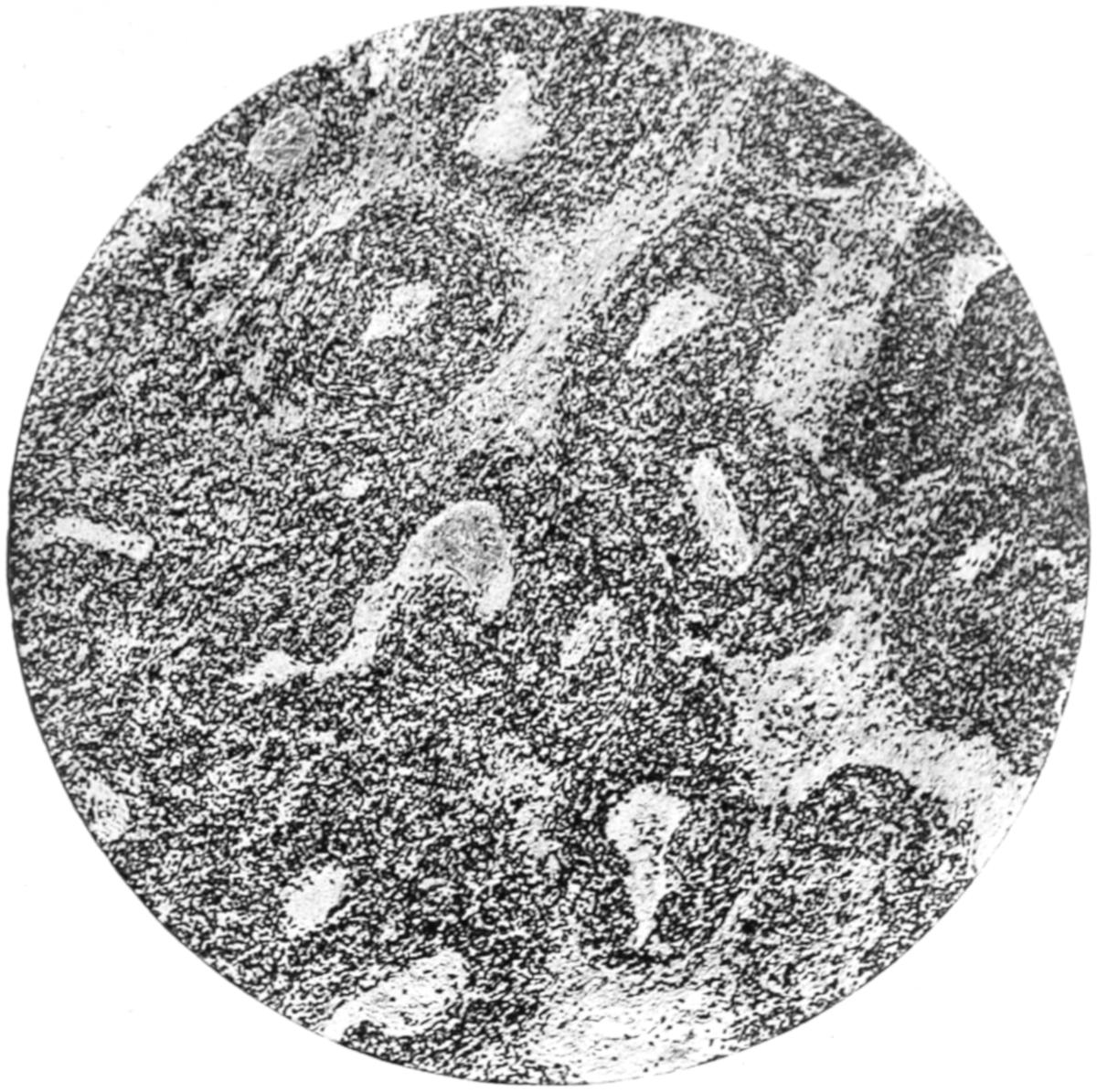
Angiosarcoma. (Low power.)
FIG. 2
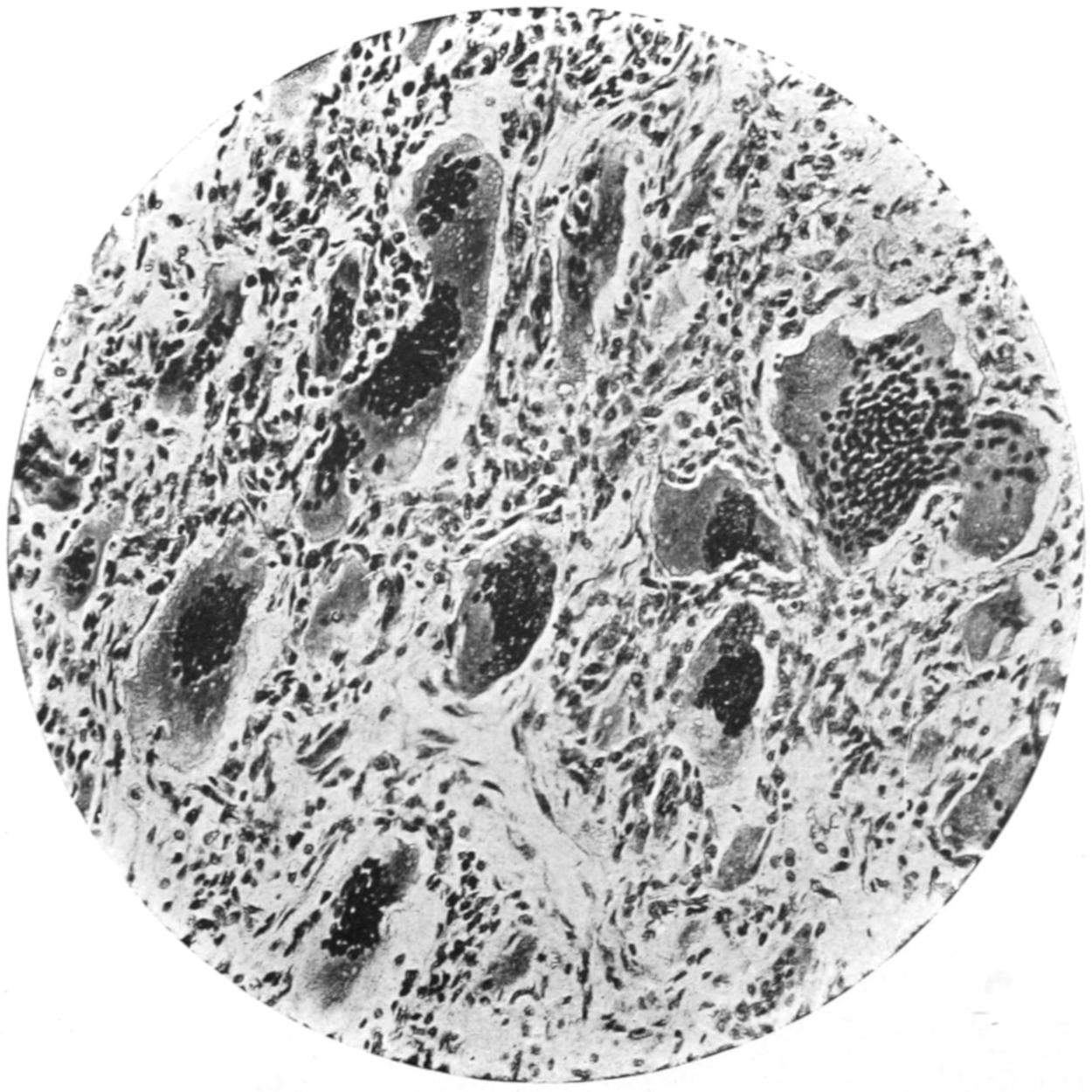
Giant-cell Sarcoma. (High power.)
PLATE XIX
FIG. 1
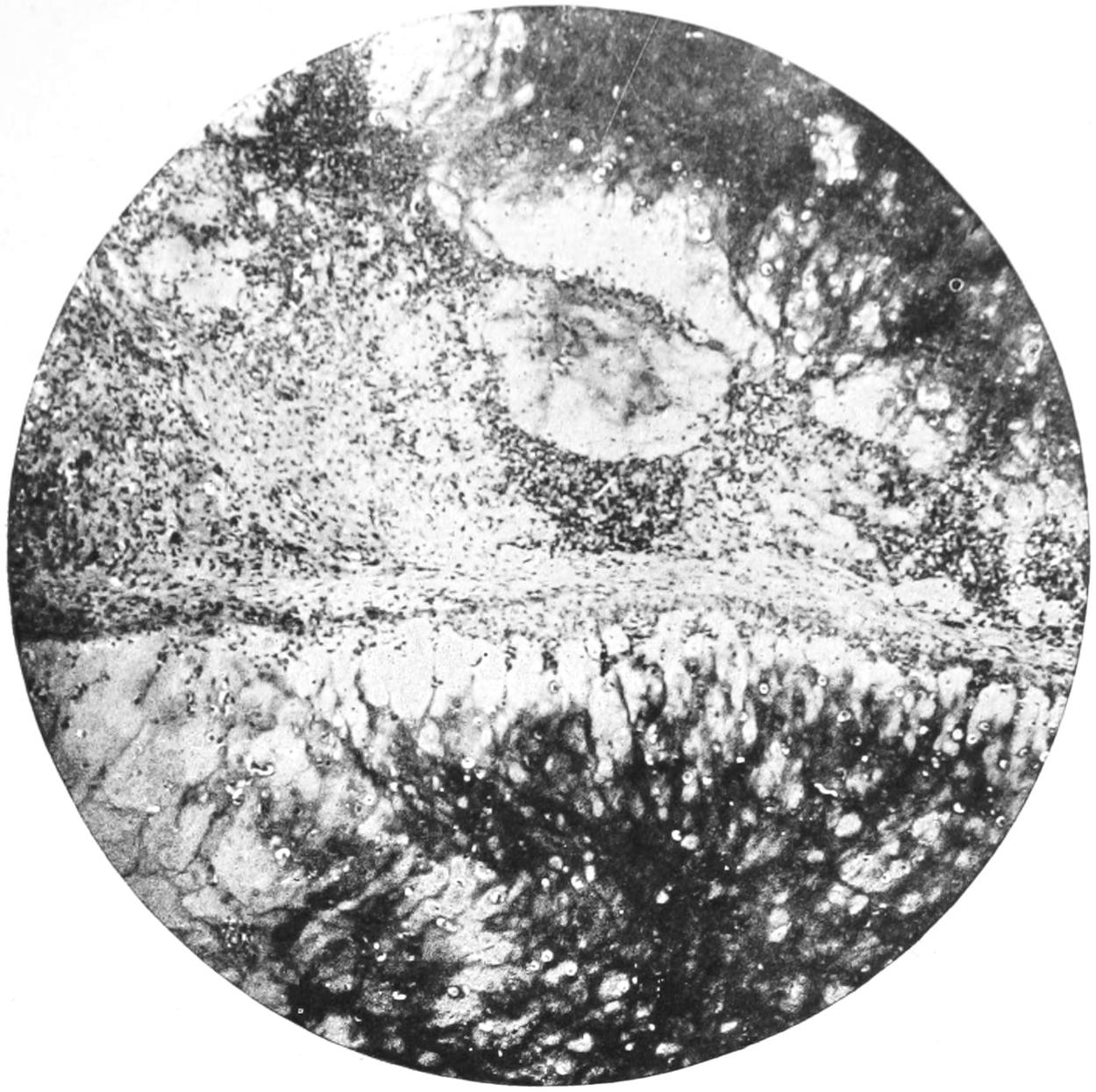
Chondrosarcoma. (Low power.)
FIG. 2
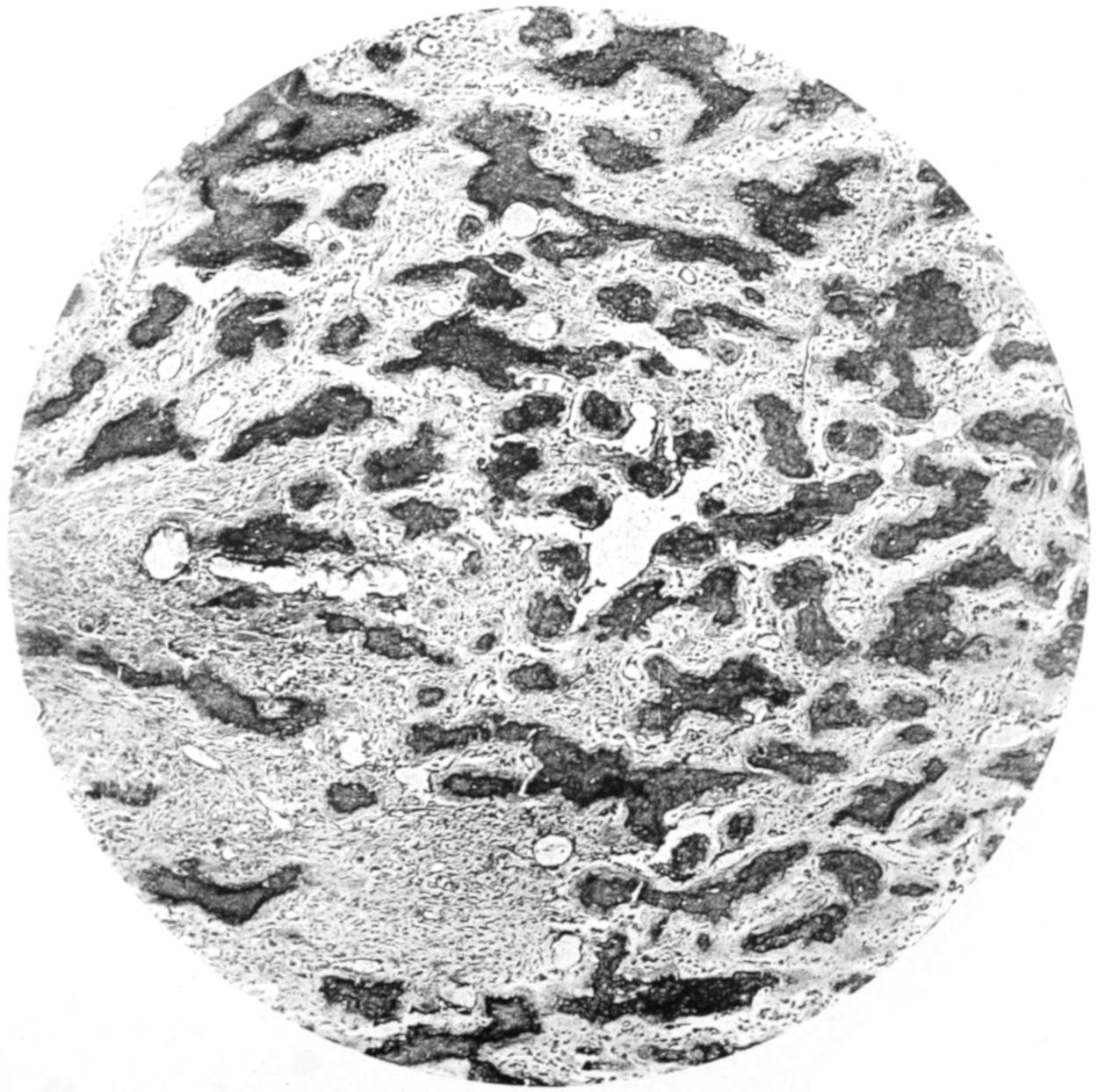
Osteosarcoma. (Low power.)
PLATE XX
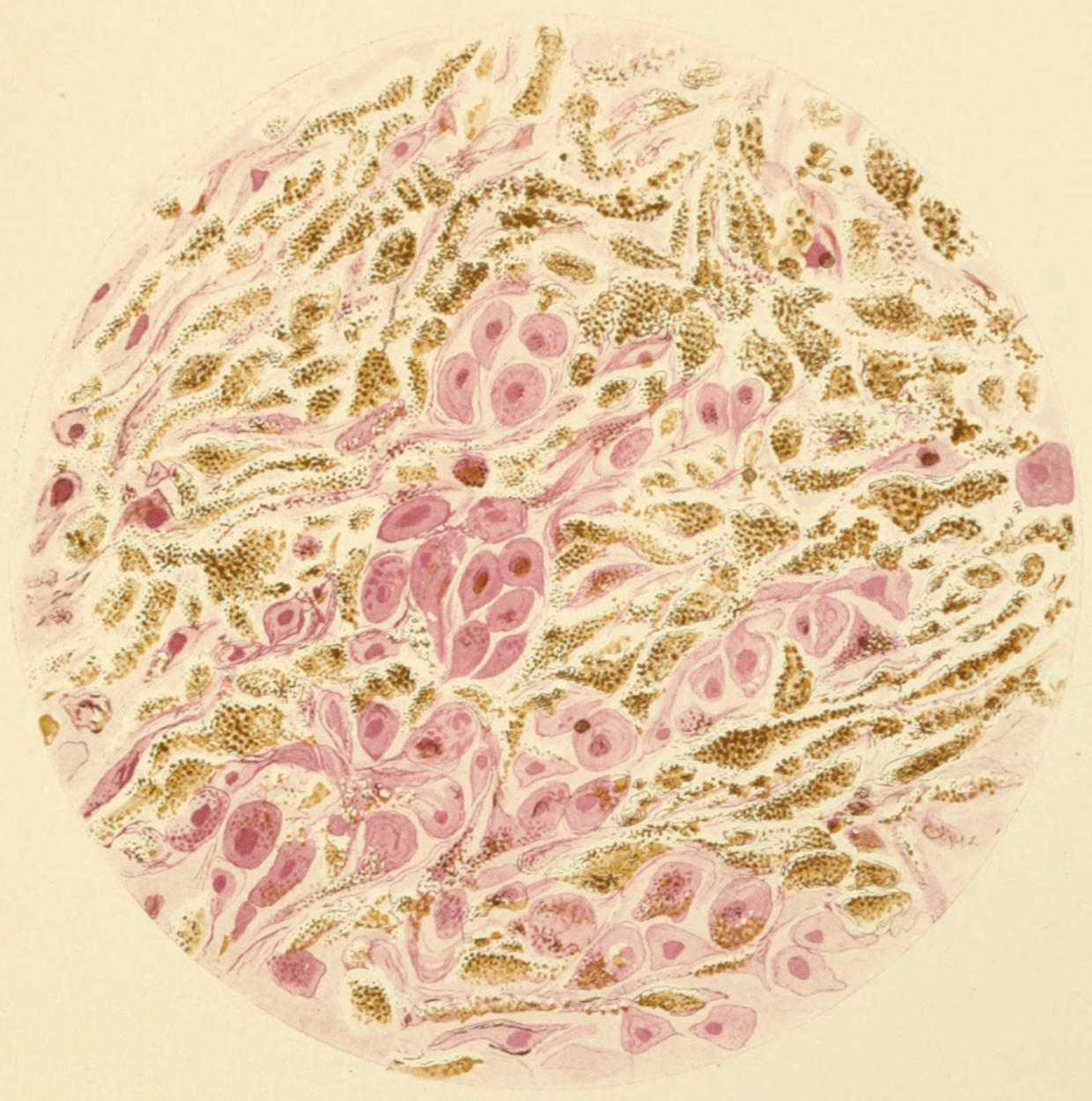
Melanosarcoma of Skin. (Dry high power.)
[275]
The microscopic picture of these tumors varies greatly, the endothelial cells often shaping and grouping themselves so as to imitate epithelioma. In doubtful cases the primary location or origin of the growth should be ascertained.
Endotheliomas are mainly of rapid growth, and often show a high degree of malignancy. If thoroughly extirpated before metastasis has occurred, prognosis is fair; but metastases happen early because of the direct connection of the tumor with the lymph current.
Fig. 80
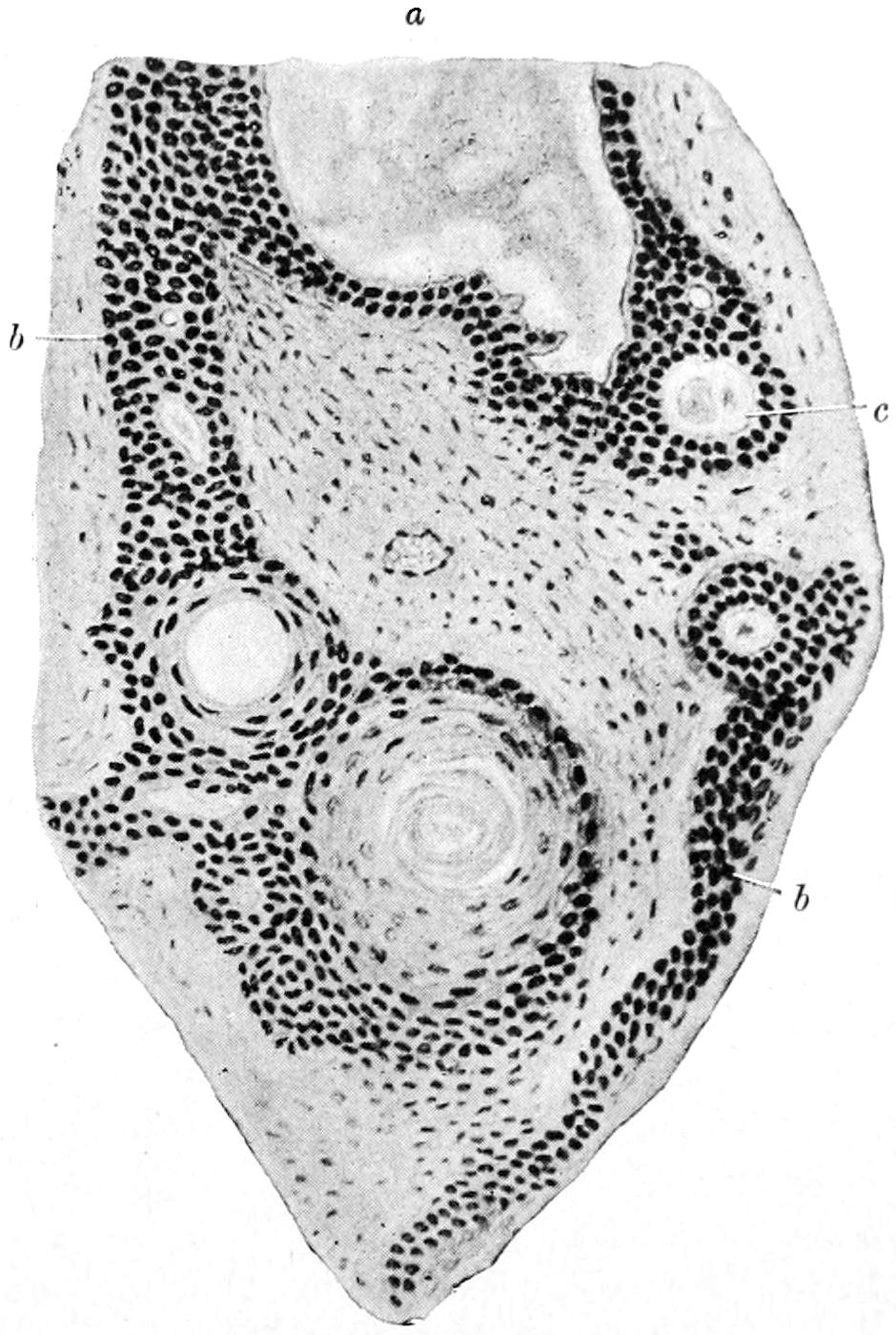
Endothelioma of the soft palate: a, dilated lymph space; b, endothelial cells with beginning cystic formation; c, completely formed cyst. (Volkmann.)
G. Angiosarcoma.
—Angiosarcoma is a sarcoma arising from the adventitia of the bloodvessels. It is characterized by its extraordinary vascularity, the ease with which hemorrhages into the structure of the tumor take place, and the frequency of pigmentation. Peritheliomas constitute a subvariety, met with especially in the kidneys, the bones, and the skin, and originate in the perithelial cells between the capillaries and the perivascular lymph spaces. They are more vascular than the angiosarcomas. The latter are common in the liver. In many cases the cells of these tumors simulate the columnar epithelium of adenocarcinoma. (See Plate XVIII, Fig. 1.)
H. Cylindroma.
—This is a term applied to tumors of the angiosarcomatous type in which hyaline changes have occurred, so that along the vessels appear cylindrical masses of altered cells. Similar appearances are noted in certain endotheliomas and are due to the same hyaline degeneration.
I. Melanosarcoma (better known as Melanoma).
—This refers to the deposition of pigment, rather than to type or shape of cell, the distinguishing feature of these growths being the presence both in the cells and in the intercellular substance of a variable quantity of blackish pigment. Of all the forms the melanotic growths are considered the most malignant. They invariably recur after removal, lead to secondary deposits at long distances, and present the most intractable and incurable forms of cancer. Deposition of pigment in carcinomas is most rare, if ever met with, and the growths of melanotic type should be relegated entirely to the class under consideration. The tumors most often develop from pigmented nevi of the skin, though primary melanoma of the deeper parts of the body is known. These will be treated more fully in the chapter on the Skin. (See Plate XX.)
This name has been variously applied by different writers to different growths. In order to avoid confusion it would be well, in using it, to be definite.
—The vascular supply of sarcomas varies within wide limits. In nearly all instances it is of capillary character, the blood circulating rather through vessels without well-marked walls. While large vessels may be found about and in the periphery of these tumors, distinct vascular structure is usually absent from the more internal portions, which will explain the frequency of hemorrhage, its persistency after operation, and the ease with which large extravasations occur. True hematocele may thus take place within sarcomatous tumors, with the usual later cystic alterations, and thus in one way we have the condition known as cystosarcoma.
[276]
In attacking these growths the vascular and bloody area may be met just about their margins, the bloodvessels expanding as they arrive at the tumor, and sometimes bleeding extensively. Under most circumstances, however, this hemorrhage can be controlled by packing or by operating at a greater distance from the circumference of the growth.
Metastasis in sarcoma is common, dissemination occurring mainly along the veins, as these growths connect with the venous channels and permit of easy detachment of fragments, which are then carried along as emboli. These emboli pass naturally to the right side of the heart, and thence to the lungs, where it is most common to find secondary growths, except in areas emptying into the portal veins, in which case the liver will be the most common site. Sarcomas are destitute of lymphatics, and dissemination does not occur through these channels.
Infiltration is also a common phenomenon with these growths. This is generally seen in muscular tissue, particularly with growths proceeding from the periosteum and projecting into it.
Sarcomas, like other tumors, tend to grow along the lines of least resistance. Hence processes of these tumors will insinuate themselves into fissures and interspaces, and penetrate perhaps even into the cavities, from which it is hazardous or impossible to remove them. Thus, sarcomas springing from the head of a rib have been known to extend through an intervertebral foramen and give rise to an intraspinal tumor, causing fatal pressure.
Secondary changes are usually seen in sarcomas, the most frequent being hemorrhage. Myxomatous degeneration is also frequent, and gives rise to cystic conditions. Calcification is common, particularly in the slowly growing tumors which arise from bone. Upon the other hand, necrosis (i. e., ulceration) is common in growths which project upon the surface or into any of the open cavities of the body. Ulceration here is growth at a rate faster than nutrition will justify, and gangrene is to be regarded as a failure to supply sufficient blood. It may also mean infection, of which it is a usual expression.
Tumors of this character, which luxuriate upon reaching the surface, and bleed easily upon the slightest touch, were formerly known as fungus hematodes. The name may be preserved for the sake of convenience, but should be held to mean, in almost every instance, a rapidly growing round-cell sarcoma.
Sarcoma is common in the lower animals, particularly so in horses—most common in those of gray color. It is met with also in cows and various other domestic and undomesticated animals.
—The myxomas are composed of mucous tissue, whose best-known normal representative is the Whartonian jelly of the umbilical cord. True myxoma should be distinguished from myxomatous degeneration, which occurs frequently in cartilage, fibrous tissue, and sarcoma, and which brings about a similar condition of affairs, though of essentially different origin. Myxomas appear under the following forms:
1. Polypi.
—These include many of those which grow in the nose. The pure form of nasal myoma proceeds from the mucous membrane of the nasal passages or sometimes from the accessory sinuses. But most of the so-called nasal polypi are due to edematous hypertrophies of the submucosa. The polypi usually hang as gelatinous tumors of grayish-yellow tint, being present sometimes singly, sometimes in clusters or in large numbers. Their principal effect is to produce nasal obstruction, with, perhaps, subsequent serious disorder, due to decomposition or to extension into the pharynx or other cavities. Similar growths also occur from the mucous membrane of the tympanum, and constitute the common variety of aural polypi.
2. Cutaneous Myxoma.
—Cutaneous myoma is not common. It presents usually as a sessile tumor, although about the perineum and labia the tumors may become pedunculated. It is often difficult to distinguish between a myoma of the skin and a sarcoma of the same which has undergone myxomatous degeneration, and which then should be called sarcoma myxomatodes. The latter tend to recur after removal; hence the importance of exact diagnosis.
3. Neuromyxoma.
Neuromyxoma is a similar condition involving the nerve trunks, and is dealt with under Neuroma.
Myxomas require complete removal, and, in the nose especially, cauterization or destruction of the surface from which they spring. When this is thoroughly done they do not recur; otherwise, they are likely to require subsequent operation.
[277]
—The true myoma is a tumor composed of unstriped or involuntary muscle fiber. Until recently it has been customary to divide the myomas into the leiomyomas in contradistinction to the rhabdomyomas, the latter being supposed to be tumors of voluntary muscle fiber. Myomas are met with only where involuntary muscle fiber is found—namely, in the uterus and adnexa, the vagina, the esophagus, alimentary canal, the prostate, the bladder, and the skin. They form encapsulated tumors composed of fusiform muscle cells with a rod-like nucleus, the size of the cells varying greatly in different specimens. The bundles of muscle fibers are much contorted, and it is often difficult in a single section to decide to just what class of cells they belong.
These tumors are most common in and about the uterus, and are referred to as intramural when developing in the true uterine tissue, and submucous and subserous when situated just beneath one or the other of the adjoining membranes. They differ in their rate of growth, are firm in composition, and are moderately vascular, sometimes containing areas of softening and becoming even cystic. In rare instances they become enormously vascular, and are then known as cavernous myomas. Aside from mucoid or colloid changes they occasionally undergo fatty metamorphosis or calcareous infiltration. The latter is possible to such an extent as to lead to a condition of uterine calculi.
Uterine myoma is liable to septic infection, which frequently follows exploration of the uterus or the changes incident to pregnancy or parturition. It then becomes a case for immediate operation. Uterine myomas do not occur before puberty, rarely before the age of thirty-five, and are most common between the thirty-fifth and forty-fifth years of life. They produce disaster not alone by their size, but by hemorrhage, by pressure on adjoining viscera (rectum, kidneys, etc.), and occasionally by torsion of a long pedicle.
Myomas are found in the esophagus, in the walls of the stomach, where they are frequently confounded with malignant tumors, in the prostate and wall of the bladder, and in connection with the skin. As soon as they give rise to inconvenience or to dangerous symptoms they are to be dealt with surgically, as no other treatment has proved of lasting benefit.
The rhabdomyomas deserve but brief description. The striated muscle fibers of which these tumors are composed have been often confused with spindle-shaped sarcoma cells. They are met with almost exclusively in the mixed tumors of the kidney under Teratomas.
Myoma or myofibroma is exceedingly likely to undergo sudden conversion into a form of growth entitling it to be called malignant myoma.
—Angiomas are tumors composed of bloodvessels, and group themselves under three headings, in accordance with the structure of the vascular system:
1. Capillary Angioma, or Nevus.
—Capillary angioma, or nevus, is the most common form of all, and is frequently seen in the skin and subcutaneous tissue. When the condition is spread over a relatively large area it gives rise to a discoloration known as port-wine mark, and called telangiectasis by the pathologists. The condition is often congenital or begins soon after birth. The color of the affected area determines whether the vessels belong to the venous or to the arterial system. These tumors may be found in all parts of the body, on the surface, on the submucous surfaces of the tongue, the inside of the mouth, the conjunctiva, and the vulva. The tendency is toward gradual increase in size; rarely, spontaneous contraction and obliteration occur.
2. Cavernous Tumors.
—These are similar in structure to the corpus cavernosum, and are called erectile tumors. They are common in connection with the skin, and are exaggerated forms of the variety first described, the vessels becoming not merely dilated but cavernous in arrangement. They occur occasionally in the tongue, in the voluntary muscles, and in the liver, and are noted very rarely in the mammæ, in the larynx, and subperitoneally.
A similar condition is met with in the so-called cavernous tumors which involve various organs, especially the thyroid and the liver. In these instances a part or the whole of the organ may be involved, and presents great increase in size and evidences of vascularity.
In cavernous growths of the thyroid are vessels, veins especially, the size of the thumb, while with the ear not touching the body of the patient a distinct venous murmur may be heard.
[278]
3. Arterial or Plexiform Angiomas.
—Arterial or plexiform angiomas, when of any particular size, are called cirsoid aneurysm or aneurysm by anastomosis. This form consists of arteries abnormal both in number, length, and diameter, tortuous in arrangement, occurring often in the scalp, but rarely in the perineum or genitalia, and seldom in other parts of the body. (See Aneurysm, Chapter XXIX.) These tumors are liable to rupture from external injury, and necessitate ligation of the main arterial trunks, with perhaps extirpation of the tumor mass.
Recognition of angiomas is not difficult unless they are deeply concealed. The effect of intermitting pressure, the emptying and refilling, and the distinction between arterial and venous growths by the result of alternating pressure and relaxation, either above or below the growth, with discoloration of the skin, and, in the larger growths, audible murmur, leave little doubt of the character of the growth.
When such growths are small they may be dealt with by electrolysis, the needles from both poles being introduced, or that from the negative, the positive being applied upon some neighboring portion of the body. The effect of the electric current is to determine coagulation of the blood in the tissues acted upon, and this is followed by organization of thrombus, conversion of vascular into cicatricial tissue, shrinkage, and possible eventual disappearance of the mass. Radical excision under an anesthetic should be made, dissecting out the mass, securing bleeding vessels, and reuniting the parts by sutures, with the expectation of securing primary union. This is the quickest and in many cases the least disfiguring method. Old methods of ligation of surrounding vessels or the subcutaneous ligature are now practically discarded. The injection methods as formerly practised, especially the use of iron salts in solution, are severely condemned, as death is liable to occur. With electrolysis and excision the surgeon has nearly all the measures which he will need to practise for the medical treatment of angiomas.
Fig. 81
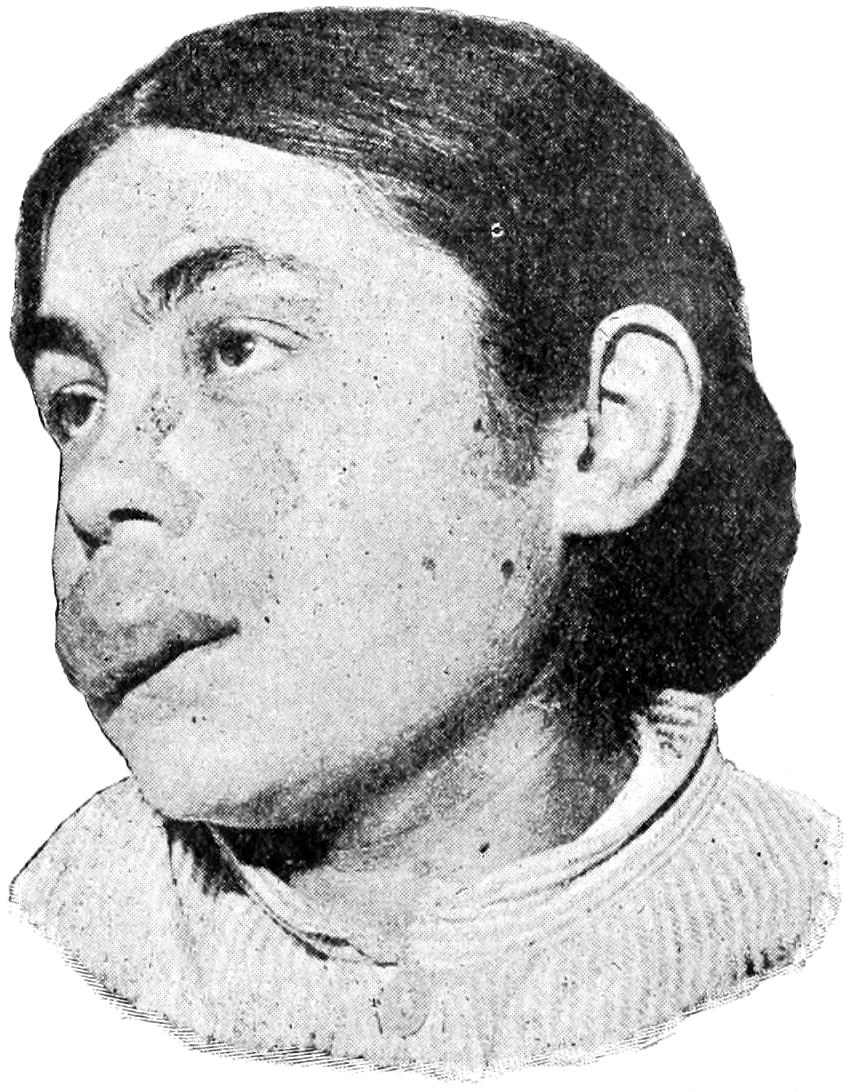
Lymphangioma of lip; macrocheilia. (Neisser.)
—Lymphangiomas are tumors composed of lymph vessels and bear resemblance to the tumors above considered. They may be divided into three varieties:
1. The Lymphatic Nevus.
—The lymphatic nevus is composed mostly of lymphatics nearly normal in size, and occasionally colored red by the presence of bloodvessels. When pricked, pure lymph or blood-stained lymph, will flow. They are usually small, and are noticed during childhood. They may occur anywhere upon the surface of the body or in the mouth, generally in connection with the tongue, where they may appear as large papillæ involving a portion or all of the dorsum. When the lymphatic structures of the tongue are thus enlarged and involved the condition is known as macroglossia, and consists of enlargement of the organ, sometimes to a degree not permitting its retention in the mouth, but leading to its constant protrusion (Fig. 81).
2. Cavernous Lymphangioma.
—Cavernous lymphangioma corresponds to cavernous angioma, and is a condition in which the lymph vessels become positively cavernous and sacculated.
3. Lymph Cysts.
—Lymph cysts are the still more aggravated form which lymphatic dilatation may attain, and are usually encapsulated, complicated with more or less tense tissue, and produce a condition of the parts, especially about the scrotum and labia, to which the term elephantiasis is often applied (Fig. 83).
The question of congenital occlusion or dilatation of lymph channels is one which has been made the subject of large separate monographs (especially by Busey). Numerous tumors, essentially of lymph-vascular origin, are found upon the lips, in the neck, and[279] elsewhere, which grow slowly, are more or less elastic and spongy upon pressure, are frequently covered with skin, from which hair grows most luxuriantly, and in which pigment or papillomatous structures are dispersed. These tumors are called cavernous tumors, are of slow growth, and undergo spontaneous involution, but usually require surgical relief. They are often confounded with branchiogenic and other congenital cysts of the neck.
—The treatment for the smaller lymphatic tumors is simple, but here electricity is less to be relied upon and excision is more urgently demanded. Electrolysis will cause coagulation of blood, but not of lymph—at least not to nearly the same extent; consequently its usefulness is restricted to blood-vascular tumors. Excision, then, is the best remedy. When this is impracticable much can be done by galvanopuncture or ignipuncture, the cicatricial contraction following multiple punctures leading to reduction in size of the affected part. The enlargement of the tongue spoken of above as macroglossia may be treated by ignipuncture or by electrolysis, if necessary under an anesthetic, the effect of the electric current here being not to produce coagulation, but apparently absorption of fibrous tissue and changes which come slowly rather than by obliterative processes.
Fig. 82

Congenital lymphangioma. (Original.)
Fig. 83
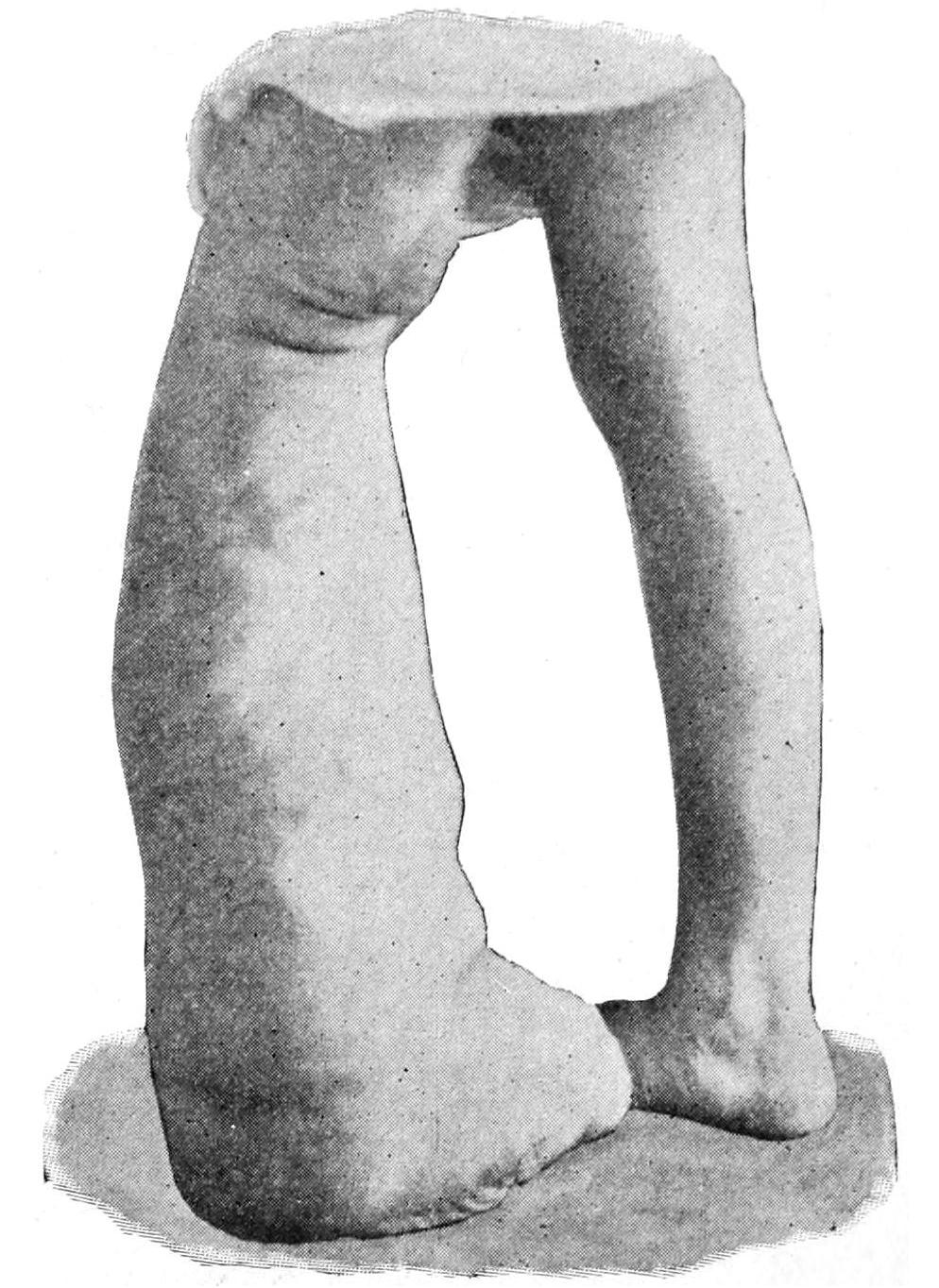
Lymphangioma of lower extremity. (Original.)
—Glioma is a malignant tumor developing directly from actual nerve structure or that of the original nerve elements, and is clinically allied to the sarcomas. It arises from the neuroglia, and hence is confined to the central and peripheral nervous system, mainly the former. It is most common in the brain, the cord, and in connection with the optic nerve and fundus of the eye. It is often extremely vascular, the vessels being sacculated, and is usually met with in solitary form. When near the surface of the cortex such a tumor may appear like a great convolution (Virchow). In the basal portions of the brain it may attain considerable size. In the cord it is rare, usually limited to the cervical region. In the orbit and eye it may produce marked exophthalmos. It is more frequent in the young than in the aged.
[280]
Glioma is an exceedingly malignant form of tumor, and operation is rarely performed sufficiently early to more than prolong life. Dissemination by continuity is the rule rather than metastasis. It kills usually by its pressure effect on the nerve centres.
—True neuromas spring from the structures of nerve trunks, which trunks may also be the site of other tumors, mainly fibromas and sarcomas, with which neuromas may be easily confounded. The most common nerve tumor is the neurofibroma, which grows from the structure of a nerve sheath, its long axis usually coinciding with that of the nerve trunk. Tumors of this class vary greatly in size, are often multiple, and in other instances affect nearly all the nerves in the body. They are extremely liable to myxomatous degeneration, which will account for many of the instances reported as myxoneuroma, etc. They attack cranial and spinal nerves alike, and no nerve or nerve root in the body is exempt. The sensory nerves appear more liable to attack than the motor. The nerve least often attacked is the optic. They are not rare upon the roots of the spinal nerves, in which location they may attain to such size as to press upon the cord and induce paraplegia. Multiple neuromas are often associated with molluscum fibrosum (q. v.). There is an instance on record in which 1600 of these tumors were found after careful dissection of the neuroskeleton, and another in which at least 2000 were found, 60 of them involving the pneumogastric trunks and their branches.
Fig. 84
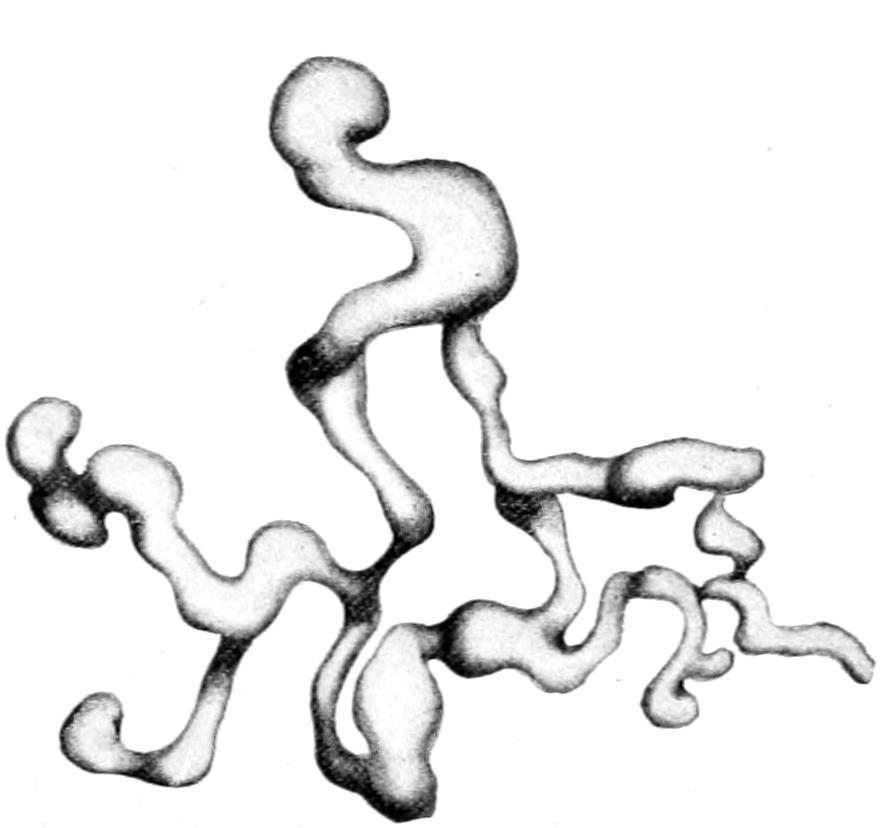
Plexiform neuroma, dissected free from all adherent tissues. (Lexer.)
Fig. 85
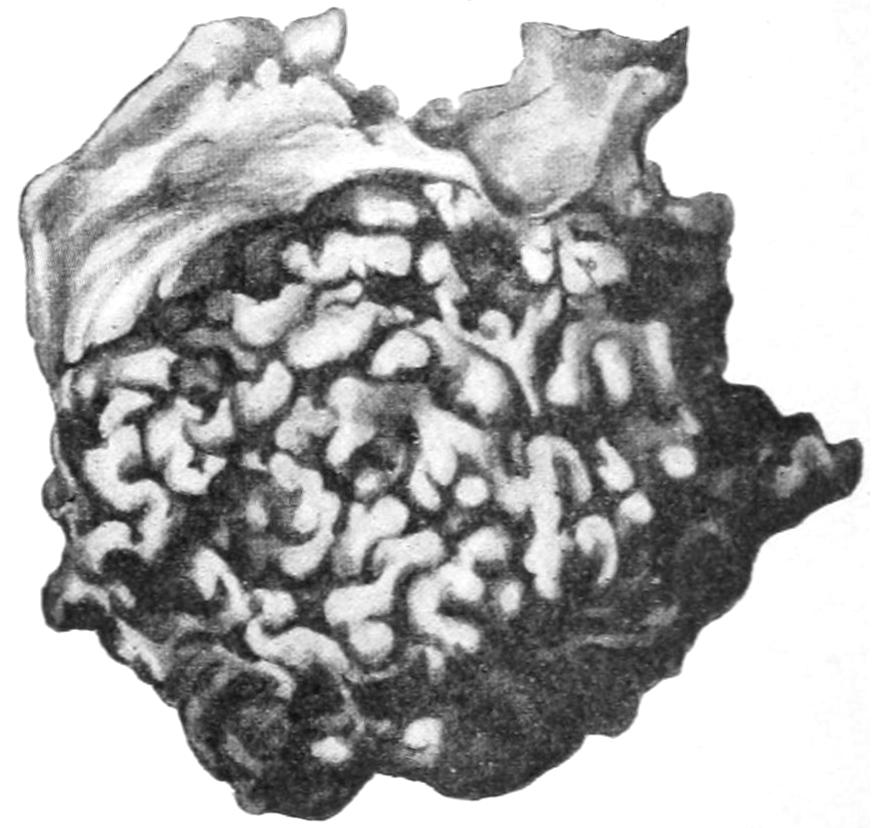
Plexiform neuroma of chest wall in a young child. Illustrating its gross external resemblance to lymphangioma. (Lexer.)
Plexiform Neuroma.
—Plexiform neuroma is relatively rare. This is a type of nerve tumor in which all the branches of a given nerve which are distributed to a particular area become enlarged and elongated, the overlying skin being stretched and thin. Such a tumor seems like a loose bag containing a number of vermiform bodies, resembling the sensation given when palpating a varicocele. On section each of the affected nerves reveals a quantity of myxomatous tissue replacing the nerve sheath. They are in large measure congenital. The skin overlying a plexiform neuroma will frequently be found to be pigmented, variously altered in thickness, and covered with fine hair. These growths have been frequently mistaken for lymphangioma (Figs. 84 and 85).
Malignant Neuroma.
—Malignant neuroma (so called) will generally be found to be a true sarcoma of nerve structures, usually of the spindle-cell variety. Traumatic neuroma is often seen in amputation stumps, where the terminations of the divided nerves become bulbous, attaining the size of cherry stones, the tumors being composed of a mixture of connective tissues and nerve fiber, from which in time the true nerve structure usually recedes or vanishes. They form when suppuration has been profuse or healing long delayed, and when sufficient care has not been exercised to prevent entangling of the nerve ends in the scar of the wound. They give rise to much pain, and often necessitate re-amputation. The bulbous enlargement is the result of prolonged irritation in a nerve, and has been noted around various foreign bodies.
[281]
True neuroma is innocent in tendency, though often painful. It is the sarcoma of nerve tissue which produces signs of malignancy. A true neuroma which causes unendurable pain should, when accessible, be removed. It is sometimes possible to separate the tumor mass from the balance of the nerve trunk, and thus to remove it without excision of the nerve. At other times it is impossible to avoid division and ensuing paralysis. Divided nerve ends should be brought together by catgut suture, by which means it may be possible to avoid permanent loss of function. Nerve grafting is also resorted to for repairing such defects. Removal of painful neuromas due to injuries to the head has more than once been the means of curing traumatic epilepsy.
These tumors consist of specific epithelial elements supported and more or less bound together by a vascular connective-tissue stroma. The only apparent exception to this statement is tumor of dental tissue. The teeth are positively modified and petrified or calcified epithelial products.
—The odontomas are tumors composed of one or more of the dental tissues, arising either from tooth changes or teeth in process of development. They may be divided, according to Sutton, as follows:
1. Epithelial Odontomas.
—These are provided with a capsule, and present usually as a series of cysts separated by thin septa, containing mucoid fluid, while the growing portions have a reddish tint not unlike sarcoma. They are most frequent about the twentieth year of life, but may occur at any age. They probably arise from persistent remains of the epithelium of the original enamel organs.
2. Follicular Odontomas.
—These are often called “dentigerous cysts.” They arise in connection with permanent teeth, and especially with the molars, sometimes attaining great size and producing conspicuous deformity. The tumor consists of a wall representing the expanded tooth follicle, and a cavity containing viscid fluid, with some part of an imperfectly developed tooth, occasionally loose and more or less displaced in location. The cyst wall always contains calcareous material. These tumors rarely suppurate. They occur also in animals.
3. Fibrous Odontomas.
—These consist of condensed connective tissue in a developing tooth, presenting as a tumor with a firm outer wall and a loose inner texture, blending at the root of the tooth with the dental papilla and indistinguishable from it. The developing tooth thus becomes enclosed within the capsule before it protrudes from the gum. These tumors are most common in ruminants, being often multiple.
4. Cementoma.
—A tumor of fibrous character whose capsule has ossified or calcified, the developing tooth thus becoming embedded in a mass of dental cementum. These tumors occur most frequently in horses.
5. Compound Follicular Odontomas.
—These are tumors containing a number of masses of cementum resembling small teeth, or even amounting to well-formed but ill-shaped teeth composed of all three dental elements. In such a tumor teeth may be found in great numbers. They occur in the human subject as well as in animals.
6. Radicular Odontomas.
—These are tumors which arise after the crown of the tooth has been completed and while its roots are yet in process of formation. The crown, being unalterable enamel, does not enter into the composition of these growths, which then consists of dentine and cementum in varying proportions. They are rare in man, but frequent in other animals, and often multiple.
7. Composite Odontomas.
—These are hard tumors, bearing little or no resemblance in shape to normal teeth, occurring in the jaws, consisting of a conglomeration of enamel, dentine, and cementum, presenting abnormal growth of all the elements of the tooth germ. So far this tumor has only been found in man.
Little is said about the odontomas in general surgical literature. These tumors, as they grow, are often regarded as due to necrosed bone or to unerupted teeth, while fibrous odontomas have been often regarded as myeloid sarcomas. No tumor of the jaw, especially in young people, should lead to excision of the jaw until it has been demonstrated that the tumor is not one of the above forms. When diagnosticated as true odontoma its complete removal is all that is necessary.
[282]
—The type of papilloma is this common wart, consisting of a central stem of fibrous tissue and bloodvessels covered by epithelial projections and proliferations. Papillomas are usually sessile and villous.
1. Warts.
[14]—These are sessile papillomas, most common on the skin, often seen on mucous surfaces, and occurring sometimes singly, often in crops. They are exceedingly common about the perineum, where skin and mucous membrane meet, and are regarded as due to the irritation of specific discharges. The papillomas occurring about the genitalia are known as condylomas. The growths in these instances are frequently so luxuriant and proliferative that they assume fungoid shape, and are called mulberry growths. Warts grow slowly or rapidly according to circumstances. Warty growths may attain enormous size and become vascular. Late in life they are frequently the starting points of epithelial ingrowths, and then become true epitheliomas—i. e., cancer. Warty growths sometimes line the buccal cavity and complicate cases of macroglossa. They occur also in the larynx, and when situated near the glottis may cause dyspnea and fatal obstruction to respiration. It is claimed by some that cutaneous warts will disappear with continued small internal dosage of Fowler’s solution. (See Plate XXI.)
[14] Warts are by many pathologists considered as mere evidences of hypertrophy from persistent irritation. They are here retained among the tumors lest too much violence be done to formerly received notions.
Fig. 86
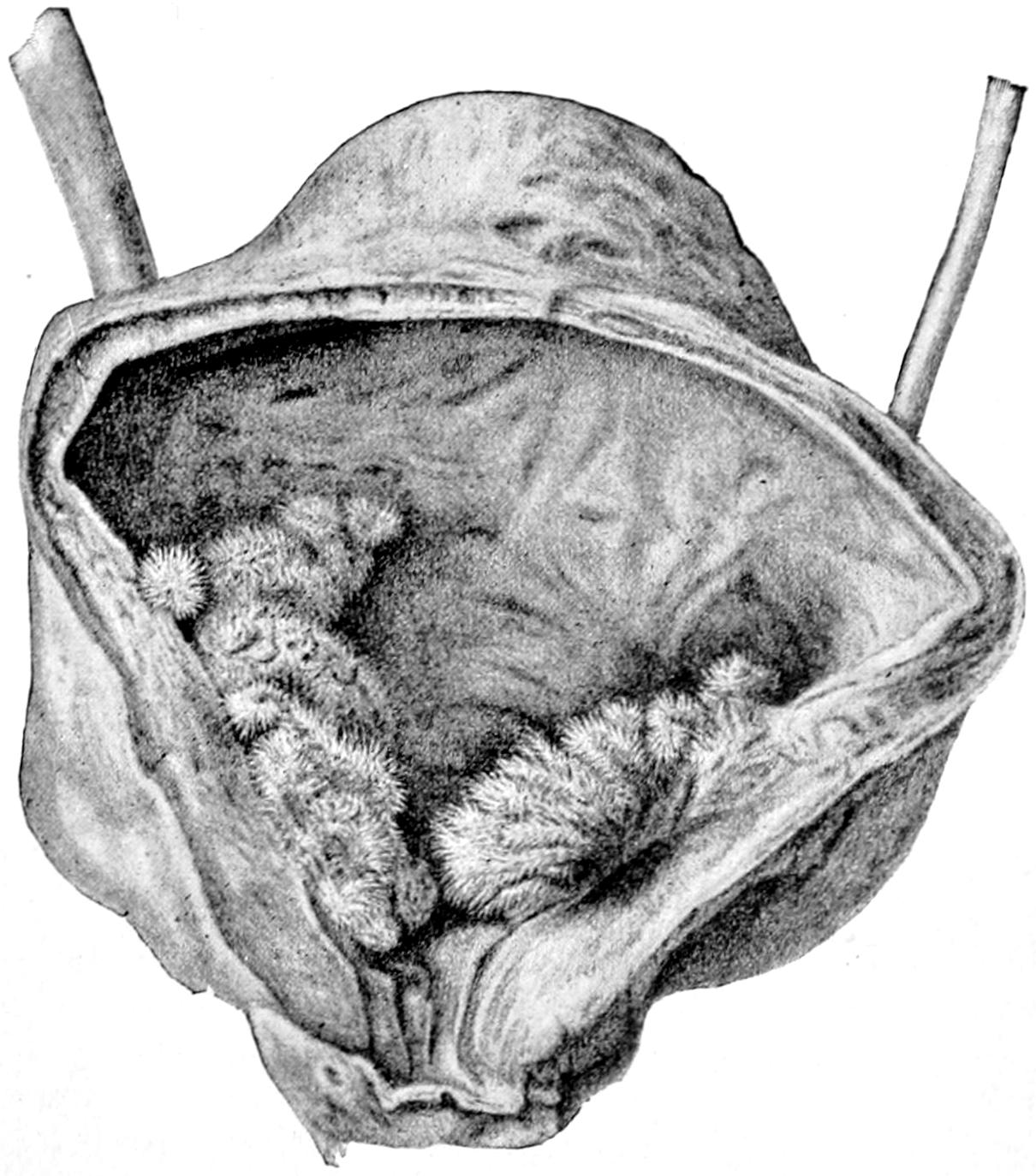
Papilloma of the bladder.
2. Villous Papillomas.
—These are met with most commonly in the bladder, occasionally in the pelvis of the kidney. They are identical with chorionic villi, and occur most often singly. It frequently happens that long, fine tufts are detached and carried away with the escaping urine. Another form of villous growth arises from the choroid plexuses of the lateral ventricles in the brain. These may grow and attain a size sufficient to produce disturbance (Fig. 86).
3. Intracystic Villous Growths.
—These are seen, for example, in mammary cysts. These, of course, are lined with epithelium, which acts here as it does in other localities, and proliferates more or less rapidly under unknown circumstances. In dealing with paroöphoritic cysts the presence of these growths has also been alluded to.
4. Ovarian Papilloma.
—There is a form of ovarian papilloma which partakes of the nature of a malignant tumor, in that separated particles seem to attach themselves to peritoneal surfaces, where they grow luxuriantly. Either this is an expression of parasitism or infectivity, or else of the implantation of tumors, which, to the writer’s mind, constitutes a strong argument for the parasitism of cancer. After abdominal section, with removal of the original focus, these growths often disappear. This affords a parallel to the instances of cure of tuberculous peritonitis after the same procedure.
PLATE XXI
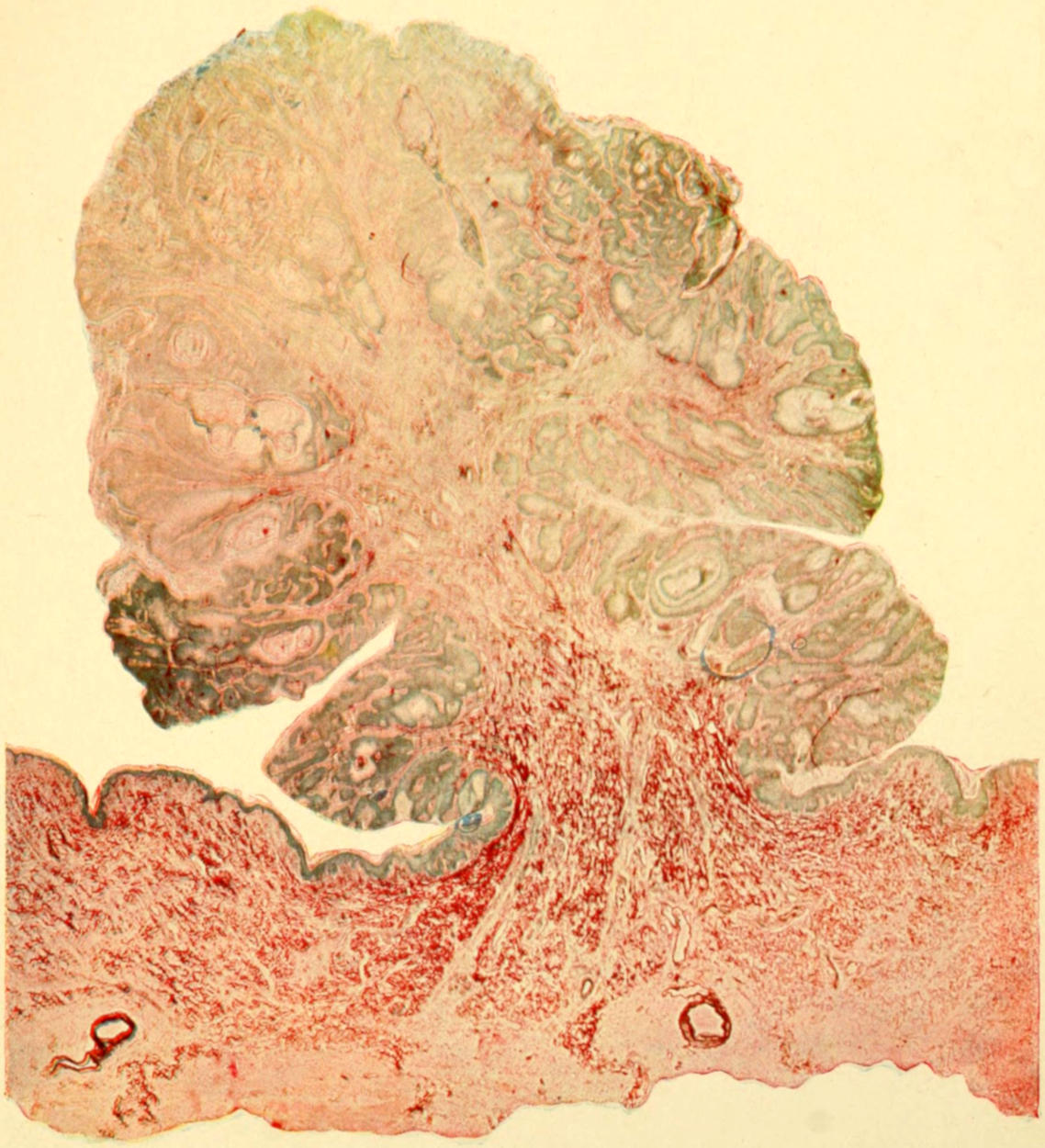
Photographic Reproduction of Papilloma. Low power. (Gaylord.)
[283]
5. Cutaneous Horns.
—These are also epithelial outgrowths, and are met with in four varieties (Sutton):
(a) Sebaceous horns, quite common, arising by protrusion of contents of a sebaceous cyst through a rupture in its wall or through its duct, with consequent desiccation by exposure to the air, while fresh material is consequently added at the basis so long as sebaceous secretion continues. These growths soften when soaked in weak liquor potassæ.
(b) Warty horns, structurally identical with the above, but growing from warts instead of from sebaceous cysts. Both these forms are often found about the head. Cutaneous horns are also met with in ovarian dermoids. They are common in the lower animals and may attain large size.
(c) Horns growing from cicatrices, especially of bones, are rare, but a cornified condition of the cicatrix itself, with formation of scales resembling those from horns, is not uncommon.
(d) Nail horns are simply overgrown nails, occurring on the digits and toes of bedridden patients who never walk (Fig. 87).
Fig. 87
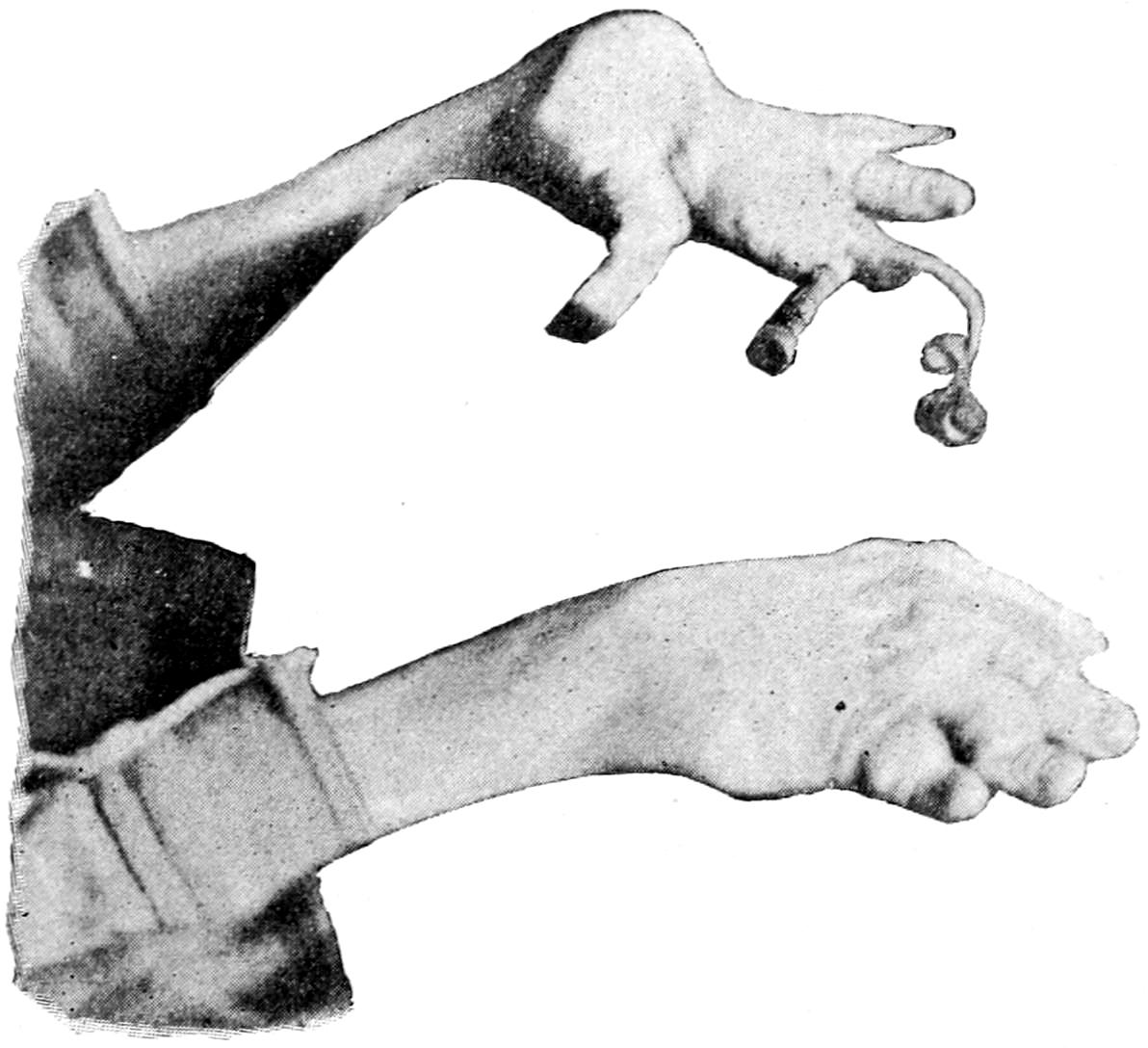
Nail horns. (Original.)
Treatment.
—All these forms of epithelial outgrowth call for radical removal, which implies complete extirpation of the membrane or tissue from which the growth occurs, after which, if effected, there is no recurrence. If some be left there is tendency to recedive.
—Similar papillary and often pedunculated epithelial tumors frequently hang or project from the mucous membrane—e. g., the rectum. The pedicle really projects from the submucosa. Between the layers of the overgrown mucosa are found altered glands. So long as the growth of these polyps is toward the exposed surface they are innocent and wellnigh harmless, unless they attain fair size; but so soon as they grow inward and the boundary of the submucosa is transgressed they assume malignant aspects at once. Such transformation is by no means rare, and constitutes a strong argument for their prompt removal.
—Pathologically the various enlargements of the thyroid known as goitre or struma constitute essential neoplasms. (See chapter on Regional Surgery of the Neck.) In this condition either the epithelial or the connective tissue may be primarily at fault.
[284]
1. Struma Parenchymatosa Nodosa.
—This includes also the colloid and the cystic varieties, and refers to an enormous overproduction of the epithelial elements (parenchyma) in distended alveoli, where they often undergo colloid softening. So marked are these changes in numerous instances that multiple cysts (minute or large) result. The collective volume of such altered tissue may be very large.
2. Struma Fibrosa.
—This presents itself in the way of dense enlargement of the thyroid, the stroma being the tissue now involved, even to the extent of causing much of the alveolar structure to disappear or become obliterated. In this condition calcification is common, and calcareous concretions or patches are often found.
Even benign tumors of the thyroid show occasionally a tendency to metastases. Cases are on record of benign goitre causing general metastases, and even of metastasis without noticeable thyroid enlargement. These occur most often in the bones, less frequently in the lungs and other organs. They are more common when the goitre has undergone colloid changes. The reasons for these changes are unknown.
In either form hemorrhages are common, with their resulting blood cysts or their solid residue, in which case pigment is usually found. Both forms are often accompanied by enlargement of the vessels, and sometimes these become enormously dilated and constitute an almost insuperable obstacle to successful removal. (See Thyroidectomy.)
—The cystomas of the ovarian region assume two types: (1) Glandular cystoma, and (2) papillary cystoma.
1. Glandular Cystoma.
—The glandular type produces the multilocular forms, with numerous small and large cavities, filled with fluid which varies in color and appearance within wide limits, having usually the consistency of mucus or thin pus, and containing a small number of cylindrical epithelial cells. The cyst wall may contain tubular glandlike structures reaching into the surrounding connective tissue.
2. Papillary Cystoma.
—The papillary type presents projections into cavities of papillomatous outgrowths from their walls, which are covered by cylindrical epithelium, which latter also lines the cavities. It is most common in the parovarium.
It is rare to find a pure type of either variety; both forms are usually blended. Malignant transformation, of the latter type especially, occurs easily and insidiously, and explains many disappointments in result.
—Adenoma is a tumor whose type is the normal secreting gland, from which it differs in being an abnormal outgrowth or product, but particularly in that it has no power of producing the secretion peculiar to the gland tissue or type from which it grows. The adenomas occur for the most part as circumscribed tumors in the mammæ, parotid, thyroid, liver, and in the mucous membranes of the bowels and the uterus. They may be single or multiple; in the intestine they are usually multiple. In certain locations (e. g., the mammæ) they attain enormous dimensions, and in the ovary tumors of this character may be met with weighing forty or fifty pounds. The true adenoma shows no tendency to infection of neighboring lymphatics, and gives rise to no secondary deposit, and when it causes death it is usually because of size or pressure upon important organs. It displays a marked tendency to cystic alteration, while the relative proportion of epithelium and connective tissue or stroma varies within wide limits. In some cases, in which the former is small in amount, the preponderance of the latter has caused the use of the term adenosarcoma, which is really a misleading name.
The distinction between adenoma and true carcinoma is in some respects but slight, and this fact will account for the conversion which many innocent gland tumors seem to undergo from one into the other. As soon as the epithelial cells lose their regularity of disposition and collect in groups, or make their way outside of the acini into the tissues, then the change from the benign to the malignant tumor has begun, and the entire clinical aspect of the case has altered. This change may be the result of external irritation, of such tissue changes as pregnancy and lactation, or of the undefined changes which advancing years seem to produce. (See Plate XXII, Fig. 2.)
Adenoma occurs in the breast as cystic adenoma or fibro-adenoma. The former often attains large size, is encapsulated, the acini are much dilated, while from the walls of the epithelium-lined cavities frequently project papillomatous processes, forming what are called intracystic growths. Cystic adenomas grow slowly, produce atrophy of mammary tissue by pressure, occur after puberty until the menopause, and rarely give rise to pain until they become large. As they grow they distort the breast until it may become pendulous. When the growth of connective tissue, peculiar to the tumor in that it is rich in nuclei, forms well-marked partitions between alveoli, the growth is called pericanalicular adenofibroma, which may assume a tubular or an acinose type. When the alveoli and ducts are themselves invaded by ingrowth of this tissue, then we have the intracanalicular adenofibroma, which constitutes a growth sometimes bordering on the malignant. When the arrangement of epithelial cells in the acini and ducts becomes irregular and atypical, then malignant transformation has begun.
PLATE XXII
FIG. 1
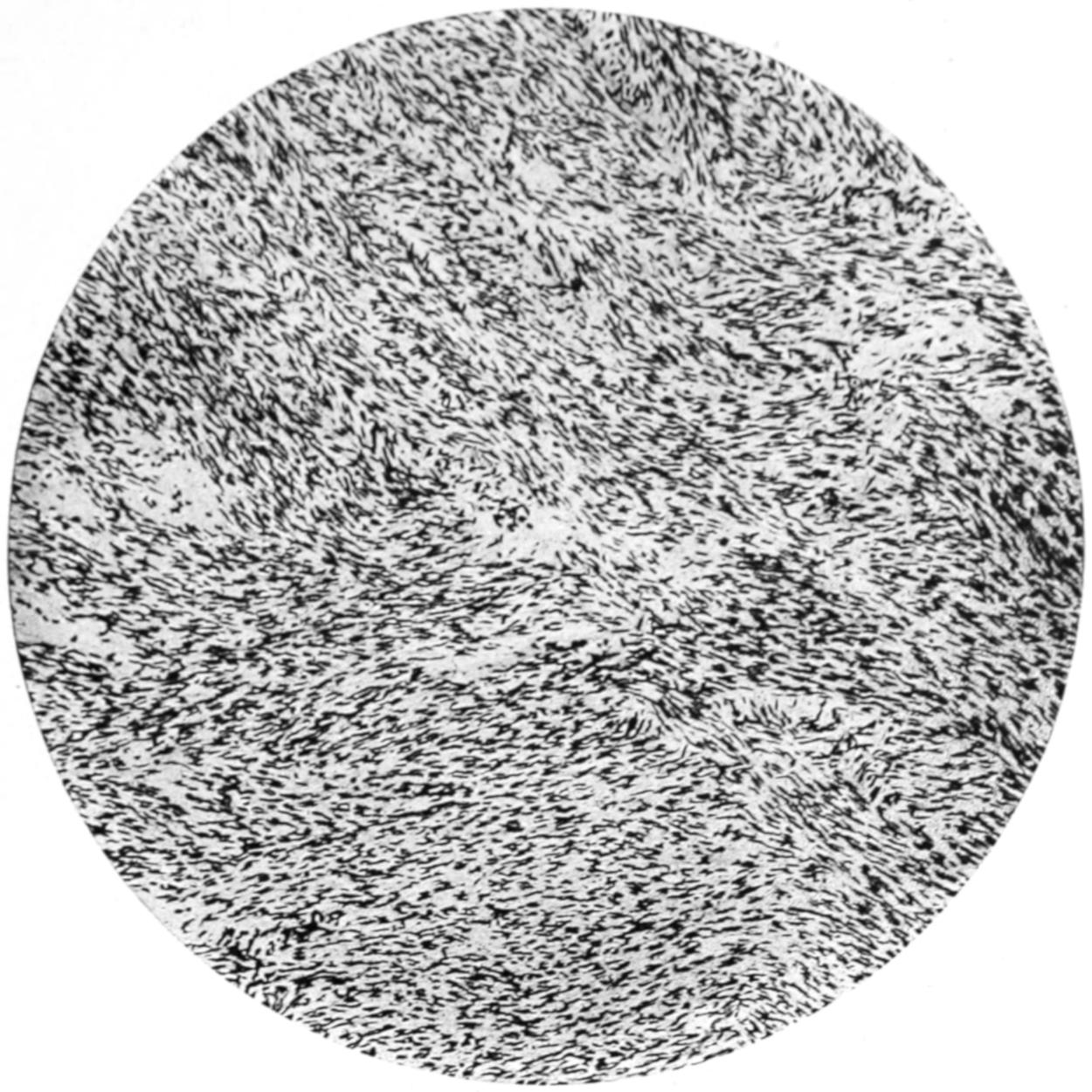
Fibromyoma of Uterus. (Low power.)
FIG. 2
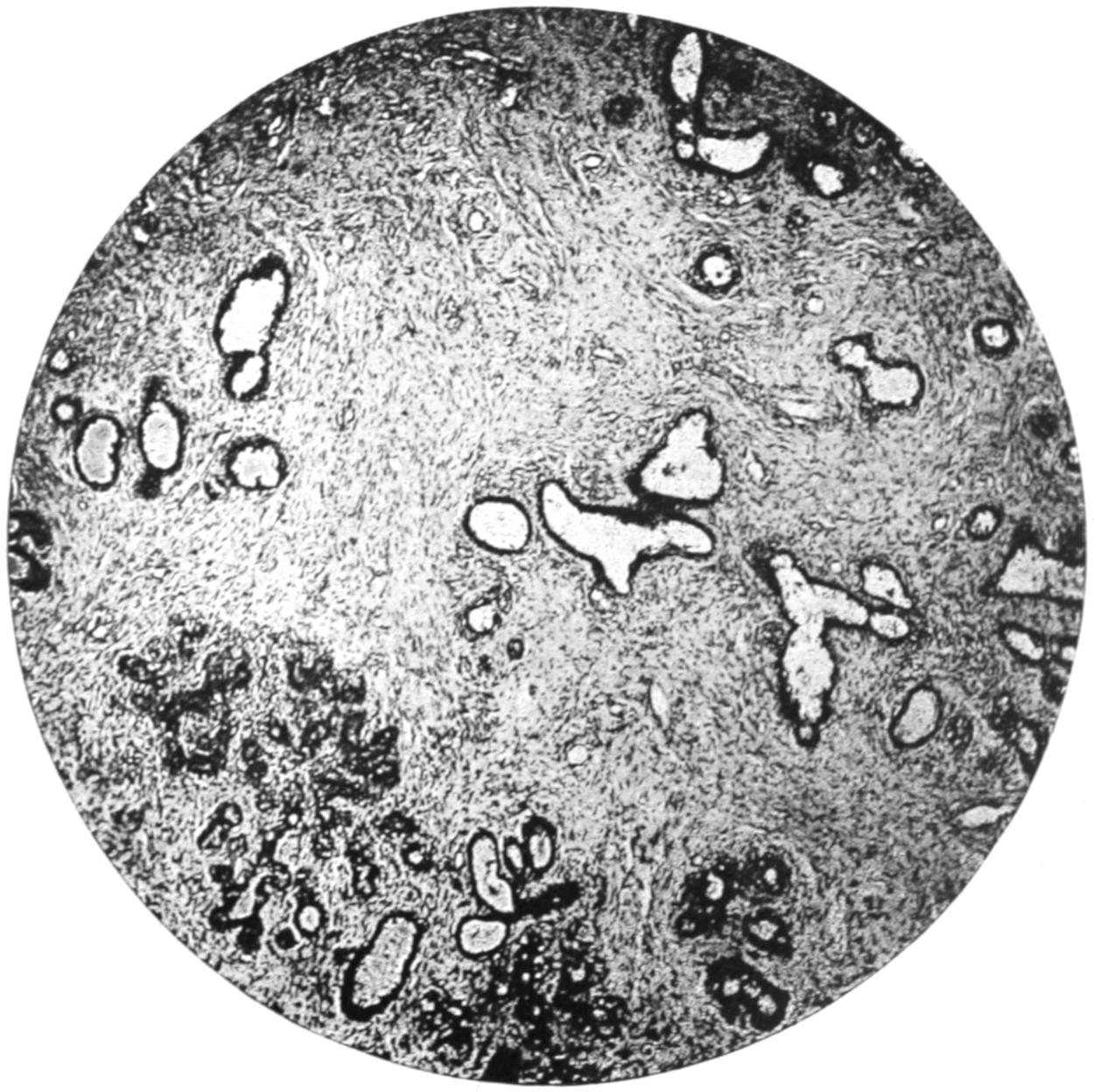
Fibro-adenoma of Breast. (Low power.)
PLATE XXIII
FIG. 1
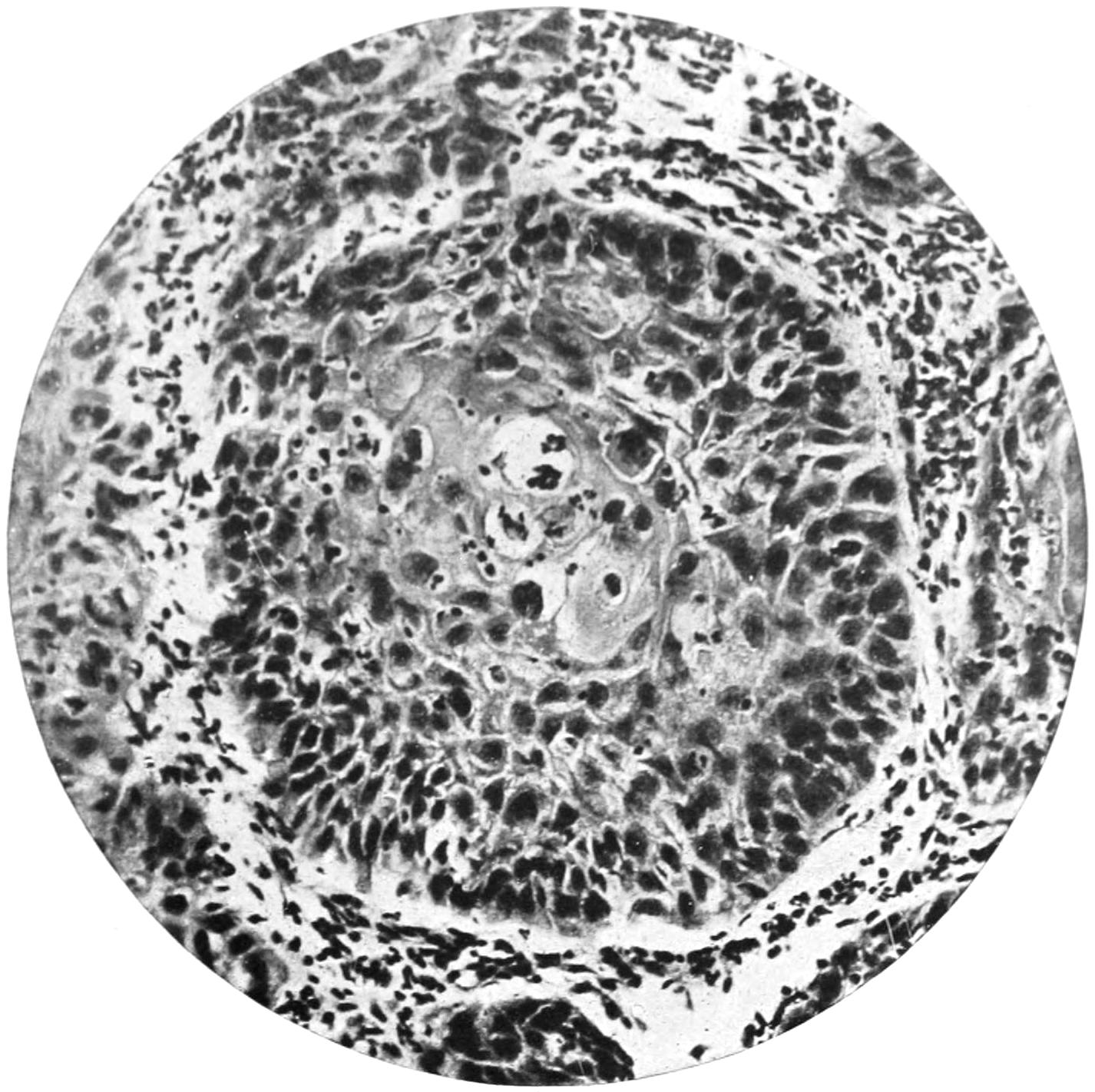
Epithelial Pearl Formation in Squamous Epithelioma. (Middle power.)
FIG. 2
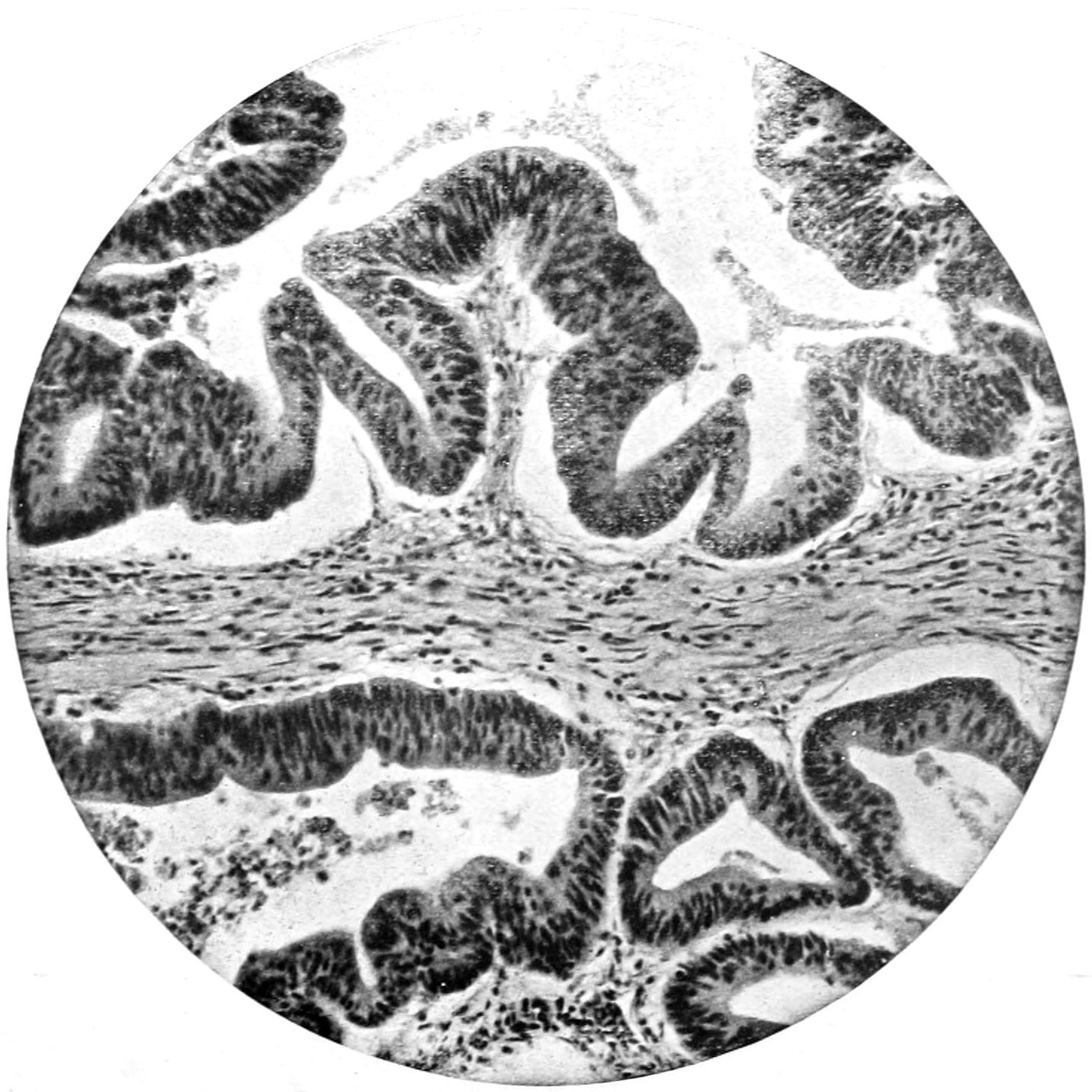
Malignant Adenoma of Rectum. (Middle power.)
[285]
Fibro-adenoma occurs also in the breast as a small tumor, encapsulated, usually superficially placed, movable in its site, often multiple; most common between the twentieth and thirtieth years of life; often painful, especially during menstruation; tender upon pressure. Both forms may occur in young men. A form of fibro-adenoma in which fibrous tissue is greatly in excess, which never attains great size, is common in the breasts of unmarried women. It gives rise to much pain and distress, but is clinically not malignant. (See Plate XXII, Fig. 2.)
Adenoma occurs frequently in sebaceous glands as:
1. Sebaceous Cysts.
—Sebaceous cysts are generally known as wens. These tumors commonly begin as retention cysts, the ducts of the sebaceous glands becoming occluded. But in many cases there is no occlusion of the ducts, and their secretion may be easily expressed. They occur wherever sebaceous glands abound, but especially upon the scalp. They are usually multiple, vary greatly in size, are easily movable over the bone, and are intimately related to the skin, while the duct orifice is frequently recognized by a black spot, after removing which sebum can be expressed. These cyst-adenomas are encapsulated, and can be easily shelled out of their matrices, save when inflamed, in which case they are often astonishingly adherent. Their contents consist of pultaceous debris resembling old epithelial scales, fat, cholesterin, etc. The contents of these cysts are very prone to decompose, and they become as offensive as anything with which the surgeon has to deal. Putrefaction may be independent of inflammation or coincident with it. When irritated these gland cysts become inflamed and may suppurate, suppuration being tantamount to cure by spontaneous processes. They may also ulcerate, without suppurating, and form foul-smelling ulcers, or give rise to cutaneous horns.
Fig. 88
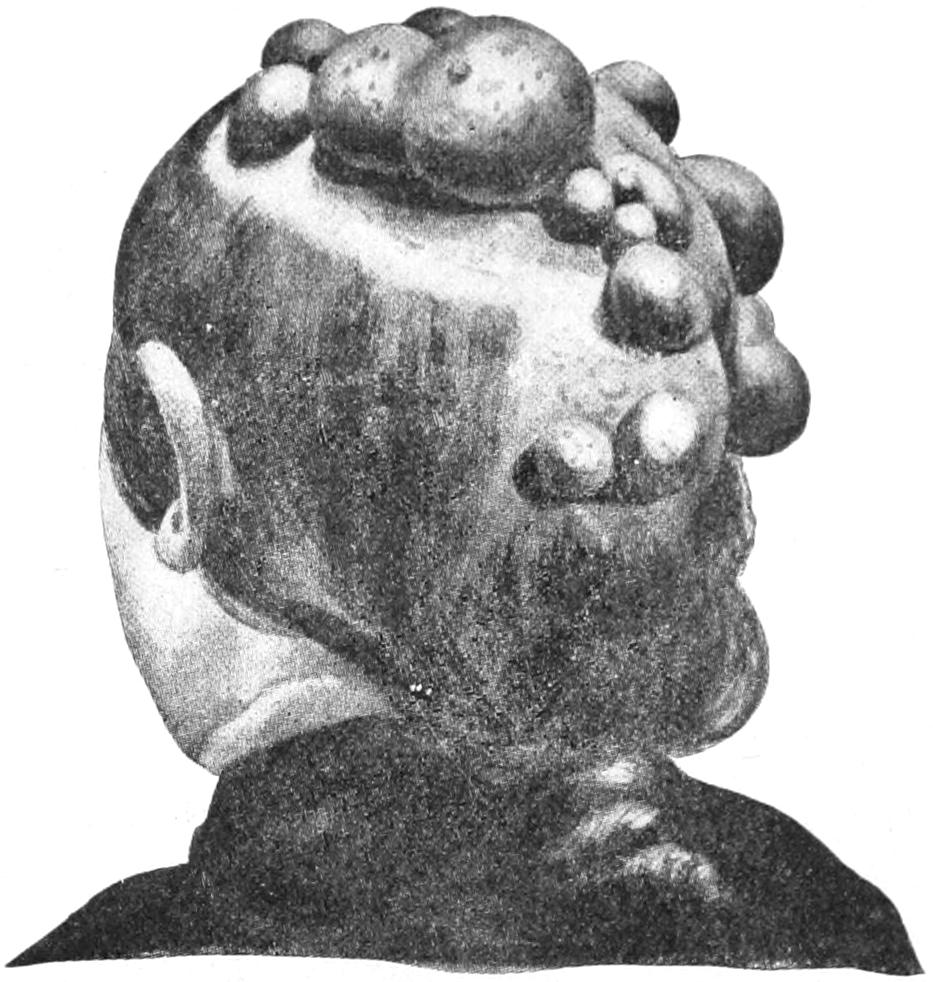
Multiple atheromatous cysts (wens). (Lexer.)
2. Sebaceous Adenomas.
—These arise from the sebaceous glands, which are lobulated, like those about the nose and ear. Adenomas from this source are extremely liable to ulceration, may undergo calcification, and are often mistaken for epithelioma because of the fungous ulcerations to which they give rise.
3. Adenocarcinoma.
—Sutton has also described an adenocarcinoma of the peculiar sebaceous glands named after Tyson. These are found particularly at the base of the prepuce, this form of tumor being rare. Adenomas arising from the mucous glands, which are usually transformed into cysts, are also known, as well as other gland tumors springing from the glands of Bartholin, Cowper, etc. (See Plate XXIII, Fig. 2, and Plate XXIV.)
Pituitary adenomas are either analogous to struma or belong to the mixed tumors of dermoid or teratomatous type.
Prostatic adenoma is in large degree fibromyoma of that body, with more or less hypertrophy of its glandular structures. Minute cystic alterations may occur also, as well as growth resembling intracanalicular fibro-adenoma.
Adenoma is occasionally observed in the salivary glands, where it is usually encapsulated, and may undergo cystic changes. It has been observed in the liver and pancreas. In the former its pseudo-ducts often contain inspissated material of bile-green tint.
[286]
The lesions of the kidney referred to as cystadenoma are now grouped among the teratomas, and are described under that heading. They present interesting examples of mixed tumors.
In the testis, as in the ovary, epithelial tumors frequently present themselves, but they partake less often of the type of pure adenoma, and incline rather to that already described under Ovarian Cystoma. Even in the paradidymis tumors of this same character are found, with cystic or even papillary alterations.
In the mucous membrane of the stomach and bowels adenoma usually presents as an ovoid tumor, attaining such size as to give rise to mechanical obstruction either by pressure or by traction. Adenoma of the pyloric region is a repetition in structure of the pyloric glands. In the rectum it presents usually as a polypoid outgrowth, often seen in young children. Such tumors are generally small, and when solitary they often hang by a distinct stalk.
Similar polypoid tumors present in the cervical canal of the uterus, where are also found sessile and racemose tumors, all of which are structural repetitions of the glands met with in the cervix uteri. Adenoma of the uterine cavity is seldom seen; it is also rare in the Fallopian tube, but occasionally presents as a dendritic outgrowth from the mucous membrane distending the tube.
—Epithelioma is common, especially where there is transition from one kind of epithelium to another, and, of all other localities, particularly where skin and mucous membrane meet—e. g., the lips, the vulva, and the anus. Epithelioma differs from papilloma in that the former is no longer limited by basement membrane, but passes beyond it into the underlying connective tissue and presents down—rather than up—growth. Characteristic of epithelioma are the so-called cell nests or pearly bodies, where there seems to be a tendency to globular arrangement of cells with such condensation or alteration that they lose their ability to take stains, and appear as a more or less lustrous mass, showing off by contrast among the standard surrounding tissue. On this account they are often called pearly bodies. Recognition of these is tantamount to diagnosis of epithelium. (See Plate XXIII.)
This form of neoplasm is essentially the same, no matter what its clinical varieties. These comprise a wart-like growth or nodule, which quickly becomes an ulcer with elevated edges, ulceration being due to necrosis of cells farthest from the periphery; or, again, the disease may start as an ulcerated fissure, ulceration and infiltration keeping pace, in which case there is a sharply defined ulcer with undermined edges. A third variety, often seen upon the lips, comprises a projecting mass, with more or less horny surface. In nearly all of these, however, the characteristic cell nests with their onion-like arrangements of cells will be found.
Epithelioma, especially when exposed to the air or to surface irritation, quickly ulcerates and tends to involve all the surrounding tissues, while occasionally the distinctive cells proliferate so rapidly as to give the ulcer more or less of a bursal or a cauliflower-like arrangement. From such a surface there is a constant discharge of foul-smelling detritus or of sloughs. Even bone cannot resist its progressive invasion and slowly disintegrates before the advancing mass. Cartilage is resistant, and usually preserves its integrity. In other words, the tendency of epithelioma is toward constant encroachment and infiltration, and toward a fatal termination from hemorrhage by ulceration, from septic infection, exhaustion, or other accidents. The wart-like forms run the slowest course of all, but even here the malignant tendency is most evident.
Lymph-node Infection.
—A striking characteristic of epitheliomas is the invasion of the adjoining lymph nodes, which attain a size disproportionate and bearing no necessary relation to that of the primary growth. This constitutes one of the most serious complications of the condition. This lymphatic invasion partakes of the malignant character of the disease, and from every focus of this character infiltration and destruction proceed. Infected nodes also show an early tendency to central degeneration and to spurious cyst formation. When the overlying skin becomes involved we have extensive sloughing and the conversion into large malignant ulcers. Dissemination to a distance (i. e., metastasis) is rare in epithelioma—much more so than in carcinoma. (See Plate XXV, Fig. 2.)
About the mouth epithelioma is not common before the thirty-fifth year, though I have seen it on the lip of a twenty-year-old woman. It is vastly more common in men than in women, and more frequent on the lower than the upper lip. In the tongue it seldom occurs before the fortieth year. It seems to be more common both on the lip and tongue in men with bad teeth and in confirmed smokers, thus giving rise to the view often held that it is purely a matter of irritation. It may, however, be due to contact infection should it be regarded as of parasitic origin. In one-fifth of the cases of epithelioma of the tongue there are preceding lesions, usually described as leukoplakia or ichthyosis of the tongue—conditions characterized by epithelial reduplication and the formation of dense plaques or scales. These lesions are usually regarded as precancerous conditions. (See Plate XXVI.)
PLATE XXIV
FIG. 1
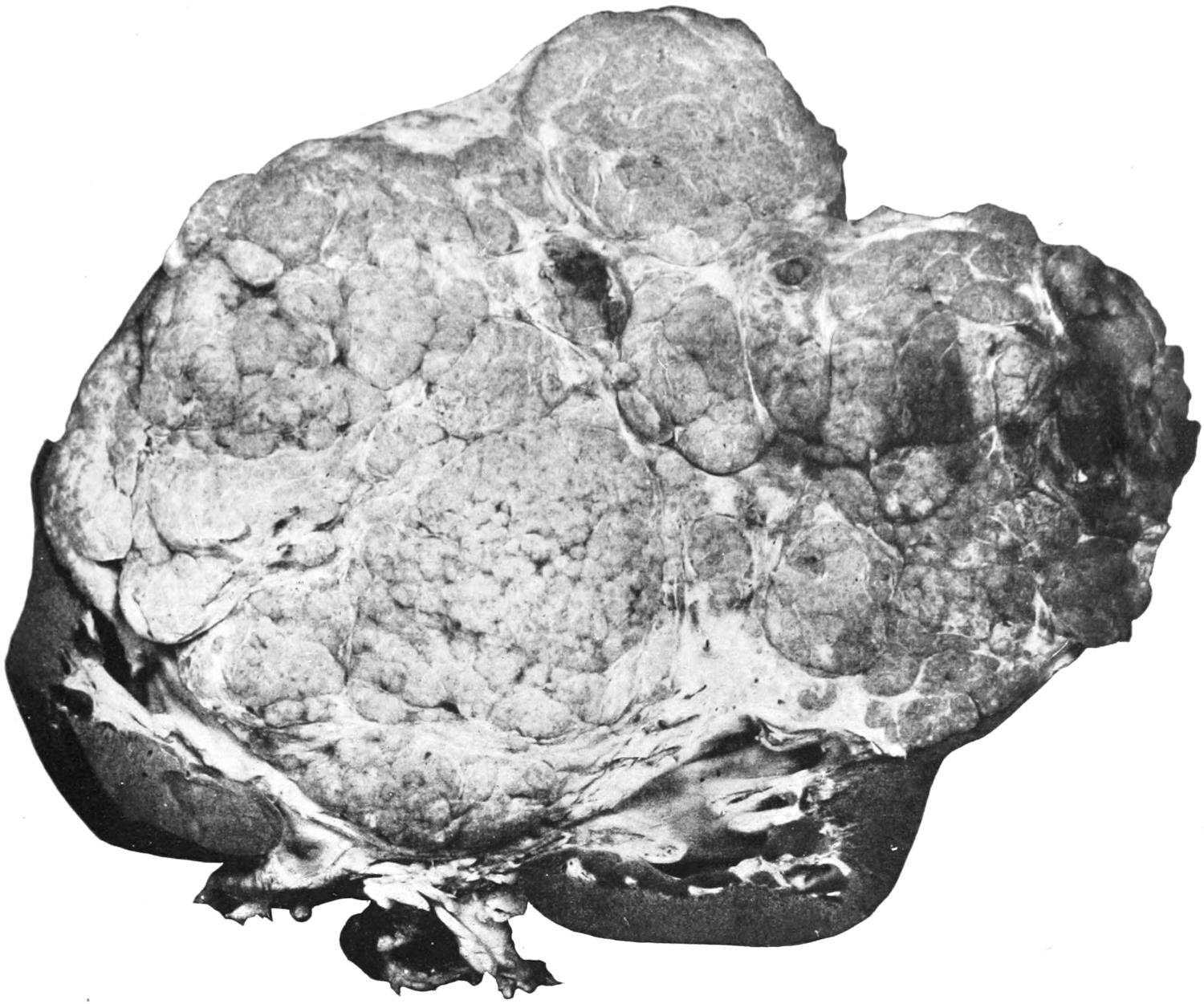
Primary Papillary Adenocarcinoma of the Kidney. (One-half original size.) (Gaylord.)
FIG. 2
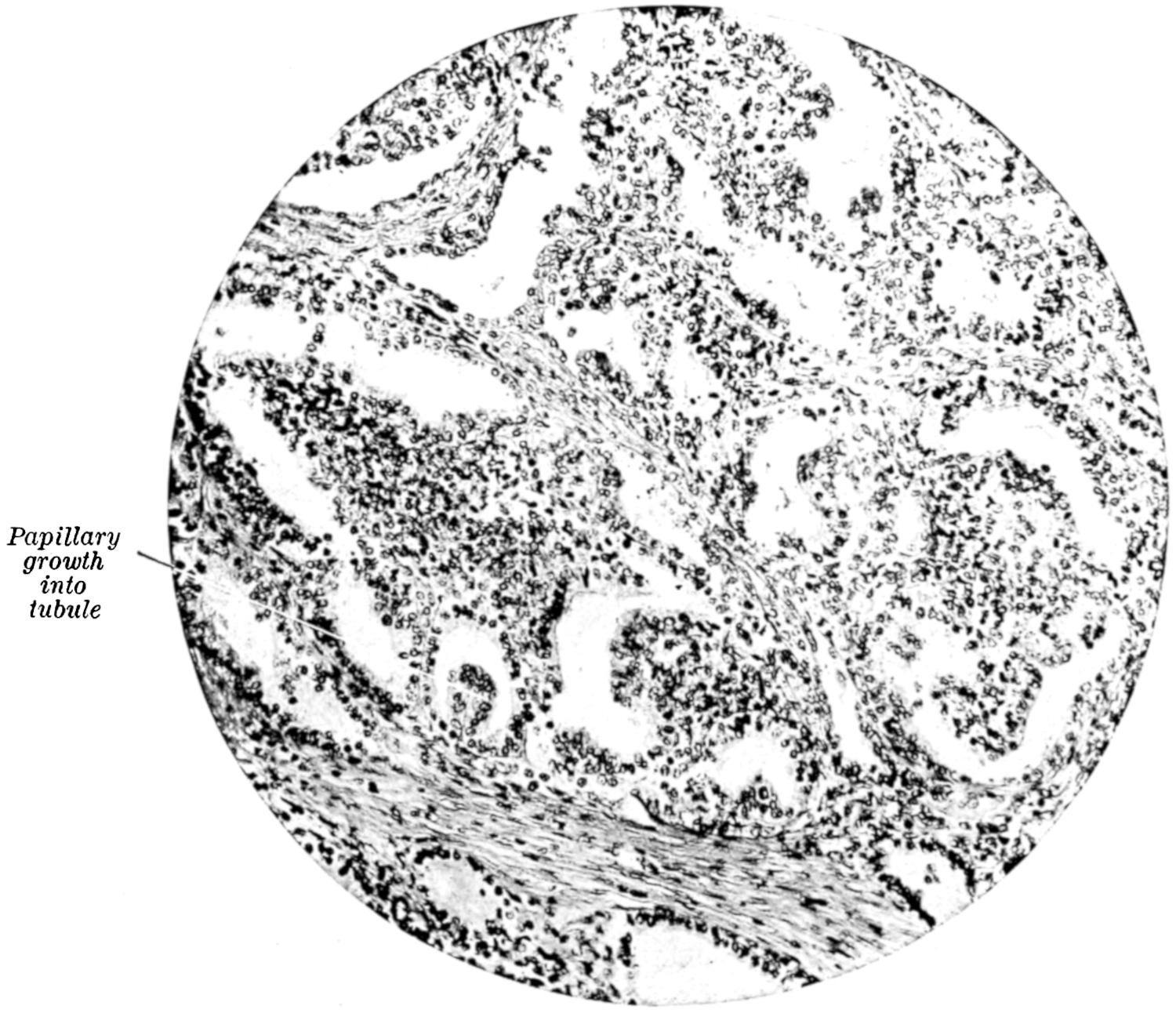
Section of the Primary Growth. (Gaylord.)
PLATE XXV
FIG. 1
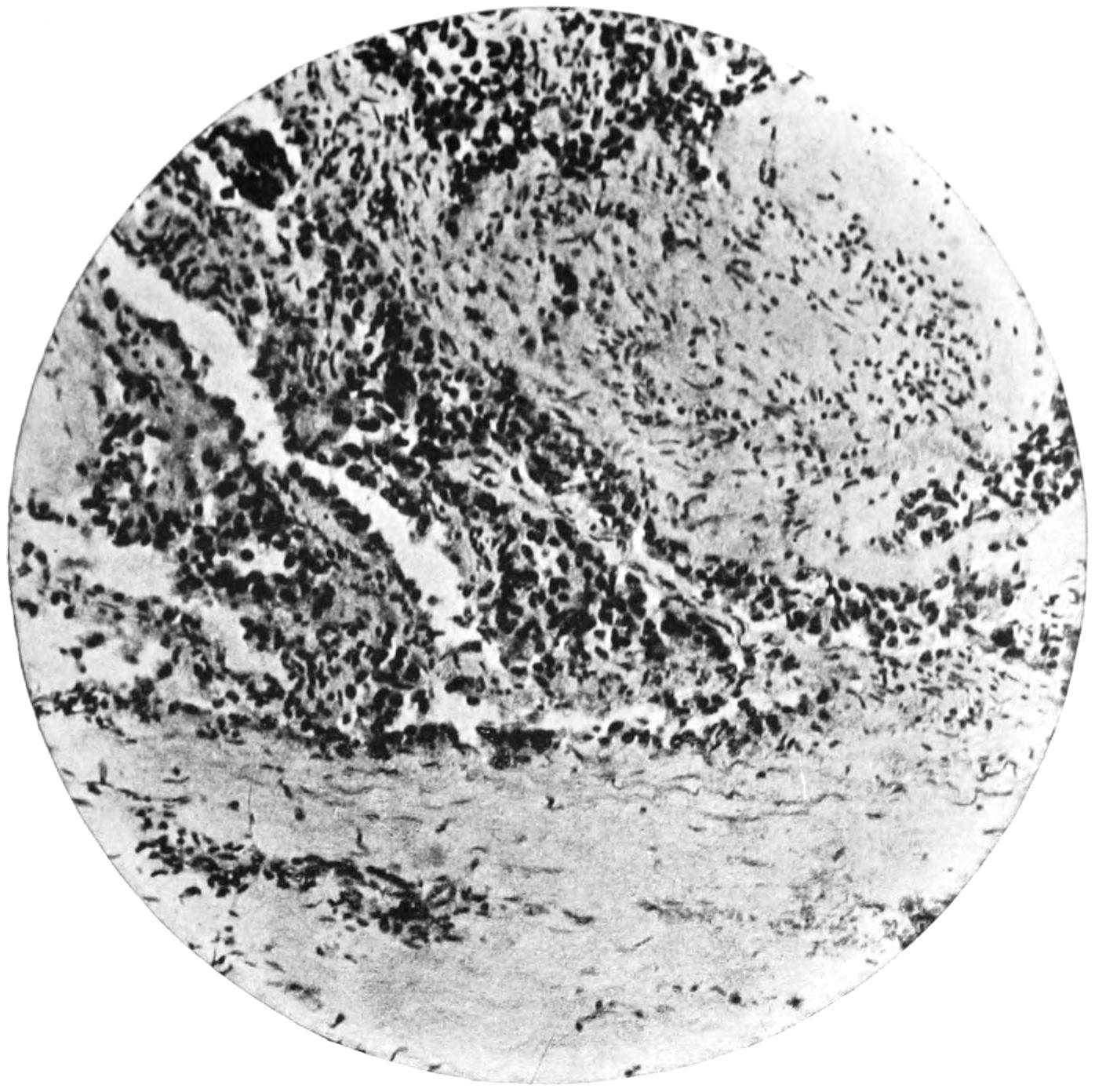
Carcinoma developing in a Thrombus in the Portal Vein. (Middle power.) (Gaylord.)
FIG. 2
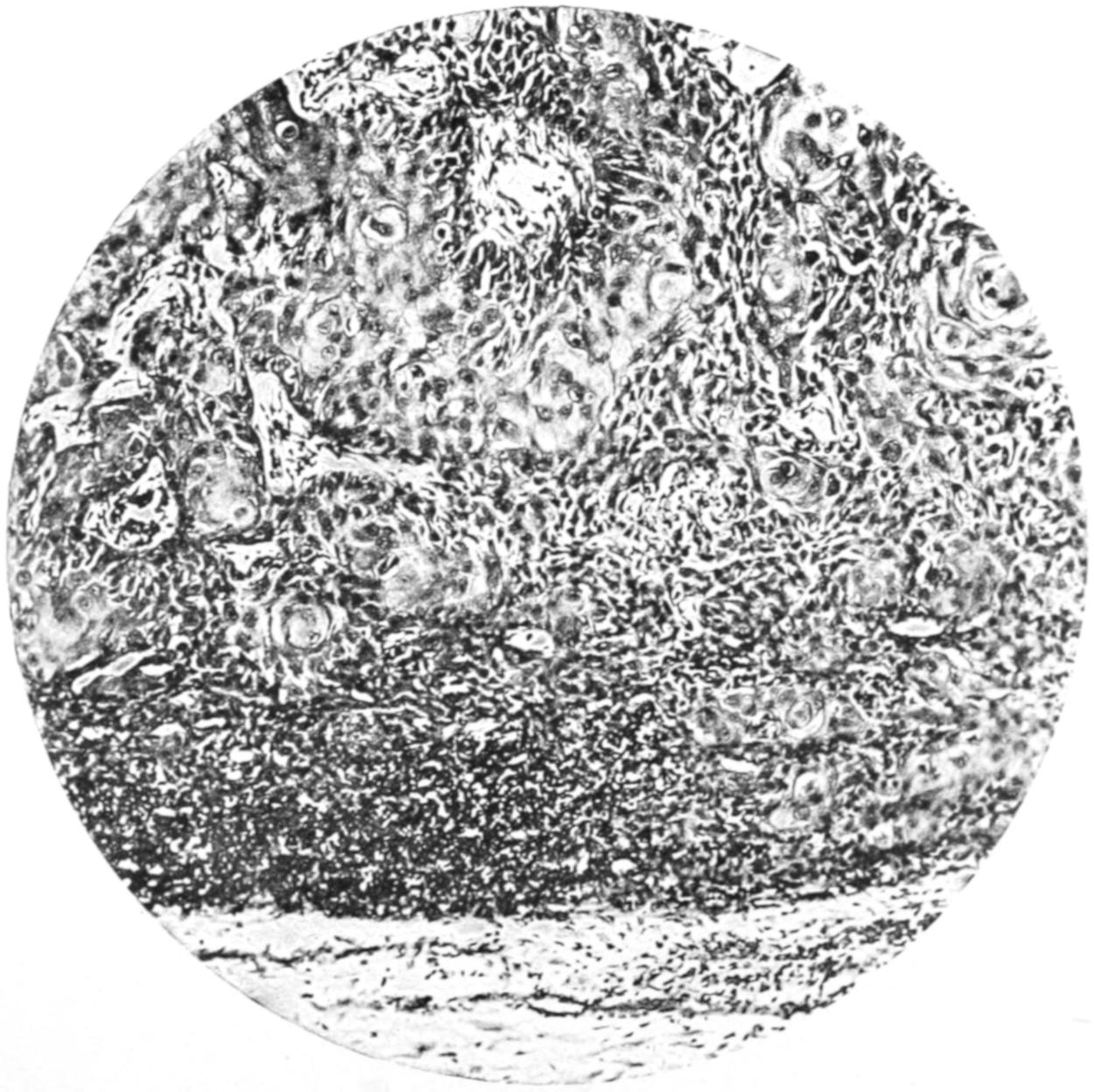
Metastasis of Squamous Epithelioma in a Lymph Node. Pearl Formation. (Middle Power.)
PLATE XXVI
FIG. 1
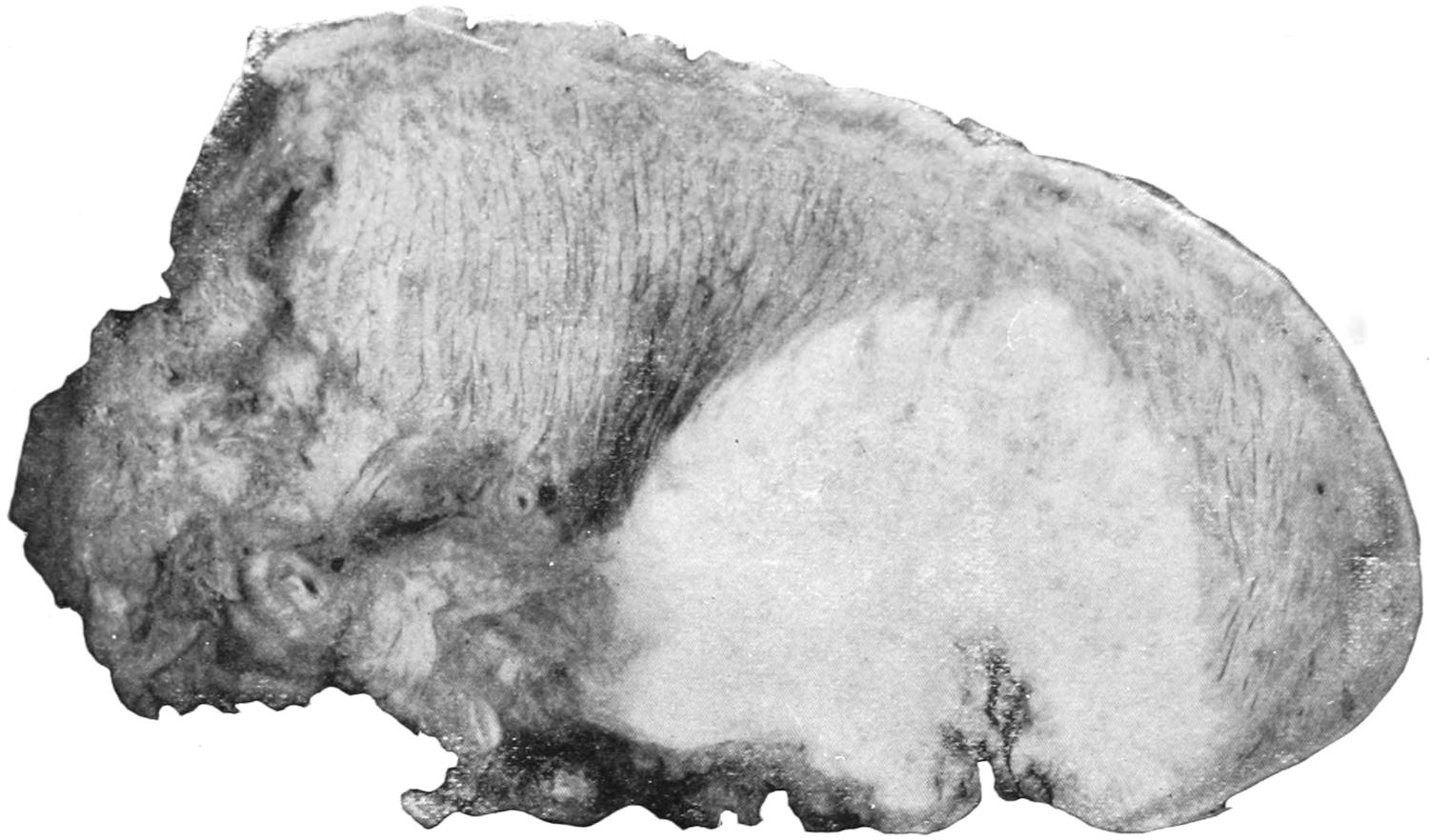
Epithelioma of Tongue. Enlarged three diameters.
FIG. 2
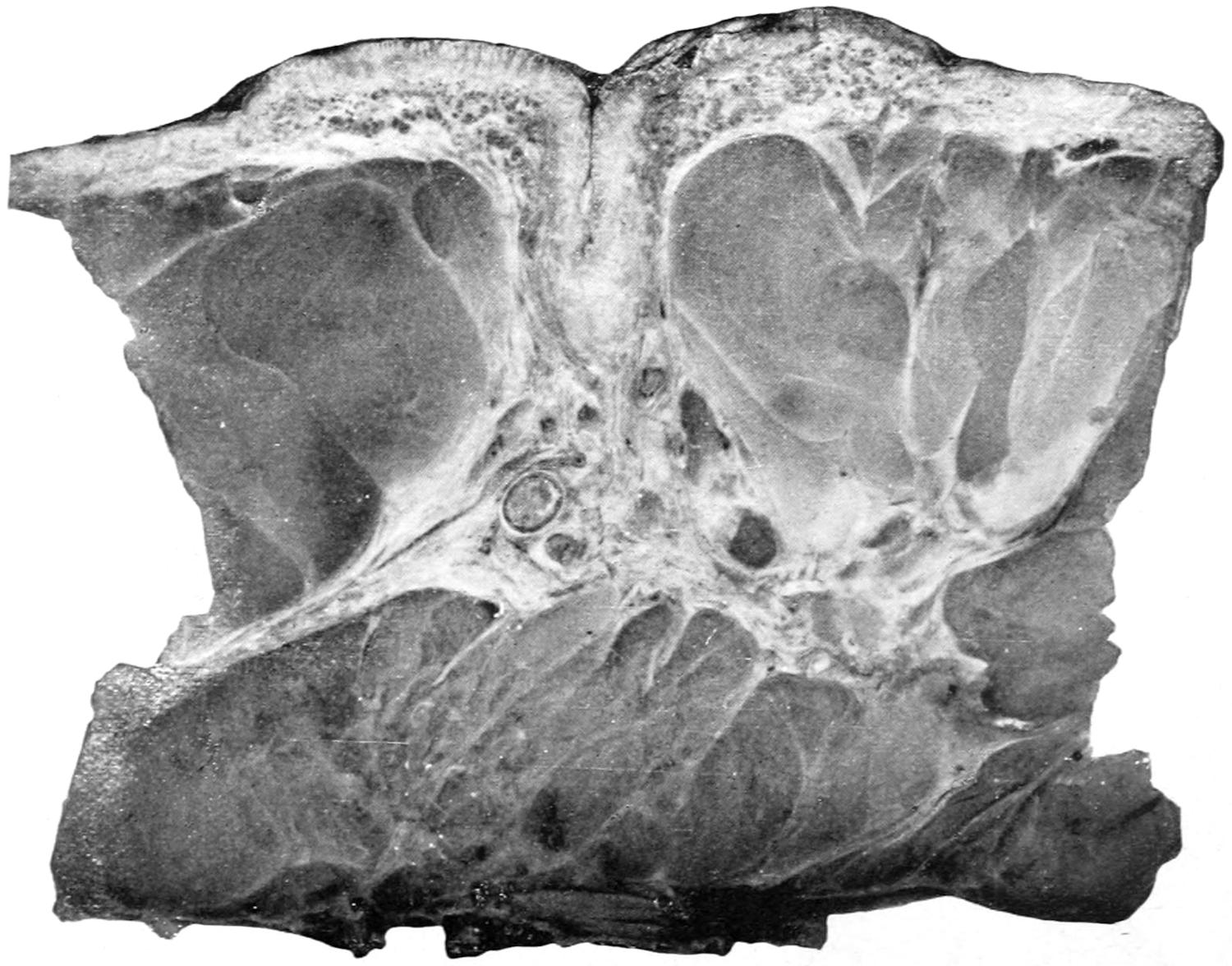
Paget’s Disease of the Nipple. Enlarged two diameters.
Photographs from hardened unstained specimens.
[287]
The disease often starts near the stump of a carious tooth, in which case infiltration and erosion begin promptly and progress rapidly. Epithelioma of the tongue has been known to follow along the obliterated track of the thyrolingual duct, and in this way to bring about a perforating ulcer.
Epithelioma of the esophagus is a common cause of stricture of this passage-way. It leads to ulceration, and usually to perforation into the trachea or some other cavity or passage (i. e., a bloodvessel). In the larynx the disease is well known, and gives rise to intense and finally fatal symptoms, but has been dealt with successfully by radical operations for extirpation of the entire organ. (See Chapter XLI.)
Fig. 89
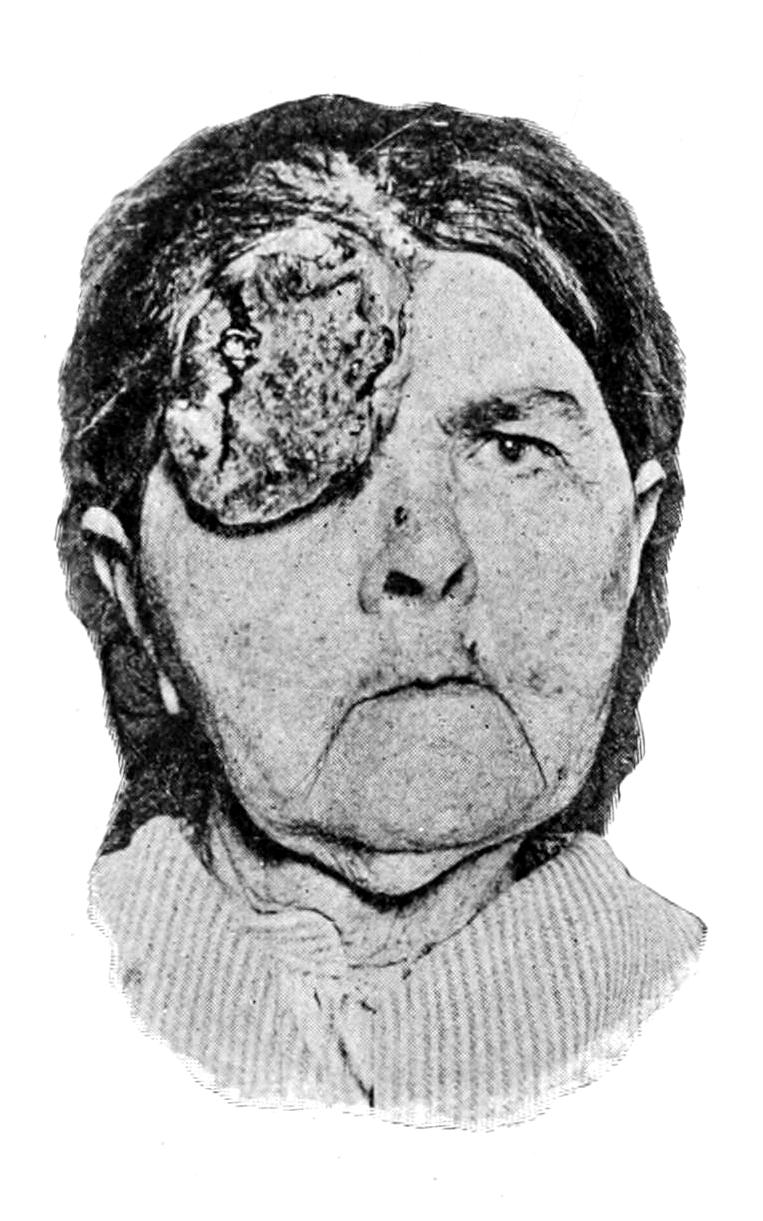
Epithelioma of forehead and eyelid. (Neisser.)
Fig. 90
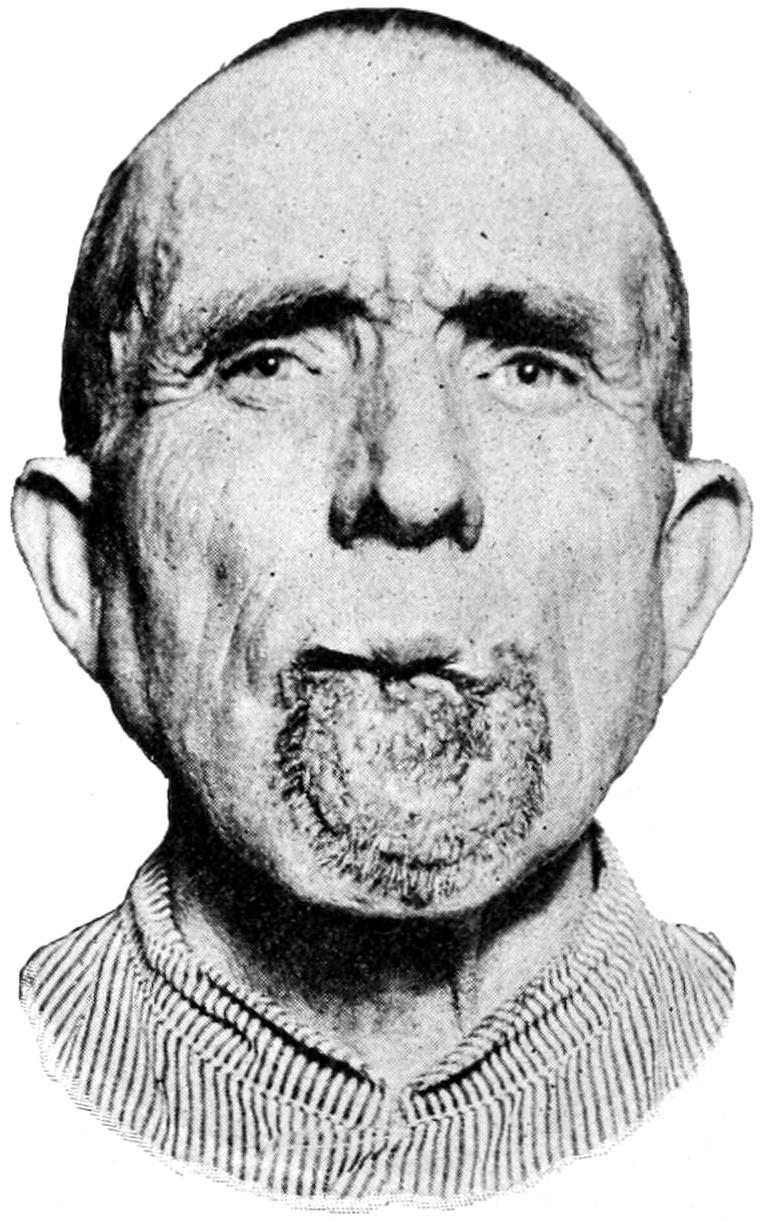
Epithelioma of lip. (Neisser.)
Occurring upon the scrotum, epithelioma has been called chimney-sweeper’s cancer, or soot-warts, and has been ascribed to the irritation of foreign material. Ulceration and infection of the inguinal nodes usually proceed rapidly and disastrously. It is believed also that tar and paraffin may produce similar irritation, and paraffin cancer has been described by various writers. It usually occurs upon the scrotum.
The skin lesions which precede the formation of paraffin cancer resemble those seen in chimney-sweeper’s cancer. The skin becomes dry, thickened, parchment-like, while the openings of the sebaceous glands become obstructed by the tar or other material, producing acne-like lesions. Warty outgrowths then occur, and these become the seat of malignant ulceration. In chimney-sweeper’s cancer the scrotum is usually first affected in a chronic dermatitis, to which warty outgrowths succeed, these enlarging and growing downward as ulceration takes place.
About the external genitalia epithelioma is not uncommon, particularly in and about the prepuce. Such a degree of phimosis as leads to retention of smegma is certainly a predisposing cause, not only in man but in the lower animals. Epithelioma of the vulva has been described under the name esthiomène, and requires to be recognized and dealt with promptly if the surgeon should attempt a radical cure. In the vagina and[288] about the cervix uteri it is common, a large proportion of cases of cancer of the uterus being essentially epitheliomas of the cervix.
In and about scars and upon granulating ulcers epithelioma is quite common. One danger to which a chronic ulcer is always exposed is that of epitheliomatous transformation. These growths also attack lupus scars, or even any tissues actively involved in the lupoid process. This is particularly true between the fortieth and sixtieth years of life.
Among the viscera the gall-bladder is probably more often involved in distinct epitheliomatous changes than any other. It presents as a uniform thickening, and causes augmentation in size, so that a distinct tumor projects from beneath the liver. In this location dessemination is rare.
Epithelioma is to be regarded as having an essential malignant tendency. Its treatment demands early removal of diseased parts and complete extirpation of involved lymph nodes. It is only the small and incipient growths which should be attacked by such destructive agencies as cancer pastes or the electrolytic current.
Rodent Ulcers.
—Under the name of rodent ulcers, lupus exedens, noli-me-tangere, etc., writers, mostly English, have described a variety of epithelioma, met especially upon the face, to which a separate classification has usually been assigned. Until recently it has been generally regarded as a local ulceration, distinct from cancer. In some text-books it is described as lupus exedens. It is preceded usually by a nodular condition of the skin, vascular, breaking down into a regular ulceration, but little elevated, the base of the ulcer deeply excavated, with a striking disproportion between ulceration and new-growth. In this particular variety infiltration seems to be continuously in advance of the rodent process, the former being excessive, the latter but slight. This variety of epithelioma rarely produces lymphatic involvement; the discharge is slight, the pain complained of inconsiderable. Occasionally it entirely alters its aspect, and may present features of the conventional epitheliomatous type.
Fig. 91

Fig. 92

Rodent ulcer. (Original.)
The development of cancer in lupus areas is now of sufficiently frequent occurrence to demand attention. Whether the epithelium which gives rise to it is to be accounted for by Cohnheim’s hypothesis, as having been cut off in the course of healing and become a cell rest to subsequently undergo malignant degeneration, is not yet settled. It has been suggested that curettage might cause fragments of epidermis to be loosened and then entangled in the cicatrix, and thus be responsible for subsequent malignant changes. When lupus thus degenerates it assumes usually the papillomatous form, which rarely involves lymph nodes, while the change which follows x-ray treatment often succeeds a hyperkeratosis and rapidly involves gland structure.
Rodent ulcer allies itself with the type of tubular epithelioma springing from the outer sheath of the hair follicle, sending out cylindrical processes which freely blend with one another. It is to be regarded as an equally malignant type of ulceration with other cancerous ulcers, and demands the same thorough and radical measures for its relief as do other forms of epithelioma. It is perhaps the most favorable one with[289] which to deal, because of the usual freedom from involvement of deep lymphatics. No distinctive measures are necessary for its relief—only those which are thorough.
—Carcinoma is a tumor springing from preëxisting gland tissue, which it more or less closely resembles in type, save that the structural similarity is incomplete, the epithelial cells now collecting in irregular clusters, or filling the acini and obstructing the ducts, or bursting beyond the basement membrane and invading the surrounding tissues. They frequently so fill the ducts as to appear in columnar arrangement when seen under the microscope, and this has given rise to the use of a term so vague as to have no place in pathology—i. e., cylindroma. Carcinomas may arise from any of the secreting glands, but more commonly from some than from others. They have no capsules. They infiltrate the surrounding tissues, usually involve the lymphatics early, are liable to spread to the superficial tissues and to ulcerate, and to undergo various degenerative changes. Nearly all cancerous tumors abound in lymphatics, which will explain the rapidity with which the lymph nodes become infected, as well as the tendency to dissemination, which is characteristic of these growths. Dissemination leads to so-called secondary or metastatic growths, which may make their appearance in any organ or tissue, even in the bones, where they give rise to changes of texture that make spontaneous fracture easy. It is characteristic of carcinoma that the metastatic tumors which it may produce will reproduce almost perfectly the type of the primary tumor whence the embolic fragments which have produced them spring. The amount of dissemination varies exceedingly: it may even become so marked and widespread as to produce a condition analogous to that met with in miliary tuberculosis—miliary carcinosis. A similar condition, much more rare, is seen in dissemination of sarcoma, and is known as miliary sarcomatosis. A constantly spreading cancerous infiltration of the superficial tissues, which is noted most often after mammary cancer, is described under the form of cancer en cuirasse, or jacket or corset cancer. Instances will be seen in which this infiltration of the surrounding structures has extended nearly or even completely around the thorax. It gives rise to a brawny induration which is unyielding, and is studded here and there by nodules that tend to ulcerate, to fungate, and to bleed easily. It is perhaps the most hopeless form of cancerous disease.
The older writers have constituted two or three clinically distinct forms of carcinoma, based mainly upon the relative hardness or softness of the tumor and the invaded tissues. The term scirrhus is thus applied to a tumor in which connective tissue preponderates and epithelial cells are relatively deficient. On the other hand, the term encephaloid has been applied to a tumor in which the connective tissue seems barely sufficient to hold the mass together, while the epithelial cells are in vast preponderance. These are all tumors of the round epithelial-cell type, and these distinctions are of clinical interest, yet have no great pathological import, save that in a general way the greater the proportion of epithelial elements the sooner will life be terminated by destructive processes. In other words, the more the tumor may partake of the encephaloid type the worse the prognosis or the shorter the probable duration of life. Again, these tumors pursue a varying clinical course. In those tumors, particularly of the scirrhus type, where the connective tissue largely preponderates, there is often an eventual reduction in the size of the part involved, and such reduction of vascularity and of nutritive activity that the rate of growth is thereby perceptibly checked. The so-called atrophying cancers of the breast are the best examples of this type of cancerous disease. Here the volume of the gland is diminished rather than augmented, and the disease may last for a number of years. It is questionable whether it is well to operate.
The so-called colloid forms of cancer are simply the expression of pathological changes occurring in growths of more distinct type. Thus colloid softening may occur in any tumor in which cancer cells predominate, and the so-called colloid cancers of the peritoneum, the ovary, etc., are either examples of such alterations or are possibly endotheliomas arising in these locations. The term villous cancer, with other terms like it, should be expunged from all scientific literature, unless these terms are used in purely adjective and clinical sense, for they imply nothing accurate as to histological structure, and are often misleading and inaccurate.
Carcinoma is most common in the following regions:
In the breast it appears particularly in two forms:
[290]
1. Acinous Carcinoma.
—Acinous carcinoma is usually of the scirrhus type. It may arise at any portion of the breast, and if anywhere near the nipple it will cause retraction of that prominence, which is always pathognomonic; elsewhere it leads to puckering and adhesion of the overlying skin. These tumors infiltrate widely, especially along the connective-tissue stroma and the fibrous tissue which intersperses the fat of the breast. They are usually firm and sometimes exceedingly dense. A form of scirrhus known as atrophying scirrhus consists largely of strands of fibrous tissue, injected here and there with epithelial cells. It is the slowest in growing of all the forms of cancer, and by its contraction tends to reduce rather than augment the size of the mamma.
Acinous cancer is rare before the age of thirty, most common between forty and fifty. It occurs in women in all conditions of life, married and single, but is rarely noted in the male breast. The most dangerous form is that which appears during lactation. Ordinarily its progress is slow. As it augments in volume it infiltrates the surrounding tissues, becomes adherent to the pectoral fascia, infiltrates the muscle fibers, and finally attaches itself to the periosteum of the ribs. The infiltrated tissues tend to shrink rather than to increase in volume. Lymphatic injection occurs early in this form, and is a pathognomonic sign. It occurs mostly in the axillary lymphatic nodes, but may often be detected in the neck above the clavicle. When the skin is involved there is a tendency toward ulceration and fungoid condition. This is preceded by the purplish appearance of the tense skin. (See Plate XXVII.)
Fig. 93
“Pig-skin” appearance of cancerous breast.
Pain is an uncertain and variable feature. It is important to emphasize this fact, as many of these conditions have been lightly regarded because of freedom from pain. Pain is not a constant phenomenon in cancer. On the other hand, it is sometimes intense, either localized or radiating and referred to distant points. Pain is particularly noticed in cases which assume the form of cancer en cuirasse. Secondary deposits in viscera frequently occur, particularly in the abdominal organs and the lungs; but any organ may be the seat of secondary infection, and this is found occasionally in the bone-marrow, not alone of the sternum or ribs, but of distant bones, and is called marrow injection. As the result of cancerous affection of serous membranes effusions of fluid frequently take place, as in the pleura, peritoneum, and pericardium, and this fluid is often blood-stained.
In consequence of pressure upon the venous trunks in the axilla there is often a swelling of the arm upon the affected side, dropsical in character, known as lymphatic edema. The arm grows heavy, the patient loses control of it, and the skin may become so distended by effusion as to cause the limb to resemble a cast. This is due not alone to pressure upon the veins but to involvement of the lymphatics, and upon careful examination positive dilatation of the lymphatic vessels may be noted. Pain is a usual accompaniment of this form of edema.
2. Duct Carcinoma.
—This appears especially about the time of the menopause, when glandular structure has disappeared and only ducts remain. It is common, without reference to cancer in these instances, to find cystic dilatation of numerous ducts, which vary in size from a mustard seed to that of a cherry. These are referred to by Sutton and others as involution cysts. They are filled with mucoid material and have a bluish tint. They occur usually upon the under surface of the gland. Such cystic breasts are common, and when appearing in diffused form may be easily mistaken for cancer. Pain is not frequent. This condition is certainly a precancerous stage, since the dilated ducts are often the starting points of cancer, and occasionally of papillomatous or villous outgrowths from their walls.
Duct cancer implies the form which arises in these dilated ducts, most commonly in the terminal branches, appearing ordinarily as a single tumor, but sometimes as a mass of separate nodules. Intracystic and intracanalicular growths of this character are often found. When assuming the truly cancerous phases they may be spoken of as duct cancers, otherwise as duct papillomas. They have generally been referred to as intracanalicular fibromas. Duct cancers are less tense than the preceding variety, and when situated near the surface often discolor the skin. It is from these cases that there is seen a more or less abundant discharge of fluid resembling bloody milk. These tumors grow slowly, lymphatic involvement is late, and in general they present the least malignant forms of breast cancer.
PLATE XXVII
FIG. 1
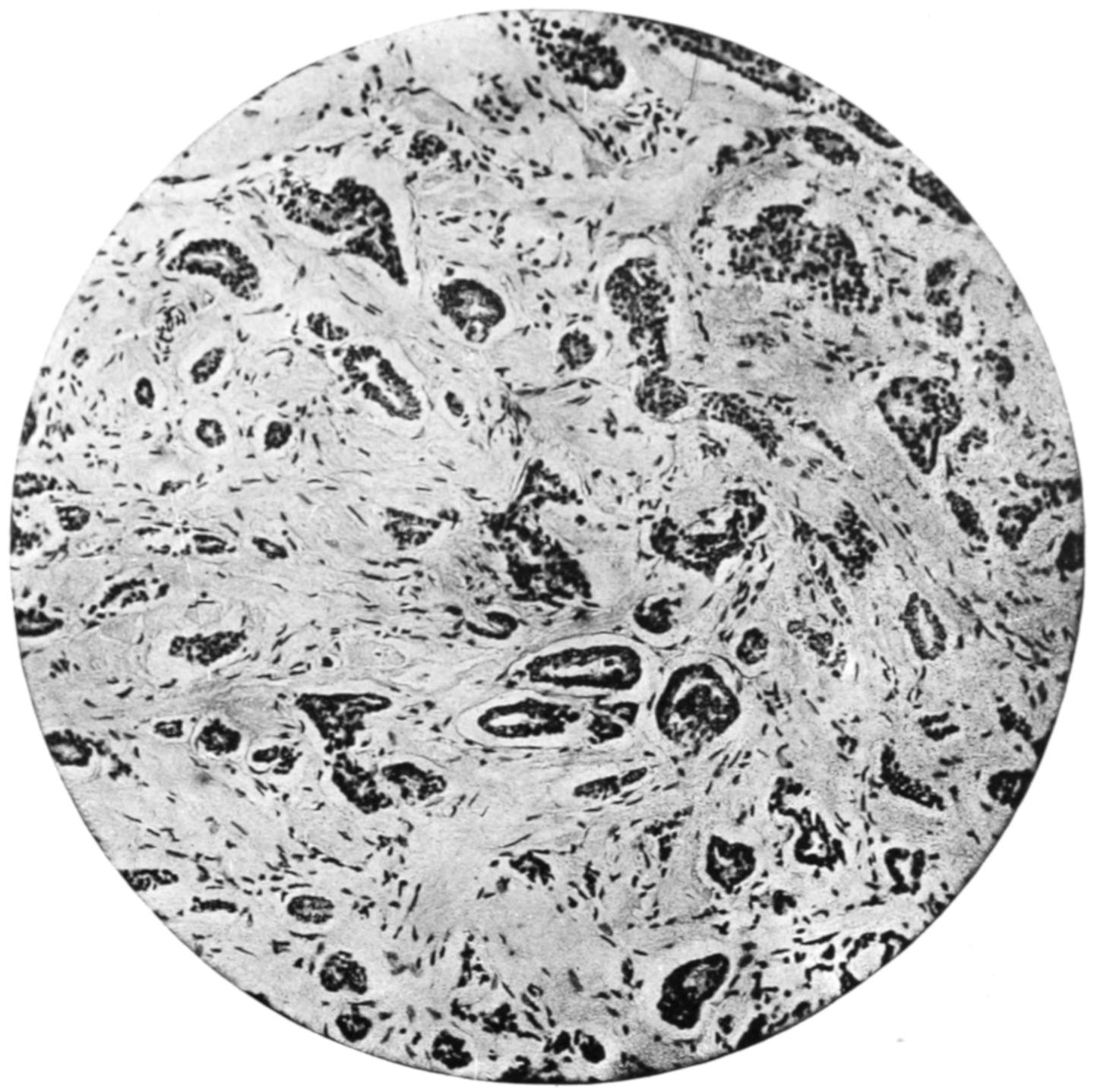
Scirrhus Carcinoma of Breast. (Middle power.)
FIG. 2

Soft Infiltration Carcinoma of Breast, showing Stroma. (Mallory’s connective-tissue stain.)
[291]
Carcinoma of sebaceous glands is by all means most common in those specialized glands named after Tyson, occurring about the prepuce. They give rise to the usual forms of cancer in this locality.
Carcinoma in the prostate is not common, and is usually confined to old men. Infiltration proceeds around the base of the bladder at the same time and binds the pelvic viscera together. The pelvic lymphatics become early infected and dissemination is frequent. (See Prostatic Hypertrophy.)
Fig. 94

Recurring carcinoma of male breast. (Original.)
Carcinoma in the salivary glands is not common; it is more frequent in the parotid region, occurring at middle life, growing rapidly, infiltrating surrounding parts, and tending to ulceration.
Carcinoma of the liver varies in its arrangement and appearance. Sometimes it appears in the form of nodules; at other times, as a more diffuse malignant infiltration by cells relatively abundant in number, so that the clinical aspects of the case conform rather to the encephaloid or medullary type.
Carcinoma of the kidney was formerly described as encephaloid, meaning thereby simply a malignant tumor of soft structure. It is probable that a large proportion of these tumors were sarcomas. Nevertheless, true carcinoma of the kidney is possible.
Carcinoma of the ovary may originate as such, or be the result of a transformation from an ovarian cystoma (see above). No better illustration can be offered of the infectivity of cancer cells (be the secret of this infectivity what it may) than the rapid dissemination of cancer throughout the peritoneal cavity, which sometimes follows the removal of an apparently non-malignant tumor which is undergoing this change.
On the other hand, in the testicle such tumors are common—more so than sarcomas. It is likely that many of them arise from the paradidymis.
Carcinoma of the stomach is a frequent disease. It involves the tubular glands, especially in the pyloric region, and conforms to them in type. After involving the mucosa it spreads to the entire coats of the stomach and infiltrates adjacent structures, while the mesenteric lymphatics are usually early and notably involved. Were it possible to recognize this involvement early in the course of the disease diagnosis of pyloric cancer and operative interference would be much more common and hopeful. Secondary involvement is generally in the adjoining viscera, but may be seen at a distance. Miliary carcinosis has been noted after pyloric cancer. This form usually occurs between the fortieth and sixtieth years of life, the duration of the disease not being long.
In the intestine, and particularly in the rectum, carcinoma proceeds also from the mucous glands, and tends constantly to extend at its periphery and involve the entire lumen of the bowel. It seems to be inseparable from a tendency to contraction of the gut and consequent annular stricture. Ulceration, favored by surface irritation and infection, occurs almost always early. Above the rectum it usually occurs in the neighborhood of the sigmoid flexure. Cripps has observed that when cancer of the rectum spreads downward and involves the anus, it loses its typical glandular character[292] and assumes the type of epithelioma, or squamous-cell cancer. In these cases the pelvic and mesenteric lymphatics are infiltrated and metastatic affections are common.
Carcinoma may appear in any portion of the uterus, but is more common in the lower than in the upper half. It assumes the type of the cervical glands, spreads rapidly, infiltrates widely, ulcerates early, and disseminates frequently. By extension of ulceration the formation of urinary and of fecal fistulæ is common. Pyosalpinx and hydrosalpinx are also favored, while the spread of the disease is, in fact, more common when it involves the cervix than when it involves the uterine fundus.
—This has also been called deciduoma malignum, a malignant growth of chorionic epithelium. Inasmuch as this tumor also includes a syncytial layer it has been known as syncytioma. Such tumors usually contain elements derived from both layers of the chorion. They follow pregnancy, generally within a few months, and are often preceded or accompanied by a hydatidiform mole. This growth constitutes a malignant neoplasm. It pertains to ulcerating uterine growths characterized by early extensive metastasis, which prove fatal. It has been shown that similar growths occur not only in the uterus but also in the testicle, and thus the scope of the term has been much enlarged. In its biology it resembles the sarcoma; in its histology, the carcinoma. It is more malignant than any other known growth. (See Plate XXVIII.)
Occurring within the uterus its most important clinical feature is a tendency to frequent and alarming hemorrhage. When occurring about the testicle this trouble rapidly becomes fungoid, bleeding easily and excessively, the lungs being among the first organs to show metastasis, which takes place through the blood as well as the lymphatic vessels, for the cells of these growths seem to penetrate the capillaries. By the time a diagnosis is made a case is likely to be too far advanced to admit of radical treatment. If scrapings could be examined early, shreds of syncytioma would be found, and it might be possible that a complete hysterectomy would be of use.
Metastatic nodules consist mostly of round, dark masses presenting a more or less pronounced fibrous structure. These are generally found in the lungs and cerebrum, where the vessels are large and the tissues soft. There is usually a sharp contrast between such a tumor and the surrounding tissues. The time which elapses between delivery and the appearance of the growth is from three to ten weeks. The tumor rapidly spreads to the upper portion of the vagina. The trouble probably begins some time before delivery.
The latest tendency among pathologists is to refer a growth of this kind to the teratomas. In women this tumor is particularly a teratoid growth, some cells of the fecundated ovum giving rise to neoplasms, while the ovum itself thus derived may misdevelop into a hydatidiform mole. The tumor may be properly regarded as consisting in effect of fetal cells; it is built up of these cells, without bloodvessels and connective tissue, and so belongs to a class by itself. Occurring in women it is almost always a consequence of pregnancy; occurring in the testicle or in the ovary it should be regarded as proceeding from ectodermal cells. For their treatment the earliest and most radical measures only will suffice.
—Grawitz has distinctly established the right of these tumors to separate consideration, for he first determined their origin and identity. Hypernephroma is a tumor, found mainly in the kidney, composed of adrenal rests, or bits of accessory suprarenal tissue imprisoned within the renal capsule. Their minute structure is often that of the adrenals, with a tendency toward the type of perithelioma. They have hitherto been considered examples of sarcoma of the kidney, but are to be abruptly distinguished from it in most instances. Tumors of this character have also been found within the capsule of the liver and along the spermatic artery. In the kidney the tumor portion is usually distinct from the renal tissue; it is often enclosed within a sort of capsule, and rarely connects with the pelvis. Hence, though exceedingly liable to hemorrhages, blood rarely escapes by the ureter. Hypernephroma is delicate in structure, and its vessels give way readily. After this has happened a true hematoma may result. (See Plate XXVIII.)
Similar neoplasms form in the adrenals themselves. These tumors vary in degree of malignancy, some of them scarcely deserving the designation malignant. They may be met at any age, but are more common in adult life. Before removal they are not to be differentiated from other tumors of the kidney. Their cells manifest this peculiarity in that they contain a notable percentage of glycogen. It should also be added that even in true sarcoma of the kidney proliferating adrenal elements may be found.
PLATE XXVIII
FIG. 1
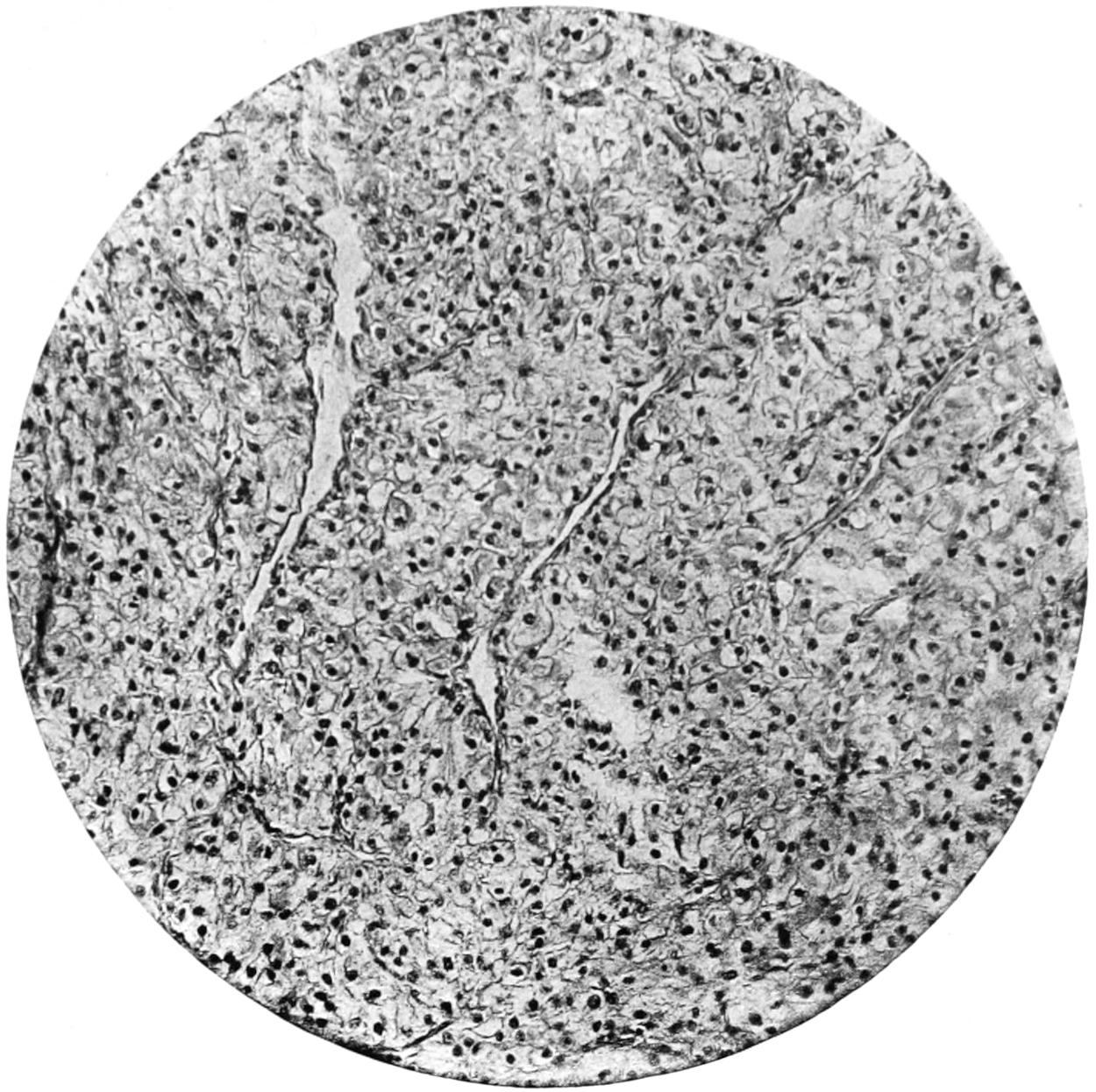
Hypernephroma Renalis. (Medium magnification.)
FIG. 2
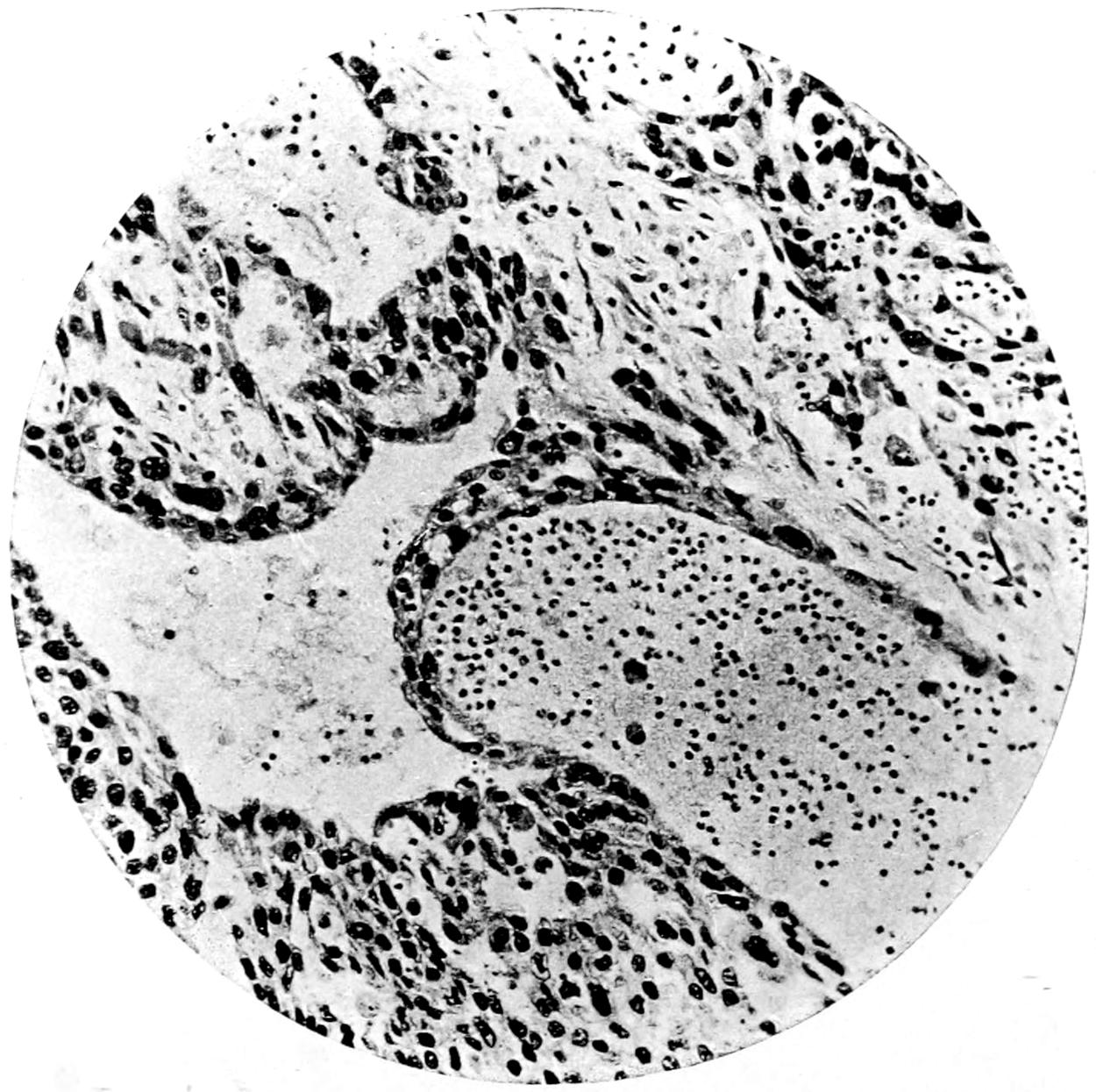
Chorion Epithelioma.
[293]
The following tables are here inserted, trusting that they may aid the young practitioner in distinguishing in a general way between benign and malignant tumors, and even in making a diagnosis between sarcoma and carcinoma. I have also inserted a table differentiating the clinical appearances of epithelioma and of lupus. In these tables comprehensiveness has not been aimed at, rather simplicity, while it is not denied that cases are met with in which diagnosis may be exceedingly difficult, and in which the common signs herein mentioned may be found either absent or misleading:
Table I.—Differentiation between Benign and Malignant Growths.
| Benign Growths. | Malignant Growths. |
|---|---|
| Common at all ages. | Rare in early life. |
| Usually slow in growth. | Usually rapid in growth. |
| No evidences of infiltration or dissemination. | Infiltration in all cases, dissemination in many. |
| Are often encapsulated, nearly always circumscribed. | Never encapsulated, seldom circumscribed. |
| Rarely adherent unless inflamed. | Always adherent. |
| Rarely ulcerate. | Often ulcerate—nearly always when surface is involved. |
| Overlying tissue not retracted. | Overlying tissue nearly always retracted. |
| No lymphatic involvement when not inflamed. | Lymphatic involvement an almost constant feature. |
| No leukocytosis. | Leukocytosis often marked. |
| Elimination of urea unaffected. | Deficient elimination of urea (?). |
Table II.—Diagnosis between Sarcoma and Carcinoma.
| Sarcoma. | Carcinoma. |
|---|---|
| Occurs at any age. | Rare before thirtieth year of life. |
| Disseminates by the bloodvessels (veins). | Disseminations by the lymphatics. |
| Arises from mesoblastic structures. | Arises from glandular (epithelial) tissues. |
| Distant metastases are more common. | Less so. |
| Contains blood channels rather than complete bloodvessels. | Contains vessels of normal type. |
| Less prone to ulceration. | More so. |
| Involvement of adjacent lymphatics not common. | Almost invariably adjacent lymphatics are involved. |
| Secondary changes and degenerations are more common. | Degenerations not common; other secondary changes rare. |
| (Sugar present in the blood?) | (Peptone present in the blood?) |
Differential diagnosis between epithelioma and ulcerating gumma will be found in Chapter X.
Table III.—Diagnosis between Epithelioma and Tuberculosis (Lupus).
| Epithelioma. | Tuberculosis (Lupus). |
|---|---|
| Preceded usually by continued irritation or warty growths. | Irritation plays no figure. Preceded usually by nodules. |
| Diathesis plays no known part. | Diathesis evident. Coincident evidences of tuberculous disease elsewhere. |
| Rarely multiple. | Often multiple. |
| Area of thickening ahead of ulceration. | Extension of ulceration not preceded by thickening. |
| Ulceration advancing from a central focus. | Various foci, which may coalesce. |
| Border usually raised and everted, regular in outline. | Border abrupt, eaten, irregular, thickened, firm, often inverted, irregular in outline. |
| Often assumes fungoid type. | Never fungoid. |
| Base may be deeply excavated. | Base nearly level with surface. |
| Usually painful. | Seldom painful. |
| Bleeds easily. | Seldom bleeds. |
| Never tends to cicatrize. | As marginal ulceration proceeds there is often cicatrization at centre. |
| Most rare in the young. | Common in the young. |
| Discharge is very offensive. | Discharge rarely offensive. |
| Lymphatic involvement nearly always. | Rarely. |
[294]
Cancer is one of the most fatal of diseases, yet has no symptomatology of its own. It produces no symptoms which may not be produced by other affections, and this lack of pathognomonic features constitutes one of the great difficulties in diagnosis. It may disturb every function of the part involved. Experimenters have sought in vain for a distinctive feature by which the disease can be recognized; neither in the blood nor in the various organic tissues have such changes been found that can be explained only on the hypothesis of cancer. The pain which it is supposed to cause is often lacking, and is extremely variable and uncertain. The cachexia of its terminal stages is not characteristic, no matter how pronounced, and may be explained by a variety of conditions, all of which may accompany the disease. The search for the suspected parasites cannot be made with such certainty as to lead to any definite conclusions. It is known by a complex of clinical conditions or by microscopic sections of tissues already removed.
When the disease is superficial it is easily recognized, but when deep-seated, recognition comes later.[15]
[15] Since the discovery of Spirochæta pallida in syphilis, Mulzer and Loewenthal have found spiral organisms on the surface of ulcerating tumors. Borrel also found spirochætæ in conjunction with helminthia in two enclosed mouse tumors, and also in a large tumor sent from Ehrlich’s laboratory. None of these authors attributed any significance to the presence of these organisms, but recently, through the publication of Gaylord, in the Journal of Infectious Diseases, who has found a characteristic small spiral organism in nine out of ten primary mouse tumors, and in all of the transplanted mouse tumors of three distinct strains in the New York State Cancer Laboratory, the subject has attracted new interest.
Fig. 95
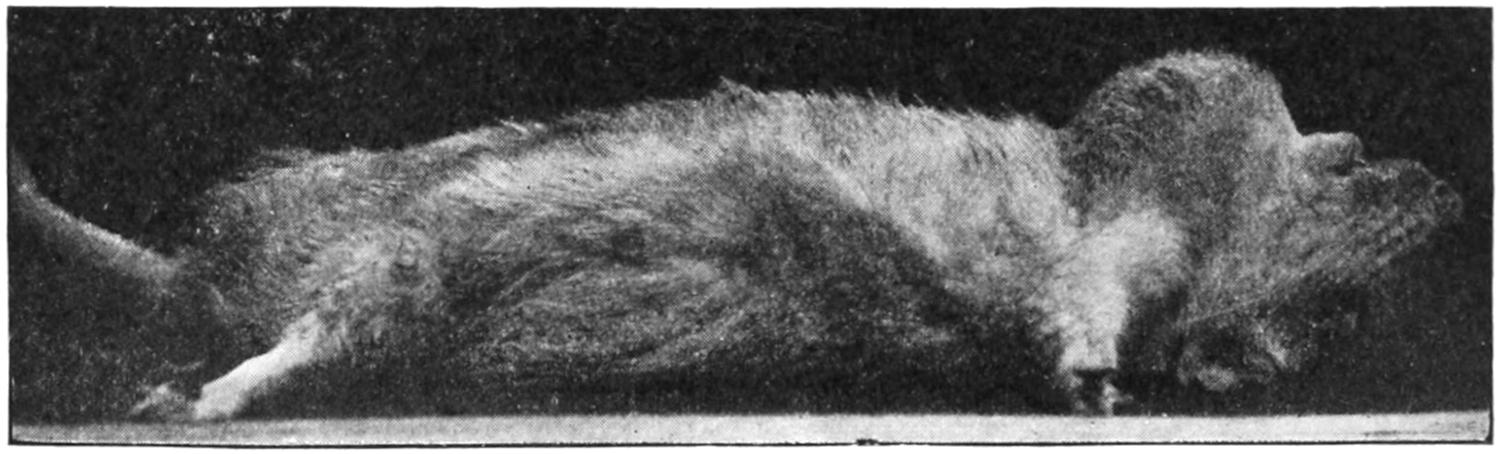
Rat with primary cystosarcoma of thyroid; cage infection in previously healthy animal kept in cage formerly occupied by rat with same condition. (Gaylord and Clowes, Jour. Amer. Med. Assoc., January 5, 1907.)
Fig. 96
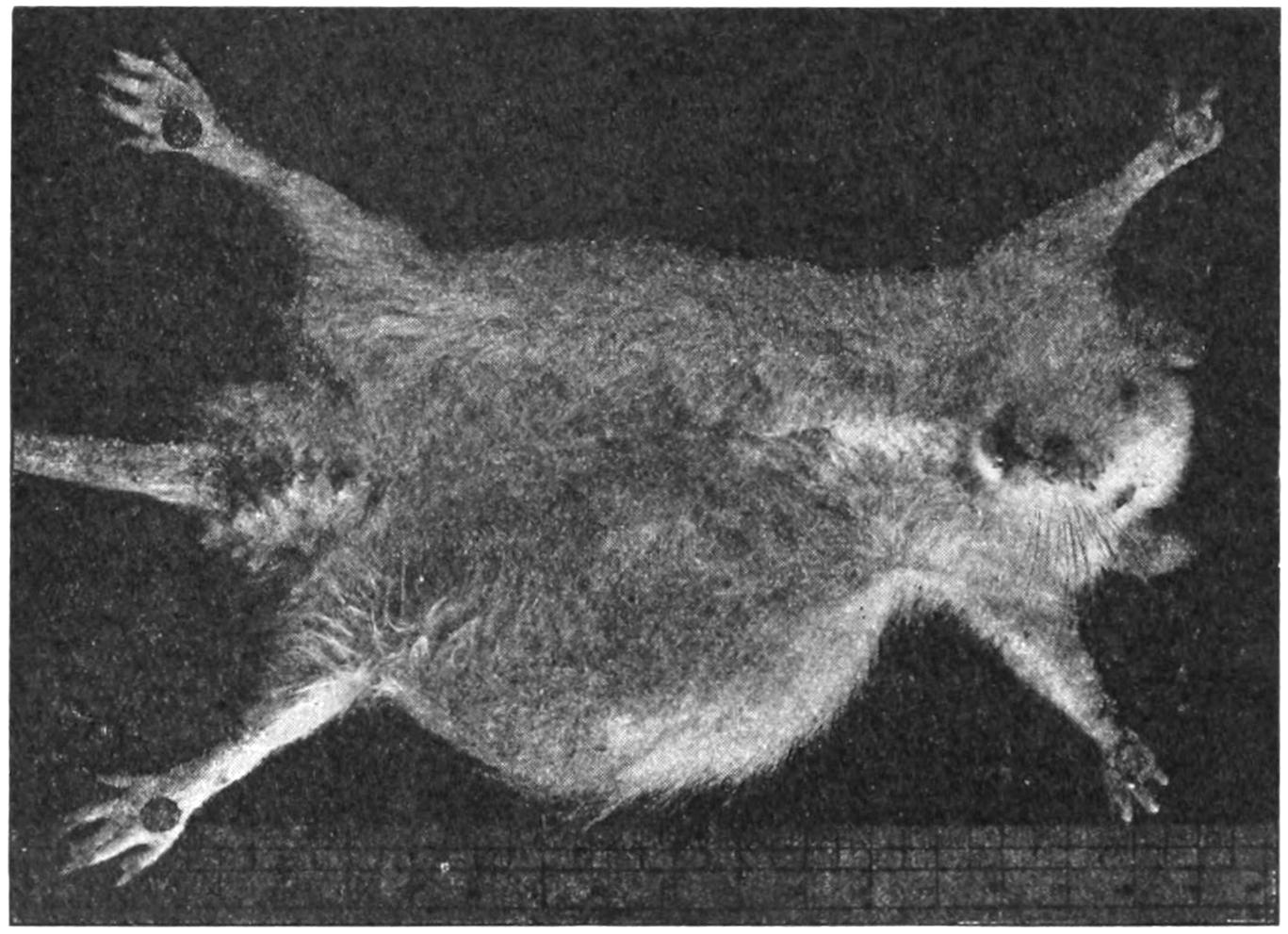
Rat with tumor produced by transplantation from that represented in Fig. 95. (Gaylord and Clowes, loc. cit.)
Gaylord’s organism is best demonstrated by the Levaditi silver method, but can be seen by experienced observers in the living fresh state. It measures from 2.5 to 7.8 microns in length, and the individuals have from four to thirteen closely packed abrupt turns. The organism measures 0.6 micron in diameter. Thus far it has been impossible to stain it with any of the aniline stains, which characteristic appears to distinguish it from the organism described by Borrel and Loewenthal. Calkins has also found this organism in a spontaneous mouse tumor in New York. The distribution of the organism in the growing periphery of the tumors, when considered in the light of Fischer’s work with Scarlet-R, would make it appear not impossible that the organism bears an etiological relation to the tumors in which it occurs.
In the light of the well-authenticated cases of cage infection and the evidence of immunity now definitely determined, the way should be prepared for the discovery of the organism or organisms of cancer. At present this organism would appear strongly in evidence as its cause.
[295]
The microscopic picture may explain considerable in regard to the future as well as the past. For instance, in a case of sarcoma the presence of small, round cells, and especially of pigment, bespeaks a degree of malignancy which probably nothing yet known can baffle. A chemical examination of the tumor after removal may make the surgeon alert regarding the future of the case, according to the amount of glycogen contained within the mass, since the glycogen content is in direct proportion to its malignancy. For a while some reliance was placed upon the percentage of urea elimination, but this is influenced by so many factors as to have proved unreliable.
The relations which cancer bears to other diseases are of considerable interest. Those between cancer and trauma have been discussed; tuberculosis perhaps is the condition which, next to pure local irritation, predisposes to cancerous invasion. The transformation of tuberculous into cancerous lesions can be best appreciated where it can be most readily inspected, i. e., on the skin, and it is well known that lupus lesions frequently undergo this change. This is also true of large ulcers, which may undergo a direct transformation into epithelioma, or pass through the intermediate stage of tuberculous infection. Cancer in tuberculous lymph nodes is also a matter of interest. Again, cancers and tuberculous lesions may exist side by side in the same organ, as in the lung or the brain. Distinct sarcomatous nodules have been found in infiltrated lungs and alongside of tuberculous cavities, while cancer of the face will not infrequently be found associated with tuberculosis of the cervical lymphatics. Lubarsch has claimed that 4 to 5 per cent. of tuberculous patients suffer also from cancer, and that about 20 per cent. of cancer patients suffer from tuberculosis.
The method of death in cancerous patients is as free from distinctive characteristics as the course of the disease. It is usually associated with two prominent features, malnutrition and some terminal infection. At the last there is usually some toxemia, which renders the closing hours free from actual pain, while if the toxemia be profound patients may linger unconscious for several days.
Accepting the views expressed when discussing the nature of the cancerous process, the following may be assumed to be true: Cancer begins as a local disease. There is therefore a period in its history when if it be recognized in time, if it be or can be made accessible, and if it be thoroughly removed, it can be frequently cured. The “ifs” in the foregoing statement afford such insuperable obstacles in so many cases that the difficulties in the way of treatment are very great. It has been said that, “The resources of surgery are rarely successful when practised upon the dying.” It happens too often that these cases are not submitted to the surgeon until long after the favorable period above indicated is past. This is explained by the difficulties of diagnosis, by the inaccessibility of many primary cancers, and by the unwillingness of patients to submit to the knife. Nevertheless the best time to treat a cancer is when its existence is first suspected, and the best way is the most radical, i. e., by thorough extirpation.
While such extirpation should include a wide area of apparently healthy tissue and of the entire organ which seems to be involved, for instance, in the case of the liver, this last may be impossible; and yet by removal of a considerable area of healthy liver around a cancerous gall-bladder the writer has seen complete and apparent final recovery follow. The principal direction is to be thorough.
[296]
That cancer so often returns after operative attack is largely due to the fact that the general practitioner, under whose observation most of these cases first come, is slow to recognize the malady, and timid to advise radical methods.
It has been recognized that in cancer the internal administration of arsenic has been beneficial. In order to obtain the best results from its use, it must be pushed to the physiological limit and in preparations of the most active and reliable kind.[16]
[16] The preparations of arsenic which have proved most satisfactory are the imported cacodylate of sodium, which comes in capsules ready sterilized for use, and the following solution, which is original and needs to be made up in accordance with the formula herewith furnished:
(1) Dissolve 7 grains mercuric biniodide with 10 grains potassium iodide in a little water. (2) Dissolve 48 grains arsenic bromide in a little water with the aid of gentle heat. (3) Dissolve 24 grains gold chloride in a small amount of water. (4) Mix the mercuric and the arsenic solutions and then add the gold solution, which will cause a whitish precipitate, becoming brownish in color. (5) Heat this mixture and decant the clear portions, setting it aside. (6) Add 2 drachms nitromuriatic acid to the above precipitate and heat gently until a clear red solution results. (7) Add to this the decanted portion of 5, which will cause a reddish precipitate. Heat the whole mixture up to the boiling point and until all residue is dissolved. (8) Add sufficient distilled water to make 15 fluidounces. The product should be bright, clear, and wine colored.
Of this solution 10 drops are supposed to represent ¹⁄₁₀₀ grain mercuric chloride, ¹⁄₃₀ grain gold chloride, ¹⁄₁₅ grain arsenic bromide. The commencing dose is 10 minims, which may be increased to 25 or more, taken in abundance of water.
—A number of years ago Fehleisen, calling attention to the fact that cancers had seemed to improve or possibly even disappear after an attack of erysipelas, suggested deliberate infection of the surface of such a growth from a case of erysipelas. In this procedure he met with some success, but there were numerous objections to it, one being the impossibility of controlling the spread of the infection thus produced. Coley, of New York, then undertook a much more systematic study of the relation between the two diseases, and devised a method of injecting the toxins produced by the streptococci of erysipelas and of reinforcing them, if necessary, by those of the bacillus prodigiosus. The intent of this treatment is to produce reasonable reaction in the hope of mitigating the rapidity of the growth, checking its progress, or even causing its disappearance. It has been on trial now for several years, and while in a few cases of sarcoma, especially in the hands of its originator, the treatment has apparently been of service, it has proved disappointing in the majority of instances.
—The application of liquid air to superficial malignant growths has proved successful in a number of instances, but inasmuch as this is practicable in only one or two of the largest cities of the country, it is not a measure which need be discussed here at length. The liquid seems to act as an almost painless escharotic, and its use produces sloughing, or a drying up under a scab, which after a day or two will loosen and be easily detached.
—This remarkable element has aroused within the past few years an amount of scientific interest and experimentation with which there is little else to compare. The enormous expense of a preparation of any great activity, and the rather bewildering contradictory statements which have been made by those who use the weaker preparations, have caused it to occupy a doubtful position in any list of reliable therapeutic agencies. It is undeniable that certain rodent ulcers, tuberculous lesions of the skin, and a few carcinomatous lesions have been much improved or apparently cured by its use. It is ordinarily used in glass or aluminum tubes or capsules, which are applied upon the surface of the growth to be treated. It has also been used sprinkled upon a plaster whose surface has been prepared with Canada balsam, and thus directly applied. Again, it has been enclosed in a capsule to which a strong silk thread has been fastened so that the former may be swallowed, retained in the stomach for a few hours, and then withdrawn. These last means of using it are of questionable value. Of still less value are the suggestions to dissolve it in water or to administer water in which a receptacle containing radium has been allowed to stand. There is much of interest and perhaps something of value in radiotherapy, but nothing as yet of positive value in the hands of the profession generally.
, or, as it is often named after its promoter, Finsen light, has proved of value in many cases of lupus, and in some cases of superficial epithelioma. Its effects, however, can scarcely be made to penetrate into the deeper tissues, and in its use it is even necessary to make pressure upon the part treated with quartz compressors, because ordinary glass shuts out a great proportion of these rays from whatever source may produce them, and because it is necessary to create a temporary anemia of the lesions,[297] as the fluids of the body have the same effect as does glass. For these reasons the method, which is of but limited value, can be made serviceable in but a small proportion of cases.
—The Röntgen or cathode rays have played a large part during the last few years in the therapy of cancer. Such varying statements have been made concerning their value as to keep them still on trial and nothing very positive can be said regarding their efficacy. It may be said, however, that the nearer the malignant growth is to the surface of the body the more promptly can their effects be produced. The superficial growths, especially of the epitheliomatous variety, often yield readily to their use; the deeper the lesion the more vague the effect, both in character and permanence. It has been the writer’s experience that they furnish the best method of relieving pain, in a large number of these growths, short of the anodyne effects produced by powerful drugs, which are in every other respect undesirable. He holds that no one can predicate with certainty what may be their effect in any given instance, but that they are worthy a trial in every inoperable, painful, or otherwise hopeless case. Occasionally improvement follows their use, while in the next, apparently a similar case, one may be doomed to great disappointment. There are as yet no indications by which the cases which are most amenable can be easily recognized. Even in cases of extensive and disseminated abdominal cancer marvellous improvement may follow, but never a cure. It is indeed questionable whether deep cancer can ever be really cured by these means. As against their undoubted and unchallenged value in some instances, certain disadvantages are met in the difficulty of selecting a proper vacuum tube, the frequency and duration of exposure, the distance, etc. Dermatitis, sometimes mild, sometimes severe, has too often followed the injudicious use especially of a “high” tube, and more painful, irritable, or intractable ulcers are seldom seen than some following so-called “x-ray burns” of the skin. Moreover this is not the worst of these cases, for efforts intended for the best have been in repeated instances turned into a travesty by the development on surfaces thus burned of epithelioma, necessitating later mutilating operation. A well-known American surgeon suffered amputation of one hand and nearly all of the other as a penalty for inattention to the destructive effects of too prolonged exposure of his hands. It has, therefore, impressed itself upon the writer that the x-rays should not be indiscriminately employed. Nevertheless in skilled hands and used with great discretion they can be made a powerful instrument for good in many cases, especially for the relief of pain. They should never be regarded as a substitute for operation if operation be feasible, but they may often be employed to advantage after operating, in serious cases, where there is reason to fear recurrence.
The efficiency of the x-rays is apparently enhanced by the simultaneous administration of thyroid extract; although the explanation for this improvement is not known, it is, however, of enough importance to be borne in mind. The extract should be given in 5-grain doses three or four times a day. All the remarks above made may pertain as well to the employment of cathode rays in non-malignant affections, i. e., tuberculous lesions, neuralgia, etc.
—A large number of suggestions concerning the treatment of cancer have emanated from various sources and from men of widely different views. Beaston, of Glasgow, being impressed by the physiological relationships and sympathies between the ovaries and the mammary glands, has suggested the benefit of the removal of the ovaries in hopeless cases of mammary cancer, holding that the nutrition of the mamma being thus influenced there would be more or less subsidence of pathological activity. He has reported instances in which, apparently, this measure had the desired effect; nevertheless it has not found general favor.
Based upon views concerning the hyperacidity of the blood and tissues in the cancerous condition, it is believed that there is a pronounced indication for the internal use of alkalies; and the hypodermic injection of 5 minims of a 1 per cent. solution of a chemically pure soap has been recommended by Webb, on the theory that it promotes the separation of cholesterin from the living cell. He would increase the dose until 60 minims are given at one time, every other day. A 20 per cent. solution of Chian turpentine, dissolved in sterile oil, has also been recommended to be used in the same way. These are recent suggestions of unknown value.
In the general management of cancer patients, two things should be kept in mind: (1) That they are entitled to relief from suffering in the least harmful way in which it may be offered, and (2) there comes a time in the history of many of these cases when[298] all other considerations may be set aside in favor of comfort and tranquillity. Opium and other “drugs that enslave” have their disadvantages, but these cannot outweigh the benefit which they may confer in the last stages of cancer. The terminal pains of malignant disease should he assuaged at any necessary cost of other considerations.
But while all this is going on elimination must not be neglected. Opiates are peculiarly liable to diminish secretions and peristaltic activity. The skin, the kidneys, and the bowels should be kept active by measures which serve this purpose, and if it be desirable to prolong life, nutrition should be regulated and frequently administered, but it is absolutely necessary to maintain elimination.
The latest suggestion, viz., to treat cancer by injections of pancreatic ferments (trypsin and amylopsin), seems to the writer to be based upon erroneous notions concerning the nature and causation of the disease, and to hold out only specious hope of self-justification.
[299]
It is proposed here to treat only of those diseases of the skin which may complicate surgical cases or call for surgical treatment.
Dermatitis may be produced by chemicals, caustics, and various irritants; the former, for instance, by the use of strong antiseptics upon sensitive skins, and the latter as when fecal matter or urine is poured over unprotected skin or allowed to remain in contact with it. Ammoniacal urine will prove irritating, as will also that of diabetes. When carbolic acid was in general use it gave rise to great trouble upon the hands of many surgeons, while iodine, iodoform, and other such remedies, as well as the stronger mercurial preparations, will cause local symptoms similar to those produced by poison ivy.
This may be prevented, when the condition has occurred, by applying soothing lotions or mild astringents, with anodynes, in dry dusting powder or in ointment form. Cocaine in small amounts, or preferably orthoform with menthol, may be employed in either of these ways. When an acid discharge is expected the skin should be protected with an ointment or with collodion or rubber cement; the latter by drying will leave a thin film upon the surface. Thus around a fecal fistula the skin will be irritated and more or less macerated, and should always be thus protected when possible.
Between sixty and seventy drugs are known to produce distinct forms of dermatitis, such as copaiba, cubebs, the various preparations of iodine, bromine, and arsenic, some of the aniline preparations, quinine, etc.; while the various antitoxic serums, especially that of diphtheria, will sometimes produce a skin disturbance. In these cases it is only necessary to recognize the source of the trouble and remove the cause by stopping the drug. Should dermatitis produce such restlessness as to interfere with the physiological rest necessary for a wound or fracture an opiate should be administered.
Dermatitis calorica means the varying degrees of irritation which may be set up by extremes of heat and cold, continuous or alternate, as in so-called chilblains. These are often seen upon the feet, but occur upon the hands and even the face, i. e., in places most exposed and least supplied with blood. The lesion occurs in patches, often with livid discoloration, and causes sensations varying from discomfort to acute pain, almost always aggravated by warmth; while the skin appears inflamed, though to the touch it usually seems cool.
—Chilblains occur most frequently in the anemic and those with uric-acid diathesis, but may be met at any time. The constitutional treatment should not be overlooked. Much pertains to good care of the feet, especially after exposure. After wetting or chilling they should be dried and then rubbed with boric-acid talcum powder, containing 1 or 2 per cent. of menthol; this may be dusted upon the feet, before going outdoors, upon return, and when there is discomfort.
It will often give relief to immerse the feet in warm water containing sufficient tincture of iodine to give it a mahogany color; or the feet may be simply dipped in this and then allowed to dry without using a towel. The use of hydrogen dioxide diluted two or three times has been highly commended. If this proportion of dioxide be added to four or five parts of hot saturated solution of sodium bicarbonate the efficacy of the measure will be much enhanced. In extreme cases frequent use of the following formula will probably give more relief than anything else: Carbolic acid 1 part, ichthyol and tincture calendula each 4 parts, and glycerin 16 parts. With this the skin may be kept constantly moistened.
The expressions of dermatitis produced by heat may vary from an efflorescent rash to complete destruction, and will be treated of under the following head:
[300]
The term “burn” is applied to lesions produced by flame or dry heat, while moist heat (i. e., boiling materials or steam) causes injuries known as “scalds.” Between the two there is but little essential difference, except that with the latter there is usually loosening of the hair of the part, and sometimes much loosening of the epidermis as well, so that it is easily detached in more or less large patches. Whether heat is relatively feeble but prolonged, or higher in degree and of shorter duration, the results of dry heat are about the same. Some differences will exist according to whether the part is exposed to actual flame or to hot or melted material, sufficiently hot perhaps to cause complete charring or carbonization of a part.
Fig. 97
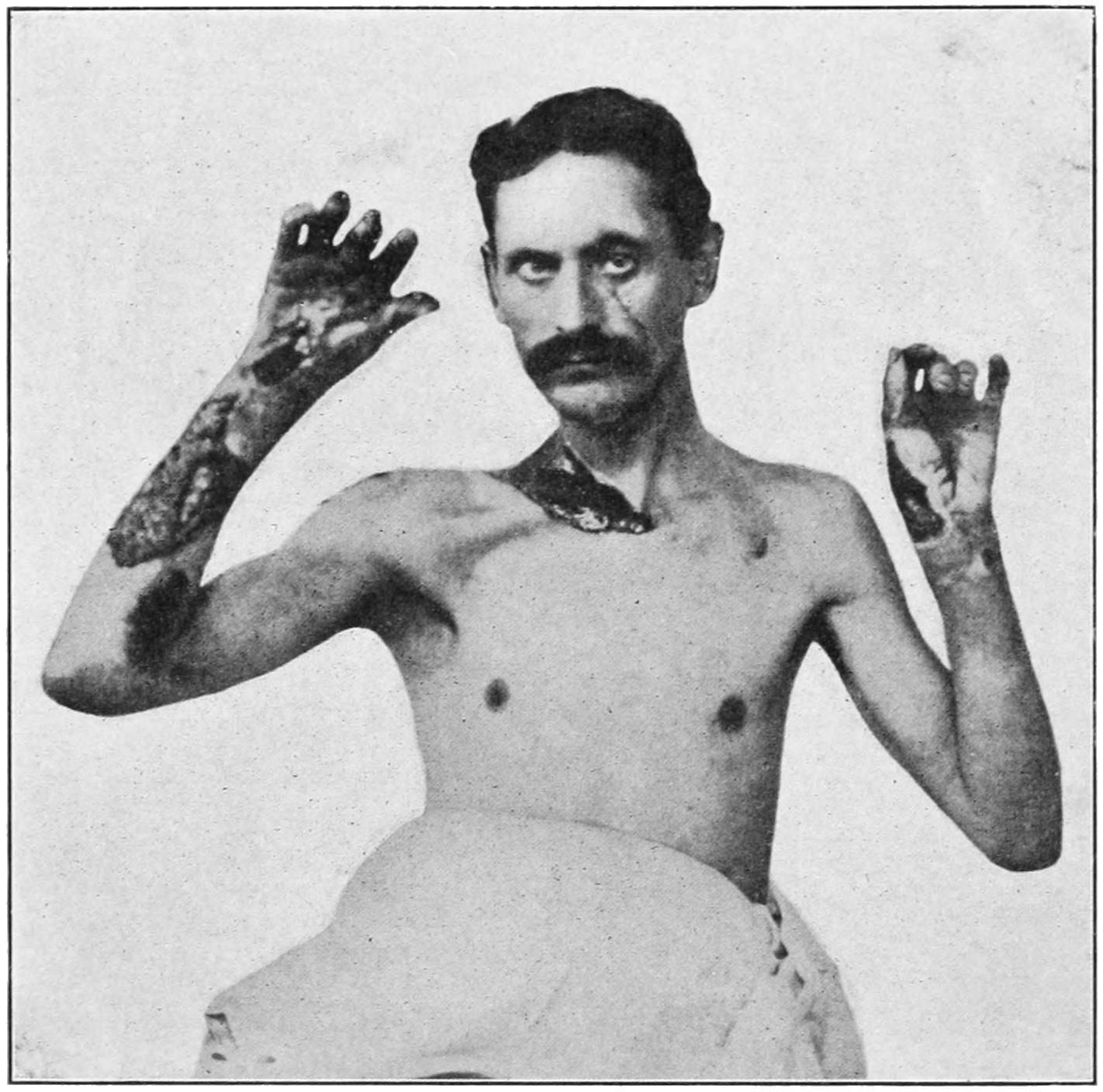
Burn by electric current from “live wire” carrying 1200 volts. (Original.)
Similar injuries are produced by concentrated caustics, acids, or alkalies, while such materials as phosphorus or sulphur produce deep burns. The burn produced by lightning is rarely deep, although it may be extensive (Fig. 97). Persons coming in contact with live wires sustain burns which partake much of the nature of the electric discharge, and are sometimes of a character to deserve the term “brush-burn.” Formerly burns were divided by Dupuytren into six or seven degrees, but this classification is too cumbersome and artificial to be acceptable. Morton’s classification is now everywhere accepted, by which they are divided into three degrees: (1) Dermatitis without vesication. (2) Vesication even to the formation of bullæ. (3) Destruction of the skin, with or without that of the deeper parts, which may include actual carbonization of a limb.
Burns may vary within the widest imaginable limits. To an extensive burn of the surface may be added the features produced by inhalation of smoke, steam, or flame; accordingly the eyes and the mucous membrane of the nose and mouth suffer, the parts becoming chemotic and disfigured, so as to make the individual unrecognizable. Burns constitute one of the most painful and distressing injuries known to the surgeon, particularly when the area is large and the case is complicated by injuries which necessitate more or less prolonged rest in bed. When the body is burned completely around it is difficult to ensure rest without the use of anodynes.
[301]
Shock is a marked feature of every serious case of burn or scald, and albumin quickly appears in the urine in these cases. Ulceration of the duodenum may follow extensive injuries of this kind, and is occasionally the cause of death. It is to be attributed to a toxic action produced by absorption of putrid material connected with the surface sloughing process. A temporary diabetes is sometimes noted. Laryngitis, bronchitis, and pneumonia may occur from inhalation of steam or smoke, while the inhalation of flame may bring about a rapid edema of the glottis, which may necessitate tracheotomy as an early and emergency measure. It is generally stated that a burn of the second degree, which even involves half of the surface of the body, may prove fatal; while this is not invariably the case, it is too frequently true, and may afford aid in prognosis.
Burns of the second degree are always followed by exudation with formation of blebs, usually within a few hours. In the more serious cases the exudate may be bloody. Burns of the third degree are necessarily followed by more or less gangrene, and this fact affords the reason for the radical treatment recommended.
—By the time the surgeon is called to treat a burn the first indications are usually relief of pain, and perhaps stimulation for shock. The circumstances attending such injury generally leave the patient in an excited mental condition, and for several obvious reasons it would be well to use sufficient anodyne to tranquillize and give comfort. An excellent application in emergency cases is a saturated solution of sodium bicarbonate, or it may be dusted over the affected surface.
The unpleasant visceral complications that follow burns are due to absorption of decomposing fluids or tissues, so retained or so in contact with readily absorbing surfaces as to produce a more or less violent degree of toxemia. In this way are to be explained delirium, convulsions, or coma, as well as the ulcerative and toxic intestinal symptoms which constitute the distressing complications.[17] For this reason the radical method of prevention is the best; hence whenever there is any prospect of sloughing, or when even the epidermis is so burned as to make it appear that it will soon separate, the best method of treatment is to anesthetize the patient and then with a stiff brush and antiseptic soap scrub the part and remove everything that is at all loose, if necessary even using a wire brush, scissors, or a razor. Beneath every sloughing area toxic absorption will go on, and it will be far better to have fresh raw and bleeding surfaces than those which cover sources of danger; the resultant scar will not be any greater, while the subsequent course of the case will be favorably influenced. Exquisitely tender surfaces thus have their sensibility blunted, and the comfort of the patient is greatly enhanced by thorough cleansing and sterilization; moreover, dressings will not need to be so frequently changed. A soothing, antiseptic ointment should be applied; there are few better than the ordinary ointment of zinc oxide, to which may be added bismuth subnitrate and orthoform.[18] Treatment of this kind would probably not need to be repeated, and the duration of the trouble would be reduced to one-quarter or one-third of the time which would otherwise be required. When actual carbonization has occurred amputation is generally necessary. Diluted solutions of ichthyol have proved satisfactory, and the dressings should be covered with some impermeable material, so as to exclude the air. Another advantage is that the amount of subsequent discharge is limited, and thus there is less need for frequent change of dressings. In extreme cases there is no method which gives so much comfort and certainty as continuous immersion in warm water; to this may be added common salt or some other antiseptic, but the water alone is sufficient, if changed frequently. In burns covering a great part of the body this treatment is the most serviceable.[302] It should be employed until the sloughs have separated and surfaces are granulating and ready for skin grafting. This implies, of course, immersion of the entire body in a bath-tub, the body lying on a sheet fastened to the sides of the tub. The advantage of brewers’ yeast dressing, when sloughs are present, has been previously emphasized in the chapter on Ulcers and Ulceration.
[17] The Poisons Produced in Superficial Burns.—The intoxication which often proves fatal in from a few hours to a few days after an extensive burn of the surface, with its attendant delirium, albuminuria, hematuria, vomiting of blood, diarrhea, etc., is very similar to the acute intoxications produced by bacterial products. The sympathetic nervous system is seriously involved in both. These toxins are evidently the result of hemolysis, and it has been shown that they are slow poisons, especially for nerve tissue, apparently eliminated by the intestines and kidneys, which thus suffer during the process of elimination. This is a more rational explanation than the theories of thrombosis or of alterations in the red corpuscles, which would not account for duodenal ulcers, necroses in the Malpighian bodies of the spleen, etc. These poisons are formed in the burnt area and not externally; hence, if this burnt area be removed immediate death may be prevented, whereas if it be permitted to remain for a few hours it may be too late. The poisons seem to be produced in the skin, as the burning of the muscle is not followed by any such degree of intoxication. They seem to be neither ptomain nor pyridin derivatives, but rather resemble the poison of snake venom. Pfeiffer believes them to be derived from the splitting up of proteids altered in composition by the heat of the burn.
[18] Cargile membrane makes an excellent covering for burns whose surfaces have been cleaned of sloughs and which are granulating. It adapts itself perfectly to all irregularity of contour, may be snugly applied and not changed until necessity requires it.
The disfigurement caused by a superficial burn will fade after a few months. In cases where the skin has sloughed there is a tendency to cicatricial contraction as soon as granulations begin to form, and the tendency then is to the formation of disfiguring scars. About the limbs the flexor muscles will always overcome the extensors, and bridle-like deformities will be formed at flexures of the joints. These are to be prevented so far as possible by two measures—proper splinting and early skin grafting. About the face splints cannot be used, but one of the grafting methods should be used.
Fig. 98

Epithelioma following ulcer due to burn. (Lexer.)
A tendency in the scars of old burns is to formation of keloid (see below) and epithelioma. The writer has seen epitheliomatous ulcers covering at least an area of a square foot, which had formed upon the sites of burns received years previously. In one case of this kind it was necessary to remove the entire upper extremity; even then the disease recurred and finally destroyed the patient (Fig. 98).
Burns produced by caustic acids or alkalies call for appropriate chemical antidotes at first and later essentially the same treatment as that already mentioned. In cases of severe burn there is danger of neglecting the ordinary rules of general treatment, which consist in maintaining elimination and nutrition.
Effects similar to those produced by heat are caused also by cold, varying from a superficial dermatitis with its surface irritation, its possible vesication, and, later, desquamation, to complete freezing of an extremity or a part (e. g., the nose, or the ear), which may be followed by gangrene. Portions which are not frozen beyond the point of restoration of vitality undergo a marked reaction and become swollen and discolored, save in rare instances where they shrivel. Gangrene is not so immediate a process as in a severe burn, as it takes a number of hours, sometimes days, for the establishment of the so-called line of demarcation, by which the dead tissue is separated from the living. On one side of this line putrefaction goes on rapidly, as in moist gangrene from any cause; on the other side there is active circulatory disturbance, with phagocytosis, by which the line becomes more marked; no portion of tissue on the distal side of this dead line can be saved. The location of the lesion and the exigencies of the case will indicate where amputation should be made. (See chapter on Gangrene.)
—A rapid restoration of warmth to the part is most undesirable. The thawing-out process in a case of severe freezing should be begun in cold or ice-cold water. Crude petroleum at a temperature of 60° F. has been recommended as a substitute for cold water, and immersion may be continuous for several hours. A rubbing with alcohol and water may be substituted for the cold water, and then a gradual restoration to the ordinary temperature of the air. Unless this treatment be skilfully managed there may be such a rapid reaction as to be painful and even injurious. By the time there is any active exudation, or putrefaction has begun, an absorbent dry dressing and suitable antiseptics may be used.
[303]
The common expression of this form of skin affection is called a burn. This is something more than its name implies, for it is understood that the active factors are the ultraviolet rays, or the rays beyond the color region of the spectrum; that it is not due to the heat rays is shown by the intense burning that is frequently seen in the Arctic regions. In the skin of the young and tender, sunburn is sometimes followed by vesication and desquamation; ordinarily it simply produces the latter. Any soothing ointment or solution is usually sufficient for the treatment of sunburn, which should, however, include avoidance of the exciting cause.
Fig. 99
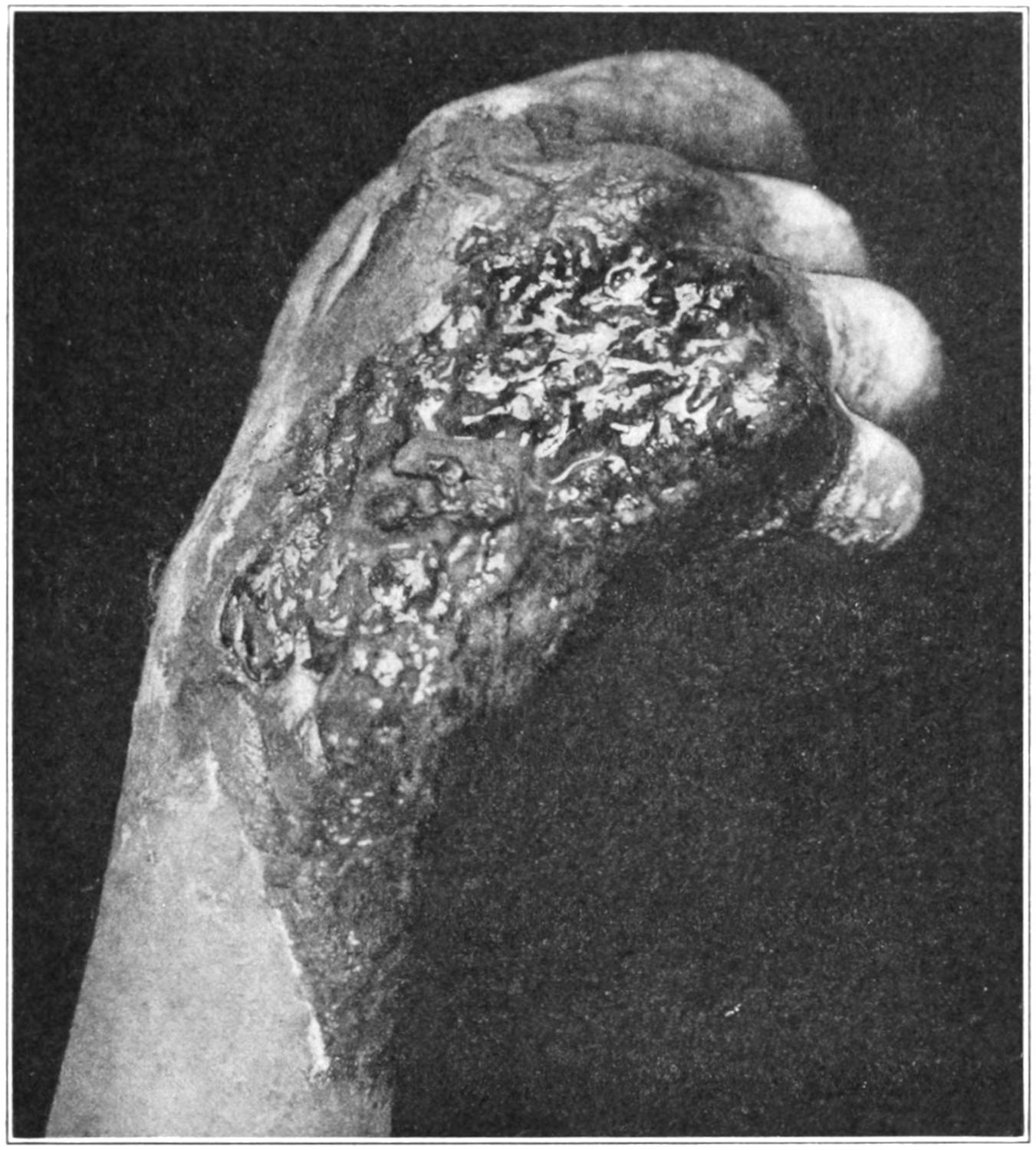
“X-ray burn,” result of nine exposures in nine days. Extensive necrosis and sloughing, with an intractable ulcer. (From collection of Dr. G. W. Wende.)
Much more intense actinic effects are produced by the x-rays, leading sometimes to complete destruction of the skin. These phenomena are usually called x-ray dermatitis. They vary from local discomfort, with itching, loss of hair on hairy surfaces, and partial anesthesia, with later a glossy appearance, to edema of the cellular tissue, by which anatomical outlines are effaced. The natural color of the skin, owing to pigmentation, appears dark. If the exciting cause be stopped before or as soon as this stage is reached complete recovery is possible, save that hair does not always grow from the surface which has lost it. The x-ray treatment should be pushed up to this stage. Careful management is now necessary, especially should any surface irritation like chafing occur. That x-ray burn, so called, may result from x-ray exposure made some time previously seems to be established by a case reported to me by Dr. L. L. McArthur, of Chicago, where he had to do skin grafting upon a lesion of this kind which did not appear until fifteen months after the last exposure.
The stage of danger is characterized by extreme itching with multiform eruptions in successive crops, desquamation, formation of minute vesicles, and ulcers; or the process[304] may be more acute and the skin begin to slough. Small lesions will become confluent, and large excavations may be formed. The sloughing process is usually slow, and by it are produced ulcers characterized by extreme pain and discomfort and a lack of tendency to heal.
These ulcers are exquisitely sensitive and applications intended for relief are of themselves most distressing. Everything about such an ulcer seems sluggish, while small areas which have apparently healed break down again; healthy scabs are not formed and granulations are extremely indolent.
—In the treatment of these lesions, so long as they are mild, the surgeon should confine himself to soothing applications and rest; at the same time discontinuance of x-ray exposures and even avoidance of light seem to be essential. Any operator threatened with such trouble should wear thick rubber gloves during all his work. The local treatment of this lesion is not essentially different from that described in the chapter on Ulcers and Ulceration, but the surfaces are often so erethistic as to demand either anodyne applications, containing such remedies as orthoform, anesthesin, or even cocaine, or else they need radical treatment with a sharp spoon.
Sloughing surfaces should be treated with brewers’ yeast until the surface has become healthy. Picric acid in solution has been recommended, a saturated solution being diluted seven or eight times before using.
The writer has rarely seen any more distressing or obstinate lesions than presented in some of these cases. In speaking of epithelioma it has been stated that some of these ulcers are prone to thus degenerate. It seems an extreme contradiction in physics that the agent used so frequently in the treatment of superficial cancers should, when used to excess, produce lesions which themselves become cancerous. It has been the writer’s privilege to witness amputation of all of one hand and a large part of the other, in the case of a well-known colleague, who carried the x-ray treatment to excess, and until he suffered to this extent. Careful and discriminating judgment is therefore necessary in the management of vacuum tubes.
Since radium has come into use it has been found to exercise a deleterious effect upon the skin. The radium emanations are known to influence living cells and tissues, and their inhibiting effect upon the growth of larvae has been well established. The prohibitive price of radium preparations will make these lesions rare. After exposure there appears an erythema followed by an active dermatitis, which so closely resembles lesions above described, in their early stages, that one description will suffice for both. Moreover, the treatment of a radium burn differs in no essential respects from that of an x-ray burn.
—A furuncle is a phlegmon having its origin in a hair follicle and involving a small area of skin and subcutaneous tissue. The infection is produced by one of the ordinary pyogenic organisms, which have easy access to the base of the follicles. Sometimes these organisms are of unusual virulence, but ordinarily there is a local condition which favors the infection, while it may be encouraged by a general diathetic condition, such as diabetes. The lesion is usually single, but may be multiple. Boils appear sometimes in groups or in crops, and when the condition has become chronic it is called furunculosis, which may be local or general. A boil commences as a tender papule, which rapidly enlarges into a conical swelling, sometimes of considerable size. Around it there is an area of dusky discoloration, while the apex becomes quite dark. Pus, travelling in the direction of least resistance, comes more or less readily to the surface, the apex of the boil yielding and pus finally escaping, if not evacuated by incision, usually with a small amount of necrotic tissue, which may be sufficiently large to justify the term “core.” With the escape of pus the throbbing pain is much relieved. A furuncle arising in tissues where swelling is not easily treated, as in the nose, the external meatus, and also in the axilla and the perineum, will produce an abnormal amount of pain.
—The domestic treatment of boils consists of poultices, usually made of hot flaxseed. These are always nauseous applications, and tend to favor the development of similar trouble in adjoining follicles. An equally comforting application can[305] be made with a piece of spongiopiline, or a compress, saturated in an antiseptic solution, and covered with rubber tissues, outside of which, if necessary, a hot-water bottle may be applied. Inasmuch as it is tension which produces pain, early incision, which can be made under a little freezing spray, or with cocaine, will give the greatest relief. This may be practised even before pus has appeared. After such incisions the same moist applications may be applied. Incisions should be made as soon as pus is shown to be present. The appearance of a whitish point at the apex of the furuncle will always indicate the presence of pus beneath.
General furunculosis has almost always an underlying diathesis as a cause, and this should be sought out and treated according to its nature. In the absence of recognized constitutional conditions the writer has never found anything equal to aromatic sulphuric acid, given in 10 or 12-drop doses, with tincture of arnica in teaspoonful doses, to be freely diluted with water.
—This differs from a furuncle in the extent of the local infection, involvement of subcutaneous tissue, and the amount of necrosis which it produces. It is in most instances a more serious affair, life often being destroyed by the extent of the resulting necrosis and the amount of toxins produced. It begins as a local process, but always with constitutional disturbance, and sometimes even with a chill. The affected surface rapidly assumes a brawny hardness, and the infiltration is often extensive; pain is severe and throbbing; the surface becomes more dusky in appearance, numerous pustules appear, development of all the features of a serious carbuncle usually taking place in a few days. Later it begins to soften and the skin gives way at several points, at each of which a small drop of pus is discharged, while after removing this there may be seen white necrotic tissue beneath. The sloughing process extends deeply, generally to the deep fascia, and this itself occasionally succumbs. A person may have a distinct carbuncular lesion where the area primarily involved is not much larger than that of a five-cent piece; on the other hand, in debilitated or dissipated subjects, a lesion of this kind may become as large as a dinner plate, while the sloughing process may expose the underlying bone. This is often the case on the back of the neck and trunk. A carbuncle may occur in any part of the body, but is usually seen on the back; when upon a limb it generally involves the extensor surface. It is especially serious and dangerous when occurring upon the face, as septic thrombosis may readily extend to a cranial sinus and rapidly kill. It was formerly believed that carbuncles of the lip always terminated fatally; while this is not necessarily true it will indicate the seriousness of the condition (Figs. 100 and 101).
Fig. 100
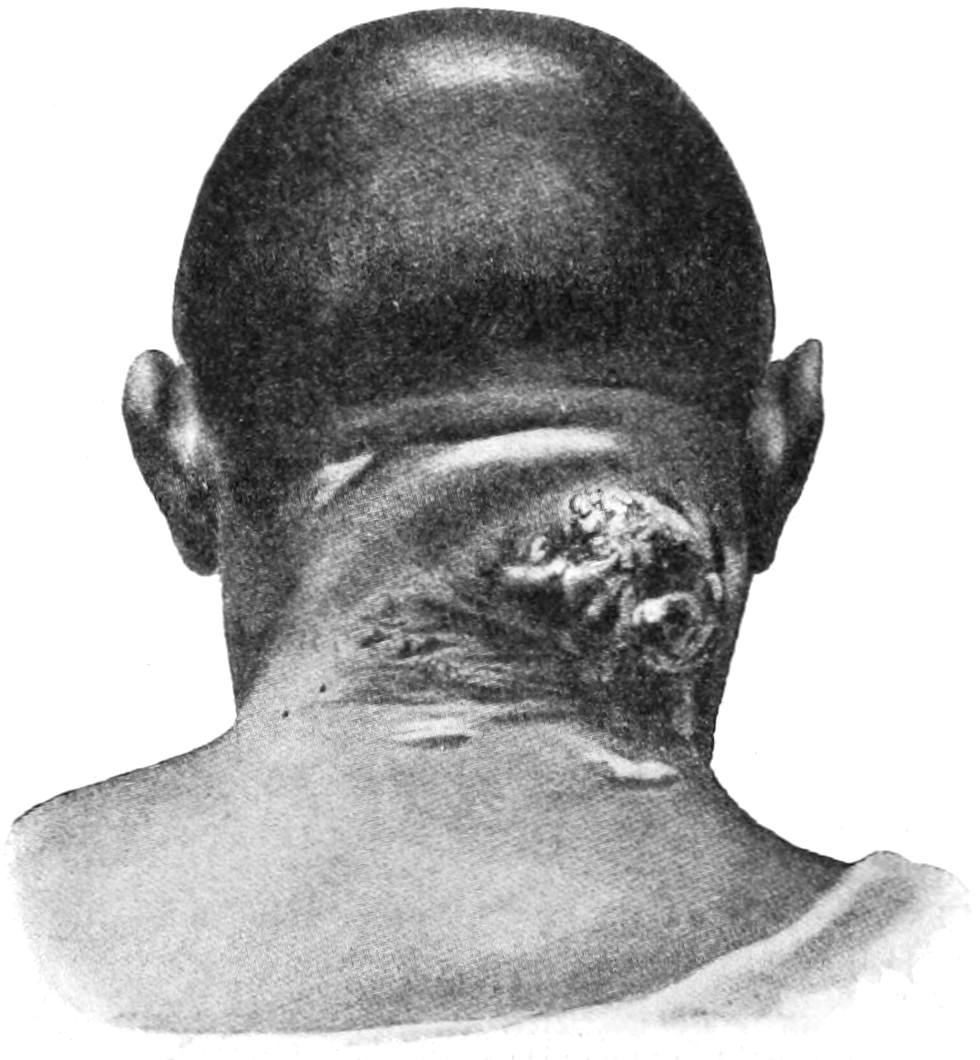
Carbuncle of the neck. (Lexer.)
—There are few lesions where both constitutional and local treatment need to be more judiciously combined. Many of these patients are diabetic, and then it assumes malignant tendencies. Others are syphilitics or alcoholics, whom dissipation has reduced to a condition of serious malnutrition. The urine should always be examined for sugar and albumin, and whatever indications it may afford carefully followed. Septic intoxication and infection may so rapidly depress the already weakened patient as to call for stimulants and tonics, and pain may be so severe as to justify the use of anodynes.
The local treatment should consist of soothing applications until the extent of the plastic exudate has declared itself, after which it should be more radical. It is better, therefore, to excise under an anesthetic, the area which ordinarily would require days or weeks to slough. The most satisfactory treatment is the radical. The knife, the scissors, and the sharp spoon constitute the best means of combating this disease.[306] In other respects the treatment was discussed when dealing with septic infection. Nothing will so hasten the sloughing and cleaning up process as brewers’ yeast. The writer’s custom is to make a thorough excision of the affected area and treat the part with yeast for some days. About the lip and face the sharp spoon should take the place of the knife, but even there, if the case be attacked early, tissue can be saved and disfigurement reduced to a minimum. The method used by some of injecting 5 per cent. carbolic solution is less satisfactory, although the measure above recommended is a rather severe operation and usually requires complete anesthesia.
Fig. 101
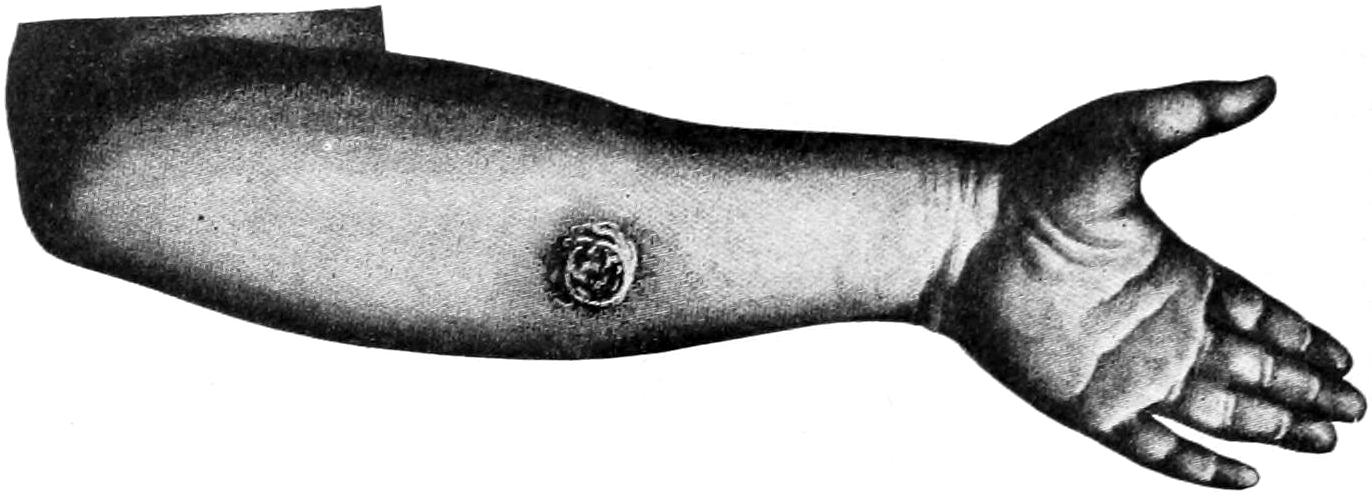
Anthrax carbuncle of forearm. (Lexer.)
—Most of the skin lesions formerly described as scrofulous are now known to be expressions of tuberculosis. So, also, are some of the papillomatous growths and the chronic ulcers, which do not assume distinctive form.
Lupus vulgaris is perhaps the most common of these cutaneous lesions, especially in certain parts of the world. It is seen more often among the young than the old. The lesions begin with a papule, which becomes the well-known lupus, smaller nodules coalescing and forming eventually a brownish-red patch, whose borders are somewhat elevated and scaly. This lesion usually goes on to ulceration, particularly in those parts of the body where it is kept moist or frequently irritated. It is in these lesions that a healing or cicatrizing tendency is seen at one point and progressive ulceration in another. Ulceration does not always occur, but the papule just described sometimes undergoes spontaneous absorption, the tissue atrophying, losing its peculiar skin functions, and the scar being depressed and scaly.
Lupus vulgaris is to be distinguished from lupus exedens, referred to under Epithelioma. It is often mistaken for the latter, and a differential diagnostic table has already been given. (See p. 293.)
Verruca necrogenica, as it used to be called, is now known as verrucose tuberculosis. It consists of cutaneous warts, surrounded by an erythematous zone or patch, which tend to break down, and covered with scabs, intermixed with pustules. The lesion rarely proceeds to complete ulceration. It occurs especially upon the hands and exposed parts of those who handle cadavers or carcasses. The lesion is usually slow and sometimes disappears spontaneously.
On or about the mucocutaneous borders of individuals suffering from tuberculosis there appear small ulcers, secreting a thin, puruloid material. These are seen especially about the nose, the mouth, the anus, and the vulva. These lesions should be regarded as local infections from a constitutional source. They are often sensitive, show little tendency to heal, and are sources of danger to others. They should receive radical treatment.
Under the term scrofuloderm are included a variety of subcutaneous tuberculous nodules which spread and involve the skin. They begin in the superficial lymph nodes. The overlying skin becomes bluish and gives way, while an ulcer remains which discharges more or less puruloid material. The edges of these ulcers are frequently undermined for a considerable distance. These are ordinarily chronic lesions, which sometimes undergo a spontaneous recovery, leaving disfiguring and discolored scars, usually irregular and more or less striped or banded.
[307]
Some of the scrofuloderms are included under the erythema induratum of Bazin, lesions which appear mostly on the calves of the legs of young women, consisting of deep-seated nodules, which break down into deep ulcers, having elevated and overhanging edges. Again, there is the so-called lichen scrofulosorum, i. e., a papular eruption seen in the young, especially those who show other evidences of tuberculosis. It consists of rounded groups of papules, usually on the sides of the trunk, at first bright in color, new papules appearing as the old ones fade. In addition there is the pustular scrofuloderm, which crusts over, heals, and leaves small cicatrices.
In all of these lesions the tubercle bacilli can be usually demonstrated. There are other skin lesions in which no bacilli can be demonstrated, which are supposed to be due to the toxins generated in tuberculous foci elsewhere. Hallopeau suggests calling all tuberculous skin lesions tuberculides and to group them as follows: (a) Those in which bacilli are present, bacillary tuberculides, and (b) those arising from tuberculous toxins, toxic tuberculides.
Fig. 102

Lupus of skin (hypertrophicus et exulcerans). Finally healed by excision and plastic operation. (Lexer.)
Fig. 103

Lupus vulgaris. (Hardaway.)
Among the latter he describes what he calls folliculitis, i. e., small papules, firm, at first red, then elevated, becoming nodules, appearing on the extremities, and gradually producing crater-form ulcers covered with black crusts, leaving small pock-like scars. This condition is chronic, lasting years. In these patients the skin is furfurated, showing a sluggish circulation.
—Inasmuch as tuberculous skin lesions tend to spread and to recur, they need radical treatment—i. e. the sharp spoon, the scissors, and caustic. Ordinarily it is best to scrape the affected surface, to trim away all unhealthy edges, and then to apply a strong caustic for a brief space of time, thereby sterilizing it and searing the mouths of the absorbents which may have been opened by the scraping. Treatment for two or three days with brewers’ yeast will usually suffice to put the surface in a healthy condition, after which it may be skin-grafted or treated by any of the ordinary plastic methods.
[308]
—The bacillus of rhinoscleroma was described in the chapter on Inflammation, under the heading Pyogenic Organisms. It is a specific infection, primarily of the skin, which appears invariably upon the nose. It begins either in the skin or mucous membrane, or both, and having once thoroughly invaded the tissues grows in all directions. It shows no tendency to heal, but gives to the tissues a distinctive brawny induration. From the nose it extends to the palate, pharynx, and antrum, making steady encroachment upon the parts which it affects, distorting the features, obstructing respiration, and often causing pain by pressure on the sensory nerves. Its first appearance is characterized by nodules, frequently covered with dilated bloodvessels. Unless it can be seen and recognized early it is a wellnigh hopeless condition with which to contend. Extirpation of the affected tissue is the only satisfactory method of dealing with it. It is a different disease from rhinophyma described elsewhere. (See Figs. 7 and 8, p. 55.)
—This form of skin infection, of somewhat uncertain origin, is met in shape of fungoid nodules, and likely to involve the upper part of the body; they tend to increase in number and size, to infiltrate, often to ulcerate, sometimes to disappear by spontaneous absorption, but in severe cases cause death, either by malnutrition or sepsis. Tumors are thus formed which attain the size of a child’s head. As soon as surface infection or ulceration begins the breaking-down process is rapid; there is early involvement of the lymph nodes, and the general health begins to suffer. The tendency in almost every case is to fatal termination. Cases may run from a few months to fifteen years, however, before this stage is reached. By some authors the disease is considered as a peculiar form of sarcoma. It is, however, generally regarded as a granuloma, whose specific organism has not been ascertained.
Fig. 104
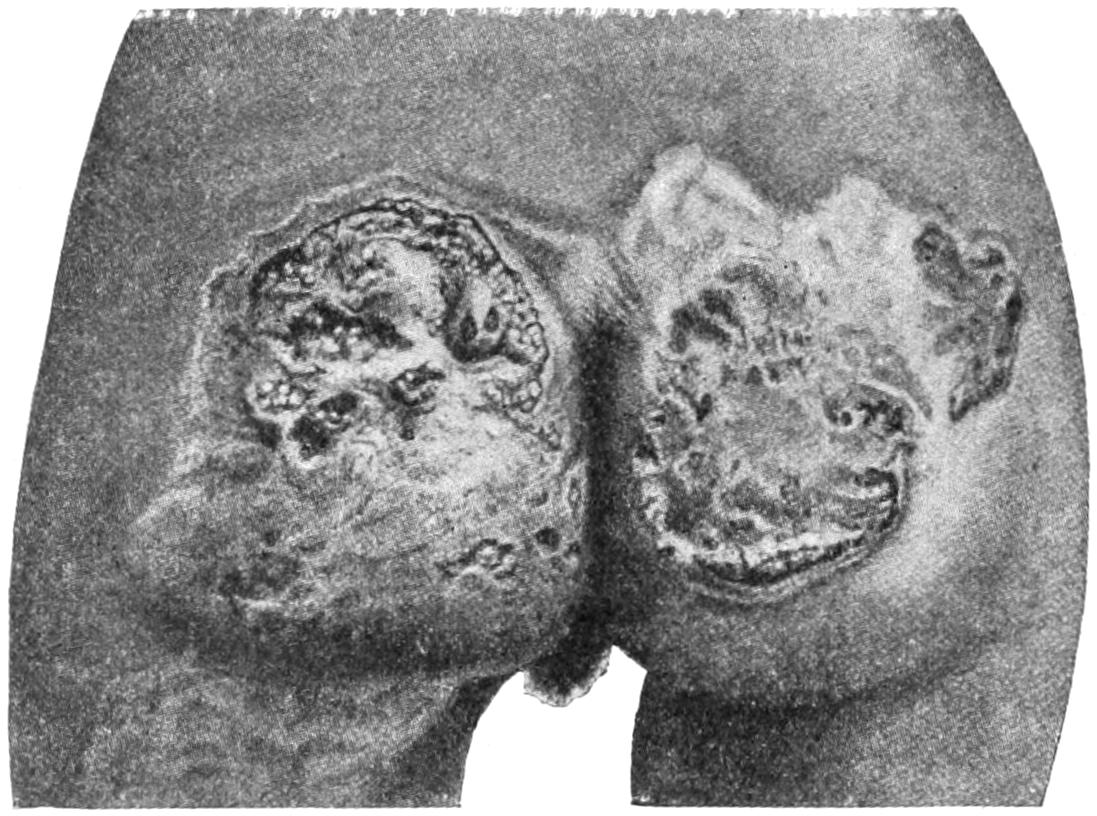
Ulcerating gumma of skin, cicatrizing in certain areas. (Lexer.)
should be included among the chronic infections of the skin, and have been described.
—Radesyge is a granulomatous involvement of the skin, peculiar to certain parts of Europe, particularly Norway, which has been by some considered to be an expression of leprosy, by others to be a disease by itself. It is generally held that the lesions which have passed under this name are really expressions of cutaneous syphilis.
—This is an endemic tropical disease, of which we see our nearest specimens in the West Indies, and involves especially the negro and Oriental races. It begins with an eruption, papules maturing in fungoid form, being met with most often at mucocutaneous borders, but appearing anywhere upon the surface. It is specific and inoculable, having a period of incubation of about two weeks, and becoming generalized in from fifteen to twenty weeks. The papules increase in size, become covered with yellow crusts, which fall off and expose a rough surface which discharges an offensive puruloid material. After remaining in this condition for an indefinite time the lesions spontaneously improve and may disappear, leaving only pigmented spots to mark their previous sites. Beyond local cleanliness and antiseptic applications the[309] lesions require but little treatment. If anything more is attempted it should be thorough and effected with the cautery or the sharp spoon.
—Mycetoma is more commonly known as Madura foot, or sometimes the fungus foot of India. It prevails especially in Southern India and about Madras, and is apparently confined to that part of the globe. Nevertheless it has been reported from Algiers and from South America. It is a specific infection of the foot, beginning in the skin; it rarely occurs on the hands, the scrotum, etc. It leads to the formation of an infectious granuloma, which gradually destroys the texture and identity of the tissues, and finally demands amputation or ablation of the part.
Russian bacteriologists have discovered parasites resembling the protozoa which they have found in the granulations and ulcerations of the Delhi boil. They were also occasionally seen in the leukocytes. By these observers these parasites have been regarded as active agents and have been given the name ovoplasma orientale.
Oriental Boil.-This also is a slow infection of the skin, met with especially in Southern India, where it is known as the Biskra button and the Aleppo or Delhi boil.[19] It appears mainly on the unprotected parts of the body at first as a papule and then a nodule, which enlarges, ulcerates, usually tends to heal spontaneously, and leaves an ineffaceable scar. It is practically a granuloma of the skin, is auto-inoculable, and is best treated by complete excision.
[19] Delhi boil is now known to be another of the local infections of exposed surfaces, occurring especially about the lower extremities and the genitals, due to the invasion of one of the trypanosomas, its actual pathology having been only recently demonstrated.
—This worm is about one line in diameter and two or three feet long, and is found generally throughout the tropics. The embryo is taken into the intestines with drinking water and migrates to the skin, beneath which it develops. The male worm has never been discovered. What is known of the evidence of its presence pertains only to the female. When fully developed it can be felt in a coil beneath the skin. It produces local inflammation, a vesicle forms, and the head of the worm then protrudes. When it is exposed it can be frequently extracted by gentle traction, removing as much each day as protrudes. Christie has suggested to destroy the worm by electrolysis, and others inject into the vesicle some antiseptic, by which the worm is killed, it being afterward absorbed without difficulty (Fig. 105).
Fig. 105
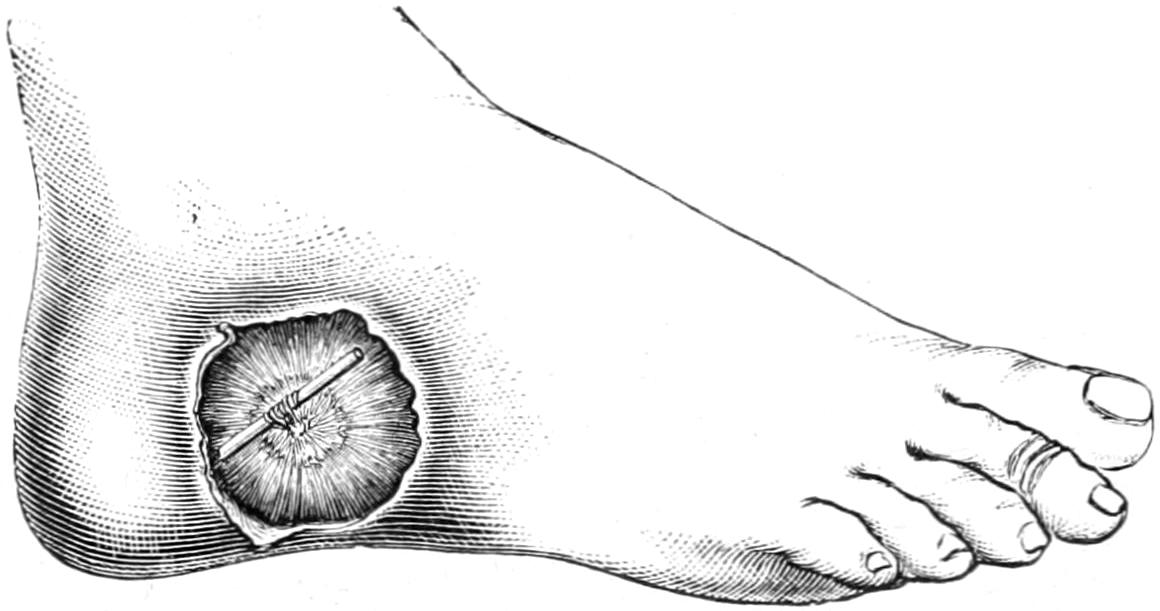
Guinea-worm bleb just cut off. (Bryant.)
—This is a true protozoan infection of the skin, first described by Wernicke in 1892, which has now become quite generally recognized and described. The parasite is a very small, spheroid protozoan, and is found in the skin elements, as well as in the pus and debris discharged from the lesions. It has been successfully cultivated and inoculated. It is classed among the yeast fungi. It produces lesions very much like some of those met with in syphilis, tuberculosis, and mycosis fungoides. Indeed it may be necessary to use the microscope in order to complete the diagnosis, which is best accomplished by teasing a small portion of tissue on the slide in liquor potassæ (Hardaway).
The lesions begin usually as small papules, which may later coalesce and become covered with a fine scab. Around these there develop thickened borders, with fungus-like projections. Between the little elevations pus may form, or an exudate occur in sufficient quantity to dry into a large-sized crust. Here, as in lupus, cicatrization may be going on at interior points while the lesion is encroaching around the margin. The affection is slow, and the ulcer may attain a size of several inches in diameter.
The treatment consists in radical measures, i. e., strong caustics, curetting or complete extirpation with the knife, which may be followed by more or less plastic work, as required.
—Under this name is described a rare form of granulomatous lesion of the skin, whose exciting cause is not one of the ordinary bacteria, but[310] a form of mold—one of the varieties of oidium. The clinical manifestations of this lesion resemble those of blastomycetic dermatitis, save that in the latter the primary focus of infection is always found in the skin and remains there localized, whereas coccidioidal granulomas may occur as well in the deeper tissues or viscera as upon the skin; in fact, the skin lesions of the latter may be described as oidiomycosis in distinction from blastomycosis. It produces miliary skin nodules which closely resemble tuberculous lesions, and may even caseate or assume an acute type and break down rapidly. The lesions are progressive, with a tendency to dissemination, both by the lymph and the blood currents. The lymph nodes are usually early affected and often suppurate.
, may be found in the subcutaneous tissue in the shape of small nodules, covered by unaffected skin. When young these tumors are tense and elastic, but are subject to calcareous changes. They occur frequently on the back.
are also found in the skin, where they may attain a size which will make them fluctuate. The treatment for all such lesions is complete eradication.
—This has already been alluded to in the chapter on Ulcers and Ulceration. The lesion apparently begins as a thickening or callosity, usually beneath the head of the first metatarsal bone, at a point where much pressure is made, owing to the natural position of the foot. Beneath the thickened skin there develops an adventitious bursa, in which, or in the skin itself, the first degeneration may take place. The result is a deep ulcer, with overhanging borders, and a thin, often foul discharge. The lesion is not painful, and patients are less likely to spare the foot. It is usually associated with some central spinal disease, or with a peripheral neuritis. It is more common in those patients who have had disease leading to loss of sensation in the foot.
The treatment consists in excision of the ulcer down to healthy tissues, with careful protection. Skin grafting is often found successful.
—Ainhum is essentially a disease of the negro and of tropical climates. It usually begins in the little toe or little finger, and goes on to spontaneous amputation, the result of an anemia caused by the formation of a sclerotic ring, which encircles the digit and shuts off the blood supply. It is an annular scleroderma, or keloid, which produces the disturbance.
The most common cysts of the skin are the sebaceous, known also as steatomas, which result from obstruction of the ducts of sebaceous follicles, and accumulation therein of sebaceous secretion. They are found where these glands abound, and may attain the size of a hen’s egg or larger. They are frequently infected and suppurate, or their contents may undergo slow change and lose their original characteristics by the time they are evacuated. Peculiar changes occur in rare instances, since they may calcify, or their bases serve even for the development of cutaneous horns, while in the other direction they not infrequently undergo malignant degeneration. In some of these cysts a small opening can be found, through which, on pressure, fatty or butter-like contents can be exposed. When their contents begin to putrefy the odor becomes offensive.
Another variety of the skin cyst is the so-called atheromatous, which is more allied to the cutaneous dermoid, and whose contents are often nearly pure cholesterin. Sometimes they contain hair or other epithelial products. They occur usually in the scalp. These are essentially inclusion cysts and purely epiblastic products. When infected their contents putrefy and smell badly. (See Fig. 88, p. 285.)
—The treatment for any cysts of the skin consists in extirpation of the sac. It is sufficient to split them thoroughly with a sharp, curved bistoury, and then, on either side, to seize the edge of the divided sac with forceps and enucleate it. All this can be done under local anesthesia. The cavity should be thoroughly disinfected and not too tightly closed.
Under the name Cock’s peculiar tumor some English writers have alluded to the offensive ulcerated surface, with raised edges, which is left after the contents of these cysts have undergone putrefaction and escaped by breaking down of the surface. Such a lesion is on the border-land between mere ulceration and malignancy.
[311]
—Clavi, or corns, vary in density. A soft corn differs from a hard one only in that it is located where it is softened by moisture of the parts. A hard corn is a reduplication or callosity, conical in shape, representing great hypertrophy, with condensation of surface epithelium. Beneath old lesions of this kind will frequently be found small cysts, while nerve fibers become entangled, and these little lesions are sometimes exceedingly sensitive. They frequently become inflamed, the process proceeding to suppuration or ulceration.
—When beneath such an indurated area of skin there forms an adventitious bursa, or a natural one becomes involved, the lesion is called a bunion. These are more frequent over the joints of the toes, where they sometimes cause intense discomfort. The bursæ sometimes connect with the joint cavity, and should one suppurate the other necessarily becomes involved. An infection of either of these lesions causes local and possibly fatal disturbance. I have seen death from pyemia follow infection of a bursa beneath a soft corn (Fig. 106).
Fig. 106

Distorted foot, from pressure and bunion. (Erichsen.)
These lesions are not met with among the savage races or those who go barefooted. They are essentially products of the footwear affected in modern society. Were shoes made to fit the natural foot and not to constrain it in abnormal positions, corns and bunions would be practically unknown.
—Preventive treatment is the most important and pertains to properly adapted footwear. Unfortunately the treatment of these minor lesions is too frequently left to charlatans and so-called chiropodists, who may give temporary relief in many instances, but have no knowledge of either the nature of the difficulty or its proper surgical treatment.
Soft corns will usually disappear if the parts can be kept clean and dry. Hard corns are essentially callosities, which should be pared down or trimmed off until the surface is almost ready to bleed. It may then be painted with a collodion containing 20 per cent. of salicylic acid and a little alcohol. If this mixture be applied to the surface of a clean and dry corn it can often be peeled away with the corn after a few days. When it is desirable to soften any callosity of this kind, previous to paring or trimming it, it can be done by applying for a few hours a mixture of equal parts of glycerin and liquor potassæ; this will so soften a callosity as, when applied over night, to make it endurable through the following day.
Bunions are so often associated with hypertrophy of the underlying bone as to entitle them to consideration under deformities of the feet. The most pronounced expressions are usually seen in connection with hallux valgus (q. v.), and their treatment comprises excision of the bunion and its underlying bursal sac, along with exsection of the joint. By this radical local measure complete relief is usually afforded.
—These have the consistence of an ordinary nail, are epiblastic products, varying in size, length, color, and shape. They have been alluded to in the chapter on Tumors. Sutton has divided them into sebaceous, which occur most often upon the head and spring from an old sebaceous cyst (see above); warty horns, which much resemble them; cicatricial and nail horns, which are instances of exaggerated growth of the finger-nails.
—A simple excision of the growth with its base is all that is needed in these cases.
—These constitute one variety of papillomas, the overgrowth having its original site in the prickle-cell layer of the rete. The most common form occurs upon young subjects on the exposed parts, as the face, hands, and feet. These are usually multiple; they frequently occur upon the surface, and retain dirt in such a manner as to be nearly always recognizable on the surrounding skin. They frequently disappear with as little known reason as that which caused their appearance.
Dilated papillary growths, like a fringe, are sometimes seen about the face and neck of elderly people. These have been known as filiform warts, while Unna gave them the name fibrokeratomas.
[312]
A form described as the seborrheic wart occurs upon the face and elsewhere in elderly people. It is frequently pigmented, may itch intolerably, and is perhaps the form which most often undergoes malignant degeneration. To the acuminate form of wart, which is usually soft, and most often met with as a venereal wart about the genital region, has been given the name condyloma. These appear in either sex, grow rapidly, are covered with a puruloid secretion, bleed easily, and assume often such shape and resemblance as to give rise to expressions “strawberry growth,” “raspberry growth,” etc. They are always produced by irritation, usually in connection with one of the venereal diseases, and are generally due to lack of cleanliness. They may grow luxuriantly and over a considerable area, and, when appearing on the surface of the vulva, conceal completely the parts underneath. They also occur in connection with the mucous patches of tertiary or hereditary syphilis, but have essentially the same structure, no matter how produced.
—In the treatment of ordinary warts nothing is better than absolute cleanliness. A dry wart touched daily with formalin solution, or covered with collodion containing 1 to 2 per cent. of corrosive sublimate, will usually shrink and become detached in a few days. Thorough excision of any true wart is sufficient to finally dispose of it. If the wart be cut through it is likely to bleed profusely, since its vessels are larger than those of the surrounding skin. Any growth of this kind can also be destroyed by the actual cautery, or by one of the strong caustic agents, which, however, should be used with great care.
Venereal warts, condylomas, are best treated radically, either with the actual cautery or with scissors and sharp spoon. Local anesthesia is always advisable in order that this may be thoroughly done. In instances of extensive growths of this kind a general anesthetic may be profitably given.
—Molluscum contagiosum, sometimes known as epithelial molluscum, is a name applied to small warty growths more or less embedded in the skin, from which, by pressure, some epithelial debris can be forced out. The lesions are rarely single and yet rarely numerous. They may be met upon any part of the body, especially upon exposed portions. They are doubtless results of skin infections by various organisms. The best treatment is excision, although they may be split and cauterized and thus made to shrivel, or the same effect may be produced by electrolysis.
Fig. 107
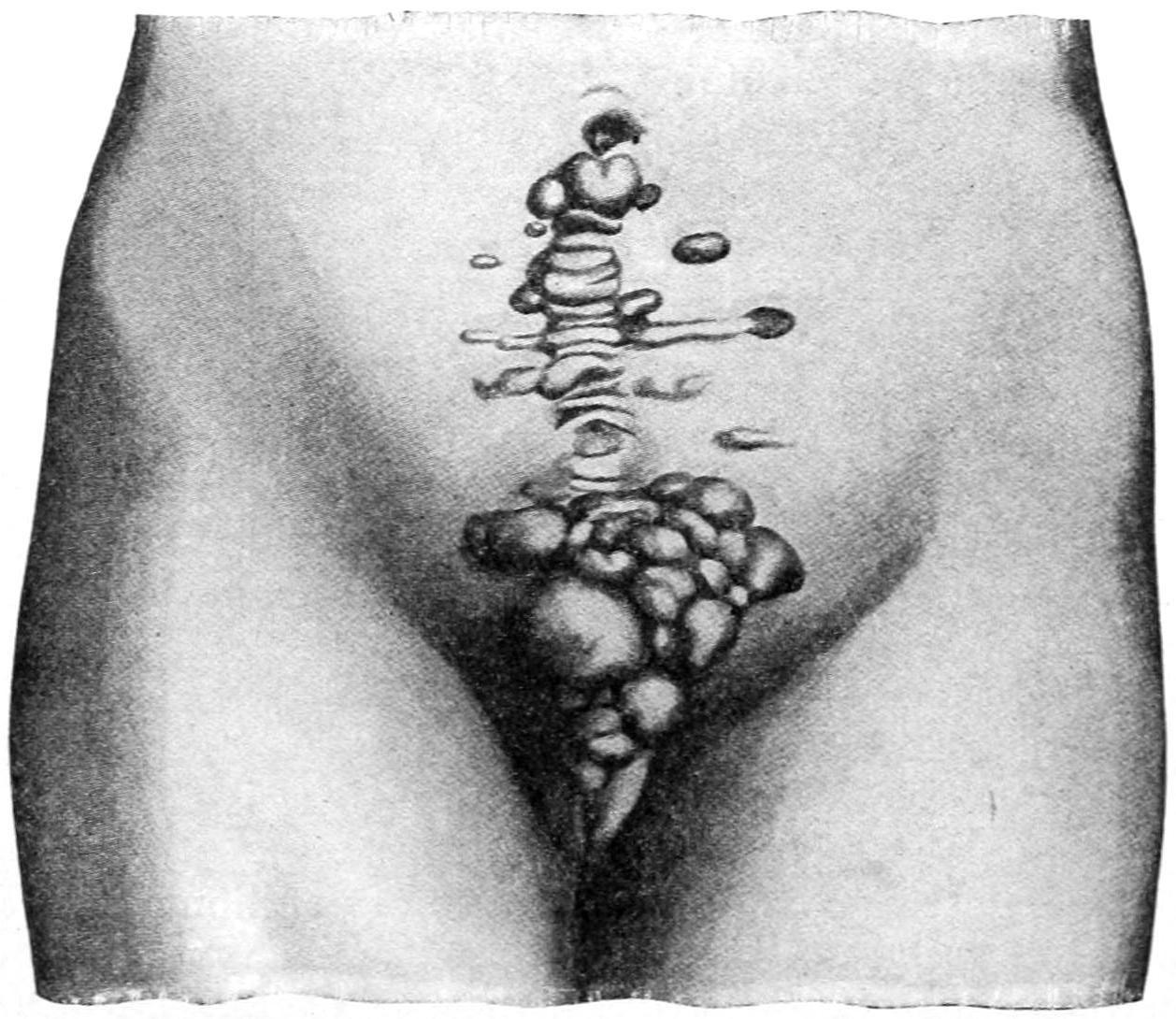
Keloid occurring in a laparotomy scar. (Lexer.)
—This has already been mentioned under the heading Fibroma, in the chapter on Cysts and Tumors. It deserves further mention here, however, because of the disfigurement produced by keloid scars, and because the spontaneous expressions of the disease may occasionally demand surgical intervention. In cicatricial tissue it often follows the scars left by burns or excision of tuberculous lesions. Since subcutaneous sutures have been introduced there is less keloid than there was years ago (Fig. 107).
PLATE XXIX
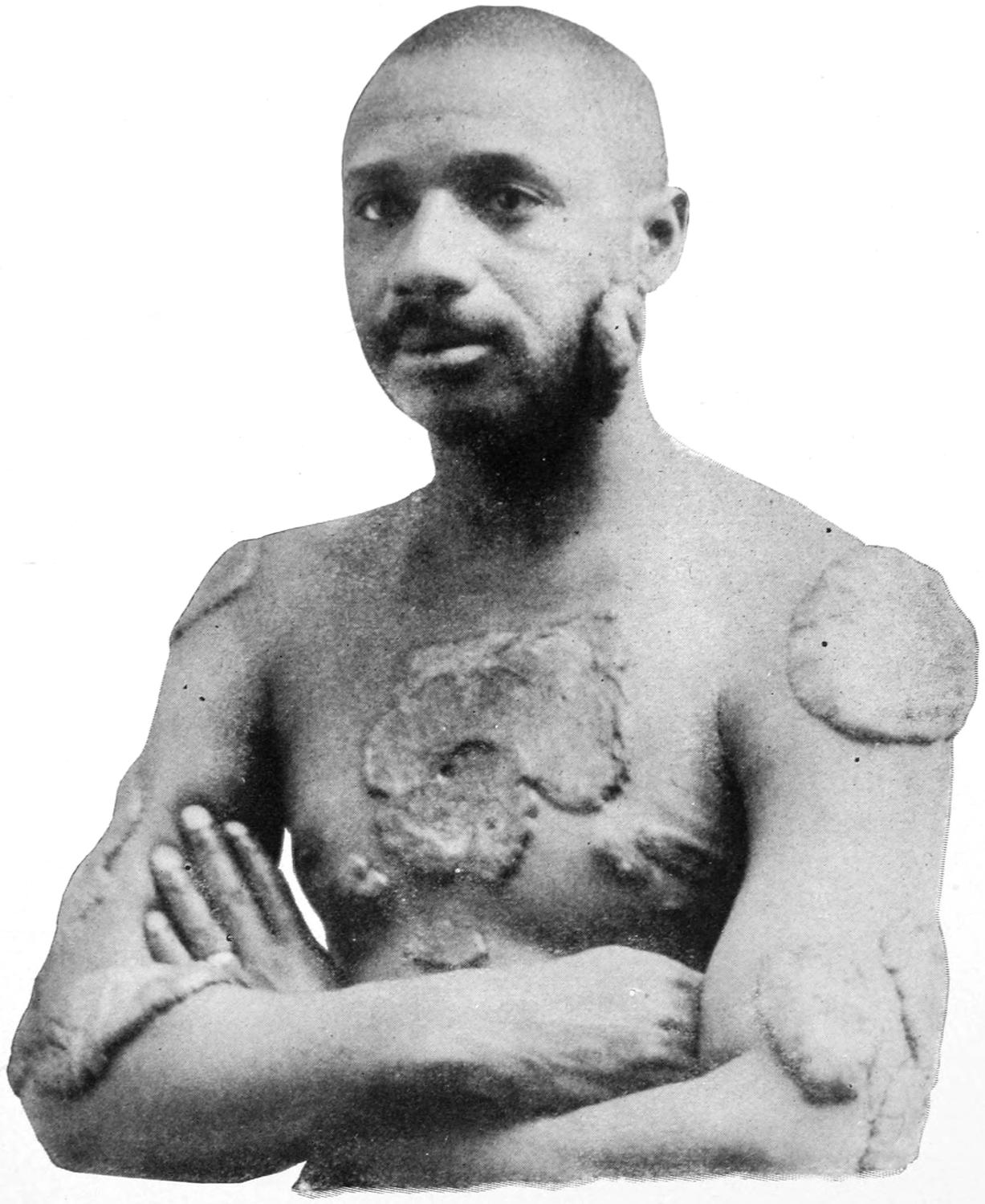
Keloid. (Hardaway.)
[313]
—The surface indication is always for excision or eradication, but one cannot give the slightest guarantee against recurrence in even worse form in the same scar. Electrolysis may have a beneficial effect on some of the lesions, but will only occasionally prove satisfactory. A number of years ago thiosinamin was introduced, and has perhaps given a larger measure of success than any other remedy. It is used in 5 or 10 per cent. solution, which is injected into and around the growth, and may lead to gradual absorption of the hypertrophied tissue. The pain which the injection produces does not last long and I have seen many excellent results follow its use.
The same injections may be resorted to in general keloidal disease, which is seen most often in the colored race. In negroes it may follow traumatism of the skin surface, and attain the size of a saucer or plate. (See Plate XXIX.)
—Fibroma of the skin may happen at any time and is likely to develop in the finer branches of the cutaneous nerves, where it will constitute a small tumor, known as painful subcutaneous tubercle. These little tumors attain the size of a pea and appear between the skin and superficial fascia. Sometimes they are painful and are always tender. Unless thoroughly removed they tend to recur. Nevertheless complete removal is the only remedy.
—A much larger, softer, and more complex tumor is that known by Virchow as fibroma molluscum. These tumors may attain large size, and may be single or multiple. Over four thousand of these lesions have been counted on one subject. They develop from the connective tissue of the cutaneous nerves, and involve later the globular and follicular structures of the skin, softening and undergoing such changes as to deserve the adjective molluscum. Changes analogous to these lead to what has been described as dermatolysis, i. e., hypertrophy of the skin, with loosening of the subcutaneous tissue, by which it is thrown more or less into folds. Another clinical expression of the same condition has been known as pachydermatocele, in which pendulous masses of skin hang from various parts of the body, especially the face and neck, and undergo pigmentation and other changes.
—These lesions can be excised, always with temporary cosmetic improvement, but not always with a guarantee against recurrence of the trouble.
—This name is given to a leathery induration of the skin occurring in circumscribed areas, which have been called “morphea,” or in diffuse patches, which shade off into surrounding normal skin. The first indication is a stiffening accompanied by some thickening and hardness. Sometimes the affection is painful, and the brawny hardening which it produces makes it irksome and uncomfortable. The skin thus affected can not be picked up between the fingers, and is more or less adherent to the tissues beneath. When the difficulty is pronounced the sweat and sebaceous glands cease to functionate. If it occur about a joint the movement of the latter may be interfered with, even to the extent of producing ankylosis. Wherever it appears there is impediment to motion and flexibility of the parts beneath. The tendency usually is to spontaneous disappearance with atrophy. While subsiding at one locality it may recur in another. Upon the hands it may effect such great disturbance of function as to produce what has been described as “sclerodactylia.” The skin over bony prominences, when irritated, may break down; ordinarily it does not go on to ulceration.
—The pathology of scleroderma is very obscure. Whether it depend upon primary disturbances of circulation, both of blood and lymph, or whether it is produced by cellular hypertrophies has not been determined.
The characteristic induration of this disease is not imitated in other affections except scleroma neonatorum, but it may, nevertheless, be confused with the infiltration of tuberculosis, of syphilis, or of malignant disease. While the disease persists, in most cases it is not often fatal.
—It is to be treated mainly by tension, the general and constitutional conditions by massage, and inunction with soothing oils or with the ichthyol-mercurial ointment. It has been successfully treated, as is keloid, by the subcutaneous use of a 10 per cent. alcoholic solution of thiosinamin. The ultraviolet rays and even the x-rays, used judiciously and carefully, may also be of service.
—This form of tumor is to be differentiated from rhinoscleroma, the latter being due to a peculiar specific bacillus, while rhinophyma is a filth disease,[314] due to hypertrophy of the sebaceous structures of the nose from obstruction of the sebaceous ducts. It is often seen among alcoholics, perhaps less frequently at home than abroad. Pathologically it consists of enormous and irregular hypertrophy of the sebaceous gland elements and connective tissue of the skin of the nose. Each hypertrophied gland secretes in proportion to its increase in size, and even the vessels of the part become engorged. In consequence there results a lobulated, distorted, most disagreeable appearance, which often becomes exceedingly offensive. The tumors thus formed sometimes increase to a size sufficient to interfere with breathing and with feeding. The resulting nasal enlargement is usually trilobed. The first impetus to the overgrowth comes sometimes from such cutaneous irritation as frostbite, or local irritation of some kind.
—The treatment of rhinophyma consists in the unrestricted use of scissors and the sharp spoon, with the preservation of so much of the integumentary structure as may serve to cover the reduced dimension of the nose. These lesions will bleed freely at first, but bleeding is usually easily checked. When a plastic covering of the defect is impossible, the surface may be left to granulate, with a certain feeling of security that the cicatricial contraction following will reduce the enlargement to normal proportions.
—This name is applied to a macular lesion, papillary or tuberculous, marked by the appearance of yellowish spots, occurring singly or in groups, often about the eyelids, but seen anywhere upon the skin. When occurring in papules it is called xanthoma planum; when in nodules, xanthoma tuberosum. There is a variety met with in diabetes which is temporary and usually disappears spontaneously.
—The treatment for xanthomatous patches is either electrolysis or complete excision, under local anesthesia.
—Keratosis is a term applied to thickening of the normal epidermis, occurring in limited areas, the skin being transformed into tense or almost horny tissue. The form which occurs in elderly individuals is called keratosis senilis. It occurs upon the face, the hands, and forearms, but may be seen on any part of the body. The involved areas become discolored, sometimes by true pigmentation, more often by a deposit of dirt. As long as epithelial reproduction occurs away from the basement membrane the lesions are simple and innocent, but in elderly people it requires but little irritation to provoke a down-growth of epithelium, and then the development of epithelioma is rapid.
—These reduplicated epithelial elements can be kept soft by an application of equal parts of glycerin and liquor potassæ. After being softened they may be easily scraped down to a normal level, but will later reform. If they begin to ulcerate they should be excised. Should excision be declined the area may be treated with the thermocautery or with one of the caustic pastes.
—These have already been mentioned in the chapter on Tumors, under the head of Angioma. So far as the skin is concerned they usually occur in the shape of nevi (called strawberry growths) or the more disseminated form, sometimes involving considerable areas, commonly known as “port-wine marks,” which are essentially cutaneous telangiectases, are almost always of congenital origin, and frequently appear in complete form even at birth. They may occur rapidly or slowly. An isolated nevus should be treated by complete excision. Large vascular areas, or port-wine marks, are best treated by repeated electrolysis. If treated early they are sometimes eradicated by the local use of sodium ethylate.
The so-called nevus pigmentosus, or pigmented mole, is generally of congenital origin, and may or may not be accompanied by vascular changes. It is not infrequently covered with hair, and sometimes forms a patch of considerable size, often upon the face. These lesions occasionally occur in such form as to entitle them to be styled nevus verrucosus or nevus pilosus. Occurring upon the back or trunk they are usually disregarded. When upon the face they should receive surgical treatment.
—Excision is, of course, the best method of treatment unless a disfiguring scar be feared. This can usually be prevented by proper plastic methods. When excision seems inadvisable electrolysis is the next best method of attack. No matter how vascular may be the lesion itself, the vessels a short distance from the margin of these growths are rarely dilated, and hemorrhage is not a feature which need deter one from radical treatment.
[315]
—This has also been described in the chapter on Tumors. A circumscribed form is occasionally found in or beneath the skin. It occurs early in life, constitutes a more or less sessile tumor, which collapses on pressure, fills slowly, its surface being often irregular, warty, or horny. Should the surface be injured lymph will escape rather than blood. An extended form of it constitutes one kind of elephantiasis. (See chapter on Lymphatics.) Any septic infection of a growth of this character is likely to result seriously and at once.
—The best treatment is excision under thorough aseptic precautions; next to this is destruction with the cautery, which will lead to resulting sloughing and cicatrization.
—All forms of cancer may appear, primarily, in or upon the skin. From the ordinary surface epithelium springs epithelioma; from the glandular elements possibly round-cell carcinoma; and from the mesodermic elements any of the radical varieties of sarcoma, while endothelioma is less common.
—This is a frequent infection of the skin, which may arise primarily as an original lesion, usually following surface irritation, or secondarily, either as the extension of similar disease from other parts or of degeneration of previously innocent epithelial tumors. Epithelial outgrowth, so long as it be an outgrowth, and do not transgress the limits of the basement membrane, is essentially innocent in character; but so soon as growth in the downward direction begins we have the beginning of a skin cancer, which may proceed to fatal extent if not promptly recognized and properly treated. These growths vary very much in rapidity and malignancy. Occurring upon surfaces which are kept constantly moist and warm they develop more rapidly, as upon the tongue, within the vulva, rectum, etc. The slowest form of growth of this kind is the so-called rodent ulcer. Epithelioma which begins in or upon the skin or mucous membrane tends to spread to and involve everything in its neighborhood; even bone and cartilage succumb to its ravages, and, becoming involved, lose all their characteristics and melt away in the surrounding ulcer. This produces in the course of time hideous and serious developments. No tissue is exempt from its ravages, and yet life may be prolonged for many years, even when the face is almost entirely eaten away. Epithelioma and rodent ulcer have been described in the chapter on Tumors.
Fig. 108
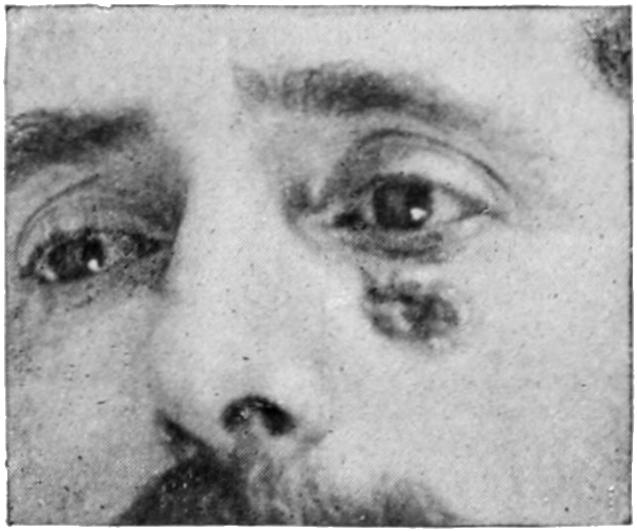
Epithelioma.
More deeply seated carcinomas of the skin infiltrate in both directions alike, and grow downward, sometimes in cylinder form, thus giving rise to a clinical type called cylindroma. Lenticular carcinoma is also described as differing from the ordinary epithelioma, in that it exhibits a true alveolar structure. This form is rare, and is distinguished from the common form by the absence of the so-called “pearly bodies,” which characterize common epithelioma. The lenticular form is most often seen in recurring cancer of the breast, or in the vicinity of scars showing where deep-seated cancer had existed.
—Epithelioma in its various forms should be distinguished from skin lesions due to syphilis and tuberculosis. A diagnostic table has been given (see p. 293) by which diagnosis as between it and lupus may ordinarily be made. The lesions of syphilis are usually multiple and accompanied by other manifestations which stamp their character. There is, moreover, usually a history which will be suggestive if not actually helpful. In cases of actual doubt, as upon the tongue and elsewhere, the therapeutic test may be applied. If resorted to, it should be vigorously made. When mercurial inunction is thoroughly practised, and the internal administration of the iodides effects no improvement within three weeks, the hypothesis of syphilis may be abandoned.
All cancerous lesions tend to advance and to destroy in spite of all local measures. There never appears about them any indication of a tendency toward cicatrization, and, while the edges of malignant ulcers may be thickened and everted, the more central portions are always excavated. They cause, moreover, involvement of the adjoining lymphatics, although this may be said as well of syphilitic and tuberculous lesions.
—Concerning the treatment of epithelioma and other malignant skin diseases there is little to be said which has not already been summarized in the general[316] considerations concerning the treatment of cancer. Radical excision of the original lesion, in its early stages, will usually lead to final recovery. If there be involvement of the lymphatics the indication is made thereby more positive for cleaning out all infected areas, while, at the same time, the prognosis is rendered less favorable. There comes a time in the history of all these cases when excision can be recommended only as a palliative measure, i. e., when it may be regarded as useless. In the more hopeless cases benefit will but rarely be obtained from the use of x-rays, ultraviolet light, or radium.
—Paget’s disease includes lesions now regarded as a precancerous stage, which appear upon the breasts and around the nipples of women during the middle decades of life. Something similar is seen in other parts of the body and in both sexes, but it is most common around the nipple on one side. For a long time it appears as an ordinary eczema, which, however, does not tend to heal but to spread, while the skin beneath becomes more or less infiltrated. A gradual retrocession of the nipple is usually seen. Certain discomfort accompanies the lesion, which may go on indefinitely until it becomes unmistakably cancerous. This is a precursor not so much of round-cell cancer (scirrhus) as of epithelioma. Eczema of the nipple is to be regarded with suspicion, especially when occurring after the menopause. Until diagnosis is fairly established it is best treated with soothing applications. So soon as the cancerous stage has been determined the breast should be removed. (See Plate XXVI.)
Other forms of malignant or border-land tumors which occur upon the skin are chimney-sweeper’s cancer, paraffin cancer, and that met with in aniline workers. Chimney-sweeper’s cancer was the name applied to epithelioma of the scrotum occurring among a class of laborers whose occupation is now almost entirely extinct. It began usually as papilloma and merged into epithelioma. Among workers in paraffin and coal-tar factories there is an analogous lesion, the result of surface irritation, the skin becoming dry, thickened, covered with acne-like pustules, and then with papillomas which ulcerate and frequently change over into true epitheliomas.
—Only the outer layers of the skin are truly epiblastic. In the depths of the integument mesoblastic elements enter largely, and from these various forms of sarcoma may develop. These have already been treated in the chapter on Tumors. They may be single or multiple, and a general disseminated sarcomatosis is occasionally observed. It corresponds to miliary tuberculosis, but presents many distinctive lesions in the skin, by which it may be easily recognized. A form of multiple pigmented sarcoma involving the hands is represented in Fig. 109. These growths are almost always tender on pressure and more or less painful. They coalesce and finally form fatal lesions.
—This term was introduced by Virchow, who made it cover all pigmented growths. By common consent it is today limited to tumors of the skin and uveal tract which contain pigment; metastases may occur in any or all of them. They occur as malignant degenerations of nevi, moles, and other small growths. Pathologists are still disputing as to whether they should be considered sarcomas or endotheliomas. The coloring matter which they contain is amorphous, finely granular material, lying between the cells in moles, but occurring free in the tissues and blood and even in the urine. It is soluble in strong alkalies, from which it can be recovered as melanic acid, containing a small proportion of sulphur. Of its origin nothing is positively known. It seems to be generally accepted that the deposit of pigment is not of itself a causative agent of the growth of the tumor, but that the growth of cells and their pigmentation are coincident processes. Johnston has offered much evidence lately to the effect that growths from nevi are really of endothelial origin. Hutchinson has described melanotic whitlow. (See below, the Nails.)
Melanoma is a pigmented ulcerating neoplasm, which possesses at first only a local malignancy like that of rodent ulcer; the more it assumes the endotheliomatous type of growth the more it tends to disseminate and to prove fatal.
The melanoma arising from a mole or nevus, thus known as melano-endothelioma, begins to increase in size and becomes more full, as well as to assume a darker tint. For a variable time it is a single, rather firm, gradually growing, flat tumor, rarely ulcerating, but sometimes exuding a thin dark fluid. Suddenly there appears rapid local spread as well as dissemination. The latter may be first noted in the adjoining lymph nodes. Thus numerous secondary tumors may be felt in and beneath the skin,[317] at first colorless, becoming more or less rapidly pigmented. Metastasis may take place to every organ in the body, but usually the liver and lungs—less often the brain—are involved. In one case known to the writer the heart was a mass of nodules of this same secondary character.
Another expression of the same serious condition is seen in a lesion called by the French malignant lentigo, which also begins with pigmented spots, on the feet of old men, sometimes upon the face. These lesions cause thickening of the skin and early ulceration.
Rodent ulcer, which is one form of epithelioma, occasionally assumes the melanotic type, and is called melano-epithelioma.
Fig. 109

Fibrosarcoma of hands. (Hardaway.)
The most marked collection of pigment in the human body, within small space, is along the uveal tract within the eye, and orbital melanomas are not infrequent. Beginning within the sclerotic they rapidly perforate this dense membrane and spread to adjoining tissues, while dissemination and metastasis occur early and rapidly.
—For melanoma there is but one successful treatment, and this is successful only when practised early, i. e., complete excision or destruction. Every mole, nevus, or other skin lesion which shows the slightest tendency to changes noted above should be promptly excised, along with a wide area of its surrounding tissue. It may be thus possible to make a radical cure. Neither x-rays nor any other less radical method of treatment will have the slightest effect. The treatment of any case left to itself until mistake in diagnosis is impossible will probably be of little avail.
The only lesions of the hair and hair follicles that concern the surgeon are those which have been described under the head of Syphilis of the Skin, or some of the congenital[318] growths, such as plexiform neuroma, lymphangioma, etc., whose surfaces are frequently pigmented and hairy, and may call for excision, along with the underlying tumor.
—Onychia implies any disturbance of the nail border and matrix. Simple onychia occurs frequently in the fingers of marasmic children. It is evidenced by softening and swelling of the skin around the nail, by more or less pain, disturbance of circulation beneath the nail, which becomes finally loosened, sometimes leaving a foul ulcer. This ulceration may extend and involve nearly the whole finger. It may occur in one or in several fingers. Lesions of this kind are regarded as local infections, occurring usually in vitiated constitutions. It is a common expression or complication of syphilis; when of such origin it yields readily to treatment; at other times it is often slow and tedious. Except in specific cases, where mercurials locally and internally will usually be sufficient, the treatment should be radical and should consist of thorough exposure of the ulcerating and fungous surfaces, thorough curetting, and the use of suitable caustics and antiseptic dressings.
—Onychia maligna implies, according to some writers, a more distinctive type of phlegmonous lesion, while the term has also been applied to malignant ulcers, sometimes pigmented (see Melanoma above) and sometimes of more ordinary type. In either type of lesion granulation tissue may be exuberant and fungating, and it is possible that at times there will be doubt in diagnosis. The finger-tips, with their peculiar tactile sensibility, should never be sacrificed unnecessarily, yet any malignant lesion calls for amputation of the finger.
—This is due almost invariably to ill-fitting footwear, the toes being crowded into too narrow shoes, with too high heels. The real lesion is not so much an excessive growth of the nail as overgrowth and overriding of the skin margin around the matrix. It is painful and annoying, sometimes even disabling. The maceration of a perspiring foot in a warm and tight shoe serves to aggravate the difficulty. Palliative treatment is afforded by chiropodists and quacks, who pack cotton beneath the edge of the nail and keep patients under treatment for indefinite periods, never remedying the footwear and never curing the case. In simple cases it is usually sufficient to excise a portion of reasonably healthy skin on either side of the terminal phalanx, in order that by cicatricial contraction the skin may be drawn away from the nail border. Serious and long-standing cases are best treated by avulsion of the nail, which may be usually performed under local anesthesia or by the aid of nitrous oxide gas. The blade of a knife or scissors is driven under the centre of the nail sufficiently to ensure its passing completely beneath the hidden matrix. The nail is then split in the middle, each half seized at its split border by strong forceps, and by a rapid movement torn loose from its bed. The border of the skin should be scraped, after which a simple dressing suffices, providing the operation has been performed with proper antiseptic precautions.
Many an individual is tattooed in youth who would gladly be relieved of the discoloration later in life. Tattoo marks are difficult to erase. The following is a method attributed to Ohmann-Dumesnil: “Wash the skin with soap and water, then with eight or ten fine cambric needles, tied together and dipped in glycerole of papoid, tattoo the stained skin, driving the needles into the tissues so as to deposit the digestive in the corium, where the carbon is located. Repeat as necessary. The pigment is liberated by the digestant.”
[319]
Fasciæ and aponeuroses are such non-vascular and indifferent tissues that they have practically no primary diseases, except such fibrous and malignant tumors as have their origin in them; nevertheless they suffer in a variety of morbid processes. They lose vitality and break down under the influence of both acute and chronic septic infections. By virtue of their resistant structure, when they slough they break down slowly and the process ends usually with the help of scissors and forceps. Many an old suppurating lesion, especially of the hand and foot, is kept active by the fact that dense, fibrous tissue remains concealed, which ought to have separated. Under these circumstances free incisions should be made and all necrotic tissue trimmed away.
Pus which has formed beneath these fibrous investments will give pain largely in proportion to the intensity of the process and the unyielding character of the fasciæ; hence the urgency of early incision in case of deep phlegmon. Moreover, the direction of least resistance may cause pus when confined to travel where its presence is most undesirable, as from the neck beneath the deeper muscle planes down into the thorax. When pus escapes from beneath firm tissue it is usually by a small opening, after which it may spread out again beneath the skin before finally escaping. This condition has been called “collar-button abscess.” Care should be exercised in opening the superficial collection not to miss the small opening. The fascia must be split sufficiently to permit of thorough cleaning out of whatever collection there may be beneath it.
In the presence of cicatricial contraction of the skin, in shortening of muscles by chronic spasm, as in wryneck, or in certain deformities—for instance of the foot—numerous signs of a shortening or contraction of fasciæ and aponeuroses are seen. In many instances of club-foot it thus becomes necessary not merely to divide tendons but to make extensive incisions through the plantar aponeurosis or elsewhere, in order to release sufficiently the parts whose extension is desired. Underneath the joint contractures which have been produced by burns and their resulting scars similar conditions will be found, which in old and extensive cases constitute bridles of dense tissue that make it almost impossible to release the parts.
Dupuytren’s contraction presents the most serious and insidious appearance of slow but almost irresistible contraction of fibrous elements which the human body presents. It is produced by contraction of the palmar fascia, with its numerous minute prolongations, rather than by flexor tendons. It is seen in the hands of men who from the nature of their occupations are subject to much irritation of the palmar surface. It begins nearly always in the fourth or fifth fingers, but may spread to and involve all the digits and even the thumb. The view held by Adams and others that it is a chronic hyperplastic inflammation, with scar-tissue contraction of the palmar fascia and of the adjoining connective and fatty tissue, which does not involve them evenly, but only at certain points, is correct, at least when small nodules may be felt in the palm which are the precursors of the disease. Either hand may be affected, but generally both are involved. It is found in from 1 to 2 per cent. of those who depend upon their hands for their support. Deformity may proceed to pressure dislocation and finally to ankylosis. Its causation then is very obscure; it is rarely the result of definite injury, but follows continued irritation of the surface. It seems to have a local origin, and yet it is frequently associated with the gouty diathesis to such an extent that the prolonged use of alkalies will relieve some cases. The first significant sign of the condition is the formation[320] of small nodules in the palm of the hand, as stated, and this usually precedes the finger contraction by a year or two.
Fig. 110
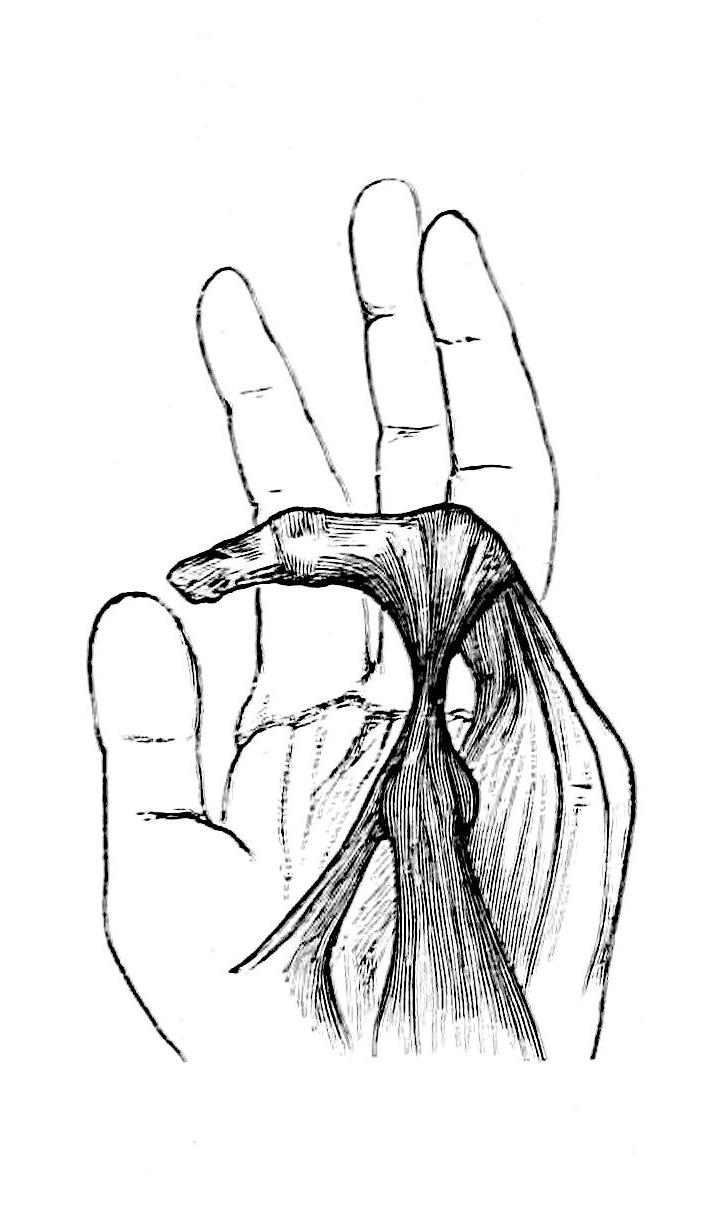
Dupuytren’s contraction. (Adams.)
Fig. 111
Dupuytren’s contraction of palmar fascia, showing contracted fingers. (Burrell.)
—There is considerable difficulty in treating these cases satisfactorily. Cooper advised subcutaneous division of the tense bands and forcible stretching of the fingers; this rarely proves sufficient. Adams advocated multiple sections made with a small tenotome, which is more effective. The best method is that of Kocher, which consists in excision of the fascial bands by longitudinal incisions along the cords, and the dissection of the skin from the underlying fascia. The cord is carefully dissected, with its prolongations and then completely removed, while the margins of the skin wounds are closed with sutures. The more thoroughly the dissection is performed the more satisfactory the result. The fingers should be straightened and kept from contraction by the use of a mechanical device. In desperate cases the entire skin of the palm has been removed, with the diseased fascia, and a plastic operation made with skin taken from the thigh or the chest, the flap being sutured in place but not detached completely for ten to twelve days.
Two somewhat allied conditions involving the hand and the foot are the so-called lock or trigger-finger and hammer-toe.
Lock or trigger-finger implies a peculiar obstruction to free movement of the finger, which requires extra effort and then is overcome quickly, as if a knot had been slipped through a small opening. It is supposed to be due to a thickening of the tendon at some point, as by a small fibroma, which becomes entangled along the course of the sheath, through which it is moved with difficulty. It is probably due to a local irritation, as in the case of Dupuytren’s contraction. Injury to the tendon sheath may also produce a similar condition.
—Should it fail to respond to rest and massage the sheath should be opened and the cause of the difficulty sought out and removed.
[321]
Hammer-toe produces deformity with more or less ankylosis. An angle is formed between the first and second phalanges, and the tip of the toe is made to bear more than its proportion of weight. This deformity is in large degree due to the use of shoes which are too short. In consequence there will develop over the protruding joint a corn or bunion.
—Should the trouble come on in childhood the toes should be fastened to a straight splint and shoes for a time abandoned, while later they should be properly adapted to the needs of the case. In troublesome cases complete excision of the involved joint gives satisfactory results.
Acute inflammation of a tendon sheath is known as tendovaginitis or tendosynovitis. It always implies an infection, and occurs about the hands and feet. It is a frequent complication of felons. Many felons begin in such a manner that it is difficult to decide which part of the fibrous structures of the finger is first involved. Infection having once occurred within a tendon sheath will travel rapidly until it meets with a natural barrier. The frequency of these lesions makes it important to recall here the anatomy of the tendon sheaths of the hand. There is a common palmar tendon cavity, which connects with the thumb and little finger and the space above the annular ligament, but communication with the first, second, and third fingers is ordinarily destroyed. This accounts for the apparent vagaries of cases where infection beginning in the thumb spreads to the little finger before the others are involved. It will also show the location where incisions should be made.
Fig. 112
Cicatricial contraction and deformity resulting from consequences of neglected phlegmon and osteomyelitis of hand. (Lexer.)
—Suppurative tendosynovitis needs prompt intervention, as adhesions may result from retention of exudate, or lest necrosis of tendon occur from perversion of its nutritive supply. Ordinarily it is the result of a local infection, perhaps through a small, trifling surface irritation, but it results occasionally as a metastatic expression of gonorrhea, or distinct septic infection. A gonorrheal tendosynovitis is, however, less likely to suppurate, but more likely to assume the plastic form and interfere with function by producing adhesions between a tendon and its sheath. The combination of virulent bacteria and susceptible tissues will produce local destruction in almost as short a time as in the appendix. The pain is intense, because of the inelasticity of the structures.
Fig. 113

Suppurative tendosynovitis (felon), with sloughing tendons and necrotic bone. Unfortunately poulticed for two weeks. (Lexer.)
Treatment.
—Every appearance of this kind calls for early incision, by which not only the skin but the tendon sheath as well should be freely incised. An incision at either end of the involved sheath, with flushing and drainage, may save a tendon and preserve function. Incision should not be delayed, as destruction may have occurred and[322] deformity be the result. When the common palmar sheath is involved a long incision from the base of the index finger, around the base of the thumb and up the wrist to a point considerably above the annular ligament, will afford considerable relief. It will, moreover, shorten the time of ultimate restoration of function.
—Chronic tendosynovitis may be the result of rheumatism, in which case it assumes the plastic form, or of gonorrhea; the same being true of a tuberculous invasion, which may vary much in intensity. In the subacute forms the deposition of tubercles may lead to a plastic outpour which, being detached by constant motion of the parts, is broken into masses whose minute portions become rounded off by friction and condensed by time, and appear as the so-called “melon-seed or rice-grain bodies.” Some of the same material may be found adherent to the walls of such a cavity. In slower forms there is less tendency to plastic outpour, but much more to the formation of granulation tissue, such as is seen in tuberculous lesions in all parts of the body. When, therefore, a case of this general character presents we have the signs of local tuberculosis, or of dropsy of the tendon sheaths, with the fluctuation somewhat modified by the presence in the fluid of rice-grain or melon-seed bodies. Should, in such a case, an acute infection be added we will have the chronic symptoms merged suddenly into acute. A tendovaginitis of this type appears as a ridge or swelling along the course of one or more tendons. It will be elastic and fluctuate in proportion to the distention of the sheath. When the palmar bursa is involved there is usually, in the palm of the hand, a bag of fluid which may be forced above the wrist by pressure, while frequently the little bodies above described are recognizable by the sensations (crepitus) which they produce. The plastic type rarely proceeds to suppuration or ulceration unless secondarily infected. The granulation type proceeds to ulceration and destruction.
Treatment.
—Treatment of the rheumatic and gonorrheal forms is at first rest, with later passive and forced motion, in order to break up adhesions and prevent their re-formation. If one wait too long he meets with great difficulty in these efforts and the cases become exceedingly tedious. Forcible motion should be practised under nitrous oxide anesthesia and should be repeated every two or three days. Meanwhile massage should be employed. If pain or reaction be extreme ice-cold applications should be applied. Extreme swelling may be combated by the use of a rubber glove. If this be worn, ichthyol-mercurial ointment should be used beneath it, in order to promote absorption.
Treatment of the tuberculous cases is often disappointing. Non-operative measures afford but temporary benefit, while operation to be effective should be thorough. It should consist of free incision, with exposure in whole or in part of the affected channel or cavity, thorough cleaning out of its contents, removal of all edematous or tuberculous tissue or granulations, and the use of an antiseptic as strong as it can be employed.
The new opsonic serum treatment, now being placed on trial as this work goes to press, promises much in the treatment of all these septic affections, though detailed statements would be premature.
It was a step in advance in surgical technique when Stromeyer and Dieffenbach, in 1842, introduced the method of subcutaneous division of tendons and aponeuroses, and showed how easily contracted tendons could be lengthened by tenotomy. From their time until somewhat recently tenotomy has held its place in the treatment of various deformities, and until Anger, Gluck, Hoffa, and others have taught the surgical profession what can be done by various plastic and suture methods in overcoming defects and atoning for loss of function in paralyzed muscles. To the surgery of tendons and muscle terminations have been added the further resources of tendon suture, i. e., tenorrhaphy, and tendoplasty, by which latter something more than the mere suture is meant, i. e., the plastic rearrangement and grafting of tendons one upon another.[20]
[20] The method of transplanting one tendon upon another is to be credited to Nicoladoni, who perfected it in 1882. Later it fell into disuse, but was revived in this country, especially by Goldthwait, of Boston, in 1896.
[323]
Fig. 114
Fig. 115
Fig. 116
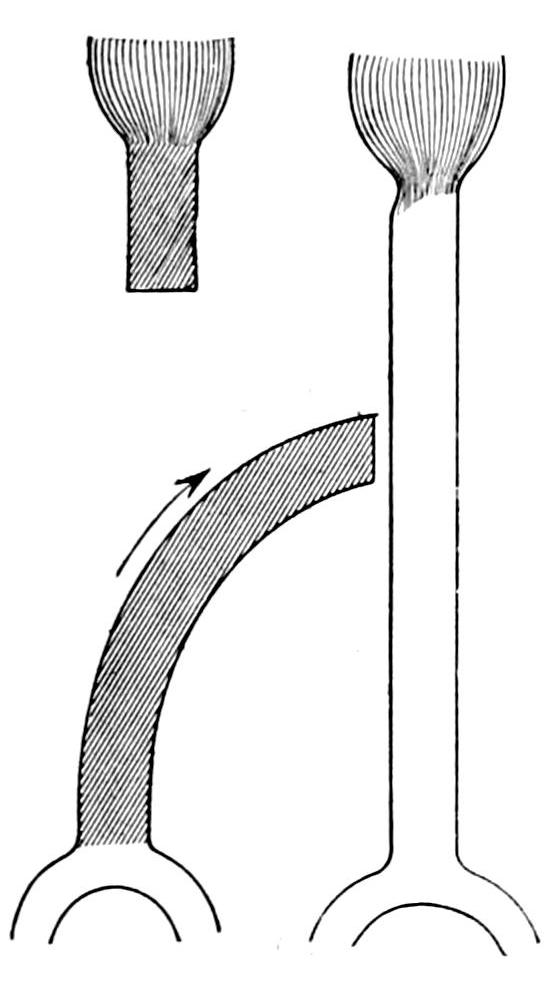
Fig. 117
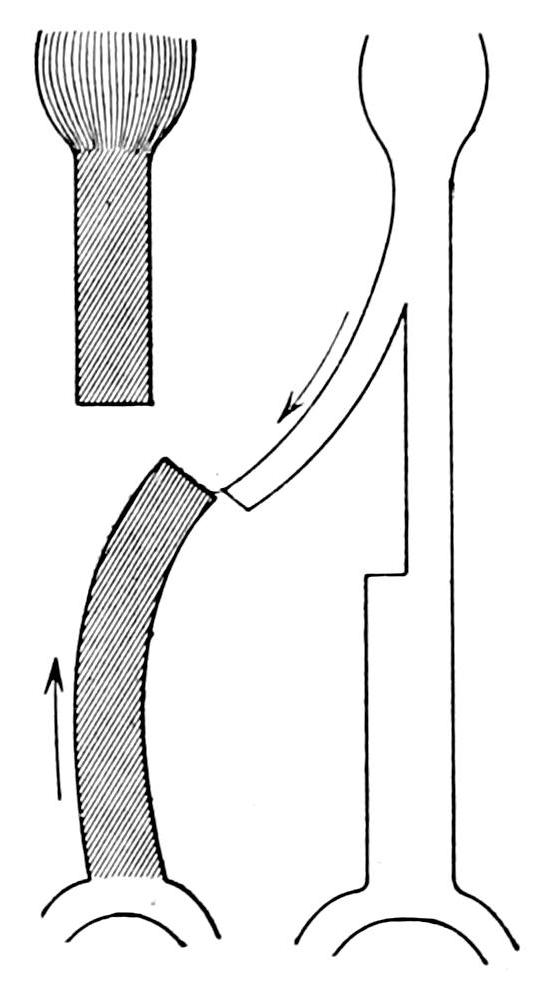
Fig. 118
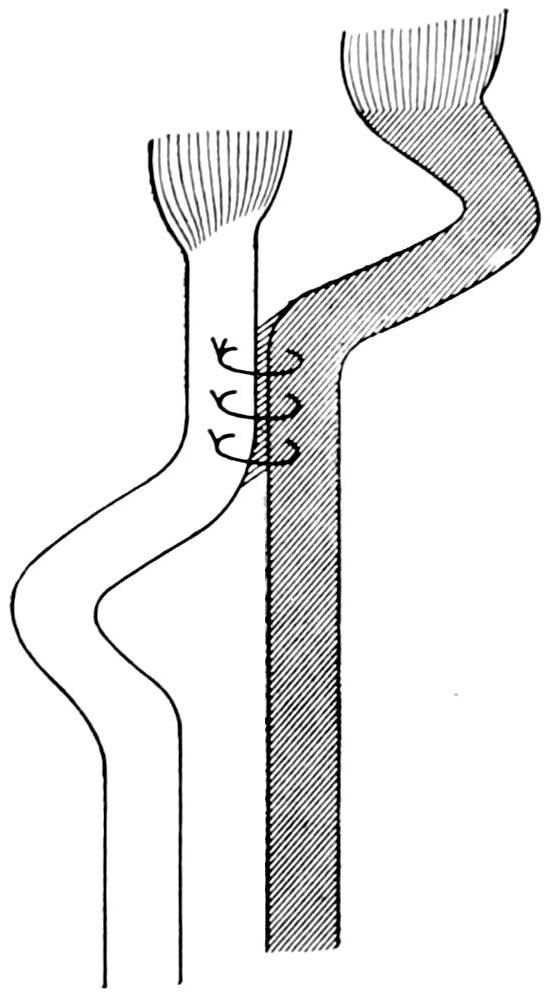
Fig. 119
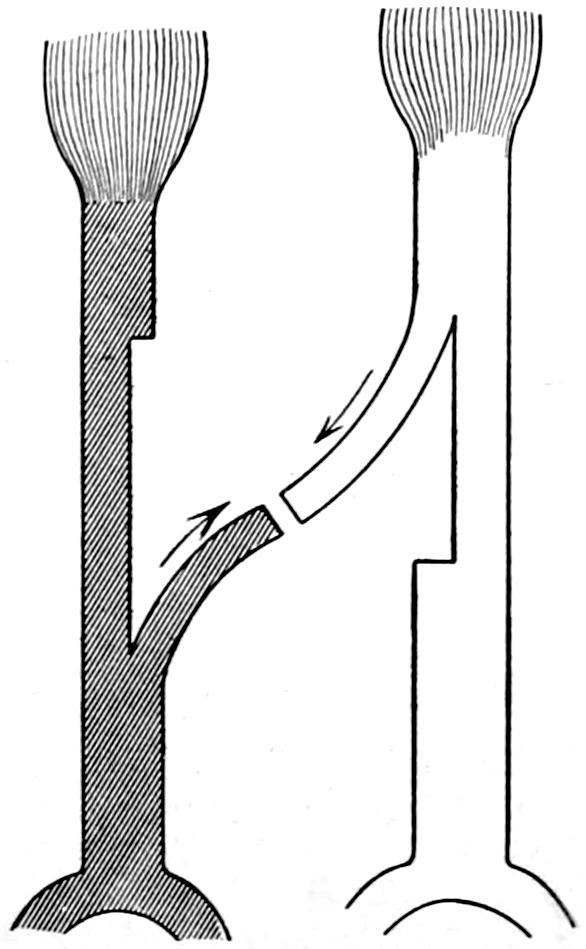
Fig. 120
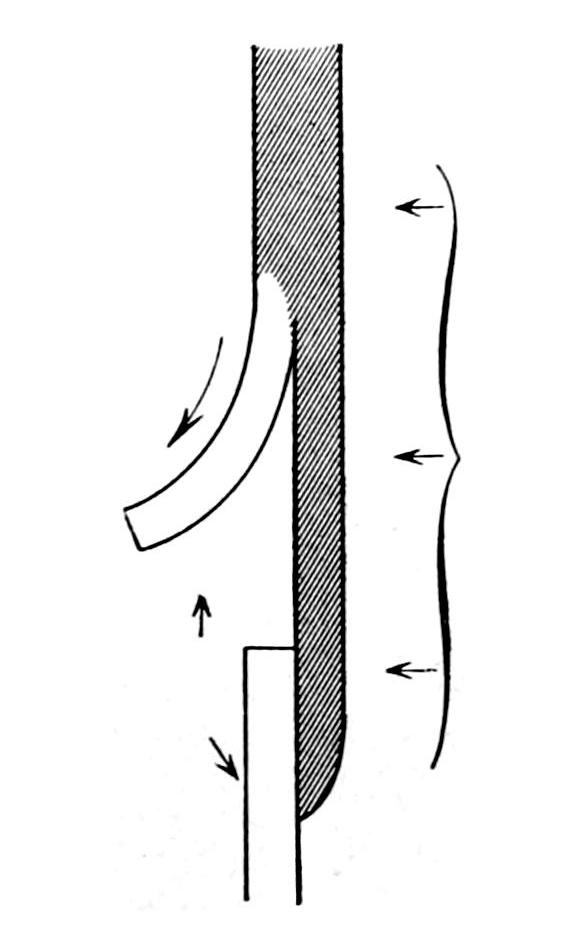
Fig. 121
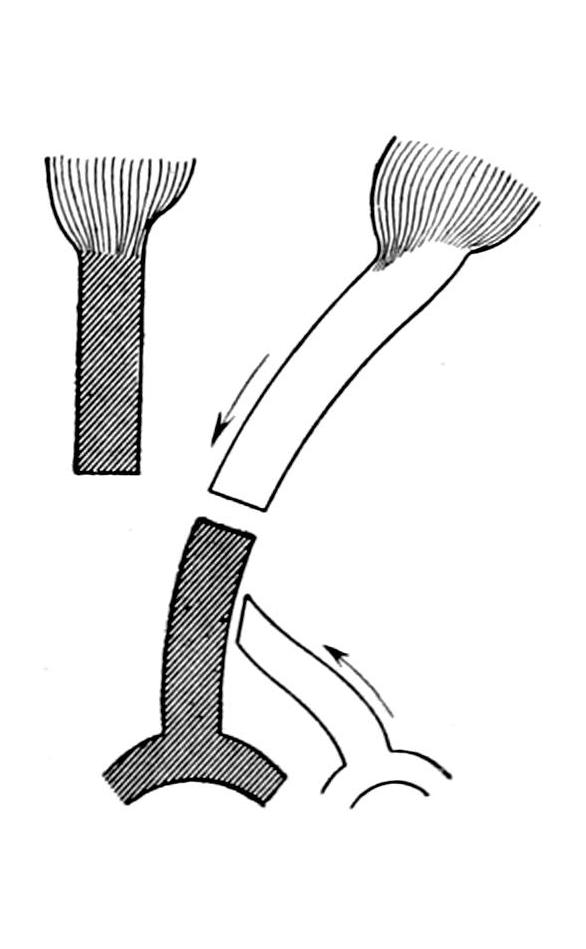
Illustrating various methods of dealing with tendons in tendoplasty. (After Vulpius.)
[324]
Tendon suture is practised as an emergency measure when one or more tendons has been accidentally divided, this being considered now as much a part of the surgeon’s duty as to close any other part of the wound. No additional resource or expedient is needed, it being necessary only to observe the principles of asepsis, which should be maintained in every case. A tendon raggedly divided should be cleanly cut and its edges brought together with formalin-gut or freshly boiled silk. A series of divided tendons should be treated after the same fashion, matching the ends as closely and completely as possible. After uniting the tendon ends, if the case be clean, the tendon sheath should be closed and the parts put at rest, in such a position that no tension is made upon the injured sinew until it is seen to have united.
Fig. 122
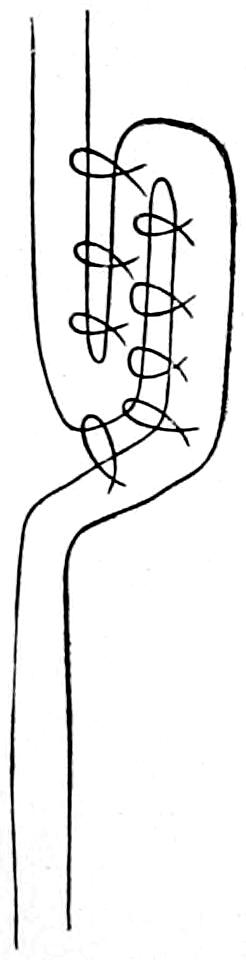
Fig. 123
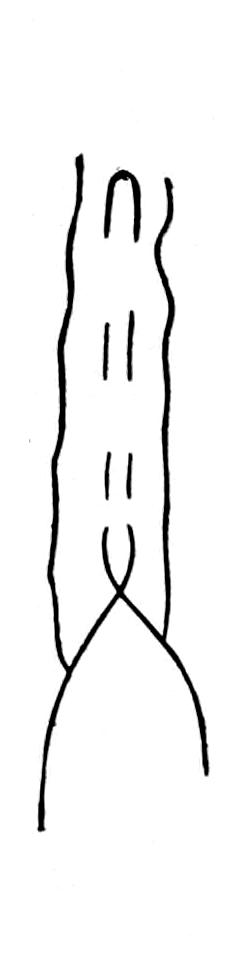
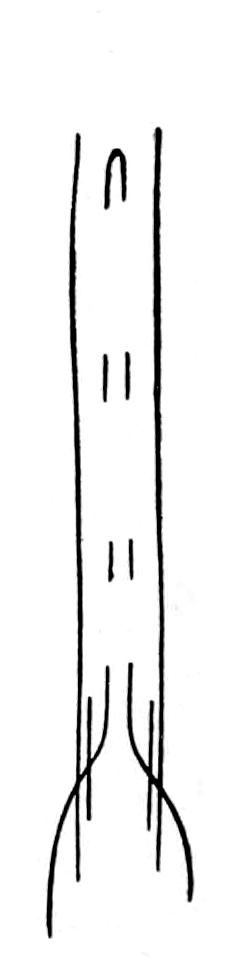
Shortening a tendon.
It was a great service, in which perhaps Gluck figured most conspicuously, to show that when tendon ends could not be neatly coapted an animal material could be interposed in such a way as to serve as a trellis along which cells could group, or around which they might organize, and thus gradually and finally become a part of the complete tendinous cord. Silk and catgut have best served this purpose, and new tendons have gradually formed around these artificial substitutes, to the length of 10 Cm. In every fresh case where there has been such loss of original structure as to justify a measure of this kind, or in certain old cases where tendons have long since sloughed away, it may be possible to resort to these expedients.
It has been possible to transplant fresh tendons from the smaller animals and to see them serve the same purpose in a satisfactory manner.
Among these methods of tendoplasty is tendon grafting, by which a part or all of the tendon of an active muscle is inserted into the terminal portion of a paralyzed muscle and thus made to assume to a greater or less extent the purpose and function of the latter; in other words it assists in ingeniously diverting the activity and direction of a given muscle to a purpose different from its original intent. By this diversion a more equal or equable distribution of muscle force is afforded the parts into which the affected muscles are inserted. For its successful performance only those muscles which are still active can be utilized. Among the simplest of cases where this expedient can be used[325] are those produced by traumatic and peripheral paralyses, or traumatic loss of a given tendon or a set of tendons. It is rarely to be practised as an emergency measure, but as an expedient to be availed of later. It finds its greatest usefulness in cases of long standing. It is equally applicable where muscles and tendons have been divided by injury, or paralyzed by injury to their nerve supply, as well as where deformities are produced by chronic neurotic disturbance, by scars, by excessive callus, etc. It proves equally serviceable in paralyses of spinal origin, particularly those due to anterior poliomyelitis.
Tendon grafting will serve both as a substitute in cases of lost function and as a provision against future deformity. In cases of the ordinary paralyses of children, tendoplasty should be deferred for several months after the occurrence of the paralysis. In the case of growing children it is desirable not to wait too long, as other objectionable features may present themselves. In the congenital and hereditary paralyses and in conditions like athetosis or the dystrophies of syringomyelia, meningocele, etc., also in such conditions as habitual dislocations of the patella, much can be accomplished by a carefully planned tendoplasty. It will be easily seen then how wide a field of usefulness lies before one who familiarizes himself with the recent technique of tendon surgery.
Fig. 124
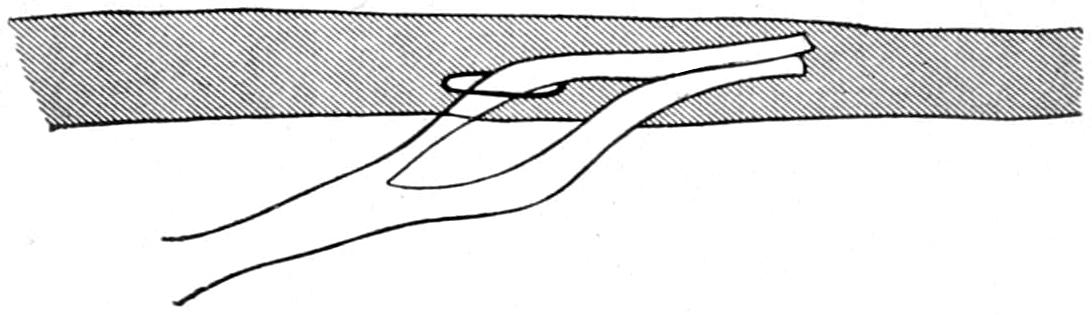
Fig. 125
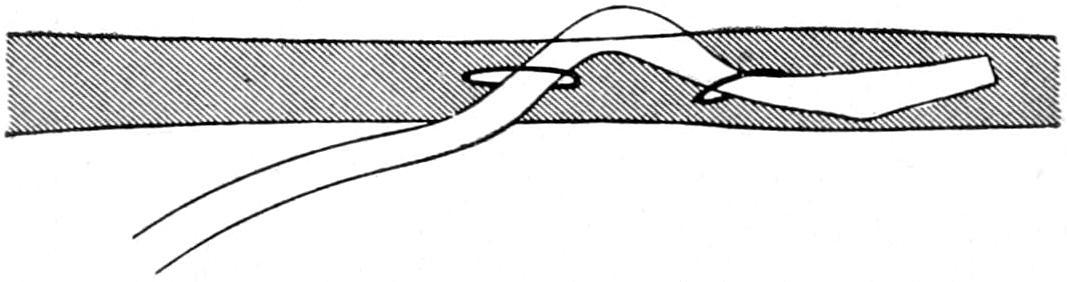
Two methods of tendon implantation and fixation. (After Vulpius.)
Fig. 126

Fig. 127
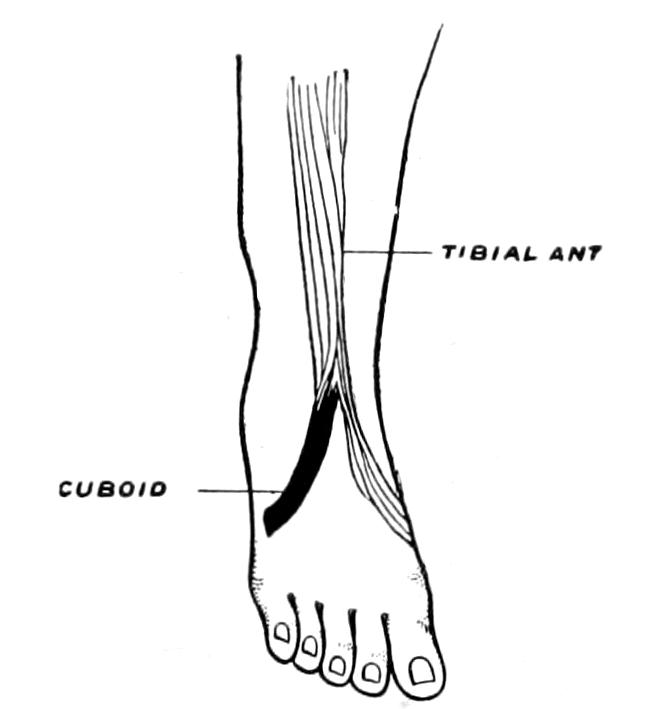
Fig. 128
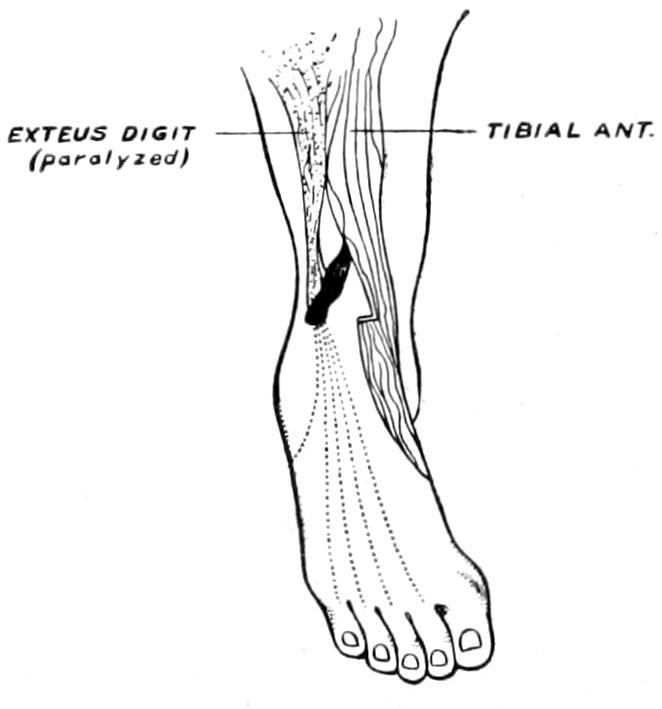
Transplantation of a portion of the anterior tibial tendon, into the bone or into the opposed group of muscles. (After Vulpius.)
So far as technical considerations are concerned these operations should be performed only with the minutest attention to asepsis. When this has been secured a permanent dressing may be applied, the limb being left in the position most desired, and maintained there for several weeks. For this plaster of Paris makes the best support. The use of the rubber bandage will permit the operation to be bloodlessly made, by which it is greatly facilitated. If careful suturing be practised, there will be but little tendency to[326] subsequent oozing or interference with repair. Fine discrimination is always needed in the matter of adjusting the length of tendon ends and the point of their fixation. A useless tendon which has been long stretched over a curved joint will have become elongated, and the tendon to be applied to it should be affixed farther down than would be otherwise necessary. The disposition of the upper portion of the useless tendon and muscle may also call for serious attention. It is rarely necessary to extirpate them. They are already atrophied, and to remove them would be to still further reduce the dimensions of the part. The excluded portions can thus be simply discarded. When there has been deformity with more or less pseudo-ankylosis the malposition should be forcibly redressed and the tendon grafting deferred until a subsequent time; the latter, to be successful, should be performed alone.
Incisions are usually made along and over the course of the tendons to be exposed, but not so close that the cutaneous scar can interfere with the tendon sheath. The lower end of a paralyzed muscle will appear very differently from that of one which is healthy; in the former instance the tissue will have lost its muscular character, and will be yellowish white and fatty. A fascia which has been stretched out of shape may be sutured in folds and will serve of itself to give support and shape to the part which is renewed.
The methods of uniting tendons are so numerous that they can be better estimated by a glance at the accompanying diagrams after Vulpius than by description (Figs. 124 to 128). It is not necessary to utilize all of the tendon of a healthy muscle, as it can be split and a portion diverted to its new function. It is not to be expected that tendons thus arranged will perfectly serve their purpose the first time they are used. There must elapse a period of education of the nerves and muscles whose relations are thus altered, and improvement in the use of the parts thus operated will accrue for months and even years. It is desirable that tendon surfaces thus applied to each other be made broad and extensive in order that their adhesion may be more firm.
Fig. 129
Showing methods of lengthening tendons. (Burrell.)
A modification of tendon grafting consists in implanting the tendon end into the periosteum instead of into some other tendon. There are various ways of making this implantation, either by simple suture or by boring into the bone or canalizing under a periosteal bridge. Fig. 129 illustrates how the tendon of the tibialis anticus can be utilized in both ways. It will thus be seen that a tendon can be given either tendinous, periosteal, or osteal implantation. Tendons thus utilized rarely undergo necrosis or degeneration. So long as the possibility of infection be excluded almost anything can be done with these structures, in spite of their apparent lack of vascularity and vitality.
There are times when it is necessary to lengthen a tendon as well as to shorten it. Fig. 129 illustrates methods by which both of these measures can be performed. Analogous methods have been practised with muscles themselves, although here the circumstances are different and nothing similar can be accomplished. Portions of the pectoralis major have been grafted into the biceps for paralysis of the latter.
Liberating the ring finger in musicians, by dividing the accessory tendons of the extensor communis digitorum, is an expedient suggested some years ago by Brinton. It is made by an incision less than a quarter of an inch long, through the skin and fascia, just below the carpal articulation of the metacarpal bone of the ring finger, and above the radial accessory slip, parallel with and on the radial aspect of the extensor tendon of that finger. The point of a narrow blunt-pointed bistoury is then inserted flatwise beneath the accessory slip down to a point just in front of the knuckles of the ring and middle fingers, where the blunt point should be felt beneath the skin. The bistoury is now turned upward, the middle finger strongly flexed, and the ring finger extended so as to make the slip tense when it is divided. The accessory slip on the other side of the[327] extensor tendon is similarly divided through a distinct incision. Snug compression is made with a bandage over the wounds, with the thumb free, and after two days the patient is permitted to use the fingers in piano-playing in order to prevent reunion of cut surfaces.
Myotomy is a measure seldom practised. It is performed either subcutaneously or by open incision. Tenotomy is indicated whenever contracted tendons need simply to be divided, either in chronic orthopedic cases or after injuries or operations when it is desired to put muscles temporarily at rest. The tendo Achillis has thus been divided to prevent the consequences of muscle spasm when dealing with certain fractures, especially compound fractures of the leg. There are obvious advantages obtaining in subcutaneous tenotomy when properly performed; the freedom from hemorrhage, the minuteness of the opening, the rapidity of healing, are all in its favor. It is performed with a small-bladed knife, known as the tenotome, with either sharp or blunt point, the cutting portion being from 1 to 2 Cm. in length. The sharp-pointed tenotome suffices for its own insertion, the blunt one being used after an opening has been made with a sharp one. The puncture is made obliquely through the skin, which should be drawn a little aside from the site of the deeper opening in order that it may be hermetically closed as it slips back into place. Whether the cutting blade should be turned outward or inward will depend largely on the preference of the operator and the location of the tendon. In some locations, as about the hamstring tendons, the puncture should be made with the sharp instrument and the deeper tenotomy with the blunt one. If the tendons alone have been divided there will be trifling hemorrhage and the puncture can be occluded without entrance of air. Similarly an aponeurotomy may be performed. Not only may the tendons be divided by the open method, but everything else which resists. This is practised more in contracted knee-joint and in club-foot, when operated on by Phelps’ method, than anywhere else. Special indications for the operation will be given in other parts of this work.
This term is applied to a cyst of new-formation, which occurs in connection with the sheath of a tendon, having a lining membrane continuous with the sheath and containing thick, gelatinous, mucoid fluid. It is termed “weeping sinew.” It is often seen on the back of the wrist in connection with the extensor tendons, but may occur in various parts of the body. It probably begins as a hernia of the synovial membrane through a weak spot in the tendon sheath, which tends to increase in size, weakening surrounding structures by pressure, and interfering more or less with the function of the tendon whose sheath is involved. These cysts sometimes connect with joint cavities, especially those occurring behind the knee-joint; as a rule, however, they do not. At first they constitute merely a disfigurement; later they produce natural impairment of function. In the majority of cases the sac becomes finally shut off from the tube with which it originally connected.
When these lesions are new they may be successfully dealt with by forcible rupture, such as can be made by firm pressure. When old, or when rupture has failed, they should be treated by incision, practised the same as a tenotomy, by moving the skin to one side, pricking the sac, turning the blade of the tenotome so as to permit the fluid to be emptied by pressure, and then, by manipulating the point, irritate and do some damage to the sac lining. Such provocation as this will be followed by a hemorrhage, and the resulting clot may obliterate the sac by organization and cicatricial contraction. This failing, excision is the only expedient which promises success. The slightest operation upon a ganglion should be done under aseptic precautions.
[328]
Felon, or whitlow, was discussed in the previous chapter, especially the form which has its origin around the root of the nail. It often originates in tendon sheaths and even in bone or close to it. It is so often accompanied by a suppurative thecitis, i. e., tendosynovitis of destructive form, especially when not primarily incised, that the necessity for early treatment needs to be emphasized. It gives rise to excessive pain, with throbbing, and to swelling of livid hue and intense degree. The parts involved are too essentially fibrous and resisting to yield, hence the intensity of the pain. Deep incision at the earliest moment, for the purpose of relieving tension, is the only proper treatment. To temporize with hot poultices, etc., is to invite necrosis and sepsis. This incision may be made with local anesthesia. Even though little pus be obtained the relief of tension will afford the greatest comfort (Figs. 130, 131 and 132).
Fig. 130

Felon of thumb. (Burrell.)
Fig. 131

Neglected suppurating thecitis resulting in palmar abscess. (Burrell.)
Fig. 132

Same, dorsal aspect. (Burrell.)
A more striking example of similar trouble is that which gives rise to palmar abscess, the suppurative process extending up the wrist beneath the annular ligament, and down into the little finger and thumb. This is not infrequently the result of infection of callosities in the palm of the hand. Infection may travel rapidly, and when confined beneath resisting structures will prove exceedingly destructive; the muscles of the forearm may melt down and great permanent damage be done.
[329]
Here, as when the finger alone is involved, early, free, and deep incision will prove the salvation of the part. These incisions should be made as indicated in Figs. 133 and 134, i. e., parallel with the nerves, tendons, and vessels, all of which should be spared, as well as the palmar arch. Should the latter be divided, the vessel ends may be ligated or the wound packed. If cavities be left by the destructive process they should be opened and the part treated by continuous immersion in warm water, or the openings may be packed with gauze saturated in brewers’ yeast. A few days of this treatment will clean up all sloughs.
Fig. 133
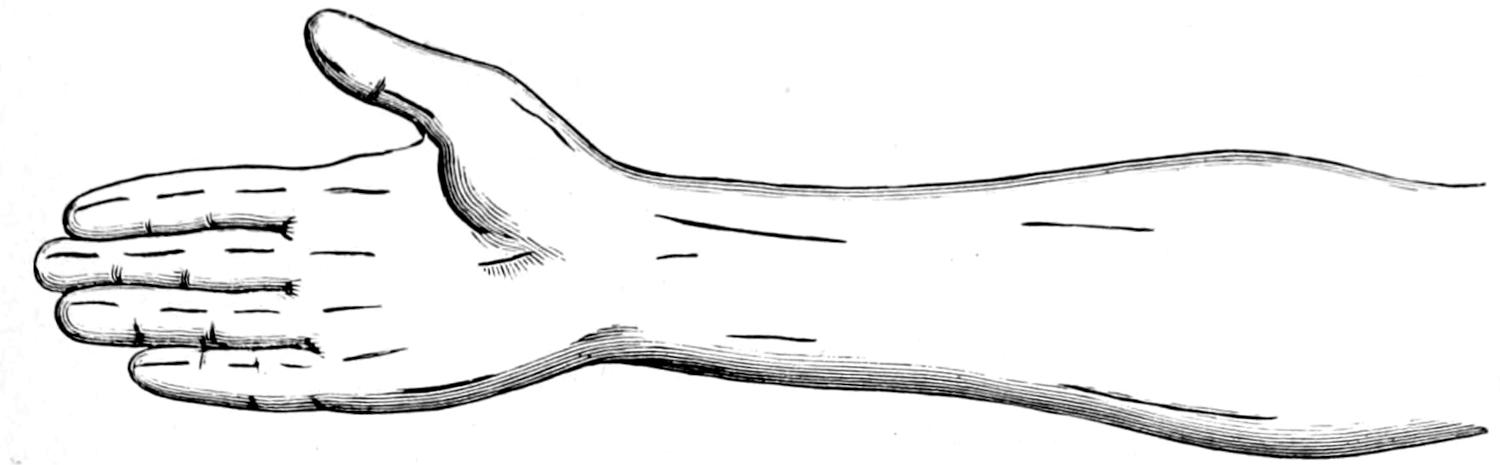
Diagram of palmar incisions.
Fig. 134
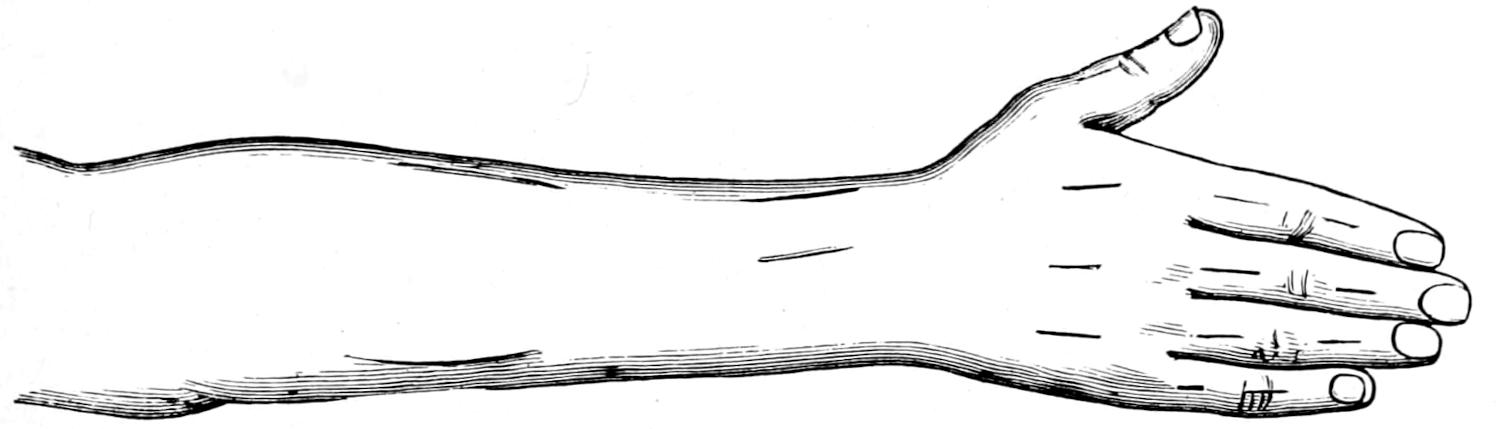
Diagram of dorsal incisions. (Burrell.)
Muscles react like other tissues under the influence of contusions. Hemorrhages not too copious are gradually absorbed, and muscle tissue repairs itself, as indicated in the chapter on Wounds and their Repair. Much outpour of blood into a muscle will temporarily seriously impair its function, while pigmentation or ecchymosis may result after a few hours or days, according to the depth of the injury. There is the same liability to suppuration after infection of muscles as elsewhere. A large hematoma can scarcely form within a muscle, save in consequence of a rupture of a considerable portion of its substance. Strains and sprains of lesser degree of violence provoke impairment of function proportionate to their severity. In nearly every instance there is a certain amount of rupture of muscle fiber and outpour of blood.
Complete rupture across a muscle is unusual. It may occur in the belly of the muscle or near one of its terminations. A tendon may be torn out of a muscle or may itself snap. These accidents are almost invariably accompanied by symptoms that indicate both the nature and location of the injury. A severe strain followed by intense pain, with a sensation of yielding, leaves little doubt as to what has happened. Unless the muscle lie deeply its parting may be appreciated by palpation, though the depression[330] or interval may be obliterated by the outpour of blood. The large tendons of the arm and shoulder have been ruptured by a violent effort, the abdominal muscles by contusions and by such efforts as wrestling, the sternomastoid by excessive traction during forceps delivery, and the tendons of the legs and ankles by jumps during such games as lawn tennis, etc.; while the frequency with which the muscles of the perineum and even the sphincter ani are torn during parturition is well known. It is also well known that muscles are weakened by the exanthemas and the infectious diseases.
—An injury of this kind and of moderate degree seen early may be treated by physiological rest and position. (See chapter on Treatment of Wounds.) When, however, there is marked impairment of function, such as will follow the yielding of one or more tendons or muscle insertions, then suturing offers the greatest promise of a cure. When the quadriceps tendon is torn away from the patella or the tendo Achillis from the heel, prompt suture under aseptic precautions will save a long period spent in partial recovery of function.
Occasionally one or more tendons will be completely avulsed, as when a finger is torn out of the hand and brings with it one or more of the tendons belonging to it. In accidents of this kind six to twelve inches of tendon and muscles may be lost. In such a case nothing can be done except to care for the wound resulting from the injury.
Tendons and muscles are occasionally dislocated, that is, forced from their normal positions. Accidents of this kind usually occur with the long tendon of the biceps, which is torn from its bicipital groove; the peronei and the posterior tibial in the leg, the extensor muscles of the thigh, and those of the back of the wrist. The lower angle of the scapula is normally held down by a small portion of the latissimus dorsi; should this be displaced the scapula rises somewhat in wing form. These injuries lead to more or less loss of function, and, when they become disabling, may justify operation, which would include incision, exposure of the tendon in its abnormal position, and its restoration to its proper place where it should be held by sutures. Such operation should be followed by enforced physiological rest of the part.
Hernia of muscle is the name applied to the escape of muscle through a ruptured fascial or aponeurotic covering. Such a protrusion will be recognized only during the contraction of the muscle and will disappear at other times. When the diagnosis is made the edges of the rent in the fascia should be united by sutures and the part put at rest.
Wounds of muscles in no way differ from other wounds which have been considered in the chapter on Wounds and their Treatment. If circumstances permit there is every indication for the suture of a divided muscle in order that its function may be less impaired after the wound is healed. These sutures, when inserted, should be made to separately include the divided fascia or aponeurosis with which the injured muscle is in relation.
There are numerous painful affections of muscles known as myalgia. It is questionable whether a rheumatism of muscle fiber ever occurs. That which patients describe as muscular rheumatism is not that which it is termed. Sometimes it is the result of previous exudate between muscle fibers, sometimes the result of hemorrhage of interstitial type. Muscles thus affected are more or less tender and give pain when used. It will usually be found that there is some marked toxic condition, such as uric acid, syphilis, or lead poisoning, behind it.
[331]
—Many of the muscle pains of which patients complain after operation, which are also toxic, are relieved by the administration of aspirin in 0.5 Gm. doses. The injection of a small amount of atropine into the body of the muscle will often give relief. Those remedies which hasten elimination, including hot baths and massage, are often of great value.
This may be non-inflammatory and be due to prolonged use of a member, as in writers’ cramp; or toxic, as in lead palsy; or traumatic, caused by minute lacerations and hemorrhage. The more acute forms may be due to extension from neighboring foci or to direct infection. A form of infection involving both muscles and tendon sheaths, and lately recognized, is the postgonorrheal. It has been shown that gonorrhea may produce an active disturbance in synovial sheaths and in muscle structures and a gonococcus myositis, as well as a gonococcus tendovaginitis, are now well recognized. These do not always proceed to suppuration, but may provoke loss of function for some time.
The suppurative form of myositis is seen more often after typhoid and gonorrhea than after the other internal infections, but may occur after any of them. In these cases abscess results in the belly of the muscle involved, while the pus evacuated will show the appropriate organism. It is met with less often in endocarditis and erysipelas.
Any or all the active and destructive infections may occur primarily in muscle structure. They are usually the result of an extension, although they maybe even in this way very disastrous. The amount of muscle destruction that may be seen in a limb after an infected and neglected compound fracture is astonishing.
—Calcification and ossification of muscles are alike due to deposition of calcium salts, but under different circumstances. Myositis calcificans may be the result of tuberculous disease following caseation, as it does in lymph nodes and in other parts of the body, or occurring as a general deposit throughout the muscles, essentially an infiltration, as is seen in the muscles of the legs. Myositis ossificans implies a formation of true bone in muscle substance. A peculiar form arising in the adductor longus results from the pressure of the limb against the saddle; this has been known as rider’s or cavalryman’s bone. Something similar in the deltoid has been called drill bone, because usually seen in soldiers who carry their weapons upon the shoulders; while a form which occurs in the brachialis anticus has been referred to as fencer’s bone, and one in the calf muscles as dancer’s bone. It occurs in two types, one of which is characterized by ossification in succession of the various muscles, this occurring first in the trapezii, latissimi, and rhomboidei. In explanation of these lesions, it has been suggested that all of these connective mesoblastic tissues may manifest certain atavistic tendencies and thus revert to bone. The question is certainly not one of periosteal origin. Binnie has shown, in a remarkable case reported by himself, that ossification is both of the fibrous and cartilaginous type. Only in the localized forms can the periosteum be suspected. In these it may be that there has been detachment of some of its tissue or escape of some of its cells into the muscle area. The ossifying lesions of surrounding muscles will sometimes interfere with the motions of joints after they have been injured. Any localized calcareous or ossific deposit which can be recognized may be removed.
—This occurs in gummatous form, no muscles being exempt; those of the tongue are most frequently involved. It is seen also in the sternomastoid. Not infrequently these gummas have been mistaken for malignant tumors. Sometimes they degenerate and sometimes suppurate. A lesion of this kind will usually be multiple, but it may have enough infiltration around it to be difficult of recognition. Lesions of this kind are also seen in hereditary cases. A more distinctively interstitial affection of muscles leads sometimes to their contracture, as seen about the arms, beginning with malaise and incoördination, and extending to disabling lesions. These will yield to properly directed antisyphilitic treatment.
—This affection is usually the result of extension from adjoining foci. As in the case of syphilis it may assume the infiltrating or the gummatous type. It is more frequently encountered than the muscular expressions of syphilis; it does not yield nearly as readily to treatment, and calls for excision of the affected area and for cauterization or other protection as against re-infection.
[332]
More or less permanent paralysis is sometimes the result of contusion or direct injury of a nerve trunk. Thus the paralysis of the deltoid which follows injury to the circumflex nerve in connection with dislocations of the shoulder is a frequent accident. It does not require continued pressure upon the nerve to produce this. It may follow a dislocation reduced within a few moments. Again, paralysis of the arm muscles is occasionally the result of pressure made by crutches. It has been known to occur from similar pressure while the patient was upon the operating table with his arm hanging over the table’s edge. This is an accident which should be carefully avoided. Moreover, it follows sometimes from mere violent muscle effort. The condition, while simple in its etiology, is difficult and sometimes impossible to cure.
—The treatment should consist mainly of massage and electricity, with the elimination of all possibility of toxemia. The resources of tendoplasty (see above) should also be considered, as well as those of neuroplasty.
Muscular paralysis is always followed by atrophy, which will lead to marked diminution in size of the part; when the atrophy concerns a single muscle or muscle group it will frequently be followed by deformity due to action of the opposing muscles. Tonic spasm of muscles unopposed may lead to contractures, often with ankylosis. The degree of deformity which is produced may eventually require amputation of a limb.
Other forms of contractures are produced either as the result of central or spinal scleroses or as expressions of irritative spasm provoked by a neighboring bone or joint trouble. The two types may cause similar deformities, which vary widely in their etiology. The former are seen in certain cases of brain and spinal-cord diseases, the latter especially in connection with tuberculous arthritis. Inasmuch as the flexors are stronger than the extensors these deformities consist largely of hyperflexion. Ultimately the shape and growth of bones and the nutrition, appearance, and function of the part are influenced.
Muscle atrophy which is the result of confinement in one position, as after the treatment of fractures, is of minor importance and tends to disappear spontaneously as soon as function is resumed.
—In most of these instances patience may be easily overtaxed while waiting the tardy results of massage and such correction as apparatus may afford. Very frequently the additional help of an anesthetic, with forced movements, often with tenotomies and sometimes with tendon grafting, will be required. When contractures can be foreseen, as they may be in connection with many lesions which produce them, such as burns and others not specifically mentioned, they should be guarded against by splints, apparatus, or whatever may best serve the purpose.
The parasitic affections of muscles are rare. Trichinosis rarely produces tumors which come under the surgeon’s hands. Still there may result from it a form of myositis with formation of cysts which may so far interfere with muscle function as to demand removal. Hydatid cysts and cysticercus are extremely rare, especially in this country.
There are two types of bursæ in the body: first, the subcutaneous, or mucous, which are loose sacs containing a clear mucoid fluid. They develop regularly when bony prominences are exposed to friction and develop adventitiously wherever undue irritation is produced. Thus beneath every bunion there will be found a good-sized and thickened bursa.
Synovial bursæ, the second type, are met with in close proximity to joints, and between tendons which play upon each other. They frequently communicate with the joint which they overlie, and infection may easily spread from one to the other. They are liable to traumatism, either extrinsic or intrinsic, the former from chafing or more direct injury, the latter by excessive muscle exertion. When infected they suppurate, forming abscesses of conventional type. As the result of contusions they are frequently filled with blood, in which case there is a bursal hematoma. Acute bursitis usually merges into localized abscess.
PLATE XXX
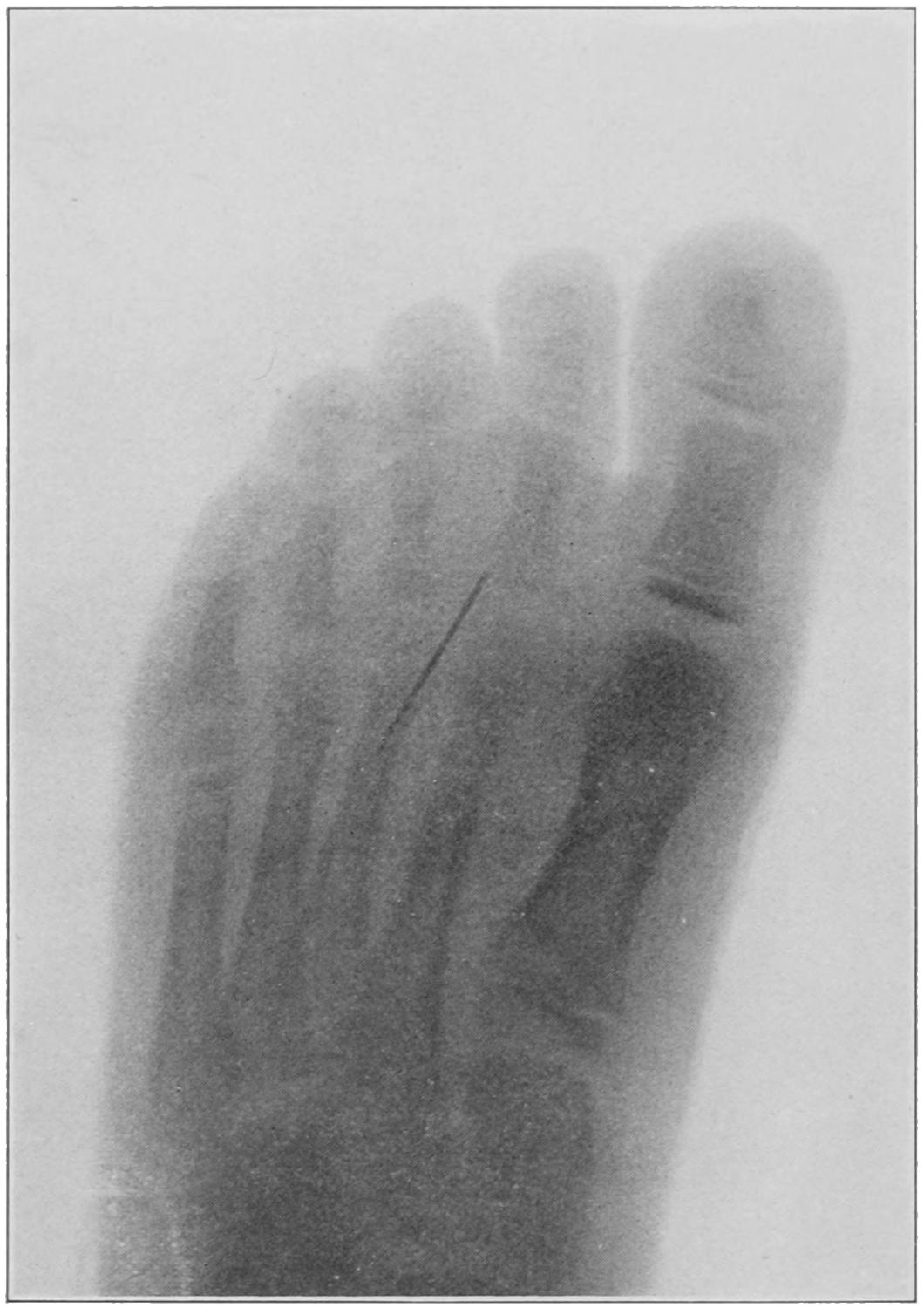
Foreign Body (Broken Needle) in Foot. Buffalo Clinic. (Skiagram by Dr. Plummer.) Illustrating the Value of this Method of Exactly Locating a Foreign Body and involving the Tissues Considered in Chapter XXVIII.
[333]
Fig. 135
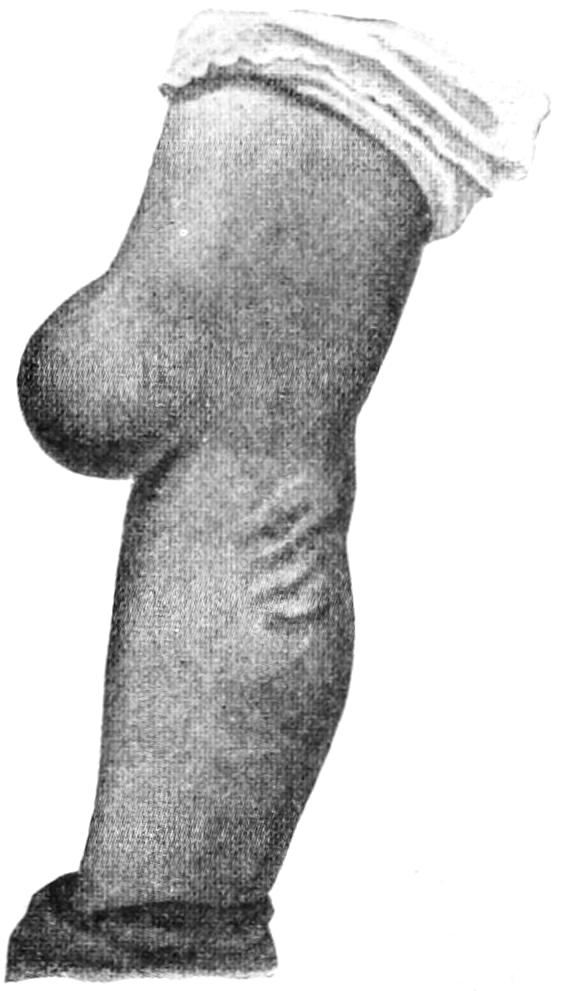
Hygroma of a prepatellar bursa (“housemaid’s knee”). (Lexer.)
Chronic bursitis constitutes a circumscribed collection of fluid, often with thickening of the bursal sac, and frequent deposition of products of exudation. Here, too, pus may form as the result of infection, while calcification sometimes takes place in old cases. A chronic bursitis is likely to be either of syphilitic or tuberculous origin. It is usually seen beneath old bunions, and in the prepatellar bursa, which is equally exposed to irritation, and which also gives rise to housemaid’s knee. This lesion used to be considered as always of syphilitic character, but this is far from correct.
Hygroma, or hydrops, is a term frequently applied to these localized collections of fluid. The former is more likely to be of tuberculous origin, and the retained fluid may contain rice-grain bodies. A chronic bursitis, originally of traumatic origin, may become infected and present a tuberculous lesion, or it may be influenced if not caused by a syphilitic diathesis, especially about the knee, where these conditions generally occur. Other bursæ which produce disturbances that eventually take the patient to a surgeon are met with in the following locations: beneath the ligamentum patellæ, which will give a prominence on each side of the ligament, particularly when the knee is flexed; over the tubercle of the tibia; beneath the quadriceps extensor tendon, which will cause a swelling two or three inches above the upper border of the patella; between the tendon of the semimembranosus and inner head of the gastrocnemius, which will present in the popliteal space as a somewhat globular swelling; beneath the deltoid; beneath the gluteus muscles, where the tendons pass over the great trochanter; between the tendo Achillis and the calcis; over the outer malleolus, occurring in tailors by virtue of the position in which they work. Large bursæ often develop on the outer sides of club-feet, on the ends of amputation stumps, and wherever there is prolonged irritation of mild degree.[21]
[21] A bunion is in many instances due to flat-foot, causing the great toe to turn out. This condition should be remedied by the usual arch, or raising the inner border of the shoes. Four out of the five tendons attached to the great toe tend also to draw it outward. If the tripod of the foot can be restored without operation this should be done.
The treatment of acute bursitis is that of threatening phlegmon in any other part of the body. As soon as the presence of pus can be determined, or even before, a free incision should be made. Such an incision should not be entirely closed after evacuation of the sac, but should be permitted to heal by granulation.
Chronic bursitis, whether with or without formation of granuloma, is best treated by excision, when the sac has become thickened and a new formation has practically occurred. Housemaid’s knee, for instance, like bunion, is more satisfactorily treated by a clean excision of all diseased tissue than by any other less radical method. Every tuberculous lesion of this kind should be rigorously extirpated, and every syphilitic lesion should be treated by constitutional as well as by local measures, the former being, save in exceptional instances, the more important of the two.[22]
[22] The Radical Cure of Bunions.—The term bunion is generally used to indicate a painful swelling over the inner aspect of the ball of the great toe; it is never seen on the feet of those who go barefooted, but is the result of badly fitting shoes, almost all of which crowd the great toe outward, thus making its base more prominent and exposing it to irritation and pressure. The inner border of the foot is nearly a straight line, but shoes are rarely made to conform to this. The result of the consequent partial dislocation of the toe, and of the pressure made at its base, is chronic periostitis, and the development of a bursa. It becomes greatly thickened and forms a small tumor, usually sensitive and painful. The dislocation often proceeds to such a degree that the great toe lies across the others, either over them or under them, in such a position as to receive and deserve the name hallux valgus, which is generally given it when this is pronounced. There is nothing to do but to exsect the head of the first metatarsal bone, and at the same time excise the bursa and some of the overlying and thickened skin.
[334]
A generation ago a chapter on the surgery of the heart would have been regarded as a surgical fantasy. Today the subject is not only a live one, but experience is constantly accumulating as to the value of surgical intervention in diseases of the heart and pericardium.
The heart may be displaced by congenital or acquired causes. Malpositions of the former type may vary from dextrocardia, where the heart is placed upon the right side, and may be accompanied by a general or partial transposition of the viscera, to those cases where there are defects in the diaphragm or the chest wall, through which the heart protrudes. Dextrocardia has an interest for the surgeon, as, for example, in the following case under the writer’s observation: Disease on the left side which simulated appendicitis, in which the diagnosis was confirmed by finding the heart upon the right side, and later by operation. It was a case of complete transposition.
The acquired malpositions may be due to intrinsic or extrinsic causes. They are pressure effects, usually found in connection with intrathoracic aneurysms and other tumors or collections of fluid, or may be due to change in the shape of the spine in pronounced curvatures. Occasionally the heart is hindered in its action by pressure from beneath the diaphragm. These cardiac displacements are surgically interesting when the cause can be removed by operative measures.
Wounds of the heart are mainly of the punctured or gunshot type. It was formerly considered that injuries of the heart were essentially fatal. This has been disproved by human and comparative observations. As far back as 1855, Carnochan reported a case of gunshot wound of the heart where the bullet was found in the heart substance after the patient had lived eleven days. The museums contain many illustrations of penetrating wounds of the heart or of foreign bodies in it, some of which had remained embedded for many years. Nevertheless the fact remains that the majority of wounds of the heart are fatal, either by arrest of its activity, by shock, by the outpour of blood between it and the pericardium or outside the latter, or later by processes which consume at least a few days, either infective or degenerative. Other things being equal the larger the wound the more dangerous, while an injury to the heart muscle which has not opened one of its cavities is less dangerous than one which perforates them. A punctured wound made by a small stiletto or knife-blade, or even by a needle used for homicidal purposes, may leave but small trace and not prove fatal, save through injury to one of the cardiac vessels, especially a coronary artery.[23]
[23] Illustrating the surgery of foreign bodies in the heart, Jordan has reported the case of a young woman who stated that she had received a blow on the front of the chest the previous day, and showed on examination a small projecting point in the lower part of the third left intercostal space about half an inch from the sternum, which was tender to the touch and seemed to move or pulsate with the heart. It gave to the finger the sensation of a hard substance beneath the skin without any external marking. Upon making an incision and dissecting partly through the muscle the broken end of a black steel pin came into view. After removal with forceps it proved to be a shawl pin, one and one half inches long, with its glass head broken off. The patient remembered having had such a pin in her bosom at the time of the accident. On the following day she had pericarditis. She apparently recovered, but had a relapse, and died on the twenty-fourth day, the autopsy showing pericarditis.
In practically all of these injuries there will be evidence of some external violence. It is of advantage to ascertain the nature of the accident and the character of the missile[335] or instrument. If the depth of penetration of a knife-blade, for instance, can be ascertained more accurate conclusions can be drawn. The special indications of cardiac injury pertain to disturbance of its own function, that is, embarrassment and uncertainty of action, bellows sounds, enlarged area of dulness owing to distention of the pericardium with blood, dyspnea, and distress, and sometimes pain and syncope. These symptoms and signs do not appear instantaneously, but increase in severity.
—In such an emergency everything possible should be done to relieve the embarrassment of the heart’s action—the head should be kept low, the body absolutely quiet, and nervous excitement should be allayed at once with a full dose of morphine. Heart stimulants should not be given. Ice applied over the chest will help quiet cardiac activity. If the patient be not failing too rapidly operation is advisable, and should be done in a well-equipped hospital, with trained assistants. The purpose of the operation is to expose the injured portion of the heart substance and close it with suture; at least to remove the fluid or partially coagulated blood within the pericardium.[24] As it is not always possible to expose the heart without opening the pleural cavity, there should be at hand not only the means for a tracheotomy, but an apparatus by which artificial inflation of at least one lung can be effected. Pneumatic cabinets have been devised for this purpose, especially by Sauerbruch, where a difference of pressure can be maintained between the outside and the inside of the cabinet, so that the chest may be widely opened and the lung not collapsed; but such a cabinet is available in few places in the United States. The improved Fell apparatus, by which a mask is kept over the face and pressure maintained with the foot through a bellows, has been found useful. Even in the absence of such apparatus the surgeon should not abstain from the effort, though it may appear less promising.
[24] Suture of Heart Wounds.—Stewart has tabulated 60 cases of suture of the heart reported up to May, 1904, with a remarkably high recovery rate of 38 per cent. (Amer. Jour. Med. Sci., October, 1904). Of the 60 cases 55 were stab wounds and 5 were gunshot wounds, 2 of the latter recovering. In 4 of the cases the coronary artery was injured, and only 1 of these recovered. The injury occurred through a puncture while suturing the heart, and an extra suture was necessary in order to control it. Of the 60 cases the left ventricle was wounded thirty times, with 30 recoveries. The right ventricle was wounded 21 times, with 7 recoveries. The operation has only been practised for about ten years. The results reported certainly justify its performance in all cases of this kind.
In the operative procedure one may feel inclined to utilize the already existing wound, either as a part of his incision or for exploratory purposes, or he may decide to disregard it. The operation consists in raising an osteoplastic flap on the chest wall, by which the pericardium and then the heart are exposed. The incision through the skin is extended to the bone and only enough of the soft structures separated from the ribs and cartilages to expose them sufficiently for division. Ordinarily it would be preferable to divide the third, fourth, and fifth costal cartilages at their rib terminations, and then to turn up the flap with its base at the sternum, though the procedure can be reversed to almost as good advantage. The cartilages and the ribs may be divided with the costotome and the rest of the structures with stout scissors. The flap, having been gently elevated at the edge, is separated from the underlying cellular tissue and pericardium until its sternal margin has been reached. When detached it may be sprung upward, and thus a complete window is made in the chest wall. When more room is desired bone and cartilage may be cut away with a rongeur.
Fig. 136
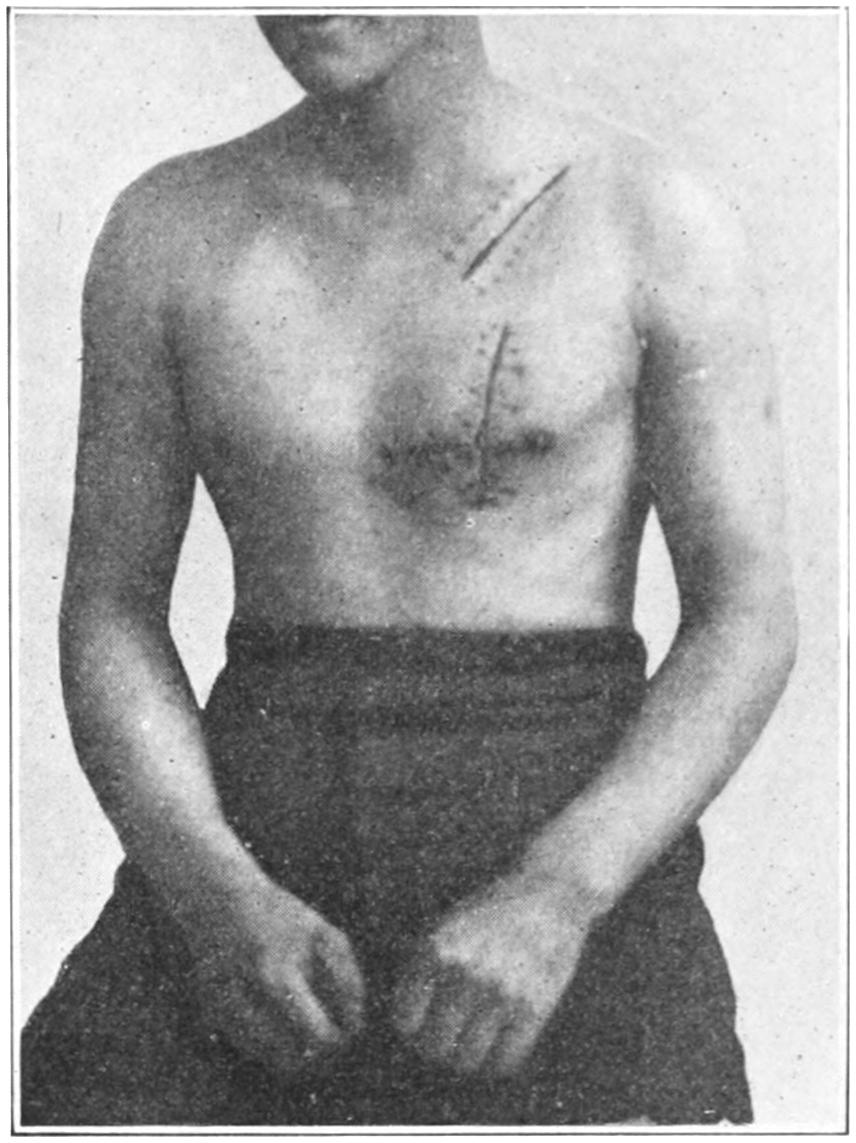
Result after thoracotomy for heart wound. (E. J. Meyer.)
The pericardium being thus exposed may be found much distended or altered by the imbibition of blood. It should be opened to an extent sufficient to permit evacuation of its bloody contents and sufficient exposure of the heart to permit not merely inspection but suture of any wound in the heart substance. This is exceedingly difficult on account of[336] motions of the heart, and the insertion of sutures will be as difficult as trying to hit a flying target. Nevertheless it may be done in many cases. Unless imperative, a coronary artery should not be included in the heart suture. Hemorrhage from the heart being checked the pericardium is then to be united, preferably with hardened catgut sutures, with or without drainage. In most instances the former is the better plan, and the drain may be of the cigarette type, that is, gauze wrapped in oiled silk.
Should it be found that the pericardium alone is injured and not the heart the case may be regarded in a more favorable light.
There are sufficient cases on record where procedures analogous to the above have been practised to justify the attempt in every case. Hardened animal sutures may be used in the heart substance, and the interrupted method will probably prove the better. A suture which will hold firmly for three or four days will suffice, as has been proved on animals.
Rupture of the heart can scarcely be considered a surgical condition, though it has frequently been one of medicolegal interest. It may, however, afford a sudden and unexpected termination to surgical cases. The cardiac muscle may be so softened by the poisons of diphtheria and other acute infections as to be greatly weakened, even though an intubation or tracheotomy has apparently afforded security.
Primary malignant tumors of the heart are very rare. Secondary and metastatic manifestation are much more frequent. True primary sarcoma has been repeatedly observed, and, with the exception of endothelioma, is practically the only primary cancer that could appear in this location. Carcinoma is found only as a secondary deposit, with which, however, the heart may become so involved as to permit of terminal rupture.
This closed sac is interesting to the surgeon in cases where it becomes filled with air; with blood, as the result of injury (see above); with fluid, as in acute pericarditis, or with pus, as a later stage of the latter, with its consequent pyopericardium. With the introduction of the aspirating needle it is possible to draw off collections of serum or pus, and paracentesis of the pericardium is now a conventional minor operation. It is managed in the same way and with the same instruments as when the pleural cavity is involved. It is ordinarily safe, and affords much relief.
The surgeon may go even farther than this and practise cardicentesis, as the writer did once by accident while hospital interne. After introducing the needle and withdrawing three or four ounces of pus he discovered that he had given great relief, which, however, was only temporary. The autopsy two days later revealed that he had passed the needle point through the pericardial sac into the heart wall and had tapped the abscess therein. This was in 1877, and was probably the first time that the heart wall was ever thus entered.
Now the operator goes still farther than this and practises intentional cardicentesis in cases of engorgement of the right side of the heart connected with lung disease which is threatening death from dyspnea with an overstrained heart. In such cases the needle may be introduced just above the fourth rib, from one-half to one inch to the right of the sternum, or entrance can be effected just above the fifth rib in an upward direction. From 100 to 250 Cc. of blood may be withdrawn.
For ordinary tapping of the pericardium the needle is inserted two inches to the left of the median line and in the fourth or fifth left interspaces, pushing it carefully until resistance is no longer felt and fluid flows through the tube. For either of these purposes the patient should be recumbent, unless the distress in this position is too great, in order that the heart may fall away from the chest wall. Aspiration can be repeated in case it gives relief. Little or no harm seems to ensue from the wound which a needle-point[337] will make upon the heart substance. As the sac is progressively emptied the needle-point should be gradually withdrawn. When aspiration, exploratory or therapeutic, reveals the presence of pus, the well-known rule will apply, i. e., that pus left to itself will do more harm than will the surgeon’s knife. For pyopericardium there is but one successful treatment when aspiration fails, and that is open incision and drainage. This is not so severe a measure as exposure of the heart, as it may not even require the removal of one costal cartilage, although it would probably be better to take out at least one, since the shape of the pericardial cavity will change to such an extent after it is emptied as to raise the opening to a higher level than is given it at first. Open incision, then, with drainage, in these cases is no longer an experiment but a life-saving procedure. It will prove successful in at least half of the cases, which otherwise would certainly perish without it.
Pneumopericardium implies the presence of air in the pericardial sac, a condition of which there are now about 40 cases on record. The air nearly always enters through an ulcerative perforation from adjoining parts or through a wound, yet in 5 of these cases no opening could be found. In these it was probably due to the presence of a gas-forming bacillus, such as may also cause pneumothorax under certain circumstances. The perforation was in the esophageal wall in 7 cases, in 4 cases it was the result of softening of a lymph node, while in other instances it has followed abscess of the left lobe of the liver, pleuropneumonia and gastric ulcer perforating through the diaphragm. Of the 8 cases of penetrating wound from without, I included the small puncture made by paracentesis, while in 7 cases there had been fracture of the ribs or the sternum, with wound or laceration of the lung or the pericardium.
The most characteristic sign is a splashing, gurgling sound, synchronous with the heart beats, such as the French have called the “water-wheel bruit.” These sounds are louder than in hydropneumothorax, and are heard distinctly over the heart. The area of precordial dulness will change with position.
In unmistakable cases operation is indicated, the trap-door exposure being the best, the inner end of the fifth and sixth ribs being elevated. Irrigation and drainage will be necessary. It is encouraging to know that 11 of the 40 cases above mentioned have recovered.
Cardiolysis refers to the operative release of the heart from adhesions which have formed between it and the pericardium or the chest wall. When with every contraction the heart itself is subjected to the strain of an adhesion the work proves excessive and it will finally succumb. It has been suggested by Delorme, Peterson, and Simon to either temporarily resect the chest wall, open the pericardium and break down or divide the adhesions, or else to resect those bony portions of the chest wall, i. e., the sternum, cartilages, or ribs, which are so inflexible as not to yield, not removing the bands but making them harmless.[25]
[25] Those interested in the modern surgery of the heart and lungs should consult Rickett’s recent work on this subject.
There are few parts of the body which adhere more closely to the normal standard than do the larger arteries. Even here malformations and congenital defects are met with. In calculating the chances of a given procedure the surgeon should consider the condition of the venous and lymphatic systems before deciding to operate on a portion of the arterial system. This is particularly true when ligating the femoral artery for elephantiasis of the leg.
Thrombosis and embolism have already been considered in the chapter on the Blood. Nevertheless it may be well to remind the student at this point that thrombus means a blood clot, while thrombosis refers to the process of its formation; that embolus means[338] something which has passed into the blood current of an artery and plugged it, the obstruction usually being a fragment of clot or tissue, though it may be a droplet of fat or a bubble of air. Emboli, like thrombi, may be sterile, and in this respect innocent, or it may be composed of material loaded with septic, tuberculous, or cancerous germs.
Fig. 137
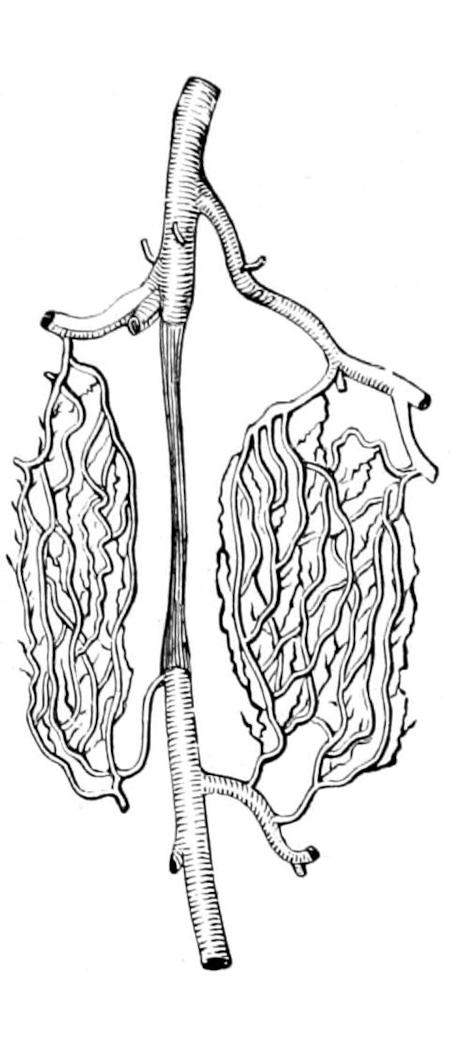
Fig. 138
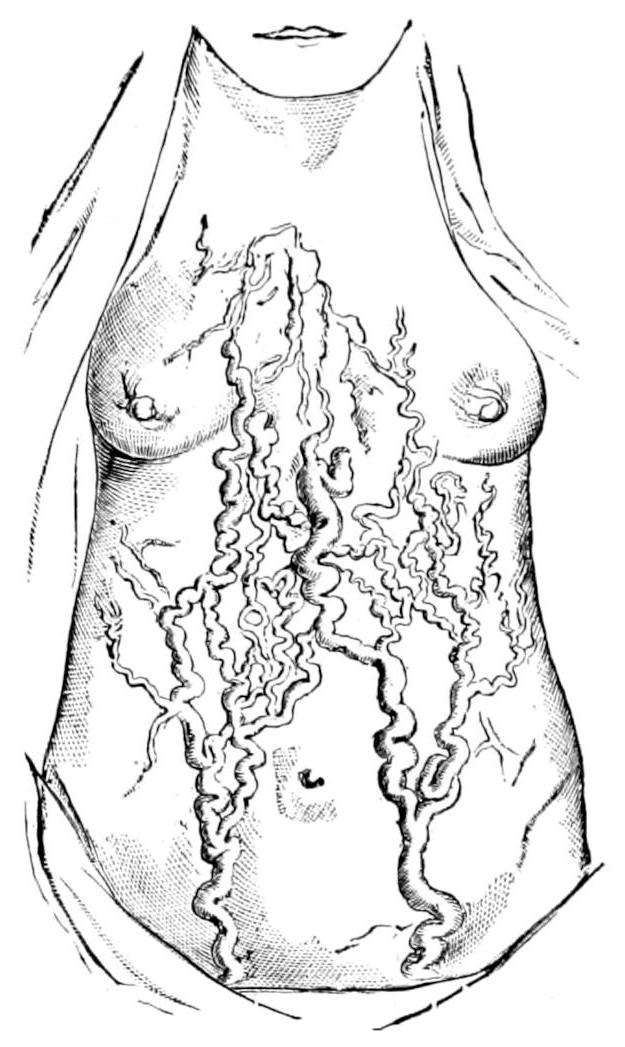
Fig. 139
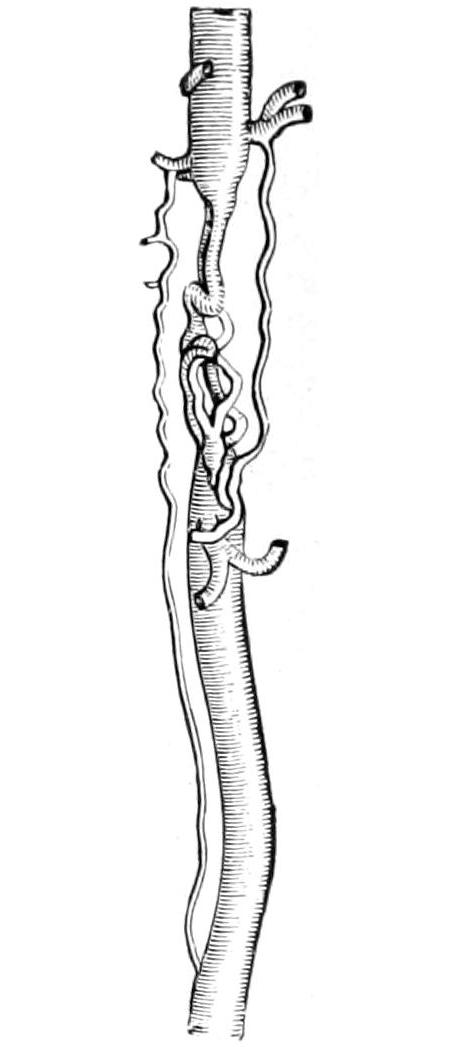
Anastomosing circulation in sartorius and pectineus of dog, three months after ligature of femoral. (After Porta.)
Collateral venous circulation, from a woman aged forty-seven, under the care of W. W. Gull, in whom the inferior vena cava was completely obstructed from cancer. (Guy’s Hosp. Mus., Drawing 44⁴⁰.)
Direct anastomosing vessels of right carotid of goat, five months after ligature. (After Porta.)
The readiness with which vessels, both arteries and veins, lend themselves to the exigencies of extra work has long been recognized, and the natural provision for collateral circulation is one of which surgeons have for centuries availed themselves. On the contrary, vessels which are no longer needed or whose function is lost will undergo atrophy almost to obliteration; thus after amputation of the thigh the corresponding iliac vessels become much reduced in size (Figs. 137, 138 and 139).
That arterial walls are resistant is shown by the fact that they are usually the last tissues to yield to gangrene. Whether a primary acute arteritis often occurs is a question of less interest in this place than the fact that even arterial walls will succumb to infection and that secondary hemorrhages from ulcerative processes are by no means rare. The pathological processes which occur in the various structures of the heart are repeated in the arterial walls; thus there may be a periarteritis corresponding to pericarditis, a mesarteritis which in many ways resembles myocarditis, and an endarteritis which corresponds more or less closely to endocarditis, and all of these in their acute or chronic forms. The acute forms which concern the surgeon are due usually to the presence of infected emboli, which have the same effect upon the arterial walls that infected thrombi have upon the venous walls, i. e., they lead to occlusion, infiltration, and suppuration.
Of the more chronic types those produced by syphilis are the most common. Here it is usually the outer and inner coats which suffer most. Tuberculous infection of an artery is of frequent occurrence and pertains only to those vessels which are in intimate relation with previous tuberculous lesions, while the syphilitic forms are diffuse and generalized and as likely to involve one part of the body as another. It is well known that arteritis in various degrees of intensity may be met with in most of the infectious[339] diseases. Whether they are due to the living germs or to toxins generated during the process concerns us at this point but little. It is of importance, however, to realize that vessels so compromised may thus receive their first impetus to degeneration and subsequently form aneurysm. The degenerative types of greatest interest to the surgeon are fatty degeneration, which occurs in the interior rather than the exterior, and calcification, which is rather an involvement of peripheral vessels and which occurs mainly in the middle and the outer coats. The latter may be limited or may involve an entire vessel. When the radial arteries are involved the condition may be appreciated at the wrist. Calcification frequently follows other degenerations, especially fatty, of the intima, and then may be seen in the interior of an artery. A true ossification has been described, but is exceedingly rare.
Arteriosclerosis is a term generally applied to a combination of these degenerations, with thickening and diminution of caliber. The changes combined are comprehended in the term atheroma, which is seen as a localized lesion in nodules or plaques in the aorta and larger vessels and in diffuse form in the smaller. Atheroma, as a complex degeneration, constitutes an interesting study, as it leads to well-marked changes in the vessel walls, which are softened at points by fatty changes, the little mass of debris resulting being called an atheromatous abscess (an unfortunate name), which may empty into the vessel, leaving a small cavity and opening known as the atheromatous ulcer. Around this occur usually the calcific changes above described. The disturbance and the roughening thus produced lead to the formation of fibrinous thrombi, which attach themselves firmly at these points. When to such a weakening of the vessel wall as is thus produced are added the elements of compensatory cardiac hypertrophy, and the sudden changes of blood pressure produced by certain occupations and alcoholic and other excesses, it will be seen how atheromatous patches constitute points of least resistance, where blood pressure may cause a vessel wall at least to bulge and thus to afford the beginnings of an aneurysm; while, by combination of various processes, final rupture may result.
The conditions are not so very different in the more diffuse forms, especially in patients who have not only a tendency to vascular disease but to increase it by the added toxemias of gout and syphilis, of various excesses and bad habits, in which not only do arterial coats suffer, but the heart muscle and lining as well. The relations then of systematic toxemias to arterial disease and finally to surgical conditions are not so circuitous as may at first appear.
An aneurysm is a tumor communicating with an artery and containing circulating or coagulated blood, or both. It may be formed entirely from the wall of the vessel, or some portion of it may be formed by surrounding tissue. Several varieties of aneurysm are indicated by descriptive adjectives. They are divided, first, into true and false, the former being composed of all the vascular coats and being small and infrequent; the false aneurysms imply those in which the entire arterial wall does not participate. Aneurysms inside the body cavities are called internal, and those involving the limbs external. The terms spontaneous and traumatic apply here as elsewhere. Fusiform aneurysm implies a spindle-like dilatation of the vessel in somewhat regular form. The sacculated aneurysm is essentially a pouch protruding from one side of the vessel with which it communicates. When the sac ruptures the aneurysm becomes diffuse. If the outer coat gives way and the inner protrudes there is a hernial aneurysm. The dissecting aneurysm is one formed by separation between the arterial coats, so that blood coagulates or flows between them. Such an aneurysm tends to assume a sacculate form and to rupture. A varicose aneurysm is a sac through which an artery and adjoining vein communicate. A cirsoid aneurysm corresponds to a varix on the venous side of the circulation, and implies dilatation of an artery and its branches. (See Figs. 140 to 145.)
[340]
Fig. 140
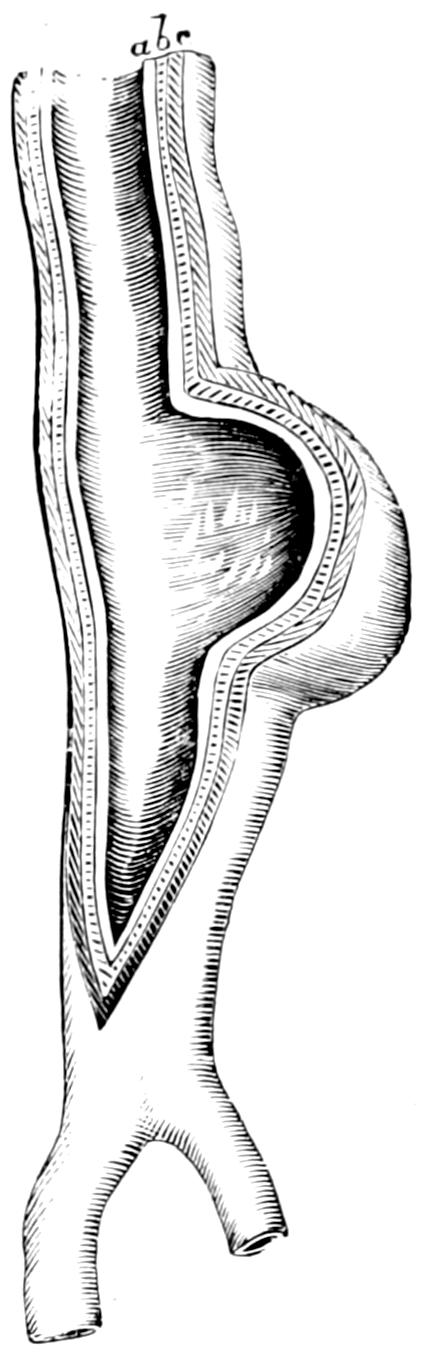
Fig. 141
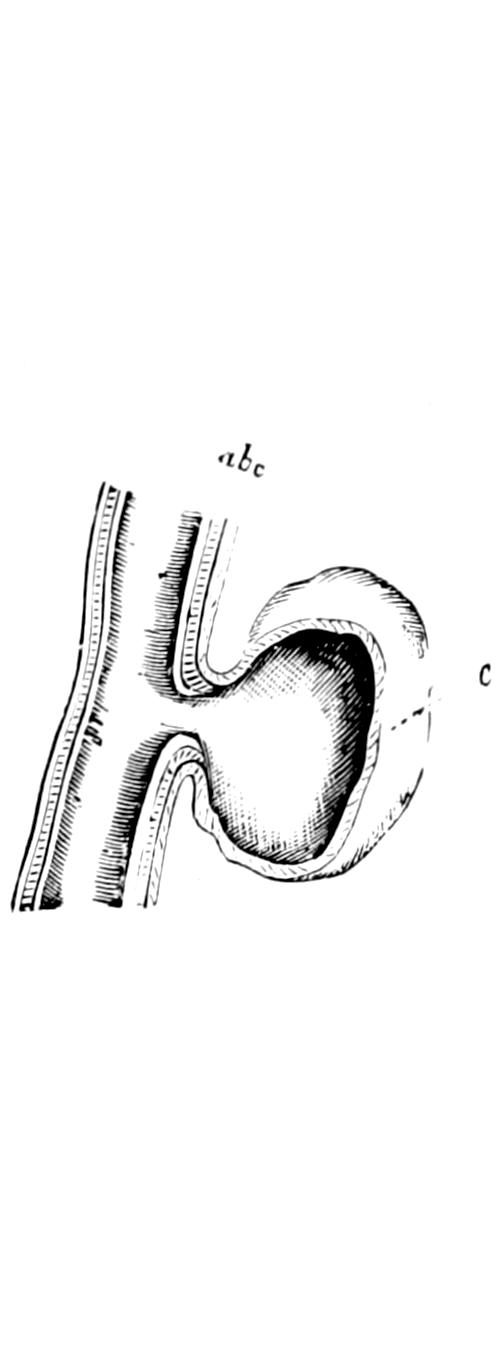
Fig. 142
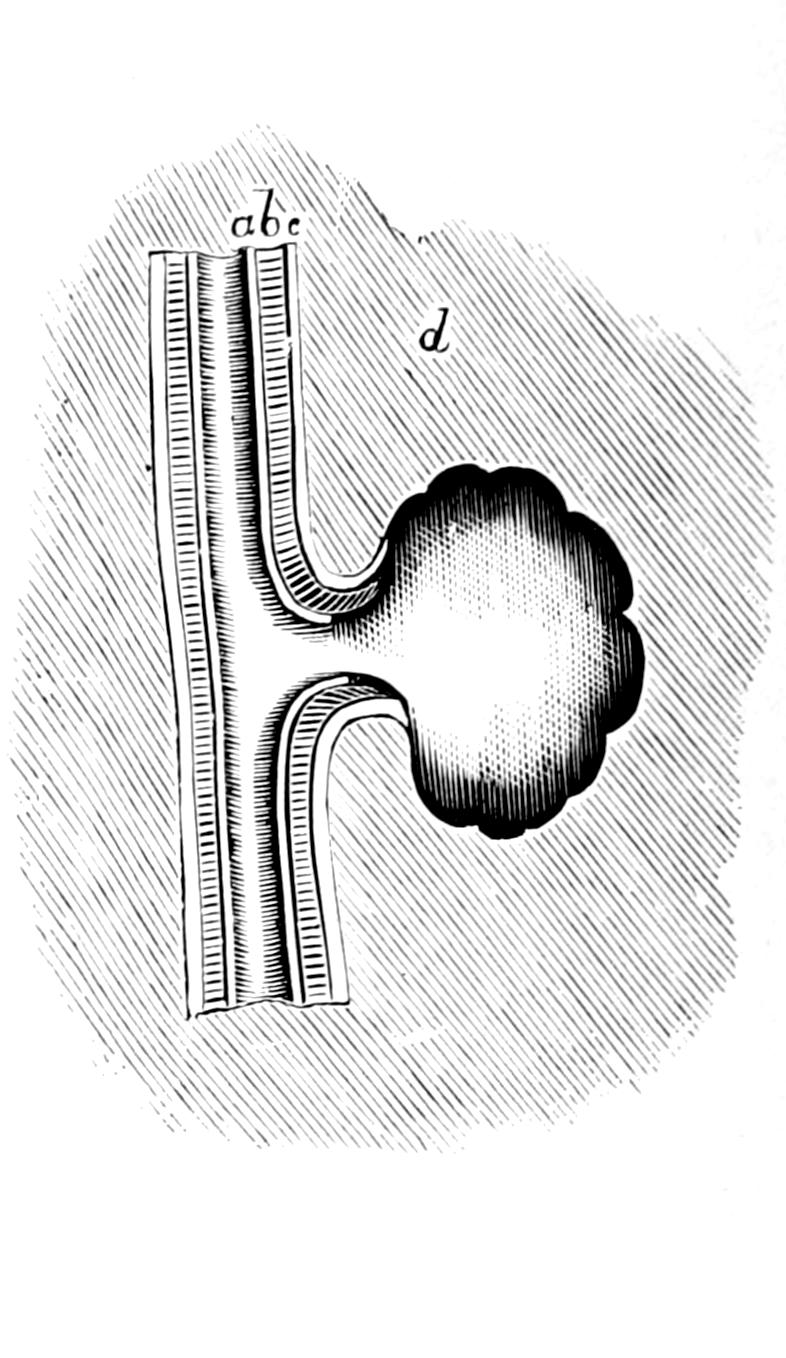
True aneurysm; the sac formed by all the coats. (Holmes.)
False aneurysm; the sac formed by the outer coat only. (Holmes.)
Traumatic aneurysm; the sac formed by the tissues around the vessel. (Holmes.)
Fig. 143
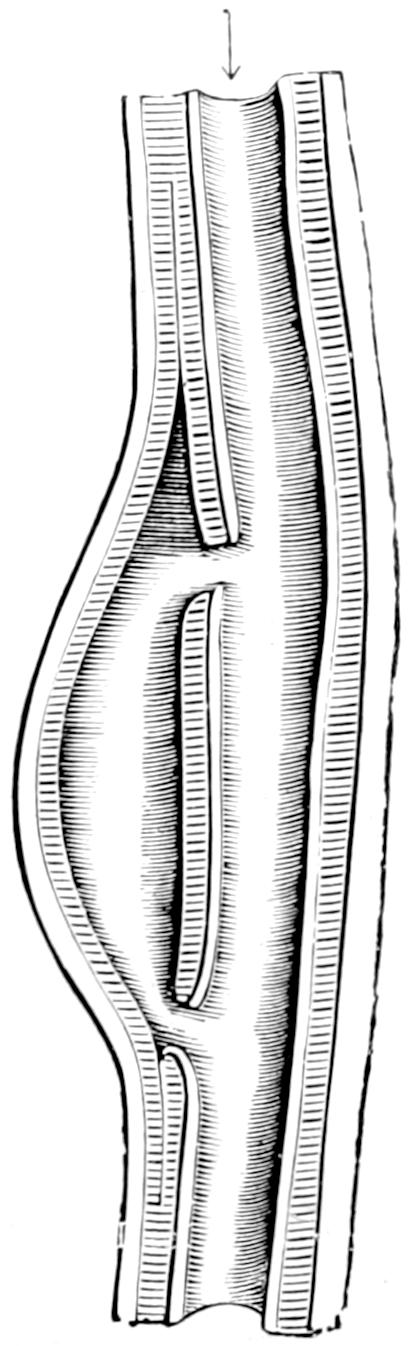
Fig. 144
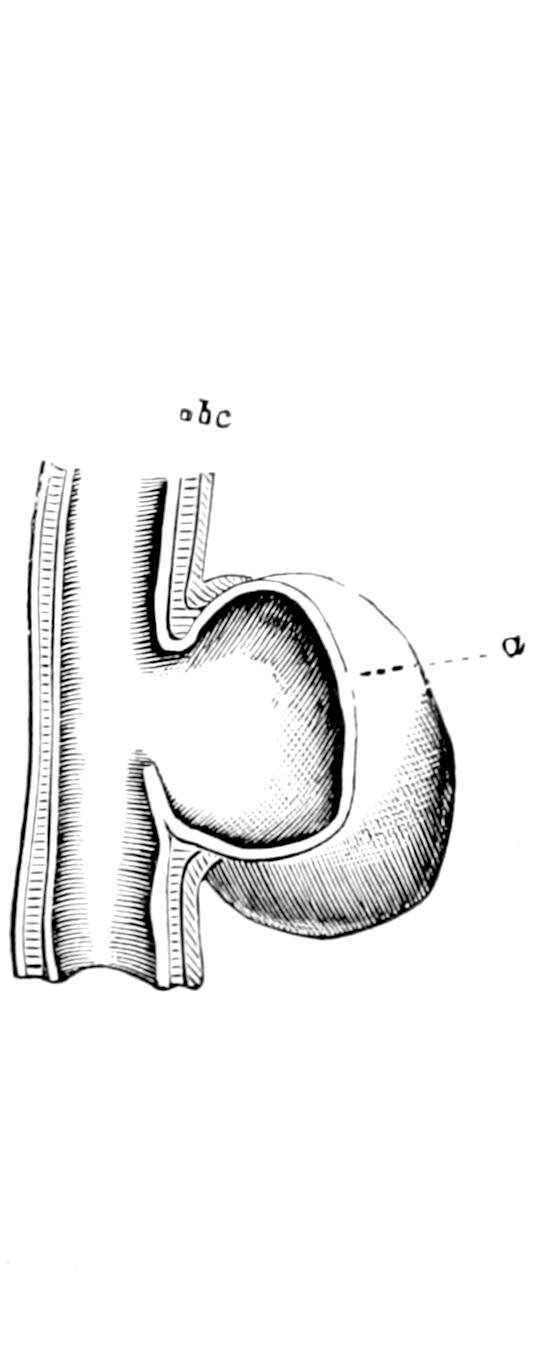
Fig. 145

Dissecting aneurysm. (Holmes.)
Hernial aneurysm; the sac formed by the inner coat only. (Holmes.)
Sacculated aneurysm of ascending aorta. Death by pressure. (Erichsen.)
[341]
The formation of an aneurysm implies previous disease of the bloodvessel or traumatism, by either of which its coats must have been weakened or divided. The previous disease which leads to this change is either of syphilitic or other toxic origin, and usually of the type of the endarteritis already alluded to, or its continuation into atheroma. A so-called atheromatous ulcer may lead to giving way of the intima and the passage of blood between the coats of the vessel. It is in this way that most dissecting aneurysms are formed. On the other hand, violent strain may stretch the vessels already weakened by increasing blood pressure, or those conditions which induce abnormally high blood pressure may produce it by slow processes. Lastly a vessel may be partly divided, as by a bullet or stab wound, or its adjoining supports may have been weakened by disease or by accident to such an extent that it constitutes a weakening of the arterial wall. The result of this will be expansion in the direction of least resistance and the formation of a sacculated aneurysm.
As a morbid condition spontaneous aneurysm seems to be less frequent now than in the past. Certain features pertain to all cases, the most essential being a pulsating tumor, giving physical signs of its presence by pressure, which causes pain, sometimes paralysis, and nearly always absorption of surrounding tissues as the tumor expands. Pulsation is characteristic and pathognomonic of aneurysm, but an aneurysmal sac may have become so filled with clots as to minimize the prominence of this symptom. The same is true of the aneurysmal bruit or murmur which is heard on auscultation. This sound and pulsation, especially of the expansile type, when present will rarely deceive. They may, however, be simulated by a solid tumor which overlies a large vessel and transmits its pulsation or even some of its murmur. Even in this case the significant expansile character of the pulsation will be lacking.
The progress of an aneurysm may be checked by spontaneous or surgical processes, but no vessel involved in this way can return to its previous condition. As the vessel expands the tendency is to fortification of its weakened walls by coagulation of the blood around the periphery of the sac. This process may be a continuous one or may occur at intervals in such a way as to produce laminated coats of blood clot, complete or incomplete, which in certain specimens can be peeled off, one after another, much as an onion can be peeled, the innermost portion representing the most recent coagulum. In this way an aneurysm is strengthened and thickened, and rupture postponed for an indefinite period. On the other hand, as the aneurysmal tumor grows slowly but steadily it tends to make way for itself at the expense of every other tissue in the body. The hardest bone will disappear before the constant advance of such a growth, and this permits aneurysms which have had their origin in the thorax to develop into large extrathoracic tumors whose walls, lacking resistance, become thinner and finally give way, death from hemorrhage being the result. In fact, rupture is the natural tendency of such lesion, the question being whether it may be averted by spontaneous or non-operative methods, or whether it should be subjected to operation (Fig. 146).
Fig. 146
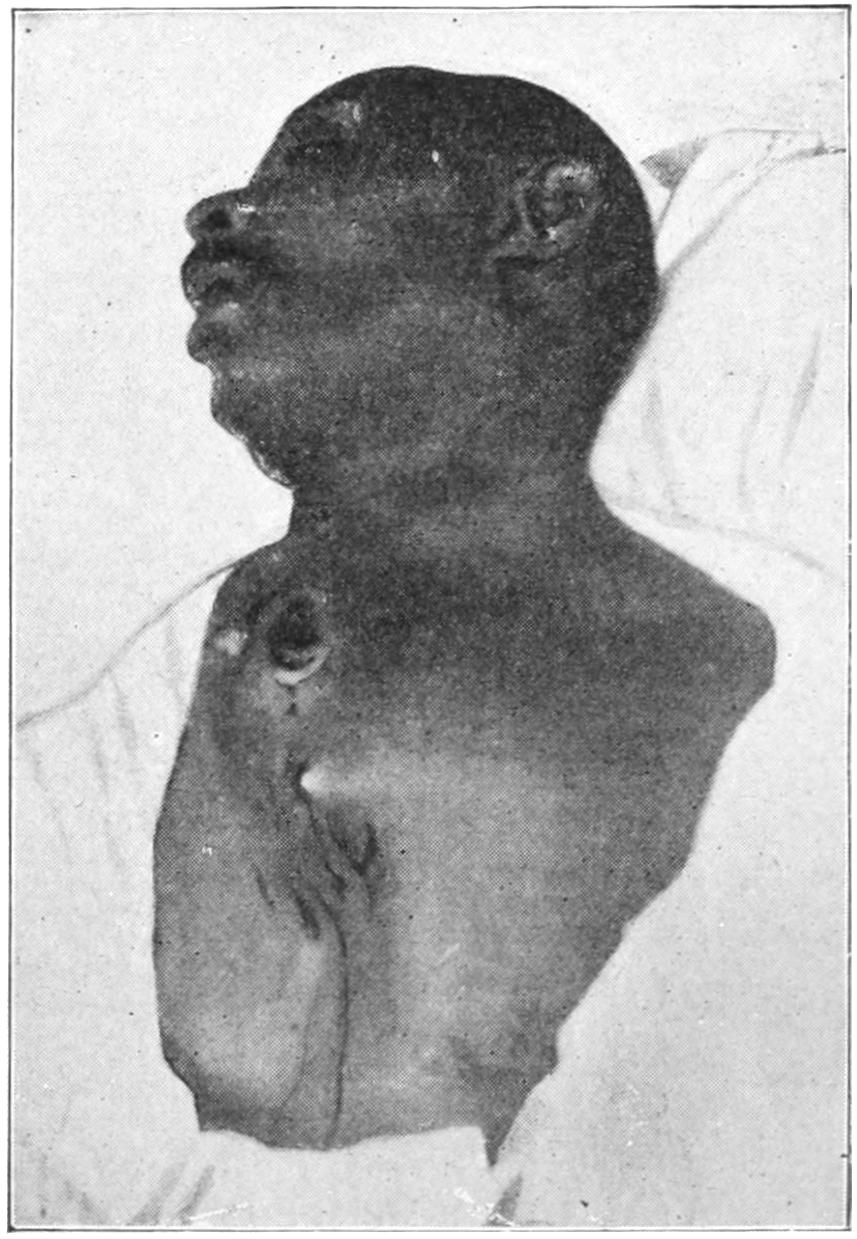
Thoracic (aortic) aneurysm. Death from external rupture.
Aneurysms may be minute and multiple, or single and large. The former are seen in the brain in connection with syphilis, and in the mesentery (Fig. 147). No artery in the body is necessarily exempt, though obviously the larger arterial trunks are the more frequent sufferers.
Spontaneous cure by natural methods is brought about in one of the following ways: (a) By consolidation of laminated clots. (b) A portion of the clot may become detached and plug the vessel on the distal side, effecting the same occlusion there that is produced with a ligature; in some cases the vessel may be occluded above the sac by a clot from the heart. (c) That which occurs naturally may be caused by accident as the result of some trifling injury. (d) The clot contained within the sac may have become infected,[342] so that suppuration with necrosis of the sac contents is produced. In connection with this there is sufficient acute arteritis to occlude the vessel, and the resulting abscess within the sac may be opened and its contents cleared out. This method is extremely rare and can only terminate happily when the surgeon intervenes promptly.
In an aneurysm in which spontaneous cure has occurred there may be progressive condensation of its contents, obliteration and partial reduction in size, and a slow process of absorption.
The importance of collateral circulation, in recovery from aneurysm, cannot be overestimated, as only by taking advantage of it is it possible to furnish blood for the needs of the part affected. There is no vessel with which the surgeon can interfere where natural provisions in this direction appear insufficient (Fig. 148).
Certain conditions predispose to aneurysm of the idiopathic type, such as age, with its accompaniment of arteriosclerosis; syphilis, with its well-known tendency to chronic endarteritis; occupation and sex, in that it is most frequent in those who are liable to violent exertion and dissipation, because of the well-known tendency to arterial structural changes after excesses of all kinds. Again, aneurysm may be the secondary result of embolism when an embolus leads to a local arteritis with disorganization.
Fig. 147
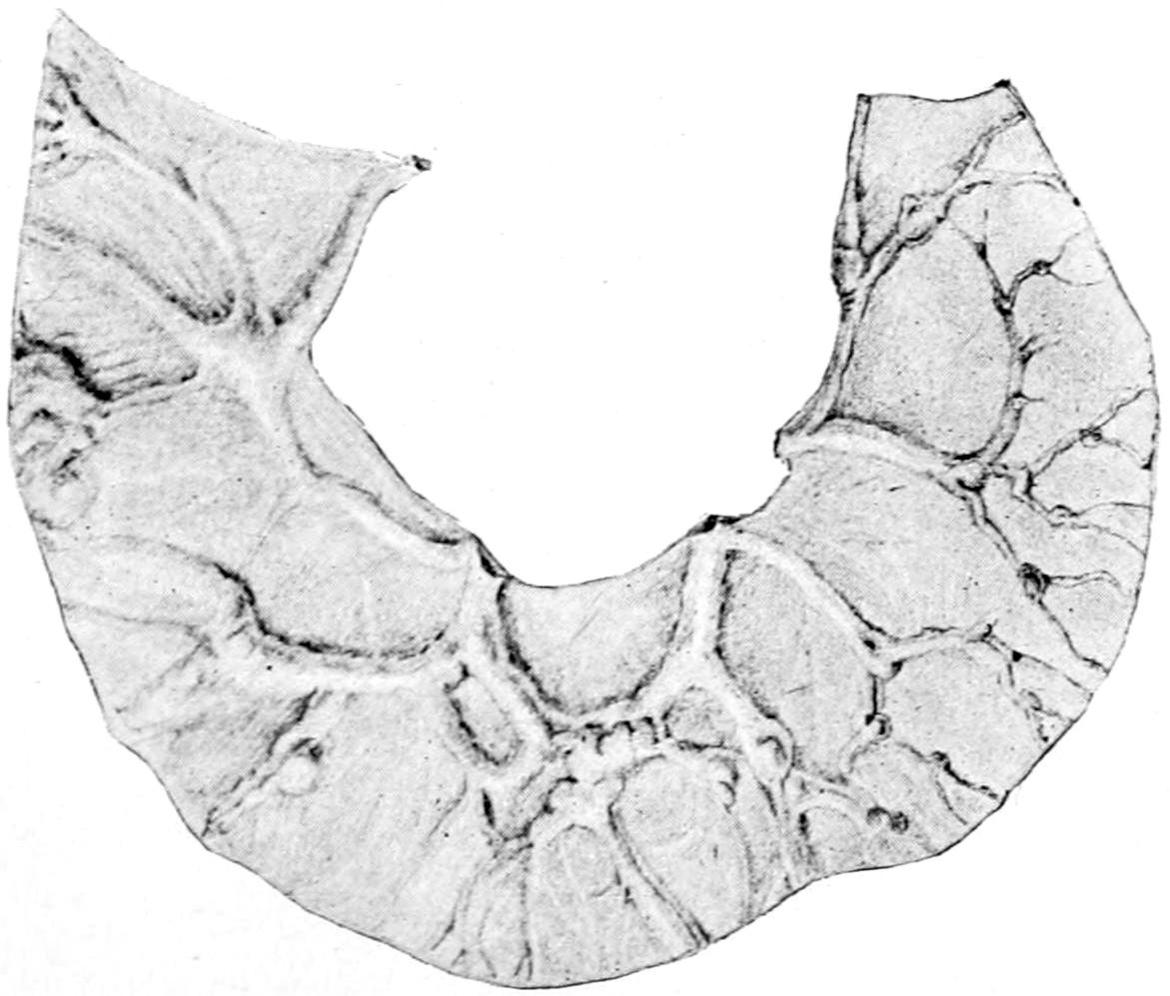
Fig. 148
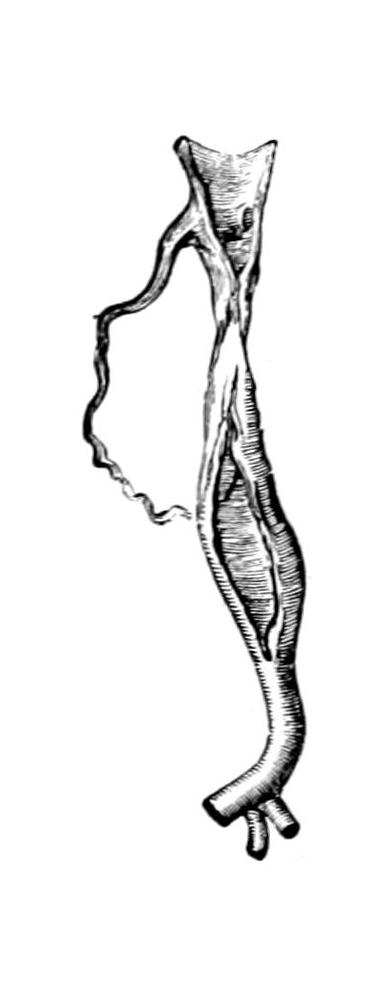
Multiple aneurysms of the mesenteric arteries. (Eppinger.)
Change in the trunk after ligature; with anastomosing vessel. (Erichsen.)
—For surgical purposes there is no better classification than the one used by Eve:
1. Sacculated Aneurysms.
—The sacculated are the most common. They assume various shapes and dimensions, and may be seen anywhere in the body. The opening between the sac and the main vessel may vary in size. These sacs are usually strengthened by plastic exudate in and around them, and condensation of surrounding tissue. In thickness they vary from 1 Cm. to the thinnest which will sustain blood pressure. In[343] old scars may be found a stratiform or layer-like arrangement, especially where the blood stream is less active. Should spontaneous cure take place the sac may be obliterated, while later calcific or other changes in the old scar may occur. When the outer portion of such a sac has disappeared and the inner coat is pushed out so as to assume, apparently, a secondary aneurysmal arrangement, the condition is referred to as a hernial aneurysm. When the ordinary sacculation gives way as the result of necrosis, of pressure from within, or loss of support from without, the opening first made is usually small and the extravasation outside the true sac will depend upon the nature and resistance of the surrounding tissues. In this way a diffuse aneurysm is formed, which is one of the varieties of false aneurysm.
2. Fusiform Aneurysms.
—Fusiform aneurysms are more or less tubular and spindle-like dilatations of arterial trunks, in whose walls may occur the changes common to all these lesions, the dilatation rarely being sufficiently large to permit of laminated coagula unless a sacculation occurs later at some particular portion (Fig. 149).
Fig. 149
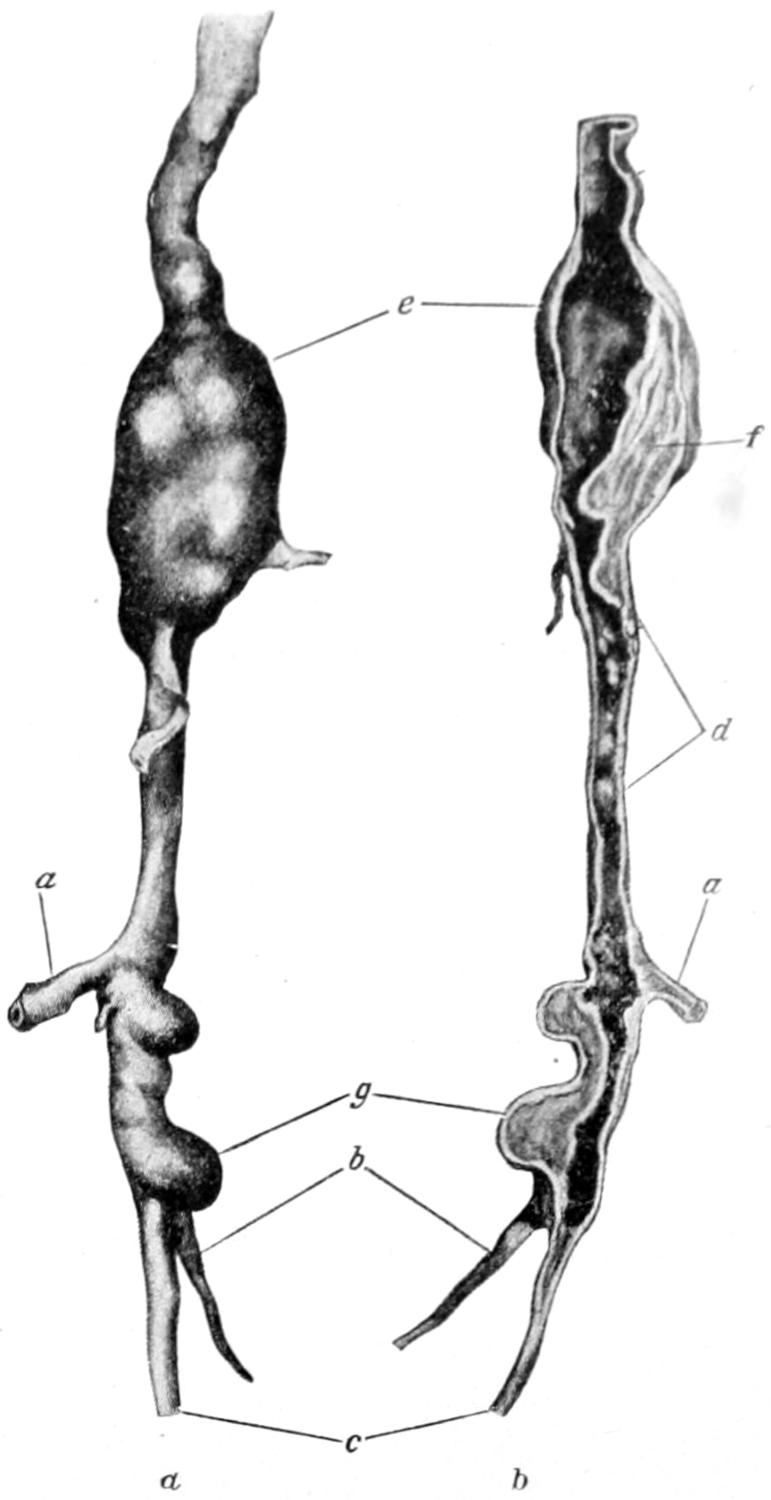
Fusiform aneurysm of popliteal artery, due to arterial disease (man aged 59), requiring amputation of thigh on account of gangrene. (Lexer.)
3. Dissecting Aneurysms.
—The dissecting aneurysms are nearly always expressions of previous atheromatous changes, by which blood is forced between the arterial coats, separating them and causing them to bulge at one or more points into sacculations or distortions. In a false aneurysm there is no true arterial coat; the sac is made up of surrounding tissue.
Fig. 150
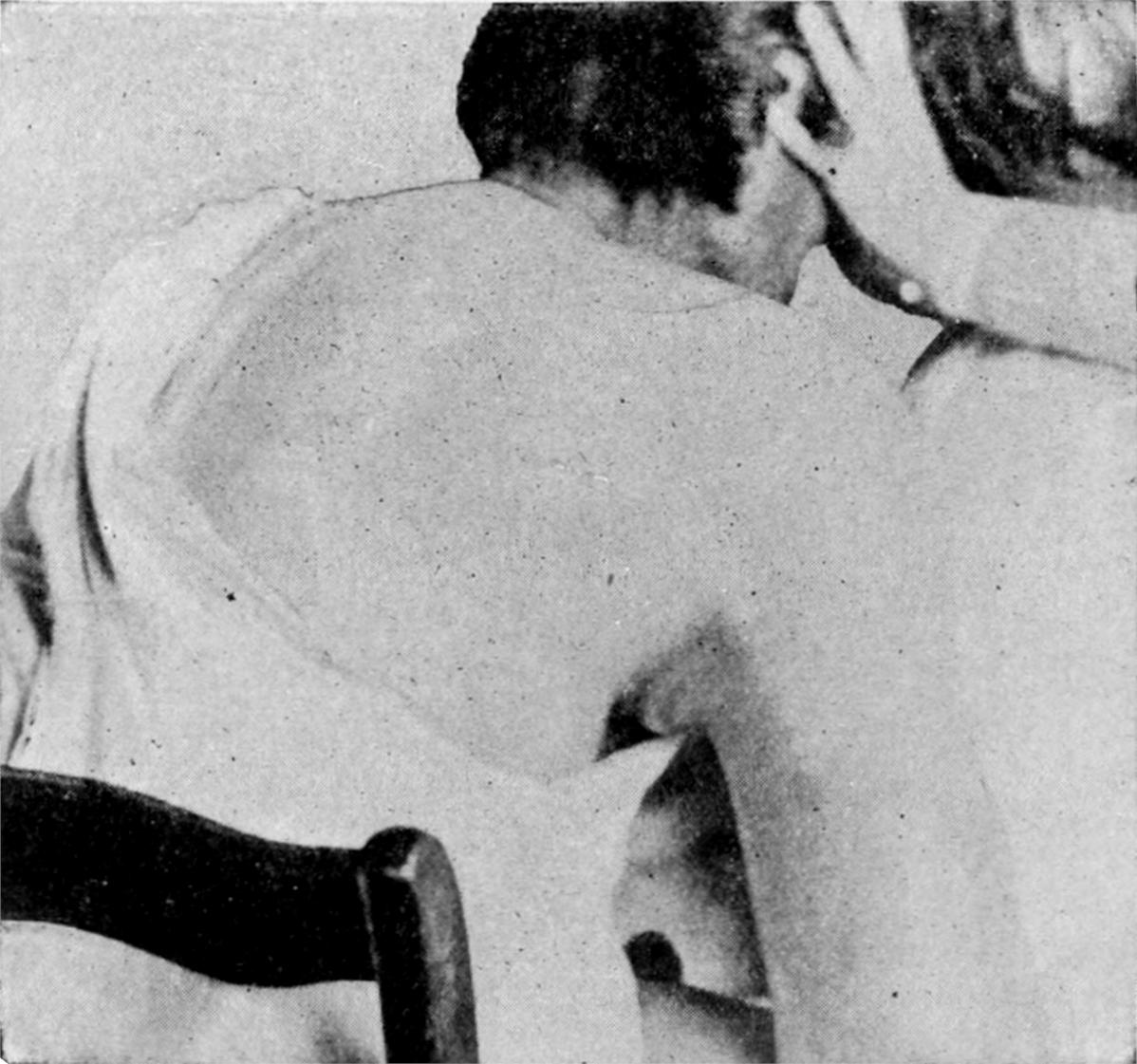
Traumatic aneurysm of axillary artery. (Park.)
4. Traumatic Aneurysms.
—Traumatic aneurysms are generally sacculated by the time[344] they come under the surgeon’s observation. They are circumscribed and diffuse. According to their age and other circumstances they may contain old and dense laminated clots as well as those which are fresh and stratified. Much will depend upon whether the artery has been extensively injured or only slightly punctured, and also upon the location and distensibility of the surrounding tissue. Such a case seen in a fresh state will show infiltration of blood and ecchymosis (Fig. 150). Arteriovenous aneurysms are now seldom seen. When venesection was more frequently performed the artery and one of the veins at the bend of the elbow were often thrown into communication, as the result of the indifferent performance of this operation and the use of the old-fashioned lancet. When the communication is direct such a condition is known as an aneurysmal varix; when indirect and through the sac it is called a varicose aneurysm (Figs. 151, 152 and 153.)
Fig. 151
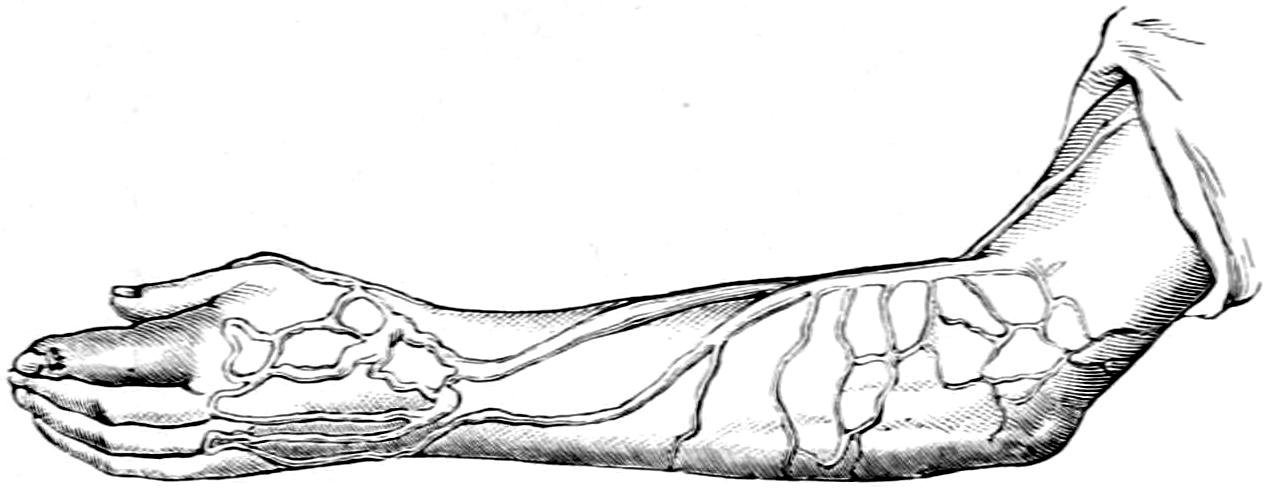
Aneurysmal varix. (Bryant.)
Fig. 152
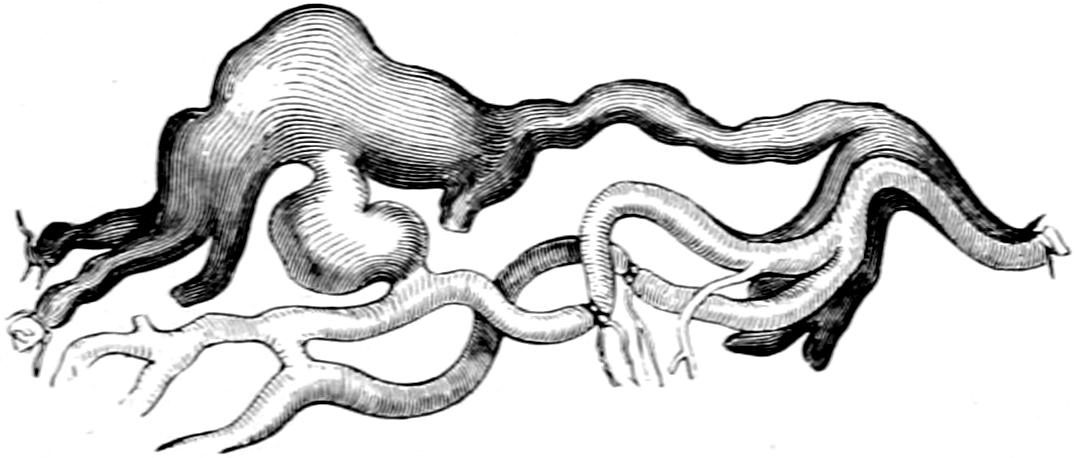
Fig. 153
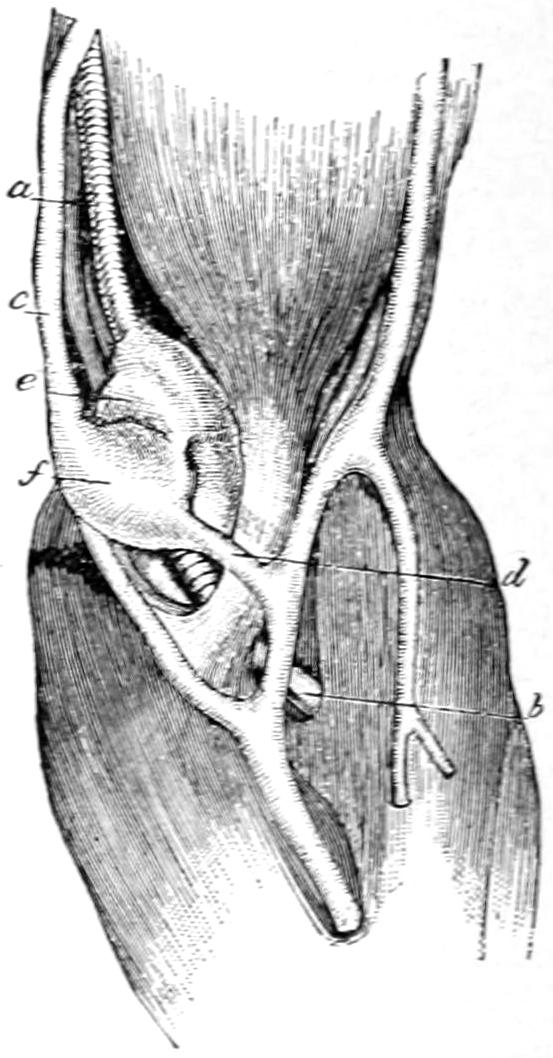
Varicose aneurysm removed from its connections. (Erichsen.)
Arteriovenous aneurysm at bend of elbow: a, brachial artery; b, radial artery; c, basilic vein; d, median basilic vein; e, aneurysmal sac; f, dilated vein. (Lenoir.)
Fig. 154
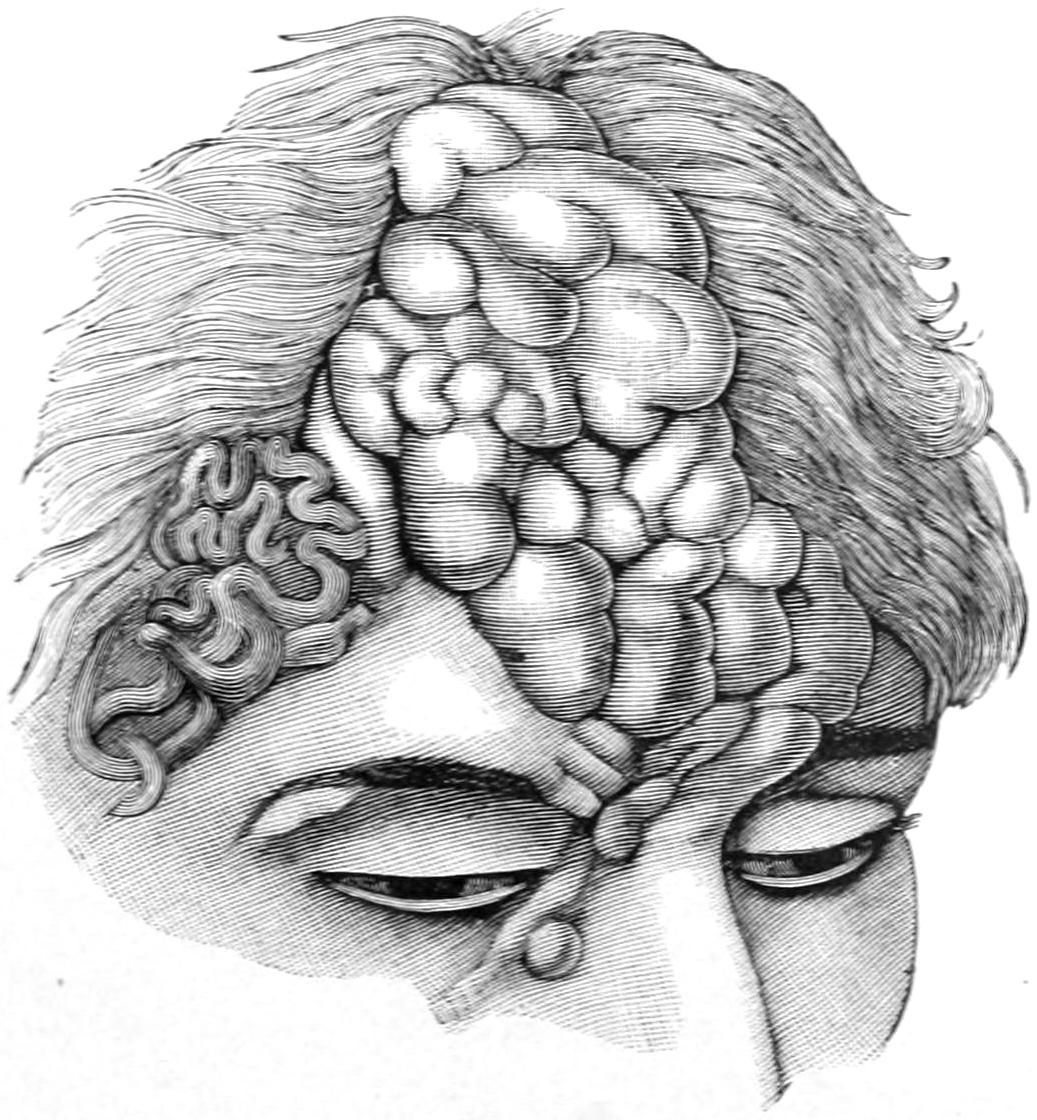
Cirsoid aneurysm. (Bruns.)
5. Cirsoid or Racemose Aneurysms.
—Cirsoid or racemose aneurysms constitute vascular tumors of irregular shape and outline, according to the extent of the arterial system involved.
Fig. 155
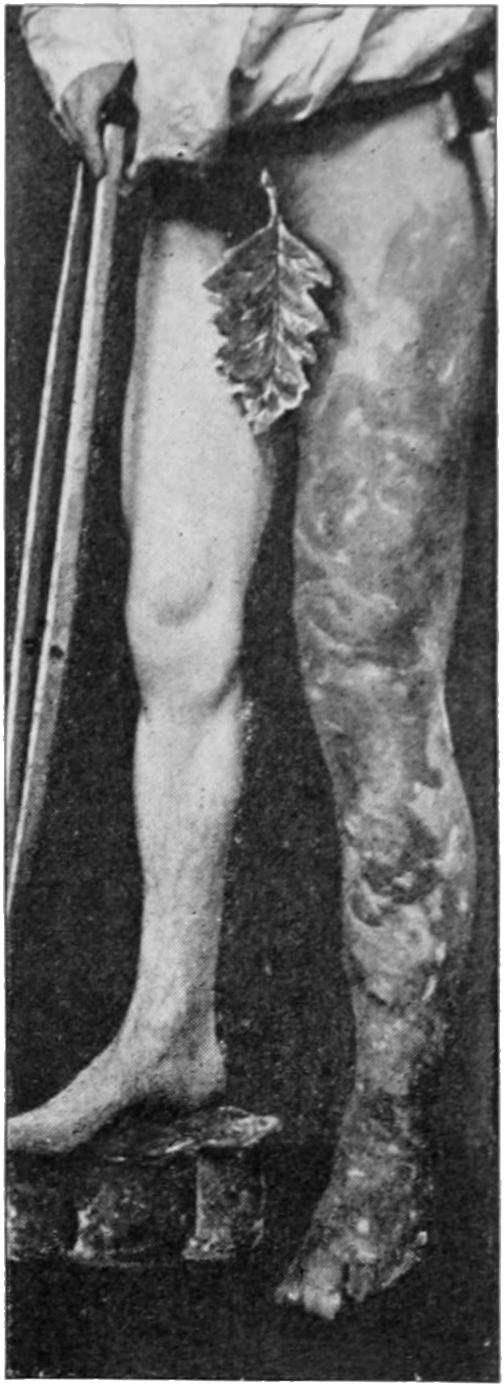
Cirsoid aneurysm of femoral artery and telangiectasis, with lengthening of affected limb from hypernutrition. (Parker.)
6. Angioma or Aneurysm by Anastomosis.
—The difference between angiomas and cirsoid aneurysms is more artificial than natural. When a single vessel is involved with all its branches it constitutes an elongated tumor and partakes of the nature of a varix. When the growth is a collection of small arteries the condition is then known as an angioma. Between these there may be all varieties of vascular changes. Fig. 154 illustrates a case of this kind in the scalp, while Fig. 155, contributed by Parker, illustrates a congenital involvement of the vessels of an entire limb, with overgrowth of the same from increase of blood supply.
[345]
—All aneurysm so constituted as to be easily palpated can scarcely be mistaken for a tumor of any other kind. It can be recognized by its circumscribed nature; its pulsation, which is always of the expansile type; its bruit, which is synchronous with systole. It can be emptied by pressure, fills somewhat slowly if pressure is made above it, but more rapidly if pressure is made below it, being in this respect the counterpart of a venous angioma. Its size and rapidity of pulsation are influenced by position, and its location is usually that of one of the large arterial trunks. The murmur, heard through the stethoscope, is sometimes more than a mere bruit, and may be of a tumultuous, almost roaring character, the sounds being modified by the smoothness or roughness of the interior blood channel as well as by the thickness of the parts outside. Naturally the sounds can be altered by pressure. The overlying integument is at first unchanged, but if an aneurysm is working its way toward the surface and threatening rupture the skin will be stretched and discolored and may finally ulcerate. Blood pressure as measured by the sphygmomanometer is not altered in a limb which is affected by aneurysm.
Signs and symptoms which are not local are also produced in most cases, their variety being great and depending upon the location of the primary disturbing cause; for example, there is generally edema with venous congestion of parts situated distally, these features being so extreme in some cases as not only to threaten but even to occasion gangrene. By pressure upon nerves both pain and paralysis are produced and important functions impaired.
The tendency in all aneurysms is to increase in size and cause atrophy or disappearance of the tissues upon which they exercise their present influence.
Innominate Aneurysms.
—Innominate aneurysms usually appear behind the right sternoclavicular joint. As they increase in size they cause pain and edema of the right arm and the right side of the face, cough, dyspnea, and dysphagia. As the swelling increases it rises above the rib and sternum, pushing forward the sternomastoid and the clavicle. After being displaced the bones and cartilages in front begin to disappear by erosion, and the growth makes its way to the surface, where pulsation can be easily seen as well as felt and heard. In proportion to their increase other significant pressure symptoms, with venous turgescence, will occur. Innominate aneurysms can sometimes be differentiated from aortic by the sign, described by Porter, of tracheal tugging. This is elicited by causing the patient to sit up and bend the head forward, after which the cricoid is grasped and drawn forcibly upward, thus stretching the trachea. If with each cardiac impulse a well-marked tugging sensation be felt it may be attributed to the pulsation of an aortic aneurysm.
Subclavian Aneurysms.
—Subclavian aneurysms of the first part of the vessel present similar features, only that the bruit is propagated down the axillary artery rather than up the carotid, and is not influenced by carotid pressure, while the pressure symptoms are limited mostly to the arm. In axillary aneurysm the radial pulse is more delayed.
Carotid Aneurysms.
—Carotid aneurysms are not always easy of early diagnosis, as at the root of the neck solid tumors often transmit a deceiving pulsation and convey an exaggerated vascular sound. They may also give rise to the same pressure symptoms as do subclavian aneurysms. Non-vascular tumors do not have an expansile pulsation, nor is the arterial sound conveyed upward along the carotid as in true aneurysm. In aneurysms of the external carotid there may be paralysis of the tongue as well as difficulties in speech and deglutition. Aneurysms of the internal carotid tend to extend inward rather than outward. Intracranial aneurysms are difficult of diagnosis, but they usually give the symptoms of brain tumor, with possibly a bruit that may be heard and described by the patient himself, especially in certain positions of the head.
Wardrop used to formulate the diagnostic features of certain aneurysms at the base[346] of the neck, as follows: Innominate aneurysms generally monopolize the episternal notch or rather its right side, taking up this whole space, even though not rising high. They first present to the inner side of the right sternomastoid, while carotid aneurysms appear in the interval between the sternal and clavicular heads, and subclavian aneurysm to the outer side of this muscle.
In the abdomen the aorta is most frequently involved, and sometimes its larger branches. An aneurysm of the renal or mesenteric arteries can easily be mistaken for an aortic aneurysm. The aorta proper terminates at the level of the umbilicus. A pulsating tumor below this level should belong to one of the iliacs. Recognition will depend largely upon the thinness of the abdominal wall and the absence of fat. In many cases expansile pulsation can be detected even here, while the pain is radiated along the well-known branches of the sympathetic, and the location to which it is referred may be of aid in deciding the part of the aorta most involved. Aortic pulsation is communicated by growths overlying it, and the surgeon is liable to be deceived by a certain abnormality of the natural pulsation through this trunk, as it is often exaggerated and appears pathological when it is not. Abnormal pulsation of the abdominal aorta was first described by Cooper, and has served as a topic for surgical essays ever since. Schede’s test may be applied here to advantage: if firm pressure be made simultaneously upon both femoral trunks the extra blood pressure thus caused inside the tumor will give rise to pain, whereas in the absence of aneurysm it produces no such effect.
Iliac and femoral aneurysms may be made difficult of recognition by obesity, but the bruit can almost always be heard, and this, with such extra aid as the rectal or vaginal examination may afford, coupled with pressure symptoms confined to one limb, will usually facilitate diagnosis. Fig. 157 illustrates what features a tumor of this kind may present when located in the upper part of the thigh.
Fig. 157
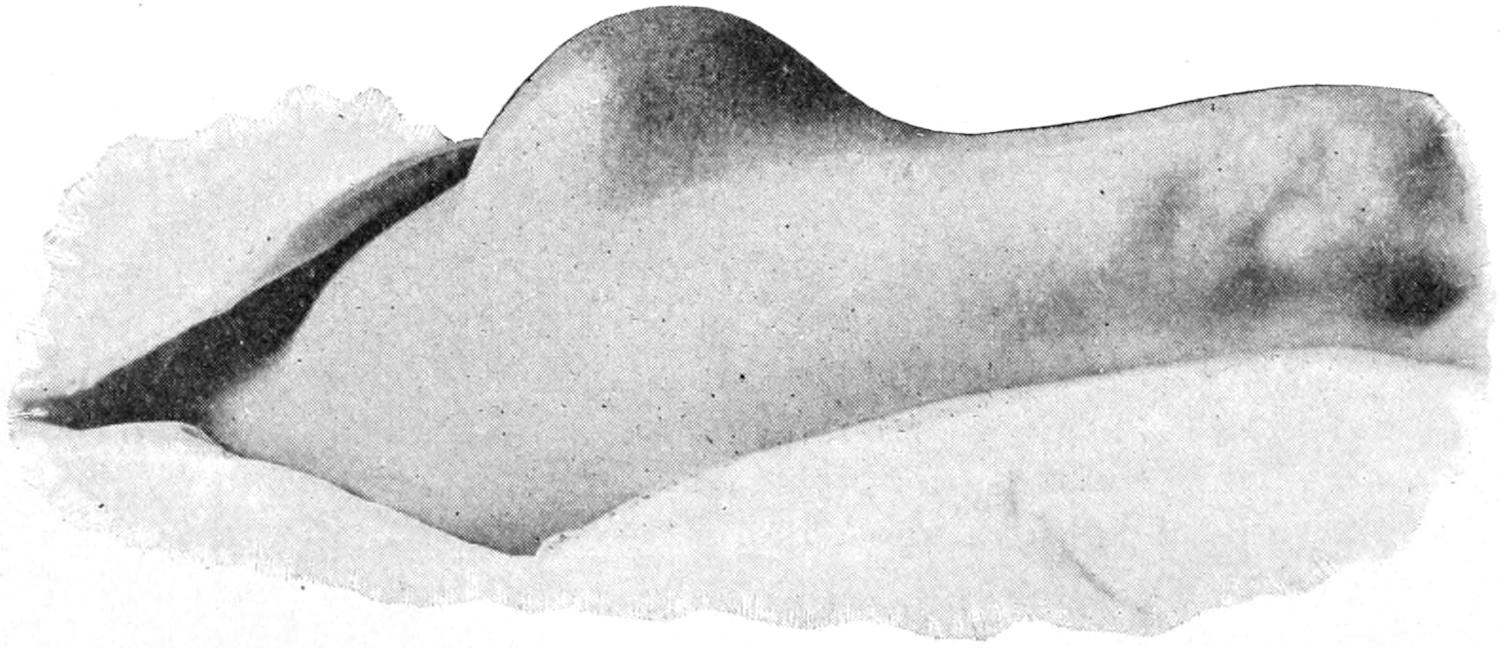
Sacculated aneurysm of femoral artery. (Parmenter.)
—The general purpose of the treatment of aneurysms is to favor coagulation and to effect a cure in this way. In the pre-antiseptic era it is not strange that men resorted to the method of starvation, by which the coagulability of the blood was much increased, or to the rest treatment, with the use of cardiac sedatives, by which the heart’s activity and power were greatly reduced. Nor was it strange that non-operative, yet mechanical, methods were used, in order to minimize the danger attending operative procedures. With the confidence, however, which Lister and his followers have given, it is generally conceded that with an aneurysm which can be made accessible[347] by an operation radical methods are more satisfactory. To the surgeon belong all aneurysms except, perhaps, those of the aorta and the innominate, and even these have not been exempt from surgical methods. The following operative measures are worthy of discussion in these cases: (1) Ligature. (2) Open operation. (3) Extirpation. (4) Opening and suture. (5) Introduction of wire, with or without electrolysis.
1. Ligation includes the application of a ligature in one of the following situations: (a) Proximal ligation (Anel’s) at a convenient point shortly above the sac; (b) proximal ligation (Hunter’s) at a distance from the sac; (c) distal ligation, either of the main trunk just below the sac (Brasdor’s) or of the highest main branch given off below the sac (Wardrop’s). Thus proximal ligation could be practised in case of aneurysm, either of the external or internal carotid, by tying the main trunk, or in the case of popliteal aneurysm (Hunter’s suggestion), by tying the femoral in Hunter’s so-called canal. Brasdor’s distal ligation may be illustrated by ligature, in Hunter’s canal, of the femoral for aneurysm in the groin, while Wardrop’s modification would consist in tying one of the tibials for popliteal aneurysm, or one of the lesser carotids for aneurysm of the common trunk. Should ligation be determined upon, circumstances will dictate where the ligature should be applied, and the surgeon will decide the character of the suture material. The methods of attack upon the large vascular trunks will be considered later. Inasmuch as it takes time to establish collateral circulation, attention should be given to physiological rest, as well as to all other general measures calculated to make any operation successful.
Fig. 158
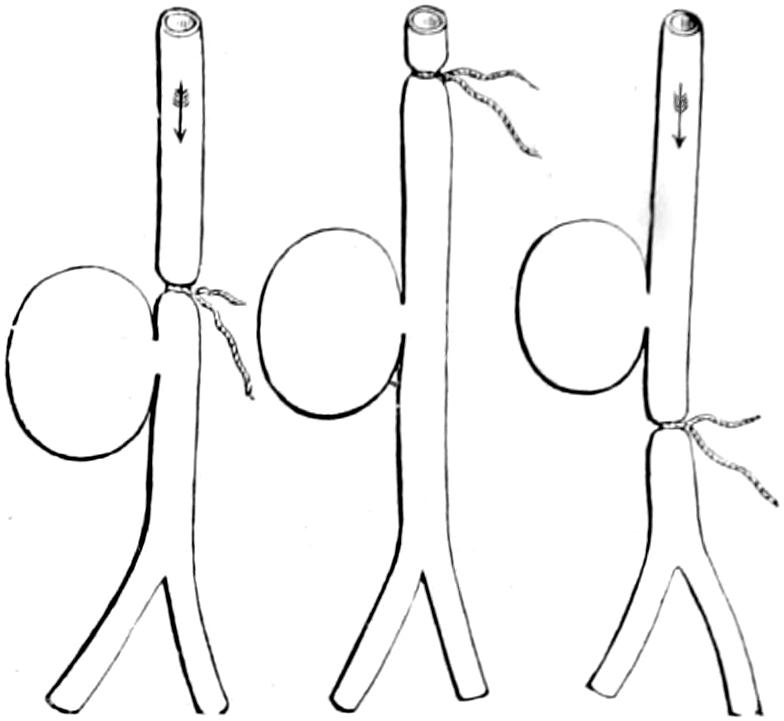
Anel’s operation.
Hunter’s operation.
Distal operation.
(Erichsen.)
Fig. 159
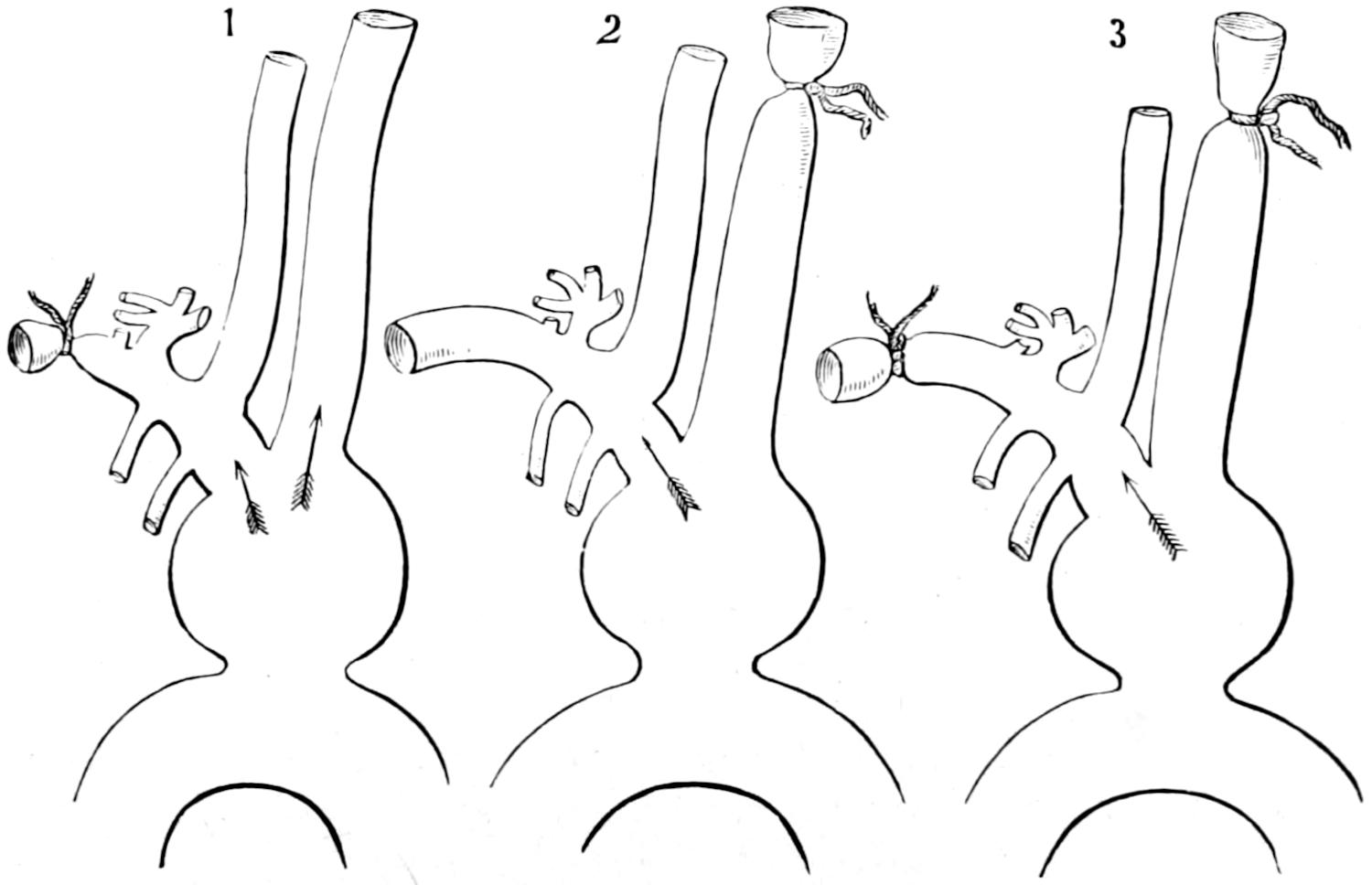
Brachiocephalic aneurysm; ligature of the subclavian only.
Brachiocephalic aneurysm; ligature of the carotid only.
Brachiocephalic aneurysm; ligature of the subclavian and carotid.
Different schemes for application of the ligature according to the necessities of the case. (Erichsen.)
2. Open division was first suggested in the fourth century by Antyllus. It soon fell into disuse and was taken up during the middle of the past century by Syme, to whom the operation has been frequently credited, although it was really the revival of an antique method; but Syme gave it so much of his anatomical exactness and brilliancy of operative skill that he almost made it his own. The method was essentially one by long and free incision, through which the interior of the sac was fully exposed, its contained clots turned out, its vascular openings plugged, while a ligature was applied above and[348] below in order to prevent further arterial communication. Performed before the days of anesthesia or of antisepsis it was an exceedingly bold procedure, yet in Syme’s hands it gave brilliant results.
3. The open division has been replaced by the more perfect procedure of extirpation of the sac, based upon the general principle that an aneurysm is a tumor and should be extirpated, the parts being sutured and expected to heal promptly. It constitutes in many cases the ideal method of treatment. There could be but one improvement on it, namely, that suggested by Matas, of arteriorrhaphy, as one of the radical methods which is often applicable to aneurysms of the extremities, or to those where rupture has occurred or is imminent. The part should be made bloodless, as in this way perfect control can be secured; should this be impracticable, the vessel should be ligated above the aneurysm before proceeding to its excision. This done, and the vessels secured above and below, the wound may be closed as after any other operation, and in this way radical cure achieved within a few days.
Fig. 160 illustrates a recent case of this kind in the author’s hands, where an aneurysm of the common carotid, of about the size of a lemon, was treated in this way, the patient leaving the hospital in eight days, and having no unpleasant complications.
Fig. 160
Aneurysm of the common carotid successfully treated by complete extirpation. (Park.)
4. Open division with arteriorrhaphy has been proposed by Matas and Murphy and in their hands has been successful. Its greatest usefulness is found in traumatic aneurysms of long standing where the arterial opening is usually small and the vessel wall healthy, so that after excision of the sac a sufficient amount of aneurysmal wall or stump may be retained in order to afford a firm surface for union. The circulation being controlled the sac is exposed, opened, and dissected down to a location near the arterial opening. Here the arterial walls are trimmed and freshened, turned in or rolled in, and a row of sutures applied, one line apart, through the outer and middle coats. Matas suggests that after the suture is complete the size of the vessel should be less than its normal, in order that pressure may be reduced at this point and more perfect union follow. The method may also be resorted to in certain fusiform aneurysms, where the arterial wall is still sufficiently healthy to sustain sutures. Here an elliptical piece can be excised, or it may be possible to infold the coats of the sac and apply sutures through a series of folds, on the same principle that they are applied in cases of dilatation of the stomach. Arterial suture as practised in these cases is similar to the Lembert suture used in intestinal surgery. It is necessary to support the tissues around the sutured artery by other buried sutures in such a manner as to fortify them against yielding of the arterial coats.
For these radical methods, either by excision or this combined with suture, the arteriovenous aneurysms afford an inviting class of cases. The parts having been made bloodless and the vessels separated, sutures may be applied, if there be sufficient room for them without too much occlusion of the vessels, which would afford but little advantage over ligatures.
In spite of what has been said about the rarity of these lesions, which is true in civil life, it has been shown, during recent wars, that bullets of small caliber having high velocity have produced instances of this character.
5. For cases so situated as to make any of the above methods inexpedient there is still the more or less promising method of treatment by the introduction of wire, coupled perhaps with the use of the electric current, and the injection of gelatin solutions. While ligation of the abdominal aorta has been practised with temporary success it has not yet proved so encouraging as to justify its performance, save in exceptional cases, but into any intrathoracic or intra-abdominal aneurysm, which appears to be otherwise inoperable, a number of feet of fine steel wire may be introduced, in the attempt to coil it up irregularly within the sac and thus to afford a sort of skeleton framework, upon which[349] coagula will more readily form and by which they may be retained. In some cases the end of this wire has been attached to the negative pole of a galvanic battery, the other pole being affixed to an external electrode, and a weak galvanic current has been passed for a period of say from five to thirty minutes, the time varying in accordance with the strength of the current. By this procedure coagulation is much encouraged. In cases of intra-abdominal aneurysm the abdomen may be opened and the sac more or less completely exposed, after which this insertion may be more minutely performed.
Occasionally surgeons have exposed an aortic aneurysm and endeavored to externalize or exclude it by producing adhesions around it, while some portion of the sac is exposed to the outer world. After adhesions have formed such methods of treatment can be repeated as may be desired. They may also be combined with the subcutaneous use of 2 per cent. sterile gelatin solution, or this may be thrown into the sac in small amounts. It is true, however, that cases of this character are desperate, and while life has been in perhaps half of the operated cases more or less prolonged, but few instances of final recovery have been recorded.
The after-treatment consists of physiological rest of the part operated upon, and rest and abstention from violent exertions of any kind. During this time elimination should not be neglected, emotional excitement should be avoided, and, in the presence of syphilitic disease or a well-founded suspicion of it, conventional antispecifics should be administered in sufficient amounts. When the aneurysm is of traumatic origin and there is no general vascular or cardiac disease, there will be a quick restoration of the integrity of parts as well as of their usefulness. Massage and an elastic bandage will be useful, in order to atone for the results of a disturbed circulation.
This is almost a new topic in surgery, especially suture of the arteries. Surgeons have learned that the walls of the arteries and of the veins, when not too much diseased, will tolerate sutures and unite easily. The larger the vessel the easier it is to apply a suture, as its walls are thicker and the method easier. The greater, too, will be the need of suture when the vessel is an important one. Small vessels are relatively so unimportant as not to demand so formal a procedure. The vessels to which the method is most applicable are the common carotid, the subclavian, axillary, brachial and femoral, with their accompanying veins, including the common jugular. It is applicable when it is an injury to the vessel which has necessitated an operation, or when, during its performance, some trunk has been torn out or torn open, as in separating adhesions. It is serviceable, also, when both artery and vein have been involved, as in the groin, where the danger of gangrene of the limb would be enhanced if both the outflow and the inflow of the blood were shut off.
Fig. 161
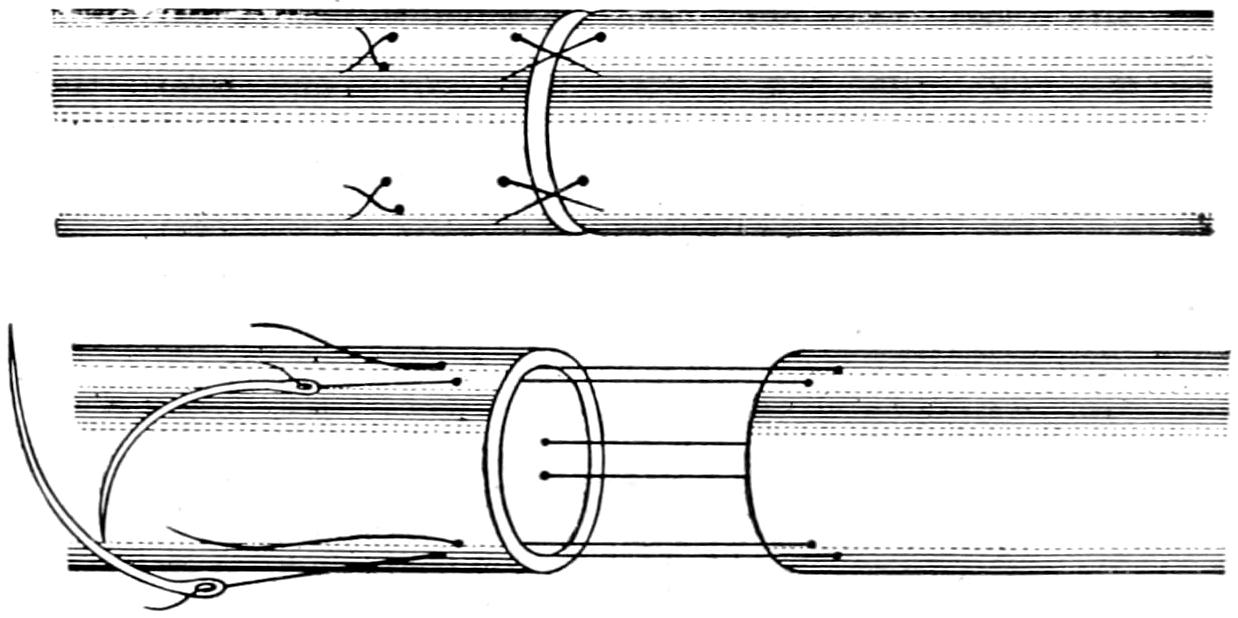
End-to-end suture of a divided artery, permitting a certain degree of invagination. (After Murphy.)
Lateral suture of injured bloodvessels may be regarded as a standard procedure, as it is nearly always possible to temporarily control the circulation on both sides of the field of operation, either by elastic constriction or temporary ligation or clamping. For this purpose fine silk makes the best suture material. It should be threaded into round needles and the sutures should include only the two outer coats. After completing[350] the suture the distal provisional closure of the vessel should be first removed. As the blood backs up in the artery it will test the efficacy of the sutures. Should there be no leakage the proximal clamp may be removed, and then if the condition appear satisfactory the arterial sheath should be carefully closed, and over this the other tissues, with buried sutures.
End-to-end suture of bloodvessels is a recent measure, for which we are indebted to Murphy. It is applicable to vessels which have been divided circularly and completely or almost completely. In the event of the adoption of this method the ends should be divided squarely and then reunited by sutures threaded upon the needles, passing through all the coats, about 1 Mm. from the margin of division, as well as about the same distance apart. If the upper end can be drawn into the lower one, and gently held there by a series of U-shaped stitches, it may be considered the best method.[26] (See Fig. 161.)
[26] There are now before the profession three methods of repairing arteries—by invagination, by suture of the two outer coats, by the through-and-through method—each of which has its advantages and disadvantages. The presence of sutures in the interior of the vessel does not seem to produce coagulation, even though the intima of the vessel is injured by the passage of the same. Nevertheless sutures must be kept out of the blood stream. Liability to secondary hemorrhage is reduced if a double line of sutures can be used.
Arteries are exposed and ligated in their continuity for the purpose of controlling hemorrhage, either for temporary or permanent purposes. The results of permanent ligature have been described in the chapter on Wounds. The application of a ligature should be so made as to thoroughly break up the intima without serious injury to the other coats of the vessel. Coagulation and organization of the thrombus soon produce a permanent occlusion and obliteration. It is a mistake to endeavor to tie the ligature too tightly. Hardened catgut or freshly boiled silk make the best ligature material. It is seldom a difficult matter to find the desired artery upon the normal individual or upon a cadaver. In some cases in practise the tissues through which search must be made will be found infiltrated with blood or otherwise altered, and the discovery of and attack upon the vessel may be thus made very trying. The vessel when exposed in its continuity will be recognized by the sense of touch rather than that of sight, and almost the entire maneuver may be made, by touch alone, by one whose tactile sensibility has been well trained and without any clear view of the vessel. The arteries which are thus exposed have their own sheaths, especially the larger ones, which should be opened with care, not alone to avoid injury to the vessel itself, but in order that the amount of separation may be as slight as possible, as the sheath is necessary for support and for nutrition. Having exposed the vessel and divided the sheath the ligature is introduced with a blunt, curved needle attached to a handle, and known as an aneurysm or artery needle. It is made to carry the ligature, or it is so insinuated and brought out from behind the vessel that the ligature may be threaded into its eye. Caution should be exercised that nothing but the artery itself is included; this is especially necessary in the neck, where the relations between the large vessels and the nerves are very intimate. As a general rule the needle should not be threaded until after it has been passed. The knot should be tied in the depths of the wound, and the vessel should not be disturbed by efforts to secure the knot. If the operation have been done as it should it will not be necessary to drain such a wound, but it may be closed by buried and superficial sutures. When one of the limbs has been involved in this operation it should be kept absolutely at rest, in a somewhat elevated position, and warm applications made, in order that the warmth previously maintained by the free circulation of arterial blood may not be allowed to drop too low.
—The innominate had been tied between thirty-five and forty times, up to 1905. A number of patients have survived the operation, and died within a few weeks of cardiac and arterial disease. Some have progressed a number of weeks, with rapid recovery from the operation and temporary improvement sufficient to justify this operation in apparently favorable cases. This vessel and the carotid also should be tied, in order that the resulting clot may be more perfect and that there should be no return pressure made upon the aneurysmal sac. The incision is made along the anterior border of the sternomastoid down to the clavicle and then[351] along the inner third of this bone, thus forming a flap whose free edges are 10 Cm. in length. The sternal and clavicular heads of the sternomastoid are divided, while the sternohyoid and sternomastoid are separated from the sternum, care being taken especially of the anterior jugular vein, which may be double ligated, if necessary, and, in the deeper dissection, of the pneumogastric and the recurrent laryngeal nerves, which wind around the innominate, and the phrenic, which is in close relation with it. In view of the great engorgement which the aneurysm may produce in the veins of the neck it would be a great help in this operation to follow Crile’s suggestion for removal of goitres, placing the patient in the semi-upright position and having him wear the pneumatic suit, in order that, by suitable pressure from without, the blood pressure may be kept at the proper degree, while, at the same time, the veins of the neck are emptied by gravity. The carotid, having been found, is traced downward and will lead to the innominate and the sac. When the ligature is ready to be drawn tight the table should be lowered and the pneumatic pressure in the suit reduced.
Obviously the deeper the surgeon dissects the more difficulties he will encounter. The innominate artery is crossed by the left innominate vein, which may be in the way, while all the other vessels may be so much disturbed as to alter their relations and make their recognition difficult. The gradual progress of the aneurysm may have caused the tissues to become matted to each other and thus lose their identity. The innominate having been found is traced downward behind the sternum and a suitable base is sought for the ligature. This search may be aided by changing the position of the patient’s head, and with the assistance of artificial light. In the depths of the wound the veins, the vagus, and the pleura can only be avoided by care in keeping the point of the artery needle in contact with the artery. If necessary gentle traction on the carotid trunk may aid by lifting the sac and making its isolation more easy.
As suggested by Bardenheuer the upper end of the sternum may be removed with sufficient of the inner end of the clavicle to facilitate approach. This has been done in this country by Burrell. The aneurysm needle is passed from without inward and from below upward, in order to avoid injury to the pleura. An artery needle made with a flexible tip, which may be bent to suit the exigencies of the case, will make the most difficult part of the work more easy. The ligature should not be tied too tightly, and for this purpose silk is the preferable material. Strips of ox aorta and other animal materials have been used, but if the knot is not too tight no harm will be done to the artery wall.[27]
[27] Sheen (Annals of Surgery, July, 1905) reports a successful case, his method being as follows: Median incision from the cricoid to one inch below the sternal notch, exposure of the carotid and innominate, then a silk ligature carried around the innominate distally and tied with Balance’s stay-knot; pulsation ceased, to later reappear. A second similar operation also failed. A third operation was performed through a five-inch transverse incision above the clavicle, the artery being twice ligated proximally. Sheen advises that ligature should always be of silk, that the incision should be central, with horizontal and vertical division of the manubrium; that the carotid should also be tied; that two ligatures be placed; that drainage is inadvisable, and that next to sepsis as a cause of death stand cerebral lesions. Statistics are thirty-six cases of ligature, with a mortality of 78 per cent.
As stated above, the common carotid should also be tied at the conclusion of the other ligation. These cases should be drained with a few strands of catgut. Absolute rest is an essential of the after-treatment.
—The common carotid may be tied above or below the omohyoid. The carotid divides at the level of the thyroid prominence, and it is more easily exposed above the omohyoid than below. It may be reached by an incision, 10 Cm. in length, along the anterior border of the sternomastoid, whose centre should be at the level of the intended ligature. The sternomastoid, after exposure, is drawn outward and the other muscles inward; bleeding veins are secured; the artery recognized by its pulsation; its sheath opened, preferably on the inner side, and the needle passed from within outward, the operator taking pains to avoid the descendens noni. The internal jugular is more likely to be in the way and to need retraction on the left side than on the right. In this operation when the omohyoid is exposed it is retracted upward.
Through this exposure temporary occlusion, either by provisional ligation or the employment of Crile’s clamps, may be practised.
Ligature above the omohyoid is performed in the same way, the veins being divided and secured. The omohyoid is now drawn downward and the other muscles separated as above. The so-called carotid tubercle is the anterior projection of the transverse[352] process of the sixth vertebra, and the ligature is usually applied at the point where the vessel can be felt pulsating upon this prominence. The same care should be exercised in avoiding the descendens noni. Nélaton is reported to have said that it would take a man four minutes to bleed to death after opening the carotid artery, but it should take only two minutes to tie it.
—The incision now is placed higher, from the angle of the jaw to the level of the cricoid cartilage, still along the anterior border of the sternomastoid, which is to be retracted outward. The posterior belly of the digastric will now appear, with the hypoglossal nerve below it, both being carefully avoided. The great cornu of the hyoid being sought and found, the artery is found opposite its tip, and ligated between the superior thyroid and the lingual branches, or perhaps below the latter. The superior laryngeal nerve which passes behind the vessel is to be scrupulously excluded.
Excision of the external carotid has been recommended, especially by Dawbarn, for the purpose of cutting off the blood supply from certain inoperable cancers of the tongue, face, and jaws. He regards mere ligature as insufficient and insists that, since anastomosis is perfected too soon after the other procedures, it is necessary to completely excise a portion of the vessel. He does this first on the side most affected, and then, say a few weeks later, attacks the other side. He advises to ligate the external carotid just beyond its origin, to divide it, to seize the upper end in forceps, and then, controlling the vessel, to isolate it up to a point where it disappears in the substance of the carotid, tying each branch as it is exposed. He would again tie it just below the origin of the internal maxillary and temporal branches.
—The internal carotid is very rarely attacked in this way. It lies at first to the outside and back of the external carotid, and here it may be sufficiently exposed to admit of ligation. The incision does not differ essentially from that for the external carotid. After the vessels are exposed the external branch should be drawn inward, the digastric upward, or divided, if necessary, and the needle passed from without inward, avoiding the jugular and the vagus (Fig. 162).
Fig. 162
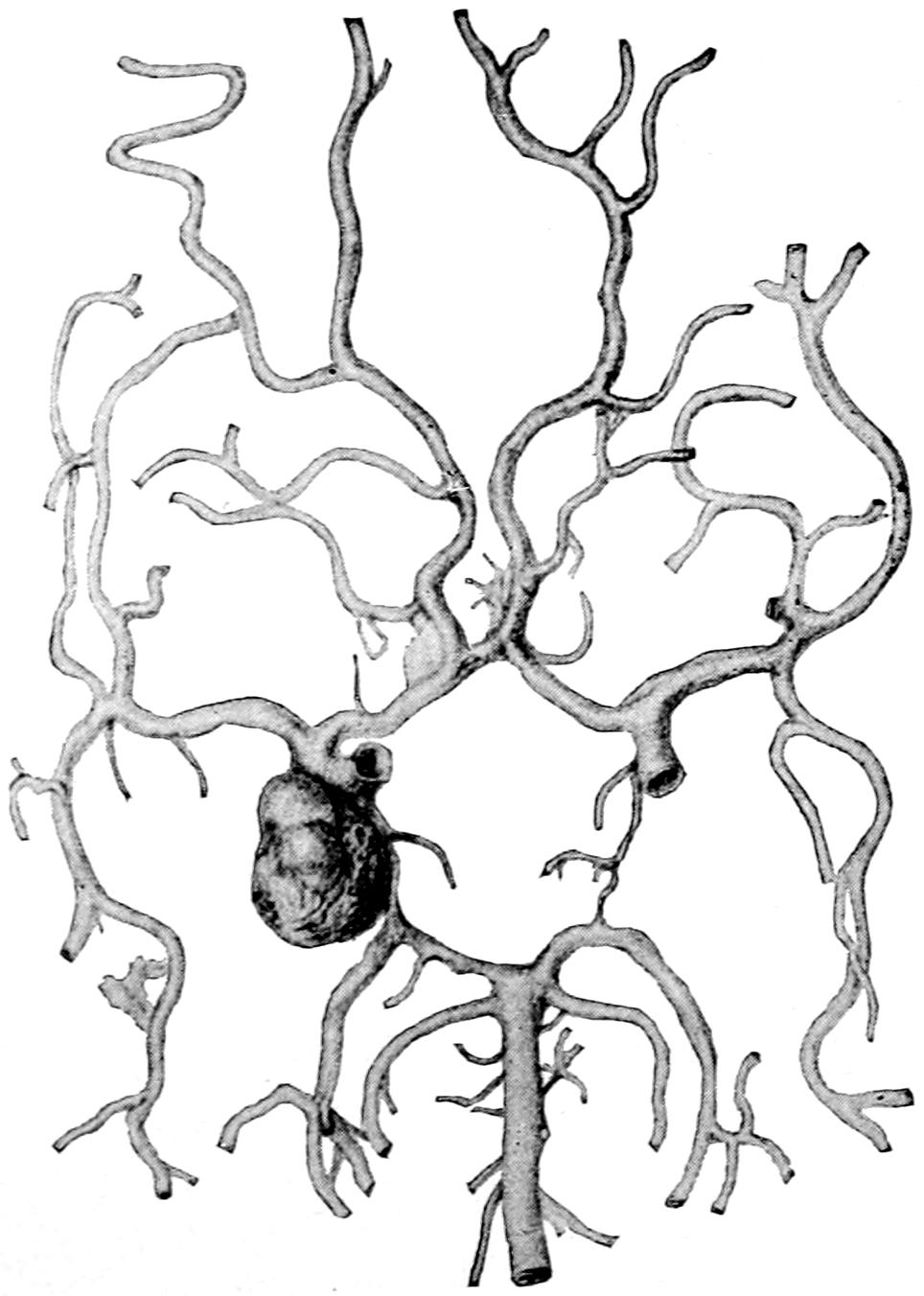
Aneurysm of the right internal carotid. (Peacock.)
—The lingual artery may be conveniently tied before some of the radical operations on the tongue, and it is also tied in cases of cancer in order to shut off nutrition. Incision is made 2 Cm. above the hyoid, parallel with it, from the middle line nearly to the angle of the jaw. Through this the submaxillary gland will be exposed and should be retracted upward and out of the way. The fascia is then divided, and the posterior border of the mylohyoid identified. The digastric tendon is then drawn upward from the hyoglossus, upon which it rests. The hypoglossal nerve is now seen, the artery lying behind it. It is, therefore, necessary to divide the hyoglossus by a short incision in order to reach the vessel. The most important precaution is to avoid injury to the nerve (Figs. 163 and 164).
Fig. 163
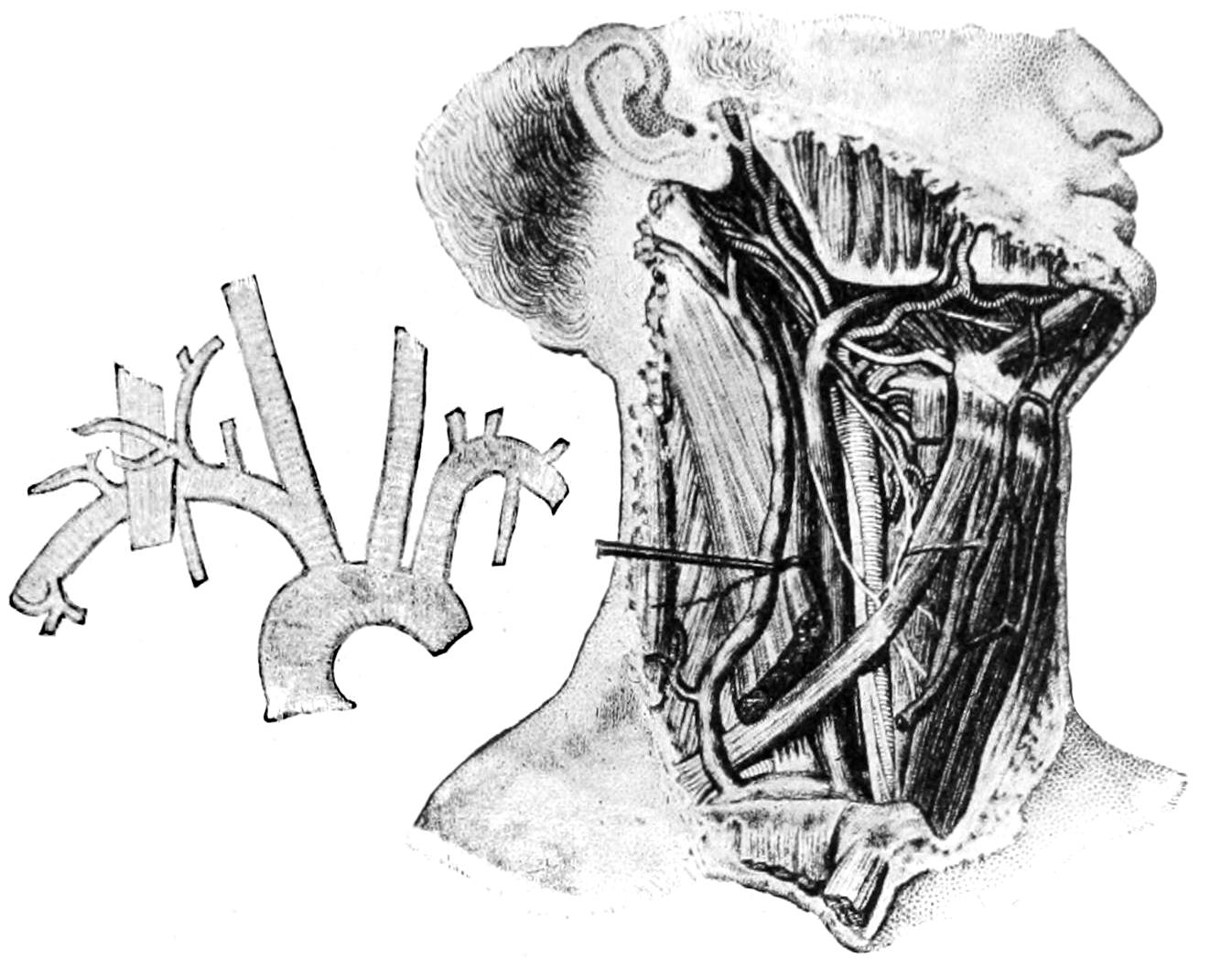
Fig. 164
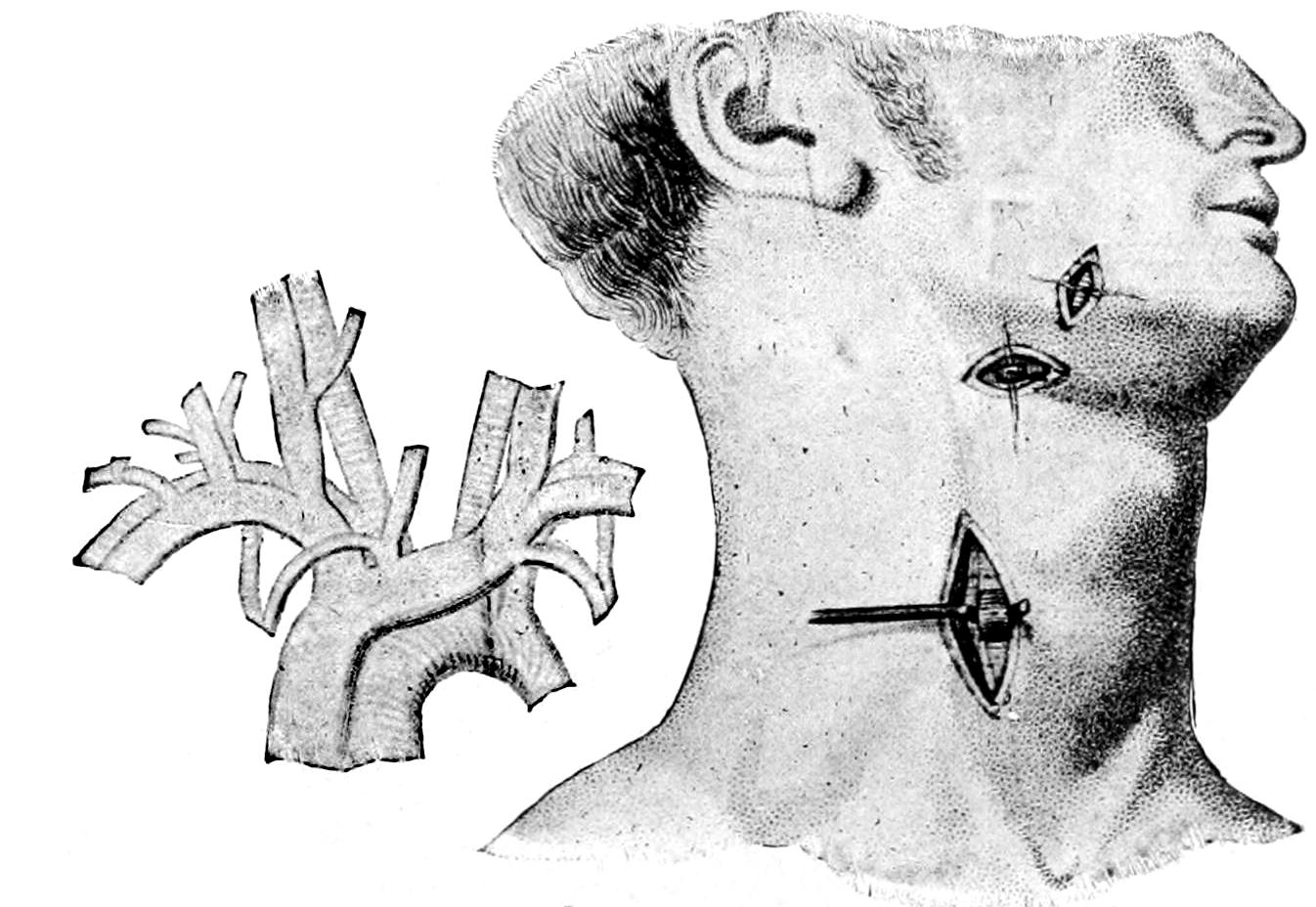
Surgical anatomy of the neck; ligation of the carotid, lingual, and facial arteries. (Bernard and Huette.)
—The facial may be tied through an incision nearly identical with that for the external carotid, or at the margin of the lower jaw 1 to 2 Cm. in front of the angle. The temporal may be attacked through a vertical incision over its course between the tragus and the condyle. Branches of the facial nerve cross the artery at right angles to it; these should be avoided. The occipital may be tied close to its origin, through the same incision as that for the external carotid, or behind the mastoid, through an incision commencing at its tip, carried backward and[353] upward. It will be necessary here to divide the posterior fibers of the sternomastoid, of the splenius, and perhaps of the trachelomastoid. The vessel is then recognized by its pulsation between the mastoid and the transverse portion of the atlas.
—The vertebral artery is tied through an incision commencing at the clavicle, extending along the outer border of the sternomastoid, some of whose clavicular fibers must be divided. This muscle and the anterior jugular veins being drawn to the inner side, the transverse processes of the sixth and seventh vertebræ should be found in the space between the scalenus anticus and the longus colli. The artery should be found below the seventh cervical vertebra as it enters the foramen intended for it. The vein lies in front of it, the pleura close to it, and on the left side the thoracic duct is not far away.
—The inferior thyroid artery may be tied through an incision along the inner border of the sternomastoid, which is retracted outward, the carotid being found and also retracted outward. The artery lies a little below the level of the sixth vertebra, whose transverse process may be easily found. It passes inward and to the rear of the carotid, close to whose main trunk the ligature should be applied, in order to avoid the recurrent laryngeal.
[354]
Fig. 165
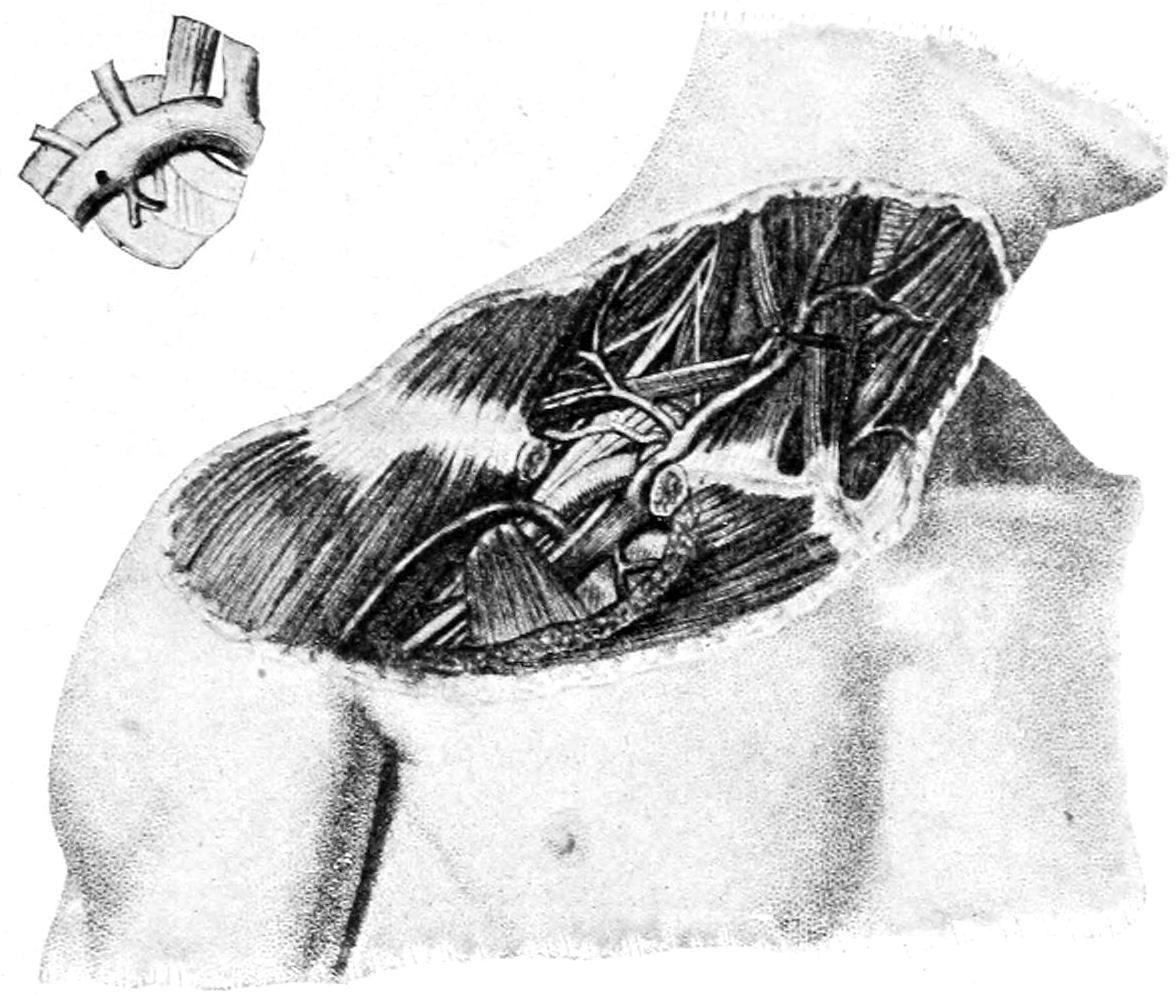
Fig. 166
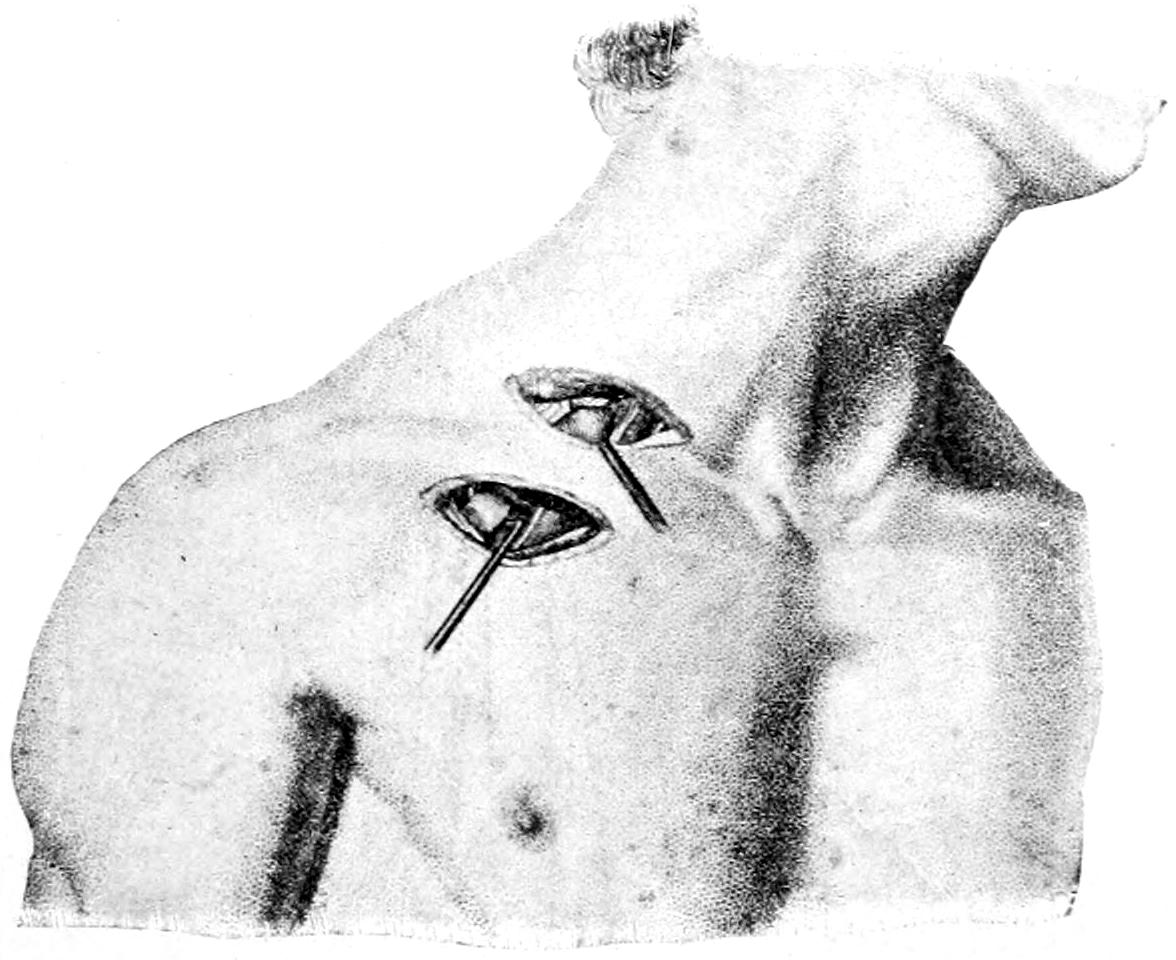
Surgical anatomy and ligation of the axillary and subclavian arteries. (Bernard and Huette.)
—This is best tied by making an incision 2 Cm. above the clavicle, beginning nearly at its sternal joint, and extending outward to the anterior border of the trapezius. In exposing it the cervical branches of the superficial nerves should also be divided. The external jugular lies here, near the posterior border of the sternomastoid, and winds around it to empty into the internal. Unless it can be avoided it should be carefully double ligated. The omohyoid should appear at the inner angle of the wound and may be drawn out of the way in either direction. The suprascapular artery and perhaps one or two other vessels may cross the wound and require retraction. It is usually necessary to remove considerable adipose tissue in which these vessels lie. The brachial plexus, of course, will be encountered. The scalenus anticus, which should be followed down to its tubercle of attachment on the first rib is of special importance. To its inner side is the internal jugular, with a somewhat bulbous enlargement. In front is the subclavian vein and behind the muscle is the artery. The phrenic nerve passes down upon the anterior surface of the scalenus anticus, and the thoracic duct ascends close to it, opening into the angle between the subclavian and internal jugular veins. While it is not impossible nor even impracticable to apply a ligature to the subclavian on the inner side of the scalenus anticus it is rarely necessary, and the ligation is almost invariably performed to its outer side, in the free part of its trunk. There must be sufficient space in which to work with safety, and, when necessary, adjoining muscles,[355] i. e., sternomastoid and trapezius, may be divided to any necessary extent. The patient should always be placed in such a position that the shoulder is pulled well down, with the arm passed behind the back, while the neck is stretched by extending the head to the opposite side. The artery needle should be passed from above downward and from behind forward, the vein being carefully held out of its way. The patient should wear the Crile pneumatic suit, in the semi-elevated position, in order that the veins in the neck may be less engorged (Figs. 165 and 166).
—The axillary artery is practically tied in its third portion, beyond the lesser pectoral. The incision is made through the middle of the axilla, over the course of the vessel, the deep fascia exposed and divided, the coracobrachialis and musculocutaneous nerve retracted outward, and the artery recognized with the finger-tip. It should be so cleared, especially from the median nerve, as to be easily raised upon the blunt hook. The accompanying veins should not be enclosed in the ligature (Figs. 167 and 168).
Fig. 167
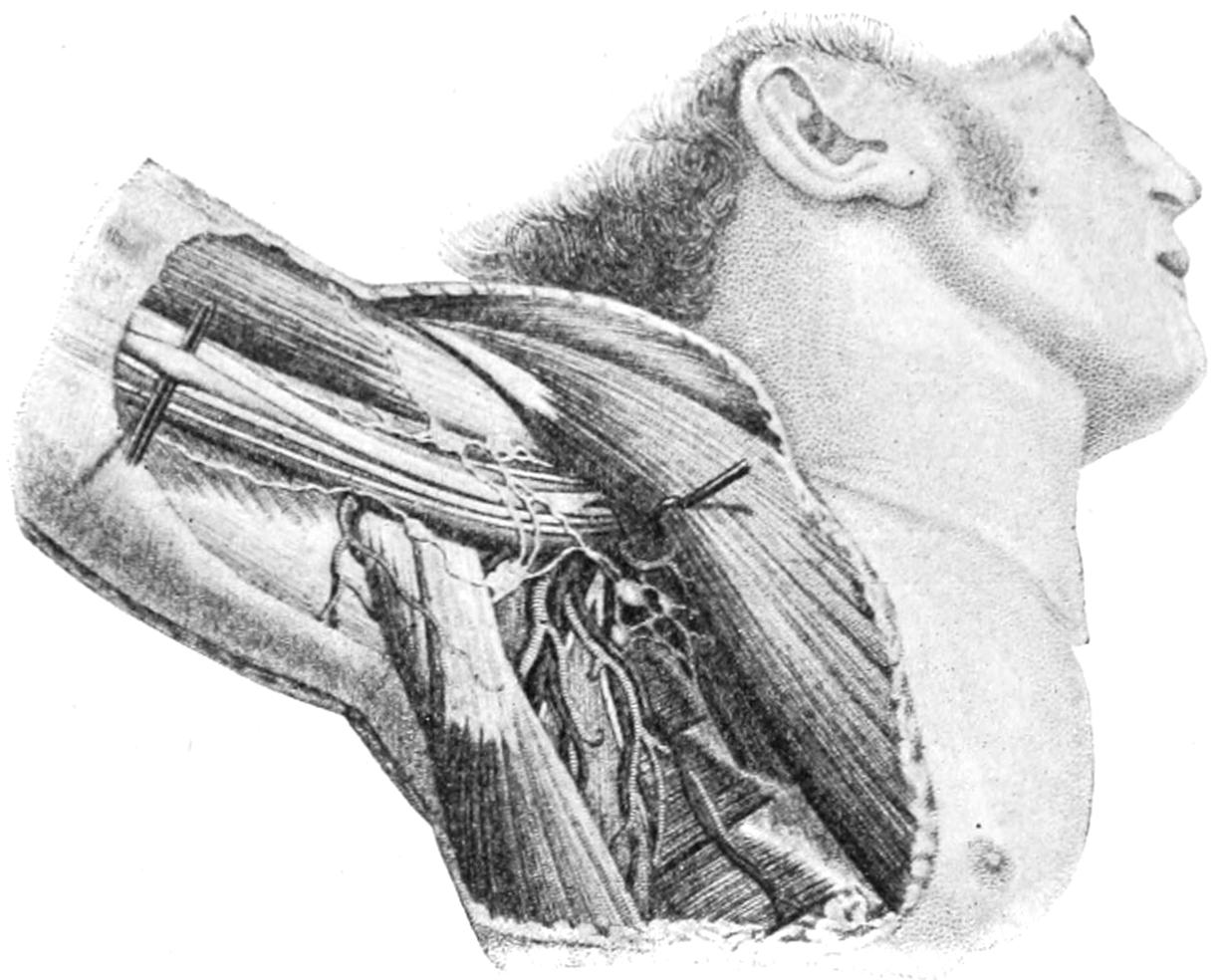
Fig. 168
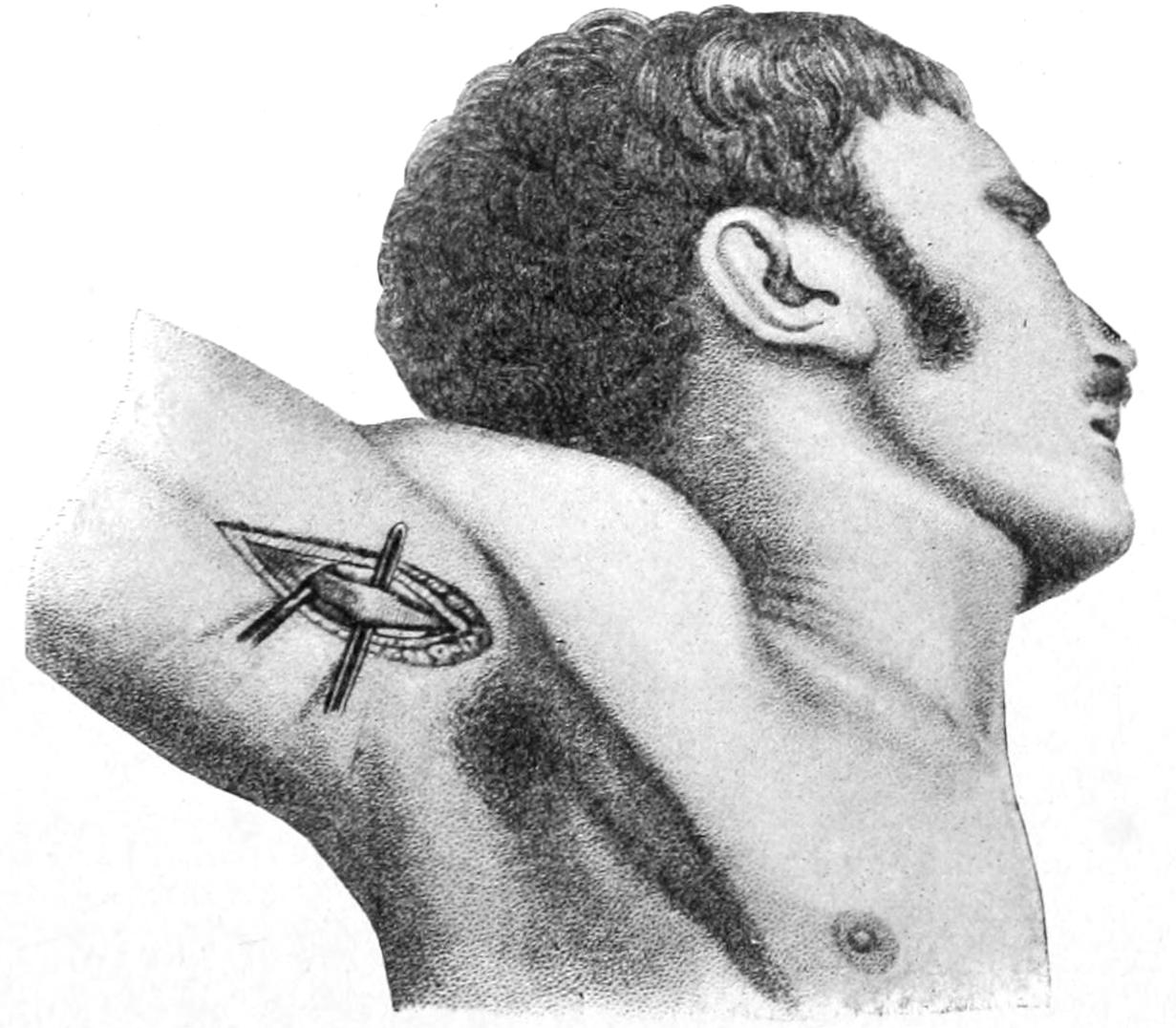
Surgical anatomy of the axilla and ligation of the axillary artery. (Bernard and Huette.)
—The brachial artery is easily found in the middle of the arm, near the inner edge of the biceps, whose inner border is identified. The median and other nerves should not be brought into view. The parts will be relaxed by[356] flexing the forearm. The venæ comites should be carefully excluded from the ligature (Figs. 169 and 170).
Fig. 169
Fig. 170
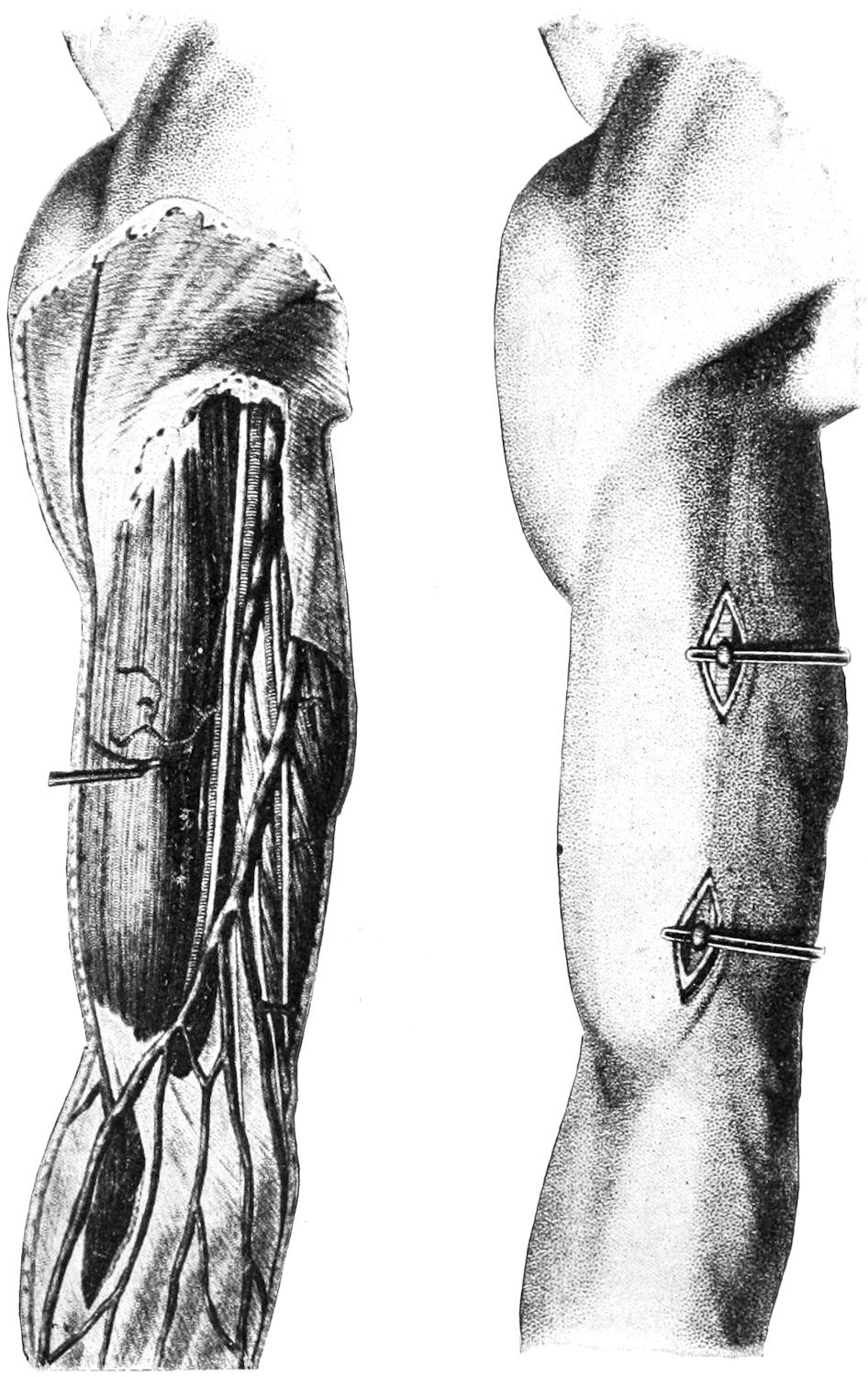
Surgical anatomy and ligation of the brachial artery. (Bernard and Huette.)
—The radial artery is the direct extension of the brachial and passes underneath a nearly straight line to the neighborhood of the scaphoid bone. High up in the forearm it may be exposed between the supinator longus and pronator teres, being found beneath the former. In the middle portion of the forearm it may be exposed along the ulnar border of the supinator longus, and lying upon the pronator radii teres. At the wrist it may be exposed with perfect ease, where it is usually outlined when feeling the pulse (Figs. 171 and 172).
—The ulnar artery is the larger of the two main trunks, and is rarely tied in the upper part of the arm, lying too deep for easy exposure. Should it be divided by a wound of this region the opening may be enlarged sufficiently for its detection and double ligation (Figs. 171 and 172).
Of the large vessels of the trunk the abdominal aorta has been tied, although it is questionable whether this would ever be a justifiable operation, as all recorded cases have succumbed from one cause or another.
—The common iliac artery is best tied by an incision commenced parallel with Poupart’s ligament and curved upward and outward. The abdominal muscles and fascia having been divided, with the least possible injury to their fibers, the peritoneum is detached from the iliac fascia, the patient being turned upon the side in such a way that gravity may assist in the exposure of the vessel behind the[357] peritoneum. A needle of medium length, and strong, with oblique lateral curve, should be passed from within outward, the vein lying behind the artery on the right side, near to its inner side, and behind on the left side. In the fossa thus formed, and lying upon the psoas, will be found not only the common trunk but the external cutaneous nerve, running downward and outward, and also the iliac branch of the iliolumbar artery.
The operator may decide, for some reason, to open the abdomen directly, and to go through from front to rear, drawing aside the intestinal loops, with the patient in the Trendelenburg position, exposing the main trunk by a small incision through the posterior peritoneum and applying the ligature there. By this same transperitoneal method the internal iliac may be attacked. Its course inward and downward, rather than outward, makes it more easy of attack in this way. The ureter, which lies in front of the artery, should be raised, along with the peritoneum, in order that it may be avoided. This vessel has thus been tied for hypertrophy of the prostate, for inoperable cancer of the uterus, during excision of the rectum, and even for the cure of vascular tumors or aneurysms affecting its terminal arteries.
Fig. 171
Fig. 172
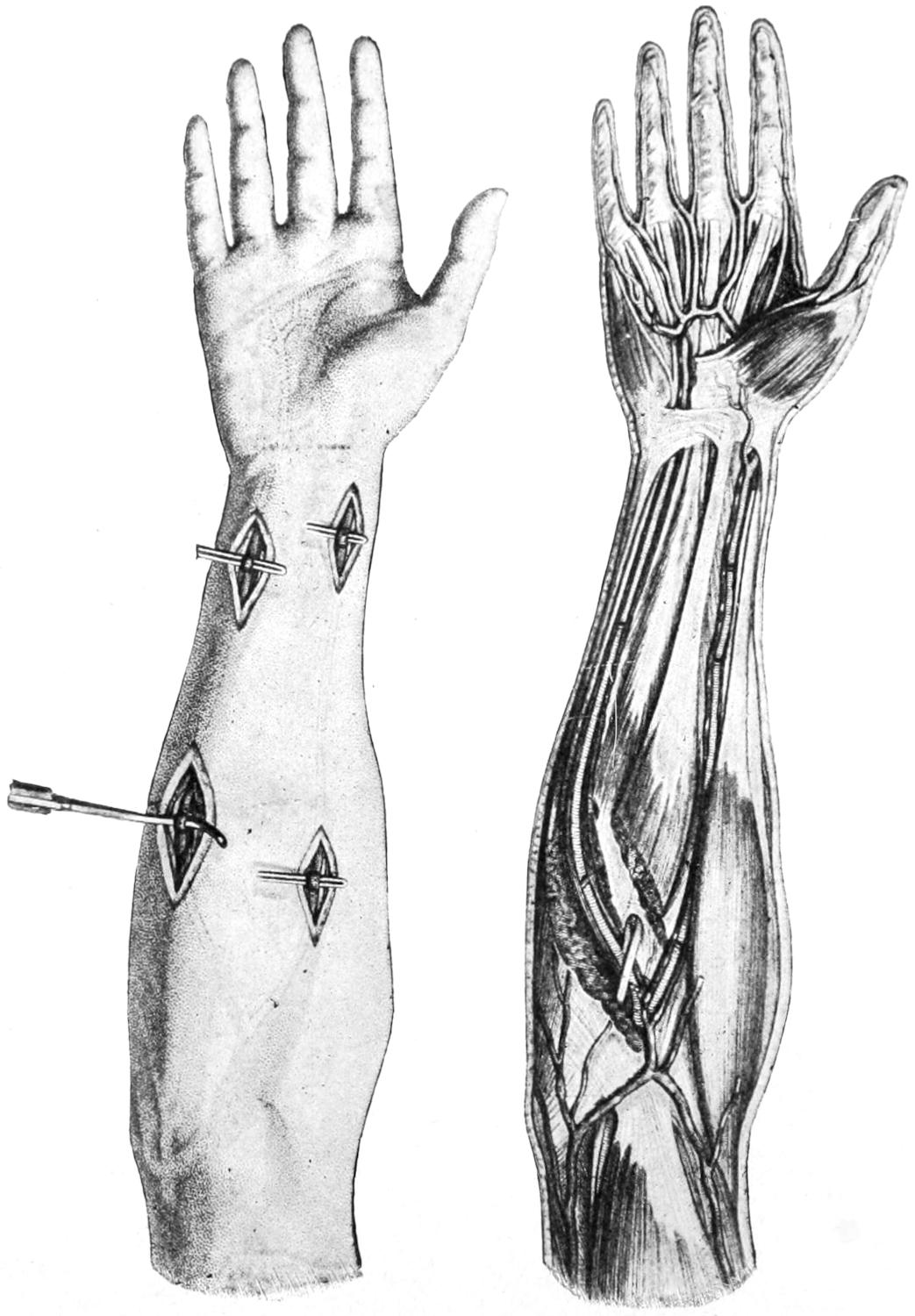
Surgical anatomy and ligation of the radial and ulnar vessels. (Bernard and Huette.)
—The external iliac artery is exposed without great difficulty by a 10 Cm. incision about Poupart’s ligament, beginning near the pubic spine, extending outward and slightly upward. It will probably be necessary to double ligate and divide the superficial epigastric artery, after which the outer border of the conjoined tendon is to be recognized at the lower and inner end of the incision. The lower fibers[358] of the internal oblique are then to be divided, the transversalis exposed and transversely divided, after which the deep epigastric artery will probably come into view. The pulsations of the external iliac will now identify it. The subperitoneal tissue should be[359] carefully detached and the peritoneum gradually separated from the vessels and properly retracted. Beneath it the areolar tissue which helps form the sheath of the vessel must be avoided, after which the artery needle may be passed from within outward. In closing the wound the deep layers should be brought together, each by itself, in order to avoid the possibility of ventral hernia. Through this same incision both the deep epigastric and the deep circumflex arteries may be exposed (Figs. 173, 174 and 175).
Fig. 173
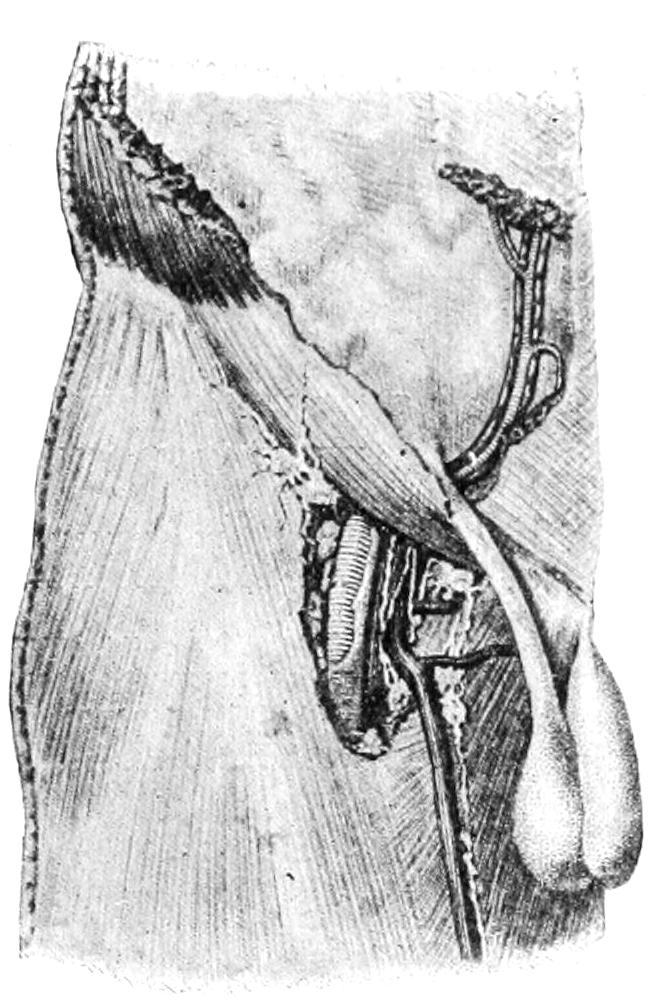
Fig. 174
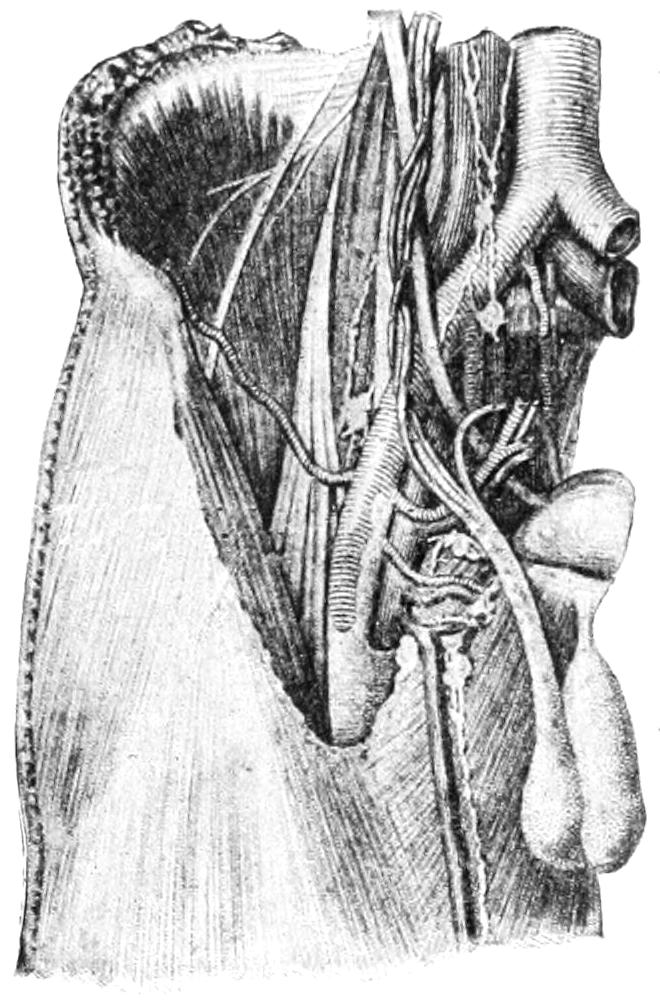
Fig. 175
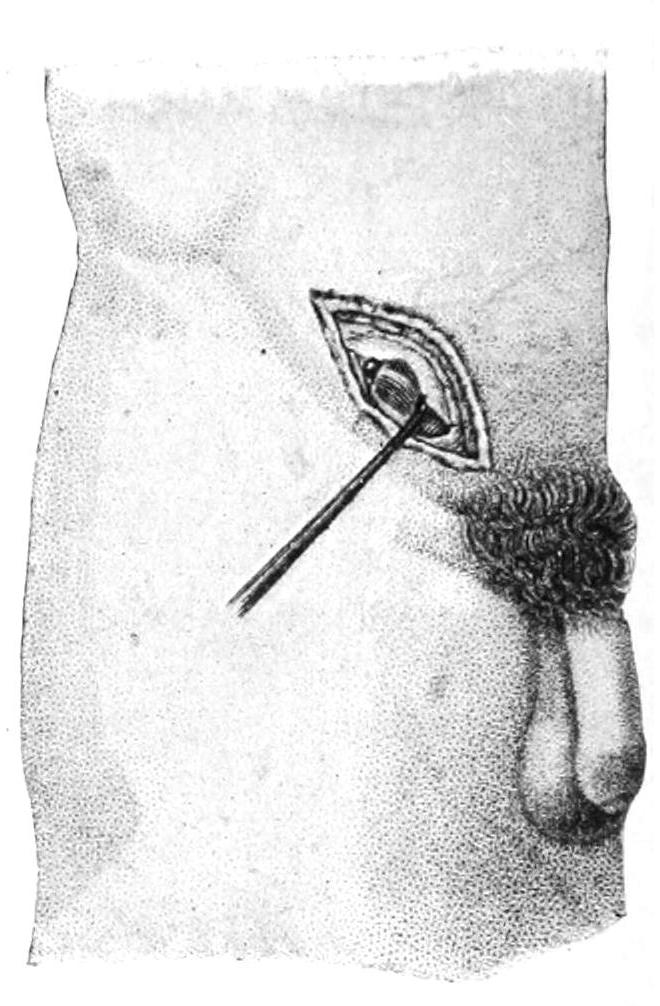
Surgical anatomy and ligation of the femoral, external iliac, and epigastric arteries. (Bernard and Huette.)
Fig. 176
Fig. 177
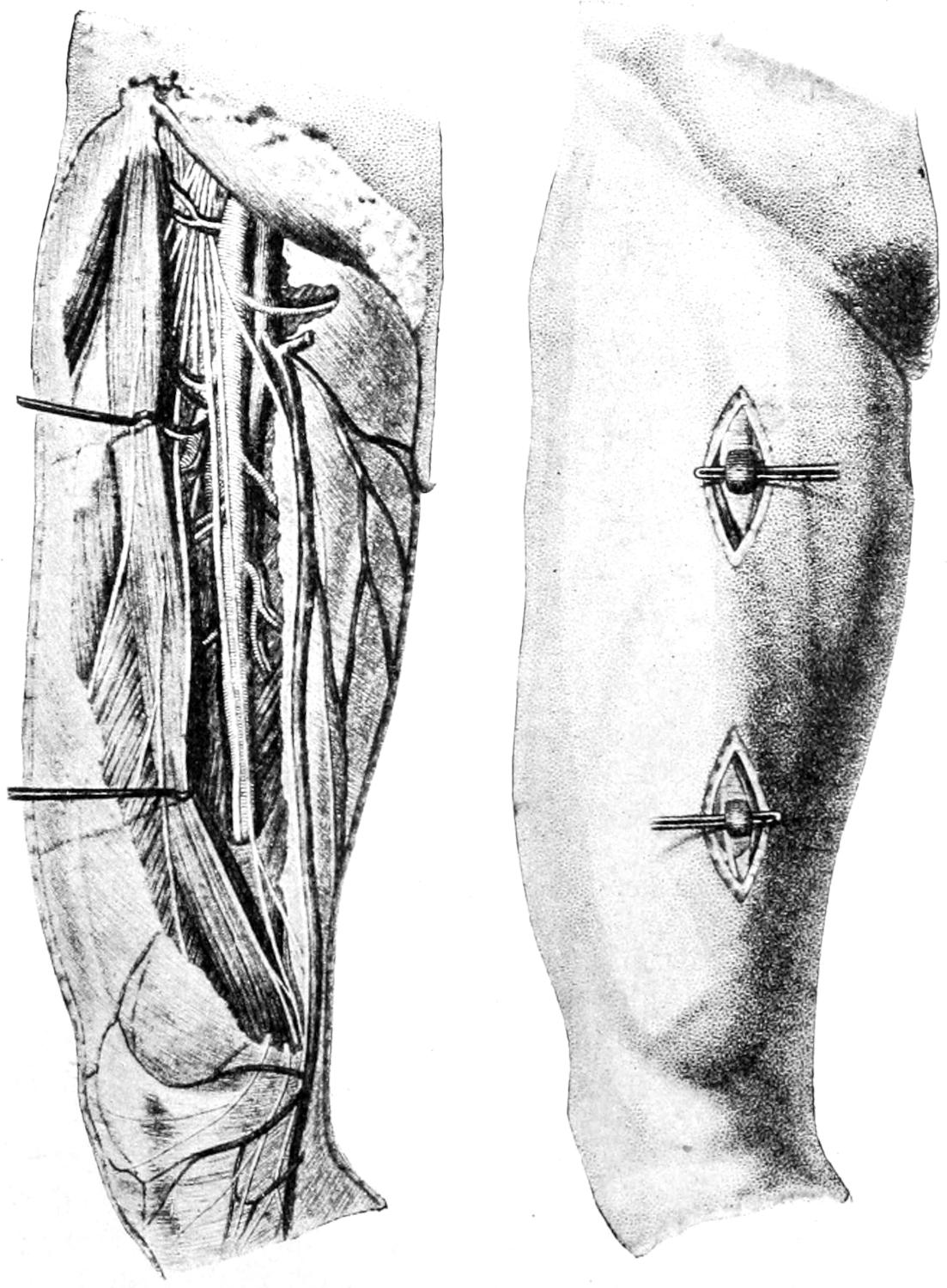
Surgical anatomy and ligation of the femoral artery. (Bernard and Huette.)
—The femoral artery is usually tied either at the base of Scarpa’s triangle, just below Poupart’s ligament, or in Hunter’s canal. In the first location its pulsation can be easily felt before dividing the skin, and will serve as the best guide. It requires an incision made downward over the course of the vessel, from the middle of Poupart’s ligament. In approaching it here a number of lymph nodes may be encountered, some of which may be considerably enlarged. They should be disturbed as little as possible, unless involved in cancerous or serious septic disease. The anterior crural nerve lies to the outer side of the vessel and the vein to its inner side. Between these it may easily be found and tied (Figs. 176 and 177).
In Hunter’s canal the femoral artery may be found nearly beneath the long saphenous vein, and near the outer edge of the sartorius. If the leg be abducted, and the adductor magnus thus stretched, the position of the canal, between the latter and the vastus internus, is easily recognized. The canal itself is partly formed by fascia which should be divided, while the artery will be found within.
Fig. 178
Fig. 179
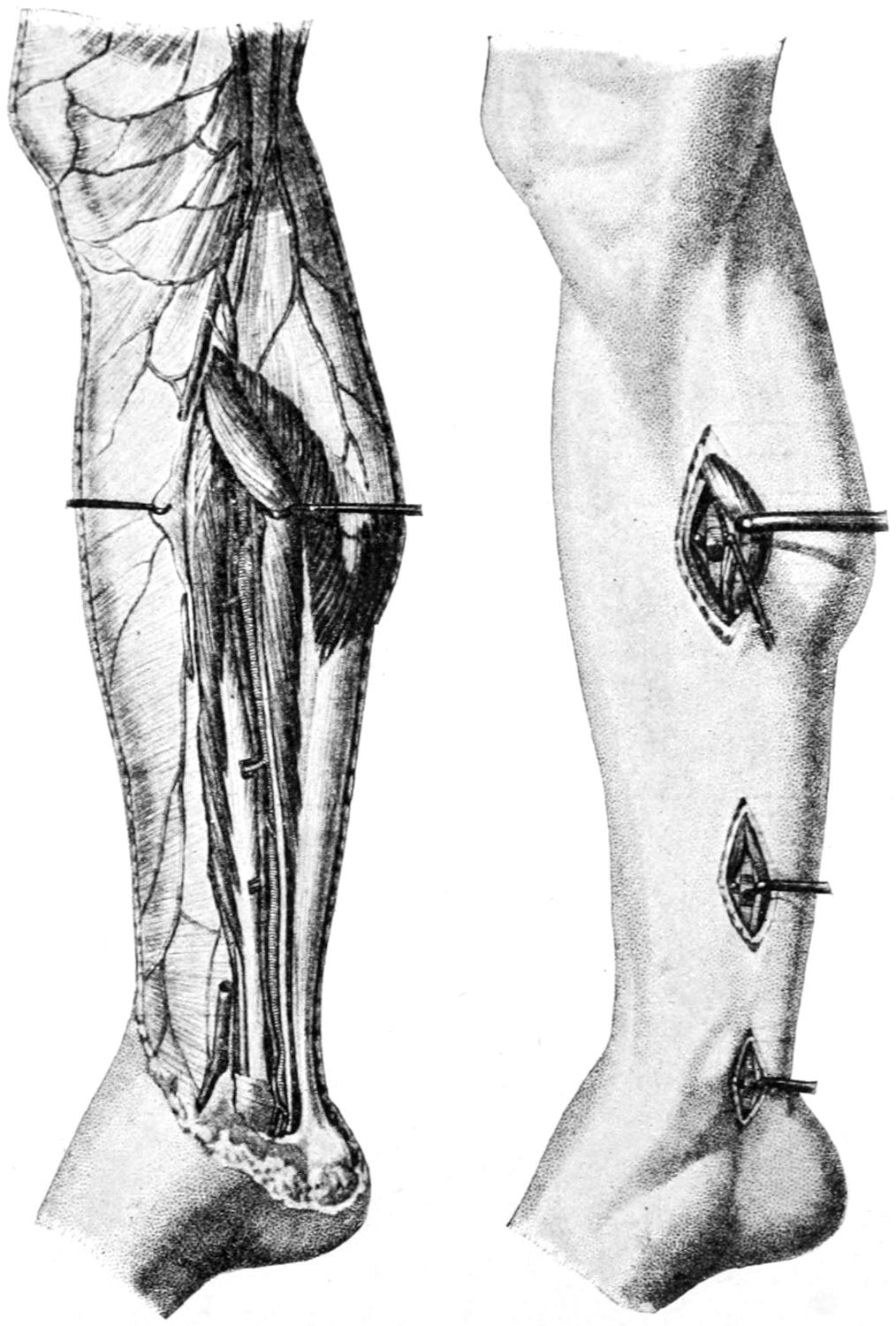
Surgical anatomy and ligation of the posterior tibial artery. (Bernard and Huette).
[360]
The lower part of the femoral artery, or practically the popliteal artery, may be found, if necessary, by an incision in the middle of the popliteal space, the operator gradually working down by blunt dissection to the location of the vessel, which is easily recognized by its pulsation.
—The posterior tibial artery nearly underlies a line from the centre of the popliteal space to a point between the inner malleolus and the heel. To expose it easily the limb, somewhat flexed, should lie upon its outer side, the patient lying nearly on his face, and incision made in the calf of the leg, beginning at the head of the fibula, after which one may expose the junction of the two heads of the gastrocnemius. Through this the tendon of the plantaris is to be sought, after which it may be necessary to divide a portion of the soleus. Here the vessel should be sought by the sense of touch, the operator seeking for its pulsation. Lower down, and in the lower part of the leg, it may be found by incision along the imaginary line which it underlies, lying on the flexor longus digitorum, with its accompanying nerve on its outer side. Still lower, at the ankle, it may be easily found, just behind the malleolus. (See Figs. 178 and 179.)
Fig. 180
Fig. 181
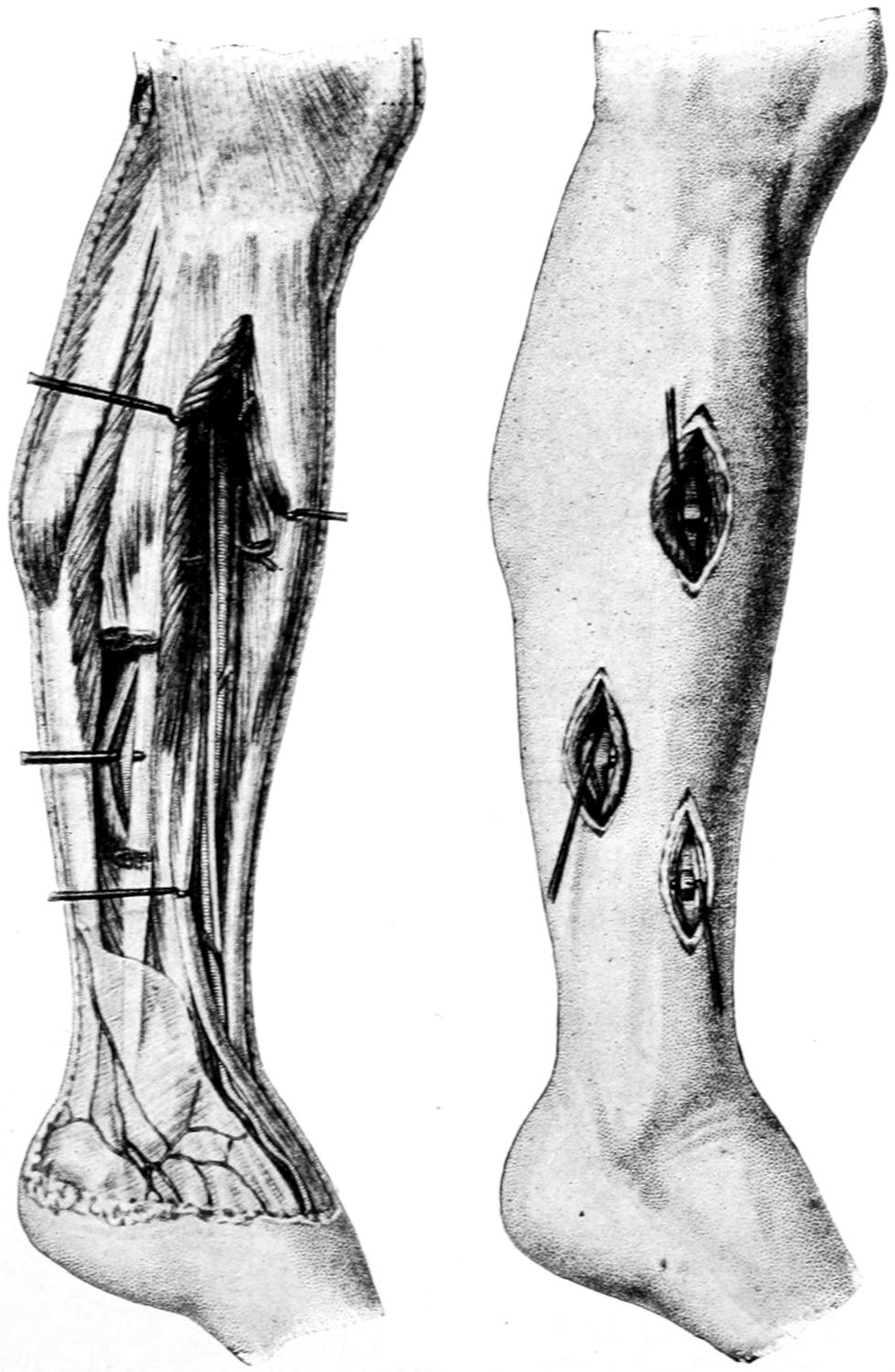
Surgical anatomy and ligation of the anterior tibial and peroneal arteries. (Bernard and Huette.)
—The anterior tibial artery underlies a line drawn from a point between the head of the fibula and the outer tuberosity of the tibia, to the front and centre of the ankle-joint. At almost any point along this line it can be exposed[361] between the tibialis anticus and the common extensor of the toes, the latter being held downward and outward and the former upward. Here in the depths it may be recognized upon the interosseous membrane. In the lower part of the leg the extensor pollicis lies to its outer side. Here the accompanying veins should be avoided. Quite low in the leg and in front of the ankle the vessel will be found between the tendons of the tibialis anticus and extensor pollicis (Figs. 180 and 181).
The veins are of interest to the surgeon particularly because of the role they play in the pathology of sepsis, especially of pyemia, and because of their various dilatations and even new formations which admit of none but surgical remedy; that is, varices, under their various names—for example, hemorrhoids, varicocele, and nevi.
The veins have an endothelial lining, between which and circulating, or more especially stagnant, blood there exist peculiar susceptibilities and relations which cannot be well described. The pathologist appreciates what disturbances of the endothelium will provoke coagulation of the blood in contact with it, but is not yet in a position to explain the relationship. Veins, moreover, are provided with valves to a more perfect degree than are the lymphatics, but the valves often become inadequate for their purpose, and then we have such conditions as varicosities; the fact that they are usually seen about the rectum and the lower extremities illustrating the disadvantages accruing from the upright position into which, by the process of evolution, man has erected himself from the quadrupedal. Even the myriads of years that have elapsed since this change took place have not sufficed to afford sufficient protection against the added weight of the column of blood inseparable from it.
Of pathological changes which interest the surgeon there may be atrophy as the result of pressure from without or prolonged distention from within, even to such an extent as to permit of rupture and serious or fatal hemorrhage. Fatty degeneration occurs in the serious intoxications and infections. Calcification occurs only in limited areas and is secondary to other changes or to thrombophlebitis. True osseous patches have been found in the walls of veins, but are great rarities. Calcification occurs in the portal and also in the femoral veins and their branches. In other directions vein walls become hypertrophied, all coats partaking in the change, enlargement or distention being especially likely to occur where there is most tendency to stagnation. The changes which lead to the varicose condition include not only absolute thickening, but increase in every dimension, the venous tubes becoming elongated as well as distended and thickened, to such an extent that they take a spiral or curved course, sometimes almost doubling on themselves.
In all forms of phlebitis, whether acute or chronic, the three venous coats are practically involved in the same manner. With enlarged knowledge of the lymphatics it is difficult to separate an acute phlebitis from a lymphangitis of the venous wall. Only in this way can descending phlebitis be accounted for, the infection travelling apparently against the blood stream. This accounts for the discoloration along the subcutaneous veins when they become involved, the same red lines appearing in the skin as when the lymphatics are involved. The relations between the intima and the blood have been mentioned above. In cases of acute phlebitis in which the intima is involved there is coagulation of the contained blood, the clot and the vein wall undergoing changes which simulate a thrombophlebitis.
—Acute phlebitis is of infectious origin. It may be seen in connection with injury, erysipelas, childbirth, and the superficial and deep infections, as from a hypodermic injection, a pin-prick, etc. It is also seen in typhoid, pneumonia, diphtheria, and gonorrhea. In most of these instances it is difficult to trace the path of infection. I have seen death from pyemia following gonorrhea, where the earliest recognizable disturbance occurred in the peri-urethral and prostatic veins. I believe it to have been my report on these cases, in 1885, which first called attention to the fact that gonorrhea might terminate fatally by the pyemic process.
[362]
When the venous system has become involved in a septic process of this kind neither its fate nor that of the patient can be regarded as secure. Occlusion, with serious circulatory disturbance, may permanently impair function, while there may be speedy death from pyemia. This is nowhere more true than in those portions of the venous system having rigid walls without valves, to which is given the name “sinuses” (cranial), in which exactly similar processes may occur, which by virtue of their location will always give rise to the gravest anxiety. To phlebitis occurring in these channels there has been given the somewhat distinctive name sinus phlebitis. It nowise differs from the same condition elsewhere, save that it is of almost invariably extravascular origin. It takes but a small venous branch, lying in the midst of an infected area, to commence the process that may extend from the basal sinus to the vena cava.
In most of the surgical infections acute phlebitis has an extravascular origin, the lymphatics of the outer wall communicating the infection to the inner coats, and so distributing it that coagulation occurs, after which the path of infection from the containing veins to the contained clot is direct. The thrombi thus formed may completely or only partially occlude the vessel. As a continuation of the lesion we have infiltration and separation of the coats of the vein from each other, and finally their necrosis. Thus in the terms of the pathologist an acute phlebitis may lead to a phlebitis desicans, and this to phlebitis gangrænosa. In every case where the patient survives such conditions as these the veins lose their identity and become obliterated by the very violence of the process in which they have participated.
A somewhat different type of acute or subacute phlebitis is produced by intravascular irritants, namely, toxins or bacteria circulating in the blood, or to some chemical or thermic agency which may produce thrombosis, such as extremes of heat and cold. These, too, may lead to partial or complete occlusion, and the latter may be followed by calcification or the formation of phleboliths. The destructive character of the entire process will, therefore, depend upon the nature and virulence of the exciting cause. As between fatal septic infection, local gangrene of a part as the result of involvement of the majority of its veins, or comparatively slight and temporary disturbance, such as edema, there may be degrees of activity, with results varying between fatality and evanescent discomfort.
—This is of the proliferative type and is followed by more or less organization. Phlebitis obliterans is sometimes seen in connection with syphilis and other chronic intoxications, and with various operations upon the veins.
Symptoms.
—Phlebitis may occur without known cause or may follow as an expected result from deep or surface lesions. The deeper the involved veins the more obscure the case. Involvement of superficial veins, especially in acute cases, is easily made known by the dark-bluish or dusky red cord which occupies the place of the previously healthy vein. As its contained clot becomes firmer the clot becomes harder. This is accompanied by more or less fever, with extreme tenderness, often pain. If a single vein only be involved the disturbance will be quite local; if thrombosis be general there will be edema of the parts to which the vein is distributed. Involvement of certain veins implies the establishment of a collateral circulation through others. If there be no others available then danger from venous insufficiency threatens, and it may not be possible to avert gangrene. “Milk leg,” or so-called phlegmasia alba dolens (“painful white swelling”), is an expression of portal, pelvic, and femoral thrombophlebitis. In many instances in which it does not kill it may cripple the individual for life. Phlebitis of the deep veins can be inferred rather than detected. Phlebitis of the hemorrhoidal veins frequently follows inflammation and suppuration of piles, while that of the pelvic veins, especially the perivesical, frequently follows gonorrhea and prostatitis. Mesenteric phlebitis and pylephlebitis frequently follow the ulcerative infections of the intestines, while in the newborn a phlebitis of the umbilical vein plays an important part in the mortality of infants. The cranial sinuses are likely to be affected in connection with middle-ear disease, while in acute osteomyelitis there are distinctive pictures of the lesion in the veins of the bone and the marrow. No matter where the lesions may centre they are of the most serious character. The role of the veins in the production of metastatic foci has been described in the chapter on Pyemia. The danger attending the liquefaction of a thrombus and the escape of its fluid debris into the general circulation stamps an acutely infected clot with a dangerous character. This fact justifies such measures as are now pursued in connection with the[363] cranial sinuses and mastoid disease, where there is not only a sinus exposed by removal of a portion of the temporal bone but the jugular opened low in the neck and the entire intervening channel freed from its putrefying contents by the probe and the irrigating stream. In other words, a recognition of the pathology of thrombosis and sepsis may lead to the performance of difficult operations.
Treatment.
—It is difficult to separate the treatment of phlebitis from that of lymphangitis, which generally accompanies it. The first essential is physiological rest for the part involved, such as confinement in bed, and the least possible disturbance of the inflamed area, which should be placed in the most restful position and handled as little as possible. Local soothing and evaporating lotions may be used, or, as seems to the writer preferable in most cases, applications of a 10 per cent. ichthyol-mercurial ointment, or of the Credé silver ointment, neither of which should be rubbed in, but spread upon the skin and covered with an impermeable material. These will, after a few days, prove irritating, and a substitution of something milder may be required; but in the acute stage they will render greater service than anything else. A phlebitis which has been provoked and is perpetuated by the presence of septic material cannot be successfully treated so long as its provoking cause remain. Puerperal sepsis which results in pelvic phlebitis calls for thorough curetting of the uterus, while an abscess in the jaw or about the mouth, resulting from diseased teeth, necessitates the extirpation of the latter, providing the jaws can be separated sufficiently to permit of it. What may be needed in cases of thrombophlebitis of the cranial sinuses has just been mentioned.
In any part of the body a vein which is filled with a breaking-down clot can be promptly and judiciously treated by exposure and removal of the involved part, or by free and open incision, with suitable after-treatment.
A chronic phlebitis that produces such lesions as varices will be dealt with under its proper head.
—Rupture of small veins is the inevitable consequence of every injury sufficiently serious to be in any sense disabling, its visible expression taking the form at least of ecchymosis, sometimes of distinct hematoma. Again, after long-continued pressure by which return of venous blood is prevented, certain degenerations take place in the vein walls which lead to their yielding on apparently trivial provocation; thus veins situated distally to large aneurysms sometimes give way, while the frequency with which they rupture in large varices of the limbs and in hemorrhoids is everywhere recognized. In the days when venesection was so frequently practised, usually at the bend of the elbow, a traumatic communication between the artery and the vein was frequently produced, with consequent anastomosis. When this was direct, the vessels being in contact with each other, it was an aneurysmal varix. When there was more or less of an intervening sac, through which the blood flowed from one to the other, it was spoken of as a varicose aneurysm. Save in rare cases produced by puncture or gunshot wounds such lesions are curiosities. Should operation be required the sac, if there be one, may be extirpated, or the vein may be ligated above and below the communication. (See above.)
—Air embolism may follow injury to the large venous trunks, especially about the head and neck. This term implies the entrance, by aspiration, of air into the veins, its bubbles being carried along to the right side of the heart, where they are supposed to more or less interfere with its action. Sometimes at the instant of the accident a sucking or gasping sound may be heard. Formerly the condition was considered alarming, but now it is almost a bugbear. It is probable that minor degrees of the accident often occur without perceptible alteration in heart action. Serious disturbance, however, is possible, especially if the longitudinal sinus or the common jugular be extensively opened, and the patient’s head is above the level of the body at the time. Such an accident might call for artificial respiration, and it has been suggested to aspirate the right side of the heart. When its danger can be foreseen precautions should be taken by pressure on the proximal side of the injury. Air embolism is said also to have followed parturition, and even exposure of veins in the stomach by the ulcerative process. (See p. 38.)
[364]
—Most injured veins can be tied in situ and their function left to the collateral circulation. Fear is sometimes felt about the axillary and the femoral veins, and serious discussions have arisen as to whether amputation might be called for should these large channels be so injured as to be made useless. Experience has shown that either of them may be ligated, with nothing worse than temporary edema of the limb beyond. Should there then occur, by accident or during an operation, an opening of these venous trunks one may apply the ligature, if necessary. Before resorting to this, however, one may consider the advisability of the application of a fine suture to the margins of the wound in the vein, which has become a standard procedure, or, if the opening be small, and it can be seized with a hemostat, it may be left in situ for two or three days, closing the wound around it, and so supporting and protecting the part with dressings that it shall not be disturbed. A small forceps or its equivalent may thus be left upon a cranial sinus, a jugular, subclavian, axillary, femoral, or other vein without jeopardizing the result.
The term phlebectasia implies an extensive affection of a portion of the venous system, characterized by more or less uniform enlargement of all its veins. A similar involvement of isolated veins is usually spoken of as varix. These conditions may be congenital or acquired. Fig. 182 illustrates a congenital varicose condition occurring in a lad aged sixteen years. Such a lesion may be explained by congenital defect in some of the deeper veins, thus compelling the venous blood to return through the more superficial channels. These congenital lesions are more common in the lower extremities, but may be seen in all parts of the body. Varices, also, by virtue of their exciting and contributing causes, are most common in the lower extremities and in the lower venous terminals, as in the scrotum, the rectum, etc. Acquired varices usually imply previous lesion in the vein walls, sometimes inflammatory, sometimes toxic. The walls of the veins thus become at first atrophied, this condition being often followed by irritative hyperplasia, by which finally the veins become thickened and strengthened, and sometimes calcified. The enlargements are irregular and sacculations frequently form. In such sacculi thrombi may occur and be followed by calcification, the resulting concretions being known as phleboliths. These can often be recognized through the skin in old and chronic cases. Sometimes adjoining sacculi become confluent and there forms what is called an anastomotic varix. By such communications cavernous conditions are produced which, when placed subcutaneously, lead to peculiar and distinctive tumor formations.
Fig. 182

Congenital varices. (Park.)
As already stated, the tendency to varices is indirectly the result of man’s assumption of the upright position, by which greater stress is placed upon the valves and the lower veins than they are prepared to bear. Naturally these conditions occur often in those who are constantly engaged in hard work upon the feet. Varices, then, are lesions, not so much of the leisurely and sedentary as of the active and working classes. Anything which predisposes to venous stasis may be regarded as a contributing cause—thus their relations with weakened hearts and obstructed lungs are indirect, but positive. Many women suffer in this way as the consequence of their first pregnancy, with its pressure upon the pelvic veins; while tight garters, corsets, and belts also predispose to overloading of the lower veins. Slight but almost permanent causes of this kind, through the influence of gravity, thus produce varices in the course of time.
To varices in certain locations have been given special names. To such a dilatation of the spermatic and pampiniform plexus has been given the name varicocele. When the hemorrhoidal veins are involved the condition is known as hemorrhoids or piles. The former is often credited with being due to the anatomical arrangement of the left[365] spermatic vein, through which blood is not as directly poured into the vena cava as on the right side, while the relation of chronic constipation, with its obstruction to the circulation in the rectal walls, will account for many cases of hemorrhoids, and the disturbance implied by the term cirrhosis of the liver will furnish an explanation for many others. A similar condition in the esophageal veins has given rise to the term esophageal hemorrhoids. Most indicative and extraordinary expressions of closing of deep circulation may be seen in some instances of intrathoracic and intra-abdominal diseases, i. e., cases in which the superficial veins of the chest and thorax become remarkably enlarged. Such expressions as these are to be regarded as natural efforts to obviate a difficulty, and no attempt should be made to eradicate such varices.
—In cases requiring surgical intervention, varicose veins present the following features, which are particularly indicative; they not only enlarge in diameter but elongate, and consequently have to assume a tortuous arrangement to accommodate their increased length; they cause a constant sense of fulness and discomfort, which often amounts to actual pain, especially after laborious effort. This pain is due to the distention of the venous trunks, to pressure upon cutaneous nerves, and often to disturbances of nutrition. In fact, nutrition is so often disturbed as to be accompanied by skin lesions, which begin as eczema and terminate in extensive ulcerations. So frequent is this association, and so distinctive its type, that such ulcers are frequently referred to as varicose. If the term be used to imply the association it perhaps may stand; if intended to typify a peculiar type of ulcer it is objectionable, as the ulcer itself is simply such as may happen on any surface whose nutrition is more or less perverted.
The most common causes of varicosities in the lower extremities are previous lesions, such as phlebitis following typhoid, injuries of the limbs or trunk, the pressure of tumors, fecal accumulations, garters or belts, laborious work in the upright position, and the possible complications of all cases from variation in the original anatomical arrangement of veins and their valves; pregnancy also should be added to this list.
The condition is rare in early life. Liability to it increases with age. Varices rarely occur in the upper limbs in connection with certain occupations or athletic sports, e. g., baseball and tennis.
The measure of the distention of veins can often be taken by the sensation of fulness and muscle cramp. In few surgical lesions do appearances give as much aid in diagnosis. This is particularly true of superficial varices. Varicosities of the deeper veins maybe suspected when patients complain of discomfort, pain, cramp, and swelling of the feet after hard work.
Varices would rarely lead to ulceration were it not for the superficial infections incurred in many obvious ways—sometimes by the finger-nails of the individual, who is constantly tempted to scratch or rub the area in which he feels such incessant discomfort.
—Suitable treatment of varices of the internal veins, varicocele, hemorrhoids, etc., will be indicated in its proper place. In this chapter only varices of the extremities will be considered. When a tendency to the varicose condition is noted early, and a cause can be discovered, removal of the cause may be all that is needed. When the condition is well established, and yet not sufficiently prominent to justify radical treatment, it should consist largely in support by bandages or elastic stockings, applied discriminatingly, with sufficient pressure to prevent undue distention and not sufficient to cause edema. It frequently affords much relief and prevents aggravation of the condition; on the other hand, once the veins become accustomed to this support they yield more readily upon its withdrawal, and the treatment by gentle constriction once begun, which is sufficient for many cases, can rarely be discontinued, even after a lapse of time.
A maximum of rest and elevation of the limb are requisite in the non-operative treatment of varicose veins. The compression exercised by elastic stockings is of only temporary benefit, and is simply such an assistance as is a crutch to a cripple. The less the patient remains upon the foot and the less he takes hot baths or indulges in other relaxing measures the better. Cold shower or tub baths are far preferable, with massage of the deeper muscles, the large veins being avoided. Such a patient should never walk slowly, but always rapidly, and rest as soon as fatigued. All diathetic conditions should receive attention.
When it is not possible to early and speedily remove the existing cause there is but one cure for varices, and that is by radical surgical treatment. A generation ago this[366] was effected by the injection into the veins of perhaps one of the iron salts, in order to produce artificial and instantaneous thrombosis, by which later occlusion of the vein could be induced. The coagulating effects were decided, and so also were the effects of the germs introduced at the same time, in the absence of ordinary antiseptic precautions. Thus it resulted that the mortality, even after this trifling procedure, was tremendous and led to its abandonment. When it had been demonstrated, through Lister’s achievements, that the surgeon could be clean about such work, it was learned also that veins could be more radically treated than had been previously realized. With the advent of the antiseptic era came more effective and extensive operations upon veins. Now we know that with strict asepsis they can be handled with absolute impunity, and open methods of treatment have replaced the subcutaneous. No hesitation is at present felt in exposing the veins at one point, or numerous points, and applying ligatures; these, however, have been found to be less effective than a long incision made over a vein, with its complete extirpation. Thus the long internal saphenous should nearly always be excised, though it take an incision twenty inches in length, in order to take off the weight of its column of blood. It is ordinarily a simple matter to clamp and tie each branch as it is divided, and, after removal of the principal trunk, to bring together the entire incision with subcutaneous or continuous sutures. In the same way numerous incisions may be made in the leg. It is possible, however, to meet with so many enlarged veins that the surgeon may feel that he cannot thus eradicate each one. In such cases it is my custom to extirpate the principal trunk or trunks involved above, and then to combine this with Schede’s suggestion to completely or partly circumcise the leg, below the knee, down to the deep fascia, cutting across every vein and tying on each side those which bleed to any extent. After all these veins are ligated the incision is usually brought together again, as above. By this means all communication between the subcutaneous veins above and below the line of incision is cut off. Wound healing is accompanied by a temporary edema of the foot and leg, especially when these are held down, and by more or less numbness of the skin due to division of the cutaneous nerves; but circulation and nerve supply both rearrange themselves in time, and the result is usually satisfactory.[28]
[28] Extirpation of the Internal Saphenous.—Keller has quite recently suggested a new method of extirpating these varicose veins without extensive scarring. He exposes the vein at two points a considerable distance apart, and ties above and below after separating it from its surroundings. The vein is then cut below the proximal end, the upper end of the section to be removed split and a strong ligature tied to it, care being taken to include no more tissue in the ligature than will pass through the lumen of the vessel. Then from the lower end a wire loop or probe is passed upward, a ligature is threaded into its eye and the probe is then withdrawn, carrying the ligature, after which traction is made upon the latter, the edges of the vein being inverted into its own lumen, it being thus extirpated by being turned inside out and withdrawn from its sheath. With the internal saphenous, when a slight puckering is seen about midway between the incisions, indicating that the anterior branch of the vessel has been reached, a third incision is made, the branch is ligated and divided, and then the traction renewed until the vein is entirely pulled through the lower opening. Several cases thus treated have been very successful.
Should ulcer, i. e., the so-called varicose ulcer, be present, it may also be attacked radically, and at the same time completely, by excising the affected area, with its indurated border, down to the level of the deep fascia, and covering the surface thus denuded with Thiersch skin grafts from some other portion of the body. Should such an ulcer require treatment after this fashion it is best to attend to excision of the infected area first, in order to clear away all material which might harbor germs. The usual procedure, then, should be excision of the ulcer, extirpation of the veins, to be concluded by skin grafting. A limb thus radically treated should be included in a comfortable dressing, and then be affixed to some splint or other device by which absolute rest and repose may be maintained.
In milder cases, where no single large dilated vein seems to call for extirpation, it may suffice to practise Schede’s operation alone. Experience has taught this fact, that in dealing with extensive varices the surgeon is more likely to err on the side of leniency than on that of thoroughness.
These have already been mentioned in the chapter on Tumors as constituting one variety of the angiomas. Many of them are of congenital origin. In many instances they produce erectile tumors. They frequently occur in the liver, in the thyroid, and other internal organs, as well as on the body surface.
[367]
A venous tumor, composed of good-sized veins, distended perhaps far beyond their normal capacity, constitutes a compound varix, of which the best expression is a hemorrhoid or a varicocele. Another form is composed almost entirely of capillary veins, which are increased not only in size but also in number. These constitute the growths called “mothers’ marks,” “strawberry growths,” etc. Technically they are venous nevi, which vary in size from trifling lesions to large tumors of varying shapes. These growths are always most conspicuous about the hands and face, because these are the visible parts of the body. They may, however, occur at any point, but mainly about the face and the orbit. A diffuse form, whose area may be almost unlimited, but usually circumscribed, is that called “port-wine mark,” which occurs more frequently about the face. It has been attributed to mental impressions during pregnancy, but there seems little to justify this view. The affected surface is sometimes pigmented and generally more hairy. Surface markings of this kind may accompany that form of neuroma described as plexiform neuroma. Fig. 183, from Holloway, illustrates another form of congenital growth of this kind. These growths rarely occur in the nasopharynx, where they not only obstruct but are sources of actual danger from hemorrhage.
Fig. 183
Congenital venous nevus. (Holloway).
—The most satisfactory treatment of a limited growth of this kind is excision, especially if this can be made at an early age. The resulting scar will be smaller, the healing more prompt, and the result in every way better. When excision seems impracticable electrolysis should be employed, one or both poles of a galvanic battery of six to ten cells being connected with needles, which are inserted directly into the growth, and whose position is constantly changed, so that the coagulating effect of the electric current may be equably distributed throughout the growth. Occasionally the growth may be so shaped as to permit of ligature, and it is best employed either with or without the use of a needle, after which it may be excised or will slough off. This is essentially one method of treating external hemorrhoids. Methods by injection of coagulants are all open to serious objection, are hazardous, and should be abandoned. A port-wine mark may be sometimes treated by a tattooing process, which should, however, be practised with strict antiseptic precautions. Electrolysis may also be practised over a small area at a time. The more destructive method, by use of the cautery, is likely to leave scars almost as conspicuous as the original condition. Occasionally a lesion of this kind will be so shaped and placed as to justify excision with an autoplastic operation.
[368]
An appreciation of the pathology of the lymphatic system requires a brief allusion here to the latest investigations and conclusions regarding the purpose of the lymph as a fluid and the channels by which it is distributed. Under the term lymph, Hall has included four different types: (1) Tissue lymph, which fills the intercellular spaces throughout the body; (2) circulating lymph, which passes through the lymphatic capillaries into the circulatory system by way of the thoracic duct; (3) chyle, or the peculiar circulating lymph of the intestinal tract, which carries into the general circulation its load of nutritive material; (4) serous lymph, i. e., the contents of the serous cavities. Closely related to the latter are the aqueous humor, the cerebrospinal and the synovial fluids. All these fluids, except chyle, contain at least 95 per cent. of water and nearly 4 per cent. of proteids.
The lymph is the only fluid which comes into contact with all the living cells of the body; it pervades every part of its substance to such an extent that it has been said that the higher animals are essentially aquatic because they practically live in a watery medium. Blood normally comes into contact only with the endothelial cells of the vessels and with those cells in the splenic pulp and perhaps other localities which have to do with its elaboration, and these are but a minute proportion of the total cells of the body. All the rest receive their nutrition and even their oxygen through the lymph, which receives them from the blood. Moreover, nearly all the waste materials of the body are emptied into the lymphatic system, and thus directly or indirectly find their way into the blood to be further extruded. Thus, with the exception of the endothelium, the lymph is the medium of exchange between blood and tissue. In this the lymph and the lymphatics play a role which even for the surgeon must be of the greatest importance.
The amount of lymph which empties into the vena cava from the thoracic duct represents only that which comes from the viscera, bearing its special load of nutritive material. When we consider the communication between the blood-vascular and the lymph-vascular systems, the promptitude with which material injected into the tissues (e. g., salt solution) is taken up by the lymphatics and its effects made known through the bloodvessels, we will better appreciate how deleterious material also can be quickly distributed through the system. The lymph then must be regarded as a fluid derived from the blood by combined filtration and osmosis, which makes its way back into the blood again with equal ease.
Lymph vessels which are sufficiently large to be recognized have thin walls and are provided with valves like the veins, the lymph stream being propelled by a vis a tergo from the heart. Any injury which permits blood to escape will also injure numerous minute lymph vessels; in fact, in such little maneuvers as vaccination the attempt is made to draw lymph alone and not blood. If a large lymph trunk be divided there may be an outpour of lymph, and if this happen to be the thoracic duct the external escape of its lymph stream may seriously interfere with nutrition. Injuries which divide it within the thorax are usually fatal, but it may be divided in the neck by a puncture or stab wound, or during a deep operation. Escape of lymph into the abdominal cavity under similar circumstances gives rise to chylous ascites, and when into the thorax to chylous hydrothorax. In the former case repeated tapping may tide over the emergency and lead to eventual recovery; in the latter, aspiration or even open incision may be necessary. When the thoracic duct has been injured in the neck it may be possible to close the opening with sutures or to suture tissues over it. In a few instances final recovery has followed the formation of a chylous fistula. Injury to this duct is to be recognized by the flow of milky (i. e., chylous) fluid from the wound or from the duct itself. When poured into the abdomen or the thorax the retained fluid has the same milky appearance. It has been suggested to withhold all food in order to favor the spontaneous closure of such an opening, supporting the patient meanwhile by rectal nourishment and by the introduction of milk into the veins. The right lymphatic duct is less liable to injury, and such lesions on the right side would be of less importance.
PLATE XXXI
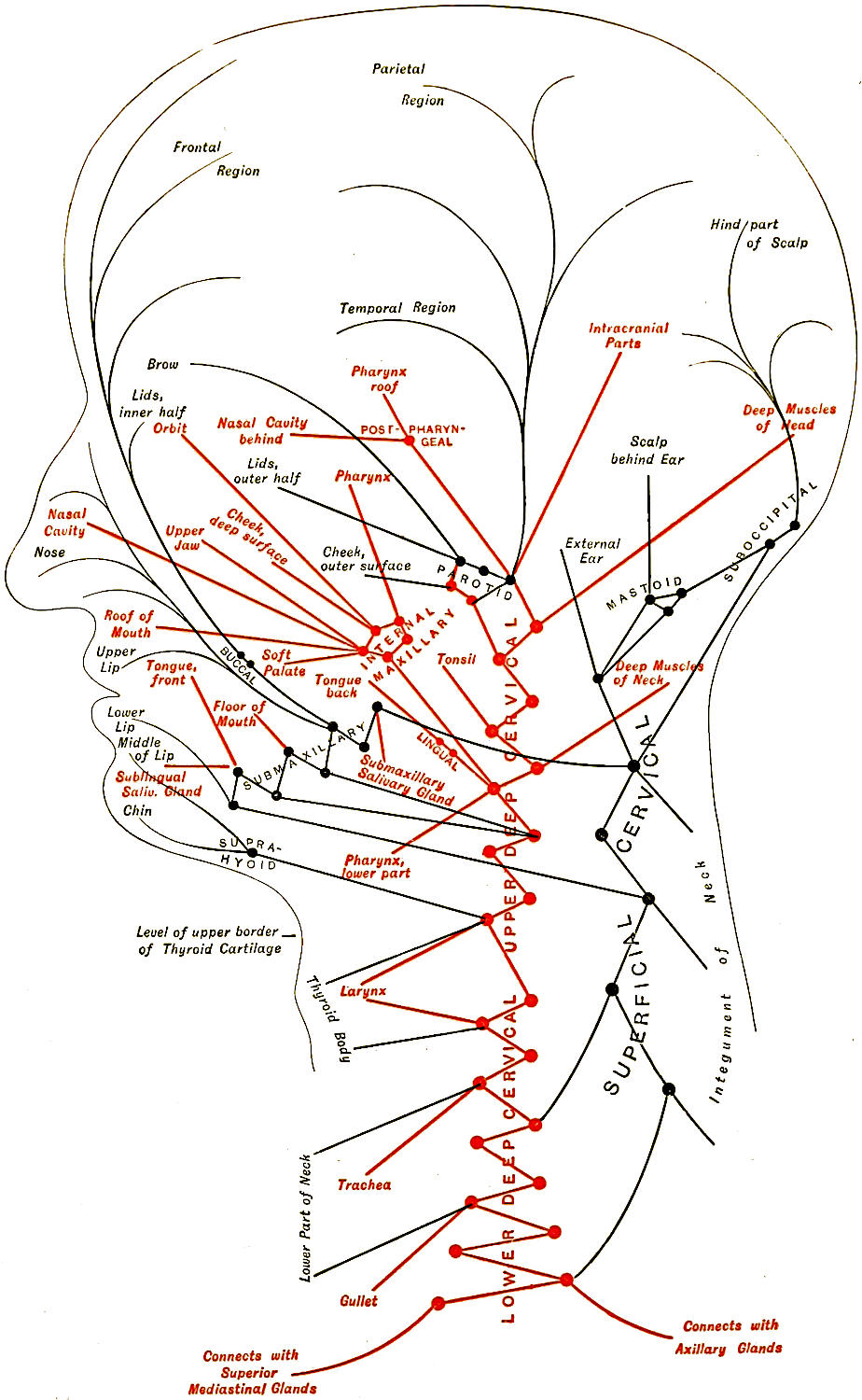
Diagram of the Nodes and Vessels of the Head and Neck, showing the Regions that are Drained into Each Group of Nodes. Deep structures in red, superficial in black. (Gerrish.)
PLATE XXXII
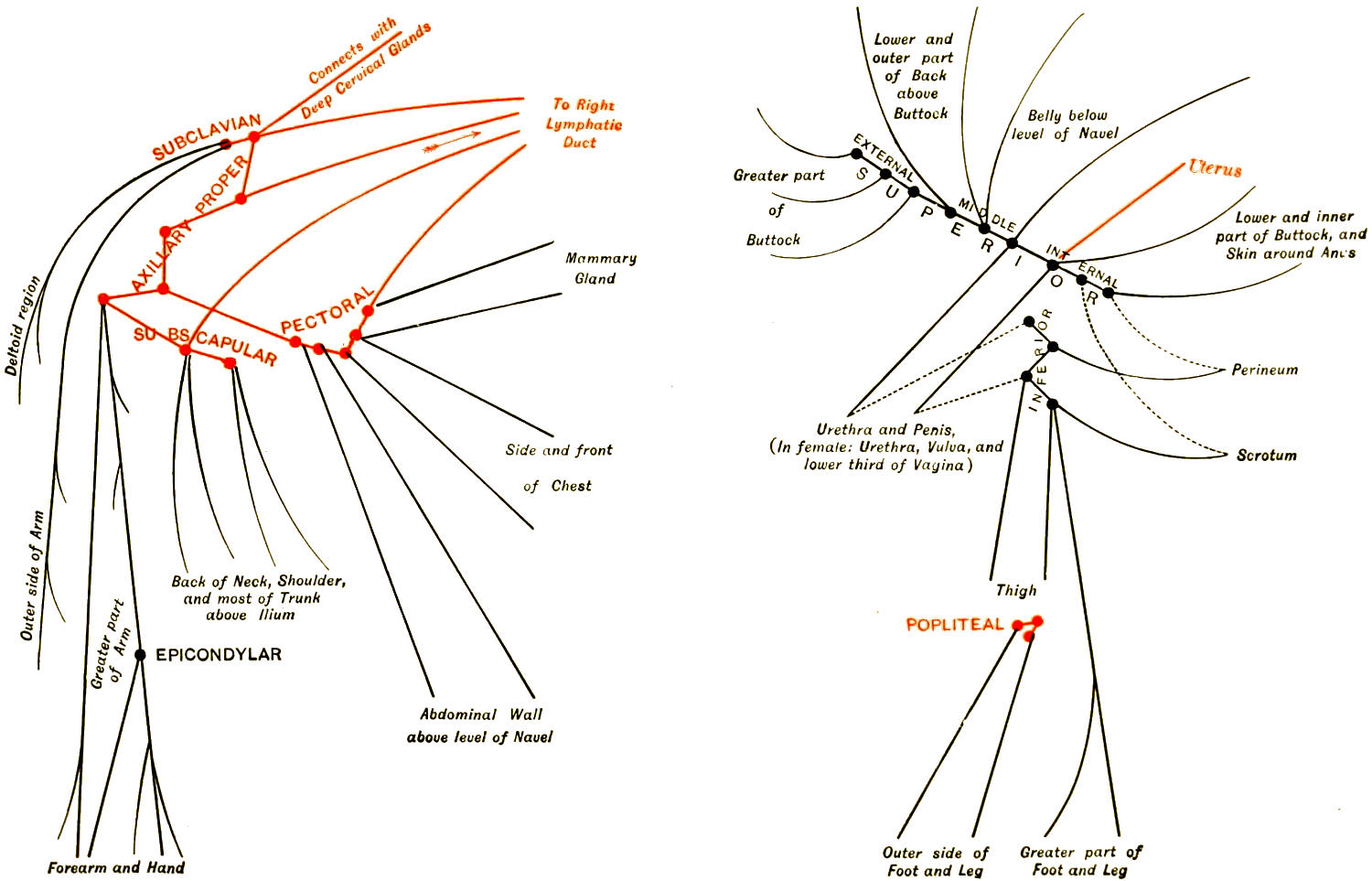
Diagram of the Nodes of the Right Upper Limb and their Superficial Tributaries, showing the Areas Drained by Each Group. Deep structures in red, superficial in black.
Diagram of the Superficial Inguinal and the Popliteal Nodes of the Right Side and their Superficial Tributaries, showing Areas Drained by Each Subgroup. Deep structures in red, superficial in black. Frequent variations in dotted lines. (Gerrish.)
PLATE XXXIII.
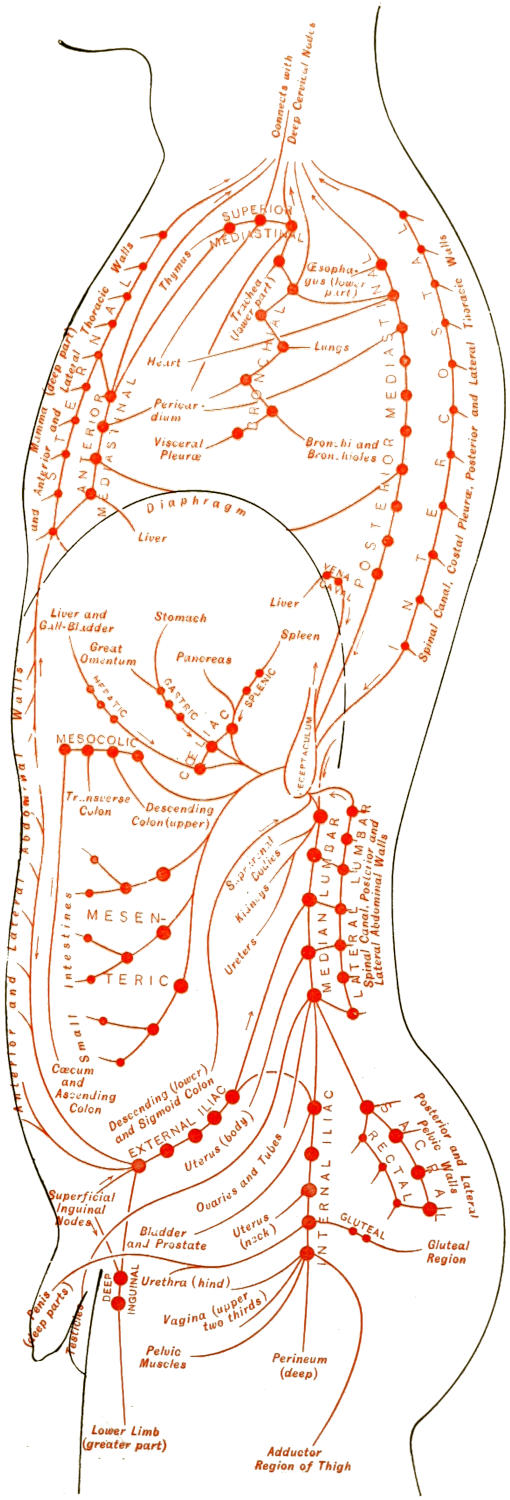
Diagram of the nodes of the trunk and their tributary vessels. (F. H. G.)
[369]
Inasmuch as most of the surgical infections, including cancer, are disseminated by means of the lymph vessels it is necessary that the surgeon should know the relation of vessels and nodes to the other parts of the body. The surgical anatomy of the lymphatics can be appreciated by reference to Gerrish’s admirable diagrams. (See Plates XXXI, XXXII, and XXXIII.) They will indicate at a glance what it would take pages to describe. The reader should also make frequent reference to these diagrams in connection with studies of septic infection, tuberculosis, and especially of cancer.
Occlusion of lymph vessel; may be either congenital or acquired. The congenital type is of extreme interest pathologically, but perhaps of less interest to the surgeon, since it rarely permits of a surgical remedy. The reader interested in this subject should consult the writings of Busey, who has contributed memorable monographs on the general subject of occlusion of the lymphatics. The acquired forms have to do with various conditions, such as thickening of vascular walls, the pressure of exudates or of tumors, or even of callus, and with the specific infections, of which syphilis and cancer are perhaps the most illustrative. The result which is brought about by these various causes is not so much the dilatation of the vessels as the saturation or water-logging of the tissues on the distal side of the obstructive lesion. The former is indicated by the formation of vesicles or bullæ which will frequently ooze or weep continuously. Should the pressure be localized and circumstances favor it, a truly cystic collection of fluid may result. The more common type is the so-called lymphedema, which, when chronic, is always accompanied by hyperplasia of the affected tissues, their overgrowth resulting from a superabundance of nutrition, the connective tissue apparently appropriating the larger amount of this material for itself. Therefore with the dimensions of a member enormously increased it will be found that almost every other tissue except the connective has been starved out. Lymphedema differs from that produced by venous obstruction by its obstinacy and the density of the infiltration; in fact, it has been sometimes spoken of as solid edema. If it continues for some time there are permanent changes which do not admit of later dispersion, and permanent enlargement is the result. The most unmistakable expressions of this kind occur in the legs and the external genitals of both sexes (Fig. 184).
Fig. 184
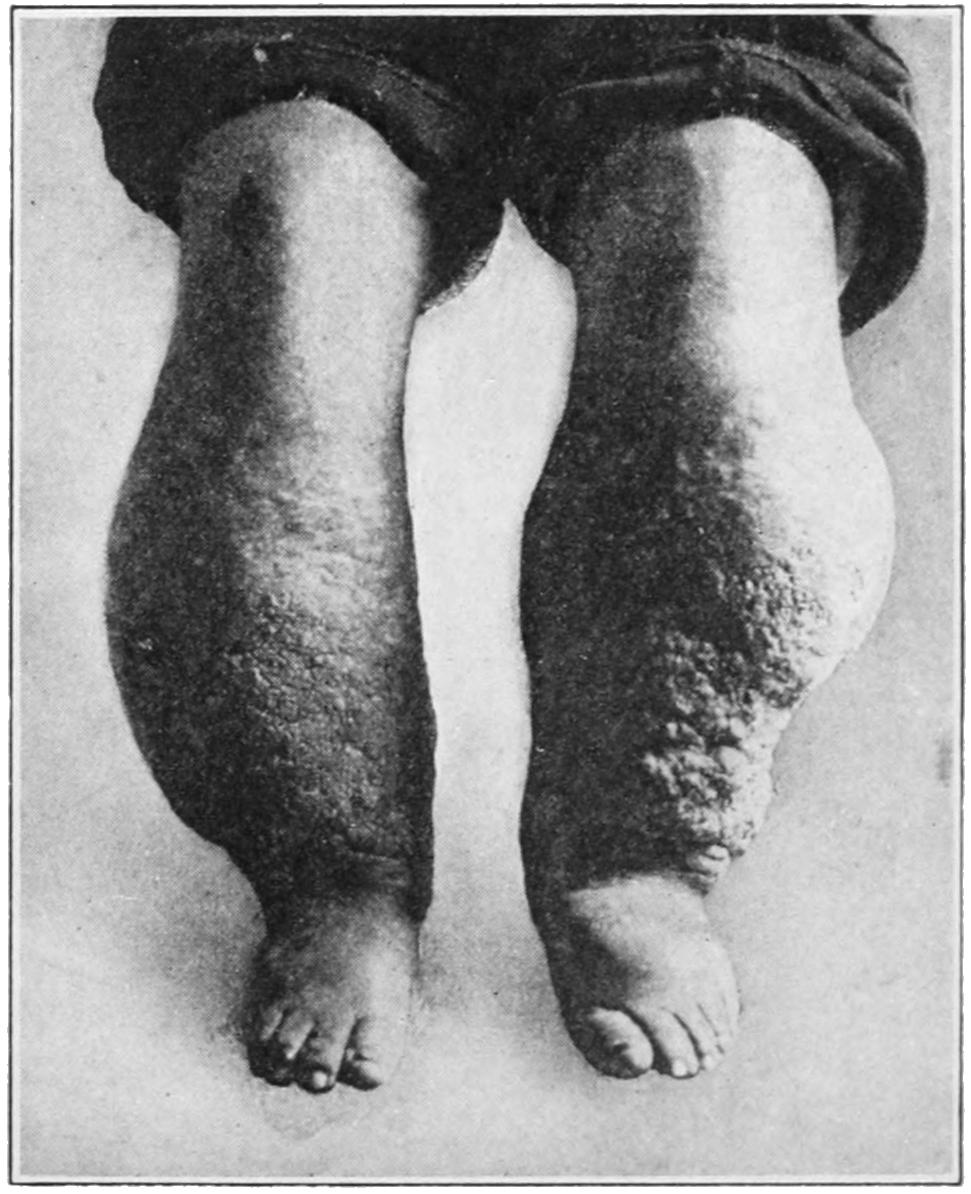
Lymphedema.
When compression, position, massage, and such measures fail the only other resort is amputation.
[370]
These terms refer to dilatation of the lymphatics, with a minimum of actual obstruction, often as a sequence of some previous lesion which has disappeared. In some of its expressions the condition is a manifestation of a widespread general disease or a parasitic infection. This is particularly true in those forms due to the presence of filariæ in the blood, in which it is not a question of the obstruction of one of a series of vessels, but plugging of a number of them by the adult worms, which reside especially in the larger lymph and chyle passages, sometimes even causing the appearance of chyle in the urine.
Elephantiasis is an expressive term given to any enormous enlargement of a part of the body, due to a combination of causes, of which lymphatic dilatation and obstruction together constitute the most important feature. The so-called congenital forms may have to do with congenital deviations from the normal standard, but should be differentiated from instances of gigantism, which have already been alluded to in Chapter I, into whose etiology different factors probably enter.
Fig. 185
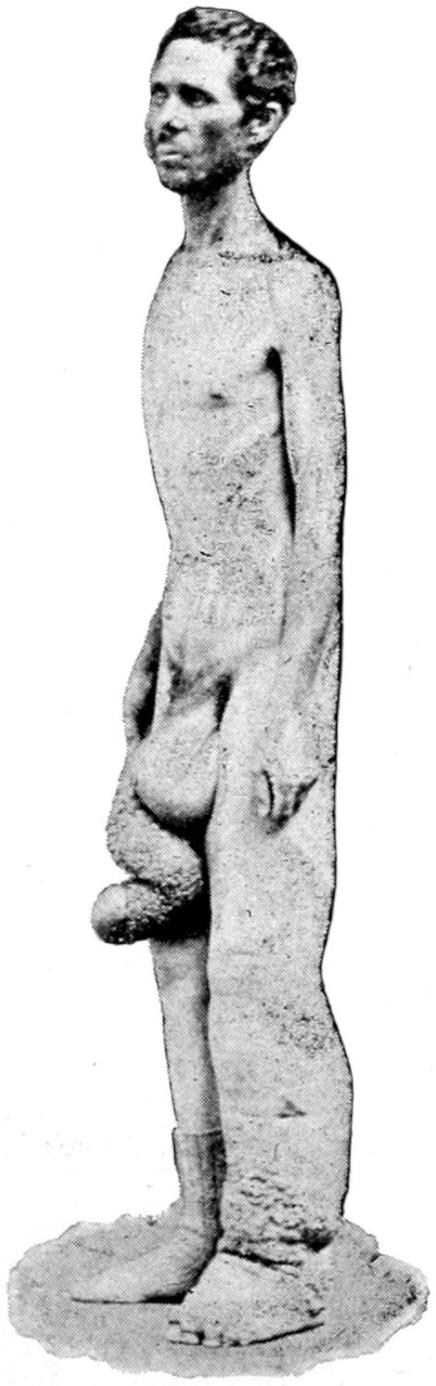
Fig. 186
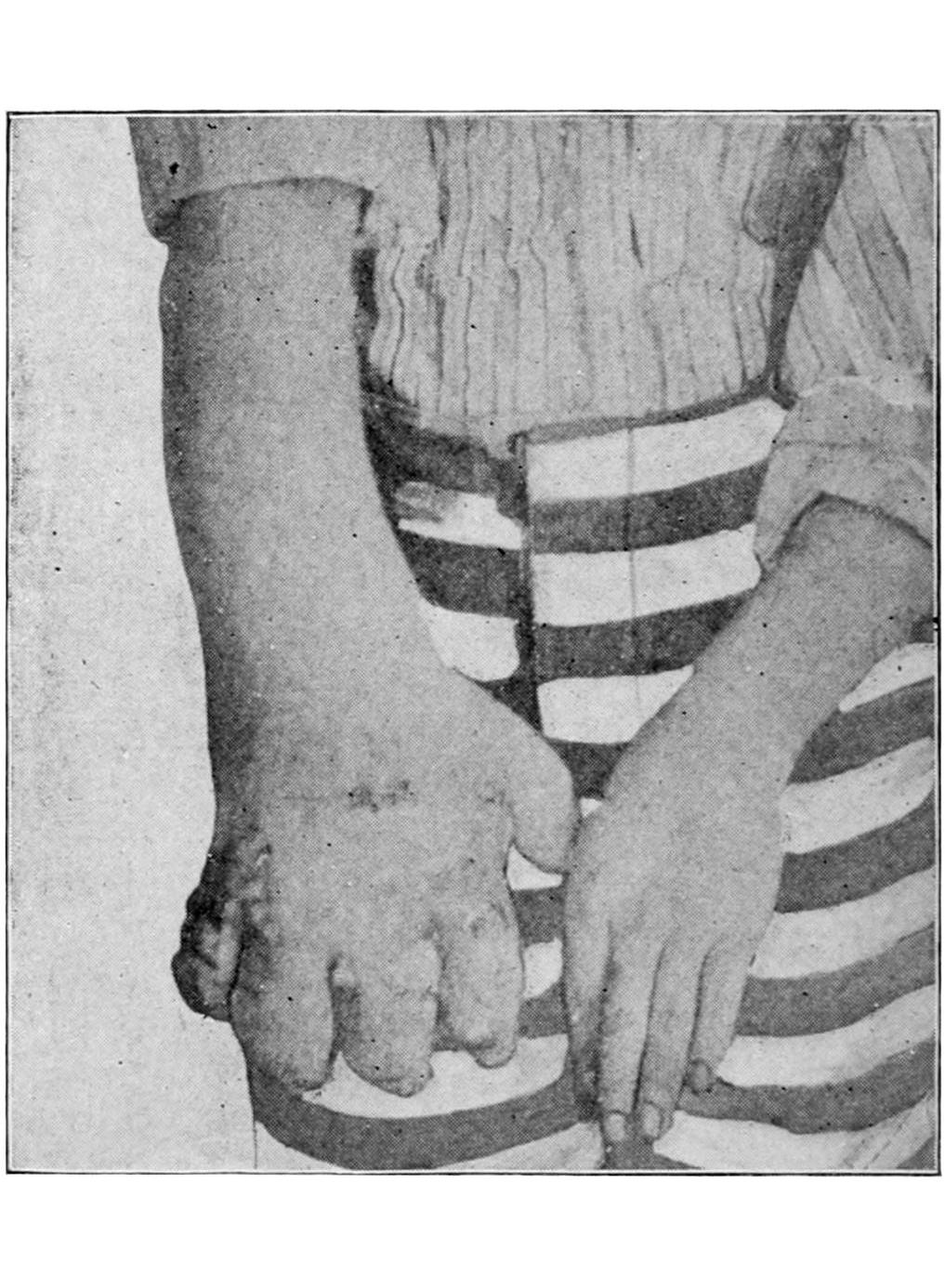
Elephantiasis of leg, scrotum, and penis.
Elephantiasis of hand, acquired.
Of the acquired forms of elephantiasis, those seen in the tropics are nearly all expressions of filariasis. Sporadic instances are met with in colder climates, and a condition resembling it is occasionally observed for which no existing cause can be detected. Such a case is illustrated in Fig. 186, which occurred in a convict in the penitentiary in Buffalo, who had never been outside the limits of the county, and in whom no parasites could be detected. Figs. 185, 187, and 188 illustrate typical instances of elephantiasis, Fig. 188 being taken from a Klamath Indian woman in the Northwest Territory, the condition being similar to that met with in the tropics.
The worms belong to the nematoids, the adult being 0.03 or thereabouts in length, thinner than the diameter of a red corpuscle, rarely remaining long in the quiescent[371] state. They can thus pass into the capillaries, which they may plug. The mosquito is discovered to be the medium of transportation, either directly or indirectly, through exposed drinking water, where the insect deposits her infected eggs. The adult worms outside the body may attain a length of 1 Cm. From the intestinal canal they pass into the lymph current and are carried until their progress is checked, where they establish a permanent home and breed and act as local irritants. The embryos which they produce are innocent; it is the adult and parent organisms that produce the damage. Lymph flow being thus obstructed the area previously drained by a given vessel will undergo various changes in the direction already described. In proportion, then, to the number of adult worms, and in accordance with their location, will be involvement of an entire member or of a more limited area, e. g., lymph scrotum (Fig. 187) or chylous hydrocele.
Fig. 187
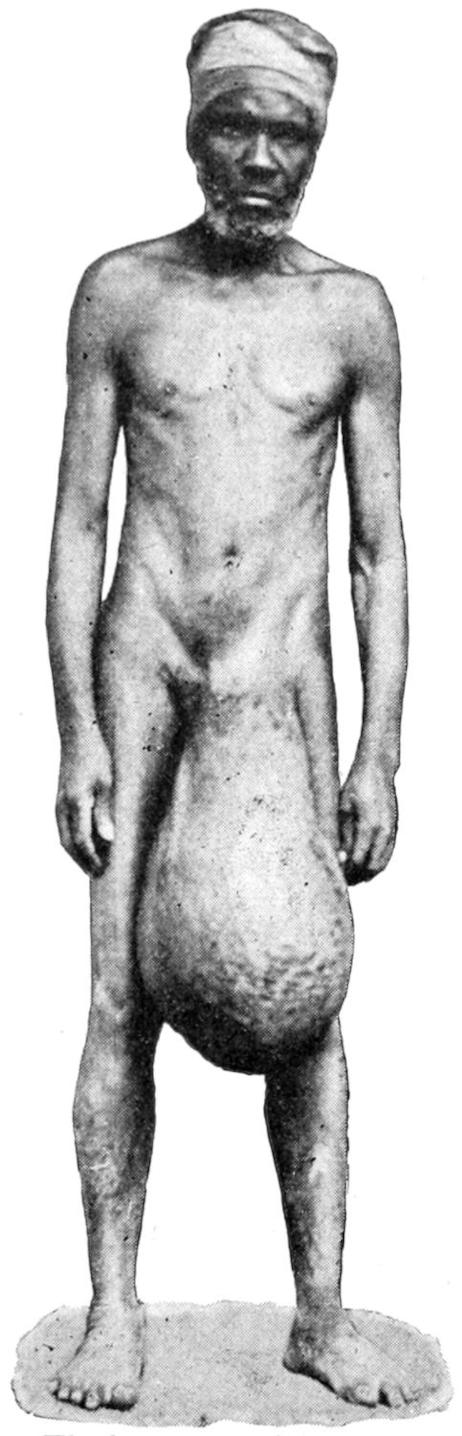
Fig. 188
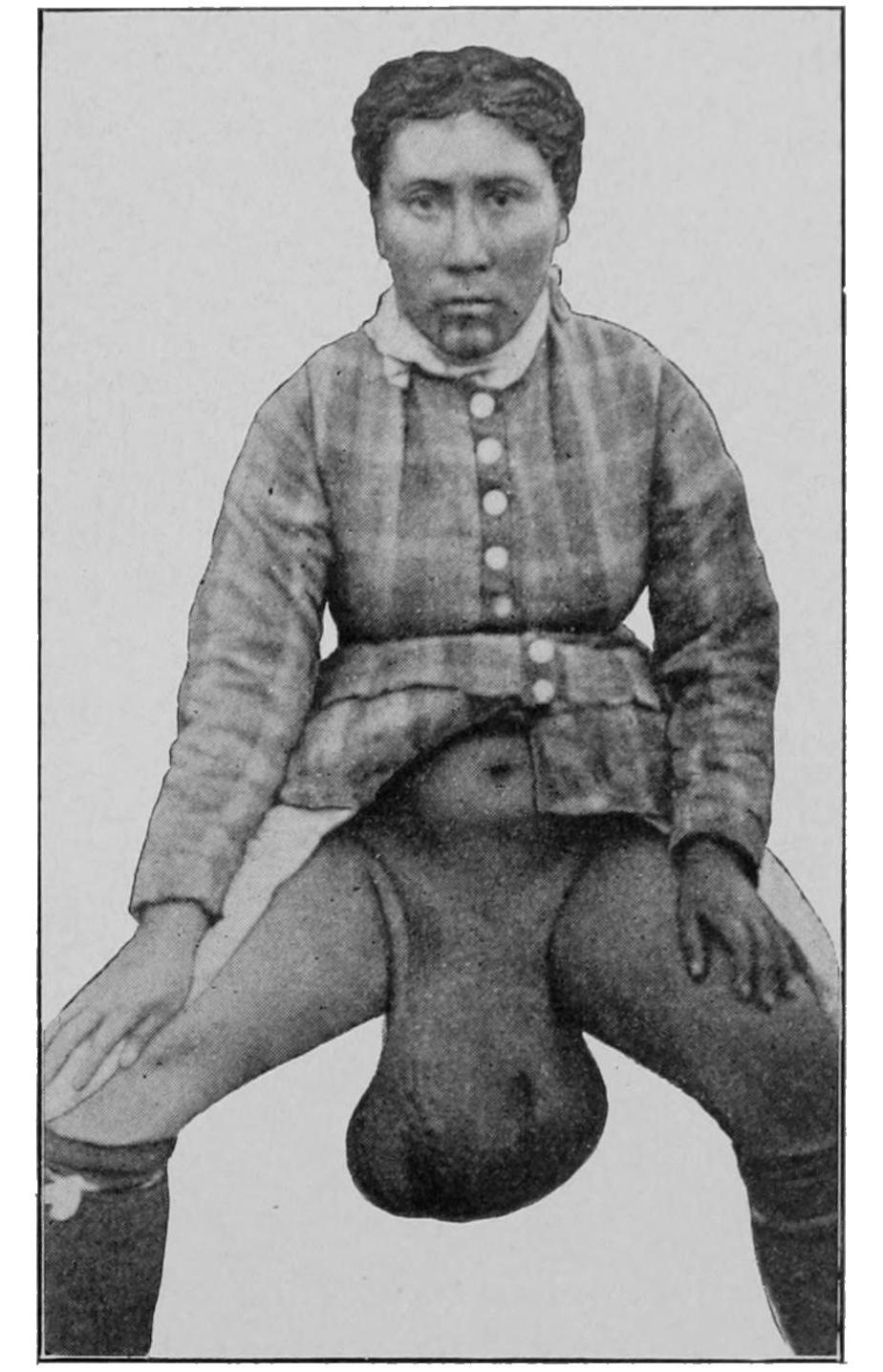
Elephantiasis of scrotum.
Elephantiasis of vulva (Klamath Indian woman).
(Contributed by Dr. H. L. Raymond, U. S. A.)
As yet there is no cure for filariasis; hence there is no relief for elephantiasis produced by it, except, when localized, to remove the part. In the tropical forms it is the lower part of the body which is usually involved. It begins in a limb, usually in the toes. It produces discomfort rather than actual pain, at least until such time as distention of the parts becomes unbearable. Along with lymphatic engorgement there is a peculiar liability to erysipelas, which becomes an exceedingly serious malady in tissues so saturated with lymph, and with such possibility for the propagation of germs. A milder degree of cutaneous and subcutaneous infection than is implied by the term erysipelas, as used in this work, may be called erysipeloid or cellulitis; it is quite common and frequently recurs. With each attack of this kind the condition is aggravated and the limits of the lesion extend. After a time the member becomes enlarged to a degree which disables, while the skin itself undergoes changes that alter its appearance; not only is it thickened, but there develop upon it papillomatous projections, with infiltration[372] of the corium, that give it an unnatural appearance and feeling. Epithelial proliferation is also rapid, and is accompanied by a sort of caseous discharge which may decompose and add extremely offensive features to these cases.
The management of these cases becomes very difficult. Total disability finally succeeds inability, and patients in the last stages are often bedridden. The repeated attacks of erysipeloid should be treated with antiseptic applications and elevation of the part, but without too much compression, as germs may be forced into the circulation.
In elephantiasis of the lower extremities it has been suggested to tie the femoral arteries, hoping thereby to deprive the limb of at least a portion of its fluid supply. This may be of some avail early, but when it is done late it is likely to be followed by gangrene of the limb, from whose consequences not even amputation can save the patient.
In the tropics, especially where the external genitals are sometimes involved, extensive operations have been of great service, and among the surgeons of India reports of operations of this kind are frequent.
Fig. 189
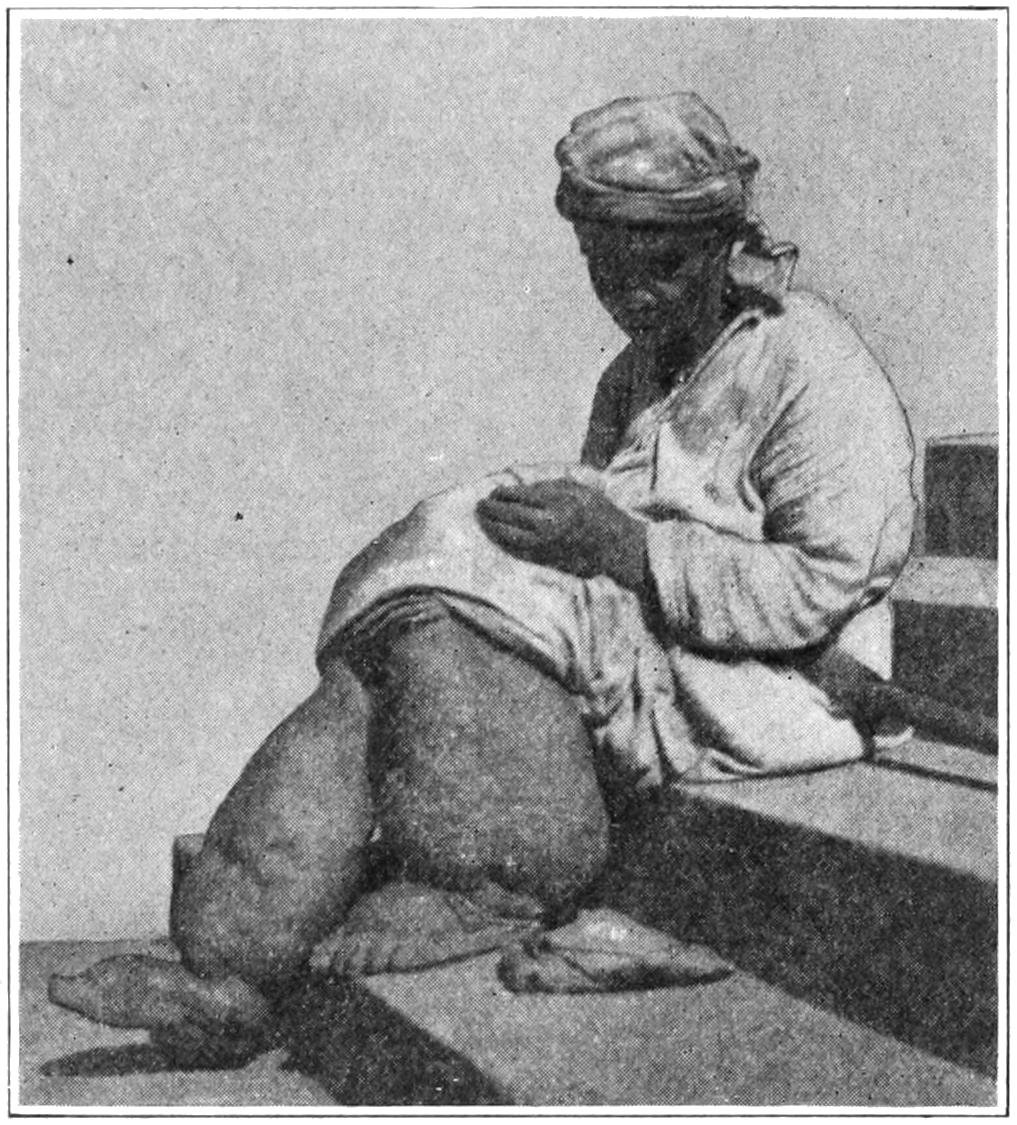
Elephantiasis (“Barbadoes leg”). (E. J. Meyer.)
Elephantiasis is most common in men; occurring in women it is not limited to the external genitals, for the writer has seen illustrations of the disease in the legs alone. In the Western Hemisphere it is met frequently in the Barbadoes, and is called Barbadoes leg (Fig. 189). The principal dangers from operations on these cases pertain to the risks of hemorrhage, shock, and infection. Nothing short of amputation of limbs or ablation of the genitals is of real benefit. In all these operations the veins as well as the arteries should be ligated, and the ligatures used en masse, introduced with a needle. There is usually copious oozing, and drainage should be provided.
This term is applied to a condition also referred to as chylous hydrocele. It implies a collection of milky fluid in the cavity of the tunica vaginalis. Occurring in a patient known to be suffering from filariasis it may be diagnosticated before exploration. In some instances where the sac of fluid is less translucent than usual, if the candle test fail when applied, chylocele may be suspected. Careful examination of the sac may show widely opened lymph vessels or lymph spaces. It is to be distinguished from spermatocele, whose contents also are milky fluid, but rarely collecting to the same amount. Chylocele may be treated by tapping, or by open division or extirpation of the sac, exactly as recommended elsewhere for the treatment of hydrocele. (See Fig. 187.)
Chylocele is to be distinguished from lymph scrotum, which is a form of localized lymphangitis of mild degree rather than a circumscribed collection of chylous fluid. It presents febrile, not to say inflammatory features, and in the chronic form the skin will be frequently seen to ooze fluid closely resembling lymph, which condition is called lymphorrhagia. The scrotum rarely becomes as large as in extreme cases of dropsy, and yet may assume an uncomfortable size. This condition, like that previously mentioned, is usually associated with filariæ. It may appear, however, spontaneously, and after persisting for a long time disappear, with as little apparent reason as that which produced it. When the condition becomes unbearable ablation may be practised. (See Fig. 187.)
[373]
The presence of chyle in the urine gives it an appearance as if emulsified oil had been mixed with it. It occurs with or without known reason. Sometimes it co-exists with lesions like lymph scrotum, etc.; at other times it seems to neither produce nor be accompanied by other disturbances. Ordinarily the urine or the blood when examined at night—i. e., the sleeping hours-will reveal the pathogenic organisms, i. e., filariæ. It is a condition but little influenced by treatment, which should be symptomatic in the absence of special indications.
The more typical congenital forms of occlusion of lymph vessels produce such changes as we see, for instance, in macrochilia, where the lips and cheeks are affected; macroglossia, where the tongue is too large to be retained inside the mouth; and sometimes macrodactylia and macropodia, where the fingers and hands or toes and feet are involved (Figs. 190 and 191). It is difficult to separate some of these cases from gigantism, as already stated. The more distinctive lymphatic lesions are frequently accompanied by pigmentary, cutaneous, or papillomatous conditions, which stamp them as something more than mere expressions of disproportionate growth. The patient of Dr. Gerrish, whose condition is illustrated in Fig. 190, presented lesions which might be assigned to either of these groups. It will usually require a careful study to make a proper assignment of such cases as macromelia.
Fig. 190

Fig. 191
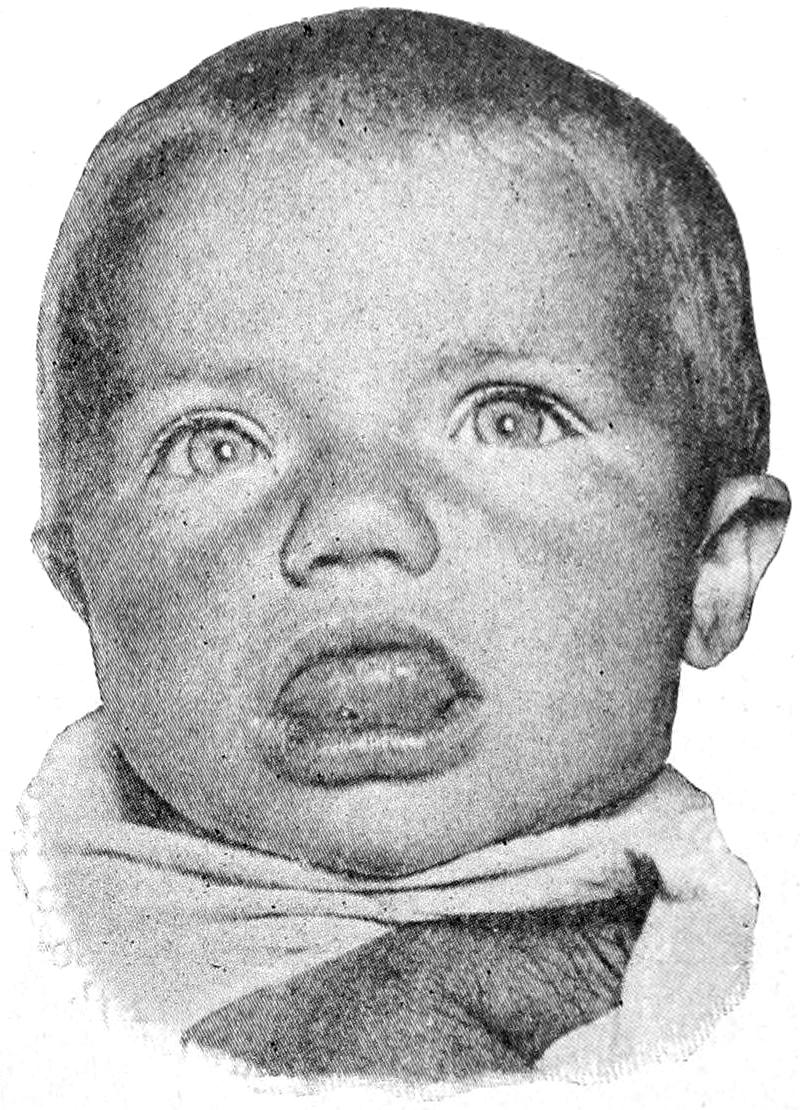
Macromelia. (Gerrish.)
Macroglossia. (Neisser.)
While this condition is usually regarded as an expression of lymphangiectasis, it has been shown that it may be due to multiple adenopathy of the mucous glands in the lips. The lips are well supplied with such glands, which lie beneath mucous[374] membrane in a mixture of more or less connective and vascular tissue. When the lips undergo marked hypertrophy in adult life, it is very likely that the affection may be explained by the hypertrophy of these collective glands, and this is particularly true when anything like nodular arrangement can be detected. A recognition of this cause will indicate the proper remedy, i. e., excision of the affected tissue. The writer has on more than one occasion made an elliptical incision both from the lower and upper lip and accomplished its purpose, with great improvement of appearance.
Lymphangioma has been described in the chapter on Tumors. It seems necessary to allude to but one expression of this kind in this place, i. e., the so-called lymphangioma circumscriptum. This presents as a cutaneous area dotted with vesicles, sometimes regularly, sometimes irregularly distributed, usually in annular form, seen most commonly on the upper limbs and in the region of the shoulders. The vesicles occasionally become sufficiently large to be called bullæ, while the contained bloodvessels are dilated and discolor the area involved, which may also be more or less pigmented. Here, as in elephantiasis, there is great liability to surface infection of low grade, which may perhaps be called erysipeloid. The tissues gradually become thickened and covered with scabs or warty collections of epithelium. It is met with early in life, rather than late, and is supposed to be of congenital origin. It may be distinguished from herpes by the pronounced vascular changes and by the discharge of lymph.
—Treatment has been too often unsatisfactory and the trouble often re-appears after apparent recovery. If the area involved be not too large complete excision will probably prove the most satisfactory method of attack.
This term applies rather to gross and visible lesions of the larger lymphatics than to the involvement of the ultimate lymph-filled ramifications. When the smaller lymph capillaries and interspaces are involved the lesion takes the type of an erysipelas or cellulitis, but as the collected products return through the lymph channels from such an involved area they will disturb and infect the lymph vessels themselves, and this leads to what is called a lymphangitis. Formerly the term spontaneous or idiopathic was given to some of these cases. Assuming, as is done throughout this work, that there is no true inflammation that is not of microbic origin, we may expunge the term “idiopathic” and say that lymphangitis is also an expression of infection, and that the inflamed vessel represents a channel through which products of inflammation are being conveyed. Histologically the walls of these vessels become infiltrated with a coagulating exudate, which may completely occlude the vessel. The bloodvessels immediately adjoining the lymphatics also become involved, and, being engorged, give rise to the peculiar red lines or streaks which are frequently seen when cutaneous lymphatics are thus involved, this appearance being due to a perilymphangitis. The infected lymph passing through this channel is filtered out in the first lymph nodes with which it communicates, which themselves become thus infected; hence the rapidity with which these enlarge and break down, so that by their own sacrifice they may perhaps protect the rest of the body from serious infection. Under these circumstances suppuration and necrosis of these lymph nodes is to be regarded as a vicarious destruction on their own part.
Lymphangitis proceeds from the periphery toward the centre, and is followed by a certain amount of pain, with great soreness and sense of stiffness in the parts; the skin overlying the infected vessels becomes reddened in streaks, which indicate their course, or becomes more or less infiltrated and involved throughout in a form of infectious dermatitis. According to the virulence of the germ, and the susceptibility of the individual and his tissues, there will or will not occur suppuration. This may perhaps be averted by prompt treatment. Should deep tenderness and pain take the place of or be added to their more superficial expressions it may be inferred that the superficial[375] lymphatics have now infected the deeper ones, and that there is greater danger of phlebitis and a generalized septic infection.
Constitutionally, at least, the expressions are those of septic intoxication, often of true septicemia or septic infection. Local appearances, increasing temperature, or accession of chills may indicate the presence of pus.
In proportion to the distance of the diseased part from the body centres the prognosis becomes more favorable. When an entire limb is involved the matter is very serious; when in the face or abdomen, still more so, the fear being of septic phlebitis and a fatal termination by a more or less typical pyemic process.
—All exciting causes, including sloughing tissues, foreign bodies, pus, etc., should be thoroughly removed. Pus, when present, should be evacuated, and when its presence is suspected suitable exploration should be made. Tension should always be relieved by incision. In cases where breaking down has already begun, continuous immersion in hot water is beneficial. Nothing, however, will take the place of removal of pus or necrotic tissue, and this should be first attended to or proved to be unnecessary. In an open and sloughing wound nothing is as satisfactory as brewers’ yeast; next to this is hot water. Over an unbroken area which is simply edematous and pits on pressure, may be applied the ichthyol-mercurial ointment (10 per cent. ichthyol, 40 per cent. mercurial ointment) or the Credé silver ointment. This should not be rubbed in, but smeared freely over the surface, and then covered with oiled silk, twice daily, in acute cases. The surgeon should satisfy himself as to the presence or absence of pus; even when only suspected it is advisable to make incision early, as tissue and possibly life may thus be saved. Constitutional treatment should not be neglected. It will consist in improving elimination, maintaining nutrition, and overcoming the acute toxemia due to absorption, the toxins being best antidoted by alcohol in some palatable form, strychnine and quinine being serviceable, but not so valuable. (See chapter on Septic Infections.)
—Chronic lymphangitis is seen in connection with the slower infections, tuberculosis—syphilis, filariasis, etc. Here the lymph vessels are not involved so much as the lymph nodes. Chronic lymphangitis does not occur without a toxic or infectious process behind it.
For the surgeon’s purpose, at least, he may assume that lymph nodes are never enlarged except in the presence of toxemic or infectious processes. The role which they play as filters of the fluid returning through the lymph vessels subjects them to daily possibilities of contamination. They may be acutely infected and actually break down by a phlegmonous process, or their lesions may be very slow, chronic, and intractable. The lymph nodes, like the leukocytes, are among our best friends; they serve as guardians at the various portals of the system, excluding, sometimes at the risk of their own existence, various deleterious elements.
The term “lymph gland” should be expunged from medical terminology, the node having, so far as known, no secretion nor any title to be considered a gland. This would mean abandonment also of the expression “lymphadenitis,” and so the writer would prefer to use the expressions lymphitis, lymphangitis, etc., which at least do not imply a wrong conception of the process. The morbid activity which the lymph nodes present will be an expression of the general virulence of the whole process which has produced it. To a tender enlargement, in acute cases, there will succeed rapid swelling, with pain and soreness commensurate with the density of the surrounding tissues and the degree of tension thus produced. The result is essentially an abscess, or multiple abscess, which necessitates prompt treatment by free incision, evacuation, and drainage, as does any other abscess. It is as often necessary to use a curette as a knife, and when so-called specific features are present, as in chancroidal bubo, a strong antiseptic should also be used. Under these conditions the collection of lymph nodes in the axilla or in the groin may become involved in multiple abscess, and it is then good practice to make a complete cleaning out of these regions. The ultimate effect of such extirpation is beneficial, and the patient does not seem to suffer from the loss[376] of the involved lymph nodes; indeed, it is probable that new ones form to replace those which are destroyed.
The chronic affections of the lymphatics which come under the surgeon’s care are expressions of tuberculosis, syphilis, gonorrhea, cancer, or of some of the other less frequent surgical diseases. In every one of these instances the disease has assumed constitutional proportions, and the lymph-node involvement will be general. The ultimate fate of these affected nodes will differ with the different diseases; in tuberculosis they sometimes suppurate by secondary infection, and they frequently caseate, or remain enlarged for indefinite periods, often throughout life. Around them will be found an area of infiltration which produces firm adhesions and frequently makes their extirpation very difficult. The lymph vessels which connect the various nodes will also be involved in a similar process, which adds to the difficulty of operation. In many cases these involved nodes can be felt where they cannot be attacked—for example, in tabes mesenterica. If, under suitable climatic and constitutional conditions, it be possible to favorably affect other tuberculous conditions, these expressions of the disease may also subside or at least cease to trouble.[29]
[29] At date of going to press I do not feel justified in lauding too highly the work done by numerous workers with the opsonins. Justice to what has been done with and claimed for them demands, however, their extensive trial, and suspension of any judgment not as yet favorable.
Syphilis of the lymph nodes has already been considered, as well as the frequency, nay, the certainty, with which the lymphatics become involved in this disease. So true is this that any general lymphatic involvement which cannot be accounted for in some other manner is usually attributable to syphilis. The condition of the lymphatics may be considered a fair index as to the success and effect of antisyphilitic treatment, for if, under such treatment, these enlargements subside completely it may be regarded as eminently successful. On the other hand, it is not felt by many that it is safe to discontinue treatment in the presence of these enlargements. Syphilitic enlargements may, moreover, undergo secondary infection, either acute or chronic, i. e., may suppurate or become tuberculous. In gonorrheal bubo the pus which the lymph-node abscesses contain will often be found almost a pure culture of the gonococcus, thus illustrating the specificity of this kind of infection.
The extent to which the lymphatics are involved in cases of cancer will often be the guide for the surgeon in advising removal or the reverse. The principal advance in the modern operative surgery of cancer has come through a better working knowledge of the area of lymph distribution of given regions. All cancerous lymph nodes which can be reached should be extirpated. If others can be discovered which are beyond reach it raises a doubt whether the operation should be performed. At all events, in these cases it should be represented as a temporary rather than an absolutely curative resort, not only because this is true, but because the surgeon may need to protect himself against charges which may be made later by disappointed patients.
The advisability of removing diseased lymph nodes is often a matter for serious discussion. There is little to justify their removal when the exciting cause cannot also be taken with them. It is a mistake to operate on nodes in the neck and leave diseased teeth through which the infection may be spread. So, too, it is a mistake to operate on nodes which may prove to be syphilitic. In many instances, then, it is best to apply the therapeutic test. In cancerous disease it can rarely be advisable to remove lymph nodes alone except for purely temporary purposes, as to check hemorrhage, remove breaking-down material, or something of the kind. In the neck, groin, or axilla the operation is not to be lightly undertaken, for it is made extremely difficult by adhesion of the surrounding structures. The surgeon should be prepared then for careful dissection, which should be made with a not too sharp knife, and he should be ready to sew up a rent in the jugular vein or tie it, as it and its large branches are frequently so displaced and obscured as to be injured, even by the most careful operator.
This is one of many names applied to a condition whose most conspicuous characteristics are a progressive anemia, with enlargement of lymph nodes, as well as usually of the spleen, with secondary or metastatic growths in the viscera, bone-marrow, and[377] elsewhere. That its etiology hitherto has been considered obscure and that its clinical characteristics vary in different cases may be shown by a partial list of the names by which it has been previously known: lymphadenoma, malignant lymphoma, infective lymphoma, progressive glandular hypertrophy, lymphosarcoma, and pseudoleukocythemia. To the writer’s mind, if the disease is to be known by any other name rather than that of the one who first described it, it might be called malignant lymphomatosis, as its tendency is downward, in which sense it is malignant in an almost hopeless degree.
The changes which occur in the blood are at first in the direction of simple anemia, followed by marked reduction in the number of red cells, with poverty of hemoglobin and increase in the number of leukocytes. In the anemia of extreme cases the red cells may be reduced 1,000,000 per Cm., while the leukocytes, especially the polynuclear forms, may be numbered by the hundreds of thousands. In one case recently under my observation the leukocytes amounted to about 300,000 when treatment was begun. (See chapter on the Blood.) It is a disease of early rather than of later life, and occurs more often in males than in females. The most pronounced objective changes occur in the lymph nodes, which enlarge steadily, the swellings thus formed being hard or soft according to the rapidity of the disease. The swellings thus formed will appear conspicuously in the neck and will be noted also in the axilla and the groin. Careful examination will show that every lymph node in the body which is accessible is involved in the course of the disease. Sometimes the tumors become so large as to cause serious pressure, and when in the neck perhaps to require tracheotomy to prevent suffocation. Fig. 192 illustrates a case under the writer’s observation, in which he had to resort to this emergency measure. The microscopic picture of this enlargement is that of hyperplasia of the tissues composing the lymph nodes, while the lymphoid cells are multiplied in number.[30]
[30] Pathologists have long suspected that Hodgkin’s disease and sarcoma have, at least, certain features in common if they are not more or less actually associated in character. Yamasaki has recently reported several cases of typical Hodgkin’s disease without any suspicion of tuberculosis, in which there were unmistakable sarcomatous formations in various parts of the body, especially in the viscera, and he believes, as do others, that the affection which begins as Hodgkin’s disease may later assume the characteristics of a general sarcomatosis.
Fig. 192
Hodgkin’s disease.
Less conspicuous but equally distinctive changes occur in the spleen in four-fifths of the cases, it becoming enormously enlarged and occupying the left half of the abdominal cavity, being universally enlarged and preserving its original outlines. This splenic enlargement sometimes is simply an hypertrophy, but in many instances the spleen itself will be occupied by tumors, i. e., lymphomas, which are scattered through it and cause part of its enormous dimensions. Late in the disease the liver also becomes enlarged and lymphomas are also scattered throughout its substance. The same lymphomatous or adenoid tissue may be met with in many other parts of the body, the bone-marrow, the alimentary canal, the ductless glands, kidney, lung, etc.
Hodgkin’s disease is doubtless closely related to other varieties of leukemia and to Banti’s disease, or splenic anemia, all of which should be regarded as expressions of an infection by organisms not yet clearly described, although their better recognition and identification are clearly foreshadowed in work now under way. Death comes as the result of the exhaustion and poisoning of a terminal infection, save when it is produced earlier by absolute starvation or suffocation. To run its entire course an average case consumes from eighteen months to two and a half years.
—So far as diagnosis is concerned the microscope will serve a certain purpose even early in the disease, enabling one to recognize an increasing anemia and leukocytosis, but not until perceptible enlargement of lymph nodes and of the spleen[378] is found can the diagnosis be made absolutely certain. One has to distinguish mainly between those forms of leukemia in which lymphomatous changes are not conspicuous, cachexia of cancer and syphilis, and the condition of lymphosarcoma, as it has been called by some, in which there is the involvement of the lymph nodes without the characteristic blood changes met with in Hodgkin’s disease. In splenomegaly we may have enormous enlargement of the spleen without the marked involvement of the lymph nodes. From lymphatic tuberculosis it is to be distinguished by absence of fever, the tendency to universal involvement of the lymphoid tissues in all parts of the body, and the absence of suppuration and caseation which occur so distinctively in tuberculous disease.
—Few drugs are of much or any avail in this disease. Of them all nothing compares with arsenic, which should be given for a long period and pushed to the physiological limit. The formula which was given in the chapter on Cancer will serve in the treatment of Hodgkin’s disease (p. 296, note). Next to this, and especially in patients with enlargement of the spleen, the x-rays are the most effective. In one case much of this character, in which I began active treatment by both methods, I saw in forty-eight hours a diminution of 100,000 leukocytes. This did not persist, however, for the proportion was later somewhat increased, but the immediate effect as well as the benefit were very pronounced. All the affected regions may be exposed to the x-rays, which should be used with great care.
The term lymphoma has been indiscriminately ascribed to various enlargements of the lymph nodes and lymphoid tissue throughout the body, so much so as to have really lost its significance. If by the term is meant simply a tumor of a lymph node it will usually fall under the proper classification as being a granuloma, a syphiloma, a carcinoma, etc. If by the term is meant a general involvement of lymph tissue throughout the body, such as is seen in status lymphaticus, then it would be best to use some other term. Finally it may be questioned whether there is any distinctly marked lymphoma, i. e., a tumor of true lymphatic structure, which is not of infectious origin. The term lymphosarcoma is still in use and probably will not be expunged until our notions of pathology are clearer. The expression lymphadenoma should be discarded. Multiple malignant lymphoma, as stated above, is but another name for the condition ordinarily described as Hodgkin’s disease. That sarcoma and endothelioma may arise in the lymph nodes is universally conceded, although as primary neoplasms in these localities they are rare. Not much can be said, then, that is distinctive about lymphoma.
In a general way, it may be said of any tumors of the lymph nodes that if isolated or not too multiple they should be extirpated.
[379]
The joints, by virtue of their function and anatomical relations, are liable to a variety of injuries and affections, most of which are essentially surgical. The joints most subject to traumatism belong to the extremities. On the other hand, the deeper joints (e. g., of the spine) are quite prone to toxic and infectious diseases and less liable to serious injury. The surgeon cannot disregard the structure of the joint when considering the pathology of its surgical affections. More or less completely protected externally, though sometimes with but a thin coating of integument and fibrous textures, it is composed largely of resistant, white, fibrous tissue, seen in its ligaments, of spongy bone in the expanded bone ends, covered with cartilage of incrustation, the articular termination of the bone shaft not being firmly affixed until a certain age has been reached, while the interior is lined with a serous membrane whose lymphatic connections are most abundant, portions of which are often loaded with fat. In certain joints—particularly the knee-there enter separate considerations in the shape of interarticular cartilages which are not so firmly attached but that they may be sometimes displaced.
Lymphatic connection between the exterior and the interior is often free, and after trifling abrasions or infections of the overlying skin the joint beneath may suffer seriously or even fatally. Many of the surgical diseases of the joints begin within the joint membranes proper, i. e., the synovia. Numerous other expressions, particularly of tuberculosis, have their origin in the bony structure contiguous to the joint cavity.
In any destructive affection of the joint in childhood the corresponding epiphyses are often involved. This is also true of fractures extending into joints or occurring near them in the young. Below will be found a table of the time when the epiphyses are usually consolidated with the main portion of the bone. In general, they unite earlier in the upper limb than in the lower, or, as Sappey puts it, the upper limb first arrives at maturity. The following table represents simply the average, there being considerable variance on either side of it in different individuals:
| UPPER EXTREMITIES. | ||
| Clavicle | 23d | year. |
| Humerus, upper | 20th | year. |
| Humerus, lower | 17th | year. |
| Radius, upper | 16th | year. |
| Radius, lower | 20th | year. |
| Ulna, upper | 16th | year. |
| Ulna, lower | 19th | year. |
| Phalanges | 18th to 20th | year. |
| LOWER EXTREMITIES. | ||
| Femur, head and great trochanter | 19th | year. |
| Femur, lower epiphysis | 21st | year. |
| Tibia, upper | 21st | year. |
| Tibia, lower | 18th | year. |
| Fibula, upper | 21st | year. |
| Fibula, lower | 20th | year. |
| Phalanges | 18th | year. |
These dates should be remembered, as an ununited epiphysis may be involved in a necrotic or suppurative process and thus break down and require removal. Moreover, these facts will also be of value in considering fractures, for up to these dates epiphyseal separations will often be met.
[380]
—A sprain is either the result of a momentary dislocation of a joint, the parts returning immediately to their proper position, or else is produced when a joint has been strained beyond its probable physiological limit without any true displacement. It may be the consequence of direct or indirect violence, or even of incessant muscular action. It always implies a certain degree of tissue injury, which may vary from minute lacerations of ligaments, fasciæ, aponeuroses and periosteum, up to a degree where ligaments are violently sundered or torn out of their bony attachments.
A sprain is generally followed by hyperemia, with its attendant phenomena, as described in a previous chapter, and as long as possibility of infection can be excluded the resulting outpour which produces the extreme joint swelling will more or less quickly disappear.
In fact, as insisted throughout this work, the differences between hyperemia and its consequences, and true inflammation with its results, can nowhere be more perfectly demonstrated than in such a case as this. Even with great damage and effusion there can be complete repair, so long as infection is excluded. Once the germ element enter, the whole aspect is altered and a serious feature is then introduced.
—The symptoms of sprain are loss of function, swelling, pain, and later ecchymosis. The first is usually immediate, the swelling takes place rapidly, and ecchymosis occurs after two or three days, unless the joint be near the surface. The degree of tenderness will afford a measure of the amount of damage done. The swelling may be produced either by serous outpour or by hemorrhage, or by both. Ecchymosis is usually due to minute lacerations, and may spread to a considerable distance. Where there has been much outpour of blood into a joint it sometimes produces a reactional hydrarthrosis, which appears only after a week or more. Such hemorrhage is serious, and is frequently the cause of more or less pseudo-ankylosis by organization of clot.
Sprain may then be of all degrees of severity. From the mildest of these one may expect perfect functional recovery in short time, while in the more severe cases chronic thickening, with hydrarthrosis, tender areas, and muscle atrophies, often persist for a long time or even permanently.
—The ordinary treatment of a sprain consists, first, in physiological rest. If the swelling be already pronounced when seen by the surgeon he will endeavor to promote absorption by elevation, gentle compression, perhaps with an elastic bandage, and by cold wet compresses. If seen early and before much swelling has occurred it will often give great relief, especially in certain joints (e. g., the ankle), to partially immobilize the part by strapping it with a series of adhesive strips, 2 Cm. in width, cut sufficiently long to encircle the foot, ankle, and lower part of the leg. The strapping should be begun at the base of the toes, and each strap as thus applied should be made to slightly overlie the preceding one. It is possible by neatly compressing the involved region in this way to almost prevent swelling, and to give such support that function is but slightly impaired, and pain reduced to a minimum. The objection to plaster of Paris or the more fixed dressings is that they are usually allowed to remain too long. Far better in most of these cases is either a splint or a dressing which permits of daily examination. With the subsidence of acute symptoms, massage and passive movement should be practised. There are cases in which swelling will be so extreme that aspiration or even incision may be advisable for the purpose of emptying the joint.
The surgeon sees many a case of this kind after it has become chronic and after domestic or simple applications have failed. Most of these cases require massage, practised skilfully, and with intelligence, by which absorption is much promoted. The same result, as well as relief of soreness or pain, follows the constant use of cold wet compresses, perhaps combined with the use of ice-bags. If the material used for these compresses be dipped in solution of sodium or ammonium chloride, say 5 per cent., the effect is much enhanced, while laudanum can also be used upon them. Tenderness and localized pain in old cases may be treated by a succession of blisters, but can be better treated by the application of the flying cautery, i. e., by the light touch of a glowing cautery point swept rapidly over the surface involved. This is one of the most powerful agents for the relief of pain. Occasionally the cautery point may be applied more[381] deeply, i. e., ignipuncture. If localized collections of fluid form they may be incised.
The statements and advice given in regard to sprain will apply equally well to the ordinary contusions of joints.
These are inflicted as are wounds elsewhere, and, while always serious, have an importance proportionate to the infection which may have occurred with the injury or afterward. In practise it may be assumed that the skin, like the clothing outside, is always dirty and infected, and that every penetrating wound should be regarded as an infected wound. Not every wound in the vicinity of a joint is penetrating, and it is advisable to ascertain whether a joint cavity be actually open, as much of the method of treatment will depend upon this fact. The majority of these injuries are of the punctured or small incised variety. The actual joint opening is usually smaller than that in the skin. It may be so small as to escape observation. Outflow of blood is not pathognomonic, but escape of synovial fluid always indicates that some serous cavity, possibly a bursa or tendon sheath, has been opened. Immediate accumulation of fluid within a joint after probable wounding of the synovial membrane is quite suggestive, as it is likely to imply that the joint is filling with blood. After any injury which may loosen them the epiphyses should be carefully examined, in order to determine if they have been loosened, while it should be estimated, so far as possible, whether the epiphyseal junction has been disturbed or is probably infected. The student should remember that punctured wounds of joints are not necessarily made from without inward. A spicule or fragment of bone may, by protruding, produce exactly the same condition, only in this case there may be a compound fracture to complicate it. Infection does not invariably follow these injuries. Their gravity is in large degree measured by the presence or absence of a suppurative synovitis. This does not necessarily instantly follow the injury, but develops within the ensuing two or three days. Therefore the fate of such a joint is not necessarily determined by inspection within the first few hours. Esmarch’s dictum regarding gunshot wounds may here be paraphrased. The fate of every punctured joint depends upon the man who first takes care of it. If the proper thing be done promptly a good result may usually be obtained.
The first indication in every such case is sterilization of the parts, including the area of the wound. If by a small elliptical incision the wounded skin can be excised, it may perhaps very much improve the prospect. A small punctured wound may be watched for a day or two, especially if it be believed that the first attention were prompt and antiseptic. Should no unpleasant features appear little need be done except to apply ice externally and maintain rest. On the first appearance of sepsis or of increasing trouble in the joint it should be promptly incised, irrigated, and drained.
In the larger openings of joints it should be assumed from the outset that infection has occurred. In such a case the wound margins should be trimmed, the joint cavity thoroughly irrigated, and explored for foreign bodies, by enlarging the existing opening. After thorough irrigation a drain should be inserted for at least a few hours. For this purpose a catgut strand or a drainage tube may be employed.
As soon as the presence of pus (acute pyarthrosis) is made clear the case takes on a larger aspect, in that drainage not alone at one point is indicated, but probably at two or three. Nothing is so disastrous to an involved joint as pus retained within its hidden recesses. Almost every other consideration is sacrificed to its discovery and to affording a means for its escape. Counteropenings in numbers sufficient for the purpose are, therefore, indicated, and it will often be best to draw through the affected joint a drainage tube, of a size sufficient to prevent its occlusion by thick pus or debris. Daily and continuous irrigation may be practised to great advantage, or, as is possible with the ankle, the wrist, or elbow, continuous immersion may be substituted as a still better measure. Wherever infection and destruction to this degree have taken place it may be presumed that the future of the joint is seriously compromised. There will, therefore, be room for display of judgment as to when to begin passive and when active motion; moreover, a guarded prognosis concerning restoration of function should be given.
[382]
Gunshot fractures of joints constitute almost a category by themselves. Under the old regime, and in the pre-antiseptic era, gunshot wounds of joints condemned one to amputation and loss of at least the part below. The mortality attending injuries of this kind, with the resulting amputations, during our Civil War, and all others previous to it, was extreme. The Continental surgeons first appreciated the value of antiseptic occlusion, and taught the rest of the world that this wholesale sacrifice of limb, and often of life, was unnecessary and could be avoided. Reyher’s first papers on this subject revolutionized previous views and practises, and established on a firm basis the general principle of primary antiseptic occlusion of those injured joints. The accumulated experience of military surgeons since his time, as well as of civil surgeons all over the world, has demonstrated that if a gunshot wound of a joint be afforded prompt antiseptic occlusion and rest the chances are in favor of restoration of function, with a minimum of disturbance and a maximum of result. It was because of these results that soldiers were provided with the “first aid to the injured” packets, so that a punctured wound might be protected immediately after its reception. Even the complete tunnelling of a joint, which the Mauser bullets so often accomplish, does not seem to be so serious an injury today as was the puncture of a needle or an awl in the pre-antiseptic era. Therefore the best thing to do with a gunshot wound is to practise antiseptic occlusion. If it become troublesome it should be treated in accordance with the advice given above.
This relegates the matter of amputation or of primary excision of an injured joint to those cases of extensive and mutilating injury where not only the soft structures are widely opened and infected, but the joint ends of the bones also are seriously involved. When it comes to the treatment of compound dislocations it is difficult to lay down principles which shall be universally applicable. As a general rule primary excision will usually be indicated, and prove not only life-saving but limb-saving. In compound dislocations of the astragalus its removal will be nearly always indicated. Only in cases of extensive damage will amputation be necessary.
Inasmuch as it is infection, leading to suppurative synovitis or arthritis, which gives to all serious cases their greatest dangers, it will be sufficient at this point to remind the reader to this effect and to describe the condition itself a little later.
The various surgical affections of a joint may be of primary or secondary origin, and of rapid or chronic type. The acute are usually expressions of serious infection, while the chronic are frequently of toxemic origin, including under this heading manifestations of a particular diathesis or defective metabolism. Others are so exceedingly slow in their course and are so intimately connected with other indications of disease of the central nervous system as to be called neuropathic. (See below.)
Nearly all the acute affections begin in the synovial sac proper. From this they may spread and involve the adjoining parts. The acute toxic lesions also arise within the synovial cavity, such as those which follow gonorrhea, typhoid, scarlatina, pneumonia, influenza, etc. Tuberculosis may primarily affect either the synovia, in which case we have a condition corresponding to tuberculous peritonitis, or it may take its origin in the expanded bone ends or in the epiphyseal cartilages. Syphilitic affections of the joints are rarely acute. They lead rather to chronic disintegrations or hypertrophy. No matter how the lesion may have arisen it will nearly always extend to and involve other parts; thus in acute suppurations the articular cartilages are soon attacked, while in the more chronic forms, which have their origin in the bone, the joint cavity is slowly encroached upon and its integrity impaired or destroyed.
So long as the type of joint disease be not destructive a complete or nearly complete restoration of function can be expected, provided suitable treatment be given early. If, however, a case occur only after fibrinous outpour has organized into adhesions, muscles have withered from disuse, and the entire joint become distorted or disarranged, then it may be too late to cure, and it is a question then of how much improvement can be effected. Even after acute suppuration, if the case be properly managed from the outset, very useful joints can be regained.
[383]
—In synovitis, as in pleurisy, there may be a minimum of serous outpour, such exudate as escapes into the joint being exceedingly rich in fibrin and coagulating easily. This material is variously disposed of, and may form adhesions which will limit motion, or masses of condensed fibrin which may be broken up into shreds or rounded off into seed-like or rice-grain bodies. When tenderness subsides sufficiently to permit it these may sometimes be felt within the joint. At other times they lead later to an hydrarthrosis, which may prove more or less disabling and require subsequent operation. Another form of synovitis sicca is met with in acute and perhaps chronic rheumatism, where masses of fibrin become loosened and can be felt as foreign bodies, or fringes, beneath the joint covering.
—The ordinary acute synovitis is characterized by more or less effusion, and corresponds to pleurisy with effusion. It is the result usually of external injury, or it is combined with what has already been described as sprain. The fluid outpour is watery, is rarely blood-stained, save in cases of lacerations, usually distends the joint capsule, often to a painful degree, but represents nothing more than the consequences of hyperemia. If this fluid collection can be protected from contamination by germs it will disappear under suitable treatment, with a return to almost normal original conditions. Let it once become contaminated, however, and the type of disease is quickly changed, for there will then be an acute inflammation with its attendant phenomena and consequences.
—Cases of simple character are of short duration, i. e., one to two weeks. If seen early they should be treated by gentle compression and the application of ice-cold, wet compresses. Heat applied at this time may give temporary comfort, but will encourage effusion. Even if a joint thus affected be not seen until the swelling is extreme, wet compresses will still afford the simplest and the most comforting method of treatment, although they need not now be kept cold; in fact, gentle heat may now promote absorption. If the compresses be moistened in salt solution, to which a little alcohol has been added, the stimulating effect will probably be still greater. Such a joint needs to be placed at rest, save perhaps in the case of an ankle-joint or wrist-joint, which may be snugly strapped after injury. In some of these latter cases the patient can resume use of the joint almost at once.
—This rarely begins as a purulent condition, but may be the result of the non-inflammatory and non-purulent form. In such a case the character of the fluid outpour soon merges into the seropurulent, and later become almost nothing but pus. If the interior of a joint could be inspected, under these conditions, the intensity and extent of the vascularity and cellular changes going on within the synovial membrane and beneath it would present a different picture from that of the non-purulent form. The appearance of a joint interior, under these circumstances, is similar to that of a well-marked purulent conjunctivitis. Articular surfaces are quickly eroded or perforated, while cartilages thus once affected are often loosened from their attachments through necrosis and remain as foreign bodies in the fluid collection. Even strong ligamentous tissues will melt down and become so weakened as to permit a looseness of motion foreign to the natural joint. In fact, as between purulent synovitis and acute suppurative arthritis it is but a matter of extent of destruction, not of character of lesion. In this way pathological dislocations are produced, sometimes even within a few days, being the combined result of destruction of ligaments and the pull of muscles which are thrown into reflex spasm by the presence of intra-articular disease. Not only do we see caries of the exposed bone ends, but epiphyseal separations are not uncommon in the young, while every structure around and outside of the joint participates, even to the extent of abscess formation. Abscesses may form without the joint and work into it, or the purulent collection within may escape at points of least resistance and burrow, forming perhaps numerous foci at some distance from the joint first affected. If such a case is to be saved it will require numerous openings and counteropenings, with free drainage, while even then there can be no expectation of restoring joint function. There is, then, in these cases at least a sacrifice of joint, sometimes of limb, and in neglected cases of life itself.
—Of the large joints only the shoulder and hip, especially the latter, are placed so deeply as not to permit of easy examination and diagnosis. Pain, swelling, and loss of function, with or without history of injury, will predominate in well-marked cases, while very early in most, and promptly in all, there will occur reflex spasm of[384] those muscles which have to do with motion of the affected parts, by which they become more or less fixed and beyond voluntary control of the patient. This condition has been described by Sayre as “muscles on guard.” It is a significant feature, and has as much to do with active joint disease as has abdominal rigidity with surgical intra-abdominal conditions. Swelling will be proportionate to the acuteness of the case. Tenderness is nearly always extreme, especially along the articular line. The joint capsule is frequently distended to its extreme and the normal contour of the part completely obliterated.
The most common position in which limbs are held is midway between extremes; thus when the knee is involved the leg will become flexed upon the thigh, at about 75 degrees. If the shoulder be at fault the arm is maintained close to the body. In disease of the elbow the forearm is carried midway between the right angle and complete extension. This is partly due to the fact that the flexors are always stronger than the extensors, as it represents a compromise between the antagonism of the opposing groups of muscles.
Pus, when present, is commonly also manifested by the usual signs of its existence. There will be pitting on pressure or edema of the overlying parts, while an acutely inflamed joint may be at any time so swollen as to impede return circulation and lead to edema of the parts beyond. To the local signs of phlegmon, then, we simply have to add in greater detail those mentioned above. Along with these there will be constitutional septic disturbances, usually proportionate to the gravity of the local condition. The opportunities for absorption afforded by a large synovial surface are great, and the lymphatics are sure to carry toxins in abundance. The signs, then, of septicemia, sometimes even of pyemia, are often pronounced. In the presence of a joint full of pus the prognosis may be regarded as exceedingly grave. Pain and tenderness seem to bear but little relation to the swelling. Usually pain is an expression of distention, yet some of the non-inflammatory forms of apparently milder type are extremely painful. Pain is influenced by the position of the joint, and the patient instinctively seeks that position in which suffering is minimized. In a joint disorganized by the presence of pus there is less sensitiveness, except on rough handling, unless the trouble have extended far beyond the joint limits, and cellulitis be present, with suppuration threatening. In metastatic joint abscess tenderness rather than pain is the common rule.
In the presence of an acute inflammation in the joint end of a long bone the other joint structures will participate to an extent proportionate to its acuteness. With an acute osteomyelitis—e. g., near the articular surface—the synovial membrane will participate, just as does the pleura in many cases of pneumonia, and we may look for fluid in the joint in one case as we do for fluid in the chest cavity in the other. Moreover, pictures of acute or chronic tuberculous affections of the synovia correspond very closely to those of the pleura. Tuberculous disease is liable to spread in every direction in both diseases. The reverse of this, however, is not true in all diseases of the chest, and there are many synovial as well as pleural affections which are confined to their respective sacs.
Fig. 193
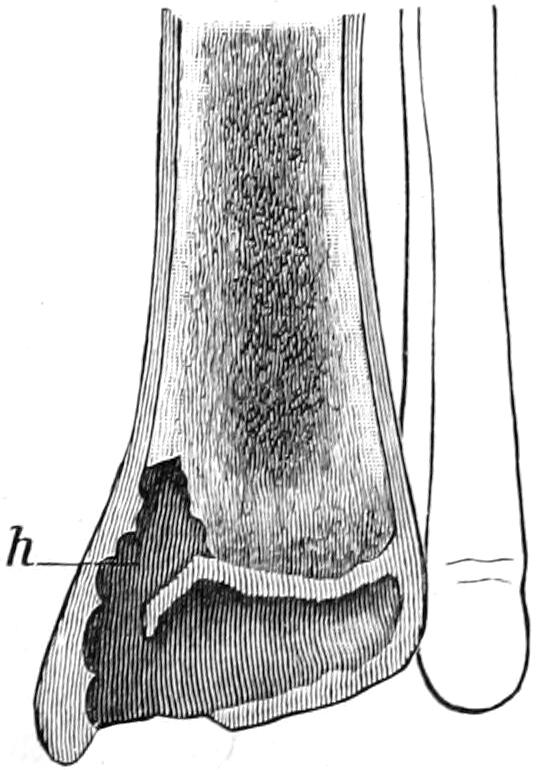
Pneumococcus infection of ankle; rapid destruction of all joint structures. Child aged nine months. (Lexer.)
The same statement, almost, can be made concerning the bursæ and tendon sheaths in proximity to infected joints. Particularly is this true when any of these connect with joint cavities.
The metastatic forms of pyarthrosis, as a collection of pus within the joint capsule is called, are more insidious, though sometimes equally destructive. They are by no means confined to one joint, and in pyemia especially many of the joints will become involved. (See Pyemia.) These secondary affections seem to be purulent from the outset. In gonorrhea the effused fluids will often be found nearly pure cultures of the gonococcus; after typhoid they contain typhoid bacilli, etc. Such expressions are less frequent after pneumonia, influenza, and the acute exanthemas, but may be seen even after smallpox. It is often in these severely destructive joint lesions that spontaneous dislocation occurs (Fig. 193).
[385]
—In the presence of a single joint lesion indications for treatment are quite clear. When we have multiple and pyemic or gonorrheal pyarthrosis it is often exceedingly difficult to determine what is for the best interest of the patient. In general it may be said that pyemia progressed to this extent will almost certainly be fatal, and we may rest content with aspirating the affected joints, or perhaps in leaving them alone; because we may feel that they constitute but a small proportion of the metastatic foci which eventually determine death. On the other hand, in other infections with pyarthrosis it would be better to aspirate or to open and drain, because these cases are slow and chronic, and the exudate is sometimes so rich in fibrin as to lead to quite firm spurious ankylosis.
Thus gonorrheal synovitis is usually monarticular, although several joints may be involved. It is readily recognized in the presence of the active disease, but there are times when recognition is made difficult by the latency of urethral symptoms or the concealment of their existence. The knee is usually the joint most often involved; next the joints about the foot, and sometimes the tendon sheaths and bursæ adjoining them.
Syphilitic arthritis is a chronic and mildly but steadily progressive affection. It rarely assumes purulent form without some secondary infection. It is frequently combined with gumma along the epiphyseal border. In hereditary syphilis numerous joints may be involved in changes of the rachitic type.
Gout or some of its allied rheumatoid manifestations may lead to a dry form of synovitis, with deposit of urates or of lymph, and the formation of tophi in the neighborhood, or it may assume the form of a chronic and intractable hydrarthrosis. The acute forms are accompanied by great pain, with redness and swelling, peri-articular and intra-articular. The tendency of these cases is to chronicity and recurrence.
—Upon the nature of the condition will depend the treatment of joint diseases. The questions of when to operate and when to abstain, when to enforce rest and when to begin passive and when active motion, call for discriminating judgment. An acute or even mild traumatic synovitis should, first of all, be protected from becoming purulent. Should injury be accompanied by a bruise, the greatest care should be given to antisepsis, and the part sterilized and dressed with every precaution. Should there be no external injury we may rely ordinarily upon cold, wet compresses, with suitable elastic compression and physiological rest. Should two or three days of this treatment fail to bring about nearly complete resorption the aspirator may be employed to withdraw the fluid. If this should be found to be bloody or too thick to run through the needle, it will be advisable to make small incisions on either side, under the strictest precautions, and to practise thorough irrigation, by which the joint cavity will be completely cleared of foreign material. As soon, however, as the presence of pus is indicated, or even suspected, the whole character of the treatment should change. The surgeon should now endeavor to be as radical as possible. The more purulent the collection the more are free incision, irrigation, and drainage indicated and the more complicated the condition the more he should make counteropenings here and there, wherever joint pockets may be emptied.
When muscle spasm not only seriously disturbs the patient but threatens to draw the limb into an undesirable position it should be overcome, either by employment of traction with weight and pulley, or by forcible reposition and fixation in suitable splints, such as plaster of Paris. Some of the most extensive operations that are called for are necessitated by neglect to observe these precautions early. Often nothing will afford so much relief as the use of traction, with sufficient weight, tiring out contracted muscles, and thus not actually separating joint surfaces, but overcoming that muscle spasm which brings them tightly together and thus gives pain.
In the more chronic form of cases absorption may be promoted by elastic compression, by massage, by wet compresses, and sometimes by blistering. Ordinarily, and especially in those cases characterized by pain, more can be accomplished with the actual cautery drawn lightly and rapidly over the surface of the joint than by blistering. This application is referred to as the flying cautery, and it is one of the most effective agents known for the relief of deep-seated pain, as well as of cutaneous hyperesthesia. Its use causes little if any unpleasant sensation, and should be repeated at daily intervals until the primary object is attained.
Should aspiration of a distended joint be practised at any time, one should atone for[386] the loss of intra-articular pressure thereby produced by external compression, preferably with an elastic medium.
In the writer’s opinion it is not advisable to use a small aspirating trocar in those cases which are likely to call for irrigation. The aspirating needle should be confined to the non-purulent collections of fluid, although some surgeons advise and practise throwing into a mildly infected joint, through such a needle, some reasonably strong antiseptic fluid or emulsion, hoping thus to gain its bactericidal effect without external incision.
The active manifestations of disease being mastered, one addresses himself naturally to the greatest possible prevention of deformity and restoration of function. Indeed, these should be kept in view from the outset, although we have, for a time, to disregard them in favor of more imperative indications. If ankylosis appear inevitable the joint should be kept in that position in which, when stiff, it will be most useful. This position will be, at the elbow, at a right angle; at the hip or knee, nearly complete extension. When, on the other hand, restoration of function is hoped for it will be obtained through a combination of massage, active and passive movements, with the use perhaps of some sorbefacient ointment, such as the compound ichthyol-mercurial, or by the nearly constant use of cold, wet compresses, combined with the other measures. The greatest care should be exercised in determining the time when absolute rest given to an inflamed joint should be changed to the gentle or more forcible movements required for restoring use to previously inflamed joint surfaces.
—A chronic serous effusion into a joint is given the term hydrarthrosis. This condition is never primary; it is always the residue of some previous acute lesion, or else it is the result of neuropathic or rheumatoid changes going on in and about the joint, accompanied by relaxation of membranes permitting passive distention with fluid. The contained fluid is ordinarily pure serum. It may contain a little blood or numerous particles or shreds of fibrin, while in rare instances there will be found in it drops of oil or even fat crystals. The degree of distention of a joint capsule is the measure of the gravity of the case, as this membrane, like any other, will yield to gradual distention, although it at the same time undergoes thickening as a protective measure. Thus the synovia may, under certain circumstances, become as thick as the pleura. The result is a tough, leathery condition of this membrane, which makes it exceedingly difficult to manage. The joint thus involved will appear more prominent than it should, because of the atrophy of the surrounding structures. Accurate comparisons can only be made by measuring corresponding joints. Neighboring bursæ and tendon sheaths often participate in the distention. These collections are ordinarily painless, or nearly so, but interfere, to varying extent, with the function of the joint. Anatomical outlines disappear or are concealed by the bag of fluid. It is rare that there are any constitutional symptoms except perhaps those of the disease which causes the disturbance. The amount of fluid which may be contained in a long-distended knee-joint, for instance, is relatively very large. The prognosis in these cases will depend much upon the underlying cause, as well as upon the age, vitality, and docility of the patient.
—Removal of the fluid is always the indication. After reasonable effort has shown that this is not possible by the employment of massage, the actual cautery and elastic compression, combined with functional rest, it should be withdrawn by the aspirating needle or trocar. The more experience, however, we have with affections of this class the more we will realize that the interior of the synovial membrane is frequently studded with deposits, fringes, etc., which are not affected by mere aspiration, and the more cogent argument will be gained for sufficiently free incision to permit inspection of the interior of the joint, removal of tags of tissue, thorough washing out and sponging, by which a change in circulation and nutrition is certainly affected; and this may be combined with excision of a liberal portion of the thickened membrane, by which the dimensions of the joint may be materially reduced when the opening is sutured. For long-standing cases of well-marked hydrarthrosis, especially in the knee, the writer would urge this method of treatment. Drainage, if called for at all, can be made with strands of silkworm, or some temporary material which will quickly disappear or be promptly removed. This is particularly applicable for the milder forms of tuberculous synovitis, in which the joint is thus treated on the same principle that is applied in washing out a tuberculous peritoneal cavity.
[387]
Fig. 194

Arthritis deformans, knee. (Ransohoff.)
Under this general name have been grouped a number of conditions, including the so-called rheumatoid arthritis, and referring to a variety of chronic progressive lesions of joints which involve the articular cartilages and synovial membranes, later the bones, and which produce more or less loss of function and deformity. Although often spoken of as “rheumatoid,” the condition has nothing to do with rheumatism as such, whatever that may be. It moreover presents no analogies to the forms of acute synovitis already described. These lesions are more common in women than in men, occurring oftener in those who have been sterile, and during or after the menopause. So far as their etiology and pathology are concerned, it is true, though it seem trite to say it, that they are the result of disturbed nutrition, which itself may be referred back to perverted trophic influences. Exposure, bad hygienic surroundings, improper food, mental perturbation, and depression are more or less potent factors in most of the cases. In some instances occurring in advanced age they seem to be due to changes ordinarily regarded as senile. When joint lesions are multiple and symmetrical, and accompanied by other nutritive changes, we may refer the cause back to the central nervous system. When monarticular they are more likely to be the residue of some previous infection or injury, such as gonorrhea, influenza, or an acute exanthem. If in connection with the joint manifestations we find the spleen and lymphatics enlarged, then the case may be regarded as doubtless infectious in nature.
The pathological changes within these joints include almost every imaginable alteration. Bones soften and atrophy at one point, or at another become enlarged and thickened, and throw out osteophytic projections by which the whole shape of the joint is materially changed. Cartilages atrophy here and thicken there, and disappear, at times, to an extent by which bone is exposed, the exposed surfaces frequently becoming polished or eburnated. The position of the joint and its general contour may be materially altered by these changes, and marked deformity or notable enlargement result. Subluxations are not infrequent, while the ligamentous structures are sufficiently strong to perform their function, and the joint yields or “wabbles.” Meanwhile the synovial membrane undergoes corresponding changes, and becomes distended with fluid so that hydrarthrosis is a frequent accompaniment.
On the other hand, there is another type of analogous changes where the tendency is atrophic throughout and little if any extra fluid accumulates. Such a joint may become smaller rather than larger, especially if, as in some cases, some part of the bone practically disappears.
At all events muscle atrophy, sometimes with pseudo-ankylosis, sometimes with actual ankylosis, will characterize most of these cases, and muscles naturally disappear as they functionate less and less.
Pain is an irregular feature, some of the lesions being quite painful, others almost free from it. The lesions are essentially progressive in their character, unless the whole body condition and environment can be changed for the better. Consequently individuals become more and more crippled. Muscle spasm is rarely present, but when such changes occur in the intervertebral joints the individual becomes gradually bent over or deformed, partly because the muscles no longer have strength to maintain the erect posture, and partly from actual changes in the bones and joints. Most of the instances, however, are characterized by tenderness, while a general myalgia or malaise is a frequent complaint. There are sometimes exacerbations, during which both severe neuralgic pains and mild fever are quite pronounced. Not infrequently on handling the affected joint pseudocrepitus or actual crepitus will be obtained. Sometimes the joint surfaces are roughened, and then this sensation is most pronounced. When the synovial membrane is proliferated, in pannus form, over the cartilages, its enlarged fringes will give a soft crepitus which is quite distinctive. Fragments of these fringes, as well as of cartilage, may become detached, and loose objects of this kind in the joint may be recognized by the sense of touch.
Fig. 195
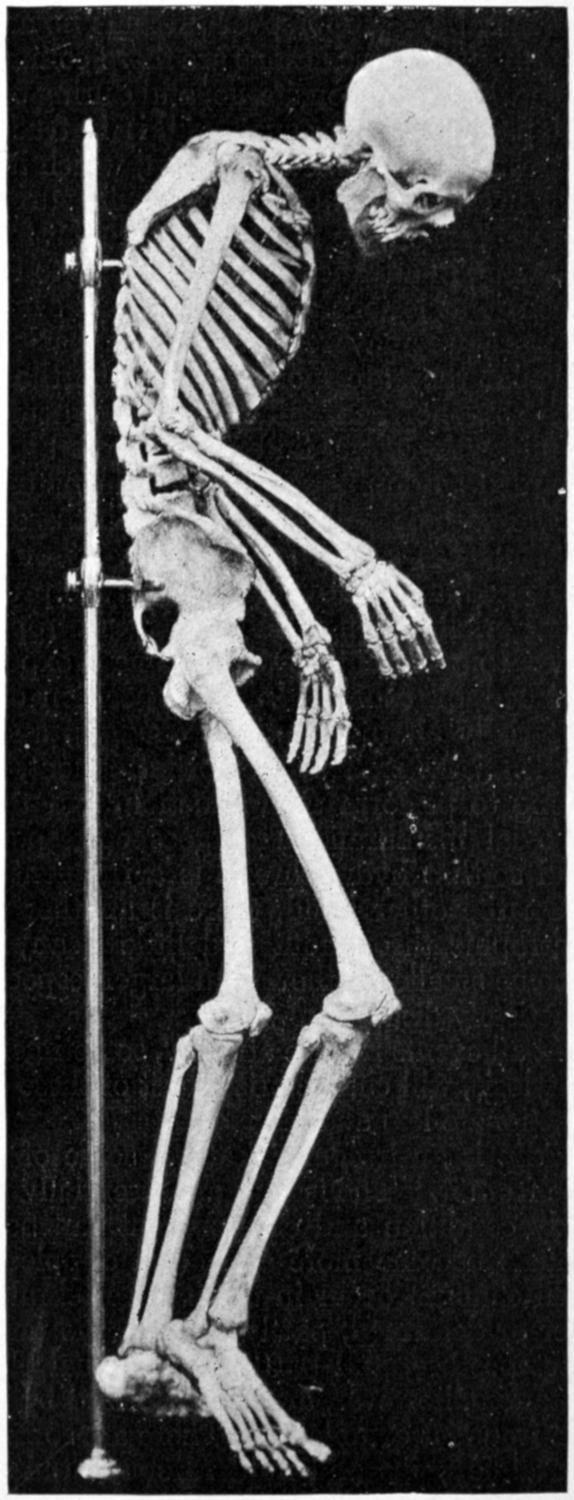
General osteo-arthritis, with multiple synostoses (“ossified man”).
While this is going on within the joint, adjoining tendon sheaths and bursæ become more or less involved, and even the periosteum will undergo considerable thickening.
The monarticular type is more frequent in men than in women, and occurs more often in a large joint or in the spine, in which latter case it is hardly to be considered monarticular.[388] The changes that may occur in the spine are distinctive, varying from trifling stiffness and limitation of motion to pronounced deformity, by which, for instance, not only the kyphosis of acute spondylitis may be imitated, but the body flexed to an angle with the axis of the pelvis and fixed there, so that the individual is bent to nearly a right angle. Some of the other deformities of this condition are more or less characteristic. In the hands the fingers are bent toward the ulnar side, and often strongly flexed, perhaps even overlapped, thus giving the hand a peculiar claw-like appearance. The feet are extended completely, the joints rigid, the toes turned outward, and also overlapping. By such changes in the hip and knee the legs and thighs may be flexed and the hips perhaps so ankylosed as to prevent separation of the knees. While these changes are, as stated, most common in the later years of life, children are not exempt, girls being more frequently affected than boys, the condition coming on at first with more or less acute symptoms. These children will often be found to have enlarged spleens and lymph nodes, to show malnutrition, while some of them will display certain symptoms of exophthalmic goitre. In other words, they are in that condition included under the term status lymphaticus, to which subject the reader is referred. (See p. 163.)
It would appear, then, that we can expunge the term chronic articular rheumatism, since by it is not meant the ultimate result of an acute rheumatic affection, but rather one of the vague conditions described above.
Fig. 195, taken from a skeleton in the author’s possession, illustrates an extreme[389] condition of this kind, characterized by multiple synostoses, nearly all of the principal joints being involved.
As between the terms osteo-arthritis and arthritis deformans it is not practicable to make such accurate distinctions as shall be acceptable to all. In a general way the more the bone participates the more we may use the former designation, whereas when other joint structures are chiefly involved we may resort to the latter.
In general, then, all these conditions are evidenced by joint deformity, especially by irregularities, by more or less effusion, by considerable tenderness, by creaking of the joints when used, by pain which is a variable feature and may be referred to nerve disturbances, occasionally by muscle spasm, but always, in cases of long standing, by muscle atrophy. A view of the interior of joints thus affected will give a complex picture of atrophy here and hypertrophy there of each or all of the component structures of the joint, sometimes with a gradual overgrowth of articular bone surfaces, sometimes with more or less complete disappearance of the same, e. g., in the acetabulum.
—So far as treatment of these conditions is concerned, it should be recalled, first of all, that the disease itself is exceedingly chronic in its tendency, and due to conditions which have probably been of long standing. Constitutional treatment is as essential as local, and must consist in restoring the environment and the nutrition of the patient to normal standards. Elimination is deficient in such cases, and should be stimulated by hot-air baths, massage, and such exercise as may be possible, as well as by the use of diuretics and laxatives to the degree indicated. The local treatment may consist also of massage, elastic compression, aspiration in rare instances, the use of wet packs, and, in many cases, the use of hot, dry air. Various forms of apparatus are now upon the market by which almost any of the joints may be subjected to the influence of dry, hot air at a temperature of 280° F. When properly used, great relief and improvement may be expected. Their use, however, calls for the best of judgment and a combination of the measures already mentioned.[31]
[31] The following types of arthritis bear little, if any, relation to true rheumatic disease, though often spoken of as rheumatoid:
The chronic villous form, most common in the knee, purely local, without effusion, and giving dry crepitus or creaking. The joint fringes are numerous, and sometimes vascular. If the crepitus be marked and the fringes too extensive the latter may be relieved by operation. Otherwise this form is to be treated by early local stimulation, with some support, at least with a bandage.
The atrophic form, of unknown etiology, causing progressive and finally crippling swelling, with later atrophy. There is little if any fluid present. Here the changes occur in both bone and cartilage, with a tendency to abnormal calcification. In this form rest and hypernutrition, especially with normal proteids, are called for, and every possible stimulus to elimination through all the emunctories.
The hypertrophic arthritis, by which cartilages are first thickened and then ossified, interfering with motion and with contour. This form causes great limitation of motion and sometimes pressure on nerves, with referred pains. It seems to have some relation to cold, exposure, and injury. Detachment of pieces of cartilage is not uncommon, so that there are loose bodies in the joint cavity. Treatment here consists of fixation, with improvement of nutrition and elimination. This form may subside under proper treatment.
The chronic, gouty arthritis, with deposits of sodium urate in and around the joint tissues, with perhaps some bone absorption beneath them, which are not connected with the bone. In the digits entire phalanges may disappear by absorption. The treatment here is essentially constitutional and directed toward the gouty diathesis.
This received its first full and classical description from Charcot in 1868. The term refers to joint lesions which follow and are apparently connected with certain injuries and diseases of the spinal cord, or the peripheral nervous system. The non-traumatic forms are mostly associated with locomotor ataxia and syringomyelia. Some of them have an abrupt onset, while others come on very insidiously. Pain is usually notable by its absence, and the involved joints show few, if any, evidences of hyperemia or inflammation. They become unnaturally mobile and relaxed and usually much, sometimes enormously, distended with fluid. The morbid changes within the joints comprise imaginary combinations of atrophy and hypertrophy, with proliferative formations in bone cartilages. Osteophytes and exostoses are met with, and ossification may occur in the neighboring tendons and ligaments. Surprising alterations take place in certain joints; thus, as shown in Fig. 197, the head of the humerus may disappear and corresponding changes may occur in other joints. While it is the knee which suffers most frequently, no joints, not even those of the spine or jaw, are exempt.
[390]
Fig. 196
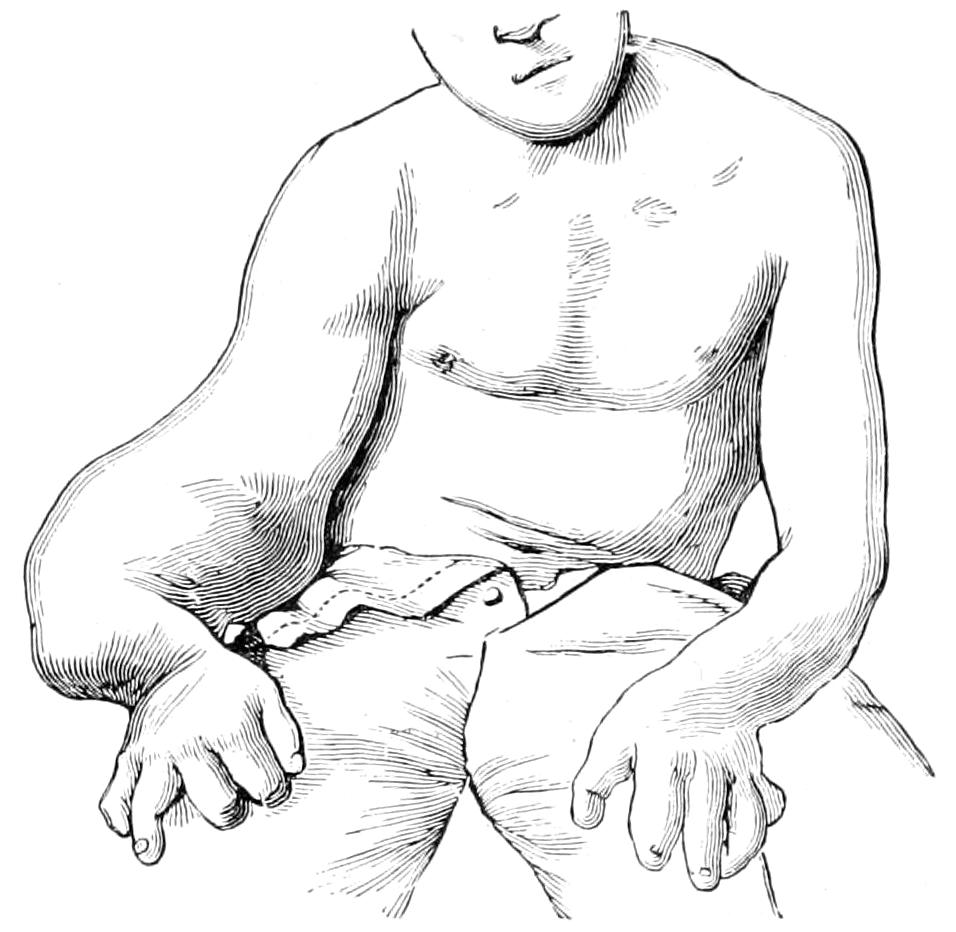
Charcot’s disease of elbow.
Fig. 197
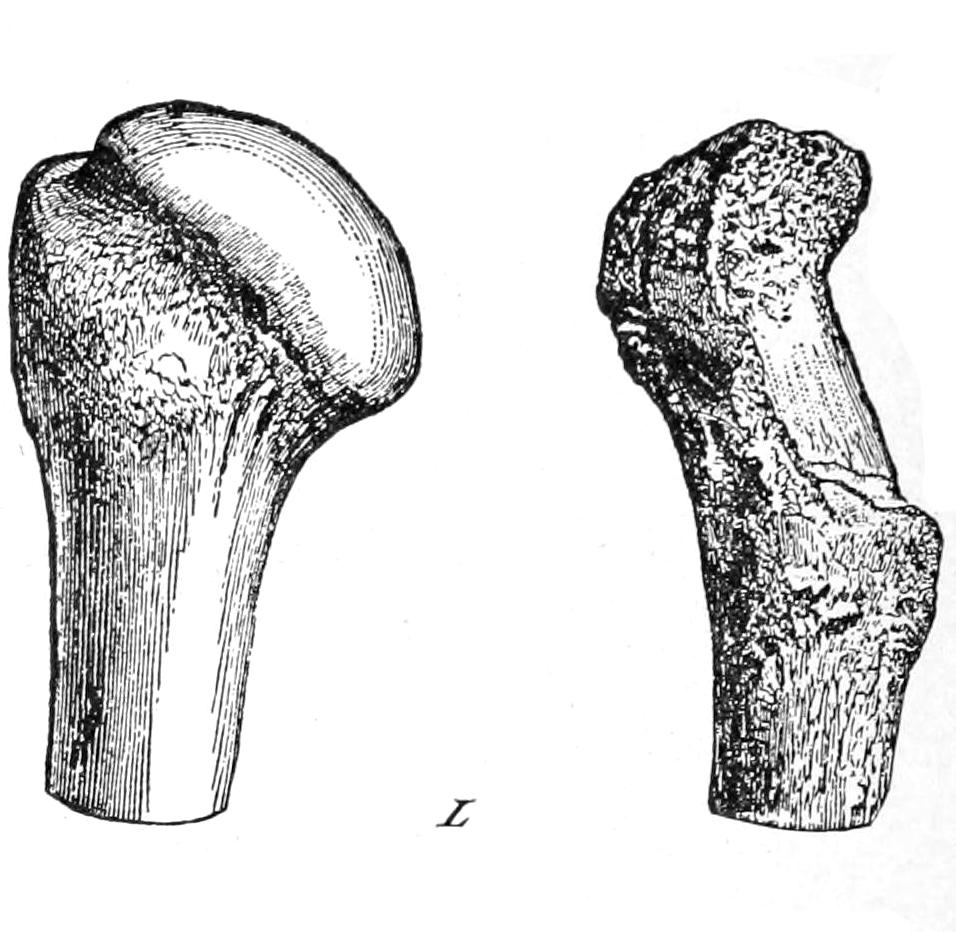
Atrophic disappearance of bone after chronic joint disease.
Fig. 198
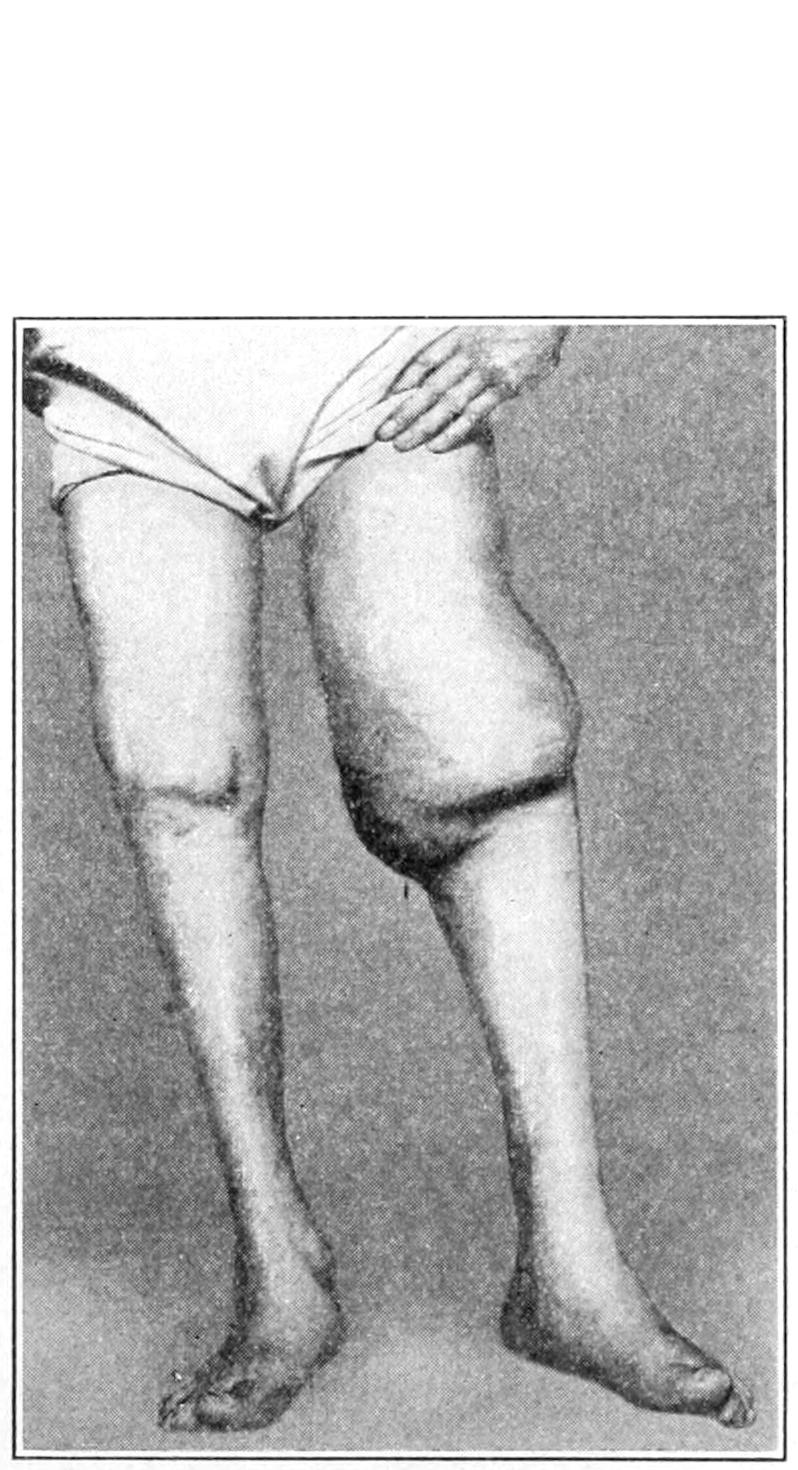
Tabetic arthropathy. (Case of E. A. Smith.)
Fig. 199
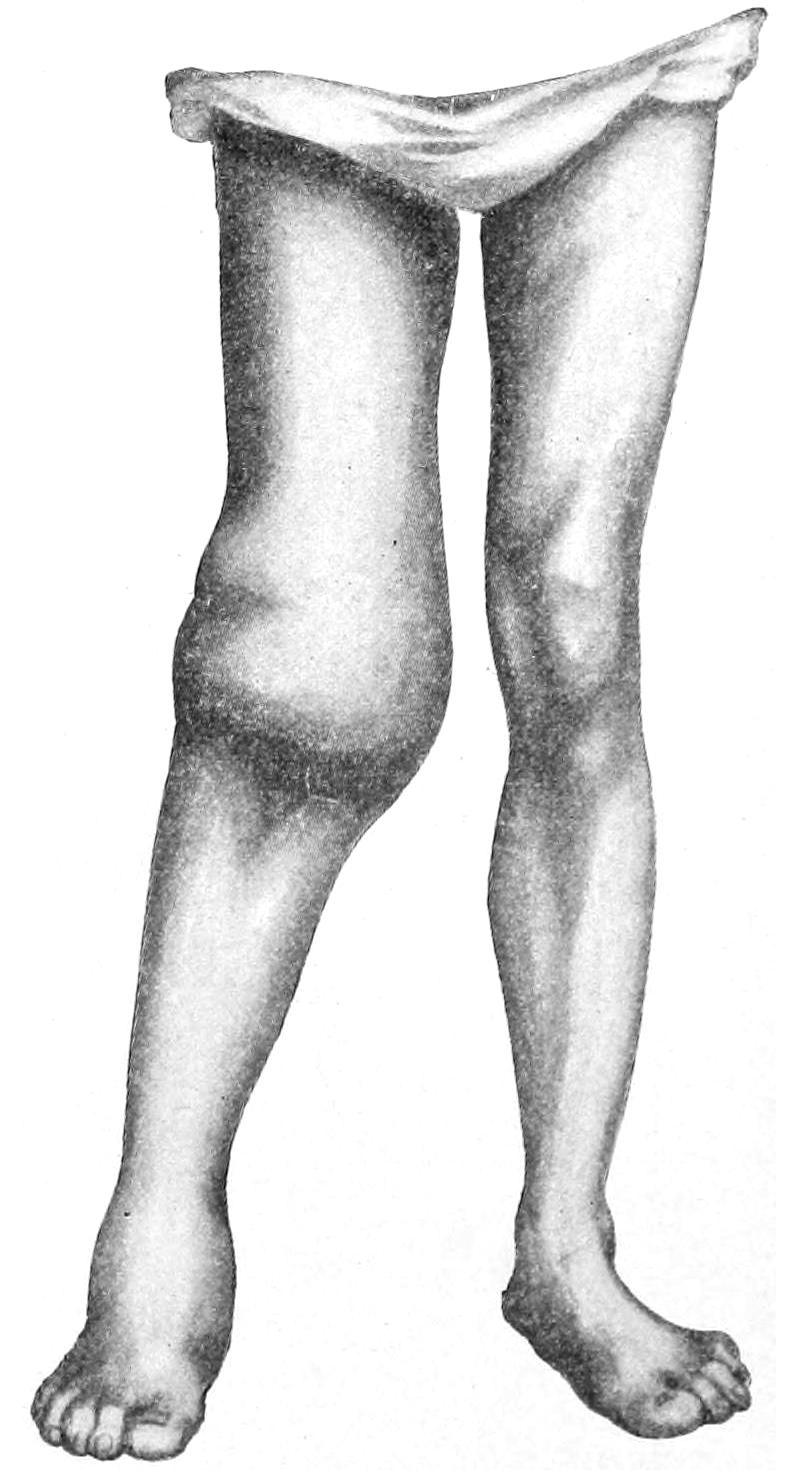
Neuropathic arthritis (tabetic joints). (Lexer.)
Locomotor ataxia is a common disease, but syringomyelia has been regarded as exceedingly rare. Nevertheless, Schlesinger has collected 130 cases of it, in one-fourth of which bone and joint symptoms were present. That the nervous system is primarily at fault is made clear, among other things, by the rapidity of involvement occasionally seen, where, for instance, an entire limb becomes edematous, with every indication of severe disturbance. In tabes the lower extremities suffer more often than the others; the reverse is true in cases of syringomyelia. While floating bodies in the joints and ossification of the muscles and soft parts are common in arthritis deformans, they seldom occur in the neuropathic lesions. Suppuration and necrosis are rare in any of these[391] forms, occurring more frequently in the finger than elsewhere, and are probably due to infection of those areas where sensibility is lost and trifling injuries less guarded against. The neuropathic lesions are more commonly symmetrical, and are often accompanied by a cretinic general appearance (Figs. 196, 197, 198, 199, 200 and 201).
Fig. 201
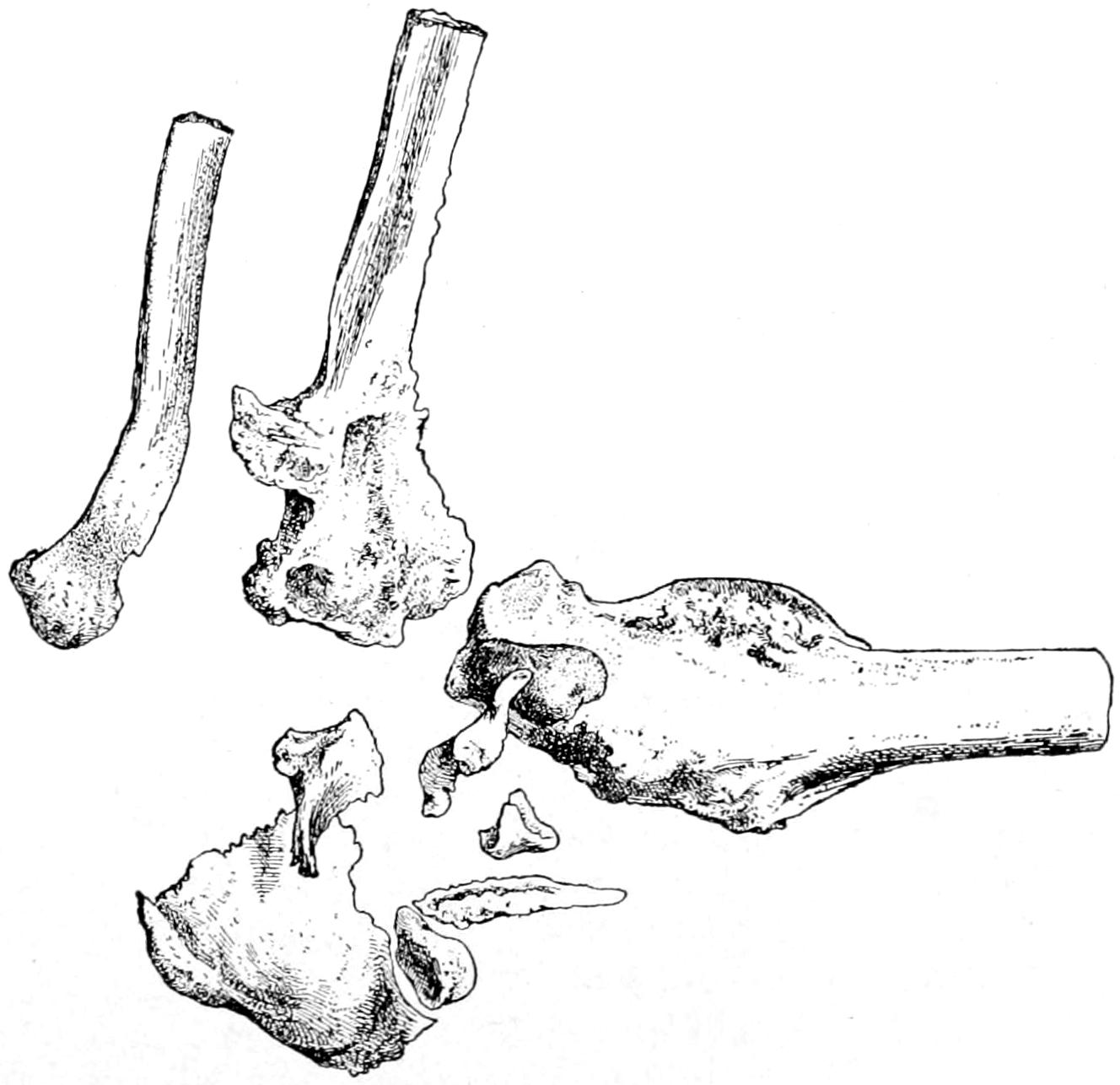
Arthropathy of syringomyelia. Left elbow, illustrating disintegration, etc., without ulceration or suppuration. (Quenu.)
The joint complications of syringomyelia are frequently characterized by skin lesions which tend to suppurate, by sudden edema, occasionally followed by phlegmon and even necrosis, also by other disturbances of innervation.
Surgical treatment of these lesions is less discouraging than would at first appear, as even in these patients serious wounds heal readily, while in healthy tissues primary union may occur. The wisdom, therefore, of incision, resection, or even amputation may be decided on their merits, and there can be no objection to open drainage when it would otherwise be indicated. Even in cases of spontaneous fracture proper treatment usually gives good results, although the amount of callus may seem disproportionate.
[392]
In any of the joints distorted by deforming osteoarthritis or neuropathic lesions, the question of partial or complete resection or exsection may be discussed upon its merits, since these operations, when duly indicated, have often given satisfactory results, even in elderly people.
—Differential diagnosis will be made more easy by the exclusion of syphilis and of the acute or ordinary infectious forms of disease. The relative freedom from pain, the relaxation of the joint structures, the large amount of fluid present, and the age of the patient will aid in excluding all but the neuropathic elements associated with spinal disease.
—Treatment is rarely curative; usually it can be palliative at best. Measures above mentioned, when they seem indicated, coupled with mechanical support, by which the parts may be maintained as nearly as possible in their proper position, will give the best result. If the disease be monarticular, exsection will frequently give a satisfactory result. Multiple lesions rarely permit of serious operations.
A different form of distinctly neuropathic joint affection is the so-called hysterical joint. This is characterized by the absence of every objective and the presence of nearly every subjective symptom. It occurs most often in young women and girls, follows perhaps some trifling injury, and involves most commonly the joints of the lower limbs. These cases are characterized by a disproportion between the character of the complaint and the actual condition. Imitation of organic trouble is a predominant feature of all hysterical complaints, and is nowhere seen to better advantage than in these cases. The pain, the tenderness, the loss of ability and even the muscle spasm and muscle atrophy of genuine lesions will be simulated. So true is this that diagnosis largely rests on the exaggeration of symptoms which have no apparent existence. Hyperesthesia is sometimes extreme, but pertains usually to the waking hours. Rarely is there actual swelling or thickening, or any objective evidence whatever of disease, save perhaps muscle atrophy due to disuse. It is possible to have the hysterical element as a complication of actual joint disease, but the truly hysterical joints usually are easily recognizable.
—The treatment of such a joint should be psychical as well as physical. Sometimes appeals to reason, at other times to fear or necessity, will be the wiser course. Restoration of self-confidence is an important feature, and these are the cases where any form of faith cure will produce its most brilliant results. Many of these cases are bedridden, and need to have elimination stimulated in every possible way. They also need sunlight, fresh air, massage, and renewed use of the parts. Hyperesthesia is best treated by continuous application of ice-cold compresses, intermitted perhaps daily for the purpose of using the “flying cautery,” as already described.
This condition may occur during the active stage of gonorrhea or after its apparent subsidence. It was probably the discovery of the pathogenic gonococcus by Neisser, in 1879, which gave to this lesion an identity of its own, and induced the profession to abandon the name gonorrheal rheumatism, by which it had been known. It has nothing to do with rheumatism, and should not be linked with it in name any more than in idea. In well-marked cases the gonococcus will nearly always be found, usually in pure culture, in the joint fluid.
It appears in different degrees of severity, from a mere hydrops, which is mild, accompanied by slight tissue changes, to a phlegmonous condition, with widespread destruction of joint structures and serious constitutional disturbances. As between these extremes there may be a pyarthrosis or empyema, which is usually the result of a mixed infection.
As a complication of urethritis it occurs in 4 or 5 per cent. of cases, the percentage being larger in children than in adults, the knee being affected in about one-third of these cases. It is not necessarily monarticular, however, and sometimes several joints will be involved. Along with the joint condition there will frequently occur cardiac lesions[393] (endocarditis) and eye complications. In fact, some of these cases terminate fatally through the mechanism of a seriously involved heart, i. e., septic endocarditis or myocarditis. When it occurs in the ankle or in the tarsal joints the ligaments and surrounding bursæ are often involved. This involvement, unless recognized and properly treated, may lead to serious deformity, e. g., flat-foot of the most painful kind. Many of these lesions at the heel are accompanied by true exostoses, which are often painful and more or less disabling (“painful heel”). Thus, Jaeger has recently reported a group of ten such cases. These may require excision. In general this form of arthritis is characterized by severe pain, often worse at night, and a peculiar distortion of the swollen joint, because it is usually complicated by a distention of the adjoining tendon sheaths and bursæ, which is rare in other forms of arthritis. It has been aptly stated that if in these cases the same zeal were displayed in seeking for gonococci that has often been shown in looking for uric acid it would be less often neglected. So far as treatment is concerned, I desire in this place only to call attention to the absolute inutility of all the so-called antirheumatic remedies and diet. However, if the urine be hyperacid it should be corrected by ordinary means. At first absolute rest, with the local use of the ichthyol-mercurial or Credé ointment, should be given. Such antiseptics as one has most confidence in may also be administered internally for their general beneficial effect. An overdistended joint should be tapped and irrigated. As soon as the presence of pus can be determined, either with or without exploration, the joint should be opened, thoroughly irrigated, and drained. If this were always done in time the more severe phlegmonous and destructive cases would rarely occur.
Tuberculous disease of the joints is one of the most frequent of surgical lesions. It has produced characteristic appearances which have been known under the name of “scrofula of joints,” until a clearer recognition of the pathology of the condition led to the abandonment of the term scrofula. Tumor albus, or white swelling, was another term commonly applied to these lesions, because of the anemic appearance of the surface of the swollen joint.
Tuberculous arthritis assumes different phases in proportion to the involvement of the different component structures of the joint. Some cases begin purely as a tuberculous synovitis, and may for a long time be limited to the synovial structures. Others begin within the spongy texture of the expanded joint ends of the long bones, the disease spreading from such foci and involving everything in the path which its products take in the effort to secure spontaneous evacuation, products of softening and infection travelling in the direction of least resistance.
It has been the writer’s custom to always follow Savory, in his suggestion to students to let their mental pictures of consumption of the lungs and pleuræ serve for illustration in similar disease of joints. Thus the cancellous bone structure much resembles the lung tissue in its spongy character. In both a capsule surrounds the mass of tubercle, and in each, by breaking down of its contents, a cavity is formed. Moreover, the pleura bears practically the same resemblance and relation to the lung and the chest wall that the synovialis does to the bone end and the joint cavity; as we may have pleuritis with phthisis, so we may have synovitis with tuberculous ostitis; and as adhesions tend to form in the pleural cavity, so also do they in the synovial cavity. Furthermore, in each case obliteration of deeper veins causes the more prominent appearance of the subcutaneous veins, and as tuberculous pleurisy often terminates in empyema, so does tuberculous hydrarthrosis often terminate in pyarthrosis, perhaps with fungous ulceration. In almost every feature, then, the progress and effect of tuberculosis in the lung and bone end may be likened to each other.
In some clinics bone and joint tuberculosis constitute nearly one-third of the total of cases treated. Joints of the lower limb are the ones most frequently involved in children, while in the adult those of the upper extremity are generally attacked. It is not often that more than one joint is involved at one time. The relation of traumatism to this disease has been frequently discussed, and is variously regarded. The disease is more common in those who are predisposed to it by environment or by heredity, in the latter case hereditary evidences usually being well marked. In such predisposed[394] individuals, especially in the early years of life, severe injuries are usually promptly repaired, while the milder traumatisms, which are often frequent and to which too little attention is paid, seem often to so far lower tissue resistance as to favor an infection to which the individual is already favorably predisposed. The true position to take, then, would appear to be this, that traumatisms rarely lead directly to joint tuberculosis, but only indirectly by affecting tissue susceptibility.
Thus lesions which begin in the epiphyses lead to what is known as osteopathic joint disease, while those which have their origin in the synovia give rise to the arthropathic forms. The former are more common in children and the latter in adults (Fig. 202).
—In regard to the pathology of these conditions it does not vary from that mentioned in the earlier portion of this work in connection with the general subject of Surgical Tuberculosis. The deposit of tubercle in the tissue whose resistance has been weakened is followed by the formation of granulation tissue, which, so long as the germs survive, tends to increase and to make room for itself at the expense of surrounding tissue. At the same time there occurs a tissue struggle by which the attempt is made to throw around an active focus a protecting barrier, which in soft tissues consists of condensed fibrous and connective tissue, and, in bone, of a sclerotic capsule, as though the intent were to imprison the disturbing cause, and, by completely enclosing it, effect protection. When this attempt at encapsulation is successful spontaneous recovery follows. It will be made successful, to some extent at least, by treatment whose most important local feature is physiological rest. On the other hand, when the attempt is unsuccessful and the barrier is transgressed by granulation tissue, the lesion will advance in the direction of least resistance, while its progress will be made known, especially as it approaches the surface, by very significant signs: adhesion of the overlying structures and finally of the skin, with purplish discoloration of the latter. Finally softening occurs with escape of granulation tissue, which, so soon as it is freed from pressure, will grow more luxuriantly and with more color, constituting the fungous granulation tissue, to which German pathologists so often allude, or so-called “proud flesh.” When this appears upon the surface it is soon infected with pyogenic organisms, breaks down, and an abscess cavity results, connecting with the original focus and its extensions. This may be so placed as to lie outside the joint capsule, which, in some respects, is fortunate for the patient. The joint function may then be compromised to only a minor degree.
Fig. 202
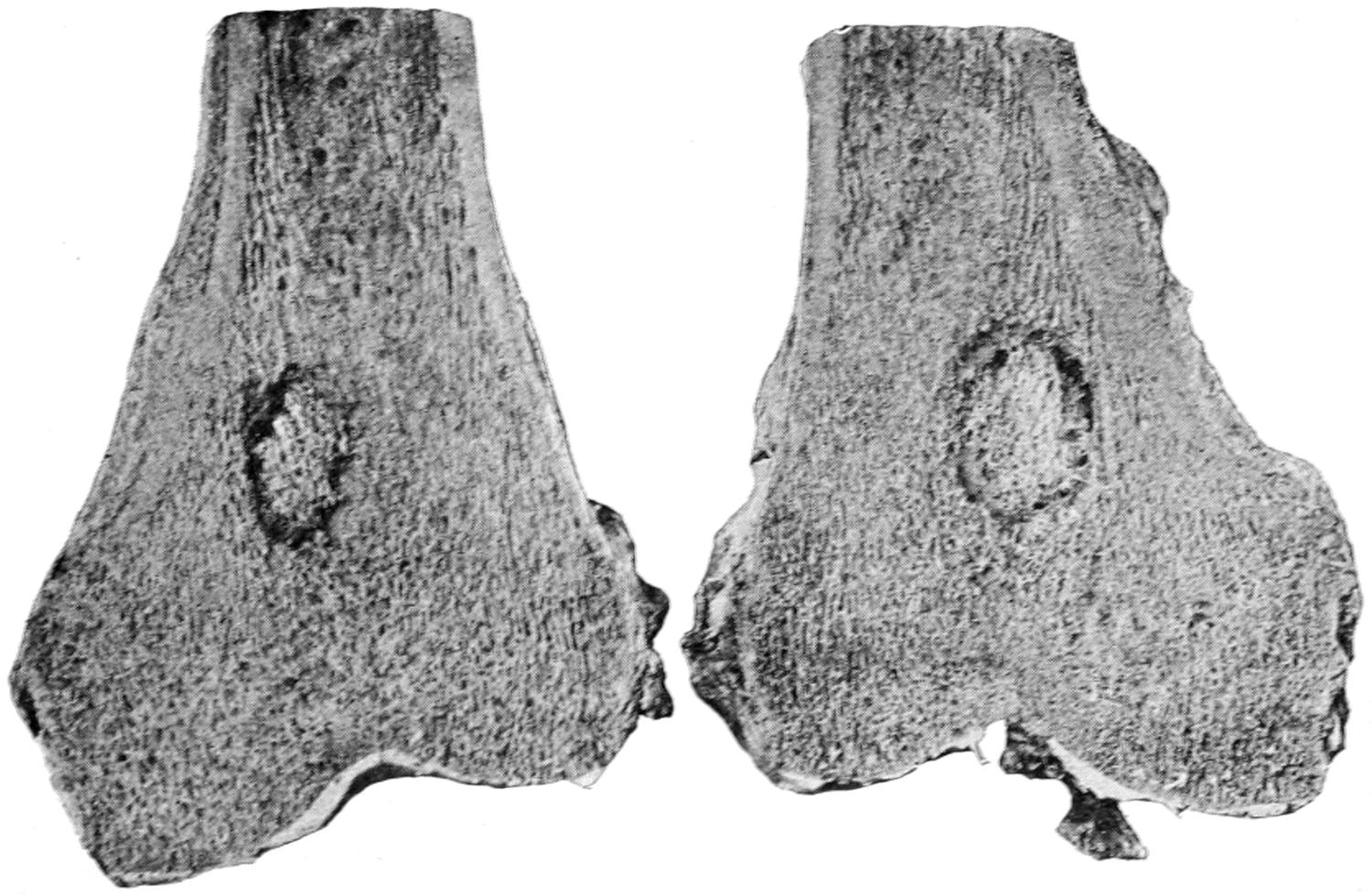
Central sequestrum. (Ransohoff.)
Often the direction of least resistance is toward the joint cavity, this fungous tissue loosening and perforating cartilage or periosteum before it enters the joint. Having penetrated it again it grows extensively until the cavity is distended, its rapidity of growth[395] diminishing with the degree of pressure produced by its surroundings. This pressure will also make it less vascular, and when such a joint is opened it at first appears pale and anemic. In proportion as the joint distends it loses in motility, while should recovery occur spontaneously or as the result of treatment this tissue will to some extent disappear, to be replaced by adhesions by which pseudo-ankylosis is produced. The extent of the intra-articular involvement will cause obstruction to the deeper return circulation, and thus is brought about the prominence with which the subcutaneous veins appear. The degree of hydrarthrosis is apparently not limited except by the distensibility of the joint. In the articular or arthropathic forms there is always more or less synovial outpour.
Fig. 203

Tuberculous panarthritis. (Ransohoff.)
To the condition already described may be added the destruction produced by suppuration, infection occurring either through the circulation, as is quite possible, or through some trifling surface abrasion. In more chronic cases caseation may occur, especially in bone foci. Finally, as the result of a combination of morbid processes, there is produced more or less complete disorganization, all of which is summed up in the term tuberculous panarthritis. To that condition in which the articular surfaces are more or less studded with fungous patches the term pannus of the joint is often applied. To reiterate, then, as between a chronic hydrarthrosis and a destructive panarthritis, perhaps even with necrosis of epiphyses, it is but a difference of degree and of combination of infectious processes (Figs. 203, 204, 205 and 206).
Among the other consequences of panarthritis may be the formation of sequestra in or near the epiphyses, and such destruction as shall lead to pathological dislocation, the latter being well illustrated in Figs. 204 and 207. This dislocation is always the result of the pull of muscles thrown into that condition of reflex spasm which is a characteristic feature of this disease. It appears conspicuously at the knee, usually as a backward subluxation (Fig. 207), and at the hip as an upward dislocation, sometimes with more or less apparent migration of the acetabulum. Another consequence of tuberculous hydrarthrosis, which frequently persists even long after the subsidence of the acute stage of the disease, is the occurrence within the joint cavity of rice-grain or melon-seed bodies, for whose presence it is not easy to account. The generally received explanation is that they are the result of fibrinous outpour, whose fluid portions have been absorbed, while the remaining nearly pure fibrin is broken up into particles and rounded off by attrition during the movements of the joint. They may accumulate in astonishing amount, thus stamping the disease as having a chronic rather than an acute character. After a time they provoke a fresh outpour of fluid, as a result of the irritation which they produce. This fluid is at first usually clear serum, but becomes turbid or seropyoid, and, if infected, becomes pure pus, in which the rice-grain bodies are dissolved or disintegrated.
Fig. 204
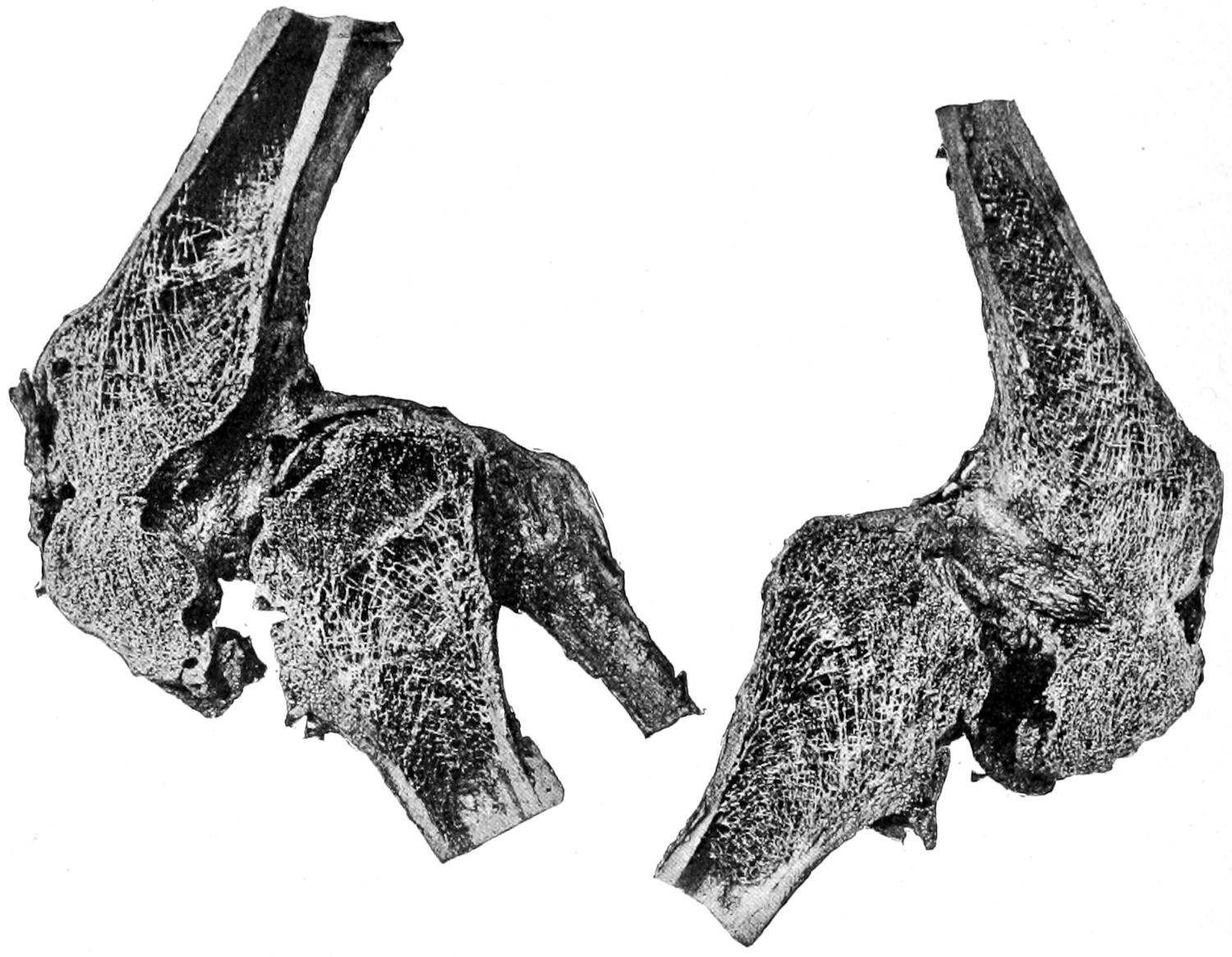
Bony ankylosis of knee. (Ransohoff.)
Fig. 205
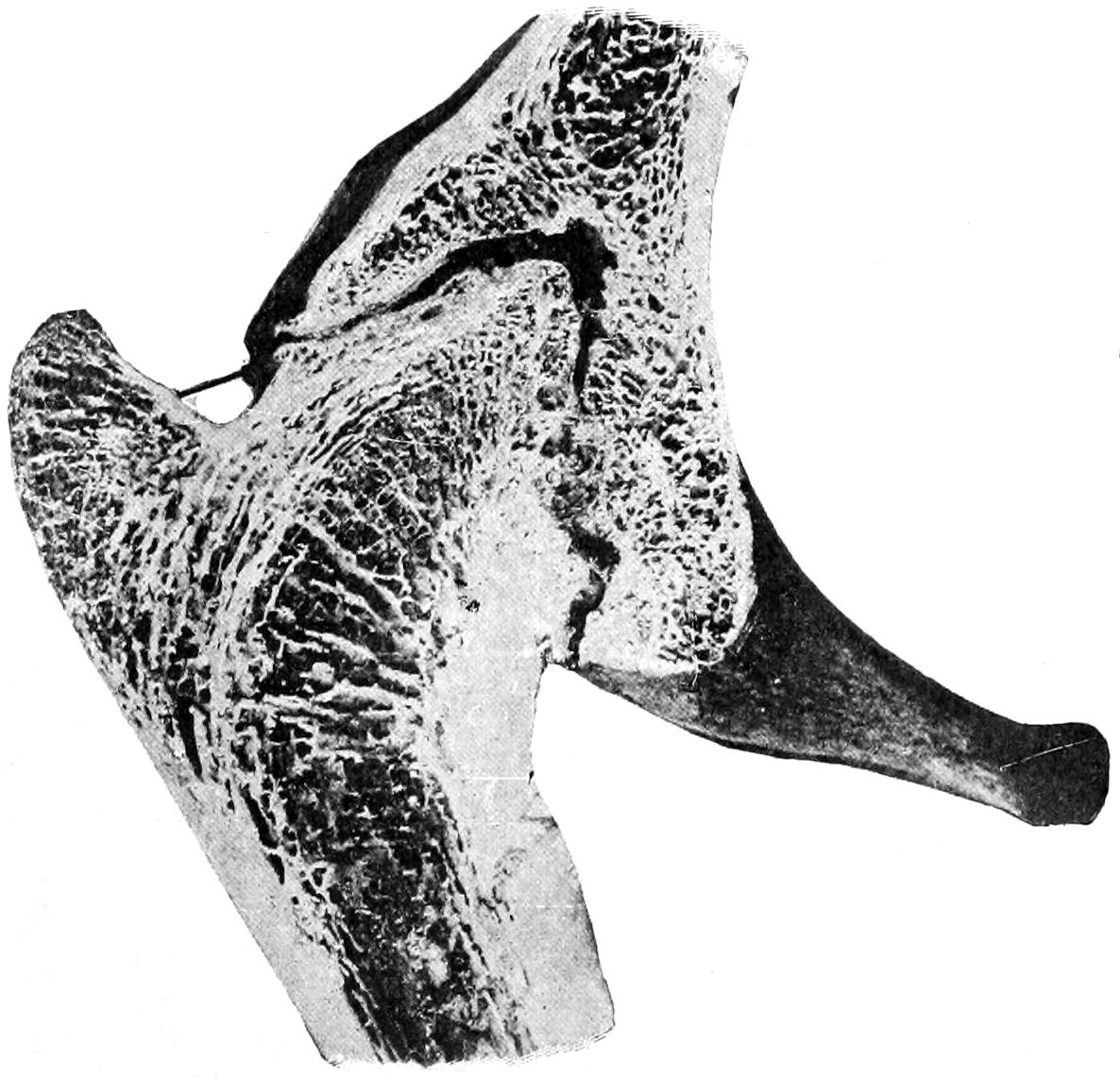
Fig. 206
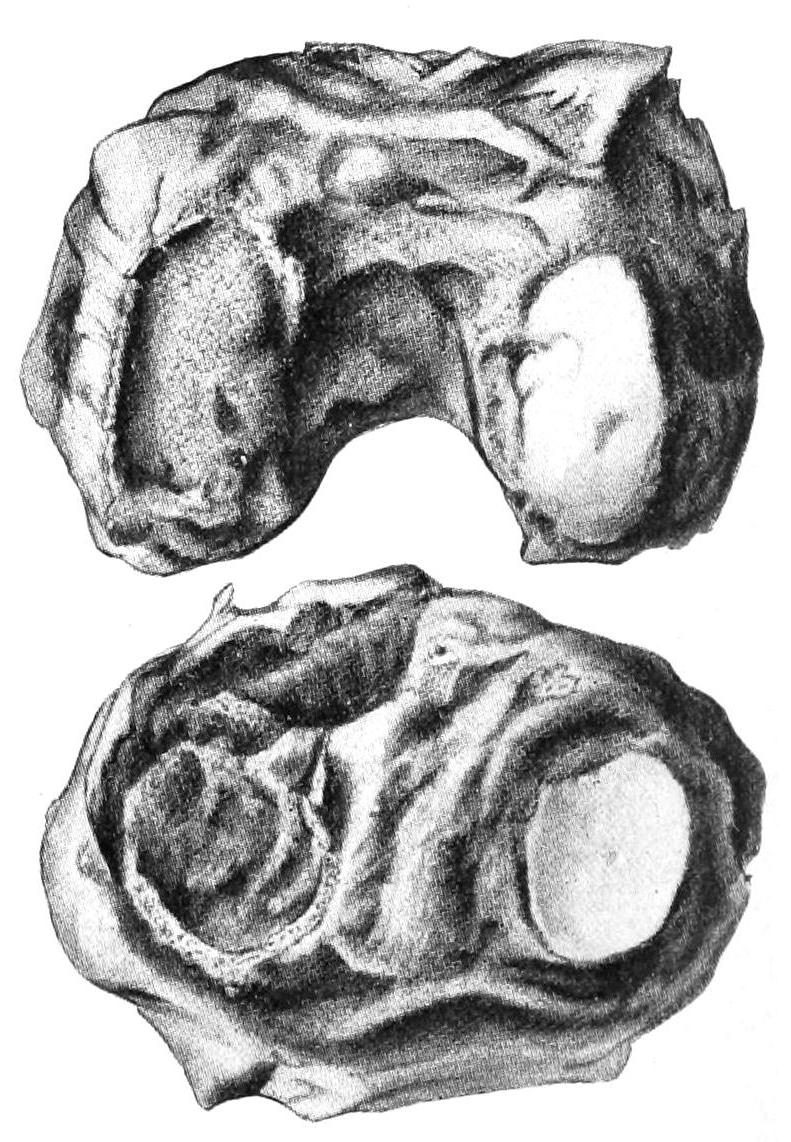
Section of bony ankylosis of hip. (Original.)
Tuberculous panarthritis, illustrating various types of degeneration and destruction. (Lexer.)
Recovery is possible in many cases when the lesions have not advanced too far. It is rarely ideal, and usually leaves some evidence of its existence in limitation of motion, thickening, or other recognizable symptom. Constitutional as well as local measures have much to do with bringing about this result. It is for this reason that it is so essential to take tuberculous-joint patients out of the environment in which ordinarily they live and get them outdoors, exposed to sunlight and benefited by the best of nutrition. Rest, oxygen, and hypernutrition are the three best general measures for combating these conditions. When recovery does occur it is by the death of all active germs, the absorption[396] to varying extent of disease products, including granulation tissue, and the organization into fibrous and cicatricial tissue of the unabsorbed residue. No tissue which has been actually disorganized is completely restored. The best that can be hoped for is substitution of fibrous or cicatricial tissue. Function may be more or less completely regained. This will depend largely upon how early treatment is instituted. In general it may be said that there is always hope for tuberculous joints if suitable treatment be instituted early and if the environment can be made satisfactory. Unfortunately this[397] is not often possible, and the best that can be hoped for is subsidence of disease at the expense of more or less ankylosis, perhaps deformity, while, at the worst, there may be loss of joint if not of life. It might be misinterpreted should it be said that there is one kind of treatment for the wealthy and another for the poor, yet so much does depend upon what the patient or the parents can afford in the way of change of surroundings that the whole plan of treatment often depends upon the patient’s circumstances. Radical measures may therefore be deemed best in those who cannot afford long delay and temporization, while at other times expensive apparatus and change of residence may bring about the desired result.
The general appearance of a tuberculous joint is one of manifest enlargement which is made more conspicuous by wasting of the limb above and below. Nevertheless by actual measurement it will usually be found to have a greater circumference than its fellow of the opposite side. Its covering skin is pale and often glistening, with prominent veins, while in proportion to the distention by fluid there will be more or less distinct fluctuation. When the joint is evidently distended and does not fluctuate the inference is that it is filled with granulation tissue. There will also be marked thickening of all the articular coverings, the synovial membrane itself being often as thick as sole leather. At points where perforation may threaten there may be dimpling and retraction of the skin, with fixation and discoloration.
—Tuberculous joint disease is characterized especially by loss of function, muscle spasm, muscle atrophy, pain and tenderness of rather significant character, and the other joint features already mentioned. Loss of function may be partial or complete. It depends on the amount of tenderness and the deformity already produced by muscle spasm. Motility is more or less restricted even under an anesthetic. This is induced by actual limitation of motion by products of exudation, by muscle spasm and wasting, and by the involuntary shrinking of the patient when tender joint surfaces are pressed against each other.
Fig. 207
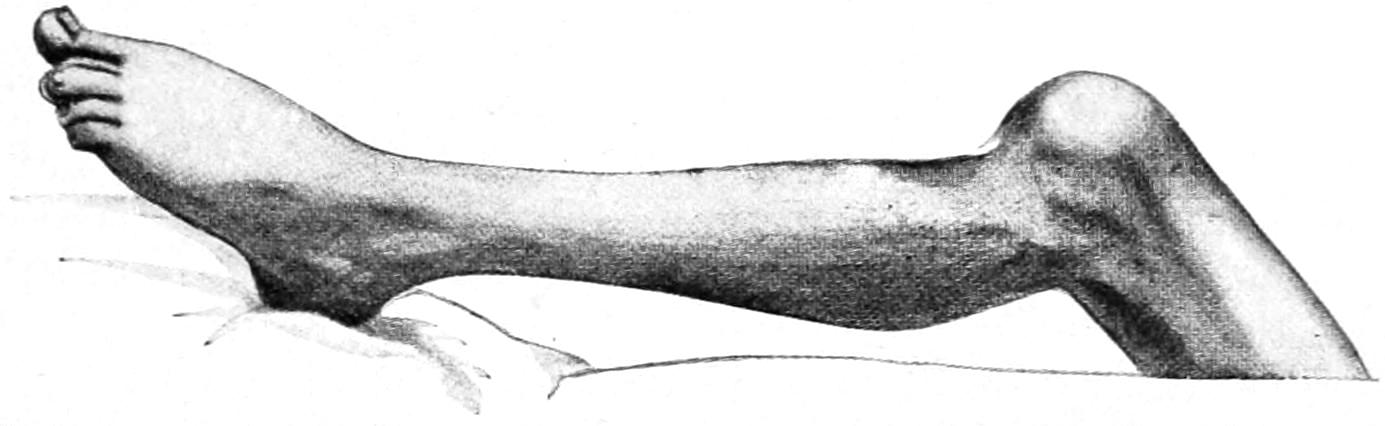
Backward displacement of tibia due to the muscle spasm of a tuberculous knee-joint, with final bony ankylosis. (Lexer.)
Muscle spasm is one of the most significant features of these cases as well as almost the earliest. It is of the greatest diagnostic value, and, if genuine, should never be neglected. It subsides under the use of an anesthetic, hence it is not advisable to employ anesthetics for diagnostic purposes. It produces at first fixation, without particular deformity, but may lead later to this or to pronounced subluxation. It is most helpful in the early stages when it does not particularly interfere with a medium range of motion, and seems to lock the joint before the extreme of motility is reached. Muscle spasm is pronounced even after muscle atrophy is well advanced, and serves more and more to fix joints until they are held by adhesions formed within. Muscle atrophy is also significant and begins about the time when diagnosis becomes fairly possible, i. e., in the early stage of the disease. With the advance of disease it becomes more pronounced and a joint which is fixed by intra-articular lesions will stand out prominently because of the notable wasting of the muscles by which ordinarily it would be moved. It is this which gives the elbow and knee especially their spindle shape. (See Plate XXXIV.)
Pain is also a characteristic feature, especially that which is produced by motion and allayed by rest and that which is accompanied by involuntary muscle spasm, and occurs during sleep, i. e., the so-called osteocopic or starting pains of tuberculous panarthritis. These occur most distinctively in children, but may be complained of at any period of life. Children thus affected will cry out sharply during their sleep and appear for a few seconds very much distressed, and yet do not awaken sufficiently to recall or describe their sensations. The explanation of this phenomenon is a sudden reflex spasm of the muscles by which tender joint surfaces have been suddenly pressed tightly together[398] and pain thereby provoked. Something of this kind may occur in syphilitic bone disease, but, taken in connection with the other signs and symptoms above mentioned, such pains are practically pathognomonic.
The various measures to which orthopedists and surgeons resort for employment of traction, by splints or weights, are directed against overcoming muscle spasm by tiring out the muscles. It must not be thought that by any reasonable degree of traction joint surfaces are actually separated widely from each other. All that it is expected to accomplish is by a steady pull to exhaust the muscles, and prevent them from thus exercising deleterious pressure by pulling joint surfaces together.
The pain complained of is by no means necessarily limited to the joint involved; in fact, some of the most significant pains are those which are described as referred. These furnish illustrations of the fact, well known to physiologists, that irritation in the course of a nerve is referred to its distribution; thus in hip-joint disease most of the pain will be centred in the knee, and when the knee is involved the ankle will be the part to which the patient will refer much of his discomfort.
There also comes an overuse of the unaffected joints of a limb by which the diseased joint may be spared as far as possible. The flexors, as a group, being always stronger than the extensors, the former will overcome the latter in time, and these joint contractures are a later expression of chronic muscle spasm. This is true even when atrophy is well advanced.
Tuberculous joint disease usually has at first no particular constitutional complications. These come on later in proportion as the general health suffers from the confinement entailed by the disease. General health will suffer quicker when the lower limb is involved than when it is the upper. By the time joint lesions are well advanced careful observation will usually reveal a rise of evening temperature and progressive anemia. The symptoms included under the term hectic are those belonging to the destructive stage and are due to a combination of causes in which auto-intoxication figures largely.
—Tuberculous joint disease is usually easy of recognition, except perhaps in the earliest stages. (See the general subject of Orthopedic Surgery.) Differential diagnosis between this condition and syphilis, or between it and hysteria, has occasionally to be made, and may at first cause some difficulty. An hysterical hip or knee may so strongly simulate tuberculous disease as to lead one at first into serious doubt. Again, as between the tuberculous and non-tuberculous forms of hydrarthrosis, there may often be doubt, even after aspiration and examination of the fluid. In fact, that which began as one may terminate as the other. Fortunately in these last cases local treatment is about the same for each, and, while the question of diagnosis may never be absolutely satisfactorily decided, the patient may nevertheless recover in either event.
—The treatment of tuberculous arthritis should be both local and general, one being about as important as the other. The general treatment for this as for every other tuberculous disease may be summed up as follows: The remedies for tuberculous disease are oxygen and hypernutrition. The best place for the patient is the place where these means can be procured. As explained above, this will, to a considerable extent, depend upon the circumstances of the patient or the family. When it can be afforded a high altitude is almost as good for joint tuberculosis as for that of the lungs. The nearest approach that can be made to it will be the most desirable. Hypernutrition will in some cases consist almost in forced feeding. Here as elsewhere in tuberculous disease it is of at least theoretical as well as of practical advantage to saturate the system with some bactericidal remedy, if such there be, and for obvious reasons. Creosote or its congeners, in more or less palatable form, seem at present to best serve this purpose. In addition to this arsenic, iron, and the iodides, the latter especially if there be any suspicion of syphilitic complication, can be used to advantage. In proportion as patients become confined to the house their elimination is usually restricted. All measures then by which elimination may be improved will be indicated.
The use of tuberculin, or some of its modifications, has been occasionally followed by excellent results. It is an agent to be employed with great discretion, but is well worth a trial in those cases where its effects may be carefully watched.
Locally the most important measure is the enforcement of physiological rest of the affected parts. This may imply confinement to bed, especially when the spine, the pelvis, and the hip are affected, but should be reinforced by mechanical contrivances, by which traction or “extension” may be carried out. The purpose of traction, as mentioned above, is to overcome muscle spasm and thus ensure rest. It is effected by many of the orthopedic apparatuses. (See chapter XXXIII.[32]) It may be enforced by fixed dressings of plaster, etc.
[32] The fundamental idea expressed in all of the methods for enforcing rest by traction is of American origin, and constitutes one of the advances in surgery for which the world is indebted to America. For a long time it was referred to in Germany as the American method, and yet now the Germans claim so much for it that one of their surgeons has written a book of 600 pages devoted to the employment of traction for various surgical purposes, in which but very little credit is given to the men who originated it.
PLATE XXXIV
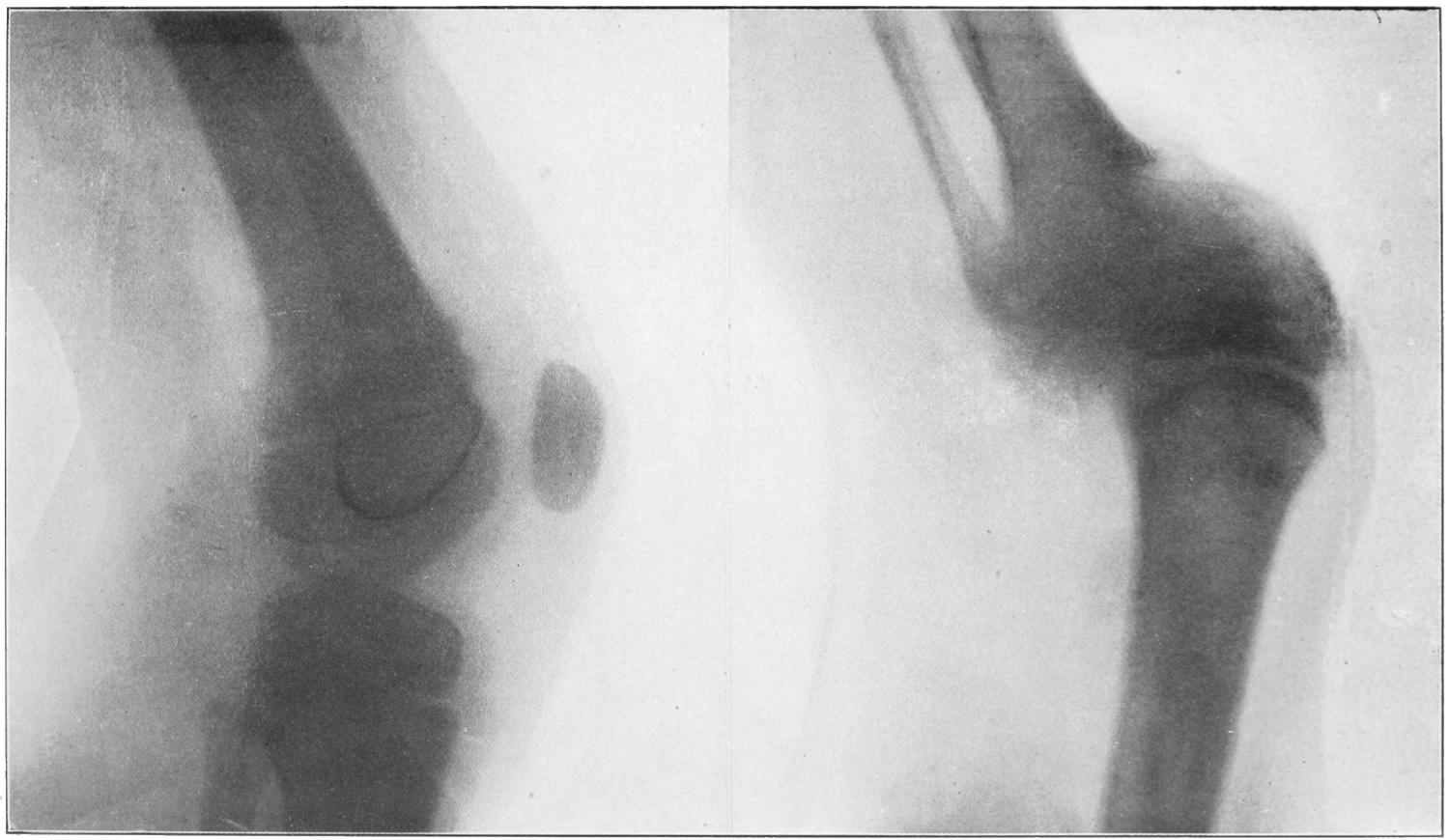
Normal Knee-joint. (Child, seven years old.)
Tuberculosis of Knee, with Partial Dislocation. (Child, seven years old.)
[399]
With a better appreciation of the pathology of the condition numerous methods were devised by which the germs should be attacked in loco. Thus various antiseptics have been injected in varying strengths, either into joint cavities or around them. Lannelongue devised a “sclerotic method,” by which zinc chloride solutions were injected into the peri-articular tissues, to so condense and harden them as to imprison and destroy their contained germs. The method, however, is an extremely painful one and has not found general favor. For a long time iodoform was employed for the same purpose, in emulsions of 10 per cent. and 20 per cent. strength, in sterilized glycerin or olive oil. It affords a curious paradox that the iodoform itself must be sterilized before being thus used. This emulsion has been injected into the peri-articular tissues or into joint cavities, which, when containing appreciable amounts of fluid, should be first emptied and washed out; all of which can be done through the same small trocar used for introduction of the iodoform. The verdict of surgeons today is rather against the employment of iodoform, since they have learned to not rely upon it because of disappointment so often following its use.
Bier, in 1891, advised the so-called congestion treatment of tuberculous joints, basing it upon the fact that tuberculosis does not develop in lungs which are the seat of venous stasis from valvular heart disease. He proposed to produce an artificial stasis, in the joint structures and about them, by which living germs should be destroyed and their disease products encapsulated, claiming that as the result of the hyperemia thus produced the alexins are thus brought into more complete contact with the bacilli. The method is applicable to the limbs below the shoulder and hip. It consists in the application of an Esmarch bandage above the affected joint, applied with sufficient firmness to obstruct the returning blood, but not to interfere with the arterial supply. If there be room the limb is also bandaged below the joint with an ordinary cotton roller. This congestion is kept up at daily intervals for increasing periods, beginning with perhaps half an hour and continuing until it is in operation at least half of the time. Meantime other methods of treatment are not interdicted. In the earlier stages of tuberculous joint disease this method has given very encouraging and pleasing results. (See Fig. 208.)
Tuberculous hydrops may be treated by aspiration and elastic compression. Should fluid distend the joint it should be opened and thoroughly cleaned, then closed and perhaps drained.
The treatment of pyarthrosis and of peri-articular cold abscess has long been a mooted subject. The orthopedic surgeons still adhere to mildly or absolutely non-operative measures, whereas the general surgeon prefers to adopt more radical methods. Each case should be judged on its own merits, and these should include a careful estimation of the general condition of the patient. Should evidences of septic intoxication be present or the ordinary general signs of the presence of pus, then these collections should be opened and cleaned out. If hectic can be excluded, then other considerations will indicate what is best. At all events there will be seen many cases where a delay in operation will be advisable, in order to permit of improvement of the general condition by measures above described. To merely open up a tuberculous focus and leave at least two fresh raw surfaces exposed to contamination is rather to invite the spread of the disease than to correctly meet the indication. Every old focus will be lined or surrounded with a more or less dense membrane formerly called pyogenic, but now more correct knowledge shows it to be pyophylactic. (See p. 113.) To leave this in situ is to leave germ-laden walls, while to dissect it thoroughly is to make a larger, fresh raw surface and to open up innumerable absorbent vessels. Thus, whether it be removed in whole or in part, or allowed to remain, some sufficiently strong caustic material should be promptly employed, by which both destruction of living residual germs and closure of the mouths of the absorbents shall be effected. This has been set forth more fully when dealing[400] with cold abscesses in general, but is of so much importance that it may be reiterated here. Whether the actual cautery, pure carbolic acid, strong zinc chloride solution, or some other agent be used should depend upon circumstances, but every portion of the surface which it is proposed to leave more or less exposed to the possibility of infection should be thus protected. In proportion to the intensity of the caustic action there will be separation of more or less cauterized and sloughing material, for whose escape provision should be made; but it will be separated by the granulation process, aided by an active phagocytosis, and when removed will leave a granulating surface which is but slightly absorbent. These facts pertain to small incisions for drainage as well as to extensive arthrectomies.
The operative treatment, then, of tuberculous arthritis varies from tapping, with or without drainage, to complete arthrectomy or amputation. When the joints of the foot or ankle are extensively diseased, and the patient, as usually happens, is in poor condition, it may appear that amputation will afford the most complete relief, and that a stump with an artificial member will be of much more use to the individual than a mutilated, tender, and disabled foot.
Fig. 208
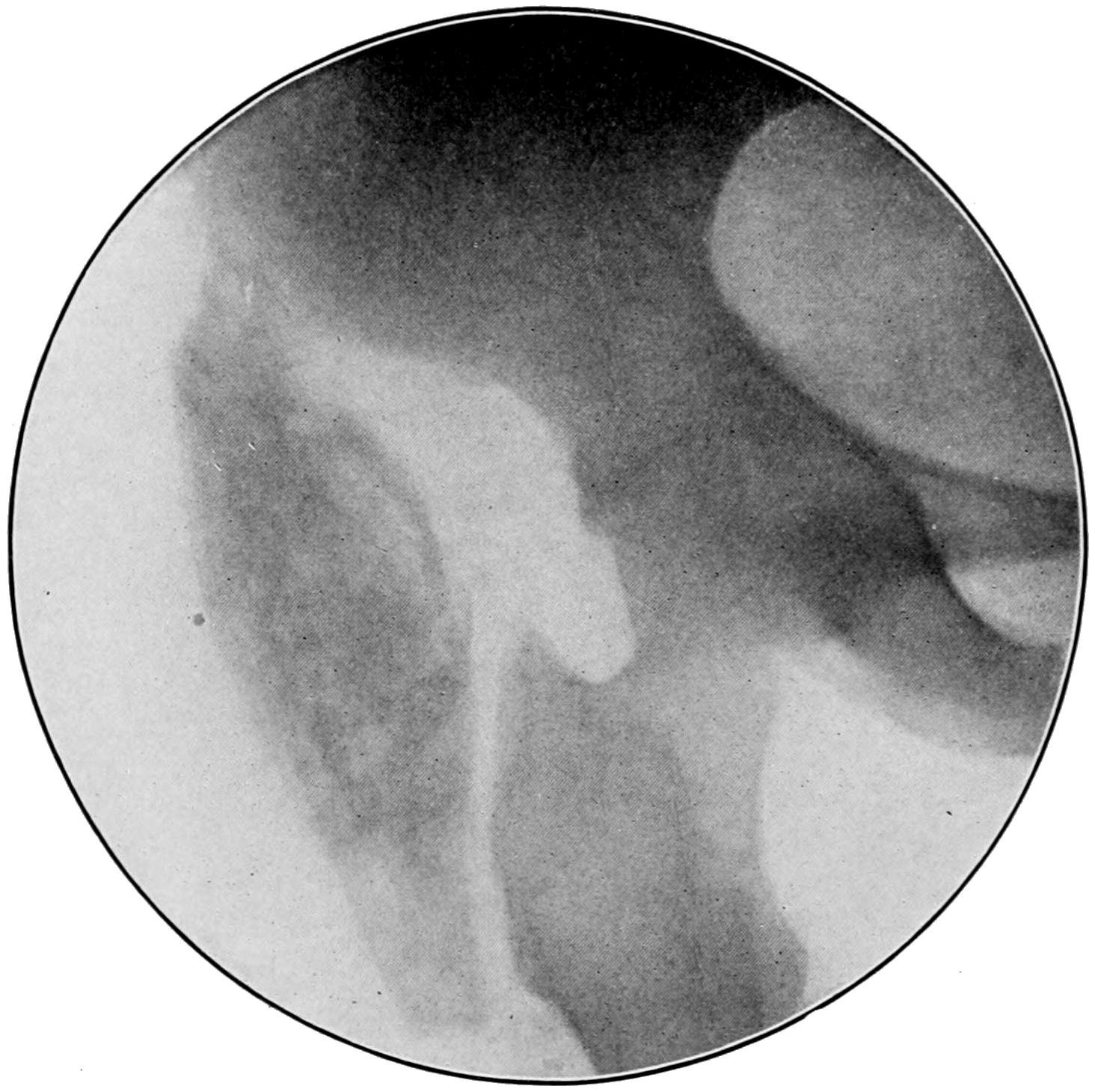
Calcified mass in old “cold abscess” about hip-joint. (Buffalo Clinic. Skiagram by Dr. Plummer.)
To incision with or without drainage is given the name arthrotomy. When the joint is widely opened and portions removed with the sharp spoon or otherwise, it is known as arthrectomy. When bone is removed irregularly the measure is called atypical resection. When entire bone ends are removed the operation becomes an exsection or resection. The ordinary arthrectomy is not sufficient when foci are present in the epiphyses. Here at least atypical resection is called for. Arthrectomy may properly include a wide exposure of articular surfaces and the removal of the thickened and diseased synovia, with its fringes, or with the cartilages, by which cancellous structure is more or less widely exposed. When arthrectomy is undertaken it should be thoroughly made and by a large incision, since the more completely the joint cavity can be inspected and attacked the better are the interests of the patient subserved. All fresh or cold abscess cavities which connect with the joint or lie in contact with it should also be attacked at the same time, and those which do not communicate with it should be separately drained. While drainage by tube or other means[401] will usually suffice, there are cases where the disease is so extensive that it will pay to pack the cavity with balsam gauze for a few days, placing secondary sutures by which the incision can be closed after its removal. In the shoulder and hip, for instance, such a method will give satisfactory results.
The advantage of avoidance of resection is the non-interference with the epiphyses and their junctions, thus permitting the growth of the bone to continue. Therefore complete and typical excisions should be practised as seldom as possible, especially in growing children. They may be practised to advantage even in advanced age, and the writer has seen satisfactory results after complete excision of tuberculous joints in senile cases. When operating upon a tuberculous tarsal joint the surgeon is likely to find one or more of the tarsal bones so much involved in the tuberculous disease that he is compelled to scrape it out and thus leave a cavity almost the size of the bone itself. Should he have to do this to a series of the bones it would be better to make a formal resection of the tarsus or possibly an amputation. The cavity should be left open with a sufficiently large incision so that it may be easily packed. A cavity of this kind left unpacked will fill up with clot, which will disintegrate and the result will be much less satisfactory. In the former case there is an open cavity which fills with granulations, but this can be kept accessible under observation and with more effect and comfort. This is equally true of those cavities where both arthrectomy and bone curettage have been practised.
Several different terms have been applied to loose and movable bodies, even in the various joints, depending on their size, arrangement, and appearance. Thus we have the rice-grain or melon-seed bodies (corpora oryzoidea), which have already been described and are now supposed to indicate a form of tuberculous synovitis which has undergone a partial if not complete subsidence. Again we have larger masses occurring singly or in very small number, especially in the knee, to which the Germans have given the significant name of joint mice. Also in the knee, owing to its peculiar construction, another form of movable body is met with, i. e., a displaced and more or less motile semilunar cartilage. This condition was first described by Hey, and especially studied by Allingham, who made it a prominent feature of what he described as “internal derangement of the knee.” Lastly, in those joints in which synovial fringes occur, the knee especially, it is held that portions may become detached by having been infiltrated and cast off or broken loose, and thus form a fourth variety of floating body. The joints most often affected are the knee and the elbow. In many instances there is a history of injury, especially when the mass is of considerable size. The theory of an “osteochondritis dissecans” has also been invoked to account for the resemblance between some of these bodies and the articular cartilages. Some pathologists have held that they may result from the organization of clots, which are subsequently rounded off and shaped by attrition (Fig. 209). These bodies then may consist of condensed fibrinous material, of cartilage, of true bone, or of hyperplastic and fatty synovial tassels. To these may be added rare instances of mucoid connective tissue.
Fig. 209
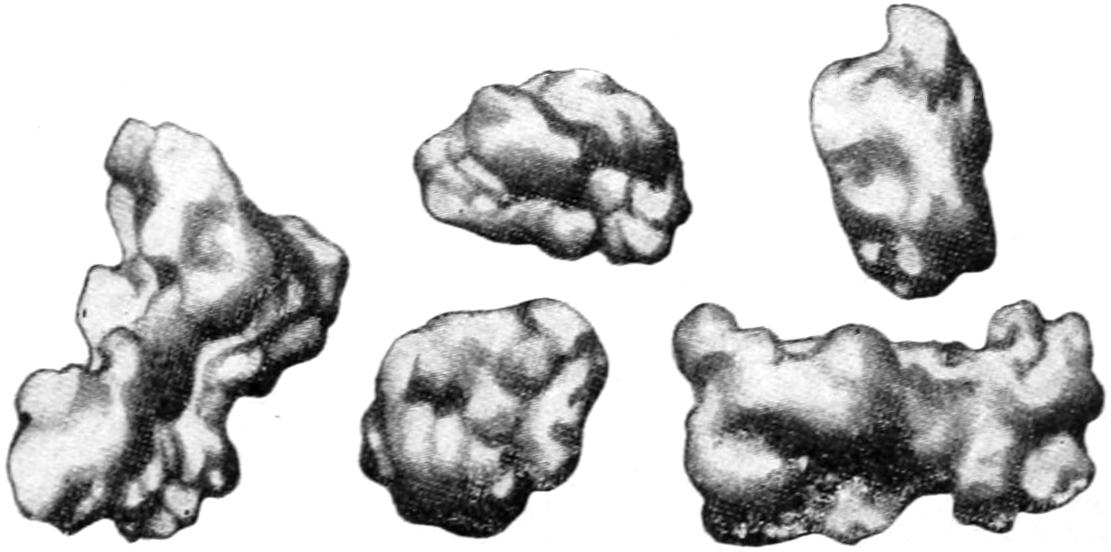
Floating bodies—“joint mice”—from knee-joint. (Lexer.)
—Rice-grain bodies may be suspected in cases of chronic tuberculosis and often in arthritis deformans, while in many instances they may be felt gliding beneath or[402] between the joint structures. A perfectly loose floating body will produce symptoms which are quite distinctive. They consist of sudden and intense pain, with such muscle spasm as to fix the joint and prevent its use, thus “locking it.” Occurring at the knee the individual is instantly disabled, but usually learns by some peculiar manipulation, with or without assistance, to “unlock” the joint, and after a few moments to resume its use. Such a complaint as this should always suggest the condition. Patients who have had it for a long time learn how to avoid it as well as how to relieve it, and will often discover and be able to indicate to the surgeon the existence of a movable body, and even to describe its usual resting place.
Partial or complete dislocation of a semilunar cartilage in the knee is usually the result of traumatism, a distinct history of which can generally be obtained. It may not have been discovered at the time, owing to swelling or tenderness, but will produce its peculiar symptoms later, i. e., after use of the joint is resumed. Here, again, so long as it remain in proper position, it interferes but little; with a misstep or sudden movement, however, the patient is seized with sudden and painful disability. Here the movable cartilage may be felt projecting near its proper location. In such cases as these it is movable only to a certain extent and makes no free excursion about the joint. When not detected it may be suspected from the description which the patient gives of his seizures.
—So far as diagnosis is concerned, when a movable body can be felt all doubt is set at rest. When it cannot be discovered its existence may be inferred with an accuracy proportionate to the patient’s description of his difficulties.
—The treatment of rice-grain bodies is essentially that of the chronic hydrarthrosis and probably tuberculous condition which have led to their formation. It will consist usually in arthrotomy, with thorough irrigation; often in some form of arthrectomy. With the larger floating bodies, the “joint mice,” the most radical measures are the best. In most of these instances there will be some degree at least of hydrarthrosis. The joint cavity being distended and relaxed, the indication for arthrotomy is the more urgent, since it will permit also of irrigation or of dry sponging, with the same benefit with which analogous intraperitoneal conditions are treated by the same measures. The joint may be opened by a sufficiently ample incision, through which the foreign body or bodies may be removed. The operator should not be satisfied with mere removal of one, but should make a thorough search for others which may have escaped previous detection.
Perhaps no operative measure in surgery better illustrates the advantages of asepsis. This operation, which now can be done with impunity, was in the pre-antiseptic era one which had a discouraging fatality, death resulting from septic infection in about 40 per cent. of cases.
“Joint mice” are of sufficient frequency and significance to justify brief separate consideration. According to Connell these may be grouped as follows:
Among the many explanations offered are the following:
Injury figures largely in the opinion of most of the authorities, it being well established that an injured portion of articular surface may become subsequently detached by a fatty necrosis, spoken of by König as osteochondritis dissecans, or by Paget as “quiet necrosis.” Others imagine that these floating bodies are rarely of traumatic origin.
Symptoms are usually marked and significant. There is sudden sharp and shooting[403] pain, sometimes so severe as to cause faintness. Along with this there is “locking” i. e., fixation of the joint, usually in the flexed position, probably due to the entanglement of the floating body between the articular surfaces or between the bone and the capsule.
Fig. 210
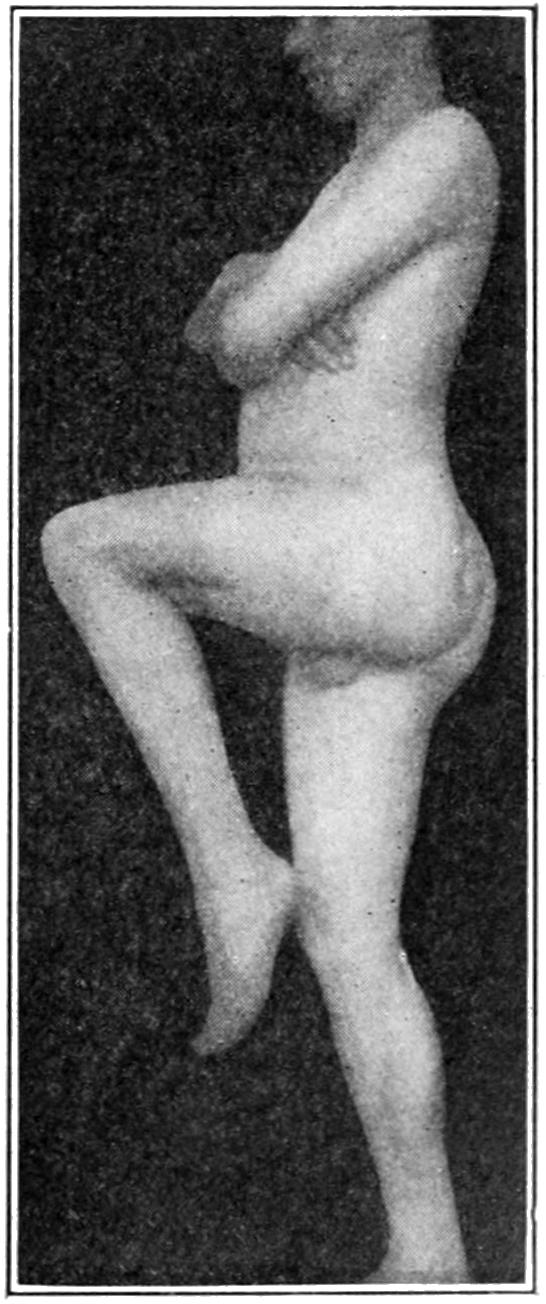
Ankylosis of hip with contracture of knee, following post-scarlatinal arthritis.
It is the smaller rather than the larger bodies which give the most acute symptoms. This “locking” may last for only a few moments or for a number of hours and may or may not be followed by acute effusion. When with the above symptoms the presence in the joint of a movable mass can be made out diagnosis is complete. Some patients discover the movable body in their own joints before they go to the surgeon.
When the diagnosis is established the removal of the offending material is imperative. In the pre-antiseptic era this was an extremely hazardous operation. It is now one involving only theoretical risks. These bodies are sometimes extremely movable and slip about within the joint in a manner to almost defy removal even after the joint cavity is open. If such a body can be felt and fixed by digital pressure, or by the method of “stockading” suggested by Andrews some years ago, i. e., fixation by forcing sterilized pins into the tissues around it so that it cannot escape, it is then an easy matter to cut down upon it and remove it. Otherwise incision may require to be sufficiently ample to permit insertion of a finger and the general exploration of the joint before it is encountered. These bodies sometimes exist in small numbers, and it may be possible to remove several through a single opening. If the joint be opened and explored it should be done thoroughly in order that nothing may escape. After removal the capsule is closed with buried sutures, the balance of the wound closed as usual, and the limb then dressed upon a splint with absolute fixation for several days, in order to ensure physiological rest (Fig. 209).
The term ankylosis implies angular deformity, but is used to designate partial or complete fixation of joints, such fixation being usually accompanied by more or less deformity or displacement. It is a name for a condition and not for a disease, but is always produced by the latter or by injury. The term itself implies nothing as to the nature, extent, or appearance of the exciting cause. The actual cause may have been disease of the joint, of the tissues around it, or may have been the result of injury rather than of infectious or other active disease.
For convenience we speak of fibrous, false, or pseudo-ankylosis, and of that which is bony or actual. A more accurate use of terms would lead us to refer to the former as contracture rather than true ankylosis.
Contractures are the result of acute, usually septic intra-articular and peri-articular processes, where muscle spasm is a pronounced factor and where the intensity of the process has more or less weakened the joint structures. The profession is hardly in the mood to accept acute rheumatism as an infectious process. If true or not the acute rheumatic affections are frequently followed by fibrous ankylosis with contractures. Disfigurements of this kind are often produced as the result of the surface lesions of severe burns or ulcerations, followed by cicatricial contraction and the formation of dense bands and scar tissue. This is a condition which can always be foreseen and which should be guarded against with very great care. (See Treatment of Burns.) Contractures also occur as the result of certain diseases of the spinal cord, either as the result of active contraction of one set of muscles, or of paralysis, by which the opposing muscles are deprived of resistance and thus draw the limb out of shape.
True ankylosis is sometimes fibrous, sometimes osseous, and occasionally both combined. The older the case the more probable is actual osseous union of joint surfaces.[404] Bony ankylosis implies a sharply destructive type of arthritis, which may have been originally of pyogenic, gonorrheal, or tuberculous character, or else indicates a series of very slow ossific and calcific changes, such as are connected with the osteo-arthritis already described. Many of these cases are to be referred to lesions of the cord, and many of them are of polyarticular character. Fig. 195, illustrating one of the cases of so-called “ossified men” under the writer’s observation, will portray a series of lesions of this kind, most of the vertebral as well as the other joints being involved in an absolute osseous union.
Fig. 211

Bony ankylosis of hip. (Ransohoff.)
Fig. 212

Bony ankylosis of knee. (Ransohoff.)
Fig. 213
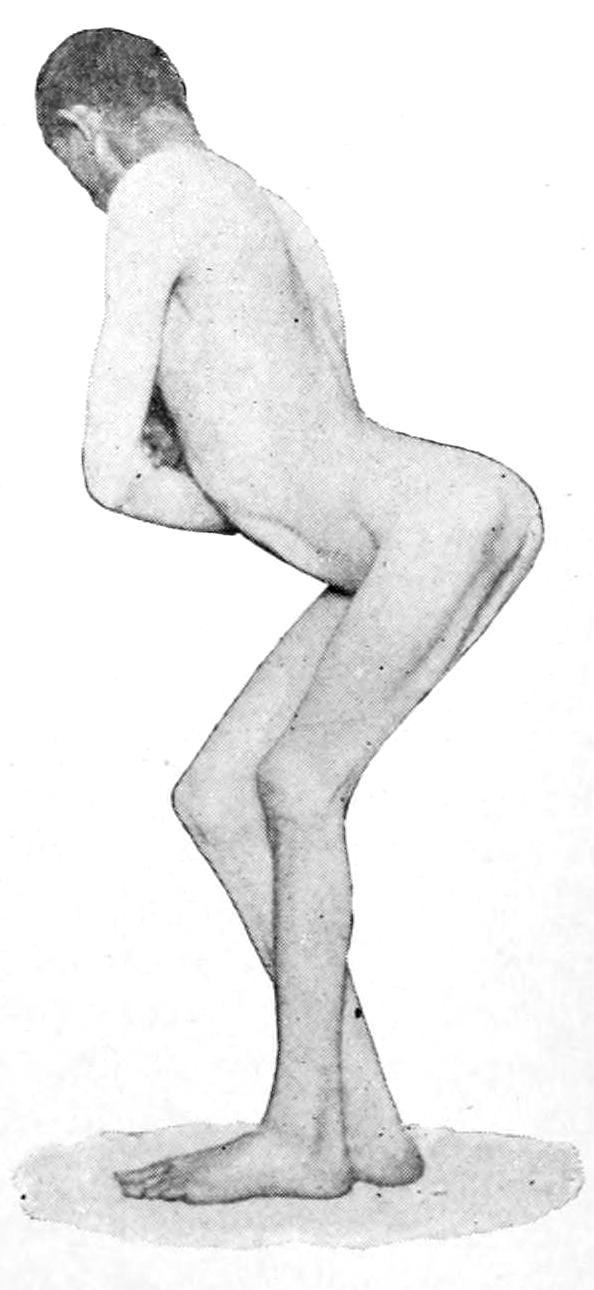
Bony ankylosis of hip with deformity. (Ransohoff.)
[405]
When a joint is stiff bony ankylosis may be inferred. So long as there is any motion possible it is essentially of the fibrous type. The condition is one easy of recognition, and is seen in all degrees of completeness. In many instances joint fixation is accompanied by adhesions of tendons and tendon sheaths, while as time passes all the structures around a joint thus fixed become less movable and more stiffened. Even the patella may become firmly attached to the bony surface upon which it normally rests, and thus interfere with motion of the knee almost as much as though the femur and the tibia were alone involved. Occasionally one of the acute exanthems is followed by contractures of a joint, with or without actual joint lesions, by which when neglected distressing deformities are produced; such, for instance, as partial flexion and fixation of the knees, or such stiffening of the hips as to prevent the thighs from being separated. While in such cases stiffening cannot always be prevented, deformity at least can be if suitable measures instituted sufficiently early.
Figs. 211 and 212, from Ransohoff, illustrate osseous union in the hip and the knee, while Fig. 213 illustrates the deformity which may be produced by contractures and ankylosis at the hip.
The following tabular presentation of the types of ankylosis will perhaps convey the greatest amount of information in small space:
| Ankylosis, true and false | - | Peri-articular | - | Capsular | ||||||||
| Extracapsular | - | Tendinous | ||||||||||
| Tendovaginal | ||||||||||||
| Muscular | ||||||||||||
| Articular | - | Synovial | ||||||||||
| Cartilaginous | ||||||||||||
| Osseous | ||||||||||||
Murphy has prepared the following table of the types of arthritis which lead to some of these varieties, and which may be classed as follows:
| Arthritis | - | (a) Primary hematogenous fibrous arthritis | ||||||||||||||||||
| (b) Dry fibrous arthritis. Non-traumatic | ||||||||||||||||||||
| (c) Traumatic fibrous arthritis | - | With fracture into joint | ||||||||||||||||||
| Without fracture (contusion) | ||||||||||||||||||||
| (d) Suppurative | - | Hematogenous | - | Cryptogenetic | ||||||||||||||||
| Metastatic | - | Typhoid | ||||||||||||||||||
| Scarlatina | ||||||||||||||||||||
| Pyemia | ||||||||||||||||||||
| Gonorrhea | ||||||||||||||||||||
| Traumatic | ||||||||||||||||||||
| Extension | - | Osteitis | - | Tuberculous | ||||||||||||||||
| Osteomyelitic (infective) | ||||||||||||||||||||
| Peri-arthritis (phlegmon) | ||||||||||||||||||||
| Panarthritis | ||||||||||||||||||||
| (e) Ossifying arthritis (primary) | ||||||||||||||||||||
| (f) Static adhesive | ||||||||||||||||||||
—The best method of treatment should be determined by the original character of the exciting cause, the duration of the condition, the amount of deformity present, and the degree of joint fixation. That which will be possible if done early will be useless if not resorted to until the case is old and chronic. In every acute or subacute condition which may threaten ankylosis every possible precaution should be taken to prevent it. If ankylosis be inevitable it should occur with the limb in the most suitable position. At the elbow, for example, this will be the right-angle position; at the knee, one with the leg almost completely extended. In the lower extremity traction with weight and pulley will serve a useful purpose in many instances, either to overcome a threatening condition or to improve one actually existant. Mechanical measures (i. e., use of various splints or forms of orthopedic apparatus) will sometimes be of great use. These may be arranged for the purpose of providing absolute rest, with fixation in a desirable position rather than in one which is undesirable, or they may be made with such devices as shall permit of frequent change of position.
The mildest operative measure which can be practised in these cases is manipulation, either gentle and frequent, combined with massage, or more violent and painful, such as requires anesthesia for its performance. The question of when to resort to these manipulations is one calling for the soundest judgment, as on one side the surgeon faces the possibility of setting up a renewed and more or less acute disturbance, and on the[406] other of seeing a joint gradually stiffen, perhaps in a bad position. There is also a third difficulty, i. e., the necessity for continuing motion in order to prevent the re-formation of adhesions, and this in spite of the fact that it may be intensely painful to the patient. Fortunately, however, the use of nitrous oxide anesthesia usually permits this to be done as often as may be necessary with a minimum of discomfort.
Firm, fibrous ankylosis will be attacked with great hesitation by the experienced surgeon. Even though he may succeed in restoring the limb to a better position, he may feel quite positive that the patient cannot undergo the pain of the subsequent frequent handling. With bony ankyloses he may feel that nothing short of radical measures will suffice. Here it is rarely a question of restoring motility but rather of overcoming deformity. At the knee a wedge-shaped portion of the joint may be removed, its angle corresponding to the angle of deformity, and thus a crooked leg may be restored to the straight position; in fact, with a raised heel under such a limb it may be made almost as useful as ever. At the hip one may do a subcutaneous osteotomy, dividing the femoral neck either with chisel or with a small and protected saw, and then bringing the limb down into the normal position of extension, allowing the bone to repair itself, and effecting improvement only in position, or, by constantly moving it, securing a false joint; or a more formal exsection may be made and by removing the head of the femur and clearing out the acetabulum a degree of motion may be established at this point. At the wrist, elbow, and shoulder-joint resections will usually give good results if the operation be performed before the muscles have almost disappeared by atrophic processes.
Danger attaches to the performance of the so-called bloodless operations, in that there is a possibility of laceration of nerve trunks or of large vessels which may have become fixed in the condensed tissues and be torn with them. There is more danger of this perhaps at the knee than in other joints, and ruptures of the popliteal vessels and nerves have been repeatedly reported. The first attempt in breaking up such a joint should be to increase the degree of flexion. If by efforts in this direction the tissues can be first released, then there is less danger of their yielding when extension is made. Another danger which threatens in all resistant cases, and especially in elderly people, is fracture of bones. The writer has seen the upper end of the tibia as well as the neck of the humerus yield under these circumstances. In the latter event one should endeavor to prevent bony union, and thus to gain a false joint in place of the original.
In regard to the nature of the operative attacks upon the above types, the following is copied from Murphy:[33]
| A. Extracapsular disease | - | 1. Tendon elongation (tendoplasty). | |
| 2. Tendovaginitis (exsection of sheath). | |||
| 3. Cicatrices (removal). | |||
| B. Intracapsular | - | 1. Adhesive synovitis (exsection of capsule). | |
| 2. Replacement by aponeurosis or muscle. | |||
| C. Osseous | - | 1. Disconnect bones. | |
| 2. Remove neighboring bony processes or prominences. | |||
| 3. Liberate soft parts. | |||
| 4. Prevent subsequent bony contact. | |||
| 5. Interpose tissue to form hygroma or fibrous surface. | |||
| D. Joints suitable for operation. | - | 1. Mandibular. | |
| 2. Hip. | |||
| 3. Shoulder. | |||
| 4. Elbow. | |||
| 5. Knee. | |||
| E. Technique | - | 1. Flap formation (skin flap with fascia, or muscular). | |
| 2. Exposure of ankylosed area. | |||
| 3. Osseous separation. | |||
| 4. Transplantation and fixation of interposition flap. | |||
| 5. Replacement of bone. | |||
| 6. Fixation of parts. | |||
| 7. Drainage. | |||
| F. Subsequent treatment | - | 1. Passive motion | |
| 2. Active motion. | |||
| 3. Forced traction. | |||
[33] Journal American Medical Association, May 20, 1905, p. 1573.
[407]
To the various expedients which may be adopted for making stiffened joints more useful may be given, in a general way, the term arthroplasty. A variety of mechanical contrivances have been resorted to in the past, operators hoping to be able to secure, for instance, a movable knee instead of one which is stiff. Artificial joints, made of celluloid, ivory, etc., have been used for experimental purposes, but while occasionally they have given good results in animals, they have rarely been satisfactory in man. For the prevention of re-adhesion, plates of celluloid, thin metal, gutta-percha, rubber, etc., have been used. These are either wrapped around a bone end or are used for lining a bone cavity, and rapidly accumulating experience is showing that this may be done with great benefit.
Thoroughness of operative work is one of the important contributing agents to the securement of wide range of motion, especially in complete removal of synovial membrane, capsule, and ligaments. Soft parts should be liberated thoroughly. Of the materials which can be interposed between bone ends in order to prevent reunion, muscular aponeurosis, with a certain amount of fatty tissue, makes the best material for interposition. When aponeurosis cannot be secured, then muscle should be tried, with some fat, as the former flattens out and undergoes structural changes, with conversion into fibrous tissue.
It should be represented to the patient as a legitimate scientific experiment, and in such a way that no matter what may happen no blame can be attached to the operator. In general it may always be stated that the older the lesion the less satisfactory will be any measure of treatment except possibly resection and arthroplasty.
This term applies to the intentional production of ankylosis in a joint previously healthy or nearly so, with the intention of stiffening a useless limb and thus enhancing its usefulness. The measure applies mainly to those cases of infantile paralysis, with loss of control of the knee or ankle, or both, when by stiffening the limb it can be made to serve the purpose of a crutch. It is the last resort in this direction when there is no possibility for tendon grafting. Long confinement of a limb in a fixed dressing will lead to considerable stiffening of the joint, yet a joint so immobilized lacks that firmness of support called for in cases above mentioned. Therefore when it is desired to perform arthrodesis the joint is usually opened and more or less of its articular surface removed, the intent being to produce the effect in the shortest time and in the best way. It can be better attained by a removal of articular surfaces with the saw and the apposition of fresh bone surfaces to each other, their retention being ensured either by sutures (tendon or wire) or accurate fixation in plaster of Paris. Under these circumstances drainage should not be necessary, and limbs can be completely enclosed in a fixed dressing.
Aside from arthrotomy and partial or complete arthrectomy, as above mentioned, the latter, including removal of synovia or cartilage, and perhaps curetting of bone foci, the formal resections or excisions of joints remain to be considered. The latter is the preferable term, as it is meant to include removal of the component parts that enter into the construction of joints, while the term resection implies rather the removal merely of portions of bone.
Joint excisions are practised especially for the following purposes: (a) To atone for the result of old unreduced dislocations; (b) in certain compound dislocations, with or without fracture; (c) in certain comminuted fractures where there is no prospect of recovery with useful joints; (d) in the destructive forms of acute arthritis where the entire joint is disorganized and the bone ends carious; (e) in tuberculous arthritis or panarthritis, with or without suppurative complications; (f) in occasional instances of disabling osteo-arthritis; (g) for relief of ankylosis, either for improvement of position (knee) or restoration of motion; (h) occasionally after gunshot injuries. Excisions required by the exigencies of traumatisms should be promptly done. If the case be complicated with septic infection the prognosis is much less favorable. For convenience of description[408] excisions may be classified as primary, intermediary, and secondary. According to the joint involved, as at the knee, the purpose underlying the operation is to effect an absolutely rigid bony ankylosis.
The development and perfection of the general method of joint excisions is a matter of but little more than a century. Previous to that time amputation was almost the only resort when destruction had occurred. The most prominent surgeons in the early development of the measure were Park, of Liverpool, and Moreau, of France. During the latter part of the past century Ollier, of Lyons, greatly improved the technique by demonstrating the importance of the periosteum and by introducing the so-called subperiosteal methods. This is of great value in uninfected cases. It is a mistake, however, to endeavor to save periosteum which has become involved in the tuberculous process; in fact, in the presence of tuberculous disease we cannot be too radical in the removal of all affected tissue.
In the so-called subperiosteal method the operator endeavors, so far as possible, to preserve the periosteum of the parts exposed to attack, and, if possible, the capsular ligament as well. Thus at the elbow the capsule, if not diseased or obliterated, should be preserved, the osseous tissue being shelled out from within, so far as possible. The less, then, the connections between the capsule and the periosteum are disturbed the better. The French apply to this method the term “subcapsular periosteal.” When the bone covering can be preserved new bone is easily formed to replace that which has been lost, especially during adolescence, while the preservation of the capsule, with its ligamentous connections, affords a better joint cavity than will the substitute which results from natural processes. Furthermore the surrounding tendons are less disturbed and the condition remains more like the original. Nevertheless one does not exsect healthy joints, and the method is not always easy nor even possible of performance. It will suffice to say that it should be adhered to only as far as circumstances may justify or permit.
Surgeons, however, have not been satisfied with the older methods, and have endeavored to still further enhance motility in operated joints. (See above—Arthroplasty.) To this end the interposition of muscle, fascia, or of foreign membrane has been suggested. Thus, after removal of the head of the femur a strip of fascia lata may be interposed between the raw-bone surface and the cavity of the acetabulum, being fastened there by catgut sutures. In the shoulder a similar procedure has been carried out, utilizing a strip of deltoid muscle. At the elbow a piece of the pronator radii teres may be detached and fixed by sutures to the brachialis anticus. In every case the method should be adapted to the demands made, the intent being to cover divided bone ends with tissue which will prevent osseous union, as it is known to do in many cases of fracture where such interposition produces non-union. In so far as one attempts here to imitate conditions which are considered undesirable in certain other traumatisms, Murphy has done more than any other American surgeon, both in the experimental and clinical study of this subject. (See above.)
For the joints below the hip and shoulder the bloodless method will facilitate operative work. In case of a septic joint, however, it would not be advisable to apply the elastic bandage below and then over and around the joint, as by the pressure thus made some septic material may be forced into the absorbents. In clean cases the rubber bandage is a great advantage to the operator. It has this objection, however, in that hemorrhage which does not occur during the operation has to be checked after its conclusion, and I have often thought it advisable to avoid the use of the bandage and to secure vessels as they are divided, in order that when bleeding has once ceased there be no fear of its recurrence later.
The question of drainage is one of importance. In a general way one may feel that in an absolutely clean case drainage is not required, save possibly a small opening for escape of blood. If practised at all it should be thoroughly done. Drainage tubes are often too small and do not permit the escape of either clotted blood or debris of injured tissue.
The after-treatment of excisions demands, first of all, physiological rest of the part involved, especially if, as at the knee, sutures or other expedients for maintaining apposition have been inserted. When motion is sought there will soon come a time when passive motion can be begun. This will vary with the size of the joint and the magnitude of the procedure. Actual rest should be maintained until firm wound healing has been[409] secured. Passive motion is then begun, to be practised daily, the sensation of the patient being the guide as to the range of the movement and extent of manipulation. Thus, after exsection of an elbow with prompt union of the wound passive motion should be begun in about two weeks, but it should not be begun for a month if the joint has been thoroughly disorganized and the cavity is still discharging. Motion should be begun as early as is considered feasible in order to guard against a false joint.
The remote consequences of joint excisions are usually very satisfactory. The best results are obtained in the young, i. e., those whose tissues are still undergoing natural changes and whose bones are growing. In the course of time, by condensation of surrounding tissues, a new joint capsule is formed, its interior smoothed off, apparently covered with endothelium and filled with a sufficient amount of fluid, similar to that of normal joints, to serve the purpose; in this way a new joint becomes gradually substituted for the old, which serves the original purpose, in a surprising and gratifying way. Even in those of advanced years a satisfactory result is often obtained. It is often necessary to afford some support, by which too great a range of motion may be avoided; thus at the elbow the result at first is what may be called a “flail-joint,” which permits much undesirable lateral movement. This can be avoided by having light leather corsets fitted to the forearm and arm, connected by two lateral hinged braces. This being constantly worn, and no motion permitted which is not an imitation of the normal, the parts in time adapt themselves to the purpose, so that all apparatus can after a while be removed.
Excisions, like amputations, may be practised and the general methods learned on the cadaver, but their actual performance in the presence of extensive disease will be found to be a different procedure from that learned upon the dead body. For reasonably representative cases typical operations can be devised, with explicit directions. It is not advisable to try to do such work through too short incisions. A long incision heals as kindly as one shorter and affords more room for operative work. The incision should be so planned and executed as to afford the maximum of exposure with the minimum of damage to important structures. The region of the great vessels is avoided in all the classical operations, while nerve trunks, if exposed, are retracted and kept out of harm’s way. After the knife has once laid open the joint it is used but little except for the division of resisting structures, e. g., ligaments. The greater part of the work is then done with elevators, or periostomes with reasonably sharp edges and sufficiently broad surface, so that the periosteum can be divided with the latter and separated with the former to the necessary extent. Obviously epiphyseal junctions should be spared whenever possible, especially in the young. To remove an entire epiphysis is to materially impair the later growth of the limb. In some of the most serious cases it will be found already loosened and lying as a sequestrum in the joint cavity. In this case it may be easily lifted out of place. Tendons should never be divided unless absolutely necessary. Incisions in their neighborhood should be so planned as to be parallel with their direction and permit their displacement without division. The sharp spoon should be employed for curetting the interior of a joint capsule or cleaning out a bone focus (erasion). A capsule involved in tuberculous disease should be completely extirpated. Diseased bone ends should be sufficiently exposed to permit of the use of an ordinary saw or a chain or wire saw.[34] Considerable force will often be necessary in making bone ends accessible for this purpose. The chisel is rarely used except in cases of bony ankylosis, where it is not possible to force bone ends through the opening in order to attack them with the saw. As remarked above, clean cases may be closed without drainage. Visible vessels should be secured, and, while a certain amount of oozing may be expected, if the part be enclosed in suitable compressive dressings and elevated, it need not cause alarm. The gentle application of an elastic bandage for three or four hours may afford additional security. It should not, however, be allowed long to remain. The terminal portion of the limb will always afford an indication as to the condition of the circulation. Should it become cyanotic or cold the dressing should be renewed and the wound examined promptly.
[34] Wyeth’s “exsector” is an admirable substitute, especially at the shoulder and hip.
—A longitudinal incision suffices for most cases (Fig. 214). This may be made posteriorly between the fibers of the deltoid or anteriorly and externally over the bicipital groove. It is better to separate the deltoid fibers than to divide them, although they may be divided. Should the straight incision afford[410] insufficient room another incision at right angles will afford ample access. The capsule, having been exposed, is opened, the wound widely separated with retractors, the arm rotated through a wide arc, while with a stout knife the capsular ligament and the various muscular attachments around the neck of the bone are divided. The greater and lesser tuberosities, with their muscles undivided, should be retained, when circumstances permit. The head of the bone, being freed, is dislocated and forced out through the wound, where it may be seized with large forceps and removed with a saw. The higher the bone is divided the better. Every other consideration, however, should be sacrificed to removal of all foci of disease. The capsule may then be extirpated and the glenoid cavity thoroughly cleaned out with a sharp spoon. Should the case be one of serious infection it is advisable to make a posterior opening, even through the deltoid, for purposes of thorough drainage. The greater part of the first incision is to be closed with sutures, the arm dressed in a comfortable position, with the elbow at a right angle, and the patient allowed to be up and around as soon as he feels in the mood for it.
Fig. 214
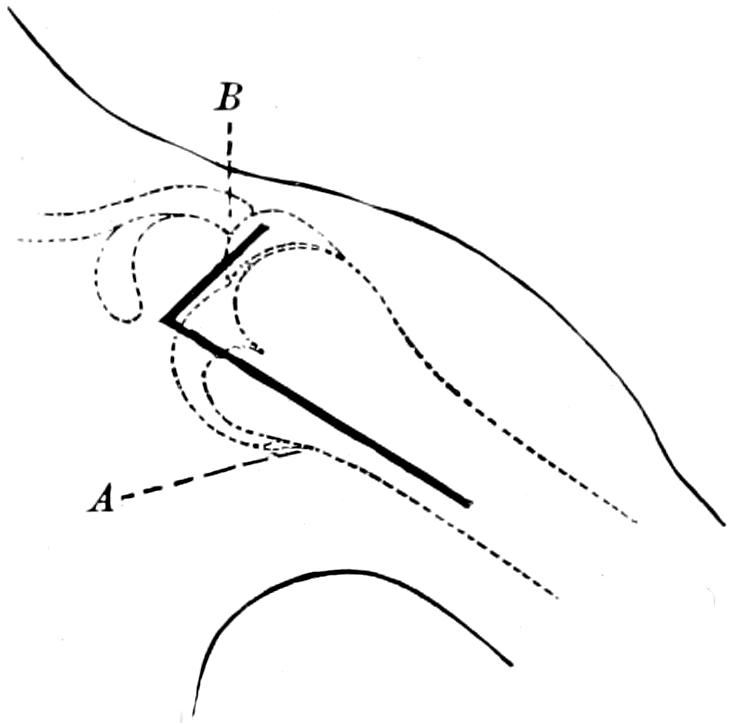
Excision of the shoulder: A, regular incision; B, supplementary. (Ollier.)
—Here a variety of methods have been advised, and the extent of the operation must depend, to some degree at least, on the nature and extent of the condition which necessitates it. Partial excisions have been recommended, though in the writer’s experience incomplete operations often give less satisfaction than those which are complete. However, when it is a question of removing callus or displaced bone fragments, which, after fracture into the joint, impair its function, then partial resections may be serviceable.
Fig. 215
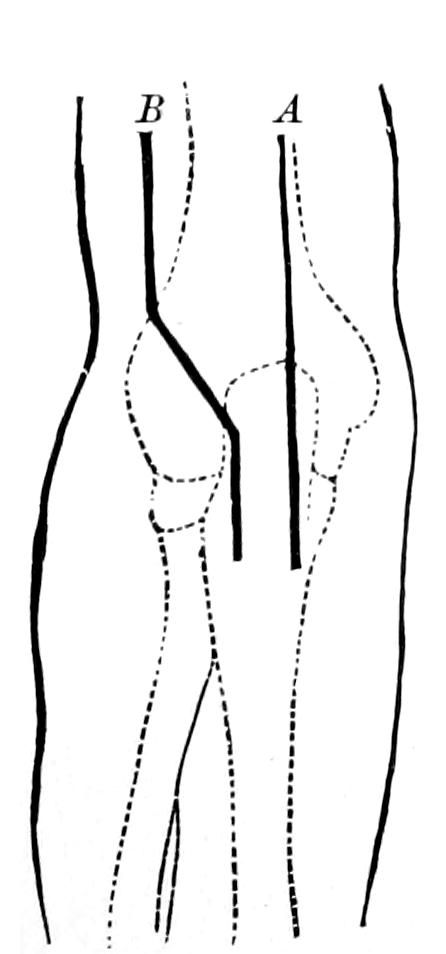
Fig. 216
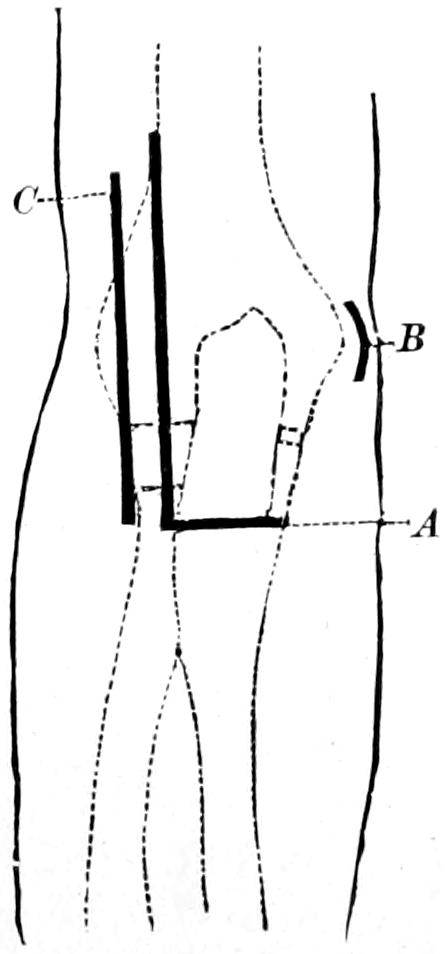
Fig. 217
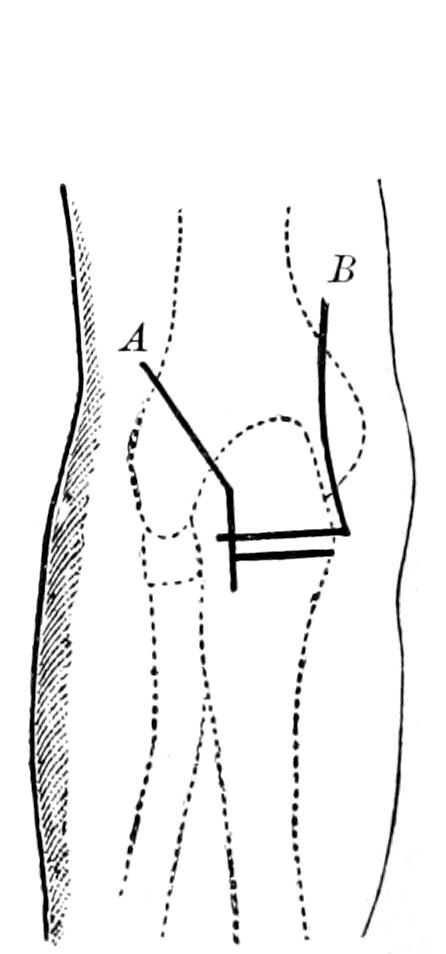
Excision of the elbow-joint: A, von Langenbeck; B, Ollier.
Excision of the elbow-joint: A, Nélaton; B, C, Hueter.
Osteoplastic method: A, by external incision; B, von Mosetig-Moorhof.
The essential incision is a long posterior one, which may be somewhat modified (Figs. 215, 216 and 217). It is essential here to avoid the ulnar nerve, which passes between the internal epicondyle and the olecranon, and the vessels and nerves in front of the joint. If it be made an inviolable rule to always keep close to the bone both of these dangers may be avoided. Ligamentous and muscular structures, among the latter the anconeus, should be spared as much as possible. After separating the joint surfaces thoroughly, by forced flexion, it is usually easier to force out the lower end of the humerus and first remove it, after which the upper ends of the radius and ulna are exposed and removed.[411] When there is bony ankylosis it is preferable to divide the bones of the forearm first. The tendon of the triceps is not only detached from the olecranon, but divided by the first long incision. After concluding the incision, the capsule, if it remains, is to be closed with chromic catgut sutures and the end of the triceps tendon or some of its periosteal attachment united to the periosteum of the upper end of the ulna.
The arm is now fixed in the right-angle position and held comfortably to the body by a suitable sling.
—It is rare that in disease of the wrist-joint this is found to be limited to a single bone of the carpus. Should an x-ray examination indicate such limitation then the focus can be exposed and cleaned by an incision upon the dorsum of the wrist, where it may seem best adapted for the purpose. Suppurative and tuberculous affections of the wrist usually necessitate removal of the carpal bones, including, possibly, the lower extremities of the ulna and radius. When the wrist-joint is involved it may be sufficient to remove the latter with the first row of the carpus.
Fig. 218 illustrates the incisions to be recommended for wrist resection, of which the Langenbeck line is to be preferred. Occasionally two lateral incisions, with through drainage, will better serve the purpose. It may be necessary to divide the short radial extensor, but this may be united again with suture. In most instances it is possible to retract the tendons to either side and thus clear the carpal region. By hyperextension the extensor tendons are relaxed and more room is thus made. The incision marked “A” combined with that marked “B” in Fig. 218, affords the best exposure when disease is extensive. The incision along the inner border of the wrist is made 5 Cm. above the styloid process of the ulna, and between the latter and the ulnar flexor down to the middle of the last metacarpal bone. Here the tendon of the latter muscle should be divided at its insertion and lifted out of its groove in the ulna. The collection of extensor tendons is then separated from the back of the wrist and lifted up, it being usually necessary to divide the unciform process of the unciform bone with forceps. The knife should be kept from the palmar surfaces of the metacarpal bones in order to avoid injury to the deep arch. After dividing the anterior radiocarpal ligament the carpus is extirpated through the ulnar incision. The ends of the ulna and radius are now easily accessible for removal with forceps or a metacarpal saw. The same is also true of the proximal ends of the metacarpals. After spreading the hand and forearm upon a flat splint drainage can be made to the desired extent and the wound closed.
Fig. 218
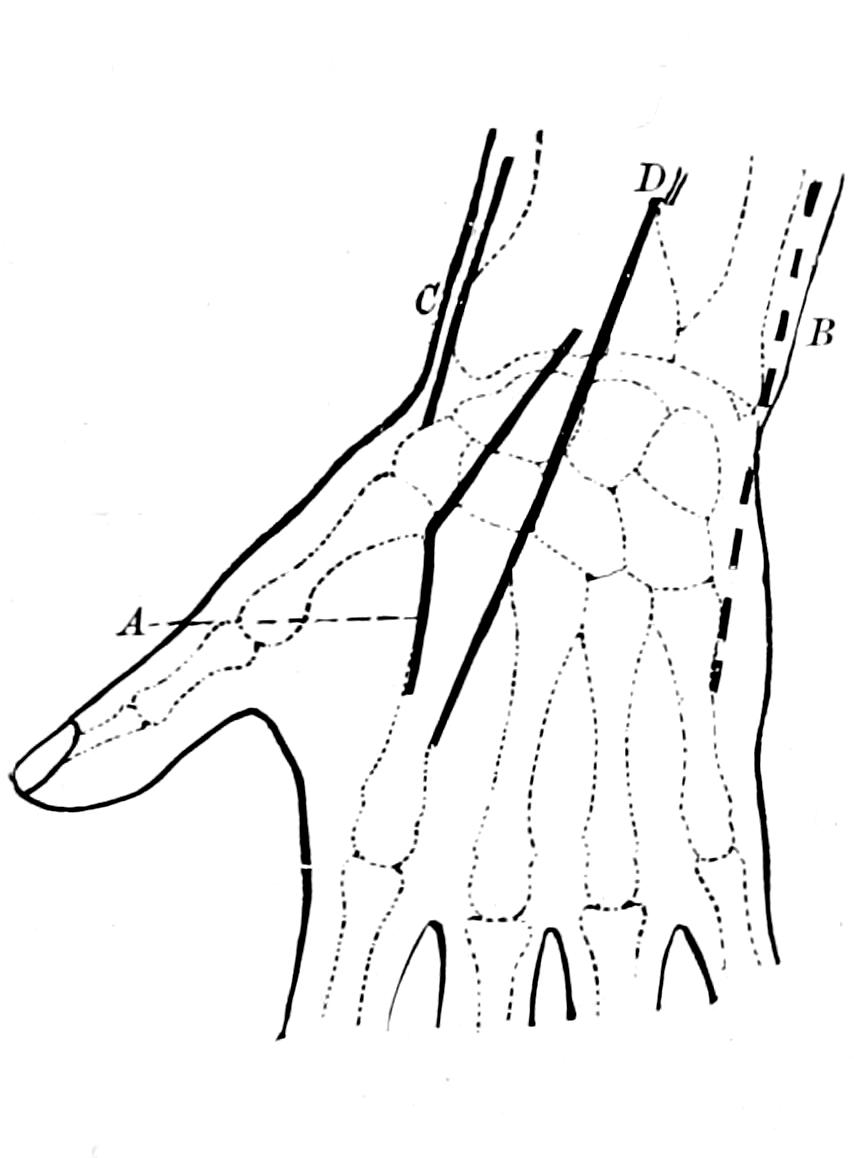
Excision of the wrist: A, Lister’s radial incision; B, Lister’s ulnar incision; C, Ollier; D, von Langenbeck.
Fig. 219
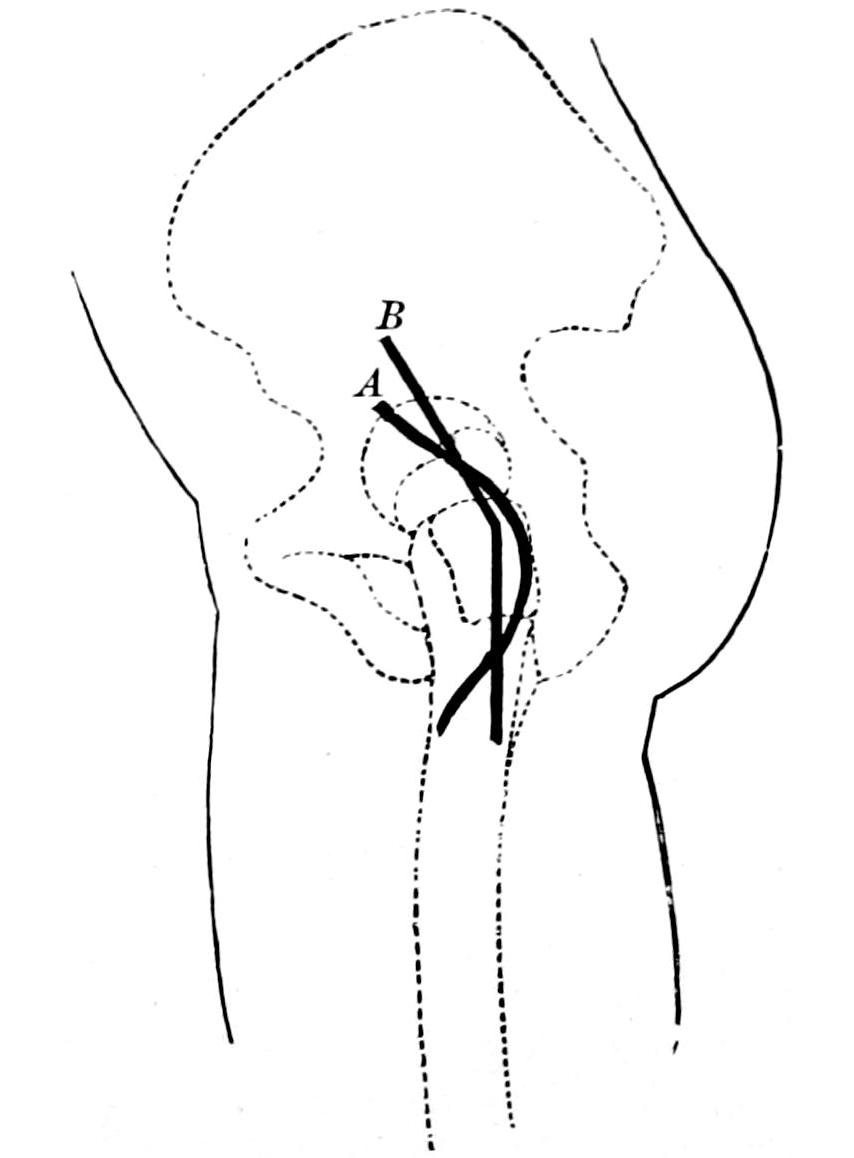
Excision of the hip: A, Sayre; B, Ollier.
[412]
So far as the hand and fingers are concerned little resecting need be done, the surgeon usually confining himself to the removal of sequestra or curetting of carious bone. In cases of compound comminuted fracture bone fragments may be removed; only in cases of lost or destroyed phalanges will amputation be necessary.
—In its structure the hip-joint is one of the simplest in the body. Although it lies deeply it is easily made accessible. Fig. 219 illustrates the incisions by which the joint is attacked for the purpose of exsection. If necessary either extremity of the incision can be extended or enlarged by a cross-cut. When the joint is disintegrated by disease, especially when partially dislocated, the parts will lend themselves to an easy and simple operation. When, however, the operation is done for ankylosis or for disease, by which great thickening and fixation have been produced, the measure may become difficult. For ordinary purposes the simplest method is to drive a sharp-pointed, strong-bladed knife directly down upon the neck of the bone from a point midway between the great trochanter and the crest of the ilium; then keeping the knife-blade in contact with the bone the incision is carried downward over the trochanter and along the shaft to a length making it sufficient for easy exposure of the bone and of the joint. Nothing is gained in these cases by trying to work through a short incision. A long one heals as readily and makes the operation more simple. It is as easy to make the entire incision in one cut as to divide the muscles layer by layer. The capsule of the neck of the femur being exposed by a wide retraction of wound margins, it is necessary next to divide muscular attachments to the great trochanter by raising the periosteum to which they are attached and saving both. To expose these insertions the femur should be rotated inward and outward, while the capsule is at the same time divided. The ligamentum teres, which offers a theoretical obstacle, usually disappears in the presence of any active disease and is scarcely ever encountered; it can be divided with curved scissors. Now by more or less powerful effort, including flexion and adduction to the extreme limit, with more or less rotation, the head of the bone is forced out from its socket and through the wound. Whether the bone should be decapitated with chain saw, metacarpal saw, or by the exsector of Wyeth will depend partly upon the freedom with which it can be exposed and on the equipment of the operator. It may be advisable to divide the neck with a chisel. The trochanter major should be preserved whenever its removal is not made imperative by the progress of the disease. The head and neck of the bone having been removed, the acetabulum is now more or less easily exposed, especially with retractors, and it should be cleaned with a sharp spoon. The capsule also should be removed, at least when the operation is done for tuberculous or other infectious condition. It is advisable to irrigate, then to wipe dry all the original joint surfaces and raw bone, and finally to cauterize either with pure carbolic or with zinc chloride, which should be washed away with the irrigating stream, the intent being to close the mouths of all the absorbents and prevent absorption from fresh exposure. Sinuses if present should be thoroughly excised, scraped, and treated in the same way. A drainage tube is usually preferable to the use of gauze.
The above is the method usually relied upon for hip exsection. Other methods have been devised, especially by anterior incision; of these the best probably is that of Barker. The cut is made along the outer border of the anterior surface of the sartorius and rectus, and through it the femoral neck is reached. By wide retraction the anterior surface of the joint can be completely exposed and opened, and through this opening the neck of the femur can be divided with a chain saw or chisel, before removal of the head from the acetabulum. The disadvantage of anterior incision is that pertaining to drainage. Nevertheless this can be obviated with capillary drains. Its advantages are that splinting and protection can be more perfectly effected, with less necessity for frequent interference. In other words it makes the subsequent care of the patient easier. Many English surgeons are in favor of it. Ollier devised a so-called osteoplastic excision, made through a curved incision with a downward convexity, the top of the great trochanter being exposed and divided with a chisel sufficiently to permit of its being turned up with the flap, and then being reunited to the main part of the bone after the removal of the neck and head. This method has its advantages in a limited number of cases, but it has not become popular in this country. It would seem to be an advantage to preserve the trochanter, although some surgeons remove it. So long, however, as disease is confined to the head and neck of the bone it is unnecessary to remove this projection.
The after-care of a hip excision is not an easy matter. Most surgeons prefer to maintain[413] the limb in position by the aid of traction, with sufficient weight to overcome all muscle spasm. If the case be such that dressings need only be made at long intervals, then it matters little, but in a septic case in which there is considerable discharge the problem is sometimes a serious one. Various beds or suspension splints have been devised, consisting essentially of frames with cross-strips of stout material, upon which the patient lies. After raising the frame one or two of these strips are released and the parts exposed. This arrangement also permits of the easy management of a bed-pan. In young children a wire splint with a fenestrum, or a plaster-of-Paris spica or breeches with large opening cut opposite the wound, will often be serviceable. The tendency is rather toward adduction, and this should be overcome. Something will depend upon whether the surgeon is working for ankylosis or for a movable joint. In the former case a rigid dressing should be employed as soon as the condition of the wound permits. In the latter passive movement should be begun as soon as the wound is healed.
While the operation is usually performed quickly, and is not regarded as serious, it nevertheless has a considerable mortality, especially in the young and the aged, because of the conditions which necessitate it. After a complete exsection, even by the most ideal method and in the most ideal case, the limb remains somewhat shortened. This may be compensated by raising the heel of the shoe worn on the affected side. In severe cases it may be necessary to supply even two or three inches of artificial support for this purpose. Unless this is done compensatory spinal curvature will ensue.
Fig. 220
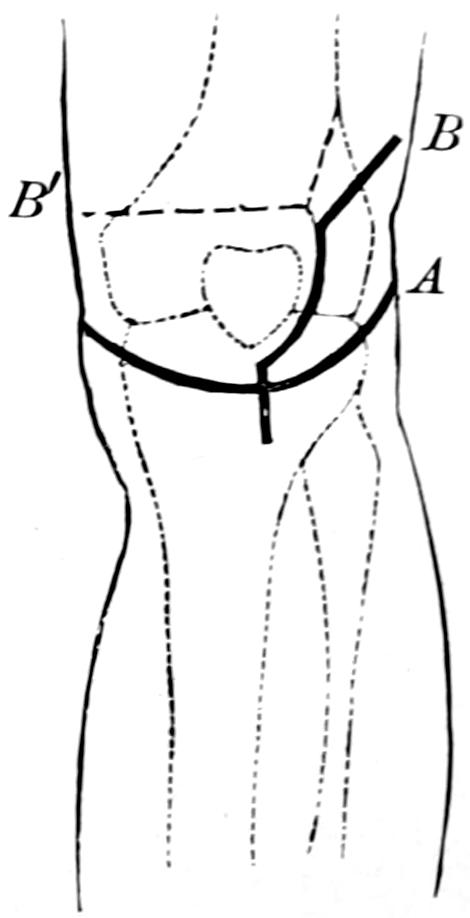
Excision of the knee-joint: A, semilunar incision; B, Ollier’s incision.
—The knee is generally more accessible for operation than the elbow, as the important structures which should not be disturbed lie grouped upon its posterior aspect. Protection for one of these is protection for all, and the freedom with which the joint may be opened makes it especially easy to do either complete or partial operation. Here the surgeon should endeavor to preserve the epiphyses, especially in children, as they have much to do with the growth and length of the limb. So long as incision is confined to the anterior aspect of the joint it can be made in almost any manner. The usual method is that represented by line A in Fig. 220, by which a horseshoe flap is raised and the joint interior exposed. Occasionally the direction of the flap is reversed, and it is turned downward rather than upward. In the former case the ligamentum patellæ is divided; in the latter, the tendo patellæ. Whichever way the flap is turned it is made to include the patella, although this bone can be removed at any time. The lateral ligaments being divided, as well as the crucial, and the limb completely flexed, exposure of the joint surfaces is made. It is now possible to do an arthrectomy, a partial exsection or a complete one, according as the disease is more or less extensive. In the complete operation the articular surfaces of the femur and of the tibia are usually removed with an amputating saw. If this be introduced from the front and made to work its way backward the popliteal vessels should be amply protected against possible injury. Here it should be borne in mind that the leg is not constructed in a straight line, but that there is a lateral angle at the knee, as the femurs diverge as they pass upward, and this angle should be imitated in directing the saw and removing the bone end. Again, a slight bend anteriorly will make the limb more useful than one which is absolutely straight. The intent thus should be to give the knee at a slight angle anteriorly and interiorly, and the saw should be manipulated with great care. In a complete operation the patella is also removed. In tuberculous and other septic disease the capsule should be completely extirpated. This offers no difficulty, save at the posterior surface, where it may approach closely to the region of the great vessels.
Various modifications have been practised in these operations. Some open the joint by straight cross-incision with division of the patella, the latter being reunited with tendon or wire sutures. Others have practised a more complicated H-shaped incision, the transverse portion being carried either through the patella or just below it. The line marked B in Fig. 220 was suggested by Ollier. It is questionable whether any of these methods offer any advantages over the one first described.
After exsection it is desirable to maintain the bone ends in an accurate position if[414] speedy reunion be desired, and for this purpose various methods are in vogue. The bones may be drilled and fastened together with tendon or wire sutures, or ivory nails may be driven in, one on each side, directing them obliquely, so that displacement cannot easily occur, or metal nails may be used for the same purpose. Another plan is to insert two long metal drills, one on either side, which perforate the skin two or three inches above the wound, and are passed downward and toward the other side so as to fix the surfaces, as it were, by a cross-forked arrangement. After two or three weeks these drills may be withdrawn. Fixation of this kind is advantageous, for when complete excision has been practised the surrounding tissues are lax and the parts are not easily held in position by external dressings alone. In a clean case, with careful hemostasis, very little drainage will be required. What is needed can be provided by an absorbable drain passed through the lower portion of the wound on either side. In a septic case it would be well to provide for ample drainage on each side.
The limb may be dressed upon a fenestrated wire or gauze splint, which is easier when frequent change of dressing can be foreseen, or it may be immobilized in a plaster-of-Paris splint.
—The ankle is usually reached by an incision on either side, three or four inches in length, extending from above each malleolus downward and forward on to the tarsus. The knife-blade should be forced to the bone, so as to divide the periosteum, which is subsequently separated and lifted by an elevator, in order that the operation may be made subperiosteally. The fibula is usually first divided, with a chain saw or a chisel, an inch above its tip. The divided fragment is wrenched from its place with forceps, and severed from the ligaments by knife or scissors, being careful not to injure the external lateral ligament. The inner incision is made in practically the same way, the periosteum separated, the internal lateral ligament divided, and the end of the tibia forced through the incision by everting the foot. Its joint end may be removed with a saw, dividing on the same level and plane with the lower end of the fibula. Through the gap thus made the astragalus may be either removed or its upper surface divided with a metacarpal saw. The fresh bone surfaces left in this way will unite and ankylosis will result, unless fibrous or muscular tissue be interposed to favor the formation of a false joint.
As in other operations methods may be varied to meet the exigencies of certain cases. Longitudinal incisions may be placed farther forward than indicated above, as is shown in Fig. 221, which illustrated König’s method. Here the bone surfaces are divided with broad chisels. A transverse incision of the front and upper part of the ankle may be made, through which the tendons are exposed, lifted in a group out of harm’s way, and curetting and bone sawing performed. Kocher makes a semilunar incision from the outer border of the tendo Achillis to the outer border of the extensor tendons, its line passing beneath the external malleolus. By this method the joint is opened and the peroneal tendons divided, their ends being reunited after the completion of the balance of the work. This method is usually applicable in children.
Ample drainage is required in these cases, for the operation is seldom performed in the absence of septic complications. The foot should be kept in proper and right-angled position by metallic splints, or by plaster of Paris, the latter preferable, fenestra being cut in order to make access to the wound.
—Removal of the tarsal bones is confined usually to cases of tuberculous disease, and may be performed by a variety of methods. Thus the tissues of the sole of the foot may be divided transversely by an incision carried from the tubercle of the scaphoid beneath the sole and across to a point one inch behind the base of the metatarsal. Through this, access can be made to the inferior surface of the tarsus. Conversely the upper portion may be exposed by a similar transverse incision across the dorsum of the foot, by lateral incisions, or by a combination of both. It is seldom necessary to divide the tendons, it being nearly always possible to gather them into a group and lift them out, while the bones are attacked with a sharp spoon or a chisel.
Occasionally the calcis becomes involved in cancerous or tuberculous disease and it would appear that removal of the heel proper would be all that is required. To meet these indications Wladimirov, in 1871, and Mikulicz, in 1880, independently devised a method by which the ankle-joint may be opened and as much of the heel and adjoining tarsus as necessary removed, the foot being later fixed in the extreme equinus position.[415] This is referred to as osteoplastic excision or amputation of the heel. Fig. 222 illustrates the line of incision, which extends from the tubercle of the scaphoid beneath the heel to a point on the opposite side, then obliquely upward and backward to the base of each malleolus, and then transversely and posteriorly, thus including within its line the region of the heel. These incisions extend to the bone, the ankle-joint is opened posteriorly, the lateral ligaments divided, the lower extremities of the tibia and fibula removed with a saw, the astragalus and calcis separated from their attachments, and the posterior articular surfaces of the scaphoid and cuboid also removed. The lines of division of bone are indicated by dotted lines in Fig. 222. Thus the lower ends of the leg bones are brought into contact with the upper end of the divided tarsus by straightening the foot in the extreme equinus position and maintaining this position with wire sutures or bone or metal pins.
Fig. 221
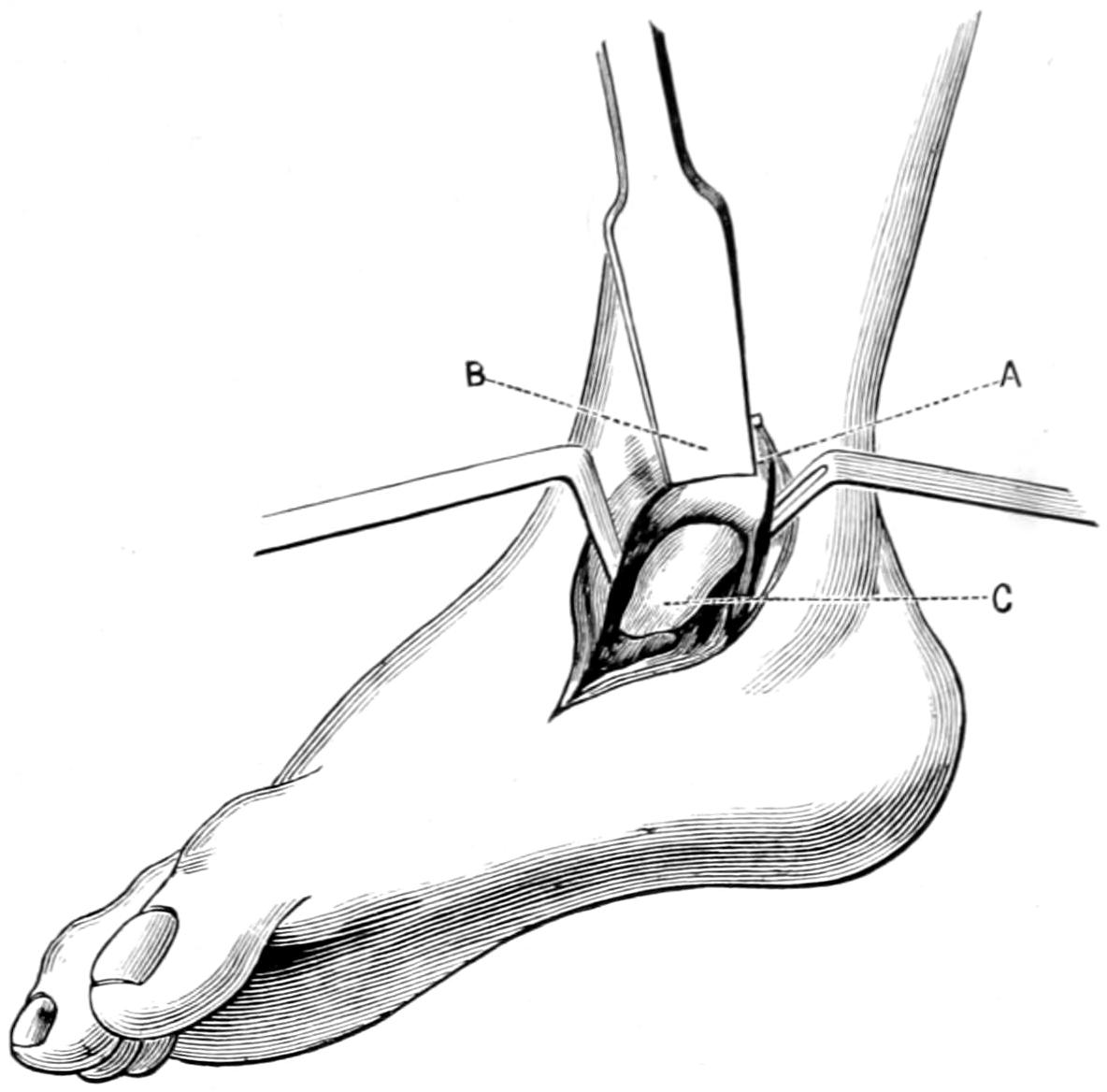
König’s incision for excision of the ankle.
Fig. 222
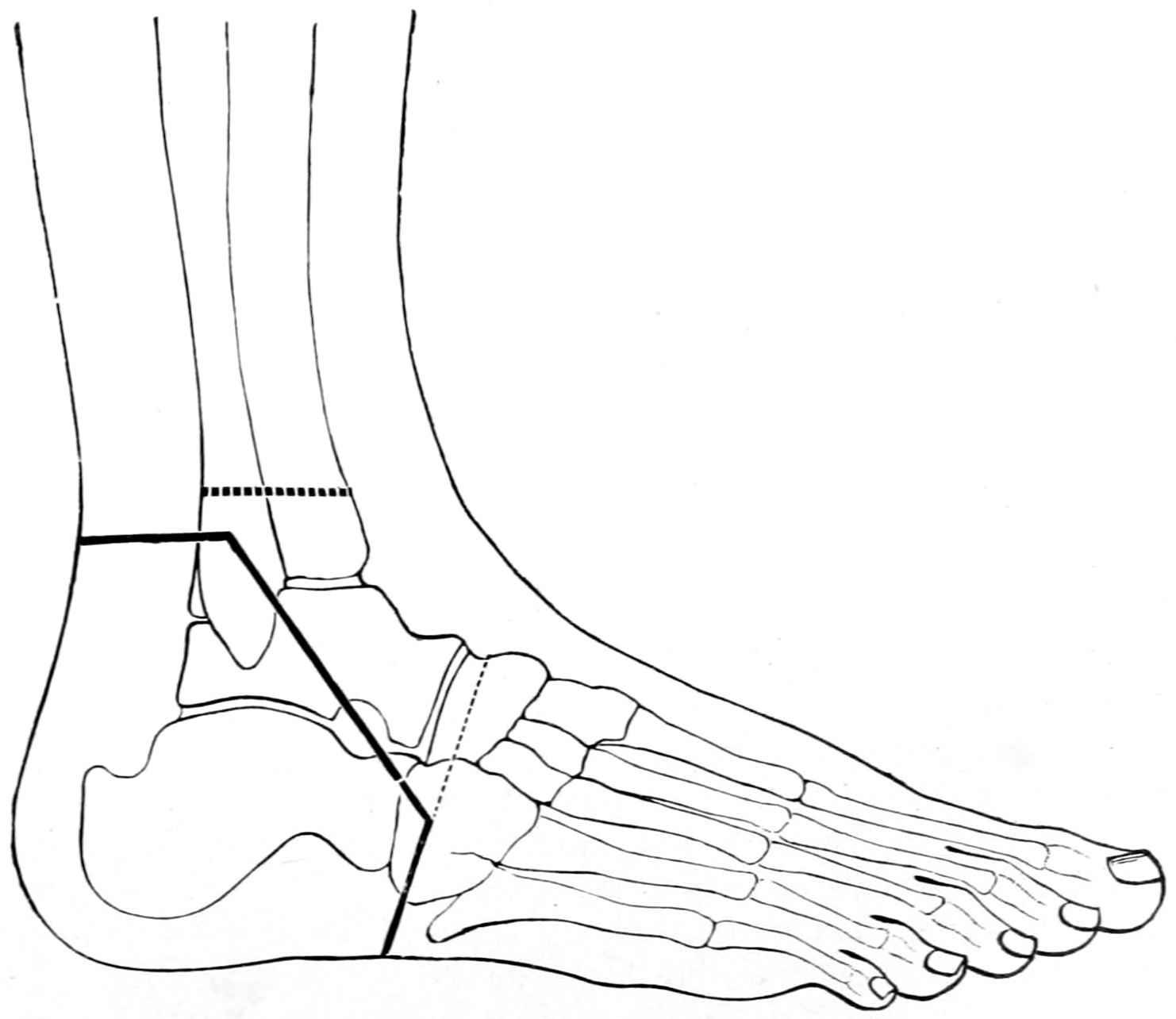
Osteoplastic excision of the foot. (Mikulicz.)
The cases in which this method is of use are rare, but when indicated it has usually given satisfactory results. It is a substitute for amputation of the leg, and it is often an open question as to which will give the most satisfactory result. It has probably not been practised a hundred times.
[416]
At the outset of a study of surgical diseases of the osseous system it is necessary to emphasize a fact which students and young practitioners are liable to forget, namely, that bone, even the densest, is a tissue, and that as such it is liable to infection, suppuration, gangrene, etc., just as is any other tissue; that all infectious processes are identical in general character, their gross manifestations varying only by virtue of the peculiar characteristics of the tissue in which the infection occurs. Bone is vascular, and even that exceedingly hard variety, which is met with in the petrous portion of the temporal, or the ivory exostosis, has sufficient connection with the vascular system to permit of its proper nutrition. The firmest and hardest bone will bleed when divided or injured, and any tissue which will thus bleed can react injuriously to various irritants.
All bone-marrow begins as red marrow, with 1 or 2 per cent. of fat, and ends by becoming yellow, with 60 or 70 per cent. of fat, and whether this change shall take place suddenly or rapidly depends upon diverse conditions. Many years ago it was claimed by Bourgery that bone is simply a large cavernous arrangement where stagnation of the blood current favors the deposition of fat. Fatty alteration progresses from periphery to centre, and the bones of the hands and feet undergo fatty alterations before those of the trunk and pelvis. In other words, the truncal skeleton remains as “red bone” longer than the balance of the osseous system, and he whose sternum has become a “yellow bone” should have reached a ripe old age. In long bones distal extremities first become fatty. Individual peculiarities seem to govern these changes. Thus the neck of the femur will sometimes be fatty and friable at the fortieth year, or reasonably firm and still red at the eightieth. This fatty condition is not to be confounded with true osteoporosis or rarefaction in bone, though it is often associated with it. When the two conditions are combined we have osteoporosis adiposa. Into this condition immobilized limbs pass more easily than those which are used. Their weeks have been equal to years of ordinary inactivity. Red bone seems to be too highly vascular to be a favorite site for tubercle, and distinctly yellow bone too non-vascular. Consequently bone tuberculosis is less often seen at the extremes of life. White bone, as those who make anatomical preparations call it, is most favorable for tuberculous infection on account of its minimum contents of blood and fat. These bones come from phthisical subjects.
This condition was never accurately recognized until described by Chassaignac, in 1853, and even he missed many of its distinctive features, although he gave to it a most descriptive name, “typhus of the limbs.”
—The disease is a distinctly infectious process, limited sometimes to the bone-marrow and internal portion of the bone, sometimes apparently involving every particle of the osseous structure. Its onset is sudden, its manifestations acute and serious, and its ravages, when not promptly checked, most extensive. The following more or less distinct varieties may be distinguished:
It is known that the virulence of cocci growing under pressure is thereby much enhanced; hence the extreme rapidity of some of these disease processes may be thereby better explained.
PLATE XXXV
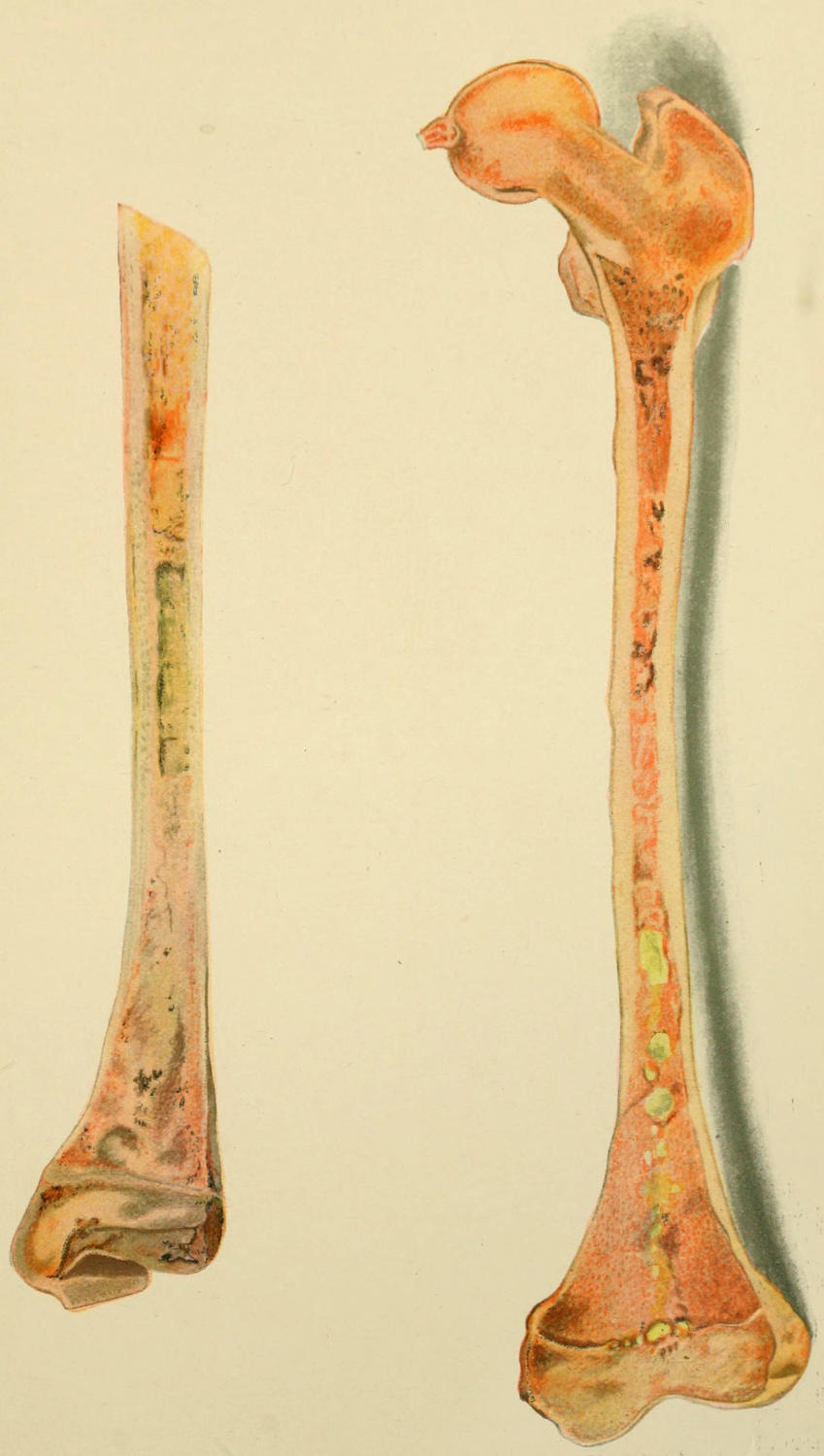
Acute Osteomyelitis, showing Purulent Foci and Accompanying Disturbance (Kocher.)
[417]
Fig. 223
Typhoid infection of bone; focus in rib. (Lexer.)
The mechanism of the infection and the lesions produced by the organism are essentially similar, and may be described together. These consist of rapid thrombosis, coagulation necrosis, and suppuration, along with the local destruction incident thereto, and with unlimited possibilities in the way of auto-intoxication from the local lesions and from the disturbance of the general economy and interference with excretion. Every severe case is accompanied by more or less of general septic intoxication, presumably from the ptomaine produced by the bacteria, while in many instances, particularly those where the bacteria at fault seem extremely virulent, the intoxication is overwhelming and the course a rapidly fatal one. Death has been known to follow within thirty-six hours after the first symptom of an acute osteomyelitis. For the average case three more or less distinct stages can usually be distinguished: first, a period of purulent infiltration, with the formation of local foci in the bone-marrow and speedy secondary involvement of the periosteum and synovial membrane; second, a period of sequestration or formation of a sequestratrum inside of an abscess cavity; third, the stage of repair.
—During this period there occurs violent inflammatory infiltration, localized areas becoming at first hyperemic, then infiltrated with hemorrhagic exudate, whose rapidity of production will indicate the intensity of the infection. Often at the same time are found enlargement of the spleen and hemorrhagic exudations in distant serous cavities, such as the pleura and pericardium. The locally infected areas of bone-marrow break down into collections of pus, which spread either toward the epiphyseal line or else along the Haversian canals toward the periosteum, which becomes both infiltrated and loosened. The loosening is particularly marked about the shafts rather than the joint ends, while, as a rule, that end of the bone toward which the nutrient artery is directed is the one whose epiphyses are first loosened. Nevertheless about the knee it would seem as though the lower end of the femur and upper end of the tibia are the particularly predisposed localities.
In many instances obliteration of nutrient vessels and thrombosis are early features. The area of separation of the periosteum is usually an index of the extent of deep destruction. From the periosteum the infection may extend toward the covering of the soft parts, in which case there may be a parosteal abscess, or it may perforate toward the joint cavity, leading quickly to pyarthrosis and destruction of joint structures. It would appear in children, particularly, that the epiphyseal cartilage often forms a barrier to the advancement of the lesion in the direction of the joint, and thus it happens that we have acute necrosis of the shaft of a long bone, with perforation through the periosteum at both of its ends. In adults this takes place less often, the joint ends being often primarily involved. Softening and separation of cartilages are usually secondary to the other processes. It is possible even to have the primary infection in the joint end proper, and extension therefrom to the epiphyses permitting of epiphyseal separation and extrusion of this fragment as a sequestrum. This separation occurs in many instances rapidly and before the attendant is aware of what has happened.
—The second stage includes, coincidently with the occurrence of suppuration, the proliferation of considerable granulation tissue, by which more or less protection is afforded; also, when time is afforded, the rapid formation of new bone, whose effect is to wall off the scene of conflict and death from the surrounding tissue, by which event prognosis, so far as the patient’s life is concerned, is improved. Intra-osseous abscesses may quickly coalesce, and the result may be one long tubular abscess extending through the shaft. At other times both bone-marrow and the cancellous tissue are bathed in pus, while if the periosteum have been totally separated the consequence will be a sequestrum whose dimensions correspond with those of the shaft. When periosteum is not loosened the necrosis will probably be central and more or less circumscribed. (See Plate XXXV.)
—The third stage is the period of efforts at spontaneous repair. There is a natural effort toward elimination of the sequestrum by the process of softening or liquefaction in the direction of least resistance. This process may extend over months, when surgical relief has been delayed, and may be accompanied by so much other disturbance as to completely ruin a bone or limb for further use. In neglected cases several[418] sinuses may lead down toward the central sequestrum. On the other hand, once this sequestrum of eliminated an extraordinary amount of activity is usually displayed in the direction of repair (Fig. 224).
Fig. 224
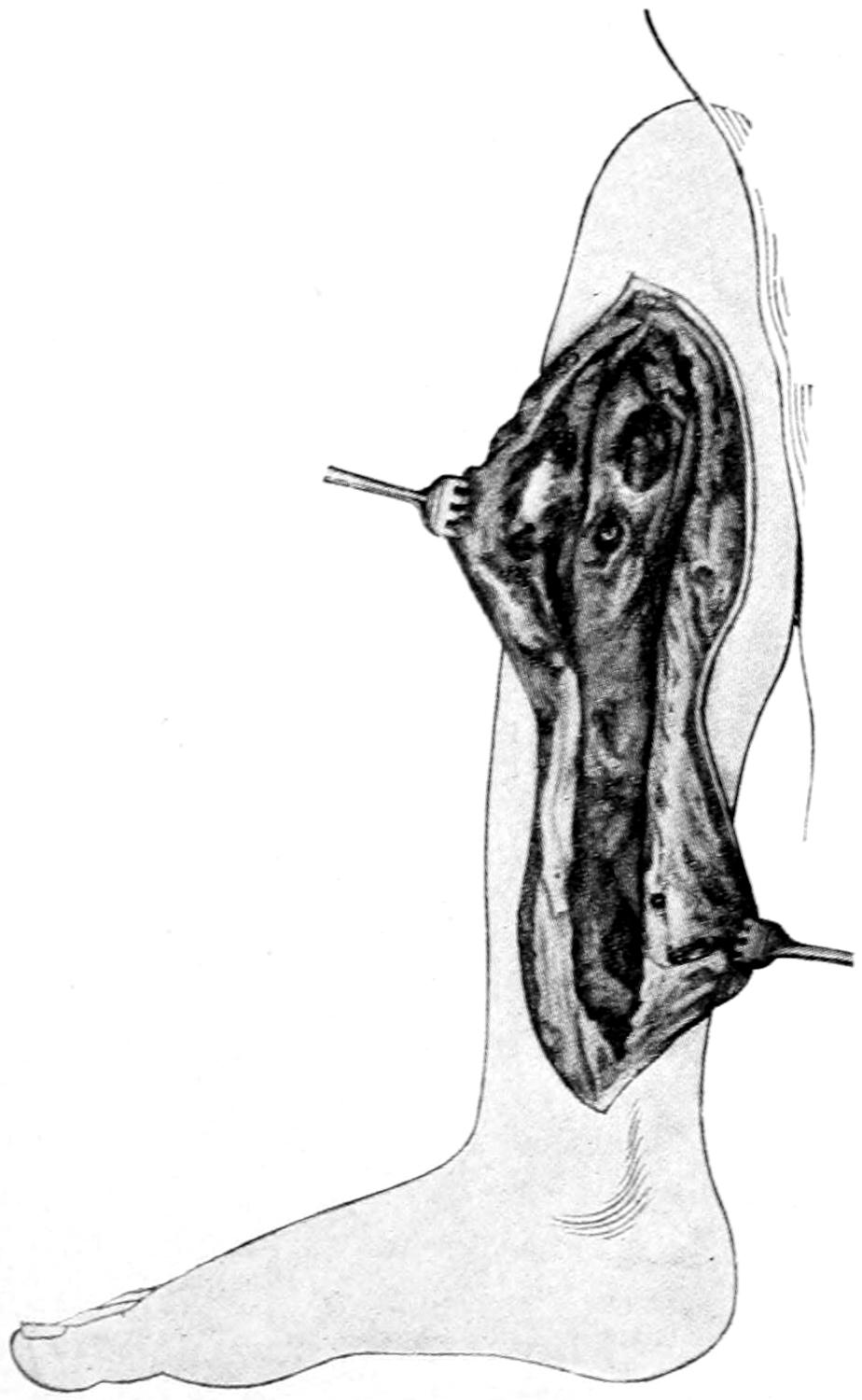
Acute necrosis of tibia, with formation of cloacæ for affording opportunity for escape of sequestra. Illustrating also the extensive openings which necrotomy may necessitate. (Lexer.)
—In a general way the signs and symptoms of acute infectious lesions in bone are strikingly similar, and are significant when construed aright. Patients complain usually first of exhaustion, followed by pain, which may become agonizing. This is often accompanied by an introductory chill with high fever, after which the general character of the disease assumes the typhoid aspect. Evening temperature may rise high and be followed by some morning remission. The spleen is usually enlarged, the primæ viæ disturbed, and often we have to do with a fetid diarrhea. In the young the sensorium is early affected and children soon become delirious. The pain, at first vague, quickly focuses in the particular bone or bones most involved, and as it increases in intensity there is a significant tenderness. Ordinarily there appear early reddening and swelling of the affected parts. With all these evidences there is also a characteristic muscle spasm, by which certain posture signs will be produced, varying with the bone involved. Pain is always intensified by the slightest degree of disturbance. In consequence the limbs (for it is the limbs which are usually involved) are contracted, and every effort to overcome the contractures is followed by aggravated pain. The more acute the pain the more vivid the external evidences of inflammation and the edema of the parts, especially below and about the lesion. Thus it may happen that within forty-eight hours there may be swelling and edema of the part involved, which should be regarded as pathognomonic.
A little later, superadded to the other signs of inflammation, there is fluctuation if parosteal abscesses have formed, or possibly the evidences of epiphyseal loosening or complete separation. When the disease is primary in an epiphysis the corresponding joint will be early involved, and the joint symptoms will assume the type of an acute purulent synovitis, but with more pain. It is probable that under few circumstances is complaint of pain more serious or aggravating than in cases of acute osteomyelitis of the fulminating type.
So far only local symptoms have been described. To these there should be added the list of those pertaining to thrombosis and metastatic infection, with their septic and disastrous consequences. The disease is frequently so acute and rapid that even within the first day or two not only are added extensive thrombosis in and along the bones, with rapid purulent degeneration and thrombi, but soon that even more serious general condition to which these lesions so easily give rise—i. e., unmistakable pyemia.
The general symptoms are common to the disease, no matter what bone be involved. Local symptoms will change in accordance with their location. While not so common, the flat bones, like the pelvis, cranium, and sternum, may be involved in active manifestations of this disease. The same is true even of the vertebræ, but, as a rule, it is in the long bones of the extremities that its ravages are most frequently seen.
—The prognosis depends upon the early recognition of the disease and prompt surgical relief. There is perhaps no disease less amenable to purely medicinal treatment, and if bones are to be saved in their entirety early and free incision is called[419] for. Consequently when the case is seen late it almost invariably entails necrosis, with more or less disturbance of function, or possibly such a serious condition as to call for amputation. The fulminant cases when not early recognized and promptly operated often prove fatal, and death has been known to follow within thirty-six hours after the onset of the first symptom, the fatal result being due to overwhelming septic infection, with thrombosis, etc. Almost every case, however, if seen sufficiently early can be saved.
—The complications are to be divided into the constitutional and the local. The former refer rather to the spread of septic infection and its more or less disastrous and remote ravages. Metastatic infections may produce serious or fatal complications, while, when less acute, important functions may suffer a serious impairment. Among the local sequels are to be considered mainly the results of destruction of bone tissue and neighboring joint structures. When the disease occurs in young and rapidly growing children partial or complete arrest of development in the bone involved is not infrequent. This may lead to inequalities in length of the femora or humeri. It may lead also to compensatory hypertrophy of bone, with perhaps considerable distortion during subsequent growth.
An entirely distinct consequence of osteomyelitis is bone abscess, in which the acuteness of symptoms has long since subsided, but in which a distinct local focus remains.
—The disease is an infection from the beginning, but the source of the infection is not always easy to trace. Two distinct causes seem to conspire to produce the majority of these bone infections—microörganisms of more than ordinary virulence, and a predisposing condition of the system, due sometimes to constitutional weakness or inherited taint, or to the results of exposure and fatigue. The causes of suppuration have been discussed in Chapter III. It is a fact, however, that the majority of cases occur in children and after a combination of exposure and fatigue—as, for instance, sitting upon the ice after being exhausted by skating—all of which would be inoperative to produce an infection were not the germs at hand ready to assail every tissue whose resistance is thus temporarily lowered.
The infection may occur from within or from without—from within perhaps through the alimentary canal or the respiratory tract, probably from the tonsils and the pharynx. Infection from without may occur through an abrasion or scratch, a blister upon the foot made by an ill-fitting shoe or by a skate-strap. These cases occur generally in the young, more often in boys than in girls, probably because in the former more opportunities for infection are permitted. Bone infections, however, are possible even in the newborn, in which case the infection may occur through the pharynx or through the umbilicus, while the local resistance may have been lowered by the injury due to mechanical delivery, turning, etc. In elderly people the disease is almost unknown.
—The disease for which this is most commonly mistaken is acute rheumatism. There may have been some excuse for this in the past because of the lack of general knowledge of bone infections; now there is none. The majority of cases of necrosis following osteomyelitis which have come under the writer’s observation were the result of errors in diagnosis.
Rheumatism is never followed by suppuration and seldom produces a septic type of disease; its painful lesions are rarely so painful as those due to osteomyelitis. Lesions of rheumatism are usually multiple; those of bone infection are mostly single. The first complaint of pain in the latter is generally along the shaft of a bone than at the joint end, while this is not true of rheumatism. Moreover in acute osteomyelitis the disease assumes from the outset a seriousness which is seldom approximated by acute inflammatory rheumatism.
—The treatment for acute osteomyelitis is essentially surgical. Anodynes may be necessary for relief of pain, but no time should be lost, when once the diagnosis is made, in making incisions to expose the bone involved, and then opening to its interior to relieve tension and to remove septic products. The incision over the femur or tibia, for instance, may be ten or twelve inches in length. The tissues will invariably be found edematous or infiltrated, with evidence of the proximity of pus; the periosteum will be thickened and infected, and between it and the bone, as well as outside of it, there may be collections of pus. If seen late the characteristic muscle appearances already described may be noted. The periosteum should be incised to the bone throughout the length of the incision, and then an ordinary bone drill may be used to perforate the bone for exploratory purposes. From the punctures in the bone[420] thus involved will exude purulent fluid, often sanious, thus indicating the condition within. A deep groove or channel should now be cut, opening into the marrow cavity, in which numerous foci will be found, or in which all distinctive structure of bone-marrow may be lost, the cavity being filled with pus. The pus cavity should be scraped and disinfected with hydrogen peroxide and cauterized with zinc chloride or its equivalent, and then packed, the wound being left open. Even this may not be sufficient, but if there be epiphyseal separation, or evidences of joint infection, the neighboring joints should be explored under aseptic precautions; if pus be found they should be opened, washed out, and drained. Meanwhile if in the soft tissues exposed by the incision the parosteal veins are found filled with septic thrombi, they should be opened as far as exposed and their contents removed.
These operations are often severe, but nothing in the way of operative treatment can be so severe nor so serious as the disease itself when left unoperated; the rule is stringent that every infected tissue, and especially every infected bone interior, should be exposed and cleaned out. Only in this way can lives be saved. Moreover, it is necessary to carry out this treatment in the fulminant cases as early as possible; and errors in diagnosis by which it may be postponed until metastatic infection or grave pulmonary and cardiac complications have set in are unfortunate. So long as the local indications are as above described, surgical treatment is desirable, whether the systemic complications are pronounced or not. The immediate effect of the operation having passed the relief thus afforded will often be so pronounced that within twenty-four hours patients may be out of danger.
Fig. 225
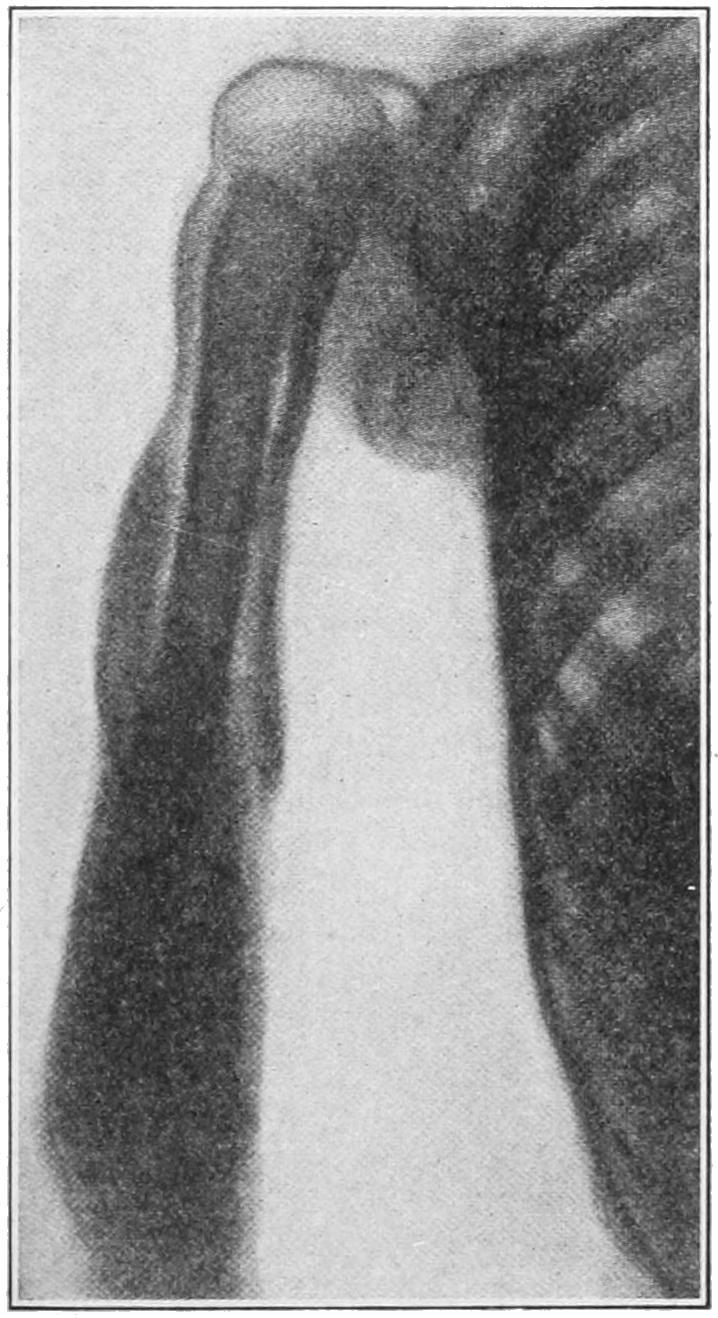
Total necrosis of humerus, as seen by aid of the cathode rays. (Lexer.)
The results of this operation are a wound which will discharge at first freely, and which so soon as septic material is out of the way will begin to granulate. Ordinarily no attempt should be made to close such a wound, though much may be done to favor rapidity of granulation. While some antiseptic dressing is always employed, it will be of advantage occasionally to change the character of the same, and to alternate between various antiseptics, the effect of any one drug being apparently lost after it has been used for some time.
There are some cases where an entire diaphysis or bone shaft will be found separated from one or both epiphyseal terminations, lying in a subperiosteal abscess cavity, bathed in pus, and dead beyond possibility of repair. This is total necrosis of the shaft from an acute infectious process, and is to be treated by complete removal of all dead and dying tissue. In the case of the forearm or leg it may be that the remaining bone, when only one is involved, as is usual, will be sufficient to maintain the integrity of the limb until new bone can be reproduced within the periosteal bed occupied by the old one. More or less complete regeneration of bone is possible, particularly in the young, and in connection with compensatory hypertrophy of the parallel bone will permit the restoration of the leg to partial or complete usefulness. On the other hand, should this later prove a complete failure, amputation and substitution of an artificial limb may be required.
When the disease has involved the articular side of an epiphyseal line, and when there is complete epiphyseal separation with consequent pyarthrosis, the probable consequence will be necessity for a complete or partial resection of the joint and the probability of subsequent ankylosis. Patients may find later that a modern artificial limb with its possibilities will be preferable to such a condition, and may readily consent later to an amputation which they would at first refuse.
—This is an infection of the same general character and type as the osteomyelitis just described, but refers to those cases where the disease apparently is confined to the periosteum and the outermost layer of the bone. In its[421] possibilities for harm it is scarcely less serious, although in its tendency to spontaneous perforation and escape of pus it is less likely to prove fatal.
—The causes and the general clinical manifestations are practically identical. The disease is perhaps less grave in its acute manifestations, the localization of pain more exact, with ordinarily less tendency to joint complications. Local tenderness is exquisite, and particularly in those bones which lie near the surface—e. g., the tibia—and early recognition of fluctuating areas is easy. It may be localized over a small area, or the entire periosteum of the shaft may be involved; in which case, so soon as pus forms and the periosteum is separated from the bone, there is probability of acute necrosis of the shaft. Here, again, there may be a tendency to mistake at least the first signs of the disease for acute rheumatism, from which it must necessarily be early differentiated as above.
—Here also there is the same necessity for immediate intervention, if possible before pus be formed, in order that there may be little or no periosteal separation and encouragement to necrosis. Anesthesia is necessary, with prompt incision, the use of the sharp spoon, and disinfecting agents: no attempt should be made to close the wound, but drainage should be favored in every way. The intensity of the pain is promptly relieved and the whole clinical picture immediately changed by such a procedure.
The ordinary bone felon upon a terminal phalanx is practically an expression of this type of disease, and experience corroborates the wisdom of deep and early incision, even in the case of so small a bone entity as a phalanx.
—This is a term applied rather indiscriminately to a form of acute osteomyelitis involving primarily and especially the epiphyseal lines, or to a condition of hyperemia and neurovascular excitement at epiphyseal junctions stopping short of suppuration, but giving rise to intense pain, muscle contraction, joint tenderness, etc. It is often seen at the upper end of the tibia. Sympathetic disturbance may extend even to serous effusion into a joint, although this is not necessarily the case. The limbs are early drawn up, and every attempt to extend them simply aggravates the distress. So long as there are no evidences of suppuration, it is sufficient in these cases to apply a sufficient degree of traction to overcome muscular contracture and to straighten the limbs. This should be applied first under anesthesia, and the patient kept under anodynes for a few hours thereafter. So soon, however, as the muscles are tired out by the steady traction, pain subsides, and the intensity of the condition may be thus relieved within forty-eight hours or less. It would be well to continue physiological rest and traction as long as there remains the slightest tenderness. Should evidences of suppuration at any time supervene, incision and evacuation of pus and exudate should be practised. Should epiphysitis occur in one of two parallel bones, there may result such failure of growth of that bone as shall cause marked deformity in the attacked hand or foot. In some of these cases, should operation be required on one bone, the other may be shortened at the time, or later, by exsection of a portion of the shaft, or even of the epiphyseal junction.
Fig. 226

Osteogenesis and osteosclerosis in slow infective processes. (Buffalo Museum.)
—This is a rare manifestation of bone disease, only given an identity of its own since 1868, when Ollier first distinguished it, since which time it has been the subject of considerable controversy. The name refers to a condition less acute than the infectious periostitis just described, almost always localized in a single bone, necessitating incision and evacuation of a fluid which is gelatinous or mucoid in appearance rather than purulent. It is because of the peculiarity of the subperiosteal collection of fluid that it received the name periostitis albuminosa, and it was not generally regarded until recently as a variety of the infectious form of periostitis. It is, however, now conceded as being a mitigated form of infection, in which the products of exudation assume the serous rather than the purulent type. In some instances it appears to be the tubercle bacilli which are at fault. At all events, the organisms which produce the disease are more or less virulent, else the clinical form of the disease would be less serious than it really is. Cultures made from these subperiosteal collections have in almost all recent instances revealed the presence of some one of the numerous pyogenic organisms. Quite recently Dor has described a polymorphic microbe, in instances of this kind, which he has called the Bacillus cereus citreus, with which he claims to have been able to reproduce the disease in animals.
—As in the lungs, however, chronic lesions are met with, and as in the lungs, again, it is possible for collections of microörganisms[422] to become more or less encapsulated and for a long time to lie latent until some provoking cause excites them again into activity. In this way are to be explained the numerous instances of recurring abscesses within the bone necessitating repeated operations, often at long intervals. (See Plate XXXVI.)
—Bone is a living tissue, calcified and stiffened by inorganic material for the purpose of giving it strength; it may suffer remotely from the consequences of local infections, the same as other tissue. Thus it may have its nutrition impaired so as to produce atrophy on one hand, or increased so as to lead on the other to hypertrophy, either regular or irregular in outline. Again in its texture it may be altered to a wide extent between the sponginess or porosity on one side (osteoporosis), or to the density attained by ivory (osteosclerosis) on the other. Similar changes are also noted in cases of bone tuberculosis, which is to be considered by itself. The densest bone has sufficient vitality to permit its nutrition and life, and may assume dimensions much larger than that of the original, and a hardness which will defy the best steel instruments should it become necessary to operate upon it. The other extreme of osteoporosis includes a condition where the bone has barely sufficient inorganic material to permit it to retain its shape and ordinary proportions. Such bone is fragile in the extreme and scarcely serviceable as a supporting tissue. The principal portion of its bulk is constituted by marrow tissue, which makes it extremely vascular, but far from strong. When spongy it is ordinarily unserviceable for its proper function. Astonishing pictures of osteosclerosis and osteoporosis side by side are present in many instances of disease, the latter being often evidence of more or less ossification of new-formed granulation tissue. This is often a happy combination, because the bone, which has been sadly weakened by disappearance of its calcareous material by liquefaction and by absorption, is reinforced along some of its lines by a pillar of osteosclerotic tissue, by means of which it still functionates as a more or less useful support (Fig. 226).
The operating surgeon should familiarize himself with the density of normal bone in various locations, as in many operations upon the deeper bones he detects healthy bone rather by the sense of touch and of hearing, and the resistance which it offers to his instruments, than by sense of sight.
In Chapter IX, on Tuberculosis in general, we entered into considerable detail in regard to the nature of tuberculous lesions, which were stated to be essentially the same whether occurring in hard or soft tissue, the active agent being the now well-known Bacillus tuberculosis, which, finding lodgement, for instance, in the osseous tissue, acts as a specific irritant, and so provokes the production, first, of a typical tubercle, and, later, of typical granulation tissue, by whose ravages the distinctive signs of bone tuberculosis are produced. This process, then, is in no respect different in bones from similar lesions in other parts, though modified to a slight extent pathologically, to a greater extent clinically, by the dense environment. Nevertheless, trifling or most extensive destruction of bone substance is produced by this tissue, while by continuity or by metastasis there is more or less involvement of the adjoining textures, either parosteal or articular. It is by granulation tissue that so-called caries is produced, and it is by the same tissue that distinct portions of bone are sometimes completely segregated from their vascular surroundings and shut off from nutrition, so that they die and form what are known as sequestra. Necrosis may then be the result of tuberculous disease.
PLATE XXXVI
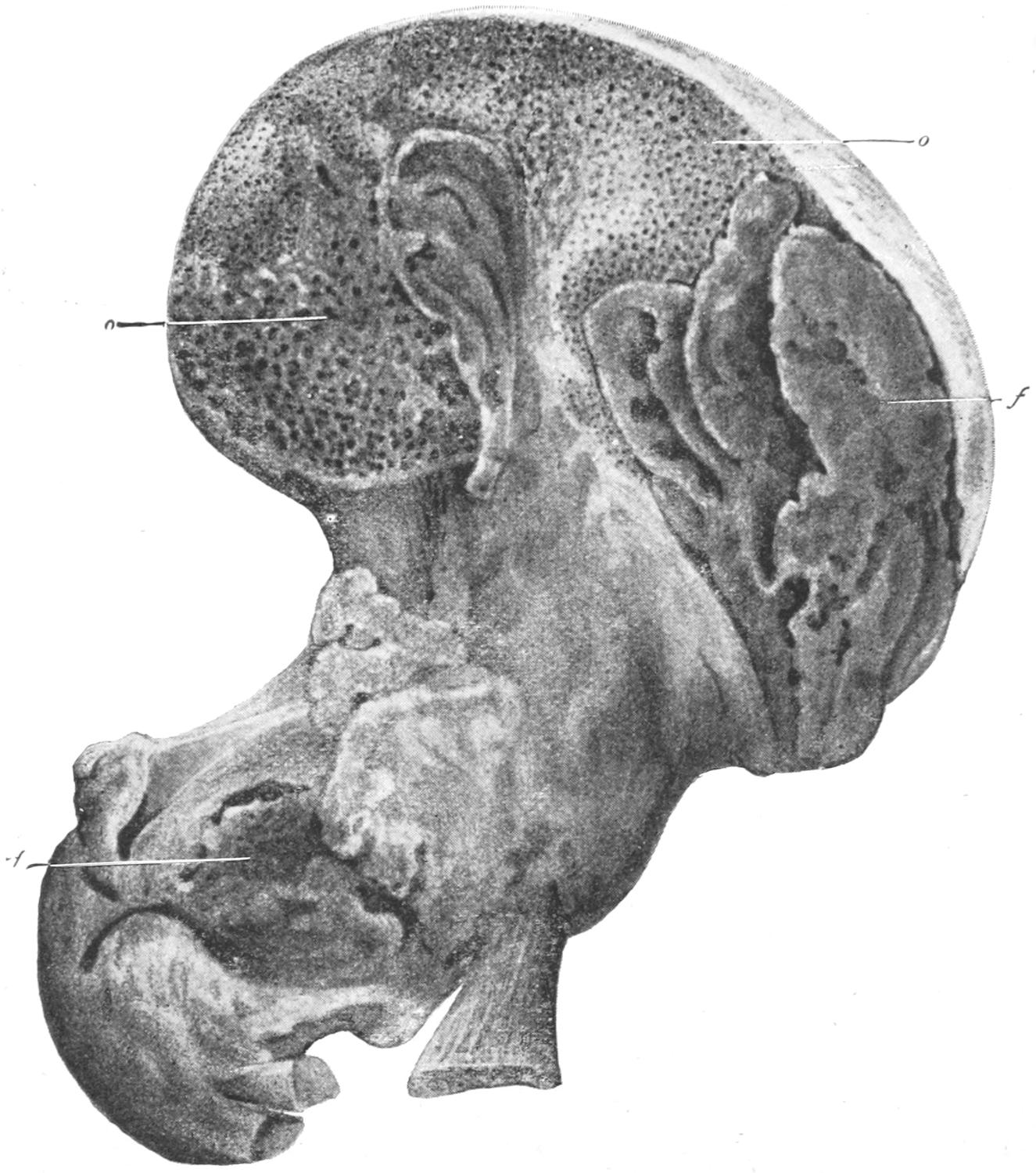
Tuberculous Disease of Hip-joint and Pelvis, involving the Muscles (rare). (Lannelongue.)
o, rarefying ostitis (i. e., osteoporosis); f, fungus granulation tissue.
[423]
So long as the process is active, this granulation tissue tends to enlarge its boundaries, and, like pus, to spread in the direction of least resistance. When produced in the shaft of a long bone this may lead to involvement of the entire shaft, or there may be liquefaction and absorption of dense bone and the formation of a sinus from the marrow cavity to the periosteum, beneath which the granulation tissue will spread, and through which it will sooner or later perforate, to resume its progress toward the surface, always in the direction of least resistance. In this progress tendon sheaths or bursæ may be involved, or dense aponeuroses may turn the granulation column aside, causing it to perforate toward the surface at some remote point; while it may spread out more or less beneath the skin before finally causing its destruction. Sooner or later, if uninterrupted by treatment, this escape will occur, and then we have the condition of a tuberculous ulcer of the skin, from which leads down, by a devious path, a sinus toward the original focus.
When this original focus has been juxta-epiphyseal there is involvement of the epiphyseal cartilage and a pathological diastasis, which may early lead to spontaneous or pathological luxation. Or, again, a focus having once originated at an epiphyseal extremity, tends usually to perforate quickly into a joint cavity, after which a considerable length of time is usually expended in filling up this joint cavity with exuberant granulation tissue. This is the material so often found in tuberculous joints, and is well characterized by the name given to it by the Germans, fungous tissue, they calling such joint affections fungous joint inflammations. (See previous chapter.)
Seen thus in joints, after it has been long exposed to friction and to more or less pressure, it may have lost some of its original luxuriant features. It is best seen when it is freshest and has been exposed to least disturbance. Under these circumstances it is vascular, dark red in appearance, friable, and easily removed from the tissue upon which it has grown. Ordinarily it is infectious, and by its inoculation into animals is capable of reproducing the disease.
—The pathology of tuberculosis of bone may then be virtually summed up in saying that it consists of the ravages produced by the presence of this granulation tissue, with the irritative hyperplasia of surrounding tissues which its presence always excites, even though they be not actively infected. This is the explanation for the majority of cases of caries, of tumor albus, of Pott’s disease, of spina ventosa, and of the condition which has been known under many other names.
—This corresponds to a similar invasion of the lungs. It might be fittingly described as an acute tuberculous form of osteomyelitis. It may run its destructive course within a short time and cause such involvement of structures as to necessitate amputation of a limb, or it may appear in the truncal skeleton as a primary disease, spreading rapidly therefrom and involving the viscera or the cerebrospinal membranes, and causing an early death, perhaps within a few weeks after its onset. This condition has been more prevalent than is generally understood, and has not even yet received the attention it deserves. It is less painful than the pyogenic forms of osteomyelitis, and may assume less of the septic and more of the typhoid or meningeal type of disease. The pain also may be less severe, though reflex symptoms, especially muscle spasm, will be an early and marked feature of these cases. When a limb is involved the case may not be hopeless; but when involving the cranium, spine, or trunk it is fatal, and little can be accomplished by treatment. The operative treatment for parts which are accessible is given under Acute Osteomyelitis.
—This is the ordinary form of the disease, and is exceedingly common. In some sections it constitutes nearly one-third of the diseases necessitating surgical treatment in clinics and hospitals. This is particularly so in the thickly settled portions of the European continent. In Buffalo it constitutes from 15 to 20 per cent. of cases found in my wards and in my clinic. The proportion some years has been larger.
—The essential symptoms of bone tuberculosis are muscle atrophy, muscle spasm and pain, direct or referred, and upon the existence of these, coupled with local tenderness and local swelling, a diagnosis can almost always be made. Muscle atrophy is distinct, and is not alone that of disuse, but is a distinctive evidence of the tuberculous process. It involves the parts above and below the lesions.
[424]
Muscle spasm is never lacking, but is most noticeable about the spine and the joints of the extremities. In Pott’s disease, for instance, the condition causes a stiffening of the back and an inflexibility of the spine. About the joints it leads gradually to fixation, usually in the condition of more or less flexion, the flexor muscles being ordinarily stronger than the extensors in all parts of the body. Thus we see the knee and the elbow drawn up, and most other joints in a condition of flexion so far as it may be permitted.
It is characteristic also that muscle spasm is frequently exaggerated, usually in a reflex way, by which pain is always augmented. These sudden but brief contractures occur more often during sleep than during the waking hours, and give rise to the so-called starting pains, usually nocturnal, which are noted in nearly every case of this kind.
The pain is in large measure the result of contracted muscles pulling tender joint surfaces together, and is consequently augmented during the muscle spasms just described to an extent causing the patient to cry out even during sleep. There is also usually a more or less deep-seated and constant pain or soreness, manifested in increasing degree as the lesion advances. These pains are also often referred, lesions in the upper ends of long bones usually giving rise to pain which patients refer to the lower ends. In hip-joint disease pain is often referred to the knee, and in Pott’s disease to the anterior part of the trunk. Slight but slowly increasing disturbance of function of a joint inaugurated by trifling muscle spasm, with complaint of aching pain, is significant and needs careful examination, it being a mistake to anesthetize patients for this purpose, as by the anesthetic the pathognomonic muscle spasm is abolished and mistakes in diagnosis favored.
Fig. 227

Tuberculous disease of the hip.
(Buffalo Museum.)
Fig. 228
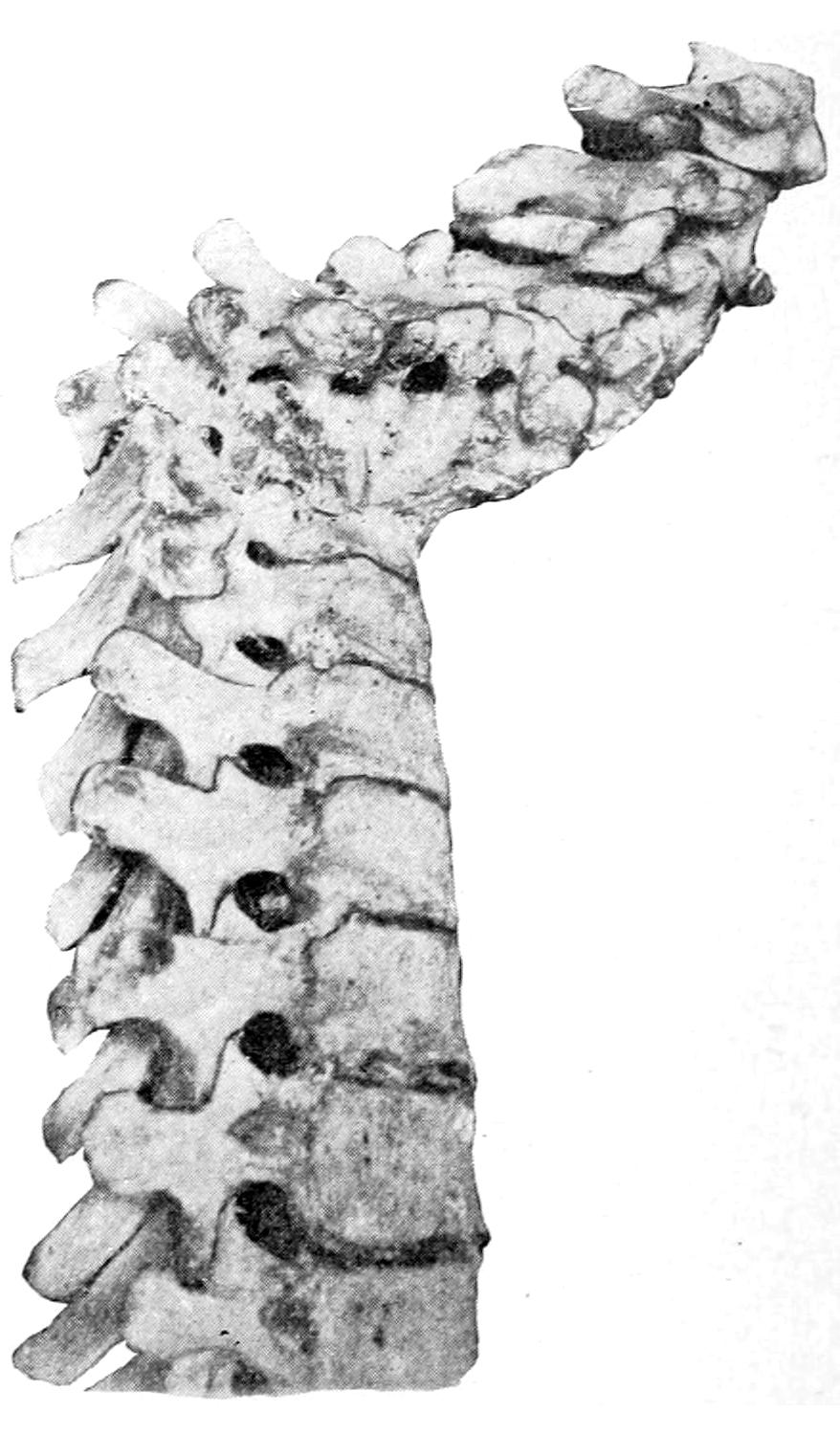
Healed tuberculosis of the spine.
(Buffalo Museum.)
It will be seen that these features are also met with in tuberculous-joint disease, the fact being the conditions are not only allied but often associated.
[425]
—The treatment of tuberculosis of bone is constitutional and local. The former consists in the best possible hygiene and in those measures which are everywhere recognized as helpful in similar conditions. I believe in the internal use of benzosol, or its equivalents, in doses sufficiently large to influence the tissues. In addition the tonics and evacuants should be judiciously used. But it is mainly with local treatment that we shall here have to deal.
The local treatment may be divided into the non-operative and the operative. The former consists in enforcing the general principles of physiological rest, which is done partly by orthopedic apparatus proper and partly by the general principles of traction, and is resorted to mainly in a class of cases treated of under Orthopedic Surgery, the best methods for the purpose, apparatus, etc., being found in the next chapter.
Aside from this a hopeful method has been that suggested by Bier, consisting of making an artificial chronic congestion, it having been long known that tubercles do not thrive when bathed in much blood. The congestion is secured by wearing an elastic bandage above the point involved, elastic constriction being made to a degree as great as may be comfortably borne. The result is venous congestion, possibly edema of the parts below, which to be made effective should be carried nearly to the tolerable extreme. Constriction may be at first enforced for only a short time, but can be later borne for longer periods, until a time is reached when the patient can wear a bandage almost continuously. Marked improvement in many cases follows this method.
The operative treatment consists in ignipuncture, curettage, or formal extirpation. Ignipuncture is the insertion into the bone focus of the glowing point of the thermocautery. It should be practised under an anesthetic, and when the bone is superficial the cautery should be plunged through the skin, making it burn its way into the depth of the bone. This is not difficult when the cancellous tissue is that at fault. If the bone be deep an incision may be made down to it, after which the cautery is applied as above. The result in almost every instance is relief from pain.
This effect seems to be brought about partly by relief of tension, partly by destruction of diseased tissue, and by the acute congestion which is the result of vigorous counterirritation. It need occasion no fear nor difficulty, and is applicable to all accessible bones. It must not be expected to cure every case, but is a measure which may be confidently expected to relieve pain and to do good.
The radical form of treatment is necessary when it can be determined that the carious process is advancing or that pus or caseated deposits are present. This is made known in various ways; but when reasonably sure of their presence it is best to begin the operation as an exploration, going as far as the findings may justify. This may include scraping out of a small focus, or it may entail removal of a large portion of a bone or resection of a joint, or even amputation, according to the severity of the deep lesion. It is best to do whatever may be necessary, and to do it all at once. The operator should not rest content with mere operative attack, but should carefully disinfect the entire tract, cutting away or removing with the spoon the sinus wall and fungous tissue, which he should follow wherever it may lead, disinfecting freely with hydrogen peroxide or caustic pyrozone, and then using an active caustic, like zinc chloride or the actual cautery, unless caustic pyrozone has already been used. In this way material may be destroyed which has escaped the instruments used, and absorbents are eared or closed and protection afforded. My personal preference is for a packing made of bismuth subiodide gauze, soaked in a mixture of balsam of Peru containing 10 per cent. of guaiacol, which I find more advantageous than anything I have used. There should be added to these measures, however, whatever may be necessary in the way of after-treatment, both local and constitutional, and the surgeon should be prepared to operate once or twice again should latent foci subsequently manifest themselves or should there be recrudescence of the active disease.
Bone abscess is a term applied to deep and circumscribed collections of pus within the bone, mainly within the shafts of long bones. They are due either to the acute ravages of pyogenic cocci or to the slower lesions produced by the tubercle bacillus. They are frequently evidences of return of disease in its acute type after a long period of latency. The manifestations are usually localized, in this respect differing from those[426] of acute osteomyelitis. The pain is deep-seated and boring, while there is local tenderness, often with considerable enlargement of the overlying bone. The lesion occurs more often in the tibia than in all of the other bones together—at least under those clinical conditions which entitle it to be called bone abscess. The pain is frequently nocturnal or osteoscopic, and patients may endure it for weeks or months before seeking relief.
The surgeon may always expect to find a layer of condensed, sometimes extremely hard bone around these local foci, and it is due to this that they do not either perforate or diffuse and cause extensive trouble.
—Treatment is always operative; it should consist in anesthesia, exposure of the bone, effective exploration by means of the bone drill, as the hypodermic needle would be used for exploration in the soft parts, and then the free use of the bone chisel or other instruments by which the area may be widely exposed. The density and firmness of the bone under these conditions will sometimes almost defy the best-tempered instruments. Care should be taken to make the external opening nearly the size of the deep focus, in order that the surface may not heal too readily and before the deeper part is filled. The same directions with regard to cauterization and packing the cavity obtain as given before.
Fig. 229
Syphilitic gummas of head and face. (After Jullien.)
Fig. 230
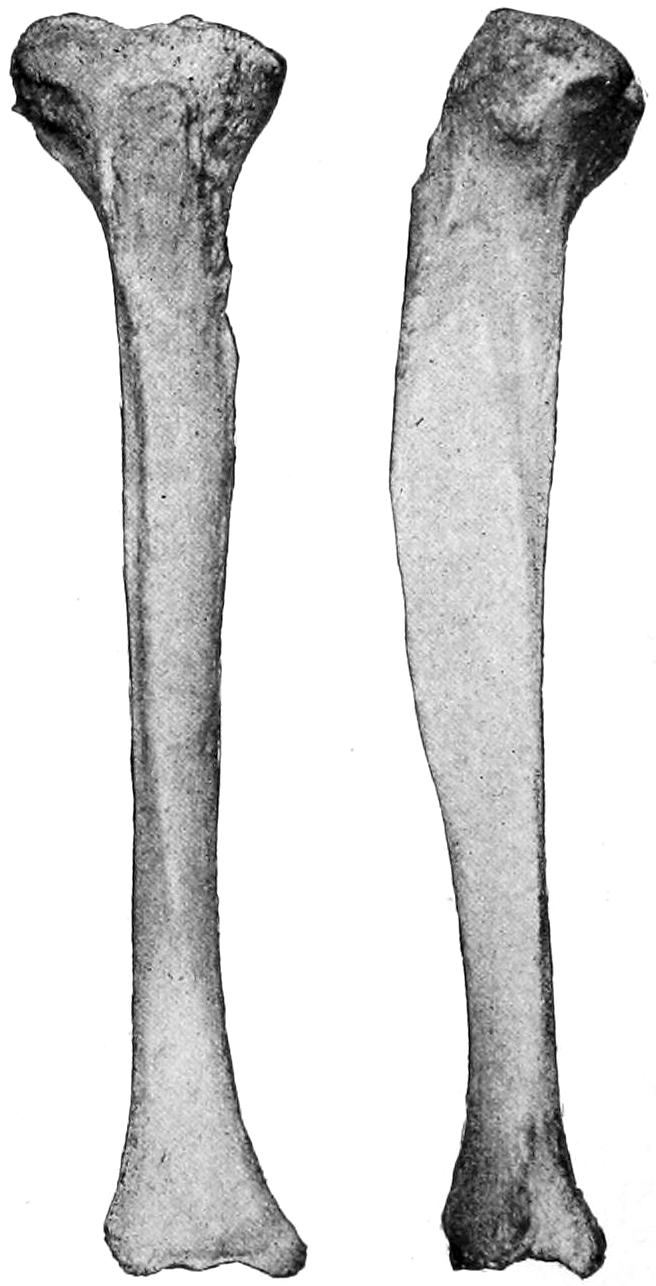
Syphilitic ostitis and osteosclerosis.
Syphilis of bone may assume the type of gummatous involvement of the periosteum or of the bone itself or of syphilitic caries and necrosis. The former appears usually as a distinct tumor, ordinarily tender and exceedingly painful, especially at night, it being characteristic of almost all cases of bone syphilis that the pain, however great during the day, is exaggerated at night. The true syphilitic gumma, or syphiloma, of bone is but little different from gumma in other tissues, which may become secondarily infected and then suppurate with the formation of sinuses, etc. Suppuration, however, is rare. Central gumma, like central osteosarcoma, is possible, and may lead to expansion of the surrounding bone. Syphilitic necrosis, so far as the bone lesion is concerned, scarcely differs from the other varieties. It is, however, almost always of the slow form, and involves more often the flat than the long bones. It is especially seen in the cranium and the sternum. Syphilis of bone is often mistaken for rheumatism or pseudorheumatism[427] because of the deep-seated and somewhat indolent pain. Syphilitic disease of bone permits occasional spontaneous fracture, the bone affected with this disease being always more friable than natural. There is also another form of bone syphilis—namely, the hereditary. It leads either to bone enlargement or to caries and necrosis, the latter usually upon the cranium, where extensive ulceration and sequestrum formation may be observed, even the dura being exposed by breaking down of the fungous tissue.
Fig. 231

Caries of lower end of femur. (Buffalo Clinic.)
Hereditary bone syphilis is also characterized by osteophytic formation, by the substitution of gelatinous for spongy bone tissue in the neighborhood of epiphyses, and by early and easy epiphyseal separations. It is characterized also by irregularity of ossification of cartilage and consequent deformity of bone ends, especially about the phalanges and the metacarpal and metatarsal bones. In almost every case where doubt would in other respects arise the other evidences of congenital or acquired syphilis are so plain as scarcely to permit uncertainty (Fig. 230).
The possible combination of syphilis and tuberculosis in the same subject may occur, the lesions partaking of one or the other character according as the tuberculous or syphilitic taint may predominate.
There is urgent necessity in all cases of syphilis in bone, whether operated on or not, for the combination of suitable internal treatment with surgical intervention. Only by this combination can the efforts of the surgeon be crowned with success. In failure to appreciate this fact operation often seems to be almost futile.
Caries is a term applied to infiltration, and substitution in healthy bone of granulation tissue, which has been in use for many centuries, from a time long before the pathology of the condition was understood. Caries never occurs except in the presence of a specific irritant, which, in general, is tuberculous and sometimes syphilitic in character. The pure type of caries is connected entirely with the formation of granulation tissue, and the slow ravages connected with its presence in and substitution for the original bone. As long as septic infection (pyogenic) is avoided it assumes the dry type, as it used to be known, called by the older writers caries sicca. When the fungous tissue is invaded by putrefactive or pyogenic organisms suppuration takes place, and then occur the moist forms of caries, the caries humida of our forefathers, connected with the presence of pus. When closed areas of bone, small or large, being thus shut off from nourishment, die as the result of its presence the complicated condition used to be known as caries necrotica. Occurring under any circumstances, caries is a result and not a cause, and is to be dealt with accordingly.
Peculiar alterations and markings in bone are the consequence of carious changes, and bones are given a fantastic and peculiar appearance in consequence. The surface is almost always irregular, tunnels or canals are formed, and the bone is often honeycombed, as it were, by the excavations just made. Along with the process of osteoporosis and disappearance of bone at one point may be seen osteosclerosis in an adjoining area, and the bone, which is apparently much weakened by the destructive process, is strengthened in a compensatory way by the artificial density of the tissue undestroyed.
The clinical evidences of caries are those of joint and bone tuberculosis or syphilis, which have been already discussed, and its operative treatment consists always in surgical attack with bone chisel and sharp spoon, according to the rules already laid down. The bone which is completely carious calls for extirpation—i. e., usually amputation. In the carpus and tarsus resection will[428] often suffice, and also when the disease is limited to joint ends. Occurring in the pelvis, ribs, sternum, or cranium, more or less extensive resections of flat bones are necessary, in the latter place leading to exposure of the dura (of which one need have no fear). The same rules with regard to cleansing and packing the wound should be observed as in operation on tuberculous bones.
Necrosis corresponds to gangrene of soft parts, and the term, when used by itself, is limited to death of bone tissue. Necrosis by itself is a distinct disease, but indicates the termination of some preceding disease process. It may be considered as:
—Traumatic necrosis is due to the discontinuance of the blood supply by accident or by separation of the whole or a part of a bone in the same way. Thus in consequence of multiple fractures fragments occasionally die and require removal. The same result has been ascribed to traumatic or non-traumatic embolism of the principal nutrient artery of a bone, but the possibility of this condition is doubtful, bone being too well supplied by its surrounding periosteum. Necrosis in connection with fracture is rare except in compound fractures, and, when a detached fragment can be seen, may be anticipated by removal of the same.
—The pathological form is due to the preëxistence either of tuberculosis, syphilis, or an acute infection, such as osteomyelitis. It may also be the result of acute infectious periostitis, where the periosteum is completely loosened from the shaft of a long bone. These conditions are connected either with the slow ravages produced by granulation tissue, or with the acute septic processes by which infected exudates shut off large areas from sufficient blood supply, or by which in consequence of septic thrombosis a similar condition results. In consequence there may be met bone dying in small visible particles, or the entire shaft of a long bone or several smaller ones may be involved in the destructive processes.
The portion which dies is known as the sequestrum, which may assume irregular and unusual shapes, varying entirely with the area involved. The general character and size of a sequestrum will depend upon the nature of the cause. In acute osteomyelitis it is either a bone shaft or an epiphysis which thus suddenly dies. In the slower processes the fragments may be of almost any imaginable size and form—irregular with jagged ends, or long, extending completely through a bone, either from end to end or from side to side.
—The toxic forms of necrosis are due mainly to two substances used in the arts—mercury and phosphorus—whose use seems to be inseparable from the manufacture of many modern industrial products.
Mercurial necrosis may come either from the volatilization of the metal in factories where mirrors are made or from refineries where amalgam is distilled. It also occurs from the internal use of the drug. Its effects are seen more frequently in the alveolar portion of the lower and upper jaw than elsewhere. It is through some unknown peculiarity that the jaws are the bones commonly involved in both of these forms.
Phosphorus necrosis, on the other hand, manifests itself almost entirely in the lower jaw, and occurs usually among the young, in factories where matches are made. It is due to the vapors of phosphorus, which cause a form of nearly distinct maxillary necrosis—a fact which has been so widely recognized as to lead to State legislation preventing the employment of the young in such work.
Phosphorus necrosis begins as a periostitis with the production of osteophytes, and is completed as a nearly total necrosis of the entire bone.
—The preventive treatment should consist of supervision of the teeth, the use of alkaline mouth-washes, inhalation of terebinthinate vapors, which neutralize those of phosphorus, and the ventilation of establishments devoted to match-making. The curative treatment consists of buccal antisepsis, opening of abscesses, and the removal of diseased bone, especially of dead bone, upon the first provocation. The occurrence of fistulas should always be regarded as pathognomonic of diseased bone. In aggravated cases, such as are rarely if ever seen since legislation has been brought to bear upon the subject, practically complete necrosis of the lower jaw, either en masse or in portions, was far from unknown, and the possibility of regeneration of the bone was for a long time discredited, until the late James R. Wood, of New York, exhibited a specimen, both at home and abroad, which proved its possibility. Since then we have learned that it is possible for bone thus to regenerate, the cause of the disturbance having been removed.
PLATE XXXVII
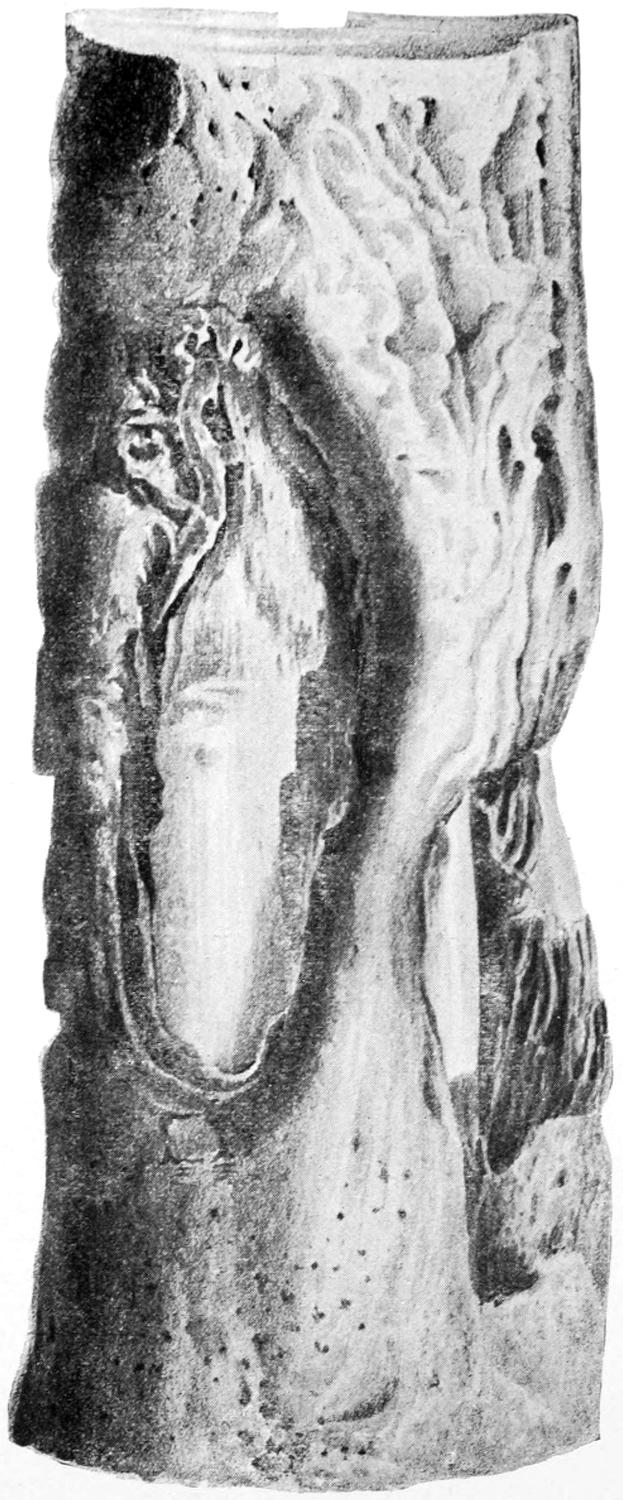
Necrosis of Shaft of Femur with Sequestra. (Life size.)
[429]
Fig. 232
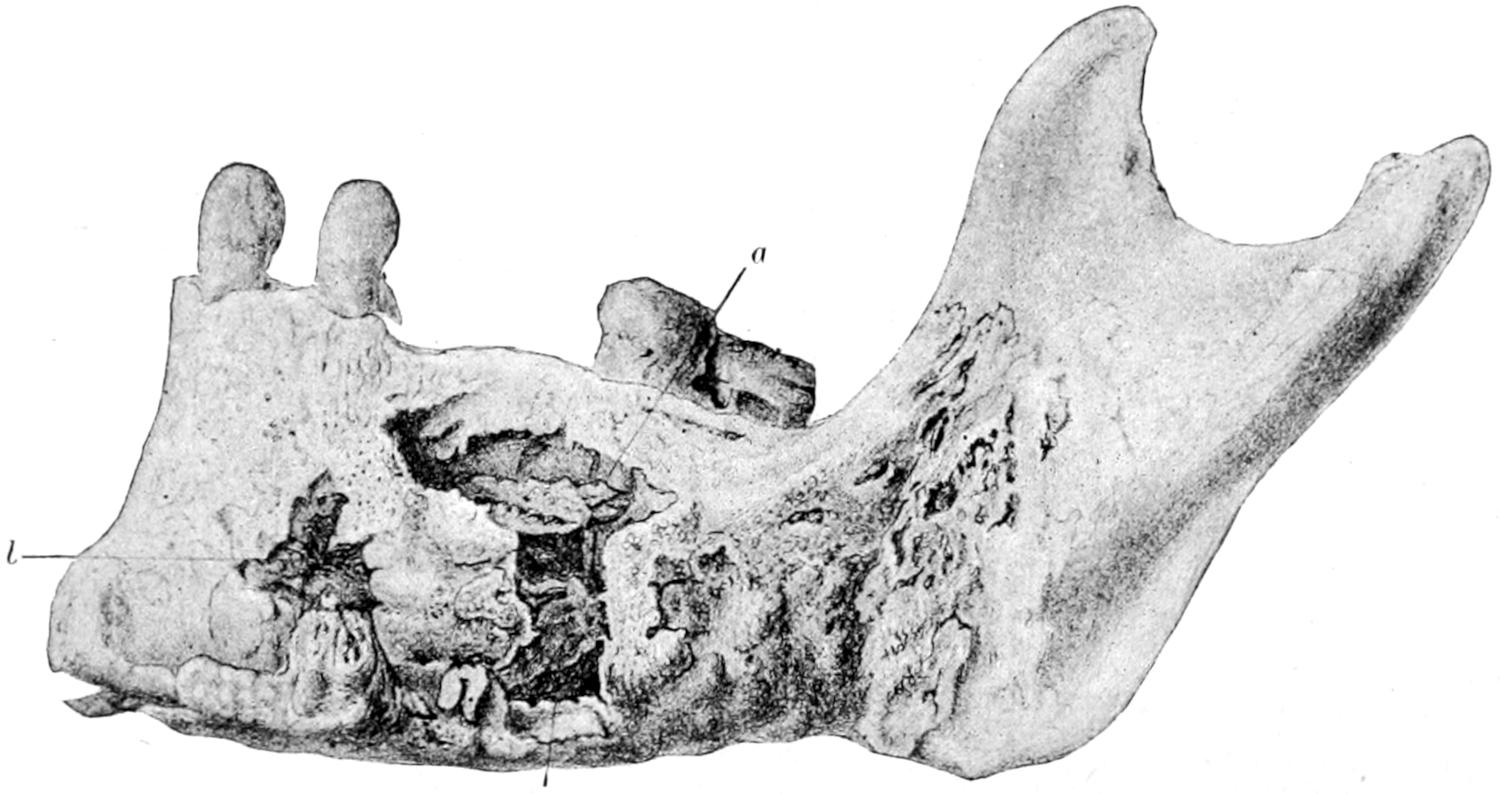
Phosphorus necrosis of the lower jaw. (Musée Dupuytren.)
—To the portion of bone which dies is given the name sequestrum, while multiple sequestra are by no means uncommon. The sequestrum is white and ivory-like in hardness when it consists of original compact structure. It is rare to find a distinct sequestrum of spongy tissue, as this yields so readily to the presence of granulation tissue and of pyogenic infection. A sequestrum may include an entire bone shaft, or epiphysis, or only a small fragment. A portion of the bone having lost its vitality becomes a foreign body which the surrounding tissues endeavor to extrude or to wall off and surround. The extrusive effort is the one which is usually seen. This is done by the continued presence of granulation tissue, which gradually perforates the surrounding bone at places of least resistance, the result being the slow formation of a sinus or several sinuses, ultimately connecting with the surface, and in which in neglected cases the dead fragment of bone can be seen or felt, or from which it can be withdrawn almost without operation. While this weakening of bone is going on in certain portions a corresponding strengthening process is also being put into effect; and the result is a quantity of new bone, which is often wrapped around the sequestrum and is simply the effort to atone for its pathological weakness and to strengthen it. This new osseous tissue which so often surrounds the sequestrum is called the involucrum, and in many instances it is necessary to remove more or less of the involucrum before the sequestrum can be lifted out of its bed or removed. (See Plate XXXVII.)
The whole necrotic process is intelligible if read aright as an endeavor on the part of Nature to get rid of dead and irritating material. When this effort is properly interpreted the natural efforts can be seconded by the interference of the surgeon at a time when disturbance is limited to the minimum and before external sinuses have had opportunity to form. On the other hand, ignorance and neglect may lead to the extreme condition, and most fantastic arrangements of sequestra and involucra are seen in all pathological museums, some of which seem to partake almost of the perplexities of Chinese puzzles. The explanation, however, is always as above afforded. (See Figs. 233, 234 and 235.)
—The treatment should be surgical, and consist in removal of the dead portions and restoration of the parts to a condition favoring rapid regeneration. It should always be radical, but is sometimes made difficult by the inaccessibility of the fragment or by the density of the involucrum and the necessity for large external openings in order to remove the sequestrum.
Large and powerful forceps and strong and well-tempered bone chisels are usually[430] necessary, while, after making the necessary opening for removal of the sequestrum, the sharp spoon should be used thoroughly to scrape away all the lining material of cavities in which fragments have been lying or all fungous tissue which may fill sinus tracks. It will be well after this to thoroughly cauterize the wall of the cavity, after which it is to be packed.
Fig. 233
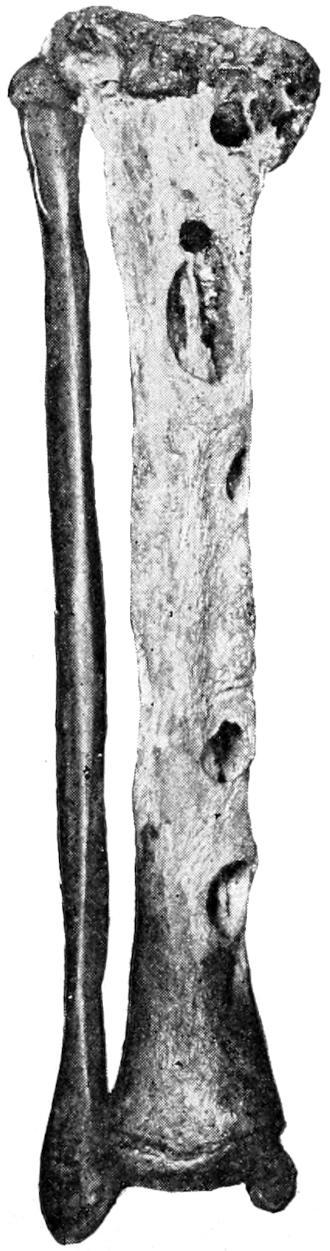
Fig. 234
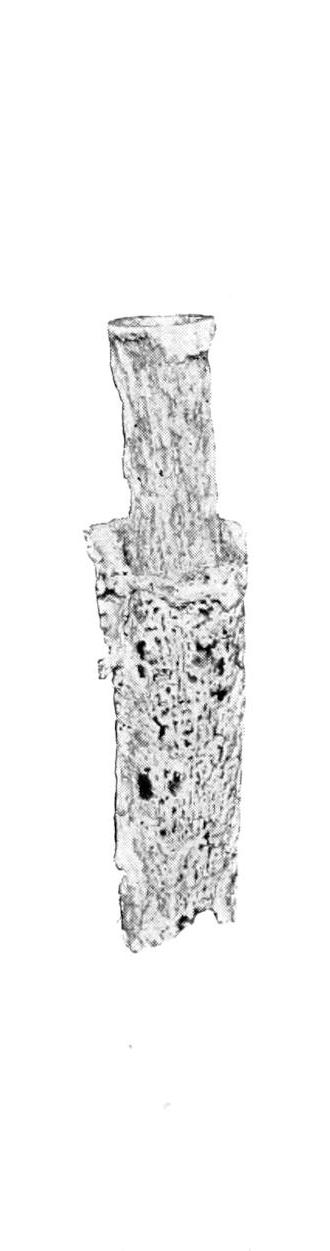
Fig. 235
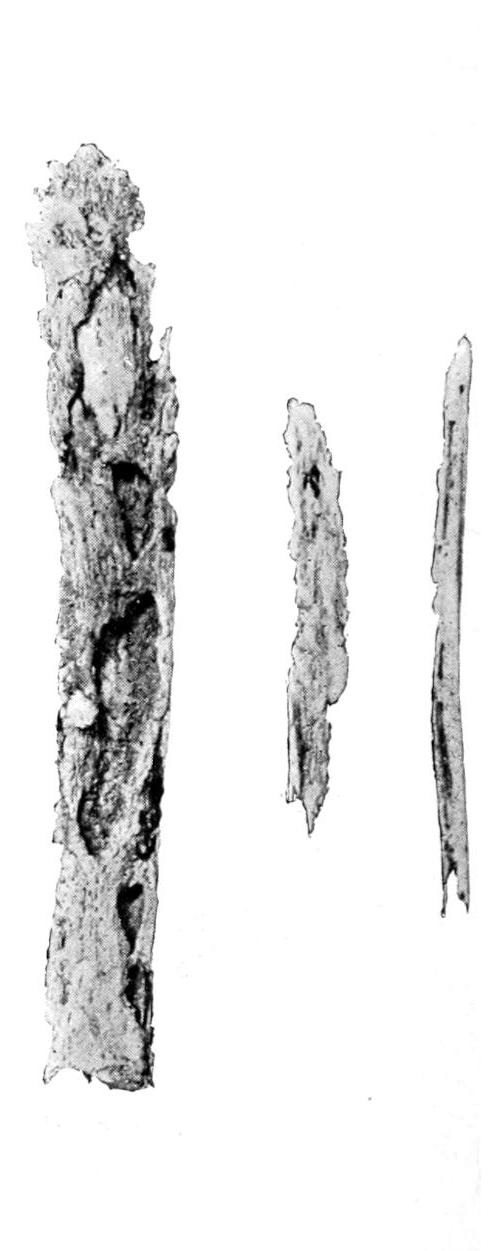
Central necrosis of the tibia, long central sequestrum.
Sequestrum inside of a core of new-bone tissue, arranged much like a puzzle.
Necrosis of tibia, showing sequestra after removal. (All three specimens from the Buffalo Museum.)
The packing of old bone cavities is of importance, and operators should appreciate the reason for so treating them. The packing is essentially a foreign material which the tissues will naturally endeavor to extrude as they did the sequestrum. The method of extrusion is by filling up beneath and around it with granulation tissue, which later may ossify. The packing is therefore a constant provocation to the formation of this tissue, which is now desirable, and is used mainly for this purpose. It is antiseptic material, and will serve to prevent decomposition of the pyoid material which would otherwise fill such a cavity as the result of waste—Nature’s effort at formative material gone to waste. A number of years ago Gunn suggested the use of wax for this purpose, wax being plastic and incapable of absorption. A piece of white wax was heated in hot water, molded with the fingers to fit the cavity, where it served the purpose of a packing, and was reduced in size with each dressing, as was necessary to permit it still to remain. It is not now used as much as it deserves to be. (See p. 431.)
In favorable cases it may be possible to so thoroughly cleanse the bone cavity without the use of caustics as to justify the attempt, after rigid asepsis, of allowing it to fill with blood, which will coagulate and organize into connective tissue. When this effect is desired the wound should be covered with green silk protective, over which the other dressing may be snugly applied. This healing by the aseptic blood clot is the ideal method when possible.
[431]
The extent to which regeneration of bone is possible is often amazing, especially in the young. Thus after removal of the entire shaft of a tibia there may result, in time, not a complete restoration to former integrity, but, in addition, the formation of so much new osseous material as to restore a great degree of strength, and which shall, with the compensatorily hypertrophied fibula, make the leg as useful as ever. In the thigh, however, complete necrosis of the femur means amputation, as it will also in the arm unless the necrotic portion is but a small proportion of the length of the humerus. The treatment of necrosis of the skull, or, in fact, of any bone in the body which is accessible, is based practically on the principles already laid down.
In the effort to atone for extensive loss of bone many experiments have been tried, first on animals and afterward on men, success with the former having lent much prospect to the latter. It has been learned, for instance, that portions of living bone can be removed from some of the lower animals and transferred into a bed of more or less healthy sterile human tissues, often with the result that a fragment thus transplanted becomes vitalized and incorporated, and serves the purpose for which it was intended; still these efforts do not in all instances succeed. However, experience has led to the effort to utilize some portion of the patient’s own osseous system. This becomes more easily possible in the case of the forearm or leg where, especially in the latter, a small or less important bone can be utilized to take the place of the greater. Thus, when the entire shaft of the tibia has been removed for necrosis resulting from acute osteomyelitis, the fibula has been sawed across, opposite the site of the ends of the lacking tibial shaft, and transplanted into the trough-shaped depression, thus making it functionate for the lost tibia. Huntington has recently reported a case in which not only was this done, but later the upper and lower ends of the fibula attached to the tibia, with good bony union and with an almost perfect functional result. This will illustrate what elsewhere may be done in this direction.
Our methods for removal of sequestra and cleaning out of infected bone cavities are now simplified and made safe. The difficulty which is still universal is to secure a rapid filling or closure of these cavities. If we could be certain of cleaning out every particle of infected tissue and the removal of every germ which might excite putrefaction, then we might resort to Schede’s plan and allow even a large cavity to fill with blood clot and await its organization, but no complicated and infected cavity in such tissue as bone-marrow can ever be so treated to a theoretical degree of perfection. Therefore disappointment often follows this attempt. Senn endeavored to improve upon the plan by the insertion of chips of decalcified bone, but this method is open to the same objection. Dentists have the advantage of surgeons because they deal with small cavities, and in tissues which can usually be thoroughly sterilized. Other things being equal, the methods to which they resort could, with advantage, be imitated by surgeons. In 1903, Mosetig-Moorhof suggested a mass containing iodoform 60 parts, spermaceti 40 parts, and oil of sesame 40 parts. When this mixture is slowly heated to 100° C. and allowed to cool, there remains a soft material which, when desired for use, is melted, being constantly stirred to keep the iodoform properly suspended, while it is poured into the cavity, where it immediately solidifies. It is claimed that its physical properties permit of its gradual absorption and replacement by granulation, and finally by new bone, as has been shown by a series of skiagrams. A cavity in which this preparation is used should be prepared as dentists prepare theirs. It is successful in proportion to the absolute disinfection of the same. For this purpose wide opening and ready access are necessary in order to dry and cleanse. Should oozing be persistent strands of catgut may permit of escape of the blood which enters the cavity. It would probably be best to use the elastic bandage and bloodless method, and to protect for a few moments the solidifying mass before allowing the blood to return to the limb. The originator uses, in his own clinic, a hot-air blast. The air is heated by an electric contrivance, and both dries and disinfects the cavity. After the cavity is thus filled the tissues are closed[432] over it and a sterile dressing applied. It is serviceable in chronic cases and after thorough work. In acute osteomyelitis it is scarcely to be thought of because of the acute character of the infection.
These are mainly of two varieties—hydatid disease and actinomycosis.
Fig. 236
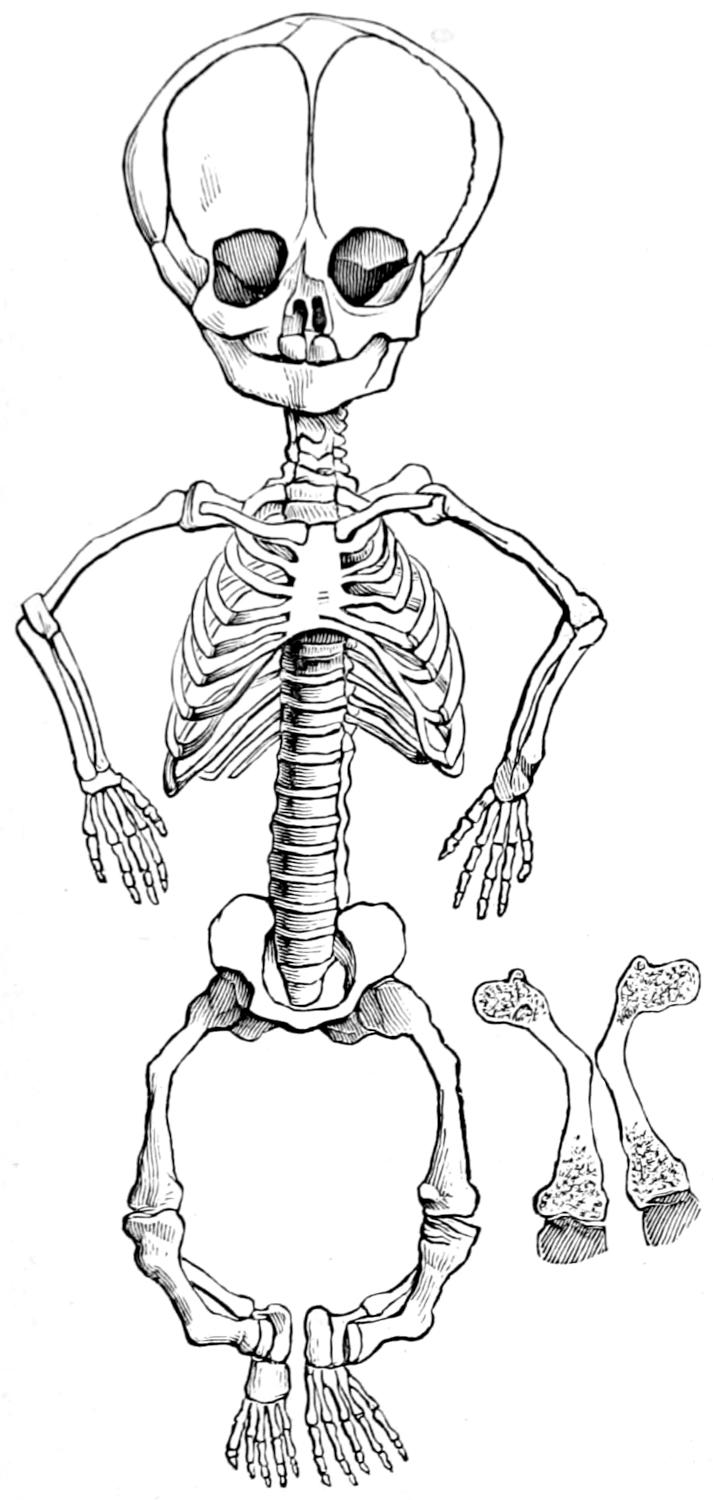
Achondroplasic skeleton. (Porak.)
—Hydatid disease of bone consists in the development of hydatid cysts, which may be either of primary or secondary origin. Almost all the bones of the skeleton are liable to cyst formation, except the short bones of the carpus, tarsus, and digits. In the long bones they occur most frequently in the region of the epiphyses. The particular vascularity of this region is the main factor in their location at this point. The cysts may be unilocular or multilocular, and around them may be a thin or a large area of infiltration. In other words, their boundaries may be abrupt or not. Their volume is exceedingly variable, unilocular cysts sometimes attaining considerable size and distending the bone beyond its normal proportions. (See Chapter XXVI for further reference to the pathology of hydatid cysts.)
—The treatment is purely operative. The contents of the cysts should be evacuated and its walls radically destroyed by caustic, spoon, etc. All sequestra should be removed; in the limbs amputation is sometimes necessitated by the extent of the affection.
—The general character of this parasitic disease has already been considered. (See Chapter VIII.)
The peculiar fungus may be found in the periosteum, in the compact outer layers of the bone, or within its more spongy depths. When the lesion is sufficiently large to be recognizable to the naked eye it assumes, for all practical purposes, the appearance of caries, like that due to tuberculous or leprous diseases, while in the pus or debris discharged from the same or contained within the invaded bones the characteristic yellow, cheesy, or calcareous particles will always be recognized. In this disease there never seems to be the slightest tendency to encapsulation nor to protect against further spreading by any process of repair. The diseased area constantly enlarges its dimensions, involving everything as it spreads, it being limited by no membrane or tissue of the body. Occurring in the bones, it is usually a secondary or metastatic infection, and may be found in any part of the body.
The symptoms will be those of osteoperiostitis, first occurring frequently in the jaws, as it nearly always does in cattle, and often in man; this is accompanied by loosening of the teeth and involvement of the submaxillary tissues. The course of the disease is slow, with little or no tendency toward spontaneous recovery.
Under this heading it is proposed to group a number of diseases whose clinical manifestations are distinct or classic, but whose underlying causes are more or less obscure.
—This is a lesion of intra-uterine life which includes a softening of primary cartilaginous structures and curvature or malformation of the bones which should be formed from them. It belongs to that period of fetal life between the third and sixth months. It is sometimes referred to as intra-uterine rickets. Under this name it was first described by Müller, in 1860, and since then under various names, most commonly as fetal rickets. It appears that in this disease the fetal cartilage contains mucus abnormally collected, quite generally, in minute cavities or cells just at its borders. The chondroblasts and osteoblasts are not regularly dispersed, and the development of the growing bone is thereby much interfered with. The periosteum appears to have nothing to do with this condition. In consequence the cartilage does not do its proper duty. The long bones fail to attain their proper proportionate length, but become thicker than normal, the periosteum being unaltered. On the other hand, those bones into whose formation cartilage enters but slightly, such as the clavicle and the ribs, retain their normal proportions—the consequence is a peculiar malformation and disproportion of the whole skeleton (Fig. 236).
These deformities are symmetrical, and pertain mostly to the bones at the base of[433] the skull and to the long bones of the limbs; therefore the distinctive appearance may be recognized even at the birth of the child. The head is disproportionately large, the spinal column short, the lumbar curvature exaggerated, all of which is rather the reverse of the ordinary rachitic manifestations. The disease is not common (Fig. 237).
Fig. 237
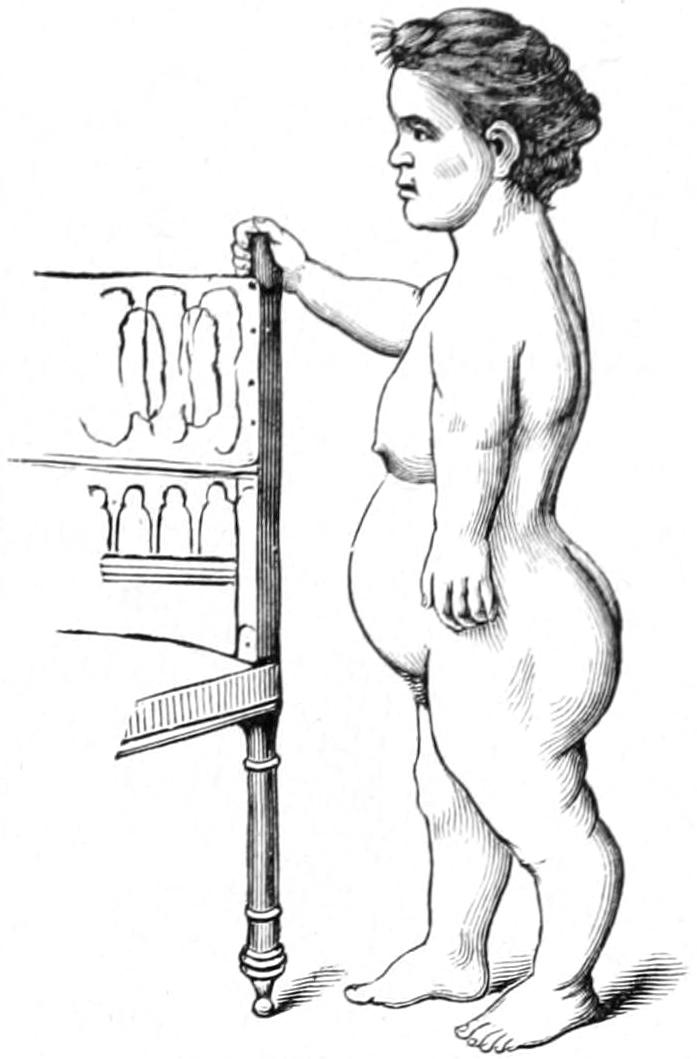
Achondroplasia. (Lugeol.)
—The prognosis is unfavorable, because it seems impossible to undo the faults of the intra-uterine condition. The disease, however, is not incompatible with a long life.
—This also is a constitutional condition, and has been described in Chapter XIII. So far as the manifestations in the bones are concerned it is a constitutional dystrophy caused by improper deposition of calcareous material in the softened and somewhat perverted fetal cartilages. It is a condition, however, pertaining rather to postnatal life, and while inconspicuous at birth becomes more and more marked as the child develops. It is essentially a disease of malnutrition, and consequently may be seen in all walks of life, as well in the bottle-fed babies of the wealthy as in the best-nourished children of the poor. The subject should be studied also in connection with the facts set forth in the chapter on the Status Lymphaticus, which bear on the relation of the ductless glands to tissue growth, and especially to rickets. The lesions are widely distributed. The disease is divided by some writers into three periods: (a) Rarefaction of bone tissue; (b) softening of same; (c) re-ossification.
The first stage is the intra-uterine part; the second and third stages are postnatal. To fetal rarefaction have been attributed intra-uterine fractures, even by Hippocrates.
The general dyscrasia and visceral alterations of rachitis interest us here less than deformities of the various bones. The head is disproportionately large, the vertex flattened, the frontal and parietal eminences pronounced; the anterior fontanelle closes very late. To the atrophic alterations of the head have been given the name craniotabes. The face is disproportionately small, the lower jaw assuming a polygonal shape. The palatal vault is of the Gothic type, dentition irregular and retarded. In the thorax the clavicular curves are exaggerated, by which the bones are shortened and the shoulders made narrow. The costochondral junctions are enlarged, the result being the so-called[434] rachitic rosary. The sternum projects and gives the peculiar appearance known as pigeon-breast. The pelvis is often deformed, and frequently distorted to such an extent as in after years to make normal delivery impossible. The spinal column may either be distorted early or is likely to undergo alterations of curvature, due to the combined results of pressure and traction upon softened vertebræ. The joint ends of the long bones are enlarged or clubbed, this being true even of the phalanges. Joint movements are often accompanied by crepitation. The axes of the long bones are distorted, and more or less marked deviations and curvatures result, giving rise to such deformities as knock-knee, bow-leg, etc. (See pp. 161 and 162.)
—As rickets is essentially a disease of early childhood, osteomalacia is practically confined to adults. The name implies a peculiar softening of the bones, by which their resistance and rigidity are weakened and deformity permitted. The disease is common to man and to animals in confinement, and is frequently noted among wild animals dying in zoölogical gardens. It commonly occurs in pregnant women, where it would appear as if the mineral elements needed for the growing fetus were abstracted from the mother’s bones rather than from the food ingested. It is brought about also by starvation, possibly by lactation, especially among those who nurse their children for unusual periods.
Fig. 238
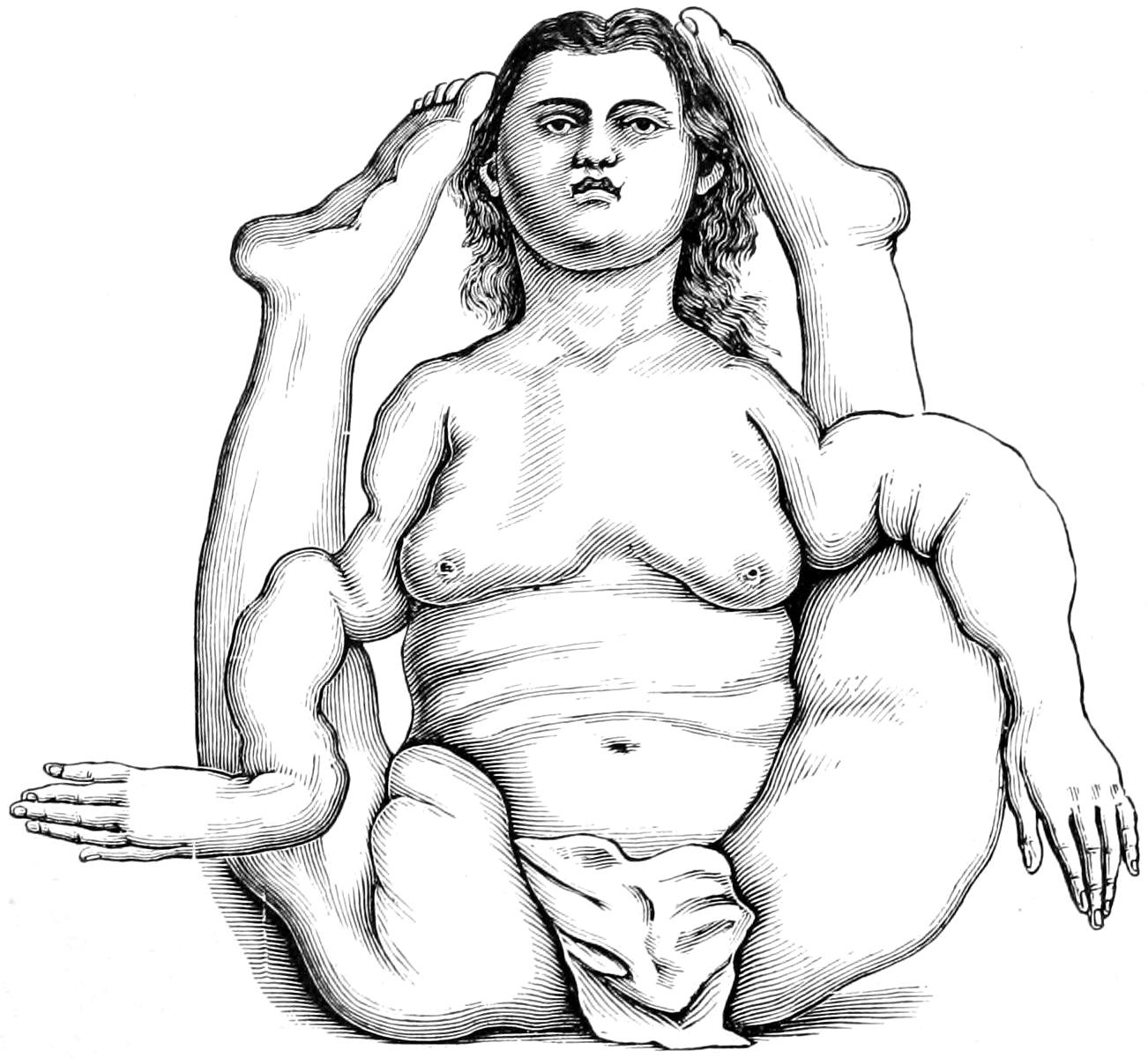
Osteomalacia: celebrated case of Moraud, 1753. (Skeleton now in Musée Dupuytren.)
Spontaneous fractures, especially of the long bones, are frequent. These may refuse to unite properly and false joints may result. The urine will under these circumstances contain an excess of mineral salts, carbonates, phosphates, and oxalates, and when these are discovered in the urine of those suffering from fractures it should always be a warning to administer calcium salts and mineral acids, preferably phosphoric, internally, and to carefully watch the excretions. The progress of the disease is slow, yet steady, and often not easily checked, if at all affected, by mineral acids. Occurring in pregnant women, it may be checked after delivery, especially if the child be not allowed to nurse from the mother. In some instances it occurs with each successive confinement in the same patient, and makes distinct advance with each fresh attack.
—The prognosis is therefore unfavorable, least so in puerperal cases.
An infantile form, as well as a fetal form, have been noted, but it is doubtful whether these forms really come under the same category, and whether they are not manifestations of rickets. A senile form has also been described which affects most frequently the sternum and thorax, which is characterized by excess of nervous excitability and by bone pains, as well as by liability to multiple fracture upon the slightest provocation. This form, however, differs but little from the osteoporosis of advanced years, and[435] scarcely deserves distinct consideration. Certain writers have also mentioned a symptomatic form—cancer, syphilis, scurvy, etc.—which, however, is unnecessary, since the fractures occurring in cases of cancer or syphilis are due to secondary lesions of the same character, while those occurring during scurvy are simply an expression of starvation and weakening, even of the bones. Cases of cancer, for instance, where bones have broken without being previously weakened by secondary growths, are exceedingly rare.
Under the name of osteogenesis imperfecta has been described the “fragilitas ossium” of certain writers. The condition has also been known as congenital fetal rickets. These cases may usually be recognized in infancy, in that the extremities are more or less bent and deformed, and the bones very fragile. Sometimes intra-uterine fractures occur, which may be recent or old, and united with more or less callus and deformity. The spinal column will be soft and friable, with marked divisions, and the ribs are often fractured. The clavicle shows lesions of this kind more frequently than any other single bone. Bones so affected will be found extremely fragile and delicate, and sometimes so thin that they may be crushed between the fingers. They are defective in every respect of structure. But these changes pertain mostly to the shafts of the long bones, and do not concern the cartilages. They are to be distinguished from chondrodystrophia fetalis, in which the extremities are shortened, the skin thickened, and the subcutaneous tissues extremely fatty or edematous.
The condition is to be distinguished from rickets, as there is no enlargement of rib ends or epiphyses and no disturbances of the alimentary or nervous systems. Osteomalacia usually occurs after puberty. Hereditary syphilis, in very rare instances, is a factor, but should give additional evidences in other parts of the body. At present there is no satisfactory explanation as to the cause of the condition.
Fig. 239
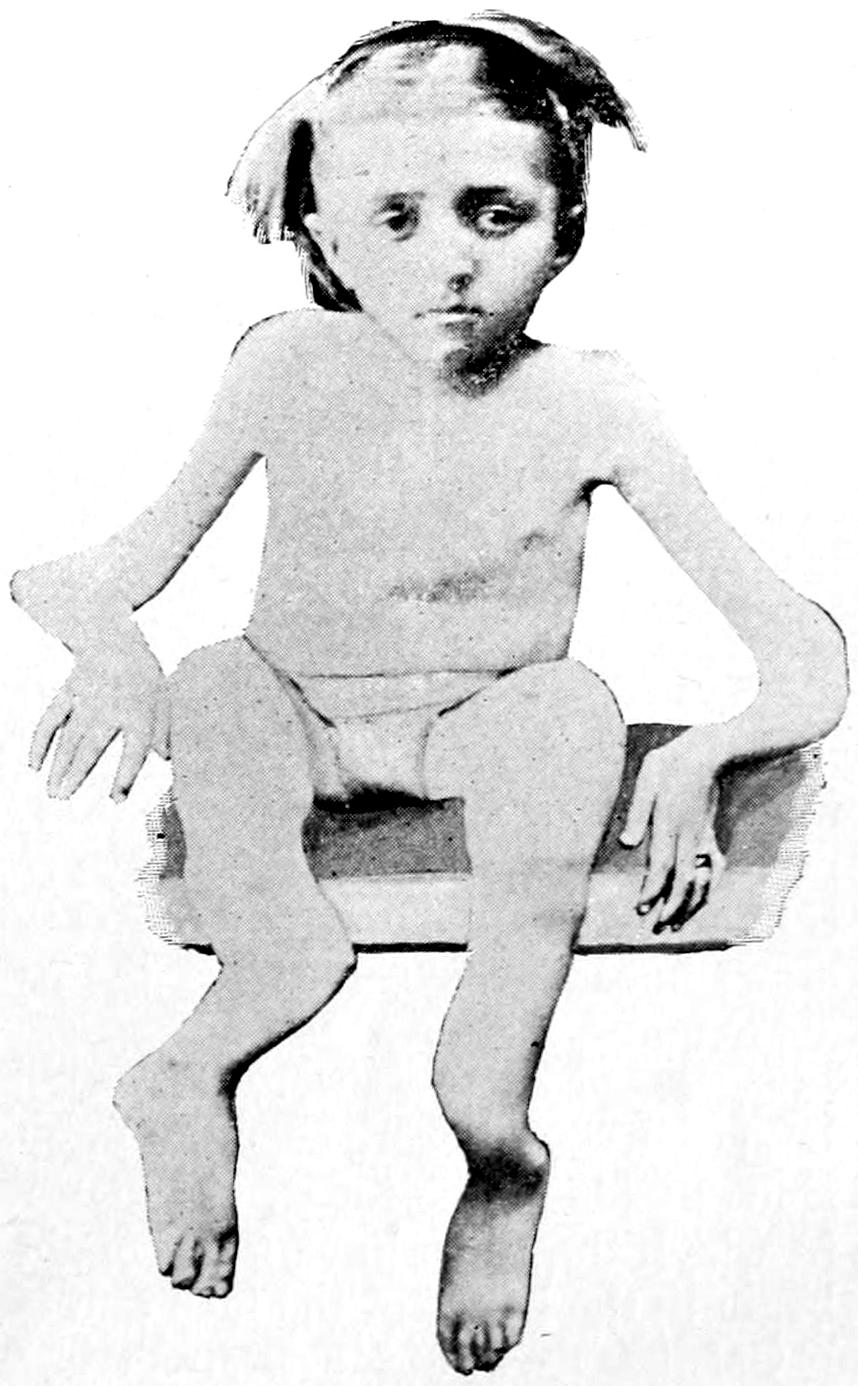
Osteopsathyrosis. (Blanchard’s case.)
—The treatment for all these conditions should be removal of the cause if discoverable and the administration of calcium salts in accessible shape, as in cases of rickets, combined with thymus or pituitary extract.
—This is a condition distinct from osteomalacia and is due to trophic nerve disturbance. The condition seems to be hereditary, often extending through several generations. It is characterized by fracture of long bones upon the slightest provocation, and is common to all ages. While apparently congenital in origin, it persists often throughout life, no impression being made upon the condition by medication. It is not characterized by distinctive histological changes, and all theories heretofore advanced toward its cause are disappointing. It is seen, at least in this country, most often in paretics and inmates of insane asylums. The ease with which the bones of such patients are broken has given rise to repeated charges of violence or homicide. From one case in which this charge was made I secured specimens of the ribs, which were so fragile that they could be crumbled between the fingers. Such patients might easily sustain serious fractures when undergoing necessary restraint, even of the gentlest nature. Allegations of undue violence are frequently made in these cases, which, especially in asylums, may be most unjust and difficult to prove or disprove.
The relationship of osteomalacia to exophthalmic goitre furnishes another illustration of the peculiar and mysterious influences which the thyroid exercises upon nutrition. The conditions have a similar geographical distribution, as well as being coincidental in the same individual. Honicke, who has recently studied the subject, believes the bone condition to be an expression of thyroidal disorder,[436] the more so in that castration does not remedy the disease, thus proving that the genital glands are not at fault.
The peculiar relationship between the bone and the thyroid in these cases is probably one of disturbance of the elaboration of the phosphorus compounds which are necessary for the proper development of bone, these compounds being excreted rather than utilized.
Osteopsathyrosis of this congenital type is perhaps best illustrated by a case reported by Blanchard,[35] of Chicago, in the case of a woman twenty-seven years of age at the time of his report, who up to that time had sustained over one hundred fractures. In her case it was sufficient to merely gently slide from the sofa to the floor to break some bone. Treatment in her case had been of no avail. (See Fig. 239.)
[35] Trans. Amer. Orthopedic Assoc.
—This means weakening of the bones which is incident to advanced age in either sex, due to and comprised under the term osteoporosis. Added to this, in certain places is a positive change in shape, also characterizing the senile condition—e. g., the neck of the femur. Under these circumstances bones will break with a minimum of violence and without invoking any theory of osteomalacia, osteopsathyrosis, or the like. As bone disappears under these circumstances fat usually takes its place, so that while the volume of the bone may not be particularly diminished, its weight and density are materially altered. (See introductory remarks to this chapter.)
—This is a term first applied by Ollier, and refers to a distinct type of alteration in long bones by which their actual volume is relatively diminished, although they increase in length. It is produced largely by lack of pressure, and is seen in many amputated stumps, in which it has much to do with the conicity of the same. It is seen in certain cases of typhoid fever or in forced confinement of the young in bed, where the bones appear to grow at a much more rapid rate than normal. It may also be due to unequal amounts, or defects, of nutritive supply, especially that furnished by the periosteum, and in certain other cases seems to be a purely reflex or trophoneurotic change which is always inexplicable. Frequently accompanying it is muscular wasting, which is to be explained rather by reflex action through the cord, produced perhaps through the mechanism of the terminal filaments of the articular nerves.
—Ostitis deformans is often called Paget’s disease of the bones, and is a condition found alike in long and flat bones, the osseous tissue being condensed in texture and increased in amount, or at other times the osseous tissue becoming quite porous and the spongy tissue rarefied without alteration in the marrow. It is due to the unknown causes which may be summed up in the expression trophoneurotic, a painful and a painless form having been described, the former the more frequent. It produces deformities, disfigurements, and hypertrophies of the long bones. It is distinguished from arthritis deformans, described in the previous chapter, which is a distinct malady.
In the skull it is usually the face bones which are most involved, although the disease often commences in the cranial bones. The skull proper may be thickened even to 3 Cm. The thorax becomes globular or cubic in form, the arms are relatively too long, and there is usually dorsal kyphosis; the pelvis is thickened and distorted; the ribs are augmented in size and the femora irregularly curved; the patellæ enlarged; the tibiæ more massive and their curves exaggerated. The disease is essentially symmetrical, commonly commencing in the cranium and radius. Fractures are rare, because the bones become stronger rather than weaker.
In many instances these changes are accompanied by severe pains, which may be exaggerated by pressure. The malady is usually regarded as rheumatism, but it may be said that even were accurate diagnosis made early it would scarcely avail in treatment, since there is none for it. It may require to be distinguished from hereditary syphilis, in which the tibiæ have more of the saber shape; from acromegaly or leontiasis, which begin in the bones of the face and involve the cranium only secondarily.
—Under this title, which has no exact equivalent in English, was described, in 1890, by Marie, a peculiar affection, often wrongly spoken of in this country as Marie’s disease. This is in large part a[437] pulmonary affection accompanied by enlargement of the extremities. There is reason to believe that there are present microörganisms, giving rise to products that are absorbed into the general circulation, the result of whose presence is an irritative hypertrophy of certain parts, particularly the joints and ends of the fingers, the elbow-, shoulder-, and knee-joints, and often the wrist. There is also ordinarily dorsolumbar kyphosis, which in acromegaly is usually cervicodorsal. The cranium remains intact; the borders of the jaw are sometimes involved.
—Acromegaly is so named from its tendency to increase the volume of the bone extremities or apices. The first case of this disease was published by Marie in 1885. It is characterized by progressive increase in weight, by enlargement of all the extremities, bones and soft tissues alike; but the most characteristic involvement is that of the lower jaw, the upper jaw being little if at all affected. The lower jaw assumes enormous size and projects so that its teeth are far in front of those of the upper. The supra-orbital ridges enlarge, as do also the sternal ends of the clavicles and costal cartilages. As the disease progresses the ribs are widened and the scapulæ enlarged, the vertebræ and the intervertebral cartilages thickened and fused together, causing usually cervicodorsal kyphosis. The long bones of the limbs suffer later, especially at the lowermost joint ends—i. e., hands and feet. The viscera are rarely affected, but there is a peculiar and characteristic enlargement, usually of the thyroid and pituitary bodies. The lower cervical ganglion of the sympathetic is also sclerosed; the mucous membrane of the nose is usually hypertrophied; the uvula is enlarged and the larynx often participates in the changes. Acromegaly is essentially symmetrical, and for each change upon one side of the body is noticed a corresponding alteration upon the other. Particular features are observed in individual cases, but the above are practically common to all.
Fig. 240
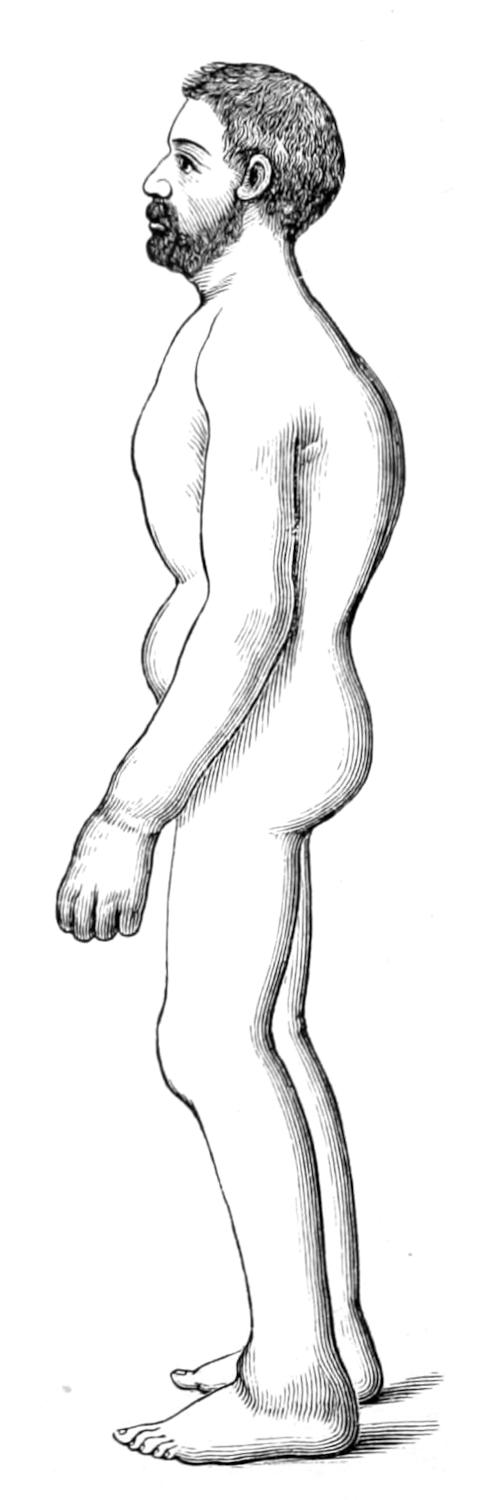
Osteoarthropathy. (Marie.)
Fig. 241
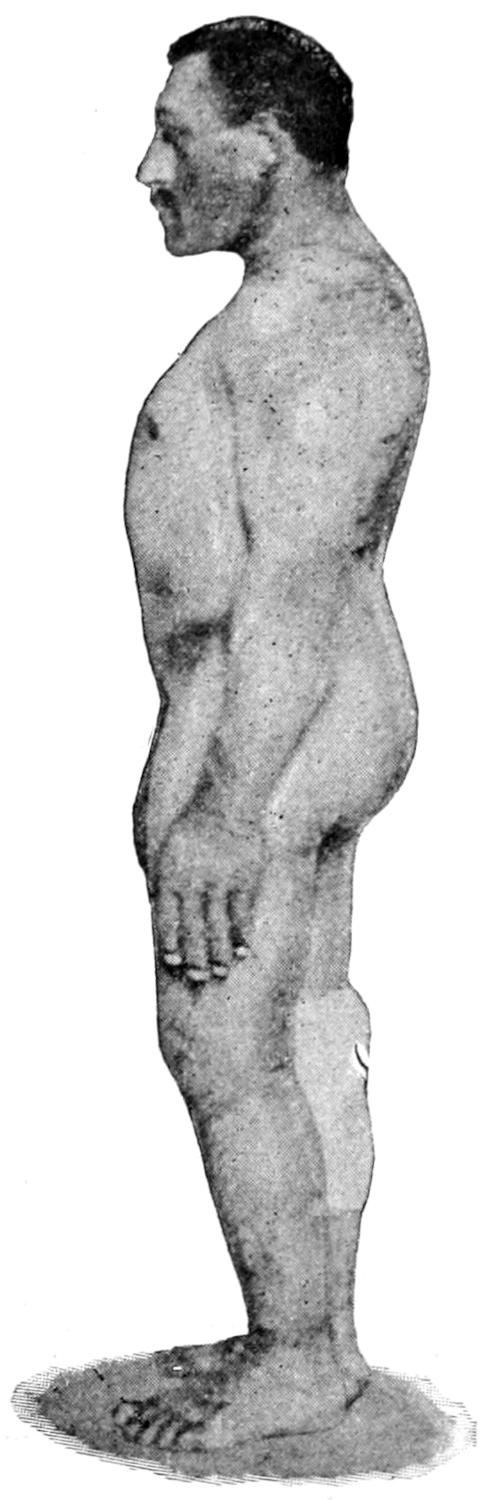
Acromegaly. (Original.)
[438]
The underlying pathological condition is as yet undetermined, though most indications point to late alterations along the original craniopharyngeal tract of the young embryo, whose remains are best known in the pituitary body and the thyroid. On this account there is reason for trying the treatment by extract of the pituitary body, or even of the thyroid. The greatest complaint usually is of headache, which is difficult of relief. The disease is steady, progressive, unaffected by treatment, and the prognosis bad, though its course is slow.
—A diffuse bilateral, symmetrical hypertrophy of the bones of the face and later of the cranium, described first by Virchow, the real origin appearing to be in the superior maxillæ, the result being a peculiar leonine appearance of the face, hence the name given to the disease. There is no distinct tumor formation in the bone, but rather the entire structure of the bones involved is affected. As it advances function of the parts is interfered with, mastication becomes impossible, headache and pain are constant. The special senses are disturbed because of involvement of their nerves, and patients die usually from inanition, because no longer able to chew and swallow food. It is distinguished from Paget’s disease, because it shows no tendency to involve the rest of the skeleton; from acromegaly, in which the general shape of the jaw is preserved, though its dimensions are magnified; from tumors of the jaw or face, because of its symmetrical enlargement. Its pathogeny is as obscure as that of the other bone affections mentioned in this list, and its treatment as unsatisfactory.
Fig. 242
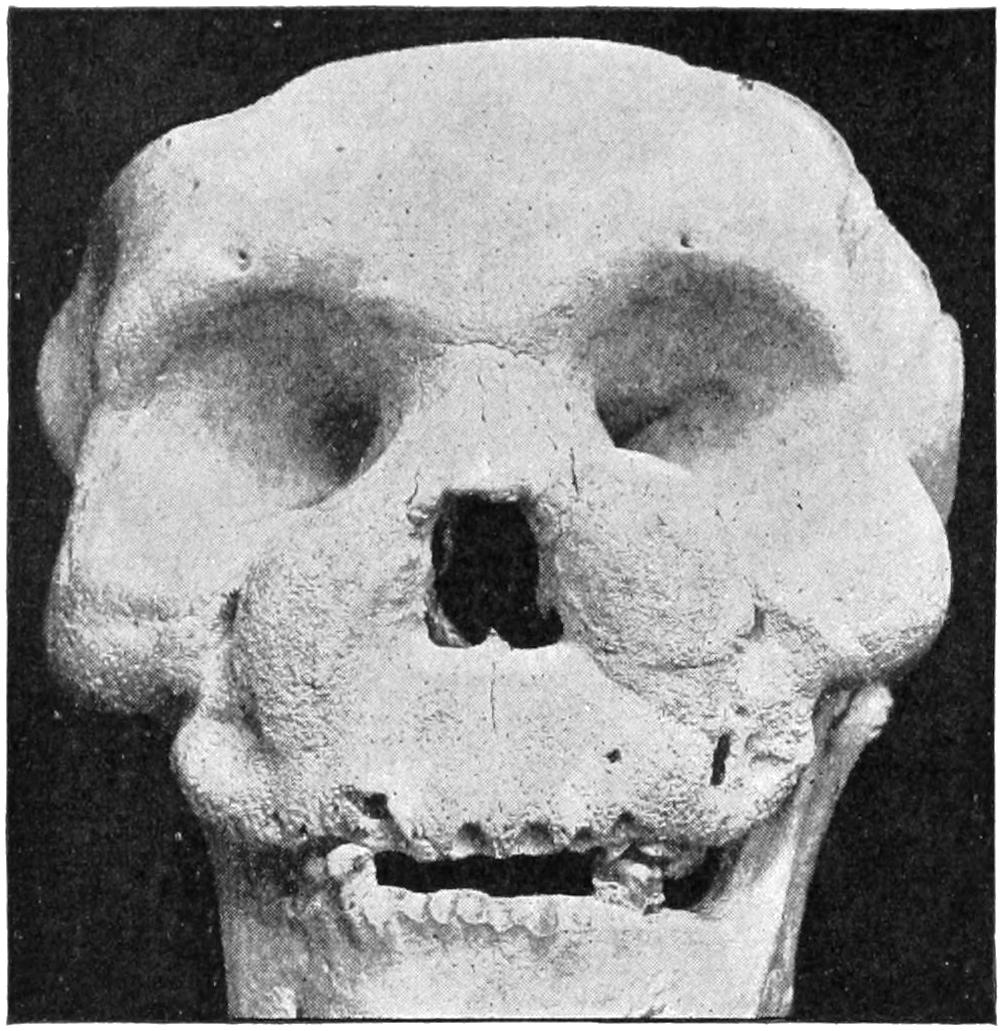
Leontiasis: skull of a Chinese woman. (U. S. A. Museum, No. 10,620.)
As between the various hypertrophic conditions of the bones above noted should be distinguished the true neoplasms, which answer all the requirements of the definition given in Chapter XXVI. There are few of the true tumors which may not be met with in bone, including the periosteum.
Fig. 243
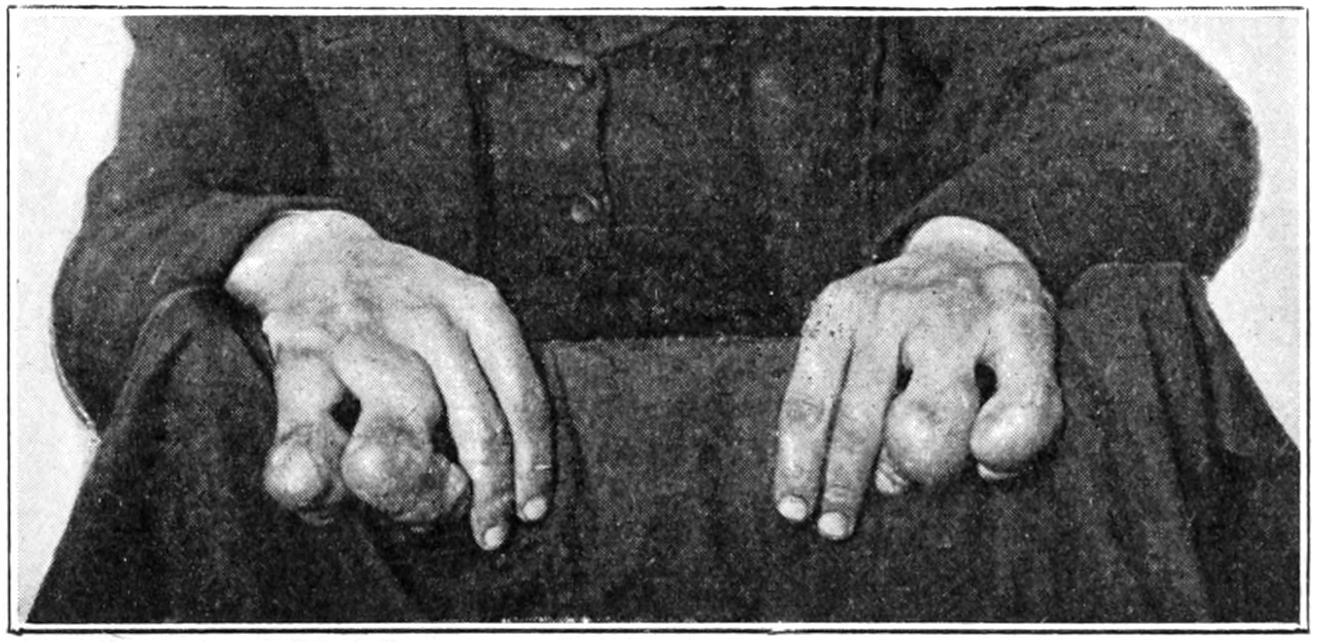
Multiple enchondromas of fingers.
—Fibromas may spring from the periosteum, especially about the jaws and from the base of the skull, from which latter place they may project into the nasopharynx and interfere with the welfare of the patient. Some of these tumors are soft and succulent, as well as extremely vascular, and I have seen death occur upon the table in an endeavor to remove a growth of this kind, hemorrhage being uncontrollable.
[439]
Fig. 244
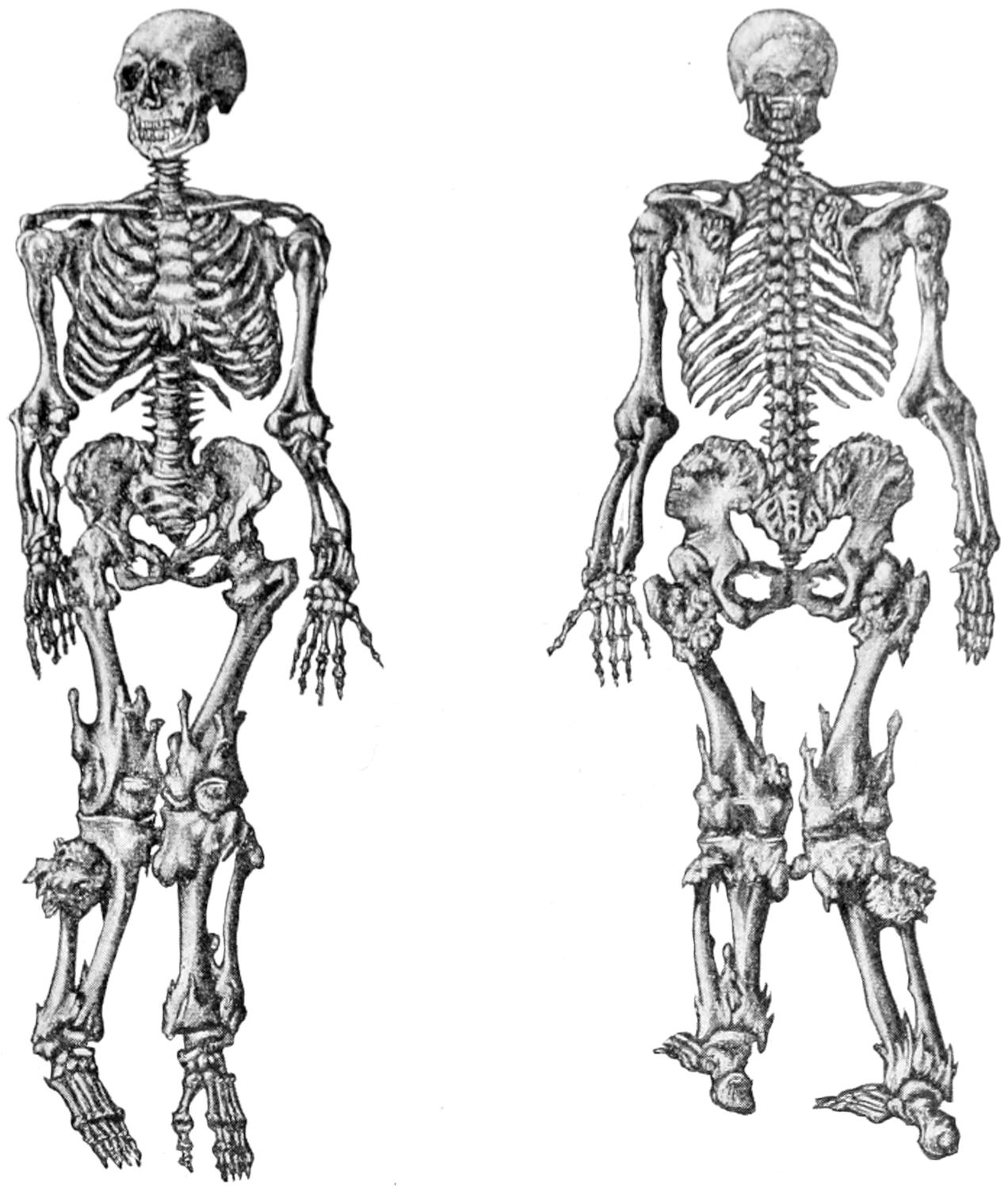
Multiple ecchondroses and exostoses.
Skeleton in the museum at Lyons. (Poncet.)
Fig. 245
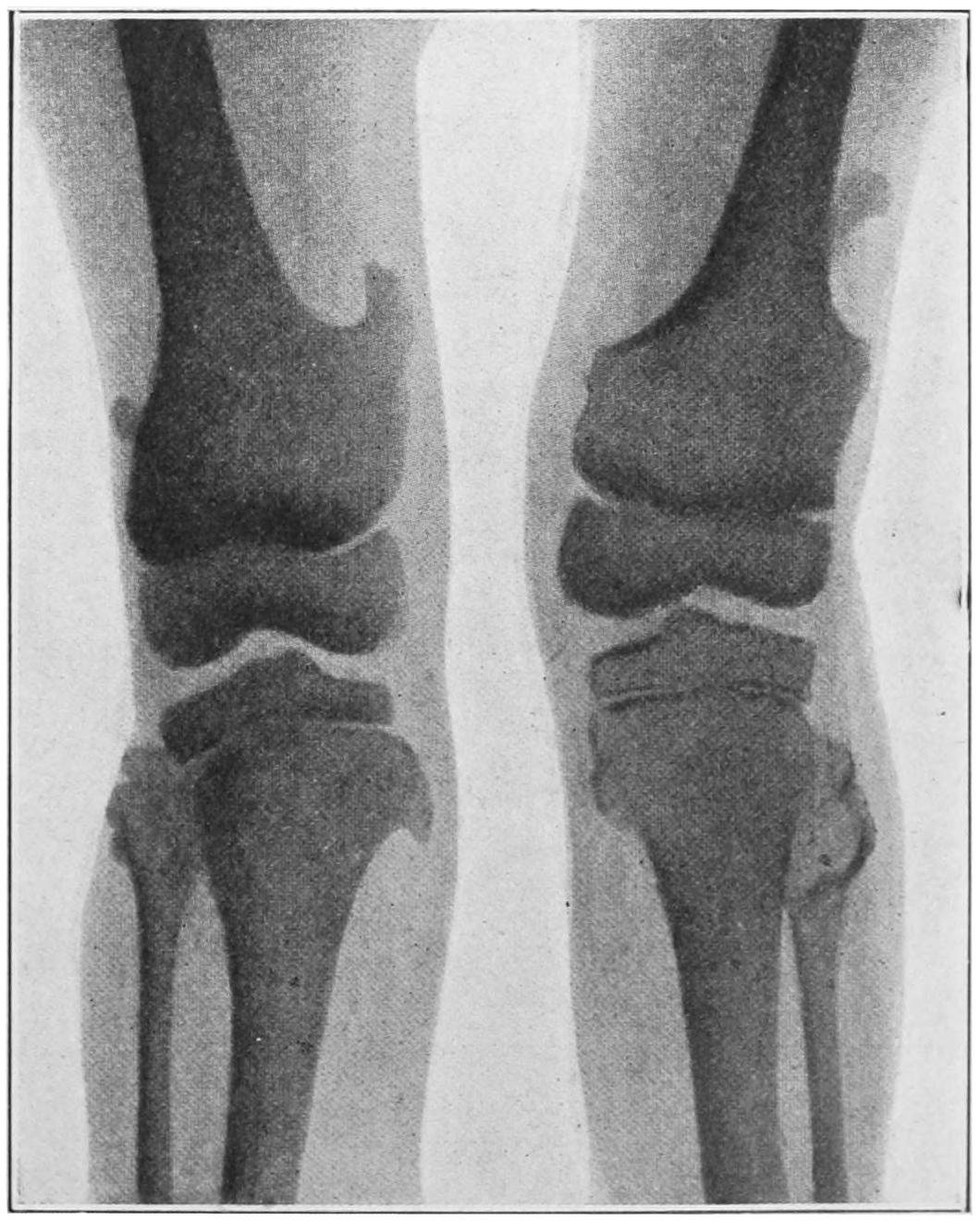
Multiple ecchondroses and exostoses. (Lexer.)
[440]
Fig. 246
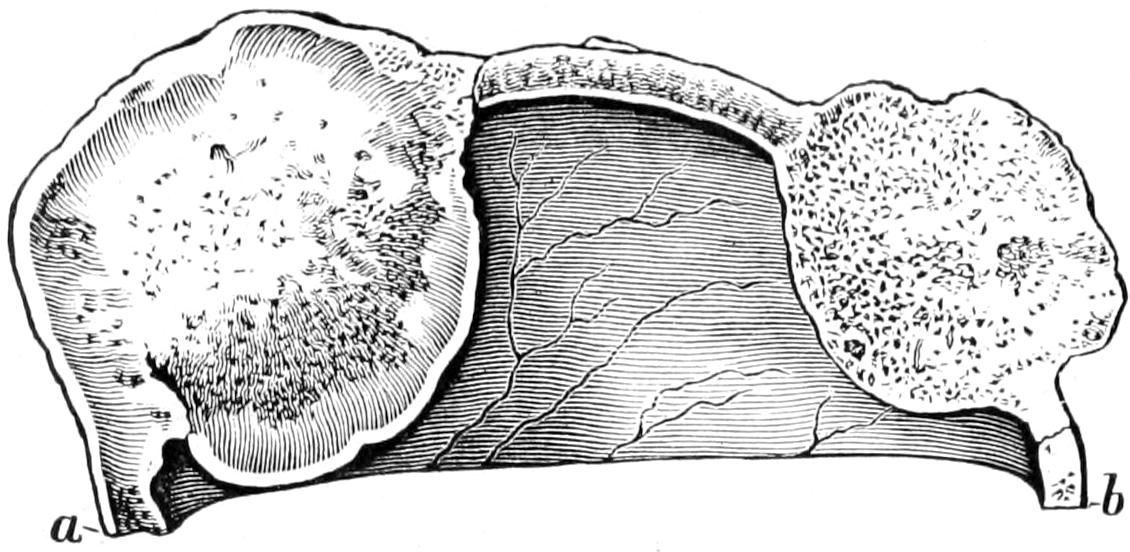
Cancellous osteomas springing from the diploë. (Musée Dupuytren.)
Fig. 247

Fig. 248

Sarcoma of femur. (Buffalo Clinic.)
Fungating osteosarcoma of cranium. (Pemberton.)
—Cartilaginous tumors, as stated in Chapter XXVI, are not often found outside of the bony skeleton. They may spring from cartilaginous extremities of growing bones, from epiphyseal cartilages, or from the interior of long and short bones, where their origin is probably due to inclusion of cartilaginous elements, as comprehended in Cohnheim’s theory. In young children they are often multiple and involve various parts of the body. Occurring in adults they are less often multiple, but may attain considerable size. (See Fig. 243.) They are found usually about the ribs, sternum, pelvis, and femora. If the entire structure of a given bone be involved in a growth of this kind, its eradication—that is, amputation—will probably be necessary.
[441]
Fig. 249
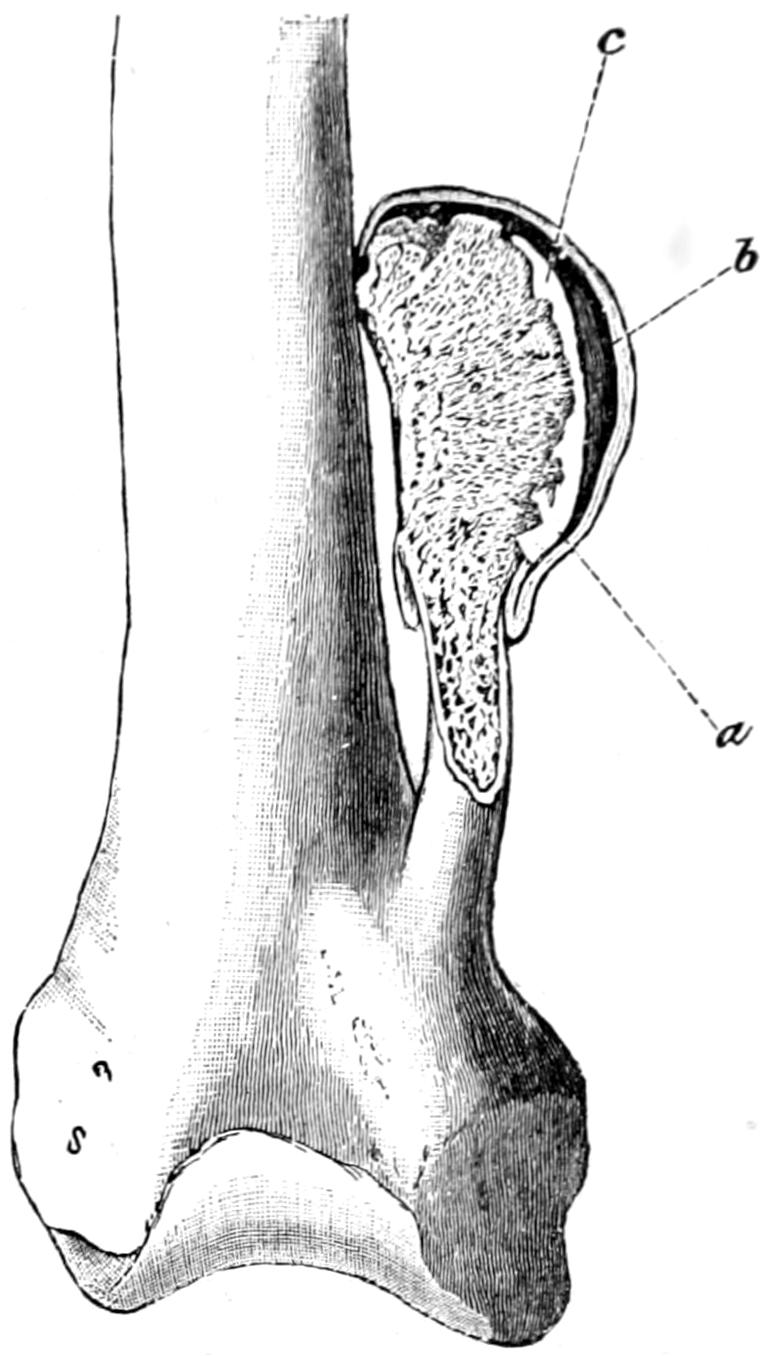
Exostosis bursata. (Orlow.)
When otherwise, complete removal with careful cauterization of the base of the growth or surface from which it sprang will usually be sufficient. These cartilaginous tumors tend on one hand to mucoid softening and cystic formation, and on the other to calcification or ossification, by which the original cartilaginous character of the growth may be concealed.
—Osteomas are by some writers made to include exostoses and hyperostoses. In accordance with the system followed in this work only those growths are considered as tumors which are of no physiological usefulness, and it is preferable to maintain a distinction between osteomas and the exostoses or bone hypertrophies, which pertain either to evolutionary relics or to constitutional affections.
There is, however, a peculiar form of exostosis which becomes covered by an adventitious bursa, whose walls become in time quite thick, which is called exostosis bursata. In the cavity of this bursa may frequently be found rice-grain or other fibrinous concretions. This lesion is common in the neighborhood of joints, and the new bursa frequently communicates with the joint cavity (Fig. 249).
—Myxomas are rare in bone, and are seen usually only as degenerated forms of cartilaginous bony or malignant growths. They lead to cystic degeneration. A primary growth of this kind has for its origin the bone-marrow.
—As already described, sarcoma of bone should not be confused with osteosarcoma. (See Sarcoma.) The former refers to sarcoma springing from the true osseous tissue or periosteum. When central the bony walls are expanded and form a shell. Osteosarcoma refers to a tumor springing from the original connective tissue which holds the bony elements together, and contains osseous tissue scattered through it. Sarcoma occurs usually in the long bones, although none are exempt; mostly single, it nevertheless may be multiple. It occurs frequently in the young, is seen even at birth, and in these instances is supposed to take its origin usually from epiphyseal structures. No period of life is, however, exempt. Tumors attain sometimes enormous size. Marsh has recently described such a tumor weighing thirty-three pounds. Microscopically these tumors may assume any of the varieties, endothelioma, angiosarcoma, etc., those of the most rapid growth being found rather of the round-cell type, while those of slow growth are usually myeloid or contain giant cells.
Sarcomas frequently arise from the periosteum. Commencing in the interior of a bone, they develop for the most part very slowly, and expand the bone more or less symmetrically, in distinction to those growths of external origin which are in evidence on one or another aspect of the bone involved (Figs. 247 and 248).
Sarcoma not infrequently has its origin from the callus of a delayed bone union, and I have had repeatedly to amputate for this sequel of fracture. (See Fig. 252.)
As the disease advances there is increase of pain, usually with increasing cachexia, while augmentation in size of such a tumor may make a limb not only useless, but the source of greatest annoyance and difficulty in management of the case.
—There is but one treatment in cases which will permit it—amputation of limbs, extirpation of tumors from certain bones, or excision of entire bones. Thus for sarcoma of the scapula we extirpate the entire bone; for sarcoma of the skull we make extensive resections of the same, removing the underlying dura when involved; for sarcoma of the lower or upper jaw we remove it in whole or in part. Sarcoma of the spine is inoperable, that of the pelvis almost equally so. In absolutely inoperable cases treatment by the toxins of erysipelas may be tested. In all cases where pain is severe opiates should be administered, which under these circumstances are[442] anodyne, stimulant, and almost nutritive. Patients in this condition should not be allowed to suffer, and opium in assimilable form should always be administered to any amount necessary.
Fig. 250
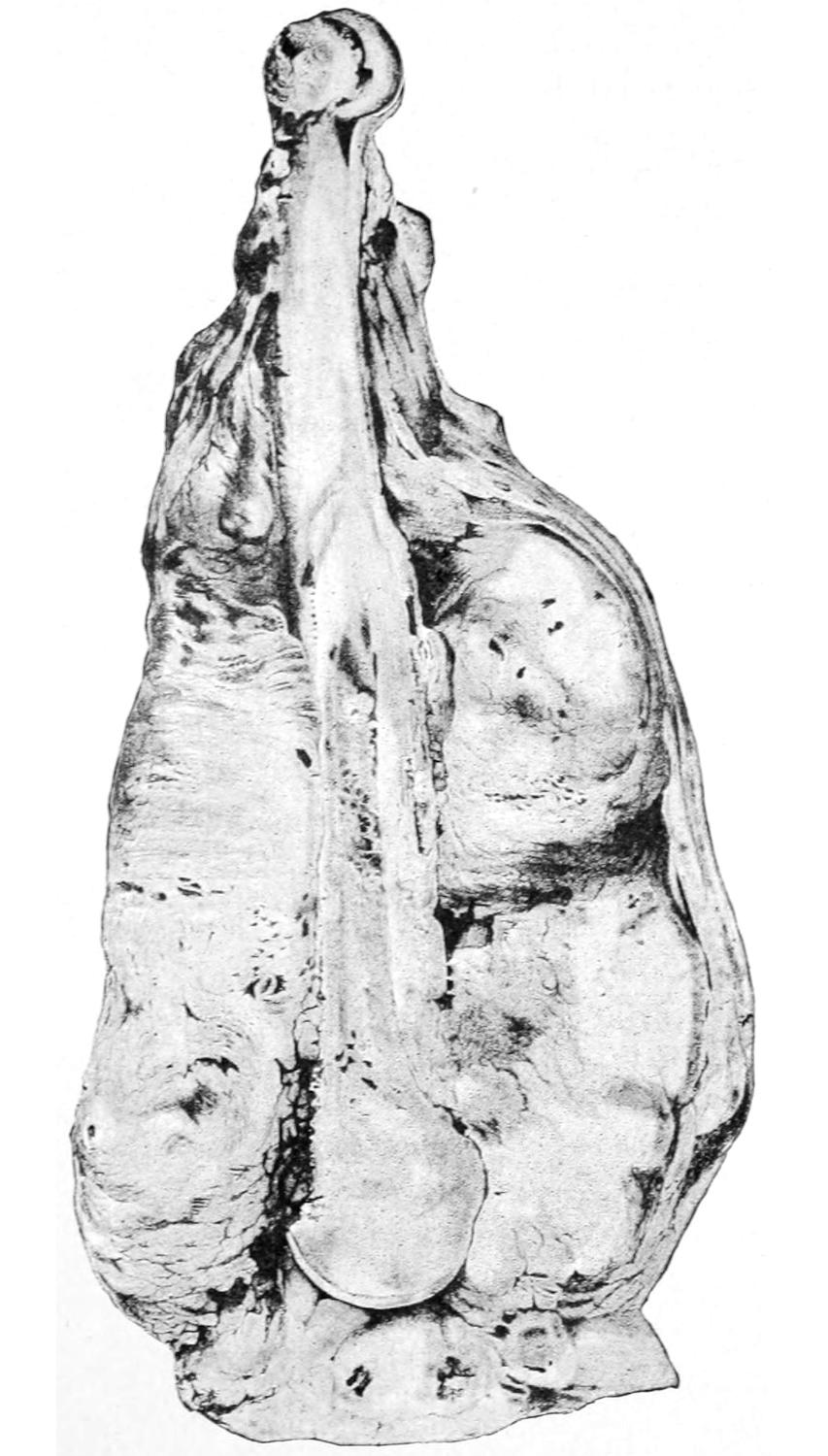
Sarcoma of periosteum of humerus. (Pemberton.)
Fig. 251
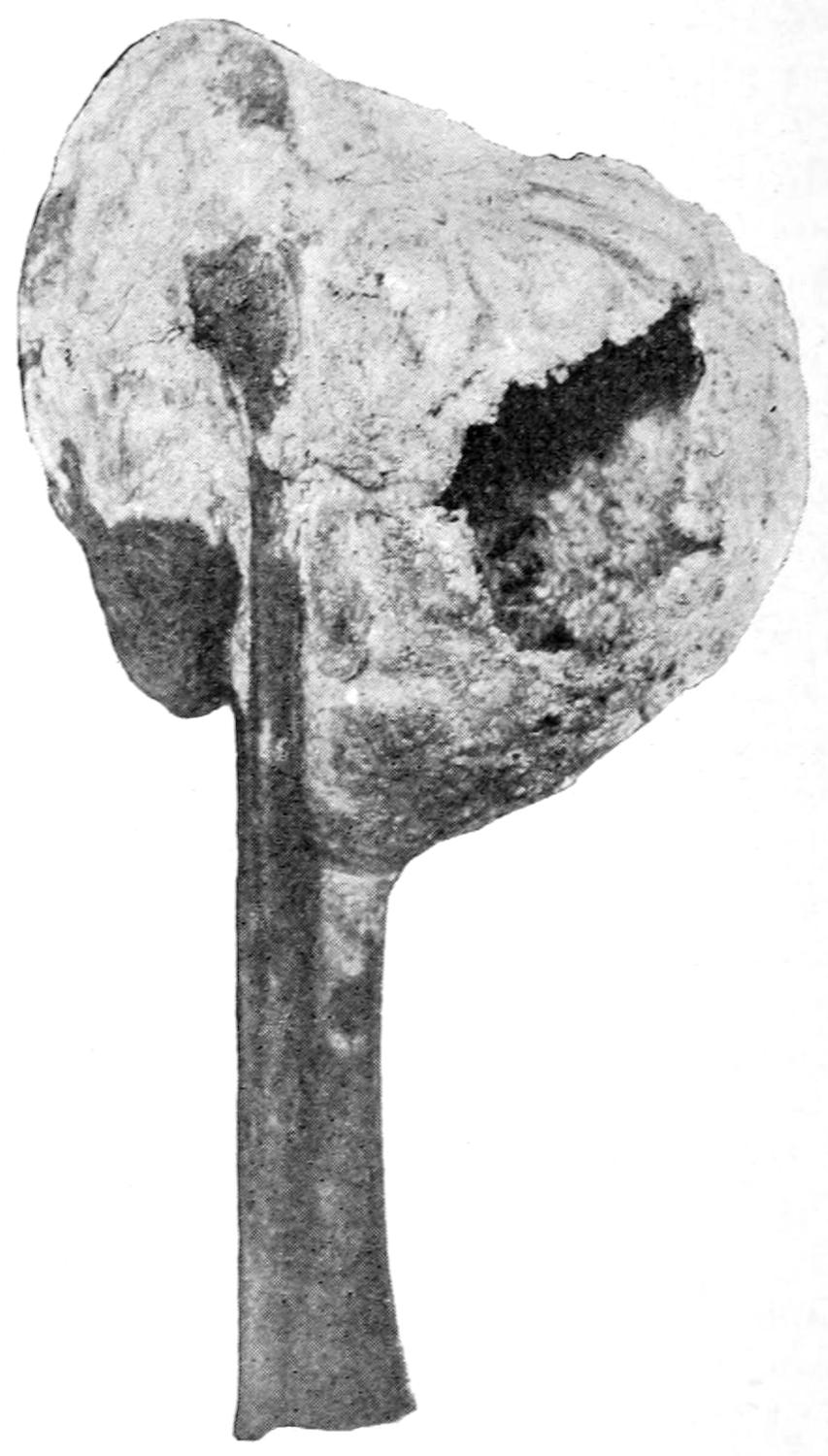
Bone cyst of tibia. (Buffalo Clinic.)
—Collins[36] reports the tenth recorded case in this country. The disease was first described by Bence Jones in connection with a peculiar proteid found in the urine. It is characterized by changes in the bones, with pain in the chest, back, and loins. In the urine albumose appears, which seems to be pathognomonic when taken in connection with such symptoms as those above. On section numerous small tumors are seen in the bones. The disease has hitherto been regarded as an expression of osteomalacia. All the bones of the skeleton may be involved without any tendency to metastasis in other tissues. On minute examination the myelomatous tumors met with seem to be found alike in the bone substance and the marrow, and to be cell proliferations of myeloid tissue. The matter is still left somewhat in doubt as to what should be meant by the term myeloma, this being a feature to be cleared up later. It is seen more often in males than in females, and in the later part of life. Aside from constant malaise, with pain in the back and side, there occur progressive weakness, with anemia, and such final softening and fragility of bones as to lead to spontaneous fractures, or to the projection of tumors, which may[443] be especially noted about the ribs, with deformity of the vertebræ. On close inspection the urine will be found turbid and albumose is detected. The disease is usually regarded as hopeless; there is no information regarding its successful treatment.
[36] Medical Record, April 29, 1905.
Fig. 252
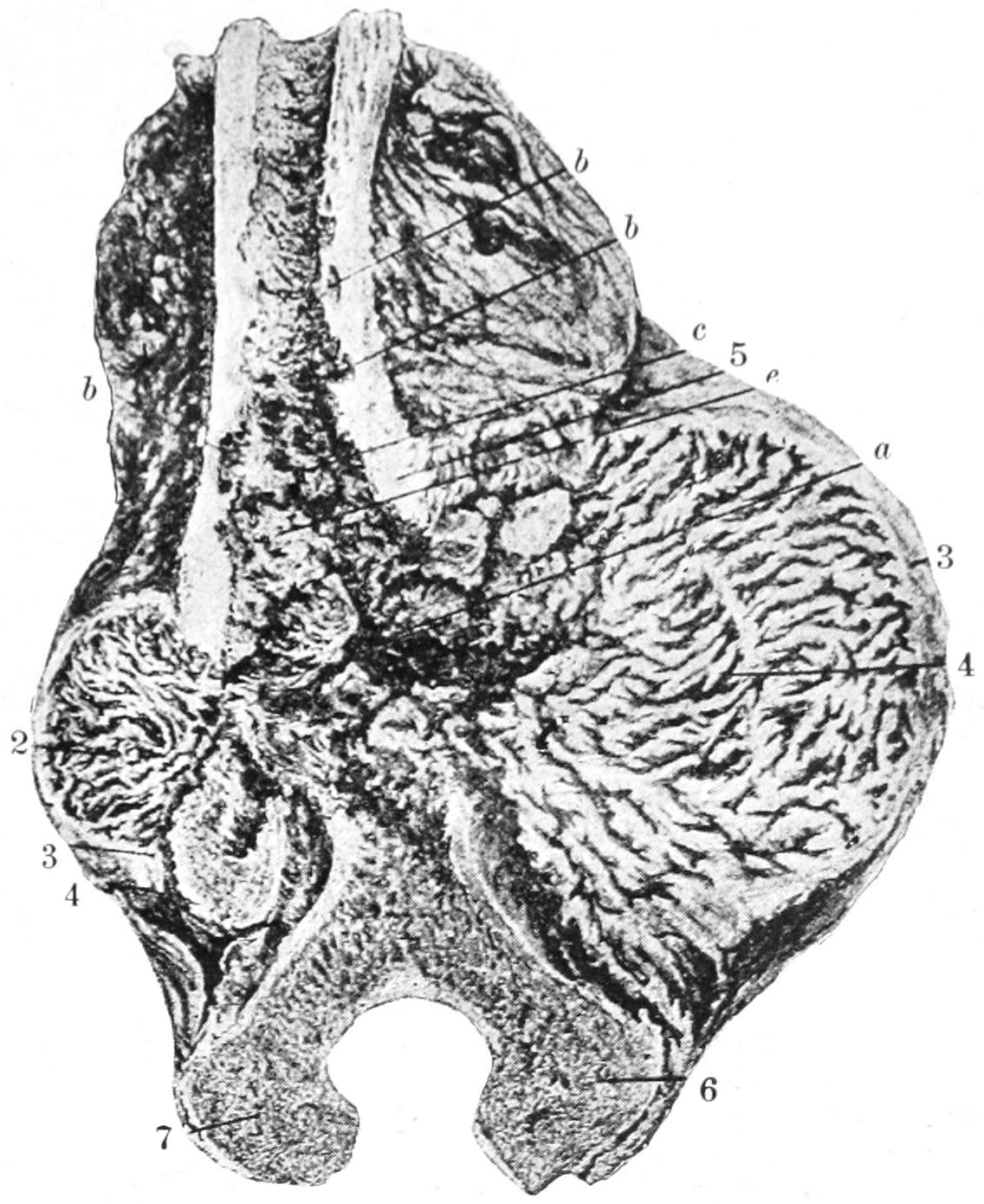
Sarcoma developing in callus. (Haberen.)
[444]
In previous chapters have been considered the various morbid conditions of bones, joints, muscles, and tissues which help to form the locomotor apparatus of the body. It would seem then quite proper in this place to insert the chapter usually relegated to the end of text-books on surgery where it stands by itself, i. e., the chapter on Orthopedics. As a subject orthopedics deals with the causation and the treatment of deformity, whether inherited or caused by disease. The term is used in a more or less elastic sense, and is made by some to cover a larger field than others would accord it. The subject divides itself into two parts:
1. The consideration of deformities produced by tuberculous or other infectious disease, and
2. Non-carious, congenital, and acquired deformities.
Tuberculous lesions do not differ in pathology or other respects from the tuberculous diseases of bones and joints described in earlier chapters of this work. Inasmuch, however, as some of them form distinct and clinical types of deformity they assume an importance which justifies reasonable consideration by themselves. Of these we shall consider spinal caries, sacro-iliac disease, hip disease, and tumor albus.
These various terms have reference to deformities of the spine of similar type, but with considerable variations, produced by caries (tuberculosis) of the vertebral column. Where osseous structures are separated by cartilaginous or more or less complete joint cavities the primary focus may form within the spongy structures of the vertebral bodies or in the softer tissues of the intervertebral joints. In other words, it is caries of the ordinary type which assumes special significance only because of the accident of its location. The entire vertebral column should be regarded as the main support of the body, while to it is due the maintenance of the erect position which raises man above the animal. When diseased and softened it yields to pressure, the result being exaggeration or distortion of its natural curves. As the instinctive tendency of the human being is to maintain the head in the line of the centre of gravity above the pelvis, any marked degree of curvature in one direction brings about, by natural causes, a compensatory curve in its opposite direction. A well-marked case of kyphosis, then, is characterized by more than one exaggerated curvature or protuberance, one being due to disease, the other to compensation.
While there may be several foci of active tuberculous disease, even in one vertebra, there may be found pronounced forms of angular curvature as the result of destruction occurring in but one or two of them. The carious process once begun may be checked at any point in its course, or it may proceed to complete softening and destruction, with formation of cold abscess. The tuberculous process once begun spares no tissue, and thus bone and intervertebral cartilage melt and disappear in the same manner. There may be a possible danger from spreading of tuberculous disease to the spinal meninges or to the cord, or of its being generalized. In the former case there is pachymeningitis and myelitis with paralysis; in the latter case it causes more or less rapid, acute general tuberculosis. Paralysis is more often induced, however, by actual compression than by mere tuberculous involvement, although the disease products which cause this pressure are likely to come from a caseous pachymeningitis.
The disease is most common in childhood, about 80 per cent. of cases occurring before puberty. Of the three regions of the spine the thoracic is the one most often[445] involved, next the lumbar, and lastly the cervical. The most common site of all is in the lower dorsal region. Deformity once established as the result of this disease cannot be expected to spontaneously disappear.
—Slight injuries occurring in those of tuberculous diathesis, by which there is produced a focus of least resistance, or secondary infections following upon such conditions as scarlatina and typhoid, constitute the most frequent recognizable causes. There can usually be obtained a history of some injury in about half of the cases. The disease once established may assume either an acute or chronic type.
—As indicated when discussing caries in joints the principal signs and symptoms are pain, muscle spasm, muscle atrophy, tenderness, deformity, and impairment of function. These are all present in Pott’s disease, to which they give that distinct clinical picture which Pott so graphically described about a century ago.
—Pain is rarely absent. It may be misleading, but is usually referred to the terminal distribution of the intercostal nerves, and thus may be complained of in the chest, the abdomen, or the legs. Many a “stomach-ache” in children is of this character and origin, and a complaint of frequent “growing pains” should be carefully investigated. Even in sleep these pains are characteristic, and have been previously described as “starting pains.” Children cry out with them in the night. They tire easily and tend to seek rest instinctively. Pain is always aggravated by excessive pressure upon the upper spine or by jars, such as may be received in jumping. It is not necessarily constant. Vertebral tenderness may sometimes be detected by pressing upon the ribs. This will especially aggravate symptoms when respiration is of a groaning character or when there is any expression of dyspnea. There may be vomiting or dysuria. A sudden increase of these painful features means a fresh focus of infection, impending abscess, or a danger of paralysis.
—It is by muscle spasm that we account for the attitudes and postures of Pott’s disease. It is a constant feature, but will vary in its expressions with the location of the disease. In caries of the cervical spine the chin is raised, the head is balanced somewhat backward, while the lower spine is straightened and given a backward curve. In the stooping posture the head is supported by the patient’s hands in the instinctive effort to protect it. In caries of the mid-dorsal region there is elevation of the shoulder, with marked tendency to support the weight of the upper part of the body by placing the hands upon the knees or thighs. Lumbar caries often produces perceptible backward curve in the lower portion of the spine.
In all cases there are stiffness and rigidity of the spine, and patients resort to all sorts of instinctive expedients to avoid motion in the affected area. When that part of the spine which is in relation with the psoas muscle is involved there is more or less psoas contraction, with characteristic flexor deformity at the hip, which is usually bilateral. This will give a peculiarity to the gait and cause it to be not only stiff in appearance, but it will be seen that the patient walks more upon the toes and with slightly bent knees, which are thus made to act as springs. An attitude assumed in stooping or in the effort to lean over as if to pick up an object from the floor is characteristic; the spine will not be curved forward and the patient will not stoop as usual for the purpose, but the spine will be more or less erect and stiff and lowered to the floor by flexing both knees and hips until the squatting position is assumed. In rising the same effort will be made to protect the spine from any motion between its component parts. (See Figs. 253 and 254.)
During sleep this muscle stiffness becomes even more pronounced, so that in the morning patients are “stiffer” than later in the day. The existence of muscle spasm can often be detected by palpation of the spinal lesion. Some lateral deviation or asymmetry of signs may often be noted, according as the muscles of one side are more pronouncedly influenced by the location of the disease focus, and it is the more common in proportion to the greater severity of the case.
The confinement caused by the disease will naturally be followed by more or less atrophy of the body muscles, but, in addition to that, those immediately involved about the centre of the disease undergo an atrophy due to it and often apparent on inspection.
—In numerous distinctive ways the patient constantly evinces tenderness and makes invariable efforts to protect against movement or even jar. Tenderness can also be evoked by pressure upon the head or shoulders, which will cause severe pain, or by causing the patient to jump down a step or to rise upon the toes and then come[446] down abruptly upon the heel. Pressure upon the spines of the affected vertebræ or upon the ribs which connect with them will also cause complaint of pain.
—This is the most striking objective feature of well-marked Pott’s disease. It is practically a backward projection known as kyphosis, the vertebra first affected being usually the first to yield, the others following or changing in shape as the disease spreads or as the growth of the individual permits accommodation and necessitates rearrangement. The more acute the disease the sharper the projection. Old and mild cases cause an abrupt curvature rather than a protuberance.
Fig. 253
Fig. 254
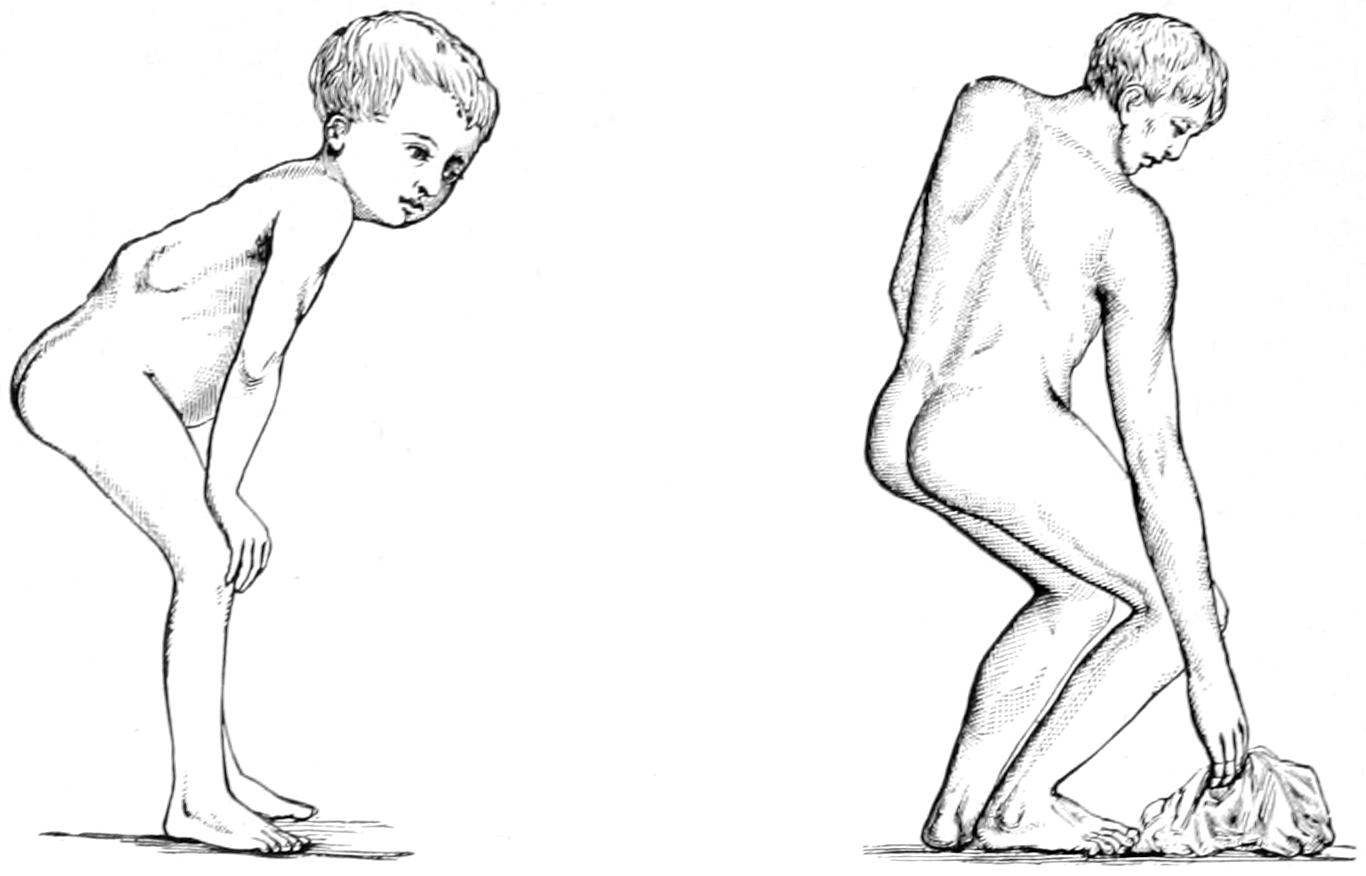
Typical postures of the spinal muscle spasm of spondylitis. (Bryant.)
It is well to keep a record of the deformity in cases under treatment. This may be graphically preserved by putting the patient flat upon the abdomen upon a straight surface and bending a strip of lead so that it shall fit the contour of the spinous processes. After it has been made to fit it may be removed and a tracing of the curve made upon a sheet of paper. Comparison of tracings thus made at intervals will afford a graphic record of the progress of the disease or of the improvement made. Kyphotic deformities lead to a shortening of the spine, so that growth is stunted and patients become dwarfed in appearance. Secondary curvatures are produced above and below the primary projection. Gradually as the shape of the vertebral bodies and of the entire spinal column changes the ribs are pressed more or less together, often being made to overlap, the shape of the chest undergoes alterations, the sternum sometimes being depressed and sometimes protruded, giving the chest, in the latter case, the so-called “pigeon-breast” appearance.
—There are but few disorders which produce more pronounced and widespread accompaniments than spinal caries. As change in the shape of the spine occurs and assumes a marked type we see changes occurring through the body, not only in the direction of anemia with general impairment of function, mental irritability, and cachexia, but there occur trophic alterations as well. The shape of the face changes, the expression assumed is one of anxiety, and the features become less mobile.
—Tuberculous meningitis, cerebral or spinal, is the most dangerous and acute condition, while other tuberculous complications may occur in various regions of the body. In fatal cases meningitis, in consequence of acute or mixed septic and terminal infection, furnishes the explanation for the great majority. Paralysis is not infrequent as a sequel, assuming the type of paraplegia and developing slowly. Motion is first impaired and a considerable interval may elapse before sensation is affected. Motor impairment varies from mere mild paresis to complete paralysis, beginning as fatigue, loss of strength, and inability to stand. Unless the disease be located in the lumbar region the reflexes are exaggerated and muscle spasm is easily provoked or occurs without perceptible cause. As above noted the muscles become atrophied, and when the cord is seriously compromised are rigid in chronic spasm. The rectum and the bladder suffer finally, especially in disease of the lower segments. Occasionally in cases of high dorsal disease the arms will suffer more or less motor[447] impairment. Sensory paralysis begins usually as paresthesia. In merely bedridden but not actually paralyzed individuals the reflexes should be normal. Of the muscle contractures, those of the psoas are the most common and distinctive. Paralysis follows rather than precedes deformity, and is noted in perhaps 20 per cent. of advanced cases. It should rarely occur if effectual treatment has been begun.
—Abscess is usually of the “cold” type. Its general character has been previously described. It may be of the purely tuberculous type, but is not infrequently the result of a secondary pyogenic infection. It is a consequence of neglect, but cannot always be prevented. Signs, both local and general, of the presence of pus or of pyoid are noted here, as under other circumstances. There is exaggeration of local tenderness, with development of tumor, which fluctuates as it approaches the surface. General septic features, proportional to the activity of the process and its location, accompany the local indications. Sometimes it occurs insidiously and with but few evidences.
Pus travels here in the direction of least resistance. The fascial planes of the body are mostly so placed as to protect important body cavities, consequently pus will travel usually around them and toward the surface, burrowing long distances, for instance, from the lower dorsal region to the groin along the psoas muscle. Cervical abscesses usually spread anteriorly toward the pharynx (postpharyngeal) and deeply into the thorax (mediastinal); they may open into the trachea or esophagus or externally through an intercostal space; or they may burrow laterally, opening behind the sternomastoid muscle. Dorsal abscesses usually travel posteriorly, opening not far from the spine, or they burrow downward and forward along the psoas so as to appear beneath Poupart’s ligament. Lumbar abscesses escape through the psoas sheath as psoas abscesses, so called, or between the fasciæ of the spinal muscles and those of the abdomen to appear upon the side; they may extend downward beneath the iliacus, escaping over the brim and into the pelvis and then out through the sacrosciatic notch. Of all these the psoas abscess, opening in the groin, is the most common. This will in time destroy the muscle fibers of the psoas, but it leaves the vessels and nerves intact, whose sheaths are much more resistant, and which can be found passing through such a cavity like cords through a chamber. This form of cold abscess, with its consequent bulging and final escape in the groin, has been mistaken for hernia as well as for abscess due to perinephritis and appendicitis. The most serious mistake would be to take it for a femoral hernia. The customary routes of all these collections of pyoid have been thus indicated. Nevertheless abscesses may burrow and appear almost anywhere. They will give rise to varying and to superadded symptoms, according to their location. For example, retropharyngeal abscess may seriously threaten respiration by pressure upon the upper air passages, while a collection of pus in the mediastinum might cause serious respiratory difficulty of another character.
Cold abscesses of spinal origin may remain stationary, the fluid portion of the pyoid material may even absorb, while the balance undergoes more or less degeneration and conversion into inert material, or they may slowly or rapidly increase in size. The best that can be hoped in such cases is absorption, with encapsulation of the solid residue. Even this may be a source of danger, as it is a focus of lessened resistance, in or about which subsequent trouble may result. Those abscesses which seem to remain stationary would best be let alone, hoping for subsidence under good treatment. Those which open spontaneously leave tuberculous fistulas behind them, which may possibly close in time, but which lead often to subsequent acute infection, and which are the bête noir of surgeons, for it is often impossible to heal them. The best that can be done in such instances is to wash them out, keep them clean, and guard them from infection from without. It is often possible to pass a tube along the sinus and through this to irrigate with a solution of iodine, of formalin, or of any other antiseptic which may be preferred. If anything be done with them in the operative way it should be as radical as possible, seeking the original lesion, thoroughly curetting its site and the whole interior of the cavity, and making ample opening so as to provide for effective drainage.
Retropharyngeal abscesses usually necessitate evacuation because of the obstruction which they cause within the pharynx. Lumbar and psoas abscesses may be let alone. When this is not practicable, then choice should be made between simple aspiration, aspiration with washing or injection of some antiseptic fluid, and free opening with radical treatment. In these cases we are to be guided by the peculiar features and surroundings of each, and by our own facilities for such work and for subsequent care of[448] the case. An abscess which will soon rupture should be opened and counterdrained; but in one where this is not impending, and where home features are such that the patient can receive no adequate or prolonged care, it would be wiser to abstain. Under the best of circumstances in these cases it is always a difficult problem to decide. Even aspiration leaves at least a needle track to be subsequently infected, while the contents may be too thick to flow through a small trocar. Aspiration with thorough washing out and then with injection of emulsions of iodoform or of other irritating antiseptics have found favor with only a part of the profession. If any radical measure is to be adopted the greatest care should be given to carry out the principles expressed in the general consideration of cold abscesses. (See p. 114.)
—Intelligent comprehension of signs and symptoms should enable one to make a diagnosis in most cases. Nevertheless the surgeon is occasionally in doubt and has to distinguish, for example, as between Pott’s disease and sprain, lateral curvature, hysterical spine, cancer, cord tumors, rheumatic arthritis, rickets, syphilis, actinomycosis, hydatid disease, acute osteomyelitis, i. e., non-tuberculous diseases, and certain abdominal affections followed by suppuration, such, for example, as peri-appendicular abscess. Moreover, spondylitis may be simulated in the course or as a complication of typhoid, scarlatina, gonorrhea, and other acute infections. Psoas abscess should be distinguished from perinephritic abscess as well as from acute appendicitis, which often causes psoas contraction, especially when the appendix is posteriorly placed and left in contact with that muscle. We may also have to distinguish this condition from sacro-iliac disease and from ordinary hip disease.
—In some degree prognosis depends on what is meant by a cure. Absolute cure, with restoration to the original condition, is exceedingly rare. Arrest of disease, with improvement of deformity, is possible in cases seen early. Even considerable motion may be restored under suitable treatment. In late cases hectic, amyloid degeneration, and dissemination of the disease make the outlook very discouraging. At best its relief is slow and in time it is always chronic, no matter how rapid the onset, except in those instances where dissemination occurs early and rapidly, in which case there is little or no hope. In ordinary cases there is a certain tendency to spontaneous recovery, but not without deformity and impairment of function, while obviously the occurrence of abscess prolongs a case to a considerable degree.
—Those general measures so necessary for the treatment of any tuberculous lesion, namely, hypernutrition, fresh air, and general constitutional measures, are needed here as in any other such disease. Physiological rest, i. e., absolute rest in a bed without springs, the patient lying flat on the back or on the face, and not on the side, and lying quietly, constitutes the best part of local treatment. In the case of children it is best to have a gaspipe frame, across which cloth may be stretched, on which a fretful child can be secured by straps across the shoulders, pelvis, and knees. This frame may be laid upon the bed and lifted from it while a cross-piece is removed for toilet purposes, or a suitable opening may be left if a single piece of cloth be stretched across it. If the patient can be made to submit to this repose, then a pad may be placed under the projection. After a sufficient length of time, with the desired improvement, a plaster shield may be molded to the back, with the patient lying upon his face; and then, after removing and suitably trimming and lining this mold, the patient can be returned in it to the previous position in bed, from which he may gradually be raised. This is the best method to follow in acute or severe cases, or when the disease is higher up in the spine. It will also best serve the purpose when the case is complicated by abscess. To it may be added, if necessary, traction upon the head (Fig. 255).
Fig. 255
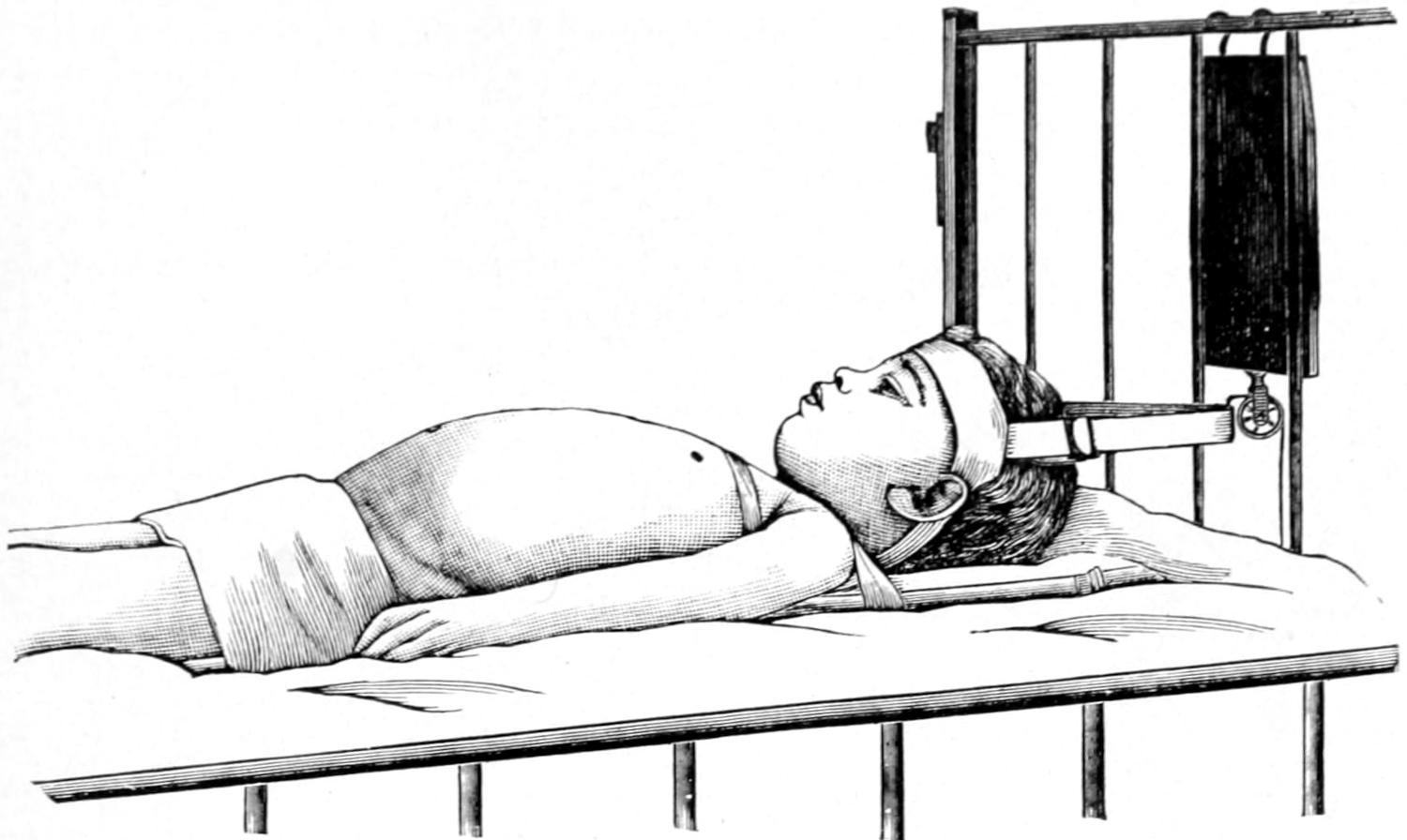
Child in bed-frame, with head traction. (Lovett.)
Fig. 256

Jury-mast for high dorsal and cervical caries. (Lovett.)
—The simplest of all apparatus is the plaster jacket, or corset, which was brought into favor in this country by Sayre, although not invented by him. It is usually applied in suspension, i. e., with the patient in the erect position beneath the frame, from which hangs a support by which firm traction can be made, both upon the head and the arms or the shoulders. The intent of such a jacket is to apply it with the patient so stretched out that a certain degree of the projection will at least be eliminated and the back made more nearly straight than it otherwise would be. In cases where this is impossible it at least affords better expansion of the thorax and supports the ribs in better relation to the spine, affording more chest room. The plaster is not applied next to the skin, but a thin undershirt or its equivalent of woven materials should be applied, care being taken to see that it fits snugly and is not allowed to fold[449] in ridges. After the patient is completely suspended to a degree where discomfort begins, then a small “stomach pad” is slipped beneath the under-jacket, in front, in order that more room may be given for enlargement of the abdomen after a full meal. Finally with the first turns of the plaster a strip of tin or a couple of strips of moistened pasteboard should be applied directly over the middle line in front and incorporated in the successive turns of bandage, in order that there may be material there which may be cut down in removing the jacket. Small pads should be placed over the iliac crests and over the protrusion if it be at all marked or tender. Now by the use of a series of bandages of gauze, in which reliable plaster of Paris has been incorporated, the entire trunk is enclosed within a corset, which will quickly harden as the plaster becomes firm. It should extend well down over the pelvis and nearly to the trochanters, since from this portion it takes its fixed support. It should then be extended as high as can be permitted under the arms and higher yet over the chest and back. Enough material should be used along with the plaster-of-Paris cream, as the former is applied, to ensure sufficient firmness and strength. If the plaster be reliable it will not be necessary to keep the patient suspended more than a few moments after the completion of the jacket. The finishing touches may be given it after he has been taken from the frame and placed again upon a soft surface.
Another method of application is to have the patient recumbent and properly supported, and this is particularly necessary in acute cases, where suspension is likely to cause faintness or unpleasant symptoms. In this attitude the spine is really put in better position. The method is not at all available in those few cases of lateral curvature which demand jackets (Fig. 256).
Substitutes for these jackets are made of various materials, such as leather, rawhide, aluminum, thin strips of veneering, celluloid, paper, glue, etc. These have to be constructed over a mold which is taken from a plaster jacket. When the disease extends above the level of the fifth dorsal vertebra there should be incorporated within the jacket a support for the head, known since Sayre’s time as a “jury-mast.” This consists of a metal upright, with cross-pieces, which are incorporated with the[450] jacket and which is curved up behind and over the head and made to carry the frame from which the leather straps and supports pass beneath the occiput and the chin, and thus give to the head a certain amount of fixation. The support is so arranged as to permit of sliding and of sufficient expansion so that traction upon the head can be made effective.
Fig. 257
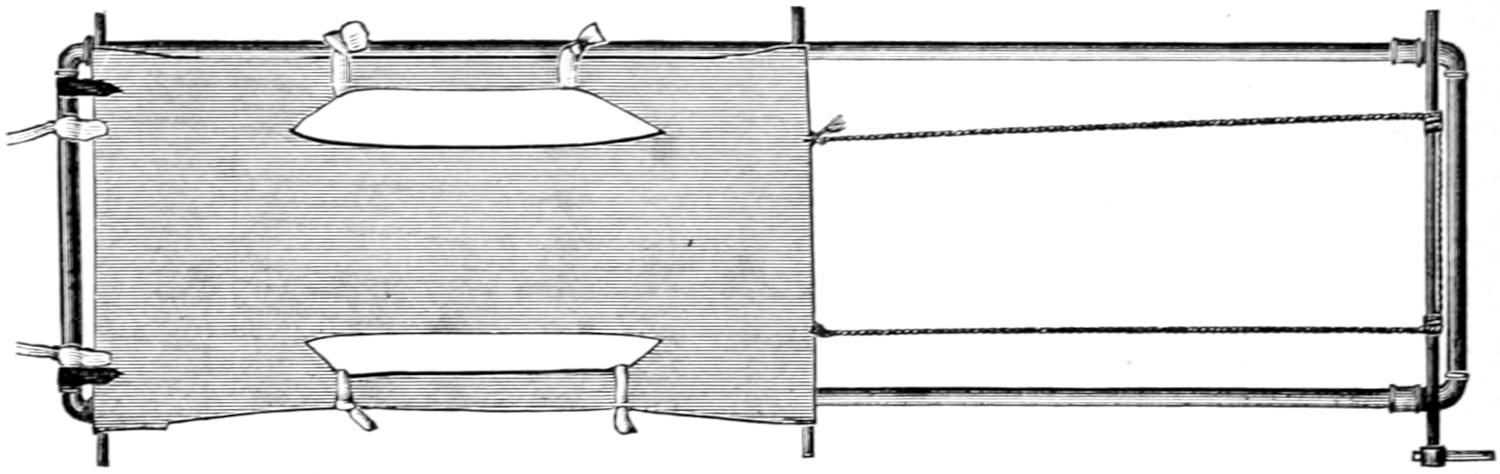
Frame for application of plaster jackets in recumbent position. (Lovett.)
Fig. 255 shows the application of traction to the head, while Fig. 256 illustrates one form of apparatus by which the jury-mast is made effective in producing traction on the head in the upright position. Figs. 257 and 258 show a convenient frame and method for making plaster-of-Paris corsets with the patient in the recumbent position. Figs. 259 and 260 show another form of apparatus intended for the same purpose.
Fig. 258
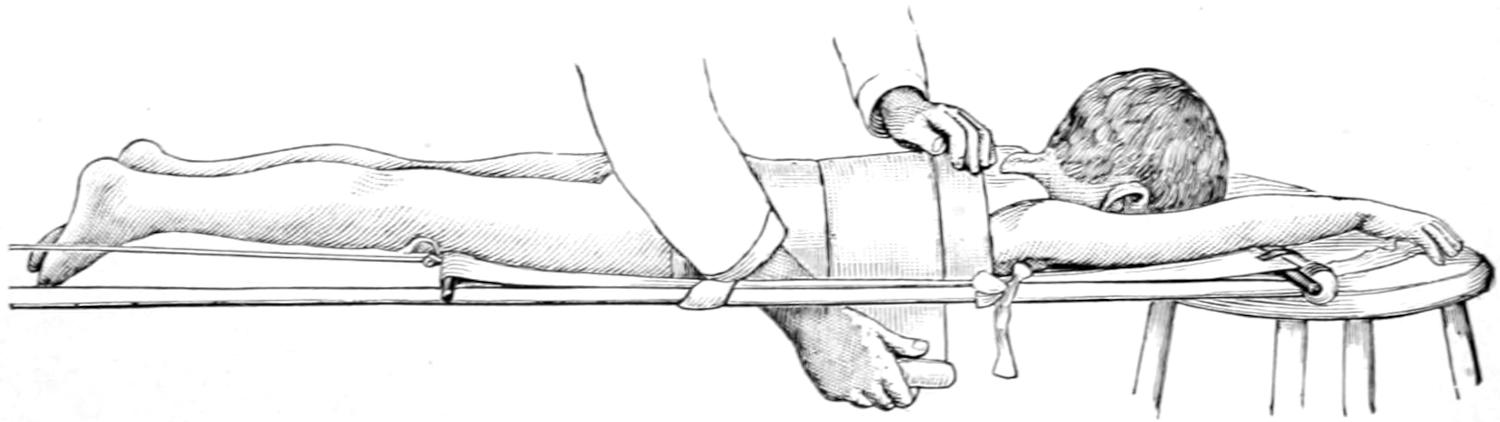
Application of a plaster jacket in the recumbent position. (Lovett.)
The variety of apparatus which has been devised for the maintenance of rigidity and correction of deformity, and, in suitable cases, traction upon the head, is to be measured almost by the number of orthopedic specialists, nearly every surgeon inclining to some device or at least modification of his own. Judson probably has formulated the best rule covering the entire matter when he says: “The apparatus may be considered as having reached the limit of its efficiency if it makes the greatest possible pressure upon the projection compatible with the comfort and integrity of the skin. It is essential that the brace is efficient; second, that it is one that can be constantly worn, if necessary, or can be easily detached from the body if not to be worn at night.” Certain ambulant cases can be treated by an effective brace through the day, and rest at night upon a reasonably hard mattress, with traction upon the head. Concerning the multitude of these special aids to treatment it hardly seems worth while to go into any elaborate description in this place, inasmuch as one who is incompetent to judge as to what is best should not retain the management of such a case, while one who is really competent will probably desire to make his own selection, and the writer’s recommendation would count for but little. Every case must be a law to itself, and every special brace must be constructed especially for the individual for whom it is meant; otherwise it loses all its serviceability.
—The feasibility and propriety of forcibly reducing the deformities due to spinal caries was first suggested by Chipault, of Paris, who suggested wiring the spinous processes of the affected vertebra, and then, by Calot, who, in 1896, described a method of forcible reduction under an anesthetic. The first to actually wire the spine under these circumstances was Hadra, of Texas, who had actually done the operation four years before Chipault. The method has probably less to commend it in actual[451] practice than in theory, and, attractive as it may be in respect to time and completeness of reduction, it is often followed by serious accidents, such as hemorrhage, rupture of abscess, fracture of the spine, etc. Bradford, in 1899, collected 610 cases performed by 29 different operators, with a record of 21 immediate deaths from local trauma and 15 cases in which there were at least alarming immediate symptoms. Of 229 of these cases complete correction was effected in 119, incomplete in 94, while no gain whatever was made in 16. Of results reported later, 66 showed some gain, there was no relapse in 17, while 49 showed more or less return of deformity. The claim has been made that the more or less wide gaps or bony defects which may result from forcible manipulation are filled in by new bone, but there do not seem to be any observations to confirm this statement. The amount of force which must be employed is a matter for the finest discrimination. The method includes complete anesthesia, traction upon the spine in each direction from the location of the deformity, and direct pressure force applied to the protection itself, as by a sling passed around the body and just beneath the projection, which can be used as a fulcrum upon which the rest of the spine can be applied as a double lever, with the application, at first, of gentle force, and, finally, sufficient to either satisfy the operator that he should go no farther or that the desired effect has been obtained. Immediately after completion of the maneuver a snugly fitting plaster jacket should be applied and the patient kept absolutely at rest in bed.
Fig. 259
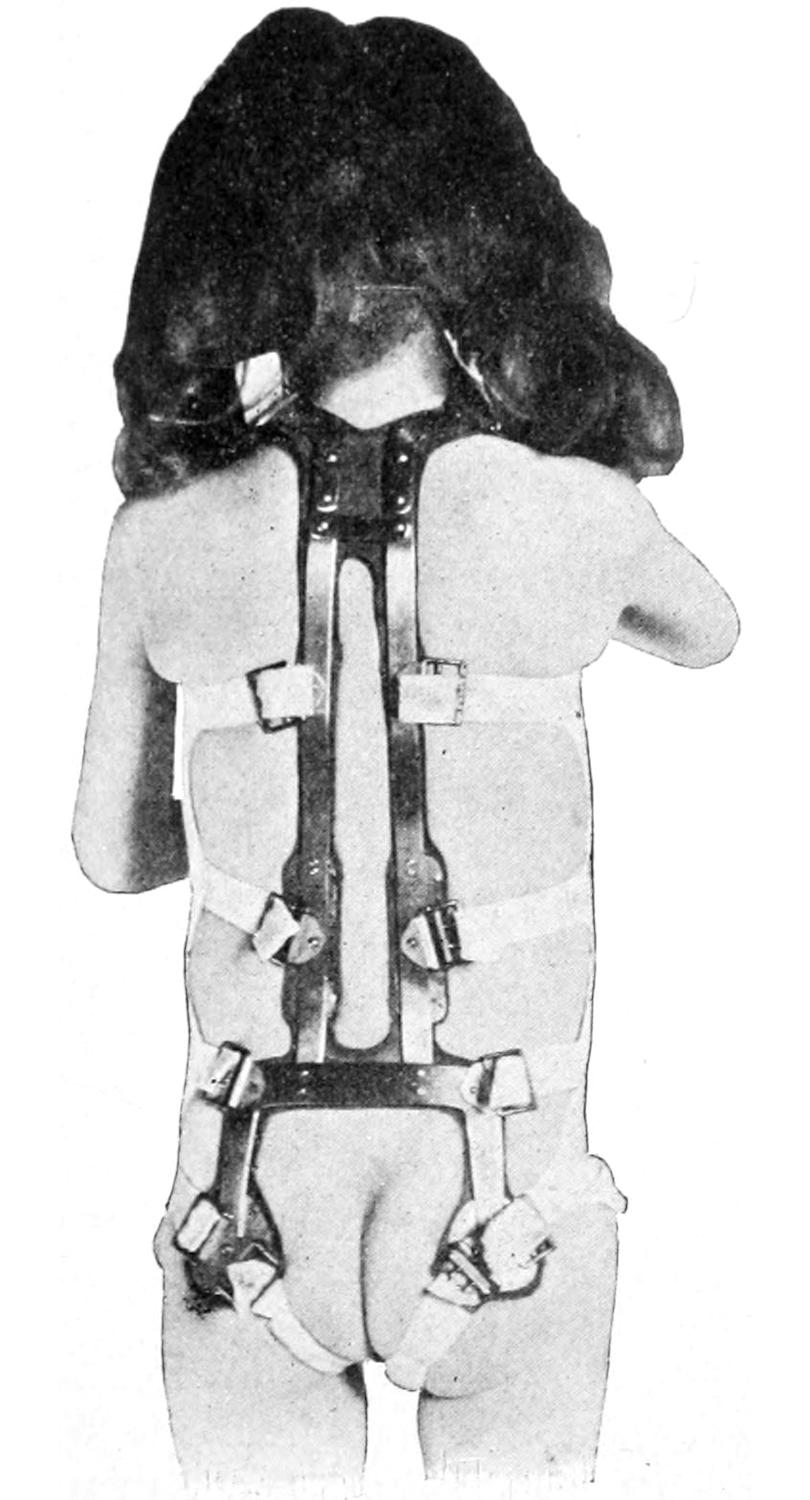
Anteroposterior support: back view. (Lovett.)
Fig. 260
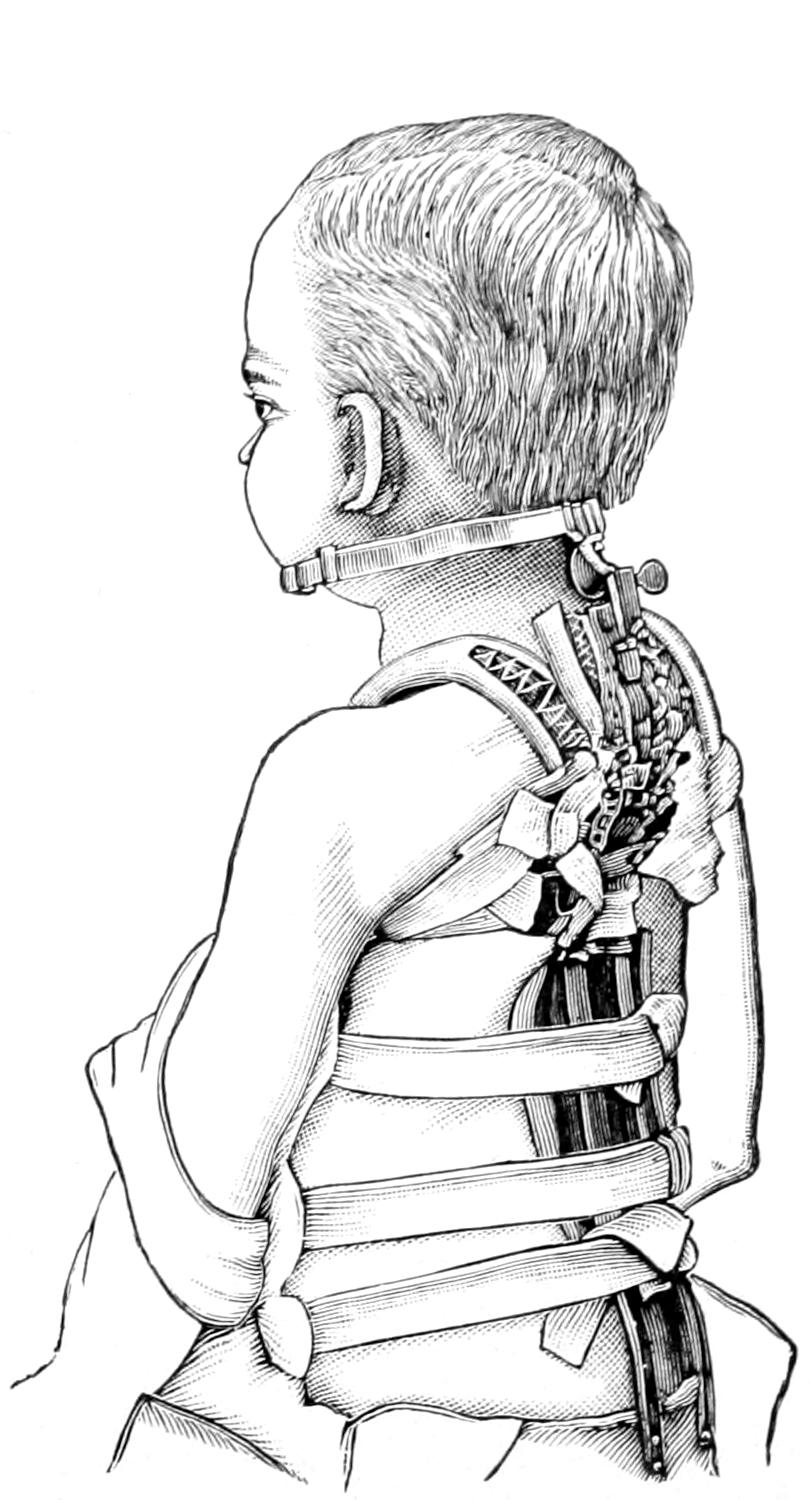
Anteroposterior support with head-ring for high dorsal caries: side view. (Lovett.)
The method seems most applicable in the presence of paralysis, even of long standing, and this feature has often been relieved.
Psoas contraction is best treated by traction, with the patient in bed, and with the maximum of weight and power applied which can be tolerated by the individual. If this seem impracticable, then the patient should be anesthetized and force applied until it is evident that more harm than good results. Should this harm appear, then open division of the tissues may be practised. Finally, as a last resort, in intractable cases, a subtrochanteric osteotomy may be made.
[452]
Pressure paralysis necessitates operative relief. This may be practised late and should consist of a laminectomy and exposure of the area compromised by bone pressure or that produced by pachymeningitis. The operation is done in the same way as for fracture, and will be described in the chapter on Surgery of the Spine.
Finally of all cases of Pott’s disease it may be said that each should be studied by itself, and for each a suitable method or apparatus devised, rather than to endeavor to apply indiscriminately unchangeable methods or forms of apparatus. Every apparatus has its disadvantages as well as its benefits. The more acute the case the more is absolute rest in bed, with traction, demanded. This is particularly true of disease in the upper spine. On the other hand, the more chronic and the lower the disease the easier it is to handle, and with such simple expedients as plaster corsets. When the sacral region is rigid, however, recumbency is usually necessary, because of the difficulty in securing adequate fixation within any apparatus that can be worn. The necessity for general constitutional, dietetic, and climatic treatment should never be forgotten, and the danger of possible acute dissemination kept ever in mind. This is particularly imminent when too much freedom is allowed. Time, patience, and discernment are the dominating factors beyond the general principles already inculcated.
Under this name is included a tuberculous condition of the bony tissues on either side of the sacro-iliac synchondrosis, or of the cartilage itself, similar to that which produces the special caries described above. It is an uncommon expression of tuberculous disease occurring often in the young, identical in pathology with other tuberculous bone lesions, and giving rise to peculiar symptoms, mainly because of its location. Early in the course of the disease these may consist of mild discomfort in the lower abdomen, irritability of the bladder and bowels, disinclination for exercise, while, as the disease becomes more pronounced, there will be actual pain, intensified by standing, relieved by lying down, often severe at night, usually referred along the course of the sciatics. A most significant symptom is the tenderness and complaint produced by firm pressure made upon both sides of the pelvis, thus forcing tender surfaces against each other. In the later stages of the disease abscess may develop and present either externally in the lumbar region or internally, breaking into the pelvis and appearing perhaps in the groin or close to the perineum. The disease is usually unilateral, and will cause characteristic limping and aggravated pain upon standing on the limb of the affected side. Naturally this limb will be spared in every possible way. It is likely to be mistaken for sciatica or lumbago, in neither of which diseases is there any tenderness at the sacro-iliac joint such as can be evoked by pressure from the sides of the pelvis. It also has to be distinguished from hip disease by the fact that motions at the nip are not interfered with, and from Pott’s disease of the lower spine, which usually causes prominence of the spinal processes and local tenderness in a different region.
The surfaces and tissues involved are extensive and the disease is always serious. It is one of the most chronic of all such affections, and too often tends to suppuration, with its slow but inevitable consequences, or to dissemination. Thus of 38 cases with abscess reported by Van Hook only 3 recovered.
—Treatment should consist of absolute rest, with traction, so long as the symptoms are active, and avoidance of all irritation when patients rise from bed. Abscess due to sacro-iliac disease should be radically attacked, especially if this can be done early. Intrapelvic pus collections may require trephining of the pelvic walls or resection of some portion of the ilium, by which complete evacuation may be made and drainage be amply provided. When the joint itself is thoroughly broken down the case will have a hopeless aspect.
Hip-joint disease, or, as it is often called, coxitis or morbus coxæ, is worthy of special consideration on account of its frequency, its importance, and the deformities which result from its existence. The most frequent site of the disease, which is of the usual[453] type of tuberculous ostitis or osteomyelitis, is on the femoral side of the joint, usually in or near the head of the bone. In a small proportion of cases the first lesions appear upon the acetabular aspect of the joint, while in some cases the primary tuberculous lesion is of the type of a tuberculous synovitis. (See chapters on Bones and Joints.) In addition to those changes already described in previous chapters there occur certain distinctive alterations about the hip-joint which are worthy of note. On the pelvic side the margins of the acetabulum occasionally become softened, and naturally yielding in the direction of pressure as the result of muscle pull upon the thigh toward the pelvis, cause, first, an elongation of the originally merely circular cavity, and, finally, considerable shifting of position, often referred to as migration of the acetabulum. Thus the head of the bone may be found in a socket thus formed on a level one inch higher than on the well side. So also perforation of the acetabulum may occur, with perhaps final escape of the head of the bone into the pelvic cavity. On the other hand, similar changes produce decapitation or marked alterations of shape in the head and neck of the femur.
—When the symptoms and signs of tuberculous disease in this location are studied in accordance with what has already been stated in general about caries of the joint ends of the long bones, we have among the most significant features:
—This is referred most commonly to the knee because of the relations of the obturator nerve to the hip-joint and to the region of the knee. Pain may also be radiated in other directions, but the complaints made of pain in the knee are classical. Pain is not, however, a pathognomonic feature and may be almost wanting, but the evidences of tenderness, if not of pain, are invariably seen in the unconscious protection of the joint afforded by muscle spasm. It is perhaps in hip-joint disease that night pains and cries are most frequently heard.
—Fixation of the affected joint is always noted. It begins as a limitation of motion, naturally first noticed in the extremes of rotation, flexion, and extension, and is perhaps the most important early sign of the disease. It furnishes the explanation for the subsequent postural features, as well as an index regarding the gravity and extent of the morbid process. It may be seen even in the lower spinal muscles, where it is detected by laying the patient upon the face, lifting first one leg and then the other, noting the freedom of hyperextension; in fact, this spinal muscular involvement is sometimes so marked as to give rise to the suspicion of low Pott’s disease, from which it is to be distinguished by the fact that the spasm affects one side rather than both.
—This involves in time all the muscles concerned about the hip. It begins early, but may not be very pronounced until quite late. It can usually be determined by measurement if not apparent upon inspection and palpation. There will also be noted more or less obliteration of the gluteal crease or fold.
The three cardinal features—pain, spasm, and atrophy—having been thus considered, we can better appreciate the characteristic gait and postures peculiar to this disease. Limping is an early feature, sometimes insidious at first, sometimes abrupt. Patients will avoid coming down quickly upon the heel, while they walk with the knee slightly flexed, in order to give more spring. Stiffness is most apparent on rising from bed in the morning, while the limp is more pronounced at night, and it is at this stage especially that night cries are most frequent. To mere limping succeeds actual lameness with more constant pain. Muscle spasm now leads to malpositions, no one of which is necessarily first to appear, and any of which may occur with others in various combinations, although flexion and adduction are usually the first to be seen, the patient unconsciously assuming that position which happens to give him most relief.
It is important to realize that a marked degree of adduction will cause apparent shortening, and of abduction apparent lengthening, and it is very important to demonstrate that these variations in length are apparent and not actual. This is to be done by placing the patient upon a hard surface with the pelvis at right angles to the spine and the limbs in absolutely symmetrical position. If there be adduction it may mean that the limbs should be crossed; while if there is abduction the healthy limb should be abducted to the same degree as the one affected. Careful measurement will show that the differences are apparent rather than real. The same care is needed in regard to rotation, and particularly in regard to psoas contraction which leads to flexion. One of the most characteristic evidences of hip-joint disease is flexion of the thigh, which, when the thigh is brought down to the proper level, will cause an arching upward of the lumbosacral[454] region. By this time also will be found well-marked limitations of motion in every direction. All of these features should be ascertained without an anesthetic, as they depend upon muscle spasm, which anesthesia would subdue. It is somewhat difficult with intractable young children to make a thorough examination of this kind, but a second or third effort will usually succeed when the first has failed.
Peri-articular symptoms affording corroboration are found in thickening of the tissues about the joint, especially enlargement of the upper end of the femur, or increase in thickness of the pelvis, which may perhaps be felt from the outside or be detected by rectal examination. There is usually involvement of the inguinal lymph nodes, and there is frequently prominence of the superficial veins, due to infiltration of the deeper tissues and obstruction to the return circulation. A good skiagram will also render much aid.
As the disease progresses there will appear evidences of deep suppuration, as abscess is frequent in the advanced stages. This may be peri-articular or may connect with the joint. It may cause separation of the epiphyses of the femoral neck and complete loosening of the head of the femur, which will then become a foreign body in a joint cavity probably filled with pus. Perforation of the acetabulum may also occur. Much of this abscess formation goes on insidiously and without marked increase of symptoms. There is no fixed date when pus may begin to form. It may occur relatively early or late. It is possible for small amounts of pus to absorb in whole or in part, or to leave a residue more or less encapsulated, which will frequently lead later to a secondary abscess, the latter tending to burrow along between the fascial planes or muscle sheaths and appear at some distance from its origin. Pelvic abscesses result from perforation of the acetabulum and may break internally or externally. Nearly all of these collections are of the cold type, and after a long time, if they have opened, may cease to discharge characteristic pus or even pyoid, and simply give vent to a watery seropus. Pus left to itself usually escapes anteriorly to the tensor vaginæ femoris, but it may travel in any direction.
The deformities and possibilities which may result from the advanced stage of hip disease are striking. Persistent muscle spasm leads to more and more flexure of the thigh, with abduction or adduction, as the case may be, while later the leg is drawn up so that the knee may almost touch the abdomen. As the bony portions of the joint change their shape there occur actual shortening and final dislocation, while all the adjoining parts show the effect of muscle atrophy and perverted nutrition. In addition to this the region of the hip may be riddled with abscesses or with sinuses, and the condition in every respect made extremely distressing.
While the disease is generally confined to one side, it may occur in both hip-joints, in which it, however, very rarely begins simultaneously. Existence of double joint disease of this character makes the case more than usually troublesome and complicates it seriously in every respect. The writer has been compelled to make double simultaneous resection of both hips.
—This has usually to be made from congenital dislocation, hysterical joint, infantile paralysis, non-tuberculous disease—such as synovitis, bursitis, etc.—acute osteomyelitis of the upper end of the femur, Pott’s disease in the lumbar region, and sacro-iliac disease, as well as from perinephritic abscess and appendicitis.
—Hip-joint disease usually tends toward recovery, but generally with more or less deformity. When the circumstances are not favorable, ankylosis, with or without deformity, is inevitable, while abscesses, with persistent fistulæ, are not uncommon, and one may in extreme cases witness death from general tuberculous dissemination or from the consequences of hectic, with amyloid degeneration, or from acute septic infection.
One may naturally ask what may be considered as constituting recovery. In cases of this kind an absolute cessation of all symptoms and indications of the disease, with a minimum of deformity and of limitation of motion, are the nearest approach to ideal recovery that can be expected to secure. In favorable cases, seen early and properly treated for a sufficient time, there may be achieved almost a restitution ad integram, but such an ideal is seldom attained; otherwise there is nearly always more or less limitation of motion, with very frequent pseudo-ankylosis or actual ankylosis. Even this is favorable and most anything may be considered so which falls short of actual suppuration.
—The essential in the early treatment of hip disease is traction, so applied and regulated as to be effective. It should not be thought that by such traction as can be tolerated joint surfaces are actually pulled apart. What it really accomplishes[455] is to tire out muscles which are in a condition of clonic spasm, overcoming thereby the deformity which they produce and thus permitting a reduction of their activity and of the harm which they have done. To do even this requires a considerable degree of traction, especially when muscle spasm is very prominent. Therefore it is best in pronounced cases of deformity to place patients in bed, and to apply traction by weight and pulley to a degree which actually overcomes the defects which we are combating. This will often require more weight than many men are in the habit of using. It should now be a question, not of amount of weight, but of effect, and of the easiest and best way of bringing this about. Physicians are very likely to use too small an amount of weight, and to neglect the use of counterextension and the benefit of more or less lateral traction, as well as that in direct line of the limb. Moreover, they often use inadequate means of applying traction, resorting to it only in such manner that traction is made at the knee and not at the hip. Even in young children it is often necessary to use twenty pounds, with a suitable traction apparatus, and four or five pounds for effective lateral traction.
Traction should be maintained until deformity has been overcome or the effort shown to be impracticable. After its complete benefit has been obtained it should be followed by fixation, the ideal method being that which accomplishes both fixation and traction at the same time; as, for instance, by the so-called Thomas splint, which permits the patient to be up and about with the use of crutches and a high shoe beneath the well limb, in order that the diseased limb may not be permitted to touch the floor, but rather to hang, and by its own weight afford a certain degree of traction. The Thomas splint is the simplest and cheapest for hospital work, while modifications in more elegant and expensive form are illustrated in works on orthopedic surgery. In cases which seem to demand it fixation can be effected by a plaster-of-Paris spica put on while the patient is standing upon the well limb and upon an elevation. The character of this work affords space neither for more elaborate description nor illustration than the hints embraced in the foregoing paragraphs.
The surgeon as such is perhaps the more concerned in the treatment of abscesses which frequently complicate these cases. Much that has been already said about psoas abscess will apply here. It is a question requiring considerable discrimination as to just how to treat a small, cold abscess about a diseased hip. Much will depend upon the environment of the patient, i. e., upon the attention and expert care which he may receive. Such abscess should be treated kindly, i. e., by nothing more severe than aspiration, until ready for more radical treatment. By the latter term is meant readiness for following it down to the joint cavity and exsecting the head of the bone, if need be, following this with extirpation of the capsule, etc. When there is actual pyarthrosis the condition of the patient is sufficiently serious to warrant radical measures. Extra-articular abscesses are apparently quite common, yet most of these, if carefully traced, will be found to lead through the periosteum at some point into the osseous structure beneath. Such abscesses are, moreover, multilocular, and have ramifications in even unsuspected directions which should be followed with the sharp spoon and the caustic, in order that absorbents may be seared and that no infectious material remain. Old and persistent fistulas should also be treated kindly until one is ready to be radical. Some long-standing cases will heal after absolute physiological rest of the joint, i. e., by fixation in plaster-of-Paris splint, with openings opposite the fistulas for dressing purposes. The general constitutional condition of patients with these lesions is a predominating factor in their improvement—a fact which should never be forgotten.
The deformity which has resulted from old, long-standing, and quiescent hip disease affords opportunity for the best of surgical judgment. It is possible to effect great improvement in position by subcutaneous osteotomy after ankylosis, but this should not be attempted during the active stages of the disease.
The question of excision of the hip-joint is one of importance. In few other instances do social surroundings or factors enter so largely into the question of surgical judgment. The wealthy can afford long-continued treatment, which to the poor is prohibited, and one may be tempted in one case to exsect early when, under other conditions, he would treat the case tentatively. Nevertheless certain indications make the operation expedient in all cases, as, for instance, when the destructive process is steadily progressing or so acute as to shorten not only the limb but life itself. It is necessary also when there is necrosis, and in most instances of suppuration extending into the joint cavity. In those[456] cases where skiagrams confirm other indications to the effect that the disease is localized in the neck or head of the femur, Huntington’s suggestion may be adopted, after exposing the upper end of the femur, to drill or tunnel in the direction of the neck until its diseased focus is reached and thoroughly clean it out. In cases treated otherwise conservatively, yet accompanied by a great deal of pain, especially those of the femoral side of the joint, one may frequently get relief by exposing the upper end of the femur and making ignipuncture in the same direction as above.
In general it is impossible to lay down succinct rules for the treatment of hip disease. Cases differ so greatly in location, in severity, as well as in environment and their personal surroundings, that what is advisable in one case is not to be thought of in another. Of the mechanical features of treatment one may say that that is the best splint or apparatus which best meets the indication in each particular case, and that none will be effective in which the element of traction is neglected, nor that of physiological rest. No patient should be released from treatment whose hip is still sensitive or in whom there remains any muscle spasm. Rest and protection should be maintained for months and even years after apparent recovery, while the same attention should be given to diet and climatic surroundings as in any other case of well-marked tuberculous disease.
This subject deserves special consideration, mainly because of the peculiar deformity produced by the disease rather than any of distinctive peculiarity in its nature. Years ago it received the name of tumor albus, and is frequently called white swelling by the laity, because of the pallor of the surface and the increased dimensions of the limb due to thickening, always of soft parts, and usually of the bone itself. The disease may begin in either epiphysis, in the patella, or in the synovial membrane, oftener in the bone in the young and in the synovia in adult cases. Its most distinctive feature is the deformity produced by excess of muscle spasm, the hamstring muscles especially producing a backward subluxation which frequently fixes the knee, not only at a right angle, but with very much disturbed joint relations, so that the head of the tibia is in contact with the posterior surface of the condyle rather than with their proper terminal areas. The soft tissues outside of the bone are frequently very much thickened and infiltrated, often edematous, while the joint cavity may be more or less distended with seropus or with old pyoid material. The exterior surface is so anemic from deficient blood supply as to make it appear comparatively white, while the superficial veins are made much more prominent by their engorgement owing to obstruction of the deep circulation. The picture, then, of an advanced case of tumor albus is quite typical.
Here the joint cavity is so large that there is early effusion of fluid, in most cases, which is in this location easily recognizable; hence the distinctive symptoms consist of pain, tenderness, swelling, limp muscle spasm, with, finally, limitation of motion, deformity, and atrophy. In addition to these features there may be added those due to the formation and the escape of pus, i. e., one may have the signs of acute or old suppuration, while the parts about the joint may be riddled with old sinuses. The deformity of these cases is usually characterized by a certain amount of external rotation of the leg, while a species of knock-knee is not uncommon. Actual lengthening of the limb due to overactivity at the epiphyseal junctions may also be noted.
—The treatment of white swelling is based upon the principles already laid down for the treatment of spinal and hip caries, the underlying feature being traction to a degree sufficient to overcome muscle spasm, unless it be too late to permit a subsidence of active changes. When seen early a few weeks of confinement in bed, with effective traction, followed by fixation with plaster-of-Paris bandage, combined with the Thomas splint (see above) or with some other form of more elaborate apparatus, by which rest and traction can be continually maintained, will be needed. The presence of tuberculous disease about the knee permits of the application of the elastic bandage above the knee, by which the congestion treatment of Bier can be more or less effectually carried out. It would, however, be a mistake to rely entirely upon this to the neglect of traction and rest, nor should too much be expected of it in severe cases. It is a method to be used early rather than late.
[457]
The final resort is excision, which is practically adapted to cases of moderate type in young adults, where the bones have attained their full growth and where it will afford a prospect of cure in a minimum of time. It is undesirable in children because it is so often necessary to remove the epiphyses, and because of the arrest of development that follows such removal and the consequent shortening of the limb. Nevertheless even in children it may be demanded and may be considered as a resort superior to amputation, the latter being reserved usually for a life-saving measure or for desperate cases where destruction has been practically complete and the limb is hopelessly useless.
Of the other large joints, all of which may be involved in tuberculous processes similar to those just discussed, it may be said that they come under the general rules of treatment already laid down.
This term includes a peculiar postural deformity by which the head is rotated and inclined abnormally to one side in a more or less fixed position. As to the causes of the deformity two will be considered:
Congenital causes include:
1. Injury to the sternomastoid muscle at birth, which is perhaps the commonest.
2. Abnormal intra-uterine position and pressure.
3. Arrest of muscular development.
4. Intra-uterine myositis, the muscles being sometimes found actually altered in structure.
5. Defective development of the upper vertebrae or such distorted growth as is often met along with other deformities, e. g., club-foot.
The acquired causes include:
1. Traumatisms, either direct, as by injury to the muscles, such as may happen from gunshot wounds, etc., or follow operations by which the spinal accessory has been injured, or by burns, and other lesions which cause much cicatricial contraction.
2. Reflex activity in connection with disease of the lymph nodes, deep cervical abscesses, parotid phlegmons or tumors, etc. Whitman states that tuberculous disease of the cervical nodes caused the condition in 50 per cent. of over 100 cases analyzed by him.
3. Reflexes from the eyes, as Bradford and Lovett have described from the orthopedist’s standpoint, and Gould from that of the oculist, refractive errors causing the head to be held in unnatural positions in order to improve vision.
4. Compensation in high degrees of rotary lateral curvature, the effort being to keep the head facing to the front.
5. Myositis, usually rheumatic, but sometimes a sequel of the infectious fevers, or even of gonorrhea.
6. Habitual deformity, the result of occupation or sheer bad habit.
7. Tonic or intermittent spasm leading to spastic contractures whose causes are difficult to seek, but appear to inhere in the central nervous system.
8. Paralyses of certain muscles, permitting lack of opposition and consequent deformity.
—According to circumstances significant pathological changes may be found in the affected muscles. These are usually the sternomastoid and the trapezius, although in long-standing or complicated cases the deeper muscles of the neck may also participate. A long contracted muscle may change almost into mere fibrous tissue.
The secondary effects of contraction of the sternomastoid and the trapezius are really far-reaching and noteworthy. The jaw may be drawn down and to one side, so that teeth do not appose each other as they should, or perhaps even do not meet. Compensatory curvatures occur also in the spine and there is well-marked change in gait and in most of the body habits. In the young and rapidly growing cranial and facial asymmetry also become pronounced. The later results and deformities of torticollis are not to be mistaken for congenital elevation of the scapula, sometimes known as[458] “Sprengel’s deformity,” which consists not merely in elevation, but in rotation of the shoulder-blade so that its lower angle is too near the spine. There may be some limitation of motion of the scapula and of the arm. Sprengel accounted for this abnormality by maintenance of the intra-uterine position of the arm behind the back. The acute forms of torticollis occur nearly always in acute phlegmons of one side of the neck, and should subside with the other and causative lesions. Nevertheless from such spasm may develop a chronic form which may persist.
The position of the head varies with the muscles particularly involved and the associated spasm. The sternomastoid muscle alone will draw the mastoid down toward the sternum, with rotation of the face to the other side. When the trapezius is involved the head is drawn backward and the chin raised. The more the platysma, scaleni, splenii, and deep rotators are involved the more complex becomes the condition, to such an extent even that in serious cases it is almost impossible to decide which muscles really are at fault. When the superficial muscles are involved they can usually be distinctly felt to be firm and contracted, while the sternomastoid will stand out like a cord. Pain is a rare complaint, but a feeling of tenderness or soreness is not unusual.
The spasmodic or intermittent form is less common, but more difficult to account for and even to treat. It seems to be due to choreiform spasm of those muscles which produce it, and here the condition is reflex, the causes lying deeply in the nervous system. In some instances, however, they are of ocular origin and can be relieved by correcting refractive errors. Intermittent spasm is usually absent during sleep and quiescent in the recumbent position; it is usually confined to one side.
—In the matter of diagnosis it is necessary mainly to eliminate only spinal caries, while as between involvement of the anterior and posterior groups of muscles the determination is made by palpation and inspection.
—There are few morbid conditions whose cause it is more necessary to discover. Could this be done operative treatment would be less often demanded. Treatment should depend, therefore, on the exciting cause and the possibility of its removal. The spasmodic or intermittent form may spontaneously subside. Cases of essentially ocular origin need the services of the oculist, and other acute cases usually subside with the successful treatment or the subsidence of their causes. On the other hand, chronic cases usually need either mechanical or operative treatment.
The most common operation for relief of torticollis is simple tenotomy of the sternomastoid, taking care to divide the sheath and everything which resists, and, at the same time, to avoid the external jugular vein as well as the deeper structures. Mere tenotomy of one or both of its lower tendons is an exceedingly simple measure, but in serious cases an open division will permit of more thorough work. Here an incision made one inch above the clavicle and parallel to it will permit division of everything which resists and also any recognition of that which should be spared. In any event the position of the head should be immediately rectified, and kept so either by plaster or starch bandage, or by a traction apparatus applied to the head, the body being in the recumbent position, while later some efficient and well-fitting brace should be worn for some time. The posterior cases, i. e., those where the posterior muscles are involved, afford greater operative difficulty, muscles involved lying too deeply and being in too close relation with important vessels and nerves to justify the ordinary wide-open division. Nevertheless in extreme cases there need be no hesitation in extirpating completely those muscles which are primarily and mainly at fault. The writer has removed the sternomastoid and the trapezius, with sections of the still deeper muscles, and has seen nothing but benefit follow the procedure. It should be resorted to when repeated anesthesia with forcible stretching and a suitable brace fail to give relief. These forms of wryneck which are due to contraction of muscles infiltrated from the presence of neighboring phlegmons, etc., will usually subside with massage and semiforcible stretching under an anesthetic. They need conservative rather than operative treatment. Attack upon the spinal accessory and the deep cervical nerves will be described in the chapter on Surgery of the Nerves. It, however, will rarely be justified, since the primary causes inhere not so much in those nerve trunks as in the nerve centres. Such operations are usually of questionable benefit, and cases should be carefully watched before being submitted to them.
[459]
Under these terms are included certain deviations from normal relationships of the vertebræ, both in their superposition in the median line and in their rotation on each other, by which are produced lateral curvatures, with more or less rotary displacement. Of these deformities there is a rare congenital form which is due to fetal, or rather intra-uterine, rickets, but practically all rotary lateral curvatures are acquired. One-half of such cases begin before the twelfth year of life. It may also come on during adult life, as the result of bad postural habits, exclusive use of the right hand, etc. Altogether it occurs in about 1 per cent. of females and in a smaller percentage of males. Scoliosis being not a disease but rather a process of irregular growth, cannot be said to have a symptomatology. It is known rather by signs. Only in the advanced stage can it produce symptoms. It is rarely seen in its incipiency by either the surgeon or the physician. Not until parents have noticed distortions of the spine are these children usually taken to their medical advisers. Exception, however, should be made to this in respect to certain gymnasia and athletic training schools, where trainers are quick to notice irregularities of this kind. The abnormal curves thus produced are at first flexible, but later become fixed. In rapidly growing girls who take but little exercise there may be some muscle weakness, which may cause fatigue or even actual soreness. Pain is rarely present. The rate and extent of deformity are not subject to any rule. Spontaneous cessation ensues in practically every case, i. e., a stage of convalescence and arrest, at a time when the deformity may be but slight, or perhaps hideous.
The nervous phenomena attending lateral curvature, like the discomforts attaching to it, are mainly due to the increasing strains and stresses that are imposed on certain structures as the deformity occurs and increases. Of these, muscles and ligaments suffer most, especially those uniting the thorax and spine. Pressure effects on nerves and tissues may be produced by distorted ribs and vertebræ or by final displacement of viscera. The conditions which lead up to spinal curvature are attended often by neurasthenic and neurotic features, both mental and physical. As deformity increases impairment of function of thoracic as well as of the upper abdominal viscera will occur, and such patients are usually thin and anemic, rather than fat.
To mere lateral distortion is added, in every pronounced case, more or less rotation of the entire trunk. The curvature consists of one primary curve, with one or two secondary curvatures, according to the location of the first. If the primary curve be located in the mid-dorsal region there will occur compensatory curvature above and below in order that the head may still be kept in the line of the centre of gravity above the pelvis. Such secondary alterations are of much less import than the primary. The most common of the mid-dorsal curvatures, which occurs in nearly four-fifths of the cases, has its convexity to the right. While the right shoulder seems higher its scapula will be more pronounced and carried backward, the back and the chest below it will be more rounded, and in front the breast on the opposite side more prominent. The whole trunk in marked cases becomes so warped that the arm on one side will hang free while the other touches the pelvis; thus the back loses its symmetry either in the erect or stooping position. In the lumbar region there is compensatory curvature to the opposite side, which makes one hip and flank more prominent. By virtue of the rotation of such a warped spinal column there result certain anterolateral curvatures that may later become pronounced. While such changes are going on in the upper part of the trunk there is sufficient rotation of the lumbar segment to lead to tilting of the pelvis, with consequent limp, or a peculiarity of gait.
The degree of torsion of the spinal column is the best index of the real severity of a given case, and to it are due the most disfiguring features of the deformity. Torsion may even precede curvature, causing a prominence of one shoulder or hip as the first visible evidence of its existence.
Those forms of lateral curvature due to rickets occur most often in the dorsal region, and as frequently in boys as in girls. In most of these cases the constitutional condition will be indicated by other significant features. Another form much less frequent, yet well known, is the result of inequality of the length in the limbs, so that patients stand ordinarily with tilted pelves; hence, the limbs should be carefully measured in every instance. A truly paralytic form of scoliosis is also known, which is of the infantile[460] type and due to some form of infantile palsy. Again, scoliosis is produced by shrinkage of tissues and contraction of old exudates occurring within the thorax and following chronic disease, as when the ribs on one side are drawn down after an old pleurisy or empyema. Extrinsic causes of lateral curvature are met with among several occupations when one side of the body is used more than the other, or when the individual habitually stands in an unsymmetrical position. In addition to this, the habitual right-hand habit, which seems instinctive, and which the majority of people exhibit, leads to excessive use of the right side of the body, with overdevelopment and consequent warping of the upper part of the skeleton. The young should be taught the use of the left hand as well as the right, i. e., to become ambidextrous.
The foreign surgeons have given the term ischias scoliotica to a form of lateral curvature involving rather the lower part of the spine and occurring usually in adults or elderly people, which is accompanied by more or less acute pain, usually assuming the type of sciatica. Its etiology is obscure, as is implied by the synonym scoliosis neuropathica. It is not a frequent malady, but usually chronic and refractory. It is best dealt with by fixation or immobilization.
—Predisposing causes of scoliosis may be both constitutional and inherited. They include general debility, rickets—with its accompanying osseous instability and liability to abnormal curvature—the consequences of various diseases of childhood, and anything which greatly lowers vitality. The actual causes include congenital or acquired defects, such as differences in the lengths of the limbs or other skeletal asymmetries; acquired abnormal position of the head due to defective vision, with its natural sequences; results of intrathoracic disease, such as empyema; faulty attitudes and bad developmental habits, such as those assumed often in school and elsewhere in sitting at a desk or standing in bad position, or at work in various ways. To these should be added the right-hand habit already mentioned. These may all be summed up as among the causes of asymmetrical growth and deformity, occurring as the result of ignorance or inattention, and allowed to go on indefinitely or until it is too late to correct the malposition. Theories of paralysis of individual muscles or certain muscle groups have been advanced, as well as of contractures, but usually these are effects which have been mistaken for causes. The bones have been blamed, but their changes are secondary results of pressure, save perhaps in some cases of rickets. The structures of the thorax have relatively considerable superimposed weight to carry, and both lateral halves of the thorax should be developed symmetrically in order to distribute this weight evenly. Nothing so influences skeletal development as exercise; thus even to assume and maintain the normal erect attitude requires a certain amount of muscular effort, and if each side be not given an equal task one will develop at the expense of the other, and thus lateral curvature is sure to result.
It is important to impress this on parents, teachers, nurses, dressmakers, and all who have a part in the care of the young, in order that they may realize the importance of ensuring symmetrical growth and of preventing the right-hand habit. It is to be expected that after deformity has occurred there may result a series of perversions of function in nerves, as well as in viscera; thus, respiration and circulation may be interfered with, the liver may be compressed, while, of course, autopsy will show all sorts of distortion of bone, among other pathological changes.
—Too often the condition is regarded as so trivial that it is likely to be outgrown, or else is quite disregarded, or, on the other hand, occasionally it is regarded as one of gravely serious import and maltreated or overtreated on this account. In the majority of instances scoliosis is a self-limited condition, whose limit may be reached at variable stages of deformity in different individuals. In slight cases any serious illness may cause such muscular weakness as to permit of serious increase of distortion. Therefore, the patient’s general condition is to be taken into account just as much as the shape of the back.
—If one may be permitted a Hibernicism, the proper treatment for scoliosis is prevention. This may be made to include the earliest possible recognition of trifling deviations from the normal. It should be made to include, in general, supervision of school desks and the way in which children work at them, as well as of children’s games and exercises, in which it should be made a point that they be taught to make as much use of one hand as of the other. It should include also supervision of children’s methods of seating themselves at the piano or at the sewing table, as well as the posture[461] which they assume during sleep, while they should be taught to stand and walk properly and to avoid a too early use of corsets. Active treatment should consist, first, of correction of bad postural and other habits by methods as vigorous as are military drill and discipline. Patients tire easily after such exercise, and sufficient rest should be taken, the patient lying symmetrically upon the back. There is usually opportunity with young children for great ingenuity in devising suitable exercises without making them too irksome. They should be taught to play games at least as much with the left hand as with the right. Gymnastic exercises, especially those with dumb-bells, will be found effective, and it is advisable to have a heavier dumb-bell in the left hand than in the right. The more severe cases should be handled with great care in order not to overdo that which should be done. Each case should be studied by itself, which means that such cases should not be taught in classes. Roth calls that “the key-note position” which is closest to the normal that the individual can voluntarily and comfortably assume. From this as a basis the surgeon should work up. Perhaps as much can be done without apparatus as with it, particularly if will power is concentrated on the effort. This is harder with the young, but pride may sometimes be appealed to as a substitute for volition. As strength is gained more strenuous gymnastics may be prescribed, including suspension from rings or the simple horizontal bar, while much heavier dumb-bells may be used, as taught by Teschner.
Mechanical corrective treatment is directed mainly to stretching shortened ligaments and contracted muscles. For this purpose many forms of apparatus have been devised. Their principal benefit lies in increasing backward flexibility at the point where curvature is most pronounced. As a substitute for such apparatus, and in private houses, padded stretchers or lounges may be supplied on which patients may lie either quietly or during massage. Finally the matter of corrective corsets and braces remains to be considered. External support takes away from the muscles and ligaments their functions and work. Nevertheless in some cases this is necessary. No appliance of this kind that may be supplied should be continuously worn. It should be removed for work and exercise, as well as for toilet purposes. Recumbency in bed is much better than too vigorous bracing. Only in old, neglected, or peculiar cases should it be considered necessary to resort to much external aid.
The relaxation and debility of old age permit of such deformities as rounded and stooped shoulders, certain degrees of kyphosis, and sometimes even pronounced stooping and deformity, whose merely senile causes are more or less combined with rheumatoid arthritis of the vertebral and costovertebral joints. These features are accompanied by more or less pain or difficulty in locomotion. Many instances of ischias scoliotica, referred to in the preceding section, would find a place among these clinical pictures. Postmortem there are found exostoses, synostoses, or ankyloses sufficient to account for the deformity. Rickets also causes skeletal deformities, in which nearly all the bones may participate, the spine rarely totally escaping. In such cases various typical and atypical deformities may be met.
Paralytics may show various curvatures, as do also subjects of pseudomuscular hypertrophy and syringomyelia. Lordosis is seen in pregnancy and in congenital hip dislocation, where it is purely compensatory in each instance and does not outlast its real cause. In fact it may be encountered as a compensatory feature of any other kind of spinal curvature.
A still more marked condition of chronic ostitic changes is seen in spondylitis deformans, which differs little from arthritis deformans of other joints, save that in these cases it usually spares the joints of the extremities. It has been known as a rare sequel of gonorrhea, even in the young. Osteophytic outgrowths occur frequently and fuse together, causing ankyloses and sometimes great deformity, even to the extent of making the spine assume a right angle with the extended limbs. Considerable pain is frequently experienced during the course of these very slow changes. The entire spine becomes more or less rigid, consequently there is little or no angular prominence, while the ribs become immobilized as well. For this condition there is little or no treatment of any avail. Sometimes paralysis supervenes and the condition is not infrequently fatal.
[462]
Acute osteomyelitis of the vertebræ is occasionally noted. It occurs nearly always in young and growing children, and is most common in the lumbar spine. It is essentially the same here as occurring in the long bones or their joint ends, and has been described in the previous chapter. Its symptoms may be severe, and it is not infrequently followed by abscess. When such abscesses point posteriorly they may be recognized and incised. When, however, pus takes the anterior path it will probably escape detection, at least until too late. The prognosis is often unfavorable.
This name was proposed by Gibney for what seems to be an infectious periostitis involving the vertebral column, of a character similar to that which has been described in a previous chapter. It is characterized by excessive pain, tenderness, and later stiffness. It may occur during or after mild as well as severe cases of typhoid.
Kümmel has shown that a traumatic and non-tuberculous ostitis of the vertebræ occurs, with succeeding kyphosis resembling that of Pott’s disease, but not so angular, usually without associated abscesses, but with occasional paralyses. This may occur without necessary reference to that curvature which may follow a healed or healing spinal curvature. Inasmuch as the condition occurs only after the lapse of considerable time after injury, it is questionable whether it represents any distinct form of disease.
Malignant disease of the spine may assume a type either of sarcoma when primary or carcinoma when secondary. The latter type is much the more common, and is not so infrequent as an expression of metastasis from cancer in various other parts of the body, even the more distant. It is most common in the lower spinal region. Pain occurs early and is usually severe. It is as often referred as localized. It may lead to curvature of the spine with some of the grosser signs of spinal caries, but the prominence, if any occurs, will be rounded rather than angular. When paralyses occur they usually assume that type described by Charcot as paraplegia dolorosa. (See Plate XXXVIII.)
When symptoms of a general type like those produced by spinal caries occur in adults who are known to have had previous or present malignant disease the inference will be that they are to be interpreted as local expressions of the same character. Under these circumstances treatment can only be palliative. There is no hope of cure.
The term spondylolisthesis implies a partial displacement forward of the body of the last lower or next to the last lower lumbar vertebra, usually the former, which slips forward on top of the sacrum with very little perceptible displacement of arches. The condition may be slight or well marked, and may or may not be followed by secondary changes. There appears to be a real fragmentation or separation of the body from the arch, which may be traumatic, congenital, pathological, or the sole result of pressure from above; later exostoses or osteophytes appear about the separation, thus forming a new fixation and preventing further displacement.
The condition is more common in females and in the young, and most cases give a traumatic history. In those which do, deformity may follow accident or it may be long postponed, perhaps until pregnancy.
—The lesion is recognized by certain alterations of gait, with a sharp lumbar lordosis and unduly prominent buttocks and iliac crests, so that these patients much resemble those having congenital hip dislocation, the pubes being higher and the sacrum lower than the normal, this diminution of pelvic obliquity being practically always pathognomonic. On vaginal or rectal examination undue prominence may be felt above the sacrum. Some of these cases complain of much pain, either local or referred, down the limb, the same being made worse by exercise.
PLATE XXXVIII

Sarcoma of the Spine and Cord. (Goldthwait.)
[463]
—Diagnosis should be made as between this condition, Pott’s disease, double congenital dislocation of the hip, and rickets.
—The condition does not admit of extended treatment, save that a certain proportion of cases are benefited by such fixation as is afforded by a plaster jacket, which firmly encloses the pelvis and supports the lower part of the trunk upon it.
The plane of the terminal articular surface of the lower end of the femur is not at right angles with the axis of its shaft; in other words, the inner condyle is placed a little lower or beyond the location of the outer. In this way sufficient angular arrangement of the leg upon the thigh is permitted so that, with the upper ends of the femora separated by the width of the pelvis, the knees and the ankles may, under normal circumstances, be made to touch when the limbs are fully extended. Thus a slight degree of angular deflection at the knee is normal. When this is exaggerated to a degree not permitting the ankles to touch when the knees are in contact the condition is known as genu valgum, or knock-knee. When, on the other hand, the angle is lessened or reversed so that the knees are more or less separated when the ankles are in contact the condition is then known as genu varum, or bow-leg. These two conditions constitute the typical and classical types of knock-knee and bow-leg. Other conditions, however, which lead to the same result occur through various and irregular curvatures or irregularities of the femur or the tibia, or both, and there thus may be produced atypical yet most pronounced instances of these same deformities. These deformities may be apparent almost from birth, may appear during early childhood, or not until adolescence. As a rule they are not manifested until young children are learning to walk. Whenever they appear before this time they are expressions of infantile rickets, which should be recognized as such and corrected by mere manipulation while the bones are still flexible, the correction being maintained, and by suitably feeding and medicating the patient. (See the general subject of Rickets.)
Fig. 261
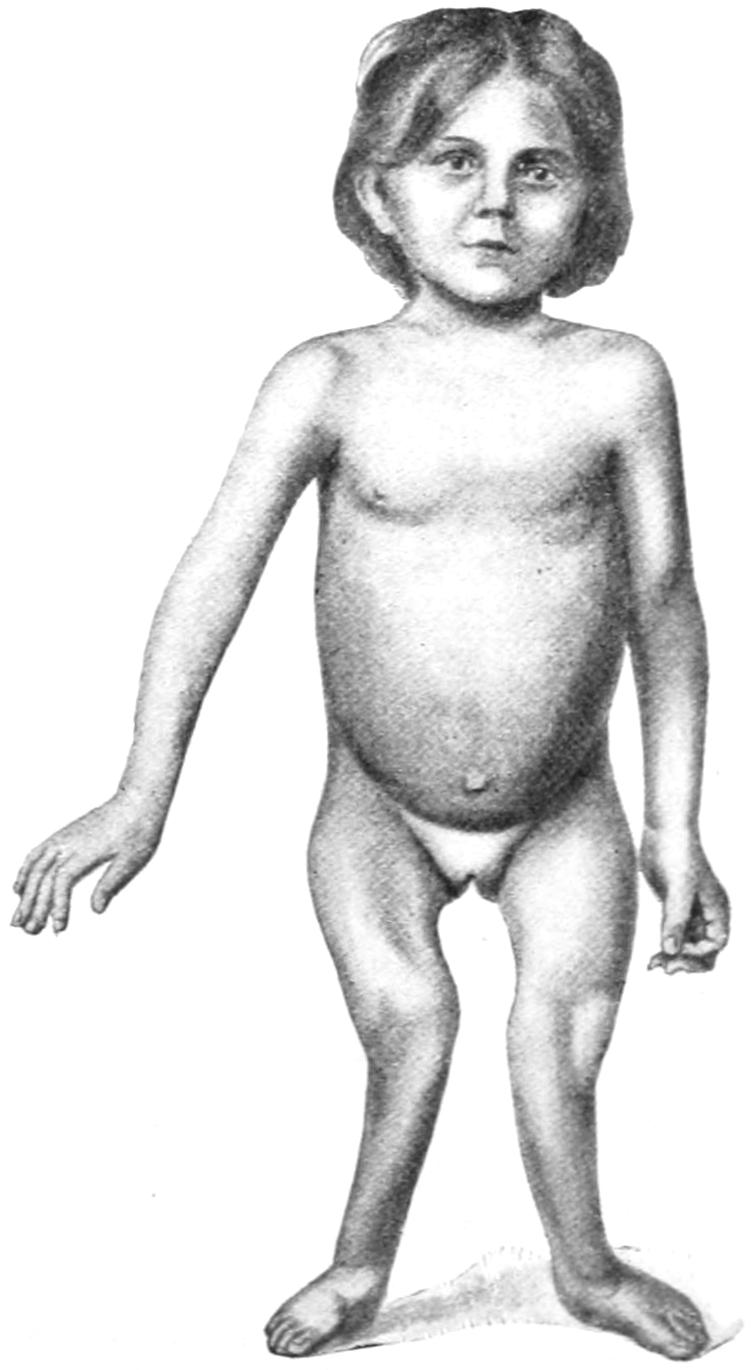
Rachitic changes in limbs. (Lexer.)
In fact rickets supplies the explanation for the great majority of these deformities; incomplete ossification and calcification of the bones accounting for the comparative ease with which they yield to pressure or other deforming influences. Rickety children always manifest a tendency to defective ossification at epiphyseal lines, and it is here that the change usually takes place. Nevertheless marked instances of curvature are seen in all the bones of the lower extremity. As deformity in any given direction becomes more pronounced the tendency to its exaggeration becomes greater. Finally these changes involve not only the bones proper but the ligaments and the other joint structures, which yield where pressure is abnormal and greatest, thus completely changing their shape and internal relations. Along with other changes in knock-knee there is a tendency to external rotation, perhaps even to spiral curvature of the tibia; the patella lies outside of its normal position, the tendons are more or less displaced, while, at the same time, there may be inflection of the feet as an effort at compensation (Fig. 261).
With the exception of spinal curvatures and torticollis there is perhaps no more conspicuous deformity than that produced by these abnormalities at the knee-joint. While[464] at first gait is not seriously affected, it is in time, especially in cases of double knock-knee. When these knees are bent to a right angle the angular deformity disappears and all that remains is the rotation of the tibia. Hence it follows that all correction of these deformities, either slow or operative, should be applied to the fully extended leg. In advanced cases there is frequently a complication with flat-foot, which may or may not be painful. The condition is rarely produced by paralytic affections, and should be differentiated from mere atrophy of wasted and contracted legs. A form of knock-knee is occasionally seen in the adult, which is of traumatic origin and is due to improper care or neglect in the treatment of the injury.
—The treatment of this condition is either mechanical or operative. Mechanical treatment varies between the gentlest expedients and the use of more or less extensive and cumbersome apparatus. When a young and growing child begins to show evidence of either of these deformities it is usually sufficient to supply shoes which are reasonably stiff, and raise one or other border of the sole and heel, according as we wish to influence the growth of the limb, i. e., in knock-knee the inner border of the foot is to be raised, in bow-leg the outer. The consequence of even slight influence thus constantly maintained when the child is upon its feet is usually sufficient to rectify slight degrees of these deformities. When, however, the case is pronounced more radical measures should be applied. Massage has been recommended along with manipulation, but should be gently performed. The different forms of apparatus in use afford various methods of making pressure against that condyle which is too prominent. It is possible to make them efficient, but only when they are both well planned and well made in the first place and intelligently applied and watched. The special forms of apparatus sold in the instrument stores are of little value. Too often it happens that when efficient they cannot be tolerated, and that when tolerated they are inefficient. Much speedier and more satisfactory results are achieved by operative methods, so that, in general, they may be regarded as the more desirable.
Operative treatment consists in some modification either of osteoclasis or osteotomy.
Osteoclasis has to do with the forcible stretching, bending, or even breaking of those parts which show the greatest effects of the deformity or are known to be its primary seat. In young children with tender and still somewhat flexible bones this may be accomplished by the hands alone, the patient being under an anesthetic. Manual power failing a simple instrument known as the osteoclast, which affords a means of applying powerful pressure by the agency of a screw at just the desired point, is used. Pressure is then applied and carried to the necessary degree, even with partial or complete fracture of the bone at fault. In this way is inflicted a simple fracture which permits of the immediate redressing of the limb, with such overcorrection of the deformity as seems desirable. The limb thus treated is completely encased in a suitable plaster-of-Paris splint, and should be held in the desired position until the plaster is completely hardened and not likely to yield. Osteoclasis, though it often appears an exceedingly barbarous procedure, is one of the most beneficent when properly managed, and is rarely followed by an undesirable result.
Osteotomy is performed by the use of the chisel and mallet, the former being introduced through a small incision made in the skin, passed down to the bone with its cutting edge parallel to the bone axis until the bone itself is reached, after which it is turned at right angles to it and the mallet used until the chisel has been driven partly or completely through the shaft of the bone or the portion which it is intended to attack. The chisel should be partly withdrawn and its position changed if it is necessary to continue its use. Thus by a partial division of the bones of the young it is possible usually to so weaken them that, without undue force, and by manual power, they are fractured at the desired point. The operation should be done with the most complete aseptic protection. The procedure recommended by Macewen is now universally accepted. The incision is made at the inner side of the thigh just above the tubercle for the adductor magnus, and the osteotome (as the chisel especially made for this purpose is called) is passed through it, down to the bone, turned at right angles, and made to cut nearly through the shaft. Lest it become too firmly wedged it may be moved a little laterally after each blow of the hammer. The operation, if properly done, is practically bloodless; the small opening made for the chisel is sealed at the moment of its withdrawal, the deformity corrected with the least amount of handling or disturbance, and the plaster-of-Paris bandage immediately applied, with the leg in exactly the position which it is[465] desired should be maintained. Such a dressing may be left for three or four weeks before being changed. One change is usually sufficient, and in from six to seven weeks the patient is allowed to slowly regain use of the member.
A special set of osteotomes, after Macewen’s pattern, is furnished by the instrument dealers for those who practise osteotomy. It consists of a set of three straight chisels, consecutively numbered, the first being a little thicker and the third the thinnest of the three, and thus made with the intent to use the thickest first in order that in the notch made by it the thinner instruments can be subsequently more easily manipulated.
Bow-legs are nearly always of rachitic origin, occurring with less angular deformity, and as the result of the warping or bending of bones which are not sufficiently rigid to sustain the weight they are made to carry. Most cases of bow-legs have their origin within the very early years of childhood. Other cases are seen in infancy and before children have ever borne much weight upon their feet. The deformity must be accounted for by muscle tonus, mere muscle activity serving to place enough stress upon the bones to swerve them from their normal axes. The bones probably bend outward because the muscles on the inner side are the stronger. Children thus affected walk not so much with a limp as with a waddle, with the feet rather apart, and some inversion of the toes. Double and complicated curves occur in many of these cases, both femurs and tibias participating, and having an anterior as well as a lateral bowing. Such complications materially increase the difficulty of any treatment.
—The treatment of bow-leg is generally considered simpler than that of knock-knee. Occurring in young and growing children it can be overcome, if taken early, by the expedient already mentioned, elevating the outer border of the sole of each shoe. The more mechanical and the purely operative methods of treatment are essentially the same as those just described for knock-knee, based on similar but reversed principles. In the very young manual force will often serve the purpose of a more formal osteoclasis, but the osteoclast may be used whenever it seems indicated. In those cases where the bowing is due to abrupt and almost angular deformity, osteotomy is indicated. This is made on exactly the same principles as mentioned above. In all instances spiral curvatures should be overcome so far as possible during the process of forcible correction and dressing in the plaster-of-Paris bandages ordinarily used. Here, as previously, all treatment should be addressed to the limbs in their fully extended position. If the rings of the ordinary osteoclast be sufficiently padded and protection afforded in this way, the skin rarely sloughs, and the damage, which is, at least, theoretically done to the tissues, is quickly repaired. Failure in union after any of these operations is exceedingly rare.
In general the term talipes is applied to any malformations of the foot by which it is more or less misshaped and its function impaired. The commonest of these is that known and described below as talipes equinovarus. Of these various deformities there are four principal types, according as the foot is inverted, everted, hyperflexed, or hyperextended. More particularly they are:
These forms may be variously blended, as well as seen in varying degrees from the slightest possible deviation to the most pronounced form. Statistics show that about one child in every five hundred is born with some form of club-foot.
Club-foot may be either of acquired or congenital origin. Acquired club-foot is essentially always of paralytic nature, following usually infantile paralysis or those injuries by which nerves have been divided or caught in callus or in tumors. As the result of such loss of nerve or muscle power, in certain muscle groups, malpositions of the feet are caused which simulate those of congenital origin.
[466]
—This consists anatomically in an inward dislocation at the metatarsal joint of the anterior part of the foot, in consequence of which the relations of all of the other component parts of the foot are deranged; the scaphoid is swerved on to the inner and lower side of the astragalus to such an extent as to touch the internal malleolus; the cuneiforms follow the scaphoid and the metatarsals follow the cuneiforms; the cuboid is shifted to the inner side and does not articulate squarely with the calcis. In infants these bones are cartilaginous, but as the individuals grow and these miniature bones develop and ossify they take similar and abnormal shapes and positions. The calcis is drawn into a more vertical position than normal by drawing up the heel, and is even somewhat rotated on its own vertical axis; thus its anterior articulating surface is made to look obliquely inward. This displacement of bones causes dislocation of tendons, the anterior group being drawn mostly to the inner side. The patient walks more and more on the outside of the foot, and as he does this adventitious bursæ develop on the outer border, which become very thick and form in time large callosities. In the most pronounced cases there occurs, in connection with all this, curvature or spiral inward rotation of the tibia, and even of the femur of the affected limb, while the contracted muscles become overdeveloped and those which are disused underdeveloped (Fig. 262).
Fig. 262
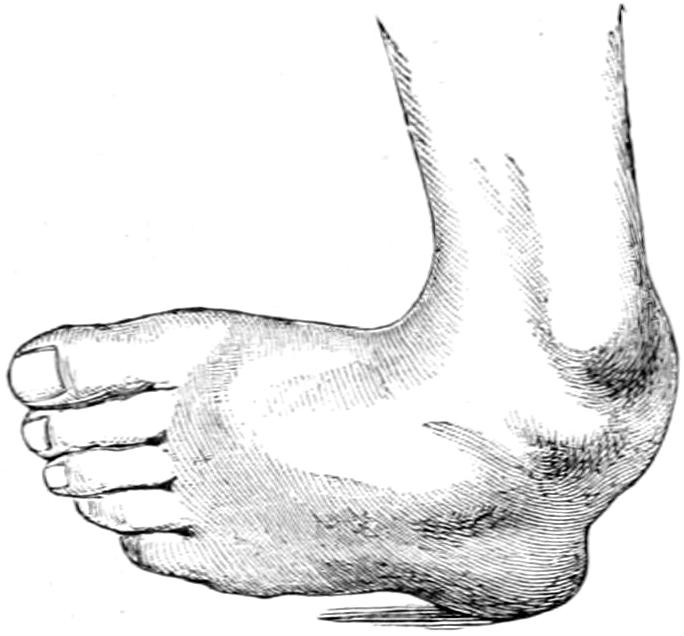
Talipes equinovarus.
Among the causes of club-foot heredity seems to play a considerable part, as it often happens that two or three club-footed children are born of one mother. The deformity has been ascribed to abnormal or exaggerated posture in utero, with compression. This theory is at least attractive and has the force of argument from antiquity, for Hippocrates thus believed. Unquestionably the normal intra-uterine position of the fetus includes a certain degree of equinovarus. Yet if this were the real cause the condition would occur apparently much more frequently. It has been ascribed also to disparity in strength between opposing groups of muscles, that group which causes the deformity being naturally the stronger, it being at the same time unimportant whether one group is relatively too strong or the other relatively too weak. Most monstrosities or seriously defective infants have also club-foot, from which some argue that the central nervous system has something to do with it; yet it has been shown in over 1200 cases of club-foot that only twice did such defect of the central nervous system as spina bifida occur. The embryologists and comparative anatomists regard it as an expression of arrested development, while evolutionists consider it an atavistic reversion to an earlier anthropoid arrangement. None of these theories really satisfactorily explains the deformity. Therefore we should hold that either there are different and variable causes or that we have not yet found the true one.
Treatment of Congenital Club-foot.
—There being in these cases no tendency to spontaneous improvement, mechanical or operative treatment, or both, are required. If these be afforded early the prospects of restoration, practically to the normal, are good, but treatment should be begun early and conducted with great care and patience. It is not so difficult to correct the deformity, but correctional supports should be worn for a relatively long time, while the older the case the more difficult become all the features, both mechanical and durational. Parents are often eager at first, but later become inattentive or careless. The main objects are to be attained by correction of position by force or by division of contracted or shortened tissues, or retention in position, with the addition of any other features which may influence growth and development according to normal standards. Of these we will speak first of rectification: (a) bloodless, as by purely mechanical force, or by means of certain apparatus, and (b) operative, as by subcutaneous tenotomy, aponeurotomy, etc., or by open incision, through which are performed osteotomy, excision, astragalectomy, tarsectomy, etc., as the operator may see fit.
In all of these the anterior part of the foot is to be forced outward as well as raised, two distinct features, which should be combined but not confused.
In the young infant gentle force applied many times a day, with the persuasion of a[467] strip of adhesive plaster, applied beneath the foot and over its outer border, and spirally upward to the inside of the leg, can be made effective in mild cases; but overstretching of the tendo Achillis is a necessary part of this maneuver every time it is practised. The more positive method consists of fixation of the foot in overcorrected position within a plaster or starch bandage, the same extending above the knee, which should be slightly flexed, the dressing to be renewed every two or three weeks, and correction increased until it has become overcorrection.
In well-marked and in resistive cases an anesthetic should be given, while by the use of sufficient force, which may be relatively great, but which should be gently applied, the resisting tissues are so stretched, if necessary to the point of something yielding, that but slight pressure is required to hold the foot in an overcorrected position. When the knife is required the tendo Achillis should always, and the plantar tendons and fasciæ usually, be subcutaneously divided, under aseptic precautions. The foot is then enveloped in suitable dressings and put up in overcorrected position for two or three days, in a rigid dressing at first of starch, but after this in plaster of Paris; this is the writer’s plan of procedure. The insertion of the point of the tenotome sufficiently deep to divide all resistive ligaments and tissues (e. g., the astragaloscaphoid or the calcaneocuboid) nowise complicates this method, but makes it more efficient.
Cases which are resistant are best submitted at once to open operation (that is, after vigorous stretching of the contracted tissues), always under strict asepsis. After decades of milder ineffectual methods it remained for A. M. Phelps, of New York, to show the benefits of this method by which all contracted tissues on the concave aspect of the foot are exposed and divided. Incision is made here from the top of the inner malleolus to the inside of the first tarsometatarsal joint. With a little care the artery can be avoided, but I have never seen any harm come from its division. Everything which proves resistant is divided, even the inner osseous ligaments. Sometimes the incisions can be made in wedge-shape, or obliquely, so that the wound does not remain so widely open. No attempt is made to close this wound. The operation may be done bloodlessly, under the Martin rubber bandage, but whether this be used or not any vessel which can be recognized as such should be tied; otherwise the wound is snugly packed with gauze (upon which I like to use Peru balsam). An ample surgical dressing is applied over it. This is covered with gutta-percha tissue, to prevent too free access of air to the blood which will ooze into the dressing, and the whole is then covered with a starch bandage, in overcorrected position; this is left, according to circumstances, for from three days to a week—the longer the better. Then everything is removed, fresh gauze placed in the wound, which will be found already largely filled up; fresh dressings are applied, and the foot put up in plaster of Paris, with or without a fenestrum or any provision by which the region of the wound may be easily uncovered for necessary renewal of dressing.
It is in the most pronounced types of cases only, with marked bone deformity, or those in which previous operations have failed, that the still more radical division or removal of some part of the tarsus is necessary. As to this no universal rule can be applied save this: take out sufficient to correct deformity. In some cases it will be sufficient to excise the astragalus (astragalectomy). In other cases it is better to remove a wedge-shaped piece of the tarsus, without reference to the name of the bones attacked (tarsectomy). I have never found it necessary to touch the external malleolus, though this has been suggested, nor to do osteotomy of the calcis or of the leg bones above the ankle, as a few have done.
Fig. 263
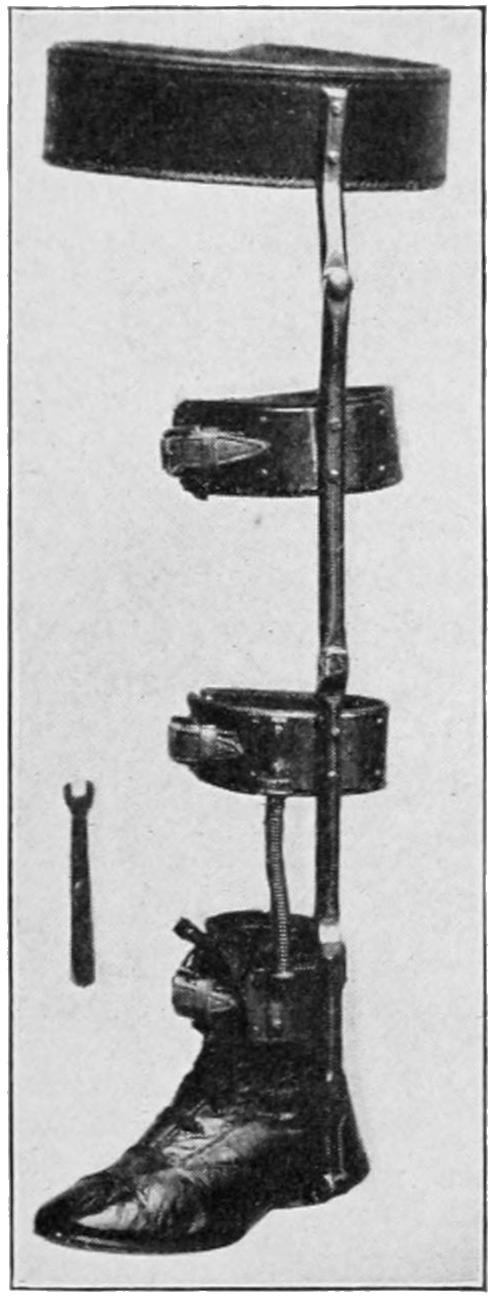
Park’s club foot brace.
These operations are usually practised, after a preliminary stretching, through a curved incision on the outer aspect of the foot, through which, at the same time, the thickened bursæ may be removed, or the callosities included in the incision. The chief convexity of the incision should be over the os calcis at its anterior portion. As the dissection is made the tendons are drawn aside and spared. If it be necessary to divide one or more of them it should be re-united later. According to the density of the structures a strong knife may be used, and strong scissors, or an osteotome manipulated either by hand or with the hammer. After sufficient V-shaped or wedge-shaped bone has been removed the defect should be held together, if practicable, by buried tendon sutures or wire; it is rarely necessary to use drainage. The external wound may be loosely closed with buried sutures, a suitable dressing applied, and the foot put up in a rigid splint; this should permit of removal, or at least inspection of the wound after[468] a few days, for renewal of those dressings which are saturated with blood and for application of new dressings. After this the foot and leg should be put up in overcorrected position in plaster of Paris.
In aggravated cases of club-foot Wilson believes combined operation to give better functional results than can be obtained by any other method. The astragaloscaphoid joint is exposed by an incision over the prominence of the scaphoid, and, being cleared, is opened with chisel or bone forceps, while sufficient of the articular surfaces is removed to destroy them as such and to take out a sufficiently large wedge-shaped piece from either bone so that the desired arch of the foot is restored, or even exaggerated. Then the tendon of the extensor proprius hallucis is exposed and divided just above the great toe, the upper end of the tendon being drawn out through the first incision. To this end is attached a strong silk ligature. The scaphoid is then perforated with a bone drill at some distance from its superficial aspect and at such an angle, with the foot in correct position, that the canal thus made shall be in line with the action of the tendon. The drill is then withdrawn and the tendon passed through the opening by means of its attached silk. One inch beyond the bony canal the tendon is cut off and split in halves, each half being turned in opposite direction and fastened to the periosteum of the scaphoid with fine silk, while the foot is held in overcorrected position, so that the tendon is sewed in its new place under moderate tension. The foot is then dressed in this overcorrected position in plaster of Paris, the splint extending nearly to the knee, and the wound area being exposed by a fenestrum cut in the splint before it is hard.
The location of the incision over the dorsum or outer aspect of the foot may be varied to suit the needs of the case and the method of the attack. In a general way a flap of soft tissues is raised and tendons, so far as possible, are held outward. This is usually practicable, and it is rarely necessary to divide the latter. After operation of any type and recovery from the same it will be necessary for a long time to have the patient wear a corrective appliance. This should be applied as early as possible, and should be worn continuously, i. e., night and day; inasmuch as growth is continuous there should also be continued correctional influences. Many types of apparatus have been devised. That which the writer has found effective and has adopted for a number of years is illustrated in Fig. 263. It may be made single or double, as occasion requires. A part of the appliance is a spiral spring and a provision for a constant outward pressure is made upon the foot, by which inversion is more easily overcome, as well as any inward spiral twist of the bones of the leg. No such apparatus can be made effective unless connected suitably with a waist-band. This is, therefore, included in the shoe shown in Fig. 263. Furthermore the appliance should be so made as to permit adjustment commensurate with the rapid growth of the patient, and in order that it need not be too often renewed. Some degree of mechanical ability is required for its application and management. The principles are, however, easily mastered and most parents can soon learn to manage it.
—This condition is known also as talipes planus, or, more briefly, pes planus, the common names being flat-foot, splay-foot, or pronated foot. A particularly painful variety has been often spoken of as pes planus dolorosus.
This type of deformity is rarely of congenital origin. It is characterized by abduction and pronation of the foot, on whose inner border there often appear two prominences, one the head of the astragalus the other the head of the scaphoid. The bones show much less alteration in actual shape than in club-foot. The scaphoid is deflected somewhat to the outer side and the astragalus turned a little outward and downward. A prominent feature is that the arch of the foot is more or less obliterated, while its inner border becomes convex instead of remaining concave. This is due in large measure to relaxation of the ligaments binding the foot to the calcis, especially that extending from the astragalus (Fig. 264).
Etiology.
—The common cause of the condition is lack of sufficient strength of the parts to carry the weight of the superimposed body. It is produced often by ill-fitting shoes, accompanied by excessive strain or rapid growth and gain in weight. It is sometimes complicated by a certain shortening of the gastrocnemius (Shaffer), which prevents flexion to its complete degree and compels some degree of eversion of the foot in completing a step. In some instances it is induced by previous morbid conditions, such as rickets, paralysis, diseases of the spinal cord, and postgonorrheal arthritis. Ill-fitting footwear is the most common cause, as it compresses the front part of the foot and prevents[469] adaptation of the foot to the position it should assume when the weight of the body is thrown upon it. The effect of this weight is to necessitate a greater divergence of the toes than such shoes permit and gradually causes the patient to walk on the inside of the foot. Flat-foot is seldom seen in those who habitually go barefooted.
The condition is best relieved by making a graphic record of each case. This is done by making the barefooted patient step first on smoked glass or on wet dusted paper, and then upon a piece of plain paper. If such a print be compared with the print similarly obtained from the normal foot it will be seen how different are the points of contact and how differently distributed is the body weight. A non-graphic but sufficient inspection may be afforded by having the patient stand upon a stool whose top is made of glass and by using a mirror beneath the feet. In any event it will be shown that the inner border of the foot is at least nearly straight or even convex, whereas it should be neither.
Fig. 264
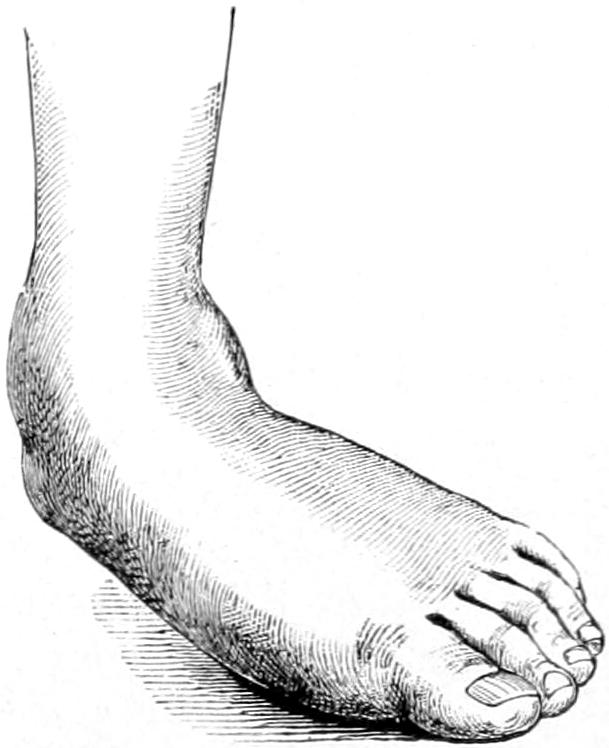
Talipes valgus.
There are tender points over the astragaloscaphoid joints, at the base of the first and fifth metatarsals, in front of the internal malleolus, as well as often beneath the heel. Patients who thus suffer find that the feet perspire very easily. In walking the feet are everted, and when tenderness is very great it is because too much weight is borne on the inner borders of such everted feet. Inspection of the shoes will also show wearing of the inner border and over the inner malleolus.
Spontaneous cure of such cases does not occur, except perhaps after long confinement in bed from other causes, but patients occasionally become tolerant after a time, though many of them grow steadily worse and avoid using the feet more than is absolutely necessary.
Treatment.
—Mild cases will be benefited, often practically cured, by simply raising the inner border of the sole and heel of the shoe. This causes more weight to be borne on the outer border than in the natural attitude of the foot. It will be sufficient usually to make from ³⁄₈ inch to ⁵⁄₈ inch difference in the level between the inner and the outer borders of the sole and heel. Shoes may be so constructed that this difference is made invisible, or suitably bevelled narrow strips of leather may be sewed beneath the sole along the inner side, or laid in between its upper and lower layers.
While this suffices for the milder cases it is not sufficient for the more severe cases, which require forcible correction, and often under an anesthetic. The best way to[470] accomplish this, after having patients thoroughly relaxed with chloroform, is to make a thorough manipulation of the foot, trying especially to so loosen its outer ligaments that it may be more easily put in proper position and finally overcorrected. The foot is then put up in plaster of Paris in this much overcorrected position. Such splints are worn for five or six weeks, after which suitable shoes should be provided, either with their inner borders elevated or with metal flat-foot plates inserted, or both. These plates are now in general use, and may be procured from instrument dealers and in shoe stores. In particular cases it is advisable to make a mold of the lower aspect of each foot, to have this cast in iron, and then over the iron model to have a suitable metal plate hammered so that it shall exactly fit the individual for whom it is intended.
Only in extreme cases, rebellious to other treatment, has it been shown necessary to resort to such treatment as division, by osteotomy, of the neck of the calcis or of the astragalus.
Most of these cases may be benefited subsequently by gymnastics and massage, i. e., by stretching the contracted gastrocnemius, if necessary, with some mechanical device, and improving the general condition of the leg muscles by suitable massage.
—Under this name has been described a peculiar painful affection of the third and fourth or the fourth and fifth toes, which gives rise to constant sensitiveness and sometimes attacks of acute pain, especially when the foot is shod, and which is often only relieved by immediately removing the boot or shoe. These affection’s are more common in the upper walks of society, especially among women who are disposed to cramp their feet in shoes which are too small for them. Aside from the location of the pain there will often be found a tender spot at the point of greatest complaint. As these cases become worse pain radiates farther and farther up the leg, and may even assume the type of a sciatica.
Fig. 265
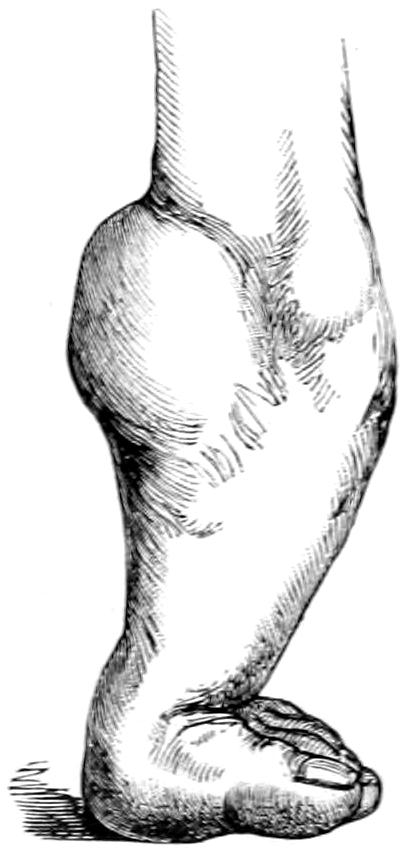
Talipes equinus.
Careful inspection usually reveals either a mild degree of flat-foot, or of distortion by which the anterior part of the foot is broadened and held in a depressed position—or else the dorsal part of the foot is depressed behind the anterior part; there is also usually limitation of dorsal flexion of the foot and plantar flexion of the toes.
Morton, who first described the affection as having a peculiar type of its own, thought it due to entanglement of the external plantar nerve between the heads of the fourth and fifth metatarsal bones, and recommended for its relief excision of the head of the fourth of these. The etiology of the affection is not always apparent, but it is sometimes due to what has been described as a non-deforming type of club-foot, while in practically all other instances it is in some way connected with the use of badly fitting footwear.
Treatment.
—Without proper treatment it does not subside. A really weak and pronated foot should be supported with a proper plate and elevation of its inner border, while a short gastrocnemius should be stretched. Only in extreme cases or when these milder measures have failed need resort be had to Morton’s suggestion and excise the head of the fourth metatarsal.
—In this condition the equinus position is simulated, and the patient walks upon the anterior part of the foot only, perhaps even upon the ends of the metatarsal bones. While the congenital form is extremely uncommon the acquired form is that which commonly occurs. Appearing thus in all possible degrees it may in mild cases cause merely a slight limp, while the extreme cases cause a pronounced deformity and alteration in gait. The actual condition is one of shortening of the tendo Achillis through contraction of its component muscles, with corresponding change in shape of the bones of the foot. There is also more or less shortening of the plantar aponeurosis, and depression of the astragalus, which is drawn down upon the calcis (Fig. 265).
Causes.
—Perhaps the most common cause is paralysis, either of infantile or cerebral and spastic type, of the anterior muscles of the leg, the condition being simulated sometimes in hysteria. The spasm which follows disease of the ankle-joint may also produce it. It may be the result of muscle contraction after fractures or even after certain fevers, the foot dropping naturally into this position and remaining there altogether too long. Hence may be seen the necessity for putting the foot in the right-angle position whenever the lower limb is dressed in plaster or other rigid dressings after fracture.[471] Talipes equinus may also be due to injury to and loss of power in the anterior muscles of the leg, or it may be compensatory, as when one leg is longer than the other. In any of these events the body weight is borne on the ball of the foot, and some degree of arching of the foot, which may be excessive, is sure to occur.
Treatment.
—In the milder cases, when seen early, it may be sufficient to thoroughly and repeatedly stretch the sural muscles, but, in the more severe forms, tenotomy of the tendo Achillis, with subcutaneous or perhaps open division of the plantar structures, will be needed. In paralytic cases tendon grafting (q. v.) will be required, probably with one or more of the measures mentioned above. In some instances nerve grafting might be profitably employed. After recovery from operation, braces adapted to each particular case will in all probability be required, at least for a time.
—In this deformity the anterior part of the foot is drawn upward by its anterior flexors and a little to the outer side, while the sural muscles are relaxed; thus the patient walks upon the heel. The condition is often more or less combined with talipes valgus. It is rarely of congenital origin, but is generally due to paralysis of the distal muscles following injury or poliomyelitis. It is sometimes of hysterical origin, and it may occur as the result of muscle spasm following bone or joint disease (Fig. 266).
Fig. 266
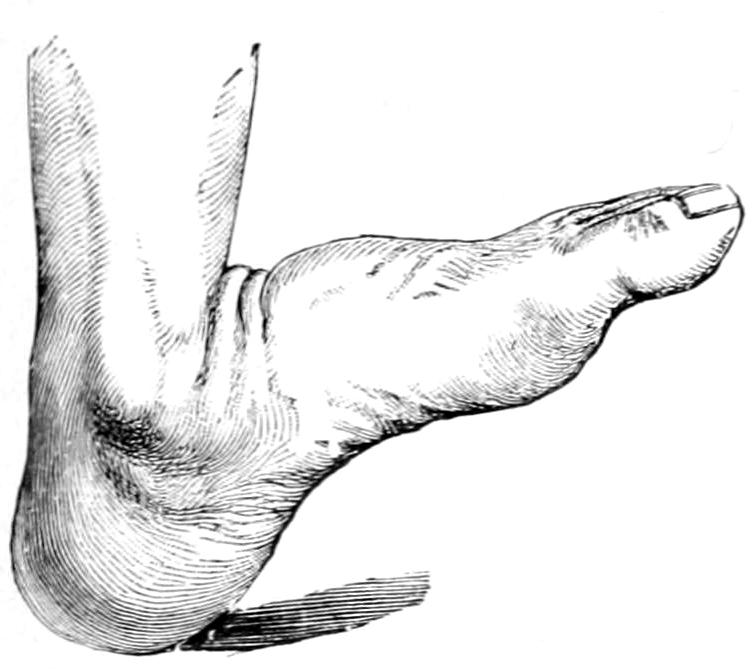
Fig. 267
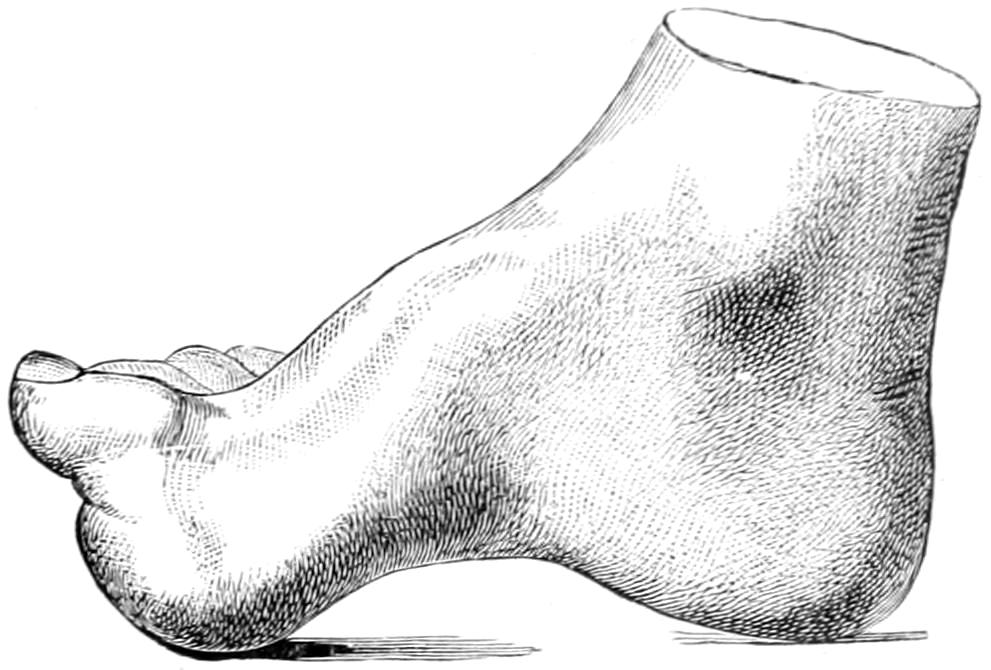
Talipes calcaneus.
Pes cavus, hollow clawfoot.
Those forms due to infantile paralysis are to be treated mainly by tendon grafting or some similar expedient, and this to be followed by a suitable shoe containing a sole plate with an upright attachment and a joint opposite the ankle. Other forms must be treated, each on its own merits, but according to general principles already enunciated.
—Here the anterior part of the foot is drawn backward and the plantar arch made much more prominent. It may even be converted into a Gothic arch. Extremes of this type are seen in the feet of Chinese women. One form is due to contraction of the peroneus longus, owing to paralysis of the sural muscles, by which the long flexors are permitted to work to extra advantage; and yet another form is often of congenital origin, having its explanation in paralysis of the interossei and other small intrinsic muscles of the foot (Fig. 267).
When an ordinary metal sole plate fails to give relief a subcutaneous or open division of the contracted structures may be practised.
Perhaps a more proper name for this congenital deformity would be “misplacement” rather than dislocation. It is seen much oftener in females than in males. It may be either unilateral or bilateral. The displacement is usually upward and backward upon the dorsum of the ilium. In rarer instances it is anterior and sometimes the head of the femur lies not far away from the anterior superior spine of the ilium.
Regarding its cause absolutely nothing is known. It represents defective development rather than arrest, and is a condition of intra-uterine life. The acetabulum is usually found incomplete, but whether this is the cause of the misplacement or whether it fails to develop because of the absence of the head of the femur from this cavity it is[472] not easy to decide. The influence of heredity in these cases is undeniable, for it is known to have prevailed in certain families. Thirty years ago but little was known in regard to the affection, and nothing could be done to atone for it. Of late years it has been the subject of special study by numerous investigators (Figs. 268 and 269).
Fig. 268

Double congenital displacement of the hip. Buffalo Clinic. (Skiagram by Dr. Plummer.)
Fig. 269

Skiagram of coxa vara; deformity most marked at the epiphyseal junction. This illustrates the mechanical limitation of abduction caused by the deformity, and the compensatory tilting of the pelvis. (Whitman.)
Fig. 270
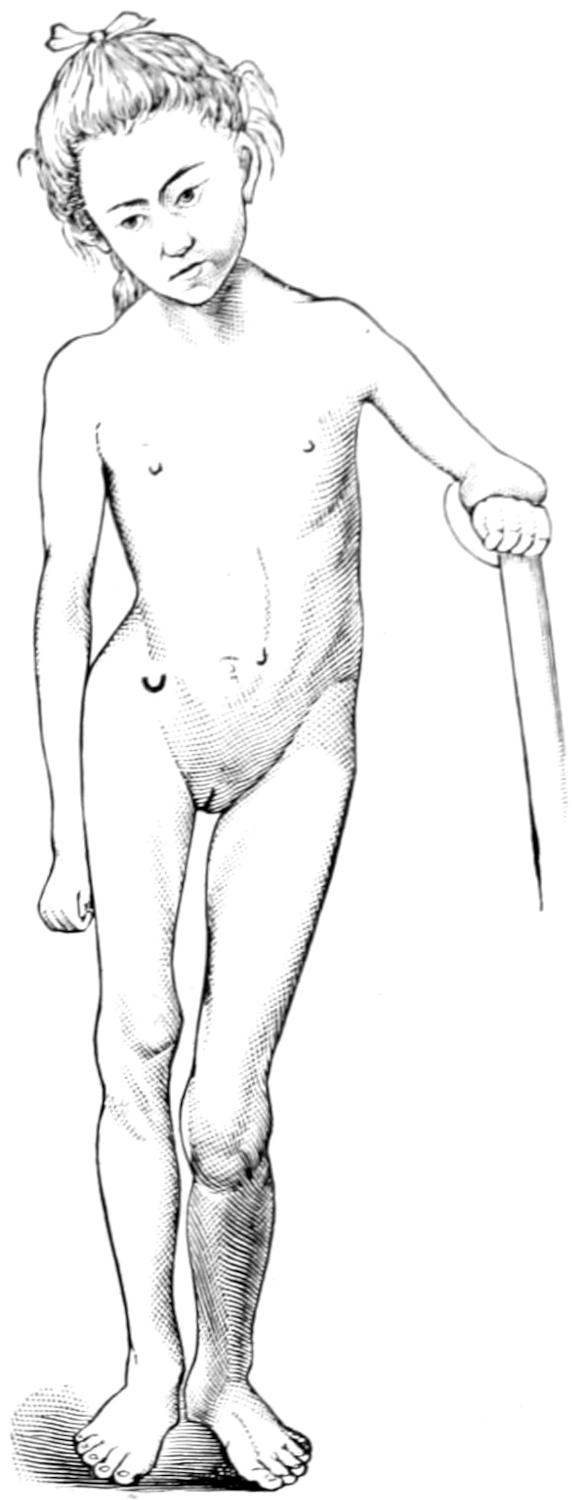
Congenital misplacement, with consequent atrophy and shortening. (Calot.)
Pathological changes are noted in the capsule itself, as well as in the bony components of the joint. Thus the capsule is usually elongated and stretched out of shape, while its lower portion may be adherent to the margin of the acetabulum or may be shut off[473] into a small cavity by itself, this cavity having but a small connection with the balance of the capsule and affording irresistible obstacles to reduction. With changed joint relations the muscular arrangements are also changed, some being lengthened, others shortened, as would naturally follow from the approximation or separation of their points of origin and insertion. Conspicuous change is seen in the upper end of the femur, which is often atrophied, while the neck is shorter than normal, its angle lessened, and the head of the bone often altered in shape. A secondary acetabulum is in time formed and is usually found upon the side of the ilium. This is shallow and insufficient to ensure firm support for the head of the femur, even were this well developed. Aside from these changes the pelvis is usually poorly developed on the affected side, its inclination increased, the sacrum forced forward and downward, the pelvic outlet widened, while a considerable degree of lumbar lordosis is present (Fig. 270).
The condition is rarely noted until a growing infant begins to learn to walk. The condition is one which has no symptoms, only signs, and these do not at first attract attention. Sometimes it will have been noted that there is an abnormality about the hip, with too free play, or a snapping sound about the joint. When the condition is unilateral there is a marked limp which increases with the age of the child. With each step the femoral head is pushed upward on the side of the ilium, and, in consequence, the pelvis is tilted toward the outside, as well as twisted downward and forward. The limb being thus actually shortened, the limp or waddling gait is easily accounted for. Along with it there is usually flattening of the tibia, while the trochanter may be felt and often seen on a level considerably above that where it properly belongs. Motility in the joint is abnormally free, and with a child on its back, by alternately pulling and pushing, the abnormally free play of the upper end of the femur may be easily demonstrated, either with the limb in its extended or the flexed position.
When the misplacement is bilateral the individual is more symmetrically deformed. The lordosis is increased, the abdomen protrudes, the thighs are separated more widely than is normal, leaving perhaps a considerable space in the perineum; the gait is of a peculiar waddling character, which makes locomotion apparently difficult, although it is free from pain. In these cases abnormal mobility of the hip may be demonstrated on each side.
As these patients grow through adolescence into maturity they sometimes improve, but usually suffer more and more difficulty in locomotion, while the abdominal protrusion and the lordosis become more and more pronounced.
Three varieties of congenital misplacement are described as backward, upward, and forward. It is in those instances where the head of the bone rests well back or well forward upon the ilium that the gait is most pronounced, but in all instances the great trochanter will be found above Nélaton’s line.
—The diagnosis offers few difficulties. The peculiar waddling gait may be seen in extreme cases of bow-legs, but then the hip-joints will be normal. Extreme lordosis may be seen in cases of lumbar spinal caries, but here again the hip-joints will be normal, while the spinal muscles will be rigid and the patient disinclined to walk. Traumatic dislocations and the results of hip-joint disease will be indicated by a history to correspond, as will also early acute joint affections following the exanthems. The diagnosis is to be made principally from coxa vara, considered below, and the various defects following infantile palsy. In coxa vara there is no corresponding abnormality of motion, while in the paralytic cases there will often be failure in muscle power, which is not present in cases of congenital misplacement. Finally in instances which offer difficulties the Röntgen rays now afford a method of diagnosis.
[474]
—For a long time after this condition was recognized its treatment was unsatisfactory, and it was not until Hoffa, about fifteen years ago, advanced his operative method of relief that surgeons felt at all like advising operation in well-marked cases. Then came Paci and Lorenz, first with improvements on the Hoffa operation, and then with a method of so-called “bloodless” reposition, which has been under severe test and testimony. Last of all come Bradford and Sherman with their improved methods of operation, which seem to me the most promising of all as well as the most scientific.
Fig. 271
A plaster bandage applied by Lorenz, illustrating the extreme thickness of the pelvic portion and discoloration of the adductor region. (Whitman.)
Lorenz was doubtless correct when he stated that the principal obstruction to reduction is the narrowed part of the capsule, just at the upper part of the acetabulum, and that if this could be torn here sufficiently to permit the passage of the head, reduction could be accomplished by manipulation alone, and maintained if the acetabulum were sufficiently deep. An almost insuperable difficulty in most cases is, however, this narrowed capsule, and the number of accidents, including not only fractures of the femur and the pelvis, but various other injuries which have resulted from too great violence, is altogether too large and too disturbing to justify the use of such force as has often been used. Of more than one hundred children upon whom Lorenz operated when making a tour through the United States, but little over 10 per cent. have given anything like ideal results; while the danger from fracture and laceration of muscles and nerves, as well as of bloodvessels, is fully as great as that pertaining to any open operation. It may therefore be maintained that the percentage of success from the use of manual force without incision does not justify the risks of the method. Sherman argues that if we may open a knee-joint without hesitation to take out a small piece of cartilage, we need not fear to open a hip-joint in order to clear away a small obstacle. The patient is thereby saved from many dangers and exposed to so few that it seems more humane and desirable in every respect.
Sherman’s method is to make traction upon the limb, drawing the femoral head down to a point just below the anterior superior crest, where it can easily be felt, and to here make an incision over it in the direction of muscular fibers so that they are not divided. After division of the capsule the head of the bone is exposed and retractors substituted by long loops of suture, put in on either side of the opening in the capsules. In many cases a tenotomy of the adductor tendons close to the pubis will also be of advantage. The leg is next released from traction and the head of the bone allowed to glide upward, while the finger is slipped into the capsule and down toward the acetabulum. Upon this finger as a guide a long, straight, probe-pointed bistoury is passed, and with it the narrower portion of the capsule is cut through, down to the bone, taking care to not cut off the ileopsoas tendon. The incision must be large enough to give free access to the acetabulum. Traction is then again made with sufficient manipulation so that the femoral head may be forced into its proper cavity. When the head is in the[475] acetabulum the retracting sutures are tied together so as to close the upper part of the capsule, and other sutures are introduced, as needed, to close the wound, leaving space for a cigarette drain. The limb is then put into a position of abduction of from 50 to 90 degrees, rotated in or not, as needed, and a comprehensive plaster-of-Paris spica applied. In this both limbs or only one may be included. The drain should be removed in two days and the dressing left otherwise undisturbed for three months.
Bradford has added somewhat to our methods by showing not only the arrangement of the capsule, but the fact that the acetabulum is often filled with dense fibrous tissue which sometimes obliterates it, and that this tissue can be curetted out, but that if it could be utilized to aid in retaining the reduced head of the femur it would be a great benefit. He operates as follows: The hip is subjected to preliminary forcible stretching of all soft parts which can be stretched by manual or mechanical force. A posterior incision is then made, which, without dividing muscles, permits free opening into the capsule and affords a channel to the deepest portion of the acetabulum. The posterior wall of the capsule is then split, after which all constricting and other obstacles at any point are carefully divided. These may be detected by the finger, and can also be seen by a small electric light passed down inside of a sterilized glass test tube. The capsular wound is then retracted by deep retaining silk sutures, placed at the lower rim of the acetabulum, thus affording a pathway for the reduction of the head. After this has been accomplished as described above, the sutures are tied closely around the femoral neck, and these retain it in position. The other portions of the split capsule are then sewed around the head and neck, to the trochanter and fascia, in such a way as to retain the bone where it has been placed.[37]
[37] American Journal of Orthopedic Surgery, October, 1905.
The earlier the operation is done the better. It is necessary to always maintain the limb in a position of well-marked abduction, and for a long time, nor can patients be released from this at the expiration of the first dressing period, usually twelve to fifteen weeks, although the abduction can usually be reduced with each dressing until at last the limbs are permitted to come together after the expiration of nine to eighteen months. Even after the lapse of this length of time it may be necessary to provide some form of apparatus by which too much rotation in either direction may be prevented, or by which pressure may still be made over the trochanter, in order that it may be kept constantly pushed into the acetabulum (Figs. 271 and 272).
Fig. 272
Unilateral congenital dislocation, showing the fixation bandage. A shoe with a cork sole about two inches in height should be worn on the operated side, while the attitude of exaggerated abduction is maintained. (Whitman.)
Fig. 273
Coxa valga, with defective development of the right femur. (Albert.)
This term is applied to an abnormality in the shape of the neck of the femur, consisting of a downward curvature or bending of the femoral neck, which is thus displaced until it stands almost at a right angle with the shaft instead of at the normal obtuse angle. At the same time there is often posterior curvature, or sometimes an anterior curve,[476] of the neck, which causes a corresponding rotation of the axis of the whole limb. The pelvic side of the hip-joint is unaffected, the change occurring usually solely in the upper end of the femur, the joint not being involved. It may appear in congenital form and then may be attributed either to intra-uterine pressure or to antenatal rickets or osteomalacia. The acquired form is usually due to a non-inflammatory softening, or to structural changes which permit of yielding, as above described. Doubtless different cases have different causes, and they are not to be included in one brief sentence. The condition corresponds to those abnormalities at the knee which produce knock-knee and bow-leg. Were the bone as easily examined at the upper end of the femur as at the knee the condition would be more easily recognized. Therefore the term has reference not so much to the results of active disease as to deformities of congenital or acquired character. Fully three-fourths of the cases are met with in male subjects, and the majority of these occur only on one side. Thus of 190 quoted by Whitman, 85 were unilateral, while only 26 occurred in females.
The more nearly the angle of fixation of the neck of the femur approaches a right angle the further above Nélaton’s line will the trochanter appear, and the more conspicuous this change the greater the difficulty in abduction. Moreover, to shortening may be added internal or external rotation, with consequent tilting of the pelvis and compensatory alteration of the spinal curves.
The disease is by no means often of traumatic origin, although traumatisms may produce an arthritis deformans, even in juvenile cases, and that this may simulate a non-symptomatic coxa valga is now well established (Fig. 273).
—Coxa vara produces certain symptoms, among them pain in the joint, radiating down the front and inside of the thigh. If the deformity be very marked, joint function is impaired. Tenderness is rarely present. When pain or tenderness occur they may lead to the mistaken diagnosis of rheumatism or neuralgia. The condition may arise as the result of an acute ostitis, in which case patients will be confined to bed for some time. Actual shortening may vary from one to one and a half inches, while the limb will be found adducted, the gluteal region flattened, with a deep curve between the trochanter and the gluteal muscles.
—The diagnosis is to be made mainly between this condition and hip-joint disease or misplacement. When abnormalities in the shape or position of the limbs in the young occur in a comparatively short time, coxa vara may be suspected, especially in the absence of that disability which coxitis usually produces. The patient should be examined in both the upright and horizontal position. Coxa vara may have an abrupt onset, but it never produces abscess. It is practically self-limited and will be followed, sooner or later, by spontaneous cessation of all acute features, while coxitis is progressive, with a destructive tendency. In coxa vara we do not have the starting pains nor muscle spasms of coxitis, while the actual shortening is much more marked. In doubtful cases the cathode rays may be employed and will often greatly facilitate diagnosis. The condition may be bilateral, but will still fail to show the muscle atrophy so significant of tuberculous disease.
As between coxa vara and that senile form of coxitis already described in the chapter on Joints as arthritis deformans, it should be remembered that the latter is a disease of advanced life, while the former occurs rather in its earlier periods. Moreover, in the[477] former there is no tendency to change in the femorocervical angle, no matter what changes may occur in other respects about the joint. When in the senile disease shortening really occurs it results from actual absorption of bone.
Coxa vara tends usually to spontaneous cessation, which may be considered recovery. Acute symptoms after a time subside, and function is regained to the full extent permitted by whatever changes have occurred in the shape of the bone. If symptoms are at all severe they demand physiological rest in bed, with traction, and the limb should not be used until pain has entirely subsided. Conspicuous deformity may call for correction by subcutaneous osteotomy made just below the trochanter. Only in exceedingly serious cases is exsection of the joint necessary.
Deformities induced by more or less acute affections of the cord and brain, or by hemorrhages, have assumed an ever-increasing importance in orthopedic work. Most of them resolve themselves into those due to acute anterior poliomyelitis and those due to cerebral hemorrhages.
Fig. 274
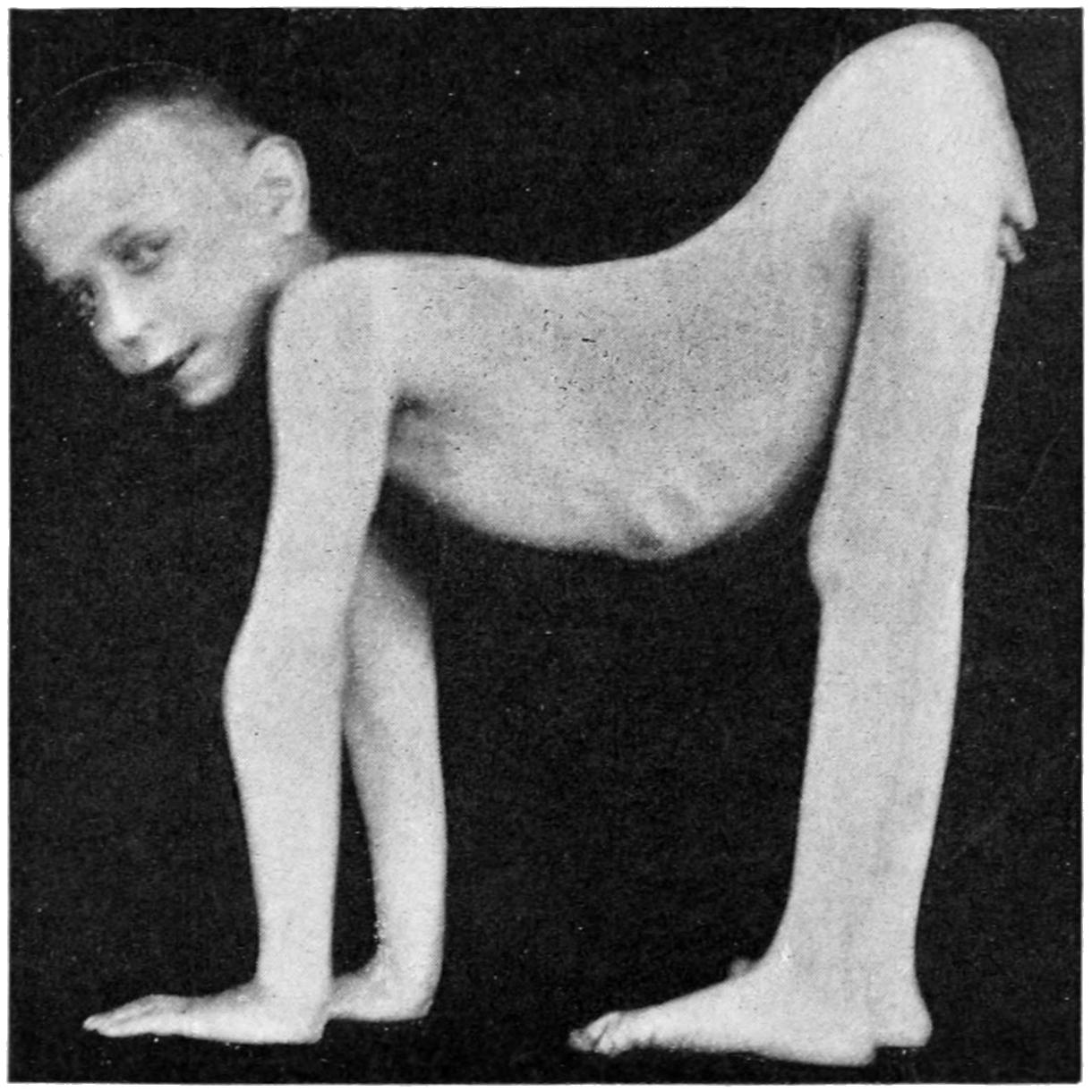
Anterior poliomyelitis. Extreme flexion deformity at the hips, inducing quadrupedal locomotion. (Gibney.)
—Anterior poliomyelitis is an acute inflammation manifested especially in the gray matter of the anterior cornua of the spinal cord, involving both the neuroglia and the cells, producing atrophy of the same and consequent paralysis of muscles supplied by the motor nerves. It may assume an acute febrile type, with rapid onset of paralysis, or it may be of slower development. Usually conceded to be of infectious origin, it still lacks the minute explanation for many of its attendant phenomena. It may appear with acute symptoms, febrile and convulsive, paralysis appearing more or less promptly. With the subsidence of other serious symptoms this paralysis remains. There may then be a period of partial improvement in the muscular condition, with disappearance of some of the most pronounced phenomena. Finally with the growth and development of the child more expressions of damage remain, and produce various distortions and deformities, varying with the muscle groups affected. Not only do deformities result, but there is more or less arrest of development, with disproportion in size between the limbs involved and those which have been spared. It is the early paralytic features which may permit diagnosis to be made in the early days of the acute febrile attack.
[478]
—The cerebral palsies, so called, are the result of hemorrhages or acute disorganization of the brain. The former are usually unilateral and give rise to a corresponding hemiplegia, with either paralysis or spastic rigidity, and usually with atrophy. The paralysis may not be complete, but is rather of the paretic type, involving the entire limb, the reflexes being increased and the muscles stiffened rather than flaccid, with loss of electrical reactions.
A paraplegia points rather to lesion in the spinal cord and hemorrhage than to cerebral lesion. Transverse myelitis is rare in children. Multiple neuritis may produce somewhat similar effects, as may also the toxic paralyses due either to drugs (especially lead or arsenic) or that following diphtheria, in which case it is the muscles of the throat and neck which are likely to be involved. Figs. 274 and 275 portray extreme types which are rare, but instances of minor degree of affection are frequent.
Fig. 275
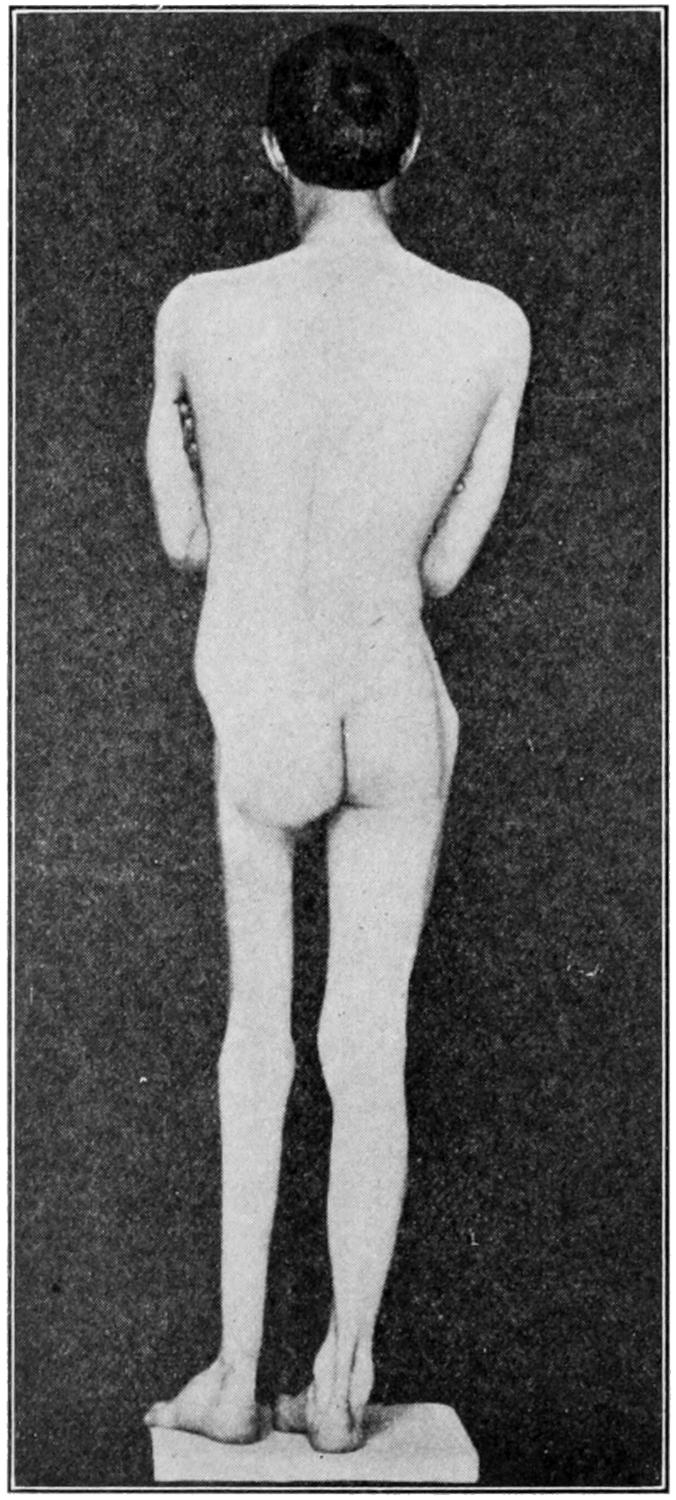
Anterior poliomyelitis. Duration seven years. Showing atrophy and slight lateral curvature of the spine; two and a quarter inches of shortening. (Whitman.)
—As two cases of this kind are seldom alike, treatment should be planned to meet the indications. Massage, electricity, hot-air baths, and similar non-operative measures find here a large field of usefulness, but, save in the milder cases, are insufficient. In no class of cases do tendon grafting and nerve grafting find a wider range of applicability, while tenotomy, myotomy, aponeurotomy, and occasionally osteotomy will permit of atonement for deformity which has not been treated. These operative measures have been considered.
[479]
The term fracture is, in surgery, applied to such injury of bone and cartilage as effects break in continuity. This injury is effected instantly, and it is rarely that fracture is produced by any slowly acting cause, although this latter may so affect or disintegrate bone as to permit fracture upon the application of a mild degree of force. Fractures are variously classified and grouped for convenience of description; thus we speak of traumatic and pathological fractures, implying by the former those which occur by violence in normal conditions of health, and by the latter those which are produced only because of some previous disease in the bone. The difference is that in the former case there is no preëxisting disease, whereas in the latter it is an essential feature of the case. Fractures are also classified as complete or incomplete, the former term implying injury to the whole thickness of the bone, while the latter are separately classified: (a) Fissure, in which there is a line of fracture by which there is no complete separation of fragment, it being essentially a crack; (b) the green-stick fracture, such as occurs in the young, where the bone is not thoroughly calcified, but is capable of bending to some extent, while a portion of it breaks; (c) depressed fracture, which is generally produced by direct violence, and occurs in a flat bone, i. e., the skull, the scapula, etc.; (d) detachment of a fragment or separation of an epiphysis; (e) partial fractures, corresponding much to the green-stick, but without deformity or change in shape or position.
Fig. 276
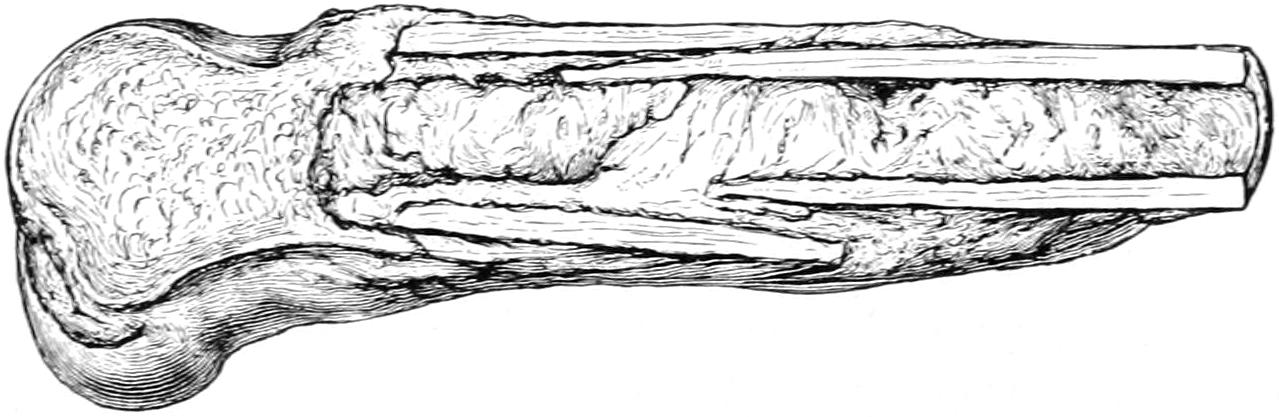
Impacted fracture of the shaft of the femur produced by a fall upon the knee in a man aged eighty-three years. Illustrating impaction. (Bryant.)
Fractures are also described by means of the following adjectives, which practically explain themselves, for instance:
A. Complete, transverse, oblique, longitudinal, dentated, etc. Spiral fracture is also described and occasionally seen. It involves only the long bones, and not only implies a considerable degree of violence, but is itself regarded as exceedingly serious.
B. In number they are single, multiple, or comminuted, as when there are a number of fragments.
C. They are often impacted, which means that one fragment is driven into and more or less embedded in the other. This impaction or interlocking of fragments occurs usually in the neck of the femur and the lower end of the radius. In the former locality it is advisable not to interfere with it; in the latter it should always be dislodged in order to restore the fragment to its proper position (Fig. 276).
D. As to their nature and location, fractures are referred to as pathological, gunshot, intra-articular, or extra-articular, etc., the latter terms referring to involvement of a joint. If blood can escape from the site of the fracture into a joint cavity, or if synovial fluid can escape from the latter into the former, then the fracture is called intra-articular.
Pathological fractures imply preëxisting disease. This may be constitutional, as in the case of the fragilitas ossium, already described in the chapter on the Bones, or it may be due to some secondary deposit of cancer or a primary sarcoma. In adults, especially those with a cancerous history, any spontaneous fracture, or even one occurring with[480] trifling violence, should lead to suspicion of a metastatic focus in the bone at the site of its yielding. The atrophic changes which notably occur in various bones as old age comes on lead also to a condition which is pathological, i. e., it permits of fracture from what would appear to be a trifling injury.
Gunshot fractures are practically always comminuted, save perhaps some of those inflicted with the modern military weapons. A Mauser bullet will frequently make an almost clean perforation, but the gunshot fractures met with in civil practice are almost invariably comminuted, especially those of the skull (Fig. 277).
E. The term compound is applied to any fracture in which there is wound of the soft tissues and so located as to permit access of air to the injured bone. There is a distinction between a compound and a complicated fracture. A fracture of the femur accompanied by a gash or extensive wound, so long as air cannot come in contact with the broken bone, would be described as a fracture of the femur complicated by a lacerated wound. On the other hand, if through the slightest puncture of the skin, even at a distance from the fracture, air can even theoretically enter and come in contact with bone surfaces at the site of the fracture, such an injury constitutes a compound fracture. This distinction is not a trifling one, for upon the exclusion of air, which to a certain extent means the exclusion of germs, depends very much the rapidity and perfection of recovery. Compound fractures are all dangerous in proportion as they permit of infection, and while air infection is not necessarily the most serious of any, it nevertheless is often sufficiently so to set up sepsis and interfere with consolidation, even if it does not prevent it. Fractures are made compound by direct violence from the outside or by indirect violence, as where a bone end perforates soft parts and the skin. Even if a sharp point of bone thus protruded from within is quickly drawn back again it is enough, since both the skin and the air in contact with it are sources of germ activity. Thus it may happen that a slight and apparently trivial injury of this kind is more serious than one which is extensive.
Fig. 277
Skiagram of compound comminuted (gunshot) fracture of elbow, inflicted with a Dumdum bullet. Illustrating the extreme of comminution. (Lexer.)
F. Epiphyseal separations constitute a somewhat distinct form of injury, having at the same time the importance and dignity of fractures in the truer sense of the term. In the chapter on Diseases of the Joints will be found a table of the ages at which epiphyses unite. In childhood and youth a fracture near the joint is most likely to partake of this character, and it is of importance that it should be recognized as such when it occurs. Injuries occurring beyond the ages mentioned in the table are not likely to be of this character unless ossification is delayed by some morbid process.
By virtue of their occupations and habits men suffer fractures more frequently than women. Fractures are, moreover, ten times as frequent as are dislocations. The aged, by virtue of their atrophic changes, are more subject to fractures than others. Fracture in the vicinity of certain joints predisposes as well to dislocation of these joints,[481] and it often happens that the treatment for the dislocation is reduction and treatment of the fracture. So far as the external causes of fracture are concerned they are frequently referred to as (a) fracture by external violence, and (b) fracture by muscle activity. The former are easily explained; the latter occur from excessive muscle action, as in violently throwing a ball, or, as in one case with which the writer was conversant, where a colored preacher in the vehemence of his gesticulations fractured his own humerus. Obviously the long or large bones are more liable to fracture than those which are short and irregular. Certain bones, especially the clavicle, are peculiarly exposed.
Intra-uterine fractures have not as yet been mentioned. These occur during the intra-uterine life of the fetus; this term does not include such fractures as may be inflicted during delivery with or without instruments. In a fetus already affected with congenital rickets it may not require any severe contusion upon the abdomen of the mother to inflict a fracture. Starvation (i. e., scurvy, syphilis, and struma) in the mother may so disturb nutrition as to weaken the osseous system of her offspring.
Such previous conditions as ensue from osteomyelitis (i. e., caries and necrosis) may often weaken the bone. Nevertheless with distinct necrosis there is usually so much new bone formation as to strengthen rather than weaken the part. Bones may also become fragile as the result of syphilis, especially when gummas develop within them.
Fractures frequently produce certain deformities which are more or less conspicuous and easily recognized. They are designated as angular, lateral, or axial (i. e., when the axes of bone are considerably displaced, even though they may be more or less parallel), longitudinal (when ends overlap), rotary, etc.; while by the interposition of muscles and other soft tissues more or less wide separation may be produced, the same result occurring when the olecranon or the upper half of the patella is widely separated from the main bone or portion by muscle pull.
Fractures give rise to subjective symptoms and objective signs. In diagnosis the history is also of value, especially in those cases where it is a question of some constitutional affection and a minimum or absolute absence of violence. The apparent immunity which the intoxicated enjoy is in large measure due to the fact that by virtue of their condition one of the predisposing causes of fracture is avoided. There can be no doubt but what muscle tension, due to voluntary or instinctive efforts to avoid harm, is a contributing factor in the separation of many bones or their processes. A patient stupidly drunk will not make these efforts, and will fall in a relaxed condition, in which violence will probably be much less extensive, and the consequences less disastrous than if he made an effort to save himself from falling.
Pain and tenderness are evidences of injury, and will often serve for its location; even the reference of pain is somewhat suggestive. It is stated as a universal rule that when pressure is applied laterally or in the long axis of a bone and evokes pain, referred to a distance from the point where pressure is made, it will indicate fracture at the point to which it is referred. There is always impairment, usually loss of function, while effort to move a thus injured limb will give rise again to localized pain and tenderness. The pain of contusion is usually diffuse, and that of fracture is referred to a limited area. The tenderness produced by handling or examination will vary with the stolidity, the age, and the character of the patient, as well as the nature of the injury.
Objective signs are crepitus, mobility, deformity, ecchymosis, redisplacement. Crepitus means the sensation of grating or rubbing produced when fractured bone surfaces are moved upon each other. It is recognized by the sense of touch, sometimes by that of hearing. Its presence is pathognomonic, but its absence is a negative sign, and an effort should be made to obtain it. To repeat the demonstration, especially to demonstrate it to others, means superfluous manipulation, which is not to the best interest of the patient. Crepitus, then, should be carefully sought for; once detected it should be sufficient.
Abnormal mobility is explained only by fracture. It is easy to detect it in the shaft of a long bone, but when near the joint it is confusing. Its determination by manipulation is not seen in green-stick or impacted fracture unless these are further broken[482] up by manipulation. When evident it should serve as a caution against unnecessary or rough handling, for if it be easily recognizable crepitus need not be sought.
Deformity is a striking and pathognomonic feature of fracture. It may be imitated by hematoma or sudden swelling of the soft parts or of joints. It may consist of shortening or of angular, lateral, or rotary displacement, or perhaps of depression or indentation. Careful inspection, then, and palpation should precede other methods of examination, as they are often sufficient to indicate the location, the nature, and sometimes even the character of the active causes.
Inspection of the injured part alone is not always sufficient. Careful comparison between the two sides of the body should be made in order that actual measurement or comparative examination may reveal what mere inspection would not. In connection with inspection it should be ascertained whether the individual has ever received previous injuries. The writer recalls a case where a physician claimed a recovery after fracture of the femur, treated by incompetent method, yet with ideal result, inasmuch as he said there was absolutely no shortening. A personal question, however, to the patient revealed the fact that he had had the other thigh broken some years previously, and that an apparently similar amount of shortening followed in each case.
The ordinary indications of fracture are frequently followed by ecchymosis. This will appear at a date corresponding with the depth of the injury beneath the skin (it may occur within an hour or three or four days). The blood will follow the fascial planes and work its way to the surface along them. The sign is of the greatest value in the diagnosis of basal fractures of the skull and certain fractures of the hip and pelvis. When it occurs after an interval it is a confirmatory rather than a promptly available sign.
Redisplacement implies that the parts when properly put into apposition quickly fall out of it unless mechanically supported—that is, they do not stay reduced. This sign is not universally applicable. It applies especially to the fractures of the long bones of the extremities, and particularly to the humerus, the femur, or double fractures of the radius and ulna in the forearm or both bones of the leg.
—Since Röntgen’s memorable discovery the cathode or x-rays have been of greater and greater use in the diagnosis and portrayal of injuries and morbid conditions in the osseous system. To such an extent is this now true that well-equipped hospitals have ample conveniences for fluoroscopic and photographic work, while many medical men are doing it in their private practice. There can be no question but that diagnosis and methods of treatment have been made more perfect since this new method of investigation has been made available. On one hand, however, it has led perhaps to something of neglect of the methods previously in vogue, which necessitated anatomical knowledge and logical reasoning. On the other hand, the knowledge thus obtained has been sometimes a two-edged sword, since the display of skiagrams, or x-ray pictures, in court has too often worked harm or discredit to the surgeon or the institution with which he was connected. Moreover, even this method of diagnosis, with its apparent certainties, is not always reliable, and disappointments have sometimes followed.
are subject to peculiar complications which enhance the difficulty of treatment and jeopardized the result. Among the more common of these are the following:
1. Too wide separation of fragments by hemorrhage or distention, with failure in resorption of fluid before fixation in bad position has resulted.
2. Complete or partial rotary displacement, preventing proper apposition of bone surfaces.
3. Interposition of soft or fibrous tissues between fragments by which bony union is prevented. This is conspicuously common in fractures of the olecranon and patella, and is of itself sufficient reason to justify operation in otherwise suitable cases.
4. Separation of a fragment within a joint capsule, by which its blood supply is cut off, making it essentially a foreign body. This occurs especially at the anatomical necks of both the humerus and femur.
5. Exuberance of callus with consequent limitation of motion.
6. Insufficient amount or absence of callus, which, when bone ends are bathed in joint fluids, is not often thrown out.
All of these are immediate consequences. The following are among the more undesirable remote consequences of the same injuries:
[483]
1. Exuberant callus, which may be the result of too early attempt to move the parts, or may result from other causes; it offers more or less mechanical obstruction to joint movements.
2. Separation of fragments to an extent precluding the possibility of repair, and interfering with function.
3. Pseudo-ankylosis, as a result of condensation and organization of blood clot between joint surfaces.
4. Adhesion of tendons to surrounding callus or within their own sheaths.
5. Displacement and distortion of bone ends with vicious union, for which the medical attendant is sometimes responsible. Unfortunate consequences of this kind are generally seen at the elbow after fractures of the condyles; at the wrist, after incomplete reduction of Colles’ fracture; at the hip, when insufficient traction has been made; at the ankle, after the complete form of Pott’s fracture.
6. Exostoses and osteophytic outgrowths, which often complicate fractures.
7. Absorption of bone, which is usually seen after fractures of the neck of the femur.
8. Involvement of nerves by pressure of callus, most often seen about the elbow.
9. Thrombosis leading to obliteration of the deeper and enlargement of the more superficial veins.
10. Edema, also the result of venous obstruction by pressure of callus.
11. Chronic hydrarthrosis.
12. Arthritis deformans traumatica. This is usually a remote result of fractures, and manifests itself by slow changes in shape and position, with deformity and disability. It occurs most often in the aged.
13. Necrosis, which may be the result of failure in the process of repair and will probably necessitate operation.
14. Malignant changes. These have to do with the occurrence of sarcoma in bone callus, a complication which is known to occasionally arise. (See Sarcoma.) It also refers to primary sarcoma, by which bone is weakened, or secondary carcinoma, which produces the same result.
15. Syphilis. Chronic syphilitic disease is well known to weaken bones by atrophic processes as well as by the deposition of gumma. It is known also to delay, or sometimes almost prevent, the process of callus formation, ossification, and later absorption. Syphilitic patients with fractures need to be kept under antispecific medicines.
The immediate consequence of a fracture is outpour of blood both from the broken-bone surfaces and from whatever other tissues may have been lacerated. This produces, first, a hematoma, which is followed by a certain degree of local edema, perhaps even of general edema of the distal parts. The latter will subside with a rapidity proportionate to the promptness of suitable treatment and the nature of the injury. The blood begins to coagulate within a short time, while with the disappearance of the more fluid portion granulations begin to form from the periosteum, as well as bone surfaces, externally and internally, and even from the marrow. The clot loses its original characteristics and is permeated more or less rapidly by granulations. With the site of the injury wrapped in a mass of granulation tissue we speak of the so-called provisional callus, whose amount will depend upon the severity of the injury and the accuracy of the replacement of the parts. If laceration has been but trifling and the bones are accurately apposed the amount of callus will be small, otherwise it may be large; so large, in fact, as to be easily palpated and even to cause edema and pain by pressure. Repair of the fracture is effected by the gradual conversion of this callus into cartilaginous tissue and then into bone. So much of it, at least, as lies on the outer side of the bone and is known as external callus goes through this change. The internal callus, i. e., that within the marrow cavity, undergoes a more direct transformation, which amounts to immediate ossification. The internal callus usually ossifies completely, and then forms a medullary plug that serves as an internal splint and affords support and strength. In time it completely disappears, this time varying in different cases.
The external callus is converted into bone by passing through the intermediary condition of cartilage. Between the broken-bone ends granulation occurs more slowly, and[484] repair at this point is delayed, partly because of poor circulation and nutrition; but the internal callus acting as a bobbin within, and the external callus acting as a solder on the outside, give sufficient support and strength to effect a final and absolute ossification of all the interfragmentary granulation tissue. When the time comes when callus is no longer necessary it begins to disappear by absorption. When everything proceeds normally callus is absorbed in a proportion commensurate with its loss of utility. When bone ends have badly united considerable callus remains permanently. When apposition has been ideal it almost completely disappears, even the medullary cavity being restored.
Fragments which are completely detached may be reunited by practically the same primary process, but fragments of considerable size usually become surrounded by granulation tissue, by which they are nourished and may be finally reunited, with more or less departure from their original shape and location. It is in this way that a comminuted fracture may heal. Fragments that are separated sometimes necrose and have to be removed.
Fig. 278
Fig. 279
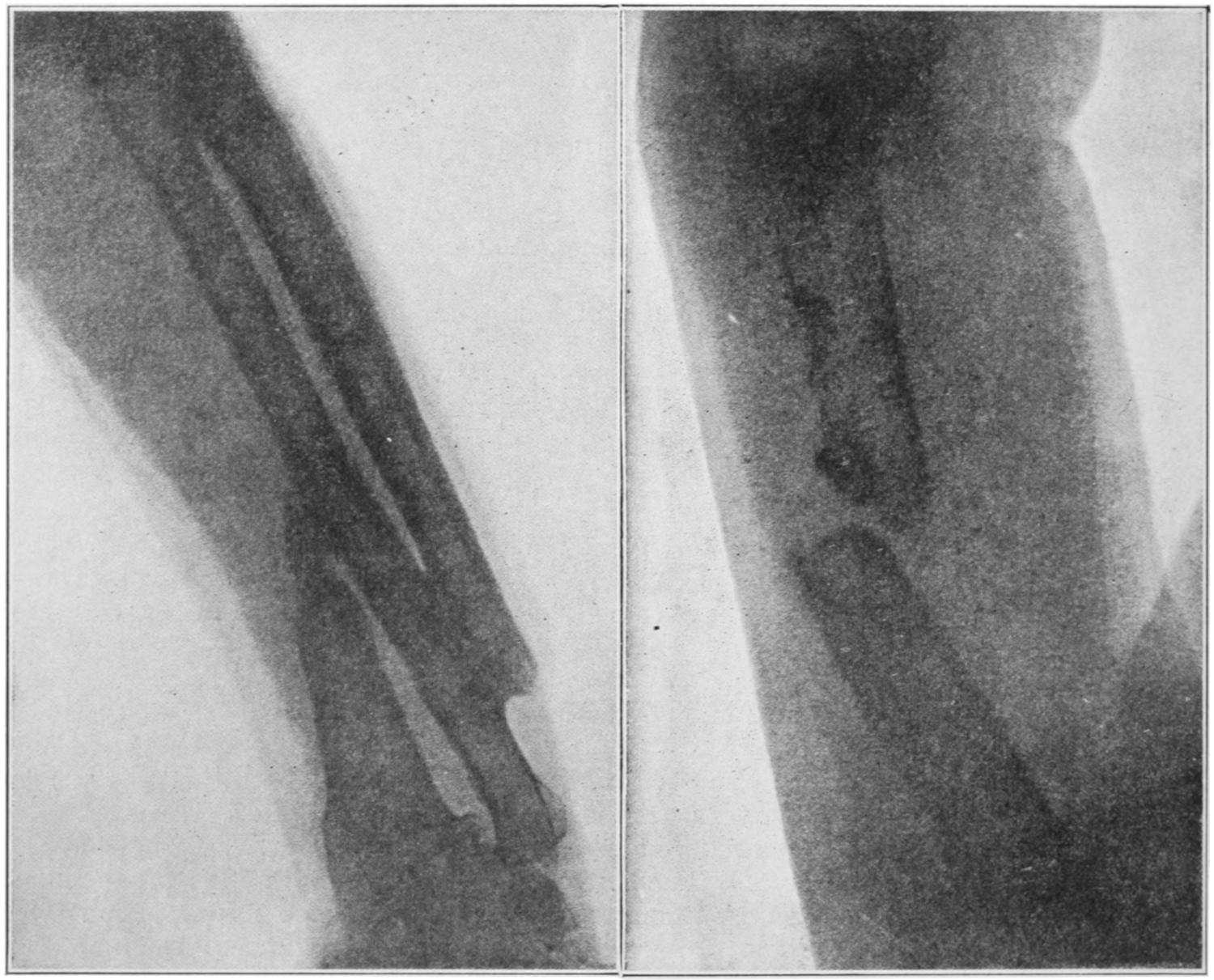
Compound fractures resulting from arm being caught in belting and wound around shafting. End of radius united to ulna and lower end of ulna to the radial fragment. Pseudarthrosis of humerus, thrice operated, the third time in the Buffalo Clinic. (Skiagram by Dr. Plummer.) (Arch. Phys. Therap., May, 1905.)
The repair of the flat bones is effected by a similar process, which is referred to as callus formation. In the skull it is brought about chiefly through the agency of the diploë, whose powers in this direction are somewhat limited. Cancellous bone tissue usually throws out but little callus. Its repair occurs from within. Cartilage heals by a very similar process, though it is not now ossific tissue but fibrous which reunites the fractured surfaces. Instances of both kinds can be seen when a fracture has crossed a joint surface.
In a compound fracture much will depend upon the existence or absence of septic complications. In a clean wound, whence blood and fluid may have escaped, there[485] will be little but granulation tissue. Should this wound suppurate the exposed bone surfaces will undergo at least a superficial necrosis, necrotic particles being removed by the same granulation tissue which will later bind the bone ends together. Here, too, the internal callus plays the largest role in the process of repair. The bone tissue first formed is always coarse and soft. Complete calcification and restoration of original density and vascularity occur slowly. Neither cartilage nor bloodvessels alone appear capable of forming bone; the latter is produced only under the influence of the osteoblasts, which penetrate from the periosteum and the bone itself along the course of the bloodvessels.
The process is one of conversion of blood clot into provisional callus, which then changes into granulation tissue or into cartilage, both of these materials undergoing subsequent conversion into bone through the medium of the osteoblasts and osteoclasts (or giant bone cells), the neighboring bone itself undergoing a rarefying ostitis, to change back into its original condition with the final changes of the callus.
Repair of intra-articular fractures has already been described as influenced by the presence of synovial fluid and cartilage. The latter does not proliferate, and the line of fracture usually appears as a groove on its surface. At epiphyseal junctions union is usually rapid and satisfactory, for the changes taking place at this point are in the direct line of what is needed for repair.
The above description refers to the process which is supposed to take place in normal bone repair. When, however, this is disturbed, as it may be from a variety of causes, there may be delayed union; when it completely fails we have non-union. General conditions have bearing on these local failures. Whatever makes a strain upon the system may interrupt the process, e. g., pregnancy, lactation, exhausting hemorrhages, acute diseases, starvation. Again, failure may result from purely local conditions, such as marked displacement, and particularly the intervention of some of the soft tissues, or any foreign body. Suppuration will also frequently cause great disappointment. The humerus is the bone most often troublesome in this direction; next the bones of the leg, the femur, and the bones of the forearm. It is necessary to distinguish between delayed union and absolute non-union. In the former normal processes may be simply retarded. When thus delayed they may be stimulated by rough handling, rubbing the bones together, or by perforating the callus with the point of a drill, from several directions. This method of drilling was introduced by Brainard, of Chicago. The existence of syphilis has much to do with delay, and should be combated by free use of antispecifics. Many patients will be found to have phosphaturia, i. e., to be eliminating phosphates which should go to repairing the bone. Such patients should be given phosphoric acid, with some of the phosphates, preferably of calcium, in order to make up for loss in this direction. Much can be done also by massage, and by everything which stimulates nutrition and general health (fig. 280).
Fig. 280
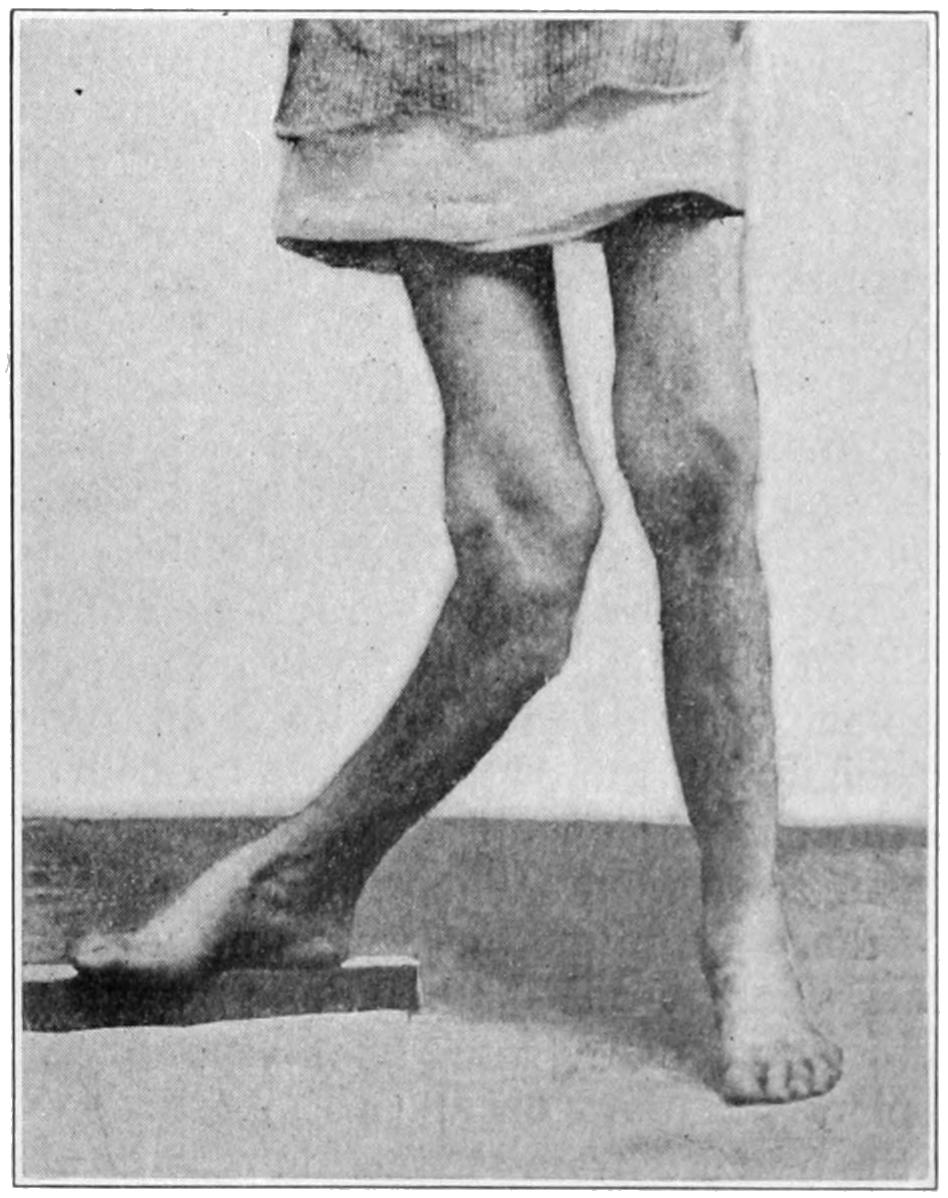
Vicious union with great deformity after fracture, requiring extensive operation. (Buffalo Clinic.)
In non-union efforts at repair are at a standstill; the bone ends become rounded off, the marrow cavity is plugged on either side, while in time the surrounding granulation or connective tissue undergoes condensation, as well as organization, and a capsule is formed in which a certain amount of fluid resembling true synovia collects, and thus is formed sometimes an almost perfect pseudarthrosis or false joint, whose perfection as a joint must be admired,[486] although its presence is so deplored. The causes of non-union are now better understood than formerly, and consist largely in the interposition of fibrous and muscular tissues, that act as a barrier and keep the granulation tissue or the callus on one side from coalescing with that on the other.
Treatment of these cases will vary with their causes. In delayed union patients should be encouraged to use the parts, thereby causing greater activity, but in the presence of an actual false joint no method is of avail except that of actual exposure, by incision, with removal of all intervening fibrous tissue, and freshening of the bone surfaces by saw or chisel, the endeavor being to so shape them that they may lie in contact, and then be so maintained, by some mechanical expedient, such as a wire nail or suture, an ivory peg, a chromicized tendon, a bone ring, a small metal brace fastened with screws, or by any other expedient which may suggest itself to the ingenuity and the means of the operator. There are, however, occasions when one deliberately endeavors to secure a pseudarthrosis, as after ankylosis of the shoulder-joint, if in making powerful effort to break up adhesions the neck of the humerus should snap it would be better to prevent union rather than favor it, as in this way something resembling the original joint, so far as function is concerned, would be obtained. At the hip, also, after such an accident, the same principles may be adhered to or more deliberately secured by a subcutaneous osteotomy, as is sometimes done for relief of deformity.
Fibrous union implies such organization of granulation tissue as converts it into simple fibrous or ligamentous tissue, the change stopping here and not going on to formation of cartilage or bone. There are three localities especially where fibrous union is sometimes the best that can be obtained and often proves sufficient of itself; these are the olecranon, the patella, and the neck of the femur. Even though the halves of the patella be separated by two inches of ligamentous tissue the patient may still have reasonable use of the limb. A separation of half an inch to one inch at the olecranon does not materially disable the arm, while at the hip-joint two or three inches of ligamentous tissue between the main end of the bone and the fragment will not totally interfere with locomotion, except so far as it permits an equivalent amount of shortening of the leg. There are, then, occasions especially when the hip is involved in elderly and decrepit people, when ligamentous union is the best that can be hoped for or attained.
In principle the treatment of fractures is very simple. It consists in putting the parts in apposition and maintaining them there for sufficient time to permit of complete repair. That which is so simple in theory is often very difficult and sometimes even impossible in practice, made so by the nature of the injury or the disposition of the patient. In the aged, who cannot lie long in one position for fear of pulmonary stasis; also in the insane, in the epileptic, and in those suffering from delirium tremens, will be met difficulties which are insuperable. In such instances the first indication is to preserve the life of the patient, the second is to get a good result, the third is to do the best we can. Good management is not the least important feature of such treatment. This will include suitable nutrition, provision for elimination, prevention of bed-sores or pressure-sores, and many other less important features.
Diagnosis having been made, the surgeon should study how he may best carry out the fundamental principle of putting the parts in apposition and so maintaining them.
The greatest obstacle to reduction and maintenance in position is muscle pull. After an injury of this kind there will be more or less muscle spasm, the more powerful groups displacing bones in the natural direction of their pull. In the humerus and femur especially all arm or thigh muscles will coöperate to produce shortening. As indicated in the chapter on Joint Affections, nothing so thoroughly overcomes chronic muscle spasm as traction. The principle underlying treatment by traction is exceedingly simple, but there are numerous ways and mechanical expedients for effecting it. In the lower limb, whether this shall be done by anterior suspension, by weight and pulley, by elastic contraction, or by some of the more complicated splints, matters little so long as it be efficiently made. Of all these methods it may be said in general the simplest is the best. In the upper extremity traction may be made by similar methods with the patient in bed, or the patient may be allowed to rise and be about with a weight hanging from the elbow or some simple expedient of this kind.
[487]
The method of traction is one to be combined usually with further protection, by which not only longitudinal but lateral displacement maybe overcome. This suggests the use of splints in addition to mere traction methods.
It is not always possible to put in operation at first that method which we may prefer a little later, as swelling is usually so pronounced as to make it advisable only to put the parts at rest and hasten absorption. The same is true of hemorrhage. In rarer instances it may be a question as to whether the distal parts may undergo gangrene from the disturbance of circulation. These are matters to be duly regarded before the later and more complete dressing. Mechanical aids, usually in the shape of splints, are therefore necessary. The physiological rest which it is so necessary to ensure will lead to a certain wasting of muscles and stiffening of joints, which are only temporary, but which by no means lessen disability when splints are removed. That splint is best for a given case which best fits it and permits the surgeon to carry out its peculiar indications. The writer is opposed to manufactured splints, as they seldom fit the part. This can be obviated by packing cotton or other compressible material into the splint. For temporary purposes they will frequently suffice. For fixed dressing, however, it is preferable to make a splint which shall fit the limb to which it is affixed. Immobilization is difficult of accomplishment and at many points impossible. Thus in fracture of the ribs or clavicle it is impossible to avoid a certain amount of motion with each respiratory effort, even though an uncomfortably tight dressing be applied.
Splints are made of various materials, metal, wood, various compositions hardened in molds, plaster of Paris, or some of its substitutes, i. e., glue, soluble glass, or a composition like one made of equal parts of powdered starch and fine isinglass, added to a solution of potassium silicate, this being allowed to stand for several days, after which a little fine boric acid powder is added; when this is painted over gauze dressings it solidifies and forms a light and rigid splint. There is one objection to all methods which comprise a solution that hardens slowly—that is, that during the time required for the purpose redisplacement may occur. It is not advisable to dress a recent fracture in a wet pasteboard splint or in such a composition as that mentioned above. Later, when a certain amount of consolidation has already occurred they may serve a useful purpose.[38]
[38] Jenkins’ packing, such as is used on some engines, has been recommended by Spotswood as a substitute for plaster-of-Paris bandages, its advantages being that it is not affected by any antiseptic washes as a plaster dressing would be, that it is lighter, and that by placing it in hot water it can be molded to assume the shape of the limb.
There are two methods of using plaster of Paris: one is gauze bandages sprinkled with it, rolled, and kept ready for use, to be placed in water at the time of their employment. A limb may be enveloped in these, after being covered with a layer of wadding or some other protective material, by which the plaster shall not come in actual contact with the skin. It is also a good plan to place a strip of tin or pasteboard along the exposed surface of the limb, over which the surgeon cuts to remove the splint. Thus one may avoid any danger of injuring the skin with the point of the knife. It is also a good plan to make at least a part of this cut before the plaster has sufficiently hardened, i. e., to do most of the work, leaving perhaps a layer or two of gauze to be cut through some time later. It is necessary to impress the fact that when a quickly hardening fixed dressing is used approximation should be ensured by the greatest attention, maintaining it until the splint is so hardened that redislocation is impossible. Another method of using plaster of Paris is by sopping strips of surgeons’ lint, ordinary canton flannel, or almost any other similar material, in plaster-of-Paris cream, then molding these to the injured limb, maintaining the same rigid precaution as to the proper position of the same while the splint hardens. In this way a splint can be adapted to the part, and, at the same time, made removable, permitting as frequent access to it as may be desired.
As already stated, it is the communication of fractured bone surfaces with the external air which makes a fracture compound in the strictly surgical sense. This may occur through a minute and tortuous opening or through a large and extensive wound. Although the communication is with the atmosphere the danger comes not so much from germs floating in the air as from those on the surface of the body and within the pores of[488] the skin, or else from foreign material admitted through the external wound. Obviously the great danger is of septic infection. Whether the tissues may prove more or less susceptible, and thus resist or break down, cannot at the outset be foretold. This leaves but one imperative ride to follow, to act in every instance as though serious injection had occurred and to take precautions accordingly. Even a small puncture made by a spicule of bone may permit germs to be withdrawn into the tissues as the bone is replaced. If, then, the surgeon seals such a puncture he necessarily takes the chances and must abide the result. Whether he shall do this or not will depend upon the patient and the injury. At all events, the site of puncture should be carefully cleansed and disinfected and the case so dressed that it may be carefully watched. Complete sterilization of every particle of exposed tissue is absolutely necessary, and for this purpose hydrogen dioxide or some of its later substitutes will prove effective. A protruding splinter of bone should be removed with cutting forceps, unless the wound must be enlarged as a part of the treatment of the fracture. In most instances it will be safer to pursue this course, i. e., to extend the wound which makes the fracture compound, to a degree permitting thorough exploration and cleansing. Not infrequently fragments of bone will be found, which when nearly or completely detached should be removed. Such a free opening permits also of wiring, or other means of fastening together bone ends, by which apposition may be more perfectly secured. A compound fracture which has been long unattended may be safely assumed to be septic. Here free incision, with cleansing and ample drainage, will be a far safer course than non-compliance with the general rule.
Compound fractures of the skull are nearly always depressed fractures, and practically always call for operation. Their proper treatment will be dealt with when considering Injuries to the Head. A fracture of the ribs may be made compound by penetration of a sharp bone end, and such injury to the lung as may permit air to escape into the pleural cavity. Such a pneumothorax may be followed by a hemothorax and hydrothorax, and these perhaps by empyema. Compound fractures of the pelvis are not infrequently complicated by perforation of the bladder or bowel, or rupture of the urethra, or some other serious visceral injury which may determine their fate. Compound fractures are difficult of treatment because they entail frequent changes of dressing and prevent the use of desirable splints. These fractures are also sometimes so serious as to necessitate amputation, which may be necessitated either by such comminution of bone as to make repair impossible, or such injury to vessels as may determine gangrene. If the circulation can be shown to be sufficient, either at the time or perhaps by delay of a few hours or a day, a limb may be saved by the resection of one or both bones, which in pre-antiseptic days would have required amputation.
The surgeon does not always see these cases in their recent or fresh state. He may be called to a case complicated by suppuration, cellulitis, and sepsis. Here though amputation may be required he may still delay it, hoping to improve local conditions, and thus to make it more promising, or he may have to resort to various expedients, such as suspension with constant irrigation, or temporary packing with yeast, in order to justify any further attack upon the parts already involved.
In the treatment of compound as of simple fractures we should never lose sight of the dangers of too tight bandaging and of pressure sores. I have seen both these lead to gangrene, with its necessary mutilation, in cases where the attendant has forgotten the proneness of injured parts to swell, and has either not allowed for this within the dressings or has not atoned for it in time when it has already occurred.
In the treatment of all these cases the operator should never forget the medicolegal aspects of such a case nor the necessity for constant attention and caution on his part. He should remember that his minutest precautions will often be disobeyed. He may, however, be cheered by the fact that only in cases of carelessness will he incur legal responsibility.
[489]
Fractures of the skull and of the vertebræ will be considered under the respective headings of Injuries to the Head and to the Spine.
The nose is the most frequently broken of all the bony parts about the face. One nasal bone or both may be broken, and each may be separated from its bony supports as well as from the other. The fracture may be compound in either direction, most frequently so into the nasal cavity, as a result of which infection may as easily take place from within as from without. The cartilages may also participate in the injury.
The injury would be easy of recognition were it not for the amount of swelling that often accompanies it. The signs are mobility and crepitus, with more or less deformity. So long as the nose can be grasped between the fingers recognition of fracture is easy. If swelling prevents this an instrument or the finger can be passed into one nostril and combined manipulation practised. There is generally more or less bleeding from the nose, and sometimes considerable emphysema. Swelling and ecchymosis are also often pronounced. This will all subside under cool and soothing applications. The most important indication is to replace the nose and hold it where it should remain. The difficulty is increased by the efforts which the patient instinctively makes to dislodge clot or secretion. The importance of accurate reposition is in some cases sufficient to justify an anesthetic and instrumental help. This will permit of the application of such force as may be necessary to elevate or to shift fragments, while a gutta-percha splint may be molded upon the outside, or a sterilized pin or needle made to transfix the nose from one side to the other (Mason), passing behind the fragments and through the septum in such a way as to keep it from dropping backward. A good plan is to introduce a tube into each nostril, perhaps a piece of silk catheter, around which a certain amount of gauze can be packed, and which can thus be used as an internal splint, while on either side and externally a little roll of gauze is held in place by adhesive plaster crossing the cheeks. The operator should take as much pains to see that the septum is in its original position as in attending to outside and cosmetic effects. The septum can be controlled by a pair of forceps.
A nose properly held in place will heal within a few days, to a point requiring little if any support. A transfixion pin should not be needed, if used, for more than four or five days. An internal splint should be removed each day, so that the nose may be sprayed with cleansing solution (Dobell’s) and retained secretions removed.
The disfigurement resulting after this injury is dropping in at the root of the nose, constituting the so-called saddle-nose defect. Such disfigurement as results can be later atoned for by subcutaneous injection of paraffin. (See chapter on Surgery of the Face.)
The more protected portions of the upper jaw are rarely fractured, save by extreme violence. The alveolar process, with one or several teeth, may be partially or completely detached. Such fractures are compound, and after replacement need antiseptic mouth-washes as well as other attention. Usually the teeth in the fragment can be utilized for the purpose of fastening it back into place by means of the uninjured teeth, retention being secured by wire or waxed silk. Extensive detachment may necessitate sutures through drill holes. The lower jaw can usually be utilized as a splint for the upper by binding the jaws firmly together and feeding the patient on fluid food. When one or two teeth are loosened or displaced it will often be possible, if they can be promptly secured, to successfully reimplant them in their sockets. Both the sockets and the teeth should be thoroughly cleansed. After replacement it will be necessary only to ensure absolute rest and retention in position.
In regard to other facial bones there is no injury which may not occur, as the result of direct violence. The zygoma and the malar bone may be broken away, or the entire collection of facial bones may be loosened from their connection with the bones of the[490] skull proper. The margins of the orbit, or its walls, may also be injured, and the sinuses opened, with perhaps more or less entrance of foreign material. These fractures are generally compound and are accompanied sometimes by injuries to the soft tissues. It becomes then a question not merely of cosmetic result, but of avoiding infection and saving life. The latter is the more important, and measures should first be directed to that object. Satisfactory results can be attained by drilling and holding bone fragments together with tendon or other sutures, and by neatly trimming and cleaning wounded surfaces and bringing them together. Subcutaneous sutures should be used for this purpose.
This bone is broken nearly as often as the nose, and almost invariably by direct violence. Here, as in the upper jaw, there may be trifling or serious fractures of the alveolar process, which should be treated on the same principle as above set forth. Fractures of the rami occur more often in those parts which are occupied by teeth, or from which teeth have dropped out by senile changes, the jaw being weakened at these locations. The most frequent seat of fracture is near the middle line. Fractures of the ascending ramus and of the upper processes are rare. Double fractures are not infrequent, the lines of separation being rarely symmetrical. The gum and the skin are often torn and the majority of these fractures are compound. The bone is considered to be weakened at the dental foramen; at all events it often yields in this vicinity. By fracture with much displacement posterior to this opening the inferior dental nerve may be injured or torn. The condyle, after extreme violence, has been known to have been driven up into the cranial cavity through the base of the skull. Gunshot fractures are nearly always comminuted (Figs. 281, 282 and 283).
Fig. 281
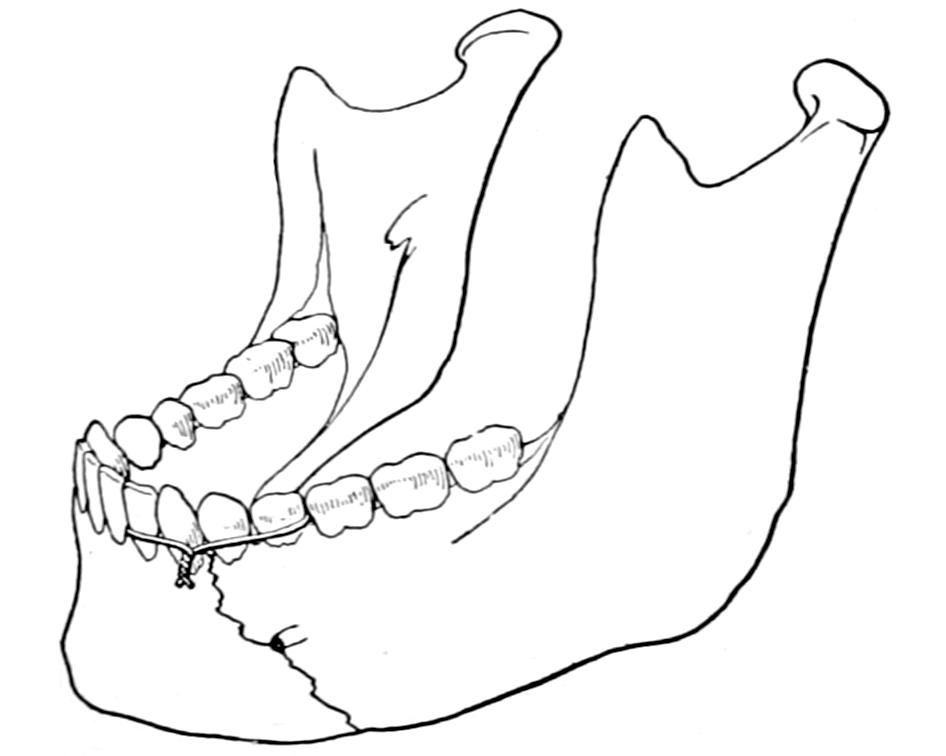
Fig. 282
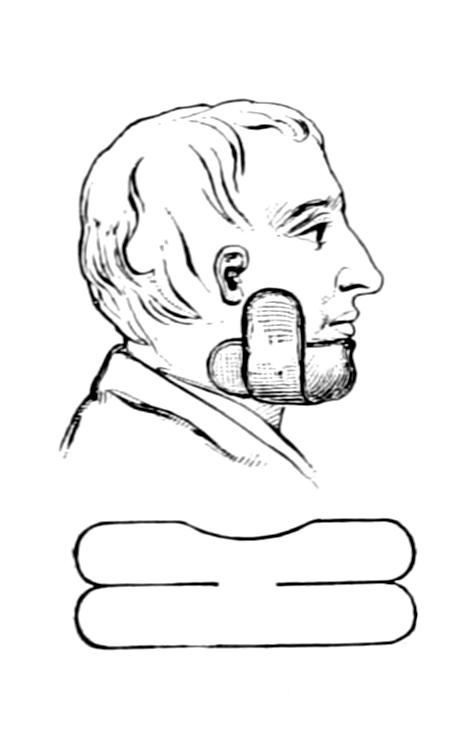
Fig. 283

Use of silver wire in fixation of fragments by utilizing the teeth.
Bandage and splint for fracture of lower jaw. (Bryant.)
The signs of fracture of the lower jaw are unnatural mobility, crepitus, displacement, pain, and loss of function. No bone in the body is more easily investigated by sight and touch, and recognition of these fractures is usually easy. Pain is provoked by attempting to move the jaw, even in talking, and depends on the extent to which the inferior dental nerve is injured. Irregularity in the line of the teeth will sometimes permit recognition. These fractures furnish excellent illustrations of the effect of muscles in producing displacement. Those of the tongue and the floor of the mouth, as well as the anterior muscles of the neck, will pull the fragments in various directions, according to the direction of the line of fracture and its location. This displacement may be trifling or serious. These fractures are often compound, internally or externally, such injuries constituting an unpleasant complication, but affording occasionally an opportunity for fastening fragments by drill or wire suture, which would otherwise require an opening to be made. In every instance antiseptic mouth-washes should be frequently used.
—The treatment is simplified when the dentition is good and regular so that the fragments may be fastened together with wire or waxed silk ligature around the[491] adjoining teeth, and then fixation accomplished with a simple molded gutta-percha or plaster-of-Paris splint, by which the lower jaw is held firmly against the upper. Such a dressing is held in position by a four-tailed bandage (Fig. 283). A silk or wire loop, used for the purpose just mentioned, should include two teeth on either side of the fracture, for by constant tension the nearest tooth will soon loosen, and if this were next to the break the effect of such displacement would be injurious (Fig. 281). When the line of fracture is oblique there is often greater difficulty in adjustment.
While the simplest means by which the fragments may be kept in position are the best, there should be no hesitation in serious cases to resort to operative measures having for their purpose the insertion of wire sutures or their equivalent. These are inserted after drilling the bone at suitable points, and are introduced with a view to their subsequent removal, the ends being left projecting in order to facilitate this. In clean cases, where the incision is made in unbroken skin, the ends may be twisted short and turned in, previously to closing the wound. Such operative treatment is required when there has been a double fracture, the central fragment being badly displaced by groups of muscles which tend to pull it downward and backward.
A dentist should be consulted, as he may be able to make a mold and then construct a plate or interdental splint, by which a more perfect reposition may be effected.
Swelling, emphysema, ecchymosis, etc., may be treated in the usual way. Irritation is likely to provoke free secretion of saliva; this may be combated by small doses of belladonna. Patients should be fed by fluid or thin semifluid food, and mouth-washes should be frequently used.
The hyoid may be broken by direct violence, either locally applied or by forcing the head backward. Fracture of the bone itself is not so serious as the lesions which accompany or follow it, either hemorrhage or inflammation, with edema of the larynx, which may impede respiration or cause strangulation. Fracture produces difficulty in breathing, swelling, and pain on talking. It is doubtful if bony union is attained, but fibrous union answers equally well. The treatment consists essentially of physiological rest. Edema may necessitate tracheotomy, and dysphagia feeding by an esophageal tube or by the rectum. Should the fracture be compound, or should a fragment be displaced so as to be detected, it may be removed through suitable incision.
This may be fractured by injuries of the same character as those which fracture the hyoid, except that it is more exposed to the direct violence of a blow, as from a baseball. In elderly people in whom calcification of the laryngeal cartilages has occurred fracture is more dangerous than in the young. Injuries which produce these lesions are of a serious nature, as prompt swelling, either from hemorrhage or edema, occurs and threatens respiration. For illustration a death occurred on the baseball field within a few minutes after reception of a blow upon the front of the neck with laryngeal fracture; the cause of death was suffocation due to swelling, which might have been averted if tracheotomy could have been performed. In the milder injuries of this kind much can be done with sprays of cocaine and adrenalin, to quiet laryngeal irritation and reduce vascularity.
Fracture of the sternum in childhood is exceedingly rare. In adults it may occur in connection with other injuries or as a solitary lesion. Such a fracture, of itself, would indicate in most cases excessive violence. It is usually more or less transverse, the periosteum being rarely so torn as to permit of much escape of blood. Cases are recorded in which it has been broken in straining during the act of parturition. It is most commonly injured by compressing and crushing injuries.
Sternal fractures are followed by much pain, aggravated by deep respiration and made worse by pressure. Sometimes displacement can be made out, while crepitus[492] may be detected with the stethoscope. Occasionally there is sufficient deformity to make the injury apparent at a glance.
Displacement should be reduced and apposition then maintained by a plaster-of-Paris jacket or other suitable apparatus. It is advisable in some cases to anesthetize the patient and to make a sufficient opening that instruments may be used by which fragments may be lifted or pried into place. This should be done under aseptic precautions.
Diastases or separations of ribs or cartilages from the sternum or from each other have essentially the dignity of fractures, are recognized by the same general signs, and are treated in the same general way. A cartilage may snap in the young, and in the old, when calcified, may break as would a bone or even a pipe-stem.
The ribs are usually broken in their lateral aspects, but rarely between the head and angle. They may be fractured by muscle action or by external violence, examples of the former being violent efforts at lifting or sneezing. Violence may be applied in so many ways that it is not necessary to specify them. Fractures may pertain to one or to several ribs in proportion to the extent and violence of the exciting injury. In some crushing injuries an entire section of the chest wall may be broken loose and depressed, this corresponding to a depressed fracture of the skull. Rib fractures are usually of themselves innocent, but may be made serious by complications, as when the pleura is torn, or an intercostal artery bleeds profusely, or when a jagged fragment of bone first scratches and then perforates a lung. This will lead first to the outpour of blood and then of pleuritic fluid, by which in a short time the lung will be separated from the chest wall. Should infection occur through the injured lung, i. e., entrance of germ-ladened air, then empyema may seriously complicate matters and later necessitate operation. Even the heart has been injured, in several reported cases, by projecting fragments of bone. Gunshot fractures of the thoracic wall imply those features pertaining to every compound fracture, plus the injury possibly done to the lungs, heart, or mediastinal contents, such as hemothorax or pneumothorax.
The first and second ribs are so protected and the eleventh and twelfth so movable that by far the greater proportion of rib fractures pertain to the eight intervening ribs.
—These are often vague, when but a single rib has been cracked through and not displaced, and comprise pain on pressure, as well as that provoked by deep breathing, coughing, and certain other movements. Should this pain be limited, or constant and made worse by pressure, fracture of the rib may be suspected. If auscultation crepitus can be heard, diagnosis is at once made. When abnormal mobility is unmistakable, or when by any means crepitus is elicited, the signs are positive. Sometimes the patient himself will recognize crepitus. This may be learned either by auscultation or by pressure with the flat hand over the affected area. Emphysema is an unmistakable evidence of fracture with perforation, while the signs of the presence of fluid in the chest cavity will also indicate fracture.
—Fracture of one or two ribs with displacement is ordinarily a matter of trivial import, the adjoining ribs acting as splints. It necessitates practically nothing but physiological rest, which may be best afforded by keeping the patient in bed, with firm compression around the chest, made either with a binder of strong cloth or a broad piece of adhesive plaster carried nearly around the body, or in more aggravated cases by a plaster-of-Paris jacket. In thin individuals the formation of callus can be recognized by the sense of touch. So soon as this is fairly formed displacement is less likely to occur and uncomfortable compression may be relaxed. Should there be external angular displacement this may be corrected by pressure. A projecting fragment which threatens to perforate should be cut away with bone forceps through a small incision, taking pains to permit as little air as possible to enter. If there be a traumatic pneumothorax the air should be removed with an aspirating needle. When it is evident that there is serious injury to the chest wall and that air has already separated the lung from it (traumatic atelectasis) the parts should be freely exposed, to permit the rounding off of bone ends, the seizure of intercostal vessels, the cleansing out of the pleural cavity, with perhaps later wiring of fragments or else their complete removal and closure of the external wound with or without drainage, as may be required. If blood or air has already escaped into the pleural cavity the blood should be speedily removed. The same plan is advisable in fractures of the cartilages. Sedatives to check cough, e. g., heroine, are also indicated.
[493]
The clavicle and the radius are the two bones most frequently broken, the former more often in the young, the latter in the elderly; the clavicle yields both to direct violence, as by blows on the shoulder, and that which is transmitted through the arm from the elbow or hand. For convenience of description the bone is divided into thirds, the most common location for fracture being near the junction of the middle and outer third. Save for epiphyseal separations the extremities of the bone are seldom broken. In spite of its subcutaneous position and its proximity to large vessels, compound injuries or other complications are quite uncommon.
The clavicle is the brace which keeps the shoulder proper from falling upon and around the thorax. Consequently when it is broken the shoulder tends to drop downward, forward, and inward, except in a green-stick fracture, while even then there may be some displacement in these directions. Deformity is usually easily recognized, one or other fragment projecting beneath the skin in such a way as to be easily palpated. There is enough spasm of cervical muscles to draw the head over toward the affected side, while there is loss of function in the affected arm. Pain is made worse by pressing the shoulder inward as well as by moving it in any direction.
In young children the bone is often broken with a minimum of displacement. Fracture of both clavicles is not so very rare. Trouble may occur later in the course of the case from pressure of exuberant callus upon nerves and even vessels. This is to be prevented by foresight and by careful attention to maintenance of parts in proper position.
—The multiplicity of dressings which have been suggested for fractures of the clavicle attest the fact that so long as primary indications are observed the treatment can be made very simple. These indications are to keep the shoulder upward, outward, and backward, as it tends to drop in the opposite way. The action of three muscles is of great importance in considering the proper treatment of these cases, i. e., the sternomastoid and the trapezius, because they tend to pull fragments upward, and the pectoralis major because advantage can be taken of its arrangement to overcome upward displacement. It was Moore, of Rochester, who taught many years in Buffalo, who showed how this could be done. The fibers of the great pectoral which arise highest, i. e., from the clavicle, are those which are inserted lowest along the bicipital groove of the humerus, because of the semi-revolution made by the tendon of this muscle as it passes to its insertion. By putting the arm in such a position that these fibers are pulled upon the operator may counteract the upward pull of the other muscles just mentioned. This is the underlying feature of Moore’s suggestion; to force the elbow far backward, into a position which is for the time being uncomfortable, in order thus to pull down fragments which jut up beneath the skin. Any dressing which permits this position to be maintained will be equally serviceable. Moore suggests for this purpose what he calls a double figure-of-eight, which is shown in Figs. 284 and 285. It is put on as follows: A strip of cloth, sheeting, or anything of the kind, about two yards in length and folded sufficiently to make a strong strip eight inches wide, is held near its middle over the surgeon’s hand. This hand is placed beneath the elbow of the injured side, so that the strip crosses the under surface of the flexed forearm at the elbow. One end, which should be the longer, lying to the inner side, is passed upward and in front of the arm, carried over the shoulder across the back and under the opposite axilla, then over in front of the sound shoulder, meeting on the back the other end, which is carried up first over the outside of the forearm, then behind the shoulder and across the spine. This bandage should be pulled tightly, while an assistant holds the elbow as far backward and upward as the patient can tolerate it, as the more the position is exaggerated the more are the clavicular fibers of the muscle pulled upon and the better are the fragments held in place. This dressing not only meets the three primary indications laid down, but gives the added advantage just described. By it the shoulders are drawn backward and fixed to each other. The elbow should be lifted as the dressing is applied, so as to lift the shoulder. Most of the cloth materials used for such a dressing are more or less elastic, and it may need to be tightened once or twice a day during the time that it is worn. After a few days, when consolidation should have occurred, it may be changed for some other less irksome form of dressing. The hand should be supported in a sling. This dressing is useful in dislocations of the clavicle, especially of its outer end, and in every[494] kind of injury in which the indication is to hold the shoulder upward and backward. In simple cases without much displacement the primary indications may be more simply met by a dressing of adhesive plaster, known in the East as Sayre’s and in the West as Freer’s. It consists of two strips of plaster of about the width of the arm itself. One of them is wound around the upper end of the arm, close to the shoulder, in such a way that, as it is passed around the back and brought over the chest, the arm and shoulder are pulled backward. The other strip passes from beneath the elbow of the injured side obliquely up and over the opposite shoulder. When it is applied the elbow should be firmly lifted. After the completion of either of these dressings the injured shoulder should appear at least one inch higher than the well one. Should the patient’s arm and chest be hairy they should be shaved before the application of the plaster strips. Like other material, plaster will stretch and slip, and these, like other dressings, should be readjusted every day or two, for the shoulder should be kept elevated for at least a week.
Fig. 284
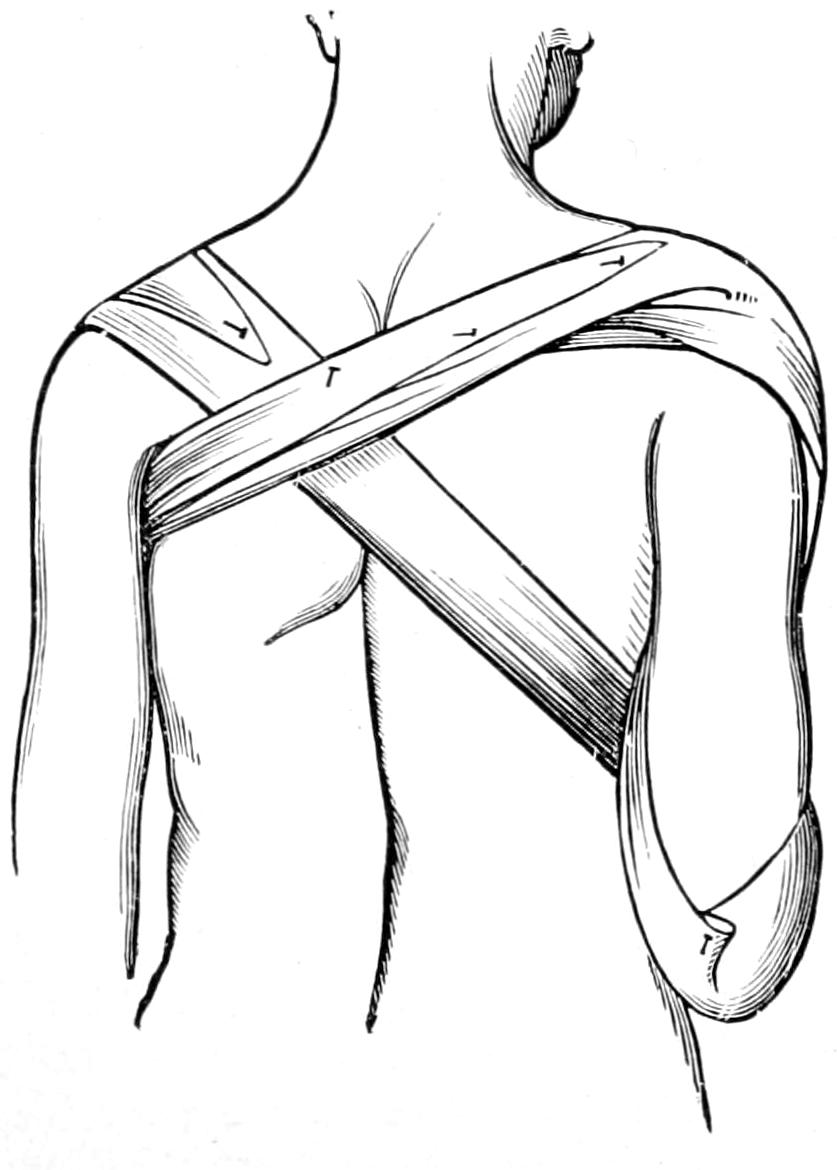
Moore’s apparatus (back view).
Fig. 285
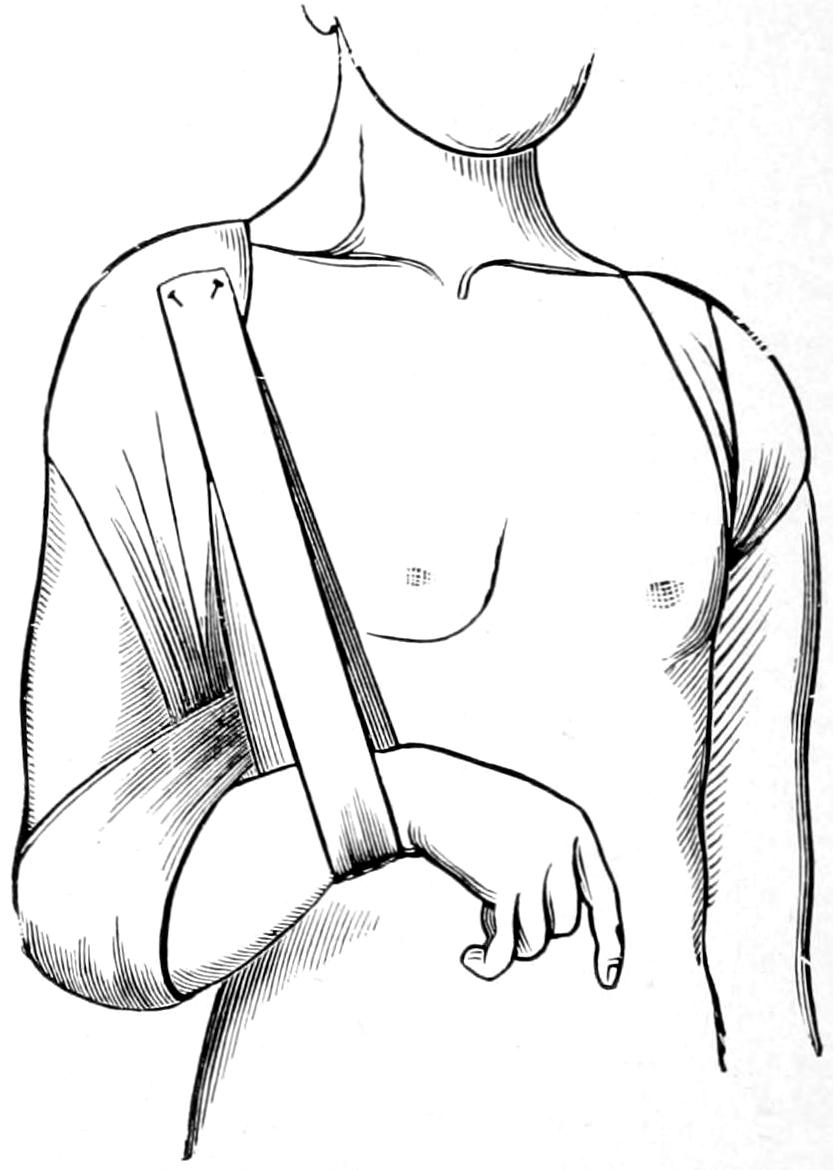
Moore’s apparatus (front view).
When the case is complicated by other injuries necessitating confinement in bed it is sufficient to keep the patient flat upon the back and without a pillow. In this position the shoulder falls naturally in the direction desired, and perhaps no other attention will be required. Many other methods are combined with a figure-of-eight bandage, crossing the back and forming a loop over each shoulder, so as to keep it from dropping forward.
While the results of treatment are nearly always good, if one is insistent upon a minimum of deformity, confinement upon the back on a hard bed is the surest way to obtain satisfactory results. Cases in which there is little or no tendency to deformity need only the simplest support by which rest may be ensured.
Epiphyseal separations are to be treated as fractures.
The most frequent fracture of the scapula is that of the acromion; this is usually the result of direct violence, such as a fall upon the tip of the shoulder. Detachment of this fragment permits a peculiar flattening of the shoulder, but without dislocation. The fragment can be easily felt, while the deltoid is displaced and its rounded contour lost. Treatment consists solely in forcing the arm upward, by dressings applied beneath the elbow, thus lifting the fragment into its place; fibrous union occurring here much more often than osseous, the latter is possible only in case a good apposition be maintained.[495] Any form of dressing, then, by which the elbow is crowded upward and rest maintained will be appropriate.
The surgical neck is occasionally detached, sometimes with and sometimes without the coracoid process. As the humerus is attached to it by the capsular ligament the arm drops with the fragment when the patient is in the upright position, and the elbow will be found lower than that of the injured side. The arm is unduly mobile, and the fragment can usually be seized and crepitus obtained within the axilla. Here it is necessary to hold the arm up, as it controls the position of the fragment. It is usually sufficient to lift the elbow up and bind the arm firmly to the side, the scapula being immobilized by broad straps of adhesive plaster.
The coracoid process is occasionally detached, usually by muscular violence, i. e., it is pulled off by the coracobrachialis and the coracoid head of the biceps which arise from it. The injury is recognized by failure to detect the process in its proper place, and usually by discovery of the fragment at a point below its normal position, to which it has been drawn out by the muscles arising from it. Ligamentous union can be secured by relaxing these muscles, which is done by placing the hand over the opposite shoulder and dressing the arm firmly against the chest. I have seen paralysis of the arm result from excessive callus after fracture of the coracoid.
The spine, body, and the angles of the scapula are occasionally broken by severe violence. In the aged comminution may occur. Crepitus can be nearly always obtained. It may be necessary to distinguish the scapular fracture from one of the ribs beneath it. The treatment consists in simply fixing the shoulder-blade upon the chest, to which it is naturally adapted, by firm bandages, which shall immobilize not only it but the arm as well.
At the upper end of the humerus we deal with fracture of the processes, i. e., the tuberosities, which may be torn off by violent action of the muscles therein inserted; of the anatomical neck, which is rare and occurs most often in the aged; of the surgical neck, which is the most common; or, in the young, epiphyseal separation, which is the equivalent of the last named. Separation of the tuberosities is diagnosticated mainly by exclusion, possibly by x-rays. The anatomical neck lies within the capsule, and should the head be thus detached it might remain as a foreign body in the joint, having no means of securing nutrition. Fractures of the head of the bone are not classical and are usually the result of gunshot injuries or extreme violence. In all of these injuries there will be swelling, loss of function, while crepitus is sometimes obtained, but is very difficult to locate, even under an anesthetic. The diagnosis is to be made mostly by exclusion.
The surgical neck is the most frequently broken; the line of fracture passing below the tuberosities and above the muscles inserted along the bicipital groove. Therefore the pectoralis and the latissimus muscles will both conspire to pull the upper end of the shaft toward the thorax to such an extent that it can be felt in the axilla. This gives its axis a different direction, while all the muscles extending from the shoulder to the forearm will tend to produce shortening. Deformity is usually distinct, crepitus is easily obtained, and undue mobility is well marked. The head of the bone can be detected in its proper place beneath the deltoid, but does not rotate with the shaft. In rare instances a certain amount of impaction may make this evidence of fracture obscure. Epiphyseal separation will give the same signs and symptoms.
—The primary indication here is to overcome muscle pull by traction in a direction toward the crest of the pelvis of the same side. At the same time, with a certain degree of coaxing of the upper end of the shaft outward and a little forward, it may be possible to so re-apply broken surfaces to each other, and so affix the arm to the thorax, as to be effective. When serious difficulty, however, is encountered the writer advises traction, applied to the arm alone, if the patient be able to be upright, or to the arm and forearm, if he be confined in bed. It will take considerable stretching to overcome the combined action of all the muscles which tend to produce displacement. Along with such treatment a coaptation splint should be applied, the best being that which can be carefully molded to the parts and adapted to their needs. For this purpose a molded plaster-of-Paris splint is preferable to one of metal made to some standard size. In the dressing it is necessary to include not only the shoulder and arm but also the forearm,[496] otherwise the principle of physiological rest would not be enforced. Fig. 286 illustrates the common tendency to displacement in these injuries.
Fracture of the surgical neck is occasionally combined with dislocation of the head of the humerus, by which such an injury is seriously complicated. Reduction may be attempted by manipulation. Until recently it was generally advised to wait for a week or ten days, and until consolidation had occurred, and then to make the attempt at reduction; but Porter and McBurney have shown that it is advisable to cut down upon the dislocated upper fragment, and, fixing it with forceps or with an instrument shaped like a corkscrew or hook, to force it back into place again. If this be done under the strictest precautions it lends no serious features to the case, while, in most respects, such a procedure would greatly simplify it, the wound being closed with or without drainage, and the usual fracture dressing being applied.
In cases of old fracture and dislocation the head of the bone should be exsected, the functional result thus obtained being excellent.
Epiphyseal separation has been too often mistaken for dislocation. Fig. 287, from Moore, shows how the periosteum is not necessarily entirely detached, but is stripped up to form a hinge, the fragment displaced forward, and its outer aspect often turned upward. This makes traction in an outward direction an essential feature of the replacement of the fractured surfaces, the manipulation being combined with fixation of the fragment so far as it can be seized through the axilla. If the epiphysis is properly slipped over upon the end of the humerus the case assumes ordinary features, and is to be dressed as usual.
Fig. 286
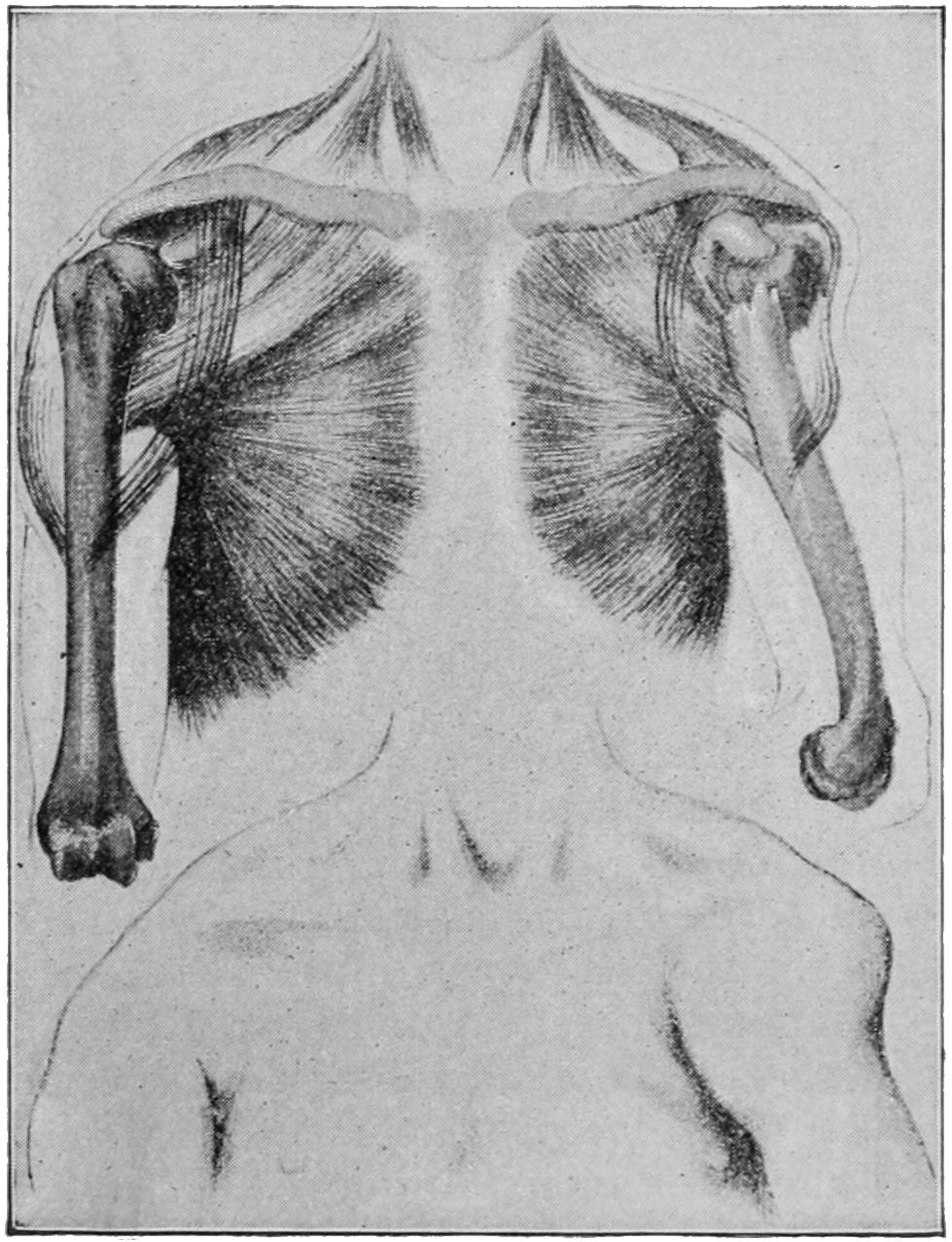
Fracture of the surgical neck of humerus. (Hoffa.)
Fig. 287
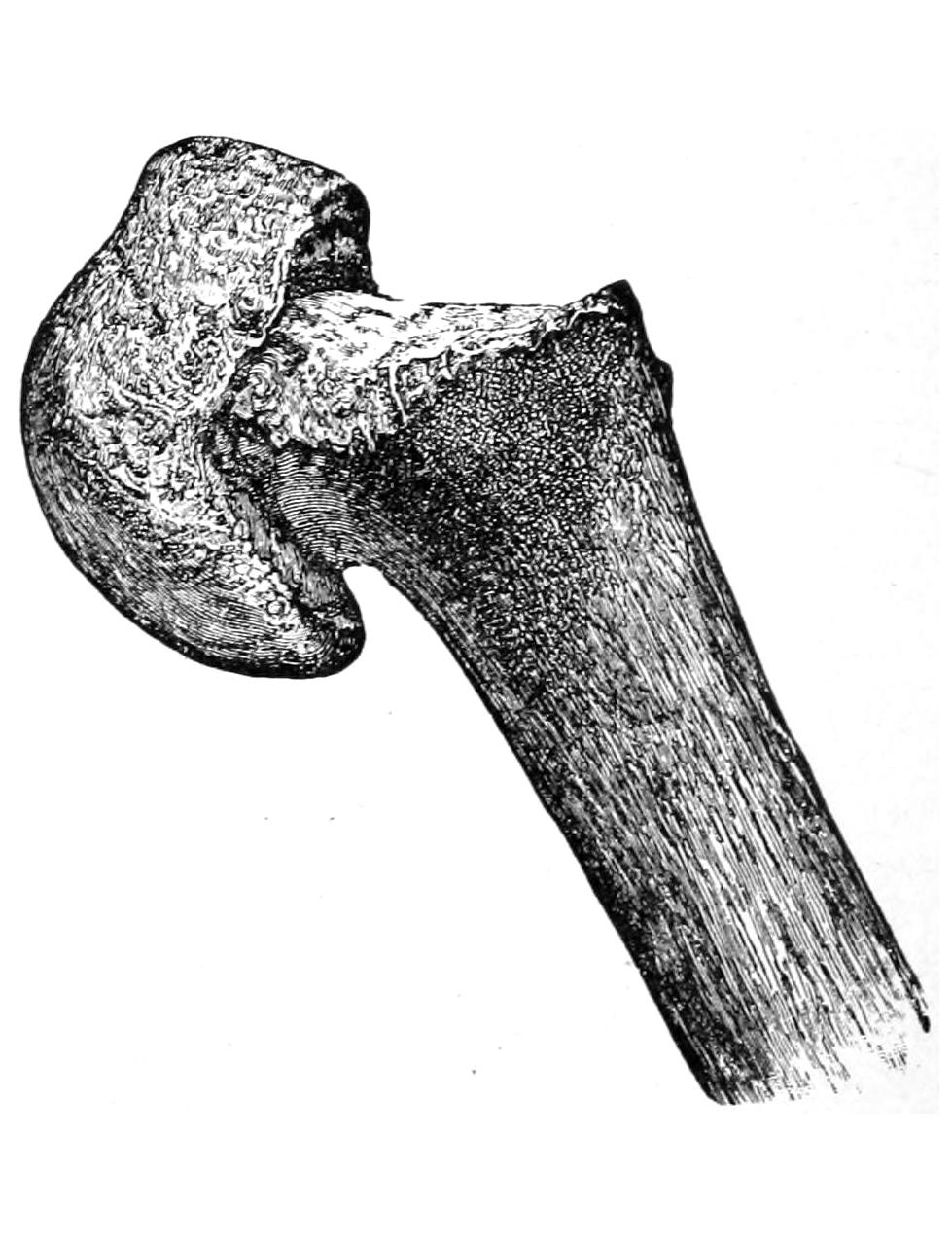
Separation of the upper epiphysis of the humerus; displacement forward of the lower fragment. (Moore.)
The shaft of the bone is frequently broken, lines of fracture running in all directions and occurring at all levels. A variety of displacement may take place. The evidences of fracture are usually recognizable and diagnosis is not difficult. The brachial artery and the musculospiral nerve are occasionally involved, either in callus or by primary injury from a spicule of bone. These fractures are more liable to delay in union or even to non-union than almost any others. These occur often without evident cause, while more or less absorption of bone has been known, by which complications are produced.
In the treatment of fractures of the shaft posture is necessary to observe, the fragments not only being held in position, but the axis of the bone being maintained. An external splint, extending up to and rounded over the shoulder, and an internal splint molded to[497] the inner side of the arm, taking in the elbow and forearm, and placed at a right angle, and then the immobilization of the entire arm by its fixation to the body will give the best result. The writer prefers to make these of plaster of Paris, by molding strips of surgeons’ lint sopped in plaster cream, and maintaining the limb in the desired position while they harden. Should comminution be extreme, or shortening difficult to overcome, a few days’ confinement in bed, with traction upon the forearm, either extended or included in the above dressing, by the usual method, with weight and pulley, will give the best result. So soon as callus has bound the ends of the bone together the patient may be released from bed and the arm left in the right-angle position, in plaster, as above. Or over such a splint as has been described, made of molded plaster, may be hung by a bandage at the elbow sufficient weight (a bag containing shot) to maintain constant traction upon the lower fragment, while the patient is in the upright position, and to influence for good any overlapping or displacement of any kind during the critical period when the bone ends are being united by callus.
The epicondyles are occasionally chipped off from the condyles, the internal being the more frequently injured. These detachments are extra-articular and are relatively unimportant, the fragments being kept from displacement by their fibrous investments. If such an injury should be compound any fragment completely loosened should be removed. It is sufficient to dress such an injured elbow with cold wet compresses in the flexed position. Supracondyloid fracture, or its equivalent in the young (an epiphyseal separation) are somewhat similar, the latter occurring nearer to the articulation than the former. In each of these injuries the arm is flexed and shortened, the fragment lying usually in front of the shaft and the olecranon protruding posteriorly. The more the arm is extended the more prominent the deformity, while by flexion it is much diminished. Hence the advantage of dressing it in the position of overflexion sometimes called Jones’ position.[39] Injury to the vessels at the bend of the elbow may occur in these fractures. If not dressed in this position the elbow should be put at a right angle, while a weight is slung over the elbow, as already mentioned above. Joint function will be greatly hampered if complete extension and reduction be not effected (Fig. 288).
[39] In supracondyloid fractures there is almost always posterior and upper displacement of the lower fragment. When the parts are found in this position, and especially when the skiagram shows the line of fracture in the usual location (from above downward and forward), the fracture should be treated by flexion of the arm in the so-called Jones’ position. By this the fragment is best restored to its proper position, being pried there by the muscular cushions of the forearm and arm. (Ashhurst.)
Fig. 288
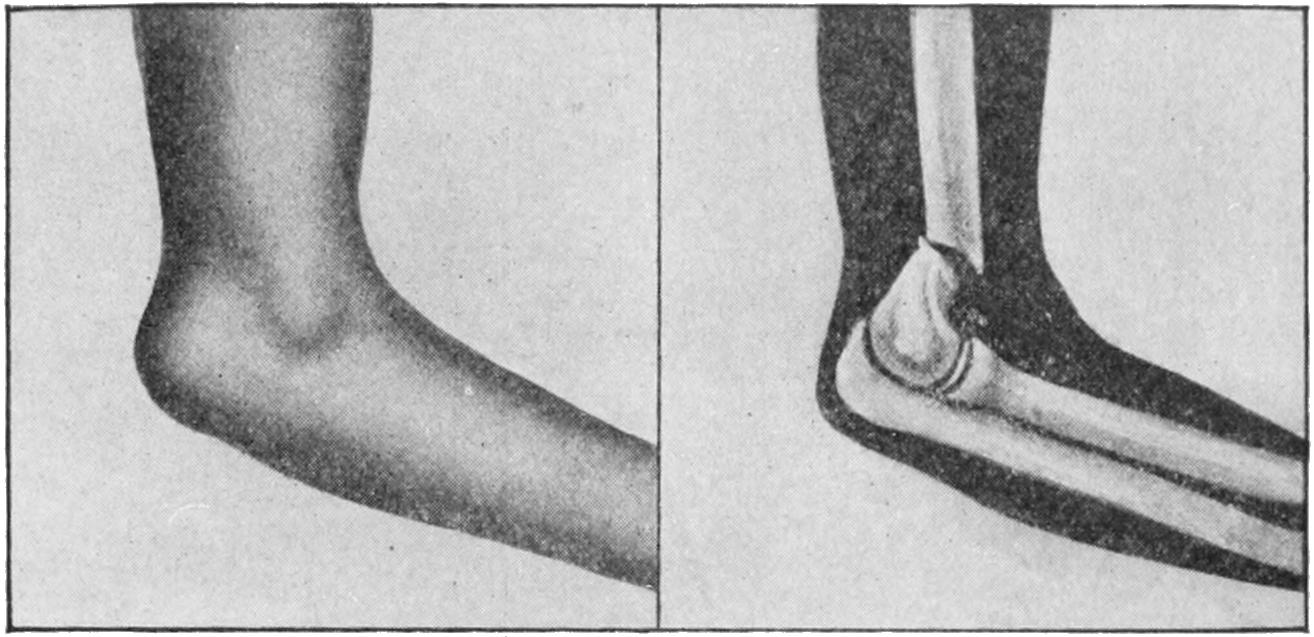
Supracondyloid fracture or epiphyseal separation. (Lejars.)
In considering fractures about the elbow no greater aid can be obtained than by a study of the relations of the three prominent or salient anatomical points to each other. These are the internal and external condyles and the tip of the olecranon. They afford a key to nearly all the displacements which may be produced after fracture or even dislocation, and the only conditions under which they cannot be made available are those where there has been tremendous swelling before the case is seen by the surgeon. A fourth prominent feature, the head of the radius, is also of much assistance, but is less often available, especially in muscular or swollen forearms. When a normal arm is flexed to a right angle and viewed from behind the three points above mentioned constitute the angles of a nearly equilateral triangle. When seen from the side the point of the[498] olecranon is just below the external condyle and in the same plane; when the arm is completely extended and viewed from behind these three points are practically in the same line. By a careful study of the variations from the above relations which are produced by injury diagnosis can be greatly facilitated.
Fig. 289
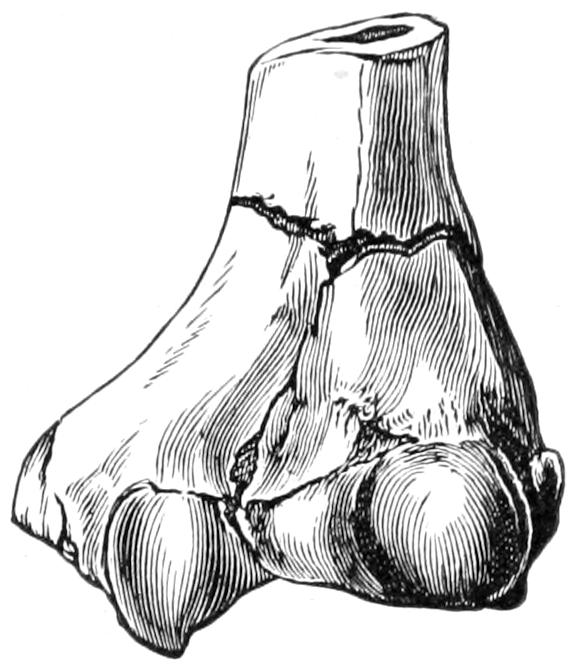
T-fracture of humerus. (Helferich.)
Fig. 290
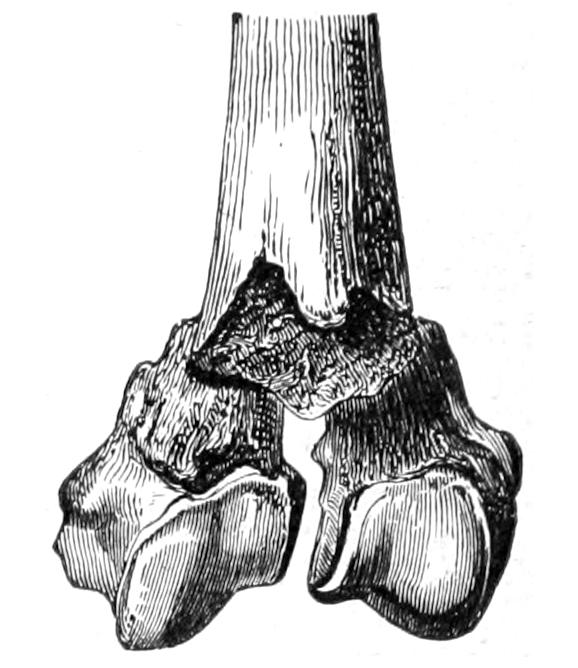
T-shaped fracture of lower epiphysis of humerus.
Fig. 291
Intracondyloid fracture of humerus. Almost perfect functional result. (Parmenter.)
Fig. 292
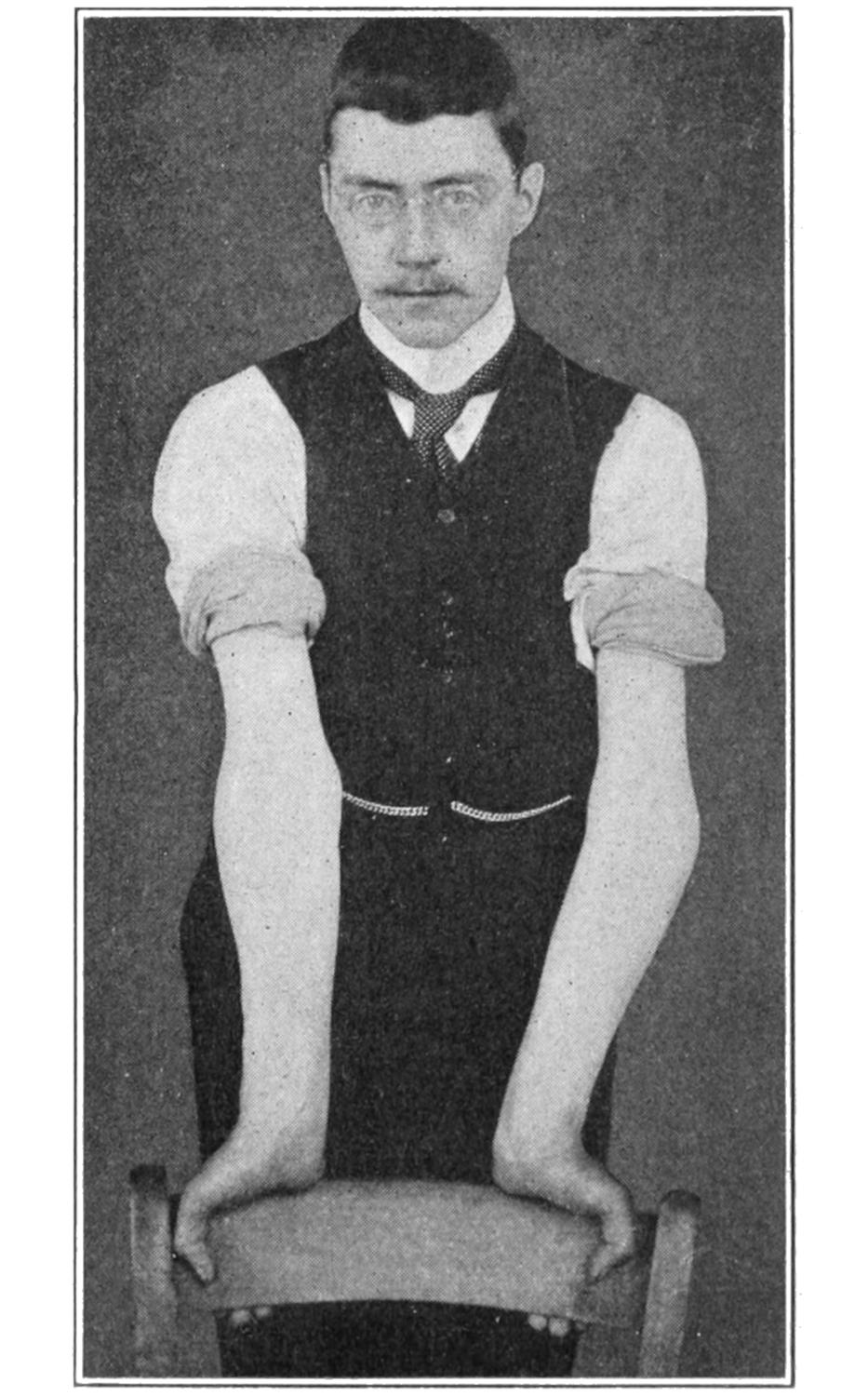
Gunstock deformity after fracture of internal condyle, illustrating neglect of precautions mentioned in text. (Beatson.)
The condyles may each be broken loose by itself, or they may be both broken at the same time. Fig. 291 illustrates what is known sometimes as a T-fracture, where the lower extremity is not only separated from the shaft but is broken into halves; such fractures imply great violence, and are particularly difficult to treat. Should the condyles be detached in such a way as to leave the lower end of the humerus in pointed wedge shape it may perforate or do much harm to the soft parts (Fig. 290). In these intercondyloid fractures the writer would advise dressing in the extended position, with a molded plaster-of-Paris anterior splint and a gentle degree of traction, the patient being confined to bed for a few days. In applying such a splint the surgeon should give extreme care to holding the fragments in proper position while the splint hardens, and in preserving the “carrying function” (Fig. 291). (See below.)
PLATE XXXIX

Supracondyloid Fracture. (Child, nine years old.) Union with deformity, fragment so joined to lower end of shaft of humerus at an angle that when forearm is completely flexed upon this fragment it yet is only at right angle with the arm. Operation indicated. (X-ray picture.)
[499]
The external condyle when fractured is displaced by muscle pull; when the internal condyle is broken the tendency is to backward displacement of the fragment and widening of the joint.
Fracture of the internal condyle is often an exceedingly serious matter, because it is so often associated with more or less dislocation and with permanent deformity, as a result of inattention to the anatomical relations of the bones. The ulna sustains peculiar relations to the inner condyle; at its upper end it is wrapped around the process, holding it much as a monkey-wrench can be made to seize an ordinary object, and being held to it by the internal lateral ligament. Herein lies the secret of success or failure in treatment, for the fragment, being so fixed to the ulna, should be controlled by it, i. e., the position of the ulna is the most essential feature of the treatment of the fracture. The forearm makes an angle with the arm proper, by which a considerable degree of divergence is maintained. This has been alluded to by Allis and others as the “carrying function.” It can only be estimated in the extended position, and be accurately judged by comparison with the other arm. If the arm be flexed all possibility of estimating it is lost; therefore to dress such a fracture in the right-angle position is bad practice (Fig. 292). The only position in which the carrying function can be preserved is the extended, or one a little short of it for the purpose of comfort. If the ulna is put in the proper position the fragment will be held equally so or as nearly as possible (Fig. 294).
Fig. 293
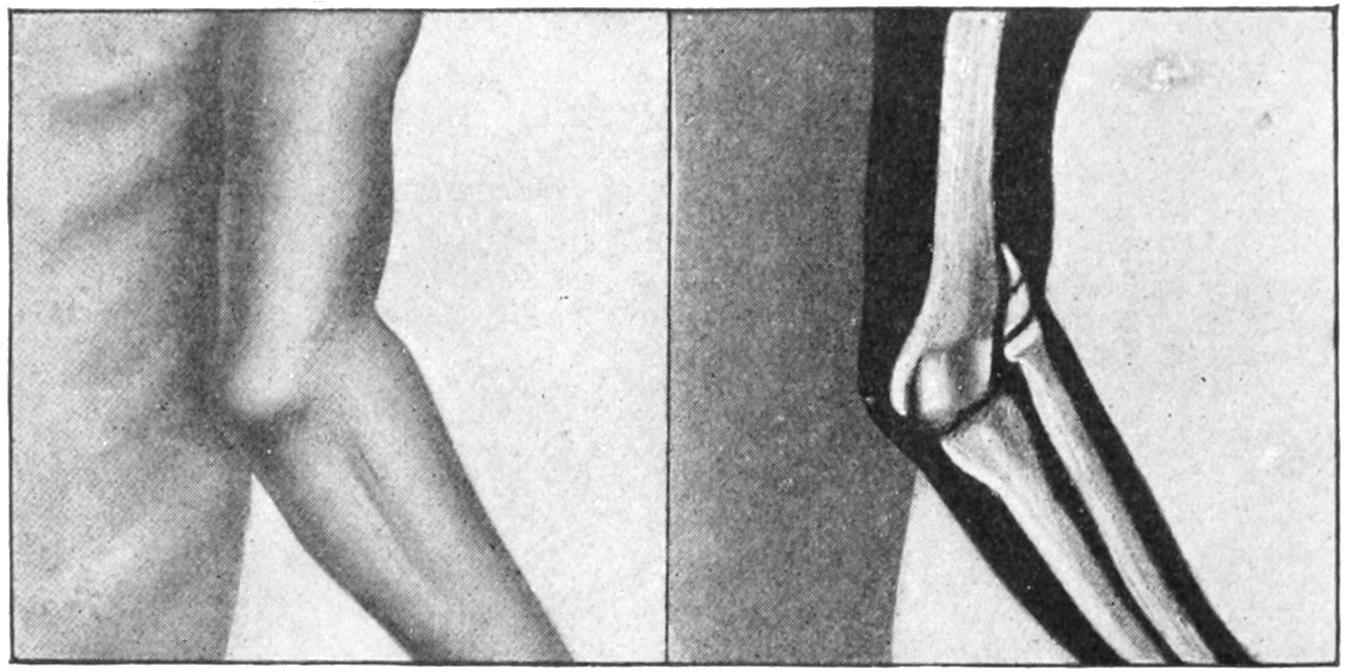
Fracture of external condyle. (Lejars.)
In the treatment of fractures of the inner condyle the patient, if a child, should be anesthetized, the upper part of the body exposed, both arms extended, and the injured arm made to correspond exactly with the other so far as concerns the angle of divergence. Upon the arm so placed an anterior plaster-of-Paris molded splint should be carefully applied, extending from axilla to wrist, and then lightly secured with bandages, the surgeon holding the arm in the proper position until the plaster is sufficiently hardened to permit no displacement. The arm should be kept in this position for at least ten days, after which the splint may be removed and gentle motion practised. It may then be reapplied for two or three days, after which we may begin to flex the arm, applying either a new plaster splint or any other that seems suitable, and in such a way that at the expiration of another week the forearm is brought to a comfortable position of right angle, where it may be maintained with a light splint or simply with a sling, according to the age and tractability of the patient. Fig. 294 illustrates the splint and the position, which is the only one in which the surgeon maintains his own security and can properly estimate the carrying function. The mistake has been in dressing this fracture, like most others at the elbow, in the right-angle position.
In fractures of the outer condyle these anatomical conditions do not prevail, and these may be dressed in whatever position best meets the indications of comfort and accurate reduction. Intercondyloid fractures are subject to the same conditions as those of the[500] internal condyle, plus others which are added, and should therefore be dressed in the same position.
Fig. 294
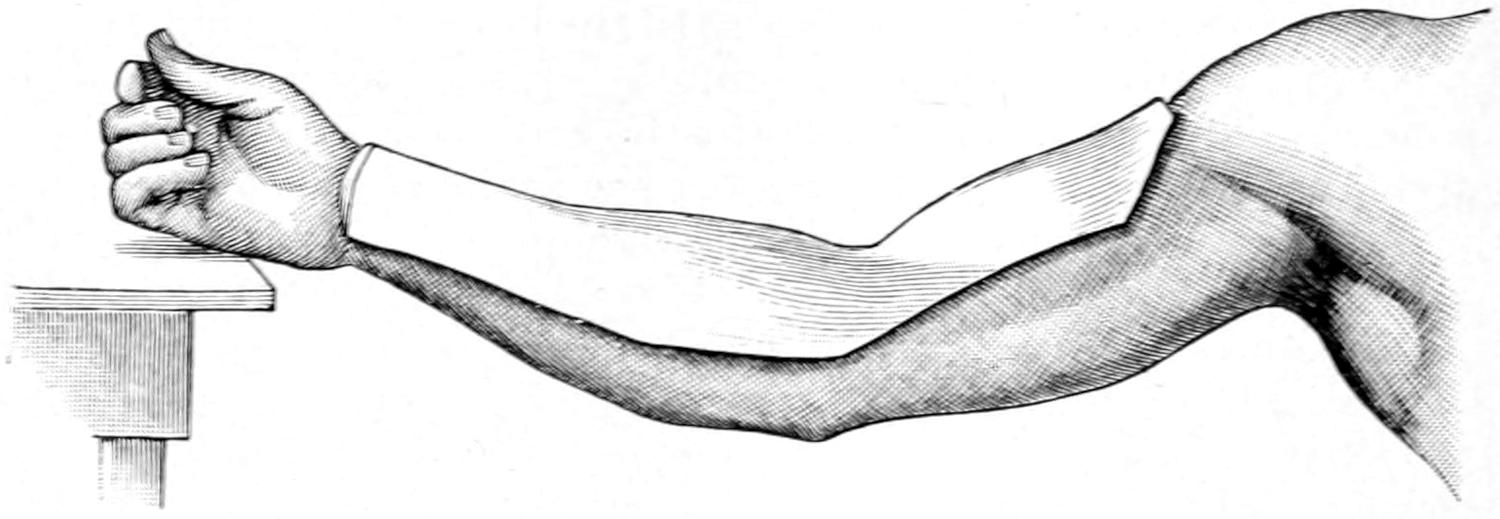
Molded plaster splint for entire arm, and especially for fractures of the internal condyle, showing proper position for dressing same.
Epiphyseal separations, as well as supracondyloid fractures, should be dressed either with traction in a somewhat extended position, or in that of extreme flexion, called also Jones’ position, according as the fragments may best fall into place in one or the other.
Fig. 295
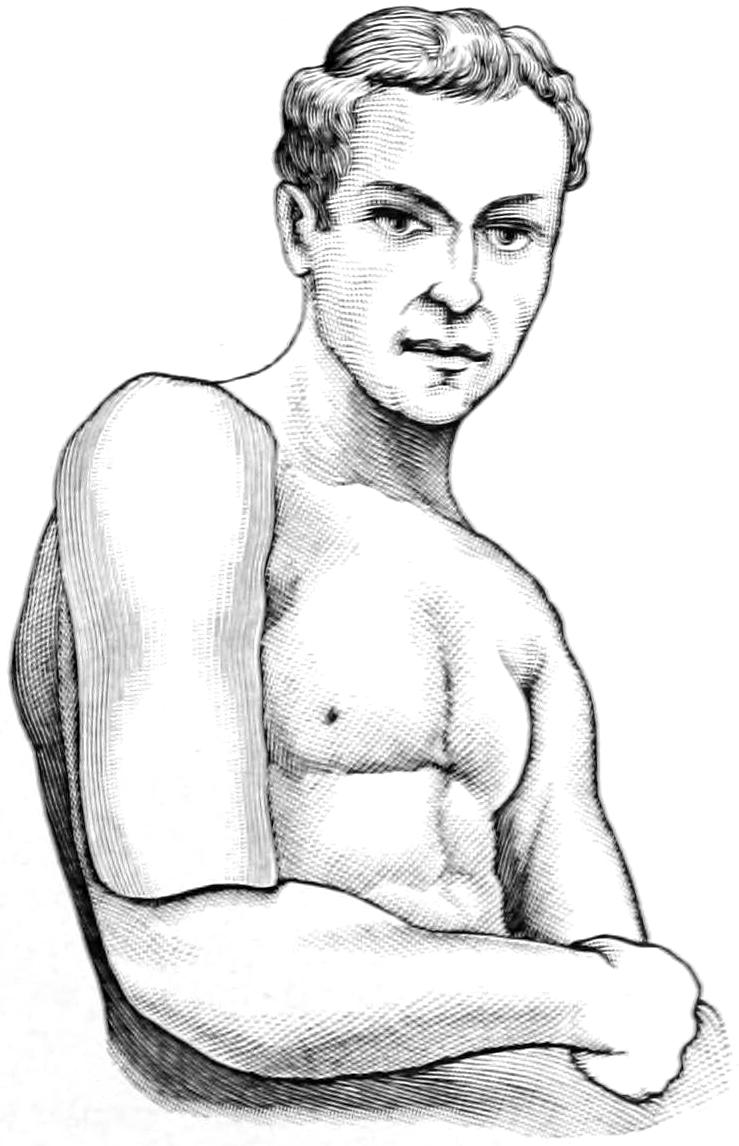
Molded plaster splint for arm.
Fig. 296
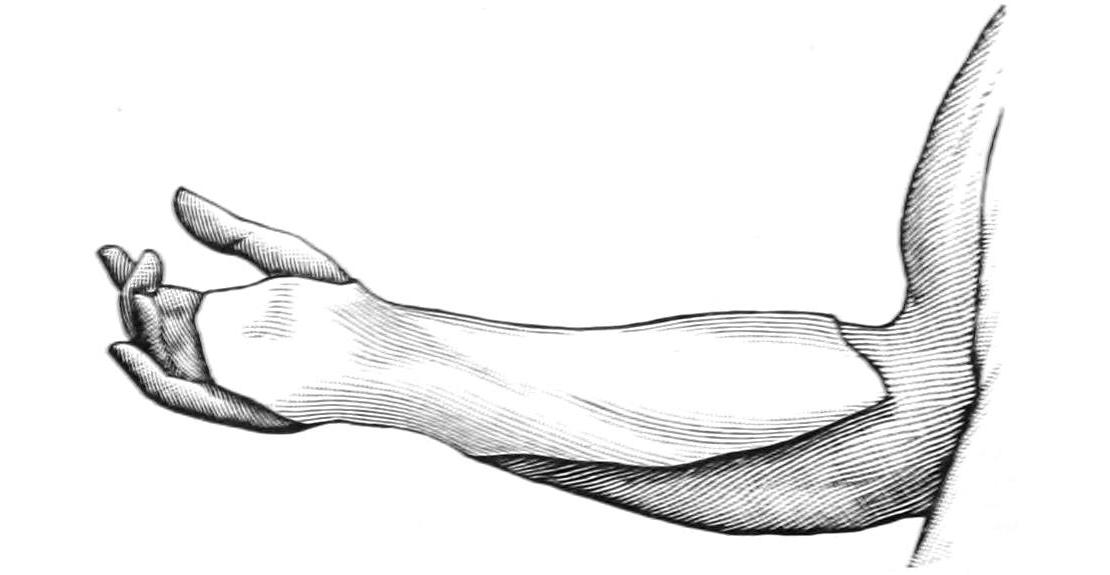
Molded plaster splint for forearm.
The writer has for his own purposes discarded almost all other splint material for the upper extremity in favor of the plaster-of-Paris splints already mentioned. Figs. 294, 295 and 296, may illustrate the method and purpose of their use; many other modifications can be devised as may be demanded. It is customary, after such a splint is hard and firm, to remove it for a few moments, trim it, smooth the edges, line it with a fresh piece of soft lint or its equivalent, and then reapply it to the arm with a roller or starch bandage, the arm meantime not having been disturbed, but maintained in its proper position, and being restored to the splint and made to take its previous position. Such a splint fits accurately the individual for whom it is made. It is worthless for anyone else; nor should it ever be used again, the intent being to mold a splint for each case which shall serve its individual purpose and none other.
Too early passive motion with the intent to regain mobility is inadvisable and often dangerous. A fractured joint should be kept at rest until the bone is consolidated. If callus be thus reduced to the minimum, and consolidation be undisturbed, the patient will, in due time, recover motion, often to the extreme limit. In fractures of the humerus five or six weeks are required for the attainment of perfect union. In spite of precaution callus formation will sometimes be excessive and interfere with motion. Absorption of exuberant material then is most desirable. This can be encouraged by constant but gentle pressure. Thus when callus in front of the lower articular surface of the humerus obstructs the coronoid process of the ulna and prevents complete flexion the patient should wear for several hours at a time an elastic sling, made with a piece of Martin[501] rubber bandage sufficiently long to make a loop around the neck, into which the hand is passed. It should be made so tight as to exert gentle but constant pressure; the result of this will be to cause rapid disappearance of the callus upon which it is made. Conditions may be reversed when necessary, and the patient may have some weight affixed to the hand by which, when the arm hangs down, reversed pressure shall be made, or when desirable these measures may be alternated. One should not, however, be tempted into resorting to them too early, since much is done, even in unfavorable cases, by purely natural processes, this being especially true of children who are growing rapidly.
At the upper end of the ulna the most frequent fracture is that of the olecranon, whose separation by direct or indirect violence corresponds to fracture of the patella. The fragment is pulled upward along the back of the arm by the triceps muscle, and the power of extension is almost lost. There is rarely any difficulty in diagnosis, except in conditions of extreme swelling, which of itself would be suspicious, as under hardly any other circumstances could a joint be so distended (Figs. 297 and 298).
Fig. 297
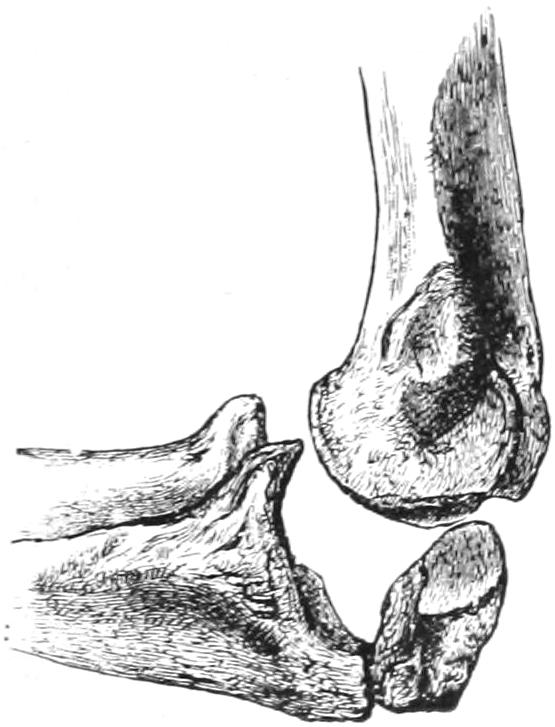
Fracture of olecranon. (Erichsen.)
Fig. 298
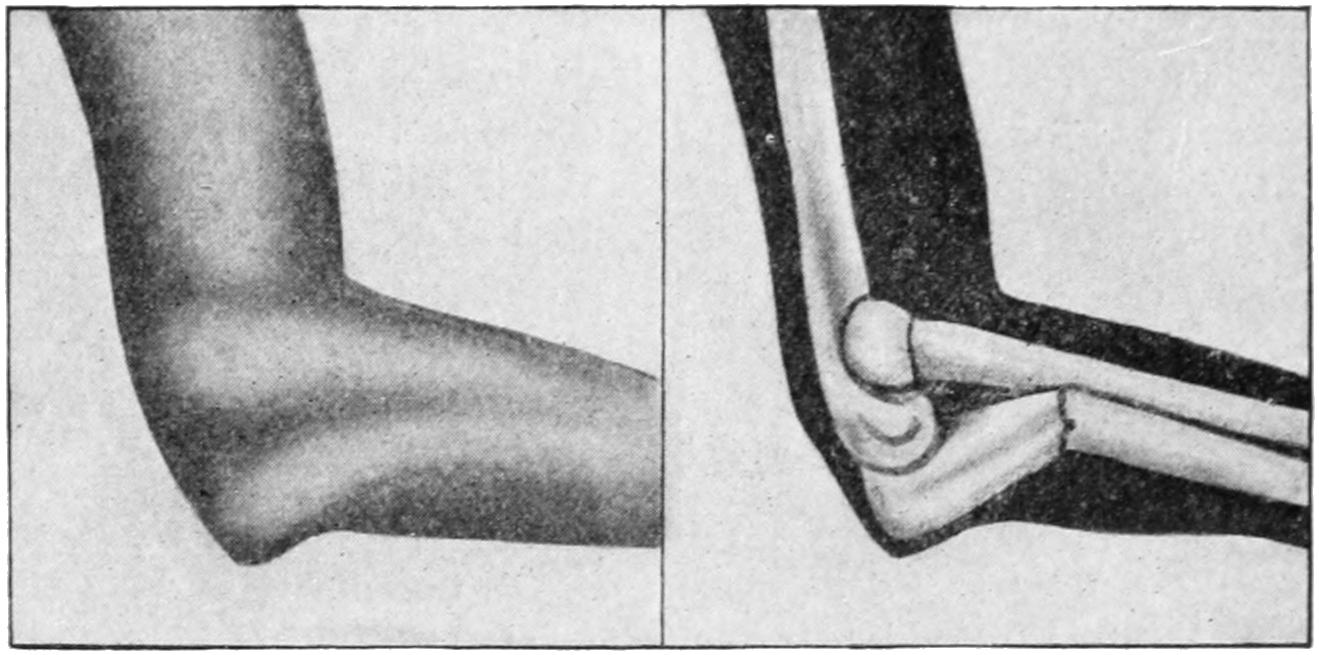
Fracture of ulna, upper end. (Lejars.)
Fig. 299
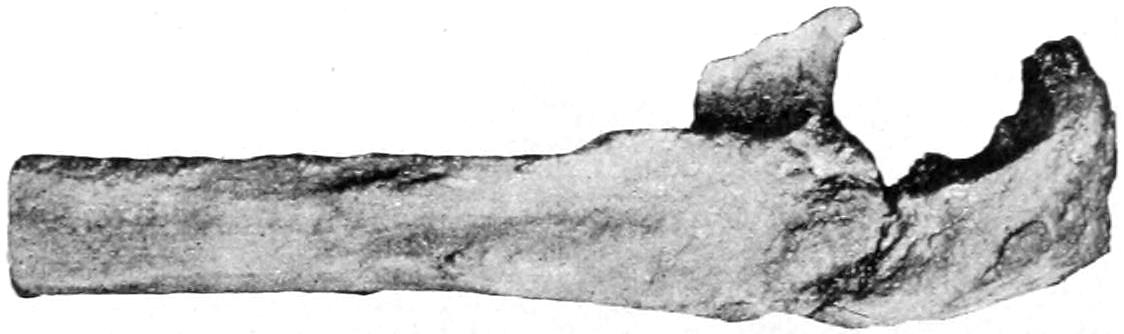
Fracture of olecranon with fibrous union. (Park.)
—The difficulty here, in treatment, consists in the necessity for counteracting the pull of the triceps. The arm first of all should be dressed in the extended position. Sometimes it is possible, by partly encircling the posterior surface of the arm just above the fragment with a strong piece of adhesive plaster, to which is attached some rubber tubing, to make a constant elastic pull upon the fragment, the tubes being brought down and attached to the sides of the anterior splint below the elbow. In the absence of swelling this can often be made quite effective. So long as much fluid is present no means will be efficient. It may, therefore, be well to wait two or three days until the fluid has disappeared, aspirating the joint if necessary. In young and otherwise healthy subjects there is strong reason for advising operation, as only by absolutely approximating the fragment to the main bone and maintaining it in position can bony union be secured. In properly selected cases, and when performed with every precaution, this measure frequently gives ideal results. A short ligamentous union is represented in Fig. 299. At other times the fibrous band will stretch out to an inch or more, not completely disabling the arm but weakening it. The extended position may be[502] relaxed within a week after operation, but not for at least two weeks after other treatment. Passive motion should not be begun too early in the latter cases.
Fracture of the coracoid process is often combined with backward dislocation of the forearm, which is no doubt an incident of the injury or may occur later by mere muscle pull. The brachialis anticus, which is inserted into it, will pull the fragment up against the anterior surface of the humerus. This fracture should be dressed in the right-angle position, in order to relax the muscle, taking care to prevent backward displacement, while ligamentous union is ordinarily all that can be hoped for.
The ulnar shaft may be broken at almost any point, usually as a result of direct violence. As it is weaker in its lower half the greater number of fractures occur here. Fracture of the shaft is easily recognized, crepitus being always obtained, unless muscle tissue has intervened, this being a condition which will occasionally prevent bony union. If it can be established by x-rays that bony surfaces are not in contact and cannot be so placed, it is advisable to cut down upon the site of the fracture, remove the obstacle, and fasten the fragments together. So long as one bone is broken in the forearm the other may be relied on to act as a more or less efficient splint. There is but one position in which any of these fractures can be dressed with safety, that is midway between pronation and supination, i. e., with the thumb pointing toward the patient’s face. Splints used for this purpose should always be wider than the forearm itself, lest by pressure the ends be forced toward the other bone. Some hold that by gentle pressure along the line between the bones, as by a narrow pad or splint, the muscles may be made to press the injured bone away from the other; nevertheless only moderate pressure can be tolerated for this uncertain purpose. It has been generally customary to use two light wooden splints, one along the palmar, the other along the dorsal surface of the forearm, padding them properly and securing them in position by strips of adhesive plaster and suitable bandages. The same plaster-molded splints mentioned above can, however, be made just as effective for this purpose, if properly applied.
When either bone is broken near the wrist, and especially when both are broken, we have to combat the tendency of the pronator quadratus, which tends to pull the lower fragments together.
The styloid process is occasionally detached, as in violent sprains, or broken off in connection with other injuries. Inasmuch as it carries the upper end of the internal lateral ligament its detachment can be quickly recognized by the abnormal freedom of motion which such an injury would permit.
Fig. 300

Obliteration of the interosseous space in a fracture of the forearm.
The radius vies in frequency of fracture with the clavicle. The head is seldom broken, its fracture being most likely when the shaft is driven against the humerus by falls upon the open hand. The neck is more frequently broken in children than in adults. These fractures have sometimes to be determined by a process of exclusion or by the use of the x-rays. In muscular forearms they lie so deeply that it is not always possible to recognize them. Ordinarily, however, if the head of the bone can be found to remain stationary while the rest of the bone is being rotated, and if, at the same time, crepitus be felt, the matter may be regarded as settled. So far as the shaft of the radius is concerned the remarks made above regarding the ulna mostly hold true for its fellow-bone. When the neck of the bone is broken the shaft will be pulled upward by the biceps tendon, while when the shaft is broken below its insertion the upper fragment is displaced by it. In either of these cases, then, the forearm should be dressed at a right angle with the arm in order to relax the muscle. The supinator brevis and the pronator radii teres should also not be neglected, for the former will tend to rotate and the latter to more or less displace the upper portion of a shaft broken high up. With a fracture near the upper end, in a powerfully muscular arm, diagnosis is not always easy. Fractures in the lower portion of the shaft are to be treated like those of the ulna. But those high up should be dressed with the elbow at a right angle and the forearm supinated. A plaster-of-Paris molded splint here can be adapted to the needs of every individual case if the surgeon will give minute care at the time of its hardening to placing the parts just as he desires them to remain.
[503]
These are not uncommon, though much less frequent than injuries to either bone alone. They may occur at the same level or be quite widely separated. The loss of function is complete in these instances, while deformity will depend largely upon whether the fractures lie near together or not. It is of the greatest importance to remember, in these cases, that the mass of muscles around the upper fragments tends to crowd them together, while the lower fragments are brought together especially by the pronator quadratus. Everything then conspires to convergence of the four fragments, a tendency which it is sometimes difficult to combat. Every large museum contains specimens showing a common callus, in which all four bone ends are involved, and illustrating the permanent loss of rotation that ensues. This is to be combated, not alone by rest, which tends to limit callus formation, but by position with the arm midway between pronation and supination, in which the bones are naturally farthest separated, and by splints applied with such gentle pressure as may hold the bones apart. This pressure should be applied between the dorsal and palmar surfaces, while the lateral aspects of the forearm should be kept absolutely free from it (Figs. 300 and 301).
Fig. 301
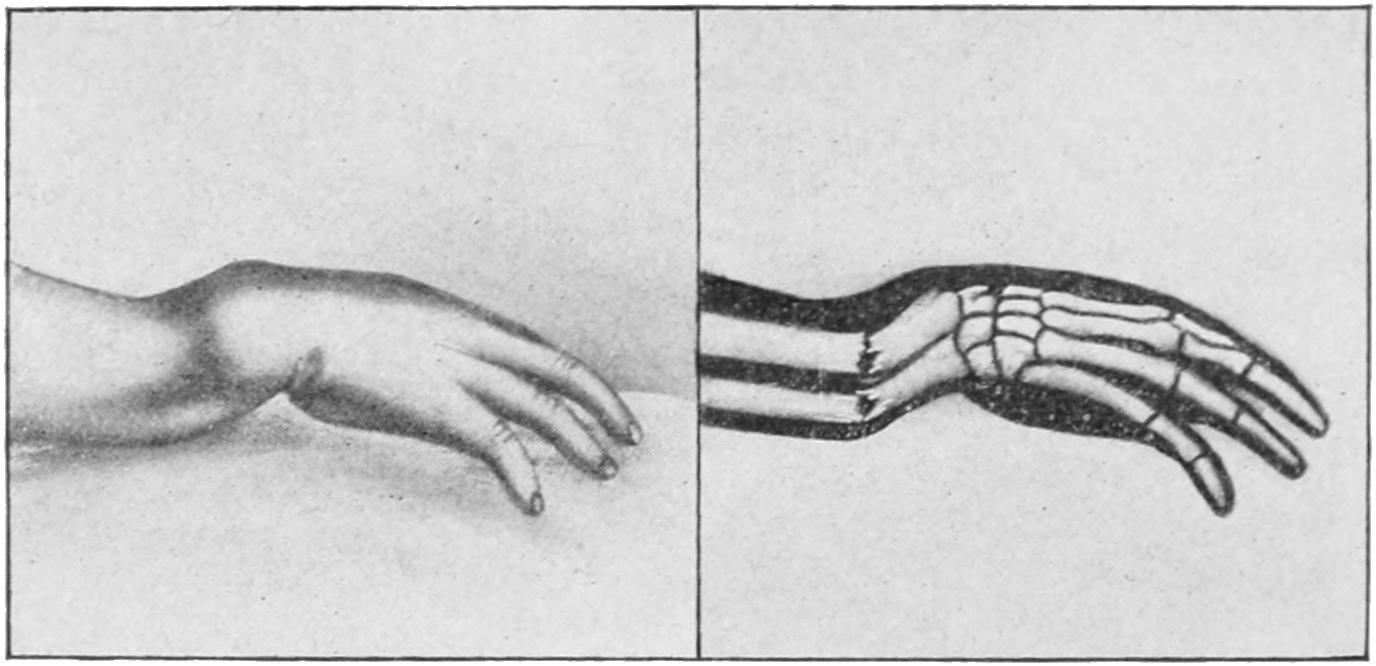
Fracture of both bones near lower extremity. (Lejars.)
It is a serious matter to dress any of these injuries with moistened pasteboard, or other material which does not take its desired shape and strength promptly, for no matter how carefully the desired position may be enforced at first the very nature of a material which remains too long plastic will permit the loss of all that should be maintained. The writer has seen malpractice suits instituted and men forced out of the State by inattention to this precaution.
This is perhaps one of the commonest fractures in the body, occurring at all ages; when seen in growing children it is to be regarded as an epiphyseal separation rather than as a distinct fracture. It derives its name from the fact that until Colles, a Dublin surgeon, over one hundred years ago, described this injury as a fracture it had been always regarded as a peculiar dislocation at the wrist. It is produced by falls upon the hand in the hyperextended position, the force being usually transmitted through the carpus to the radial end. The name is usually limited to those fractures which occur[504] within one and a quarter inches of the articular surface (Fig. 303). Here the structure of the bone is cancellous and impaction may easily occur, this being a decided feature in many of these accidents, and making replacement more difficult. The deformity which results from the fracture is characteristic and more or less uniform. This is called the “silver-fork appearance,” the lower fragment being so displaced, and usually more or less tilted, as to raise the tendons and the structures on the back of the wrist; at the same time it is usually drawn toward the radial side. The more the fragment is impacted or driven into the shaft of the bone the less easily is crepitus elicited.
The fracture is more common than is supposed, and there is no doubt but that many alleged sprains of the wrist illustrate cracks in the bone without displacement, which, nevertheless, are slow to heal and are sometimes followed by thickening and impairment of function. (See Plate XL.)
Along with the radial fracture separation of the styloid process of the ulna may also occur, or, as Moore has shown, the process itself may perforate the internal lateral ligament so as to protrude through the skin; and the surgeon has occasionally to withdraw the styloid from the ligament which has been impaled upon it. The radio-ulnar ligament is also frequently injured, and this permits the ulna to become more prominent than normal. If the styloid has perforated the skin it lends a compound feature to the case. The interarticular fibrocartilage may also be displaced.
—The secret of obtaining a good result and the explanation for failures lie in the completeness or incompleteness of the reduction of the fragment. If the latter be absolutely and accurately replaced it makes but little difference what dressing is applied. On the other hand any fragment not completely restored will lead to subsequent deformity and impairment of function. Successful reduction, then, is the keynote to success, and should be accomplished at any reasonable cost. Sometimes it is not difficult, and then no anesthetic is required; sometimes it is extremely difficult, and the operator has to exert all the strength he has in his arms, aided by profound anesthesia. Moderate cases can usually be dealt with successfully under nitrous oxide gas. The surgeon grasps the hand as if to shake hands, i. e., with his corresponding hand, the elbow being firmly held by an assistant. Traction is then made upon the hand to which the fragment is affixed, while with his other hand the operator makes such pressure, rotation, or coaxing manipulation with his thumb and fingers as may assist in restoring the fragment to its place. With whatever other effort may be made traction should be combined. Forcible swaying movements, combined with hyperextension, may be necessary to dislodge an impacted fragment. Any degree of force is preferable to failure in this respect. Perfect reduction is the key of success; without it, no dressing is efficient; with it, almost anything will suffice.
Fig. 302
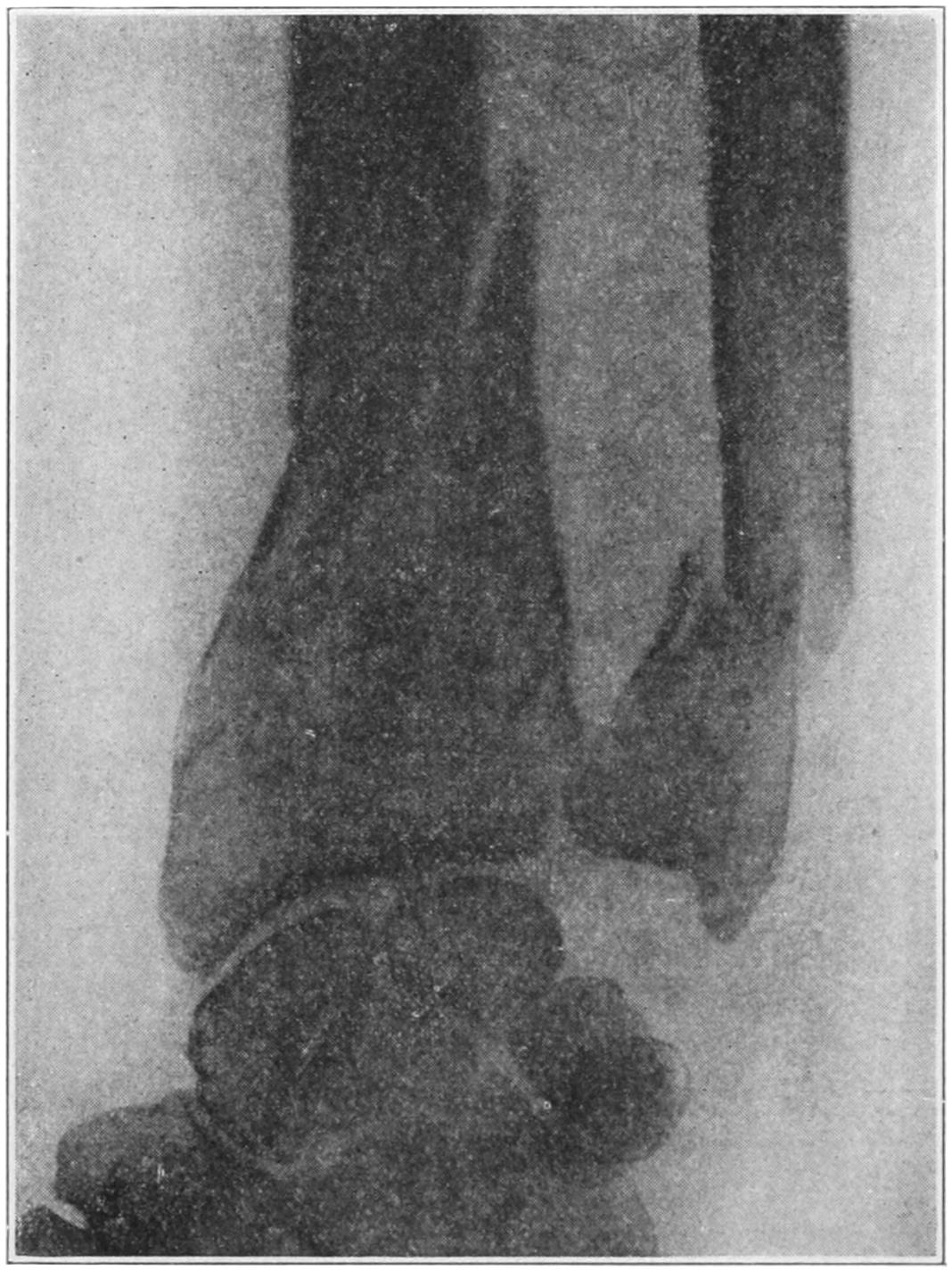
Comminuted but not compound fracture of wrist. (Beatson.)
Reduction once accomplished it is usually an easy matter to hold the arm in position. The writer prefers above all other means a molded plaster-of-Paris splint, which should extend from the line of the knuckles upon the palmar surface well up toward the elbow. It should be fitted neatly to the hand and forearm, bandaged comfortably upon it, while as it solidifies the surgeon should hold the hand slightly flexed to the ulnar side as well as anteriorly. When the splint is hardened and bandaged a simple sling will suffice. The hand should be dressed with the thumb pointing toward the face, while upon the back of the wrist an ice-bag can be applied. Ecchymosis is sometimes extreme; I have seen it extend even to the shoulder after an apparently simple break (Figs. 304 and 305).
PLATE XL
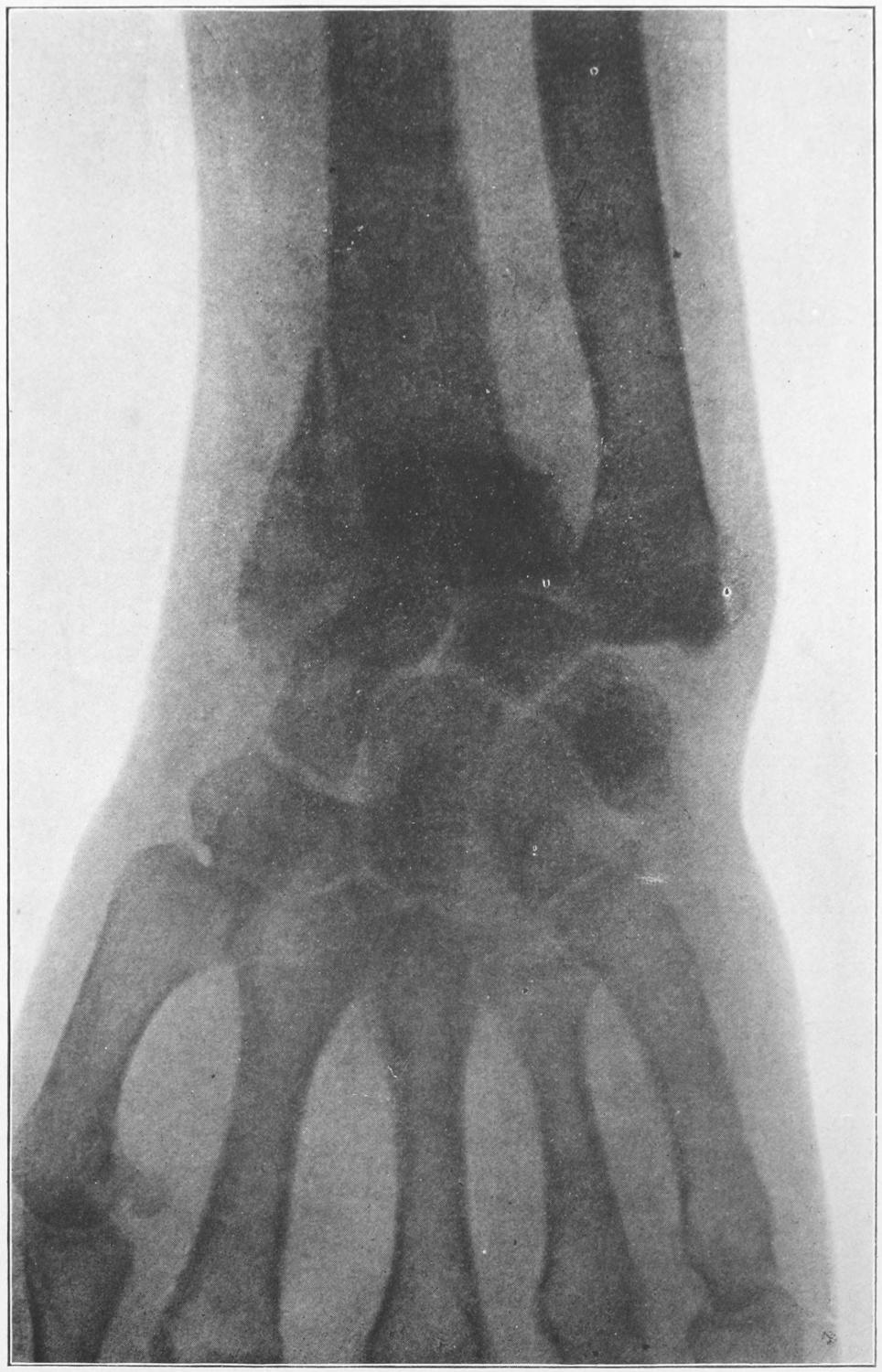
Skiagram of a Fracture of the Lower End of the Radius. (Wharton.)
I have not described other splints for dressings, at this point, for two reasons: the dressing given above is ample and sufficient for all cases, and, aside from it, the number of splints and methods devised is so large as to be confusing. It is much better to know one method well than to have a slight working acquaintance with several.
[505]
Fig. 303
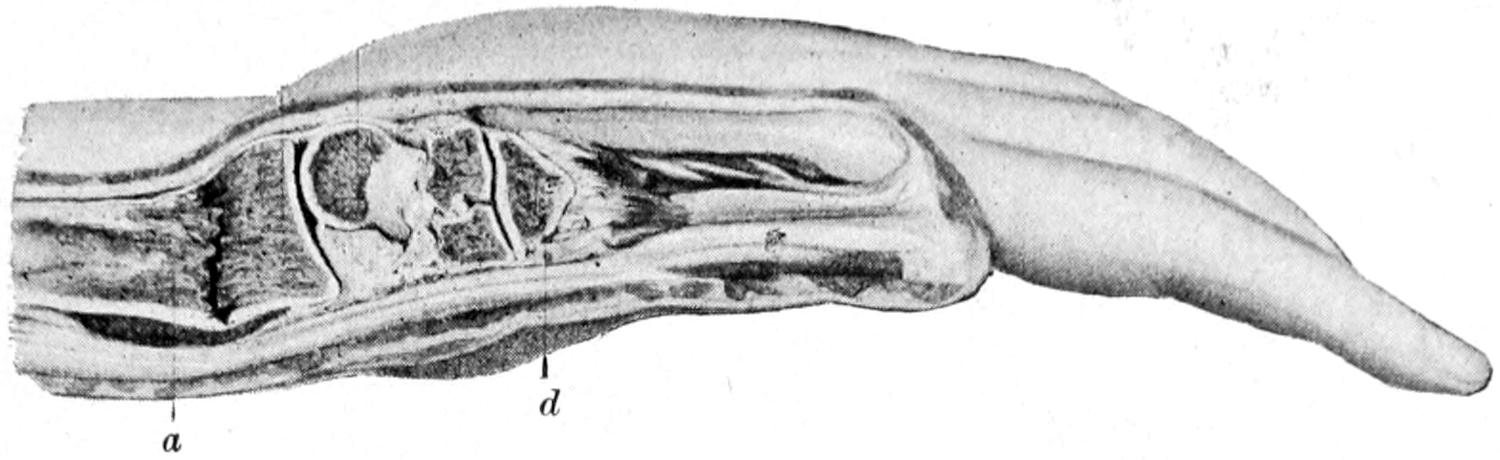
Colles’ fracture. (Anger.)
Fig. 304
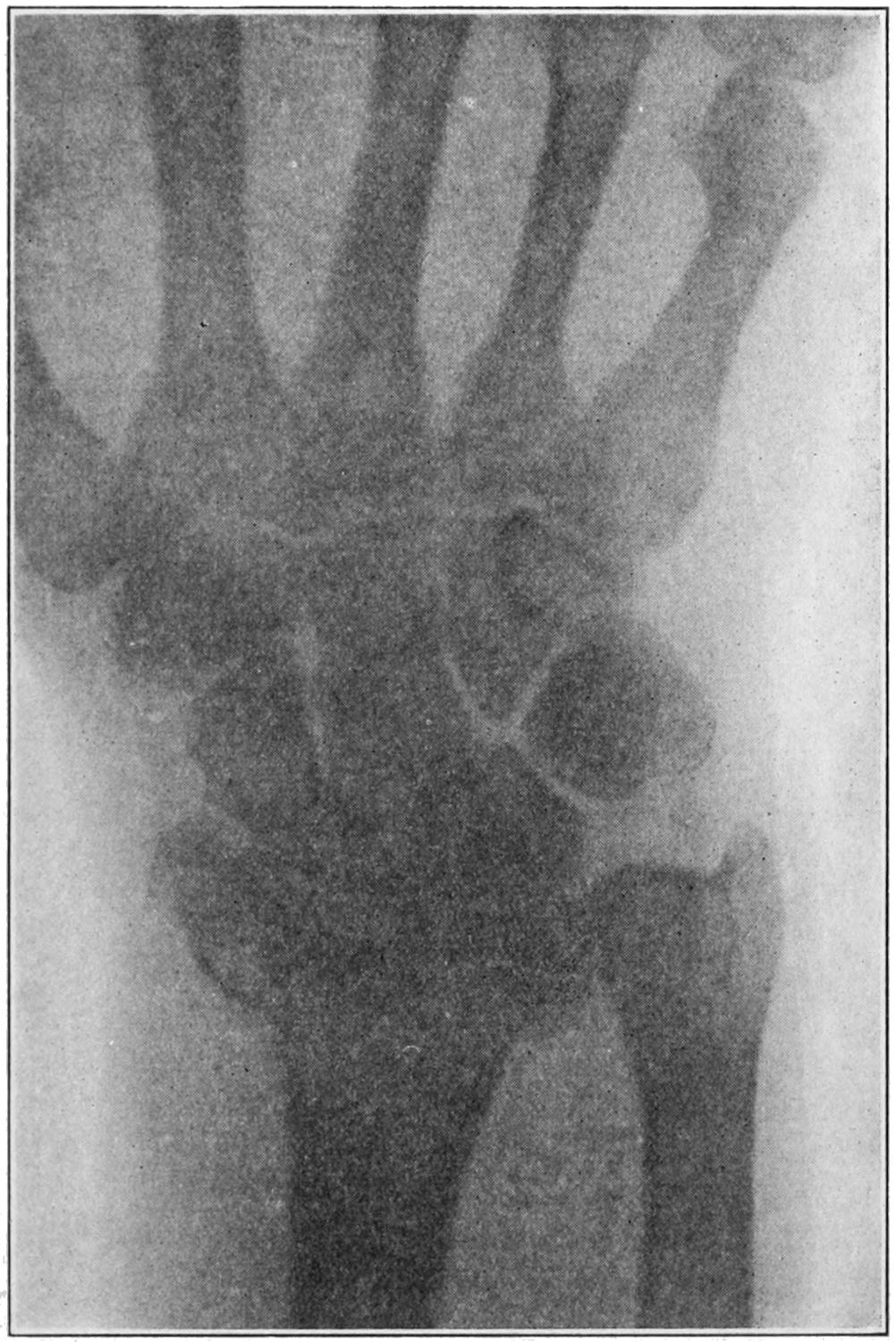
Fig. 305
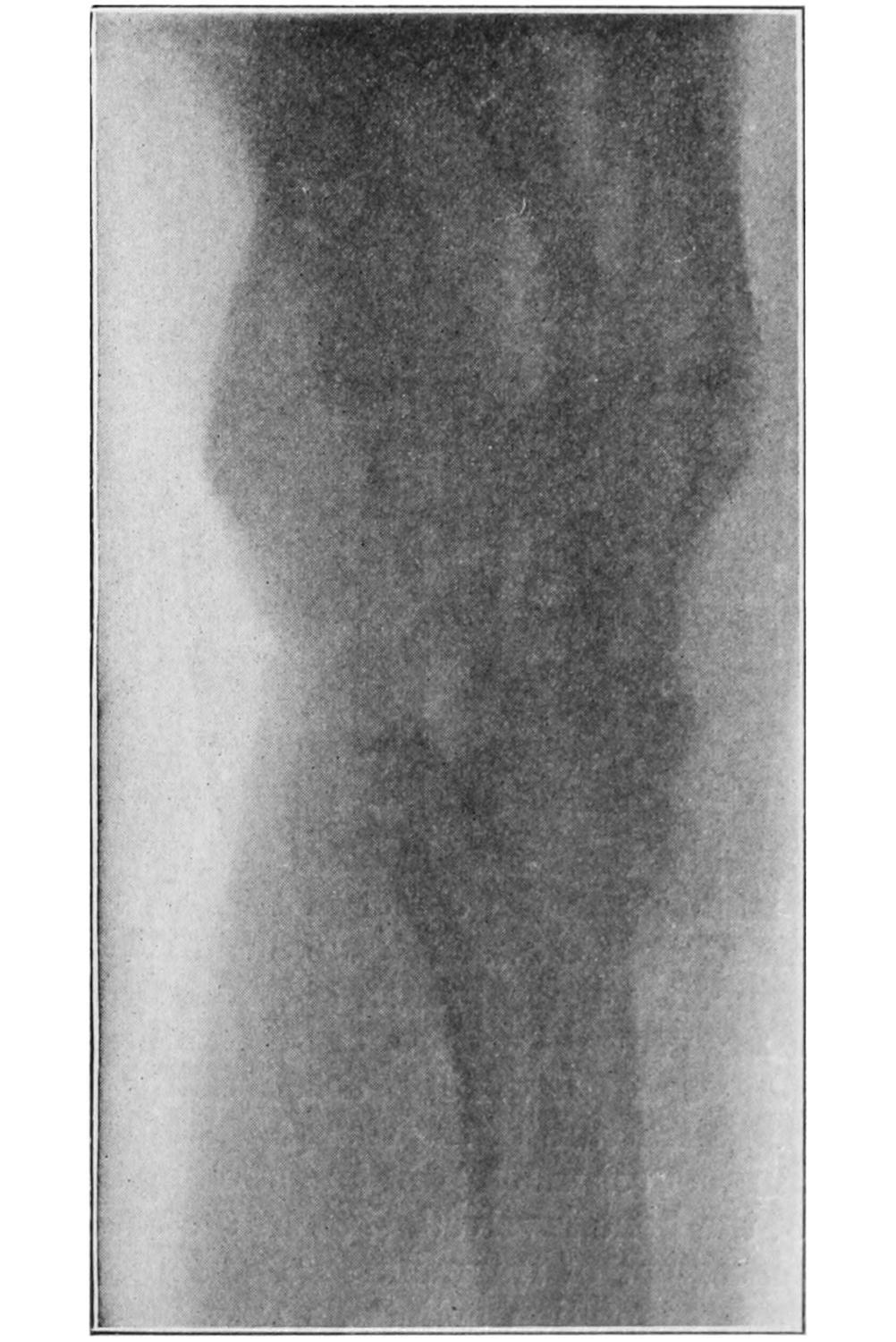
Deformity from faulty union following fracture of wrist. Buffalo Clinic. (Skiagrams by Dr. Plummer.)
While Colles’ fracture is far more frequent than all other fractures about the wrist, it is possible to have less-known forms with different displacements; thus a fracture the reverse of Colles’ has been described by Barton and by R. W. Smith, being occasionally produced by falls upon the back of the hand instead of upon the palmar surface.[506] Figs. 306 and 307, from photographs given me by Dr. Beatson, of Glasgow, illustrate both the clinical picture and the actual condition of the bones. Of all these fractures it may be said that accurate reposition, as in the case of Colles’ fracture, is the key to success. Once the fragments are reduced the same plaster-of-Paris molded splints will answer for these as for the others.
Fig. 306
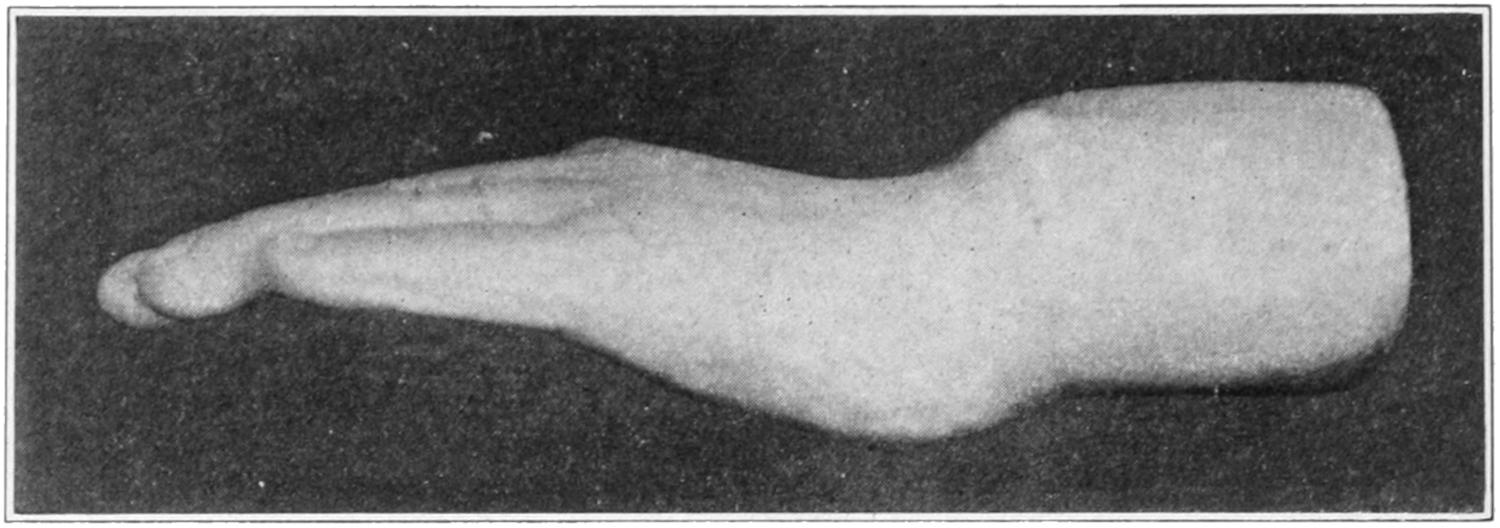
A Barton or Smith fracture at wrist. (Beatson.)
Fig. 307
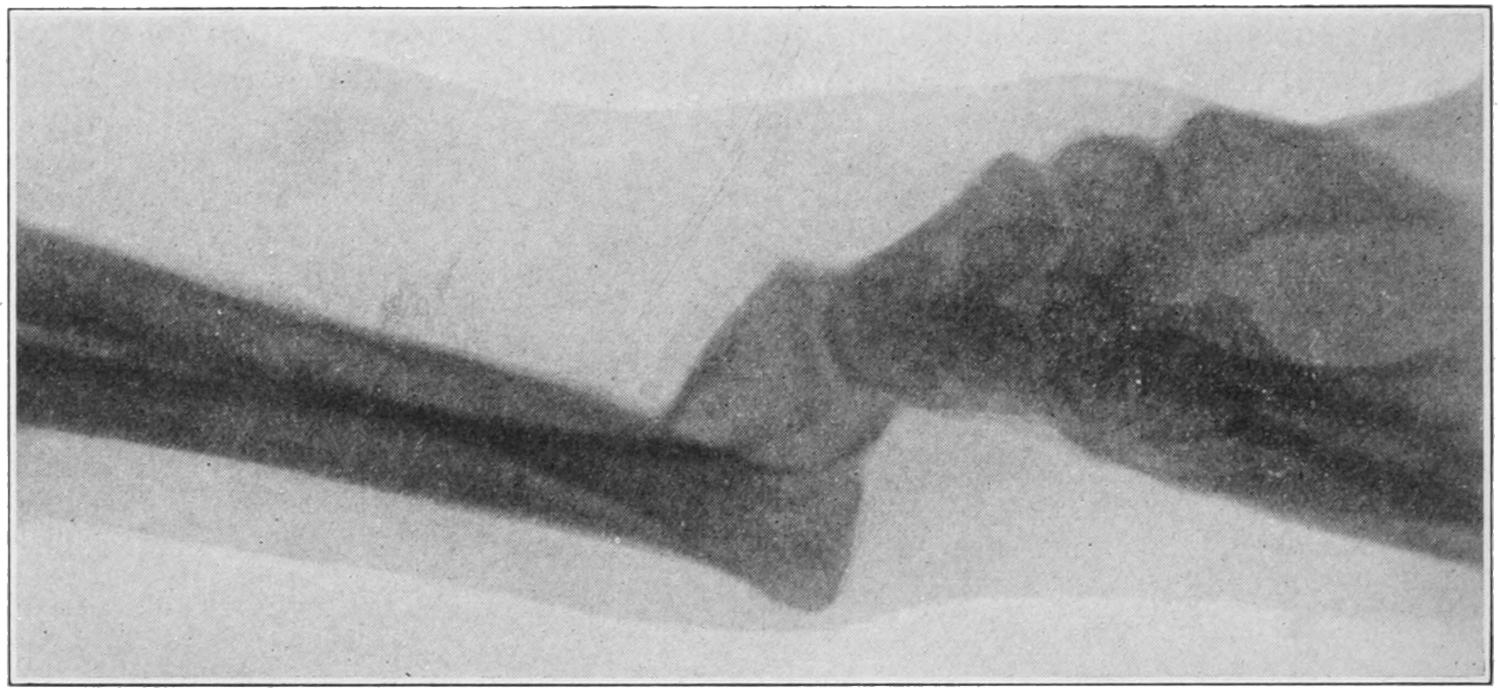
Smith’s fracture; reverse of Colles’. (Beatson.) (Skiagram of case represented in Fig. 306.)
When considerable force is applied to the distal end of the first metacarpal, as in striking with the clenched fist, or, as in a fall upon the outstretched thumb, the first metacarpal is often fractured transversely at its neck or longitudinally, its interior basal projection being broken off, both injuries being often associated. This is a condition lately proved by Russ, of San Francisco, to be more common than has been generally supposed. It was first described by Bennett, of Dublin, in 1885, and is known as Bennett’s fracture of the thumb. Its peculiar features can be best seen in a radiograph. It produces much pain and swelling of the hand, with tenderness, especially at the base of the bone involved, i. e., at the root of the thumb. There may be more or less displacement of fragments. The injured thumb should be treated by traction and with such coaptation splints as may be extemporized or prepared for the purpose, in the position of abduction. If accurate coaptation and sufficient traction be made to overcome both deformity and muscle spasm the result obtained will be satisfactory. Otherwise more or less loss of function and local tenderness may long persist.
PLATE XLI
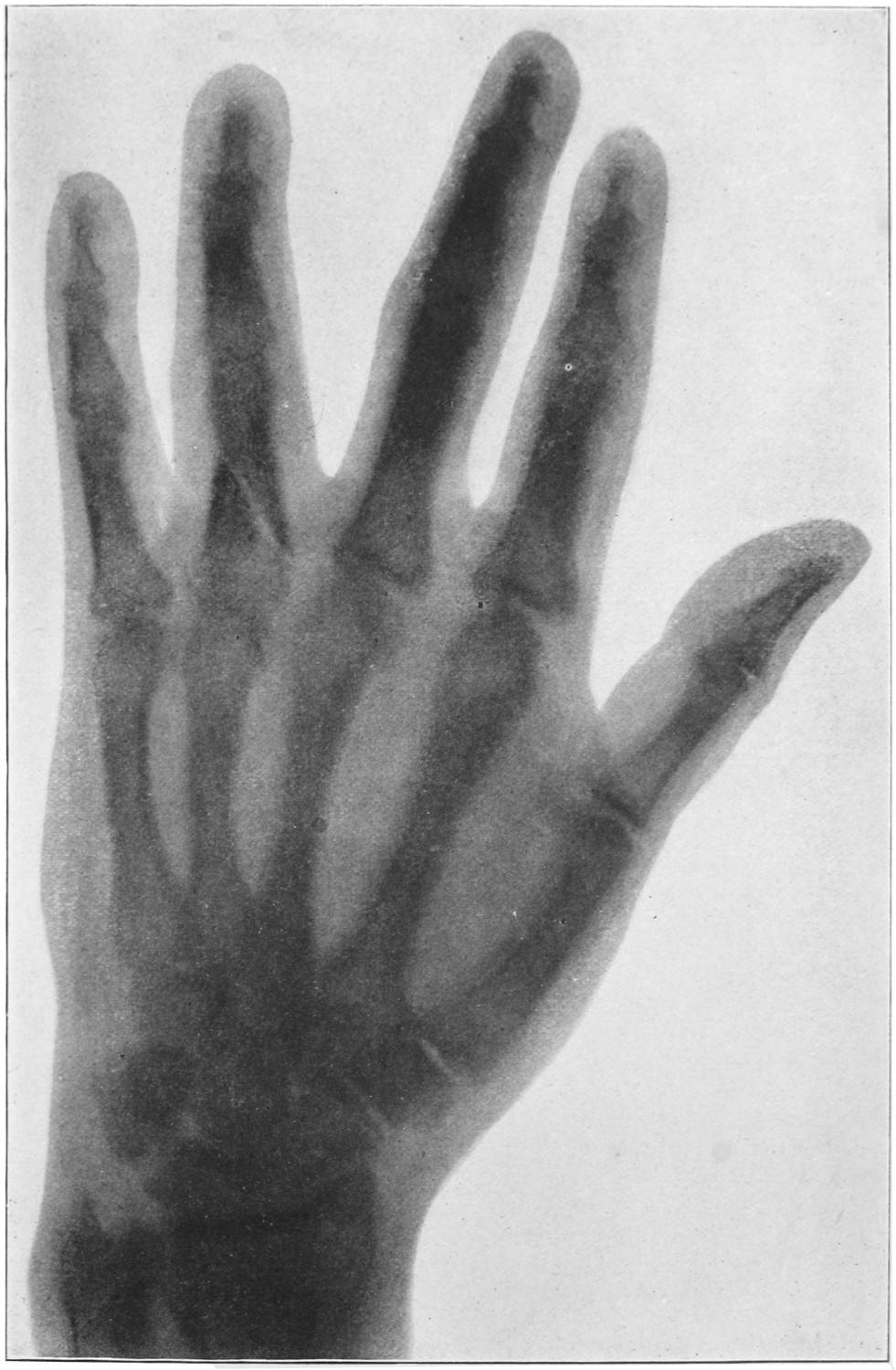
Skiagram of Fracture of the Proximal Phalanx of the Ring Finger. (Wharton.)
[507]
Fractures of the carpal bones seldom occur, except when the parts have been crushed. The scaphoid is, however, broken much more often, and doubtless many cases of so-called severe sprain include this injury. The use of the x-rays has done more to teach the relative frequency of carpal fractures than was ever previously appreciated. The scaphoid ossifies by two centres, which do not appear until the eighth year. When the bone has been thus cracked the usual signs of sprain are present, which subside and leave a tender wrist and hand whose fingers can be normally moved, but whose wrist movements are reduced one-half, while attempts at motion beyond these limits produce great muscle spasm and pain. Codman and Chase[40] have shown that the sheaths of the radial extensor tendons are in close relation to the periosteum of the bone at this point, as well as to that of the radius, so that by injury here blood may escape into the sheath without appearing at other parts; the result being a tense, fluctuating, triangular swelling over the radial half of the wrist, the blood being effused so deeply as not to discolor, or at least not at first. They regard the presence of such an engorged bursa as diagnostic of fracture either of the radius or the scaphoid.
[40] Annals of Surgery, March, 1905.
While carpal fractures call ordinarily for treatment by absolute rest, Codman and Chase have advised removal of any loose fragment, especially of the scaphoid, by incision along the back of the wrist just to the inner side of the long radial extensor. The annular ligament is to be divided between it and the long extensors of the fingers, and without opening tendon sheaths; inasmuch as this ligament does not retract when divided its borders must be held apart. In this way the joint may be completely exposed over the proximal half of the scaphoid. The line of fracture being made out, a blunt hook is introduced into the fissure and the fragment elevated, loosened by a tenotome, and removed, its removal seeming nowise to interfere with the function of the whole bone or the usefulness of the wrist.
The metacarpal bones are frequently broken, usually as the result of violence, the distal portions suffering more than the proximal. The diagnosis is best made with the fingers closed, when any lack of symmetry in the row of knuckles may be seen or any protrusion of a fragment noted. Here the x-rays are useful. Such injury should be treated by placing the hand upon a palmar splint extending well up the forearm and maintaining rest by suitable pressure, with or without traction upon the finger of the bone involved. For this purpose adhesive plaster may be passed up and down the finger and attached to an elastic band which is fixed to the end of the splint.
The same is true of fractures of the phalanges, which are often made compound by the injury. Here the danger is not so much to the bone as to the tendon sheaths or thecæ, along which infection may easily spread. Widespread and prolonged suppuration might disable a hand thus injured unless properly and promptly dressed. Ordinarily adjoining fingers can be utilized for splints, and if the outstretched hand be fastened upon a palmar splint and the injured finger kept in position by its neighbors a good result can generally be obtained. Occasionally distinct splints for one or more fingers are required, and occasionally also the suggestion made above with regard to traction may need to be enforced.
Fracture of the pelvis may be serious not only in and of itself but because of frequently accompanying injuries to the various pelvic viscera. Save in the possible separations that may occur during parturition it is always the result of direct violence. Such injuries are usually divided into fractures of the pelvic girdle and those of the more exposed prominences, such as the iliac crest, the ischiac tuberosity, the coccyx, etc. Lines of fracture may run at any point, although it is at the synchondrosis that the pelvis is usually broken loose from the sacrum. As in the skull and the lower jaw double fractures or even comminutions may occur. The same considerations concerning the transmission of serious violence may account for some of the vagaries seen in these cases. The sacrum is[508] usually broken as the result of great violence. The pelvic girdle is perhaps weakest opposite the joints and in the neighborhood of the pubis. Here there may be a separation of the symphysis, but the break usually occurs a little to one side of the middle line. In rare instances the head of the femur has been forced through the acetabulum (Fig. 308).
In a general way fractures of the pelvic girdle can be recognized not merely by local evidences of injury and shock, but by the resulting more or less complete loss of function; patients will be disabled in proportion to the violence and extent of the injury. The more unilateral the symptoms the easier it is to localize the site of the injury. Mobility can often be detected upon examination, sometimes crepitus. This is essentially true of fractures of the pubis. Occasionally combined manipulation, with a finger in the rectum or vagina, will permit more accurate localization of the injury. When the crest of the pelvis is fractured, or any of the parts to which the abdominal muscles are inserted, then the patient will be still further disabled in movements of the lower part of the body, while by palpation the fracture is sometimes easily determined.
Not the least serious features of these injuries are those which pertain to the viscera. These include not only the ordinary results of abdominal contusions which may produce all sorts of harm, for example, ruptures of the kidneys, spleen, or liver, but also more localized lesions, such as ruptures of the rectum, bladder, or urethra, or even the pelvic connective tissue. If the urinary passages be torn there is always opportunity for urinary infiltration and infection. The same is true of the rectum so far as possibility of infection is concerned. Therefore one of the earliest maneuvers in dealing with such a case should be the passage of a catheter, to determine if the urine be bloody or the urethra obstructed. In such a case, in the male at least, it will usually be wise to make a perineal section and to open widely and then drain the bladder. In not a few of these instances the laceration takes place internally, and a pelvic crushing injury, which is followed by collapse and abdominal rigidity, without satisfactory explanation as above, should be promptly explored by abdominal section, the danger of doing it being considerably less than the risk of leaving it undone.
Fig. 308

Fracture of pelvis. (Mudd.)
Fig. 309
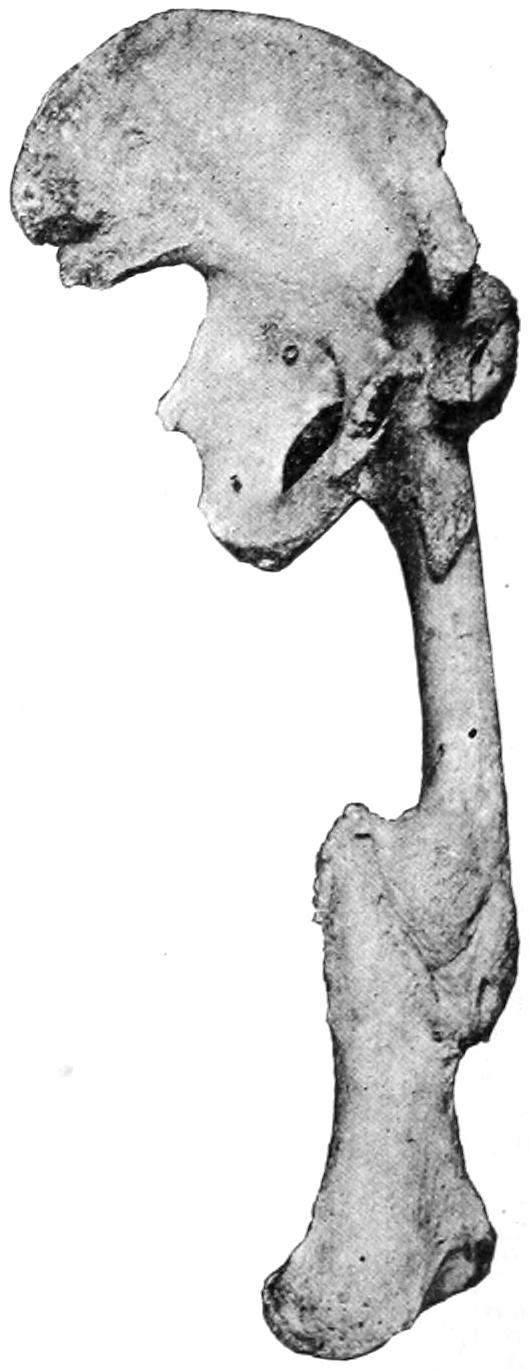
Great deformity after multiple fracture of femur, with synostosis. (From the Buffalo Museum.)
Some of these fractures are conspicuously compound, and the treatment for the external wound will permit of more careful exploration of the bone injury, as well perhaps as the insertion of wire sutures or other means of fixation.
Fig. 309 illustrates a serious complication that ensued in one case after multiple fractures of the pelvis and hip, with synostosis at the hip, as well as extensive deformity following fracture of the shaft of the femur.
—Treatment of pelvic fractures should comprise, first, absolute rest. This means not merely confinement in bed, with traction applied to one or both limbs,[509] but probably fixation of the pelvis and perhaps the thighs, either in a compressing bandage or in a plaster-of-Paris double spica, the pelvic jacket running as high as may be necessary upon the trunk of the body. Cases which seem to permit of operation and suturing are entitled to it, but they will constitute but a small proportion of the total. While patients are so rigidly confined provision should be made for free elimination, and possibly conveniences provided for receiving the evacuations without possibility of infection. Recovery is in many instances complete; occasionally it occurs with considerable displacement. If the viscera escape injury much may be expected in the way of repair of the bones under suitable treatment.
The margin of the acetabulum is occasionally chipped off, sometimes by itself, sometimes as a complication of dislocation of the hip. The posterior margin of the brim is the part which usually suffers. Diagnosis should be made by the ease with which such a dislocation recurs after manual reduction. Sufficient traction to keep the limb from displacing the fragment, and snug bandaging with pressure, especially around the injured hip and above the trochanter, is indicated in such cases.
The coccyx and even the lower portion of the sacrum are occasionally broken loose, either by external violence or during parturition. Here the fragment is drawn forward by the levator ani, displacement is marked, and pain and soreness are great. Should there be doubt as to the nature of the injury, combined manipulation, with a finger in the rectum, will make diagnosis positive. Fibrous union is about all that can be expected in either of these cases. The fragment may be justifiably removed at any time.
Fractures at the upper end of the thigh are more common than those at the lower. At the upper end there may be fractures of the head, of the neck, those which pass between the trochanters, and epiphyseal separations. All of these are rare except those of the neck.
Fractures of the neck of the femur occur most commonly in those who have passed the fiftieth year of life. They occur, however, during the middle period and even in children, and, as Whitman has shown, are by no means so rare in the young as was until recently supposed.
The shape and structure of this portion of the bone, and the peculiar changes which occur with advancing years, constitute the explanation for the frequency of this injury in late life. As the jaw begins to change in shape, and the teeth to drop out, there occur also unseen changes within the cancellous structure of the head and neck of the femur by which the strength of the latter is materially reduced. It is still further weakened by the change in shape which the bone also undergoes as it loses its obtuse angle and becomes set more at a right angle with the shaft. The reduced ability to resist strain produced by these changes is remarkable, and accounts for the ease with which fractures occur, even from so apparently trivial an accident as tripping on the floor. With all the violence directly transmitted there is usually present an element of twist or torsion by which fracture is still further favored.
As between so-called intracapsular and extracapsular fractures surgeons have made distinctions to which unnecessary importance has been attached. Anteriorly the capsule is attached to the intertrochanteric line, while posteriorly it does not extend nearly so far outward; it can thus be seen that many fractures are partly intracapsular and partly extracapsular. These lines vary in different individuals, especially that of the posterior insertion; it is not usually possible to make minute distinctions of this kind. The principal importance which attaches to them is in the direction of prognosis, for if the fragment be absolutely intracapsular it can derive its blood supply only through the ligamentum teres, which is, to say the least, a precarious method of existence and usually disappointing. In general it may be assumed that a fracture close to the head is intracapsular, but that when it occurs well out toward the shaft it may partake of both characters. In this connection the x-rays will afford, usually, more satisfactory information than can be obtained by even extensive or rude manipulation.
Impaction occurs with considerable frequency in these cases, and, unless accompanied by too much deformity or displacement, is rather a fortunate occurrence, since by it is afforded an automatic splint which it should be the surgeon’s endeavor to not break apart.[510] There can be no doubt, moreover, but that trifling degrees of impaction with incomplete fracture occur, especially in the aged, in many injuries to the hip. It would be the greatest misfortune to the patient in one of these cases to complete the separation, and when assured of the existence of such a lesion it is best to treat the case as though it were a fracture. I am sure that many cases which have gone into court have been due to incomplete fractures with impaction, where there has been later absorption of bone, by which the femoral neck has been much shortened, so that recognizable deformity as well as more or less disability have resulted. Other changes comprised among those already described in the chapter on Joints, under the section on Arthritis Deformans, may also occur. Callus which has been at one time abundant may also undergo too great absorption.
Fig. 310
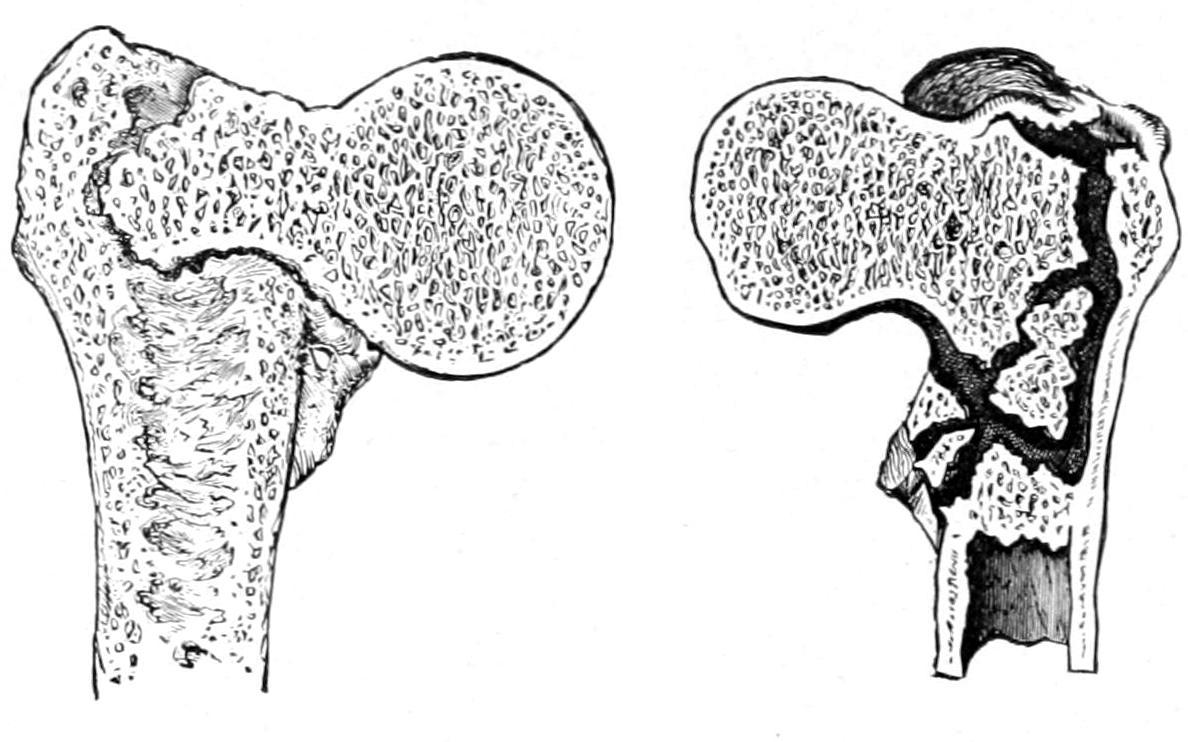
Fig. 311
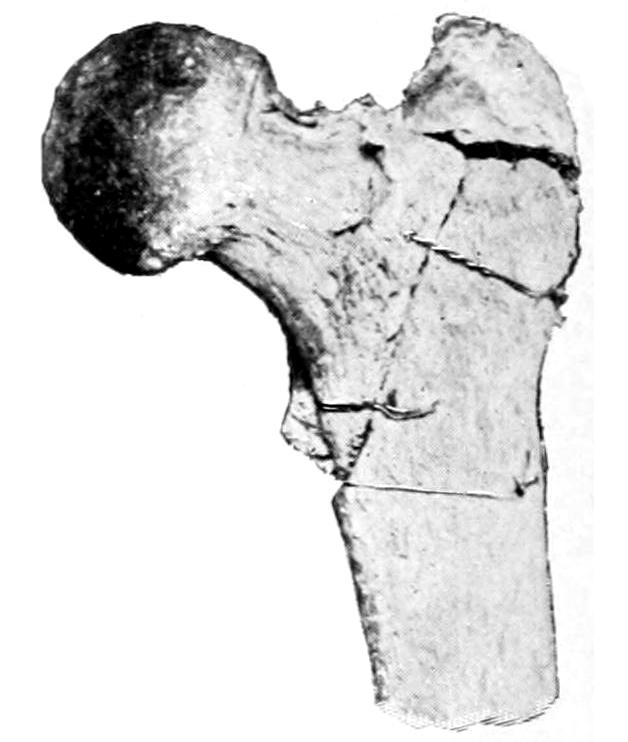
Sections of impacted extracapsular fractures of neck of femur, showing the degree of impaction and of splintering in different cases. (Erichsen.)
Extracapsular fracture of thigh.
Fig. 311 illustrates extracapsular fracture and comminution. Figs. 312 and 313, also from specimens in the author’s collection, show some of the changes described above, including impaction, displacement, and some osteophytic outgrowth.
Fig. 312
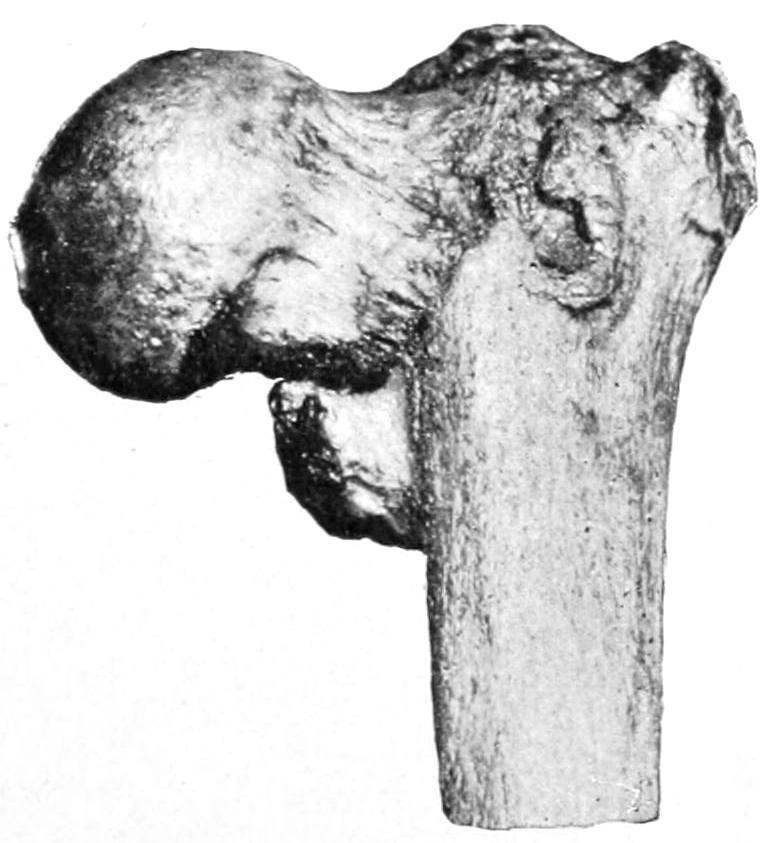
Fig. 313
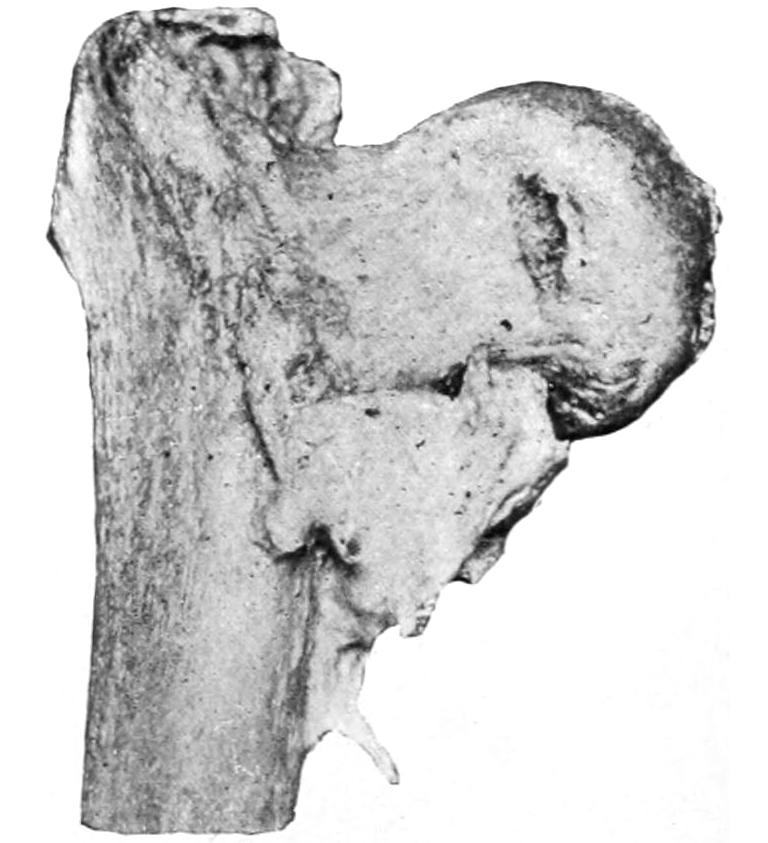
Impacted fractures of necks of femurs.
Signs of fracture of the neck of the femur of special import are history of injury, pain, loss of function, shortening, rotary displacement, usually eversion, crepitus, relaxation of the fascia lata, and disarrangement of the lines of triangulation between the bony prominences of the pelvis and the trochanter. Diagnosis should be attempted with as little manipulation as possible lest impaction be dislodged. The patient should be placed upon a comfortably hard surface. Anesthesia will sometimes afford important aid. It should be ascertained, first, that there had been no previous injury which[511] could produce shortening. If, then, shortening be apparent it is of itself almost a diagnostic sign. Such a limb is practically helpless, and unless the neck be so driven in upon itself as to produce impaction the foot will be usually everted, while the tension of the fascia lata will be relaxed and there will be fulness in Scarpa’s triangle. Absolute inability to use the limb implies fracture without impaction. Should the patient have been able to help himself or work after the injury, impaction may be safely assumed. The parts are exceedingly tender and pain is easily produced. Shortening is to be assumed only after placing the limbs and body in a perfectly symmetrical position (the pelvis being at right angle with the spine), after which the measurement most usually made is from the anterior superior spine to the internal malleolus. Nélaton’s line is the shortest line which can be made to pass around the hip, in one plane, from the anterior superior spine to the tuberosity of the ischium. While the line is curved it should lie in the same plane. Normally this passes just over the great trochanter. If there be real shortening the trochanter should rise above this line to an extent corresponding with the shortening made out by other measurements. Still another method of measurement is to hold a straight edge opposite to the superior spine and perpendicular to the surface upon which the patient is lying; the distance between this edge and the great trochanter should be as much less than the distance found by similar measurement on the other side as the amount of shortening measured by the other methods. This is the easiest way to measure the lines included in Bryant’s iliofemoral triangle. Both are illustrated in Fig. 314. Impaction can sometimes be determined by comparing triangles drawn between three points on either side, these points being, respectively, the great trochanters, the anterior spine, and the centre of the pubis, which is common to both. The lower line of the triangle on the injured side should be shorter than on the other, in proportion as the head and the end of the shaft have been driven toward each other.
Fig. 314
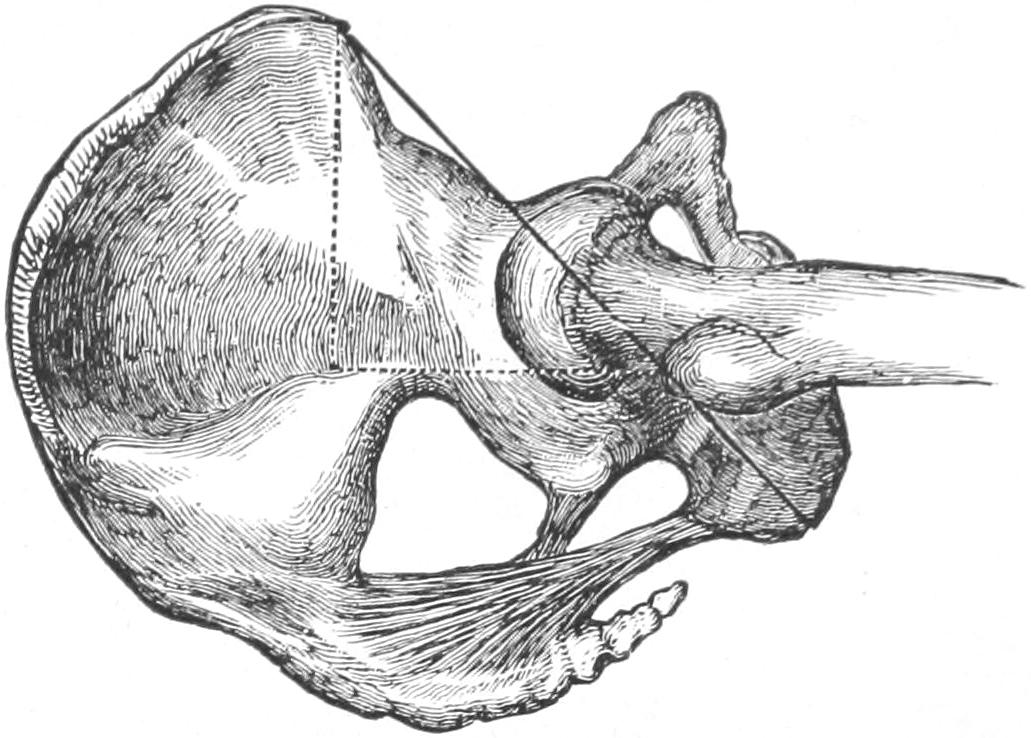
Nélaton’s line, dark. Bryant’s iliofemoral triangle, dotted. (Erichsen.)
Crepitus is a sign to be elicited with care and gentleness. Up-and-down movements of the thigh upon the side of the pelvis or gentle rotary movements, combined with circumduction of the knee, will yield it if it is to be easily detected. Every effort of this kind disturbs the injured bone and should be minimized as much as possible. One other sign of considerable value is the fact that if the patient be turned upon his face a fractured femoral neck will permit the leg to be hyperextended to a degree not permitted by the normal condition. In making this test the pelvis should be held firmly; it should be made but once, the intent being to disturb the parts as little as possible.
—The diagnosis of fracture is often easy, but in some cases it is accompanied by many difficulties. It would be better to give the patient the benefit of a doubt and treat him for a fracture with rest than to subject him to excessive manipulation. Such an injury is not likely to be mistaken for anything else save a dislocation of the hip, although occasionally separation of the margin of the acetabulum might cause confusion.
—The prognosis depends upon the age and vitality of the patient, the location and extent of the fracture, the method of treatment, and upon causes which seem at first foreign to the subject. Patients with pulmonary or cardiac trouble, who need frequent change in position, or perhaps absolute rest, are likely to develop something hurriedly which will disarrange ordinary calculations. Sometimes they die suddenly or they may develop pulmonary edema or hypostatic pneumonia. The circulation may be so poor as to lead to early development of bed-sores, while ordinary complications in prostatics, or habitual constipation in the aged, may make care and treatment exceedingly difficult. It should be emphasized, then, that treatment of the fracture alone is by no means all that these patients require, and prognosis means something more than what[512] may merely happen to the bone. In this last respect, however, the better nourished the fragment the more likely is bony union to take place if good position can be maintained. When osseous union has failed patients get fairly useful limbs with fibrous or ligamentous union, even with one or two inches of shortening, and such patients may hobble about for years, with a cane or a crutch, with limbs that are semiserviceable.
—Of these cases it may be said that interests of life are paramount to those of limb, and the treatment should be directed to that which the patient can tolerate. Reasonably healthy, muscular people can bear the application of adhesive strips and traction such as the thin and delicate cannot tolerate. The ideal method is that by which sufficient traction is made to overcome all muscle pull which shall produce shortening, the measure of weight to be used in these cases being the effect thereby produced. Thus if twenty pounds be sufficient, well and good; if not, it should be increased to thirty or forty pounds, providing that the patient can tolerate it. At the same time a broad binder around the pelvis may afford sufficient support with a tractable patient, while many will require a long side splint, extending from the axilla to beneath the foot, to which both body and the injured limb should be fastened, in order to more perfectly maintain that physiological rest which is so necessary. This last is the so-called “Physick” splint, which has been variously modified, while the method of traction has been usually spoken of as Buck’s extension. It seems well thus to commemorate the names of the American surgeons who showed the value of these methods. When a long side splint cannot be borne, sandbags 15 in. or 20 in. in length and 3 in. in diameter may be used to give support. Any decided tendency to eversion of the limb should be corrected as well as the shortening. When the long side splint is used the foot can be held in place with it and thus the position of the shaft of the femur controlled. At other times this may be done by flexing the knee and thus preventing upward rotation. In all methods of traction it is advisable to keep the heel free from the bed, in order that the effect of the method may not be lost by the obstruction of the mattress.
Fig. 315
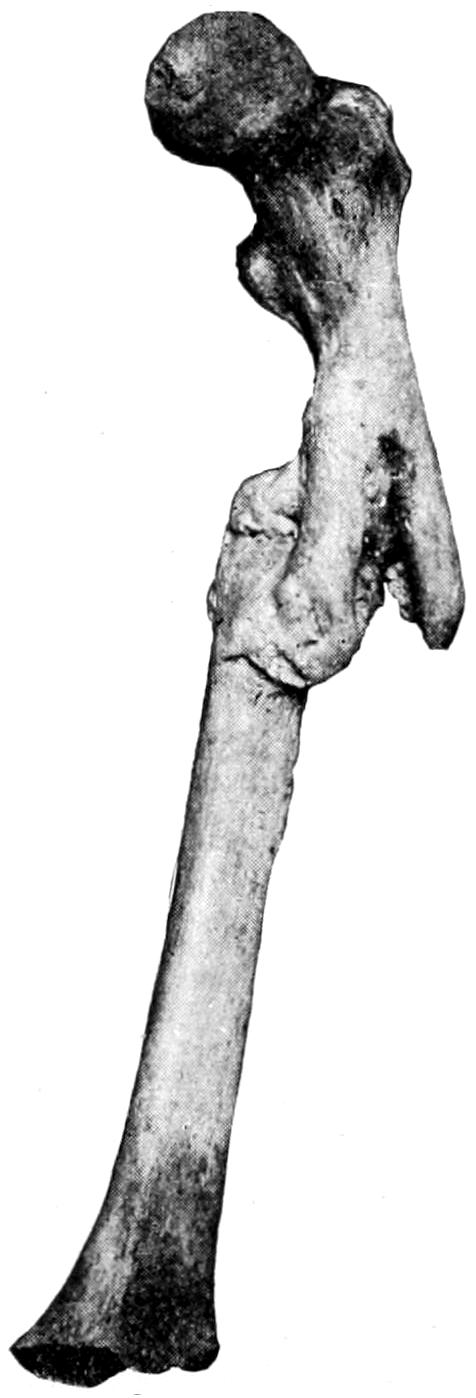
Fig. 316
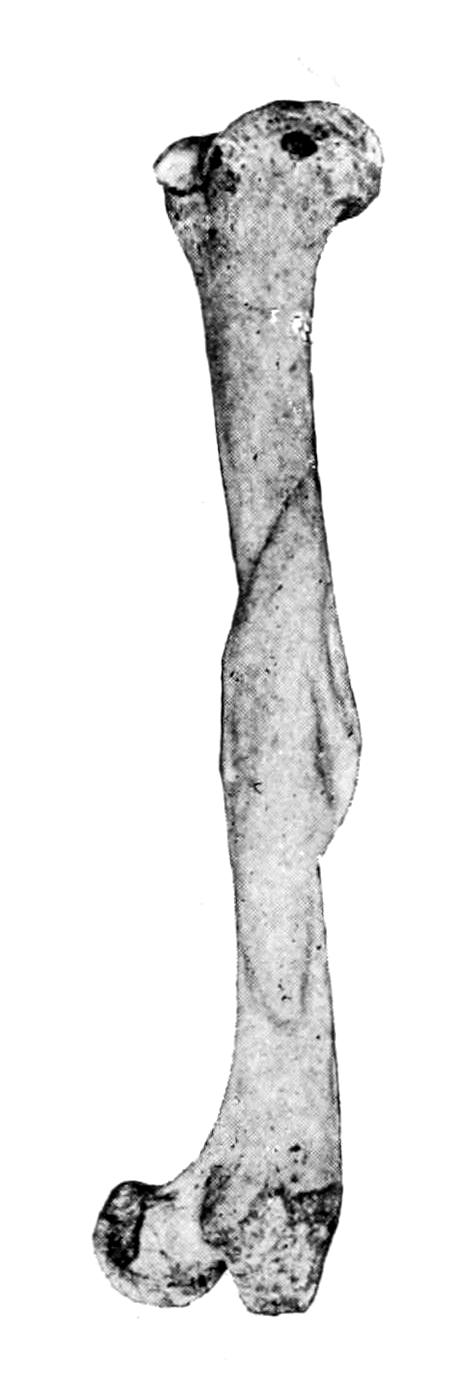
Fig. 317

Fracture of upper third of femur. Vicious union.
Shortening resulting from overlapping.
Overlapping fracture of femur.
Other methods of treatment of these fractures are common as well to those of the shaft, and will be considered later. These include the single and double inclined plane and the method by anterior suspension. In general the first indication is efficient traction. This should be made as efficiently as possible. When the patient cannot tolerate any[513] of the usual methods, then the double-inclined plane may be used, the knee being hung over its apex, or anterior suspension may be practised. In severe cases patients should be simply made comfortable, with such local treatment as they can bear. It may be even necessary to place them in the semi-upright position in bed, in order to free the lungs, or to frequently change their position to avoid the formation of pressure sores.
Fig. 318
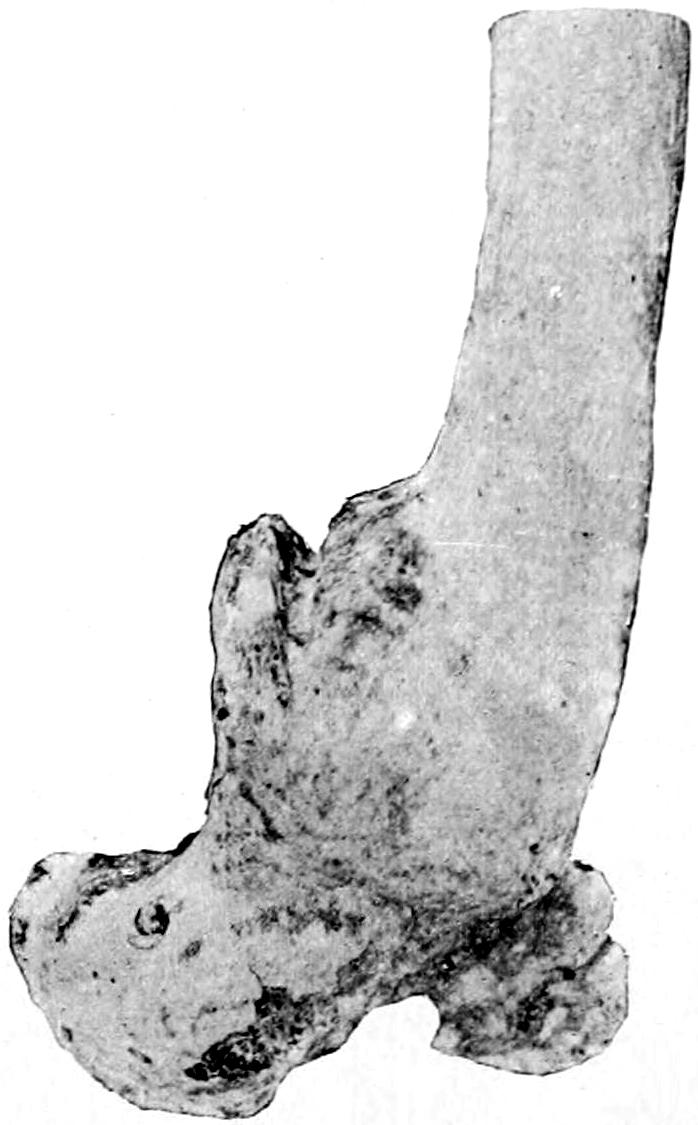
Fracture of lower end of femur, with great displacement of condyles.
—Fractures of the shaft of the femur are usually oblique and accompanied by considerable displacement, because of the powerful thigh muscles which tend to shorten the limb. These fractures are often compound, and occasionally the femoral fragment causes serious damage to important vessels or nerve trunks. When the fracture is just below the insertion of the psoas into the lesser trochanter this muscle tends to not only pull up but to externally rotate the upper fragment. Inasmuch as there is no way of controlling this muscle or the fragment, the fractured limb should be dressed upon an inclined plane, or in anterior suspension, in such a way as to make the axis of the shaft fall into line with that of the fragment. When the fracture is in the middle of the thigh, or lower, there is sufficient length of the upper portion so that pressure can be made upon it, or that psoas activity can be overcome. Fig. 315 illustrates the tremendous deformity that may result from neglect of these precautions. Fig. 316 illustrates a certain degree of overlapping without conspicuous other deformity. Fig. 317 shows the shortening which is often inevitable.
Muscle spasm should be overcome as an essential part of successful treatment, the most important feature in making traction being to use force sufficient to tire out and overcome the irritated muscles.
—Fractures of the lower end of the femur are usually the result of extreme violence, and may be classified as were those of the lower end of the humerus. When there is a supracondyloid fracture the two heads of the gastrocnemius will help to displace backward the upper end of the lower fragment to an extent permitting injury to the bloodvessels, while there is always marked shortening. Here the patella will be made unduly prominent, and there will be depression above it. Either condyle may be broken loose alone, or there may be intercondyloid or T-fractures which are serious because the amount of force required to produce them may have played serious havoc with the soft tissues. The joint capsule will probably be filled with blood, the ligaments rent, and perhaps the blood supply of the limb compromised. In such a case as this the joint may be opened, the contents turned out, and the fragments readjusted and wired or fastened in place (Fig. 318). Epiphyseal separations, which may occur up to the twentieth year, are not essentially different, although lateral displacement is perhaps more common, while they are often compound.
Treatment.
—Oblique fractures of the femoral shaft can be more easily adjusted under the influence of powerful and continuous traction than the transverse, where lateral displacement and overlapping tend to occur. A more general application can be made of the method described above when dealing with fractures at the upper end of the shaft, i. e., when the upper fragment cannot be controlled the balance of the limb must be adjusted to it in whatever position it may be required to maintain. By the use of sufficient traction, combined with molded or other splints, a fair result may usually be obtained. In stout individuals it is by no means easy to determine just how the fragments lie, save by the use of the x-rays. If traction be so adjusted as to maintain the limb at equal length with the other the surgeon may feel that, with certain coaptation splints, he is doing the best he can. Application of the same rule given above would lead him to place the limb on a double inclined plane, in case of fracture near the knee-joint, in order that in this position the sural muscles (the calf) may be relaxed and backward displacement of the lower fragment be adjusted. If the apex of this plane be arranged sufficiently[514] high, so that the patient’s knee is practically hung over it, and that the weight of the body makes sufficient countertraction, then the use of weight and pulley may not be necessary. Here, however, pressure which will be efficient may produce numbness, as will any long-continued pressure in the popliteal space, and after a few days it may be necessary to assume some other position. Fractures which loosen the condyles will need lateral pressure, while the position of each condyle may be controlled by the position of the leg, through the medium of the corresponding lateral ligament.
Fig. 319

Extension band and foot-piece.
Fig. 320

Same, folded and ready for use.
The standard “Buck’s extension” (for which latter word I prefer to substitute the term “traction”), by weight and pulley, with the limb in the extended position, is still the resort of the majority of surgeons, but combined with other support by long side splints or coaptation splints as may be needed. Fig. 321 illustrates the method of its use, except that the ends of the adhesive strips should be extended upward to a point nearly opposite the site of the fracture. The amount of weight to be used should be graduated to the effect produced. From ten to forty pounds, or even more, may be needed. After the muscles are thoroughly tired the amount of weight may be somewhat reduced[41] (Figs. 319, 320 and 321).
[41] Before applying the strips of adhesive, the best for the purpose being that made of moleskin spread with material with which zinc oxide is incorporated, the limb should be carefully washed and shaved and then completely dried. A little cotton should be placed over each malleolus, in order to avoid pressure-sores, while the strip of wood beneath the foot should be sufficiently wide to prevent or minimize this pressure. The heel should be kept off the mattress.
Fig. 321
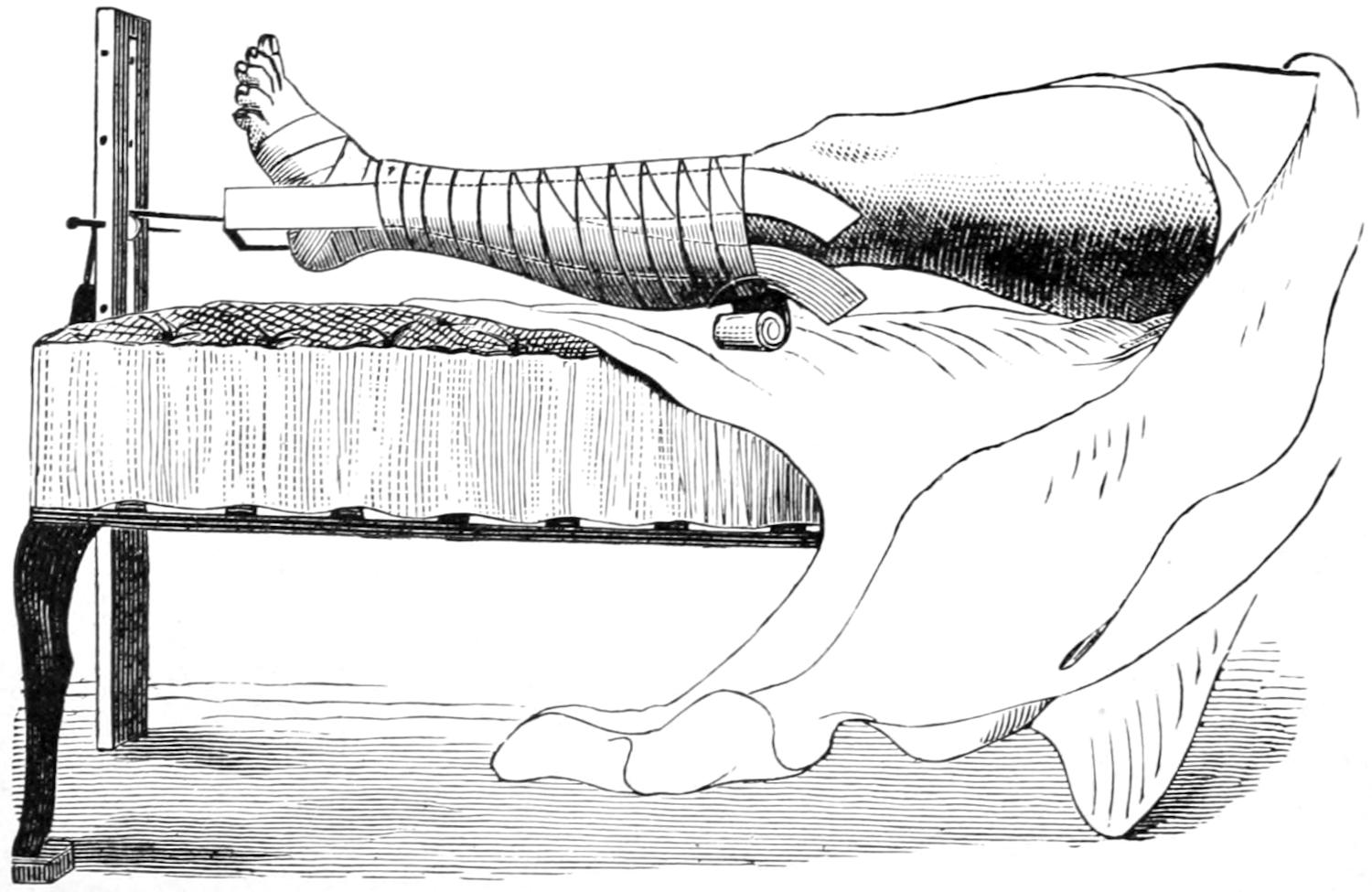
Mode of applying adhesive plaster. (When the dressings are completed the limb should not be allowed to rest on the bed.)
Continuous and anterior traction was devised by Nathan R. Smith, in the use of a so-called anterior splint, which was later modified and improved in device by Hodgen. The method of its use is shown in Fig. 322. Adhesive strips are used in this method as well, permitting the leg and foot to be attached to the lower bar of the wire frame. The[515] position of the frame which contains the limb, swung within it upon turns or strips of bandage, is then controlled by a suspension apparatus, as shown, which tends to constantly pull the frame and its attached lower part of the limb away from the patient, the effect being to make a constant but gentle traction. If the point of suspension were placed directly above the limb there would be no traction whatever. The essential feature of the method, then, consists in arranging it as shown, so that the pull shall be oblique, and that, according to the obliquity of the suspension cords, the amount of traction shall be regulated.
Fig. 322
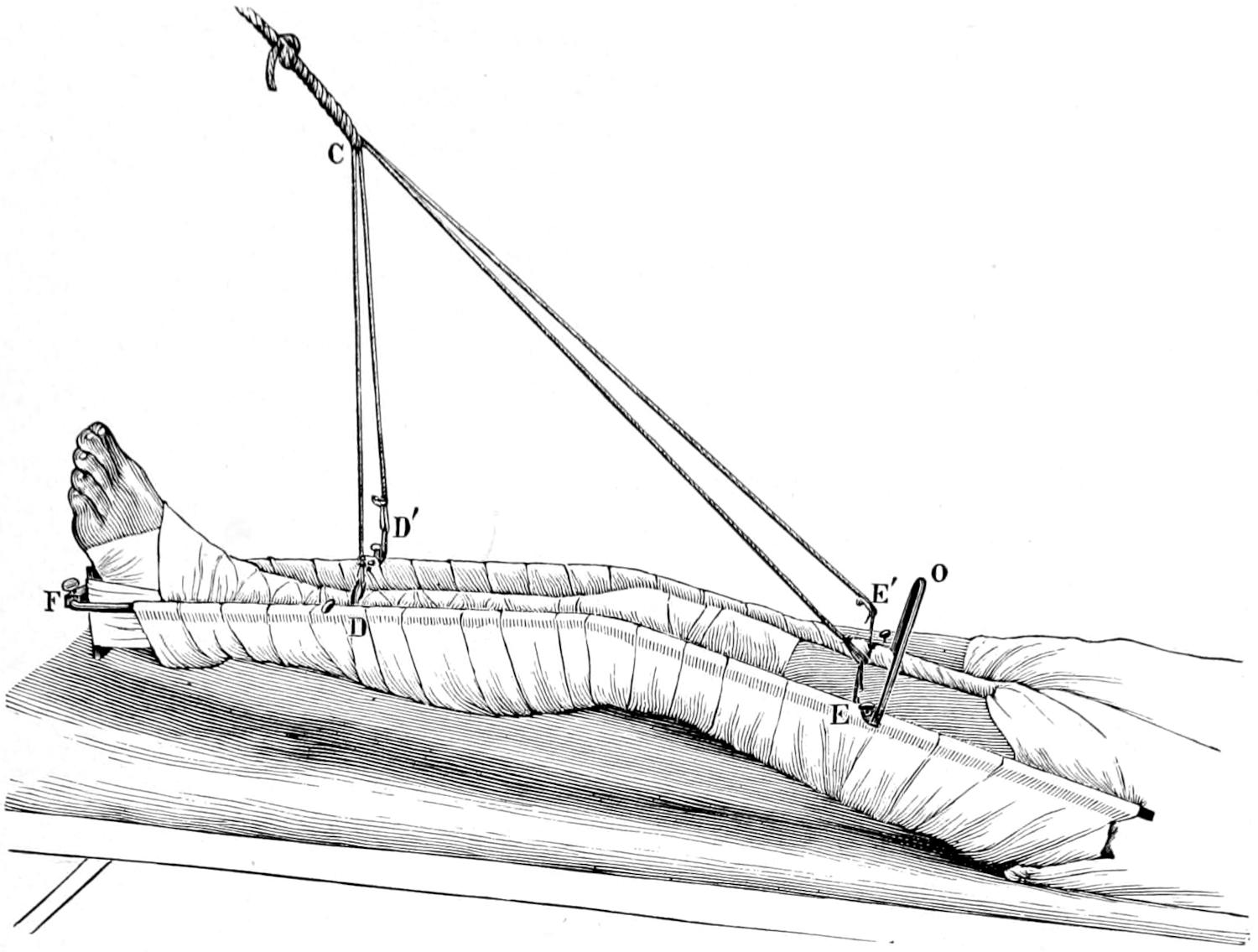
The Hodgen suspension splint.
In this method of treatment there is no violent attempt made at reduction or overcoming displacement, but dependence is placed, at least for two or three days, on the effect of the constant pull and its overcoming muscular activity. After this such added splints or expedients may be adopted as the case may require. The knee is usually flexed at a comfortable angle, the intent being not to lift the foot too high, so as to avoid being compelled to overcome this added weight, but to regulate the tension by the obliquity of the suspending cord.
Fig. 323
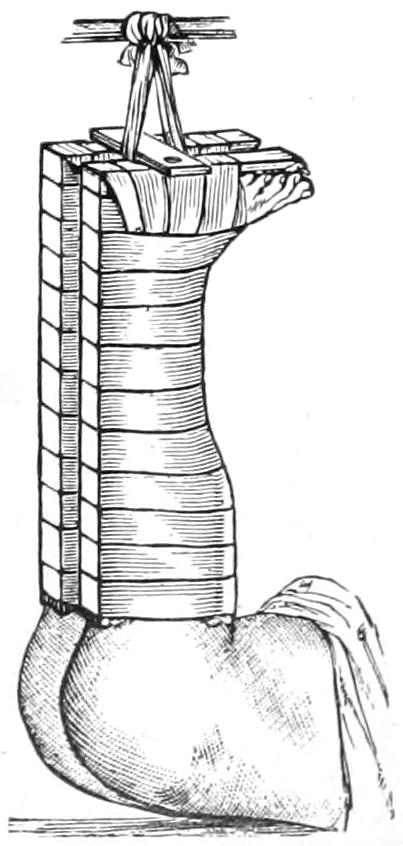
Fracture of the femur in a child treated by vertical extension. (Bryant.)
This method has found favor in the West under the enduring influence of Hodgen’s teaching. In the East it is not so generally practised. It has, however, several advantages, as follows: (1) Equably perfect and comfortable extension; (2) easy adjustment; (3) easy exposure for inspection; (4) when a fracture is compound it permits of easy application of dressings; (5) adaptability to nearly all fractures of the femur. It is peculiarly serviceable for feeble and aged patients who chafe at restraint. If it be desirable to flex the knee to a considerable degree this can be done, e. g., in fractures near the lesser trochanter.
In fractures of the thigh, patients are frequently disturbed by muscle spasms occurring during sleep. This can usually be obviated or minimized by suitable doses of sulphonal, given early in the evening.
Fractures of the femur in children are not uncommon. In those who still wear diapers, and perhaps in those a little older, these injuries may be best treated by vertical suspension, with sufficient weight to overcome all shortening. Here the adhesive strips and the suspending cords should be attached to both limbs alike, in order to have sufficient access to the perineum, and[516] in order to judge of the effect which we are obtaining. Figs. 323 and 324 illustrate this method.
Plaster-of-Paris dressings for fractures of the thigh appeal especially to those who are most familiar with the use of the material. Some patients with fracture of the neck of the femur may be early put in the erect posture, upon an elevated surface, allowing the injured limb to hang down while the patient rests upon crutches. In this upright position, with the down-hanging leg, to which traction can be made by an assistant, a plaster-of-Paris spica may be applied, extending from the waist-line down to or below the knee. As a limb is thus dressed so it will heal, and it is of importance that complete reduction be effected as a part of the procedure.
Fig. 324
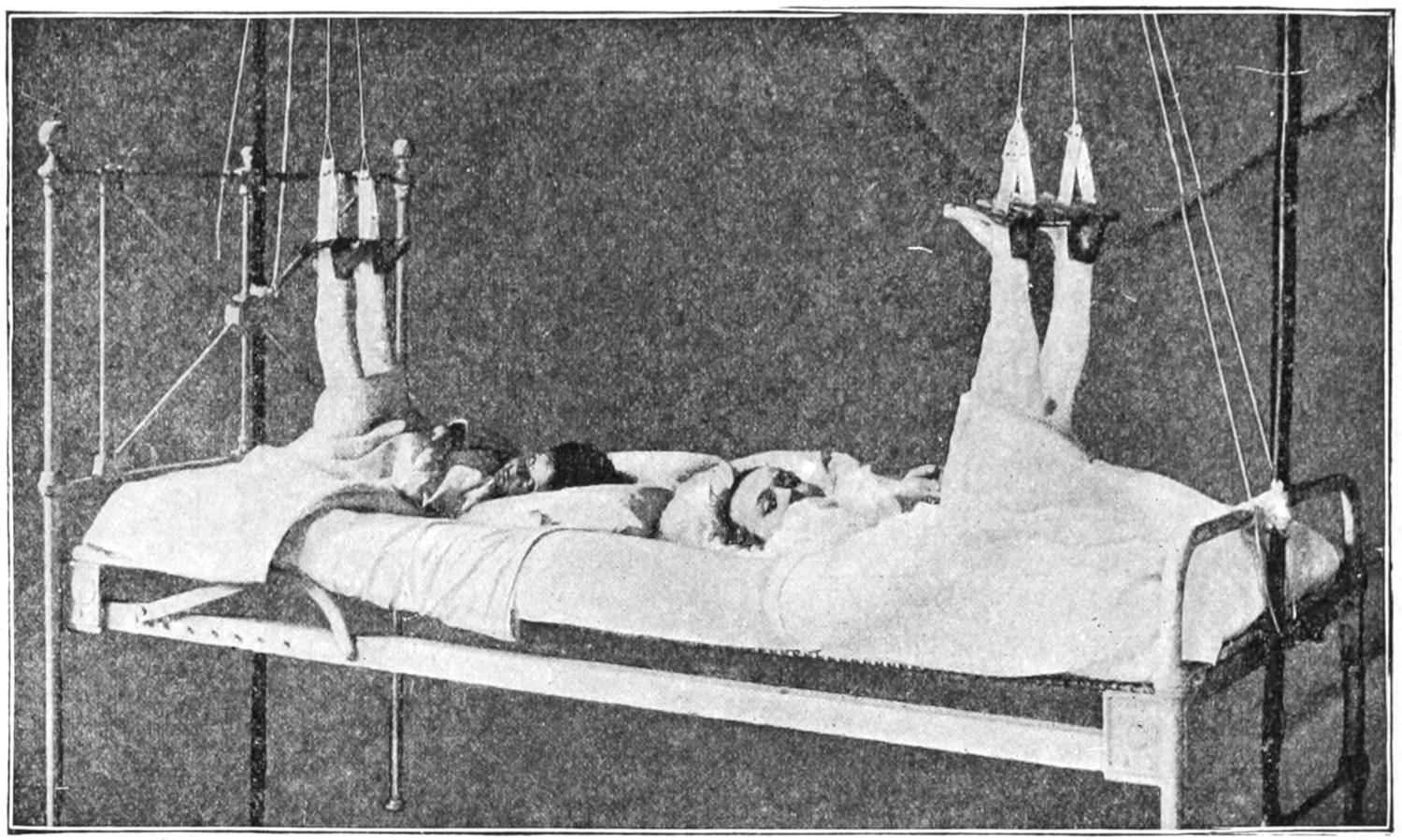
Fracture of the thigh; vertical suspension. The fracture is compound in the patient on the right. (Stimson).
During the active period of middle life the patella is the bone most frequently broken by muscular violence. In many cases it is practically cracked over the condyles, as one would crack a piece of wood over the knee. If direct force be applied, as by a fall, in connection with the above, the effect is even more marked. In such cases the fracture is sometimes comminuted (Fig. 325), or the line of fracture may run more or less perpendicularly rather than horizontally. Ordinarily, however, these fractures are transverse, while the upper fragment is pulled upward, sometimes to a considerable distance, by the powerful extensors of the leg. When the fracture runs vertically the displacement is very slight. Occasionally these fractures are compound, a most undesirable complication, since the knee-joint is thus exposed to infection, from which it suffers unless first attention be prompt and scientific. There is usually sufficient hemorrhage to distend the joint cavity, and it may at first be quite impossible to bring the fragments near enough to each other to get crepitus, but the loss of the power of extension and the evident gap between the fragments will serve to make diagnosis positive, at least in all transverse fractures. A vertical fracture without much separation is a milder form of injury which may be regarded in a much more favorable light (Figs. 326, 327 and 328).
In these transverse fractures it is rare that bony union can be secured by non-operative methods. This is not only because of the difficulty in maintaining parts in apposition, but because it is notably the case that fragments of periosteum or other tissue drop in between bony surfaces and tend to prevent their actual contact, no matter how firmly they may be pressed toward each other. Osseous union then may occur without operation, but is rare. The best that can be expected is fibrous union, the intervening fibrous band being short or long, according to the success met with in treatment and to the[517] amount of strain later put upon it by too early use of the limb. Even with two inches of fibrous tissue intervening patients are not completely disabled. The usefulness of a limb under these conditions, however, is seriously impaired. Something will depend, also, on the extent to which the joint capsule and the aponeurosis terminating the vasti muscles may have suffered.
—The non-operative treatment consists in placing such a limb upon a single inclined plane, for the purpose of relaxing the quadriceps extensor group. In this position the limb should be maintained for at least from ten to fourteen days. Some expedient should be added, so soon as swelling has subsided, by which the upper fragment can be coaxed downward toward its fellow. A neatly molded splint, formed out of gutta-percha or of plaster of Paris, may be fitted to the thigh above the fragment, held in position, and then drawn downward by elastic traction on either side of the leg, the principle of traction being thus given a special application. Something of this kind should be done if the fragments are to be approximated to each other.
Fig. 325
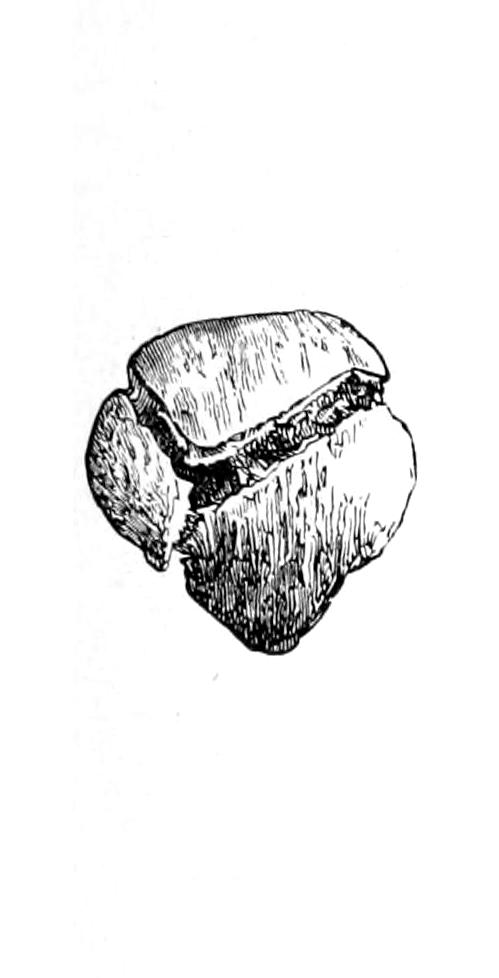
Fig. 326
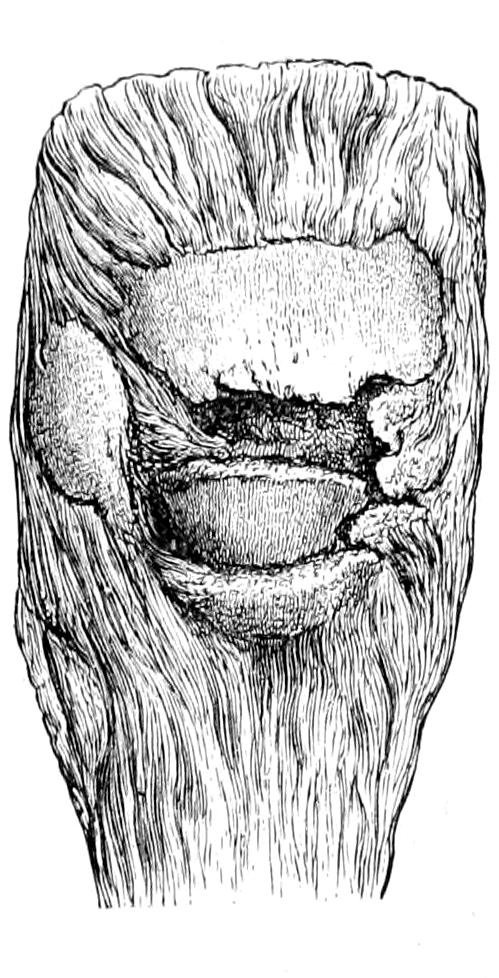
Fig. 327
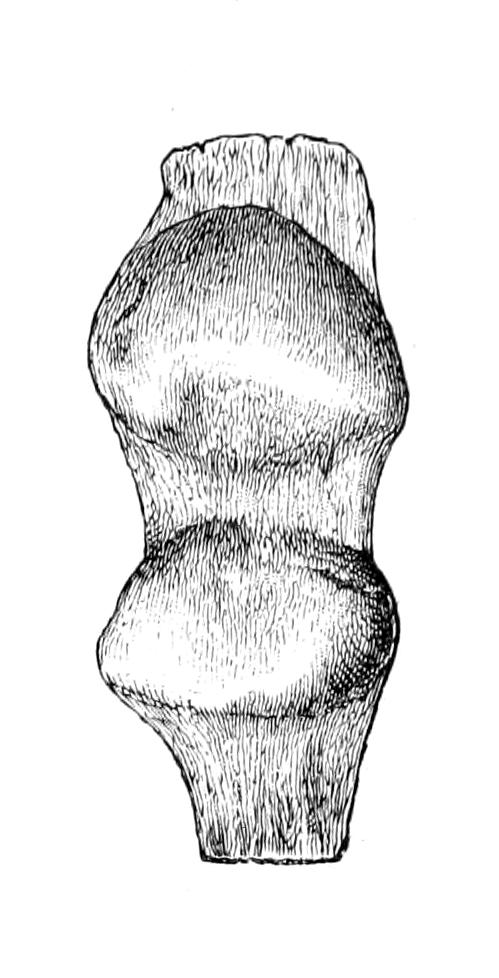
Fig. 328
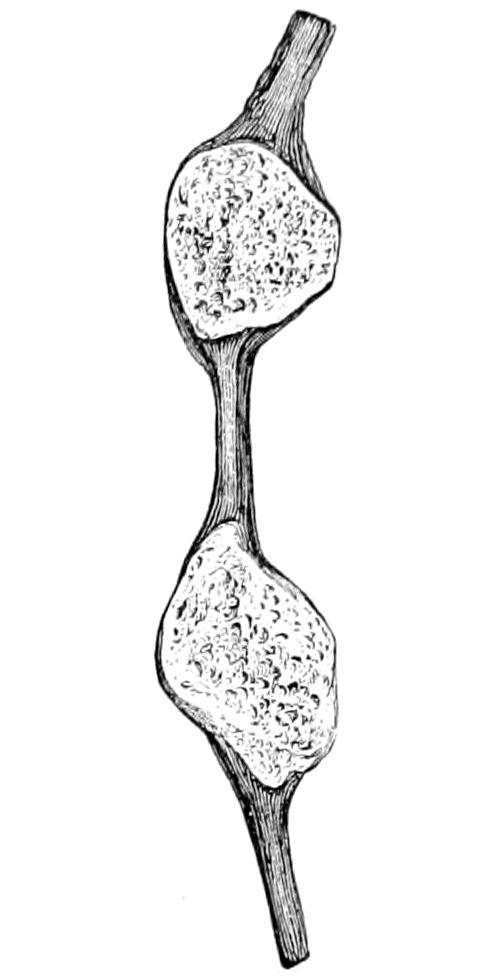
Comminuted fracture.
Stellate fracture of the patella. (Erichsen.)
Fracture of patella, united by ligamentous tissue. (Erichsen.)
Side view of same.
The more completely mechanical method, partaking of the operative, is afforded by the use of certain hooks, whose points are permitted to pass through the skin above and below the fragments and to engage in the bone. By a screw mechanism these points are drawn toward each other, and thus approximation is effected. This method was first devised by Malgaigne and is usually known under his name, although his device has been much improved. This is far from ideal, and yet has given good results in some cases. The surgeon should constantly guard against infection through the punctures.
By far the most ideal method, when it can be suitably carried out, is the open operation, a transverse incision being made across the front of the joint, which is completely opened; this affords an opportunity to empty out clots and to thoroughly cleanse it, which of itself is a great advantage, since these clots often produce subsequent adhesions. The exposed surfaces may now be freed from clot and all soft tissue, or they may be neatly sawed as near to the fractured surfaces as possible, the intent being to permit them to come into absolute and complete contact, and to hold them there by wire or other sutures, for a length of time sufficient for absolute bony union. When properly performed this operation gives ideal results; it, of course, exposes to great danger if improperly done.
Treatment by non-operative method rarely affords a useful member under an average period of from thirteen to fourteen weeks, while the operative method permits a reduction of this time to less than half. It, therefore, has obvious advantages for those (e. g., laboring men) to whom time is of great importance. The operation, however, is not[518] to be practised as a rude emergency affair, but only when we may be absolutely certain of everything pertaining to aseptic technique. After operation it is rarely necessary to use a drain, and such a limb can usually be dressed in a plaster-of-Paris splint. Compound fractures, however, will probably need drainage at least for a day or two, and because of this need may as well be operated at once. In comminuted fractures the method is desirable, since by a loop or by some other expedient fragments can be held together as in no other way (Figs. 329 and 330).
Fig. 329
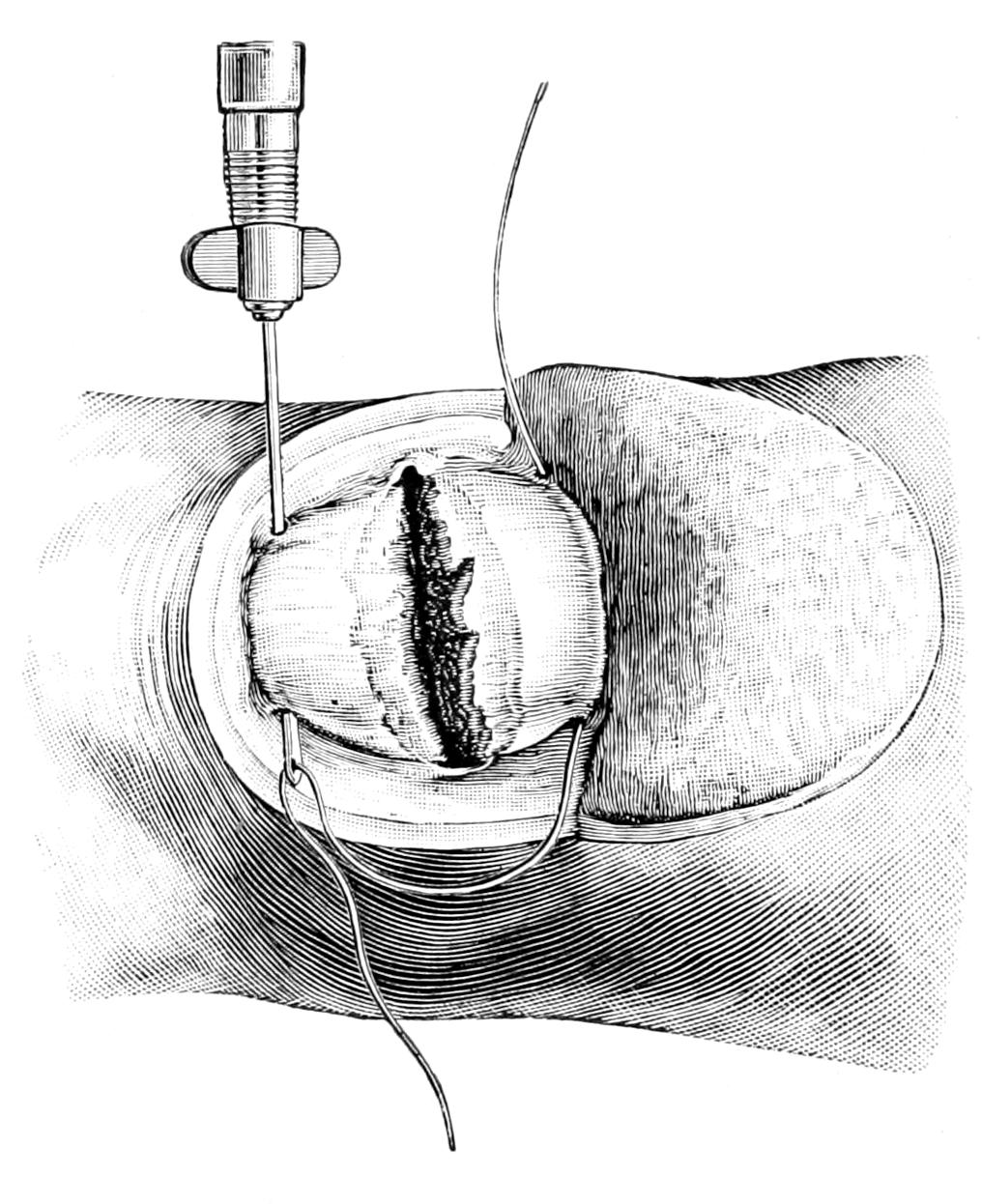
Fig. 330
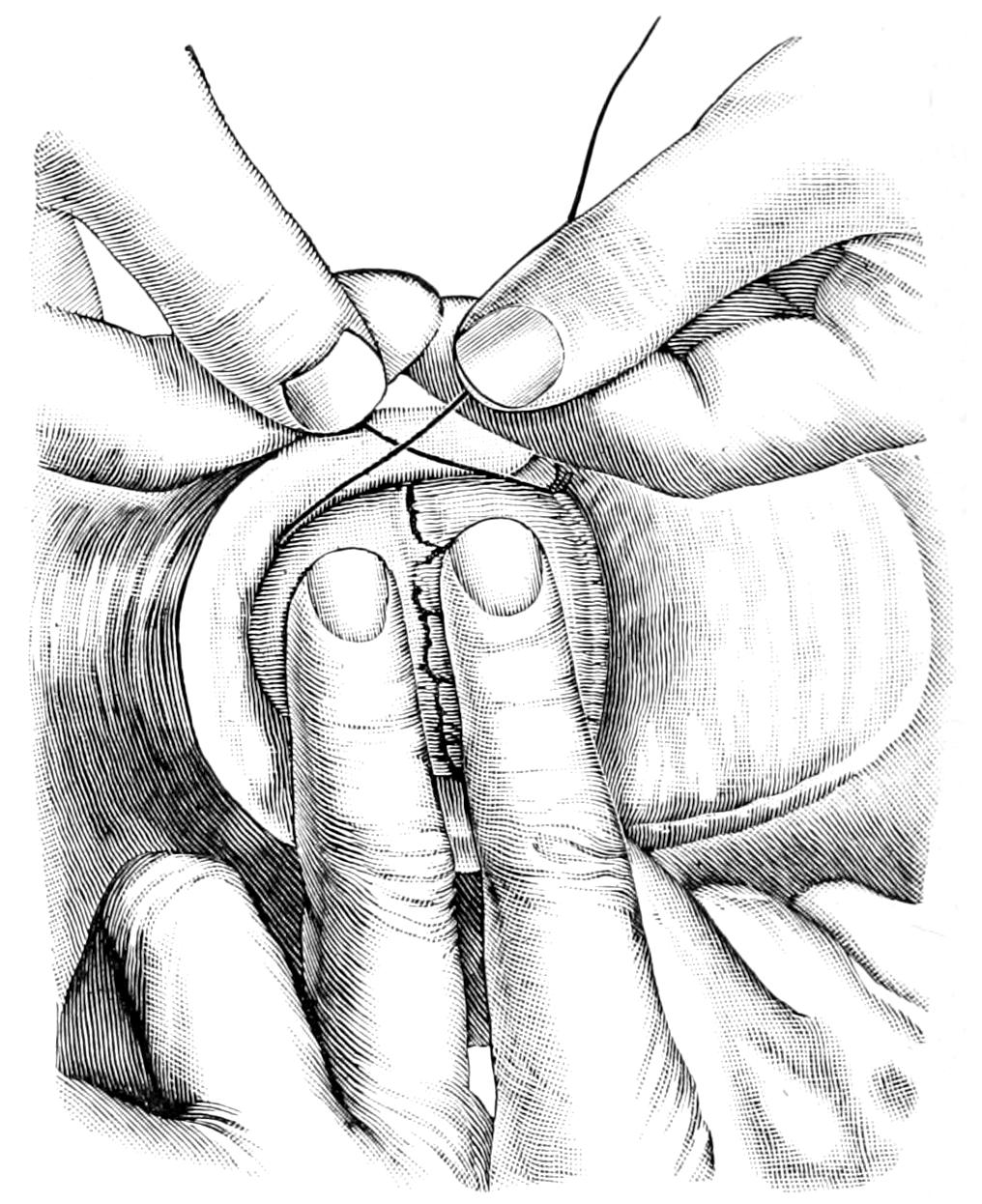
Wiring patella. (Lejars.)
Injuries to the patellar region, equivalent to fractures, are separations, either of the tendon from the bone, or of the bone from the ligament which holds it to the tibia. Such injuries can be recognized by the fact that the contour of the bone itself is preserved; in the former case it is not drawn up, although the extensor muscles have lost their power while in the latter it is drawn up, leaving a well-marked gap below it.
Remarks concerning the treatment of fractures apply equally here. Choice can be made between the operative and the non-operative treatment. In well-selected cases the former seems much the more desirable, the fibrous end of the tendon or ligament being held to the bone by strong sutures of silk or wire.
The head of the tibia is occasionally broken as the result of extreme violence, the fragment being usually held reasonably in place by one or other of the lateral ligaments. Hemorrhage into the joint will be profuse, with swelling extreme, while disability will be complete. Not a few of these cases justify operation, directed toward opening the joint, removing all clot, and fastening the fragment in place with suitable sutures (Figs. 331 and 332).
Transverse fracture below the tubercle is less rare. The insertion of the terminal ligament of the quadriceps extensor group will, in all of these injuries to the upper portion of the tibia, tend to pull up the upper fragment and make it project beneath, even protrude through the skin. Fractures of the lower part of the tibia are freer from such distorting influences. Fig. 333 illustrates the distortion produced as above, while Fig. 335 shows one of the tendencies in fracture of the lower end of the tibial shaft, which has to be overcome by correct emplacement of the foot within the dressing. Fig. 334 illustrates synostosis as the result of fracture of both bones at about the same level.[519] Torsion is a factor of no small importance in the production of most of the fractures of the leg, to such an extent as sometimes to make a completely spiral fracture, a condition generally held to be more serious than fracture of the ordinary type. The line of fracture often extends in such a direction as to leave a sharp spicule of bone close beneath the skin; here rough handling, or carelessly made pressure in the dressing, may cause a perforation within a few hours or days after the injury, by which a simple is converted into a compound fracture. Such a complication should always be avoided.
Fig. 331
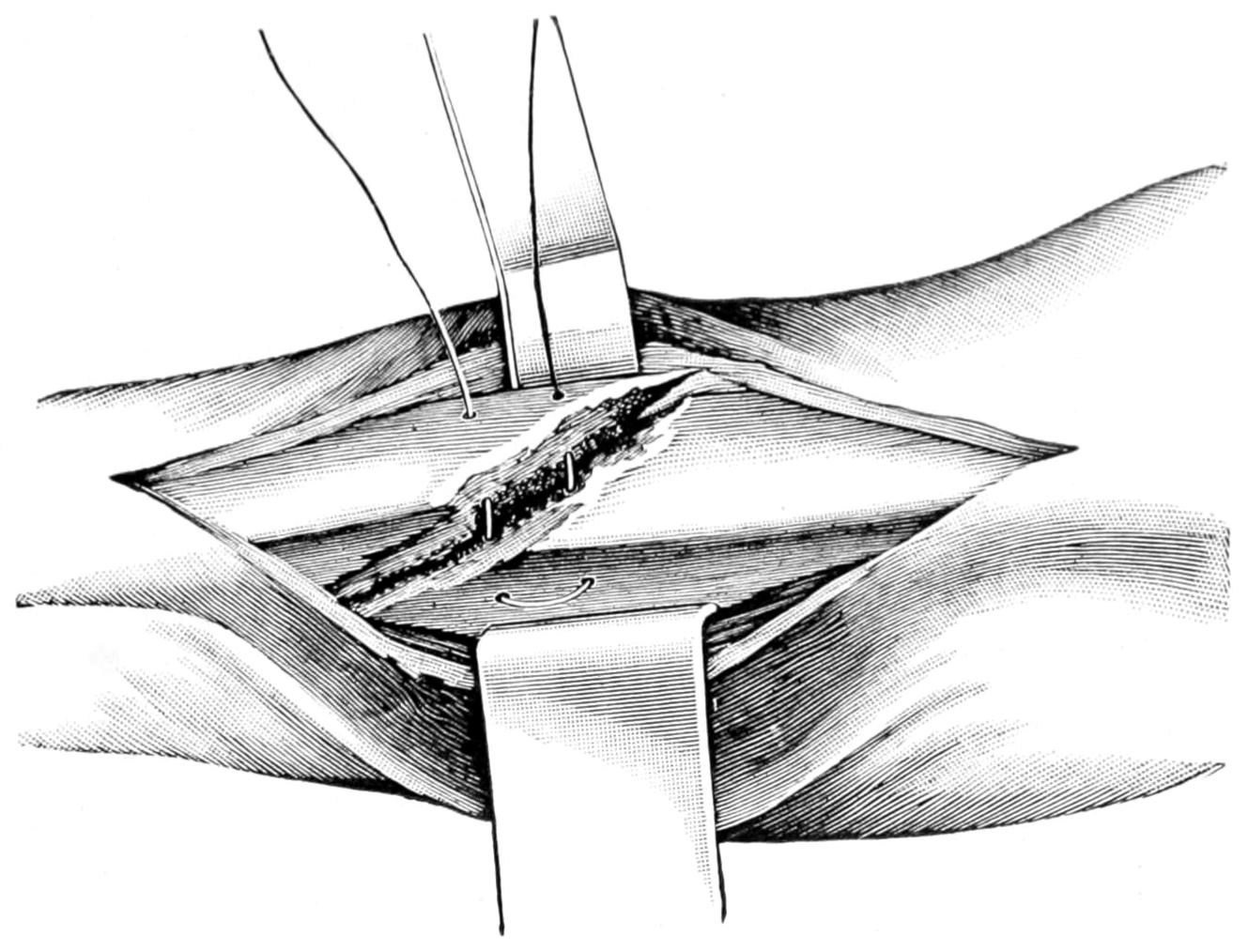
Fig. 332
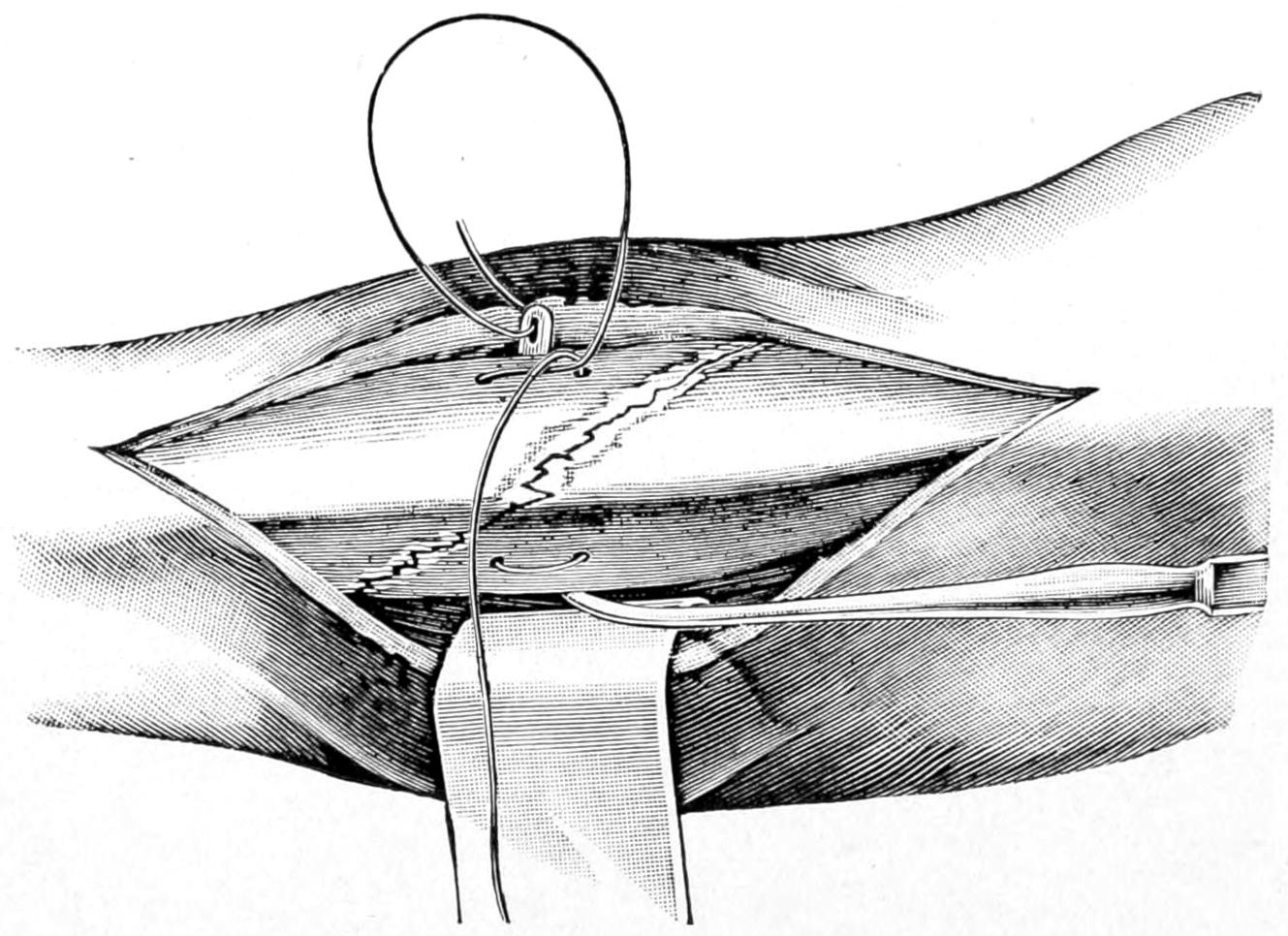
Wiring tibia. (Lejars.)
The lower end of this bone is much more often fractured than the upper, although it may be broken at any point. Into its upper termination is inserted the external lateral ligament, and this insertion may be torn off from the bone in cases of violent sprain of the knee, damage occurring which is similar to that which happens in injuries about the ankle. The upper portion of the bone lies well buried beneath muscles, and fractures here are not so easily recognized. A good maneuver for their recognition is to seize the bones at the lower portion of the leg and press them together; if such pressure gives[520] severe pain above, or if it be shown that the fibula is more movable than natural, fracture may be practically diagnosticated, even though crepitus be not detected. A skiagram would, of course, clear up such a diagnosis.
Fractures of both bones of the leg occur almost as frequently as of either alone, usually as the result of direct violence, with or without more or less torsion; as, for instance, when the foot is more or less entangled, and, at the same time, twisted at the time of injury. These double fractures are by no means necessarily placed upon the same level; thus the tibia may be broken low down and the fibula high up, so high indeed that the latter fracture may escape observation. With fracture of both bones disability becomes complete, while shortening is very likely to occur, all the muscles passing from the leg to the foot conspiring to this effect. These fractures, moreover, are often comminuted and compound, sometimes to an extent necessitating exsection of fragments or of an inch or more from the shaft of each bone. In exsection of the tibia an equivalent amount should for obvious reasons be taken from the fibula. Displacements are extremely likely to occur, and in every compound fracture the presence of the opening may be utilized for the emplacement of sutures or suitable means for enforcing approximation. Indeed, other means failing, resort may be had to this measure in order to secure an ultimately good result.
Fig. 333
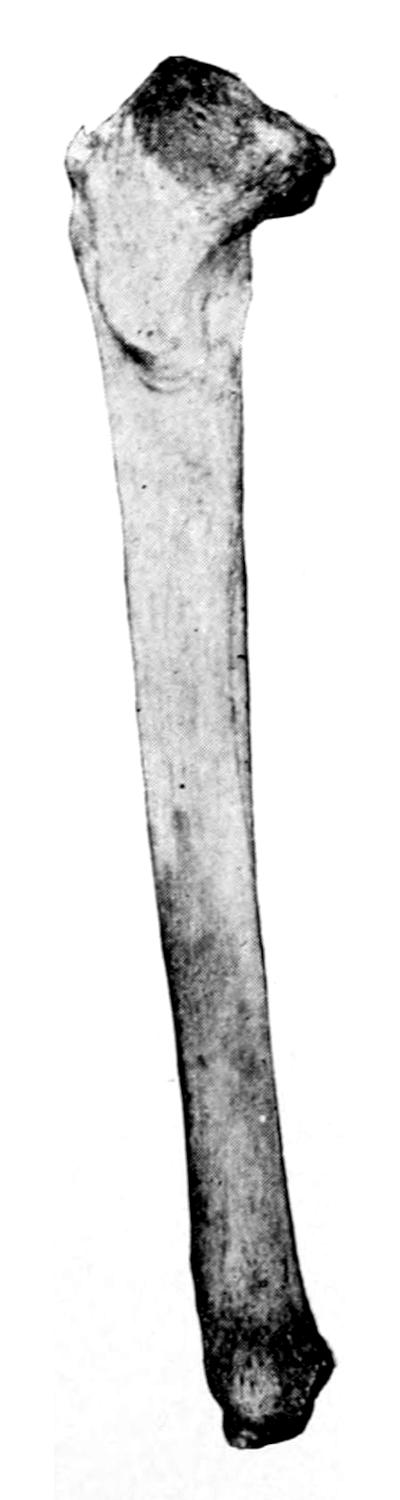
Fig. 334

Fig. 335

Fracture of upper end of tibia.
Transverse fracture, with anterior displacement. (From the Buffalo Museum.)
Line of fracture at junction of lower and middle thirds of tibia.
While wire sutures may be used as freely as may be indicated it will be well, at least in the majority of cases, to leave the ends protruding in such a way that they can later be untwisted and removed. The presence of wire after a certain length of time rather interferes with the process of ossification than helps it.
Fractures of the lower end of the leg nearly always involve the joint, to some extent at least, in respect of being accompanied by sprain if nothing else. They are accompanied by displacement of the foot, and are produced by violence, which first involves[521] the foot. The term “Pott’s fracture” is meant to include the injury originally described by Pott himself. In the typical Pott’s fracture, as shown in Figs. 336 and 337, there are a chipping off of the internal malleolus, of the outer portion of the articular end of the tibia, and fracture of the fibula a little above the joint. In spite of the classical description which Pott gave fractures of the fibula alone, those accompanied by tearing of the internal lateral ligament, or chipping off of the malleolus, are frequently referred to under the same term. The more complete the injury the greater the possibility for displacement. Eversion and outward displacement, of course, are conspicuous. Lesser degrees of injury are accompanied by less displacement, but all of these injuries will be followed by extreme swelling of the ankle-joint, which may at first make diagnosis somewhat difficult, because of the extreme tenderness which prevents the handling necessary for careful determination. It is not always easy to so completely replace the bones, when we have the combination of three fractures as above, as to get an ideal result. Nevertheless with suitable treatment usually very useful limbs are secured. When the injury has been made compound the difficulties are increased. Such a result will not be obtained, however, unless the tendency to backward and lateral displacement be overcome, when the limb is placed in its permanent plaster-of-Paris splint, as it should be after a few days. Great care should be given to this point in the management.
Fig. 336

Pott’s fracture. (Hoffa.)
Fig. 337
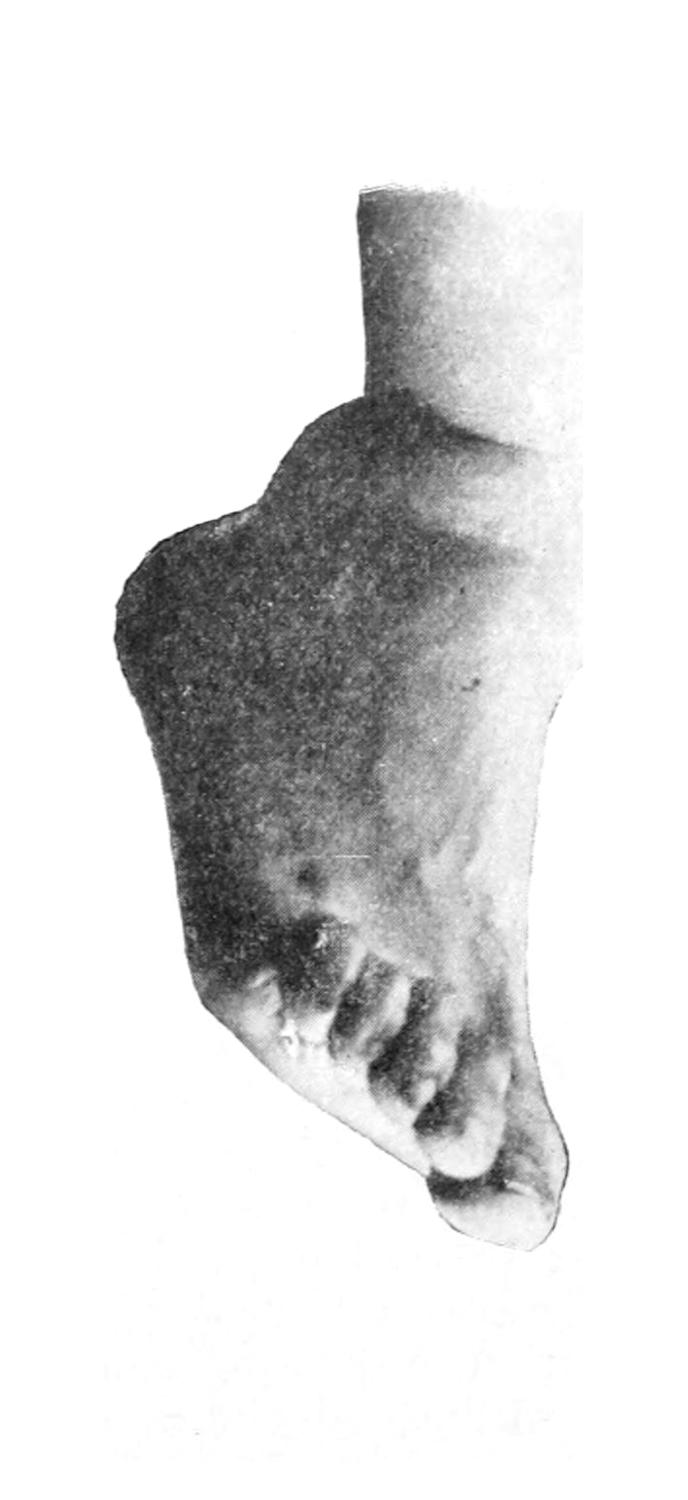
Exaggerated deformity in Pott’s fracture.
—Nearly all these fractures are likely to be followed by swelling, even to a degree which makes it impracticable to put them up in permanent dressing until the swelling has subsided. This means a period of two to several days, during which the limb should be kept absolutely at rest, and the bones maintained in apposition by side splints, while the limb is restrained within a folded pillow or other comfortable cushion. More frequently here than in any other part of the body there will form blebs or large blisters, which are most liable to occur in alcoholic subjects. The leg should be scrubbed and shaved before putting on dressings, in order that the skin may be reasonably clean before its surface epithelium is raised. Ecchymosis, infiltration, and sometimes general edema may become somewhat pronounced,[522] and the splint which would be required to fit a limb under these circumstances would soon be too large when this disturbance has subsided. The limb should not, therefore, be placed in a fixed or permanent dressing until it is in every respect ready.
While these disturbances are subsiding, or perhaps being encouraged to subside by the use of an ice-bag or of cold wet applications, extreme care should be taken that proper position and apposition are maintained. This will at times need considerable ingenuity. A delirious or maniacal patient would need restraint far beyond that required for one who is rational and docile. Moreover in all of these fracture cases which entail confinement to bed there is a tendency to deficiency of elimination which will require judicious use of laxatives and other eliminatives.
The writer prefers a well-molded set of side splints, properly padded, to any other first dressing for fractures of the leg. A limb thus dressed may be supported on a pillow and even made adaptable for transportation should it be necessary to remove the patient from one place to another. The fracture box can be well superseded by this method.
So soon as swelling has subsided, plaster of Paris should be used for a fixed dressing. The limb should be enveloped in a layer of cotton, by which the skin is protected, within which swelling may occur without much strangulation. Over this and down the front of the leg a strip of thick pasteboard should be placed, which can be moistened and made to adapt itself, or a strip of sheet tin, an inch wide, which can be made to fit the part, and upon which one may cut down later in removing the splint. This refers especially to the use of the roller bandage saturated with plaster of Paris. Molded splints can be made, as recommended for the upper extremity, out of surgeons’ lint, canton flannel, or old blanketing, while at the lower end of these splints may be incorporated, with the plaster, a strip of bandage or other material, by which a loop is formed beneath the foot, which may be utilized for the purpose of traction.
The foot should always be placed at a right angle to the leg. If there be too much muscle spasm to permit this, or make it too uncomfortable, the tendo Achillis may be divided. This position should be maintained during the period of repair, in order that so soon as one resumes the use of the limb the foot may be planted naturally upon the ground. In addition to this precaution it must be noted that backward displacement is completely overcome, and that eversion is perhaps a trifle overcorrected.
In all fractures of the lower end of the leg the foot and entire leg should be enclosed in a bandage. In fractures near or above the middle not only the leg but the lower part of the thigh should be immobilized if the promptest and most satisfactory results are to be obtained.
The limb being immobilized it soon becomes a question as to how quickly the patient can leave the bed and begin to move about on crutches. This will depend to some extent on the patient’s temperament. Timid women are less desirous of getting out of bed than are active men and children. Some patients acquire facility with crutches very slowly. Others are so tenderly built that crutches give pain and even produce crutch paralysis. It is advisable to get patients at least into the sitting posture so soon as the immobilization has been secured, while those inclined may be encouraged to use the uninjured limb and move about with crutches. A foot and leg too long kept off the ground will swell when again lowered. The later this dependent position is attained the greater the liability to edema. Patients should be cautioned about this.
The so-called ambulatory method of treatment has found favor with some surgeons. This implies something more than merely permitting motion with crutches; it means really such dressing as to permit use of the injured limb in locomotion. The various forms of splints used for immobilizing the limb in hip-joint disease may be used in this way. A useful splint is made with body and perineal bands, or an inside steel bar with ischiatic crutch and a cross-bar below the sole of the foot, on which the weight of the body may be supported. This is to be combined with a plaster-of-Paris support.
The ambulatory treatment is occasionally of value, but the advantages claimed for it have not been generally sustained.
[523]
The astragalus and the calcis suffer more often than the other tarsal bones, partly because of their size and partly because they are in the line of transmission of force as usually directed after accident. When the posterior end of the calcis is broken off there remains a fragment which is easily palpated, and which would be displaced backward and upward by the tendo Achillis were it not for the plantar fascial fibers which are inserted into it. The bone may also be comminuted, in which case that part of the foot will lose much of its shape and distinctive peculiarities. The sole will be flattened, but swelling and hemorrhage will at first be so great that there will be much difficulty in recognizing the exact nature of the injury.
The astragalus is usually broken by being caught between the calcis and the lower end of the leg. It is generally broken through the line of its so-called neck. Not infrequently one or more of the fragments is forced out of place, usually beneath the anterior tendons. When such extensive displacement occurs the fragments should be removed if the fracture is compound. In both of these bones results are generally satisfactory when displacement is not marked, also after removal of the entire astragalus. The foot and leg should be immobilized in the best possible position, and this can be best accomplished within a plaster-of-Paris dressing.
In regard to the tarsal bones, diagnosis can now be made accurately by the use of the x-rays. These bones, according to Eisendrath, may be fractured in any one of the following ways: (1) Compression, as when the weight of the body is violently thrown upon the feet; (2) sudden dorsal flexion, often with fracture of the inner malleolus; (3) forced supination or pronation, the interosseous ligaments being stronger, the bones forcibly pulling the latter apart; (4) violent traction upon the heel through the calf muscles, by which the tuberosity of the calcis may be torn from the rest of the bone; (5) extensive crushing injuries, in which several tarsal bones may be involved; (6) gunshot fractures. Some assistance in diagnosis may be obtained by computing the distance from the malleoli to the bottom of the heel, which will be shortened when the bones are compressed; or shortening of the length of the foot, or by fixed abnormal positions.
The metatarsal bones are broken by direct violence, the first and fifth being most exposed. As in other fractures of the foot contusion will be a serious feature, and swelling and laceration will frequently seriously complicate, while the fractures themselves may be compound. The same is true, also, of fractures of the phalanges, crushing and comminution being common. The matter of treatment often includes an estimation of the blood supply and of the vitality of the distal portion. The operator may sometimes temporize with an antiseptic dressing until this matter is settled. Simple fractures require only immobilization in good position.
[524]
A sprain has already been described as a momentary change of emplacement or disturbance of the normal relations between joint surfaces, which, so far as displacement is concerned, is but a momentary affair and is promptly overcome. The term dislocation implies something more permanent as well as complete in both respects. It indicates an absolute and direct separation of articular surfaces of much more than momentary duration and requiring skilled assistance for its reduction. It pertains to articular surfaces which are enclosed within a capsule. The term luxation is synonymous with dislocation. When the condition is evidently partial or incomplete it is often referred to as subluxation. As compared with fracture dislocations are about one-tenth as frequent.
Dislocations are described as compound when through a co-existing wound air may enter the cavity of the joint, and as complicated when accompanied by other lacerations or injuries. When unaccompanied by these conditions they are described as simple.
To dislocations which result from external violence or from sudden muscular action is given the term traumatic. Pathological dislocations are those which are brought about by slow morbid processes, muscle spasm being the most prominent factor in their production. A third variety of dislocations, the so-called congenital, do not belong strictly in this class; by common consent the term is applied to congenital abnormalities where, from errors in development, normal emplacements and relations are altered.
The distal bone is the one described as that which is dislocated; thus we speak of dislocations of the forearm upon the arm, of the leg upon the thigh, etc.
Subluxations or incomplete dislocations are frequently accompanied by fracture of a bony prominence, e. g., the rim of the acetabulum, the coronoid process of the ulna, etc. The direction in which the distal member of the joint has been displaced is indicated by one of the common terms, as forward, inward. A consecutive or secondary dislocation implies a shifting of position from that at first occupied by the displaced bone end. These injuries may occur at any age, although usually during the more active period of life, from childhood to middle age, when mankind are more subject to injuries.
Certain conditions predispose to dislocations. Abnormalities or previous injury or disease of joint structures figure especially in this respect. A joint already relaxed by hydrarthrosis will exercise a relatively small restraining influence and a subluxation, at least, may easily occur.
The immediate cause is violence, either from without or within, generally the former. This may be direct, as from a blow, or transmitted, as when the shoulder is displaced by a fall upon the open hand. It occasionally happens that the component bones of a dislocated joint were in a position of extreme flexion or extension at the time of injury. The factors of leverage and spiral tension or wrenching are also important ones. Luxation from muscular activity is occasionally met with; most frequently when the lower jaw is dislocated by the act of yawning or violent laughter. The shoulder has been displaced in a violent effort at throwing or pitching a ball, or in wild gesticulation.
A few individuals have been in the habit of exhibiting themselves whose normal ligament and joint arrangements are so lax that they can voluntarily displace one or more of them and as easily replace them. These may be spoken of as instances of voluntary dislocation.
A joint once displaced may never fully recover its normal degree of tension, and will yield more readily to subsequent similar injuries. In this way there may occur so-called recurrent or habitual dislocations. Expressions of this kind are seen most often in the lower jaw and in the patella.
Actual injury to tissues is to some extent unavoidable. In arthrodial joints the capsule is nearly always lacerated, at least upon one side. In hinge joints both lateral ligaments are likely to be ruptured. It is probable, however, that about the maxillary[525] joints the ligaments may stretch without tearing to any extent. Not only are ligaments torn, but bony prominences are frequently detached, while sometimes there is extensive tearing away of tissue.
In connection with these injuries to joints proper other complications may occur, such as fractures of prominences about joints and epiphyseal separations, or such injuries as compound fracture of the neck of the humerus with dislocation of its head. Furthermore, bloodvessels are occasionally lacerated and nerves are frequently injured. This latter lesion is liable to occur after shoulder dislocations, the head of the bone injuring the circumflex nerve, paralysis of the deltoid being the consequence. This is a feature of the injury, and yet the result has often been unjustly imputed to the physician in attendance. Even a momentary contusion of the nerve may be followed by lasting effects, for which the medical attendant should be held blameless. Other injuries, e. g., contusions or lacerations of nerves, may occur about any of the joints.
Dislocations of the spine subject the cord to a special class of injuries which will be dealt with later in this work. In very rare instances the head of the humerus has been forced within the thorax or the head of the femur within the pelvis, these, injuries being practically always fatal.
Compound dislocations rarely occur about the jaw or shoulder. They pertain usually to the joints below. In every case of such character the question will be promptly raised whether a more or less complete exsection of the joint will not be preferable to mere reduction with the ensuing probability of ankylosis. Such injuries will, under all circumstances, require aseptic measures.
So far as repair is concerned, dislocations by themselves are so rarely fatal that there have been but few opportunities for a study of tissue recovery under these circumstances. It is apparent that repair is complete, for after almost any simple dislocation there is restoration of function.
The obstacles to reduction are spasm of muscles pertaining to the injured limb, by which the dislocated bone end is firmly held in its abnormal position, and, in those joints provided with a capsule, the fact that the head of the bone is frequently forced out through a comparatively small opening, through which it is only with the greatest difficulty reduced. It is a part of the manipulation in most cases to enlarge this rent in the capsule, after which reduction is comparatively easy, although impossible until it is accomplished.
Dislocations which have long gone unreduced are called old, inveterate, or ancient. By common consent a period of six weeks has been fixed, beyond which the dislocation is spoken of as old or ancient; up to that time it is usually described as unreduced. In proportion to the length of this period the difficulties of reduction are materially enhanced. So soon as a dislocated joint has been put at rest, i. e., fixed by muscle spasm and by the timidity of the patient, the blood which has been poured out will begin to coagulate and conditions are soon favorable for organization of clot and formation of adhesions in abnormal position. In the course of a few weeks these adhesions become strong, and in the course of months they are frequently stronger than the bone itself, which has been disused and has undergone a certain amount of fatty atrophy. Thus it happens that even with well-directed effort the bone will yield before the adhesions, and thus, in spite of every precaution, fracture sometimes complicates the effort to reduce these ancient dislocations.
So generally is this fact now recognized that surgeons do not hesitate to make open incisions for the purpose of separating adhesions and reopening what remains of the capsule in the endeavor to replace the head of a bone. Nor do they hesitate sometimes to cut down upon the latter and exsect rather than run the risk of more extensive injury.
Efforts at reduction under these circumstances subject the patient not only to risk of failure, or of fracture of bone ends, but to rupture of vessels or laceration of nerve trunks. I recall seeing one case of enormous traumatic aneurysm of the axillary artery which was brought about by unsuccessful attempt in this direction.
The cardinal indications of a dislocation are deformity with alteration in contour and position of the affected joint. It usually happens that the dislocated bone ends cannot be felt in normal position, but are felt somewhere else in the vicinity. About the[526] shoulder and hip of stout or fat individuals it may not be easy to feel the head of the bone, but unless the case be complicated by a fracture it can usually be detected by aid of anesthesia. The deformity may include a lengthening or shortening of the limb, apparent or real, as well as abnormal eversion or inversion, or other peculiarity of position.
Whatever alterations in position appear will be accentuated by spasm of the muscles which pertain to the movement of the affected joint or even of the entire limb. These are usually so tightly contracted as to form a complicating feature of such cases and to lead to that loss of mobility which is diagnostic of every dislocation. Limitation of motion is not entirely a matter of muscle spasm. It is not under voluntary control and subsides only under anesthesia. To some extent motion may be limited by escape of the head of a bone through a small rent in the enveloping capsule, by which it is afterward tightly clasped. This is particularly true of the shoulder and hip. Certain dislocations of the fingers or thumbs are also made more rigid by fixation of the tendons, which become tightly stretched within the neighboring tendon sheaths.
A sort of crepitus, which may be easily mistaken for that of fracture, is occasionally detected during the examination of a dislocated joint. It lacks the peculiar grating character of true bony crepitus.
In addition to these features there are certain subjective symptoms, of which loss of function is the most prominent, while pain is a more or less frequent but variable accompaniment, and dependent on the amount of tissue injury or pressure upon nerves. Moreover, the displacement once completely rectified (“reduced”) does not tend to recur, as is the case with fractures.
The statements made above refer almost entirely to recent and traumatic dislocations.
Pathological dislocations are those which are produced gradually and through the mechanism of disease affecting the joint structures. The head of the bone is gradually drawn out of the acetabulum, in tonic spasm of hip-joint disease, by the continuous action of muscles, the result being the complete displacement of the bone from its original socket, or what is known, at the hip, as the migration of the acetabulum, where its upper margin, being softened by disease, is gradually extended and altered, so that the femoral head rests an inch or more higher upon the side of the pelvis than is normal. Pathological dislocations, then, may occur both in the course of the infectious joint diseases as well as in the neuropathic.
Congenital luxations are those which occur from defect in the shape or arrangement of joint structures, permitting a departure from the normal standard. While no joint in the body is exempt from abnormalities of this description, the congenital hip dislocations are those which have attracted attention by their frequency and the disability which they produce.
While the general character of these changes is easily made out by the ordinary methods of examination, coupled with a suitable history, a well-made skiagram will tell at a glance a story which it may take some effort to elicit by other means; hence radiography has here been of great value to the surgeon. Congenital dislocations are devoid of nearly all the features which characterize traumatic dislocations, and their consideration will be found in the chapter on Orthopedics.
Differential diagnosis as between fractures and dislocations is not always easy. Furthermore it is frequently the separation of a prominence by fracture which permits of dislocation, this being particularly true of the elbow and the ankle. The extent of a fracture may seriously complicate the problem of treatment, as, for instance, when the head of the humerus is not only dislocated below the clavicle but separated from the shaft by fracture at the surgical neck. A dislocation made possible only by fracture will not remain reduced as will one which is simple and uncomplicated, while it will display even a greater amount of motility and displacement. Other complications may occur, many of which are common both to dislocations and to fractures in the vicinity of joints, such as lacerations of bloodvessels or nerve trunks, pressure upon the latter, compound injuries with infections, etc.
[527]
The essential requisite of every case is complete reduction or replacement of the dislocated bone end. The earlier this is attempted the better the result. Brief as such a statement is, dislocations frequently offer considerable difficulties, both in reduction and in maintenance in proper position with the necessary physiological rest of the injured part. Thus dislocations of the clavicle, which can hardly occur without considerable injury to the ligaments, may be reduced with slight effort, but are kept in place with difficulty. The simplicity of the after-treatment is proportionate to the difficulty experienced in reduction, so that while “to put the part in place and keep it there” sounds very simple, it will often perplex the ingenuity of the surgeon.
Reduction having been effected, rest is the essential feature of the after-treatment, which should be absolute for a few weeks and relative for many months. Should reaction be extreme, ice-cold applications will afford relief.
The causes which prevent reduction of dislocation are either those attributable to ignorance, carelessness, or failure in diagnosis on one hand, or, on the other, mechanical difficulties, including “button-holing” of the capsule around the expanded end of a bone or the interposition of some of the adjoining tissues. Dislocations of the class referred to above as unreduced or ancient, offer great difficulties, proportionate to their duration, which are due to the formation of adhesions that sometimes take place and become very dense. Judgment, skill, and effort are needed in their management. A dislocation which has become unreducible is only to be treated by arthrectomy and the establishment of a false joint. Nevertheless in a small proportion of cases, especially of the hip and shoulder dislocations, the adhesions which first form gradually relax, and in time there is formed a natural substitute for a joint which may be regarded as a nearthrosis, and which will sometimes prove as serviceable as any result afforded by arthrectomy. The duration of time after which reduction is impossible or impracticable varies so widely with different cases that it can scarcely be stated. It rarely is more than a few months and often but a few weeks. It is greater when it is a ball-and-socket joint which is affected.
Nearly everything that has been stated in the previous chapter concerning compound fractures applies here to compound dislocations. They are subject to the same dangers, both of infection and of injury to important adjoining structures. There is the same necessity for aseptic management if the case be seen early, and for antiseptic treatment, including drainage, if seen late. In many instances there is so much liability to subsequent ankylosis that the first treatment may well be made to include an arthrectomy, or the total removal of a small bone, e. g., the astragalus. Fortunately compound features are less frequent in dislocations than in fractures.
Unless accompanied by fracture there is but one direction in which the condyle of the inferior maxilla can be dislocated, i. e., forward. One side or both may be affected, i. e., dislocation may be unilateral or bilateral, the latter being more frequent. It is rare during the extremes of age, and most common during middle life. There is considerable variation in the degree of tension of the capsule of the maxillary joint. In some it is so loose that dislocation may occur during the act of yawning or vomiting. Ordinarily it occurs only as an expression of violence from without. By a blow which shall thrust the jaw forward, whether the mouth be closed or open, the ramus may be made to carry the condyle over the articular eminence. The capsule is not necessarily torn, but is always tightly stretched, while as a reflex result the temporal muscle is thrown into a condition of tonic spasm by which the jaw is fixed and firmly held in its abnormal position. This produces the symptoms, then, of a more or less widely opened mouth, with rigidity and inability to close it, with protrusion of the chin and tense contraction of the temporal muscle, which can be easily recognized. When the dislocation is[528] unilateral the symptoms are essentially the same, save that the protrusion is toward the side that is injured.
—The method of reduction is simple and consists in depressing the angle of the jaw, while, at the same time, the chin is supported and carried both upward and backward. If temporal spasm be not too pronounced the reduction is rather easy and may be effected while the patient is seated in a chair, the surgeon standing in front of him and grasping the jaw with the fingers of each hand, while the thumb is utilized within the mouth to press the angle of the jaw downward and backward. At the same time the fingers should lift the chin. The operator should protect his thumbs by wrapping them with some material in order that they may not be injured by the patient’s teeth. Should muscle spasm offer much resistance it would be well to administer nitrous oxide or one of the other anesthetics, at least to the point of primary anesthesia, with sufficient relaxation of muscle to make reduction easy. When once this has been effected the lower jaw should be bound to the upper and kept at rest for at least two weeks. When this injury has taken place it is likely to recur with much less effort until it becomes almost a habit.
Fig. 338
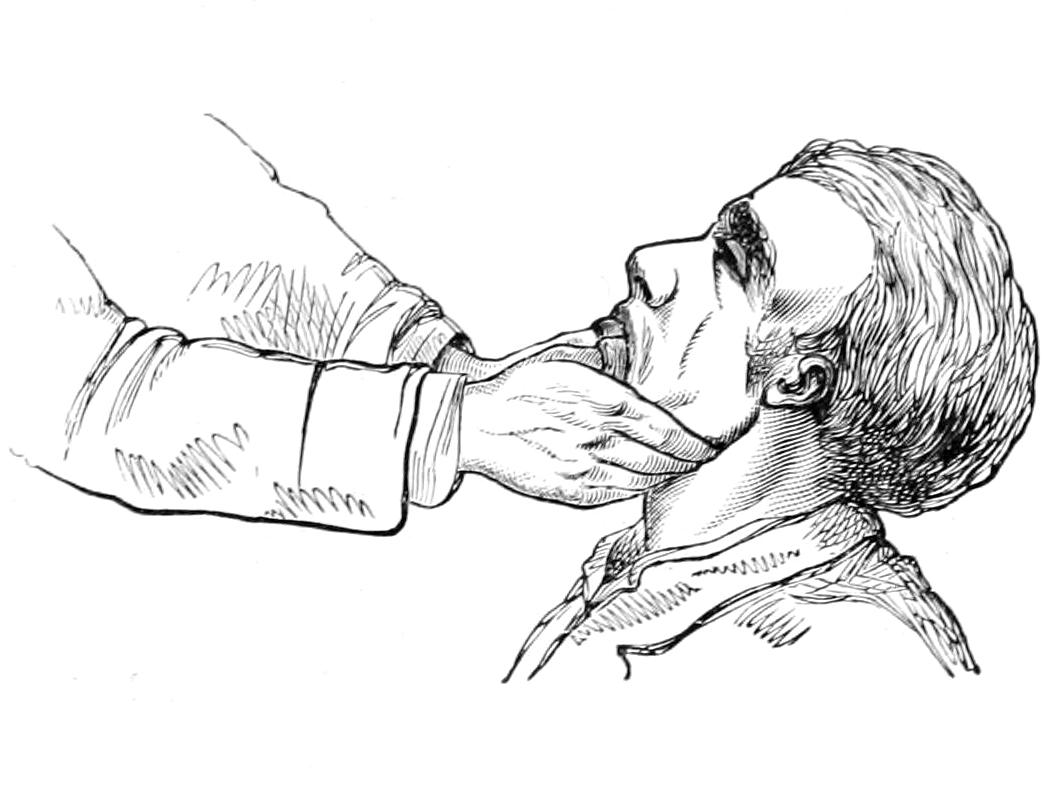
Fig. 339
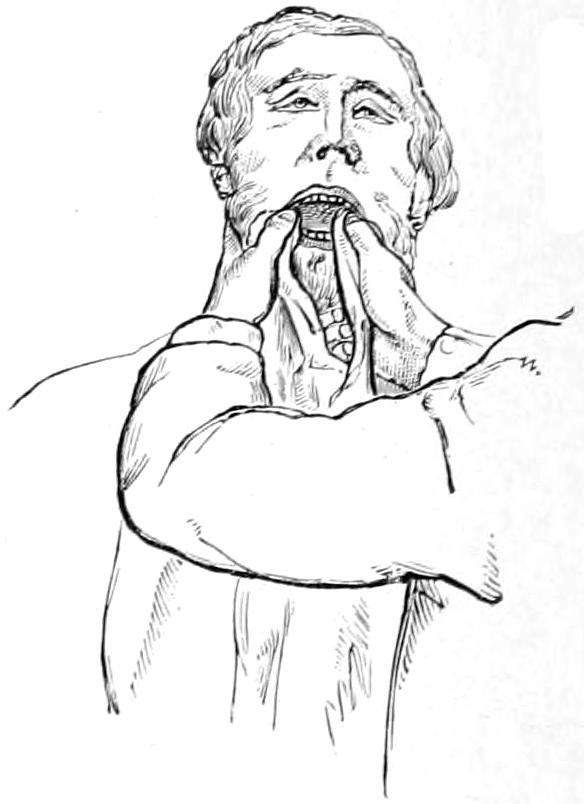
Reduction of dislocation of lower jaw.
There is a condition of relaxation of the capsule and elongation, with abnormal loosening of the interarticular fibrocartilage, peculiar to this joint, by which it has too free play, to such an extent that a clicking sound in its movements may be frequently heard by others than the patient. This condition is either congenital or the result of previous injury, and is one for which little can be done, although this explanation should be afforded to all who suffer from it.
The cartilages of the larynx are sometimes displaced as the result of direct violence applied to the anterior region of the neck. Almost any lesion of this character may take place between the independent cartilages of the larynx or the attachments of the larynx to the hyoid. The injury may simply give rise to pain and soreness, or may cause so much interior damage as to be quickly followed by edema of the glottis and suffocation. If the latter be impending a quick tracheotomy should be done, after which time may be afforded for such replacement as may be required, by manipulation, and subsidence of swelling with relief from occlusion of the respiratory tract.
The various portions of the sternum, especially the upper and the lower, may be displaced as the result either of direct violence by forcible backward flexion, or by muscular action accompanied by flexion of the trunk and neck. When the latter, it is usually forward; when produced by violence, it is usually backward.
[529]
These displacements are sometimes so easily reduced by mere pressure as to make it almost impossible to retain them. At other times anesthesia with firm pressure, accompanied by flexion of the trunk backward or forward, may be required; reduction has been possible sometimes only through incision and by the use of instruments applied as levers, or by the use of a screw driven into one of the fragments, thus affording a handle by which to manage it. Serious dislocations are frequently accompanied by fractures of the ribs or of the sternum. The same fixation of the thorax is required as in fractures of these parts, and should be conducted in the simplest manner possible.
To displace a rib from its sternal connections requires actual fracture of bone or cartilage. Forward dislocation at its posterior and spinal connection, especially of the eleventh and twelfth ribs, has been described. Considerable effort is necessary for its production, and the case should be treated on its individual merits.
Either end or both ends of the clavicle may be dislocated. Its sternal end may be thrown in any direction but downward; its acromial end in any direction, although usually upward. Dislocations of the sternal end can only occur in consequence of serious damage to the sternoclavicular ligaments, because of which, and in the absence of a socket, it is extremely difficult to maintain the parts when restored to position. Violent backward traction upon the shoulder permits anterior displacement when the joint is thus weakened. Backward displacement is usually the result of indirect violence when the shoulder is forced forward and inward, while upward displacement is the result of tilting which occurs when the shoulder is violently depressed. Respiration is generally more or less disturbed, while in backward luxations deglutition may be made difficult and painful.
Reduction is not difficult to effect, but extremely difficult to maintain. Pressure in the proper direction, accompanied by traction upon the shoulder, suffices for the former. For the latter there should be a combination of fixation of the shoulder and arm with proper traction, and at the same time pressure upon the end of the clavicle. For all of the clavicular dislocations the dressing and position advised by Dr. Moore, of Rochester, and referred to in the chapter on Fractures as his double figure-of-eight, serves admirably for maintaining the proper position of the shoulder, while pressure can be made by a pad, retained either by adhesive plaster or by some further addition to the dressing itself. (See p. 494.) Acromial dislocation is usually in the upward direction, and is produced by violence upon the shoulder, which has expended itself in rupturing ligaments rather than in fracturing the acromion process. The indication here is to keep the shoulder elevated by any dressing which will accomplish the purpose and the clavicle bound down.
Fig. 340
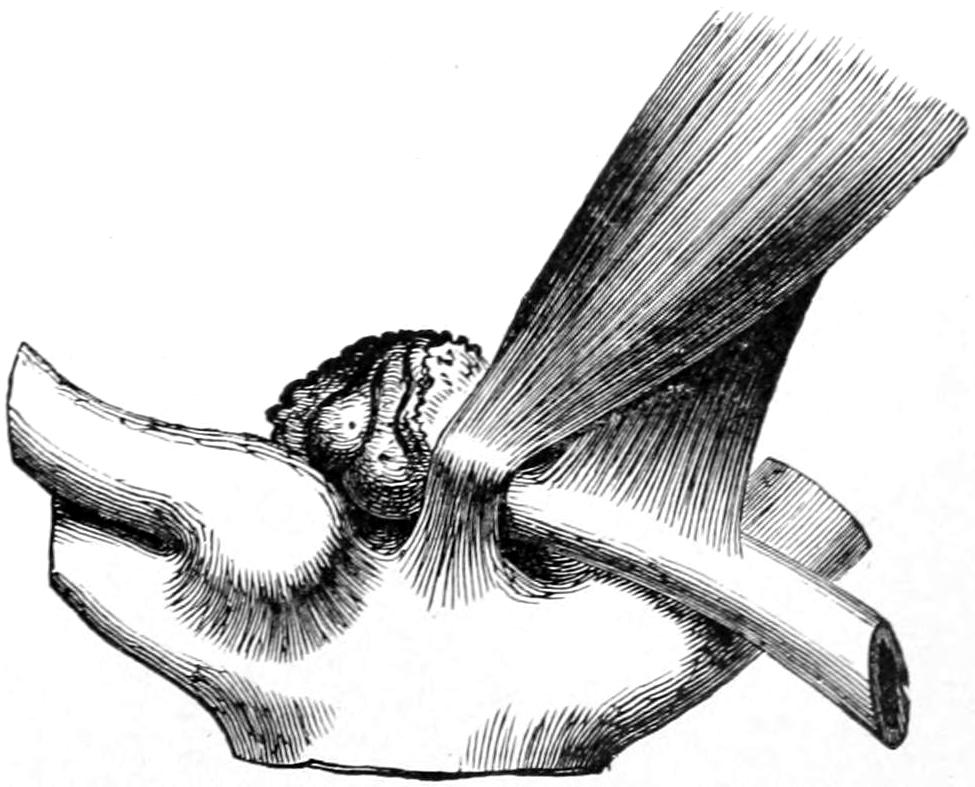
Position of clavicle in dislocation of sternal end upward.
Dislocation of both ends, i. e., complete loosening of the bone, occurs occasionally, in which case the indications already given are reinforced, while the difficulties of treatment are considerably aggravated. Here the shoulder should be kept upward, outward, and backward, and the clavicle retained by pressure or some other means.
—Clavicular dislocations yield fair results to intelligent treatment. Ideal results are difficult to secure without coöperation on the part of the patient. Functional results, however, are usually satisfactory.
[530]
The upper end of the humerus is attached to the margin of the glenoid cavity by a capsule which has a certain degree of elasticity, and which resembles a short section of a sleeve or a cuff. It is sufficiently loose to permit a wide range of motion, and were it not for the acromial process above it there would be as much motility in the upward direction as in any other. It is not the capsule which keeps the articular surfaces together, but the tension of the muscles which are wrapped around the shoulder-joint, all of which contribute to this effect. The glenoid cavity is made a more complete socket by a fibrocartilaginous rim. Thus a certain degree of subluxation or displacement may be permitted without very serious damage to this rim and capsule, but a complete dislocation is hardly possible without more or less laceration. The prominence and exposure of the joint and its natural freedom of motion help to account for the fact that more than half of all dislocations occur here, and that this rarely ever occurs in children or in the aged, in whom the violence which may be expanded produces either epiphyseal separations or fractures of the surgical neck. The relation of structure to function also accounts for their far greater frequency (i. e., four to one) in men than in women. The influence of atmospheric pressure should not be forgotten, as in the shoulder this affords a force of some fifty pounds, and in the hip of nearly double that amount, of pressure.
Fig. 341
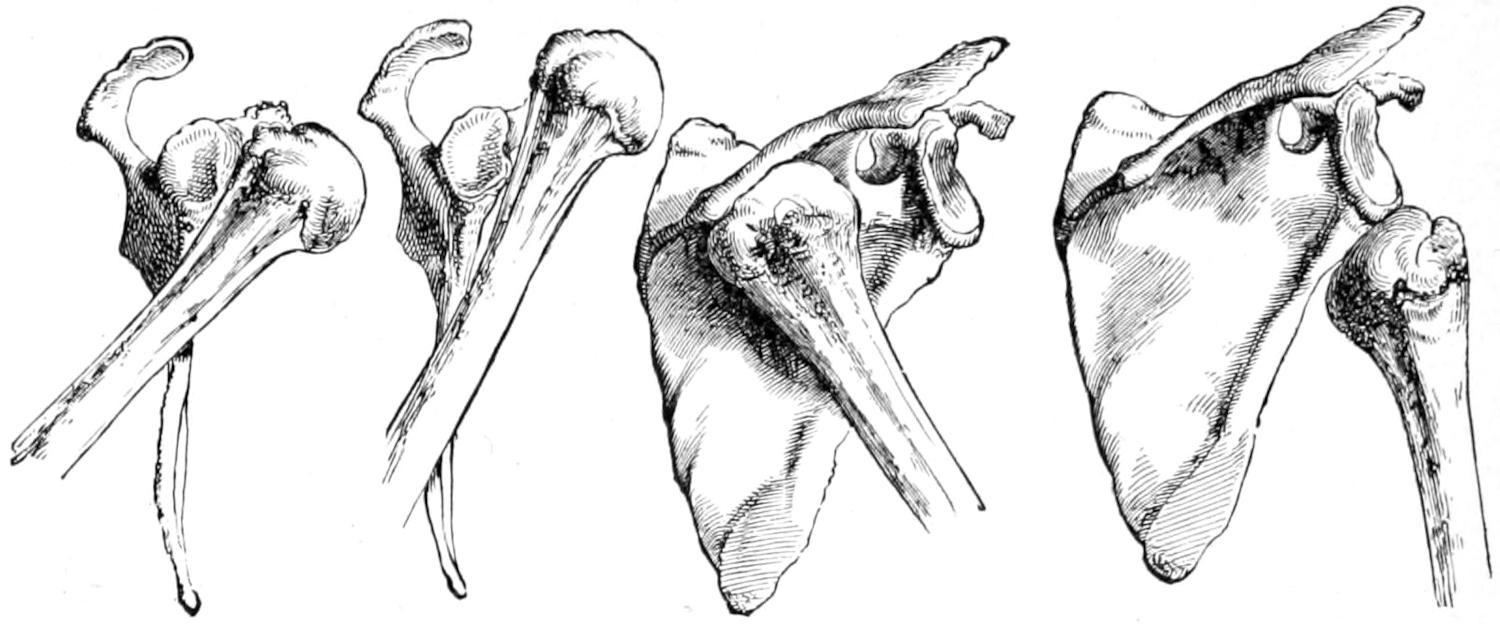
Subcoracoid.
Subclavicular.
Subspinous.
Subglenoid.
Dislocations of the head of the humerus. (Erichsen.)
Fig. 342
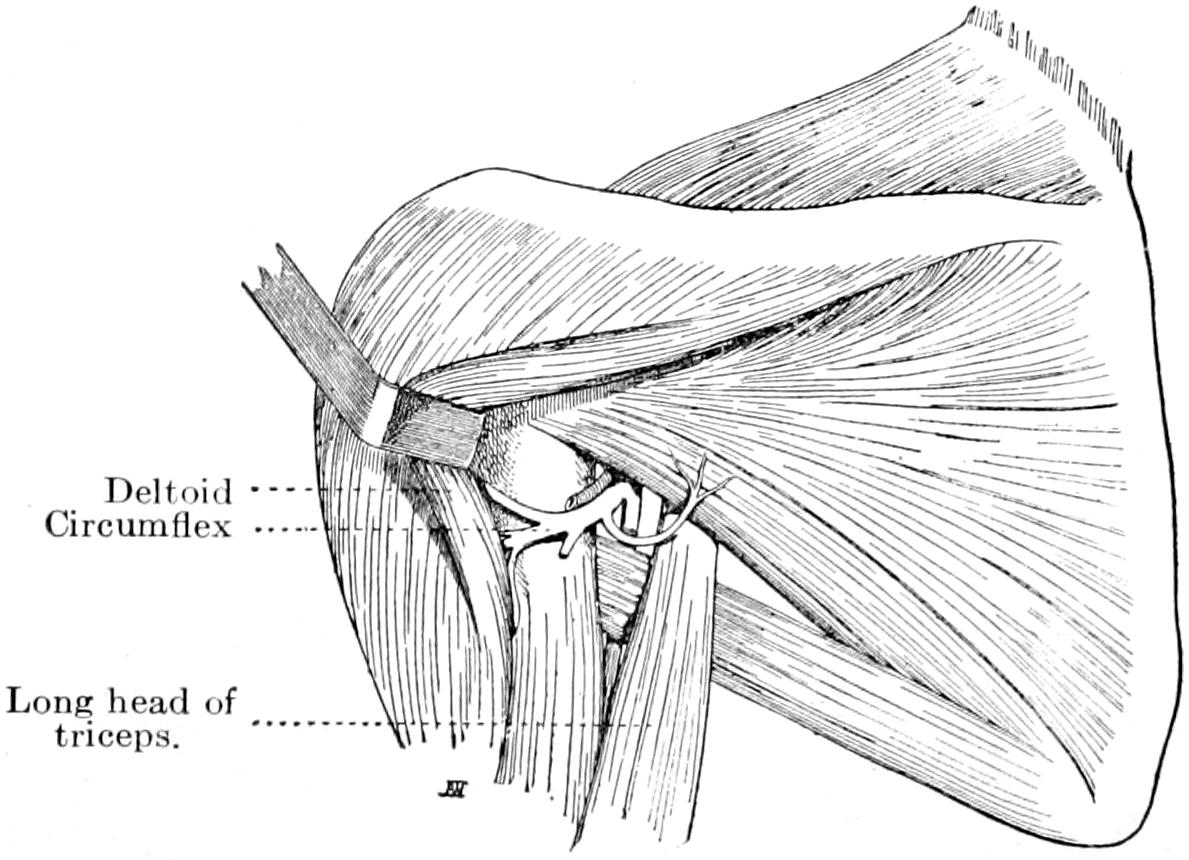
Relation of circumflex nerve to the head of the humerus, explaining mechanism of deltoid paralysis. (Marion.)
For convenience of description, and in the order of their frequency, shoulder dislocations are referred to as anterior, downward, posterior, and possibly upward, when combined with acromial fracture. Anterior displacements vary in degree, so that they[531] are described as subcoracoid or subclavicular. Complete displacement in this direction can only occur through a rent in the anterior portion of the capsule, while the subclavicular muscle is pushed away or torn. The nearer the head of the bone rests to the sternum the greater the amount of laceration of the capsule, while its posterior portion is either stretched tightly or torn. In aggravated cases the tendon of the biceps is also torn out of its groove (Figs. 341, 343 and 344).
Fig. 343
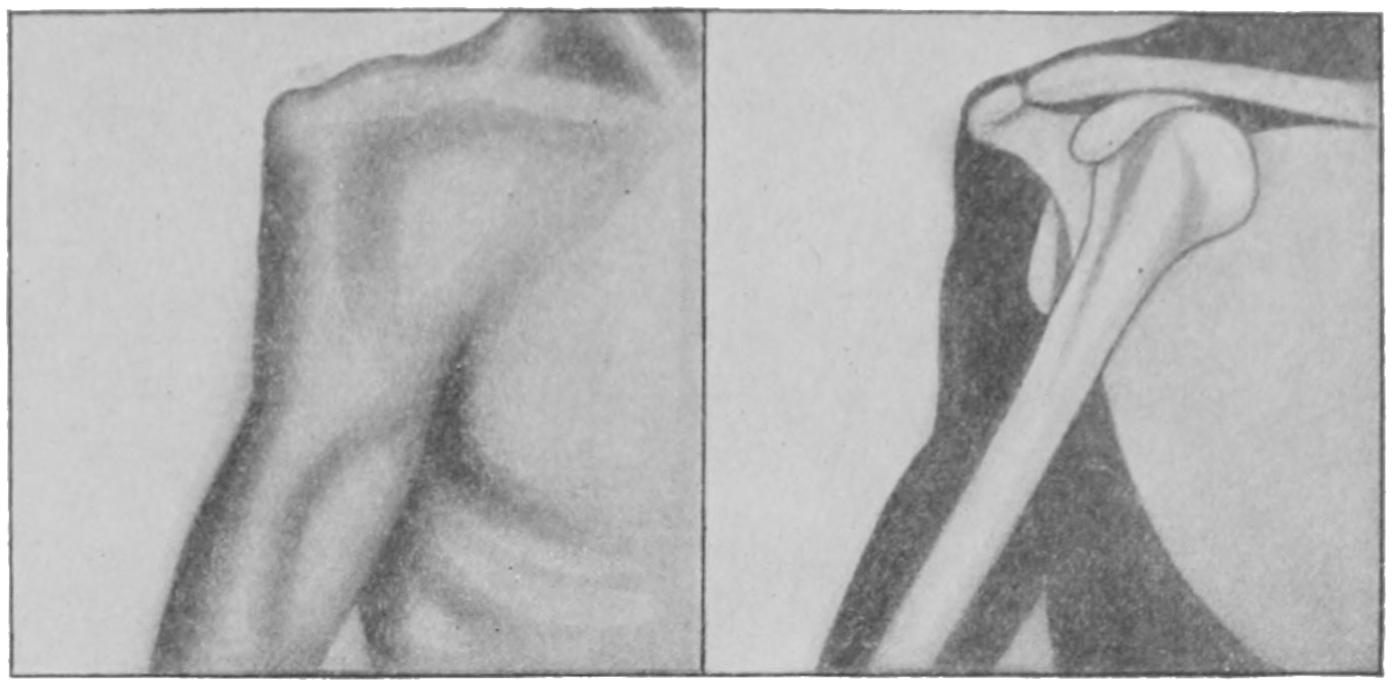
Subclavicular dislocation. (Lejars.)
Fig. 344
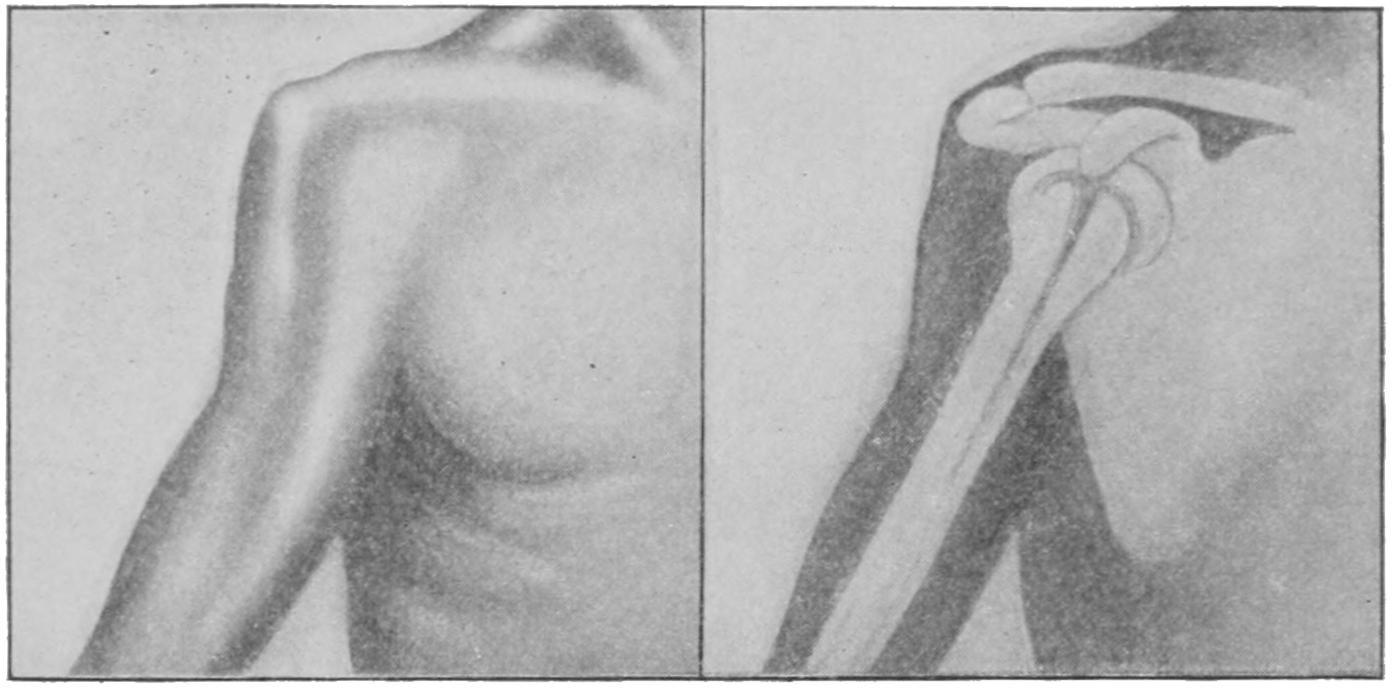
Subcoracoid dislocation. (Lejars.)
In the downward or subglenoid luxations the capsule is lacerated lower down. These displacements occur when the shoulder has been dislocated with the arm in the extended and elevated position. Here the head of the humerus is found in the axilla, resting against the border of the scapula, and the axillary structures, especially the circumflex nerve, usually sutler, while the external rotators are either ruptured or their insertions detached (Fig. 345).
Fig. 345
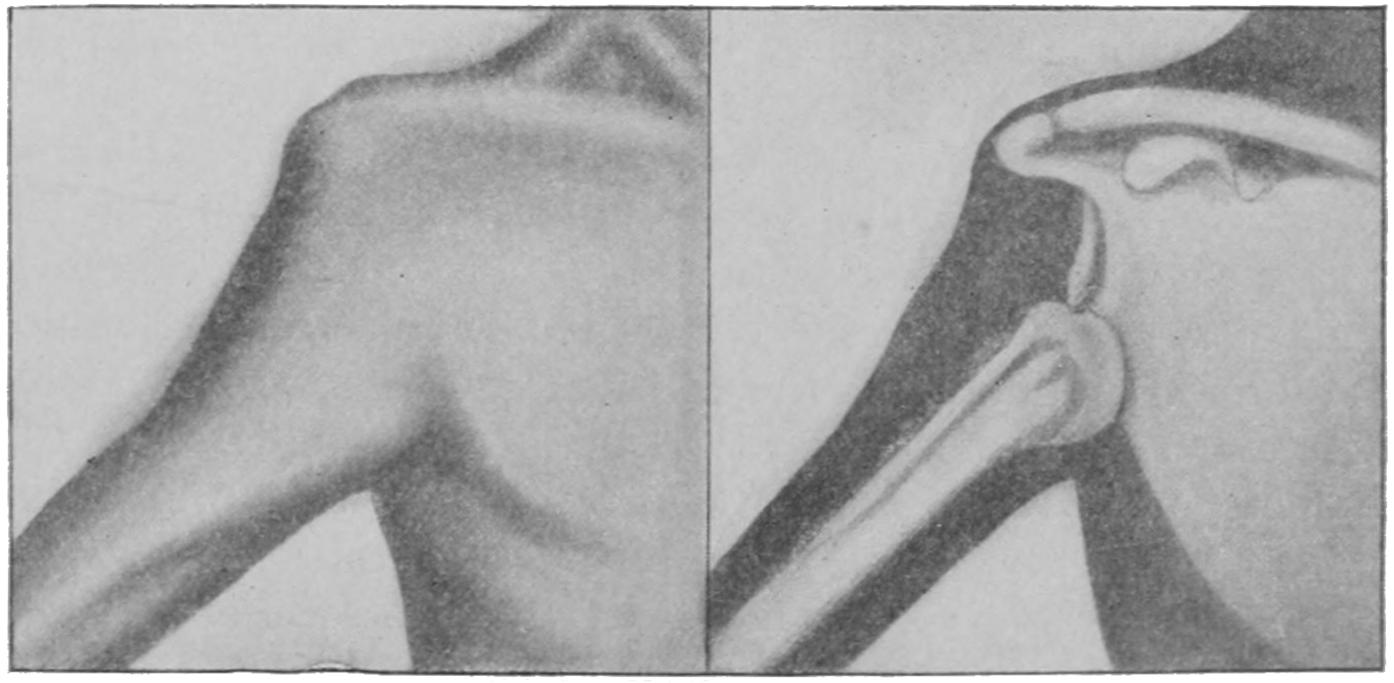
Subglenoid dislocation. (Lejars.)
[532]
The posterior or subspinous dislocation is the least common of all. In its production the arm is apparently adducted and the elbow raised. Here the humeral head is found beneath the posterior surface of the acromion or beneath the spine of the scapula (Fig. 341).
—The indications of shoulder dislocation are pain; flattening of the shoulder; undue prominence of the acromion; depression opposite the glenoid cavity, with loss of the rounded contour due to the presence therein of the head of the humerus; appearance of a more or less globular mass in the position now abnormally occupied by the head of the humerus; change in the axis of this latter bone; inability to bring the elbow to the side; more or less complete loss of function, and more or less spasm of the muscles about the joint. Owing to the fact that the thorax presents a curved or warped surface, to which a straight line can be tangent only at one point, it results that the hand of the injured side cannot be made to wrap itself over the opposite shoulder while its elbow still touches the chest or side (Dugas’ test).
—As between fracture and dislocation the surgeon may be greatly helped by deciding that the head of the humerus is still in its proper position; that the deltoid is not flattened as in dislocation; that the arm is shortened rather than lengthened; that motility is increased rather than diminished; that bony crepitus is usually obtainable, and that replacement, which may be comparatively easily secured, is maintained only so long as the parts are held in position by the operator’s hands. An additional sign of value is the fact that a straight edge cannot ordinarily be made to touch the tip of the acromion and the external condyle of the humerus at the same time, because of the protrusion caused by the presence of the head of the humerus in its socket. When the straight edge can be so applied it must be either because the head of the bone is out of the socket or the upper end of the bone broken. A still more crucial test which should, however, only be applied when others prove unsatisfactory, may be furnished by passing a sterilized hat-pin through the sterilized skin over what seems to be the displaced head of the bone and into the globular mass. Rotation of the humerus will then cause its end or head to make an excursion which will be quite distinctive.
Fig. 346
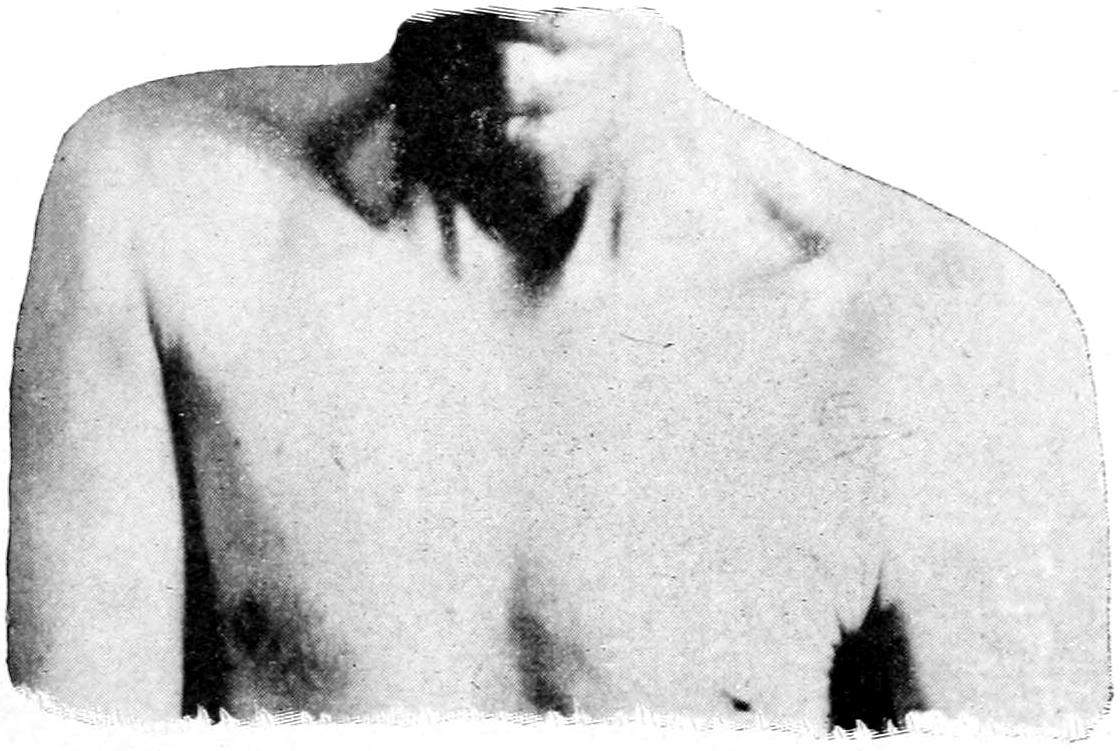
Exhibits a subcoracoid dislocation and the position of the patient in his endeavor to find relief from pain. (Mudd.)
—Prompt reduction is the only treatment for shoulder or other dislocations. This may be first attempted without anesthesia. Should muscle spasm prevent easy reduction it should be relaxed by an anesthetic, for which purpose nitrous oxide will often suffice. In the forward or forward and downward dislocations it will sometimes be sufficient to simply make firm traction in a direction obliquely outward and upward, with rotation. When this is insufficient it may be assumed that there is more or less laceration of the capsule and entanglement of the head of the bone, as well as that it is caught around the border of the glenoid cavity, against which it is firmly held.
The above simple maneuver failing, the luxation is to be reduced by a more scientific manipulation, in which traction figures largely, the method now generally in vogue being that suggested by Kocher, by which rotation and leverage are added to traction, and a minimum of power made to do a maximum of good. Kocher’s method is especially[533] applicable to the anterior displacements. It consists of a triple manipulation whose three stages are portrayed in Figs. 347 to 349. The first procedure is to flex the forearm to a right angle with the arm, apply the former firmly to the side, and then, while keeping the elbow at the side, forcibly rotate the limb outward until the forearm points away from the body (Fig. 348). This having been done the arm is abducted and the elbow moved upward until the limb is in the horizontal plane of the shoulder, the scapula being held firmly during these movements, as shown in Fig. 348. After the arm has been brought to the level of the shoulder it is rotated inward and brought downward by a process of circumduction, the elbow being made to describe some part of the arc of a circle as it comes down. The displaced head should slip into place during this movement, and will do so unless the capsular tear is too small. In that case the movements should be repeated, perhaps with more force, until the opening is sufficiently enlarged to permit the button-hole in the capsule to slip over the head of the bone.
Fig. 347
First position in Kocher’s rotation method.
Fig. 348
Arm is being carried forward and upward toward second position.
Fig. 349
Completion of third movement in Kocher’s method.
This method of manipulation, with such modification as circumstances may require, or such addition as pressure with the hand or fingers of the assistant, has superseded all the older more crude and forceful methods, and proves sufficiently applicable for all cases. It is assumed that the operator has sufficient judgment to modify any method to fit the exigencies of a given case, else he should not proceed with it. For instance, in the axillary dislocations upward traction affords valuable assistance. In the subspinous form the arm is raised to a level while extension is made upward and forward. In other words, all these methods depend upon the combination of traction, rotation, and leverage. The old method of Astley Cooper, with the foot in the axilla, the shoe having been removed, coupled with traction upon the arm and swaying movements, combined with rotation, abduction, and adduction, may be made effective, but is not nearly as elegant as the simpler manipulation above described. On the other hand, old, unreduced dislocations, complicated with adhesions, are often exceedingly difficult.
In rare instances dislocations several months old have been reduced after adhesions have been broken up by more or less violent manipulations. When forcible efforts of this kind prove futile fair restoration of function may be obtained by maintaining[534] regular motion, at first passive, later active, to prevent reformation of adhesions, the head of the bone gradually forming a new and false socket for itself. Finally, the method of excision can be employed should occasion demand. The experience of a number of surgeons has shown that in old cases, or those impossible of reduction by justifiable force, an open division of the joint, with severance of those tissues which prevent reduction, may be profitably, safely, and satisfactorily practised. Porter and McBurney, among the American surgeons, have devised a corkscrew instrument which may be driven into the head of the bone, by which manipulation after arthrotomy is materially facilitated.
The simultaneous occurrence of fracture and dislocation has been treated of in the previous chapter. When difficulty presents the best result will be obtained by open incision, replacement of the head of the humerus, and fixation of fragments by sutures, wire or otherwise. If seen late the upper fragment should be removed. The possibilities of aseptic surgery have led to the abandonment of the old method of first permitting the fracture to unite and then attempting to reduce dislocation.
Physiological rest is the essential feature of the after-treatment of all these cases, a sling and a retentive bandage being sufficient for the purpose. Function should be restored by an increasing degree of motion.
One of the most serious complications of shoulder dislocations is deltoid paralysis from injury to the circumflex nerve. The momentary pressure of the head of the bone upon the nerve is sufficient to more or less permanently impair its function. In its medicolegal aspect it should always be maintained that the surgeon is never to blame for the accident, and is only to some degree blamable in case he has failed to diagnose the dislocation so soon as opportunity was afforded and has thus permitted prolonged pressure to possibly intensify the effect which has already been produced by the injury.[42]
[42] The shoulder is liable to numerous injuries that produce disability. Pain in some of these conditions may be almost constant and spread upward to the neck and be aggravated by even passive motion. Loss of power varies from moderate paresis to complete paralysis. When the circumflex nerve is especially involved it is the deltoid which shows the effects. More severe injuries may involve the muscles of the arm and the forearm. Muscle atrophy may be greater than can ordinarily be accounted for by mere disease. In rheumatic patients a dry synovitis may be added to the other complications. Most of these features are due to traumatic neuritis. When aggravated they may result from rupture of nerves or cicatricial formations around them. The best treatment consists of immobilization for three or four weeks to favor nerve repair, counterirritation, especially with the flying cautery, over the roots of the branchial plexus, with massage, electricity, and even deep injections of strychnine to stimulate the paralyzed muscles. When paralysis is persistent and scar tissue seems to press upon nerves, exposure of the plexus and freeing its branches from all source of pressure will be necessary.
The irregularities of the elbow-joint have permitted a complicated dovetailing of its component parts which would seem to make dislocations almost impossible without fracture. Nevertheless, and especially in the tender years of childhood, both bones may be dislocated in either direction, or either bone of the forearm alone in any direction save toward the other. Diagnosis will be greatly aided by observance of the anatomical facts stated in the section on fractures of the elbow-joint and by an estimate of the relative positions occupied by these bony landmarks. When, however, intense swelling prevents this then we should either wait for its subsidence or depend upon a skiagram.
The most common dislocation is that of both bones backward, one of the possible consequences of a fall upon the extended arm and palm of the hand. The coronoid process may rest beneath the joint end of the humerus, making the dislocation incomplete, or back of it, making it complete. If the coronoid process has been broken off the dislocation can be made and reduced as often as desired. The fan-shaped lateral ligaments are always more or less lacerated. The arm will be partially bent and there will be prominent deformity upon the posterior aspect of the joint while the axes respectively of the arm and the forearm will be somewhat disturbed. Usually the lower end of the humerus can be felt in front of the normal situation of the elbow-joint (Figs. 350, 351 and 352).
Reduction is more or less easily accomplished by traction with an easy movement, by which the upper end of the forearm shall be directed toward its proper position.
[535]
Lateral displacements result also from falls in extreme positions. Lateral dislocations are rare and the result of violence, and may compel amputation. In these cases the lateral diameter of the joint is markedly increased, while the normal relation of the condyles to the olecranon is greatly altered. In these cases movement is painful and limited.
Fig. 350
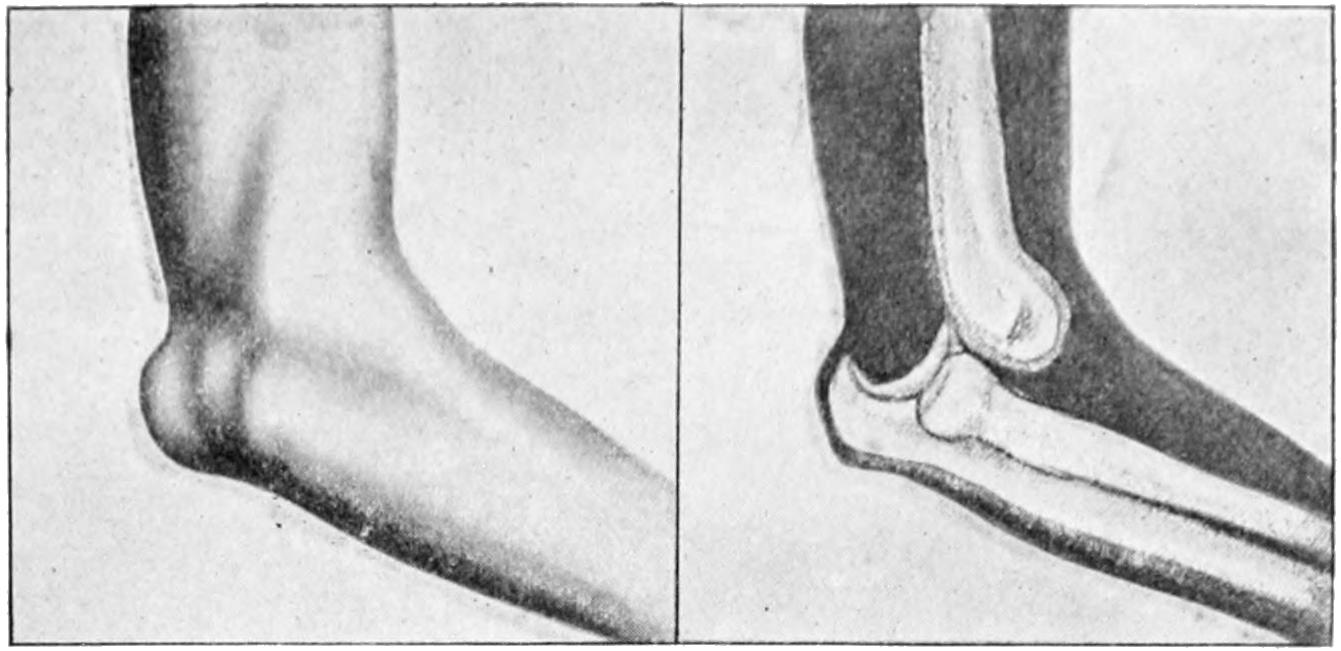
Backward dislocation of both bones. (Lejars.)
Fig. 351
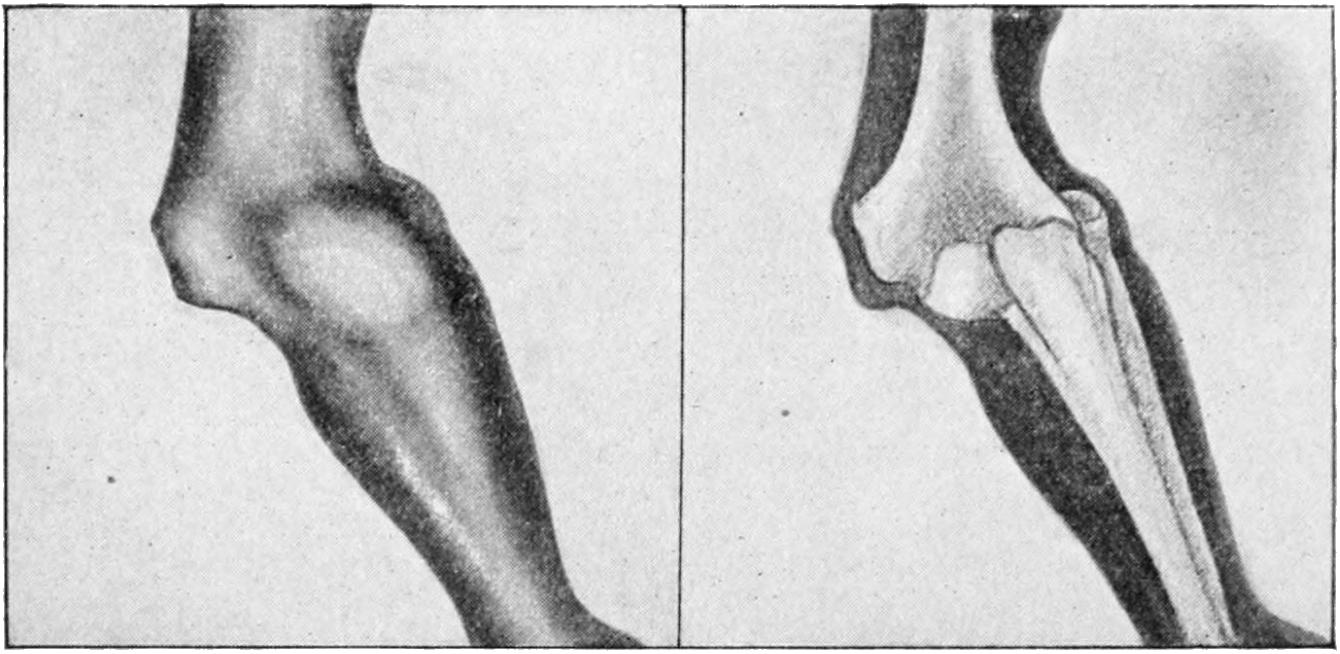
Outward displacement of both bones. (Lejars.)
The ulna alone may be dislocated backward, in which case the orbicular ligament must be lacerated and the upper ends of the adjoining bones forcibly separated. The olecranon will present back of its proper position, while the head of the radius will rotate where it belongs.
Fig. 352
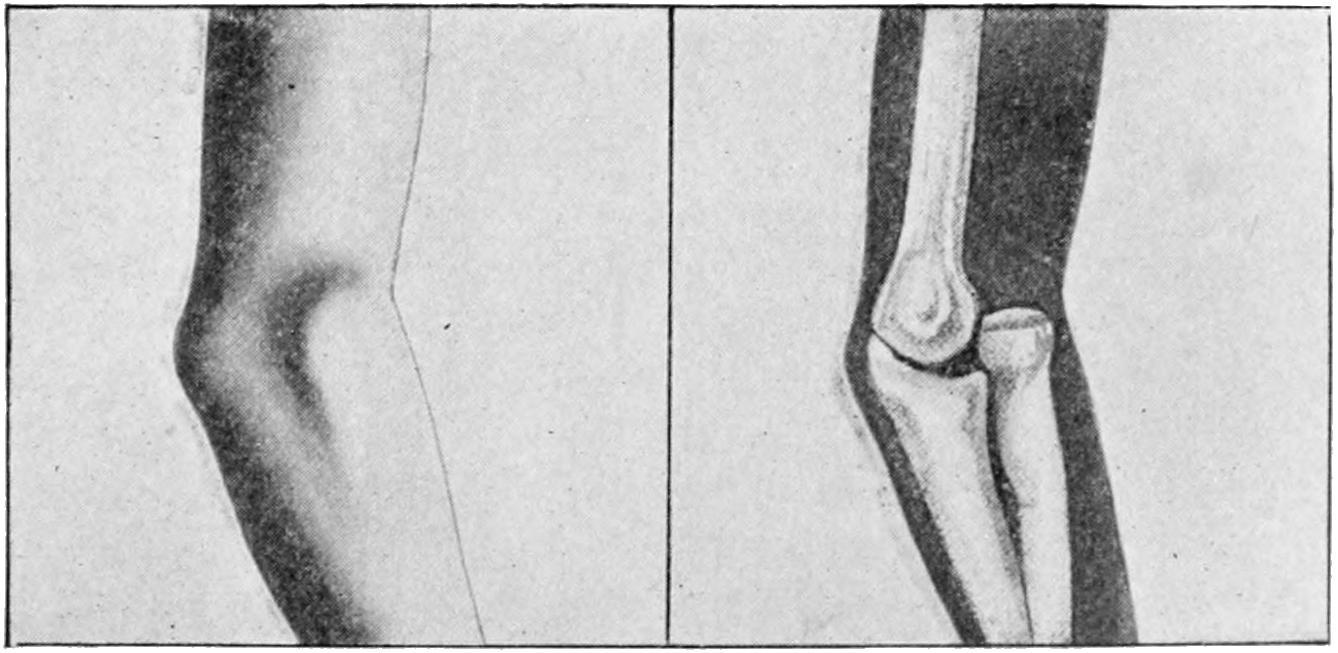
Dislocation forward and outward of head of radius. (Lejars.)
Anterior dislocation of both bones is exceedingly rare unless complicated by fractures of the olecranon. When thus injured the forearm is lengthened and fixed. The posterior surface of the humerus here has only a skin covering, the condyles are bulging, the olecranon fossa empty, and the upper ends of the forearm bones felt in front of the elbow.
[536]
The head of the radius alone may be displaced in any direction save toward the ulna. The forward dislocation is the most common, which may be produced by a fall upon the overextended and pronated hand. The orbicular ligament here is lacerated or the head of the radius is slipped out of it. In the latter case it may be difficult to replace it. When dislocated backward the capsule is torn posteriorly as well as the orbicular ligament (Fig. 353).
Fig. 353

Position of the bones in an old unreduced dislocation forward of the radius. (Erichsen.)
—The treatment of elbow dislocations is based upon general and but slightly differing principles. It consists of a combination of traction with sufficient force, made with one hand, while with the other pressure should be made upon one or both bones in the desired direction; at the same time by a combination of swaying and rotary movements more or less massage may be given to the parts, by which complete reduction may be more easily effected. Anesthesia is nearly always necessary, not alone for the relief of pain, but to produce muscular relaxation, by which manipulation is materially assisted.
A peculiar form of dislocation of the head of the radius in young children has received considerable attention. It is produced by a firm pull upon the wrist or forearm, as in lifting or jerking a child by the forearm or hand. Pronation of the hand is usually a feature of the injury. It is probable that the head of the bone is pulled out of the orbicular ligament and displaced forward. The forearm is slightly flexed, movements of the elbow are very free, except that supination of the forearm meets with resistance. The displacement is rectified by a forced supination with traction. An epiphyseal separation of the head may simulate this injury. Such cases necessitate a few days’ rest in a splint, with the arm flexed and supinated, although recovery often occurs without particular restraint.
Wrist dislocations are rare, the posterior being more frequent than the anterior. It simulates the deformity of a Colles fracture, and is produced in a similar way. The deformity is more marked, the outlines of the various bones more distinct, except in front, where they may be masked by the flexor tendons. There is no alteration in the relations of the styloid processes. The forward dislocation may possibly simulate Smith’s fracture, the symptoms being the reverse of those above mentioned.
Firm traction, with pressure in the proper direction upon the carpus, will suffice for reduction of these cases. The subsequent dressing may be practically that of a Colles fracture.
The lower ends of the ulna and radius are sometimes dislocated from their proper relations. Reduction is easy, but rest and restraint are required for some time until the ligaments have recovered their tonus.
Of the carpus the os magnum is the only one likely to be displaced, it being occasionally forced backward so that it forms a projection on the dorsum of the hand. It requires extreme force to displace the carpal bones, enough frequently to produce other injuries at the same time, some of which may be compound. A carpal bone which cannot be reduced to position by pressure may be safely removed through an incision.
Of the carpometacarpal dislocations, the thumb is the most frequently displaced, usually in a backward direction. Traction and pressure suffice for its reduction. When the bone is forced forward it is usually as the result of direct violence. Wherever the base of the bone may rest it is easily detected, while pressure with traction suffices for its replacement.
Of the dislocations of the phalanges upon the metacarpus those of the thumb are the[537] more frequent. This may occur as the result of a fall, by which the thumb is forced backward into a position of hyperextension. Nearly all of these dislocations are accompanied by a rupture of capsule. Those of the thumb are difficult of reduction; this appears to be due to the tendons of the short flexor, which surround the head of the metacarpal bone. The sesamoid bones also furnish a source of difficulty, while the long tendons, when contracted by their respective muscles, increase it (Fig. 354).
Fig. 354
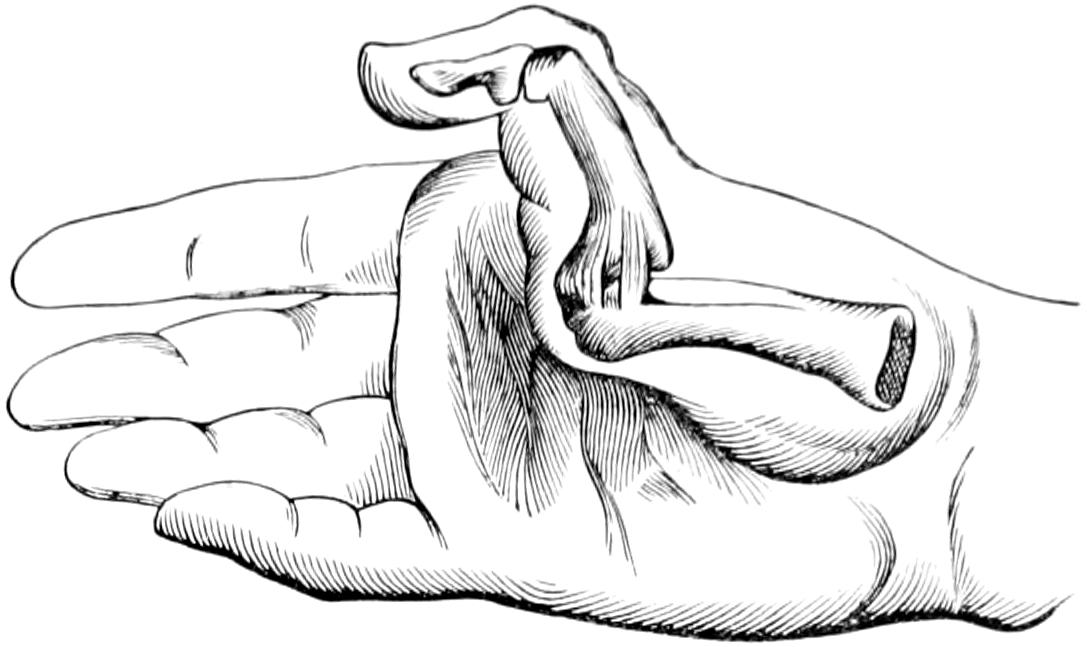
Metacarpophalangeal dislocation.
Treatment, especially of the thumb dislocations, is facilitated by first exaggerating the abnormal position, then making traction and pressure in the proper direction at the same time. Special forceps have been devised for seizing and holding the digits, or a clove-hitch can be thrown over the thumb or finger. Extension should not be first made in the axis of the metacarpal bone, but rather at an abrupt angle to it in order to relieve the expanded phalangeal end. The majority of writers concede that in some cases reduction is practically impossible. When effort has proved futile the parts should be sterilized and incised, the incision being utilized for open reduction or for excision, as deemed best.
Dislocations of the other phalanges are usually easily recognized and treated by traction and pressure.
Hip dislocations constitute about 5 per cent. of the total. As they are produced by violence they are much more frequent in men, and occur mostly between the ages of twenty and fifty years. Before the twentieth year epiphyseal separations often take place, while after the fiftieth year violence will usually break the neck of the femur. Nevertheless dislocations may occur at any age. The hip is a ball-and-socket joint, with a deep socket still further extended by cartilage, in which the head of the bone is not only retained by the ligamentum teres, but by atmospheric pressure, which in the natural state furnishes a factor of perhaps one hundred pounds. The strongest muscles and tendons of the body envelop the joint. When dislocation occurs the capsule is usually torn along its inferior aspect. The limb is usually in an extreme position, or it would require more violence to tear the head from the socket. The anterior dislocations occur during abduction without outward rotation; posterior dislocations occur during flexion. Thus when a person is stooping over in work and a heavy weight falls upon the back the head of the bone is more easily pushed backward, especially if the feet be close together.
While hip dislocations are classified for convenience, and because of their final form, the head of the bone may rest upon almost any segment of the margin of the acetabulum, though within a short time it will assume a position justifying a designation as anterior or posterior, meaning thereby in front of or behind Nélaton’s line. This is, moreover, a convenient distinction, as the symptoms vary between the two groups. Another classification is into the forward, the backward or backward and upward, and the downward, which are again referred to as iliac, ischiatic, dorsal, and supracotyloid among the posterior, and perineal, obdurator, suprapubic, etc., among the anterior (Fig. 355).
Allis, however, has simplified the subject by showing that all forms of dislocation escape primarily from the lower segment, shifting their position later either upward or downward. He classifies them as follows:
| 1. Lower thyroid. | - | All present the general characteristics of adduction and rotation outward. | |
| 2. Middle thyroid. | |||
| 3. High thyroid. | |||
| 1. Low dorsal. | - | All present the general characteristics of abduction and rotation inward. | |
| 2. Middle dorsal. | |||
| 3. High dorsal. | |||
[538]
The relation of the so-called Y-ligaments to the successful reduction of these dislocations, as well as to their formation, is of considerable importance.
Fig. 355
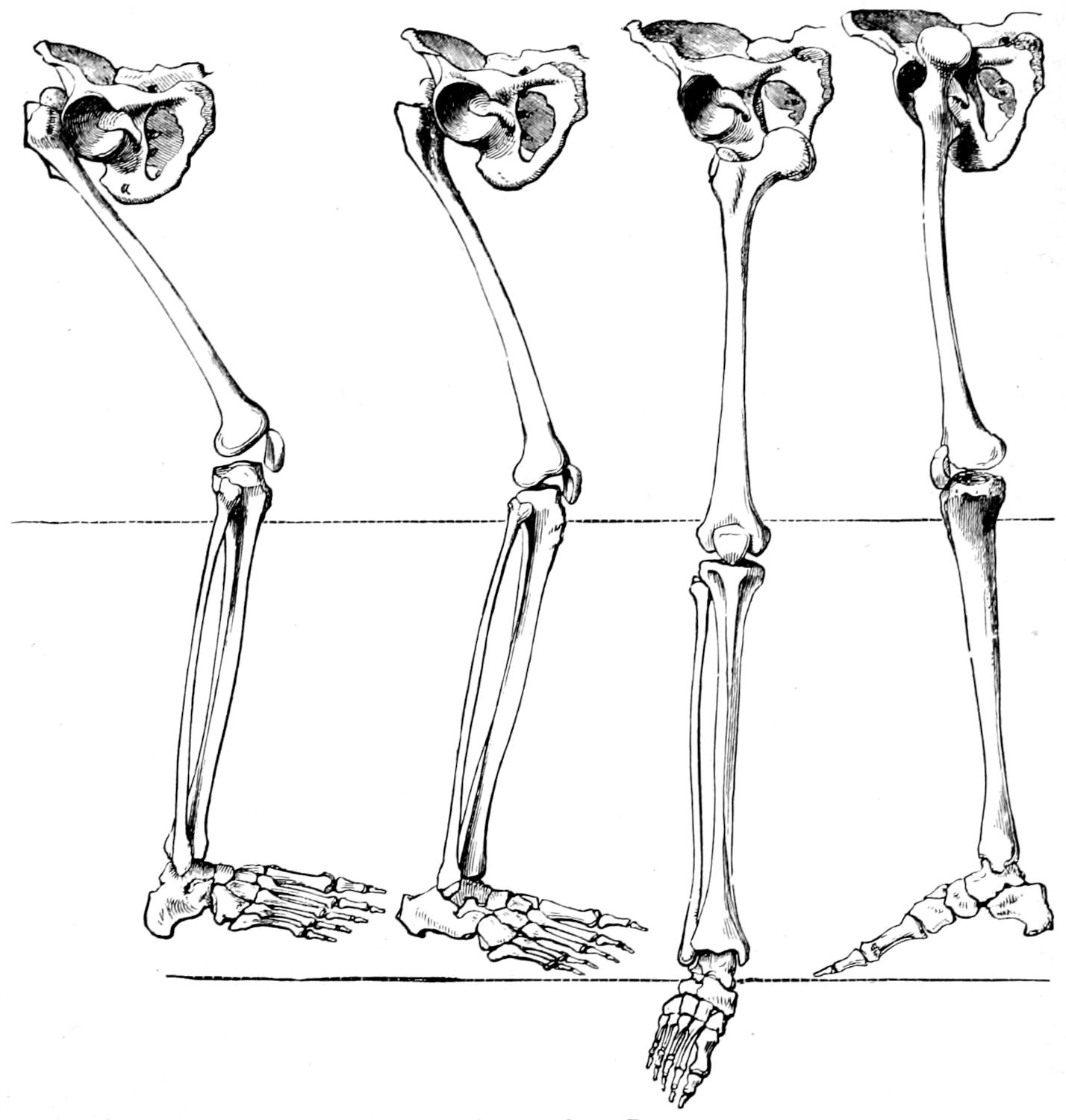
Upward and somewhat backward on dorsum ilii.
Backward toward sciatic notch.
Downward into foramen ovale.
Forward and upward on the pubic bone.
Dislocations of the head of the thigh bone, according to Astley Cooper’s classification. (Erichsen.)
Fig. 356 illustrates the manner in which this ligament receives its name, it being simply a reduplication of fibers which strengthen the capsule and which are arranged in the shape of an inverted Y. No matter how serious the injury it is seldom entirely detached. While it prevents too great displacement it is of special service in that it may be made to serve as a fulcrum for the leverage required in certain manipulations. American surgeons are entitled to the credit for the establishment of the importance of this ligament in this consideration, and while Bigelow’s name is most prominently mentioned, the names of Gunn, of Chicago, and Reid and Moore, of Rochester, New York, deserve almost equal prominence, not only for their anatomical studies, but for working out the entire method of manipulation which has completely supplanted the old and more violent methods in which the use of pulleys and tackle was not infrequent. The Jarvis “adjuster,” a powerful mechanism, which was formerly employed for this purpose, is not now seen except in museums.
Fig. 356
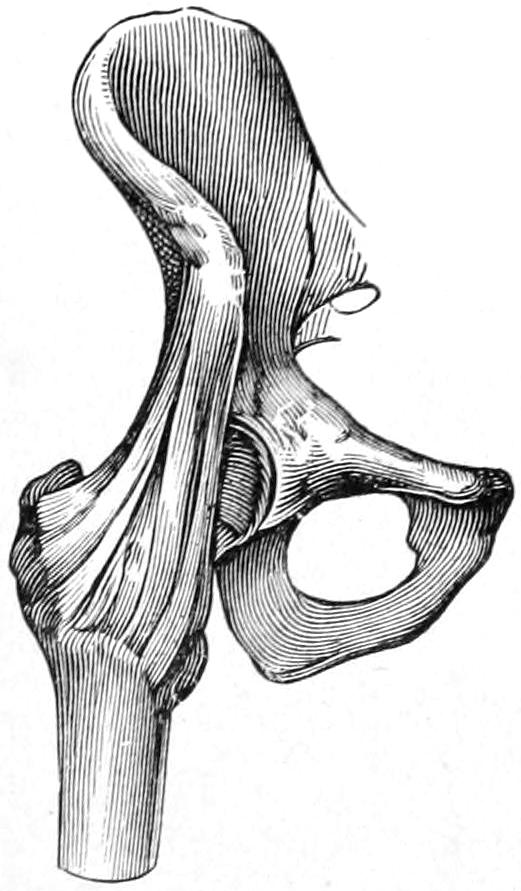
Inverted Y-ligament.
—These vary decidedly in the different forms. In every case where the head of the bone rests on a higher level than the acetabulum there will be shortening. In nearly every instance a certain degree of flexion is present. In[539] anterior displacements there is generally abduction and outward rotation. When the head of the bone is beneath the pubes or in the obturator foramen the limb may be lengthened as well as flexed, while the trochanter is shifted to a correspondingly lower position. In most instances the head of the bone can be felt in its abnormal position, and muscle spasm is always a pronounced feature, especially when there is actual elongation and muscles are really stretched. In the backward displacements adduction and inward rotation are the conspicuous features, the reverse of those of forward dislocation. When the head of the bone is actually in the ischiatic notch, and even when it is on the dorsum of the ilium, the limb is the more flexed, while the trochanter will be found above Nélaton’s line. Figs. 357 and 358 illustrate the two types of anterior and posterior displacement, with the usual and predominating postural features, while Figs. 359, 360, 361 and 362 (from Lejars) portray the anatomical features of the four principal types in graphic form. By these can be determined the class to which the dislocation belongs.
Fig. 357
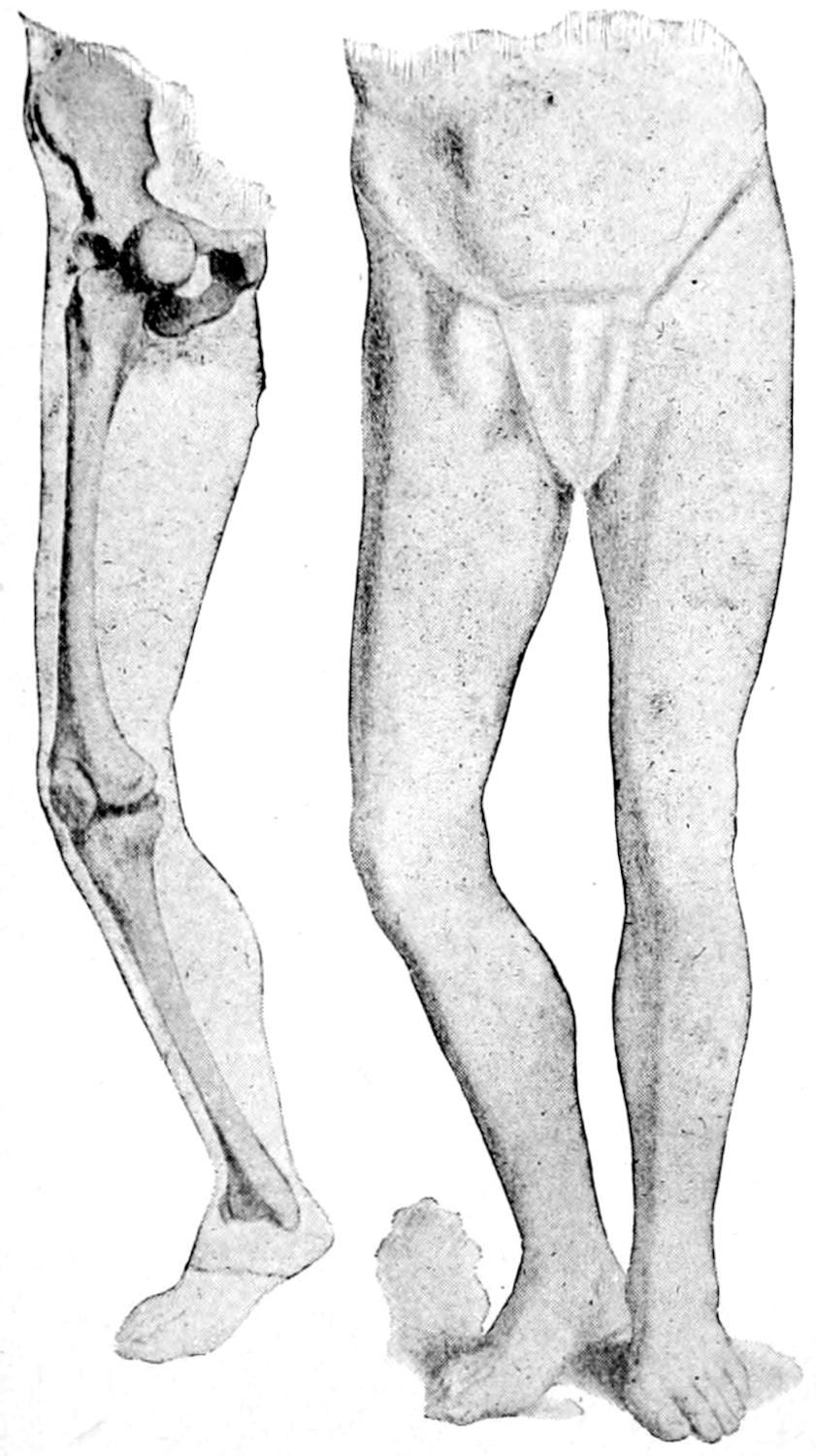
Anterior dislocation of head of femur. (Lejars.)
Fig. 358
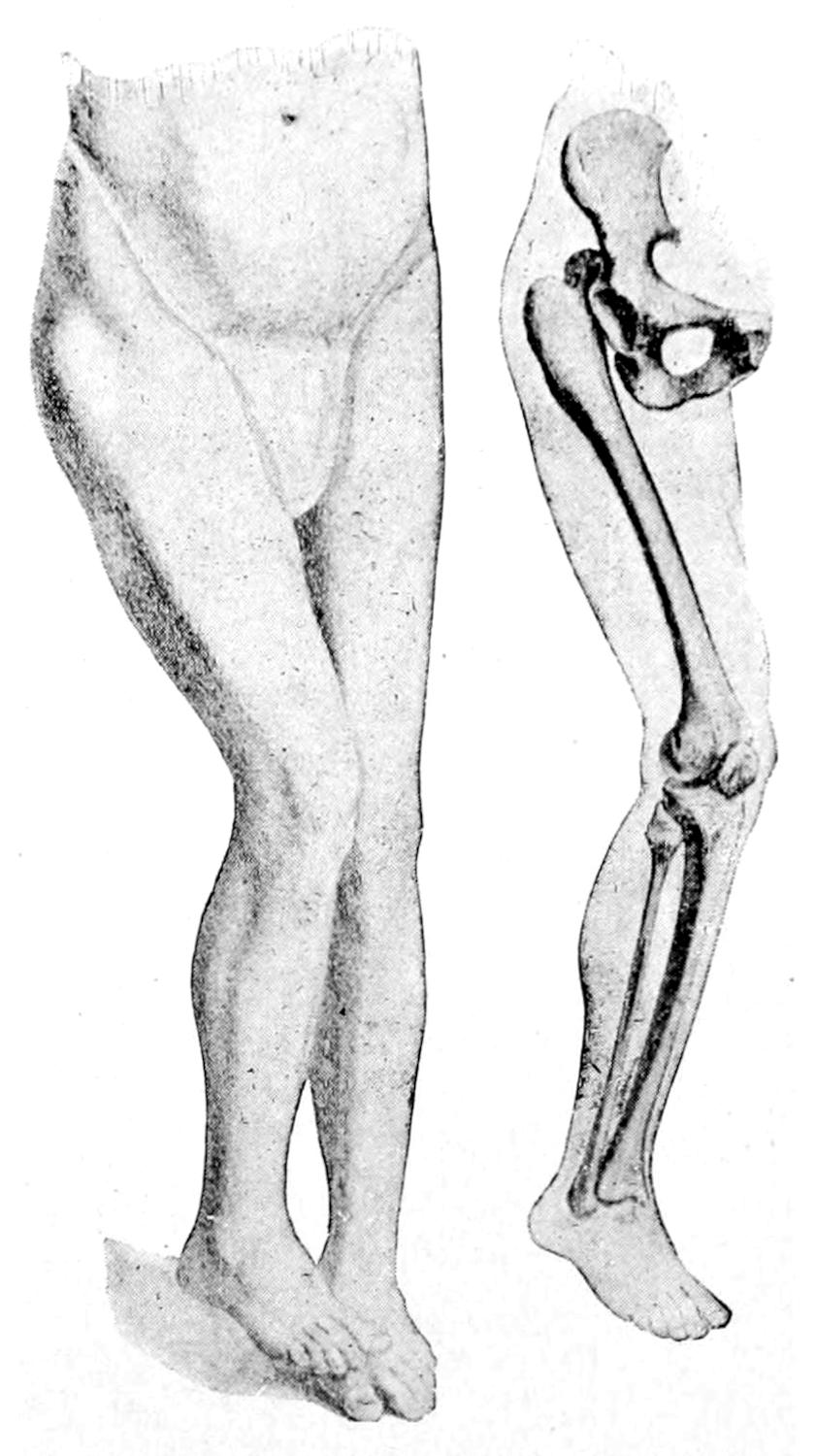
Posterior dislocation of head of femur. (Lejars.)
This classification into the anterior and posterior seems to the writer to simplify the general subject and to be serviceable for its particular purpose and place. Inasmuch as anesthesia is nearly always required for these injuries it may be expected to clear up difficulties in diagnosis by its aid.
—Through the anatomical researches of the surgeons above named, as well as those of Allis and others, the method of reduction of hip dislocations is practically always that by manipulation, and is in nearly every instance commenced with flexion. In fact a considerable number of backward dislocations can be reduced almost alone by flexion and rotation with traction, the patient being upon his back, preferably upon the floor, and the surgeon standing over him. While anesthesia is not necessary in all cases it affords sufficient assistance to justify its general employment.
In the backward dislocations, the patient and surgeon being in position as above, it is well to employ the Kocher method, which consists of (1) inward rotation, by which the capsule is relaxed and the head of the bone carried from the pelvic surface; (2) flexion to a right angle, preserving the existing adduction and inward rotation; (3) traction, by which the capsule is made tense and the head of the bone raised to the level of the socket; (4) outward rotation, by which the posterior part of the capsule and the outer band of the Y-ligament are tightened and the head turned forward into the socket.
[540]
Fig. 359
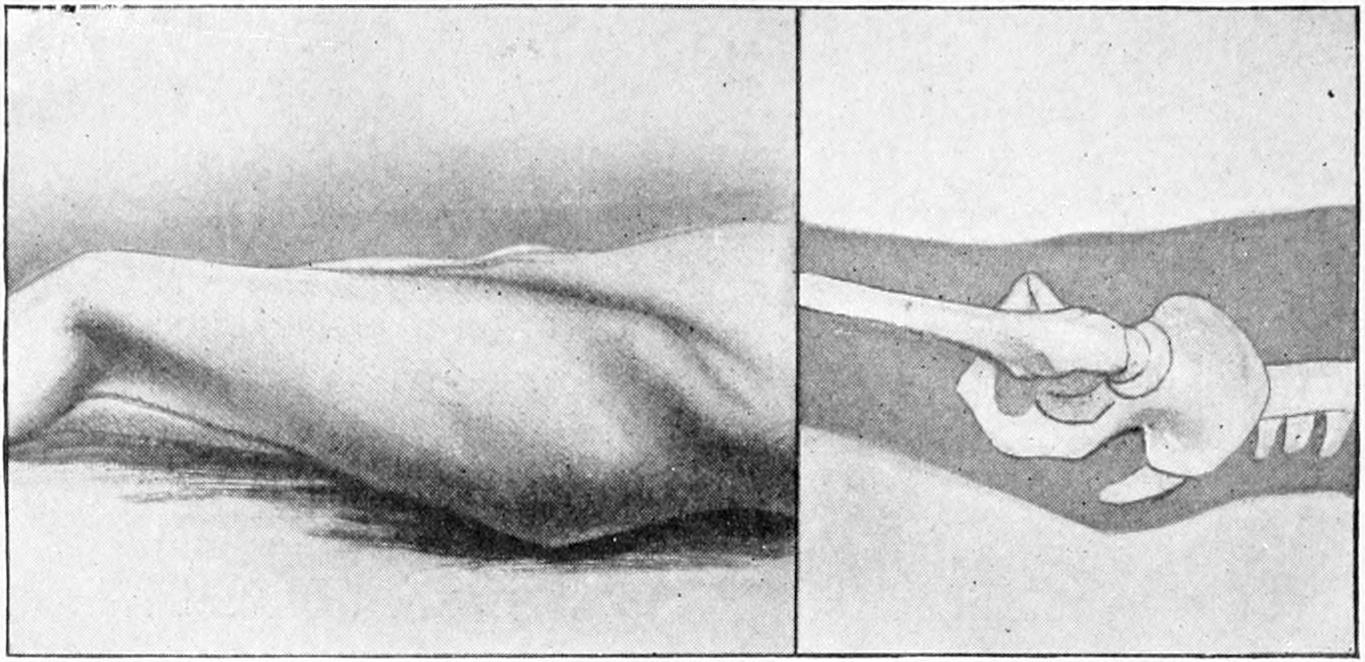
Fig. 360
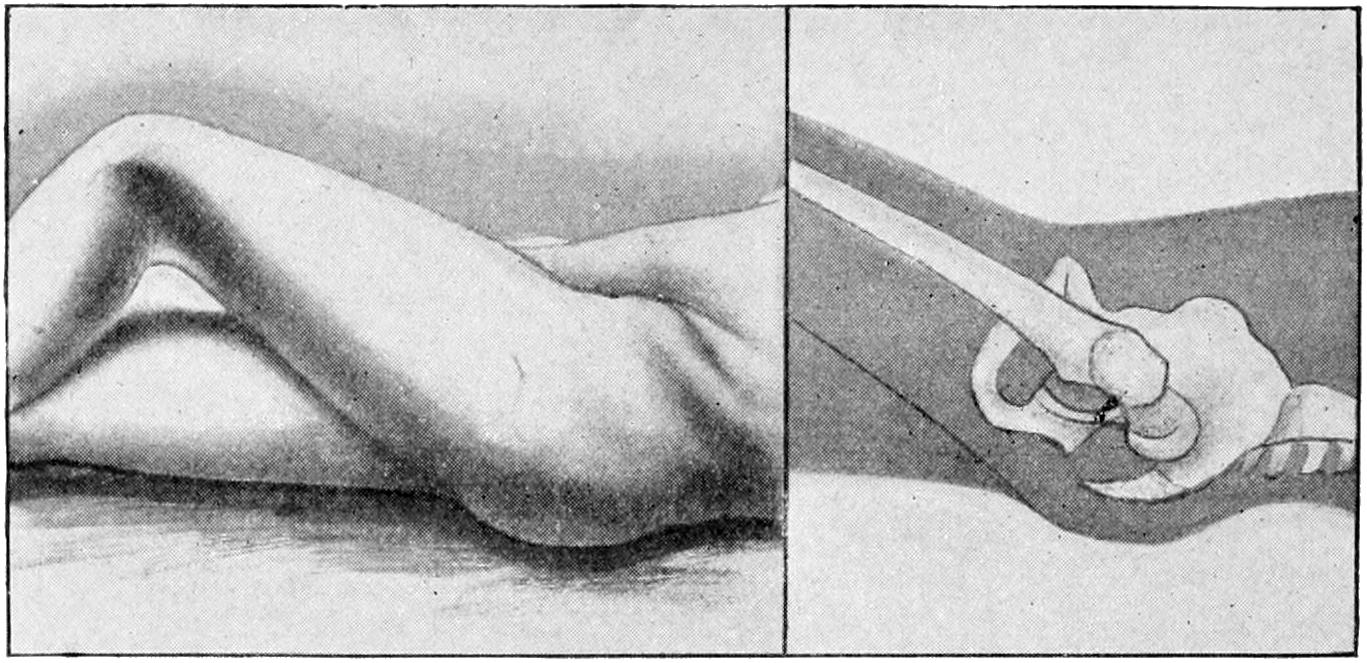
Fig. 361
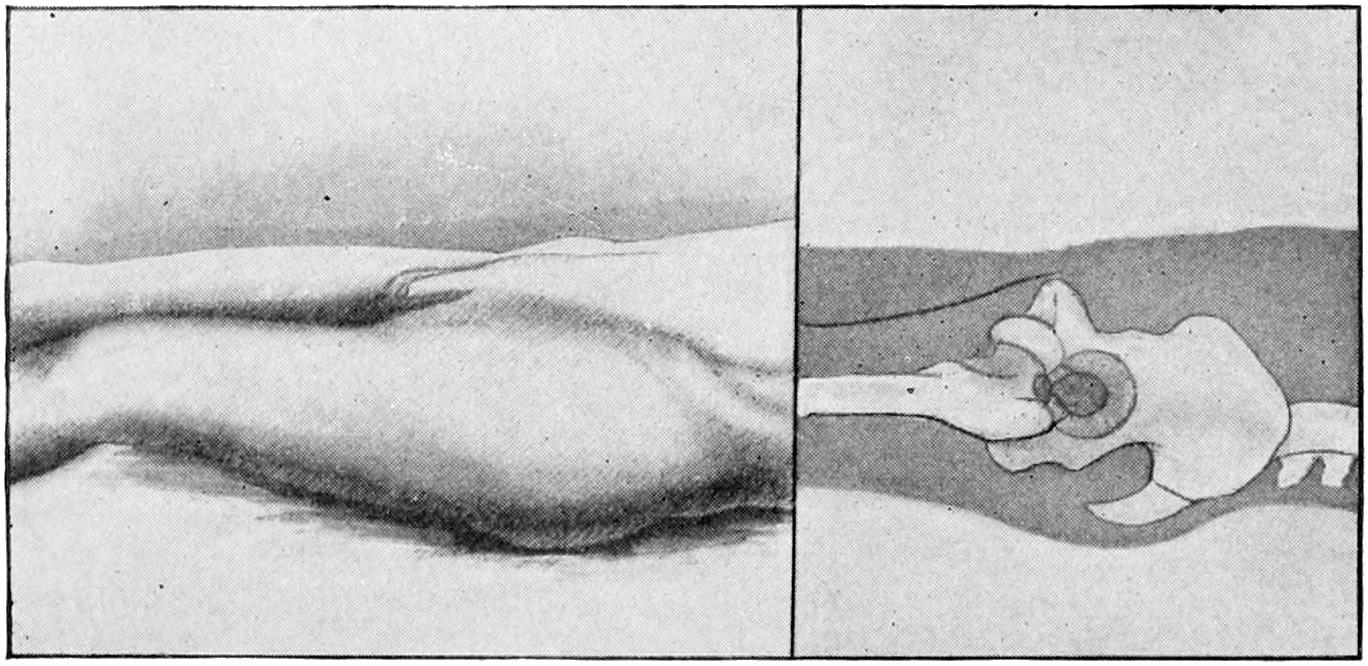
Fig. 362
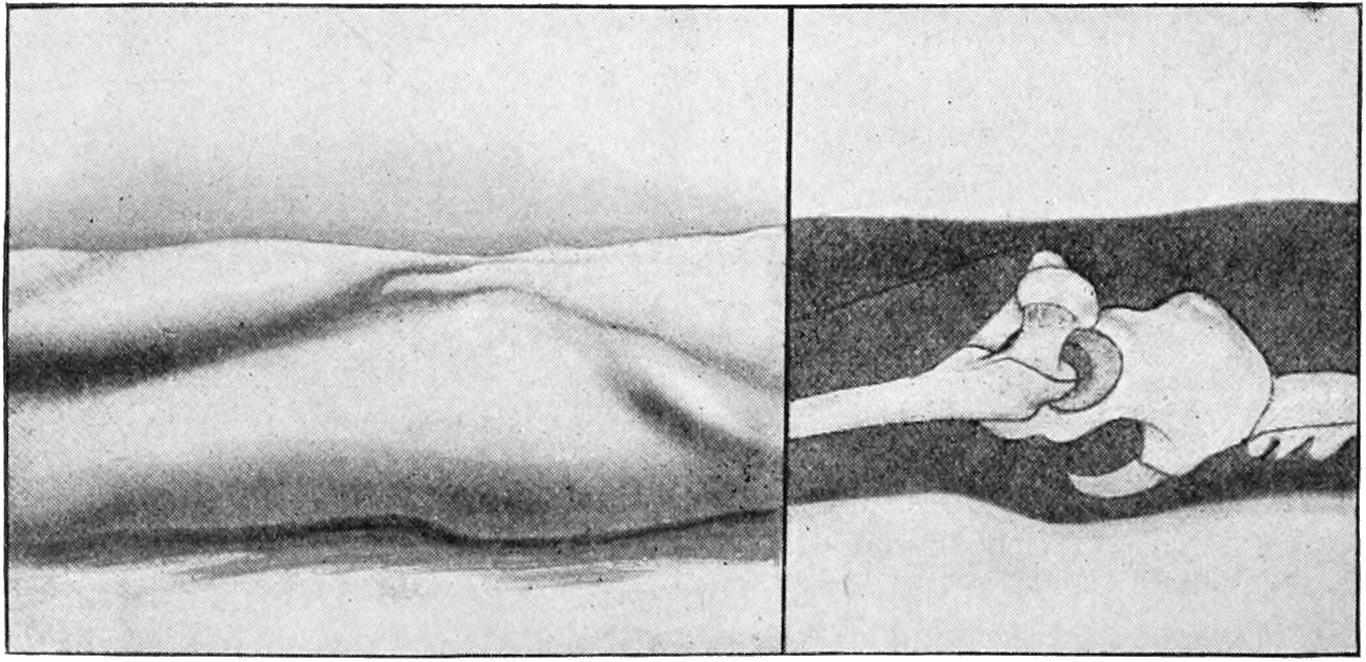
Illustrating various types of dislocation at the hip. (Lejars.)
[541]
During the practice of this or any other method the pelvis should be firmly held in place by assistants, who may seize it with the hands and hold it down. If the patient lay upon the table the pelvis may be bound to it. The surgeon may need help in making a sufficient degree of traction. This can be furnished by a strong loop passed under the patient’s knee and over the surgeon’s shoulders, the hands thus remaining free for manipulation, traction being the most important feature.
Stimson accomplishes the same purpose by placing the patient, face downward, upon a table, the dislocated limb hanging downward as represented in Fig. 363. Traction is here partly affected by the weight of the limb, while in some instances the surgeon has to wait only for the muscles to relax and the bone to resume its place without much further effort than a slight rocking or rotation. Stimson claims that this often succeeds without anesthesia, and sometimes so quietly that there is scarcely any jar or sound to indicate the effection of the reduction.
Fig. 363
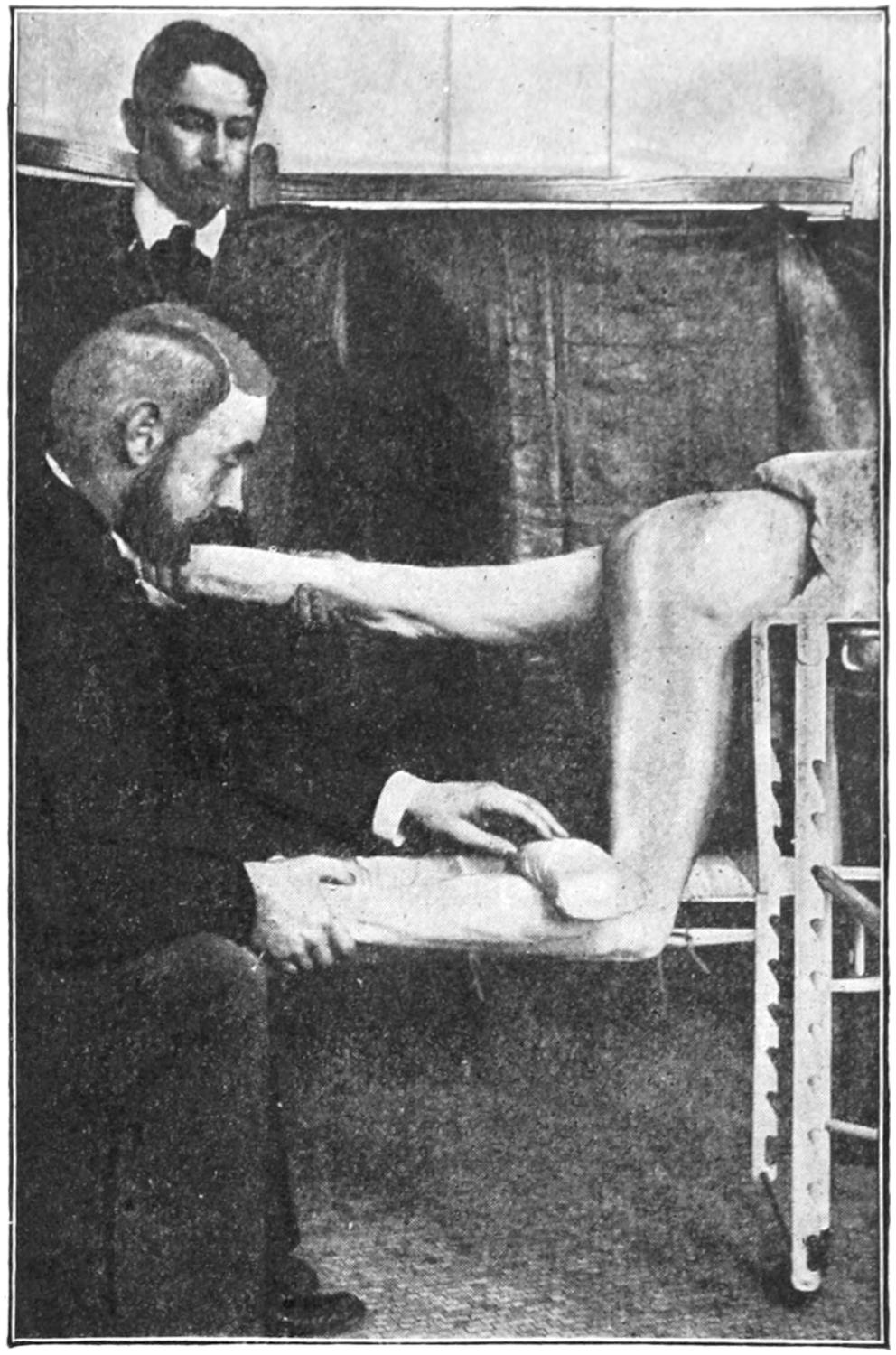
Reduction of dorsal dislocation of the hip by the weight of the limb. (Stimson.)
In those forms of dorsal dislocation which are accompanied by eversion instead of inversion it is necessary only to convert them into the ordinary dorsal type before proceeding as above.
In high displacement of the head of the bone traction should be made in the extended position, by which the head will be brought back of the acetabulum, and then proceed as above.
Of the anterior dislocations the obturator is perhaps the more common, while for its reduction the following directions usually suffice: The limb is flexed toward the perpendicular to disengage the head of the bone, then rotated inward and adducted while the knee is carried to the floor. As Bigelow suggested, in this maneuver we may need the aid of a towel passed around the upper part of the thigh, an assistant making upward and outward traction while the operator is bringing the limb downward. Inward rotation is likely to transform the dislocation into a posterior one. On account of this fact, Kocher would give the following advice: (1) Flex the thigh to a right angle with the pelvis, preserving abduction and outward rotation until (2) traction is made, by which the posterior part of the capsule is tightened and the head brought nearer the socket; then (3) forcible outward rotation is made, which should bring the head upward and backward into place.
A perineal dislocation is usually accompanied by laceration of the capsule. This will permit of easy reduction, which can probably be effected by traction in the axis of the limb in its abnormal position and by direct pressure, with some rotation or rocking.
The pubic and suprapubic dislocations require forcible flexion with traction in the axis of the limb, followed by inward rotation and circumduction of the knee. Some of these maneuvers are illustrated in Figs. 364 and 365.
So of the other dislocations of the hip; an application of principles similar to the above, coupled with such assistance as may be afforded by manipulation, practised by the operator, or by traction, with the help of an assistant, will usually suffice.
If a general rule could be formulated covering all cases it would be of great assistance. I have been in the habit of quoting a rule of this character, which I first saw mentioned[542] in the American edition of Bryant’s Surgery, edited by Roberts, to the following effect: (1) Flex the leg on the thigh and the thigh on the body; (2) carry the knee as far as it will go in the direction in which it already points; (3) carry the knee to the extreme in the opposite direction and combine this movement with circumduction and traction. In the backward dislocations these manipulations should be accompanied by traction made with one of the operator’s hands in the popliteal space. In the anterior displacement backward pressure instead of traction can be made by pressing upon the knee. I have found this an admirable working direction.
Fig. 364
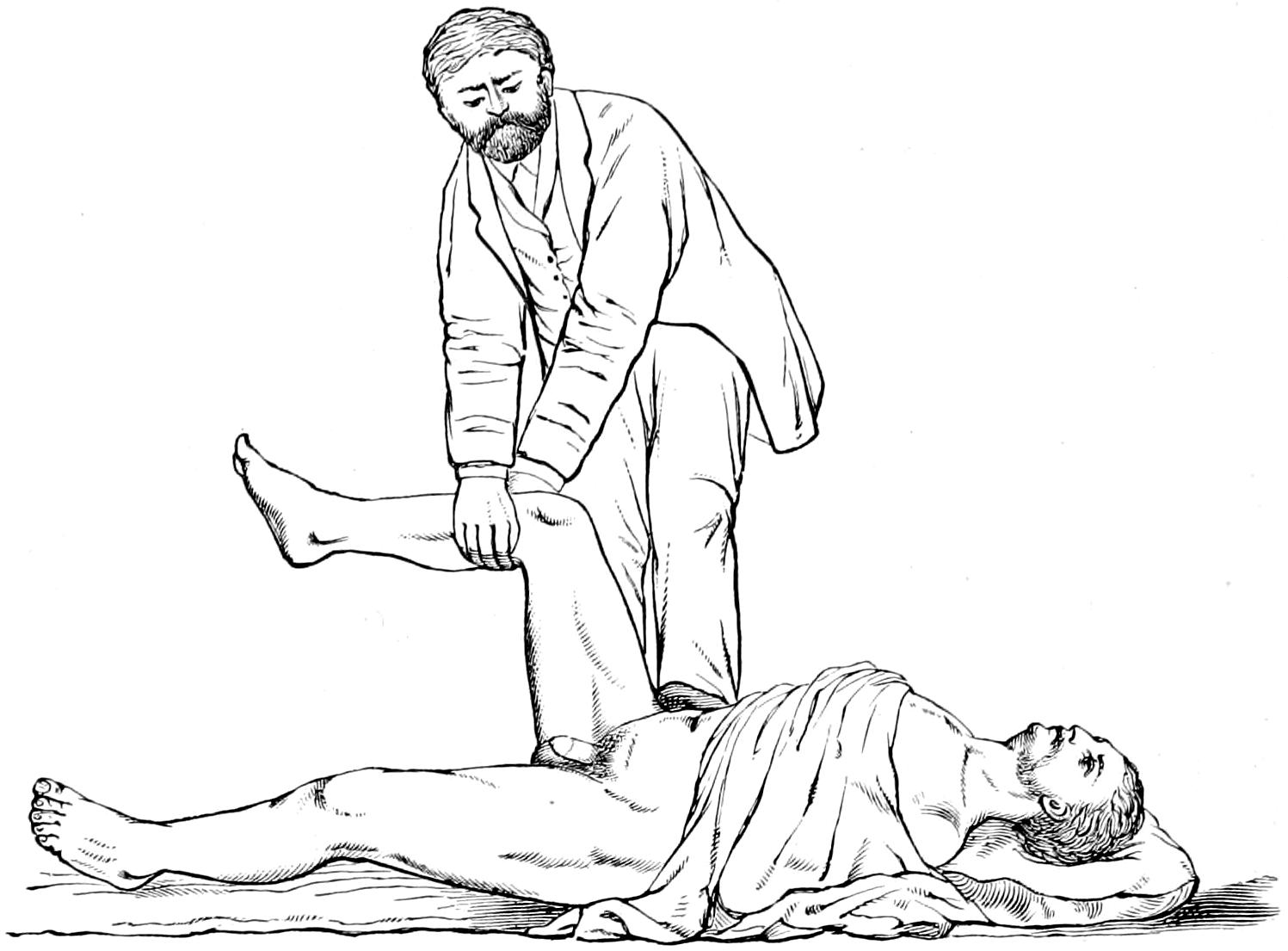
Reduction of a dorsal dislocation of the hip by traction. (Erichsen.)
Fig. 365
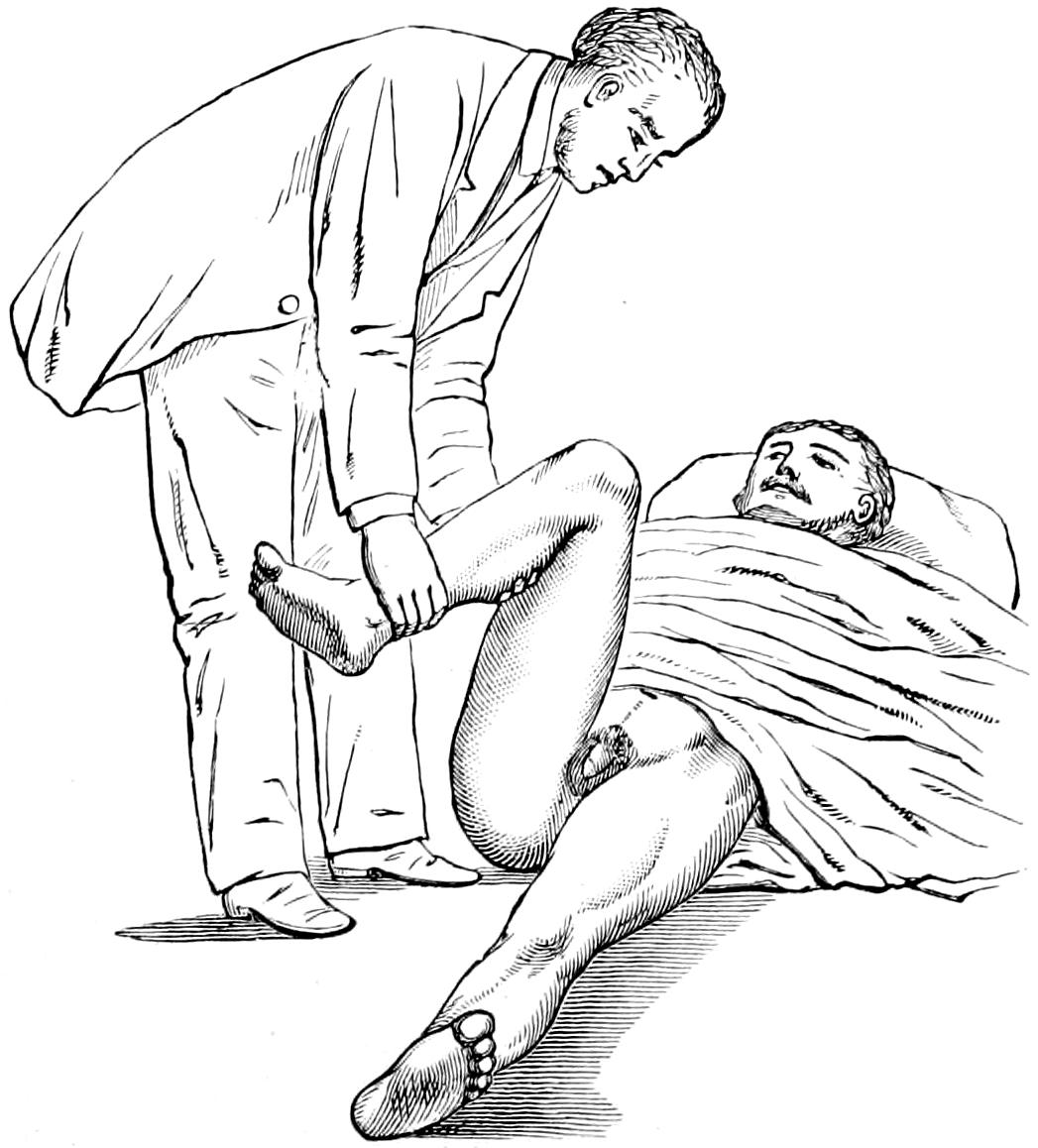
Reduction of a dislocation by rotation. The thigh is flexed, slightly adducted and rotated inward, as in the first stage of reduction of a dorsal dislocation. (Erichsen.)
The after-treatment of hip dislocations consists mainly in rest and quiet. These should be enforced, at least by a binder around the pelvis, and, if necessary, a starch or plaster-of-Paris protection. The anterior suspension splint affords a comfortable and efficient method of treating these cases after the first few days. (See Fig. 322.) Very little liberty should be allowed the patient until the expiration of the first month.
—The longer a hip dislocation is allowed to go unreduced the more difficult is its replacement. The expiration of six weeks will usually make a hip reduction very difficult, while after a lapse of three or four months it becomes wellnigh impossible. The longer a limb is disused the more do its osseous structures atrophy. Therefore a fracture of the neck of the femur or upper end of the shaft may occur in attempting to reduce an old luxation. The most marked obstacles are offered by formation of adhesions about the femoral head in its new position, and the shrivelling or change in shape of the[543] capsule, whose opening may be distorted or obliterated, so as to make reëntrance impossible within it of the head of the bone.
Other things being equal, then, more force and wider range of motion are necessary in reducing the older dislocations, while success may be attained only by the expenditure of wellnigh all the muscular energy of a powerfully built man. Attempts prolonged too far produce serious laceration, with hemorrhages, which tend to encourage new adhesions in case of failure. If a dislocated hip cannot be reduced by any apparently safe procedure the operator should decide whether to leave it, in the hope of securing a false joint, or to cut down the parts and make such further division of tissues as may be necessary. Should this be contemplated it implies, of course, that each case should be adjudged upon its merits.
By various contractions of the quadriceps muscles the patella may be displaced outward, it being practically slipped over the external condyle. The same result may be produced by a blow from the inward direction and in the extended position of the limb. These displacements may be complete or incomplete; in the former case the flat plane and inner edge of the bone are directed forward instead of sidewise. Inward displacements are unusual and usually produced by direct violence. Such previous disease as shall have weakened the capsule, or caused its distention, permits these dislocations to occur with a minimum of violence. In fresh cases the capsule is usually torn.
Reduction is easily effected by lifting the limb, thus relaxing the quadriceps muscle and making pressure and manipulation in the indicated direction. An anesthetic may be given if thought admissible.
When the limb is partially flexed, and a blow is received on the edge of the patella directly from the front, it is occasionally rotated on its tendinous axis, so that without being displaced from its position in front of the condyles its articular surface looks inward and it rides the knee upon its edge. This is referred to as vertical rotation. It is relieved and replaced by suitable manipulation, a feature of which may be sudden and forcible flexion with external pressure.
The patella once displaced the joint structures are left more or less permanently impaired, and recurrence of the lesion is by no means uncommon. Some individuals, the young especially, have the habit of “slipping the knee-pan,” this implying that at least partial displacement occurs easily with comparatively slight provocation. Sometimes children become so accustomed to this that they learn how to care for it themselves.
—After every knee dislocation protection should be afforded for a considerable period. In habitual dislocations it may be justifiable to make lateral incisions and to excise an elliptical portion of the capsule, by which its dimensions may be reduced and its undue laxity abolished.
The head of the tibia is occasionally displaced as the result of accident, though frequently this is the result of joint lesions. A traumatic dislocation can scarcely occur without considerable injury and internal derangement of the joint structures proper. Anterior dislocation may occur when the femur is forced backward or the leg forward in severe accidents. Here the popliteal vessels may undergo such pressure and injury as to constitute a serious complication. The backward dislocations are less common, though likewise the result of violence. It matters not whether the thigh be fixed and the leg forced in either direction, or whether the leg be caught and fixed while the body is made to displace the femur; such injuries are not likely to be mistaken. They are likely, also, to be accompanied by displacement of the semilunar cartilages. Lateral dislocations are practically the result of force, often combined with torsion. Injury to the lateral ligaments, usually extensive laceration, should accompany them.
Dislocations of the knee are more or less easily reduced, in theory at least, by forcible traction and manipulation, and with the aid of an anesthetic. Absolute rest, preferably in a plaster-of-Paris splint, is requisite.
The semilunar cartilages are occasionally torn loose and more or less displaced, either toward the notch or toward the exterior of the joint. A cartilage so displaced will[544] project, as a rule, at the upper margin of the tibia. These injuries may occur alone or as a complication of more serious forms described above.
—These displaced cartilages produce symptoms simulating those of movable bodies in the joint—that is, disability depending upon the extent of the original injury and the direction of the displacement. The movable cartilage may be either pulled into place by flexion or manipulated until it returns there, but will frequently reappear when the leg is straightened. It sometimes becomes so entangled in the joint as to cause almost complete disability. When movable anteriorly it may be recognized along the upper border of the tibia. The same sudden disability may be produced here as when there are other loose or movable bodies in the joint. The patient may be able to indicate that there is something movable in the joint.
—Non-operative treatment consists in sufficient limitation in the motion of the joint with abstention from use of it. In cases not amenable to non-operative measures the joint may be opened and the cartilage fastened in place to the head of the tibia either with absorbable or non-absorbable sutures.
—The upper end of the fibula, although firmly bound to the tibial head, may be dislodged by direct or indirect violence. Forcible inward rotation of the foot, in full extension, will sometimes displace it forward, while forcible traction on the biceps may dislocate it backward. Displacements at this joint may occur when the leg bones are broken, while when the tibia alone is broken and shortened upward displacement may occur in consequence. Should displacements be discovered it will not be difficult by traction upon the foot and leg, in the normal direction, and by pressure to replace them. The backward displacement is the more unstable of the two. The lower end of the fibula is by itself rarely dislocated or distorted except in connection with violent sprains, accompanied by the laceration of ligaments or fracture of one or both bones.
Backward and forward displacements of the foot are possible without fracture; as, for instance, when violence is applied to the leg after the foot is caught and fixed. Even here, however, the lateral ligaments must suffer partial or complete laceration, while one or both malleoli may be broken. The most frequent displacements of the foot are those which accompany and are permitted by fractures of the lower part of the leg, notably that originally described by Pott, with its troublesome form of bone lesions. An inward dislocation of the foot is described as produced by extreme supination and adduction.
It is necessary in studying these injuries to the ankle region to make out the existence of fracture, if any be present, as the treatment hinges largely upon such complication.
The astragalus may be dislocated from its relations with the lower ends of the leg bones, as the result of wrenches or twists or of violent injuries, as falls or blows upon the feet. When displaced it is nearly always forward. A backward dislocation is exceedingly rare. The rest of the foot itself is sometimes dislocated backward beneath the astragalus, although some portion of its lower surface still remains in contact with the upper surface of the calcis. These displacements occur in consequence of combined torsion and excessive violence. The foot here will be shortened anteriorly. No matter in what direction the astragalus may be displaced it is easily recognized.
—Reduction of ankle-and-foot dislocations accompanied by fracture is not a difficult matter, although their retention may be; but astragalus dislocations which are complicated are usually difficult of replacement. They will require relaxation of muscle tension by anesthesia or tenotomy and forced manipulations. When accomplished good function results. Better results may be obtained by exsection.
Many of these more serious forms of dislocation are compound. In such cases removal of the astragalus, or a more or less typical resection of the ankle-joint, may be judicious. In crushing injuries, either primary or secondary amputation may be necessary.
In general it may be said of the bones of the foot that one which resists reasonable effort at reduction, when displaced, should be removed. Various displacements of the tarsal bones, as the result of direct violence, may occur, as well as of the metatarsal and phalanges. Many of them may be reduced by judicious pressure and manipulation, but the violence which inflicts the displacement will frequently make the injury so compound that excision or partial amputation may be necessary.
[545]
Erysipelas and cellulitis of the scalp are the result of the same infections and conditions as when encountered in other regions, but are peculiarly prone to occur here because of the liability to infection from the hair with the material concealed in and upon the surface. They frequently lead to suppuration, in which case abscesses form that may extend inside the cranium, or into the frontal or other sinuses. These are common about the orbit and in the upper eyelid, and unless speedily incised may lead to gangrene. Multiple abscesses are also common. Disturbances of sight and hearing as sequels of these infections occasionally occur. The principal danger from these purulent collections pertains to intracranial infection or general sepsis, usually of pyemic type.
Fig. 366
Pneumatocele of cranium. (Warren’s Surg. Obs., 1867.)
The most common of these tumors is ordinary emphysema, which may result from injury to the upper and lower air passages. Thus fractures of the nasal bones or of the base of the skull may permit of distention of the subcutaneous cellular tissue by forcible inspiration of air. Emphysema of the scalp may be a valuable diagnostic feature in certain instances, as after fractures of the upper bones of the face. When connected with a wound it should be enlarged in order to permit the escape of contained air. Otherwise these puffy swellings disappear spontaneously by absorption of air into the veins. In cases of malignant or gangrenous emphysema early and numerous incisions are necessary, after which antiseptic solutions, etc., should be used.
—A pneumatocele is a chronic gaseous tumor, being a cavity distended with air which has escaped from the cells of the underlying bone, bounded on the outside by the scalp and beneath by the cranium. They are found about the mastoid or the frontal regions. Not more than three dozen cases are on record. In consistency these tumors are elastic, while the escape of air upon pressure is sometimes heard on auscultation. Their explanation is usually a defect of the inner wall of the mastoid cells, through which air may be forced from the pharynx through the middle ear by violent[546] effort, or similar defect in the ethmoidal cells by which air is forced anteriorly. Bony defects which might permit this condition are seen in a small percentage of craniums.
Treatment.
—The best results in the way of treatment have been achieved by puncture, with the injection of weak iodine solution (Fig. 366).
Tumors of the scalp may be divided into the congenital and the acquired, as well as into the benign and malignant.
Of the congenital tumors the dermoids are of most interest. Originally the dura and the skin were in contact, and the cranial bones develop later between them. This explains the occurrence of dermoids either beneath or outside of the bone or their simultaneous appearance and possible connection. Many of the so-called atheromatous cysts or wens are of dermoid origin. Those which are extracranial need only antiseptic incision or excision. It will often be sufficient to split such a cyst with a bistoury, after which each half of the sac can be detached from the bed in which it has lain. Should intracranial connection be discovered the bone chisel and sharp spoon will be necessarily called into employment. Some of these dermoids perforate into the orbit, and may have to be followed into that location.
Most varieties of tumors, benign or malignant, may be met with in this region. Subcutaneous collections of fat are not so common, nor are fibromas. Various bony growths may be met, while in certain cases the signs of brain pressure are to be explained only by their extension within the cranium.
Malignant tumors are common about the scalp and the cranium; they assume, however, no conventional appearance, and are seen in any shape or form, those of the scalp alone occurring either as carcinoma or epithelioma from its epithelial elements, or as sarcoma from its mesoblastic elements. Tumors primary in the periosteum or bone are necessarily of sarcomatous nature, while those of the type which perforate to the surface may be either sarcoma or possibly endothelioma. The general character of these growths has been referred to previously. In regard to their extirpation (for there is no other treatment than this) operations of varying degrees of severity may be required. (See Cysts and Tumors and Tumors of Bone.)
Fig. 367
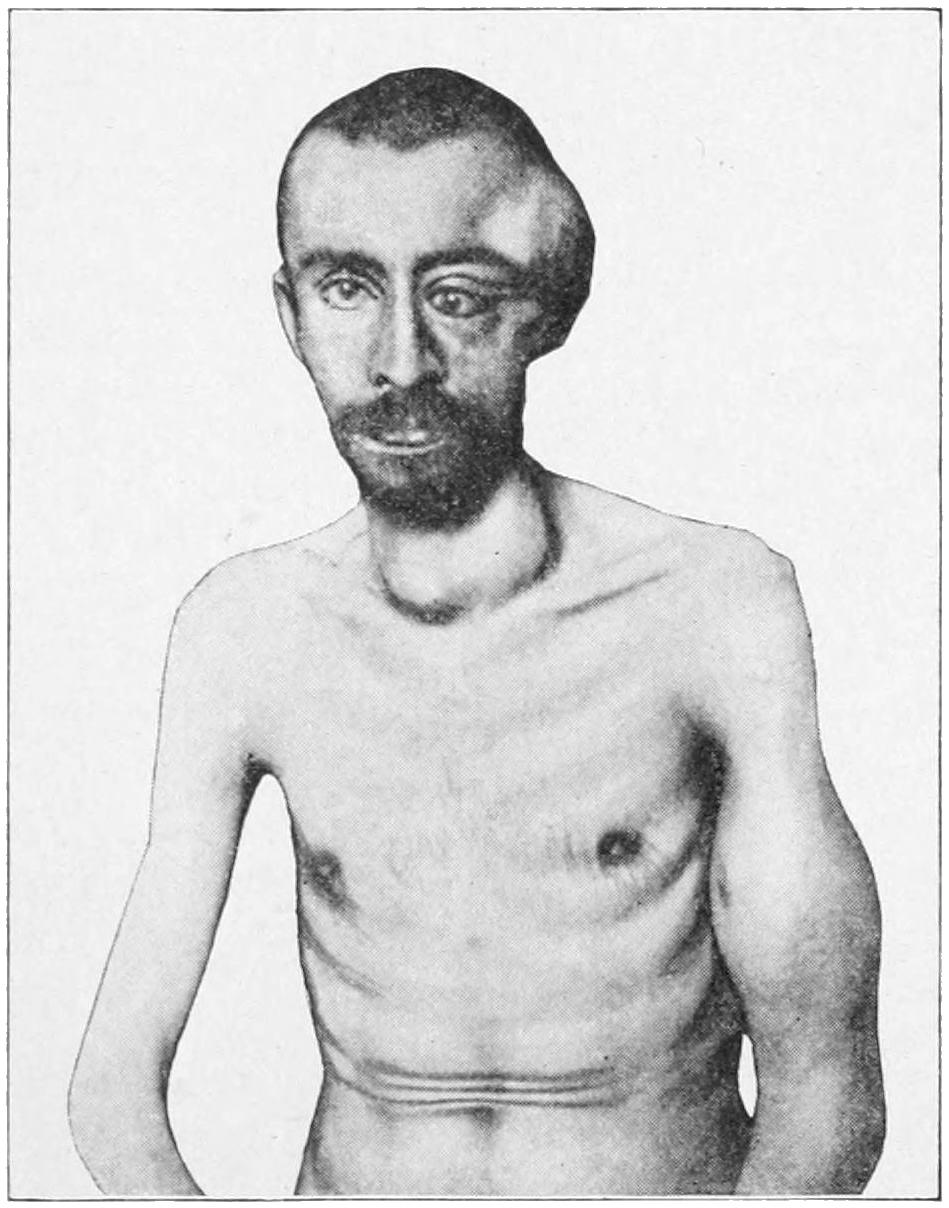
Osteosarcoma of the temporal region. Metastatic tumor in the arm and thyroid. (Parker.)
The superficial epithelioma should be attacked before it has become adherent, in which case everything should be removed down to the underlying periosteum, after which a plastic operation will permit the repair of the defect, so that primary union of the whole surface may be secured. Any malignant growth which is adherent to the underlying cranial bone calls not only for removal of its own substance, but for that of the bone to which it is attached. To fail in this is to invite recurrence. This may necessitate more or less extensive osteoplastic resections of the bone, but the condition permits of no middle course. Extensive resections of bone have been made with success, and need not be abstained from unless there be good reason to fear involvement of the dura or cortex. In this case the advantages and dangers should be carefully weighed before proceeding to operation. During operations on the bone great care should be taken, especially in certain regions, to avoid injury to the intracranial sinuses, although it has[547] been learned that these may be ligated and intervening portions removed. But the wounding of the sinus by the point of an instrument or spicule of bone may lead to a hazardous and annoying complication, and is to be prevented when possible. A small wound in a sinus may be plugged with gauze, which may remain for two or three days. There is always a possibility of air embolism (see pp. 38 and 363) when the sinuses are opened, as their walls do not easily collapse. Hemorrhage from the soft parts may be almost entirely controlled by the use of an elastic tourniquet stretched around the skull. Oozing veins in the diploë or in the bone may often be secured by pressing the tables of the skull together with bone forceps, while at other times an antiseptic wax can be forced into the interstices of the bone and hemorrhage thus checked. In certain cases where it seems impracticable to slide flaps and cover defects the desired end may be obtained by skin grafts, after Thiersch’s method.
A rare and specialized form of blood tumor, seen only on or within the cranium, is the so-called hernial dilatation of the superior longitudinal sinus. It may present through openings in the bone; sometimes pressure upon it will cause vertigo and perhaps greater prominence of adjoining veins, even of the jugulars.
—Incomplete formation of bone is occasionally met with. The bone is a secondary formation in the skull, the dura and skin being originally in contact; consequently this condition can be easily explained as a failure to develop bone where it is normally produced. These defects are most common in the frontal and temporal regions. The bone may fail also to develop to ordinary thickness, and may be found as thin as paper or ossifying only in certain directions. Supernumerary bones may also develop, apparently to take the place of those previously lacking. Aplasia may also be a unilateral defect and contribute toward the formation of meningocele. Atrophy or anostosis—i. e., complete disappearance of cranial bones—is occasionally observed. It may be an interstitial or an eccentric process, and may happen at any point or at several spots. Up to a certain extent it is the rule in the skulls of the aged, when the bones become reduced to the thinness of paper or may in certain places completely disappear. Senile atrophy, in other words, is a normal process, and is to be expected after the sixtieth year of life, its possibility being not forgotten when operations are undertaken upon the skulls of those advanced in years. Eccentric atrophy may also occur from pressure of soft or hard tumors, among them the so-called Pacchionian bodies. It is also stated that increasing hydrocephalus may produce an internal and eccentric anostosis.
—It is particularly in the skull that the manifestations of rickets are most common, the bone becoming unduly thick and the general shape being changed. Usually there is a flattened vertex with delayed ossification, with an abnormally firm union along the suture lines. In spite of these changes, the bone often becomes affected by pressure to such an extent that a rachitic or hydrocephalic child, confined to bed and moving little or not at all, will develop a skull showing the effect of such pressure. Many rachitic skulls show areas of atrophic thinning, dispersed irregularly, while the inner surface may show the markings of the convolutions impressed upon it by the softness of the bone (Fig. 368). (See Rachitis.)
Fig. 368

Craniotabes (rachitis). (Bruns.)
[548]
The acute affections of bones have been considered in Chapter XXXII. Acute periostitis is, in the main, due either to syphilis or to an infection following injury. In the latter case it proceeds from the margin of the wound, and may spread to a considerable distance. It is in some instances secondary to deeper infection extending from the middle ear, and then is found posteriorly to the ear and externally to the mastoid cells. Congenital openings or defects of the sutures about the mastoid seem to have much to do with the travelling of infectious lesions in these localities.
Fig. 369

Osteoma of skull. (Mudd.)
have been considered on pages 437 and 438.
—Acute osteomyelitis is due to essentially the same causes as those just discussed. In this case it is especially in the diploë that the principal ravages occur. Unless promptly recognized and relieved by surgical measures this is likely to[549] lead to sepsis of the pyemic type and at a relatively early period, the venous arrangement of the diploë favoring such type of disease.
—Necrosis of the skull is ordinarily the result, directly or indirectly, of injury, in which case it is usually of the acute form, a fragment, which has been too much separated from its surroundings to live, giving evidence of early and easily recognizable death. This necrosis is mainly confined to the external table. Necrosis of slow origin is due either to tuberculosis or syphilis, perhaps more often to the latter. Under a cold abscess of the scalp or subperiosteal abscess will often be found a small area of dead external table which needs complete removal. Necrosis has also been observed to follow severe burns of the scalp. It is usually combined with caries of adjoining bone. The caries produced by syphilis is illustrated in Fig. 371.
Fig. 371
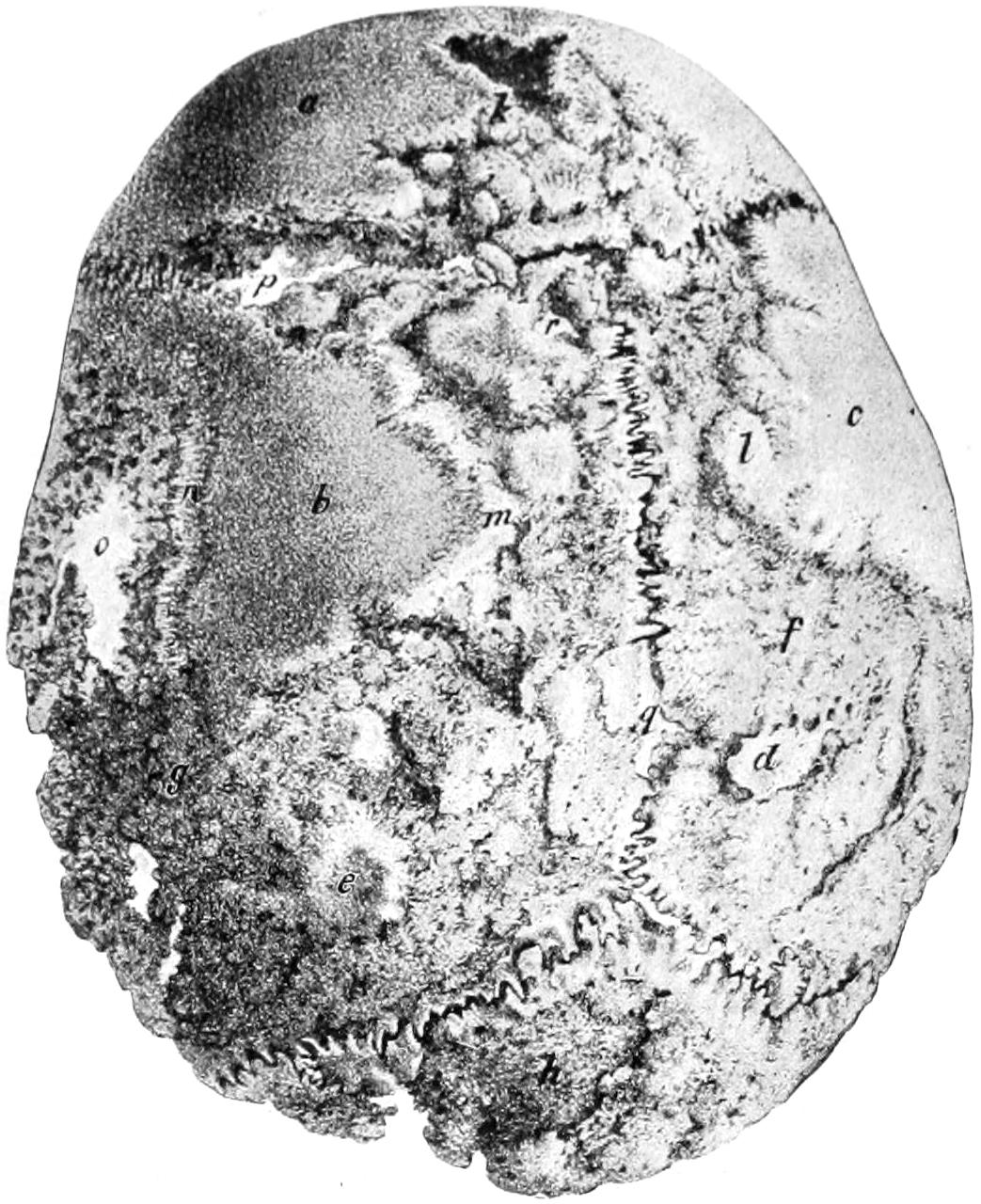
Syphilitic caries of cranium. (Bruns.)
In utero the head is surrounded by amniotic fluid and is well guarded against injury. Nevertheless as the result of penetrating wounds or of falls on the part of the mother real injuries do occasionally occur. Most of the cases of skull fracture reported as occurring before birth have occurred during delivery. Multiple fractures of the skull of either character have been observed.
During the process of parturition there nearly always appears a tumor of the scalp in the newborn, known as the caput succedaneum, at the point where pressure upon the head has been least. It usually disappears quickly after birth. It is due to a collection of blood, partly an extravasation, as the result of compression or injury. It is composed also of edematous soft tissues of the surface. If incised, blood-stained serum is poured out. When this fails to rapidly resorb during the first days of the infant’s existence, and especially if it fluctuate, it may be incised under antiseptic precautions and blood clot be turned out. In rare cases it suppurates, by which is produced an acute abscess, which should be promptly evacuated.
A collection of fluid blood between the periosteum and the bone is known as the cephalhematoma neonatorum, such a lesion occurring on an average once in two hundred cases. It is generally found over the fissures, and appears to be produced by the sliding[550] of the bones. This collection also usually promptly disappears. In case of failure it may be aspirated or incised. Before resorting to any operative procedure it would be well to make a careful distinction between a possible meningocele or encephalocele, as a congenital defect, and cephalhematoma as an accident of delivery.
Fig. 372
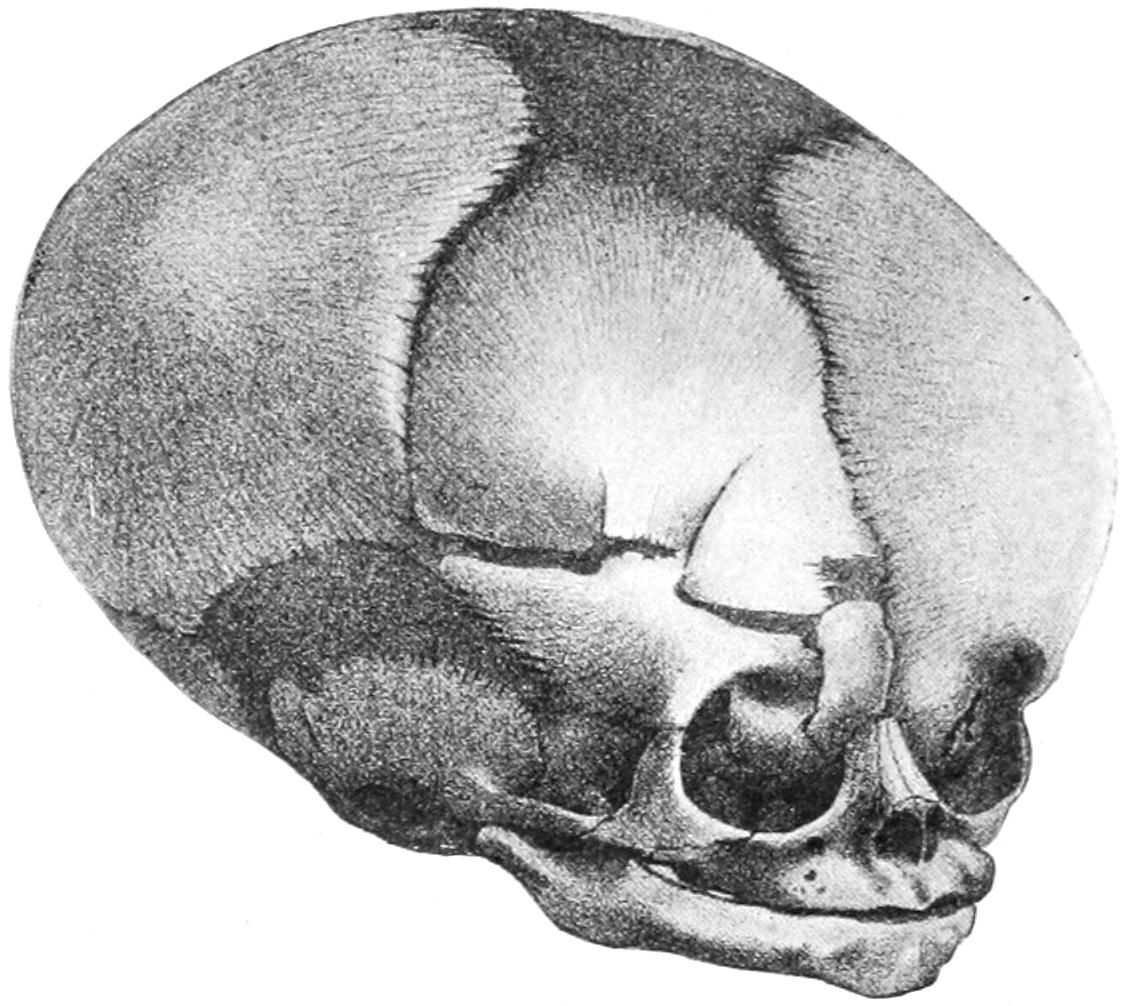
Fracture of right frontal bone in a newborn infant; fracture extending into orbit. (Bruns.)
A depression in the skull of a newborn child which does not quickly right itself or yield to expanding influences from within should not be allowed to go uncorrected, as serious lesions ordinarily of paralytic type may result therefrom. In these days of aseptic surgery there is no reason why such operation as may be necessary to elevate a fragment or an entire bone should not be performed, with the usual precautions.
The young and the aged have no distinction of tables of the skull, but the diploë which separates the two tables is an affair of middle age, develops slowly, and disappears after the same fashion—sometimes to such an extent as to leave the skull of almost paper-like thinness. In all operations, then, upon the young and the old the surgeon should proceed with extreme caution, as if expecting to find the skull quite thin. The lower limit of the squamous bone proper is the so-called mastosquamosal suture, and operations confined to the squamous plate alone are safe from injuring the sigmoid sinus on its inner side. The ridge at the posterior root of the zygoma indicates, by its lower border, the level of the mastoid antrum. A few lines above this is the level of the base of the brain. The mastoid is present at birth and appears externally by the second year. Its antrum is present also at birth, though its air cells do not develop until after puberty, their location being previously occupied by cancellous tissue. Most of these cells open into the antrum, a few directly into the tympanum. They are not always separated from the sigmoid sinus by bone. The partition between them is perforated by minute veins, forming an easy communication between the sinus and the antrum. Air escaping from the mastoid cells into the overlying tissue may cause emphysema from a basal fracture. In all operations upon the mastoid antrum the operator should keep to its outer side, and the higher and the more closely to the posterior zygomatic ridge he makes the first opening the more sure is he to escape injuring the facial nerve. The groove for the sigmoid sinus extends to the jugular foramen from a point on the outside corresponding to the asterion. The lateral sinus may be indicated externally by a line from the superior border of the mastoid to the inion—i. e., from the asterion to the inion.
The frontal sinuses are usually separated by a septum, which is often incomplete or wanting. They are variable in size and outline, and do not develop until after the seventh year. The infundibulum, by which they empty into the nasal cavity, is often so small[551] that when the lining membrane is involved it becomes closed, and retention, with its accompanying symptoms—pain, tenderness, swelling, etc.—may ensue. Ulceration and erosion, however, may cause perforation internally through the supra-orbital plates, so that pus may penetrate through the inner half of the orbit.
Aside from its direct communication the superior longitudinal sinus connects with the basal sinuses through the middle cerebral and the Sylvian veins, while communications with the middle meningeal veins are abundant. Where the frontal and diploëtic veins enter the longitudinal sinus there frequently are dilatations in which marasmic thromboses often originate. This sinus is also connected with the veins of the nasal septum, so that a septic phlebitis may be propagated from the nose. So much of the lateral sinus as is contained in the sigmoid groove is known as the sigmoid sinus, which connects directly with the exterior through the mastoid and the posterior condyloid veins. In sinus thrombosis this mastoid vein is likewise affected. One or more condyloid veins accompany the hypoglossal nerve through the anterior condyloid foramen, and may also serve for the propagation of infection or exit of pus.
While septic particles may be carried from any part of the lateral or sigmoid sinuses—usually through the internal jugular—they may also be carried by way of the other veins above mentioned or the occipital sinus, all of which empty directly into the subclavian without passing through the internal jugular. These sinuses are all rigid tubes, always open, while the veins are thin and flexible, their caliber constantly varying with inspiration and expiration. The sinuses contain no valves, and these are very rare in the cerebral veins.
So far as the lymphatics are concerned there is free and easy communication between the internal and external plexuses and nodes. Into the superficial nodes, along the external jugular, outside of the deep fascia, empty all the external lymphatics of the head. Intracranial infection shows itself in swelling of the deep cervicals beneath the deep fascia. Lymphatics are abundant in the dura, and pathogenic organisms, once housed within the dura, find it easily open to invasion. The potential interval between the dura and the arachnoid is termed the subdural space, when considerable effusion may occur without marked symptoms, owing to its easy diffusion, while blood here poured out may travel even to the lowest parts of the spine and cause death by pressure upon remote points.
The arachnoid bridges over the convolutions and does not extend into the sulci. It is not vascular; at certain points it is adherent to the pia, at others it does not touch it. The subarachnoid space is formed in the latter way, and within it most of the cerebrospinal fluid is contained. This space is unevenly distributed over the brain surface, most prominently beneath the posterior two-thirds of the brain, where there is a wide interval between the arachnoid and the pia, extending forward around the medulla and pons and as far forward as the optic nerves. This space connects with the ventricles by the foramen of Magendie, as well as with the sheaths of the cranial nerves. Where these nerves escape from the brain or cord they are covered by all three membranes, the layers being most distinct along the optic nerves. Fluid injected into the subdural space may pass along the spinal nerves as far as the limbs. It is essential to realize this in order to appreciate how extensive is the surface exposed in leptomeningitis.
Internal hydrocephalus is often the result of closure of the foramen of Magendie. The cerebrospinal fluid is rapidly reproduced after traumatic escape. External hydrocephalus or accumulation in the subarachnoid space, is a condition frequently due to tuberculous infection.
The pia is the vascular coat of the brain, supplied with an extensive network of fine nerve fibers derived from the sympathetic and the cranial nerves, having intimate relations with the brain, to such an extent that leptomeningitis and encephalitis are almost inseparable. The nerve supply to the cerebral membranes explains the severe pain of meningitis.
In direct connection with what has been stated above it is well to emphasize that the venous communications between the exterior and interior of the cranium are numerous, and that the frequency of these anastomoses explains the ease with which extracranial[552] infections are propagated within; in other words, these explain the frequency of septic mischief in the brain after external injuries.
—Penetrating and incised wounds are frequent about the head, their prognosis per se, as well as their proper treatment, varying but little from that of such wounds in other parts, so long as the skull proper and its contents escape injury. Hemorrhage from scalp wounds may be profuse and even fatal. The most dangerous hemorrhages occur from the temporal vessels. Penetrating wounds are short, and the periosteum and underlying bone are usually also injured. Such small articles as blades of penknives, particles of dirt, etc., will often be found when the parts are carefully inspected, a measure never to be neglected. Contusions of the scalp and skull are spoken of as subcutaneous, subaponeurotic, or subperiosteal, and are most frequent in the frontal and lateral regions. Ecchymoses following them may be extensive and discoloration may spread over a large area. In traumatic hematomas resulting from various injuries incision should be an early resort should blood clot fail to resorb.
All conceivable degrees of injury to the bones, from a trifling division of the periosteum down to most extensive denudation or mangling of the external table or the entire thickness of the bones, may be encountered. These lesions may be spread over a large area or may be the result of penetrating wounds. In other words, we may have linear, penetrating, or large surface wounds, with such injury to the scalp as perhaps to amount to a total loss of covering for the same. All of these, moreover, may be complicated by fractures of the bone at the point of injury, with or without brain lesions, or by other and more remote lesions.
In regard to most of these, it may be said that non-penetrating injuries, when promptly and properly attended to, have, in most cases, a favorable prognosis. Every penetrating wound of the cranium is a condition justifying grave prognosis, on account of the great danger of infection incurred. Other features of these wounds, with more in regard to prognosis and treatment, will be given under the head of Compound Fractures of the Skull, etc.
It is necessary, however, to say in this place that penetrating wounds of the cranium are often received in a way which does not permit actual diagnosis, as, for instance, when received through the nose or the orbit. Every wound whose history and appearance indicate that penetration may have occurred should be subjected to the most rigid scrutiny and care. Points of fencing foils, umbrella tips, etc., have been forced into the brain cavity through the orbit and elsewhere in ways which left little external evidence of the severity of the injury.
Following the anatomists, and for general convenience, these are divided into fractures of the vertex, of the lateral region, and of the base, the former being the most frequent as the vertex is the most exposed. A fracture in a given region may be confined to that locality or may radiate widely or extend nearly around the cranium. Of all the fractures of the bony skeleton those of the skull constitute about 2 per cent.
Fractures of the vertex are, in most instances, due to actual violence, the force being often expended at the point of application or producing radiating fractures. Those which are limited to the neighborhood of the injury are referred to as direct fractures, in distinction to which we have indirect or radiating, often producing remarkable results. Fractures may vary between the simplest crack or fissure, accompanied by but trifling brain symptoms and never recognized, to the most extensive comminution and destruction of cranial bones which can be imagined.
—Splintered or comminuted fractures refer to the formation of numerous bony fragments, which are often more or less[553] loosened, sometimes completely so, occasionally dovetailed together, and often driven in or depressed. Such fractures are direct. It is possible to have comminution without depression; the latter makes it the more grave condition.
Fractures with absolute loss of substance may be made by gunshot injuries or by any extensive splintering or by a penetrating body. It is possible to have fracture of one table without that of the other, this being often true of the external table. In isolated fractures of the inner table there is often dislodgement of small fragments which may injure the dura and possibly produce later epileptic or irritative disturbance. When the external table is chipped off the diploë is exposed, and this with its wonderfully fine venous communications opens up a wide area to infection and subsequent pyemia.
—Gunshot fractures are always depressed and almost invariably comminuted. The bullet of the modern army rifle possesses a great initial velocity, and the cranium struck by it will probably be disrupted into fragments, causing instant death. The majority of gunshot fractures of the skull seen in ordinary civil practice are due to revolver or pistol bullets from weapons of the prevailing type. In these instances there will usually be penetration, perhaps with perforation of the skull, and the formation thus of one or of two compound fractures, the wound of entrance being always comminuted and depressed, while fragments of bone may be scattered along the course of the bullet, which may also carry infectious material from without, such as hair, particles of hat, and the like (Figs. 373 and 374). (See also Figs. 52, 53 and 54.)
Fig. 373

Fig. 374
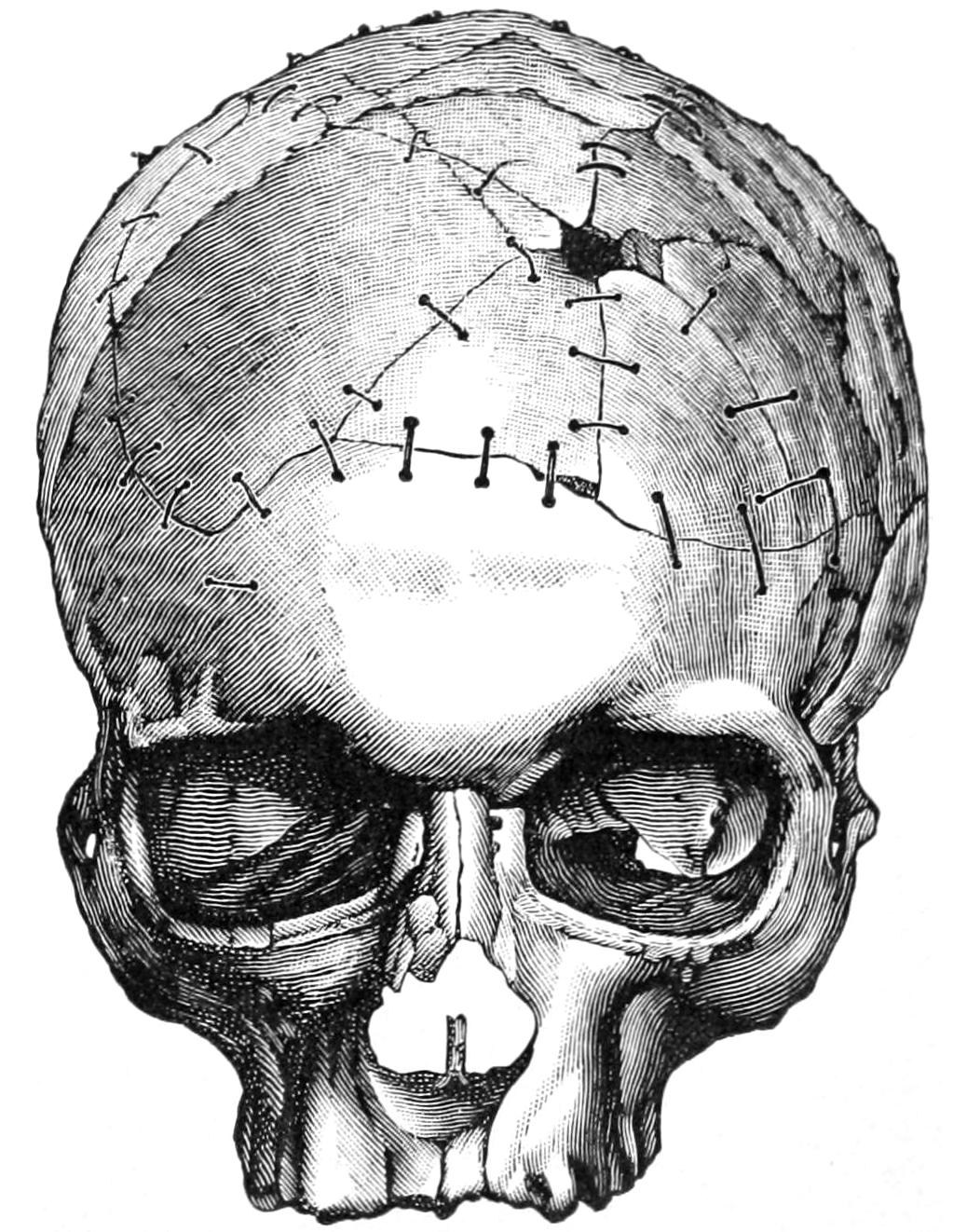
Gunshot fracture of skull. (Helferich.)
Whatever may be the wisdom of operating in other cases where there is room for doubt as to the proper course there rarely is uncertainty as to the proper treatment of gunshot wounds of the skull, which should be invariably subjected to operation.
It will thus be seen that fractures of the skull may be simple or compound, or complicated with other injuries, or depressed, without any reference to whether they are simple fissures or more extensive injuries. On the other hand, depressed and comminuted fractures may occur without being compound in a surgical sense, and with each one of these injuries there may be accompanying disturbance of the brain of any degree of severity, from the mildest concussion or shock up to rapidly fatal compression. Any imaginable complication of these head injuries is not beyond the bounds of possibility.
The essential features in explaining the mechanism of fractures of the vertex are the area involved and the violence of the impact. The skull is often surprisingly elastic, even in the oldest individuals, and fractures occur ordinarily when the natural limits[554] of elasticity have been exceeded and bone cohesion overcome. Children particularly suffer from depression without fracture, which formerly was never operated upon, but which is now regarded as requiring operation. On the other hand, certain skulls are abnormally fragile (see Fragility of the Bones, Chapter XXXII), and among the insane may be found so porous and yielding as to be easily pressed out of shape. In injuries of slight extent it is sufficient that the skull be regarded as composed of an elastic substance, while for injuries produced by greater violence the skull is to be considered rather as a globe or arch possessed of high resistance and elasticity, whose shape will probably yield more or less before a fracture results. Much may be learned from such experiments as those of Félizet, who filled skulls with paraffin and dropped them from varying heights, and then divided the bone, to note in numerous instances that, although the bone had not been fractured, it had yielded at the point of impact to a degree producing a marked depression in the paraffin beneath. After various injuries, especially to the top of the head, the shape of the skull may be altered and its diameters affected. Many fractures, then, are the result of a bursting force, which may be shown by the fact that hair has been found included within apparently closed fissures, and even on the dura. Moreover, particles of bullets have been found within the skull without any visible opening through which they could have entered, showing that the bone has yielded under impact for a fraction of a second. In certain injuries to the head, as when a man is struck to the ground, there is injury at two points nearly opposite.
Fractures of the skull, especially of the vertex, possess surgical interest mainly as they are accompanied by more or less evidence of intracranial complications. So long as there is no evidence of hemorrhage or laceration within they are ordinarily regarded as a feature of the external wound with which they are usually found, and unless there be comminution, depression, or some other good reason for operating they are covered over as the wound is closed and are left to the natural process of repair by formation of minute callus or by the ossification of granulation tissue.
It is unfair to contrast the results of the surgery of today with those of the pre-antiseptic era. Rules then enforced are now abrogated. One respect in which we violate precedent is in our disregard of the periosteum or pericranium. This is sacrificed without hesitation when found to be infected or torn or lacerated beyond repair. A flap of scalp will adhere as readily to denuded bone as to periosteum, and skin grafts can be applied and will adhere to this same bone—if not upon the first day, a little later when granulations have appeared. In the various plastic operations necessitated about the head we may also transplant flaps upon otherwise uncovered bone without the slightest hesitation. Fractures should be treated mainly in accordance with intracranial complications, or through what can be seen either through the wound or through an opening intentionally made under antiseptic precautions for purposes of exploration. It is conceded to be better policy to remove fragments of bone whose vitality is uncertain and to sacrifice tissue injured or lacerated to such an extent that sloughing would probably follow or be so exposed as to have become infected.
—In the absence of an open wound, and unless incision be made, diagnosis of fractures of the vertex is necessarily conjectural. In the presence of a wound diagnosis is usually easy. In case of a small puncture it will be better to enlarge it sufficiently to permit the introduction at least of the finger. With the finger and the eye we seek to detect differences in level, depressions, fissures, etc. Mistakes arise from the formation of an exudate or a clot, by which a depression of the soft parts may be regarded as depression of the bone. Error occasionally arises from the existence of previous atrophy of the bone or any congenital defects in ossification of the skull; also in the skulls of syphilitic patients where disappearance of a gumma is often followed by absorption of the underlying bone. In case of doubt exploratory incisions should be made under aseptic precautions. These should not be made, however, unless the attendant is ready—i. e., has the facilities immediately at hand—for carrying out any further operative procedure that may be necessary, as elevation of fragments, removal of foreign bodies, etc. Error also may arise from mistaking for fracture a deceptive circular effusion of blood which frequently occurs beneath the scalp after injury. Areas of bloody infiltration often have abrupt margins which are calculated to easily deceive. In children, more especially, we often have a circumscribed bloody tumor which may contain cerebrospinal fluid rather than pure blood. In some of these cases after exploration there will be found material resembling brain matter,[555] which, however, is not always such, although real brain substance may escape, caused by rupture of the overlying membranes. Should it be noted that the fluid used for irrigating and cleansing such a wound begins to pulsate, it will imply connection with the cranial cavity, and, obviously, fracture. A suture should not be mistaken for a line of fracture. This mistake is more easy when Wormian bones are present. Blood may be wiped away from a suture line, but not from that indicating fracture. It is not often possible to diagnosticate an isolated fracture of the inner table. It happened, however, once to Stromeyer to notice that so soon as an injured patient assumed the horizontal position he began to vomit, and that nausea subsided when he was placed in the upright position. On autopsy it was found that there had occurred a depressed splintering of the inner table with perforation of the dura—less irritation was produced in the upright position than when the patient was lying down, which accounted for his vomiting when in the horizontal posture. When a comminution has been produced it is always of prognostic value if an unbroken dura be found. Prolapse of brain substance is a serious complication. Escape of cerebrospinal fluid is relatively rare. Rising temperature after these injuries is always a sign of danger.
—Treatment comprises attention to the local injury and the suitable dealing with the condition of the brain within when injured. The treatment of simple fractures is expectant. In the absence of indication for operation it should be simple, and should consist of physiological rest, aseptic dressings, ice applications to the head, the administration of such laxatives, diuretics, antacids, etc., as may be necessary to favor free excretion and to guard against autointoxication. Whenever there is reason to suspect a depression, exploratory incision should be made. Actual depression, whether the fracture be compound or not, requires operation. This course is justified by the numerous instances in which later consequences have been noted, such as traumatic epilepsy, insanity, etc.
Compound injuries should always be operated upon in some manner, which includes the removal of loosened splinters, the elevation of depressed bone, the removal of foreign matter, the checking of hemorrhage, the excision of bruised and lacerated tissue, and the proper closure of the wound, with or without drainage.
In serious and lacerated cases it is inadvisable to close the wound with the view of attempting primary union. It should be packed with gauze and temporarily closed with secondary sutures. These measures should be seconded by physiological rest (quietude of the head, which may even be enforced by the posterior plaster-of-Paris splint to the head and neck), attention to the primæ viæ, the avoidance of transportation, the prevention of auto-intoxication, etc. The surgeon should use discrimination as to the amount of bone to be removed, the wisdom of opening the dura when not lacerated, of examination of the brain with the exploring needle, the matter of drainage, and the time during which it shall remain. With reference to all these matters exact rules cannot be given. When drainage is made in recent cases it is usually sufficient to drain the scalp wound. Only in cases where there is probability of meningeal infection is it advisable to attempt to drain the dural cavity. This is better accomplished with gauze, catgut, or folded rubber tissue than with drainage tubes.
Skull fractures where the injury is limited to a small area are treated according to a bolder method than was in vogue a number of years ago. There should be careful and judicious operating in every case where distinct depression can be made out, as well as in every case where indications point to injury of parts within the bone. The statistics of trephining in the pre-antiseptic era are valueless as arguments in this consideration. If done according to aseptic precautions, and if good surgical judgment be used in every respect, the operation is per se almost devoid of mortality and should not be regarded as a last resort, but rather in such cases as a first one. I have seen so many instances of later untoward consequences resulting from delay, which corroborate the experience of others, that I would not be misunderstood in this matter. My advice might perhaps be summed up in the following words: Where there are no brain symptoms and no skull symptoms, in fractures of the vertex, let the case alone; when either of these are present, especially the former, it will always be advisable to operate.
[556]
In the majority of these fractures the violence is applied at some more or less distant point, and, by transmission through the arch-like structure of the skull, expends itself in fissuring or comminuting the base. The most frequent location of the indirect injury is upon the convexity. The mechanism of these fractures has been a problem for many centuries, but has been cleared up mainly within the past three decades. Félizet has shown, for instance, how the handle of a hammer may be forced into its head by striking it in either one of two different ways, and has compared the mechanism of basal fractures to this fact. The secret of these fractures probably resides in the elasticity of the skull, which varies within wide limits in different individuals, and which breaks, as do the ribs and the pelvis, at points more or less distant from that at which the injury occurred. Were the skull everywhere equally thick and elastic, there would be much less variation in these fractures, but lacerations frequently extend between the most resistant parts; and when violence is applied upon the forehead we find that the resulting fissure extends between the crista and the wings of the sphenoid, upon the same side, in its course toward the base; that when the lateral region of the skull is injured the fissure extends between the sphenoidal wings and the occipital bone; and that when the occipital region receives the first injury the fracture lies between the pyramid and the occipital crests. The analogy between fractures of the skull and cracks made in nutshells (cocoanuts, etc.) when struck with a hammer is too self-evident to be disregarded. Many years since the French introduced the term fracture by contre-coup (counter-stroke)—a practical admission of the occurrence of fracture at a point more or less opposite to that struck.
Fig. 375
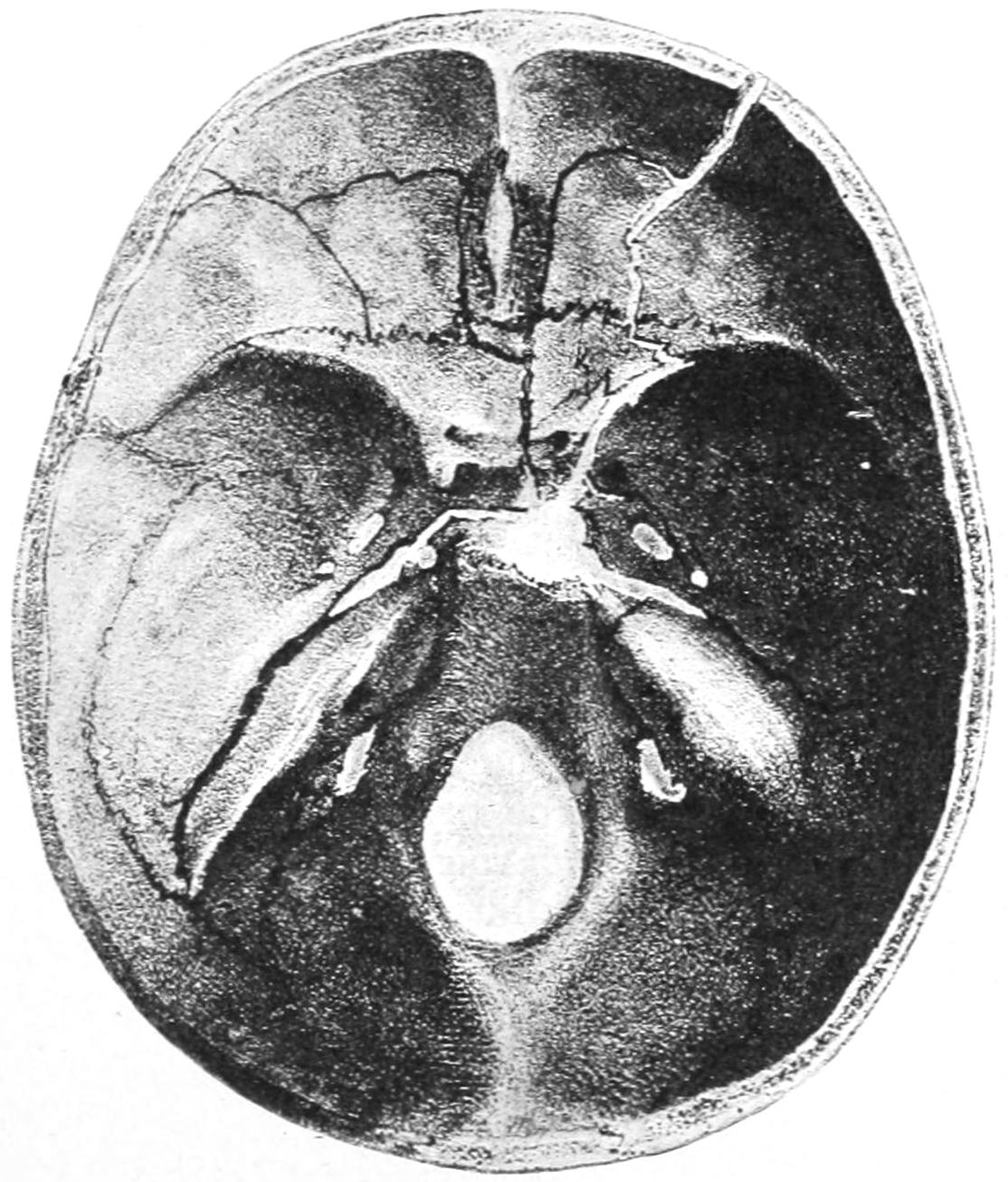
Fracture of base of skull. (Bruns.)
Fig. 376

Fracture of base by fall on vertex. Both condyles broken off and driven in. Vertex was fissured.
There is, however, no certainty about these fractures. Extensive fissures of the vertex are almost always extended to the base of the skull, while the reverse is seldom true. There are doubtless also many cases in which a bursting force compromises the bone rather than mere radiation of unexpended violence; but so long as skulls conform to no fixed mathematical figures nor proportions, and are composed of bones varying in shape, density, and strength, it will be impossible to formulate any laws which are sufficiently comprehensive to be satisfactory. Fractures in the posterior fossa occur most often through violence applied posteriorly and from below. There is a ring form of basal fracture produced mainly by the impact of the vertebral column, as when an individual falls upon his head the weight of the body forcing the cranial base in upon the brain.
PLATE XLII
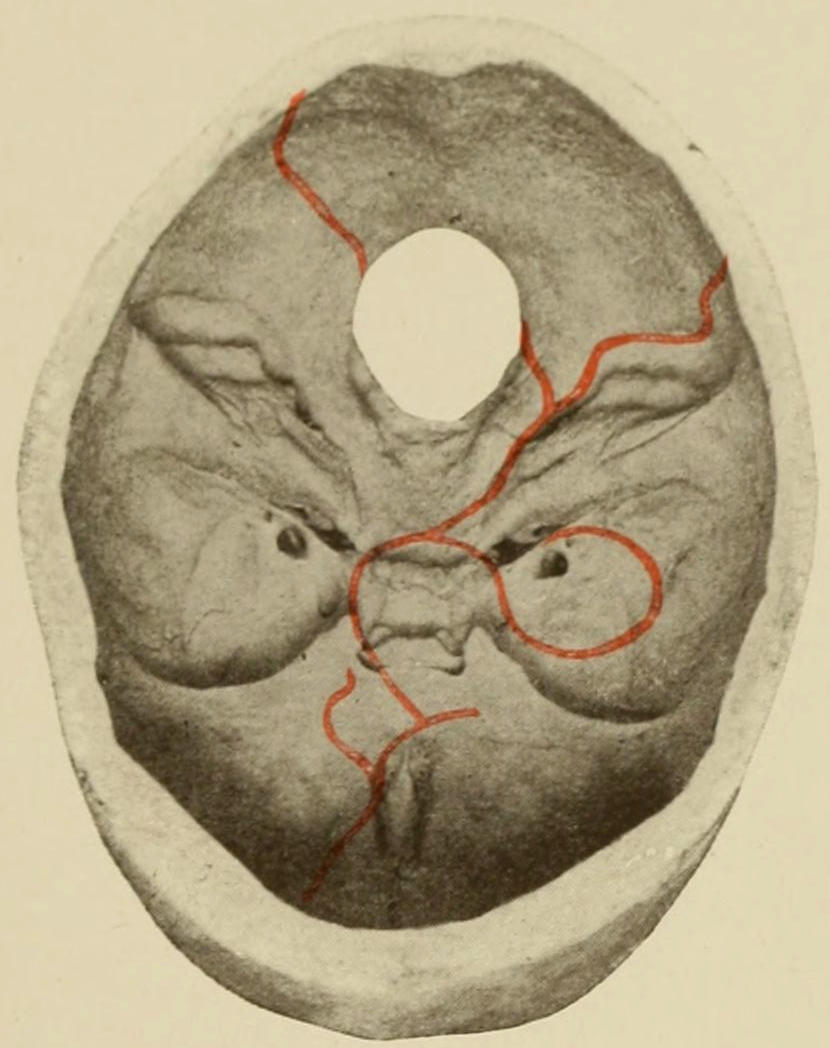
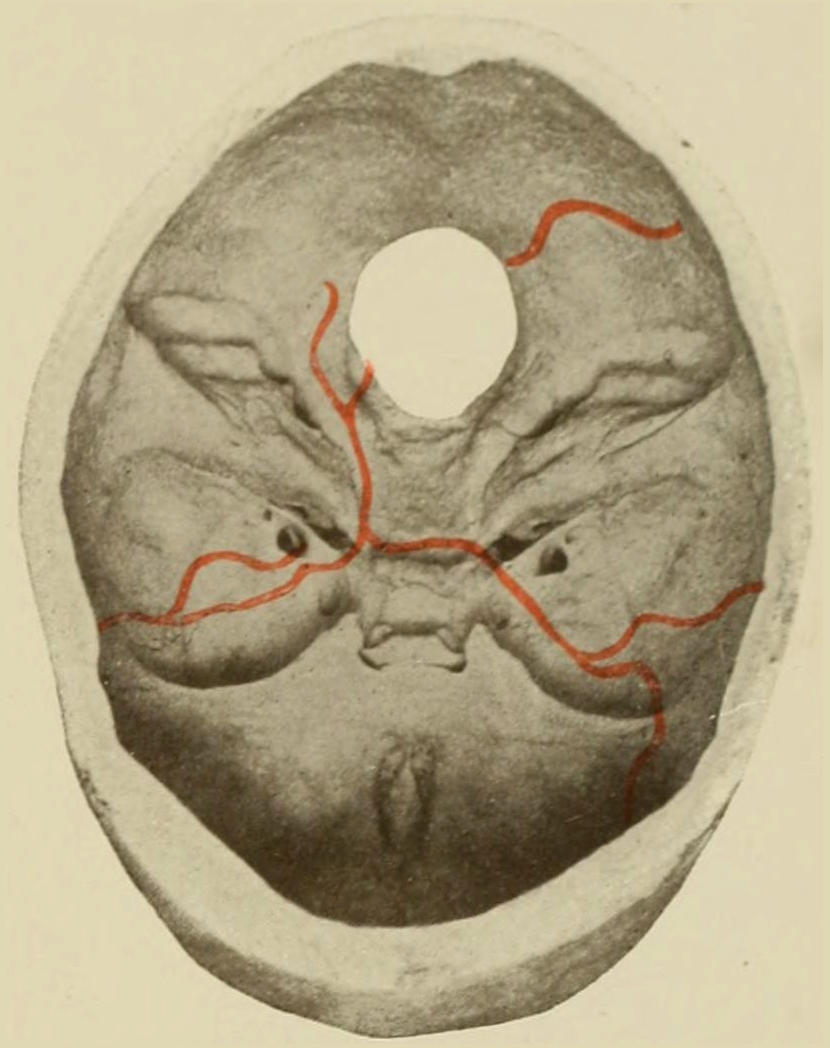
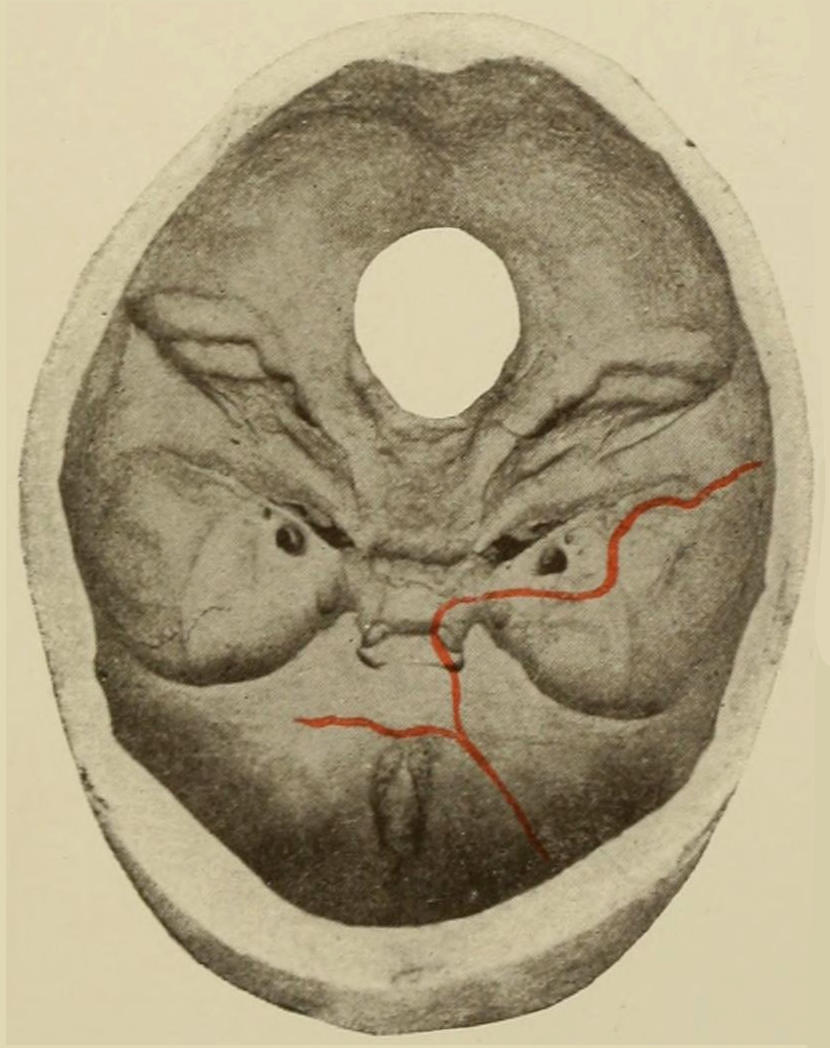
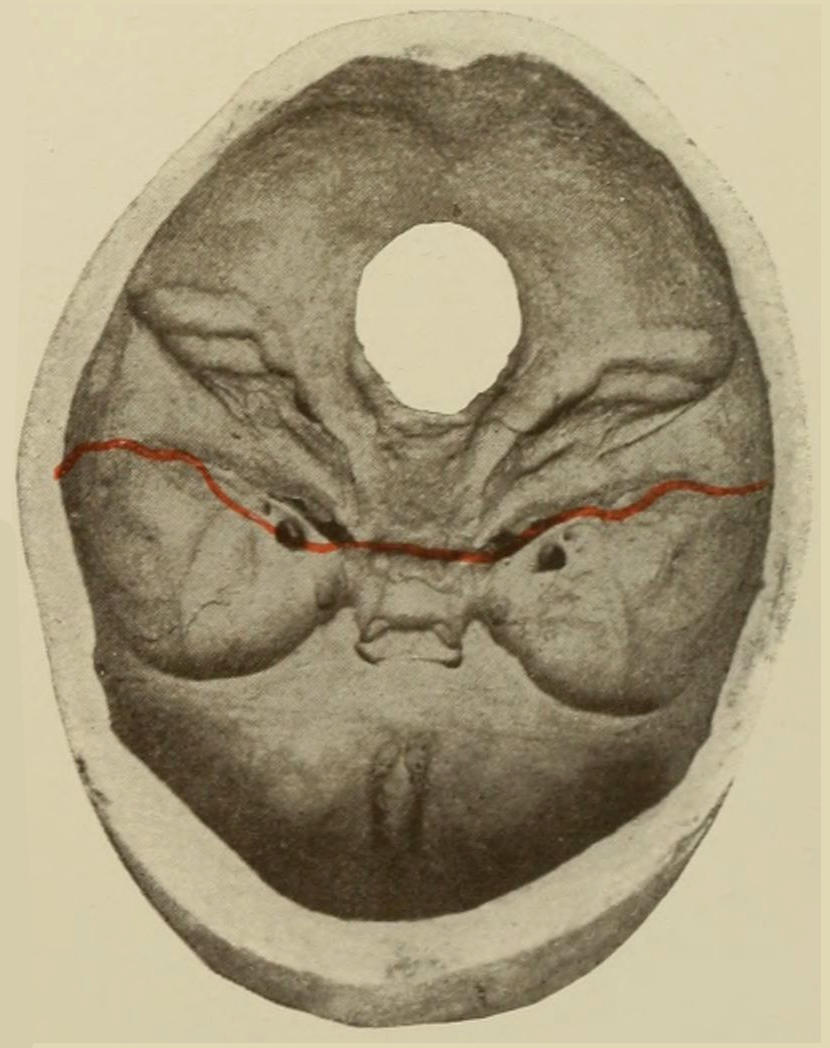
Fractures of the Base of the Skull. Illustrative lines of fissure or fracture are printed in red.
[557]
Fractures of the anterior fossa may involve the roof of the orbit; even facial bones may participate in the injury. These considerations are not without importance, for if a patient presents symptoms of injury of the petrous bone, and if these be accompanied by injury to the lateral region of the skull, we are in a position to make a diagnosis of fracture of the middle fossa. (See Plate XLII, and Figs. 375 and 376.)
By all means the majority of basal fractures are mere fissures which open and close instantly upon their production—close so quickly, in fact, as scarcely even to include blood between the broken bony surfaces.
—The majority of basal fractures are fatal, either because of injuries to the brain, or of hemorrhage or violence along the nerve trunks, or from infection extending along the newly opened paths. Other things being equal, the longer the fissure the greater the danger, particularly so when it takes its origin in the vertex, and because of greater ease of infection. Air infection may occur in any basal fracture by fissures extending into the various air-containing cavities—nose, ears, sinuses, etc. They are then practically compound, though invisibly so. The general prognosis will depend, first, upon the injury to the cranial contents; second, upon the possibility of infection. Statistics are absolutely unreliable, although always possessing interest. Numerous museum specimens show the perfection with which bony repair may occur and the admirable way in which compensation is afforded for defects. Suppuration after basal fractures is mainly that due to purulent basal meningitis, in which case the brain symptoms dominate in the clinical picture, while the appearance of a single drop of pus in the ear or upon the surface is of the greatest significance. The conversion of a serous outflow (e. g., from the ear) into purulent fluid is also pathognomonic. Various paralyses, principally of the cranial nerves, may follow this injury and prove temporary or permanent. Diagnosis is often made by a study of these special nerve lesions.
—The most significant diagnostic features are:
1. Spread of blood from the point of fracture until it appears as an ecchymosis at certain points beneath the skin: This will occur early in some cases and late in others. It may appear beneath the skin or beneath the conjunctiva or other mucous membranes, even in the pharynx. Occurring about the mastoid, it implies fracture of the middle or posterior fossa; about the eyelids, of the anterior fossa. Beneath the bulbar conjunctiva it means extravasation along the optic sheath, probably from within the dura. In fractures of the posterior fossa it will come to the surface of the neck, but only after two or three days. The ecchymoses about the lids or orbits occurring after two or three days mean more than those occurring within these days, for the latter may be caused by external bruising. The globe of the eye may be pushed forward by blood accumulating within the orbit. Exophthalmos thus produced is therefore most significant, though not common.
2. Escape of serous fluid, blood, or brain substance from the cavities of the skull: Hemorrhages from this cause occur most often from the ear, the petrous bone being tunnelled with various canals through which blood may thus escape. The surgeon should, however, assure himself in every instance that the blood is escaping from the ear and not from some trifling wound of the external soft parts, the soft walls of the meatus, or the tympanum. Profuse hemorrhage can probably only come from a basal fracture. Escape of serous fluid is usually noted as a sequel to hemorrhage, although it may begin almost immediately after an injury. Rarely more than twenty-four hours elapse before it begins to flow. The quantity of fluid discharged is sometimes considerable. It may occur in frequent drops or during expulsive efforts, like coughing, or may ooze in such a way as to be insensibly collected by the absorbent dressings. In average cases the amount in twenty-four hours is from 100 Cc. to 200 Cc.; 800 Cc. have been noted in occasional instances, and in a very few still more. Occasionally violent expiration will increase the flow.
In some cases the fluid may escape through the Eustachian tube into the pharynx, whence it may escape by the nostrils or be swallowed.
The escape of brain substance is rarely noted, but obviously implies such serious injury as to make the prognosis of the worst.
[558]
3. Disturbance of function along particular cranial nerves, paralysis of which is often produced by fractures of the base, especially those involving the foramen of exit of the nerve involved: The nerve may be lacerated or injured in such case by the fragment of bone.
In addition to these distinctive features there will be in the majority of instances brain symptoms, either of contusion or compression, varying in severity within all possible limits, but adding their weight to the value of the testimony.
Other and unusual signs of basal fracture may occur, such as communication between the cavities of the petrous bone and the mastoid cells, leading to the formation of pneumatocele (see page 545), or emphysema of the overlying soft parts, observed mostly about the orbits, when the nasal cavity is involved.
—The treatment of basal fractures is mainly symptomatic. The first effort should be to make antiseptic all those parts of the skull involved, which means to shave the scalp; to thoroughly cleanse and irrigate the external ear and the auditory meatus, using a head mirror and ear speculum for this purpose; to tampon the meatus with antiseptic cotton; to provide a copious absorbent dressing for such fluid as may escape and to change this frequently; to cleanse the nasal cavity as well as the conjunctival sac, for all of which the peroxide of hydrogen is serviceable. All of this should be done promptly, while at the same time studying the patient for evidence of brain injury or of involvement of special nerves. By the time these measures are thoroughly performed a decision as to the necessity for immediate operation should have been reached. Evidence of brain compression wanting, and in the absence of external or compound injury the patient may be left at rest, with cold applications to the head and active purgation. In many of these instances benefit follows the application of a number of leeches to the mastoid region and to the occiput. Operation is necessary later only when brain symptoms supervene, these consisting of evidences of compression, either from blood or from pus, as compression from other causes should have been acting at the time of the first examination, and should have been recognized at that time. When direct fractures are evident the possibility of the entrance of foreign bodies should be also remembered. Thus penetrating fractures of the base have occurred through the orbit as the result of accident or assault, and such weapons or implements as foils, ramrods, drumsticks, canes, umbrella points, etc., have been known not only to penetrate into the brain, but perhaps to leave some portion of their substance—e. g., a foil tip or an umbrella tip—within the cranium after their withdrawal.
Separation of sutures, known also as diastasis of the same, is the occasional result of injury instead of, or complicated with, fissures or other fractures. It is the result of violence, and is virtually a specific form of fracture, from which it differs in no essential particular. Diastasis can only take place along lines of previous suture, but it is possible that Wormian bones may be thus loosened. Sutures thus separated ordinarily heal by fibrous repair rather than osseous union. Diagnosis is possible only as they are exposed to view, although displacement in the middle line or along known suture lines may be regarded as diastasis. The treatment differs in no respect from that of other fractures.
Injuries to the frontal sinuses occasionally complicate fractures of the skull. These sinuses vary in different individuals, are rarely truly symmetrical, and are not found in the young. They connect with the nose in such a way that emphysema of the frontal region is quite possible, while air may be blown beneath the periosteum or may communicate with the interior of the cranium. In wounds of the frontal region the sinuses are occasionally opened—a fact of importance, for infection of the Schneiderian membrane may occur and endanger life, mainly because of the retention of infectious products within its cavities. Moreover, by such wounds the ethmoid may also be injured. Pus which escapes from these sinuses and from the ethmoidal cells is usually thin and bad-smelling. Long continuation of suppuration after such injuries probably means necrosis and formation of sequestra.
By better acquaintance with certain portions of the brain whose function is now generally recognized and described, as well as with the more exact knowledge regarding the entire encephalon, the outcome of many recent studies, the teaching of the past in regard[559] to the nature of various brain lesions has been essentially modified. Especially is this true in regard to the distinction formerly emphasized as between concussion and compression. In discussing brain injuries we should, first of all, distinguish between traumatic disturbances of the entire endocranium and localized injuries to the brain or particular vessels and nerves entering into its composition. In regard to the first, it is possible that the entire blood or lymphatic circulation within the cranium may be affected in such a way as to influence its nutrition and function, by which means activity and function are mildly or seriously perverted. The immediate effect of severe injury to any part of the body is reflex vasomotor spasm, which constitutes the essential feature of the condition known everywhere as shock. It is this condition, with its marked local expressions, which was formerly known as concussion of the brain. When studied upon its merits it is found to be indistinguishable from shock produced by injuries to other parts. The condition for so many years taught and recognized as concussion is but shock following injury to the head. This makes no further demands upon the question of pathology than those prompted by any traumatic disturbance.
Through the mechanism of the cerebrospinal fluid rapid alterations of pressure and of the volume of the brain are produced. There is an easy path between the inelastic cranial cavity and the exceedingly elastic and accommodating spinal canal, which latter serves as a reservoir for the fluid which may be pressed out of the cranium when brain pressure is increased. While the subdural and subarachnoid spaces are each of them absolutely closed sacs and do not communicate one with the other, there is ample accommodation within each to permit a constant equilibrium of pressure under ordinary circumstances, as between the spinal canal and the cranial cavity. The brain expands in volume with every systole of the heart, while with every diastole it contracts. Its size is, moreover, modified by the motions of respiration. Under these extremely accommodating conditions it is scarcely credible that external injuries which leave no internal evidences of violence should do anything more than disturb the equilibrium of fluid distribution.
We inherit this term concussion from the earlier masters of our art, by whom, however, it was used in a much broader sense than of late. Its modern significance was given to it by Boirel, who made it apply to a group of cerebral symptoms the result of injuries not accompanied by fracture or perceptible laceration of vessels, symptoms varying in intensity and duration.
Our present position is practically this: The possibility of pure concussion of the brain—i. e., disturbance of brain function without gross mechanical lesions—is admitted, but its general frequency is denied. When present it should either pass away quickly, the condition being equivalent to that called “stunning,” or, if it assume distinct form, its signs and symptoms are indistinguishable from those of shock, consisting essentially of rapid and feeble pulse, quick and shallow respiration, pallor of the skin, copious perspiration, complete or partial unconsciousness, muscle incoördination, with lack of sphincter control, occasional vomiting, the pupils usually reacting in light.
—The treatment for this condition is essentially that for shock, and whatever may be called for in the way of attention to injuries about the head—e. g., sewing up a scalp wound, etc. (See Chapter XVIII, on Blood Pressure.)
The condition of shock (cerebral concussion), when of pure type, passes away with reasonable promptness, especially when aided by surgical treatment. Anything which persists in the way of muscle paralysis, disturbance of function of nerves of special sense, or other sign of importance, indicates something more than mere vibratory disturbance: it implies mechanical lesion which could be perceived by the eye were the parts exposed, and constitutes the condition known as contusion. This implies the existence of trifling exudates, or hemorrhages, which lead not only to absorption but even cicatrization. Contusion pure and simple differs from ordinary laceration as a contusion elsewhere may differ from a wound. It cannot be separated, however, from conditions[560] in which there are minute separations of continuity and actual lacerations. It may be divided into three postmortem forms—general hyperemia, with or without edema; punctate or miliary hemorrhages; and thrombosis of minute vessels, which may occur separately or together. Moreover, there may exist similar lesions in the meninges, constituting meningeal contusion. Ordinarily minute vessels of the pia are ruptured and blood is effused in small and thin patches over various parts of the brain. The so-called compression apoplexies of certain authors are inseparable from the conditions above described. Such minute blood clots are only to be distinguished upon very careful sectioning of the brain, and are found most often in the region of the medulla and along the floor of the fourth ventricle. They are probably caused by the forcing into the fourth from the lateral ventricles of the fluid contained in the latter.
—When the ordinary symptoms of shock, which follow all severe injuries to the head, especially when the deep lesions are not too severe, fail to disappear in a short time under proper treatment, and when new and irregular symptoms are superadded to those of shock alone, it is reasonable to suppose that the intracranial condition is one of contusion rather than of shock. When mental agitation changes into delirium, when the rapid, feeble pulse becomes stronger and slower, the respiration deeper, the limbs move in incoördinate ways, the speech disturbed from muscle incoördination, the patient selects wrong words, or when the mental condition becomes more serious and stupor or coma take place of the delirium, while external irritants have less and less effect, and when the pupils gradually enlarge while failing to respond to light, it may be said that the condition of contusion is making itself apparent. If along with muscle uncertainty there is also muscle spasm or rigidity, with fixation of the fingers in the athetoid position, the evidence to this effect is increasing. If with all this the thermometer fails to show that an active inflammatory condition—i. e., meningitis—is prevailing the diagnosis may be regarded as certain. Error may possibly arise when there are evidences of alcoholism. Coma following head injury ought not to be ascribed to the alcoholic condition except by the strictest process of exclusion. Temperature alone will be of the greatest service in this direction, since in alcoholism it is usually subnormal. In apoplexy and non-traumatic hemorrhages it is also usually subnormal at the commencement of the attack, rising to normal, and remaining there if the patient recover, but continuing to rise in cases where the prognosis is bad.
—The treatment of brain contusion should be managed largely in response to special symptoms. Physiological rest, attention to scalp wounds, fractures, etc., shaving of the scalp, application of ice to the head, with such stimulation to the heart as may be necessary in extreme cases by subcutaneous administration of adrenalin, atropine, etc., by local fomentations over the epigastrium, or by immersion in a hot bath when surroundings permit it—these in a general way constitute most of the methods of treatment in contusion. When only symptoms of diffuse and minute lacerations can be recognized the use of the trephine is impracticable except when indicated by some external marking—i. e., compound fracture or the like. When localizing symptoms are present the trephine is, of course, indicated. When the skull injury is recognized as a basal fracture, venesection or the application of leeches behind the ears will be most serviceable. In every such case there is the greatest necessity for regulating the excretions and preventing auto-intoxication. For this purpose diuretics and laxatives should be used, often in conjunction with intestinal antiseptics. The catheter should be employed whenever indicated by the condition of the bladder, which should be carefully watched. As the days go by, and patients lie more or less helpless and inert, the greatest care should be exercised for the prevention of bed-sores. When mental inertness, muscle rigidity, etc., fail to disappear, potassium iodide should be used internally.
That the cranial contents—brain, blood, lymph, and cerebrospinal fluid—completely fill the cranial cavity has been already amply shown, as well as that there is no room for anything in the shape of a foreign body without seriously affecting the equilibrium between the brain and the contents of the spinal canal. When, however, any foreign substance exerts pressure upon the brain the results are invariably the same, be this substance what it may, and compression signs are always the same, no matter what the compressing cause. Reduction in capacity of the cranial cavity (i. e., compression) may be produced—
PLATE XLIII
FIG. 1.
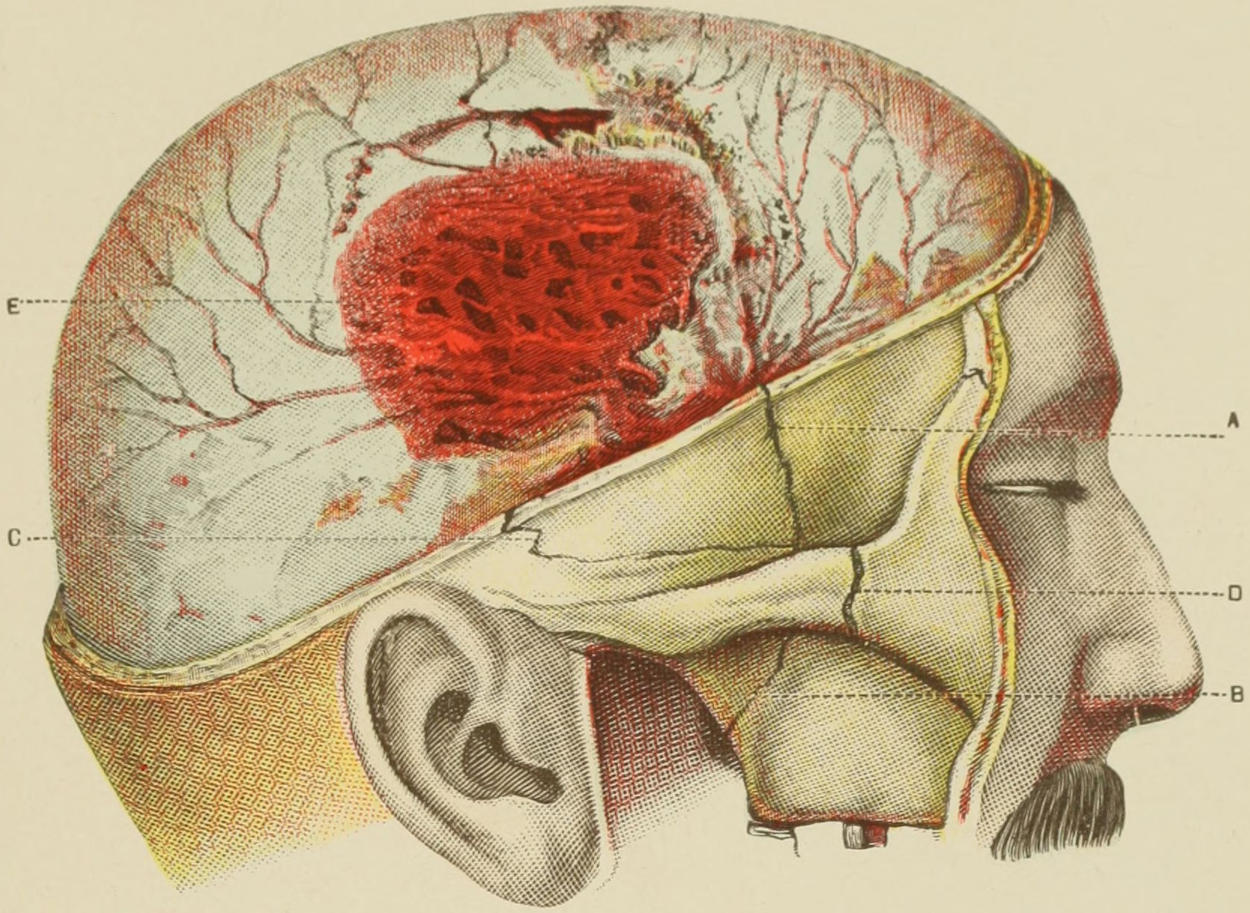
FIG. 2.
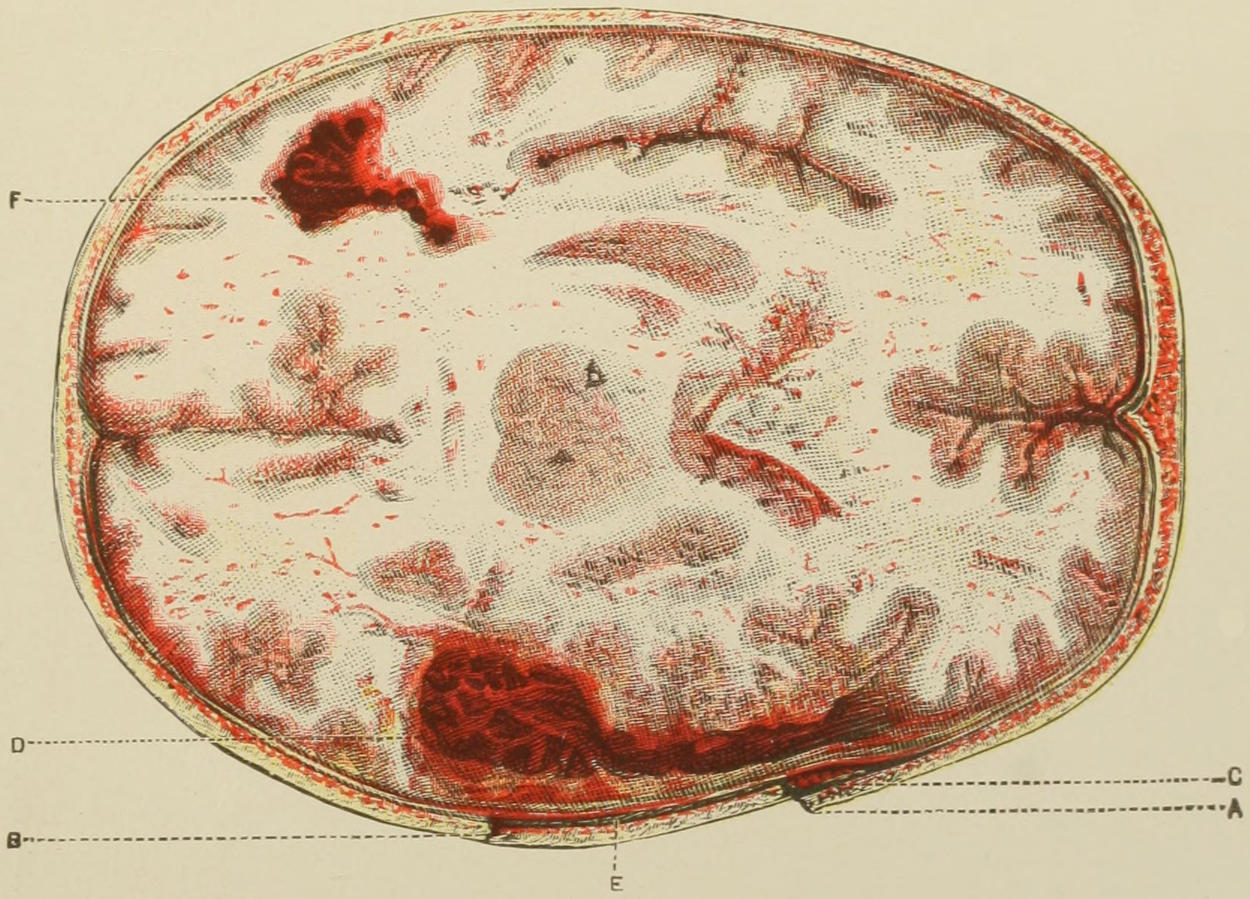
Fig. 1. Compound Fracture of Cranium, with Depression; Fracture of Bones of Face; Extradural Clot from Rupture of Middle Meningeal Artery.
Fig. 2. Horizontal Section of same, showing Depressed Fracture of Bone. (Anger.)
C, extradural clot; D, laceration of brain substance, with extensive intracerebral clot; F, same condition produced by contrecoup. Punctate hemorrhages and minute lacerations at numerous points, characteristic of contusion of the brain.
[561]
1. By reducing the dimensions of its enclosing walls (e. g., depressed fractures or by direct pressure);
2. By increase in the quantity of cerebrospinal fluid or of the volume of the brain, which latter may be produced by edema, by serous exudate, or by actual hypertrophy;
3. By foreign bodies, which may enter the skull from without;
4. By pathological conditions—collections of blood or pus, tumors, etc., which may be produced either from the brain substance, its containing bone or membranes, or its vessels.
In every one of these conditions the size and tension of the brain are affected. The cerebrospinal fluid is mainly involved in acute not in chronic conditions. A slow reduction of the diameters of the skull produces such slow alterations of pressure as to cause a minimum of disturbance. So far as compression from traumatic influences is concerned we distinguish mainly between compression—
1. By extravasation of blood (see Plate XLIII);
2. By fractures of the skull with depression, or by foreign bodies penetrating from without;
3. By products of acute infectious inflammation due to septic infection from without.
The result common to all of these is increase of intracranial tension, and its consequence is a less rapid flow of blood and an altered blood supply to the brain and its membranes.
Experiment has established that in compression of the brain cerebrospinal fluid is forced by pressure into the spinal canal, whose membranes are more elastic, and which thus help to accommodate it; it has been also established that compression of the brain by one-sixth of its volume, by any material, is fatal, and that much less is at least serious. That fractures with depression produce sometimes serious, at other times trifling, symptoms is due to the varying accommodation of the spinal canal. Both experiment and observation seem to confirm the view that consciousness pertains to the cortex as a whole, and that unconsciousness is an inhibitory or paralytic condition which is produced in compression.
Temperature is a matter of great importance in studying compression and foretelling its consequences. Elevation of temperature is an early, continuous, and constant symptom in these cases. If temperature be subnormal and subsequently rise, prognosis is bad. Variations of temperature are more reliable guides than conditions of consciousness. As Phelps has remarked, in no condition except sunstroke is temperature so uniformly high as in cases of serious encephalic lesions.
—As indicated above, the symptoms and signs of compression are practically identical, no matter what the compressing cause. When this cause acts instantly there is no time afforded for differentiation, but when it occurs slowly we note the following symptoms, and about in the order here presented: Irritability or restlessness; visceral disturbances; pain; intense cephalalgia; congestion of the face; narrow pupils; augmented pulse, often seen in the carotids. If compression occur more rapidly, torpor quickly succeeds erethism, after which patients vomit, have convulsions or at least convulsive motions, speech is disturbed, and stupor comes on, from which they neither awake nor can be awakened until the compression is relieved. All of these indications refer to involvement of the cortex, which is generally regarded as the seat of consciousness as well as of projection and imagination. During the night, of the senses produced by pressure upon the cortex only the automatic basal apparatus and that of the spinal cord continue in more or less disturbed operation. Of all the general functions consciousness vanishes first and returns among the last. When intracranial pressure has reached a certain point, epileptiform convulsions result, varying in intensity, affecting all the limbs, and terminating perhaps with rigidity. These form an expression of high pressure. Similar convulsions occur in various head wounds, explanation for which is the result of pressure, which, though not extensive, may produce alteration in the circulation, with its disastrous consequences. The later and constant evidences of compression, and those which in aggravated cases supervene at once, are reduction of pulse rate, due to the action of the pneumogastric, which suffers first an irritation and later a paralysis. The pulse becomes not only slackened but full; the respiration rate is correspondingly reduced, so that breathing during coma is deep, slow, and often stertorous. This feature of stertor is an expression of paralysis[562] of the palatal and pharyngeal muscles, which flap, as it were, in the air current. Vomiting, which may occur before brain tension has risen high, does not occur in the most serious cases. Coma is absolute.
Along with these signs the most important other indications are the paralyses, which may consist of monoplegia, hemiplegia, or paralysis of individual muscle groups, according as pressure is made upon a limited area or upon an entire hemisphere. By the division of the cranial cavity by the falx and the tentorium it is divided into chambers, in any one of which pressure may be more manifest than in the others. Nevertheless a serious compressing cause will affect the tension of the cerebrospinal fluid and produce general expression of pressure. The pupils often vary, and responsiveness to light is occasionally noted. Nystagmus and ocular rotation may be occasionally seen. Choking of the optic disk is also a frequent phenomenon, to be recognized only by ophthalmoscopic examination. This is due to pressure in the subdural and subarachnoid prolongations along the optic nerve. In milder cases of chronic compression disturbances of vision are of very great clinical importance. These pertain especially to diagnosis of hydrocephalus and of brain tumors. When they occur immediately after injury and remain, they depend upon laceration or other severe injury of the optic nerve. Those which quickly disappear depend mainly upon pressure of blood, which is reabsorbed, while those which are later in their appearance depend upon later intracranial complications. A unilateral lesion of the optic nerve depends most often upon injuries to it within the optic canal. When the lesion is bilateral the cause lies deep. General paralysis may be of the type of hemiplegia, single or double—i. e., by “double” I mean paralysis of the entire voluntary musculature of the body, which necessarily implies serious and often fatal hemorrhage.
—This depends in large degree upon the nature of the compressing cause and of the possibility of its removal. While the nature of the same may ordinarily be determined, how much can be accomplished by way of removal may often not be foretold before the operation at which this should be attempted. In every acute case it is desirable to make this attempt early, for high pressure, which may be borne for a short time, is fatal if continued. Compression to any serious degree is usually fatal. So soon as paralysis of circulatory and respiratory centres is apparent the beginning of the end is at hand. Another reason for hastening operation is that acute softening of brain tissue comes on promptly, as well as general cerebral edema, which has destroyed many a patient during the second to the fourth day after injury.
—The treatment of compression is summed up in one phrase—i. e., to remove the cause when possible. The only cases in which this rule may be safely disregarded are those where the attempt to remove the cause means more danger than to leave it unremoved. This is not true, however, in the ordinary cases of bone depression, meningeal hemorrhage, etc. Before operation, however, or as a substitute for it in cases of minor severity, it may be well to assist venous outflow by venesection, by which blood pressure is reduced. In these cases this may be done from the temporal veins or external jugulars, with the patient in the semi-upright position. Drastic purgatives may also be employed in order to utilize intestinal outpour as a stimulation to resorption of cerebrospinal fluid. The physiological action of cold (ice-bags) may also be secured for the purpose of contracting the cerebral arteries. But all these measures are only to be resorted to when there is uncertainty as to the wisdom of operating, since when operation is indicated it should be done at once, and should take precedence of everything else. This operation means ordinarily the procedure to which the now general term trephining has been, by common consent applied, and comprises any measure by which the skull is opened at a suitable place and the dura or the underlying cortex exposed to such extent as to permit removal of the compressing cause. Whether the opening be made with trephine (annular saw) or with the straight or revolving saw, with bone chisel, with bone forceps, or with anything else, is a matter of choice on the part of the operator. So, too, removal of the compressing cause should include the elevation of depressed bone, the removal of dislodged particles as well as of all foreign bodies, the cleaning out of blood clot, the checking of hemorrhage, and the closure of the wound, with or without drainage or counteropening at some other part of the skull, as may seem desirable in special cases. This entire procedure comes now under the name of trephining, and should in most instances be painstakingly followed.
The operative maneuvers will be discussed in another portion of this chapter.
[563]
Intracranial hemorrhages may occur—
(a) From internal sources through the broken bone or between it and the dura (extradural);
(b) Beneath the dura, between or into the membranes (subdural);
(c) Into the brain substance proper or the ventricles (subcortical or intraventricular).
The vessels whose injuries are most often under consideration are the meningeal arteries, the sinuses, the small vessels of the membranes, and the internal carotid. The arteries, like the sinus walls, may be ruptured either by substances forced in from without or by sheer laceration. The longitudinal sinus is most liable to injury from without. When this sinus is exposed, it may be dealt with either by suture if the wound be small, or by ligation, or by tamponing with prepared gauze. Hemorrhage from this source is ordinarily not difficult to check. Fatal air embolism has resulted through an opened sinus not properly plugged. The other sinuses are more rarely injured, as by gunshot wound, fracture of the base, etc. The sinuses have also been injured by compression of the skull during parturition. Bleeding from a sinus is usually indistinguishable from that from a meningeal artery, except that the former occurs more slowly.
—Injuries to the middle meningeal artery naturally occur in the immediate neighborhood of this vessel, which is not infrequently ruptured by contre-coup. The artery runs sometimes in a groove of the bone, sometimes in the dura, and sometimes entirely in the bone. The more it lies within the bone the more likely it is to be ruptured when this part of the skull is fissured. Basal fractures often follow the groove for this artery. The anterior branch is more often injured than the posterior. Extravasations from this source are more common than from all others combined, the amount of blood varying within wide limits. 240 Gm. of blood clot have been known to collect and the dura to be separated down to the base of the skull. I have repeatedly taken away a small teacupful of blood clot in such cases (Fig. 377 and Plate XLIII).
Fig. 377
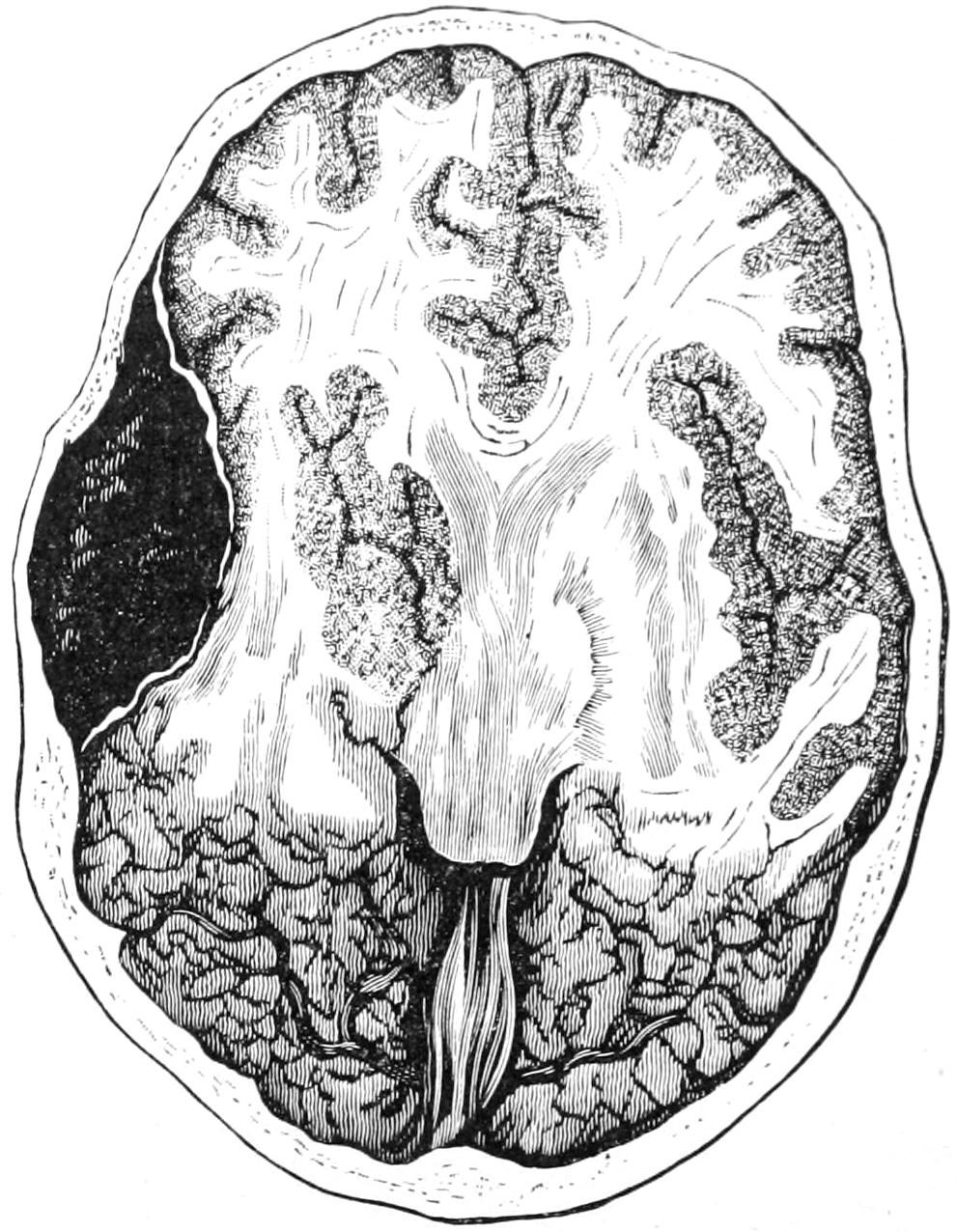
Compression following hemorrhage from the middle meningeal artery. (Helferich.)
Symptoms.
—The symptoms of this hemorrhage are those of compression, while extravasation may be rapid and quickly fatal, delayed for some time, or may take place in two stages, the first but slight and producing no coma. New clots are always dark and disk-shaped, thick in the middle, with a definite margin. As the clots become older they become more adherent and difficult to remove. The symptoms of meningeal hemorrhage consist of an interval of consciousness or lucidity after injury, followed by epileptic or spastic symptoms, alterations in the pupils and pulse, unconsciousness passing into coma, and stertorous respiration. There may or may not be external evidence of head injury. The character of the paralysis (hemiplegia) may indicate that the clot is really upon the side opposite to that of the skull which shows evidence of injury. In this case arterial laceration is the result of contre-coup. According to the rapidity of the symptoms is the extent of the primary lesion. Meningeal hemorrhages involve immediately the motor area, which makes diagnosis all the easier.
—Injuries to the carotid within the cranium are exceedingly rare. Still, it has been injured in basal fractures and penetrating wounds.
[564]
—Development of arteriovenous aneurysms after basal injuries is occasionally noted. They will occasionally give rise to pulsating exophthalmos. Pulsating tumors within the orbit which push the eye forward not infrequently occur after serious head injury. Of 77 cases collected by Rivington, 41 had a traumatic origin.
—Subdural hemorrhages are not infrequent in the skulls of the newborn, and constitute the so-called apoplexia neonatorum. They may occasion convulsions and paralyses of irregular type, while if the extravasations become infected multiple abscess may result.
In adults subdural hemorrhages are most commonly connected with brain lesions which have been already spoken of as contusions. They may be the starting points for pachymeningitis. Their most common results are disturbances of consciousness and mentality. Paralytic dementia follows in some of these cases. Extensive subdural hemorrhage may give a clinical picture corresponding to extradural. Disseminated minute ecchymoses constitute minute focal lesions, which are, however, usually so distributed as to confuse and prevent accurate diagnosis. Apoplexy or intraventricular hemorrhages, especially from the lenticulostriate artery (Charcot’s “artery of hemorrhage”), have until very recently never been regarded as warranting surgical interference. Of late, however, especially in the ingravescent or progressive forms, ligature of the common carotid has been of some service, though in order to render this effective ligation should be done early.
—Traumatic intraventricular hemorrhage occurs in much the same way as meningeal, by contre-coup. Individuality of symptoms is lost in the general comatose condition of the patient, but when operation is performed, as it is usually best to perform it, if no extradural clot be found and if brain tension be evidently increased, the dura should be opened; after which, if no subdural clot be seen, the ventricles should be tapped with an exploring instrument. In this case, if blood be removed by aspiration, a knife should be passed directly into the ventricle, after which blood, if present, will promptly escape. Dennis was the first to diagnosticate the presence of intraventricular clot and to deliberately incise into it, and I have myself repeatedly imitated this procedure, both with and without success.
In every case in which superficial or cortical hemorrhage can be recognized—or even suspected—or intraventricular hemorrhage as well, one should insist upon exploration. This means trephining, with perhaps aspiration of the ventricular contents. Tapping of the ventricle is described under Treatment for Hydrocephalus, while trephining is described at the end of this chapter.
These have been mentioned under contusion of the brain. They may be divided into those which occur with or without fracture of the cranial bones. The term contusion was first suggested by Dupuytren. The condition comprises all degrees of injury, from the most minute local disturbances to lesions involving the entire hemisphere. The milder forms show a sprinkling of punctate hemorrhages, numerous in the centre of the injured area, the surrounding tissue taking on a more or less diffuse tint, which fades out toward the periphery, discoloration being due to the imbibition of the coloring matter of the blood. In more extensive injuries clots as large as peas, or larger, are embedded at various points, each surrounded by its area of discoloration. When foreign bodies have been driven into the brain the tissue is also discolored, while various foreign materials may be met. In instances of great violence there may occur absolute rupture of brain tissue extending from cortex to ventricle.
—Prognosis depends in large degree upon escape from or occurrence of infection. In infected cases the principal dangers are from blood pressure and from later edema or acute softening as well as from meningitis. Brain lacerations may heal by cicatricial repair, but usually with some perversion of function.
The possibility of cystic degeneration of large or small clots is one of great importance. (See Cysts of New Formation in Chapter XXVI, page 264.) A blood clot within the cranium which fails to resorb is essentially a hematoma, in whose interior softening and conversion into a cyst may easily occur. These cysts make room for themselves at[565] the expense of surrounding brain tissue, and when located in the motor area give rise to localizing symptoms as well as to epileptic convulsions. They may be often diagnosticated with certainty after an accurate history of the case and a study of the phenomena which it presents. As they grow older their walls become firmer, and it is often possible to dissect them out.
That foreign bodies may be encapsulated and remain without producing disturbance is now well known. This is particularly true of bullets. As a rule, however, though encapsulated, they produce symptoms like headache, vertigo, etc. (See Plate XLIII.)
—The general features of brain lacerations are those of contusion. So long as the disturbances are minute, even if multiple, or the foreign body small, compression symptoms are not produced, or at least in very incomplete degree. Minute diagnosis is not easily obtained. The most essential thing is to decide upon the question of operative interference. In the absence of distinctly localizing symptoms or other external markings it is not usually performed. Upon the other hand a lesion which can be localized is probably due to extravasation sufficiently large to be easily reached by opening the skull; and, unless there be other and sufficient reason to the contrary, this should be done (Fig. 378).
In many instances, however, contractures or paralyses of muscle groups occur later, and are followed by spastic conditions which may be permanent. More can be done in these cases by massage, by internal medication, perhaps with external counterirritation, than by distinctly surgical procedures. Tendoplastic or neuroplastic measures for their relief may also be considered. Both albuminuria and glycosuria are known to be the result of injuries herein described, as well as bulbar paralysis and disturbances of special senses. More immediate dangers after these head injuries are those of bronchopneumonia or hemorrhagic or edematous infiltration of the lower lobes of the lungs—conditions often spoken of as hypostatic pneumonia, much resembling those produced experimentally in bilateral division of the pneumogastrics. Some of them are produced by paralysis of the glottis, the result of which is incomplete closure, with aspiration of fluids and solids from the mouth, whose decomposition sets up an infection within the lungs, and is often referred to as aspiration pneumonia. Some form of pulmonary disturbance follows in perhaps one-third of the cases of the injuries above alluded to, and should be anticipated and prevented.
Fig. 378
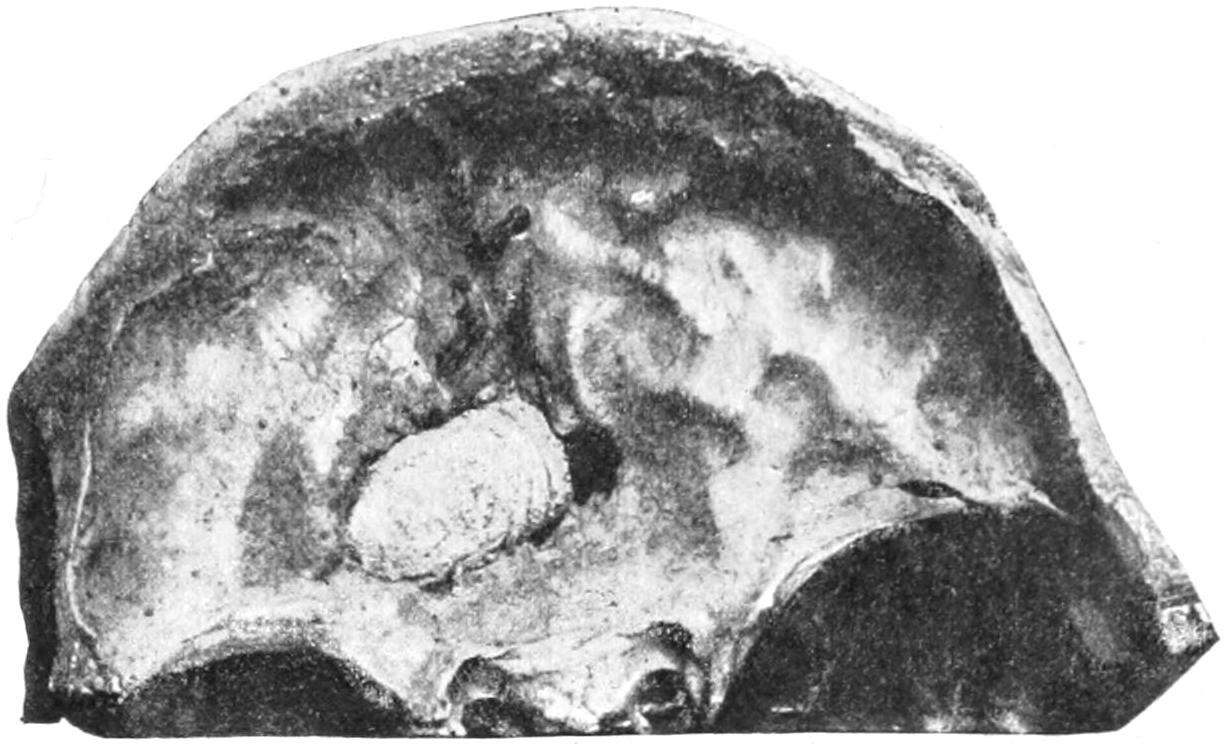
Bullet embedded in anterior fossa. (U. S. Army Med. Museum.)
These have already been extensively considered in a previous chapter, so that but little more need be said of them here. Such wounds in the scalp are likely to be followed by sloughing. So far as gunshot fractures of the skull are concerned, there is frequently a marked discrepancy between the wounds of the inner and outer tables, that last perforated by the bullet being almost splintered. Penetrating wounds of the cranium by Mauser and similar bullets are not necessarily fatal. Many men were shot through the head during the Cuban and South African wars and yet did not die as a result of the wound. (See Chapter XXII.)
—So far as treatment is concerned, gunshot injuries of the skull necessitate trephining or exploration, for checking of hemorrhage, disinfection of the bullet track when possible, often for a counterdrainage opening with through drainage either by tube or gauze. The bullet, if it can be found, should be removed. In searching for it the old porcelain-tipped probe of Nélaton has almost completely given way to Fluhrer’s[566] aluminum probe, which is larger and longer and when rightly directed will by slight weight usually glide gently along a bullet track, thus leading often to the missile, and at the same time indicating by its direction where the counteropening should be made. Two other methods of detecting bullets are now in vogue. Girdner, some years ago, invented a telephone probe, by which, so soon as the instrument touches the missile, a telephone circuit is completed and the operator with a telephone receiver applied over his own ear hears the tell-tale “click” indicating the fact. This has been further improved by the substitution of a bell or “buzzer,” which tells its own tale when the probe touches the bullet.
A still more ingenious application of electricity for the purpose is that afforded by Röntgen’s discovery, and during the American and English campaigns of the past few years skiagrams of skulls showing bullets in various locations have become quite common. (See Plate XIII., p. 229.)
Escape of brain matter beyond its normal level is not uncommon in connection with compound fractures or their sequels. It may be primary, escaping with the blood at the time of the accident, or secondary, occurring during the ensuing days. Any lesion of this kind in which the brain appears or can be handled is entitled to the term prolapsus, in contradistinction to hernia, which implies that, though escaping from the proper cavity, it is nevertheless covered by other textures—e. g., the dura or scalp.
The protrusion may vary in size from a small tumor to one the size of a fist. It is always the result of uncontrolled intracranial tension, and may be produced by hemorrhage, by serous imbibition, or as the result of brain abscess. When immediate it is of the first variety; when later, of the second or third. When abscess is present it usually delays protrusion, which is produced by degrees. Prolapse occurs through large openings, such as those made by gunshot wounds, the trephine, etc. Prolapse proper implies laceration of the dura. It pertains obviously to the convexity of the skull, occurring, however, in exceedingly rare cases into the orbit (Fig. 379).
Fig. 379
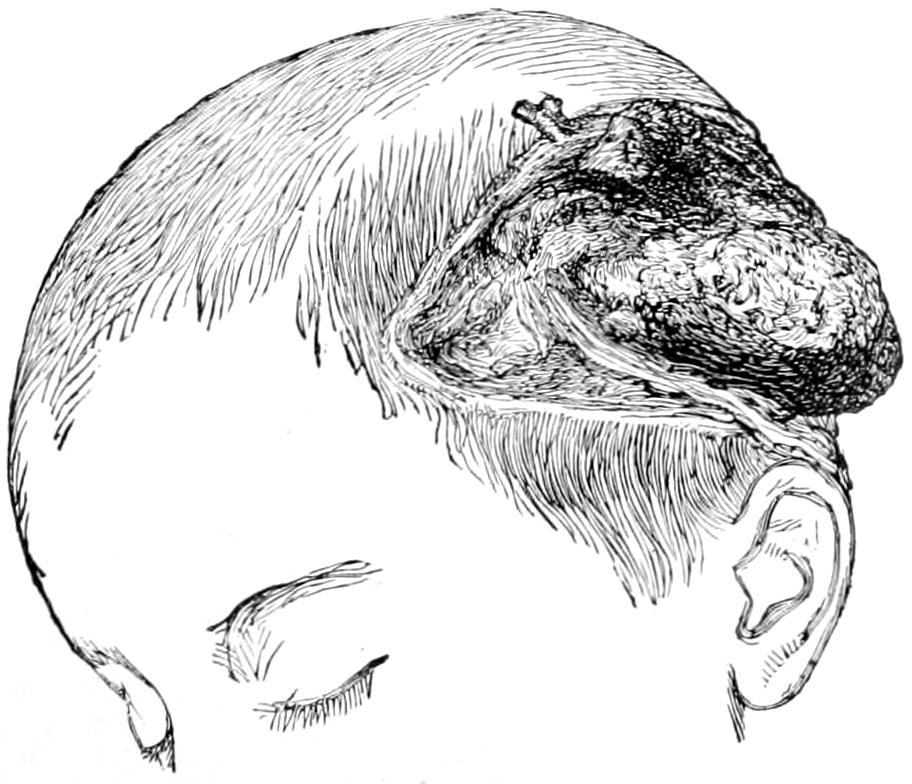
Prolapsus cerebri. (Bryant.)
—The prognosis is generally unfavorable. There is always risk of edema or infection, either of which may prove fatal.
Infiltration, gangrene, suppuration, or repair by granulation may so disfigure and disguise the real brain substance as to lead to error of diagnosis. It by no means follows that every tumor presenting through an opening in the skull is of this character. When gangrene and spontaneous separation occur, spontaneous recovery may follow, the stump being covered by granulations and finally roofed over by connective tissue.
—Treatment in the primary cases should include the most rigid asepsis with removal of all foreign particles. Localized pressure does some good, especially in those cases where it can be tolerated. Signs of abscess should always be watched for, and deep exploration is often justified or indicated. While excision or cauterization are often heralded as successful, they are by no means without their dangers. Nevertheless in selected and suitable cases excision may be freely practised. Cases that admit of it should wear a protective shield properly molded to the part. Skin transplantation, or even osteoplastic repair of the defect, may give good results in favorable cases.
[567]
Under the general term septic infection are included:
These are different manifestations of infection, the clinical picture differing according to the tissues and localities involved. For the production of these infectious conditions no special bacteria other than those already catalogued in Chapter III are comprehended. Their method of activity is there discussed at sufficient length, and we need here only consider the various paths of infection. These may lie along the bloodvessels, the lymphvessels, nerve sheaths, and prolongations of the membranous sacs which extend from the cranial cavity proper.
The most common of all the paths of infection is afforded by the middle ear, especially when involved in a chronic suppurative lesion, which is by no means necessarily connected with a patulous tympanic membrane, and which may consequently be undiscovered, though in more or less constant activity.
—This may be traumatic or non-traumatic. The former variety is most often due to the direct result of injury, infection displaying its consequences promptly or sometimes not until long periods have elapsed. The ordinary form occurs within the first two weeks, usually as an acute cortical abscess beneath a more or less compromised membrane, surrounded by a zone of red softening, and this by another of brain edema. The chronic traumatic abscesses are less often cortical, but are deeper. They are marked by prolonged suppuration of the external wound, but may occur through some mechanism not understood. Only the chronic abscesses show encapsulation, the capsule partaking of the character of the pyophylactic membrane, elsewhere described. (See Chapter VIII.) It may cover a long period—to my personal knowledge at least nine years, while others have mentioned twenty and more. The non-traumatic abscesses are in the main due to middle-ear disease. When the roof of the tympanum breaks down it is the middle fossa of the skull which is infected; when the posterior wall, naturally the posterior fossa. The most common result of perforation of the tympanic roof is involvement of the mastoid antrum or the sigmoid groove and sinus. In the former case we have temporosphenoidal abscess; in the latter, cerebellar, if any. Previous to actual perforation there is thinning of bone with thrombosis along the minute veins connected with the sinuses. When the dura is exposed by the carious process, granulation tissue often protects it against further inroads, while masses of the same projecting into the tympanum have been mistaken for prolapse. If the sigmoid groove be the site of the first disturbance, extradural abscess may form between the sinus and the remaining bone, the granulating process then involving the whole bony groove. Its later consequence is sinus phlebitis, sinus thrombosis, or intradural infection. If there be adhesion between the dura and the cortex we have actual brain ulceration without formation of a true abscess; but if once the perivascular sheaths have carried infection to the substance of the brain there is a rapid purulent disintegration of the same, and formation of a true subpial or deep abscess, which latter is in effect a purulent encephalitis. Macewen has shown how important it is not merely to evacuate such abscesses, but to eradicate the path of infection from the point of origin, which is rarely easy.
Extradural pus may escape into the mastoid cells by erosion of their inner walls. Such pus may escape suddenly, and serious symptoms thus be mitigated. Even abscess of the bone may thus empty itself by the process of adhesion and pointing toward the surface. Pus from the mastoid cells may perforate the temporomaxillary joint or escape along the digastric groove and form deep cervical abscesses.
When the arachnoidal tissue is involved, both subdural and subarachnoidal spaces participate in the infection, and the brain floats upon a pus-bed rather than a water-bed. Leptomeningitis under these circumstances becomes quickly diffused and fatal. Serous fluid may accumulate so quickly as to produce death by mere obstruction to the cerebral bloodvessels, while distention of the ventricles and an acute infectious internal hydrocephalus[568] is possible. Leptomeningitis may be propagated wherever anatomical paths may carry it, even to the cauda equina and along the spinal nerve sheaths.
The pus within cerebral abscesses is often discolored, sometimes offensive. A greenish color is usually imparted by the Bacillus pyocyaneus, while the offensive odor comes mostly from the Bacillus coli. Around such an abscess is a zone of inflamed cerebral tissue. If within this zone a pyophylactic membrane is produced by condensation the abscess may become encapsulated and life be prolonged. When a capsule fails to form, the process being too acute or rapid, death is the speedy termination of such a case. These abscesses are generally single, but may be multiple. There is also a metastatic expression of abscess formation, seen in typical cases of pyemia, where numerous miliary abscesses are found within the brain. Pressure symptoms are less likely from abscess than from a tumor of the same bulk, while there is much greater liability to edema and sudden infection. Gradually extending paralysis implies pathological activity around the abscess. Large collections of pus are often met in the least vital parts of the brain, as in the frontal or temporosphenoidal lobes.
Symptoms.
—Aside from causal indications (e. g., injury to the head, middle-ear disease, recent operations upon the air-containing cavities, etc.) the first symptoms may be slight. They consist usually of headache, often ascribed to cold or trifling injury, becoming exaggerated, rarely definitely located, radiating widely. In time it is spoken of as “excruciating,” and may be continuous or intermittent. Vomiting is not infrequent, rarely accompanied by nausea. Chills come on early in the history of the case, varying in intensity, duration, and frequency. The more frequent, the more likely is it that the abscess results from some general infection. Temperature is seldom much elevated; it is often subnormal. When exalted it is in proportion to the degree of meningeal involvement. If pressure symptoms become marked we get the usual slow pulse due to increased tension. After evacuation of pus pressure symptoms may subside, but temperature rise. Such discharge from the middle ear as may have been previously noted usually diminishes. A history of cessation of discharge and of increased pain and fever occurring at irregular intervals is very characteristic.
These patients seldom come under the surgeon’s notice until the condition is serious. If they are still conscious, pain is the dominating complaint. This may be aggravated by percussion over the affected region. Rigidity of the sternomastoid on the affected side is a sign of lesion of the sigmoid sinus. Pain elicited by deep pressure in the posterior cervical triangle is also significant. There is mental hebetude, with progressive failure of mental and physical power, as the stupor increases, or coma becomes marked.
Abscess may be often distinguished from infectious thrombosis, as in the latter respirations are quickened and vomiting occurs when the patient is in the upright position.
Vomiting accompanied by cephalalgia is always indicative of intracranial mischief. If it be a special feature throughout the case it may indicate cerebellar lesion. Convulsions are also frequent, but rarely distinctive. They are the result in most cases of secondary irritation of motor areas. Paralysis is the consequence of destructive rather than of irritative lesions.
The ear should be examined, and the use of a probe may give much information.
Brain abscess connected with middle-ear disease will usually be found in the temporosphenoidal lobe, but occasionally occurs beneath the tentorium, in the cerebellum. Many of these cases are connected with self-evident indications of purulent otitis media and mastoid disease, and operation for the latter has often to be combined with the recognition of and suitable treatment for brain abscess. The surgical treatment of mastoid disease will be discussed in separate paragraphs and under a separate heading. Whenever there is any reason to suspect the existence of pus within the cranium the operator should expose the dura by opening above the mastoid; or his operation may already have taken him as far as the sigmoid sinus, in which case, with the dental engine or with other bone-cutting instruments, he may much enlarge the field of operation and thus make access both to the sinus and to the brain itself. An extradural collection of pus may be found within the sinus or above it. Drops of pus may escape as the operator cleans away or even presses apart the granulations. He has often to decide upon further exploration, either to open the sinus expecting to find it filled with disintegrated blood clot and products of decomposition, or to open the dura proper, expose the cortex, and perhaps explore here with the aspirating needle for pus located more deeply. In those cases where evidences of brain abscess are more pronounced, and those of mastoiditis[569] less so, the lateral region of the skull may be exposed and the cranium opened with a trephine before working downward and exposing the mastoid region. In not a few instances both operations are combined and the area of bone to be cut away is relatively large. Thus complete tympanic eventration, with removal of much of the mastoid, may be combined with trephining and opening of a brain abscess, or opening of the sinus, in which latter there may be found such a condition as to make it advisable to ligate the common jugular low in the neck, and irrigate from the sinus to the location of the ligature, where the vein is laid open, or even to pass a small swab upon the end of a flexible probe. Nothing can more predispose to typical pyemia than a breaking-down clot within a sinus or vein involved in thrombophlebitis.
Temporosphenoidal abscess will often be indicated by the escape of pus through the dura, above the roof of the tympanum. Although such an abscess might be evacuated by enlarging the tympanic approach to it, it would ordinarily be much better to open the skull above the ear, and thus make free access and provision for drainage. In any part of such an operation when the dura has once been exposed its appearance should be carefully noted. The coarse of the pial vessels can usually be traced through it. Therefore when it is sufficiently opaque to prevent any appreciation of conditions beneath, or sufficiently distended, it may be opened.
When cerebellar abscess is suspected the trephine should be applied about midway between the tip of the mastoid and the external occipital protuberance (inion), i. e., one inch beneath Reed’s base-line and one and a half inches back of the mastoid. The instrument should here be used with care, as the occipital bone is of irregular and variable thinness. In a brain abscess which can be freely opened gauze packing will be found serviceable, even though its use necessitates the employment of secondary sutures or perhaps leaving the wound open in order to permit of its removal.
Localizing symptoms are only occasional in connection with cerebral abscess, because the majority of these lesions are located without the motor area. Pupillary alterations are indefinite. As an abscess enlarges the size of the pupil may increase. Infective thrombosis rarely affects the pupils, save that when located in the cavernous sinus it may produce ptosis. In temporosphenoidal abscess pain is usually localized in or near the ear upon the same side. As the motor area becomes involved there is a gradual development of localizing phenomena, referred to the opposite side. Facial paralysis is common in advanced destructive lesions in the mastoid and tympanum. When produced by cortical lesion it is rarely so pronounced as when by direct paralysis of the nerve. In frontal abscess there are few localizing phenomena. Abscess in the parietal region is most commonly of traumatic origin, and is to be suspected in accordance with external surface markings. Occipital abscess is exceedingly rare, and cerebellar abscess furnishes few localizing symptoms. Its most prominent clinical features are retraction of the head and neck; slow, feeble pulse and respiration; subnormal temperature; violent yawning; rigidity of the masseters; slow speech; optic neuritis; vertigo and vomiting. If accompanied by thrombosis there is pain upon pressure in the upper part of the neck. In all of these cases when abscess is near the surface there is more or less leptomeningitis, which becomes diffuse at once when the abscess bursts. If meningitis be present we have high temperature without marked remissions, rapid pulse, and general irritability, rapidity of pulse indicating predominance of leptomeningitis over encephalitis, since the more marked the latter the slower the pulse. As distinguished from sinus thrombosis we have in the latter high temperature with marked remission, rapid and weak pulse, frequent chills, profuse sweats, and often symptoms of pulmonary infarct or diarrhea, with cervical and submastoid tenderness and involvement along the jugular vein upon the affected side. If all three conditions be associated the symptoms of thrombosis usually prevail, although there may be retraction of the head due to basilar meningitis. As between tumor and abscess we have in the former absence of explanation of infection, slow progress of symptoms, more definite localizing phenomena, progressive involvement of nerves, pronounced optic neuritis, absence of chill, and alternating periods of mitigation of symptoms. Temperature and pulse afford little help, save that subnormal temperature points rather to abscess.
Prognosis.
—From every direction come statements that the tendency of cerebral abscess is invariably toward fatality. No matter what the cause, unless relief be promptly afforded, death is the sure result. Of the acute cases those not promptly operated usually die within a few weeks. The more chronic or prolonged cases rarely come[570] under surgical treatment; most of those which do are the result of disease in or about the middle ear. Were it possible to early diagnosticate formation of these abscesses prognosis would be much more favorable. When seen before necessarily fatal complications have arisen, in instances where the position can be reasonably well determined, surgical attack is likely to give good results. After proper evacuation even complete mental and bodily recovery is possible. Anchoring of the brain by adhesions may leave a train of disquieting symptoms, which, however, are not so bad as fatality. Abscesses may remain for a long time encysted, and yet be a fruitful source of danger. Multiple abscesses may complicate both the diagnosis and the treatment and produce a condition beyond help.
The operative treatment of these cases will be discussed by itself.
—The sinuses are predisposed to thrombosis by virtue of their size, inflexibility, shape, and the fact that they are not emptied during respiration, all of which tend to retard blood flow. If to these be added defect in the blood supply, then everything predisposes toward marasmic thrombosis. This occurs much less frequently than the infective form, is mostly confined to the longitudinal sinus, is noted mainly at the two extremes of life, and is often seen in cases of death following exhausting diarrhea in children. In the marasmic form the clots are dense, firm, stratified, and non-adherent; they rarely occupy the whole caliber. In old cases the clots may be tunnelled sufficiently to permit reëstablishment of circulation. Their principal evil consequences are edema of the frontal lobes and serosanguineous effusion into the ventricles or orbits—in the latter case producing exophthalmos. Sometimes epistaxis is produced. Strabismus, tremor, muscle rigidity, or contractures are more often seen conjoined, especially in children, with convulsions, sometimes unilateral, and choked disk.
Diagnosis.
—The diagnosis in adults is difficult, but in children, when convulsions occur after exhausting illness, with the signs just noted, marasmic thrombosis may ordinarily be diagnosticated.
Infective thrombosis, the other variety, is due exclusively to the invasion of pyogenic organisms. It is observed mostly in the basal sinuses; its origin is local, and it is always secondary to some external infection. Its most frequent cause is middle-ear disease; consequently the sigmoid sinus is the one most often involved. It may follow carbuncle, erysipelas, or cellulitis of the external parts, or nasal ulceration, as well as dental caries, suppuration of the tonsils, etc. Infection may be propagated by tissue continuity, or through the circulation.
Symptoms.
—Infective thrombosis presents few distinctive symptoms. Local ischemia, perversion of function, extracranial edema are too vague. Headache is nearly always constant and vomiting is frequent; temperature runs high, with marked remissions; the pulse is small and rapid, and remains so even under an anesthetic. Chills are frequent, of the pyemic type, and are followed by copious sweats. Should pulmonary infarct occur there will be typical thoracic signs, although at first physical examination may give negative results. Later, however, we get prune-juice expectoration, putrid sputum, etc. Cerebral function is disturbed late rather than early. The duration of the disease ordinarily is from two to four weeks. Should meningitis complicate the case there is more violent headache, persistent high temperature, great excitement, muscle spasm, strabismus, delirium, and coma; if the sigmoid sinus be involved there is usually retraction of the head. Should leptomeningitis extend down the spine, complaint of girdle pains will be made.
Differential Diagnosis.
—The two conditions which are most likely to be confused with sinus thrombosis are meningitis and brain abscess. In thrombosis there are pain and tenderness over the mastoid, extending down the neck. Fever is high, pulse rapid, respiration not affected, rigidity not usually present. Chills are frequently followed by profuse perspiration. The general picture is one of sepsis and the typhoid state. There are no special eye symptoms. Death is finally due to pyemic processes. In meningitis pain is an early, constant, and severe symptom. Headache is frontal or general, fever is not characteristic, pulse is rapid until the accumulation of pus causes slowness by pressure, breathing is short and rapid, and finally of the Cheyne-Stokes variety. Rigidity of the neck and back, with retraction of the head, is nearly always present, with spasmodic contractions or convulsions about the neck. Chills are not so pronounced, vomiting is almost invariably of the projectile type, optic neuritis is frequent, and the intellect is early impaired. In brain abscess pain is at first localized and[571] severe, extending and becoming excruciating. This increases on pressure, and does not disappear until relief is obtained or the patient becomes unconscious. Temperature is normal or subnormal until the abscess ruptures. The pulse is slow, as in compression from other causes; breathing is slow and stertorous. Rigidity and vomiting are like those of meningitis. Eye symptoms are almost always present, photophobia at first, later inequality of pupils, with dilatation on the affected side, optic neuritis and irregular movements of the eye and lids. Drowsiness, dizziness, and impaired intellect are features when the abscess is in the cerebellum. Death occurs in coma unless the case be complicated by meningitis.
We may also have exophthalmos on one side or both, with conjunctival injection, edema of the lids, and disturbances of vision, due to thrombosis of the cavernous sinus and stasis in the ophthalmic vein. In thrombosis of one transverse sinus only the internal jugular on that side will carry less blood. So long as that on the other side is free it will take that which cannot pass through the obstructed one. Consequently the jugular on the other side will carry more. But if the contained clot extend so far that direct communication with the internal jugular is interfered with then the internal jugular of the affected side will be almost empty, while the external of the same side will be the more distended. When the eye is protruded and the frontal vein distended it is evident that the cavernous sinus on that side is involved. If the superficial veins of the scalp be distended it is the superior longitudinal sinus which is at fault. When the veins of the mastoid region are involved, we may locate the thrombus in the transverse sinus; when there are no localizing symptoms, it can only be said in a general way that thrombosis has occurred.
Prognosis.
—Prognosis is always unfavorable, though recovery is not impossible. The therapeutics are in the main prophylactic. By actual physiological rest the possibility of pulmonary complications can be diminished. The treatment, aside from this, is purely operative, and will be discussed elsewhere.
—This may be the result—
Symptoms.
—The symptoms are seldom diagnostic. Sinus phlebitis is often accompanied by meningitis, even encephalitis. The first symptom is usually severe headache, often localized, made worse by pressure. Anorexia with early mental disturbance and often delirium follows, with vomiting, restlessness, and mania, changing to stupor and coma. Rigidity or spasm of cervical muscles, or of those of the extremities, followed by paralyses, is often seen. Evidences of irritation of special nerves, particularly the oculomotor or the vagus, are not rare. When pyemic symptoms occur they are vague and are most conspicuous in the lungs and liver. Taken in conjunction with aggravating brain symptoms they make prognosis unfavorable.
Symptoms will in large measure depend upon the sinus most involved. They are characteristic if this be the cavernous sinus. There are disturbances in the eye on the same side, congestion of orbital veins, pain and photophobia, and, later, cloudiness of the cornea and edema with exophthalmos. Finally the pupil becomes paralyzed and dilated, the cornea loses its polish, the upper lid cannot be raised, and, if the case persists, the cornea ulcerates. Along with these local evidences there will be complaint of frontal pain, usually with paralysis of the hypoglossal nerve and consequent thickness of speech. When the transverse sinus is involved there are, first, vagus irritation, then paralysis with paralytic sequences in the muscles of the jaw, the tongue, palate, pharynx, etc. Diaphragmatic motions are interfered with and the character of the respiration altered. As the trouble extends to the internal jugular we have further paralysis of accompanying nerves, especially of the hypoglossal. As the irritation extends down the vein there will be tenderness, rigidity, and often swelling. The local signs and symptoms vary obviously as the lesion extends from one sinus to the other, for when one cavernous sinus is involved the trouble nearly always extends to the other, and local symptoms are repeated upon the opposite side.
—The dura has a duplicate anatomical character. Its outer surface, having the structure of periosteum, functionates as such; its inner surface, being lined with endothelium, partakes of the nature of a true serous membrane. When the former texture is mainly at fault we have pachymeningitis externa, or endocranitis, which is rarely a primary, but usually a propagated lesion met with after injury or external[572] infection. It may lead to infiltration with purulent products, and, if speedy exit for pus be not provided, to involvement of the pia within. Extradural suppuration without external injury is very rare, but should there have been a subdural hemorrhage with external lesion the blood clot may become infected and break down. Pachymeningitis externa is most common after chronic lesions of the cranial bones—i. e., caries and necrosis. Symptoms are not characteristic and often not distinguishable. When chronic there will be local tenderness, evidence of the presence of pus, with focal symptoms.
Treatment.
—The treatment is always surgical, save possibly in certain cases due to syphilis, where delay may be justifiable for the purpose of testing the action of antispecific drugs.
—Pachymeningitis interna is often confounded with chronic hydrocephalus. It is frequently the occasion of a firm, membranous exudate upon the internal surface of the dura, which forms in time a new membrane rich in small and extremely friable vessels, from which hemorrhages easily occur, thus giving rise to the condition of pachymeningitis hæmorrhagica. Trifling hemorrhages will produce little or no disturbance; when of greater extent they may give rise to localizing brain symptoms. These extravasations may absorb or undergo fluidification—i. e., produce localized or cystic collections of fluid. The condition sometimes occurs after other acute infections, especially pneumonia, pleurisy, typhoid, whooping-cough, etc. Recovery is possible, but usually at the expense of adhesions, which lead to subsequent complications.
The symptoms of pachymeningitis hæmorrhagica are headache, which will increase in intensity with every new escape of blood, usually localized in the vertex, with more or less paralysis following each new extravasation. The final result may be atrophy. Absence of disturbance in the cranial nerves points to lesions in the convexity rather than basal or ventricular. In chronic cases there is optic neuritis, and toward the end coma, usually coming on slowly. Dennis has recommended trephining under these circumstances, and has practised it with great benefit.
Treatment.
—The treatment should be in a large degree surgical, for little short of eradication will bring about the desired result.
—This term refers to inflammation (i. e., infection) of the pia mater, in whose texture we encounter tissue quite different from that composing the dura, and in which, when inflamed, distinction as between the arachnoid and pia has disappeared. Leptomeningitis suppurativa is an exceedingly common expression of intracranial infection, and may result not merely by extension, but as a primary infection. When begun it spreads rapidly, the fluid contained within the meningeal cavities, mixed with pyogenic agents, helping to disseminate the active agents to the ultimate limits of the membranous involvement. Consequently basilar meningitis usually extends down the spinal canal. Next to injury the most frequent cause is middle-ear disease, with its infectious complications and extensions. Next to this come sinus phlebitis and endocranitis. Infection from the teeth and the nasal cavity may occur. It is also known to result from panophthalmitis: in traumatic cases, when primary, it sets in early, even from four to thirty-six hours after injury. So rich is the pia in loose connective tissue that even from the outset the inflammation may assume the phlegmonous type. The cerebrospinal fluid, as well as that of the ventricles, becomes cloudy, contains numerous flocculi, and is often blood-stained.
Symptoms.
—When the disease is limited to the vertex and follows several days after injury it usually begins with chills and malaise, with increasing temperature; after which the symptoms assume the pyemic type, distinguished from true pyemia by their comparatively early onset. The pulse becomes frequent, first full and then small; patients are disturbed, restless, or uncontrollable, and complain of headache, moan, grate the teeth, become delirious, with glistening eyes and congested face. After a while delirium subsides into stupor and restlessness into insensibility. The pupils contract and remain inactive to light. Paralyses and cramps are not infrequent. Traumatic basilar leptomeningitis occurs often with fracture of the base. Signs and symptoms are less distinctive here; paralyses occur more easily and are less distinctive, save those which involve the special cranial nerves. When ptosis occurs with dilatation of the pupils and glossopharyngeal paralysis we should be quick to suspect extension of the process along the brain. Cramp or stiffness of cervical muscles mean the same thing, and are signs of grave import which may be considered pathognomonic. Albuminuria is frequent, with marked increase of phosphates in the urine.
[573]
In the non-traumatic cases the symptoms of leptomeningitis are those of increasing brain pressure and temperature. The disease usually commences with headache followed by vertigo, hyperesthesia, restlessness, delirium, insomnia followed by somnolence, muscle spasm, paralyses, coma, and death. If the disease extends from the middle ear there is frequently facial paralysis before the meningeal symptoms appear.
The type of fever is one of gradual increase, though before death temperature often falls even below the normal. Pathognomonic fever should not be mistaken for the elevation of temperature which often accompanies absorption of intracranial hemorrhages. In these latter cases temperature may mount to 39° C., but if rising higher than this meningeal complications should be suspected.
Diagnosis.
—The diagnosis as between sinus phlebitis and leptomeningitis depends principally upon the existence of pyemic symptoms. When the latter are entirely wanting we may at least say that the predominating symptoms of sinus phlebitis are absent.
Prognosis.
—The prognosis is unsatisfactory. Many cases end in forty-eight hours; others may live for two weeks or more.
Treatment.
—Treatment seems almost futile, though one should endeavor by energetic purgation, venesection, etc., to do what he can. The only prospect or hope comes from the possibility of relieving the compression from effusion of purulent fluid, and of irrigating and draining what is now an enlarged abscess cavity. Since we do not hesitate to open and wash out other serous cavities when thus affected—e. g., peritoneum, pericardium, joints, pleura—we should no longer hesitate to open the dura and wash out the subdural space, even though this necessitate more than one trephine opening. The measure was suggested by S. W. Gross, in 1873, when he reported cases thus treated with success, and has since been practised by other surgeons, among them by Souchon, who has advised multiple puncture with the small drill and irrigation and disinfection through numerous small openings. Of 11 cases collected by Gross more than twenty-five years ago, 45 per cent. recovered.
—The etiology of this condition is practically that of leptomeningitis. It may proceed from sinus phlebitis or from the veins emptying into the sinus, infection travelling backward rather than forward. In many cases the primary infection occurs from without, as in gunshot fractures. It is also transmitted along the lymphatic channels, since I have operated on abscess in the frontal lobe following intranasal operation. It assumes practically always the suppurative type, and may run either an acute or a chronic course. When acute the lesion is usually limited in area, and the result is an acute abscess with irregular boundaries. It may be distinguished from uremic coma by examination of the blood (leukocytosis) as well as that of the urine.
In dealing with pus the surgeon can never follow a safer rule than to go according to this dictum: i. e., that pus left alone is a greater source of danger than the surgeon’s knife judiciously used. Consequently ubi pus, ibi evacua, applies to intracranial collections as well as others. For its detection and evacuation operations are now regarded as not merely justifiable, but indicated whenever there is presumption of its presence. Discussion now hinges entirely upon the wisdom of exploration when absolutely no diagnosis can be made. Save where an opening already exists, trephining is a necessary preliminary. Among other indications is spontaneous escape of pus through a previous opening or any of the natural outlets of the cranium, with or without localizing phenomena. Further indications are those pertaining to the bone—i. e., loosening of pericranium; or to the scalp—i. e., edema, puffy tumor, etc.; and certain other indications are those of a more general character, chills and pyrexia. When the dura is exposed much can be determined by the existing brain tension, it being now well established that brain pulsation is often intensified by the presence of pus beneath the dura. The most feasible method for detection of subdural or deep collections is the use of the aspirating needle—a method now generally in vogue and everywhere accepted.
[574]
In all cases of infection and suppuration of the middle ear the adjoining portions of the cellular structure of the mastoid undoubtedly participate. Fortunately morbid activity is usually so limited that the clinical evidences of what is called mastoiditis occur in a relatively small proportion of cases, but otitis media purulenta is so common that mastoiditis is consequently a complication of sufficient frequency, and occasionally of such severity, that it is as likely to come under the supervision of the general surgeon as that of the specialist. Moreover, the region affected is such common ground, as it were, between the broad field of the former and the restricted field of the latter that it seems to me that every general surgeon or student of general surgery should be familiar with the condition and its surgical treatment.
Several of the specific germs, of diseases like pneumonia, la grippe, etc., are known to set up acute mischief within the tympanum as well as the commonly known pyogenic organisms. They have easy access to the middle ear through the Eustachian tube, as well as by the deeper blood and lymph channels. The nasopharynx is never free from the presence of organisms, while the specific fevers, like scarlatina, and notably such infections as diphtheria, predispose to germ activity in the region into which the inner end of the Eustachian tube opens. The Schneiderian membrane, which is practically continuous from the ethmoid cells to the membrana tympani, affords easy travelling, and in all directions, for infecting organisms. The violence of reaction will depend upon two uncertain and indeterminable factors, the virulence of the organism and the susceptibility of the patient. To what extent the mastoid cells and antrum, around an infected tympanum, shall participate may be, to a considerable degree, a matter of their anatomical arrangement. When, however, they do participate to any great extent the fact is made known by symptoms of unmistakable character. These constitute the added features of what is known as mastoiditis.
The cavity in the mastoid known as the mastoid antrum, no matter what may be the arrangement of the other cells, is always present, and in the presence of deep disease the antrum should be first opened. In close proximity to the antrum are cavities like the sigmoid sinus, the horizontal semicircular canal, the facial canal, and the interior of the cranium. While opening the antrum care should be taken to avoid encroachment upon the other cavities or structures, except in those instances where there is evidence of intracranial mischief, in which case it may be desirous to expose the sinus wall, or even a considerable area of brain surface. The mastoid prominence varies in different individuals, extending outward to accommodate the sigmoid groove for the lateral sinus.
According to the intensity of the process the pathological condition of the mastoid may vary between an empyema of its cavities, an osteomyelitis of its osseous structure, or osteoperiostitis of its external surface. Nevertheless all three of these may be combined in the same case.
—The symptoms of mastoiditis are pain, referred to the mastoid, as well as to the region around it, although when pressure is not made by retained pus pain may not be intense; local tenderness is present in nearly all cases, and will depend upon the proximity of the trouble to the surface. This tenderness is evoked by gentle pressure, which will sometimes produce pitting, or by tapping lightly with the finger. When the trouble is superficial there will often be edema, with all the local evidences of suppuration. In addition to this there will be coincident symptoms of disease of the middle ear, with discharge, earache, etc., and frequently edema or actual phlegmon of the auditory canal.
The different directions in which destructive processes may extend, and their consequences, are as follows: (a) Externally, with well-marked local evidences of the proximity of pus; (b) anteriorly into the meatus, with phlegmonous appearances in that canal; (c) upward, through the roof of the tympanum or the antrum, with disastrous cerebral symptoms or extradural abscess; (d) inward, toward the sinus, with consequent thrombophlebitis, extradural abscess, and perhaps cerebellar abscess; (e) downward, and away from the mastoid, with phlegmon deep in the neck.
The first appearance of symptoms of any of these complications should awaken apprehension and demand scrupulous attention. Any collection of pus along the auditory canal should be promptly incised, and the first indication of mastoid tenderness or[575] inflammation should cause a prompt application of leeches, followed by antiseptic irrigations. In this way it may be possible to avert serious symptoms, provided these measures be instituted early.
But with either the access of local symptoms indicating the presence of pus, or of more general symptoms, elevation of temperature, acceleration of pulse, headache, or anything else suggestive of dural irritation or cerebral complication, no time should be lost in making free and radical operation. The mastoid operation, so called, is then demanded in these cases. When thus indicated the first objective point should be the antrum. In order to reach this the customary incision of many writers, back of and parallel to the posterior convex border of the ear, is insufficient and uncertain. The antrum lies within what Macewen has described as the suprameatal triangle, and is to be regarded as the key to the situation. It is necessary to recognize the posterior zygomatic root, which projects behind and above the ear, as well as the tip of the mastoid process, and then to make a perpendicular linear incision, about a quarter of an inch behind the posterior border of the external osseous meatus, extending from this posterior root down to or nearly to the mastoid tip. The surgeon should cut down directly upon the bone, without dissecting or scratching his way through the different tissue layers. The posterior auricular attachments are thus fully exposed, and should be reflected forward, so that the posterior aspect of the external meatus is fully exposed. After thus exposing the bone the surgeon notes the position of the superior meatal triangle, which is formed by the posterior zygomatic root, the upper posterior segment of the external osseous meatus, and an imaginary line uniting these two, extending from the most posterior portion of the osseous meatus to the zygomatic root. Within this triangle the mastoid antrum may be entered, its depth being proportionate to the depth of the middle ear from the surface. So long as care is exercised the sigmoid groove will not be injured. The depth at which it lies from the surface varies. It is more superficial in children, while in adults with chronic ostitis of the region it may have a thick covering. When opened it should be thoroughly cleansed, for it may contain not only pus but granulation tissue or masses of cholesterin. After cleansing the antrum the passage between it and the middle ear should be noted, as well as the position of the facial canal, which traverses its inner side obliquely from without inward as it passes into the inner wall and roof of the tympanum. It is recognizable by a ridge of harder osseous tissue. If changes have occurred in the surrounding bone it may not be recognized. If the operator keeps to the upper and outer part of the antrum he will avoid the nerve. Any injury to it will produce facial twitching. The bony canal may be eroded by granulations, so that the nerve itself may be exposed when the antrum is being cleansed.
The mastoid cells lie posteriorly and below this antrum, and should be exposed, when cleaning out their morbid contents, by removing the external mastoid wall. In this part of the operation the sigmoid groove should not be forgotten, as it may have been disintegrated by granulations which have extended into the fossa and separated the dura from the bone. When granulations have thus formed there is usually more or less thrombosis of the sigmoid sinus in addition to the localized pachymeningitis.
The instruments which may be employed during this work are a matter of choice. It can be done with the ordinary bone instruments of the general surgeon, which should, however, include gouges and curettes of small size as well as delicate chisels and mallet. A dental or surgical engine is advisable, which will serve admirably and for the desired purpose. Just what instrument should be used and how manipulated will depend upon the more or less pneumatic (i. e., cellular) character of the bone. Some mastoids are richly cellular. Pus or granulation tissue should be followed wherever it may lead.
When both mastoid cells and tympanum participate in the morbid process, and are practically filled with pus, debris, or granulations, there may then be added to the operation those features which entitle it to be called tympanomastoid exenteration, as devised by Schwartze, Zaufal, Stacke, and others, and frequently described under their names. It is an extension of the measures already described, and results in converting the mastoid cells and antrum, the tympanic cavity, and the auditory canal into one common cavity. Not only is the bony barrier between the antrum and the tympanum removed, but the ossicles as well. This leaves a large cavity, which should be partially closed and lined by granulation and cicatricial tissue, epithelial lining being furnished so far as it may extend from the exterior.
The operation may be begun practically as already described, the incisions being more[576] extensive and the auricle more freely detached, so as to be reflected forward. There need be no particular effort to save the periosteum over the area of the attack, although there is no objection to reflecting it with the softer tissues. Some operators prefer to detach the cartilaginous meatus and the ear from its osseous insertion and to shift them all farther forward. The antrum and the mastoid cells having been exposed, opened, and cleaned out, the surgeon next passes forward and upward to the external wall of the epitympanum, and the dividing barrier of bone between the tympanum and the mastoid. This cavity being uncovered, the incus, if present, may be lifted out of its position, or all of the ossicles removed in as gentle a manner as circumstances will permit. All the bony prominences and partitions between the tip of the mastoid and the anterior wall of the tympanum are then smoothed off with a curette, or surgical engine, while granulation tissue is followed in to any recesses which may be occupied by it, or along any of the cranial outlets which it may be seen to traverse. One gives the greatest care to avoidance of injury to the horizontal semicircular canal, to the aqueduct of Fallopius, or to inadvertent puncture of the sigmoid groove. The Fallopian aqueduct, or canal, lies in the ridge between the mastoid and the meatus, along the floor of the aditus, and it should be spared in the process of cutting away the bone.
If the membranous portion of the meatus has been split, as advised by some operators, its margins may be brought together with chromic gut. At all events the auricle should be brought back into place after the cleansing is finished, where it should be fastened and retained by sutures as well as by the dressings. Should there be insufficient skin to cover the opening thus made, slide a flap, or even cover the exposed raw area with a skin graft. The former will usually be the better plan. The cavity left after such closure should be packed with gauze, on which balsam of Peru should be used. This may be left for two or three days, after which a daily dressing, with irrigation or suitable cleansing, will suffice.
Most of the mechanism of the middle ear is apparently destroyed, but loss of hearing is not complete.
The term cephalocele is applied to tumor of the endocranium, presenting through defects in the cranial bones, of essentially congenital origin, and containing more or less of intracranial contents. It comprises—
A. Meningocele, which means a tumor consisting of a membranous protrusion and containing cerebrospinal fluid; and,
B. Encephalocele, referring to tumors which contain also more or less of actual brain substance.
Fig. 380
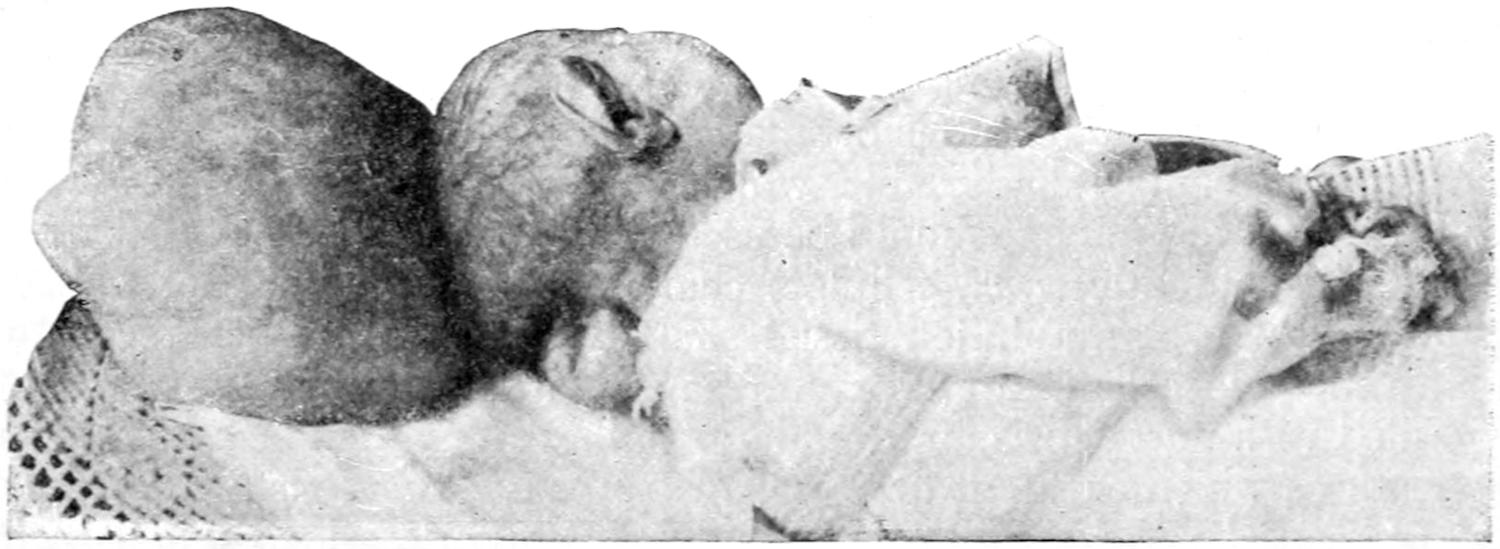
Occipital cephalocele.
Such tumors of non-traumatic origin can only be explained by the existence of congenital defects which permit the escape of that which the normal bone retains within normal limits. In most instances the defect is in the middle line, at either one or the other extremity of the skull. In some instances the arches of the atlas, or even of other cervical vertebræ, are lacking. The most common cephaloceles are the occipital, which are known as inferior when below the occipital spine, or superior when above it. Those appearing anteriorly are known as sincipital, and are met with most often at the root of[577] the nose, where they may communicate with the orbit or the nasal cavity. Other and irregular forms are laterally or unsymmetrically located (Figs. 380, 381 and 382).
Cephaloceles have an elastic feeling, many of them an exquisite fluctuation. Sometimes by touch alone we recognize both their fluid and solid contents. A meningocele with thin walls is translucent. By pressure they can be reduced in size, such pressure usually producing brain symptoms, often paralysis or convulsions. Many children thus affected cannot lie upon the tumor without becoming restless. When the patients cry or make violent straining efforts it becomes larger and its covering more vascular, while during quiet sleep it is usually reduced in size or tension.
Fig. 381

Sincipital meningocele.
A large proportion of patients with these congenital defects die shortly after birth. The tumor, when large, may be ruptured during delivery. Occasionally the sac ruptures spontaneously, which accident is usually followed by purulent meningitis from infection, though it may possibly lead to spontaneous recovery. The principal danger is the liability to such accident.
Fig. 382
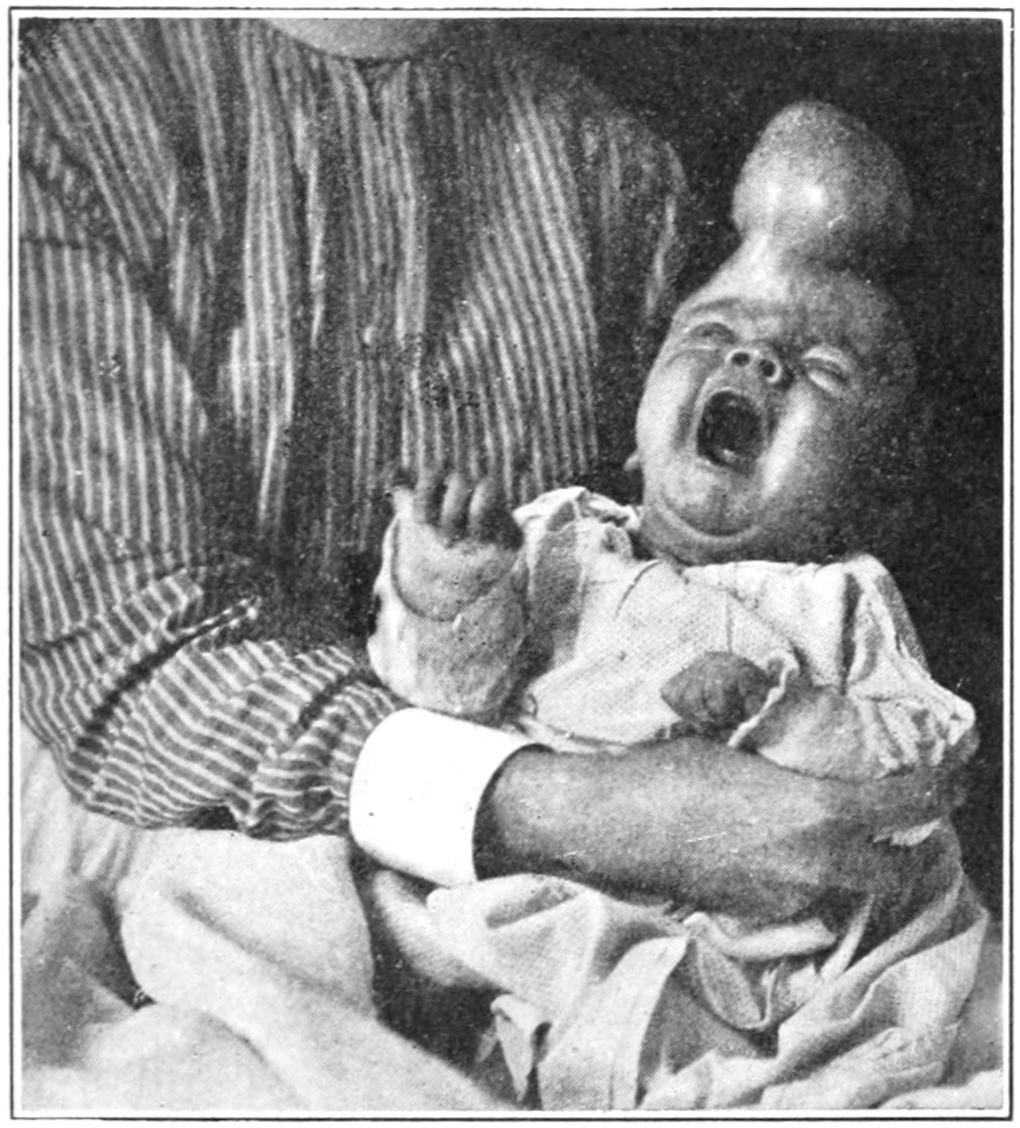
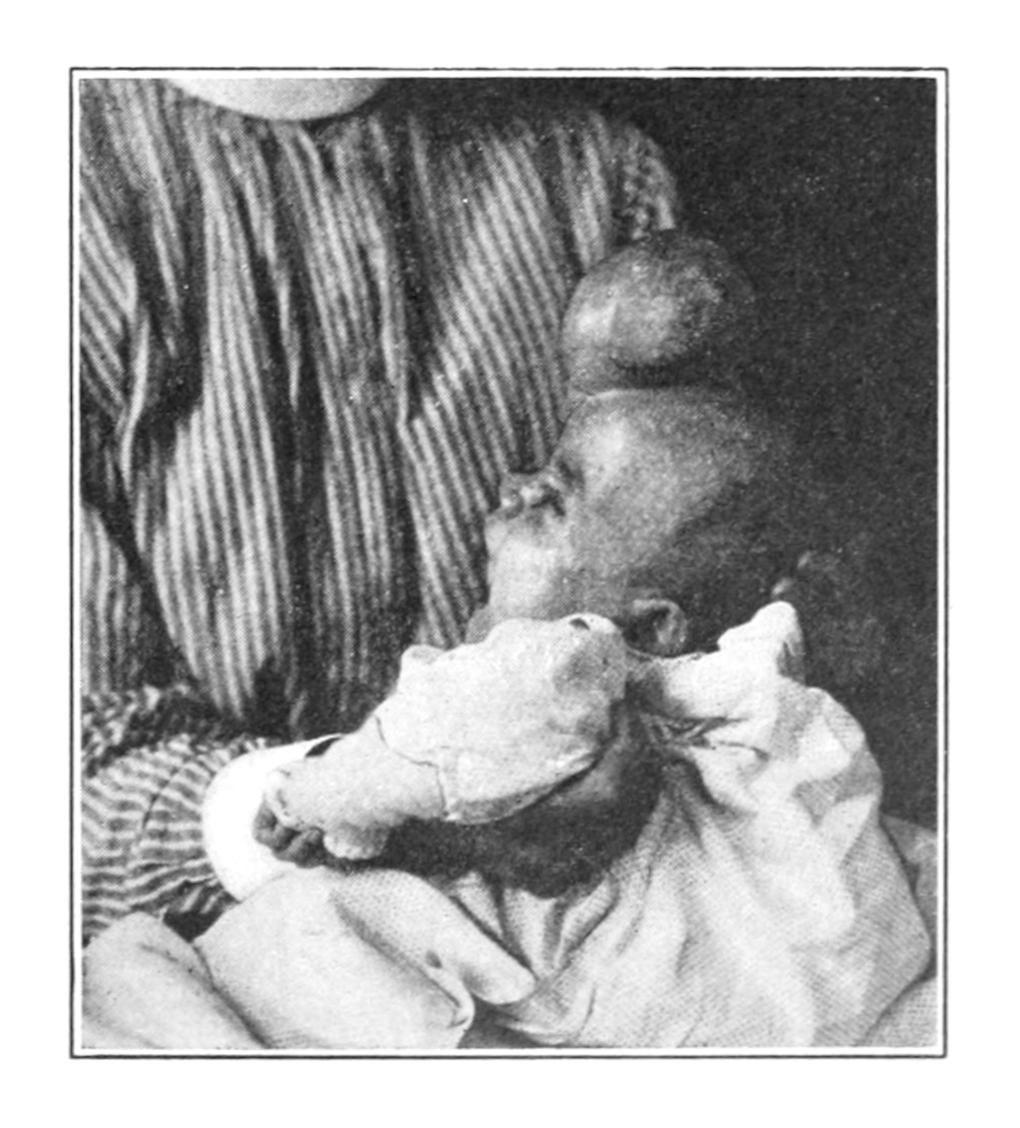
Sincipital hydrencephalocele; two views. (All of these from the Buffalo Clinic.)
The encephaloceles are divided into the cenencephaloceles, containing solid brain substance, and hydrencephaloceles, consisting of the protrusion of a dilated brain cavity—i. e., a thin area of brain enclosing fluid communicating with one of the ventricles. Most of the large tumors pertain to the latter class. The more brain material such a tumor[578] contains the more it pulsates, especially if the patient cry or strain; the smaller, too, is the skull—i. e., the greater the tendency toward microcephalus.
Congenital cysts of brain and membranes, in a measure traumatic, are classified by Rawling, as follows:
1. According to situation: (a) within the calvarium, subosteal, subdural, subarachnoid or intracerebral; (b) projecting through an opening in the skull, with or without ventricular communication.
2. According to origin, i. e., whether they arise from blood clot or other causes.
3. According to contents, whether they contain clear fluid, altered clot, or brain substance.
Cysts of this character are to be differentiated from the cephaloceles already considered because there is about most of them the element of traumatism, although this may have been intra-uterine or produced during parturition. Those which are associated with premature synostosis and microcephaly, with hydrocephalus, with marked deformity, or situated below the external occipital protuberance, are generally considered inoperable, while those considered operable consist of limited protrusions without any of the above defects. This practically excludes the greater proportion of these cases from operation, which is always dangerous. Nevertheless if success is to be achieved the risks should be taken. Osteoplastic methods of closing cranial openings may be perhaps of value in rare cases, although in the young the skull is too thin to furnish an external table which can of itself be detached. In inoperable cysts of this kind, with a tendency to increase, while the rest of the brain lags behind in the rate of growth, the edges of the opening become everted, and operation is thus made more difficult and less desirable.
—Treatment should, first of all, be protective, by a shield of some device held in place by a suitable bandage or dressing. Compression, with or without puncture, has given at times satisfactory results, but not much should be expected from any method or combination. Most of the cases are such that extirpation would seem applicable, but the impossibility of absolute asepsis in young infants and the liability to fatal shock preclude many of these attempts. In some instances ligature of a meningocele has been successfully applied. Operation may be attempted in young children in selected cases. Plastic operations may be resorted to, or plastic maneuvers combined with extirpation. It may be possible by the insertion of a celluloid plate to atone for a small defect in the skull after extirpation of a tumor of this kind. I have successfully practised this method in spina bifida.
This term is applied to abnormal collections of cerebrospinal fluid within the cranial cavity. We speak of—
A. Hydrocephalus ventriculorum or internus, when the fluid is confined to the dilated ventricles of the brain; or of—
B. Hydrocephalus meningeus or externus, when the fluid collects between the brain and the dura.
The former condition is much the more common. The cause of hydrocephalus in the young is essentially congenital, and inseparable from imperfect development within the cranium. The forms are occasionally combined. At the time of commencing trouble the skull may be of natural size, but yields to the accumulation of fluid within until it attains relatively enormous dimensions. Most children thus affected die early, some shortly after birth. It is most common in rachitic children. Hydrocephalus developing in the adult is the result almost solely of atrophy of the brain. Pachymeningitis interna (see p. 572) may also produce subdural exudate leading to hydrocephalus externus. Encapsulated collections of cerebrospinal fluid due to pachymeningitis interna are known as hygromas of the dura. A ventricular form of hydrocephalus may also result from meningitis and tuberculous disease. The condition is essentially chronic, the fluid collecting in the dilated lateral ventricles, though the third or forth are sometimes also distended: 4000 Cc. of cerebrospinal fluid have been found in more than one instance. As the result of the presence of the fluid there is atrophy of brain, with arrest of development, to such an extent even that the hemispheres are changed into great sacs, being merely spread out upon the outer wall of cystic cavities; all the surface markings are lost, and gray and white substances are scarcely to be differentiated.
[579]
In the cranium itself the bones of the vertex separate, and instead of sutures there is a tightly stretched membrane. There is also congenital or acquired aplasia—i. e., absolute defect of bone between the dura and pericranium. All these changes give to hydrocephalic heads a distinctive appearance. Other developmental defects—hare-lip, club-foot, etc.—are common in these patients. Many infants thus affected die during delivery unless skilful help is at hand. The resulting disproportion between the enlarged head and the small face is most distinctive. Children in this condition suffer from disturbed digestion, are emaciated, with rachitic curvatures of the long bones; special senses are seldom developed perfectly; strabismus and nystagmus are frequent, while cramps and stupor are by no means infrequent.
—While spontaneous recovery is possible, as already stated, the tendency is always toward fatality.
—Treatment by compression of the enlarging skull, with elastic bandages or their equivalent, is an abandoned method since compression which can be effective is too great to be tolerated. Treatment by mere aspiration is also useless. Tapping is an old operation long discontinued, recently revived, but again proved disappointing. The establishment of permanent drainage is a more recent suggestion. It depends upon the demonstration of the fact that the tension of the cerebrospinal fluid and of the blood in the cerebellar veins is the same, and that intracranial pressure forces fluid into the veins and away from the skull. Thus subdural or autodrainage was suggested. Sutherland and Cheyne, in 1898, were the first to operate in this manner. They opened the dura near the lower angle of the anterior fontanelle, through the opening carried a strand of catgut into the ventricle, and passed the outer end beneath the dura; but the method again proved disappointing. Mikulicz passed a gold tube into the right ventricle, leaving its outer end in the subcutaneous tissues about 5 Cm. from the middle line. After being three weeks in this position it ceased to drain, and was then inserted into the other ventricle. The child died, unbenefited, in six weeks. In another case he used a glass-wool drain, making it subdural rather than subcutaneous. This case seemed to be benefited. Senn has modified the method by making a large pocket in the subcutaneous tissues of the cervical region, inserting one end of a rubber tube into it and carrying the other into the ventricle between the temporal and frontal bones. Even this proved disappointing. I have twice tried conducting fluid by a small rubber tube from the ventricle into the cellular tissue in the neck, passing the tube beneath the skin by suitably curved forceps. This method, however, showed no advantage over the others mentioned above. Taylor has endeavored to make a permanent fistula between the ventricles and the subdural space by passing chromicized catgut into the ventricle and letting it drain into the latter. His results, however, were not encouraging, in spite of the plausibility of the theory upon which they were based. Drainage through the spinal canal into the abdominal cavity has also been practised by a very few surgeons. The ingenuity and theory of the method are most attractive, though but very few little patients are in condition to bear the abdominal section which is necessitated for the purpose.[43]
[43] In March, 1906, Cushing informed me that his present routine in effecting such drainage was to make a laminectomy and expose the spinal canal from the rear, then to do a laparotomy, and, exposing the bodies of the vertebræ, pass through from in front backward a silver tube, whose end should reach into the spinal canal, draining it into the abdominal cavity, the posterior wound being always snugly closed. The spinal canal is thus exposed in order to ensure the accurate performance of the other part of the operation.
Permanent drainage, then, has been a most disappointing procedure, although there need be no hesitation in tapping the lateral ventricles when there is indication for it. This can easily be done at any time by an opening about 3 Cm. behind the external auditory meatus and the same distance above the base-line of the skull. By directing the puncturing instrument to a point on the opposite side, 6 Cm. above the meatus, the lateral ventricle will be entered. (This same general direction will serve for opening an abscess in the temporosphenoidal lobe.) The best results in hydrocephalus seem to have been obtained by lumbar puncture, as first suggested by Quincke, the method being the same as that now in general use for intraspinal cocainization. As directions for entering the spinal canal with the aspirating instrument would be identical with those mentioned in the chapter on Anesthesia, when describing intraspinal cocainization, the reader is referred to that section for further direction (p. 208). The only case of well-marked hydrocephalus which I have ever apparently cured was one repeatedly tapped in this fashion, a considerable amount of fluid being withdrawn at each little operation.
[580]
There are numerous causes which produce imbecility and kindred conditions in the young. Some are in effect congenital, some are postnatal. Within the past few years a number of these cases have been subjected to surgical operation, in many instances with more or less success. Mental defect may occur from injuries at the period of birth—mainly hemorrhages, more commonly cortical, though sometimes deep. In either case the clots thus formed frequently undergo cystic alterations. The term porencephalon is modern, and applied to changes comprising disappearance of real nerve tissue with partial substitution by connective tissue, often with other degenerations, the result being atrophic alterations which apparently permit of no remedy. In a case of true porencephalon the outlook for operation is not at all encouraging, nor is it in any cases which are accompanied or caused by a genuine arrest of cerebral development. On the other hand, when the mental condition can be ascribed to the result of injuries, to hemorrhages, to meningeal irritation, to premature ossification, or too early closure of the fontanelles, or when it is accompanied by evidence of meningeal irritation or symptoms which point to a definite area of the brain as being the site of the principal disturbance, operation as a legitimate experiment may be conscientiously suggested and performed.
Fig. 383
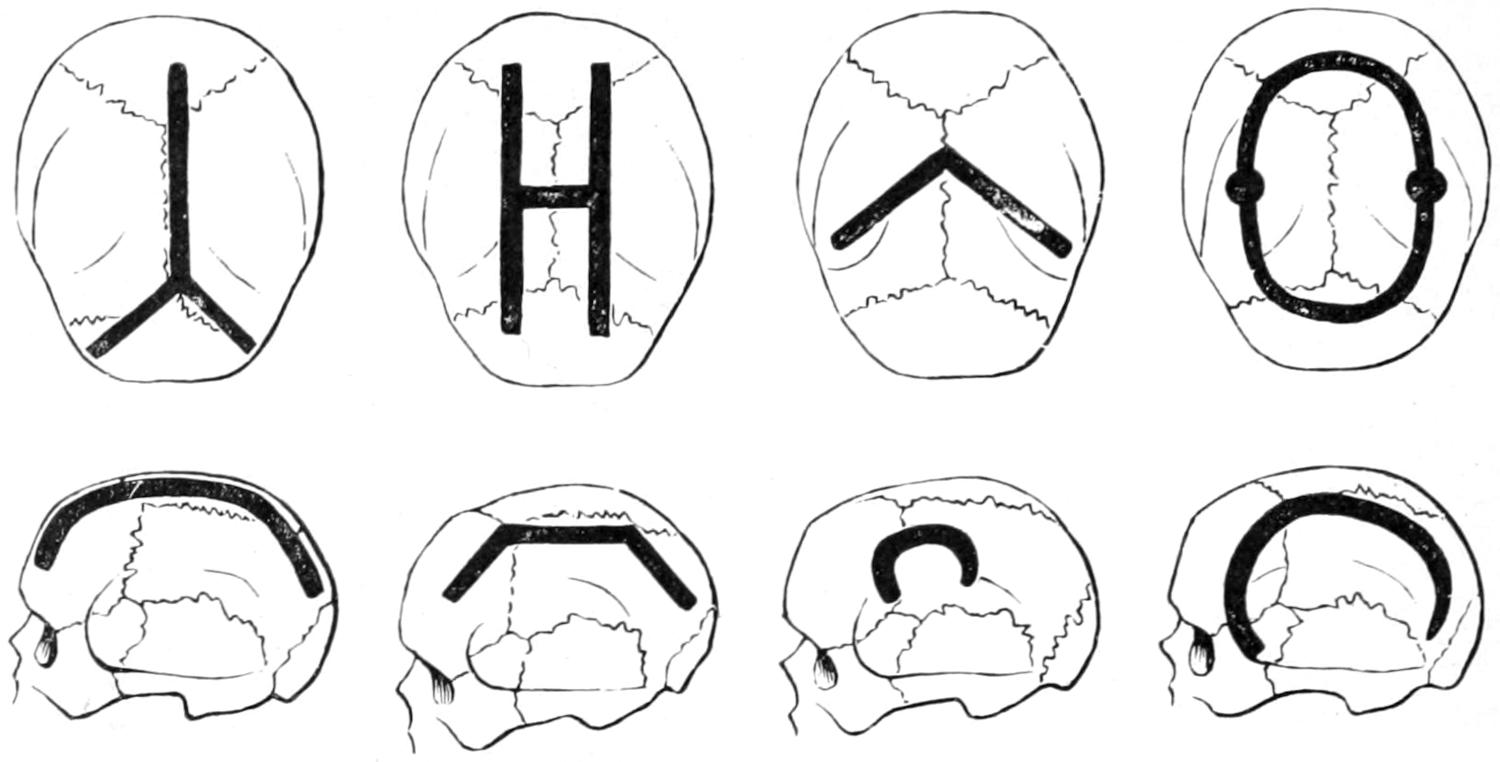
Lines of removal of bone as practised by the author, by Lannelongue, and by others.
Fig. 384
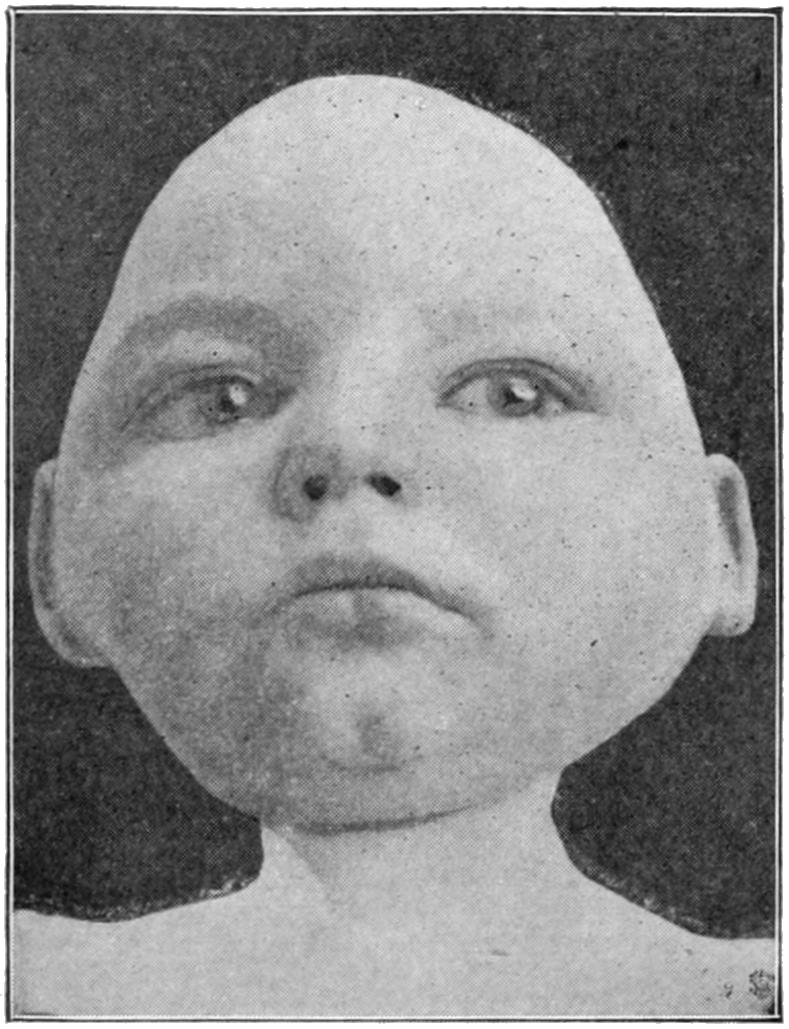
Defective cerebral development. (Buffalo Clinic.)
The operation is usually described as craniotomy or craniectomy, and is apt to be successful in many cases of microcephaly combined with idiocy. An acquired form will give a better prognosis than will the congenital condition. The danger of the operation is often great, and especially so since it is called for in puny, ill-nourished, and badly cared-for children. To be successful it ought to be extensive. It should vary in character and degree—from simple division of the skull along the middle line, from near the root of the nose to the occiput on one or both sides, to the formation of large bone flaps by cutting away a wide groove of bone so as to relieve pressure upon the hemispheres. Fig. 383 presents the various ways of performing the operation.
It can usually be made bloodless, or nearly so, by an elastic tourniquet around the skull. The incision in the skin should not correspond to the groove in the bone, but[581] should overlap it some little distance. For my own part I prefer to do most of these operations in two sittings. I would advise, as a rule, to prepare the scalp carefully for operation, to divide the skin along the proposed line, separate it from the pericranium and check all oozing; then, after opening the skull with the trephine, to cut away with proper forceps (rongeur) along the desired line, or, if provided with it, to remove the bone by some surgical engine or revolving saw operated by electricity. The strip of bone thus removed should be at least half an inch wide, and the overlying periosteum should be removed with it, as only in this way can the undesirably rapid regeneration of bone be prevented. By this means the dura is exposed, but not opened. In some cases this will be sufficient.
In many others, however, it will be insufficient; and, could this be foreseen, it would be well to combine the above measures in one as a first operation, and then, a few days later, to open the dura as the second procedure—this, however, only on the discovery by careful inspection that the wound is absolutely free from possibility of infection. Could infection be prevented, this is certainly the safer procedure, since in weak, puny young children to make a long scalp incision, to remove a long strip of bone, and then to widely open the dura is more than can safely be done in the majority of instances.
It should have been carefully explained to those interested in the case that improvement will in all probability be extremely slow, and that little or nothing is to be expected at first, even if prompt recovery from the operation ensue. Neither would I advise any one to perform the operation unless parents are willing to assume all risks and abide by the results.
Operations for relief of epilepsy seem to date back even to the prehistoric era, and were for centuries done as a purely empirical measure; later, to have been practised with more or less plausible reason; then to have fallen into discredit for long periods of time, with occasional revivals of the practice, until within the past twenty-five years the operation has been again revived upon its merits and upon the recognition of more or less accurate indications.
Operations of this character are based upon two fundamental facts: the first, the widespread experience that after various operations epileptic patients have been benefited; and, second, that a certain proportion of these cases, especially those of traumatic origin, are characterized by a localized and definite aura, and by a systematic and practically invariable order of muscle involvement, according, it would seem, to some fixed law, and pointing definitely to a certain area of the brain from which apparently the irritation arises and spreads. This form of epileptic seizure is that generally known as the Jacksonian, and is that in which operation is most often of real service. The statements of patients regarding these phenomena should never be accepted; only those made by a trained observer (nurse or physician) are reliable.
In spasms of the Jacksonian type there is a certain order of progression which is scarcely ever violated. Thus, irritation beginning in the leg centre can hardly reach the face centre without traversing that of the arm. It is possible also to have sensory equivalents for Jacksonian attacks, as when they commence with peculiar sounds indicating irritation in the centre of hearing, or with optical phenomena, or with disturbances of smell or taste, the former indicating occipital irritation, the latter irritation in the temporosphenoidal region.
The surgeon will often be consulted as to the wisdom of operation in the presence of this condition. In brief, and in a general way, the following statements may be made: It is necessary, first of all, to establish a traumatic origin, and epilepsy which has preceded a severe head injury can in no sense be ascribed to it. If it can be clearly established that it has followed injury, and if a distinct scar—especially a scar which is adherent—or depression can be discovered, or any area which is always irritable and which seems epileptogenic when irritated; or if, again, by close study of the case it can be determined that the aura and the initial muscle symptoms arise always in the same part—as, for instance, a finger, thumb, foot, etc.—and proceed according to a constant program—then it may be said that operation is not merely justifiable, but advisable. On the other hand, when neither distinct scar nor history of localizing phenomena can be obtained operation should rarely be attempted.
[582]
Again, in epilepsy of the non-traumatic type, operation may be advised when it assumes the distinctly Jacksonian form—i. e., when everything points to irritation proceeding from a localized portion of the brain. In the absence of Jacksonian symptoms operation is even more of an experiment than in the traumatic form. Such cases should be studied a long time on their merits before a decision is made to trephine.
The operation itself is directed to excision of irritable scars, to exposure of the dura at the point of opening, to the detection and suitable treatment of depressed fragments, dural adhesions, tumors, foreign bodies, etc. It is essential in every case that it be represented to those interested that the operation itself removes the cause, but cannot be, per se, expected to complete the cure, especially in cases of long standing, and that the final cure must depend in large measure upon the avoidance of subsequent irritation, upon the establishment of perfect habits of diet and excretion, which are often perverted, and perhaps upon the long-continued administration of drugs, of which the bromides are those most constantly given. The reader need not be reminded that old cases are the least favorable, and that recent cases are the most so for operation, and that the longer the diseased condition has existed the harder it will be to cure by any method.
Besides these direct operative attacks it has been suggested by Alexander to tie the vertebral arteries (now practically abandoned) and by Jonnesco to excise the superior and middle cervical sympathetic ganglia. This seems to me particularly indicated in those cases where a convulsion can be aborted by prompt administration (by inhalation) of amyl nitrite as soon as the preliminary aura is recognized. The operation is described in the chapter on Surgery of the Cranial and Cervical Nerves. Many encouraging results of this treatment have been reported.
I believe thoroughly in operating in selected cases. I am equally confident that indiscriminate operation must lead only to disappointment and to occasional disaster. In the presence of long-standing lesions, like bone depressions, cystic degeneration of old clots, etc., the brain may have been so long pressed upon as to have become atrophied.
The whole subject of the modern surgical treatment of epilepsy is inseparable from the topic of prompt and efficient treatment of all head injuries. Were the indications in these always met at the time of the accident we should have a much smaller proportion of cases of traumatic epilepsy.
Inasmuch as one object of many of these operations is to break up adhesions between the dura and the pia, there is generally anxiety to know the result after such operations as to whether they do not speedily form anew. There is always this theoretical danger, and it is my custom in such cases to insert beneath the dura, at the point where such adhesions have been divided or torn, a piece of delicate gold-foil, duly sterilized, in order that it may separate these surfaces and prevent the recurrence of the old condition. Foil used for this purpose is harmless, and I have numerous patients in whom it has been used, apparently without producing the slightest disturbance. (Foils of silver or aluminum answer as well or better.)
Mental and psychic disturbances after head injuries have been long known and the suggestion to operate upon the skull in cases of so-called traumatic insanity is not new. In a general way it may be said that whenever distinct mania follows a recognized lesion of the vertex of the skull, and fails to subside within a reasonable time and under proper treatment, there are the best of reasons for raising the scalp, trephining, and exploring as to the deeper conditions. Patients might be released from asylums who have long been inmates had this measure been practised at the beginning of their mental alienation.
The same measure will give relief in certain cases of cephalalgia, or headache, where the pain is always ascribed to a particular region, and especially when there is tenderness over this region. These operations are, of course, empirical, yet, as the result of altered nutrition and allayed irritation, relief follows in a fair proportion of instances.
Until within recent years these were regarded as having interest mainly for the pathologist and clinician, but as essentially hopeless so far as surgical help is concerned. Recent discoveries in the field of cerebral localization and recent experience with extensive openings into the cranium have shown, however, that a small proportion of intracranial tumors are of such a character and so located as to make them amenable to[583] surgical relief. These tumors occur with about equal frequency in childhood and adult life. In the order of frequency they stand about as follows: Tuberculous gumma, glioma, sarcoma, cysts, carcinoma, and syphilitic gumma, with a small proportion of fibroma, etc.
Of 100 cases of brain tumor selected at random not more than 5 to 7 per cent. are so placed as to justify surgical attack. In as many more, at least, the tumors are so located as to justify opening the cranium for mere relief of pressure without any notion or endeavor to attack the tumor itself. Before opening the cranium diagnosis should be made as carefully as possible—first, as to location; second, as to whether cortical or subcortical; third, as to the number of tumors present; fourth, as to their general character. Location is determined in the main by study of pain complained of, by watching patients during convulsive seizures, by determining the extent of local or general paralysis, by careful history which shall reveal the method and rate of extension of these symptoms, and by the study of the optic disks, of vision, and by noting the presence or absence of stupor, nausea, coma, slow pulse, or other compression symptoms.
—A brief epitome of the principal features attending cases of brain tumor will include:
1. Pain and headache, rarely localized with much accuracy; the former sometimes increased by percussion or pressure, occasionally periodical and usually intense. The location of the pain sometimes corresponds with that of the tumor.
2. Vomiting, usually without pain or nausea, and often projectile. I have repeatedly seen obstinate constipation in brain-tumor cases which has gone almost to a degree of acute obstruction, and which has caused serious error in diagnosis.
3. Vertigo, independent of indigestion or the condition of the stomach or bowels. It is most frequent in cerebellar tumors, but occurs in about 50 per cent. of all cases. It is sometimes quite severe.
4. Eye symptoms such as optic neuritis, choked disk, usually double, indicating pressure, but telling little or nothing as to the location of the tumor causing blindness. Ophthalmoplegias are of little value by themselves as symptoms. Hemianopsia, when homonymous, usually indicates a lesion of the cuneus of the same side, the blind half, according to the patient, indicating the side.
5. Localizing symptoms which may be due to the destruction of brain tissue or to indirect pressure. Those of importance comprise paralysis or spasms, indicating involvement of the motor area; sensory aphasia, indicating trouble in Broca’s area, ataxia or staggering, due to cerebellar lesions; loss of sense of position, sometimes seen in lesions of the parietal regions; anesthesia, which is rare unless the internal capsule is involved. Other symptoms are: word-deafness, which indicates a lesion of the posterior part of the first temporal convolution; agraphia, indicating deep lesions under Broca’s speech centre, and alexia, usually produced by lesions of the lower left parietal lobe. Tumors in the sensory zone affect vision and speech, and reveal themselves by irritative symptoms. For instance, a patient with verbal deafness and marked hemiplegia probably has tumor involving the left superior or dorsotemporal gyrus, which, as it grows, would involve loss of muscle sense and anesthesia on the opposite side of the body. A patient with headache, vomiting, choked disk, stupor, increasing hemianesthesia, lateral hemianopsia, without spasm or hemiplegia, probably has a tumor in the white substance of the occipital lobe. If hemianopsia alone be present there is almost always a tumor upon the inner aspect of the occipital lobe, on the side opposite to the dark half-fields, which by downward growth may cause cerebellar symptoms. Psychic and mental disturbances are present in many cases, but not in all; most frequently in frontal lesions. They are met with in about one-third of the cerebellar tumors and two-thirds of the temporal tumors; they assume the epileptic type, with hallucination, mania, or sometimes convulsions of Jacksonian type, the latter, of course, indicating lesions of the motor area.
6. Finally there are frequent constitutional disturbances, including anomalies of thirst and appetite, and disturbances of heart and respiration. In two or three instances the writer has seen such serious obstruction of the bowel as to lead to mistake in diagnosis, the obstruction in each case being finally fatal, but apparently not justifying operation.
The above symptoms pertain to the brain tumors in general. When it comes to tumors of the cerebellum these constitute, in a measure, a class by themselves. Those which are operable comprise tumors located in one lateral lobe, or invading the vermis[584] or middle lobe, or those found at the junction point of the cerebellum, medulla, and pons, those first mentioned being by far the more favorable for attack. It is not relatively difficult to decide upon the presence of a tumor in the cerebellum, but to minutely locate it is extremely difficult. In addition to the symptoms already rehearsed above the following features may be mentioned: Headache is often intense, sometimes agonizing. While usually referred to the back of the head it is occasionally frontal. Nausea and vomiting are generally present, at least for a time. Sometimes they subside to recur later. Optic neuritis and choking of the disk occur earlier and oftener than in other tumors. Blindness sometimes comes on promptly. Vertigo, as in other brain tumors, is commonly due to irritation of those branches of the fifth nerve which supply the inner surface of the dura, this irritation being reflected to the bulbar nuclei of the fifth, and thence to the nuclei of the pneumogastric. This is partly true of those growths which are in relation with the dura, though sometimes it is true of tumors which make pressure at the base of the brain. It is important to distinguish, if possible, between mere vertigo and cerebellar ataxia. The more directly focal symptoms are: nystagmus, which may be present when the eyes are quiet or only when they are in use; paralysis, when the pyramidal tracts are involved; muscle weakness, seen more often in the legs, which is nearly always a cerebellar symptom; and sometimes a peculiar posture of the head, where the spinal column becomes concaved toward the affected side, the face looking almost backward. Incoördination is a common indication; in about four-fifths of the cases patients stagger in their gait.
To determine whether a given tumor is an irritative or destructive lesion special study should be made of the spastic or non-spastic condition of the limbs, and note to which side the eyes are turned. Tonic spasms and contractures are rare in cerebellar tumors. A tremor of the head and upper part of the body is not infrequent, and muscle sense is rarely lost.
Between cerebellar tumors and those of the parietal region the chief diagnostic points are muscular and cutaneous sensibility in the former, with nystagmus and peculiar and extreme vertigo. From frontal growths they may sometimes be differentiated by the clearness of the mental processes and the absence of those symptoms which point especially to involvement of the temporocortical region, e. g., aphasia. In cerebellar tumors convulsions, one-sided or general, are not infrequent, and incontinence of urine and feces is often noted. The convulsions are accompanied by subjective sensations and noises, vertigo, and by sudden blindness, with loss of consciousness, while such tonic spasms as occur are generally of the extensor type, and last from one to ten minutes.
Basal tumors of the cerebrum produce a collection of symptoms which sometimes are significant. Owing to their location they involve the functions of several of the special nerves. In tumors in the anterior fossa there is involvement of the optic, the oculomotor, and the first branch of the fifth. In tumors of the pituitary body there is involvement of the optic, the chiasm, the oculomotor, and the first branch of the fifth, as well as the abducens. In tumors resting on the middle fossa and situated above the dura the oculomotor, the patheticus, and the chiasm are involved. If situated beneath the dura there is paralysis of the three ocular nerves and also the fifth nerve. In tumors of the posterior fossa there is involvement of the facial, the trigeminus, the auditory, the glossopharyngeal, the vagus, the accessorius, and the abducens.
—Fränkel and Hunt have recently shown that basal tumors spring from the acoustic nerve, which are essentially neurofibromas. They have their site upon the nerve at the point where it merges from the junction of the pons and the medulla; in other words, where the function of the nerve is more or less disturbed, and the patient thereby made to complain of deafness, tinnitus, and vertigo. They slowly displace surrounding tissues. They vary in size from a cherry to that of a robin’s egg, are loosely attached, and when exposed easily enucleated. Their general symptoms are those common to all brain tumors, but focal symptoms may include ataxia, paralyses (especially of the fifth, sixth, and seventh nerves), inequality of the pupils, and loss of coördinate movements of the eyes; these symptoms are in addition to those of the auditory already mentioned.
Access to these tumors is a serious matter. It should be undertaken in two stages: the first including a large lateral exposure, with or without an osteoplastic flap, comprising the lower portion of the squamous, a part of the occipital, and perhaps even the[585] posterior aspect of the mastoid. Drainage will be required for a few hours as in other similar operations.
As to depth and number the former may only be learned by studying the nature and location of the signal symptoms, the presence and order of appearance of the same, presence or absence of headache, and local changes in temperature. Tumors occurring in tuberculous individuals are probably multiple. When different centres or systems are involved multiple lesions are usually present.
It has been held that the three cardinal symptoms of brain tumor are optic neuritis, headache, and vomiting; and while each of these is significant, and all of them are corroborative, they are not necessarily present nor does their absence exclude possibility of tumor. Other signs indicating the presence of tumor, it is a mistake to wait for the development of these three. The most distinctive feature of intracranial neoplasms is the progressive character of such symptoms as are present.
There is but one form of brain tumor which is amenable to internal treatment—namely, syphilitic gumma; and in case of doubt it may be justifiable to keep the patient actively under the influence of iodides for a reasonable length of time. This, however, need never be prolonged beyond six weeks, after which time, should no improvement occur, operation should not be delayed.
—Brain tumors are operated for two purposes: First, for relief of pain and other distressing symptoms in incurable cases; second, for radical cure. Operation is justifiable in any case when pressure symptoms become severe, particularly so when pain is localized to a reasonable extent. Choking of the optic disks is not infrequently relieved and threatened disability postponed. The complete operation consists in the exposure of the tumor and in its removal.
The osteoplastic method should be used in exposing the tumor, by which a bone flap is raised, along with the overlying scalp, from which it is not detached. The centre of this flap is supposed to be calculated to overlie the centre of the deep lesion which it is proposed to attack. In many instances the operation should be divided into two distinct procedures, the first consisting in removal of the bone and exposure of the dura; this exposure should be ample, including the whole lateral region if necessary, as Horsley has shown; the second, a week or two later, comprising the balance of that which is to be done. But comparatively little shock attends removal of the tumor in the second stage of such a divided operation. After removal of the growth its cavity is best packed with a gauze tampon, after prompt ligation of all bleeding vessels within the field of operation, although it is usually required merely on account of venous oozing, as it is often possible to cut to the depth of an inch in the brain without a single artery spurting except those in the pin. The tampon is of value if allowed to remain for forty-eight hours, as preventing filling of the cavity with clot or excessive bleeding during the vomiting which may follow the administration of the anesthetic. The vasoconstricting properties of adrenalin may prove of great service here; it should be used in the standard 1 to 1000 solution, diluted 1 to 3. I have no hesitation in spraying this upon the brain or in saturating tampons with it, which may be left in situ so long as necessary. A number of the old-fashioned small serrefines, properly sterilized, can also be resorted to, if needed, for securing vessels, which may not be easily tied. They can be left in place along with the tampon and all may be removed together.
Next to the danger from hemorrhage is that of rapid edema of the brain, which may result from increased tension in the arteries or through venous stasis, which later produces lymph stasis, by which fluid collection in the tissues is still further facilitated. Another reason for using tampons is to prevent such relaxation of veins as may predispose to this edema. In most respects the operations for removal of brain tumors differ slightly from those whose general principles are elsewhere mentioned in this work. I am greatly in favor of using secondary sutures (i. e., those tied with bow-knots), which may be loosened on the second or third day, permitting the raising of the flap, removal of tampon, etc., and I employ them largely after all sorts of operations upon the cranium. If we desire to prevent any attempt at union of wound margins we may employ the green silk protective introduced by Lister, which should have been previously carefully sterilized by boiling.
The operative treatment of cerebellar tumors is made doubly difficult by their protected position and the large sinuses with which this part of the brain is surrounded. The cavity is restricted in size, intradural tension is greater than above the tentorium, and there is[586] no room for easy displacement or retraction of parts. The occipital bone varies much in thickness and at points is somewhat thin. Operation which is begun either as an exploration or with a fixed purpose may prove palliative, even should the original purpose fail of accomplishment, as relief may be afforded by reducing tension, such relief consisting perhaps in freedom from headache, vomiting, and vertigo. Incision should extend from the tip of the mastoid process, a little above the superior curved line, to beyond the median line, with a vertical median incision by which a flap sufficiently large may be reflected downward. It is best to reflect the periosteum with the other soft tissues in order to expose the bone. The bone should be bitten away with forceps or removed with a reliable engine as rapidly as possible, hemorrhage being controlled with Horsley’s wax.
The operation may be divided into two stages, confining the first stage to the exposure of the cerebellar surface, or the operator may attempt all at one time.
The second stage consists in raising a dural flap, by which the cerebellar surface is exposed for inspection. It will protrude promptly through the opening, so that, with the finger, it may be possible to detect a tumor by the sense of touch. If no tumor appear on or near the surface deeper exploration should be made, with the aid of a retractor and by removal of a portion of the cerebellar hemisphere. This may require further exposure of the lateral region of the skull. Tumors situated deeply or at the junction of the cerebellum and pons require all the room that can be afforded from the outside, and are better approached from the lateral region than from above or below. It is comforting to realize what considerable portions of the cerebellum can be removed without serious or extensive disturbance, but as the medulla and pons are approached there is need of great care. The opening may be extended across the middle line, and either the lateral or the longitudinal sinus, or both, may be doubly ligated and divided. The tentorium may also be divided nearly to the petrous portion, after the lateral sinus has been thus divided, and so better access given to the deep location.
These remarks apply especially to operations for tumors of the cerebellum. The other features of such operative attack are those common to brain tumors in any location.
In all operations for brain tumor, but particularly for cerebellar tumor, it will prove of the greatest advantage to have the operating table so inclined that the patient’s head will be three or four feet above his heels. In this position the veins are drained by gravity, and the operation is complicated by but little venous oozing. Crile’s pneumatic suit, or at least the lower part of it, should be worn, and an assistant should watch and report on the blood pressure. These two precautions permit such an operation to be conducted with an ease and safety hitherto unknown.[44]
[44] New York Medical Journal, February 11 and 18, 1905.
Cushing, dealing especially with a group of brain tumors in which radical procedures are impossible, where nevertheless relief from symptoms would prove a therapeutic desideratum, has proposed to afford this by removal of a portion of their bony covering, in order to allow a part of the brain to protrude, and thus provide a means of relief for the constantly increasing pressure. The incomplete union of the bones in infancy permits something of this kind to occur through natural causes, but after fusion of the elements of the cranial vault it is no longer possible, save in those rare cases where an opening results from the process of slow pressure absorption, which comes only when the tumor is in actual contact with the bone.
It would be mechanically ideal if, during adult life, a dislocation of cranial sutures could be produced similar to that observed in very small children. The dangers of such operation are many, among them being the possible injury to the functions of that portion of the cortex which protrudes through the opening thus made, by which, for example, preëxisting paralyses might be aggravated. For this reason it is preferable to establish the hernia over some “silent” or unimportant part of the cortex and to avoid making it unnecessarily large. Cushing, after various trials, recommends to make the bone defect under the temporal muscle, which not only affords a certain degree of protection, but exposes an area where few important motor centres are involved. He has reported several cases, with gratifying results, with a minimum of undesirable sequels.
Obviously in tumors below the tentorium the opening would best be made in the suboccipital region. Nevertheless, Cushing believes that even here the final result would be no more effectual than were the defect placed elsewhere.
Beck has called attention to the value of the temporal fascia as a substitute for the other firm coverings, by which the brain should be left enclosed after exposure, and when these latter are not available. For the purpose he would fold over a flap made from the temporal muscle and the adjoining periosteum in such a manner that fascia originally external should now be placed deeply and in contact with the cortex.
PLATE XLIV
FIG. 1
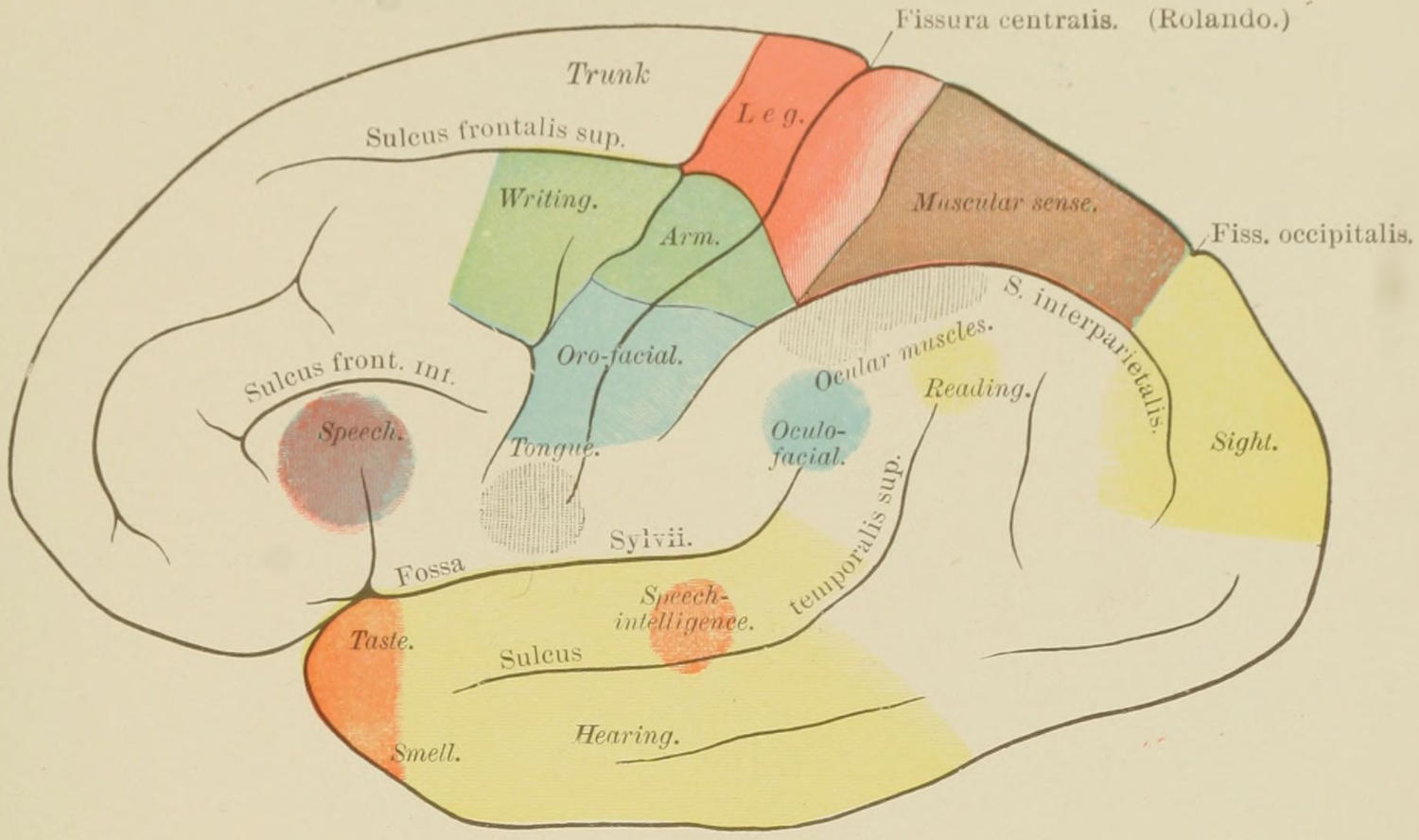
Topographical Anatomy of Cortex. Localization of Functions. (Ziehen.)
FIG. 2
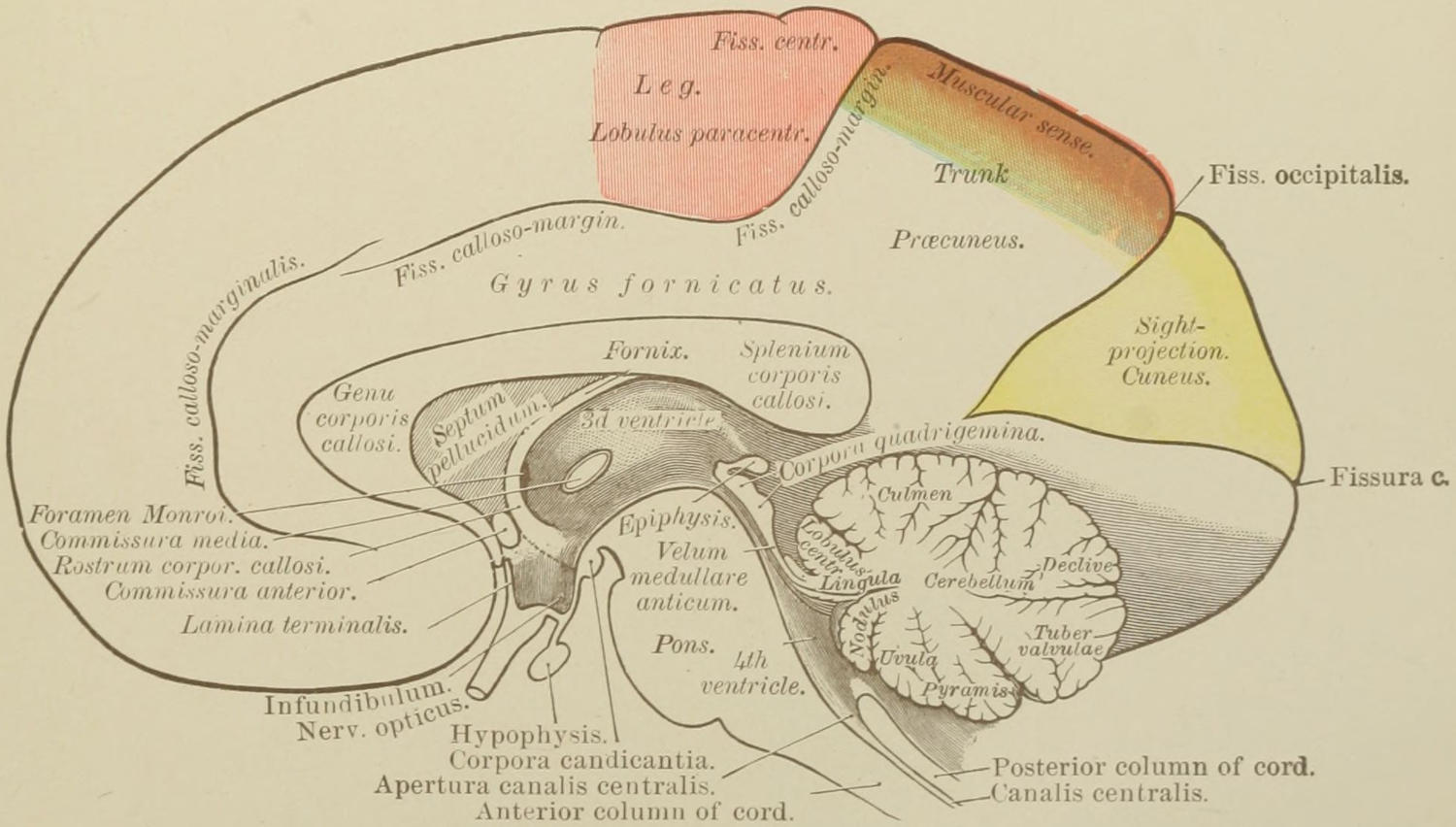
Topographical Anatomy of Inner Surface of Right Hemisphere. Localization of Functions. (Ziehen.)
[587]
The fissure of Rolando is the anatomical landmark whose position it is important to determine with reference to a number of modern surgical procedures, for around it cluster most of the motor areas or centres. It commences at the middle line about 56 per cent. of the distance backward from the glabella (root of the nose) to the inion (occipital protuberance), and, passing downward and forward, makes with the middle line an angle of 67 to 69 degrees. For most purposes it begins half an inch back of a point midway between the glabella and inion. It may be easily found by Chiene’s method, which consists in folding a square piece of paper diagonally and folding this again; after which it is three-quarters unfolded, the acute angle then representing 67¹⁄₂ degrees. If this be properly applied to the skull, one edge of its surface can be made to fall directly over the Rolandic fissure. The fissure may also be located by a simple instrument known as the cyrtometer—a gauged metal strip having a sliding arm upon it, which, when the long strip is placed over the longitudinal sinus (i. e., the middle line of the skull), can be made to fall directly over the fissure. While neither of these methods is invariably and minutely exact, either of them is sufficiently accurate for all practical purposes.
The fissure of Sylvius may be indicated by a line drawn from a point 3 Cm. behind the external angular process to a point 2 Cm. below the most prominent part of the parietal eminence. The short and ascending limb of this fissure is of relatively small importance in this connection.
Reid’s base-line, so called, is a line drawn from the inferior margin of the orbit backward through the centre of the external auditory meatus. It is a line often alluded to in cranial topography. The colored plate (see Plate XLIV) will indicate with reliable accuracy the relations of the motor centres to each other and to the principal fissures and convolutions. It pertains merely to the left hemisphere of the brain, in whose third frontal convolution is placed Broca’s centre for speech, the corresponding area upon the right side having no exactly corresponding function. The centre for vision, it will be seen, is located in the cuneus, the most basal portions of the hemispheres being the seat of the special senses of taste, smell, and hearing.
—The word trephine is at present used both as a noun and as a verb, the older term trepan being now wellnigh discarded. The instrument consists of a section of a tube, one of whose extremities is arranged with sharply cut saw teeth, the whole provided with a grip or handle, which revolves in a plane parallel to that in which the saw teeth cut. The best instrument is that arranged in a slightly conical manner, so that it may less easily burst through the skull and do harm to parts within. The trephine proper is manipulated by the hand. A variety of substitutes have resulted from applications of human ingenuity to the problem of opening the cranial bones. Some of these are operated by foot or hand power, with reduplicated mechanisms, and others by electricity. The more complicated the mechanism the more likely it is to get out of order, and there are but few of these substitutes which give anything like lasting satisfaction.
The operation of trephining is made to include any method by which an opening is made in the uninjured cranium or by which an opening already existing is enlarged and made to subserve the surgeon’s purpose. Aside from the saws already alluded to, there are in use a variety of cutting bone forceps, rongeurs of various device, and a variety of chisels, which are to be used in connection with the mallet or hammer. In order to use any of the latter instruments to advantage the first attack should be made with a trephine of reasonable size, say 2 to 3 Cm. in diameter, after which forceps, chisel, or saw may be used. Straight saws also are of occasional usefulness. I do not favor the use of the chisel and mallet, feeling that the concussions resulting from blows of the hammer add to the shock of the operation. The common trephine is provided with a centre pin, which can be withdrawn after a shallow groove has been cut. To prevent slipping of the centre pin the point to which it is to be applied should be marked by cutting a nick with the point of a chisel.
[588]
The Gigli saw should be in every surgeon’s outfit. It consists of a piece of steel wire having a thread cut around and along it by a die, by which it is made as effective as a series of saw teeth. Two small trephine openings are made, and it is then passed into one and out of the other, the dura protected by depressing it, and the wire then handled as though it were a chain saw. It can thus be made to cut its way quickly through the bones of the skull.
Other aids in mechanical procedures are revolving small saws and the surgical engine.
Fig. 385
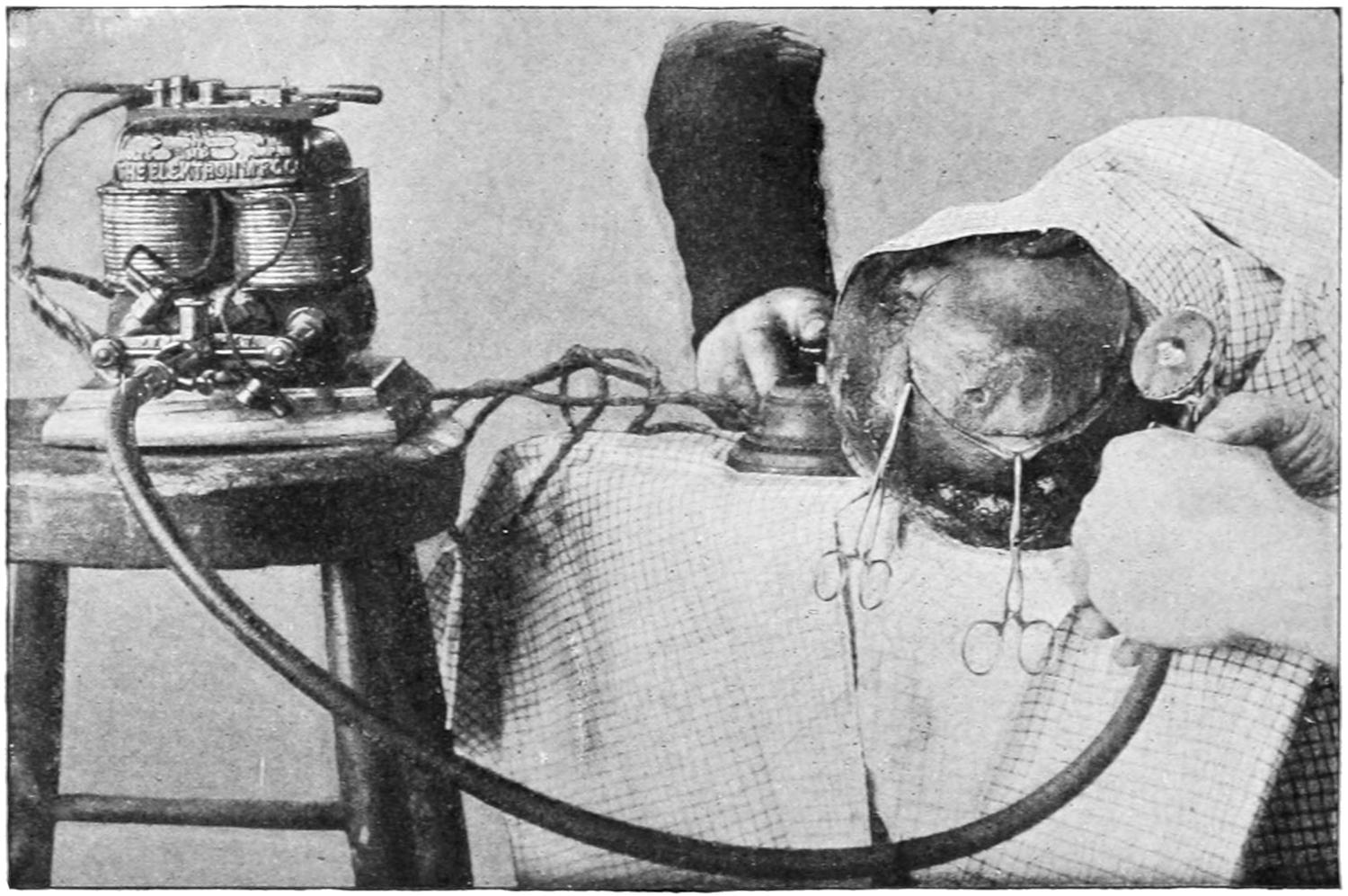
The Powell electric saw cutting a “trap-door” in the skull. (Illustrating the operation upon a cadaver.)
In the absence of a wound a flap of scalp is raised before applying the instrument. This flap is ordinarily of horseshoe shape, and should be made with its convexity pointing toward the occiput, as drainage is best afforded later by this arrangement. The old crucial incisions are now wellnigh abandoned. The pericranium is detached, after incision, with the periosteum elevator, and it should be turned up with its overlying scalp without completely separating it. The scalp flap can be held out of the way by temporarily sewing it to some other part of the scalp, every portion of which should be previously shaved closely and thoroughly scrubbed. The operator has his choice—to seize vessels as they bleed or to make the operation in large degree bloodless by applying an elastic tourniquet tightly around the scalp above the eyebrows and beneath the occiput, the ears preventing it from sliding. If the tourniquet be used the vessels will often bleed in an annoying way after the wound is closed. If the operation be performed for fracture of the skull, should there be an opening already made by the depression of fragments, it may not be necessary to use the trephine, but with suitable bone forceps fragments may be removed or detached. In this case, however, there are often sharp points of bone which will require removal by cutting bone forceps, for the surgeon should leave the margin of the bone opening comfortably round and smooth. Should there be no opening into which the point of an elevator or of bone forceps can be inserted, then one should be made; it is for this purpose that the trephine is mainly used in cases of fracture of the skull. It should now be applied upon a firm and undetached surface of bone, one which will bear the pressure necessary in the process of perforation. As used for this purpose it should be so applied that at least two-thirds of the circle cut by its teeth will be upon unbroken skull; the remaining segment of the circle may be over the fractured area. After it has begun to cut a distinct groove the centre pin should be withdrawn and the instrument maintained in its position during its work by a firm and steady hand, which will force it evenly through the bone and not exercise undue pressure. As the diploë is perforated the bone-dust becomes soft and bloody and the resistance is diminished. As the instrument sinks deeper the operator should frequently intermit its use, and determine his position by means of the irrigator and of the probe or other[589] instrument. The nearer the inner surface is approached the more caution must be exercised, remembering that the bone is likely to be of unequal thickness. When the skull has been completely perforated at one or two points around the little circle the operator should introduce the point of an elevator and pry up the disk of bone, or by rocking the handle of the trephine he may be able to remove the button with that instrument. When the operation is performed in the ideal manner the dura is scarcely touched, certainly not raggedly injured by the teeth of the instrument (Figs. 386, 387 and 388).
Fig. 386
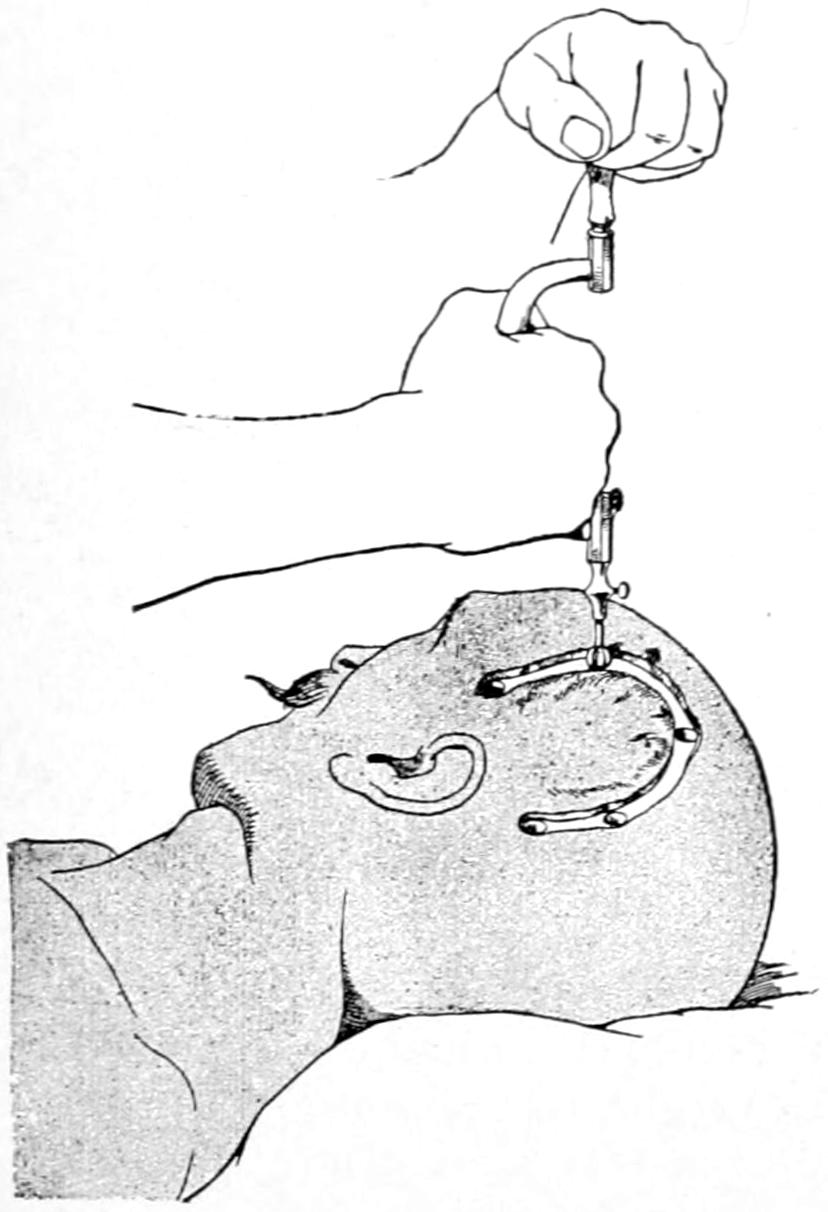
Construction of an osteoplastic flap; bone is exposed; first openings are made with a hand trephine or burr. (Marion.)
Fig. 387
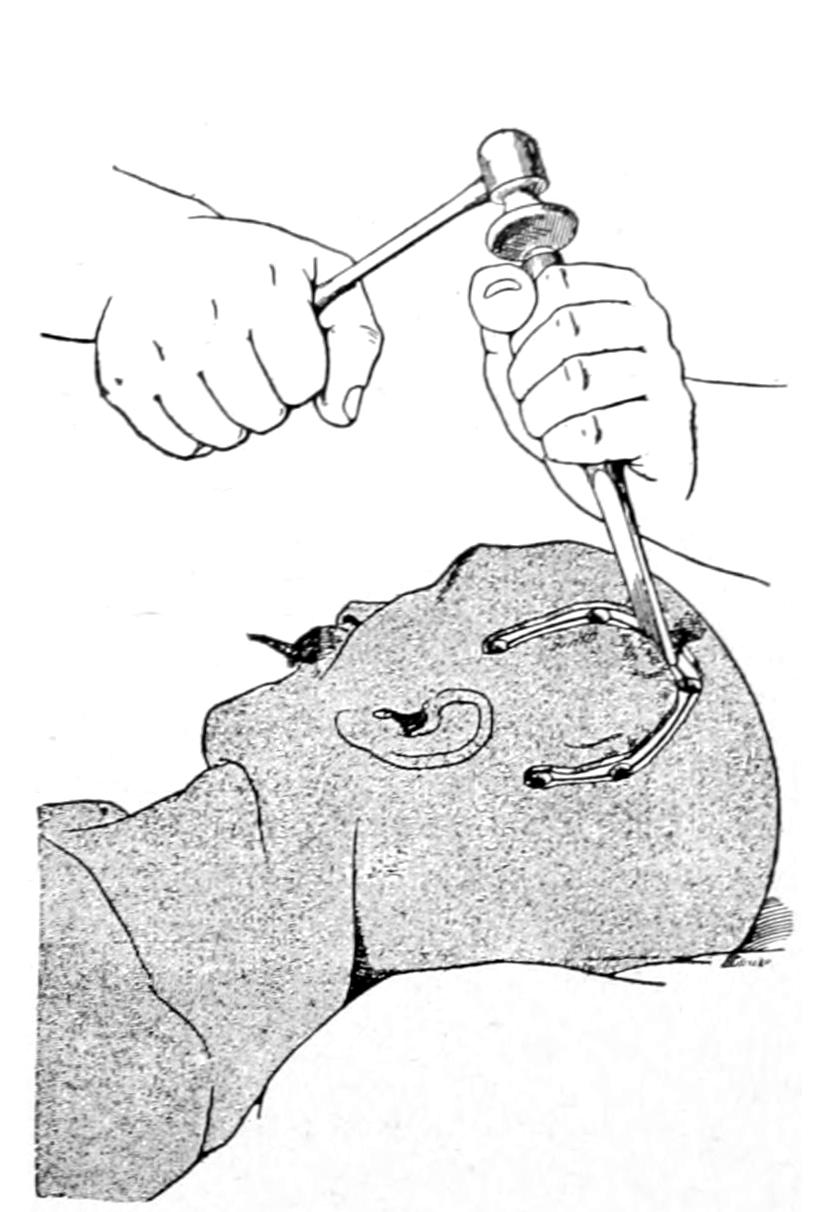
Division of bone by use of hammer and chisel. (Marion.)
Before opening the dura every loose particle of bone and every splinter should be removed, depressed fragments should be picked out, and those which are semidetached should be raised to their proper level. Through the opening thus made the dura is carefully examined; extradural collections of blood are recognized instantly, while some idea as to the amount of intracranial tension may be secured, even through a small opening. Absence of pulsation means probably the presence of cyst, tumor, or abscess deeper. Edema of the membranes usually subsides after nicking or opening them. A yellowish discoloration of the dura often indicates the existence of a tumor beneath. Nothing abnormal being discovered outside of the dura, should brain tension be great or should the dura be discolored, as by blood beneath, the membrane should be opened, by a triangular or horseshoe flap, and the subdural condition accurately estimated. In some cases of meningeal hemorrhage clots will be ejected with some force the instant the dura is opened. In other cases of intracranial pressure, either from tumor or from intraventricular hemorrhage, the brain will instantly protrude to such an extent as to make its reposition difficult or even impossible. Horsley’s dural separator is exceedingly useful, both outside and inside the dura, for detecting and separating adhesions, and as a retractor.
Incisions in the dura should be made, so far as possible, parallel with its vessels rather than across them. When accessible, dural vessels can always be secured and tied. Vessels of the pia can also be picked up and secured with fine catgut ligatures. When the brain tissue itself is diseased it should be carefully excised. The cortex itself is not so vascular as to afford much trouble. Upon any portion of the membranes or cerebral surface a sterilized solution of adrenalin can be sprayed or applied without hesitation. In all deliberate operations sinuses are avoided. When exposed or when necessary to attack them they may be ligated and divided, or may be packed with tampons of sterilized[590] gauze, or may be seized with serrefines or light hemostatic forceps, which may be left for a day or two included within the dressings.
Any of the exposed motor areas or centres can be stimulated, when desired, if the patient be not too deeply anesthetized, by the faradic current of mild degree, applied to surfaces which have not been bathed with antiseptics, nor long exposed to the vapor of the anesthetic, through a double brain electrode made for the purpose, or by sterilized probes connected with the battery.
Buttons of bone or chips of the skull may be replaced after suture of the dura, when desired, though this is seldom advisable. When fragments are thus to be replaced they should be placed in warm sterile salt solution at once after removal, and kept warm. When a button is thus put back the periosteum may be sewed over it with buried catgut sutures.
The dura should be stitched with fine catgut as closely as possible. I have often placed beneath the dural opening a piece of gold, silver, or aluminum-foil, carefully sterilized, with a view to preventing dense adhesions between the dura and the membrane or cortex beneath. I have never known it to do harm.
Fig. 388
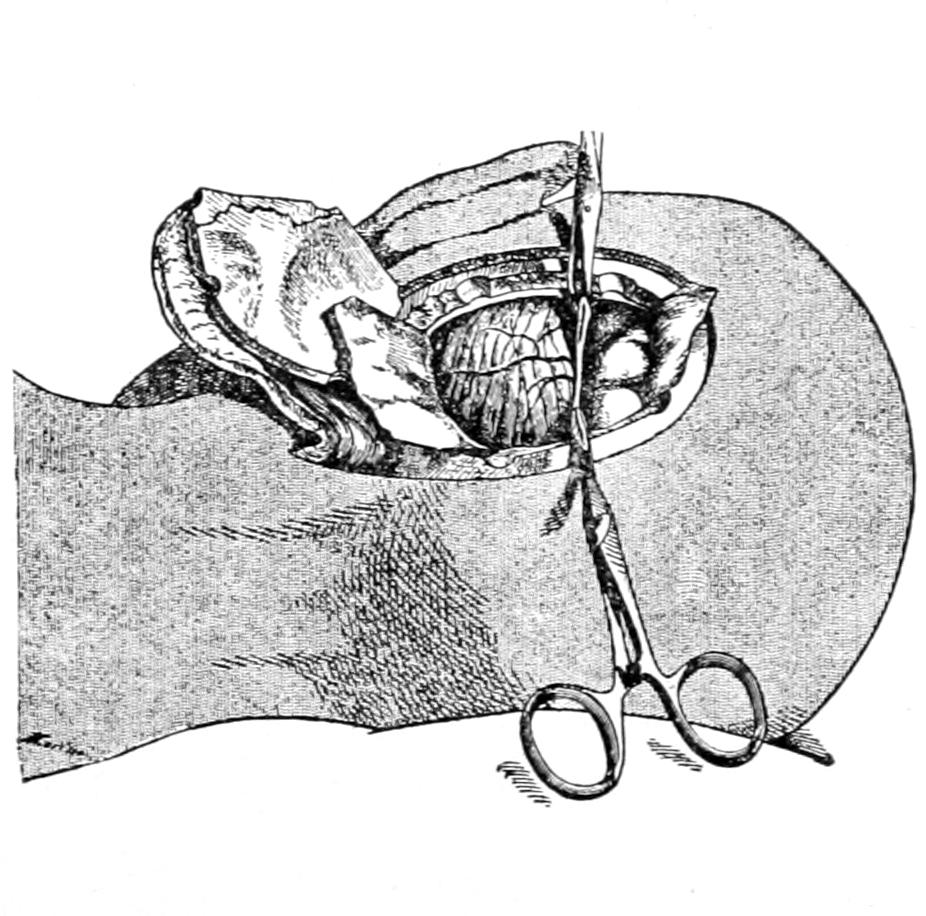
Exposure of cortex or of cerebellum after division of dura. (Marion.)
Fig. 389
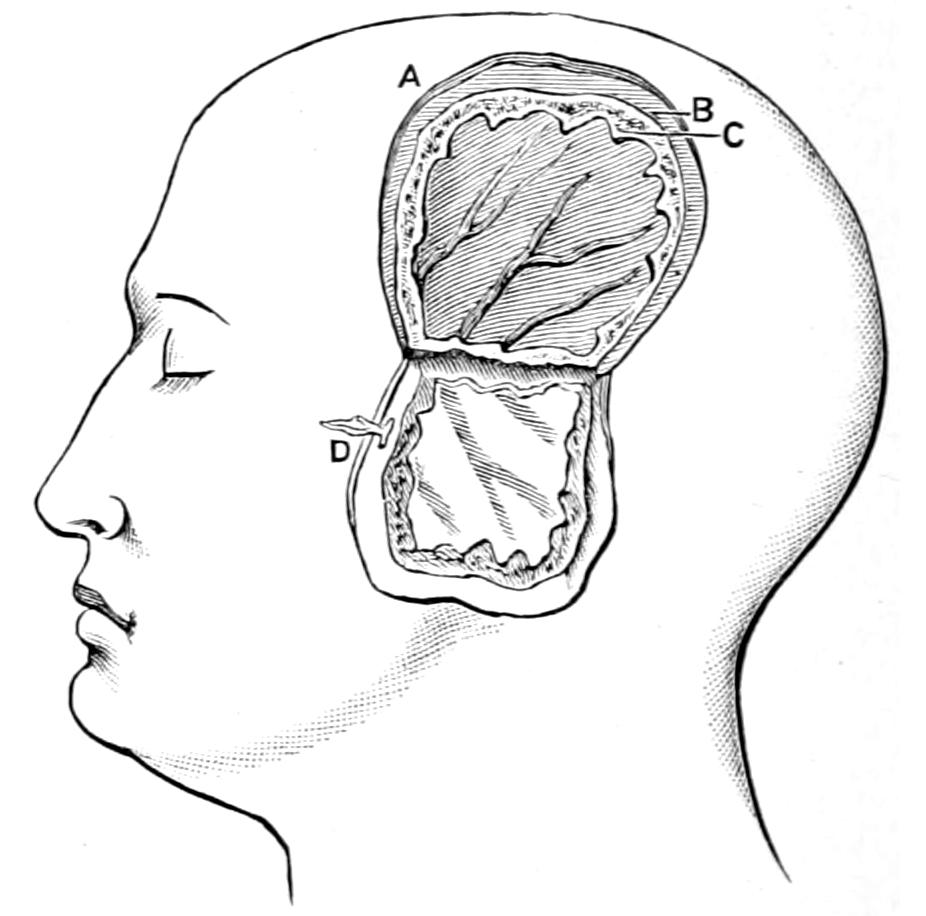
Osteoplastic resection after Wagner. (Chipault.)
Drains and drainage are to be avoided when possible, and should be removed early, except in cases of abscess. They may be made of catgut, horse-hair, gauze, rubber, or even of glass, like those short ones which Kocher inserts after extensive operations, their outer ends flanged to prevent their slipping beyond control.
Opening the skull, or, in general terms, trephining, is at present resorted to for the following purposes:
1. For relief of compression—
2. For removal of foreign bodies.
3. For relief of intracranial irritation—e. g., epilepsy, the psychoses, etc.
4. For removal of tumors.
5. To compensate for defective development.
6. For exploratory or purely empirical reasons, including the making of “relief openings” for relief of pain, etc.
Aside from the ordinary methods of trephining as applied for common conditions, modern surgery comprises the resort to essentially new methods for raising areas of skull of considerable size and then restoring them to their previous position. These are ordinarily spoken of as osteoplastic resections, and have added very materially to the art and resources of the surgeon. These consist, in a general way, of the formation of a window,[591] as it were, in the vertex or lateral region of the skull by outlining a quadrangular or horseshoe flap of scalp, which is detached only for a slight distance around the incision, after which, by use of the revolving saw or by chisel and mallet, a groove is cut through the bone running parallel with the margin of the scalp-flap, but perhaps a centimeter within it. After this bone area is completely cut through on three sides it is then sprung up or elevated in such a way as to be broken across the base of the bone-flap. It is not at all detached nor separated from the scalp, and so when subsequently lowered into position retains its vitality by virtue of its vascular connections.
When some particular measure seems indicated in order to atone for a large defect in bone it has become quite customary to insert some artificial substitute, mainly either celluloid or a thin aluminum plate, previously absolutely sterilized and cut at the time into such shape as may be called for, but a trifle larger than the real defect, being let in or sprung in, as it were, either completely beneath the bone or into the bony opening, so as not to be easily detached or slip out of the way. By this heteroplastic method most admirable results have been achieved. I have used celluloid for this purpose in the spinal column also, closing with it the defect which remained after the extirpation of the sac of a spina bifida. It is rarely necessary to resort to this practice in the skull, as dense fibrous tissue in due time firmly protects the endocranial contents from external harm (Figs. 386, 387, 388 and 389).
[592]
Intra-orbital hemorrhage is not uncommon after injuries to the head. It may result from rupture of orbital vessels proper or by escape of blood from within the cranium, either outside or beneath the dural prolongation which constitutes the sheath of the optic nerve. When extensive it may produce a pulsating tumor, and this may, in time, become practically a traumatic aneurysm. After basal fractures blood frequently will escape forward so as to appear beneath the conjunctiva. Collections of blood in the orbit may also interfere with the return circulation in such a way as to lead to extensive chemosis of the conjunctiva or edema of the lids and orbital contents. Pressure may cause temporary disturbance of vision. Should there be absolute blindness it may be inferred that there has been injury to some part of the optic tract. Protrusion of the globe is an indication of the degree and amount of extra-ocular hemorrhage, which may be very pronounced. When visual symptoms are bilateral, while external evidences are confined to one orbital region, it may be assumed that there has been intracranial disturbance as well, with laceration along the optic tract. Such immediate damage will in time be followed by the ordinary symptoms of neuroretinitis and atrophy.
The more external the injury the more quickly will it yield to ice-cold applications. There are times when incisions for relief of tension may be desirable. An extensive clot in the orbit which seriously displaces the eyeball, and which does not quickly absorb, should be evacuated by an incision, either directly through the lid or beneath the lid and outside of the globe.
Penetrating injuries, like gunshot wounds, are usually easy of recognition. If vision be instantly and completely lost the harm done to the optic nerve or the globe will probably prove irreparable. Foreign bodies penetrate from various directions, and sometimes to such a depth that they are difficult to find. I have seen a large chip of wood completely lost within the orbit, and such bodies may enter either from outside or from within the nasal cavities. A foreign body will nearly always limit the motility of the globe and usually displace it. If its presence can be ascertained or revealed before operation it should be sought and removed at the expense of almost any and every other indication. If its presence be suspected it may be sought for, even though a skiagram fail to reveal it. When the usefulness of the eye is destroyed it will be advisable in such case to remove it in the progress of this search.
Aside from the traumatic hematomas above mentioned extravasation occurs, due to constitutional or vascular disease, as atheroma, especially when coupled with violent straining efforts. Subconjunctival effusion and exophthalmos, with limitation of motion, will be unfailing expressions of such damage. Orbital aneurysms, spontaneous or traumatic, are occasionally seen. They will cause a more or less pulsating exophthalmos, while, in some instances, a bruit may be detected with the stethoscope. Cases may be imagined where it would be suitable to cut away the external wall of the orbit and expose such a tumor. Ordinarily, however, ligature of the internal or common carotid will be required. Angiomas occur also in the orbit, producing exophthalmos, usually without pulsation. Such tumors will prove compressible and the globe may be gently pressed backward into the orbit to immediately protrude again when pressure is removed. These lesions will prove very difficult, usually impossible of treatment, and no general rule can be made therefor.
Orbital cellulitis, i. e., infection of the cellular and other tissues in the orbit, may occur, either from without or from within, but usually in connection with some traumatism.[593] Sometimes this involves first the cornea or the structures of the globe; at other times infection is by a more direct method, through the conjunctival sac or the orbital coverings. It varies in intensity between extreme limits. It may even be bilateral. While cases occasionally undergo resolution it usually terminates by formation of abscess. It is met with in the infectious fevers, in facial erysipelas, by extension upward of infection from diseased teeth, after primary infection of the ethmoidal or sphenoidal sinuses, or by extension from external phlegmons. There will be edema of the lids, usually with chemosis, fixation and protrusion of the eyeball, commonly with divergence. In proportion to the severity of the lesion there will be present septic symptoms, with deep-seated pain and headache. Vision is disturbed in proportion to the pressure upon the nerve and globe, as well as the involvement of the ocular structures proper. When the disease is begun within the eye it will usually terminate by a combination of panophthalmitis with orbital abscess.
—The application of the compound ichthyol or Credé’s silver ointment, with ice, preceded perhaps by the use of leeches, will be suitable local treatment unless the presence of pus be distinctly made out or until tension threaten serious harm. In either of these events, however, free incisions are required at points of greatest tension, the knife being so directed as to avoid the globe. These incisions should be free and sufficiently deep. Should there be accompanying panophthalmitis the eyeball itself should be freely incised through its anterior aspect and its contents completely evacuated. Such emptying of the contents of the sclerotic is called evisceration of the globe. While theoretically indicated, experience has shown that it is a disastrous practice to enucleate the eye at such a time; evisceration first and enucleation later, should it prove desirable.
The orbit is the site of many primary tumors which originate within its proper tissues as well as those which encroach upon it from neighboring cavities or from the face. Prognosis is better in the former than in the latter, but unfavorable in all malignant cases.
Of the primary cystic tumors there may be nearly all the known varieties, including those of parasitic origin. The pseudocysts of the cranial cavity sometimes project into the orbit, forming orbital encepholacele. Dermoid cysts are not at all uncommon. Around the bursæ of the orbital muscles exudation cysts occur, while the retention cysts, including the cholesteatomas, are not infrequent. The true dermoid cysts may contain all the ordinary epithelial products, just as in any other part of the body. Parasitic cysts include the echinococcus and the cysticercus, the latter being rare, while the former may extend into the frontal sinus or cranial cavity. It produces almost constant ciliary neuralgia. Vascular tumors of all types are found in the orbit and the various expressions of telangiectasia of the lids and orbit are often seen. These are always of congenital origin. Of the more simple types of mesoblastic tumors the osteomas are perhaps as common as any. These assume all the types described in the chapter on Tumors, and are of all degrees of hardness. Sarcoma and osteosarcoma, originating within the orbit, are unfortunately too common. Naturally they spread to and involve all the adjoining structures. True endothelioma is rarely recognized as such until after removal and microscopic examination. Epithelioma commencing upon the surface of the eye, or about the skin and spreading inward, is also quite common.
Exophthalmos is an expression of intra-orbital tension common to all forms, while by the extent of protrusion and its direction the site of the tumor may to some extent be determined. Other disturbances of position, with limitation of motion and consequent diplopia, are further expressions of pressure and dislocation. Ptosis, or drooping of the upper lid, is a feature of tumors which proceed from the upper part of the orbit. The vascular tumors, as already mentioned, produce more or less pulsation. Ocular tension is usually increased, and when circulation and enervation have been seriously affected necrosis and even perforation of the cornea may occur. Pain is a variable feature, but is sometimes pronounced. An exploring needle may be passed into a tumor which seems to be cystic, but it should be done with every precaution, both against infection and injury to the eye.
Tumors of the optic nerve proper originate more often in its sheath than in its true neural tissue. They may occur at any point, but usually within the orbit. These tumors[594] are usually of the sarcomatous, gliomatous, or endotheliomatous type. Cystic changes are not infrequent; they occur usually in the young. All of these tumors will involve the optic nerve in such a way as to produce signs easily recognizable with the ophthalmoscope, such as optic neuritis and nerve atrophy. Moreover, they affect or completely destroy vision. They are not so painful as most of the other intra-orbital tumors, and, while causing a direct forward protrusion of the eye, affect its motility less than other forms. Nevertheless they grow with great rapidity and evince destructive tendencies. In theory the treatment for all tumors of the orbit is complete extirpation, while the malignant tumors require emptying of the orbital contents. Benign tumors and cysts are usually successfully treated by this method. Of most malignant tumors it may be said that the prognosis is unfavorable. The lymphatic and vascular connections are so free, and extension into surrounding cavities so easy, that recurrence takes place in the larger proportion of cases. Too often by the time a patient is willing to sacrifice the eye and the orbital contents it is too late to effect a radical cure.
The term exophthalmos simply implies protrusion of the eyeball beneath and even between the lids. Usually it is in a downward and outward direction. In some cases the displacement is accompanied by an easily recognizable pulsation, and occasionally by a bruit or audible sound. The latter instances are spoken of as pulsating exophthalmos. They are connected in most cases with vascular tumors or intra-orbital aneurysms, although sometimes the aneurysm may be primarily intracranial. For instance, arteriovenous aneurysms, by communication of the internal carotid artery with the cavernous sinus, will produce pulsating exophthalmos. Whatever be its cause exophthalmos is an expression of pressure from behind. This is true even of the ocular symptoms accompanying Graves’ disease or exophthalmic goitre, only here the protrusion is permitted by general fulness of the vessels and undue vascularity of the orbital tissues.
In proportion to the amount of projection there will be swelling and edema of the upper lid, the skin being more or less shiny and the veins distended. In extreme cases the lids are everted and the conjunctiva extremely chemotic, while by exposure of the cornea it becomes vascular, infected, and often necrotic. Should it be possible to replace the globe by pressure it will protrude so soon as pressure is removed. In vascular cases a bruit may be heard and pulsation detected with the finger. Audible sounds are lost by making firm compression on the common carotid of the same side, and return instantly when this pressure is removed. By the ophthalmoscope both arterial and even venous pulsation may be perceived at the fundus. Vision is only slightly affected by a well-marked protrusion, especially when the latter has occurred slowly. The pulsating forms will frequently give subjective symptoms of sound and sense, e. g., vertigo.
A history of injury, coupled with external evidences, may give a clue to some of these cases as an indication of traumatic aneurysm or communicating vascular tumor. Soft and vascular tumors, without history of injury, are usually malignant, this being true also of multiple growths.
—The treatment of exophthalmos should depend entirely on its nature. When due to arteriovenous aneurysms, or to the consequences of injury alone, a ligation of the common or of the internal carotid will give the best result. When compression of the carotid gives temporary relief to at least some of the features of the case its permanent ligation is indicated. Bilateral exophthalmos implies a more serious condition, especially in Graves’ disease. When thyroid symptoms are prominent a thyroidectomy is indicated. When the thyroid participates but slightly such a case may be treated by excision of the cervical sympathetic on both sides.
These tumors may assume most of the known types and may spring from practically all of the tissues of the eye.
From the iris there may develop cysts of traumatic or even of congenital origin. In the former such a foreign body as an eyelash may be found, having entered through an[595] external wound of the cornea. Vascular tumors are occasionally met with, many of which are full of pigment, while melanomas, with a minimum of vascular structure, are also observed. The actively malignant tumors of the iris usually assume the sarcomatous or endotheliomatous type, and when melanotic assume an exceedingly rapid and serious phase and course. In the iris, also, tuberculous or syphilitic granulomas are occasionally encountered.
In the choroid are seen expressions of tuberculosis, especially the more acute, as a complication of tuberculous meningitis. The most common malignant tumor here is sarcoma of the melanotic variety. Of the retina, glioma is the most common as well as the most malignant tumor, occurring usually in the young. All of these tumors when malignant spread from their primary site to the adjoining tissues. When extremely malignant they kill too quickly to show many metastatic expressions. At other times they will appear in other parts of the body.
All intra-ocular tumors tend to impair, and the malignant to quickly destroy vision. Tension is increased and the natural contour of the globe may be lost. Fixation to and involvement of the surrounding orbital tissues depend in some measure on the rapidity of growth and its location. They occur sooner or later in malignant cases.
A malignant growth of any part of the globe calls for enucleation of the eye, as well as removal of the orbital contents. When the orbital tissues are thus involved it is too late to secure more than temporary benefit. If the eyelids are involved they should also be sacrificed and the orbital opening covered by some plastic procedure.
The term panophthalmitis implies a phlegmonous process involving the entire contents of the sclerotic, by which the eye is destroyed. It is usually traumatic in origin, but may occur as an extension of infection from ulcer and abscess of the cornea, or from thrombotic or metastatic processes. Its course is usually rapidly destructive, while it is accompanied by more or less orbital cellulitis. These signs, therefore, are not confined to the orbit proper, for the lids become edematous, the conjunctiva chemotic, and there is more or less purulent discharge from the entire conjunctival sac, which will escape beneath the lids. If the cornea is at first clear it rapidly becomes cloudy, and to the signs of intra-orbital mischief are added all those above described under the heading of intra-orbital cellulitis. The sclerotic is an unyielding membrane; hence pain in these cases is usually intense, while septic features are added according to the nature of the cause. When the lesion has begun in the cornea it usually ruptures early and the ocular contents may escape in this way.
—Panophthalmitis is dangerous to life as well as to the eye when not promptly treated. The same rule prevails here as well as elsewhere in the presence of pus. Prompt evacuation offers the greatest safety and relief. Evacuation of the entire contents of the eye through a free incision and by means of a sharp spoon, with antiseptic irrigation, affords the only safe measure in these cases.
As previously remarked, the general consensus of opinion among oculists and surgeons is that, under these circumstances, enucleation should never be done, the danger being that of a purulent meningitis or thrombosis by extension backward along the sheath of the optic nerve.
This, too, is a matter of interest common to the eye specialist and the general surgeon. The term refers to lesions of one eye which follow sooner or later upon injuries or infections of the other. These expressions of so-called sympathy occur in irritative or inflammatory lesions. The former are more or less neurotic and include pain, often referred to the region beyond the orbit, photophobia, blepharospasm, too free lacrymation, and various subjective phenomena of impaired vision. These features will be accompanied by more or less tenderness of the globe, with ciliary neuralgia and injection. These may subside under treatment, but will recur when the eye is again used.
Contrasted with these lesions is another form whose features are most pronounced along the uveal tract, though the retina may also suffer. Its subjective features are those[596] of uveitis, to which are added actual exudates in various parts of the globe, some of which may be seen with the ophthalmoscope, with intra-ocular tension, which reduces the anterior chamber, and with partial or complete loss of sight that may end in total atrophy. In some instances these lesions occur rapidly; in others the course of the disease is chronic.
The oculopathologists have striven hard to explain these phenomena. Most of them believe in the continuity of the subdural or subvaginal sheath of the nerve from one orbit around into the other, and believe that the germs passed along this subway. Involvement of the yet unaffected eye may follow the entrance of foreign bodies, occurrence of traumatisms, punctures, existence of corneal lesions as minute ulcers, constant irritation of the presence of an artificial eye upon the stump, the performance of some of the common operations upon the globe, and even the much less frequent conditions of pathological changes in the choroid, the ciliary body, the optic nerve, or the existence of intra-ocular tumors. A recognition of the possibilities in these cases will lead to more radical treatment of the lesions which may produce them. Even a minute foreign body should be promptly removed and an ulcer of the cornea should not be regarded as a trifling lesion. Under all circumstances the surgeon, as well as the general practitioner, should be alert to the possibilities of these lesions, quick to recognize the symptoms, and prompt in urging the only satisfactory relief. It will be seen that the earliest suggestive features are those of involvement of the uveal tract.
—There is usually but one efficient method of treatment for these cases, and this consists of removal of the injured or diseased other eye, more particularly if it be more or less already impaired by the consequences of the original lesion. The exceptions to this statement occur in the event of well-marked sympathetic inflammation, as it may be possible that there will be better vision in the originally injured eye than in that secondarily infected; but so long as it is a matter of simple sympathetic irritation enucleation is the proper course. While this is extremely radical there is no satisfactory substitute for it. The only excuse for delay should be threatening phlegmonous processes by which communication posteriorly might be afforded. Bull has laid down the following indications for enucleation of the first eye before the outbreak of sympathetic inflammation in the other eye:
1. When the wound is in the ciliary region, and so extensive as to greatly damage or entirely destroy vision;
2. When the wound is in the ciliary region, and is already accompanied by iritis and cyclitis;
3. When the eye contains a foreign body, and attempts at its removal have proved futile;
4. When the eye is atrophied or shrunken and tender on pressure, or is continually irritated.
The conditions which justify enucleation of the eye have been pointed out. For the operation, which is usually done under general anesthesia, the lids should be widely separated with the ordinary eye speculum or by suitable retractors. A circular incision is then made through the conjunctiva, around the margin of the cornea. This is carried down to the sclerotic at a little distance from the corneal margin, by which Ténon’s capsule is opened; then a strabismus hook is inserted in each direction and the tendon of each muscle raised upon it and divided close to its insertion. By pressure upon the surrounding tissues the eye is now made to protrude. Should the globe have been already collapsed it should be drawn forward with forceps, one blade of which may be thrust within it. After thus firmly withdrawing it a blunt-pointed, curved scissors is passed behind and around it, the blades being made to open in such a way as when closed to divide the optic nerve at a little distance from the globe. After this enucleation by pressure is easy, and any further tissues requiring division may be readily cut. The principal source of hemorrhage is the artery extending through the nerve, but this is readily controlled by pressure.
Should there have been any inflammatory or septic condition about the orbit or the conjunctival sac the parts should be cleansed with hydrogen peroxide or other antiseptic. Sutures are seldom required. A compress should be applied outside the eyelids, removing it sufficiently often to be certain there is no retention of fluid or blood.
[597]
Recovery is usually rapid. Granulation tissue sometimes forms at the bottom of the conjunctival sac and becomes exuberant. In this case it should be removed with scissors and cauterized, after which it rarely recurs.
As already described, many expressions of the various stages of syphilis pertain to the eye. Thus there may be chancre upon the eyelid or conjunctiva, or ulceration of the same; syphilitic iritis as a secondary expression; syphilitic retinitis, neuroretinitis, choroiditis, as tertiary lesions; and the formation of gummas in the later stages of the disease, and in almost any imaginable locality, especially the uveal tract. Syphilitic tumors are seen upon the iris more often than anywhere else within the eye. Outside of the globe and within the orbit the ordinary expressions of syphilitic periostitis and of gummatous tumors occur. These constitute also the more common intra-orbital expressions of this disease.
The symptoms of syphilitic lesions in this location do not vary from similar lesions elsewhere, save so far as they involve special tissues or disturb the special sense of sight. The prognosis in nearly all of them is relatively good if suitable and active treatment be promptly instituted. It is, however, too much to expect that annular destruction of areas of the retina or choroid can be completely repaired.
Cataract is a subject of primary interest to the general surgeon only so far as it pertains to the consequences of injury to the orbital region. The term implies opacity of the lens or of its capsule, or both, which may be partial or complete. Its pathognomonic feature is slow and progressive failure of vision. Examination by direct as well as bilateral illumination will show the opacity to be located behind the iris. Everyone should be able to recognize it; its excision should be relegated to the trained specialist, since it is one of the most delicate special operations.
The term glaucoma implies a collection of more or less variable pathological conditions within the eyeball which lead to increased intra-ocular tension. Because of this increased pressure, with its disturbance of circulation and the peculiar coloration often given to the cornea or the pupil, the disease has received this name. Among its symptoms are pupillary changes, including both size and mobility of the iris; turbidity of the cornea, as well as the fluid humors of the eye; pain, corneal anesthesia, impairment or final loss of vision, engorgement of the visible vessels of the globe, and a peculiar cupping or excavation of the optic disk. Unless checked by operative intervention the course of the disease is steadily toward blindness. It varies in acuteness, the favorable cases being the acute ones, in which early operation can be practised. It admits of no other treatment.
—The operation almost universally practised by the oculist is either iridectomy or sclerotomy. The condition is briefly mentioned in this place for the double reason that the student may be made aware that the condition may follow certain injuries to the eyeball or the head, and that the more chronic forms have been successfully treated by excision of the cervical sympathetic, on one side or both, the operation being based upon anatomical and physiological facts pertaining to the distribution and function of those sympathetic fibers which pass to the orbit from the cervical trunk. The operation is described in the section on the Cranial and Cervical Nerves.
[598]
These lesions are frequently the result of blows and of penetrating injuries, as well as of syphilis. Moreover, motility of the iris is so essential to the normal function of the eye that where it may possibly be effected the surgeon should protect against those adhesions between the iris and the lens or cornea, which are very likely to occur, by instillation of a sufficiently strong solution of atropine, a ¹⁄₂ to 1 per cent. solution being usually sufficient for this purpose. These adhesions are referred to as synechiæ, and are anterior when the iris becomes affixed to the cornea, or posterior when affixed to the lens. They occur easily after minute punctures of the cornea, the result being a limited mobility or a dislocation of the pupil, along with opacity of the cornea, all of which work to the detriment of vision.
The iris is so visible that the mechanism of an exudate on or in it can be observed almost from beginning to end when it occurs in the form of iritis. Occasionally an exudate will merge into an actual collection of pus which will gradually fill up the anterior chamber, and which is then spoken of as hypopyon. Under the most favorable circumstances a disappearance of this pus by absorption may be noted. It may prove destructive or may necessitate evacuation.
The iris and the ciliary body are intimately connected, and inflammation beginning in one point may easily spread to and involve other tissues. These structures with the choroid constitute the so-called uveal tract, and when they participate in inflammation it is called uveitis.
The symptoms of iritis consist of pain, lacrymation, photophobia, which is often intense; increasing turbidity of the aqueous humor, as well as of the cornea, by which vision is impaired; visible discoloration; irregularity and sluggishness in movements of the iris, and circumcorneal injection. A congestion which assumes an annular form about the cornea and does not involve the conjunctival sac indicates trouble in the ciliary region, while a true conjunctivitis is limited only by the extent of the membrane itself.
Iritis due to syphilis, whether assuming the plastic or the gummatous form, requires the most active antisyphilitic medication, in addition to local treatment. The non-specific and traumatic forms need absolute rest in a dark room, with cold applications about the eye and the free use of atropine, to completely dilate the pupil and prevent the formation of synechiæ.
The cornea being the most exposed part of the eyeball will be frequently subjected to minor or serious injury in connection with violence to the orbital region. It is an exceedingly sensitive membrane, whose reflex excitability is heightened by the presence of a small foreign body, this accident being one of frequent occurrence. It is a lesson in neurophysiology to watch the relatively local and general disturbances which the presence of a minute speck of foreign material embedded in the cornea may cause. Every extraneous body should be removed at once, the procedure being now facilitated by the local use of cocaine, for any abrasion or serious injury of the cornea occurring in surgical cases offers a possible source of infection to the deeper ocular structures. Careful attention should be given to the use of antiseptics of suitable strength in the conjunctival sac, whenever this region is involved. This statement cannot be made too positive. There is danger both to the cornea and to the iris in perforating ulcer or traumatism of the cornea, and there is as much occasion for the use of atropine in these instances as in those pertaining to the iris proper. To the protrusion of the cornea, which is produced by weakening of its structure and tension from within, is given the name staphyloma. It is frequently combined with adhesions of the iris and dislocation of the pupil. It constitutes not only a cosmetic disfigurement, but a serious impediment to vision.
PLATE XLV
FIG. 1
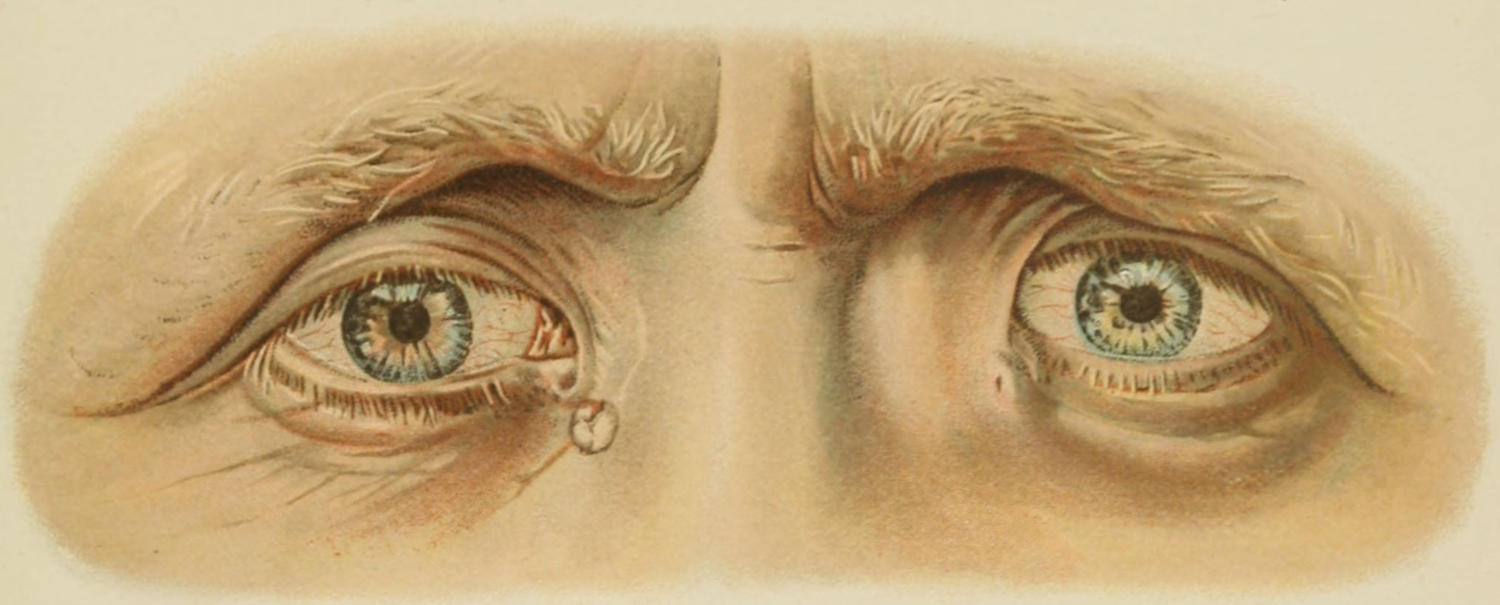
Lacrymal Fistula on the Right Side; Ectasia of the Lacrymal Sac on the Left; Bilateral Epicanthus. (Haab.)
FIG. 2
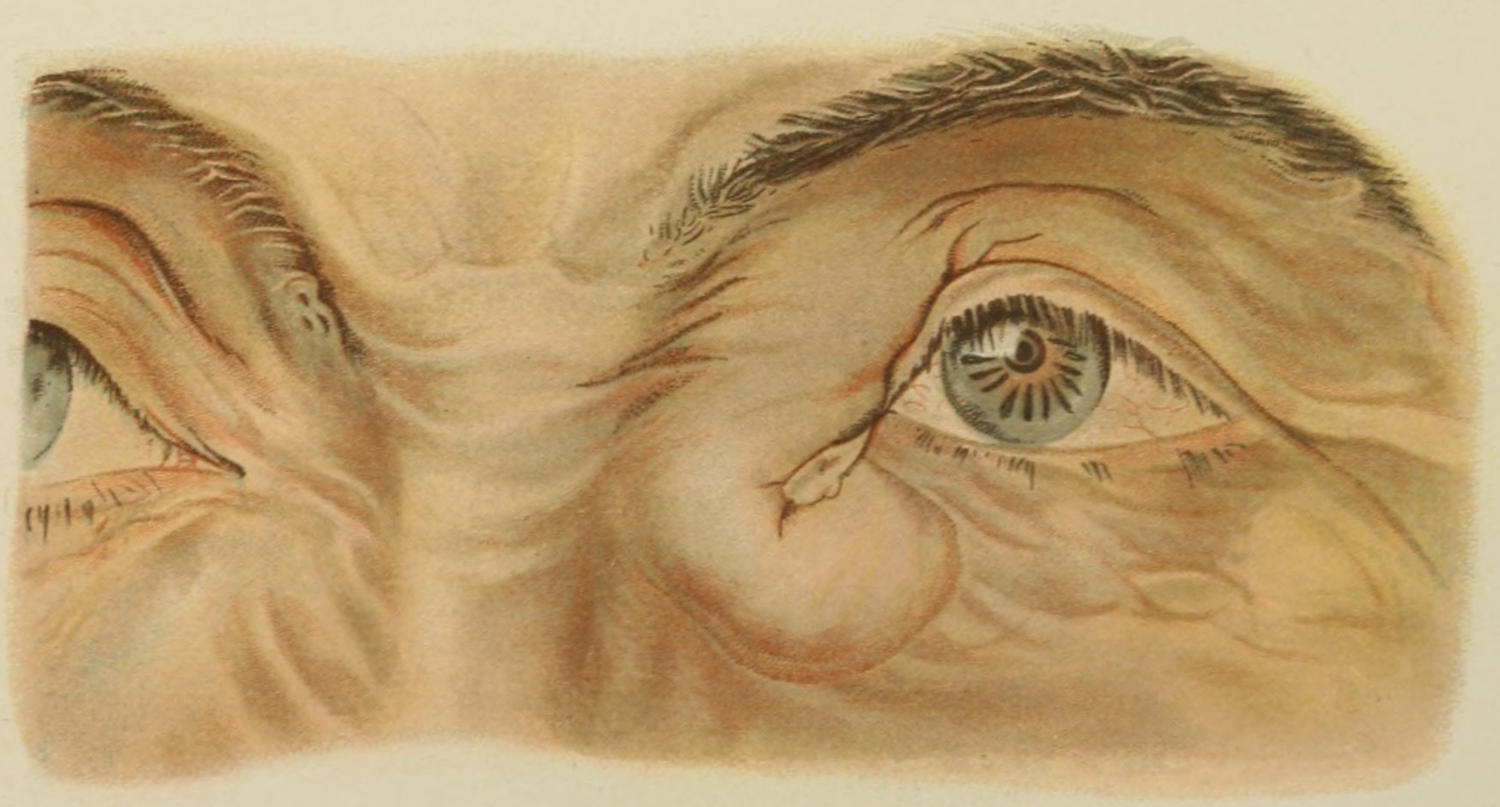
Dacrocystitis. (Haab.)
[599]
The mucous membrane lining the conjunctival sac is perhaps the most exposed to irritation and even infection of all mucous surfaces. It is not strange then that conjunctivitis is the most common of all eye affections. Whether irritated by constant exposure to dust and dirt, or raw and cold winds, or by the heat of a blast furnace, by the dazzling brilliancy of electric lights, or contact with bacteria, it displays a surprising degree of accommodation and resistance. It has peculiar susceptibilities, particularly to the germs of gonorrhea and diphtheria. To these it is peculiarly sensitive, and under their influence it may quickly succumb. The harm done in either of these conditions is by no means limited to the conjunctiva, but may extend in such a way as to eventually cause loss of vision.
Nowhere else may the phenomenon of hyperemia be so easily studied as by watching the ocular conjunctiva for a few moments after the occurrence of irritation. The rapidity with which the vessels dilate and become visible, the occurrence of the consequent redness and swelling, and the reflex phenomena attending it become appreciable within a short time. In the chronic conditions the tissues become thickened and less mobile. A chronic conjunctivitis is the constant condition in certain laborers whose eyes are exposed in their occupation.
A peculiar granulomatous condition of the conjunctiva, especially the palpebral, is that known as trachoma, which appears to be due to a specific form of infection that leads to exudation, organization and thickening, intensified in punctate areas, and giving the surface the appearance of an ordinary granulation. This condition has assumed such importance as to be sufficient for the exclusion of aliens and immigrants.
The milder conditions of acute or subacute conjunctivitis subside under cold applications and mild antiseptic and astringent eye-washes or collyria. These should be frequently instilled, beneath the lid whenever this area is involved as a complication of injuries to the head or face. In acute cases of the infectious type, such as the gonorrheal or diphtheritic, atropine should be used locally, so that the iris may be drawn out of harm’s way and the pupil left free should resolution and recovery ensue. Individuals suffering from either gonorrhea or diphtheria should be cautioned and protected from possibility of conjunctival infection. The eyes of the newborn are not infrequently infected during the process of parturition. The parturient canal of women suspected of having an infectious lesion of this kind should be cleansed before the passage of the fetal head, and in all suspicious cases instant and constant attention should be given to the eyes of the newborn infant.
The lacrymal gland, though situated in the anterior and upper part of the orbit, and beneath the upper lid, where it is ordinarily well protected, is nevertheless liable to both acute infections and chronic irritations. When acutely inflamed it usually goes on to abscess formation. We have then acute dacryo-adenitis, which will produce the ordinary symptoms of phlegmon, with the added ocular features of vascularity and chemosis of the conjunctiva and more or less edema and immobility of the upper lid. Displacement of the eyeball may be produced by great inflammatory swelling. These abscesses tend to discharge either through the skin near the external angle or sometimes through the conjunctiva. While in the former case a scar results, it nevertheless is a preferable point either for spontaneous opening or for incision. If the case be seen in time it will be advisable to make this incision early and so limit destruction. (See Plate XLV, Fig. 1.)
The lacrymal gland suffers occasionally in instances of constitutional syphilis, undergoing chronic and obstinate enlargement. It may also be the site of tumors either non-malignant, usually adenoma, or cancerous, most instances of the latter being expressions of extension.
The tear passages proper are composed of the canaliculi, the lacrymal sac, and the duct. These are altered, occasionally, in their relations, or absent, as the result of congenital defects. The passages proper frequently become obstructed, as the result of any chronic irritation which produces thickening of the conjunctiva, and in many[600] laborers and others who are exposed to dust, dirt, or cold winds there will be a more or less constant stillicidium or overflow of tears. In some of these cases it is sufficient to slit up one or both canaliculi with a fine probe-pointed bistoury.
The lacrymal sac proper is frequently the site of both acute and chronic disease, known as dacryocystitis, which is the result of infection spreading from the conjunctival sac, rarely from the nose, or the exaggeration of conjunctival thickenings, like those mentioned above. The first symptoms are overflow of tears, accompanied by swelling or enlargement in the region of the sac. By pressure upon this a mixture of water, mucus, and sometimes pus may be expressed. As the disease goes on the fluid becomes purulent. If the sac, by pressure, can be emptied into the nose the nasal duct may be regarded as patulous and the treatment is simplified. If not there is stricture, usually at the upper end of the duct, which requires division and dilatation. The more chronic forms of trouble in this region are frequently intensified into acute phlegmonous lesions which, if neglected, will lead to spontaneous perforation and the formation of a lacrymal fistula at a point below the inner angle of the eye. (See Plate XLV, Fig. 2.)
—The treatment should consist of exposure of the sac by incision of the canaliculi and its irrigation by means of a syringe and antiseptic fluid. Unless this fluid passes easily into the nose the stricture should be divided and Bowman’s probes passed, the principle of treatment being the same as that in treating urethral stricture. This part of the treatment should be referred to an oculist.
In acute dacryocystitis with suppuration the sac along the natural passages should be opened. When a diagnosis of an acute lesion of this kind is made nothing but the most radical treatment is advisable.
Congenital deformities of mild degree are not infrequent about the eyelids.
Epicanthis is a term implying folds of redundant skin extending from the internal end of each eyebrow to the inner canthus and over the lacrymal sac. It varies much in degree, is a more or less hereditary feature in certain families, and is not infrequently associated with other defects. The palpebral fissure varies in length in different individuals, giving a longer or shorter window through which the eye proper shall appear. Sometimes the fissure is much too short and requires division or extension, which is easily made by incision at the outer angle.
Coloboma is a term applied to various lesions of the eyelid, the iris, and the choroid, implying a defect in structure, which, in the eyelid, leaves a V-shaped deficiency, corresponding to harelip, whose edges may be brought together by a simple operation.
The eyelids are subject to certain painful or disfiguring lesions, which frequently come under the notice of the general surgeon. Of these the most common is stye, or hordeolum. This is a phlegmon of one of the minute glands along the margin of the lid, which has become infected and violently reacted. It forms a miniature furuncle, often associated with conjunctivitis, and giving a disproportionate reaction. So soon as the presence of[601] pus can be detected a puncture should be made and the contained drop of pus exvacuated. Threatening suppuration may sometimes be aborted by local use of 1 or 2 per cent. mercurial (yellow) oxide ointment.
A somewhat similar but non-inflammatory cystic distention of one of the Meibomian glands, which pursues a slow and painless course, is called chalazion. It presents rather beneath the mucous surface, but is often visible through the skin. Its contents are mucoid or dermoid. When it attains troublesome dimensions it should be exposed through a small incision, usually external, and thoroughly extirpated.
Small, elevated areas of dirty-yellow color are met with in the skin about the eyelids, more often near the inner angle. Such a lesion is called xanthelasma, the lesion being a fatty metamorphosis of a portion of the skin structure. While harmless, it is amenable to excision for cosmetic effect.
Any of the ordinary tumors which affect similar tissues elsewhere may be seen about the eyelids. The more common are the vascular tumors, especially small nevi. Epithelioma occasionally commences along the palpebral margin, but is more often an extension from neighboring tissues.
The margins of the lids are frequently involved in a mildly infectious inflammatory condition called blepharitis, in which nearly all the structures participate; when the borders alone are involved it is referred to as blepharitis marginalis. The condition is largely due to dirt, and to irritation in which the Meibomian ducts seem to share. It is accompanied by chronic conjunctivitis. The condition is seen more often in the ill-nourished, the rickety, and the tuberculous. The best local treatment consists in the use of an ointment of yellow oxide or yellow sulphate of mercury. The former may be used in 2 per cent. strength, and the latter not stronger than 1 per cent. This should be applied along the lid margins at night, and thoroughly rubbed in. A commencing phlegmon and stye may be aborted by one of these preparations.
Another very annoying complication, and usually the sequel of the condition already mentioned, is trichiasis, or turning inward of the eyelashes. Chronic irritation and cicatricial contraction on the inner aspect of the eyelids, or a chronic blepharospasm, which may be the result of corneal infections, serve to draw the lids inward, especially with the margins of the hair follicles, so that the eye-winkers grow toward the ocular surfaces, which they constantly irritate. The result is a vicious circle, each morbid condition intensifying the other. In time there is produced a condition of entropion, which is to be remedied only by operation. It is not sufficient to treat trichiasis by epilation, as the hairs will grow again and continuously cause trouble. The cause should be removed and the effect treated.
By this term is meant a condition of inversion of the margin of one or both lids, by which the external surface is brought into actual contact with the surface of the eyeball. It is a chronic condition brought about through the action of several contributing causes. Any condition of the cornea or deeper portion of the eye which leads to photophobia and spasmodic closure of the eyelids will produce in time hypertrophy of the orbicularis, with corresponding strengthening of the muscle and exaggeration of its activity. Chronic[602] blepharospasm will thus in time lead to a mild degree of entropion, while any affection of the inner palpebral surfaces which leads to cicatricial contraction will still more intensify it. So soon as trichiasis or irritation by the eyelashes is added to what has gone before, every feature is exaggerated and the cornea is made to lie practically in contact with the skin surface of the eyelid. A further consequence is corneal disease, often with ulceration and opacity, with even worse structural changes.
The condition is really a serious one and is to be treated not alone by operation upon the lid, but care should be given to all the contributing features. So far as the lid condition alone is concerned, I have found the operation suggested by Hotz the most satisfactory of any, at least in average cases. An incision is made from one end of the lid to the other, along the distal border of the tarsal cartilage, and down to it. Through this a bundle of those orbicularis fibers which run parallel with the incision is dissected away. In extreme cases the tarsal cartilage, which is incurved as the result of the old condition, may be either incised or a strip excised from its structure. Sutures are then inserted which include not only the borders of the skin incision, but the exposed border of the tarsus and the tarsoörbital fascia. By applying the central suture first, and then one on either side, it will usually be found that as the sutures are tightened the edge of the lid is drawn outward and the desired effect obtained.
The large number of operative methods which have been suggested for the cure of entropion bespeak the variety of causes which may produce it and the many devices to which different ingenious ophthalmic surgeons have resorted.
Fig. 390
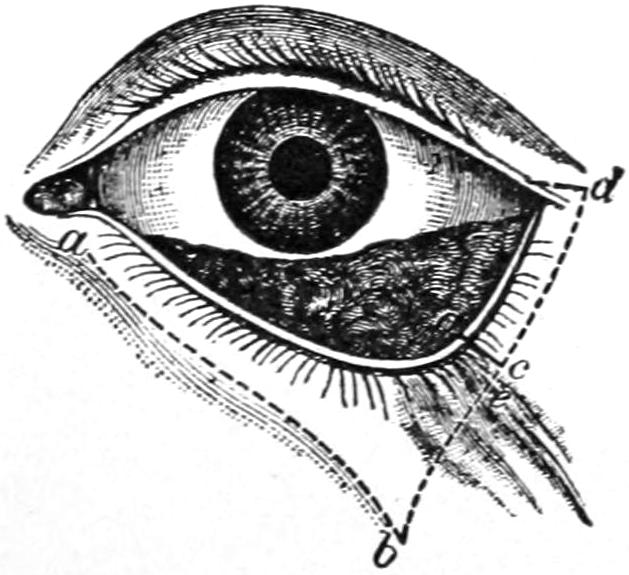
Arlt’s operation for ectropion. (Arlt.)
This condition is the reverse of entropion, and implies eversion of the margin, or of a considerable portion of a lid, with consequent exposure of its conjunctival surface, which undergoes changes in consequence of which it becomes thickened, contracted, and irritated. Ectropion may possibly be produced by violent orbicular spasm, especially in children, the lids being so tightly shut as to be everted. Ordinarily it is the result of external lesions which produce cicatricial contraction, like burns, or of chronic ulcerative lesions along the palpebral border, such as are met with in tuberculous and syphilitic disease. The lower lid is much more frequently involved than the upper.
For the relief of ectropion plastic operations are practised, usually on the lower lid. The milder cases require a V-shaped incision, its apex downward, with free dissection of the integument up or near to the margin of the lid, by which it is released from the scar tissue which has bound it down. Fig. 390 illustrates the general principle of such an operation. The lower portion of the V-shaped defect is then brought together with sutures, the triangular flap being fastened in a position much higher than that in which it originally rested.
All of these operations upon the eyelids are included under the term blepharoplasty, of which the above is the most simple. When necessary new flaps may be raised from the temporal region, from the forehead or from the cheek, as may be required, and turned into place, their pedicles being so planned as to carry a sufficient blood supply for nourishment of the same. If this supply be properly provided these operations are practically always successful. It is necessary only to make the transplanted flap at least one-third larger than appears to be necessary, judging from mere size of the defect, for experience shows the necessity of allowing at least one-third for primary and cicatricial shrinkage. A heteroplastic operation is occasionally performed for this purpose, by which the flap of skin is detached from an entirely different part of the body, or from the body of another individual. Skin thus transplanted should be prepared by removal of all of the fat upon its raw surfaces, skin alone being desired and not other tissue. Figs. 391, 392, 393 and 394 illustrate blepharoplastic operations of various types, which may be modified or made more extensive. These are but a few of the various plastic devices, and are intended to serve merely as suggestions or examples rather than methods to which one is limited.
[603]
Fig. 391
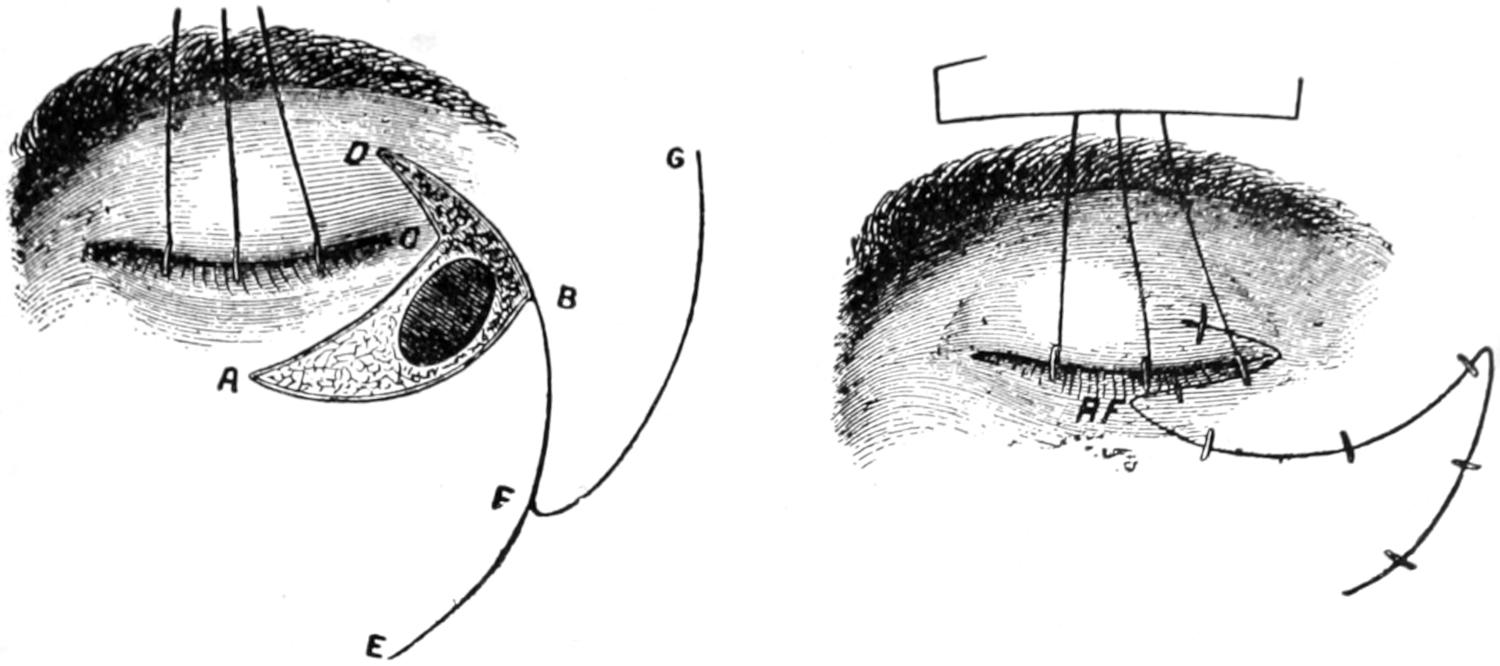
Richet’s operation for ectropion. (Arlt.)
Fig. 392
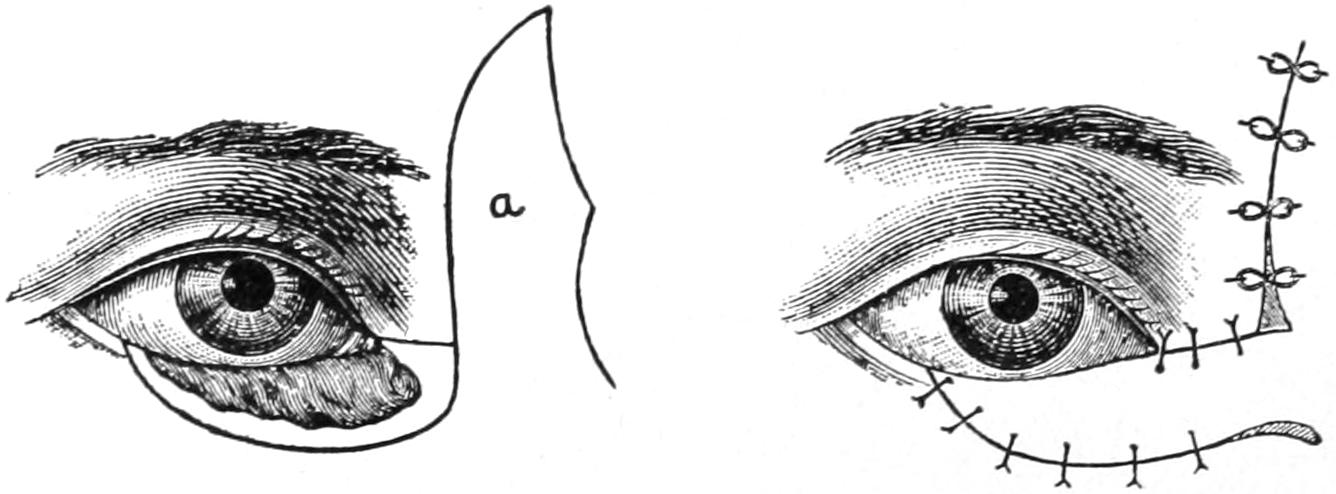
Fricke’s method of blepharoplasty. (Arlt.)
Fig. 393
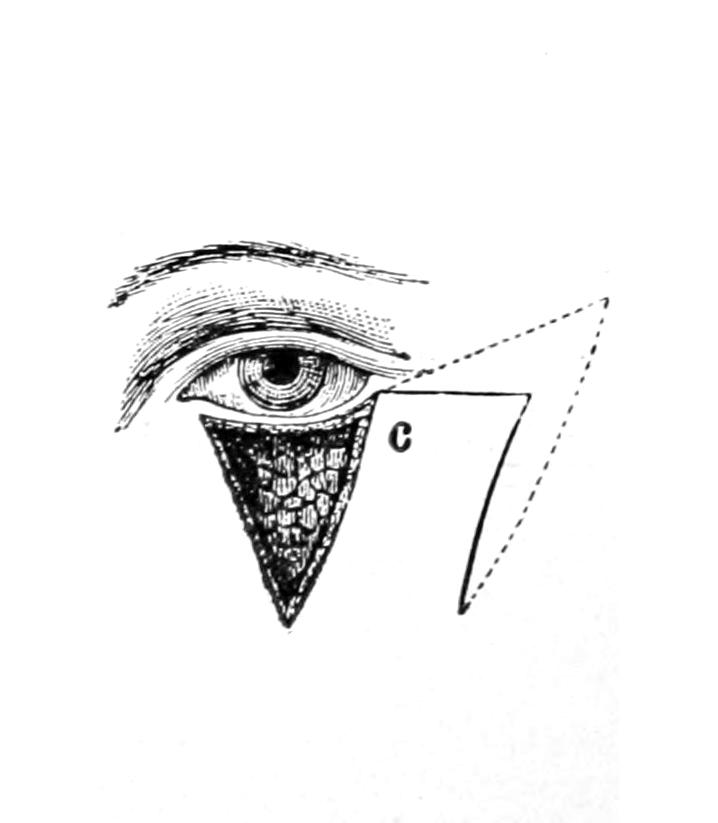
Dieffenbach’s method of blepharoplasty. (Arlt.)
Fig. 394
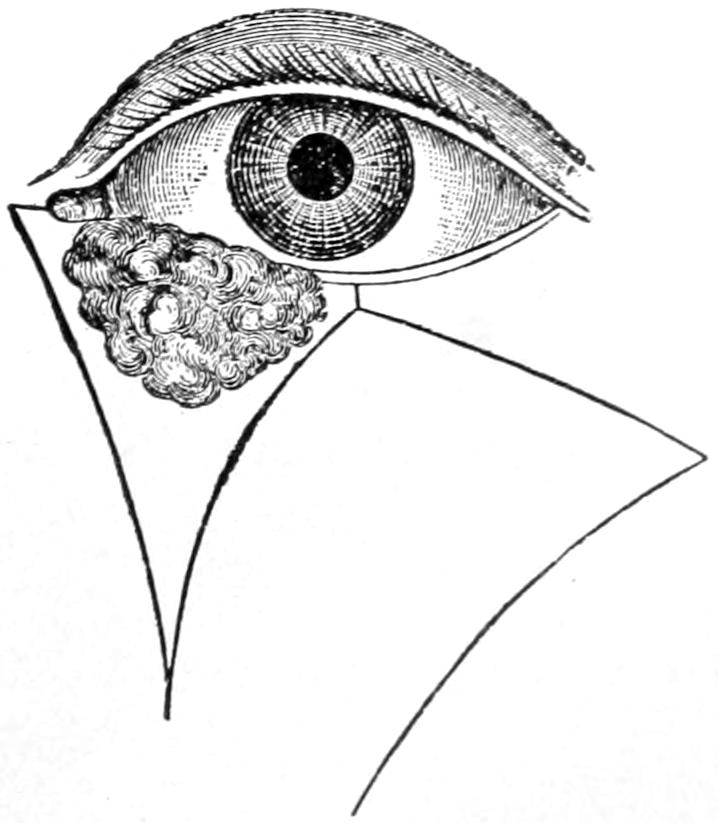
Arlt’s method when a portion of the eyelid is to be sacrificed. (Arlt.)
This topic has already been considered. It seems advisable, however, to summarize some of the results of such injuries in order to call attention to their dangers and methods of treatment. Burns of the orbital regions, for instance, are liable to cause not only opacity of the cornea following ulceration, but adhesions between the conjunctival surfaces and the palpebral margins. The term symblepharon is applied to those lesions where the lids are more or less fixed upon the globe and their motility partly or completely impaired. When the edges alone of the lids have grown together the condition is known as ankyloblepharon. Both of these conditions are the result of adhesion of granulating surfaces and of cicatricial contraction, and should be avoided.
[604]
By a concussion of the orbital region, and especially of the eyeball, all sorts of injuries may be inflicted, from those involving the cornea to deep lesions which leave little or no superficial evidences, but cause partial or complete blindness. Detachment of the retina, for instance, is one of the possibilities of such conditions. Intra-ocular hemorrhages or dislocation of the lens, with traumatic cataract, may also occur.
The sclerotic may be ruptured with or without the presence of a foreign body, in which case the contents of the eye may have partially or completely escaped. An eye which has collapsed from these causes offers an almost hopeless field for the general or special surgeon, and little can be done, save possibly for cosmetic purposes. There is danger of sympathetic ophthalmia, and it may be a question whether evisceration, i. e., completion of the evacuation, may not be the wiser course.
Perforating wounds, even when inflicted by minute bodies, have dangers of their own, including the possibilities of infection. The interior mechanism of the eye is so easily disturbed, and its transparent media so easily clouded, by the results of accident or hemorrhage, that even apparently trivial injuries may be followed by disturbances of vision.
—The general principles of treatment of all such injuries should include, first, the removal of every detectable foreign body, followed by the application of cold, and the use of antiseptic eye-washes, which, however, must not be used too strong lest they irritate. Saturated boric-acid solution is perhaps as strong as anything which is permitted, while even this may occasionally require dilution. In addition to this the use of atropine solution is always indicated. It has the double effect of soothing and allaying pain and of dilating the iris into a narrow ring. With such measures as these it may be possible to save vision; at all events it will limit reaction and prevent harm.
The nerves which supply the eye and its adnexa may undergo injury, either within the orbit or within the cranium, or in their course from one to the other. The paralyses may be caused by syphilis, by intracranial tumors, or by injury. A careful study of the areas and nerves involved will sometimes lend considerable help in diagnosis, both in traumatic and pathological cases. Thus diplopia, or double vision, may be caused by paralysis of the external rectus on one side, by which its antagonistic internal rectus is permitted to swerve the eye too much to the inner side and away from the normal axis of vision required for single sight. When there is complete paralysis of the third nerve there may be drooping of the eyelid, called ptosis, with impaired motion of the eye, upward, inward, or downward. The eye will roll outward because the external rectus is supplied by the sixth nerve. There will also be dilatation of the pupil, with loss of accommodation. When the upper lid is raised there is also double vision. This third-nerve paralysis, however, is not always complete, and diplopia may result only when the eye is directed in a certain way. When the sixth nerve is paralyzed the eye is rolled inward, and again there is diplopia. When the fourth nerve is paralyzed the eye is but slightly displaced upward and inward. When the sympathetic nerve is involved there will be protrusion of the globe with dilatation of the pupil. This will be accompanied by flushing of the face.
Detection of errors of accommodation is practically a specialty within a specialty, while the various forms of strabismus, or deviation of the eyes from their normal axes, depend largely upon regulation of accommodative errors.
The region of the ear is subject to congenital malformations, deviations, and defects, which include anomalous shapes of the auricle, malpositions of the organ, defects in the cartilaginous structure with resulting deformity, and congenital excesses or redundancies[605] by which there are made to appear supernumerary auricles or portions thereof. These latter have been described by Sutton and treated in his work on Comparative Pathology. They bear relation as well to the branchial clefts, and are of great interest from a phylogenetic point of view. Some of these defects result from absolute arrest or excess of development, others from injury during intra-uterine life; some are accentuated by lack of care during the early months of infancy. The most common deformity of the ear is that by which it is made unduly prominent and deflected outward or forward, the cartilage being thick and abnormally curved. Such overlapping or overprominent ears can be made to assume their proper position on the side of the head by the excision of an elliptical piece, either of skin or of skin and cartilage, at the point of junction of the ear and the scalp. The amount to be removed should be proportionate to the desired effect. The parts may be brought together by sutures, and the auricle should then be bound upon the head.
Fig. 395 illustrates a common form of defect, inherently of the cartilage and of the overlying skin. This is but one illustration of many, two cases being rarely found exactly alike. Not infrequently these arrests of development include the structures of the middle ear as well. The auditory meatus may be entirely covered and concealed, or may be absent, having failed to develop.
Fig. 395
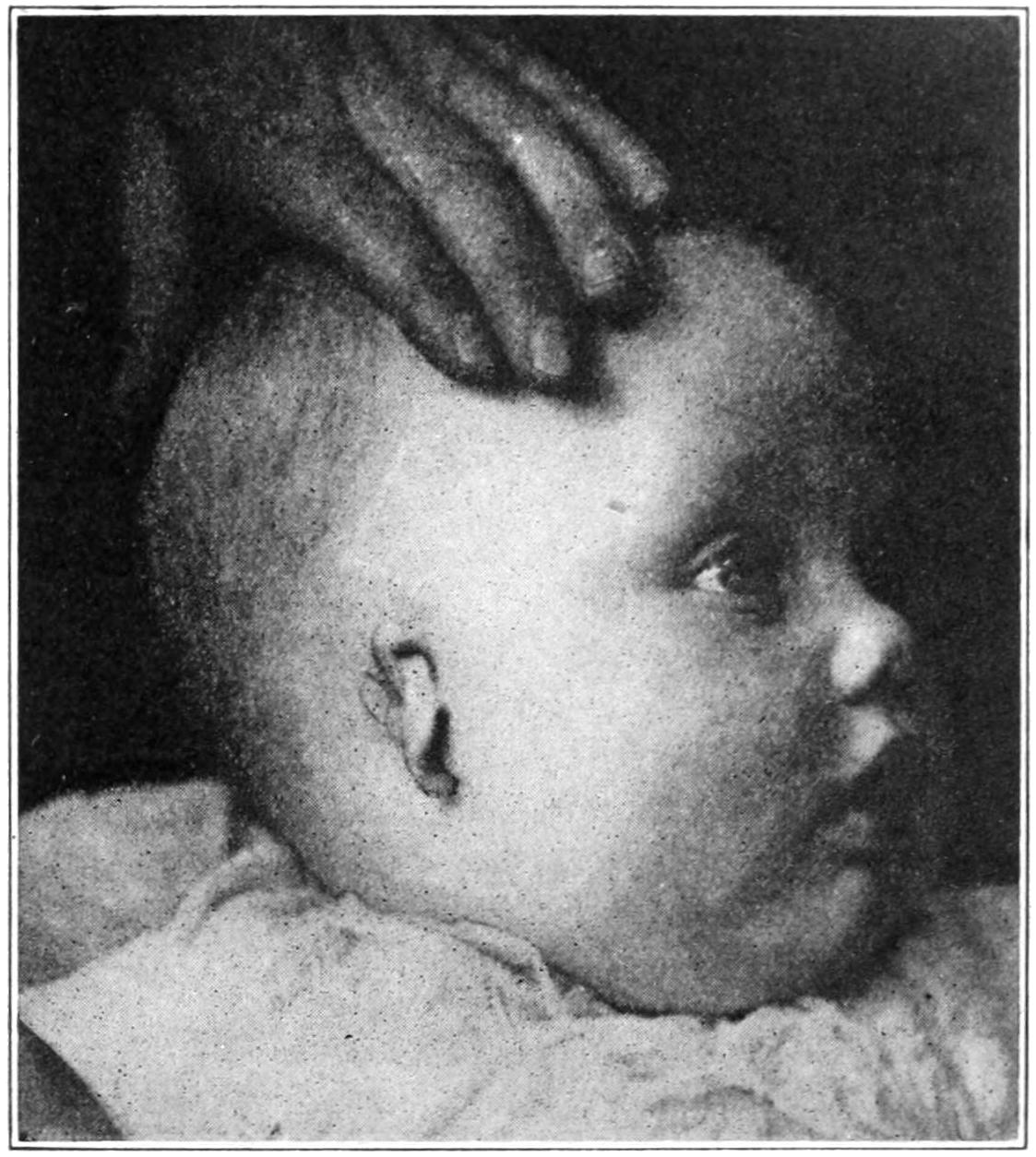
Developmental defect of external ear. (Broome.)
Supernumerary auricles are usually found as small tags of skin and cartilage in front of or below the ear. They are easily removed and leave no disfiguring scar.
The external ear is also exposed to injury, which it frequently receives in the way of contusions and lacerations. It is occasionally detached. The ordinary wounds of these parts require only the conventional treatment, while it may be possible, by replacement and approximation of a completely detached portion, to see it re-adhere. This happened to the writer after his horse had completely bitten a piece out of the ear of his groom. Here, as with detached finger-tips, cleanliness is necessary, and the parts must be kept warm and protected after dressing. The cartilage of the ear is covered by a perichondrium which corresponds to the periosteum. Beneath it, or beneath the skin alone, blood may be extravasated as the result of contusions. When such collections fail to promptly resorb they should be incised and the contained blood released. Such lesions are referred to as traumatic othematomas.
A peculiar lesion of this general character occurs occasionally in the insane. If due to injury the latter is but trifling. It makes a conspicuous tumor, involving usually the lower end of the auricle, and is known as the othematoma of the insane. It is scarcely amenable to surgery, nor does it often need it, but it constitutes a disfigurement which is not only easily apparent, but diagnostic as to the cerebral or mental condition.
The ear is the site of many neoplasms, both innocent and malignant. Small papillomas are common, while fibrous tumors are likely to develop, especially about the fibrocartilaginous lower end of the auricle, where the ear has been pierced for ear-rings. Keloid tumors, of still more conspicuously fibrous nature, are common about the ear, especially among negroes. All innocent tumors may be excised, through incisions which should be so planned as to leave a minimum of disfigurement. (See Fig. 397.)
Of the malignant tumors epithelioma is perhaps the most frequent. It pursues a course here similar to that which characterizes it elsewhere, save that the dense structures[606] of the cartilaginous ear yield but slowly to its encroachment. The form known as “rodent ulcer” is slower here than elsewhere. Fig. 396 illustrates a case under the writer’s care, showing complete destruction of the external ear by a growth of this kind, which had attained a degree and extent that did not permit of successful treatment, and which eventually proved fatal. When growths of this character have not progressed too far they should be radically removed, the question of cosmetic effect being secondary to that of their eradication. By a well-planned plastic operation much can be done to atone for disfigurement resulting from radical operation.
Fig. 396
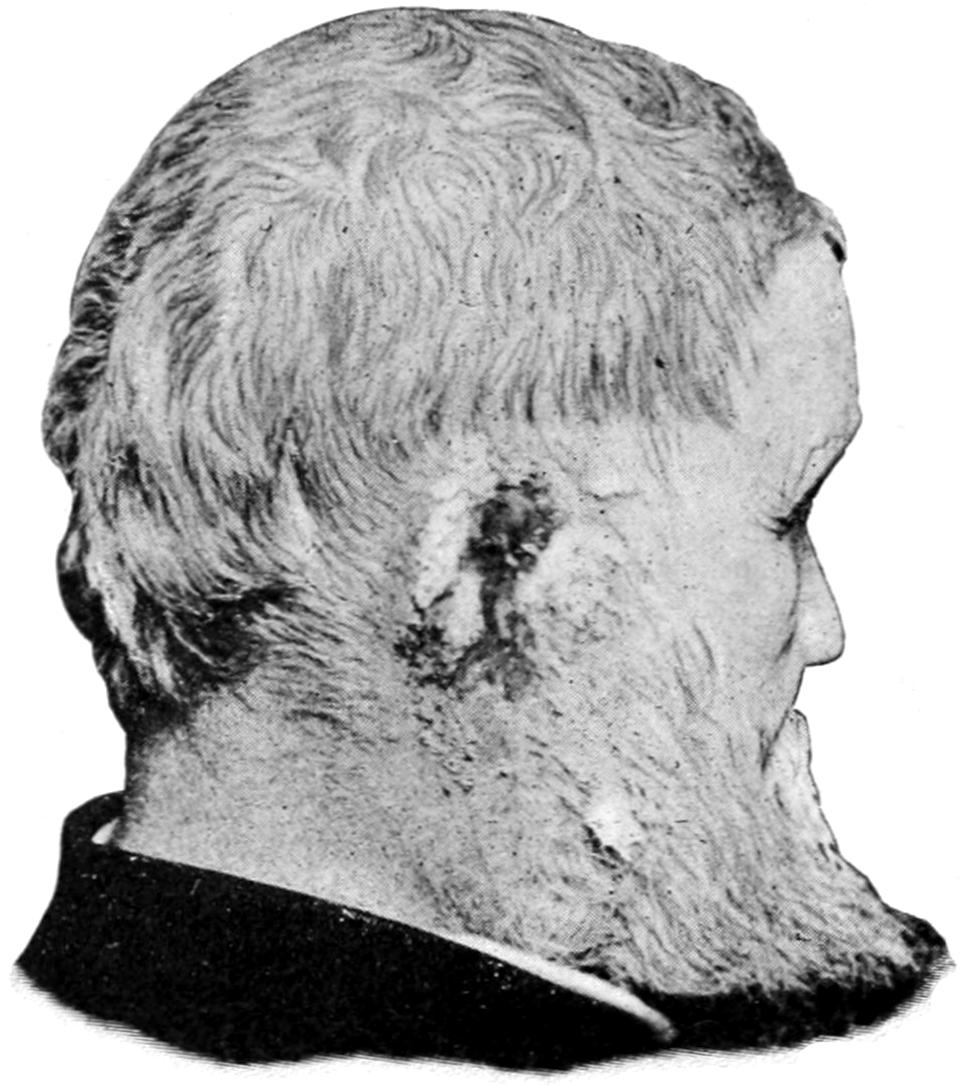
Complete destruction of auricle by rodent ulcer. (Buffalo Clinic.)
Fig. 397
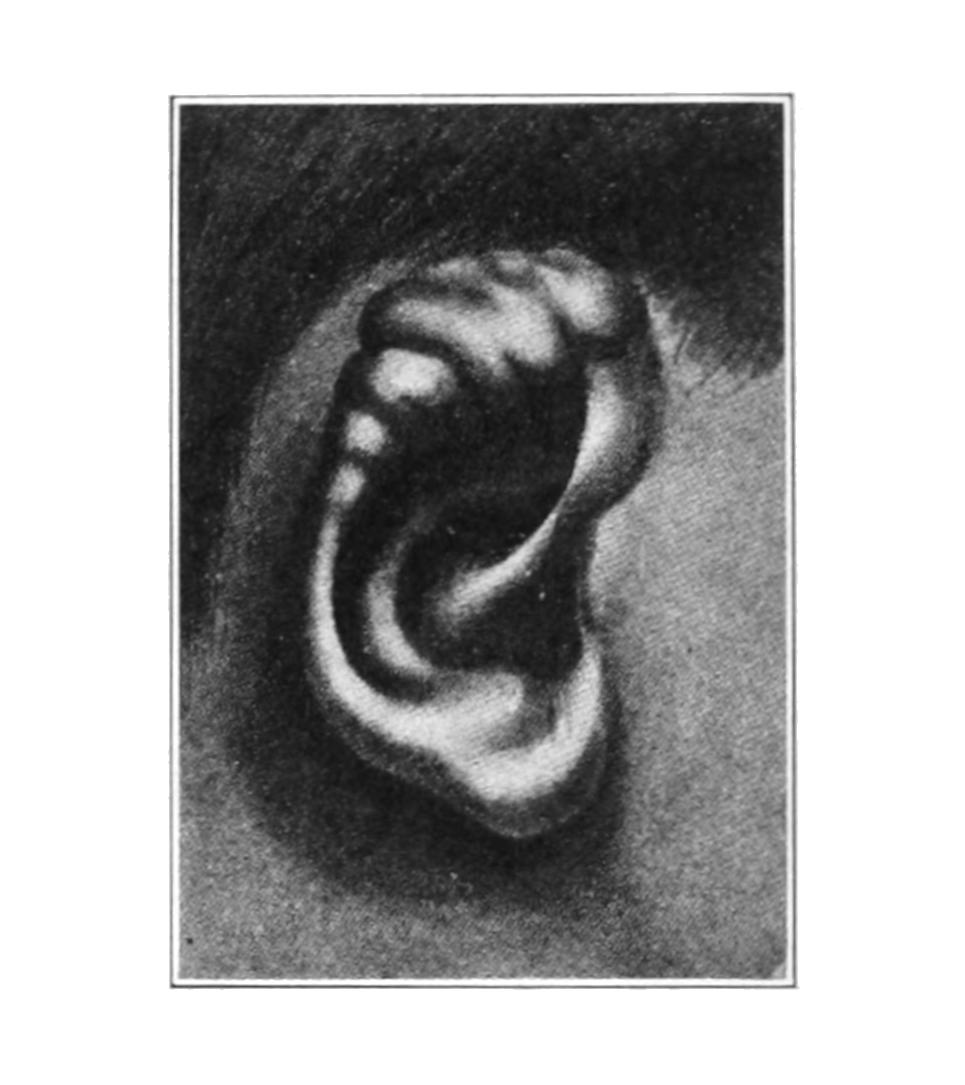
Congenital lymphangioma of ear. (Lexer.)
All sorts and descriptions of foreign bodies may enter the ear. Young children have a tendency to introduce all kinds of bodies into the ear, as into the nose, and sometimes intrude them to such a distance that their removal is made difficult. Living insects make their way into the meatus auditorius and even deposit their larvæ, which may subsequently go through their developmental phases and fill the passage-way with young insects. Among the inanimate materials which children introduce are small buttons, pebbles, beans, peas, beads, etc. Such a foreign body may not be at once discovered, and some of those which easily undergo decomposition, like fresh vegetable substances, may not be detected until they have set up trouble by decomposition. Therefore it may be hours or days before its presence is recognized. Sometimes it may be easily seen, again it may be concealed. When the auricle is drawn upward and backward the external meatus is somewhat straightened, and bodies within it are more easily made visible, especially by reflected light. Therefore the head mirror is usually required for their detection and removal. The substance may be one which is easily seized and withdrawn, after certain turning or shifting motions have been attempted, or it may be impacted so as to offer considerable difficulties. It should never be pushed farther in, for injury might thus be done to the membrana tympani, and the effort should be to remove it with the least possible damage to the lining of the canal. So essential is it to have the head kept perfectly still during these maneuvers that it will be advisable, with young children, to administer an anesthetic. Instances occasionally occur which necessitate incision and liberation of the auricle, with its deflection forward, and the consequent more complete exposure of the auditory canal.[607] Forceps of various fashions may be used, or occasionally a blunt hook may be made with a probe, which may be used to advantage.
Of living foreign bodies information can be obtained more promptly, as the annoyance caused by their movements will at once disturb the patient.
Relief has often been promptly afforded by filling the meatus with water or glycerin as warm as can be borne, by which the insect is killed, after which it may be removed by irrigation or by forceps, assisted by good illumination.
That which is essentially a foreign body may be produced by an accumulation of cerumen in wax-like form within the auditory canal. Neglectful patients sometimes allow this to accumulate until it constitutes not only a source of irritation but an obstacle to hearing. Its removal is not ordinarily accompanied by difficulty, but requires patience and often considerable effort, not only with instruments, but with irrigation, especially with an alkaline solution, by which the waxy substance is softened.
A phenomenon noted in many of these cases, where instrumentation has to be practised within the vicinity of the middle ear, is coughing or sneezing, sometimes to a degree which interferes with the work to be done. This is a reflex to be explained through connection with the pneumogastric nerve.
In the fibrocartilaginous as well as in the more richly cellular portions of this passage-way small phlegmonous processes frequently occur. They give rise to an amount of suffering, and even of sympathetic reaction, disproportionate to the extent of the difficulty. They are called furuncles, or boils, sometimes occurring singly, often in groups. A commencing process of this kind may be cut short by the use of an ointment of 1 to 2 per cent. yellow sulphate of mercury, but after the furuncle is well developed it is best treated by free incision, which can be made with the freezing spray, and without much pain to the patient.
More extensive phlegmonous destruction, assuming even carbuncular form, is occasionally met with in this region. There will be more or less necrosis of tissue in such cases, which will require removal, usually with the sharp spoon. These cases are not without their danger, since the veins connect so freely with the interior of the cranium.
Hyperostosis and exostosis produce either a narrowing of the auditory canal or its complete obstruction, and sometimes even the formation of an osseous tumor of considerable size. A thickening and even new formation of bone may be the result of the chronic irritative processes which frequently occur in the middle ear, but many of these conditions occur in the newborn, in whom they are to be regarded as congenital excesses and in whom they frequently cause permanent impairment or loss of hearing. Some of the osteomas in this region are of bone-like hardness, their density being sufficient to dull or even to break the finest tempered steel instruments.
A small exostosis may be removed with the ordinary instruments of the surgeon or the dental engine, but the larger and more dense growths offer formidable difficulties for the operator and uncertain results for the patient. When growths of this kind attain considerable size they should not be attacked through the natural passages, but the auricle should be separated and pushed forward and the auditory canal opened.
The middle ear has for its external boundary the membrana tympani, which, for clinical purposes, constitutes a limit beyond which the general surgeon should not trespass, the structures within being those within the field of the aural surgeon. Nevertheless the student of surgery should realize that the membrane of the drum may be ruptured in consequence of a blow upon the external ear, or perhaps by the sudden condensation of air produced by explosions, etc. It may, moreover, be lacerated in consequence of various injuries to the head, basal fractures, etc., even those involving the opposite side of the head; it may also be injured by foreign bodies, introduced usually from without and through the canal. While this membrane has normally an opening[608] by which air pressure is equalized on either side, this seems to play but a small part in the liability to or exemption from injury such as just described. The membrane has its own blood supply, which can become congested to a degree permitting considerable escape of blood after laceration. It does not follow that bleeding from the ear is necessarily an indication of basal fracture, after injuries of the head, unless the hemorrhage is continuous and considerable, in which case it may be stated that the injury must be deeper and more extensive than one of the membrane alone. If, however, cerebrospinal fluid can be detected as escaping with and diluting the blood, or escaping independently, then the diagnosis of basal fracture may be regarded as certain.
After such injuries as lead to hemorrhages from the ear the external auditory canal, should be irrigated and protected against infection by light tamponing, etc.
It is the writer’s opinion that the general surgeon should abstain from operative intervention in the ordinary diseases of the middle ear, save in the presence of symptoms which accompany mastoiditis, acute infections of the sinuses, or even of the brain itself. When it comes to an extensive operation, such as is often required in such instances, including not merely opening of the mastoid antrum and cells, but exposing the dura and judging of the condition of the sinus, with perhaps the simultaneous ligation of the jugular in the neck and washing out of the intervening portion, then these are measures requiring such surgical judgment and operative skill that it would seem that the general surgeon should be peculiarly equipped for this task. But the ordinary office operations should be left to those who make a specialty of these diseases.
When the cavity of the tympanum is involved in a suppurative condition, with caries of the surrounding bone and extension into the spongy tissue of the adjoining mastoid, this abscess cavity should be cleaned out. Therefore the more radical operations of the aurist, by which the membrana tympani is destroyed, the ossicles of the ear removed, etc., are but applications of broad surgical principles to a limited region of the body, but made justifiable by their results. Moreover, in a more chronic type of cases, where the tympanum is filled by redundant granulation tissue and by polypoid formations, which are producing more or less circumscribed caries or necrotic processes in the bone, by which bony partitions between the cranial cavity and the ear proper are gradually thinned or lost, and by which encroachment on the intracranial sinuses with all its dangers is incurred, they are still to be subjected to the same general radical methods of treatment, no matter whether it be carried out by a specialist or a general operator.
While these cranial cavities are connected with the respiratory tract there are, nevertheless, good topographical and physiological reasons for considering their lesions in this place. There is free venous communication between each of them and the cranial cavity, and free lymphatic communication as well from at least three of them. Infection, therefore, may and often does travel from the smaller to the greater cavity, and thrombophlebitis, brain abscess, or purulent meningitis may be the ultimate result of apparently trifling infection of one of the sinuses.
They are four in number—the frontal, the ethmoidal, the sphenoidal, and the maxillary, or antrum of Highmore. They are all connected with the nasal cavity, and all lined with the same Schneiderian membrane, which affords a continuous pathway of infection. At least two of them are cellular in character, much resembling the mastoid cells. Their means of communication with the nasal cavity are small, and often obstructed by catarrhal swelling and inspissated discharge. If thus plugged their retained contents may undergo decomposition and intensify the trouble. It has been shown that the effect of inward currents of air through the nostrils is to suck out from these sinuses more or less of their secretion. In this way perhaps may be accounted for the strings of tenacious mucopus which slowly make their way out of especially the anterior sinus openings. Some surgeons believe that if one sinus is affected all the others on that side of the head are more or less involved; while this may be true in many cases, and is easily explained on anatomical grounds, it is not strictly true of all instances, least of all in cases of chronic empyema of the antrum, which often long remains simple and uncomplicated.
Surgical lesions within the accessory sinuses result from infective processes, proceed[609] often to suppuration, often, too, with caries of the surrounding spongy bone as well. These conditions may result from the ordinary acute catarrhs, or follow the more specific fevers, like influenza and the exanthems, and frequently follow diphtheria. Traumatic causes may also conspire to produce the same effect. In the maxillary sinus disease is often due to extension upward from carious teeth. In syphilitic and tuberculous patients these affections will partake to a greater or less degree of the specific nature of these diseases.
Symptoms differ according to location and are often obscure enough to make diagnosis difficult. Perhaps the most prominent symptom is pain, either deep-seated, vague, or disquieting, located in the neighborhood of the diseased sinus; or intense and neuralgic in character, radiating from the source of the trouble. Its severity is proportionate to the acuteness of the case. When the frontal and maxillary sinuses are involved there occur external swelling and tenderness. If the sinus openings be patulous there will be more or less purulent discharge into the nasal cavity, that which comes down from the upper sinuses appearing beneath the middle turbinate body. Transillumination by means of a small electric light, passed into the nostril, will demonstrate an opacity in the region of the affected sinus which does not appear on the healthy side. The condition is frequently associated with nasal polypi, small or large; while granulations in time spring up within these cavities and may even escape therefrom as these become filled. The general clinical picture is one of nasal obstruction, with more or less constant discharge, sometimes mucopurulent, sometimes offensive, which perhaps may be favored by certain positions of the head, this being especially true of the maxillary antrum. Along with these features go a degree of headache, of local pain, and even of mild or severe febrile disturbances, proportionate to the severity of the lesions which produce them.
When the anterior ethmoid cells are involved pain is usually referred to the temples rather than the forehead, though both may suffer alike.
Treatment should be based upon the fact that we have affected and infected cavities whose interiors are diseased, and whose outlets are blocked. The more free and thorough the drainage and the cleansing which can be given, the more prompt the results. In all well-marked cases, then, radical treatment is indicated. The ordinary treatment by sprays, inhalations, etc., is useless, as the source of the trouble is not reached.
Special treatment for each sinus will now be considered.
Frontal Sinus.—Most of the symptoms of affection of the frontal sinus are objective, and there is frequently external swelling, with tenderness and edema. For its relief intranasal methods will often suffice. In almost all cases we may expect to find hypertrophic conditions within the nose. When empyema exists there is often a deviated septum. It is impossible to avoid the conclusion that there is a strong relation between hypertrophic lesions and sinus retention. The difficulty may arise from many causes, most of which lead to sneezing, coughing, and hacking, by which the mucous membrane of the nasopharynx is both thickened, loosened, and predisposed to polypoid changes. The irregularities thus produced harbor more germs than usual and their effect is, in a measure, proportionate to their numbers. For the examination of the upper part of the nasal cavity Killian’s speculum is of great help.
The frontal sinus differs very much in shape and size, not only in different individuals but on opposite sides of the same individual. It may be rudimentary upon one side and large upon the other. It is usually more capacious in those individuals who have prominent foreheads and resonant voices. Here, as elsewhere, it will usually be found that the most radical operation is the best, although one endeavors naturally to preserve cosmetic features of the nose, so far as he can, without sacrificing the patient’s interests. The nasopharyngeal duct is so often connected with the ethmoidal cells, as well as the frontal, that the former may be easily affected when the frontal sinus is diseased.
In case of sinus disease, especially when the frontal sinus is involved, it is better to encourage patients to snuff materials back into the throat rather than to forcibly blow the nose or expectorate them, as the latter would tend to force into the sinus that which it would be better to have aspirated out of it.
The frontal sinuses may be attacked from within the nose or externally. It is perhaps the least open to mild and conservative treatment, as it is the most difficult of access by non-operative methods. The anterior ethmoid cells are usually connected with it and infection rarely spares one part to involve the other alone. Therefore if it be necessary[610] to operate on the frontal sinus the anterior and upper cells should be exposed at the same time. Thus operations which have for their object continuous drainage have usually as an objection the necessity for wearing the drainage tube for months. After opening the sinus from without the nasal duct may be enlarged to any size and desired degree, and a tube inserted which shall afford ample drainage downward. This may be covered with a flap and allowed to remain for a number of weeks. Nevertheless it is a foreign body which has to be subsequently removed from the nose. Killian’s method is doubtless the best for most cases, as the most anterior of the ethmoid cells, and those which extend over the orbits, cannot be easily reached through the nose, and if disease involve the posterior ethmoid cells its extension to the sphenoid may be expected. The operation includes an incision from the temporal end of the shaved eyebrow, along its curve to the side of the nose, and down to the middle of the nasal processes. The periosteum is divided along a line a little higher, and again in the centre of the frontal process, the intent being to so remove it that a bony bridge may be left after removal of the anterior lower wall of the sinus. The first periosteal incision should correspond to the upper border of this bridge, either above or below it. The sinus is opened at first with a chisel, afterward with bone forceps or surgical engine. It is then completely scraped out, leaving the supra-orbital ridge for a bridge. Its floor is resected along with the frontal process of the superior maxilla. Through this opening the anterior and middle ethmoid cells may be reached and cleaned out to the middle turbinate. The ethmoid cells may then be attacked, the sphenoidal cells inspected, and also attacked if necessary. The opening into the nose should be made free, and a flap should be formed from the nasal mucoperiosteum, so that there may remain a permanent opening of sufficient size. This method may be modified to suit various needs. After doing all the work necessary the external wound is closed, with a tube for drainage, while the formation of the bridge above alluded to prevents much of the sinking in of the anterior wall of the sinus, which would otherwise occur. If the little pulley over the superior oblique muscle has been interfered with in the operation or loosened from its attachment there will be at least temporary and perhaps permanent diplopia. This should be carefully avoided. There is also danger of injury to the contents of the orbit. For some time after the operation there will be some drooping of the upper lid. Nevertheless the results are usually satisfactory. After the operation the patient should be permitted to lie upon the healthy side and be forbidden to blow his nose; he should rather attempt to aspirate the fluid from the wound. If necessary both sinuses can be attacked at the same time and after the same fashion, the septum being removed.
Here as with the other sinuses the test of the efficacy of the treatment will be furnished by relief of the headache, pressure, and pain. Should carious or necrotic bone be exposed, or should there be indications of malignancy, much more radical surgery would be indicated.
The Ethmoidal and Sphenoidal Cells.—For the exposure of these, especially the latter, it is necessary to make room for work. This would be true even in normal cases, and is still more so when the parts are hypertrophied and the passage-way is obstructed. It is necessary at least to remove all deviated portions of the nasal septum, and to clear away not only all hypertrophies of the turbinates, but to remove more or less of these bones. With a free passage-way it is possible to expose the opening of the sphenoidal cells, whose anterior wall may then be broken down, after which granulations may be removed with an appropriate small spoon, or the purulent contents cleaned out with swabs.
In dealing with the ethmoidal cells by intranasal methods it is necessary to break down the slight compartments between them, one after another, because of the fact that they all constitute foci of disease. An opening at least 2 Cm. in length will usually be required, and can be comfortably made, under suitable illumination, if all obstructions have been removed; after this a probe is gently passed upward and alongside of the nasal septum until it rests against the ethmoid, then passed backward until it meets the posterior wall, which will be in the immediate neighborhood of the sphenoidal opening, through which, by gentle manipulation, it may be passed. At this point the presence of polyps or a greatly thickened mucosa may be detected by palpation with the finger within the nasopharynx, while should pus be removed by the end of the probe it would indicate empyema of this cavity.
In all these accessory nasal sinus examinations and operations the greatest aid will be[611] afforded by cocaine solution, which has the double advantage of not merely abolishing sensation, but of contracting and rendering anemic the mucous membranes, and thus to a certain extent shrinking them. When necessary for this latter purpose, or for the control of hemorrhage, adrenalin may be added to the cocaine. For all these purposes a spray of a mild solution may be first used, for its general benumbing effect, after which it would be advisable to use a strong solution, even saturated, very sparingly, applying it by the aid of illumination just to the area where the effect is desired, and not allowing it to come in contact with other parts of the nasal cavity; this is done to avoid unpleasant symptoms from cocaine absorption. Another benefit obtained from the use of cocaine is in thus abolishing sensation to an extent which does away with reflex vasomotor symptoms, shock, etc. Therefore even when a general anesthetic is used it will be well to use at least a small amount of it for this latter purpose.
The question of instruments and of methods will depend much on the equipment of the operator and his expertness in the necessary technique.
The Maxillary Antrum of Highmore.—This is the largest of the accessory sinuses, the most easily approached, and the one whose disturbance is most quickly and easily appreciated. It may be infected by continuity, along the Schneiderian membrane which lines it, or by extension upward of disease from carious teeth, as well as after a variety of injuries involving its integrity. So long as its opening into the nose be not plugged it will, when involved in catarrhal or suppurative inflammation, discharge into the latter a characteristic fluid, which is especially likely to escape when the head is held downward and to the opposite side. Any statement of this fact, coupled with evidences of local inflammation, should enable an easy recognition of antral disease. In more chronic cases it becomes blocked by thickening of its membrane, the production of granulations or of polypi, which sometimes completely fill it. When thus plugged and filled there is a tendency to protrusion of its anterior outer wall and floor, while the overlying cheek may become somewhat edematous, the parts at the same time being tender. The pain from a diseased antrum will often induce the patient to go to the dentist for extraction of a molar tooth, which, however, affords little relief.
The relief for chronic antral disease is surgical, as in the case of the other sinuses. Opening the antrum through a tooth socket would seem judicious only when a diseased tooth is the cause of the lesion. It is useful only for such otherwise uncomplicated cases. The argument usually used in its favor is that it affords better drainage. This, however, is not the case, since the position assumed by the head for the greater part of the time does not locate such an opening in the most dependent part of the cavity. Moreover, the discharge is not always fluid, nor does it flow freely; on the contrary it is often thick, and so adherent to the wall or roof of the cavity that it takes a strong irrigating stream or swab to dislodge it. If the antrum is to be opened through the mouth it would seem more surgical to open it widely, cleanse it, and then either drain it or close it again. Other things being equal, the best method is that which permits of both examination and subsequent treatment. Jansen’s method is frequently most serviceable. It includes careful cleansing of the teeth, with disinfection of the mouth, and walling off the area to be exposed by gauze strips in order to prevent hemorrhage into the throat. An incision is made through the anterior mucoperiosteum, beneath the floor of the antrum, from the first incisor to the first molar. Its edges are then separated and the entire front wall of the antrum removed. Through such an opening its interior can be carefully inspected and cleansed. Should it seem desirable to go farther the inner wall may be removed by forceps, and through this opening the ethmoid cells can be seen and curetted up to the insertion of the middle turbinate. Then the sphenoid surface can be inspected and the lower portion of the sphenoid cells resected. Finally a good-sized counteropening is made inward, onto the floor of the nose, the antrum is loosely packed, the ends of the gauze extending into the nose, and the mucoperiosteal wound closed, in order to secure primary union. All bone edges should be made smooth and non-irritating; the sphenoidal cells should not be packed, but left open for subsequent treatment.
In the presence of bone disease, malignant growth, etc., it may not be possible to shut off the mouth again from the antral cavity. In such cases the packing may be made more snug and the granulation process will have to be substituted for sutures.
Special flaps or plastic methods should be devised for special cases, as, for instance, the formation of a mucoperiosteal flap from the outer side of the antral wall and its[612] union posteriorly within the cavity of the antrum with another made from the antral floor. By turning the latter in the necessary direction a line of suture may be made through the mouth. Any such cavity, long diseased, will call for a radical method of attack and opening, which latter can be maintained to permit of subsequent treatment, as an early closure would sometimes be undesirable. Antral cavities thus left more or less open should be treated with cleansing sprays or applications, and with such stimulating applications as silver nitrate in various strengths of solution, or similar antiseptic stimulants.
While most of the affections of the nerves are considered to be non-operative, and to belong rather to the internist than to the surgeon, there are, nevertheless, some nerve lesions which are only to be relieved by surgical intervention. These may be divided into: (1) Wounds and injuries. (2) Morbid conditions, such as (a) neuralgia, and (b) muscle spasm.
Wounds of nerves have been considered in the chapter on Wounds, and the possibility of nerve regeneration and repair therein discussed. In every division of a nerve trunk of importance or size the nerve ends should be trimmed and reunited by a suture, passed either through the sheaths or through the nerve itself. The ends should be brought together securely and the tension should not be too great. If this be promptly done the best of results may be expected. This is equally true of cranial and peripheral nerves. Clinical experience has long since established the necessity of this procedure after all such injuries, and nerve suture, or neurorrhaphy, is now a standard operation. Later there was added to this measure the analogous one of nerve grafting, and it has been found that nerves can be juggled with just as can tendons, as described in the section on Tendon Suture. Indeed the methods of nerve suture and nerve grafting are strikingly similar to those employed with tendons, where can be made either end-to-end junction, lateral implantation, or a more properly termed grafting, a trimmed end of one nerve being inserted into another. In the arm, when the ulnar nerve has been caught in callus and completely destroyed, both the upper and lower portions may be grafted into one of the adjoining nerves, e. g., the median; this procedure seems to reëstablish communication and serve the double purpose, in a manner corresponding to duplex or quadruplex telegraphy over one wire. Nerves which have been divided and entangled in scars may be disengaged, their ends trimmed off and approximated, success being proportionate to the length of time during which nerve degeneration may have been taking place.
Another operation is practised on nerves, solely for the relief of painful or disturbing symptoms, i. e., neurectomy. In cases of intractable and hopeless neuralgia, where other measures fail, sensory or complex nerve trunks are divided, a portion of the continuity being resected. This operation is practised more often upon the trifacial nerve than upon all others. It is generally successful, but in those cases where pain is due to some central lesion it is often palliative rather than curative. In the case of the trifacial nerve the operator endeavors to be as radical as possible in its practice, and to remove the Gasserian ganglion rather than portions of any of its branches.
The neuralgia for which these operations are performed may be due either to central or constitutional causes, as well as to local irritations, compressions, or degenerations. The term neuralgia itself is so vague and covers such widely differing changes that nothing which can be said in this place would clear up the problems of its pathology; consequently attention will be directed here solely to its surgical relief in connection with the various nerve trunks which are usually attacked.
One other operation is practised upon nerves for the relief of pain and spasmodic affections—namely, nerve stretching, or nerve elongation. This is practised more often upon the sciatic than upon any other nerve, but has been done for the relief of choreic spasm of the arm and shoulder, by exposing and stretching the various cords of the brachial plexus, for the relief of spasmodic torticollis, and in various other places.[613] Nussbaum was the first to note that obstinate intercostal neuralgia was relieved by accidental stretching of an intercostal nerve, and introduced the procedure.
Fig. 398
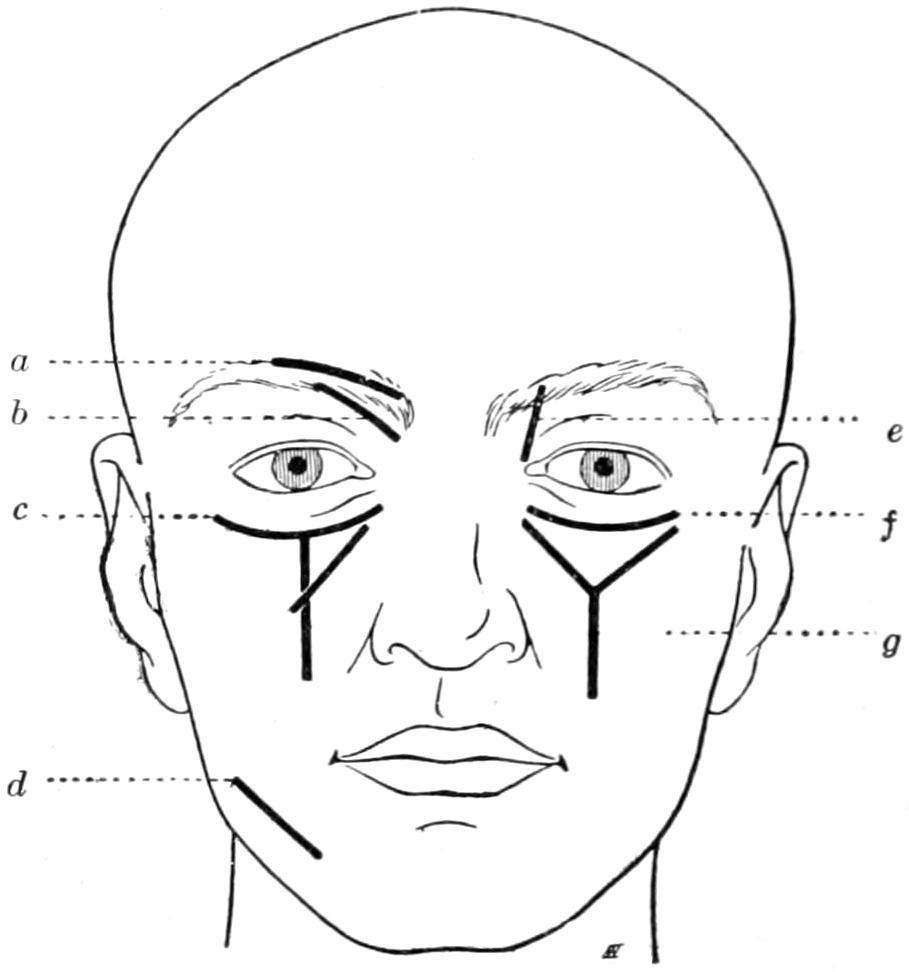
Various incisions for reaching different branches of the trifacial nerve: a, supra-orbital; b, external nasal; c, Bruns’ incision; d, inf. dent. at mental foramen; e, internal nasal; f, infra-orbital; g, Carnochan’s incision. (Marion.)
Operations upon nerves, then, include suture, grafting, stretching, division, and resection. After any operation upon a nerve trunk the parts pertaining to it should be placed in a position of rest; and, furthermore, such position as will prevent stretching and favor relaxation of the sutured trunk should be maintained. The writer is credited with the first primary suture of the sciatic nerve, which was done immediately after its accidental division, during the course of an extensive operation. Recovery was prompt and complete. The limb was immobilized in the extended position and physiological rest thus maintained.
Nerves can be stretched, it has been found, to one-twentieth of their length. Nerve trunks have much more strength than has been generally appreciated. The sciatic trunk of a full-grown individual will bear a stress of more than eighty pounds, while even six pounds’ pull are necessary to tear the supra-orbital nerve. The benefit which follows nerve elongation is ascribed to the improvement in its nutrition produced by the damage done to its substance, and the consequently enhanced blood supply, as well as to the severing of adhesions between the sheath and its surroundings and between the nerve bundles within the sheath.
The operation of nerve stretching consists simply in exposing the nerve at a site of election, detaching it from its surroundings, and then hooking either the finger or some smaller instrument beneath it and pulling firmly, yet gently, in both directions; in the case of the sciatic, for instance, the entire limb should be lifted from the table, and even this does not entail upon the nerve trunk anywhere near a breaking force.
The cranial nerves are sought, found, and treated as follows, in their respective cases:
The supra-orbital nerve is attacked at its exit from the supra-orbital notch, which can usually be felt, or foramen, when such exists, either by a straight incision made directly over it, where it can be felt, or by a curved incision through the region of the eyebrow, which should have been shaved for the purpose, the resulting scar being hidden by the hair as it grows again.
The infra-orbital nerve is similarly treated at the infra-orbital foramen, where it lies under the levator labii superioris. It may be exposed by either a curved incision, parallel to the orbital margin, or by a vertical incision, which will leave a more disfiguring scar.
The second branch of the fifth nerve may be attacked from the front by Chavasse’s modification of Carnochan’s original method, consisting of a T-shaped incision from one corner of the eye to the other, the vertical branch extending from its middle well down to the mouth. After the infra-orbital nerve is identified it is secured with a piece of silk. The anterior wall of the antrum is then removed, the cavity opened, and a small trephine applied to its posterior wall. The nerve, being exposed in its canal or groove, is divided anteriorly, pulled down into the cavity by means of a ligature previously applied to it, and now made to serve as a guide into the sphenomaxillary fossa. Here it may be followed directly into its connection with Meckel’s ganglion, which may also be extirpated. The nerve trunk is forcibly pulled out of the foramen rotundum, through which it escapes from the Gasserian ganglion.
Horsley does not open the antrum but lifts the orbital contents, including the periosteum, follows the nerve along the canal by means of sharp-pointed bone forceps, and thus follows it up to the foramen rotundum, where it is evulsed as above. (See Fig. 399.)
Luecke years ago devised a method of lateral approach, attacking the ganglion and the nerve from the temporal region. An incision is made from the external angle of[614] the orbit straight downward in the direction of the molar teeth, where it is met by another extending from the middle root of the zygoma, downward and forward. Through these incisions the zygoma is exposed and divided. Thus an osteoplastic flap is formed which is laid up over the temporal region, the divided piece of bone being raised with the overlying skin and not detached. This exposes the temporal and zygomatic fossæ. The temporal muscle is then drawn backward with a hook, the fatty tissue which fills these fossæ cleaned out, and the nerve sought for in the sphenomaxillary fossa, where both it and Meckel’s ganglion may be extirpated. The flap is then turned down and fastened in place (Fig. 400).
Fig. 399
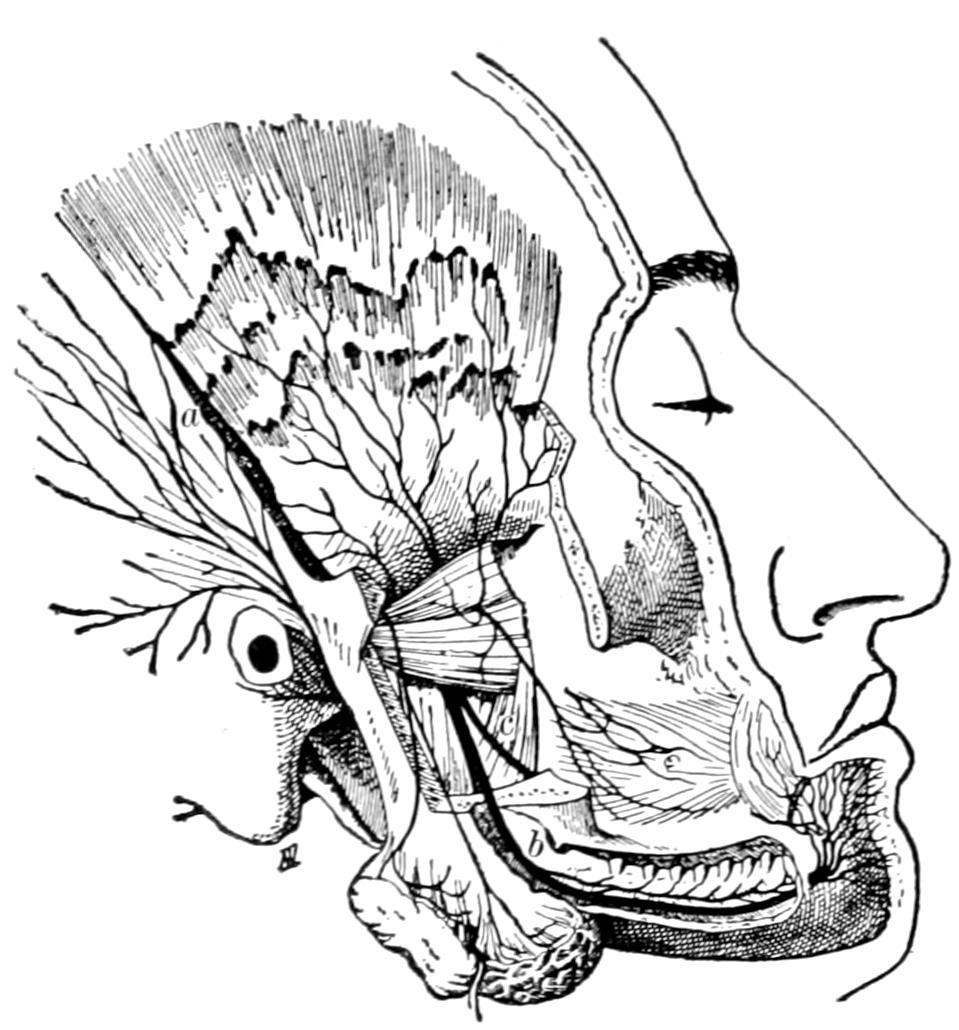
Branches of the inferior maxillary nerve which most concern the surgeon: a, auriculo-temporal; b, inf. dental; c, buccal. (Marion.)
Fig. 400
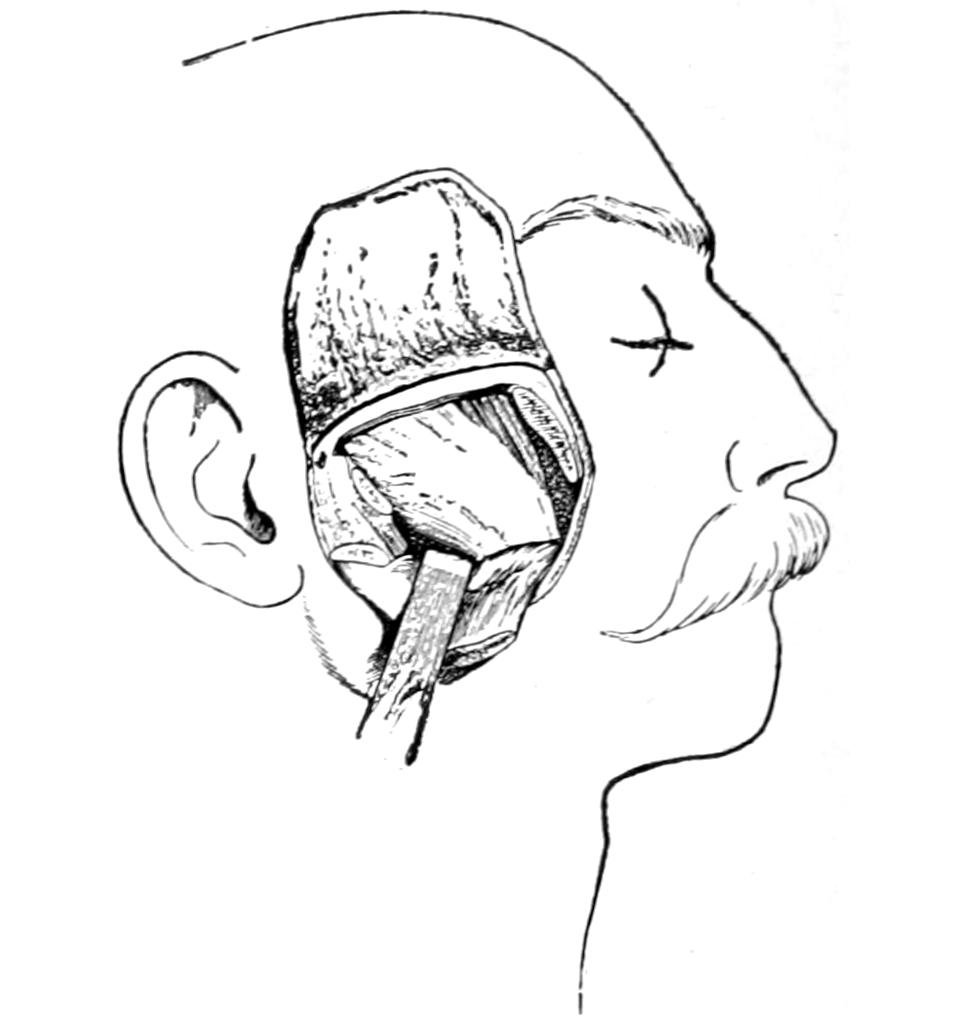
Exposure of Meckel’s and the Gasserian ganglia by temporary resection of the zygoma; Luecke’s method. (Marion.)
The inferior dental, or third division of the fifth nerve, may be reached in several ways: Its terminal portion where it escapes at the mental foramen; its upper portion by an incision two inches along the lower border of the jaw and above the angle, the masseter muscle being separated from the jaw, and the ascending ramus opened with a ³⁄₄-inch trephine at a point 1¹⁄₄ inches above the angle, its upper edge ¹⁄₄ inch below the sigmoid notch. The nerve is here exposed before it enters the canal. The lingual nerve may also be found resting upon the internal pterygoid muscle. A ligature tied around each nerve, for traction purposes, permits easy tracing of their trunks to the foramen ovale, where, after vigorous stretching, they are divided. They should then be traced downward and at least one inch of their trunks removed.
—When all three branches of the trifiacial nerve are involved in painful tic, or when operation has already been practised upon one or more of them and the tic has recurred, it becomes necessary to attack the Gasserian ganglion itself.[45] This may be approached by either one of two methods. Both are difficult and[615] serious, having a mortality of from 15 to 20 per cent. As Cushing has pointed out, however, its mortality rate is scarcely as great as the death rate by suicide in neuralgic cases of this kind. The attack from below was first carefully worked out by Rose and then by Andrews, and is begun in much the same way as the operation for the removal of Meckel’s ganglion by resection of the zygoma, described above. A flap is laid up, larger and wider, including the zygoma, with the most complete possible exposure of the zygomatic fossa. The coronoid process is drilled in two places, divided between the openings, which are to be used for subsequent suture, and the temporal muscle pushed upward and forward, out of the way, with the upper fragment. The foramen ovale is then identified by following into it the inferior maxillary nerve, the base of the skull being cleaned away in that neighborhood, and a small trephine opening made between it and the foramen rotundum, connecting these two openings by a much larger one. Through this opening the ganglion is exposed and destroyed piecemeal or extracted as completely as possible. The operation is exceedingly difficult, and hemorrhage, especially from the middle meningeal artery at the foramen spinosum, maybe so troublesome as to make it impracticable unless the carotid be tied. I have preferred in doing this operation to make preliminary ligation of the common carotid, which facilitates the balance of the procedure. The exposure by this method, however, is not as satisfactory as by that next to be described.
[45] Osmic Acid and Other Treatment of Trigeminal Neuralgia.—While it hardly pertains to operative surgery, it may be worth while to say that it seems to me that no case of trifacial neuralgia should be subjected to radical operation until at least two or three remedies have been given a fair trial. One of these is castor oil its use being based upon the theory that such neuralgia is of toxic origin and that a prolonged evacuant treatment should benefit it. This would mean the administration of two or three good-sized doses of castor oil every day for a period of two to three weeks. It is not such a drastic remedy, thus given, as would appear, for after the oil has once thoroughly produced its laxative effect it ceases to distress, but serves as a very effective eliminant. The second remedy is gelsemium, the best preparation being the tincture of the green root. It seems to exercise a selective affinity for the trifacial nerve. It should be given in large doses, pushed to the physiological limit, i. e., until the patient begins to see everything in yellow colors. Its effect on the heart must also be guarded. Fifteen drops of the green tincture given every two hours, and for a few days, will usually suffice to thoroughly test its efficacy.
Osmic acid is used only for intraneural injection, its efficiency now being under trial. Ten to twelve drops of a 2 per cent., freshly prepared aqueous solution are directly injected into the nerve trunk after its exposure. Murphy has been its particular advocate, and has reported relief of pain in a number of cases thus treated. It seems to depend for its effect upon two factors—the destruction of nerve filaments and their substitution by connective tissue. All the nerve branches that can be exposed should be injected; the palatine and lingual through the mouth; the intra-orbital and supra-orbital by incisions upon the face; orbicular-branches, as well, should be injected, if possible. Most of those who have used it advise also to inject a few drops into the foramina of exit, around the trunks, which are thus infiltrated with the solution. The procedure is painful and usually requires a general anesthetic, but it seems to be free from danger. While the treatment has been successful in some cases it has been equally disappointing in others, and the method will scarcely supplant the more radical method of ganglion exsection.
Hartley and Krause, about the same time and independently, devised a method of attacking the ganglion, after raising an osteoplastic flap from the side of the skull, which affords a better exposure and a more satisfactory method.
Within reason the larger the osteoplastic flap the easier the balance of the operation. Whether it be square or horseshoe in shape, whether it be made by chisel, by Gigli saw, or by surgical engine, matters little. In fact experience has shown that the conservation of the bone is not a matter of serious import, and there is no good reason why there should be any hesitancy to remove the bone should the formation of such an osteal flap present too many difficulties. After the dura is completely exposed it is to be separated from the base of the skull until the foramen spinosum and middle meningeal artery are reached. It is better to do this quickly and with the finger than slowly with instruments. After this separation the brain with its dural covering is lifted by a spatula or retractor, so as to afford a good view of the region of the ganglion. It will be necessary to double ligate the middle meningeal artery unless preference has been given to make a preliminary temporary or permanent ligation of the carotid. Should this artery have been injured in raising the flap it should be secured before going any farther, either by plugging the opening or canal with gauze or with antiseptic wax (Fig. 401).
The upper surface of the ganglion is adherent to the dura, and these adhesions should be separated. The second and third branches should be identified and divided near their exit. The first branch is in too close relation with the cavernous sinus to justify much interference. The ganglion itself is then seized, after complete isolation, with forceps and evulsed, with as much of its longer and shorter roots as possible. Hemorrhage is checked by adrenalin or by pressure with gauze, as may be required. If gauze be used for the purpose it may also be utilized for drainage. The brain is restored to position and the flap sutured in its proper place.
Before doing either of these operations I should prefer to place the patient within the Crile pneumatic suit and then tilt the body to an angle of at least 45 degrees, thus prompting emptying of the cranial and cervical veins by gravity, while at the same time blood pressure is maintained by the pneumatic pressure (see p. 180).
Abbe has endeavored to lessen the shock of the operation by not formally tearing out the ganglion, but by taking out a section of the nerve trunks between it and their foramen of exit, and then interposing a piece of thin, sterile, rubber tissue, inserting it in such a way that it shall effectually prevent regeneration of nerve trunks across the interval, this rubber being intended to remain and become encapsulated. This method of Abbe[616] seems to have made operative attack upon the Gasserian ganglion less formidable and less dangerous. It remains to be seen whether it is permanently as effective as more complete extirpation.
—In some cases of cancer of the tongue there is such intense pain that not only has the lingual artery been tied but the lingual nerve been stretched or exsected. It can ordinarily be reached where it lies on the floor of the mouth beneath the mucous membrane, at the fold between it and the tongue, where it can be felt if the tongue be forcibly stretched. Through a small incision a blunt hook may be passed and the nerve thus secured. Close to the first lower molar the nerve lies in the tongue near the surface, where it can also be found.
—This nerve has sometimes to be stretched for spasmodic affections. When the desire is simply to reach its trunk it may be sought through an incision behind the ear, by which the posterior border of the parotid is exposed, the sternocleidal insertion identified, the nerve lying in the interval between these two landmarks. A more easy method of reaching it would probably be by an incision in front of the ear just before its main branch divides as it enters the parotid gland. If necessary this may be followed backward until the main trunk is reached.
Fig. 401
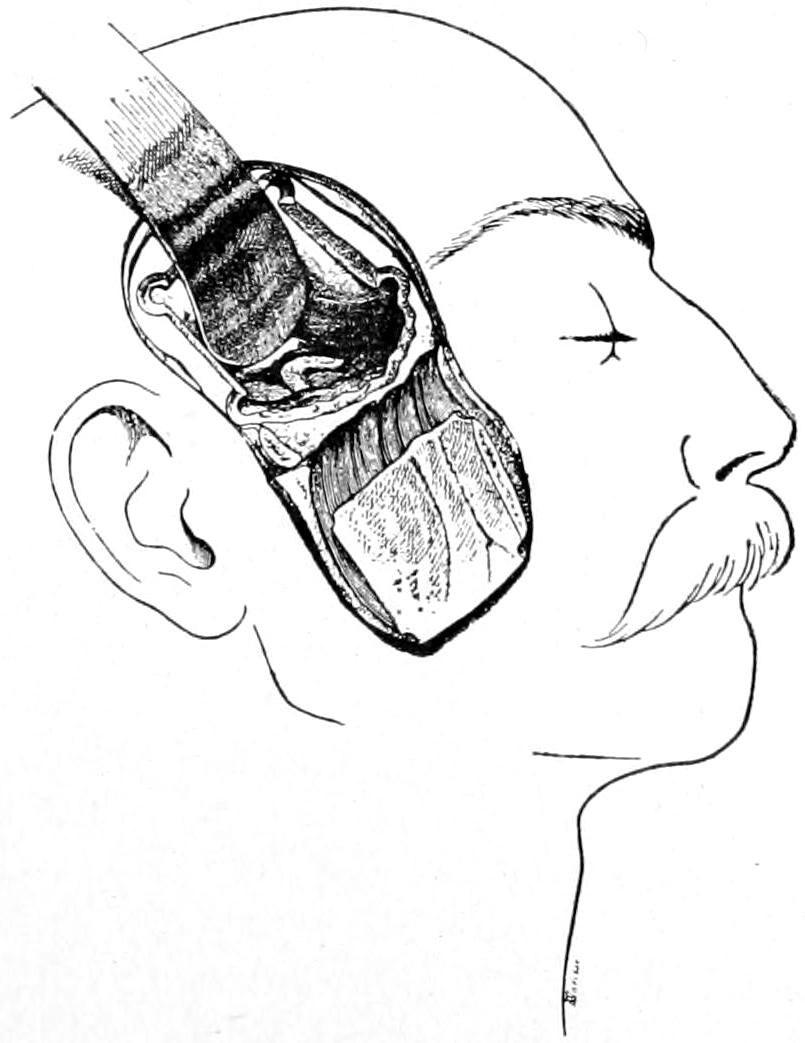
Intracranial exsection of Gasserian ganglion; dura open, brain lifted up. Hartley-Krause method. (Marion.)
Fig. 402
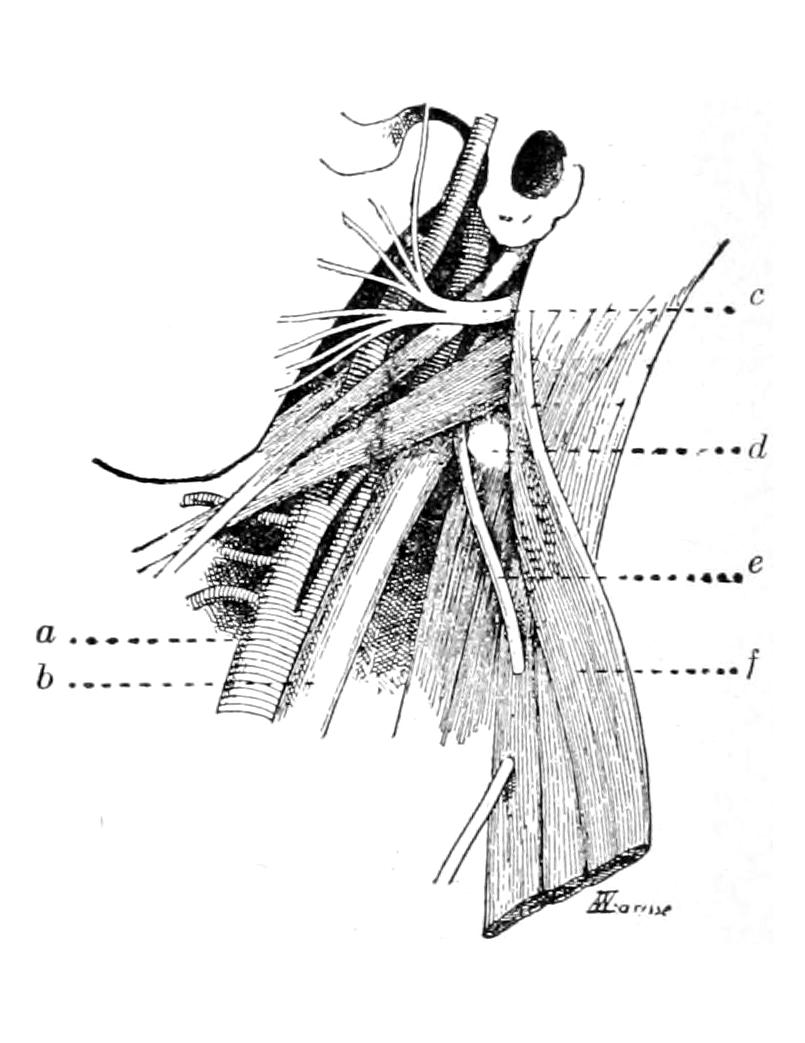
Relations of the facial and spinal accessory nerves: a, carotid; b, int. jug.; c, facial nerve; d, transv. proc. atlas; e, spinal acces.; f, stern. mast. muscle. (Marion.)
—In view of the hopelessness of facial paralysis, when resulting from destructive injuries to the nerve trunk, the introduction of anastomotic methods has marked a very distinct advance. Ballance, in 1895, was the first to apply neuro-anastomotic methods to the facial nerve. He attached the facial to the spinal accessory. His own experience, as well as that of half-a-dozen later operators, proved that nerve regeneration is possible, but that in this particular instance voluntary movements of the face were often accompanied by distressing and unsightly associated movements of the shoulder, and vice versa. Hence, Taylor and others suggested the use of the hypoglossal instead of the spinal accessory, the former being a purely motor nerve running near the facial, intimately associated with it in function, and arising by nuclei, which are equally closely associated in the cranial centres. The operation is indicated in all cases of paralysis caused by lesion of the nucleus within the brain, or the nerve trunk at the base of the brain, or along its course. It is justifiable in Bell’s palsy, when there is complete reaction of degeneration in the facial nerve after several months of treatment (Fig. 402).
The steps of the operation are practically as follows: Incision is made along the anterior margin of the mastoid and the sternomastoid muscle, and the parotid gland is retracted forward and the posterior belly of the digastric is exposed. It should then be[617] pulled downward and backward and divided if necessary. The styloid process is identified, and the facial nerve which emerges from the stylomastoid foramen near its base is then sought and isolated. It should be separated as high as possible and divided close to its exit, so that one-half inch of its free trunk may be secured before it enters the gland. Two fine silk sutures are then passed, one on either side, through the peripheral end of its sheath and tied, the ends remaining long, to be subsequently used. This nerve end should be trimmed to a wedge shape. Next the transverse process of the atlas is identified and the deep cervical fascia divided. This will expose the internal jugular, which should be separated and held out of the way. There will now be seen the spinal accessory nerve, which runs obliquely downward and outward, sometimes in front of and sometimes behind the jugular (Fig. 403). When the vein is held forward and the fascia well retracted both the hypoglossal (Fig. 404) and the pneumogastric nerves are seen, with the internal carotid to their inner sides. The former may be identified either by the electric current, which will cause contractions in the muscles supplied by it, or it may be followed down to where it turns forward around the occipital artery and gives off the descendens noni. Here it should be separated until its trunk is sufficiently free, so that the facial stump can be inserted into it without tension. The nerve being elevated by a hook a slit is made in it, about ³⁄₄ inch long. Into this the wedge-shaped end of the facial trunk is introduced, and held there by utilizing the sutures which have already been passed through its sheath. When the nerve is thus firmly held in the cleft, with its end turned toward the direction of nerve supply, a little cargile membrane may be wrapped around the junction and the wound closed.[46]
[46] Taylor and Clark, New York Medical Record, February 27, 1904, p. 321.
Nerve regeneration has been known to follow this procedure in a number of cases, and it has given encouraging results. Considerable time, however, is required, and the patients should be warned that results are not to be quickly expected.
Fig. 403
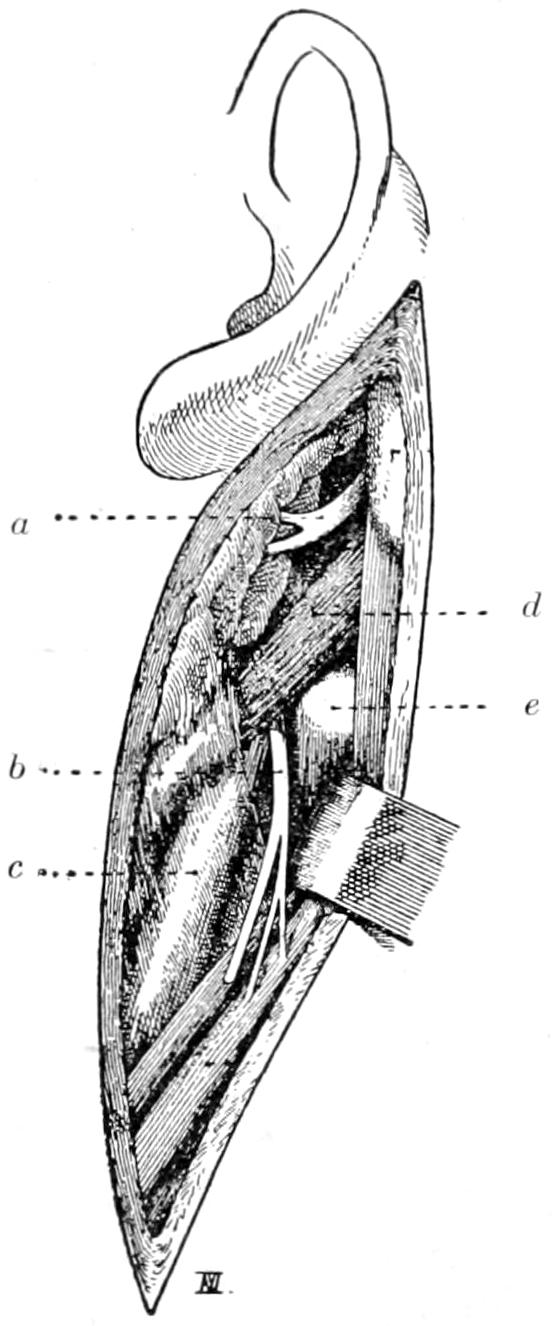
Fig. 404
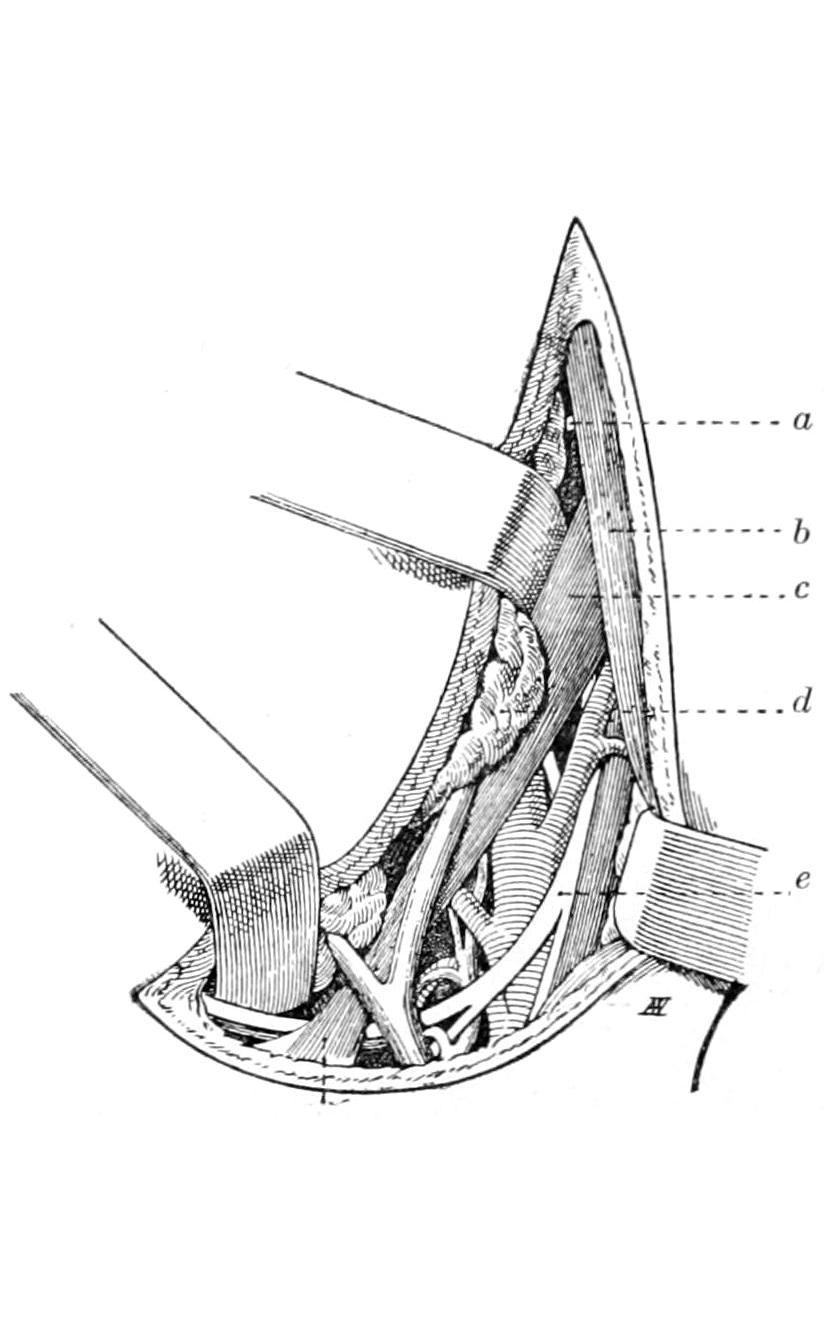
Exposure required for anastomosis of facial and spinal accessory nerves: a, facial nerve; b, sp. acces.; c, int. jug.; d, digastric muscle; e, atlas, trans. proc. (Marion.)
Exposure required for anastomosis of facial and hypoglossal nerves: a, facial nerve; b, sternomastoid; c, digastric; d, parotid; e, hypoglossal. (Marion.)
—The principal reason for attack upon this nerve is spasmodic torticollis, or wryneck. It is exposed through an incision along[618] the anterior border of the sternocleidomastoid muscle, extending two inches downward from the ear. The nerve is found a little above the level of the hyoid bone; or, again, it may be found by an incision along the outer border of the muscle, opposite its centre, just above which it will be detected (Fig. 405).
The Deep Posterior Cervical Plexus.
—When operation upon the spinal accessory has failed to relieve long-standing and serious spasmodic torticollis, Keen has suggested to divide the first, second, and third cervical nerves. The operation is difficult and not always successful; still it is worth trying. A transverse incision is made below the level of the lobe of the ear, the trapezius being divided and dissected up until the great occipital nerve is found. It is followed after the necessary division of the complexus until its origin from the posterior division is reached. The suboccipital or first cervical nerve, which lies in the triangle close to the occiput that is formed by the two oblique muscles and the posterior rectus, is excised. The exterior branch of the posterior division is found lower down, and should be divided close to the bifurcation of the main nerve (Fig. 406).
Fig. 405
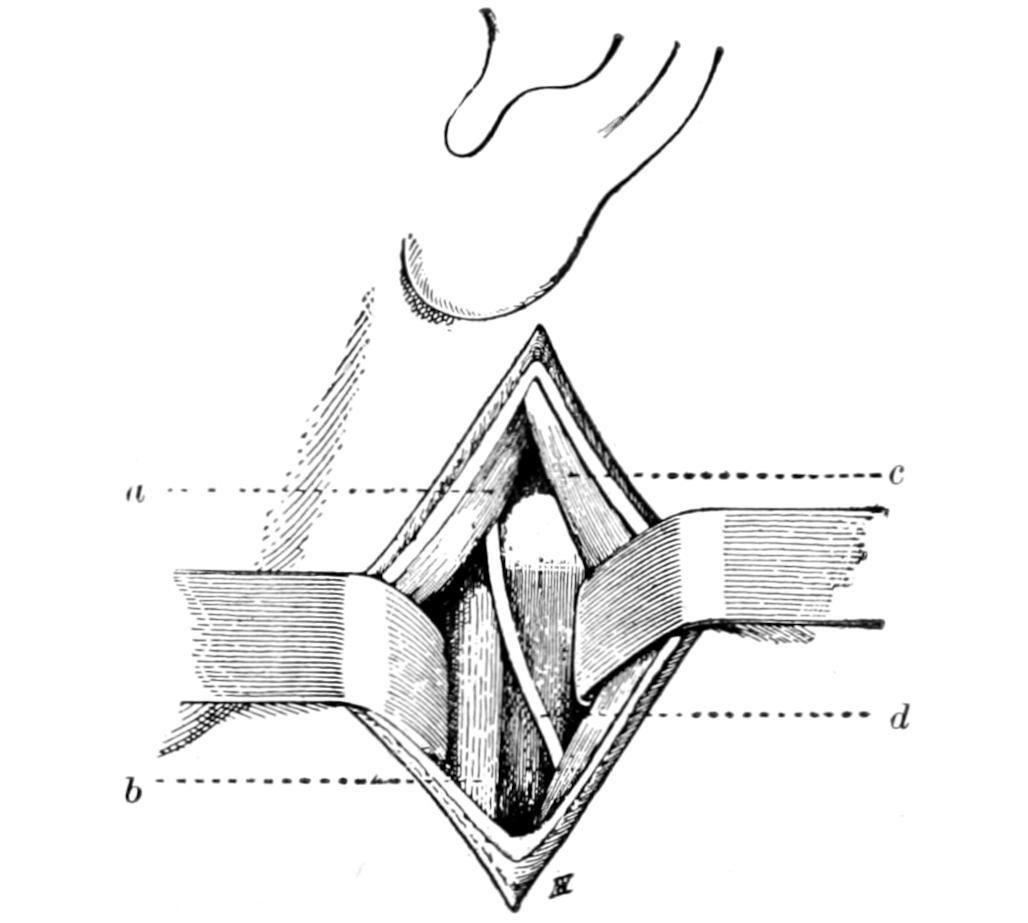
Exposure of the spinal accessory nerve alone: a, digastric; b, jugular veins; c, sternomastoid muscle; d, spinal accessory. (Marion.)
Fig. 406
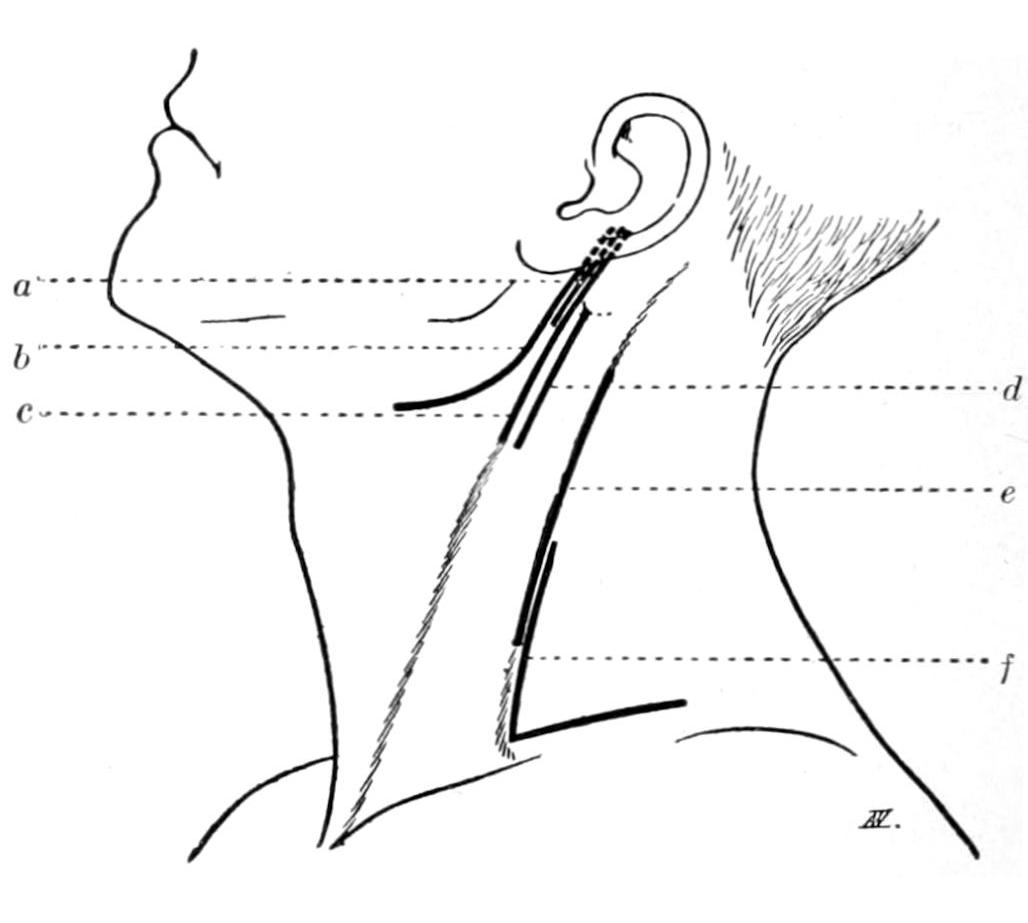
Incisions through which the various nerves in the neck may be sought: a, facial; b, facial and hypoglossal; c, facial and sp. acces.; d, spinal accessory; e, cervical plexus; f, brachial plexus. (Marion.)
—The cervical sympathetic is a most complicated nerve trunk, furnishing fibers of various functions to the skin, and to the deeper parts fibers which are vasomotor, vaso-inhibitory, pilomotor, and secretory in function. It supplies the various glands, the upper viscera, the heart and bloodvessels, and connects with nerves below, which supply even the genital organs and the non-striped muscles of the body. The upper part has a very important oculopupillary function, as it supplies the dilator pupillæ, the non-striped part of the elevator of the upper lid, and the orbital muscle of Müller, i. e., a small bundle of non-striped muscle which lies behind the globe and projects across the sphenomaxillary fissure at the back of the orbit. (By contraction of this muscle the eye may be pushed forward.) It also supplies the submaxillary gland, the cutaneous bloodvessels, and the sweat glands of the head and neck. The pupil dilating fibers arise in the medulla, run backward in the lateral columns of the cord to the ciliospinal centre, emerge through the anterior roots of the first and second dorsal segments, and enter the inferior cervical ganglion, thence passing upward through the sympathetic trunk to the orbit. Therefore ocular and other symptoms are produced not only by lesions of the external trunk, but also by lesions within the cord at the level of the upper dorsal segments. These nerves may be injured anywhere in the neck, or compressed by inflammatory deposits or new-growths, or even by cicatricial tissue at the apex of a tuberculous lung. Many cases of phthisis show inequality of the pupils. One nerve may be injured in operations on the neck, the result being slight drooping of the lid and flushing of the face, as well as excessive perspiration on the injured side;[619] the corresponding pupil being smaller than the other because of paralysis of the dilators, but contracting to light, as the third cranial nerve which supplies its sphincter is unaffected. The eye will then sink back somewhat, owing to paralysis of Müller’s muscle, and thus permit a nearer closure of the lids. These oculopupillary symptoms are pathognomonic of paralysis of the cervical sympathetic. Cocaine will not dilate a pupil whose dilator has thus been paralyzed. The area of skin supplied with sweat fibers by the cervical sympathetic includes the corresponding side of the head, neck, shoulder, and upper part of the trunk (Fig. 407).
When the cervical sympathetic is unduly stimulated we have dilatation of the pupil, exophthalmos, widening of the palpebral aperture, delayed descent of the upper lid when the patient looks downward, all of which can be imitated or produced by dropping into the eye a solution of cocaine, which stimulates the nerve.[47]
[47] Stewart, Some Affections of the Cervical Sympathetic, The Practitioner, February, 1905.
The surgical sympathetic is attacked surgically for three widely variant conditions: epilepsy, glaucoma, and exophthalmic goitre—the first, because of its vasomotor control of the vascular supply of the brain; the second, because of the relation of the nerve to the orbital circulation and nutrition; and third, because of its relations to the thyroid and the heart. In the latter case it is especially desirable to remove the lower cervical ganglion and the first dorsal, if it can be reached, although the procedure here is exceedingly difficult.
The tachycardia of Graves’ disease is due apparently to irritation of the accelerator nerves of the heart, which come from the sympathetic, or else to paralysis of the regulator (pneumogastric) supply. The former spring from the lower part of the cervical cord and the upper dorsal segments, and pass to the third cervical ganglia and to the first dorsal, terminating in the cardiac plexus.
The operation described below is practically that advised by Jonnesco, more or less modified by other operators, and may be varied to some extent to meet the exigencies of particular cases. Thus whether it shall be done through one or two incisions will depend on the will of the operator. It is made about as follows: A long incision is made along the posterior border of the sternomastoid. The latter may be either retracted forward or its fibers separated, in order that the fascia on its inner side may be reached and separated from the deeper muscles. This fascia should be divided as high as the base of the skull. The upper ganglion of the cervical sympathetic lies on the inner side of the anterior tubercle of the transverse process of the second and third vertebral processes, resting upon the muscles covered by this fascia. The ganglion, being recognized by its shape, and the sympathetic trunk being thus identified, the nerve should be divided and made free, as high as possible and just beneath the base of the skull. (See Fig. 408.)
Fig. 407
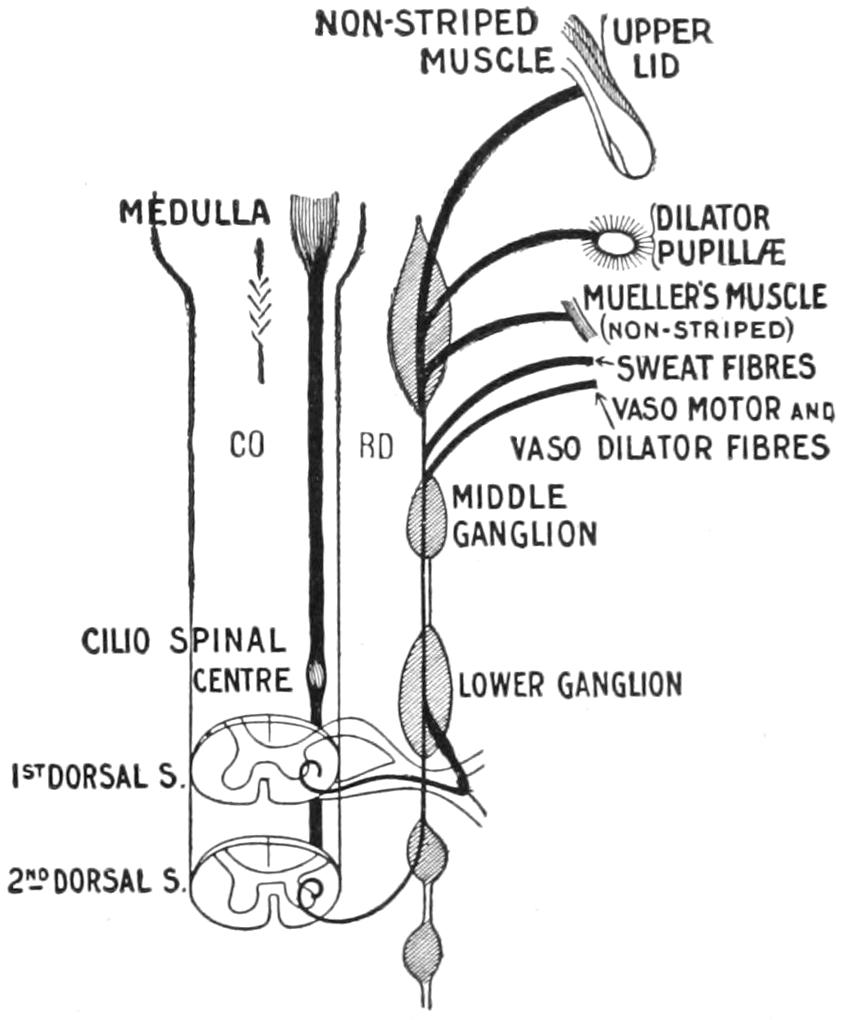
Diagram to illustrate the relations of the cervical sympathetic and the mechanism of the various disturbances following lesions of its trunk. (Stewart.)
The lower end is to be exposed by continuation of the first incision, or by another beginning 1 Cm. above the clavicle and extending along the posterior border of the sternomastoid for 4 or 5 Cm. The platysma should be entered and the tissues separated upward until the fingers can meet in a channel thus made by connection with the upper incision. The tissues should also be loosened downward until a point has been reached behind the clavicle. They then should be widely retracted and the inferior thyroid artery sought. The middle cervical ganglion is found inside of its curve. Occasionally this ganglion is replaced by a plexus, or the main trunk may pass behind the artery. At this level it is to be seized and its upper divided end pulled down and out through this opening. The nerve trunk should then be followed downward. The artery should be[620] freed from any plexus of sympathetic fibers around it, all of which should be destroyed, and especially those fibers which constitute the middle cardiac nerve, which pass to the inner side. The main trunk is to be drawn down beneath the artery and then followed downward and outward to the lower ganglion, where it lies behind the clavicle, on the neck of the first rib, between the scalenus anticus and the longus colli. The ganglion and the trunk should be separated from the efferent and afferent branches which connect with it, as well as from the vertebral artery; being thus made free it is again drawn outward. Here one should divide especially the cardiac branches which form the lower cardiac nerve, as well as the vertebral branches which have so much to do with controlling the supply through the vertebral artery. The ganglion, after being identified, should be finally removed. The nerve should be traced still farther down to the first thoracic ganglion, which has much to do with supplying the heart, and this also should be separated and destroyed (Fig. 409).
Fig. 408
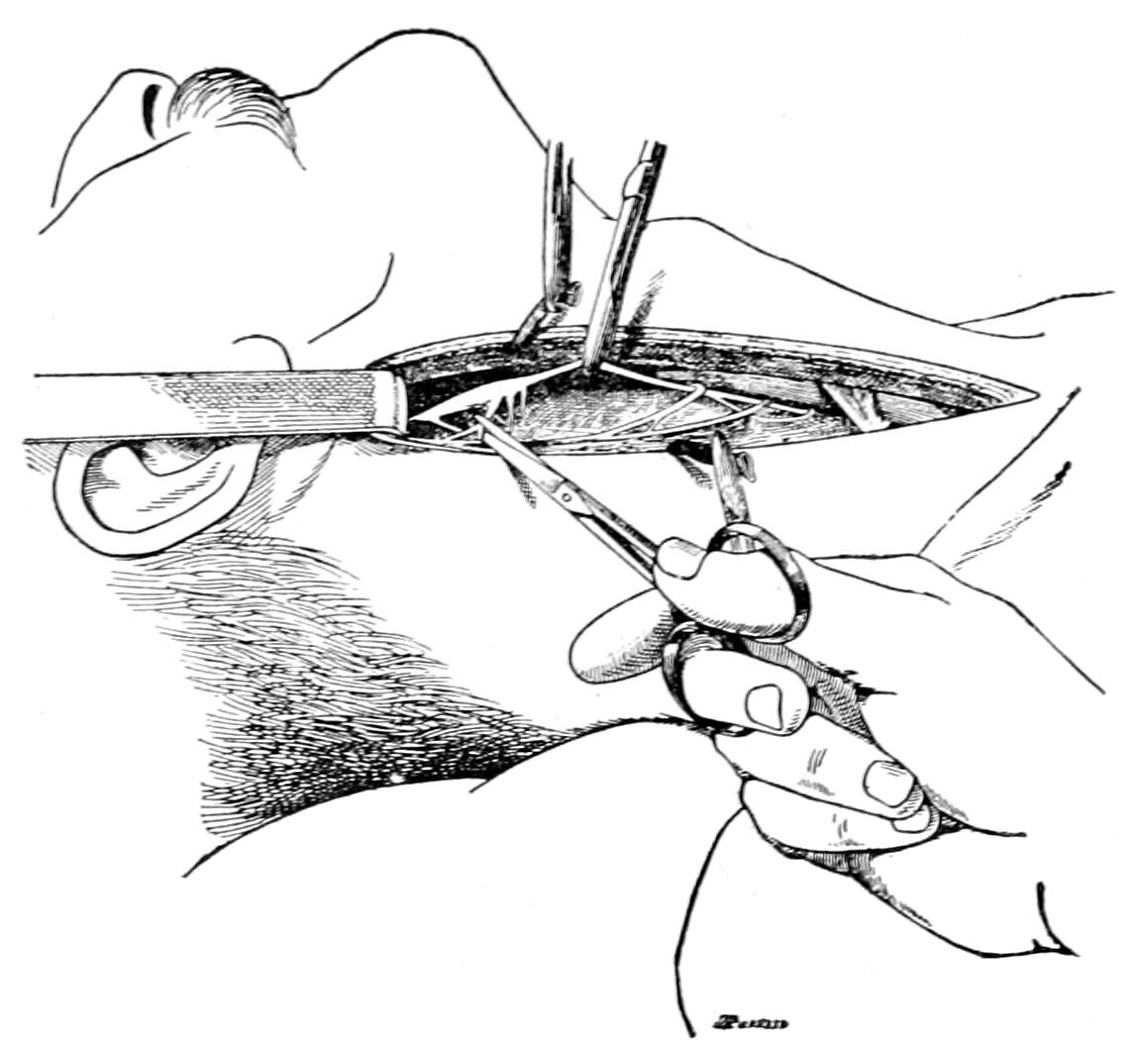
Sympathectomy. Exposure and removal of middle and upper ganglia. (Marion.)
Fig. 409
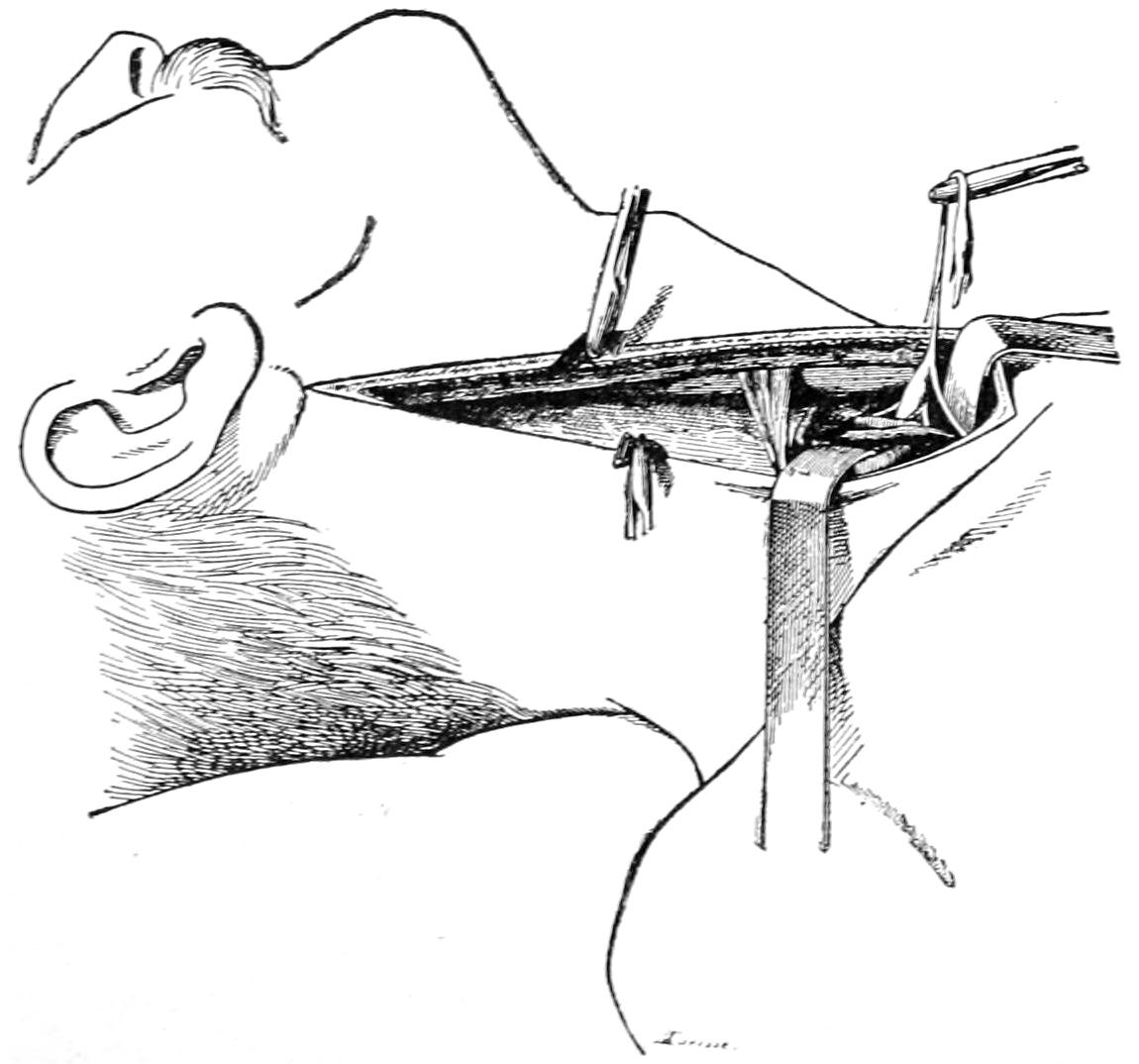
Sympathectomy. Seizure and removal of inferior ganglion. (Marion.)
It is rarely necessary to provide for drainage after the operation, unless the retraction and laceration of tissues have been very great. My own preference is to make one long incision along the posterior border of the sternomastoid, by which the dissection is facilitated and the operation made less complicated and difficult. When done for glaucoma on one side it will be sufficient to attack one nerve, but when for epilepsy or for exophthalmic goitre the operation should be bilateral. When for epilepsy or glaucoma it is not so necessary to remove the lower cervical ganglion; this is indicated rather in those cases where it is desirable to control the accelerator nerves to the heart. The operation has given good results in all three affections named, yet it is one of considerable difficulty. It would be made extremely difficult by the presence of a large goitre, and in such case it would probably be better to extirpate the thyroid rather than to attack the nerve. (See Glaucoma, Epilepsy, and Exophthalmic Goitre.)
[621]
The term syringomyelia implies irregular dilatation of the central canal of the spinal cord, having a congenital origin, tending to relative increase later in life, with corresponding disturbance of function, the latter including paresthesiæ, loss of sensibility to heat and cold, more or less motor impairment and disturbances of nutrition, more noticeable in the region of the joints than elsewhere, the latter having been already considered in the chapter on the Joints. The dilatation is by no means regular, may occur in various regions of the cord, and attain a size permitting encroachment upon, and even atrophy of, the structures of the cord itself. When functional disturbance, especially paralytic, has become very pronounced a few surgeons have ventured to expose the cord by a laminectomy, and endeavored to make a more or less permanent opening with drainage of the dural cavity. Thus Keen has operated twice, Abbe once, and Munro three times, including twice on the same patient. Only in this last instance was any permanent relief obtained, and this was at the expense of a second operation. It is doubtful if any of the peculiar joint lesions of this disease will be in any way affected by operation for this purpose.
Tumors of the spinal cord may be classified as follows (Krauss):
1. Tumors springing primarily from the envelopes of the cord: (a) Tumors of the vertebral column, and (b) tumors of the meninges, the latter including those arising from the external surface of the dura, or from the periosteum of the spinal canal, i. e., extradural tumors, and those from the inner surface of the dura and the other membranes, that is, intradural tumors.
2. Tumors developing in the cord proper, intramedullary. These are generally gliomas and do not present so much the symptoms of cord tumors as of syringomyelia.
Vertebral tumors may be carcinoma (secondary), endothelioma, sarcoma, osteosarcoma, as well as the non-malignant and cartilaginous or osseous tumors, and parasitic cysts, i. e., echinococcus. The sarcomas are the most common of all.
—The symptoms of tumor of the spinal cord depend upon the part involved and differ according as it involves the cervical, thoracic, or lumbar portions or the cauda equina. They are to be classed as root symptoms and cord symptoms. Root symptoms include pain, paresthesia, and hyperesthesia. The pain is usually persistent, burning, and severe, affecting one side or the other, if the tumor be laterally placed, or both sides if central. The pain follows the distribution of the spinal roots rather than the course of the intercostal nerves, i. e., is more horizontal and less oblique. These pains persist and have the characteristic feature of not presenting painful points on pressure. They are commonly referred to the abdomen, and may thus give rise to serious mistakes in diagnosis, e. g., they have been regarded as due to hepatic colic, dry pleurisy, appendicitis, etc. Pain may assume the girdle character, which is usually accentuated by movement, and is frequently accompanied by herpes zoster. The greater the involvement of the posterior roots the more painful the condition. When the anterior sensory roots are involved pain may be wanting and the disturbance assume a type of paresthesia, with final anesthesia, in which case the patient would at first complain of numbness and prickling sensations. There is sometimes noted a zone of hyperesthesia on the proximal side of the anesthetic area, or this zone, if not hyperesthetic, may be replaced by a condition of uncertainty of sensation.
[622]
The cord symptoms are the reliable ones, varying according to the segment involved. The portions of the cord where lesions can be best localized are, for instance, the third to the fifth cervical, including the origin of the phrenic nerve; the fifth to the seventh cervical, where the posterior thoracic nerve comes off; the seventh to the eighth cervical and first thoracic segments, where originate the dilator nerves of the pupil. The upper border of the anesthetic area points to a lesion of the next or second higher spinal segment than the level really represents. The lowest level of the lesion corresponds to the highest level of the sensory disturbance. The level of the segment area of the skin of the back does not correspond to the level of the spinal segment involved, the latter being higher up. The point of greatest sensitiveness over the spine is in many cases a good guide to the segment involved, but is applicable only where the lesion is posteriorly placed. The absence of pain or tenderness along the spine means little or nothing, but their presence has great significance.
—The diagnosis of a cord tumor covers, according to Krauss, a first or subjective period, indicative of irritation along the posterior roots, and is characterized by pain and paresthesia. This is followed in time by a second or objective period which points to invasion of the spinal cord, characterized mainly by weakness and later by paralysis, with disturbed tendon reflexes. Diagnosis early is extremely difficult, for pain and disturbances of sensation are produced in many ways.
—The treatment of spinal-cord tumors is purely surgical and should be instituted promptly so soon as diagnosis has been made. Only in tumors of syphilitic origin will internal treatment be of any avail. The therapeutic test having been made, should it seem wise, and proved futile, the case should be regarded at once as surgical. According to Krauss’ statistics nearly 40 per cent. of all operated cases have resulted in recovery, while in 35 cases of sarcoma 8 have resulted in recovery and 6 in improvement. This is really a more gratifying statement than can be made with regard to brain tumors, and should be regarded as lending encouragement to surgical procedure.
The operative details will be discussed later in this chapter.
The remarks made concerning the surgical affections of and operations upon nerves contained in the previous chapter, pertaining to the cranial nerves, will apply equally well to the peripheral nervous system.
Constant pressure as well as contusions of nerves will cause more or less paralysis. The surgeon occasionally sees manifestations of this kind in the so-called “crutch paralysis,” due to pressure upon the brachial plexus by the use of crutches, and in another form so generally associated with administration of an anesthetic as to be called “ether paralysis.” It is another form of pressure paralysis due to indifference in letting the arm, for instance, hang over the edge of an operating table during anesthesia or operation. It does not call for operation so much as for electricity, massage, and similar measures. Extreme consequences of nerve and vessel injury are portrayed in Fig. 410.
Tumors of nerves are both benign and malignant, the former assuming the fibromatous type oftener than any other, and frequently involving more than one nerve trunk, attaining also considerable size and impairing or destroying function by pressure. In addition to the true fibroma of nerve sheaths we have the peculiar type of fibromas of nerve stumps seen after amputations, and the multiple neuromas, again largely of the fibromatous type, which involve many and in rare instances nearly all the peripheral nerves. Cases are on record where as many as 1600 small and large tumors have been found, strung like beads upon wires, along all the peripheral nerves throughout the body. Another variety of fibromas of nerves involves those of the skin and produces small painful subcutaneous nodules, although these may attain a considerable size. Within the past few years there has been a much better familiarity with that form of growth known as plexiform neuroma, in which entire nerve trunks are involved, so that they become elongated, thickened, and tortuous, and resemble a varicose condition of the veins. The plexiform neuromas are found in any part of the body; they produce little or no pain, but lead to disturbances of function, as well as to peculiar irregular swellings that may be mistaken for lymphangioma, and which are often accompanied[623] by pigmentation of and growth of hair upon the overlying skin. (See chapter on Tumors.)
For the various purposes already mentioned different nerve trunks and plexuses are made accessible for operation by the following methods.
—The brachial plexus is reached through an incision similar to that for ligation of the subclavian artery. After opening the deep fascia the nerves are sought and found behind the subclavian vein and lying around the artery. This plexus is stretched especially for the relief of choreiform spasm or painful nervous affections. The various nerves of the upper extremity, after leaving the brachial plexus, are made accessible to operations for grafting or suture as below. (See Fig 406.)
—The median nerve lies in front of the brachial artery and is exposed through an incision as if the artery were to be tied in its course. It may also be found on the inner side of the tendon of the palmaris longus, where it lies beneath the deep fascia.
—The ulnar nerve is reached through practically the same incision as the median, when it is sought in the middle of the arm, but is farther back. It lies near the surface, just behind the inner condyle, between it and the olecranon, and at the wrist it is on the radial side of the tendon of the flexor carpi ulnaris.
Fig. 410

Gangrene (mummification) of arm resulting from injury to nerves and vessels. (Preindlsberger.)
—The musculospiral nerve is found between the heads of the triceps, where it lies in the groove which winds obliquely around the humerus.
—The radial nerve lies to the outer side of the radial artery, three inches above the wrist. Should any of the nerves of the arm or forearm have been cut by an accident which has produced an incised wound they should be sought for in the wound if fresh, and in the neighborhood of the scar if older, and should be reunited by suture, as already described.
—In the lower extremity it is the great sciatic nerve which is usually made the subject of operation. An incision midway between the great trochanter and the tuberosity of the ischium, by which the lower border of the gluteus muscle is exposed, will enable the surgeon to identify the biceps, to divide the deep fascia, and find the sciatic nerve at the outer border of the muscle. It is sought for the purpose of nerve stretching, and it may be pulled completely out of the wound, while the entire weight of the limb may be suspended by it.
—The tibial nerves may be exposed through incisions identical with those indicated for ligation of the tibial arteries.
—The anterior crural nerve lies in Scarpa’s triangle, near Poupart’s ligament, on the outer side of the femoral artery.
Tetanus should be treated by injecting antitoxin into the main nerve trunks, as well[624] as into the spinal canal. The individual nerve trunks of the brachial plexus may be exposed in the upper arm, where the point of the hypodermic syringe needle may be inserted into their substance. The same expedient may be employed with the sciatic or anterior crural trunks, through the incisions just described. The same measures may be used in cocainizing the nerve trunks, as suggested by Crile and others, and described in the chapter on Alterations of Blood Pressure (p. 181).
Abbe has suggested to treat certain cases of inveterate neuralgia of the peripheral nerves by an intraspinal division of the posterior nerve roots.
There has been added to the standard operations on nerves another measure. This consists of grafting by means of foreign material; using a section of nerve trunk removed freshly from some animal, or inserting catgut loops between nerve ends which shall serve as trellises upon which the growing nerve tissue may arrange itself. Powers, of Denver, has, for instance, reported the implantation of four inches of the great sciatic nerve of a dog into the external popliteal of a man. The results seemed to be good so far as sensation was concerned, but negative as regards motion. Probably no method of nerve grafting will give so good results as the utilization of a part of the nerve itself to be operated upon, by partially detaching and turning back a portion of its central end and uniting it to a similar flap made from the other end. Various operators have made use of different materials for the purpose of forming a tube around the nerve ends, and thus excluding other tissues. For this purpose cargile membrane is perhaps as serviceable as any. When all other measures fail the method by long catgut sutures may be adopted.
A few of the nerve trunks may be displaced by injury in such a way that they are liable to subsequent redislocation. The condition is recognized by the mobility of the nerve trunk under the skin, by peculiar sensations when the trunk is irritated, and often by tingling sensations referred to its distribution. The condition is most common in connection with the ulnar nerve, just behind the inner condyle. Should nothing else give relief the trunk should be cut down upon and retained in place by suture or by fixation of other structures around it.
—Penetrating wounds of the spine occur both in military and in civil practice. Sometimes the vertebræ alone are injured; occasionally the spinal canal will be opened, with little injury to the bone, only the cartilage suffering. All such injuries are serious in proportion as the cord itself may be injured. Such injuries may be direct or indirect. Should a large vessel have been divided the cord may suffer from pressure of clot, and should this injury occur high in the spine, death may be caused by pressure. The severity of such an injury is generally estimated by phenomena pertaining to the nerve supply of parts below the wound. Should anything indicate partial or complete division of the cord, or that a single nerve trunk has been divided, then an operation is indicated for relief of symptoms, and for nerve or cord suture except in those instances where destruction seems to be too complete to warrant it.
—Gunshot injuries vary from small punctures and penetrating wounds to extensive laceration. The lower the injury the lower the mortality, other things being equal. Such injury to the cervical region generally proves quickly fatal. The symptoms here are not essentially different, save that the bullet may have done still more harm by passing beyond the cord, and that to the signs of a penetrating wound may be added those of a traumatic hemothorax or some other serious complication. It is necessary to distinguish between mere stiffness of the back and disinclination to use certain groups of muscles and absolute loss of motility. The former may indicate contusion and the latter severance or pressure. After some perforations cerebrospinal fluid will escape. In one instance I opened a spinal canal for perforating gunshot wound with complete paralysis, and found not only that the bullet had divided the cord but had passed through the vertebra into the lung beyond. A very curious phenomenon presented in this case is that when the passage was well opened air passed backward and forward through the spinal wound, the patient thus partly breathing through his back.
PLATE XLVI
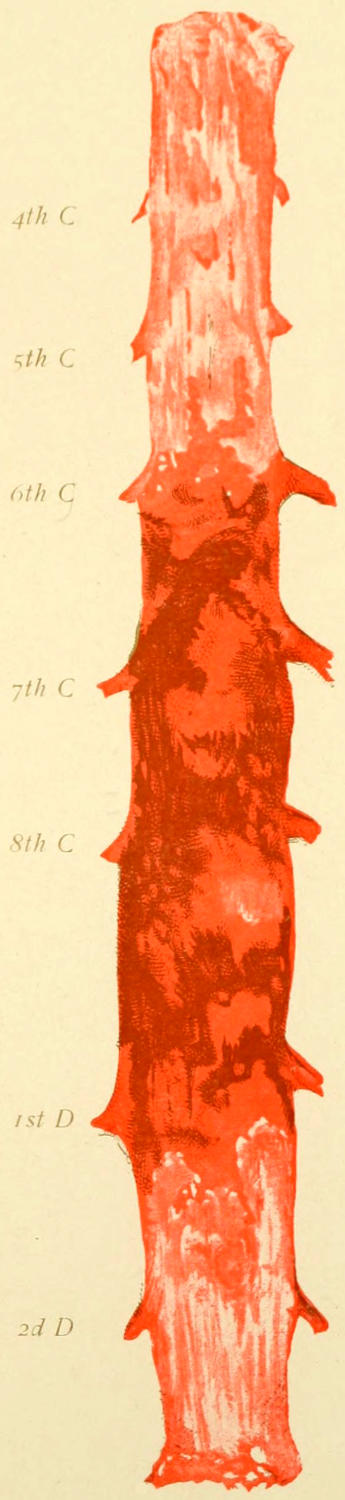
Intraspinal Hemorrhage, mostly Subdural, with Minute Subpial Ecchymoses.
[625]
The effect of pressure from hemorrhage is practically the same whether it be intradural or extradural, or occurring within the structure of the cord itself. The presence of blood in the spinal canal is known as hematorrhachis, and when occurring within the cord itself is termed hematomyelia. The typical symptoms of sensory and motor paralysis, which serious pressure upon the cord always produces, occur when produced by mere presence of fluid more slowly than when due to the introduction of a foreign body or to comminution of the bone. Diagnosis is then much facilitated if by the personal history it can be learned that there was an interval after the reception of the injury and before the occurrence of paralysis, during which the patient had reasonable use of the parts later paralyzed. This interval may be one of but a few minutes’ duration or may have extended over several hours.
When, on the other hand, such an interval lasting several days has been noted, then the intraspinal lesion must be either one of acute degeneration or of suppurative character. (See Plate XLVI.)
The question of operation in spinal hemorrhages will frequently be raised, and is to be decided in part by the intensity of the symptoms and in part by the character of the injury. Incomplete paralysis would indicate a lesser degree of pressure and justify a hope that the outpoured blood may be resorbed. This hope may be further encouraged should symptoms improve. On the other hand symptoms of complete paralysis, indicating serious and extensive pressure upon the cord, would justify a laminectomy, and make it even more encouraging than though it were done for a crushing injury. The more serious cases, then, of spinal hemorrhage would seem to justify exploration.
Until very recently it has been held that a complete cross-division of the spinal cord must necessarily be followed by a hopeless paralytic condition, plus the changes due to ascending degeneration of the upper segment. The results of laboratory experiments have made this quite plain, and therefore it was a startling innovation in surgery when Harte could report an experience contradicting all that we had learned to believe in this regard. In spite, then, of the fact that experimental suture of the cord after its division had not been successful in animals we are now confronted by three more or less successful cases reported by American surgeons, Estes, Harte, and Fowler, where the spinal cord was sutured after division, with at least partial recovery of function. In Harte’s case the operation was done three hours after injury; in Fowler’s case ten days had elapsed. Fowler used chromicized catgut sutures in the cord itself, with separate sutures of the dura with the same material, the principle here being the same as in nerve suture, and the effort being to do as little harm as possible with the needle and the suture material. After a simple division there is but little tension, and the ends of the cord are easily approximated.
It has thus been proved that there is at least some possibility of regeneration of the cord after such destructive lesions; but the cases which permit of or justify this measure will be rare, although it is gratifying to learn that there has been so much encouragement afforded by experiences reported.
Spina bifida is the result of a congenital defect in the construction of the spine with incomplete closure of the spinal canal. The defect lies in the posterior arches of the vertebræ; the bodies are rarely involved. For this reason these lesions are centrally placed, i. e., in the middle line. The essential feature of a spina bifida is protrusion of the spinal membranes, and they are, to all intents and purposes, spinal meningoceles. These tumors sometimes have only the thinnest of skin coverings; at other times they will be covered by considerable masses of overlying fat or fibrous tissue.
These congenital tumors when more definitely described should be classified as—
1. Meningocele, where there is simply a protrusion (hernia) of the dura, which may be lined with some branches of the vertebral nerves;
[626]
2. Meningomyelocele, where some portion of the spinal cord proper is included within the sac;
3. Syringomyelocele, where the central canal of the cord is dilated into a cyst of some size, over which the structures of the cord proper are more or less thinly spread out, the whole being covered with the spinal dura.
The first form is by far the simplest and most amenable to treatment. The other forms are much more serious, and the third form is hopeless so far as operative surgery is concerned.
The greater proportion of these cases occur in the lumbar region, at least 70 per cent. being met with in the lower region of the spine, including the sacrum. It occurs occasionally in the neck and in the mid-dorsal region.
Fig. 411 illustrates the general appearance of such a tumor. The opening of communication may be very small or may involve the arches of several vertebræ. So with the tumor itself, it may be small and almost imperceptible, or it may attain almost the size of a child’s head. The overlying skin is rarely absent; it is usually covered with a growth of hair, and its presence in the region of the spinous processes, coupled with the presence of any perceptible tumor, should cause suspicions of the so-called spina bifida occulta.
Fig. 411
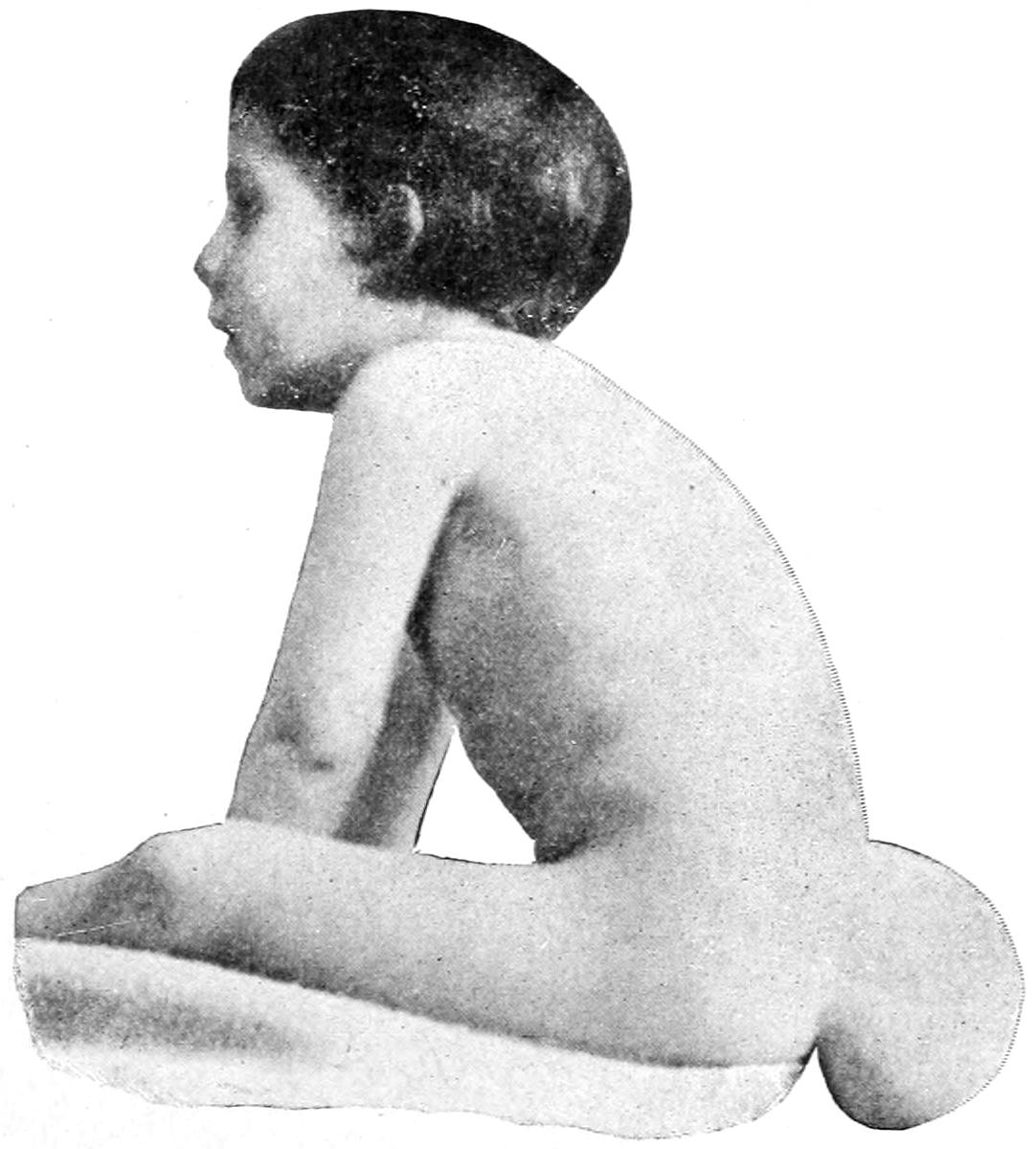
Spina bifida. (Bradford.)
These tumors are situated in the middle line or very near to it, and are compressible in proportion to the thinness of their coverings. When small they can be collapsed by pressure, the same not infrequently causing pressure symptoms, as the fluid is forced into the cranial cavity, such as coughing, vomiting, vertigo, etc. If the fluid can be easily expressed from the sac the opening may be regarded as relatively large. If pressure makes no alteration in the size of the growth the case should then be regarded as one where the small original communication has been closed by natural processes. Some of these tumors have more or less of a pedicle and others are broadly sessile. The tendency is ever toward increase in size, being rapid or slow according to the thickness of the protecting membranes and the size of the opening. While spontaneous occlusion may occur there is practically no spontaneous repair of the bony defect. The surgeon should beware of a tumor of congenital origin situated in or near the middle line, anywhere from the root of the nose, over the head, and down to the tip of the coccyx. Such a tumor should be regarded with suspicion until shown to be harmless. Many cases of spina bifida are accompanied by other congenital defects, such as club-foot, or hydrocephalus. Symptoms may or may not be present. When present they will be of the paralytic type and affect those parts of the body below the level of the growth. They are due to the involvement of the cord or the nerves. The ever-present danger in such cases is of rupture with escape of the contents, with its proportionate reduction of intraspinal pressure, and the possibilities of infection, with rapid death from meningitis. Inasmuch as some of these cysts have such thin walls that transillumination is possible it will be seen how great may be this danger.
—Treatment should be made to meet the indications. Only in cases which are deemed inoperable should some protection be relied upon and worn. This may be afforded by a common surgical dressing or by means of a plaster-of-Paris or waxed gauze. A molded shield may be prepared and so arranged upon a band or girdle as to protect the cyst from external harm. Efforts to reduce the size of the tumor[627] by pressure are futile and useless. The skin may be protected by covering with collodion.
The radical treatment of spina bifida should only be attempted in favorable cases, but in such instances can be made exceedingly satisfactory and successful. A tumor with a small pedicle may be treated by ligation, the skin being divided by elliptical incisions, the pedicle proper being surrounded by a chromicized or silk suture and the sac then excised. When the pedicle is too large to be treated in this way and yet not very large, it may be closed by sutures after removal of the sac, and dropped downward into the spinal opening, and the adjoining tissues made to close over it by buried and superficial sutures. It is the larger and more sessile sacs which give rise to the greatest difficulties. The attempt may be made to excise a greater portion of the sac, to fold in its edges and to approximate these with sutures of fine chromic catgut. The fold thus formed may be laid downward and upon the spinal groove, the aponeurotic and other firm fibrous tissues in the neighborhood being loosened sufficiently so that they may be brought together by buried sutures, and the balance of the wound closed. I have a number of times been able to introduce either strips of metal foil or thin pieces of celluloid, or, better still, ivory trimmed to fit the bony defect, and so arranged as to be sprung into grooves made on either side of the osseous canal. If ivory be used for this purpose the thin small sheets which are used by miniature painters should be procured.
Such operations should be made at the earliest practical moment; in infants especially, but probably with all young patients, the head being maintained at a much lower level than the sacrum in order that only the smallest quantity possible of the cerebrospinal fluid may escape. I have also used a small amount of weak cocaine solution after exposing the cord in the spinal canal, in order that reflex impressions may be avoided so far as possible and shock thus prevented. With a young patient the amount of cocaine to be thus used should not exceed more than 2 or 3 Mg.
Osteoplastic methods have also been devised for the purpose and may be practised in cases permitting them.
Many of these cases do not come to operation until the skin is excoriated or ulcerated. It is exceedingly difficult under these circumstances to make an aseptic operation. The subsequent difficulties of maintaining asepsis should also be foreseen, especially when lesions are located low in the spine and in little patients, as soiling from diapers and discharges is so easy. After such operations oiled silk, or gutta-percha tissue should be fastened around the pelvis by rubber cement, in such a way as to make a water-tight covering for the deep surgical dressings, and this line of junction should be scrutinized frequently. These operations often give satisfactory results.
Many congenital tumors are met with about the region of the sacrum and coccyx, some of which have the essential characteristics of meningocele, while others are rather of the dermoid or embryonal variety. Tumors of great size develop from the region of the coccyx, and many are of interest to the pathologist.
True dermoids often begin to develop within the pelvis and then escape therefrom in this vicinity, some of them containing soft epithelial products, others being dense and hard. (See Figs. 72 and 73, p. 266.)
Fig. 412
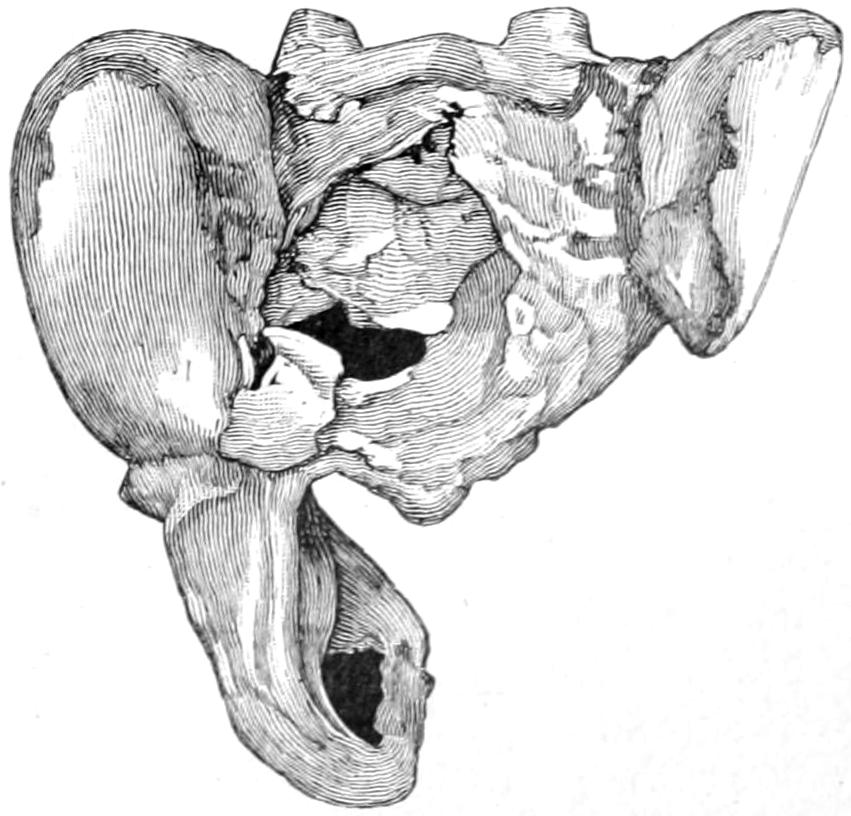
Sacral cyst, showing defect in sacrum. (Warren Museum.)
Every tumor of this general character and in this location should be removed as early as possible unless it can be determined that it is not only cystic but dangerously large. Of even these, however, it may be said that to leave them is to expose the patient to more danger of infection than is incurred during a legitimate surgical operation. There should be, then, about such a case serious complications and perplexities, which would tend to make a competent surgeon decline to operate (Fig. 412).
[628]
—In 1866 Erichsen published a series of lectures dealing with “Certain obscure injuries of the nervous system commonly met with as the result of shock received in collisions on railways.” In 1875 he expanded these lectures into his celebrated monograph on Concussion of the Spine, a work which served first to arouse the greatest interest in a hitherto neglected subject, and which has unfortunately served in later years as a basis for many a damage suit. The injuries described by him may occur as the result of railway accidents, hence the name often applied to the condition which they cause—railway spine. Cynical observers have noted the frequency with which these cases appear in court and have stigmatized the condition with the name litigation spine. Erichsen’s original work is now superseded by much better monographs, although his clinical descriptions were full and complete. Nevertheless he had no knowledge of minute changes in the nervous system and many of his explanations were based upon theories then prevalent but now abandoned.
These injuries involve the spine as a whole, and the spinal column is so firmly held together by powerful ligaments, and so abundantly protected by muscular and aponeurotic coverings, that its contents are exempt from injuries which would easily involve those of more exposed joints. An injury which would cause serious disintegration within the spinal cord must be so severe as to inflict other and well-marked damage upon the surrounding structures. Consequently a large part of the injury received consists in what may well be called strain and wrenching of all of these component structures. These may be accompanied by minute hemorrhages into the cord, with or without laceration, while exudates may result therefrom which may press upon the spinal nerve roots or cause adhesions within or without their sheaths, all of which may lead to signs and symptoms which may persist for a long time. But the theory to which too many have held in time past, that a mere concussion of these parts, without other injuries, can be followed by such extensive and durable lesions is not tenable.
Obviously these cases are of a character frequently to appear in court. Unfortunately the signs and symptoms are so vague, so variable, and the latter so subjective that opportunity is afforded for deception, opportunity of which both dishonest patients and dishonest lawyers too frequently avail themselves; this to an extent which has almost brought the condition into disrepute among the better class of practitioners and caused it to be in some sense neglected. That serious lesions do follow injuries to the back is undeniable; that many of the resulting conditions can be simulated is unfortunately too true.
Nervous demoralization and more or less chronic invalidism frequently follow these injuries, producing symptoms which are mainly functional and maybe grouped among the traumatic neuroses. These symptoms are mostly ill-defined, often contradictory, and accompanied by very few objective features.
If malingering can be excluded the best way to regard these clinical pictures is to consider them as indicating a traumatic neurosis—that is, a nervous disturbance, with perversion rather than abolition of function, comparable with similar conditions from other causes. As Angell has said, its symptomatology is largely built up of the emotional features, with such grotesque nervous disturbances as to be quite inconsistent with any true organic malady. In the latter there will always be definite indications with positive changes and normal reactions, while each segment of the spinal cord will have its own definite features. Quite the reverse is the case in a so-called railway spine, where paralyses are incomplete, where loss of sensibility fails to correspond with anatomical relations, where the reflexes are contradictory and the complaints out of all proportion to the injury received. Such a condition is, therefore, a psychosis or neurosis rather than a somatic disease. (Angell.) As a mental perversion it is often dependent upon the dominating influence of an imperative conception, which may or may not have an honest basis. Even if a patient be not tempted to malinger or simulate, his troubles may be exaggerated by expectant attention, which of itself has nothing to do with the injury, but rather with his mental attitude. This is a predominant feature of those cases which go to trial, and while it may persist after a settlement is reached, it should be admitted that the morbid condition usually subsides when litigation is terminated.
[629]
These imperative conceptions are intensified by emotion, fear, sympathy, or anxiety, while attention becomes more and more self-centred, the condition finally terminating in a more or less self-induced hypnotic state—a species of autosuggestion. Similar cases of non-traumatic origin are frequently observed, which are then called neurasthenia or hysteria. When in an individual already neurasthenic injury occurs it almost invariably produces exaggerated symptoms. To use Angell’s own expression: “Railway spine is a convenient and picturesque term which hypnotizes juries, even as shock has hypnotized patients. It is dramatic, but not accurate. The damage is not to the spine nor to the spinal cord, but to the mind. It is a psychical disorder, not a physical one, although it has a physical expression in its symptomatology.”
—Viewed in this light it will be seen that there is the greatest value attaching to physiological rest, beginning immediately after the injury and continuing until the subsidence of the symptoms. This should be combined with measures which improve elimination and nutrition. Confinement to bed or the room will reduce elimination, which should never be allowed to decrease in any way. Bodily and mental rest, combined with the above features, followed later by massage, cold spinal douche, electricity (either for its actual or suggestive value), and mental encouragement, constitute the principal methods of treatment. A case of this kind tinctured by a hope of securement of ultimate damages will be not only resistant but difficult of successful treatment.
The principal injuries to the spine proper to be considered here consist of:
Fig. 413

Fracture of body of the vertebra. (Warren Museum.)
Fig. 414

Crush of cord and its membranes. The result of a fracture of the spine. (Erichsen.)
The spinal column is so strongly put together and its bones so protected that fracture of any one of its component parts is inconceivable except as a result of violence. This may occur by objects falling upon it or by the body falling a distance, or from violent twisting or wrenching. These injuries constitute but a small percentage—about 3 per cent.—of all fractures. They occur more easily and commonly in the upper portion than in the lower, where the vertebræ are larger. As a result of their occupations adult males suffer much more frequently than women or children.
Diagnosis.
—The diagnosis of fracture of the vertebral column is rarely difficult. The disability produced is instantaneous if the cord itself be compressed. If the cord escape pressure there may be serious symptoms, but without paralysis. The most serious feature, then, of any fracture of the vertebræ is the amount of damage done to the cord proper. The so-called gunshot fractures of the spine have already been partially treated of above and in the chapter on Gunshot Wounds. They constitute a somewhat different class of lesions, but have, in common with those above alluded to, the actual fracturing of the bone and the question of damage to the cord. In most respects they may be considered with the non-penetrating injuries. Fractures of the spine, therefore, may be divided into (a) fractures with injury of the cord, and (b) fractures without such injury. In many cases it is difficult to state whether the cord is crushed or simply more or less compressed by bone, fluid, or exudate, until the spinal canal has been opened and explored.
When the cord is totally destroyed there will be total loss of reflexes, with motor and sensory paralysis complete. (See Fig. 413.)
In some instances there is visible or palpable deformity. This is by no means necessarily the case. It is more likely to be noted in the upper portion of the column, where the vertebral spines are more easily palpated. If sufficient time have elapsed there will often be ecchymosis. The principal feature, however, of spinal fractures is the paralysis, which results in most instances as above. Its careful study is requisite both for minute[630] diagnosis and localization of the injury. Paralysis, then, whether of motion or of sensation, along with the condition of the reflexes, deserves careful consideration in each instance. It is of the greatest importance, because by it, rather than by other causes, death is brought about in the majority of cases which outlive the first twenty-four hours after injury. Even injury low down, which causes paraplegia with loss of control of the bowels and bladder, may terminate fatally in time, through an ascending infection of the urinary passages, which may finally lead to pyelonephritis and death. This has often occurred as the result of inattention to precautions in the use of the catheter, and to carelessness on the part of the patient. Death, then, may be caused by roundabout methods of infection which have only accidental connection with the original injury. Other cases die of septic infection in consequence of lack of proper attention to bed-sores. Again, with cord involvement high up in the dorsal region there is very likely to occur a rapid ascending degeneration, by which, one after another, the roots of the phrenic nerves are involved in their order from below upward, until finally the patient dies of asphyxia from paralysis of all the respiratory apparatus (Fig. 414).
Aside from such evidences as actual displacement of the vertebral spines may afford the localizing diagnosis is made mainly by a study of the paralysis. In regard to this paralysis it should be remembered how it is produced from the very nature of the injury itself. That occurring within from a few minutes to a few hours after the injury is due to hemorrhage; that which occurs still more slowly is due to exudate or the presence of pus; while a late paralysis may result from poliomyelitis. The first form of paralysis may be produced by hemorrhage either within the central canal (hematomyelia) or hemorrhage within the membranes or structure of the cord itself (hematorrhachis).
There is another form of paralysis due to embolism which, however, has but little to do with the ordinary injuries. The following table, inserted by the courtesy of Dr. Dennis, will assist in localizing the lesion by a study of these paralyses and reflexes due to spinal injury:
Paralyses and Reflexes due to Spinal Injury.
| Spinal Nerve. |
Motor Paralysis. | Anesthesia. | Reflexes. | |||
|---|---|---|---|---|---|---|
| Cervical. | - | 1. | Death from pressure of odontoid. | |||
| 2-3. | Death from paralysis of diaphragm. | |||||
| 4. | Deltoid muscles of upper arm. | Upper shoulder, outer arm. | Pupil. | |||
| 5. | Supinators of hand. | Outside of arm and forearm. | Pupil, scapular, supinator, triceps. | |||
| 6. | Biceps, triceps, extensors of wrist. | Outer half of hand. | Pupil, scapular, triceps, post. wrist. | |||
| 7. | Pronators of wrist, latissimus dorsi. | Inner side of arm and forearm. | Pupil, scapular, post. wrist, ant. wrist, palmar. | |||
| 8. | Flexors of wrist, hand, muscles. | Inner side of hand. | Scapular, post, wrist, ant. wrist, palmar. | |||
| Dorsal. | - | 1. | Thumb.[631] | Ulnar supply to hand. | Scapular, palmar. | |
| 2-12. | Muscles to back and abdomen. | Skin over the back and abdomen in areas corresponding to distribution of spinal nerves. | Epigastric, 4-7; abdominal, 7-11. | |||
| Lumbar. | - | 1. | Psoas and sartorius. | Groin. | Cremasteric. | |
| 2. | Quadriceps extensor femoris. | Outside of thigh. | Cremasteric, patellar. | |||
| 3. | Abductors and inner rotators of thigh. | Front and inside of thigh. | Cremasteric. | |||
| 4. | Adductors of thigh, tibialis anticus. | Inside of leg, ankle, and foot. | Gluteal. | |||
| 5. | Outward rotators of thigh, flexors of knee and ankle. | Back of thigh and leg; outside of foot. | Gluteal. | |||
| Sacral. | - | 1-2. | Muscles of foot, peronei. | Outside of leg. | Plantar. | |
| 3-5. | Perineal muscles. | Perineum, anus, sacrum, genitals. | Ankle clonus. | |||
Injuries low in the lumbar segments cause incontinence of urine and feces because of the location of the centres for the rectum and bladder at this level. Injuries higher up cause retention by paralyzing the expulsive muscles of the abdomen. The reflexes which most interest the surgeon and which are of importance to him in diagnosticating these and other traumatic conditions are the following, with their method of detection (Bradford):
| Pupillary: | Dilatation produced by pinching side of neck. |
| Scapular: | Scratching skin over scapula causes muscles to contract. |
| Supinator: | Tapping tendon at wrist causes flexion of arm. |
| Triceps: | Tapping tendon at elbow causes extension of arm. |
| Posterior wrist: | Tapping tendons causes extension of hand. |
| Anterior wrist: | Tapping tendons causes flexion of wrist. |
| Palmar: | Scratching palm causes flexion of fingers. |
| Epigastric: | Stroking mammæ causes retraction of epigastrium. |
| Abdominal: | Stroking abdomen causes retraction. |
| Cremasteric: | Stroking inner side of thigh causes retraction of scrotum. |
| Patellar: | Striking patellar tendon causes extension of leg. |
| Gluteal: | Stroking buttock causes dimpling in gluteal fold. |
| Plantar: | Stroking sole of foot causes flexion and retraction of leg. |
| Ankle clonus: | Forcible extension causes rhythmical flexion. |
Much will depend upon the minute character of the injury, its location, and the amount of displacement of fragments. Fracture of a spinous process causes irregularity of the tips of the spines, with frequently the displacement of a fragment which may be moved beneath the skin, with or without crepitus. Fracture of one or both laminæ will permit mobility of the spinous process, with perhaps displacement. It is difficult to elicit crepitus. The neural arch may thus be broken without serious involvement of the body of a vertebra. On the other hand, the body itself may be fragmented, compressed out of shape, or so loosened as to permit of easy displacement.
A limited proportion of serious and paralyzing injuries to the spine consists of dislocation of some of its component parts without fractures. These may be considered as pure types of dislocation, but they constitute less than one-fourth of such cases. In a large proportion of these spinal injuries the actual lesion consists of the combination of fracture with the displacement which it permits. Such conditions are referred to as fracture dislocations. Unilateral dislocation in the cervical region produces a distortion of the neck simulating wryneck, the face being turned to the opposite side. Except in very fat individuals irregularity will be perceived in the line of the cervical spines.[632] When high up dyspnea is a constant feature. Traumatic dislocations are sharply differentiated, so far as the treatment is concerned, from those of slow production as the result of cervical spondylitis. In the acute cases the muscles are spasmodically contracted on the dislocated side. Irregularity of contour may be detected with the finger in the pharynx.
Fig. 415
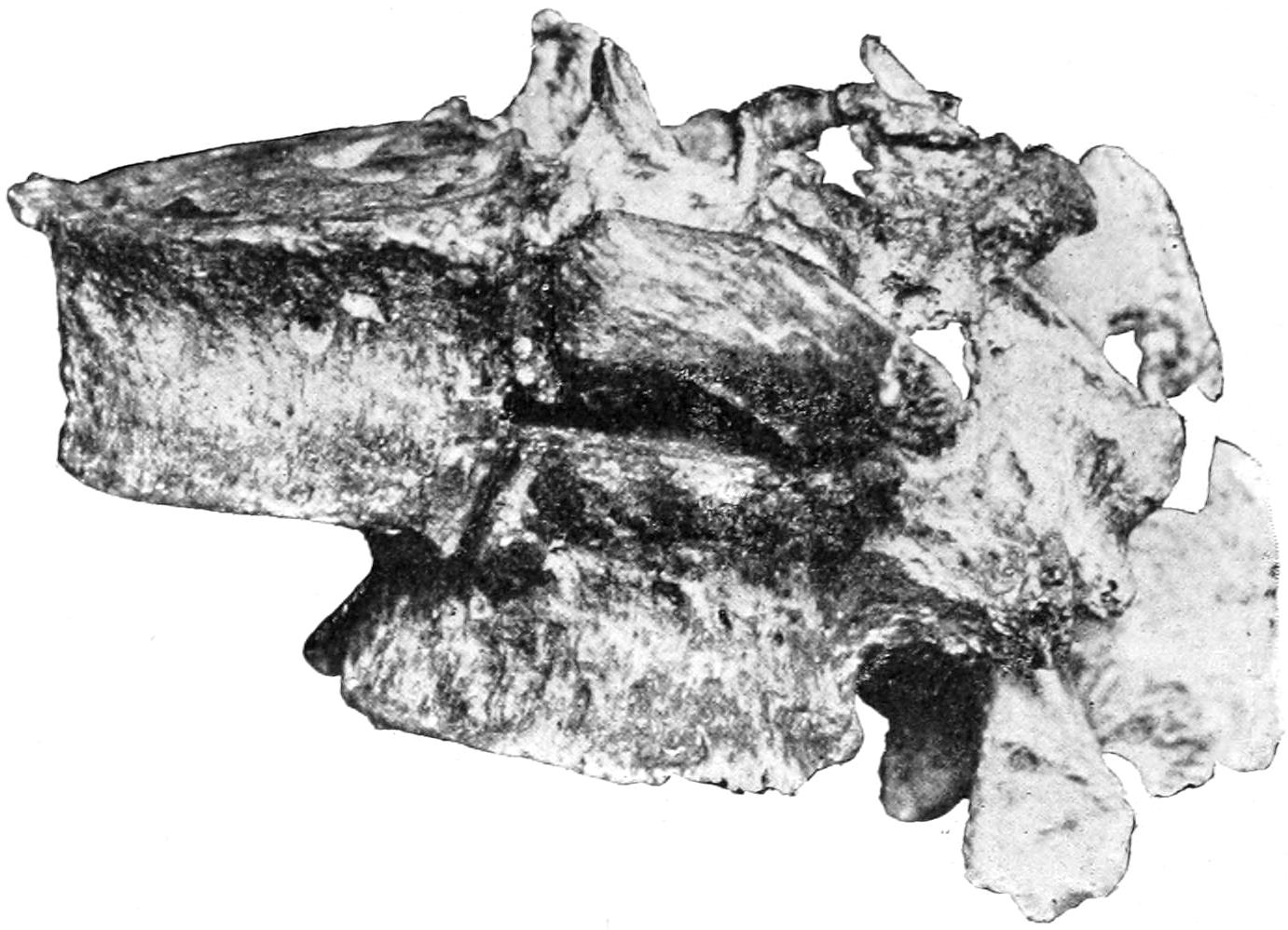
Fracture dislocation with great displacement—patient almost completely recovered. (Buffalo Museum.)
In the lower portions of the spine, which are both larger and more protracted, are more frequent combinations of both injuries and fewer instances of the single type of either. Except in the cervical region it is exceedingly difficult to distinguish between these lesions, for the question of operation or no operation is decided by other and more conspicuous features (Figs. 416 and 417).
Fig. 416
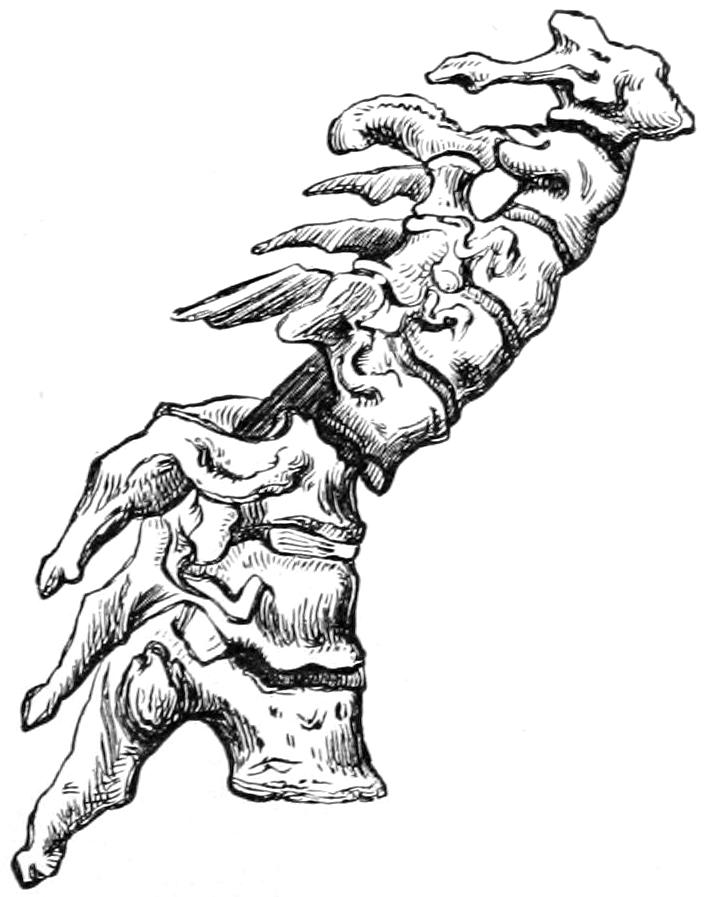
Dislocation between the fifth and sixth cervical vertebræ. (Erichsen.)
Fig. 417
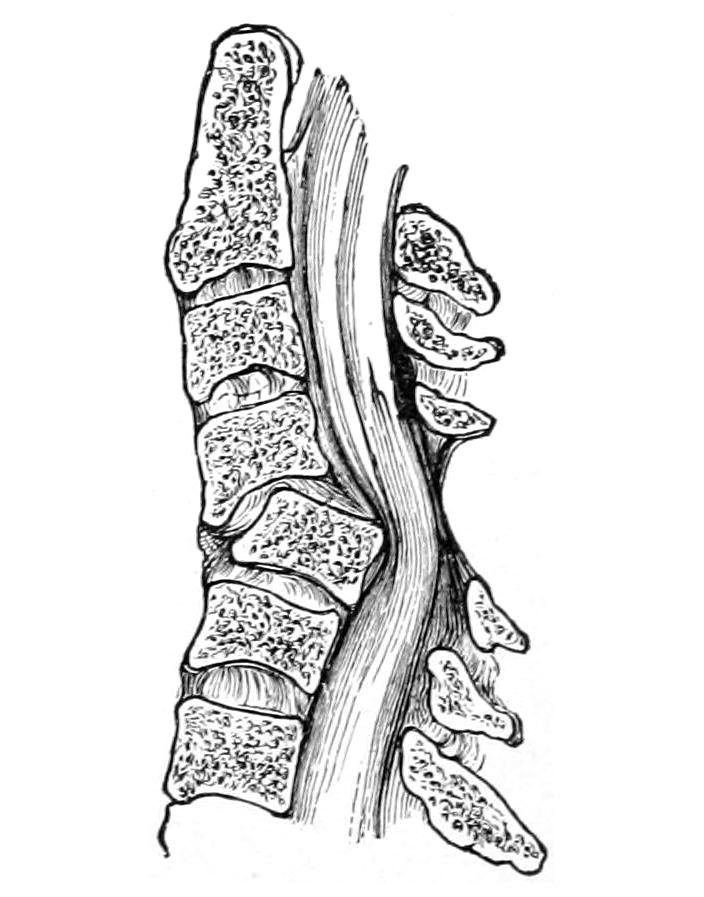
Dislocation of the spine forward (Bryant.)
Treatment.
—The injury having been localized, so far as deformity and careful study of its paralytic features will permit, the questions of prognosis and treatment become insistent. In the pure type of dislocation the prognosis will depend, first, upon whether reduction can be accomplished, and, secondly, upon the amount of damage suffered by the cord previous to such reduction. Every injury of the cervical spine is of most serious import because of the possible damage to the phrenic nerves. Rapidly ascending changes may terminate life in two or three days even though reduction be[633] accomplished. The injuries to the lower part of the spinal column which produce paraplegia threaten life much less directly, but too frequently terminate fatally after the lapse of weeks or months, as the result of infections from spreading bed-sores, or infections through the urinary tract permitted by the constant necessity for and carelessness in the use of the catheter. The prognosis, then, in almost every case of these severe spinal injuries is unfavorable, at least if it be let alone (Fig. 415).
It becomes, then, a question of what can be done to improve the local conditions. Certain cases of cervical spinal dislocation have been reduced by forcible traction upon the head, assisted by rotation and manipulation with the hands in the direction indicated by the displacement of the patient’s head, as well as by such indications as may be secured in the pharynx. A considerable degree of traction may be necessary in this effort, and there is the possibility not only of failure but even of serious harm, and perhaps immediate death, since a fragment loosened may be made to produce promptly fatal pressure upon the cord. Such a measure, then, should be undertaken with the greatest care, and not without a complete understanding with those interested regarding its dangers (Fig. 418).
Fig. 418
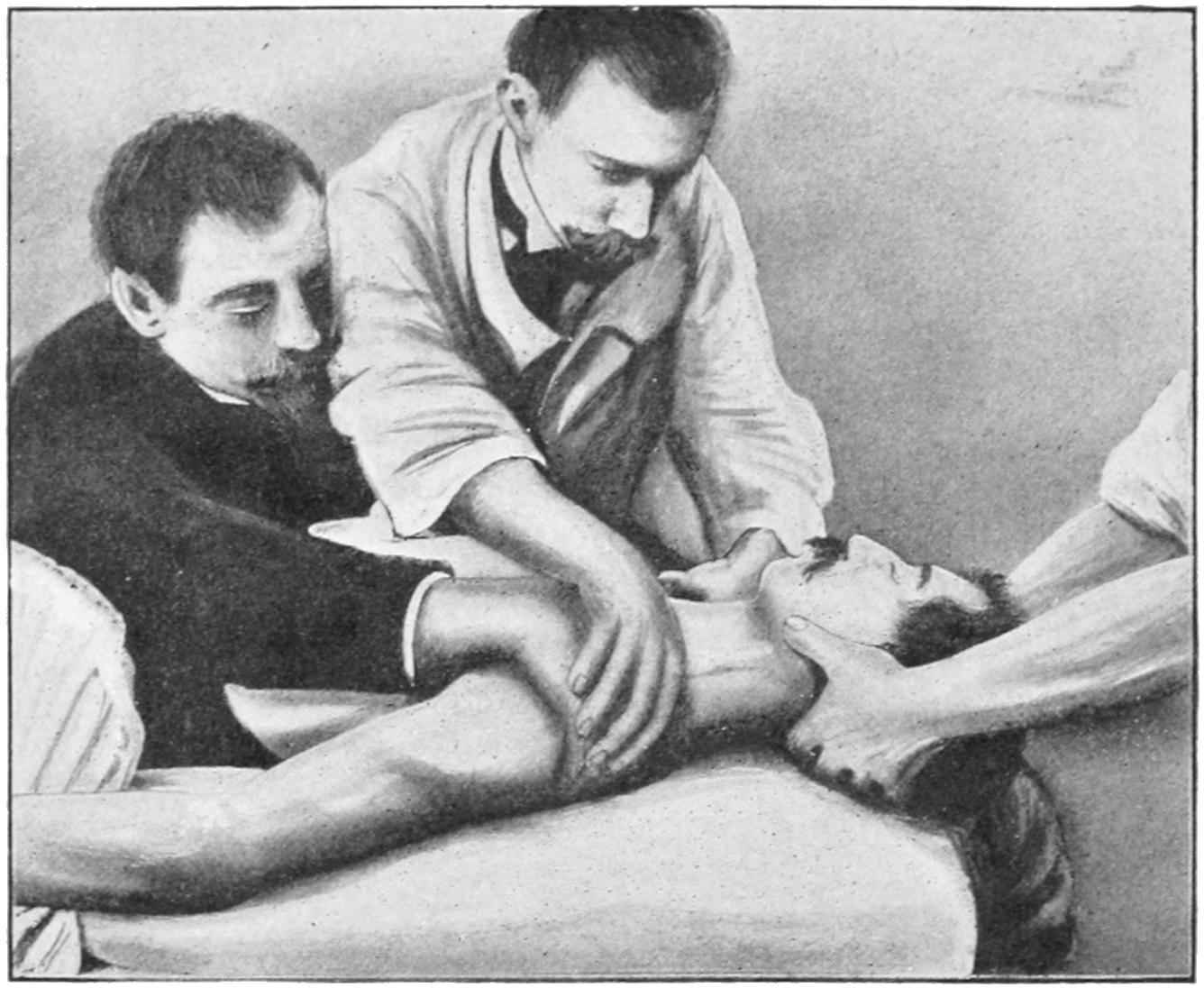
Method of reducing dislocations of the cervical vertebræ by manipulation. (Lejars.)
In most cases it is impossible from the exterior to estimate either the damage to the cord or the amount of fluid outpour until the spinal canal be opened. If there be complete loss of reflexes, with absolute insensibility and motor paralysis, then complete transverse destruction of the cord may be inferred. In these instances it may be decided not to operate. On the other hand it may be felt that unless the damage appear irremediable an open operation for inspection and relief should be performed at the earliest possible moment, since pressure on the cord allowed to persist even for a few hours causes damage for which there is no compensation. These cases may then be viewed in this light—if left to themselves they are almost hopeless. It therefore is a question simply of what can be accomplished by operation. On one hand the patient’s condition may be materially improved; on the other it is scarcely possible to make him worse. The dangers of such operations inhere especially in the anesthetic and in the possible introduction of sepsis; not that the operation itself cannot be properly conducted, but that it is often difficult to keep these cases free from contamination during the subsequent course of events. To operate through bruised or infected skin would probably be fatal. These operations, then, are begun as explorations intended to reveal deep conditions. When one has freed the spinal cord from pressure and has removed the products of hemorrhage he has done nearly all that can be accomplished in such a case.
[634]
Until recently it has been supposed that complete transverse division or crushing of the cord was necessarily hopeless and fatal. As previously mentioned, Estes, Harte, and Fowler have reported instances of complete division of the cord, with subsequent approximation by suture and with at least partial restoration of function, that have lent an element of hope to cases previously regarded as hopeless.
For my own part, although I regard these cases as discouraging, I do not feel like withholding from patients the only possibility of improvement which can be offered them, but I am more and more impressed with the necessity for prompt intervention if this benefit is to be obtained. To wait a few days, then, until it has been made evident that nothing can be done, save by operation, or until a tardy consent is obtained, is to rob the patient of the hope which it may afford. The operative treatment should be begun immediately after the diagnosis is made, providing that this be promptly done. Delay is more than inexpedient—it is absolutely dangerous. As Burrell has pointed out it is scarcely fair to decide upon a course of treatment from a study of statistics alone, as lesions vary within widest limits, as do also results of individual operators. Let each case, then, be decided upon its merits, but let whatever is done be done promptly. If there be excuse for delay it is in those cases where paralysis is incomplete and where the cord apparently has not been seriously compromised. But these would afford the most promising results after operation.
The operation itself will be described at the conclusion of this section, and in connection with other operations practised for exposure of the cord when involved in other lesions.
These occur, as do hemorrhages within the cranial cavity, with or without serious other lesions of the investing structures. They are expressions, of course, of transmitted violence, depending so far as known essentially upon injury, whether the hemorrhage occurs within the central canal of the cord, within its structure, or within the subdural or even extradural spaces. Everywhere within these regions bloodvessels abound, from which may occur sufficient outpour of blood to make pressure upon the cord to a degree producing complete paralysis. The duration of time between reception of injury and the occurrence of diagnostic paralysis will be to some degree a measure of the rapidity of such outpour, while a study of the paralyses themselves will permit of localizing the injury. The symptoms consist mainly of pain in the spine radiating to some distance, often referred to the distribution of the nerves most involved. This pain is often associated with muscular spasm, while paralysis may be a very early or somewhat tardy symptom.
Treatment.
—Once the fact of pressure upon the cord is established these cases come under practically the same rule as above. While there is a possibility that a moderate amount of bloody outpour might be absorbed there is nearly as much danger of its organization and of permanent involvement of the cord. In fact there is more reason for operating in cases of spinal hemorrhage than in cases of fracture, since it may be possible to thereby accomplish more.
The non-operative treatment of fractures or dislocations consists mainly in external support, preferably by a plaster-of-Paris corset properly applied, and by maintaining elimination and nutrition, while affording physiological rest for a sufficient length of time. These cases will need massage and electricity, i. e., stimulation of the compromised muscles, and extreme care should be given to the prevention of bed-sores, to which they are peculiarly liable. Every precaution should be taken also against any possible retention of urine or feces. The incontinence of an overdistended bladder should not be mistaken for that of paralysis of its sphincter apparatus. The specimen of dislocation from which Fig. 415 was taken was removed from a patient who almost completely recovered from the effects of the injury, but who became careless about the condition of his bladder and who suffered an ascending urinary infection that terminated his life.
Of these cases it may also be said, then, that a much better prospect of exact diagnosis and atonement for harm done is afforded by exploration, since as between compression of the cord by clot or by bone there is little essential difference.
[635]
The subjoined table may afford assistance in the diagnosis of the injuries above considered:
Differential Diagnosis of Diseases and Injuries of the Spine and Spinal Cord.
| Fracture. | Dislocation. | Hematomyelia. | Hematorrhachis. | Acute Poliomyelitis. |
|
|---|---|---|---|---|---|
| Onset. | Immediate. | Immediate. | Immediate. | Progressive. | Slow. |
| Anesthesia. | Immediate. | Immediate. | Immediate. | Incomplete. | Absent. |
| Paralysis. (Is of hemiplegic type when compression is unilateral, paraplegic when bilateral, and local when single nerve roots are involved.) | Hemiplegia or paraplegia. | Hemiplegia. In partial dislocation may be absent. | Paraplegia. | Hemiplegia or paraplegia. | Paraplegia. |
| Deformity. | Usually present. | Present. | Absent. | Absent. | Absent. |
| Temperature. | Rises after second or third day. | Same. | Same. | Same. | Precedes the paralysis of degeneration. |
| Bowels and Bladder. | Paralyzed. | Paralysis usual. | Same. | Affected late if at all. | No paralysis. |
In the neighborhood of the coccyx, usually below its tip, between it and the anus, sometimes above the tip, a small depression or sinus mouth is occasionally seen. This is usually known as the pilonidal sinus. It is the persistent remnant of the original fetal termination of the spinal canal. It varies in size from a mere dimple to a cul-de-sac, in which sebaceous matter, with any other epithelial products, hair, etc., as well as foreign material and dirt from the skin, may collect and excite suppuration. In this way an abscess of considerable size may form. Sometimes its contents will be found to be principally hair; hence the name pilonidal. Frequently this sinus can be traced down to the periosteum and into the remains of the original neurenteric canal. When it is distended so as to give trouble it needs only to be freely incised and thoroughly cleaned.
In the region of the coccyx and lower part of the sacrum there appear tumors of congenital origin which are often present at birth or may not develop until later. These assume various sizes and aspects, varying from mere protuberances to large pendulous tumors. While covered with integument their internal structure varies within wide limits, and they are usually made of such a mixture of embryonal elements as to entitle them to be considered true teratoma. Even organized tissues or rudimentary organs may be found therein. They are rare and constitute practically surgical curiosities. Such a tumor, if troublesome, calls for removal, which should be accomplished with the strictest precautions, as the spinal canal may perhaps be opened during the procedure and most inflammable tissue thus exposed to infection from the perineum.
The sacrum, like the coccyx, is also the site of numerous congenital cysts and tumors which may appear posteriorly or anteriorly. Occasionally they form within the bone itself. Cysts that connect with the spinal canal will be found filled with cerebrospinal fluid, and some of them are essentially spina bifida occulta. The sacral region is also the site of predilection for those teratomas which consist in whole or in part of vestiges of an attached fetus. The advisability of operation must be determined for itself in each of these cases. (See Fig. 412, p. 627.)
[636]
Under this name are included severe and chronic neuralgias of the coccygeal region, including its joint, which occur most often in women, and usually as the result of contusion or direct injury. Occasionally it results from an injury inflicted during parturition. It gives rise to a degree of pain and tenderness which sometimes is almost disabling. Because of the insertion of the levator ani into the tip of the coccyx defecation may become distressing, to an extent which leads to fecal impaction in the rectum from postponement of evacuation as long as possible. The symptoms are subjective, but the tenderness is frequently exquisite.
In regard to treatment subcutaneous division of the tissues around the bone may afford relief, but in most instances, particularly those of traumatic origin, an excision of the coccyx will afford the only cure. (See below.)
These are included under the general heading laminectomy, which is used in a comprehensive sense, as is also the term trephining.
In a general way the measure is about as follows: Through a long median incision over the spines of the region where the lesion is localized their tips are exposed, while the muscle groups on either side and posterior to the laminæ are separated by the knife and by retractors. Dense fibrous bands may be nicked. In this way the posterior aspect of the neural arches is exposed to the desired length. The exposed spines should be removed by cutting them off at their bases with bone forceps, although they may be left and later removed with the posterior bony arches. To clear them away, however, affords a better view of the field of operation. The ligamenta subflava are then divided transversely at their upper and lower margins, after which, either with cutting forceps, saw, or chisel, the laminæ are divided on either side, and the section which is loosened pried out from the bed in which it rests. More or less fatty tissue will be found outside of the dura and in this tissue veins, sometimes of considerable size, freely ramify. These may be seized and divided, those of considerable size being tied. Great care should be given during the procedure to avoid perforation of the spinal membranes by the points of the instruments used. The cutting forceps are preferable to the saw or chisel, except for work in the lower lumbar region, where the parts are stout and strong. Especially in case of fracture, and at the upper end of the spine particularly, care should be given, with the force used, that no loose fragment be so handled as to increase the damage already done to the cord.
The dura being thus exposed and the blood cleared away, inspection may or may not reveal the nature of the lesion. A probe, gently handled, passed upward and downward into the canal, will reveal whether the cause of the pressure has been cleared away or not. According to the nature of the lesion it can then be decided whether to open the dura. To open it is to pave the way for fatal infection, unless the strictest aseptic technique has prevailed. On the other hand, to leave it unopened is to fail to appreciate the actual condition of the cord and to leave an important matter still undetermined. The dura if opened should be closed by suture.
Reference has already been made, in three cases now on record, to suture of the cord as a whole. Such sutures may be applied, if necessary, in a manner to do the least possible damage to the structures of the cord. If cerebrospinal fluid escape too freely the patient may be operated in a position with the head lower than the trunk, avoiding leakage.
Osteoplastic methods of temporary resection of the posterior arches of the vertebræ have been devised and practised, but they offer no particular advantages, and are attended by disadvantages which have caused them to be almost abandoned, save in rare instances and by individuals of large experience. (See Plate XLVII.)
In regard to wiring fragments of a fracture or displaced spine, Hadra, of Texas, was perhaps the first to carry out the measure. It comprises simply the fixation of fragments by wire sutures or ligatures which bind them together after they have been replaced through a more or less open wound, such as is included in the term laminectomy. But resort to wire is to be left to the judgment of the operator and the needs of the case. There is no reason, however, why it may not be used here, as in other fractures which are thus made compound, if there would seem to be prospect of benefit attaching to its use.
PLATE XLVII
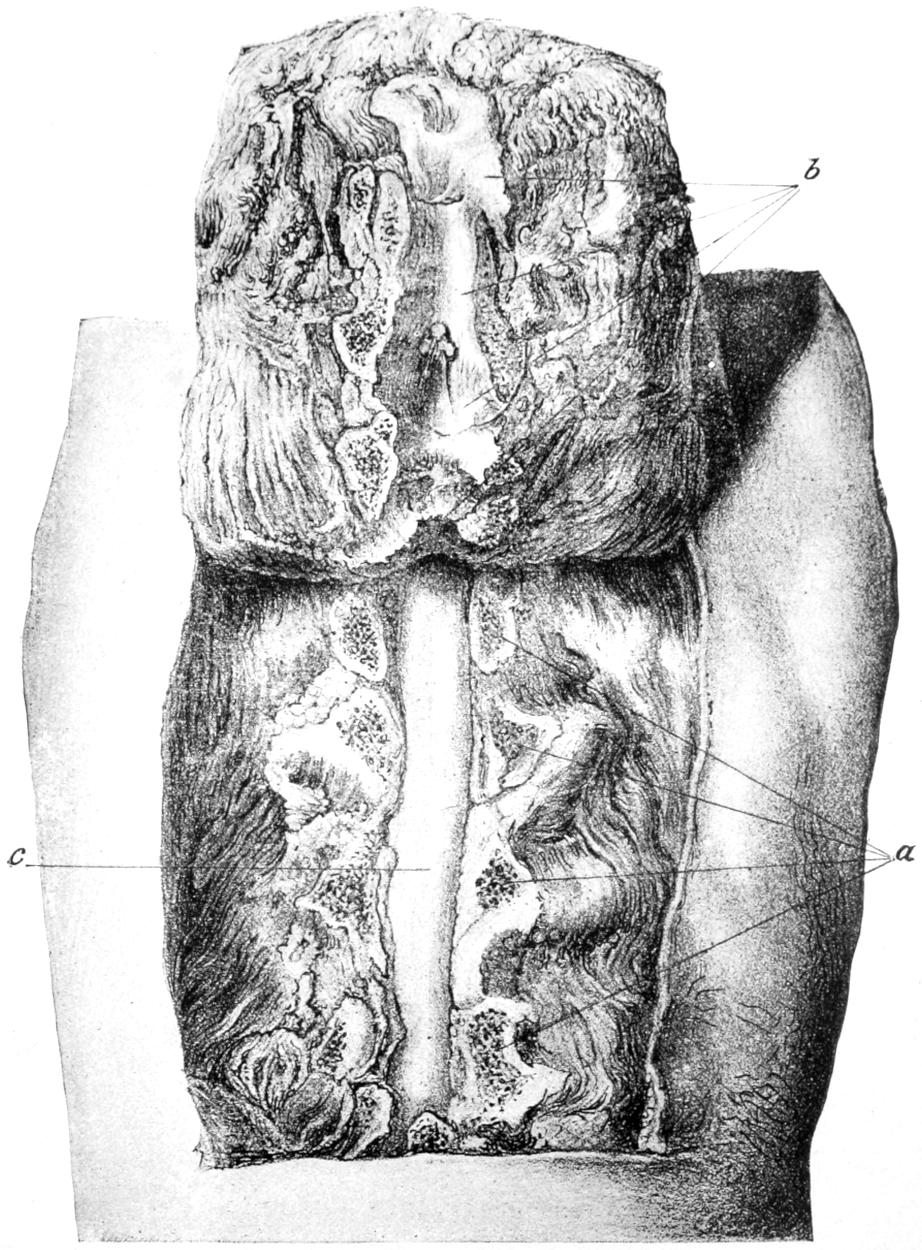
Osteoplastic Resection of Posterior Vertebral Arches. (Urban.)
[637]
Laminectomy is practised also in Pott’s disease, with the hope of relieving pressure upon the cord, due to the deformity or to the presence of tuberculous foci. It is possible that in some of these cases an incomplete operation will serve the purpose. Sufficient should be done, however, to relieve pressure if such a measure be indicated.
When laminectomy is practised for the purpose of attacking a tumor of the spinal cord the exposure of the cord should be followed by the removal of the tumor. Some of these are so placed as to make the procedure simple, while at other times it will be exceedingly difficult, if not impracticable. If the growth has so extended as to involve the bones themselves, then the measure will be futile and should be abandoned; but an isolated tumor, either within or without the dural space, in or on the substance of the cord, can usually be removed by a process of blunt dissection. Sometimes the small wounds thus made will ooze considerably and hemorrhage may prove troublesome; it should be checked before the parts above it are closed. Pressure forceps and ligatures and the occasional use of adrenalin solution will afford the necessary means for combating bleeding.
For nearly all of these operations upon the spine the chisel and the cutting forceps will suffice. Some operators, however, prefer a small saw, like that suggested by Doyen, which has a guard that can be so set as to determine the depth to which the instrument may pass. No matter what instrument be used, great care should be taken lest it pass through and beyond the bone in such a way as to lacerate the dura or the plexus of veins outside of it.
The sacrum is rarely attacked except in connection with some of those tumors already described.
The coccyx is easily removed through a median incision, the parts around it being entirely separated and the bone thus freed removed at the joint with stout scissors or cutting forceps. The instruments used should be kept in contact with the bone and not allowed to injure the veins between it and the rectum. Such a wound should not be closed completely, as a cavity always remains, which it is better to pack and permit to heal by granulation. (See Coccodynia.)
[638]
Monsters are born with almost complete absence of the face, which is called aprosopia. They have also been observed with double faces. Again a condition of congenital hypertrophy is known involving one or both sides. On the other hand congenital atrophy is also occasionally noted, affecting one or both sides. The former is likely to be of syphilitic origin (hereditary), in which case it will be accompanied by other indications such as corneal opacity, irregularity of teeth, or other evidences of its luetic origin.
Among the most interesting congenital defects are those connected with imperfectly closed branchial fistulas and the various outgrowths therefrom. These may lead to fissures extending from the ear to the mouth. Fibrocartilaginous growths occur along the regions of the original branchial clefts, either as tags of skin upon the face or so-called supernumerary auricles or auricular appendages. While these are covered with skin they usually contain a cartilaginous nucleus. They are most common in front of or on the tragus. They may be single, multiple, or symmetrical. They sometimes increase in size and at others remain stationary.
Fissures are seen more often upon the central portions of the face, especially in the nose or between it and the cheek. About the root of the nose and the orbit dermoids are somewhat common. They may be connected with fissures or fistulas, and extend upward and involve the dura.
Absence of the mouth is known as astomia, and of the lips as acheilia. These malformations are exceedingly rare. Atresia, or narrowing of the mouth, is more common. While the lips and mouth may be apparently well formed there may be imperfections. These conditions of narrowing call for division on each side and union of skin to mucous membrane. Fistulas of the lip are extremely rare, but are found occasionally, especially opening upon the lower lip. Branchial fistulas opening upon the lips have also been observed.
A condition of arrest of development of one or both jaws leads to unnatural smallness of the mouth known as microstoma. The opposite condition, macrostoma, is produced usually by fissure of the cheek on one or both sides, extending upward and backward from the labial junction and due to incomplete closure of a branchial cleft. The most common congenital defect of the lip known as hare-lip is a median fissure involving the upper lip. This occurs in all degrees, from a trifling notch at the vermilion border to a hideous defect, in which, through a wide cleft, projects a relatively overdeveloped intermaxillary bone, with a small downward projection of skin, known surgically as the philtrum. This defect may involve much more than the lip alone, for there may be failure to unite, along the median line between the lip and the uvula, of those portions of the superior maxillary which should develop symmetrically, and coalesce as they are formed from the rudimentary maxillary processes. Any portion, then, of the hard or soft tissues may show failure to unite in the middle line.
Hypertrophy of a lip is known as macrocheilia. It is not uncommon in strumous subjects. Another form is known as mucous ectropion. (See p. 373.)
The chin may be malformed in the direction either of atrophy or the reverse, as in the so-called double chin. A deviation forward, known as galoche chin, is also recognized. A peculiar malformation, consisting of the implantation of a supernumerary inferior maxilla by its own symphysis upon that of the subject, is known as hypognathy. Such a tumor will occasionally develop to considerable size, with cystic degeneration or other irregular changes.
Aside from the common forms of hare-lip most of the congenital defects that occur about the face are to be explained through incomplete closure of the branchial clefts[639] or the development of dermoid cysts and tumors therefrom. Deviations rather than defects appear more commonly about the nose than anywhere else. They produce disfigurements known as pug-nose, saddle-nose, parrot-nose, etc. Again, double noses exist, each being more or less well formed. In such a case the surgeon should endeavor to remove a part of each and unite the remaining portions in one, unless one of them be placed away from the middle line, in which case it may be extirpated.
These are usually the result either of mutilation or of some ulcerative morbid process. Injuries of the face, unless extremely carefully and promptly attended to, are commonly followed by scars, which may cause great disfigurement. This is invariably true of severe burns, which, by subsequent contraction, draw features badly out of shape, and sometimes close the mouth or pull the lower jaw down upon the neck and the chin upon the chest. Serious contused wounds are frequently accompanied by fracture of parts beneath, and should be treated as a compound fracture. Considerable portions of the facial mask are sometimes torn away, producing hideous appearances. By punctured wounds the maxillary sinus, orbit, or brain cavity may be perforated and foreign bodies carried in. A wound may be so placed as to sever Stenson’s duct. All of these injuries may be accompanied by serious brain disturbance, as the result of the contusion. Gunshot wounds will present either punctures or extensive lacerations, according to the proximity and the weapon. In no part of the body are gunpowder stains more observable or more deplored than upon the face. In order to prevent them each grain of powder must be picked out with a small spud or needle, after a careful scrubbing of the face. Every grain of gunpowder allowed to remain will produce a minute area of staining.
Injuries to the nose may require plastic reconstruction or the formation of a new nose by one of the rhinoplastic methods later described, or an artificial nose, carried by spectacles, may be worn. The cartilages of the nose are frequently dislocated, thus producing deformity, and the same result may follow fractures. As already indicated in the chapter on Fractures, prompt and complete replacement with support are usually sufficient to give a satisfactory result.
Deviations of the nose, and especially cosmetic defects which result from injuries or disease, producing the so-called saddle-nose, when not extreme, may often be remedied by the injection of paraffin, the patient being either under cocaine or general anesthesia.
Burns, injuries, and serious ulcerations about the cheeks and lips produce conspicuous disfigurement (perhaps none more so than a serious form of cancrum oris) with a considerable loss of substance. In this way may be produced an acquired microstoma, or adhesion of cheek to jaw, which is known as syncheilia. More superficial lesions may produce ectropion or eversion of the lips, or acquired macrostoma. Cretins, idiots, and patients with facial paralysis acquire gradually a chronic swelling of the lower lip with drooling of saliva. The lip may enlarge to such an extent as to ulcerate as the result of exposure. Frostbite also produces serious deformity by ulceration of the skin. When a puncture of the cheek occurs at the opening of Stenson’s duct, i. e., opposite the second upper molar tooth, there may occur a salivary fistula. In a recent clean wound the duct ends may be stitched together. In old wounds Souchon recommends to introduce catgut into the distal end, and then by pressure on the parotid to discover the proximal end and stitch it with the catgut in the divided portion; or the wound may be enlarged and the proximal end turned into the mouth and there retained.
Considerable emphysema may follow contusions of the face, especially those causing fracture of the nose. In this way a face may be so distended as to produce almost a caricature of its former appearance; this, however, will subside within a few hours.
By virtue of its extreme vascularity wounds and injuries of the face heal with a surprising degree of promptitude and certainty. This affords the reason for the satisfactory results of extensive plastic operations. For the same reason secondary hemorrhages may easily occur and additional precautions should be taken. Exact hemostasis, before closure of wounds, will afford protection as against this event. Wound edges should be neatly trimmed and subcutaneous sutures may often be used to advantage to minimize[640] the resulting scars. A lesson “how not to do it” may be learned from the faces of German university students who have indulged in the common but senseless sport of duelling, and who are said to rub salt and alum into their cuts in order to make the scars as conspicuous as possible.
Anesthesia of parts supplied by the trifacial necessarily follows division of its various portions. It may also occur as the result of a deep-seated or central lesion. In course of time more or less sensibility will return, apparently due to an anastomotic process. Facial paralysis, so-called Bell’s palsy, may be of central origin, or be due to the effects of a “cold” following exposure, apparently with inflammation of and an exudate around the trunk of the facial nerve as it passes through its bony canal in the temporal bone. It is also the result of a division of the nerve trunk either outside of the bone or in the bony canal, where it is occasionally wounded in operations upon the mastoid or in removal of the parotid for malignant tumor. Facial neuralgia is an affection of one or more of the branches of the fifth nerve, and, when assuming a spasmodic and intermittent type, is often spoken of as tic douloureux. Its exciting cause may be a carious tooth, even though it give no pain, while other causes are lesions in the neighborhood, such as callus, foreign bodies, tumors, bone disease, and the like. Its special treatment has already been indicated in the chapter dealing with the Cranial Nerves. Many of these cases of neuralgia gradually diminish the patient’s strength.
The serious ulcerative lesions of the face are usually due to tuberculosis, syphilis, or malignant disease. In all of these conditions there will be enlargement of the neighboring lymphatics. This is true also of the lesions of actinomycosis, which should not be forgotten as a possible cause. The free border of the lips is occasionally ulcerated in patients with pulmonary tuberculosis. Otherwise tuberculous lesions are uncommon upon the lower lip, while in the upper lip they show a tendency to invade and spread. Syphilitic ulcers may be either primary chancres, which are most common on the lower lip, or the results of mucous patches, or other secondary or tertiary lesions. Of the cancerous ulcerations, which tend always to break down and spread, without any tendency to healing in the centre, epithelioma is the most common form. It is a frequent disease in men, occurring much oftener on the lower than upon the upper lip. In women it is exceedingly rare at this point. The difference is explained by the liability to constant irritation incurred by those who smoke pipes or are particularly careless about their teeth. Of epithelioma there are, as is well known, various types, including the so-called rodent ulcer, which, however, is less frequent here. The location of the lesion subjects it to constant irritation, as well as maceration from the moisture of the mouth. Such a growth may be superficial and raw, or it may be covered by scale or crust. It will nearly always have an indurated and raised periphery. A papillary form, with non-indurated edges, is also known, as well as a diffuse form, where several minute lesions seem to coalesce, with elevation of the central portion. This is perhaps the most malignant of all, as it has no well-defined boundaries. In nearly every well-marked case involvement of the submaxillary lymphatics can be detected. All of these cancers of the lip and face should be removed, with plastic re-arrangement of the parts. Growths of this kind seen early, before much tissue is involved, can be removed with permanent success. Error is made on the side of not doing sufficient rather than doing too much. (See Chapter XXVI.)
Cancrum oris has already been described in the chapter on Gangrene. The extensive destruction which it may cause is also described there. The condition, when seen and recognized early, has been successfully treated by local applications of bromine and the actual cautery. It is, however, a destructive and unpromising condition with which to deal, as it rarely occurs in healthy children, but usually in those with a constitution already vitiated by heredity or environment. (See p. 75.)
[641]
The parts described in this chapter may be the site of almost every tumor which is met with in any other part of the body; in addition to which there are two which are peculiar to the nose and adjoining tissues. These are rhinophyma and rhinoscleroma. They have both been described briefly in the chapter on Tumors, and each is to be differentiated from the other, having a very different etiology.
Rhinophyma consists of vascular engorgement, with hypertrophy, especially of the glandular and connective-tissue elements of the skin, which begins about the tip and the alæ of the nose, and produces disfiguring deformity. It is, however, at first, quite innocent in its character. It occurs most often in hard drinkers, and is to be regarded as an overgrowth, coupled with a large amount of secretion, of the sebaceous glands of that portion of the skin. This secretion is often so great as to escape and lead to the formation of scabs, as it dries, until more or less ulceration takes place. The nasal enlargement is rarely symmetrical, and is nearly always lobular, so that the overgrowth may consist of a series of nodules whose escaping secretion becomes offensive. The parts are often discolored, even to a purplish color, in consequence of venous stasis. Frostbite frequently predisposes toward it.
Fig. 419
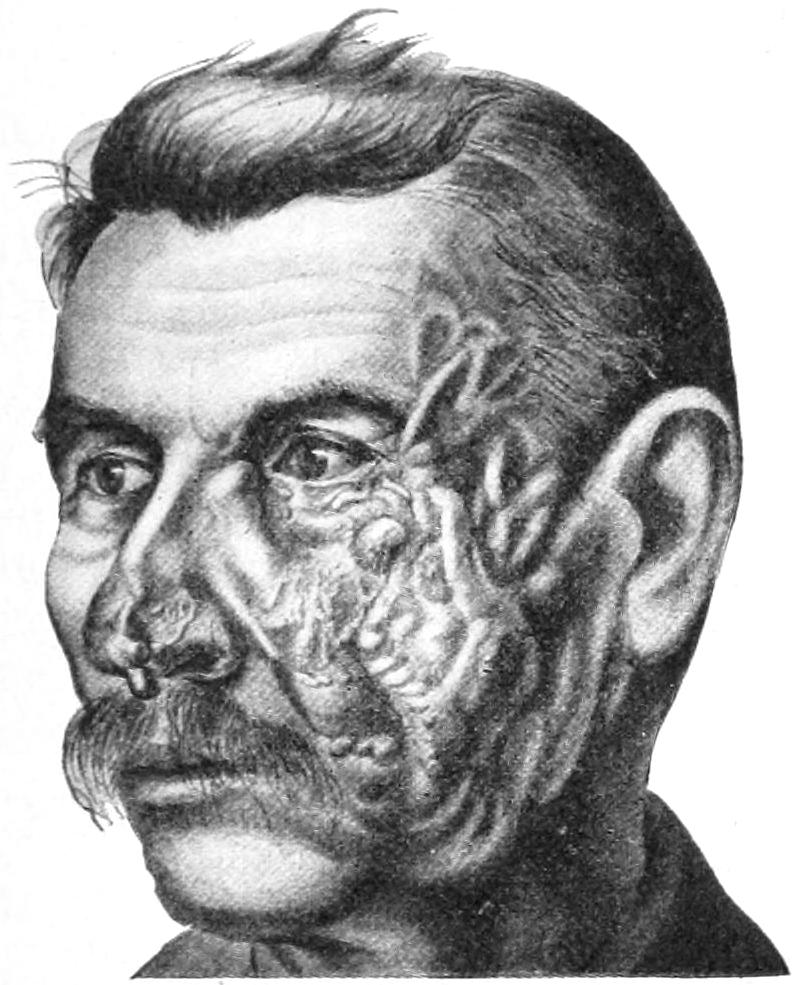
Fig. 420
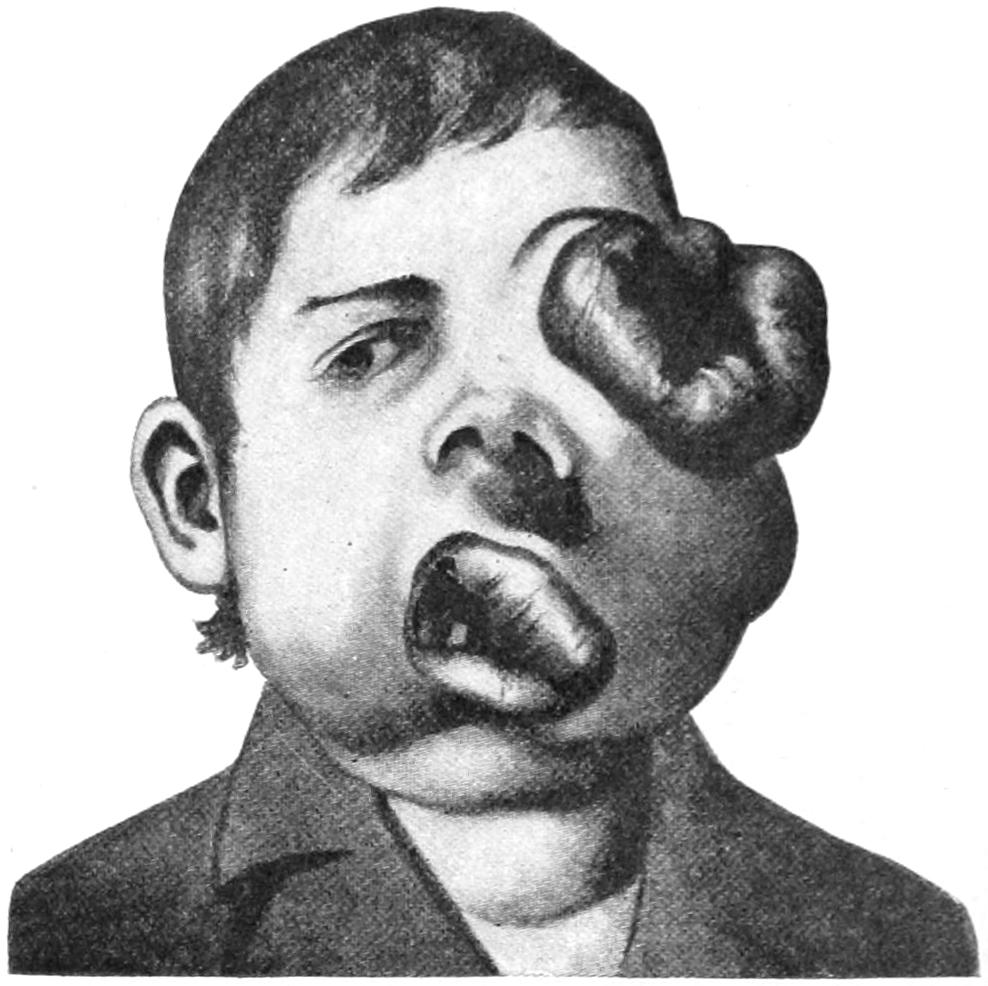
Plexiform angioma of face; cirsoid aneurysm. Not benefited by ligation of external carotid. (Lexer.)
Illustrating ravages of rapidly growing vascular sarcoma of face, involving all the cranial and facial cavities. (Lexer.)
Treatment in incipient cases may consist of a sort of massage, by which the overloaded glands are emptied. In more serious instances the diseased tissue should be extirpated, and either left to granulate or be covered by a plastic operation.
Rhinoscleroma is a serious and fatal lesion, consisting of a parasitic invasion by a peculiar bacillus. It begins as a painless induration, either at the edge of the nostril or upon the upper lip, grows slowly, the tissue affected becoming firm and dense. The growth is usually lobulated, with fissures or excavations between the lobules, which may crack and give rise to a yellowish discharge that dries into crusts. While the affection may begin in the deeper parts of the nasopharynx its occurrence there is usually the result of extension from the anterior growth. The disease may occur either in the young or in the adult. A case illustrated elsewhere (see p. 55), for which I am indebted to Dr. G. W. Wende, proved fatal after a couple of years. In this country it is rare, but occurs frequently in some portions of Russia.
For treatment there is but little encouragement, least of all for operative intervention. Growths nearly always recur after removal.
In the cheek cysts of Stenson’s duct and dermoid tumors and cysts have often been observed near the parotid region. The so-called “fatty ball of Bichat” is occasionally[642] the site of an angioma, which may press upon Stenson’s duct and be accompanied by calculus in the parotid gland, the superficial veins being much dilated. (Souchon.)
Fatty tumors, as well as sarcoma in this same tissue, are prominent. The most frequent tumors of the face are the epitheliomas of the lip, nearly always of the lower lip, occurring oftener in men than in women. A growth of this character at this site is regarded as an expression of the result of irritation, which may be produced by a carious tooth or by constant friction of a pipe-stem, or from many other causes. It frequently develops at the site of an old chronic fissure. These growths spread from small beginnings, and if, when small, they were extirpated there would be fewer cases of cancer of the lip spreading to and involving the face and neck. Every ulcer of the lip whose base becomes indurated, and from which the syphilitic element can be excluded, should be excised, the ensuing defect being repaired by a plastic operation. (See above.)
Fig. 421
Fig. 422
Fig. 423

Fig. 424
Fig. 425
Fig. 426

Fig. 427
Fig. 428
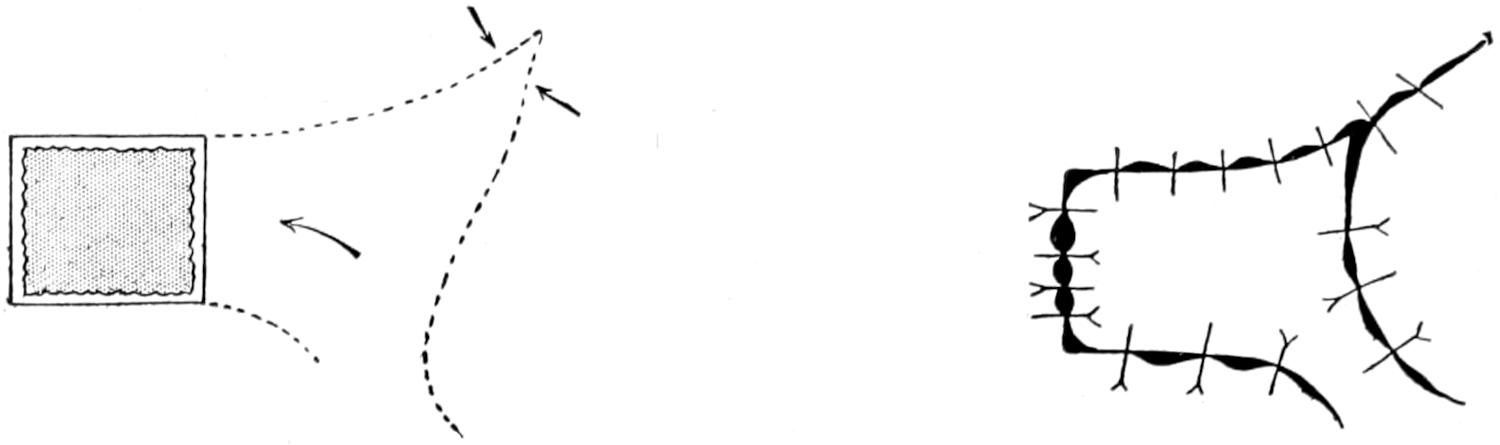
Fig. 429
Fig. 430
Fig. 431
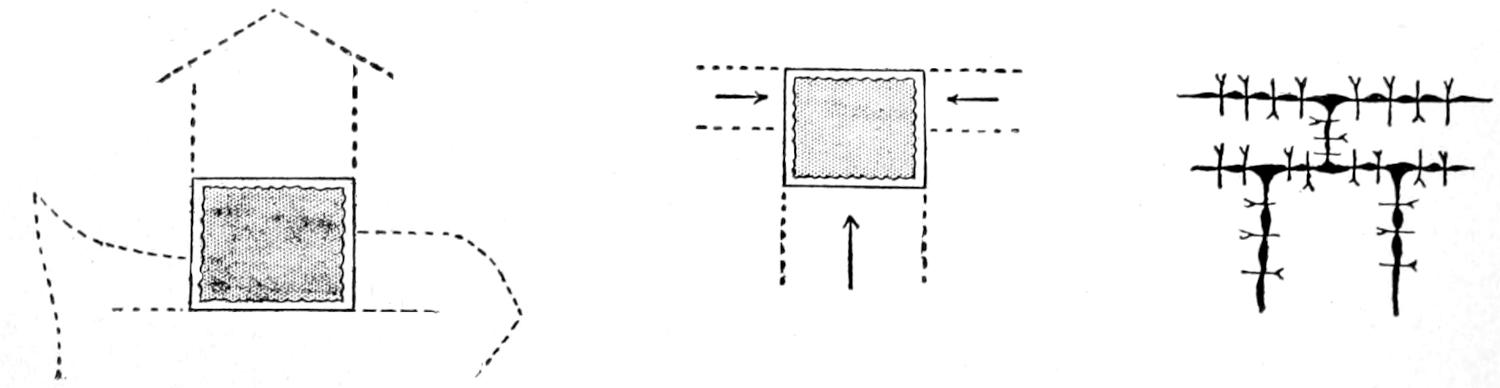
Utilization of rectangular flaps.
The tissues composing the face are extremely vascular, hence hemorrhage is profuse and hemostasis should be exact. By virtue of this same rich blood supply the process of repair is prompt and satisfactory, if sources of infection be avoided. Patients here, more than anywhere else, desire a minimum of scar. Incisions, then, should be so planned as to permit the utilization of the natural folds or grooves of the face. They should also be so made as to avoid injury to main trunks of vessels and nerves, as well as to Stenson’s duet. Sharp knives and the least possible bruising of the tissues help to ensure the desired result. When possible a subcutaneous suture should be employed. When this is not sufficient fine needles and fine suture material should be used. A reasonably[643] short, clean wound upon the face, especially in the neighborhood of the mouth, should be protected from the air until it is dry, using a dusting powder and then covering with collodion. In extensive operations provisional or permanent ligation of the carotid may be necessary; usually the external branch will suffice. In every instance plastic repair should be made, as it will always be required after the excision of growths involving the surface.
Space does not permit of detailed or specific directions for all possible methods of plastic repair of facial defects, but Figs. 421 to 441 illustrate the principal methods which may be utilized in planning and sliding flaps which shall serve this purpose. These may be modified or combined to meet special indications.
Fig. 432
Fig. 433
Fig. 434
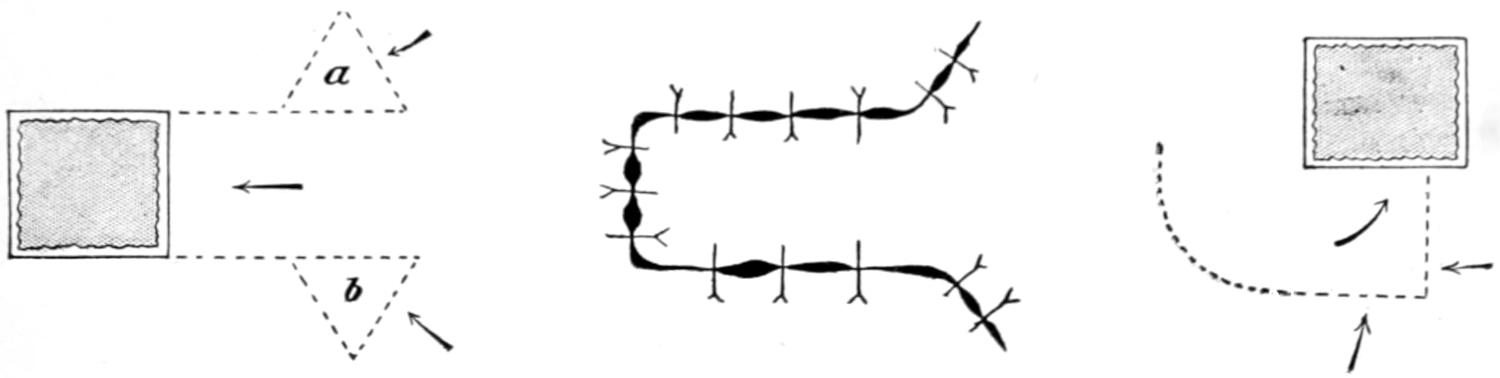
Fig. 435
Fig. 436
Fig. 437
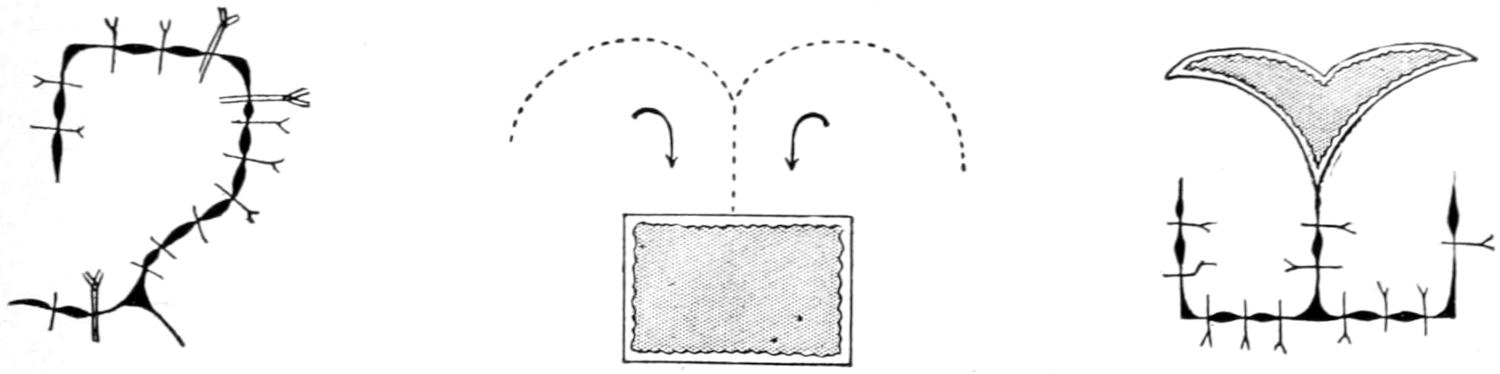
Fig. 438
Fig. 439
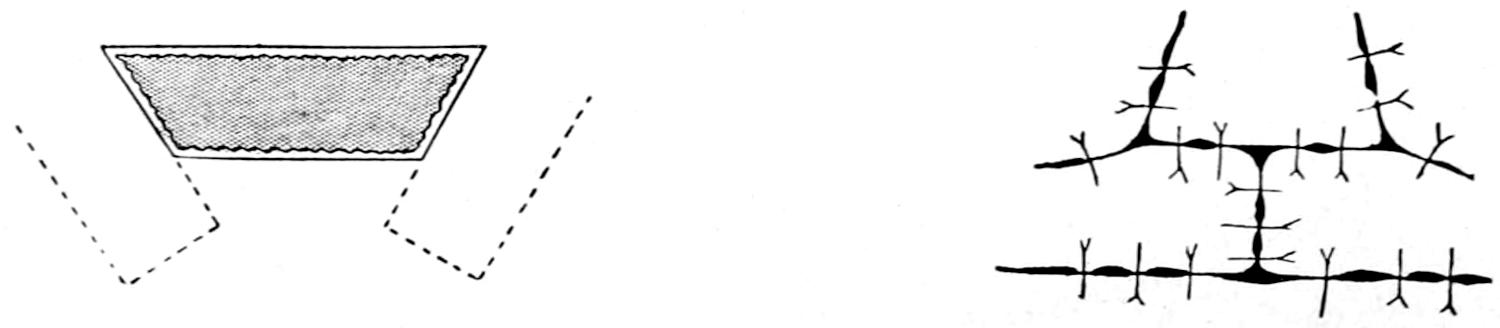
Fig. 440
Fig. 441

Sliding rectangular flaps into desired position.
It is often necessary to intermit the anesthetic because the operator must displace the mask in order to do his work. Souchon advises an apparatus by which most of this delay can be avoided. By means of a rubber bulb a current of air is passed through the bottle containing the anesthetic and then directed through a tip which is passed down in the pharynx through a nostril. This may be connected, if so desired, with a bag of nitrous oxide gas, which is illustrated in Fig. 442, and its use in Fig. 443.
Ligation with excision of a section of the external carotid has been suggested by Dawbarn as a means of cutting off the blood supply in cases of inoperable malignant tumors of the face, thus reducing their rate of growth. In tumors of the jaw, for instance, he would also tie the inferior dental artery, with its mylohyoid branch, just before it enters the inferior dental canal. He advises, also, the removal of one inch of the[644] inferior dental nerve, thus avoiding pain and distress, occluding the artery on the less diseased side first, waiting for two or three weeks before attacking the more diseased side, for should there be noticeable benefit after operation on the more affected side many patients would be unwilling to be again subjected to the other operation. Other operations include those made upon the various nerves for relief of neuralgia or for nerve suture of divided trunks. These have been described in a previous chapter.
Fig. 442
Fig. 443
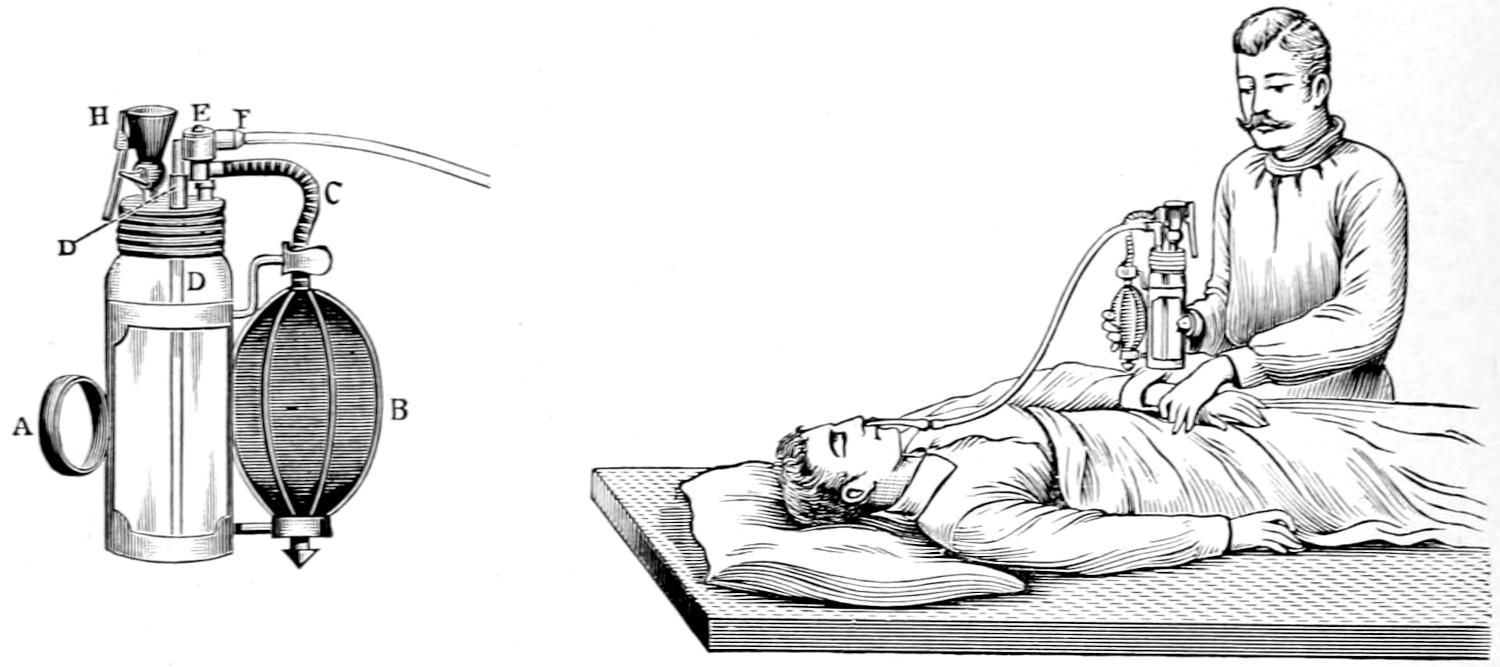
Souchon’s intranasal inhaler.
Plastic operations upon the nose appear to have been practised early in the history of surgery. The East Indians had a method by which the skin of the forehead was made to furnish a flap from which a new nose was created. This was known as the Indian method. It has been somewhat modified of late years by raising with the skin flap the periosteum, or, as suggested by König, the outer table of the frontal bone, with the intent and hope that something resembling the nasal bone might be secured. The so-called Italian method (named the Tagliacotian operation, after Tagliacozzi) consists in utilizing the skin of the arm, which is loosened according to a pattern previously made, leaving it connected only by a pedicle through which its blood supply is to be afforded. This flap is usually cut out and perfectly formed, then left loose upon the arm for about fifteen days until its viability has been thoroughly proved and its under surface is granulating. Then the edges of the defect in the nose are pared, as well as those of the flap, and the arm is brought into such position as to allow fitting the latter to the former, where it is held by stitches. The arm is held in proper position by cushions and by bandages of plaster of Paris until union has taken place, after which the pedicle is severed and the arm then released.
Fig. 444

“Saddle-nose” due to syphilitic destruction of bone. (Lexer.)
Lesser deformities of the nose may be remedied or repaired in various ways. Angular deformities may be excised, while a sunken bridge may be raised, as Weir has suggested, through a bevelled incision at the junction of the nasal and maxillary bones, they being held in place by a transfixion pin. One of the most common and objectionable deformities is the so-called saddle-nose, which may be treated by Weir’s method, or which[645] has afforded satisfactory results after the injection of paraffin. Roe, of Rochester, New York, has succeeded in remedying many of the more trifling nasal deformities by operation from within the nose, as, for instance, in case of pug-nose, where he dissects from within superfluous fat and connective tissue (Fig. 444).
Hare-lip, or coloboma of the upper lip, is due to a failure in coalescence of the developing maxillary processes, which should unite early in fetal life to form the lip, alveolar process and roof of the mouth. This failure may involve but a trifling part of this line of normal junction or may be complete. Thus anywhere along it defects may be noted, such, for instance, as a little notch in the lip, a small opening in the hard or soft palate, or a bifid uvula. The defect in the lip alone is known as hare-lip because of its normal occurrence in the hare, and occurs on either side of the median line, absolute median fissure being extremely rare. It may occur alone or in combination with deeper fissures which involve the gum or the alveolar process alone or the entire palate. In extensive fissures of this character development is rarely symmetrical, and one side is usually not developed sufficiently to match the other. This makes operative treatment the more difficult. The more complete and extensive fissures are often complicated by excessive development of the intermaxillary bone, apparently from lack of pressure. This permits a projection of the septum, and especially of the central portion of the alveolar process, with a small part of the skin and connective tissue, which should have been blended into the lip proper. It represents the original intermaxillary bone with the portion which should have been developed downward from the nasal process of the midfrontal region. This gives a snout-like appearance to the face, and nearly always necessitates doing an operation for closure of the lip in two sittings. In Figs. 445 and 446 will be seen wide clefts with projecting intermaxillaries, while Fig. 447 illustrates a much more complete coloboma of the face, with complete bilateral fissures. Figs. 448 and 449 show the double form with philtrum or snout. Figs. 450 and 451 give the palatal conditions of irregularity and projection of the intermaxillary bone. (See Cleft Palate.)
Fig. 445
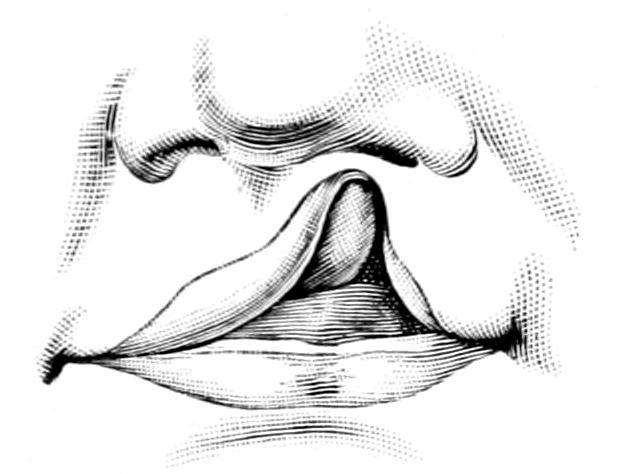
Incomplete hare-lip.
Fig. 446
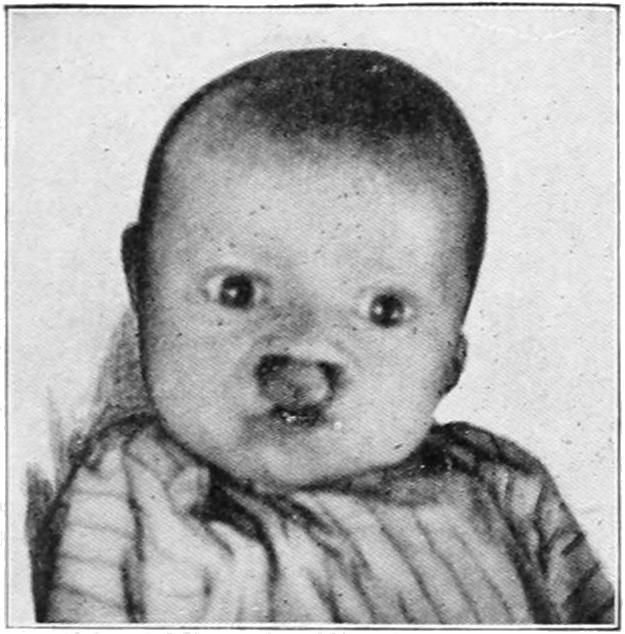
Fig. 447
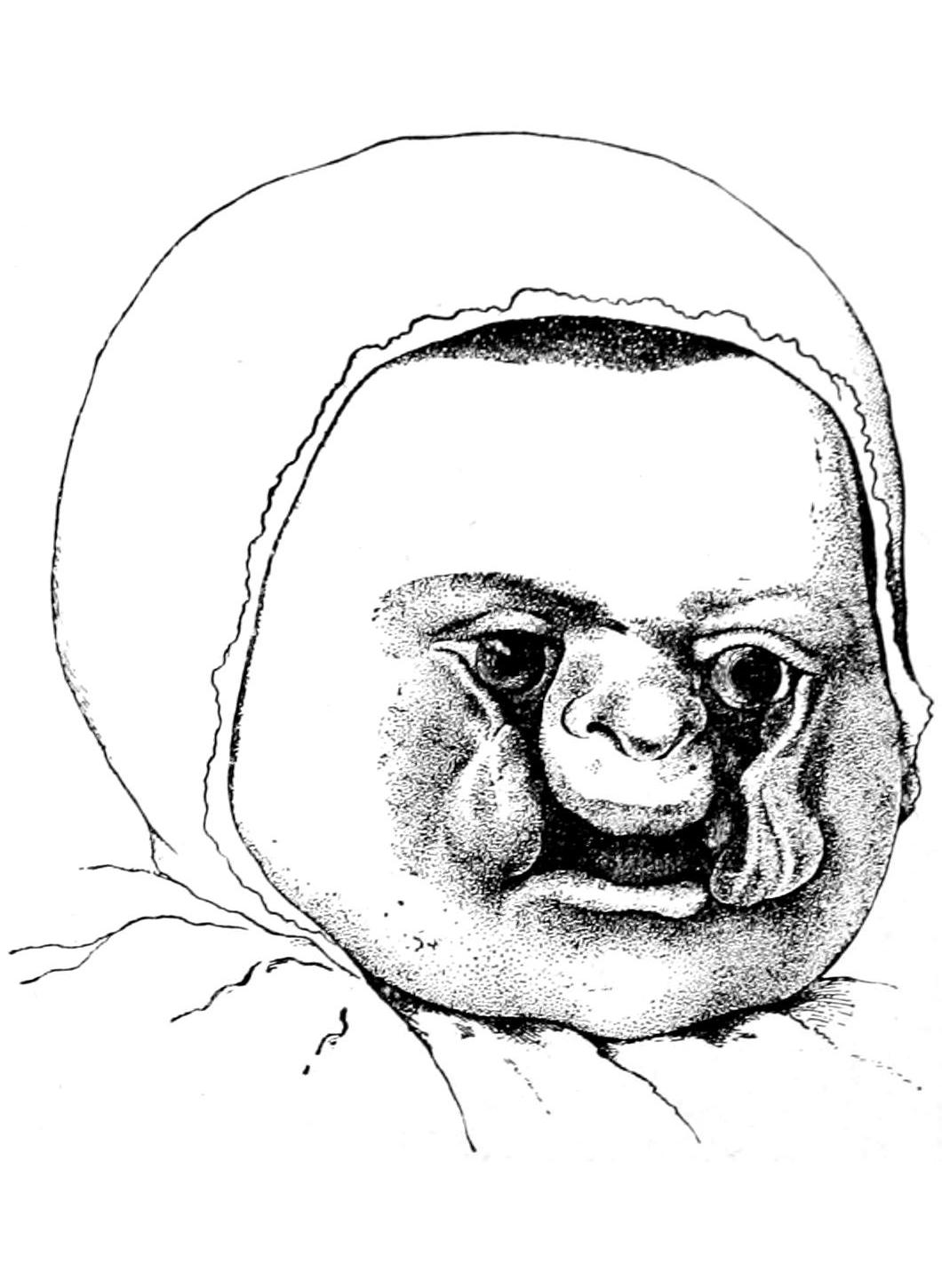
Complete fissure in double hare-lip.
Complete bilateral fissures (coloboma) of face. (Guersant.)
All forms of hare-lip call for operation not alone for cosmetic purposes, but so that patients can nurse, drink, eat, and talk to better advantage. Obviously the earlier[646] such operations are done, other things being equal, the better the results. When the cleft does not include the deeper tissues it may be closed within the first week or two of infancy. When the roof of the mouth is involved the surgeon is perplexed in deciding which is the better of two courses—to operate or to wait. Unquestionably by early closure of a fissured lip a gentle but constant influence is maintained to press the divided upper edges together, or at least to influence their more rapid growth toward each other. For this reason it would be desirable to operate early. On the other hand with a bad palatal defect it is a difficult thing to operate until, with the increasing age of the child, the mouth has attained a size which will permit the manipulations required for the purpose. Nevertheless, unless there be some special reason for delay it would appear wise, at least as a general rule, to operate early. (See Cleft Palate.)
Fig. 448
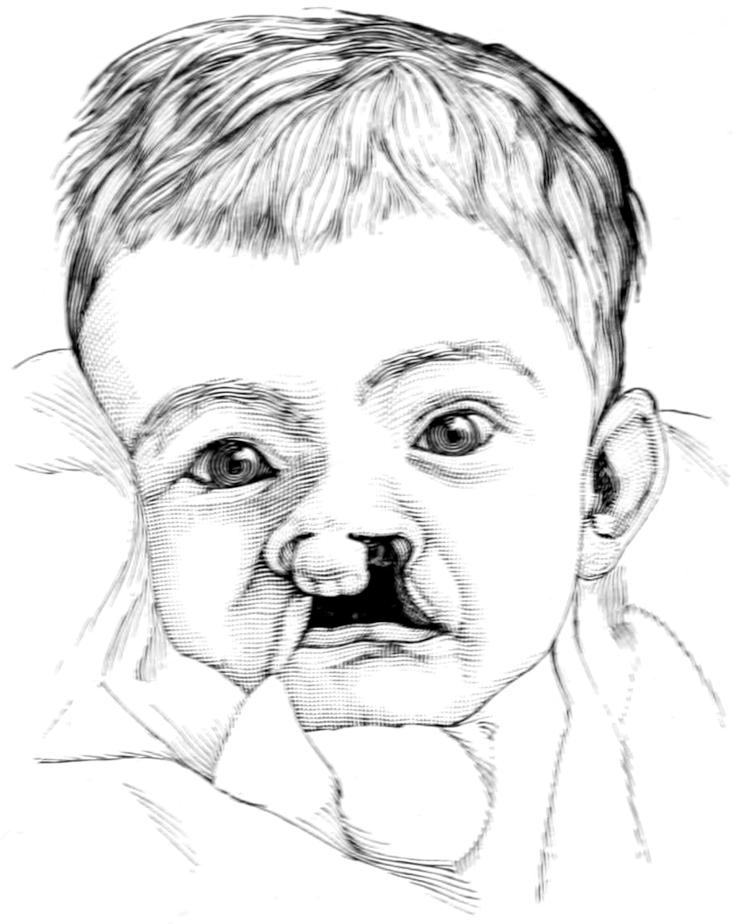
Double hare-lip with philtrum or snout.
Fig. 449
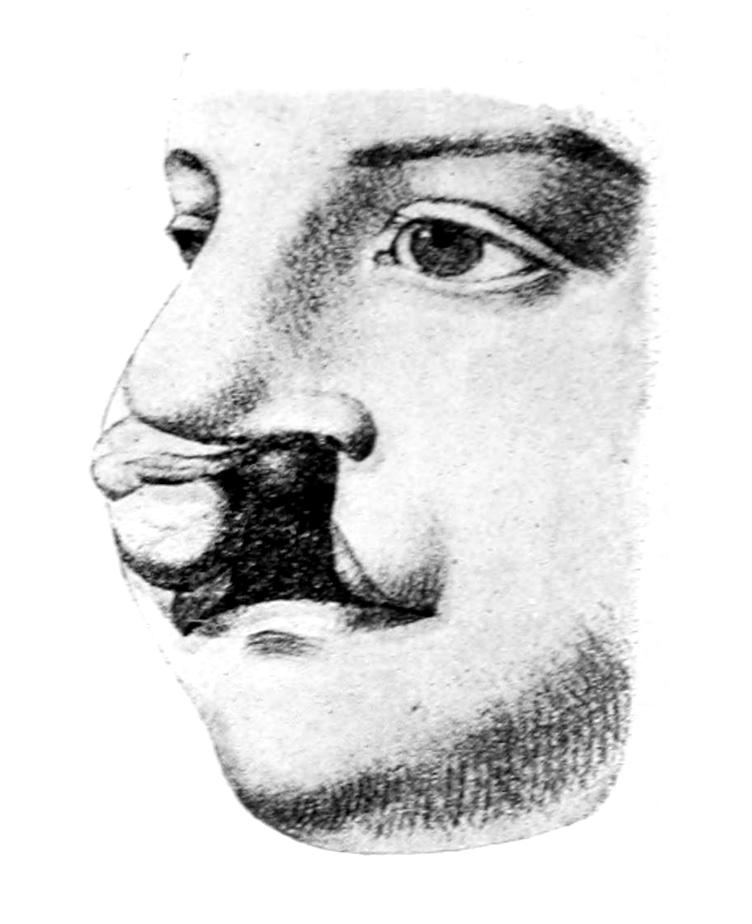
Complete fissure, with labial defect and projecting intermaxillary. (Bruns.)
Fig. 450
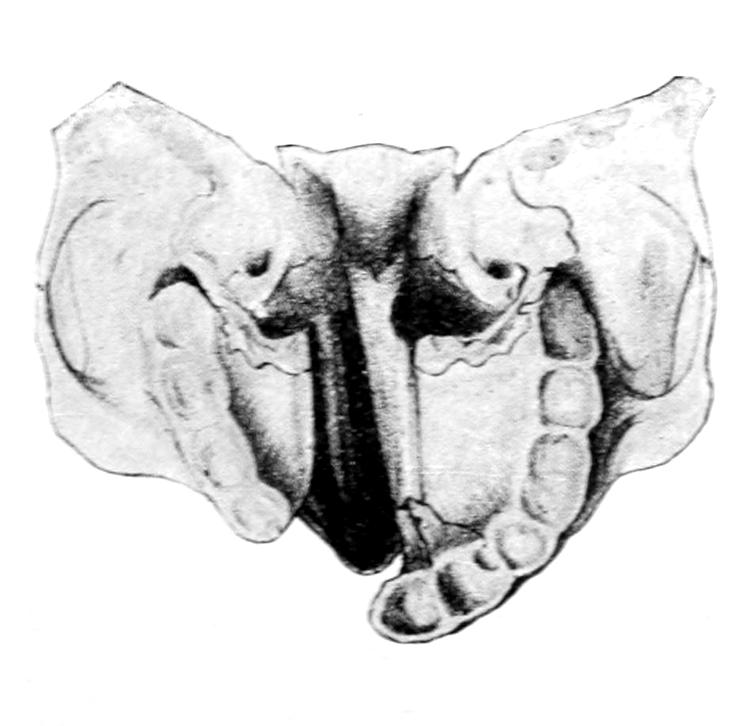
Illustrating the osseous (palatal) defect in complete fissures. (Bruns.)
Fig. 451
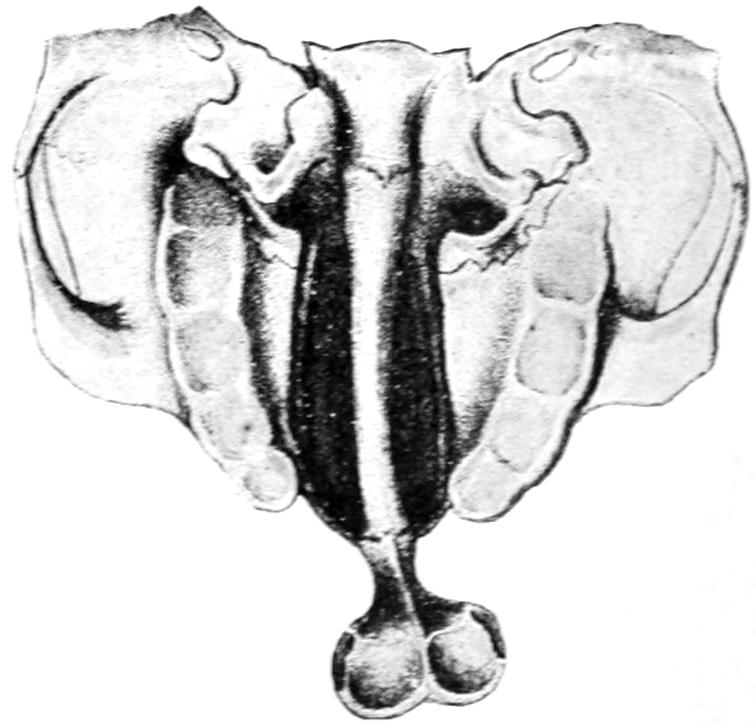
Projecting intermaxillary bone. (Bruns.)
The underlying principle of these operations is easily and briefly stated. The edges of the defect should be freshened and brought together by sutures. Extreme care should[647] be taken that the vermilion border of the lip be maintained. A little particle of mucous membrane in the lip of an infant, dislocated to a level higher than that where it belongs, will appear later in life as a reddish patch upon the skin, which will prove quite a disfigurement. Simple fissure of the lip is easily managed by Nélaton’s procedure (Figs. 452 to 457). The deeper and more extensive the fissure the more plastic reconstruction is required.
Fig. 452
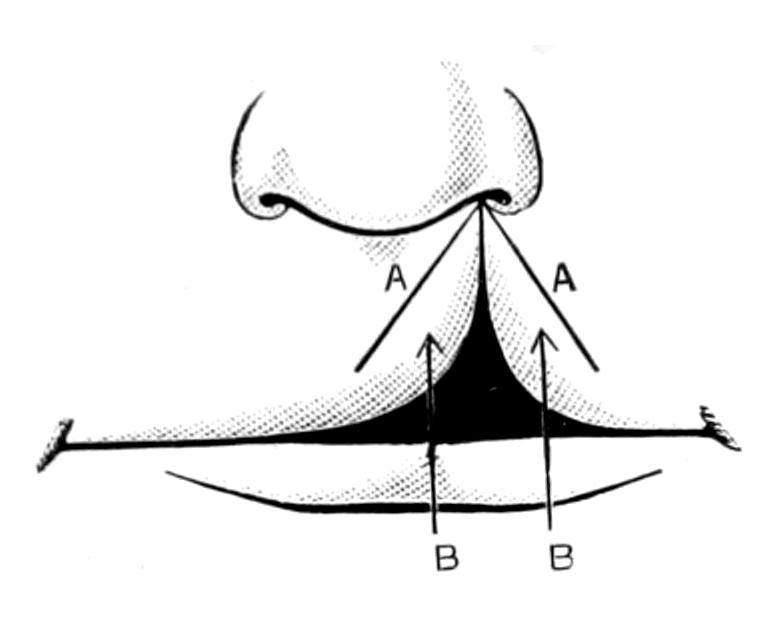
Malgaigne’s operation: the incision.
Fig. 453
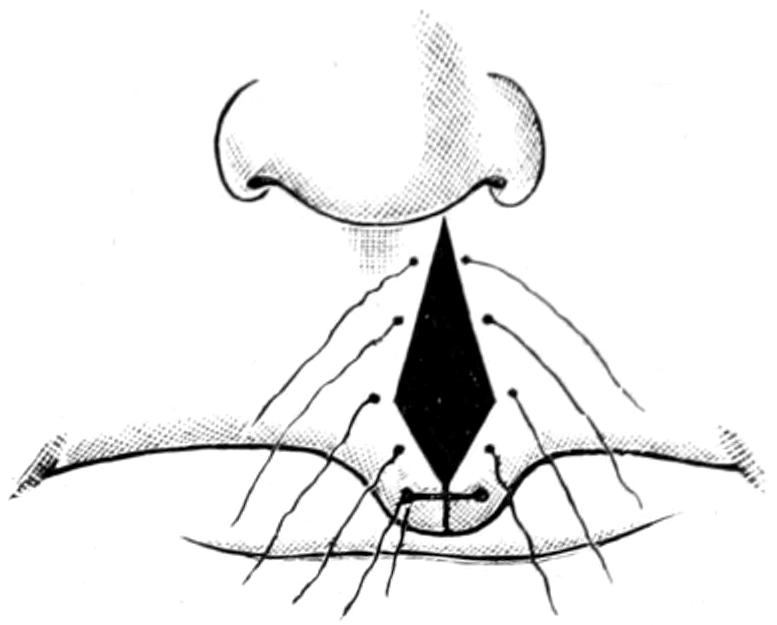
Malgaigne’s operation: the sutures in position; the lower sutures tied.
Fig. 454
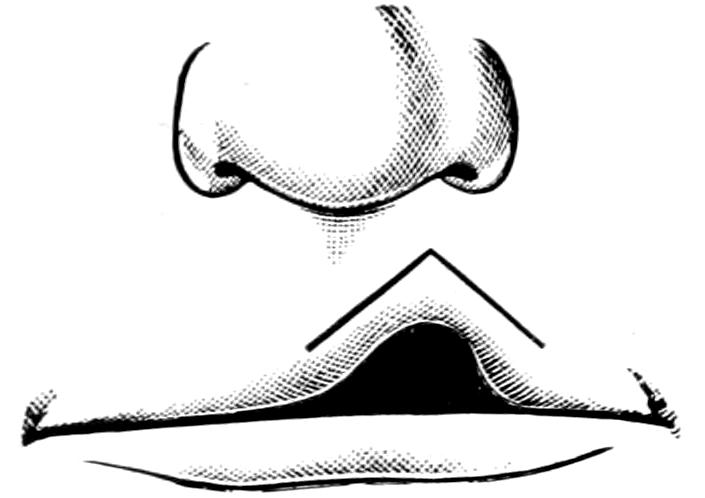
Nélaton’s operation: the incision.
Fig. 455
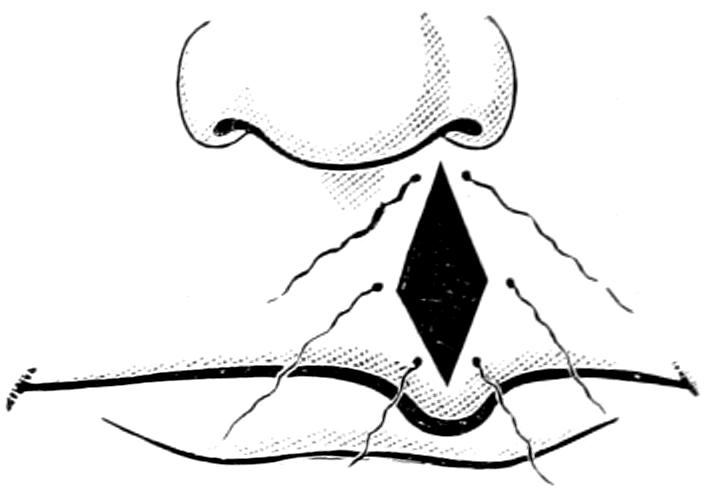
Nélaton’s operation: the sutures.
Incision, when necessary, may be extended around the angle of the nose on one side or both, and the lip should be dissected away from the bone sufficiently to make it movable. Operations by which a certain dovetailing of the little flaps is performed afford more security than a perfectly straight incision, but the resulting scar is rather more marked. The more perfectly the mucous membrane can be preserved upon the under side of the lip the better will be the result.
Fig. 456
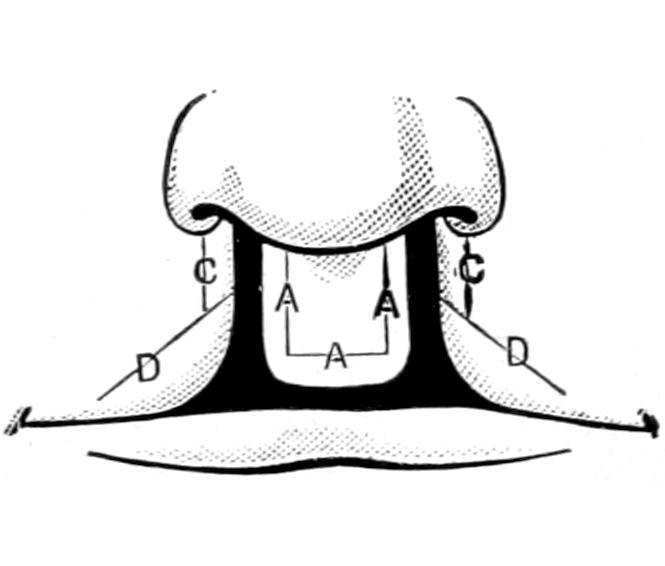
The operation for double hare-lip.
Fig. 457
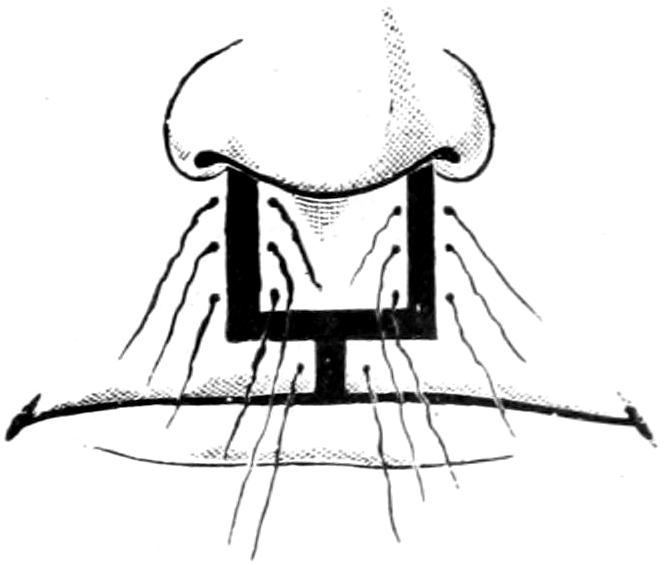
Operation for double hare-lip: the sutures in position.
Hare-lip pins have been abandoned. Sutures only are used, which may be of thread or horse-hair, catgut absorbing too rapidly. It is my custom to pass a retaining suture of stout silk through the cheek on either side, at a distance of one inch or so from the wound margin, to bring this forward in front of the alveolar process, and, by using a plate and shot on either end, to prevent tension upon the line of junction. This is very[648] important, for children will fret and cry in a manner to tear out many a stitch not thus fortified. After operation young children should be snugly enclosed in a protective bandage around the chest, by which it shall be made impossible for them to get their hands to their mouths. It is vitally necessary to maintain absolute rest of the face and protection from any possible source of harm.
Fig. 458
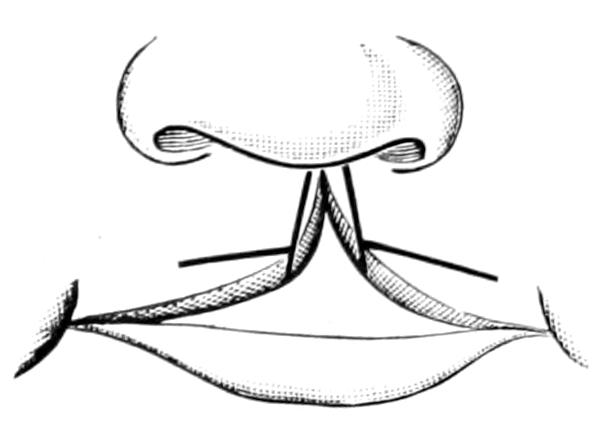
Fig. 459
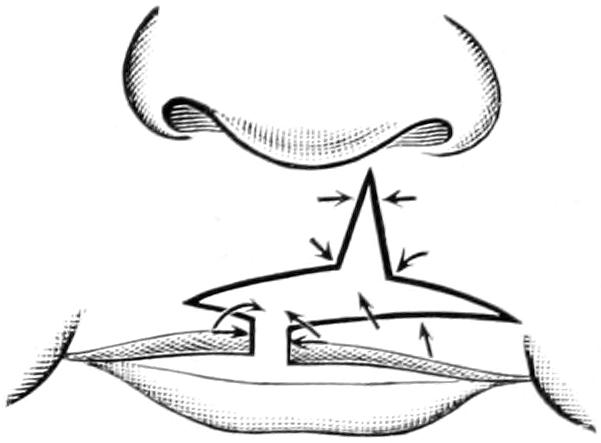
Line of incision, according to König.
Fissures of the lower lip are surgical curiosities. Should one be met it may be treated on the same general principles.
Fig. 460
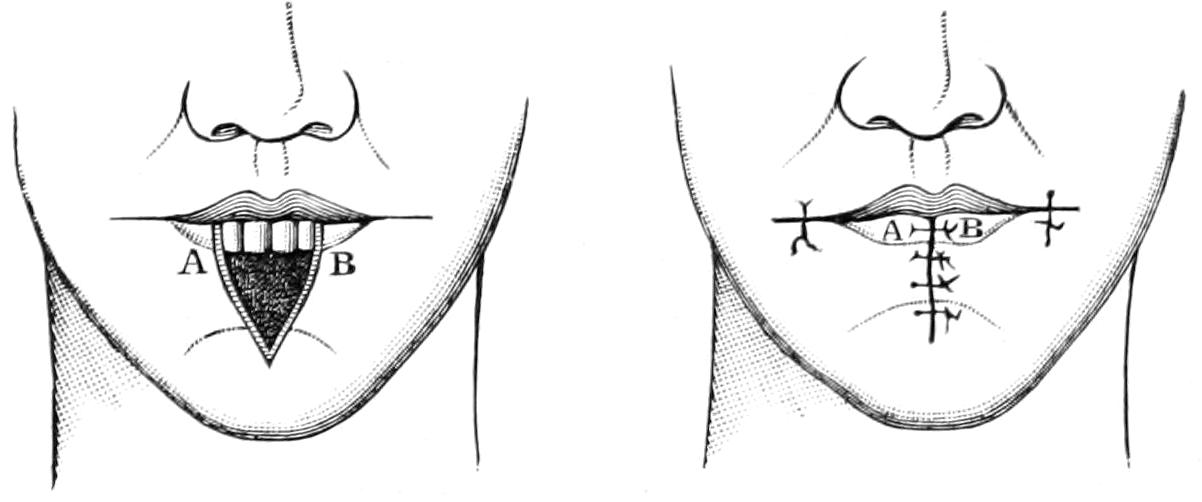
Cheiloplastic operation on lower lip. (Tillmanns.)
The other cheiloplastic operations upon the lips are those made necessary by excisions of malignant growths, or by deforming cicatrices such as follow burns, syphilitic lesions, and the like.
Fig. 461
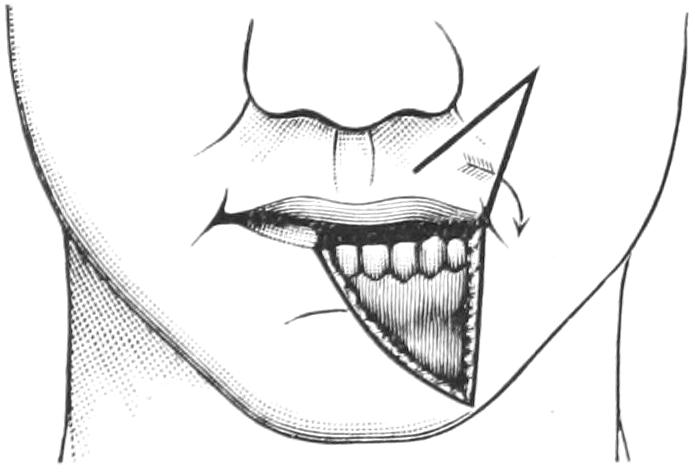
Fig. 462
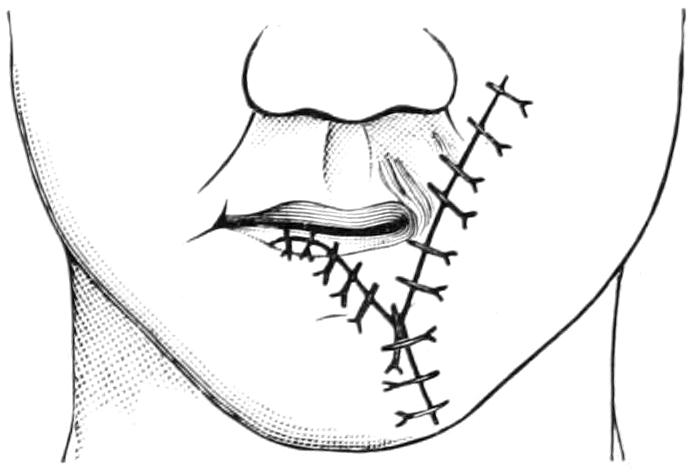
Estlander’s cheiloplastic operation.
Fig. 460 illustrates one method of filling a defect of the lower lip, while Figs. 461 and 462 indicate a method of bringing down a flap from the upper lip for the same purpose.
Foreign bodies occasionally enter the salivary ducts, especially Stenson’s and Wharton’s, where they may set up an inflammation known as sialoductilitis. These may consist of bristles, fish-bones, and the like. Abscess, in consequence, may form in the gland or between it and the foreign body. Calculi also lodge in the ducts, where they remain as foreign bodies, producing sometimes a disproportionate amount of irritation.
[649]
Fistulas of the salivary ducts involve Stenson’s duct. They open on the inside of the buccinator muscle, back of the orifice of the duct, which is opposite the second upper molar tooth. These fistulas of the parotid gland may be recognized by the passage of a probe from within the mouth. When they open externally they result nearly always from injury, and it is only the external forms which are troublesome. One may resort to the mildest measures first, and experiment with cauterization of the orifice or compression by occlusion. These measures will be ineffective if there be no opening upon the inside of the mouth, in which case one must be made by reëstablishing the original canal or forming a substitute. For this purpose a suture may be passed around the duct, back of the fistula, using a curved needle, and making it come out near the point of entrance. It should hold the duct in its loop. This suture may then be tightened and the distended duct punctured on the inside of the cheek. When once the flow of saliva is diverted to the mouth the edges of an external fistula may be pared and closed. In obstinate cases which have resisted all other methods it has been suggested to remove or destroy the gland which connects with the duct at fault. Even this is not an easy matter, but it can be done in the case of the parotid by careful dissection, with separation of the branches of the facial nerve and removal of the greater portion of the gland itself.
Congenital anomalies of the salivary glands are rare and of small import. Any one of them may be displaced, or either of them may connect with an accessory gland separated from it by an appreciable interval. Abnormal duct openings have also been noted.
Inflammatory affections of the salivary glands give rise to sialoadenitis. Among these by all means the most common is parotitis (mumps), which often occurs in epidemic form. It is an infectious and probably contagious disease, usually attacking the young, though no age is exempt. The period of incubation is about fourteen days. The condition begins with a stomatitis and with swelling of the affected parotid, with edema of the overlying tissues. It is accompanied by moderate fever. Swelling may be extensive and involve the entire neck region. The parotid on the other side becomes affected within a few days, although usually not to a similar extent. The other salivary glands occasionally participate. The febrile stage lasts for about a week, after which the swelling recedes and is gone within from two to four weeks. Occasionally the affected glands suppurate, in which case the condition may be very serious, since it may simulate Ludwig’s angina, or may be followed by sloughing and gangrene.
Save when abscess threatens the treatment should consist of warm antiseptic mouth-washes and the external application of an ichthyol-mercurial ointment or of Credé’s silver ointment. When suppuration threatens early incision should be made for the relief of tension and prevention of destruction.
A frequent and important complication of parotitis is orchitis, or swelling of the testicle. This is an unexplained feature of these cases, and occurs mainly in sexually mature individuals. It is the testis proper which suffers and not the epididymis. Suppuration here is rare. More or less atrophy is a remote consequence in many cases, estimated at about one-third. When both testicles are affected to a marked degree impotency may follow. Treatment of this orchitis consists in absolute rest in bed, with elevation of the parts affected, often with the application of an ice-bag. Painting the scrotal skin with guaiacol in small amount will often relieve pain. A similar complication occurs in the female, the ovary being involved. Aside from this, other complications may occur in the breast, the vulvovaginal glands, the prostate, the heart, the eye, and the ear.
Apart from this somewhat specific affection the parotid and the other salivary glands may become involved in swelling and inflammation on account of surrounding local infections, or the presence of foreign bodies, stones in the ducts, etc. Metastatic abscesses, especially in the parotid, are not uncommon. Considering the open pathways offered it is surprising that these glands are not oftener involved in septic conditions of the mouth.
[650]
Mikulicz has described a not very infrequent simultaneous affection of two or more of the salivary glands, occurring in middle age, characterized by uniform swelling which may involve even the palatine, labial, and buccal glands. It is spoken of in German literature as Mikulicz’s disease. The swelling progresses slowly, so that the glands reach a varying size in the course of years. Thus the parotid glands may attain the size of the fist, and other glands a corresponding increase. Sometimes the adjoining lymphatics are also involved. The enlargements are not tender, but may interfere with movements of the tongue and jaw. These tumors have been known to recede after an intercurrent acute disease. Nothing is as yet known of the cause or nature of the affection. In its treatment arsenic and potassium iodide have given perhaps the most favorable results.
The salivary glands, especially the parotid, are as likely to be involved in the manifestations of tuberculosis, actinomycosis, and syphilis as are the other structures of the body. Lesions of these various natures will be appreciated without further description.
Tumors of the salivary glands are not uncommon. The parotid is more frequently affected than either of the others. These tumors may be of cystic character, either large from obstruction of the excretory duct, or small and numerous. Almost all the tumors described in Chapter XXVI may be found in this region. Simple adenomas are common and the parotid especially is often the site of tumors of mixed character, in which the various mesoblastic elements mingle in a confusing manner. Cartilaginous tumors here are frequent. The presence of cartilage is to be explained on Cohnheim’s hypothesis. Endothelioma, sarcoma, and carcinoma are also common, especially as primary tumors in the parotid. Any or all of the glands may also suffer by extension of malignant disease from primary foci in their neighborhood (Figs. 463 and 464).
Fig. 463
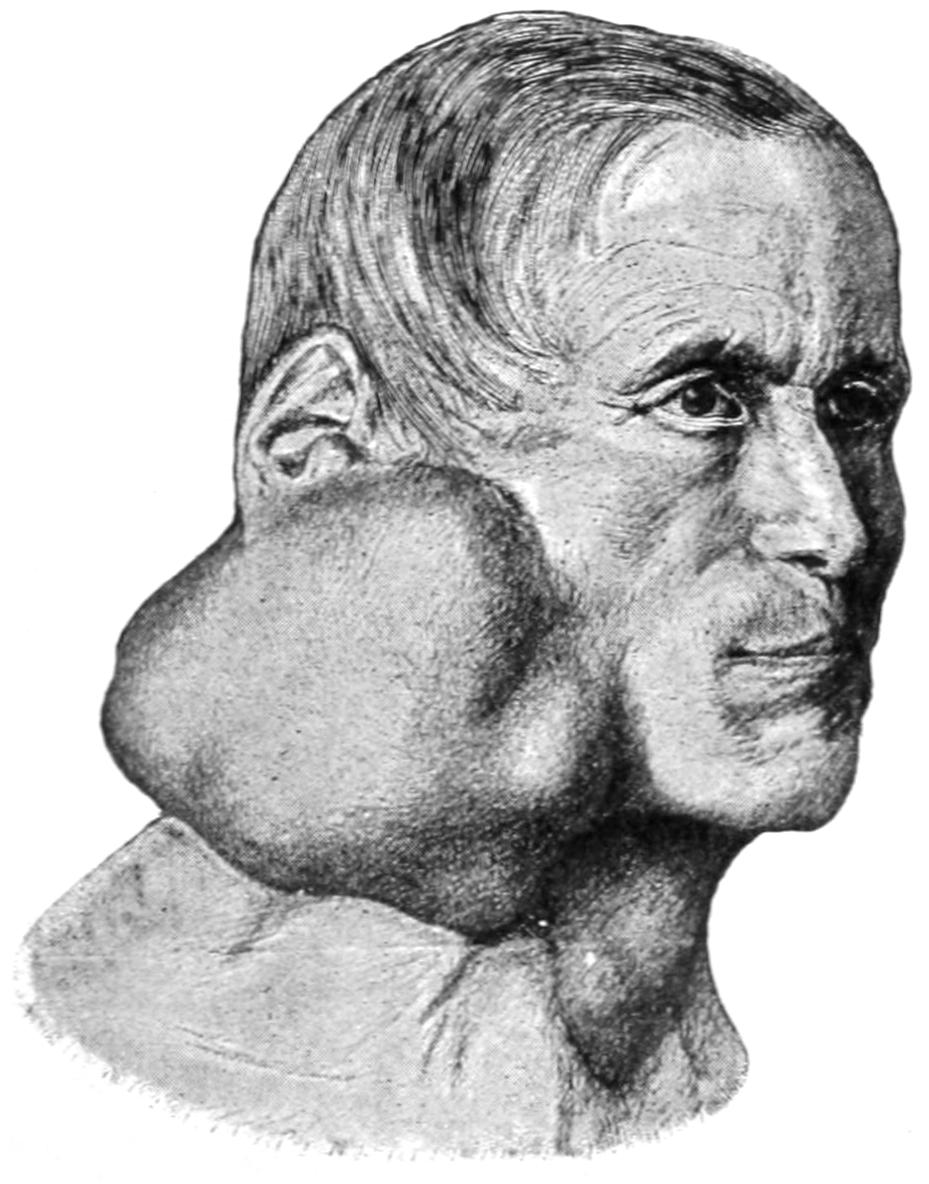
Mixed tumor of the parotid. (v. Bruns.)
Fig. 464
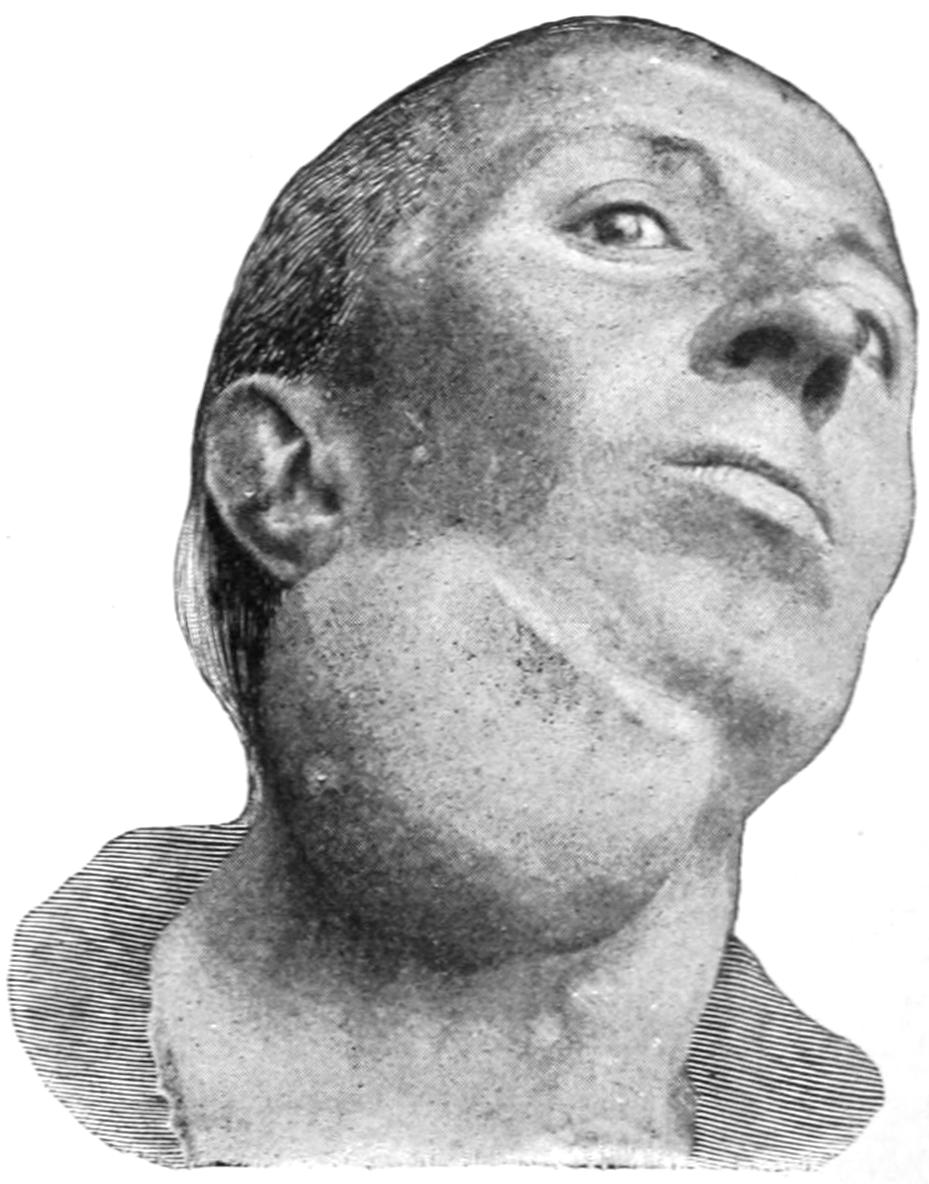
Mixed tumor of the submaxillary gland. (v. Bruns.)
Cancer of the parotid is especially serious and discouraging, because, while radical removal is necessary, it is impossible to effect this without destroying the facial nerve and producing consequent paralysis of the face on that side. Such an operation should not be made without explaining to the patient beforehand its inevitable result.[651] Only when seen in their very early stages can these tumors be so effectually removed as to not leave the patient liable to secondary or metastatic affections. This also should be explained to them in order that the surgeon may protect himself from blame.
Calculi which form either in the substance of the glands, or much more commonly in their ducts, by precipitation of those salts held in solution by the saliva, are of the same character as the accumulations of the so-called tartar upon the teeth. They are met with frequently in Wharton’s duct and occur more often in men than in women. They may vary in size from that of a rice-grain to a stone more than one inch long. They are always ovoid in shape and with a rough exterior. They are believed to grow much as do gallstones, as the result of some previous infection, a clump of bacteria perhaps affording the nidus on which calcareous material is deposited. The affection may be spoken of as sialolithiasis.
They usually give rise to pain and swelling, and lead occasionally to the formation of abscess and fistulous openings. They may be revealed by the x-rays, or the operator may search for them as for stone in the bladder, with a small probe passed through the duct opening. The discharge of mucopus or blood into the mouth would suggest infection of this kind. They may also be recognized by thrusting a needle through the overlying tissues in the direction of the swelling which they produce. Their removal through the smallest incision on the interior of the mouth which will suffice for the purpose is indicated. No attempt need be made to close the opening.
Operations on the parotid region are difficult and severe. In case of large tumors the external carotid and the common carotid may be ligated. By separating the patient’s jaws the parotid space is increased and deep dissection is more easily made. Caution should be taken not to open the maxillary joint. Souchon has called attention to the fact that the safest plan is to proceed so long as the surrounding tissues are easily removed en masse, and to stop when they become too resistant as the deep surface is approached. Then the portion of the tumor which has been cleared should be cut off. The stump thus left will, in growing again, become more superficial, and it is sometimes possible to effect a radical removal by a second operation.
[652]
Aside from anomalies due to incomplete closure or erratic development from the branchial clefts, the principal congenital defects of the regions included in this chapter are as follows: The mouth is essentially a coalescence of the upper end of the foregut and a recess known as the stomodeum, which are at first separated by membrane, the latter disappearing early in fetal life. Some remains of it, however, may produce a narrowing of the oral fissure and cause one form of microstoma. Some of these facial defects are due to formation of amniotic bands and adhesions, which restrain or interfere with the normal development from the branchial fissures. Malformations of the tongue may accompany other anomalies. A median cleft, called also a bifid tongue, and defective development and undue adhesions to the floor of the mouth, are known, whose most trifling expression may be seen in the so-called tongue-tie, where the frenum is too short and needs to be divided in order to release the tip and more movable part of the organ. Adhesive bands may also attach the tongue laterally to the cheek, bands between the cheek and the gums being also occasionally seen. An extreme type of tongue-tie is known as ankyloglossum. Abnormally long tongues are also met, and cause an actual menace from danger of the tip being swallowed, as children have suffocated from this cause. Congenital macroglossia has been described; it is usually due to lymphangioma of the tongue. A condition known as lingua plicata is characterized by moderate enlargement of a number of either longitudinal or transverse folds or rugæ. The covering mucosa, however, is normal. Complete absence of the tongue has been noted.
Aside from malformation of the upper jaw, cleft palate, there are arrest of development in one or both sides of either jaw and a failure of union in the two halves of the lower jaw. Anomalies about the temporomaxillary joint interfere with its function and may prevent separation of the jaws.
Malformation and misplacement of the teeth are extremely common. Thus a tooth may develop in an abnormal position by displacement of its body, or it may project in an abnormal direction; while teeth may be lacking in number or in eruption, so that a given tooth, usually a molar, completely fails to appear. Absence of a number of teeth is more rarely noted. Numerous cases are on record where a third set of teeth has succeeded the second instead of the latter remaining permanent. Abnormalities of tooth formation extending to the dignity of tumors of the dental tissues have been referred to in the chapter on Tumors, under the head of Odontomas. Cysts of congenital origin not infrequently develop around unerupted or misplaced teeth, and constitute tumors which at birth are scarcely noted and which may not develop until later in life.
Persistent remains of the thyroglossal or thyrolingual ducts may be seen early in childhood, or not until late in life. Their consequence is occasionally noted in the existence of fistulas, but more often of cysts or dermoid tumors, which, though having their origin in the middle line, may become displaced to one side, and when seen by the surgeon have a lateral position.
Cleft palate is a congenital defect due to failure of coalescence between the nasal and maxillary processes, which, proceeding from either side, should meet and unite in the middle line. The defect may be so slight as to produce only a small notch in the alveolar border, or a small opening in the roof of the mouth, or it may be so complete as to constitute a separation with the formation of but a small part of the roof of the mouth, leaving[653] but little tissue serviceable for any possible operation. The relation between the products of lateral growth and the downward projection and formation of the intermaxillary bone by the midfrontal and nasofrontal processes is too complex to be described here (Fig. 465). In some instances there is but little evidence of the formation of such a bone, while at other times it has not only bone formation but is relatively overdeveloped, in such a way as to make the lower anterior angle of the septum and its own part of the alveolar process project far beyond the level of the surrounding tissues, thus producing a snout-like appearance, which not only makes the case more disfiguring, but seriously complicates operative procedure. Usually the lower border of the nasal septum will be found attached to one side of the cleft (Fig. 466). The soft palate presents the same fissure, and the uvula is often neatly separated into halves.
Fig. 465
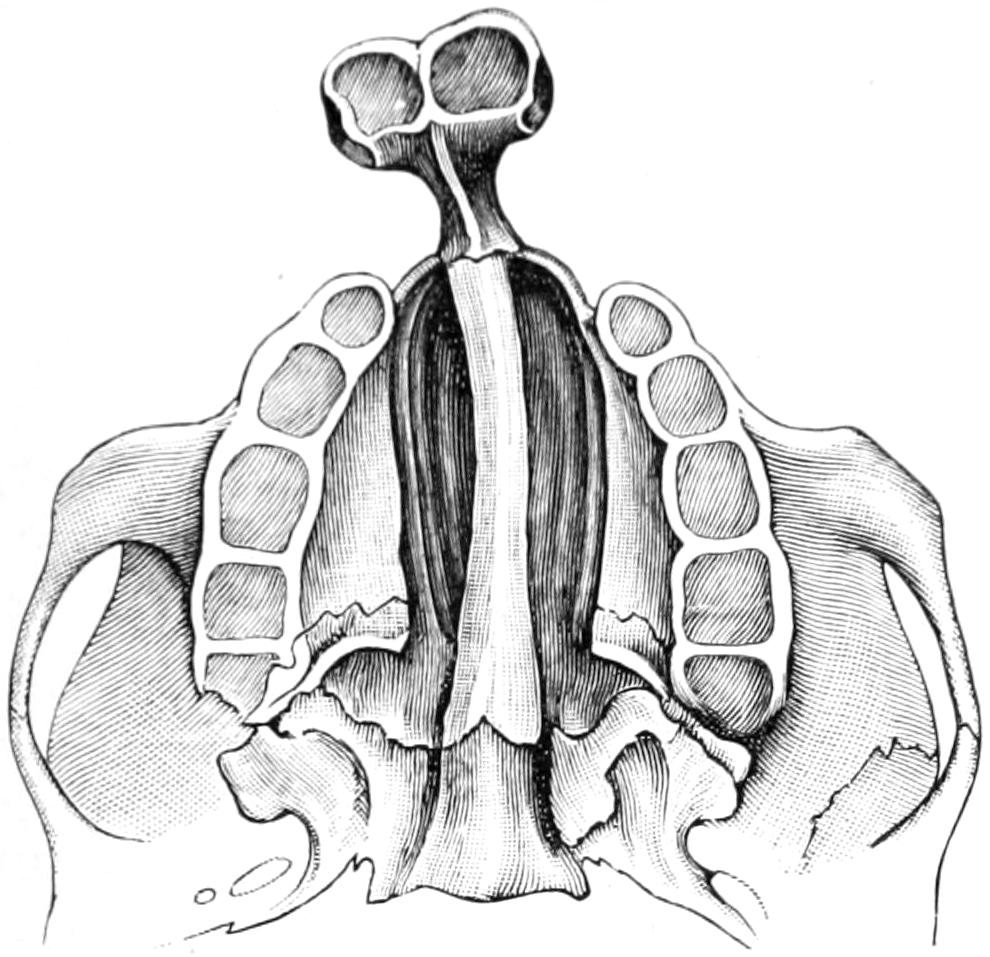
Double cleft palate.
Fig. 466
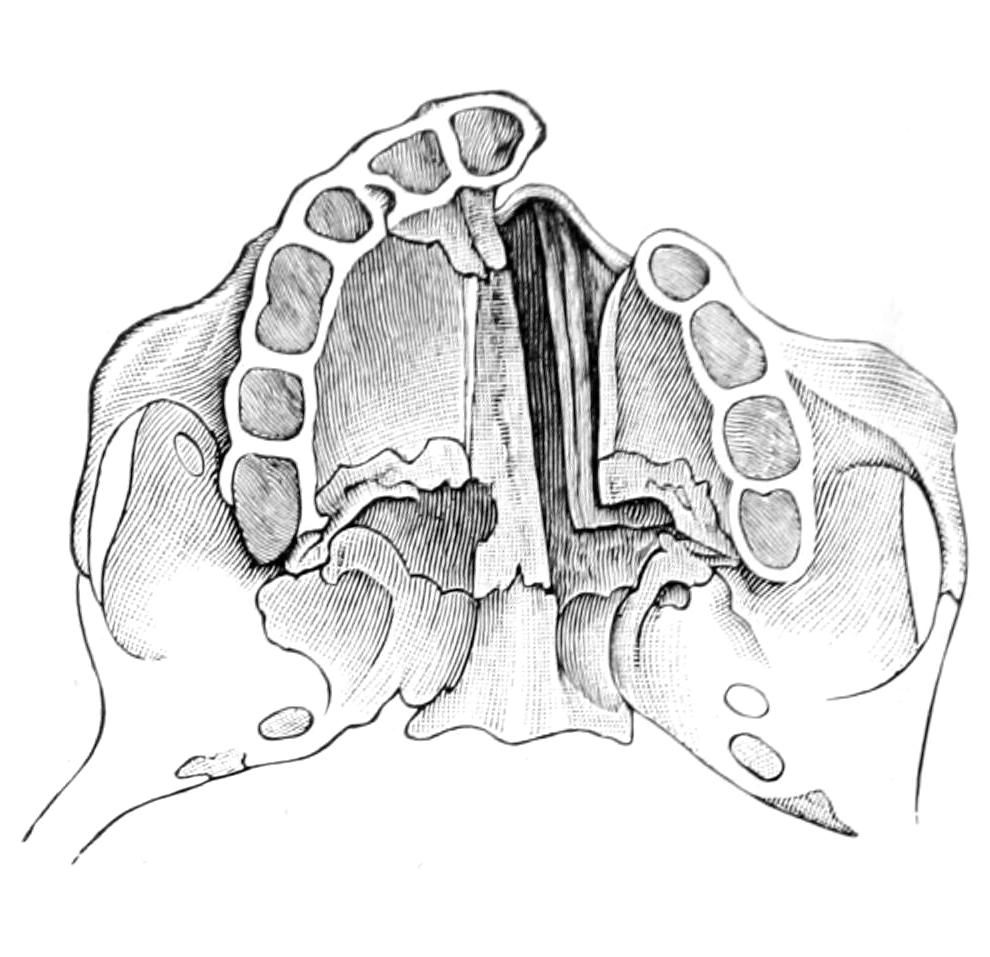
Left-sided cleft palate.
The coincidence of cleft palate with hare-lip has been described. (See p. 645.) While they often are combined, either may occur without the other (Fig. 467).
Fig. 467
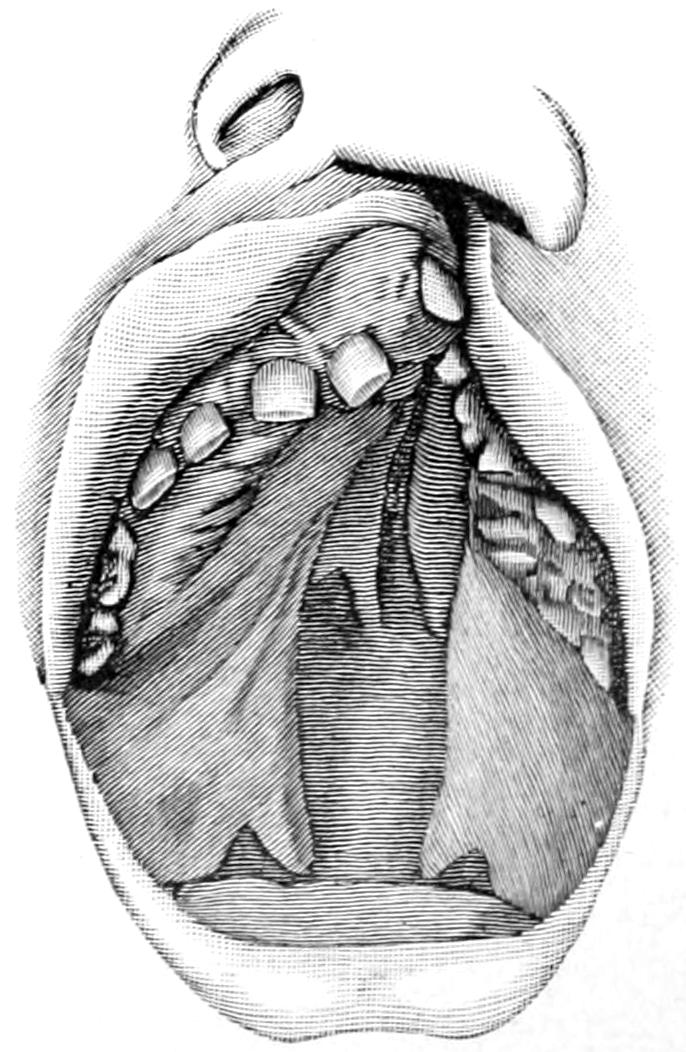
Left-sided hare-lip and cleft palate. Marked displacement of intermaxillary bone. Boy, aged six years. (Bevan.)
No matter how incomplete the palatal cleft may be the nose and the mouth are converted into a common cavity. Suction, as from the breast, is impossible. Infants with this defect should be carefully fed by hand; as they develop, food passes readily from the mouth to the nose, while there is corresponding difficulty in swallowing. With lapse of time speech becomes defective or almost unintelligible. There is, therefore, every reason for any possible closure of such defects. Against the mechanical difficulties on one side should be weighed the desirability of such closure on the other. One argument advanced in favor of operation on hare-lip is that the influence of the pressure thus afforded will tend to hasten the natural attempt on the part of the halves of the upper jaw to grow toward each other instead of in the opposite direction. On the other hand, by closure of the labial defect, the space within is materially diminished and manipulation made more difficult. It then becomes a serious problem when to operate upon a given case of cleft palate. The operation itself is usually one of no small mechanical difficulty, the space required for manipulation is most restricted, the procedure relatively a long one because of the anesthetic, and necessity for its frequent suspension in order that the operator may proceed, and, because of these difficulties and delays, the attendant shock to the patient. A puny child, unable because of the defect to take sufficient[654] nourishment, is then in far from a favorable condition for a serious operation. Without a general anesthetic no child will endure it, while local anesthesia in the young is insufficient on account of their timidity and involuntary resistance. When to operate, then, should depend upon the condition of the child, the dexterity of the operator, and the width of the cleft—that is, the amount of work to be done.
Brophy, of Chicago, has taken a radical and advanced position in this matter, and believes that these operations should be performed in early infancy, a fact which his own large experience would appear to demonstrate. Yet this same experience has developed in him a facility possessed by few, and that which such an operator may do with impunity can be duplicated by but few. He finds, however, unanswerable argument in this: that in infancy the bones of the jaws are scarcely developed, are not only friable but very flexible and yielding; that even in the very young the tissues unite kindly, and that very young infants seem to be less liable to extreme shock than those several months old; that the earlier the muscles of the palate are brought into contact and action the better performed are the functions of deglutition and of speech, and that if they are not used they atrophy; that the teeth are more likely to erupt normally, and that the extreme liability to pharyngitis produced by such wide-open fissure is obviated. To all of these statements no objection can be raised, and the only argument which can be adduced against Brophy’s position is the actual danger of the operation.
In the matter of time it may be said that in extremely competent hands operation in infancy is the ideal method, but that when children reach the age of two or three years and still have very small mouths, not much is lost by waiting until they are five or six years of age, while considerable room is gained for ease of manipulation. Much depends also on the temperament and obedience of the child. These children, like most of those born with congenital defects, are usually pampered and spoiled by indulgent parents, so that at a time when implicit obedience is most needed it seems almost impossible to do anything with them. In dealing, therefore, with such a child one should insist upon its being thoroughly disciplined, and, at the same time, accustomed to manipulation within the mouth, as the presence of a finger, tongue depressor, etc., so that when need comes for their use the child shall not be totally unaccustomed thereto. Every case should also be prepared so far as possible by antiseptic and astringent mouth-washes. A nasopharyngeal catarrh which shall compel such a patient to be constantly swallowing and spitting may defeat the object of the operation itself.
The terms usually used in this connection are uranoplasty, which means closure of the hard palate, and staphylorrhaphy, which means the closure of the soft palate.
—The responsibility of the anesthetist in these cases is great. Considering that he has to work through the same cavity as the surgeon it is sometimes very difficult to keep the child in a consistent state of narcosis. The inhaler devised by Dr. Souchon serves an admirable purpose. (See p. 644.) I regard chloroform as the safest of the anesthetics, as it is less irritating and provokes less flow of saliva. It is a good plan to cocainize the parts previous to incision, in order to so benumb them as to make reflex impressions less pronounced.
The theory of these operations, like that for hare-lip, is simple. It consists in freshening the edges of the cleft, bringing them together and holding them in position; this requires clean work and a mouth kept clean—in other words, it calls for efficient antisepsis, for strict asepsis is impossible. All carious teeth should be removed or put in good condition, and large tonsils, with their distended crypts and reservoirs of decomposing material, and all adenoid tissue should be removed.
Owen has shown the benefit in nursing infants of using an old-fashioned “slipper bottle,” having a soft giant teat with a hole on the under surface. As the infant sucks from this the teat fills the cleft, and as the child compresses it in sucking the milk is directed downward. When this does not suffice milk may be given in a warm teaspoon, passed far back over the tongue, or from a medicine dropper.
Owen sustains Brophy in the contention that the most favorable time for operating on a cleft palate is between the age of two weeks and three months, there being at that time less shock, and the bones are extremely flexible. Accepting this statement as authoritative the operation upon young infants will be described.
Previous to the operation a warm, nourishing, and stimulating enema should be given the patient. After the infant is anesthetized the tongue is drawn forward by a long suture and the mouth kept open by a mouth-gag. The edges of the cleft are then[655] pared with a sharp knife, after which effort should be made to press the upper maxillæ together, in order to test their flexibility and the possibility of approximating them in this manner. This will rarely be sufficient, however, and it becomes necessary to raise the cheek, on each side, toward the posterior extremity of the hard palate just behind the malar process, and pass a knife through the outer bony surface, making a sufficient division of the antral wall through a minimum of opening. Rather than cut too much bone at first the knife may be re-introduced. The actual approximation of the maxillæ is produced by silver-wire sutures. A firm, stout needle carrying a thick, silk pilot suture is passed through at the point above mentioned and made to appear in the fissure, where the loop may be pulled down, after which it may be again passed through the other side and made to emerge at a point corresponding to that at which it entered. The suture thus passed in one way or the other is made to carry a strong silver wire from one side across to the other, on a level above the hard palate, emerging on each side within the cheeks. Another wire suture is similarly passed more anteriorly. Two small oblong leaden plates, 1.5 Cm. in length and 35 or 40 Cm. in width, drilled with two holes, are then provided, one of them laid along the outside of each maxilla, the wire sutures passing through the holes which they contain. On one side the ends of the wire are then twisted firmly and cut short, thus forming a complete grip upon the plate on its side; then the jaws are pressed firmly together, while the wire sutures on the other side are similarly fastened over the lead plates and twisted tightly to make permanent the effect produced by pressure with the fingers. These sutures should be made sufficiently tight to permit of approximation of the borders of the mucoperiosteal surfaces, already freshened, in such a way that they may be held together with fine wire or horse-hair sutures and without undue tension.
The lead plates are left in situ for three or four weeks. If necessary the wire suture may be tightened to allow for relaxation produced by pressure effect. Some ulceration may occur beneath the plates, but this heals after their removal. Theoretical objection to this method may be made because of the tendency to narrowing of the upper jaw. In fact, however, it is only restored to its proper dimensions, as that part of the face has been previously widened by the width of the cleft. Irregular eruption of teeth or irregularity of development may be treated by a dentist.
When the vomer affixed to the intermaxillary bone projects in a snout-like manner it is necessary to remove a V-shaped section from it, the base of the triangle being along the margin of the cleft, in order that the projection may drop backward and the corresponding part fall into line with the rest of the alveolar process. This is best done as a preliminary and distinct operation.
Uranoplasty in older patients consists essentially of forming two anteroposterior mucoperiosteal flaps, from the hard and soft palates, on either side of the cleft, with their inner edges neatly pared, which should be separated from the bony roof of the mouth, and slid toward each other until they can be held together by sutures. These operations are best performed with the patient’s head hanging over the end of a table, so that blood may not find its way into the trachea or stomach, but be sponged away. This is the position of the so-called “down-hanging head” described by Rose. In fat-necked individuals it may be impracticable. After paring the borders adjoining the fissure an incision is made just within the alveolar border, close up to the teeth, parallel to the former, of sufficient length to permit of the formation of the flap above mentioned; then with raspatories or elevators it is detached from the hard palate. In a mouth with a gothic arch or roof it is often easier to form these flaps and to bring them together than in others. It may be possible in such cases to not only suture the edges, but also some portion of their raw surfaces, thus ensuring better union. (See Fig. 468.)
Branches of the anterior palatine artery will bleed freely during this part of the performance. Firm pressure and the use locally of adrenalin solution will usually overcome this difficulty. As the incision is extended backward the posterior arteries will cause the same difficulty. The wider the defect the farther backward should the lateral incisions be extended. Here the principal obstacle to easy approximation of edges is the activity of the levator and tensor palati muscles. Formerly it was a part of operations to divide the tendon of the latter as it passes around the hamular process. It has been found, however, that this is often unnecessary. A tenotomy of this tendon, however, may be made just as that of any other tendon with the expectation that the gap thus made will be filled with fibrous tissue. While, on one hand, it is of great[656] advantage to spare this tendon, on the other hand its muscle may be the principal factor operating to pull apart those surfaces which have been neatly brought together.
Fergusson and Langenbeck have not hesitated to make osteoplastic flaps when necessary, dividing the hard palate along the line of the lateral incisions with a fine chisel. This is not often required, and complicates the case to an undesirable extent, although it may be necessary in wide fissures with a minimum of tissue (Fig. 469).
Sutures are best made of fine silver wire or of black silk, as the ordinary silk is usually too absorbent, and permits infection of the stitch holes. These sutures are introduced with any one of a variety of needles devised for the purpose. A complicated needle is not necessary for this purpose, for with an adequate needle holder even the ordinary needles can be used. Silver wire may be fed directly into the needle or through a hollow needle devised for the purpose, or sutures of silk may be passed, by which a wire suture is pulled after them.
Great assistance can be obtained from packing strips of gauze between the flaps and the bone from which they have been detached. These may be inserted for pressure effect and prevention of hemorrhage during the operation, and later may be substituted by smaller packing of antiseptic gauze left for the purpose of helping to minimize tension, flaps being crowded toward each other by their use.
Fig. 468
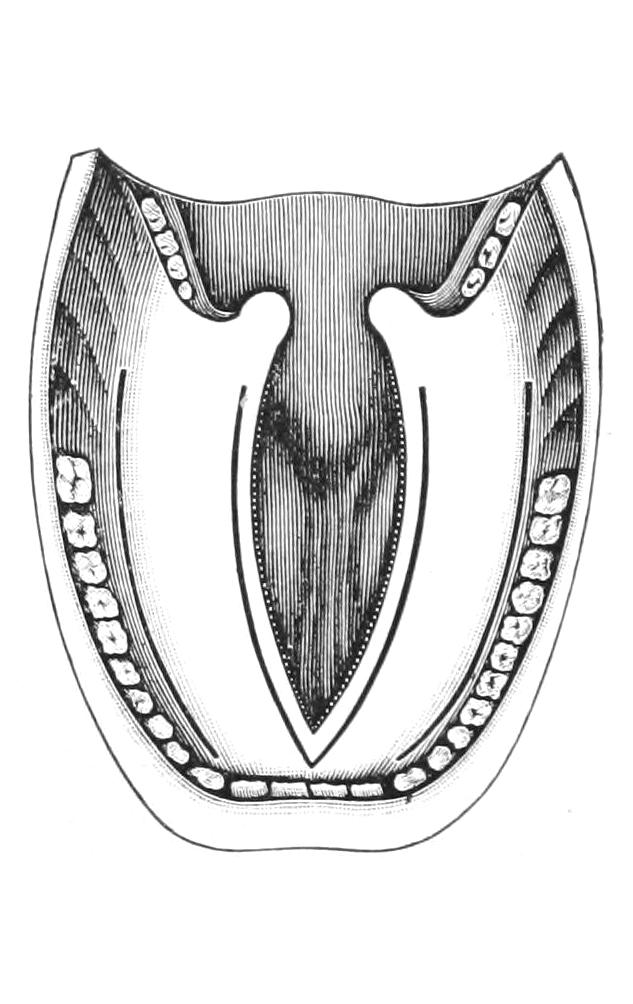
Fig. 469
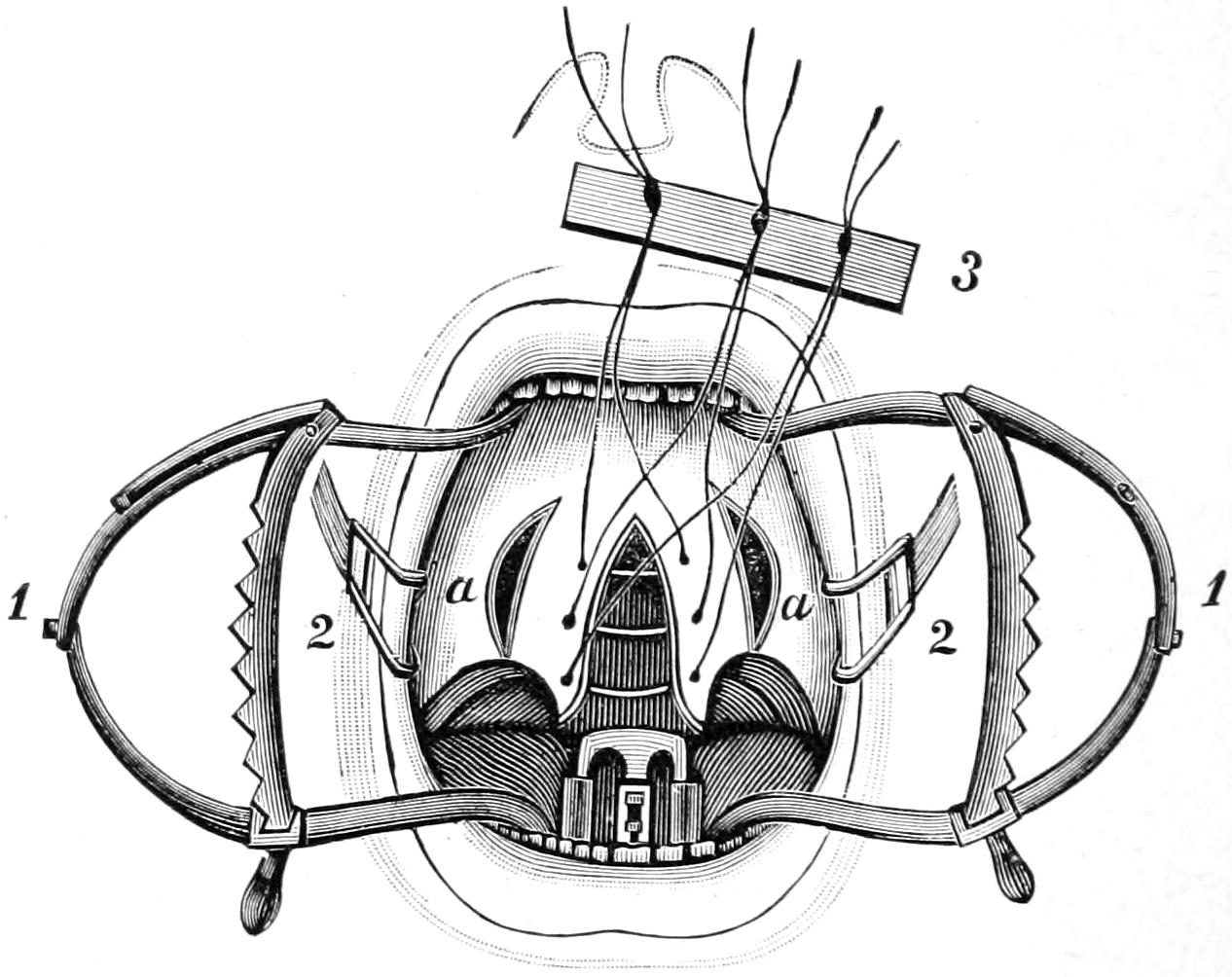
Uranoplasty, showing incisions. (Tillmanns).
Staphylorrhaphy, sutures placed. (König.)
The parts being approximated and the wound suitably tamponed it is necessary to keep the patient as quiet as possible. Young infants tend to keep up a constant sucking motion with the tongue, which may interfere with the quietude of the palate. Small doses of bromide or chloral may be administered either by the mouth or rectum, for every effort at crying, coughing, or vomiting tends to make a stress upon the line of sutures. Vomiting immediately after the operation is not necessarily serious, and yet should be avoided. Patients sufficiently old to talk should be cautioned not to converse. Water is better for the patient than milk, as the latter does not allay thirst so well and may form curds. Most of the nourishment for the next few days should be administered by the rectum, giving only water through the mouth. Children should be watched continuously lest they get fingers or toys into their mouths, and fretfulness should be guarded against. Thread sutures should only be removed with scissors and forceps after the expiration of five or six days. A useless suture is a foreign body which does more harm than good. When lead plates are used with strong wire sutures they should remain from two to four weeks. In young or undisciplined children it may be necessary to give an anesthetic for removal of the sutures. The tampons or pledgets of gauze should be removed from day to day. An antiseptic mouth-wash or spray should be frequently used.
The two results most desired are prevention of passage of food from the mouth to the nose, which is always commensurate with the success of the operation itself, and improvement in speech and voice. The earlier the closure the more natural the voice.[657] Patients in adolescence or adult life rarely note much gain in this respect, while those operated in early childhood may learn to talk almost perfectly.
There are cases, especially those which have gone for years unattended, where the arch of the mouth is of such gothic shape and the defect so wide that disappointment is sure to follow in at least one of the above respects. The art of the dentist has now reached a point where plates or obturators may be constructed for unsuitable cases, which will give better functional and vocal results than any which the surgeon can produce.
Another form of palatal defect is the result of the late manifestations of syphilis, and small and large perforations may occur, usually in the hard rather than in the soft palate. They are to be dealt with surgically, but not until after the patient has been subjected to a course of antisyphilitic treatment.
The mouth more than any other part of the body is the habitat of a large fauna and flora of minute organisms. Over one hundred different kinds of bacteria from this region have been identified by Miller, and it will be easily seen how prone fresh wounds or old lesions may be to infection from these sources. Fortunately but few of these microörganisms have decided pathogenic propensities. They lurk especially in two localities—the crypts of the tonsils and along the gingival borders and alveolar processes. Along the gingival border of the teeth tartar accumulates, by a precipitation of mineral salts from the saliva, where by irritation, coupled with germ activity, the gum is loosened from the teeth beyond the level of the enamel, and the sockets thus exposed to various kinds of infection. In consequence the teeth thus undergo dental caries, become loosened in their sockets, while, at the same time, infection travels along lymph paths until the germs are filtered out in the adjoining cervical lymph nodes, which thus suffer enlargement and often suppurative destruction. An interstitial gingivitis, therefore, is always a serious menace to the integrity of the teeth. This will furnish another argument for a semi-annual inspection of the mouth by a competent dentist, that he may clean away all tartar accumulations and treat the gums in such a way as to prevent disintegration. In elderly people, especially, there is a marked tendency toward retrocession of the gums. In young or old, when this condition is noted, it may be treated by applications of zinc iodide, either of the dry, minute crystals or of a saturated solution, which may be used daily or weekly. By such precautions the teeth may be preserved to old age, the importance of which is not generally appreciated, since the teeth are necessary for suitable mastication of food which the enfeebled stomach of an aged person can more easily digest.
Infection may also occur during the period of eruption of teeth in young people, and serious trouble sometimes accompanies the appearance of temporary or permanent teeth. Gingivitis of toxic origin is not uncommon, as among the possible effects of overdosage of mercury and phosphorus.
All that has been said of the teeth and their sockets is in the main true of the tonsils, which afford numerous crypts or lacunæ in which germs may be harbored for a long time. The explanation of probably 75 per cent. of enlarged and tuberculous lymph nodes is afforded by infection spreading from the tonsils and teeth. It may not be tuberculous at first, but it becomes so later.
In the mouth may be seen expressions of actinomycosis, tuberculosis, and especially of syphilis, among the more chronic lesions, as well as of diphtheria, erysipelas, and the result of the oidium albicans of thrush. Tuberculosis is more common in the pharynx, while the syphilitic infections may appear anywhere and in any form, as chancre on the tonsil or the lip, mucous patches of the tongue, destructive lesions of bone, all of the earlier and most of the later expressions of the disease offering serious dangers of contagion.
Stomatitis is a term generally applied to the lining membrane of the mouth and indicates little regarding its nature or seriousness. It may be of traumatic origin, as when strong caustics have come in contact with the mucosa. Ulcerative stomatitis is a disease of childhood, due to the activity of the oidium albicans or some kindred microörganism, it being usually a more serious expression of the condition known as “thrush.” Washing[658] the mouth frequently with dilute solutions of hydrogen peroxide or of tincture of iodine will usually be all that is necessary. Resistant ulcerations may be treated with 10 per cent. solution of silver nitrate. Stomatitis gangrænosa is another name for noma, or cancrum oris, which was described in the chapter on Gangrene. In these cases the surgeon should hasten the tedious separation of sloughs by use of scissors, curette, or the actual cautery (Fig. 471).
Blastomycetic lesions of the mouth, and especially of the lips, have been recognized. Bevan has reported extirpation of granulomas provoked by the blastomycetes, or yeast fungi, which are known to produce similar effects elsewhere (Fig. 471).
Fig. 470
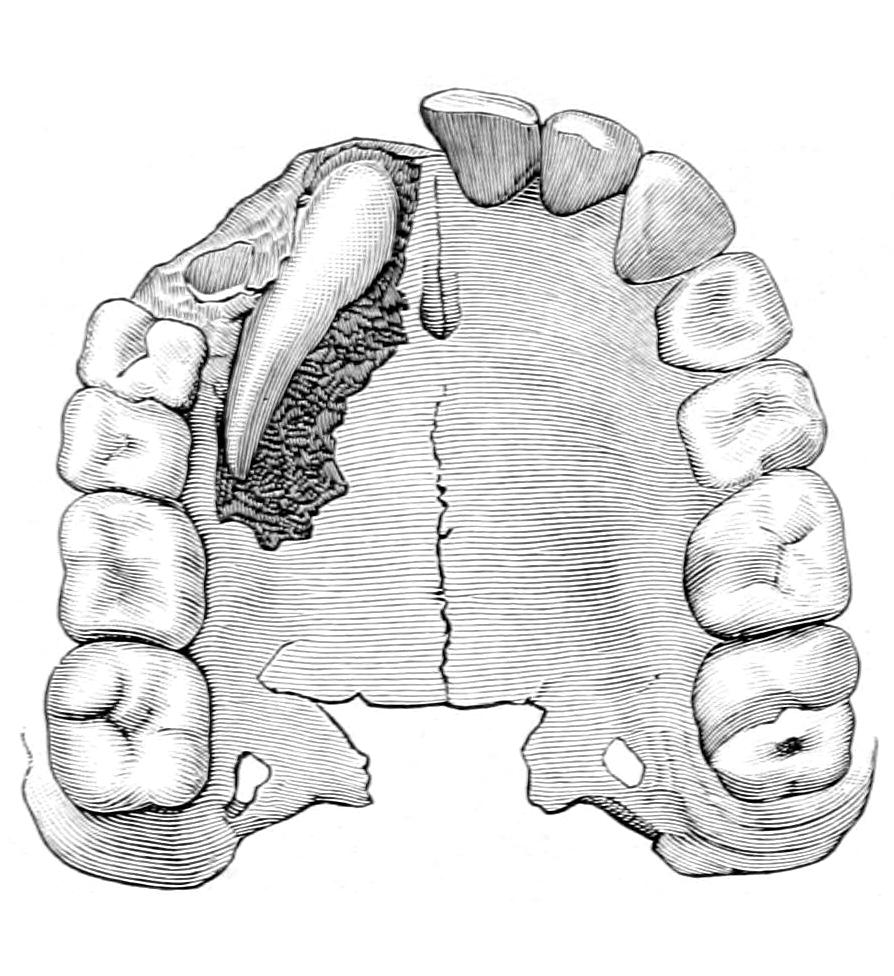
Misplaced and imprisoned tooth. (Forget.)
Fig. 471

Destruction of cheek the result of cancrum oris. (Tiffany.)
Severe infections of the mouth may also involve the tongue and thus produce acute glossitis or may spread to the connective tissue, or the submaxillary region, and there produce that type of phlegmon called Ludwig’s angina, described in the chapter on the Neck. The source of infection in most of these cases is a tooth or tooth-socket.
Injuries and wounds of the mouth are liable to septic infection, whether they occur from mechanical, chemical, or traumatic causes. Injuries inflicted by the mouth, or rather by the teeth, upon others constitute infected wounds of a serious type. Burns, scalds, and similar lesions inflicted by violent caustics, such as carbolic or nitric acids, may be followed by cicatricial contraction and produce serious consequences. So far as the latter can be foreseen they should be prevented, while for their more extreme results various plastic operations may be performed.
What has been said above with regard to the possibility of infected wounds in the mouth applies also to the tongue and other parts. It is often lacerated by being caught between the teeth in falls and blows and is sometimes bitten by epileptic patients during their convulsions. Free hemorrhage from such wounds may occur and may require ligation of vessels at the site of the wound, or of suture of tissues en masse with catgut, or ligation of the lingual artery just above the hyoid bone. Lacerated wounds should be closed with sutures, and antiseptic mouth-washes should be frequently used.
Glossitis, or inflammation of the structures of the tongue, may appear in either acute or more chronic form. To some extent it is a part of a general stomatitis, but no matter in what form occurring it is an expression of infection from a source easily recognized, and may be limited to one side of the tongue. Its principal features are swelling, which may be so extensive as to prevent movement of the tongue, infiltration of the floor of the mouth, and extension of a phlegmonous type down the structures of the neck. The[659] swelling may also involve the epiglottis and larynx, causing edema and even suffocation unless tracheotomy be performed. Thus acute glossitis may frequently lead to abscess formation either in the tongue or the adjoining tissues. When swelling is extreme its formation may be anticipated, and free incision should be promptly made to permit of its evacuation. Naturally the region of the large vessels should be avoided, and, after external incision the focus should be reached by blunt dissection. Some of these cases are due to extension of an erysipelatous process commencing externally. Even hemiglossitis may be accompanied by serious swelling and high fever. One form of this affection is supposed to be analogous to herpes zoster. The relation of phlegmonous glossitis to Ludwig’s angina, the latter being described in Chapter XLI, may be readily appreciated. Sometimes it is due to the entrance of foreign bodies, as fish-bones, bone-splinters, and the like.
Most urgent danger is that of asphyxia from pressure, and of inspiration pneumonia, for the infected saliva in these cases will trickle down within the larynx and trachea. Even gangrene of the tongue has been observed as the result of pressure, while the teeth will leave their impress upon the sides of a swollen tongue.
The more chronic infections of the tongue are syphilis, tuberculosis, and actinomycosis. Syphilis may assume a primary type and occasionally typical chancres may be seen on the tongue. It is frequently the site of mucous patches and of other ulcerative lesions. Tuberculous ulcerations of the tongue assume less indurated and irregular borders, and may be suspected in connection with well-marked tuberculous lesions of other parts of the respiratory tract, being particularly common in consumptives. These ulcers yield best to cauterization and antiseptic mouth-washes, whereas syphilitic lesions rarely disappear without active antispecific medication. Both syphilis and tuberculosis produce gummatous tumors, the former more frequently than the latter. The former will disappear equally readily under suitable treatment.
Actinomycosis of the tongue is rare in man. It constitutes a granuloma which may soften and present a ragged, ulcerated surface. (See Actinomycosis, Chapter VIII.)
Leukoplakia implies the appearance of opaque, white patches upon the mucous surfaces of the tongue as well as on the lining membrane of the mouth, lips, and palate. They are far more frequent, however, on the tongue and generally appear there first. Here they appear almost as if thin scales could be separated from the surface upon which they lie, but this will not be found possible when the effort is made. The patches are irregular, but sharply outlined, occasionally confluent, involving the entire upper lingual surface; while the plates become harder and more roughened as they grow older, and furrows, subsequently ulcerating, may appear between them. The affection is chronic and intractable. It occurs often in the mouths of smokers during middle and advanced life. While its etiology is unknown it may be due to chronic irritation.
Between leukoplakia and epithelioma of the part involved there seems to be a strong relation, and the former is often regarded as a precancerous stage of the latter. Epithelioma is a frequent terminal feature of leukoplakia. There often seems, moreover, a predisposition to it in syphilitic individuals. It is mainly to be distinguished from secondary syphilitic lesions, which may be done by recalling its chronicity and its obstinacy to the treatment which would disperse the latter.
In the way of treatment smoking must be prohibited, antiseptic mouth-washes often used, with cauterization to a mild degree. These methods, however, suffice only for the milder cases. If any caustic be used it may be either 10 per cent. chromic acid, chemically pure lactic acid, or nitric acid, caution being used in their application. The more serious forms of leukoplakia will usually yield to local anesthesia, followed by curetting of each patch until the raw surface beneath is exposed, and then the application of the actual cautery. Rigorous treatment is necessary when ulcerated and fissured patches are present.
The benign tumors of the tongue include nevi, often in connection with single or multiple papilloma, or which may assume the type of multiple papillomas, each of which is extremely vascular. Occasionally the tongue will be seen almost covered with these small growths. This condition is noted usually in young children, and is practically of congenital origin. It frequently subsides spontaneously, but may require the actual cautery or something equally radical. The other benign tumors are of occasional occurrence, even an enchondroma having been occasionally seen. Much more common are the retention cysts, especially that particular form of cyst occurring beneath the tongue[660] or at its base, known as ranula. This term is vaguely applied to cysts produced by obstruction of one of the salivary ducts or by cysts of congenital origin. It is caused mainly by incomplete obliteration of the thyroglossal duct. A so-called ranula may contain colorless fluid, more or less thick, and mixed with epithelial or dermoid products.
Fig. 472
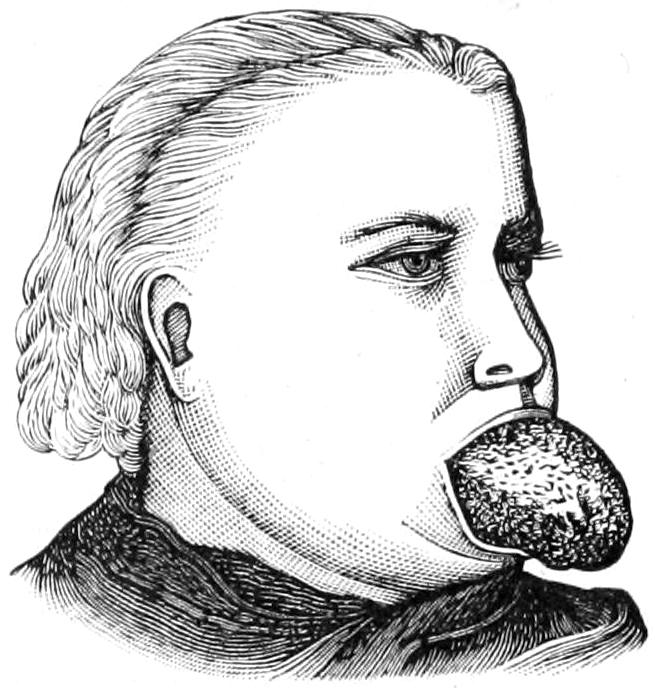
Macroglossia. (Tillmanns.)
It is possible to extirpate nearly all of these growths through the mouth, with aseptic precautions.
Macroglossia is a condition of congenital enlargement of the tongue, due mainly to a form of lymphangioma, which may be accompanied by vascular papillomas or alteration of the mucous covering. Such a growth will produce enlargement of the tongue to an extent that does not permit of its retention within the mouth. Excision of a V-shaped portion sufficiently large to reduce the tongue to proper dimensions is usually requisite in these cases (Fig. 472).
Of the malignant tumors of the tongue epithelioma is by far the most common. It is rarely seen in women, and not often before middle life. Here more than in almost any other part of the body the possible causative factors of irritation and trauma are present, jagged teeth furnishing the usual source of each. It is known also to be a frequent sequel of leukoplakia and of various chronic ulcerations and other lesions. Other benign growths occasionally alter their type and become epitheliomatous. It occurs usually on the exposed surface, and tends quickly to an ulceration whose border is indurated and often fissured. It is ordinarily distinctive in its appearance, but occasionally needs to be differentiated from lesions of syphilis, tuberculosis, and actinomycosis. Lymphatic involvement occurs early in each of these conditions and may be confusing. A suspicious ulcer which tends constantly to deepen and increase in dimensions, accompanied by marked induration and lymphatic involvement, and not benefited by antisyphilitic treatment, will generally prove to be epitheliomatous. As the lesion extends there is involvement of all the surrounding structures—the floor of the mouth as well as the pharynx, the salivary glands, and even the lower jaw itself. When pain is felt it is usually referred to the region of the ear. There will be, naturally, interference with all the functions of the mouth, as well as with speech, while starvation, septic infection, and hemorrhage may terminate the case.
In no part of the body is prognosis more unfavorable. Recurrence, even after early and radical operations, is usually unavoidable, and it is doubtful if 10 per cent. of cases of epithelioma of the tongue are free from disease at the expiration of three years after removal.
Treatment should be prompt and radical. It consists of extirpation, which must be extensive to be effectual. A small cancerous ulcer on one side of the tongue may justify removal of one-half of the organ, but, under nearly all circumstances, it is best to make a complete removal of the tongue. This may necessitate a formidable operation, and may be expected to materially interfere with speech; but that it does not prevent it is shown by the fact that in medieval days, when tearing out the tongue was a means of punishment or torture, men were often still able to speak intelligibly.
Inoperable cases should be made comfortable with cleansing mouth-washes and applications of local anesthetics, coupled with such anodynes as it may be necessary to administer. Resection of the lingual nerve will sometimes relieve the intense pain, while proximal ligation of the lingual artery may arrest rapidity of growth. It is in these inoperable cases that Dawbarn’s suggestion of the extirpation of the external carotid artery, first on one side and then on the other, may be put into practice, the intent being to so completely shut off circulation as to check growth. In some forty cases or more it has given results as satisfactory as could be expected.
[661]
Operations upon the tongue include partial excision and complete extirpation, perhaps with much of the adjoining tissues. Here, as in every operation, the mouth should be thoroughly cleansed. Before extensive operations a preliminary ligation of the lingual artery should be made on both sides, just above the hyoid bone. (See p. 352.)
A small lesion at the tip of the tongue may be excised by a wide V-shaped removal of the anterior part of the tongue, under cocaine anesthesia, the edges of the opening being brought together with sutures of silk or of chromic catgut, for ordinary catgut would be too quickly macerated when thus soaked in the mouth. The lesion may be so placed as to not permit of this V-shaped opening being symmetrically placed. The same rules, however, will apply, the operation being performed with a sharp-bladed bistoury or with sharp scissors, bleeding vessels being seized with forceps as they are cut. These clean removals give more satisfactory results than the old operations performed with the écraseur or cautery. A complete excision of the lateral half of the tongue is easily made through the mouth, the organ being controlled by a stout suture passed through the other portion. The vessels and lymphatics of the tongue do not cross its septum, and all the hemorrhage that need be anticipated will come from the side attacked; but when it is necessary to remove an entire half of the tongue the case has usually progressed to such an extent that its complete removal will be usually indicated and will be more effectual.
Of the various complete operations upon the tongue but three will be described here.
Whitehead’s operation comprises an almost total extirpation made through the mouth, without division of cheeks or lips. The patient is placed in a semi-upright or upright position. The mouth is held open with a mouth-gag, for which purpose none serves better than the O’Dwyer gag used for intubation. The operation is begun under brief but complete anesthesia, and is usually completed before the patient has recovered from it.
The tongue being secured with a stout suture passed through it, its frenum and its attachment to the fauces are divided, along with all other reflections of the mucosa. Vessels which spurt should be caught at once. General oozing may be disregarded. After being thus freed the tongue is pulled forward, a strong suture passed through the glosso-epiglottidean fold, and then with sharp, slightly curved scissors the entire organ is cut away from its base, the lingual arteries being seized the instant they are divided. The operation is bloody for the few minutes required for its performance, but is quickly done and with a minimum of disfigurement. By the last-mentioned suture the stump can be pulled forward, should the epiglottis tend to drop backward and disturb respiration, or should hemorrhage require. After its conclusion, and during the after-treatment, frequent warm, antiseptic solutions should be used for washing the mouth, and it is the practice of some to paint the raw surfaces with a styptic varnish, made of balsam and saturated solution of iodoform in ether. In order to avoid the passage of saliva downward the patient is encouraged to sit up and to expectorate freely rather than swallow infected saliva.
The Regnoli-Billroth operation is performed by turning down a horseshoe-shaped flap, its convexity being taken from the symphysis of the jaw, and thus opening into the mouth from below. After making the opening sufficiently wide, the tongue, through which a traction suture has been passed, is pulled through the submental wound and its base divided with scissors. Should it be difficult to locate bleeding points in the stump a finger may be hooked in the pharynx and the latter pulled forward. The submaxillary wound is then closed with sutures, with one drain.
Fig. 473
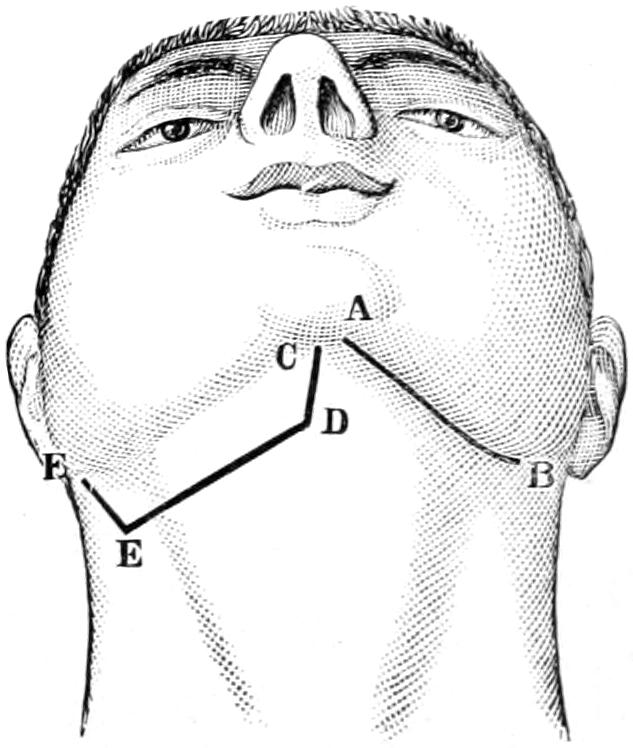
Lines of incision for total excision of the tongue. (Chalot.)
The most complete of these operations is that described by Kocher. It permits of removal of the tongue, of the floor of the mouth, of all infected lymphatics, and even of a portion of the jaw if this be necessary. A line A-B, Fig. 473, may offer sufficient exposure by incision, but the line C-D-E-F will permit more complete attack. Through[662] this incision a flap is raised, the facial vessels being ligated. All lymph nodes are extirpated, as well as the salivary glands, if necessary. After separating the mylohyoid from its insertion in the inferior maxilla the mouth is opened and the tongue drawn out through the incision, where it may then be kept under perfect control. It will facilitate matters if the lingual arteries be secured before the entire tongue is cut away. In some cases a preliminary tracheotomy is considered advisable, largely because the performance of the operation interferes with the administration of the anesthetic in the ordinary way. Should it be done the pharynx should be tamponed until the conclusion of the operation. The trachea tube may be immediately removed or left, as seems advisable, while the patient is fed for several days with a stomach tube.
Operations suggested by Sédillot and Langenbeck include division of the lower jaw in such a way that by separation of its portions a more complete exposure of the floor of the mouth is afforded. They are at present rarely adopted, unless extension of the disease to the bone should necessitate excision of some portion of the jaw itself.
The tonsils are the most conspicuous portion of the ring of lymphoid tissue which extends completely around the original opening connecting the exterior of the face with the upper end of the neurenteric canal. This tissue is particularly inflammable, and this may account for the frequency with which severe infections of the tonsils occur, and the marked toxemia which complicates even mild degrees of the same. In this lymphoid, or, as it is usually called, “adenoid” tissue, crypts and follicles abound, and in these latter all sorts of infectious materials accumulate. Thus acute infections, as well as chronic hypertrophies due to pressure and irritation, are extremely common.
The various forms of angina, i. e., sore throat, have to do largely with expressions of these infections in varying degrees of severity. The adjoining mucosa and other tissues frequently participate, and it is possible to produce a painful degree of chemosis of the membranes involved in a short time. Adjoining lymph involvement, with discomfort or even distress in the region of the throat, and sometimes pronounced general malaise, are extremely common accompaniments.
The “cynanche tonsillaris” of the older writers implied an acute expression of this kind, often with more or less exudation, which, accumulating upon the exposed surfaces, produces there a membrane, the condition being most noticeable in the pronounced types of diphtheria. At other times activity is manifested rather in the peritonsillar structures, and acute and suppurative types of cellulitis, leading either to abscess in the tonsil or deep in the neck, are the result. A surprising degree of toxemia accompanies these lesions and sometimes severe and fatal general septic infection, perhaps with endocarditis. Abscess of the tonsil may produce so much occlusion of the pharynx as to make breathing difficult and even almost impossible, perhaps even to a point requiring tracheotomy. Tonsillar abscesses usually evacuate themselves in time; if they are opened by the surgeon relief comes promptly, with evacuation of pus, no matter how brought about.
Many such abscesses could be easily recognized and incised were it not for the surrounding inflammation, which prevents the patient from opening the mouth sufficiently wide to expose the pharynx. Suffering in these cases is acute.
A swollen and fluctuating tonsil, if it can reached, is easily perforated by a sharp, straight knife. Erasion and fatal perforation of the carotid artery has been known to be a sequel of such a case unrelieved. Again, pus having its source within the tonsil may burrow in such a direction as to produce a retropharyngeal abscess.
The tonsil is rarely the site of primary syphilitic lesions, more often of the secondary, and occasionally of tuberculous lesions.
The most common chronic affections of the tonsils result from failure of absorption of inflammatory products after acute inflammations, which leaves a permanent enlargement, and which is constantly irritated and provoked into further growth by the retained contents of the tonsillar crypts. It is in this way that chronic hypertrophy, or the so-called enlarged tonsils, result. These conditions are especially common in children, presenting the milder forms of the status lymphaticus. (See Chapter XIV.) These enlargements are seldom seen alone in the tonsils. Similar involvement of the lymphoid[663] or adenoid tissue in the vault of the pharynx, and even at the base of the tongue, is quite common, the entire original lymphoid ring being more or less involved.
The consequences of chronic enlargement of the tonsils have much to do with the subsequent welfare of patients. Not only is speech interfered with and made peculiarly “throaty,” but, owing to encroachment upon the natural breathing space, children suffering in this way contract a habit of carrying the head forward and stooping the shoulders, in order thereby to increase the dimensions of the nasopharynx; thus they become “mouth-breathers” and hard of hearing, which is deleterious to their intelligence as well as to their physical well-being. Such children, in time, become stupid, unintelligent, and defective in many ways. There is, then, every reason for removing these obstructions to respiration and for doing it early.
Children thus suffering will present such peculiarity of voice as to suggest immediate examination of the oropharynx, while the posture above described and the existence of the mouth-breathing habit should also prompt investigation. An instant inspection through the widely open mouth should permit the detection of this condition. Should it be desired to estimate it more thoroughly it may be done with the finger, although it will provoke the act of coughing or vomiting and be resisted by most children. Frequently the enlargements can be felt from the outside. There is but one suitable treatment for such a case, i. e., tonsillotomy.
Tonsillotomy may be effected with any one of several different patterns of tonsillotomes on sale in the instrument stores, most of which are neat and speedy in their work, but the surgeon need not refrain from the purpose of removal because of the lack of such an instrument, as it may be easily accomplished without one. Young and timid children are probably best anesthetized, although if one can establish perfect confidence it may be possible to do it by the aid of local anesthesia. In adults the latter will always be sufficient.
An anesthetized patient should be placed in a chair or semi-upright, and the mouth widely opened. The circular loop of the instrument should be fitted over the tonsil, this, if necessary, being drawn into its grasp by a small hook or forceps, after which by a quick motion of the cutting blade the projecting mass is removed. All instruments are made to be used with either hand and to cut on either side. The practised operator will, therefore, use his left hand when operating on the right tonsil of the patient, and vice versa, it being best to adopt this order, for should he be a little clumsy with his left hand and the patient be thereby somewhat disturbed, the right hand may more dexterously perform the excision on the other side. The surgeon should be thoroughly familiar with his tonsillotome before using it. It is not, however, necessary to employ such an instrument, and it will often be more satisfactory to grasp the projecting tonsil in the bite of a suitably constructed tenaculum forceps, or even hold it with a common tenaculum, while with blunt scissors, long handled and curved upon the flat, the tonsil itself is cut away.
None of these methods gives promise of complete extirpation of the tissue, which is often chronically diseased, and it is often well, therefore, to complete the extirpation with the sharp spoon or even to use the finger-nail as a curette. Hemorrhage will be active for a few moments, but is nearly always controlled with either iced water or water as hot as can be borne. Only rarely does it give rise to serious trouble. In such cases adrenalin may be used. Cases are on record where it has been necessary even to tie the carotid, but such instances are mostly bugbears which need not deter one of good judgment from a properly devised operation. Antiseptic gargles, and avoidance of speech and swallowing of hard food, will be all that are needed in the after-management.
The young and the timid will need complete anesthesia, which should be complete in order to abolish reflexes, and cocaine locally to ensure this condition. Many of these subjects are, however, those presenting minor degrees of the status lymphaticus, to whom anesthetics should be administered with caution. In such children tonsillotomy should be combined with the erasion and removal of other involved adenoid tissue in the nasopharynx. Inquiry should be made as to whether the patient bleeds unduly freely after minor injuries. In a bleeder it would be well to proceed with caution or abstain from operating.
Foreign bodies in the tonsil are as often fish-bones as any kind; they all give rise to serious irritation. True calculous formation in the tonsil is known. Every foreign body which can be detected and exposed should be removed.
[664]
Tumors of the tonsil are usually of the malignant type, either epitheliomatous or sarcomatous. A cancer of the tonsil should be recognized as such very early if operative or other relief is to be effectually afforded, and if operation is made it should be done more thoroughly than can be done through the mouth.
External pharyngotomy is the measure usually required for this purpose. This is usually performed by making a long incision along the anterior border of the sternomastoid muscle, and, after retracting it, making careful and blunt dissection down in the direction of the tonsil, separating tissues which are evidently not involved, but excising everything in which infiltration can be recognized. An extensive operation of this kind would justify preliminary or provisional ligation of the common or at least the external carotid artery. Care should be taken to avoid wounding the nerve trunks, especially the hypoglossal.
Subhyoid pharyngotomy is performed by a transverse incision just below the hyoid bone, with division of the platysma, the omohyoid, the sternohyoid, and the thyrohyoid muscles, leaving enough of their insertion into the bone to permit of subsequent reunion by suture. The thyrohyoid membrane is then divided in such a way as to also permit of its reunion by sutures. Then the mucous membrane, which will probably now protrude into the wound, is caught and divided, retraction sutures being inserted in the edges of the wound. The epiglottis may be retracted or a suture may be passed through it, to be used as a retractor. The lower portion of the pharynx is now exposed and through this opening the tonsil may be removed. After completion of the deeper work the different layers of the tissues are reunited with chromic gut and the deep wound is drained.
Transhyoid pharyngotomy. Vallas has suggested a central method of approach to the pharynx by a median incision, through which the mylohyoid muscles are separated, the body of the hyoid exposed, and its division effected with stout scissors or with cutting forceps. When its two halves are retracted a space over an inch long is made, through which the mucous membrane of the pharynx may be opened, this being done by making it protrude with the finger passed into the throat, which shall thus serve as a guide. In closing the wound it is not necessary to make suture of the hyoid bone.
The alveolar process, which furnishes the actual sockets for the teeth, and which carries that peculiar fibrous texture with its mucous covering known as the gum, is a frequent site of ulcerative disease and fertile source of infection. While the toilet of the mouth is much more generally attended to at present than in times past, the majority of people are extremely inattentive and indifferent to the condition of the teeth and the gingival borders. As elsewhere stated the mouth is the habitat of an extensive flora and fauna, and deposits of tartar along the gingival border afford excellent hot-beds for their development and growth. This accounts for the marginal ulceration of the gum, or ulcerative gingivitis, seen in so many mouths, and it may be regarded as the beginning of a disease process, pyorrhea alveolaris (Rigg’s disease), that will eventually cause the loss of the teeth and extensive infection of the lymphatics in the neck. In almost every mouth where such accumulations of tartar have taken place the expressions of local infection may be traced by a bluish or purplish line along the gingival border, with some degree of sponginess and mild ulceration.
The enamel covering the teeth is extremely resistant, but when the dentine is exposed below the enamel line, as happens in such instances as those just described, bacteria may easily enter the dental tubules, and dental caries or alveolar suppuration is the result. In order to prevent such disease the services of the dentist should be secured at least as often as every six months, in order that all tartar may be removed and the gums placed in a healthy and resistant condition.
For the marginal ulcerations thus produced there is no better treatment, after removing tartar, than the local application of zinc iodide, either in fine crystalline form or in saturated solution. It is not so much the visible surfaces which need such application as does the gingival tissue in concealed locations and between the teeth. Zinc iodide is not only an excellent antiseptic, but a powerful astringent, and meets a double indication. It may be applied once a week or oftener.
[665]
The dental enamel is the protective medium which, being once injured, exposes the dentine beneath to the possibility of infection. Such injuries are mechanical, but usually minute. The practice of putting hot food into the mouth and immediately following it with a drink of iced water is calculated to crack the enamel on a tooth as it would on any other material. Such a crack, although microscopic in dimensions, permits the entrance of bacteria into the dentine, in whose tubules they multiply and produce minute amounts of lactic acid. The enamel will resist this acid almost indefinitely, but the softer dentine is dissolved by it, and in this way cavities are formed within the teeth, and the condition known as dental caries is engendered. While it requires the special art and training of the dentist to cope with such conditions, every general practitioner should be familiar with the circumstances under which these lesions are produced. Congenital defects of the enamel afford also the same opportunities for infection.
When infection has extended to the delicate pulp cavity and when one of the terminal fibers becomes exposed the condition is accompanied by more or less distress, and when the alveolar socket becomes involved the tooth is loosened, either temporarily or permanently, according as the condition is treated. Thus a small alveolar abscess, referred to as “gum-boil,” may result. In the former case there is usually a small sinus which leads down to the root of the tooth, either through the spongy bone or alongside the tooth itself.
Plate III illustrates the conditions in teeth undergoing various forms of caries, there being numerous bacterial forms responsible for different types of the disease.
Treatment here does not differ in principle from that for treatment of caries in bone. Its essential feature is actual removal of all infected dental tissue, with a combination of protection against further infection, and that substitution for lost tissue which is effected by the use of gold, amalgam, or some of the other fillings in common use among dentists. American ingenuity has reached its acme in the discovery of means and methods for atonement of tissue thus lost by disease, and American dentists certainly lead the world in the mechanics of their art. They go much beyond the mere filling of diseased teeth, but have devised substitutes for teeth actually lost, and much of the plate work of the past is now substituted by what is known as crown and bridge work.
Dentistry as a part of oral surgery has now become a specialty by itself. A competent dentist, therefore, is a necessary coöperator in the treatment of all diseases of the teeth.
It is mainly when disease has spread from the teeth to the surrounding bone and tissues that the surgeon as such intervenes. Caries and necrosis of a small or large part of either jaw may be the result of extension of disease processes having their beginnings as above. In the chapter on the Neck, when dealing with the subject of tuberculosis of the lymphatics, it is stated that a large proportion of such cases due to the propagation of infection from the oral cavity and often from the teeth.
There are two substances used in medicine and in the arts which have a proclivity for the tissues of the mouth and jaws. These are phosphorus and mercury, the former usually affecting the bone and the latter the softer tissues. Before legislation had been enacted by which the young were prevented from working in match factories phosphorus necrosis of the lower jaw was not uncommon. Today it is rarely seen. Again, in the older days when mercury was given in large amounts, and its effects were not as well guarded against as now, mercurial stomatitis proceeding to ulceration and even loss of teeth was not an uncommon event. Now it is seen only in those who have an idiosyncrasy which makes them peculiarly liable to its effects. The mechanism of phosphorus necrosis is supposed to be an ossifying periostitis, with formation of small osteophytes in the alveolar periosteum, which lower tissue resistance and permit easier invasion of bacteria from the mouth. (See p. 428.)
The extension of disease from the teeth, especially of the upper jaw, upward into the antrum of Highmore, with its consequent infection, is elsewhere discussed, and the reader will find the treatment of empyema of the antrum considered in Chapter XXXVII.
The teeth are also subjects of certain tumor formations which in general are spoken of as odontomas, and have been mentioned in the chapter on Tumors. (See p. 281.)
Teeth, moreover, show at times excessive development or marked displacement or defects of development. Thus they erupt in abnormal positions, or fail completely in eruption, or they project in abnormal directions or are sometimes amalgamated. The art and science of the dentist permit of wonderful control of abnormal development of those teeth which once appear upon the surface. Children whose teeth are irregularly[666] placed, or which are abnormal in any respect, should be placed under the care of a competent specialist. The most serious tumors of the teeth are those connected with cyst formation, which may assume considerable size. A dentigerous cyst is proper material for the surgeon rather than for the dentist, inasmuch as while the operation can be usually done through the mouth it may require external incision and removal of a considerable shell of bone, perhaps with plastic restoration of tissues.
The general practitioner has often to remove diseased teeth as well as the surgeon. The theory of tooth extraction is simple. Its performance, especially when the tooth is diseased, may be exceedingly difficult, for such teeth may be crumbled in consequence of the force needed for their removal.
Forceps of different shapes are required for the various teeth. At least half a dozen different patterns are requisite. A form of elevator is also of use in elevating stumps which may lie beneath the alveolar border.
The tooth to be removed should be seized along the fang and beyond the crown. The blades of the forceps should be pressed firmly down and along the tooth, in order to separate from it the softer tissues of the gum and the firmer tissue of the alveolar socket. This is thinner upon its outer aspect than its inner, save in the location of the wisdom tooth, and it is the outer border which is more easily broken away by force applied toward the cheek rather than toward the interior of the mouth. Using first one blade of the forceps and then the other to split the socket and separate the osteofibrous tissues, the tooth being then firmly grasped between them, the operator makes a series of rocking movements, by which it is itself loosened and its further attachments torn, until by a lifting effort it can be extracted from the socket. In this minor operation the head must be firmly held with the disengaged hand, or better between the forearm and the operator’s body, while with that hand he supports and manipulates the lower jaw, if it be a lower tooth which is to be removed.
The operation is painful for the moment. With timid patients local anesthesia may be produced with cocaine or one of its substitutes, the solutions being sterile, and either locally applied around the socket or injected into the surrounding tissues with the ordinary hypodermic syringe needle. Such attempts are not without their own danger, for I have seen serious infection follow the introduction of unsterile solutions by dentists not familiar with aseptic technique. Again, nitrous oxide gas may be administered, it being usually necessary to employ a mouth-gag. Recovery from anesthesia is prompt and muscle spasm may not be entirely abolished; therefore, the gag should be inserted before the gas is administered. It may be sufficient for the purpose to employ a good-sized piece of cork, to which a cord should be attached in order that it may not disappear down the patient’s throat during a violent effort at inspiration. The horizontal position is the safer for this purpose.
It is especially the removal of fangs or roots which gives the greatest trouble in these cases. For this purpose special forceps are devised, but for their use it is necessary to clear away the gum and periosteum and to cut away a portion of the alveolar process. Such broken fragments of teeth allowed to remain give rise to curious reflexes, such as convulsions, neuralgia, etc., all of which makes it apparent that the extraction of a tooth being undertaken it should be thoroughly performed. After its removal the patient should rinse his mouth with water as hot as can be borne, to check hemorrhage. The removal of the tooth having left an open pathway for infection, antiseptic mouth-washes should be frequently used and the socket packed with antiseptic gauze. Except in rare instances granulation tissue fills the cavity and the process of repair is rapid.
Among the accidents which may follow extraction of teeth are hemorrhage, which may be checked by plugging and the use of adrenalin. Adjoining teeth are occasionally injured in clumsy efforts at extraction, while not infrequently a patient who has not sufficiently described his symptoms has indicated to the dentist the wrong tooth, whose consequent extraction has, therefore, not relieved him of his difficulty. Some teeth have such spreading roots as to make their removal extremely difficult, and even careful operators have occasionally inflicted fractures, especially of the lower jaw. The treatment of such an accidental fracture will not be different from that of fractures otherwise[667] produced. Such an accident as forcing a tooth upward into the antrum of Highmore should be followed by its removal, even at the expense of further operation, while excessive tearing of the alveolar border, or especially of the gum, may be treated by suitable packing or by suturing. The accident of aspiration into the larynx of part or all of a tooth just removed has been known to be followed by suffocation. The operator, therefore, should not release the tooth from the grasp of the forceps until the latter are entirely out of the mouth.
By accident or from indifference it may happen that a healthy tooth has been removed instead of one diseased. Should this happen the tooth may often be re-implanted after being cleansed, and will usually resume its previous position and function. So feasible is such re-implantation of teeth that they have been frequently removed or transplanted from one mouth to another, for a compensation, a new socket being made for the reception of the healthy tooth just removed from the mouth of the individual willing to part with it.
While the jaws are not subject to affections peculiar to these parts, there may be seen in them peculiar expressions of general conditions, made so by virtue of environment or complexity of tissues. Most of the acute infections of the jaw bones are propagated from the teeth or the tooth sockets. There may be periostitis and osteomyelitis, and these may be followed by a sclerosing process or acute suppuration. The jaws are prone to be thus affected in consequence of the acute exanthems and the infectious fevers, while the effects of mercury and phosphorus have been mentioned. The treatment of the inflammatory affections here is the same as elsewhere, i. e., early incision and complete evacuation of pus, with removal of necrotic bone or other tissue. Many sequestra may be removed from within the mouth in such a manner as to avoid disfiguring scars. When external sinuses complicate the case, incisions through the skin should be made. These may be so planned as to coincide with the natural wrinkles or folds of the face.
The temporomaxillary joint is a locality of considerable interest. Dislocations take place here in consequence of blows or of violent muscular effort, and are easily recognized because of the fixation and displacement which they produce. Ordinarily they are easy of replacement. These luxations may be unilateral or bilateral. As the result of violence the condyle has been driven upward through the base of the skull, the violence producing such injury usually being fatal. Aside from these injuries to the grosser structures the temporomaxillary joint is not infrequently the site of acute synovitis, or more extensive inflammation, usually propagated from surrounding tissues, but sometimes the result of distant infection. In phlegmons of this region the structures of the joint rarely escape a sympathetic participation, while parotid abscess and similar collections of pus may penetrate the joint and destroy it. Again it is occasionally the site of a postgonorrheal arthritis, or it may suffer as do other joints after the exanthems and acute fevers. It also occasionally becomes involved in the disturbances accompanying irregular eruption of the last molar, i. e., the wisdom tooth; in other words, it may suffer just as may any other joint in the body, and from similar causes.
Ankylosis of the temporomaxillary joint is an infrequent result of its involvement in serious disease, or may result from lesions of the adjoining tissues, as from the cicatricial deformity following noma, burns, and the like. Thus we may have either a true or a spurious ankylosis of this joint, in either case the resulting condition being intractable and exceedingly difficult to manage. When it can be foreseen as a consequence of extrinsic disease it may be prevented by the insertion of a mouth-gag, and more or less frequent and forcible stretching, or by wearing some suitable apparatus between the teeth which shall keep the jaws apart, and which may be used at night. A pseudo-ankylosis produced by cicatricial bands, and long neglected, will become genuine, and require as radical an operation as though it had been interosseous from the outset.
For the relief of such conditions various operations have been devised, in each of which the formation of a false joint is contemplated, it depending upon the exigencies of the case whether this shall be produced by the division of the horizontal ramus in front of the masseter, or of the ascending ramus behind the masseter, or whether there shall[668] be actual resection of the temporomaxillary joint, with division of the neck and removal of the condyle. The latter procedure is the more ideal, at the same time the more difficult, and the more likely to permit injury to the branches of the facial nerve, with consequent paralysis of the orbicularis and the facial muscles.
I have elsewhere described a peculiar condition of relaxation of the temporomaxillary ligaments, by which there is a recurring subluxation of the joint, noticed most often during eating and accompanied by a snapping sound. This is usually unnoticed by the patient, but is often observed by others. It is painless, harmless, and not ordinarily amenable to treatment. (See p. 528.)
Tumors of the jaws proper include mainly cysts, which are often connected with odontomas, benign tumors, such as fibroma, chondroma, and osteoma, most often of mixed type, and the malignant tumors, i. e., sarcoma, carcinoma, and endothelioma. Malignant tumors primary to the bone are usually of sarcomatous type, though these may include the endotheliomas. Carcinoma and epithelioma do not originate in bone texture, but may easily spread to and involve it. Thus many cases of advanced epithelioma of the lip involve the bone as well as the other neighboring tissues.
Epulis is a somewhat vague term, which has been applied to tumors which spring from and mainly involve the fibrous texture of the gum and the periosteum covering the alveolar process. The term itself simply implies a tumor upon the gum. Microscopically these tumors are usually of the giant-cell type of fibrosarcoma, and are among its least malignant varieties. They pursue a slow course, gradually loosening one tooth after another as they invade the tooth sockets, show very little tendency to spread rapidly, and are usually sharply circumscribed growths, tending to ulceration. They seem to be products of irritation. When removed they rarely recur. The surgeon should excise involved tissue in order to be on the safe side, sacrificing teeth, gum, and alveolar process as widely as necessary for the purpose. Formerly the epulides were made to include different expressions of fibroma and sarcoma involving the gum, but the name is so vague that it would be better to speak of each of these cases as its histological characteristics may indicate.
Benign tumors involving the entire bone may necessitate its removal, but most of the dentigerous bone cysts may be laid open, their contents evacuated, their size reduced, and the remaining cavity allowed to fill with granulation tissue; while malignant tumors call for sacrifice of every portion of tissue involved, often including the skin, and in the upper jaw much of the complicated structure of the nasal cavity, or in the lower jaw the loss of the tongue or a large portion of the floor of the mouth. A cancer of the lower jaw may be removed, with permanent good result, but a true cancer of the upper jaw should be seen early and mercilessly extirpated if the result is to be more than temporary.
Aside from those already mentioned the principal operations upon the jaws consist of partial or complete excision.
Removal of the upper jaw is a rather formidable procedure, frequently made so by extent of the disease which requires its performance. The presence of an extensive and ulcerating tumor, by which normal anatomical outlines are obliterated, will cause mechanical difficulties as well as unusual liability to hemorrhage. During some portion of its performance a temporary control of the vessels of the neck may be of assistance. This can be usually afforded by external digital pressure. In serious cases a ligation of the external or the common carotid may be of assistance. If soft, vascular tumors protrude into the nasopharynx a preliminary tracheotomy should be performed, tamponing the pharynx in order to prevent escape of blood down the throat. The position of the patient with the down-hanging head may be also of assistance in these cases. Of the various incisions employed one should be selected according to the nature of the case. Most of the operations include a splitting of the upper lip near the middle, with continuation of the incision along the margin of the nose, upward toward the orbit and outward along the orbital border, as originally suggested by Fergusson. This permits of completely raising the cheek from the underlying bone in one extensive flap and turning it backward, with complete exposure of the anterior surface of the superior maxillary. The operator next proceeds according to the desired[669] extent of removal. If the roof of the mouth is to be sacrificed the osteoperiosteal and soft tissues composing the palate should be divided as far from the middle line as may be permitted, then reflected, and the bone divided with chisel or with cutting forceps. It may be necessary to remove one of the incisor teeth to permit the insertion of the chisel for division of the anterior part of the jaw. Bone forceps or a chain or wire saw will serve for division of the zygoma and the external or lower wall of the orbit, while with chisel or forceps the nasomaxillary region is divided. The loosened bone can now be seized with strong lion-jaw forceps and wrenched from its attachments, which may then be divided with scissors or knife as they are encountered (Fig. 474).
Fig. 474
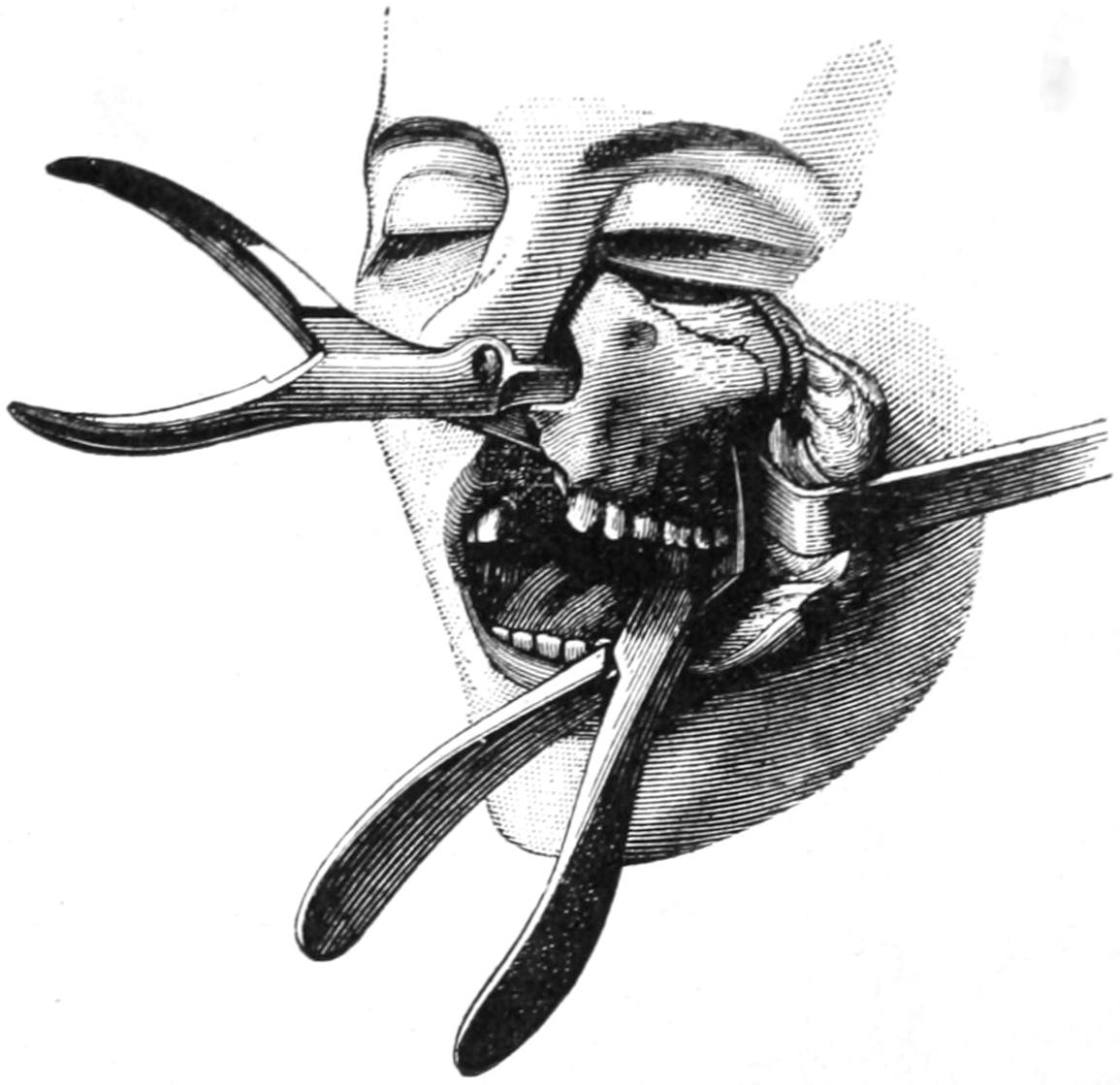
Resection of superior maxilla. (Farabeuf.)
Hemorrhage will be profuse at this juncture, when the internal maxillary artery is, with many of its branches, thus torn across or severed. The surgeon should be ready with tampons and forceps to check the bleeding and secure the vessels. The complete Fergusson operation includes removal of the entire upper maxilla, but oftentimes much less than this will suffice. On the other hand it is necessary sometimes to go still farther and remove more bone from the orbit or the nasal cavity, or perhaps to clean out the orbit entirely. A case which necessitates one of the more formidable operations is too unpromising to make it often judicious to perform it.
When the tumor involves the overlying skin this should also be sacrificed, and a plastic operation should be made to cover the defect. The skin flaps required for this purpose may be taken from the temple, the forehead, the neck, or adjoining parts of the face.
Bardenheuer has suggested the raising of osteoplastic flaps for removal of tumors lying within the jaw, and their replacement at the conclusion of the operation. He has also devised ingenious methods of making immediate plastic repair which are worthy of study, but which are so seldom required as to not justify description in this place.
After operation the bleeding should be checked by torsion, by ligation, by sutures en masse, by application of hot water, and by securely tamponing with antiseptic gauze, by whose pressure oozing is checked and protection from infection afforded. The patient is allowed to sit up as early as possible, meanwhile being made to lie upon the affected side in order to avoid danger of aspiration pneumonia, and using an antiseptic mouth-wash with relative frequency.
It is sometimes possible to perfect an artificial substitute for tissues removed, which can be inserted after the operation. The loss of tissue will cause more or less disfigurement by sinking in of the cheek and side of the face. After the parts are healed an apparatus made of gutta-percha or metal, and adapted to each case, by which most of the lost symmetry may be restored, should be worn, in the same manner as an artificial denture.
The lower jaw seldom requires complete removal. It is rarely necessary to go so high as the joint or the coronoid process, although occasionally the condyle must be avulsed and the coronoid either cut away or its temporal tendon detached. Most of the exsections in this location are confined to some portion of the horizontal ramus. Except in rare instances it is not possible to make a complete excision of the lower jaw through the mouth, and nearly all operations are practised through external incision, carried along the lower border for a sufficient length, and extended upward along the posterior border beyond the angle, if necessary. In most instances the facial vessels are directly exposed and should be secured before division. Masseteric attachments are separated and the instruments are kept as near to the bone as the circumstances of the case will justify.[670] In well-marked ulcerating cancer, however, the surgeon should go nearly an inch beyond its apparent border and remove still more if it be visible, taking everything which seems involved. Here the bone is usually divided with a chain saw, although stout cutting forceps may suffice. It may be necessary to remove a tooth in order to clear a place for the action of the chain saw. Growths involving the skin necessitate not merely linear incisions, but extensive oval excisions of the overlying tissues. All the involved structures should be removed in one mass; if it be necessary to remove the floor of the mouth the divided bone section is seldom cut away until it can be removed with the rest of the tumor. The healthy mucous membrane should be preserved and brought together with catgut sutures at the conclusion of the operation, as the more carefully the cavity of the mouth can be shut off from the balance of the wound the more prompt and satisfactory the healing (Fig. 475).
Fig. 475
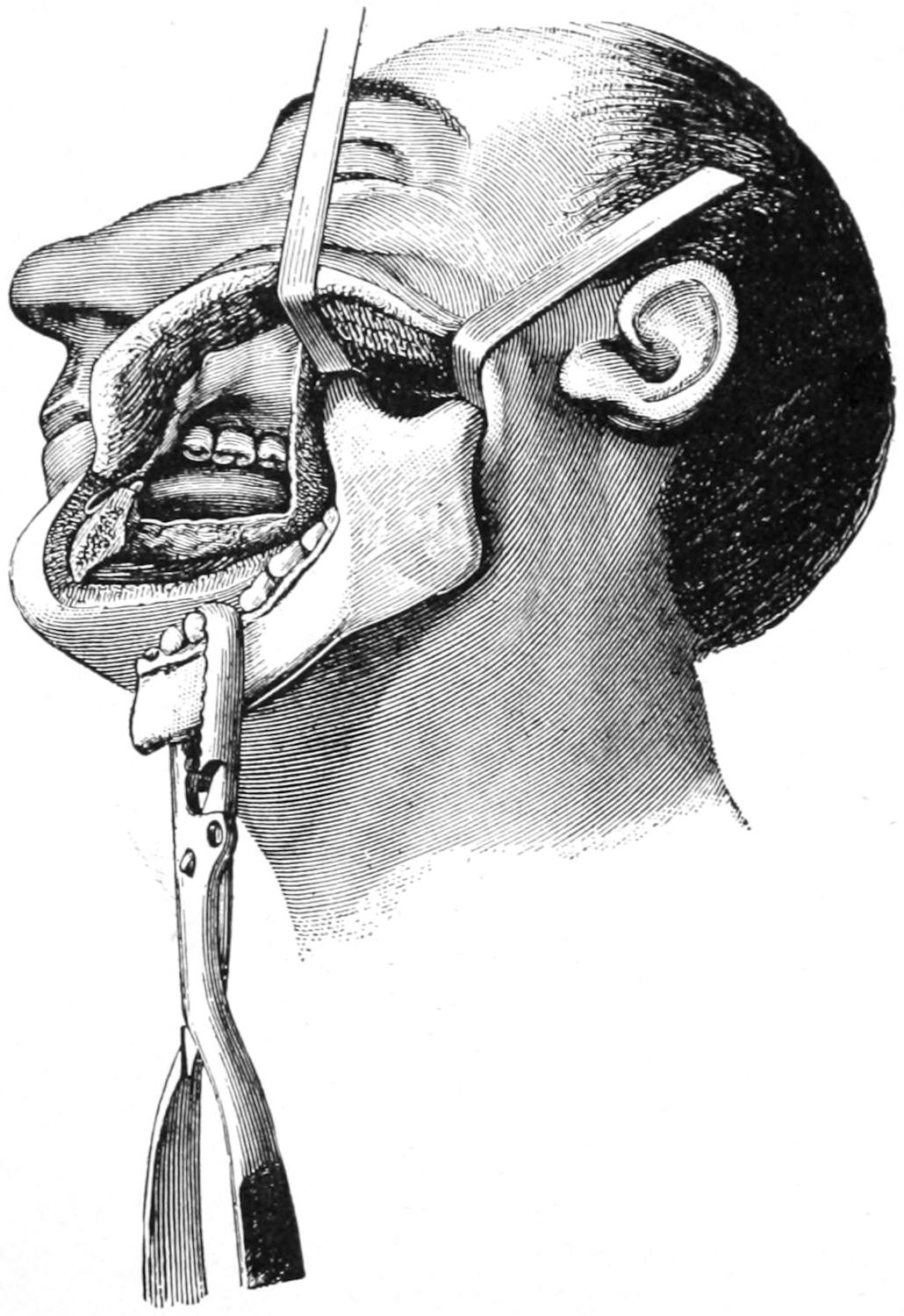
Resection of inferior maxilla. (Farabeuf.)
In a few cases it may be possible by the use of stout silver wire, or some other substitute, inserted between bone ends to keep them apart and thus nearly preserve the contour of the lower part of the face; but this can be expected to succeed only when the cavity of the mouth can be completely closed, so that the wire or other material may be quickly incorporated in granulation tissue, where it is expected to remain.
When it is necessary to remove the joint end of the bone the operator should work carefully along the bone toward the joint in such a way as not to injure the facial nerve, the external maxillary artery, or Stenson’s duct. With a sharp separator it is possible to thus expose the joint, and after opening it to avulse the articular surface. In operating for necrosis the healthy periosteum should be preserved, while in the removal of cancer it should be sacrificed to the same extent as the bone itself.
The same rules apply here as above with reference to the closure of the wound and the construction of flaps; an extensive plastic operation being sometimes necessitated, as when a large portion of the lower lip, the chin and the bone are removed for extensive epithelioma. Dead spaces should be avoided, any cavity should be packed sufficiently, opportunity for drainage afforded, and the mouth cavity closed. Mouth-washes should be frequently used.
These cases should be prepared for operation by a careful cleansing of the mouth and the local use of antiseptics. During any of these operations, diseased teeth which may require it should be removed, whether they occupy the site of the operation or some other portion of the jaws. The cleaner the mouth the more prompt will be the healing process.
[671]
The congenital malformations of the upper respiratory passages pertain mainly to the nasal septum and the interior of the complicated nasal cavities, which are rarely symmetrically arranged, and which often differ considerably. The nasal septum is frequently deviated or warped to one side, often to an extent making one nostril too restricted for easy breathing purposes. The nostrils are occasionally seen to be abnormally retracted. Malformations of the pharynx are of rare occurrence. The soft palate is occasionally found to be more of a diaphragm than is natural, and imperforation is sometimes seen. Pharyngeal fistulas have been mentioned in connection with incomplete closure of branchial clefts. They occur more commonly on the right than on the left side, and are usually incomplete. A fistula placed in the middle line and opening into the larynx or trachea is also occasionally seen, its inner opening being generally found on the side of the pharynx and just below the tonsil. This is not necessarily a persistent remains of the thyroglossal duct, but may have a different origin. Cystic distentions not infrequently occur along these fistulous tracts. Malformations of the larynx are rare and consist mainly of narrowings or stricture formations.
Acquired malformations of the respiratory passages are common and are the result usually of previous disease or injury. They may assume the obstructive type, as when the tonsils or the other adenoid or lymphoid tissues of the nasopharynx become hypertrophied, or they may assume the constrictive type, as when strictures result from ulceration, produced either by disease or by caustics. Such diseases as diphtheria cause not only paralyses, through the nervous system, but cicatricial deformity in consequence of ulceration. The latter is also true of burns, while fractures may permanently displace parts, this being particularly true of the nose, but holding good also for the hyoid, and even for the larynx. Nearly all these malformations permit of more or less surgical improvement by operations, some of which are simple and easy of performance, while some will need the highest degree of trained skill.
—Ozena is a general term applied to ulcerative lesions, especially involving the Schneiderian membrane in the nose, and causing more or less discharge of mucus, pus, and crusts, nearly always offensive, and accompanied by evidences of deeper ulceration, involving the fragile nasal bones or the nasal septum, and constituting expressions of caries or necrosis in this region. Ozena may be the consequence of a milder catarrhal inflammation, occurring in patients of vitiated constitution and bad habits of life, with insufficient attention or no care whatever. Another type of ozena is from the beginning of syphilitic origin, and it is especially the syphilitic cases which present the most offensive types of lesions, yet which are the most satisfactory to treat, because of the relative certainty with which they yield to properly directed treatment. Any case characterized by profuse and offensive nasal discharge, in which by suitable illumination and examination ulcerations can be detected, should be considered ozena.
—The treatment for all these cases should consist of local cleanliness, alkaline solutions in spray or by irrigation being especially indicated because of their cleansing properties. Warm sterilized salt solution may also be used for the same purpose. All visible ulcerations should be treated by local applications of mild silver nitrate solutions, or some other combined antiseptic and stimulant; or these may be alternated with local applications of an ointment of the yellow oxide of mercury in strength of 0.5 to 1 per cent. Local treatment, however, is but a part of that which should be instituted. In every case where the syphilitic element can be recognized, or where there is good reason for even suspecting it, vigorous antisyphilitic treatment should be begun and prosecuted. While these cases nearly always need one of the iodides, administered[672] internally, there is no way of so quickly bringing them under the desired influence as by inunction with the ordinary mercurial ointment. Both measures should be carried along simultaneously until the combination proves to be too active, when the inunction may be discontinued.
In addition to these measures such cases need improvement of elimination and of nutrition, and the best restorative tonics may be combined to advantage with any other special medication which may seem to be indicated.
Nowhere, except perhaps in the ear, are foreign bodies more likely to find entrance, and become impacted, than in the respiratory passages. They are introduced either through the nose or the mouth. They consist of almost all imaginable substances, introduced either by accident or design, and belonging to all three kingdoms—animal, vegetable, and mineral. According to their nature, size, and lodging place, symptoms of more or less severity will ensue. Migratory bodies, especially small insects and parasites, may escape from the nasal cavity into one of the accessory sinuses, where they will give rise to great irritation, and necessitate perhaps serious measures for relief. The presence of a foreign body is not always promptly recognized. In some instances it is discovered only by accident, as when, having been present for some time, it has produced irritation, with or without ulceration and offensive discharge. Thus a shoe-button may have been pushed up the nose of a little child, and remain there undetected for some time, perhaps to be spontaneously extruded in the act of blowing the nose. The presence of a foreign body in the nasal passages, then, will be manifested by symptoms of obstructed nasal respiration and by other evidences of local irritation, with pain, tenderness, swelling, and discharge.
An object easily seen is ordinarily easily removed, unless it has some peculiar shape which impedes its easy withdrawal. Local cleanliness is the first prerequisite, and then in most instances local anesthesia, which may be produced with cocaine or one of its substitutes. After this a probe, bent into the shape of a blunt hook, or forceps of various patterns and shapes may be required, and will usually suffice for all ordinary cases which can be detected by inspection through the nostrils or with the rhinoscope. In more difficult and unusual cases the fluoroscope or the skiagram may be made to render great service. Should some larger object be found, particularly in the antrum, deeply within the cranium, then a more formal operation will be demanded, whose details should be made to suit the needs of each individual case. When a mass of inspissated secretion or of granulation tissue more or less conceals the outline of the foreign body, everything should be cleaned away with irrigating spray, or with cotton wrapped around a probe or held within the forceps.
—A rare condition of calculus formation is occasionally met with in the nose, the concretions being formed by precipitation of the mineral elements from the nasal mucus, and constituting the ordinary rhinoliths. These become, in effect, foreign bodies, and are to be recognized and treated as such. After syphilitic ulceration portions of bone may be loosened spontaneously, and dropped into locations where they are caught instead of being spontaneously expelled.
It is known, also, that, especially in tropical climates, there are several species of insects which enter the nostrils and there deposit their eggs, which later are hatched into the resulting larvæ, the latter sometimes being expelled, or perhaps developing and burying themselves further within the nasal recesses. Any living organism may be killed by administration of chloroform or ether, and then expelled as an ordinary foreign body; or, in most cases, such larvæ or eggs can be washed away with an irrigating stream to which a little extract of tobacco should be added. Thus maggots have been found buried within the nasal mucosa, and requiring extraction by means of forceps. When larvæ have invaded the sinuses the case becomes more serious, for it will require free exposure by perhaps a somewhat formidable operation on the interior of the sinus, which should then be carefully cleansed and suitably drained. Living organisms within the nasal cavity or the sinuses will cause headache, lacrymation, sneezing, nasal discharge, perhaps with epistaxis, and almost every possible expression of local discomfort.
[673]
—Foreign bodies in the pharynx are usually, when small, lodged in the neighborhood of the tonsil, or caught in the lymphoid tissue of the tonsillar ring. According to their size they may become impacted at almost any point, and may even cause suffocation. They may be detected sometimes by the finger alone, or, at other times, only with good illumination and local anesthesia. The irritation which they produce leads to frequent acts of swallowing, the latter always exaggerating the former. Such objects as small fish-bones and the like, which may cause irritation, may easily escape or defy detection; moreover, such objects may be multiple.
For the sake of comfort pellets of ice may be frequently swallowed and cocaine may be used locally. Their extraction should be promptly practised. In rare instances emergency may call for prompt tracheotomy, but this is rarely the case unless the object be impacted below the epiglottis. Curious instances of impaction in the nasopharynx, of strange foreign bodies, have required the administration of anesthetics and even serious cutting operations for their removal, by combined manipulation through the nostril and the oropharynx. Such bodies, however, can be in some way always removed.
Liquids may be aspirated through the nose, and cause strangling attacks of coughing. They are then more easily drawn into the larynx or trachea, where they will cause reflex phenomena and actual obstruction, according to their nature. Again by free inhalation of steam, natural or superheated, burns and scalds of the respiratory passages may be produced, which will be followed by edema of the glottis or by pneumonia. The inhalation of extremely strong vapors, like that of ammonia, may cause spasm of the glottis. The entrance of blood, as from rupture of an aneurysm, or of pus, as from a bursting abscess, or the escape of pus from one side of the chest into the other lung by way of the trachea, may cause serious symptoms or may produce actual suffocation. In operations for pyopneumothorax, for instance, with one side of the chest well filled with pus, one should be careful to avoid turning the patient in such a way that pus may run over into the other lung and thus suffocate him. I have seen death occur on the operating table from this cause, in spite of every precaution, when the accident itself had been anticipated.
Solid objects may be of all shapes, sizes, and materials; living insects are occasionally aspirated and may not be at once killed, the local irritation caused by their presence producing intense spasm of the glottis. I have personally known of two cases of suffocation in restaurants, where men eating hastily died as the result of impaction of pieces of meat within the rima glottidis. Again, bodies may pass beyond the glottis proper and enter the trachea, or even one of the great bronchi; shoe-buttons, for instance; and in one case in my knowledge a small hat-pin passed down and was only removed after a low tracheotomy and careful search, aided by a skiagram. Owing to the anatomical arrangement the right bronchus is more frequently entered than the left. Immediate danger of suffocation, of obstruction, or spasm having passed, there is still serious menace from pneumonia, with or without abscess or gangrene of the lung. Such condition occurring in a young child, in the absence of the history of passage of a foreign body, may cause some difficulty in diagnosis. The greatest help would be afforded by the use of the Röntgen rays, although the laryngoscope alone will sometimes be sufficient. To use the latter to advantage it will probably be necessary to allay local irritation with the cocaine spray. (See Figs. 476 and 477.)
—Treatment should be operative, although in some cases it is sufficient to invert the patient and slap him on the back. With an object impacted in the glottis relief may be afforded with the finger, but this may be exceedingly difficult, for in the later stages of suffocation the jaw may be convulsively shut and it will be almost impossible to effect entrance. In such case the jaw should be hastily pried open and the index finger carried down behind the base of the tongue, lifting the epiglottis and dislodging the object. If this fail and respiration have ceased, attempt should be made to hastily open the trachea, even with the blade of a penknife, and to follow this with artificial respiration. Under these circumstances the vessels of the neck will be engorged with venous blood, which will escape freely; this may, however, be disregarded, the primary indication being to get into the trachea, which may be held open by turning the knife-blade at right angles, while artificial respiration is practised, and until a couple of hair-pins, for instance, can be secured, bent into shape of blunt hooks[674] and made to act as temporary retractors. This is an illustration of what may be done in emergencies.
Fig. 476
Toy-pin (actual size) removed by external pharyngotomy from pharynx and esophagus of a two-year-old child. Recovery. Skiagram by Dr. Plummer. (Buffalo Clinic.)
On the other hand these operations should, when possible, be done deliberately and with local anesthesia. Foreign bodies should be located with the laryngoscope, after which they may be removed with the aid of the illumination thus afforded, or by mere sense of touch. An object impacted in the larynx proper may be extracted by thyrotomy, whereas when it has passed below the larynx it will be necessary to open the trachea, perhaps even low down, making more than an ordinary opening for purposes of manipulation. Numerous forceps have been devised for these purposes. Roaldes reports having[675] removed a piece of impacted iron from the bifurcation of the trachea, by means of a powerful electromagnet.
In the ensuing chapter there will be mentioned a method of exposing both the trachea and the esophagus by posterior incision or resection of the thoracic wall.
Fig. 478
Tack in bronchus of young child, removed after a low tracheotomy. Case of Dr. Parmenter’s. Skiagram by Dr. Plummer. (Buffalo Clinic.)
Besides those inflicted by foreign bodies injuries may be produced here from external conditions, gunshot wounds, fractures, and a variety of causes which need not be specified. The inhalation or the entrance of violent caustics, either fluid or volatile, may produce edema at least, or actual destruction of tissue. The glottis, being the narrowest portion of the respiratory tract, offers the greatest danger under conditions of obstruction, and fatal dyspnea may ensue. Thus, for instance, burns caused by inhaling steam, or hot vapors or flame, will be followed by most intense reaction, often extending beyond the trachea and to the air cells. Edema will be prompt, while pain, shock, dyspnea, and loss of voice will be instantly produced. If the patient survive the early complications he may succumb to pneumonia or other disastrous sequels in the lungs.
—Wounds are nearly always complicated by other injuries of the neck or face, which may involve vessel or nerve trunks of primary importance. Moreover, such wounds are mostly infected and lead to extension of phlegmonous involvement, which may later cause mediastinal or deep cervical abscesses, and all sorts of septic and pyemic complications. Even when recovery ensues cicatricial contraction may produce laryngeal or tracheal stenosis, with defective voice, or sometimes fistulas, connecting usually with the trachea.
—In the treatment of such wounds provision should be made for drainage, and it is seldom advisable to make too accurate a closure lest its very intent be thereby defeated. Unless the patient be suffocating the first indication is to check hemorrhage, then to cleanse the wound, and later to make such approximation of its surfaces as the case may permit. Occasionally in order to obtain a good result in the upper part of the respiratory tract it would be good practice to make a tracheotomy below. At other times an O’Dwyer tube may be inserted.
The occurrence of edema may be prevented, or at least its severity in a measure controlled, by the use of adrenalin solution, 1 to 10,000, while the local use of mild cocaine[676] solutions will be frequently indicated, in order to check irritability and the reflex phenomena to which it will lead. Local symptoms may also be combated by inhalation of vapor, with soothing solutions, such as weak preparations of cocaine or of one of the opiates, followed by mild astringents and antiseptics—tincture of benzoin or oil of eucalyptus, or some of their equivalents, being nebulized and used in a spray. Opiates internally should be prescribed; while with delirious, drunken, or maniacal patients every effort should be made to secure physiological rest and to subdue restlessness or frenzy.
—Fracture of the larynx is a somewhat uncommon accident, due to direct violence, which may instantly precipitate symptoms of the greatest severity. It may be simple or compound, the thyroid being obviously most often involved and the cricoid next. These injuries will occur more frequently in the aged, in whom the external cartilages of the larynx are prone to calcify and thus become more brittle. A fracture of the larynx precipitates extreme danger of suffocation, either from displacement or edema, and will usually require a prompt tracheotomy, which may be performed with a penknife in the absence of any better instrument. It may be indicated also by expectoration of bloody mucus, with froth, with stridulous respiration, dyspnea, pain—which is increased by pressure or motion, as in swallowing—and the local indications of injury. Thus death has occurred upon the field during a game of baseball, from a direct blow of the ball upon the larynx, no one who knew sufficient to perform it reaching the patient in time to do an emergency tracheotomy as above. Edematous laryngitis, which is not sufficiently serious to call for operation, is characterized by dyspnea, aphonia, dysphagia, cough, laryngeal irritability, and by more or less chemosis and congestion of the mucosa. The specialists treat certain of the milder forms of this condition by local scarification (i. e., with a knife made for the purpose), in order that by considerable local hemorrhage the vascular engorgement may be relieved.
These consist in large measure of deviations of the nasal septum, with or without turbinate hypertrophy, due to previous disease of the Schneiderian membrane, and followed by thickening and structural change. Nasal deviations are either of congenital or acquired origin. An absolutely symmetrically arranged and divided nasal cavity is a rarity. Thus, though one side is rarely a replica of the other, deviations which are sufficiently marked to cause nasal obstruction are commonly the result of rapid or slow disease. They will be seen in connection with other body deformities by which the head is habitually held in an abnormal position, so that growth in one direction is thereby favored. Such conditions may be caused either by irregularities of vision, by enlarged tonsils, or by spinal deformities.
The acquired deviations are frequently the result of injuries, not necessarily of those sufficiently severe to produce fractures. The nasal septum proper is made up of the cartilaginous or purely nasal portion, the vomer, and the perpendicular plate of the ethmoid, any one of which may be separated from its connections or warped from its perpendicular plane. Dislocation of the cartilages may also occur in the young, and, having once taken place, is rarely reduced unless treatment has been both prompt and scientific.
Angular deviation to an extent which often produces a spur is not necessarily of serious inconvenience unless it protrude sufficiently from its proper plane to come in contact with one of the turbinates, in which case a nearly complete obstruction may result, with symptoms of constant nasal irritation. Absolute symmetry being rare, and mild deviations being very common, it is only those which produce either visible deformity or local irritation which require surgical treatment. Obviously after injury to these parts attention should be given to overcome present and prevent further dislocation. This may be conveniently done by the introduction of small, tubular, nasal splints, of celluloid or caoutchouc, made for the purpose. In their absence short pieces of a stout, silk catheter may be used, one inserted on either side of the septum, and packed around with a light tampon of antiseptic gauze. All intranasal splints, no matter how made, will cause considerable local irritation, with tendency to discharge, and will need to be renewed every day or two.
Deviation having resulted in permanent deformity, no matter how produced, it can[677] be relieved by operation. Except in the young this may be performed under local cocaine anesthesia. These measures fall under two heads—those made for removal of projections, or spurs, and those directed to straightening of warped or deviated septa, which do not show much thickening.
For the treatment of projections caustics and the actual cautery were formerly much in use. They have been now almost abandoned for the use of instruments, such as a strong knife, a small intranasal saw, or cutting forceps of various patterns, adapted for use within the nose. Only these latter means will be mentioned in this place. Cutting instruments may be actuated by hand or by electric motors. When the field of operation is small cocaine anesthesia is nearly always sufficient. Extensive operation involving both nasal cavities may often be better performed under a general anesthetic. The nasal cavity should have been previously thoroughly cleansed by the aid of irrigation with alkaline solutions, and then just previous to operation with hydrogen peroxide. Instruments should be absolutely clean and sterile. When local anesthesia is complete it is sufficient to seat the patient with the head supported, opposite to the operator, to illuminate the nasal cavity with the head mirror or some substitute therefor, and to introduce the knife, saw, or forceps in such a way that the removal may be effected with one movement, while injury to surrounding tissues is avoided. An intranasal saw should be blunt-pointed, and should never be pushed so as to touch the posterior wall of the pharynx. After division of bone the final detachment of the mucosa should be made with scissors or knife. Bleeding after these operations is rarely severe, although free at first, and may be controlled by a tampon made of a narrow, continuous strip of antiseptic gauze, either packing it into the nostril and occluding it, or inserting a nasal tube and packing snugly around it. Only in rare instances is it necessary to tampon the nose from the pharynx by the use of the Bellocq cannula. (See below.)
Warped and deviated septa, without angular projections, may be sometimes successfully treated by dividing the septum, either with knife or scissors, or with cutting forceps whose blades make a stellate incision, by which the curved surface is so much weakened that it can be pressed back into normal shape, where it is retained by tamponing the nostril on the affected side. The pressure required for this purpose is, however, sometimes irksome or even intolerable. A method of using a long pin, like a small hat-pin, has been suggested, it being passed through one nostril into and out of and again into the septum, in such a way that it serves as a splint, to keep it straight for a sufficient length of time. Later this pin may be removed without difficulty, its enlarged head lying meantime concealed within one of the nostrils.
This was first suggested by Killian as affording a method not subject to the objections of the older authorities. It may be performed under cocaine anesthesia, each side of the septum being swabbed with a 20 per cent. cocaine solution. A semilunar incision made through the mucous membrane and perichondrium on one side is the more convenient. Through this opening the coverings are separated from cartilage by means of a sharp and a plain elevator. Unless the perichondrium be itself elevated the mucous membrane will be torn in the pressure of loosening. The cartilage is then cut through with suitable instruments or burred away with a dental engine, the instrument being guarded by a finger in the opposite nostril, which acts as a guide, it not being desirable that the membrane on that side shall be cut through. In this way any spurs or ridges may be removed submucously with such instrument as the operator may select. The separated membranes then fall together and may be retained by light gauze packing without any suture.
Of true neoplasms in the nose the most common are those myxomatous or fibromyxomatous developments from the Schneiderian membrane, which are called nasal polypi. Histologically most of these are of myxomatous character. Clinically, however, they seem to be in large degree products of inflammatory and irritative conditions. At all events they constitute sessile and later pendulous outgrowths, occupying different[678] areas or occurring in clusters, those from the upper part of the nose being covered with columnar cells, while those of the lower pharynx are covered with flat epithelium. They are firm or soft, according to the amount of connective stroma which they contain. They are poorly supplied with blood and their contained fluid is largely composed of mucin. When involving a considerable area the condition is referred to as polypoid degeneration. They are observed at all ages and in both sexes. Their most common seat is the middle turbinate, toward its posterior extremity, and they also hang from the septum, but may be found in any part of the nasal cavity. From it they may spread to fill the adjoining accessory sinuses, even producing absorption of their bony walls by pressure. They also produce distortion of the nose, with such obstruction as to prevent nasal respiration. They may involve one side or both, and may hang so loosely attached that a flapping, valve-like sound is heard on respiration.
—They produce nasal obstruction, with irritation; more or less discharge of watery or acrid mucus, the latter sometimes leading to excoriation; while by pressure they produce headache, especially when located high in the nose, or deafness, as when they press upon the Eustachian outlets, or symptoms of sinusitis according as they invade one or other of the sinuses. Other reflex symptoms, such as facial neuralgia, reflex cough, lacrymation, and conjunctivitis, frequently accompany them, and mouth breathing and snoring are almost inevitable consequences. The voice becomes impaired, as does occasionally the sense of taste.
In most cases they are easily revealed by artificial illumination and exposure with the nasal speculum. In color they are usually pinkish, and may be seen to move with the respiratory effort. While it is usually easy to see at least some of them, when present, it is difficult to detect their exact point of origin. With the rhinoscopic mirror they may be seen projecting into the nasopharynx. Occasionally one will be detached by violent effort at sneezing or blowing the nose.
Fig. 479

Jarvis snare.
Aside from the danger of retained secretion, which they may bring about, and that attending their extension into adjoining cavities, there is in elderly people at least an actual possible danger of their undergoing malignant transformation, although this is not common. There is, however, good reason for their removal, and none for allowing them to remain, for they are always both irritant and obstructive.
—Almost every other method of treatment has yielded to that of removal by the Jarvis snare, or its equivalent, supplemented by the occasional use of forceps. In order, however, to expose them sufficiently to permit of removal it is often necessary to cut away a portion of the middle turbinate. In extensive polypoid disease this would be practically always required, and it should be done thoroughly, for nasal polypi tend usually to recur unless radically attacked. Local anesthesia is sufficient for the majority of cases, but an aggravated instance will call for complete anesthesia and thorough work, especially if the accessory sinuses have been infected.
The snare figured in Fig. 479 is a type of instrument which can be used to great advantage in dealing with these cases. When, however, it cannot be made effective by being applied around the actual base of each growth its use should be supplemented by that of the curette. No actual assurance can ever be given that there will be no subsequent development of polypi. Nevertheless it does not follow that new polypoid development is of the actual nature of recurrence. It may occur independently from the same causes that produced its first appearance.
It should hardly be necessary to insert here the caution that no operation of even this degree of simplicity should be effected without careful cleansing of the nasal cavity.
Of the other tumors that may occur within the nasal cavities none can be said to frequently occur here, but all varieties may be encountered. Of the more benign tumors the most common are the vascular growths and the fibromas, or mixed form of fibromas and papillomas. Epithelioma and sarcoma occur occasionally.
[679]
Fibroma of the nasopharynx is much more common than in the nasal cavity proper. Here it assumes its usual characteristics as a more or less firm and dense tumor, growing slowly, sometimes from a large base and again in pedunculated form. A form occasionally met with springs from the periosteum of the base of the skull and slowly extends into the nasopharynx, causing in time a complete obstruction, with disappearance of the surrounding structure by its pressure effects. Some of these growths are of a considerable degree of vascularity. When arising from the base of the skull they become almost inoperable after obtaining considerable size. I have seen death upon the operating table, in one of the foreign clinics, from uncontrollable hemorrhage occurring during the removal of one of these growths. A growth thus situated should be attacked with extreme caution, and preferably after easier access has been made to it by division of the soft palate, and removal of a portion of the hard, or perhaps by a temporary or permanent resection of the upper jaw; the route being left in each case to the decision of the operator. Provisional ligation of the carotids may be also made.
The same is true of the other tumors of the nose and nasopharynx. The less malignant they are the more they justify radical attack. By the time a sarcoma or adenocarcinoma of deep origin has declared itself it is usually too late to justify its removal.
A new-growth of different form, occurring in the vault or around the outlines of the pharynx, is frequently seen in the shape of great hypertrophy or overgrowth of the lymphoid tissue, already and elsewhere alluded to as composing a part of the original lymphoid ring which marks the site of the embryonic nasopharyngeal canal. This lymphoid hypertrophy, whose commencing expressions are seen in the tonsil, is referred to as adenoid growth. Associated with it occurs more or less hypertrophy of the other tissues, fibrous, etc., according to whose proportion the growths will be soft and spongy or more dense and resistant. The so-called adenoids occupy more or less of the nasopharynx proper, reducing its dimensions, encroaching upon the vault of the pharynx, materially reducing the breathing space, thus leading to the establishment of the mouth-breathing habit, as well as to alteration of voice and the accompanying disagreeable features of increased secretion of the parts. It leads to characteristic appearances which may be recognized at a distance, consisting of a mouth habitually open, with more or less projecting teeth, pinched nostrils, Gothic roof of mouth, stooped shoulders, deformed thorax, loss of hearing, irritative cough, and possibly remote reflex effects, such as laryngeal spasm, general neuroses, chorea, and epilepsy. The effect of these changes is to give not merely an appearance of stupidity, but actually to interfere with mental development. Save in exceptional instances, a child with the mouth-breathing habit, and with that peculiarity of voice which indicates nasal obstruction, will nearly always be found to be defective in cerebral activity, if not actually stupid. The longer the condition is allowed to persist the greater the permanent alterations and damage permitted.
Pronounced degrees of the condition may be easily recognized by the habitually open mouth and the character of voice. A moment’s inspection will usually reveal the character and the degree of involvement. When adenoids in the nasopharynx attain a size sufficient to produce these results the tonsils are also usually involved, and the clinical picture is thereby made more pronounced. The rhinoscopic mirror, if it can be used, will give a picture of the condition, while the finger-tip passed upward behind the soft palate will give an idea as to the extent to which the cavity is filled.
By virtue of the interference with the vital function of respiration thus produced, and because of the retention of secretion and the greater exposure to irritation through the constantly open mouth, individuals with this condition are usually anemic, while many of them give evidence of the status lymphaticus, to which attention has been called in the preceding pages. To such an extent is this true that the administration of an anesthetic is frequently attended by extra danger, and the operator should give the necessary relief only after careful preparation. This should consist not only of general measures, by which the condition of the patient may be improved, but by local cleansing of parts; and finally, as a preparation for the anesthetic, of the local use of a weak cocaine[680] solution, by which reflex excitability may be controlled. Just before administering the anesthetic in these cases it is well to spray into the nostrils and pharynx a weak cocaine solution, after which the anesthetic may be administered. In most instances it would be better to use ethyl chloride or ether than chloroform, not because the latter is necessarily more dangerous, but because one is placed less upon the defensive in case of accident, owing to the belief that it is not so safe as some other anesthetics. (See p. 164.)
—Local applications being of small avail in producing either condensation or resorption, the treatment of this condition is essentially surgical. With children an anesthetic is always necessary. With adults cocaine may be sufficient. The best position for the patient is that with the down-hanging head (Rose’s), as blood is not swallowed nor passed into the lungs, but may be removed as fast as it collects. The hemorrhage in these operations is generally profuse but of short duration.
Adenoids are removed either with a snare, the curette, or by special instruments constructed on the type of a tonsillotome, and having a concealed blade. The curette is also used as forceps. Two or three curettes and forceps are sufficient for nearly all purposes. In operating the instruments are guided entirely by the sense of touch and the operator’s knowledge of anatomy, for he relies upon his finger-tip for information as to whether the tissue has been completely removed or needs further attention. These instruments are used until the entire vault of the pharynx and its openings into the nasal cavities (choanæ) are freed from all hypertrophied tissue or excrescence. The posterior wall of the pharynx should be scraped until it is smooth. In addition the tonsils should be removed if it be necessary, while the lingual tonsil may be also removed with curette or forceps if it be involved. For a few moments there will be a free flow of blood through both nose and mouth. In some instances there will be indications for cutting away hypertrophied turbinates and removing nasal polypi. Hemorrhage, at first profuse, quickly subsides. A mixture of 1 per cent. cocaine solution with a little adrenalin is the best hemostatic for local use. The nostrils may be packed if the turbinate has been cut away, or the entire passage-way may be left open for the purpose of permitting the later use of an irrigating stream, by which blood clot may be washed away and antiseptics applied. While using and relying upon instruments for the greater part of this work there is no better curette for concluding the work than the finger-nail of the index finger. The finger being introduced recognizes the degree of relief afforded, and the finger-nail may be used to scrape away any remaining projecting tissue.
Various operators have devised formidable operations, varying from the temporary resection of one upper jaw to Cheever’s ingenious method of dividing and separating both upper jaws in one piece from the cranium, and thus exposing the nasopharynx from in front and above. Such operations are rarely performed.
Other neoplasms in this region are cysts and dermoids of congenital origin—those involving the original craniopharyngeal canal, and those produced from pharyngeal diverticula. These produce only the ordinary manifestations of tumor and are of pathological rather than surgical interest.
The escape of a small amount of blood from the nose, especially in childhood, is a common occurrence, and may occur in consequence of slight traumatisms or even spontaneously. The so-called nose-bleeding of children, then, is scarcely of sufficient importance to justify consideration here, nor would it were it not for the fact that it may become severe and even dangerous. Children in whom it frequently recurs will lose sufficient blood to become anemic, while the effect of its frequent occurrence may bespeak a depraved condition of the blood as well as of the tissues which permit of its escape. A history of repeated nose-bleed should prompt an investigation into the general condition of the patient as well as a local examination of the nasal passages, where some explanation may be afforded. For instance, a polypus may be found whose removal will then be indicated, or an exceedingly spongy and vascular area may be revealed, which will call for a touch of the actual cautery or the use of the curette.
Besides the frequent expressions of this kind in childhood, some of which may occur during sleep, there are other forms of nasal hemorrhage. A vicarious menstruation is known to assume this type, individuals thus losing blood every month. This is a rare but well-known phenomenon. A plethoric individual may suffer serious epistaxis at[681] any time, and this may be beneficial unless it be too extensive. Nasal hemorrhages may occur with certain fevers. Individuals with a hemorrhagic diathesis are peculiarly liable to it, and it is seen in connection with purpura hæmorrhagica. When this occurs in the debilitated or dissipated it may be fatal. Thus epistaxis may terminate fatally in spite of all that can be done. This statement requires some explanation. The nasal cavity may be tightly plugged, but such plugging cannot be made permanent because of decomposition of products thus retained and their absorption, with consequent septic infection. Nasal tampons should be removed every day or two, for the purpose of cleanliness, although their removal is contra-indicated when the necessity for physiological rest of the part is realized. The treatment, then, of epistaxis may be trying, at least, and in rare cases will prove absolutely disappointing and ineffectual. I have even been compelled to tie the common carotid to save life.
—The ordinary nose-bleed of a young child will usually subside with the application of cold to the nose, elevation of the arms, or firm pressure upon the upper lip just below the nasal septum. It may be also checked by an irrigating stream of cold water, or by a spray of cocaine or weak adrenalin solution. A 5 per cent. antipyrine solution also makes an excellent styptic for the purpose. Within a day or two after a serious hemorrhage, after the remaining clots have been cleaned away, a thorough inspection of the nasal cavity should be made in order to reveal the source of the hemorrhage and permit local treatment.
Nasal hemorrhage may be subdued by plugging the anterior nares with strips of gauze, or, better still, after the introduction of a tube through which air may pass freely, and around which packing may be firmly inserted. The ordinary dry styptics should not be used, for they may produce such a crusting of tampons as to make it difficult to remove them. More efficient materials can be used in solution. No tampon should be introduced into the nostrils which is not tied with a ligature of silk in such a way that it may be by it more easily withdrawn, and, at the same time, prevented from going too far. If the source of the bleeding be in the anterior part of the nasal cavity anterior packing may be sufficient. The surgeon should not, however, be deceived by the apparent cessation of bleeding, which cannot escape through the nostrils under these circumstances, but may continue into the nasopharynx, the patient swallowing the blood as it trickles down. Inspection of the pharynx should be made after the use of tampons. A much greater degree of safety is afforded by posterior tamponing of each side of the nasal cavity, which is most easily effected by means of the little instrument known as Bellocq’s cannula, whose use is illustrated in Fig. 480.
Fig. 480
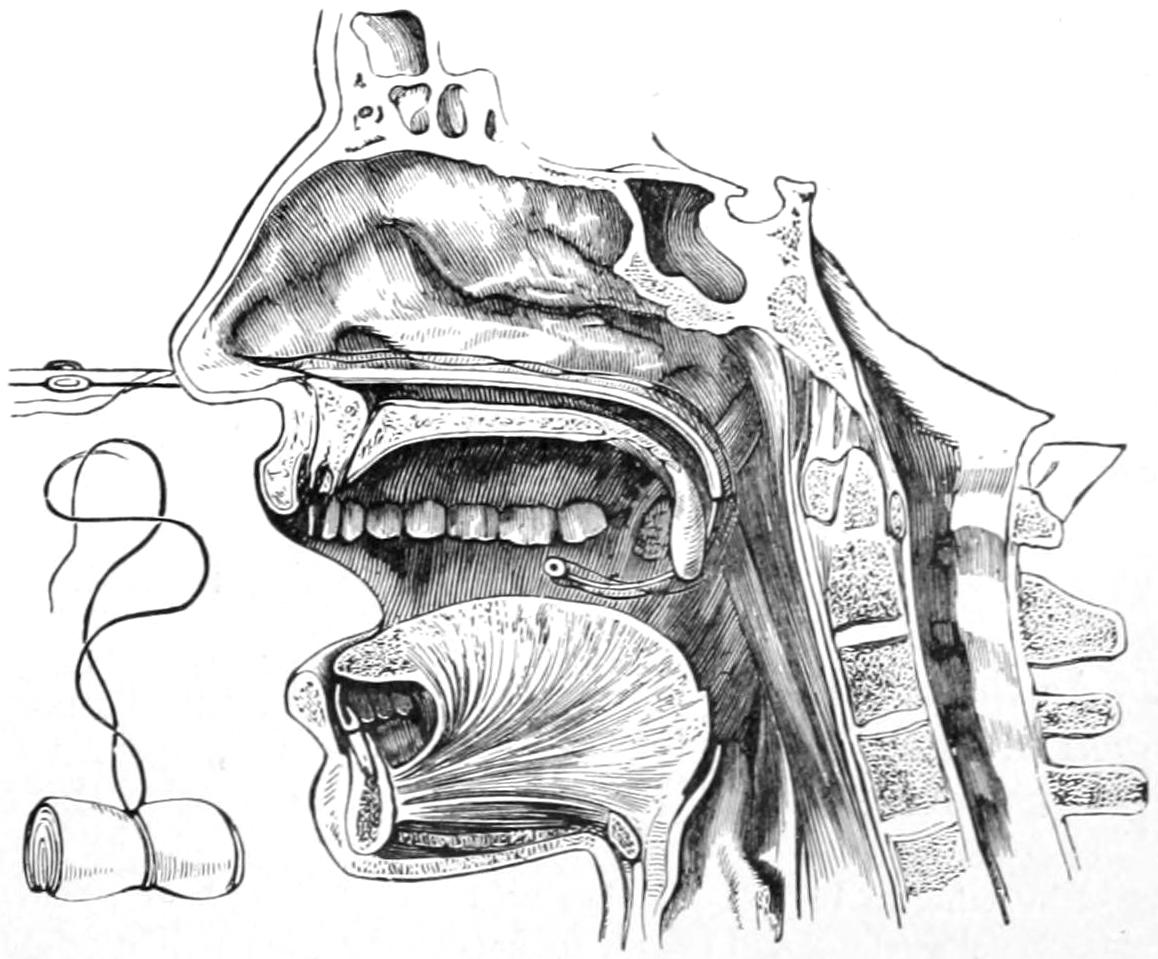
Plugging the nares with Bellocq’s cannula. (Fergusson.)
It is, however, by no means necessary to have this special instrument in order to accomplish the purpose. A soft catheter may be passed backward through the nostril until its end appears in the nasopharynx, where it is caught with forceps and drawn into the mouth. Here, by means of a needle or knot, a piece of silk is fastened to this end. When the catheter is drawn out from the nose it pulls up after it and out through the nostril this bit of silk, to whose middle is tied a tampon, made of a sufficient amount of gauze or similar material, folded or rolled into the desired shape. By combined manipulation, as the silk thread is drawn upward and outward through the nostril, it pulls up the tampon into the nasopharynx, where it should be guided into its place by the tip of the index finger of the disengaged hand. If necessary this procedure is then repeated upon the other side, and thus a complete double tamponing can be effected. If the procedure be made difficult by the extreme sensitiveness of the part this can be overcome by local anesthesia. The tampon may be[682] saturated with a weak adrenalin solution if desired. Ordinarily such a tampon can be easily disengaged and removed by again passing the finger up behind the soft palate and dislodging and withdrawing it, using curved forceps for the purpose of securing it. A tampon inserted for the control of hemorrhage should be left in situ for at least forty-eight hours, possibly longer. The case should be watched for a while after its removal, lest it might require re-introduction. This maneuver is made easier by fastening the tampon in the middle of a long piece of silk as described; one end being brought out through the nostril is tied to the other portion, which is allowed to come out of the mouth. The latter will provoke some discomfort, and patients should be cautioned not to disturb it, its purpose being explained to them.
Mulford, of Buffalo, has suggested a method of dealing with cases of epistaxis by injecting two or three drops of reduced adrenalin solution into the tissues at the base of the upper lip, in close proximity to the course of the arteries which pass upward on either side and supply the septum. The injection should be made in the fold of the mucous membrane just beneath the septum of the nose.
This has already been referred to as the product of tuberculous disease in the upper cervical vertebræ, or in the neighboring lymph nodes, or as the possible sequel of more acute infections occurring in the upper portions of the neck, proceeding usually from infected tooth sockets or other lesions within the nose and mouth. Collections of pus in this location may be circumscribed or may be extensive and rapidly assume serious phases. A chronic abscess is essentially a tuberculous expression. Acute abscesses, either in the tissue behind the pharynx or to either side of it, may be seen in cachectic children and assume serious phases.
The first evidences in these cases are those of pharyngitis, but swelling and edema occur rapidly, septic indications become unmistakable, and, finally, almost complete nasopharyngeal obstruction may occur. The discovery by the palpating finger of a fluctuating swelling will make the presence of pus practically positive. If the operator be still in doubt he may use the exploring needle. The experienced practitioner will at once plunge the point of a knife into such a swelling, and, at the same time, plan his opening in such a way as to afford the best possible drainage.[48] For the purpose it may be necessary to have the patient in the position of down-hanging head, or, in extreme cases, the patient may be almost inverted in order that pus as it gushes forth may escape through the mouth rather than into the larynx or down the esophagus. The operation should be done without an anesthetic. The mouth may be opened with the O’Dwyer mouth-gag, or it may be forced and held open with the ordinary tongue depressor. When pus has travelled to such an extent as to give the case the importance and aspect of a deep cervical phlegmon, such as described in the chapter on the Neck, then anesthesia is necessary in order that by external, combined with internal, incision, escape of pus and provision for drainage may be permitted.
[48] Nevertheless in one instance an eminent American practitioner thus hastily incised a fluctuating intrapharyngeal swelling and found, to his dismay, that he had opened a carotid aneurysm, the patient dying within five minutes.
Two dangers attend inexcusable delay in such acute cases—one is of suffocation from pressure or from sudden spontaneous rupture of abscess; the other is of invasion of large blood trunks in the vicinity and possibility of hemorrhage after erosion, either into the abscess cavity or directly into the outer world.
As the result of constant irritation by coughing, or other reflex motions of the pharyngeal muscles produced by local irritation, the uvula frequently becomes elongated to a point which permits it to rest upon the base of the tongue and there to produce still more[683] irritation and reflex phenomena. Patients suffering in this way will be noticed to make frequent attempts at swallowing and coughing, which may be depressing, and may lead to disturbed sleep and even an asthmatic form of breathing. The uvula is a useless organ when it has attained such dimensions, and its amputation, or at least its shortening, are indicated in all such cases as those above described. Local anesthesia is sufficient. Its tip is caught with a pair of forceps and it is clipped off, not too near its base, by long-handled and sharp scissors. This is a much neater and more expeditious method than to include it within the grasp of a wire snare and somewhat slowly crush it off.
Upon the uvula, as upon the soft palate, papular lesions of syphilis are frequently seen, rarely the primary chancre, but very often mucous patches or the deeper ulcers, which characterize the secondary and tertiary lesions. Gummas also may form within the thickness of the palatal tissues, which will in time break down and form ragged ulcers, while the destruction may extend to the bony portions, either of the nose or roof of the mouth, and then necrosis will be added to the evidences of ordinary ulceration. The rapidity with which these specific lesions will disappear under prompt and vigorous constitutional treatment, along with that local cleanliness which should include removal of necrotic tissue, is surprising and gratifying.
The epiglottis is composed of yellow elastic cartilage and it does not tend to calcify during the later years of life, as does the white or fibrocartilage of the balance of the larynx. Thus its elasticity and flexibility are fortunately maintained throughout life. It may be sometimes injured by the incised wounds elsewhere described under the term “cut-throat,” and is at least often thus exposed when not actually injured.
The epiglottis seems to be exempt from most of the primary diseases, but is occasionally involved in lesions of surrounding tissues, in which it may then participate. Thus it may be deformed by cicatricial tissue and unduly bound down, or it may succumb to advancing ulceration of syphilis, tuberculosis, or cancer. Injuries which break the laryngeal box rarely affect the epiglottis because of its elasticity.
While an extremely useful portion of the body, the epiglottis is not an absolute necessity, for even after its removal individuals can swallow, although the act requires some extra care. Should the epiglottis become involved in cancerous disease it should be removed with the rest of the diseased tissue, while syphilitic and tuberculous lesions will usually prove amenable to a combination of local and general treatment. New-growths in this region are extremely uncommon, but will prove relatively easy of removal when present.
The laryngeal cartilages, save the epiglottis, are composed of white fibrocartilage which manifests a tendency in the later years of life to undergo calcification. This makes the organ less elastic, changes the tonal qualities of the voice, and makes it more brittle and subject to possible fracture by external violence. Fractures of the organ, as of the adjoining hyoid bone, have been elsewhere discussed, with the indications which may make an emergency tracheotomy necessary because of hemorrhage or edema of the narrow laryngeal passage.
Of the inflammatory affections of the cartilages chondritis and perichondritis are most common. These are usually seen in connection with other expressions of tuberculous, syphilitic, and malignant disease. Nevertheless they are known to occur as sequels of the exanthems and ordinary infectious fevers. They may be followed by destructive ulceration, which will lead to a necrosis of the cartilage corresponding closely to death of bone under similar circumstances. In due time there may form a cartilaginous sequestrum, and this will require removal as though it were bone. Dangers attend these lesions in two peculiar directions. The very condition which produces the destructive inflammation may also produce either hemorrhage or edema, with suffocation which can usually be prevented by an emergency tracheotomy. On the other hand, when repair follows spontaneous recovery or successful treatment, it may be accompanied by such cicatricial contraction as shall materially change the shape and impair or possibly[684] destroy the function of the larynx itself. In this case either thyrotomy, tracheotomy, or laryngotomy may be called for, the opening thus made being expected to permanently remain.
Various forms of stricture of the larynx may be similarly produced. Such strictures, then, are due to previous disease or to injuries, and here as elsewhere stricture is a consequence rather than itself a disease. It occurs in consequence of syphilis and of the destruction following laryngeal diphtheria.
What is, in this respect, true of the larynx is also true, though less often, of the trachea, where constrictions may occur at various points, with reduction of caliber or such distortion of shape as to produce partial or even finally complete obstruction. The peculiar scabbard-shape which the trachea may be made to assume by compression between the lobes of a growing goitre has been elsewhere described. While the trachea itself is in this case free from disease the obstruction is none the less pronounced. Similar effects are produced by pressure, as from aneurysms or tumors, even at a distance. Loss of voice, shown to be due to paralysis of one or both vocal cords, should always prompt an examination of the chest, in order that the presence of an aneurysm or other tumor making pressure upon the recurrent laryngeal may not be overlooked.
—Symptoms of laryngeal and tracheal stricture comprise (1) those of the primary and active disease which produces them; (2) those of obstruction; (3) those of suffocation in emergency cases. The earlier symptoms are those of increasing dyspnea, which may vary in rapidity and extend over weeks and months, or which may become most pronounced within a few hours. There is also a change in the character and sometimes complete loss of voice, hoarseness of the speaking voice changing into a whisper. The condition is frequently complicated by attacks of serious dyspnea, often at night, which are due to an added spasmodic feature, and in which death may suddenly occur. Usually, however, with asphyxia comes muscular relaxation, and individuals may pass through a large number of these attacks, which are accompanied with extreme mental and physical suffering, in which death is only avoided by final relaxation. Again the heart may suddenly give out, and then the case becomes practically hopeless. In recognition of causes and location of such troubles it may be held that when hoarseness precedes dyspnea the lesion is in the larynx; when the reverse, it is in the trachea. Careful auscultation of the chest and thorough laryngoscopic examination will usually enable the lesion to be recognized. The lower the location of the stenosis the worse the prognosis, because of its inaccessibility. So long as the trachea below the stricture can be opened life may be prolonged indefinitely; but when due to a mediastinal tumor or an enlarged thymus, the case assumes desperate aspects and may baffle the best-directed efforts.
—Strictures in the larynx proper may be treated by dilatation, as by the introduction of intubation tubes of increasing size, a method which ordinarily gives satisfactory results. Nevertheless such laryngeal strictures manifest an almost permanent tendency to recontract, and whatever measures are addressed to them have to be frequently and thoroughly practised and over a long period. Fortunately, however, these patients are able to wear an O’Dwyer tube nearly all the time. When these internal operative methods fail there remains only an external opening, which may be made through the larynx proper (thyrotomy), or a low tracheotomy, which may require the insertion of short or long tubes, according to circumstances. Long trachea tubes are made, their lower portion being composed of rings fastened together in such a way as to cause them to be called lobster-tailed, and such a long tube may be passed through a low tracheotomy opening and made to extend beyond the point of pressure produced by an extrathoracic or an intrathoracic tumor. By the use of such an expedient life may be prolonged, although the exciting cause may prove fatal.
Tuberculosis of the larynx may appear in a generally disseminated form, involving nearly all the structures, or in circumscribed localized form, as a tuberculous ulcer, which may produce symptoms depending upon its exact location. Laryngeal tuberculosis[685] may, moreover, be but a local expression of the disease, apparently primary, or as often happens, it may be an accompaniment of pulmonary tuberculosis, the laryngeal trouble appearing as a local infection, taking place by the constant passage over the surface of tuberculous sputum which the patient is expectorating at frequent intervals. Thus, clinically, we may have a miliary, an ulcerative, or a gummatous form of the disease.
The condition is frequently referred to as laryngeal phthisis, and is mainly to be distinguished from syphilitic laryngitis, or occasionally from commencing malignant disease. Local symptoms include those of chronic laryngeal catarrh, with hoarseness, impairment of voice, sensation of dryness within the larynx, and frequent short, hacking, unsatisfying cough. To these features are later added more or less pain, especially in deglutition, while aphonia will finally succeed dysphonia. When the epiglottis and the structures near it are involved there are more irritation and pain. Dyspnea is a measure of the encroachment upon the breathing space left by the progress of the disease. Infiltration of all the parts within and later of those around the larynx finally takes place, and with further implication nervous reflex symptoms are added to those above mentioned. Cough is usually a distressing feature; the sputum varies in amount; saliva is increased in flow, and the expectoration is frequently streaked with blood. In advanced disease the sufferings of the patient become excessive, while constitutional symptoms keep pace with those of the local disease. Thus anemia, emaciation, debility, insomnia, and general malaise cause the patient great discomfort, and, coupled with his terminal local symptoms, make death an absolute relief.
With the laryngoscope varying pictures may be seen, either of ulceration or of general involvement of the entire interior of the larynx, which will be tumefied, irregularly swollen, ulcerating here and there, while the vocal bands show thickening and roughenings as well as ulcerations. Gummatous outgrowths may be seen at almost any point and in various stages of ulceration. A more distinctly lupoid form of tuberculosis is also occasionally seen in the larynx, where it assumes more of the nodular appearance characteristic of lupus, the nodules coalescing or disappearing by ulceration, which may leave a dense, cicatricial tissue after healing. Primary lupus of the larynx is rare.
Tuberculous lesions of the larynx are mainly to be recognized with the laryngoscope, but they, like all other local diseases in this location, produce alteration and final loss of voice, with difficulty of breathing, reflex cough, and are accompanied by general constitutional symptoms, according as the disease is purely local or an expression of a general affection.
—Treatment should be both local and general. The latter may be summarized by stating that all measures, including proper climatic environment, which are found to be of advantage in ordinary tuberculous disease, will prove of equal advantage here. There should be avoidance of exposure to all irritation—coal gas, tobacco smoke, vitiated air, etc.—while absolute rest of the vocal organs should be prescribed and all attempts at singing or unnecessary speaking be prohibited. All measures regarded as of value in general tuberculosis will find an equally wide field for their activities.
Local treatment is directed toward amelioration of discomfort and improvement of local lesions. The former may be afforded by steam inhalations with some soothing, volatile antiseptic added to the spray, such as methol, oil of eucalyptus, some gentle opiate, or anything that may give local anodyne effect. Cough may also be treated by the milder anodynes, of which cocaine or heroine will serve for most instances. Sleep is to be secured by some of the ordinary hypnotics. Local applications may be made by an applicator guided by the laryngoscopic mirror, by the medical attendant, or through watery or oleaginous solutions in a spray. For absolute local relief a mild cocaine solution, followed by the use of a very weak solution of silver nitrate, lactic acid (C. P.), or even the more thorough treatment of local ulceration by means of the laryngeal curette or touching with the point of the galvanocaustic loop, may give relief. The treatment of laryngeal tuberculosis rarely comes within the domain of surgery proper, until the disease has reached a degree necessitating some radical measure, such as thyrotomy, with erasion of the affected tissue, or possibly a laryngectomy, with complete removal of an organ which is too thoroughly diseased to warrant hope of repair.
[686]
Syphilis of the larynx is more common than tuberculosis, the lesions usually belonging to the later stages of the diseases, including especially mucous patches, and the ulcerative expressions, with or without the formation of small gummatous tumors. The loss of voice is rarely as pronounced, and the entire course of the disease is accompanied by less irritative and offensive features than is tuberculosis. Diagnosis will be materially assisted by the discovery of suggestive expressions of syphilis, either in adjoining or distant parts. Thus if mucous patches appear within the larynx they will also be seen within the mouth. Ulcers which are produced by syphilis have well-defined edges, and are rarely multiple; while those produced by tuberculosis are more often multiple, are seated upon an anemic base, produce more distortion of laryngeal structures, and more residue of cicatricial tissue at points where healing has occurred.
—The treatment of laryngeal syphilis is essentially constitutional, for nearly every local expression will clear up under the influence of properly directed remedies. However, when local symptoms are uncomfortable or depressing they may be treated as are those of tuberculosis, by soothing sprays and the local application of anesthetics, astringents, and the like.
Within the larynx tumors may occupy the space beneath the glottis, where they are referred to as subglottic; they may grow from the structure of the vocal cords and become intraglottic, or they may spring from above the glottis and from the aryteno-epiglottic fold. Certain forms of benign tumor are relatively common in this location, while others are almost unknown. The former include cysts, papillomas, fibromas, angiomas, and adenomas, as well as the ordinary granulomas.
A nodular lesion seen upon the vocal cords, especially in singers, which is hyperplastic in character, irritative in origin, and often called “singer’s node,” is frequently found upon the edges of the cords, either as a single or bilateral lesion. The adjoining structures are usually quite vascular. These lesions occur in those who abuse their voices, as, for instance, in amateur singers and newsboys. The nodules themselves vary in size from that of a pin’s head to that of a split pea. The condition produces hoarseness and impairment of the voice, is recognized with the laryngoscope, and is amenable to treatment, which should consist in absolute rest from vocal effort and gentle astringent and stimulating applications. If the node project very far it may be removed by the intralaryngeal guillotine.
Laryngeal polypi include the forms of benign tumor above mentioned, most of which assume in time a polypoid form, and cause impairment of function according to their location.
Fig. 481
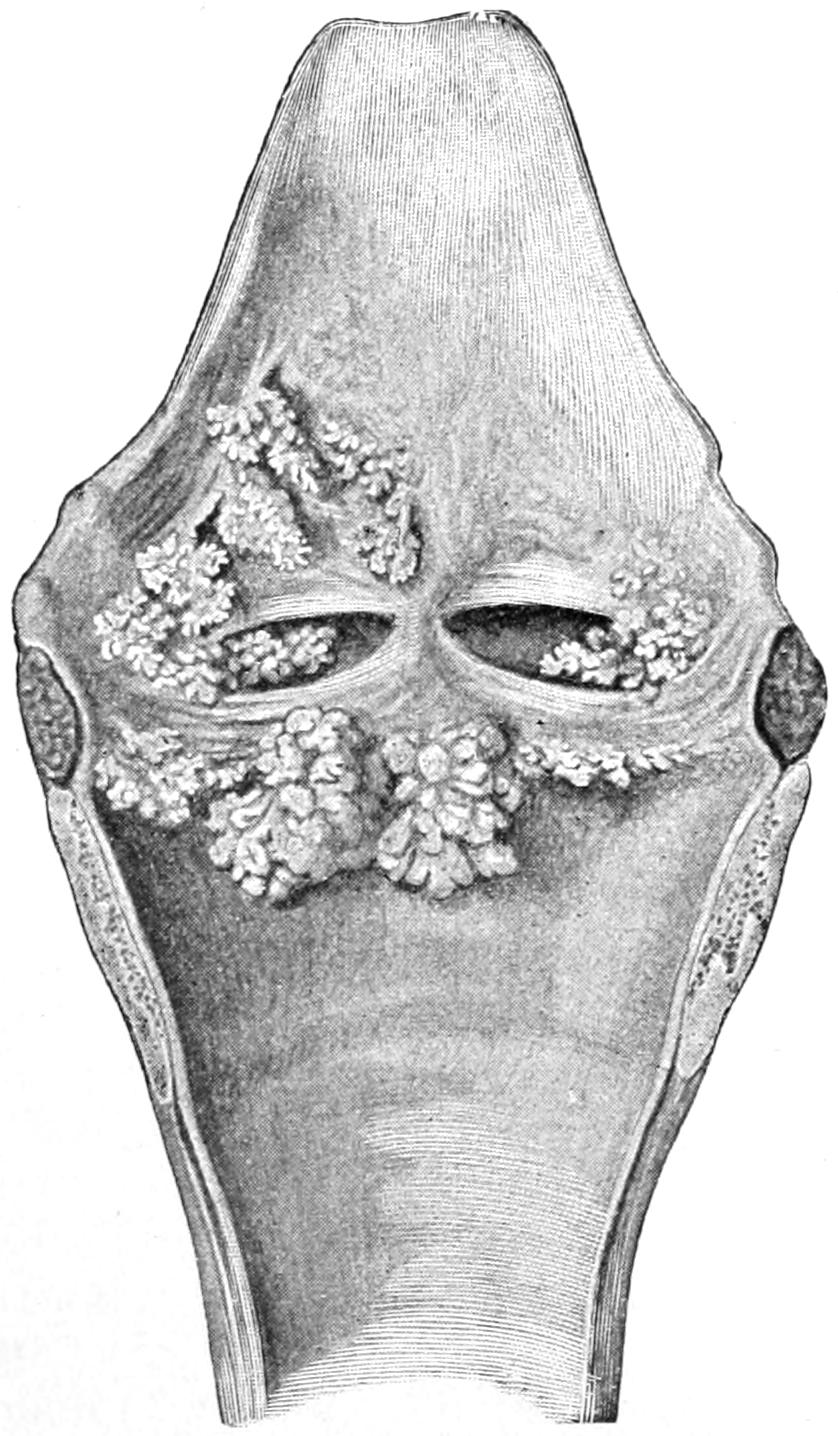
Multiple papilloma of larynx. (Bergmann.)
Papilloma is by all means the most common of these growths, and may present either the vascular type, bleeding easily and growing rapidly, or the firmer and denser type from admixture with fibromatous tissue. It occurs frequently in the young, and may even be present in the newborn. Here it can scarcely be detected with the laryngoscope, but may be felt with the finger. Cysts take their origin from the mucosa, save those which, possibly of embryonic character, protrude into or encroach upon the larynx from without (Fig. 481).
[687]
—The symptoms of benign intralaryngeal growths are largely irritative, including cough, with hoarseness and change of voice, and going on to production of dyspnea in proportion to the size which they attain. Later complete aphonia, with spasm of the glottis, may be the result of their presence, while pedunculated growths, or polypi with long pedicles, may cause aggravated symptoms by circumstances of position, the patient being much of the time relatively free. Hoarseness, dyspnea, and cough, without other evidences of inflammation or epidemic disease, should always lead to careful inspection with the laryngoscope, and this will reveal the size and situation of the growth. These examinations can be made with cocaine and give satisfactory information. Only in young children are they difficult, or sometimes impossible. Even in an infant with a hoarse cry and spasmodic or suffocative attacks the condition may be suspected.
—The prognosis will depend upon the character of the tumor and the local conditions—i. e., size, fixation, location, etc. In the young it is serious because of the danger attending its removal. Rational adults can be usually put in excellent condition for endolaryngeal operation by the aid of local anesthesia, and expert specialists become dexterous in their manipulation of the specially shaped forceps, curettes, and the like which are required for removal of these growths. As elsewhere a truly innocent tumor in this location does not recur after complete extirpation.
Of these tumors the most common is epithelioma within the larynx. Sarcoma occasionally originates from the vocal bands, true or false, and will usually form a nodular tumor, of rugose surface, until it begins to ulcerate. Once it begins to break down it is difficult to distinguish from the other varieties without the aid of the microscope; but epithelioma may be met with in any part of the larynx, generally arising from the ventricular bands. Here, as ordinarily upon mucous surfaces, it begins as a small nodule with a definite zone of infiltration about it; if seen early it may be mistaken for innocent papilloma. As infiltration progresses the hoarseness resulting from its presence will change to loss of voice, because of the fixation of the tissues whose mobility is essential to voice production. Pain may be an early feature, depending upon ulceration and exposure of sensory nerve endings. Later when the ulcerated surface has become deep, irregularly covered with fetid discharge, and more or less concealed by edematous surroundings, the picture is more complete in one respect, although the details may be obscure. From the mucous and softer tissues the disease will spread and invade the cartilages themselves, as well as the tissues outside, and so with the progress of the cancer the entire larynx becomes fixed in a bed of infiltrated tissue extending in all directions, involving the upper part of the trachea, the epiglottis, and the base of the tongue. Meantime the loss of voice, the distressing cough, and the other evidences of local invasion will have kept pace with the progress of the disease, and dyspnea will come on sooner or later as the passage-way becomes blocked, while from sudden, violent efforts at coughing acute attacks of edema, which may result fatally, are liable to occur.
Tumors of the trachea proper are far less common. They may be benign or malignant. In either event they will prove to be of about the same type as those already discussed above as occurring within the larynx. They cause less interference with speech, but as much or even more difficulty in respiration.
When tracheotomy was a frequent resort in croup and diphtheria a peculiar form of new formation in the trachea was occasionally encountered, resulting from the irritation of the trachea tube, whose presence sometimes provokes excessive formation of granulation tissue, whose subsequent contraction brings about not only the formation of a dense granuloma, but cicatricial contraction. Hence in the older literature references to granulation stenosis were common. Now that intubation has almost completely replaced tracheotomy for these purposes the latter is rarely performed, and tubes are seldom left more than a day or two in situ, so that this kind of local provocation, with its consequences, is rarely encountered.
It may be possible by expert use of the laryngoscope to see a tumor located within the trachea. If the patient cannot tolerate its use the parts may be made tolerant by the use of a weak cocaine spray. Such a growth, if accessible from above, may be removed[688] through the glottis by forceps. Most operators, however, prefer to make an opening through the trachea and thus profit by the larger surgical opportunities thus afforded. Such an operation should be made with the patient’s head low in order that blood may gravitate to the pharynx rather than to the lungs.
Cancer of the larynx was regarded, until the last quarter of the previous century, as an absolutely hopeless condition for which nothing could be done until it became necessary to do a tracheotomy, this simply affording relief from some of the distressing features, but aiding nowise to check the progress of the growth. The first demonstration of the possibility of successful removal of the larynx was made by Czerny, in 1870, upon dogs. Watson, of Edinburgh, had removed a syphilitic larynx in toto in 1866, but this summary operation only became known to the world through a publication of Foulis in 1881. Meantime, Czerny’s experiments were so successful that Billroth was induced to attempt the removal of the entire larynx in a case of cancer, with results which astonished the profession of that day. Thus introduced, nevertheless, the mortality rate was great, the principal cause of death being inspiration pneumonia—that is, rapid infection of the lung through the widely opened trachea and the entrance of saliva and fluids from the mouth. Hahn, of Berlin, undertook the improvement of the technique and was able to reduce the mortality from this cause. Meantime another radical method—namely, thyrotomy, i. e., opening the laryngeal box—had not fared much better than the measure just mentioned. Thus until about twenty-five years ago the radical treatment of laryngeal cancer stood in an unpleasant light, partly because diagnostic methods were unsatisfactory and our general knowledge of the disease incomplete, partly because operation was always delayed until late, and because operative measures had yet to be much improved. Tremendous impetus was given to the whole subject by the celebrated case of the Emperor Frederick, and the acrimonious criticisms concerning its conduct were not without benefit, since they led to a careful re-study of the whole situation, with its numerous subsidiary questions, among which was the possibility of transformation of a benign into a malignant tumor. At present, largely through the labors of Hahn and Billroth, in Germany, and Semon, in London, the question of operative procedures is fairly settled, everyone now believing that the disease should be radically attacked at the earliest possible moment, opinions differing only in regard to the route which the surgeon should adopt, i. e., whether he should make an intralaryngeal operation, as is now favored in Germany; a thyrotomy, as preferred in Great Britain, or a laryngectomy, as some of the general surgeons in all parts of the world prefer.
The different methods of attack upon the larynx for cancer may then be summarized as including intralaryngeal extirpation through the natural passages, thyrotomy, and partial or complete laryngectomy.
The intralaryngeal method, seen from the general surgeon’s view-point, can only be suitably applied to a limited class of cases which are recognized early, and may be best performed by an expert laryngologist, i. e., one accustomed to instrumentation within the pharynx and larynx. It includes the use of various instruments for the excision of small areas, for the application of the galvanocautery, etc. The writer agrees with Semon in regarding it as irreconcilable with the principles which should guide us in dealing with malignant growths, the fundamental one being the removal not only of the growth itself but of an area of surrounding tissue. This intralaryngeal method may then be satisfactory in the removal of benign growths, but will seldom appeal to the operating surgeon when he deals with cancer. Epithelioma may commence at the accessible tip of the epiglottis, but intrinsic cancer of the larynx should be dealt with in a more radical manner. Thyrotomy is the operation of choice, especially among the British laryngologists. It seems rational to believe that in cases where diagnosis is made early a thyrotomy, with removal of the growth and a wide area of surrounding tissue, including portions of cartilage, if necessary, may prove the ideal operation, while vocal results are better than after extirpation. It is necessary, however, that diagnosis should be made early and that operation be made thoroughly; while if, after opening the thyroid, it should appear that complete extirpation of the growth is otherwise impossible, then the operator should make a complete laryngectomy.
[689]
All of these operations are best preceded by use of a cocaine spray, by which extreme irritability of the interior of the larynx is allayed, and the reflex lowering of blood pressure prevented. (See p. 178.)
Thyrotomy is performed as follows: The patient is preferably in the position with down-hanging head. An incision in the median line, about three inches in length, is made from the upper border of the thyroid cartilage down to a point below the cricoid. With but slight separation of the tissues it is made to extend directly down upon the abrupt ridge-like anterior border of the thyroid cartilage, below which will be exposed the cricothyroid membrane. Into this the knife may be inserted and made, with cutting edge up, to split the halves of the larynx exactly in the middle line, the blade passing between the vocal cords, unless they have been much distorted by the growth. In that case the dissection may be made more deliberately. The larynx being thus split, the cricoid should be divided, after which, with suitable retractors, the interior is exposed to such an extent as to permit both inspection and palpation. Through the opening thus afforded all suspicious tissue should be removed, from one side or both, the primary question being not what will be the resultant effect upon the voice, but how best to completely eradicate the cancerous tissue. With the patient’s head hanging downward there is less likelihood of the entrance of blood into the trachea. Nevertheless the tampon cannula should always be accessible so that it may be inserted should it be required. The tampon cannula is a trachea tube around which there is a small rubber bag, with a tube through which it may be inflated, so that after the cannula is introduced into the trachea it may be tamponed by air pressure in such a manner as to permit no passage of blood.
In the absence of one of these specially designed tubes an effective substitute may be made by the ordinary trachea tube wrapped with a covering of antiseptic gauze, the latter held in place by a few turns of fine silk or catgut.
The thyrohyoid membrane bears the superior laryngeal vessels and nerves, and it should be entered through the middle line in order not to disturb these. Whatever operation may be required upon the tissues within the laryngeal box may be conducted with knife, scissors, curette, and the fine point of the actual cautery. The interior of the larynx should be cleaned, leaving it simply as a part of the respiratory tube, without reference to what may become of the structures within it devoted to voice production. The cartilaginous shell, with or without a part of its previous contents, having been rid of the suspicious tissue within, it may be held together by one or two sutures of silver wire or by superficial sutures of chromic gut, while the trachea tube which may have been used may be left for a day or two, or removed at the time. Ordinarily the latter course will prove the better.
Laryngectomy, or total extirpation of the larynx, is the most severe procedure of all, but will be requisite when there is evidence of escape of malignant growth from within the true confines of the laryngeal box. Not only the larynx but more or less of the surrounding tissue may be removed, with infected neighboring lymphatics, the upper portion of the trachea, and the base of the tongue.
The operation may be preceded by a low tracheotomy or otherwise. If necessary this should be done several days in advance, in order that the patient may have become tolerant of the tube and of the new method of breathing. If requisite the ordinary trachea tube may be substituted for the tampon tube above described, in which case it will not be necessary to lower the patient’s head. Otherwise the operation is perhaps best performed with the head and neck in the Rose position.
The incision is a long median division of tissues from above the hyoid to an inch or more below the cricoid cartilage. Through it the anterior border of the thyroid should be easily exposed. It is then necessary to separate on either side the sternohyoid and sternothyroid muscles, the lateral mass of the thyroid body being drawn to either side along with the musculature, the isthmus having been previously doubly ligated and divided for this purpose. Now as rapidly as may be the larynx is completely isolated from all the structures around it, the dissection being bluntly made. After freeing it on both sides it is drawn forward, first to one side, then to the other, so that on either side the superior laryngeal artery may be exposed and secured, the superior laryngeal nerve being necessarily divided. The cricothyroid branches need also to be secured, as well as any other vessels which may spurt blood. Circumferential isolation of the larynx is now completed by dividing the inferior constrictor of the pharynx and separating[690] it from the side of the thyroid, keeping close to the cartilage. After this isolation is completed the surgeon has the choice of first dividing the respiratory tube either above or below the larynx. This will depend largely upon his own choice, but usually the procedure is easier when the first division is made either through the cricothyroid membrane or between the cricoid and the upper ring of the trachea or even below this point, if necessary. With a low division first the patient will immediately begin to breathe through the opening thus made unless a previous tracheotomy has been done. Ample time will be afforded for the introduction of a trachea tube and protection around it to prevent entrance of blood, when the larynx may be lifted and separated with knife or scissors from the tissues remaining attached. The esophagus begins at the level of the cricoid cartilage, and if the cricoid is to be removed the esophagus should be separated from it; otherwise it is not disturbed. Last of all, in this order, the thyrohyoid membrane will require division, and then the extirpation is completed.
The wound is large, the communication with the oropharynx is unobstructed, and there will be constant escape into the newly formed cavity of secretions from the nose and mouth. At first the patient will be unable to swallow, although there may be constant desire to reflex attempts in this direction. The questions to be decided are the management of the wound in gross and the suitable treatment of the upper end of the trachea, as well as of the esophagus, if this has been touched. The greatest danger is that of inspiration pneumonia. Other consideration should be secondary to that of prevention of the escape of fluids down the trachea and the consequent production of pneumonia. General experience is rather to the effect that the best results are obtained with a minimum of sutures, the large cavity being lightly packed with absorbent material, while the upper end of the trachea should be sewed to the skin as high as possible on either side, the esophagus being allowed to take care of itself. The patient should wear a trachea tube for several days after the operation. Through the exposed upper end of the esophagus a tube may be passed three or four times a day, and sufficient nourishment be thus introduced into the stomach. The patient may be kept lying upon the side for the greater part of the time, so that saliva may escape from the mouth.
The question comes up later as to what substitute, if any, may be afforded for the lost larynx. Gussenbauer devised an improvement on what was called the “artificial larynx,” devised originally by Foulis and then modified by Hahn, which afforded an ingenious mechanical substitute for the larynx, permitting the production of voice by vibration of a metallic reed, such tone as it produced being, like that produced by the vocal cords, modified by the vocal organs above into perfectly intelligible speech, but always in a monotone. It consisted of a tracheal tube through whose external opening another tube could be passed upward to a point where it lay beneath the epiglottis, if this were left in situ, or behind the base of the tongue, if the epiglottis had been removed. Through this the patient could breathe under ordinary circumstances. By a little device at the external opening the touch of the finger upon a spring would throw into the air current a thin, metallic reed, by whose vibrations tone was produced, to be modified as mentioned above. This was the principle of the artificial larynx which was worn by many patients and which in many gave good results. One patient of my own wore one for seven years, although he discontinued using the reed because the peculiarity of the tone attracted more attention than did the loud “stage whisper” which he had cultivated. Around the instrument there is always more or less moisture or discharge, and there are many disagreeable features attending its use, even though it permit the act of swallowing without any difficulty.
Solis Cohen introduced a method of treating these cases by fastening the trachea to the external wound and permitting the cavity above to close as rapidly as possible. In this way the trachea is permanently terminated in the middle of the neck and patients breathe through this opening. It has been found that with practice they can retain sufficient air in the mouth and pharyngeal cavity to permit them to whisper several words at a time. This simplifies the procedure, and is now usually adopted after extirpation of the larynx.
Partial laryngectomies have been practised through external openings, one lateral half or more of the larynx being removed. These operations have been few in number and often unsatisfactory. They should be reserved for cases with favorable indications. When required they are performed on the same principles as those already outlined, only the extirpation is incomplete. Certain modifications have been proposed by individuals,[691] as, for instance, the suggestion made by Gluck, to suture the opening in the trachea to a buttonhole opening made in the overlying skin, by which means he thought to prevent inspiration pneumonia.
Tracheotomy is the general term made to cover any opening into the lower air passages between the larynx proper and the upper end of the sternum. Laryngotomy, cricotracheotomy, tracheotomy, etc., may be described as implying by these names the exact location of the opening. The principle is, however, the same, and the details of the operation vary but little.
Fig. 482
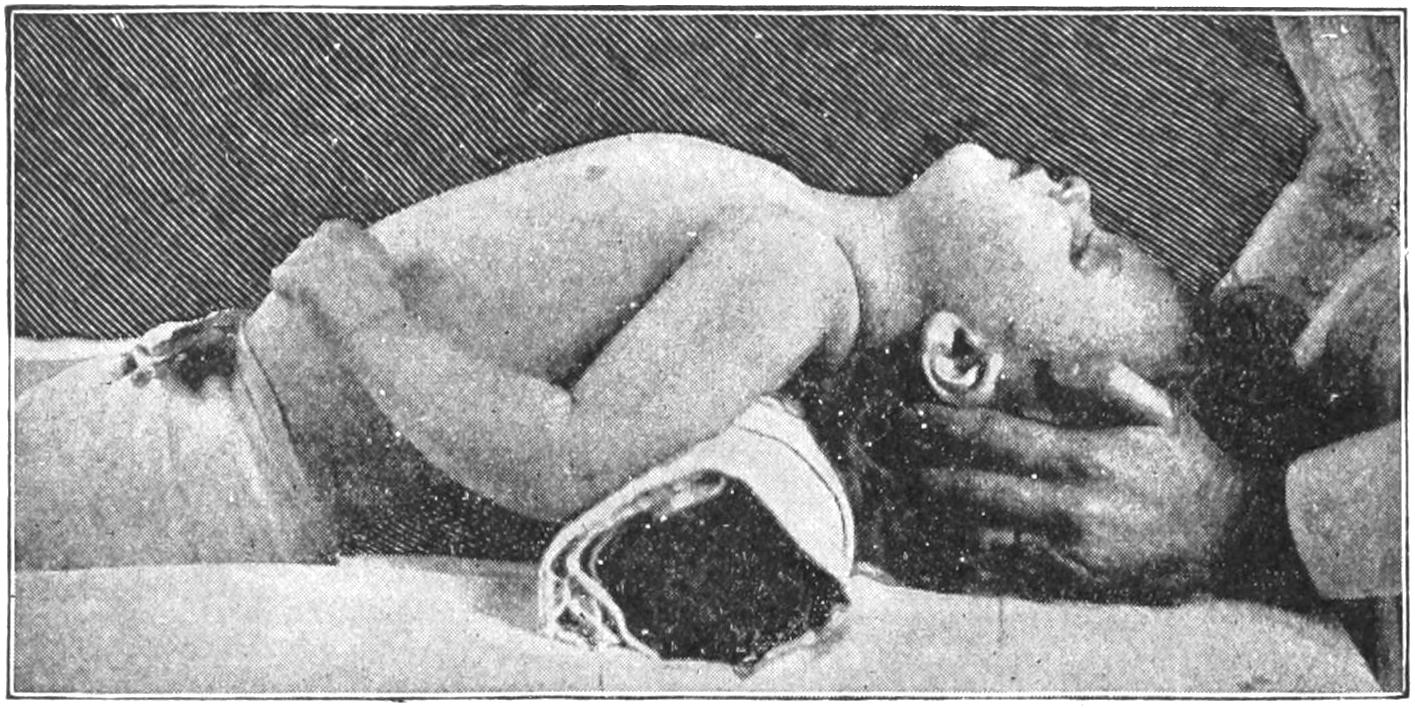
Position of patient for tracheotomy. (Wharton.)
Tracheotomy as a deliberate operation is different from tracheotomy as it was formerly practised for diphtheria, and as it is yet done in emergencies, some cases being so serious that suffocation will occur if the opening be not promptly afforded. In the former case preparations can be made; in the latter, operation may have to be done with the blade of a penknife. It makes considerable difference also whether an anesthetic can be used. To administer chloroform to a child with a heart already weakened by the toxins of diphtheria is almost to invite disaster, and yet to do the operation without an anesthetic is perhaps impossible.
The middle line is the line of safety in all of these operations. The danger of heart failure from the anesthetic, or of suffocation from tardiness of relief, being passed, the other principal danger is that of hemorrhage. The isthmus of the thyroid may be divided, but always with preliminary ligatures, or it should be caught between the blades of pressure forceps on either side before dividing it. A patient with a short, fat neck, whose cervical veins are dilated and engorged with venous blood owing to partial asphyxia, makes a difficult and undesirable subject. The trachea lies nearer the surface at its laryngeal end than in its lower portion—i. e., if the operation be low in the neck deep search will have to be made for the tube. The first incision should be made sufficiently long, never less than two inches, and should be so planned as to bring the operator down upon the tracheal rings. By this time sufficient engorged veins may have been divided to cause a serious oozing of dark, venous blood, by which the field of vision is much obscured. Except in emergencies the surgeon may wait for this engorgement to be relieved. The trachea, being recognized by the finger-tip, is seized with a tenaculum, by which it may be held forward, and then at least two of its rings divided with the knife-blade. The instant the opening is made, if the patient be still breathing, bloody foam and frothy blood will be ejected, and for a moment or two the bleeding may be uncontrollable. Under these circumstances the normal blood color soon returns. Artificial respiration should be practised at the same time. Supposing this to be an emergency case, with little or almost nothing at hand, sutures should be passed through the tracheal opening and through the skin margin on either side. If no other retractor be at hand the suture materials may be left long and tied behind the back of the neck, sufficient tension being made to prevent the wound edges from coming together. Formerly when the surgeon was called to do this operation with little or no[692] help the writer has extemporized a couple of retractors out of hair-pins, bent for the purpose, hooked into the tracheal wound, then tied with tapes, which were united behind the neck, while the wires were kept from being pulled out of place by a skin suture on each side. There is now less occasion for these crude methods since the introduction of O’Dwyer’s intubation.
With tracheotomy done deliberately, and at the point of election, usually above the thyroid isthmus, with or without division of the cricoid, the vessels may be secured as they are exposed or bleed, and the trachea should not be opened until all oozing from its exterior has been checked. For this purpose the patient is placed upon the back, the shoulders raised, the head thrown backward, and the neck exposed, a pillow being placed beneath. (See Fig. 482.) The operation may be done under cocaine local anesthesia or with a general anesthetic. Incision in the middle line, below the lower border of the thyroid cartilage, is made two inches or so downward, the fascia beneath being divided in the same line and the tissues retracted to either side from this median exposure. Thus one makes access to the cricothyroid membrane, the cricoid, the upper tracheal rings, and the thyroidal isthmus. According to the size and location of the latter (it usually lies in front of the second tracheal ring) it may be retracted or doubly ligated and divided in the middle. The difficulty now afforded is from the upward and downward play of the larynx, which may occur during forced efforts at respiration. To steady it a tenaculum should be introduced just above the cricoid, a little to one side of the middle line, firmly fastening it. With this held in the left hand, thus steadying the parts, a sharp-pointed knife is so employed as to divide the cricoid and one or two upper rings of the trachea, being cautious not to wound the posterior wall. The opening thus made should be about one-half inch in length. Through it a second hook is now passed into the other side of the cricoid and the incision held open by their agency while the trachea tube is introduced.
This procedure may be modified in accordance with any local indications, and may be made according to the needs of the case. When the opening is made into the trachea below the isthmus it is called a low tracheotomy. Here the anterior part of the trachea lies free from the skin, but may be covered with a plexus of veins connecting with the inferior thyroid. Farther down the arteria thyroidea ima may be encountered. There is always reason for operating as high as the case will permit. The trachea may itself be displaced by the growth which compresses it and necessitates the operation. Thus it may be crowded to one side, other anatomical relations being disturbed, or it may be compressed into scabbard shape, and thus be difficult to find or to open.
The moment the trachea is open more or less marked expulsive efforts will drive blood and foam in all directions, and may for a moment obscure the field of vision. Every precaution should be taken to prevent the entrance of blood into the trachea. Pressure of the tracheal walls against the tube to be inserted may check hemorrhage from its margins. The operator should be ready to suspend all other procedures and make artificial respiration, and he should also be prepared to open the trachea suddenly, should impending suffocation require it.
In a general way, then, the indications for tracheotomy are symptoms of rapidly or slowly threatening obstruction to respiration from causes either within the larynx—e. g., diphtheria, foreign bodies, tumors, and the like—or causes external to it, such as tumors, phlegmons, cicatrices, etc. Any cause which interferes with the free play of air through the respiratory tube, which can be either relieved or atoned for by the operation, will always justify it.
Tracheotomy tubes are mechanical devices for not only keeping the tracheal wound open but permitting the unobstructed passage of air. They are made of various materials, of which silver is the most satisfactory, as aluminum is too easily acted upon by the fluids of the body, and rubber occupies too much space. The tracheotomy tube is a double tube, the inner one slipping easily into and out of the outer, and being necessitated by the ease and abundance with which secretions may collect and dry, and thus obstruct. Were it necessary to remove the entire tube for each cleansing, difficulty might be met in re-introducing it, whereas the inner tube is easily removed, quickly cleansed, and restored to place within the outer without disturbance or pain to the patient.
Aside from the tracheal tubes ordinarily used there are others made exceptionally long, and with flexible lower ends, which may be used in case of tumor low in the neck or high in the mediastinum—for instance, in cases of enlarged thymus, where it is necessary to go beyond an obstruction.
[693]
In the after-care of these cases it should be remembered that air passes directly into the lung without being warmed, or moistened, by passage over the mucous membrane of the upper respiratory tract. The patient, therefore, should be kept in a warm room, and the air should be kept moist by the use of a croup kettle or a spray machine. The inner tube should be kept unobstructed, the length of time during which it should remain depending on the nature of the case. So soon as its usefulness is passed it should be removed. A tracheotomy wound kept open but for a day or two will quickly close, but one which has remained open for weeks may close with difficulty, and then there may be trouble from granulation stenosis or cicatricial contraction. (See above under Stricture.) In instances where a permanent opening is to be maintained it is desirable to remove the tube as early as circumstances may permit.
The perfection by Joseph O’Dwyer of a method, at which others had worked, of substituting intubation of the larynx for the old tracheotomy, not only shed the greatest luster upon his own name, but has afforded a speedy and bloodless method of accomplishing much more than had been previously possible by the older procedure. The method comprises the emplacement of a suitably sized and shaped tube within the larynx, by a manipulation guided almost entirely by the sense of touch, for the relief of suffocative symptoms due to disease at this level, and leaving the tube in situ for a sufficient time to permit morbid activity to subside and justify its removal.
It is advisable to have a half-dozen tubes, varying in size from 1¹⁄₂ inches to 2¹⁄₂ inches in length, and of corresponding increase in other dimensions, each of which affords a passage-way for respiratory purposes, and is also provided at its upper end with a flange, which shall rest upon the false vocal cords and prevent the descent of the tube into the trachea below. The complete set of instruments as now furnished by all the manufacturers provides an assortment of these tubes, with a scale indicating which one to use upon a patient of a given age, and includes a mouth-gag, which may be used for many purposes, and two handled instruments—one intended for the introduction, the other for the extraction of the metal tubes.
Fig. 483
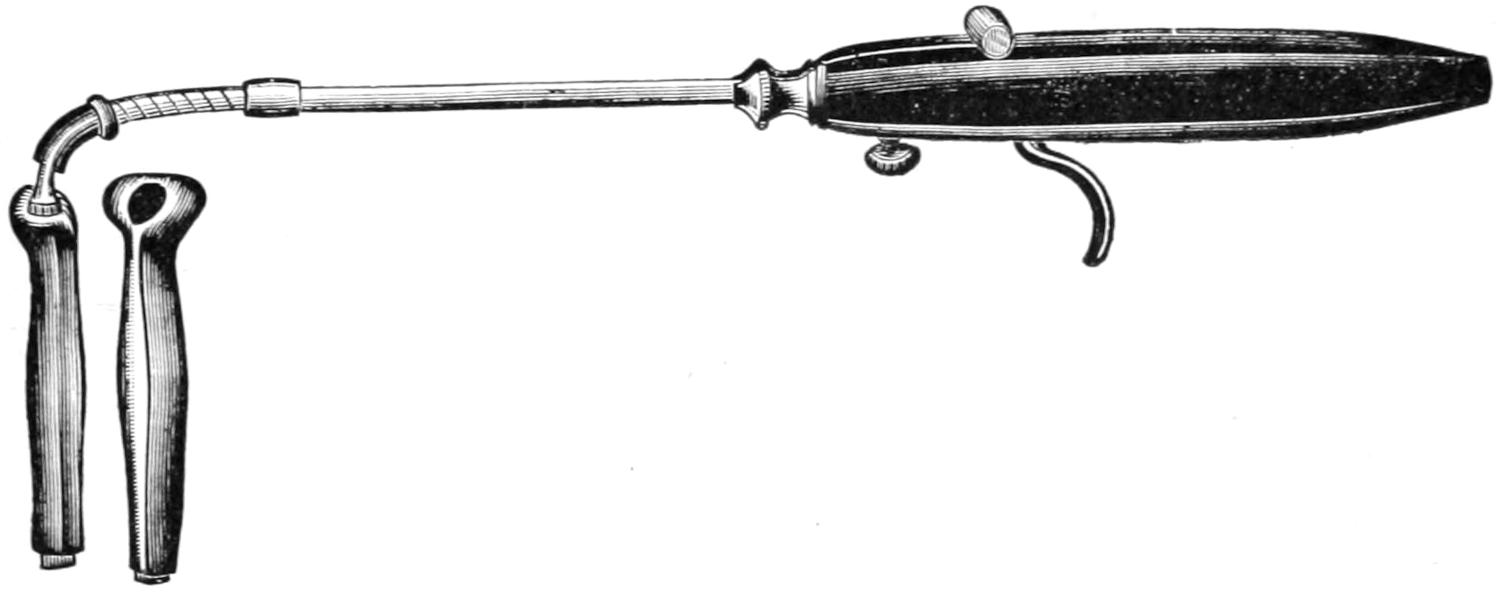
O’Dwyer’s laryngeal tube and introducer.
Fig. 484

Mouth-gag.
Fig. 485
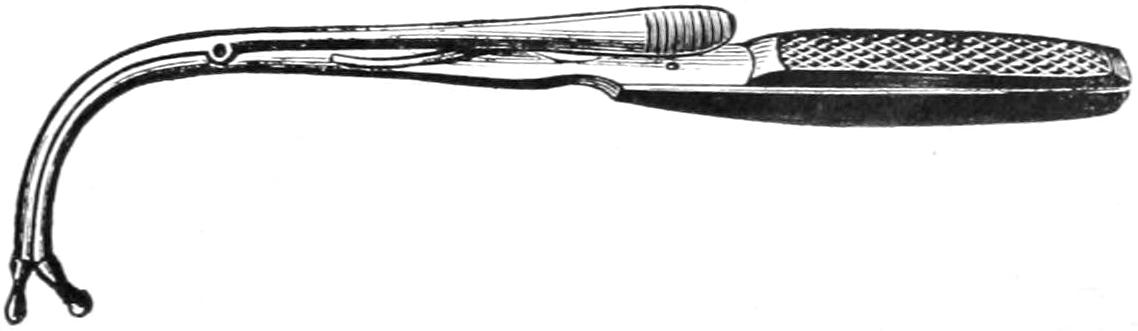
Extractor.
[694]
Fig. 486
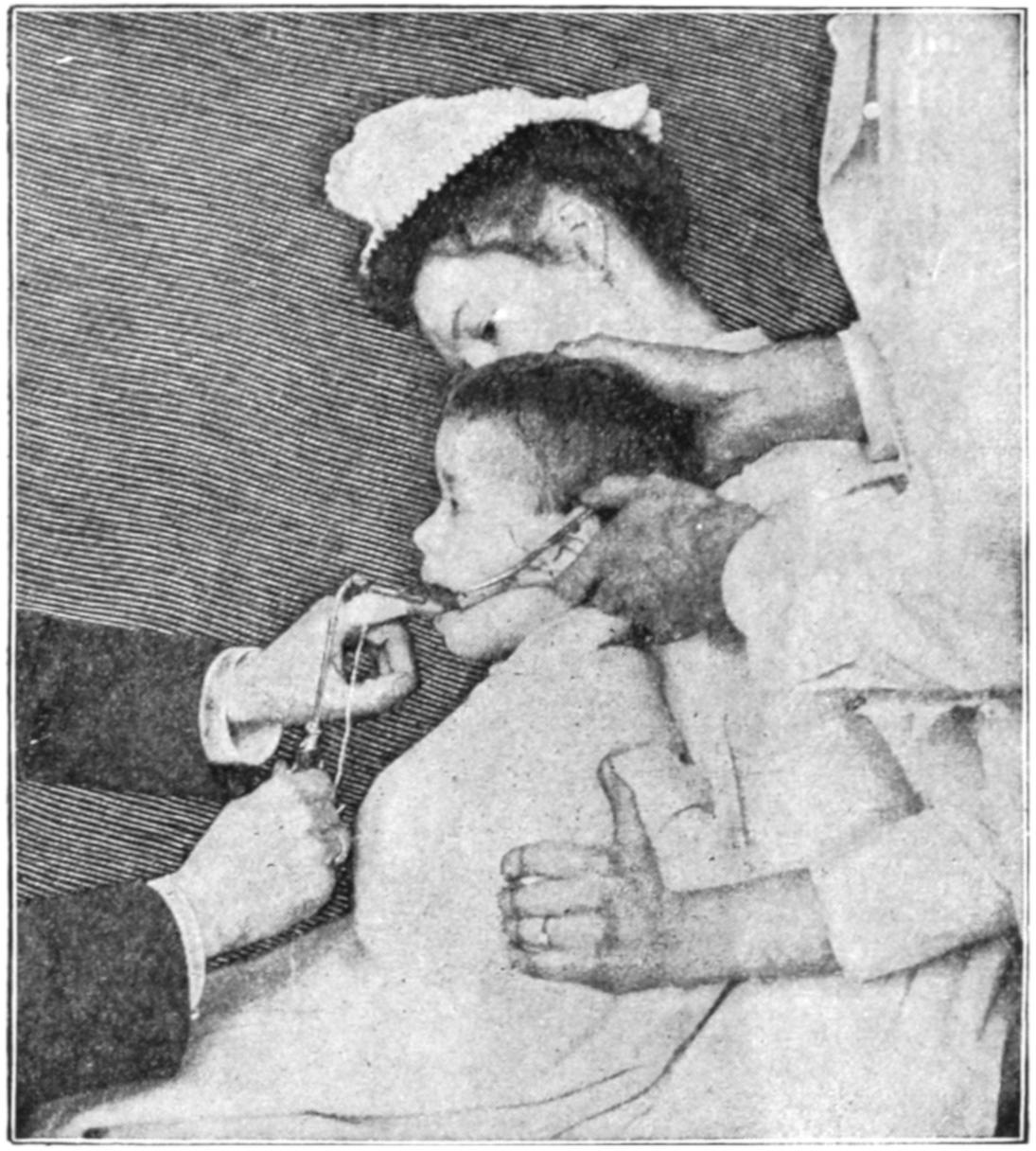
Intubation of the larynx.
Fig. 487
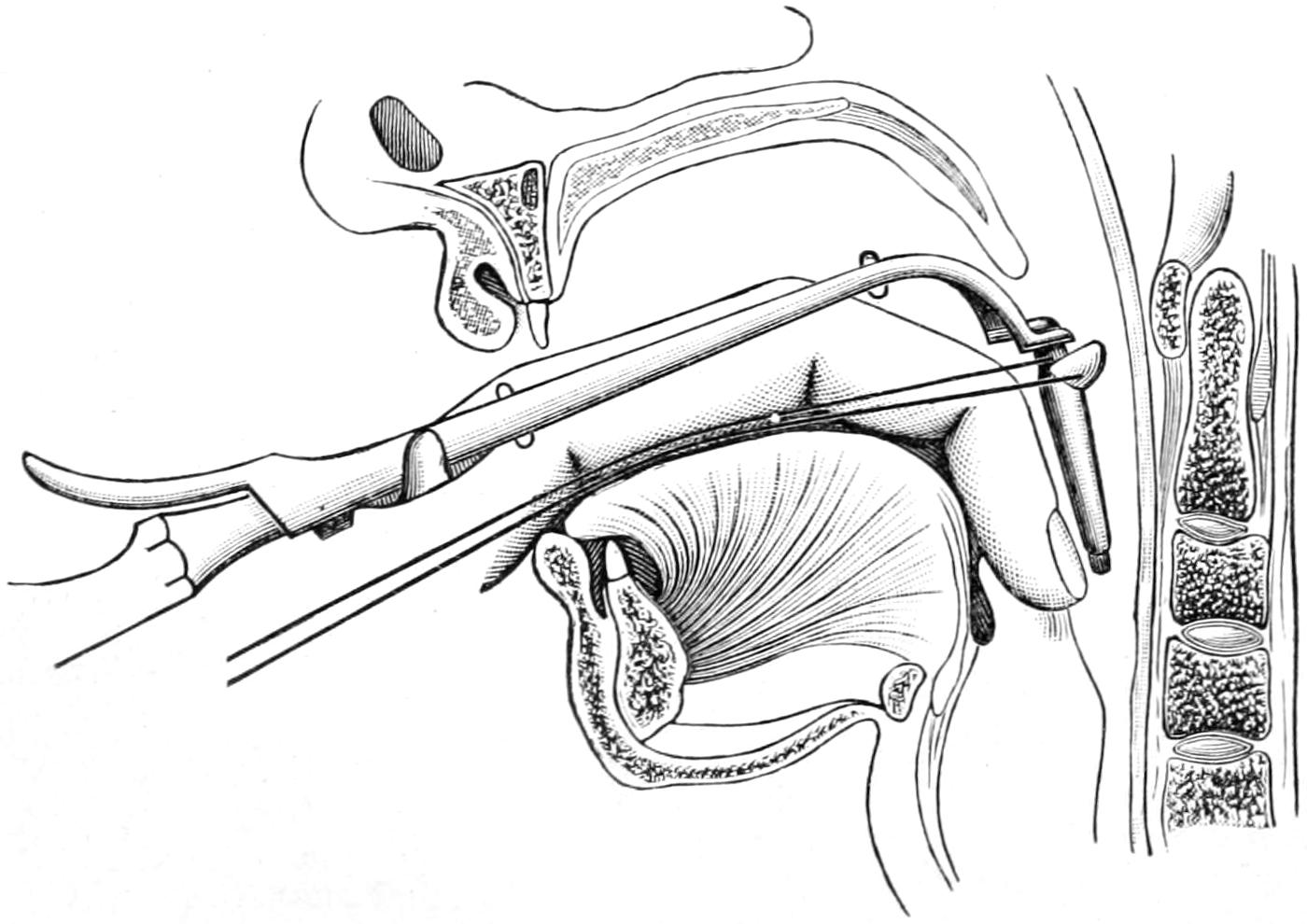
The tube in the pharynx.
A suitable tube having been selected, a strong thread is passed through a small opening near its head, thus affording means for withdrawing it should there be need before it is finally left in its resting place. The particular obturator meant for the tube to be used is then firmly fastened upon the handle and over it the tube is slipped. The instrument should then be tested to make sure that disengagement of the tube will easily take place. Everything being ready, the patient is then held in the arms and on the lap of an assistant, in the position indicated in Fig. 486. The individual holding the patient should be perfectly reliable in the matter of presence of mind and self-control, for a great deal depends upon having a child firmly and properly held during the moment of intubation. The arms and hands of the patient should be well wrapped with a towel and firmly held by the side of the chest, for the temptation is inevitable to put the hand to the mouth and interfere with the operator. A second assistant should stand above and behind, holding the mouth-gag in position, as represented,[695] and steadying it as well as the head. It is necessary that the mouth-gag be held firmly in place, for if it should become disengaged the child may bite the operator’s finger.
Fig. 488
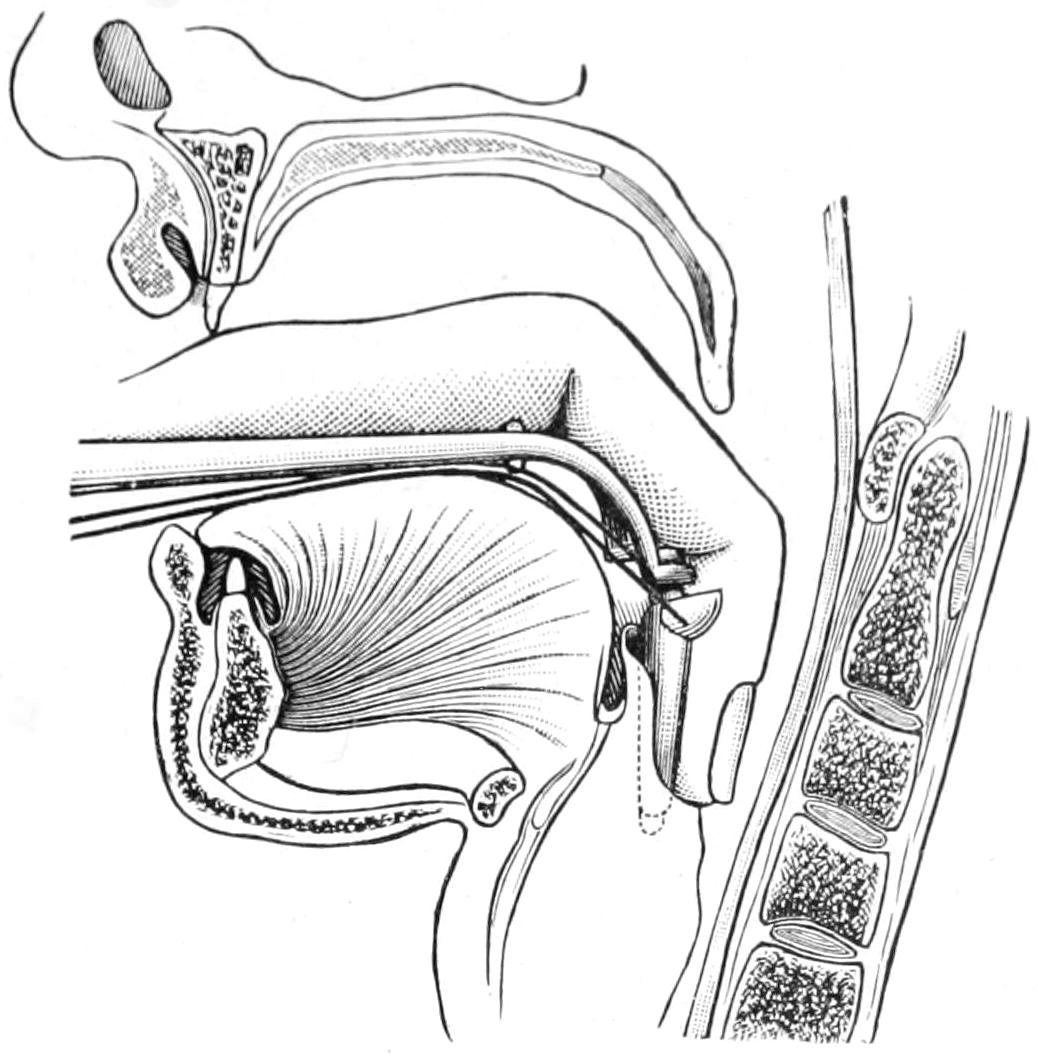
The tube penetrates the larynx. (Lejars.)
Fig. 489
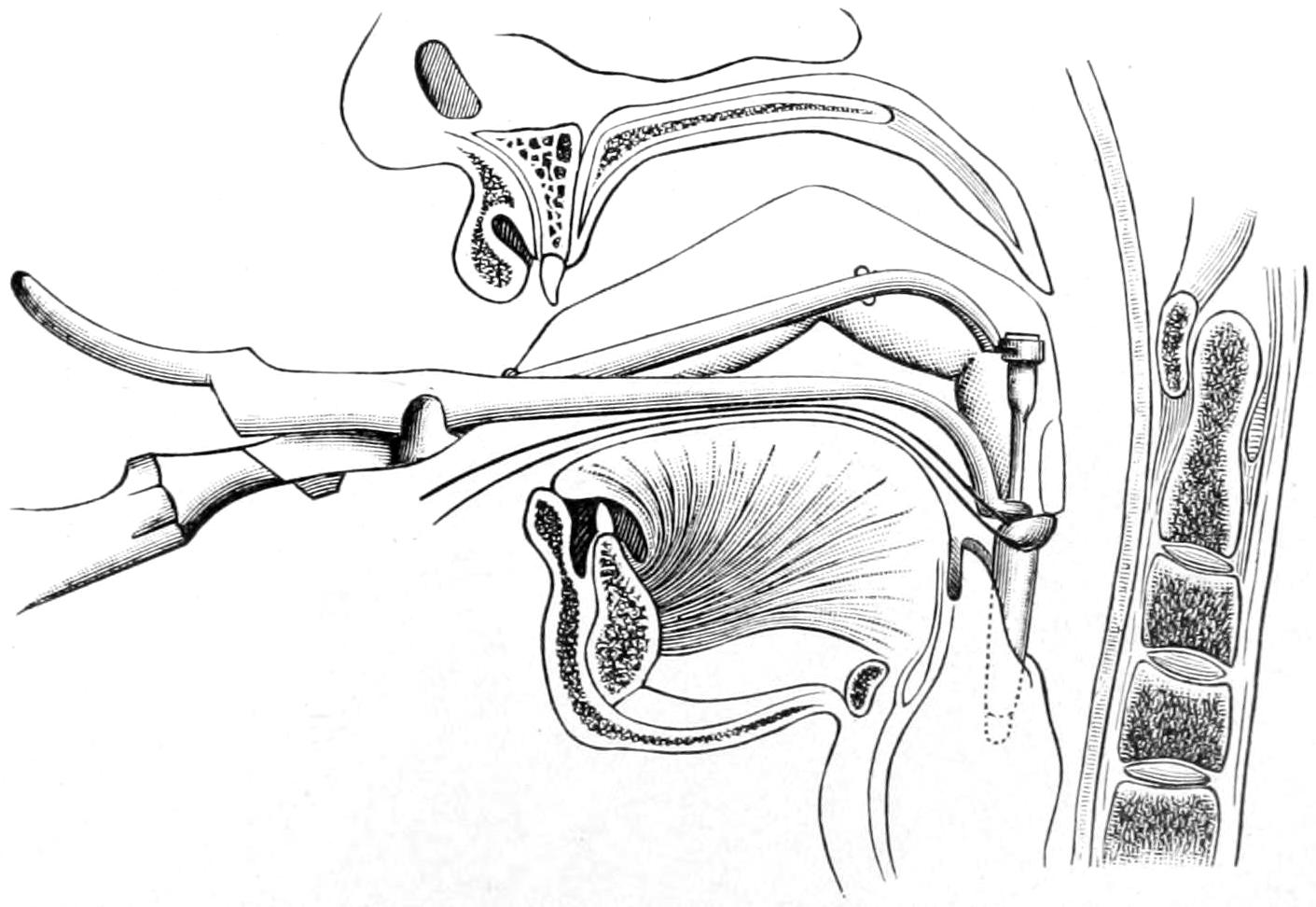
The stem is withdrawn while the finger fixes the tube. (Lejars.)
Standing in front of the patient the operator identifies the tip of the epiglottis with the forefinger of the left hand in the pharynx, this finger being used at the same time to raise and fix the epiglottis and also to serve as a guide to the tip of the tube, which is passed downward alongside it, by a maneuver similar to that by which the laryngoscopic mirror is used in the pharynx (Fig. 487). When the tip of the tube reaches the location behind the epiglottis the finger may be passed a little farther downward, plugging the entrance to the esophagus, while at the same time the handle of the instrument is so manipulated as to bring the tube forward. With gentle movement in the right direction it passes into the larynx (Fig. 488). It is then pressed downward until the flanged upper end has passed the epiglottis, after which the tube is disengaged, the handle and the obturator withdrawn, and the upper end of the tube pressed gently into place by the finger which still rests in the pharynx (Figs. 488, 489 and 490). During the manipulation there is almost complete obstruction of the glottis for two or three seconds. The effort, therefore, should be to shorten the procedure, and at no time should[696] it occupy more than two or three seconds. If the landmarks are not easily recognized, and the tube is not placed at the expiration of three seconds, the operator should discontinue for a few more seconds in order that a few inspirations may be taken, after which he should try again.
Fig. 490
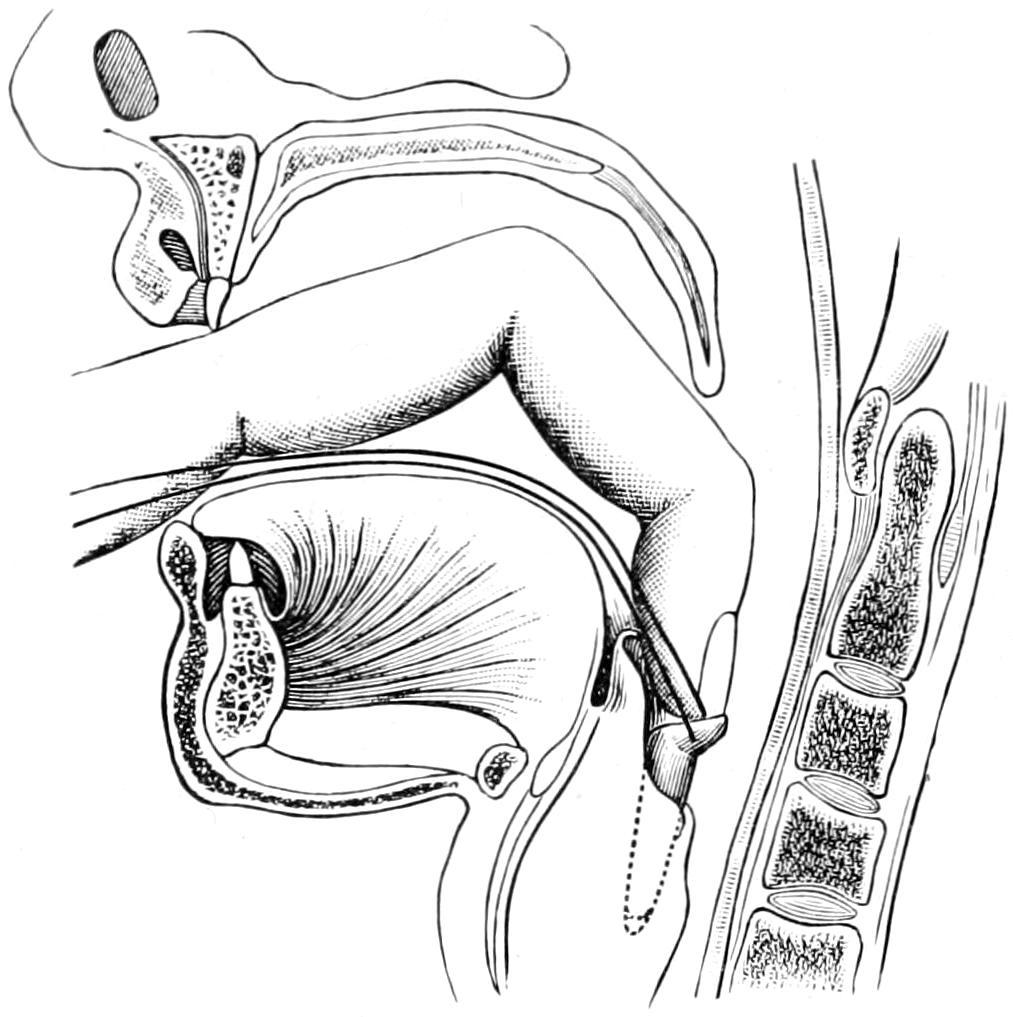
The finger pushes the tube into place. (Lejars.)
Fig. 491
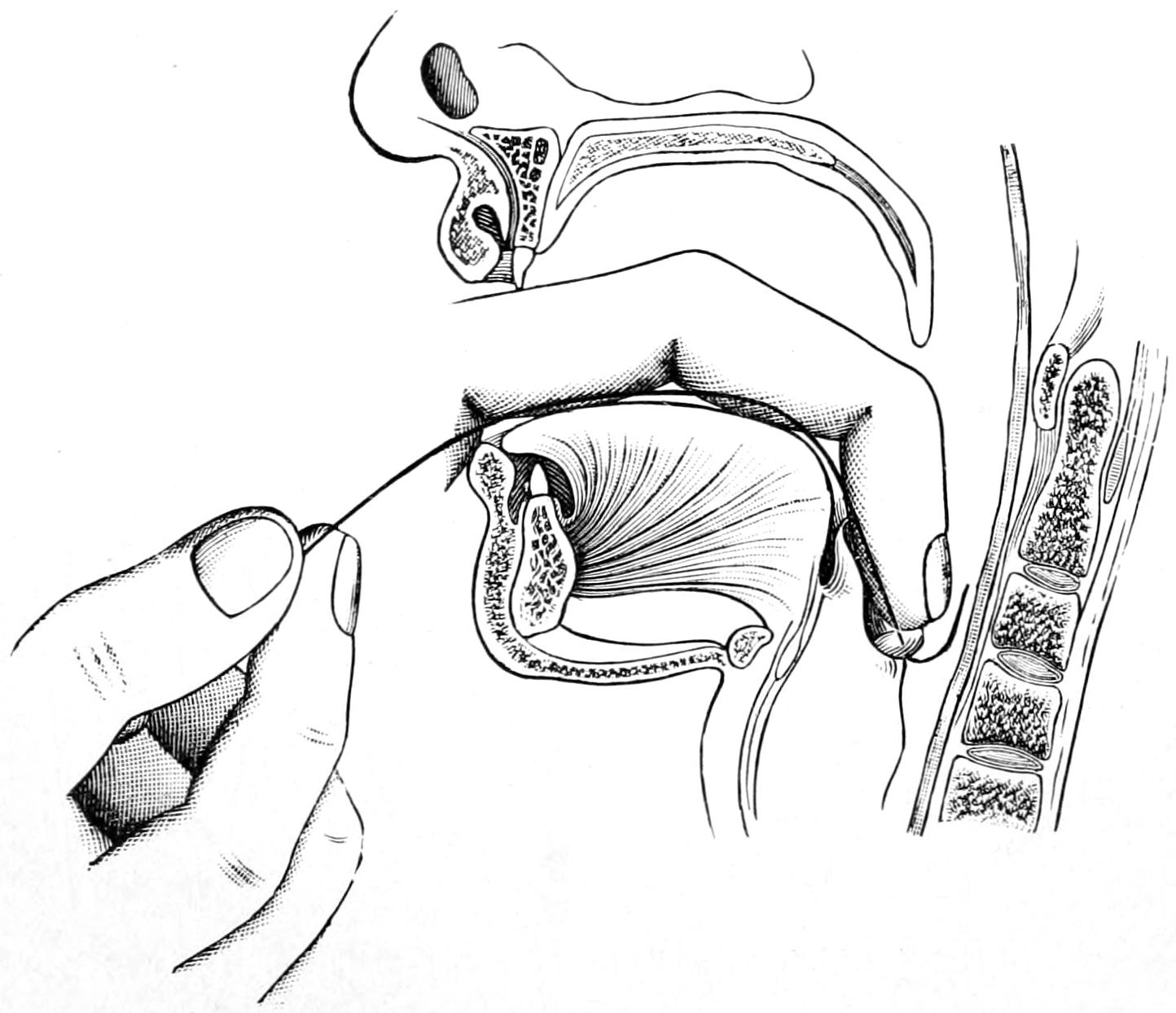
Withdrawal of the thread. (Lejars.)
When the tube is in place there will come ease of respiration, at the same time violent coughing efforts, because of the irritation thus suddenly produced. So soon as it is apparent, both to the finger in the pharynx and from the relief of obstructive symptoms, that the tube is in its proper place, the finger may be once more passed into the pharynx, the tube pressed down, while the silk thread is withdrawn, since it is not intended to leave it for more than the time necessary to be assured that the tube will not have at once to come out again (Fig. 491). Before removing the thread the gag should be removed for a few moments, so that the effect of the excitement may pass, after which it may be re-introduced for the purpose of withdrawing the thread.
[697]
The procedure is by no means a simple nor necessarily easy one, and it should be practised with the instruments upon the cadaver before resorting to it on the living child.
The tube being placed it will remain to be decided by the subsequent course of events how long it should be allowed to remain—in some cases a few hours, in others a few days. With young children it should remain for at least a week. The time having arrived for its removal, the procedure is similar to that required for its introduction. The assistants hold the child in the same position as before, while the operator substitutes the extractor, guiding its tip again by the sense of touch along the left index finger, which, passed down into the pharynx, is made to discover and identify the upper end of the metallic tube. So soon as the point of the extractor is engaged within the tube the blades are separated and it is then drawn out, while the finger is withdrawn along with it in order to make its removal easier and to prevent its loss should it slip off the instrument. Unless the patient struggles violently the whole procedure should be conducted so as to scarcely cause the slightest staining of the expectoration with blood.
Various causes may require abrupt removal of the tube. Thus it is possible for its caliber to be become occluded with tenacious secretion. This may produce a violent fit of coughing, during which there may occur spontaneous expulsion of the tube. At any time, when it is seen that asphyxia is increasing, or when violence of respiratory effort would indicate obstruction within the tube, it should be removed, cleaned, and re-introduced. After its introduction and removal the operator should remain within easy reach for a short time, to be sure that no unpleasant effects result and that no re-introduction may be suddenly required. Should obstructive efforts occur the child should be held head downward and be slapped vigorously upon the chest. This may loosen membrane or it may permit dislodgement of the tube and its spontaneous expulsion. The latter may also occur during the act of vomiting.
The above description is meant especially to apply to intubation as performed upon young children for the relief of the laryngeal obstruction consequent upon diphtheria. It has given better results than tracheotomy, which was the only resort previous to O’Dwyer’s device. It is usually performed easily, and is devoid of the horrors frequently attendant upon an emergency tracheotomy. But intubation is not necessarily limited to children nor to cases of diphtheria. The emplacement of such a tube may be called for at any time in cases of threatening or actual edema of the glottis, as, for instance, from inhalation of steam or flame. It may be advisable in other forms of intralaryngeal disease, both acute and chronic, while individuals suffering from laryngeal stricture or stenosis find that they can wear an O’Dwyer tube almost constantly, not only with relief, but that they are thereby saved from the more serious measure of opening the trachea or removing the larynx.
Impending suffocation having been relieved by intubation, the question of feeding arises. The principal disadvantage attendant upon the use of the tube is partial or complete inability to swallow, for the epiglottis does not always easily close over the tube and prevent entrance of fluid into the larynx. It is necessary to feed patients, especially the young, with extreme care. For this purpose there is no food better than ice-cream, while little children should be placed upon their backs, with the head lower than the body, and made to swallow in this position, at least until they have been accustomed to the presence of the tube and instinctively learn how to avoid irritation by involuntary regulation of the act of swallowing.
[698]
These consist largely of defects due to arrest of development along the lines of the branchial clefts. Necessarily of embryonic origin, they do not reveal this until varying periods after birth, sometimes not until old age. They consist of fistulas, opening either externally or internally, or more commonly of cystic dilatations of the interior portions of the original fissures. External openings are usually seen along the sternomastoid, either in front or back of it, or between the larynx and the clavicle. Vestiges are also present in the shape of little tags of skin containing portions of cartilage or bone. They frequently occur together, the tag indicating the location of the fistula, whose opening may be found obstructed with crusts. Internally the openings are usually found in the pharynx, perhaps in the larynx or trachea, generally near the tonsil and base of the tongue. An external fistula may be tested for its completeness by injecting a colored fluid and inspecting the pharynx. The fistulous portion is usually marked by a cord-like mass which extends inward, usually toward the hyoid bone. Internal blind fistulas may gradually expand and constitute one variety of the so-called pulsion diverticula of the pharynx and upper esophagus, their dilatation being due to accumulation of food, and gradual stretching in this way.
All of these embryonic relics are of interest because from their small beginnings large growths may take place, constituting even serious surgical problems. These growths may present in almost any region of the neck and frequently extend into the mouth, where they give rise to certain forms of ranula. Almost every cystic tumor beneath the tongue or jaw is open to the suspicion of having an embryonic origin. Most of these vestiges are amenable to surgical treatment should they give rise to discomfort or trouble. The operations required are sometimes quite extensive, as any tumors of branchiogenic origin are especially liable to adhesions to the large vessels; moreover, they are nearly always firm and the dissection thus made difficult. A dermoid cyst may be evacuated and its wall or sac destroyed or dissected out. It may then be made to heal by packing.
—In the treatment of fistulas of the neck, König has advised that a curved probe be passed through the tract to a point close to the tonsil, at which point on the inside of the mouth or pharynx the mucous membrane is incised, a silk thread is fastened to the end of the probe, pulled out with it, then made to pass to the external end of the fistulous tube, which is then invaginated and pulled back into the mouth, where it is reduced to a short stump which is fastened to the margins of the opening of the mucous membrane. The external wound is then made to heal as usual. This treatment suffices for blind internal fistulas of the cervical region.
It is a matter of great surgical importance and interest that certain branchiogenic remnants persist in a perfectly harmless manner until advanced life is reached, after which there take place therein cancerous changes which convert them into the so-called cancers of branchiogenic origin. These are too often of hopeless character by the time they are seen by the surgeon.
Other congenital defects consist of atrophies, such, for instance, atrophy of the sternomastoid muscle, or of certain hypertrophies which may be unilateral or symmetrical.
The neck is everywhere exposed to incised and perforating wounds, partly as the result of pure accident, too often as the result of homicidal efforts. The most exposed parts are supplied with veins of large caliber which connect directly with the heart, and whatever[699] danger there may be of entrance of air into the veins, under any circumstances, is in this region enhanced. This entrance of air has been regarded as a serious and often fatal accident. The writer’s experience and research have shown that it may often occur in mild degree with but little temporary disturbance. Should it occur the fact will be indicated by a slight gurgling sound, with tumultuous action of the heart, dilatation of the pupils, embarrassed breathing, and every indication of lowered blood pressure. Every competent operator will secure these large veins before dividing them, but if anything of this kind should be noted during an operation, pressure or plugging of the wound, with artificial respiration, perhaps even massage of the heart, and tracheotomy if necessary, should be practised until the patient has revived. If in the course of an exceedingly deep dissection the accident can be foreseen it may be avoided by keeping the wound filled with warm sterilized salt solution. This, however, will seriously embarrass the operative work, as it obscures vision.
The lower in the neck a serious wound be received, other things being equal, the more dangerous it becomes. Thus penetrating wounds above the larynx are of less importance than those below it. All injuries or wounds about the larynx are not only likely to dislodge its interior cartilages, but are especially likely to be followed by pressure of effused blood, or the consequences of a rapid edema of the glottis, which may prove fatal unless the trachea be opened below. It is this fact which makes fracture of the larynx so dangerous an injury.
A wound of the trachea rarely occurs by itself, as it lies deeply, and it may be especially serious if vessels in this neighborhood have been so injured that blood may be easily poured or escape into the lungs. If the trachea be completely divided its ends will be separated and gap, while the lower end will be drawn out with each deep inspiration. In this way suffocation may quickly occur. In all such cases the head should be placed lower than the body (Rose’s position), the lungs emptied completely, the wound enlarged, and the tracheal wound be sutured or else a tube be inserted. The treatment must largely depend upon the number of hours which have elapsed since its infliction, and the condition of the wound itself. In these cases it may be assumed that such a wound is infected, therefore it should not be closed without provision for drainage.
Any injury to the respiratory tract proper will be indicated by the character of the expectoration and the sounds heard on auscultation. Such injuries are likely to be complicated by a subsequent bronchitis, pneumonia, deep abscess, or various other undesirable sequences. Under the suggestive term “Schluck-pneumonie” the Germans have described a condition which we describe in the term “inhalation pneumonia.” It implies a septic type of pneumonia caused by the passage downward of foreign material, including septic wound secretions, which, not being expelled promptly, cause a type of inflammation, with consolidation, which will give most of the ordinary physical signs of pneumonia.
A rather distinct type of incised wound is that included in the term “cut-throat.” It implies a homicidal, usually suicidal, attempt on the part of the ignorant to sever the large vessels in the neck. This is but rarely accomplished, the injury being done to the larynx and the trachea and the tissues anterior to the vascular trunks. Usually inflicted with the right hand, one side of the wound may be deeper than the other. While the trachea is usually cut and often divided, the injury may be to the larynx instead. At all events, a wide gash is made and there is considerable hemorrhage, the external jugulars being nearly always severed. By the time such a wound is seen by the surgeon it is an infected wound and it should not be closed too tightly. The trachea may be sutured by itself, but it will be best to place therein a tracheal tube. Ample provision should also be made for drainage. In some instances the wound may be left open, at least for a few days, until it is granulating, and then be closed by deep sutures. Care should always be given to those of desperate suicidal intent and to the maniacal, that they do not reopen the wound in continuation of their previous efforts. This requires careful watching.
Rupture of the trachea, either due to violent coughing or straining efforts or to external violence, is known. It will call for tracheotomy, because of the emphysema which will ensue. Penetrating wounds of the large arteries and veins are always serious. When not extensive they may be followed by diffuse or circumscribed hematoma or by aneurysm. Nélaton is reported to have stated that it takes four minutes for a man to bleed to death from the carotid artery, and that two minutes should suffice for its ligation. Any[700] injury to the vessels should be followed by their exposure, and probably by ligation or suture, in order to prevent the conditions above mentioned. If the wound be low in the neck it would be proper to remove the upper end of the sternum or to divide the sternomastoid sufficiently to expose it.
The vertebral artery is occasionally injured, mostly in the osseous canal through which it passes. At the base of the neck a wound at or near its origin is an exceedingly serious injury. The same rules apply as above.
Wounds of the large veins are supposed to be of a more serious nature because of the possibility of inspiration of air, i. e., air embolism. These vessels are occasionally injured during removal of deep-seated and adherent tumors. It has been possible in some instances to make a lateral suture of the jugular vein at the point of injury, providing this be not too extensive. Effort at reunion of this kind is always legitimate if the operator feel himself equal to the task. The jugular vein is also occasionally exposed and tied low down, then opened above the ligature, for the purpose of cleaning out its upper portion when filled with infective thrombi, a condition occasionally seen with mastoid abscess, etc. To open it before tying would be a surgical mistake. By this process it is practically obliterated as recovery ensues.
If such a muscle as the sternomastoid be partially or completely divided muscle suture should be practised and the head and neck kept at rest for the ensuing few days.
Injuries to the cervical nerves may be followed by peculiar and interesting features. That of the recurrent laryngeal will cause paralysis of the laryngeal muscles on one side, with consequent difficulty in speech; injury to the cervical sympathetic will be followed by dilatation of the pupils and protrusion of the eyeballs with flushing; of the spinal accessory, by mastoid and trapezius paralysis; of the phrenic, by paralysis of the diaphragm on one side; and of the pneumogastric, by embarrassment of respiration, with pupillary and abdominal symptoms, which are variable. Of all of these injuries that to the phrenic is probably the most serious. Some years ago I tabulated the then recorded cases of injury to the pneumogastric and was able to show that only about 50 per cent. of such cases were immediately or tardily fatal. The phrenic nerve is then the only one within the neck which can scarcely be spared. Any of these nerves when divided should be reunited by sutures, as elsewhere described.
When any portion of the brachial plexus has been injured a corresponding paralysis of the arm will follow. Wounds of these nerves should be sutured at once. A distinction should be made in all cases between hysterical anesthesia, malingering, and the actual paralysis of injury. Sometimes the amount of callus thrown out after a fracture of the clavicle will include a nerve of sufficient size to produce a neurosis, usually neuralgia, or possibly a paralysis. Excessive callus, or, in effect, the bony tumor which is thus produced, may be removed by operation, and any entangled nerve should be hunted out and liberated.
Pressure of a tumor upon a nerve will cause paralysis corresponding to its degree. When this comes on gradually, even though it involve the phrenic nerve, the consequences are not so serious. Repeated irritation or pressure may cause paralysis, as in the cases of the strap of letter-carriers or those who carry burdens slung from the neck.
Injuries occur to the cervical muscles during parturition and a hematoma of the sternomastoid in the newborn is described. The muscle is contracted and the head bent over. It usually disappears by resolution within a short time. This muscle is also ruptured by violence in the adult; again, hematoma is the result, with at least temporary torticollis, pain, and tenderness. When an abrupt division can be recognized, exposure of the ends and muscle suture would be indicated. At any time, in the presence of clot, it would be proper to cut down and turn it out.
Syphilitic myositis is often seen in the sternomastoid, where it may affect the entire muscle, transforming it into a cord-like mass, or where it may occur as gummatous infiltration. These cases occur without pain and without known cause save the disease itself, whose possibility should be established by the history of the case. Again, these muscles are sometimes contracted because of reflex excitement from adjoining inflammatory foci. Such an affection subsides shortly after due attention to the exciting cause, unless it has been allowed to continue too long. Inflammation, even of the destructive type, may be propagated to the muscles by continuity from a neighboring suppurating focus.
Serious phlegmons of the neck may be followed by phlebitis of the internal jugular[701] vein, which may be recognized by the presence of a palpable cord-like clot within its lumen. Such a condition is serious because of the ease with which pyemia may ensue. It would be better to expose the vein, to tie it low down, to freely excise and turn out such a clot, than to leave it to create serious disturbance a little later.
Of the posterior portions of the neck we have fewer injuries, and these less serious, excepting those by which the vertebral column or the enclosed spinal cord are injured. These injuries have been referred to in the chapter on the Spine. A high perforating injury of the cord, especially if it involve the medulla, is promptly fatal. Infanticide has been produced by a long needle driven between the occiput and the vertebræ, corresponding to the pithing of small animals in the laboratory. An injury above the origin of the phrenic, on one side, is not necessarily fatal. Injuries to the posterior portion of the high cervical cord, as well as to the membranes, may be followed by more or less atrophy of the genital organs, with corresponding impotence, Larrey claiming that this may take place even when the cord itself is not affected.
Ruptures of muscles and separations from their insertions or origins are occasionally noted. The scapular muscles are occasionally torn loose. A reflex spasm of the trapezius which follows some of these injuries will produce a posterior form of acute torticollis (wryneck) described in the chapter on Orthopedics (XXXIII). The resulting deformity and stiffening might be confounded with arthritis of the upper vertebral joints. It is to be overcome by traction and by suitable apparatus, save in extreme cases, when division or excision of a sufficient portion of the muscle may be practised.
Fig. 492
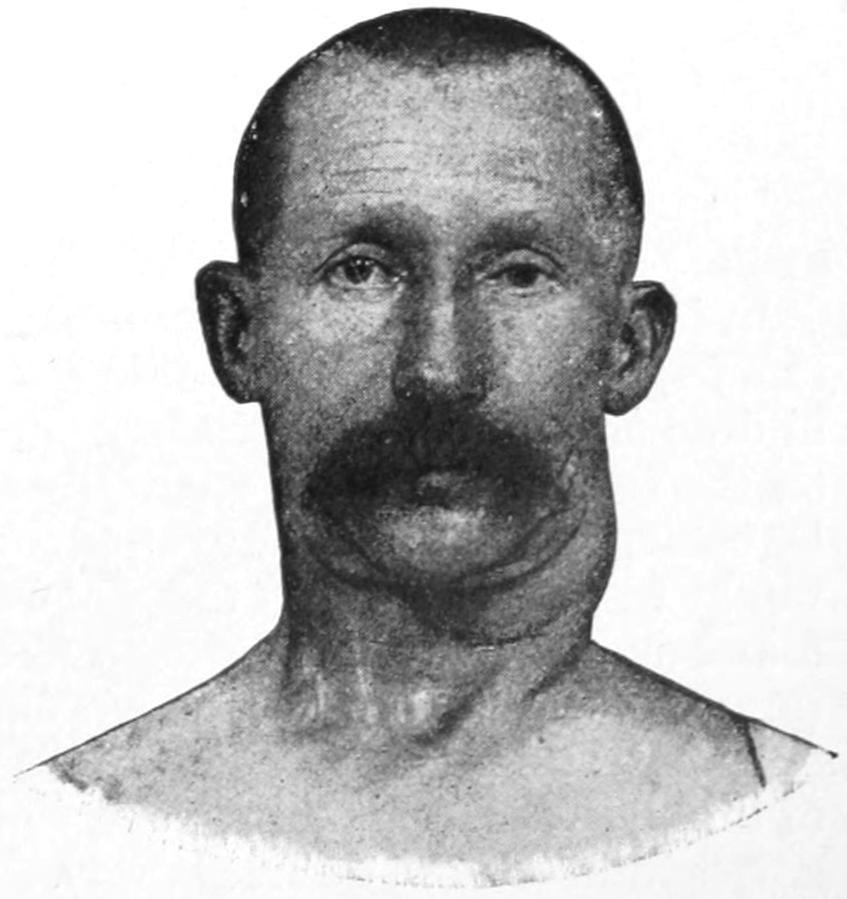
Carotid aneurysm successfully treated by complete extirpation. (Author’s Clinic.)
Of great interest are the blood vascular tumors of the neck, both those of spontaneous and of traumatic origin. Large angiomas, either of the arterial (cirsoid aneurysm) or of the mixed or venous type, are seen about the neck. Here more than anywhere else are found peculiar venous dilatations, especially of the smaller veins, which form cavities in a tissue that becomes thereby almost erectile. Should these tumors connect with the arteries they will pulsate. If composed of larger veins they will prove quite compressible. These tumors should be extirpated, care being taken to place a provisional or permanent ligature upon the large vessels connecting therewith before the tumor itself is attacked. Occasionally the ampullæ of these growths become sufficiently large to entitle the growths to be considered as sanguineous cysts. The neck is also frequently the site of the smaller varieties of these growths which constitute the ordinary nevi. (See chapter on Tumors.)
Aneurysms of the cervical vessels are more frequently of spontaneous than traumatic origin. They may, however, result from contusions or penetrating injuries. While no vessel in the neck always escapes, it is the common carotid which is more frequently affected than the others. The general subject of aneurysm has been considered. Care should be taken not to confuse the vascular and pulsating goitres, or other pulsating cysts of the thyroid. It is necessary also to distinguish aneurysmal pulsation from that which is transmitted through a tumor overlying the vessels or which may be seen in some of the extensive malignant tumors of the neck. When the diagnosis of aneurysm is made the surgeon should decide what vessel is primarily affected. This, however, is not always possible, as an aneurysm of the vertebral artery projecting forward is liable to be mistaken for one of some other trunk.
Aneurysm in the neck, unless very deep, and in a very unfavorable subject, is always an indication for operation. While operation necessarily includes ligation, either on the proximal or distal side, if this can be practised the sac itself may be treated just as though it were a tumor of any other character, and extirpated. I have myself had satisfactory results by the last-mentioned procedure (Fig. 492). The existence of laryngeal paralysis, especially unilateral, which is not easily accounted for in other ways, should excite a suspicion[702] of aneurysm, with consequent pressure upon the recurrent laryngeal nerve. Its possibility should be excluded as part of the diagnosis.
Wounds of the subclavian vessels give rise to serious hematomas which may be converted into spurious traumatic aneurysms of arteriovenous character. When such a tumor pulsates it is probably connected with the subclavian artery, which should be ligated. It may be possible to make this ligation above the clavicle, but a portion of the sternum should be removed as well as the inner end of the clavicle for a more complete exposure. On the right side at least the artery can only be reached above the bone after dividing the scalenus anticus, where a provisional ligature may be placed. After this the sac should be incised and the vessel ligated, on either side of it, so that the provisional ligature may be removed. On the left side it is safe to ligate the second portion of the artery at once. The clavicle should be divided to afford better exposure, and its ends reunited with silver wire (Fig. 493).
Fig. 493
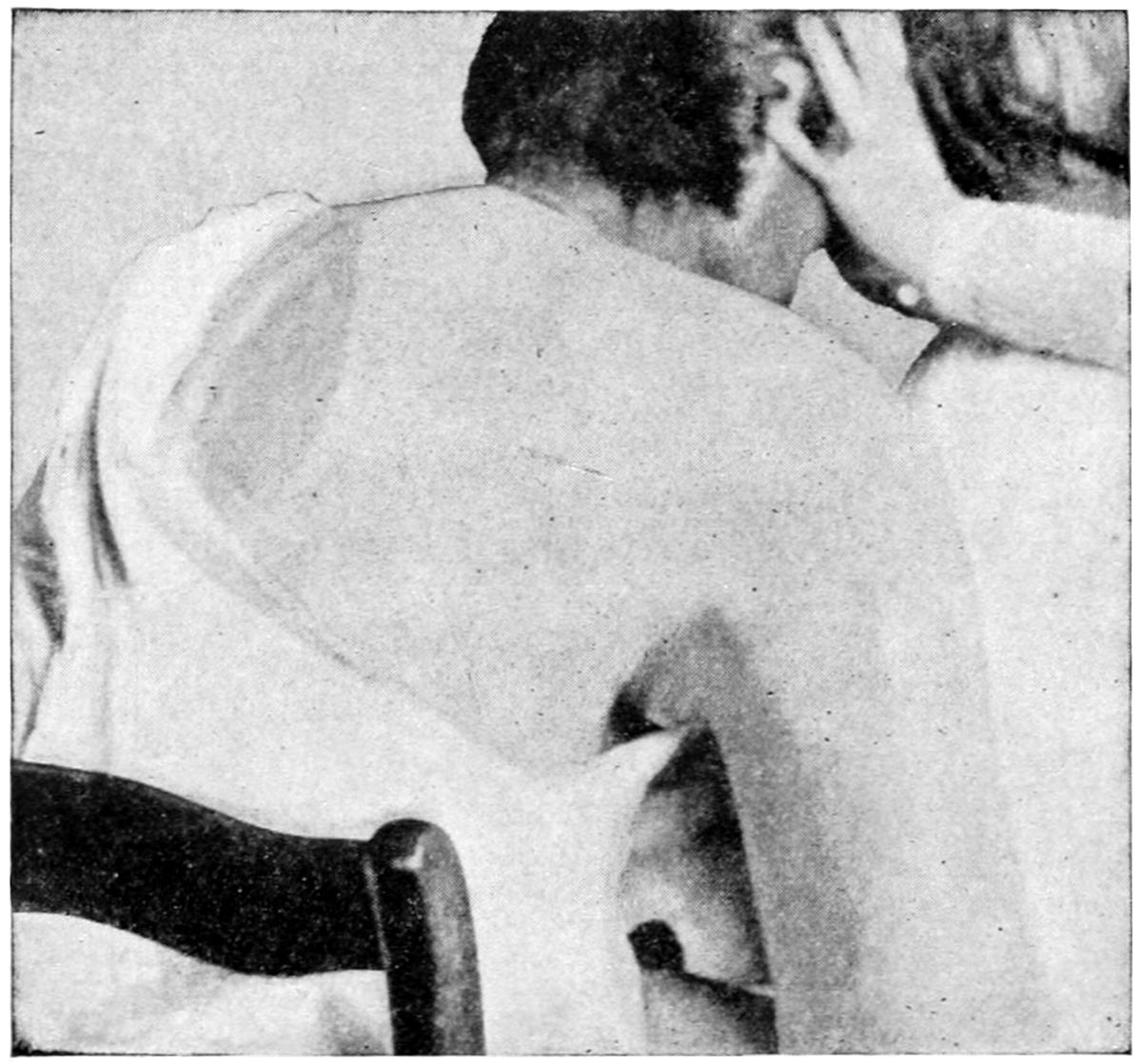
Traumatic aneurysm of axillary artery.
Any open wound of the subclavian vein is a serious affair, as bleeding will be profuse, and there is also danger of air embolism. Immediate occlusion with an antiseptic dressing would probably afford better prospect than any attempt to enlarge the wound and secure the divided vessel. If the vein be thus attacked its proximal portion should be first secured in order to avoid the entrance of air. Meantime much of the hemorrhage from the distal end may be prevented if pressure be made in the axilla upon the axillary vein. If the vessel be secured both ends should be tied.
In instances of accidental injury, or that included in the removal of large and deep tumors, the thoracic duct on the left side and the lymphatic duct on the right have been injured or divided. It is one of the possible dangers in performing extensive operations on the root of the neck, especially on the left side. Its occurrence would be indicated by oozing of the milk-like lymph. The accident has not been frequently reported. It would render closure of the wound without drainage impracticable, but it has been found sufficient to place a deep packing and to rely upon the natural healing process (granulation) by which such a wound would be gradually closed.
It may be said of vascular lesions that when it appears to be necessary the upper part of the sternum may be resected, as it adds little to the danger and exposes the operative field in a more desirable way. There is no better operative method for ligation of the innominate artery than that which includes removal of the upper end of this bone. Incidentally it may be added that this is also justifiable in certain penetrating wounds of the trachea and in attacking retrosternal goitres or lesions of the thymus.
[703]
Phlegmonous affections in the region of the neck are serious because of the complications which may ensue. The more deeply they lie the greater this danger. This comes not only from septic processes which may follow veins and lymphatics, but from burrowing of pus along and between the deeper muscle planes, which may carry it into one of the mediastinal spaces or within the thorax. These phlegmons may be primary, or may follow infection spreading through the open crypts of the tonsils, or the open pathways afforded by diseased teeth and by superficial ulcerations. An infection of a tonsil may cause an abscess which presents beneath the jaw, while a deep axillary abscess may be the consequence of a phlegmon beginning in the neck. Not infrequently they come about through the mechanism of infected lymph nodes, which may sometimes produce multiple or extensive single abscesses. These phlegmons occasionally follow the exanthems, especially scarlatina, and the variety of directions in which infection may spread from the middle ear is well known, since it may cause phlegmon in the neck or empyema of the mastoid antrun and even fatal disturbance within the cranium. When the resulting pus travels downward in front of the thyroid and sternum it will appear upon the thoracic wall; when behind the trachea and the oesophagus, or along the large vessels of the neck, it will be seen either within the thorax or at the root of the neck, possibly opening into the esophagus or spreading to the axillary space. Retropharyngeal abscesses are often the result of caries of the vertebræ, but may occur in consequence of a deep cellulitis caused by extension from some focus within the nasopharyngeal cavity. This is an illustration of the rule that pus travels in the direction of least resistance.
—The diagnosis of cervical phlegmons is usually not difficult, especially when they are superficial. The ever-present indications of redness and edema of the surface, pitting upon pressure, tender swelling, and loss of function of the surrounding parts, often with fixation through muscle spasm, coupled with the general systemic disturbance, and, in desperate cases, the indications afforded by the blood and the urine, will enable a diagnosis to be made, usually without the use of the exploring needle. This, however, may be employed if necessary. The same is true in lesser degree of tuberculous collections of pus and pyoid, which have been earlier described as “cold abscess.” Only in the beginning of its course can any doubt arise concerning the nature of a carbuncular process.
A somewhat typical type of deep phlegmon is often referred to as angina and Vincent’s angina. Semon regards these manifestations as expressions of an acute septic cellulitis which has been described as abscess of the larynx and as erysipelas of the larynx, and which other writers refer to as cynanche tonsillaris, acute peritonsillitis, etc. The disease may occur in healthy individuals, more often in the diabetic. A violent sore throat is followed by serious dysphagia, with considerable edema of the pharynx, whose surface is of a dark-blue color. Patients may become unable to swallow, while hoarseness with aphonia will result from edema of the glottis. The epiglottis will be darkly discolored, greatly tumefied, and nearly obscuring the entrance to the larynx. Dyspnea may necessitate tracheotomy. A light-colored false membrane may be seen in the throat. There is always marked lymphatic involvement. The disease may be more confined in some cases to one side. Vincent has described a particular spirillum or bacillus which he found in some of these instances. The infection here doubtless proceeds from the mouth or the tonsils, its activity being due to symbiosis of various organisms. It is to be distinguished from Ludwig’s angina, which is rather a submaxillary affection than a retropharyngeal. It infrequently leads to retropharyngeal abscess.
Ludwig’s angina, also called infectious submaxillary angina, is an infectious cellulitis of the mouth. The tongue is swollen and immovable; the mouth more or less fixed, with difficulty of swallowing, and the condition is one of extensive infiltration, with formation of pus, which is likely to burrow. In some of these cases the Micrococcus tetragenus is the organism at fault. In my experience when present it leads to a brawny infiltration which is slow to subside or disappear.
—The early recognition and evacuation of pus are called for in all cervical phlegmons. The presence of pus may be assumed before it can be recognized from external evidence. Therefore when swelling begins to mask anatomical outlines, or to[704] produce difficulty of swallowing or breathing, free external incision, with deep dissection, will prove much safer than to leave such a case to itself. Retropharyngeal abscesses, or such collections as may be recognized in the tonsil or in the pharynx, may be opened from within the mouth. That there should not be too much haste in this direction, however, was indicated to me when a well-known surgeon plunged a bistoury into what he supposed to be an abscess of the tonsil and found it to be an aneurysm, the patient dying within five minutes in his office.
Early and free incision will relieve tension, and do good by a certain amount of bloodletting, even if pus is not reached, while an easier outlet for it will be afforded when it does form. However, the surgeon will rarely fail to find it if he goes sufficiently deep or in the right direction, when the existing symptoms and signs are of serious import.
The operator should incise freely in the beginning, after which deep dissection is best effected with some blunt instrument. The exploring needle may afford valuable information, but if the deep tissues be edematous we may feel quite sure of the presence of pus in the neighborhood. Souchon has described a method of guided dilatation which requires a series of dilating instruments, and which will give good results. Search for pus can be made without them by using the blade of a dissecting knife or hemostatic forceps, or the blades of a pair of scissors to stretch a small opening. The less tissues are cut and the more they are thus separated the better.
Perilaryngeal or peritracheal abscesses are likely to cause dyspnea and show a tendency to extend downward along the trachea into the thorax. In these locations they produce a peculiar diffuse cellulitis, which was described by Dupuytren. Such phlegmons may extend from the ear to the clavicle or from the back of the neck to the larynx. Pus will collect in many small interspaces, and purulent infiltration will affect many of the tissues, and may produce gangrene. This condition has also been described by Gray-Coley and by Hannon. The surface not infrequently seems to be involved in erysipelas. In fact it is doubtless true that most of these affections are of the streptococcus type, where it is impossible to distinguish between erysipelas and cellulitis. Tracheotomy as well as the other free incisions may be indicated. An early tracheotomy should be made whenever suffocation threatens from any swelling or edema. The latter occurs so suddenly that a tracheotomy should be made early rather than wait for its necessity, especially when patients cannot be kept under constant observation. The operation may be done under cocaine, while the presence of the tube will then permit the administration of one of the ordinary anesthetics without embarrassing respiration.
All of the other phlegmons, no matter what type they assume, are to be treated on the same general principles. If seen, however, before incision and drainage appear these cases may be treated locally with the compound ichthyol-mercurial ointment, or with Credé’s silver ointment, re-inforced by hot external applications; and the mouth should be frequently rinsed with warm antiseptic solutions. Any lesion within the mouth should receive its own proper treatment.
—Carbuncles, which appear perhaps more frequently upon the back of the neck than elsewhere, should be treated by the radical method, i. e., excision of all tissue which is evidently so involved that it will subsequently slough. Even an extensive carbuncle several inches in diameter, with numerous crater-like openings, and presenting large amounts of already necrotic tissue, is best treated in this same way. The more quickly the dead and dying tissues are removed the better for the patient. Such an operation requires an anesthetic and the free use of scissors and a sharp spoon, even the scalpel. After being freed of necrotic tissue the exposed surfaces should then be dressed with brewers’ yeast. In general, of all these phlegmons, it may be said that nowhere does the general rule elsewhere laid down in this work better apply, i. e., that pus left to itself will always do more harm than will the surgeon’s knife if judiciously used.
The various fixations of the neck by muscle spasm or muscle infiltration due to these phlegmons, i. e., the temporary forms of wryneck, will nearly always subside as infiltration disappears. Some degree of permanent contracture may follow neglected cases and may call for massage, stretching, and the use of a suitable brace.
[705]
The cervical lymphatics are abundant in number, as they need to be to serve their purpose, considering the variety and extent of the possible sources of infection, both from within and without. They become enlarged even in a trifling case of tonsillitis, while in more serious infections they participate with the surrounding tissues, but sometimes suppurate independently of them. They are involved in nearly every case of constitutional syphilis, and serve as an index of the saturation of the system with the specific poison. Treatment for the same should never be discontinued so long as they are perceptibly enlarged. They participate, then, in both the local and the constitutional infections.
In no respect is this more true than in local tuberculous infections, or in others which have become tuberculous through the process of mixed or secondary infection.
Tuberculosis of the cervical lymphatics is then one of the results of previous mild or severe infections. They constitute the so-called “scrofulous glands” or swellings of writers of the past generation. There may be seen repeated within these structures those processes which in the lungs cause at one point softening, at another caseation, and at another sclerosis. An acute suppurative process may also be going on, or there may be found, in broken-down cavities, that pyoid material which is often seen in cold abscesses, and to which elsewhere in this work is given the name archepyon, indicating that it was originally of a truly purulent type, which it has lost in course of time.
Fig. 494
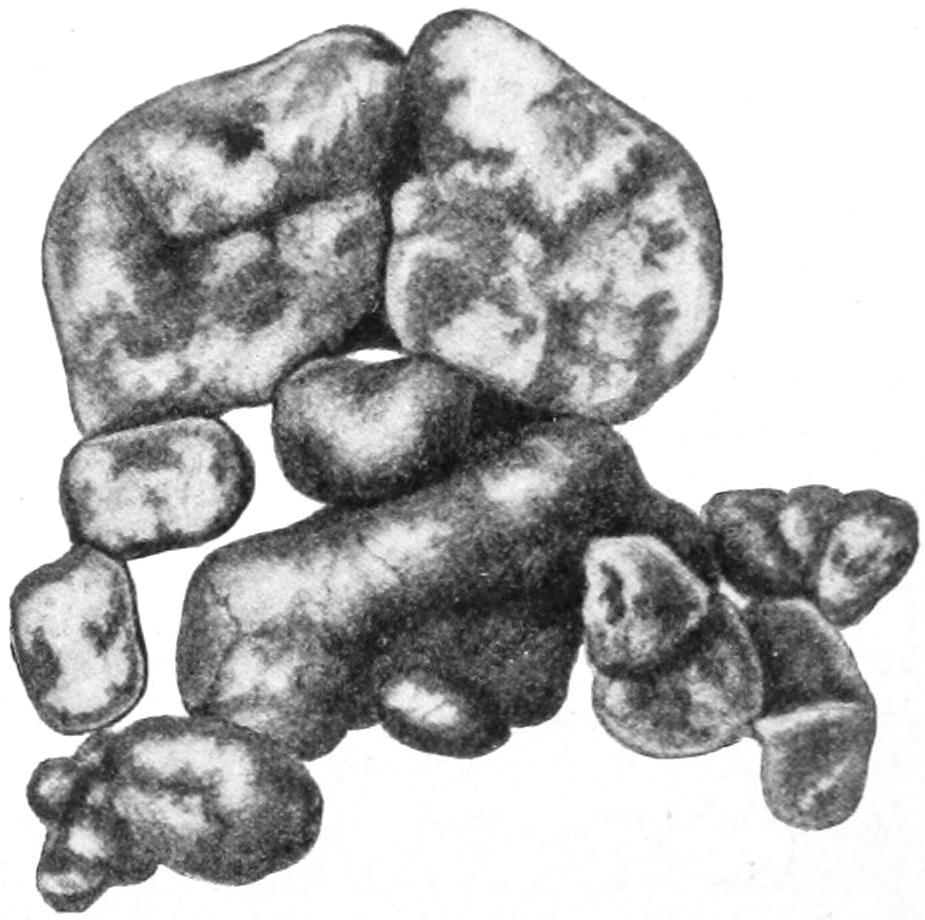
Cluster of tuberculous lymph nodes removed by dissection, and showing the usual and various changes. (Lexer.)
Tuberculosis of the cervical lymph nodes may be a limited and almost single expression of disease, or one involving both sides of the neck, and to a degree that may produce large and disfiguring swellings. It is nearly always a secondary infection, the original lesion being found upon the surface of the skin, more frequently in the middle ear, the pharynx, the tonsils, the nose, the teeth, or other parts within the mouth. The first measure in every instance should be to trace this source of the infection, since to leave it uncared for is to invite a continuance of the disease. The course of events often is an acute exanthem, a chronic tonsillitis, a mildly septic involvement of the lymph nodes, followed later by tuberculous invasion through a port of entry opened by the previous process (Fig. 494).
Most of the acute septic infections of these lymphatics will be followed by local abscess and by one of the extensive phlegmonous manifestations described above. This usually means an acute abscess formation, which should lead to early incision and speedy recovery. It is the more chronic and less suppurative types which cause serious trouble. They occur more frequently in the young. There is a distinct form, however, occurring in the aged, which is called senile tuberculosis. Its pathology nowise differs from that of the type occurring in the young, although it has a different clinical expression.
When the lymph nodes are but recently involved they are simply so encapsulated as to be easily shelled out from their beds; but when degenerating and slowly suppurating they become so firmly embedded in the surrounding tissues by dense infiltration that their extirpation is exceedingly difficult. This condition has been spoken of as peri-adenitis, a bad term, because nowhere in this work are lymph nodes spoken of as “glands.” Not infrequently the operator will find large masses affixed to the carotid sheath, or surrounding the vessel and nerve trunks, so that it is almost impossible to separate them. During the dissection the internal jugular may be torn, or one of its branches severed at its base, while an important nerve trunk may be so lost in the mass that it is almost impossible to distinguish it, and it may not escape injury.
[706]
—Search should be first made for the source of the infection, since to attack the consequences of the disease and to leave the cause untouched would be a mistake. If it be a chronic nasopharyngeal catarrh it will require considerable local treatment. If an enlarged tonsil this should be removed. If due to dental caries, or ulceration in connection with faulty dentition, or to pyorrhea alveolaris, the patient should be sent to the dentist; if the trouble be in the middle ear, to the aurist; if the infection come from the skin, as in various ulcerating skin diseases, again appropriate external measures should be adopted. When the patient is otherwise in good condition and freed from liability of further infection, then the question of surgical intervention is to be decided. Decision will rest somewhat upon the general condition of the patient and the extent of the lesions. A consumptive patient, for instance, is not a good subject for surgery, and it may be held that the lymphatics will be benefited by such change of climate as is indicated for his tuberculous lungs. A puny or anemic subject is not a favorable one for an extensive surgical operation, such as the removal of a large mass of those nodes often necessitates. It may be deemed advisable to delay while the patient is temporarily sent to the mountains, or is placed upon treatment, including arsenic as an alterative, and the best restorative tonics. Some cases not favorable for operation are benefited by x-ray treatment. This should be judiciously administered, in such manner as not to produce a dermatitis nor increase the infiltration in the tissues of the neck. It is to be advised rather in cases considered inoperable than in those favorable for operation.
Excision is the measure usually resorted to because of the promptness of its effect, as well as the extent. Excision, however, necessitates an exceedingly careful and tedious dissection. When the whole side of the neck is involved I would advise an S-shaped incision, by which a double flap, with much better exposure, is afforded. There may perhaps be found two quite different sets of involved nodes, the superficial lying rather to the outside and to the front of the sternomastoid, which will be adherent to the carotid sheath, and a deeper set lying back of the sternomastoid whose removal will usually take one down to the transverse processes of the cervical vertebræ. In an average case there may be found all possible combinations of degeneration, with softening and cold abscess on one hand, and caseation and calcification on the other. Proceeding more deeply masses will be found whose existence had not been appreciated from the surface. Nevertheless, such cases usually do well and often recover. Thus a wound extending from the mastoid to the clavicle may be entirely healed within a week if the wound has not been infected by fresh pus. Such extensive wounds should be treated with at least one drainage provision, a drain being brought out through the wound or a special opening made for it, at a point where the resulting cavity will empty itself with the patient lying upon his back in bed.
For all these operations the patient should be prepared in the best possible manner. It will be of advantage to send patients to the woods, while, under any circumstances, they should be kept under those surroundings most favorable to tuberculous individuals, where hypernutrition, lively elimination, and oxygen fulfil the general requirements. They may also take such alteratives as arsenic, and such drugs as creosote or its derivatives, which are supposed to have more or less specific effect.
A distinct type of involvement of the cervical lymphatics is seen in connection with the spread of malignant disease from adjoining structures. Nowhere is this more marked than in epithelioma of the lip, but it may be seen in cancer spreading upward from below, as in connection with cancer of the breast. When the cervical lymph nodes are involved in a case of cancer of the breast a hopeless aspect is thereby put upon it. Although operation may be justified for temporary relief it should be so understood.
Aeroceles of the neck are sacs formed by air distention of an adventitious pouch, and constitute a species of local emphysema, due to weakening and yielding of some portion of the respiratory tract, produced by such strains as cough, labor, etc. A congenital dilatation of a laryngeal ventricle may produce the same effect. It may also follow a distinct wound of the trachea, or the expansion of a cavity in one of the mucous glands produced by its ulceration or breaking down. They may also result from abscess cavities opening into the respiratory tract. According to their location they may be referred to[707] as laryngoceles, tracheoceles, etc. The term pneumatocele implies a protrusion of the pleura and the lung into the region above the clavicle. It will give distinct signs here on percussion, will disappear under pressure, and quickly recur as the result of forced expiration, coughing, etc. It may even follow the respiratory movements. This latter form is scarcely amenable to treatment unless tissues can be brought together over it and the opening closed. The other aeroceles are more or less amenable, according to their location and exciting cause. It is rare that there is any contra-indication to their exposure and extirpation.
Of the many true cysts of the neck a large proportion are due to incomplete closure of some portion of one or more branchial clefts. These have already been mentioned in the chapter on Tumors. The lesions vary from trifling submaxillary dermoid tumors to extensive hydroceles of the neck, such as those illustrated in Figs. 495 and 496. Not every congenital tumor, however, is of branchial origin. There is a possibility of the development of others along the thyroglossal duct, along the great vessels, and in the neighborhood of the pharynx and larynx. True bursal cysts, as well as true atheromatous cysts, also develop at various ages. The former will be found filled with serous fluid. They occur on the anterolateral aspect of the neck and generally on the left side. Dermoid cysts also abound here. They have an epithelial lining, which always indicates their congenital origin. They frequently do not develop until puberty. They may contain various epithelial products, which may escape by suppuration or perforation. These growths sometimes extend into the mediastinum. A form of median thyrohyoid cyst of this character often grows rapidly after confinement. Such a cyst if incompletely treated will be followed by persistent fistula. All of these growths should be thoroughly extirpated if attacked at all, or widely opened and packed, and then made to heal by granulation. Fig. 497 illustrates another type of cystic growth of the neck connecting freely with the lymph spaces and vessels and regarded as a congenital lymphangioma.
Fig. 495
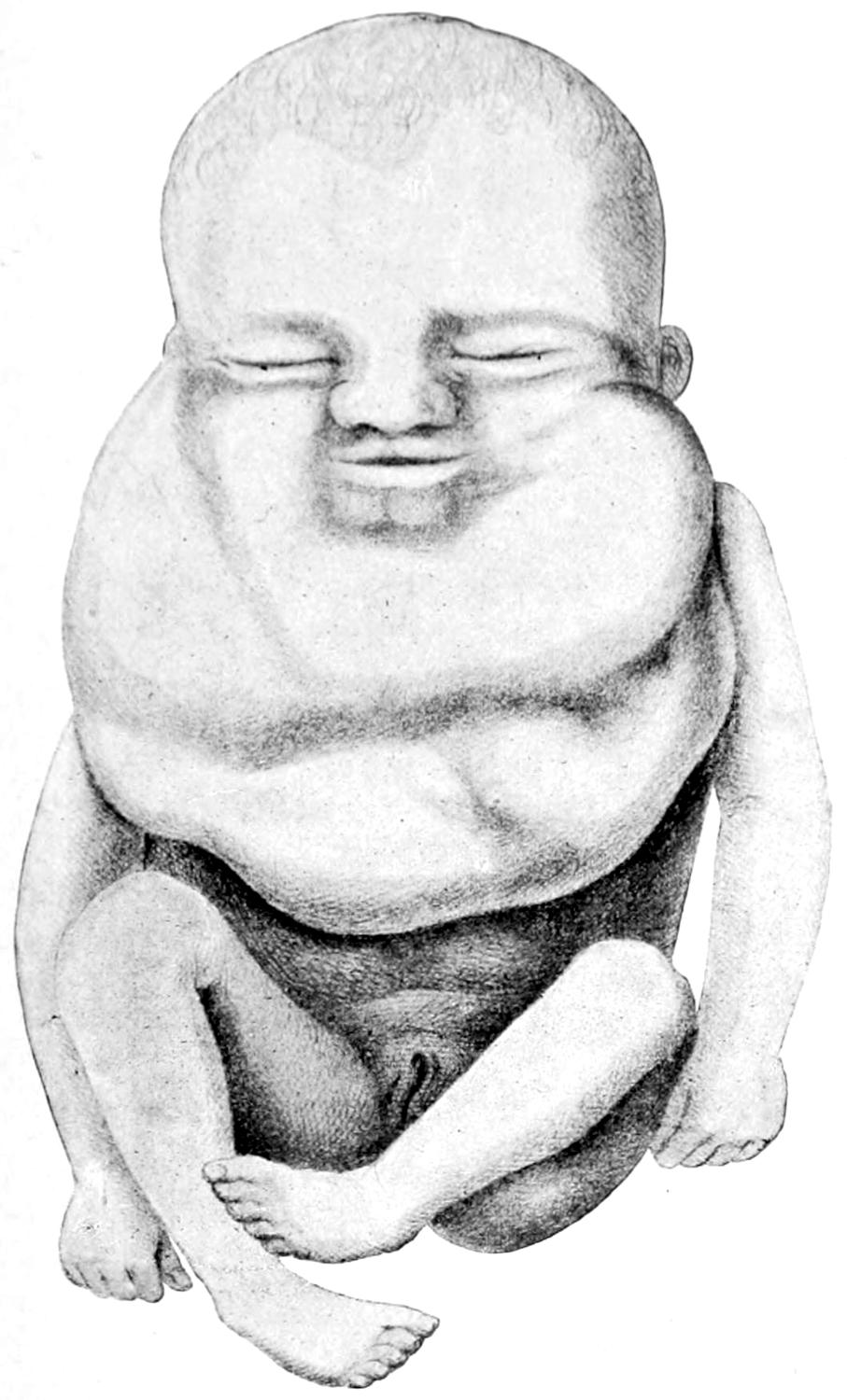
Congenital multilocular serous cysts (hydrocele) of neck. (Lannelongue.)
Fig. 496
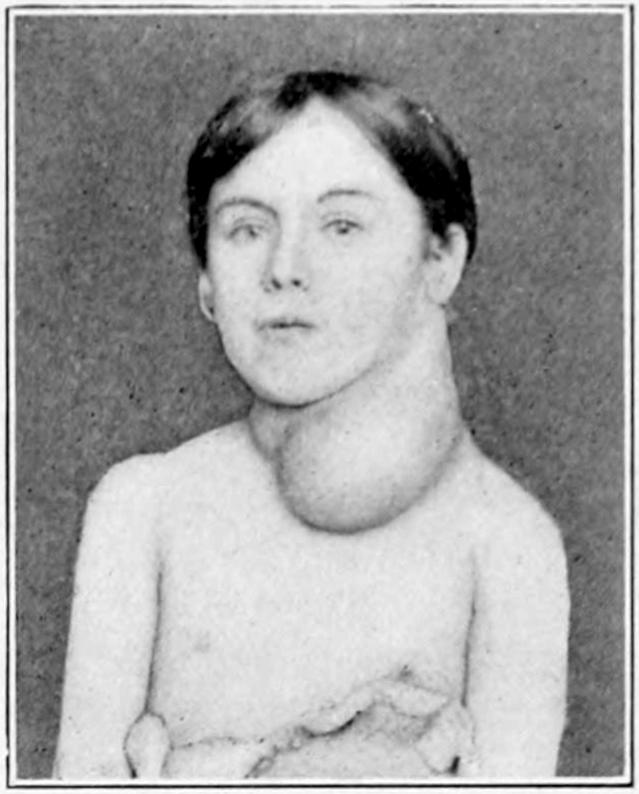
Branchial cyst. (Case of Dr. Parmenter.)
Still another type of cystic growth is connected with the anterior jugular vein. It contains sanguineous fluid, and sometimes true venous blood. Connection with the vein may be determined by making pressure. A growth easily emptied and rapidly refilling will be distinctive. It should not be mistaken for an aneurysm, as it does not pulsate. It is known as a sanguineous cyst.
[708]
Fig. 497
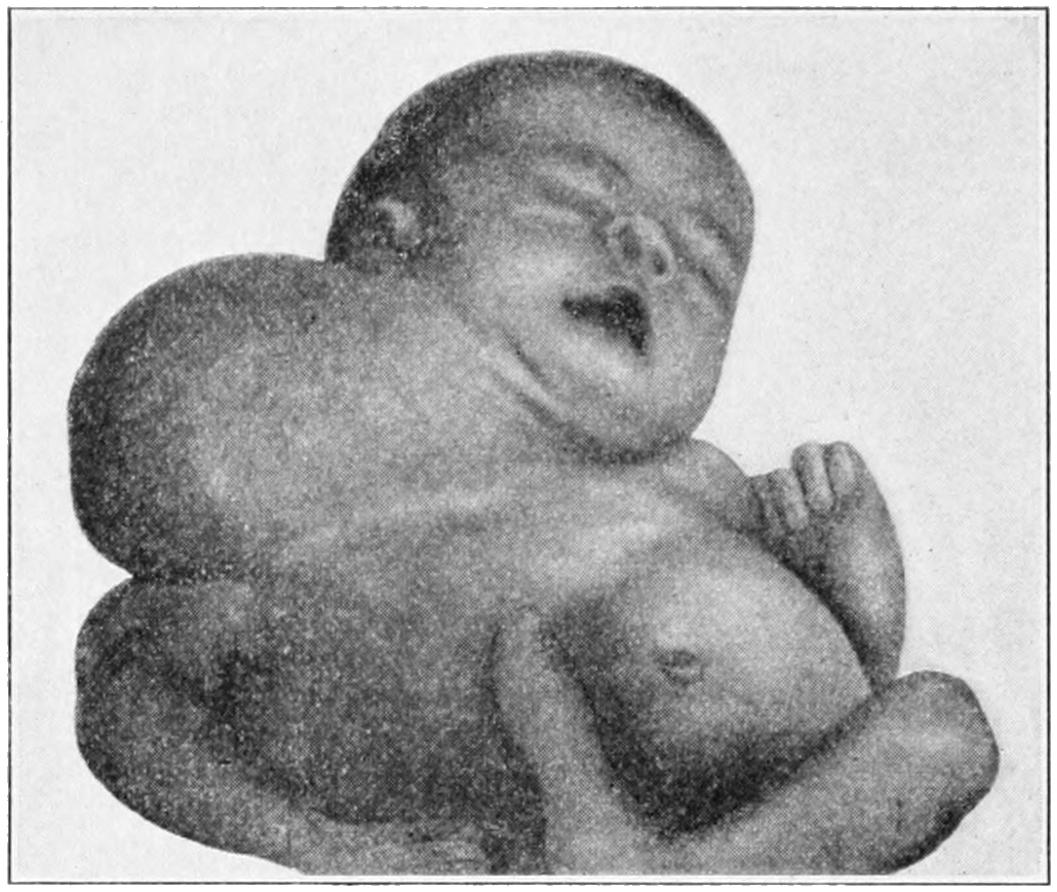
Branchial cyst or hydrocele of neck. Baby six weeks old. (Case of Dr. Parmenter.)
The difficulty of distinguishing between dermoid cyst and dermoid tumor has been mentioned in the chapter on Tumors. The distinction is one of small importance, for no matter what its character such a growth calls for extirpation. A similar dermoid in the course of the thyrolaryngeal duct is represented in Fig. 498.
Fig. 498
Fig. 499
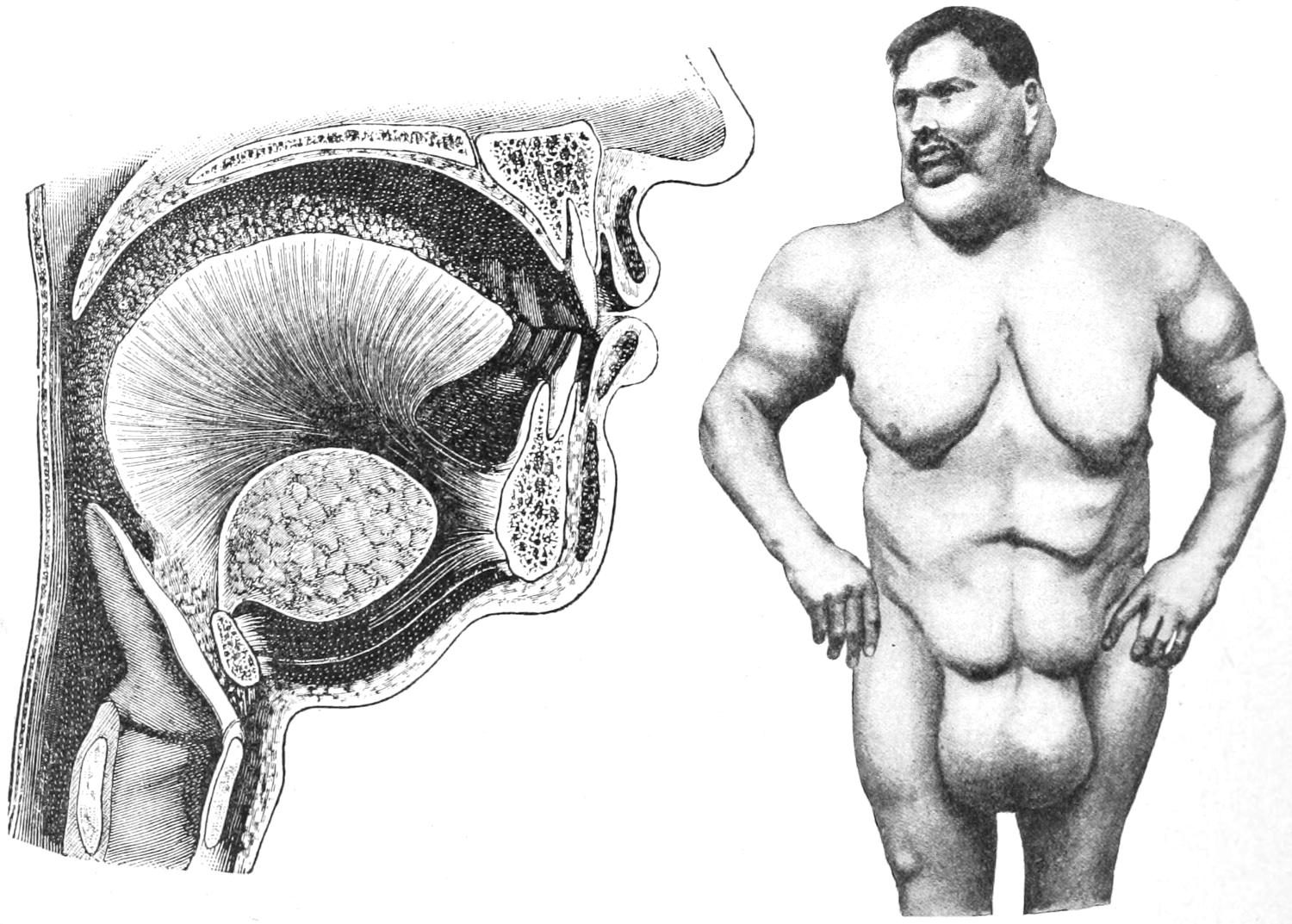
Dermoid (ad-hyoid) cyst at base of tongue. (Marchant.)
Diffuse symmetrical lipoma, multiple. (Lexer.)
In the neck, more often than in any other part of the body, may be seen well-marked cases of diffuse lipoma. These are painless overgrowths of fatty tissue, unencapsulated and consequently liable to spread to an unlimited extent (Fig. 499). They form disfiguring clinical pictures, but cause no unpleasant symptoms. They are scarcely to be attacked surgically, as they have no anatomical limit. They are rarely operated. More circumscribed growths can be more or less easily removed.
Of the true tumors of this region little need be said here. There is a form of fibrochondroma, springing from a branchial cleft, which occupies the external orifice of a congenital fistula a little above the clavicular joint. This makes it of interest, and, at the same time, distinctive in character.
Any of these growths may give rise to serious pressure symptoms and may be so located as to make tracheotomy difficult. They often extend downward behind the sternum, in which case the upper part of that bone should be removed in order that they may be safely followed. Such a tumor, if it so extends and is a true cyst, should be treated by free incision and packing; but when solid, no other resource than extirpation is left.[709] On their posterior aspect the greatest caution should be exercised, and it may be well to leave a part of their posterior walls to avoid the danger of injuring the large veins.
The majority of tumors that present on the floor of the mouth which are not of malignant type, nor adenomas of the salivary glands, are embryonic relics, a type alluded to above. A small vestige of this kind may long remain dormant and then suddenly assume a rapid growth.
Of the malignant tumors there are many expressions in the neck of endothelioma, of sarcoma, and of carcinoma, the latter only arising from epithelial structures like those of the skin, the glands, or the mucous membrane. They may extend in all directions. Many cancers of the neck are metastatic, the primary growth not necessarily being in the immediate neighborhood. A distinct form of cancerous degeneration of embryonic vestiges is known under the name of branchiogenic carcinoma. It is seen usually in elderly people and along the line of the branchial clefts. If possible it constitutes a more hopeless variety than others, because of its origin and depth. Certain sarcomas of the neck are prone to assume the type of fungus hematodes. Any tumor of this character should be attacked with spoon and cautery, for the vessels which bleed so easily are only those of the growth itself, those which lead up to it and around its margin not being enlarged.
The carotid body seems to have been first described by Haller, in 1743, although his description has attracted but little attention. In 1833 Mayer recognized that, aside from the well-known cervical ganglia, there was met at the bifurcation of the common carotid a small, so-called glandular structure, about the size of a grain of rice, red, firm, and vascular, much resembling the superior cervical ganglion, which receives sympathetic filaments as well as branches from the vagus. Luschka, in 1862, spoke of it as a glandlike appendage of the sympathetic system in the neck. It is usually wrapped in a sheath from the adventitia of the carotid and perhaps by more or less fat, the former having to be divided before the gland becomes visible. It seems to be a common meeting-place for fibers from the superior laryngeal, the glossopharyngeal, the sympathetic, and certain ganglion nerve fibers. It is not always present and may vary in position, lying either below the division of the artery or considerably above it upon the external carotid. In any case it is enclosed by a sort of capsule.
Its principal surgical interest obtains in that it is the occasional site of tumors, which as they grow will have intimate and perplexing arrangements to the surrounding tissues, which may necessitate most painstaking dissection, or may call for sacrifice of the large vessels. In one case reported by Scudder the tumor became larger and more tender whenever the patient caught cold. Such a tumor will not of itself pulsate, but will transmit pulsation from the carotid in a perplexing manner. They move sidewise, but not vertically. When vascular they may diminish upon pressure, or they may pass in between the other tissues in a way to simulate collapse on pressure. They lie in front of the sternomastoid, above the level of the thyroid cartilage, are usually of slow growth, and are sometimes accompanied by such vasomotor disturbance as flushing of the face and irregularity of the pupil. They are likely to be mistaken for tuberculous lymph nodes, or for common tumors of the neck. While views concerning their absolute malignancy differ, one may be certain that at least they rest upon the border line, and should in all cases be removed. Instances are reported, however, where the tumor has shown an extremely malignant tendency.
By virtue both of its complex functions and complicated affections the thyroid is an object of surgical interest. Between it and some of the most important body changes there is intimate relation, and its effects on disposition, mentality, voice, general appearance and behavior, sexual function and the development of the sexual organs are matters of common knowledge. The latter features are abundantly illustrated by the effect upon these parts of removal of the thyroid. Embryologically it develops from the floor of the pharynx, between the upper branchial arches. Within it there forms a duct,[710] known as the thyroglossal duct, whose glossal portion opens upon the base of the tongue, where it is of great surgical importance, because of growths of embryonic origin occurring along its path, and because downward growth of cancer of the posterior portion of the tongue usually takes the same course. In the early days of its existence it contains no iodine, at least in mankind, this lack of iodine being supplied from the mother’s milk, the babe thus receiving from its mother that which its own thyroid at first fails to supply.[49]
[49] This may afford an explanation of the unsatisfactory character of artificial foods, as well as of cows’ milk, since, unlike the babe, the calf is born with a functionating thyroid. Cows’ milk does not contain in this respect that which is found in human milk, all of which may afford a reason for adding minute amounts of thyroid extract for a short time to artificial foods for children.
That the thyroid normally produces substances of vital import in the human economy is shown both by the bad effects of their overproduction, as in tetany and certain spasmodic affections, with final clonic rigidity, and in thyroidism or the hyperthyroidism of Graves’ disease or exophthalmic goitre, with its tachycardia, mental depression, and numerous other symptoms, and by those of its underactivity, as in myxedema, cretinism, cachexia strumipriva, and certain of the toxemic neuroses.
The relations between the thyroid and the genital organs, especially in the female, are in many instances pronounced. Menstrual suppression and pregnancy are often followed by thyroidal enlargement, and nearly every woman having a goitre notes its temporary enlargement with each menstrual epoch, and its permanent enlargement with each succeeding pregnancy. The most specific constituent of the thyroglobulin, which is supposed to be the substance formed within the thyroid, is iodine, which is present in variable amounts.
In general it may be said of the thyroid: (1) That it secretes some material requisite for normal nutrition; (2) that it has much to do with the assimilation of oxygen by the tissues as well as with phosphorus metabolism; (3) that its peculiar secretion has a marked effect in lowering blood pressure and quickening the pulse, in the former respect being the direct antagonist of adrenalin.
The parathyroids have only recently assumed importance either in surgery or pathology. Their existence as separate structures with an identity of their own was first demonstrated by Sanström in 1860. Up to his time they had been assumed to be small accessory thyroids. In 1884 they were described by Horsley. Since that time they have been an object of the greatest interest to experimenters. They are of different character from the thyroid proper. Nevertheless the two are not absolutely independent of each other, for removal of either one causes changes in the other; the symptoms caused by removal of the parathyroids, especially, including tremors and various nervous symptoms, of which tachycardia and sometimes exophthalmos are the most prominent. Experimental animals will usually survive removal of the thyroid alone, but to take away all four of the parathyroids is almost invariably fatal. Anatomically they consist of two pairs of small bodies, with an average diameter of ¹⁄₂₅ inch, having color and texture much like the thyroid in gross appearance, but containing epithelioid cells, lying in man in close relation to the lateral lobes of the thyroid, behind them and to their inner sides. In minute structure they resemble that of the pituitary body. Their relatively trifling size and deep position in man have caused them to be neglected in pathology, and to be seldom recognized during operations or except by a careful dissection made for the purpose. The present trend of opinion, especially among the experimenters, ascribes to them an important role in the production of exophthalmic goitre, it being made to appear that by some neglect of duty their function of indirectly regulating the heart and controlling the sympathetic system is not properly performed.
Congenital affections of the thyroid may assume the type either of defect or of absence of the organ, or an hypertrophy which may involve one side or both. Presumably when the thyroid is lacking its function is to some extent assumed by the thymus and perhaps by other portions of the body.
Anatomical alterations are met in the so-called supernumerary or accessory thyroids, which may be due to separate development of one of the original lobules, or they may arise independently. These vary in size, location, and importance. They may be seen[711] as high as the base of the tongue or as low as the upper end of the sternum or behind it. Tissue of this kind has been seen in the body of the hyoid bone. These accessory masses are subject to the same type of affections as those which involve the principal thyroid, and thus tumors may develop in the anterior region of the neck, which may cause some perplexity.
An extraordinary feature of thyroidal tissue is that when affected it may infrequently produce metastases, even to distant parts of the body. Thus cases are on record of benign goitre, with universal metastases, and, on the other hand, of numerous metastases without any noticeable thyroidal enlargement. They occur frequently in the osseous system, and in the lungs, and when the thyroid is the site of a colloid type of goitre. The same is equally true of the malignant growths of the same tissue.
The immediate results of a total removal of the thyroid, as by operation, are myxedema, or cachexia strumipriva, conditions which require a few weeks for development and which may be preceded by an acute mania. These conditions are indicated by anemia with weakness, defective circulation, swelling of the extremities, usually first in the fingers, the swelling being of a hard, inelastic type, and not pitting on pressure, appearing later in the face so that the features become altered. Later appear also muscular tremors, with tetanoid convulsive attacks. These results of thyroidectomy may be combated by feeding thyroid extract, or by transplantation of thyroid tissue from a sheep into the tissue of the body or into the abdominal cavity. While Horsley and others have been successful with the surgical procedure, it is usually now sufficient to resort to continuous administration of thyroid extract, this being indicated only in cases where thyroid activity is defective and being contra-indicated in instances of overactivity, such as exophthalmic goitre.
Thyroiditis as a more or less acute affection is occasionally noted, being due to one of the infectious fevers, or occasionally following dermatitis, local infections, etc. It may assume a hemorrhagic type and be followed by production of hematoma. It may also assume a suppurative type and lead to the formation of abscess. This, if impending, is always of a serious nature, as it is sure to be followed by local cellulitis, perhaps with serious pressure symptoms, and escape of pus along the deeper fascial planes into the thorax.
An acute idiopathic hypertrophy in children has been noted by the writer in one instance, in which the enlargement was rapid, occupying but a few days, and had already caused such compression of the trachea when the case was first seen that even a tracheotomy promptly performed did not serve to save the patient’s life.
Intra-uterine hypertrophy of the thyroid is also known. There are at least five cases on record of this condition following the administration of potassium chlorate to the mother during pregnancy. In one case reported the tumor attained a size sufficient to constitute a serious complication in delivery of the child.
Among the special symptoms produced by these acute affections are: difficulty of swallowing, which may lead to great thirst; head symptoms due to obstruction to the return circulation, with congestion of the face and epistaxis; while pressure upon the pneumogastric may cause nausea or vomiting. The treatment of such a case when seen early should consist of wet and ice-cold applications for several hours; but when seen later, especially if suppuration be already threatening, pus formation and its localization may be encouraged by hot applications, followed by free incision, thus relieving tension and evacuating pus.
Thyroiditis occurring in goitrous thyroids is usually referred to as strumitis, as the enlargement itself was formerly known as struma; it follows the exanthems and fevers, and may cause sudden and distressing complications.
Aside from those thyroidal enlargements to be considered under the heading of goitre may be met tumors of congenital origin, especially the simple or complicated cysts, which may grow slowly or rapidly, or may not appear at all until puberty or adult life.[712] An apparently innocent cyst may suddenly increase in size and produce serious symptoms, or hemorrhage may occur into it, or it may rupture, in either of which instances severe pressure symptoms will ensue. All cystic tumors of the thyroid should be enucleated, an operation usually easy of performance unless the collection be multilocular and extensive. If an entire thyroidal lobe be occupied by growths of this character it may be assumed that its function has been so much impaired that it should be completely removed.
The thyroid body is occasionally the site of teratomas, i. e., tumors containing tissue of each blastodermic layer. No two such tumors are alike. They may assume various sizes and shapes, growing in various directions, and will hardly define themselves until removal.
The benign solid tumors consist mainly of the various types of goitre.
Of the malignant tumors, sarcoma is perhaps the most frequent, and is met here in all its varieties. Endothelioma occurs here also, while true carcinoma can hardly be primary in the thyroidal tissue, but may frequently extend to it and invade it, thus seriously complicating a case already made desperate by its presence in the neck. Metastatic forms of true cancer may also occur here as elsewhere. For a growth of this kind there is but one resort, i. e., extirpation, but this will be difficult and usually inexpedient.
The enlargement or hypertrophy of a part or the whole of the thyroid, now known universally as goitre, has been known also as bronchocele and trachelocele. The condition is one of unilateral or symmetrical affection, met with much oftener in women than in men, and particularly in certain regions. It is most prevalent in Switzerland and in Upper India. It is occasionally known to assume an endemic or epidemic form, the affection disappearing from the region of the country concerned after a period of some years. Practically nothing is known of its cause. Many theories have been advanced, that which finds perhaps widest acceptance referring to the character of the water supply.
For present purposes goitre may be understood to include the following forms:
The parenchymatous form consists essentially of an overgrowth of the ordinary thyroid tissue. It is diffuse and unencapsulated, all the thyroidal tissues participating in its structure. Sometimes whole families suffer from this form of goitre, and occasionally an apparently hereditary influence may be traced. The tumor thus produced may attain great size. According as it involves one side or both will it be symmetrical or otherwise. It is elastic, smooth, rounded, sometimes apparently subdivided by furrows which mark the original lobar arrangement. It displaces the structures around it, and may attain a large size without producing serious pressure effects. When these occur they assume the type of dyspnea, dysphagia, and laryngeal paralysis. The growth is insidious, usually increases markedly with each pregnancy, and may spontaneously recede. Within it changes may occur which lead either to cystic softening and formation of cysts, or fibrous trabeculæ may appear and thus make it more firm and dense. The denser the growth the earlier the pressure symptoms appear. Occasionally the isthmus alone will appear involved, in which case there will be a central growth.
The so-called thyroid adenoma (the term adenoma being used on the supposition that thyroidal tissue is true gland tissue) is often of cystic type. It consists of more or less isolated tumors of general thyroid character, but circumscribed, often encapsulated, perhaps undergoing cystic degeneration, occurring frequently in multiple form, and producing cysts of all sizes. Such a growth will displace the other thyroidal tissue and may give a decidedly irregular aspect to the resulting tumor. The cysts often contain cholesterin. In recent cases the capsule is thin; in old tumors it may be calcified, and so may be the tissue within the capsule. These growths are seen in successive generations of the same family. They have their beginnings usually in the earlier years of life.
Similar growths may also arise from the outlying portions of the thyroid, or from accessory[713] thyroids, so that they may be found back of the sternum, or lying deeply in the neck or near the base of the tongue. If near the surface and cystic they give a sense of fluctuation which the harder forms do not afford.
—A recent study of Enderlen has shown that small, goitrous growths make their appearance within the trachea more commonly in females than in males, and in patients of middle age. The known duration of growth has varied from a few weeks to fifteen years. He believes the majority of the cases begin to grow at the age of puberty. These growths have been found on the posterior wall of the larynx or in the trachea itself. They have usually rounded bases and broad implantation, with smooth surfaces, covered with intact mucosa. In most instances the thyroid itself is also enlarged. The only recorded symptom is dyspnea, proportionate to the degree of obstruction. They are probably to be explained by the inclusion theory, some thyroidal rest being disintegrated and so entangled as to grow in this direction. The only satisfactory treatment is ablation of the tumor, after tracheotomy, as endolaryngeal operations are more dangerous.
These constitute the ordinary types of goitre. Diagnosis is not difficult, as the resulting tumors are more or less prominent, involve the region of the thyroid, and rise and fall with each act of swallowing. When the entire organ is involved the tumor may have a horseshoe shape. Large veins appear upon the surface, while pressure symptoms will correspond with its size and location. They pursue an irregularly slow course. Many patients attain old age and a considerable size of growth without such discomfort as to require operation. Any goitrous enlargement in which considerable softening occurs, with formation of colloid material, is entitled to the term in frequent use, “colloid goitre.” By accident of location any growth of this kind behind the sternum may cause serious pressure effects before attaining large size. In symmetrical enlargement of both lobes the trachea may be so compressed as to be narrowed and to entitle it to the term scabbard trachea.
Iodine has been used externally and sometimes with benefit. The favored method in India is to use an ointment containing one grain of red iodide of mercury to the ounce. This is daily rubbed over the goitre and then the parts exposed to the bright sunlight for an hour or more. Iodine has also been used by parenchymatous injection. It is mainly used, however, by those who object to operation or do not dare perform it. The iodine treatment, whether externally or internally used, is usually disappointing. So also is that by the Röntgen rays, and, for that matter, all other non-operative measures. Operative relief alone is complete and final. It is described below.
As a clinically distinct type of disease this was first described by Graves, of Dublin, in 1835, and five years later by Basedow, of Magdeburg; hence it is frequently called by their names. Although the thyroid participates in the clinical picture it cannot be stated that it is primarily at fault. Three marked objective features characterize pronounced cases—thyroidal enlargement, more or less pronounced tachycardia, and exophthalmos.
So far as known there is an essentially toxemic feature behind these lesions, which is mysterious, nor is the nature of the toxemia certain. No constant lesions have been found in the nervous system, although the sympathetic nerves are always involved when the heart and the eyes are affected. The three cardinal symptoms or signs above mentioned are nearly always associated; but with pronounced rapidity of the heart’s action there may be but little involvement of the thyroid or slight protrusion of the eyes. Whatever the original toxemia, or its source, a prominent feature of the condition is hyperthyroidism—i. e., hypersecretion of the substance which regulates nutrition—whose overproduction materially disturbs the heart and vasomotor nerves. It stands in strong contrast to myxedema and cachexia strumipriva, which are considered to be due to hypothyroidism or diminished secretion. Consequently it is not to be treated by feeding thyroid extract. A recent view which has much to support it is that at the basis of this condition the parathyroids are so concerned that any operation which includes their extirpation would be a serious menace. At present it may be held that the parathyroids are intermediate factors between the primary toxemia and the hyperthyroidism.
[714]
Aside from mere thyroidal enlargement, which is influenced by pressure and shows an increased pulsation, always palpable, sometimes visible, there occur increased heart activity, with a rapid and easily influenced pulse; widening of the palpebral fissures, the upper lid not following the motions of the globe, with defective convergence; rhythmic muscular tremors; increase of general sensibility; insomnia, with disturbed sleep; psychical disturbance, sometimes amounting to melancholia or mania; digestive disturbances, including diarrhea, vomiting, and thirst; cough, with frequent and shallow respiration; loss of hair and nails; sweating, flushing of surface and sometimes leukoderma or pigmentation of the skin. Terminal symptoms consist of all those mentioned above, with acute mania, high temperature, vomiting, profuse sweating, dermatitis, jaundice, and final convulsions with exhaustion, all these resembling those of death in experimental animals after the removal of the parathyroids.
A sign recently described by Teillas, which he considers pathognomonic, consists of deep-brown pigmentation of the outer surface of the eyelids, the color being evenly diffused, bounded above by the eyebrow, below by the margin of the orbit, the conjunctiva being not affected. Its effect is to apparently increase the degree of exophthalmos and to intensify the fixity of gaze observed in these subjects.
—This is not the place in which to consider in detail either the pathology or the drug treatment of this affection. By many surgeons it is regarded as a surgical disease, i. e., one to be treated by one of two operative methods, either thyroidectomy or excision of the cervical sympathetic. When such measures as electricity, Röntgen rays, and hydrotherapeutic treatment, and such drugs as belladonna, sodium phosphate, arsenic, iodine, phosphoric acid, etc., have failed, and when the antithyroidal serums or preparations, such as thyroidectin and antithyroidin have proved insufficient, then surgery remains a last resort. Unfortunately this is too long delayed. To remove the thyroid so soon as it is shown to be producing an injurious amount of oversecretion is neither a difficult nor a dangerous procedure, but to wait until the heart beats 150 times a minute and the patient is nearly maniacal is to wait until he is almost moribund and until it is too late. Nowhere does the remark, “The resources of surgery are seldom successful when practised on the dying,” apply more forcibly than to such cases as these.
As between sympathectomy, already described, and thyroidectomy (see below) it may be difficult to choose. By the time such a case comes to operation each will present its distinct difficulties. The question is mainly one of choice. A large tumor will obscure access to the sympathetic trunk in the neck, while, on the other hand, the neurectomy itself is probably a less dangerous procedure. The decision should be based on the predominance of the features due to vasomotor disturbances. Thus when the eyes are prominent, the pupils dilated, the palpebral fissure widely open and difficult of closure, there is reason for attacking the middle and upper cervical ganglia, which are not so difficult of access. Again when the heart is affected there would be a special indication for extirpating the inferior cervical ganglion, as well as the first dorsal; but the former will always be difficult in the presence of a thyroidal tumor, and the latter wellnigh impossible. When, however, thyroidal symptoms are pronounced, with difficulty in respiration or other purely pressure effects, thyroidectomy is indicated. This should be performed as described below. An effort should be made to preserve the capsule, at least on the inner and posterior aspect of the thyroid, in order that the parathyroids which lie in close relation to it may not be disturbed. Operations upon the vessels for the purpose of controlling the circulation are rarely practised, and the question in these cases is as between partial and complete extirpation.
Curtis has recently collected from the statistics of two German and two American operators 136 cases of exophthalmic goitre treated by thyroidectomy, with 17 deaths, chiefly from acute thyroidism. The most marked improvement realized was disappearance of tremor, nervousness, and insomnia, and of a feeling of anxiety, so common to the disease. To these may be added the more extensive experiences of Charles Mayo, which present extirpation as an almost ideal method of treatment.
As remarked above, all attempts at feeding with thyroid extract should be avoided, the case being one already suffering from hyperthyroidism. It should be noted that in few instances the thyroid seems to suffer from its own overactivity, and passes into a stage of physiological atrophy, with more or less subsidence in volume. In such a case the symptoms of Graves’ disease would gradually change into those of myxedema.
The thyroid itself is extremely vascular under all circumstances, particularly under[715] these, to such an extent that pulsation becomes a prominent feature. This, however, should not be mistaken for that form of ordinary goitre in which the vessels undergo increase in dimensions and in which sometimes a loud bruit may be heard.
Malignant goitre implies a generalized involvement of the thyroid in one of the malignant forms of neoplasm. (See below.) It is of rapid growth, with more or less infiltration of surrounding tissues, which is evidently not of inflammatory character but more distinctive.
This may be partial or total. It is important to leave a portion of the thyroid in order that the patient may not suffer from the consequences of athyroidism, i. e., cachexia strumipriva. It is generally understood that if one-sixth or one-seventh of the total mass can be left in situ, with sufficient blood supply, it will suffice. Thus it may be possible to leave the isthmus, after removing both lateral lobes, or a portion least affected of one of the latter may be left in place.
The character of the incision will depend on the size and position of the enlargement. For complete thyroidectomy a horseshoe-shaped incision, convexity downward, should be made, extending along the anterior border of the sternomastoids and then across the neck. This should be carried through the platysma and superficial fasciæ, the anterior jugular veins being secured when cut. The flap thus made is then raised, after which a large part of the subsequent procedure is made by blunt dissection, and separation of the surrounding muscles, which are held aside with retractors. When the tumor is so shaped and placed as to make it possible it is well to approach it laterally and secure the upper and lower thyroidal vessels on one side or both, dividing between double ligatures. If this be done the mass can be drawn forward in such a way as to avoid injury to the nerves and vessels, the operator keeping in close contact with the capsule, or, for reasons specified above, perhaps dividing and shelling out the mass from within it. Although the tumor may be occupied by large vessels, those which lead up to it—i. e., the thyroids—are rarely much enlarged. Nevertheless it is wise to secure them first. While the anterior muscles may, in many instances, be separated and the tumor mass exposed between them, there are cases which will require transverse division of the sternohyoid and sternothyroid, in which case they should be subsequently sutured.
One of the complications is to find the tumor mass extending down behind the sternum or the clavicle. From these locations it should be separated by cautious blunt dissection, else the pleura or one of the deep veins might be wounded. The former accident would be instantly denoted by the passage of air and its entrance into the thorax, the latter by severe hemorrhage.
In exophthalmic cases it may be held to be especially desirable to enucleate the thyroid from within its capsule. This makes the performance easier in some respects and more difficult in others.
Extreme caution should be taken in two particular respects: First, that the trachea be not compressed, nor its caliber interfered with, by the traction efforts used in removing the mass. The second caution necessary in exophthalmic cases is to make the least possible amount of pressure upon the thyroid during the operative procedure, since, as mentioned above, its secretion is depressing to the heart, and it would complicate matters to force more of this material into the circulation at a time when everything conspires to reduce blood pressure and the reliability of the heart’s action. A certain amount of manipulation is unavoidable, but this should be made as gentle and as slight as possible. Moreover, these cases are to be drained to permit of free escape of thyroidal secretion. (Mayo.)
In performing thyroidectomy for Graves’ disease advantage should be taken of the pneumatic suit devised by Crile, and the patient placed in the semi-upright position. These are advisable precautions to take in every such operation. The position allows more natural emptying of the veins at the base of the neck and the suit permits of the blood pressure being maintained by mechanical means. In order to use the suit to best advantage the blood pressure should be noted throughout the course of the operation.
The enucleation or extirpation concluded, hemostasis should be observed, as with returning cardiac vigor secondary hemorrhage is by no means an impossible event. Every vessel which can be recognized should be carefully tied, and tissues which ooze should be caught up with suture and tied en masse. All the deeper portions of the wound[716] should be brought together by buried sutures in such a way as to leave no dead spaces. Cases where a retrosternal pit has been left, by removal of a low-lying growth, should be drained to avoid the accumulation of blood. Where doubt exists as to security from secondary hemorrhage it is the writer’s custom to place secondary sutures, and to pack the cavity with gauze dipped in balsam of Peru, leaving this packing in place for two days, then removing it and closing the wound by utilization of the sutures.
Shock after these operations may be extreme, and is to be combated by transfusion or infusion of salt solution, with small amounts of adrenalin.
Should the surgeon attack a so-called malignant goitre he must be prepared to meet with greater difficulties and perhaps to abandon the operation before its completion. Death on the table is not unusual in such cases.
Operation under cocaine local anesthesia is often most advantageous, and is the rule in such clinics as that of Kocher, in Berne. The patient should be well narcotized with morphine, after which a weak cocaine solution is injected along the proposed line of incision. The pain produced by the balance of the work is not beyond endurance, while the dangers are certainly minimized, especially in cases where there is compression of the trachea or excessive heart action, the latter being particularly true in Graves’ disease. There is less fulness of veins, and there is neither coughing nor vomiting. The operative features are the same as those described. As the anterior thyroid artery is approached all possibility of including the recurrent laryngeal nerve in the ligature is avoided by having the patient talk, injury to the nerve producing instant hoarseness. If the growth extend low and into a pit behind the sternum it may be possible to extirpate it from above downward, and finally to lift it from its bed, securing its base or pedicle with an elastic ligature.
Fig. 500
Patient placed in semivertical position, and enclosed in Crile’s pneumatic suit, as recommended for many cases of goitre, brain tumor, or other serious operations about the head and neck. (Crile.)
A danger common to all thyroidectomies is that of injury to the trachea. This is avoided when there are no abnormal adhesions, but when the growth surrounds the trachea, or is firmly fastened to it, such an accident may happen in spite of the greatest care. According to its size and location the surgeon may endeavor to close the opening with sutures, or he may insert a tracheotomy tube or leave the wound open sufficiently to pack it snugly, preventing entrance of fluid into the trachea, at the same time expecting the wound to be subsequently closed by granulation tissue.
Sympathectomy as a measure directed toward the treatment of exophthalmic goitre, as well as of glaucoma and certain forms of epilepsy, has been described in Chapter XXXVII.
[717]
Strumitis is a term applied to actual inflammation of an already goitrous thyroid. It may follow such infectious diseases as typhoid, or it may be an apparently spontaneous infection without known cause. It may run an acute course, tending rapidly to suppuration, in which case there will be not only pain and tenderness in the thyroid itself, but all the local evidences of pyogenic infection, with infiltration and rapid formation of pus, perhaps with widespread phlegmon of the neck. This is a serious condition and may call for early and free incision of the infected area. A hemorrhagic form of strumitis is also known. The thyroid may also be the site of metastatic abscesses in cases of pyemia, in which case there will be but few local indications.
The thymus figures but rarely in surgical interest, but when seriously affected it causes most pronounced symptoms. Its principal activity is shown previous to birth and during the earliest months of infancy, and it should have disappeared by the age of puberty. Instead of atrophying, as it should, it may undergo hypertrophy, by which, on account of its location, serious pressure is made upon the trachea and the base of the neck. This may occur suddenly, so that a tumor in its location rapidly develops and will prove fatal unless surgical relief be afforded. This constitutes an acute hypertrophy of the thymus, which is more than a mere surgical curiosity. In one case seen by me a long trachea tube was with difficulty inserted just in time to prevent death by asphyxiation. In case of such tumor the upper end of the sternum should be removed and the tumor enucleated, or the thymus should be sewed up to the sternum and the tumor thus raised out of its bed.
The thymus is of special interest in connection with the status lymphaticus, which has been referred to in a previous chapter. Its connection in such cases with hypertrophied lymphoid elements all over the body, and especially of the adenoid tissues of the nasopharynx, was therein described, and the seriousness of the condition, with the menace which it offers to anesthesia, as well as the extreme cautions to be observed, were fully rehearsed. The significance of laryngismus stridulus and its relations thereto were also mentioned. All this is of extreme importance to the surgeon, as every child with so-called thymic asthma, and with symptoms of lymphatism, should be watched carefully and anesthetized cautiously. (See Chapter XIV.)
Acute inflammation of the thymus as well as hemorrhages within it have been observed. It may also be the site of cystic tumors, perhaps of hemorrhagic origin. Suppuration in these cases is possible. In brief, the thymus, when acutely inflamed and suppurating, may be excised, when the tumor may be removed; but when simply somewhat involved, as in the status lymphaticus, it is best let alone, except in the presence of urgent indications to the contrary.
[718]
Fig. 501
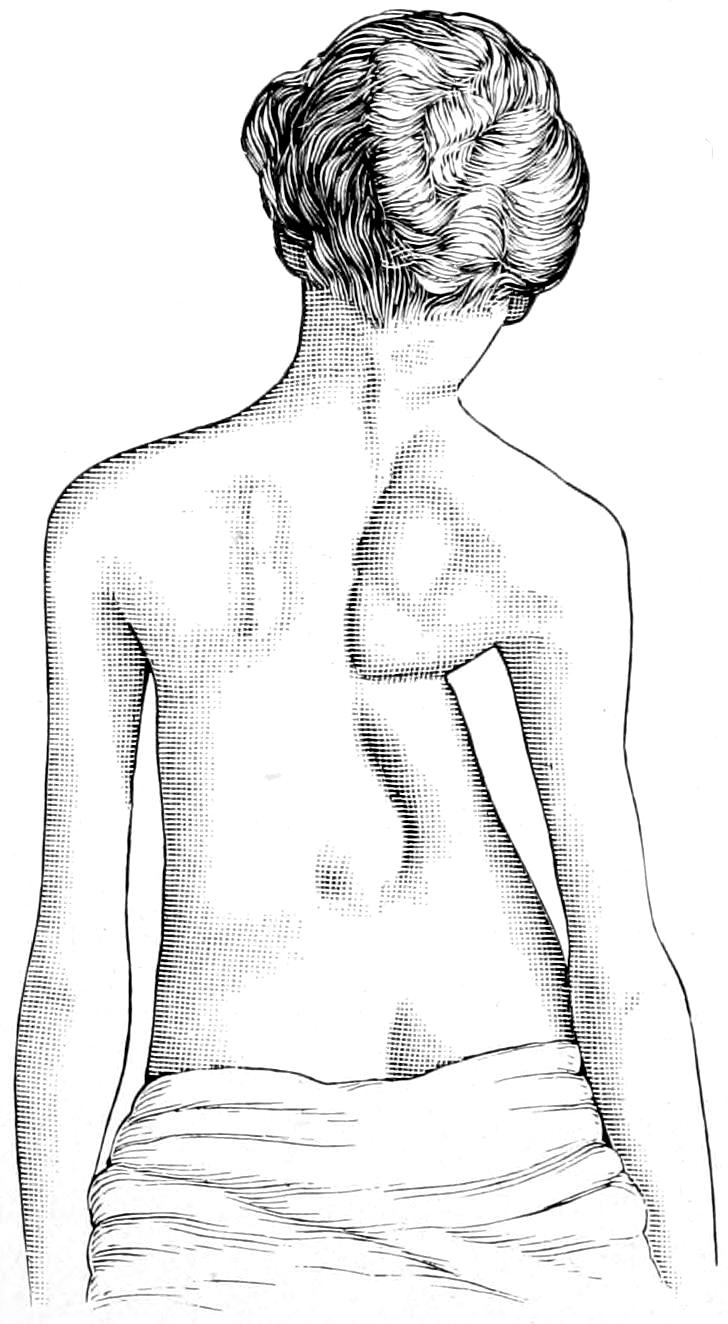
Congenital malformation of chest. (Sayre.)
Congenital malformations of the thorax are not uncommon, yet but few of them permit of surgical remedy. One or more of the ribs may be absent or defective in formation and produce lateral distortion of the spine. The clavicle also may be defective on one or both sides, or absent. This is a defect which causes but little inconvenience, in spite of its prominence. The chest as a whole may develop defectively or irregularly, some of these conditions being expressions of intra-uterine rickets and others being due to unknown or uncertain causes. Thus we have the absolutely flat chest seen most often in connection with an unduly rounded back, the flattening appearing rather in front, while perhaps the anteroposterior diameter is actually increased. As Hutchinson has shown, this may be a persistence of the fetal type of chest. Pigeon-chest or keel-shaped chest may be regarded as a reversion to a more primitive type, the anteroposterior diameter being increased at the expense of the lateral. The reverse of this deformity is the so-called funnel-shaped chest, where the sternum is depressed and the lateral dimensions increased. In addition to the defects thus noted in the ribs and sternum, absence of a vertebra has been known, the condition not producing deformity, but rather an appreciable shortness of the spine. Malformations are seen frequently in the sternum, which may be fissured in either direction, or may present perforations. With these similar defects of the ribs may also be seen, even to a degree permitting congenital hernia of the thoracic contents.
Supernumerary developments find their expression usually in an added rib, either in the cervical or in the lumbar regions. This condition is practically never noted at birth and may pass unnoticed. Nevertheless a cervical rib may, in adult life, produce discomfort or actual interference with function, partly by pressure upon the subclavian artery or the brachial plexus. When found it is in relation with the seventh cervical vertebra, and the space between it and the first dorsal rib is occupied by muscle developed for the purpose. The scalenus anticus may be inserted into its anterior edge. When sufficiently prominent to produce troublesome symptoms it may be recognized by palpation, and cases of doubt may be made clear by a radiograph. Should it prove troublesome it may be removed, an operation requiring considerable caution, because of its close relation to the pleura, which might easily be opened. It may be exposed by such an incision as would be used for ligation of the subclavian artery.
The thoracic muscles occasionally show anomalies, either in arrangement or by their absence, the pectoralis major being occasionally wanting in whole or in part, and furnishing the most frequent illustration of these defects, which are usually unilateral. (See Fig. 502.)
Congenital luxations of either extremity of the clavicle are also occasionally seen, particularly of the inner end. A peculiar displacement and relaxation are thereby permitted, with some degree of functional loss.
[719]
The acquired malformations of the chest may be produced from a variety of causes. Thus in connection with non-closure of the foramen ovale and the consequent disturbance of heart action, with its overdevelopment of the right auricle, the left side of the chest may be pushed forward and the apex beat found far below its normal position. Asymmetry in the young may also be produced by several different intrathoracic conditions, the most common being pleurisy and empyema, with their consequent distention of the pleural cavity, and later a tendency to cicatricial contraction. In this way marked forms of lateral curvature are produced. In a previous chapter it was stated that overgrowth of lymphoid tissue in the nasopharynx, ordinarily spoken of as adenoids, with consequent embarrassment of respiration, leads in time to stoop shoulders and poor development of the thorax. Deformity may also be produced by such defective vision as shall compel a peculiar or abnormal position of the head.
In chronic emphysema there is noted a peculiar barrel-shape of the chest, which is also to be regarded as an acquired deformity. Paralyses of the internal thoracic muscles will also permit of asymmetrical growth, and projection of the lower angle of the scapula, giving it a wing-like aspect.
Fig. 502
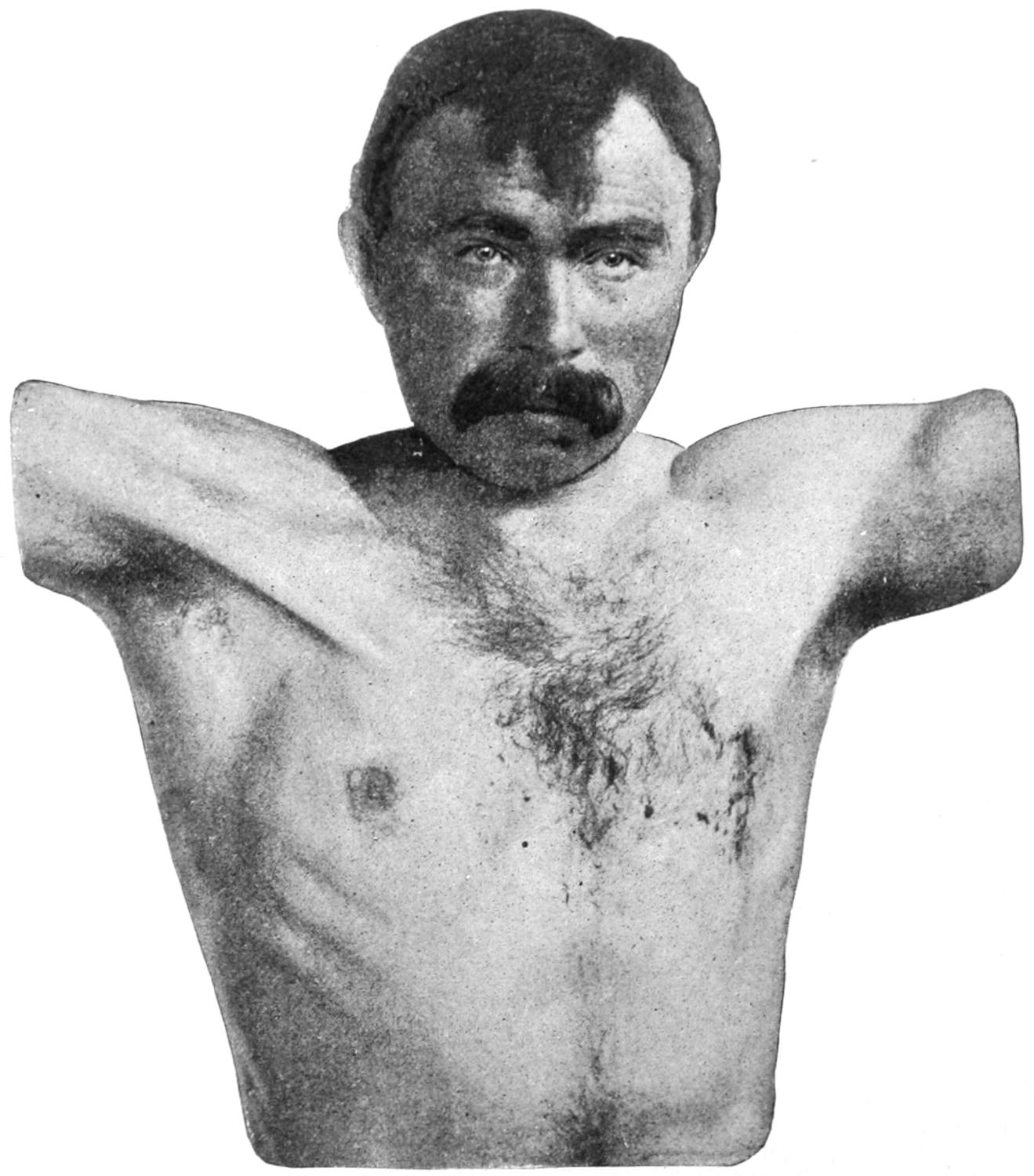
Congenital absence of the pectoralis major muscle of right side. (Richardson.)
The most common cause of thoracic asymmetry or deformity is rickets, which may be an early or a late manifestation. By the ordinary changes permitted in the epiphyses and along the costochondral junctions is produced the peculiar appearance known as “rickety rosary.” In these cases the effect of the weight of the upper part of the body upon the soft and changeable structures of the osseous and cartilaginous ribs, as well as the vertebræ and the sternum, are to be noted. Pronounced types of deformity result from such changes, producing extreme cases of pigeon-breast, or of hollowing in front known as birds’ nest deformity, while alterations occur in the vertebræ, producing various expressions of kyphosis and scoliosis. (See Fig. 504.)
[720]
These deformities of the back thus produced require to be differentiated from those produced by Pott’s disease, the former being unaccompanied by symptoms and occurring slowly, while the latter are usually accompanied by pain and are progressive in character, as well as more or less disabling. With a softened skeleton in a rapidly growing child such trifling influences as the position assumed in the nurse’s or mother’s arm, or that habitually taken in sleep, may affect and modify symmetrical growth. Rickety deformities of the spine and thorax, if not too far advanced, permit of being checked and much improved by braces, along with the measures indicated in rachitis. Without the latter, however, the former would be almost ineffectual.
Fig. 503
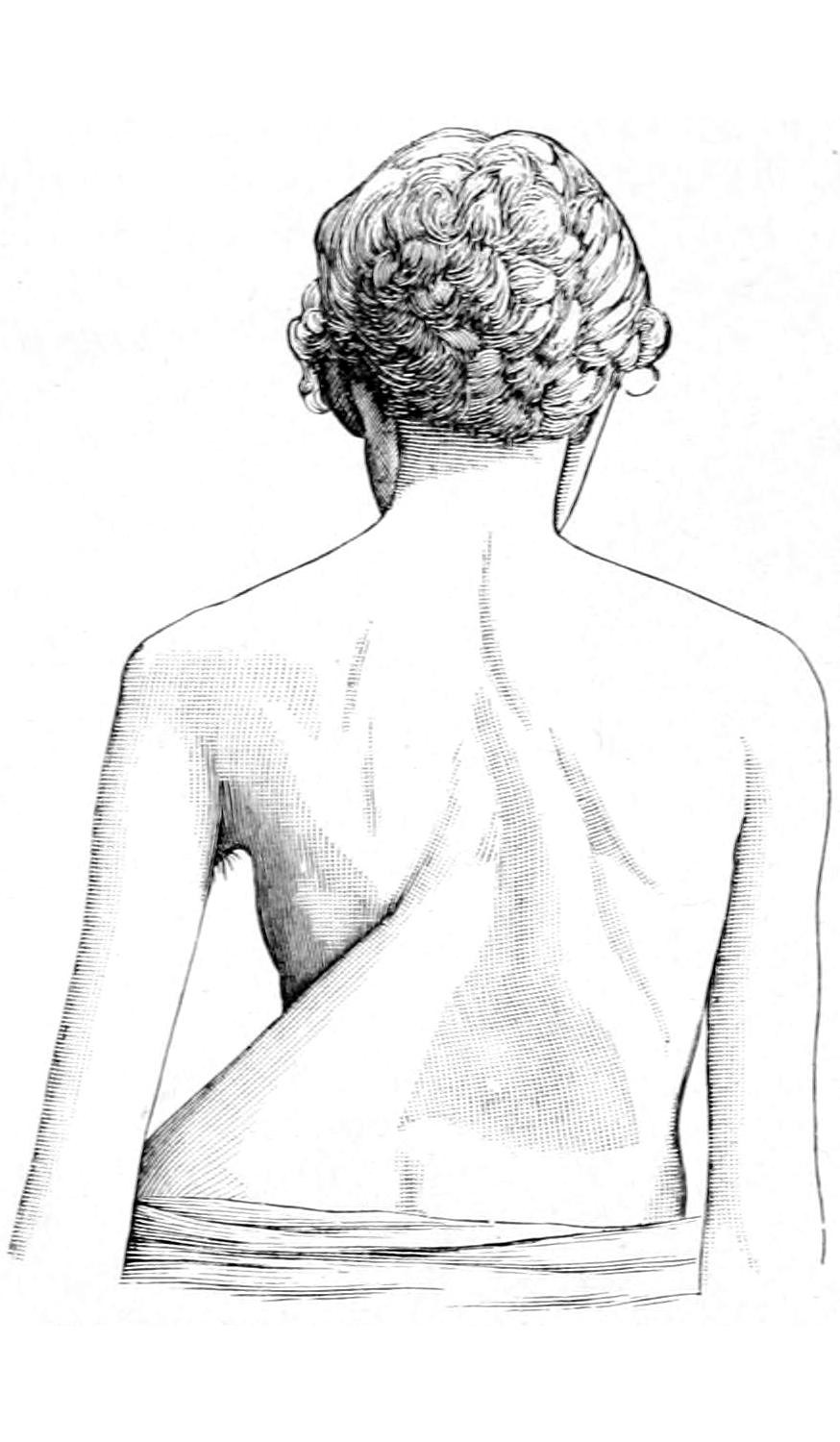
Malformation of chest following empyema. (Sayre.)
Fig. 504
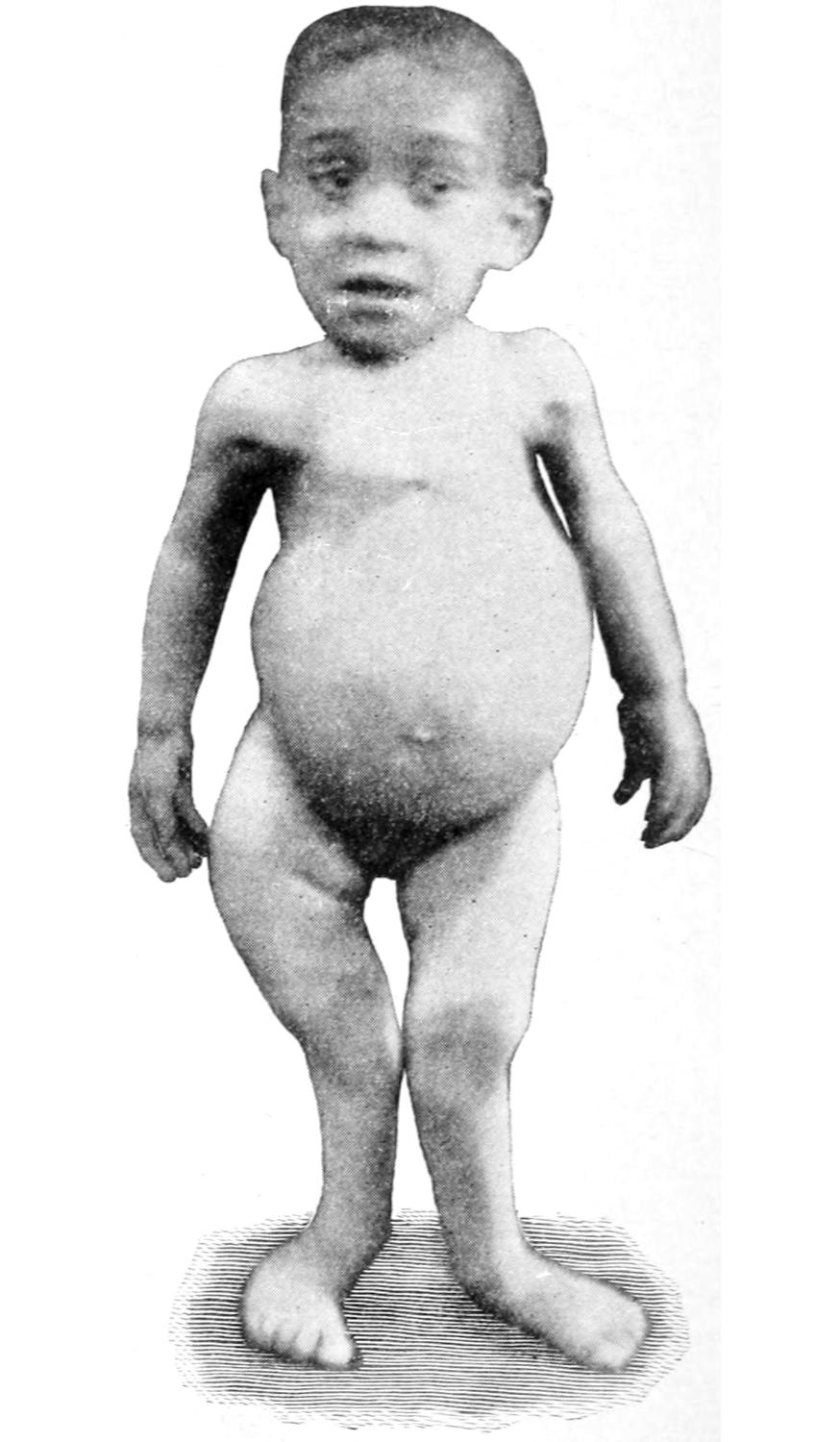
Deformity of the thorax, the result of rickets. (Gibney.)
Malformations may also be produced by injuries or certain occupations. Extensive burns may cause cicatricial contraction; contusions may produce paralyses, and more serious lacerations may leave extensive scars, which will gradually warp the chest out of shape. Burns, for instance, which may involve the axilla and the upper arm, may be followed by such dense scars as to limit the motion of the arm. Skin grafting should be resorted to early in the treatment of lesions thus produced.
Tight lacing is the source of a mild form of thoracic deformity, by which the chest capacity is reduced, the respirations made peculiar in character, the liver displaced downward, and the general welfare of the individual materially affected. Influence of the right-hand habit is frequently quite apparent in that the right side of the chest becomes overdeveloped as compared with the left. This may be seen in a large number of workmen who use heavy tools especially with the right hand. Certain occupations, as well as sports, lead to constant assumption of the stooping position, with the inevitable round shoulders and drooping head so apparent in bicycle riders.
Tattooing.—As a local expression of a bad habit, or in some instances almost of a criminal instinct, tattooing may be mentioned. This is seen usually upon the chest and arms. It is a prevalent custom among sailors, and is regarded by alienists and anthropologists as a habit indulged in by criminals and the insane. La Cassagne has spoken of tattooing as “an uninterrupted and successive transformation of an instinct.” Among[721] the inhabitants of the Pacific Islands it is almost a mutual practice, and among them the tattoo marks are often found upon the back and upon the sexual organs. The materials usually employed are lamp-black, indigo, and India ink for the black or blue tints, and cinnabar or carmine for the red. Practised as it is by the unschooled and the ignorant it may be followed by all forms of local infection, while syphilis has been thus transmitted.
For the removal of tattoo marks many methods have been suggested, but few have been found satisfactory. The minute particles of pigment have become so deeply lodged that, like powder marks, it requires infinite patience in their detection with the lens and individual removal, or those portions of the skin must be destroyed which contain them. Mechanical methods should be limited to localized stains, unless a plastic operation is preferred, and, after removal of the affected area, healthy skin may be transplanted by one of the plastic methods or we may resort to skin grafting. Actual cauterization with strong caustics or with the actual cautery will be followed by superficial sloughing, which may remove the disfigurement. It is questionable, however, if the resulting scar will be considered much of an improvement upon the previous condition.
As a result of a severe blow made by a blunt object there may result a form of concussion or commotion, similar in its results to the conditions which were formerly described in the cranial cavity as concussion of the brain, but which are now known to be due to reflex vasomotor disturbances, by which blood pressure is seriously affected and extreme degrees, perhaps fatal, of shock or collapse produced. It is possible for fatal injuries thus produced to leave little or no evidence that may be discovered at the autopsy. Hence the term concussion of the chest may be retained as descriptive of what has taken place, and implying serious symptoms produced through the agency of the nervous system, especially through its sympathetic plexus. In such instances the heart is seriously affected and may continue to beat feebly for some time, as in shock from other injuries.
Severe blows upon the chest also disturb the function of respiration, and it is possible that asphyxia, even to a fatal degree, may result from a momentary paralysis of the entire respiratory apparatus thus produced. In such cases artificial respiration will be required. In many instances patients will complain of not merely distress, but severe pain, which may require local anodyne measures as well as the administration of an opiate.
Contusion of the chest leaves more visible and lasting effects upon the tissues of the chest wall. Thus extensive hemorrhages may result and hematomas form, or ribs may be broken, with or without injury to the pleura, or internal hemorrhages may occur, as from a ruptured intercostal or internal mammary artery, the consequences of such injuries not necessarily appearing at the time, but developing later. Along with these injuries to the chest there may occur other injuries to the abdominal viscera or to other portions of the body. Something will depend upon the distention or relative emptiness of the lungs at the time of injury, and whether there may have been at the same time a sudden closure of the glottis, in which case, by an external blow, something resembling an explosive effect may be produced within the air passages. The degree of stomach distention may also have its own effect. Laceration of lung tissue will usually be shown by appearance of bloody froth at the mouth, as well as by more or less dyspnea. Rapidly developing symptoms of pressure upon the lung would indicate the accumulation of blood within one pleural cavity and cause the ordinary physical evidences of the presence of fluid. The diaphragm may be ruptured, and the proper viscera of one cavity be displaced into the other. When emphysema of the tissues of the chest occurs it is usually safe to assume that a rib has been fractured, even though the injury cannot be located or even otherwise recognized.
A series of later lesions may result from such contusions, which may be of serious character. Thus there has been described a so-called contusion pneumonia, whose symptoms are similar to but milder than those of the genuine disease. It is a result of inflammatory and hemorrhagic infiltration. It may lead to a pleuropneumonia, with subsequent hydrothorax or pyothorax, or these may take place more directly and without its occurrence. The products of this disease afford foci in which, later, tuberculous expressions are commonly met. It has been shown experimentally that the blood[722] serum of animals subjected to severe injuries of the chest and abdomen has well-marked toxic properties. Thus the appearance of sugar or albumin in the urine or of other toxemic indications may be perhaps explained.
—The treatment of these injuries should include the relief of pain; the performance of artificial respiration, along with the inhalation of oxygen; the customary treatment for shock, with the use of adrenalin, when needed, for raising blood pressure; absolute rest, and especially the enforcement of local physiological rest by bandaging or the application of broad strips of adhesive plaster about the thorax. In addition to these general measures special indications should be met when they arise. The occurrence of phenomena indicating the development of pneumonia or collection of fluid should be noted, as the latter may call for removal, with perhaps ligation of a vessel, if it be bloody, or later evacuation, should it be serum or pus. External extravasation will usually disappear under soothing, warm, and moist applications. No hesitation need be felt in opening a hematoma which does not show a disposition to prompt resolution. Other non-perforating injuries include, for example, severe burns or scalds, which may need the same treatment as when occurring in other parts of the body. Fluid may accumulate within the chest when there has been any such serious external disturbance.
Penetrating wounds of the chest are generally inflicted by stab or gunshot injury. Two serious elements of danger accompany these injuries: the first immediate, that of hemorrhage from division of some vessel of importance concealed from sight; the other that of infection, for either by the penetrating object itself or by air or clothing which may follow it, infection may ensue, which may result in septic pneumonia, pyothorax, or some deep phlegmonous process, with always dangerous and sometimes fatal results. Gunshot wounds vary, and according to the character of the missiles and the weapons from which they are discharged. Those occurring during warfare and made by bullets of the Krag or Mauser type are usually driven with such velocity that they produce a minimum of laceration, even though they pass through the chest. Such injuries have in the late wars in different parts of the world been frequently observed, and have shown a surprisingly low mortality rate, providing only that the heart itself, the pericardium, the large vessels, and the spine be not injured. Stories of the battle-field afford abundant illustration of men shot through the chest being scarcely affected by the injury, but continuing in action, at least for some time, and finally recovering. On the other hand, the ordinary revolver or pistol, with which most affrays in civil life are terminated, does not drive its bullet with nearly the same velocity, and is more likely to inflict a serious or even fatal wound. (See Plate XLVIII.)
A bullet or a stab wound almost invariably so opens the thorax as to permit the immediate entrance of air. In theory this should be followed by prompt collapse of the lung; in fact, however, this is only partial, and often surprisingly so. If such a bullet wound be occluded the air thus admitted is more or less absorbed, disappearing into the bloodvessels, and the lung once more expands to its natural dimensions. Much will depend, therefore, on the size and character of the wound as to whether occlusion may occur spontaneously, or may be practised through the first-aid dressing or its equivalent.
The entrance of air may be recognized by a certain degree of embarrassment of respiration, by alteration in the percussion note, and often by its passage to and fro through the opening.
The principal indications of possible injuries, in addition to those just noted, will be the occurrence of paroxysmal coughing, with inspiration of blood, and the added physical signs of the presence of blood in the pleural cavity. Thus dulness on percussion, with the line of dulness altering with position, will indicate the presence of fluid, and should this occur soon after the injury it can only be regarded as an evidence of hemorrhage into the pleural cavity. A combination of abnormal tympanitic condition, as above, with the physical signs of fluid beneath, will indicate a condition of pneumohemothorax. These signs will change from hour to hour or from day to day in accordance with altering internal conditions. If they become rapidly more pronounced they indicate a condition which will probably call at least for free incision, evacuation of blood, and very likely determination of the source of its escape and proper attention thereto.
PLATE XLVIII
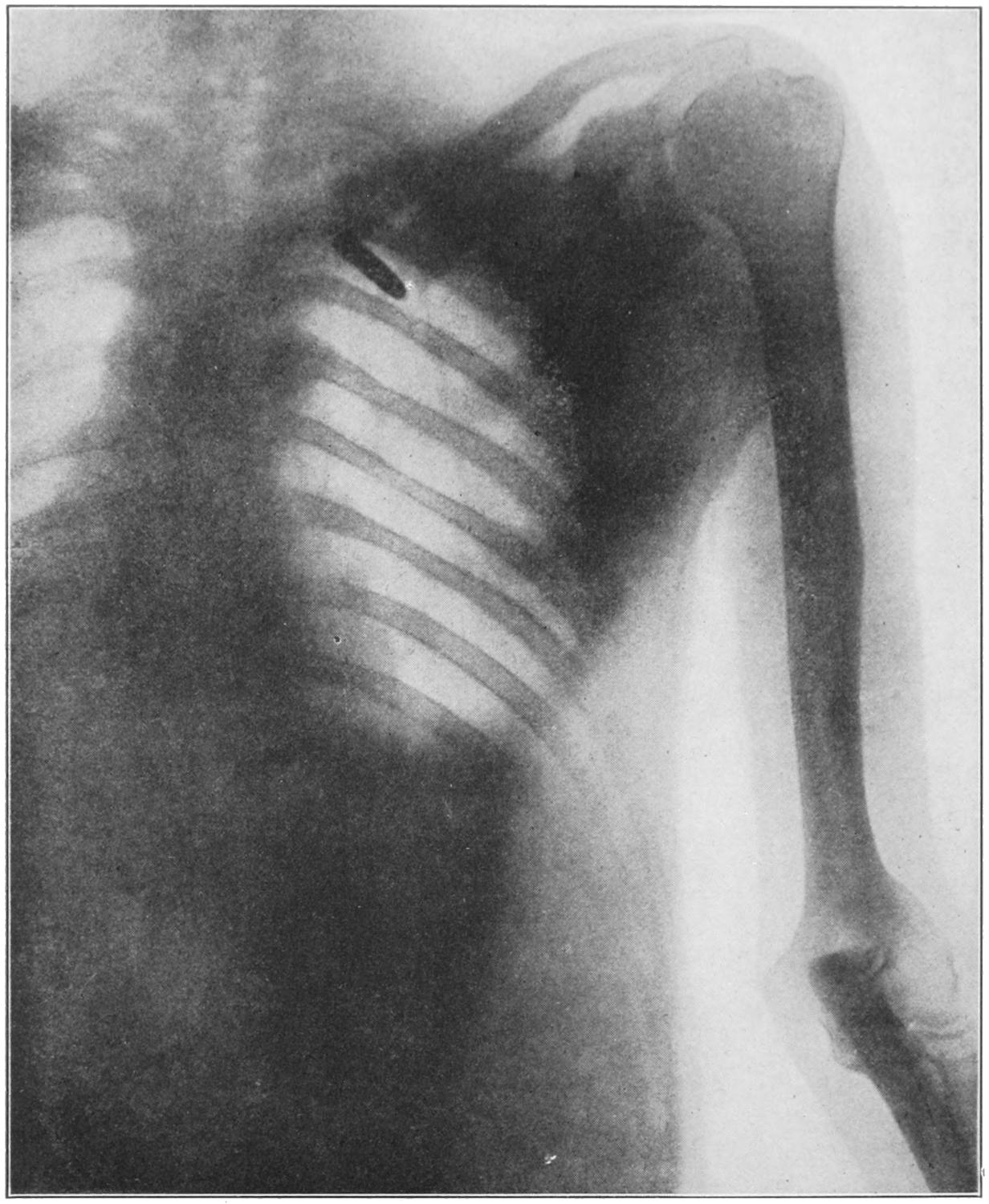
Radiograph of Chest, showing Mauser Bullet.
(From Plate X, “Use of Röntgen Ray by the Medical Department of U. S. Army in the War with Spain, 1898.”)
[723]
An intercostal artery is of itself a small vessel, but when cut across by the edge of a knife or torn by the passage of a bullet it may pour sufficient blood into a pleural cavity to cause serious dyspnea and perhaps fatal result. To discover at the coroner’s inquest that a patient has been allowed to die because no one had the judgment to enlarge the wound and assure himself whether such a hemorrhage was not occurring is not at all creditable to those in charge of the case. The combined dangers of infection and of collapse of the lung are not so great as those of possibly fatal hemorrhage, or intrinsic disaster through septic infection from neglect of this kind.
Aside from the injuries thus produced to the respiratory apparatus there are those especially involving the heart. It has been supposed that gunshot wound of the heart was necessarily fatal. There is now reason to think that this is not invariably true, even in individuals not promptly operated upon, while the resources of modern surgery have enabled the surgeon to save a number of cases of absolute gunshot injury to the pericardial sac and even to the heart itself. (This subject has already been considered in the chapter on Surgery of the Heart and Great Vessels.) Every case which is not promptly fatal is worth attempting to save, if suitable help be at hand, by a resection of the chest wall, exposure of the pericardium, and of the heart itself, with the introduction of sutures or the use of the ligature wherever these may appear to be needed.
The occurrence of more special forms of traumatic lesion may be indicated by particular features. Thus if the esophagus has been wounded the patient may expectorate or vomit blood, whose presence in the stomach could not be explained by other features of the case. On the other hand blood which comes into the mouth from the lungs may be swallowed and its appearance in the ejected materials thus accounted for. A violent disturbance of cardiac regularity or evident paralysis of the diaphragm may be accounted for by injury to the pneumogastric or phrenic nerves.
—In regard to the general treatment of these injuries the use of the probe should not be encouraged, at least in the way in which it was formerly used. It is a serious matter to stir up clot or to open up a wound with a probe, thus inviting free entrance of air. Nearly all the information desired may be more accurately obtained by careful physical examination and study of symptoms. It should never be used except with aseptic precautions. It affords little information as to the course, and practically none as to the location of a bullet which has penetrated the chest wall. It may possibly be of service in searching for a bullet in the muscles of the back, but the only information it is capable of furnishing is afforded by a skiagram. Miscellaneous probing should be condemned, and in these injuries is rarely justifiable.
The first measure to adopt in cases of gunshot wound of the chest is to determine that the heart has not been disturbed; the next to estimate what injury may have occurred to large vessels, then a general determination of the other surgical features of the case. The patient who shows no depressing symptoms nor develops them during the ensuing few hours may be left with only a temporary occlusive dressing placed over the wound; but increasing embarrassment of respiration, or weakening and increasing rapidity of pulse, should be carefully watched to guard against internal hemorrhage. If it be learned that there is such internal bleeding prompt action should be taken for its control. This means anesthesia and perhaps thoracotomy, with resection of one or two ribs, in order to afford space through which to practise deep suture or ligation. So long as one side of the chest alone is involved—i. e., one lung thus exposed—the surgeon may widely open the chest and meet every surgical indication without the necessity for artificial respiration or the use of the Fell apparatus. It is, however, advisable to have this at hand for such work, while cases demanding such extreme measures can scarcely be made worse by the performance of a tracheotomy and resort to some means for forced and artificial respiration.
To simply enlarge a small bullet opening or punctured wound, in order to be sure that an intercostal artery has not been injured adds but little to the danger and much to the security of such a case. In case of doubt give the patient the benefit of that doubt and operate to any necessary extent. When hemorrhage is slight and not alarming it may be sufficient to make the occlusive dressing include a tamponing of the opening between the ribs, gauze being packed in the opening in such a way as to prevent hemorrhage.
A study of the escaping blood will permit of differentiation between arterial and venous hemorrhage, that which escapes from the lung being ordinarily of the latter type. Richter[724] has suggested an ingenious method of deciding whether hemorrhage comes from an intercostal artery or lung tissue, by introducing a sterilized piece of pasteboard, similar to a visiting card, rolled up in the form of a circular tube and flattened with a crease; should blood flow out along the groove it shows that it is an intercostal artery which is bleeding; but if it flows out of the wound through the tube the source of the bleeding is the pulmonary tissue itself. (Dennis.)
The question of the presence of a foreign body, bullet or otherwise, is important. This is less so when it is a question of the bullet itself than of driving in some fragment of rib or of foreign body introduced from without. A bullet, a broken knife-blade, or anything of such character will be revealed by an x-ray picture. The probe will rarely give this information. Clothing, objects carried in the pocket, or various other foreign material may escape detection.
The first measure of importance is the determination of the occurrence of serious internal hemorrhage, the second is the emergency treatment of the injury itself, which should include primary aseptic occlusion, to be followed later by other measures. A withdrawal of fluid is also indicated. Escaped blood may be contaminated and produce later a pyothorax. As the result of a traumatic pleurisy serum may collect within the ensuing few days, and it too should be removed. It should be first found with the exploring needle. If seen to be free from pus it may be withdrawn by the aspirator; but if it be destined to become pus, then the sooner it is evacuated by incision the better.
Increasing embarrassment of the heart’s action, which is not caused by the collection of blood, may be due to pyopericardium. So soon as the physical signs indicate gradual enlargement of the cardiac area the exploring needle should be used. A traumatic pericarditis may simply require aspiration of the pericardium, whereas the presence of pus in the pericardial cavity will not only necessitate aspiration, but occasionally open incision, with or without drainage. The appropriate manner of affecting these procedures will be found more fully discussed in the section on the Heart.
In general, and without regard to the nature of the accident, injuries to the thoracic viscera include wounds of the pleura, the lung, the diaphragm, the various large and small vessels, the pericardium, the heart, the thoracic duct, and the nerves.
—Injuries to the pleura, including rupture, are produced by severe blows which do not inflict fractures, although these are rare in the absence of such injuries. They are usually not accompanied by external markings, but are indicated rather by dyspnea and cough, with involuntary limitation of respiratory motions and by the physical signs of escape of blood (hemothorax) or air (pneumothorax), or by some crepitation at the site of fracture, which may be recognized with the stethoscope. In many instances lacerations of the pleura are accompanied by more or less injury to the lung, perhaps with perforation of air cells or small bronchi and the inevitable pneumohemothorax. With a wound situated near the twelfth rib the lung, which extends normally only to the tenth, may escape injury. A small wound of the pleura is of little consequence. By itself it is of serious import only as it is accompanied by more serious disturbances of the lung which it envelops, or the heart which it contains.
When air passes freely to and fro through the opening in the chest wall, without expectoration of froth or bloody mucus, it may be assumed that the lung itself has not been injured. To this condition the name traumapnea has been given.
Uncomplicated cases of pneumothorax usually take care of themselves, the air being gradually absorbed by the bloodvessels. In certain cases this air may be withdrawn by the aspirator. A small amount of blood within the pleural cavity is usually absorbed. An amount sufficient to embarrass respiration should be withdrawn either with the aspirator or by incision. For the latter purpose the wound may be utilized when properly situated.
—Wounds of the lung are made immediately dangerous by injury to its bloodvessels or are given a serious aspect by the possibilities of various forms of infection, including septic pneumonia. In serious cases this may proceed to abscess formation or gangrene. Should either of these be sufficiently localized no surgical procedure directed to evacuation or to excision or removal of the gangrenous tissue can[725] be more dangerous than the condition left to itself. The surgeon may, therefore, be impelled to perform a pneumotomy or a pneumectomy.
When the lung tends to protrude or prolapse through an external injury the condition is referred to as pneumocele, or sometimes as hernia or prolapse of the lung. This is rare, and occurs usually in connection with punctures or stab wounds placed anteriorly and generally low. The lung may be entangled, after having been forced out by violent coughing, and the external portion has been known to be strangulated in such a way as to slough off. Should this occur the mass may be permitted to slough, or it may be removed by cautery or by ligature, the wound being left to heal by granulation. In rare instances the pneumocele has been covered by the parietal pleura, as is abdominal hernia by parietal peritoneum.
Another form of pneumocele is the later consequence of injury, the soft, crackling, or crepitating tumor presenting beneath the skin and returning the usual breathing sounds when auscultated. It may increase and diminish in size with the respiratory movement. Such a hernia may occur beneath a scar or through ruptured intercostal muscles. It is of small surgical consequence, and, if troublesome, may be retained by a suitable pad.
The lung is occasionally ruptured by a violent concussion of the chest, as is also the heart. Its consequences will be emphysema, pneumohemothorax, with vomiting of blood, and later infection.
The later consequences of hemothorax, simple or uncomplicated, may be troublesome pleuritic adhesions, by which freedom of respiration is impaired, and, it may be, chest motions interfered with and chest development limited. The pleural surfaces are usually gradually drawn toward each other by the development of granulation tissue and its subsequent contraction and condensation.
—The diaphragm may also be lacerated by the compressing effects of violent blows, either upon the chest or abdomen. In consequence there may be passage of viscera (hernia) from either cavity into the other. Accurate recognition of these cases will scarcely be possible, but the development of distinct abdominal symptoms or noticeable displacement of the heart or of the abdominal viscera may lead to exploratory section, which shall reveal the location of the rent and possibly permit of appropriate repair or suture.
—The thoracic duct is occasionally injured by penetrating wounds, while, at the base of the neck, it has been known to be divided in the course of the removal of deep and adherent tumors. In the latter case the escape for a short time of the milk-like chyle, which it carries, will give evidence of the injury. Several cases on record show the comparatively innocent nature of the injury and its tendency toward spontaneous recovery without the necessity for further intervention. The very low pressure of the fluid in the duct is a contributing cause to this exemption from serious harm. Should the duct become obliterated near its upper end doubtless collateral circulation will enable the right and smaller duct to take up its work and continue it.
—In regard to injuries of the upper nerve trunks in the chest it is necessary to add but little to statements made regarding injuries to the same nerves in the neck. The writer has collected over fifty cases of destructive injury to the pneumogastric, in over one-half of which recovery followed. It has been shown that unilateral resection of the vagus is almost devoid of danger, though when it is required the nerve is rarely in a normal condition. Unless the nerve be attacked or involved below the branch which forms the recurrent laryngeal, laryngeal symptoms may be certainly expected. Irritation to the cervical sympathetic is usually followed by dilatation of the pupil, widening of the palpebral fissure, some degree of protrusion of the bulb, and paresis of that side of the face, while absolute sympathetic paralysis, such as follows division, will produce dilatation of the pupil, ptosis, and increased flushing of that side of the face. The sympathetic nerve may have to be extirpated in certain cases of excision of malignant tumors. Again, it has been deliberately resected, as recommended by Jonnesco and others, for the cure of epilepsy, of exophthalmic goitre, and of glaucoma. This will demonstrate the fact that injury to it is not necessarily of itself a severe accident.
In certain injuries to the chest branches of the brachial plexus will be divided or compromised, or displaced by fragments of bone or otherwise. When nerve pressure can[726] be recognized the compressing cause should be removed. If a nerve be divided every attempt should be made to suture it.
Partial or complete division of the large vascular trunks is usually too promptly fatal to justify much consideration here. On the other hand, injuries to the intercostal and internal mammary vessels are not uncommon and should not be fatal if only they can be properly recognized and treated. It is stated that even an intercostal artery may pour four pounds of blood into the pleural cavity in case of gunshot or stab wound. The presumption would be that one of these vessels, if injured, is wounded at the site of the evident puncture. While this is usually true it is possible that a bullet penetrating may have divided an intercostal on the opposite side. If a ligature is to be applied it should be done on each side of the wound, whereas a tampon used to check hemorrhage may be packed in such a direction as to completely meet the indication. While many methods have been suggested for arresting bleeding, the surgeon will enlarge the puncture, seek out the source of the hemorrhage, and then resort to ligature or to tamponing, as the case may indicate. When the tampon is used it is well to push ahead of it a piece of gauze like a glove finger and fill this with the tampon, in order to ensure complete removal of the whole mass at the proper time.
This is true also of injuries to the internal mammary. Dennis mentions five cases, quoted to him by Langenbeck, of perforation of the chest with a sword-blade, as the result of duels among university students of Göttingen, of which number two died. The latter also stated that up to 1876 there never had been a successful ligation of this artery. The vessel, leaving the subclavian between the two heads of the sternomastoid muscle, lies in its course just to the inner side of the sternum, with the vein on its inner aspect. Near the clavicle it lies on the pleural sac, where if injured the pleura will not escape. Lower down the pleura is not necessarily opened, although it rarely escapes. As Dennis shows, the inference from this is that tamponing the wound in the two upper intercostal spaces is impracticable, while below these it might succeed, as the triangularis sterni lies between the pleura and the artery. The mortality of the injury has been stated to have been nearly 70 per cent. Diagnosis is not difficult so long as the blood escapes externally. With a wound properly situated and rapid accumulation of blood within the chest, and increasing collapse, assumption of the injury or provisional diagnosis will scarcely prove fallacious.
The internal mammary when injured should be secured. The operator need never hesitate to resect a portion of the sternum, or the rib ends or cartilage, in order to expose it, since no danger can be so great as that of not finding it. Incision may be made along or between the ribs, parallel to them, or over the known course of the artery. After retracting the tissues down to the bone a sufficient amount of the bone should be removed to afford space for the examination. The pleura should be first separated, care being taken not to inflict upon it more than a minimum of injury. A T-shaped incision will afford more room when the case is complicated. The ends of the vessel having been found and secured, it becomes then a question of emptying the chest of the blood already accumulated. This is preferably done by incision placed laterally and sufficiently low, with the introduction of a drainage tube. Should the blood be already coagulated the incision should be made sufficiently wide to permit of breaking up the clot and completely removing it.
—In general, with regard to the treatment of all these injuries, it should be said that, in addition to whatever local measures may be indicated, general rest of the parts should be secured by as complete immobilization of one or both sides as can be effected. This should be made a part of the treatment of all fractures, simple or compound, as well as of all perforating injuries. Anodynes, hypnotics, and the like need to be used both to restrain motion and to allay cough, either of direct or reflex origin, by which harm is always done.
The complex structure of the thoracic walls is not exempt from the infections and other diseases which may involve skin, muscle, cartilage, and bone. Thus upon its surface all sorts of phlegmonous lesions may occur, assuming carbuncular or localized type, or occasionally ending in widespread gangrene, usually of that particular type[727] which is due to the morbid activity of the gas-forming bacilli, whose first expression is a gangrenous emphysema. These infections occur not only in consequence of some external irritation, but are seen after the infectious fevers, as well as in connection with syphilis, tuberculosis, scurvy, actinomycosis, and other forms of infection. Tuberculous disease beginning on the exterior of the chest wall may spread to the interior and even deeper, and, vice versa, tuberculous lesions beginning within the chest spread to the adjoining bone, producing caries, and then to the exterior surface, the resulting sinuses being irregular and sometimes opening at a point at considerable distance from the origin of the trouble.
All the infectious processes, whether slow or rapid, need radical attack, including free incision, curetting, removal of diseased bone, cauterization of the affected area, and suitable dressing and packing. Carious ribs or portions of the sternum may be removed without fear, it being necessary in certain advanced cases to remove nearly the entire sternum. Any concealed focus of disease is sure to spread and do more harm than will a well-directed attempt to eradicate it. Infection originating within the bone may spread in either direction, and may give rise to pleurisy, with adhesions, and possibly even subsequent abscess of the lung. The same is true of the diaphragm, while products of infection travelling in the proper direction may cause the beginning of an extensive subphrenic or hepatic abscess.
Fig. 505
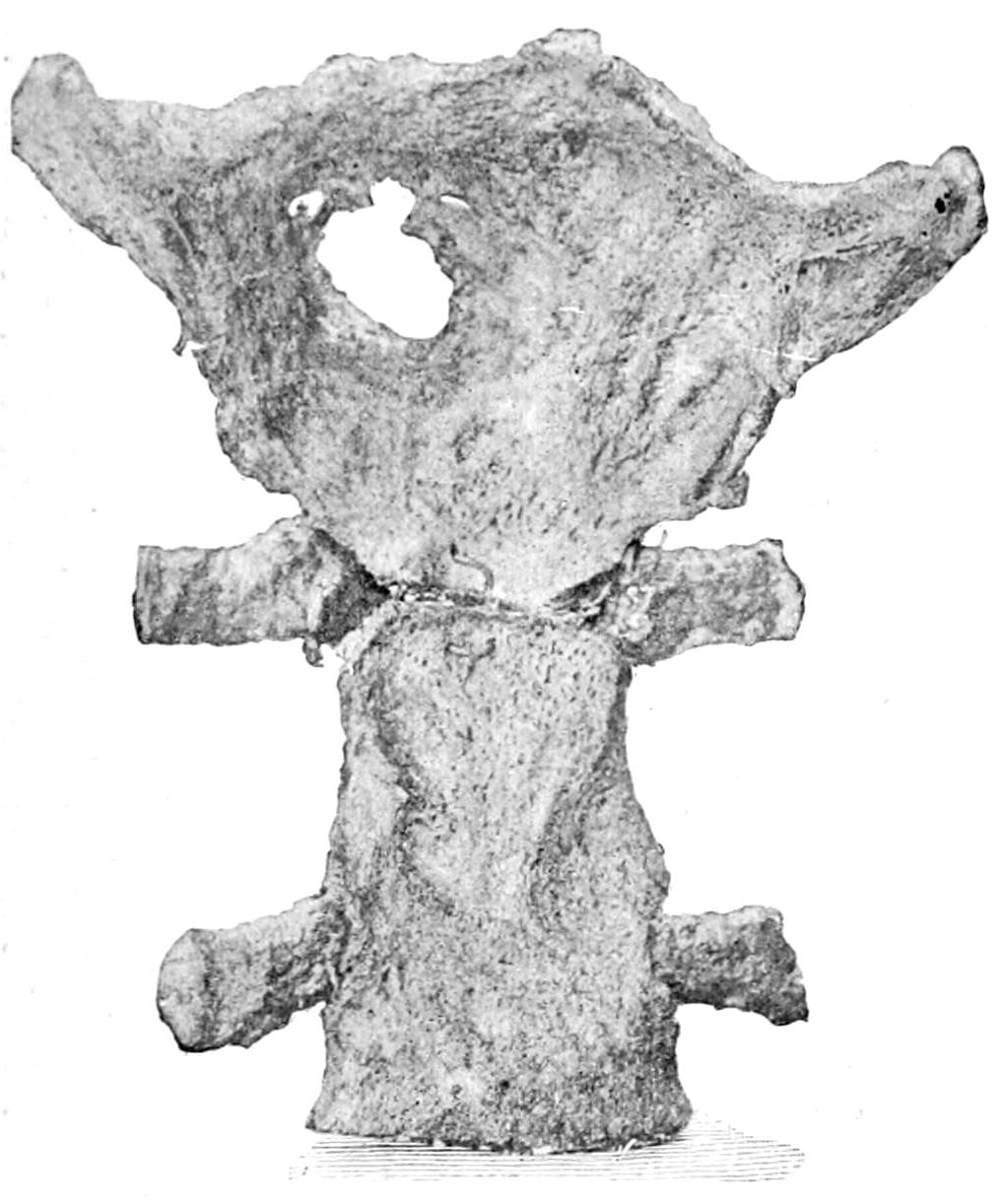
Erosion of sternum, the result of pressure of an aneurysm. Wood Museum. (Dennis.)
Fig. 506

Erosion of vertebræ, the result of pressure of an aneurysm. Wood Museum. (Dennis.)
The pressure of advancing tumors will sometimes cause surprising changes, not so much the result of ulceration as of mere absorption in the path of the advancing mass. Thus aneurysms will gradually erode the sternum or the ribs, and in time form bulging projections from within the chest, which may ultimately rupture and thus terminate the case. Even upon the vertebral column the effects of such pressure are pronounced. Figs. 505 and 506 illustrate what may happen under circumstances just detailed.
Remarkable expressions of subcutaneous emphysema may be seen in certain cases of fracture of ribs, with perforation of the lung, air escaping into the tissues and puffing up the whole upper part of the body and neck, giving it an appearance and shape very different from the original. For this condition there is no particular treatment, save immobilization, by which respiratory efforts shall be limited. Ordinarily the tissue distention quickly subsides. Should, however, putrefactive organisms enter with the air there may arise emphysema, terminating in gangrene, with fatal septicemia.
Painful affections of the thoracic walls are associated with lesions, either of the intercostal nerves or the ganglia or special nerves with which they are connected, which produce[728] intercostal neuralgia of various types, including that with its peculiar eruption known as herpes zoster, or as the laity call it, “shingles” (being a corruption of the Latin cingulum, meaning a girdle). Neuralgia may also be caused by inclusion of nerve branches in callus which is formed around a badly united fracture of the ribs. The diseases of the vertebræ which lead to softening and changes of shape will also permit of pressure upon nerve centres and trunks, which cause more or less pain, referred more often to the distribution of the nerves involved than to their origin. Thus the referred pains of spondylitis (Pott’s disease) are to be thus explained and are sometimes very pronounced. We give the term “neuralgia” to those painful affections for which there is no satisfactory explanation, and thus we are told that in intercostal neuralgia there are three points of tenderness, known as those of Valleix, whose determination confirms the diagnosis—the first being at the point of exit of the spinal nerve from the vertebral canal, the second in the axillary line, and the third close to the costosternal articulation. Abrams has shown that if a freezing spray be applied over the first spot the neuralgia will at once subside if it be of peripheral, but not if of central origin. Again, if one pole of the galvanic current be placed on the affected side and the other upon any one of the above spots the pain, if neuralgic, will disappear. If the current employed be the Faradic, and the pain subside, its cause is located in the muscles, as the induced current does not influence the pain of a genuine neuralgia. (Dennis.) So far as the treatment of these painful affections is concerned it is rarely surgical; although it was the relief afforded by the accidental stretching of an intercostal nerve which first suggested to Nussbaum the utility of nerve stretching as a more general procedure, and it was thus introduced to the profession. The treatment of herpes, i. e., of that form of neuralgic affection which is characterized by the appearance of papules which soon become vesicular, which collect in clusters and appear along the course of certain intercostal nerves, is rarely surgical. It is not difficult to distinguish this from ordinary eczema, which does not follow the nerve distribution and is not accompanied by the severe pain of herpes.
The principal interest attaching to diseases in either mediastinum pertains to the consequences of spreading infection, which will be practically always of the phlegmonous type, and which will produce clinical expressions varying much with its location and the direction of its course. These are included under the general head of acute or chronic mediastinitis, which might be the result of an extension from above, as from cervical abscesses, spondylitis of the cervical vertebræ, deep cervical phlegmons, and the like; or the result of perforation, or of foreign bodies impacted in the esophagus or elsewhere; or may again come from the osseous structures of the chest proper, spine, ribs, and sternum. Doubtless certain cases of subphrenic abscess are the result of suppuration begun in the mediastinum. Instances are also occasionally seen after typhoid and the other infectious and contagious fevers.
The indications of mediastinitis consist of intrathoracic soreness and pain, increased upon coughing and deep inspiration, difficulty of deglutition, disturbances of respiration and of heart action. Any irregularity of the pupils is evidence of irritation along the sympathetic nerves. Displacement of the heart means accumulation in its neighborhood and pressure disturbance. The lesion which will produce this will probably give dulness on percussion, and alterations of the ordinary chest sounds. With trouble high in the thorax the recurrent laryngeal may be involved, with the inevitable change in the voice. If the pneumogastric be compressed there will be rapid and irregular heart action. If the esophagus thus suffer dysphagia will result. Should the presence of pus be suspected a differential blood count may do much to clear up the diagnosis. Should pus come near the surface it will probably give the ordinary surface indications which one should be quick to appreciate and to relieve. Collections of pus within the chest tend always to migrate and pus may burrow to a considerable distance.
—The treatment of phlegmonous mediastinitis mainly depends upon recognition of the lesion and its degree of accessibility. Certain deep forms are hopeless, since they tend to kill before even pus can be located and evacuated. So soon as there be found any surface indication surgical attention should be promptly given. Any of these cases may be complicated by septic conditions within the lung or accumulations within the pleural cavity. The latter at least may be recognized and relieved. The proper use of the exploring needle may afford much information, and, in the presence of suitable indications, the sternum should be trephined and exploration made behind it. The main thing in all these cases is to distinguish between pressure effects produced by phlegmon and those due to aneurysm or tumor. Only rarely, and then only by surgeons of wide experience, should radical measures be attempted for the latter. Chronic processes, of tuberculous character and leading to formation of cold abscesses, will usually produce symptoms much less urgent, while the nature of the relief to be afforded will scarcely be left in doubt.
PLATE XLIX
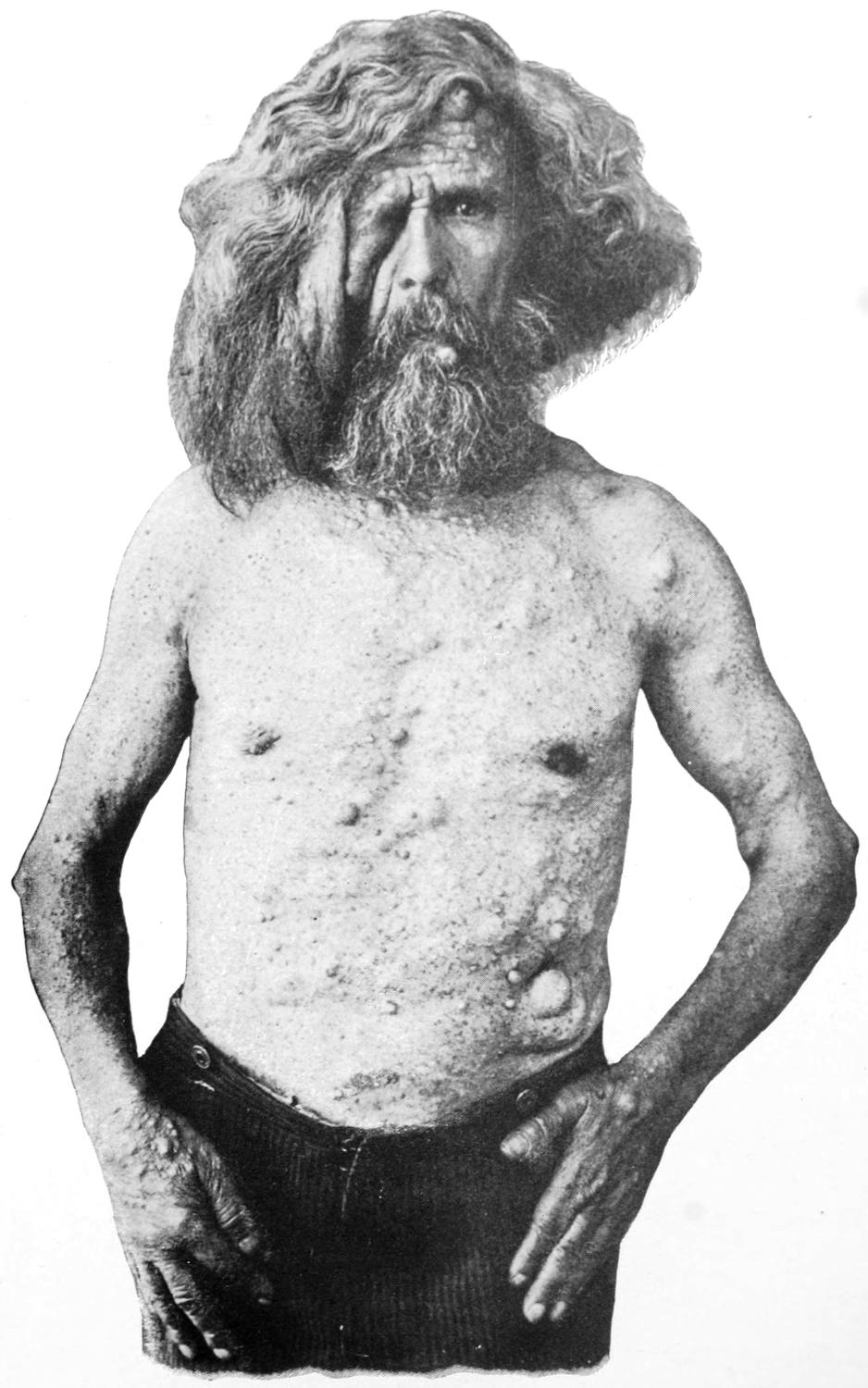
Neurofibroma of Skin.
[729]
Primary tumors of the chest wall constitute less than 1 per cent. of those occurring in general practice; this, of course, not having reference to secondary developments from cancer in the breast, which are somewhat frequent. Of the benign tumors those which most frequently appear upon the surface are the lipomas, which are seen either in circumscribed or diffuse form, as illustrated in Figs. 507 and 508.
Fig. 507
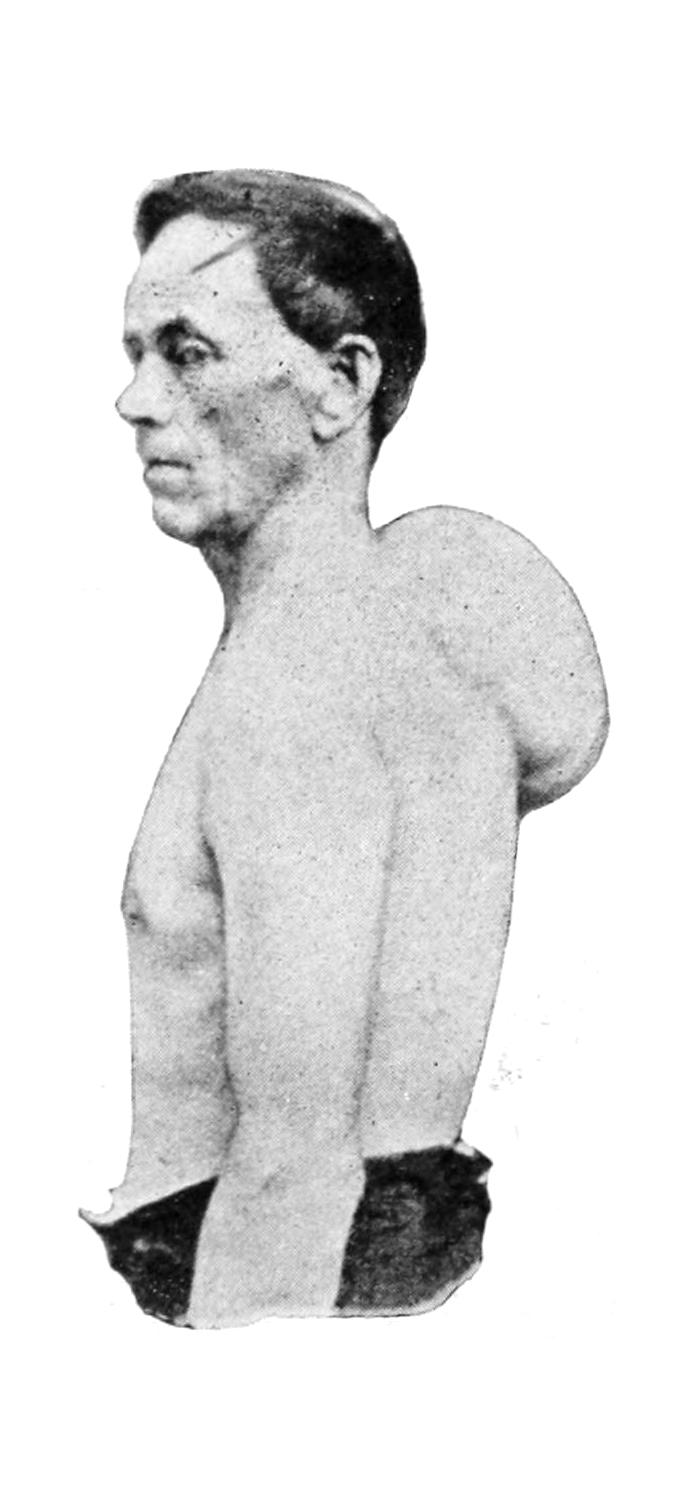
Circumscribed lipoma of back. (Dennis.)
Fig. 508
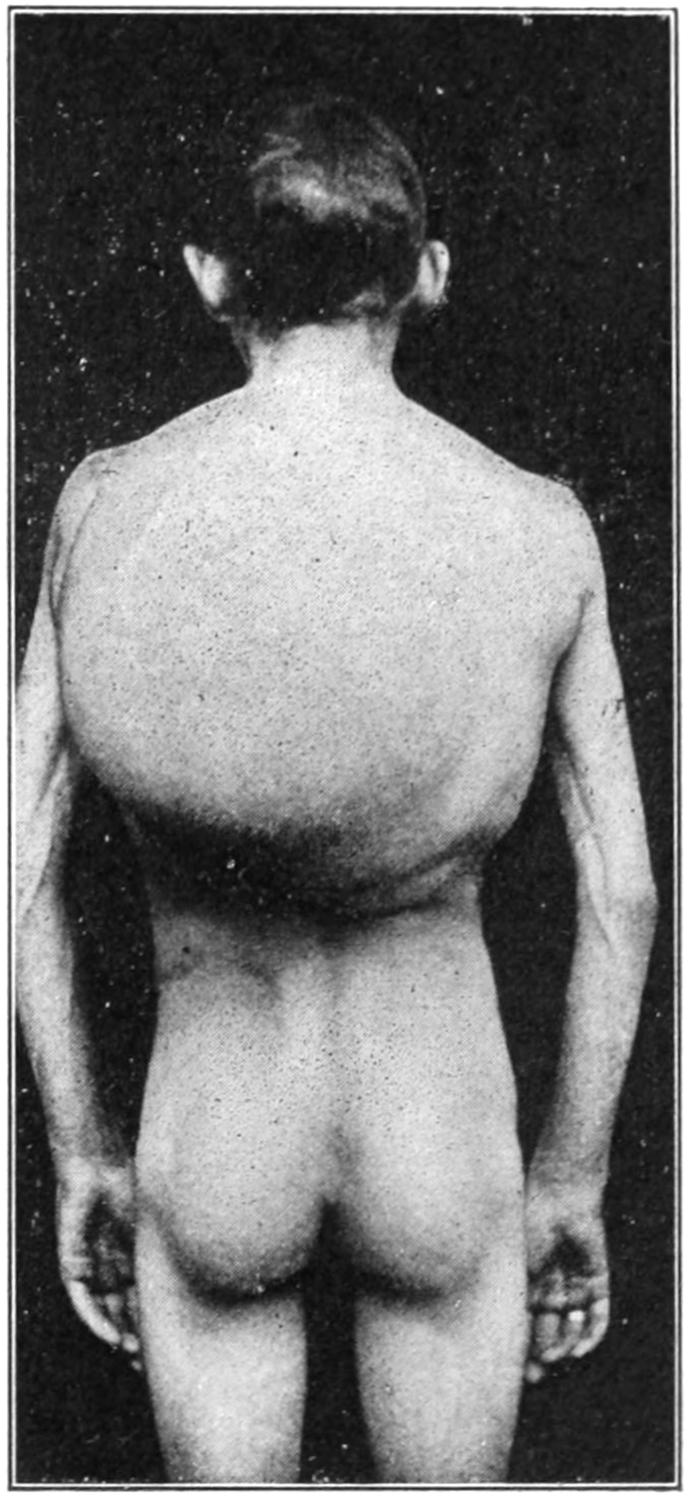
Congenital diffuse lipoma of back. (Mixter.)
They are sometimes multiple and perfectly innocent, save as they may attain large size or ulcerate from surface irritation. The granulomas, especially those of syphilis and tuberculosis, are common, appearing either as superficial tumors which ulcerate, or as deeper ones which may break down in the course of months or years, after perhaps involving the ribs or a considerable portion of the chest wall. Actinomycosis is perhaps as often seen in this region of the body as anywhere.
The fibromas are seen more commonly in the axilla and beneath the thoracic musculature. The chest is a frequent site for those pedunculated fibromas which have been described under the term keloid. A most striking case of neurofibroma of the skin is portrayed in Plate XLIX.
[730]
Chondromas of the chest are slow-growing, usually painless, may involve a considerable area, both of bone and cartilage, are not infrequently the seat of cystic changes, and often undergo a final sarcomatous degeneration. All this is true in lesser degree of the osteomas, which are of the cancellous type.
The malignant tumors of the thorax proper are mostly sarcomas which assume various types, according to their cellular characters, the round-cell sarcomas growing rapidly, becoming extremely hemorrhagic and fungous, and tending to kill early, while the larger and more spindle-cell and the giant-cell forms grow relatively more slowly, and may even be successfully removed (Figs. 509 and 510.)
Fig. 509
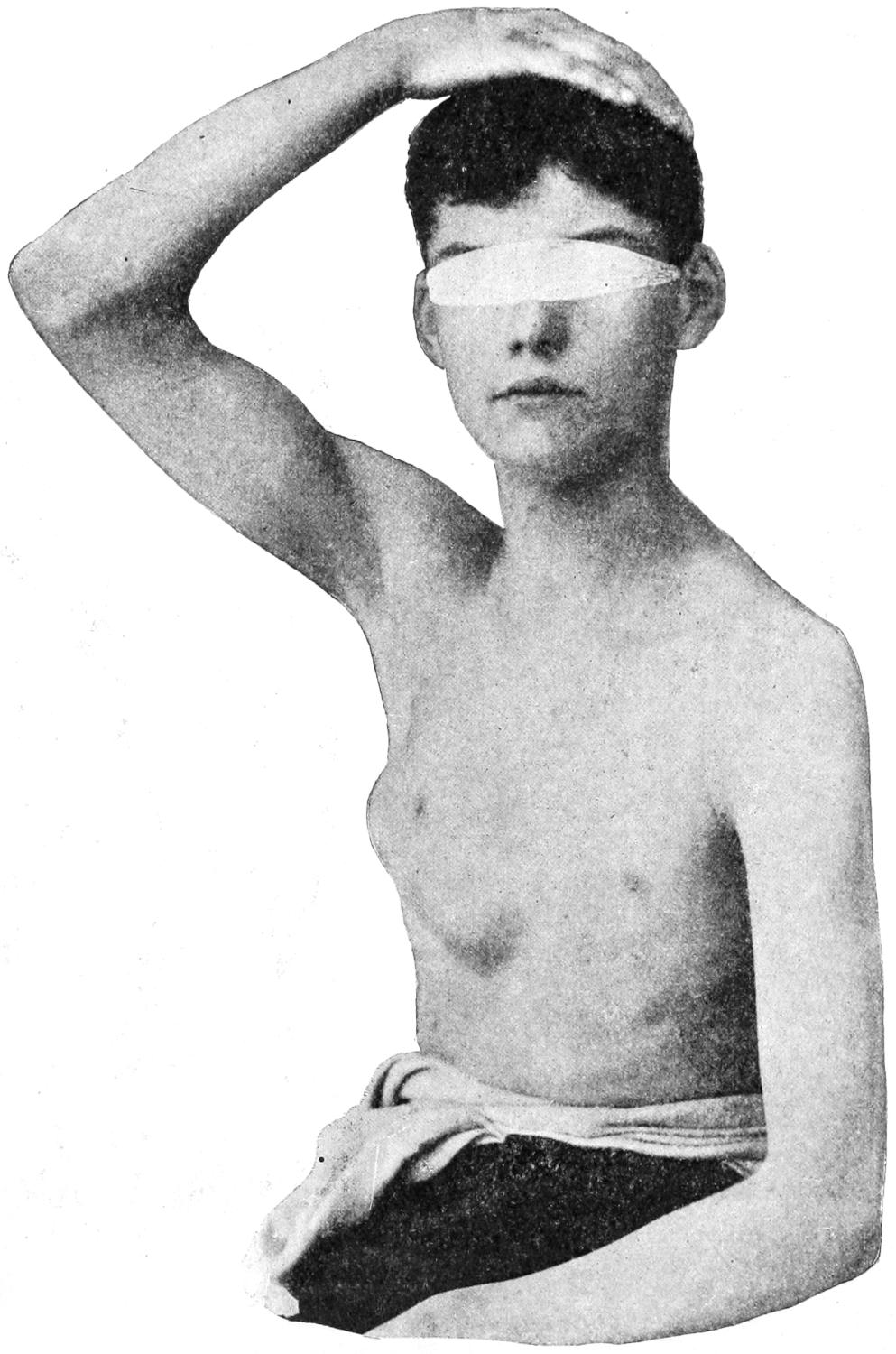
Sarcoma of rib and pleura, result of injury by a base-ball. (Dennis.)
Carcinoma of the chest wall is generally the result of extension from cancer of the breast or of some other epithelial structure. Advancing carcinoma spares nothing, and may not only perforate the chest but involve the lung beneath, with or without later ulceration, and the occurrence of pneumothorax.
Fig. 510

Skiagram of a large sarcoma of the thorax and humerus, whose bloodvessels were injected previous to taking the x-ray picture. (Lexer.)
While these are the more common forms of tumor of this region there are no known growths which may not occasionally be met here.
—The treatment for all these tumors is extirpation. With benign growths outside of the ribs proper this is usually a simple matter. When the whole[731] or nearly the whole thickness of the chest wall is involved it becomes then a serious problem how far to proceed in the effort to extirpate. This is true alike whether sternum or ribs are involved. The entire sternum may be separated from its surroundings and lifted out of place, and this would be justifiable when dealing with an osseous or cartilaginous growth. If, however, it were distinctly sarcomatous it would be hardly worth while. If in such an operation the pleura be spared and air not admitted to the pleural cavity almost anything is allowable. If, however, it appear that it will be necessary to open the pleural cavity caution should be observed. Of late years, however, less hesitation has been felt in this regard, and Parham and others, including myself, have shown that extensive portions of the thoracic wall may be resected without the necessity for employment of the elaborate operative methods suggested by some recent experimenters. For instance, Sauerbruch has devised a “pneumatic cabinet,” the patient’s head resting outside when the anesthetizer administers the anesthetic. The balance of the body rests within the cabinet, which is sufficiently large to accommodate the operator and two or three assistants, and which, being closed, is subjected to a lowering of atmospheric pressure equivalent to 10 Mm. of mercurial column, or to a difference in atmospheric level of 1000 to 1200 feet. The patient breathing air at external pressure does not suffer the collapse of the lung, thus exposed, which would otherwise take place. The operation being completed within the cabinet, the dressings are applied and hermetically sealed, and the door then opened and pressure equalized. Subsequent dressings can be made in the same way. Thus has been afforded a scientific method of doing that which the experience of many American surgeons has shown to be only theoretically indicated. Sauerbruch’s device is ingenious in theory and complicated in operation.
A simpler method is to apply the Fell-O’Dwyer apparatus over the face and thus keep up artificial respiration. It is not, in theory, so ideal as to open the trachea and practise this procedure as is done in the experimental laboratory, but is much simpler and will usually suffice, should anything of the kind be required.
A malignant tumor of the chest wall whose overlying skin is seriously involved, and whose removal would leave a defect which it would not be possible to cover with integument, should not be disturbed. It might be possible in certain cases to partially transplant the breast in such a manner as to permit closure of a defect thus made. Nevertheless it is questionable if any cancer advanced to the extent of requiring this procedure is to be considered operable.
Nor should any malignant tumor of the chest wall be operated if, in addition to its own presence, there be indication of the involvement of the lymphatics or other structures within the chest, such indications including, for instance, cough, loss of voice, dyspnea, dysphagia, disturbance of pneumogastric control of the heart, displacement of the latter, or great accumulation of fluid in any of the chest cavities. The only exception to this statement is possibly when the lung has attached itself to its interior surface, but yet not so extensively but that removal of a small amount of lung tissue will not interfere with extirpation of the growth. Cases of recurring carcinoma where the chest wall is completely involved rarely justify operation.
[732]
Tumors of the lung proper might be made amenable to surgery, in certain instances, if an exact diagnosis could be made. Occasionally this is possible, though but very rarely. Particles of lung tumor have been expectorated and their minute character recognized, so that actual diagnosis has been made. As in the abdomen, cancer of the thoracic viscera will usually lead to an accumulation of serous fluid, and, in both instances, thus obscure rather than simplify recognition. Quincke has shown that the presence in such pleuritic effusions of fat cells (hydrops adiposus) is significant, since they rarely if ever occur in any other exudates.
Primary tumors of the lung are usually sarcomas or endotheliomas. Carcinoma is exceedingly rare, save as secondary to cancer in the breast. Even sarcoma is itself usually secondary to disease in some other part of the body, metastasis having occurred through the blood channels, instead of through the lymphatics, as is the case with carcinoma. Tumors arising in the pleura may be of endotheliomatous type and are usually accompanied by the presence of bloody serum. Extremely rare tumors within the chest are those of dermoid origin, connected more often with the pleura than with the lung proper. These may suppurate and communicate either externally or internally. One known case mentioned by Dennis was that in which such a tumor communicated with a bronchus, so that the patient coughed up hair. Syphilitic gummas are also found in the lung, either in multiple small form or in masses of considerable size. They are slow in development and may give rise to no special disturbance. Dennis has described instances in which these growths have become encapsulated.
Two other forms of tumor are not very rare in this situation: one is that produced by actinomycosis; the other occurs in echinococcus disease and in the formation of hydatid cysts. The former, developing within the lung proper, tends to migrate toward its surface, to include the pleura, and finally to invade the chest wall. Such a tumor when exposed in either location can scarcely be differentiated from a breaking-down sarcoma, except by the recognition in it of the small, calcareous particles which are so pathognomonic of this disease. (See Actinomycosis.) In the living patient the sputum will frequently contain these particles, while under the microscope the peculiar club-end, thread-like fungus formation may be recognized. The disease is usually of slow development, but occasionally, especially when mixed with a secondary infection, may be rapid. Significant tumors may also occur in other parts of the body. Actinomycotic tumors upon the surface may be attacked with curette and cautery. Injections of iodine are also of value. For actinomycosis of the lung proper potassium iodide and Lugol’s solution are indicated as well as copper sulphate.
Hydatid cysts occur within the lungs in about 10 per cent. of cases of echinococcus disease. Their contained fluid is alkaline, of low specific gravity, colorless, and contains the characteristic hooklets which are pathognomonic of this disease. A circumscribed collection of fluid within the chest, shown to be due to this condition, may be tapped or incised and drained. When occurring in the lung it not infrequently leads to secondary pyothorax, while operation for the latter may reveal the existence of the former. Any hydatid cyst of the lung which can be recognized, or be made accessible, may be treated by incision and drainage, the lung, if not already adherent, being first fastened to the chest. Inasmuch as the condition develops in the lower lobe and on the right side this is occasionally a practicable procedure. As the diagnosis is usually made only after the primary cyst has ruptured and small cysts are cast off, producing more or less pleuritic effusion, the attempt may still be made to do this by a free incision of the chest wall, perfecting the diagnosis and completing the procedure at this time.
There is but little to be said about the heart in addition to that elsewhere stated, where such injuries as gunshot wounds, stab wounds, etc., are considered. Rupture of the heart without external injury is possible under conditions of fatty degeneration or softening produced in consequence of embolus or thrombus. Aneurysms of the heart are also known by which it is weakened and permitted later to give way. The final[733] rupture is usually the consequence of some emotion or extra exertion, although it may occur with injury to some other part of the body, as after a blow upon the abdomen. Death may be instantaneous, or occur more slowly as the result of filling of the pericardial sac and rapidly increasing embarrassment of heart action.
Wounds of the heart produce syncope and shock, restlessness, extreme anxiety, with dyspnea and such disturbance of heart activity as to materially change the sounds heard on auscultation.
The treatment of such cases not primarily fatal should include opium narcosis, but not stimulants intended to excite the heart to extra activity. The operations justified under these conditions are elsewhere described.[50]
[50] Borchardt has collected 83 cases of operations upon the heart, of which 78 included heart suture. Of these 78, 46 died and 32 recovered. He quotes a statement of Billroth, made when this surgeon was sixty years of age: “Paracentesis of the pericardium is an operation which, according to my view, closely approaches to what might be considered a prostitution of surgical art, or, as some surgeons would call it, a surgical frivolity, an operation which altogether has more interest for the anatomist than for the physician. Possibly a later generation will regard it differently. Internal medicine is constantly becoming more surgical, and those physicians who concern themselves especially with internal medicine will find themselves compelled to make the most daring operation.” The rapid advances made in surgery during the past three decades cannot be better illustrated than by contrasting Billroth’s statement of a few years ago with the standard practice of today.
Pericarditis, either of idiopathic or traumatic origin, may produce a degree of distention, either hydropericardium or pyopericardium, calling for surgical intervention—in the former case with the aspirating needle, in the latter either with the needle or the knife. When a pericardium is greatly distended with fluid there is marked change in the position of the apex beat, with embarrassment of heart action, accompanied by distress and distention of the veins of the upper part of the body, as well as much alteration of the ordinary physical signs, the area of dulness being correspondingly enlarged and the lung sounds being lost over the area occupied by the distended sac. Great distention, with marked precordial trouble and distress of heart and lung function, always requires paracentesis.
Paracentesis pericardii is performed ordinarily by puncturing (a previously sterilized area) 3 to 5 Cm. to the left of the left border of the sternum, and in the fifth intercostal space, with a sterilized needle. Here are found the internal mammary artery and the pleura. Too rapid withdrawal of fluid may lead to syncope. It should, therefore, be allowed to escape slowly. Should it prove purulent it may be incised, passing the knife-blade along the needle; or the sac may be emptied, when, if fluid re-collect, a free incision should then be made. Roberts has shown that recovery follows in at least 40 per cent. of cases of empyema of the pericardium thus treated. Gauze drainage may be provided, but irrigation of the cavity should not be practised.
Allingham has suggested to open the pericardium from below by an incision three inches in length, carried along the lower margin of the seventh left costal cartilage, to separate the cartilage from the abdominal muscles, pull outward and upward the lower surface of the diaphragm, expose the cellular interval between its attachment to the cartilages and to the tip of the sternum, to expose and enlarge by blunt dissection, until there appears a mass of fat which belongs above the diaphragm in the interval between the pericardium behind, the sternum in front, and the diaphragm below. When this is removed the pericardium is exposed and can here be opened. Throughout the procedure injury to the pericardium which lines the upper surface of the diaphragm should be avoided. By this method the pleura need not be opened and better drainage may be secured. (Dennis.)
Abscess in the heart wall is an exceedingly rare lesion, usually accompanying pyopericardium, but occasionally met without it. It was the writer’s experience in one case, in puncturing for what was supposed to be a pyopericardium, to withdraw pus and give temporary relief. Later postmortem examination showed that this pus came from a large abscess in the wall of the heart, which had been thus entered by the aspirating needle without immediate bad consequences, but, on the contrary, with temporary relief.
In the fact that the lung never completely fills the pleural cavity we find explanation for the kindred fact that small effusions produce little if any compression symptoms.[734] Collapse of one lung after opening the chest is never complete if the other lung be uninjured and functionating. Moreover, a partial collapse on the affected side will be quickly atoned for when the pressure of the external atmosphere is taken off.
Two or three serious pathological conditions of the lung occasionally require surgical intervention.
Hydatids of the lung have been mentioned (see above). Seventy-five per cent. of these cases terminate fatally without surgical help, and in reality more prospective benefit can be offered by it than without it. Serious and even fatal collapse has attended the sudden withdrawal of fluid from hydatid cysts in this location. Aspiration may be made, but even this is scarcely less dangerous while it is less satisfactory than free exposure and drainage.
Actinomycosis of the lung may be recognized by the sputum and also by the pus discharged from any breaking-down cavity within the affected area. (See section on the Pleura.) If a localized focus could be diagnosticated or recognized after exposure the portion of the lung thus involved might be removed.
Abscess of the lung is always the result of some local or distant infectious process. The mechanism of production of the multiple metastatic abscesses which characterize pyemia has been described in the earlier portion of this work. For such conditions surgery affords no aid. Circumscribed abscess may be the result of the presence of a foreign body—i. e., a bullet or a parasite—or it may result from embolism with infarct, in consequence of such affections as ulcerative endocarditis, puerperal septicemia, sloughing fibroid, an otitis media, or a septic pneumonia produced from any cause. It may be the result of extension from an osteomyelitis of some portion of the bony wall of the thorax, which itself may result either from injury or from local infection. Abscess of the lung is seen not infrequently in connection with empyema, and often results from suppurating tuberculous bronchial nodes. It may be produced, also, by extension of trouble from below the diaphragm, as hepatic abscess, subphrenic abscess, and the like. It is always a secondary rather than a primary affection.
Such abscesses are to be recognized by the character and offensiveness of the sputum, the pus discharged being colored green or brown, containing shreds of tissue, with masses of bacteria and crystals of fat. Some believe the presence of elastic fibers to be pathognomonic. When pulmonary abscess is diagnosticated it is necessary, in addition, to determine whether multiple lesions or a circumscribed collection are to be dealt with. In the former instance it is of little avail to intervene. In the latter the physical signs will usually furnish evidence of adhesions between the lung and the chest wall, by whose presence the operative procedure is simplified.
The term pneumotomy is applied to the exposure and evacuation of pus in the lung, whether it be found in connection with an ordinary abscess or a suppurating hydatid cyst. It is essentially a thoracotomy, plus the added measure of whatever may be done to the lung itself, and will be described in connection with other operations upon the chest.
If a tuberculous abscess could be located it also might be treated upon the same general principles. Thus Lane and others have suggested early operations for relief of tuberculous lesions. For obvious reasons, however, the method has not found general acceptance.
Gangrene of the lung is the terminal stage of a local infection, and unless relieved may prove fatal to the patient. It is due to the causes above mentioned as producing[735] abscess in the lung, while to them may perhaps be added a few others, especially expressions of embolism or thrombus of the pulmonary circulation by which, the blood supply being cut off, death of tissue occurs before there is time for phlegmonous development. Thus it is met with occasionally after the acute exanthems and the infectious fevers and after violent pertussis. When diffuse it is of the miliary type. When circumscribed it may be due to more localized causes. In any event it is more frequent in the lower portions of the lung.
Pulmonary gangrene may be recognized by the extreme condition of the patient, offensive odor of the breath, and expectoration of sputum which may at first be frothy and bloody, but becomes rapidly purulent and finally necrotic in type. Meantime, the function of the lung being materially interfered with, respiration is rapid and there will be more or less cough, pain, and finally collapse. When the sputum is allowed to stand in a test tube there will form an upper layer, opaque and frothy; a middle, more frothy layer; while the lower and denser portion will be of a dirty green color and contain shreds of dead tissue with bacteria, crystals of triple phosphates, fat debris, and pus. According to the nature of the case the cavity or the area of dead lung may be outlined by physical signs. There is a form of fetid bronchitis which has been mistaken for pulmonary gangrene, but the character of the sputum and the progress of the case will be quite different.
Gangrenous areas of limited size have in certain favorable cases cleared up and the patients have recovered, but ordinarily for this condition surgery affords the only prospect of relief, the operation being begun with a thoracotomy and completed by the removal of the gangrenous lung tissue. The operative procedure is essentially the same as that for abscess and above described.
Septic pneumonia is the term applied to those forms of pneumonitis which occur in connection with septic lesions in other parts of the body, or with the less typical forms—e. g., aspiration pneumonia, due to the passage into the finer bronchioles of material from the mouth or nose. It gives rise to the same physical signs, though it is perhaps more often irregularly located than is the consolidation of the ordinary lobar pneumonia. Viewed in this way it will be regarded as a serious complication of various other conditions, many of which are surgical, and it is frequently a primary expression of infection. The physical signs by which it may be recognized are scarcely different from those of ordinary pneumonia, except that, in addition to the latter, there may be distinct expressions of general septic infection and of profound toxemia, and that the disease may progress to the point of producing pulmonary abscess or gangrene. While the milder types of septic pneumonia are not necessarily fatal, it is always a serious complication, and, as such, dreaded by the surgeon. It is not, however, essentially a surgical complication, but calls for the treatment generally given to pneumonia, plus whatever may be needed for the primary condition behind it.
This implies a collection in one of the pleural cavities, usually the left, of fluid which is practically unchanged chyle, which has probably escaped from the thoracic duct. The number of cases on record is not over fifty, of which about one-third have followed unrecognized injury with probable rupture of the duct. Most of these cases have occurred in connection with fracture of the spine. The duct may be opened by the progress of ulcerative disease, and carcinoma is often the predecessor of chylothorax. Rupture may also occur in connection with tuberculous lymphatics about the course of the duct, and when the condition occurs in children this is the usual explanation. It should be differentiated from so-called chyloid effusions into the pleural cavity, which are more often seen in connection with cancer than tuberculosis, the fluid in this case being mixed with fat and degenerated leukocytes or cells. Pure chyle contains sugar, while chyloid fluid contains but a trace of it. The former also is thicker, and compares with the latter as does cream with skimmed milk.
The prognosis is not usually favorable. Nevertheless recovery has ensued without operation. Mere pressure of the effusion may occlude the opening through which it occurs until the latter shall heal. When the fluid gives rise to severe symptoms the chest should be aspirated.
[736]
Under these terms are included the presence of fluid in the pleural cavity, between the lung and the chest wall; this fluid, in the first instance, being serum, which may be slightly admixed with pus and blood; in the second, blood; and in the third, pus.
Hydrothorax may be a primary condition, the result of pleurisy with effusion, or of pleuropneumonia. It may also occur as does a similar collection in the abdomen, as the result of disease of the chest wall, the lung itself, or in consequence of serious cardiac or renal disease, with tendency to dropsical accumulations in various parts of the body. Thus it is seen in connection with tuberculous disease or cancer of the lung, as well as cancer of the chest wall. There is, moreover, a miliary expression of tuberculous pleuritis in which hydrothorax is always a complication.
The serious features of hydrothorax result from the compression which it may make upon a lung with consequent embarrassment of lung function and from the possibility of infection by pyogenic organisms and the consequent conversion of a hydrothorax into a pyothorax.
Collections of serum within the pleural cavity which manifest a kindly tendency to disappear by resorption do not require surgical intervention, but all such accumulations which do not quickly evince this tendency should be removed by the operation of paracentesis, which, applied to the thorax, is called thoracentesis, i. e., aspiration through the hollow needle. No lung should be allowed to have its capacity long reduced by compression.
Hemothorax may be idiopathic or traumatic. In the former case it is an expression of malignant disease, or of advanced septic lesions which have permitted erosion of bloodvessels and escape of blood. It may also result from rupture of an aneurysm, and will then prove fatal. It is seen in surgical cases in connection with injuries to the chest wall or its contents, as in compound fracture of a rib or perforation of a rib fragment into the chest, with injury to the lung.
In case of the sudden escape of fluid into the chest, with symptoms of collapse and lung compression, it may be assumed that an acute hemothorax affords the explanation. Fluid accumulating rapidly under any circumstance is more likely to be blood than serum. The exploring needle may be relied on to furnish the deciding test, in addition to the ordinary physical signs afforded by auscultation and percussion.
Pyothorax is frequently referred to as empyema, the latter term indicating a collection of pus in a previously existing cavity, and, by common consent, made to refer to the pleural cavity unless some other be mentioned. Empyema is seldom a primary condition. Generally it is the result of a hydrothorax, which has become contaminated either by direct or by indirect access of germs. Under these circumstances it indicates the conversion of a relatively innocent collection of serum into a collection of pus, with all its attendant dangers. It may be looked for in cases of perforating injury of the chest, e. g., compound fracture of the ribs, gunshot wounds, and the like.
While returning the ordinary physical signs met with in fluid collections in this location, and being discoverable with the exploring needle, empyema has this additional feature, that the pus may, when long retained or accumulated in large amount, burrow and attempt to escape through whatever path may offer least resistance. In this way strange freaks will occur, as when it escapes behind a mammary gland and pushes the latter forward, thus forming a large retromammary abscess, which requires not merely the ordinary incision, but a thoracotomy and ample drainage as well. It may penetrate at other points and thus escape. The most remarkable illustration that the writer personally has known of this travelling of pus was in a colored man, in whom it perforated the diaphragm, then separated the peritoneum from the abdominal wall over a large area, collected in large amounts between the peritoneum and the abdomen in front, and even extended down into the pelvis. This man had such a peculiar abdomen that he was supposed to have dropsy. When the trocar was inserted there was a discharge of over a pailful of almost pure pus.
In addition to the ordinary embarrassment which a considerable amount of pus thus collected causes, there should be reckoned the peculiar septic and toxic features, which can be easily accounted for by the nature of the contained fluid. Pyothorax will nearly[737] always have septicemic in addition to local features, which give it an individuality of its own.
The operations practised for relief of these conditions are discussed at the conclusion of this chapter.
Anatomically, the esophagus is a musculomembranous tube with downward projection into the thorax, its uppermost portion blending with the lower constrictor of the pharynx, the tube proper beginning at the level of the cricoid cartilage, and opposite the sixth cervical vertebra. Its conclusion opposite the tenth dorsal vertebra marks the cardiac orifice of the stomach. In its upper portion it is placed centrally, then inclines a little to the left, and, at the level of the third dorsal, lies about half an inch to the left of the middle line. This furnishes the reason for approaching it upon the left side in doing external esophagotomy. From here it passes to the middle line again until opposite the ninth vertebra, where it once more inclines a little to the left. It has an anteroposterior curve corresponding to the shape of the spine. Between it and the trachea, in the neck, lies the recurrent laryngeal nerve. Its nervous supply is derived from the sympathetic and the pneumogastric, and its lymphatics connect with the mediastinal nodes, the latter point being of importance in connection with cancer of the esophagus. Its average caliber is about three-quarters of an inch, save where it is crossed by the left bronchus and at the diaphragmatic opening. There is also a slight constriction at its upper opening.
Congenital malformations include its absence, at least throughout some of its course. Communication between it and the treachea, so-called tracheo-esophageal fistula, has been noted. Its upper portions, into which may open the incompletely closed branchial clefts, are also subject to malformations with incomplete obliteration of the latter and consequent diverticula. Irregular dilatation is also occasionally of congenital origin, as well as acquired, in the latter case being due to fatty degeneration of muscle fibers. These dilatations should be differentiated from those which are mostly found on the proximal side of any constricted tubular passage, and which are produced by accumulation and distention from behind of whatever should be passed through it.
The most common malformations of the esophagus which are not of the stenotic character are so-called diverticula, which appear in two forms—namely, distention and traction, these being both acquired forms, while congenital formations of this character are also occasionally met.
Congenital diverticula may appear anywhere along the course of the tube, but are probably more common in its upper portion. They constitute more or less irregular tubular sacs which lie alongside of and parallel to the main tube. The openings by which they connect may be large or small. These saccular defects, always small at first, may assume increasing proportions, because of the entrance therein of food and their consequent distention by foreign material, as well as by products of decomposition of the same. Thus slowly and insensibly a very mild form of such defect may in time assume serious proportions.
The acquired diverticula of the distention type are usually met with in the upper part, and are practically hernial protrusions of at least the mucosa through the fibers constituting the muscular portion of the tube, and cannot occur save by some preceding pathological change. Traction diverticula are the results of adhesions to breaking down lymph nodes or other pathological conditions, by which the esophageal wall is first pulled out of position, then gradually sacculated, and the condition still further aggravated by accumulation therein of foreign material. The acquired diverticula attain considerable size, and when emptied one may be astonished at the accumulation which has occurred. Such a tube having been completely emptied may be again filled by the first food which is subsequently taken. After being filled, the balance of the food may then pass into the stomach, with partial or complete comfort or satisfaction to the patient.
The principal indication of an esophageal diverticulum, beside dysphagia, is regurgitation[738] or vomiting of food. When food which has undergone decomposition is occasionally rejected, and when, at the same time, the stomach is shown to be not dilated and not at fault, the suspicion of a diverticulum may be considered well founded. Its opening into the esophagus may be so placed as to always engage the instrument which may be passed down for examination, either bougie or stomach tube. Should this be a constant phenomenon the diagnosis may be easily established. In such a case it may be possible to first empty and then distend the sac with food mixed with bismuth subnitrate, or perhaps to inject it with an emulsion of the same. If this can be done, the fluoroscope or a good radiograph will show a distinct shadow, and in this way a pictorial outline of the condition may be obtained.
—The treatment of these diverticula is of great difficulty, especially when the sac has attained a size which permits of retention of material. Sacs which contain decomposing matter should be emptied by the stomach tube and washed out at frequent intervals. If it be then possible to pass the tube beyond them the patient should be fed through it, or it may be possible to place the patient in the recumbent position, with the head lower than the body, and cause food or fluid to be swallowed in this attitude. It will then probably enter the stomach instead of the sac. Such measures as these failing, and nothing else affording relief, operations are occasionally undertaken. Much will depend upon the location of the sac, especially its height. A diverticulum in the neck may be more easily reached than one in the chest, and Richardson and myself have had remarkable success in the relief of aggravated cases of this kind. Cushing has shown the advantage of the administration of atropine before these operations, in order to limit the flow of saliva and keep the parts dry. The sac having been exposed by a long incision in front of the sternomastoid, it may be filled with a solution containing methyl blue, by which it may be identified, or it may be filled with paraffin, which, solidifying, will serve admirably for its identification. It then may be attacked as would be any solid tumor. The sac having been identified and extirpated its opening into the esophagus is then closed by sutures and the neck wound cared for as usual, with provision for drainage (Figs. 511 and 512).
Fig. 511
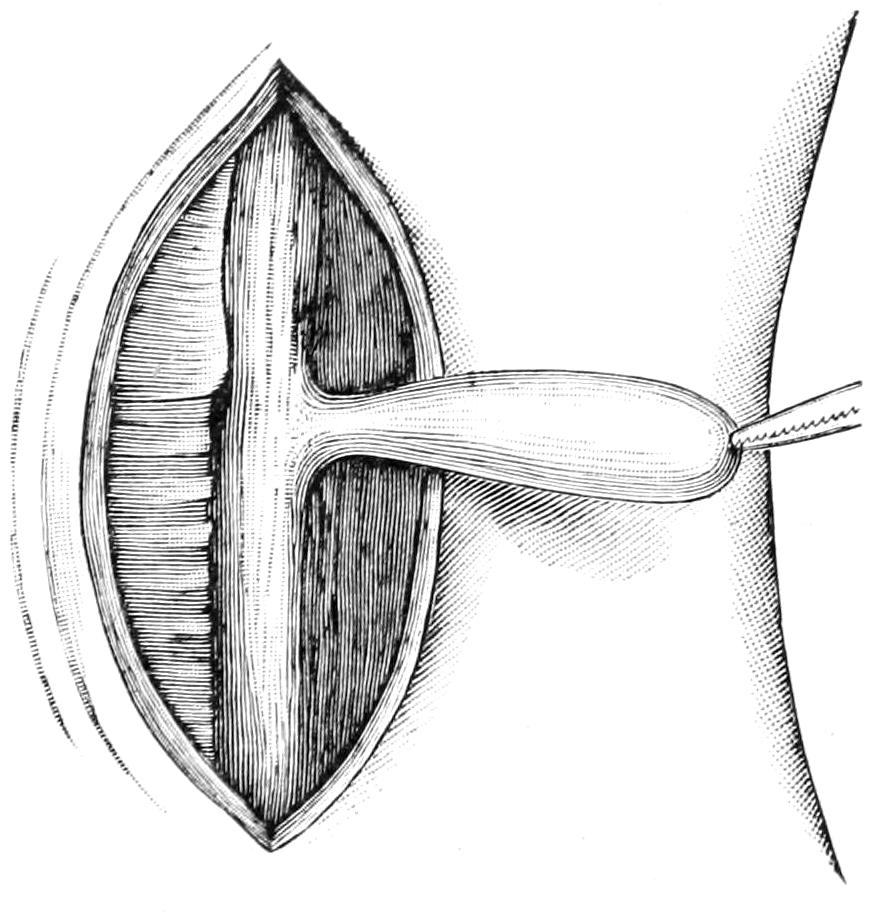
Diverticulum freed from its attachments and delivered from the wound. (Richardson.)
Fig. 512
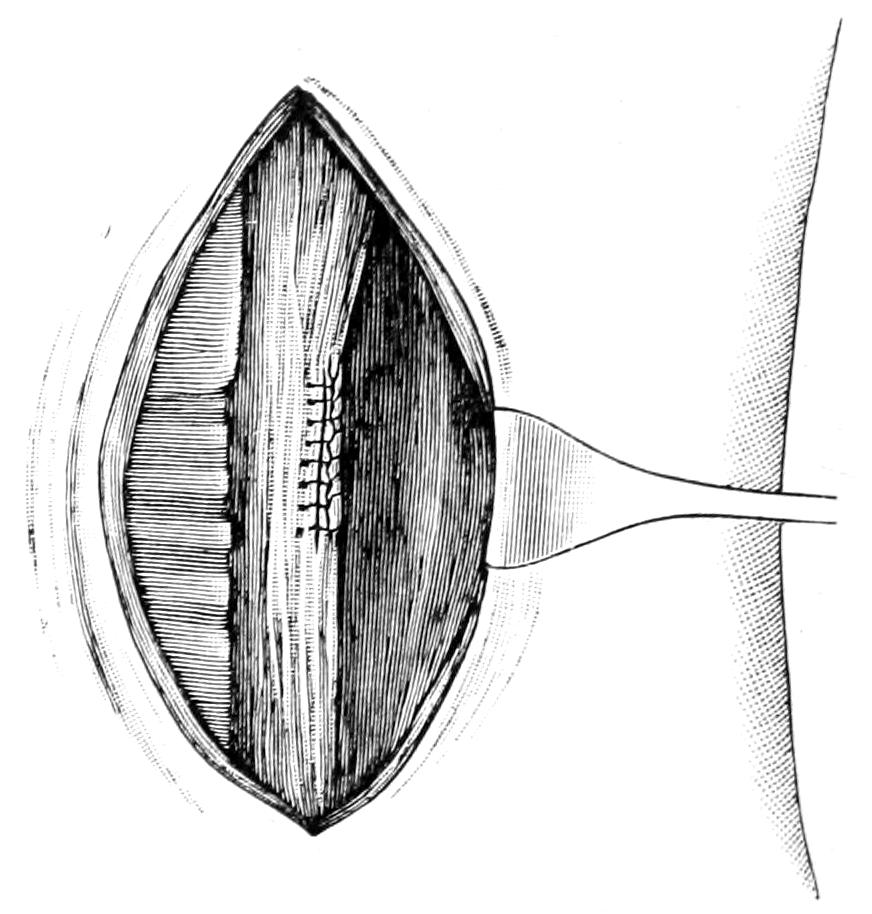
Shows the external layers of the esophagus closed by interrupted Lembert suture of silk. (Richardson.)
Traction diverticula may be amenable to surgical intervention. Should the esophagus be diverted by adhesion to an advancing aneurysm nothing should be attempted. Among the operations which may be practised upon the thorax there may be mentioned a method of posterior exposure and attack upon some of these conditions which may or may not afford advantages, according to the nature and location of the various conditions.
Cardiospasm (see chapter on the Stomach) produces a sacculation of the gullet often mistaken for diverticulum, and requiring to be differentiated from it.
[739]
Foreign bodies may be lodged in any portion of the esophageal tube and cause a variety of troubles, according to their size, shape, location, and nature. There is scarcely any conceivable object which may be introduced into the mouth which has not been known to be impacted in the esophagus and produce more or less serious symptoms. Young children, imbeciles, and the insane may suffer unwittingly in this way, while the condition is usually accidental and unintentional.
The accompanying figures (Figs. 513 and 514), portraying in one case a jackstone lodged in the esophagus, a coin in the other, a case of my own, will furnish illustrations of what has just been said. (See also page 674.) The young and the insane may make no statement which will furnish a clue for the distress caused in attempts to swallow or the actual impossibilities of the act. In most instances, however, a history of impaction and a statement as to the nature of the foreign body may be obtained. The symptoms produced are those of partial or complete inability to swallow, of more or less pain accompanying the act, and of the regurgitation often of blood or of bloody mucus. The object may be sufficiently large to produce dyspnea and suffocative symptoms, e. g., a plate with false teeth.
Fig. 513

Jackstone lodged in esophagus. (Phelps.)
Fig. 514
Coin lodged in esophagus, successfully removed by external esophagotomy. From the Author’s Clinic. (Skiagram by Dr. Plummer.)
The condition being suspected or made known, the location of the foreign body may be determined by the esophageal bougie and by the use of the x-rays. With certain[740] irregularly shaped objects the latter prove a desirable help, especially when irregular plates containing false teeth, or toys have been passed into the esophagus. They afford an indication not only as to their exact situation and emplacement, but also as to the best method of attack, that is, whether from without or within. Considerable distress may be produced by even small particles, as chips from an oyster-shell, small pieces of glass, and the like.
Fig. 515
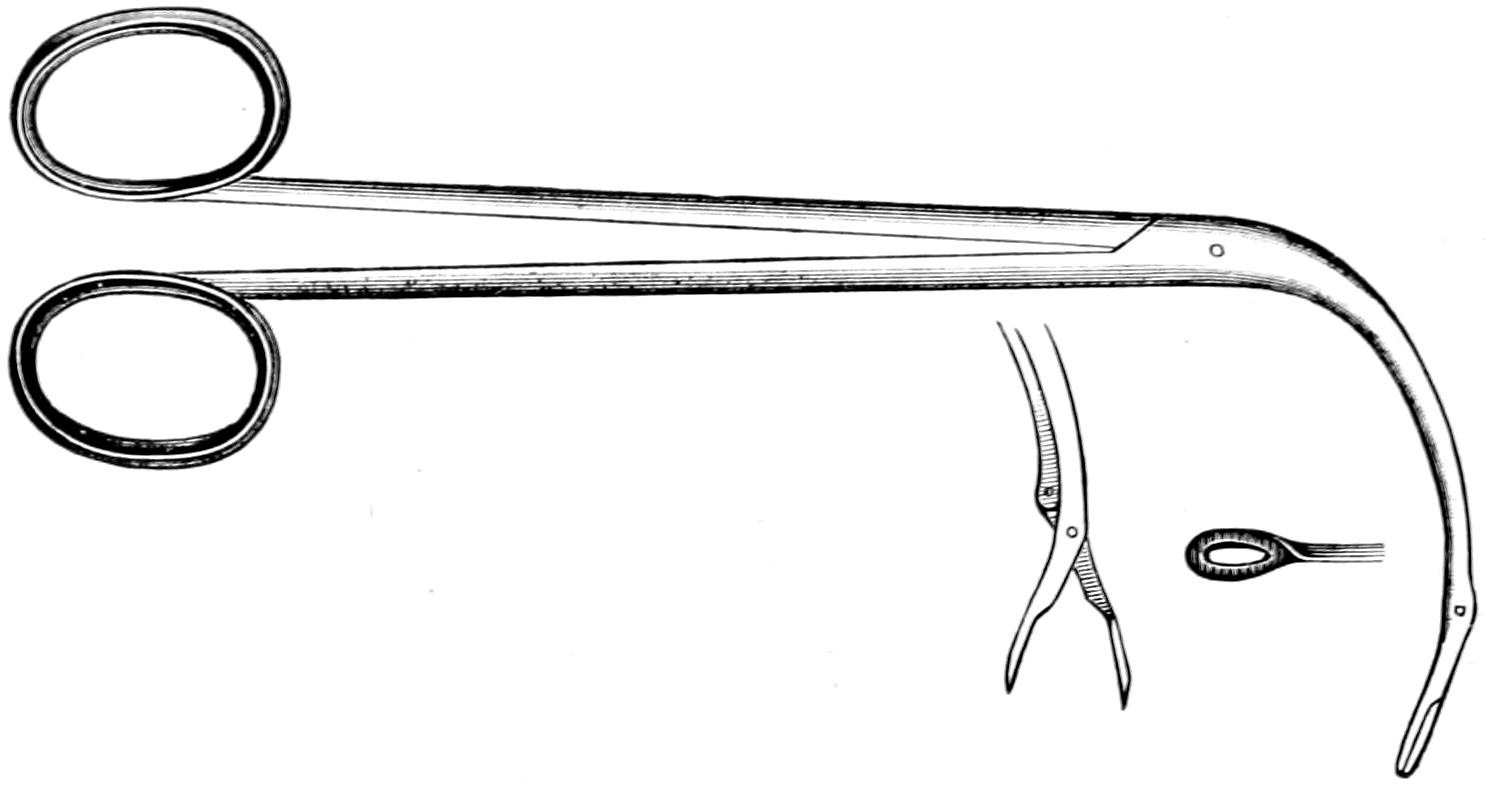
Esophageal forceps.
Fig. 516
Horse hair probang, expanded and unexpanded.
—A foreign body which produces the slightest discomfort or recognizable symptoms should be removed. Only occasionally can this be done by making the patient endeavor to swallow something else, this being too uncertain a method of procedure; although I have known a peach-stone impacted in the esophagus to be pushed into the stomach by the passage of an esophageal bougie. The situation and the nature of the object being known, one then decides how best to proceed. The available methods of operation are:
The esophagoscope is an instrument of comparatively recent device and perfection. We owe it largely to the ingenuity of Mikulicz. It is to the esophagus what the endoscope is to the urethra, and may be regarded as essentially an enlarged endoscope. Its introduction is comparatively easy, but its retention is distressing to the patient, so that opportunity may thus not be afforded for profiting by its use. The employment of cocaine anesthesia, and perhaps of morphine hypodermically, will sometimes enable it to be used satisfactorily. It may also be used for exploratory purposes previous to commencing a formal operation under general anesthesia. There are furnished with the instrument itself forceps and extractors, by which it may be possible, when the object is once seen, to grasp and withdraw it. The use of the esophagoscope is, moreover, not limited to these lesions, since it can be used in revealing the character of strictures, small wounds, diverticular openings, and the like. Endeavors may be first made to locate the body by those possessing such an instrument and expert in its use.
The esophageal snare is a simple instrument which, after being introduced, is shortened in such a way as to cause to protrude a basket-like meshwork of bristles in which, as the instrument is withdrawn, a small object may be entangled and so withdrawn. In the same way an ingeniously made coin catcher is furnished, which, in cases of impacted coins or similar shaped objects in the esophagus, may be introduced beyond them and[741] then withdrawn, the object being caught in a miniature cradle, from which it cannot escape until brought up into the pharynx. Esophageal forceps are made with long blades, curved like all the instruments used within the pharynx, and serving admirably for grasping objects impacted high in the tube (Figs. 515 and 516).
Dislodgement being impossible by either of the above-mentioned expedients, recourse may be had to the operation of external esophagotomy. This may require to be done as an emergency measure, but is practically always indicated when an impacted object cannot be otherwise removed. A dangerous location for a foreign body in the esophagus is at a distance of about nine inches from the upper incisor tooth, at which point it will be located directly behind the arch of the aorta, at which level ulceration would perhaps result disastrously, as Richardson has shown. The operation was devised by Goursault, in 1773, and has proved a satisfactory surgical measure. It is performed upon the left side of the neck. The incision is made along the anterior margin of the sternocleidomastoid from the middle of the neck downward. The larynx and trachea are separated to the inner side, the muscles and the large vessels to the outer side, the omohyoid divided, the descendens noni and the recurrent laryngeal nerves, which lie in the groove between the trachea and the gullet, are protected from injury, and the esophageal tube thus exposed. The surgeon will feel more secure in opening it if he now pass downward through the mouth a bougie or instrument upon whose beak or tip he may cut down. The esophagus being opened, the margins of the wound are secured by sutures which serve as retractors, and the interior of the tube is then subjected to the necessary manipulation. Even now it may not be an easy matter to dislodge a pointed object, which may have become partially impacted. Thus it may be dislodged at first by pushing it down a short distance and turning it, the direction having been already indicated by an x-ray picture. The manipulation should be as gentle as possible. Extraction having been accomplished, the esophageal wound is closed by the sutures introduced for traction purposes. Over this the external wound is closed, with suitable provision for drainage, as it is almost certain to have been infected during the procedure. In rare cases it has been necessary to combine a gastrotomy with this operation, in order that by combined manipulation a peculiarly shaped object may be dislodged.
Gastrotomy will be necessary in but few instances, as, for instance, when an object known to be one which cannot pass through the pylorus has been dislodged into the stomach by pressure from above—as plates containing false teeth, and various similar objects. It will probably be safer to open the stomach and remove the object than to leave a patient to his otherwise uncertain fate. On the other hand objects which are sure to be in time dissolved or disintegrated by the stomach juices may be allowed to remain to await this event.
Wounds of the esophagus occurring in other ways than those above indicated may be the result of gunshot and various perforating injuries. The tube may be also partially cut across in so-called cut-throat.
Any external wound of the esophagus which can be recognized should be closed with sutures, and the parts brought together, if possible, with provision for drainage. Those lacerated wounds constituting some forms of cut-throat, however, permit of very little in this direction, for when seen they are too infected. Through an esophageal opening thus inflicted the patient may be fed for a time by a tube, the wound being left to close later by granulation or by a secondary operation. When the esophagus has been anywise injured it would be better to abstain from feeding or else to introduce food through an esophageal tube.
Rupture of the esophagus has been known to occur in consequence of severe vomiting, there being some twenty-five cases of this character now on record. (Dennis.) A tear is rarely complete, but it may be followed by hernia and formation of a diverticulum. The accident will be indicated by violent pain following severe vomiting in connection[742] with an effort to dislodge a foreign body. There will be more or less shock and perhaps collapse, with escape of blood. Emphysema of the neck and upper part of the chest may result and the injury prove fatal. The condition being suspected, it would be advisable to do an external esophagotomy or else to carefully introduce a stomach tube and leave it in situ.
Perforation—i. e., rupture without traumatism—may result from the existence of ulcers or from the advance of malignant disease. It may occur in either direction. Thus while the mediastinum may be infected from entrance of septic material into it the direction may be reversed and an abscess or other lesion of the surrounding tissues may evacuate itself into the esophagus. Should this prove to be an aneurysm the patient will die with uncontrollable escape of blood. The treatment of such a case, if any be permitted, will depend entirely on the nature of the exciting cause. Perforation has also followed injudicious use of bougies when exploring or treating strictures (especially cancerous) of the esophagus.
Esophagismus, or spasmodic contraction of the esophagus, is usually an expression of hysteria, or else is a reflex spasmodic effect due to the presence of some neighboring irritation. In the esophagus, as in the urethra, there may be spasmodic stricture, which will afford considerable obstruction. Thus I have seen it as a functional neurosis, absolutely without explanation, in an apparently healthy workingman. It is noticed also in connection with hemorrhoids and with hepatic lesions. It is seen in pregnancy, and a certain degree of it will complicate many cases of gastric ulcer, gastritis, or esophagitis such as is produced by swallowing mild caustics. While producing dysphagia and obstructive phenomena it is intermittent and interposes little real obstacle to the passage of a full-sized bougie or tube. It is frequently accompanied in the hysterical by globus hystericus, and by regurgitation of whatever food the patient attempts to swallow.
The local treatment consists of dilatation by the passage of full-sized instruments at frequent intervals. If a neurosis the patient may require other treatment, addressed either to the nervous system or to any well-marked constitutional condition.
Stricture of the esophagus has an etiology practically identical with that which pertains to stricture of any other passage of the body. It may be due to extrinsic or intrinsic influence. Among the former may be mentioned the presence of tumors, either benign or malignant, or of cicatricial tissue, while among the latter should be mentioned the injuries resulting from the presence of foreign bodies, the extensive ulcerations due to the swallowing of various caustic fluids, and the cicatricial contraction which may follow other lesions like ulceration. Those cases which are due to serious congenital defects will usually die early. Of the ulcerative lesions which lead to stricture the most common are the cancerous. Syphilitic and tuberculous ulcerations may occasionally produce the same effect. By far the most common causes are the traumatic, which are connected either with foreign bodies or with the unfortunate accidental use of caustics.
Esophageal strictures are recognized by the difficulty in swallowing which they produce and the later dilatation of the esophagus above, which is the frequent result of their long existence. The degree of difficulty experienced by the patient in deglutition is to a considerable degree a measure of the extent of contraction. It may be nearly always assumed that such a stricture as is produced by the swallowing of caustic fluids will leave a tortuously contracted passage-way, and the instrument passed for its recognition, while arrested in its upper portion, may give little or no correct idea as to the arrangement below. In some instances it may be possible here, as in the case of diverticula, to introduce sufficient bismuth emulsion into the esophagus to make it cause a[743] shadow in an x-ray picture, and in this way to give pictorial information not otherwise attainable.
The surgeon should distinguish between hysterical spasm or esophagismus and cicatricial stenosis. The former will offer but little obstacle to the passage of a full-sized bougie. In fact it will be frequently benefited, usually cured by it, while in the latter instance this is almost impossible.
Fig. 517
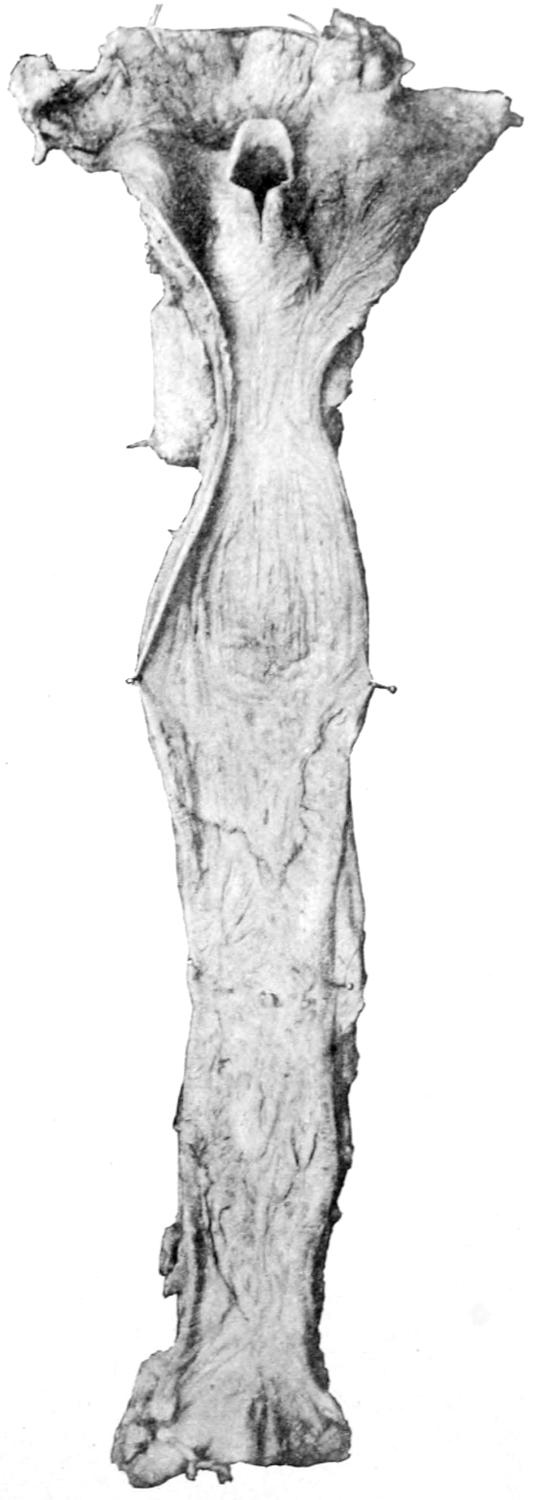
Stricture of the esophagus. (Dennis.)
Fig. 518
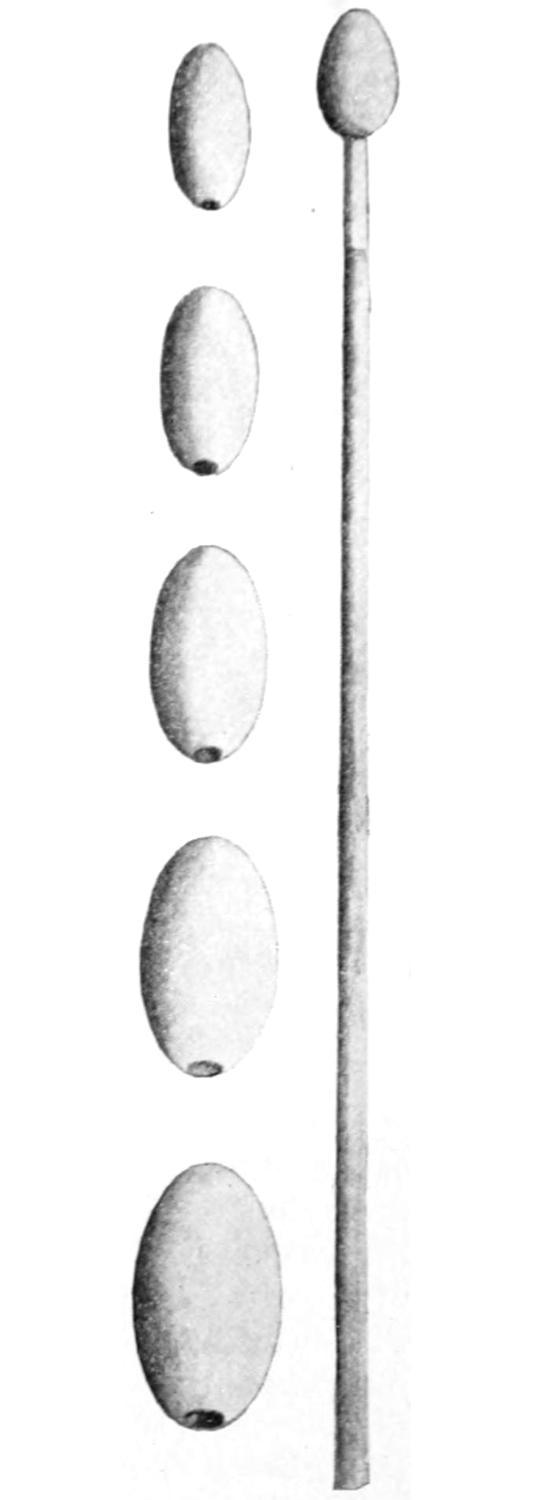
Esophageal bougies.
Fig. 517 shows the possibilities in a case of actual obstruction, and how different such a condition is from mere esophagismus or globus hystericus. It has been recently shown, especially by Dennis, that during or just after typhoid fever, ulcers occur in the esophagus which may produce serious stenosis. At present writing I have under observation a little girl of nine years who has an extreme condition of this kind. It is with difficulty that she can swallow fluid nourishment, and she was so nearly starved that her life was only saved by a gastrotomy. Those congenital defects which may produce esophageal stricture are usually of such a serious and extensive character as to afford no opportunity for relief.
The location and caliber of these strictures may be ascertained by the use of esophageal bougies, such as represented in Fig. 518. These are made of various sizes, and are fastened upon the end of a flexible rubber handle, which affords a degree of elasticity in manipulation. They should be used with care and caution, as minor degrees of injury produced by them may cause a spreading infection, while still more harm may be done by rupture of an ulcerated area, or perhaps the perforation of an aneurysm.
The patient should sit before the surgeon, with the head thrown backward, the mouth comfortably widely opened, while the surgeon, standing, introduces the left forefinger into the pharynx and with it depresses the tongue and guides the tip of the instrument, be it bougie or tube, along this finger, which serves as a guide. Unruly or hysterical patients will not only gag, but may attempt to bite the operator’s finger. To prevent such accidents a metal thimble is made, which, being inserted between the teeth, protects the finger, but makes the manipulation more awkward. Should the patient show any tendency to folly of this kind, it should be remembered that when the finger is forced back into the pharynx the mouth is instinctively opened. If necessary, at the same time, the nostrils may be grasped and held closed, in which case the patient is sure to open the mouth widely and thus release the finger. After the tip of the instrument[744] is engaged in the pharynx it sometimes assists in the manipulation if the patient’s head be now tipped a little forward. This manipulation is not very different from that by which a small and long flexible rubber tube may be inserted through the nostril into the stomach for the purpose of feeding, as is frequently done with the insane who refuse to eat, or may be done in the presence of certain diseased conditions.
The intent in this exploration is to determine the distance from the upper incisor teeth of the obstruction, as well as its caliber. When the instrument is withdrawn the surgeon marks the location of the teeth by grasping it at this point with the thumb, and the distance is measured off afterward so that it may be read in inches if desired. The caliber is determined by the success or non-success met with in passing an instrument of given diameter. The size with which the attempt should be made may be determined largely by the history and statement of the patient. With a patient who cannot swallow no ordinary bougie should be expected to pass, while a small solid instrument might produce a perforation. Flexible bougies are also provided by the instrument makers, made as are the silk catheters, some of them being loaded with small shot in order to give them a certain degree of weight. A small, soft, flexible instrument may be thus passed when the ordinary probang would fail. Here, as in the urethra, an olivary bougie may pass, after which the same sort of resistance will be offered upon its withdrawal. In this case the stricture is passed twice, going and coming. A slight degree of constriction is met opposite the cricoid cartilage at the entrance to the esophagus. This should not be mistaken for a pathological condition. Information may be afforded by material brought up by the instrument, such as shreds of tissue, blood, etc. A small bougie coated with sponge may be used for the purpose of retaining and bringing back such material as it may engage.
It will be of assistance to let the patients dissolve in the mouth a tablet containing a little cocaine and swallow it, or to spray or gargle the pharynx with a weak solution. It prevents the gagging and discomfort of an operation which otherwise is almost painless.
Esophageal hemorrhage occurs especially in connection with cirrhosis of the liver. Stockton and others have called attention to a peculiar varicose condition of the esophageal veins in certain of these cases, and the possibility of repeated hemorrhages which may terminate fatally. The same is true of obstructive jaundice with Riedel liver.
Cancer of the esophagus may be either primary or secondary, and may be either sarcoma or carcinoma. Its first expression will be ulcerative or stenotic, according as it originates on the inner surface or not. Sooner or later it will produce stricture, with the ordinary evidences thereof, and is to be detected in the same way. Cancer is usually of the carcinomatous type or squamous epithelioma. The disease is more common near the lower than the upper end of the canal. The disease spreads and involves the adjoining lymphatics, as well as various other structures. In addition to the ordinary evidences of stricture it is accompanied by a certain degree of pain, which is likely to be referred to the interscapular region or the back of the neck. The emaciation which always accompanies it is not merely an expression of the disease itself, but of the starvation which stricture in time produces. Frequent expulsion of bloody mucus or shreds is extremely indicative.
Esophageal cancer admits only of esophagectomy, as a very unusual method of relief, or gastrostomy, which is a palliative measure intended to prevent death from starvation, but not affording exemption from the advance of the disease.
[745]
Operations upon the esophageal canal include:
1. Dilatation is practised ordinarily with olivary or conical-tipped bougies. The former are usually metal or ivory tips fastened to a firmer handle, while the latter are fashioned like silk catheters having more or less conical tips. These are introduced until they are engaged within the stricture, after which the amount of pressure or force used should be graduated to the character of the trouble, the density of the tissues, and the tolerance of the patient. Daily dilatation may be practised either for the prevention or relief of strictures following cicatrices due to caustic fluids and the like. A small passage may in time be stretched up to nearly the normal diameter, after which instruments may be passed at regular intervals, as the tendency to recontraction is inevitable. These methods of dilatation have taken the place of more complicated mechanical procedures performed with instruments like those intended for use in the urethra. The writer has, however, in one or two instances used with advantage the Otis dilating urethrotome in cicatricial strictures of the gullet.
2. Internal esophagotomy is practised either with instruments carrying concealed blades, like those used within the urethra, or by a method suggested by Abbe, where the stomach is first opened, and a retrograde divulsion effected, or at least a small bougie is pushed upward from beneath. When its tip is felt in the mouth there is firmly attached to it a strong silk thread which, as the instrument is withdrawn, is brought down into the stomach and then out through the stomach opening. With one hand in the stomach and the other in the mouth this thread is then manipulated in such a way as to saw through the strictured passage. It is well, should the surgeon use silk in this way as he would use a Gigli saw, to pass it through a piece of rubber tubing, both above and below, in order that its sawing effect may be limited to the esophagus proper. This is a procedure which should be done with great precaution. The operator should stop at short intervals, and, by using a bougie, satisfy himself whether the strictured passage has been enlarged. When the desired result has been attained the thread is withdrawn, the stomach and abdominal wounds closed, and dilatation resorted to every day or two in order that the benefit gained may be maintained.
The use of the esophagoscope may permit the exposure of a cicatricial band or an annular stricture, so placed that it may be divided by a fine knife directed through the tube. Whatever cutting is done in this region should be done cautiously, so as to avoid injuring adjoining structures.
3. External esophagotomy is easily performed for the removal of foreign bodies. When done from below it may be combined with a gastrotomy, the cardiac end of the esophagus being thus exposed and exploring instruments or those intended for either removal of foreign material or division of stricture being thus introduced. After the measure is complete the stomach is first closed and then the abdomen.
4. Esophagectomy is an operation undertaken from without, and is seldom performed for other purposes than for the removal of malignant growths. A cancer of the esophagus should be seen early and be favorably located in order to be amenable to such a radical measure, yet cases of this kind have been successful. Too often, however, they are done too late. The esophagus is exposed by the same incision as that described for esophagotomy, namely, on the left side along the anterior border of the sternomastoid, the vessels and nerves being retracted to either side in such a way as to permit its clear exposure. The portion to be removed is then isolated by blunt dissection and resected. This leaves two ends of the canal, which can usually be brought together by sutures, after the fashion of an end-to-end intestinal anastomosis. The principal difficulty met with will be adhesions and infiltration caused by extension of disease, and these of themselves in well-marked cases would be contra-indications to operation.
—Bryant and others have shown how the esophagus may be exposed from the posterior aspect of the thorax by a posterior thoracotomy, made in the third and fifth intercostal spaces, where, by resection of the[746] ribs and dissection, the esophagus may be exposed behind the hilum of the lung. The azygos vein which crosses it at about this level should be either retracted or divided after a double ligation. Experimentation has shown that it is possible at this point to stretch the tube in such a way as to permit of restoration of its caliber, if but a small amount have been removed, but great care should be exercised, otherwise tension would be extreme. Because of the doubt regarding the success of such a resection Mikulicz has suggested the following procedure of externalization of the esophagus: After exposure the distal end of the esophagus is closed and dropped back. An opening is next made along the anterior border of the sternomastoid, where the esophagus is exposed, pulled up and out of its situation—i. e., dislocated—and brought out through the upper opening, which can be done because of its loose connective-tissue surroundings. A third incision is then made over the second intercostal space in front, where a bridge of skin is lifted up, the esophagus drawn down beneath it and fastened, the intent being to connect this opening with the stomach through a gastric fistula by means of some special apparatus, thus making it possible to again feed the patient through the mouth. The incisions in the back are closed by layer sutures. The principal objection to this method is that the passage of fluid through the externalized portion of the esophagus would have to be accomplished by massaging the part and forcing it down through the tube. Sauerbruch and others have shown that in animals at least it is possible to make a transdiaphragmatic anastomosis of the stomach and esophagus. By much the same method as that last above described, i. e., through a posterior opening, the esophagus can be exposed near its lower end, resected, and then turned into an opening in the stomach, the latter having been brought up through an opening in the diaphragm. It is hardly necessary to go into details of this operation here, since the occasions which would justify it are almost as rare as the individuals who could be entrusted with its performance.
Exploratory puncture, either of the pericardial sac or of a pleural cavity, is an exceedingly simple matter, the ordinary hypodermic needle sufficing for many instances, while in some cases the contained fluid will be too thick to flow through a finer needle and will necessitate the use of a larger one. Such needles are furnished, with so-called exploring syringes, and their use is a convenient preliminary to the use of the aspirator—i. e., thoracentesis—or open division—i. e., thoracotomy. It is essential that both the patient’s integument, the instrument, and the operator’s hands be absolutely clean. When several points are explored at one time and fluid is found at but one it is well to indicate this with a little nitrate of silver or tincture of iodine, which will make a temporary mark. Thoracentesis implies a withdrawal of fluid through a hollow needle, which will make a small puncture that will promptly close, a vacuum apparatus of some kind being attached to it. The needle may be introduced at various points to enter either the pericardium or the pleura. Ordinarily no harm pertains to exploratory puncture and but little to withdrawal of fluid, providing certain precautions are used, though fatal syncope has been known to immediately follow it. Beyond absolute sterilization the most important feature is to withdraw fluid slowly rather than rapidly, and to desist so soon as symptoms of a serious nature appear, such as faintness or collapse. When a collection of fluid has existed for some time in one of the pleural cavities it may have gradually so displaced the heart that its too sudden withdrawal may permit a too sudden restoration to its normal position—so sudden, in fact, as to place extra stress upon it and perhaps to seriously embarrass or completely check its action. This is always a matter requiring attention. The position of the patient also should be regarded, and a patient who is seated in a chair, in order that fluid may gravitate to the lower part of the chest cavity, should be promptly placed in the recumbent position so soon as alteration in pulse or coughing or serious embarrassment of respiration are noted.
The skin over the point selected for puncture may be anesthetized with the freezing spray or with a sterile cocaine solution. The needle point should be driven in sufficiently to secure fluid and not such a distance as to puncture the heart or the lung within. The better aspirating needles are provided with rounded points rather than with sharp ones, in order that scratching with a sharp end may be thus avoided. When using a more[747] blunt needle of this type it is well to make a trifling puncture in the skin with a small knife-blade. While the more elaborate instrument outfits sold by the dealers are pleasing to use, fluid may be siphoned through a needle and tube with a fountain syringe just as in lavage of the stomach. Consequently it is not necessary in emergency cases to have anything more than a satisfactory needle. Care should always be given that no air is introduced. Thus in managing the last-named expedient the tube and the needle itself should be filled with fluid before the latter is introduced. Then the bag may be lowered in order that no fluid escape into the chest. It is an advantage to have a piece of glass tubing connected with the apparatus, in order that the character of the fluid first withdrawn may be easily ascertained. If the patient begin to cough or to have a feeling of oppression the operator should temporarily cease, and if symptoms are not ameliorated he should withdraw the needle, renewing the procedure a day or two later. A lung too suddenly forced to expand by removal of fluid may not only give distress to the patient, but there is a possibility of hemorrhage.
—The term thoracotomy implies an incision made through the chest wall, usually for withdrawal of fluid, with or without removal of some portion of its bony structure. Thoracotomy performed for pericardial collections of fluid has been described. That for removal of ordinary empyemic collections is usually a simple measure. It may be practised under local anesthesia. In a general way the extent of the fluid collection is made out by percussion, and its character by exploratory puncture. The endeavor should be to make the opening laterally and posteriorly near the lower aspect of the cavity to be emptied in order that it may drain by ordinary force of gravity with the patient in the dorsal position. Unless it be intended to remove a portion of rib the incision need not be more than one inch in length.
Ordinarily the skin is pushed a little one way or the other so that a rib can be seen underlying it, in order to steady it for the external incision. Then it is allowed to glide back to its normal position and the knife-blade is so directed as to at once enter the thoracic cavity. Only rarely is it necessary to make a careful dissection. It is not often that vessels of importance will be divided, and one may usually proceed boldly with the incision. It will be promptly followed by appearance and usually by forcible expulsion of fluid, perhaps even in a jet, for which a basin should be provided. In fresh cases this fluid will be thin; in old empyemic cases there will be so much caseous material mixed therewith that it may obstruct the opening and check escape of fluid. In these cases it may be pushed aside with forceps or by the introduction of a finger. When such material is present, however, there is need also for its evacuation, and in such cases the incision should be extended and an inch or more of rib may be removed in order to afford sufficient exit.
The objection above mentioned regarding speedy evacuation applies theoretically rather than practically to this procedure, for when it is necessary to open the chest cavity widely it is because the walls of the cavity thus opened have already become so thickened or stiffened by the disease process that there is not the danger of sudden change of position of the thoracic viscera which obtains in the less serious and more acute cases.
The fluid having been removed the next question is one of irrigation. This is only rarely necessary or even justifiable. Even in cases where the evacuated pus has a more or less offensive odor it is found sufficient to remove it, while experience shows the inadvisability, sometimes the practical danger of prolonging the procedure and trying at this time to wash out the chest cavity. If irrigation be practised it should be with a bland fluid, for antiseptics are here peculiarly irritating.
The third question is one of drainage. In recent cases it will often be sufficient to insert some flexible material, like a piece of oiled silk folded upon itself, secured externally by a safety-pin, or stitched to the skin in such a way that it shall not be lost within the cavity. In the older and more serious cases more complete drainage should be provided. This is usually effected with a short piece of rubber tubing, which needs to be amply secured against loss, either with a large safety-pin or by being stitched to the skin with silk rather than with gut, lest the latter soften too soon. This tube should ordinarily be quite short, in order that it may not irritate the pleural surface of the expanding lung. It is rarely necessary to make valve-like protection of the opening, nor is it usually advisable to insert any sutures in the external wound. These openings in most instances close too soon rather than too slowly.
The surgeon should avoid making the opening too low, lest the diaphragm, having been[748] pushed downward by the accumulation above it, rise and cover the end of the tube. Well-marked cases of empyema will often improve more quickly if a counteropening be made. It is an easy matter to introduce the end of a long forceps and determine the best point at which to make this opening. The forceps being then held at this point, one may easily cut down upon its end, force it through, and utilize it for drawing backward, completely through the chest, a long piece of perforated drainage tube, which perhaps may be eventually replaced by a few strands of silkworm gut. A very large and copious external dressing should be applied, and changed as often as need be, in order to receive and provide for such discharge as may take place. Sometimes this will be quite considerable, and necessitate, for the first two or three days, a change every few hours.
Some surgeons have endeavored to make drainage more complete by a vacuum irrigating apparatus, on the Bunsen pump principle. Should it be necessary to resort to this the more complicated older methods may be supplanted by the simple procedure, illustrated later in this work, for continuous drainage or siphonage of the bladder.
One should never attack a case of this kind without being prepared to remove a section of one or more ribs. Indications for this will be found in the character of the contained fluid, or in the thickness of the wall of the abscess, i. e., the old pleural cavity. The difficulty usually is that these openings tend to close too promptly, and that, especially in children, the proximity of the ribs to each other affords too small space for the maintenance of drainage. When it becomes necessary to remove a piece of one or more ribs there is little object in trying to preserve the periosteum, and the operation may be made within a few seconds by simply retracting the skin wound and the musculature, introducing the bone-cutting forceps, with which the rib or ribs are divided at points one inch or more apart, the intervening portion being promptly lifted out with forceps and cut away with strong scissors. The operation of dividing the rib will often so compress the intercostal arteries that there will be little hemorrhage from this source. Should they bleed too much strong forceps should be used to compress the lower edge of the rib, and, by crushing it produce hemostasis, as though the artery were itself seized with forceps, or the vessel itself may be seized and secured. A special form of forceps for dividing ribs, known as the costotome, has been devised and has proved serviceable, since it is so made as to prevent easy slipping of the rib from the grasp of the blade.
The larger opening thus made is treated in practically the same way as the smaller. Through it the fingers or a blunt spoon may be inserted and any cheesy material lifted out, or a sponge or gauze swab held in the grasp of a long forceps may be introduced, and with it the cavity thus opened may be wiped out or swabbed. In this way a considerable amount of caseous material or shreds of membrane may be removed. The more that can be removed the better, since there is so much less to come away later. Such manipulation is, however, sometimes attended by embarrassment of respiration, and one should use discretion in the extent to which he practises it. Hemostasis having been secured, it will depend on the case and its extent whether any effort is made to partially close the wound or whether it should be left open. Even large defects thus made usually heal kindly and fine or careful suturing is rarely needed.
The subsequent management of such a case is usually simple. After the first few days it may be advisable to practise irrigation. According to the age of the case will be found the expansile capacity of the lung. The lung itself expands by relief of pressure and by its own inherent tendencies and returning function. Again by a process of granulation it is gradually made to attach itself to the chest wall and is thus withdrawn toward its surface. The combination of these agencies will usually in time produce satisfactory results. The functionating power of the lung may be determined by filling the cavity with fluid, the patient lying upon the other side, and then noticing the difference between the amount of fluid held in extreme inspiration and extreme expiration.
—In old and neglected cases of empyema, especially of tuberculous type, the pleura itself becomes more or less thickened and stiffened, and affords such an obstacle to lung expansion as to justify more radical measures. These have sometimes to be undertaken as secondary operations, while in other instances, where there has been spontaneous perforation and escape of purulent overflow, perhaps for months or years, the necessity for such measures may be foreseen. This necessity was first appreciated by Warren Stone, an American surgeon, but the procedure was first formally placed before the profession by Estlander, of Helsingfors. The principle[749] upon which it and all similar operations has been based may be likened to the various efforts which it is necessary to make when a person tries to collapse an ordinary barrel whose heads have been knocked out. So long as the hoops of the barrel are intact the staves cause it to retain its cylindrical form. If, however, the hoops be divided it easily falls apart. In the case of a human chest, the lung, having been so long bound down, is incapable of expansion, and the chest walls are rigidly maintained by virtue of the hoop-like arrangement of the ribs. It is necessary then to divide and remove a section from several of these ribs, in order that the wall, falling in, may meet, at least half-way, the lung, which may be expected to partially expand to meet it.
Fig. 519
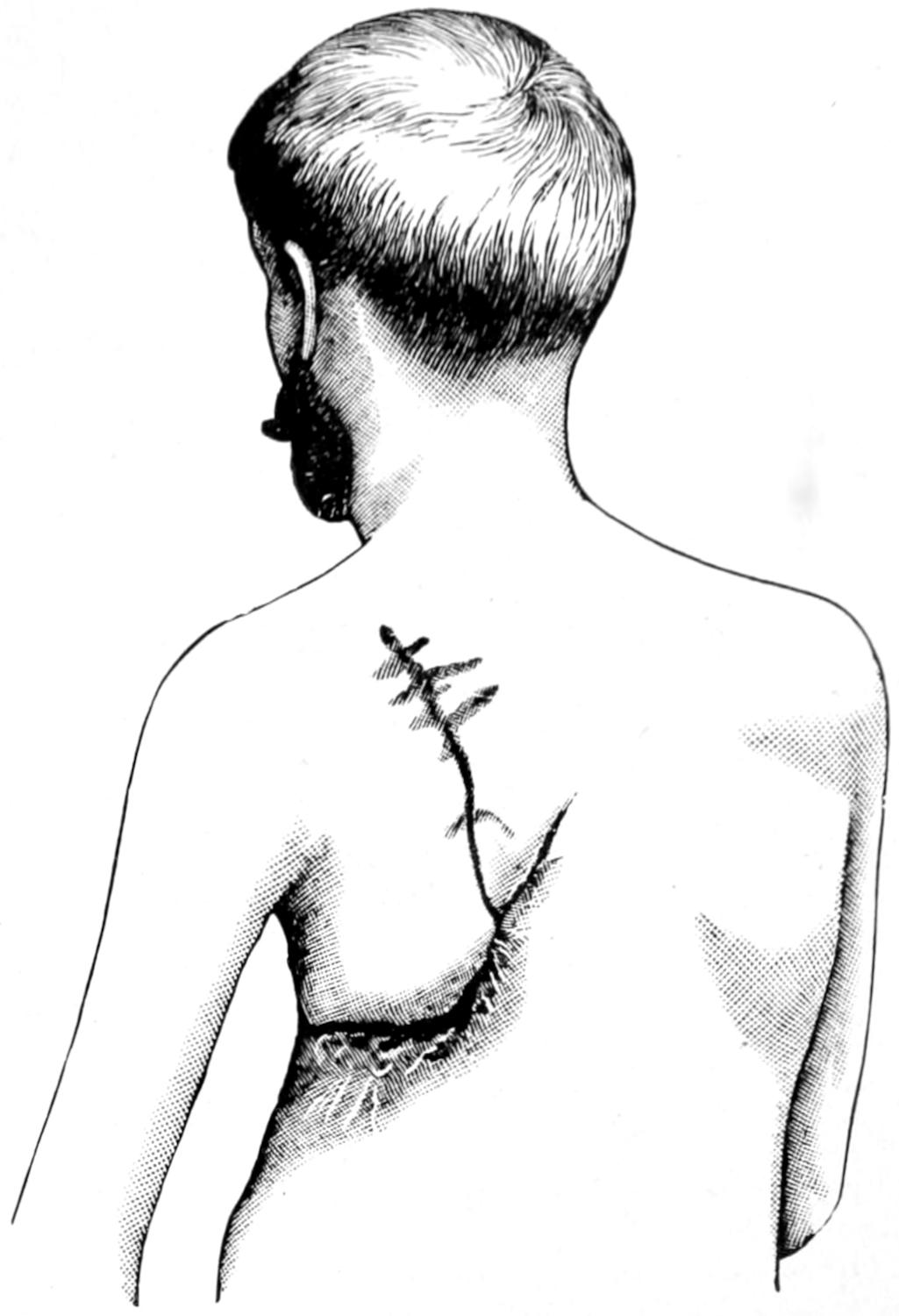
Incision for resection of thorax. (Bergmann.)
Fig. 520
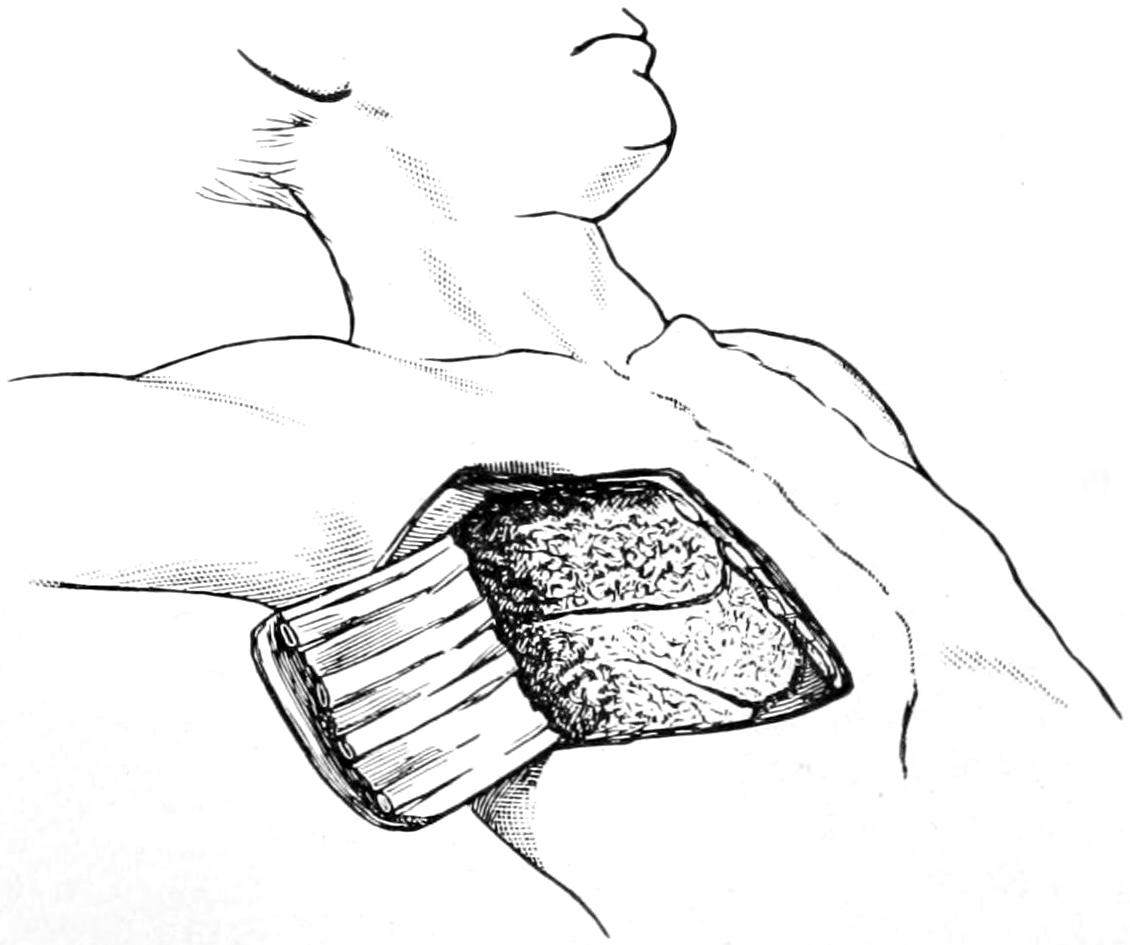
Trap-door thoracotomy. (Lejars.)
The original Estlander operation has been modified by Schede, and as now practised is made by a long incision passing obliquely across the lateral aspect of the chest, from the origin of the pectoralis major, at the level of the axilla, to the tenth rib in the posterior axillary line, and then ascending to a point between the spine and the scapula. The large flap thus outlined is made to envelop all the tissues outside the ribs. The ribs thus exposed are resected from the tubercles forward to their insertion into the costal cartilages. The large area of the chest wall thus exposed is then removed with the underlying pleura, and all hemorrhage checked. This flap includes the periosteum, the intercostal muscles, the ribs, and the pleura, and thoroughly uncovers the entire abscess cavity. It makes a formidable procedure, but is more often life-saving than the reverse. Over the opening the skin flap may be later drawn down and tacked in place at points sufficiently near to each other to properly hold it in place (Figs. 519 and 520).
[750]
This procedure may be modified to suit the indications of any given case, and simply includes what may be done in extreme cases. The surgeon who thus for the first time uncovers such a cavity will be surprised at its interior appearance, and at the shreds of tissue and debris which hang from its walls. The measure thus described provides for collapse of the chest wall. Fowler and others have shown, however, that even now the principal obstacle to expansion of the lung is not removed, and have suggested what Fowler has aptly described as decortication of the lung—namely, a removal of its thickened pleura by a process of dissection and stripping, which may be made partial or complete, as circumstances permit. In some respects this adds to the gravity of the case and will perhaps better be done at a second operation. Should it, however, be justified by the condition of the patient it is best done in connection with the resection of the chest wall.
When decortication cannot be practised Fowler has advised that a series of incisions be made, and that by thus gridironing the thickened membrane it may be weakened or caused to lose its inelasticity and thus a mild degree of similar effect secured. Fig. 521 illustrates the end result of such an extensive thoracoplasty.
Fig. 521
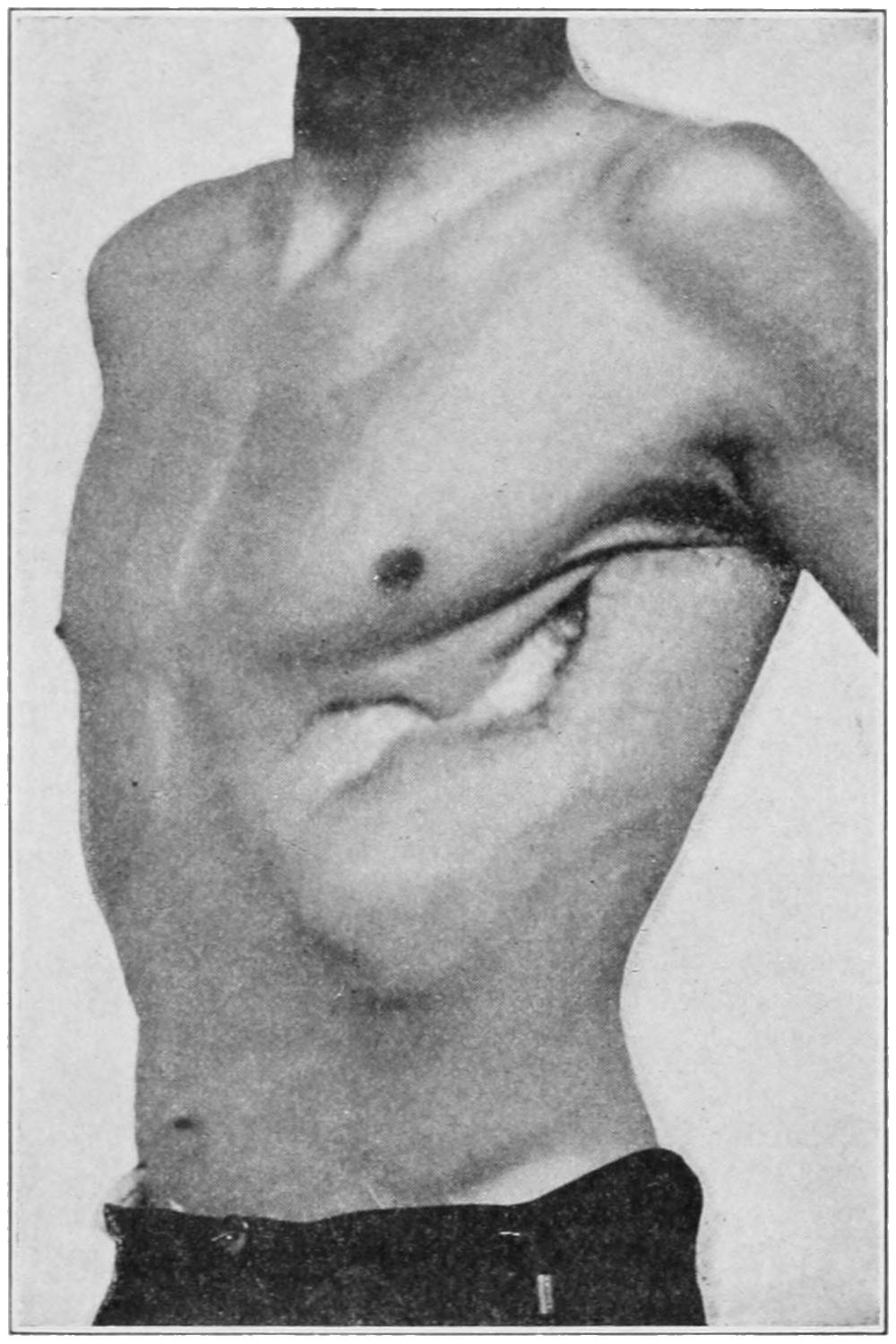
End result of an extensive thoracoplasty. (Park.)
—This is a term applied to an attack upon the lung itself, it having been exposed by a thoracotomy. It is necessary in cases of gangrene, abscess, hydatid cyst, and occasionally in large bronchiectatic cavities. It is not ordinarily a difficult procedure when the lung has attached itself to the chest wall in the course of the disease process. Here the lesion having been located a part of one or more ribs is removed, as may be needed, thus exposing the lung surface, the cavity is then opened either with a knife or by dilatation with the blades of a forceps, or preferably with the thermocautery blade, by which hemorrhage is better controlled and possibilities of absorption reduced. If such a cavity can be located it may be opened with a large trocar and cannula, which should be introduced with great care, lest it be thrust too far, the method by incision being therefore preferable. If after opening the chest the lung be found non-adherent, it depends on the character of the lesion whether adhesion should be provoked or the cavity itself attacked. In the former case adhesions may be produced by stitching the exposed lung surface to the margins of the wound, and waiting for sufficient exudate to be poured out to ensure that the pleural cavity has been hermetically sealed. The same result may be obtained more crudely by packing gauze around the opening.
In case of urgency it would probably be best to attach the lung to the chest wall with sutures and secure it there. This is a comparatively safe method in dealing with hydatid cysts, and will give a fair measure of success in many other instances. The suppurating or gangrenous cavity being opened its contents should be removed, dead or sloughing tissue excised, and the cavity then packed for drainage purposes, the external wound being kept open until it can be safely allowed to close.
Pneumonectomy, that is, removal of a portion of the lung substance, may be done with comparative safety upon animals, but rarely upon human patients. It is occasionally required in connection with the removal of malignant tumors of the chest wall, to which the lung has affixed itself. In exceedingly rare instances it may be justified for localized tumors of the lung itself. It would be equally valuable for circumscribed, primary[751] tuberculosis of the lung, were it possible to recognize this in time. This an Italian surgeon once thought that he had done, in the case of his fiancée, and proceeded to resect the upper lobe of one of her lungs. His lack of success quickly led to his own suicide a few days later.
The lung is exceedingly vascular and at the same time bears sutures well. The suturing, however, should be accurate in order to prevent secondary hemorrhage and favor the process of repair.
Other operations may be practised upon the chest wall for relief of such conditions as acute osteomyelitis of the ribs or sternum, caries of the ribs, necrosis, and the like. It should be scarcely necessary to give explicit directions, save that the pleural cavity should never be opened unless the pleura itself be involved in the disease. Every case demanding such operative relief should be measured by its own needs, and the operative procedure adapted to them. Necrosed portions of bone may be completely removed. The suppurative and carious conditions necessitate rather a sufficiently wide exposure from without and then a judicious use of the bone curette. One need never hesitate to remove so much bone as is diseased, this being true even of the sternum.
The possibility of suffocative and other disturbances proceeding from enlargement of the thymus has been discussed, as well as the use of long trachea tubes in cases of this character which call for tracheotomy, as they usually do if they permit of any surgical intervention. The thymus is seldom the site of primary malignant disease. Certain acute lesions are due to a peculiar form of hypertrophy in the young, which takes place instead of that spontaneous disappearance which should have occurred during the earliest months of infancy. Its connection with the status lymphaticus, with thymic asthma, and laryngismus stridulus has already been mentioned. While it can hardly be considered absolutely exempt from ordinary infections and the like it nevertheless is rarely involved.
The thymus has been removed by operation, usually with success. Should it become necessary to resort to such a measure it should be preceded by the removal of the sternum, for only in this way can sufficient exposure be obtained, and sufficient opportunity for checking such hemorrhage as might result from its enucleation.
The axilla as a surgical region belongs as much to the thorax as to any part of the body, although none of its diseases are peculiar to this area.
It is frequently the site of furuncles of local origin, which occasionally assume carbuncular type, and which are expressions of local infection along the hair follicles or mammary ducts. It is full of lymph nodes, through which are filtered the lymph streams coming from the upper extremities. In this way there are entangled therein septic germs, which frequently give rise to small or large phlegmons proportionate in size to the magnitude of the lesion beyond them. It takes but a trifling infection of the finger, for instance, to produce such involvement of axillary lymph nodes as to make them palpable under the finger. Such lymph nodes once genuinely inflamed frequently coalesce, and the resulting abscess cavity may be large, especially if neglected. The sooner these phlegmons are incised and cleaned out the better for the patient. In order to do thorough work an anesthetic is usually required.
In the axilla also are frequently seen tuberculous manifestations, the result of propagated infection from some part of the arm or hand. These may be involved in a mixed infection and quickly break down, or may assume the type of the chronically enlarged nodes, which undergo caseation and more or less encapsulation, with such infiltration of the surrounding tissues that when extirpated considerable difficulty is met in the dissection.
In syphilis, also, the lymph nodes become involved, frequently enlarging to a degree making them palpable, and sometimes participating in a mixed infection in such a way as to break down into abscesses.
[752]
Again, in the axilla are occasionally seen conspicuous evidences of Hodgkin’s disease. Any disease of constitutional character which precipitates trouble in one axilla will cause nearly duplicate alterations in the other, whereas disease of local origin is usually confined to one side.
Any phlegmonous cavity or tuberculous lesion which has been incised through the axilla should be carefully cleaned out and then drained, lest the external incision close before the deeper parts are ready for it. Incisions made in the axilla should be parallel with the great vessels and nerve trunks, by which they are better exposed and avoided. A wound made in the axillary vein may be sutured or the vein be doubly ligated. The former is much the better course, very fine silk sutures being employed. In some lesions where it has not been possible to discover the bleeding point the writer has not hesitated to secure it with the ends of pressure forceps and to leave these forceps included in the dressings for forty-eight hours. He has never seen harm result from this procedure.
Fig. 522
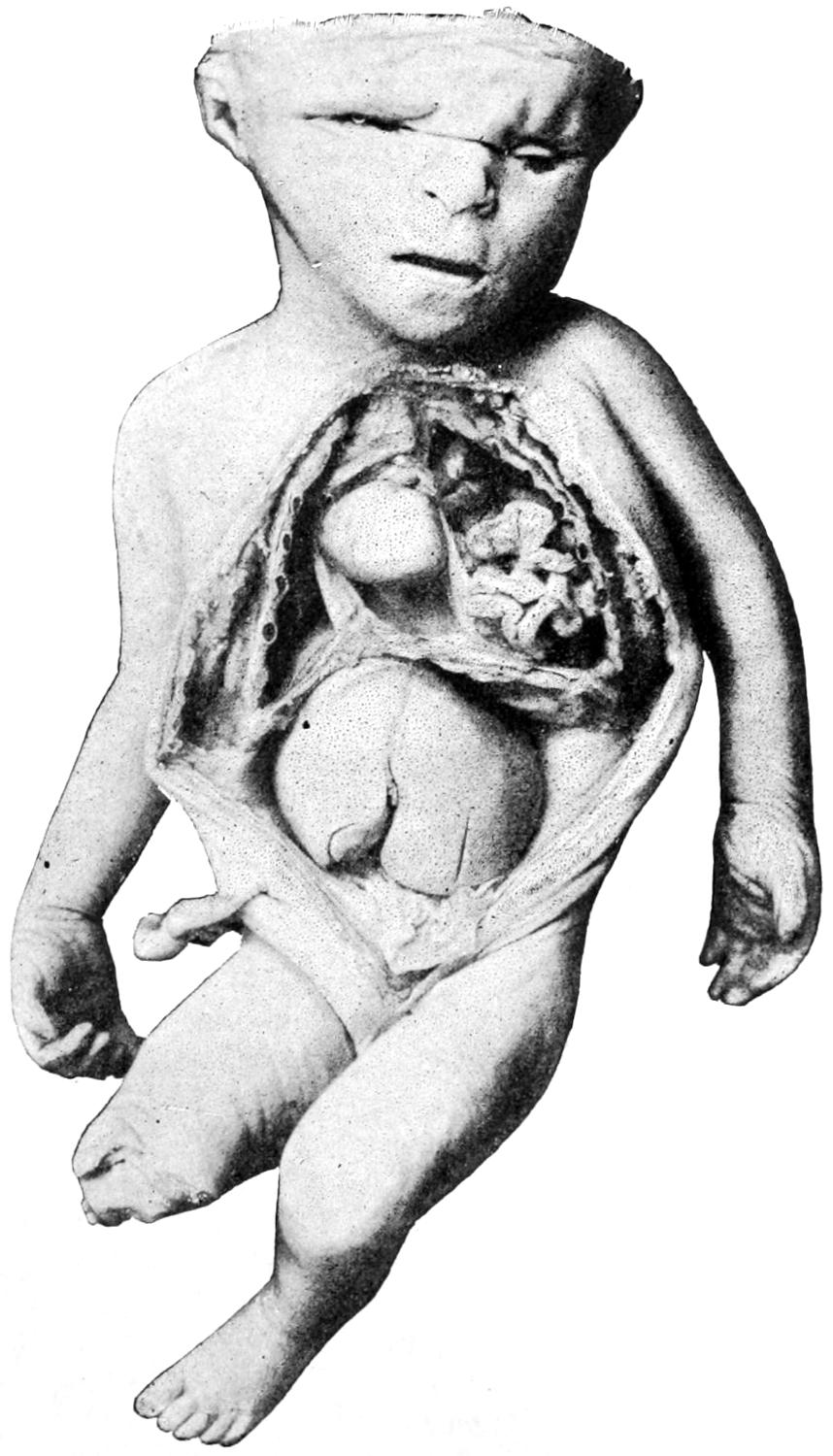
Congenital diaphragmatic hernia, with other congenital defects. Wood Museum. (Dennis.)
Finally the axilla is almost always involved in cases of malignant disease of the breast, of the arm itself, and sometimes of the regions adjoining. Primary malignant disease in this region is rare, while secondary cancer is not unusual. According to the modern plan of treatment of cancer there is reason for scrupulous extirpation of every particle of infected tissue and all involved lymphatics, and in dealing with such cases the surgeon need not hesitate to divide or extirpate the pectoral muscles, in order to permit of thorough work. The disease being present nothing can be so serious for the patient as to allow any particle of it to remain.
The diaphragm may show certain congenital defects, consisting mainly of fissures or openings which permit displacement of viscera, usually from the abdomen below into the thorax above. This is often fatal, constituting a form of diaphragmatic hernia, which is particularly liable to strangulation. Fig. 522 indicates a case of this kind, showing the hopelessness of the condition.
Anatomically it is worth while to recall that the diaphragm may rise to a level with the third cartilage during forced expiration, and descend to the level of the fifth intercostal space on the right side, and a little lower on the left, during forced inspiration. When forced upward by pressure from below it may rise even higher than stated above. These facts are of surgical interest in considering the possibility of injury or perforation of the diaphragm in connection with gunshot and other perforating injuries to the thorax or abdomen.
[753]
Diaphragmatic paralysis is the necessary result of injury to the phrenic nerve. It may occur as the result of injury to the thoracic viscera, especially those of the posterior mediastinum, or injuries to the cervical or upper dorsal vertebræ, usually fractures or dislocations, followed by ascending degeneration and involvement of the phrenic nerve roots. Double phrenic paralysis is in these cases obviously fatal. Paralysis of a single side will cause at least serious embarrassment of respiration. An hysterical form of diaphragmatic paralysis has also been described.
Primary tumors are exceedingly rare in this muscular partition. Advancing growths, however, attach themselves to it or perforate it, as may also aneurysms.
Aside from the ordinary injuries which the diaphragm may suffer from without, and already mentioned, there are peculiar forms of rupture, the result of force applied from below, usually at right angles to the surface of the body, this being permitted on account of the dome-like shape of the muscle. When thus ruptured abdominal viscera may be forced into the chest and even out through openings between the ribs. A gunshot wound of the diaphragm will be serious mainly in proportion to other injuries involving the viscera above or below it. These injuries produce no typical symptoms, but are nearly always accompanied by severe pain radiating toward the shoulders, with dyspnea and a substitution of abdominal for diaphragmatic respiration. When the viscera have been forced upward they will displace the heart, and this may produce cardiac symptoms. It is said that the so-called “sardonic grin” is still observed on the faces of corpses who came to sudden death from some injury to the diaphragm.
Thus diaphragmatic wounds are not of themselves of serious import. When inferentially present they may, therefore, be disregarded so long as no serious symptoms are produced. On the other hand, exploratory celiotomy should be performed at any time, should conditions seem to justify it.
While this is a condition pertaining, strictly speaking, to the abdominal cavity, it nevertheless arises so frequently from intrathoracic causes as to justify its consideration here, as well as because of its close relations to the diaphragm. It was Volkmann who, in 1879, first showed how these abscesses could be successfully and surgically treated. The term is applied to collections of pus beneath the diaphragm, usually between it and the liver, which, however, may extend to and later involve surrounding viscera.
The causes may be divided into those met with above the diaphragm and those below. The former may include empyema, pus having escaped beyond the normal pleural limits, advancing tuberculous disease from any of the structures above the diaphragm, echinococcus in the lung, or suppurative mediastinitis. From below the diaphragm the infectious process may travel from the direction of a gastric or a duodenal ulcer, hydatid disease in the liver, phlegmon around the liver or kidney. The contained pus may, on culture, show the presence of colon bacilli or pneumococci, as well as the ordinary pyogenic cocci and tubercle bacilli. If connected with hydatid disease hooklets may be seen in pus which is not too old.
Subphrenic abscess may result in large collections of pus, which may travel a considerable distance, separating the peritoneum from the diaphragm and from the lateral abdominal walls, appearing even low down in the pelvis. The same is true of escaping pus from a case of empyema. The primary trouble gives rise to a localized peritonitis or perihepatitis, by which are produced certain barriers that serve to retain pus within bounds, and to keep it from spreading save as above mentioned. Should it be due to extension of abscess or disease within the liver it may be confined by adhesions about it. Fig. 523 illustrates the relations which such a collection may sustain to the liver and the diaphragm, as well as how the opening by which it may be best evacuated should be made through the thoracic walls. Even with this condition produced by disease below the diaphragm it is not infrequent to find some collection of fluid or evidence of exudate above it.
A study of this condition will nearly always lead one back to a history of some illness which may furnish the explanation for the commencement of the trouble. Thus, there may be obtained a history of pulmonary tuberculosis, of empyema, of gastric ulcer, of gallstone trouble, or of abscess in the liver or in or about the kidney. When the[754] result of perforation from above, the chest wall may furnish signs which will be sufficiently indicative.
The symptoms will include swelling, pain, tenderness, with fixation of the liver, and apparent enlargement of its boundaries, because it is pushed away from the diaphragm. The abdominal wall will frequently be edematous. The ordinary signs of the presence of pus are rarely absent, including the evidences furnished by a differential blood count. Diagnosis is proved by the use of the exploring needle. The disease is nearly always situated upon the right side. The more distended the abscess cavity the less respiratory murmur will be heard over the lower part of the chest, while the line of the hepatic dulness may be considerably above the normal. Sometimes a succussion sound may be obtained.
Should pus be withdrawn from the lower part of the chest by the exploring needle there might still be doubt as to its actual location, whether above or below the diaphragm. The absence of cough and of indications of pleural involvement would prove much in favor of the latter.
Subphrenic abscesses tend in time to evacuate themselves. Thus they sometimes perforate the diaphragm and escape into the pleural cavity, or through a lung which has attached itself at its base, and thus afforded an outlet for pus through the bronchi and the mouth. On the other hand, pus may burrow downward and appear in the flank or beneath the skin near the liver and in front of it. The nearer it comes to the surface the more easily it is recognized.
Fig. 523
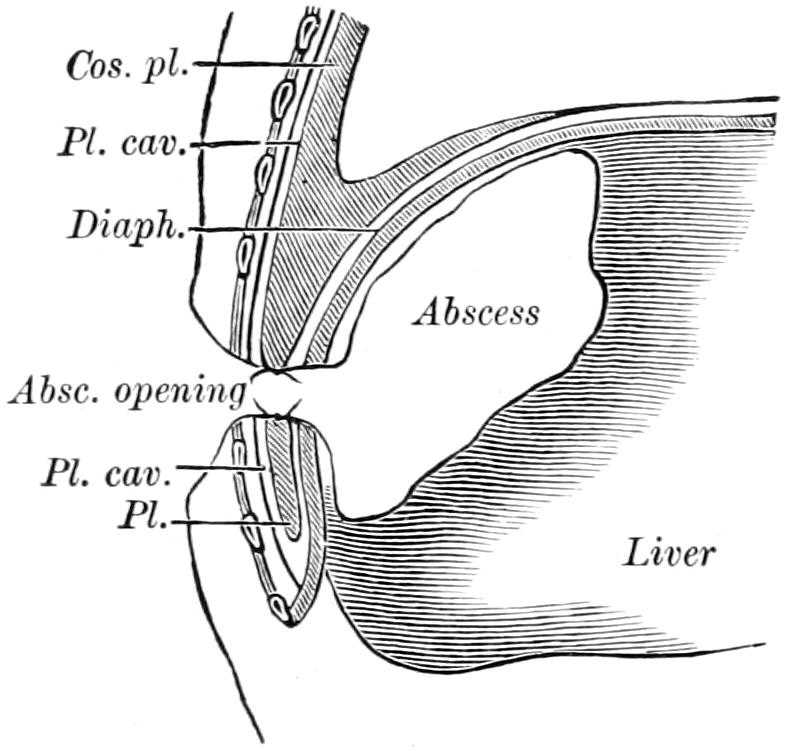
Transthoracic opening for subphrenic abscess. (Beck.)
—The treatment of subdiaphragmatic abscess, like that of all other abscesses, consists in evacuation of the contained pus, with provision for drainage. In some instances this may be done with an ordinary trocar and cannula, but serious cases are best treated by incision, with resection, if necessary, of a portion of a rib. When the chest wall is entered the best place is between the ninth and tenth ribs in the axillary line. Nevertheless pus which is presenting at any other point may be best reached by taking advantage of the indication thus afforded. An opening having been made the question of counteropening may be raised. This should be decided in each instance upon its merits. While an opening made in front does not drain so well as one placed posteriorly it may be made to drain by keeping the patient upon the side or face for a portion of the ensuing few days. When it seems desirable to go through the chest wall it should be incised carefully, and if the pleura has been opened before reaching the abscess, the pleural surfaces may be either stitched together or packed; after waiting a day or two for protective adhesions to form the abscess may then be opened. The less extensive operations may be performed with local anesthesia. Rib resection and extensive incision will usually require general anesthesia.
[755]
Amastia, or complete absence of one or both breasts, is a rare defect. Polymastia, or the occurrence of supernumerary breasts, is more frequent.[51] These may be found on any portion of the thorax or abdomen, and may constitute masses of trifling size or may bear considerable resemblance to the normal breast. A supernumerary breast has even been found upon the thigh. The condition is to be regarded as atavistic, and a return to the polymastia of animals, which produce a litter at one birth. Similarly absence of the nipple, amazia, is occasionally seen, or more frequently polymazia, the occurrence of more than one nipple, either upon the normal breast or in some abnormal position. Some of these lesions are so small as to escape observation, or to be considered moles unless carefully noted and recognized when found.
[51] History records interesting examples of the importance attached to these conditions. Thus the beautiful Anne Boleyn fell under the displeasure of King Henry because of a supernumerary breast, and it is said that the mother of the Roman Emperor Alexander Severus was given the name of Julia Mammæ because of a similar abnormality.
Ordinarily supernumerary breasts are met near the middle line and below the normal mammary gland. A more common condition is one of defect of the nipple, which fails to assume its normal prominence and remains ill-developed, so as not to be seized by the infant in the act of attempting to nurse. Nevertheless with the physiological activity which occurs in the breast at the time of pregnancy these ill-developed nipples usually expand sufficiently to fulfil their function, even though imperfectly.
Hemorrhages from the breast sometimes take place idiopathically, at others as vicarious efforts at menstruation. There is a peculiar sympathy between the pelvic organs of women and the mammary glands, and the latter evince this in more than one way, becoming sometimes extremely tender or swollen at the menstrual period, or at other times peculiarly sensitive or even neuralgic, while at times congestion will proceed to the point of hemorrhage. These conditions do not require particular attention, but are not to be confused with a bloody discharge that may occur later in life, in connection with certain forms of malignant disease occurring in the interior of the breast.
Fig. 524
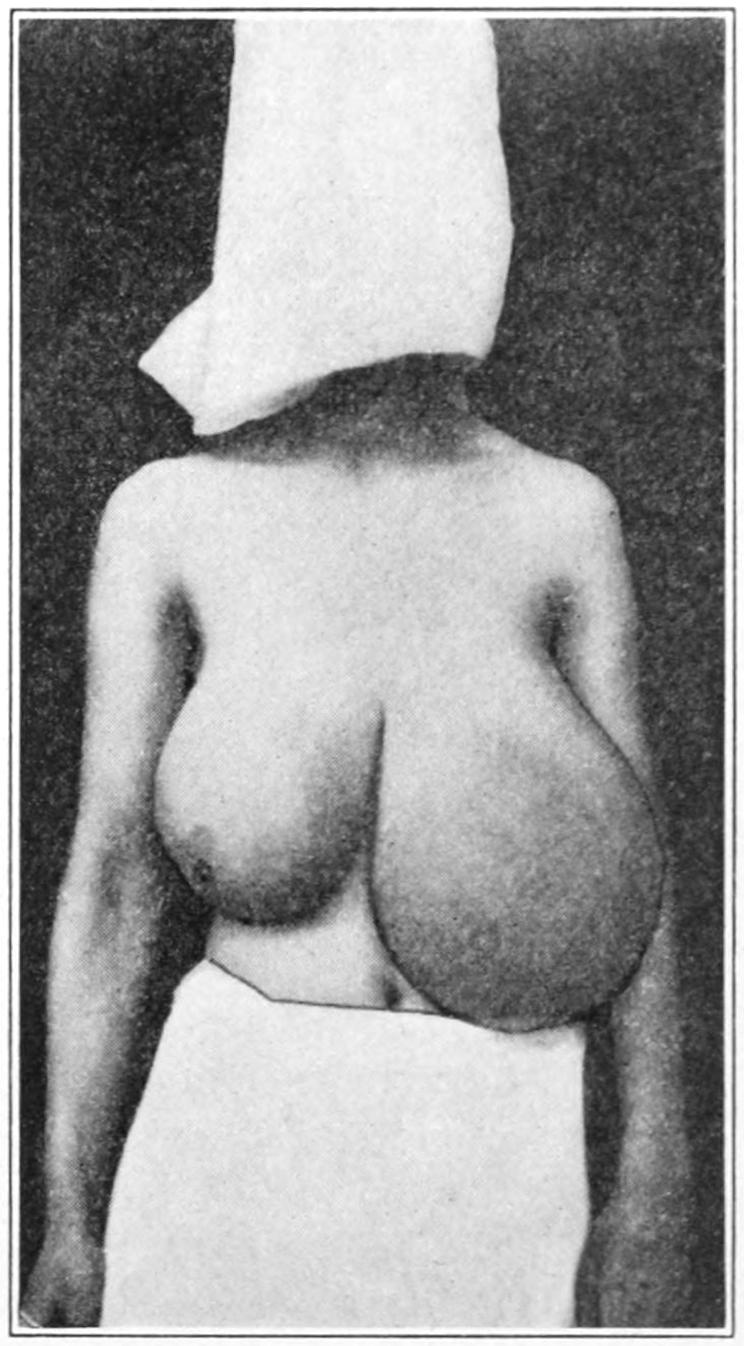
Idiopathic hypertrophy of breasts in a girl of sixteen. (Bebee.)
There exist the widest differences in development of the breasts in different individuals. The term “breast” is used intentionally, since the difference is not so much in the actual glandular development as in the surrounding connective tissue and fat. Thus a plump breast may contain very little more secreting structure than one apparently ill-developed. Nowhere outside the uterus save in the breast do such compensatory changes take place under the stimulus of pregnancy. In fact, a mammary gland in preparation for lactation is a physiological adenoma. At conclusion of lactation there is absorption and atrophy from disuse, usually not to the original degree, although in some instances the[756] fatty tissue disappears irregularly and leaves the breasts in quite different shape from their originals. In this way the breasts may become exceedingly pendulous, so much so as to lead to pain and soreness from traction, and to call for their support.
Idiopathic hypertrophy of one or both breasts is a rare deformity, occurring usually in the young, sometimes in girls, involving them to an indefinite degree, but in some producing enormous overgrowth, with corresponding deformity. For such hypertrophy no known cause has been assigned. Fig. 524 illustrates an instance of this character in a young girl, occurring under the observation of my colleague, Dr. Bebee.
These consist largely of contusions to which, from their positions, the breasts are peculiarly exposed, and these may be followed by hemorrhage, by extensive ecchymosis, or by any of the consequences of infection. They may also be followed by more or less permanent induration. The fact that in the course of time certain contusions of the breast are followed by development of cancer is incontestable, although the relation which may exist between the accident and the neoplasm has not yet been made clear. The breasts are also subject to the same possibilities of injury as other parts of the thorax, which has been considered in the previous chapter. The nipples are more often injured by efforts of the nursing infant, or by the friction of ill-fitting stays or rough clothing, than in any other way. These injuries, at first of a minor character, are not infrequently followed by serious results, erysipelas, septic infection, or tuberculosis being conveyed through trifling abrasions thus inflicted.
The nipple of a nursing woman once excoriated, or its surface broken, is kept constantly liable to maceration and surface infection. In this way a trifling lesion may result in a linear ulcer known as a fissure (“cracked nipple”), or in a more extensive involvement. These fissured nipples are very erethistic, and great pain is caused by each attempt at nursing. On this, account the mother postpones the act as long as possible, and until her breast has become overdistended, the result being injury to the breast itself, with a greater possibility of infection and of subsequent abscess formation.
The slightest excoriation of the nipple, under any circumstances, should lead to the adoption of every precaution for its cleansing and protection. Both before and after nursing it should be carefully washed, while, after removal of the child from the breast, it should be carefully dried and dusted with dry boric acid or a similar antiseptic. Any abrasion which fails to heal should be treated with silver nitrate. More pronounced abrasions and ulcers should be cocainized, then cauterized, and afterward treated as above. Finally in extreme cases it may be necessary to discontinue nursing and allow the breast to dry. If this policy be adopted it should be applied to both breasts, for such is the sympathy between them that the use of one gland seems to stimulate the other. The local use of such preparations as belladonna ointment, etc., is to be avoided. Pressure, rest, and the care above described afford more relief.
Paget’s disease of the nipple implies an eczematous condition, first described by Paget as a precursor of many cancers. It is a more or less chronic affection, involves the nipple and the areola, is quite intractable to treatment, gives more or less discomfort, and is to be dreaded when noted. It seems to sustain about the same relation to later cancerous involvement as does leukoplakia in the mouth and on the tongue.
There is no reason why any person may not have an attack of eczema about the nipple, but cases in which the condition is persistent and obstinate, and especially in which the underlying tissues gradually become infiltrated or indurated, should be viewed with suspicion, and should be treated by eradication of the area involved, even though this may require extirpation of the nipple or of the entire breast. When the condition is developed no ordinary treatment will suffice, although a fair trial might be given to the cathode rays.
A true inflammation of the mammary gland may occur at one of three periods: (1) At birth, when the tiny breasts of the newborn infant secrete a milk-like fluid, become more or less congested and tender, and when they are unintelligently treated by massage or interference of any kind; (2) at puberty, when a perfectly natural turgescence and[757] congestion occur, which, however, rarely proceed to suppuration unless infected or unless violence or some indiscreet treatment have been received; (3) during pregnancy and lactation, this being the time when mastitis is most common.
Considering that the nipple affords a number of open paths, from an area which it is difficult to keep clean, extending into the depths of inflammable tissue, it is strange that infection through the milk ducts does not occur in most cases. Such a path of infection affords the explanation for at least a large proportion of mammary abscesses. Again the presence of excoriations, abrasions of any kind, and especially of deep fissures which are not easily cleansed, will account for infection through the lymphatics. In these two ways nearly all cases of mastitis and of mammary abscess are to be explained, and both these accidents are likely to occur during pregnancy and lactation.
The consequence of such infection is mastitis, which begins with painful induration and local indications of inflammation, but which may under suitable treatment undergo resolution. This failing, the infectious process proceeds to suppuration, and the consequence is a superficial, deep, or retromammary abscess, all but the last named often in multiple form. The lobular construction of the breast permits the independent occurrence of distinctive suppuration, occurring synchronously at several different points, and hence it may be that a breast is riddled with abscesses, which form successively or almost simultaneously.
There is a superficial form, which occurs usually near the nipple, and in which the deeper structure of the breast is scarcely involved. This comes usually through infection of some surface lesion. Simple incision is usually sufficient, and the local lesion is thus quickly terminated. Deep or intramammary abscess, single or multiple, is always painful, sometimes distressing and occasionally an extremely serious condition. Occurring in a breast already well developed and fatty, abscesses may form at such depth as to be recognized with difficulty. The surgeon infers their existence rather than discovers it. This is unfortunate, for the longer the delay the greater the local disturbance, with a tendency to burrowing, and the worse are the consequences for the patient. It is, therefore, far safer to early note the minor signs of deep suppuration and to freely incise, than it is to wait for pus to come toward the surface and give its ordinary surface indications. The amount of induration, sometimes dense and brawny, which such conditions will produce within the breast, the size which the latter may assume, and the consequent suffering to the patient from neglected conditions of this kind, need to be seen to be fully appreciated.
Retromammary abscess may be the result of conditions not primary to the breast itself. Thus the writer has seen spontaneous perforation of the thoracic wall in a case of empyema, with escape of pus into the loose cellular tissue behind the breast, and the consequent protrusion forward of the latter until it presented as an enormous tumor. Treatment in such cases would mean not alone evacuation of the retromammary collection, but emptying the pleural cavity of its accumulated fluid.
An infected breast will produce not only the ordinary local indications, but will be characterized by extreme tenderness, with enlargement of the lymph nodes in the axilla and later abscess formation in this location. In proportion to the amount of pus thus imprisoned, and the virulence of the infecting organisms, constitutional symptoms may be mild or extreme.
Nowhere is there greater need for release of an imprisoned amount of pus than under these circumstances, although the incisions necessary for the purpose may be sometimes multiple and deep. Every incision made for evacuation of a mammary abscess should be placed radially—i. e., in a line radiating from the nipple—in order that lobules may be incised along their course, and that neither they nor vessels be cut across transversely. There is also need for complete drainage, and several tubes may be used for this purpose, being passed completely across or beneath the breast.
—Chronic mastitis may be the termination of a partially resolved acute process, or of injury, or of apparently unknown causes, being in these instances of apparently spontaneous origin. Pathologically it comprises induration, with more or less infiltration of the interacinous and interlobular tissue, and with some infiltration of the other structures of the breast, by which fixation, retraction of the nipple, or condensation of the surrounding structures and adhesion of the overlying skin are produced. The result may be to produce either an enlargement or diminution in size of the breast. One or both glands may be involved. It is a disease usually of late adult life.
[758]
Breasts thus affected are often tender and painful, especially during menstruation, and upon palpation are found to be irregular in shape, more or less nodulated, extremely firm in some cases and places, and perhaps so infiltrated as to strongly simulate cancer. The changes which are thus produced are slow, and it is important to note that the lymphatics are usually not enlarged, and that after attaining a certain degree the diseased condition becomes stationary. The general health usually does not suffer beyond a certain point; at least even in the more chronic cases there is no characteristic cachexia. While the condition is more frequent in women who have nursed it may be met in those who have never borne children nor have been married.
Suitable examination of all these cases can only be made with the upper portion of the patient stripped, the body in the horizontal position, and both breasts compared and examined, first with the flat hand in order that differences of shape, size, mobility, and fixation may be determined. Subsequently the patient should be raised to the sitting position, the surgeon standing behind to examine each breast with one hand and simultaneously, in order that differences may be more accurately noted. Any tumor present will be more easily discovered with the flat hand than with the finger-tip, while chronic induration will not give the sensation given by neoplasms. The axillæ should also be carefully examined, as well as the supraclavicular regions, for evidences of lymphatic involvement. When the entire breast is involved diagnosis is less difficult than when one or more lobules alone are concerned. These constitute the painful nodular conditions to which so many names have been given by different writers.
Significant features in their differentiation from cancer are the disproportionate pain and tenderness, their diffuse leathery hardness, and the fact that both breasts are usually similarly involved, though perhaps not to the same extent. Cancer is, on the other hand, somewhat dense and confined to one breast, and affords a sensation of infiltration of the surrounding tissues, with the peculiar “saddle-skin” retraction or adhesion of the overhang skin and nipple. Moreover, the growth is more rapid and localized, and the lymphatics are involved in nearly every instance. Some of these cases are so obscure that diagnosis previous to operation is impossible, while innocent lesions may gradually merge into malignant, and no one can say when the transition begins or has begun.
—The milder forms of chronic mastitis gradually improve under the influence of local applications such as the ichthyol-mercurial ointment, to which menthol may be added for its soothing effect. Pendulous or painful breasts should be supported as much as possible. Otherwise these cases are best let alone—i. e., they should not be rubbed or massaged. There is usually a constitutional condition which is closely related, and in nearly every instance there is more or less failure of elimination. These features should be studied and treated as they are identified. Finally there are some intractable forms of innocently indurated breast which give so much trouble that it is best to remove them as though they were cancerous.
Many women suffer from annoying and painful affections of the breast for which no sufficient excuse is found, while others who have small fibrous nodules or innocent lobular tumors will suffer an amount of pain which is disproportionate, and in instances of either type we are prone to point to the neurotic or hysterical features of the case and to say that it must be, at least to a certain extent, neurotic. Inasmuch as these cases usually occur in young and otherwise neurotic women, often of the more impressionable type, it is generally proper to consider them as to some extent hysterical, while in others there are pelvic accompaniments which may perhaps account for neuralgic breasts, because of the well-known intimate relations between the pelvic organs and these glands. In some cases, again, are found actual small tumors, single or multiple, but of innocent character. In other cases there are hypersensitive areas of entire breasts, to a degree where the patient cannot stand the slightest handling. These cases are hyperesthetic, even if not hysterical, and some are unsatisfactory to treat. The pains are more or less periodical, and often radiate down the arm or the side of the thorax; this may be explained through the intercostohumeral and other nerve connections.
—The treatment of mastodynia should include constitutional, local, and moral measures, but of these the local are the least important. The excision of painful[759] nodules is often disappointing, the remaining scars becoming even more sensitive than the original lesions. Women who under these circumstances have insisted upon the removal of an entire breast have still suffered from intercostal neuralgia or other remaining painful conditions, so that their ultimate condition has not been much improved. Each case should be studied upon its merits, and while one may be benefited by some pelvic operation, or another by Turkish baths and improvement of elimination, others are best let alone, or given a minimum of drugs with a maximum of general and sexual hygiene.
I cannot agree with writers like Fowler, who claim that tuberculosis of the mammary gland is extremely rare. I think it not infrequent. In the breast may be noted the presence of lesions, either separate or coalescing, and gummas as such, or breaking down into caseous masses or into cold abscesses. In connection with the local lesions there may be more or less involvement, even to ulceration, of the overlying skin, with the formation of lupoid ulcers, while the axillary lymphatics will be nearly always involved. In some instances the disease may have gone on to suppuration and burrowing of pus, with its discharge, and the existence of tuberculous sinuses; or in others may be seen results of a secondary infection of the remains of multiple mammary abscess. The condition is most often met with in the young and fair, but may be seen in elderly women. Around the distinctly tuberculous lesions there may be considerable tissue sclerosis. The actual proportion of cases is about one of this condition to fifty of cancer. Lesions are more frequent in the outer quadrant of the breast than the inner, and they occasionally produce retraction of the nipple or adhesion of the skin, above described, before its distinct involvement.
In any of these circumstances secondary purulent infection may occur, and an acute phlegmonous process may seriously complicate the previous chronic condition.
—There is but one satisfactory method of dealing with tuberculous disease of the breast—i. e., its extirpation. The entire breast, or so much of it as may be distinctly involved, should be extirpated as though it were cancerous, while the axilla should be opened and its contents cleared out, if it appear in the slightest degree involved. Moreover, every other tuberculous lesion in the neighborhood should be eradicated, either with the knife, the scissors, or the sharp spoon. After such radical treatment results are usually satisfactory.
Actinomycosis is not common in this location; nevertheless tissue conditions are such that it would furnish accessible and diagnosticable features which would be distinctive, at least until some secondary infection had occurred.
Syphilis appears in this location in many of its protean manifestations. Chancres about the nipples and on the surface of the breast are not uncommon, the disease being often conveyed from syphilitic infants through cracked nipples, while many other methods of contamination have been reported. Near the nipple the chancre may not have those characteristics which usually distinguish it upon the genitals, but may appear rather as an indurated, intractable ulcer, with firm base, accompanied by distinct involvement of the axillary and supraclavicular nodes, and unless early recognized and promptly treated as such will so endure until the occurrence of the first significant secondary eruption, whose appearance should dispel doubt and lead to radical treatment.
There is difficulty, sometimes, in distinguishing between tuberculous and syphilitic skin lesions upon the breast, especially near the nipple. When other methods fail the therapeutic test will nearly always clear up the difficulty. All truly syphilitic lesions here, as well as elsewhere, yield promptly to well-directed treatment.
[760]
The mammary gland is a frequent site for tumors, although neoplasms of embryonic origin are not as frequent here as might perhaps be expected. Nearly one-fifth of all tumors occurring in the body will be found in this location, while the larger proportion of breast tumors are malignant.
Cysts abound in this locality, occurring in one or both breasts, and singly or in exceedingly multiple form, the latter being small and containing but a few drops of fluid. Their cystic contents are colorless and of a serous consistency, sometimes thick and mucous, occasionally discolored, and in rare instances almost like unchanged milk. In the latter case the condition is known as galactocele.
In an organ so thoroughly provided with ducts it is easy to understand how retention cysts may readily occur from plugging of some duct and the accumulation of secretion behind it. Should it occur at a time when milk is forming galactocele may be readily explained. At other times it is in every respect an abnormal development. This occlusion of the ducts may be the result of disease or of injury, and is not always complete, for it often happens that from a distended duct more or less accumulated material may be expressed by gentle pressure. In this case it will be found thick and loaded with the epithelial cells which line the passages. These retention cysts are spoken of as serous, mucous, or sanguinolent (blood cysts), according to their contents, while the lacteal contain material more or less resembling butter. True galactocele seems to be rare. While the original contents are milky it is claimed that through changes taking place in the neighborhood induration and proliferation in the surrounding membrane may result, or that mammary tissue may soften and break down into pulpy detritus.
Cystic tumors in the breast may be of innocent character, or may assume all degrees of malignancy. A cyst whose lining membrane is smooth, without reduplications or irregularities, may be regarded as innocent, while the complete extirpation of its walls will be all that is required. This may be made more complete after injecting it and staining it with methyl blue, or filling it with melted paraffin in order to occupy the place of the fluid, which should have been drawn off. On the other hand, every cyst whose interior is roughened, or presents the slightest papillomatous appearance, or which is unduly adherent, or has about it any mark of infiltration, calls not only for its own eradication, but for practically the complete removal of the breast.
The signs of cystic tumor in the breast are essentially those of any other neoplasm, except that it is frequently possible to recognize its cystic character by fluctuation. A cyst ordinarily presents as a distinct tumor, and when innocent is circumscribed and non-adherent, lacking the clinical evidences of malignancy. Pain is an uncertain feature. Most cysts develop slowly, but a cyst developing suddenly after parturition or during lactation, without previous local inflammatory changes, is probably a galactocele. The small multiple form of cyst, with which one or both breasts may be studded, is frequently confused with chronic mastitis, from which it is difficult to separate it. The escape of sebaceous material or of milky fluid from the nipple, or the possibility of making it appear by gentle pressure, will probably afford the best indication. If along with this possibility the nipple be found ulcerated, or if the extruded fluid be bloody, complete extirpation of the breast would be the only suitable measure.
—The general treatment of cyst has been indicated. It is a question simply of how extensively the eradication should be made. The advice of the older text-books is misleading, and it is the studies of very recent years which have shown how early the lining membrane of apparently innocent cysts may undergo malignant changes, by which the breast is soon compromised and which necessitate its entire removal.[52]
[52] It will be a safe rule to follow if it be assumed that every cyst whose contents are bloody, unless this can be traced to recent accident, and especially every cyst whose interior is papillomatous, is on the border-land of malignancy, if not malignant in character. All such tumors then should be extirpated. If they occur in the breast a complete operation, as for cancer, should be done.
Of the benign tumors lipomas in the substance of the gland are rare, while they may frequently develop in its fatty surroundings. Adenoma and fibroma, with their various combinations, are the most common of the innocent tumors, and they constitute single[761] or multiple nodules, located in the substance of the gland, or in evident communication with it, constituting masses of well-marked density, slow growth, nearly always mobile and non-adherent to the skin, causing neither retraction of the nipple nor lymphatic involvement, and being frequently accompanied by a very disproportionate amount of pain and tenderness, some of them being, in fact, exquisitely sensitive. While these growths are rare previous to puberty they are frequently met in girls and young women, and, occurring in these neurotic subjects, they cause considerable mental as well as physical trouble. In these patients there may be found coincident pelvic disorder. The removal of these sensitive masses, which seems to be plainly indicated, is often disappointing, as the remaining scar may retain the original hypersensitiveness, and patients often suffer as much as before the operation.
The enlargement of the breast, which normally prepares it for lactation, is to be regarded as the development of a normal or physiological adenoma. Anything which simulates this under other conditions is abnormal, and any overdevelopment of true mammary gland tissue, when localized and circumscribed, should be referred to as adenoma. In such tumors cystic changes often occur, as well a later transformation into adenocarcinoma, something always to be dreaded. These changes are more likely to take place during lactation, at which time the blood supply to the breast is more free. The development, then, of an adenoma in the breast of a nursing woman should be regarded with suspicion, and unless benign it should be regarded as demanding removal of the entire organ. These tumors also are non-adherent and lack the ordinary signs of malignancy.
—Cancer occurs in the breast more often than anywhere else, and carcinoma constitutes about 85 per cent. of these malignant tumors, the balance being mostly sarcomas, the remaining small number being made up of endotheliomas and the other rare forms. The most common type of carcinoma is the so-called scirrhus, in which there is a large amount of dense stroma, and which forms a strong contrast with the rare forms of rapidly growing, true soft cancer—i. e., the encephaloid or medullary as they used to be called—in which the cancer cells proliferate with greater rapidity and in which there is a small amount of stroma, so that in consequence the tumor itself is soft or almost gelatinous.
Sarcoma of the breast may assume either of its well-known types, and is a tumor seen in the earlier rather than in the later years of life. It sometimes grows rapidly and attains large size, seeming to approach the surface more rapidly and readily than ordinary forms of carcinoma. In consequence it may be mistaken for abscess. As a rule, however, the skin is not so likely to be adherent to the tumor as in carcinoma, and the lymph nodes are not so early involved, while in a cut section of the tumor the fat is not so disposed as in carcinoma, where it may be seen in layers, while in the former case it has been transformed into malignant tissue.
The two principal forms of carcinoma are the acinous and the tubular, in the former the cells being packed into the alveoli and surrounded with a firm and adventitious stroma, while in the latter the primary development seems to be within the milk ducts, which being first involved cause a more multiple minute invasion and a less distended tumor formation.
The general indications of cancer in the breast are as follows:
The presence of tumor, sometimes of regular and definite outline, sometimes diffuse and not easily outlined.
Fixation of this tumor in the surrounding tissues in such a way that it cannot be moved without disturbing them.
Fixation of the general area, either to the skin above or to the pectoral fascia below, or both. This gives to the part an immobility in contrast with normal conditions.
Retraction of the nipple, when the growth is large or located near it. This is a feature perhaps not noticeable in the primary stages when it is so important to recognize the disease if present.
Retraction of the overlying skin, at points if not over a considerable area, giving it a peculiar “saddle-skin” or “pig-skin” appearance. This indication of itself is always suspicious and one which should be noted if present.
In addition to the local evidences in the breast the involvement of the nodes in the axilla and of the lymph vessels leading up toward it. These should be carefully studied, the patient’s arm being held loosely away from the body, and somewhat to the front,[762] in order to relax the pectoral muscle. In fleshy subjects it may not be possible to discover them even if present. The supraclavicular region should also be examined, and enlargements may be felt here or along the cervical chain.
In addition to the above features others which are more indicative, because they point to advanced disease, are the appearance in the skin or just beneath it of shot-like nodules, more or less red, or of any mass which causes the skin to protrude and to have an unnatural appearance, usually one of lividity or threatening ulceration. Pain is an uncertain and variable feature, upon which little stress should be laid. The laity have incorrect notions about the constancy and significance of pain, and many a woman has deluded herself into the notion that she had no cancer because her tumor was not painful. Pain is sometimes pronounced and severe, even radiating down the arm; at other times it is absent until almost the terminal stage.
Any tumor in the breast which presents any one of the above characteristics is to be regarded as at least suspicious, while the occurrence of two or more of the above features should stamp it as malignant, and consequently condemn it. This is equally true of the cancers which rarely appear in the male breast.
Cancer is supposed to be a disease of middle and usually of advanced life. This, again, is an error. To be sure, carcinoma is rare below the age of thirty, and yet one sees it not infrequently in women much younger than that. One of the saddest cases I have ever known was one of carcinoma of both breasts in a young mother of twenty-two, advanced to hopeless condition because her physician had held that it could not be cancer at her age, and because she had coincided with his belief, since she had not suffered pain.
The course of a cancer in the breast depends on several factors. There is a rapidly growing type which tends to kill within a few months, this occurring usually in younger patients. On the other hand there is a slowly growing type which may last over a period of years. This is the so-called atrophic cancer, and its slow growth is due to the perfection of the protection afforded around the cancerous masses by the density of the stroma. Occurring in a fatty breast it leads to a diminution of its total mass, even though the cancerous features themselves be advancing, and this makes it sometimes hard to convince patients that a breast which is actually diminishing in size is becoming more and more seriously involved. Cancer tends ever to advance, and sometimes, as it were, by leaps, the method of invasion being usually one of steady progress and infection of the adjoining tissues; while metastases are to be expected as the case goes on, and occur sometimes in unexpected forms. Thus in cancer of the breast there is a well-known metastatic invasion of the bones, even of the extremities, with the consequent liability to so-called spontaneous fracture. In cases of the latter the former condition should always be suspected. There is a possibility always of invasion of the sternum and the ribs by continuity. It has been shown that invasion of the pectoral muscle, and even of the firm pectoral fascia, was a common result, and this demonstration has led to the adoption of the more recent radical methods of removing both of these structures along with the involved breast. In rare instances both sarcoma and carcinoma assume the miliary type, and evince it by a miliary invasion of the skin of the thorax which becomes gradually infiltrated, softened, and perhaps finally ulcerated, the involved skin thus having the aspect of a corset of diseased tissue, and being spoken of as “jacket cancer” or “cancer en cuirasse.” Such a condition may before the patient’s death involve the entire circumference of the thorax. Any of these miliary expressions of malignancy stamp a case with a hopeless aspect. General miliary carcinosis is also known to occur.
Nearly all cancers grow faster in the young. Other things being equal, there is a somewhat better prognosis for the condition in elderly people, and this applies equally to prospect of recurrence after removal.
In regard to the curability of cancer the reader is again referred to an earlier chapter on the general subject, but doubtless there is a time when if the growth were recognized and thoroughly removed it would not recur and the patient might be cured. This time is, unfortunately, too often past when the case comes under the observation of one competent to deal with it. This is due partly to fear and ignorance on the part of the patient, and unfortunately too often to failure on the part of some practitioner to appreciate the significance of the early manifestations, i. e., to a failure in early diagnosis.
Cancer also occasionally occurs in the male breast, and I have record of a number of fatal instances of this kind. It is, however, quite rare. It is usually of the scirrhus[763] type, but may be the result of epithelioma commencing about the nipple and spreading. It cannot assume marked size without becoming thoroughly distinctive, and probably ulcerating, and there should be no difficulty in diagnosis. It demands the same radical operation as cancer in the female (Fig. 525).
—In regard to the method of treatment there is but one which needs to be seriously considered, all others being fallacious and irrational. It is by operative removal alone that every hopeful case should be treated at the earliest possible date. Patients may dread the knife and some men may fear to use it. Nevertheless the above statement holds true. Even then cure is not obtained unless the knife be used thoroughly. Treatment by plasters is barbarous and unscientific, as well as uncertain and absolutely unsurgical. None of the popular remedies is of the slightest value. Treatment by the Röntgen rays should be reserved for the hopeless cases or for postoperative protection. Eradication is, therefore, the only scientific surgical relief.
Any growing tumor in the breast of a woman which cannot be clearly recognized as perfectly innocent demands operative removal, and the operation itself should be made thorough if success is to be attained. In the presence, then, of lymphatic involvement, of any adhesion or infiltration of the overlying skin, or of the surrounding textures, or of retraction of a nipple, or of fixation of the breast upon its base, operation should be advised without any reference to the question of pain. Equally important is it to decide when not to operate. When the condition is disseminated, when the presence of cancer in any other part of the body can be demonstrated, when the lymphatics of the neck are notably involved, when the arm is already swollen from obstruction to the return circulation, when the skin presents numerous miliary nodules, or when from disturbance of the heart or of respiration—i. e., chronic cough—it might appear that there is involvement of the bronchial nodes, with consequent pneumogastric irritation, then it may be held that the case is so far advanced that it is useless to subject the patient to the risk entailed by operation. There are exceptions, however, even to this statement; such as an evidently hopeless case that has reached the stage of ulceration, in which discharge is offensive or hemorrhage recurring, when operation may be done for temporary and with humane purposes.
Fig. 525
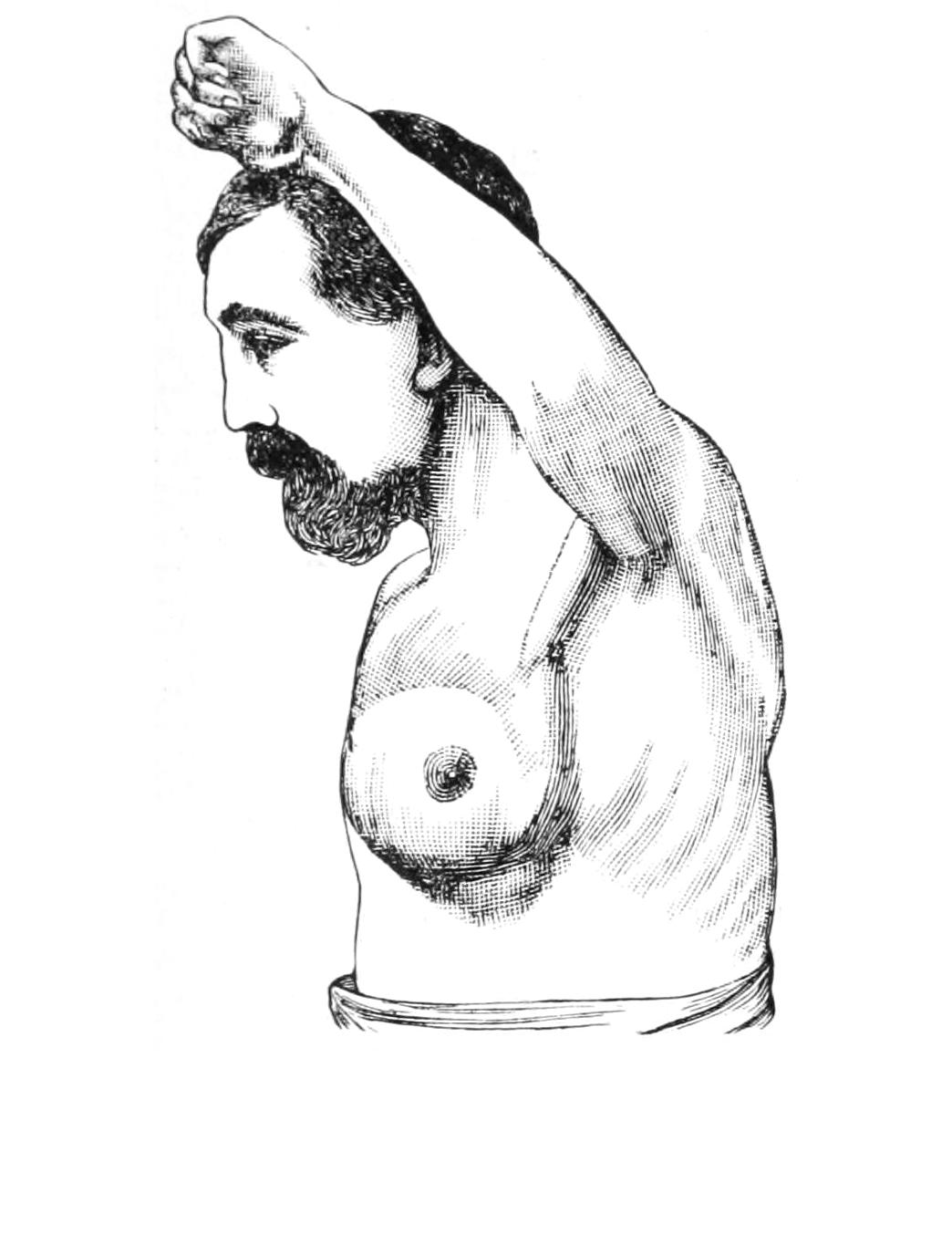
Cancer of male breast. (Buffalo Clinic.)
Fig. 526

Recurrent carcinoma eight months after incomplete operation in a woman seventy-five years of age, showing the extensive nodular, ulcerating surface surrounded by cancerous masses under the skin. The edema of the right arm from the circulatory obstruction occasioned by metastatic growths about the axillary vessels is well shown. (Parker.)
[764]
Recurrence is to a large extent inseparably connected with the matter of both early and thorough removal. Only when this can be practised should any hope of radical cure be offered. While the results attained by modern methods are very encouraging, they nowise contradict this statement. The discreet operator will, therefore, be guarded in giving a favorable prognosis or making promises. Fig. 526 illustrates many of the sad features pertaining to recurrence.
Every precaution having been taken the operator should decide whether the operation is to be enucleation of the tumor or complete excision of the breast, with dissection of the axilla. An evidently innocent tumor of small size may be removed, either through a straight incision, which should be placed radially, or by raising a flap with an ovoid incision, by which more perfect dissection is permitted. Small nodules and superficial growths may be removed under cocaine anesthesia. The first essential is to leave behind nothing of the mass which it is desired to remove; the second is exact hemostasis, and the third is the closure of the wound. It is possible to remove portions of the gland itself, as well as to enucleate tumors from within its substance. V-shaped incisions may be coapted with sutures, by which the size of the gland is reduced, but its general proportions maintained. Tumors situated posteriorly may be removed by making an incision beneath the breast, around its border, raising it from the thorax, and returning it to place after the necessary excision. It is advisable to provide a small drain for these cases, as in the more or less loose tissues of the breast blood is likely to accumulate, and by distending the wound to interfere with its repair.
Operations for cancer of the breast are performed more radically than a few years ago. This is due to a more thorough knowledge of the pathology of the disease, and to the better appreciation of the value of thorough extirpation of all affected tissues, especially if this can be done early rather than late. Therefore the modern operation includes not only the removal of the breast and of the axillary nodes, but of the pectoral fascia and muscle, the fatty tissue in the neighborhood, and everything in which the disease may lurk.
The essential feature, then, of every case is the removal of all tissue which may be involved. It is therefore necessary to remove the skin covering the mamma, as well as the structures above mentioned. This is done by elliptical or ovoid incisions, the amount thus included being sufficient to take in every particle of skin which shows the slightest possibility of infection—i. e., every nodule or dimple which may be in any way connected with the primary disease. Inasmuch as only in cases seen early is it at all safe to be less radical than just mentioned the pectoral fascia and muscle should be removed. For these purposes large and long incisions are necessary, extending from the anterior border of the axilla down toward the costochondral junction, while the lower part of the opening is divided and the incision made elliptical, in order that the breast, with its coverings, may be completely removed. The upper end should follow the lower border of the pectoral tendon, or at least be placed near it, extending as far as the insertion of this tendon, since that portion belonging to the muscle excised should be divided at its insertion and removed with the rest of the mass. The incisions then are usually carried down first to the deep fascia, and then through this, in such a way that the underlying muscle may be lifted from the thorax and detached therefrom. The result is that there is dissected from the chest wall a total mass of gland, fat, fascia, and muscle, which is continuous upward and outward toward the axilla, from which the final dissection is made. Then, commencing on the outer side of the axilla, so much of the pectoral tendon is divided as may be necessary; close beneath it will be found the axillary vein, and this is next to be freed from its cellular and fatty surroundings. The dissection is now carried toward the deeper part of the axilla, vessels being secured before division, and the entire contents of the axilla being carefully removed in one continuous mass. This requires careful and sometimes tedious dissection, which is made much easier by exact hemostasis. If the greater part of the great pectoral muscle be removed, complete exposure of the axilla is easier. When this is not sufficient, because in the uppermost portion of the axillary cone may be felt enlarged lymph nodes, at the level of or beneath the clavicle, then the lesser pectoral should be divided at its middle, and[765] its ends held apart, this affording a still better exposure of the axillary depths. By this measure the vessels and plexuses may be easily followed up to the level of the emergence of the former from the thorax, especially if the arm be held upward and forward, much depending upon the position in which the assistant thus holds it.
Everything which is actually involved should be sacrificed. This might even apply to the axillary vein, which may be doubly ligated and exsected. It will occasionally happen that it is cut or torn in some deep dissection. In this event, before resorting to final double ligation, an effort should be made to suture the opening with fine silk sutures passed with a round needle, which may be successfully done, or to secure a small tear within the jaws of a curved hemostat, may then be left within the dressings for forty-eight hours or longer; by this time a clot will have formed which will permit its detachment. While much work may thus be done upon the axillary vein the writer nevertheless has the feeling that when a case is advanced to such a degree as to demand this it is scarcely worth while, because recurrence is practically sure to follow. Nevertheless in the interest of general thoroughness, if the work has been begun, it is usually well to finish it as completely as possible.
Fig. 527
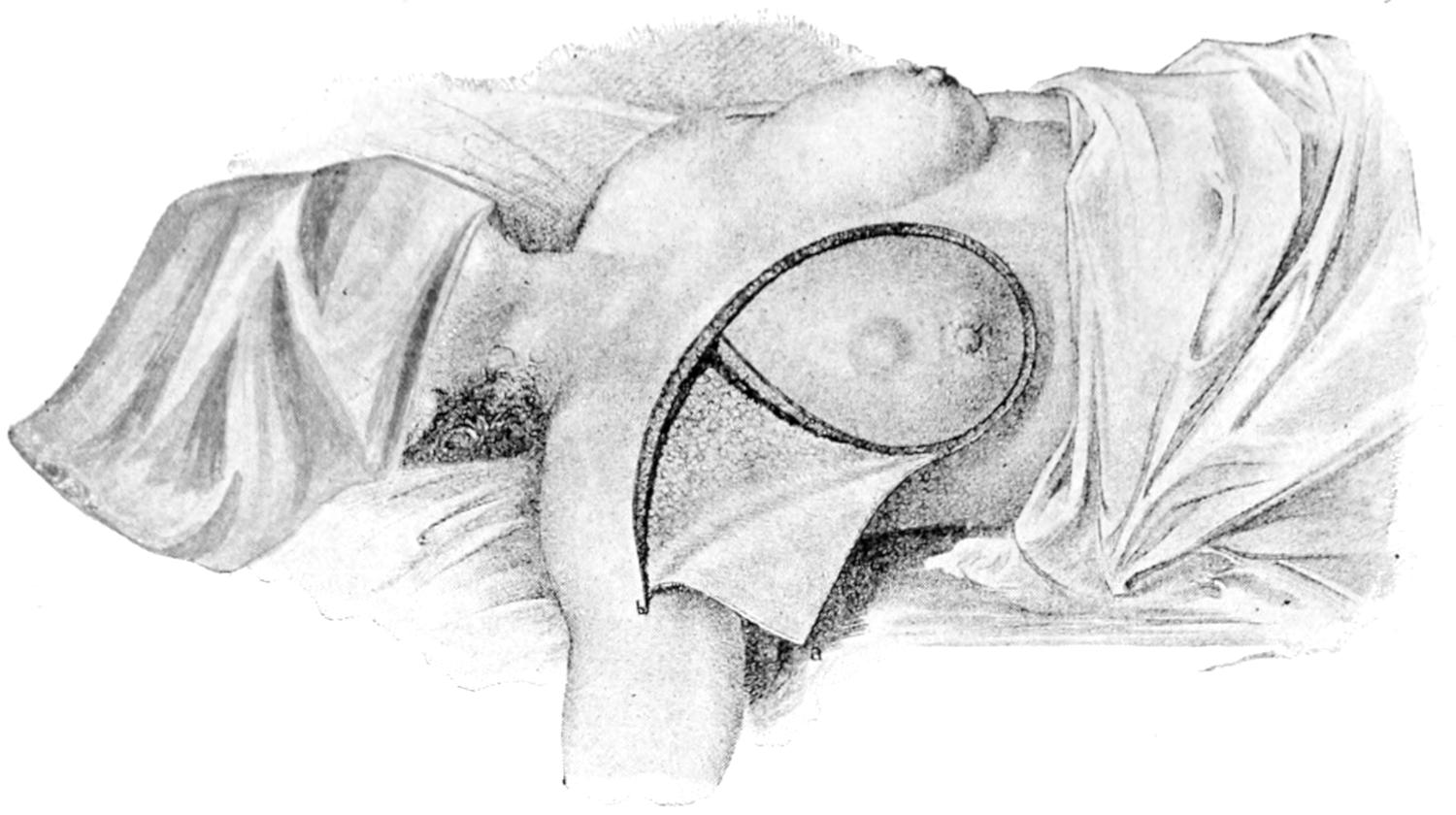
Diagram showing skin-incisions: triangular flap of skin, a b c, and triangular flap of fat. (Halsted.)
Fig. 528
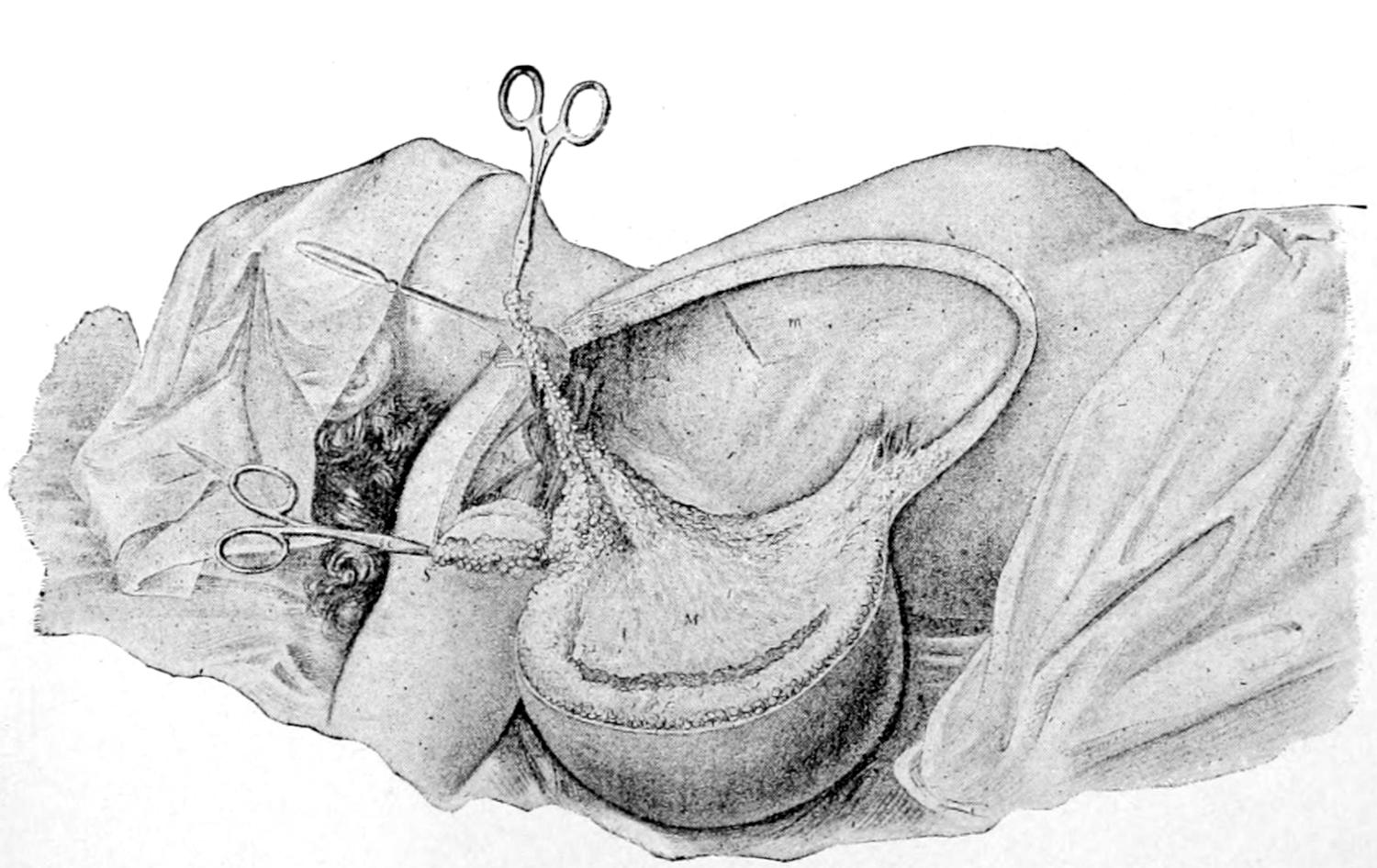
Breast and pectoral muscle completely separated from thorax; axilla exposed. (Halsted.)
The operation as thus described has been extended by Halsted to a degree which requires often much more work, and which has furnished even better results, since he[766] includes in it, if necessary, the removal of both pectoral muscles, and even the division of the clavicle for better exposure of the axillary and lower cervical regions, and the more thorough extirpation of involved lymphatics. In other cases he makes a vertical incision along the posterior margin of the sternomastoid, exposing the junction of the internal jugular and subclavian veins, and removes the supraclavicular fat by a downward dissection and the infraclavicular fat by a dissection from below. This is facilitated by elevating the shoulder, by which the clavicle can be removed one inch or more from the first rib.
Figs. 527 and 528 illustrate the incision recommended by Halsted and the general method of attack.
Throughout these operations the primary question is removal of disease, the matter of subsequent closure of the wound being a secondary consideration. Nevertheless the extirpation being completed, there arises the question of how best to close the extensive defect thus created. This will depend on its size and upon the amount of loose skin in the vicinity furnished by the patient’s general physique. With emaciated patients, whose skin is tightly drawn, it is not easy to furnish flaps, whereas in those who are fatty, with flabby flesh and skin, it is easy to rearrange the latter. Beck has suggested to make quadrilateral instead of elliptical incisions, leaving a square defect, which can then be closed by sliding flaps from two directions. The names of Warren and Meyer are also connected with elaborately described plastic operations. Years before any of these were published the writer was doing similar sliding of flaps, but never endeavoring to make them conform to a single pattern, raising semilunar flaps, or those of any other shape, as might best fill the demand, and taking them from that portion of the thorax, side, or even the abdomen, which would seem best to furnish them. There is, therefore, no one method to be especially recommended, for every operator of good judgment will be able to secure sufficient integument from some surrounding location, so that it is rarely necessary to leave such a wound uncovered. In those cases which require an amount of dissection not permitting this it is a question if operation be advisable. Nevertheless should it happen that for some reason a sufficient skin covering is not thus easily available, Thiersch skin grafts may be applied to any uncovered area at the time of terminating the operation or later, and may be nearly always relied upon for their destined purpose.
At least one opening should be made in the lateral flap in such a location as to drain the axillary cavity when the patient is lying upon her back, and through this a drainage tube of sufficient size should be inserted. This should rarely be left more than forty-eight hours. Inasmuch as there will sometimes be considerable tension upon flaps a certain number of strong and reliable sutures (silkworm or thread) should be used, to prevent parting of the wound margins, while long retention sutures may be inserted if required. The balance of the suturing may easily be done with catgut. The intent should be to leave no dead spaces. Any isolated mass of fat which stands out by itself after the dissection is complete should be pared down to the common level, in order that it may not perish from ill-nutrition, nor disturb the general level of the adjoining surfaces. It is rarely necessary to keep patients in bed more than two or three days after even extensive operations of this kind, but it is necessary to ensure that equable pressure be made with the dressings, and that the entire arm be bound to the side and immobilized in such a way that the patient cannot move it nor disturb the dressing.
[767]
That large portion of the human body which with its contents we term the abdomen was for a long time terra incognita to the surgeon. Despite the sporadic success of such men as McDowell and others there was felt, until the latter part of the last century, a universal and well-merited fear of intrusion upon the peritoneal cavity, because of the tremendous probabilities of infection and fatal peritonitis. Until the memorable researches of Lister and the introduction of an antiseptic, later of an aseptic technique, there was, therefore, the best of reason for regarding the abdominal cavity as a sanctum to be entered only when dire necessity required. In spite of the complexity of its anatomical arrangements, as well as the peculiar and widespread ramifications and connections of its vessels and its sympathetic and spinal nerves, with the almost innumerable complications thus permitted and favored, and the resulting uncertainty of symptoms and distant disturbances of function, the abdominal cavity became, first, a favorite seat for laboratory study and experiment, and then a fascinating field for surgical endeavor. Today this region is invaded by the surgeon in a manner and with a freedom which would have been criminal and unjustifiable when the writer of these pages was a student; and yet, while we have in the main lost our fear of the peritoneum and our dread of peritonitis, we nevertheless see the latter occur now and again, as it were as a punishment for forgetfulness or inattention, the patient unfortunately paying the penalty for the errors of which he is not guilty. Abdominal surgery has now become a specialty which has attracted too many of those not thoroughly fitted by training and by experience. One hears today of many, the older practitioners especially, insisting that the abdomen is too often opened; perhaps it would be more just to say that it is opened by too many. By this expression is meant simply that enthusiasm has not always been tempered by discretion, and that this is a department of surgery which has been too enthusiastically cultivated by men who have not waited to ripen their judgment or perfect their methods. My own feeling is that not merely large observation should be regarded as an essential preliminary for such work, but extensive experimentation in a surgical laboratory; while even here the tyro has to learn, perhaps by severe experience, that not all human beings can recover after manipulations which some of the lower animals bear with apparent impunity. Previous experience as assistant to a skilled operator is of the greatest value.
While uttering this caution we must, at the same time, candidly acknowledge that accurate diagnosis of deeply seated lesions is by no means always possible, and that the tendency, especially among the practitioners of internal medicine, has been, and often is, to waste valuable time in the application of methods of physical diagnosis, all of which are valuable, many extremely ingenious, and yet which prove insufficient or misleading. To give but one illustration—cancer of the stomach, for instance, is a disease absolutely without a special symptomatology. If we are to wait for the development of a recognizable tumor or other features which are unmistakably significant, we wait until the period for successful surgical attack has nearly or quite elapsed. Thus rather than permit months of valuable time to be wasted, it seems to the modern surgeon far more humane to make an early exploration, in order that he may attack the disease while it has involved but a minimum of tissue.
The general practitioner has seen himself robbed, as it were, of one part of the body after another, by the application of this general principle, until there has developed a feeling of irritation or one even more pronounced, in certain cases, of rebellion, as it were, against the cession of this territory to the surgeon; but this is wrong, and such feeling should not exist. Rather should there take place the heartiest coöperation[768] between physician and surgeon, while the operative procedures directed toward the early recognition of these more or less vague conditions should be regarded more kindly and the procedures themselves regarded rather in the light of operative therapeutics. A recognition, then, of the limitations of physical diagnosis, combined with an earnest desire to do the greatest good to the patient at the earliest possible time, when cheerfully combined, and practised by those of ripened experience and cultivated skill, will redound to the greatest credit of all concerned and afford the greatest prolongation of human life. It is to be hoped that the day when the physician shall charge the surgeon with killing his patient, and the surgeon shall have it in his power to retort that the patient did not reach him until he was almost dead for lack of surgery, may soon pass away.
Diagnosis of abdominal diseases requires, first of all, a comprehensive knowledge of anatomy and physiology, as well as familiarity with all the methods of biochemical and mechanical research, on which large volumes have been written, along with a peculiar tact which in some individuals amounts to a gift, and includes the cultivation alike of the senses of touch and sight, and the power of analytical reasoning.
While some of the intra-abdominal lesions may be recognized within a minute or two, others defy a study prolonged over hours or days. The general methods to be applied do not differ here from those available elsewhere, save that they find perhaps an even wider application.
Transposition of the viscera is one of the rare anatomical anomalies with which we may at any time meet most unexpectedly. This applies equally well to the thorax and to the abdomen, but the condition is met with oftener in the latter. It may be met as a surprise or it may be diagnosticated before operation. In one case upon which the writer operated for appendicitis he found the thoracic viscera transposed and the heart upon the right side. The occurrence is so rare as to figure but seldom in the consideration of a given case, but its possibility should not be forgotten. Thus acute pain upon the left side, with other indications of appendicitis, has been known to have an anatomical basis of this character. It will usually be easy to determine whether the liver and the spleen have changed places, and if so it may be expected to find relative rearrangement of all the other abdominal contents.
Inspection should be made with the patient well exposed, in the dorsal position, divested of clothing, and with fear and hypersensitiveness allayed as much as possible by tact, and perhaps even by the administration of some soothing remedy. Inspection should concern not alone the abdomen but the attitude of every portion of the body, the character of the breathing, the motility of the chest, the expression of the face, the degree of muscle spasm, and the fact whether pain impels the patient to move and toss or to lie quietly. Any irregularity of abdominal contour, with or without the legs flexed, should not fail of observation. The cause of any great increase in normal proportions should be promptly sought and assigned, either to collection of fat outside of the peritoneal cavity, of fluid within it, to gaseous distention of the bowels, or to the presence of some intra-abdominal growth. Any bulging in either side or loin should also be noted, as the latter may be due to some renal condition. The existence of a distended bladder should be recognized, while the appearance of the umbilicus sometimes affords valuable information, it being flattened in tumor cases or bulging and perhaps containing fluid in dropsical conditions or tuberculous peritonitis. When the superficial veins are enlarged it may be felt that there is deep obstruction to return circulation, which may be often located in the liver. When the veins of the limbs show the same result it may be believed that the obstruction is rather of the general circulation than of the hepatic, and when involving one side alone a unilateral lesion may be expected. The coexistence of hemorrhoids will indicate obstruction to the hepatic return, while varicosities of the external genitals would probably indicate it in the general circulation. Much importance may sometimes attach to the presence or absence of the lineæ albicantes, or of those pigmented areas which almost invariably indicate a previous pregnancy. Fixation of superficial tissues or of viscera implies either an infectious or a malignant process, while recognizable local edema may point to a suppurative condition if the disease be recent and acute, or to venous obstruction if it be old.
Palpation will afford information in proportion to the tactile sensibility and ability of the observer, and the relaxed, rigid, collapsed, or distended condition of the patient’s abdomen. It may afford aid in one case and little or none in another. The value of[769] what it may reveal is also greatly influenced by the pain and tenderness which its practise may cause. Its value may also be limited by hypersensitiveness or reflex contractions, from which some patients can never voluntarily free themselves. So completely may the value of palpation be limited or destroyed that every means of producing relaxation or of abolishing spasm may have to be employed. When these are present in lesser degree nothing is more efficacious than to examine the patient just after removal from a hot bath or even while submerged in hot water. In extreme cases the aid of complete anesthesia may have to be sought.
Bimanual palpation is of special service in examining the region of the kidneys or the loins, and may often be advantageously combined with the finger of one hand in the vagina or rectum. Special rigidity, like special tenderness, is always a sign of great significance. When the neurotic or hysterical feature can be eliminated one may almost hold to the view that it points unerringly to something wrong within. Palpation should include the recognition of abnormal pulsation in the aorta, and determination whether this is due to the presence of an overlying tumor or is one of those cases in which the aorta pulsates more prominently than it ordinarily should. Any abnormal pulsation should be estimated as to its expansile or non-expansile character. The recognition of a bruit may be supplemented by its further identification with a stethoscope. An intra-abdominal growth once discovered, the surgeon should obviously learn about it all that he can, regarding its real location, its origin, its movability, its density, its fluctuation, etc.; also whether there is free fluid in the abdominal cavity. It is not infrequently necessary to differentiate tumors in the lower abdomen and pelvis from pregnancy, either normal or abnormal, and one should be familiar with the ordinary evidences of this condition, as well as alert to the possibilities of such a case. The value of palpation is often enhanced by changing the position of the patient from that upon the back to the lateral or the genupectoral position.
The value of added vaginal and rectal examinations is sometimes inestimable, even in conditions which apparently do not involve the pelvic organs proper. In cases of obstruction of the bowel, for instance, the finger in the rectum may discover an intussusceptum, while in the female every tumor of the lower portion of the abdomen can be better examined and estimated by this combined bimanual palpation.
The value of palpation is increased by the addition of percussion as part of the procedure, although conditions made evident by the latter are usually detectable by the former. The surgeon will, however, rely but little upon percussion alone, although it may be possible in a large hernia to decide as to the probable nature of its contents by this test. Auscultation is of especial value in recognizing fetal heart sounds and placental or aneurysmal bruit. Friction sounds with splashing in stomach dilatation, and gurgling sounds in certain subdiaphragmatic abscesses which contain gas, are also discernible through the stethoscope.
Measurement affords ordinarily small help, save as one may in this way record the progress of a chronic or inoperable case.
Inflation by means of carbon dioxide or hydrogen was first suggested, as an aid in abdominal diagnosis, by Ziemssen in 1883, and was applied especially to recognition of perforating wounds of the intestine by Senn. Nevertheless it is but little employed, except in estimation of the degree of dilatation of the stomach or of the lower bowel, as when, by distending the colon, the kidney may be pushed backward toward the loin and the gall-bladder up beneath the ribs, the bulging thus produced settling the question of diagnosis as between enlargement of one or the other. Even this is not, however, always accurate.
The aspirating needle is now but rarely used, especially by those most experienced. In those instances where such grave doubt exists as might indicate its use it generally appears that the welfare of the patient is better observed by an exploratory incision rather than by puncture with a needle.
Pulse and respiration nearly always, and temperature frequently, give information of great value in abdominal conditions. A rising pulse or a rate over 112 to 120, occurring during any serious intra-abdominal condition, will stamp it as one of considerable severity, the gravity being proportionate to the increase above the figures just given. This is particularly true in acute appendicitis, with or without prominent local symptoms. A rising pulse rate, then, should always be considered as a warning. A very rapid, feeble, thready pulse will usually indicate a condition seen too late to justify surgery,[770] the patient being then in a condition of practical collapse. Nevertheless if it appear that this be due to hemorrhage, either from injury or by rupture of an extra-uterine pregnancy, it may be felt that so long as the pulse is perceptible the indication is present.
Respiration is markedly affected in many intra-abdominal diseases. The more thoracic it becomes—i. e., the more the abdominal muscles are disused—the more it bespeaks a serious condition below the diaphragm. A rigid abdominal wall accompanying frequent thoracic respirations bespeaks a condition of grave danger. It should never be forgotten that some of the acute diseases, especially of the lungs above the diaphragm, cause symptoms and pain referred to the viscera below. Thus in the early stages of pneumonia and of diaphragmatic pleurisy there may be thoracic respiration, abdominal spasm, and pain referred even below the waist line, with strong simulation of acute appendicitis or of localized or general peritonitis.
Temperature is an uncertain feature. Rapid elevation is usually of serious import, but one is constantly surprised at the revelations of an operation, or an autopsy, where temperature is not significantly elevated or is even subnormal. Small matters may suddenly send it up—a stitch abscess, for instance—and it is often difficult to distinguish between the pyrexia of intestinal toxemia and that of actual septic infection. When elevated temperature is intermittent and accompanied by chills the surgeon is justified in suspecting the presence of pus, although the reverse of this is not true, and pus may form within the abdomen without causing chills or even fever. Intermittent fever, with tenderness in the upper abdomen, points as often to infection of the biliary tract, usually with gallstones, as to all other conditions combined. Pyrexia with chills and enlargement of the liver may indicate hepatic abscess.
When pulse, temperature, and respiration rate seem to keep pace with each other, no matter what the rate may be, they together afford a fair indication as to what is going on. A careful blood count, especially a differential count, will often be of service, though it will occasionally mislead.
The significance and importance of pain in abdominal diseases are very great, since nearly all of them are characterized, at least at some stage, by more or less suffering. Much value attaches to the history, when it can be accurately obtained, as to the suddenness of onset, the location and character of the pain; as, for instance, whether it could be accurately localized or was diffuse. Unusual intensity of pain may afford an index to the acuteness of the trouble, but in its location or reference it may be exceedingly misleading. A large proportion of patients are unable to describe their pains with sufficient accuracy, and a neurotic patient suffering severely will evince a widespread hyperesthesia which will be deceptive. It should be ascertained whether previous and like pains have ever been experienced, and, if so, where. The pains of acute appendicitis, for instance, are widely referred, and will sometimes be complained of as intense in the left side or high up in the abdomen. I have known patients to refuse operation because they could not be convinced that, with pain on the left side, it was possible to have acute appendicitis, while even an experienced practitioner may be tempted to wait too long for similar reasons. Pain, accompanied or followed by jaundice, or a history of pain so associated in time past, will point significantly to the biliary passages. A history of previous pains constantly associated with taking of food will indicate gastric or duodenal ulcer. Still pain is probably more often associated with mechanical rather than chemical conditions. Pain arising from the gall-bladder radiates usually toward the right infrascapular region, and with adhesions between the stomach and the gall-bladder pain is frequently referred to the right shoulder, while when these adhesions are between the stomach and the colon it is more commonly referred to the left shoulder. Pains due to kidney lesions usually are referred along the corresponding genitocrural nerves, although, by association of the renal nerves with the semilunar ganglia (and thus indirectly with the phrenic and pneumogastric nerves) we may hear of shoulder pains even in these cases. In most cases of acute appendicitis the first complaint of actual pain will be in the umbilical region, since the appendix receives its blood supply from the superior mesenteric artery and its nerve supply from branches which accompany this vessel, which are given off from the spine at a higher level than those which supply the colon and sigmoid. Thus the reflected pain involves the tenth and eleventh dorsal nerves.
The pain of colicky affections is usually relieved by pressure, while that of true inflammation is made worse and is continuous. When pain is accompanied by tenesmus it[771] is generally supposed that the disease will be found in the lower third of the intestinal tract.
In this connection we may perhaps be a little more specific, and, following Hemmeter, make out a catalogue somewhat after the following fashion:
Gastritis will cause sudden abdominal pain, with sensitiveness, made worse by ingestion of fluids, by which, in all probability, vomiting will be promptly produced.
Duodenitis will cause constant pain and increased sensitiveness, especially in the right hypochondriac region, with mucus and perhaps blood in the stools.
Enteritis causes rather a colicky pain, more widely referred, with a general unpleasant sensation of pressure, accompanied by distention, diarrhea, anorexia, and thirst.
Colitis will produce more diarrheic symptoms, with more accurate limitation of pain and tenderness on pressure, while sigmoiditis and proctitis will cause characteristic stools, in addition to the localized pain which they produce. A chronic colitis may cause backache, sometimes quite sharp, while the same may be produced by a well-marked condition of enteroptosis.
The more chronic forms of enteric disorders cause irregularly recurring pains, having definite relation to errors in diet, exercise, excitement, and environment. The membranous form of colitis nearly always produces abdominal pain, referred along the course of the transverse and descending colon. The complaint of pain and the condition of the stools will be found to have a close relationship. Fecal impaction rarely produces sharp pain until it proceeds to the degree of actual obstruction, but does cause feelings of discomfort and distention, especially in the right iliac region, with more or less tenesmus.
Lead poisoning produces severe abdominal pain, distention, and tenderness, with vomiting and alternating constipation and diarrhea, which may lead to confusion, especially as a subject of lead poisoning may be a sufferer from one or the other acute abdominal conditions. Of course, in its chronic forms the characteristic line upon the gums and the nature of the occupation would aid in diagnosis.
Tuberculosis of the intestines and peritoneum produces more or less colicky pain, especially in children, with enlarged mesenteric nodes; while in consumptive patients recurring abdominal pains, with alternating constipation and diarrhea, would suggest secondary intraperitoneal involvement.
The possibility of abdominal pain being caused by parasites, especially by tapeworms, should not be overlooked.
The intestinal ulcerations produce nearly always continual pain, associated with localized tenderness on pressure. The higher in the intestinal canal the ulcer be located the more regularly will it produce pain from one to two hours after eating, while the lower the location of the ulcer the more likely are we to find recognizable blood in the evacuations. During typhoid any sudden onset of abdominal pain associated with bladder irritability, and often with pain in the penis, may be regarded as indicating perforation.
In appendicitis the pain is usually first referred to the more central portion of the abdomen, later becoming localized in the right iliac fossa. Frequently the overlying muscles will be already in a condition of spasm before this pain is localized beneath them. In this disease, no matter where pain may be referred, the tenderness will usually be felt and the resulting tumor detected in significant position. Constant mild pain and tenderness in McBurney’s region are usually indicative of a chronic catarrhal and more or less obstructive appendicitis. In the chronic and relapsing forms the pain is intermittent, but tenderness is nearly always significantly located.
Strangulated hernias, when external, will usually attract attention by their presence without reference to pain, even though the latter be referred to some relatively distant part. Whatever might be characteristic of strangulation will more or less quickly merge into symptoms of intestinal obstruction, but no case presenting local indications should escape detection. Internal strangulations nearly always defy accurate detection before operation.
Intestinal obstruction from any cause, when acute, produces early sharp and severe abdominal pain, sometimes localized vaguely, but nearly always becoming general, and so quickly followed by muscle spasm with distention and the soreness of vomiting, that, with the accompanying general disturbances, it lends little aid in accurate diagnosis.
Acute pancreatitis of either clinical type produces a pain which is central and agonizing[772] and is quickly followed by collapse, with abdominal rigidity. The resulting pain and tenderness are usually confined to the upper abdomen and may be expected at least to attract attention to this part of the belly.
Mesenteric embolism and thrombosis also produce intense pain, with pronounced depression and speedy collapse, the complaint usually so widespread as to be suggestive.
Pain made suddenly worse by extra exertion or straining, as perhaps in defecation, may be due to pressure or to rupture of some part previously involved. When this is complained of in the lower bowel it is usually due to some ulcerative condition in the rectum.
Aside from conditions briefly specified as above, there may be numerous other causes of acute abdominal pain, as, for instance, in connection with various tumors, either those which involve the bowel, where there is suddenly precipitated a condition of acute obstruction, or ovarian cysts and pelvic or other tumors which have undergone a sudden deprivation of blood supply, as by twisting of a pedicle. In nearly all of these instances the previous existence of such a tumor has been learned, or else may be made out by such physical examination as may be permitted with or without anesthesia. Again rupture of an extra-uterine gestation may produce intense pain, followed by speedy collapse and a condition widely referred. I have been repeatedly called to operate for acute appendicitis when the actual lesion was of this character.
In general, of abdominal pain, it may be said that, excluding hysterical cases, when severe it is usually an indication of a more acute condition, while mild, chronic and intermittent pain, accompanied by more or less tenderness, indicates a chronic condition which may not amount at any given time to an emergency, but which may precipitate one that may call for immediate intervention. The nearer, anatomically, the morbid condition to the stomach and the great ganglia the more likelihood there is of nausea and vomiting of purely reflex character. When these occur with conditions low in the abdomen or pelvis, vomiting may be an expression of obstruction rather than a neurosis, pregnancy, of course, forming a well-marked exception to this statement.
In the presence of severe pain the general practitioner and the surgeon alike feel inclined, from humane motives, to do everything in their power to relieve it. While, on one side, it is kind and rational to give sufficient anodyne, usually morphine, to relieve intense suffering, it may be felt sometimes that the practise is not to be too widely extended or commended, since by relief of pain the significant feature of the disease is masked, and there may be temptation to wait longer than would be advisable. While wavering, then, as between advice in either direction, my own view is that most of these cases, when symptoms are so severe, can be classified by themselves as those justifying or demanding surgery.
One last caution in this respect is needed, lest the inexperienced regard the sudden subsidence of pain as necessarily a good sign. When a patient who has been suffering from acute obstruction or acute peritonitis becomes suddenly relieved the fear is rather that the disease has gone beyond all possibility of help, and that such relief will soon be followed by coma and death. Such cessation of pain, then, is not necessarily a favorable indication.
Localized tenderness is the next most important sign of value in determining the location and nature of abdominal diseases. The more accurately it can be localized the better, since it permits us to select, in all probability, one organ or one location as the site of the disease. When it is accompanied by radiating and diffuse tenderness it may be suggestive rather than indicative.
Muscle rigidity or spasm is the third of the trio of symptoms which give the surgeon his most imperative indications. Excluding the hysterical and purely neurotic cases there is no occasion for pronounced muscular rigidity save some disease concealed beneath it, which produces these reflex phenomena. This, too, may be localized or generalized. In the latter case it may indicate, for instance, a general peritonitis or a local process tending to become generalized. Of the trio of signs and symptoms it is perhaps the most significant and reliable.
Pain, tenderness, and muscle spasm constitute the tripod upon which the surgeon has most to rely, and which are never absent in serious disease, while conversely it may be said that serious disease is rarely ever present without producing them. These with such other phenomena as special conditions may produce—e. g., vomiting, intestinal hemorrhage, etc.—are our principal aids to diagnosis. When present and progressive[773] they nearly always indicate necessity for surgical intervention, the most pronounced being in those instances where abdominal distention and collapse with other grave features have already taken the case beyond the help even of the surgeon.
In more deliberate cases aid is also to be obtained from examination of the discharges from the various viscera, and by examination, for instance, of stomach contents, as well as by differential blood count. All of these, however, take time, and the experienced surgeon may see clearly his indication to operate at once rather than to wait the time which they require. The whole intent of this paragraph, as, in fact, of this section, is not to make light of the ordinary means of diagnosis, but to insist upon the necessity for early appreciation of important signs and symptoms in order that one may know when it is not safe to wait, since too many lives are even now sacrificed to this kind of delay.
Abdominal section, generally called laparotomy, though more properly termed celiotomy, is often begun as an exploratory measure, and then called exploratory laparotomy, whose wisdom and safety may be properly explained to even an ignorant patient, the underlying intent being a relatively small and safely made opening for the purpose of orientation and decision. It is with me a rather favorite expression that the danger of such an operation is insignificant, and that the danger of whatever may be required, as revealed through the opening, is proportionate to the gravity of the condition thus indicated.
Abdominal section having once been decided upon, careful general and local preparation should be made, as indicated elsewhere in this book, if time be afforded. There are, however, emergency cases in which moments are valuable and when there must be omitted almost everything but the considerations of cleanliness. More and more I am impressed with the value of sterilization of the entire trunk, both front and rear, since should necessity for posterior drainage be revealed we need not halt in order to disturb everything else and sterilize the skin of the back. It is presupposed, then, in this place that all the ordinary measures have been carried out and that the ordinary equipment is at hand. There should always be a supply of warm, sterile water (112°) in order that the intestines may be protected, should it be necessary to temporarily remove them from the abdominal cavity, and saline solution at proper temperature should be ready for irrigation purposes, if needed.
The abdomen may be opened at any point, and by incision in almost any direction. Nevertheless there are provisions which should be observed. When there is no special reason for a lateral incision it is to be opened in the middle line; any incision, including the umbilical region, should be made to pass to the left of the navel rather than to the right. There is no reason why the entire navel may not be excised. It is a difficult point at which to insert sutures and in most individuals is at best an infected region. Therefore there need be no hesitancy to include it in an oval incision and completely remove it. It is, furthermore, a wise precaution to drop into the umbilical region a few drops of tincture of iodine just before the operation, in order the better to sterilize it. It is my custom to use one knife for the skin and then lay it aside and employ another for the deeper work, in order that no germs may be transplanted from the skin. The surgeon has to cut deeply in fleshy individuals before reaching the deep aponeurosis, and sometimes it is necessary to pass through two or three inches or even more of fat. This necessitates a long, superficial incision. The deep aponeurosis being reached we have to either go through or between muscle fibers, at least in most places. It is desirable rather to separate muscle fibers longitudinally. When opening in the middle, or parallel to the middle line, this may be done with the fibers of the rectus, the transverse tendinous intersections, however, always requiring division. Operating in either iliac fossa, and coming down upon the broad and flat abdominal muscles, there may be adopted the so-called “gridiron method,” and, after exposing those fibers which run at a right angle to the line of incision, one may endeavor to spread rather than divide them. This is done when making the small openings required in removing the appendix, or in making an artificial anus. For removal of considerable tumors, or for temporary disembowelling, large incisions, however, are required.
By suitable disposition of the patient’s body much assistance and comfort are afforded[774] the operator. When the upper abdomen, especially the region of the gall-bladder, is to be attacked, the upper part of the body should be raised with dorsal flexion above the pelvis, thus permitting gravitation away from the liver and facilitating the retraction which may be required. Again, in operations upon the pelvic viscera the reverse position was suggested by Trendelenburg, and it is of the greatest help, the pelvis and the limbs being elevated until the body assumes a position at an angle of some 45 degrees. The intestines then gravitate toward the diaphragm, and the pelvis is more easily emptied and kept empty. When, however, there is no particular need for either of these positions the ordinary dorsal position is the best. With an operation begun in the latter there should be no reason why position may not be changed, when the exploration reveals necessity for the same, and all good modern operating tables are so constructed as to permit of this being rapidly done.
Of late the transverse incision has been received with growing favor. In 1896, Küstner reported a number of cases where he had used a transverse suprapubic incision down to the aponeurosis solely for a cosmetic effect, the method being adopted by Rapin about the same time. Others went farther and made use of an incision above the pubis and parallel to it, carried down through the aponeurosis, over the recti, with vertical separation of the muscles, in order to diminish the chances of hernia. The incision is made just below the margin of the pubic hair or in the natural fold of the abdomen. The fascia being divided in one direction and the muscle in another, there is less tendency to hernial protrusion, the disadvantages being that there is limited space through which to work and that more time is required in its performance. All vessels should be secured so soon as divided. The incision through the fascia may be somewhat curved, if necessary, at the outer edges of the recti, by which a sort of horseshoe flap may be lifted up if desired. The fat should not be dissected from the surface beneath. Scissors will be required to separate the aponeurosis from the muscles in the middle line, this separation being made high in the same line. The peritoneum is opened in the middle with the usual vertical cut. When more room is required the aponeurosis should be incised farther on each side, outside of the recti. The method finds its greatest serviceability in those cases where not more than four inches in a thin woman and two inches in a fat woman of vertical separation of the recti muscles will be required.
Ordinarily when the peritoneum is reached there will be no difficulty in recognizing it. It is a membrane easily shifted, both upon its attached surfaces, beneath the fat, and over the bowel or whatever may cause it to protrude into the wound. Unless one is very sure of his work he will, however, pick it up very carefully, nick it slightly, and convince himself that he has the desired membrane, and then will dissect it with care, since the bowel beneath will lie closely in contact with it, and might easily be wounded were the operator careless. The peritoneum in the presence of such disease as tuberculous peritonitis becomes very much thickened, and is then not easy of recognition. Again, it is sometimes slightly adherent in the presence of recent exudate, or firmly adherent in the presence of old disease, to the tumor or viscera beneath. When the tissues are edematous and become more so as the peritoneum is approached, pus may be found beneath, and extreme caution should be exercised, making at first a small opening through which pus may escape, and endeavoring not to tear adhesions apart nor thus permit escape of pus into the peritoneal cavity.
The true abdominal cavity once opened, the first endeavor should be to ascertain the conditions within. Through a small opening this is done with the finger. This measure, trifling as it seems, requires a knowledge both of normal and pathological anatomy which cannot be too great. Unless the normal arrangement, size, density, and location of all its contents is known and the way which they should feel when healthy it will be somewhat difficult to distinguish between health and disease. Again, unless the surgeon is familiar with pathological conditions he will not know how to interpret what he may thus discover. Through a small opening it can usually be discovered whether or not there is a serious condition within. According to knowledge thus gained there may be justification for enlarging a small opening or closing it. One caution here is of the greatest importance—an exploratory operation should never be begun unless the operator is provided with means for meeting any indication which should thereby be disclosed, else the patient would be subjected to two ordeals when one should suffice.
The “diagnostic finger,” having once entered the abdominal cavity, should be used with extreme gentleness, especially in the presence of adhesions, which yield easily, and[775] which may point to the existence of a purulent focus in the neighborhood, as scarcely any disaster could be more fatal than to rupture such a focus and permit escape of its contents in every direction before surgical protection has been afforded. Much will depend upon whether there is reason to suspect the presence of pus, and it is always best to proceed as though such a contingency might happen. Again, adhesions which seem firm may be met with in the presence of malignant or ulcerative disease. In some instances they will be so firm that surrounding normal structures will yield before they part, or are closely associated with a dense adhesion which will be found a weakened area that will tear easily. The process of separating adhesions, then, should always be conducted with extreme caution.
When the presence of pus is suspected the adjoining parts should be protected by “walling off” with gauze. Gauze pads, either of sufficient length to be secured with forceps or provided with tapes for the same purpose, by which their loss in the abdominal cavity may be prevented, are now used almost to the exclusion of the flat sponges formerly employed, for they are more reliable when properly sterilized. With a sufficient number of these spread out as carefully as may be, a neat padding or protective wall of gauze is made and formed around the focus of disease, into which any discharge of blood or pus may take place, and by means of which contact of surfaces is prevented. Sometimes a large amount of gauze is needed for this purpose, and when the abdomen is widely open sterile towels may be used. The greatest care should be given that nothing be left within the abdomen at the completion of the operation, and every loose piece of gauze should be secured with forceps and every towel accounted for. By this protective “walling off,” spreading of an infectious process may be prevented, as also the distribution of infectious material. The gauze should be changed as often as needed and there is often no apparent limit to the amount that may have to be employed. Advantageous as the process may be, it has its disadvantages, in that material so employed is a source of irritation and is practically a foreign body, intruded within the abdomen in such a way as to have always a depressing influence. This depression, however, is but temporary, and is the lesser of two evils, and in the presence of pus can scarcely be avoided. Instruments, especially the smaller ones, should also be counted before and after operation, or be so accounted for that none may remain or be lost.
The general indication having been met, the next question is one of local cleanliness and resort to irrigation. If the protection above described has been sufficient there will be a minimum of local cleansing required. This may be effected with hydrogen dioxide, or with or without other antiseptics, according to the choice of the operator. Obviously every focus of disease should be as thoroughly cleansed both of clotted blood and debris or pus. When this can be accomplished by gentle wiping or swabbing it may be sufficient. When this is not possible irrigation and drainage should be provided.
Irrigation of the abdominal cavity has been widely practised, and has advantages as well as disadvantages which have caused it to be differently regarded by different operators. While little hesitation need be felt about washing out a well-localized cavity, it is felt by many that to use a quantity of water within the complicated peritoneal cavity is to more widely distribute that which would best be not disturbed. On the other hand, it is maintained by some that infectious material so diluted and scattered is more easily capable of disposition by natural processes. The general trend of opinion is that a localized condition is best treated by local measures, and that general abdominal irrigation should be limited to cases of generalized infection. The temptation to use antiseptic solutions is very strong. Yet one must remember that any solution, of which a portion must remain, used in such a cavity and having sufficient strength to kill bacteria, will prove at least profoundly and perhaps fatally toxic to the individuals, because the peritoneum is a membrane of tremendous potential capabilities in the matter of absorption, and those chemicals which are toxic to germs are also harmful to the human tissues. Strong, then, as the temptation may be to use antiseptics under these circumstances, solutions used for the purpose should be made extremely weak if we are to do more good than harm. Warm sterile water or saline solution is then the generally accepted irrigating fluid, while a few use such antiseptics as acetozone in the strength of 1 to 10,000, or others of the more harmless drugs. In cases of tuberculous peritonitis exception may be taken to this and a solution used which is sufficiently strong to have some perceptible immediate effect.
When general abdominal irrigation is practised quarts and even gallons of fluid should[776] be used, sufficient to accomplish the desired purpose. Various tubes have been devised for the purpose of conducting the fluid into the deeper recesses, and yet these, while convenient, are not essential. Practice varies somewhat as to whether to leave a considerable amount of saline solution within the abdominal cavity or try to free it of all fluid. The former practice is desirable, in theory at least, for if readily absorbed it will help in relieving shock and keeping the kidneys active. In general it may, however, be said that unless an isotonic saline solution is employed it is advisable to remove all that can conveniently be withdrawn before closing the belly.
The next important question is one of drainage, and here, again, men differ widely in their opinions. A distinctly purulent focus is doubtless always best drained. The question is argued rather with regard to the matter of possible spread of infection or in cases of general doubt. Drainage is always a confession either of fear or of impossibility of ideal removal of the primary difficulty. It certainly is less practised than in years gone by, but will always find a certain field of usefulness. Thus after some deep, extensive pelvic operations, where the separation of adhesions almost ensures a certain amount of leakage of blood, one should insert a glass or metal drain for a few hours, or a day or two, and through it aspirate at intervals such amounts as may accumulate in the cavity thus emptied. Nearly all cases of abdominal traumatism require drainage, best applied posteriorly, and practically all instances of acute pancreatitis, whether purulent or otherwise, will also require it, posteriorly as well as anteriorly. All old abscess cavities also demand drainage, no matter where located. No case of septic peritonitis, general or local, can be safely closed without similar provision. Drainage through the cul-de-sac is the best method of all, when available.
Drainage methods include the use of hard tubes made of glass, aluminum, or celluloid, perforated with numerous openings through which fluid may escape into their interior. These are used mainly for drainage of the pelvis through an abdominal wound. Soft-rubber tubes of varying sizes may be used in many ways, either by themselves or when split longitudinally, and made loosely to enfold a strip of gauze, or when lightly wrapped with gauze and covered with perforated oiled silk. Except when it is desired to drain a gall-bladder or some similar circumscribed cavity, which can be closed around the tube, such tube should have numerous large openings cut in it. Cigarette drains consist of small rolls of gauze wrapped with oiled silk, then fenestrated and secured with a piece of catgut tied around it to prevent it unwrapping.
Ordinary absorbent gauze or prepared gauze may be used by itself to any desired extent, but when so used it is usually well to make the amount sufficient to effect the purpose. Thus a drain at least one inch in diameter or even exceeding that size will be much more effective than two or three small strips. In using this it is well to protect the wound margins with strips of oiled silk, between which the gauze is deeply passed, as in this way its adhesion to the wound edges is prevented, such adhesion being undesirable both because it helps to prevent the escape of fluid and causes pain when the gauze is removed. In this way it is well to combine the double purpose of drainage, and pressure to check oozing, by packing in sufficient gauze to accomplish both. These gauze drains, when well soaked with discharge, are easily removed. Otherwise they frequently adhere and cause much discomfort during the act of removal. In such a case it is an advantage to wet them from the outside, perhaps three or four hours before withdrawing them. Even with such a gauze drain there is always the danger of causing fecal fistula if it be left too long in situ. It is, therefore, always undesirable to leave a drain, even of this apparently innocent character, longer than absolutely necessary.
In not a few cases through-and-through drainage—i. e., by a counteropening—will be of great value, this especially in many cases of peri-appendicular abscess, where pus has collected behind the cecum. So-called posterior drainage of the abdomen is also advisable in cases of acute pancreatitis or deep retroperitoneal phlegmon. Here the opening is made from the back, by an incision two or three inches in length, just outside the upper part of the quadratics lumborum and near the costovertebral angle. In stout individuals a distance of two or three inches, or even more, must be traversed. After the more superficial incisions this opening may be effected by blunt dissection, and is best done with conjoined manipulation, one hand working on the exterior and the other in the interior of the abdominal cavity. Occasional necessity for such posterior drainage shows the wisdom of the practice of sterilizing the back as well as the front of the body as part of the preparation for operation.
[777]
Drainage having been effected by one of the above methods, the best of good judgment will be called for in determining how long it should be continued. First of all, no drain which fails to effect the purposes intended should be allowed to remain, and any drain around rather than through which material is discharged may be regarded as useless and a mere deleterious foreign body. Gauze which is supposed to drain by osmosis often fails, and in some of these drains it may be well to insert a few strands of silkworm-gut in order that material which is to become moistened may not collapse and adhere, thus destroying its own capillarity. A pelvic drain in a non-septic or but slightly septic case, inserted for removing escaping blood or collecting serum, may be removed in from twelve to sixty hours, according to the amount of discharge, which when collected with a syringe should be carefully estimated. Any cavity which is not filled at a rate faster than 2 or 3 Cm. in an hour may be regarded as capable of disposing of all the fluid which may collect within it, and every tube which is no longer needed is an irritating foreign body, whose lower end may press upon intestine, and even produce ulceration if allowed to make pressure too long. Appendicular abscesses usually require to drain from two to three or four days; gall-bladders and hepatic abscesses for a much longer time. In nearly all instances it may be expected that within from forty-eight to sixty hours after the establishment of drainage a natural passage will be formed, by exudate appearing first around the drain, and remaining after its removal, which should serve drainage purposes as would a canal. Sometimes the outer end of such a canal tends to close too quickly, and then with accumulation in the deeper part there may come retention, with later spontaneous escape, or possibly rupture into the abdominal depths, which may be serious. In nearly every instance, however, a large drain may be substituted within a short time by a smaller one and final removal be thus accomplished. Any localized cavity whose discharges are offensive or putrefactive should be cleansed each day, either with hydrogen peroxide or by gentle irrigation, or with a reasonably strong antiseptic solution—iodine, silver nitrate, etc. While no such cavity will close until all such material has escaped, it nevertheless is well to keep the external opening wide open, in order to hasten the whole process. This may be accomplished by gauze packing or the insertion of a short tube.
Cavities which persist, with apparently permanent fistulas, require more radical treatment, which will consist at least of a thorough curetting and considerable enlargement of the fistulous opening, in order to permit of this. Such a cavity, then, may be comfortably packed with gauze for a few days.
The use of massive tampons and the introduction of large-sized pieces of gauze into the abdominal cavity have been generally discontinued, largely through the writings of Morris, who stigmatized such practice as “committing taxidermy upon patients.”
Abdominal drainage may be favored by one other expedient—i. e., position. The peritoneum possesses unusual powers of absorption and is capable of taking care of morbid material up to a certain point. It has been shown that the peritoneum of the upper abdomen especially, even that lining the diaphragm, is particularly potent in this direction—next to it perhaps that of the pelvic cavity. Septic processes in the upper abdomen are then sometimes advantageously dealt with by placing the patient in bed in a position with the pelvis considerably elevated and the head dependent. This is the more valuable after irrigation has been practised, where there may be considerable fluid which may thus gravitate. On the contrary, in serious septic pelvic infections it is often good practice to keep the patient in the semisitting posture, so soon as sufficiently recovered from the anesthetic. (Fowler.) These expedients are perhaps the more valuable when provision is made in either one of the dependent portions for drainage, gravity thus favoring the accumulation of fluid where it can be best cared for.
In what may be termed a clean abdominal operation it is seldom that drainage is provided. Such cases are expected to heal promptly and the wound to close immediately and without pus formation. It is only in cases where drainage has been necessitated that there is a really legitimate excuse for subsequent yielding of the scar, and the production of postoperative ventral hernia. These at least are the ideal and theoretically correct notions, although it should be acknowledged that in the practice of even the[778] most competent such undesirable sequels as ventral hernia do sometimes occur. Foreseeing the possibility of their occurrence and realizing the conditions which permit the same, every known precaution should be taken. The question then of the method of closure of even a small abdominal wound is one of great importance, which has long engaged the attention of the most experienced operators, who have not yet united upon what all consider the ideal or perfect method. In general it may be said that suture of each separate tissue layer comes nearest to this ideal, along with the employment of a suture material which should serve its purpose sufficiently long, and yet not remain as a possible future irritant. When time is afforded, and there are no contra-indications, the following may be given as the best directions in this regard: A suture of the peritoneal edges, with or without the deep fascia. In or near the middle line the posterior sheath of the rectus may also be included in this row. These sutures should be inserted with extreme care so as not to include any peritoneum of the bowel surfaces. Then the muscle edges are brought together by a second row, over which the deep aponeurosis is covered and brought together with a third row. Rather than fail in accurate approximation of this third row it would be better to overlap the edges and fasten them together in this position. These sutures should be made with hardened catgut, of whose sterility and durability there is no question. It should have been so treated that reliance may be placed on its remaining for at least twenty days. The method with the balance of the wound may depend to some degree upon its thickness. In individuals with fat abdominal walls it is better, in order to avoid dead spaces, to insert one or two rows of buried sutures, by which the fatty surfaces are brought into contact. Finally the skin margins may be approximated, either with a subcutaneous chromic or silkworm suture, or by the ordinary continuous or interrupted suture, which may be made, according to choice, of celluloid thread (Pagenstecher’s linen thread soaked in a celluloid solution and thus made non-absorbent), sterile silk, or fine wire.
The nature and the location of the incision and the thickness of the tissues, along with the degree of tension which may be made upon them, will to some extent determine how the more superficial stitches may be placed. The depressing effect of postoperative vomiting may be forestalled by placing another set of three or four mattress or quilted sutures, which may be brought out at a distance of two or three inches from the incision and guarded with shot, plates, or rolls of gauze. These sutures have a tendency to take off tension from those immediately closing the wound and are a valuable means of securing primary union.
Ordinarily, as stated above, one never drains the abdominal wound proper. Nevertheless if it has been infected by contact with gangrenous or infectious material it is better to leave some opening for escape, or else, as a final precaution, to trim the surfaces which have been exposed and bring into contact only those which are absolutely fresh and uncontaminated. In gunshot wounds, for example, unless the track of the missile has been cleanly excised some provision should be made for drainage thereof.
A further protection should be, however, afforded in the dressings, by strips of plaster placed over the deeper dressings, by which again tension is taken off the wound, and still further by such snug bandaging and arrangement of compresses and dressings as shall complete this protection.
There are occasions when this procedure, which necessarily consumes a little time, cannot be completely carried out, and when there must be haste in order to get the patient off the table in suitable condition. In such cases the operator usually contents himself with the application of silkworm-gut sutures, which include the whole thickness of the abdominal wall, or the use of secondary sutures, which can be tightened and utilized later. As Binnie has said: “Inexperienced surgeons, after completing a prolonged operation on an exhausted individual, sometimes forget that it is better to have a postoperative hernia in a living patient than a perfectly closed wound in a corpse.”
While in the general principles regarding the after-treatment of abdominal cases practitioners are well agreed, the world over, they differ so in regard to minor points that it is difficult to give explicit directions which shall be acceptable to all. Much will depend upon whether the patient has had suitable preliminary preparation. If, for instance,[779] the bowels have been thoroughly emptied there need be no haste to administer laxatives, as though this had not been the case. In many instances where this precaution has been neglected catharsis is, after operation, the most important consideration, and yet this may be difficult to secure, the difficulty being enhanced by the fact that an individual just operated on and extremely tender finds it difficult to give natural assistance to the process of defecation. The matter is particularly complicated by the difficulty of selecting an active cathartic which may be retained by a sensitive stomach. One of the greatest needs of the surgeon, as well as of the physician, is a suitable medicament of active cathartic properties which can be satisfactorily administered with a hypodermic syringe. Nothing of this kind is as yet known.
It is good practice in many cases to throw into the intestine, through a fine needle connected with a large syringe, a considerable quantity of saturated solution of Epsom salt before closing the abdomen. This places it where it will not be rejected by an irritable stomach, and where it must have the desired effect. The needle so used should be carefully introduced, in a very oblique direction; while should the minute puncture bleed or seem to leak it may be included in a suture or ligature loop, which should take up the peritoneal coat only. In addition to this, an occasional expedient, the writer usually administers, before the patient leaves the table, a subcutaneous injection of ¹⁄₅₀ Gr. of eserine sulphate, the active principle of Calabar bean, this being a powerful stimulant to the muscular coat of the intestine. The bowels should be thoroughly emptied in the easiest manner after every operation.
The next question is one of pain. Patients should not be allowed to suffer when morphine is at hand, and this would always be true were it not that morphine has, at times, undesirable effects, both in checking intestinal activity and in “locking up the secretions.” Moreover, it frequently nauseates. On the other hand, patients who have undergone serious operations need to be kept absolutely quiet, and to be prevented from tossing and moving themselves in bed. Some expedient then is called for in many cases, and one may, if he choose, begin with the milder of these—such, for example, as the administration of 2 Gm. each of chloral and sodium bromide, with or without chloretone, in a little saline solution or sterile water, thrown high in the rectum. When pain is not severe this is frequently sufficient to soothe and allay, and often to produce sleep. It reduces or prevents the nausea with which many patients suffer. This, too, may be given before the patient leaves the table. Such an enema, with or without asafetida or other soothing drugs, may be repeated as often as indicated, and does much to quiet a rebellious stomach.
It is assumed here that the reader is already familiar with the precautions advised before the administration of anesthetics and that it is now simply a question of after-treatment. (See Chapter XX.) My own advice is not to withhold morphine in those cases which seem to require it, remembering, at the same time, that suitable management of the stomach is required. It is inadvisable to permit the patient to take any fluid in the stomach for several hours, for even plain water will upset a stomach which has seemed to be perfectly calm and controllable. According to the degree of nausea and discomfort should the stomach be used, the patient’s need for fluids being supplied by more or less copious saline enemas. So soon as the stomach becomes quiet ice pellets or small quantities of water, as hot as can be borne, may be used, the latter frequently proving the more acceptable.
Until the bowels are freely moved whatever food may be administered should be fluid, and, under most circumstances, not more than forty-eight hours should elapse after any operation before the intestinal canal is emptied. Milder degrees of nausea may be treated by the use of milk of magnesia, of small doses of orthoform, or by a mixture which the writer is fond of using, in each dose of which the patient receives 0.02 of cocaine, one minim of carbolic acid, and one or two minims of dilute hydrocyanic acid, in a small amount of water. I have found this in many instances very soothing.
The after-management of many of these cases includes also the treatment of shock and collapse, which have been considered in a previous chapter. It should include, also, suitable attention to the bladder, and a catheter should be used within the first ten or twelve hours if no urine be passed, and as often thereafter as may be necessary. Catheterization should be conducted with the same precautions as indicated at any other time. Other details of after-treatment, such as the removal of drainage materials, change in position of the patient, etc., have been discussed. Stitches of chromic catgut[780] need no further attention, while those of silk or thread will need removal. It is to be emphasized that the great danger of the so-called stitch-hole abscesses comes not so much from the material first employed as from failure to protect it and guard it against the possibility of subsequent infection. Non-absorbable sutures in the abdominal wall are usually allowed to remain from ten to twelve days, but any stitch which is seen to fail in accomplishment of its purposes should be immediately removed, as should also stitches around which a drop of pus is seen to be escaping.
Certain abdominal wounds, especially in fleshy individuals, seem to heal perfectly, then part a little and give vent to material which is hardly pus, but appears more like liquefied or altered fat. Such, in effect, it often is, and the condition implies a necrosis of a certain amount of fatty tissue, with its liquefaction and escape instead of absorption. In this way a small cavity will be left which should heal by granulation, and this may be hastened by the use of mild nitrate of silver solution.
A patient having been removed from the operating table in a satisfactory condition the principal danger is that of internal hemorrhage, which, though fortunately rare, is disturbing when it does occur. In fact, severe abdominal hemorrhage is one of the most serious of surgical accidents, either primary or secondary. It may occur from wounds of all descriptions, as the result of erosion, perhaps of a foreign body, even of a drainage tube, from the slipping of a ligature, from reaction after shock, the heart recovering its vigor and pumping blood out from the vessels which had not previously oozed. In other instances, of course, it may be the result of rupture of an abdominal aneurysm or the twisting of the pedicle of an abdominal tumor. Constitutional causes which contribute toward it are jaundice, both with or without accompanying cholemia (mentioned more particularly in the section on the Biliary Passages), hemophilia, scurvy, and that form of myelogenous leukemia for which splenectomy has been occasionally performed. In all these cases the patients are abnormally prone to bleed freely. When this condition is suspected it is well to determine the coagulation time of the blood. If this be over six minutes the calcium salts, with iron and fruit acids, should be administered some time previous to operation.
The most important symptoms of postoperative or internal abdominal hemorrhages are rising pulse, with fall in temperature, pallor, and that marked reduction of blood pressure which gives rise to the ordinary symptoms of shock or collapse, along with extreme restlessness and disturbance of vision or almost complete blindness. When there has been any notable collection of blood within the abdomen there may be found dulness on percussion over the flanks. Richardson has spoken of the nurse’s duty and the surgeon’s duty under these conditions, the former being to recognize the indications of increasing shock and alteration in pulse rate, the latter being to adopt every expedient for the checking of hemorrhage, including, in many cases, prompt re-opening of the abdomen. The more promptly this measure is instituted when demanded the greater the probability of saving the patient.
The principal danger after all abdominal operations, next to the possibility of hemorrhage, which rarely occurs, is that of peritonitis, a danger so imminent in the pre-antiseptic era as to have made the abdomen an almost sacred cavity, but one which is now almost abolished by perfection of aseptic technique, yet calling for never-ending care and attention to detail, and occurring occasionally in spite of all the precautions which the most experienced and conscientious operator can take. This condition is to be feared when vomiting continues or comes on afresh, and in the presence of tympanites, with a steadily rising pulse. The first appearance of these threatening signs will be always a warning, although not invariably an indication of danger, since the condition producing them may be averted by catharsis or by meeting some special indication. Septic peritonitis, the great dread of the abdominal surgeon, and practically the only form with which he as such has to deal, will be considered by itself a little later. Yet it is always a question whether it is advisable, even in these cases, to administer powerful cathartics which provoke undue intestinal motion and favor the distribution of infection. While it is true that opium masks symptoms and leads to erroneous conclusions the same is frequently true of cathartics. From them a really obstructed or really paralyzed bowel suffers harm rather than good. They are too sparingly absorbed, and if absorbed their effect is bad. It is much better in these cases to wash out the stomach with a weak soda solution, and then keep it empty, emptying the lower bowel by the same means, and thus placing as much as possible of the intestinal tube at rest.[781] With from 1000 to 2000 Cc. saline solution introduced beneath the skin each twenty-four hours patients can be kept from starving for a sufficient length of time to permit of other treatment for the condition.
—Contusions of the abdominal wall may be followed by serious consequences, even though they have the appearance of being trifling. The injury that may be done implicates not alone the abdominal wall proper, but the viscera beneath. A blow upon the abdomen, followed by immediate collapse of temporary character (as the history of many a prize fight has shown), indicates a sudden reduction of blood pressure, the nausea and other features being due to the mechanism of the semilunar ganglia and the sympathetic nerves.
Contusions of the abdominal walls alone are serious largely in proportion as they are followed by extravasation or hematoma, since from failure of absorption of the latter there may result a cyst, or possibly an abscess should local infection occur. In either event evacuation and suitable local treatment are demanded. But any blow, even without penetration, may give rise to serious disturbances within the abdomen. Thus, as Richardson has said, the hollow viscera are liable to rupture, with extravasation, the solid to fracture with hemorrhage, while lacerations of the omentum or mesentery may produce immediate hemorrhage and subsequent possibility of intestinal obstruction. When extravasation has occurred distention and the ordinary evidences of peritonitis supervene. When the spleen or liver has been torn or crushed there will be obtained evidences of extensive internal hemorrhage.
Of the hollow viscera much will depend upon the degree of their fulness—especially with fluid. In a small tear there may be eversion of the mucosa, which may hinder or even prevent extravasation. Escape of infectious material into the cavity of the lesser omentum may produce local peritonitis, with subsequent development of what is practically a subphrenic abscess. When the patient vomits blood it shows that there has been rupture of the gastric mucosa. Intestinal rupture will be made known by rapid distention and the ordinary evidences of acute peritonitis. These injuries rarely lead to vomiting of blood, but when occurring low in the bowel may lead to the occurrence of bloody stools. Rupture of the spleen or pancreas is rarely diagnosticated previous to exploration, save as a severe abdominal injury. It is not so likely to lead to rapid peritonitis. Rupture of the liver permits of more or less escape of bile, as well as of blood, and rupture of the gall-bladder permits the free emptying of bile into the upper abdomen. As this is usually harmless, in otherwise healthy individuals, the injury is not necessarily so serious as might appear. In such a case the resulting peritonitis will probably be local rather than general.
In this connection may be considered ruptures of the kidney, which are produced by similar injuries to those under consideration, and which may permit escape of urine or blood into the abdominal cavity, as well as the appearance of blood in the urine. While these will be considered in another place the possibility of their complicating abdominal injuries cannot be overlooked.
Considerable laceration will predispose to subsequent hernias, either direct or indirect, in the latter case by absorption following injury. The more serious consequences of abdominal contusions—i. e., the deep hemorrhages and lacerations of viscera—may then include all degrees of such injury, from trifling subperitoneal ecchymosis to extensive ruptures of such organs as the kidney or liver, or perhaps multiple perforations of stomach and bowel. These deep injuries will be considered by themselves when dealing with special organs. It is sufficient here to indicate their possibility and to warn that every severe contusion of the abdomen which is followed by local symptoms, or those which are grave and progressive, may at any time demand exploratory section, which should be made early rather than late. It is advisable to pass a catheter to make sure that there is no blood mixed with the urine, and to make a rectal examination in order to discover blood should it have escaped.
Penetrating wounds of all descriptions, punctured, incised, and gunshot, are again of importance largely in proportion to the damage done to intestines and great vessels. Some of these injuries are so evidently superficial that exploration may be abstained[782] from, but every penetrating wound which has truly penetrated is to be treated either as they are treated on the battle-field, by mere inspection and occlusion, or by careful exploration under all aseptic precautions. What the operator would do deliberately may not be what he can do in an emergency, but if he cannot reach one extreme he would best be content with the other.
Abdominal contusion has been found by Makin to be the cause of about 70 per cent. of the cases of intestinal rupture which have followed sudden or sharp blows, while the other 30 per cent. have been due to the passage over the abdomen of heavy objects. Le Conte has well summed it up in the following words: “If the force be circumscribed, and of high velocity and of small inertia, such as a kick or blow from some rapidly moving object, crushing of the intestine is more likely to occur; while if the force be diffuse, as from a slowly moving, ponderous object of considerable inertia (e. g., a wagon wheel), the belly is more apt to be torn at one of its fixed points or the mesentery injured. Thus out of 61 cases of horse-kicks of the abdomen in 59 intestinal rupture occurred. When the abdominal muscles have been braced in expectation of a blow less harm results than when it has been suddenly inflicted upon a relaxed musculature.” Crile has shown that the more specialized and abundant the nerve supply to a given viscus the more will it contribute to the production of shock when injured.
Pain is not always an immediate symptom. It may be delayed for hours, or possibly even for days. When intestinal rupture has occurred pain is most often referred to the central portion of the abdomen. In rupture of the spleen it is complained of in the left side, while when the kidneys have been ruptured pain follows the course of the ureters to the genitals and there is usually retraction of the testicle.
Muscle rigidity is a sign of equal diagnostic value with pain, and immobilization of the abdominal wall nearly always indicates intestinal rupture. The facial expression is also of importance, it being in the more severe cases almost distinctive. A steadily rising pulse is always a bad sign, usually indicating a developing peritonitis. Vomiting, if long continued, after a patient has rallied from the immediate shock, is considered of itself to justify operation. The same is true of paralysis of peristalsis.
Such injuries to the abdominal walls proper may divide important vessels, such as the epigastric, and give rise to hemorrhage which may be internal rather than external. The first and most important danger of hemorrhage having been passed or being avoided, the next and always urgent risk is of infection. This may come from non-penetrating injuries, as well as those which open a wide path into the interior, and it is sometimes the small punctures which prove most disastrous.
From any wounded abdomen there may protrude omentum, intestine, or portions of some other abdominal viscus, while extensive abdominal incisions permit more or less evisceration. There are cases on record of pregnant women being injured by the horn of an infuriated animal and having the entire abdomen, as well as the pregnant uterus, ripped open, everything thus escaping. The omentum is the most likely to escape through small openings of all the abdominal contents, and this is fortunate for the patient for reasons to be mentioned in connection with the omentum and the peritoneum.
When the nature or the appearance of the wound make a complete perforation of the abdominal wall probable it will always be safer to be satisfied regarding deeper conditions. The parts having been thoroughly sterilized the ordinary probe is rarely sufficient, the best method of orientation being the sterile finger. Its use may require enlargement of the incision, and this should always be made. Such an opening being made and proving insufficient should be enlarged to any desired extent. Possibly a deep condition will be thereby revealed, which will make it expedient to open the abdomen freely in the middle line, and to deliberately practise one of the many expedients called for in such an emergency, such as ligation of vessels, intestinal suture, removal of a foreign body, and the like. The indication once met the incisions are closed, an infected wound being suitably drained.
In general it may be said that laparotomy is the wiser course in nearly every instance, and that it should be done when the surgeon is in actual doubt as to its necessity, it being better to give the patient the benefit of the doubt and operate. In all cases with serious symptoms it is certainly safer than to wait for further symptoms. This will appear advisable in view of Curtis’ collection of 116 cases of intestinal rupture which were left unoperated, all of which died.
[783]
—In regard to gunshot wounds the principles of treatment in civil life are different from those obtained in an active military campaign. In the former the patient is usually given the best chance by an early exploratory section, with thorough examination of the abdominal contents, done with every aseptic precaution and every means for correct work. This is not possible upon the battle-field.
—Foreign bodies are occasionally met with in the abdominal wall. These may be introduced from without by accident or design, such as needles or splinters, or may result from the escape by slow process of some foreign body from within, such as a fish-bone, a needle, and the like. Thus in an abscess of the abdominal wall I once found a stick-pin over five inches long with a large glass head. This had been swallowed by an insane patient, who, subsequently recovering from her mania, went home and developed this disturbance a year or so after her release from the asylum.
Abscesses may develop within the abdominal wall, without reference to deeper phlegmonous processes within. Thus they are occasionally seen after typhoid and the exanthemas, appearing perhaps as often in the rectus as anywhere. They may at any time result from superficial abrasions and travelling infections. They may occur sometimes as the extension of suppurating bubo, especially after phagedenic chancroid. They are recognized by signs which are usually unequivocal, and when once detected should promptly be evacuated.
Gummas, both tuberculous and syphilitic, frequently break down and form abscesses of mixed type. These may burrow deeply behind fascial planes, and require one or more counteropenings. As the result of a particularly virulent infection with the specific organisms that produce it one sees, rarely, about the abdomen expressions of gangrenous cellulitis or malignant edema, which may spread here from some adjoining part and involve wide areas. Abscesses also result from infection of hematomatous or other cysts, while collections of pus arising in the chest, travelling far, may spread downward along the subperitoneal connective tissue and appear even low within the abdomen or externally upon it. Acute osteomyelitis of the bones of the pelvis, or acute suppurative spondylitis, may produce abscesses which will also involve the abdominal wall, while it frequently suffers in the effort of pus to burrow toward the surface, as in large perinephritic collections and the like.
Erysipelas not infrequently involves the abdominal surface, and, spreading deeply, may produce suppuration or a virulent type of peritonitis. The latter is more likely to occur in connection with wounds and other injuries.
Aside from burns of the minor type, which may involve large areas, there may be seen, especially upon the abdomen, extensive and distressing expressions of x-ray dermatitis, so called, followed by ulcerations, perhaps with the later development of epithelioma. These results of injudicious exposure to the cathode rays are always of the most painful and erethistic type, and most difficult to heal. Resistant cases are probably best treated by complete destruction of the surface with knife or spoon and skin grafting.
Upon the abdominal surface are seen some of the characteristic expressions of the ulcerative syphilide and of tuberculosis of the skin. The former will require active antispecific medication and the latter call for the curette or complete excision. In either case radical treatment is usually promptly successful.
Actinomycotic lesions are also seen, perhaps as often about the abdomen as anywhere. They are likely to be mistaken at first for tuberculous or syphilitic disease, but may be differentiated by appearances elsewhere noted. They require active eradication, combined with the local and general use of iodine and copper sulphate.
The abdominal walls are not exempt from tumors which involve similar textures in other parts of the body. About the ordinary hernial outlets it is advisable to proceed cautiously with any tumor, lest it may prove to contain or to be combined with a true hernia in disguise. This is especially true at the umbilicus. Congenital cysts in the[784] walls are usually met with along the middle line, and will prove to be remnants of embryonic cysts, vitello-intestinal, urachal, echinococcus, or dermoid. Cysts should be distinguished from fatty tumors and sometimes from hernias or from cold abscesses.
Fatty tumors are common in all shapes, locations, and sizes. Among the benign tumors frequently observed are the fibromas, especially those of the type spoken of in Chapter XXVI as desmoids—i. e., those arising from the dense, fibrous, aponeurotic tissues, growing slowly, being exceedingly firm and hard in character, intimately connected with the fascia or aponeurosis, but not with the overlying skin nor with the viscera beneath. They are practically painless, may attain great size, and should always be removed while yet small, in order that the abdominal wall may not be weakened more than necessary by taking away the fibrous structures which especially give it strength.
The vascular tumors which call for surgery are uncommon. Pigmented nevi, however, are occasionally met, and these should always be promptly removed lest they degenerate into melanosarcomas. Varices and venous angiomas, sometimes of extensive dimensions, are also not infrequently found here. Extensive varicosities may have a congenital cause, the deep venous channels being insufficient, or they may be due to thrombotic occlusion of the abdominal veins following typhoid, puerperal fever, or injury.
Primary carcinoma originating within or upon the skin, epithelioma of similar origin, and sarcoma arising from the deeper mesoblastic tissues, may occur as primary tumors of the abdominal wall. We may also have endothelioma springing from the peritoneum, with possible origin elsewhere. Occurring secondarily we may see any of the ordinary metastatic expressions of any of these forms of growth, as well as those spreading by continuity, the most frequent example of the latter being so-called cancer en cuirasse following cancer of the breast.
Finally, for those enormous overdevelopments of fat and connective tissue which accompany exceedingly pendulous abdomens, such as most commonly follow pregnancy or elephantiasis, the surgeon has occasionally to excise large areas, closing the defects thus made by numerous tiers of buried with strong superficial and retention sutures.
It is well known that these conditions occasionally follow parturition and then lead to sudden death. A similar condition is now generally appreciated as occasionally following abdominal operation, and sometimes leading to the same fatal result. It has been said that thrombophlebitis follows about 3 per cent. of abdominal sections. It occurs oftener in the left than in the right leg, and its etiology is obscure. It begins with pain in the calf and groin, the leg rapidly swelling and then becoming edematous. Various writers have called attention to the occurrence of pleurisy and pneumonia during convalescence from appendectomy, and ascribe them to the presence of small emboli detached from the thrombi formed around the immediate site of the operation.
Two rather opposite theories prevail at present regarding the condition—one that it starts as a phlebitis due to infection at the time of the operation, the other that thrombosis is the primary lesion and therefore responsible for the phlebitis. Clark and others have contended that injury to the epigastric veins, by retracting and holding open abdominal incisions during protracted operations, is the cause of the trouble.
It would seem rational to hold that mechanical violence to the vessel walls, at or about the site of the operation, is the actual exciting cause in non-septic cases. On the other hand, the cases of infectious type should be accounted for either by local infection or as an expression of toxemia such as we see when similar thrombophlebitis occurs during the course of typhoid fevers and the like.
Years ago, Agnew, for instance, stated that after operations in which much blood has been lost there is always more or less tendency to the formation of coagula, but certainly the majority of these operations today are accompanied by very little loss of blood. Embolic pleurisy and pneumonia may appear without preliminary symptoms, while abdominal thrombophlebitis rarely shows itself until at least the end of the first week and sometimes not until the fourth week after operation, and then more often in the left than in the right leg.
In the treatment of these cases palpation and massage are to be strongly avoided, lest thrombi be dislodged and thereby produce pulmonary infarcts. Rest and sorbefacient ointments constitute the best treatment.
[785]
Were the peritoneum spread upon a flat surface it would be found to equal in area that of the skin which covers the body. In man it is a closed sac; in woman it is exposed to exterior contamination through the Fallopian tubes by way of the uterus and vagina. Hence the frequency with which infections of the latter are transmitted to the membrane itself. Thickened in some places, or duplicated, for the purpose of forming ligaments and membranous visceral supports, it is usually thin, connected with the structures which it lines or covers by a more or less delicate, cobweb-like connective tissue. In some of its duplications relatively large amounts of fat may be collected. While freely supplied with bloodvessels it may be regarded as an enormous lymph sac, its capabilities of absorption being relatively immense. It is because of this that human beings escape many of the possibly fatal consequences of infection. Along it infectious processes travel, sometimes with wonderful rapidity, while again it throw’s out exudates and rapidly walls off a serious disturbance, imprisoning it, as it were, and often effectually. Fluid may escape from it (fluid exudate) with great rapidity, or it may exude a fluid rich in fibrin which rapidly accumulates and forms a dense, firm exudate that serves to bind surfaces together and is often the surgeon’s best friend. In fact, the surgeon looks for a minimum and desirable amount of this exudate to ensure the result of whatever sutures he may pass through the peritoneum and the tissues which it covers. Thus after an ordinary intestinal suture it is expected that within some six hours the exudate thus formed will be of itself almost sufficient for the purpose of safety.
Peritoneum is said to possess the power of absorbing from 4 to 8 per cent. of the weight of the individual within an hour, but this only under normal circumstances, since inflammation or previous lesions delay or interfere with the process. Increased peristalsis hastens it, the reverse being also true. On the other hand, conditions may be easily reversed, and the presence of sugar or glycerin within the peritoneal cavity causes a diluting fluid to be thrown into it at about the same rate. It is by virtue of a firm, fibrinous exudate that foreign materials, e. g., ligatures, sutures, and even larger substances, are encapsulated, those which are capable of disintegration finally disappearing from within this investment. Occasional instances are on record of instruments, sponges, or pieces of gauze being left within the peritoneal cavity, in consequence of inadvertence during or when concluding an operation. Such bodies as these often encapsulate in this way and have been found years after at postmortem examination, or have been slowly extruded during life by natural processes. Such unfortunate occurrences as the latter afford the greatest reason for care during all such operations.
The term peritonitis has been made to cover so many conditions, of widely differing pathological character, that it is intended here to consider only those which have a practical interest for the surgeon. It is unfair both to terminology and pathology to include under the same name conditions that may be brought about slowly, or without any participation of bacteria, with those which are due solely to bacterial invasion. No attempt will be made here to go into a minute or complete classification of the various conditions included by different writers under this name. For instance, they have spoken of an idiopathic form of peritonitis, thus confessing by use of this adjective ignorance of the etiology of the condition. The surgeon has neither use for such an expression nor belief in such a possibility. The thickening of the peritoneum which may result from the proximity of an old hemorrhage, or the irritation produced by the circulating fluids in cases of Bright’s disease, is for him an entirely different entity, and is neither an idiopathic form nor peritonitis itself.
[786]
For surgical purposes we mention especially the following forms:
Forms A, B, and C may merge into one another or be confused from the beginning, or they may themselves be consecutive to D, while E, the malignant form, is hardly a distinct type, but rather a peritoneal expression of a more widespread general condition.
Again writers have endeavored to make distinctions by the use of such terms as “virulent,” “septic,” “putrid,” between which, however, no lines can be clearly drawn nor sharp distinctions made. They depend to some extent on the nature of the bacterial invasion, and again upon the actual virulence of the bacteria involved. The most distinctive type of surgical peritonitis is the tuberculous, which is usually relatively slow and recognizable as such, but as between the cases produced by spreading erysipelas, gonorrhea, intestinal perforation or postoperative infection one can make few, if any, distinctions which are serviceable or useful.
Anatomically considered there are two types of great importance—the circumscribed or local and the general or diffuse—prognosis depending in no small degree upon the extent of limitation of the active process, while at any time the former may merge into the latter. Consecutive peritonitis may include that which is the result of direct extension, as from erysipelas, appendicitis, acute cholecystitis, pyosalpinx, or other acute infections which have spread to and involve this membrane. Under this head also may be included those cases due to thrombosis or embolism, of mesenteric or other vessels, which lead to speedy gangrene of a part or all of the intestine.
Traumatic peritonitis refers rather to those cases where infection has been carried directly inward from the exterior. Traumatic peritonitis may be the result of extension of the same conditions which produce the first, the consecutive form, or only occur more directly, as, for instance, those cases produced by rupture of the stomach or duodenum after ulcerations of the same, or perforation of typhoidal ulcers, actual rupture and escape of the contents of a suppurating gall-bladder, appendix, tube, or any other collection of pus, or perforation due to the gradual extension of tuberculous, syphilitic, or malignant disease, with final rupture of a viscus.
The nature of the bacterial invasion is of more interest to the pathologist than to the surgeon as such. In general, however, it may be said that, in addition to the ordinary pyogenic organisms, the colon bacilli are perhaps the most frequently to blame, while the more putrid types are the result of actual escape of bacteria from the intestine, as through a perforated appendix, and the addition of a mixed type to one which began perhaps as a simple one. Thus in the so-called putrid forms multiple bacterial contamination is usually discovered upon making cultures. The pneumococcus, the capsule bacillus, and the gonococcus are also not infrequently found, in cases of peritonitis whose nature and origin will be suggested by the discovery of the particular germ involved in each case.
—While varying much in time and intensity, and even completely changing their type during the successive stages of the disease, there are, nevertheless, certain cardinal symptoms which are universally recognized in cases of surgical peritonitis. These include vomiting, pain, tenderness, with more or less shock, followed sooner or later by abdominal spasm and distention, while to these symptoms there is sure to be added bowel obstruction of some type which becomes, toward the end, perhaps the most profound feature, and which may even mask the significance of other symptoms. According as the lesion is localized or generalized pain may be referred to a particular area or may be general and intense. Local pain, with tenderness, usually implies, at least at first, a localized lesion, and is not so likely to be accompanied by vomiting as the more diffuse form. Depression is found to correspond largely to the type and degree of sepsis, while collapse is a prominent feature in the more severe cases. The pain, which is sometimes intense, subsides, and it should be emphasized that a speedy subsidence is not necessarily a favorable symptom. It too often marks the transition of an ordinarily acute case into one of intensely septic or even putrid type. Tenderness may be acute and localized, or diffuse and only evoked on deep pressure. One of the[787] most significant symptoms is abdominal rigidity, which persists throughout the active state of the disease, and which, when followed or accompanied by meteorism, may to some extent mask and obscure all conditions within. If the patient be not seen until this stage is reached diagnosis can be made only by history and conjecture, for it is almost impossible to determine anything by palpation.
Temperature is an uncertain factor. It sometimes rises high at first, and then falls, while if it fall too low the prognosis is serious. The pulse also shows very irregular variations, usually rising, however, as the disease becomes more severe, and being often almost uncountable at the end. A combination of rising pulse and falling temperature is of serious import.
In addition to the vomiting, which is a pronounced early feature of the disease, we have, as bowel obstruction comes on, an added fecal character to the vomitus, which sometimes is most characteristic of complete obstruction. This obstruction is due in part to toxic paralysis of the muscular coat of the bowels, and in part to the result of adhesions or fixations by which bowel motility is completely prevented. Thus in many instances of peritonitis following acute appendicitis there are loops of intestine glued together by exudate in such a way as to practically occlude or disable them.
The depression, shock, and final collapse of the disease are characteristic, as is also the facial appearance, the cheeks becoming discolored and the orbits hollowed out, so that the eyes early sink back. Other expressions of diminished blood pressure are not lacking—coldness of the extremities; cold, clammy perspiration; lividity of the skin, and the like.
While this is a picture of the most common expressions of acute septic or surgical peritonitis, it is occasionally found that conditions equally serious arise without such marked symptoms, and that the patients become rapidly worse, finally dying, who neither vomit continuously nor show extreme meteorism nor abdominal rigidity. Such cases are thereby stamped as those of more extreme toxicity, where systemic reaction is paralyzed almost from the outset, and are accordingly the more hopeless on that account.
Ordinarily it is not difficult to recognize the onset and the course of peritonitis in surgical cases. The condition may be confounded with one of septic intoxication from some focus which has not involved the peritoneum; otherwise differentiation is rarely difficult. The occurrence of such a condition does not necessarily indicate faulty technique on the part of an operator, as the condition is too often present when the surgeon begins his work. On the other hand, it too often follows faulty technique and constitutes the strongest argument for vigilance both in preparation, performance, and after-treatment.
—But little will be said here about non-operative treatment, although first it should be emphasized that treatment in the past was too often of the non-operative type. Many cases of peritonitis could be saved by operation were it performed while the infection is still localized, but this is at a period when they too rarely reach the surgeon’s hands, he being called in as such when the inefficacy of drug treatment has been already demonstrated. Without denying that the surgeon is not blameless in all these respects, blame should, nevertheless, be placed where it properly belongs, at the door of the man who fails to recognize and carry out plain surgical principles.
The opium treatment for peritonitis, with which the name of Clark will always be associated, was introduced at a time when many things were considered as peritonitis which were not necessarily such. It was furthermore an advance on previous methods and gave better results. That, however, is no excuse for adhering to it when better means are at hand. On the other hand it must not be denied that much can be done medicinally to give comfort and meet certain indications. In spite of the many disadvantages attaching to the use of opiates it seems unnatural to let patients suffer as they would without them. It is justifiable, then, to use them in cases which are hopeless, or in those which refuse operation; but given indiscriminately and early they often mask symptoms which, if properly appreciated, would lead to early diagnosis, and, it is to be hoped, early operative relief. Views also differ regarding catharsis. It is a great disadvantage to permit the intestines to retain fecal matter for days and add a consequent copremia to the other features of the disease. On the other hand, intestinal activity tends to disseminate infection, and is, consequently, most undesirable. If at the outset the intestinal canal could be emptied and then left at rest it would best meet the somewhat contrary indications.
[788]
Ordinarily, however, it is of small advantage to keep bombarding the stomach with repeated doses of laxatives which are more often rejected than retained, and which have little effect.
One of the most distressing features is vomiting, and here it is well to follow Berg’s suggestion and test the vomitus with litmus paper. If it be found alkaline small doses of morphine should be given, each with a drop or two of aromatic sulphuric acid, in a little chopped ice. If it be found acid small doses of milk of magnesia are advised or some such preparation, with minute doses of morphine, frequently repeated. The greatest relief in these cases, where the upper bowel is emptying itself into the stomach, will be obtained from lavage. In the same way tympanites and meteorism are best treated by passing a rectal tube high, leaving it in place, and utilizing it for lavage of the bowel, using warm water with a little sodium salicylate. Not the least distressing feature of such a case is the reflex hiccough which is produced by diaphragmatic spasm, since the phrenic nerve distributes sensitive fibers as well to the peritoneum. For this there is no really effective remedy. Small doses of Siberian musk, with or without morphine, beneath the skin will sometimes quickly relieve it. Depression and lowered blood pressure are best treated by adrenalin and digitalis, rather than by strychnine, which stimulates peristalsis. Fever, when high, should be treated by cold sponging rather than by antipyretics. The kidneys should be kept active, if necessary by hypodermoclysis, and the skin equally so by hot-air baths, as through both of these emunctories much elimination may be effected. The question of catharsis comes up again in considering what can be done to improve elimination of ptomains by watery stools, but these are hard to secure; it is, after all, questionable whether their effectiveness in this regard has not been greatly over-rated. Richardson, for instance, is inclined to believe that cases reported as cured by free catharsis would, in all probability, have recovered without it, it being doubtful whether the really infectious element be present.
Surgical treatment of peritonitis includes a recognition of the cause, and, if possible, its removal. Richardson has grouped in the following suggestive manner the indications for operative intervention in the early stages, when cases are not without hope:
On the other hand, in cases of fully developed peritonitis, where the surgeon may still consider the possibility of intervention, but where prognosis is far less favorable, the conditions include:
In such cases the decision rests largely upon the degree of collapse. To operate upon a moribund patient is hopeless and brings discredit upon surgery. Before operating upon any serious case of this kind the circumstances should be fully explained to those concerned, and they should be impressed with the fact that should the patient die he dies not in consequence of the operation but in spite of it.
The operation itself will in a large measure depend upon what can be learned of the etiology of the disease and the diffuseness of the resulting infection. To reach a localized focus the incision may be made at any point which will best afford access; but in dealing with a generalized process the middle line, and an extensive incision, will ordinarily afford the best opportunity for doing whatever is necessary.
The preliminary incision may be made short, as for exploratory purposes. Unless a loop of distended bowel be at once blown into the opening there will be prompt escape of fluid, whose character will reveal much of what has gone wrong within. If reasonably clear the operator is fortunate. If it be purulent he has to combat a most serious[789] condition; if it be offensive, it is probably due to contamination from a septic abscess or from intestinal gases, while if the fluid be nondescript and contain floating particles of fecal matter there is an intestinal or gastric perforation. So soon as one comes upon fixation or adhesion of viscera he will find lymph, in condition of greater or less organization. Inside the masses thus bound together he will probably find the greatest centre of pernicious activity.
The more one sees of these intra-abdominal conditions the more respect he, as a surgeon, feels for the omentum. Only recently have surgeons learned to appreciate the kindly activities of this duplicature of the peritoneum, with its slight or heavy load of contained fat. It manifests a tendency which may be almost regarded as a sagacity or instinct for shifting itself toward a local focus of infection, and there throwing out lymph by which it becomes attached and helps to form a protective barrier that often is most effective. Were it not for this tendency many cases of acute appendicitis, for instance, which now recover would be lost during the early days of the attack, in consequence of a quickly disseminated infection. Thus a gangrenous appendix, or hernia, or gall-bladder, is frequently so wrapped up in a protective layer of omentum that the operator has first to detach this, or go through it, before he comes upon the actual site of the trouble. Some such disposition of the omentum, then, may be easily discovered during the earliest moments of his exploration, and if later he conclude to remove a portion of it, because of actual or impending gangrene, he nevertheless sacrifices it with a feeling of regret because of the good it has already done.
The further treatment of these cases is essentially a matter of what can be done to remove the exciting cause. Questions of gravest import, and often difficult of immediate decision, will present in nearly every case; as, for instance, whether to resect a portion of intestine, to remove a gall-bladder, to hunt for an appendix when embarrassed with the difficulty of the effort and necessity for widely separating intestinal coils, or of the treatment of distended bowel, which it may perhaps be impossible to restore to place, of extensive and complete flushing of the abdominal cavity, or of mere local cleanliness. And after these questions have been decided, and action taken, there comes still the question of drainage, with the wisdom of or necessity for counteropening, as in the loin or in the cul-de-sac, and the character of drain to be used. As to what should be attempted in general there will rarely be much room for doubt. As to how best to accomplish it should be decided according to the training, the experience, and the opportunities of the operator, and the nature of the environment. When the entire peritoneal cavity is invaded, and flooded with more or less infectious material the more thoroughly it can be washed out the better. At the same time to do this with any degree of even apparent thoroughness requires practical evisceration of the patient, and an amount of time spent and shock produced by handling the viscera, which are exceedingly depressing and may of themselves be more than can be borne. The meteorism, which is so conspicuous a feature of most of these cases, means the distention of the bowel to such a degree that when once the intestines lie upon the surface of the body they can usually be restored with the greatest difficulty; and this would raise the question of the desirability of either one or more punctures, through which gas should be allowed to escape, or a sufficiently wide opening, with the introduction of a Monk tube, and the complete emptying both of gas and putrefying fecal matter. The latter is certainly in theory the much more desirable measure, if the patient’s condition will only justify it. Probably after pelvic drainage the Fowler semi-sitting posture in bed would be desirable, while after high drainage the Trendelenburg position, with the pelvis higher than the thorax, would be preferable.
If free abdominal irrigation is to be practised a large quantity of warm sterile saline solution should be used, to which may be added perhaps a small proportion of acetozone or of mercury bichloride. The silver salts also make equally effective and less irritating fluid, the nitrate being used in the proportion of 1 to 10,000, or the citrate or lactate in proportion of 1 to 500 or 1 to 1000. These metallic salts will coagulate the albuminoid fluids and give to the peritoneum an opaque appearance, which, however, need cause no alarm.
Another question of importance is that of enterostomy. In some of these cases the acute bowel obstruction is the most predominating and distressing late feature, and an enterostomy may be attempted, even though it be known it will serve but a temporary purpose, in order to relieve distress. There never can be more than sentimental objection to it,[790] in such cases, with the possibility of something more than mere temporary relief. It can be effected under local cocaine anesthesia, by attaching to the parietal peritoneum the first loop of distended small intestine that presents, and, after firmly fixing it in place, making a small opening, and then preferably inserting a glass or other tube for better drainage purposes.
These constitute the precautions to be followed and the advice to be given in cases of septic or surgical peritonitis. How successful they may be, or how satisfactory the termination of the case, cannot be foretold by statistics nor by reports of cases in the hands of others. Success will depend in large measure upon the early or late period at which the case is thus treated, and upon the general surgical discretion and experience of the operator. It is probable that disappointment will result more often than success. Nevertheless every life thus saved is one snatched from a certainly fatal termination without it, and if successful but once in ten times one life has thereby been saved that may be worth saving, without saving the other nine. While I would advise to make the attempt in any case which offers a reasonable prospect of success, caution should be used against doing it without a full understanding with those concerned that it is an effort in the right direction, concerning which no promise can be made; death results not from the operation so much as in spite of it.
Summarizing, briefly, the best methods of treating a diffuse septic peritonitis we may agree with Le Conte,[53] that they consist of the following measures: The least possible handling of peritoneal contents, the elimination of time-consuming procedures, most perfect drainage of the pelvis by a special suprapubic opening, as well as free drainage through the operative incision, the semi-sitting posture of the patient after its conclusion, the prevention of peristaltic movements by withholding all fluids by the mouth, and perhaps by small amounts of opium, and the absorption of large quantities of water through the rectum, by which there may be produced a reversal of the current in the lymphatics of the peritoneum, making it a secreting rather than an absorbing surface and increasing urinary secretion. It is inexpedient to waste time sponging peritoneal surfaces or wiping away lymph, for danger of septic absorption is increased rather than diminished. Patients with diffuse septic peritonitis bear brief operations fairly well, but prolonged ones badly; therefore a minimum amount of work should be done.
[53] Annals of Surgery, February, 1906.
One of the most valuable procedures in carrying out the above advice is Murphy’s method of slowly introducing large quantities of water into the rectum. The rectal tube used for the purpose ends with a sort of nozzle containing three or four openings, and the reservoir containing the solution is elevated but a few inches above the level of the bed, the intent being that it shall simply trickle into the bowel no faster than absorption can occur. In this way from a pint to a quart may be absorbed each hour, the pressure being continuous, and the flow so regulated that no accumulation of fluid takes place in the bowel. Murphy claims that by this method the lymph current in the peritoneal lymphatics is so reversed that the peritoneum is bathed with free discharge and that this should be afforded escape by suitable drainage methods, coupled with Fowler’s (the sitting) posture.
Acute or chronic tuberculosis of the peritoneum assumes usually, first, the miliary form, after which, in the slow cases, infiltration and great thickening occur to such an extent as to alter the appearance, texture, and behavior of the peritoneum itself. It is rarely a primary condition, but is usually secondary to some other tuberculous focus, which may be one or more of the mesenteric nodes, these being involved in consequence of infection from the alimentary canal; or the peritoneum may be easily infected either from the genito-urinary tract or directly from the intestine. In children, the most common path of infection is through the mesenteric nodes; in females, through the Fallopian tubes, and in males, either through the intestine or the kidneys or ureters. The peritoneum, under these circumstances, behaves very much as does the pleura, in the presence of acute or chronic tuberculous lesions which extend to and involve it. Thus it may become so thickened, and even “leathery,” as to have lost all its original characteristics, and to appear more like a dense, firm membrane than in its original semblance.
[791]
Peritoneal tuberculosis appears in three different types: A fibrinoplastic type, characterized especially by adhesions; an ulcerative and sometimes absolutely suppurative form, marked always by the presence of pus and pyoid; and an ascitic type, characterized by leakage of increasing amounts of serum and the development of well-marked ascites.
The first, or fibrinoplastic, is a localized lesion, and leads to the formation of dense adhesions, as, for instance, between a Fallopian tube and the pelvic walls or the other viscera. As the disease spreads all the tissues become matted together in a mass which renders them almost indistinguishable, frequently much resembling malignant disease. In some instances it may be possible to remove the entire affected area. At other times it is best to let it alone.
The ulcerative form is characterized by more general symptoms of conspicuous febrile type. It produces rapid loss of strength and weight, frequently attended with evidences of intestinal ulceration and with abdominal tenderness and pain. A certain proportion of these cases justify exploration, though but few of them will be found favorably disposed for radical surgical measures.
The ascitic type is characterized by rapid accumulation of fluid, with accompanying malaise and debility. As the abdomen distends and the diaphragm is pushed upward respiration becomes more difficult and rapid. A certain protrusion of the umbilicus also characterizes many of these cases. Their course is not so febrile, but it may be possible, especially in the early stages, to make out some enlargement of mesenteric nodes, or involvement of the viscera, which will aid in diagnosis. It is most common in children, but it may be met with at any age. In general such a collection of fluid, which cannot be accounted for by recognizable disease of the heart, liver, or kidneys may be suspected to be tuberculous.
—Treatment of tuberculous peritonitis should be surgical when possible. This statement is based partly upon the fact that it is so commonly a secondary condition. Such treatment will depend, in large measure, upon the extent to which it may be possible to remove any exciting foci of the disease; but experience shows that even this is not always necessary to bring about a cure, as in those cases of the ascitic type where it is desirable only to wash out the abdominal cavity and close it again, this simple procedure seeming to suffice.
It is the cases of the ascitic type which seem most benefited by incision and irrigation, usually without drainage, and it is these which are perhaps as hopeless as any under non-operative treatment. It was Van de Warker, of Syracuse, who, in 1883, first recognized the value of simple irrigation in these cases, and while at present we find it impossible to explain the benefit which so often and so rapidly accrues, the measure is universally recognized as that offering the most hope. This, like every other surgical procedure, should be practised early rather than late, preferably so soon as diagnosis is made, or, when this is difficult, it should be made a part of an exploratory operation intended partly for diagnostic purposes. The measure itself is simple. A small opening in the middle line, between the pubis and the umbilicus, permits free escape of all contained fluid, which should be facilitated by changing the position of the patient, thus preventing plugging of the opening by presenting bowel. Every drop which can escape having been removed, the abdomen is then flushed repeatedly with either warm saline solution or a plain watery solution of acetozone, 1 to 1000, or silver lactate or citrate, in the same proportion or a little stronger. My own preference has always been for the latter, and with a silver solution I have obtained a large degree of success. There is no objection to leaving a small amount of either of these fluids in the abdominal cavity—i. e., no more than an ordinary effort to empty it before closing the wound. An incision one inch long, made for this purpose, will serve nearly every indication. Through it the parietal peritoneum, as well as that covering numerous loops of intestine, can be inspected, and through it also a finger may be inserted for exploratory purposes, for the detection of mesenteric nodular disease or of any other focus. Should any serious local condition be revealed which might be benefited by radical measures, this would be the time to practise them.
Before closing the wound margins it would be well to thoroughly disinfect them, for over them has flowed infected fluid, and we sometimes see tuberculous foci develop at this point. This fact explains also the disadvantage obtaining in these cases of making drainage openings. They serve their purpose admirably for a short time, but, becoming[792] thus infected, lead to the establishment of tuberculous fistulas and sinuses, which may call for subsequent operation. Fecal fistula may even be a more remote consequence. As the peritoneum is approached it will be found more or less altered, and there may even be observed bowel or omentum adherent behind it; therefore caution must be observed.
A final caution should also be given in order that we may avoid mistaking that form of ascites which is frequently seen in connection with cancer of the abdominal viscera extended to the peritoneum, and particularly that form spoken of as miliary carcinosis or miliary sarcomatosis, for a tuberculous collection. While surgeons are occasionally deceived, one will usually find much in the history of the case, and in the results of local examination, which may save making this error, if it be so regarded; but, in effect, the opening and the evacuation will give relief, even though this character of the disease makes it less amenable to help from any such source.
[793]
These malformations are quite rare, at least those raising the question of possible surgical remedy. Transposition does not require relief, nor does a stomach abnormally small allow it. More or less stenosis of the pylorus as a congenital defect has been observed, but it is extremely rare. Along with it is often associated a certain hypertrophy of the stomach muscle. Hour-glass deformity may be of congenital or acquired origin. The latter two conditions permit of easy surgical remedy. Pyloric stenosis may be atoned for by gastro-enterostomy or treated directly by a plastic operation, while the hour-glass stomach permits of an anastomotic rearrangement, either of its dilated portions with each other or with the bowel below.
The acquired malformations are connected with the consequences of ulceration and stricture. They include more or less complete stenosis, either cicatricial or malignant, various forms and types of gastroptosis and gastric dilatation, in which sometimes enormous degrees of distention are produced, with disturbed or practically destroyed stomach digestion. These cases will be considered by themselves a little later, along with their surgical relief.
The anatomical relations of the nerves supplying the stomach are worthy of the surgeon’s especial consideration. Its sympathetic nerve supply is in particular and intimate relation with the seventh, eighth, and ninth spinal roots, by which we account for the tenderness of the overlying surface in ulcer of the stomach, and the pain which is often referred to the region of the left shoulder-blade. When the stomach is adherent to the gall-bladder, in cases of biliary calculi, the pain is often referred to the right shoulder, but so soon as the pylorus becomes entangled and bound down pain is referred also to the left side as well.
Hour-glass stomach is now more common, and is to be attributed more to results of pathological conditions than to any congenital anomaly, it being now well established that it is usually the result of perigastric adhesions of chronic ulceration, with cicatricial constriction, as well perhaps of subsequent malignant implantation. Cancerous infiltration may produce the so-called “leather-bottle” stomach. Moynihan suggests, among other methods of diagnosis, the passage of a stomach tube and lavage with a quantity of fluid. If there be loss of a certain amount of this, when it is returned, it will indicate that a portion has escaped into the distal sac of the stomach. Again if the stomach be washed until the fluid returns clear, and then if there suddenly comes an amount of offensive fluid, or if the stomach be washed clean, the tube withdrawn and passed again a few moments later, and if then offensive fluid escape, the facts can be best explained on the hypothesis of an hour-glass constriction. “Paradoxical dilatation” may also be noted, i. e., the fact that palpation will still elicit a splashing sound after a stomach tube has been passed and while the organ is apparently empty.
Moynihan has suggested still another method of recognition. The area of stomach resonance being outlined, a Seidlitz powder in two halves is then administered. After about twenty or thirty seconds great increase in resonance of the upper part of the stomach will be found, while the lower part remains unaltered. If now a bulky pouch can be felt or outlined the diagnosis is determined, as the increase in resonance occurs in the distended cardiac segment.
The method of treating an hour-glass stomach will consist either, in selected cases, of a plastic operation by which an incision made in one direction is closed in the opposite,[794] i. e., a measure like that practised at the pylorus for benign stricture, or else the separate sacs of the stomach must be united by an anastomotic opening and a gastrogastrostomy thus performed.
These are most commonly those which have been swallowed, either by design or through inadvertence, and may consist of almost all imaginable substances. In those animals that have the constant habit of licking their own fur or that of others, and thus scraping off a quantity of hair, hair-balls in the stomach are frequently formed, and, as may be seen in museums, these sometimes obtain relatively enormous size—a foot or more in diameter. Hair-balls in the human being are of rare occurrence, and are the result of the habit of chewing the hair, observed in some hysterical or insane patients. There are several instances now on record of successful removal of such hair-balls from human stomachs. Artificial dentures, partial or complete, are not infrequently passed into the stomach, sometimes during sleep. In dealing with a case of this character extreme caution should be exercised, because many individuals have deceived themselves, or have been deceived, and the missing teeth supposed to have been swallowed have been found in some place where they have been mislaid and forgotten. Children have a habit of swallowing almost anything left loose in the mouth, and all sorts of toys and small playthings have disappeared into their stomachs, sometimes causing death, and occasionally passing through the alimentary canal. The insane sometimes show a maniacal tendency to swallow foreign bodies, such as nails or anything else which they can get into the mouth. Hysterical patients and museum freaks evince the same habit, and it is wonderful how tolerant the stomach becomes in some of these individuals, and what objects seem to pass the pylorus and escape externally without doing serious harm. Still, sooner or later nearly every one of these individuals comes to grief. Thus from one patient at the Erie County Hospital, in Buffalo, Gaylord removed an astonishing amount of junk, including nails, screws, pieces of glass, knife-blades, and the like. As a general rule, any reasonably smooth object which can pass through the esophagus may also pass through the pylorus.
—The symptoms produced by these foreign bodies will vary according to their size, number, and character. A hair-ball may lie for a long time within the stomach, producing few symptoms, and none by which it may be recognized. So long as no perforation of the entire thickness of the stomach walls occur, nor any infection which may produce a local peritonitis, the disturbances they set up may be limited to those included under the name “dyspepsia.” So soon, however, as pain, tenderness, or septic indications, or those of local peritonitis supervene, the abdomen should be promptly opened. Today we have the cathode rays as an aid in diagnosis, which will clear up doubt in most instances, and afford a definite indication for operation. Nevertheless a negative result does not necessarily imply that no foreign body is present.
—The operation indicated is gastrotomy, i. e., opening of the stomach at a suitable or convenient point, removal of the foreign body or bodies, and the complete closure of the wound as well as of the abdominal incision, without drainage. If due care be maintained throughout, and the element of previous infection be excluded, prognosis is good. When perforation with local peritonitis, and perhaps abscess, has already occurred, there is a local indication as to exactly where to open; one should then complete the operation with the establishment of suitable drainage.
As already indicated, the stomach maybe ruptured, especially if weakened by previous disease, by severe abdominal contusion. It is subject to all possible wounds by perforation, either gunshot or by puncture. As it is more protected than the bowel below it is less liable to perforating injuries. Much will depend upon the nature and the extent of the injury. A small perforation may be protected by prolapse of the mucosa in such a way that little escape of contents takes place. On the other hand it may be extensive, and nearly the entire gastric contents may be poured out into the upper abdomen. The location of the stomach lesion by no means necessarily corresponds to that of the[795] abdominal wall, this being particularly true in gunshot cases. Extravasation depends in amount and rapidity upon the stomach contents and their fluidity. If the posterior wall alone be injured it will empty rather into the cavity of the lesser omentum. Stomach injury may always be diagnosticated if, after abdominal injury, the vomited matter contains blood. The pain is usually severe and involves generally the entire upper abdomen. In proportion as the lesion lies near the diaphragm the breathing may be affected. Collapse is usually prompt and may be due to hemorrhage from a vessel of considerable size. Pain, collapse, and hematemesis constitute indications for the promptest possible opening of the abdomen and investigation, with suitable suture of the stomach wound, toilet of the peritoneal cavity, and drainage, which should be posterior as well as anterior. Every ragged or compromised margin of a stomach wound, especially gunshot, should be neatly excised, and sutures applied in such a way as to only bring clean and fresh surfaces together. An external opening of sufficient length should be made to permit easy and complete withdrawal of the entire stomach, and a complete search over both its surfaces in order that no lesion may escape detection. If the opening made into the stomach be sufficiently large to permit, it would be best to thoroughly empty its contents and gently wipe it out, in order that it may be left not only empty but clean. Should the puncture be very small it would be well to pass a stomach tube from above and wash out the stomach, protecting the opening by pads and pressure, and thus preventing contamination of the peritoneum.
While apparently spontaneous rupture, i. e., without previous ulcer or disease, is most rare, there are a few cases on record where patients have been seized with intense paroxysmal pain and have died more or less quickly, and where the condition has been found with little or nothing to explain it. Immediate operation might possibly have saved some of these had the possibility of its occurrence been recognized. Perforation from within may also occur, as it is known to have happened in the cases of sword or knife swallowers.
Suture of the stomach is practised in exactly the same way in these cases as for other purposes and the method will be described later, along with the other operations upon this viscus.
The gastric mucosa presents a remarkable contrast to that of the intestinal tract, the latter being exceedingly likely to succumb to tuberculous infection, which is exceedingly rare in the former. Primary tuberculous ulceration of the stomach, then, is most unusual. When tuberculous ulcers are found there they are usually the result of a secondary or perforating process. Such ulcers may attain great size, as in one case reported by Simmonds where the ulcerated area measured four by eight inches, yet produced no symptoms during life. This would correspond almost to a lupus of the gastric mucosa. Tuberculous gummas are even more rare, and, occurring in the stomach, are pathological curiosities rather than surgical possibilities.
Syphilis of the stomach is met with either as gumma or ulcer, the latter leading almost inevitably to more or less stricture as recovery follows suitable treatment. Although it is claimed that 10 per cent. of cases of chronic ulcer of the stomach have suffered from syphilis at some time, it by no means follows that such ulcers are to be considered as of genuinely syphilitic origin, as a syphilitic patient is not exempt from other stomach conditions. However, symptoms of gastric ulcer, associated with actual manifestations of syphilis, might well indicate associated syphilitic lesions and would probably yield, with the others, to suitable treatment.
Lesions of either character, which do not subside under proper medical treatment, and which require a surgical operation, would be equally benefited by it whether of one of these types or of the other.
The acute form of gastric dilatation was described by Fagge in 1872, the chief symptoms being excessive vomiting and anuria, and the disease proving fatal within three days, the dilatation being enormous. For a condition occurring as rapidly and[796] progressively as this does there is as yet no satisfactory explanation, careful autopsy failing to disclose a sufficient reason. It has been known in at least twelve instances to follow surgical operation, four only of which were upon the abdomen, and none of them upon the stomach proper, in all instances the patients apparently progressing favorably. The stomach becomes rapidly and enormously distended, and bent upon itself with a sharp kink in the lesser curvature. Thus it seems to occupy the entire upper abdomen. Two factors at least seem to assist in the condition: A paresis of the gastric musculature, and the fact that as it becomes distended it itself produces obstruction of the duodenum, and thus aggravates the primary condition.
It has been suggested that these acute cases of postoperative dilatation are closely connected with certain cases of ileus and obstruction after abdominal operations, the dilatation once initiated tending to more and more obstruct the duodenum, as well as cause upward pressure on the diaphragm and embarrassment of the heart’s action. Hence the value of the stomach tube in treatment of such conditions.
—The symptoms are usually sudden and fulminating, beginning with intense pain, which finally involves the entire abdomen. Vomiting comes early and persists, the vomited fluid being greenish in color and large in amount, changing later to a brownish color and having an offensive odor. The act of vomiting is passive rather than active or violent. In spite of it the stomach never seems to empty itself. The outline of the dilated stomach may be seen through the abdominal wall, bulging being often extreme. With the passage of the stomach tube there may be escape of a large amount of gas as well as of fluid. Thirst is intolerable and never satisfied. The amount of urine is almost always reduced and sometimes anuria is practically complete.
—The treatment is too often ineffectual, since the condition itself is lethal almost from the beginning. Early and frequent lavage, or perhaps leaving the stomach tube in place, would be indicated. It might be practicable to pass a small tube through the nostril and leave it, as is done with the insane. Gastrostomy would be theoretically indicated, could it be done sufficiently early. The same is perhaps true of gastro-enterostomy, although it has never had a fair trial, these cases coming to the surgeon too late to permit of much help.
—Chronic dilatation of the stomach, often spoken of as gastrectasis, is a frequent complication of various other conditions, being essentially a consequence rather than a primary condition. It may be due to:
1. Pyloric stenosis or its equivalent in the first part of the duodenum:
2. A dilatation due to old lesions which have subsided, the atonic stretching not having been repaired.
It will be seen, then, that the condition may be met as a sequel to many different pathological processes. As such, therefore, it has no constant etiology nor necessarily distinctive features. In general it is recognized by tardiness in escape of gastric contents, associated with vomiting, the vomitus being distinctive, consisting often of old and undigested food, or perhaps of food which has rested in the stomach until putrefaction has occurred. The vomitus also contains evidences of fermentation, with sarcinæ and yeast cells and much mucus. In cases of ulcer it is usually very sour, owing to excess of free hydrochloric acid. When due to cancer the acid is usually due to excess of lactic acid, while hydrochloric acid may be nearly or totally absent. Even if vomiting does not occur after ingestion of food, heaviness and discomfort, with much eructation of gas, are produced. Constipation and diminished urine secretion are almost invariable accompaniments. When the obstruction is of the mechanical type a visible peristaltic wave can often be seen and felt, and this is a sign which should be regarded as always indicating operation.
[797]
Patients gradually lose flesh and become anemic and run down, suffering from what has been often vaguely called indigestion, their lives sometimes being terminated by starvation, occasionally by gastric tetany. The question of diagnosis can usually be settled by having the patient swallow the dissolved separate parts of a Seidlitz powder, one after the other, when the carbon dioxide released within the stomach will cause it to balloon up and assume that shape and position which the amount of its dilatation permits.
Gastric dilatation which does not quickly yield to lavage and suitable medication is of itself always an indication for operation. When accompanied by a tumor, especially if this move and change position with the stomach, a cancerous condition may be assumed, which, while not permitting a cure, may nevertheless be ameliorated by a gastro-enterostomy. In the absence of actual cancerous conditions the surgical treatment of chronic dilatation is exceedingly satisfactory.
This surgical treatment consists in the application of one at least of the following expedients:
The methods in vogue a few years ago for opening the stomach and merely stretching the pyloric outlet have been supplanted by other plastic operations which have proved more satisfactory because of the greater permanency of their results.
The downward displacement of the stomach, to which the term gastroptosis has been given, implies not only more or less actual dilatation, but also a stretching or lengthening of the upper attachments and peritoneal folds which should hold the stomach up in place. When these yield and the stomach is thus permitted to drop, more or less obstruction of the pylorus and kinking of the duodenum are apt to occur. The condition regarded surgically is not essentially different from that of chronic dilatation. When the stomach is distended with carbon dioxide its normal position may be easily recognized, while, at the same time, it is determined that it is perhaps but little dilated.
The causes which lead to this condition, aside from those which affect the stomach proper, include tight lacing, by which the supporting viscera are forced downward and the stomach permitted to fall with them. In addition to such a cause any previous disease by which the abdominal viscera have been affected or ligaments weakened would be of more or less effect. The condition leads sooner or later to one of dilatation, and always merges into it. Its symptoms are those of dilatation, only in milder degree. On account of the dragging upon the upper supports patients frequently complain of intense lumbago, and they nearly always become neurasthenic.
—The ordinary routine treatment failing to give relief, one may, in mild cases, adopt an external mechanical treatment, consisting of a suitable abdominal bandage which should press the viscera up from beneath, and thus relieve splanchnic congestion and weight.
Mechanical support failing and symptoms persisting, the surgeon is able to afford relief by gastropexy, first suggested by Duret, and consisting of an exposure of the stomach through the middle line and its fixation to the anterior abdominal wall. This, however, has its theoretical disadvantages, since it might be followed by symptoms similar to those resulting from pathological adhesions. The method has been more or less modified, sutures being passed through the gastrohepatic omentum and gastrophrenic ligament in such a way as to bring them into close contact and looking to their complete union. Thus, Beyer, of Philadelphia, has reported four cases apparently successfully operated upon in this fashion. Bier has added four others, all of which seem to afford much encouragement to operative treatment of gastroptosis. Furthermore, Coffey has modified the technique in such a way as to include a sort of suspension of the stomach[798] by making a hammock out of the great omentum. He did this by stitching the omentum to the abdominal peritoneum, about one inch above the umbilicus, with a transverse row of sutures about one inch apart.
Gastric tetany has but relatively small interest for the surgeon, save as it may complicate some of his results or prevent his endeavor to secure them. The condition is usually characterized by peculiar, disturbed sensation in the extremities, with a feeling of coldness or numbness in the limbs, and drowsiness, vertigo, and disproportionate weakness after exercise. Somewhat severe attacks are sometimes precipitated by lavage, and are then begun with a complaint of formication, followed by tetanic contraction of the muscles of the extremities. Instead of tonic spasm the muscles may be in more or less constant motion. The muscles of the face, neck, and abdomen are also involved. The facial expression changes, and patients may complain of loss of vision. During these paroxysms they may even mutter or speak unintelligibly. Chvostek some time ago showed how to produce these spasms, when the condition is present, by tapping over the facial nerve just at its exit from the cranium, and Trousseau demonstrated that during the attack the paroxysms may be produced at will by compressing the affected parts in such a way as to impede venous or arterial circulation through them. Some of these spasmodic attacks are accompanied by severe pain, while spasm is usually made less painful by gently yet forcibly overcoming it by pressure. The condition is essentially toxic, usually autotoxic, and yet, inasmuch as it may complicate the best efforts of the surgeon or complicate the case upon which he would wish to operate, it is deserving of this brief description here, largely in order that it may not be mistaken for true tetanus or be misinterpreted in any other way.
This is a term recently suggested by Mikulicz for a peculiar contraction of the lower end of the esophagus and the cardiac orifice of the stomach, which is occasionally met with, and until fully described by him was somewhat misunderstood. In consequence of the spasmodic stricture thus produced there occurs dilatation of the esophagus above and formation of a sac, which may be discovered by the bougie or tube, or by a good radiogram, after having been filled with a weak bismuth emulsion. Such sacculation had always been previously regarded as due to esophageal diverticulum, which it greatly simulates at first and in time practically becomes. It is due either to primary and unexplained spasm of the muscular coat at this level, or to a primary atony for the esophageal muscle above the stricture. It has been ascribed also to paralysis of the circular fibers and spasm of the cardia, due to vagus involvement and to primary esophagitis. The view that it is of congenital origin can scarcely be sustained.
—The symptoms and signs produced are not widely different from those of a capacious diverticulum. It is difficult, often impossible, to pass a stomach tube into the stomach, it being diverted into the upper cavity. The patient moreover, vomits material which is undigested and more or less putrefactive, and, at the same time, without evidences of actual stomach disease. Such a sac may hold even two pints, and thus it will be seen how much material may be vomited or washed out by lavage which, at the same time, never entered the stomach. Should it be possible to enter the stomach the two sets of contents will be found quite different.
—While more or less benefit and relief may be obtained from frequent washing of the abdominal sac thus produced the real cure will only come, as shown by Mikulicz, from opening of the stomach and dilatation of its constricted upper orifice.
[799]
Reduction in caliber of the pyloric opening, amounting in extreme cases to absolute closure, may be met with at various ages and following various conditions.
A congenital stenosis has been observed, although very infrequently.[54]
[54] Fiske (Annals of Surgery, July, 1906) states that there are at present on record 121 cases of hypertrophic stenosis of the pylorus in infants. The three theories advanced to account for the condition as occurring before birth presuppose either a true malformation with muscular hypertrophy, a secondary hypertrophy due to prenatal pyloric spasm, or a spastic condition of the pyloric region without definite gross anatomical lesion. None of these theories satisfies the condition in any but a small proportion of cases, although either of them doubtless is or may be correct in certain instances; 71 of these cases have now been operated upon, of which 33 died, gastro-enterostomy giving 57 per cent. of recoveries and pyloroplasty 54 percent.
Pyloric constriction following cicatricial contraction of healed ulcers is perhaps the most common non-malignant form. This rarely proceeds to absolute closure, but is frequently sufficient to lead to dilatation.
Conversely any condition of the stomach which drags it out of shape and leads to kink or abrupt angulation near the pylorus may lead to early postural and later to actual structural contraction.
The pressure or alteration of shape produced by neoplasms, either within the substance of the stomach or more frequently without, will cause more or less irregular contraction of the pyloric end amounting to pyloric stricture.
By old adhesions similar conditions are produced, while a definite form of spastic contraction, corresponding much to cardiospasm just described, will cause more or less pyloric obstruction.
Finally malignant tumors involving the pyloric region invariably spread to the pyloric ring, and not only infiltrate it but cause it to become inflexible and diminished in size, to a degree finally amounting to almost complete or to absolute obstruction.
—No matter what the cause the symptoms are essentially the same, in that they produce dilatation of the stomach and frequent vomiting. According to the cause there will also be a history of pain and hemorrhage, suggesting ulcer, or of biliary colic, denoting perigastric adhesions, or of pancreatic disease, accounting for adhesion of the duodenum and displacement of the pylorus. The discovery of tumor or the results of examination of stomach contents may also suggest or corroborate the diagnosis of cancer.
The essential feature being the failure of the gastric contents to pass onward into the bowel, and their accumulation in the stomach or rejection by vomiting, the condition will be seen to have a purely mechanical as well as a pathological aspect. The case, therefore, must be extreme in which a mechanical remedy will not afford at least temporary relief.
—This remedy obviously is either to overcome the stricture by dilatation, or plastic operation upon the region involved, or to form a new opening by which the stomach shall connect with the upper intestine—i. e., gastro-enterostomy. The latter has gradually supplanted the former in the choice and in the hands of most surgeons, although occasionally a case may be met which invites the performance of a pyloroplasty, by either the Heinecke-Mikulicz or the Finney operations, which will be described later. In the absence of malignant disease few serious operations give more satisfactory results than do these.
During the past few years the studies of internists, of pathologists, and of surgeons have all served to show that gastric ulcer in any form is a more common lesion than was suspected by the previous generation. At first it nearly always comes under the care of the internist, but too often, becoming chronic, it is too long continued under his care until a serious, perhaps almost fatal, hemorrhage makes operative relief more dangerous, if not impossible, or until a chronic ulcer has degenerated into a cancer, and this is permitted to go on until the patient pays with his life the penalty for such inattention.
Ulcers in the gastric mucosa vary from a simple fissure (such as may be seen in the mucosa of the lip or the anus) to extensive and deep ulcerations, which weaken the[800] stomach structure in spite of protective infiltration and even adhesions, until a final perforation may terminate the case, either by hemorrhage or septic peritonitis. While surgical teaching has of late pointed more and more definitely to the importance of ulcers resulting from simple erosions, or apparently mere abrasions which have not been appreciated, most pathologists and surgeons fail to realize that even from so trifling a surface alarming hemorrhages may occur. Such lesions appear upon the postmortem table to be minute and unimportant, but, occurring during life, they have an importance of their own.
Gastric ulcers, then, should be referred to as erosions, as simple or complicated ulcers, and as ulcerating cancers, in addition to which there may be mentioned the rare lesions produced by tuberculosis and syphilis. These ulcers are always to be regarded seriously, because in their milder expressions they cause pain and various forms of dyspepsia and indigestion, while their more serious consequences include hemorrhage, which may be fatal, and perforation, which is essentially so unless surgical intervention be prompt and complete.
—The symptoms and discomforts which they produce include pain, which is nearly always most pronounced within a short time after the ingestion of food, and which may be accompanied by local tenderness more or less constant. As the case progresses, with the pain usually comes vomiting, by which the former is relieved, the vomitus nearly always containing excess of hydrochloric acid and sometimes fresh or old blood. The pain of gastric ulcer is usually referred to the back. The indigestion and the frequent vomiting together are sufficient to produce a well-marked anemia, which is more pronounced when much blood is lost. Blood may not be vomited but escape into the duodenum, and will then give to the stools a tarry character, which should always be looked for and identified when discovered. The greater the loss of blood in either direction the more pronounced will be the anemia. Pain, vomiting, and evidence of loss of blood constitute the most distinctive features of gastric ulcer. When these are accompanied by tenderness in the epigastrium, and by pain in the back, the diagnosis is almost complete. In the more chronic cases there may have already occurred contraction of the pylorus and consequent dilatation of the stomach. Thus symptoms of the latter may be added to those of the previous condition.[55]
[55] In doubtful cases accompanied by pain it will sometimes be of value to try the effect of orthoform in ¹⁄₂ Gm. doses, to see if it will relieve it. This remedy will not anesthetize nerve endings which are protected by skin or mucous membrane. The fact, then, that it affords relief implies an ulcerated or exposed area.
The two ever-present and alarming dangers are those of hemorrhage and perforation. Serious hemorrhage permits the escape by the mouth of large quantities of bright, fresh blood, with a corresponding degree of shock or collapse, and depression. Perforation is indicated by sudden onset of intense pain, with collapse, rapidly spreading tenderness, with abdominal rigidity and increasing distention. In other words the symptoms of perforation are those of acute local peritonitis of abrupt origin.
In either of these events the paramount indication is for prompt intervention, unless the patient is already too weak to withstand the shock of any operation. In one case this will consist of gastro-enterostomy, with or without a gastrotomy for the purpose of discovering the bleeding vessel and making local hemostasis. In the other it will consist of free incision, complete toilet of the peritoneum, with removal of all escaped material, and local attention to the site of the perforation, doing there whatever may be needed.
—Should the surgeon see a case of gastric hemorrhage due to ulcer after the apparent cessation of the active loss of blood he may easily decide to wait for a few days until the patient has in some degree recovered strength and atoned for such loss. On the other hand if he see the case during its active stage he need not hesitate to open the abdomen, withdraw the stomach, open it sufficiently for exploration, and then attack the source of hemorrhage, be it large or small, in such manner as he may see fit—either with the actual cautery, with a sharp spoon, with complete excision of the ulcerated area and union of its borders by suture, or by merely including a bleeding vessel in a loop of suture, addressing himself at once to the formation of an anastomosis, preferably posterior, between the stomach and the uppermost loop of the small intestine. This procedure, which is wise in all instances, would be imperative in nearly all save those perhaps where an ulcerated area could be cleanly excised and its margins neatly sutured. Should it prove that suture of the stomach wall were impracticable its edges[801] might be fastened to those of the abdominal wound, a gastrostomy thus resulting, which could be later closed by another operation.
For perforation the surgeon might have to rely, in emergency, on a gastro-enterostomy as a relief opening, accompanied by local gauze tamponage; the point of perforation could not be made accessible for suture, but one should prefer suture for all cases that permit of it. In these cases a considerable margin should be enfolded and included within the grasp of the suture, or else the margins should be completely excised until healthy tissue is reached. In rare instances it has been feasible to fit into a perforation a drainage tube, or to pack about it a gauze strip which should conduct from the stomach cavity directly to the abdominal wound. The question of excision of the entire ulcerated area should rest entirely upon the possibility of repairing the defect by sutures, and this will depend in large degree upon the location of the ulcer and the freedom with which the stomach can be manipulated, especially with which it can be withdrawn into the wound.
Practically every case of perforation thus operated will demand posterior as well as anterior drainage. Aside from the treatment of the stomach itself the general peritoneal cavity needs the same thoroughness of cleansing and the same care in every manipulation that would be given in a case of well-marked peritonitis already established.
This term has reference especially to external fistulous openings, which are an exceeding rarity save as relics of injury or of operation. They have been known to occur spontaneously by perforation of an ulcerated and adherent stomach, such perforations occurring either in direct line or irregularly in the direction of least resistance. Traumatic fistulas result usually from gunshot or stab wounds, or are due to incomplete union of an opening deliberately made. In any event they permit of the escape of more or less of the stomach contents. Their tendency is usually toward spontaneous repair, but this is often so slow or so incomplete that it needs to be hastened by stimulation of the fistulous tract with silver nitrate, the actual cautery, curetting, or by a complete resection of the entire tissue involved, and a neat reunion with suture.
Intra-abdominal gastric fistulas result usually from perforation of gallstones or the escape of foreign bodies. Produced in this way they empty usually, though not always, into some neighboring portion of the intestinal canal.
Benign tumors are occasionally found in the stomach, and are most often of the adenomatous type. Papillomatous growths into the stomach have also been observed. Beneath the peritoneum, or in the submucous tissue near the pylorus, fatty tumors have also been seen. Myomas of mixed type have been described, and cysts have been met in the walls of the stomach. These have rarely attained a size larger than a hen’s egg. All of these non-malignant tumors are of pathological rather than surgical interest. Every one of them, however, will admit of successful surgical remedy when once recognized, operation consisting of excision, with suitable suturing.
Carcinoma is perhaps as frequently seen in the stomach as in any part of the body, the breast possibly excepted. In about three-fifths of the cases it involves the pyloric region, in one-tenth of them the cardiac end, the balance occurring in the intermediate part. It is usually of the round-cell or scirrhous variety, and is generally supposed to be a disease of adult or advanced life. While this is generally true there have been exceptions. It is occasionally met in the young, and has been reported even in early childhood. True sarcoma of the stomach is exceedingly rare. It spreads especially in the submucous tissue and evinces a tendency to involve especially the lesser curvature.
The duodenum evinces an extraordinary immunity from malignant disease, even[802] that involving the pyloric region. When the pyloric end is involved the lesion is frequently complicated by adhesions, which are present in considerably more than half of the cases. The lymph nodes of the adjoining mesentery are nearly always involved, practically always in cases which come to the surgeon for operation. As the disease advances it spreads in several directions, and adjoining viscera may be involved, or even those at considerable distance, while metastases to other parts of the body are common. It is somewhat more common in males than females. In proportion as the pyloric ring itself becomes infiltrated and involved pyloric obstruction is an early feature, with the inevitable gastric dilatation and greater frequency of vomiting. Pathologists and surgeons are learning that the most frequent cause of gastric cancer is gastric ulcer, and recent investigations are to the effect that in at least 80 per cent. of cases there has been ulceration which has been followed by this malignant change. This affords additional reason, then, for regarding gastric ulcer as a surgical disease and operating upon it early and before such transition has occurred.
—As repeatedly emphasized throughout this work cancer is a disease without a pathognomonic symptomatology. For this reason it is rarely diagnosticated in its early stage, the symptoms which it produces being those of indigestion or dyspepsia.
The most distinctive features met with in gastric cancer are pain, vomiting, more or less dilatation, and presence of tumor. Pain is an early and constant symptom, the complaint at first being of heaviness and oppression, made worse after the ingestion of food, and later referred to as actual pain, which may be limited or may radiate to either side or to the back. Much will depend upon whether the cancer develop from the site of a previous gastric ulcer or independently.
Individual complaints are variant regarding the intensity and reference of this pain. In large measure it is due to the formation of adhesions, and its reference will depend much upon their location.
Vomiting is an equally constant and perhaps even more important symptom, being met in nine-tenths of the cases. When the growth involves the pyloric end the vomitus is copious in amount, while the intervals between attacks of vomiting are relatively long. When the more central areas of the stomach are affected and its capacity is thus reduced vomiting is more frequent, usually following soon after taking of food, and the amount of vomitus is consequently less. In general the character of the vomited material depends upon the length of time it has been retained, upon the possible presence of bile or blood, the presence of small amounts of blood giving to it a somewhat characteristic appearance, indicated by the term “coffee-grounds.” As the ulceration proceeds the amount of blood may be increased, and it may even come up fresh and red. The degree of actual ulceration will be indicated by the odor and the more or less putrefactive character of the materials ejected.
Too much reliance has been placed upon examination of the stomach contents. The amount of hydrochloric acid present therein depends in large measure upon the area involved. The same is true of pepsin. The glands which produce these digestive materials are found especially in the more central area, and when this is involved their amounts will be much reduced, whereas as long as these are free they are not necessarily so affected. The presence or absence, then, of hydrochloric acid may prove most misleading. The Oppler-Boas bacilli are perhaps of more significance, but even here the surgeon is often deceived. I regret thus to appear to belittle the significance of features upon which internists place so much reliance, but I have so frequently seen their unreliability that I think it is a sad error to wait for weeks in order to make a diagnosis by means of material secured through a stomach tube.
McCosh believes that for diagnostic purposes the stagnation test is of greater value than any examination of stomach contents. This consists simply in the discovery by lavage of food within the stomach when it should have left it. Thus an ordinary meal should pass out of the stomach within five hours, but if after six hours undigested food still remains there it denotes sluggishness of digestion. Food remaining ten hours makes positive the fact of stagnation. This being once established it should be determined whether it is from atony, spasm, pyloric stenosis, peritoneal adhesions which kink the opening, or cancer. In all of these except the first, surgical intervention is necessary.
[803]
Tumor in the stomach region, in connection with symptoms already mentioned, is corroborative. In nearly every case it can be felt sooner or later. Too many have waited, however, for this corroborative symptom before considering the case a surgical one, or even one of unmistakable cancer. Anyone can make a diagnosis when he can discover the tumor. What is needed is recognition of the condition before it has advanced to that stage. When it escapes detection it is usually because it is situated in the posterior stomach wall, high up, or else because the abdomen is enormously fat. The tumor when felt will be found firm and usually tender, sometimes regular in outline, sometimes quite the reverse, usually movable, but occasionally firmly attached either to the abdominal wall or to the viscera, usually the liver. Such a tumor, changing its position with the change in shape of the stomach produced by its inflation with carbonic dioxide, may be regarded as almost certainly a cancer of this organ. One rarely detects lymphatic involvement through the abdominal wall, but in many instances it may be noted at the root of the neck. The tumor usually rises or falls with respiration. Occasionally it will not be discovered until the stomach has been washed out and completely emptied.
However, further aids to diagnosis may be furnished, for instance, by the discovery of cancer cells in the vomitus or washings, by the presence of adventitious materials, such as lactic acid, whose especial significance is rather that of stagnation and motor paresis.
It is of great importance, when possible, to decide as between ulcer and actual cancer. In general the following aids to diagnosis may be considered: Ulcer is a disease of the earlier years of life, cancer rather of the later; in ulcer the pain is direct and boring (extending to the back), in cancer it may be widely referred to the shoulders; in ulcer the vomited blood is usually fresh, in cancer it furnishes the so-called “coffee-grounds;” in ulcer there is ordinarily no tumor present, in cancer this is a late but sure sign; the history of a case of ulcer will often be a long one, that of a case of cancer is rarely long, but steadily progressive; in ulcer there may be distinct anemia, whereas in cancer it assumes rather the type of a peculiar cachexia; and the free hydrochloric acid which is increased in ulcer is usually diminished or absent in cancer.[56]
[56] Sahli has suggested what he calls a desmoid test for free hydrochloric acid. A small amount of methylene blue is enclosed in a small gutta-percha bag, and this is tied by means of a small strand of raw catgut. This catgut will not be affected by pancreatic juices, and will only dissolve in the stomach in case there be free hydrochloric acid present. The fact of its solution and the liberation of the methylene blue is made evident by the peculiar color given to the urine in a short time. If, therefore, this appears within an hour or so after the material has been swallowed one maybe sure there is free hydrochloric acid present in the stomach. The test is not absolutely accurate, but will often serve as a fairly reliable one and a substitute for the more disagreeable and ponderous method of a test meal and lavage. In some respects it is perhaps even more reliable.
The question in cases of gastric ulcers is whether they have yet advanced to actual malignancy. Probably no surgeon has ever attacked a case of gastric cancer which has not been under treatment for a time for so-called “dyspepsia or indigestion,” perhaps with a more definite diagnosis. Too many internists have waited for the discovery of a tumor before thinking of surgery. It is the business and the duty of every surgeon to impress upon the profession that the only way to treat cancer successfully is to treat it radically, and the only way to do this is to operate early. This applies equally well to the viscera or to the external portions of the body. Gastric cancer is essentially a surgical disease, and could it be recognized early and treated radically it could often be cured.
What are we to do then in the absence of early and indicative symptoms? The following rule may be laid down as one to which there is no exception: A well-founded suspicion of cancer of the stomach (or of any part of the alimentary canal) justifies an exploratory operation for its detection and recognition, which then should be extended into an operation for its complete removal should circumstances justify it. If this rule were followed we would not hear of cases of this description remaining for months or years under drug treatment, and then perhaps being finally turned over to the surgeon for relief of pyloric obstruction at a period when strength is so reduced that no operation should be seriously considered.
Gastric cancer is, then, at least in its earlier stages, a surgical disease. How is it to be recognized? By exploratory incision when there is serious doubt as to the nature of dyspepsia or indigestion which fails to promptly improve under suitable treatment. In an early stage even this might not be easy, especially for the inexperienced. Nevertheless[804] any cancer of the stomach which produces distinct disturbances of digestion will have advanced to a degree of infiltration and thickening which will permit of its recognition by the touch of a practised operator. The discovery, then, of thickening in the stomach wall will imply the presence therein of either an ulcerated or cancerous area, which will in either event demand relief. In such a case the stomach may be opened and the mucosa exposed to sight and touch. Should the lesion prove to be malignant the same rule will apply with greater force, with the sole difference that the area should be much larger and that the surgeon should keep clear of suspicious tissue. This may necessitate a more or less complete removal of a considerable portion of the stomach. The greatest care should be exercised in the discovery and removal of all infected lymph nodes, which will be found especially along the curvatures and within the peritoneal fold. When retroperitoneal lymph involvement is discovered a hopeless aspect is put upon the case. Life may be prolonged for two or three years, even under such circumstances, and the patient is certainly entitled to whatever can be afforded him. If the cancerous process has advanced to a point or a degree making radical removal impossible, one may at once select the other alternative and perform a gastro-enterostomy at a point of election, by which relief may be afforded for at least a number of months.
Only by exploration, then, can it be decided whether to attempt a radical measure or a palliative procedure. It is scarcely fair to quote statistics in this regard, especially any but the most recent, as only lately have these cases been referred for early operation. Obviously the less wide the removal the less reduced the patient, the more favorable is his condition to withstand operation, and the more favorable the aspect of his case. Thus pylorectomy before gastric dilatation has occurred is more promising than pylorectomy when half the stomach is involved. In proportion, then, as these cases are submitted to early operation, statistics will improve and better results be attained, while if physicians and surgeons can be made to coöperate early an ever-growing number of cases will be seen and operated at a favorable time.
The various operations practised, including gastrectomy, pylorectomy, etc., will be discussed with the other operations upon the stomach.
To this term attaches about the same force and significance as to perihepatitis or perisplenitis. The expression implies the consequences of a local peritonitis, usually of low grade, by which adhesions are produced that may anchor the stomach in whole or in part, in any possible direction and to any of the surrounding viscera or part of the abdominal wall. Such adhesions are more common at the pyloric end than elsewhere. Their causes may be intrinsic or extrinsic, among the former ulceration and cancer being by far the more common; among the latter gallstones, tuberculous processes, and occasionally the remote consequences of typhoid ulceration. In the majority of cases the adhesions thus produced are protective and purposive, although they often constitute a serious obstacle to surgical work. While they may be suspected in almost any of the conditions above named, they are rarely discovered or identified until the abdomen is opened. Nevertheless, distention of the stomach with gas and the discovery of its irregular movements or shape because of fixation will afford good ground for suspicion as to the condition itself. When it can be shown that these adhesions are producing pain or discomfort, as they often do, operation, gastrolysis, affords the only legitimate and reasonably certain relief. Time sometimes permits a stretching of adhesions or the possible absorption and amelioration of symptoms, but only by surgical intervention can anything radical or prompt be offered.
Under this term is included a suppurative or necrotic inflammation of the stomach wall, beginning probably in the submucosa, but extending in both directions. It appears in two forms—the circumscribed and diffuse.
—The symptoms of the latter are those of an intensely acute gastritis with rapid, almost inevitably fatal course, beginning with severe pain, quickly followed[805] by faintness and collapse, with early vomiting, vomited matter being first bile-stained, then containing blood. The sensation of nausea is extreme and a complaint of thirst constant. Frequently there are hiccough and peculiar and uncontrollable general restlessness. Pain is, however, a variable feature, and some cases are too rapidly necrotic to afford much pain or tenderness. The pulse is rapid, weak, and poor, and the temperature usually runs high. After a short time the abdomen may be much distended, while symptoms of paralytic ileus (i. e., obstruction), supervene, though occasionally there is offensive diarrhea. A well-marked case of this type comes on with fulminating suddenness, patients later becoming apathetic and dying in stupor.
About all this there is nothing peculiarly characteristic, and similar symptoms might be caused by mesenteric thrombus, by acute pancreatitis, or acute gangrenous cholecystitis.
Symptoms of the more circumscribed form are similar to those just described, but of less severity. The pain and vomiting appear suddenly, but are less intense. If time be afforded for formation of abscess a distinct tumor may be felt. Appetite is lost and food regurgitated. A localized lesion favorably placed might lead to adhesions and circumscribed collection of pus, assuming the subphrenic or some less typical form. The pyloric end of the stomach is more commonly involved in such a process and affords evidence to the effect that it begins as an infection, the port of entry being usually a gastric ulcer.
—Treatment would be surgical if any were available, but has never yet been applied sufficiently early to save an acute, generalized case. On the other hand, when the lesion has been local and has led to subsequent phlegmon, cases have been successfully opened and drained.
In every instance, when time is afforded, certain preparations should have been made by which the stomach has been put in an aseptic condition. Not only should it be emptied of food in the ordinary sense, but it should have been washed out at least once, and in most instances repeatedly, first with cleansing lavage and then with a fluid containing a small proportion of borax, with the intent that by a mildly alkaline solution its contained mucus may be more thoroughly washed away. This alone, however, is not sufficient, for quantities of septic material may be introduced by the patient from his nose and throat. Frequent use of the toothbrush, with a strong antiseptic powder or solution, and frequent rinsing of the mouth with a suitable antiseptic mouth-wash, should be practised at frequent intervals for two or three days before such an operation. If offensive mucus be dropping from the nasopharynx this also should be cleansed and sprayed. In other words the possibility of contamination from the nose and mouth should be prevented as completely as possible.[57]
[57] The first deliberate operation upon the stomach seems to have been that by Crolius, in 1602, for removal of a knife, and a similar operation was made eleven years later by Günther. Up to 1887, however, only thirteen such gastrotomies had been reported. The first unsuccessful gastrotomy was done by Sédillot in 1839; the first successful one by Jones, thirty-five years later. While pylorectomy was suggested by Merrien in 1810, it was not actually performed until 1879 by Péan. Gastro-enterostomy was first done by Wölfler in 1881. The first operation for hemorrhage from gastric ulcer was performed by Mikulicz in 1889. It will thus be seen how recent is the whole matter of modern surgical attack upon the stomach.
—When the stomach has been opened by gunshot, stab, or other wounds it should be closed at the earliest possible moment. The operation intended for this purpose may be simple or difficult, and may be complicated by the fact of injuries to other organs. A simple opening is easily closed, when exposed, by sutures, of which there should be at least a double row, the internal devoted entirely to the mucosa, whose edges should be brought together and held by a continuous chromicized catgut suture, with stitches at intervals sufficiently short to prevent the possibility of hemorrhage, and interrupted occasionally to prevent puckering. A second row of sutures, of fine silk or thread, is then applied, by which the serous and muscular coats are firmly approximated, care being taken that the needle is not allowed to perforate a vessel and thus produce hemorrhage. The stomach walls are so thick that two layers of sutures thus applied usually suffice. If thought advisable a third suture[806] may be applied after the manner of the second. A round needle is usually preferable to a flat one with cutting edges.
Great care should be maintained to prevent escape of stomach contents or infection of the peritoneal cavity, if this has not already occurred. In some cases after exposing the stomach wound it may be advisable to pass a stomach tube and wash out the stomach, holding the wound with a compress in order that no leakage at this point can occur. Unless there is some good reason for not doing this it should be the method of choice. Two dangers particularly characterize cases requiring gastrorrhaphy: the first that of assuming that there is but one wound and failing to discover others which may co-exist; the second that of infection by the stomach contents which have already escaped. The first is to be avoided by careful observation and examination; the second by a careful toilet of the peritoneum, both before and after suturing. Drainage may be provided according to the necessities of the case.
A gunshot wound produces more or less contusion of the tissues in its immediate vicinity. Liberal allowances should then be made in suturing that gangrene and subsequent perforation may not occur; or, better still, when it can be properly done, the margins of gunshot wounds should be smoothly excised and fresh clean surfaces thus brought together.
—The stomach is opened for purposes of exploration or for removal of foreign bodies, as may be needed, and then promptly and completely closed when the opening has permitted such diagnosis or removal, or after a diseased area in its interior has been exposed by incision. Such may be the procedure in certain cases of gastric ulcer, where the stomach is opened, its entire lining examined and the sharp spoon or cautery applied, with or without linear suture. The stomach is also opened for dilatation of its orifices as in cases of cardiospasm or pyloric stenosis, although the latter procedure has given way to anastomotic methods, which are more permanent in their results.
The stomach having been exposed, usually by a sufficiently long median incision, it is brought out and divided at a point of election, the incision being made of sufficient length to permit introduction of forceps or finger, or even of more or less eversion of its interior surface in order that it may be carefully inspected. The purposes of the opening having been achieved, it is closed as indicated above, with at least two layers of sutures. A perfectly clean wound will scarcely call for drainage. One which has been infected should be protected in this way.
Gastrotomy has also been done in order to permit of the retrograde division of strictures of the esophagus, when it has been impossible to pass even the smallest bougie from above. In these cases it has been occasionally possible after exposing the stomach to introduce a whalebone bougie which, passing upward, may follow the tortuous passage and be made to appear in the pharynx. To its upper end may then be attached, by strong silk, the small end of another bougie, and thus guide it downward as the first one is withdrawn. This procedure has been improved on by Abbe, who has thus been able to pull down from the mouth a stout piece of coarse silk, bringing it out through the stomach opening, and then, by a species of sawing manipulation, divide the tightest and densest part of an esophageal stricture sufficiently to permit of the passage of some other instrument. This having been accomplished the stomach wound is immediately closed.
—This term implies making an opening into the stomach by which its cavity may be directly connected with the exterior abdominal surface, and the communication thus established maintained indefinitely. The procedure itself is necessary in cases of dense stricture or malignant disease of the esophagus, or the growth of such a tumor in its vicinity as shall occlude it, and thus cause slow starvation unless atoned for in some manner. In one instance recently, where I expected to do a gastrostomy, because the stomach itself had been so destroyed by powerful caustic that not only was the esophagus ruined as such, but the stomach decreased in size and motility, I found the stomach too immovable to permit of this procedure, and accordingly utilized the duodenum just beyond the pylorus, thus making essentially a duodenostomy; the indications, however, being the same as for gastrostomy. We have, in other words, to effect a permanent gastric fistula, the older method being to make the most direct possible communication between the stomach and the surface of the body, and then to introduce a tube, or resort to some similar expedient for preventing cicatricial contraction, and perhaps even subsequent closure. Silver tubes were formerly used, whose openings were corked and kept closed when the tube was not in use. In consequence of this foreign body with[807] the irritation it produced there was always more or less leakage and discomfort. The more recent methods have been devised with an intent of making a tunnel rather than a direct opening, through which, as needed, a soft rubber tube may be introduced, whose walls shall collapse at other times and close themselves, if necessary, with a little assistance, by pressure, thus preventing leakage. Sometimes it is possible to attain this ideal. At other times a rubber tube is worn a greater part at least of the twenty-four hours.
Fig. 529
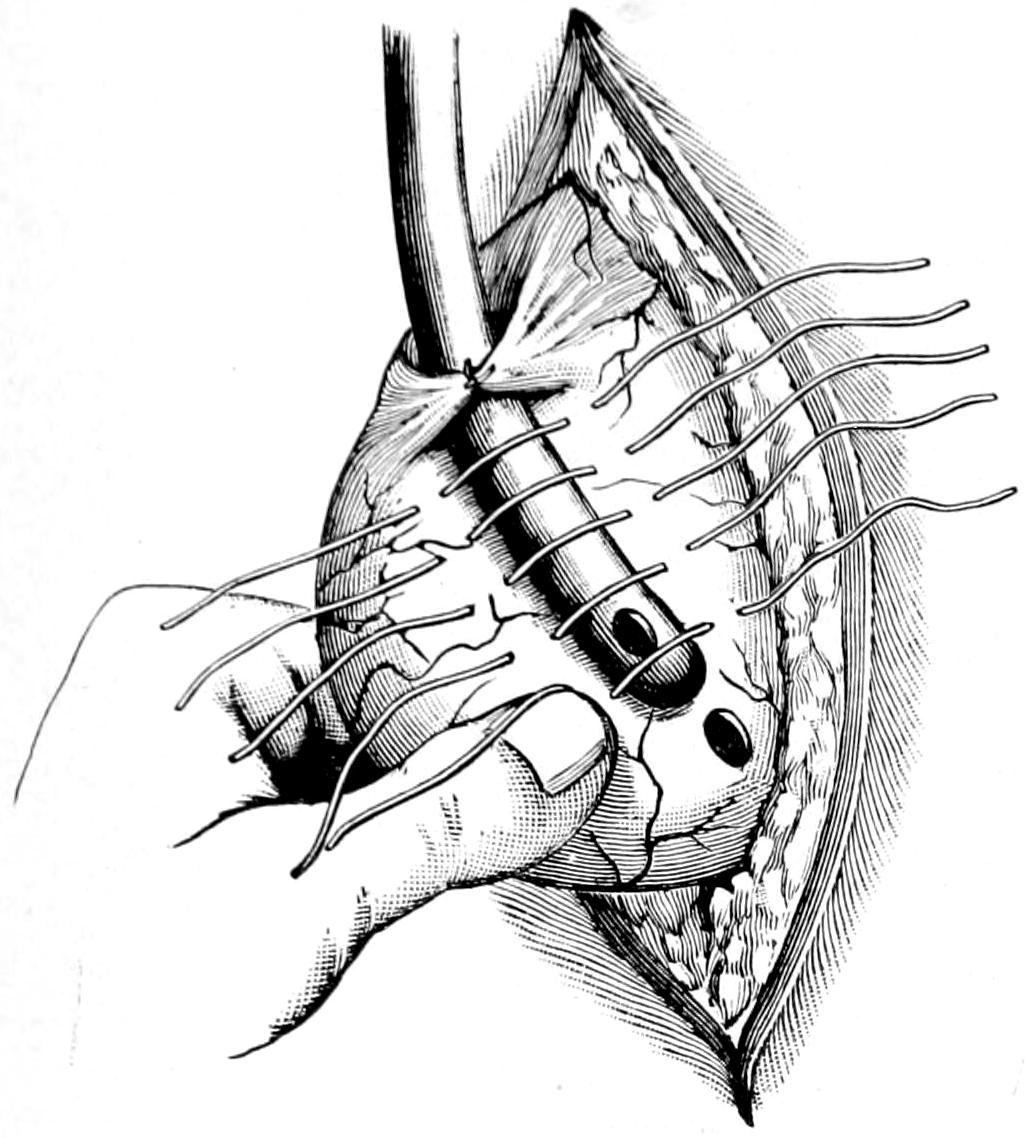
Gastrostomy: Witzel’s method. Tube in position; sutures ready to tie. (Richardson.)
Fig. 530
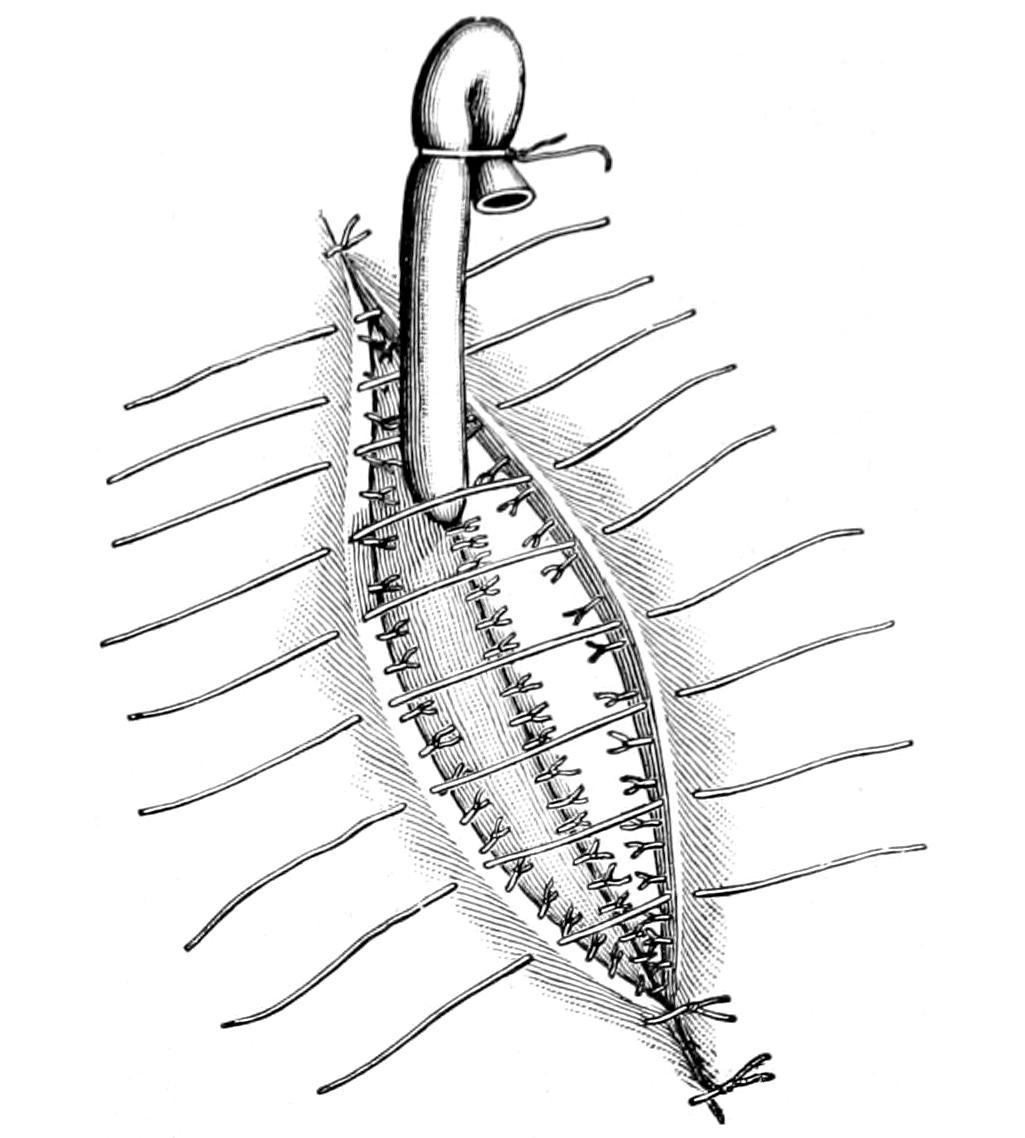
Gastrostomy: Witzel’s method. Tube in position; sutures ready to close abdominal wall. (Richardson.)
Fig. 531
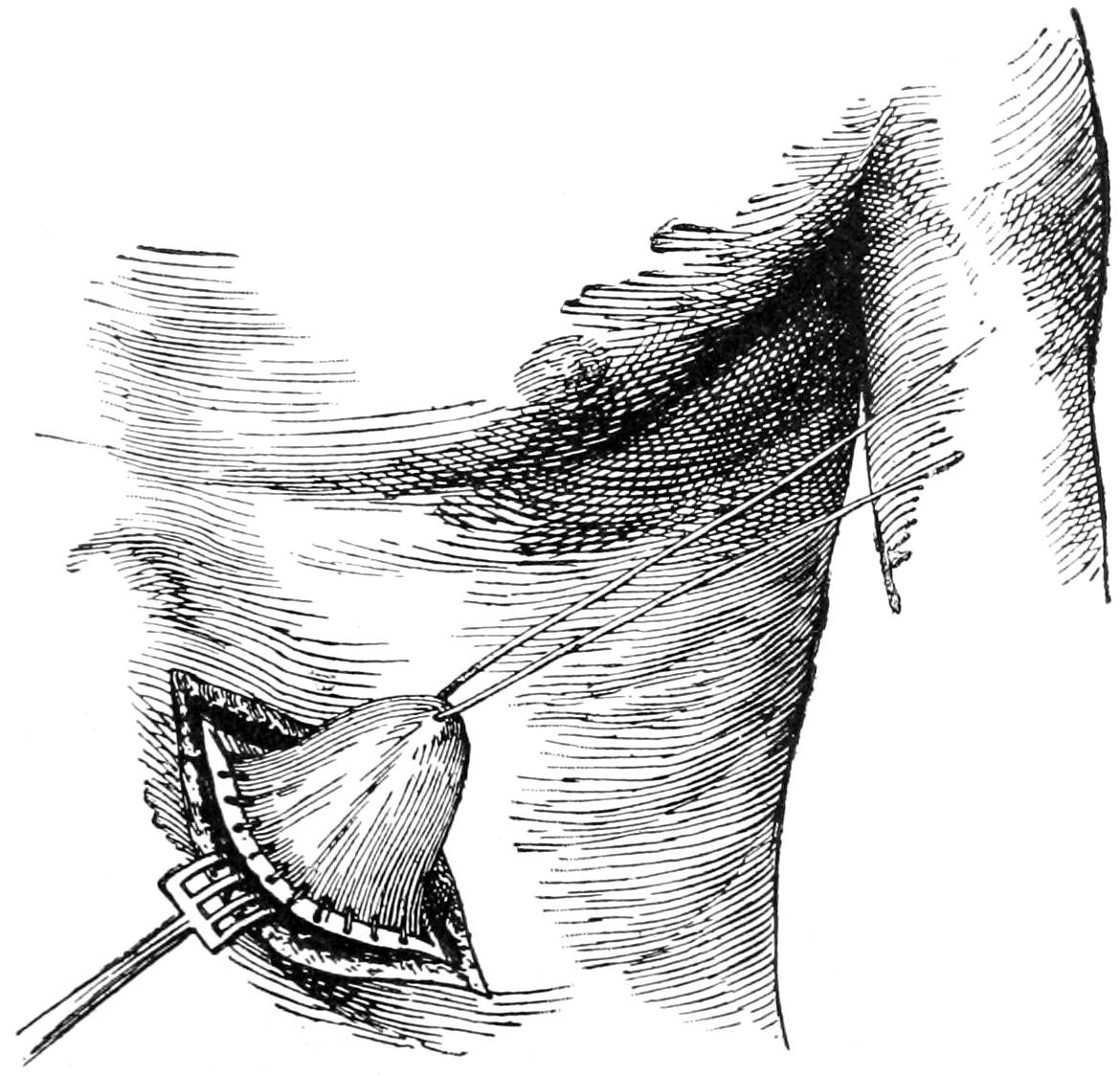
Gastrostomy by Frank’s method: cone of stomach stitched into the peritoneal wound. (Richardson.)
All operative methods include fixation and consequent adhesion of the anterior stomach wall to the parietal peritoneum, just below the border of the ribs. Of the many methods employed the following will be described, most of which can be easily appreciated in diagram:
Figs. 529 and 530 illustrate, for instance, Witzel’s method, where a sterile, soft rubber catheter is infolded in the stomach wall, and finally passed into its cavity through the[808] smallest opening that may suffice for the purpose, after which the outer layer of the stomach is completely closed over it. The stomach itself is stitched to the deep margins of the external wound, and these are then closed without drainage. If everything has been neatly done feeding may be begun within a few hours. Care should be exercised about passing into a stomach which has long been without much food a quantity which may disturb it, or of a quality which may distress it. A procedure very much like Witzel’s is that described by Marwedel, who first sews the stomach to the abdominal wound after drawing it partly into the wound, in order to afford sufficient working material, and then infolds the tube and inserts its lower end through a small opening. This is perhaps preferable, since the stomach being so fastened up at once there is no possibility of leakage into the abdomen.
Figs. 531, 532 and 533 illustrate Frank’s method, where the stomach is pulled up through a sufficiently long incision and drawn out into a cone, whose apex is then brought out through a second small incision, parallel to the first and at a distance of an inch or so from it. Here an actual opening is made into the stomach, while the cone is fastened to the skin here and to the peritoneum through the other opening, which is then completely closed. This method cannot be applied to a contracted stomach.
Fig. 532
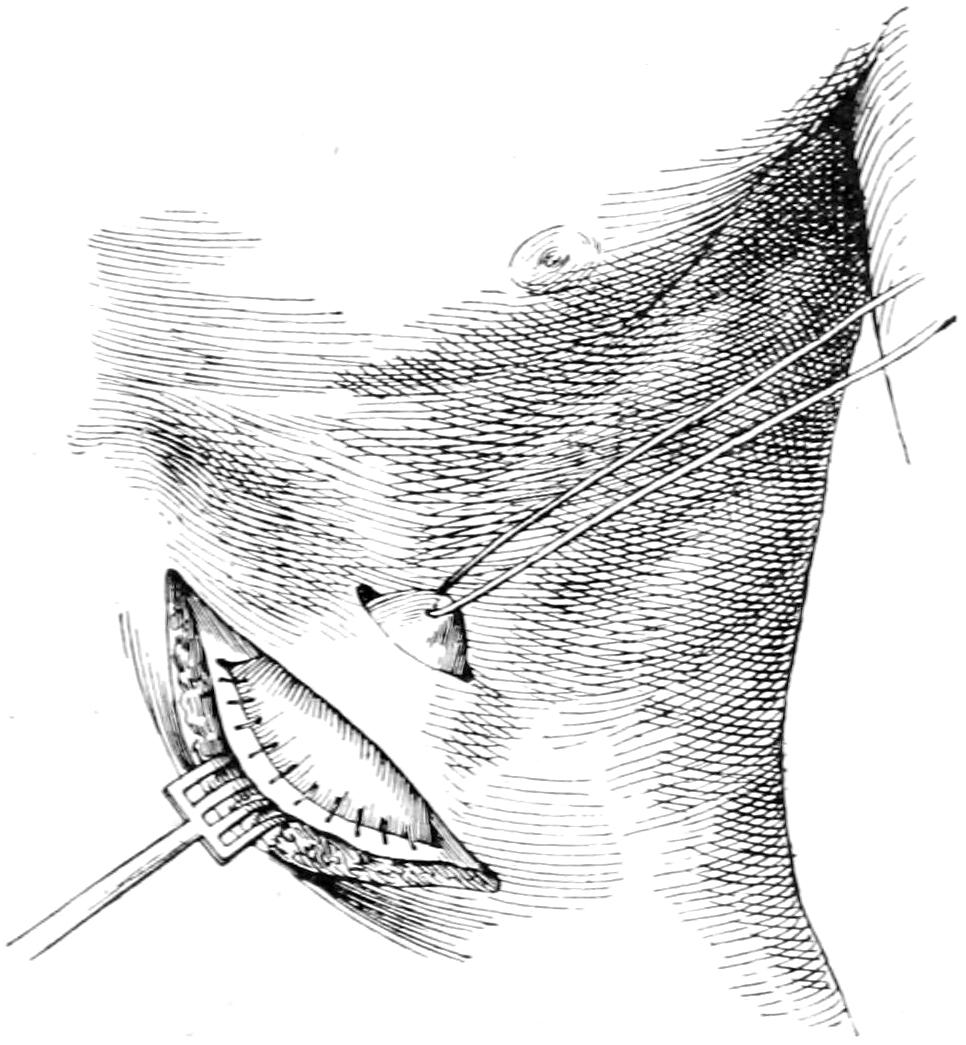
Gastrostomy by Frank’s method: cone of stomach pushed through the second skin incision. (Richardson.)
Fig. 533
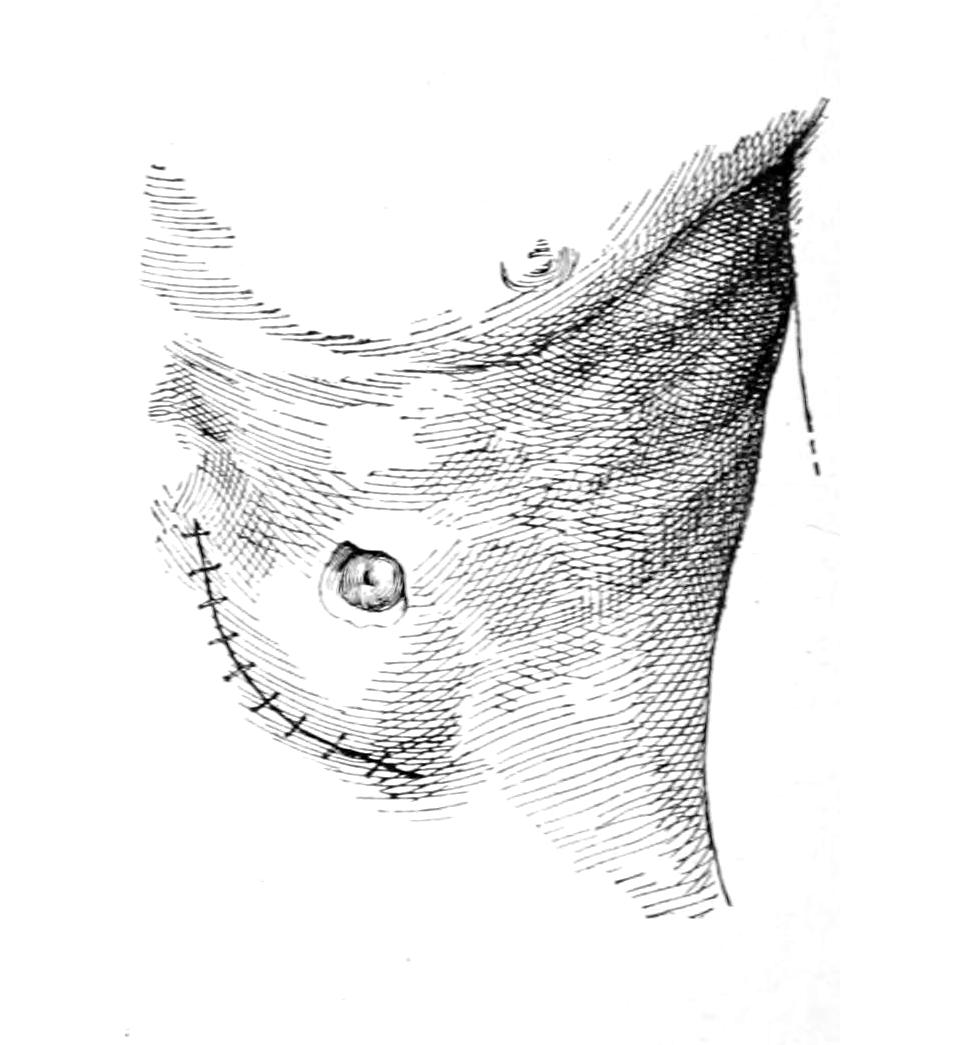
Gastrostomy by Frank’s method: suture of abdominal wound; stomach stitched in the skin incision. (Richardson.)
—Operation for this condition consists essentially in a gastrotomy as above, the opening being made sufficiently near to the cardia in order that either with finger or with suitable dilating instrument passed upward from below, the contracted cardiac orifice may be stretched, or, if necessary, nicked at several points, and then forcibly dilated, in this latter procedure great care should be given that stress be distributed as much as possible. If it be practicable to introduce any dilating instrument a four-bladed uterine dilator would probably be ideal for the purpose.
—Among the earliest suggestions of a method of pylorodiosis was that of Loreta, who opened the stomach near the pyloric end and deliberately introduced through the constricted pyloric ring a dilating instrument, fashioned much after the shape of the ordinary glove stretcher, which, in fact, might be used for such a purpose should emergency require. The operation is simple and but slightly dangerous, but it was found that strictures here as elsewhere tend to contract, even after forcible dilatation, and that the method, while temporarily successful, was but seldom permanently so. It was applicable only to the cicatricial, i. e., the non-malignant cases.
A plastic method was then suggested independently by Heinecke and Mikulicz, with which their names are often connected and which is referred to as pyloroplasty. It[809] consists essentially in making a buttonhole incision in one direction and then closing it in the opposite, as illustrated in Figs. 534, 535 and 536.
Fig. 534
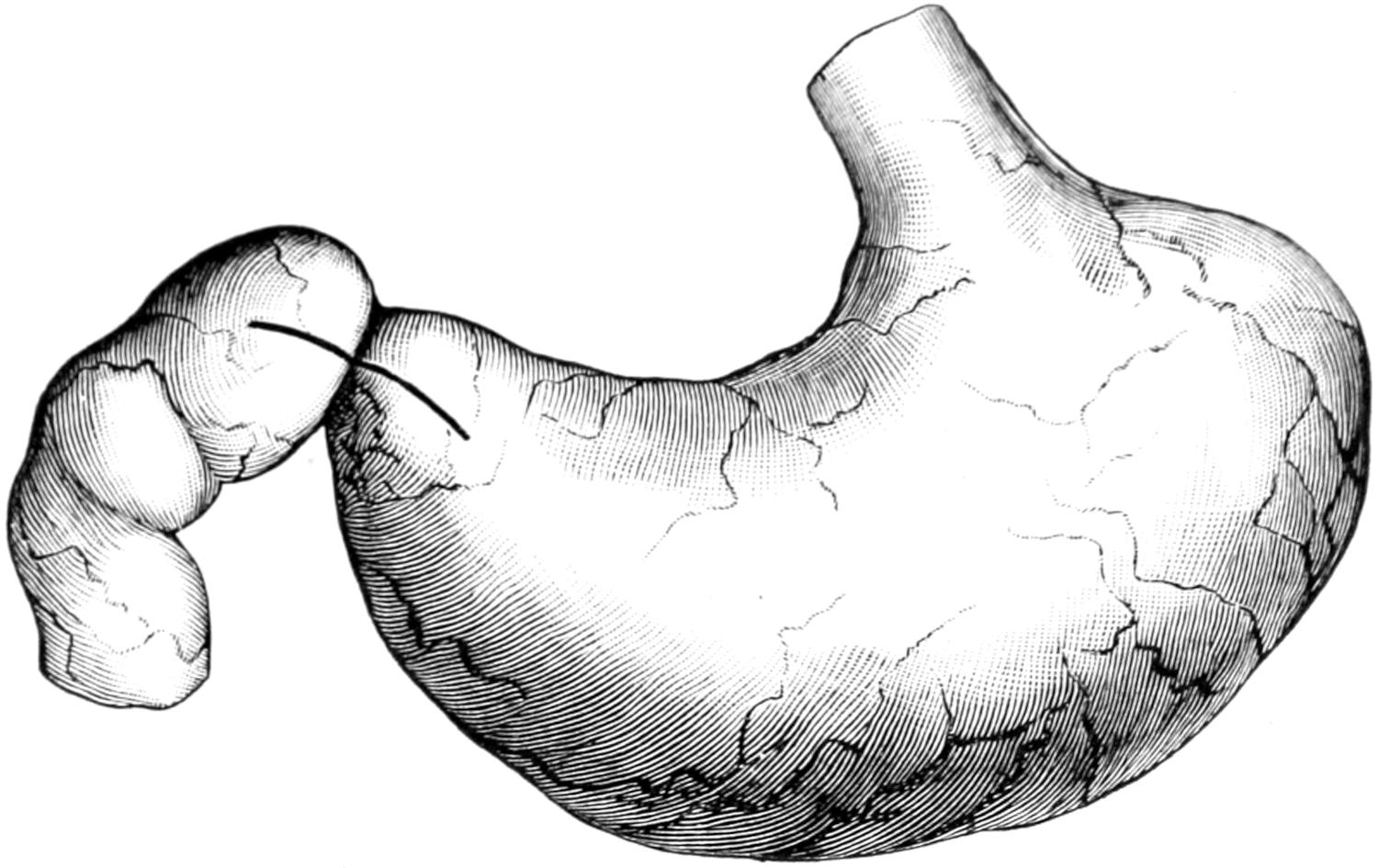
Linear pyloroplasty. Seat and length of cut. (Richardson.)
Fig. 535
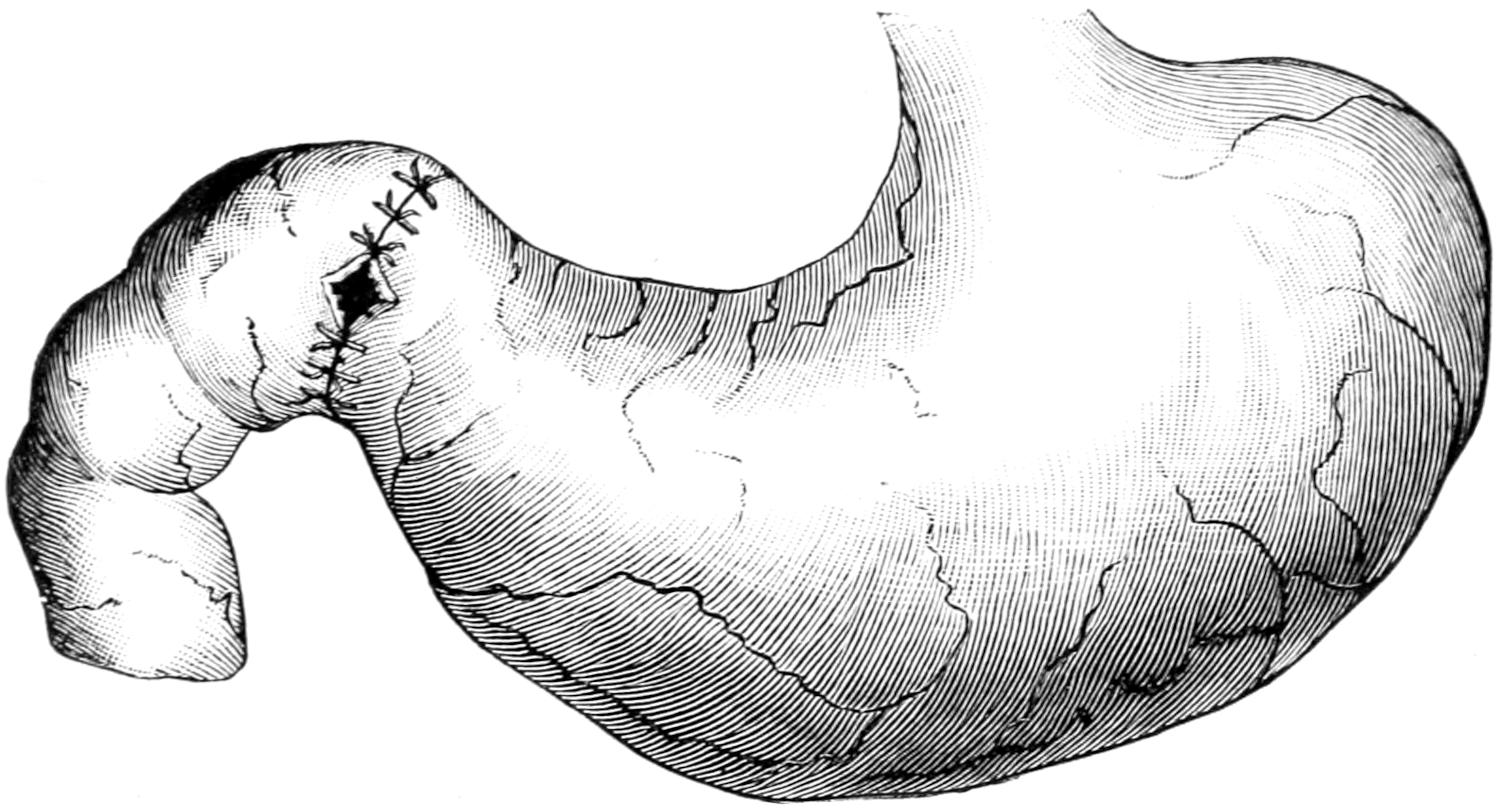
Linear pyloroplasty. Appearance of cut sutured transversely. Two more sutures to be applied. (Richardson.)
Fig. 536
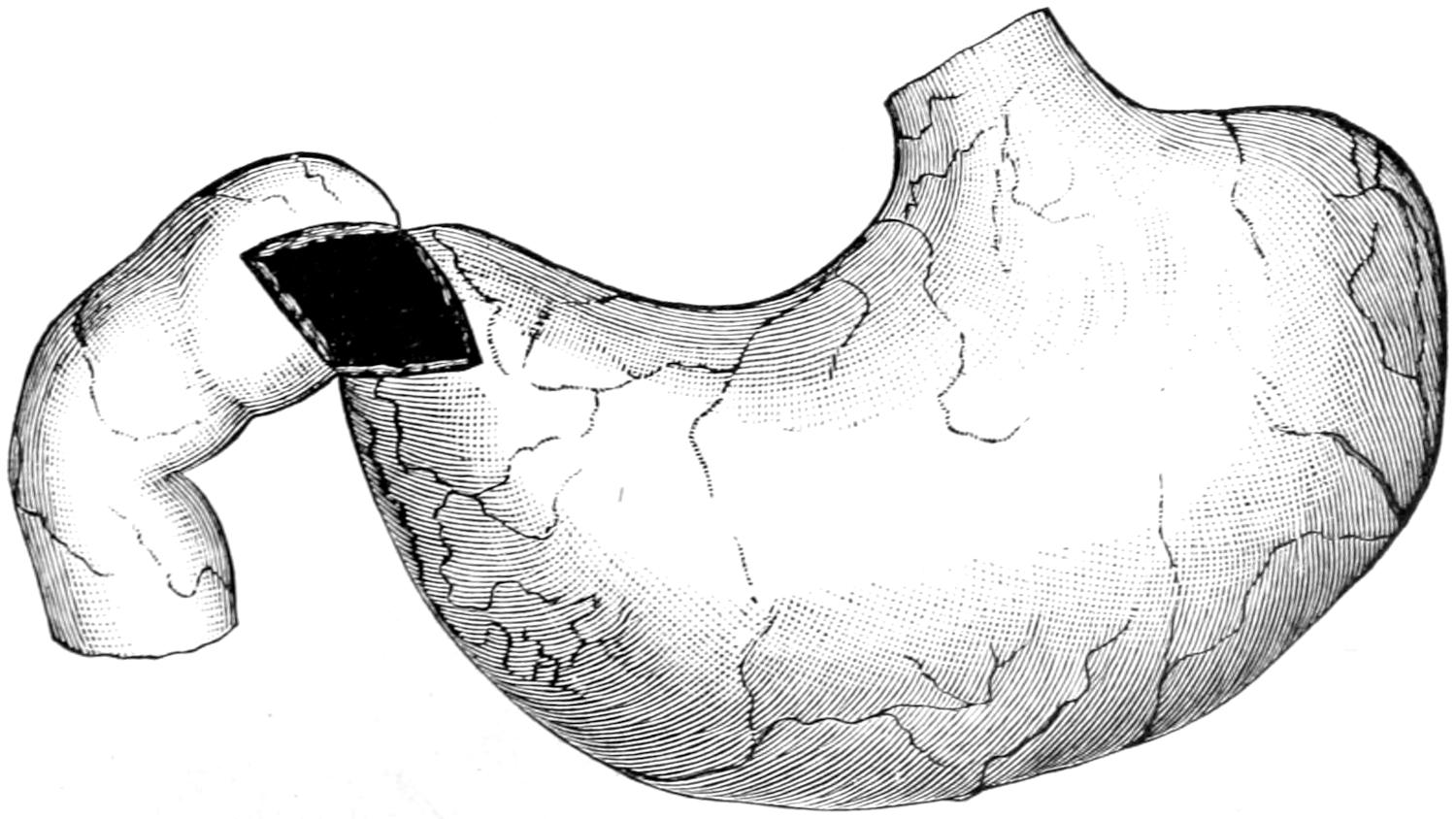
Pyloroplasty. Shape of cut when more than a linear incision is desirable. (Richardson.)
[810]
When cicatricial tissue is not too dense, and the parts not infiltrated, it has given satisfactory results. Even here it has been found to be frequently reduced in size by subsequent contraction, and the method suggested by Finney is more serviceable.
Fig. 537
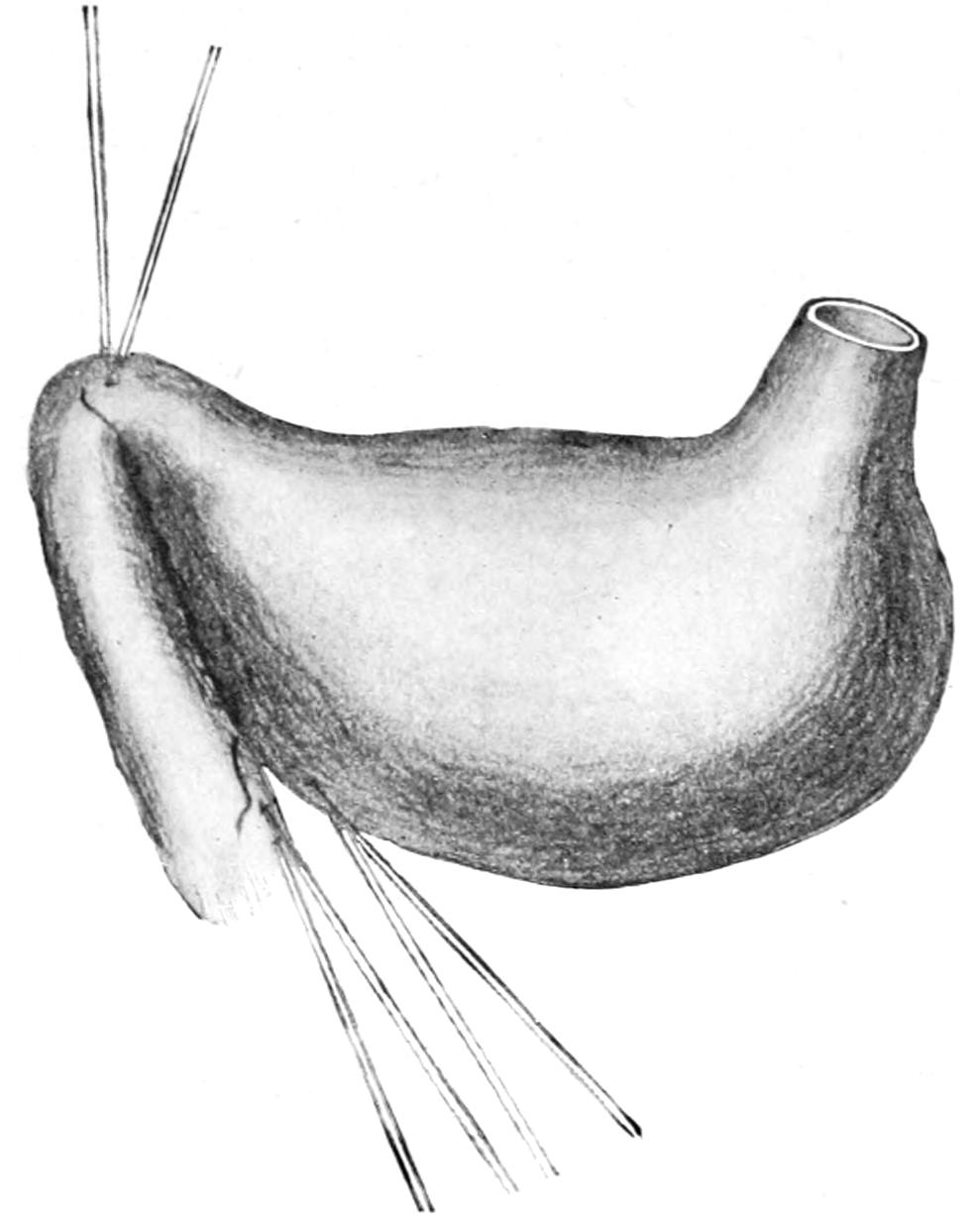
Finney’s pyloroplasty: posterior suture. (Bergmann.)
Fig. 538
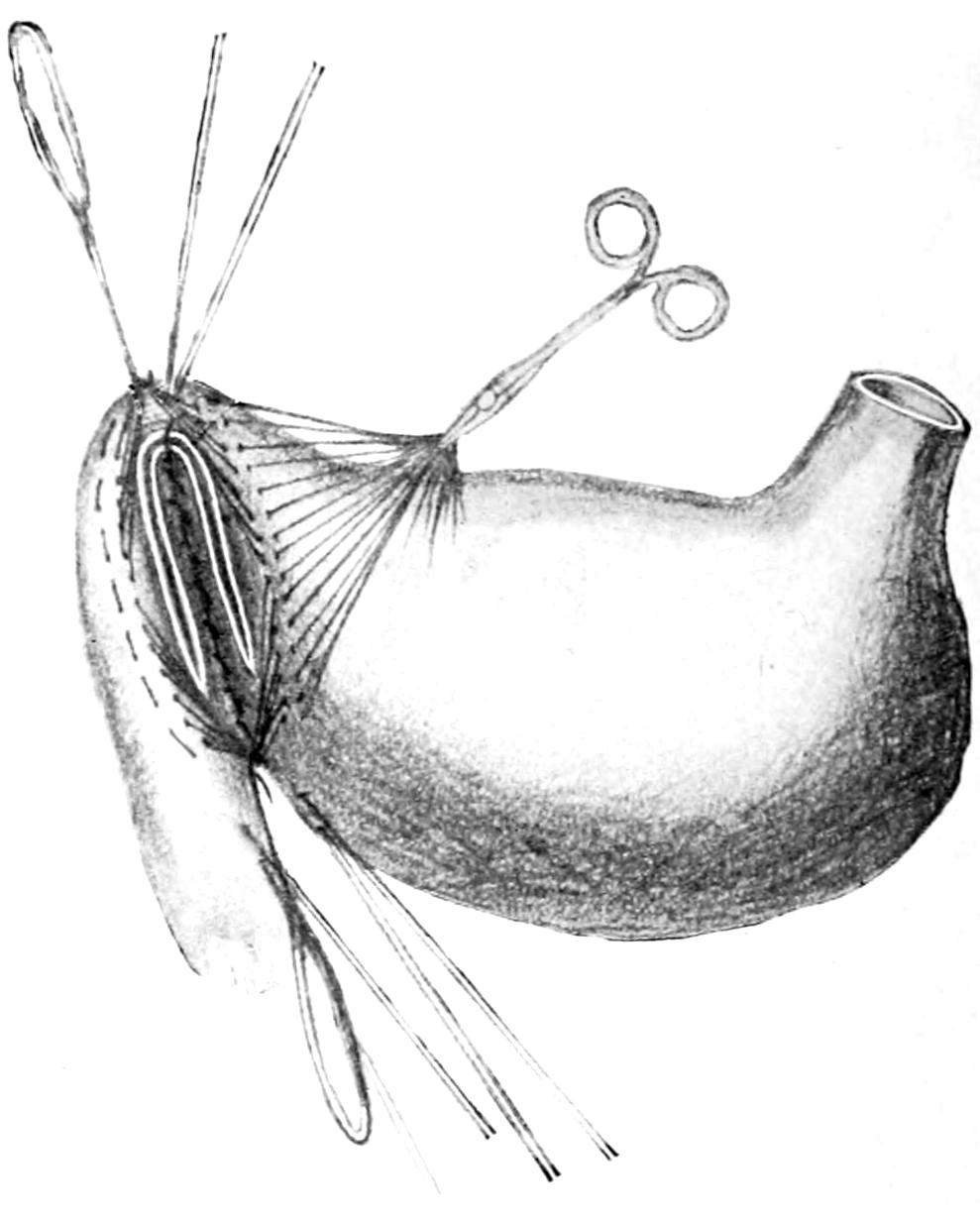
Finney’s pyloroplasty: anterior sutures drawn aside; incision made. (Bergmann.)
Fig. 539
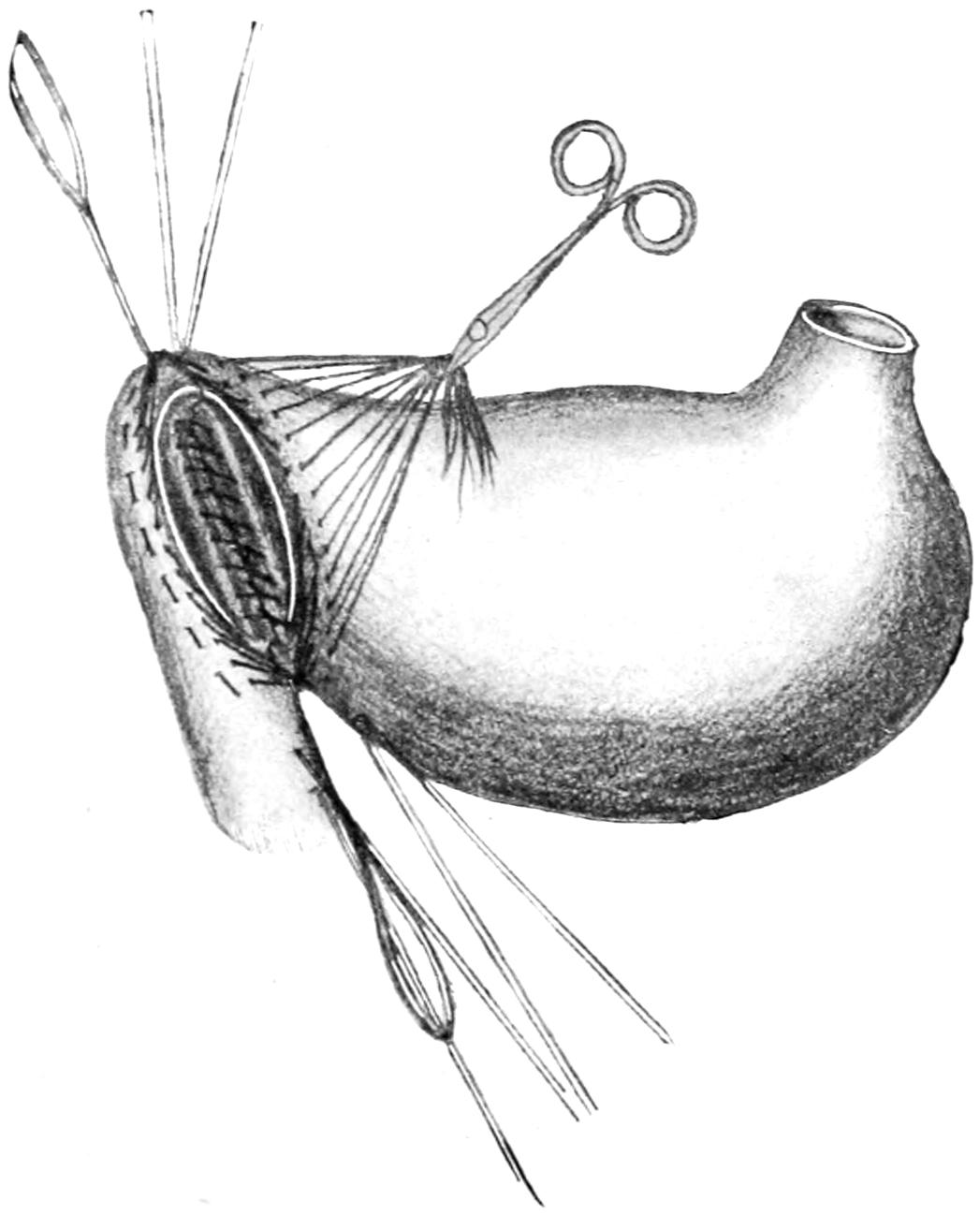
Finney’s pyloroplasty: posterior suture of mucous membrane. (Bergmann.)
Fig. 540
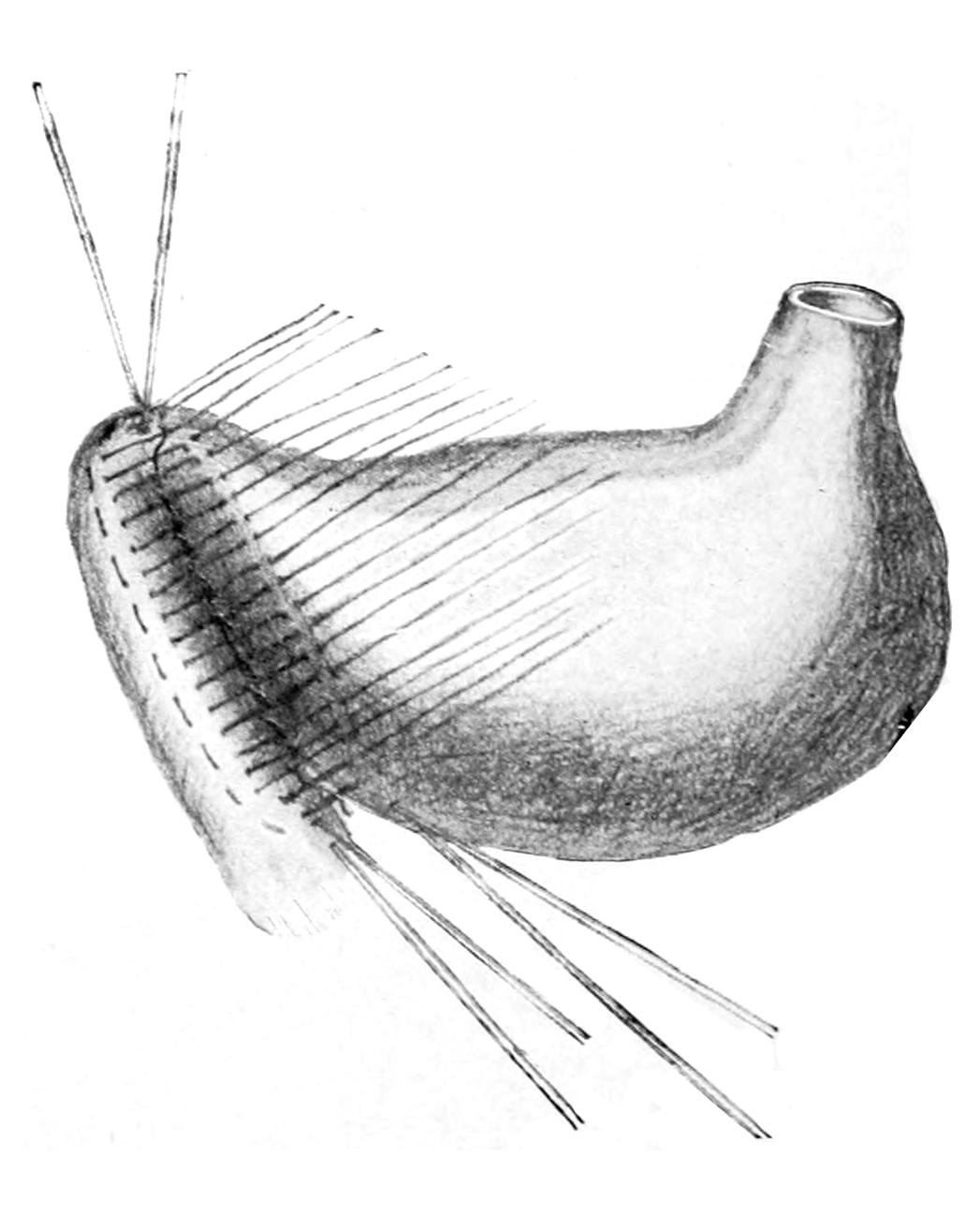
Finney’s pyloroplasty: anterior stitches inserted but not tied. (Bergmann.)
Finney’s pyloroplasty consists in making an anastomotic opening between the pyloric end of the stomach and the first part of the duodenum, and will be best appreciated from the accompanying illustrations (Figs. 537, 538, 539, 540 and 541).
[811]
Fig. 541
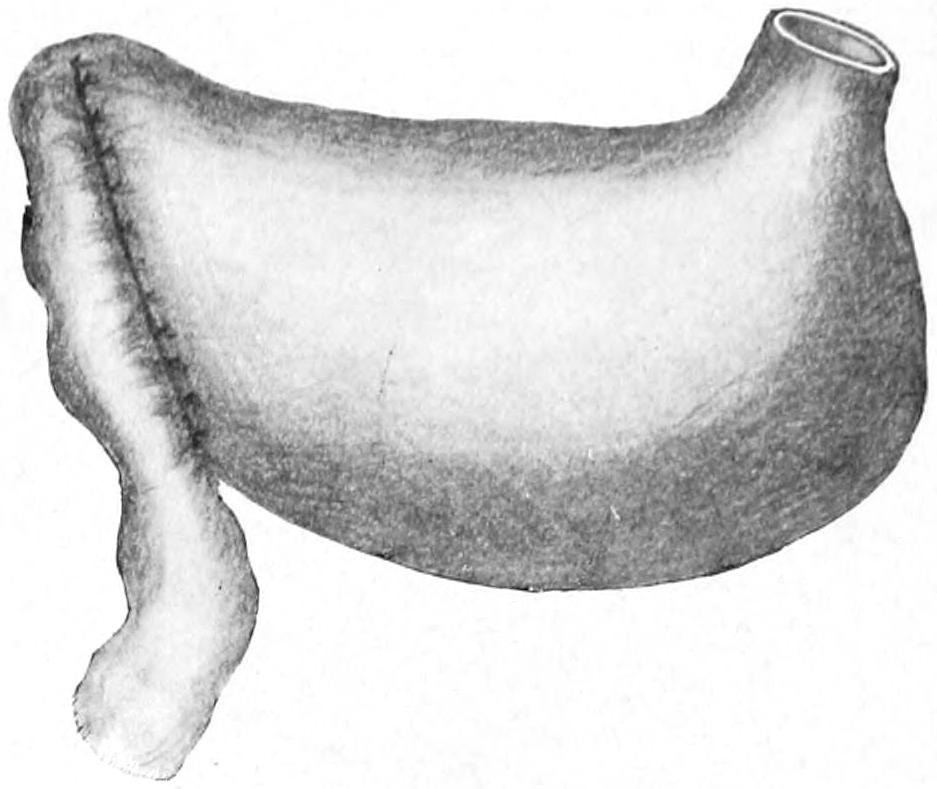
Finney’s pyloroplasty: anterior suture completed. (Bergmann.)
The opening can be made as extensively as desired, and it is not easy to see how it can be subsequently reduced to a degree disadvantageous to the patient.
Gastro-enterostomy may be needed in non-malignant cases, because of fixation and the impossibility of bringing the pyloric end of the stomach out sufficiently to make operation feasible. It will be required in cases of cancer when pylorectomy is not indicated. The method of making gastro-enterostomy will be described later.
—Gastroplication consists of taking a number of “tucks” in the stomach wall and thus reducing its capacity. The purpose and the method of the operation will be appreciated by the accompanying illustrations. These operations are mainly indicated, however, in the absence of pyloric stenosis, for if a free opening be afforded from the dilated stomach into the upper bowel the gastric enlargement will usually be spontaneously reduced (Figs. 542 and 547).
Gastropexy is a term applied to fixation of the stomach to the anterior abdominal wall. It has been thus stitched up in a few cases when greatly dilated or depressed into the lower abdomen. Fig. 548 illustrates the method. The stomach has also been suspended by shortening the gastrohepatic and gastrophrenic ligaments, as illustrated in Fig. 549.
Fig. 542
Fig. 543
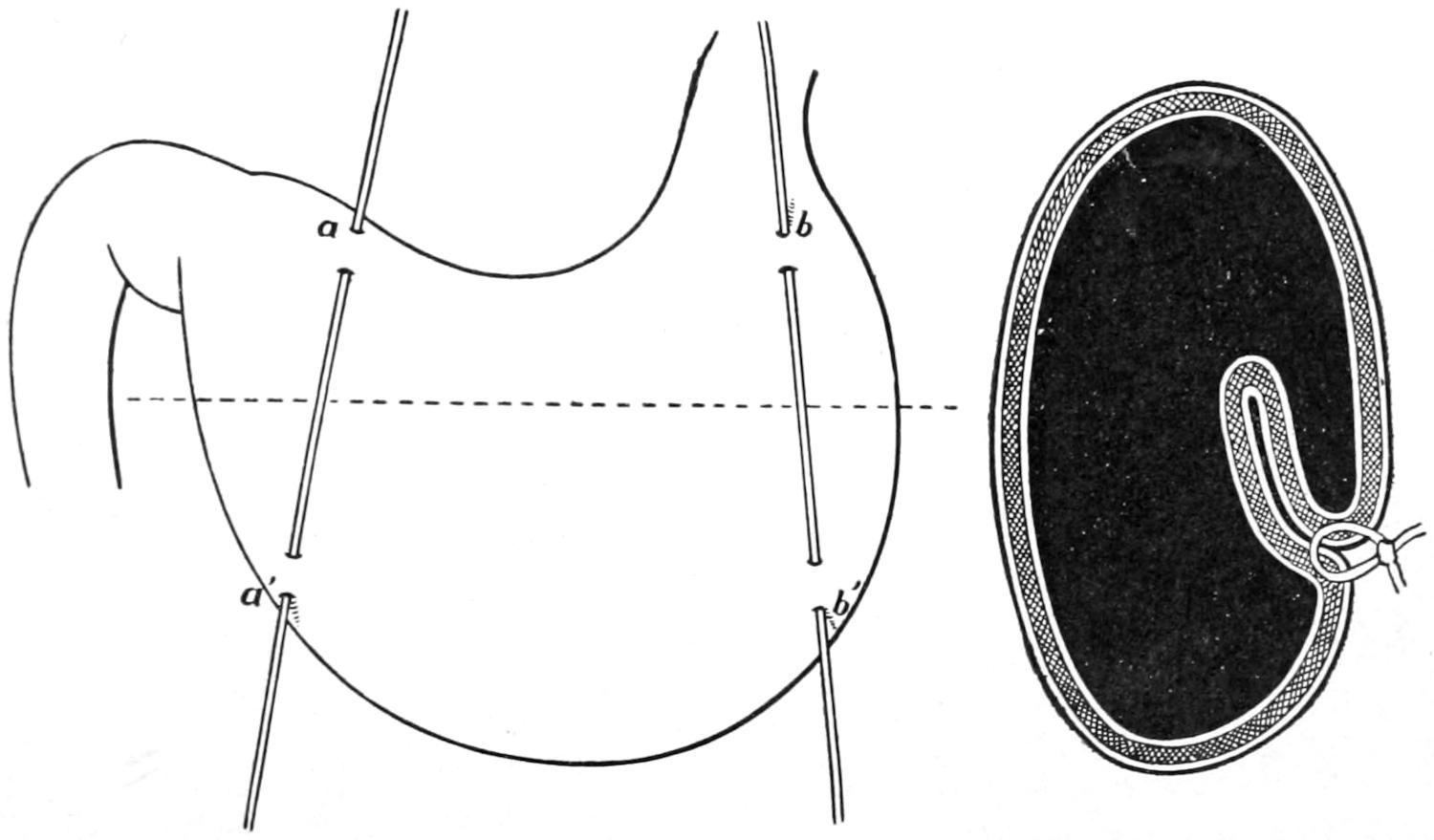
Gastroplication. When the threads a a´, b b´ are drawn up a fold is formed. (Bircher.)
Sectional view to show result of operation.
—In dealing surgically with an ulcer of the stomach the selection has to be made between anastomosis and direct exposure of the stomach wall with the performance of a gastrotomy (i. e., opening the stomach) and then discovering the site of the ulcer, either treating it with the actual cautery, the curette, or, preferably, when this general method is adopted, completely excising the involved area and bringing the margins of the wound thus made together with sutures, which over the mucosa only may be of chromic gut. Should it seem advisable to excise the entire thickness of the stomach wall it would be better to suture in two layers, making the external one of thread or silk, while the inner one may be made of reliable chromic catgut. If this operation be attempted the incision into the stomach should be made sufficiently large to permit of thorough exploration. Nothing being found in the anterior wall, the gastrocolic omentum should be opened and the entire stomach palpated between[812] the operator’s hands. Any suspiciously indurated spot on the posterior wall may then be so manipulated as to be brought into view through the anterior opening. Other surgeons besides myself have noted the occurrence of serious hemorrhage, which, upon exposure, must have come from small fissures or cracks in the mucous membrane. In fact the lesion which may furnish a considerable amount of blood may thus be so small and concealed as to be really difficult of exposure. However, exploration should be made as thoroughly as possible. The stomach having been opened and the ulcer found, it should be treated by one of the above methods. If, on the other hand, nothing be found the surgeon still has the measure of gastro-enterostomy. Any ulcer, however, which is threatening perforation can usually be recognized by the sense of touch alone, corroboration being afforded by inspection. An ulcer which is recognized and found to be favorably situated may be completely excised. It has been found, however, that this ideal measure of local attack gives but little better results than does the general procedure of gastro-enterostomy, while, on the other hand, it is less satisfactory in some respects and seems to be an equally if not more dangerous procedure.
Fig. 544
Fig. 545
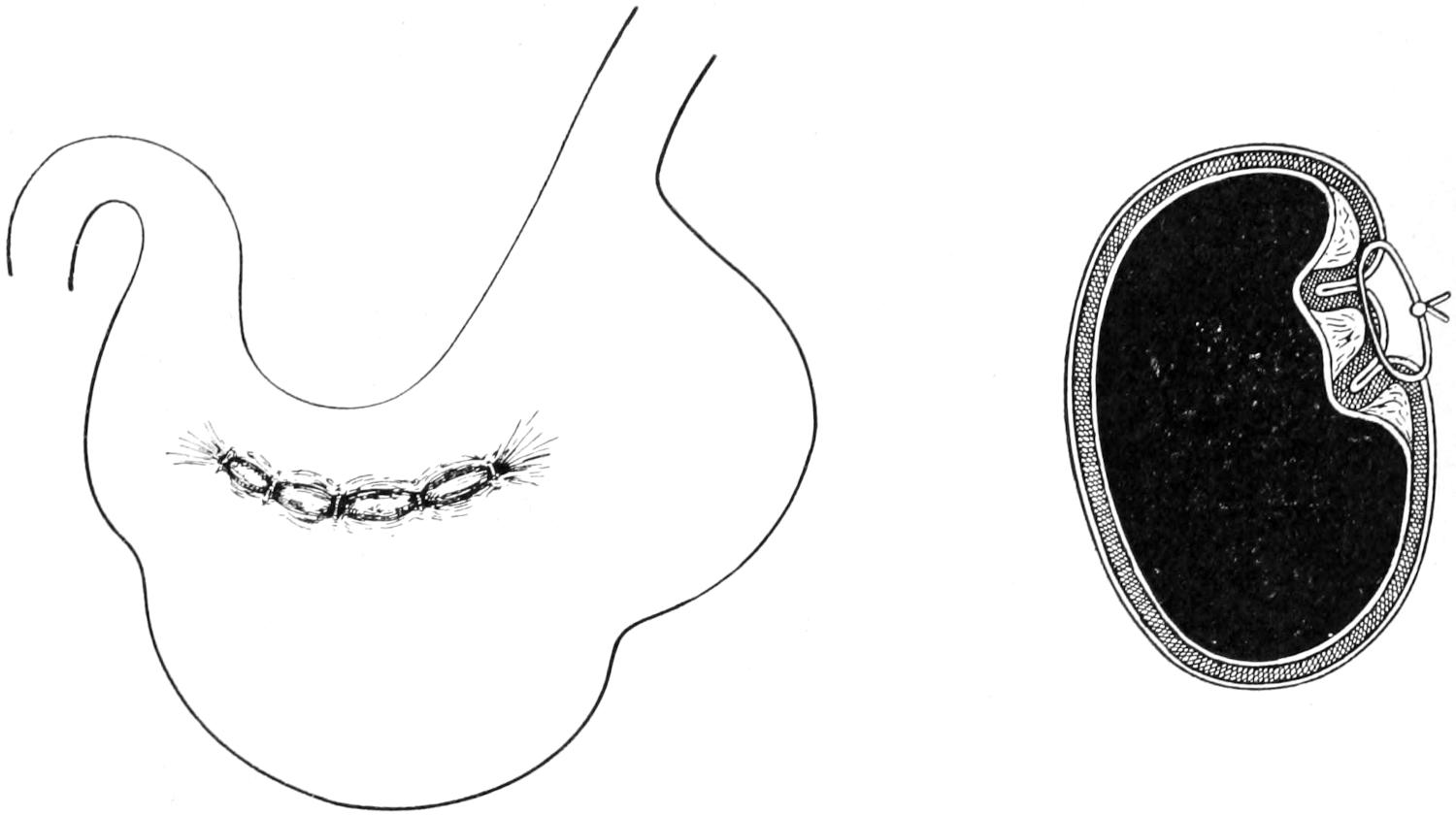
Surface view of the result.
Sectional view of the result when two folds are turned in.
Fig. 546
Fig. 547
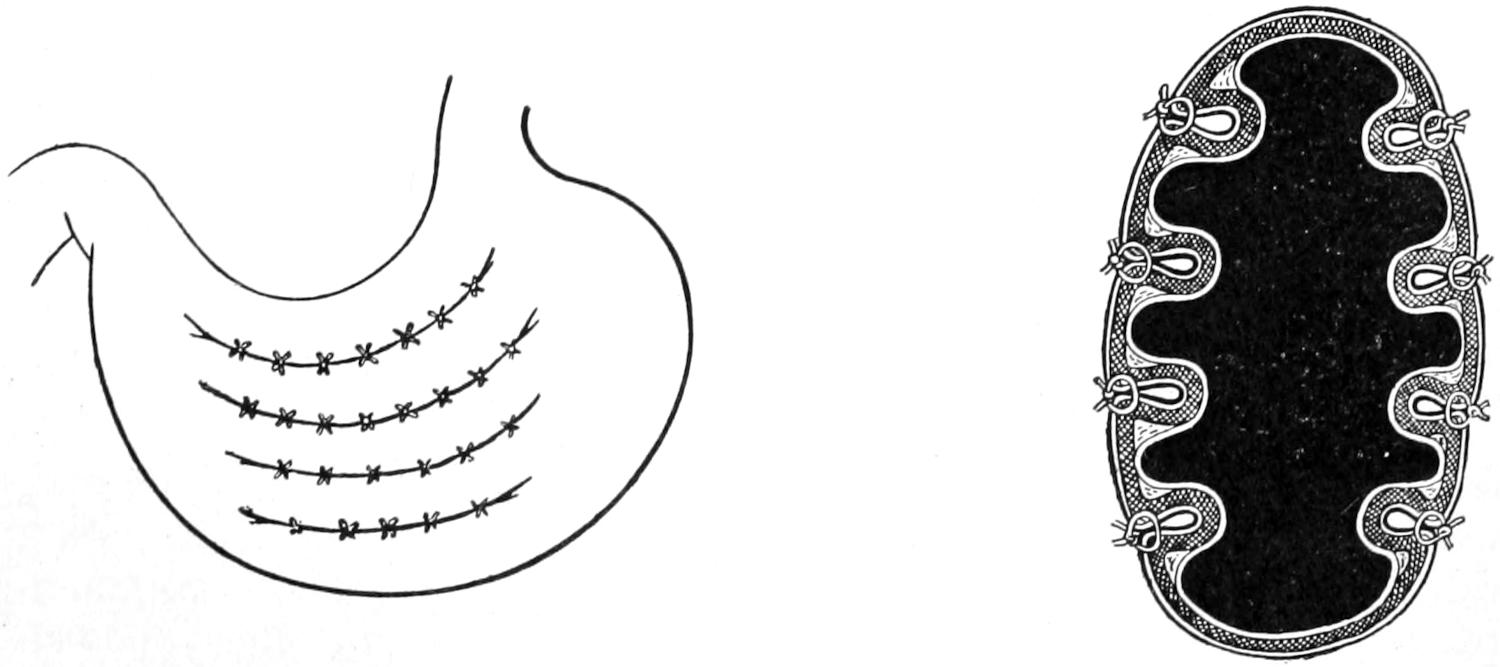
Gastroplication. (Brandt.)
Sectional view of the result.
The rationale of making an anastomotic opening between the stomach and the upper end of the bowel is simply this: that thereby the stomach is given a degree of physiological rest to which it has long been a stranger, and that food may pass easily from the stomach into the upper bowel without irritating or aggravating the ulcerated portion, which is[813] usually at the pyloric end. It should be understood, then, that gastro-enterostomy, done for this purpose, is simply a means of carrying out the universally applicable canon of physiological rest for diseased organs or surfaces. The operation of making this anastomosis will be described below.
—A complete removal of the pyloric end of the stomach is usually referred to as pylorectomy, while still more extensive extirpation of portions of the stomach proper are spoken of as gastrectomies. In a few instances it has been possible to practically remove the entire stomach, this having first been done by Schlatter. Such an operation would be spoken of as total gastrectomy. These operations are done almost exclusively for removal of areas involved in cancerous growth. Obviously the more extensive the growth the greater the amount of stomach which should be removed. For some reason as yet unknown cancer of the stomach rarely transgresses the pyloric ring, and thus the first part of the duodenum usually escapes involvement, even though the stomach be extensively diseased. All these operations, therefore, include simply the removal of a part terminating with the pyloric ring proper. It is seldom necessary to take away any of the duodenum. Removal of the pylorus may be also applicable in certain cases of benign strictures, where the mere plastic operations would seem insufficient, as well as in the cases of ulcers encroaching upon the pyloric ring itself.
For all of these operations the stomach is exposed through a median incision, or, if a tumor presents distinctly upon the right side, the incision may be made even far to the right and near the semilunar line. Through an opening sufficiently liberal the stomach and the movable part of the duodenum are withdrawn and carefully examined. When the pylorus is so fastened by dense adhesions within the abdomen that it cannot be withdrawn it is best to abstain from this particular procedure, as the mechanical difficulties too greatly enhance its dangers. Suitable clamps, whose blades are protected with soft rubber, are essential in order that the duodenum may be clamped beyond the line of its division, and that the stomach as well may be fixed between their blades, for the double purpose of controlling hemorrhage and preventing escape of contents. The omentum along the involved part of the stomach should then be carefully tied off, in a series of loops, before its vessels are cut, and one should take great pains to hunt out enlarged lymph nodes and include them in the area to be removed, or else make a separate incision for those that cannot be thus extirpated. To leave lymph nodes which are perceptibly involved in the cancerous process is to invite the speediest possible return of the disease, even though the operation should be successful. The upper and lower borders of the stomach being thus freed, the surgeon is then at liberty to cut away all the diseased portion, going at least an inch beyond the apparent limit of the disease. There will result from any such operation two divided ends of the alimentary canal, i. e., one, that of the divided stomach, much larger than the other, which is the upper end of the duodenum.
Fig. 548
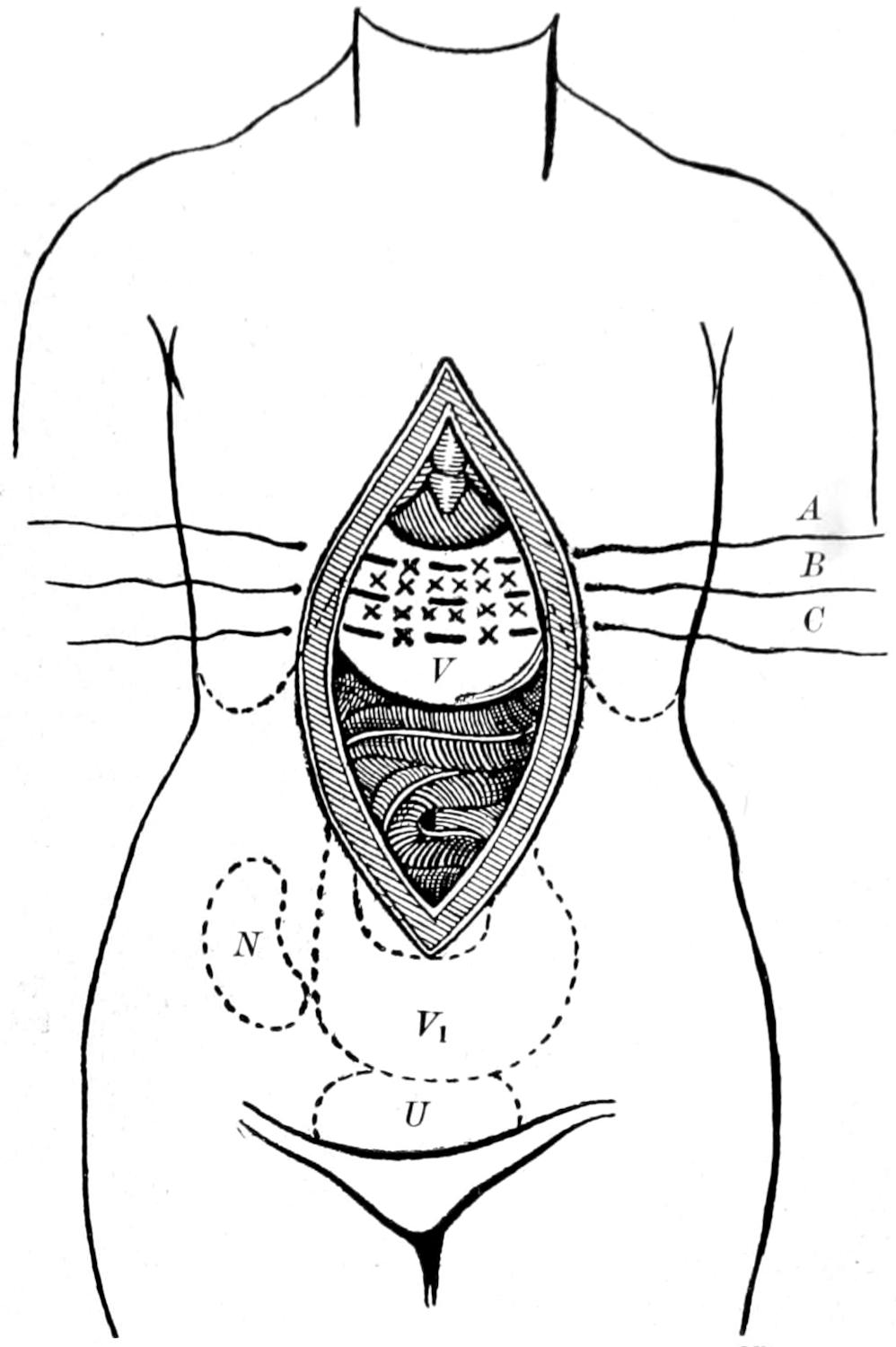
Rovsing’s operation for gastroptosis: V, stomach; V₁, position of the stomach before operation; U, urinary bladder; N, right kidney; A, B, C, silk sutures; x, x, scarifications. (Bergmann.)
Two procedures are now open to the surgeon: He may entirely close each of these openings with sutures and then make a posterior gastro-enterostomy, making new openings[814] for this purpose, and by the common method described below, or he may reduce the size of the stomach opening and endeavor to fit it to that of the duodenum in such a way as to bring the two openings opposite each other, where they are then approximated as in ordinary end-to-end resection of the intestine. The earlier operation of Billroth and his followers was made according to the latter plan. It has been found usually easier and more successful to adopt the former method, as it is easier thus to prevent leakage and consequent infection; that is, the majority of operators would today probably completely close the stomach and the duodenum, and proceed at once to make a posterior gastrojejunostomy.
Fig. 549
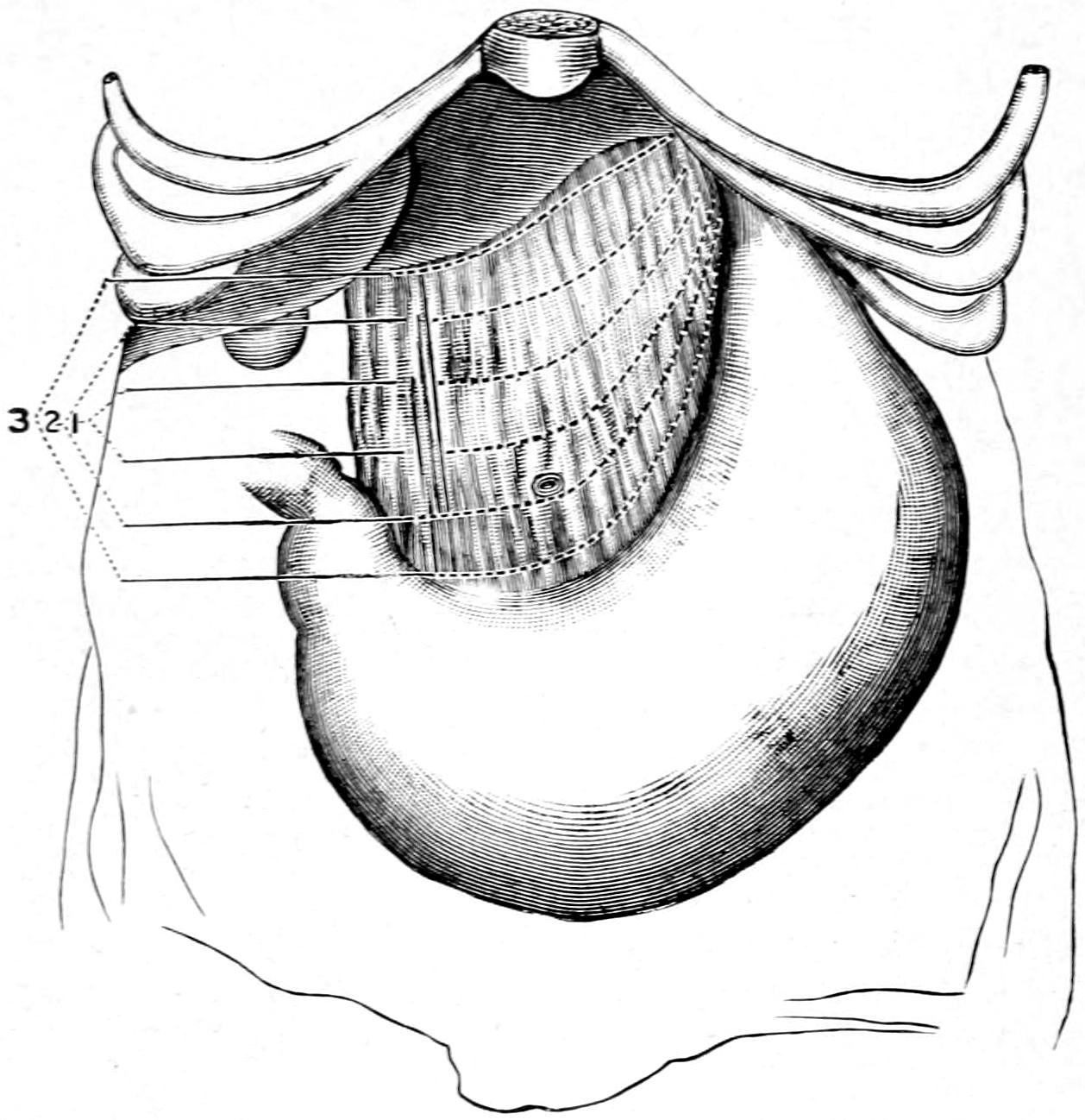
Suspension of stomach by three rows of interrupted stitches through the gastrohepatic and gastrophrenic ligaments: 1, 2, 3, single stitches of the three rows. (Beyea.)
Fig. 550
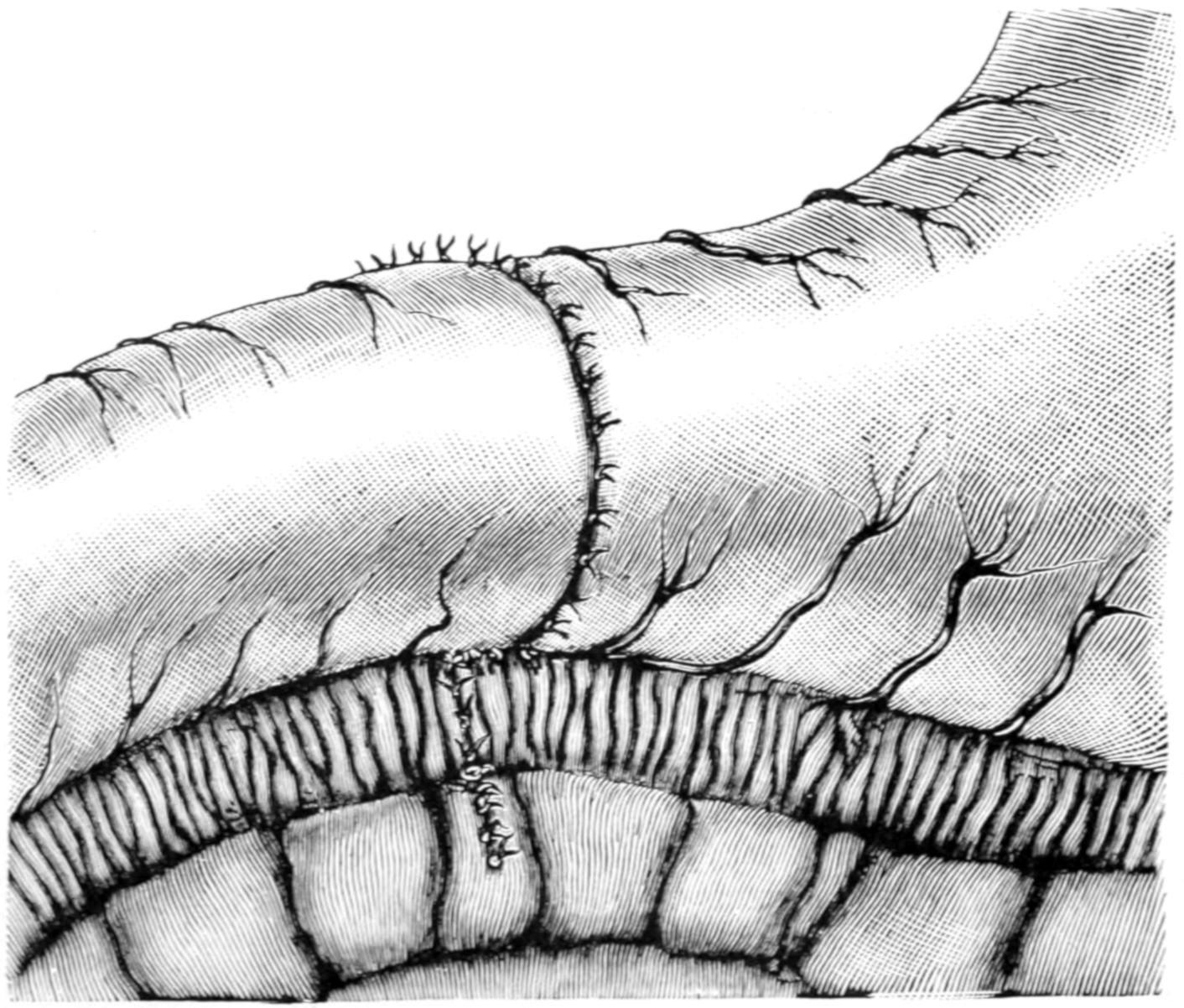
Resection of the pylorus. Suture completed. (Richardson.)
[815]
Figs. 550, 551 and 552 give a fair idea of the procedure of end-to-end reunion. The edges of the mucosa should be united with chromic gut, the stitches being close to each other, to prevent leakage and to control hemorrhage from small vessels. The external sutures of silk or thread should be placed sufficiently deep to afford a strong bond of union, and, at the same time, to escape the mucosa. Some difficulty is met here, for the thin wall of the duodenum should be attached to the thick wall of the stomach, but with care it can be done. When the divided stomach end has been reduced or trimmed off in such a way as to leave only a portion to be matched with the duodenal opening, there is need for extreme care at the corners and angles of the suture margins, as here tearing of stitches or separation by tension, perhaps during the act of vomiting, are most likely to occur. Fig. 553 indicates the first of the procedures above mentioned.
Fig. 551
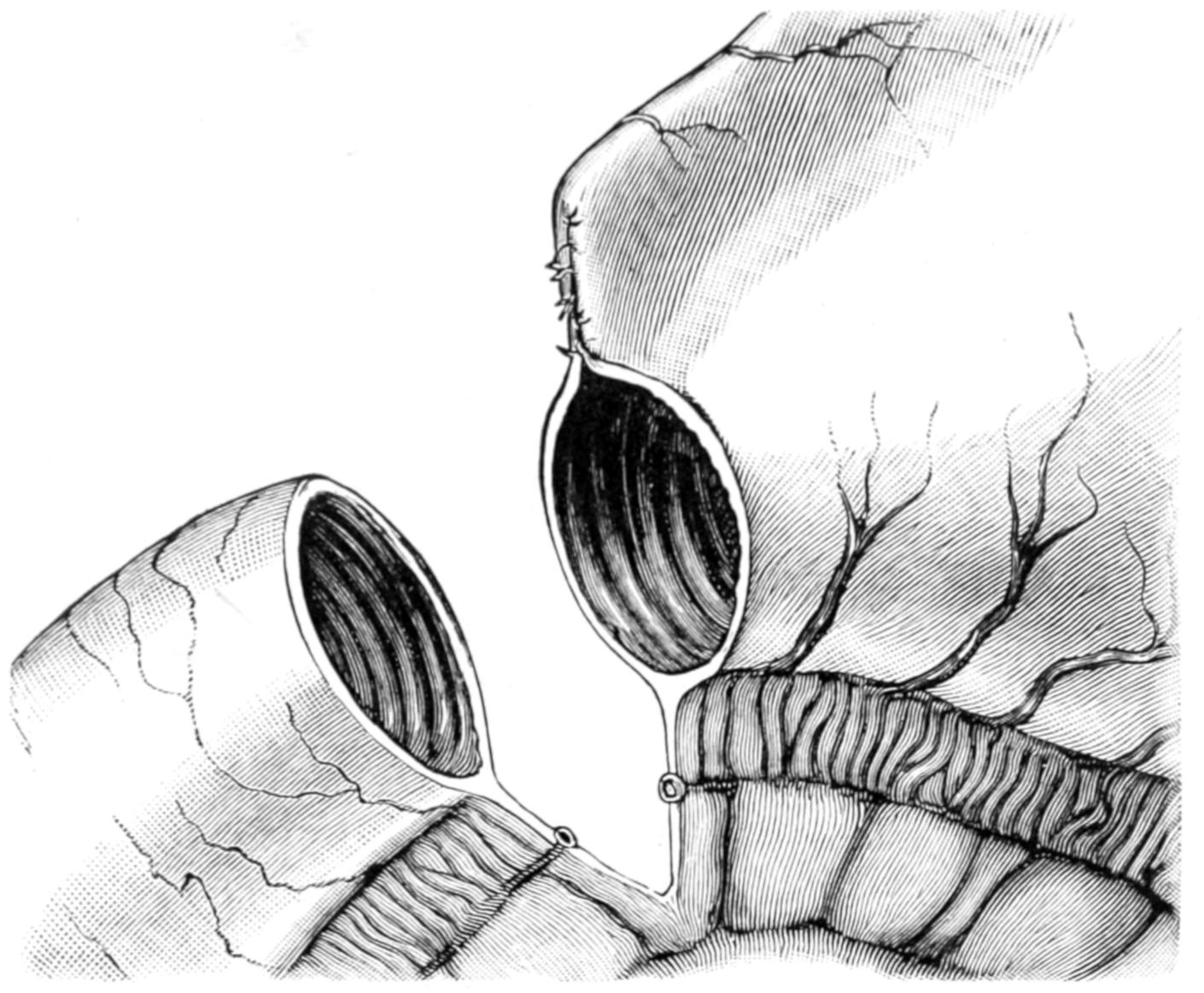
Resection of the pylorus. This figure illustrates the method of fitting the duodenum to the stomach when the gap in the stomach is too large to fit the duodenum. (Richardson.)
Fig. 552
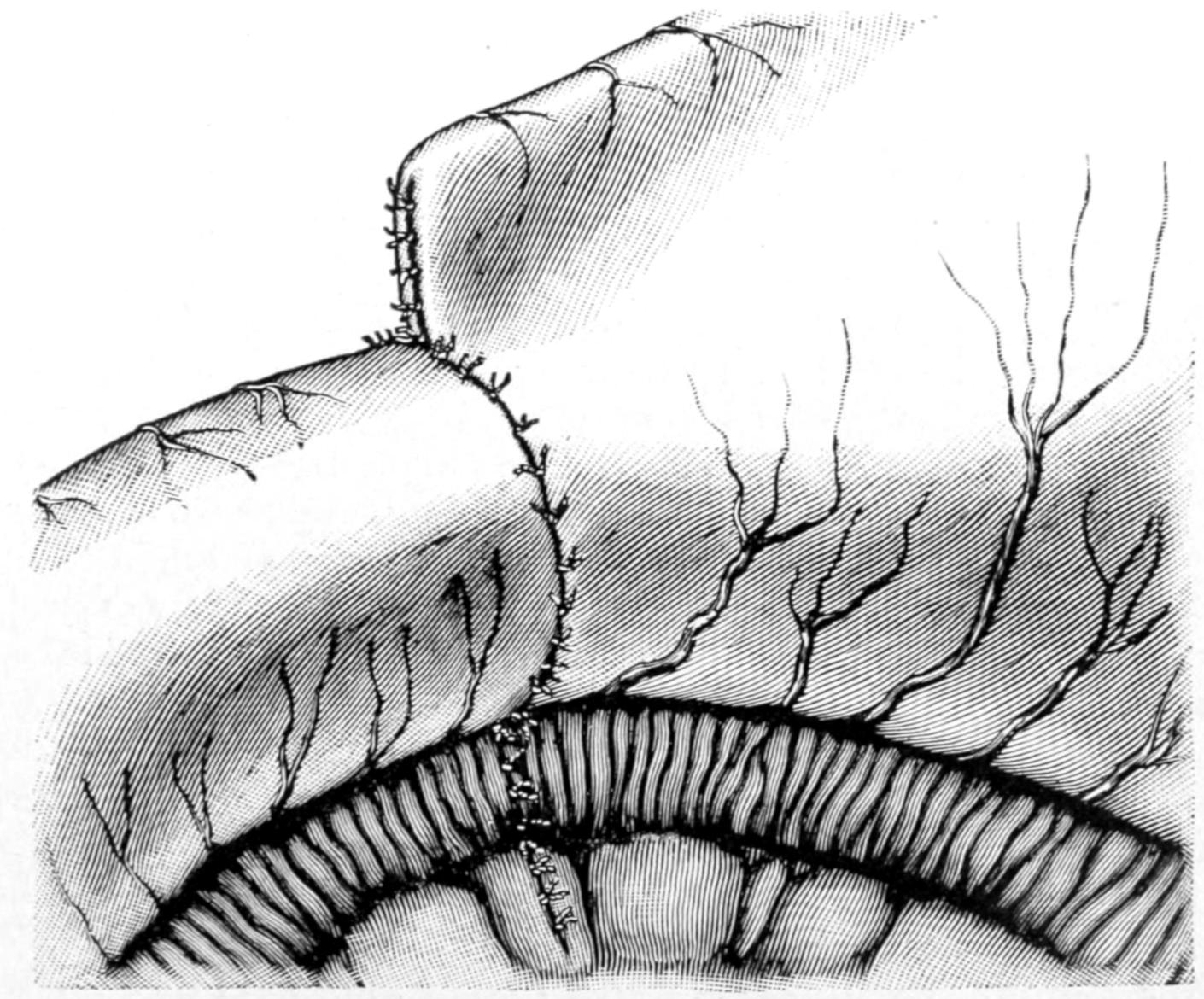
Resection of the pylorus. (The same as Fig. 551). Suture of the stomach to the duodenum completed. (Richardson.)
[816]
Fig. 553
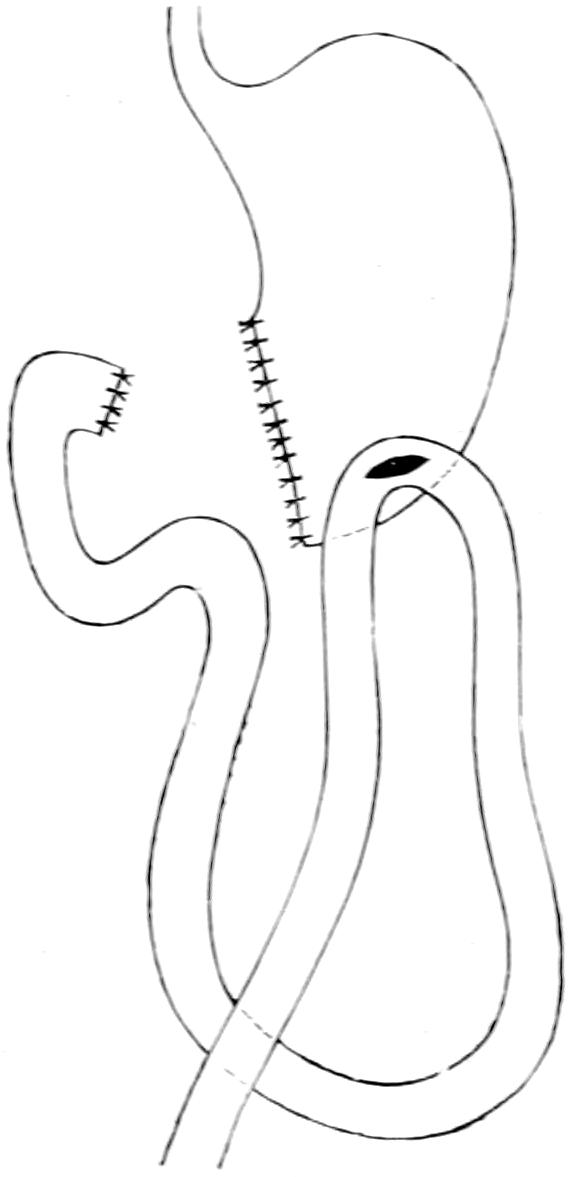
Resection of the pylorus according to Billroth’s second method. (Bergmann.)
In performing complete gastrectomy the cardiac end of the stomach is brought down and fitted to the upper end of the divided duodenum, after removal of the stomach, which will usually be possible under favorable circumstances, but which exposes the patient to great risks of tearing apart reunited surfaces by undue tension.
—This consists in making an anastomotic opening between the stomach and the uppermost part of the jejunum, the duodenum proper being too bound down in its course to permit of its utilization for this purpose. Gastro-enterostomy, then, should be referred to as gastrojejunostomy. In brief, it consists in making an opening by which the stomach shall empty directly into the upper bowel, and while, for this purpose, one of the uppermost loops would theoretically suffice, it has been found that the shorter the loop, i. e., the portion between the duodenum proper and the upper part of the bowel used for this purpose, the better for the patient.
Gastrojejunostomy is, first of all, referred to as anterior or posterior, according to whether a loop of bowel be brought up in front of the omentum and around it, and attached to the anterior and exposed wall of the stomach, or whether the lesser peritoneal cavity be opened by perforating the omentum behind the colon and below the stomach, so that the posterior wall of the latter is found, drawn into the wound, and made accessible and utilized for the purpose. The anterior operation is the easier of performance, but the posterior is far preferable in most instances. Should it be found that the posterior wall of the stomach is far more involved in cancerous infiltration than the anterior, the anterior operation should be performed.
Simple as is the procedure in theory there are about it one or two complications which were not at first foreseen. Perhaps the most important of these is that bile emptied into the duodenum passes downward until it has an opportunity to escape through the opening directly into the stomach, usually in the direction of least resistance. This may then carry it where it is a most undesirable fluid, and prevent its passage onward into the intestine, where it is physiologically needed. This circulation of bile has been spoken of as the “vicious circle” and it is the formation of a vicious circle which has complicated not a few of the anastomotic stomach cases, and which has engaged the attention of not a few clinicians and operating surgeons.
The second objection is that the contact of stomach contents with the mucous membrane at a point below where the bowel is normally prepared for it, and before intestinal contents have been prepared by bile or materials alkalinized by this fluid, sometimes leads to the formation of ulcer just opposite the opening, and this has been referred to as peptic ulcer of the jejunum. This is a possible though not a frequent complication, but has added weight to the other considerations regarding the best way of performing anastomosis. Again, it has been feared that this anastomotic opening would contract in time, or sometimes completely close. This objection obtains especially with anastomosis, made with a Murphy button, or its equivalent, and can rarely be made against the ordinary suture methods. Again, if the opening in the intestine be made too long the intestine itself may be narrowed, for too much of the circumference of the bowel may be taken up in the formation of the anastomosis, and thus there will be mechanical obstruction with vicious circle.
“Vicious circle” produces symptoms which do not appear until the lapse of at least three days after the operation. If vomiting should persist and retain a bilious character it is to be feared that some complication of this kind has occurred. Under these circumstances when lavage is practised a large amount of fluid mixed with bile, perhaps blood, may be returned.
Much depends also on the exact location of the attachment of the intestinal loop to the stomach. Other difficulties arise from possible twisting of the loop of small intestine, or its strangulation by being entangled beneath the bridge of the jejunum, which is[817] always made in every anastomosis. Again the small intestine may become incarcerated in an imperfectly closed opening made in the mesocolon. It will thus be seen that the posterior method has disadvantages which need to be fully appreciated. On the other hand it has this great advantage, that it permits of drainage or emptying of the stomach into the jejunum by gravity, in almost any position which the patient would ordinarily assume, either sitting or lying. Many operators have devised methods of preventing formation of the vicious circle.
Fig. 554 illustrates how valves may form which there is no sure method of preventing. Fig. 555 represents the suggestion of Braun, to make a second anastomotic opening between the small intestine above the stomach opening and below it, hoping that in this way bile, for instance, may pass directly through this opening, which it will first meet, into the intestine below, and thus not pass on and into the stomach. Others have divided the loop of jejunum after making the second anastomosis, in this way planting the efferent portion of the bowel in the stomach and then planting the afferent portion of the bowel into the side of the efferent part. This is the so-called Y-gastrojejunostomy. Roux does much the same thing, save that his method is all carried out behind the colon instead of in front of it. The principal argument in favor of the use of the Murphy button, in this procedure, is that vicious circle is less frequent after its use than after most of the suture methods, all of which would simply indicate that vicious circle is largely a matter of valve formation, and that by the time the button is loosened and passed on the danger period seems to have elapsed, and the current in the new direction to be well established. Nevertheless the button is now discarded by almost everyone in favor of the suture.
Fig. 554
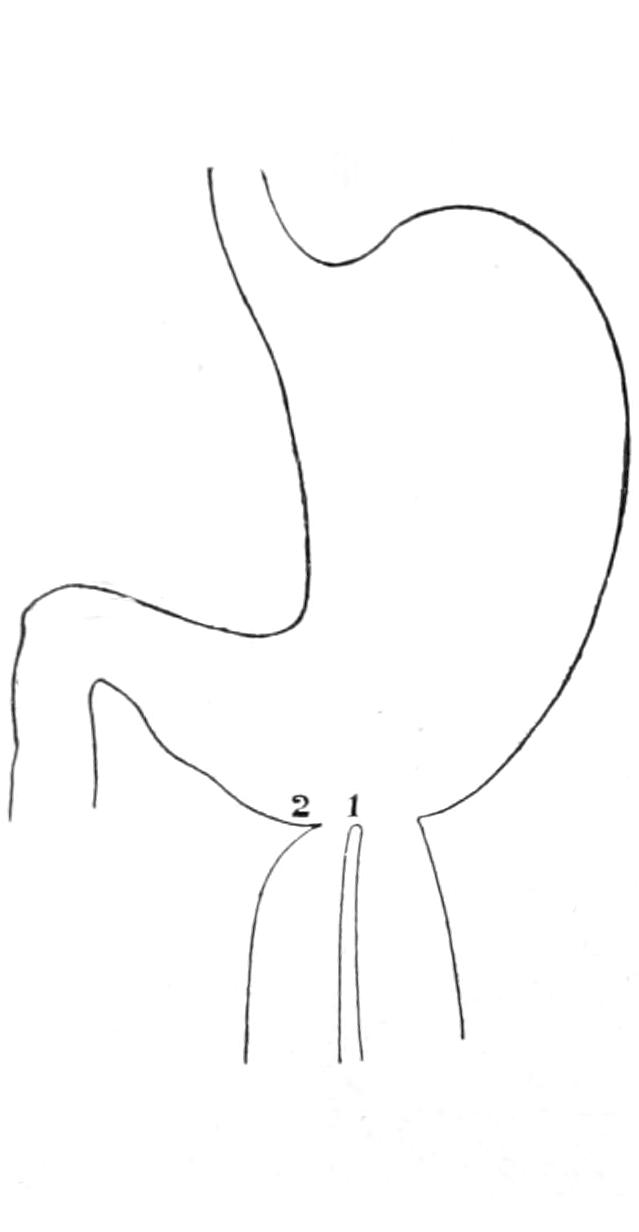
Formation of valves in gastro-enterostomy: 1, intestinal valve; 2, right-sided gastro-intestinal valve. (Bergmann.)
Fig. 555
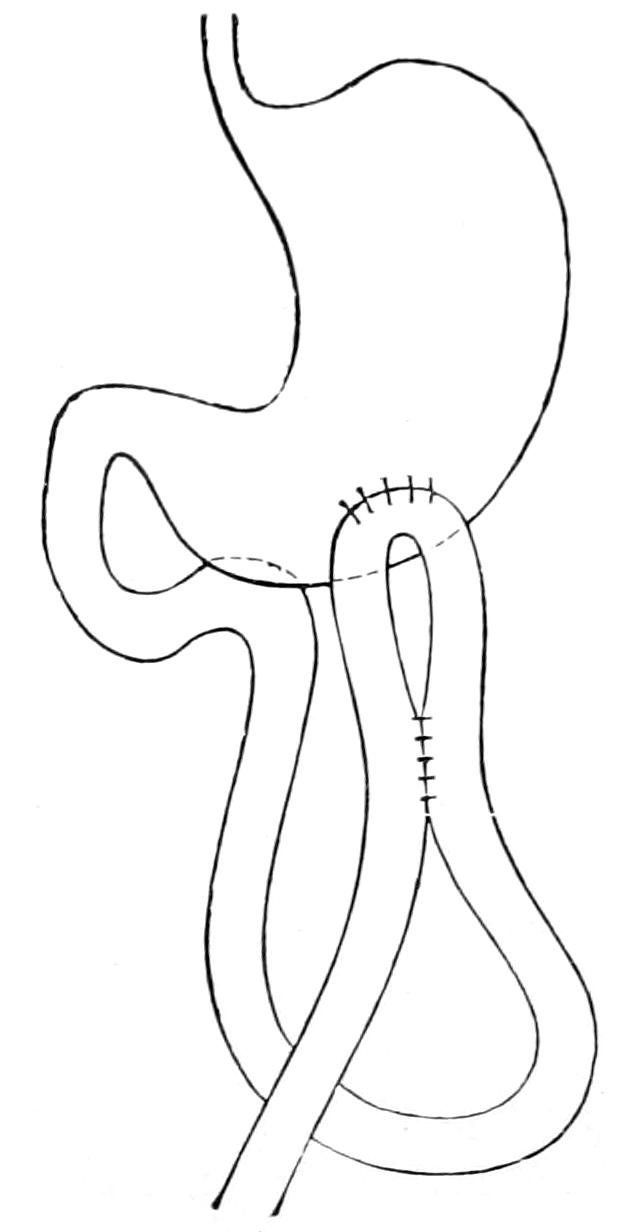
Gastro-enterostomy with entero-anastomosis according to Braun. (Bergmann.)
—Artificial anastomotic opening between the cavity of the stomach and some part of the intestine below is indicated in a number of conditions, which have been discussed. It is done mainly, however, for two good reasons: first, to atone for pyloric stenosis, and, secondly, to give the stomach a more physiological rest in cases of gastric ulcer, permitting food to pass readily from it into the jejunum, with a minimum of gastric activity or disturbance. This particular form of anastomosis is but the application to these viscera of a general principle, which in various ways, in different parts of the body, has constituted one of the greatest features in the advance of modern surgery.
The operation is practised in two ways. In the anterior operation the highest accessible loop of small intestine is brought up in front of the omentum, or else the omentum[818] is fenestrated in such a way that the bowel shall be brought through its window, and then attached to the anterior wall of the stomach, where the latter is much more accessible. In this operation there is less handling of the stomach and bowel, and, in general, it is easier of performance. Nevertheless the bowel loop itself may become adherent to the abdominal wound and give rise to pain, or even obstruction simulating the vicious circle. Volvulus of the jejunum has also followed it. Another objection is that as the patient gains flesh the weight of the transverse colon and omentum sometimes causes dragging upon the loop, which may cause serious trouble. The opening thus made is not where gravity will afford the best drainage of the stomach, and it is now considered undesirable in almost all cases save those where one is compelled to its performance, either by necessity for haste, or because the posterior wall of the stomach is so involved in cancerous infiltration as to afford no suitable area for fixation and opening. This method is of use mainly in dealing with malignant disease.
The posterior operation calls for all the resources of a perfected technique, and takes longer in performance. Nevertheless when once the anastomosis is safely effected it is more satisfactory.
The posterior operation alone, therefore, will be described at length in this place, and only that form of it which discards the anastomotic loop, the writer quite agreeing with the Mayos, who have had larger experience with this operation than any other surgeons, and who advise the direct attachment of the jejunum, as near as possible to the termination of the duodenum, without further complication by operative procedure. The direction of active propulsion from the stomach comes from its pyloric end, the larger end of the stomach being mainly for storage purposes and having thus a forceful action; consequently the preferable site for the stomach opening is on a line with the longitudinal part of the lesser curvature, with its lower end at the bottom of the stomach. The Mayos have abandoned reversing the jejunum and now apply it directly to the posterior wall of the stomach from right to left exactly as it lies under normal conditions, having had better results with this method than with any other.
In brief the operation is as follows: Incision is made a little to the right of the median line, the transverse colon is withdrawn by steady traction to the right and upward, and the mesocolon made to follow it until the jejunum comes into view. The latter is then grasped at a distance of three or four inches from its origin. When, now, it is drawn tight the fold of peritoneum which covers the so-called ligament of Treitz is demonstrated; this is a small band containing muscle fibers, having its origin on the transverse mesocolon and extending down to the beginning of the jejunum, thus acting as a suspensory ligament. It leads to the base of the vascular arch of the middle colic artery, and indicates the place where the mesocolon should be torn through in order to expose the posterior wall of the stomach. At this point, in the least vascular area which can be discovered, the mesocolon is first incised and then torn, until a good liberal opening is made, through which the posterior wall of the stomach is easily exposed, and, later, drained. It should be forced through this opening by combined manipulation with one hand introduced above it and gently urging it through the opening where it presents. It may be easily identified by its resemblance to its anterior surface in its thickness, the arrangement of its vessel and the like. The posterior wall alone is then secured and drawn through the mesocolic window, in such a way that after the jejunum is attached to it the anastomotic opening can be made at a point one inch above the greater curvature and ending at the bottom of the stomach two and a half inches to the left of the pylorus. This area having been exposed and prepared, a considerable portion of it is drawn into a pair of specially constructed clamps (Doyen’s or Moynihan’s), whose blades are usually protected with rubber. The Mayos prefer to have the handles lying to the right and to direct the forceps transversely to the body axis. Moynihan prefers to reverse this direction and make them point to the right shoulder. The stomach being thus protected, and prevented from slipping by suitable tightening of the clamps, the jejunum is similarly secured with forceps lying in a direction parallel to the first, having within their grasp a portion of the gut extending between points one and a half and three and a half inches from its origin. If this be properly effected the left low point of the stomach lies in the grasp of one pair of clamps and the first part of the jejunum in that of the other, and these two portions should be easily brought into close contact with each other. A gauze pad having been placed behind the damps in order to avoid soiling, should there be any leakage of intestinal contents, the clamps should now be carefully and[819] attentively held by an assistant, and their distal ends may even be bound together in such a way that, after the suturing process has once begun, nothing shall disturb the perfect contact between the surfaces thus mutually applied. The first row of sutures, usually of the ordinary continuous type, is made of silk or thread, the serous and muscular[820] coats being seized and united over a line some two inches in length, the suture being carefully secured at either end of this line. Next, with a scalpel, an incision is made through the serous and muscular coats, parallel to the line of sutures, at a distance of about one-quarter of an inch, and over a length a trifle less than that of the line which they occupy. Here the vessels will bleed freely and forceps may be momentarily used for their securement. Through the opening thus made the mucous membrane will prolapse. Moynihan especially has shown that it is not enough to merely incise this membrane in the same direction as the other coats, but that a narrow elliptical portion of it should be excised, since it tends to prolapse. Therefore with knife or scissors a strip of the mucosa, perhaps a half-inch in width, should be cut away from either surface, thus widely opening into and exposing the interior respectively of the stomach and of the gut. Extreme pains should now be given to prevent both leakage and soiling, and instruments used upon the mucosa should be discarded after it has been divided and sutured. Now with reliable chromicized catgut a row of continuous sutures is applied by which all three coats of both cavities are bound snugly together, the needle passing through six distinct layers as each stitch is made. These sutures should be drawn sufficiently and secured at frequent intervals so as not only to ensure perfect application but sufficient pressure to prevent hemorrhage when the clamps are released. The lower side having been first closed the same character of sutures is continued until the upper margin of the buttonhole-like opening is thus completely closed. The fourth line of sutures, this time of the same material as those used in the first, is applied in a similar fashion, and with it the serous and muscular coats are accurately affixed to each other in such a way that there can be no leakage. Two or three extra sutures at either end of the line may be inserted for greater security. The clamps are now withdrawn, the gauze behind the anastomotic opening is removed, and it should be found that the smaller bowel is neatly and perfectly fastened to the posterior stomach wall and that no possibility either of hemorrhage or of leakage remains. This being accomplished there remains only to tack the margins of the mesenteric opening to the posterior wall of the stomach, at a distance sufficient to prevent all possibility of subsequent constriction or strangulation, after which the parts are carefully cleansed, restored to the abdomen, the colon and omentum dropped back and made to cover them, and the abdominal wound closed as usual. (See Figs. 556, 557 and 558.)
Fig. 556
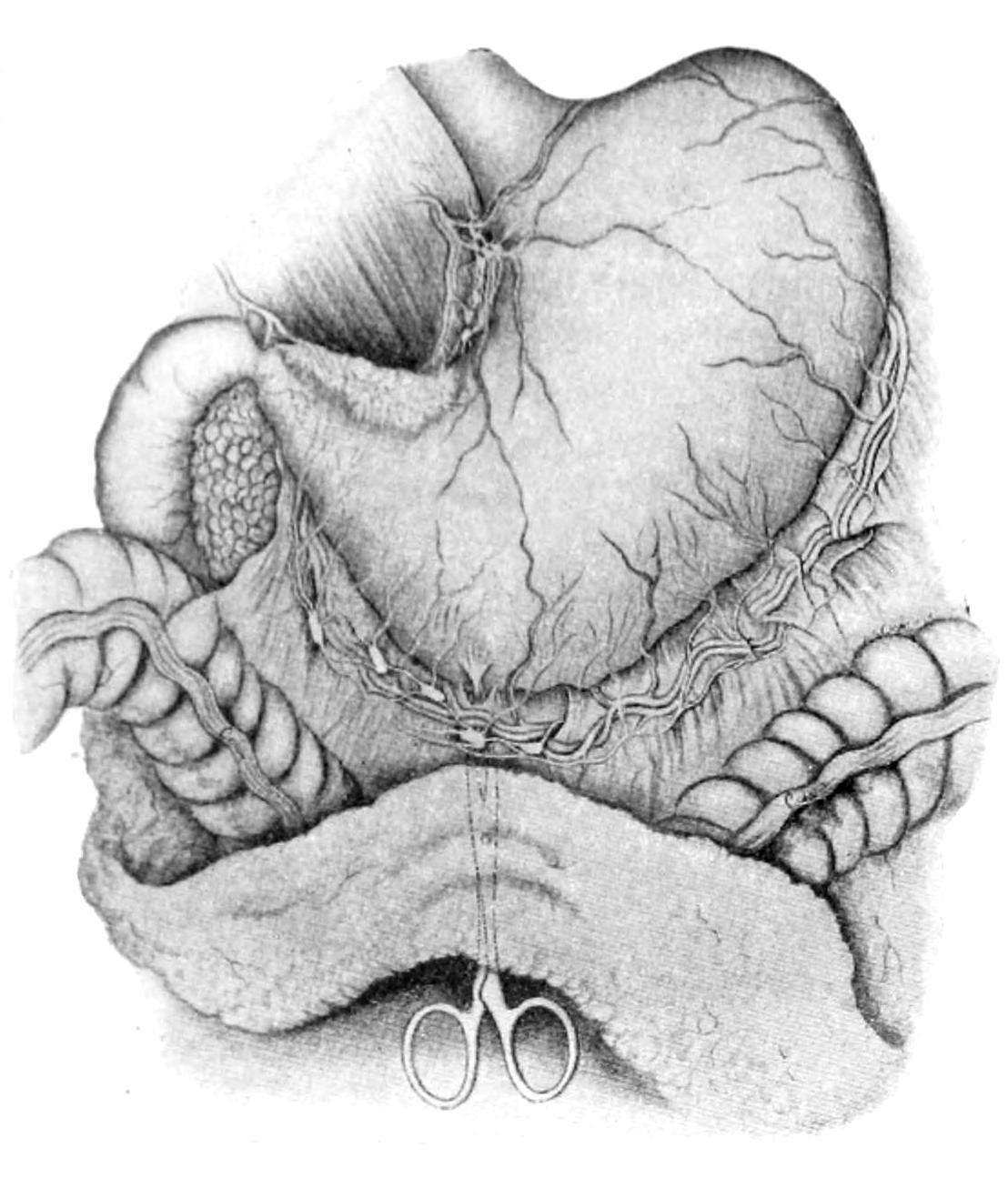
Anterior wall of stomach grasped by forceps passed through from behind. (Case of saddle-ulcer of lesser curvature near pylorus.) (Mayo.)
Fig. 557
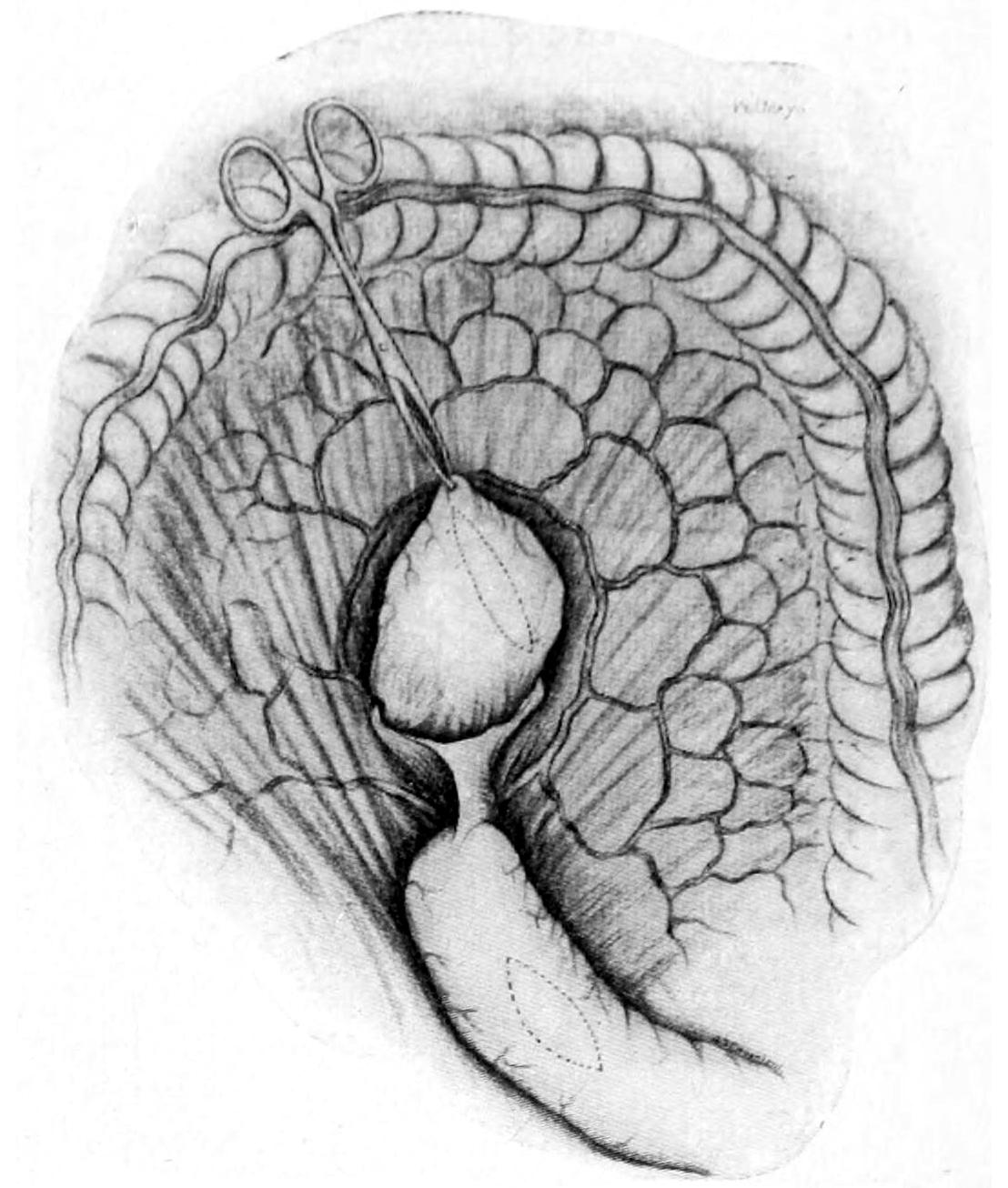
Mesocolon lifted and posterior wall of stomach drawn through the opening made in it. Dotted lines show site of proposed anastomotic openings. (Mayo.)
Fig. 558
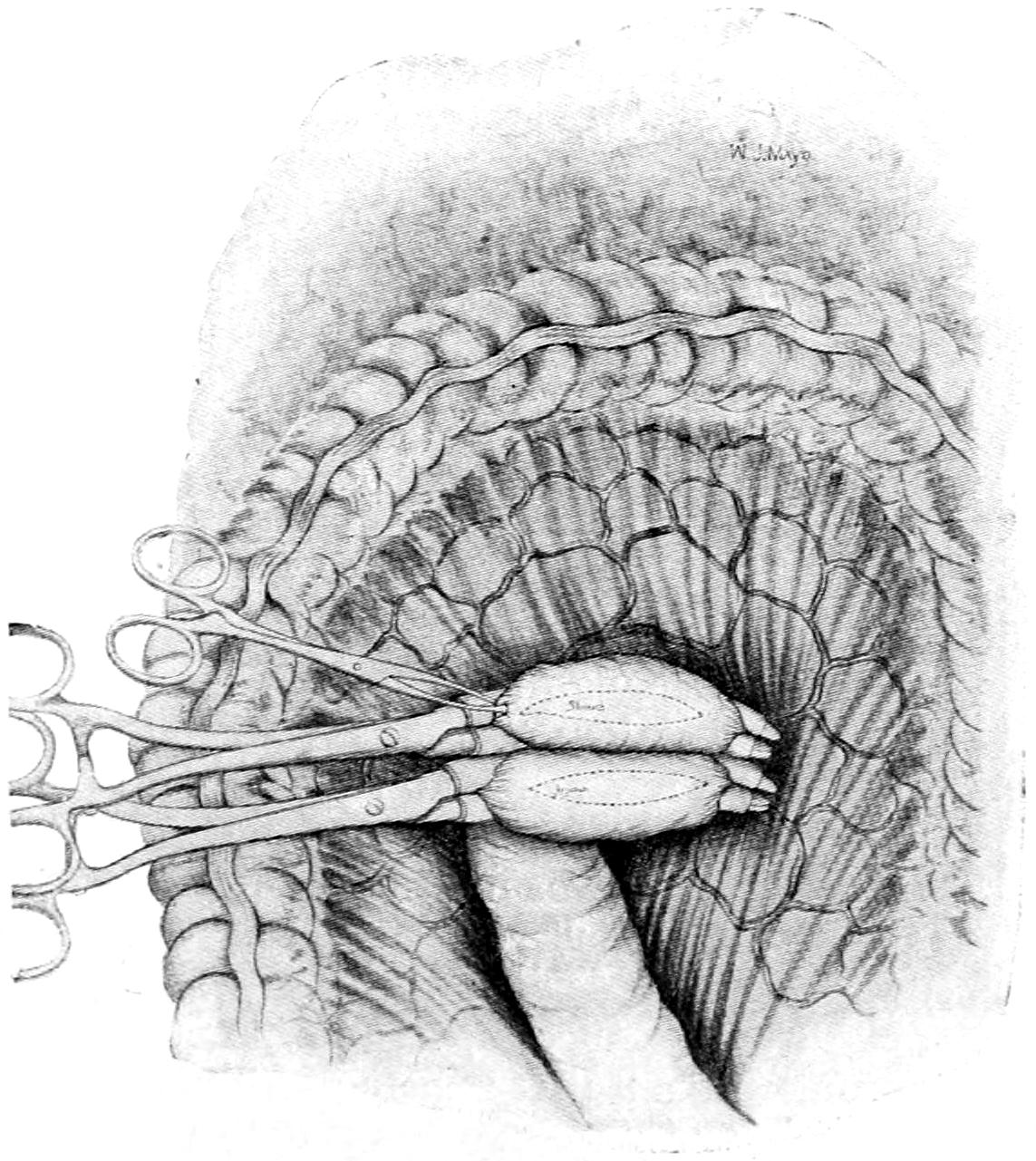
Stomach and jejunum in the grasp of the large clamps, made ready for suturing. Small forceps still marking low point of stomach. (Mayo.)
Such is the operation with suture, which may occupy from thirty to forty minutes in performance, it takes a little longer than the methods either with the button or with the elastic ligature, but seems to be the method generally used. In this method, as stated at the outset, no special provision is made as against “vicious circle,” because it has been found that it is seldom that this unpleasant complication ensues. If, however, the anastomosis with the jejunum has been made at a point twelve inches or more beyond its beginning, there is a likelihood of finding that vicious circle will cause later complications, and perhaps necessitate the performance of a second anastomotic opening in the small intestine above and below the stomach opening.
Of course all the precautions mentioned previously for prevention of infection, such as washing out the stomach previous to the operation, and ensuring both its emptiness and that of the upper bowel, are a part of these procedures and cannot be safely neglected in any of them.
Many an ingenious device for effecting the same kind of communication between the stomach and the bowel, or between various parts of the alimentary canal, has been placed before the profession, though but a few will be considered more in detail when dealing with the operations upon the intestines proper. The most prominent of them, and the one which has found the most lasting favor in the eyes of the profession, is the Murphy button, or some similar expedient, by the use of which time is economized and the operations in some respects simplified. All devices of this character, however, depend upon a necrotic process for their eventual success, as the intent is that parts compressed between the halves of the button shall first adhere and then slough, the button falling through the opening thus made and passing on. But to rely upon a necrotic process is much like relying upon a criminal for the performance of a serious duty. The button, therefore, has gone out of general favor for purposes of gastro-enterostomy, although for other intestinal work it is still frequently used.
McGraw, of Detroit, has devised a different and equally ingenious method of keeping surfaces in contact with each other until adhesion shall have occurred, and then effecting[821] a further necrotic process by which opening shall be finally accomplished. This is the so-called method with the elastic ligature. In many respects it is simplicity itself, and permits of ready and rapid employment. One needs especially a round rubber cord, about 2 Mm. in diameter, of the purest gum obtainable and sufficiently fresh to be reliable. The surfaces to be united are first approximated by a posterior row of silk or thread sutures which shall include their outer surfaces. Then a long straight needle armed with this rubber cord is passed into the intestine and out again at a distance of from 5 to 10 Cm. An assistant now holding the intestine, the operator stretches the rubber suture until it is very thin and then draws it rapidly through the bowel. This same step is repeated in the opposite direction within the stomach. A strong silk ligature is next passed across and underneath the rubber between the latter and the point where the stomach and the intestine are to come together and a single knot is then made in the rubber after it has been tightly drawn. Another silk ligature is passed around beyond the ends of the rubber ligature where they cross and is here securely tied. The rubber ends thus released are then cut off. The original silk suture is next continued around in front until the point of its beginning is reached. In this way the rubber ligature and the parts which it includes are surrounded with an elongated ring of silk sutures, and with this the operation is complete. Here it is the continuous pressure of the elastic suture which first shuts off the circulation and finally cuts its way through both coats, and permits the communication between the bowel and the stomach. This method is as applicable to other portions of the alimentary canal as to the stomach.
[822]
The entire intestinal canal is sometimes too short and sometimes fails to develop sufficiently in caliber, or sections of it may remain undeveloped. None of these changes have interest or importance for the surgeon as such, save those which produce acute or chronic obstruction or conduce to acute inflammatory affections.
Intestinal diverticula are usually of that type described by Meckel and everywhere known by his name. Aside from these the others usually met are irregular sacculations or hernial protrusions which may be due to previous disease or to some congenital anomaly of structure. These are sometimes seen in multiple form, and in one case recently under my observation over one hundred of them were found scattered along the intestinal canal, but, inasmuch as the patient died practically of old age without a history of serious previous disease, it could not be ascertained whether the pouches were of congenital or acquired origin.
The genuine Meckel diverticulum is a relic of the tubular structure which leads from the primitive intestine to the vitelline or yolk sac, and which should persist until about the end of the second month of embryonic life. After this time it should be completely obliterated and disappear. When this does not happen there may result a fecal fistula at the navel, which is then usually referred to as persistent omphalomesenteric duct, and which implies a continuous passage-way between the skin and the interior of the bowel.
When the umbilical portion alone persists there results a small cyst on the posterior side of the navel.
When the intestinal end alone persists a protrusion or sacculation will remain to mark its site.
The duct may become obliterated and yet fail to disappear, thus leaving a fibrous cord which represents the original omphalomesenteric structures and vessels, which will be probably mistaken for an inflammatory band and may serve as a later cause of acute obstruction. If such bands lead to the umbilical region their identity may be easily established.
The presence of Meckel’s diverticulum may cause serious abdominal mischief. It may become involved in a localized process exactly as the appendix often does, which may then be referred to as a diverticulitis, where ulceration and perforation may occur. It may constitute the whole or a portion of the contents of a hernial sac. I have twice found it in inguinal hernia, once in umbilical hernia, and by others it has been reported in all the ordinary hernial locations. Porter has collected from literature 184 cases in which its presence caused serious abdominal crises. The condition itself is probably present in at least 1 per cent. of mankind, and is stated by Halsted to be the cause of intestinal obstruction in 6 per cent. of cases. In the 184 collected cases above mentioned it caused obstruction in 101. Out of 21 cases of the above collection it was not only found in the hernial sac, but in all but 1 was shown to be the actual cause of the trouble. In 5 of these cases the diverticulum was open at the umbilicus. In such a case if the opening be large the gut wall might prolapse and thus form a hernia.
Diverticulitis has been repeatedly mistaken for appendicitis, its symptomatology not being distinctive. Exact diagnosis is seldom possible before operation.
On general principles, considering their possible dangers, it would be well to remove all diverticula which are found in the course of ordinary abdominal operations, whether they appear to be causing trouble at the time or not.
[823]
While the average length of Meckel’s diverticulum is three inches it may exist as a mere nipple-like projection, or it may be a free tube attaining a length of several inches. Its attached end is usually larger than its distal portion and its diameter usually less than that of the gut from which it arises. It may be provided with a scanty mesentery or may hang independently. While ordinarily its distal end is free it may nevertheless be continued as a solid cord attached, as above mentioned, to the umbilicus. This cord frequently contracts secondary adhesions, and it is under these conditions that it most often constricts the bowel by forming a loop within which the intestine becomes entangled. Free diverticula of sufficient length are sometimes found tied in a genuine knot in a manner which is absolutely inexplicable. There are numerous ways by which such a diverticulum may produce strangulation of the normal bowel; thus, by formation of a ring in which its own free end projects, in which is later entangled a bowel loop, or by surrounding the pedicle of an intestinal loop as might a noose. Again bowel is sometimes tightly drawn over such a diverticular band, just as a shawl may be thrown over the arm, obstruction following in the displaced bowel. When much contraction is brought to bear the gut may be so acutely bent as to become occluded. Finally the bowel at the point of origin of the diverticulum may undergo gross structural changes, the result of long-continued traction, which may lead to cicatricial narrowing. More indirectly diverticula seem in some unknown way to predispose to intussusception at their point of origin, or they have been found inflated and hanging from the intestine after obstructing it (Fig. 559).
Fig. 559
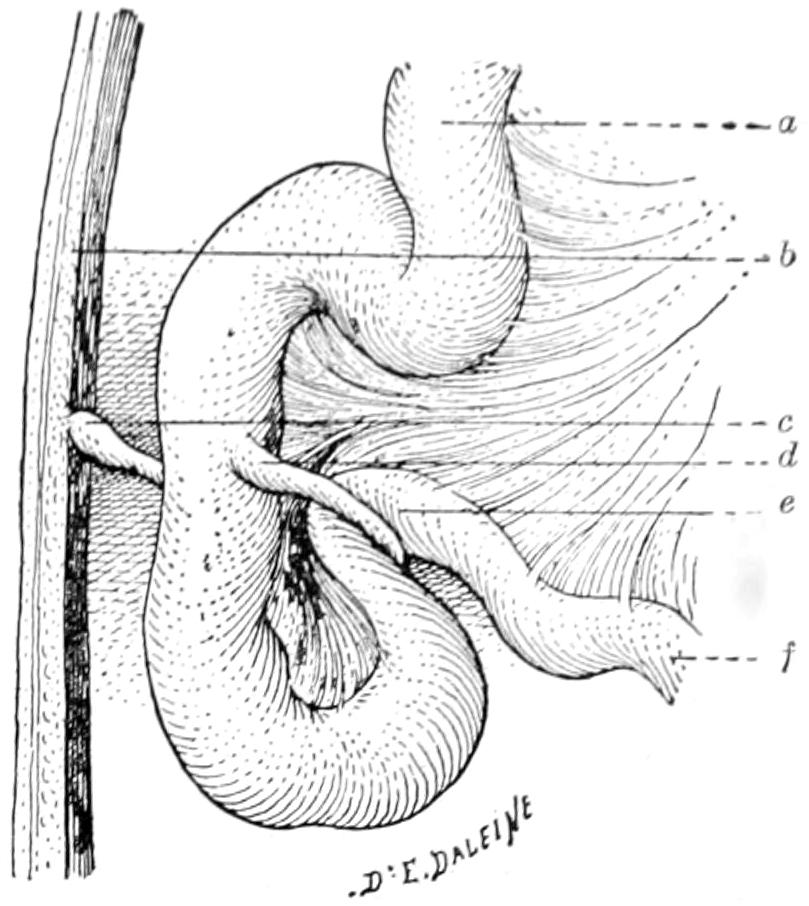
Meckel’s diverticulum still attached at the umbilicus and producing obstruction. (Lejars.)
Of acquired malformations of the small intestine we have mainly to deal with those which are produced by injury or disease. Among the former would be the results of violent contusions or of any of the lacerated, incised, or gunshot wounds to which the bowel is so often exposed. Should recovery ensue cicatricial contraction is likely to result. On the other hand, such previous disease conditions as ulcerations—tuberculous or typhoidal—or the so-called chronic catarrhal or malignant, may in one way or another occlude and thus finally obstruct the lumen of the bowel. Distention diverticula may also result, which correspond to the traction diverticula of the esophagus already described.
The small bowel, like the larger or the stomach, may be ruptured in consequence of abdominal contusions, the condition depending on the nature of the injury, the degree of fulness of the bowel itself, and other obvious causes. This character of injury has been already sufficiently considered in dealing with rupture of the stomach. Their symptoms are not essentially different, neither are the principles of ordinary surgical treatment. Of all gunshot wounds those of the abdomen constitute about 6 per cent., being more frequent than stab wounds.
—Gunshot wounds of the intestine would by themselves fill an interesting chapter in a work on surgery. In such an epitome as this they can be given but short consideration. The condition was for centuries hopeless, until the American surgeons Parkes, Bull, and Senn took up the subject and taught the profession how to[824] more quickly recognize the injury as well as to treat it. The special dangers of all punctured wounds of the bowel, like those of the stomach, are hemorrhage and escape of fecal contents. The great length of the intestinal tube, and its coiled arrangement within the abdominal cavity, subject it to the possibility of multiple punctures, from a dozen to twenty having been inflicted by the passage of one bullet. The multiplicity of these injuries, therefore, gives a still more formidable character to their presence. Much will depend upon the size and velocity of the bullet and the distance from which it is fired. The perforated gunshot wounds of the abdomen which occur in civil life are usually inflicted by a smaller bullet than those occurring in actual warfare, while, at the same time, the distance is usually short.
Gunshot wounds are followed by an apparently disproportionate amount of collapse. There is no accurate method of recognizing from the exterior the amount of harm done by the passage of a bullet into or through the abdominal cavity. This constitutes one of the greatest arguments in favor of immediate exploration, an argument which is strengthened by the fact that almost every penetrating wound of the abdomen is complicated by injury of some abdominal organ. The greatest danger attaches to perforation of the transverse colon or of the small intestine, because these are the most movable parts of the intestinal canal. The dangerous wounds are those which lie in the frontal plane. Bullets which pass through the abdomen obliquely are perhaps less likely to produce fatal result. Astonishing differences prevail between the severity of those accidents received upon the field of battle and in civil life. In battle men are shot through the abdomen and not conspicuously disabled, recovering sometimes with no other treatment than antiseptic occlusion. It is impossible to assume that the bowels have not been injured, and yet they recover. The fact thus stated best indicates the reason for abstention from intervention on or near the firing-line in battle, and its most prompt and early performance when the patient is in a well-managed civil hospital.
—The symptoms of intestinal perforation in these cases are not so prompt as when the stomach is wounded. Blood may occur in the vomitus or in the stools, but only ordinarily after the expiration of a few hours. Should fecal matter be found within the external wound evidence would be complete, but this is rarely the case. The probe may show whether the abdominal wall has been completely perforated or not; beyond this it will give little information. By far the best probe is the sterile finger, introduced through the opening enlarged for the purpose. With this more distinct information may be gained. Some years ago Senn proposed the method of inflating the colon and small intestine with hydrogen gas, on the expectation that it will escape through any intestinal perforation into the abdominal cavity, which it would distend, and that then by inserting a small glass tube in the abdominal wound it could be lighted and made to thus identify itself at the distal orifice of this tube; but this method requires special conveniences which are rarely at hand in emergency cases, and has been practically abandoned.
A study of the direction of the abdominal wound which may be sometimes made from an accurate account of the accident, and at other times by noting the location of the wounds of entrance and exit, will do much to determine whether intestines were probably in or out of harm’s way. If it can be established that the bullet has probably avoided them then some would wait for the inception of the first serious sign of mischief before exploring. On the other hand, if it should seem inevitable that such injury must have occurred, or, without such reasoning, if the patient present a serious condition, he should be promptly operated unless practically moribund.
The general principles of recognition and treatment of gunshot wounds have been considered in an earlier chapter and the subject will not be further considered here except as regards treatment.
—The principles of surgical treatment for gunshot wound of the intestines include a free abdominal incision, an inspection of the entire length of the intestinal canal, which can only be made by passing it through the examining fingers while exposed to sight upon the abdominal surface, the accurate securement of all bleeding vessels, and the closure of all punctures. Any portion whose blood supply has been so completely cut off as to threaten or produce gangrene should be removed by resection, with end-to-end or a lateral anastomosis. The patient having been thus eviscerated and the intestinal viscera examined, the abdominal cavity should be further explored, not so much to find the missing bullet as to discover what further harm may have been done;[825] while if such be found the indication should be met. Then after an exceedingly careful toilet of the peritoneum the intestines may be restored, it being of course assumed that every puncture has been fully recognized and properly sutured and secured. Nearly all of these cases will call for some abdominal drainage, which may or may not be posterior, as shall seem best.
The location of the bullet is a matter of minor importance. Should it lie where it can be easily identified and removed this should be done. Otherwise one should not waste valuable time in hunting for it, remembering that he is performing not an autopsy but an operation.
There is no point of the intestinal tube between the pylorus and the anus which may not be involved in an ulcerative process, either acute, chronic, or malignant. Acute ulcers of the upper bowel are usually of typhoidal origin, while those of the lower bowel may be due to either typhoid, tuberculosis, or syphilis. At certain points ulcers assume somewhat distinctive character. Thus the acute catarrhal ulcer, so called, seems to have a more definite entity than a declared pathology, it being somewhat difficult to account for its existence. The peculiar duodenal ulcers which have been met with after operations or burns have been elsewhere discussed, and are to be regarded as of an acutely toxic origin. A special type of ulcer of the duodenum has also been noted opposite the anastomotic opening which is made in the ordinary gastro-enterostomy, for whatever purpose performed. This appears to be due to the outpour of the gastric juice upon a surface not normally prepared for it, upon which it acts as an irritant, in time producing more or less acute ulceration. This is the so-called peptic ulcer of the duodenum, an occasional complication of gastro-enterostomy.
—Duodenal ulcer of a type corresponding to gastric ulcer has been recently determined to be a more frequent lesion than has been supposed. A series of over fifty operations for this condition, reported by Moynihan, in 1905, thus occurring in the practice of one surgeon, will dispose of the question as to its great rarity. Its symptoms are often so characteristic as to admit of reasonably easy diagnosis, and it has, therefore, become more and more a matter of greatest interest to the surgeon, since duodenal like gastric ulcer is essentially a surgical condition.
These ulcers are usually located in the first portion of the duodenum, i. e., in at least 90 per cent. of cases. They may be solitary or multiple, and may be associated with gastric ulcers. In the ordinary postoperative peptic ulcer the sequence of events is usually gastric ulcer, hyperchlorhydria, and duodenal lesion. It may occur at any age, and is the frequent cause of melena of the newborn or of the young.
—Symptoms of duodenal ulcer include pain, hematemesis, and melena. Pain may be a vague uneasiness or may be severe. It is usually described as of a burning character, felt mainly in the middle line or along the right costal margin. It becomes gradually more severe and may finally disable. It is sometimes described as cramp-like. When severe it is referred to the right of the middle line. In cases where there are adhesions to the liver or gall-bladder, pain radiates upward to the right breast, or even around the chest to the back. The pain is associated, by more or less marked time limit, with the ingestion of food, coming on from two to four hours after a meal, whereas that of gastric ulcer comes soon after eating. Sometimes it is even regarded as a “hunger pain,” and patients find that the taking of a little food will give relief. So soon, however, as this is digested pain returns, when they again call for more food. Hematemesis and melena may be present together or either may appear without the other. Small quantities of blood in the vomitus is more likely to attract attention than considerable quantities in the stools. It has been estimated that in from 25 to 30 per cent. of acute cases hemorrhage is frequent, and occurs in 40 per cent. of chronic cases. In the stools blood is found in perhaps one-half of the instances. The amount of blood may be considerable, even sufficient to produce faintness. In fact, the intestine has been found full of blood when the abdomen was opened, and Moynihan has seen even the colon distended with blood.
The more serious complications of duodenal ulcer, aside from hemorrhage, are those of perforation, cicatricial contractions or stricture formation (obstructing the bowel or[826] the common duct, or both), local peritonitis, cancer, and indirectly gall-bladder or pancreatic disease. Next to hemorrhage perforation is more likely to occur in a duodenal than in a gastric ulcer and with more disastrous consequences. Such perforation affords a peculiar mimicry of acute, gangrenous appendicitis which, as Moynihan has shown, is due to the direction taken by the extravasated fluid down along the right of the transverse mesocolon toward the iliac fossa. In fact, the condition is more likely to be mistaken for one of acute appendicitis than for anything else.
With a primary ulcerative lesion in the duodenum it is easy to realize that infection may readily travel up the common duct, involving both the pancreas and the biliary passages, while the resulting cholecystitis will intensify and spread the local peritonitis previously produced, and all combined will cement the viscera in this region into one common mass in which anatomical identity is easily lost. A good history, when obtainable, will help very much in diagnosis, especially when the absence of previous gastric symptoms can be established. This, with the symptoms already given above, and the tenderness over the duodenum, which is rarely absent, will afford good basis for diagnosis in the more chronic cases. Duodenal perforation may even be mistaken for rupture of an extra-uterine pregnancy, as well as for perforation of the stomach or of the gall-bladder, or, as mentioned above, of an appendix.
Quite recently attention has been called to a condition of the duodenum resembling that known as hour-glass stomach, and produced in much the same way. It seems to be the result of cicatricial contraction of an old ulcerated area, and may cause almost complete constriction. Hour-glass duodenum is amenable to surgery only, and should be treated either by gastrojejunostomy or possibly by a resection with end-to-end suture.
—For duodenal ulcer when recognized before perforation, there is but one treatment, i. e., gastro-enterostomy, preferably posterior, performed exactly as for gastric ulcer, for the same reason, and with the same prospect of relief, inasmuch as it affords physiological rest for the diseased area. In rare instances it may be possible to so expose the duodenum as to make it justifiable to attack the ulcer directly, but the simplest and, in general terms, the best procedure is that just mentioned.
For perforated ulcer of the duodenum the indication is not alone for a gastro-anastomosis, but for exposure of the site of perforation, removal of all extravasated material, a most careful toilet of the peritoneum, and suture of the perforated area, this being the indication when possible. Provision should be made for drainage, while at the same time affording a direct outlet from the stomach into the first portion of the jejunum beyond. Should the surgeon operate apparently for appendicitis and discover that he has to deal with a perforated duodenum he should extend far upward the incision made for the former purpose, and, having thus widely opened the abdomen, should thus find himself perhaps better provided with space in which to work than had he opened at first directly over the duodenum.
—Typhoidal ulcers of the intestines have a tremendous surgical interest in that they not infrequently lead to perforation, and that this almost always is fatal if let alone. It may be possible, however, by prompt recognition of the occurrence of the perforation and by immediate intervention to cleanse the peritoneal cavity of extravasated feces and close the opening thus made.
—The symptoms of perforation are at first not unlike those of hemorrhage, in that shock is immediate and profound, and pain, usually intense, is produced. These are quickly followed by abdominal rigidity, while a blood count will show a rapidly increasing and high leukocytosis. To the expressions of local peritonitis are quickly added those of one which is generalized, with well-marked rigidity and great meteorism.
The condition having occurred admits of but one remedy—namely, operation. One of the latest collections of statistics includes 63 operations for typhoid perforation, with 11 recoveries, although probably today the percentage is somewhat better than in 1903. Operations to be effective should be immediate. Patients are usually too profoundly collapsed to justify general anesthesia, unless perhaps this may be secured with ethyl chloride or somnoform. Many of them have been operated under local anesthesia. This has its disadvantages, however, in that it is so difficult to make free opening and exploration or free toilet. Opening having been effected, the loops of intestine must be successively examined until the site of the perforation is discovered. Here sutures must be applied, if possible. Should the condition of the bowel render it absolutely[827] unreliable, i. e., should it be too extensively gangrenous to retain sutures, it should be brought out and an artificial anus made, at least for temporary purposes. In addition to these measures the most careful toilet of the peritoneum is needed, perhaps including extensive irrigation, unless it can be shown that the area contaminated by extravasation is localized and shut off.
Perforation of tuberculous, dysenteric, cancerous, or other ulcers will cause symptoms very much like those of typhoidal perforation, and the case will differ essentially only in this respect, that in most of the latter the general condition of the patient will not be so extreme, and the danger of administering an anesthetic or of operating not so great. Otherwise the indication, the necessity, and the method do not differ.
—Tuberculous lesions of the small intestines produce less destructive features than when situated in the colon. Tuberculous infection of the intestinal tract occurs more often through the swallowing of infected sputum, and, consequently, is a frequent condition among consumptives. Such lesions in the small intestines will lead to infection of the mesenteric nodes which, in time, may become serious or even fatal, or it may lead to tuberculous peritonitis with its finally disastrous consequences. As a rule, however, tuberculous ulcers are not so likely to perforate, this being in large measure due to the frequency with which they contract adhesions or affix diseased surfaces to others, thus rather guarding against such an accident.
—Tuberculosis may also appear throughout the intestinal tract in miliary form, or we may find tuberculous gummas, either in the folds of the peritoneum or subperitoneally in the wall of the bowel. Any of these lesions may lead to any of the others, and by the time the case has been diagnosticated or has come to operation or autopsy it is sometimes difficult to say what was the primary lesion. Diagnosis is made partly with the thermometer and partly by inspection and palpation, where one may be able to discover mesenteric enlargements or the presence of fluid, as it usually collects in tuberculous peritonitis; and perhaps partly by the general appearance of the stools, in which a careful search may possibly, although by no means with certainty, reveal the tubercle bacilli.
—The treatment of such tuberculous lesions is largely constitutional. When the case assumes the aspect of tuberculous peritonitis much more can be accomplished by abdominal section and irrigation, at which time it may be possible to remove some localized focus without thereby doing more harm than good. The usual constitutional measures, including oxygen, are indicated; but there maybe difficulty in forcing hypernutrition because of the actual state of ulceration. In this case foods which are cared for by the stomach should be given in preference. Such intestinal antiseptics as creosote or other remedies of its class may also be pushed to the point of toleration.
The other granulomas produced by either syphilis or actinomycosis may give rise to ulceration and its consequences and sequels, in a way resembling those of tuberculosis. While the lesions they produce may give rise to uncertain symptoms, a diagnosis can hardly be made without accurate history and without the co-existence of other lesions in more accessible parts of the body, by whose character they may be determined. Primary actinomycosis of the intestinal tract is more common than is generally realized. As it develops it tends to spread to adjoining viscera and form tumors which later may break down. The debris thus resulting will be indicative, especially when the characteristic calcareous particles are felt in it, or the characteristic ray fungus discovered with the microscope. (See Actinomycosis.)
Save in rare instances where stricture may be due to congenital defect the condition is never primary, but is secondary to some previous and active disease. Stricture proper should be distinguished from obstruction produced by compression from without and should usually be made to include those cases due to intrinsic disease of the intestinal wall. Here it is in the vast majority of cases either due to cicatricial contraction, following the healing of some previous lesion, or else to the infiltration and progress of malignant disease. In the former instances a great deal may be accomplished by operation. In the latter much will depend upon the relative period at which the case is seen by the surgeon.
[828]
—The symptoms of stricture are those of bowel obstruction. The tumor which produces it may be identified by palpation, or by the fecal impaction, at least accumulation, which is likely to occur above it, which may appear as a tumor and be mistaken for it until cleared away by suitable cathartic measures. Ordinarily the surgeon never recognizes stricture of the small intestines, then, save by its obstructive features.
—The treatment consists in what can be done by radical surgical measures, and this can only be determined after exploratory abdominal section.
Benign tumors of the small bowel are relatively infrequent, perhaps the most common being the lipomas which develop along the mesenteric border, usually as excessive epiploic appendages. But circumscribed and even pedunculated lipomas are seen occasionally in this location and are of surgical interest largely because, at points where they are located, intussusception is peculiarly liable to occur. In fact, the condition figures as one of the predisposing causes of invagination. Fibromas develop occasionally in the intestinal walls and adenomas grow from the glandular structures which abound therein. Other benign tumors are exceedingly rare.
Besides predisposing to intussusception these tumors are innocent, save that in time they constrict or obstruct the lumen and produce one form of stricture with obstruction, which will first be chronic and then terminate acutely and fatally unless promptly relieved.
All benign tumors of the bowel should be removed with the least harm possible to the bowel itself, but when a neat extirpation without reduction of intestinal caliber is not possible no hesitation should be felt about resecting a sufficient portion of the gut; or should this be impracticable in making an anastomosis, thus excluding that part of the bowel involved.
—In the small intestines by far the most common type of malignant tumor is the round-cell carcinoma, epithelioma rarely appearing except in the lower part of the rectum, where flat epithelium is met. Adenocarcinoma, then, is common, and sarcoma relatively rare, the latter arising, of course, from mesoblastic elements. A diagnosis is made by first noting symptoms of intestinal obstruction plus certain added features of cachexia, lymph involvement and possibly of metastasis, for which a benign stricture would not account. Sometimes a tumor is easily felt within the abdominal wall; at other times one simply makes the general diagnosis of intestinal obstruction, presumably cancerous, because of age and cachexia, and leaves the rest to be determined by operation. Cancer of the bowel will naturally spread in the direction of the lymphatics at the root of the mesentery, and these will nearly always be found involved. It is fortunate if a case may come to operation before this invasion has occurred.
—Cancer of the bowel permits of but two methods of treatment, one excision of the entire infected area, both of bowel and of mesentery, in cases not too excessive, the other an anastomosis, by which temporary relief at least may be afforded. In all cases I am strongly inclined to advise the use of the x-rays, for a long time after operation; in favorable cases because it exerts a prophylactic influence, in the unfavorable cases because it nearly always relieves pain and retards growth, seeming sometimes even to disperse it. Such treatment should always be tempered by the best of judgment, lest x-ray dermatitis complicate or prevent it.
The somewhat badly derived and indefinite term “ileus,” in common use abroad, is coming into more fashionable use in the English-speaking profession, which is rather unfortunate, for it has not always meant exactly the same thing in the writings of different authors. It will be used, however, in this chapter as practically synonymous with acute obstruction or strangulation.
[829]
Acute obstruction may be classified in two ways, as to types and as to causes. For the first purpose the best classification is perhaps the simplest, and, as recently rehearsed by Murphy, is as follows:
Conditions which permit the adynamic type may include those of spinal origin, those interfering with mesenteric nerve supply or that of the walls of the intestines (for instance, in cases of fracture of the spine), or, again, where extensive operations have been performed on the mesentery, or where there have been extensive wounds. Thus in removal of mesenteric tumors, unless care is exercised in separating the mesentery from the tumor and in ligating bloodvessels without including nerves, a paralytic ileus may promptly result. Gunshot wounds of the chest or of the spine may also include injuries to nerves, by which paralysis of the bowel ensues. So, too, adynamic ileus sometimes results through the paralyzing reflexes which follow strangulation of the omentum—as, for instance, in a hernial sac—or it may be due to biliary calculus acting in the same way.
The dynamic forms, as well as the mechanical, are much more likely to be characterized by pain and violent symptoms than are the paralytic. Gastric tetany is a condition to be differentiated from reflex ileus. Enormous distention of the stomach immediately after operation leads perhaps to a belief that a patient has acute obstruction of the intestine, when the fact is that such a case may be relieved by vomiting or passage of a stomach tube. Local peritonitis of septic type, as well as peritoneal traumatism, tends to weaken if not to paralyze peristalsis. In general peritonitis the entire intestinal tract is involved, partly from reflex paralysis, partly from inflammation of the intestinal wall. The embolic type of paralytic ileus may be due either to interference with nerve supply or with blood supply. In thrombophlebitis symptoms develop more slowly, especially when this follows abscess of the liver or spleen. Here there is not so much meteorism, and the bowel may be even nearly empty, while we have the other symptoms of pain, nausea, and vomiting. Borborygmus is one of the most pronounced manifestations of mechanical ileus and the stethoscope will then give much assistance. In fact auscultation of the abdomen, with a recognition either of active motion within or of absence of peristalsis, should not be neglected; when one can hear intestinal waves the condition is much more likely to be one of purely mechanical obstruction.
Classified by causes, we may make out the following well-marked groups:
—By far the most common of all the causes of acute obstruction are strangulated hernias. These are, however, treated by themselves in a distinct chapter.
—These terms imply a protrusion or prolapse of one part of the intestine into the lumen of an immediately adjoining portion. This is found to be the cause of perhaps one-third of the total number of cases. Enteric invaginations occur along any portion of the small intestine, being more common in[830] the lower portion and rare in the uppermost. They seldom attain great length and are often very short. The ileocecal is the most common variety, since obviously it is the easiest of occurrence, the ileum protruding into the cecum or the ileum and cecum together passing into the ascending colon. Colic invagination may occur anywhere along the large bowel, being again more common near its distal termination. The colon may descend into the colon or the sigmoid into the rectum, even to such an extent as to present at the anus or possibly protrude. Statistics show that the ileocecal occurs in 44 per cent., the enteric in 30 per cent., the colic in 18 per cent., and the ileocolic in 8 per cent. of cases.
While the surgeon is concerned only with the obstructive form of intussusception it is of interest to know that the condition occurs occasionally shortly before death and is then spoken of as the intussusception of the dying, being usually due in these cases to irregularity and uncertainty of peristalsis during the concluding hours of life; paralysis occurring at one portion of the intestinal tube and abnormal activity just above it. These conditions are discovered at autopsy, and can be recognized as such by the absence of exudate or of any attempt either at repair or inflammation. They occur most commonly in the young and may also be multiple. In direction intussusception is practically always descending, although there may be a secondary and associated ascending movement, the latter being unimportant.
Double intussusceptions are somewhat common, and triple or multiple have been described.
Cross-section of an invaginated bowel will show that on each side one must pass through three distinct layers of bowel wall. That portion which is intruded is spoken of as the intussusceptum, while that portion which receives the latter is known as the intussuscipiens (Fig. 560). Obviously when invagination occurs the mesentery should be drawn in with the intussusceptum, while traction upon it should increase with advance of the included bowel. This is particularly often seen in ileocolic varieties where the ileum, with its mesentery, may travel the whole length of the colon and even present at the anus. Moreover, this may occur within a relatively astonishing short time, and the fact that the intussusceptum may be felt in the rectum within a few hours after the occurrence of the first symptoms is a fact not easily to be explained.
Fig. 560
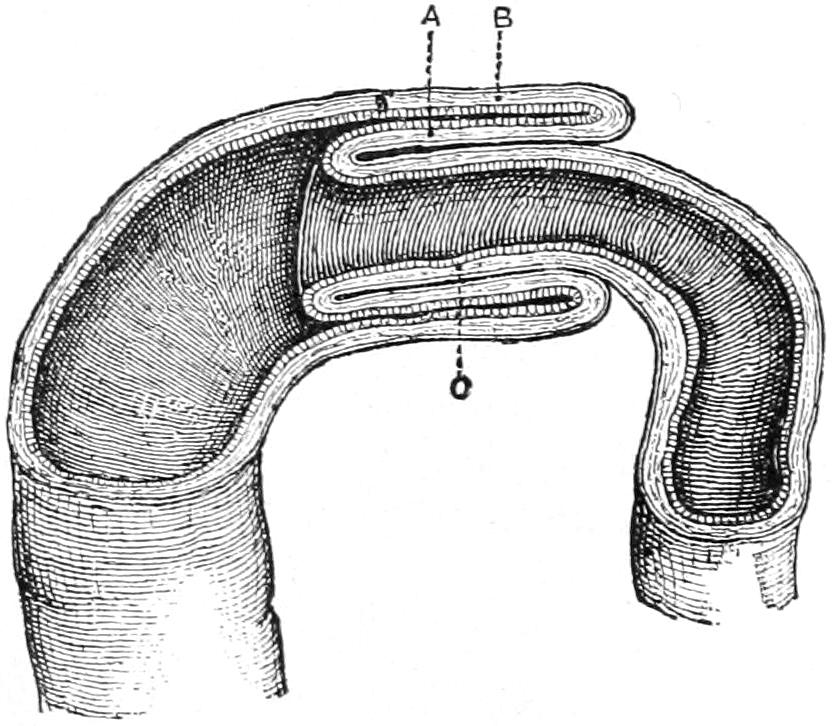
Diagrammatic section of an intussusception: A, reflected tube; B, receiving tube or sheath; C, entering tube.
—The causes of intussusception are obscure, postmortem findings or even the revelations of a laparotomy demonstrating conditions, but not often affording explanations. The presence of tumors, especially lipomas, which may even be pedunculated along the small intestine, has been demonstrated in a number of instances, and they have been supposed to be active factors in the first disturbance. Everything points to the association of disordered intestinal movements with the mechanical condition of obstruction, and the former are more frequently seen in the intestinal complaints of the young, along with the presence of masses of undigested food or impacted feces within the bowel, or the occurrence of intestinal polypi. The most complicated case of ileocecal invagination which ever came under my notice was associated with the presence of a polyp in the ileum. All of these conditions, save the presence of tumors, pertain more frequently to the young than to the aged. The influence of the ileocecal valve is also undeniable, and that at this region parts are more predisposed to invagination than elsewhere is quite obvious. In at least half of the cases that have been recorded no satisfactory cause could be shown. Any condition which causes severe intestinal colic may give rise to intussusception; the next most common causes are paralysis or weakening of some part of the bowel, such as may follow injury or disease, or the presence of tumors, while even the role which they play is not entirely explained (Fig. 561).
That invagination will produce mechanical obstruction is obvious, while the fact that such obstruction is not always nor necessarily complete incites surprise. The orifice of the intussusceptum is distorted, while the included portion may be greatly bent or[831] curved upon itself, in addition to which the obstruction to the circulation leads to congestion, exudation, and swelling, and predisposes to active inflammation, all of which tend to still further narrow the passage-way. If, in addition to this, some tumor or hardened fecal mass be included in the grasp of the bowel involved it may be seen how complete shutting off of the intestinal tube may occur within a few hours. Invagination having occurred tends quickly to become irreducible; most commonly by the formation of adhesions, as lymph quickly exudes and bowel surfaces are by it thus glued together. Such adhesions may persist throughout the whole involved length of bowel or may occur at various scattered spots. As pressure becomes greater circulation of the invaginated portion is impeded and finally shut off, gangrene of the intussusceptum thus resulting. Cases occasionally terminate favorably through this actual condition, the included portion being finally cast off as a slough and passing onward and outward. It is on record, for instance, that six feet of invaginated bowel have thus been obtruded from the rectum after having sloughed, the patient eventually recovering. While this possibility, then, is present it is never safe to wait for it, and it is to be regarded simply as a happy accident when it occurs. Unless, then, a case of intussusception be very early and promptly operated, the included portion of the bowel may be regarded as dangerous and unsafe, unless upon disengagement it prove to have been but very slightly affected. Even then there is danger of immediate recurrence of the previous condition because of distention of the bowel above, paralysis of the part disengaged, and stretching of the part below. In proportion as obstruction becomes more complete distention of the bowel above the lesion, from accumulation and gas formation, will cause more and more distress, until finally complete paralysis of the muscular coat and possibly eventual rupture may terminate the case.
Fig. 561
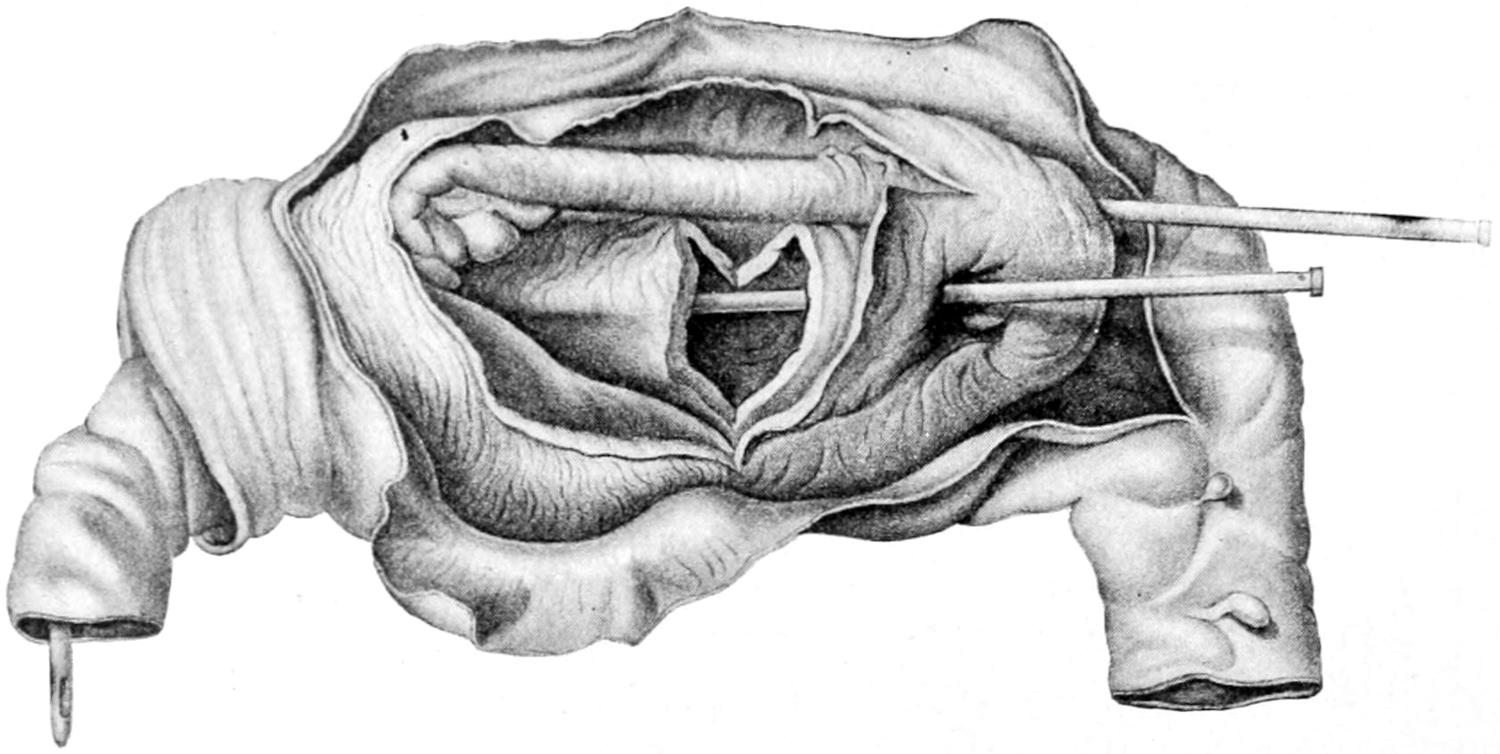
Invagination of ileum, cecum, and ascending colon into transverse colon. One probe is passed into the appendix, the other into the invaginated portion of the ileum. (Rafinesque.)
In addition to the conditions above described, all of which are acute, there is known also a chronic form of intussusception, whose whole course is much slower and less severe, where symptoms of obstruction never become more than partial, but may involve any portion of the bowel, and with about the same relative frequency as the acute forms. Such a condition in the rectum, for instance, has been mistaken for cancer.
—The special symptoms by which intussusception may be recognized, or at least by which suspicion is aroused, are, in addition to those common to all forms of acute obstruction, the abrupt onset, which may even occur during sleep, the late rather than the early occurrence of vomiting, complaint of tenesmus, the wave-like or colicky character of the pain, and the fact that along with the violent peristalsis of which this colicky pain is an indication diarrhea is a common accompaniment, the actual local coprostasis being masked by this fact. As the lumen of the bowel becomes occluded and fecal matter fails to pass, the evacuations become more bloody and contain little but mucus. Finally, almost pure blood may be passed. In no other form of obstruction is the passage[832] of blood so distinctive as in this. Urine elimination is but slightly influenced, and strangury is an exceedingly rare feature. Meteorism is also less pronounced. The discovery of a tumor formed by the invagination will lend further aid in diagnosis. It may be felt either through the abdominal wall or by the rectum, and may be noted in about half of the cases. It is most frequently found in the ileocecal and colic varieties, and felt in the rectum with the lower colic forms. In children it is more distinct than in adults. The tumor may even take the outline of the involved bowel, is usually movable, but may be fixed. When such a tumor is felt within the rectum it may have to be distinguished from some intrinsic neoplasm of the lower bowel; but the history of the case should prove satisfying if the physical examination leaves one in doubt.
—Spontaneous cure of an intussusception by a sloughing process has been mentioned above. Cure may also occur by spontaneous reduction. It would seem possible also only in recent cases and in the enteric forms. Cure may also occur by formation of a fecal fistula, although this is most rare.
—The term “volvulus” implies some form of twisting or of revolution of a part of the bowel upon itself or its mesenteric axis, the result being knotting or intertwining of intestinal coils to an extent causing their partial and finally complete obstruction. A common site for volvulus is the sigmoid flexure. Still no part of the intestine which hangs loosely is exempt.
The most common causes of volvulus are chronic constipation and fecal impaction, with distention and ptosis. Intestine thus displaced and overloaded becomes more or less paralyzed, its circulation more or less impeded, and any twist which has once occurred is not likely to right itself. The twisted loop having been engorged becomes distended with gases, and thus tends to increase the difficulty. In these cases the bowel loop is closed at both ends. Unless relief be afforded by operation it is a question merely of how soon the loop will become gangrenous from aggravation of every one of the features above recounted. Bowel thus involved permits easy passage of bacteria, and thus to the other features are rapidly added a septic peritonitis. The resulting abdominal distention may appear early and will become more prominent.
—A condition of extreme coprostasis, or fecal impaction, to a degree producing actual obstruction, may occur without necessary volvulus or twisting of any portion of the bowel. As fecal impaction increases the overloaded bowel becomes more and more paralyzed until there may occur final and complete arrest of peristalsis, with gradual development of symptoms of obstruction. The longer the condition persists the less the prospect of restoration of peristaltic movement. Moreover the condition may be complicated by the development of ulcers above the obstructed segment, known as stercoral ulcers, due partly to gangrene from pressure and partly to the chemical effects of long-retained decomposing material. They may appear as sloughs of the mucous membrane and finally lead to perforation.
This form of ileus is more common in the large than in the small intestine, and especially so in the cecum. Here there is little chance of retrograde movement, while fecal matter coming down from above will continue to pack the colon, and thus the cecum may have to bear the brunt of great pressure. The amount of fecal matter which may be thus collected is sometimes astonishing, for the bowel may dilate to the diameter of six or even ten inches, and contain many pounds of impacted feces. Such masses of collected feces can usually be palpated through the abdominal wall, and will at least indicate the location of the principal disturbance, if not its actual character.
—The most common causes of cicatricial stenosis in large or small intestine are the results of cicatricial contraction following recovery from local ulceration or repair of injury, as, for instance, after reduction of a strangulated hernia. The exact character of the ulcer does not matter. Any lesion which may granulate and heal will also contract, and the extent of the stricture will be proportionate to the area first involved. Should this extend well around the mucous membrane there may be a distinct annular stricture. Stricture may also result from infiltration and thickening in connection with a more active diseased process, and such a condition may be multiple. This is particularly true in cancerous involvement of the bowel.
Previous history of the case will shed much light on the probable existence of intestinal stricture. Thus a history of typhoid, of dysentery, of tuberculosis, or of syphilis will be most suggestive, for in any of these diseases there may be numerous intestinal ulcers. A history of hernia, reduced or operated, or of injury, is also of importance, as also is one of operation upon other viscera, especially within the pelvis, the lower bowel being often involved in a disease process within this cavity which may have left its marks.
PLATE L
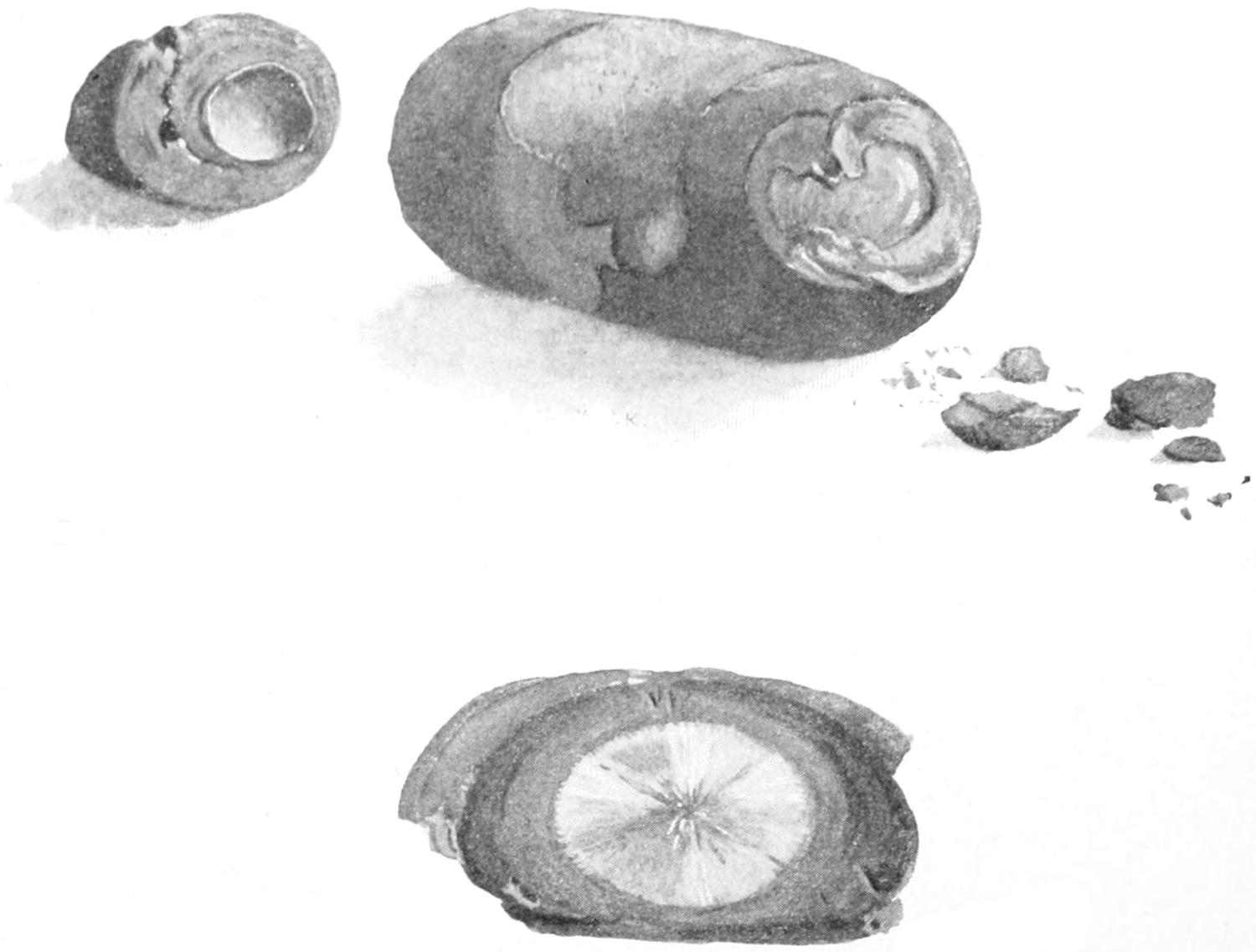
Enterolith with Gallstone for a Nucleus; Removed by Enterotomy. (Richardson.)
This patient was a man of sixty-nine, with symptoms of complete intestinal obstruction. There was no previous history whatever of gallstone. The impaction was high up in the small intestine. The gallstone was removed by a small linear cut which was satisfactorily sutured. The patient died in the course of twenty-four hours.
[833]
Stricture may be recognized by the gradual course of the case and by a history of increasing difficulty or of increasing constipation. A stricture as such is not formed within an hour, and in this sense is the result of a previous more or less active disease. This is true, also, of cancerous stricture.
—The possibility of both innocent and malignant tumors occurring within the intestinal structures has already been considered. It is obvious that any such growth will cause gradual obstruction by the usual process, or may precipitate by its presence the occurrence of intussusception, of volvulus, or of some kinking by which obstruction is suddenly produced.
—What has been said above applies equally well to growths not primarily involving the intestine, but encroaching upon it. Thus obstruction may gradually result from retroperitoneal growths, or from the impaction of a growing uterine myoma pressing upon the rectum and finally occluding it. Also cancers growing in various locations encroach upon and finally involve the bowel in conditions which nevertheless were originally quite external to it.
—In the section devoted to the biliary passages the accidents which may occur during gallstone disease have been summarized, and it has there been related how large ones may ulcerate through and drop into the small or even into the large intestine. Enteroliths may be thus produced, which were originally small gallstones that have lodged and grown by accretion until they have reached considerable size, or by gallstones which have suddenly entered the intestine by ulceration above, or by other material which may have collected in some sacculation or diverticulum, where it has received more or less calcareous deposit and has grown by accretion until it produces obstruction, either by occlusion or by causing the intestine to kink. Other foreign bodies may also produce obstruction. Although it has been generally held that whatever may escape through the pylorus may be evacuated from the rectum, nevertheless peculiarly shaped objects become entangled in such a way as to be checked in progress and serve as impacted bodies upon which an accumulation may take place. (See Plate L.)
—While coprostasis is a feature of almost every case of acute peritonitis the obstruction referred to in this paragraph comes rather from the adhesion and fixation of bowel from outpour of lymph than from paralysis and ileus in consequence. It may be doubted whether acute peritonitis is ever idiopathic. As seen by the surgeon, at least, it has some point of origin which furnishes ample excuse for its existence. The most common cause in the male is the appendix, and in the female the appendix or the tube. At least one-half of the cases occurring in general practice originate in one or the other of these ways. Infection may also easily spread from the mesenteric nodes, beginning locally and resulting in adhesions, the disease spreading by a natural process until perhaps the whole abdomen is finally involved. While healthy bowel is ordinarily impervious to germs, when it becomes diseased germs may easily travel from its interior to its exterior and thus set up peritonitis. In this way a purely mechanical original condition may bring about a fatal septic peritonitis. It is known also that intestinal diverticula are subject to exactly the same lesions as is that one in particular which is called the appendix, and the symptoms and sequences of the diverticulitis may simulate those of an acute appendicitis. In acute appendicitis coprostasis and even apparently fatal obstruction are frequently met with. Their occurrence is to be explained not alone by toxemic paralysis (i. e., toxemic ileus), but by the actual mechanical impediments offered by loops of bowel strongly bound together around the appendix in the actual protective effort.
—Bands of tissue which may cause obstruction of the bowel are neither necessarily long nor large, and one will frequently be astonished to see how trifling a tissue cord may produce intense disturbance. The bands which may be found within the abdominal cavity under these circumstances include those produced by peritoneal adhesions, where the cohering lymph has organized and at the same time stretched, such bands being found to arise from and connect with the bowels alone, to arise from the omentum from any other causes, particularly traumatic, or to occur at any point within the peritoneal cavity. They may be single or multiple. When speaking of Meckel’s diverticulum it was stated how it might be mistaken for a band extending to[834] the region of the umbilicus, and acting as one cause of obstruction. (See Fig. 559.) An adherent appendix or tube tightly attached at its free extremity may also act as a band, and the former is known to very frequently produce at least a mild form of intestinal obstruction, which may at any time assume acute proportions. The pedicle of an ovarian or other tumor may also, if long, by becoming twisted, include an intestinal loop and thus produce obstruction.
—The mesentery is the occasional site of fenestra which apparently are of congenital origin. Through such openings or slits a loop of bowel may easily pass and become strangulated. The same is true of the omentum. Openings in either of these structures are perhaps more frequently the result of traumatisms. Similar conditions result where omental or mesenteric surfaces have united over small areas, leaving pockets or openings in which bowel might be caught. Quite a similar condition results in so-called hernia of bowel into and through the foramen of Winslow.
—These causes are not perhaps independent of some of those above mentioned, yet presuppose a certain looping or abnormal festooning of intestine, with the further stretching that occurs as the result of greater loading and the final entanglement of such loops, or their adhesion, in such a way as to become completely occluded. To this result some local inflammatory process may contribute. The condition is often met in connection with pelvic disease of females. Much that may happen to a loop of bowel which has become attached to a growing tumor during its migration, as it gradually changes its shape and position, may be imagined.
Fig. 562

Strangulation of bowel by a long diverticulum. (Lejars.)
—Certain congenital defects predispose to acute obstruction. Among these are diverticula, as already mentioned, which may produce trouble, either by incomplete obliteration and separation from the umbilicus, in which event they act as bands or cords, or by becoming acutely inflamed, then attaching themselves and indirectly producing the same effects (Figs. 559 and 562). Even the smaller diverticula or sacculations which extend between the folds of the mesentery may, when infected and inflamed, thicken and cause angular bending of the intestine, with consequent partial obstruction, which later is made complete by the consequences of local peritonitis, with its dense inevitable adhesions. Statistics show that acquired diverticula occur twice as often as Meckel’s, and nearly as frequently in the small as in the large intestine. They are mostly of the traction variety and occur at the mesenteric border, where they have close relation to the bloodvessels, thus increasing the dangers of operative measures because of possible gangrene from shutting off circulation. Porter has recently collected 188 cases of violent and even fatal trouble thus produced within the abdominal cavity, returning an exceedingly high death-rate after operation, which unfortunately was almost always done late. In nearly all of these cases the diverticula were found within the lower four feet of the ileum. In one case of my own an unobliterated hypogastric artery caused acute obstruction.
—Finally cases of postoperative obstruction are met with in a way to bring disappointment and disaster when everything else has seemed favorable, and constitute a clinical type without any distinct pathological foundation. Most of them are due either to some form of paralytic ileus, or else to local or general peritonitis with its combined sequels of paralysis and adhesion by the gluing of portions covered with exudate. Some of these cases will justify reopening the abdomen, while in others the condition is absolutely helpless because of the septic element present.
—Certain symptoms and signs characterize all cases of acute intestinal obstruction and may be, therefore, included as common to each; consequently they may be considered collectively. The cardinal indications are pain, vomiting, constipation, distention, and collapse.
[835]
Pain may be the first indication, and usually is so in invagination, volvulus, and mechanical obstructions generally. It is usually of violent paroxysmal character, continuing at least during the earlier stages, rapidly wearing away the patient’s strength, diminishing as distention increases and nerve endings become paralyzed.
Vomiting is an early or late feature, according to the portion of the alimentary canal obstructed. The more prompt its occurrence presumably the higher in the small bowel the defect. In consequence of the remedies usually administered it will be found that when nothing but stomach contents are ejected it is easier to produce fecal evacuation from below, while the greater the difficulty in securing a return from the lower bowel the lower the obstruction and the more likely the vomited material to become fecal in character. Vomiting once begun is usually continuous until relief is afforded or the patient utterly exhausted.
Constipation or obstipation sooner or later characterize these cases. The tenesmus of intussusception, with the passage of bloody mucus, which may occur in this form, or in volvulus, for instance, does not imply that the bowel itself is not obstructed, nor does the emptying of the larger bowel of an accumulated load necessarily imply that the fecal stream is in motion. Even the passage of flatus usually is promptly shut off, and it is the gas which forms and cannot escape that produces the distention.
Distention gradually becomes excessive, the abdomen becoming ballooned and extremely tympanitic on percussion, while its surface becomes shiny because so stretched. This meteorism is in large degree due to the formation of gas within the bowel proper, but is permitted by the additional features of paralysis of intestinal muscle and weakening of that of the abdominal wall. As it increases the diaphragm is pressed upward and respiration is much impeded, while even the bladder may be compressed below. It affords another reason why fluid which is taken into the stomach is quickly ejected.
Characteristic collapse comes on more or less promptly, according to the nature of the exciting cause, and the date of its occurrence is in some degree an index of its violence.
In dealing with obstructive cases any history that may bear upon the conditions, as of previous peritonitis, appendicitis, of so-called dyspepsia which might indicate gallstone disease or gastric ulcer, or of pelvic conditions which might indicate pyosalpinx or the like, should be obtained. The manner of onset should be learned, whether acute or gradual, with the relative date of the occurrence of pain, vomiting, and stools, along with their character, if there be anything distinctive therein. Past and present history being secured, the most methodical examination of the body should be made, including the physiognomy and general conditions, the attitude (e. g., whether the knees are drawn up, whether the patient is able easily to turn), the type of respiration, and the amount of restlessness. The character of the abdominal movements during respiration should also be noted, as well as the presence of any prominence or the indications of violent peristalsis. By palpation the degree and location of greatest tenderness, the presence of muscle spasm or of tumor may be learned. Careful examination of all the ordinary hernial outlets should be made and the rectum and vagina explored. Revelations thus obtained may also prompt a careful physical examination of the chest. Percussion will show the presence of free or localized fluid or gas, while localized dulness may denote a loop of intestine distended with fluid or impacted feces. Auscultation will enable the surgeon to hear the sounds produced by violent peristalsis or to note the absence of movement within the bowel. A study of the temperature and the pulse may reveal much in certain cases, especially the inflammatory, and particularly in appendicitis, while the urine may be examined for indican, and a differential blood count made.
Meteorism, constipation, and fecal vomiting of themselves indicate acute obstruction, but furnish no aid as to the nature of the exciting cause. They are, however, sufficient to indicate the wisdom of immediate intervention.
Pathologically every case of intestinal obstruction has an interest of its own. Surgically, however, they are readily grouped as a class of cases in which operation should always be performed early, inasmuch as it offers the better prospect of relief and in which death is the inevitable spontaneous termination. It can scarcely be imagined how a more distressing case than an acute strangulation can be allowed to go to its fatal termination without being offered the prospect of a judicious operation, if only performed early. The disfavor with which operation is received by the general physician, as well as by laymen, is due to the fact that too much time is wasted with futile[836] drug treatment, and that the golden hours when surgical intervention might save are allowed to pass unutilized. Of most of these cases it may be said that dying after operation they have died in spite of it rather than in consequence of it.
This is particularly true with intussusception and volvulus in young children or infants. Within six hours, in such cases, the harm which may be done is necessarily fatal, and to keep them for a day or more, dosing them with cathartics or making strenuous efforts to relax invagination, is to deprive them of the only measure which offers them any chance. The disrepute into which operative treatment of these cases has fallen in certain quarters is due, then, solely to the fact that the physician does not call the surgeon early, because there is a time in the history of nearly every one of them when it could be saved were mechanical relief afforded.
—There are certain cases of obstruction by fecal impaction or lodgement of enteroliths which may be successfully treated by internal or non-operative means. Could these always be diagnosticated it would be known when not to operate. But to wait until paralysis of the bowel has occurred, or gangrene due to stasis, or perforation have taken place, or septic peritonitis has set in, is to wait far longer than circumstances justify and reflects on those responsible for the delay rather than on the operator or the operation. In general terms, acute intestinal obstruction is always a surgical disease.
It is not necessary to wait for accurate diagnosis—recognition of the existence of obstruction alone is all that is required. Conditions rapidly aggravate themselves, and strength is rapidly lost, if we wait for more than distinctive symptoms. There is no palliative treatment save operation, and the drugs and other harsh measures which are often prescribed serve to intensify and aggravate rather than to relieve. Anodynes given, though administered with the most humane intent, serve only to mask conditions and lead to delay.
Exploration once resolved upon, careful judgment must decide as to where to place the incision. If local indications be present they may be followed. If there be good reason to believe that the original cause was an acute appendicitis, then the incision may be placed upon the right side. In the absence of all indications the surgeon operates most safely in the middle line by an incision below, above, or around the umbilicus, as circumstances may indicate. Edema of the subserous tissue or of the abdominal muscles indicates the presence of pus beneath. Peritoneum should be sought and opened with care, as in the presence of much distended bowel injury to the same may easily occur. The opening once made the operator will be embarrassed from that time until the conclusion of the operation by the distention of the bowels—at least those above the obstruction, and by their being constantly in the way. If a mechanical cause for obstruction be found it will be noted that the intestine above is more distended than that below, which latter may be collapsed and apparently smaller than natural. Thus if a constricting band be found, or an internal hernia, the removal of the obstructing cause will permit of prompt restoration of equal gaseous pressure between the parts above and below.
Scarcely any surgical emergency requires wiser discretion than do cases of this kind. Bands may be double ligated and divided, kinks straightened out, twists untwisted, invaginations withdrawn, if this be possible by reasonable effort. On the other hand the surgeon should be prepared to find bowel which has apparently lost its vitality or is actually necrotic, either for a few inches or for several feet, and he will soon realize that to leave such gangrenous masses within the abdomen is to accomplish naught, while to remove them is to subject the patient to a procedure longer and more severe than he can bear. He must, then, decide whether to close the abdomen for form’s sake and let the patient die a natural death, or whether to undertake the risk of resection, or perhaps to leave a considerable portion of the intestinal canal upon the outside of the body, opening it and establishing an artificial anus in the hope that the sloughing portion may be cast off, and that the artificial anus, having served its purpose, may be subsequently closed by another operation. Such cases live, though not very often. Here, perhaps as often as anywhere, can be seen the most desperate expedient succeed and the most trifling measure fail.
Another question is what to do with distended and paralyzed intestine, especially when it appears impossible to restore it to the abdominal cavity. Paralyzed as it is, it is almost too much to hope that it may recover its tone, and distended as it is, it is practically unmanageable. To open it at one point would be to empty several loops, at least of[837] gas and probably of fluid fecal matter, all of which will help. One cannot but reflect on the toxic nature of all fecal matter so retained and feel that could it all be evacuated the patient would, other things being equal, be in vastly better condition. And so operators have often made openings, taking all possible precautions to prevent contamination, and have not only evacuated a considerable length of the intestinal canal, but, as suggested by Mixter and others, have washed it out.
A more perfect method, however, of accomplishing this purpose has been suggested by Monks, of Boston, in the use of a large glass tube, from twenty to twenty-four inches in length, strong and with smooth ends. He has shown how, an opening having been made, say just above the obstruction, it is possible by manipulating the bowel with gauze pads to draw it over the tube (as shown in Fig. 563), to an extent of several feet, and to thus more completely evacuate it than could be accomplished in any other way. Monks is undoubtedly entitled to priority for this suggestion over Moynihan, who has elaborately figured and described it. All in all this permits better management and more complete effect than any other method. The bowel having been emptied, the opening is closed by the usual double row of sutures and is then easily dropped back into the abdominal cavity. Cases occur where this procedure might be carried out at two different points, say above and below the obstruction.
Fig. 563
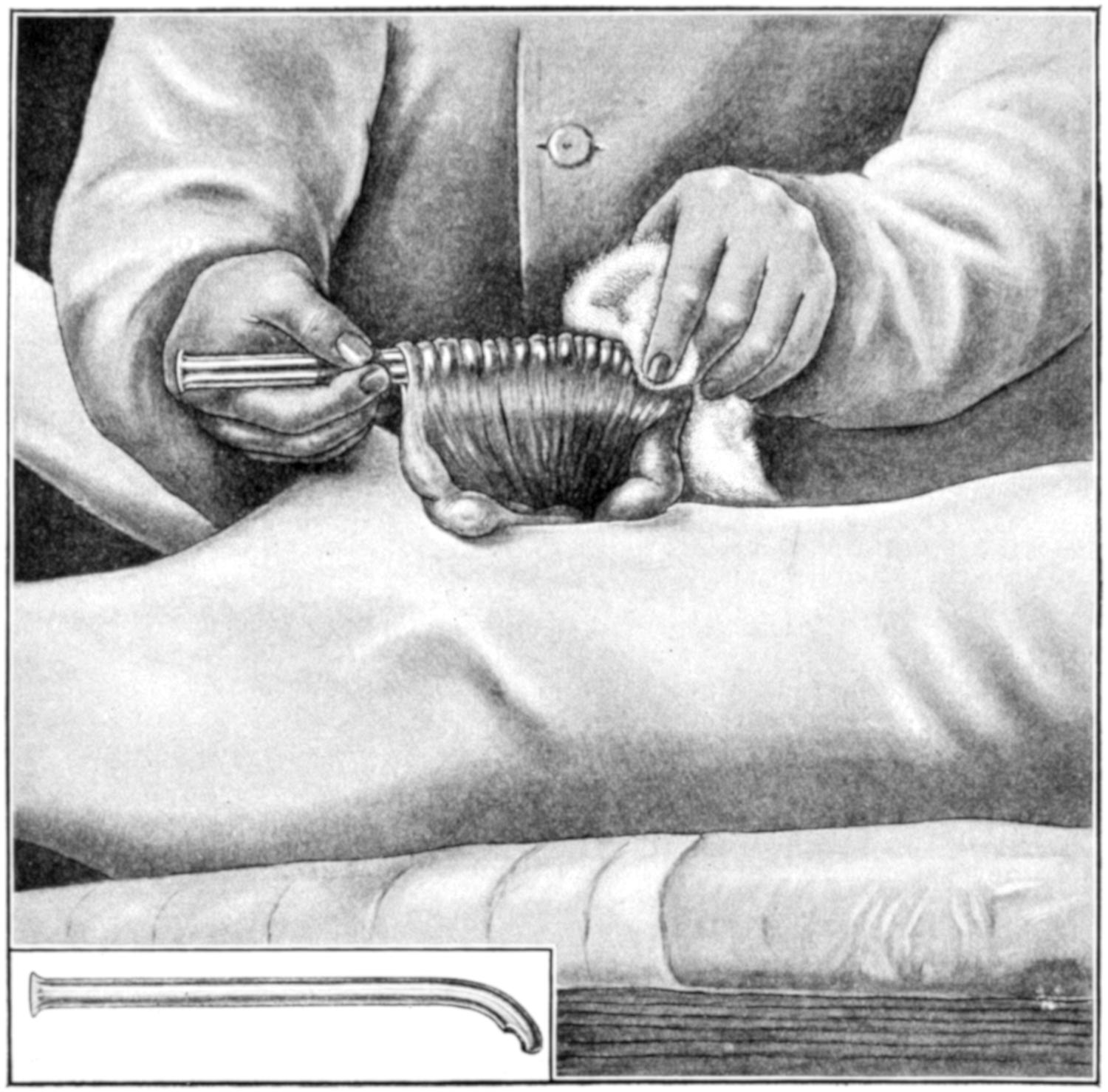
Method of inserting a tube (through an enterostomy opening) a considerable distance into the intestine by drawing the intestine around it with the help of a piece of dry gauze. The tube used in this case has a curved extremity, the opening being on the concavity of the curve. It is shown entire at the lower left corner of the illustration. The longer the abdominal incision and the longer the tube the greater the length of intestine which may be drawn upon it and emptied of its contents. (Monks.)
What may be done with the obstruction produced by local and septic peritonitis, such as is especially seen in acute cases of cholecystitis, appendicitis, and pyosalpinx?[838] Here the surgeon deals not only with twisted, kinked, and obstructed bowel, tensely distended, but with much infected lymph and perhaps a collection of pus and a gangrenous appendix. Such a condition becomes appalling and every such case should be dealt with upon its merits. Any collection of pus should be evacuated and drained, and it must then be decided whether to endeavor to withdraw entangled loops, disengage and straighten them out, or to be content with an artificial anus for temporary purposes, the latter often being the safer course, even though it may lead to a tedious convalescence and the necessity for subsequent operation. It might even be advisable to evacuate pus and remove a sloughing appendix, if it were easily found, and then make an enterostomy, opening at some other point, in order to keep the two procedures and fields of activity quite distinct.
A case may occasionally be seen where the question of affording some relief is paramount to every other consideration, and where, at the same time, the patient’s condition is such as to make anything extra-hazardous. I have saved life under conditions of this kind by making a simple enterostomy under cocaine, the intent being only to attach a loop of distended bowel to the parietal peritoneum and to open it then or a little later, thus establishing an artificial anus. This may be done with local cocaine anesthesia. I have even seen the fecal fistula thus produced close spontaneously in the course of time, and, while the exact character of the lesion was never known, have had the satisfaction of thus saving a life which I believe would otherwise have been lost.
One of the most unfortunate accidents that can occur during operation for acute obstruction is to have the patient practically drown in his own fecal vomit. This may occur either on the operating table or soon after leaving it. The term implies simply this—that there is regurgitation of fecal matter into the stomach, and that as this is ejected by a patient in his unconscious condition he is not able to prevent its aspiration into the trachea, with the occurrence of all that essentially constitutes drowning. Even a few ounces of fluid material drawn into the lungs, under these circumstances, would be sufficient to cause asphyxia and death.
The accident is to be prevented not alone by lavage, both before and at the conclusion of the operation, but by placing the patient upon his side in such a way that any gush of fluid into the mouth may escape from it and not be sucked into the lung. The amount of fluid that may arise is sometimes astonishing. The introduction of harmless fluid, under these circumstances, would be sufficient, but the entrance into the lungs of a viscid, offensive, and septic fluid, even in small quantity, would quickly serve to induce a septic pneumonia if nothing else. The accident once having occurred, resuscitation is almost impossible. Under the relaxation of anesthesia it may occur without outcry and almost unsuspected, and with the patient on his back, death may be determined even before the attendant has noticed anything particularly wrong. To prevent this accident tubes have been devised having balloons around them which can be inflated with air, to the desired degree, and the esophagus thus be plugged.
Hence it will be seen that the surgeon should temper his measures to the condition of the case, its exigencies and its surroundings. Operation, therefore, may be exceedingly mild or exceedingly severe, taxing the resources of the best-equipped clinic.
Strangulations recognized from surface indications are usually dealt with according to standard indications. Those discovered only after abdominal section are to be dealt with each on its merits.
The expressions of chronic obstruction are essentially those of acute, in which they usually terminate, occurring meantime in milder degree. Their causes are nowise different from those tabulated above.
—The symptoms of chronic obstruction are those of intermittent colic, constipation, perhaps with local tenderness, with change in shape of the abdomen due to the primary cause or to intestinal distention, and in many instances with some characteristic appearance or shape of the feces. Thus the stools are often loose, or scybalous masses when removed by cathartics, and these are followed by diarrheal stools containing many gaseous bubbles. Obstruction of the lower bowel will frequently cause the hardened fecal masses to assume a tape-like shape. With increasing obstruction there is increasing severity of symptoms, until finally they become acute.
[839]
—The treatment of chronic obstruction is also operative, either radical or palliative. When the exciting cause can not only be detected on exploration but removed, it should be radical. If, however, this be not possible then enterostomy or entero-anastomosis only can be practised. Thus in cancer of the rectum or sigmoid, colostomy is the last resort. In cancer of the bowel above the sigmoid anastomosis may relieve the obstruction and permit the patient to linger until he dies of the natural progress of the disease.
Here, as elsewhere, operation should not be too long delayed. To wait for a chronic obstruction to merge into one of the acute forms, and then to wait until the patient is moribund, is to have deliberately deprived him of that which otherwise might have prolonged his life.
For chronic obstruction whose cause is not easily revealed the hypothesis of cancer affords the most common explanation. This may be intrinsic or extrinsic, so far as the bowel itself is concerned, the results however not differing. It matters but little whether cancer is producing an annular stricture or involving a considerable extent of bowel, something should be done. When health has gradually failed, and obstructive symptoms have come on slowly, and when distinct cachexia is present the presence of cancer within the abdomen may be suspected. When a distinct tumor is palpable or when the abdomen gradually fills with fluid there is little doubt. When to these signs is added pigmentation of the abdominal wall the diagnosis may be considered certain. Even now exploratory section is justified, in the hope that some operative measure may offer comfort and at least temporary relief.
On the other hand, when obstructive symptoms appear and increase without the accompaniment of other serious indications, it may be hoped that the condition is benign rather than malignant. Obstruction with ascites may possibly be due to tuberculous lesions, which are not uncommon, especially in children. The recognition of enlarged mesenteric nodes would corroborate this diagnosis. A history of typhoid fever or of injuries or foreign bodies might confirm the theory of cicatricial stenosis. The possibility of enteroptosis of the colon and impaction of hardened fecal matters should not be disregarded and that of enteroliths, especially gallstones, not forgotten.
A fecal fistula implies any communication between the intestinal tract and the exterior of the body or one of its other cavities. Thus it is possible to have a rectovaginal fistula as well as a vesicovaginal. In rare instances we may meet also with intestinal communication with the bladder, the other viscera, or even the pleura or lungs.
Fecal fistulas are always abnormal productions, and result either from congenital causes, previous injury, or disease. Among the traumatic causes may be mentioned penetrations or ruptures of the intestines, injuries to the bowel occurring in the course of abdominal operations (for instance, the inclusion of some part of the bowel wall within a ligature or suture), while the pathological causes include the possibilities of perforation of any form of ulcerative lesion, cancer, actinomycosis, or the secondary sloughing which may follow appendicitis, or even the pressure of a drainage tube. Fistulas result also from escape of foreign bodes (for instance enteroliths or bone fragments), which may work their way into some other viscus, or out through the abdominal wall to the body surface. Old pelvic and abdominal abscesses also occasionally cause perforation and fecal fistulas. These fistulous tracts may be long or short, and direct or indirect. They may also permit the escape of a large amount of fecal matter or the smallest appreciable amount. The majority of them tend to close spontaneously in the course of time, but this time is sometimes so prolonged that a surgical operation is preferable to waiting for natural processes. The communications may be high in the intestinal canal. In such a case matter that escapes will be but partially digested and will have the character of chyme rather than of feces; and patients suffer in consequence, as products of digestion are not complete and opportunities for absorption have been too limited, and they are deprived of all that should normally happen further along in the bowel. In such a case there is temptation to operate much earlier than is advisable. Another form of fistula results from certain cases of strangulated hernia, in consequence of necrosis of the strangulated loop of bowel. In fact this is true of any of the mechanical causes[840] of acute obstruction, where this expedient may be resorted to under compulsion and we produce a fistula as an emergency measure.
The difference between intestinal or fecal fistula and artificial anus is that the former is an undesirable and untoward event, whereas the latter is deliberately produced by operation practised for the purpose. Artificial anus is in the main limited to cases of cancerous or other hopeless or inoperable obstruction of the lower bowel, and in such case is purely a palliative measure. It is made occasionally at the upper end of the colon in order to give a diseased colon physiological rest and permit of more perfect irrigation of that tube, the intent being to later close the opening. It is an inevitable emergency measure in certain cases of acute obstruction, where the patient is in no condition to bear anything more extensive or prolonged.
The operation for making an artificial anus, usually referred to as enterostomy or colostomy, will be described below.
Fecal fistulas should be treated largely according to their causes; when they are the product of actinomycotic or cancerous disease little can be done, and perhaps nothing should be. On the other hand, when resulting from traumatism, from sloughing of some portion of the bowel, or from strangulation, much can be accomplished.
A small, fistulous tract should be kept clean and stimulated occasionally with silver nitrate or something of the kind, and perhaps by introducing into it every day a small piece of gauze, which provokes the granulation process as well as fills the opening. It is bad practice, however, to simply close the outer end and let the lower portion distend with feces. Much will depend upon whether it now connects with the bowel. This may be determined by injecting into the fistula some methyl blue and then noting the subsequent stools. When communication with the bowel is evidently free the surgeon may feel like making a deeper operation, perhaps with intestinal suture or even intestinal resection, whereas if there be little or no actual fecal leakage it may be sufficient to enlarge the outer end of the fistula, to thoroughly scrape it with the sharp spoon, and then, lightly packing it, see it close with granulations. A passage-way which is exceedingly short may be treated by simple superficial plastic operation, including freshening of the entire margin of the opening and the passage around it, and a purse-string suture, with or without a circular incision of the skin. By drawing this suture tight the external opening may be closed. This is a neat way in which to dispose of a small fistulous opening resulting from a previous enterostomy or appendicitis operation.
A rectovaginal fistula may be closed by formal operation, similar to that for closure of a vesicovaginal fistula, based upon the simple principle of freshening the edges of the opening and then holding them together with suitably placed sutures. A rectovesical fistula would, in most instances at least, require a laparotomy, with careful separation of the rectum from the bladder, and then a separate suture of each opening. Such an operation might be quite difficult, made so not by its plan of performance but by the conditions which necessitated it. Any bladder thus attacked should be kept perfectly empty for several days by the use of a self-retaining catheter. Every case of fecal communication with any large abscess cavity, or through the diaphragm, directly or indirectly, as with a bronchus, should be treated on its individual merits, it being a grave question whether operation would be indicated or not.
Certain fecal fistulas will justify more formidable operation, in which, after opening the abdomen and carefully protecting its contents against contamination, the adhesions should be separated entirely and that portion of the bowel which is involved removed, making either an end-to-end suture or a lateral approximation. If this be done it will be best also to completely excise the old fistulous tract through the abdominal wall, and to remove everything that was involved in the previous condition.
It is possible to atone for almost every opening of this character, save those produced by some seriously malignant disease. If such a condition be the result of cancerous extension then it is practically hopeless.
—Intestinal suture is by no means a new or modern operation. It was spoken of by the ancient writers and was evidently practised in the middle ages by the “Four Masters” of the School of Salernum and their followers. But until[841] it was reduced to a science by the French surgeons, Jobert and Lembert, during the first quarter of the past century, it was always a hazardous measure. Success with intestinal suture depends upon exact hemostasis of the edges to be united and their accurate approximation in layers (i. e., mucosa to mucosa and serous and muscular coat to its like). Save when haste compels, this accurate application is effected by two distinct suture rows, the first or deeper (of hardened gut) made to include the mucosa alone, the suture being usually continuous, but knotted at intervals, with stitches close together and drawn tightly to amply secure against leakage from the relatively large vessels of this membrane. It is better to apply this row by itself, as any suture drawn through the mucosa and out again through the serous coat is liable to contaminate the latter, it being much better to keep the contaminated row of sutures distinct. The first row having been applied and the surface carefully cleansed the operator may then coapt the balance of the annular wound by a continuous row of fine silk sutures, made to include the serous and muscular coats and to avoid the mucosa. The stomach and the colon are sufficiently thick to take a row of rather coarse sutures for this purpose, but most of the small intestine is so thin-walled that these need to be applied with caution as well as with dexterity.
Every row of sutures should be so applied and directed that the lumen of the bowel be not reduced by its presence, it being a serious matter to greatly encroach upon the diameter of the bowel, since obstruction will thereby be favored and extra tension made upon the sutures (Figs. 564 and 565).
Fig. 564
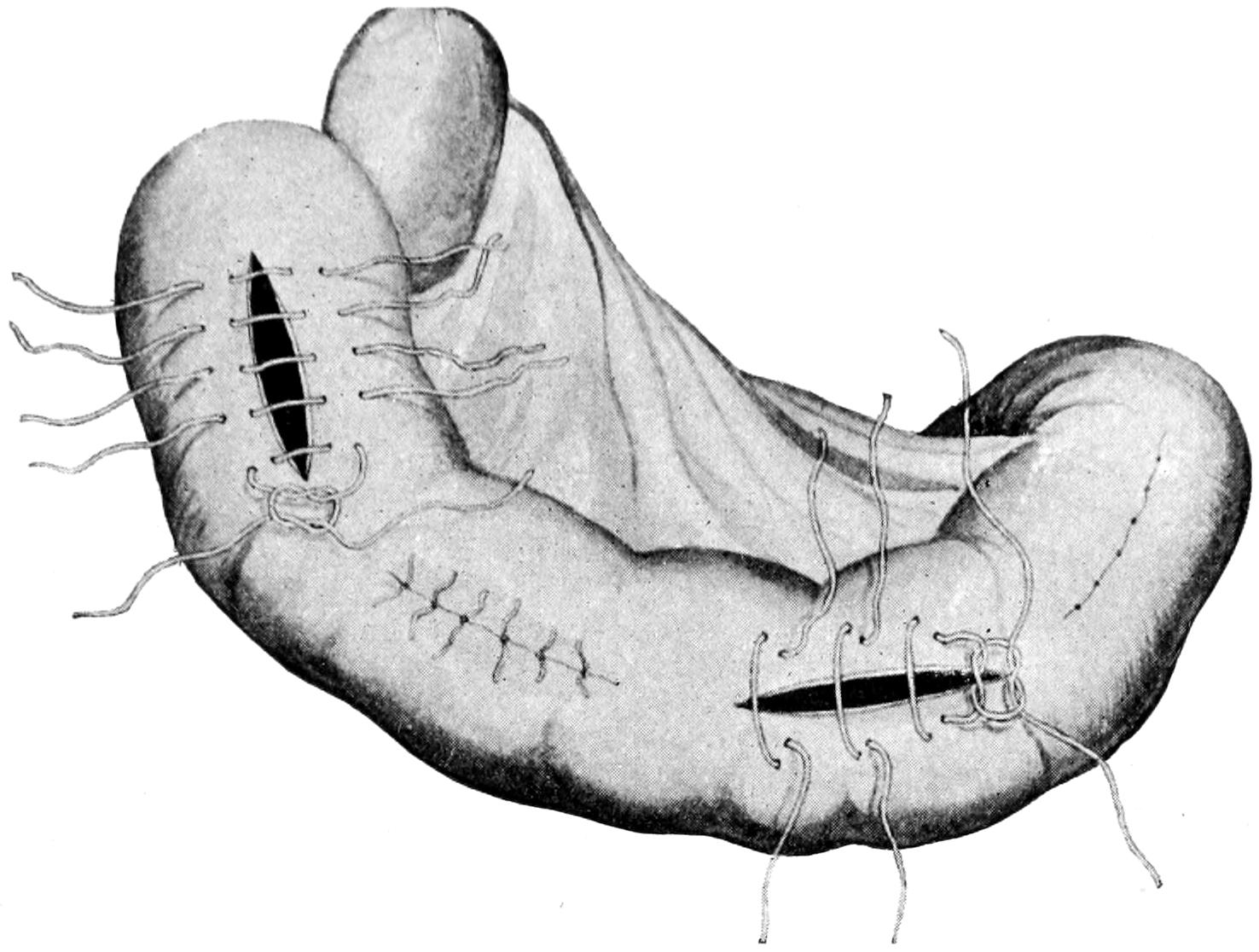
Application of the interrupted Lembert suture. (Richardson.)
Fig. 565
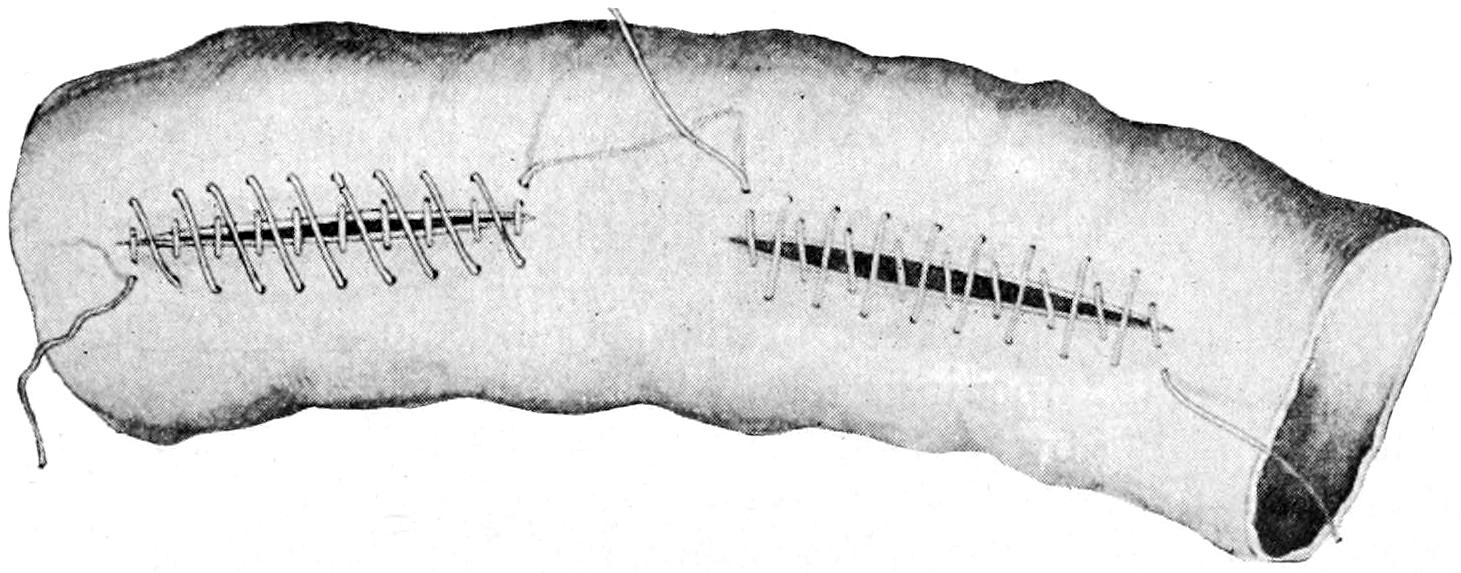
The continuous Lembert stitch. (Richardson.)
So many different forms of intestinal suture have been devised that it is useless to attempt here to describe them all.
[842]
Any minute puncture of the bowel may be closed by purse-string suture. Any perforating wound should be not only first carefully cleansed, but also slightly enlarged, cutting away its more or less contused margins in order that fresh, viable tissue may be exposed. This is particularly true of gunshot wounds. Many of the operations now practised include inversion of the end of the bowel, a method illustrated in Fig. 566, showing a method equally applicable to burying the stump after removing the appendix, closing the end of a portion of the small or even the large bowel.
Most operators now use for the mucosa a carefully prepared and reliable chromicized catgut, the smaller size being preferable, with the ends cut short after the knots are tied. It is well also to use for intestinal suture needles which are round rather than made with cutting edges, as by the latter openings are made larger and vessels sometimes cut, this requiring the insertion of extra sutures for their securement. Whether the operator shall use curved or straight needles, and shall do the work with his fingers or depend upon various forms of needle holders, is purely a matter of choice and training. Success or failure depend not so much upon the needle holder as upon the holder of the needle, and his care and attention to detail. In the presence of multiple lesions the procedure may have to be repeated to meet each indication.
—For the general application of the principle of anastomosis to intestinal work the profession is largely indebted to Senn. The principle having been once recognized will never be rejected, but methods have already varied much from those first introduced, and will be improved by the substitution of simpler procedures for the more complex.
In general an anastomotic opening may be made between any distinct portions of the alimentary canal, and almost any one part may be thus, as it were, connected up with any other. Gastrojejunostomy has already been described. Only under compulsion does one thus connect the stomach with any other part of the alimentary canal. From the jejunum down to the rectum one may, however, effect attachments of this kind at any desired point. These operations are in the main done for one of the following purposes:
The method of performance will depend not so much upon the nature of the difficulty requiring the operation as upon the condition of the patient, the equipment, and the operative skill of the surgeon. With a patient in extremely serious condition that method which may be most quickly performed is obviously the best. When time and method are under control, then that is best which can be most perfectly performed by the operator, or that which he is compelled to adopt, as when, for instance, he resorts to a suture method because he has no button at hand.
In order to simplify the subject as much as possible the following methods alone will be mentioned here:
The method by suture is essentially similar to that described as gastro-anastomosis, the surfaces which are to be brought together being properly placed, and approximated, first, by a row of silk suture, the openings being then made with excision of a strip of mucosa, and the mucosa being next sutured with chromic gut, first on the further side, then on the near side of the opening, after which the serous membranes are accurately sutured around the opening by continuation of the first row of silk sutures. The actual opening made for the purpose should be at least an inch in length, preferably an inch and a half or more, while when the lower bowel is attached to the colon such an opening may well have a length of at least 2¹⁄₂ inches, for if successful it will be followed by a certain degree of cicatricial contraction and will never remain of its original size (Figs. 566, 567, 568 and 569). The suture may be combined with the elastic ligature, the method again being similar to that for uniting the jejunum with the stomach, already described. The rubber ligature used for the purpose is of the same size, and there is no difference to be made in the directions already given. The elastic ligature, however, can not be relied upon in emergency cases where it is necessary to effect a communication at once. It is serviceable only in instances where there is a leeway of at least three or four days. This method has for one of its advantages the fact that in its performance it is not necessary to clamp or secure the bowel by any instrument, simply to empty it[843] for the moment with the fingers, it not being opened during the operation by anything save the needle puncture, which is promptly filled with the rubber. It does require, however, that the rubber used for the purpose shall be reliable and new, it being[844] unfortunately the case that pure rubber which will last for a long time is seldom found in the market.
Fig. 566
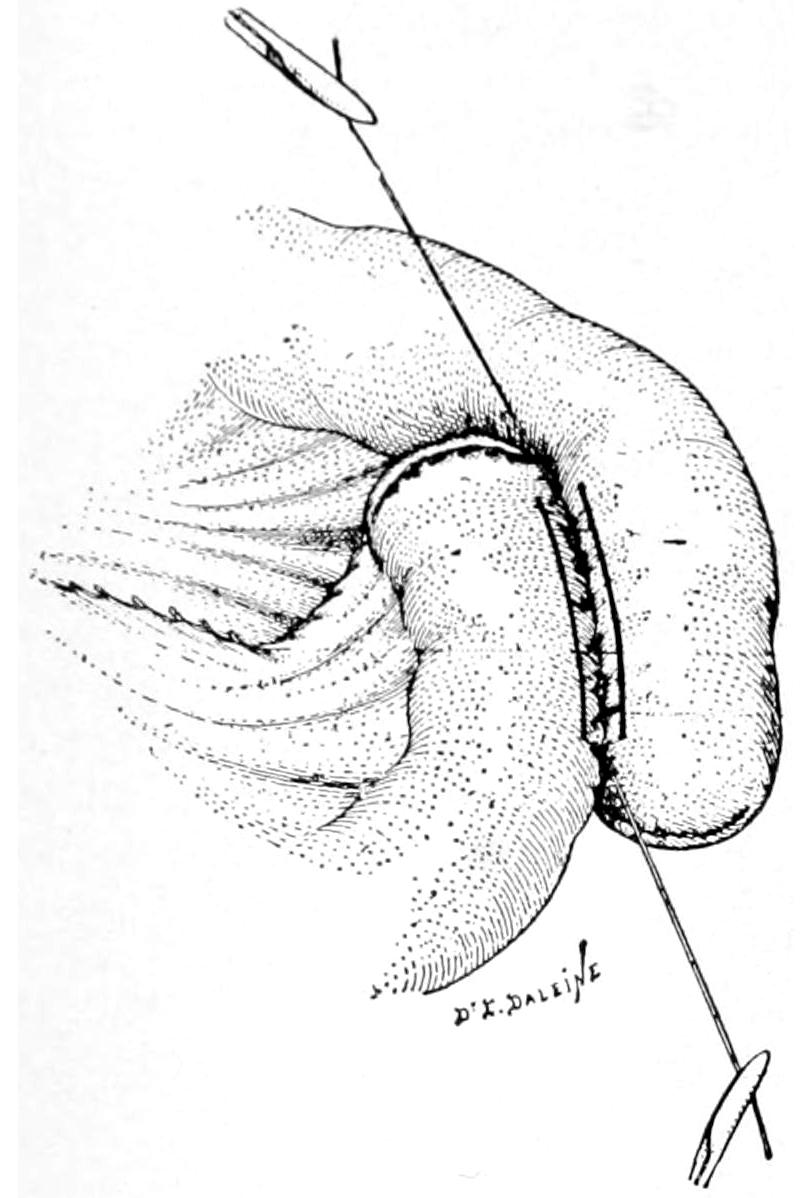
Entero-anastomosis of intestinal loops which have been resected and the bowel ends closed; the first row of sutures has been applied and the line of opening indicated. (Lejars.)
Fig. 567
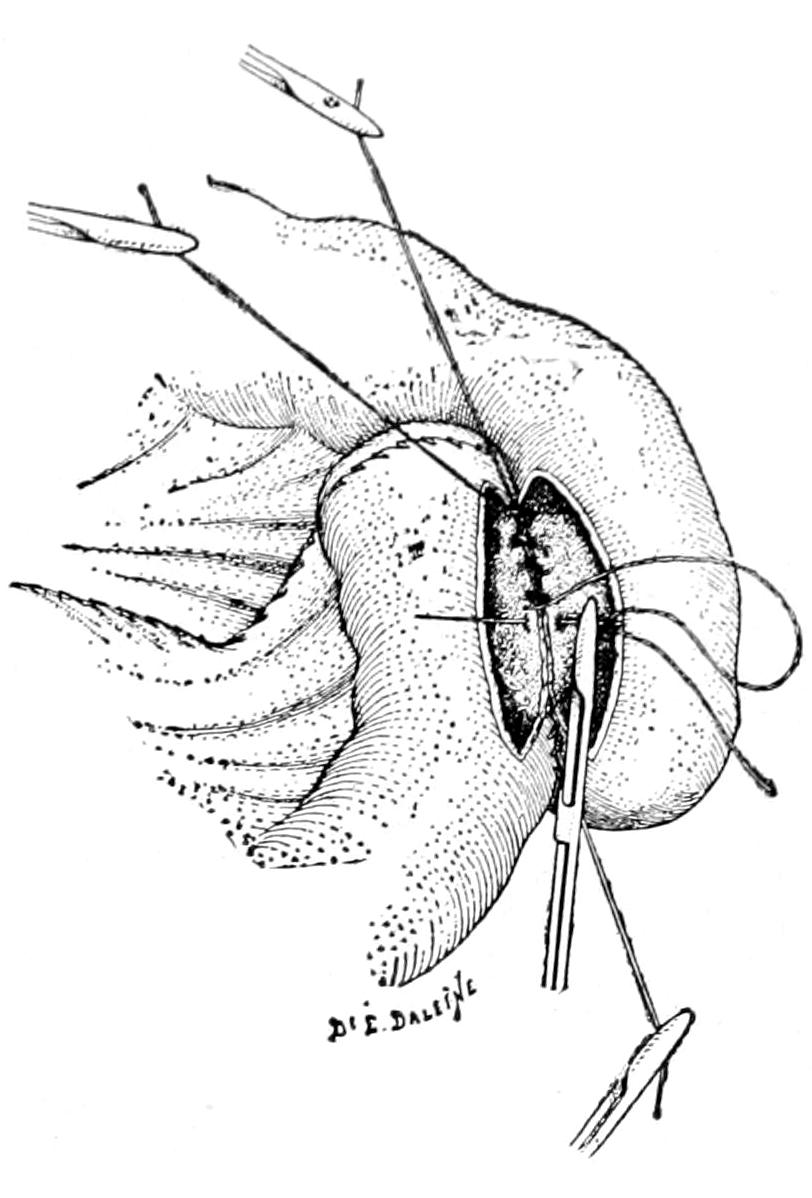
Suture of the distal edges of the mucosa.
Fig. 568
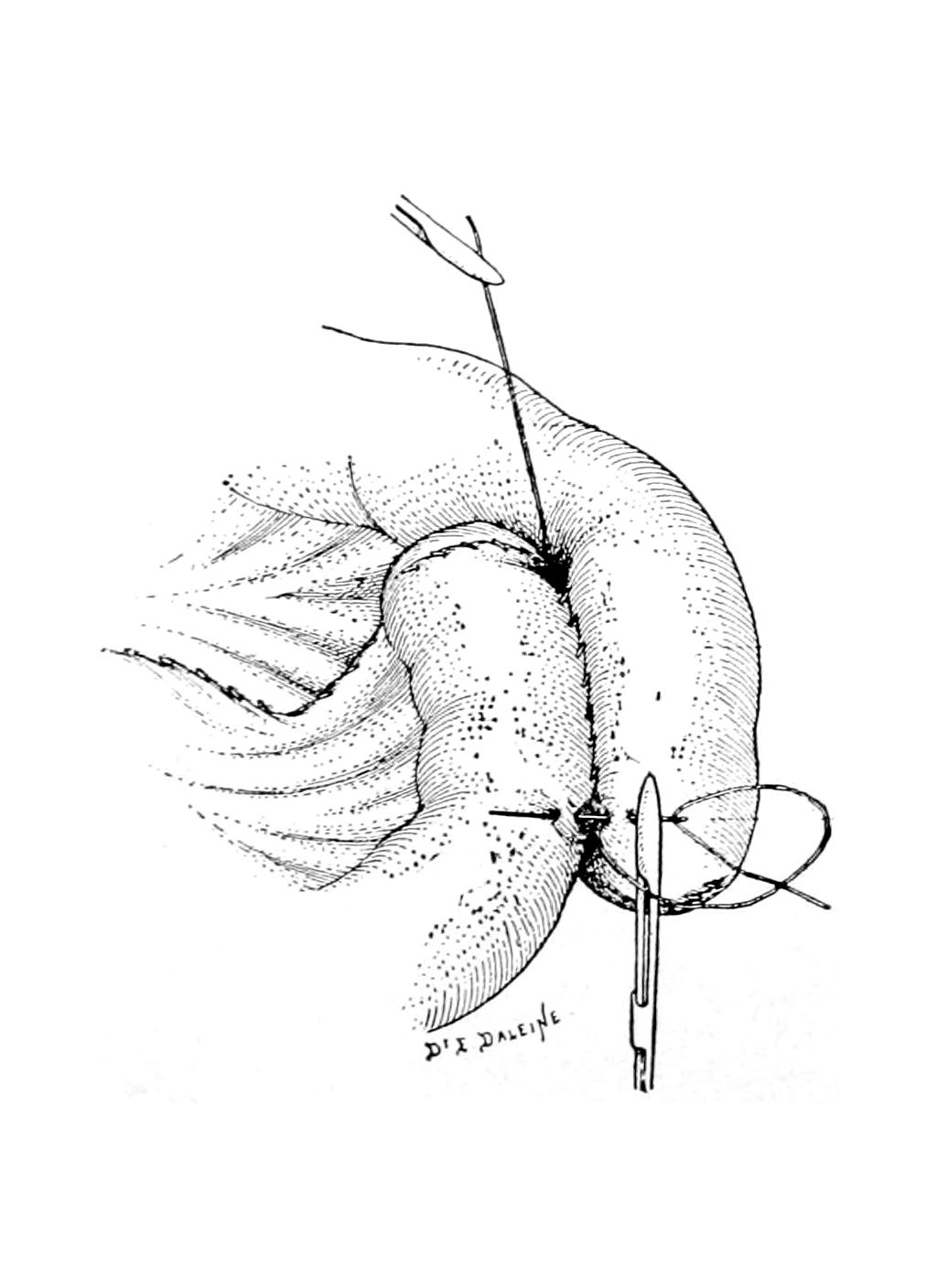
Insertion of the last (fourth) row of sutures. (Lejars.)
Fig. 569
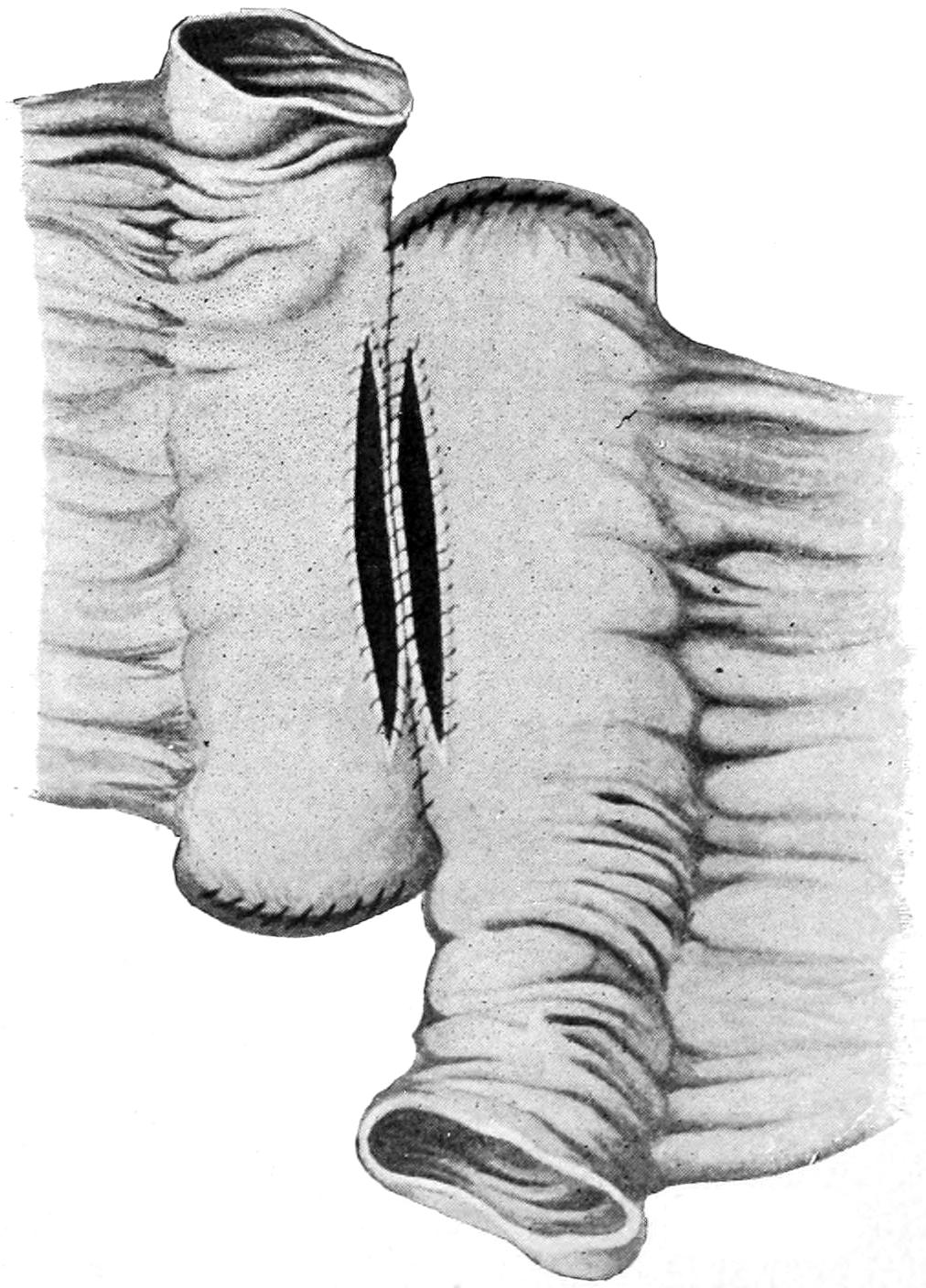
Resection of intestine with lateral anastomosis. Posterior suture inserted. The free ends of the bowel inverted and sutured. (Richardson.)
The button method depends for its success upon a mechanical device of Murphy, known everywhere as the “Murphy button,” or upon one of its modifications. Fig. 570 illustrates the component parts of this device, which is made in various sizes and, in fact, in various shapes for different purposes, though the circular forms suffice for practically all cases. In Fig. 572 it is seen in actual use, while Figs. 573 and 574 illustrate the method of its insertion and securement.
Fig. 570
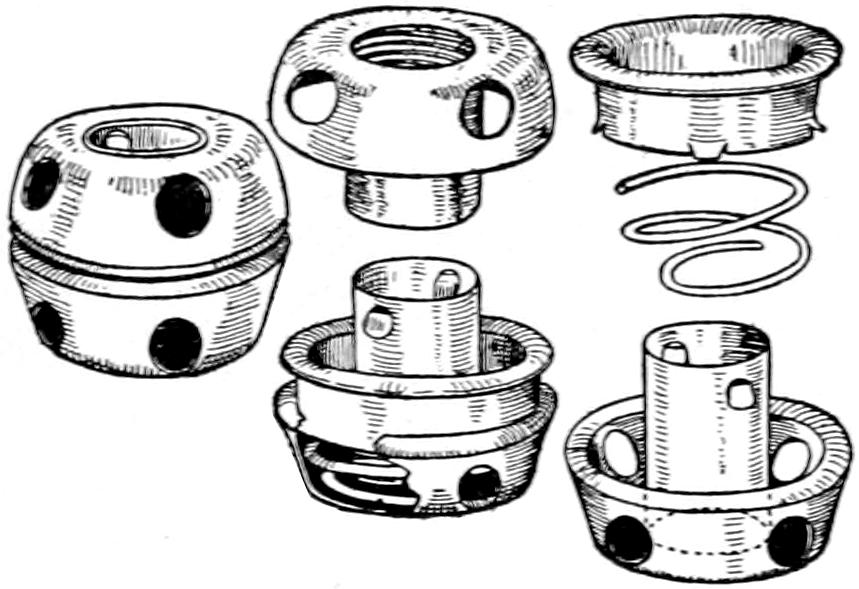
The Murphy button.
Fig. 571
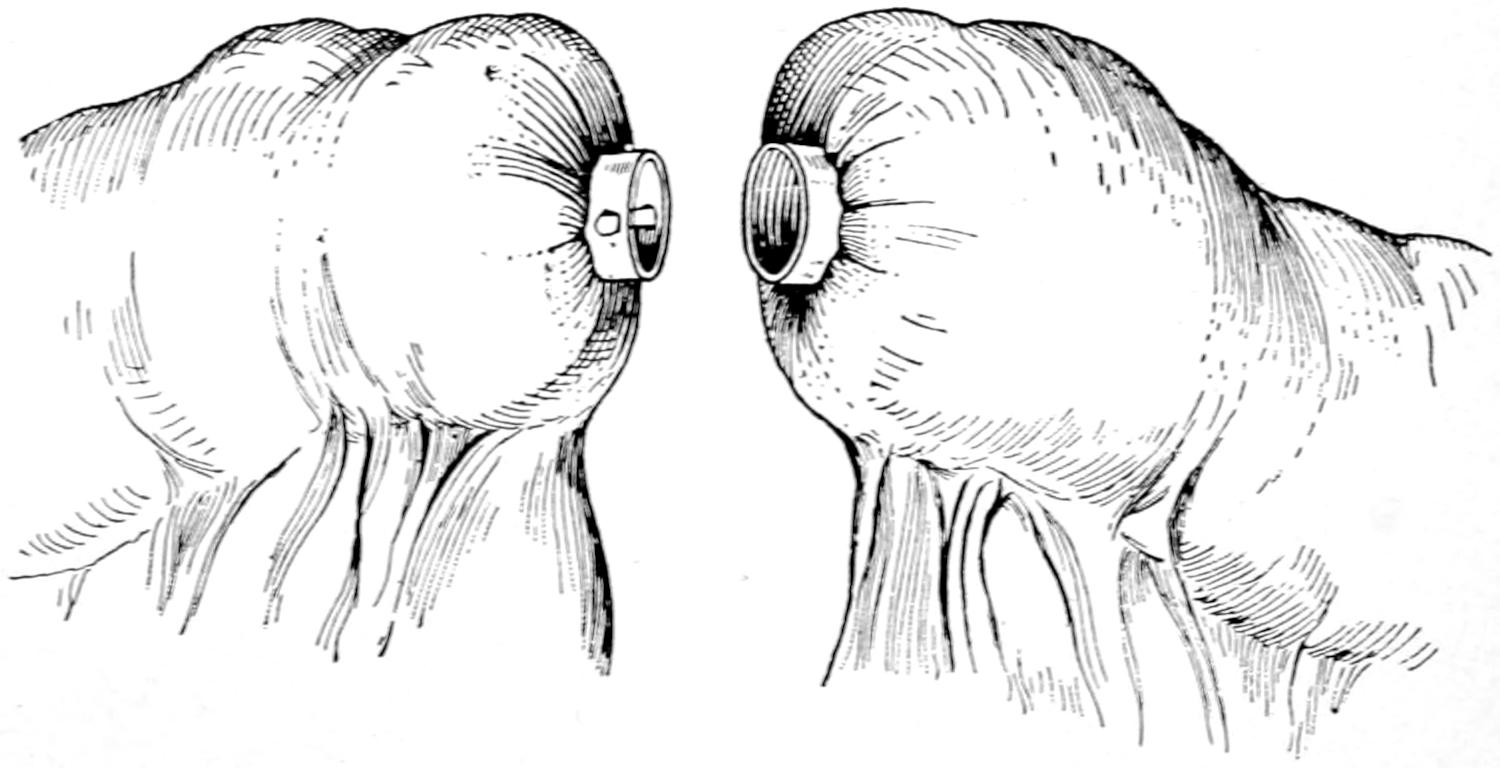
End-to-end union of intestine by means of the Murphy button: the two portions of the Murphy button, held in position by purse-string sutures, are ready to be pressed together. (Richardson.)
Fig. 572
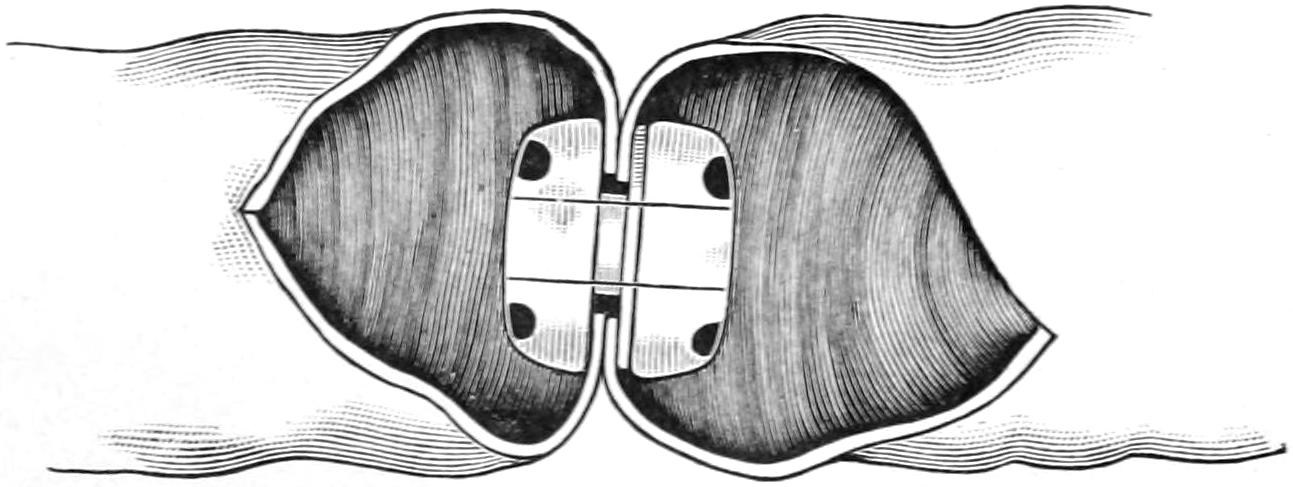
Union—end to end—with the Murphy button.
The underlying principle of the Murphy button is that each half can be inserted separately and that then, by pressing these halves together, an opening is at once afforded from one part of the bowel to the other. If the halves be pressed together with the proper degree of firmness they produce, first, adhesion between considerable areas around their circumference, followed in the course of a few days by a necrosis of the central portion, which sloughs because deprived of its circulation by the pressure. So soon as this separation or sloughing is complete the button drops into the intestinal canal, being completely loosened, and is now carried along by peristalsis and by the fecal current from above, its position shifting as would that of a scybalous mass or a fecal concretion, until it finally emerges from the intestinal tube, being passed from the anus. How soon it will thus appear will depend in large measure upon the point of the intestinal canal into which it is thus intruded. If this be high up it will be slower in appearing. If low down it may be expected sooner. While it usually appears within ten days or two weeks it may, however, be longer retained, and in one case of my own was not[845] passed for three months, although the anastomosis was made with the ascending colon, into which it must have dropped.
Fig. 573 shows one of the halves held in the grasp of a forceps, being inserted into a small buttonhole opening just large enough to receive it, around which there has been passed a buttonhole or purse-string suture of silk. This portion once thus inserted should not be lost within the bowel, it being necessary to retain control of it by the forceps until its application to the other half. Both halves being inserted and brought opposite to each other, as in Fig. 574, the smaller is introduced into the larger, and they are then pressed together until the included serous surfaces are brought into contact, with sufficient pressure inflicted to bleach them, in order that their subsequent necrosis may be ensured. A circular row of sutures should now be placed around the surfaces thus applied, in order to more widely secure them in contact. The procedure being completed in this way, the parts are dropped back into the abdomen and the abdominal wound closed.
Fig. 573
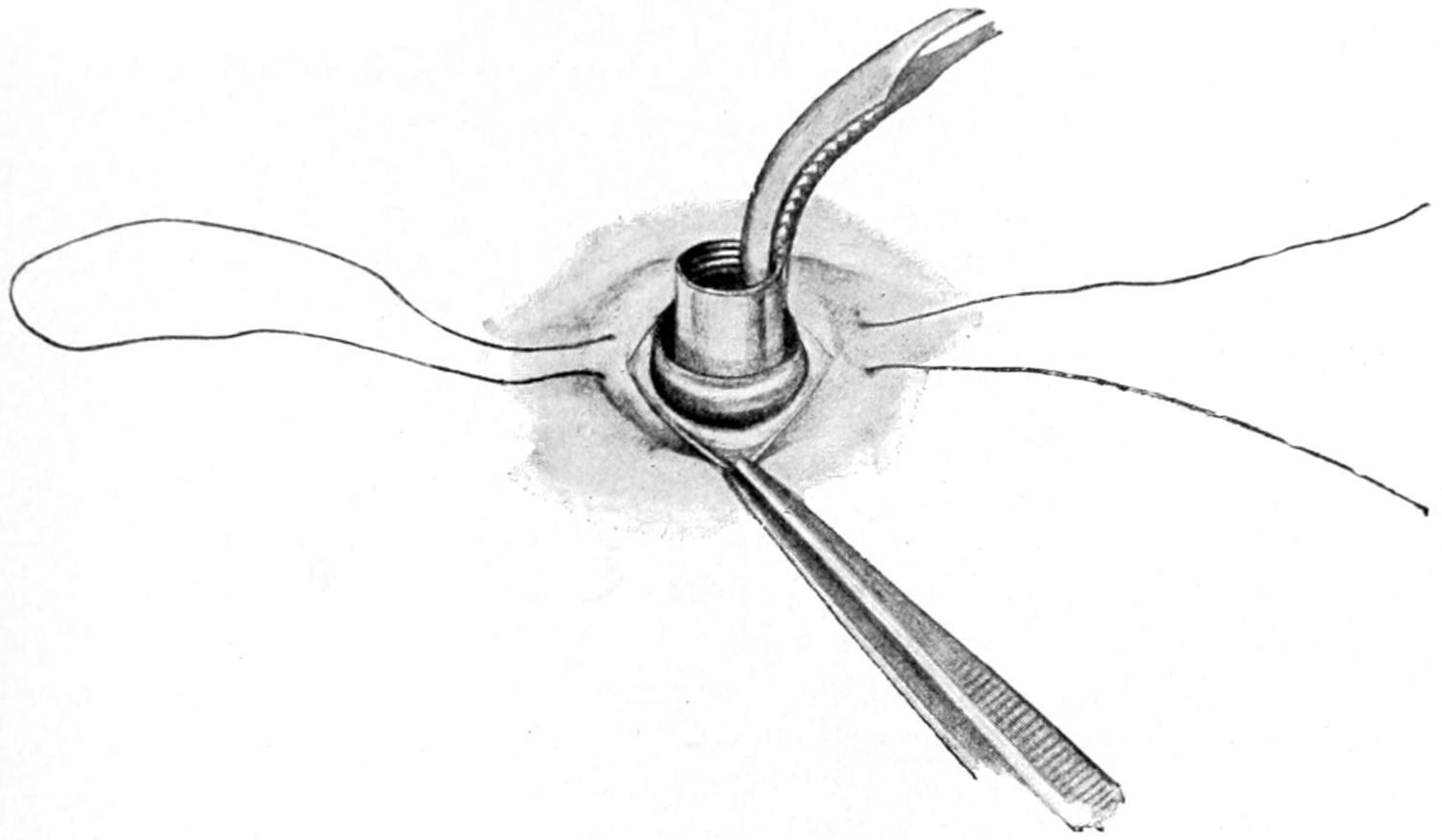
Introduction of one-half of a Murphy button. (Bergmann.)
Fig. 574
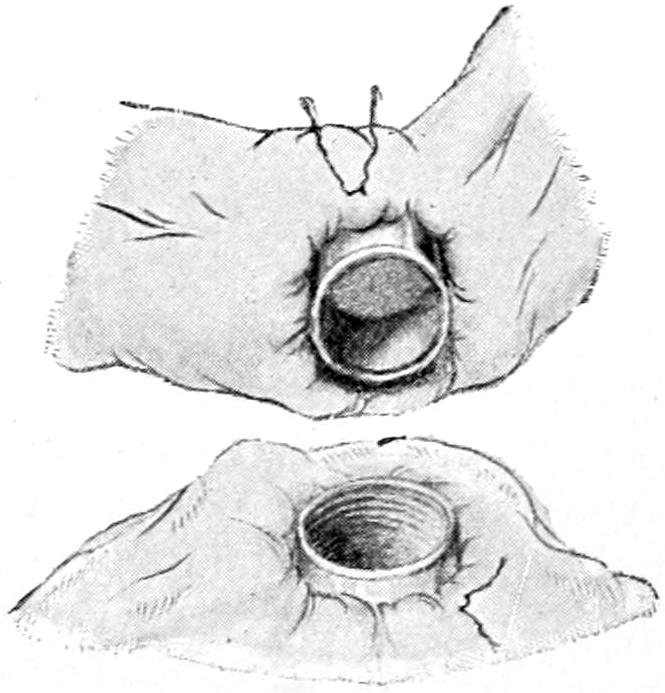
Intestinal anastomosis with a Murphy button, showing the halves in position ready to be pushed together. (Bergmann.)
End-to-end reunion can be accomplished by the same method, or the end of the small intestine may be applied to the side of the large, after a method which will be best understood by reference to Fig. 571, it being necessary here to draw the squarely cut end of the intestine around the button with a circular suture, and, at the same time, to so grasp the button that it shall not recede into and be lost in the bowel.
Small buttons have been made for the purpose of uniting the gall-bladder to the upper bowel and extra large ones are made for the large intestine.
The particular advantage of the button method is the shortness of the time required for its performance, as it can be conducted in a few moments by one who might take four times as many minutes in using sutures. The disadvantages attaching to it are these: (1) That it depends for its success upon necrosis, i. e., of the part of the bowel included within its grasp; (2) that it might itself serve as a foreign body and produce acute obstruction, a not unknown event; (3) that it is not always at hand, especially in emergency cases, and that to rely upon it is to be limited in one’s abilities.
There is but little question that, when properly performed, the simple suture methods are the best of all, and the operator who has never seen a button used should abstain from its use. Still it has given many good results. My belief is that the better the surgeon’s judgment, and the more developed his skill, the less he will rely upon any[846] mechanical expedient of this character, and the more upon what he can accomplish with the needle in his own fingers.
End-to-side anastomosis is in no essential respect different from resection, only it may be done for the purpose of exclusion when nothing is absolutely removed. Thus in case of cancer of the cecum a lateral implantation can be made of a lower loop of the ileum upon the side of the ascending colon, using for this purpose a button, having divided the ileum on the proximal side of the ileocecal valve, and turned in both ends and invaginated the stumps. Here one resects nothing, but makes a direct communication between the bowel above and below the cancer, short-circuiting the intestinal canal, as electricians would say, and all for the purpose of giving temporary relief. Thus end-to-side or end-to-end anastomosis may be made, according as circumstances dictate, and, if one chooses, with the Murphy button.
Resection of some portion of the large or small intestine is required under a variety of different circumstances. Thus after certain injuries, contusion and rupture, or numerous punctures or gunshot perforations, it may be decided to remove a considerable length of bowel rather than be compelled to give special attention to a number of distinct lesions, believing it a time-saving measure, and, therefore, for the welfare of the individual. The same measure will be indicated when, either by injury or disease, the blood supply of any portion of the bowel is apparently compromised or certainly shut off. Here necrosis is so certainly to be expected, or perhaps has already occurred, in such a way as to necessitate removal of whatever length of bowel may thus be involved. Several of those cases, already mentioned, which produce obstruction of the bowel will demand resection, as, for instance, when reduction of an invagination is impossible, with gangrene threatening. In a few instances extensive gangrene, precipitated by embolism or thrombosis of the mesenteric vessels, has been successfully treated by resection of considerable lengths of bowel. Again, the bowel is resected for closure of fecal fistula or artificial anus, as well as for relief of stricture due to various causes. Finally, nearly all of the tumors of the intestine itself, and especially all of the malignant forms, will require removal of at least a few inches of gut, save in those cases where this is shown to be impracticable because of the presence of cancer elsewhere, in which case it may be sufficient to make an anastomosis.
When intestinal resection is not an emergency measure there should be as much preparation as the case will permit, including lavage of the stomach, the ingestion of sterilized food, the use of antiseptics and the most thorough emptying of the bowel which can be accomplished.[58]
[58] Sanderson has suggested a new method of sterilization of the interior of the bowel at the time of operation. He injects a solution of acetozone through a hypodermic needle, or, after opening the bowel, freely irrigates with the same.
One of the greatest difficulties attendant upon the operation is the avoidance of all contamination by contact of peritoneum with intestinal contents. Against this the most minute precautions should be taken. This is never an easy matter, and in the presence of distended bowels and the emergency of acute obstruction it sometimes taxes every resource at hand. A variety of clamps have been devised by different operators, the intent being to so clasp the bowel beneath their blades as to completely occlude it. These blades are covered with sterilized rubber tubing to keep them from acting too harshly, and it is necessary to use pressure upon the handles with great discretion, lest permanent injury be done to the bloodvessels. The bloodvessels of the bowel are essentially terminal, and the blood supply should be kept sufficient for every part which is not removed. These vessels are, moreover, numerous and relatively large, and hemorrhage is not always easy of control, especially when clamps are not at hand. As a substitute for clamps tapes of sterilized gauze may be used, being tied around the bowel, or the fingers of a reliable assistant may be substituted. Such use of the fingers is not easy nor simple, not only because they become tired and relax their grasp, but since they slip so easily, and because the escape of one drop of fecal matter may cause a fatal contamination.
Resection of the bowel may imply in one case a removal of but two or three inches of its length, while the other extreme is not reached until several feet of bowel have been removed. I have been able to successfully remove eight feet and nine inches of intestine, the lower part including the cecum and a portion of the ascending colon, and there are now on record nearly twenty cases where over 200 Cm. of bowel have been resected, nearly all of them recovering. Success in this procedure depends partly upon the condition[847] necessitating the operation, as well as the general condition of the patient, but in no small measure hangs upon the perfection of the operator’s technique.
Fig. 575
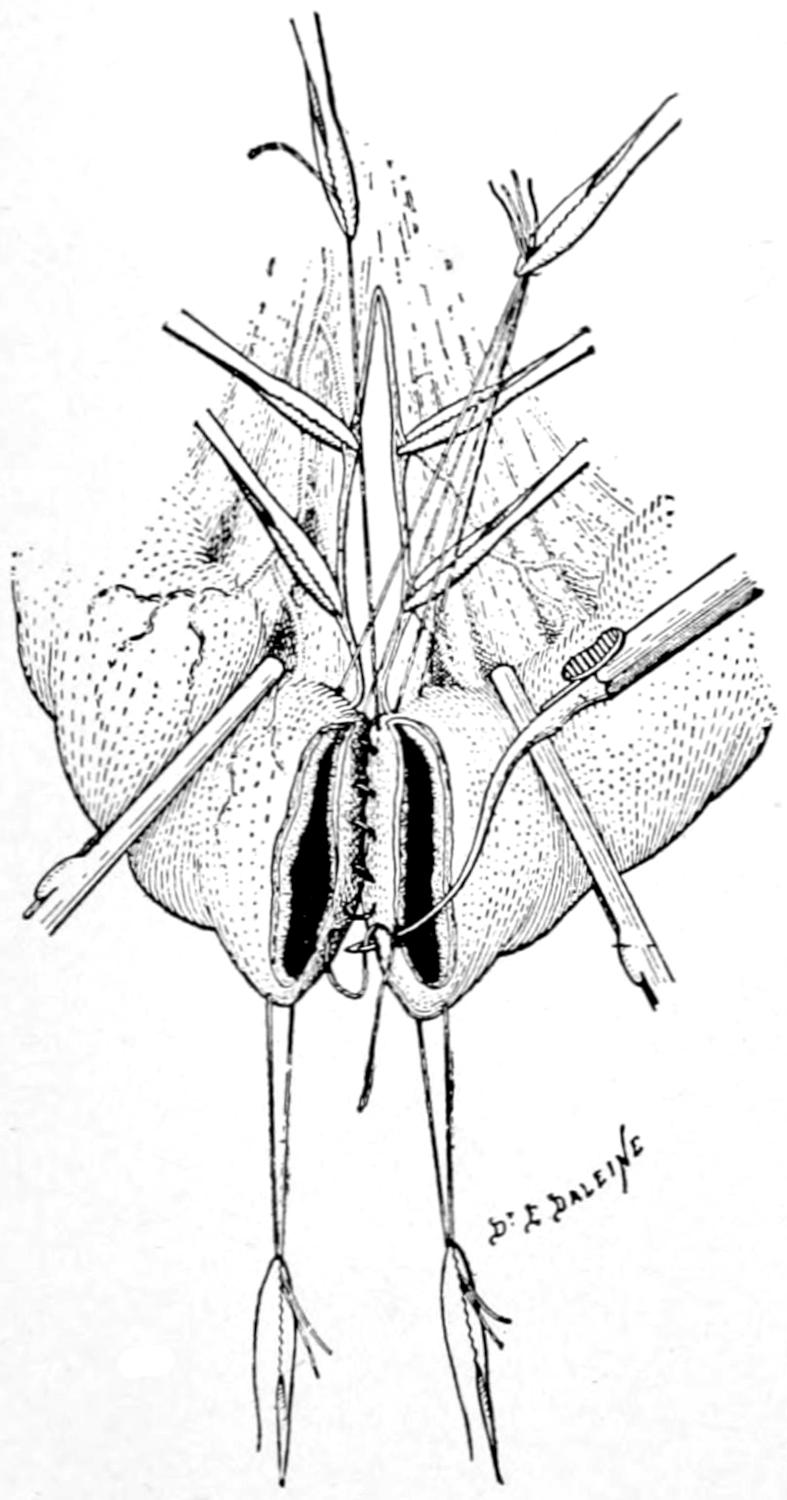
End-to-end or circular anastomosis by enterorrhaphy. First row of distal sutures in serosa. (Type of needle differs from that used in this country). (Lejars.)
Whatever be the condition which requires such resection it should be made sufficiently extensive to completely include and permit the total removal of the diseased or injured portion. The abdominal incision should be large enough to permit the delivery upon the surface of the body of all that portion to be removed. Unless this be done the difficulties are greatly enhanced. Save where there is some distinct indication for opening elsewhere, this incision is made in the middle line. The compromised bowel having been sought and thus delivered and one having decided exactly where to divide it, clamps are so placed both above and below each line of division as to prevent leakage. Underneath the bowel to be thus divided gauze is placed in such a way as to receive the small amount of discharge which will escape from the portion between the clamps. The exposed bowel surfaces should then be thoroughly cleaned, the contaminated gauze removed, fresh pieces substituted for it, and the other division of bowel made in the same way. While in some cases it may be well to tie off the mesenteric border and secure all its vessels before dividing the bowel, this may at other times be delayed until after the division. At all events it is the next step. Whether the mesentery shall be simply separated along the intestinal border and tied off in small portions, one after another, or whether a triangular resection of a portion of the mesentery itself should be made, securing the larger vessels nearer to its root, will depend on the nature of the case and upon whether the mesentery itself be involved in the disease. In dealing with cancer it is often necessary to remove, at the same time, every enlarged lymphatic. It may be inferred that no incision or tear, no matter how short, can be made in these tissues without danger of subsequent hemorrhage unless the parts be secured against it. A series of ligatures[848] and sutures is therefore called for here which may consume no small proportion of the entire time of the operation. (See Figs. 575 and 576.)
All that portion of bowel which has been condemned having been removed and a careful toilet of the parts having been made the surgeon next proceeds to restore the bowel lumen. A V-shaped defect in the mesentery should be united with sutures. The line of former mesenteric border left after removal of bowel should be not only carefully protected with ligatures, but the whole margin should be overcast and so folded in or drawn together in tucks as to make it easy to bring the bowel ends together without undue stress.
Fig. 577
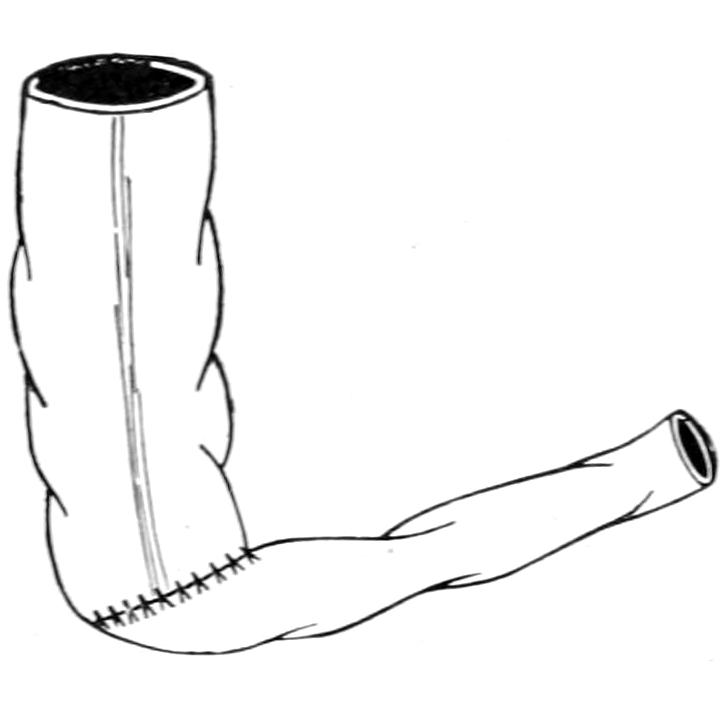
Fig. 578
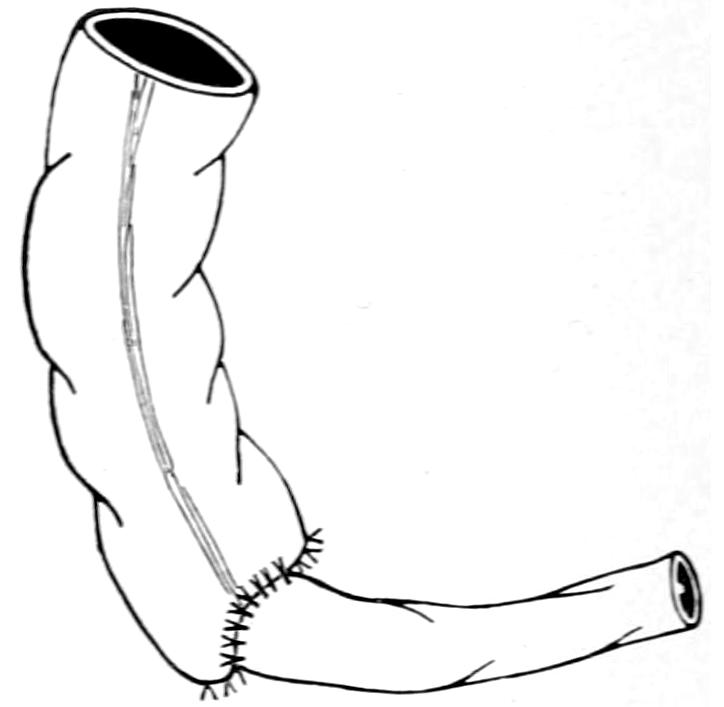
Circular anastomosis of portions of the bowel having different lumina. (Bergmann.)
The sutures by which the divided bowel is restored should begin at the mesenteric border, and every care should be taken to make the joint at this point absolutely water-tight. Suture methods have been described. To unite bowel ends of the same diameter it is an easy matter to suture together first the mucosa and then the outer layer, so long as the intestine is on the outside of the body and equally accessible on all sides (Fig. 578). The surgeon is sometimes compelled to do this work within the body cavity, as in resection of the rectum for cancer. It may be advisable to first place a row of sutures between the serosa and muscularis on the further side of the margins to be united, then to close the mucosa completely around, and then to finish the outer layer of sutures. So long as differences of size are not conspicuous, end-to-end approximation can be made almost anywhere. When, however, it is necessary to attach small bowel to large, the size of the larger opening should be reduced to fit the smaller, or one or both ends may be closed, turning in the stump, as already described, and then making lateral or end-to-side anastomosis. Any such anastomotic opening should be so placed, and bowel so directed, that there shall be no interference in the direction of the natural bowel stream, failure to observe this precaution producing not only added immediate danger but more or less permanent obstruction (Figs. 579 and 580).
Fig. 579
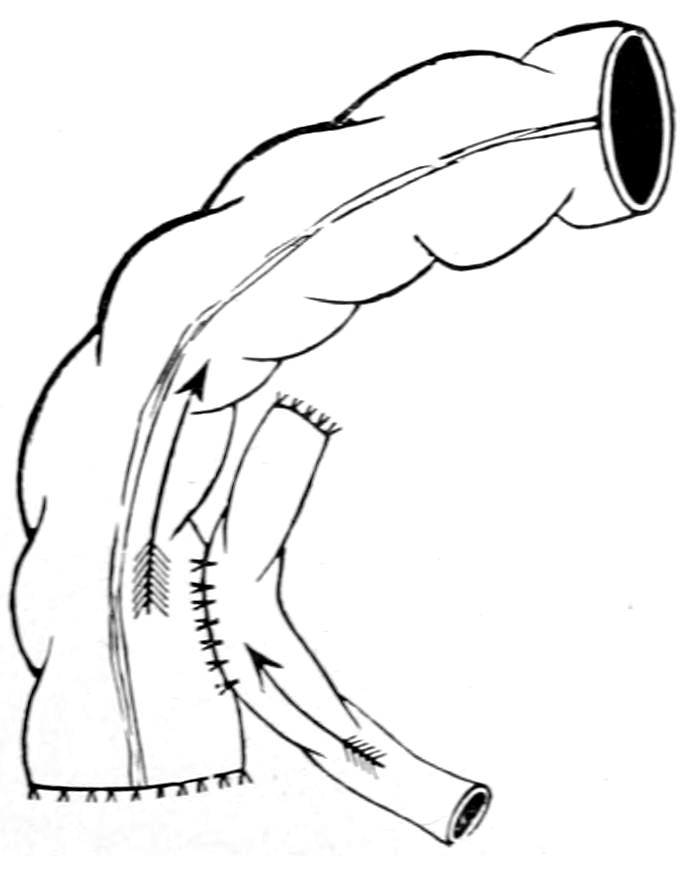
Isoperistaltic lateral apposition.
Fig. 580
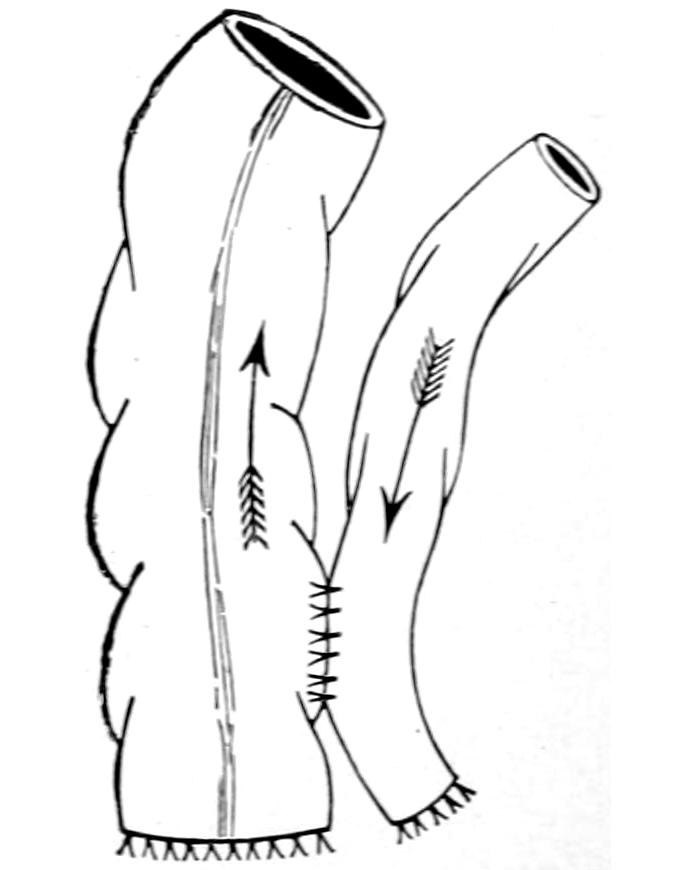
Antiperistaltic lateral apposition (bad).
[849]
All that has been said above with regard to the Murphy button and its use in anastomotic operations holds equally good here with regard to its usefulness after resection.
Numerous devices, either instruments for the purpose of holding the bowel together while it is sutured, or of affording substitutes for the Murphy button, have been planned by operators all over the world. There are few of them, however, which give any better results than the simple methods above described, to which I prefer to limit description here because of their very simplicity.
Intestinal suture or any other method of completing the resection having been finished, a careful toilet of all exposed parts should be made, by which bowel may be dropped back into the abdominal cavity and the latter closed without drainage.
The subsequent management of these cases will consist in two or three days’ starvation, in order that peristalsis may be reduced to a minimum, the patient being meanwhile fed by the rectum. Then will come a time when both fluid food, and cathartics a little later, should be gently and discriminately administered. Any satisfactory suture method will rarely give way after forty-eight hours. Buttons, on the contrary, may break loose after many days or even weeks, and this fact affords another argument against their use.
Fig. 581
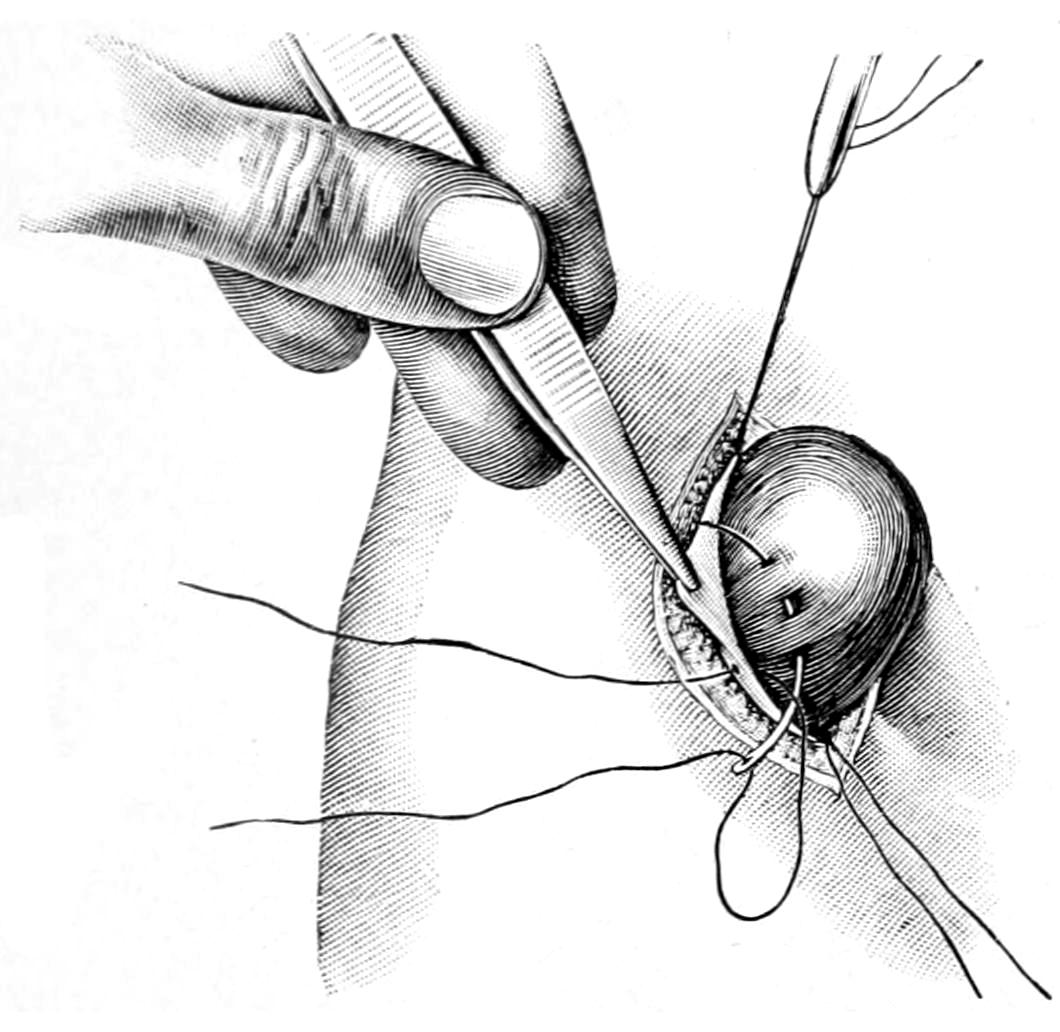
Enterostomy; preliminary fixation of a loop of bowel to the peritoneum. (Lejars.)
Fig. 582
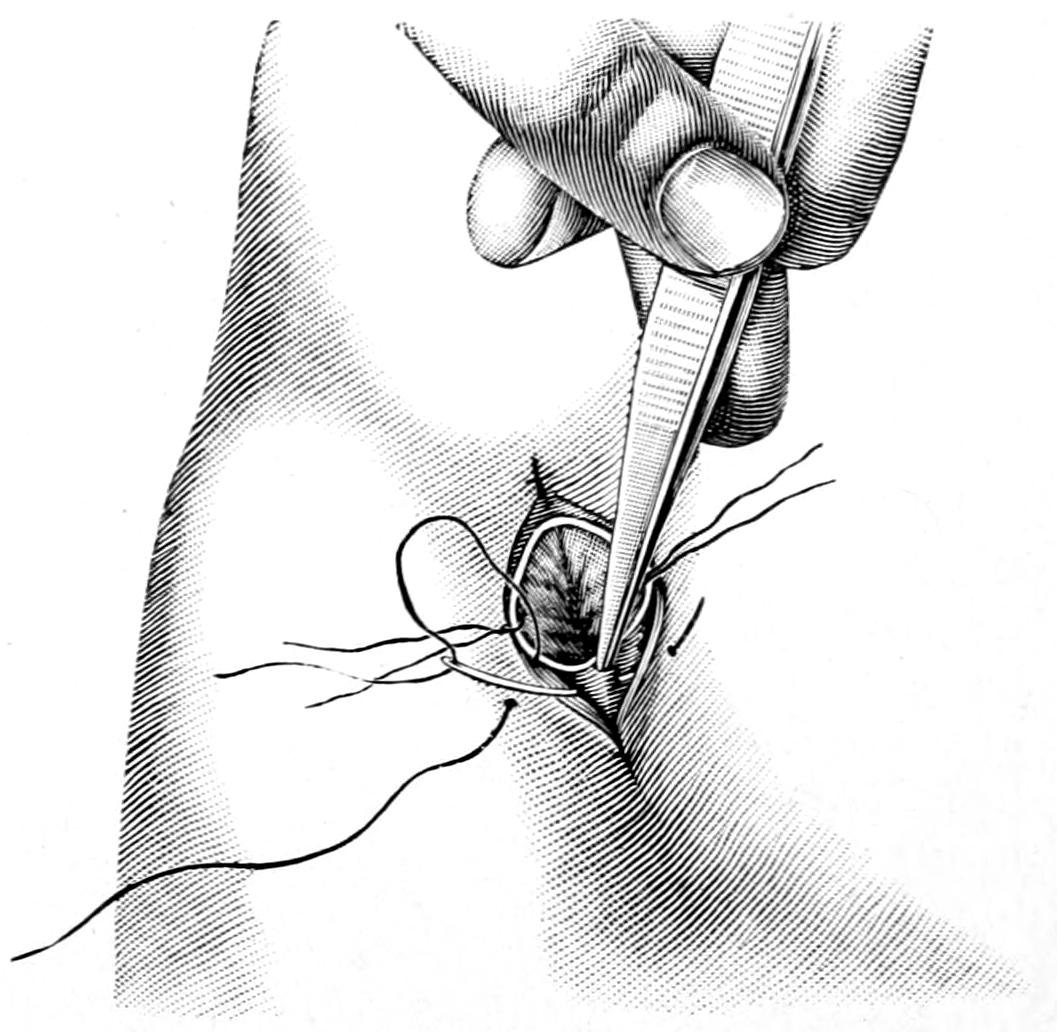
Enterostomy; fixation of margins of opened gut to skin. (Lejars.)
—Enterostomy for establishment of fecal fistula, or artificial anus, is performed for relief purposes and sometimes as an emergency measure. It consists in attaching some portion of the bowel, naturally that above the constriction or disease which compels the operation, to the parietal peritoneum through a small wound in the abdominal wall. When the large intestine is opened for this purpose the operation is usually referred to as a colostomy, and this preferably is done in the left iliac region. When enterostomy of the smaller bowel is preferable it may be done at any point on the abdominal surface. Thus if through a median incision a condition be found necessitating it the bowel should be attached at the lower end of the abdominal opening, for here drainage will be better and contamination less likely. When enterostomy is done for acute obstruction, it is preferable to place the opening in one iliac fossa or the other.
Enterostomy consists essentially of the following steps: opening through the abdomen, recognition of the parietal peritoneum, which is seized with forceps on either side, opened and secured with these forceps, after which the first tensely distended loop of bowel which presents is taken, and, with a series of fine sutures in a round needle, the serous surface of the gut is attached to the margins of the parietal peritoneum (Figs. 581 and 582). In the more desperate cases a portion of the bowel may be brought out through the wound and fixed there in such a way that it cannot recede. If the emergency is great the bowel may be immediately punctured, the patient so placed and so protected that fecal contents shall escape away from the body rather than over it. If one can take a little time he may wait a few hours for the adhesion which is sure to take place between the peritoneal surfaces[850] and the consequent shutting off of the abdominal cavity from the outer wound. Thus after twelve hours the surface of bowel exposed through the wound may be punctured either with a knife, scissors, or the actual cautery, and this may be done without causing pain to the patient. Escape of bowel contents will instantly ensue after puncture. After permitting all to escape that will, abundant protection should be provided for the reception of the discharges, which will continue at reduced rate. The best way to do this is to pass into the bowel in the proper direction a rubber tube, as large as it can accommodate, or a glass tube, bent at an angle, which shall connect with a flexible tube, and thus conduct away all discharge.
Another method of performing the operation is to bring out the loop of bowel, open and empty it, then to introduce a glass or rubber tube, around which is snugly fastened the bowel margin. The intestine is then stitched in place and the tube so arranged as to conduct away all discharge.
Just how much may be expected of such a relief opening will depend upon the case. These operations, especially for cancer of the rectum or the lower bowel, may prolong life for two or three years. An emergency opening into the small bowel for relief of acute obstruction may need to be kept open for but a few days, after which the tube may be removed and the fecal fistula be allowed gradually to contract. According to the case an intestinal resection may be made or the opening may be closed by one of the plastic methods.
—Appendicostomy is the more complete form of carrying out a suggestion first made by Hale White, of opening the colon on the right side in cases of intractable colitis. Gibson suggested to accomplish this by a method similar to Kader’s for gastrostomy, making a valvular colostomy through which the colon might be irrigated, without escape of feces. In 1902, Weir, intending to do this operation, found the appendix rising so invitingly into the wound that the inspiration occurred to him, and was promptly acted upon, to utilize it for the purpose.
In performing the operation the smallest possible incision should be made through which the appendix may be delivered, its mesenteric artery is tied, and its mesentery stripped down to its origin. At the latter the cecum is fastened to the parietal peritoneum by a suture on either side, avoiding the appendicular artery itself. The balance of the wound is then closed as usual, the appendix being fastened to the lower angle by suture, the protruding part then wrapped with gutta-percha tissue and included in the dressing. At the end of two days the external portion may be divided about 1 to 4 inches from the skin, after which a catheter is passed along its lumen and the stump tied around it. This serves the double purpose of preventing leakage and severing the appendix flush with the skin. The catheter is introduced from 2 to 4 inches, and its external portion left open to allow escape of gas, or doubled and fastened to prevent leakage, as circumstances may require. Irrigation may be begun on the third or fourth day.
When the appendix is used for the purpose of forming an artificial anus it will be probably in instances where there is more of the emergency element present, and it may be sufficient then to simply utilize it for the purpose of anchoring the cecum to the abdominal wall, or with the purpose of dilating it after the expiration of a few hours. In other words, the method may be modified to meet the indication.
It is scarcely necessary to devote space to any other operative procedures upon the small intestine. Consequently it will simply be mentioned here that the upper part of the jejunum can be used for artificial feeding and jejunostomy made to take the place of gastrostomy under those rare circumstances which may demand it.
Upon the large intestine colopexy may be practised, attaching it to the anterior abdominal wall or to the border of the liver or the gastrohepatic omentum. Andrews’ suggestion to attach the colon to the lower border of the liver, after certain operations upon the biliary passages, will be described in connection with the latter. In cases of extreme dilatation, with loss of muscular tone, etc., involving especially the colon, an enteroplication may be practised corresponding to gastroplication, and having the same purpose, with a technique practically identical with the other. Thus when the sigmoid flexure is so dilated as to largely fill the abdominal cavity, with an enormous S-shape, much can be done by thus reducing its dimensions, the only objection being the fear that the causes which produced the condition will conspire to reproduce it even after enteroplication.
[851]
[59] The laity, as well as part of the profession, having not yet ceased to wonder at the great importance attaching today to appendicitis, when twenty years ago it was practically unknown, it is worth while to insert here the following brief historical account: The term “appendicitis” was coined by Fitz for a condition which had not been hitherto unknown, but to which he gave a classical description. That the appendix might be primarily diseased had been known for one hundred and fifty years; that peri-appendicular abscesses were frequent may be seen by reference to works of the middle and latter part of the past century on perityphlitis and perityphlitic abscess, Willard Parker, of New York, being the most prominent writer of his day upon this subject. In the Transactions of the Medical Society of the State of New York for 1875, Gouley reports a case of so-called perityphlitic abscess due to perforation of the appendix, with remarks upon its surgical treatment. The curious feature attaching to this case was that two years previous to its occurrence the patient had swallowed one of his teeth. Although this tooth was not found at the time Gouley alluded to the possibility of it or any other small body lodging in the appendix and finally causing ulceration. He referred also to the case published in 1856 by Dr. Lewis, of New York, who reported an individual dying at the age of eighty-eight, whose appendix was found to contain one hundred and twenty-two deer shot, it appearing that he had been exceedingly fond of game; he supposed that the shot found in the appendix were contained in meat which he had eaten. Lewis also referred to forty-seven cases of foreign bodies which he tabulated, all but one of which died.
Fitz’s article appeared in 1886. In it he claimed that operation should be done much earlier than was then the custom, and he showed that 34 per cent. of these cases died during the first five days of illness. But the first real operation for appendicitis as such was done by Krönlein, of Zurich, according to a suggestion made by Mikulicz in 1884. The second was done by Symonds, in England, in 1885, this being an interval operation. The first operation in the United States was done by Hall, of New York, in May, 1886, although to Morton, of Philadelphia, the credit must be given of the first operation in this country on a case deliberately diagnosticated. This was in April, 1887, Sands doing the next one in December of the same year.
McBurney had assisted Sands in a large number of cases, and in 1889 published his classical paper with an account of “The First Recorded Case where an Acutely Inflamed Appendix had been Removed while Full of Pus.” In the same year Weir also published an elaborate paper, making similar recommendations. It is not necessary to follow the subject later than the year 1889, since to it every surgeon of note has probably contributed.
—The vermiform appendix is an embryonic relic, and, like all such remains, is not merely superfluous, but often troublesome. That at some time it may have had an ordinary function is not to be denied; that now, in quadrupeds at least, it has one cannot be successfully maintained. Its past importance may, however, be perhaps indicated by the fact that in the ostrich, for instance, it is said to assume a length of six feet. Because of its relatively wide variations in size, length, and emplacement, as well as because of its mesenteric and other anatomical arrangements, its affections are often complicated and variable in the symptoms they produce. The appendix is, in fact, a miniature intestinal tube, having the same structure as the small intestine, though but greatly reduced. Its average length should be 8 to 9 Cm., the shortest on record being 1 Cm., and the longest perhaps 24 Cm. Its average gross diameter should be that of a No. 16 French catheter, but it may be found 1.5 Cm. in size. The average diameter of its lumen should be 1 to 3 Mm. The appendicular artery is given off from the right colic branch of the ileocolic artery, and it ordinarily divides into four or five branches, according to the length of the appendix and the extent of its mesentery. It derives its nerve supply from the superior mesenteric plexus of the sympathetic ganglia, which itself is connected with the right pneumogastric, this fact explaining many of the reflexes accompanying its diseases. In it lymph abounds and lymph follicles are numerous. Around its neck, as around the origin of every other embryonic canal (as Sutton has shown), is found a collar of lymphoid tissue corresponding in structure to that seen in the pharynx. This tissue is inflammable, and succumbs easily to infection. Hence probably the apparent ease with which infection and gangrene occur in this locality. The position of the appendix is variable, and depends in effect on the development of the cecum and the degree of its rotation during this process. Its most frequent location (40 per cent.) is behind the cecum. In 30 per cent. of cases it occurs on its anterior surface or just at its lower end. It may lie as a free pouch with a loose mesentery, movable in the abdominal cavity, or it may be essentially a retroperitoneal affair not only[852] not free, but even difficult to find. In direction it may vary correspondingly. Thus it may lie behind the colon, perhaps pointing straight upward toward the liver; it may hang in the pelvis, it may point toward the sacrum, or it may coil up anteriorly; and, according to the extent and freedom of its mesentery, in any of these locations, it may either be unattached and movable or quite bound down. Again, it may lie nearly straight or it may be kinked, bent, or coiled. It is necessary that the surgeon appreciate these possible variations, for they account for vagaries in symptomatology. In brief it should lie in the iliac fossa, at least, and to the outer side of the iliac vessels, but it may hang over into the pelvis in 20 to 25 per cent. of cases, or its tip may rest in a pocket or even in a subcecal fossa. In other words, it may be found in almost any attitude or position, these variations being explainable by peculiarities of fetal development. Furthermore it may even have its own diverticula, as has been recently shown. Normally it should be practically empty, save perhaps for a little muddy mucus. Very frequently, however, it contains fecal matter, and upon this fact depends much of its importance. If from retained fecal matter fecal concretions gradually result, then these become irritants and may produce either appendicular colic or may predispose to acute infection. Upon the retention of fecal contents should depend also a miniature peristalsis, and imitation of what goes on in the intestine above, in the production of a genuine appendicular colic. How annoying, painful, or even disabling this may be may be learned from the history of many a patient. On the other hand the appendix may become gradually occluded or obliterated, in whole or in part. If this process begin at its distal end and involve the entire tube it might be considered a fortunate occurrence for the patient. If, however, it be due to previous inflammation, or to subinvolution of the previous process, and if fecal concretions be thus imprisoned, it is hardly desirable and will frequently lead to trouble. More or less occlusion occurs in probably at least one-fourth of mankind.
Like the bowel above, the appendix may suffer in various as well as in similar ways. Thus in it may be seen pathological conditions which involve the bowel proper. Tuberculosis and actinomycosis may even occur here as apparently primary lesions, while cysts have been discovered within its walls, and such tumors as fibromyomas or primary adenocarcinomas are also met here. I have seen three or four instances of primary cancer of the appendix, and have now living one patient from whom six years ago I removed an appendix and adjoining portion of the cecum involved in most distinct cancer.
Again, the appendix participates in certain hernias and has been found in instances of strangulated or non-strangulated inguinal and femoral hernia, and has been seen also in cases of umbilical hernia. Twice I have found it in the inguinal canal and once in the femoral.
Furthermore when diseased the appendix, like the bowel, may contract adhesions to certain viscera, while it is now well known that it may attach itself to the kidney, the bladder, the right ovary, the tubes, or the uterus. This is of more than mere passing interest, for by such adhesions cases are not only surgically complicated, but diagnosis is made difficult, because of associated symptoms pointing to the organ thus involved.
—Foreign bodies are occasionally found. This expression refers not merely to the fecal concretions above mentioned, which are practically small enteroliths. Thus, Kelly has mentioned cases in which ordinary pins have been found in this location, two of these cases being my own. In one instance I found the appendix to contain a round-worm at least three inches in length, and other intestinal parasites have been found by other observers. The laity have been greatly impressed by the reputed frequency with which grape and other seeds are found in the appendix, these figuring in their eyes as exciting causes of disease. In truth seeds are seldom found, that which has been mistaken for them being fecal concretions of various sizes and degrees of density. I have found actual seeds two or three times, but probably not oftener.
—Acute appendicitis being essentially an acute infection one inquires naturally which are the organisms most commonly involved. Answer to this question should be sought rather in the text-books on pathology, and should be summarized here by simply saying that the colon bacillus is perhaps more often found in connection with these cases than any other one organism. Streptococci and staphylococci rank perhaps next in frequency, while the pneumococcus, the capsule coccus, and all of the other pyogenic forms may be present, either as contaminations or in almost pure cultures. The fauna and flora of the intestinal tract afford ample opportunities for contaminations with many forms of microbes. If pus found here be a pure culture of any one organism it is most often of the colon variety, which is known to vary much in virulence, even when occurring alone. Mixed infections, however, are more predominant and more serious, especially in proportion as the more active pyogenic organisms appear in greater numbers. The bacteriology of appendicitis is then of great pathological interest, but concerns the surgeon very slightly, unless he have to do with some peculiar form, such as pyocyaneus, or a particularly virulent streptococcus.
PLATE LI
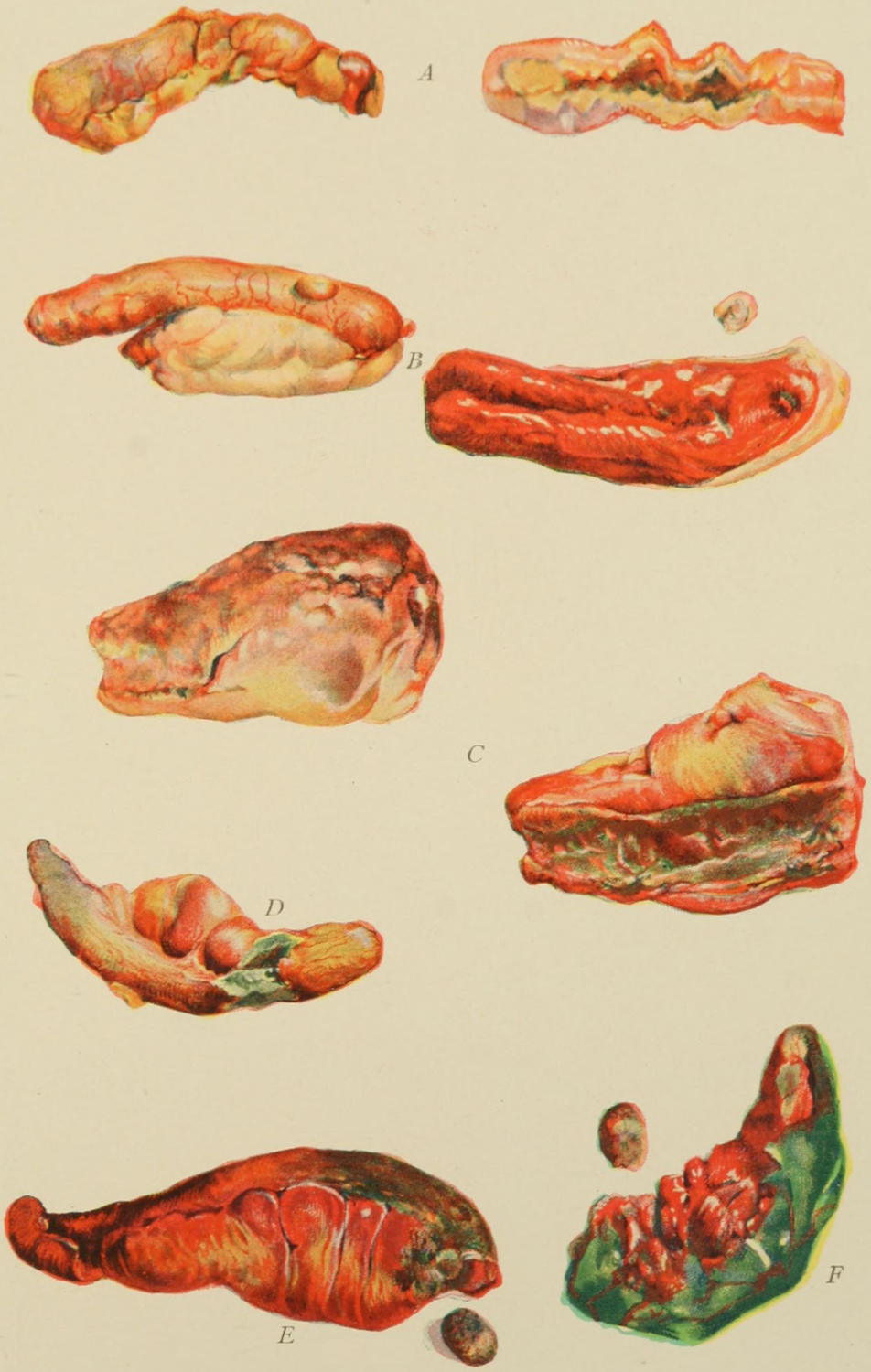
Illustrating Various Degrees of Involvement of Appendix Vermiformis. (Richardson.)
A. Chronic, recurring.
B. Chronic, much thickened.
C. Acute, with necrosis and rupture.
D. Showing necrosis of mucous membrane.
E. Gangrene and perforation, permitting fecal extravasation.
F. Total gangrene without perforation.
[853]
—Sufficient has been said above regarding the appendix as a miniature intestine, its outlet guarded by the little valve of Gerlach, to afford an anatomical reason why conditions even in the larger bowel should be imitated here. Some writers have not placed as much stress upon appendicular colic as I would here. One sees many instances of it if he will only recognize it, the frequency of its occurrence not only disturbing the comfort of patients, but keeping ever before their minds the necessity for operation. An absolutely empty appendix will be free from all abnormal activity of this kind, but when a little fecal matter has become imprisoned, and when by its long retention fecal concretions have formed, they may give rise to considerable disturbance without actually producing inflammation, the former being due to the spontaneous effort of the appendix to expel them. This effort may be excited by other conditions in the bowel adjoining, but by itself it may be the essentially relatively violent muscular effort which produces pain and is followed by soreness. That not a few cases of acute appendicitis commence with an appendicular colic is extremely probable, and that it may occur at frequent intervals and never pass the colicky stage is equally true. Appendicular colic, then, may be a precursor of an infectious appendicitis, acting as a predisposing cause, or either may occur independently of the other.
Indications of this form of colic are frequent, viz., nagging pains in the region of the cecum, which may last a few moments or a few hours and then subside, leaving a tenderness which persists for a day or two, after which the patient seems to be free for a longer or shorter interval, to suffer again and again in the same way. These attacks may be accompanied by some nausea, will be found frequently associated with whatever may have disturbed ordinary intestinal activity, and may even produce a mild degree of fever, which latter is partly due to mental perturbation and partly to a mild degree of toxemia, the latter being possible in connection with abnormal appendicular activity, as the appendix itself is a closed sac and the very materials which it is trying to expel may furnish the toxins.
It is difficult to distinguish between appendicular colic and mild attacks of catarrhal appendicitis. The transitory nature of the former is its particular diagnostic feature, coupled with absence of all lasting indications.
The following would seem the simplest working classification of lesions of the appendix.
| A. Acute. | - | Catarrhal. | Endo-appendicitis. | ||||||
| Diffuse. | Parietal or interstitial. | - | Hyperplastic. | ||||||
| Obliterative. | |||||||||
| Purulent. | - | Intertubular. | |||||||
| Intramural. | |||||||||
| Peri-appendicular. | |||||||||
| Any of these may lead to | |||||||||
| Gangrenous or | |||||||||
| Perforative lesions. | |||||||||
| B. Subacute. | Recurrent or relapsing. | ||||||||
| C. Adhesive or obliterative. | |||||||||
Almost any of the above forms may be associated with diseases of other abdominal viscera, as, for example, with typhoid. Thus out of 119 autopsies on typhoid patients 19 showed changes in the appendix corresponding to those produced by the typhoid organisms in other portions of the intestines. (Kelly.) Of 3770 autopsies on tuberculous patients tuberculous lesions were noted in the appendix in 44 instances. The appendix may also become involved with any form of ileocolitis, either in the young or in the adult. Again an infection of the right tube and ovary may easily extend to and involve the appendix, just as infection may travel in the opposite direction. (See Plate LI.)
[854]
Before discussing the causes of this condition it is advisable to take a comprehensive view of the entire subject in its pathological relations. As Dieulafoy has shown, appendicitis is the consequence of the transformation of the hollow conduit into a closed cavity, whose length and narrowness make it liable to such changes, for which various causes are to be assigned: for example, the formation of calculi or concretions which are quite comparable to renal or biliary and which lead to a true appendicular lithiasis. There is even reason to believe that a calculous appendicitis may be hereditary and belong to the patrimony of gout. At other times it is the consequence of local infection, followed by tumefaction, and corresponding to obstruction of the Eustachian or the Fallopian tubes. Again it results from slow, progressive fibrous alterations or from the strangulations due to twisting or formation of adhesions. In any event the closed cavity varies in size and shape, and does not necessarily lead to self-destruction unless the bacteria thus pent up are sufficiently virulent. At all events the attack declares itself only when the cavity is actually closed, and it is then that imprisoned bacteria, previously harmless, multiply and intensify their virulence, as they do in a blocked loop of bowel. At times an acute intoxication from toxins is produced, and may be so pronounced that patients succumb to it almost before the characteristic lesions, or any local peritonitis, has become fairly outlined. On the other hand if retained bacteria be but slightly virulent, or have been successfully conquered by phagocytes, or if the canal has become pervious again, the attack may spontaneously subside, although there is great probability of recurrence. In many instances the infection ends in ulceration, abscess, gangrene or perforation, all of which may give rise to peritonitis of varying extent and severity. Germs may traverse the walls of an affected appendix without perforation. It may then become the direct cause of peritonitis, septicemia, or hepatic abscess.
—Every attack of appendicitis, no matter how mild, predisposes to a repetition of the trouble, in mild or in fulminating form. Every appendix once inflamed has had its blood supply compromised and may break down easily upon a second attack. While not every patient who has once suffered in this way should necessarily suffer again, the majority who have had one attack may have another. No one can be prophetic in this regard and no one may truly assert that several mild attacks may not be followed by another most severe. That an appendix has been once inflamed is sufficient to justify its subsequent removal. That it has been several times involved makes operation next to imperative. Even repeated attacks of appendicular colic predispose to trouble in this region. In any appendix which has in this way frequently excited suspicion, or which gives rise to frequently recurring though mild colicky pain and local tenderness, especially when coupled with mild stercoremia, indications are for removal. It may be safely laid down, then, as a rule, to which there should be few exceptions, that any appendix which causes frequently recurring or almost continuous trouble should be removed.
—It is impossible in any brief summary to include all the possible causes of appendicitis. Those mentioned below are perhaps those most commonly recognized or pronounced, yet the list is far from complete. First of all it should be remembered that the disease occurs in a vestigial organ, containing relatively considerable lymphoid tissue, especially around its neck, that it is comparatively poorly supplied with blood, and that such tissue under such circumstances inflames easily and breaks down quickly. Doubtless the trouble in some instances commences within the tiny intestinal tube. At other times its originating cause lies without, as, for instance, when its blood supply is interfered with by pressure of an overloaded cecum, by tumors, or by violent intestinal activity; this especially in connection with an appendix firmly anchored and not freely movable, it being so fixed in many instances that it cannot readjust itself easily to varying conditions. Thus an overloaded cecum may first press upon the appendix and then by violence of activity so displace it that it may easily succumb. Again in those appendices which hang downward into the pelvis there is little or no drainage by gravity, and they may easily become overloaded. A movable kidney may also disturb the integrity of an appendix in certain locations. Foreign bodies frequently excite pernicious activity, especially fecal concretions, and actual calculi or miniature enteroliths. Traumatism sustains a certain relation to some cases of violent activity of the psoas muscles in athletes, which may upset the circulation of appendices which lie directly upon the muscles involved.
[855]
Many of the causes mentioned above are predisposing rather than actual. The actual exciting causes of acute infection have mainly to do with germ activity and with vascular supply. It is well known that the more virulent the organisms the more acute the resulting inflammation, and it is also well known that colon bacilli and the ordinary pyogenic organisms vary in virulence within wide limits, and that mixed are often more acute than simple infections. Typhoid bacilli, tuberculous bacilli and the like vary in the same way, and, in company with other germs, may easily light up serious disturbance.
—Of the complications which may accompany or ensue upon appendicitis the most common are those which involve the peritoneum, either local or general. Acute peritonitis is to be feared not only because of its autotoxic expressions, but because of the acute obstruction which it may produce by gluing intestinal loops together and paralyzing their motility. When to more or less widespread peritonitis are added general sepsis, with all its possible complications, and such further local expressions as cellulitis, which may be pericolic, subphrenic, perineal, or pelvic, or phlebitis which, involving the portal system, would soon lead to formation of hepatic abscess, it will be seen how easily the case may become serious. Furthermore not only may the ovary and tube suffer, but cystitis and nephritis may occur as toxic complications, while finally, by violence of the ulcerative process, a fecal fistula may form. This is by no means a complete list, but includes some of the more frequent complications.
—Pain with nausea, tenderness, and rigidity constitute the triad of the most indicative early signs and symptoms, each of which needs to be considered by itself.
—Pain is at the same time an important yet variable feature. In few other acute lesions does it vary as much in degree and location. Generally it is referred at first to the more central portion of the abdomen, as around the navel or between it and the right side of the pelvis. Later it may be localized at some widely distant point, as, for instance, far over upon the left side. Such vagaries may be held to be due to peculiarities of emplacement of the appendix, and would indicate that the organ will probably not be found in its most common location, but rather extending to the left or hanging over into the pelvis. When the appendix is attached to or lies near the bladder there may be considerable pain in the pelvis and in the bladder. It should be remembered that the parietal peritoneum is much more sensitive than the visceral, and in proportion as the lesion approaches the surface more exact information may be gathered from location of pain. Occasionally it may be referred to the region of the gall-bladder, or even to the chest above the diaphragm. In some instances it is agonizing, almost from the outset; in others it is never very severe. The rapidity of the process may be measured to some extent by the intensity and character of the pain. When the disease resolves slowly and kindly pain gradually subsides, but the sudden subsidence of pain, especially without equal improvement in other respects, is a bad rather than a good sign, indicating probably that perforation has occurred.
—Tenderness is a more constant and persistent and, therefore, a more reliable indication than pain, and, as well, less misleading. No matter where the patient may seem to feel pain the actual tenderness will indicate the location of the appendix itself. Thus even if pain on the left side be severe, tenderness will not accompany it, but will be found centred at the location of the appendix. This is a fact of great importance. In his first paper on appendicitis McBurney showed that the appendix is most commonly located at a point beneath a line drawn from the umbilicus to the anterior superior spine and one and a half or two inches away from the latter. This has since been known as McBurney’s point. To it, however, too much importance should not be attached, since the appendix is often not found under this area, and tenderness may be found at a distance two or three inches away from it. Over the actually tender area the skin will also be hypersensitive, and this intense hyperesthesia is also an indication of considerable value.
—Rigidity and muscle spasm are to be carefully studied, and upon them much reliance may be placed. With the first onset of pain they may be general, but they usually become more and more localized, unilateral, and finally limited, save in those instances where general peritonitis has begun and is spreading. For instance, Richardson regards it in this light: “Rigidity with distinctly localized pain strongly[856] suggests appendicitis; with fever it almost proves it; with tumor it fully establishes diagnosis.” When to ordinary abdominal rigidity is added actual muscle spasm, provoked by even light palpation, and occurring in the rectus or one of the flat muscles lying in close relation to the appendix, then a still more important indication has been obtained. When true muscle spasm involves all the abdominal musculature general peritonitis has probably begun.
—The presence of tumor in the suspected area will nearly always be a corroborative sign, but diagnosis should not depend upon its presence. It is hardly to be looked for during the early hours or perhaps days of an ordinary attack. It may be due to fecal impaction in the cecum, to outpour of exudate, to binding together of omentum and intestine, or to the presence of pus. If a considerable mass can be detected within the cecum during the early hours of an attack this should be regarded rather as an expression of coprostasis and impaction, to which the attack itself may be due. Tumor, therefore, is significant when present, while in some instances its absence is still more so.
—Vomiting is an irregular and uncertain feature. Probably the majority of cases begin with nausea (after the initial pain) or with vomiting, either one without the other, or with both combined. Likely through the course of the disease vomiting may be an occasional disturbing element, though patients may have no nausea whatever.
—The condition of the bowels and their behavior will depend very much upon their actual state at the moment of attack. Some attacks seem precipitated by violent intestinal activity; here diarrhea or dysentery will be an early feature. Others are precipitated rather by overloading of the cecum; in these cases constipation would be a well-marked feature. Bowel inactivity is to some extent an expression of bowel paralysis due to toxemia, which in some instances is profound, in others slight.
—The temperature is also a variable and uncertain feature. It may be normal at first or very high. At any time it may rise gradually or suddenly, and may subside in the same atypical way. Taken by itself it is an unreliable feature. When, however, temperature steadily rises the surgeon may take alarm, and if the pulse rate goes up correspondingly the case takes on a serious aspect. A sudden fall of temperature is almost as serious a feature as a sudden rise. A normal or subnormal temperature may be seen when a large amount of pus is present, or but a minimum of disturbance may be found when operating upon a patient whose temperature is 104°.
—The pulse is a more reliable guide than any obtained with the thermometer, its rapidity being proportionate to the gravity of the disturbance. A constantly rising pulse is a serious indication, especially if accompanied by vagaries of temperature. Some operators regard the pulse as a sufficient indication for operation, holding that when it rises above 112 operation should be made. I hold this to be a good rule, but would not have it interpreted as indicating that operation should not be done unless the pulse attains this figure, and believe that, no matter what the other conditions, the final indication has arrived when the pulse goes above 112.
—Abdominal distention may be due to gas formation, to constipation, or may indicate the paralysis of peristalsis. When it becomes well marked it is a serious indication, and when toxemia is profound no sound whatever will be heard within the bowels thus distended. It usually indicates the onset of general peritonitis. It is unfortunate in more than one respect, since intra-abdominal conditions are masked by it and operation complicated, it being sometimes impossible to restore the bowel to the abdomen without at least partially emptying it.
—Jaundice, when occurring, is a toxic expression, possibly due to temporary obstruction of distended or paralyzed bowels.
Finally the general appearance of the patient will be suggestive, patients with serious conditions having always an anxious or haggard facial expression, rarely moving themselves easily or freely in bed, or smiling at anyone or anything, their faces being perhaps somewhat flushed, their expression and action being apathetic, while perhaps later there will be delirium with restlessness. When the face is pinched, the eyes sunken, the nose sharp, the skin dusky, and respirations rapid and unsatisfying, as well as of thoracic type, any intra-abdominal infection may be regarded as serious and unpromising.
What shall be said about the value of the blood count? It is possible in nearly every instance to make a diagnosis of appendicitis without the aid of the microscope, as well as even to judge of the advisability of immediate or postponed operation. Nevertheless an indicative differential blood count, an affirmative result of the iodine test, or the[857] discovery of indican in the urine, may afford positive corroboration in cases where doubt may have existed. In reality, however, any case which will furnish satisfactory and distinct responses to these tests should be recognized without them. A leukocyte count above 12,000, in connection with other indications, is usually sufficient to justify operation. A very high leukocytosis—e. g., above 24,000—is a matter of great importance. In the more chronic cases the leukocytosis is but slight.
—Obvious and indicative as many cases of acute appendicitis are from the outset, there are still others when one may be in serious doubt, even for some days, either because patients do not clearly state their own symptoms, because of peculiar reference of pain, or because of the co-existence of complications, each of which may mask the other.
Colitis of adults and enterocolitis of children will produce sometimes severe attacks of pain, with cramps and local tenderness, that may at first mislead. There is a form of mucous colitis which is now more generally recognized than in time past, in which diagnosis is sometimes quite difficult. The onset is often sharp, while the right iliac fossa may be occupied by an elongated, resistant, tender mass, showing fecal impaction within the cecum. On the other hand the same condition may be met in the left iliac fossa, and will thus indicate that the sigmoid is especially at fault. In these conditions there is often actual exudate around the inflamed bowel, and this may even break down; it is proper then to speak of a circumscribed colitis, and there is reason to think that in certain cases it arises from infection of a diverticulum from the large bowel. The pain is not infrequently complained of at the so-called McBurney point. In not a few instances the appendix has been removed when under perfectly natural suspicion, and found so slightly involved as to show that the actual trouble was in the cecum rather than in the appendix itself. Dieulafoy believes, in fact, that formerly the cecum was made too much of and the appendix disregarded, while today these conditions are sometimes reversed.
From gallstone disease and cholecystitis its symptoms are sometimes quite difficult to distinguish. Especially is this true when pain is not accurately localized, and when, on the other hand, muscle spasm and tenderness are widespread. The previous history of the case will give much aid in this matter, while the pain in gallstone trouble radiates rather toward the right shoulder, in appendicular disease toward the umbilicus or downward. When dulness on percussion shades directly into liver dulness the gall-bladder is naturally the more to be suspected. When patients themselves cannot make minute distinctions in description of pain and tenderness the condition may be difficult of recognition.
—The majority of all attacks of so-called idiopathic peritonitis spring from appendicular disease, at first and perhaps throughout unrecognized. A condition of peritonitis, then, for which other explanation is not found may be considered as, in all probability, due to appendicitis whose peculiar features may have been masked. It is not difficult to recognize a condition of general peritonitis. The great difficulty is to ascribe its proper cause. As already and elsewhere indicated these conditions merge into expressions of acute obstruction which still further complicate the case, and it is by no means infrequent to have this order of events: an acute gangrenous appendicitis followed by local peritonitis, with adhesions, which, becoming dense, rapidly produce obstructive symptoms, the condition going even farther and gangrene spreading from the appendix proper to any or all of those intestinal loops which come in contact with the primary focus, so that when the condition is thoroughly revealed it is found to be one of multiple gangrene of the bowel as well as of fierce and septic peritonitis.
Gastric and intestinal ulcers with perforation are easily mistaken for appendicitis, especially when the duodenum is involved. In at least half of the recorded cases of perforating duodenal ulcer the condition has been at least at one time supposed to be one of acute appendicitis, while after perforation has occurred and the matter which has escaped has worked its way down toward the right iliac fossa the similarity of conditions will be all the more striking. If an accurate history can be obtained there will probably be learned from it that which will tend to avoid mistakes. The exceedingly abrupt and acute onset of symptoms will also be more pronounced than in most cases of commencing appendicitis. This is true also of the perforations of typhoid ulcer, especially of “walking typhoid.” While acute appendicitis during the course of typhoid is by no means unknown, the abrupt onset of pain, rigidity, and tenderness during the third[858] week or later would suggest perforation very much more than the possibility of an appendical lesion.
Acute obstruction of the bowel due to other causes than appendicitis—e. g., volvulus or intussusception—might give rise to symptoms which would be regarded as indicating appendicitis. This is true also of strangulated hernias, especially the internal forms, since there will be no excuse for failing to discover an external strangulation of this kind. Lead colic may simulate some of the milder and more chronic forms of appendicitis, from which it should not be difficult to exclude it by its history, the occupation of the patient, and the appearance of the gums.
The kidneys and ureters are sometimes so involved as to occasion doubt. A floating kidney, with its possible crises, displaced into the right iliac fossa, where it might be mistaken for an inflammatory mass, might thus cause some hesitation. So also might the acutely suppurative forms, the formation of a sudden phlegmon about the kidney, or the entanglement of a calculus, either at the hilum or along the ureter, produce severe pain, tenderness, and fever, which would at first easily perplex. The pain of renal colic, however, is usually more agonizing, beginning in the flanks and referred down along the ureters to the genitals and the inner side of the thigh. It may also be intense in the back, and may be accompanied by nausea and vomiting. Renal colic is also nearly always accompanied by frequent urination and sometimes by the appearance of blood in the urine. With an impacted calculus at the lower end of the ureter at the level of the appendix diagnosis may be very difficult. Here the x-rays may afford some assistance.
Acute pancreatitis begins with intense abdominal pain that may at first suggest appendicitis. The pain, however, is usually epigastric; abdominal distention comes on early; vomiting may be profuse, and the tenderness is most marked along the left costal border. There is, moreover, a more profound prostration, sometimes accompanied by cyanosis. An acute suppurative pancreatitis may soon be followed by peritonitis, which when seen will so completely mask all symptoms that diagnosis as between the two is quite impossible, but symptoms which can be accurately localized will usually point to the upper rather than to the lower abdomen.
Mesenteric thrombosis and embolism are rare conditions which commence usually with fulminating symptoms and produce intense agony, with tenderness and rigidity all over the abdomen. Their onset is so profound that patients fall into a condition of extreme collapse within the first few hours, and their tendency is so rapidly to the bad that they are not likely to be mistaken for acute appendicitis.
The pelvic viscera of women also furnish acute inflammations, such as pyosalpinx, with or without rupture, that sometimes precipitate very acute symptoms which may point to the abdomen rather than to the pelvis. In many of these instances the appendix is more or less adherent to the adnexa on the right side, and infection in either one may easily travel to the other, so that both become ultimately involved. Local examination will reveal the existence of pelvic conditions, in whose absence there may be justification for inferring that the trouble has not originated in that cavity.
Ruptured extra-uterine pregnancy has been in numerous cases mistaken for acute appendicitis. It usually begins with violent pain and pronounced muscle spasm, with more or less shock. I have repeatedly been called to operate for appendicitis and found the other condition present. The operator may be prepared to find it if he elicit a suggestive history or if a vaginal examination reveals a pelvis more or less filled with semisolid material. Amenorrhea does not always signify ectopic gestation, yet when doubt arises it would be advisable to inquire carefully into the menstrual habit of the patient. On the other hand it is known that acute appendicitis may bring on uterine hemorrhage. When, however, the possibility of pregnancy exists, along with a history of menstrual irregularity, or of hemorrhages unaccounted for, and one finds within the pelvis the uterus pushed forward or displaced, or perhaps an irregular tumor, he may suspect the condition if not actually diagnosticate it.
A peculiarly unfortunate combination is that of acute appendicitis occurring during pregnancy, or still worse, as I have seen it, e. g., in a woman with a large uterine myoma, gone to about the seventh month of pregnancy, and then suffering from an acute peri-appendicular abscess, the whole proving more than she could withstand.
With an appendix placed behind the cecum it will usually rest upon the psoas muscle, where it may be disturbed by violent exercise, or where it may lead to mistaken diagnosis[859] either in case of acute inflammation of the muscle itself or of acute appendicitis. When the right limb is drawn up, and especially when all motions of the limb give pain, we may believe at least in the participation of the muscle in the inflammatory activity. On the other hand, an insidious psoas abscess may give rise to a certain degree of tenderness in the right iliac fossa, with flexion of the thigh, and gradual development of tumor, which may be mistaken for chronic appendicitis.
The possibility of appendicitis occurring during typhoid has been mentioned. Differential diagnosis between the two conditions will ordinarily not be difficult when one can obtain an accurate history. In classical appendicitis pain is always the first symptom, and temperature rarely rises until a number of hours at least after the first attack of pain. Even the milder typhoid cases may show tenderness in the right iliac fossa, but one should look for the characteristic eruption and make a Widal test. The presence of splenic enlargement would point to typhoid, as would also the occurrence of bronchitis, epistaxis, or headache, with perhaps albuminuria. The most perplexing cases will be those of perforation, perhaps even of typhoid ulcer of the appendix. In these cases acute pain will usually indicate perforation.
Intrathoracic affections sometimes begin with or are accompanied by severe pains which are referred to various parts of the abdomen and cause great confusion. Thus I have repeatedly seen pneumonia, even on the left side, regarded at least at first as acute appendicitis, because patients referred most of their pain to the abdomen rather than to the chest, while the abdominal muscles participated to such an extent as to produce pronounced rigidity. Here a blood count would scarcely help, but careful physical examination of the chest would reveal the difficulty. Such examinations should be made when respirations become irregular, or when the breathing is evidently in any way embarrassed. Acute pneumonia and acute pleurisy, especially diaphragmatic, may have then to be differentiated from acute appendicitis.
Finally, hysteria is an element not to be disregarded in some of these cases; not that it is likely often, if ever, to lead to serious doubt, but that patients with the hysterical or neurotic temperament are constantly tempted to so seriously exaggerate their complaints as to lead to at least a more serious view regarding themselves than circumstances justify. Thus a mild appendicular colic in a neurotic patient may produce a disproportionate complaint, and one must be ready to assign to hyperesthesia or exaggerated complaints their proper value.
The symptomatology of appendicitis may then be summarized briefly as follows: When pain comes on suddenly and is referred to the lower part of the abdomen, or even its central region, becoming perhaps more localized as the hours go by, is shortly followed by nausea or vomiting, and this by general abdominal sensitiveness, with an increasing degree of rigidity; and when temperature, which at first is not elevated, begins to rise in from twelve to twenty hours, then it may be held that this is a classical picture of an attack of acute appendicitis. So strongly does Murphy, for instance, hold to this order of events that he even questions diagnosis when symptoms are not thus timed, and especially if vomiting precede pain.
When pain which has been severe subsides, and comes on afresh after an interval of perhaps thirty-six hours, it is to be regarded as due to fresh peri-appendicular involvement, and is an unfavorable feature. In fact the subsidence of pain and apparent improvement often noted do not always mean actual improvement, but may be the forerunners of a still more dangerous condition. Thus the “perilous calm” of appendicitis should hasten operation, or at least increase watchfulness, rather than beget confidence. Should one rely too much upon them and procrastinate he will find that his mortality rate will rise accordingly. The statement elsewhere quoted in this work that “the resources of surgery are rarely successful when practised upon the dying,” will apply here.
There is scarcely any equally limited area of the body in which as many varied and widely different pathological conditions may be exemplified as in the appendix and the space immediately around it. The mildest degree of hyperemia or vascular engorgement, the most destructive form of inflammation, with fulminating necrosis, may here be observed. Moreover, conditions commencing under one type may quickly change and the whole type of an attack may within a short time be merged from the mildest into the most severe.
In catarrhal or endo-appendicitis it is mainly the mucosa which suffers. This may undergo merely a congestion, with increase of discharge, and, so long as the outlet be[860] not completely obstructed, may be a purely temporary matter of but a few hours’ duration, or it may extend over a few days. The purulent or more destructive forms may commence in either of the coats of the appendix. It is no uncommon thing to find a necrotic mucosa with a still unbroken serosa, or a perforation of the outer coats and a hernial protrusion of the inner, perhaps just ready to give way. In location and extent the suppurative and destructive process may also vary. Whereas ordinarily the distal portion, being less supplied with blood, will suffer first, it is not uncommon to find perforation at the junction of the appendix with the cecum, or even gangrene of a limited area of the cecal wall itself. Again, at times, the trouble seems limited to accumulation of pus within the appendix, i. e., an empyema of the appendix, without great tendency to involve the structures adjoining, and an appendix may be found containing a few drops of pus or distended almost to its bursting point still free or but slightly attached by exudate. In the milder cases there may be found strictures indicating the site of previous lesions. Again, aside from pus, there may be more or less fluid or semisolid fecal matter or dense concretions, in addition to the possible foreign bodies whose presence has been elsewhere considered. In the more subacute or chronic forms there will be found relics of previous rather than active expressions of present trouble, such as strictures, thickenings, contortions, old adhesions, sometimes quite dense, and contained concretions, or other foreign bodies, or one may find appendices shrivelled up or more or less obliterated (appendicitis obliterans).
The role of the omentum has elsewhere been mentioned, but must be alluded to again at this point, since it participates more or less in almost every case of acute appendicitis. The moment the appendix is acutely inflamed the omentum tends to shift itself over toward it and finally around it, and it is not uncommon to find a gangrenous appendix wrapped in a roll of this kindly disposed fatty apron. In fact this may constitute the tumor which may have been already discovered and found to be fixed or movable. The inner surface at least of the omentum thus applied will nearly always have sacrificed itself and one has need usually to remove a considerable area of gangrenous omentum, as well as the appendix itself, feeling as he does it that he is necessarily sacrificing the best friend that the incriminated appendix has had.
Aside from what may concern the appendix itself the two most serious complicating local conditions are abscess and gangrene with perforation. Abscess is not necessarily the result of perforation, at least at first, but may be due to infection by continuity, the sequence of events being acute appendicitis, with exudation, fixation, and adhesion of surrounding tissues, followed by pus formation, perhaps first within the appendix and then perforating, or perhaps having its origin in the infected exudate exterior to it. So long as this process is localized by a protective barrier of surrounding lymph, with intestinal adhesions and the assistance of the omentum, there is to be dealt with a more or less complicated peri-appendicular abscess, such as in the past was frequently seen and spoken of as perityphlitic. Concerning the frequency of perityphlitic abscess in days gone by the literature of the previous century will afford ample illustration, but in spite of the surgical acumen and advice of Willard Parker, who taught the profession how to deal with it, its proper explanation did not come until the researches of Fitz, alluded to at the beginning of this chapter. Even now it is perhaps not quite correct to say that every typhlitic abscess, i. e., every collection of pus around the typhlon or head of the large intestine, is of appendicular origin, for the tendency has been to forget the possibility of phlegmonous cellulitis about any part of the bowel without reference to the appendix.
Such a peri-appendicular abscess may be small, containing but a few drops of pus, or extensive, even to the degree of holding a pint or more. The pus is usually offensive and sometimes one will find floating in it shreds of tissue, or even a completely separated and sloughed-off gangrenous appendix. According to the original location of the appendix, and the disposition of the adjoining parts, such a collection of pus may form a tumor in the iliac fossa, which may also fill the pelvis, or may present in the loin, closely simulating a perinephritic abscess.
It is unfortunate when the natural walling off process has failed and we have to deal with a spreading, generalized, septic peritonitis. A partial compromise between these conditions sometimes appears as a widespread yet practically localized peritonitis, in which several loops of bowel have become affixed, and, what is worse, infected to such an extent that they are themselves breaking down, so that there may be impending or[861] actual gangrene of the intestine. Such a condition bespeaks the intensity of the infection and the destructiveness of the infectious process, and produces a condition which may appall the operator. The result is not only acute obstruction of the bowel but such a local condition that one scarcely knows where to begin or terminate his operative efforts. It was in such a case as this that I removed eight feet and nine inches of bowel, the last nine inches including the colon, turning in both ends and making a lateral anastomosis, because of multiple gangrenous patches, each of which taken alone would have required a distinct and laborious intestinal resection, it seeming better to remove the entire amount involved. This patient recovered and was well years after the operation. Still other complications may disturb the surgeon’s calculations. Thus fecal fistula may have already occurred, or suppurative thrombophlebitis may have already produced the beginnings or an hepatic abscess, while septic expressions within the lungs, the heart, or elsewhere may have also occurred. In addition to this general peritonitis, with all of its terrors, may put a hopeless aspect upon the case.
—Viewed in the above light it will be seen that appendicitis is essentially a surgical disease, and that while mild attacks may at times be successfully conducted to resolution, or tend in that direction without treatment, the danger of spreading infection with all its possible disasters is ever present, and even a mild case is at no moment free from the danger of becoming acute. Considering its widest relations, and believing in the greatest good to the greatest number, the surgeon may easily maintain that, save when it is too late, it is never a mistake to operate, providing operation be properly performed. This, however, is sometimes out of the question, and the laity occasionally assume responsibility for a decision against the better judgment of the profession. We have to accept, then, the fact that, no matter what the theory may be, we are not always allowed to operate when we desire. Nevertheless if a universal rule could be established it could be laid down in terms such as these, that more lives would be saved by operating upon every case of appendicitis as soon as the diagnosis has been made or even in the presence of good reason for suspicion.
With conditions such as they are, and the fact that these cases are usually first seen by general practitioners whose surgical judgment has not been cultivated, and whose prejudices often actuate them, it may be said that every case should be seen early by a surgeon, no layman and no ordinary practitioner of small experience being in position to assume responsibility for delay. It then remains for the judicious and competent operator who may see such a case early, as thus advised, to study it carefully in order to convince himself whether there be about it good and sufficient reasons for not operating. The most honest operator does not gainsay the possibility of mild cases recovering without operation. He does, however, question by which course they run greater risk.
The following may serve as a brief summary of conditions which justify waiting:
Under the above conditions the conservative surgeon will be justified in waiting; being prompt, however, to intervene, should there be change for the worse in any one of the features specified. Even here it may be said that with conditions all as favorable as above represented pus may be present (in small quantity) and the whole picture may suddenly change into one of local disaster.
Finally it may be summed up in these words: When there is no doubt as to the advisability of waiting, then wait; but in case of doubt operate, i. e., give the patient the benefit of the doubt, which he in this way the more certainly obtains.
[862]
—While thus waiting in cases which justify it, what should be done? Absolute rest in bed, even to the extent of using bedpan instead of commode, is the first essential. The second comprises abstention from all food, and practically the temporary starvation of the patient, who may be allowed water in abundance and nothing else. Altogether too much stress has been placed upon the so-called starvation treatment as “saving patients from operation.” Active therapeutic treatment is limited mainly to the use of cathartics and of anodynes, according to reason therefor. On one hand it is not advisable to rudely stir up the large intestine, one part of whose structure is already involved in a serious and questionable inflammatory process; on the other hand it is not for the general welfare of the patient to permit him to continue with a condition of coprostasis and the ever-increasing stercoremia which it encourages. On the whole it would seem better to clean out the lower bowel at the earliest possible moment, after which if the patient be properly starved there will be less necessity for subsequent active catharsis. The question of anodynes is one of equal importance. Those who bear pain badly, or those who suffer intensely, will demand anodynes, which every physician knows both help to mask the symptoms and interfere with elimination; but such cases seem to be of themselves so violent that the extreme expression of pain should of itself be regarded as an indication for operation. It should be held, then, that cases which demand opiates for relief of pain demand operation even more strongly. In the mild cases, expectantly treated, the local application of ice may be of some value. In effect these cases are to be treated expectantly, and, while expectant treatment is a confession of weakness or of ignorance, it may be unavoidable because early operation is flatly refused.
—Sufficient reasons for not operating being absent or having passed, the following may be considered among the more urgent indications for immediate surgical attack:
Such are the indications by which the surgeon may say upon the instant of their recognition that a given case requires immediate operation. Fortunate are both he and the patient if the case be seen early, when these conditions have but lately shown themselves, and before it be too late. It has been said that almost every death from appendicitis means the loss of a life that might have been saved and for which someone is responsible, this responsibility being divisible among the patient, the parents or family, and the general practitioner who first saw the case and was tardy in recognizing its essential features. While patients die after late operations the surgeon himself is rarely censurable, it not being his fault that he was called in too late, and the patient dying of the progress of the disease in spite of an operation and not because of it.
Operation for appendicitis may be one of the simplest and easiest of the abdominal operations, especially when the acutely infectious element be not present, or it may be one of the most trying and difficult of all possible surgical procedures, taxing alike the judgment of the experienced operator and the resources of the clinic. Much will depend upon the time at which it is performed. If within the first forty-eight hours the surgeon may expect to find but a small amount of pus; if from the second to the fifth day, he may find a well-marked collection, while later he may have not only localized abscess but extensive complications. Again, he who operates between attacks, during the interval or interim stage, will find conditions of adhesion and results of old disease rather than its active products.
These operations should then be considered under these different headings:
[863]
Under the above headings conditions vary so widely that they can scarcely be spoken of or described under the same name. The seat of the disease should first be approached. Here there is wide range for choice of location of incision and even the method of its performance. Some prefer the outer border of the rectus, others go through the rectus muscle proper by an incision parallel to its fibers, which when exposed are separated, its sheath both anteriorly and posteriorly being divided separately. Others go through the abdominal wall by incisions more or less oblique, and made near the anterior superior spine, where are found the different layers of the abdominal muscles arranged in proper order, their fibers being disposed at right angles to each other. That incision is best in each case which affords the shortest and easiest route to the site of the lesion when it can be located. If tumor be present it is ordinarily best to go in directly over it. In the absence of tumor the point of greatest tenderness is the best guide. The possibility of subsequent hernia at the site which is weakened by operation should be taken into account. If it be possible to avoid drainage hernia may usually be avoided. When drainage is necessary hernia is sometimes unavoidable. The advantage of operation through the rectus is that the muscle fibers can be separated without dividing them. Incision here may, however, carry the operator so far from the site of the appendix that he must necessarily disturb the interior arrangement more than is advisable, and thus increase the danger of infection. The oblique exterior incisions near the ilium always permit of separation of the fibers of the external oblique. The deeper muscle fibers which cross at nearly a right angle may sometimes be nicked and widely separated by firm traction, as in the so-called “gridiron method,” or they may require division. A short external incision is desirable when it suffices for the purpose. Considerations of safety (i. e., the better exposure and easier removal of the appendix) may call in some instances for long incisions, and they should be made sufficiently long for his purpose.
It will often happen that as the surgeon passes more deeply toward the peritoneum he will find the tissues more or less edematous. This is a reliable indication of the presence of pus beneath, and should make him open the peritoneum with care and then use extreme caution in his further manipulation, lest by separating recent adhesions he permit pus to escape. The peritoneum being opened sufficiently the finger is gently insinuated, and thus the first orientation concerning internal conditions is obtained. With the exploring finger there should be ascertained, first, the existence of any adhesions; second, their location and relative firmness, and, third, in a general way, the amount of surrounding disturbance. With an appendix placed anteriorly we may thus come directly upon it, while when placed deeply and posteriorly we may have much to do before reaching it. After the first general exploration the next procedure should be to protect and wall off the region involved from the rest of the abdominal cavity by strips of gauze. These should be long and so secured that none may be lost by being left within the abdomen. The introduction of gauze for this purpose will sometimes increase depression and decrease blood pressure, but it is a necessary procedure in nearly every instance. Moreover, several strips may be needed, and the incision may have to be extended to a limit of two or three inches, according as further exploration reveals a more complicated situation. The fluid pus which may escape should be gently removed with dry gauze, or, if present in considerable amount, be carefully conducted toward the surface. Loops of bowel or tissue bound together by lymph should be gently separated, as they may easily tear, or since imprisoned between them there may be found small collections of pus. If found gangrenous the situation is thereby seriously complicated, and it is advisable not to restore such a loop to the abdominal cavity.
The omentum, as already indicated, may serve as a valuable guide to the location of the appendix, which may be found wrapped within it. It should be handled with great caution, while, at the same time, it is made to reveal the desired information. When the omentum is infiltrated, contorted, and adherent we may be sure of finding pus concealed within the cavity which it helps to wall off. That which is already gangrenous should be removed, with use of sutures in such a way that there shall be no subsequent bleeding. It may be found easily, or not until many other details have been mastered. The involved appendix, when found, may be in one of the conditions described above, all of which demand its removal save those where this has been already accomplished by violence of the disease, in which case the opening in the cecum may have to be closed, or one may employ it for the purpose of an artificial anus. The appendix is often so[864] hard to find that any reliable guide will be welcomed. Such a guide may be found, first, in the location and relation of the omentum, and, secondly, in the cecum if this can be exposed, or in either one of its firm, longitudinal, white tissue bands, which, leading down on either side of the colon, meet and blend at the point of origin of the appendix. Either of these followed in the right direction leads to this spot. Conditions may be such, however, as to obscure both of these guides, and then the colon should be followed downward toward the ileocecal valve, or the small intestine up toward it, in the belief that in this vicinity, and probably in the centre of the tumor, the appendix will be found. What the surgeon shall next do depends on the details of each case. He has not only to remove the diseased appendix, but to ligate and separate from it its mesentery; furthermore to separate either or both of these from surrounding tissues or organs, e. g., the wall of the pelvis, the ovary, the bladder, the retroperitoneal tissue above the sacrum, or from the lateral or anterior abdominal wall. This separation may be easy, or in its performance the tube may rupture and both pus and fecal matter escape; or perforation may have already occurred and the operator will be conducted into a cavity containing matter, pus and fecal mixed, in which perhaps fecal concretions of considerable size will be found loose. He is fortunate who, finding a condition of this kind, finds at the same time that he is still within a circumscribed cavity. This he should respect, and, while endeavoring to clean it thoroughly and drain it, he will avoid doing further harm by breaking down its walls.
Another condition which may arise after the peritoneum is opened is that of escape of a quantity of seropurulent fluid or of almost clear pus which is free within the abdominal cavity. There may be little or much of this. When present it should be removed by gentle sponging before the gauze packing is introduced. Some operators are inclined to irrigate freely and endeavor to wash out all this contained fluid. Others are opposed to this method and believe that gentle dry sponging is preferable. When the appendix is found free and movable, and when the tissues in previous contact with it are free from evidences of destructive infection (as, for instance, when peritoneal surfaces have not lost all their glimmer or sheen), one should carefully remove it, cauterizing its stump, burying it beneath the surrounding peritoneum, and close the abdomen without drainage. In spite, however, of the assertions and actions of some operators, I believe it to be the wisest rule to lay down for general application that it is safer to drain in every case where free pus or breaking down exudate is discovered.
The question of drainage thus raised is as important as any connected with this subject. When and how shall one drain is a question upon which hundreds of pages have been written by various operators, and one which, while settled for individuals, can hardly be settled for the profession at large by any brief statement. Inefficient drainage is almost as bad as none. Efficient drainage may call for the insertion of a tube into the depths of the pelvis, even for counteropening in the cul-de-sac, or for additional opening in the loin, or for the employment of two or three tubes and drains of various kinds. A large tube loosely packed with gauze, perhaps split through its length and abundantly provided with openings, is probably the most effectual drain for most purposes. The cigarette drain, of gauze wrapped in oiled silk, or a few folds of oiled silk loosely tied together, along which fluid may percolate, may be sufficient for cases of lesser extent. Large foul cavities are better left more widely open, and abundantly drained with gauze packing, in spite of the humorous stigma which has been cast upon some of these methods by Morris with his expression “committing taxidermy upon patients.” The depressing reflex influence of such packing being readily conceded it may be regarded as the lesser of two evils.
Another almost equally important question is that of treatment of the peritoneal cavity when involved. Here methods and opinions have varied widely. A peritoneal cavity once inflamed cannot be made absolutely clean in any way, and much reliance should be placed on the properties of the membrane itself, which, to a large extent, should act as its own scavenger. When, however, by removing the parts evidently diseased we have taken away the main source of infection we may feel like relying upon the natural protective forces of the human body; still even here opinions differ. Thus some would flush the abdomen with hot saline solution and even leave some portion of it there, closing the external wound, while others would carefully avoid the introduction of anything by which infectious material may be spread; and while each method has much to justify it one is scarcely found preferable to the other. I believe, however, in thoroughly[865] cleaning out any distinct abscess cavity, and if the pelvis be such then I would irrigate it. I would also thoroughly drain it.
The attention of the reader is here directed to the general considerations found earlier in this work concerning the general technique of abdominal operations, and the matters of drainage and after-care, it being scarcely necessary to reiterate what has been there said regarding the general use of saline solution locally and by the rectum, the advantage of the Fowler position, or of Murphy’s method of slow and gentle introduction of saline solution into the rectum, providing for its continuous absorption, etc.
The possibility of appendicitis leading to general peritonitis, this to acute obstruction of the bowel, and this possibly even to multiple gangrene, has been mentioned. What should best be done under these circumstances must depend upon the patient and upon the surroundings. With a patient too much reduced to justify any prolonged operation the surgeon would probably content himself with evacuation of pus which may be readily reached, and then perhaps by the formation of an artificial anus. Cases which will justify such extensive operation as that above reported by myself in this connection, where it was possible to successfully remove nearly nine feet of intestine, will be exceedingly rare, as well as impracticable in the ordinary private house.
A condition perhaps a little less serious but always perplexing is that of gangrene of a limited area of cecum around a gangrenous appendix. To remove the appendix alone in this condition is to accomplish nothing, while to meet the indication may require the exsection of a small area of cecal wall or the resection of the entire cecum, or perhaps in cases of limited extent the enfolding of the gangrenous area and the suture of its edges in such a manner that when it sloughs it may slough into the bowel cavity.
When the surgeon sees a case of peri-appendicular (the old perityphlitic) abscess late, and after it is easily recognized, he should operate according to the local indication, making incision perhaps short and placing it at a point where pus will apparently be most easily reached and best drained. Most of these instances present rather on the side or even in the loin behind the colon, and here a posterior incision might be sufficient. This may here be more liberal, since there is little danger of postoperative hernia, while through it one may possibly expose the cecum freely and often reach even the appendix itself. In making this opening it is well, if possible, to separate the fibers of the transversalis by blunt dissection. Here, as in all of the other incisions made toward the outer side of the body, the opening should be made, if possible, obliquely and parallel to the branches of the iliohypogastric nerves, which are thereby avoided and loss of sensation thus prevented. In fact this posterior method is sometimes even more rapid, and preferable in exceedingly fat patients, while it will always cause less shock and abdominal distress than does an anterior section; moreover, drainage takes place in the most desirable direction.
Fecal fistula is sometimes the immediate and unavoidable, sometimes a more or less delayed and apparently inevitable, result or complication of some of these operations. In the former instance it will be because of more or less gangrene or the necessity for an immediate enterostomy. In the latter case it results from conditions which are concealed, but may be imagined, comprising the giving way of tissues already compromised or else being a continuation of the ulcerative or gangrenous process. These complications are always unpleasant and untoward, though they rarely reflect upon the method or judgment of the operator, being essentially inevitable. If only the fecal outflow escape externally the condition may be regarded as inconvenient and temporary. Only in those instances in which the peritoneal cavity is contaminated does septic peritonitis ensue. The majority of these fecal fistulas close spontaneously by granulation tissue. Sometimes closure is rapid, sometimes delayed, in which latter case it may be stimulated by the use of silver nitrate, as already indicated above. In a few instances the condition is so extensive or so permanent as to justify or require further operation, which may be in the nature of a curettement of the fistulous tract, a slight plastic procedure, including a buttonhole suture about the opening, or possibly a complete intestinal resection. I have seen small, fistulous tracts discharge occasionally, even for years, and then finally close spontaneously, and have far oftener seen some form of spontaneous closure than necessity for operative intervention. The danger of infection around any such fistulous tract is ever present, and when it has occurred the fact will be made known by increase of edematous granulations, with swelling and tendency to[866] breaking down. In every such case active cauterization, or, better still, the use of the curette, will be required.
A tuberculous form of chronic appendicitis, as well as tuberculous infection of a subacute exudate, is possible, the case being converted into one of greater chronicity, with more or less mild but constant septic features (hectic). In any event, so soon as the tuberculous element can be recognized radical measures should be instituted.
Fig. 583
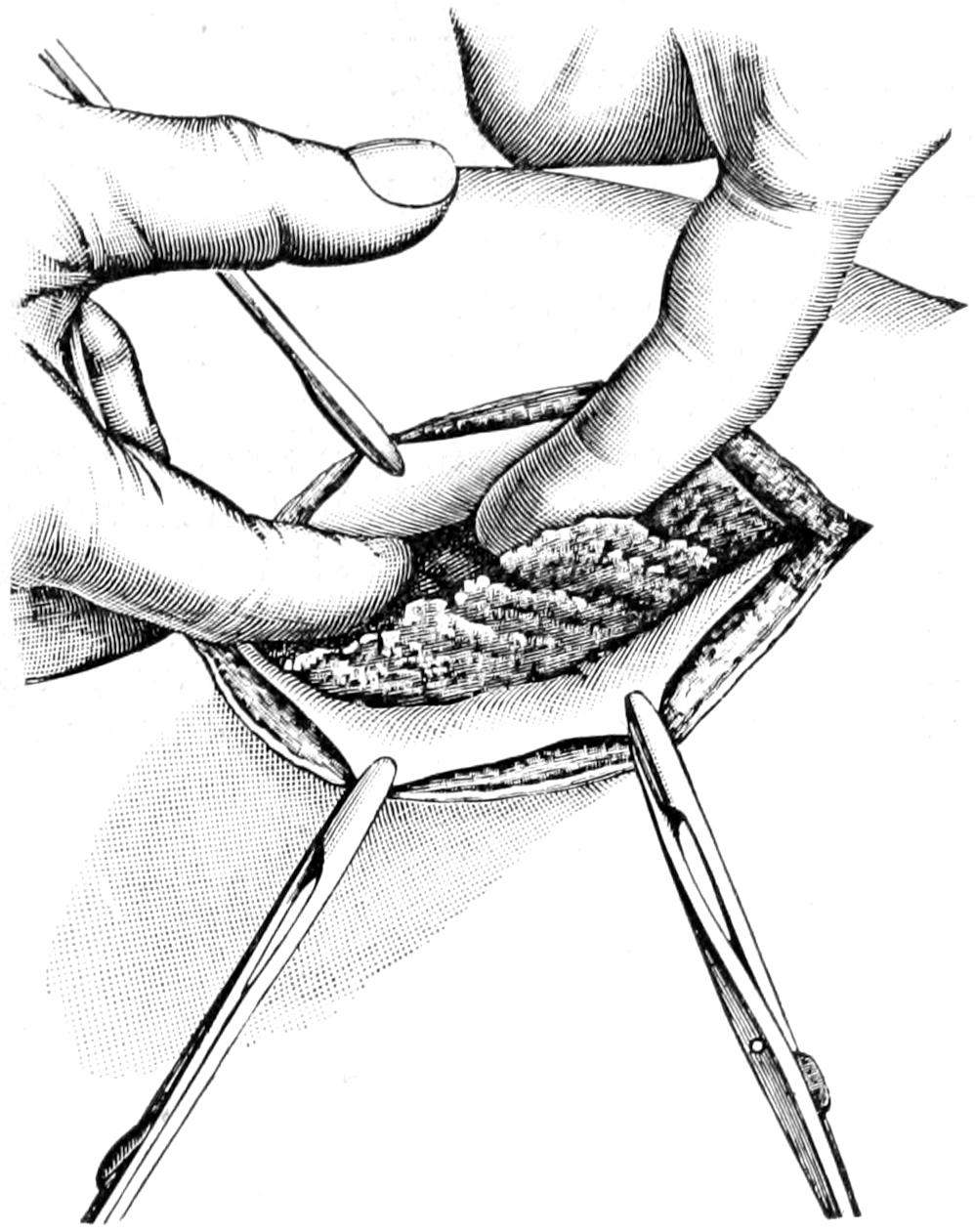
Omentum being gently lifted in order to uncover the appendix enclosed with its fold. (Lejars.)
Fig. 584
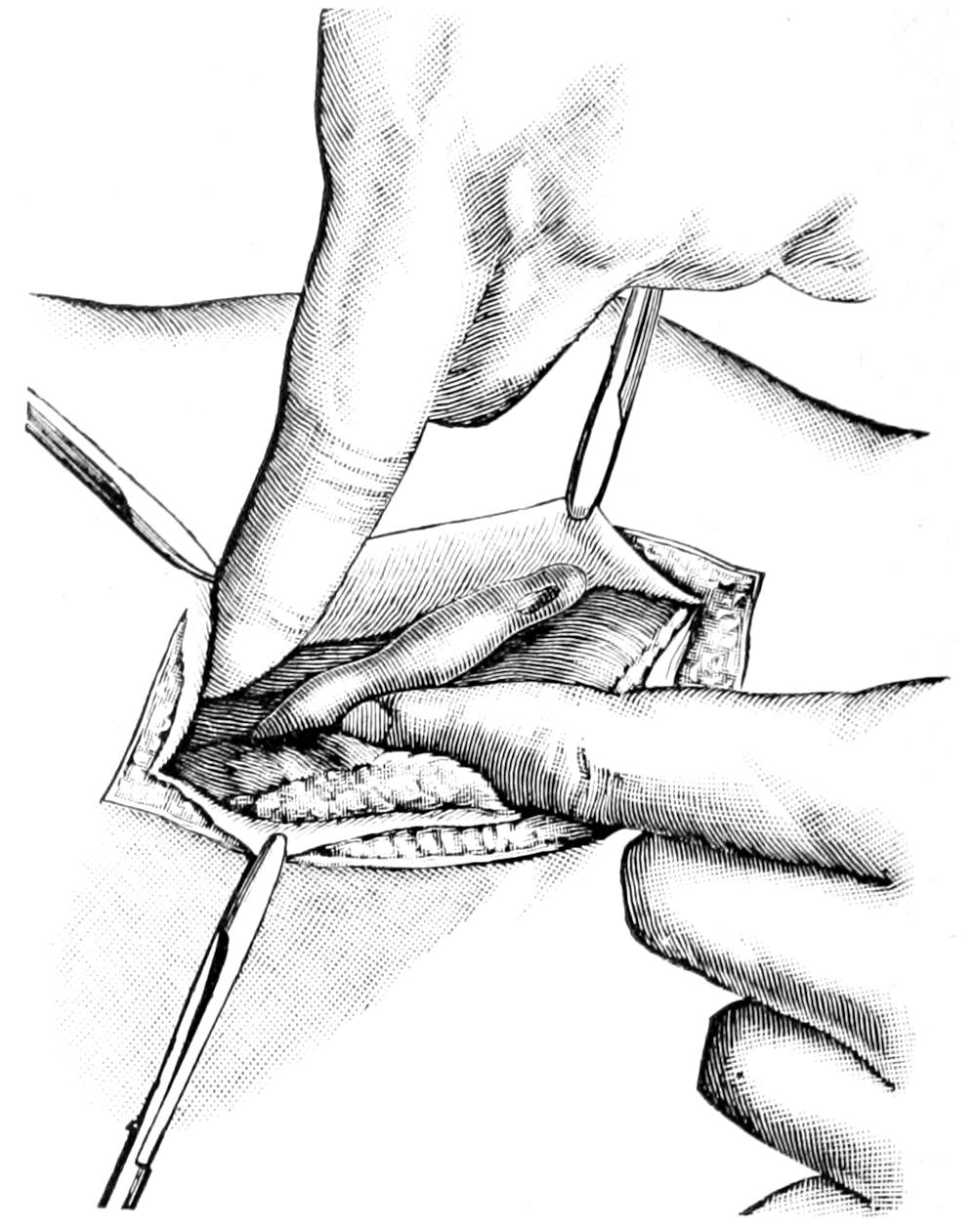
Appendix delivered from the abdominal cavity and brought to view. (Lejars.)
Fig. 585
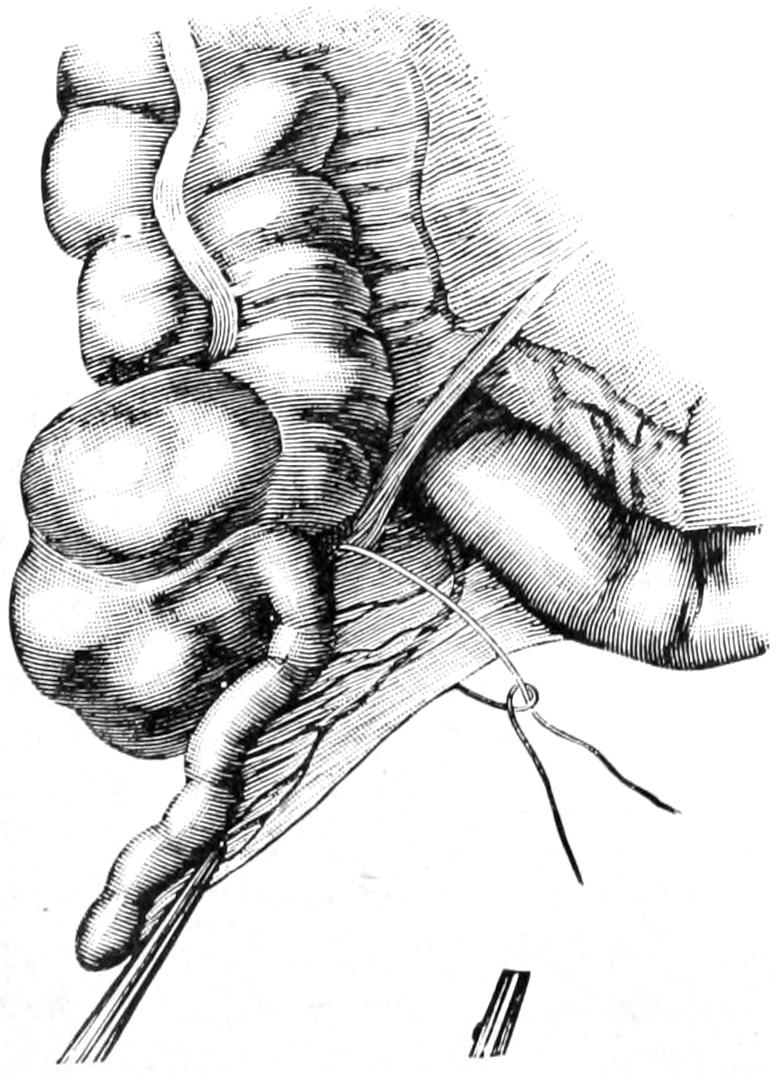
Separation of the meso-appendix. (Gosset.)
—Other things being equal the most favorable time at which to remove the appendix is that when pathological processes are least active. If, therefore, there be a choice the interval of quiescence rather than the stage of active infection would be chosen. Interval operations, so called, are usually comparatively simple, both in principle and technique. There are times, however, when it is difficult to find a partially obliterated appendix which has been covered up in thickened peritoneum or partially organized exudate. In such a case considerable blunt dissection or separation may have to be done before it can be removed. In those instances is this particularly true where it had originally a retroperitoneal location, and at no time a free or movable position. When difficult of recognition we may be unerringly led to it if we but follow the bands of white fibrous tissue on either side of the cecum to their junction.
The opening by which the appendix should, under these circumstances, be reached may again be made at the point of election, and should best be located over the area of greatest tenderness. Whatever incision is selected we should endeavor to separate muscle bundles as much and incise as little as possible. The appendix being delivered[867] through the wound, either before or after ligation of its mesentery, and being thus completely isolated, is removed close to the large intestine, its base being tied and its structure being seized within the blades of a forceps in such a way that none of its contents may escape. The scissors with which it is divided are contaminated by its contents and should not be used again until cleansed. The stump on the proximal side may be touched with the actual cautery, or scraped and then cauterized with pure carbolic acid or formalin solution in order to thoroughly disinfect it. Subsequent treatment of this stump differs with different operators. Some are satisfied to leave it thus cauterized, while others cover it with the adjoining peritoneum, which is brought together over the stump end by either a purse-string or a continuous suture. Yet others have been satisfied to invert the ends of the stump into the cecum and thus leave it with or without further protection. It seems to make really very little difference how the stump is treated, providing only it be disinfected and prevented from leaking. Nevertheless it would appear preferable to give it at least a peritoneal covering to prevent adhesions (Figs. 583 to 588).
Fig. 586
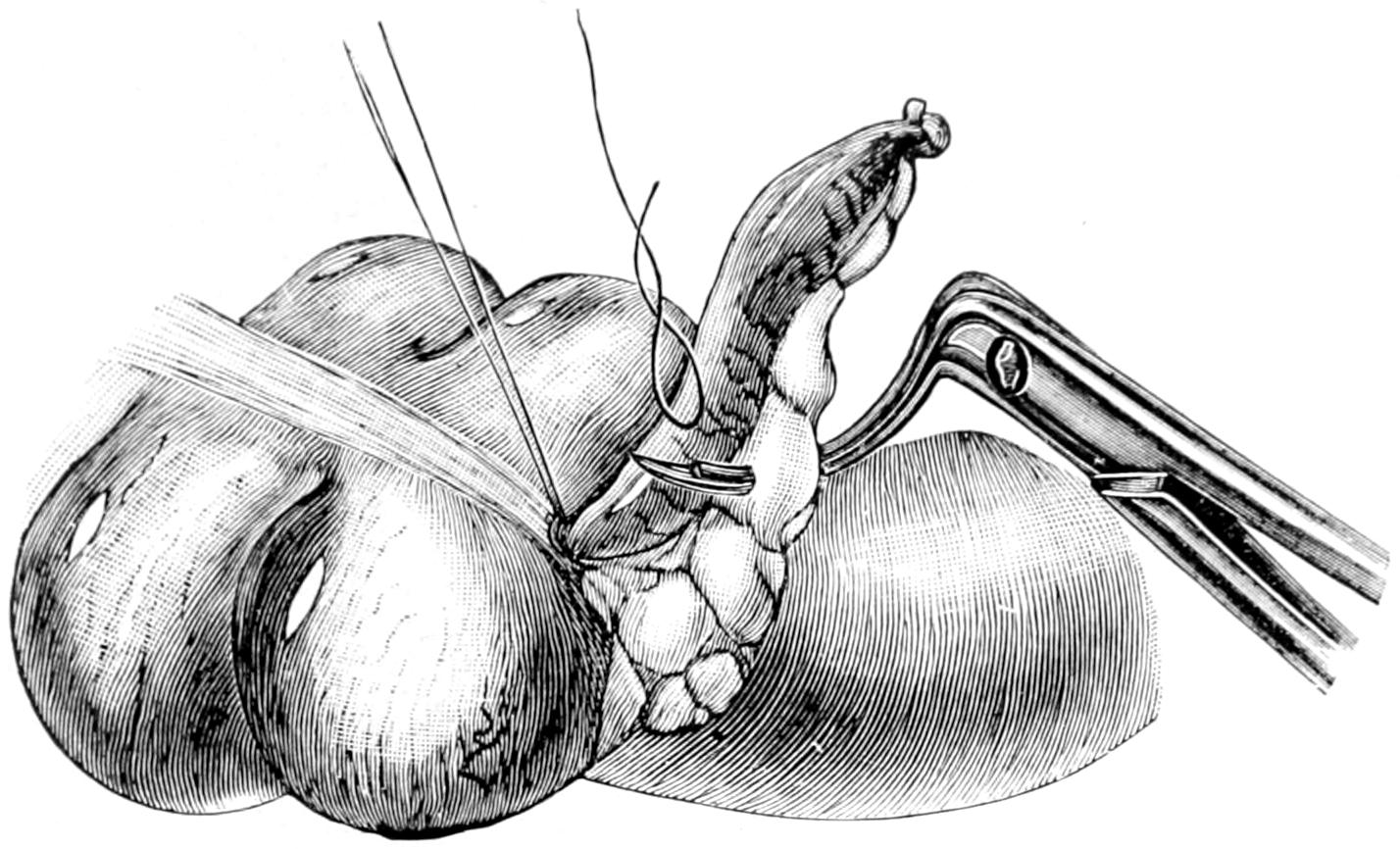
The base of the appendix is tied with silk. The meso-appendix is being tied in sections with the Cleveland needle. (Richardson.)
Fig. 587
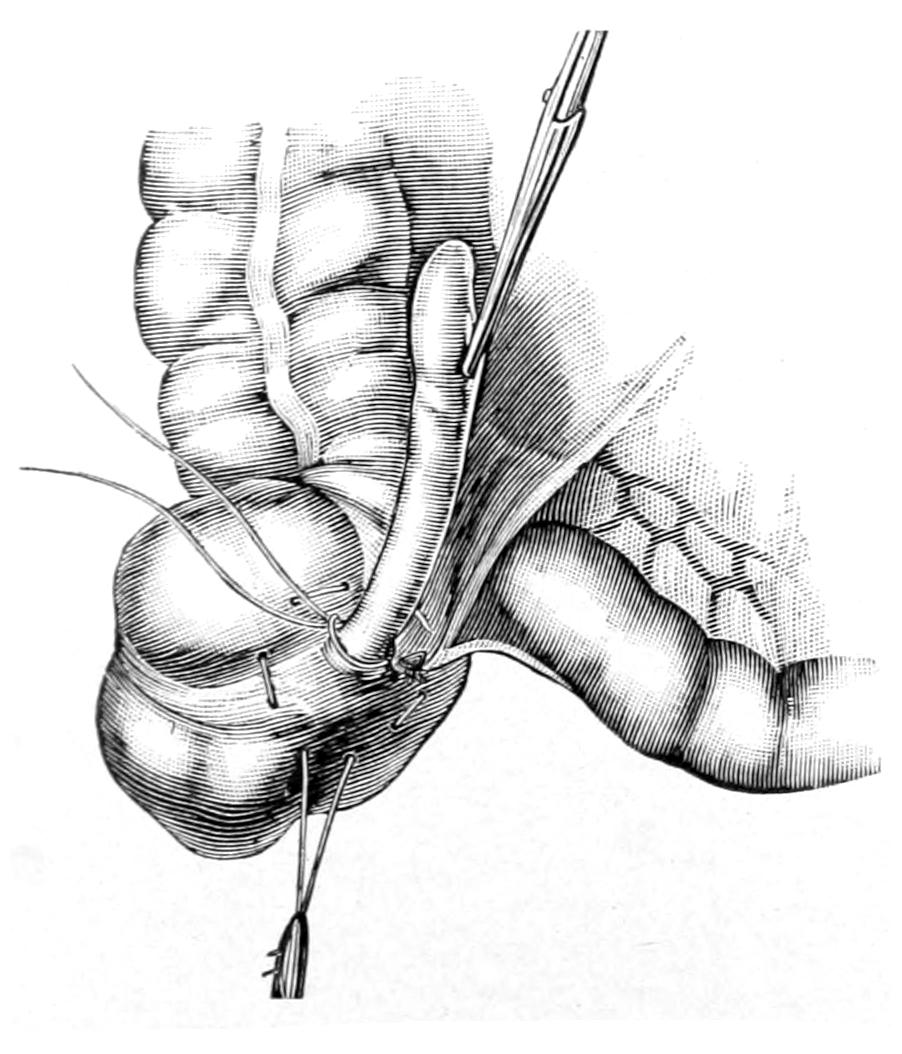
Appendix surrounded with ligature at its base, after its isolation from its mesentery. Purse-string suture in place. (Gosset.)
Fig. 588
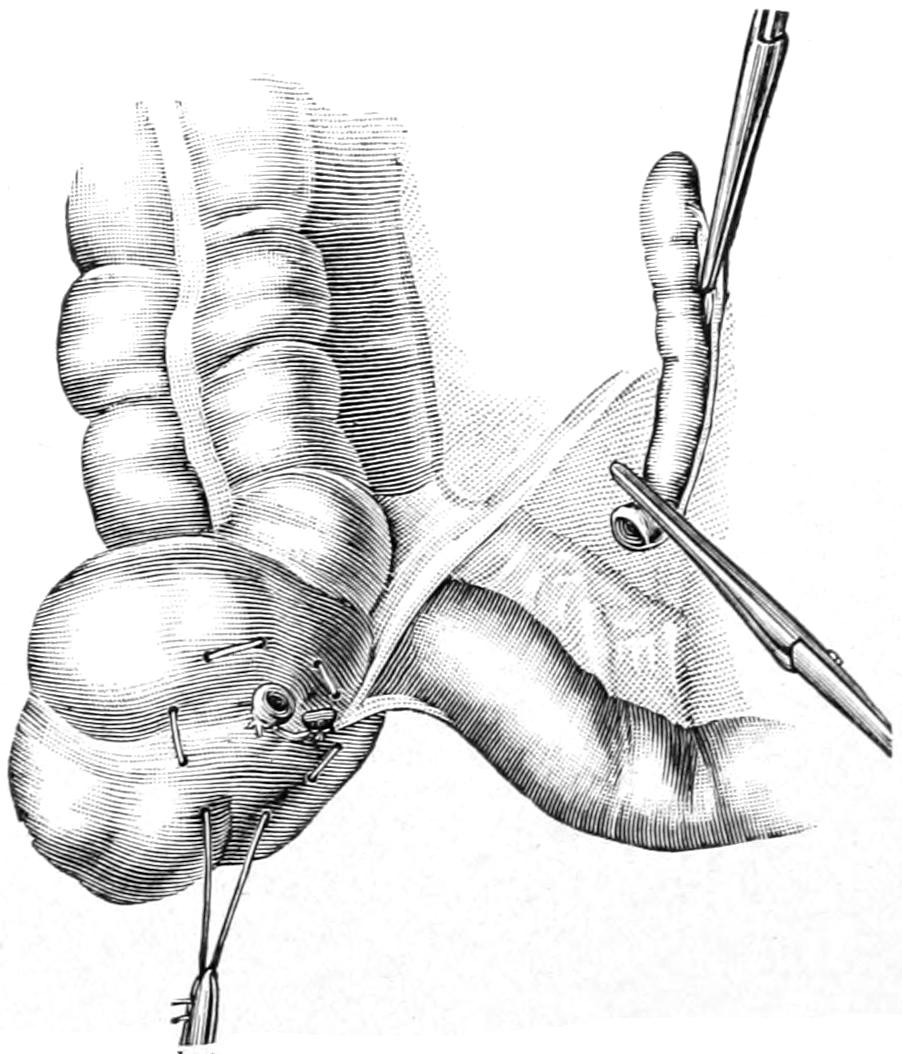
Complete detachment of appendix. (Gosset.)
In the subsequent closure of the external wound drainage is not made, there having been no pus to call for it; while the more perfectly the wound layers be closed, each with[868] a row of chromicized catgut sutures, the peritoneal incision being first carefully approximated and over it the muscle and aponeurotic layers, each by itself, the less the tendency to subsequent postoperative hernia. On general principles, also, the shorter the incision the less the danger of this undesirable event. Nevertheless other considerations should not be sacrificed to shortness and beauty of the cutaneous scar.
The essentials of after-treatment of these cases have been already summarized in the previous section, and to these little exception may be taken in cases such as those above described. Every precaution should be taken to prevent vomiting, as every muscular effort involved in the act tends to disturb a freshly sutured wound. While violent muscular efforts of defecation are also to be deprecated, there is perhaps as much or more to be dreaded from the abdominal distention which may result from inattention to free intestinal elimination. Until the bowels have been moved it is best to restrain the diet to the simplest fluid nourishment. So soon as elimination becomes free more liberality in diet may be allowed. There is the same liability to and danger from other possible complications, such as postanesthetic pneumonia, anuria, or lack of expulsive power of the bladder, which requires the use of the catheter, in these as in other abdominal cases. Principles of treatment, however, do not vary, and the reader is referred to the previous section already indicated.
Paratyphlitic abscesses are to be distinguished from perityphlitic or peri-appendicular abscesses in that they arise from a phlegmonous process in the cellular tissue around the colon not due to intra-appendicular infection. In consequence of such a cellulitis more or less considerable collections of pus may form, which are most likely to present either in the loin or just in front of the cecum, which may burrow either upward or downward, or appear elsewhere. They are mentioned here, not because they are to be differently treated or surgically regarded, but because it is worth while to remember that here about the cecum and ascending colon, as on the left side, such pericolic abscesses may form without reference to the appendix.
[869]
The more common congenital anomalies of the various divisions of the colon have to do mainly with the presence of diverticula and atresiæ, or possibly total absence, due to defects in development. Diverticula are much the more common. Some degree of constriction is not particularly infrequent, but complete absence of even a section of the colon is an extremely rare anomaly.
The acquired anomalies have to do with disease processes or results of injury. Displacements may be the result of old adhesions and distortions; of chronic constipation, i. e., fecal impaction and resulting overloading, with sagging, stretching, and complete change in shape and position; with displacement due to enlargement of other organs, e. g., the liver, stomach, spleen, uterus, or, in milder degree, with the gradual but inevitable and chronic results of tight lacing. The causes which produce a gradual enteroptosis of the transverse colon are not supposed to concern the surgeon, yet the condition may precipitate acute obstruction which will necessitate his urgent participation in its final treatment.
There are no diseases peculiar to the large which do not also concern the small intestine, and no surgical diseases peculiar to it which have not been considered in the foregoing pages. It is not, therefore, necessary to make even a brief summary of the surgical diseases peculiar to the large intestine. Of well-known lesions, however, in this location there is perhaps a little worth emphasis in this place. The most serious surgical conditions of the large bowel, aside from the acutely obstructive, are those pertaining to expressions of tuberculosis, syphilis, actinomycosis, dysentery in one or other of its tropical forms, and cancer. There is a condition also of either acute or chronic colitis or mucocolitis which may assume such extreme degree as to necessitate a colostomy made at the cecum (appendicostomy) for the purpose of more perfect irrigation and physiological rest. The amount of suffering, as well as of toxemia, which may proceed from a seriously inflamed colonic mucosa, must be at least once seen in order to be fully appreciated. Such a condition is characterized by local and general suffering, with septic and copremic symptoms, as well as by tenesmus and the passage of numerous small or larger and more infrequent amounts of blood-stained mucus, sometimes of almost pure blood. As an illustration if one recall what may be seen in case of a violently inflamed conjunctiva or pharyngeal mucous membrane, and realize that this condition is duplicated through a large portion of the colon, a more vivid picture of what it actually represents can be afforded. When exposed to inspection, as it may be when the rectum and the sigmoid are involved, it will be found to bleed at the slightest touch and to freely discharge large quantities of thick mucus. While such a colitis is usually treated by non-operative methods an anesthetic is sometimes required for its more perfect diagnosis and recognition, as well as for such local applications as can scarcely be made without it.
Tuberculous and syphilitic ulcerations of the colon may be localized and relatively insignificant, or numerous, disseminated, extensive, and serious. In extreme cases of this kind the entire colonic mucosa will be involved and the amount of distress thus occasioned be scarcely controllable. These are the cases which, failing to yield to ordinary therapeutic measures, justify colostomy at the cecum, for the purpose of temporary exclusion of the large intestine and its physiological rest, as well as its more perfect local treatment by the irrigation and suitable local applications thus permitted.
[870]
Strictures of the large bowel have the same etiology as those of the small bowel, and are to be recognized by the same general indications, of which increasing obstipation, perhaps with alternating attacks of diarrhea and increasing difficulty in evacuation, are unmistakable features. The nature of a stricture is not always to be foretold before the exploration which it will necessitate. No stricture of the large intestine which is above easy reach from the anus can be successfully treated by any save operative methods, i. e., by abdominal section and proper attention to whatever may be thereby revealed. Thus at one time bands may be divided or some external mass removed by pressing upon the bowel (e. g., a uterine myoma), or there may be found an associated tumor, malignant or benign, whose complete removal is both possible and permissible, or at other times a malignant stricture so complicated that only an entero-anastomosis, for temporary relief, can be effected.
Cancer of the large intestine spares no part of its length or lumen. Primary cancer of the cecum may commence in the region of the appendix, and has frequently been mistaken for a chronic appendicitis. If the transverse bowel be involved there may be more or less sagging or fixation, while at the flexures obstruction is more easily produced. Such growths in time become sufficiently prominent to be easily recognized from without, but then they have usually gone beyond the time when radical operation can hold out much promise. In the large, as in the small, intestine radical operations are, however, often successful, and always in proportion as they are made early and thoroughly. When extirpation is impossible anastomosis will offer a temporary substitute (Fig. 589).
Fig. 589
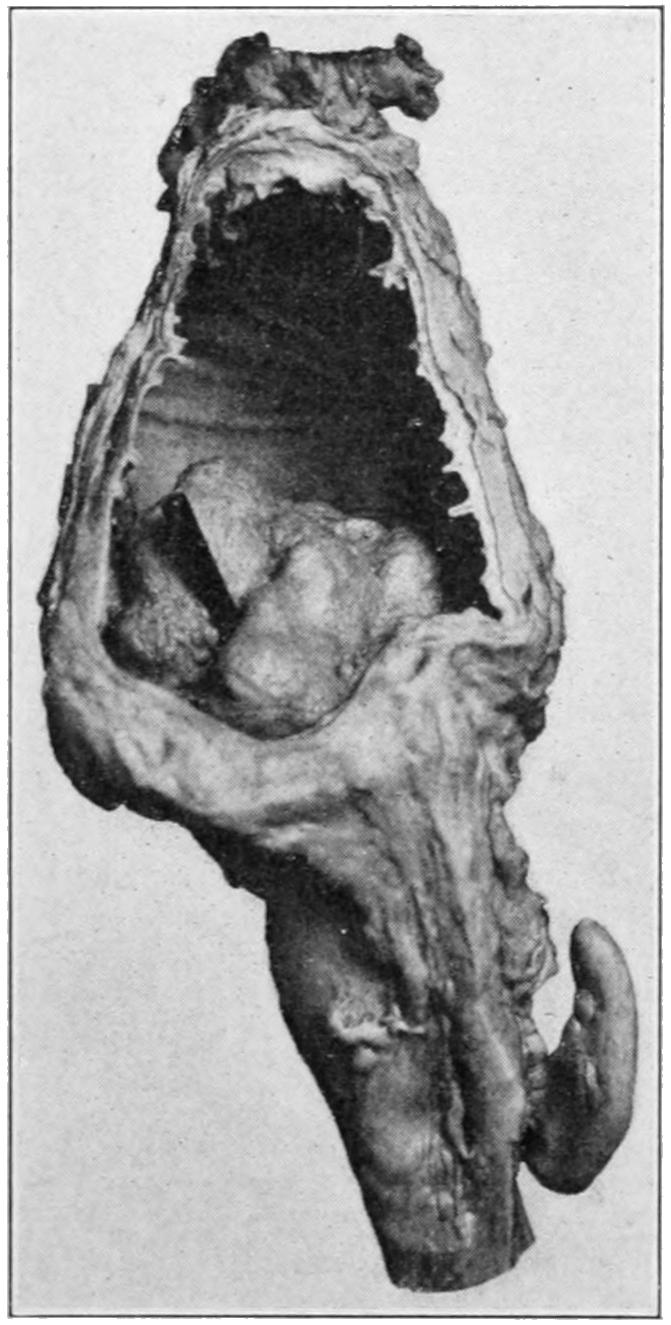
Cancer of cecum, showing ulcerating growth protruding interiorly and obstructing. (Dr. E. A. Smith.)
Chronic obstruction of the large bowel is usually due to one of the causes above considered. Acute obstruction of the colon is the result either of precipitation of an acute condition upon the base of an old chronic trouble, of invagination, of volvulus, or possibly of one of the other mechanical contortions not included in either of these expressions.
Intussusception is most likely to occur either at the ileocecal valve or in the region of the sigmoid. Volvulus is more common in the latter region. It is here due to relaxation of natural ligamentous supports, to overloading and stretching, or is possibly permitted by some congenital condition. Volvulus in this section having once occurred the patient is liable to its subsequent recurrence. So well known now is this fact that surgeons have endeavored to take special precautions against it, which unfortunately have not been brilliantly successful. It has been suggested, for example, to anchor the sigmoid to the anterior abdominal wall, or to resect a portion of it, to anastomose it with the cecum, as well as to reef the mesosigmoid. Desirable as such operative relief may be, all of these methods present inherent objections, while those which include absolute fixation of the sigmoid perhaps predispose it to subsequent obstruction from other causes. At present it would appear that a sigmoidopexy is probably the best procedure, in order to prevent local recurrence, in a sigmoid volvulus[871] which has once been exposed by operation, care being taken to fasten it well up to its outer side, as well as posteriorly, in order that there may be no vacant spaces in these directions.
The rectum was for too long a time relegated to the care and almost sole interest of the itinerant charlatan, or the somewhat ambitious, though scarcely more honest, specialist, who preyed alike upon the suffering and ignorance of patients, until the practice of rectal surgery was almost a mark of disgrace. From this unfortunate condition it was rescued by the organized effort of honest men, until now, in the light of their researches, the rectum has been shown to be both the site of numerous, easily discernible, and serious, alike mysterious and reflex lesions, all deserving careful study. The connection between the sensory nerves with which its terminal inch and a half are freely endowed and the vasomotor nerves throughout the body is easily shown by their influence, for instance, upon the respiration and the circulation, and in these respects some important lessons have been learned from the charlatans. We have learned, for example, that general vasomotor spasm, with its evidence in coldness of the extremities and pallor of the surface, may often be overcome by so simple a measure as stretching the sphincter; while to cure lesions which produce more or less sphincteric spasm is to frequently restore general circulatory tone. Again, what may be accomplished in stimulating respiration by dilatation of the sphincter has been shown to be of the greatest value in patients breathing badly under an anesthetic.
The “orificialists,” then, while making absurd and impossible claims, have nevertheless taught us considerable concerning the value of recognizing the importance of sphincteric spasm. Their claims concerning so-called “pockets” and “papillæ” are untenable and absurd, and the expression which they have taught many of the laity that they are sufferers from “rectal pathology” indicates alike their ignorance of good English and good surgery. That papillæ do become, under certain circumstances, exquisitely sensitive and are occasionally in need of the cautery or the scissors, as well as of the general relief afforded by stretching the sphincter, is undoubtedly sometimes true.
The itinerant “pile-drivers” and charlatans of their class have done more harm than good, and yet even from them the honest practitioner has learned that “it pays” often to give attention to the rectum. As a source of various disturbing and particularly distressing reflexes there is scarcely any portion of the body of equivalent area which can furnish so many. The relief to mental conditions, amounting often to pronounced melancholia, which follows cure of rectal lesions, is often astonishing, all of which shows that the rectum is well worth the attention of the scientist, and especially of investigation in every case where the slightest complaint is made.
All of which properly leads up to the subject of rectal examination and how to make it complete. Much can be learned here by use of the educated finger, as well as in the vagina, and the surgeon should cultivate that tactile sense which will orient him so soon as the finger-tip comes in contact with a morbid or diseased surface. In this way it is possible to detect ulcers which are within reach by the finger alone, without having to use the speculum, at least to make a diagnosis sufficient to indicate what further procedure is required. The rectum and lower bowel should be thoroughly emptied. It is safe to assume that exquisite sensibility and pronounced sphincteric spasm are the result of morbid conditions. The use of a local anesthetic will in many instances be sufficient to permit at least of a preliminary digital examination, the suggestive characteristics especially sought being the general size of the rectal tube, infiltration or fixation of its walls, and the presence of stricture, tumor, or other impediment to insertion of the finger, including pronounced spasm at the anus. The presence of bloody mucus or pus should also be noted. In addition the rectal surroundings should be examined and the presence of any phlegmon, fistula, sinus or other evidence of present or past disease, including old scar, either of ulcer or incision, should be noted. The degree of pain as well as of hypersensitiveness produced should also be noted. With tact and gentleness satisfactory knowledge of the condition of the parts within reach may be obtained.
[872]
A rectal bougie may be used should suggestions of the presence of stricture be present. Rectal bougies are usually made of soft rubber of various sizes, with tips variously shaped, of which the tapering and conical are the most useful. One of these may be anointed and gently introduced, the endeavor being to guide it first in the middle line along the course of the rectum and then gently toward the left as the rectum swerves in this direction as it comes down from above. With such a bougie the presence of a stricture beyond reach of the finger may be detected. When recognized its nature is, however, still left in doubt, to be decided by the history or other features of the case. There is never excuse for roughness in handling a rectal bougie, since perforation or serious injury might result.
The next method of more complete examination of the rectum is through one of the various forms of specula, from the so-called rectal speculum, with its blades only a couple of inches long, to the more formidable proctoscope or sigmoidoscope, with their possibilities or artificial illumination, etc. According to the nature of the lesion and the sensibility of the surface exposed various specula may be used, with or without an anesthetic. For the majority of purposes local anesthesia is sufficient. One will furthermore often need the aid of position. The ordinary digital examination may be made with the patient upon the side or back. When an ordinary speculum is used a position corresponding to Sims’ for gynecological work is far preferable. For more thorough work when the long, tubular instruments are used, the knee-chest position is necessary. The specialists have devised certain elaborate chairs, instruments, and methods by which exceedingly complete and satisfactory exposures of twelve or fifteen inches of rectal and colonic mucosa can be made. What is written here, however, is not for their purposes, but rather for those of the general practitioner, who must work with ordinary means and methods. The knee-chest position, for instance, can be assumed upon the ordinary table or it may be facilitated by certain additions made to a regular operating table. With all these facilities and the peculiar skill which specialization produces it is possible to make striking demonstrations of the valvular arrangement of the rectal mucosa, and of the varying degrees of obstruction which mucous folds or cicatrices may produce, as well as to successfully dilate or divide them. In the hands of a limited number of skilled surgeons local treatment of obstipation, as well as of various other conditions of the sigmoid or upper rectum, has become extremely satisfactory. These are, however, in the writer’s estimation, methods and procedures which are scarcely within the domain of the general practitioner or even the general surgeon, as they require a degree of peculiar facility and an amount of time which can scarcely be expected of him. Therefore the conditions and methods of treatment here considered will be limited to those intended for general use.
The lowermost portions of the intestinal tube are by far the most common sites of congenital anomalies and defects. These rarely occur in the direction of excess, rather of atresia or entire deficiency. The lower end of the alimentary tube is differentiated from the balance of the original neurenteric canal, and connected with the exterior, in ways similar to those followed at its upper extremity. The canal itself should early become obliterated at a point whose site is marked by that small collection of lymphoid tissue known as the coccygeal or Luschka’s body, corresponding in this respect and location to the pituitary body at its other extremity. The rudimentary rectum is then connected with the surface by the formation of a depression and disappearance of tissue in just the same way that the mouth is formed, and as about the mouth we find atresia or incomplete communication, so we may find the same condition in various expressions about the termination of the rectum. Moreover, there may occur also more or less arrest or abnormal development of the tissues which eventually shut off the rectum from the genito-urinary tract. In consequence, we have various degrees of rectal atresia, and, finally, actual imperforation. Beyond this we may more rarely meet with complete absence of the rectum, and even of some portion or of nearly all of the entire large intestine. In one case under my observation this entire tract was represented by little more than a mere cord.
PLATE LII

Cancerous Stricture of Rectum. Bowel Laid Open for Inspection.
[873]
The mildest degree of such malformation refers to partial occlusion of some portion of the rectum, or extreme smallness of its natural opening, either of which constitutes essentially a stricture of congenital origin, which may be sufficiently tight to barely allow passage of meconium. Such strictures may escape notice for a considerable length of time and will always tend to produce dilatation and consequent displacement of bowel above.
Ordinary imperforate anus is produced by its closure by a more or less thick, membranous diaphragm, which may act, in some cases, like a thin but imperforate hymen, or, in others, be so dense and massive as to act more like a plug than a partition. The thinner the diaphragm and the more perfect its structure as such the simpler the case, for it simply needs perforation, with sufficiently frequent subsequent dilatation to maintain the proper size of the aperture.
Complete absence of the anus and the lower end of the rectal pouch may be so marked that scarcely a dimple indicates the point where the anus should be found. In these cases the external sphincter may or may not be present, while the rectal pouch may present loosely in the pelvis, or be defective, or attached to some portion of the abdominal wall, the intervening space being filled with indifferent tissue. The fact that there appears to be a slight anal depression is to be taken for nothing more than an indication of what should be found, and signifies nothing regarding the deeper condition.
A somewhat mitigated expression of this last defect is seen when the anus is normal, with a more or less complete sphincter, but where a distinct partition separates this pouch from the rectum above. This, again, may vary considerably in thickness. If, then, fluctuation be detected the condition may prove less unfavorable for the little patient, since at this point communication may be easily established. Too often, however, this diaphragm is dense and tough. When successfully perforated, like the hymen, it may allow a slow dribbling of material, and will require constant attention and dilatation. Figs. 590 and 591 portray these conditions in some of their expressions.
Fig. 590
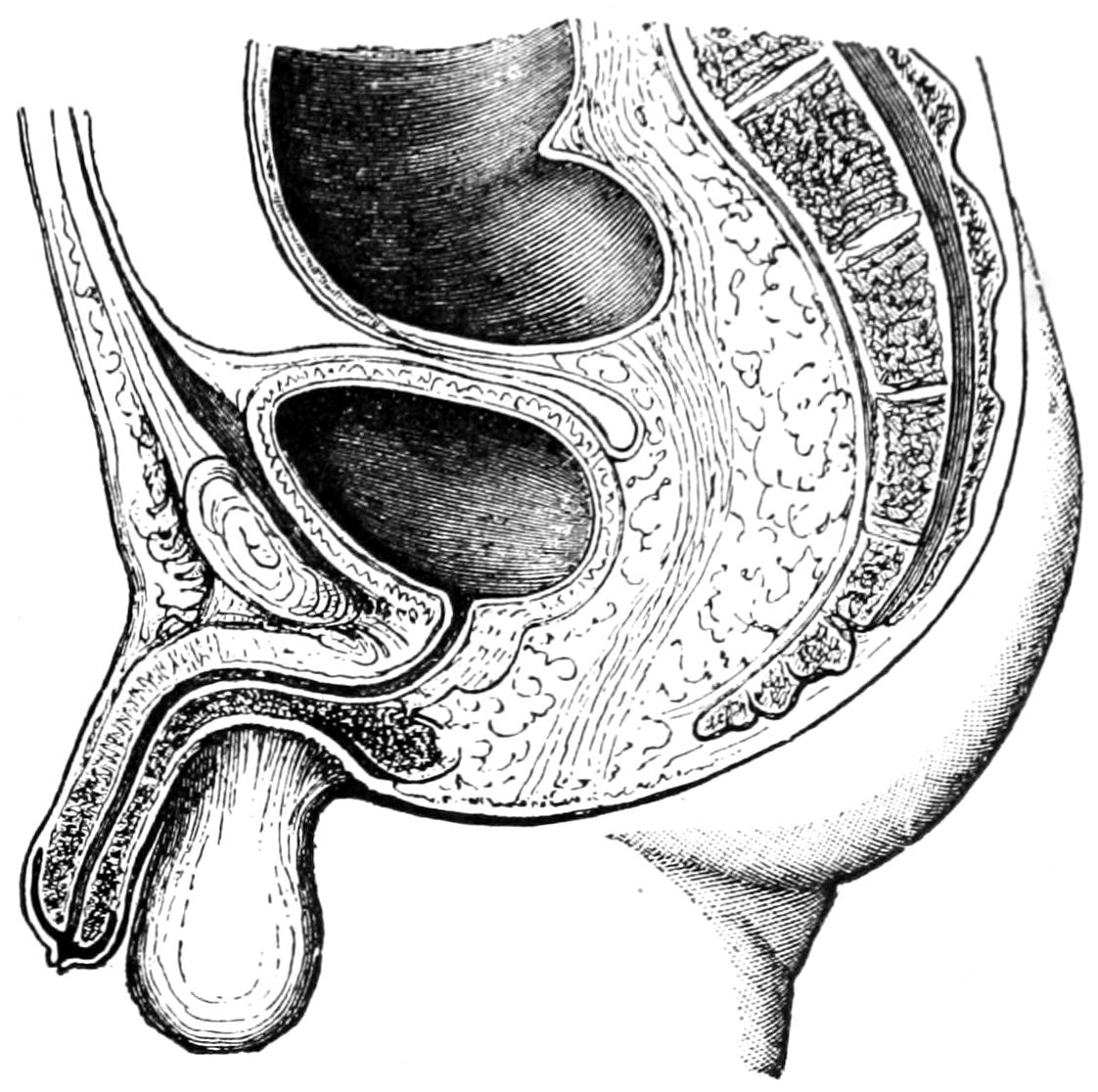
Rectum ending in a blind pouch. (Kelsey.)
Fig. 591
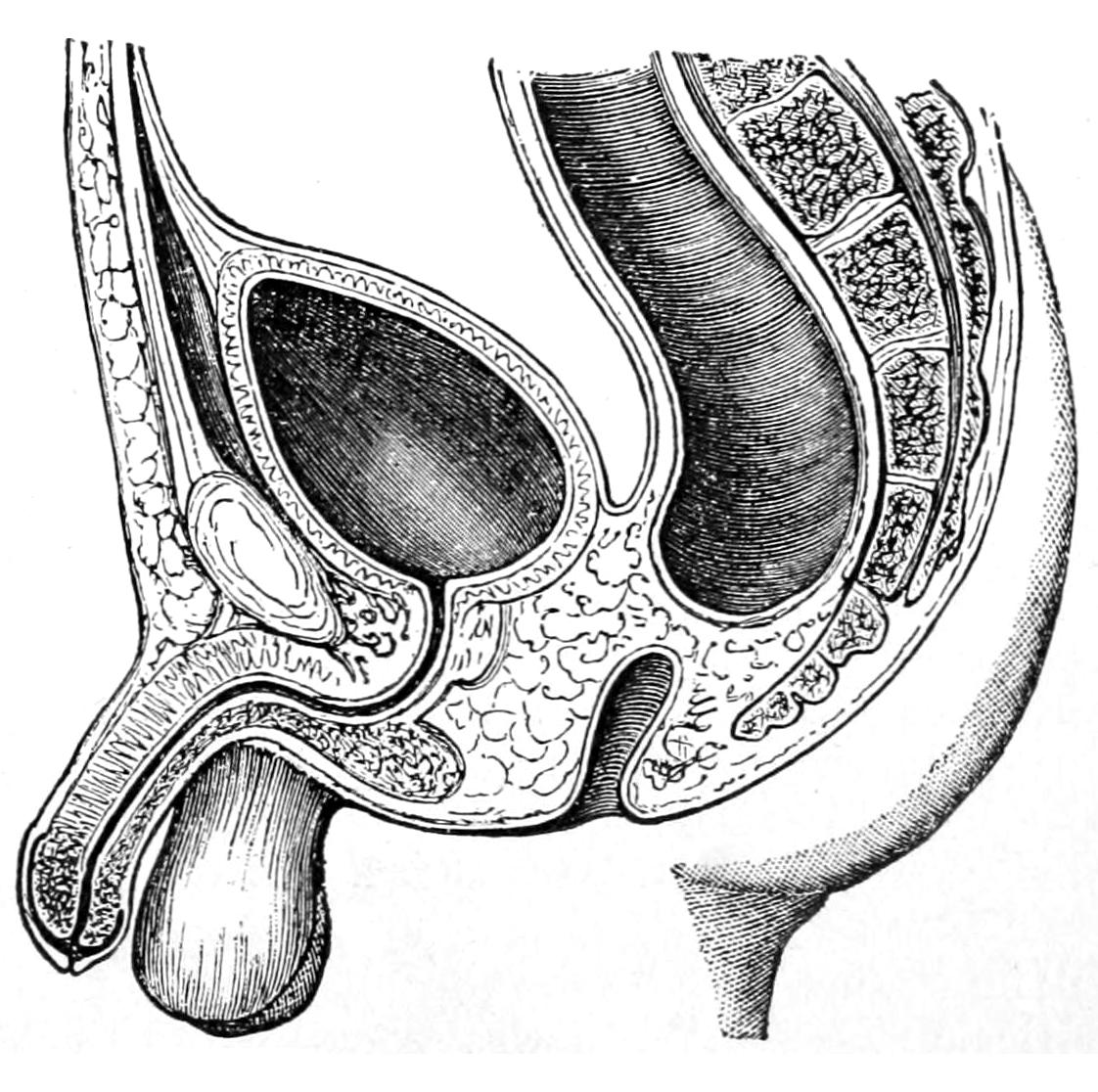
Rectum ending in pouch; anus normal. (Kelsey.)
The anus itself is by no means a fixed anatomical opening, and its position may vary considerably. It may be found anywhere along the middle line of the perineum or even in the sacral region.
Another variety of complication is, with the conditions represented as above, a practically imperforate anus or rectum which nevertheless opens into one of the other pelvic cavities—the vagina, the bladder, or the urethra. In female infants an[874] opening into the vagina may be of a size sufficient to serve its purpose, even throughout life. This condition has occurred in ignorant women who became wives and mothers, and were never conscious of anything abnormal. When the rectum communicates with the urinary passages meconium will escape with the urine. When the opening is in the urethra it is not so serious, and patients live to adult life, whereas when the bladder is thus involved the ureters will become infected and the patient eventually dies of a terminal infection of the kidney.
There is a somewhat reversed condition similar to this where the urinary passages connect with the rectum or with the colon.
Most of the anomalies above catalogued produce conditions of acute intestinal obstruction within the first two or three days of the newborn infant’s life. The condition is perhaps first made known by the nurse’s failing to note the presence of meconium upon the diapers. A suspicion of such a condition should prompt immediate investigation, which should be made with the little finger or with a soft catheter properly anointed; the finger making the best probe for purposes of orientation. The first thing is to determine the patulency of the anus. This established, the next procedure is a determination of the rectal condition and of possible communication with other passages. In this the presence of a small sound or metal catheter in the urethra and bladder may be of assistance. If a fluctuating sac presenting downward can be discovered in the location of the rectum its character may be assumed, and, after exploring with an ordinary aspirating needle, one may, if meconium be discovered, leave the needle in situ for a guide and with sharp scissors or pointed knife passed along it carefully cut into the sac, and then gradually enlarge the opening until it be given a sufficient size. The surgeon is fortunate in this respect who has a case of imperforate rectum so simple as to permit of doing this and finding it sufficient.
Every completely obstructed case becomes instantly a surgical one, whose outcome depends not on the operator alone, but on the actual anatomical condition. There is justification, therefore, in going to almost any extreme in the endeavor to open up a passage-way, for no danger can be greater than that of failing to establish it. After a careful search of the pelvis, aided by anesthesia and a metal instrument in the bladder, if no trace of large bowel can be found or if tissues be so dense as to completely mask the anatomical details, then as a last resort an artificial anus may be made in the left inguinal region, if there be no reason for not violating the usual rule and opening the large bowel in the right groin. Colostomy in an infant, under these circumstances, is always a hazardous and serious matter, but it offers the only resource. It is made in exactly the same way as enterostomy described previously, and the operation requires no special description here. Very young infants thus affected make bad subjects, and operation should be performed as expeditiously as possible. Considering the danger of leakage it would be well if practicable to wait a few hours after attaching the intestine to the abdominal surface before opening it, in order that the peritoneal cavity may be more perfectly protected.
Even those cases where the rectum communicates with the urethra or bladder should have a natural anal opening. In cases where communication is into the vagina it may be proper to wait until youth or adult age is reached, when more may be accomplished.
The rectum may be the site of injuries of various kinds from both extrinsic and intrinsic causes. When weakened by disease it may be burst by accumulation and straining, or it may be the site of perforation of ulcer, just as may any other part of the intestine. Although well protected from most directions it may suffer from penetrating wounds, such as stab or gunshot. It is occasionally injured in fractures of the pelvis, and possibilities of such injuries should be excluded in such cases. It may also be lacerated during parturition. The sphincter and even the muscular tube itself sometimes suffer. It has been indifferently wounded or punctured in operations, especially for stone in the bladder and in prostatectomy.
In the absence of disease a laceration occurring in any of these ways may be repaired by prompt suture, although to make a suitable exposure may require an extensive removal of sacrum, or the performance of a laparotomy with the patient in the Trendelenburg[875] position. The rectum is also frequently injured by accidental or intentional introduction of foreign bodies from without. Museums, especially the foreign, are full of collections of foreign bodies which have been removed from the rectum, most of which have been placed there with intent, malicious or otherwise. They include objects of all imaginable character, shape, and size, some which are easily introduced and are also easily removed; others which have been passed inward under no small difficulties are removed only with a more or less formidable operation, or have even determined the death of the individual. The ignorant have peculiar superstitions, and the criminal most vicious tendencies, toward the insertion of such foreign bodies, and the complications that may be brought about are too numerous to be rehearsed here.
On the other hand, by actual accident serious injuries may be produced; as in one case under my observation where a boy of twelve fell, in the squatting position, over an iron picket nearly one inch in diameter in such a way as to permit it to pass into the anus, scarcely bruising the mucous membrane, yet entering the pelvis for nearly six inches, penetrating the anterior wall of the rectum, the posterior wall of the bladder, and bruising its anterior wall without perforating it. One feature of the accident was the carrying into the bladder of a piece of his trousers. In this case I opened the abdomen in order to be sure that there was no abdominal complication, closed the major part of the wound, and drew a good-sized drainage tube through from just above the pubes out through the anus, after removing the piece of cloth above mentioned. The boy made a perfect recovery.
The danger in all these cases is of infection, either of the bladder or of the pelvic cellular tissue. In the female similar perforating injuries may involve the vagina or the other female organs.
Some of these accidents or conditions above recounted take place during intoxication. The recurrence of tenesmus, pronounced rectal pain, the appearance of blood either at the anus or in the urine, should in every instance prompt a thorough investigation of the rectum, if necessary under an anesthetic.
Under the term proctitis are comprised acute inflammations of the rectal mucosa, which are characterized by discharge of mucus, mucopus, and perhaps blood, and accompanied by more or less tenesmus, pain, and sphincteric spasm. The conditions which produce proctitis are those which lead to ulceration. It may be the result of a downward extension of trouble from above, as in mucocolitis, dysenteric, tuberculous or other forms of colitis, or it may be the result of infection from below (e. g., gonorrheal). An inflamed rectum may be more or less easily exposed for study through some form of speculum (see above), and a more perfect picture of the actual condition thus presented to the eye than can be seen elsewhere, save in the mouth and pharynx, of the effects which serious and even ulcerative inflammation may produce in the way of congestion, swelling, bleeding, and actual breaking down.
Gonorrheal proctitis is not common, yet it may occur either by extension or by direct infection, and will be of an acute type. The other forms may vary in severity according to their cause and duration.
—The symptoms differ only in degree, and include the features already mentioned. There are soreness, tenderness, and often pain, especially when the lower part of the rectum, with its numerous sensory nerves, is involved, while reflex pains are referred to the sacrum and the lower part of the back. Sensation of local heat and of soreness is generally noted, while the patient is more or less tortured by frequent desire to evacuate the bowel, but passes perhaps a little bloody mucus with the accompaniment of tenesmus and straining. In acute cases the condition is an exceedingly painful one.
—Treatment should be begun by a search for and removal of the cause. Relief is afforded by local anodynes, of which the hot sitz bath is one of the most comforting, and by hot rectal lavements of soothing antiseptic fluid, such as linseed tea, to which a little thiol or ichthyol has been added. These should be retained as long as possible, then ejected. Local anodynes may be furnished through the medium of suppositories containing opium, or preferably some of the milder local anesthetics, such as[876] orthoform. Cases which do not quickly yield to this form of treatment should be anesthetized in order that complete exposure of ulcerated areas and vigorous local treatment may be accomplished. A brushing of the entire surface with a 2 or 3 per cent. solution of silver nitrate will frequently be followed by relief, which will be further furnished by sufficient stretching of the sphincter to overcome its painful spasm. The diet should be so regulated as to leave a minimum of undigested residue that may irritate the lower bowel, and laxatives should be so administered that there shall be no coprostasis in the colon, but that whatever enters it shall be speedily extruded. The specific forms of proctitis require specific treatment, for which there is perhaps nothing better than the silver preparations, either the mild, like argyrol, or the active, like solutions of silver nitrate.
The causes of the formation of ulcer in the rectum nowise differ from those of ulcer elsewhere about the body. They may be summarized as catarrhal, i. e., more pronounced and local extensions of non-specific inflammation of the mucosa, which, in certain areas, assume more intense and later infective and degenerative form (in this way are formed the so-called catarrhal ulcers); specific, including primary chancre, which is rarely met with high up in the rectum, or the later expressions, varying from mere mucous patches which may abound both within the rectum and around the anus, to the deeper, more destructive, and usually tertiary ulcerations, with destruction of tissue, extensive involvement of surface and most pronounced tendency to subsequent cicatricial contraction when they begin to repair.
What has been said regarding syphilitic ulcer is true also of chancroid, which when found in this region involves most frequently the anus, but which may extend or even be seen as a primary lesion higher up.
Tuberculous ulcers are not infrequently primary, usually the accompaniment of advancing and ulcerative infection of the intestine above, or secondary, as frequently occurs when the more innocent forms suffer a secondary tuberculous infection, becoming thus converted into lesions of pronounced type.
Typhoid ulcers in the rectum are rare, but those connected with dysentery are common, especially in localities where tropical or other forms of the disease prevail. The innocent tumors within the rectum, such as polypi and adenomas, etc., tend to break down because they are kept continually macerated and exposed to contamination. Even innocent hemorrhoidal tumors are extremely prone to suffer in this way because their epithelial covering is thin and they are exposed to both external and internal contamination. Finally every malignant tumor which grows into the rectum tends to break down, and sooner or later to present an ulcerating surface. The causes of rectal ulceration are then seen to be various. Nearly everyone of them may be an exaggeration of a condition first producing an acute proctitis.
Ulcers occupying the anal region are usually compressed into a linear form and present rather as cracks or linear abrasions. These are known as fissures and are spoken of as fissures in ano or rectal fissures, according to their situation. These fissures occupy the most sensitive portion, i. e., the lower inch and a half of the rectum, and become in time irritable, erethistic lesions, whose sensibility is constantly enhanced by the reflex spasm of the sphincter which they produce. An essential part of the treatment of every such case is dilatation of the sphincter, as well as the destruction of the irritable surface, even the former alone often sufficing for the milder cases. Anal fissures, like corneal ulcers, give rise to exquisite pain and annoyance, and produce irritability and general distress. Their treatment is so simple that there is no excuse for allowing patients thus to suffer.
To a peculiar form of combined infiltration and ulceration involving the lower part of the rectum, the anus, and, in females, more or less of the vulva, the French have given the name esthiomene. It has been considered due to more or less mixed forms of infection, including those of chancroid, syphilis, tuberculosis, and other undescribed types. It is a mixed infection, and not necessarily of the same type in all cases. It is usually seen in old syphilitic subjects or in prostitutes. It produces more or less deforming lesions, and sometimes such active and protuberant granulations as to cause it to be mistaken for epithelioma or condyloma. It is essentially chronic, and its most[877] striking characteristic is the combination of ulcerative and hyperplastic processes which it presents. Clinically it is a chronic ulcer, with thickened and deformed base and with all the possible consequences or complications of ulcer in this region.
The other forms of ulcer above mentioned appear singly or multiply in any and every possible location, pronounced types presenting extreme pictures of an ulcerated, inflamed, partially destroyed tube, which needs only to be seen before recognizing the advisability of a colostomy for the purpose of rest of the inflamed surfaces.
—The symptoms of rectal ulceration are essentially those of proctitis, mild or severe as the case may be, with local pain, and escape of pus and blood. Much depends upon their location, i. e., whether within the sensitive area or not. Ulcer low down in the rectum, no matter how produced, will always cause a disproportionate amount of suffering, because of the reflex sphincteric spasm which it produces. On the contrary, ulcers high up give rise to little or no suffering, and may be discovered only after a history of discharge of blood or pus prompts a thorough local examination. Therefore, without reference to the feature of pain, every statement that mucus, pus, or blood is discharged from the rectum should lead to an examination, sufficiently thorough to detect and expose the cause and permit of proper treatment. Should local anesthesia prove unavailing for this purpose a general anesthetic must be administered. Thus the non-specific, the syphilitic, and the tuberculous ulcers may be scraped and cauterized, care being taken not to perforate. If ulcerating tumor is found it should be operated upon at once. Sometimes, however, by these examinations unsuspected conditions are revealed such as to give the case a serious aspect. In this event a second anesthetic, with operation, will be necessary. For all ordinary purposes, however, sufficient specula, curettes, the actual cautery, and applicator, by which suitable local treatment can be made to the affected surfaces, should be provided.
—As indicated above in the treatment of proctitis there is need also for various local anodynes and soothing applications. Physiological rest for the inflamed bowel is imperative. Finally, in extreme cases, it has been shown that it is best to open the colon above the seat of the principal disturbance, doing this even on the right side should the whole large intestine be involved, and by thus relieving it of its duties enable more complete physiological rest and local treatment.
The inevitable consequences of any of the serious forms of ulceration above described are, if recovery ensues, and usually even if it does not, the formation of cicatricial constrictions by which varying degrees of rectal stricture are produced. Rectal strictures, then, are to be grouped as:
The symptoms and signs of rectal stricture include those of ulceration and obstruction, or difficulty in defecation. A history of alternating constipation and diarrhea, with perhaps tenesmus, and with discharge of pus or blood, will prove the presence of some obstruction. One characteristic feature met with in some strictures is the passage of stools which when solid or semisolid have a characteristic tape- or cord-like shape, as though extruded through a constricted passage-way. This is not a feature necessarily present, and may be produced even in non-malignant cases, as when the rectum is obstructed by uterine myomas.
With respect to any suspected rectal or colonic stricture it is necessary to determine: (1) Its existence; (2) its location; (3) its character; (4) any other circumstances bearing upon the case which might affect the question of treatment. The latter is particularly important when the question of syphilis is raised.
The above features are determined by careful physical examination for which the finger alone may be sufficient, or which may require instruments and postures already described.
—Treatment of rectal strictures is necessarily mechanical, but will depend in large measure upon their cause and extent. Thus a stricture produced by[878] conditions extrinsic to the rectum proper might require abdominal section and removal of a pelvic tumor or other similar operation. Many a patient with retroflexed uterus will complain of a rectal condition which is essentially one of stricture, the overturned uterine fundus being forced against the rectum and pressing upon it, demanding not a rectal operation but one for suspension of the uterus. The obstipation which is produced by ptosis of the sigmoid, or by hypertrophy and abnormal arrangement of the folds and rectal valves, may necessitate operation upon the colon (coloplication or colopexy) or a careful division of hypertrophied mucosa through the proctoscope, as used by one skilled in its manipulation.
Fig. 592
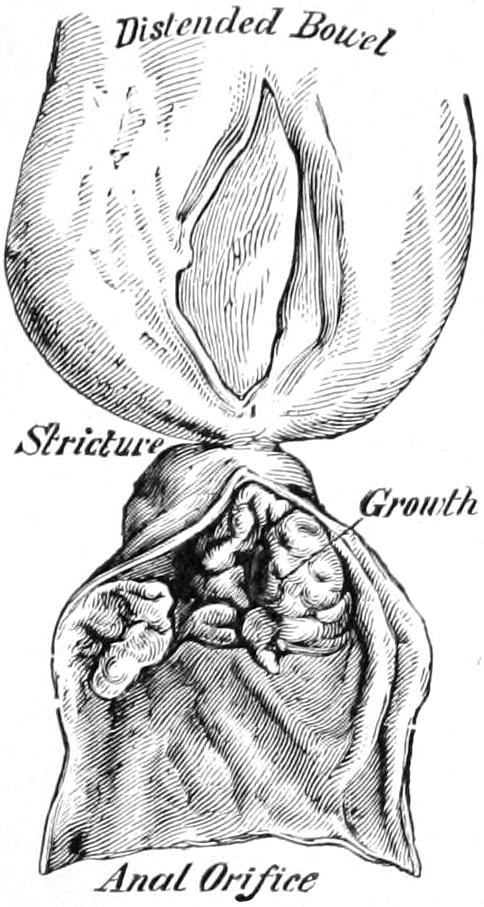
Stricture of rectum. (Bryant.)
Strictures of recent origin may yield to a forcible dilatation, which should, however, be systematically repeated in order to maintain the desired effect. Old, dense, and chronic strictures will require more radical procedures, according to their location and extent. Strictures practically impassable may indicate conditions so extreme as to necessitate colostomy, while in a small proportion of cases conditions will be found so favorable as to justify a resection of the rectum, either from below and from without, or through abdominal section with the patient in the Trendelenburg position. Nearly every stricture is accompanied by more or less ulceration, sometimes in extreme degree.
Dilatation or expansion by some mechanical method is the necessity in every case. Simple in theory its performance is often difficult because of density of the structures, and its danger often pronounced because of the serious surrounding conditions and the possibility of rupture or perforation of the bowel at some weakened part, or of infection and phlegmon following division of the stricture and exposure of fresh, raw surfaces. Various instruments have been devised for dilating rectal strictures, some of which are ingeniously arranged to be used at a considerable height above the anus. Danger attaches to their use in proportion to the amount of force employed and its distance from sight and touch, i. e., from intelligent means of control. The best method is that which permits of exposure through the speculum and more accurate division with knife, scissors, or actual cautery, the latter often being preferable, as hemorrhage is less after its use.
It should be remembered that “once a stricture always a stricture,” and that the tendency of cicatricial tissue to contract is continuous and never ceasing, and that wherever there has been a stricture (and this is true of any tubular portion of the body) there is necessity for constant and more or less frequent later attention. If possible, then, milder methods and those more capable of repetition should be adopted. The best of these is the use of the finger for cases within reach of it, and of the soft-rubber, conical bougies for those placed higher, and for the patient’s individual use. Dilatations should be gradual and increased as rapidly as circumstances permit, and with tight strictures the endeavor should be with each sitting to make some gain until a sufficient size has been attained. Local anesthesia may be required, and is justifiable when needed.
This condition, usually accompanied with irritative or ulcerative conditions of the lower end of the rectum, the verge of the anus, and the surrounding skin, is one of intense itching, leading to an uncontrollable desire to rub or scratch, by which temporary relief may be afforded, but which tends to produce excoriation and ulceration. The condition is not primary, but secondary to something else, although the conditions which produce it are widely variant, ranging from the neuroses due to anemia or other causes, to the toxemias of uric acid origin, the local irritations produced by lesser degrees of internal disturbance, or eczema or other itching eruptions on the outside. In corpulent persons eczema and intertrigo from friction are common, and these, combined with irregular tags of skin or remains of old piles, permit of irritation and maceration which still further complicate. Annoyance is usually greatest at night, when the attention is less distracted by other things.
[879]
—The treatment should consist in removal of the cause and local relief. The former may be difficult and require prolonged effort. Local relief may be afforded by frequent applications of water as hot as can be borne, with local application, after the parts are thoroughly dried, of a powder containing menthol, a solution containing camphophenique, with the addition of a little chloroform, or by soothing ointments containing carbolic acid, menthol, and orthoform. When there is abrasion of the skin applications of silver nitrate, in 5 per cent. solution, may be made; but when there is multiple ulceration, stretching the sphincter and thoroughly cauterizing or excising the ulcerated surfaces will be more radical and effective.
On either side of the rectum, between the dividing folds of the deep pelvic fascia, is situated the ischiorectal fossa, a pyramidal-shaped cavity filled with fat and cellular tissue. This is not only in close relation with the outer rectal surfaces, but is peculiarly liable to infection and acute inflammatory disturbance. Thus it happens that ischiorectal or perirectal abscesses are of frequent occurrence, often of marked violence, and not without their peculiar dangers. Infection may travel from the rectum, or the first excitement may occur in one of the mucous or skin follicles at or near the anus. The consequence is what the patient ordinarily calls a boil, which to the surgeon is a phlegmon, first limited by the walls of the cavity within which it rises. So long as the phlegmonous process be confined within these walls it is acutely painful.
The local signs of such an abscess are redness and infiltration of the exterior surface, swelling, which becomes quite distinct, and pain and tenderness, of which the patient may complain bitterly. The local soreness is so extreme that defecation becomes difficult or almost impossible. Any attempt at digital examination of the rectum will give rise to extreme pain.
—Could every perirectal abscess be distinctly recognized and properly treated in its comparatively early and localized stage there would be few cases of residual trouble. This treatment consists of early and extensive incision, made externally and directed to the centre of the phlegmonous mass, sufficiently deeply also to reach it. The evacuation of even a small amount of pus, followed by more or less blood, will give prompt and immediate relief, and bleeding may be encouraged rather than checked for purposes of local depletion. Such incision may be in most instances made with freezing spray or local anesthesia. In children and exceedingly nervous patients it would be better done under general anesthesia, in order that it be done thoroughly. It is in patients who decline such early relief, or who, from ignorance or inattention have not received it, that ischiorectal abscesses sometimes assume serious proportions and become extensive phlegmons, breaking down anatomical partitions in the pelvis, burrowing extensively in various directions, since there is considerable fatty and cellular tissue both inside and outside of the pelvis in this region. Thus the surgeon may not see such a case until the entire buttock is involved, or until the process has gone perhaps even farther. Relief now must come from radical application of the same principles, by the aid of general anesthesia, multiple incisions with counteropenings, use of drainage tubes, etc. The patient now is fortunate if perforation into the rectum has not already occurred so that no pus is discharged from the bowel. If this has not yet happened it will probably be prevented by the above measures; but when it has, and a fistulous communication has already been established, it may be sufficient to thoroughly cleanse the infected cavity to see both it and the fistula close by granulation in the course of time. Wide external incisions are necessary in these cases, for complete access to the deep fossæ must be made. In more pronounced cases the pus evacuated will be extremely offensive, and there will be found masses of necrotic tissue, sloughs of fascia, and evidence of extensive local gangrene. Such putrid cavities must be thoroughly cleaned out, and will then be found to quickly resume a healthy aspect when treated by packing with gauze saturated in brewers’ yeast.
The more chronic and slower expressions of this condition are usually connected with local tuberculous disease. In fact every phlegmon which has passed the acute stage is favorably situated for tuberculous infection, and becomes in time a tuberculous lesion, which is to be treated on the general principles elsewhere enunciated. These fistulas[880] are often seen in consumptive patients, and apprehension has widely prevailed that the pulmonary disease might be aggravated by radical attention to the fistula. This was only when such attention was made incomplete. To divide the fistulous passage and leave its raw surfaces unprotected and in contact with tuberculous tissue is to invite the spread of infection. To do the proper thing, on the other hand, i. e., to radically dispose of all tuberculous tissue and so treat both fresh and old surfaces that a new infection is not invited, is not to make a patient worse in any respect, but to relieve him of at least one focus of disease. There is, therefore, no reason why rectal fistulas should not be radically treated even when they occur in consumptive patients.
Rectal fistulas are always the consequence of ischiorectal abscesses left to open spontaneously in either or both directions. They may occur also without the preëxistence of a distinct phlegmon, as, for instance, when a small ulcer in the rectum gives way and permits the gradual extension into the perirectal tissues of a mildly ulcerative or suppurative process.
Rectal or anal fistulas are classified as blind external, blind internal, or complete, according as they open and discharge themselves or show a complete passage-way from the rectum to the exterior. They may be small and single, or numerous and extensive. Old and especially chronic tuberculous cases are seen when the whole gluteal region is honeycombed and perforated by numerous fistulas, some of which probably connect with the interior of the bowel. I have seen such openings as low as the knee and as high as the dorsal spines, as the result of extremely insidious advance of tuberculous granulation and its subsequent breaking down. In such cases a history of an acute phlegmon occurring years previously may be obtained.
A blind external fistula, simple or complicated, naturally discharges its pus upon the exterior. It may be accompanied by little or no local tenderness or pain. A blind internal fistula makes itself known by a certain amount of rectal tenderness and by the discharge of pus with the stool, or at other times of pus which may possibly be blood-stained. Here there may be a history of old trouble, with external evidences of it, which suggests that exterior communication has been shut off while that with the bowel remains. In complete fistulas there is discharge not only of purulent material, but of more or less of that which is distinctly fecal, while gas sometimes escapes through them. Such a statement made by a patient is of itself significant. A fistulous passage may be surrounded by more or less infiltrated and inflamed tissue, or it may appear much like a duct. While always causing more or less annoyance, it may produce symptoms which seriously disturb. (See Plate LIII.)
—The treatment of rectal fistula in any of its forms is distinctly surgical and should always be radical. A blind internal fistula can be discovered only with the speculum.
Every such fistulous passage should be split up and its tubular portion thoroughly excised or destroyed with a sharp spoon or caustic. Furthermore it should be followed to its ultimate ramifications. For this purpose it is of great assistance to first inject it with methyl-blue solution, or something else which shall stain it and make it recognizable wherever it may extend. To incise a superficial and external fistula is a simple matter, for which local anesthesia alone may suffice; but to deal radically with an extensive fistulous tract requires dilatation of the anal sphincter and such thorough investigation, with complete relaxation of the patient, that general anesthesia is needed. Now with a probe identifying the tract, and the knife and spoon made to follow it, or by identification of the stained tissues colored as above mentioned, the surgeon should proceed to the extreme of every morbid passage-way, dilating, cutting, trimming, scraping, as may be needed; while after the work is done every particle of disturbed raw surface should be cauterized with some reliable caustic (such as pure carbolic followed by alcohol) so as to sear the surface and prevent the possibility of reinfection.
To do this operation thoroughly necessitates sometimes multiple and extensive incisions, with a fierceness of action which may cause surprise. It is, however, the only effective way in which to proceed.
PLATE LIII
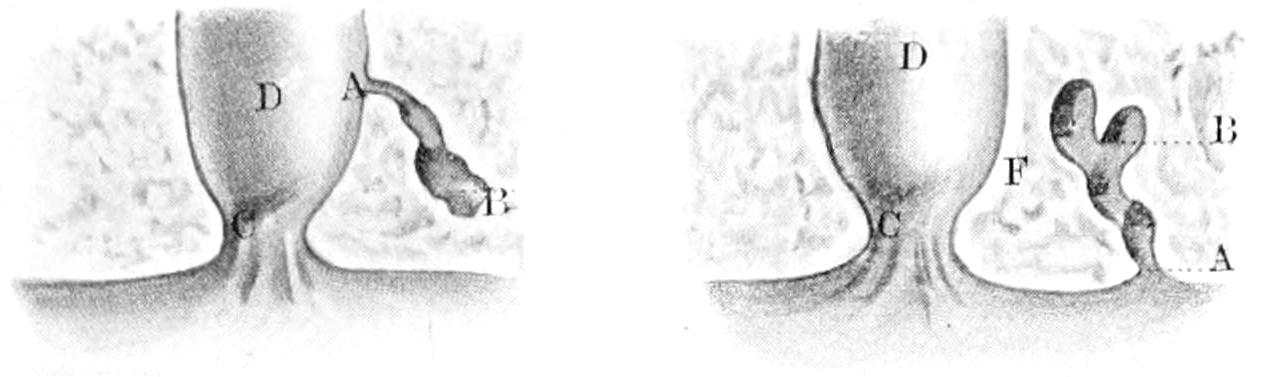
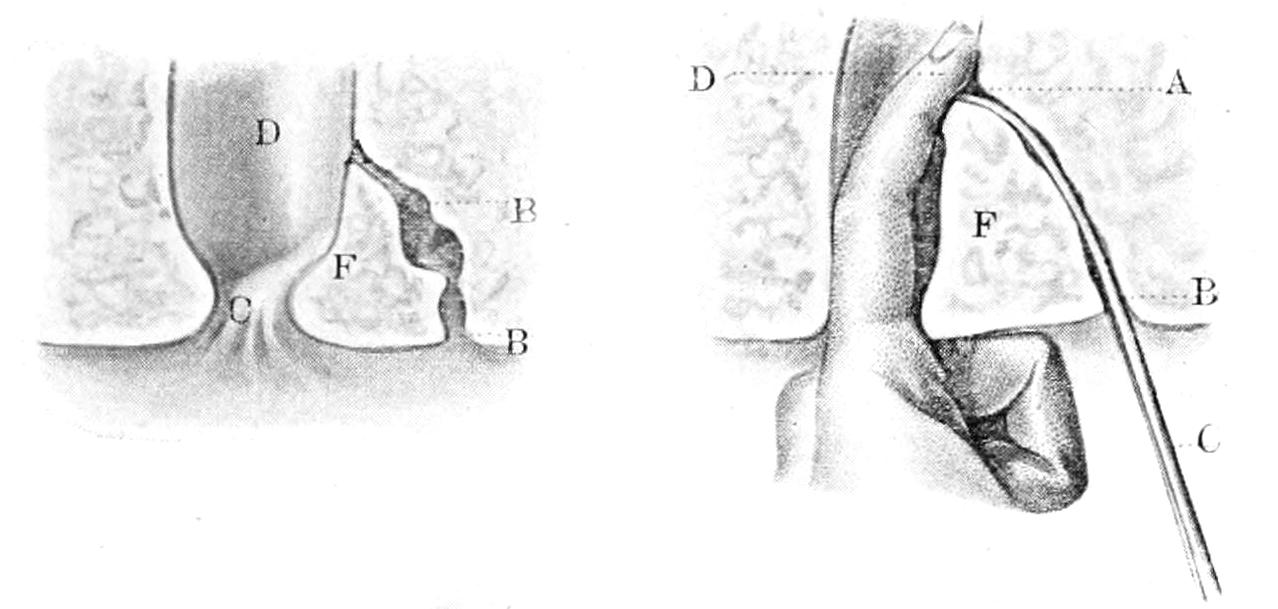
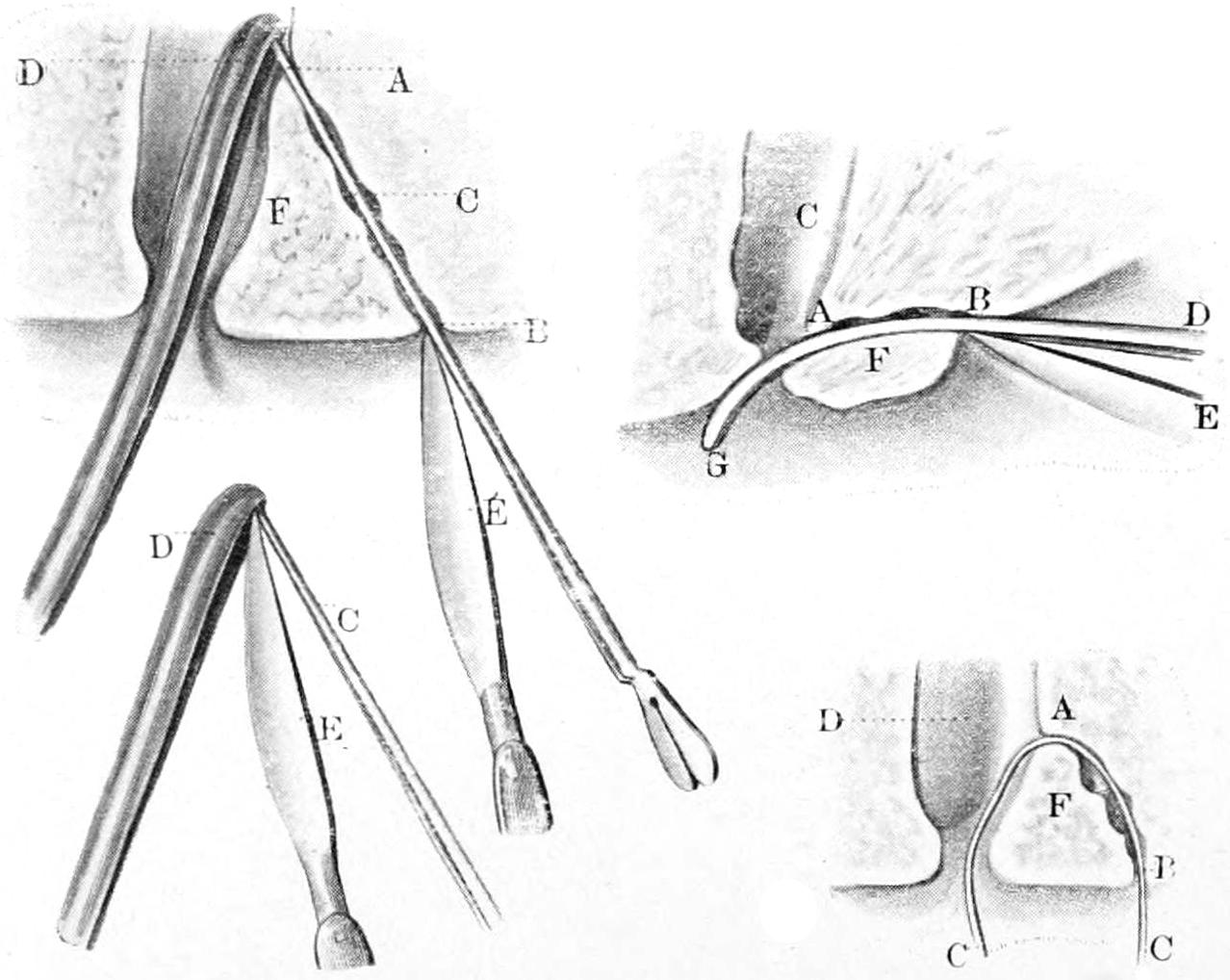
Illustrating Various Forms of Rectal and Anal Fistulas, and the Conventional Methods of Dealing with Them. (Bernard and Huette.)
[881]
One source of doubt and disappointment is met occasionally in the radical treatment which requires division of the sphincter, for to completely divide this muscle is to practically paralyze it and leave the patient thereafter with fecal incontinence more or less marked. Such accidents leave more or less disabling consequences. Usually they are avoidable, for it is rarely necessary to cut completely through a sphincter muscle, it being possible to avoid the necessity by partial division, with perhaps more complete exposure above and below. Even in those instances where it seems unavoidable if the muscle be first vigorously stretched, and thus temporarily paralyzed, it may then be safely divided, provided it be neatly and completely sutured at once, and the parts kept at rest for a few days, the intent in stretching the muscle being partly to so weaken it that it shall be temporarily disabled. It was suggested years ago by Jenks, of Detroit, and later by Kelly and others, to make a complete excision of the entire fistulous tract and then to treat this as any other fresh wound, closing it completely with sutures. The method is good in theory and occasionally applicable, and should not be neglected when circumstances favor its practice.
Every fistulous tract, simple or complicated, not promptly and neatly closed, should be dressed with gauze, with or without yeast, balsam, or some one of the other local applications recommended elsewhere in this work.
Prolapse of the rectum is observed in two degrees, either as a mere eversion of its mucosa, which, however, may be profuse and extreme, or as an actual escape by process of invagination through the anus of some portion of the rectal tube, with all its coats, including in well-marked cases even its peritoneal covering. The former is more common in children as the result of diarrhea, colitis, the presence of pin-worms, or other parasites, or any other cause which produces tenesmus and frequent straining, with consequent relaxation of the anal sphincter. It is amenable to treatment and is usually of insignificant proportion. It is also frequently seen in adults in connection with internal hemorrhoids, which are extruded with every stool, carrying with them more or less mucosa, and which are usually returned within the rectum by the patient at the conclusion of the act of defecation.
The more complete form of prolapse by true invagination is rarely seen, save in adults, and in consequence of some serious preëxistent condition, such perhaps as complete laceration of the perineum in the female, paralysis of the sphincter from previous accident, or from the existence of spinal-cord disease. Here and in extreme cases several inches of bowel may be extruded from the anus, and to an extent scarcely permitting spontaneous or even individual restoration. So complete a form is permitted only by some previous lesion of the pelvic floor, while the mesorectum and even the mesosigmoid become gradually stretched and useless. The lower portion of the rectum is by far the more muscular, and such a condition requires that its intrinsic muscles yield also with those around them.
Prolapse is a condition of general and usually slow development rather than of abrupt onset. It is made known by the presentation at the anus of the bright-red mucosa of the rectum, where it pouts and protrudes, forming a tumor of varying size, with more or less tender surface, which, with gentle coaxing pressure, is easily made to return within the rectum. It can usually be made to appear by straining effort on the part of the patient. Boys with phimosis, who are in consequence made to strain every time they urinate, will frequently present minor degrees of the condition, perhaps oftener than when the rectum itself is at fault, as the act is so frequently repeated. The oftener such protrusion occurs the more relaxed becomes the anus and the more irritated the presenting surface, until ulceration and even keratosis may result. Chronic constipation of children or adults will also produce the same effect. The presence of hemorrhoidal tumors or of polypi, or even of parasites, causes the same result.
The most pronounced and complete types of invagination produce a condition in which reduction is perhaps not possible and procidentia is constant. There may form here a pouch around the rectum, containing loops of bowel, bladder, or ovary, or there may even occur a perirectal hernia.
While patients nearly always become more or less accustomed to the condition it nevertheless is distressing in proportion to its size and the individual’s temperament.
[882]
—Treatment depends entirely upon the nature and extent of the condition. Mild forms occurring in young children may be easily obviated by attention to their stools, by circumcision if needed, or by the use of a five-grain capsule of ergotin inserted as a suppository, it having the effect of invigorating the involuntary muscle and stimulating the sphincter. Cases not amenable to the milder methods become surgical and the treatment is then apportioned to the extent of the lesion. If connected with hemorrhoids or other tumors it becomes a part of their treatment and is to be dealt with at the same time. Occurring apparently independently the milder forms will often yield to the proper use of caustics. The actual cautery being preferable, it is applied in streaks up and around the rectum, in such a way that, when the ulcers thus formed cicatrize, the rectum shall be shortened by cicatricial contraction as by a series of loops drawn up to shorten it. When permitted by rupture of the perineum and more or less combined perhaps with cystocele, repair of the perineum, rather than attention to the rectal condition itself, will be demanded, while the latter may be combined with an operation for rectocele by excision of an elliptical portion of the vaginal mucosa and the approximation of its edges into a line of sutures. This will reduce the capacity of both the vagina and the rectum and a double indication be thus met. Acute inflammation sometimes follows exposure of a prolapsed rectum and it may slough, thus leading to spontaneous recovery, the process not being without its dangers of thrombosis and septic infection. This procedure may be imitated by a surgical excision of the entire prolapsed portion, always with great caution so that if peritoneal surfaces be exposed they be protected from infection. It has been possible in many instances to completely excise the protruding portion, and then to apply a double row of sutures similar to those used in intestinal resection, only with attention first to the peritoneal rather than the mucous surface, in such a way as to excise several inches of the prolapsed bowel and thus meet the indication. Nevertheless cases where this can be done are exceptional.
Pratt has suggested a temporary purse-string suture of the anus, effected by a curved needle, completely circumscribing the anal opening, but kept between the skin and the mucous membrane, to be brought out through the same puncture at which it was inserted. The finger of an assistant being passed into the anus, the suture is now tied around it. This may be used as supplementary to linear cauterization above mentioned.
Numerous methods of proctopexy, or elevation and fixation, have been devised. Fowler, for instance, made an incision half-way between the anus and the point of the coccyx, and after separating the rectum from the latter and the sacrum inserted two fingers in the rectum, holding it up while its posterior wall was forced into the external wound and there held by heavy sutures of kangaroo tendon. By further incision he brought out the ends of these sutures on each side of the coccyx and tied them across the bone, thus by traction bringing the rectum up into position.
Colopexy has been practised as a more radical measure for the same purpose. As advised by Bryant the abdomen is opened by an incision parallel to Poupart’s ligament on the left side and one inch above it, and the prolapse is reduced by firmly pulling the rectum upward. It is then secured to the peritoneum about it, and is held by quilting sutures, which include the entire muscular coat of the bowel. Save in exceptionally favorable cases one or the other of these methods may be considered preferable to the complete amputation above described.
Hemorrhoids constitute perhaps the most common and, in some respects, uncomfortable or distressing disease of the rectum. The term implies a varicose condition of the lower veins, sometimes those of one set of hemorrhoidal veins being involved, at other times nearly all of them participating. They are spoken of as external or internal. In the former case it is the external hemorrhoidal veins alone which are involved, and usually only two or three of them, although occasionally one sees outside the anus, as within, a general involvement of the entire venous distribution. A pile, then, is essentially a venous angioma, or a single varicosity, and its peculiar features are due solely to its location.
Any vein thus involved is liable to the same dangers and accidents as veins in other parts of the body. Thus it may undergo dilatation, thrombosis, and suppuration, while[883] the ordinary consequences of the latter condition may follow here, as elsewhere, with this difference alone, that when the middle and upper hemorrhoidal plexuses are involved the thromboseptic process, should it occur, follows the portal vein, and the first metastatic abscess that forms occurs within the liver. Thence it may spread to other parts of the body in classic form.
The hemorrhoidal veins, save those at the verge of the anus, are more or less entangled among the fibers of the levator ani and the sphincter. These muscles are thrown into a condition of more or less spasmodic contraction when the veins are so involved. In consequence more pressure is made upon the veins themselves, and the conditions of spasm and venous engorgement react upon each other in a vicious circle, each tending to make the other worse. Hence the great advantage of stretching the sphincter in any operation save that for a small external pile.
Hemorrhoidal angiomas may appear as single tumors or in multiple form surrounding the lower part of the rectum. The most common cause for their occurrence is chronic constipation. Occasionally the first exciting agent is some violent strain in defecation, or possibly the actual rupture of a small vessel, but such constant overloading of the rectum as obstructs its return circulation conduces to engorgement and the other conditions may easily follow. A small pile may be brought into existence in brief time, but a general hemorrhoidal condition is one of slow development. Chronic cases are always accompanied by further changes involving the surrounding connective tissue and the overlying mucosa, both of which become thickened and infiltrated, while ulcers form frequently upon the latter, and the occurrence of those linear ulcers which are ordinarily called fissures is very frequent. This gives an additionally distressing feature to these cases. As the condition goes on and the angiomas increase in size there is an increasing tendency to prolapse. This may be temporary or constant, i. e., it may occur with the straining effort at stool or it may result in a condition of permanent protrusion at the anus of the engorged mucosa; or, if the sphincter has finally become prolapsed a true prolapse of the rectum may result. A mucous surface thus constantly exposed to irritation will nearly always be more or less ulcerated and tender, while hemorrhages in either variety are common. It is not an infrequent event, then, for a patient to lose a number of ounces of blood with or just after stool, and sometimes the blood loss is even excessive. There is then added to the local condition a secondary feature of anemia and its attendant consequences which are sometimes extreme, and may even make operation somewhat hazardous. The lower inch and a half of the rectum is the portion particularly supplied with sensory nerves, and, under these circumstances, the irritated area becomes erethistic and painful and the patient’s suffering may be extreme. This is the so-called “pile-bearing area,” as it is within it that the hemorrhoidal condition is practically confined. Even a small individual pile connected with one of the little external veins may give rise to a disproportionate amount of discomfort.
There has been so much quack literature upon this general subject that ignorant patients are very likely to say that they have piles, no matter what may be the local condition. A statement to this effect should, first of all, provoke a physical examination with the finger, then with the speculum. The educated finger will easily detect the presence of the rugosities or tumors produced by internal piles, the external being always self-evident. The coexistence of ulceration will be indicated by an extreme degree of sphincteric spasm and of tenderness. It should be remembered that, along with hemorrhoids, there may coexist fissure, ulcer, painful spasm, prolapse, and, in long-existent cases, even cancer. The average patient with cancer of the rectum will go to his physician saying that he thinks he has piles.
—Treatment needs to be something more than merely local in aggravated cases, as it should also be more comprehensive. Patients who have thus long suffered have almost inevitably contracted the constipated habit, postponing defecation whenever possible because of pain and tenderness, and perhaps the hemorrhage accompanying it. The large bowel has, therefore, become weakened, and attention should be given to it as well as to the general digestive process.
Locally very mild degrees of purely temporary disturbance may be sometimes acceptably and temporarily treated by the use of suppositories containing some soothing and anodyne drug, as well as ergotin, the latter being valuable because of its constringent effect upon the bloodvessels. A five-grain gelatin-coated pill of ergotin makes a satisfactory suppository for the young, under these conditions.
[884]
A freshly formed, external hemorrhoid, which may attain a size no larger than that of a pea, but which will seem to the patient as large as a bird’s egg, is best treated by open division, turning out the blood or clot contained within the dilated vein, which will quickly obliterate, so that recovery will be complete within two or three days. This may be done under local anesthesia and with prompt relief. There have been methods in vogue, especially among the charlatans and some of the specialists, of treating external and the more localized internal conditions by injection of carbolic acid, either pure or reduced with a little glycerin. A few drops are thrown into the tumor with a hypodermic needle, the effect being to promptly coagulate the contained blood, the intent being to produce a final cure by absorption of the clot and obliteration of the veins. This, in fact, is the secret method long employed by the travelling charlatans and often connected with the name of Brinkerhof. It is uncertain in action, and the production of a clot under these conditions is by no means always free from danger, nor is the relief prompt. What is desired is to empty the vein and turn out the clot rather than to provoke its production. The method is rarely practised by judicious surgeons, who have too often seen serious sloughing and even general septic disturbance follow it.
For the radical relief of distinctly hemorrhoidal conditions there is no satisfactory method save the operative. So many measures have been devised in time past that it is necessary here to be selective and only mention one or two. On general principles every pile is a venous tumor, and there is no reason why it should not be treated like any other tumor, i. e., by enucleation or excision. The same is true of the area which contains a number of such tumors, i. e., the so-called pile-bearing area. Hence, surgeons of the largest experience have practically discarded the more bungling methods and have applied to these conditions the same radical measures which they recommend elsewhere.
One important feature which should always be practised is thorough dilatation of the sphincter, not only for reasons above described, but because of the facility with which the surgeon then exposes the diseased tissues. Any distinct tumor or series of them may, for instance, be seized, isolated, and dissected out, either by an elliptical incision of the mucosa or by a more blunt dissection with scissors. The base, or pedicle, if sufficiently large to justify it, may be ligated before the incision is completed, after which catgut sutures may be used to close the opening in the mucosa. When the tumor is small the suture may be made to include the bleeding points so that even a ligature is not required. A more radical method of extending this same principle to the entire pile-bearing area, especially when prolapsed, or to so much of it as is affected, is the so-called Whitehead’s operation of excision, which practically consists in trimming off a ring of exposed mucosa, with its clusters of enlarged and more or less pendulous veins. This ring extends from the mucocutaneous border, at the verge of the anus, to a point perhaps 1¹⁄₂ inches above, the intent being to separate the mucosa and the tumors from the fibers of the sphincter, which can be practically effected in such a way that sphincter control is not lost. Hemorrhage will be free for a few moments, but is always within control. Larger vessels which spurt may be twisted or tied, while oozing surfaces are included within the row of catgut sutures, which is later placed in such a way as to unite the divided mucous tube with the skin border at the anus. The operation is, in effect, an annular excision of the lining of the rectum, and as such proves satisfactory. There is about it this temporary disadvantage that the pile-bearing area thus removed is also the sensitive area, and that for a few weeks, at least until nerve communications have been reëstablished, there is a lack of peculiar or normal sensibility about the parts which is annoying, and may perhaps lead to some incontinence, but this soon passes away. The measure is the most satisfactory of all for well-marked cases of hemorrhoids associated with more or less ulceration and prolapse.
An occasional dilatation, scattered here and there around the lower end of the rectum, perhaps with a mild degree of ulceration, is usually very satisfactorily treated by a method which it must be confessed would be rarely used on the exterior of the body, and yet which proves quite serviceable here, namely, the actual cautery. The consequences of its application are obliteration of the vein, cicatricial contraction of the overstretched tissues and eventual relief.
Fig. 593

Multiple polypi of rectum. (Potherat.)
Other methods of operation include the use of the clamp and cautery for removal of considerable masses, a method ordinarily less satisfactory than excision, and the use of the ligature, with or without incision of the mucosa at the base of the tumor, it being thus cauterized and expected to separate by sloughing, an uncertain procedure.[885] None of these methods, nor others not worth mentioning, compare with the newer methods of excision.
Much has been recently written concerning the advantage of local anesthesia in doing these operations. This seems to have been advocated largely for effect, although external tumors can be treated by cocaine applications or by the ordinary injections of cocaine or one of its substitutes. It is claimed that the infiltration of the surrounding tissues with normal salt solution affords an effective local anesthetic. Mere local anesthesia is not sufficient for thorough work upon parts not easily visible, and the actual stretching of the sphincter is half the battle in dealing with these conditions. This cannot be thoroughly accomplished without general anesthesia. Consequently for any well-marked hemorrhoidal condition chloroform offers decidedly the preferable method, not alone from considerations of comfort, but from the standpoint of permitting more thorough and effective work to be done.
After these operations it is advisable to place within the grasp of the anus a stiff rubber tube wrapped with gauze. It permits the escape of flatus without distress to the patient, and it effects a better coaptation of surfaces recently united by suture than would otherwise be secured. Such a tube may be left in situ for from six to thirty-six hours.
The rectum is the frequent site, more especially in children, of polypoid degenerations similar to those seen in the nose. In consequence there are formed the so-called rectal polypi, which, in origin, consistence, and course correspond to the common nasal polypi. Such a pedunculated tumor may attain considerable size, especially when solitary, while, on the other hand, the mucosa may be studded with small pedunculated growths, giving the appearance represented in Fig. 593.
Pathologically these polypi are originally of myxomatous or adenomatous type. They may bleed easily and may be passed with stool. In their multiple and smaller expressions they give rise rather to rectal uneasiness and tenesmus than to more distinct symptoms. On the other hand an isolated tumor, so pedunculated as to become gradually stretched out, may attain considerable size and give rise to all the sensations of a foreign body in the rectum, with constant tenesmus and desire to expel it, while it may even present at the anus or bleed freely.
Only exceptionally will these tumors be recognized previous to examination, which, however, should easily disclose their characteristics. Isolated polypi should be removed, either by being twisted off or by excision and ligature of their bases. General polypoid degeneration may be treated with the curette or with the actual cautery. In all these instances surgical intervention in some form will be required.
Other benign tumors in the rectum are mainly of the adenomatous type. Owing to their location it is rare that they are seen early by one competent to judge of them. In consequence the surgeon sees them usually as more or less ulcerated, sometimes extensive growths, perhaps bleeding freely, and much changed by maceration and by compression from their original condition.
In such cases it becomes a question of importance to distinguish between the benign and the cancerous growths. This is not always easily done, especially when they are high up and ulcerated. The matter is usually decided by the presence or absence of actual infiltration around the base of the growth, and perhaps the involvement of lymph nodes. A movable tumor with an infiltrated base is usually clinically benign, nevertheless it should be radically removed.[886] It is in many of these instances that one may see expressions of transformation of adenoma into carcinoma.
—This will be considered here rather from its clinical side; hence what is said refers alike to sarcoma and carcinoma, the latter being far more common. Carcinoma of the rectum may assume the type either of epithelioma, as when it begins low and spreads upward, or of adenocarcinoma, when it arises from that portion of the tube not lined with squamous epithelium.
It usually begins insidiously, and for a considerable length of time furnishes scarcely any recognizable symptom. The first indications noticed by the patient are usually more or less frequency of stool, with tenesmus, and the passage of mucus, perhaps stained with blood, rather than of fecal matter. By the time those conditions are noticed there will usually be more or less mechanical difficulty of defecation, due to the presence of the tumor and obstruction of the rectal tube. Pain may be a long-deferred feature, and local soreness may be absent until late in the case or until its terminal stage, when the growth is above the peculiarly sensitive part of the rectum, i. e., when it does not approach to within 1¹⁄₂ inches of the sphincter. As time goes on there is more and more suffering in the rectum, with backache, referred pain, while the tenesmus and other local conditions cause increasing distress. It often happens that it is not until this period is reached that the patient consults a physician, and then he usually goes with the statement that he is suffering from piles.
Fig. 594
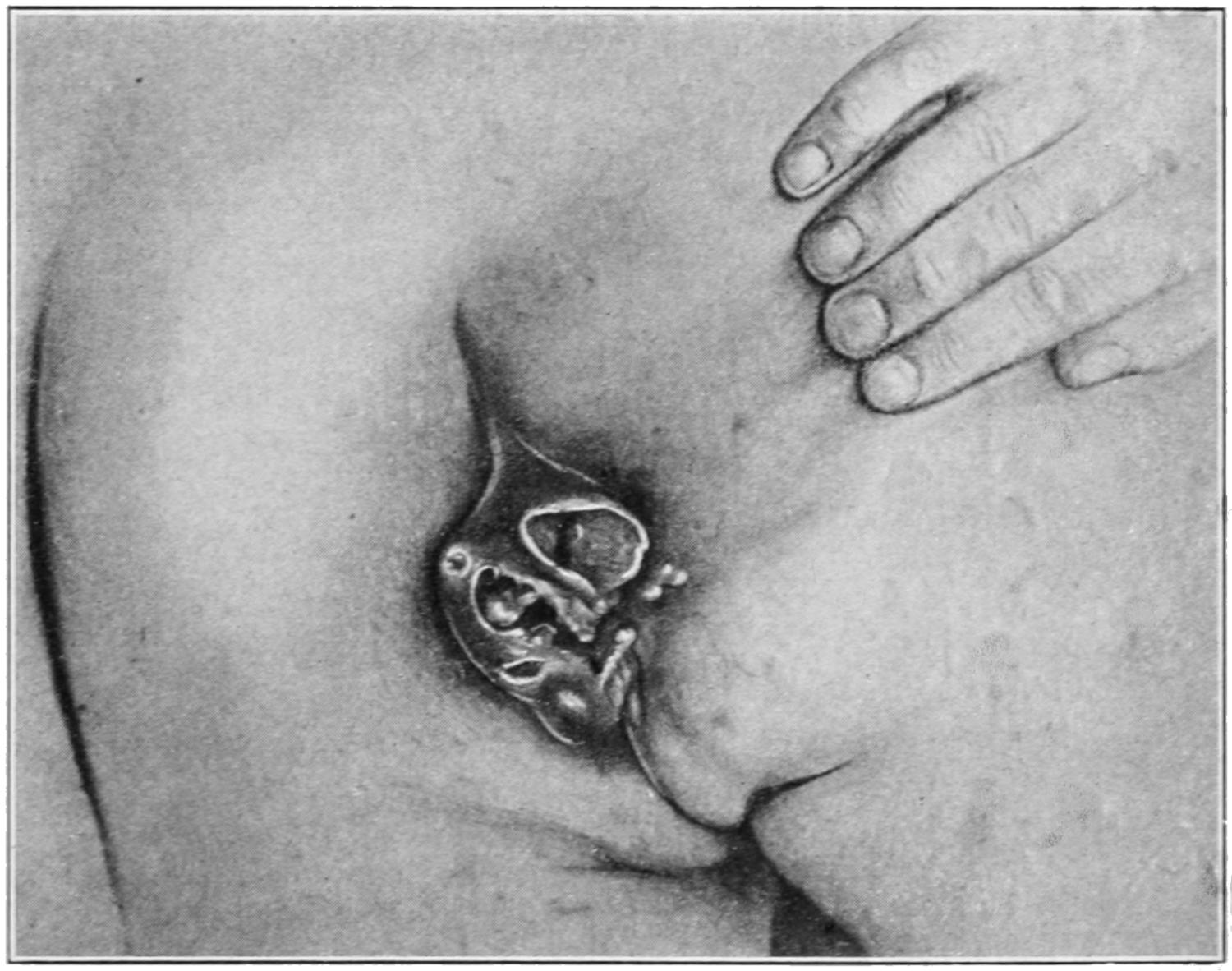
Epithelioma of anus and rectum. (Grant.)
So frequently is this the case, and so prone are many practitioners to accept such a statement, that the proper examination which should permit the recognition of the condition is perhaps not made until the patient is really in a pitiable condition. I do not recall ever having seen a case of cancer of the rectum which had not been regarded, by some physician as piles, and in most cases locally treated by him, usually without any adequate local examination, and usually also until the time had passed when a radical operation could be practised with any degree of hope. The first examination at least will be digital, and if the malignant growth be within reach of the finger it should be possible to appreciate it, to estimate its size, degree of attachment, and the amount of infiltration, as well as the extent to which it is breaking down. A soft, rapidly growing cancer will give a fungous sensation to the finger, while the more dense, scirrhous forms produce hard masses, growing in irregular shapes, sometimes involving one side of the bowel, sometimes appearing in annular form, and tending sooner or later to produce malignant[887] destruction. The only difficulty would be in cases seen exceptionally early or in those beyond reach. The circumstances above detailed should lead to a careful proctoscopic examination with suitable instruments, perhaps in the knee-chest position, when the growth is not easily appreciated from below. Any complaint of tenesmus, with discharge of blood and mucus, with more or less pain and tenderness, local or referred, demands an examination sufficiently careful to reveal the nature and extent of the lesion and indicate the treatment. If such an examination call for an anesthetic, it should be administered. Practically every rectal cancer is a malignant ulcer by the time it is recognized, ulceration being favored by warmth and moisture.
Treatment.
—There are few malignant lesions anywhere about the body which require more good judgment in treatment than cases of cancer of the rectum. So much depends upon their location, their extent, the degree of infiltration, the age and general condition of the patient, that it is almost impossible to lay down succinct rules. The question of treatment hinges, first, upon the location and extent of the lesion; is it operable or is it not? When the lymph nodes of the pelvis or the groin are noticeably involved it is practically too late, under any circumstances, to hold out prospect of radical cure. When the disease has extended far above reach of the finger it is again late to expect much even from radical measures. When the prostate, the floor of the bladder, the vagina, or any of the pelvic viscera are involved it is again too late to justify them. There are wide differences of opinion between surgeons as to the propriety of extensive operations in serious cases. Mild cases are certainly much benefited and even actually cured by early and thorough removal, but this occurs too infrequently, because such cases are rarely seen sufficiently early.
The class of cases universally acknowledged to be inoperable, so far as radical measures are concerned, are nevertheless much benefited and their lives prolonged by a colostomy, the effect being to provide an easy and manageable outlet for fecal discharge, and to avoid the irritation and attendant difficulties associated with an obstructed and malignantly ulcerated rectal outlet. The surgeon has to select between some method of excision and colostomy. My own opinion is growing in favor of the latter, save when the prospect of complete excision is good. The opening is more manageable, the progress of the disease seems much checked, patients have better fecal control and live in far greater comfort, while their lives are placed in less jeopardy, and, in general, are actually prolonged. Thus a colostomy performed in a well-marked case of inoperable cancer of the rectum may permit of prolongation of life for two or three years, something not often attained by any other method of treatment.
Of the various radical operations some are made from below, i. e., by the perineal route, some by the so-called sacral route, and some from above. Of the latter it may be said that occasionally an annular cancer of the rectum is seen so favorably located that by opening the abdomen with the patient in the Trendelenburg position it is possible to make a complete excision of the growth, to remove enlarged lymph nodes, and to make an end-to-end reunion with success. In a case in my own practice nearly six years have elapsed since this operation was done, and the patient, a young woman, is still absolutely free from the disease.
Through the perineum the lower portion of the rectum may be attacked either by splitting the sphincter and dividing it posteriorly, completely dissecting out the gut from its surroundings, removing all infiltrated tissue, and then, by dividing the bowel above the growth, amputating the lower part. It may be possible to bring down the upper end and attach it to the mucocutaneous border of the anus, reuniting the divided sphincter, and aiming for a restoration to something like the original condition, which under quite favorable conditions is attainable. At other times it will be impracticable to thus attach the lower end of the tube because it has been too much shortened, and in these cases it should be brought out through a posterior incision just below the tip of the coccyx, or higher up if the bone has been removed. Here the rectal outlet is placed posteriorly, but is devoid of a sphincter. Something like sphincteric action can be provided by giving it a third or half of a revolution on its axis before fastening it to the external wound. After this expedient more or less control of solid fecal matter is afforded.
The more complete and radical operations, associated with the names of Kraske and other operators, include removal of the coccyx, and of the lower portion of the sacrum, which are usually completely excised, although certain “trap-door” operations have been devised. If the sacrum be not cut away above the third sacral foramen there is[888] not much damage done to the nerves, while sufficient room is afforded for any removal that is justifiable. Some operators open the peritoneum, others attempt to avoid it. If the growth be attached to that membrane it becomes necessary. If peritoneal invasion can be avoided it is desirable. It is possible to completely expose the contents of the pelvis through such an opening, while from this direction, the gut being withdrawn after the peritoneum is divided, the pouch of Douglas may be opened and further removal of diseased tissue be effected. In all these operations the endeavor should be to disturb the mesosigmoid and the mesorectum as little as possible, in order to not interfere with blood supply, for reasons already mentioned when discussing the mesentery.
In all these operations contamination of the wound should be avoided, especially of the peritoneum, by clamping or ligating the bowel, or by amply packing and by every possible additional precaution. Bowel should be divided between two clamps and the divided edges at once thoroughly cleansed with compresses and with hydrogen peroxide.
One may read in the works on operative surgery descriptions of most extensive and elaborate operations of this general character, and of extensive and even daring feats of removal, where portions of the bladder, of the tubes, of the ovaries, even the uterus, have been removed. It has seemed to me that the surgeon should avoid operative gymnastics, especially in this region, so far as possible, and confine himself to measures which if successful would improve conditions rather than complicate them. My own judgment then is that in any case where so formidable an operation would be attempted by some, the best interests of the patient will be served rather by simple colostomy.
Early operations upon cancer of the rectum afford comforting prospects. It is not so much to the discredit of surgery as to the discredit of the patient’s judgment, and of the carelessness of the practitioners who first see these cases, that cancer of the rectum has become such a bête noir and is justly regarded as so serious and unpromising a measure.[60]
[60] It becomes a question of importance just when and where we should cease to attempt operation on the colon from above or on the sigmoid from below; in other words, the exact location of the tumor should decide the measure when it can be accurately determined. Moreover, a wide margin of bowel on either side of any new-growth which is about to be resected should be excised. The question of blood supply to the margins of the wound thus made is also of importance, as the most ideal operation in appearance may be marred by gangrene due to lack of sufficient blood supply. When there is sufficient uninvolved gut below the tumor to permit of complete operation within the abdomen it is not advisable to do anything from below; but there are some cases in which anything like complete removal can only be effected by a combination of abdominal and sacral routes. A thorough extirpation should be made above the growth as well as of the involved tissue below. Those vessels which require ligation should be tied accurately at the level of their division, and no ligation of trunks or larger vessels should be attempted at any distance from the line of division. If this be carefully carried out and the divided mesentery, with its ends, and all the fat between the rectum and the sacrum be carefully dissected out, there will rarely be difficulty in making an end-to-end reunion of the divided bowel.
It is rarely necessary to include a colostomy with this procedure; in fact, when a permanent opening has become necessary there is little possibility of removing the main growth. Colostomy is a procedure for the hopeless cases; resection is rarely to be thought of as an alternative. It should be an early not a late measure, the reverse being true of colostomy, though even this should not be too late.
Colostomy.
—Colostomy for relief of rectal cancer is not a radical operation, but in many cases is far more humane and satisfactory than are those alluded to above. The intent is to make an opening in the left side of the groin at a point where it is easily made. There are two methods of performing colostomy here. One is to make an opening through the abdominal wall, attach to it the presenting surface of the sigmoid or colon, and either open it at once or some hours later, when adhesions have cemented the desired union. Such an opening may be made for emergency purposes under local anesthesia, but when the colon is movable, and when the disease has not yet involved the area thus exposed, or any portion above it, a more desirable method is a deliberate one. An opening is made such as is usually made on the right side when operating upon the appendix. The bowel thus being accessible is divided between two clamps, while the end of the lower segment is inverted and closed with chromic or silk sutures, after which it is dropped back. This leaves the upper portion with its open end corresponding to the abdominal opening, into which it is fastened by a series of sutures, being attached to the peritoneum and to the deep musculature rather than to the skin, for if it be brought out too freely and attached externally there is greater tendency to prolapse and subsequent discomfort. Into the opening thus afforded a large-sized rubber or bent glass tube is inserted for a few inches, around which gauze is packed, and every effort is made to conduct fecal matter to the exterior, as well to protect, at least for a few hours,[889] the wound itself from fecal contamination. Improvements in this technique have been suggested, such as tying into the bowel a curved glass tube, thus conducting its contents into a rubber bag or receptacle placed outside the dressing. Another method which has been suggested by Stewart is to connect the interior of the colon by a Murphy button with a rubber bag or rubber dam upon the outside of the abdomen, by which protection for this purpose can be afforded.
This operation makes a complete and final division of the colon, and permanently excludes the rectum with its cancerous involvement. It is not, therefore, in this respect, a radical measure. The result, however, is that if the rectum be washed from below each day it is kept far cleaner and freer from contact with irritative foreign material than it otherwise would be. Furthermore, being disused it tends to undergo to some degree a species of physiological atrophy, and, in consequence, the cancer grows more slowly, if there do not occur an apparent temporary cessation of malignant activity.
By suitable management of the artificial anus, including the deliberate emptying of the bowel every morning and the use of protective pads for receptacles, it can be made far less disagreeable than patients ordinarily fear (Figs. 595 and 596).
Fig. 595
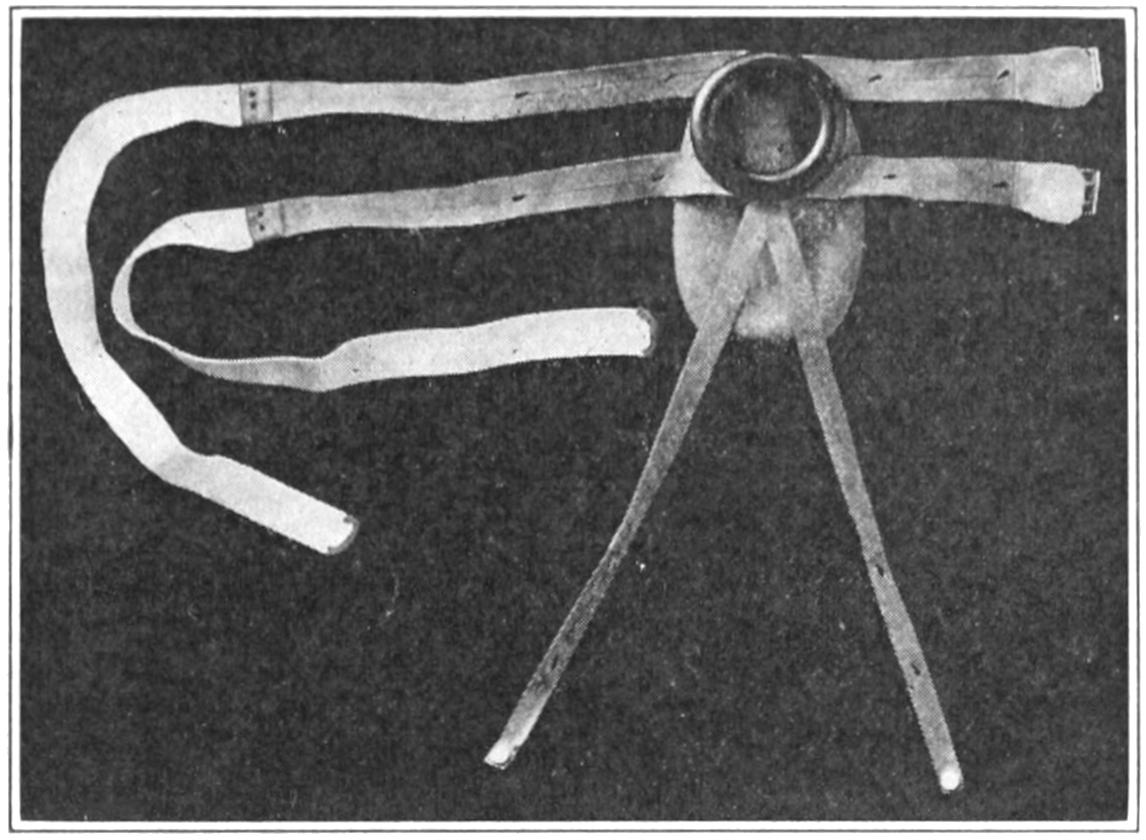
Gleason’s pouch and supporter.
Fig. 596
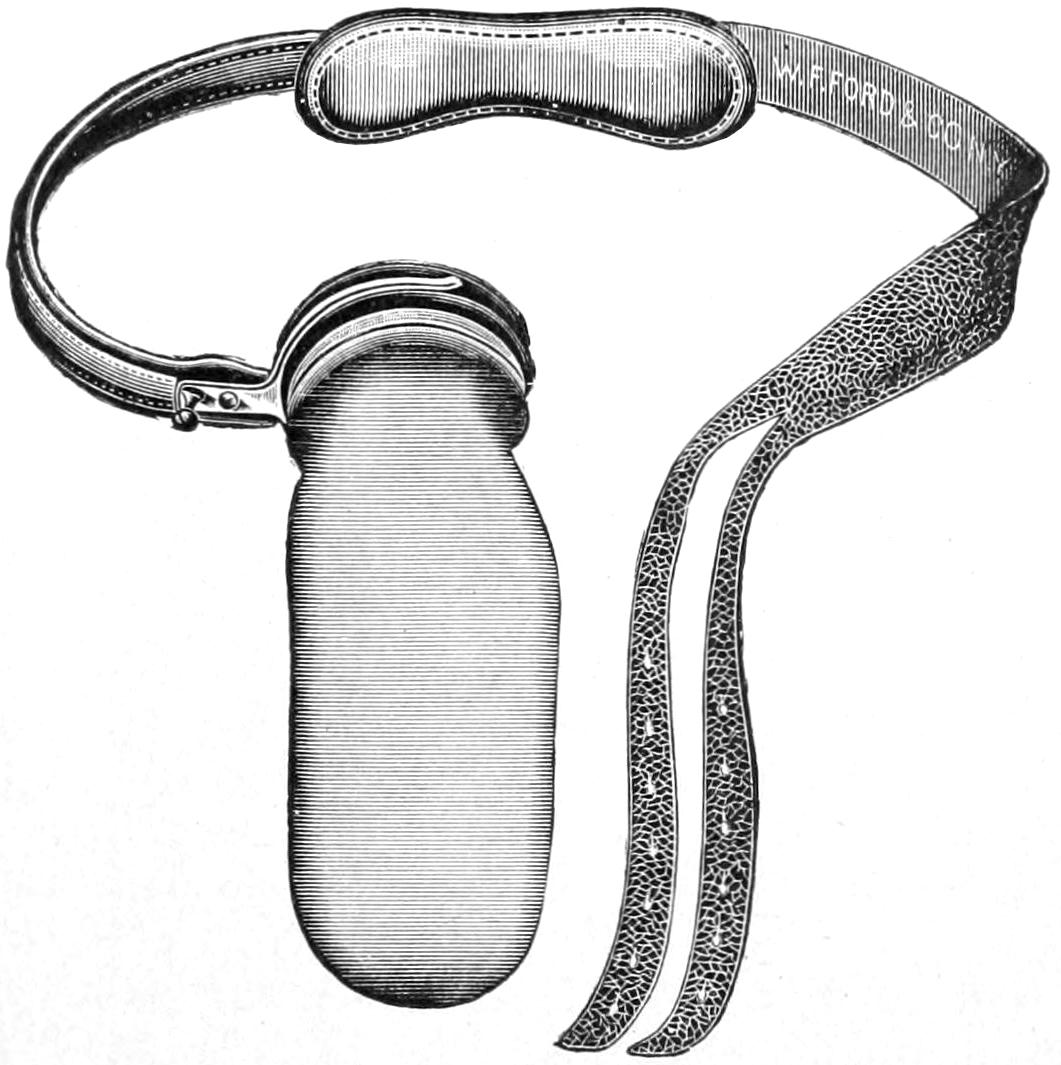
Colostomy pad and bag, worn as is a truss. (Kelsey.)
The colostomy opening in the abdominal wall should be made as small as practicable lest there occur not only more or less ventral hernia through the weakened outlet, but even, as I have seen in one case, a most extensive prolapse of the colon, in which two or three years after performance of the operation the colon could be made to prolapse to an extent of twelve or fifteen inches.
[890]
The term hernia of itself implies protrusion or escape of a contained organ or part through its containing walls, yet covered by some of them. Thus we may have hernia of the iris, of the brain, and the like; but when no particular part of the body is specified, by common consent the term is understood as implying hernia either of the intestine or the omentum, or of both. Such hernia may be either of congenital or acquired character, the former condition being permitted by some defect or abnormality in the abdominal parietes, the latter being the immediate or remote result of accident or of operation; and in the latter case they are referred to as traumatic or as postoperative. Of these the former is usually of rapid and the latter of slow development. Increased abdominal pressure doubtless has much to do with the occurrence even of a truly congenital hernia, as this would hardly develop were it not for the former. Such pressure may be the result of occupation, of pregnancy, or of certain morbid conditions—for example, those which cause constant coughing or straining at stool, or straining during urination—as from prostatic hypertrophy or phimosis, or such intra-abdominal conditions as tumors, which distort the abdominal walls, or accumulations of fluid which weaken them. Accident produces hernia mainly by causing the effects of pressure to be manifested in a brief space of time. Thus pressure or strain on abdominal muscles may part them in such a way as to permit the immediate appearance of a hernia, or its more slow development. The postoperative hernias are usually of the so-called ventral type, and occur most often after wounds which could not be immediately closed because of necessity for drainage, or in those which were closed in such a way as to permit of gradual warping or stretching of the resulting scar.
The surgical anatomy of hernia is described in works on anatomy. It is necessary, therefore, here only to remind the reader that the conditions existent in an old hernia may be different from those so described, for the original anatomical outlines may perhaps have long been lost and the original coverings more or less blended together so as to become indistinguishable. Particularly is it true of strangulated hernia that the more minute details are lost, and that in such cases there is great difficulty in the effort to recognize distinct anatomical layers and coverings. In old cases the sac—namely, the original peritoneum—may be greatly thickened, while in strangulated cases it will be discolored, perhaps even gangrenous, and will bear but slight resemblance to the original condition. The same is true of its contents, which may be adherent, strangulated, or gangrenous, according to circumstances.
The opening through which the hernia appears is usually referred to as the ring, to which, however, it may bear very little resemblance. Thus it may be an elongated buttonhole-like, or a warped, irregularly rounded sac opening, whose margins are thick or thin and easily distinguished or otherwise.
By all writers hernias are classified according to their anatomical characteristics as follows: Inguinal, indirect and direct; femoral, umbilical, ventral, diaphragmatic, gluteal or ischiatic, obturator, perineal, lumbar, sacrorectal, retroperitoneal (including the recently described paraduodenal or Treitz variety), and properitoneal.
Of these the most common are the inguinal and the femoral, the umbilical ranking next, while the other forms are rare.
—Regarding the cause and nature of the common forms—namely, the inguinal and femoral—I propose here to introduce the views enunciated by Russell, of Melbourne, which seem to me to furnish the actual explanation for nearly all instances. This explanation refers to the congenital origin of the condition, even though it do not appear until the middle years of life. In the case of inguinal hernia it refers also to the persistence of the canal of Nuck, or of at least incomplete obliteration of the original vaginal process or prolongation of the peritoneum, which comes down with the migrating[891] testicle and whose lower portion furnishes the cavity of the tunica vaginalis. It is more rational to explain the occurrence of hernia in connection with this preformed sac than by the view that there are so many instances of congenital weakness of the abdominal wall. That such weakness exists in many cases of hernia is undeniable, but this is to be regarded as the effect rather than the actual condition. From this last statement it follows also that there is great advantage in early operation, and in complete removal of the sac, which when performed early will not only cure the hernia but prevent the weakening of the abdominal wall itself. It follows, further, that the use of a truss, save possibly in the case of young infants, is an improper method of treatment. In other words, upon it is based the crux of the whole matter of successful treatment, i. e., operative removal of the sac.
It will be seen, then, that the cause of inguinal hernia is closely related with the cause of so-called congenital hydrocele of the cord (q. v.), the latter condition being one of sacculation of the canal, with accumulation of fluid; and it is interesting to recall that such sacculations are occasionally found in the ordinary so-called congenital hernias, when they are seen early, and before all anatomical surroundings have been merged together. The existence of a hernia implies the presence of a sac, and a congenital defect furnishes this latter, while the variations in the type of hernia are due mainly to the variations in the sac itself, i. e., in its location.
Fig. 597

Congenital hernia.
Fig. 598

Infantile hernia.
Russell has traced out the relations between the peritoneal pouches of the lower abdomen and the principal bloodvessels, and has shown how the former arrange themselves about the latter and are carried with them as they develop, assuming in consequence the type either of inguinal or femoral hernia, according as they are placed to the inner or outer and lower side of the same. He has insisted, and I think properly, that the variations observed in the clinical manifestations of a hernia are mainly determined by the size and the position of the sac, and that these depend upon its relations to the femoral and epigastric vessels, the associated sac and vessel being subject to the same vicissitudes in development. In this way the occurrence at one time of a congenital and at another of a so-called infantile type of inguinal hernia may be easily explained, as well as the differences between the so-called funicular and the partial form, and also the occurrence of the retroperitoneal or properitoneal forms, which, as variations are rare, and as clinical manifestations perplexing, but which nevertheless are easily explained when viewed in this light (Figs. 597 and 598).
Fig. 599
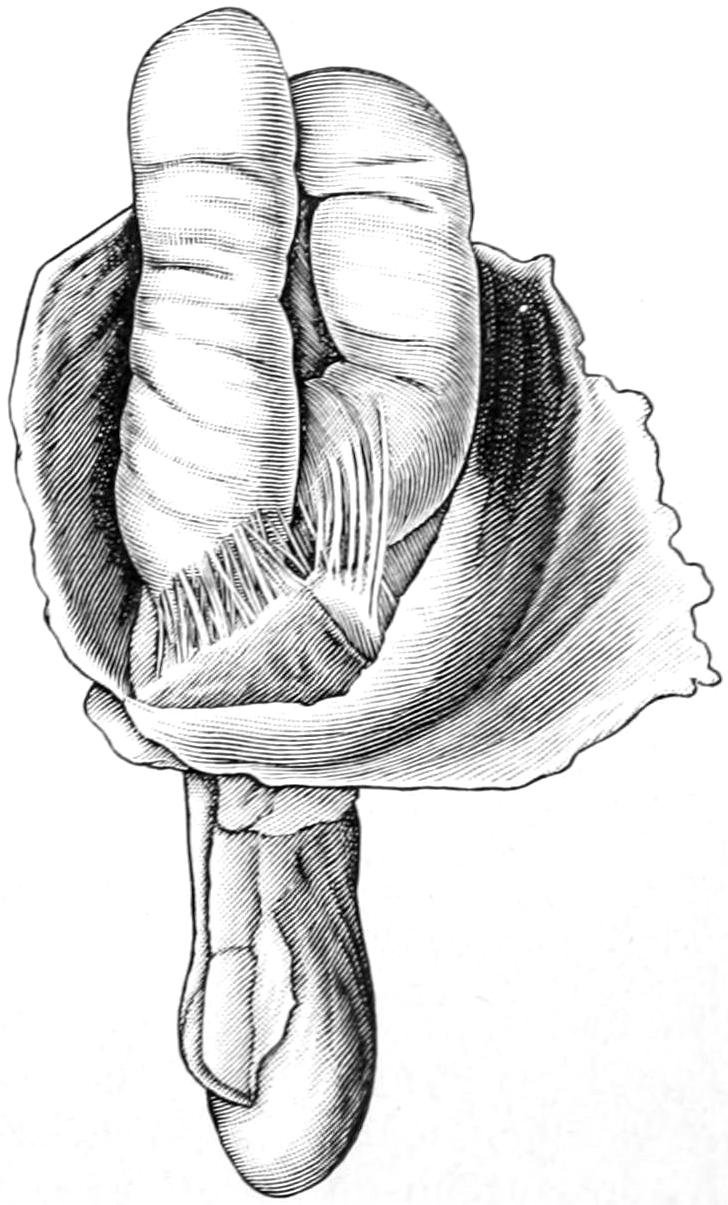
Adhesions in hernial sac. Scarpa. (Lejars.)
Thus viewed, then, what are the relations of traumatism to congenital defects? When thus explained they seem to be as follows: By no means every individual who sustains an injury to the abdomen suffers from hernia, but when the parts are already weakened or prepared by the preëxistence of these congenital defects, then a small amount of strain or injury may serve to open them up and to produce a condition apparently due to accident which otherwise could not have occurred. The more I have studied the entire question the more I have come to the conclusion that hernias of the ordinary type, save[892] in case of extreme violence, would not occur were it not for such a congenital prearrangement and tissue permission, as it were; so that we are justified in assuming that inguinal and femoral like umbilical hernias are really of congenital origin.
—The signs of hernia include the existence of a tumor, usually at one of the common outlets, which may be variable in size, and fixed, changeable, or otherwise, according to whether it consist of intestine or omentum. To a hernial protrusion consisting of intestine alone may still be given the old term enterocele. One consisting of omentum is known as epiplocele. Hernial protrusions may attain tremendous dimensions, especially those appearing at the umbilicus, and some of these sacs contain perhaps the larger proportion of the intestine or even of the entire abdominal contents. Scrotal tumors, again, may attain large size, e. g., that of the individual’s head or even much larger. According to the nature of the contents such a tumor will be more or less resonant on percussion, and more or less compressible as well as reducible. Reducibility—namely, the ability to be returned to the abdominal cavity—is the most characteristic feature of a hernia and one possessed by nearly every such tumor, at least at its inception. It may, however, be lost.
Loss of reducibility, when occurring gradually, is replaced by what is known as incarceration, i. e., more or less complete fixation, at the same time without such pressure on bloodvessels as to produce necrosis. Incarceration may be the result of reduction in caliber of the hernial outlet, or of the formation of adhesions between the walls of the sac and its contents, such adhesions being common alike to omentum and large or small bowel. (See Fig. 599.) Strangulation is an acute process which may terminate either a reducible or an incarcerated hernia. It implies some sudden change, such as overcrowding of the bowel within the sac, or some peculiar kinking, by which intestinal caliber is shut off, as well as blood supply affected because of pressure, by which the vitality of the gut and of the sac is compromised or perhaps quickly lost. Strangulation, then, includes at least the possibilities and usually the simultaneous occurrence of acute obstruction of the bowel with more or less gangrene of the sac itself, as well as of the compromised gut.
Reducibility as an ordinary feature of hernia is one with which the patient himself is quite familiar, most patients with reducible hernias being able to effect reduction in the horizontal position, accompanied by some manipulation or maneuver. When in such cases reduction cannot be accomplished incarceration or perhaps strangulation has begun and the case immediately assumes serious proportions. Reduction is usually accompanied by a peculiar gurgle, as well as disappearance of the tumor itself, while the opening through which it has disappeared can usually be identified with the finger, by invagination of the scrotum, or by pressure over the femoral region. Such a tumor usually reappears when the patient stands, or particularly when he coughs or makes any straining effort, and the occurrence and recurrence of these phenomena clearly establish the diagnosis of hernia.
Irreducible or incarcerated hernias usually give some impulse upon the patient’s coughing, as do the reducible forms, yet in some cases they lead to more difficulty of diagnosis. Ordinarily in the male the question is mainly as between inguinal (or scrotal) hernia and hydrocele. In the latter there is a pear-shaped tumor whose apex should be found below the level of the inguinal outlet; a tumor which will fluctuate, whose shape does not change, which gives no impulse when the patient coughs, which is not influenced by pressure, even with the patient in the horizontal position. It is only in incarcerated or in peculiar types of congenital hernias, or in those combined, as they may be, with hydrocele, in which doubt should not be easily dissipated. While incarceration predisposes to acute obstruction it is not always followed by it, but may produce a more chronic type of constipation, with tendency to fecal impaction, because of the mechanical impediment to freedom of bowel motility. This condition is more frequently met in the aged.
Inflammation of the hernial sac, as well as of its coverings, leads to a condition described as inflamed hernia. It is essentially one of circumscribed cellulitis. It may be due to the irritation of a badly fitting truss or to other external causes. The inflammation may extend so as to involve the sac wall itself, and thus produce adhesions and later incarceration, or it may set up actual peritonitis, which may extend to the general abdominal cavity and terminate fatally. The more superficial and less acute forms are scarcely distinguishable from a local erysipelas which may terminate by abscess. Such a condition might be mistaken for one of suppurating bubo. Nevertheless the existence[893] of the hernia itself should guard one against this error and make him extremely cautious in using the knife, even though it be necessary for the evacuation of pus.
Fig. 600
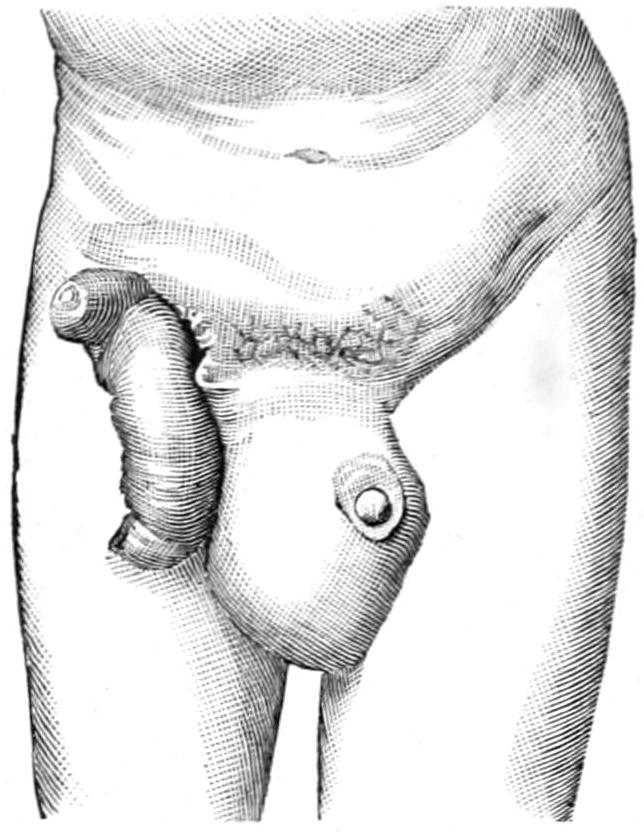
Gangrenous strangulated hernia; artificial anus; prolapse of bowel requiring intestinal resection; eventual recovery. (Preindlsberger.)
Strangulated hernia has already been considered as the most common cause of acute obstruction of the bowel. Its possibility should be excluded in every case of this serious condition. While such are its general features, locally there is added to the general bowel obstructive condition that of more or less local destruction, which may vary from the presence of exudate, fluid or solid, with infiltration of adjoining tissues, to the most prompt and disastrous consequences of venous stasis, namely, extensive gangrene, which, involving first the bowel itself or the omentum, will later spread to the sac wall and its surroundings. In this instance around the loop or loops of gut involved will be seen a tight constriction or sulcus, above which the bowel will be more or less discolored and distended, while below it will be completely necrotic and perhaps actually sloughing. Minor degrees of strangulation may produce conditions which would lead up to this, but have not yet actually reached the stage of gangrene. Around such bowel will be found more or less fluid, the result of transudation, which will be swarming with bacteria and often offensive. The sac wall closely corresponds in appearance to that of the bowel, and everything about the sac and its contents will be infected and contaminated with bacteria, often of most virulent activity. The gangrene may involve an area of exceedingly small size, or the entire contents of the hernial sac. In the former instance the condition is comparatively simple as compared with the latter, which may require resection of several feet of necrotic bowel. The proper treatment of these conditions will be more fully dealt with below (Fig. 600).
—The symptoms of strangulation are those of acute obstruction, plus the local evidences of a hernia, usually with added pain and tenderness, sometimes acute. These symptoms may come on as the result of strain or accident or without any known cause. Their intensity will depend in some measure upon the completeness of the blood stasis and the rapidity of the consequent gangrenous process. The latter may vary in degree. Thus the death of the compromised bowel may be practically determined within a few hours or within two or three days. The hernial tumor, within which strangulation has occurred, becomes more tense and incompressible, and, at the same time, more tender. Sometimes there is marked augmentation in volume; at other times this changes but little. So soon as a loop of bowel has lost its blood supply and become actually necrotic it will have also lost, when exposed, all of its luster or “sheen,” and will appear not only black and lusterless, but will be more or less offensive in odor, and of extremely septic character. The surrounding fluid will be found swarming with bacteria, and will seriously and perhaps fatally infect anyone inoculated with it.
Concerning the color of the exposed bowel and its appearance, it is a fairly safe rule to follow that gut which has not lost its luster, even though darkly discolored, is still viable, and may with safety be returned to the abdomen, which is probably the safest place for it; but when its sheen is actually lost the case becomes one either for resection or for artificial anus. It is possible that such a case may be seen only after absolute necrosis and fecal escape have occurred. When actual sloughing is thus met it is a question for resection or some other expedient.
—The inguinal form of hernia comprises nearly four-fifths of cases in males, a much smaller proportion in females. The hernial protrusion is always through the external abdominal ring, either by way of the inguinal canal, which it enters through the internal ring, or directly through the abdominal wall. The former is called indirect, the latter direct. Such a hernia is considered complete or incomplete according as it descends below the lower margin of the inguinal canal. An incomplete and direct hernia is often referred to as bubonocele. (Fig. 601.)
Holding the views above enunciated, regarding the congenital origin of practically every inguinal hernia, it is necessary to pay less attention to the distinctions insisted[894] upon by the earlier authors concerning the congenital, the infantile, or the encysted forms of hernia, which depend upon the extent and degree of closure of the vaginal process or the canal of Nuck, which is carried down with the testis during its migration from the lower margin of the Wolffian body, and which is normally obliterated at birth. Nevertheless these conditions, however explained, are actually met during life and are represented by the diagrams seen in Figs. 602, 603 and 604.
Fig. 601
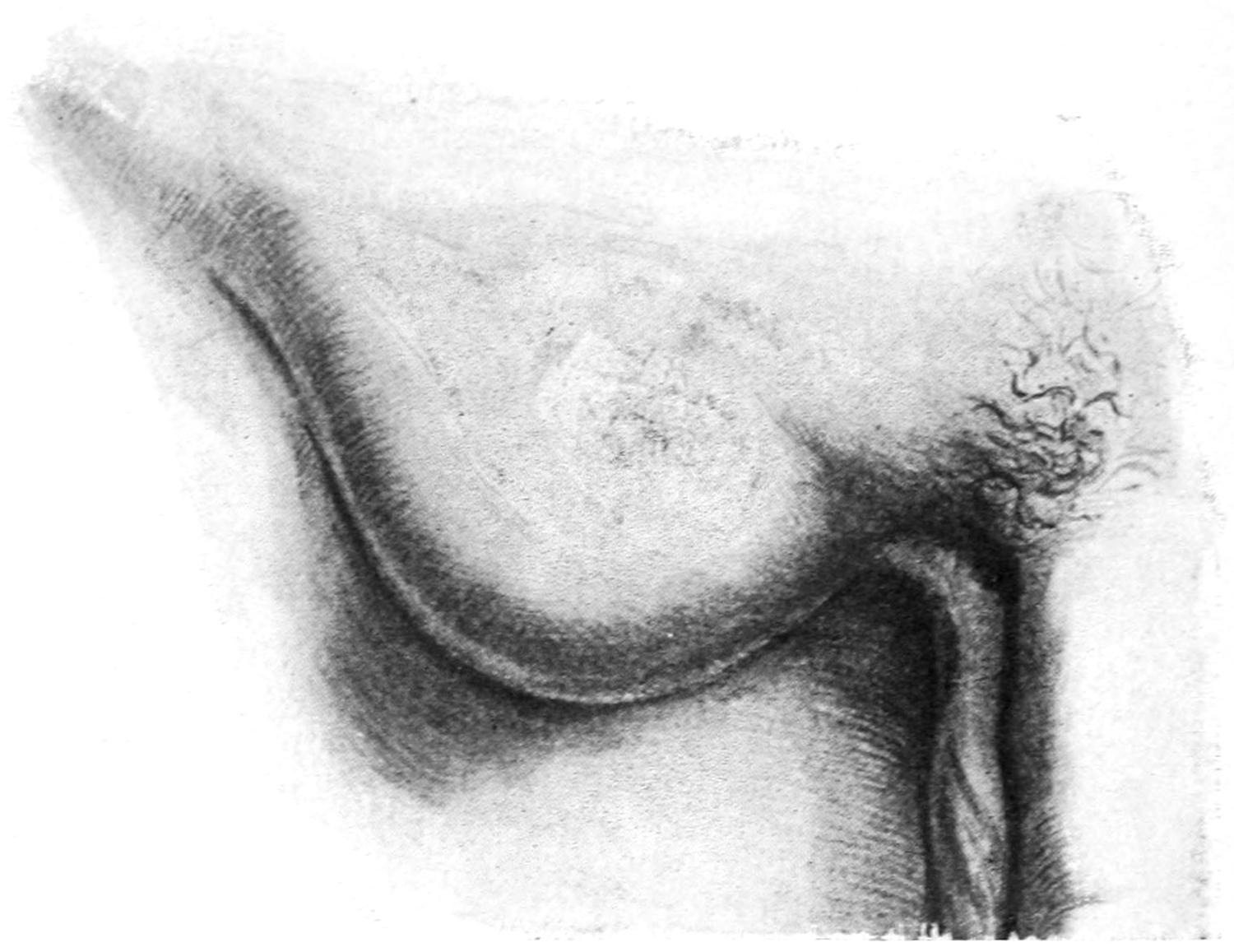
Indirect inguinal hernia (bubonocele.) (Richardson.)
Fig. 602
Fig. 603
Fig. 604
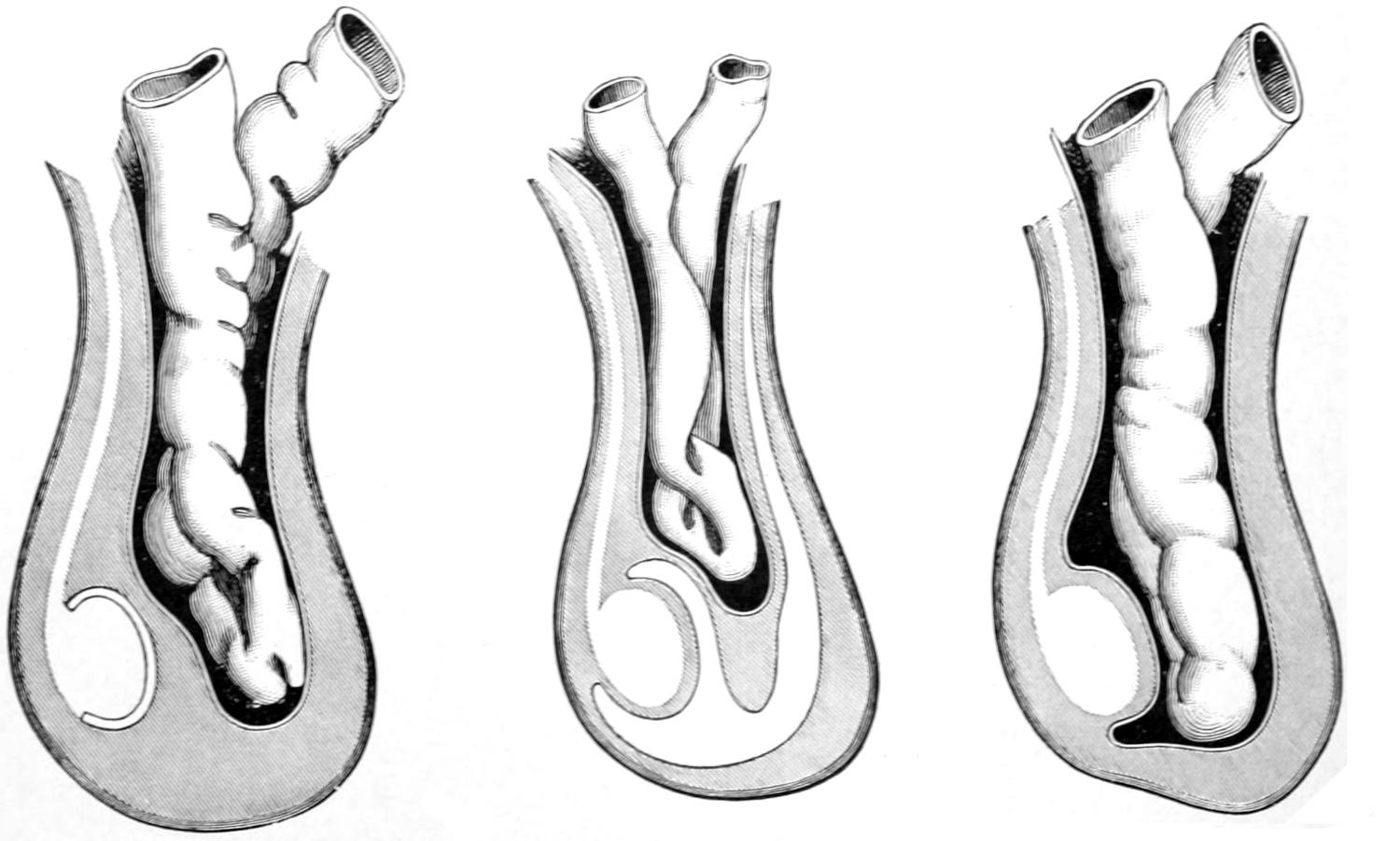
Congenital inguinal hernia.
Infantile or encysted hernia.
Hernia of the funicular process.
In the female the canal of Nuck is a matter of minor importance, containing only the round ligament. Nevertheless along it may proceed an indirect inguinal hernia corresponding to that in the male.
The so-called acquired indirect hernia, according to the above views, would not occur were it not for the opportunity—as it were, the temptation—already afforded by some deviation of the peritoneal arrangement in this locality. In these cases, however, the[895] sac appears to be new and is pushed along the inguinal canal anteriorly to its normal contents. This may be the result of violent strain, or of one which is apparently disproportionately small, but frequently repeated.
Direct inguinal hernia is generally an occurrence of adult life, takes place commonly as the result of accident, is a direct protrusion through the abdominal wall at the triangular weak spot, whose outer limit is the deep epigastric artery, with the obliterated hypogastric artery to the inner side and Poupart’s ligament below, i. e., the so-called triangle of Hesselbach. This hernia appears always at the external ring, from which it may descend and become scrotal.
Fig. 605
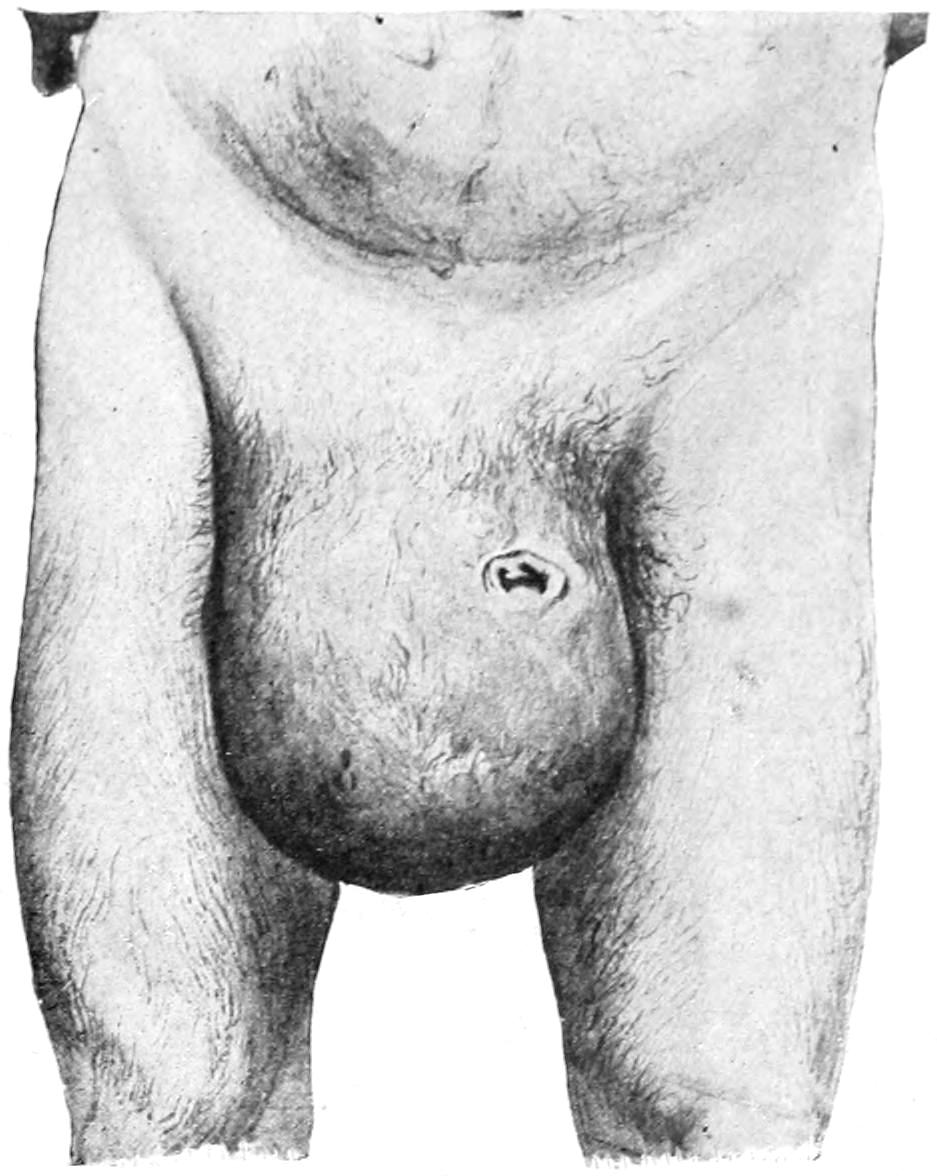
Scrotal hernia. (Richardson.)
With complete or scrotal hernia there is usually little difficulty of diagnosis (Fig. 605). An incomplete hernia, protruding at the external ring, covered with considerable fat, and perhaps shifted a little in position, is sometimes hard to distinguish from a hernia through the femoral opening. The inguinal form escapes above Poupart’s ligament, the femoral always below it, and Poupart’s ligament is to be located by a line drawn from the anterior superior spine to the spine of the pubis. The inguinal forms are usually nearer the middle line. If the epigastric artery can be identified, either before or during operation, the character of the hernia will be promptly demonstrated by its relations to the neck of the sac.
Hernial protrusions give a familiar impulse on coughing unless the incarceration of an epiplocele may mask this feature. By it they are to be distinguished from hydrocele, varicocele, aneurysm, undescended testicle, and the like.
Fig. 606
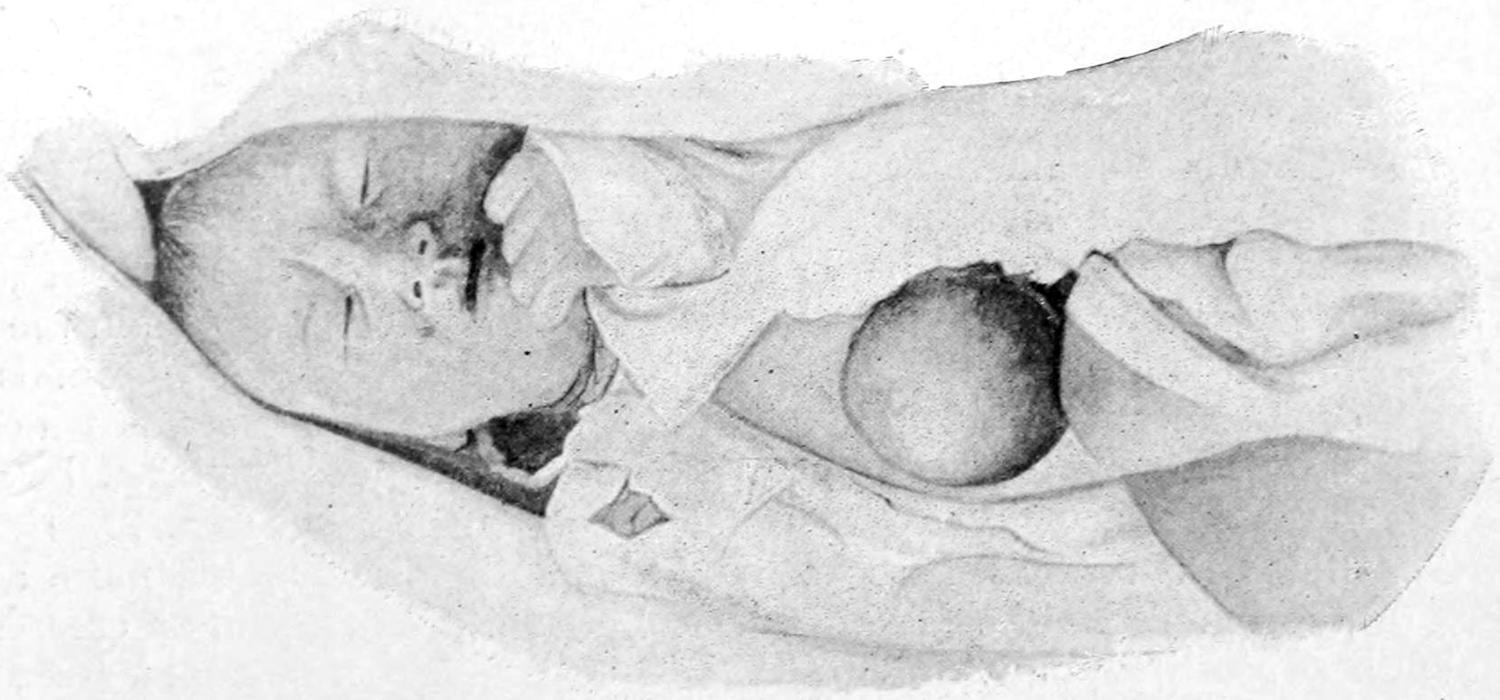
Hernia of liver through congenital opening in the umbilicus. (Richardson.)
—Femoral hernia is much more common in women than in men, and constitutes about one-tenth of all cases. This form is also nearly always congenital in the above sense, and is particularly liable to strangulation. It escapes through the femoral ring into the femoral canal, to the inner side of the femoral vein, and then, passing forward through the femoral opening, finds its direction of least resistance upward. In consequence a loop of bowel thus escaping from the abdomen may first pass downward, then forward, and then upward, which will illustrate the futility of the ordinary methods of taxis in the effort to reduce it by manipulation. These hernias are usually small, hence their greater danger. These cases have especially to be differentiated from[896] psoas abscess, from inguinal lymphatic enlargements, and tumors. If the sac be entirely filled with omentum diagnosis is often difficult.
—Umbilical hernia is primarily permitted by failure in obliteration of the opening at the navel for the omphalomesenteric duct and for the urachus. Originally small, it may yet assume enormous dimensions. Though actually of congenital origin, as just stated, it may not be discovered until the later years of life. It occurs much more commonly in females than males, and usually in connection with a large deposit of fat in the abdomen, by which its existence, or, at least, its limits and dimensions are masked. Through the umbilical opening, which in the majority of cases is small, may escape other of the abdominal viscera, as is shown in Fig. 606, illustrating hernia of the liver. Fig. 607 illustrates the pendulous form which many of these cases assume.
Fig. 607
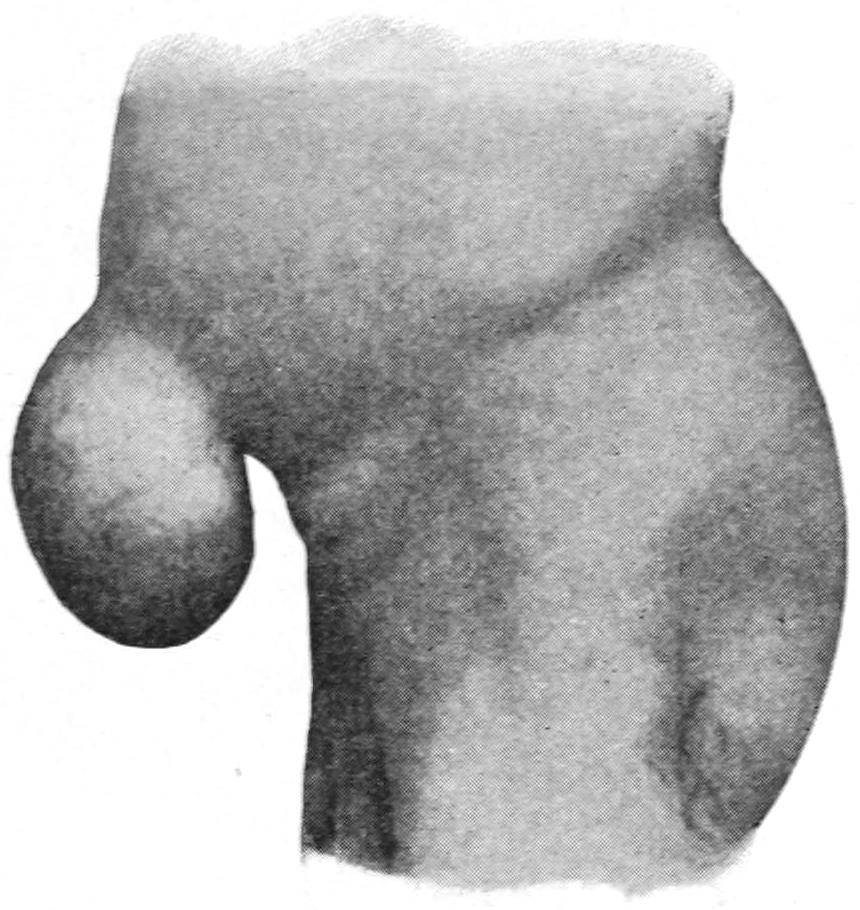
Umbilical hernia of pendulous form. (Park.)
An infantile form (umbilical) is known, in which the actual protrusion does not occur until the infant is several months old, and which appears to be due to frequent strain, on a weak or incompletely closed fenestrum, by coughing, crying, efforts to expel urine through a strictured prepuce, and the like. These tumors at first are small and always intestinal. It is often possible to so adjust a small pad over these openings as to secure subsequent closure by natural processes. On the other hand, the forms which come on in later life, acquired during pregnancy, ascites, or in connection with excessive obesity, assume sometimes relatively enormous size. Here the hernial contents may be solely omental, but are usually at least partially intestinal. Strangulation occurs in a large proportion of these instances and incarceration is nearly always observed. Naturally, in consequence, the patient complains of gastric disturbances, as well as of chronic constipation, with frequent colicky attacks.[61]
[61] A rare form of hernia into the umbilical cord has been described by Moran. It has been known as hernia funiculi umbilicalis, and has been held to be due to abnormal persistence of the vitelline duct, which holds the loop of intestine to which it was attached inside the abdominal wall, the intestine continuing to grow, the umbilical ring remaining open and the hernia thus enlarging. Occurring in this way it happens about the tenth week of fetal life. Such a hernia has no covering except the peritoneum and the amnion—i. e., is without muscle or skin covering. It would be probably first noted when the cord is about to be tied, when at its loop, as a translucent tumor, varying in size from that of a small cherry to a lemon, the cord being distended and assuming its own natural size only after it has left the hernial tumor. The bloodvessels will run on one side of the amniotic sac. Such sacs rupture easily, perhaps during crying efforts or even during parturition. The condition is serious, and when present no traction should be made on the cord. If easily reduced by taxis an antiseptic compress should be fastened over the opening. Should anything like strangulation occur operation is imperative and should be done immediately.
—Ventral hernia is of two types—the spontaneous, usually epigastric, which is an omental escape in the middle line above the umbilicus, occurring most often in fat women, in whom it is likely to be mistaken for a hernia of ordinary umbilical type. By fixation of its contained intestine and omentum there is more or less dragging upon the upper abdominal viscera, with consequent disturbance of function.
—Postoperative hernia often also spoken of as ventral, occurs through the cicatrix of the wound which has permitted it, whether this be in the middle line or elsewhere. It is an unfortunately frequent sequel of laparotomy wounds which have required drainage, but occasionally occurs in perfectly clean wounds which have closed satisfactorily in the first place, but which have subsequently parted because of unsatisfactory methods of bringing together their deeper portions. (See p. 778.) Consequently it should be sufficient here to remind the reader that the more accurate the method of approximating the margins, layer by layer, and effecting a complete and perfect union between them individually the less the tendency to this unpleasant sequel.
Postoperative hernia may be so small as to be kept under subjection with some[897] form of abdominal support, or it may call for operations for radical cure, as do other cases. They are subject to the same dangers of strangulation of their contents.
—Diaphragmatic hernia may be congenital, as when occurring through a defect in this partition, or acquired, as when under stress or strain some of the abdominal contents are forced into the thorax, either through natural openings or through a rent or tear. Such escape may include but a small portion of bowel; in congenital cases one-half the abdominal contents have been found within the thorax. The left side seems more often involved than the right. Serious wounds of the diaphragm may be followed by this condition. Under these circumstances the thoracic viscera are more or less displaced, and the heart may be pushed considerably out of place. In cases with a history of violent accident the surgeon may more readily suspect and recognize the condition than in congenital cases, where anatomical relations have long been disturbed, but apparently more or less adjusted or compensated.
—In the lower part of the pelvis, under rare circumstances, hernial protrusions occur either through the sacrosciatic foramina, in which case they are known as gluteal or ischiatic (Fig. 608), or through the obturator foramen, when they are known as obturator hernias, the latter occurring more often in stout women. Unless these constitute some form of recognizable tumor, or produce acute obstruction by strangulation, they will pass quite unrecognized. A perineal form of hernia is also known, which occurs in Douglas’ cul-de-sac, behind the bladder or uterus, the levator ani muscle being more or less disturbed, and the protrusion occurring somewhere between the labium and the anus. In such hernial sacs the ovary has been found, as well as intestinal loops, and the so-called ovarian hernia includes some anatomical anomaly of this kind.
Fig. 608
Fig. 609
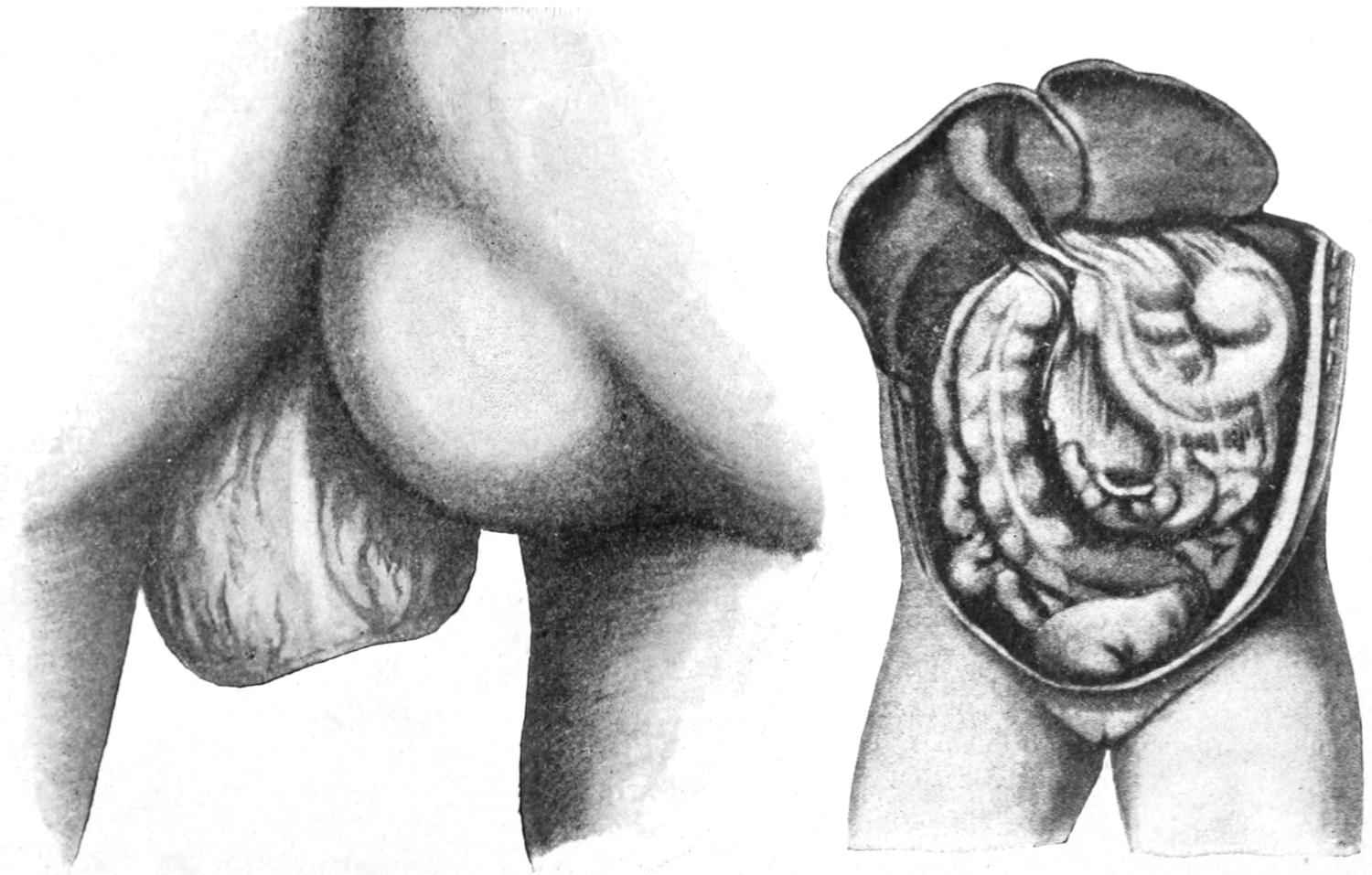
Ischiatic hernia. (Richardson.)
Hernia into foramen of Winslow.
—In so-called lumbar hernia, which is very rare, the hernia escapes along the outer border of the quadratus lumborum muscle into the triangle of Petit. Such a tumor, usually small, may be easily mistaken for lipoma or for cold abscesses.
Other anomalous types of hernia may occur in connection with congenital defects of the bones or the less dense structures of the pelvis proper.
—Retroperitoneal and properitoneal hernia are types which seem to corroborate the views already enunciated concerning the essentially congenital origin of the ordinary forms. The former implies a protrusion into an internal peritoneal pouch, and is usually found in the upper abdominal cavity in the duodenojejunal fossa, although it may also occur lower down on either side. It will[898] not be recognized save by its effects, which will usually be those of acute intestinal obstruction, and even then will only be diagnosticated after the operation which the condition will necessitate. Hernia through the foramen of Winslow has already been mentioned in the chapter on the Small Intestines. (See Fig. 609.)
Properitoneal hernia implies usually the existence of a double sac, with a common opening, its inner portion lying between the peritoneum and the abdominal musculature, while its outer portion takes the usual position of the hernial sac, either the inguinal, the femoral, or the umbilical form. It may be suspected when reduction which has been apparently successful has later evidently failed. It occurs most often in the inguinal region, where it is usually referred to as inguinoproperitoneal hernia, and where it was first recognized by Parise, and later fully described by Krönlein. It may be with equal propriety called interstitial hernia, and is often associated with imperfect descent of the testicle, which perhaps has served to deflect the descending hernia in an unusual direction. The properitoneal sac is most often found between the internal ring and the anterior spine, although it may be directed downward and inward toward the bladder, or backward toward the iliac fossa. In size it is usually small as compared with the external portions. Its existence may be suspected when a patient with a hernia previously easily reducible suddenly develops strangulation, which is apparently relieved by taxis, only to recur a little later. So far as its radical treatment is concerned all that is necessary is the extirpation of the extra sac, with perhaps separate treatment of its neck, when dealing with the greater and more completely filled pouch in front (Fig. 610).
Fig. 610
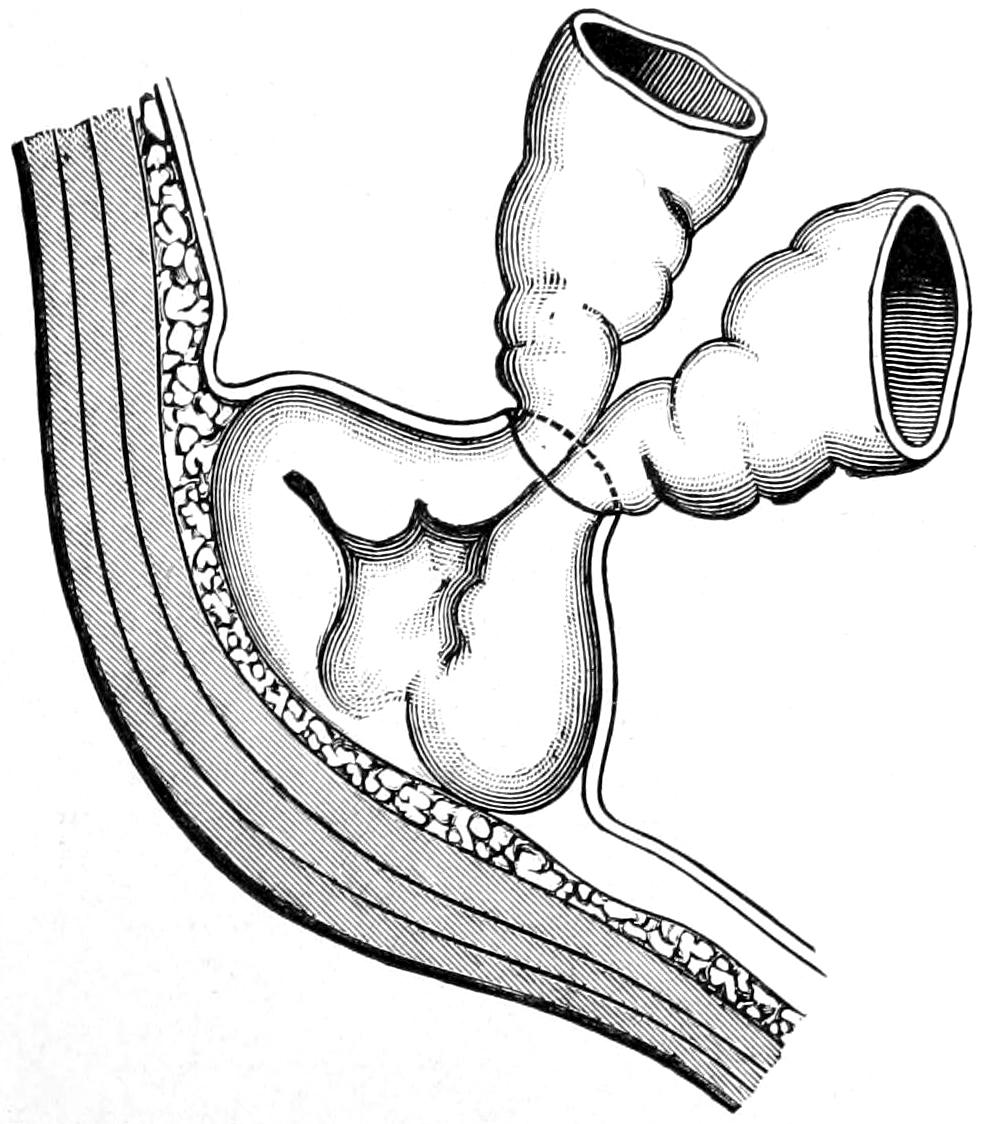
Properitoneal hernia. This illustrates also incomplete reduction of hernia. (Richardson.)
—These terms have reference to strangulation of intestine in which, nevertheless, the entire lumen of the bowel is not completely involved, rather only a small area, which soon becomes sacculated, or perhaps by a diverticulum becoming involved in the occlusive and later gangrenous process. These forms are most frequently seen in women and at the femoral ring. They are peculiarly dangerous in that they produce symptoms which do not include those of total and acute bowel obstruction, and hence are often allowed to go unoperated until gangrene has already occurred. These forms, then, will produce signs and symptoms of partial strangulation, with incarceration, followed after hours or perhaps days by those of local cellulitis, with perhaps necrosis; conditions which when opened may expose gangrenous bowel and promptly become fecal fistulas.
—Hernia is treated for three different purposes: for the relief of strangulation, i. e., as an emergency, for palliation, or for radical cure, according to the nature of the case and the wishes of the patient.
The relief of strangulated hernia becomes a measure of instant importance so soon as the condition is recognized, mortality being due to delay, practically every case being curable could it be recognized and operated promptly. The symptoms of strangulation, as repeatedly indicated, are those of acute obstruction of the bowel, including fecal vomiting with meteorism, and the local indications which may be trifling, as in very small hernial protrusions, or unmistakable, as in large hernial masses. The indication in every instance is to restore the occluded bowel to the abdominal cavity. Occasionally this may be effected by the method of manipulation or by taxis, which should never be thought of save at the very outset, and which may be aided by the local use of cold, or especially by the Trendelenburg position, which may be exaggerated. Under these circumstances, as Richardson has said, minutes are precious and delay adds materially to the danger, so that usually all non-operative methods are to be condemned.
PLATE LIV
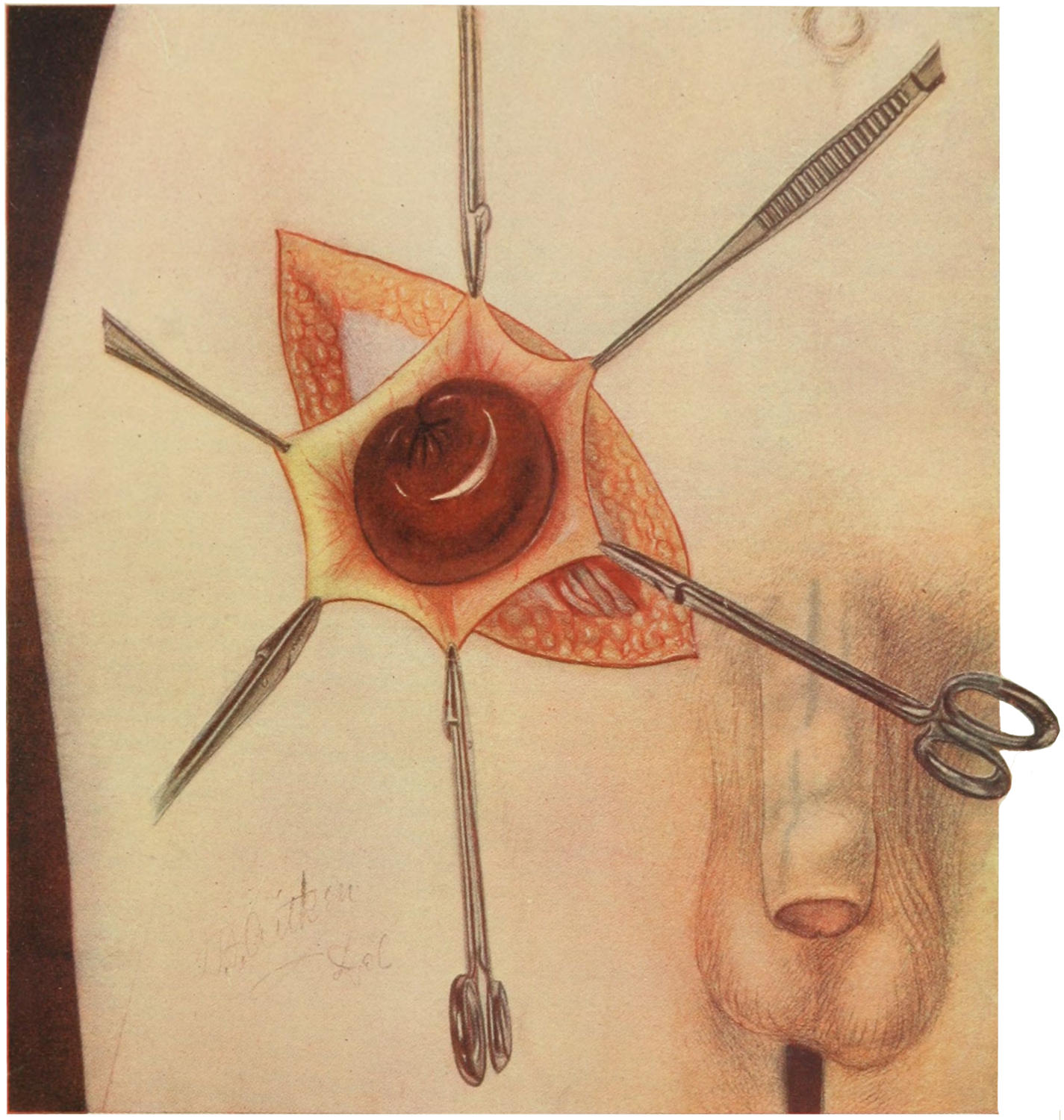
Strangulated Right Inguinal Hernia. (Richardson.)
The sac has been opened and its edges are drawn apart by means of forceps. The inguinal canal and spermatic cord have been dissected.
[899]
—The principal danger in connection with taxis is that of doing harm to the occluded bowel by rough manipulation. The method includes a coaxing pressure in the proper direction, with more or less compression of the external mass, the effort being to gently persuade it back into the abdominal cavity. In this effort the temptation, especially among the inexperienced, is to use too much force, by which extravasation is produced, exudate increased, and the local condition in every way made worse. That which is possible during the first hour after strangulation has occurred may be impossible a little later, when edema and exudate have distorted the parts or cemented them together. The effort should not be prolonged, but rather very brief, and if after a very few moments no gain be made it should be discontinued.
Reduction “en bloc” is an unusual but ever-present danger. It implies forcing back the peritoneal sac as well as its contained intestine unreduced, so that while the external tumor is dissipated the actual condition of strangulation is not influenced. Its effect would be in no way to diminish the danger of the condition, but rather to more seriously menace the patient, under the supposition that reduction had been accomplished satisfactorily.
Two or three axioms in the treatment of strangulated hernia are imperative:
Very little time, if any, should be wasted in manipulation or taxis.
Taxis failing or there remaining any suspicion of reduction en bloc, open operation is imperative.
The time to operate is just after the diagnosis has been made and the condition recognized. Every hour of delay increases danger of obstruction and of gangrene.
Operations for strangulated hernia should thus always be done early and before much exudate or local disturbance has occurred, as when thus performed they may be combined with measures for radical cure, which are hardly to be thought of when infection has occurred. (See Plate LIV.)
Strangulated hernia, then, being always a dire emergency, is in nearly every instance best treated by herniotomy, whose principles are the same, no matter whether applied to inguinal, femoral, or umbilical hernia. By a suitably planned incision the sac is exposed. In the inguinal region this follows the general direction of the cord and inguinal canal. In the femoral region it is best to raise a flap, while in umbilical hernia, although the first incision may be in the middle line, it will usually be found necessary to make an elliptical excision of the overlying skin, in order that both it and the sac may be removed. Under conditions of long existent hernia, plus strangulation, the original anatomical conditions are much altered, and it is not necessary to waste time in the endeavor to recognize the various coverings of the sac. One cuts directly down upon it with such care that he may recognize it as he comes upon it, usually by its color and by the sensation of proximity to its strangulated contents. This is ordinarily not a difficult matter; all bleeding vessels should be secured before the sac is finally opened. Final and complete identification may be made by finding that the sac itself may be pinched up between the fingers or forceps, while the underlying contents slip away. Only when parts are bound together in exudate will there be difficulty in this regard. The surgeon should still proceed with caution, although the sac will usually contain sufficient fluid of transudation to protect against injury to the enclosed bowel. Nevertheless the greatest care should be observed not to wound the intestine, which sometimes lies very closely under the skin, especially in the middle line of an umbilical hernia, although there may be masses of fat on either side of it. Sometimes the sac distended with discolored fluid is itself mistaken for the bowel. Error can usually be avoided by following it upward and identifying its continuity with the surrounding tissues.
When opened its contained fluid may be found quite clear, blood-stained, purulent, extremely offensive, or even fecal, according to the relative age of the condition and the degree and results of strangulation. Under all circumstances it is advisable to disinfect the sac and its contents before endeavoring to release them. This may be done with dilute peroxide of hydrogen or with any ordinary irrigating fluid.
Within the sac, when thus identified and opened, may be imprisoned omentum or bowel, or both, in any degree of preservation from that which is almost normal, and with circulation but slightly disturbed, to that which is absolutely gangrenous. Congested bowel will nearly always be more or less discolored. So long as it is dusky or even almost black, but has not lost its luster, it may probably be safely returned to the abdominal cavity; but if green or if luster be gone, or if the contained fluid be[900] distinctly putrefactive, then serious doubt as to its viability will arise. In case of actual perforation, gangrene, or fecal abscess there will be no doubt as to the danger of returning such bowel, and other measures should be adopted.
The viability of the bowel having been determined and the sac disinfected the location and degree of tightness of the constricting ring should now be determined. In inguinal hernia the constriction may occur either at the external or internal ring; in femoral hernia it is usually at the femoral ring; in umbilical hernia, at some portion of the umbilical opening; while in all three forms constriction may occur within the sac itself and with little reference to the ordinary hernial outlets; all of which needs to be clearly kept in mind. This identification is usually done with the tip of the little finger, gently insinuated and used as a probe. The operator who is sure of his methods does not necessarily need to expose the constricting ring in order to nick it or divide it, but he who is not as proficient should extend and deepen his incision until the parts are clearly exposed, so that he may be sure of not doing more harm than good.
Ordinarily it is necessary only to nick at one or two points the margin of the ring, which will feel much like a wire loop, and then to use the finger as a dilator, stretching and perhaps tearing, i. e., making the knife do as little and the finger as much work as possible, in order to so loosen up the constricted canal that by gentle taxis or manipulation reduction can now be accomplished. The text-books on anatomy give minute descriptions of the relations of these hernial outlets to important bloodvessels, with which even the student should be perfectly familiar. Nevertheless by following the subjoined rule, and never departing from the principle thereby indicated, the operator may safely proceed in practically every instance. This is to cut in the direction of the patient’s nose. The knife used for this purpose is ordinarily the herniotome, i. e., a blunt, slightly curved bistoury, with but a small exposed cutting blade, whose dull point is passed along the finger until the constriction is reached, and then, by the sense of touch, beneath and beyond it, until the wire edge of the ring rests upon the cutting part. The handle is then turned until this edge points upward and is moved with a gentle sawing action always in the above-specified direction, until the peculiar resistance is felt to have yielded. It may then be turned a little and another nick be similarly made. These nicks should not be more than one-quarter of an inch deep, after which the knife is withdrawn and the finger now made to dilate and tear. With these precautions there is very little danger of dividing an anomalously placed vessel.
Dilatation of the ring being now sufficient it is well to pull the hernial mass a little downward, in order that the condition of the bowel at the point of constriction may be exactly noted. It should therefore be gently coaxed into the wound, once more subjected to inspection, and then to disinfection. The surgeon should now determine what to do both with the bowel and the omentum. Omentum which is covered with exudate or darkly discolored, or surrounded by offensive material, should be first liberated, then ligated, above the original point of constriction, and the undesirable part removed, the stump being returned to the abdominal cavity. The bowel, if decided by above indications to be viable, may then be gently coaxed back if handled with care.
But gut which has perforated, or is so compromised as to be threatening gangrene, should not be returned into the abdominal cavity, but treated by resection, or by fixation and the formation of an artificial anus, decision depending both upon the condition of the patient and of the bowel. Some of these cases are too nearly moribund when operated to justify such procedures as resection, and are suffering too profoundly from the consequences of obstruction to make it advisable to do more than open the bowel for its immediate relief. Artificial anus is, therefore, the inevitable necessity in some forms of strangulation. When the bowel is gangrenous it is not necessary even to endeavor to draw it farther down into the sac, but it may be simply opened in situ.
Intestinal resection and suture instituted under these circumstances are essentially the same as those already described in the chapter on the Small Intestines. With the formation of an artificial anus there results the inevitable fecal fistula which will require subsequent operation, probably secondary resection.
In non-septic and favorable cases, the reduction having been accomplished, the operator then may proceed to extirpation of the sac and the closure of the hernial outlet, i. e., operate for radical cure, this being a modern extension and addition to the old operation for relief.
If obstructive symptoms should persist after operation the possibility of twisting of[901] the intestine, or a possible reduction en bloc, may be feared, which is not likely to occur if the open part of the operating have been done thoroughly.
Clean cases of strangulation may be closed without drainage. In case of doubt, however, it is advisable to provide at least a capillary drain, while every case known to have been contaminated should be perfectly drained.
Fig. 611
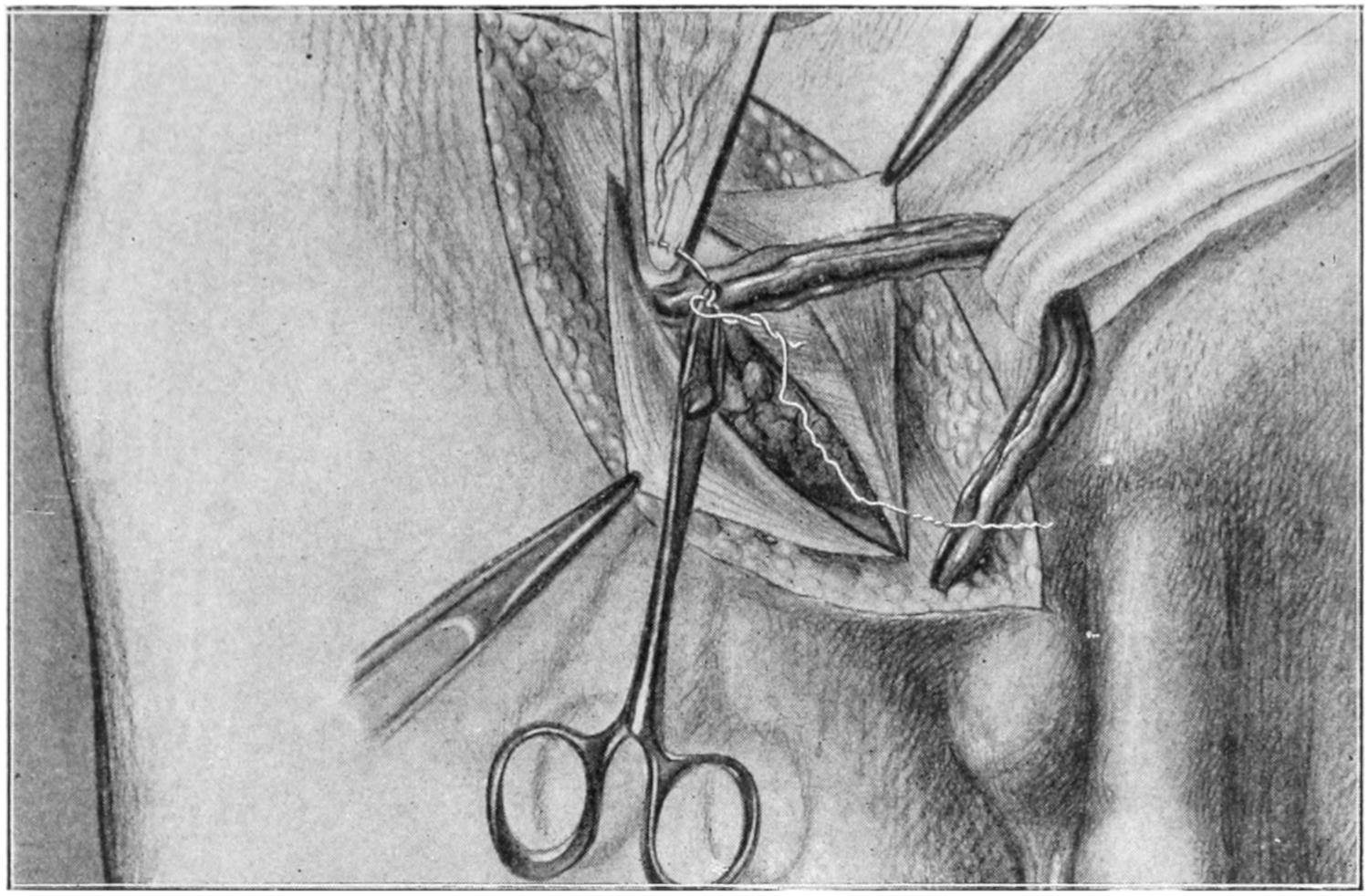
Bassini’s operation. Ligation of the sac by means of a purse-string suture passed through the internal surface of its neck. The cord is drawn to one side. The aponeurosis of the external oblique is drawn apart with forceps. (Richardson.)
Fig. 612
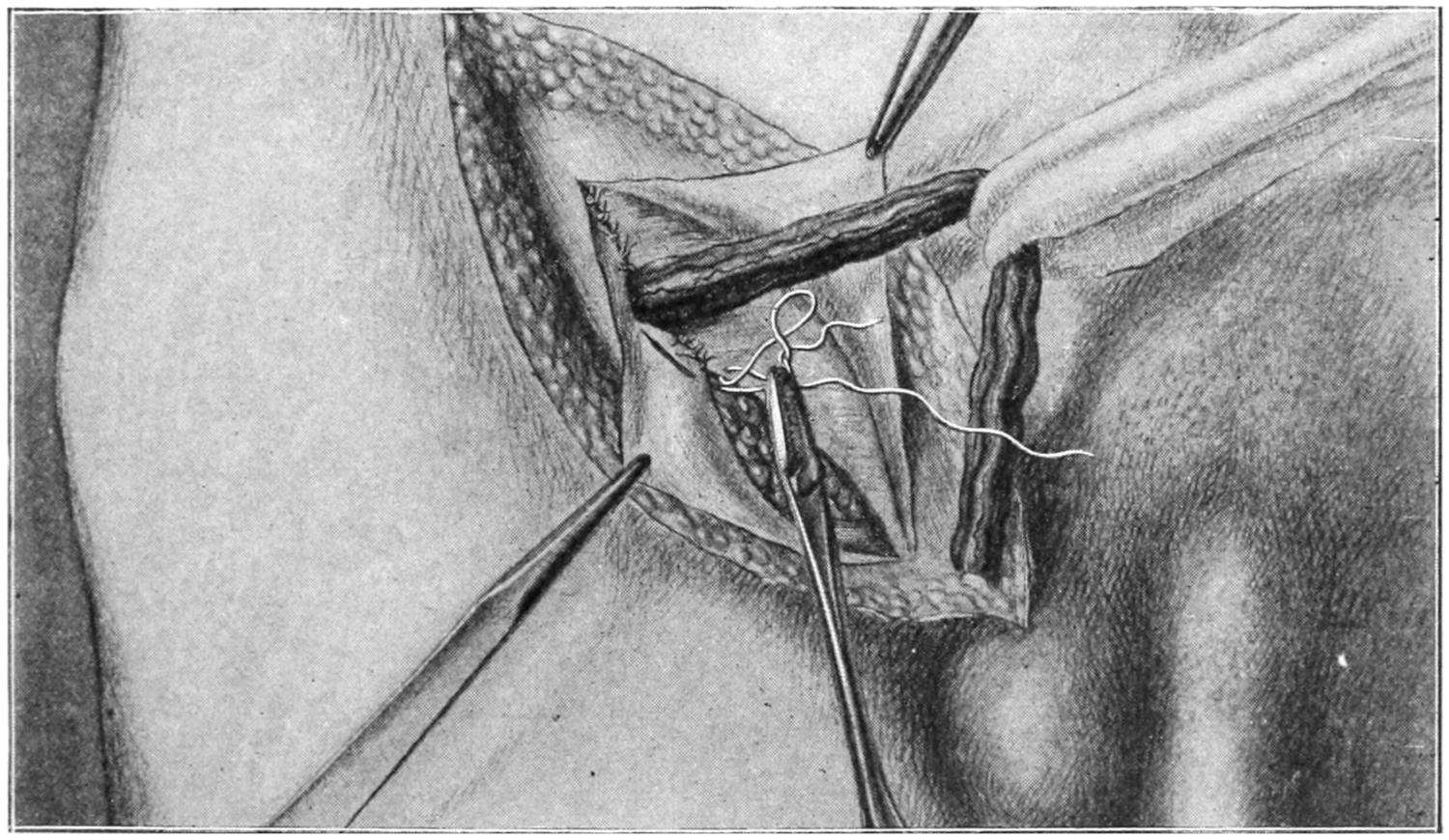
Bassini’s operation. Suture of the conjoined tendon to the internal surface of Poupart’s ligament. Fortification of the posterior surface of the canal. (Richardson.)
—From the earliest times rude and crude methods of endeavoring to effect a radical cure of hernia have been in vogue. While sometimes effective they have always been dangerous and always clumsy. Not until the antiseptic method was introduced could they be regarded as in any way safe or reliable. With the introduction of Listerism it became practicable to do this work, upon principles simple in character and ordinarily easy of performance, which may be summed up in the formula: Isolation and obliteration of the hernial sac, with permanent closure of the hernial outlet. Easy as such description may sound it has been found more or less difficult in practice, and numerous methods, apparently both simple and ingenious, have proved defective and have called for the most pronounced modification. Considerable space could be devoted to operations for radical cure, but the intent here shall[902] be to simplify the subject as well as the method, and consequently but two or three will be described. Suffice it to say that while all are based on the same principle they vary somewhat in detail, and that some of these details have to be adapted to the special requirements of individual cases.
With increase in experience has come enlarged confidence in the operation, and it is now regarded as justifiable in nearly every instance among individuals otherwise in good condition. It has a double purpose—namely, the avoidance of the danger of sudden strangulation and the riddance of necessity for wearing trusses, or suffering the discomforts of hernia without any mechanical control. Some modern methods include the utilization of some portion or all of the sac, while in others it is entirely cut away. Consequently some operators have endeavored to utilize such portion of the sac as could be made available for either purpose, either as plug or suture material.
The method of Bassini for relief of inguinal hernia, more or less modified to meet individual demands, seems to have become of late years the most popular and widely adopted. The incision is made over the most prominent part of the tumor, extending as far downward upon the scrotum as necessary, and upward to near the anterior superior spine. Through it the external ring, with its pillars, is exposed, and then the sac, by a dissection long and sufficiently wide to fully reveal it. The exposure is made more complete by dissection of the aponeurosis of the external oblique from the level of the external ring upward and outward for an inch or so above the external ring. By seizing the edges of the aponeurosis on each side with forceps and retracting there is now afforded an excellent view of the hernia proper. (See Fig. 611.)
Fig. 613
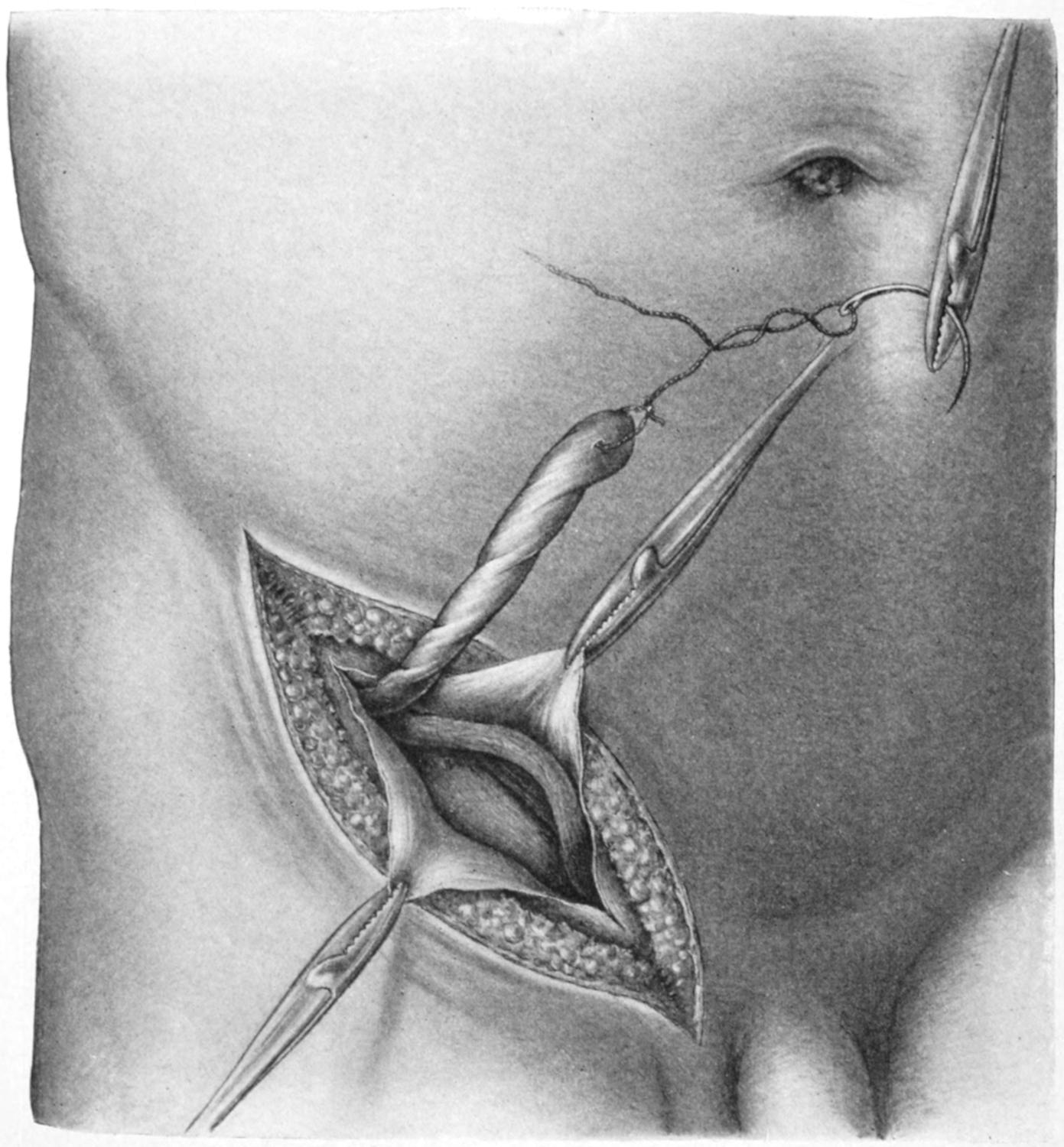
Park’s method of utilization of sac, showing its isolation and one way of employment in making the suture further represented in Fig. 614.
[903]
By careful dissection the sac and cord are identified and isolated, while the sac is opened and its edges held apart by forceps, after which it is carefully separated from the other structures of the cord. After thus isolating the sac, and with the least possible disturbance of the cord and of the testicle, it is ligated as high as the internal ring, or, if possible, higher yet. This leaves the cord uninjured; its size should next be reduced by cutting away all superfluous tissue. Some operators remove all the veins, but this seems unpromising and dangerous.
Fig. 614
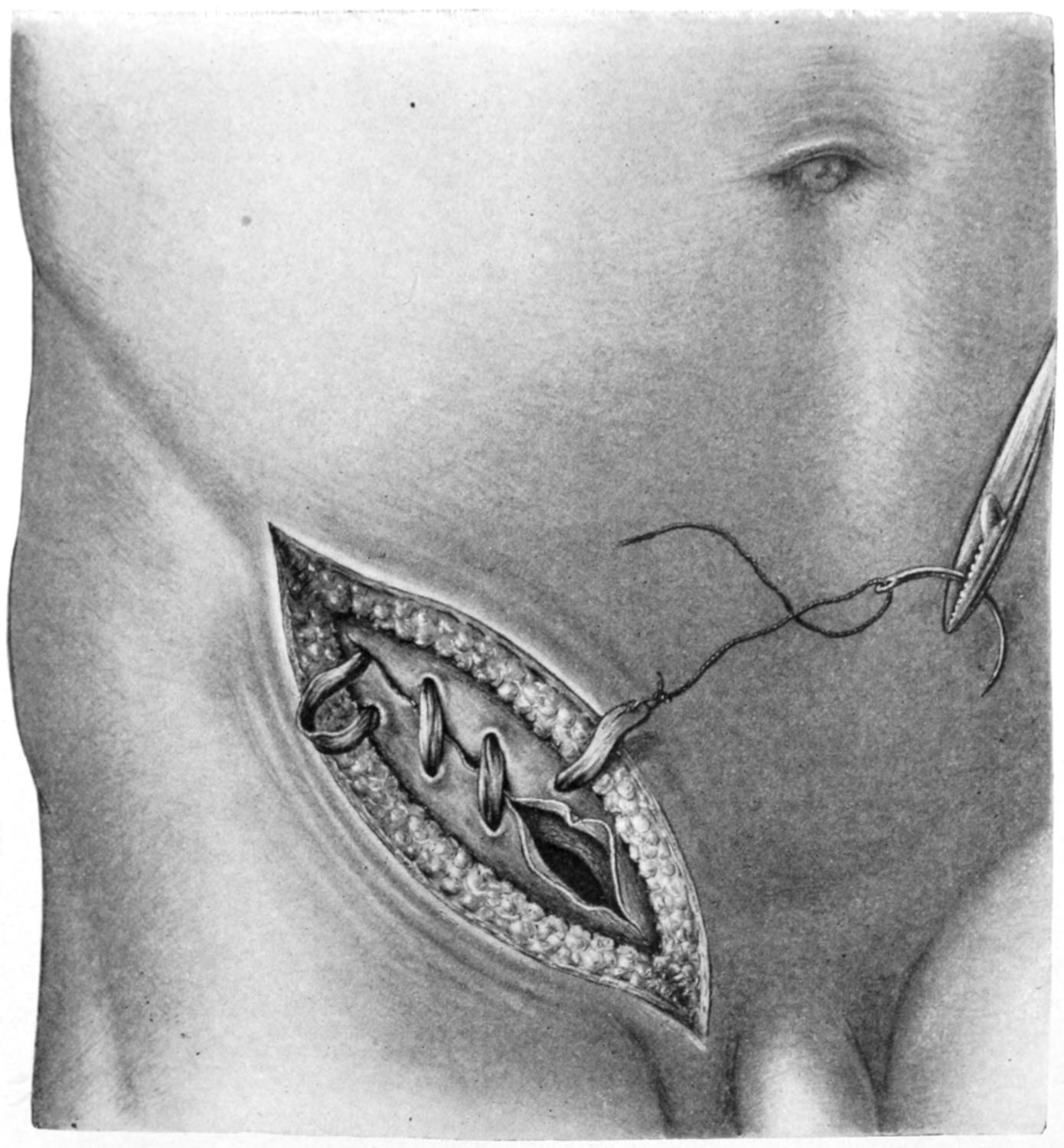
Park’s operation. Continuous suture made with a long thin sac.
By all this dissection and reduction the inguinal canal has been temporarily, cleared, and the sac having been elevated, ligated, and cut away it becomes now a question of what to do with the cord. The lower surfaces of the external oblique and of Poupart’s ligament are next freed, the edge of the internal oblique, of the transversalis with its fascia, the outer border of the rectus and the conjoined tendon being all exposed to view by whatever dissection may be required, all fat and areolar tissue being removed. The cord is finally disposed of by holding it out of the way, usually by a loop of gauze, while the deep layer of the external oblique and the external portion of Poupart’s ligament are sewed to the muscle edges of the internal oblique and transversalis, as appears in Fig. 612, by a line of sutures which include the conjoined tendon, at the lower angle of the wound, which should be affixed to the outer border of the rectus. In the deeper portion of every such wound there is danger of injury to the external iliac vessels as well as to the epigastric. For the escape of the cord, and to avoid its undue constriction, an opening should be left for it, i. e., a new internal ring, adapted for the purpose and not too small. This is made by not suturing the upper part of the wound. The cord being afforded this exit is now dropped, and the edges of the external oblique are brought[904] together over it, the sutures extending well downward, but being omitted at the lower portion, where a new external ring is thus left, only not of its original size, but sufficiently large to accommodate the cord.
Such are the essentials of the Bassini method, which has been modified by Halsted in such a way that the cord, reduced as much as possible, usually by removal of most of its veins, is now not left within the inguinal canal, but transplanted entirely outside of the external oblique, escaping at the upper part of the incision and requiring no further accommodation in its course toward the testicle. In children, or even in adults with very small veins, he does not so reduce the cord. After isolation, opening and transfixion of the upper end of the sac, and its secure ligation, he drops the stump back into the abdomen. The muscular and tendinous layers of the ring and abdomen are united also, by layers, with quilted sutures.
Fig. 615
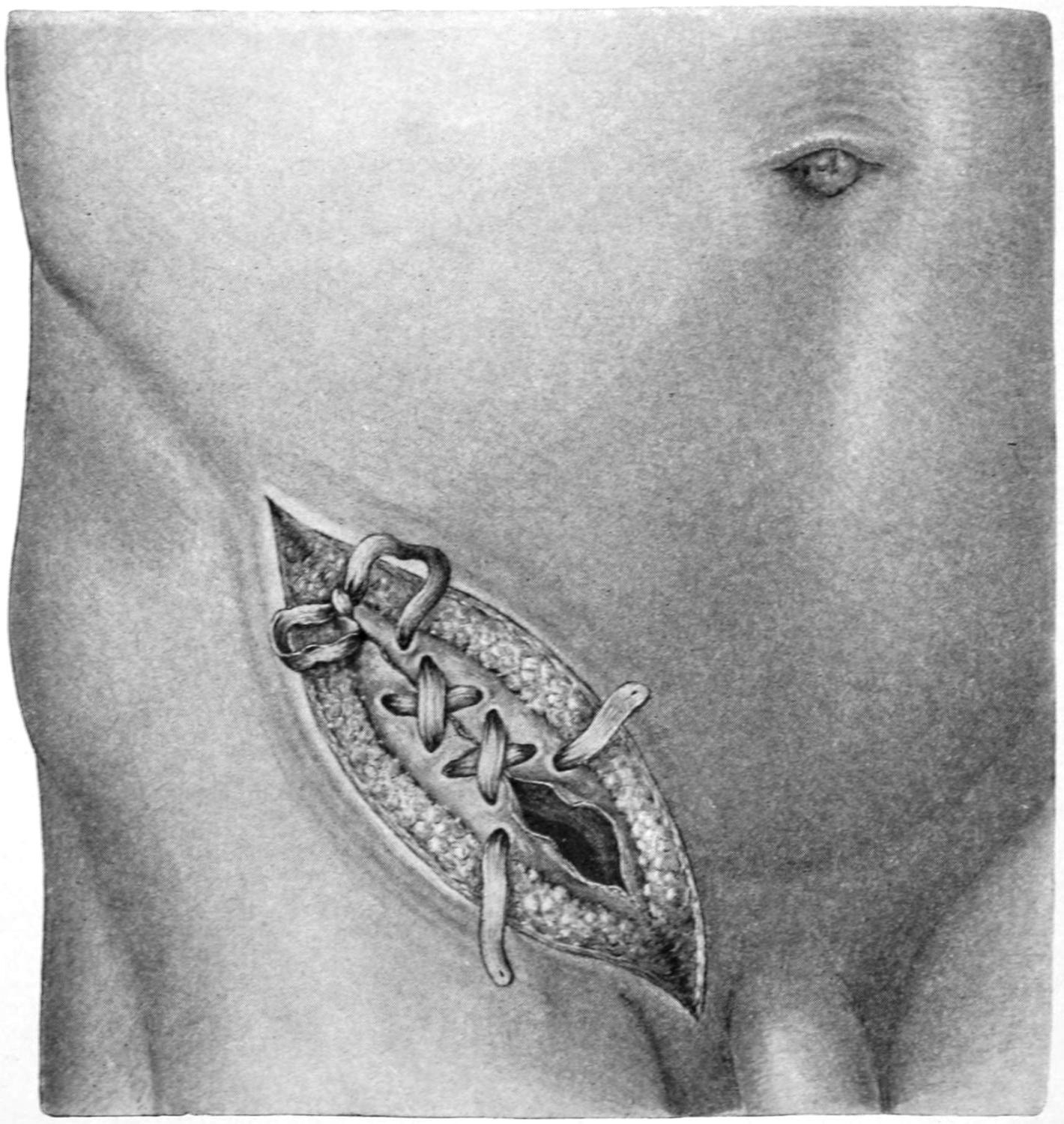
Park’s method. Shoelace suture made with a sac split into two strips.
In these as in many other methods, much, practically everything, depends upon the certainty and durability of the sutures used for disposal of the inguinal canal. For some years surgeons used silver wire, which has now been abandoned. The choice now seems to depend on silk, thoroughly and freshly boiled, or animal sutures, such as kangaroo or reindeer tendon. McArthur suggested to dissect off a strip from the margin of the opening in the external oblique, or from the aponeurosis, and to use this strip of the patient’s own tissue for suture material. I have modified this method, as will be described later. Kocher devised a method of isolation of the sac, without such complete emptying of the inguinal canal, the sac being drawn up through the canal, then through the internal ring, and finally through an opening in the external oblique, over the internal ring, where it was twisted and fastened, after which the external portion was removed.
[905]
My own preference in operations for radical cure has been, until recently, an exposure similar to that of Bassini’s, with complete isolation of the sac, which is separated up to the level of the internal ring or even higher. At this point it is drawn out through an incision made in the external aponeurosis, twisted and fastened. The inguinal canal is then closed, its deeper layers by a shoelace suture of tendon, threaded into two stout curved needles, by which the deeper margins of the canal are brought accurately together. Sometimes I have transplanted the cord and again have dropped it back, the layer of shoelace sutures closing the external aponeurosis over it. It has not seemed to me to make any difference which method was adopted, and I have practically never seen any atrophy or permanent disturbance of the testicle.
More recently it has occurred to me to utilize the sac itself for suture material, and this is the method which I now adopt in those cases that permit of it.
Figs. 613 to 616 show the method of thus utilizing the sac. A long thin sac may be twisted into a cord and used as an over-and-over suture, by which the margins of the canal are brought together. If found thick and unwieldy it may be trimmed down into a single suture, or it may be split, with more or less trimming, into two portions, by which the canal is then braided together or closed with a shoelace suture, the ends being tied or fastened at the lower portion. Fig. 616 shows how a short sac not otherwise available can be lengthened and made sufficient for the purpose.
Fig. 616
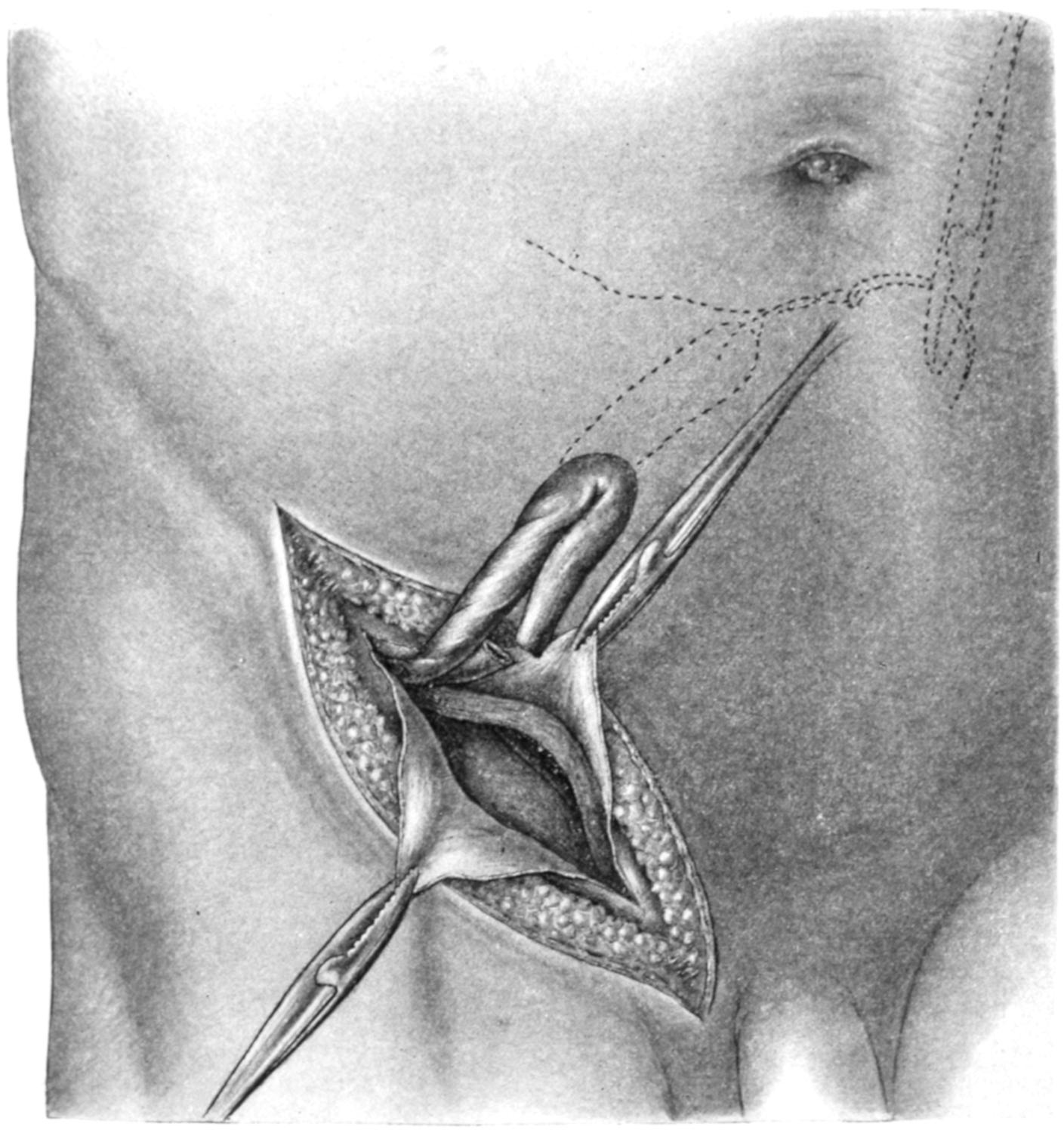
Park’s method. A short sac is so divided as to be elongated sufficiently for use as a suture.
This again is utilization of the patient’s own tissue, he himself furnishing his own animal ligature, which, being fresh and sterile, may be regarded as reliable. The method, furthermore, has this advantage, that there is reason to believe that tissue so utilized becomes organized, in time, and that the union becomes more reliable rather than otherwise. At all events in a considerable number of cases it has yielded satisfactory results, and in no case has it caused any disappointment.
[906]
Fig. 617
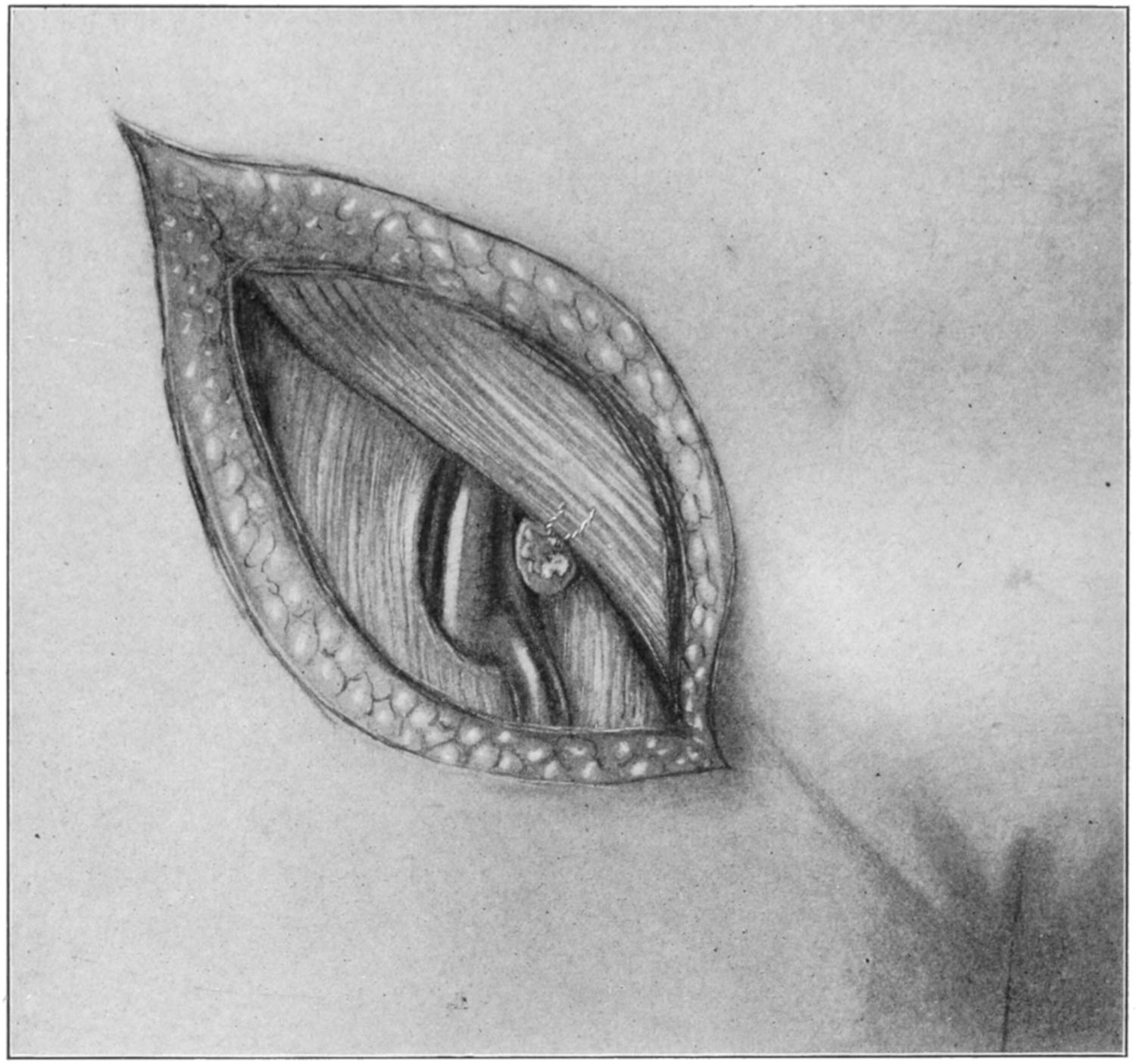
Radical cure of femoral hernia. Dissection of the saphenous opening. The sac of the hernia has been tied. (Richardson.)
Fig. 618
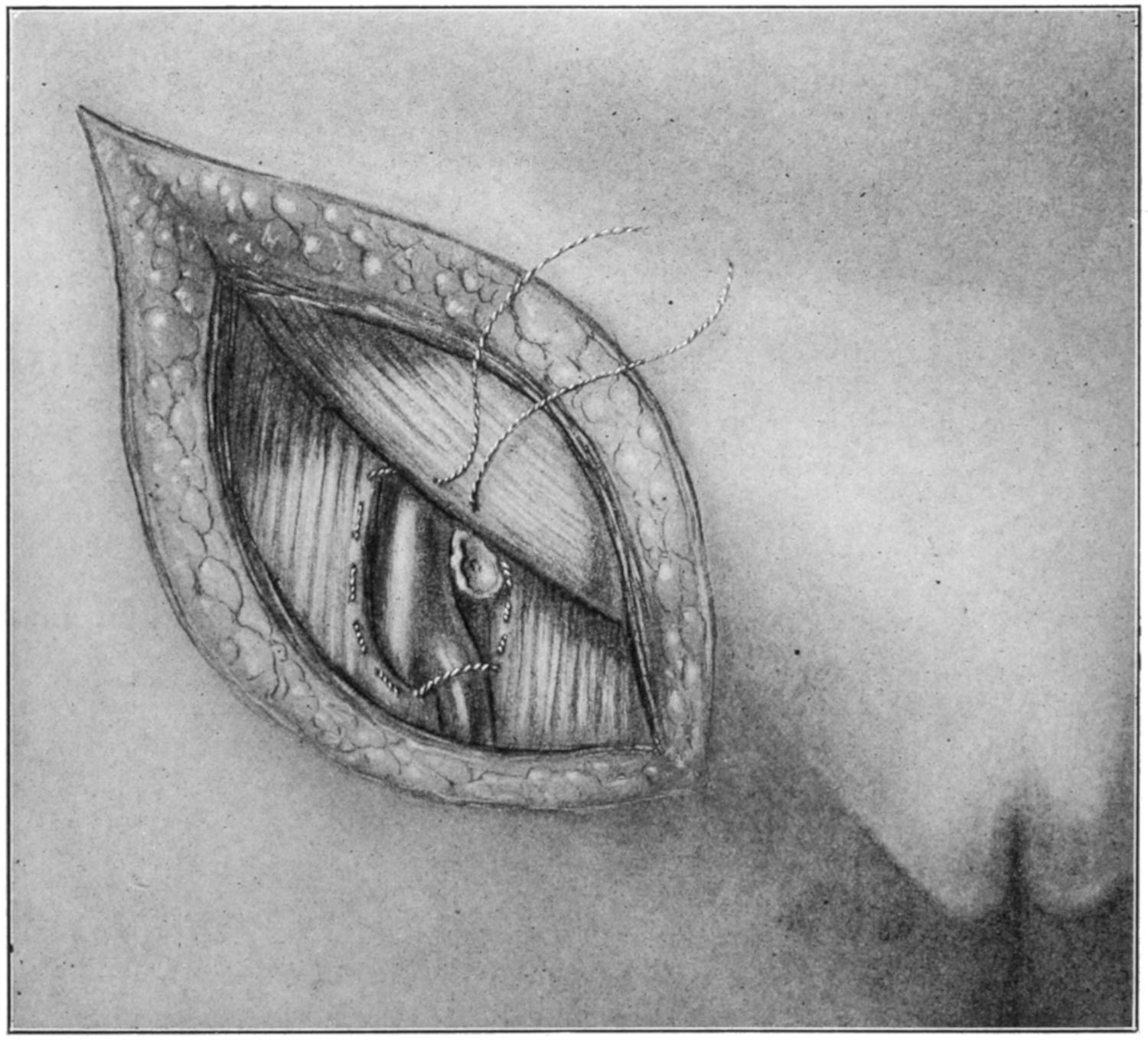
Radical cure of femoral hernia, showing method of application of purse-string ligature to close saphenous opening. (Richardson.)
[907]
Fig. 619
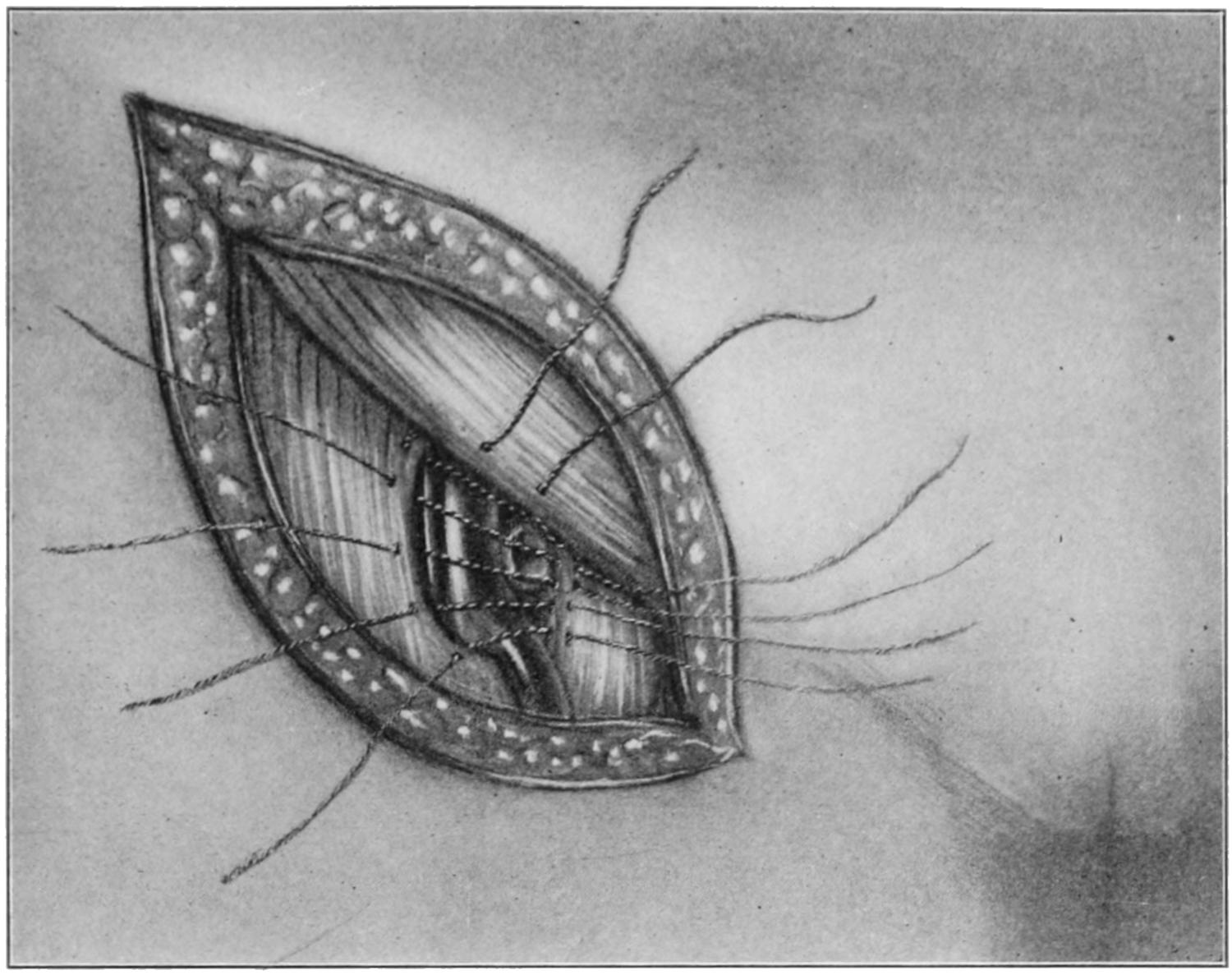
Radical cure of femoral hernia. Sutures applied to pectineal fascia, fascia lata, and Poupart’s ligament. (Richardson.)
Fig. 620
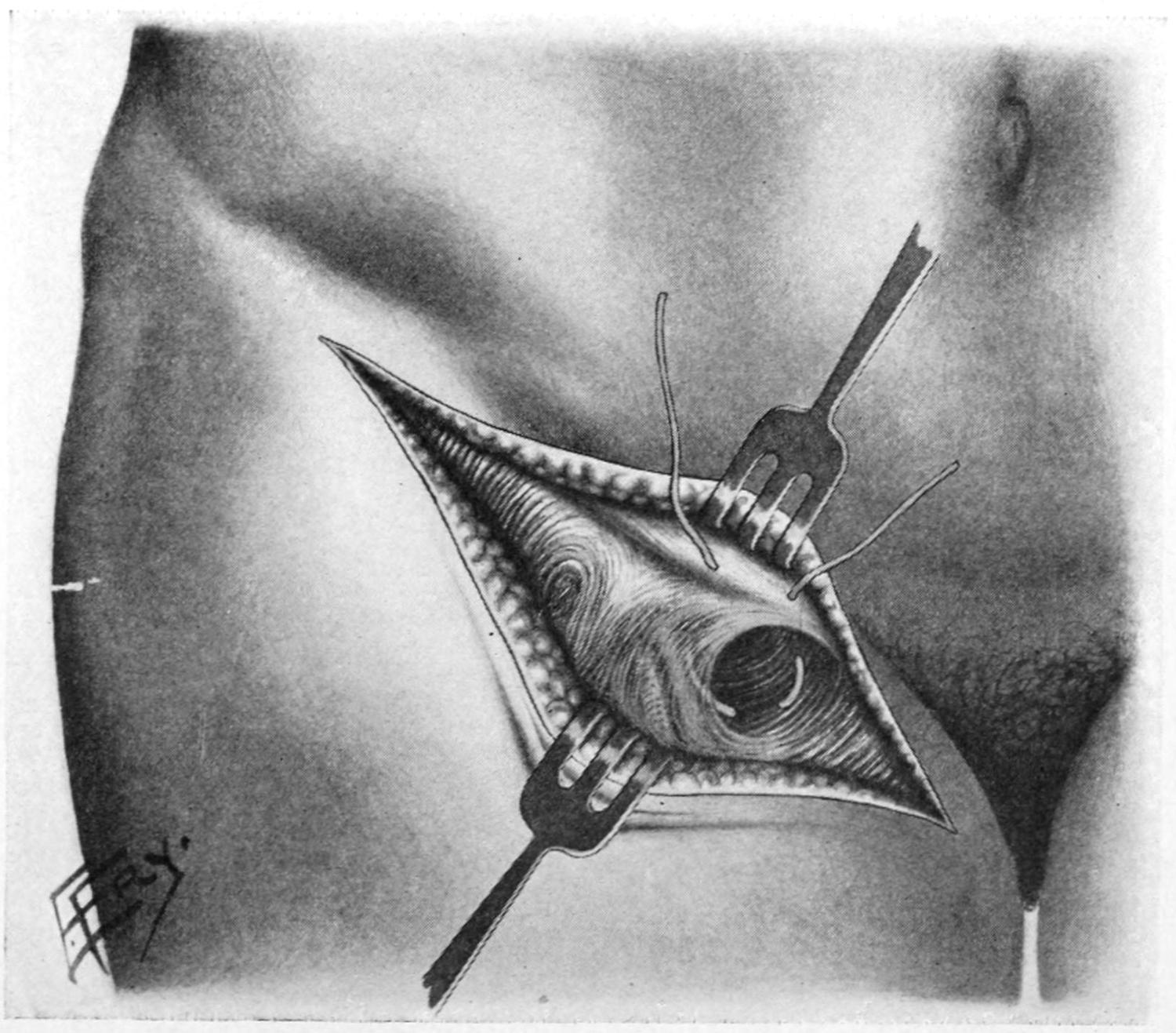
Obliteration of the femoral opening by purse-string suture. (Coley.)
Recurrence after these operations occurs less and less frequently as operators gain in experience and technique is improved. At all events the procedure has now become[908] standard and disappointments are relatively rare. It is useless to quote statistics of individuals, for they necessarily differ. In general, however, it is probable that from 90 to 96 per cent. of cases properly operated suffer no recurrence.
In the female inguinal hernia is treated in practically the same way, conditions being simplified by the absence of necessity for making any provision for the blood supply of the testicle or cord. The canal and rings may, therefore, in the female be absolutely closed.
Femoral hernia is radically treated on the same general principles, but with greater difficulty, as anatomical conditions are less favorable. A flap is raised below Poupart’s ligament, with its centre over the tumor, and the sac exposed and completely dissected, then opened, as in inguinal hernia. Its contents being reduced obliteration of the sac and its utilization, if possible, are in order. It is rarely difficult to separate it from its surroundings well up in the femoral canal. It may be twisted and its neck ligated, or it may be possible in some cases to either infold or reduce a sufficient portion of it to thus form a plug, which, being pushed upward, serves as a means of closing the femoral opening from above. Whatever use may be made of it it should be obliterated as a pouch, and its descent prevented by closure of the canal around it. This is difficult because of the proximity of the femoral vein and the somewhat unyielding character of the falciform and crural fasciæ. By some form of purse-string suture, or by a little dissection and sliding of aponeurotic flaps, it is usually possible to bring the surrounding structures snugly together. Even here I have been able to apply my principle enunciated above, and, by cutting away a strip of the sac, utilize it for the purpose of closing the femoral canal; but it is not often that a femoral pouch will be sufficiently large to afford tissues for this purpose. Figs. 617, 618, 619 and 620 will save the necessity for further description.
Fig. 621
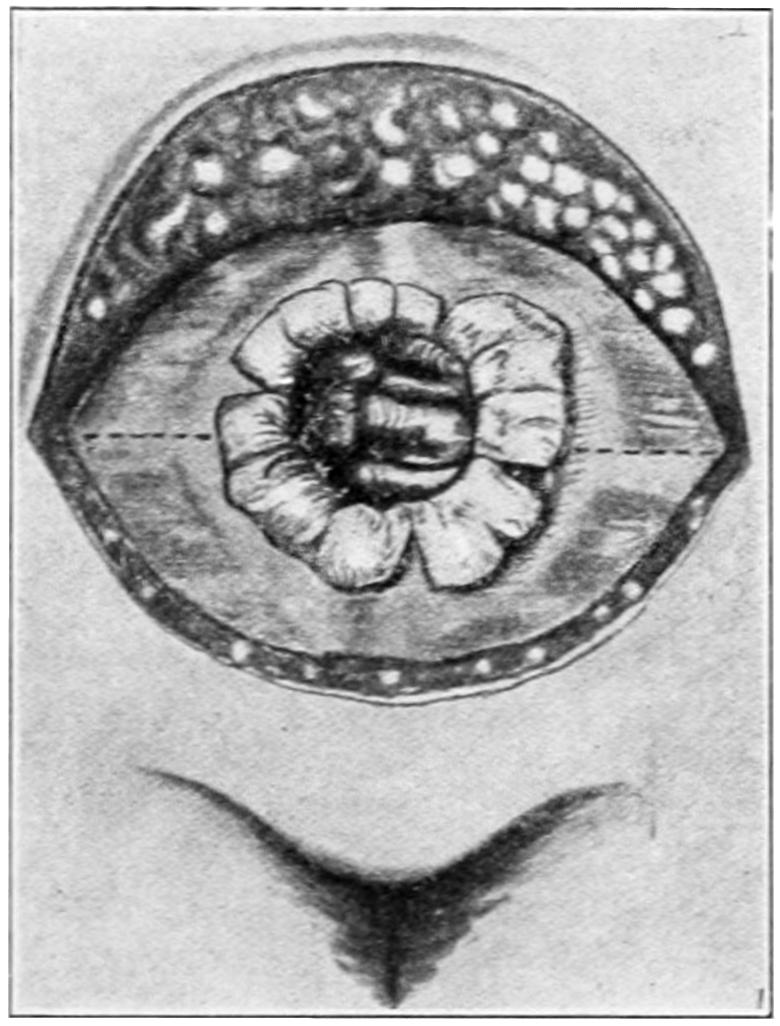
Fig. 622
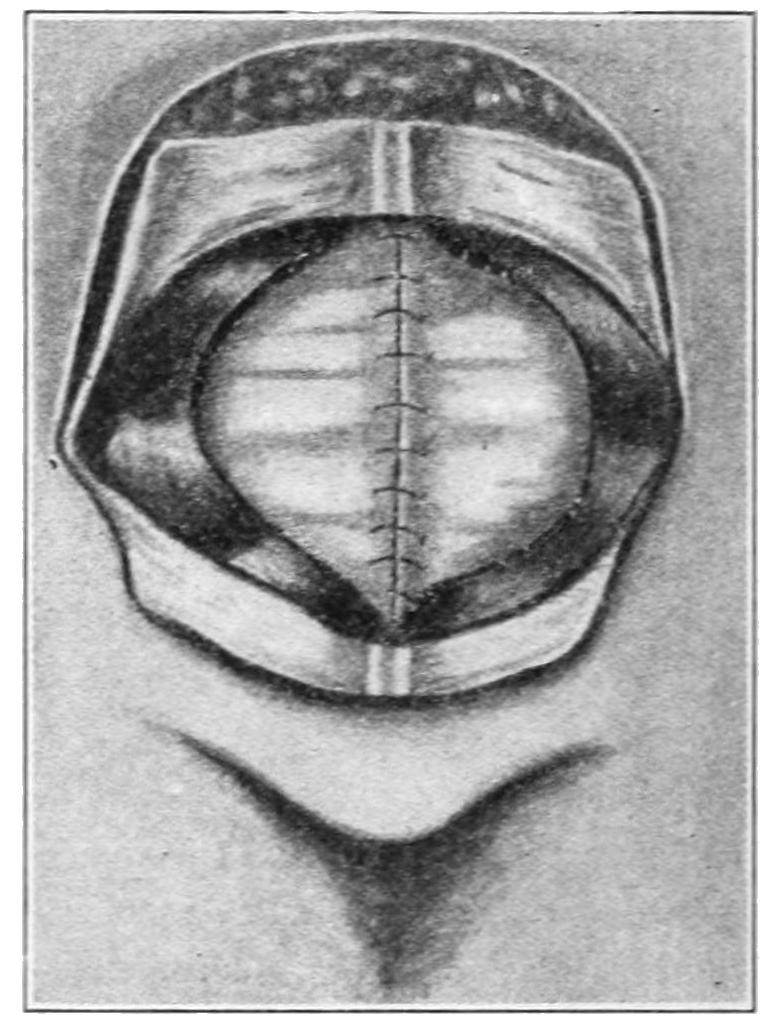
Graser’s method of dealing with umbilical hernia.
In many inguinal and umbilical and in a few femoral hernias the operator will be hampered by adhesions between the omentum or between the bowel and the sac wall. These may be infrequent and slight or extensive and dense. They are relatively unimportant so long as they involve only the omentum, which may at any time be cut away, the stump being dropped back into the abdomen, after being suitably secured; but when bowel, especially large intestine, is thus adherent, great care should be exercised, avoiding all possibility of shutting off the blood supply while securing every divided vessel.
Particularly is this true in treatment of umbilical hernias, either radical or under conditions of strangulation. In stout individuals, usually women, umbilical sacs sometimes contain several feet of bowel, and adhesions may be met at many points, difficulties arising not only in their separation, but in the final disposition and accommodation of[909] all this bowel within the abdominal cavity, from which it has been so long absent. Radical cure will in these cases leave intra-abdominal viscera in a rather overcrowded condition.
The essential details of radical treatment of umbilical hernia are the same, modified by the extent of sac which has to be removed, and by the wisdom in many instances of a large elliptical excision of the overlying skin and removal of much superfluous tissue. After freeing the contents and reducing them, the sac wall being completely separated, there is the choice of two or three methods of closing the umbilical opening, either by overlapping of flaps, which may be cut from the thickest portion of the sac, which will be close to the outlet, or by dissecting them from the aponeurosis, as suggested by Mayo, and turning the upper down over the lower, or by any other expedient which individual peculiarities may suggest (Figs. 621 to 624). I have been able to employ, to apparent advantage, my method of securing suture material for this deep closure from the sac wall itself, this not preventing the employment of any other method or improvement.
Fig. 623
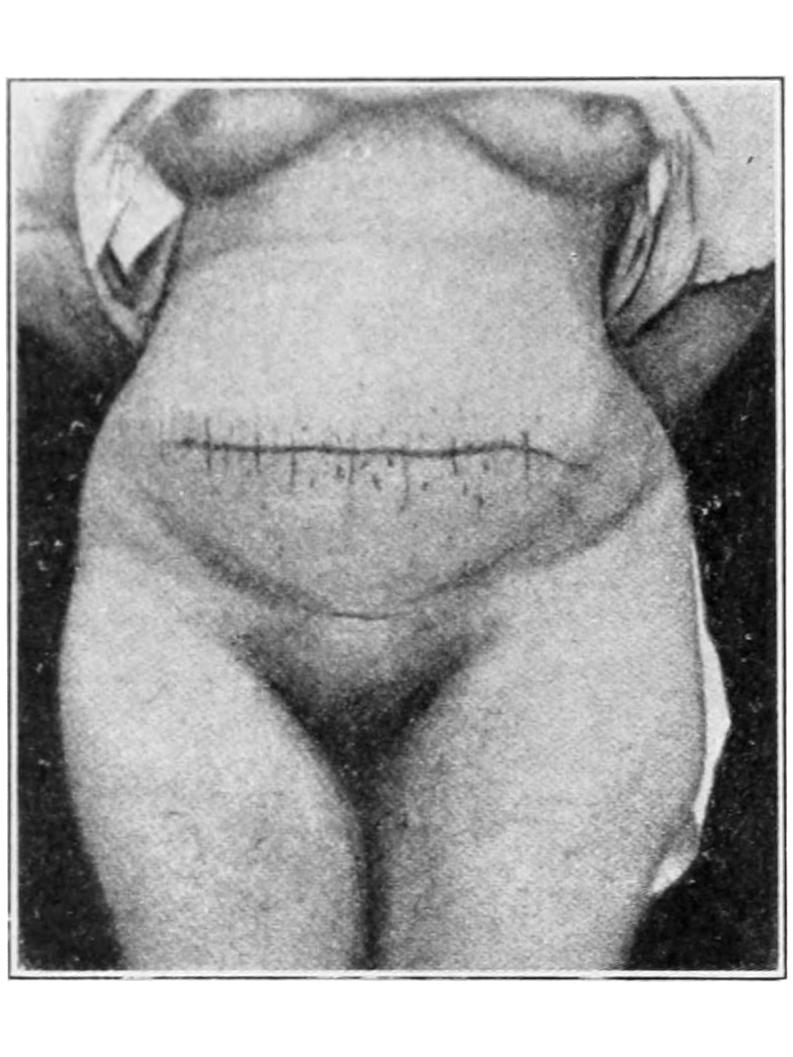
Fig. 624
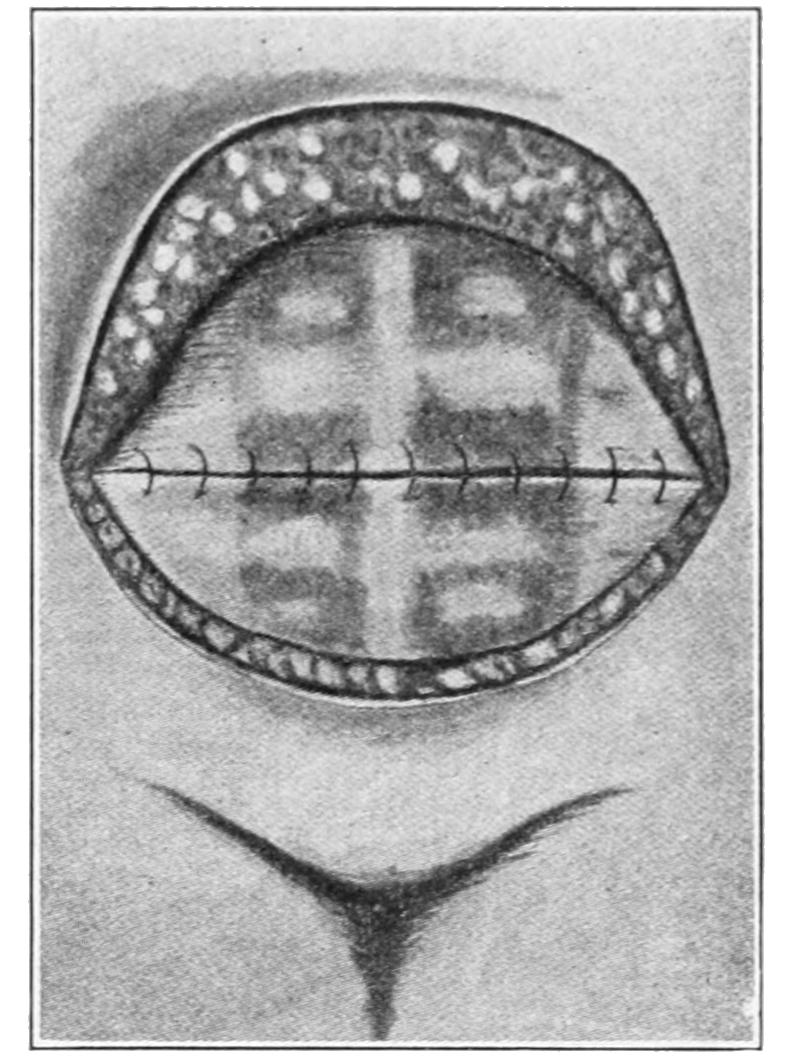
Method by transverse closure of both deep and external incisions.
Ventral and postoperative hernias are operated on in essentially the same manner as the forms above described. Adhesions may be found in these cases, and plastic methods should be devised for bringing together irregularly shaped openings and holding them in the firmest possible manner. In any extensive abdominal hernia, umbilical or ventral, it is advisable to use buried sutures, closing the abdominal walls, layer by layer, and finally to insert at some distance a sufficient number of through-and-through retention sutures, guarded by plates or small rolls of gauze, these taking off tension from the wound and affording protection against any special strain, such as vomiting.
[910]
The congenital defects and displacements of the liver which interest the surgeon are few. More or less transposition, sometimes complete situs transversus, is encountered. The same is true of more or less hernial protrusion into the chest, through a defect in the diaphragm, or such displacement as may be permitted by some defect of the abdominal walls or other viscera. Hammond has recently shown that the left lobe of the liver is sometimes congenitally enlarged to an extent sufficient to cause symptoms, a condition alluded to by very few writers. In this way the liver may cover the stomach and even extend over the spleen. Similarly the right lobe may be affected, but giving a different train of symptoms. Under these conditions mistakes may arise. Thus the left lobe might be mistaken for a large spleen, from which, nevertheless, it should be separated and differentiated by its free movement during respiration. Hammond even reports one case of this kind where, instead of removing the elongated portion of the liver, it was held up against the abdominal wall by sutures. For a similar condition Langenbuch has successfully resected a portion of this viscus. What is said here pertains to a true congenital variety, and not to acquired displacements or enlargements. In Fig. 625 is represented the case of xiphopagous twins united by a band of liver tissue and operated (by division of the band) by Baudouin.
Fig. 625
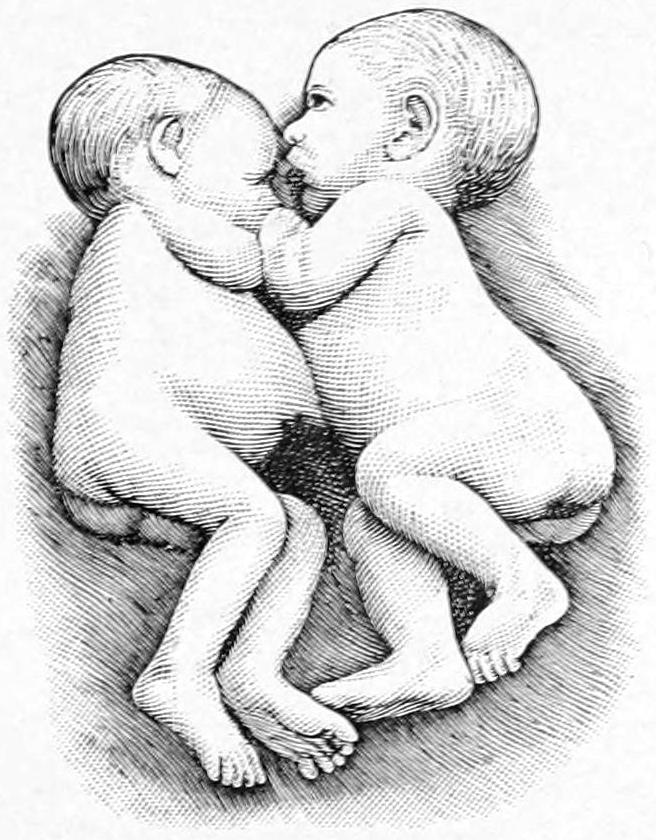
Xiphopagous twins, separated by division of a band of common liver tissue. Case of M. Baudouin. (Pantaloni.)
The relations between congenital laxity of the natural supports of the liver and certain morbid conditions, especially those produced by marked enlargement followed by great reduction in size, to the so-called wandering or floating liver are very indefinite. The term “wandering” implies a mobility far beyond the normal, with more or less yielding of ligaments, especially the suspensory, which permits undue displacement. We often fail to realize that the liver, which is the heaviest of the viscera, is nevertheless, in man, placed at their top, and hence that it has, in at least some respects, very meagre support. This is one of the disadvantages of the upright position, and it does not prevail in animals. In addition to this may be mentioned the peculiar enlargement of the right lobe, very rarely of the left, so often seen in connection with biliary obstruction, and often spoken of as Riedel’s lobe. Floating liver is more common in women than in men by four to one, and is often ascribable to the ill effects of tight lacing. Repeated pregnancies, with the consequent relaxed and pendulous abdominal walls which often follow them, also conduce to the condition by weakening, in fact almost removing, its lower supports.
—The symptoms produced are those of indigestion, dyspnea, perhaps with cyanosis, nausea, vomiting, and occasionally biliary obstruction and jaundice. In addition to these the patient will show the ordinary physical signs of a displaced or displaceable liver, noticeable in the upright or in the knee-elbow position.
[911]
—The treatment of milder cases will consist of support from below by suitably adapted and well-fitting abdominal binders or supports. Serious cases may necessitate surgical relief. This consists of hepatopexy, i. e., fixation of the liver to some of its upper surroundings. The operation is performed through an incision such as that used for exposure of the gall-bladder. The lower surface of the diaphragm and the upper surface of the liver are scarified until they ooze perceptibly. The anterior edge of the liver is then fastened to the abdominal walls, as also the gall-bladder, if it can be utilized for the purpose. The patient is then placed in bed with as much compression of the abdomen below the liver as can be tolerated, in order that the scarified surfaces may be kept in contact until adhesions result.
By its size and construction the liver is made peculiarly liable to certain injuries, while from others it is made more or less exempt by its protected situation, especially by the ribs, which nearly enclose it. From contusions it may undergo different degrees of laceration, sometimes even to the degree of fragmentation and pulpifaction. Again it is frequently involved in punctured wounds (stab, gunshot, etc.), which may be inflicted from any possible direction, perforation sometimes taking place from above and through the chest, and involving the tissues beneath.
General indications of injury to the liver will be furnished by its nature and location, the degree of collapse, and the consequent abdominal rigidity, with the common signs of internal or intra-abdominal hemorrhage. There is no doubt but that minor injuries of the liver are nearly always repaired, and that they occur much oftener than is generally appreciated; but a severe tear of the liver is a source of great danger because of hemorrhage. In general, of these injuries it may be said that any traumatism which produces profound or increasing symptoms should be regarded as indicating a careful exploration, done with every precaution at hand for carrying out any possible indication. What the liver may safely bear in the way of ligatures, sutures, and operative disturbance will be indicated later. Many fatal cases show a period of a few hours of temporary amelioration of symptoms which may have lulled to a sense of false security, and during which internal mischief is still increasing. Moreover, any blow sufficiently severe to rupture the liver may do other harm. In such instances, then, it becomes a simple question of whether there can still be sufficiently early intervention to save life. To what extent this intervention may be required in stab and gunshot wounds it is difficult to state. If hemorrhage and puncture of any hollow viscus can be excluded and if no other serious symptoms be present, it may be advisable to wait; otherwise the possible harm of a judicious early exploration is so small, while the prospective benefits are so great, that it is far the wiser course. Here, again, the general rule may be applied. When in doubt operate. Further details of operative procedures will be given below.
While abscess of the liver is, like all other abscesses, due to germ activity, it may yet definitely follow injury or be the result of a primary disease, or an extension from some one of the adjacent tissues or organs; as from above (empyema, pyopericardium, subdiaphragmatic, spinal), from below (gall-bladder and ducts, pancreas, stomach), from the portal circulation (superficial or ulcerating piles, typhoid and other intestinal ulcers, peculiar or tropical parasites like amebas), from the appendix, from the general circulation (pyemic, metastatic), through the lymphatics (mesenteric nodes), from the intestinal tube (ordinary round-worms and various parasites), from cancer breaking down, as well as from degenerating gumma or granuloma and from hydatid cyst.
Hepatic abscess may be acute or chronic, small or large, solitary or multiple. The tendency is to enlarge and finally to kill. This they do usually by rupture, e. g., either into the pleural cavity or the lungs, after adhesions have been contracted, the pericardium, the mediastinum, the peritoneum, any part of the upper alimentary canal, or the biliary passages. Finally they may open externally and perhaps be followed by spontaneous recovery.
[912]
A certain convenience of description is afforded by dividing these cases into the so-called solitary abscesses and the multiple forms, the latter being more commonly associated with tropical diseases of the amebic type or with pyemic processes. In most solitary cases the abscess is located in the right lobe, its extent varying within wide limits, especially when the subphrenic space has been involved. Its contents may be of almost any color and the pus is often thick and foul in odor. (See Subphrenic Abscess.)
—Symptoms of the solitary type may be at the onset acute, with or without history of previous sickness, the patient being suddenly seized with severe epigastric or hypochondriac pain, which is followed by prostration, with fever, chills, and sometimes cough. Characteristic rigidity and tenderness follow and the liver increases in size, the whole type of illness being one of acute abdominal infection. The slower forms appear to come on without early liver symptoms, patients complaining of cough and discomfort in the chest, with loss of flesh and appetite. Gradually the indications point to the hepatic region, while chills or intermittent fever occur, the liver gradually increasing in size and becoming tender. Again, in some cases, the trouble begins with irregular fever, patients running down rapidly, yet showing few local signs until the abscess invades the subphrenic region. In such instances examination of the chest gives negative evidence, save that there may be found elevation of the diaphragm due to accumulation below it. In nearly all instances there arise, sooner or later, severe chest pains, with enlargement of the liver, tenderness, and often indications of fluid in the right pleural cavity, which on aspiration may be found clear or purulent. Tenderness along the liver border will be most marked among characteristic features. Sometimes there is intercostal tenderness. Any indication of local peritonitis should be taken as evidence of approach of pus toward the surface. Jaundice is an occasional accompaniment. Previous malaria should be excluded if possible and a careful case history is a great help.
Diagnosis is usually to be made between hepatic and subphrenic abscess and between the single and multiple forms of the former. The possibility of empyema or of one or two subphrenic abscesses should be carefully determined. In fact, first of all, the surgeon has to determine whether the lesion is above or below the diaphragm. Some of the subphrenic abscesses contain gas, and, should indications of its presence be found below the level of dulness due to the presence of fluid, interpretation of the facts is easy. Localized edema of the chest wall, or of the region of the liver, is of importance when present. It is necessary, also, to exclude phlegmons of the abdominal wall. These are cases where it is justifiable to use an exploring needle repeatedly, if necessary, in order to determine the presence and location of pus. After anesthesia the needle may be used even more freely, its use being not only of assistance in diagnosis, but it appearing to be an agent of great value in the relief of pain. I have known painful affections of the liver to be much relieved by such exploration.
The accompaniment of dysentery of amebic type, and the discovery of amebas in the stools, would quite settle the question of the origin and nature of such abscess. Hydatids are of slow growth and are almost symptomless until they produce pressure disturbances or those due to the presence of pus. The fluid withdrawn from them is clear and may contain hooklets. Cancer eventually produces jaundice and the resulting enlargements are nodular, while the lower border is irregular, and the liver itself less tender and more movable, and there is usually more or less ascitic fluid present. Syphilitic gumma may cause enormous enlargement of the liver, with difficulty in diagnosis, especially in the absence of a significant history. Under vigorous mercurial treatment it will steadily improve; without it such gummatous tumors may suppurate. It will often be advisable, in case of doubt, to make this therapeutic test. Actinomycosis produces granulomas which tend to increase, infiltrate, produce adhesions, and gradually work toward the surface, as well as eventually to break down, the débris thus produced containing not only pus, but the peculiar calcareous particles characteristic of this disease.
—Multiple foci in the liver scarcely admit of successful operative treatment and are nearly inevitably fatal. The solitary liver abscess, even though large, is, on the other hand, usually satisfactorily treated by the general method of free incision and drainage, although, in exceptional cases, aspiration alone has seemed to suffice. Any collection of pus, no matter what the internal condition, so long as it be not distinctly cancerous, which tends to present externally, no matter at what point, should be thus treated. Incision may be made over any protruding or edematous area where pus seems[913] to be nearing the surface. With a considerable collection of this fluid in the right lobe, especially nearer its diaphragm-covered portion, it is usually safe to assume that the upper surface of the liver has become adherent to the diaphragmatic dome above it, and that there one may follow the costal border or may enter between the lowermost ribs, or may even resect one or more ribs if necessary, and drain posteriorly or by counteropening, as may be indicated. When approached from beneath, the lower surface of liver thus affected will usually be found more or less matted to the colon, omentum, or pyloric region, as the case may be, so that by carefully opening the abdominal cavity, and walling it off with gauze, pus may be evacuated from below and cavities satisfactorily drained. In this work it is of advantage to use an exploring needle, the operator guiding his further procedures largely by what it may reveal. Vessels which may be divided and spurt should be ligated or secured en masse, while oozing is overcome by gauze pressure. Drainage of a cavity already protected is simple; otherwise it may require a very careful combination of large fenestrated tube, if possible sewed in place, with the margins of the opening carefully puckered and secured around it and protected with gauze. Counteropening may be made, as well as drainage of any neighboring purulent focus.
Fig. 626
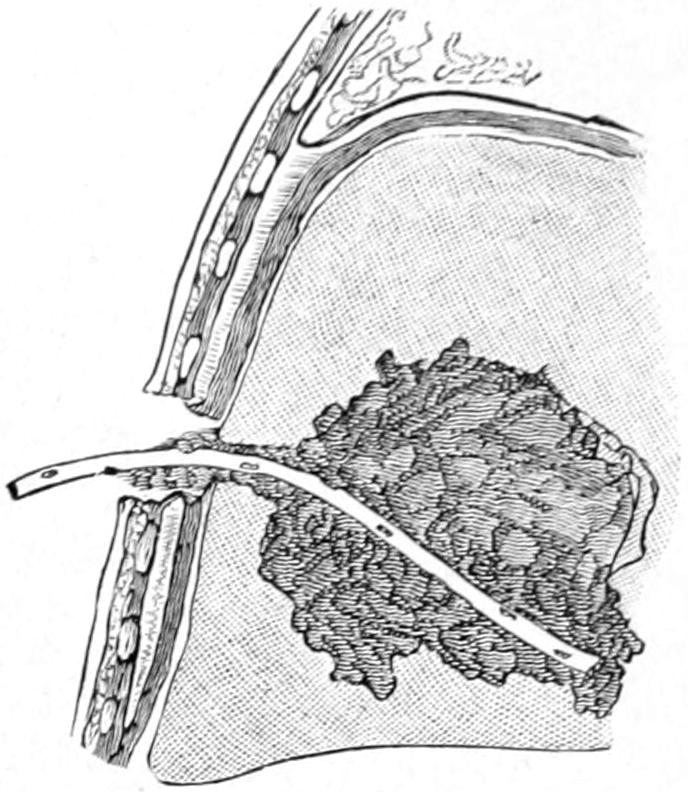
Abscess of liver, opened by transperitoneal hepatostomy. (Pantaloni.)
Echinococcus disease is almost a surgical curiosity in the central portions of the North American continent, whereas in some parts of the world it is extremely common. Thus while very rare in the United States, in Winnipeg it is an exceedingly common disease, being brought there by immigrants from a locality where it is still more prevalent, namely, Iceland, where it is said that nearly half the inhabitants die of some form of hydatid disease. In New Zealand, also, as elsewhere, this form of parasitic invasion is very common. With most American practitioners, however, it is so seldom seen that its mere possibility may be overlooked. In the liver it produces cystic disease whose symptoms are rarely significant until the cysts have attained considerable size and have begun to suppurate. That the liver is so frequently affected is easily understood, as the parasites make their first invasion along the duct from the intestinal tract. The history of these cases is always slow, as four years is a short time and twenty-five years not an exceedingly long one in which hydatid cysts run their course. Small cysts may even undergo spontaneous retrogression and calcify. These cysts when large may rupture, just as do hepatic abscesses, and in various directions. (See above.) Ordinarily it is only when suppuration occurs that the general health suffers, and not until that time are they, at least intentionally, seen by the surgeon.
Hydatid cyst of the liver appears as a tumor, evidently cystic or fluctuating, growing painlessly and attaining considerable size. It may usually be excluded from abscess, cancer, dilated gall-bladder, aneurysm, gumma, hydronephrosis, renal cysts, or tumors of unknown origin. A tumor peculiar to the liver will move with that organ. The aspirating needle will probably need to be used before diagnosis is complete, the fluid withdrawn being clear unless suppuration has begun.
—Hydatid cysts require radical treatment. Aspiration does not remove the mother-cyst nor any of its semisolid contents. Even the injection of iodine and resort to electrolysis hitherto in vogue have been abandoned. Open incision, first, of the abdomen, and then, after careful protection of the abdominal cavity, of the cyst itself, with scrupulous attention to prevention of escape of its contents save externally, is the only radical and promising procedure. These precautions should be taken because of the possibility of implantation of some living fragment of the parent organism, or its offspring, elsewhere in the abdomen and the growth of the same in this new location. After free evacuation of such a cyst it should be explored and thoroughly cleaned out, after which its edges are to be affixed to those of the parietal peritoneum if practicable,[914] a large tube inserted and suitably connected up for drainage, while the opening around it is closed with sutures or packed with gauze. This connection of an interior cavity with the exterior of the body is called marsupialization.
The operating surgeon as such is only concerned with gummatous tumors, not with diffuse expressions of syphilis which produce interstitial hepatitis or cirrhosis. The latter are often met in cases of general syphilis, and yield to suitably directed treatment. Either the diffuse or the gummatous form may produce enormous enlargement of the liver, with suspicion at least of an abscess. In one case of this kind, known to the writer, the lower border of the liver extended below the crest of the ilium, and yet within a short time, under vigorous treatment, the liver resumed its normal size. Gummas have, then, an interest for the surgeon, as no other similar enlargement ever reduces its volume so speedily under any other circumstances. Moreover gummas may occasionally break down and produce abscesses requiring incision and drainage. If syphilis can be recognized as the etiological factor prognosis is satisfactory in nearly every instance.
The specific fungi of this disease may be easily carried from the alimentary canal to the liver through the portal circulation, and its peculiar granulomas, appearing first here, may spread to the diaphragm, to the abdominal wall, or in any other direction. Unless aided by the presence of other distinctive lesions diagnosis is rarely made until the presence of a granulating tumor and its ulceration, with the escape of the distinctive calcareous particles, makes it recognizable to touch as well as to sight. This often might be secured by an exploratory operation, which circumstances might justify. (See chapter on Actinomycosis.)
Benign tumors in the liver are rare. So-called adenomas of somewhat indistinct type, and fibromas, have been described as occurring here. The former are of uncertain origin and probably do not deserve the name given here. Nevertheless they have a structure more or less simulating true gland tissue. Fibromas may spring from any of the fibrous structures. Other benign tumors occur here so rarely as to scarcely warrant mention. Aneurysms and large venous dilatations also occur occasionally in the liver. Any of these lesions may justify exploration, and those favorably situated may be enucleated or excised, with subsequent suture of the liver and drainage of any remaining cavity.
Of the malignant tumors the sarcomas and endotheliomas may arise in almost any part of the organ. Primary carcinomas have their origin only about the gall-bladder and its ducts, from whose epithelial lining they may spring; otherwise they are products of extension or metastasis. By far the larger proportion of cancers arise from the gall-bladder, within which they begin to grow, either as the expressions of irritation or of parasitism. The presence of gallstones in the gall-bladder is now known to be an extremely common provocation of cancer, and the relation obtaining between the two is certainly more than accidental or casual. (See Cancer of the Gall-bladder.)
That an associated and solitary cancerous growth of this kind may be successfully removed has been proved in my own experience, by the good health persisting at least six years after operation upon a woman from whom I removed a large cancerous gall-bladder containing two large calculi, and with it a considerable amount of the adjoining liver tissue. It is, therefore, possible to successfully remove some benign tumors, as well as occasionally a malignant one, from the liver when other conditions are favorable; but this should always be done before it be too late, as a comparison of cases will demonstrate. If the lymph nodes or any other viscus be involved in malignant disease, then it is too late. The tumor is to be attacked from its most accessible aspect. A pedunculated[915] growth, like a distinct benign hypertrophy, may be tied off, sutures being also used if needed. The actual cautery furnishes the best means of division of liver tissue, while with a sessile growth elastic constriction may be of assistance. The principal danger in these operations is from hemorrhage. Methods of meeting it are discussed below, as well as other general procedures. A tumor stump may be fastened to the abdominal wound, or it is better treated by being packed around with gauze, the latter being allowed to remain for three or four days.[62]
[62] As a means of preventing the ligature cutting in liver sutures Gillette has suggested the use of a piece of rubber tube drawn over a No. 10 catheter and placed along the proposed line of sutures, which are passed around this, and through the abdominal wall, making exit between the ribs, after the manner of a staple.
Von Bruns, in 1870, was probably the first to resect liver tissue, after injury, with good results. Modern surgery has done much to improve the prognosis in these injuries and to show that it can be attacked much more freely than previously supposed. Within the past fifteen years Ponfick and many other experimenters have shown the regenerative capacity of the liver by removing as much as three-fourths of it. The fear of cholemia, due to escape of bile, has also passed, and it has been found that peritoneal complications do not result from its presence, for bile, unless actually mixed with pus, is not septic, although its antiseptic properties have been much overrated. Most of the expedients which have been suggested by various operators for controlling hemorrhage have been abandoned for the more simple methods of the tampon and the suture, although the actual cautery is still generally used for the operative attack. For suture catgut is preferable to silk. Even large wounds may be successfully fastened in this way. Arterial bleeding is easily distinguished from venous oozing. Spurting arteries may be ligated en masse, while continuous oozing usually subsides under pressure. In contusions of the liver, when it is not practicable to bring hepatic surfaces together, loops of catgut may be passed with a large needle through the liver structure in such a way as to bind its edges whenever they are bleeding. The sutures or loops may be drawn tightly to check hemorrhage before they cut through the liver structure. When the attempt is made to actually suture liver tissue it is necessary here as elsewhere to avoid dead spaces. If liver surfaces can be brought into actual contact they will heal kindly. In fact when there is access, and the emergency is not too pressing, the portion to be removed may be excised with ordinary knife or scissors, and this is better when suture methods are to be employed. There are times, however, when the Paquelin cautery knife will perhaps be preferable. It is a mistake in these cases to try to work through too small an incision. For wounds located posteriorly Lannelongue has suggested resection of the thoracic wall along the anterior portion of the eighth to the eleventh costal cartilages, since the pleura does not extend down to that level. He makes an incision parallel with the costal border, 2 Cm. above the same, beginning 3 Cm. from the border of the sternum, and terminating at the tenth costochondral junction. After retracting the muscles the costal cartilages are to be resected. If, now, the rib ends be firmly retracted and pressed apart a large portion of the convexity of the liver can be made accessible.
In order to make better access to the upper margin of the liver it may be well to adopt Marwedel’s suggestion of retracting the rib arches by a curved incision, parallel with the costal margin, with complete division of the rectus and the external oblique, which latter is to be separated from the internal and transverse. The cartilage of the seventh rib is divided at its sternal junction and the cartilages of the eighth and ninth are also exposed and divided by blunt dissection. After thus loosening the lower ribs the lower part of the chest wall can be retracted, and much better access made to the region below the diaphragm. When necessary the left side of the abdomen may be treated in the same manner.
From the liver we pass to the consideration of the surgical aspects of cholelithiasis and other affections of the biliary passages.
The gall-bladder is a convenient but more or less superfluous receptacle or reservoir for bile, whose normal capacity is from 50 to 60 Cc., but which, when distended, may, by virtue of its elasticity, contain at least 200 Cc. of fluid. Its normal position is beneath[916] the ninth costal cartilage, at a point where it crosses the outer edge of the rectus. Only its lower surface is covered by peritoneum, in average cases, but when it is distended or hangs well down in the abdomen the peritoneum may enclose the larger amount of the sac. Its neck is bent into an S-shape, and contains two folds of mucous membrane, which serve as valves. When this neck is mechanically obstructed the sac itself may be distended with glairy, bile-stained mucus, amounting even to 500 Cc., but in patients who have had repeated attacks of gallstone colic and have suffered for a long period of time, the gall-bladder is usually contracted, shrivelled, and sometimes almost obliterated. Under these conditions there is a strong resemblance between it and so-called appendicitis obliterans, and when so contracted and buried in adhesions it may not be easily found. In certain cases of cirrhosis of the liver the gall-bladder is carried up well beneath the ribs and then descends with whatever motion depresses the liver. On the other hand when distended it may hang down into the abdominal cavity as a pear-shaped mass, which may even cause doubt and uncertainty in diagnosis, for it may be then found in the cecal region or in the pelvis.
The common duct is from 6 to 8 Cm. long. Its size is about that of a No. 15 French sound. It is both extensile and distensible, and may be dilated even to the size of the small intestine. About one-third of it is in intimate relation with the pancreas, whether wrapped within its head or lying in a groove upon it. This is of surgical import, for in enlargement of the pancreas the duct may be first pushed away and then obstructed; this explains why biliary drainage is indicated in so many pancreatic cases. The part which passes obliquely through the duodenum is expanded into a reservoir beneath the mucosa, into which opens also the pancreatic duct, the latter lying lower and being separated by a fold of mucous membrane. This dilatation, the ampulla of Vater, is 6 or 7 Mm. long, and is surrounded by an unstriped muscle fiber—a miniature sphincter. Its opening constitutes the narrowest portion of the entire biliary canal. Seen from within it forms a little caruncle or papilla, distant 8 Cm. from the pylorus. The duct of Santorini opens normally about 2 Cm. above this papilla, and is patent in about one-half of these cases, while in about 80 per cent. of cases it communicates with the duct of Wirsung. Many variations from the normal, as above epitomized, occur—especially in and about the ampulla. They are both congenital and acquired. Thus an hour-glass gall-bladder is occasionally seen, or one so divided by a partition that one part may contain mucus and the other calculi. It is worth remembering in this connection that along the free border of the lesser omentum there are three or four lymph nodes which, when enlarged, may be easily mistaken for calculi. The gall-bladder lies in a peritoneal pouch, having the colon below it, the spine and the pancreas to its inner and posterior aspects, the liver above and the abdominal wall on its outer side. When this pouch is seriously affected it may be drained not only from in front but often to great advantage from behind, i. e., by posterior drainage. This pouch may hold a pint before it overflows into the pelvis, or through the foramen of Winslow into the greater peritoneal cavity. The right lobe of the liver is sometimes enlarged so as to form a tongue-shaped projection which may extend some distance below the costal margin. This is frequently called Riedel’s lobe. (See Plate LV.)
The gall-bladder is essentially a biliary reservoir, convenient but not essential, storing bile between meals and expelling it during digestion. It is absent in the horse and in many animals, and individuals from whom it has been removed seem to suffer thereby no inconvenience. Consequently there need be no hesitation in removing it when necessary. Bouchard claims that bile is nine times more toxic than urine, and that the liver of man may produce sufficient in eight hours to kill him if it cannot escape. Consequently biliary obstruction may become a very serious matter. Besides containing bile the gall-bladder has numerous minute glands of its own, which secrete the ropy mucus with which it is so often found distended. A mixture of bile and pancreatic juice seems ideal for perfect emulsification and digestion of fat. Hence the disadvantage of anything which interferes with the escape of bile into the duodenum. Bile possesses by itself slight antiseptic properties, yet when uncontaminated is not septic. It may be regarded as mainly excrementitious, and its function as an intestinal stimulant has been much overrated. The average quantity secreted in twenty-four hours is about thirty ounces. Its excretion is constantly going on, but is more abundant by day, is not much influenced by diet, nor nearly so much by the so-called cholagogues as has been generally supposed. All these points have a practical interest for the surgeon who has to do with the consequences of biliary obstruction, or who has to watch its progress for lack of a biliary fistula.
PLATE LV
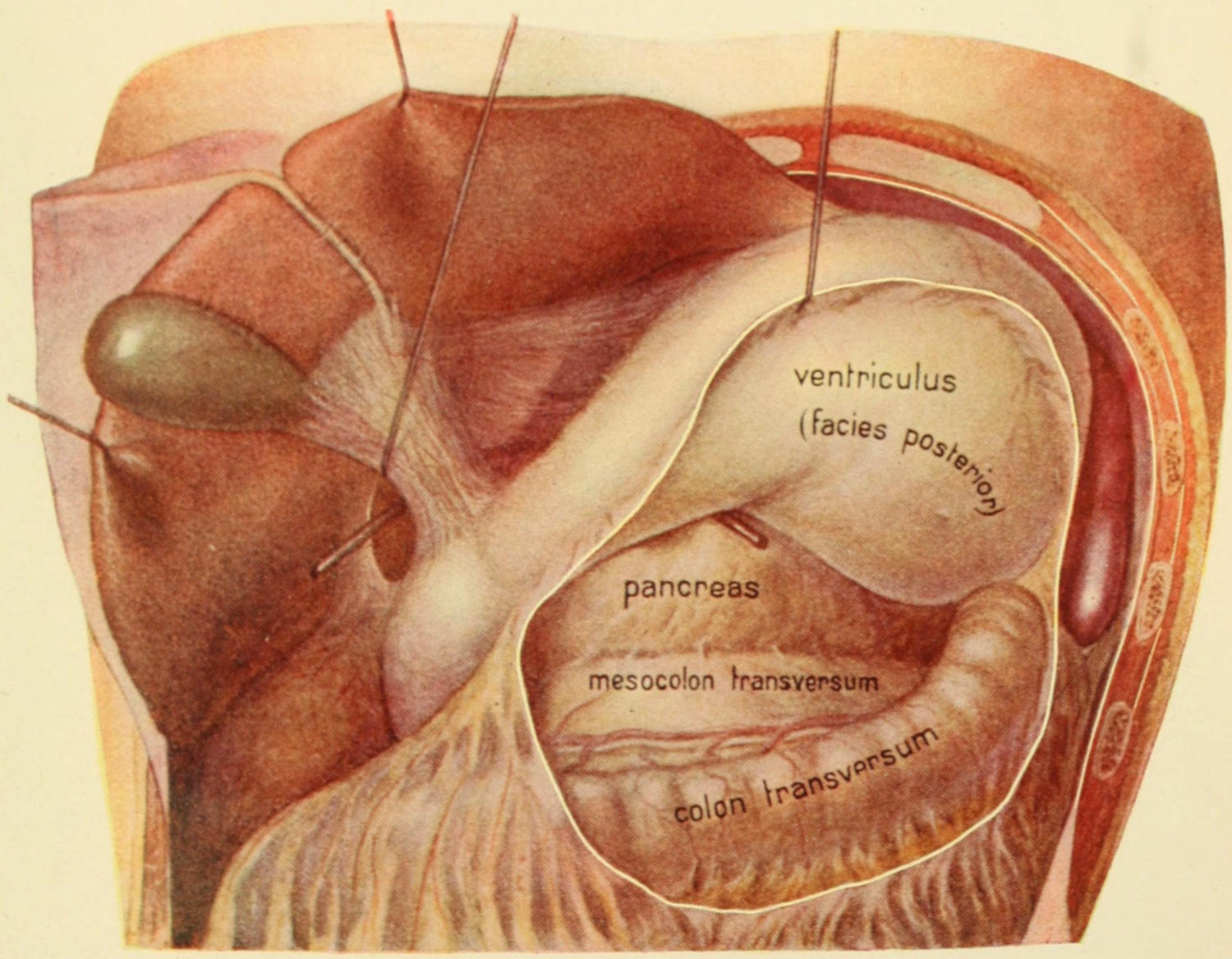
Surgical Anatomy of the Gall-bladder and of the Omental Foramen and Cavity. (Sobotta.)
The probe enters the omental (epiploic) foramen. By retraction and removal of its anterior covering the cavity of the lesser omentum (omental bursa) is exposed, revealing especially the pancreas in situ.
[917]
These may be due to accidental injury during operation or to disease processes. They may be direct or indirect, and internal or external. An example of direct, external traumatic fistula is afforded by a cholecystostomy or a cholangiostomy; of indirect internal when the gall-bladder has burst into an abscess and this into a hollow viscus. A fistula might arise from a local abscess outside the biliary passages, later communicating in both directions, or it may be connected with the thoracic organs, with evacuation into the bronchi or esophagus, and cases are on record where gallstones have been passed from the mouth. The external or cutaneous fistulas tend in most instances to spontaneous healing, but the time required is often long. They may discharge thin, biliary mucus or true bile.
Mucous fistulas result from cholecystostomy where the obstruction in the cystic duct has not been overcome, as when it is the seat of stricture or extrinsic pressure. They cause but little inconvenience. Nevertheless if allowed to close the mucus accumulates and pain results from distention. In these cases either a small tube or drain should be worn, or a cholecystenterostomy may be made. Sometimes after the discharge of some foreign body, such as a silk ligature or small stone, such a fistula will close of itself, or it may be possible to frequently cauterize its interior with a bead of nitrate of silver melted upon the end of a probe, or perhaps by using a long curette to so destroy its mucus lining as to do away with the condition and its consequent discharge. Ordinarily cholecystostomy will not be followed by permanent or even long-continued fistula if the common duct have been thoroughly cleared, and if the gall-bladder be fastened to the aponeurosis and not to the skin. Postoperative biliary fistulas, with discharge of large amounts of bile (one to two pints per day) and their consequent inconvenience, will ordinarily not be long tolerated by the patient, who will insist on some further procedure for relief. If possible, in every such case, the real cause of the difficulty should be removed. If the ducts be cleared and stimulation with caustic be not sufficient, then the abdomen should be opened, the gall-bladder detached, and its fistulous opening freshened and sutured. If the patency of the common duct can be established this will be sufficient. Otherwise, after closing the gall-bladder, it should be anastomosed with the small intestine as near the duodenum as possible.
Spontaneous or pathological fistulas often open at the umbilicus, the disease process having followed the track of the umbilical vein up to that point. Here, too, calculi are thus spontaneously extruded, one case on record including the discharge in this way of a stone three inches in diameter. In any such case as this the fistula cannot be expected to close until the calculi are all extruded. In the treatment of any such lesion the margin of the wound and the entire track of the fistula should be carefully curetted and disinfected, as at least a part of the procedure.
Biliary intestinal fistulas, due to escape of calculi into adherent intestine, are also occasionally seen. These often form without marked disturbance until perhaps at the last, when there may be destructive symptoms, both biliary and intestinal, symptoms which will suddenly subside when perforation or passage of a calculus occurs. After their occurrence patients may enjoy some relief for a considerable time, or until the contraction of the fistula may necessitate a subsequent operation. At other times their formation by ulceration is often accompanied by severe pain and fever, and possibly even by hemorrhage. Impaction of a gallstone in the intra-intestinal portion of the common duct is perhaps the most frequent cause of this kind of trouble. Fistulas into the colon are less common than into the small intestine. Such fistulas should never be intentionally made if it be possible to utilize any part of the small intestine. Although the pylorus and the gall-bladder often become firmly united to each other gastric biliary fistulas are rare. If, however, there be vomiting of gallstones, such a sign would make it quite certain. Mayo Robson has reported one such case where he separated adhesions, pared the stomach opening, closed it with sutures, and utilized the opening in the gall-bladder for the removal of calculi and subsequent drainage, the patient recovering.
[918]
These are less common than injuries to the liver proper. They may be caused by penetration or by severe blows and concussion. In those already suffering from local disease accidents are more likely to be followed by rupture. Injuries have also been attributed to traction and later adhesions. The fundus of the gall-bladder is the most exposed portion; therefore, that part is most often injured; while neighboring organs may suffer simultaneously—for example, the liver, stomach, and colon.
Injury will either produce such damage as to lead to acute local peritonitis, with extensive exudation for protective purposes, and with all the possibilities of subsequent infection, or there will be actual rupture, with extravasation of bile, and perhaps of blood, and the development of well-marked local as well as general symptoms. Fluid thus escaping will first fill the abdominal pouch, already described above, where it will then be confined by the mesentery until it begins to overflow. A small opening may be sealed by lymph, and a small collection of fluid may even be encapsulated, so that it may be subsequently opened and drained. The symptoms of such injury will include shock, pain, fever, fulness in the right side and hypochondrium, abdominal rigidity and the development in certain cases, after a few days, of jaundice, indicating absorption of bile. Should this bile have been aseptic, no great harm may ensue, but if infected a general and probably fatal peritonitis will result.
In any case where the condition may be recognized or where it is strongly suspected, abdominal section should be promptly made. According to the conditions thus disclosed the opening may be sutured, if possible or the gall-bladder or other cavity containing bile may be drained. It has been possible in some such cases to successfully suture a tear or wound in the duct, while in a few cases the duct has been doubly ligated and the bile flow been turned into the intestine by an anastomosis.
The formation of bile takes place under low pressure and therefore is easily hindered by slight back pressure. In this way jaundice may be easily produced with no greater degree of chemosis of the duodenal mucosa than that produced by a relatively small amount of activity in the duodenum. Inasmuch as the common duct traverses the intestinal wall obliquely its small outlet would be the first to suffer. In minor catarrhal duodenitis it is of small surgical importance, but when the condition becomes chronic the obstruction then becomes a matter to be dealt with by the surgeon. Such conditions may occur in connection with typhoid fever, pneumonia, influenza, ptomain poisoning, and other diseases, and are often accompanied by vomiting and diarrhea, with referred tenderness and possibly enlargement, while even the spleen is sometimes enlarged.
—In the early stage of such a condition the treatment is medicinal, but when the condition has become chronic biliary drainage may be required.
This is frequently a sequel to the above acute condition, and generally accompanies jaundice, no matter how produced. It is a frequent concomitant of cancer and often the actual cause of its accompanying jaundice. It has been known to lead up to suppurative lymphangitis, the lymph nodes along the border of the lesser omentum, already described, being nearly always involved and occasionally suppurating. Pylephlebitis may also have this origin. Gallstones nearly always provoke a certain degree of cholangitis and cause the formation of thick, ropy mucus which causes pain when passing, this pain being often mistaken for that produced by calculi. Riedel believes that two-fifths of the cases of jaundice occurring in connection with gallstone disease are really produced by accumulations of mucus and thickening of the mucosa, rather than by the stones themselves. Moreover, there is a form of membranous catarrh, both of the ducts and gall-bladder, where actual casts are shed, this condition corresponding to[919] fibrinous bronchitis or enteritis. Thudichum believes that these casts often form nuclei for gallstones. The condition has been spoken of as desquamating angiocholitis, and casts of the duct or even of the gall-bladder have been found in the stools.
The surgical interest attaching to these conditions lies in the fact that the symptoms produced are often identical with those caused by gallstones, and the desired relief is to be sought in the same way—i. e., by operation. The operator should not feel chagrined if on opening the abdomen he finds the gall-bladder containing such material rather than calculi.
This is often mistaken for cholelithiasis, although when the gall-bladder is opened only thick, ropy mucus will be found. This, as just remarked, may give rise to very painful spasm. The trouble when present is usually connected with similar trouble in the ducts. Moreover, around such a gall-bladder numerous adhesions are formed which give rise to much pain, tenderness, and local distress. Under these conditions the gall-bladder is enlarged and thickened.
Here, too, the curative treatment is essentially surgical, although pain may sometimes be temporarily relieved by aspirin in doses of from 0.5 to 1 Gm.
Cholecystitis obliterans corresponds closely to appendicitis obliterans, and is a condition characterized by a reduction in the size of the gall-bladder or its almost complete obliteration. In order to account for this it is seldom necessary to assume a congenital defect. The morbid process which produces it begins early, perhaps even during fetal life. The bile ducts are extremely small at birth and further stenosis is easily produced. The accompanying enlargement of the spleen will illustrate the toxicity of the condition which led up to it, and which may have occurred in infancy or early childhood. In a small proportion of cases early constriction of the ducts produced by local peritonitis and infection along the track of the umbilical vessels may account for the condition.
A suppurative condition within the gall-bladder is necessarily an expression of an infection, in nearly all instances proceeding from the intestine. The colon bacilli and those of typhoid are the organisms usually at fault. As has already been shown in the earlier part of this work they are facultative pyogenic organisms. Mixed infection with the ordinary pus-producing germs may also occur here. Such infections may spread through the walls of the gall-bladder and cause at least local and sometimes fatal general peritonitis. The condition is an especially frequent complication of typhoid fever, occurring sometimes relatively early, at other times after apparent recovery from the disease. In most of these instances it is supposed that the bacteria reach the gall-bladder by migration along the ducts, although direct penetration or infection through the blood is not to be denied. Impacted gallstones especially predispose to such infections. The result of all such cases is the formation and retention of pus—i. e., empyema of the gall-bladder—save in those rapid virulent or fulminating infections when it quickly becomes gangrenous, as does the appendix when similarly infected.
—In acute infections of the bile passages patients suffer severe pain, made worse by movement, with general malaise, rapid loss of appetite and flesh, extreme tenderness over the gall-bladder and often around it, because of the accompanying local peritonitis. It is frequently possible to make out enlargement of the gall-bladder, which will move with the liver during respiration—this at least until it has become fixed by local inflammation—after which the patient will have thoracic rather than abdominal respiration. As such a case progresses local indications of disease will be added, with finally visible tumefaction and redness of the overlying skin. Jaundice is an uncertain feature, depending on the patulency of the common duct.
Pus when formed may escape and burrow in various directions; thus it may follow the suspensory ligament of the liver and appear at the umbilicus, or it may pass along other reflections of the peritoneum and appear about the cecum or above the pubes, or it may pass into the liver and appear as an hepatic abscess, or around it and thus give rise to a perihepatic or subphrenic abscess. It may even perforate the diaphragm[920] and produce such collections of pus or such phenomena as have been described in the previous chapter, including empyema, pericarditis, abscess of the lung, etc. Again it may burst into the hollow viscera, stomach or intestines, or into the general peritoneal cavity, where it will cause speedily fatal peritonitis. Pulmonary abscess, with discharge of pus and bile, has been cured by Mayo Robson by removing a stone from the common duct. Gallstones have also been found in the pleural cavity and have even been passed by the mouth. Finally pus collecting in the right abdominal pouch may also be mistaken for perirenal abscess.
Acute phlegmonous cholecystitis, with gangrene, corresponds to the fulminating form of gangrenous appendicitis, and only received its first description in 1890 by Courvoisier. This is not common, but when met with becomes a disastrous lesion. It is essentially a still more virulent expression of infection and consequent necrosis than the condition described above. It may be so rapid as to destroy the gall-bladder before it has had time to fill with pus. It may occur with or without a history of previous trouble, in the absence of which a diagnosis will be made more perplexing. As the condition declares itself and progresses there will usually form about its site a protective barrier of lymph and omentum, which may prove, when present, the salvation of the patient, especially if the surgeon who makes the operation, and this should be early, recognizes the value of these protections and does not break them down. The condition occurs in connection with gallstone disease, but may follow typhoid fever, cholera, puerperal fever, or other intense infection.
Symptoms of gangrenous cholecystitis are essentially those of the less severe types of infection, only more pronounced. They include severe pain of sudden onset, rapidly growing worse, spreading over a larger area, extreme tenderness and muscle spasm, rapid thoracic respiration, quick pulse, intense depression and collapse, vomiting, rapidly increasing tympanites, anxious facies, with every expression of intense sapremia. Jaundice is an inconstant symptom, while fever is usually present, but is of little importance. The disease may be so rapid as to quickly kill. At all events local destruction occurs early, either with abscess or gangrene, or both.
—The diagnosis consists virtually in a recognition of the cause of the intense local peritonitis, after which a history of previous disease, if obtainable, may help. The condition is to be differentiated especially from perforated ulcer of the stomach or duodenum, from acute pancreatitis, and from acute mesenteric embolism or thrombus with gangrene of the intestine. It is also occasionally to be distinguished from an acute appendicitis, and this may be difficult, since the appendix is sometimes found high up and the pain widely referred or not accurately localized. In acute cholecystitis the pain is more likely to be subcostal, and the tenderness and muscle spasm are more marked in the upper part of the abdomen, to which the various local expressions of the disease are referred rather than to the lower. In any or all of these troubles symptoms of acute peritonitis are likely to be present and paralytic ileus or bowel obstruction may complicate the case.
Ransohoff has called attention to a hitherto unnoted sign of gangrene of the gall-bladder—namely, a localized jaundice about the umbilicus, apparently brought about by staining of the fat beneath the peritoneum, and noted after incision, if not previously. He considers it the result of imbibition, and that it appears at the navel first because here the abdominal wall is thinnest, it being also possible because of the anatomical relations of the round ligament of the liver to the transverse fissure, where there may be a retrograde flow of bile through the lymphatics and toward the navel.
Fortunately all of these acute conditions as between which doubt may arise are to be dealt with in only one way—namely, by prompt operative intervention—and minute diagnosis is of less importance than ability to appreciate necessity for immediate operation as it may arise.
Gangrene is the extreme degree of disaster in these cases, and its occurrence may be marked by sudden cessation of the pain, a most important symptom, which may be deceptive to the uninitiated. Gangrene may be due to thrombosis of the vessels of the gall-bladder, to bacterial invasion, to extreme tension because of obstruction of the duct, or to all three.
Acute cholangitis was first described by Charcot, who called it intermittent hepatic fever. It is usually due to the presence of one or more gallstones in the common duct, but any obstruction of the hepatic or common ducts may favor infection of retained bile[921] and involvement of the duct. Thus it has followed chronic pancreatitis, cancer, hydatid disease, pancreatic calculus, typhoid fever, and the presence of the parasites. Mertens has collected forty-eight cases in which ascarides have been found in the bile-duct, their entrance having probably been facilitated by the previous escape of gallstones and enlargement of the duct end. Round or lumbricoid worms have also been found in the duct, as they are occasionally met with in the duodenum, and I once saw a long one in the appendix. Cancer in this neighborhood is also a not infrequent exciting cause in producing acute cholangitis.
Symptoms.—There is usually a history of spasmodic pain covering a considerable period, and then of such an attack followed by chill and fever, with more or less jaundice, which may persist for some time. Such attacks as these become more severe and more frequent; the gall-bladder enlarges if it contain no stone, or contracts if calculi be present. This association was especially noted by Courvoisier, who formulated a statement to this effect, often absurdly known as his “law.” Later the entire liver or its right lobe may enlarge, while patients complain of tenderness over the gall-bladder, as well as of loss of appetite and flesh, and those vague symptoms included in the term “dyspepsia.”
Such a condition may possibly subside in time, but is more likely to be followed by acute trouble of one of the types already described. In the matter of diagnosis it may be distinguished from malaria, especially in districts where malaria prevails by absence of relief from quinine, and the results of a carefully completed examination, combined with the fact that in the former it is usually the gall-bladder which is enlarged, and in the latter the spleen. When the condition has proceeded to its suppurative form the occurrence of still more significant symptoms and signs should lead to prompt operation.
—In the acute infections and affections, both of the gall-bladder and of the duct, operative intervention is imperative. The more acute the case the more urgent the indication. Free evacuation and drainage are the indications to be met, and as early and completely as possible. These cases call for cholecystostomy, often for choledochotomy, with drainage of both gall-bladder and duct, and perhaps of the peritoneal cavity, while possibly even posterior drainage may be indicated. So true is this that the back should be as carefully prepared for operation as the abdomen, in order that no time be lost during the operation, should one decide on the wisdom of a posterior counteropening. Of course much will depend upon the patient’s condition at the moment and what it may appear he can endure. By free opening of the gall-bladder evacuation of its septic contents and removal of calculi are secured, if present, while the ducts are permitted to empty themselves and free flow outward of all septic material is invited and permitted, pressure is relieved, the tumor is disposed of, respiration allowed to become normal, and no small load removed from the kidneys; and the chronic pancreatitis which so often accompanies many of these cases is allowed to subside by virtue of the other relief thus afforded.
These may occur anywhere along the biliary tract, and vary as between the superficial and the perforating, the former being sometimes multiple, the latter solitary. Of these lesions cholelithiasis is the most common cause, while typhoid and cancer should be ranked next. They are all of pathological import, because of their possible sequels, i. e., not merely perforations with fistulas, but possible strictures or hemorrhages, or peritonitis with sepsis. When ulceration is extensive a previous local difficulty may be supposed, with more or less adhesions, but as the trouble becomes more serious the local excitement will extend to the peritoneum, at least that of the area involved. In fact most cases of gallstone disease are accompanied by more or less peritonitis, and adhesions which are protective, although they may cause other troubles as well, such as dilatation of the stomach from displacement of the pylorus. Hemorrhage is not a frequent event, for thrombosis usually precedes erosion. Some degree of sapremia or septicemia will be present in nearly all cases.
Stricture of the ducts is the most common result, especially of the cystic duct. If this occur and the mucous membrane be still active the gall-bladder will become distended with pus or mucus, or both. These are the cases which perhaps give the best results after ideal cholecystectomy.
[922]
Perforation is a constant possibility whose menace cannot be estimated, but which is always actual, the great danger depending on the virulence of the extruded material and the consequences of delay in operating. Although healthy bile is but slightly toxic, these cases do not furnish it, and one may always look for consequences of infection. Nevertheless if diagnosis be made sufficiently early to bring about immediate operation prognosis is good. Occasionally during such an operation there will be found a gallstone endeavoring to extrude itself, but not yet completely escaped. It might be, in rare instances, possible to utilize the opening which it has partially made for subsequent drainage purposes.
It is not advisable to permit patients with distended gall-bladders to go unoperated, even in the absence of serious symptoms, because the risk of operation is small and that of rupture is large.
Acute intestinal obstruction due to gallstones will usually, but not invariably, involve the upper intestinal tract. It may be due to the actual occlusion of a large stone which has escaped from the gall-bladder or duct, or it may be caused by volvulus due to intense colic accompanying peristaltic effort, or it may depend upon adhesions after a local peritonitis due to previous disease of the gall-bladder or to stricture following ulceration; or again it may be purely paralytic, and in this way result from a local peritonitis. Impaction of a biliary concretion may happen at any point, but most often at the ileocecal valve, where the intestinal tube is narrowest. The size of the stone is not the only consideration. Obstruction depends perhaps as much upon spasm above and below as upon any local disturbance that its presence may have caused. Biliary concretions may enlarge as they pass downward, growing by accretion of calcareous and of fecal matter. The larger the calculus the more likely it is to obstruct the upper intestine. The majority of these calculi have escaped from the gall-bladder by a previous process of ulceration, and usually into the duodenum, rarely into the colon.
—Symptoms of this condition, thus produced, will obviously be those of acute obstruction from any cause, the most marked features being severe pain and early frequent vomiting. Bile may be raised in quantities because of the biliary fistula so near the stone, and from which it is supposed to have escaped. The higher the exciting cause the more violent the symptoms and the less the distention of the abdomen by gas. A significant history may help in assigning the cause for the evident obstruction.
—Since more than half of these cases treated expectantly die without relief early operation is to be urged. It should always be preceded by lavage in order that the stomach may be thoroughly emptied. When a stone has been exposed within the intestine it is advisable to open the bowel a little below where it rests, so as to make the division at a point where the chances of repair are not compromised by previous excitement. In severe cases a temporary enterostomy may be made, but this should of necessity be high. The volvulus may be relieved by untwisting the kink or by an anastomosis. Obstruction due to adhesions will require separation of these adhesions, with perhaps an anastomosis.
There is so much which may be said about the formation of gallstones and the troubles which they may produce that it is necessary here to epitomize as much as possible and to refer mainly to the surgical features of this condition. Gallstones are of all sizes, from the most minute to that of a hen’s egg, are present in numbers varying from a single calculus to thousands of calculi, are found commonly in the gall-bladder, in the cystic duct, or in the common duct, but occasionally are met with just escaping into the duodenum, through the duodenal ampulla, or in the smaller ducts of the liver or the main hepatic duct (Fig. 627). In at least 99 per cent. of cases they will be seen in one of the locations first mentioned.
Fig. 627
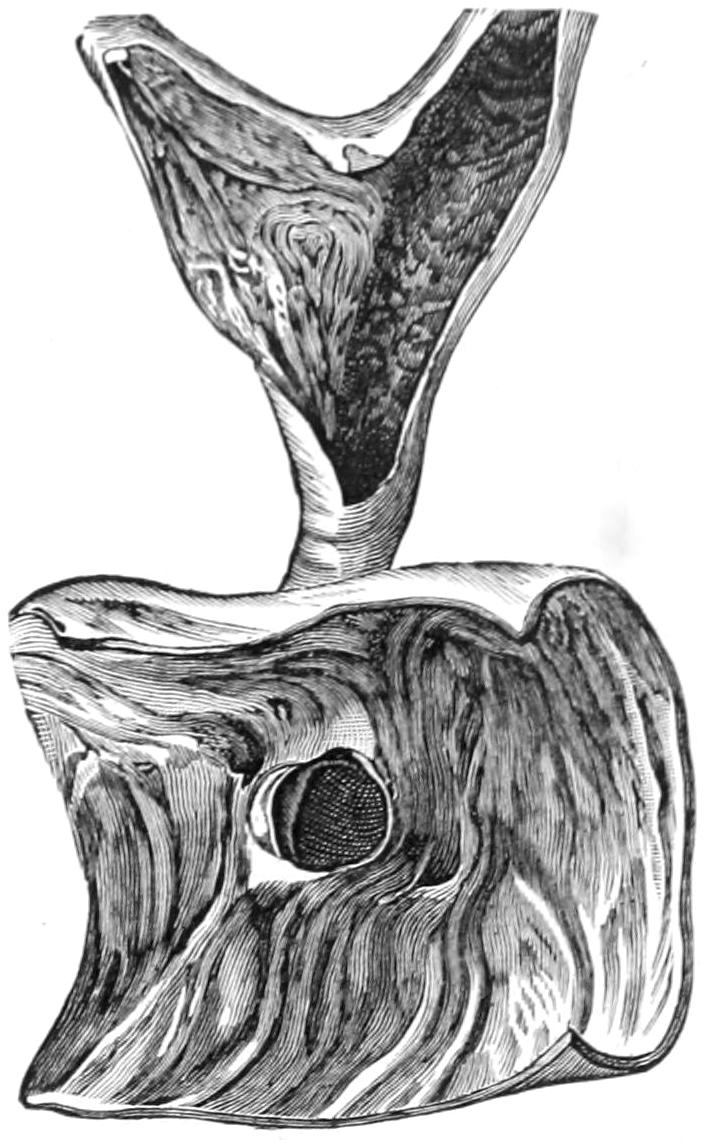
Gallstone presenting at the ampulla of Vater, i. e., endeavoring to escape into duodenum. (Pantaloni.)
Pages might be devoted to a discussion of the reasons for their formation. That cholesterin, their principal component, should more readily deposit in such a way as to produce these calculi, and more often in some individuals than in others, is hard to explain, but may be held to be largely due to its formation in excess in certain individuals and to concentration of those fluids which hold it in solution. Increase of cholesterin seems to be connected with catarrh of the membrane which produces it, and thus[923] stagnation of bile may predispose. That bacteria have much to do with biliary calculi is now conceded, and a history of typhoid is obtainable in many cases. It has been shown experimentally that aseptic foreign bodies introduced into the gall-bladder remain indefinitely without becoming covered with precipitate, while virulent organisms set up disturbance, and only the attenuated or moderately infectious organisms produce calculi, and usually then only when some trifling foreign body is introduced at the same time. It will thus be seen that a nidus may be afforded by a clump of epithelial cells or débris.
It is not at present so much a question of what organisms are at fault, although they are usually the colon and typhoid bacilli and the ordinary pyogenic organism. It has been shown, moreover, that in typhoid fever the gall-bladder is often invaded, and that the typhoid bacilli may live there indefinitely, and that they tend to clump or agglutinate themselves in a very suggestive way into trifling masses which may serve as minute foreign bodies. Thus each predisposing factor reacts upon the other, and by a vicious circle either an acute lesion may be established or calculi may be formed in varying numbers.
Gallstones have been found in the newborn, but are relatively infrequent below the age of twenty-five, and are most common in the later years of life. The condition is by four to one more frequent in women than in men. The only predisposing habit seems to be such lack of exercise as gives no expulsive movement to the gall-bladder by action of the abdominal muscles. They are more common in the gouty and in those predisposed to uric-acid diathesis, while abundance of nitrogen seems rather protective. Biliary calculi have never been found in the wild carnivora.
McArthur has formulated the following conclusions of interest in this connection:
Biliary calculi are serious menaces to a patient’s welfare, not alone because of the obstructive symptoms which they may produce, but because of the acute or chronic conditions to which they indirectly give rise. These have been in some degree already mentioned. Thus cholecystitis and cholangitis of all degrees of severity, from the milder chronic forms to the phlegmonous and fulminating varieties, may be at least associated with the presence of such calculi and seem to be to a greater or less extent due to their presence. Around such foci of excitement there will always occur local peritonitis, which will result in adhesions, and the consequent tenderness with referred as well as local pains to which it necessarily gives origin. The viscera suffer not only in this direct way, but functional disturbances are produced, and are usually covered under those vague terms “dyspepsia” and “indigestion” with which patients crudely describe their discomforts, and under which physicians too often conceal their failure to appreciate the actual condition.
Furthermore there is always a possibility of cirrhosis resulting, because of distention of the hepatic ducts and backing up of the hepatic secretion. Thus the liver becomes larger and more dense, is colored green, its edges become more rounded, this occurring especially in the right lobe, or at least attracting more attention in that location because[924] more easily recognized from without. Again the more acute inflammatory conditions sometimes cause paralytic ileus, or at least paralysis of the lower bowel, and thus lead to conditions almost identical with, and difficult to distinguish from acute intestinal obstruction.
Of equally great and growing importance is the fact that, according to Schroeder, some 14 per cent. of gallstone sufferers develop cancer, the presence of these irritating foreign bodies in the biliary passages having much the same relation to cancer of the liver as does the existence of previous ulcer to cancer of the stomach.
—There is scarcely any morbid condition which is at one time characterized by such significant symptoms and at another by none at all as cholelithiasis. In rehearsing the list of the ordinary symptoms produced by the conditions exceptions should be made, for no matter how complete the list something may be omitted which has been noted in some particular case.
Gallstones confined within the gall-bladder proper may produce few or no symptoms, this being particularly true so long as the ducts are free and there are no persistent consequences of previous acute trouble. A stone may grow in the gall-bladder to a large size and cause little or no distress until it begins to work its way by the ulcerative process. Doubtless small concretions pass with little or no disturbance, or only that which would be considered a “temporary dyspepsia.”
When, however, gallstones produce symptoms these usually include more or less paroxysmal pain, occurring unprovoked and at irregular intervals, referred not alone to the upper abdomen, but radiating to the rest of the trunk, as well as in the direction of the right shoulder-blade. (The shoulder pains of biliary and renal lesions are due to the connection of the pneumogastric nerves with the ordinary sensory nerves above, and below with the sympathetic ganglia.) Attacks of pain are usually followed by nausea and vomiting, and if extremely severe by more or less depression and collapse. At times there will be a sensation as of distention in the region of the gall-bladder. Tumor in this location may or may not be present, and jaundice is an uncertain symptom, not occurring unless the ducts are occluded. The stomach so far sympathizes that digestion is at least temporarily disordered. In proportion as angiocholitis is produced by the passage of calculi we may meet with more or less septic features. The pain produced is uncertain in severity and duration, and is often relieved by the relaxation which may accompany or follow vomiting. After subsidence of severe pain there remains a dull ache for several days, lasting perhaps until another acute paroxysm. These pains are sometimes referred to the left side and over the stomach, in which cases it will usually be found that the gall-bladder is adherent to the stomach, while when the pain is felt in the right side of the thorax it is usually because there are numerous adhesions between the lower surface of the liver and the viscera below it. Such pain may even simulate angina pectoris or may involve the genitocrural distribution. In fact it may be referred to almost any part of the body.
Vomiting which is at first paroxysmal and colicky may become persistent, continuous, and even dangerous. It is essentially an expression of pneumogastric irritation. The vomited matter may contain bile or even, by retrostalsis, fecal matter. The depression which at first occurs may merge into complete collapse; it may even be fatal. It will necessarily be more marked when the paroxysms are more frequent.
A significant feature in nearly every case is muscle rigidity, especially of the upper abdominal muscles on the right side, but not necessarily confined to these. This muscle spasm is a symptom common to many serious conditions and is not of itself indicative. It simply implies a serious condition within. Tumor or enlargement in the region of the gall-bladder may be met with, but are by no means constant. These may become more pronounced with each attack, being reduced between times because of the escape of bile between paroxysms. It is a valuable symptom when noted, but no importance should be attached to its absence.
The presence of gallstones in the stools is, of course, indicative, but most valuable time is often wasted when waiting for their discovery. Moreover, a number of hours, or even days, may elapse, the time depending on the activity of peristalsis, between the escape of calculi into the duodenum and their appearance in the stools. A convenient way to search for them is to let the stool be stirred with a 1 per cent. solution of formalin and then strained through a sieve which has about sixteen meshes to the inch. The question of the wisdom of operation can practically always be decided without reference[925] to the appearance of calculi. In this way the surgeon may feel that his diagnosis is corroborated by it, but in no sense weakened without it.
Jaundice is always a significant sign when present, but is absent in at least four-fifths of cases which nevertheless should be subjected to operation. Its occurrence is a matter of interest along with the previous history of the case. It is, however, of great value if it were noted in connection with the first pains or cramps. In chronic obstruction by stone in the common duct it is important to determine the intensity of the jaundice, since this may indicate whether we deal with calculous disease or obstruction from tumor. In chronic obstruction by stone the color changes are less marked, and often clear up entirely, while when produced by tumor they become gradually more intensified.
Deep and persistent jaundice is suggestive of malignant disease. The degree of cholemia rather predisposes these patients to hemorrhage or persistent oozing during operation. Jaundice gradually deepening with each attack of pain is also very suggestive. Such attacks, coming on with symptoms like those of malaria, chill, sweating, and pyrexia, are extremely suggestive and always call for surgical intervention, i. e., drainage. In brief it may be said that jaundice, with enlargement of the gall-bladder, is at least suggestive of cancer, while a history of gallstone colic, without much enlargement of the gall-bladder, is indicative of stone in the common duct. Although this statement is probably true for the majority of cases there are occasionally marked exceptions to it, as, for instance, when a gall-bladder is distended with hundreds or even thousands of small calculi, or to such an extent that it may form even a pear-shaped tumor hanging down within the abdomen.
In addition to these features thus rehearsed there might be made a long list of possible “extras,” by which the original condition is complicated and made to appear in unusual aspect or even life endangering. Such a list would include nearly every imaginable lesion of the upper abdomen. Suffice it to say that the liver, stomach, and the pancreas especially may suffer, while other viscera and the larger veins, with the surrounding tissue, may any or all of them become involved.
—Diagnosis has to be made mainly from non-calculous obstruction; from the acute gastric conditions, ulcer, etc.; from renal colic; from the acute or subacute pancreatic affections, duodenal ulcers, renal lesions, localized peritonitis from some other cause; from cancer, lead colic, angina pectoris, pneumonia, pleurisy, and even hysteria. Not so rarely pneumonia and pleurisy begin with pains which are referred to the upper abdomen and are suggestive of gallstone disease, while they seriously perplex the medical attendant. Much stress is to be laid on the first location of the pain, especially if this be in the direction of the right shoulder, and upon concomitant vomiting and jaundice, if present, as well as on the location of the greatest tenderness and muscle rigidity. Recurrence of more or less similar attacks is also suggestive. Diaphragmatic pleurisy may cause pain, referred especially along the esophagus, and intensified during the act of swallowing or vomiting. Affections of the appendix and gall-bladder may co-exist, as well as be easily mistaken one for the other. The former is so true that when operating for one condition it is always advisable to explore in regard to the other. When the appendix is placed high, especially behind the colon, confusion may confound. Biliary colic is usually free from the associated ordinary symptoms which are so often met with in renal colic, while in the latter the urine will contain no bile pigment and the pain will usually be referred to the external genitals. In lead colic the characteristic line upon the gums and the habitual constipation which always accompany it will be suggestive. When the stomach is at fault and the pylorus obstructed this viscus will usually be dilated, and the vomit is of a different character, while, at the same time, actual stomach movements may or may not be made visible. With gastric or duodenal ulcer pain it is more regular and associated with food taking after a definite interval, longer in the latter case.
Chronic pancreatitis is so often associated with cholelithiasis that it is impossible to disassociate their symptoms, but the referred pain is rather midscapular or even on the left side. It will be particularly suggested by rapid loss of flesh. In acute pancreatitis the symptoms are usually more excessive, the distention earlier and greater. Cancer of these various organs does not commence with pain, but has a more gradual, distinctive downward course, with cachexia. These are some of the considerations which may aid in differential diagnosis.
[926]
The detection of bile pigment in the urine and blood will have corroborative value.[63]
[63] Hanel has shown that a small capillary tube filled with blood, sealed at both ends, may afford a convenient corroborative test. After standing for a few hours in a vertical position its separated serum can be examined against the light. Normal serum is colorless, while even a trace of bile pigment will give it a distinctive yellow tint.
Baudouin’s test for the urine will be the most satisfactory in the matter of precision and simplicity. If two or three drops of a ¹⁄₂ per cent. solution of fuchsin be dropped into urine containing bile it immediately develops a fine orange tint, in marked contrast with its own red. No other coloring matter in the urine gives this reaction; which is very delicate. (Mayo Robson.) Methyl blue and methyl violet each give a reddish tint; Loeffler’s blue solution gives a green tint which vanishes on heating, to reappear on cooling. There are numerous other tests, but these are the simplest and most satisfactory.
—The general subject of cholelithiasis and its associated lesions constitutes an important topic in the so-called “border-land” between medicine and surgery, where views and advice regarding prognosis and treatment will depend on the experience and the training of the medical attendant. Surgeons now recognize, and physicians are being gradually converted to their view, that gallstone disease is essentially a surgical disease, i. e., one to be combated by surgical intervention. While it is not to be gainsaid that many patients live and die with gallstones who are never conscious of their presence, and while others who have had serious attacks live to die of some other disease, nevertheless the general statement may be boldly made and easily defended, that when the disease is well marked and when patients suffer more or less constantly from it the only successful method of treatment is the surgical, and that, in other words, operation offers the only prospect of permanent relief. Regarding its associated dangers it may be said that danger comes from delay rather than from operation, and that here, as with many other conditions, patients often wait too long, partly from lack of proper advice, partly from timidity, and that a septic and moribund patient, allowed to become so for lack of earlier application of the resources of surgery, is a reflection on the one who waits rather than on the surgeon, who, endeavoring to save, still unfortunately loses his patient.
This is not the place to discuss non-operative measures—i. e., medicinal and dietetic treatment—valuable as they may be in certain cases. Most of the drugs which are supposed to be effective in their power of solution of gallstones or of facilitating their escape are disappointing, and at best are vague and uncertain in their action. The hydrotherapeutic treatment, such as carried out, for instance, at Carlsbad, will do good in many cases, especially for those who have been indulgent in their appetites and careless in their habits. Cases of any description not too far advanced would be benefited by a careful regimen of this character, but that Carlsbad or any other waters will certainly cure cholelithiasis is now absolutely disproved. As a preparation for operation a sojourn at some such place may be advised; as a substitute for it, never. Large doses of glycerin (50 to 150 Cc.) often temporarily relieve the pain of biliary colic.
In general, then, it may be said that cases which give a history of recurring attacks of biliary colic, with or without recurrent jaundice, and with those varied concomitant symptoms which are usually grouped under the term “indigestion,” in which there is definite tenderness over the region of the gall-bladder, with or without muscle spasm, and with the other referred pains so often present in this condition, should be regarded as legitimately surgical, where operation is more than justifiable and usually decidedly advisable, even too often imperative. The same is true of those cases of distended gall-bladder with obstruction of the duct where perhaps no calculi are present, but where the patient suffers in much the same way as though they were present. Biliary drainage is equally called for, and the presence or absence of calculi is but a minor feature upon which too much stress should not be laid nor too much disappointment expressed if they be not found.
Many cases of chronic cholelithiasis have become more or less toxemic, as well as cholemic. It is a well-recognized fact that cholemic patients are more likely to cause inconvenience to the surgeon from free hemorrhage or persistent oozing, because of the slowness with which coagulation of their blood takes place. When time is afforded for preparation it is of great value in these cases to administer calcium chloride, of which several doses may be given each day, in considerable water, the former varying in amount from 1 to 2 Gm. When time suffices, too, it is always of value to prepare these patients for the operation by measures already discussed, improving their elimination, reducing the degree of their toxemia, and fortifying their circulatory systems by well-known[927] measures. The value of such preparation is perhaps more apparent in such instances than in most others. On the other hand, many cases calling for operation are almost as imperative as those of acute appendicitis, where every hour’s delay is to the disadvantage of the individual. The operations which are practised upon the biliary tract will all be discussed together in a section by themselves.
This expression refers rather to actual neoplasms of the gall-bladder itself than to distention of the sac by which an intra-abdominal tumor may be formed. The latter subject may be dismissed with the mere statement that the gall-bladder may become distended with bile, with mucus, with pus, with concretions, or with the products of such disease as echinococcus, actinomycosis, etc. In this way it may be so much enlarged as to be easily felt through the abdominal walls or to be even mistaken for other conditions. In the latter case it may have to be differentiated between such a condition and a movable right kidney, a tumor of the kidney itself or of its capsule, as well as from tumors of the stomach, especially the pylorus, of the liver, or of the intestine and from the enlargement of the right lobe which often accompanies cholelithiasis, or from fecal impaction. It would be best to abstain from the use of the aspirating needle in these cases, as more harm might be done by the escape into the abdomen of deleterious fluid than would be atoned for by the information which the procedure would afford. Even when the abdomen is open the gall-bladder should rarely be punctured in this manner, unless one is prepared at the same time to open it and drain. In other words, there is less risk about a small exploratory incision than in puncture.
Nearly all varieties of malignant and many of benign tumors have been reported as occurring in this location. It will be sufficient in this place, however, to say that cancer of the gall-bladder, which, of course, may extend in various directions, is by no means an uncommon affection, and is usually a complication of gallstones. In fact, it may be doubted whether primary cancer of the gall-bladder ever occurs in the absence of such a source of irritation. These cancers vary in type between the round-cell and the squamous, most of them, however, being of the former character. Although Musser has put the percentage at 65 and Zenker as high as 85 of instances where gallstones are found within cancerous gall-bladders, it does not follow that the above statement may not be true regarding their almost universal association and causal relation, for any gall-bladder found empty at a given time may at some other time have contained a calculus. This frequent association is justly among the valid arguments which surgeons may now use in making a plea for earlier operation, and for making it a more standard procedure.
Cancer may be suspected in cases of progressive and unintermittent jaundice, especially when there can be felt in the region of the gall-bladder a distinct tumor or an enlargement of the liver. Pain is a frequent but by no means a constant or reliable symptom. As the disease spreads the adjoining textures will become matted together, and a low grade of local peritonitis may still further cement them into a mass which will occupy a considerable portion of the upper part of the abdomen.
But few cancers of the gall-bladder which are so apparent as to be recognized without exploration can be considered as still amenable to surgery, which for them can hold out but little prospect save perhaps a temporary relief by biliary drainage. It is the cases in their earlier stages, when the condition is made out by exploration, and by it alone, which still afford prospects of more or less permanent relief. The very impossibility of detecting the condition in these earlier stages without exploration affords one of the strongest arguments for such a procedure in every vague case of the kind. That cases of this character are not necessarily hopeless is instanced by an experience of my own, where on opening the abdomen of a large and fleshy woman I found a distinctly cancerous gall-bladder containing two large calculi, and removed the entire mass, with a considerable portion of the surrounding hepatic tissue, the removal being effected with the actual cautery. At present date of writing, nearly six years after the operation, the patient is apparently perfectly well and doing her own housework.
[928]
The small area included under the above title has been made the field for a variety of operations, dignified with formidable names, the entire list of which might be made quite long. In order to simplify their arrangement and illustrate their purposes they may be referred to as (1) operations upon the gall-bladder proper; (2) those upon the ducts; and (3) the more complicated operations upon one or both of these in connection with some other part of the intestinal tract; or, to catalogue them somewhat definitely, the operations upon the gall-bladder include cholecystotomy, cholecystostomy, and cholecystectomy, according as the surgeon opens the gall-bladder and closes it, makes a more or less permanent opening, or completely removes it. Again, upon the ducts he may make cholangiotomy or cholangiostomy, or, using their practically equivalent synonyms, choledochotomy or choledochostomy, these terms referring to operations upon the cystic and the common ducts; while when similar procedures are applied to the hepatic duct they have been spoken of as hepaticotomy and hepaticostomy. Cholecystenterostomy refers to an anastomosis between the gall-bladder and the upper bowel, while when this is effected between the common duct and the bowel it is referred to as choledochenterostomy. When a stone lies partly in the common duct and partly within the wall of the duodenum, and it becomes necessary to incise the latter, it may be spoken of as duodenotomy. The operation of merely crushing biliary calculi, hoping that the fragments will be passed on with the flow of bile, and spoken of as cholelithotrity, is now almost abandoned, and the term has historical rather than present value.
To even attempt to epitomize directions for these various operations into space available here would be impossible, for large volumes have been devoted to this subject alone. The main thing for the student and the junior practitioner is to appreciate the indications for their performance, at which he should certainly have assisted before attempting to perform them himself. General directions, however, may be given as follows, the usual preparations having been made both of the patient and the environment: A woman who has borne children and who has, in consequence, relaxed abdominal walls, makes a more favorable subject for operation than a muscular man whose abdominal muscles cannot be relaxed until a profound degree of anesthesia has been obtained. In many instances exposure is made better by placing a sandbag behind the region of the liver, especially on the side to be operated, by which the costal angle is more outlined and the parts pushed forward.
A preliminary incision should be made of, say, three inches in length, and is best placed a little to the inner side of the outer border of the rectus, whose fibers are separated and its tendinous intersection divided. This incision may be extended upward and curved toward the middle line, as recommended by Bevan, or downward, as the exigencies of the case may require. The beginner especially should provide himself with sufficient space for manipulation. The posterior sheath of the rectus and the peritoneum are best divided together. Sufficient opening being thus made, a finger may be inserted for the purpose of exploration. In the presence of adhesions, and especially in acute cases in which pus is likely to be present, this should be done with great caution. When no adhesions are present gauze pads may be inserted and so disposed as to permit exposure to view of the lower surfaces of the liver. The operator should be prepared for any and all conditions—one of dense adhesions or their complete absence, as well as for cobweb-like adhesions which surround foci of infected exudate or of pus. The more reason he may have for suspecting the presence of pus the more carefully should the region be walled off with protective gauze. Adhesions are most likely to form between the omentum and the colon, in front and below, and with the stomach, duodenum, and colon below and behind. Those who have had experience with abdominal operations will appreciate whether these adhesions are recent and likely to cover purulent foci, or old, and will proceed accordingly. Occasionally tissues will be so matted that even an experienced operator will scarcely be able to differentiate them.
The endeavor should be, if possible, to expose the gall-bladder itself, both to touch and sight, in order that after orientation concerning its actual condition its duct may be followed into the common duct, and this into the intestine. This is sometimes an exceedingly easy matter, and again impossible. The presence or absence of pus will of itself indicate what should be done. When, for instance, the gall-bladder is found[929] black or partly gangrenous the surgeon will content himself with doing the least possible amount of separating, endeavoring rather to provide the widest outlet for drainage. It might be better to make simply a small opening and permit the escape of fetid débris, and to postpone until a later day further attempt to remove the calculus, which presumably has produced the difficulty. Local indications, then, should be considered along with the general condition of the patient.
The lower surface of the liver will afford the guide to the location of the gall-bladder, and when the latter is nearly obliterated its discovery sometimes taxes the resources of the surgeon. When not contracted it is usually easily exposed, and so far freed that it may be even drawn up into the wound. After having thus isolated and perhaps secured it, it must be decided by further exploration how it shall be treated. It is of great importance to liberate the ducts from surrounding adhesions.
—Cholecystotomy, sometimes fallaciously spoken of as ideal, consists in simply opening the gall-bladder, emptying it of calculi or other contents through a small incision, and closing this by sutures. The operation is ideal in but one way, but conditions which permit it rarely justify it, for any gall-bladder so diseased as to call for operation needs either removal or drainage.
—Cholecystostomy includes provision for drainage over a considerable length of time. A distended gall-bladder which permits of easy manipulation and isolation may be sufficiently long and large to justify uniting its surface to the peritoneum and deep margins of the wound, in such a way as to permit discharge of its contents through the latter. The old method was to unite it to the skin. This should never be done, as fistulas thus resulting are more likely to be permanent. If the gall-bladder be thus affixed to the parietal peritoneum the better way is to insert a drain, its arrangement being left somewhat to the choice of the operator. For my own part I prefer a rubber tube, not too flexible, inserted two or three inches into the gall-bladder, through a small opening closed around it, with invaginated edges, by a purse-string suture of chromic gut, by which it is intended to prevent leakage into the abdominal cavity. By another suture of common gut the tube may be so fixed as to avoid danger of being lost in either direction. If the gall-bladder be sufficiently long to permit additional fixation to the depths of the abdominal wound the operation is made still more ideal; but in the case of a short and contracted cavity the tube may be left to follow it into the abdominal recesses. Within forty-eight hours the exudate which has been thrown out around it will have become sufficiently organized and well ordered to form a canal in which the tube shall rest, and which shall serve later as a conduit to conduct bile to the surface after removal of the tube itself. Into such a tube, after the application of the dressings, may be conducted another more flexible tube, whose upper end shall connect with a receptacle of some kind, which may later be a bottle held within the dressing, to receive the discharge, and thus avoid soiling.
This operation has been done occasionally in two sittings, the gall-bladder being brought into the upper part of the wound and fastened to the peritoneum by sutures, which should not perforate its walls, as that leakage would occur which the method is intended to avoid. After waiting a day or two for adhesions to form the cavity is then opened with a knife or scissors and drainage thus accomplished. This method has been practically abandoned, for the reason that it permits no digital exploration by combined manipulation.
—Cholecystectomy includes the removal of the whole or the greater part of the gall-bladder. It has already been stated that this is a reservoir, convenient and advantageous, but not needed in a way, and not essential to life. It figures as a superfluous organ, then, similar to the appendix, and there is no reason why, when diseased and troublesome, it should not be extirpated. Its removal will sometimes be a matter of choice, and at other times a necessity. The former is the case when the surrounding conditions lend themselves to its dissection from the lower surface of the liver without too much violence to other tissues; the latter when it is involved in malignant processes or when its interior is seriously infected. An incomplete method of treating the gall-bladder under the latter circumstances might include the scraping or removal of its thickened mucosa, without removing the entire thickness of its structure. In this case, however, drainage would be required. That the gall-bladder may be completely separated and thus isolated, with comfort and speed, requires that its wall be sufficiently strong to stand the ordinary manipulation. This may not be true of[930] the perfectly normal gall-bladder, but in such case no one would think of removing it, whereas the cyst, which is diseased sufficiently to justify removal, will usually permit of the necessary manipulation. Even if somewhat torn in the process the procedure may be effected without much added difficulty. This procedure consists essentially in separation of the overlying peritoneum and enucleation of the gall-bladder from its bed or the depression in the liver in which it lies, which, as already indicated, may be narrow or wide and deep. Actual separation from liver tissue will be followed by oozing and at least two or three vessels in the surrounding structures and at the neck of the gall-bladder will require to be secured. Removal should not be attempted in cases which do not permit of it, but may be practised in those cases not too infected, when after emptying the sac (full of calculi, for instance) it can still be established with the probe that the common duct is patulous. These are ideal cases for such complete work. The gall-bladder having thus been isolated down to its cystic termination, the surgeon proceeds much as though it were the appendix, by firmly ligating the duct with chromic gut, guarding against escape of contents while it is divided on the distal side of the ligature thus applied. The stump of the duct is then cauterized with pure carbolic, after which oozing is checked by tamponing for a few moments. It then is often possible to bring together the peritoneum beneath the torn liver surface and almost completely cover it anew. The liver tissue will bear a ligature or suture not too tightly drawn. If the case have been one otherwise surgically clean, and the operation properly conducted, the abdominal wound may be closed without drainage. If, however, doubt be felt a small cigarette or a tubular drain may be placed, to be left not more than thirty-six hours. Every infected gall-bladder, if not removed, should be thoroughly cleansed, its interior being mopped with gauze, preferably with the addition of hydrogen dioxide. An important step, next to attention to the gall-bladder proper, is to demonstrate the patency of the ducts. This is done by gently passing a probe, which should be bent to suit the case, along the duct and into the intestine. This, of course, cannot be done if calculi are discovered by manipulation, neither can it always be done when calculi are not present. Gallstones in the duct can usually be distinguished by the fingers with which the exploration is made, and failure to thus pass a probe may be brought about by stricture rather than by calculous obstruction. The importance of this determination will be seen in removing the gall-bladder, as to remove it in an obstructed case is to leave no outlet for bile except into the abdominal cavity, whereas to fail to drain such a case is to plainly neglect to meet the indication.
Fig. 628
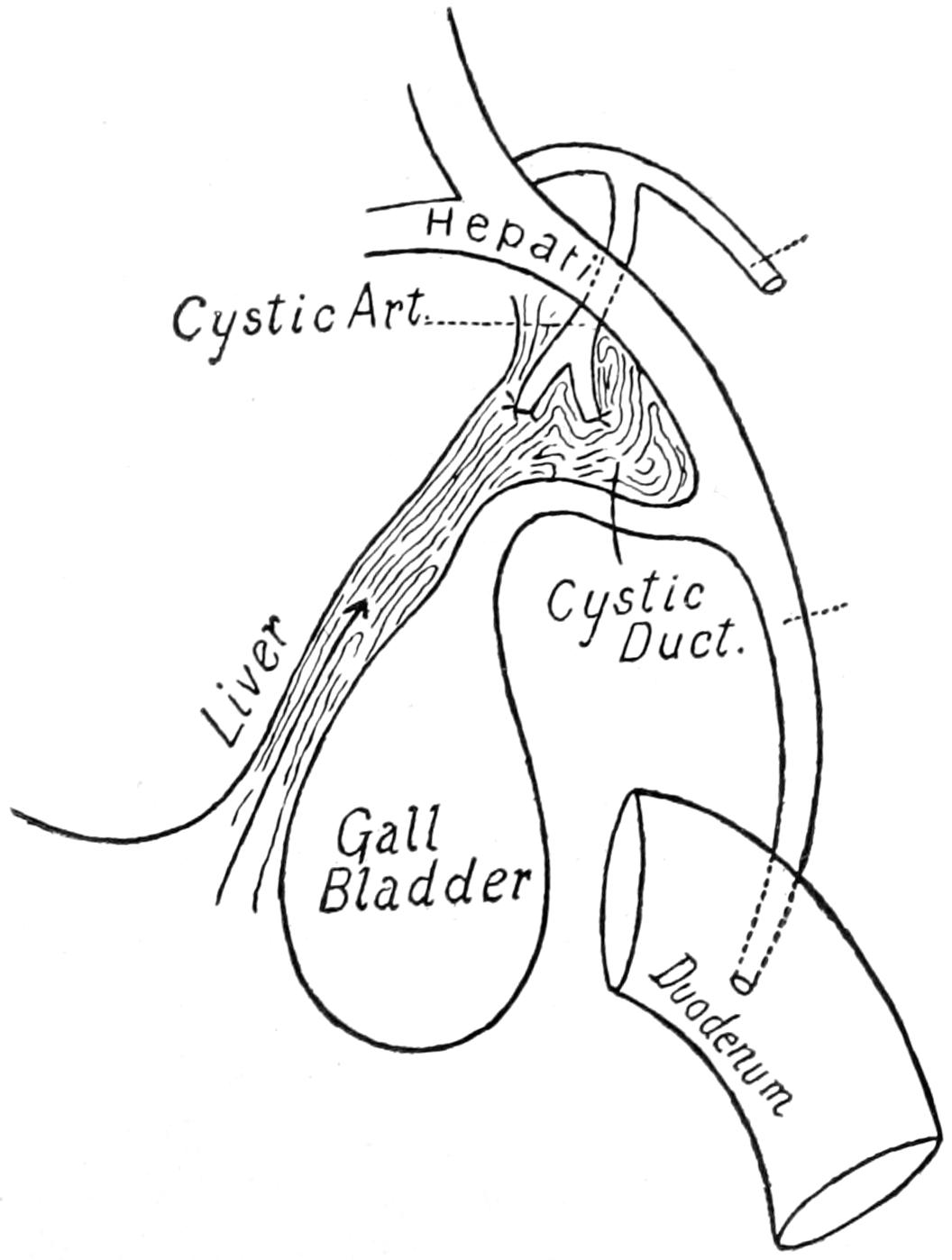
General scheme of cholecystectomy; detachment of gall-bladder and duct from their investments; ligation of cystic duct and arteries. (After Kehr.)
—The term cholecystendysis, now almost obsolete, implies practically a cholecystotomy with drainage, the gall-bladder having been opened for the purpose of removal of one stone or more and then united to the abdominal wound.
Of the operations upon the ducts there is something to be said in addition to the directions already given. Inasmuch as they lie more deeply they are more difficult of access, and variously shaped retractors, with walling off the cavity with gauze, are more often required, while in proportion as deep adhesions have enwrapped the structures they are made more difficult of exposure. At present surgeons have less hesitation in leaving duct incisions unclosed than was formerly felt. It was formerly held that every incision[931] into a duct should be closed with sutures. It has been later found that satisfactory results ensue when the end of the drainage tube is left resting, or even fastened, within the duct opening, the operation being thus made shorter and simpler and the difficulties of deep suture thus obviated. As elsewhere noted the common duct may become enormously dilated, and may be almost mistaken for the small intestine. The passage-way between this duct and the gall-bladder may be so obstructed that double drainage will be of advantage, or this may be a case where partial removal of the gall-bladder may be effected, with drainage of the common duct. Such cases should be judged upon their merits. The more infectious the existing condition the more is free drainage demanded. When a stone is impacted in the ampulla of Vater there should be no hesitation in dividing the walls of the duodenum in order to extract it. In such a case the duodenum is sutured, but the duct or the gall-bladder must be drained (Fig. 629).
These deep operations require free incision, several inches in length, and it will astonish the beginner to see how the liver may be delivered from the abdominal cavity through such an opening. Much assistance will here be gained by a large pillow or sandbag placed beneath the back. Bleeding vessels need to be secured, at least temporarily, with forceps, and usually with sutures or ligatures en masse. The exposed or torn surfaces of the liver will ooze freely at first, but bleeding usually ceases with the pressure of a gauze tampon. From the uninflamed gall-bladder the peritoneum is usually easily separated, with but trifling hemorrhage. For deep work traction on the middle portion of the duodenum makes more prominent the junction of this part of the bowel with the gastrohepatic omentum, at which point the peritoneum may be incised and separated along the free border of the duodenum until this portion is free from external peritoneal covering. There will be exposed here the second portion of the common duct where it lies upon the pancreas, it being more or less embedded in the latter further along. When it is necessary to cut away more tissue it is better to sacrifice a portion of pancreas rather than of duodenum itself. Blunt dissection alone should be made here. When it is necessary to cut it will be better to use the thermocautery.
Fig. 629
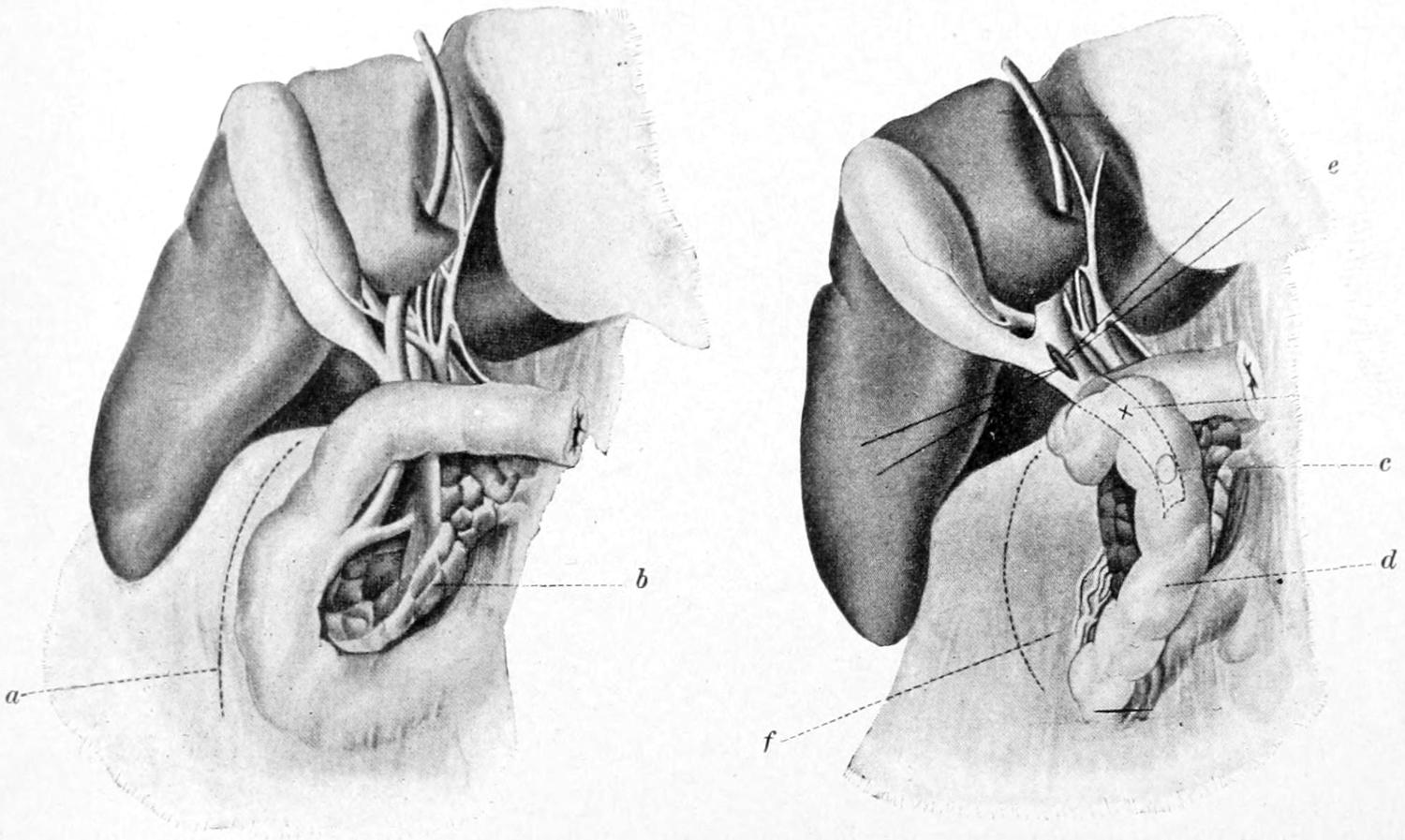
Removal of gallstone entangled at the papilla. Kocher’s method of displacing the duodenum: a, incision in the paraduodenal peritoneum; b, pancreas; c, location of the stone; d, duodenum; e, sutures used either for retracting or closing opening in the common duct; f, retroduodenal venous plexus. (Kehr.)
These various cutting operations have superseded the previous methods of endeavoring to crush stones within the duct and force the fragments along by pressure. The Mayos have recommended the use of two fine parallel sutures, introduced longitudinally into the duct, between which the incision should be made, and which may be used as tractors, or subsequently for purposes of closure.
[932]
Practically every gall-duct case should be drained with a tube extending down to the deepest portion of the site of the operation. This may be done with what has been called a “dressed tube,” made by surrounding an ordinary rubber drain with a few layers of gauze and covering this with oiled silk. The lower end of the tube is then bevelled or trimmed in fish-tail fashion. This may be passed into the depths, or it may be used for gall-bladder drainage as well.
Of the anastomotic operations there is less heard now than a few years ago. There are now considered to be but a few conditions which are not better dealt with by biliary drainage as made above than by any other method. Occasionally, as, for instance, when the common duct is strictured or involved in pancreatitis or cancerous deposit, and bile is backing up into the gall-bladder, it may be of great advantage to effect an anastomosis between the latter and the bowel. At one time the colon was used for the purpose, but this prevented the utilization of the bile in the upper bowel, where it is most needed. Consequently it should always be made into the upper portion of the bowel, the duodenum, or one of the upper loops of the jejunum. For this purpose a small Murphy button is probably still the speediest and best expedient. This is true also when it seems necessary to drain the common duct into the bowel, since the field of operation in most cases lies too deeply to permit of accurate and satisfactory suturing. A further and more difficult as well as later application of this principle has been suggested for certain cases of permanent obstruction of the common and main hepatic ducts. Under these circumstances the operation last mentioned would be useless and a cholangiostomy would be objectionable, as it would constitute a permanent fistula. As practised by Kehr and others this hepato-cholango-enterostomy is performed by removing from the lower surface of the liver a strip of its tissue about 7 Cm. long and 2.5 Cm. wide. The hemorrhage is checked with the thermocautery, and with it an opening is made into the liver, of such a depth that several of the bile ducts are thus divided and opened. The uppermost loop of bowel which then can be utilized without tension is opened and sutured to the margins of liver wound. The method is still on trial, and yet in at least one successful case it was shown that the liver tissue tolerated this unavoidable contact with the contents of the upper abdomen (Fig. 630).
Fig. 630
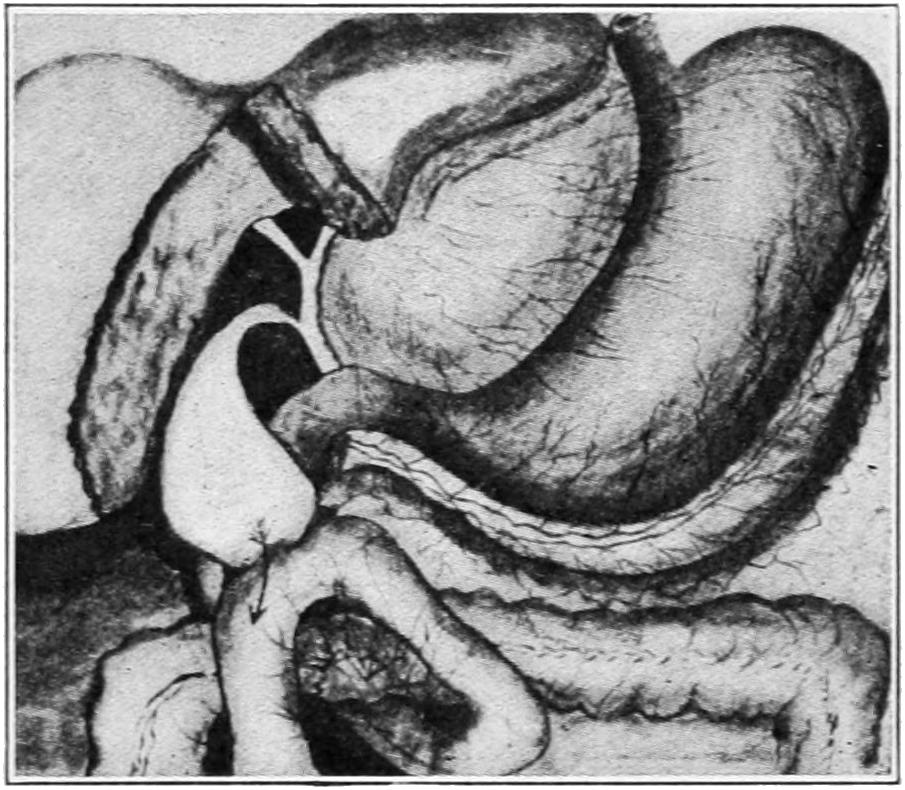
Demonstrating the technique of anastomosis between the gall-bladder and the jejunum. (Cordier.)
—What to do with these cases of biliary drainage after it has been effected is sometimes a serious problem. No hard-and-fast rules can be laid down regarding the length of time during which drainage should be maintained. In instances where the gall-bladder has been removed the drain should be taken out within thirty-six hours, but in those cases where a tube has been fastened into the gall-bladder for so-called permanent drainage the term “permanent” may be regarded as elastic, and covering a period of from ten days to perhaps ten weeks. In the majority of instances three weeks or so of such drainage suffice to meet the original indication. In cases, however, of chronic pancreatitis a long period of easy outflow will be demanded, while in rare cases of cancer drainage once thus made cannot be abandoned.
[933]
When the gall-bladder has not been fastened nor allowed to adhere to the skin, but only to the peritoneum, the fistulas thus made will usually close and rarely need stimulation. Should, however, the granulation process by which closure is effected be too sluggish it may be stimulated by the application of nitrate of silver, either in solution upon a swab, or in solid form, as when melted into a bead upon the end of a suitable probe. Firm pressure will also assist in final closure.
It is not reasonable to expect that after so much intervention, within the rudely triangular potential cavity occupied by the gall-bladder and the ducts, adhesions will not form as a part of the reparative process. In fact it may rather be expected that as it becomes obliterated adhesion must necessarily follow. In consequence there may result an agglutination around the gall tract, and into a common mass, of the liver, the colon, and the pyloric end of the stomach. In spite of these adhesions bad symptoms rarely ensue, and when discomfort persists it is usually in those cases in which no stone was found or those in which stones have been overlooked. Andrews regards such postoperative adhesions as unavoidable and even desirable, and, having no faith in any measures to prevent their formation, differs from Morris in regard to the technique of their subsequent removal. It appearing from observation and experience that the stomach is the organ which suffers most by extensive adhesion to the liver, he has proposed to substitute the colon for the stomach in this necessary union of surfaces, and would even practise it in old cases after separation of old adhesions.
The operation suggested by Andrews, and which he calls cholehepatopexy, or colon substitution, is made with an incision through the middle line of the right rectus, avoiding any old scar, long enough to afford plenty of room. The stomach is then carefully separated from the liver, tearing liver tissue rather than that of the former, if something must be torn, and checking bleeding by hot sponges. The pylorus having been exposed the stomach is invaginated into it in order to demonstrate its patency. The freshly separated viscera will now fall again into immediate contact unless the transverse colon be pulled up and held in place between the liver and the pylorus, this not being so much of a displacement as would appear, as the bowel is not rotated and does not cross over the stomach. The colon is held in its new relation by attaching its omentum to the gastrohepatic ligament, to the liver surface, or to remnants of old adhesions in the angle between the pylorus and the liver. The looser the omentum and the more easily it can be interposed in this way the better. Andrews’ conclusions are that gall-tract adhesions are unavoidable, both in disease and after operation, that they are harmless except in a very few cases, and often beneficial, and that in the few cases where they do harm this comes from malposition rather than from adhesions per se. He even believes that certain vague gastric adhesions which might have been benefited by this operation have been previously treated by gastro-enterostomy.
[934]
The omentum is something more than what it generally appears, i. e., a more or less thick and extensive apron of fat, hanging down in front of the small intestines, although in this respect alone it serves as a sort of reservoir or storehouse for fat, which is always drawn upon as the needs of the system may require. The omentum varies within wide limits from being the flimsiest veil of peritoneum, whose four original layers have become so blended as to be lost to recognition, and which may even be perforated in places with openings through which strangulation of the bowel is possible, to the thickest and grossest mass of fat found in the human body, resembling a coarse mat rather than any finer texture, and having a thickness, in obese individuals, of two to four inches. Under these circumstances it makes a formidable obstacle to nearly all abdominal operations. The thickness of the omentum sustains usually a pretty constant proportion to the amount of adipose between the skin and the abdominal muscles. In certain enormously fat individuals one has then to go through from four to six inches of tissue, mostly adipose, before reaching the rest of the abdominal contents. This necessitates a longer incision and is always a disadvantage and impediment. To the operating surgeon, then, the omentum sometimes appears a nuisance.
It does not deserve, however, to be so regarded, and when properly viewed the omentum will frequently appear in the role of the surgeon’s as well as the patient’s best friend. This is due to its power of shifting itself, and, as it were, enclosing actively dangerous foci due to any variety of infection, the natural intent being, as it were, to wrap itself around and thus completely imprison the source of the trouble, a fact which is often actually accomplished, and by which life-saving protection is frequently afforded. This is true of the omentum whether thick or thin. By virtue of the adhesions which often annoy the surgeon, and which necessitate separation and perhaps considerable work before the actual trouble is exposed, a protective barrier is formed and the greater portion of the abdominal cavity shut off from danger of spreading infection. Moreover, that the omentum has a really valuable purpose appears from the fact that its removal from young animals seems to cause retardation of development, and from adult animals a diminution of resistance to the action of poisons introduced into the peritoneum. It is the omentum which, to a large extent, absorbs foreign corpuscles, such as those from extravasated blood. It helps, moreover, to dissolve blood clots and to facilitate their disappearance, and after the removal of the spleen it would appear to vicariously perform at least some of its duties. Thus when the complete blood supply of the spleen is cut off the organ almost completely disappears as the result of its absorption by the omentum. (This at least in experimental animals.)
The omentum serves further useful purpose by plugging various openings and wounds in the abdominal walls, and thus affording at least a temporary protection, just as the mucosa sometimes acts in reference to the stomach. Moreover, it is so vascular, so flexible, and so available that it may be used for plastic purposes in covering weak spots, lines of sutures, and the like, in the small intestine or even elsewhere. These same physical qualities make it extremely prone to escape through the natural outlets. Hence the frequency of epiplocele or omental hernia (q. v.). By a species of such hernial protrusion it has saved many a life after bursting open or re-opening of recent abdominal wounds. Sometimes it will escape after removal of a gauze drain which has not been judiciously placed and protected, this accident then constituting one variety of postoperative or traumatic hernia.
By virtue of its adhesions, which at first are short and flat, but which later become stretched into bands, obstruction of the bowels may be produced, or by atrophic or absorptive[935] processes openings or windows may occur in it with the same result. When participating in septic processes it becomes infiltrated, is often covered to a large extent with breaking-down lymph, and may become gangrenous. All portions thus compromised are best tied off and removed when exposed during operation. Nevertheless the omentum should be gently handled, because its venous walls are thin and liable to rupture, and its bleeding points should be carefully secured, especially after separation of adhesions.
By contusions, lacerations, and punctures various injuries to the omentum may be inflicted, naturally more commonly when it is the anterior abdominal wall which has sustained the traumatism. As result of lacerations, hemorrhages or strangulations may occur. The immediate danger is, then, from hemorrhage. Indications of such lesions of the omentum are not specific, but grave symptoms after any abdominal injury require exploration, and that minute punctures or lacerations should be repaired, while other injuries should be treated according to obvious indications.
Torsion of the great omentum was first described by Oberst, in 1882, as a condition found in the sac of a large irreducible hernia. As a distinct and serious condition it has been reported in about sixty instances. The condition occurs within the abdomen as simple torsion, also within hernial sacs, or in both, where the torsion is not limited to the sac, but extends upward into the abdomen. It is more frequent in males, and its onset is usually sudden. Of all its symptoms pain is the most constant and the earliest. This is usually acute and persistent, and in a large proportion of cases is referred to the right iliac fossa. Vomiting is not constant; bowel conditions are not significant. Absolute obstruction is usually rarely noted. In most of the recorded cases some tumor can be felt on examination, which is hard, tender, dull to light percussion, and irregular in shape. Meteorism is not common. Death has occurred in about 15 per cent. of known cases. Diagnosis previous to exploration can be inferential only, but such symptoms as above noted should lead to exploratory laparotomy.
The most common of the omental tumors are cysts of inflammatory origin, such as may, for instance, be formed by inclusion between surrounding adhesions or by previous hemorrhage; lymph cysts, often large and multiple, and sometimes of congenital but often of lymphatic origin, are also occasionally seen. The so-called omental dermoids are usually ovarian products. Hydatid cysts have been found in the omentum, but only as secondary products. Omental cysts are difficult or almost impossible of diagnosis previous to operation, which latter should always be performed, and without previous aspiration, as the presence alone of any such tumor requires removal. If large they are most likely to be confused with ovarian cysts. Those which may prove not to be removable should be drained, after being fastened to the abdominal wall—that is, marsupialized. Angioma in the omentum is rare, but has been recorded by Homans and others. Fatty or other benign tumors are also rare. Primary sarcoma is rarely seen here, but most of the sarcomas, and all of the carcinomas which never arise here primarily, but are often seen, are either metastases or direct extensions. In these forms cancer of the omentum is common.
With extensive involvement of the omentum radical operations in these cases are seldom advisable. A circumscribed involvement may, however, be removed, while such operations as anastomoses, enterostomies, and the like are often necessitated.
Omental tumors are difficult of diagnosis, although they are usually superficial and overlie the intestines. They are not affected by respiration. They move laterally and[936] upward, but not downward. If confined to the omentum proper they cause no functional but only mechanical disturbances. Obviously in the presence of extensive adhesions every distinctive feature may be confused.
The effect of stasis in the portal circulation is to produce outpour of varying amounts of serous fluid into the pleural cavity. This condition, long known as ascites (dropsy), is the most distressing terminal feature of such diseases as cirrhosis of the liver, cancer, and the like. The osmotic direction of fluid seems to be reversed, and transudation tends to go on until intra-abdominal pressure equals that within the vessels. Absorption is always impeded and finally prevented. Reflecting on the biophysics of this condition Talma and Morrison, independently, and at about the same time, suggested an expedient by which a portion at least of this fluid might be brought back into the general venous circulation. The plan was to attach the epiploön (the omentum) to the peritoneum of the anterior abdominal wall in such a way and over such an area that, by virtue of the adhesions thus produced and the new vascular anastomosis thus established, a new line of vascular connections should be formed, so that fluid not returnable to the vena cava by the usual route should be given a new and artificial direction. To this fundamental proposition much detail has been added.
Thus Schiassi has shown that, so far as the supply of toxins which shall pass through the liver is concerned, there are really two portal veins—the superior mesenteric and the splenic—or he would call what we usually name the portal system the splenoportal. Consequently he would include the spleen in the above mechanical procedure, especially in those cases where it participates in the morbid process—e. g., in the hepatosplenic or pre-ascitic form of Banti’s disease, and the splenomegalic cirrhosis described by Gilbert. In 1904 this problem was studied from its surgical aspects by Monprofit (French Congress of Surgeons), who collected 224 operated cases. Of these 84 died, 129 recovered from the operation, and 11 could not be traced. In 25 cases relapse occurred, in 26 there was improvement, while in 70 there was claimed complete recovery.[64] In other words about one-third of the cases thus reported have recovered. He insists, as would every other surgeon, that with this showing the results would be far better were cases seen and operated earlier. His statistics are not widely variant from those of Zesas, who found that out of 254 cases which he collected 67 recovered and 82 died, while 42 were greatly improved.
[64] It is but fair to add that, at the same time, Delagenière maintained that since, in his opinion, cirrhotic processes in the liver are due to intestinal infection, the treatment should consist of combating this and its possible consequences, to which end he would make a temporary cholecystostomy, having found it of benefit even in the atrophic, but mostly in the hypertrophic, forms of disease. Thus in two cases of this procedure, combined with hepatopexy, the patients survived eight and two years respectively. Nevertheless he acknowledged that the best results would probably be secured from combination of cholecystostomy, hepatopexy, and omentopexy.
In brief, we may hold, with Rolleston and Turner, that it is no longer advisable to treat ascites by repeated tappings, when the patient is otherwise in fairly good general condition, for numerous surgeons have warned against repeated punctures. When liver cirrhosis can be diagnosticated with fair certainty in the pre-ascitic stage, and when there is evidence of splenic enlargement or hematemesis, operative intervention would probably succeed far better than in the later stages. So far as special indications for operation are concerned they may perhaps be listed as follows:
If these indications be met by reasonably early omental fixation there would seem to be a well-marked place for the procedure, while they cannot give rise to any worse results than the repeated puncture methods of old.
Among contra-indications to such operations may be mentioned the presence of[937] much biliary pigment in the urine, its absence from the feces, jaundice, or marked pigmentation of the skin, while distinct renal insufficiency would also make any surgical procedure hazardous.
The operation itself, done according to the simpler and earlier recommendations of Morrison and Talma, consists in median abdominal section, withdrawal of all ascitic fluid, and the deliberate provocation of adhesions between the diaphragm and the upper surfaces of the liver and the spleen. This is produced by vigorous swabbing to a degree sufficient to cause a little oozing from the surfaces attacked. The margin of the liver may then be fastened to the costal border. After this the anterior surface of the omentum is also scarified or swabbed and affixed to the anterior abdominal wall, which has been similarly treated over as large an area as possible, by means of catgut sutures placed to the best possible advantage for the purpose. Some operators have preferred to close the abdomen without drainage, some to insert a tube in the lower margin of the wound for a day or two, and others to drain the lower abdominal cavity through a small, distinct opening above the pubes. Theoretically much advantage attaches to permitting no immediate re-accumulation of fluid. Practically, however, danger also attaches to it, i. e., from the difficulty of so managing the dressings as to avoid infection.
Schiassi has modified the above procedure and has made an omentosplenopexy of it as follows: He makes a right-angled incision across the median line and then another several inches downward along the left semilunar. The tissues down to the peritoneum are reflected toward the umbilicus, and a transverse deep opening is made just below the horizontal skin incision. Through this the omentum is drawn upward and spread over the right portion of the exposed peritoneum, where it is sutured in place. Through another vertical opening in the peritoneum, near the vertical skin incision, the spleen is then exposed, a piece of gauze is placed under each pole of that organ, and, while thus lifted, by means of a long curved needle three to six catgut sutures are passed through it, including also the peritoneum and all the superficial structures except the skin, this being closed later and separately.
Finally, whatever operative method be selected it is important that it be done early rather than late, bearing in mind that “the resources of surgery are rarely successful when practised on the dying.”
No one has done more to forcibly place before the surgical profession those anatomical features of the mesentery which most concern them than Monks, who, for instance, has demonstrated the fact that the mesentery is practically an enormous fan, composed of two layers of peritoneum, between which are spread out the vascular structures and more or less fat, and whose border contains the intestinal tube. This fan at its base is but a few (six) inches in length, while along its outer border, when completely unfolded, one may measure a distance of twenty-one to twenty-three feet. Not one of the structures contained between its layers can be regarded as a negligible quantity. The arterial distribution in the mesentery is terminal in the same sense that it is in the brain. Consequently dependence can be placed only on a sufficient blood supply for any given portion of the intestinal tube when its mesentery is intact. If necessary to sacrifice a portion of the mesentery it is requisite to resect that portion of the bowel which is dependent upon it for blood. This will explain the reason why thrombosis or embolism of the mesenteric vessels so quickly determines the death of that portion of bowel supplied by the occluded branches, this being equally true of the tiny fragment known as the appendix or of the entire bowel.
The root of the mesentery is placed obliquely across the spinal column, arising from the left side above and crossing obliquely to the right side below. Monks has shown how easily we may make practical application of this fact in determining approximately to what part of the bowel tube a given loop may belong, since it is necessary only to follow it down to the mesenteric insertion, and from this estimate what proportion of the entire distance is represented.
[938]
Obviously the mesentery may be injured in the same way as any other of the abdominal viscera, either by contusions, lacerations, punctures, or otherwise. Here the immediate danger is from hemorrhage, while a more remote but quite possible danger is that of thrombosis of some of the vessels and its consequences in the direction of necrosis.
Erdmann has recently reported two cases of complete detachment, for several inches, of the mesentery at the intestinal border, as well as a case of multiple lacerations in the peritoneal coat of the mesentery with hematoma. While the latter might not be so serious, the former will almost invariably determine gangrene of bowel from lack of blood supply; all of which shows the difficulty of diagnosis, and furnishes a further argument for intervention when, after an abdominal contusion, the patient has abdominal rigidity or pain, with or without evidences of hemorrhage, either from the stomach, rectum, or bladder. These features are sufficient without the addition of those by which a more certain or minute diagnosis can be made.
Mesenteric occlusion was first described by Virchow in 1859. Whether it involves first the arterial or the venous circulation seems to matter but little. Of course in one case it is to be regarded as embolic, in the other as thrombotic. In this location either condition is harder to explain than in many other places. The mesenteric veins have no valves and collateral circulation is poor. Mitral stenosis and arterial sclerosis will often account for the former. For thrombosis search has to be made for some local infectious process, either in the veins of the pelvis, the kidney, or the intestines. It seems to occur least often when it might be most expected, i. e., after typhoid.
The blood supply may be simply shut off from portions supplied by one of the mesenteric vascular branches, or, should the main branches be involved, from the entire intestinal tract. I have myself reported two cases of practically complete rapid gangrene of the entire alimentary canal, due to lesion of this kind, explanation being forthcoming in neither case.
—The more complete the occlusion and the more extensive the area deprived of blood the more sudden and overwhelming will be the onset. This is always sudden and characterized by intense and often paroxysmal pain, so agonizing, in fact, as scarcely to be quieted even by morphine. While this is common, instances have been known in which the disease has run an almost painless course. Diarrhea is frequently an early symptom, evacuations being profuse and bloody. Symptoms of obstruction are not uncommon, perhaps followed later by loose stools. Vomiting occurs usually early and becomes fatal in a few hours. The general physical signs are intensely acute, with rapid pulse, subnormal temperature, and meteorism, beginning early and becoming more pronounced. Abdominal rigidity also constitutes a distressing feature, which, while indicating the gravity of the condition, masks its diagnostic features. If the patient live long enough fluid will accumulate in the peritoneal cavity. The cases terminate with complete collapse and delirium. When the inferior mesenteric vessels are involved tenesmus is a more prominent characteristic than when the lesion is confined to the upper, as the colon and rectum are supplied from the former.
The surgeon may have to distinguish between the condition just described and the following: Perforating ulcer of the stomach or duodenum (which will have a previous history), possibly so-called phlegmonous gastritis; acute obstruction of the bowel (whose onset is rarely so acute); pancreatitis, which would, at least at first, produce almost identical symptoms; acute splenic infarct (when the early symptoms would probably be referred to the region of the spleen); acute appendicitis; acute cholecystitis, and that acute peritonitis to which either of these might lead; a ruptured ectopic pregnancy; and possibly certain intrathoracic lesions, especially pneumonia in the lower lobes. Mesenteric occlusion is essentially a fatal condition, at least when extensive. There have been known cases where so limited an extent of the bowel and mesentery were involved that an exsection, made early, has proved successful, but when anything like the entire alimentary canal or its major portion becomes necrotic there is no hope for the patient.[65]
[65] Annals of Surgery, April, 1904.
[939]
Abscess formation may take place within the mesenteric structures, as an expression of acute septic infection or of a mixed infection of old tuberculous foci in the nodes. A careful case history or some peculiarity of local conditions may occasionally furnish a clue to the conditions, otherwise it will not be distinctly revealed until such operation as may be necessitated by unmistakable indications of the presence of pus or by autopsy. Inasmuch as operation can scarcely exaggerate the danger of the condition it would be best attempted when such abscess is suspected. When the meso-appendix is involved, as is often the case, the trouble may be so walled off that it is almost a purely local affair.
Aside from the common miliary expressions of acute tuberculosis which are seen so frequently dotted all over the bowel surfaces and the expanse of the mesenteric folds, there is a peculiar form of involvement of the mesenteric nodes, i. e., those which are especially clustered along its root. These are always involved in general tuberculous peritonitis, though but slowly in the absence of such generalized features. To the slow forms of this condition the early writers gave the name tabes mesenterica. The more limited the involvement the greater interest the lesion has for the surgeon, since it may be so limited to the nodes of a single coil as to justify extirpation. In fact, if such a focus could be easily and thoroughly removed without too much disturbance of circulation, tabes might be remedied by surgery. Not very frequently, however, do the location or the arrangement of a collection of tabetic nodes permit of their enucleation. They are usually too numerous, too large, too degenerated, too adherent, or the patient otherwise too extensively infected.
The acuter expressions of mesenteric tuberculosis may be considered as already sufficiently discussed under the caption of Tuberculous Peritonitis.
Occasionally a localized, slightly mobile tumor, especially in the ileocecal region, may cause suspicion, or may be correctly diagnosticated, by taking note of other symptoms, along with a good case history. Especially is this the case in patients known to be tuberculous. This is particularly true of the appendix and its mesentery, where a tuberculous gumma may attain considerable size before there is any active breakdown. The relation between this condition and tuberculous ulceration within the bowel will also be obvious. Moreover, it is of interest to recall that calcification of mesenteric nodes is not impossible, and that occasionally chalky tumors in this location may be thus explained.
There is also a possibility of involvement of the mesenteric nodes in constitutional syphilis and in actinomycosis.
The treatment of mesenteric tuberculosis should consist of exploration and orientation, followed by whatever procedure the condition thus revealed may require—e. g., abdominal irrigation, with or without antiseptics, extirpation, drainage, or even resection of a portion of the bowel (appendix, cecum, etc.).
The other condition in which the mesenteric nodes are especially involved is the cancerous. In this location, as in the omentum, sarcoma may be primary and endothelioma may occur, but carcinoma is never primary, although it invariably occurs as an extension from epithelioma or adenocarcinoma of the bowel. Otherwise cancer will appear here as an expression of metastasis. In all primary cancers of the intestine early involvement of the mesenteric nodes may be looked for, while involvement of everything in the vicinity, even the aorta or spine, will occur in due time, often with more or less breaking down. There would be little justification for attacking any cancerous portion of the mesentery or any cancerous nodes unless the primary lesion could be radically removed. Generally speaking, in bowel cancer invasion of the deep-seated nodes imparts to the case such an unfavorable aspect as to justify only palliative (anastomotic) rather than radical measures.
[940]
Cysts of the mesentery are, in the main, similar to those met with in the omentum (Fig. 631). A peculiar form of mesenteric cyst is produced by obstruction and consequent dilatation of one or more of the lacteals, and is known as chyle cyst. It may attain considerable size and occur in multiple form. The contained fluid is naturally milky and corresponds to that seen in chylous ascites and hydrocele. These lesions are only recognized after exploration. When found they are to be extirpated, on general principles, usually by enucleation, with ligature of the connecting lacteals and avoidance of all unnecessary disturbance of blood supply.
Fig. 631
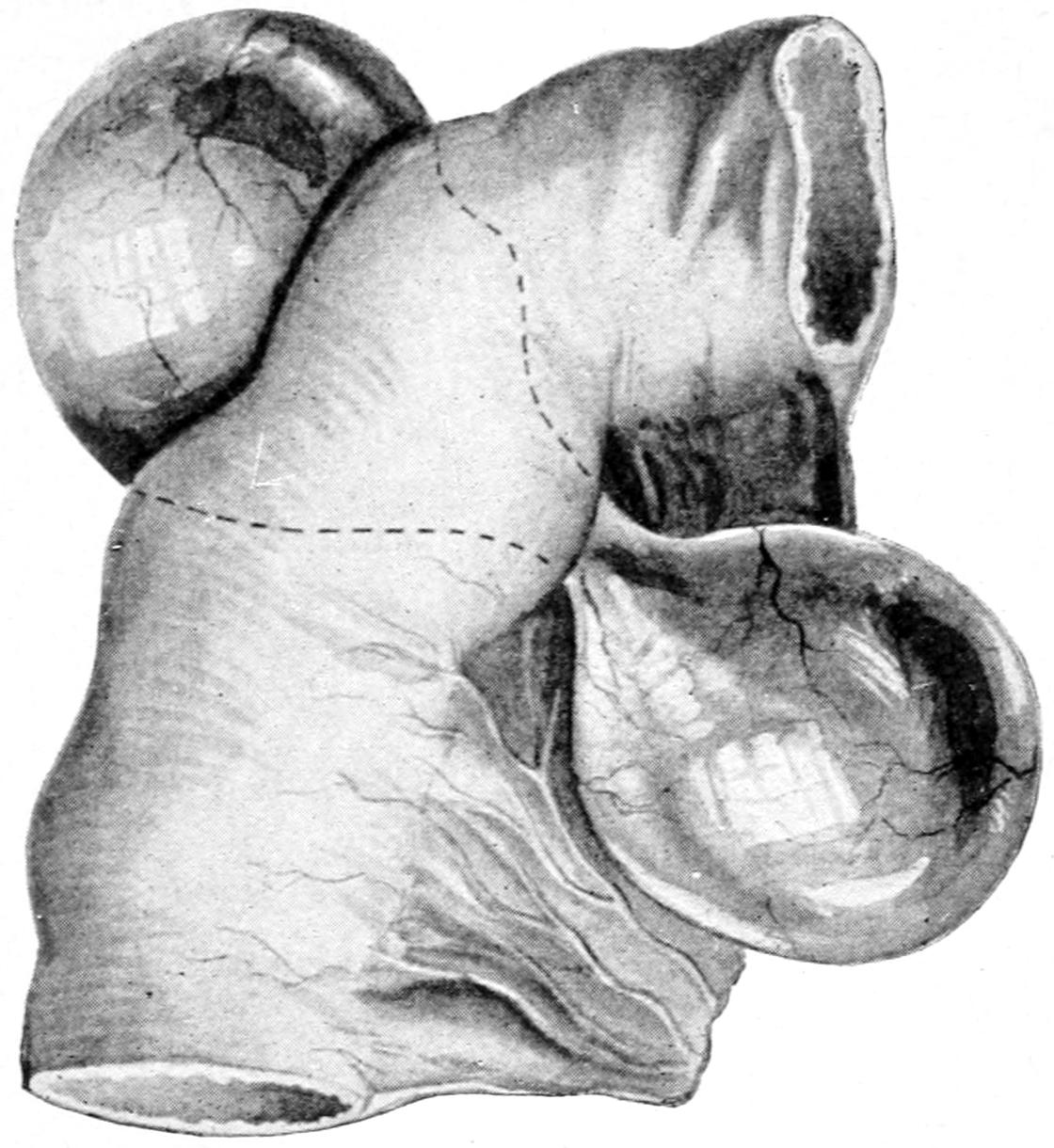
Cyst of the mesentery, containing clear fluid. The hour-glass constriction passes through the layers of the mesentery. (From a case occurring in Richardson’s practice.)
The spleen is often an object of surgical interest, not alone because of the frequency with which it is enlarged in the course of the acute surgical infections, but because it is something more than a reservoir for blood. Thus it seems to enlarge to accommodate blood forced in from the exterior under conditions of extreme exercise, etc., and in the higher vertebrates it seems to be a place where blood corpuscles are destroyed, especially those which are already disintegrating, rather than one in which they are manufactured. It is claimed by Ehrlich that the splenic enlargement of the infectious diseases is produced mainly by the products of disintegrating leukocytes which are allowed to accumulate.
Of the congenital anomalies or defects the surgeon is mainly interested in the fact that supernumerary spleens are common, being found perhaps in one out of four bodies varying in number up to thirty or forty, located near the hilus in the gastrosplenic omentum, in the great omentum, or even in the pancreas. Doubtless after some splenectomies no peculiar symptoms are produced, which is due to the fact that some of the supernumerary organs have taken up the splenic function. The spleen varies in shape to such an extent that the notch upon which so much stress is often laid in[941] diagnosis will not always be found along the anterior border. In cases of transposition of the viscera the spleen may be found on the right side. It has been found in the sacs of large umbilical hernias and in the left thorax after defects of the diaphragm.
The spleen may be injured by itself or along with other viscera. The most common injury is from contusion, which produces more or less disintegration or rupture and hemorrhage. The organ is so friable that it may literally burst under a comparatively slight force, other conditions being favorable. Doubtless minor degrees of these injuries pass unnoticed or are followed by some local peritonitis and adhesions. On the other hand the spleen may be actually fragmented, with necessarily fatal consequences unless promptly operated. Rupture is especially likely to occur after those infectious diseases which cause its enlargement—e. g., typhoid.
In case of injury there is, in addition to the history, a prompt location of pain in the region of the spleen, with signs of intra-abdominal hemorrhage, but without blood in the urine; perhaps with tumor or dulness on percussion, and always with abdominal rigidity, all of which point to the serious nature of the injury and demand exploratory section. Should this reveal a slight injury it may be repaired with ligatures or sutures. More serious tears or perforations are treated by gauze packing through a sufficiently open wound, while the most serious cases of pulpifaction call for complete extirpation. When the blood supply of the spleen is left in doubt its total removal will be far the safer course to adopt. Obviously such an operation should include examination of all the viscera and a careful toilet of the peritoneum.
Pus may form within the spleen in consequence of septic infarcts or thrombosis, or it may be due to the extension of trouble from adjoining foci, or to pyemic metastasis. Splenic abscesses are usually localized, but the pyemic forms are always multiple, miliary at first, but coalescing into larger collections, and practically destroying the organ if the patient live long enough. The infectious fevers may be followed by suppuration of the spleen, which is also known to occur rarely in malaria.
—The symptoms of splenic abscess are indeterminate until the capsule is involved and a perisplenitis—i. e., a local peritonitis—results, after which pain becomes severe. These collections occasionally discharge spontaneously into the colon or even into the stomach.
On general principles any abscess which can be located, even somewhat vaguely, should be attacked. After the abdomen is opened, preferably through the left semilunar line, the exploring needle may be used, especially if adhesions be present.
Gangrene of the spleen is the result of a still more rapid, otherwise similarly septic or thrombotic process, or of severe injury, by which circulation is practically cut off. It is a condition which rarely permits of any surgical help, though if it could be foreseen it might be prevented by an early splenectomy.
Enlargement of the spleen occurs during numerous acute and chronic infections—e. g., typhoid, malaria—in connection with certain affections of the liver; in consequence of interstitial or gummatous forms of syphilis, with or without similar lesions in the liver; in acute peritoneal infections; in general septic and pyemic disturbances; in rickets and the status lymphaticus; in the various forms of leukemia, Hodgkin’s disease, and pseudoleukemia, and in that somewhat peculiar type known as Banti’s disease, or splenomegaly.[942] In fact the spleen enlarges under so many conditions that its hypertrophy is an expression of a general infection rather than of any pronounced or particular type of the same. Minor degrees of enlargement have often passed unnoticed or given little or no trouble. When seriously overgrown its principal features are its inconvenience, weight, and size. The condition is recognized by its characteristic shape and notch (See above.) By its extension upward it can be usually distinguished from a tumor, of the kidney.
Every splenic enlargement, especially chronic, should lead to a careful blood examination, by which, among other things, malaria may be recognized or excluded, while the degree and form of leukemia, if present, may be estimated. The lymph nodes throughout the body should also be carefully examined. Splenomyelogenous leukemia, for example, is progressive, severe, and marked by cachexia and anemia of peculiar type. In many of these cases there is a tendency to hemorrhage, both from surfaces and into the tissues. The hemoglobin is much reduced and prognosis after any operation is unfavorable. (See chapters on the Blood and the Lymphatic System.)
Banti’s disease, or splenomegaly, seems also a somewhat peculiar type of lesion which is probably due to an infection proceeding from the intestinal canal, and involving the liver in its later course. In its last stage there is a tendency to hepatic cirrhosis, with ascites, and hemorrhages in any part of the body are frequent.
Removal of the spleen for any of these conditions is usually a precarious procedure. It has been more successful when performed for malarial hypertrophy than for other conditions, the patient’s chances being then about three out of four; but here, too, the lesion is usually amenable to other treatment. If done in the early stages of Banti’s disease it would seem to be strongly indicated, but not in the later stages, when the liver is involved and the abdomen full of fluid. In the leukemias it has succeeded in a few instances. It is mostly indicated in those cases where hemorrhages occur early.
The Röntgen rays have recently been shown to have an excellent effect in many of these cases and are worthy of trial. Especially in the leukemic forms, in connection with arsenic internally, they offer probably the best prospects.
While, under ordinary circumstances, the supports of the spleen may seem equal to ordinary needs they prove insufficient in many cases of marked enlargement. Hence results displacement, or the so-called “wandering spleen,” which may be due to the results of injury, to tight lacing, possibly to congenital relaxation of ligaments, but mainly to hypertrophy, with increase in size and weight. When the spleen enlarges it descends toward the umbilicus, but it has even been found in the pelvis. As it prolapses it brings down with it the stomach and the pancreas, thus interfering with the circulation of all three organs and producing a train of distressing secondary consequences. A long-drawn-out splenic ligament may be much stretched and may even become finally twisted, thus causing gangrene of the spleen from torsion of its support. Moderate displacement and stretching produce discomfort, pain, and disturbance of function. Such a displaced spleen is to be recognized by its shape, size, and notch, and is occasionally to be distinguished from a wandering kidney. When displaced its normal location will not be dull upon percussion.
—Palliative treatment, which may be tried first, calls for whatever drugs may be needed to unload the bowels, but especially for rest in bed and support by suitable abdominal binder, with or without a pad. If the spleen itself be much enlarged it may also be subjected with a judicious frequency to the x-rays.
Operative help, which is the only measure when other treatment fails, should come either through a splenopexy or splenectomy, preferably the former, save in the presence of serious disease which may call for its extirpation. Nevertheless splenopexy, which seems so simple and so promising, is often unsatisfactory because of the friability of the spleen itself and the weakness of its capsule. Here, as in hepatopexy, the intent is to produce adhesions, by scarification of the external peritoneal surroundings, which is made through a suitable incision, directed usually along the left costal border; after thus intentionally provoking adhesions, sutures may be used if there be any prospect of their being serviceable.
PLATE LVI
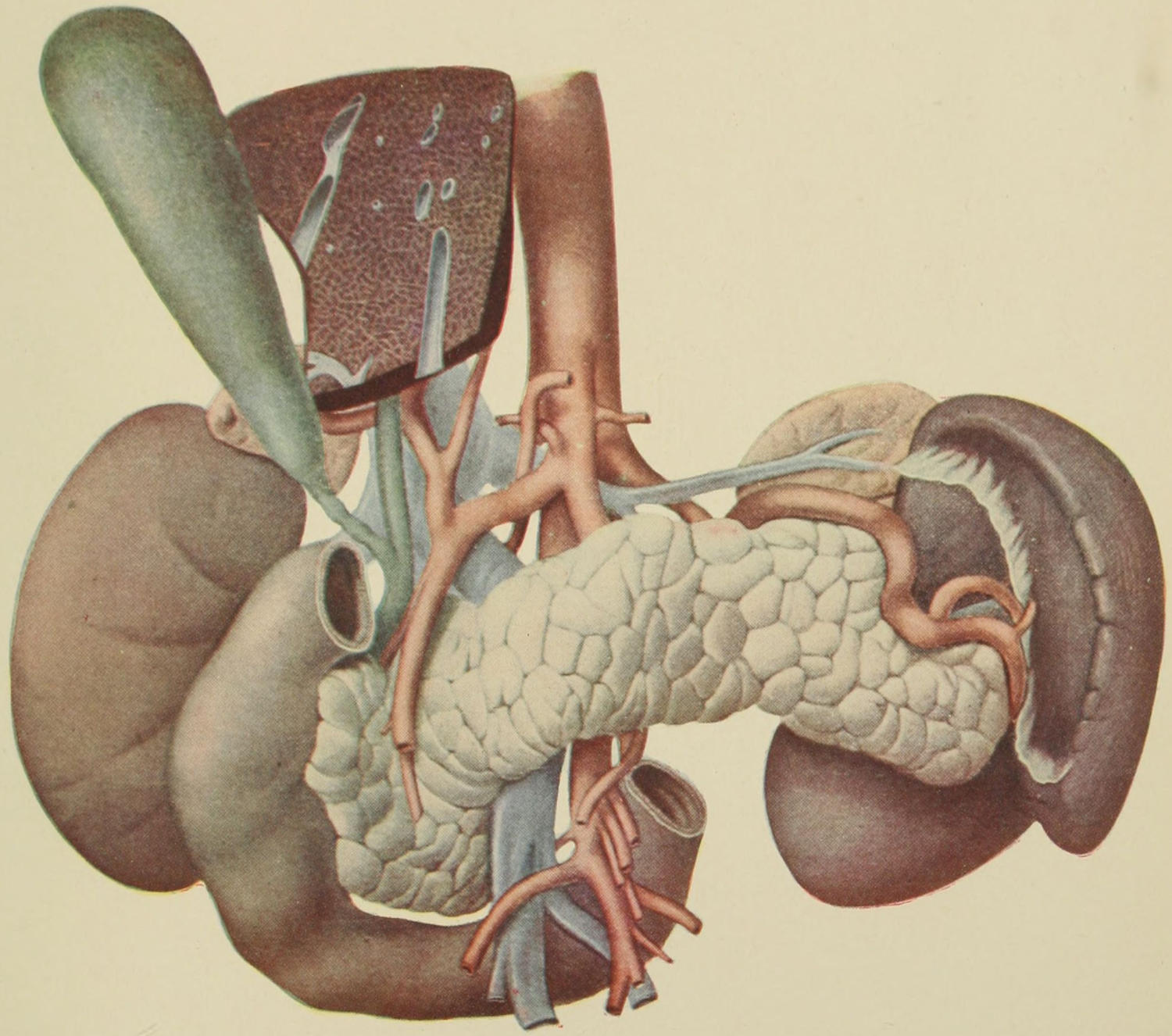
Upper Abdominal Viscera, showing their Normal Relations. (Sobotta.)
[943]
Splenic cysts of the serous or blood type are seldom seen. Even hydatids here are uncommon. Sarcoma of the spleen may be primary; carcinoma is due to extension or metastasis. In proportion as splenic tumors develop they may be recognized as involving this particular organ. While a careful blood examination may permit the exclusion of certain conditions, exact early diagnosis will scarcely be made without exploration, which is justifiable whenever the blood count would indicate it. After exposing the lesion the surgeon is for the first time in a position to judge whether to drain or extirpate a cyst, or remove part or the whole of the spleen itself.
Besides those operations addressed toward fixation of a more or less enlarged or wandering spleen a splenotomy can be made—i. e., incision and drainage at any suitable point, anterior or posterior, which can be satisfactorily exposed; and evacuation of fluid may be followed, with or without suture of the deep to the external wound, by gauze packing or tubage, combined, if necessary, with counteropening or posterior drainage.
—Total removal of the spleen is performed through an incision which should be made ample for the purpose, either along the costal border or the left semilunar line or by combination of both. A median incision may be also utilized if it will permit better access. Splenectomy, under ordinary circumstances, would not be a difficult operation, but with the organ enormously enlarged and the vessels dilated, as they may be, it becomes usually a formidable procedure. The most serious difficulty and danger arise from the numerous adventitious vessels which may connect the spleen with the diaphragm or with some of its other surroundings, and whose location is to be made out before an attempt is made to remove it. Thus, in one instance, I have seen an adventitious vein, the size of the little finger, between the upper splenic surface and the diaphragm. Through such large vessels torrents of blood will pour unless they be first secured. All such connections then with the stomach and the diaphragm have to be ligated and separated with great care, while gentleness of manipulation is requisite throughout the operation. The spleen may be reached and adhesions be located with great speed of manipulation, but in the depths of such a wound valuable time may be consumed and much blood lost, all at a time when the patient can least tolerate them. Oozing from vessels which cannot be secured should be checked by gauze packing.
The anatomical features of the pancreas which have most interest for the surgeon are the facts that its head is in contact with the duodenum, and lies usually so closely against the second portion of the former as to surround from one-fourth to one-third of its lumen. Becoming adherent at this point it may then produce obstruction high up in the intestine. In rare instances it may even completely surround the duodenum, and thus may, when swollen, cause tight constriction of the latter. Should this condition be met with a gastro-enterostomy would be the proper measure for relief. These intimate relationships account for the spread of disease from the pancreas to the intestine, rarely in the reverse direction. The pancreas lies also in contact with the stomach along its anterior peritoneum-covered surface, and malignant disease travels easily from one to the other. Ulcers of the stomach, favorably situated, may also be followed by adhesion and inflammatory infiltration of the pancreas, by which the viscera are cemented together, the same result following duodenal ulcer, as well as serious disease about the biliary passages. Thus under a variety of circumstances the operator may find these parts so cemented as to be separated only with the greatest difficulty, or perhaps not at all, without causing laceration or rupture of one or more of them, with escape of contents which are often septic. Therefore when there is reason to fear this accident it will usually be safer to simply make a gastro-enterostomy. (See Plate LVI.)
[944]
The relations of the biliary ducts to the pancreas are most important, the association of the common duct with that of Wirsung having the greatest bearing upon a variety of conditions, which are nearly all essentially surgical. The former, descending along the head of the pancreas, comes in contact with the duct of the latter, and passes alongside of it for a short distance before entering the intestinal wall. In about two-thirds of individuals it is completely enclosed by the pancreas. In the other third it lies in a deep groove upon it. Resting here, as it were like Siamese twins, it will be easily seen how disturbance in one duct or its source may be reflected to the other. When the common duct lies in a groove it is less likely to be seriously compressed by pancreatic engorgement than when actually embedded in pancreatic tissue. The degree of resulting jaundice may thus be dependent upon anatomical conditions not determinable before exploration. Such pressure doubtless accounts for many cases of so-called catarrhal jaundice. When the condition becomes constant, or nearly so, a chronic interstitial pancreatitis may be assumed, which really warrants an operation—i. e., cholecystostomy with drainage. When a gallstone is passing through the common duct, especially when lingering or impacted, it may have in turn reversed this condition, and, by obstructing the pancreatic duct, set up as a consequence pancreatic stagnation and consequent digestive disturbance, and such other internal conditions as invite infection from the duodenal cavity, with a more or less lively pancreatitis, perhaps even of fulminating type, by which life may be jeopardized.
The pancreas, however, being usually provided with two ducts, the second (that of Santorini) is often represented as an additional safeguard, since it usually has a separate opening into the duodenum below the ampulla. Opie carefully studied 100 cadavers and found that in more than 50 of them the accessory duct could be of no use or relief, and that in only 10 instances did two independent ducts enter the intestine, while in the other 90 they were united, and in 21 of the latter the accessory duct had become obliterated. Moreover, in only 6 of the 100 instances was it larger than the duct of Wirsung. This will show, then, how little reliance may be placed upon the duct of Santorini. Moreover, no matter which duct is opened, or whether both are, so long as pancreatic fluid can escape there is an open channel for infection, and when it cannot escape it may be seen that infection has already occurred and is manifesting its pressure consequences. Chemosis of mucous membrane may be the first mechanical result of such infection, but this is sure to be followed by interstitial sclerosing and compressing effects.
The normal duct opening in the duodenum is also a matter of surgical interest. The ampulla of Vater, within the second portion of the duodenum, is usually described as a conical protrusion or papilla, having an average length of 4 Mm., with an opening 2.5 Mm. in diameter, this being the narrowest portion of the common duct, but from this arrangement there are many variations. The ducts may join at some distance from the intestine, or they may open independently into a depression or into a protrusion, and the ampulla be thus totally wanting, all of which has the greatest possible bearing upon what may happen during the passage of gallstones, for instance, or by infection and according to its direction; and may account for the difficulty met in certain cases, as when, for example, it becomes necessary to incise the duodenum and open the ampulla for the removal of a pancreatic or biliary calculus. It will emphasize, too, the necessity for always exploring the common duct by opening the biliary passage and thus making sure of its patency.
Congenital anomalies include not only those of the ducts above mentioned, but the presence of accessory masses, like the accessory thyroids, which may occasionally lead to confusion and perplexity. Furthermore, accessory nodules of pancreatic tissue may be found alongside the ducts, or even in the walls of the stomach and intestine, where they are probably present more often than is generally appreciated, and are to be explained by the embryology of the parts, since the pancreas is known to take origin from a cluster of cells in the wall of the upper end of the developing intestinal canal. They have been seen also along the line of a persistent vitelline duct. Such small accessories, when present, usually empty by minute independent ducts into the intestine. On the same embryonal grounds are to be explained other anomalies occasionally met, such as[945] separation into detached portions. The existence of accessory pancreatic glands is also held to account for the absence of glycosuria in certain cases where the principal portion of the pancreas is itself extensively diseased.
Glycosuria is so associated with the popular conception of pancreatic disease that it seems imperative to state what importance should be attached to it. It is now clearly established that the so-called “islands of Langerhans” have to do with the elaboration of a certain glycolytic ferment, and that the failure in its supply to the blood (it being regarded as an internal secretion) is followed by the appearance of sugar in the urine. These islands are not connected with the ducts, at least not in the vertebrates, and usually escape pressure effects in chronic interstitial pancreatitis of the interacinous as well as of the interlobular form. This explains the accompaniment of diabetes in some instances of pancreatic disease and its absence in others. Again, if only part of the pancreas be affected, as in cancer, the remaining healthy portion may still afford a sufficient amount of this ferment to supply the body needs.
The uncertain symptomatology of the slower forms of pancreatic disease is to be accounted for by the fact that, with the exception of its glycogenic function just mentioned, all its other functions may be vicariously assumed by other organs of the body. Thus as a compound racemose gland it furnishes—
The first of these functions may to some extent at least be assumed by the stomach and the others by the bile and intestinal juices. (Mayo Robson.)
Injuries to the pancreas may occur with or without external traumatisms. By any kind of injury which affects the gland it is probable that its glandular structure may be so disrupted as to set free an autodestructive secretion, which, by softening and weakening vascular walls, may lead to hemorrhage and to the accumulation of a collection of inflammable material, which is a good culture medium, and which needs only the spark of infection to be easily aroused into a conflagration. That possibility of infection is imminent is apparent from the relations of the adjoining viscera and their ducts, as already outlined. However, the same is true of even a first and spontaneous hemorrhage, as of the clot, however produced. It has been held that the manipulations to which the pancreas has been unavoidably submitted during many operations may lead to its acute inflammation or destruction. On the other hand, there seems no doubt but that it is sometimes much relieved or benefited by a mild massage as a part of the operative procedure. Mayo Robson has suggested that concretions may thus be pushed along or adhesions removed, or, as it seems to me, circulatory equilibrium restored and autonutrition improved.
Aside from the injuries which the pancreas may receive during operations it is unquestionably the site of hemorrhages produced by contusions of the abdomen, although these are rare, and of injuries produced by deeply penetrating wounds, especially those caused by a stab or gunshot. The immediate result of a serious wound might be hemorrhage, perhaps even a large escape of blood filling the lesser cavity of the peritoneum. Such injuries are always to be treated surgically, as any external contusion followed by serious collapse and evidences of internal hemorrhage should be promptly explored, and, even more so, every case of penetrating wound. Should blood be found to be escaping from the pancreas the bleeding vessel may be sought and secured, or, if necessary, a portion of the organ extirpated, since no danger can be greater than that of uncontrolled bleeding. It is on record that through an extensive gash in the abdomen the pancreas has not only been exposed, but has partially escaped, and one case report, apparently authentic, details its subsequent sloughing and spontaneous separation.
[946]
Any wound of the pancreas which needs no further attention may at least be sutured if it can be exposed. Nearly all surgical attacks upon this viscus will require extensive incision and more or less emptying of the upper abdominal cavity. It may now be of great assistance to place the patient in the semi-upright position in order that the viscera may gravitate toward the lower part of the abdomen—i. e., to reverse the ordinary Trendelenburg position.
These diseases include especially the acute infections, the chronic lesions, and the occurrence of neoplasms or calculi.
Certain local and general conditions predispose to pancreatic disease of any type. Among them are to be reckoned—
The principal exciting causes are the various infections which may proceed from the blood, as in pyemia or syphilis, or from the alimentary canal, which is never free from bacteria, either by adhesions and continuity, as from gastric ulcer and cancer, or by those natural passage-ways, the ducts.
When summed up the most common of all the causes of pancreatic disease, acute or chronic, will be found to be cholelithiasis, with some of its variant consequences or complications. This will help to make clear the reason for operating on the biliary passages in most cases of pancreatic disease, especially the more chronic forms. A stone impacted in any portion of the common duct, especially in its terminal portion, after it has come into relation with the duct of Wirsung, may cause an amount of disturbance disproportionate to its size. Moreover, a stone impacted at the orifice of the duct will permit the entrance of bile into the pancreatic canal, where it does not belong, and where of itself it may cause trouble.
These include—
—Acute pancreatitis is a distinct form of disease, like appendicitis, with an etiology and symptomatology of its own, which has been recognized only within the past twenty-five years. This statement will account for the fact that so little reference to it is made in any but the recent text-books. In fact it is to the writings of Fitz, of some fifteen years ago, that the world owes its first keen interest in the subject. By no means a frequent disease, it nevertheless occurs with frequency sufficient to make it inexcusable for the practitioner to fail to take it into consideration, although he may waver in diagnosis.
The predisposition to infection which previous injuries, especially minute hemorrhages or previous pathological conditions, seem to afford has been already mentioned, and a history of previous injury or digestive disturbances will aid in diagnosis. The[947] exciting cause is, however, in nearly every case when not distinctly traumatic, connected with previous disease in the biliary tract, either cholelithiasis or cholangitis. Reference to what has been said above, and a consideration of the anatomical relations, will show how readily an infectious process can travel upward from the duodenum into the pancreatic duct, as well as into the common duct; or how, passing down the latter, it may speedily find its way up the former. The previous condition of the tissues, and the activity or virulence of the infective organisms, have to do with the degree of acuteness of the resulting pancreatitis. This is sometimes of such overwhelming toxicity that the entire gland dies almost as does the appendix, within a few hours, the result being an acute necrotic condition that of itself is necessarily fatal.
Symptoms.
—Acute pancreatitis gives rise to symptoms which, in general, assume the clinical form of an acute peritonitis of the upper abdomen. It commences with sharp pain in the epigastrium, accompanied by faintness, nausea, vomiting, and collapse, while tenderness over the pancreas is an early symptom, and swelling or enlargement can sometimes be detected. Constipation is so frequently a feature that the diagnosis of acute bowel obstruction is sometimes made, but it will be found that obstruction is not complete, for flatus may pass and enemas may be successful. The pain becomes paroxysmal, is increased by movement and pressure, while the tenderness becomes more localized. Meteorism may so quickly succeed the other symptoms as to make physical signs uncertain, while rigidity of the abdominal muscles makes them still more vague, yet affording in itself a sign of value. Vomiting intensifies the pain and the vomitus changes from food to bile, and then to blood, which is dark and altered. Hence jaundice may be an early feature, in which case it becomes more marked as the disease progresses, and may become intense. This is likely to be the case if the exciting cause prove to be a stone impacted at the ampulla. The face indicates profound distress and disturbance. The temperature affords no certain indication, save that in the most serious cases it may be subnormal. On the other hand, as the case progresses, the pulse becomes small and rapid. Every expression of overwhelming toxemia is added, and delirium usually precedes death. In fact death may follow the first expression of pain, in unrelieved cases, in from two to three days. Other less acute expressions of the same general character are met with in the so-called subacute forms of pancreatitis.
While the postmortem findings differ in various instances the symptoms above noted do not vary conspicuously. They differ rather in intensity only, in accordance with the gravity of the case.
The pathologists have described various forms of pancreatitis as the hemorrhagic, the gangrenous, the suppurative, and those distinguished by fat necrosis, as well of the omentum as of the pancreas itself. These distinctions have the greatest interest for those engaged in minute research and are not to be regarded lightly. They have no small interest for the clinician, since prognosis is in some measure dependent upon them. Nevertheless the symptoms of the condition are but slightly modified, whether the destructive process assume one or the other of these types, and the therapeutic indication is the same for all—namely, the earliest possible operation.
If pathologists were better agreed on their pathology it might be worth while to give more space here to this aspect of the subject. It is, however, not yet certain, for instance, whether in a given case inflammation precedes hemorrhage, or whether hemorrhage occurs first and the outpour of blood is suddenly invaded by bacteria. In fact it is probable that sometimes one thing occurs and sometimes the other. Certain it is that the pancreas is not only loosely held together, and consequently disrupts easily, but that it quickly succumbs both to its own digestive juices and the disintegrating effect of bacteria, so that putrefaction quickly occurs hours before life is extinct. The morbid excitement quickly spreads to the adjoining peritoneum, and along it, so that a more or less generalized peritonitis soon complicates the case. Mayo Robson inclines to the view that in the most fulminating cases the hemorrhage is the prior lesion.
Diagnosis.
—The diagnosis should be made mainly from perforating gastric or duodenal ulcer; phlegmonous or gangrenous cholecystitis or cholangitis; rupture of the biliary tract, with escape of contents; fulminating appendicitis; acute intestinal obstruction, including internal hernias, and acute mesenteric thrombosis or embolism. Fortunately in every one of these conditions prompt operative intervention is alike demanded, save possibly in the last named; while even in the latter diagnosis cannot be made without it, and it may still be possible to accomplish something if the occlusion be not too widespread.[948] A history of previous “dyspepsia” or “indigestion” may point to the stomach or the biliary channels; repeated hemorrhages to gastric ulcer, and repeated attacks of pain to gallstone trouble. General tympanitis would indicate intestinal obstruction, especially if no flatus were passed, while when limited to the upper abdomen it would be more suggestive of pancreatic disease. This would be corroborated by vomiting of blood, while fecal vomiting would indicate obstruction. Tenderness and tumor located in the region of the gall-bladder would point rather to it as the source of trouble, while in pancreatitis something distinctive may be perhaps made out by palpation and percussion, and the tenderness will be complained of alike on each side of the middle line. Abdominal rigidity, while general, is usually most pronounced near the site of the most important lesion. Much importance is attached by Halsted to excessive pain, and to cyanosis of both the face and the abdomen. The latter may be helpful as a corroborative indication, but is certainly not always present, and, on the other hand, is seen in many cases of general peritonitis. Glycosuria is rarely a feature of the acute cases.
Treatment.
—This is of necessity not only surgical, but, to be effective, should be prompt, every added hour of delay causing increased danger. While arranging for this it is possibly justifiable to allay pain by giving morphine hypodermically. The colon should be emptied by a copious enema. Collapse is to be combated by the usual means, including hypodermoclysis or infusion, perhaps with the addition of a little adrenalin to the saline solution. The preparation of the patient, both before and during anesthesia, should include the same scrubbing of and attention to the skin of the back as that of the abdomen, as there is much probability in any such case that posterior drainage will be needed.
The operation is begun as an exploration, through a median incision above the umbilicus, some three inches in length, through which the operator may inform himself as to the state of affairs within the abdomen. Should fat necrosis be revealed, and first noticed in the omentum, no doubt need be felt as to diagnosis. Any tumefaction by which the stomach or colon is displaced, or the gastrocolic omentum placed upon the stretch, calls for further and deeper exploration. The upper abdomen should next be walled off with gauze and a small rent made through the gastrocolic omentum; or it may in rare instances prove wiser to push down an already depressed stomach, or more likely to lift up the greater omentum and enter the lesser peritoneal cavity through the mesocolon. In the majority of instances the condition can be best appreciated and relieved by separating the stomach from the colon.
The condition may be one of extensive fat necrosis, disseminated, but with its most abundant expressions in the neighborhood of the pancreas, or there may be found evidence of extensive gangrene, the pancreas itself sloughing and involved past any possibility of repair, surrounded by disintegrating clot and debris; or there may be found a more or less localized abscess, and perhaps evidences of putrefaction. In at least two instances reported by Muspratt and Porter the pancreas itself was not yet dead, but was so darkly discolored and swollen, as well as so dense, that it was freely incised, the bleeding vessels being tied and the clot removed. Both of these cases recovered. Such incisions, if made in the gland, should always run parallel with the duct and not across it. Whether pus be found or not will depend in large degree upon the time that has elapsed since trouble began. It is most desirable to expose the focus before pus has had time to form, just as it is in acute appendicular disease.
The further operative treatment consists essentially in checking and preventing hemorrhage, in removing all sloughing tissue which can be safely taken away (and this may involve the greater part of the entire gland), in disinfection of the cavity and general toilet of the upper abdomen, with ample provision for drainage. This may be anterior or posterior, and in bad cases should be both, unless procedure is hastened by collapse. Posterior drainage is effected by having the patient turned upon the right side, then making an incision 3 or 4 Cm. long at the left costospinal angle, where, if the advice above given have been followed, the skin will have already been prepared. Here the outer border of the erector spinæ group of muscles is quickly exposed and the blades of a pair of stout forceps entered and pushed toward the inner cavity, within which the operator’s left hand is acting as a guide. In this way it is possible to quickly insinuate the blades so that the large vessels and the upper end of the kidney are preserved from harm. A suitably prepared drain, preferably tubular, may then be introduced deeply enough through the anterior wound to be seized by the forceps and pulled through[949] the tunnel made by their introduction. It is thus drawn backward and outward to such an extent that its inner end shall rest just where it is desired in the cavity of the lesser peritoneum, the unnecessary external part of the drain being now cut away. The whole procedure consumes but little time. Anterior drainage will also be necessary, and the wound may then be closed.
It has been suggested to make the exploration as well as the drainage from the loin, but this procedure cannot be here advised, since it leaves too many features in doubt and affords insufficient means whereby to appreciate and cope with many grave complications. Calculi, either biliary or pancreatic, which are so often an exciting cause of these troubles, should be carefully sought for and removed if present. They could not be revealed nor removed through any small posterior opening. Other good reasons are also advanced, since the intensity of the symptoms is an expression of an intraperitoneal rather than retroperitoneal lesion.
The reader will note that but little has been said as to the distinction between the hemorrhagic, gangrenous, and other forms of acute pancreatitis, as these are for the surgeon, as such, side issues. His paramount duty is to open the abdomen of every such case, so soon as he can possibly effect arrangements.
—Under this term are included disease processes and lesions similar to or identical with those described as causing acute and even fulminating expressions of pancreatic obstruction, but less severe in their manifestations, less rapid in their course, and more localized in their boundaries. They are often so associated with a protective and natural walling off of the area of excitement by barriers, which outpour of lymph and its consequent condensation into adhesions afford, that they appear more often as abscess of the pancreas or hematoma of the lesser cavity of the peritoneum.
So far as concerns its etiology the causes are essentially the same as in the acute cases, only the results are brought about more slowly, weeks being in these cases as days in the others. Gallstones are by all means the most common cause, and the pancreatic disease is itself an expression of an infection travelling up its duct.
Symptoms.
—The symptoms usually include pain, which, however, lacks the agonizing intensity noted in the more acute cases. Vomiting is usually associated with constipation, but the vomitus is rarely or never bloody; jaundice of variable degree is a common feature, and collapse is rare. Distention of the upper abdomen and tumor formation come on more slowly. Tenderness is less extreme and muscle rigidity less marked. While the pulse is less affected the temperature is usually more so, often running high. Even early in the case we may note general expressions of septic intoxication, such as mild chills and a characteristic appearance of the tongue and face. Constipation is followed by diarrhea; at least the stools which are fetid contain blood, pus, fat cells, and undigested meat fibers. Pain is more or less constant, but increased in paroxysms. Loss of appetite and rapid emaciation are apparent from the outset. Albumin will be found in the urine, but rarely sugar. The peculiar reaction described by Cammidge will, according to Mayo Robson, give uniformly positive evidence. As abscess gradually or rapidly develops it will cause a swelling, which has its origin behind the stomach and may displace this viscus, as well as the colon, upward or downward, presenting usually toward the abdominal wall. In rare instances the direction of least resistance takes it toward one loin or the other, where it may appear as a perirenal abscess, or around the crus of the diaphragm and above the liver, where it would appear as a subphrenic abscess. It has been known also to burrow along the psoas muscle and appear at the groin, or even in the left broad ligament. Abscess of the pancreas may also burst into the stomach, when pus will be vomited, or into the bowel, whence it will be evacuated. A sudden relief, with disappearance of tumor, followed by diarrhea and purulent stools, would indicate this latter termination. Under these circumstances the abscess cavity may repeatedly refill and reëmpty itself. Spontaneous recovery in this way is possible, but septicemia and hectic usually persist until obviated by operation.
Diagnosis.
—The history, the evidently septic type of the case, and the distinct signs above noted will make almost certain the presence of pus, and Mayo Robson insists that the pancreatic reaction in the urine (Cammidge) will make clear its location and origin; but, with or without the latter, the important feature is that there must be a deep collection of pus somewhere in the neighborhood of the pancreas.
[950]
Treatment.
—This is necessarily operative, and in such cases as those now considered there will be plenty of time afforded for all the precautions known to careful surgeons. The aspirator should never be used, at least not until the abdomen has been opened, then usually with caution, lest pus escape along the needle track. The operation is made as described above for the acute form of this disease. The greatest care should be given to protecting the general peritoneal cavity against infection. When adhesions to the anterior abdominal wall are met they should be separated as little as possible, only to such an extent as will permit direct approach to the collection below. Only after the abscess cavity has been thoroughly emptied, disinfected, and packed with gauze should the surgeon proceed to clear away or break down adhesions so as to permit a suitable exploration of the lower surface of the liver and the biliary passages.
And now perhaps comes the necessity for operative attention to these latter, as one or many stones may be recognized in the gall-bladder or the ducts. In this case there must be followed those general directions elsewhere given in regard to the technique of operations upon the gall-bladder and ducts. Biliary drainage will in these cases be nearly always indicated, for which a separate small opening in the usual position may be made, if desirable, as it probably will be, for one wishes usually to continue such drainage for several weeks, whereas it is desirable to have a median incision heal as rapidly as possible. The question of posterior drainage will also be raised. Ordinarily it is of advantage, as the time required for anterior drainage can be materially shortened, the abdominal wound be encouraged to close, and because the natural effect of gravity is thus afforded. Moreover, by it the whole period of confinement to bed may be materially reduced. Therefore, unless the condition of the patient absolutely contra-indicate, it will usually be a wise measure. In a few instances it has been possible to drain a pancreatic abscess by a tube in the common duct, after removal of the stone which has been obstructing either it or the duct of Wirsung.
Chronic affections of the pancreas which interest the surgeon are:
—The interlobular and interacinous forms can both be considered under one heading so far as we are concerned, their symptoms being similar, save that in the former the compressed connective tissue by its presence causes atrophy of true glandular elements, and thus by preventing their function interferes with digestion; while in the interacinous type the proliferations of this same sort of tissue invade the islands of Langerhans, impair their glycolytic secretion or suppress it, and add a glycosuria to those features common to both forms—moreover, their treatment is essentially the same. In the advanced form of either type the pancreas may be reduced in size and somewhat cirrhotic. This chronic affection may be the result of an incomplete recovery from one of the more acute conditions previously described; it may also have its origin in the chronic irritation of the poisons of syphilis, typhoid, alcoholism, and the like; but by far the most common causes are obstruction of the pancreatic duct, either by biliary or pancreatic calculi, cicatricial stenosis, the presence of tumors or the encroachment and erosion of gastric ulcers and cancers. The morbid condition may involve the whole gland or be localized, in the latter case particularly about its head.
Symptoms.
—These should be studied with particular attention to the case history, for a previous record of pain, cramps, chills, fever, jaundice, very slight digestive disturbances, soreness, or local tenderness will be suggestive and valuable if obtainable. As symptoms gradually arrange themselves it will be found that tenderness over the pancreas becomes constant, and is accompanied by at least a mild degree of muscle[951] spasm, that pain increases and is referred more widely, often to the left side or even the scapula, while there may be some fulness in the epigastrium. Dyspepsia and emaciation become more marked. By the time the obstruction of Wirsung’s duct has become complete, perhaps previous to it, fat and undigested muscle fibers will be found in the stools, which are light-colored, bulky, and sometimes contain blood. As pressure effects become more prominent evidences of biliary obstruction, if previously lacking, present themselves; the gall-bladder usually distends; the liver enlarges or may even become cirrhotic from the irritation of pent-up toxic bile. Even the spleen may become enlarged. In the urine sugar will be found in cases of the interacinous type, though usually only at a late date; while bile pigments are usually present and Cammidge’s test may reveal his peculiar pancreatic reaction.
Diagnosis.
—If the peculiar symptoms above rehearsed are present diagnosis is not difficult. In many cases it is not easy to go beyond the point of recognizing that both the pancreas and the biliary tract are at fault, without deciding as to the exact degree of culpability of each. The question of possible cancer arises in almost every one of these instances. Should the ordinary pancreatic reaction in the urine prove all that has been claimed for it, this grave problem can often be settled previous to operation. If the operator satisfies himself by any method short of actual operation that he has to do with cancer of the pancreas, then operation may be considered inadvisable unless for some special reason.
Treatment.
—At least a reasonably long trial will usually be made, in these cases, of medical, hydrotherapeutic, and other non-operative treatment, with little or no benefit. When after appreciation of the condition and intelligent treatment but slight relief accrues, the case may be regarded (as it really is upon its commencement) as surgical. Treatment, then, consists of removal of the obstructing cause by drainage of the biliary passages. The operative procedure will therefore take the form elsewhere described for this purpose. Should deep exploration reveal no calculi it will be well to make sure at least of the patulency of the ducts, by opening the gall-bladder or common duct and exploring with the probe, or possibly even opening the duodenum in order to do the same with the pancreatitic duct. Whether calculi are discovered or otherwise a gentle stripping or massage of the pancreas may be made to advantage. Biliary drainage should then be established, and usually externally.
It has been difficult for the profession to appreciate why and how these measures, which seem to be directed rather to the biliary passages than to the pancreas, have given such brilliantly satisfactory results as are everywhere reported. These are to be accounted for by the facts that the primary cause most often lies in the former rather than the latter, and is thus removed, and that one source of constant irritation—namely, infected bile—is thus done away with, while tension is removed and pancreatic juice again permitted to flow on as it should; that a chronic toxemia (cholemia) is relieved, and that physiological rest is afforded to the affected and disturbed organs. When the operation is thus performed benefit may be expected; even when done late it may be capable of great good.
—In addition to true cysts of the pancreas there have been described so-called “pseudocysts” in the lesser peritoneal cavity, and more or less surrounding the pancreas. They are rarely of congenital origin, but are probably due rather to traumatism than to any other cause. By many they have been likened to ranulas, or the cysts which form in the salivary glands in consequence of obstruction to ducts or their branches. Anything which obstructs any portion of the pancreatic duct may lead to the formation of a retention cyst, the true proliferation cyst—adenomas being practically unknown. That traumatism figures so largely is due to the fact that injury is followed by hemorrhagic extravasation, and this by more or less liquefaction or degeneration, both of contents and of surrounding tissue, with the secondary formation of a cyst whose walls are made of new connective tissue.
A true pancreatic cyst is a retroperitoneal tumor, while pseudocysts are intraperitoneal. In front of the former lie four layers of peritoneum, which may be completely merged together, but through which a passage must be made when opening into it from the[952] front. The etiology of old pancreatic cysts may be completely concealed by the changes which have slowly occurred since their origin. They may be single or multiple, occur in any portion of the gland, and increase even by coalescence. Within some of them, especially those of the duct type, papillomatous excrescences may be found. The more distinctly traumatic cysts occur perhaps oftener near the tail of the pancreas, while into them repeated hemorrhages may take place, and the sac will become quite thick, even exceptionally calcifying in places. These have been described as apoplectic cysts.
Altogether, up to date, at least 150 of these cysts have been subjected to operative intervention.
Pancreatic cysts contain a fluid which may be variously colored or sometimes colorless, which is usually alkaline, and contains fat globules, cholesterin crystals, blood crystals, albumin, and various salts, most of these being evidences of their hemorrhagic origin. The fluid may also contain the specific pancreatic ferments, of which the diastatic is the more common, tryptic ferment being met occasionally, while the fluid may also possess emulsifying properties. In size these cysts vary from minute sacs to enormous collections of fluid.
As such a cyst attains marked size it will displace the adjoining viscera, pushing the diaphragm upward and impeding heart and lung action, obstructing the pylorus and duodenum and causing gastric dilatation, pressing upon the intestines and perhaps even compressing the ureters, thus producing hydronephrosis. Other peculiar pressure effects may be met in particular instances. A sudden increase in size indicates a fresh hemorrhage, which may lead to its rupture and to death from peritonitis. These cysts rarely empty spontaneously into the bowel. Their contents are liable to infection, and thus a cyst may become converted into a large abscess.
Symptoms.
—Symptoms include especially pain, which may have been sudden, but becomes more or less constant, accompanied by a sense of oppression, according to the size and the pressure effects produced in each case. Digestion is always more or less disturbed; this may be attributed to the stomach dilatation, which is itself a sequel of the condition. The stools show little which is significant save that they are occasionally bloody. Undigested muscle fiber would indicate loss of pancreatic function. Other symptoms will vary so much with individual cases that it is not necessary to consider them here.
The physical signs, coupled with a suggestive history, especially one which includes an account of injury, are of the greatest importance in diagnosis. These physical signs will include usually a yellowish tinge of the skin, marked emaciation, dry skin, and the presence of a tumor in the upper abdomen, which is usually centrally placed, but not necessarily so. If the patient has carefully noted the development of his own symptoms it will be found that the enlargement commenced above and usually a little to the left, and developed in other directions from that location. Palpation reveals a smooth, elastic, usually fluctuating tumor, sometimes movable with respiration, rarely pulsating.
It must be remembered that a pancreatic cyst may rise above the stomach, may rest entirely behind it, or may protrude either below it and above the colon or else quite below the colon. Distention of the stomach will afford accurate location, in these respects, upon percussion, while percussion without distention may mislead. A tumor which gives dulness below the stomach and above the colon is extremely suggestive.
Diagnosis.
—Diagnosis by aspiration is inadvisable, even dangerous, for death has followed the introduction even of a needle into such a cyst. Aspiration, then, should be reserved for tumors already exposed through an abdominal incision.
For the purpose of differentiation it will suffice here to remind that tumors of the kidney, as well as hydronephrotic cysts, grow downward and forward from the loin, and can be pushed backward to their proper place unless too large, that they are not accompanied by digestive disturbances, while the urine is usually more or less indicative. A hydronephrotic cyst can scarcely be made to occupy a position between the stomach and the colon and present in the middle line in front. Ovarian cysts rise from the pelvis and will rarely occur in the upper location, save those provided with extremely long pedicles. Hydatid cysts of the liver show a continuity and fixation to that viscus which are usually diagnostic.
Treatment.
—The only treatment for pancreatic cysts is surgical, it remaining with the surgeon to decide as between drainage and extirpation. While it is indisputable[953] that extirpation is the ideal method of dealing with all cysts and tumors, most of these cases are of such long duration that the adhesions contracted between their exteriors and the surrounding viscera are so dense and firm that much greater danger attaches to a radical operation than to one for simple incision and drainage. I have been able in at least one case to completely extirpate such a cyst, but it was one exceedingly favorably situated and surrounded.
Incision and drainage may be effected in one operation or in two sittings, and as between them it must be decided according to the merits of the case. It is undesirable to permit the escape of the contents of these cysts into the abdomen. In some instances, therefore, it would be much better to make a small abdominal incision and through it attach the surface of the cyst to the margins of the parietal peritoneum, reserving the actual opening into the tumor until a day or two later, when it may be expected that firm adhesions will have attached the sutured surfaces. In this way any leakage within the abdomen may be avoided. Care must be exercised, even in such cases, as a large cyst too suddenly emptied may cause sudden displacement of the heart or of other viscera, which would not be to the advantage of the patient. In this case fluid could be withdrawn in portions as desired, or, making a small opening, one could arrange for its gradual escape. On the other hand, there are cases where it would be of great advantage, if the cyst could not be emptied, to so open it as to permit posterior drainage to be made, by which the period of recovery would be much abbreviated.
No case of this kind can be treated without drainage, the explanation being that the cyst being emptied will collapse, its walls coming into more or less close contact with each other, that the presence of drainage material will provoke exudate and the formation of granulation tissue, and that a complete obliteration will thus in time occur—but drainage in the natural direction of gravity as the patient lies upon the back will permit of much more speedy fulfilment of one’s hopes; hence its advantage. Better still, perhaps, would be through-and-through drainage, with such irrigation as might be needed, practised daily, or oftener if necessary.
—While sarcoma and other forms of malignant disease, as well as adenoma of the pancreas, have been described, they require no special consideration here, since the surgeon has so rarely to do with anything of this character save adenocarcinoma of the pancreas. This is a disease of middle or advanced life, more common in males than in females, usually of scirrhous type, and localized, though it may appear in softer forms or be disseminated. It takes its origin from the epithelial cells lining the acini and the ducts. Metastasis is common and direct extension by continuity most easy and frequent. It is made known by its pressure effects rather than by any other important signs or constant features. It has been known to lead to chylous ascites.
It is difficult in many exploratory operations to decide as between a chronic induration or cirrhosis of the pancreas and that due to cancer, and, in fact, in certain cases it may be impossible to clear up the difficulty, leaving it to be solved either by recovery or death in consequence of extension of malignant disease. Thus when operating for biliary obstruction, where the parts are surrounded by adhesions and the organs are only indistinctly palpable, it may be impossible to decide as to the nature of a hard mass felt in the head end of the pancreas, especially when other distinct expressions of cancer are absent.
Cancer of the pancreas is at present a primarily hopeless disease, and is of interest to the surgeon only in that some of the most distressing features which it causes may be temporarily relieved by biliary drainage. The symptoms which will bring such a patient to him will be essentially those of biliary obstruction, perhaps with the accompaniment of glycosuria or the discovery of fat in the feces. Neither of these, however, is an invariable symptom. Diarrhea is but an occasional feature, and colorless stools may be discharged when there is no jaundice. A perfectly painless progressive (bronzing) jaundice, with distention of the gall-bladder, would perhaps more than any other single feature indicate pancreatic cancer. When such a growth has attained a size sufficient to make it discoverable on palpation it might be mistaken for a biliary cancer, from which it would have to be differentiated especially by the movability usually noted in the latter.
The only treatment for pancreatic cancer is operative, and consists in drainage of the gall-bladder, and after a manner elsewhere described in the section on Diseases of the Biliary Passages.
[954]
From the true pancreatic secretions precipitations of mineral salts, combined with organic elements, may occur, just as from the saliva, the latter thus furnishing the salivary calculi elsewhere described, the two varieties having many points of resemblance. Again, calculi, evidently of biliary origin, may be met with in the pancreatic duct. The former consist largely of calcium oxalate, combined with calcium carbonate and phosphate. They may be single or multiple, and vary greatly in size up to that of a robin’s egg. Hypothetical calculi, with consequent duct obstruction, have been held to be responsible for many pancreatic cysts. Thus one may explain cyst formation, even though no calculi be found at the time of operation.
Calculi reposing within the structure of the pancreas have much to do with the acute and subacute, as well as the more chronic types of pancreatitis, the latter when they act alone, the former when to their essential disturbances are added the possibilities of bacterial infection.
When pancreatic calculi produce symptoms they resemble those of cholelithiasis, causing paroxysmal pain, with vomiting, and perhaps transient jaundice. Glycosuria is an occasional feature.
The condition is rarely diagnosticated previous to operation. Should a calculus be met in this location during the progress of any operation it should be removed by an incision made parallel to the duct, with such closure of the wound in the pancreas as can be subsequently effected and with ample drainage of the deep wound, in order that pancreatic fluid may not escape into the peritoneal cavity. If encountered during operation for pancreatic cyst the same advice will apply.
[955]
Recent embryological studies have established the fact, in regard to the kidneys, and given rise to the inference in regard to the other viscera, that the primary cause of congenital variations has much to do with the earliest development of the bloodvessels. The general inclination has been to view the vessels as following the organs. This should be reversed, as we are now learning that organs develop around the bloodvessels, and that so-called congenital variations arise from departures of vascular arrangement from the ordinary types. Without pursuing this subject further it is sufficient to say that, aside from defects of such character that the newborn infant can live but for a few hours or days, those which have most surgical interest mainly comprise variations in number and in size, including every possible combination, from absence of an entire kidney to horseshoe forms, and various anomalies of the ureters including defects and redundancies, double ureters, and the like. While supernumerary renal tissue or kidneys are extremely rare, the presence of supernumerary adrenal tissue in one or both kidneys (even in adjoining organs) is not uncommon. Here it may lead to the development of a distinct form of tumor, hypernephroma, which will be discussed later. The complication of absence of an entire kidney is sufficient to give it actual surgical importance, since it has repeatedly happened that the remaining kidney has been removed for disease, the inference being that its work could be carried on by its fellow, which proved to be lacking. This accident might be prevented by a careful cystoscopic examination. Nevertheless the rarity of this condition permits it to be almost excluded from ordinary consideration. After removal of one kidney the other undergoes compensatory physiological enlargement and does double duty, if indeed this has not already occurred.
Acquired defects may be due to intrinsic or extrinsic causes, e. g., disease within the renal structures or ureters, or lesions in adjoining organs and tissues, producing mechanical or other disturbances. Thus the functionating capacity of one or even both kidneys may be seriously compromised by either internal or external conditions, and it behooves the surgeon to estimate the degree of renal disability or inadequacy before operating upon either of these organs. On the other hand if the disease be confined to one kidney he may feel that it is doing so little good and so much harm that the patient will be really relieved by its removal. Nearly everything, then, depends upon a determination of the precise existing conditions. They should be ascertained by means of the catheter, the cystoscope, the microscope, and by the careful chemical study of the urine. These methods have been developed into a specialty of considerable complexity, but of great practical importance. The surgeon should not fail to employ them. If he is not familiar with the technique he should seek special assistance.
Fig. 632
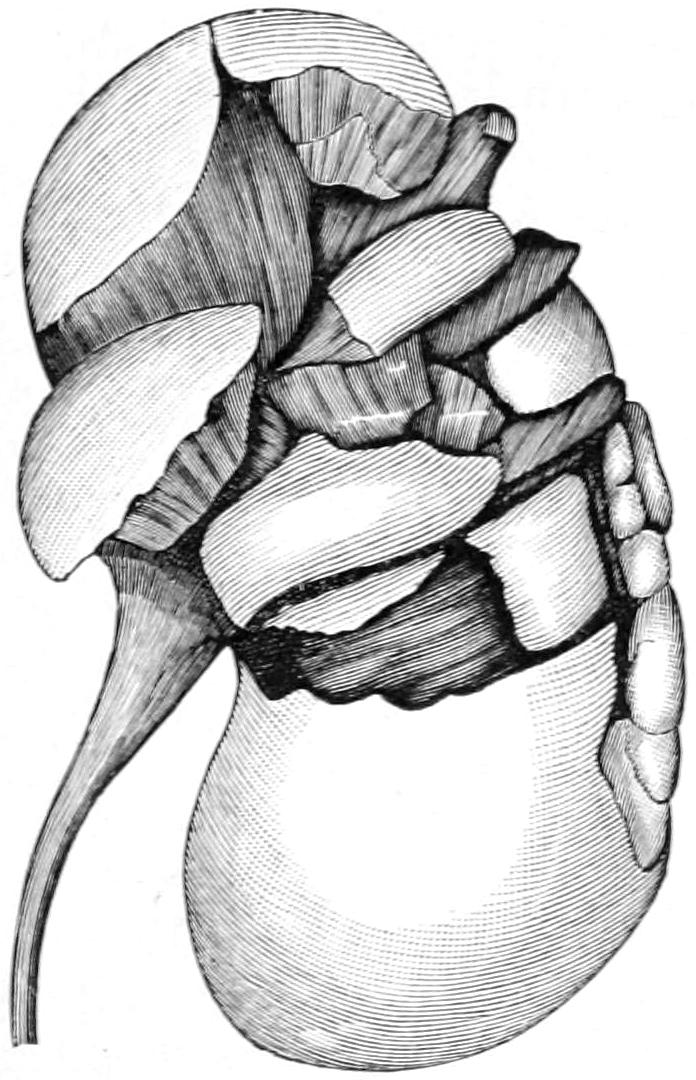
Laceration fragmentation of kidney. (Güterbock.)
Although the kidneys lie in a protected position they are not infrequently injured, both by contusions and by penetrating wounds. From the latter blood will escape externally. In the former it can only extravasate when the cortex and capsule are torn, or escape through the ureter into the bladder, when it will be seen in the urine, which, however, may have to be drawn by the catheter on account of retention. Blood in the urine after a local injury denotes serious mischief inside the kidney or along the urinary tract. If continuing for several hours, but especially if accompanied by local indications, swelling or other evidences of extravasation, by muscle rigidity or by severe pain, with general symptoms, it should be assumed that these fluids are escaping[956] into the perirenal tissues, perhaps into the peritoneal cavity, and that an immediate exploratory operation should be urged. When once this indication is clearly recognized the condition brooks no delay. The same is true of penetrating wounds. On general principles, with a patient in such a condition and showing no improvement, or especially if the reverse, exploration offers the safer course in by far the greater number of cases. The surgeon need only convince himself that such blood as the urine contains does not come from the lower tract, but rather from the kidney or ureter. Exploratory nephrotomy is by itself so harmless that one need never hesitate to urge it. A kidney found slightly lacerated may be repaired with sutures, while one found seriously disorganized should either be sutured and drained or totally removed, as the case may require. There is little room for doubt that it is better to institute such a measure early rather than to permit the dangers and even ravages of infiltration of blood and urine. In fact it may almost be laid down as a precept that every patient who has received an injury in the loin or flank and who repeatedly passes blood in the urine should be explored.
This is a vague term, implying pain or neuralgia in the kidney, and can refer only to symptoms, not to any particular disease. Yet it must be confessed that for certain cases of so-called nephralgia no physical cause is easily discovered. Pain in the kidneys—or, as patients will often say, in the back—may be associated with excess of oxalic and uric acids and salts in the urine, and is then relieved by a steady course of alkaline diuretic treatment, with plenty of fluid, the severe pain being combated with aspirin. Nephralgia may be expected in connection with many renal disorders, but the term should ordinarily be confined to cases of pain without known cause.
When such pain is uncontrollable and intolerable the indication is to make an exploratory operation, by which the kidney should be at least exposed, perhaps delivered upon the external surface of the body, and carefully examined. Its capsule should be split (capsulotomy), as Harrison and others have suggested, and if on palpation or needling (using a needle as a probe) there be any good reason for opening it this may be done, so that with the finger its pelvic cavity may be carefully explored, in order to find any previously unrecognized calculus or other surgical lesion. The mere operation of capsulotomy or capsule splitting has proved of such great value that I always practise this measure upon any kidney which for any reason it may seem wise to expose.
Under this head it is intended to consider (1) acute or subacute specific infections of the upper urinary passages, due to bacteria, with the effects of which we are familiar, i. e., septic, gonorrheal, and tuberculous lesions, and (2) chronic nephrites of irregular or uncertain type, for which operative treatment has been recently proposed.
—Septic infection of the kidney is usually the result of a process ascending from the lower urinary passages, particularly when these are obstructed by calculus, tumor, prostatic enlargement, or ureteral stricture. It may follow catheterism either once or prolonged, especially when done without strict precaution; or the infection may come from the other direction via the blood stream, as in typhoid and various other fevers, the exanthems, and diphtheria. Gonorrhea is a frequent cause, acting insidiously and by a creeping invasion, with the intervention of a rather more abrupt cystitis. Nevertheless when[957] gonorrhea is followed by pyemia and metastatic abscess these form early in both kidneys, and disaster quickly follows. These types of infection spreading upward along the ureters do not spare the pelvis of the kidney, but expend their first violence there. Beyond this they may extend to the renal tissue proper, where they set up a true nephritis, which may prove fatal.
—Clinical symptoms do not vary greatly except in detail. They include fever, chills, and similar expressions of toxemia, with more or less pain in the kidney, down the ureter, and even referred to the ultimate distribution of the nerves sympathetically or anatomically involved, e. g., to the testicle on the same side, often with retraction of the scrotum, and down the thigh. There is a tendency to thamuria (frequency of urination) when the bladder is involved, as it always is sooner or later. Pus and mucus are recognizable in the urine by the naked eye, while a microscopic study of this fluid will reveal, from the character of the cells, the extent and type of the invasion. The tuberculous type will be considered separately. Suffice it to say that in this form, however pure may have been its original type, it becomes sooner or later converted into a mixed septic infection, with which renal abscess is often connected. The gonorrheal type is nowise clinically distinct, so far as the kidneys are concerned, but is to be recognized either by the microscope or by other clinical evidence.
—Such cases as the above may even perplex the surgeon, since they complicate many other surgical conditions. Yet if they go no farther than above described they are to be treated rather by internal methods, i. e., diluents, with hot-air baths, and especially by urotropin, the remedy of greatest value, while such drugs as aspirin, benzosol, sodium benzoate and the like, in moderate doses and at rather short intervals, may be administered to great advantage.
—The conditions above described do not necessarily nor often terminate with resolution. Not infrequently suppuration follows, with resultant abscesses, which may be solitary and possibly large, but are more likely to appear in multiple and perhaps punctate form. Should this condition occur in one kidney alone, it determines probably its ultimate destruction; if in both kidneys, the prognosis is very grave, since later, if not immediately, such a case will succumb to renal failure, due to the extra load put upon the portion still capable of secreting. It is to kidneys thus crippled by acute or subacute infections, with punctate abscess and similar lesions, that in the past the term “surgical kidney” was applied, because such kidneys were seen oftener in surgical than in so-called medical cases.
Brewer has recently called attention to a type of acute hematogenous renal infection, to which he has given an identity of its own. The possibility of renal infection through the blood has been long recognized, but it has been generally supposed to produce bilateral lesions. Of late, however, it has been shown that these may be unilateral, on account of the diminished resistance of one kidney as the result of previous disease or injury, among the former being calculus, renal retention, and floating kidney. While the colon bacilli are most frequently at fault the infection is often of the pyogenic or mixed type. It seems to be more frequent in women than in men. The symptoms are those of an acute infection, often ushered in by a chill, with sudden rise of temperature, sometimes followed by such marked remission as possibly to suggest malaria. The pulse ranges high. Abdominal pain is an almost constant symptom, although it is usually vague and often shifting or referred. Sometimes it will cause such a complaint as to lead to mistaken diagnosis in favor of an acute appendicitis. Occasionally it radiates along the course of the ureter. Tenderness in the costovertebral angle is nearly always present. Muscle rigidity is frequent but inconstant. There is nearly always a leukocytosis, with a percentage of about eighty polynuclears. Frequency of urination may accompany these cases, but they will ordinarily be diagnosticated by physical and urinary examination. The urine will usually contain albumin, perhaps with pus, and occasionally a few red blood cells. Urine obtained from the affected kidney by ureteral catheterization will contain more of these evidences of abscess than that from the other side. Brewer has had far better success in entirely removing the affected kidney than in exposing and simply draining it. He has thus done a great service in demonstrating the possibility of unilateral acute and suppurative disease of the kidney, where diagnosis is most obscure and the clinical picture one of acute general abscess rather than of local affection, showing as well that the more acute cases tend rapidly to terminate fatally unless promptly arrested by complete removal of the affected organ.
[958]
As we consider the above infections, with others yet to be mentioned, it becomes more necessary to appreciate those constituents and characteristics of the urine which have for the surgeon the greatest significance, and those methods of investigation which furnish him the promptest and most satisfactory results.
The following include methods in present use for determining renal capacity and function, i. e., the matters of greatest importance:
1. By cystoscopy, with ureteral catheterization, we determine whether urine is secreted by both kidneys or but one, while the secretion of each kidney may be separately collected and studied. Even this method leaves much to be desired. Though one kidney be actively diseased it may still contain sufficient tissue to make it partly competent for its purpose, and undesirable to remove; or an organ with very defective structure may, nevertheless, yield a certain amount of nearly normal urine. These, then, are aids to determine the character of the morbid process, and the information they furnish is valuable, but not always sufficient.
2. Cryoscopy, based upon the physiochemical law that the freezing point of the solution is proportionate to the number of molecules it contains, i. e., to its molecular concentration, has revealed that the blood of a person with severe kidney lesion freezes at a lower temperature, while the freezing point of his urine would be much higher than in a normal individual, because those materials which should have been excreted in the urine are, on account of impaired renal function, retained in the blood and do not get into the urine. The freezing point of normal urine varies from -0.09° to -2.3° C.; the freezing point of normal blood from -0.55° to -0.57° C. The reasoning employed in the method is sound, but the method itself difficult, requiring special apparatus and experience. Moreover, the limits of the possibility of error are such that this method alone should never be relied on. It is essentially a test of the ability of the kidneys to act as filters, but does not test their serviceability as secretory organs.
3. The phloridzin test is one of the most trustworthy for estimating the secretory function of the kidneys, as it shows how much active working epithelium remains in the organ. It consists in the subcutaneous injection of 0.005 Cc. sterilized phloridzin with an equal quantity of sodium benzoate, to hold the former in solution. The bladder must be emptied just before the injection is given. About an hour after its administration sugar should appear in the urine, if the kidneys are acting normally. If they are to be studied separately, catheterization of the ureters is necessary. The test is, of course, worthless in diabetic subjects. It depends upon the amount of sugar excreted, the time of its appearance, and the duration of its elimination. If no sugar be present the kidneys are seriously affected; if it be delayed, renal insufficiency is present. The average quantity of sugar eliminated during the first half-hour, when the kidneys are normal, is about 0.5 per cent. If the kidneys be diseased, this quantity is reduced by a half, and there is very little more secreted in the first than during the second half-hour. This valuable method is unfortunately difficult of application and requires minutely careful chemical tests.
4. Chromocystoscopy, introduced by Voelcker and Joseph, is perhaps the simplest of all methods of estimating renal capacity. 20 Cc. of a 0.4 per cent. solution of indigo-carmine is injected into the gluteal muscles. In fifteen or twenty minutes, if the kidneys be normal, the cystoscope will reveal dark-blue urine flowing from the ureteral orifices toward the median line, with a peculiar jet at regular intervals of about twenty-five seconds, and lasting for perhaps five seconds. There is both rhythm and force about this ejaculation. If the color be pale, the jet weak, or the rhythm irregular, the intervals prolonged or late, or if no flow whatever occur, there must be hindrance in the secreting and filtering structure of the kidney, or occlusion of the ureter. The results given by indigo-carmine in these cases are superior to those furnished by methylene blue, since it is not so much a solution as a mixture which is formed and ejaculated as such. Moreover, in passing through the body the indigo-carmine undergoes no reduction. By this method there is no necessity for catheterization of the ureter. One needs only to[959] use the cystoscope with reasonable dexterity, and there is no necessity for chemical tests of separate specimens. The method is generally useful in cases where ureteral catheterization is made impossible by growths. It affords an easy means of differentiation, for instance, between ovarian cyst and hydronephrosis.
5. The toxin test is one only to be carried out by the use of animals, since it depends upon the amount of filtered urine required to kill an animal after injection into its veins, the number of cubic centimeters necessary to kill, divided by the weight of the animal, being called the urotoxic co-efficient. It has greater laboratory than clinical interest.
6. Electroconductivity of urine is of value in determining the capacity of the kidney for eliminating inorganic cells. It depends on the resistance offered by the urine to the electric current. It is complicated in method, requires special apparatus, and its results are still of questionable value.
For ordinary purposes the most trustworthy data for the surgeon who is not provided with ample laboratory facilities are afforded by an estimate of the amount passed in twenty-four hours, its specific gravity, its color and acidity, and by the presence or absence of albumin. The test-tube and the microscope then still afford satisfactory means of deciding those matters which the surgeon needs to know. If applied to urine collected separately from each kidney, they may be regarded as trustworthy. If catheterization be impossible, then it is advisable to inspect the ureteral orifices while elimination of indigo-carmine is taking place.
—The significance of blood in the urine is rather that of a symptom than of a disease, although it should be admitted that there are occasional patients who lose blood in this way, more or less frequently, even periodically, without seeming to suffer in the least. Hematuria may also be present as an expression of vicarious menstruation. Again, blood may thus appear in scurvy and similar conditions, especially in tropical climates; in certain of the domestic animals its presence may be due to infection of the kidneys by macroscopic parasites (the so-called “black-water fever” of men and horses). Such cases as these are outside the pale of surgery. Nevertheless general experience has shown that many cases of hematuria, without perceptible changes in the kidney, have been benefited or cured by exploratory nephrotomy. Among the causes ascribed for these so-called “essential hematurias” have been incipient tuberculosis, renal retention from prostatic enlargement, congestion from venous obstruction (due to tight lacing or displacement from any cause), and even the congestion of chronic nephritis.
—When known or recognizable causes are absent, and the ordinary therapeutic agents, the special styptics (cotarnin), and such measures as hypodermoclysis with a 2 per cent. gelatin solution (see Control of Hemorrhage) have failed, an exploration may be advised. It is of the greatest advantage to be certain that but one kidney is involved, or it may be necessary later to operate on the second kidney.
—The various changes included under this head are usually bilateral. The term implies a non-pyogenic infection of the renal bloodvessels, interstitial tissues, and glomeruli or tubules, which produce changes, often spoken of in this country as constituting interstitial parenchymatous or diffuse forms of nephritis, and inducing gross changes which cause the kidney to be spoken of as contracted, large, white, waxy, etc. Discussion of the pathology of these conditions here is out of place. They have all been grouped, most loosely, in common parlance as forms of “Bright’s disease.” Apart from the significance of albuminuria and the many terms implying peculiar features, the apparent hopelessness of many of these conditions, and the disappointment following internal treatment, finally led surgeons to attempt to ascertain what they could accomplish. It was in 1886 that Péan operated on a case of chronic nephritis with nephralgia and removed the kidney. Ten years later Harrison made three nephrotomies, and, though under a wrong diagnosis in each case, it was noticed that the symptoms all cleared up and that albumin disappeared from the urine. About the same time Newman showed that albumin and casts have often appeared in movable kidney, because of torsion of the vessels, and that they disappeared after nephropexy. Then Pousson, in 1899, reported some twenty-five cases of hematuria and nephralgic nephritis, operated upon by nephrotomy and nephropexy, with great benefit. In 1899, Israel was, perhaps, the first to formulate rules for nephrotomy for these conditions. In 1899, also, Ferguson claimed that chronic nephritis should be treated as are inflammations elsewhere, by relief of tension and even drainage.[960] Meantime, Edebohls had been doing partial decapsulation and fixation in cases of so-called unilateral nephritis (the possibility of which is disputed by the best authorities, like Kümmel), and later extended his method to complete decapsulation (capsulectomy), with replacement of the kidney in its fatty bed, claiming that by and through the new adhesions thus produced new and more complete as well as additional blood supply was furnished, and that regeneration of the slightly altered parenchymatous tissue, as well as absorption of exudates, was produced. (Guiteras.) The fact that it seems now well established that these forms of chronic nephritis are always bilateral does not of itself affect the cogency of Edebohls’ reasoning, if it be otherwise correct.
Accurate diagnosis has much to do with this problem. Israel has shown that chronic nephritis is even more difficult of recognition in the living than in the dead, not only after ordinary examination of the capsule, but also after opening into the kidney. Age is not a serious contra-indication, and enlargement of the heart is said frequently to subside after these operations. If cardiac compensation be good operation is permissible, if not otherwise contra-indicated. Edebohls’ method is to anchor the kidney to the muscles of the back, whether it was previously movable or not. Primary healing is desirable, since “nephritics” do not bear suppuration well.
—At present a satisfactory summary is impossible. It is of the first importance that operation should be undertaken early, since to wait until anasarca or other grave conditions supervene is to invite disappointment as the result of a procedure which is by many considered capital. The coincidence of pronounced disease of any other type would be a contra-indication. Bacteriuria, pyuria, etc., would perhaps make it more desirable rather than otherwise. Cases of operative toxemia (postscarlatinal, typhoid) and of cirrhotic type, without other contra-indications, are the most favorable. When a careful examination of the patient and the urine leads the surgeon to think that preparatory treatment may be of advantage, he should find therein almost his only excuse for delay, if operation is to be done. Low hemoglobin percentage should also lead to postponement.
Operation may consist of nephrolysis, or breaking down of adhesions, by which pain is frequently relieved, of decapsulation, of nephrotomy, and, finally, of nephrectomy, in case serious lesions are disclosed. It is doubtful if benefit is due so much to formation of new vessels as to a freer circulation of blood within the kidneys, with their consequent improved opportunity for repair and elimination. Guiteras, for instance, does not believe in total decapsulation, but in partial exposure of a sufficient area on the posterior kidney surface to assist in its fixation, if movable. Otherwise he considers that simple division of the capsule over the convexity will be sufficient. In cases of unilateral nephralgia and hematuria he advises nephrotomy, not so much as an approved therapeutic measure as for exposure, perhaps for revealing the possible existence of deep lesions.
Fig. 633
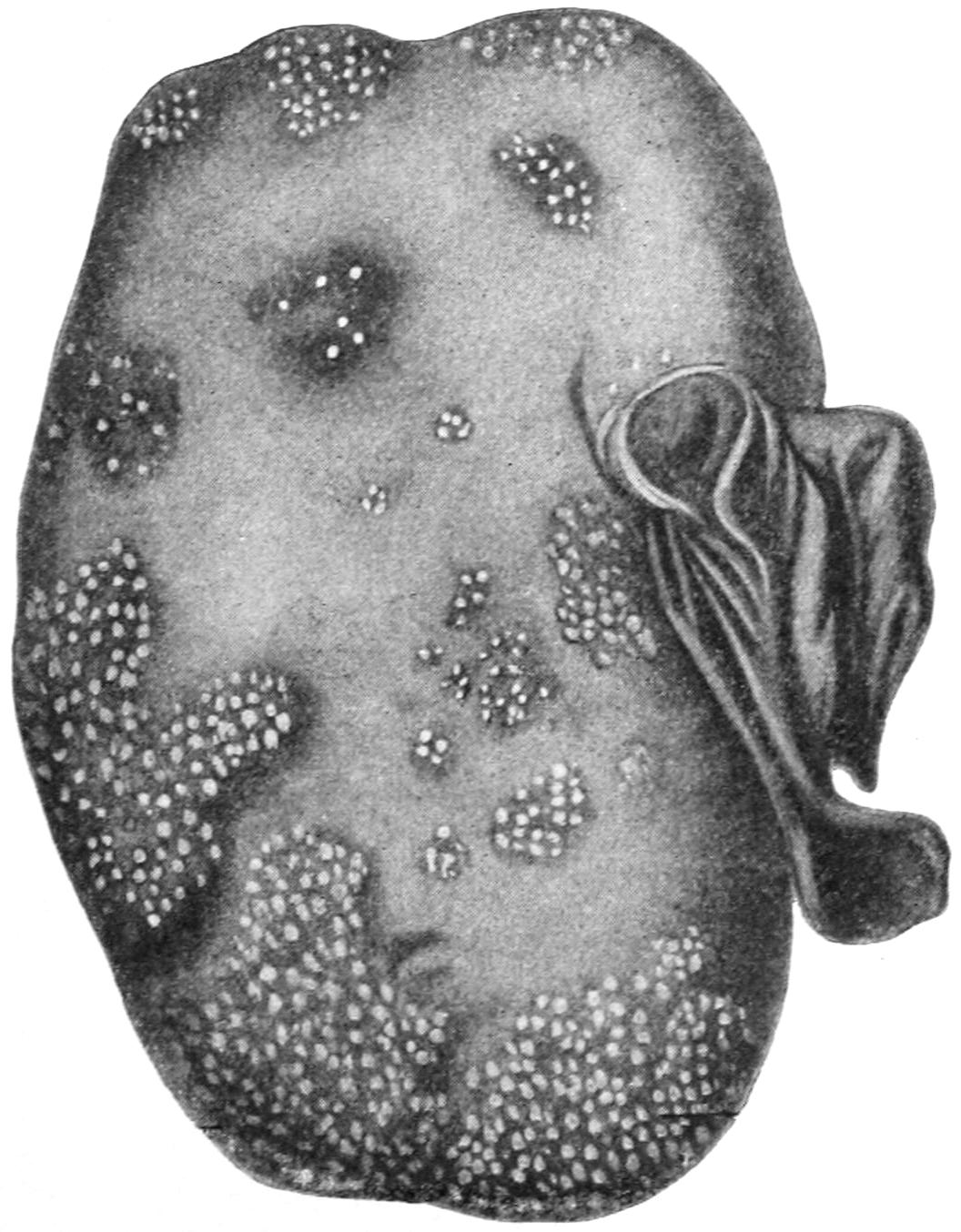
Acute pyelonephritis with multiple miliary abscess formation. (Israel.)
The recent reports from various surgeons concerning the value of renal decapsulation alone are by no means unanimously favorable, although a majority of writers are in favor of exposure of the kidney, capsulotomy and fixation, either by suture or tampon. Still, it does not seem at present justifiable to maintain that decapsulation can be expected to cure diffuse or deep-seated arteriosclerosis or degenerative processes within the kidneys.
[961]
The question of the suitable anesthetic is here one of importance. For reasons set forth earlier in this work, ether should always be avoided. If the operation be one that can be speedily performed, nitrous oxide gas alone may suffice. Otherwise it should be done under chloroform, preceded perhaps with ethyl chloride, or under somnoform.
—As a condition this is to be distinguished from ordinary abscess of the kidney, in that it implies the retention in the renal cavity or pelvis of pus with eventual destruction of kidney tissue. In other words it is an empyema rather than an abscess. It results from septic or tuberculous invasion, plus ureteral obstruction, regardless of the obstructing cause, e. g., calculus, plugs of mucus, stricture, kinking of ureter, or extrinsic tumor causing pressure. Occlusion may be so complete that no urine escapes from the affected kidney, while that from the other is clear, or the phenomenon may be intermittent. There results more or less enlargement and often great dilatation of the diseased kidney. Pus thus retained has been known to be discharged into the intestine or even into the lung. Spontaneous recovery is rare. Aspiration from the back in these cases is proper for diagnostic purposes.
—Pyonephrosis, like any other collection of pus, calls for incision (nephrotomy) and drainage, with removal of any possible foreign body, such as calculus. If the entire kidney be found destroyed, or so compromised as to jeopard its future, a nephrectomy may be done at once, while it may be a secondary measure in cases of permanent urinary fistula following drainage. So, too, if the kidney be found tuberculous, it is better to remove it than to temporize.
—To pus formed in a perirenal phlegmon is given the term perinephritic abscess; this is sometimes due to external or penetrating injuries; sometimes it appears as a primary condition difficult of explanation; but it usually follows inflammation of adjacent structures, such as the kidney itself (tuberculous pyelitis), the liver, the colon, and the appendix. While perinephritis usually terminates by suppuration, spontaneous recovery, with more or less absorption of exudate, is known to occur. These perinephritic collections sometimes attain enormous size, and are then sure to migrate, always along lines of least resistance, which takes them usually downward, either toward the loin or the groin. I once tapped below Poupart’s ligament a collection which exceeded a gallon. These abscesses may also, more rarely, burst into any of the adjoining cavities, and discharge either by the mouth, bowel, or bladder, or even externally.
—In addition to the usual systemic indications of the presence of pus there may be tumor in the lumbar region, sometimes with distinct fluctuation, usually with rigidity of the lumbar and psoas muscles, perhaps even contractions of the thigh muscles which may simulate hip disease. These abscesses have been mistaken for peri-appendical phlegmons. If necessary to establish the presence of pus the exploring syringe may be used, but this is rarely necessary.
—While in the early stages the local application of guaiacol may be of use, every collection of pus thus formed here, as well as elsewhere, needs evacuation and drainage. This latter is to be provided by opening through the loin, in order that gravitation in the dorsal position may be of greatest assistance. A more or less free incision, such as is made for exploring or removing the kidney, will usually be sufficient, but may be combined with a counteropening at any point where the latter would be of advantage. Thus should pus present in the groin an opening should be made both posteriorly and at the point where it appears to be coming toward the surface.
—At no age are the kidneys exempt from tuberculous lesions, although these are more frequent in the earlier years of life. Here as elsewhere they may assume the disseminated miliary type or occur as a solitary focus. The infection may proceed upward from the bladder, or it may be a local expression of a widely diffuse process. In the latter case it has passed beyond the control of the surgeon as such, and calls for general therapeutic measures, judiciously selected and actively maintained. Not a few cases of renal abscess, of pyelonephritis, and even of perinephritic abscess, are due to primary tuberculous lesions.
—About the earliest symptoms that a patient may complain of are thamuria (frequency of urination), with blood or pus in the urine. Even at this early stage the condition is essentially surgical, so the diagnosis should be established. Cryoscopy alone is hardly sufficient, although if the freezing point be studied it should be regarded along[962] with the amount of fluid ingested and the quantity of carbohydrates taken with the food. Ureteral catheterization is valuable, although until it came into vogue we were content to study the cystoscopic appearance and to judge by the ureteral orifices, assuming that if one appear healthy and the other not so operation is indicated.
The question of removal of a totally diseased kidney when the other is more or less affected is one demanding greatest judgment. Some of the more recent operators endeavor to determine this by the cryoscopic test of the urine from the less affected organ. If this stand the test they do not hesitate to remove the one which is totally diseased. Thus it would appear that the ideal method is one of careful study of the urine from each kidney, although it is acknowledged that when the question is still in doubt the associate kidney may be explored before deciding to remove the one most diseased.
—The most frequent and significant symptoms of renal tuberculosis are pain, local and referred; hematuria, polyuria, and pyuria. In young adults suffering from bladder irritability, painless pyuria usually indicates tuberculosis of the bladder, secondary to that of the kidney, this being particularly true when the urine is hyperacid. This urine, if noted, will be found at first faintly cloudy or smoky, while later the admixture of pus becomes more evident. The frequency of micturition (thamuria, pollakiuria), which is frequently noted early, may be due mainly to polyuria; the final test is the discovery of bacilli in the urine. There is another form of thamuria which is associated with tenesmus, constituting the painful cystitis of Guyon, which depends on complications in the bladder itself. A search for bacilli is often disappointing, and tuberculin may be used in the endeavor to make a diagnosis, as well as animal inoculation. Tuberculin might, however, give rise to error were there tuberculous foci elsewhere about the body.
Fig. 634

Tuberculosis of kidney, nodular form. (Israel.)
Renal tuberculosis may run a painless course, or it may be accompanied by a severe renal colic or renal crises, the latter sometimes due to plugging of the ureter with cheesy debris. Pyuria may be masked by hematuria, the latter trifling, apparently spontaneous, and occurring even during repose.
More accurate diagnosis can be rarely made without resort to the cystoscope and catheterization of the ureters. When in the cystoscopic image the ureteral orifice is enlarged, congested, and even hemorrhagic or ulcerated, it may be regarded as evidence of tuberculous disease in the corresponding kidney. Meyer has claimed that in the descending[963] form of tuberculosis the mouth of the ureter is ulcerated, while in the ascending form it is apparently healthy. When both outlets are apparently healthy, and urinalysis indicates renal disease, the case must be one of ascending lesion. Fenwick has described what he calls a “golf-hole ureter,” the orifice being dilated and patulous, and the appearance being to him pathognomonic.
Ureteral catheterization is perhaps less necessary on the suspected side than it is to prove the healthfulness of the kidney on the opposite side. The disease is more common in the female, and usually occurs in early adult life. It is more often a descending than an ascending affection.
Fig. 635
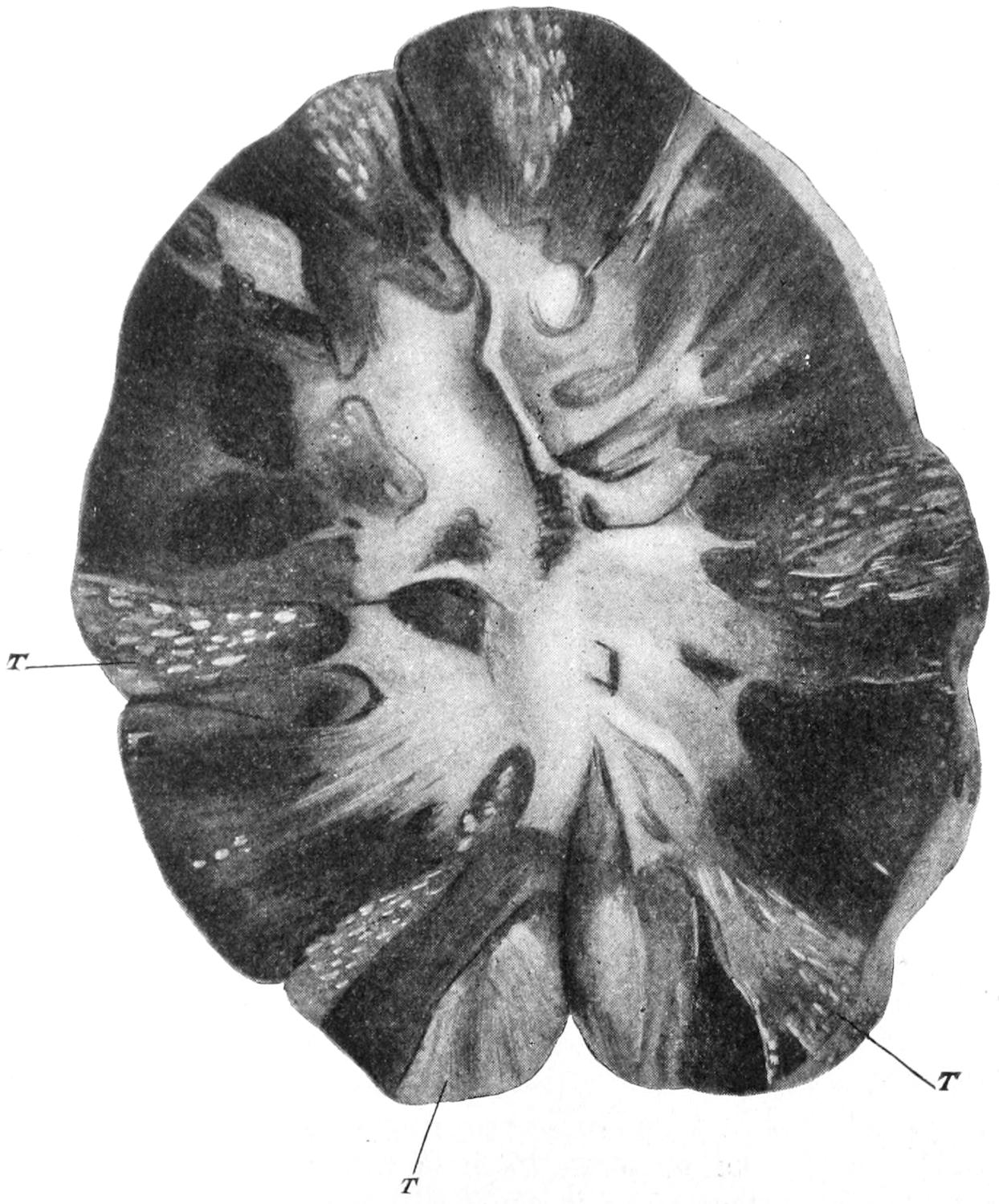
Renal tuberculosis as seen on section. Papillary granulomata seen at T. (Israel.)
Treatment.—Radical treatment of renal tuberculosis is possible only when the lesion is limited to one organ. What shall be done with the kidney involved, when exposed and the disease revealed, may depend to some extent upon the actual degree of involvement. More and more surgeons are agreeing that anything like partial nephrectomy is of questionable value, and that an organ distinctly tuberculous should be removed. In other words, partial nephrectomy is of doubtful merit. Of course, the kidney should be opened before its removal, unless from its exterior it is seen to be hopelessly involved. A further question of great importance is that of involvement of the ureter. With a few associated lesions in the kidney the ureter may easily escape, but with a kidney thoroughly degenerated, and with infected urine or tuberculous debris passing constantly down through the ureter it cannot escape contamination. It is not a difficult procedure, nor does it add to the gravity of the operation, to extend the incision sufficiently to permit not only the delivery of the kidney but the exposure at least of the upper portion of its ureter. In this way the renal pelvis may be opened and the ureter itself examined. When thus involved, and especially if it be determined to sacrifice the kidney, as much of the ureter should be removed with it as can be reached. While theoretical considerations would always require these measures to be combined, many mild tuberculous[964] lesions of the ureter undergo spontaneous retrocession after removal of the diseased kidney from which it has become contaminated.
The incision intended to expose the ureter should begin about a half-inch forward and in front of the lower costal cartilage, parallel with the last rib, and terminate on a level with the anterior superior spine, about one inch toward its inner side. This incision will then be about four inches in length. The use of a pillow is of assistance in the easy performance of this operation. The body should be rolled as far as possible without losing negative pressure upon the abdomen. The more abdominal fat there is present the further over the patient should be rolled; a stout patient should have the hips raised from the table by a cushion, in order that the abdomen may be pendent, while the foot of the table is somewhat elevated and the operator is facing the abdomen. After exposing the fat which is adherent to the peritoneum, and the knife is laid aside, the peritoneum is separated from the abdominal wall until the kidney and the perinephritic fascia are recognized. Then with a short retractor the posterior edge of the wound below the ribs is elevated, after which, under the influence of gravity, the cavity opens widely, the fascia may be torn through, and the kidney exposed and freed. The retractor is then removed, the anterior edge of the wound pressed backward, and the kidney is easily delivered from the abdominal cavity; or if its delivery be impracticable, it may be at least so drawn up that the renal vessels are easily exposed, tied, and divided. After their division care should be given that the weight of the kidney does not drag injuriously upon the ureter. The latter is then cleared of peritoneum, especially to its outer side, by blunt dissection, after which a medium-width Sims speculum, with a long bill, may be passed downward between the peritoneum and the abdominal wall and made to draw the latter upward. Thus an extensive view of the ureter is afforded, while its lower portion may be still further freed toward the base of the broad ligament. By a continuation of this process of separation and exposure it is possible to release the ureter almost to its junction with the bladder, where it is tied, its stump being disinfected with pure carbolic.
—These lesions may be briefly dismissed so far as they pertain to the kidneys. Gummas are rare, renal syphilis being usually of a disseminated type, which should be treated by internal therapy, except when abscess results or when there arises some peculiar surgical complication. Actinomycosis is rare in the kidneys, and is not recognized until the peculiar fungi are found in the urine, or until some granuloma, developing toward the surface, breaks down and discharges its characteristic products.
Renal colic implies severe and often agonizing pain, which follows spasmodic contraction of the renal pelvis and ureter, in the effort to expel an obstructing object from one or the other. It may be produced by calculi, by clots of blood, clumps of pus and debris, by particles of sloughing tissue (as in breaking-down tuberculous or cancerous foci), by extrinsic pressure of various morbid products, or finally by kinking or alternating stricture and dilatation of the ureter. Pain is the constant and significant feature, marked by spasmodic exacerbation. It is usually well localized, and referred along the course of the ureter and the cord to the testicle in the male, with retraction of the scrotum, to the labium in the female, and down the thigh in both sexes. With it there usually occur more or less sympathetic disturbances, such as nausea, with most pronounced local tenderness and sometimes abdominal rigidity.
—Treatment, while palliative during the intensity of the attack, should be later made radical. For the former hot applications, morphine, and chloroform inhalations may be used. It may happen that an almost complete inversion of the patient will be followed by relief. Large does of glycerin, and sometimes of aspirin, will also occasionally prove beneficial. Meantime the case should be carefully studied and a skiagram be taken, in order that one may intelligently advise and carry out whatever indications may be revealed.
[965]
Renal and vesical calculi are the result of the precipitation of material previously held in solution by the urine as it escapes from the tubules, their nuclei or nidi being usually a clump of cells, particles of blood clot or of tissue. They are composed mainly of uric acid, urates or oxalates, less abundantly of phosphates, and rarely of cystin or xanthin. They vary in size from the smallest visible particle to those weighing ounces, and in number from one to hundreds. They occur more often in males, and usually late rather than early in life. They may be found in one or both kidneys. When the latter it may be assumed that some systemic defect underlies their formation. In shape they vary greatly, the small, sharp particles often causing as much pain as do large stones, or even more. Diathetic conditions produce them in some de novo, while in others they result from previous morbid processes.
Small calculi escaping into the bladder cause intense renal colic (see above), and, within the latter, unless they escape through the ureter, as they usually do when small or are not retained behind a large prostate, they increase in size, and become then the common vesical calculi, those with uric acid nuclei. Calculi long present in the kidney usually set up what is known as calculous nephritis or pyelonephritis. It is quite possible, however, for such a concretion to first form within the tubules or at the apex of one of the pyramids, so that it does not fall free into the renal cavity. In such locations it may produce great pain, with hematuria and tenderness, yet not for a long time escape into the renal pelvis. Such a stone may be shown by a good skiagram. Calculi long retained will cause other troubles, whose characteristics will be revealed by careful study of the urine, especially of that drawn from the affected kidney, albuminuria and pyuria often figuring. The symptoms include pain and tenderness, which may be referred; colic, hematuria, and pyuria. Symptoms of less frequency include thamuria (sometimes painful), nausea, and vomiting. The accompanying features include pyonephrosis, tuberculous or movable kidney, or possibly various neoplasms.
—Stone in the ureter may cause symptoms likely to be mistaken for appendicitis, especially when lodged on the brim of the pelvis, or an inflamed appendix may hang over into the pelvis and cause bladder and rectal symptoms, while on palpation through the vagina the tenderness and thickening may be misleading. In such cases the urine offers the surest guide. Acute pancreatitis should hardly be mistaken for renal trouble, as there would be a history of former attacks of indigestion, probably associated with typical gallstone colic, while the location of pain and the presence of pancreatic enlargement would be significant. In pancreatitis, moreover, the urine might show sugar. Renal or ureteral colic is sometimes followed by such reflex paralysis of the bowel, with meteorism and tenesmus, perhaps even with nausea and vomiting, as to suggest intestinal obstruction. Again, the crises of Henoch’s purpura, and of angioneurotic edema, sometimes accompanied by hematuria, may mislead.
Inspection of the entire body will probably reveal purpuric spots or areas of edema.
Finally, x-rays afford very convenient means of diagnosis under many circumstances, although mistakes have occurred from misinterpretation of shadows. Nevertheless, when a well-taken picture shows unmistakable evidence it may be considered as quite reliable.
—In the matter of diagnosis few diseases, as Hunner has shown, present such protean symptoms. Between calculous nephritis and tuberculosis the only positive indication is the discovery of bacilli in the urine or the reproduction of the disease in animals by inoculation. Blood occurs in both, but is more likely to be influenced by exercise in cases of stone. Pus occurs also in both, while pain is unreliable. Palpation shows nothing, unless it may reveal thickening of the ureter in the female as felt through the vagina. In pyelitis the presence of a stone may cause any of these conditions, or it may develop because of them. If trouble have begun soon after an acute infection, or during pregnancy, it is more likely to be a case of infected kidney. When tumor is suspected, urinary examination is the best guide. The sudden occurrence of hemorrhages, with their abrupt cessation, rather favor diagnosis of tumor, as does also the absence of pus. Still the latter may be absent when the ureter is obstructed. Intermittent hydronephrosis is usually due to kinking of the ureter connected with a movable[966] kidney. During the attacks the kidney will be enlarged and misplaced, while blood may appear. With return to place comes subsidence of enlargement, while increase in the amount of urine is characteristic. Idiopathic hematuria or “renal epistaxis” is sometimes connected with the chronic interstitial forms of nephritis. The urine shows blood, if dealing with renal calculus, and bile if with biliary calculus. In the former pain is more likely to radiate down the ureter, while in the latter it is upward and backward. In biliary trouble the gall-bladder may be enlarged and movable or even pendulous. Kelly has suggested a method of differential diagnosis by catheterizing the ureter, and forcibly injecting into the pelvis of the kidney a bland, sterile solution. If the pain which it produces be identified by the patient as the same which is usually suffered it may be regarded as diagnostic; if somewhat different, then the actual attacks are more likely to be biliary. A normal renal pelvis should hold about 7 to 8 Cc. before the patient begins to complain.
—In the milder cases, and those where small concretions are repeatedly passed, medicinal treatment may be given a trial. While the alkalies, especially the lithium preparations, have repute in certain quarters, there is probably nothing superior to piperazin in its power of dissolving small uric calculi. Its physical properties and its expensiveness, however, make it disadvantageous to use. It is so sparingly soluble that part of the benefit obtained from it may be due to the volume of fluid ingested with it, and to the consequent dissolving and washing down of small particles. Glycerin is also an analgesic here, as in biliary calculi, and a half-ounce, administered every two or three hours, will often give relief. Attention to the diet is also necessary, especially in acute and uric acid patients.
When there is reason to believe that the kidney contains a calculus which cannot be passed, and especially when an x-ray picture reveals such a condition, then surgical treatment alone offers prospect of complete relief. This includes nephrotomy and what has been named nephrolithotomy, i. e., exposure and opening of the kidney and removal of its contained concretions. When these are easily felt the procedure is simple. However when only a small concretion has been shown in the skiagram, and it is not easily palpable, even with the kidney between the fingers, it is sometimes a difficult matter to locate. One method of doing this is with a small needle, passed repeatedly in the direction of the supposed calculus—used, in other words, as a probe. When such a stone is thus recognized it should be removed.
In cases of long-standing, renal pelves are dilated into relatively large sacs, containing numerous concretions, or sometimes a large stone in branching form, resembling coral. If a considerable degree of pyonephrosis or of disintegration accompany such a stone a complete nephrectomy should be made. It remains, then, for the surgeon’s judgment to decide as between nephrolithotomy or nephrectomy, a question which will be settled, in large measure, by what has been ascertained regarding the condition of the other organ. If considered fully competent little hesitation need be felt in removing the diseased one; if its condition be distrusted, then it were best to not carry out the surgical indication, but to substitute for it good general treatment.
In most of the serious and in many of the milder degrees of unnatural mobility of the kidney to which the adjectives “movable” and “wandering” are applied, the surgeon has to deal with a somewhat anomalous condition, which, while it attains serious and alarming symptoms during life, leaves little evidence after death. Thus, Ebstein found it in only 5 out of 36,000, and yet it is said to occur in at least 20 per cent. of all women examined. In women and children the kidneys lie lower and deeper in the gutter on either side of the spine, beneath the seventh to the tenth cartilage, the upper end of the left kidney belonging at the level of the ensiform cartilage. The kidneys are supported by perirenal fascia, by the renal vessels, by pressure of the surrounding viscera, their anterior peritoneal covering playing but small part. Abnormal mobility below the twenty-fifth year of age is rare; its etiology is still obscure, it being found in women at least six times as often as in men; more commonly in those who have borne several children, or who have become suddenly emaciated after long illness, while in men it is most[967] common on the left side. The kidney is afforded a small, distinct peritoneal covering, the so-called mesonephron, which, with its other supports, may be more or less lax, permitting differing degrees of abnormal mobility, the milder being spoken of as movable kidney, the more serious as floating kidney. As Belfield has shown, in every case of functional disturbance of the urinary organs the possibility that a floating kidney may be the cause of the trouble should be borne in mind.
—The symptoms vary from vague discomfort to agonizing pain. Ordinarily they include dragging sensation in the abdomen, with indefinable discomfort, a feeling of weakness, sometimes radiating down the legs and across the back, these symptoms frequently accompanied by dyspnea, flatulence, constipation, and frequency of urination, all of which may be intensified by increased activity. In the more severe forms we find abdominal tenderness, severe pain and vomiting, with collapse and the occurrence of peculiar crises, sometimes of intense agony, which may occur gradually or suddenly, ceasing in the same fashion. Not one of these symptoms is pathognomonic of movable kidney, nor can they be with certainty attributed to it until the suspicion is confirmed by physical examination. The severe crises are described as coming on with intense pain, nausea, vomiting, collapse, chills, and sometimes considerable temperature, especially in hysterical subjects. Osler and Atlee think that too much stress has been laid upon the condition, especially after the patient’s realization of it, the severer symptoms often dating from the first knowledge of the facts. Obviously, temporary hydronephrosis may be caused by temporary obstruction in the ureter, from displacement, while temporary venous obstruction may cause pain in a different way. Actual alimentary disturbances are very closely simulated, and sometimes it is difficult to distinguish between a movable kidney on the right side and a chronic appendicitis.
A great deal of attention has of late been given to nephroptosis and to the effects of enteroptosis, and their production. The peculiar crises were long ago described by Dittel, and include sometimes a feeling of suffocation, with a desire to loosen and remove clothing, when, after lying down, the kidney resumes its position. When after urination relief quickly follows, there is much to suggest kinking of the ureter and distention of the renal pelvis. Much less frequent features are jaundice, from contraction of adjacent viscera, and persistent nausea from the same result, or hematuria from a disturbed circulation. The more marked forms in women are usually accompanied by certain neurotic features, which give them a feature to which they are not properly entitled, while the entire digestive process and the vasomotor innervation of the viscera seem more or less disturbed, with consequent toxemia.
The actual indication of floating kidney is its discovery by palpation, the degree of displacement being in some cases quite noticeable; thus it may cross the middle line, or may be felt even in the pelvis. In the female the kidney should lie above the twelfth rib, posteriorly, and above the costochondral border of the eighth rib anteriorly, and, therefore, not be easily palpated during respiration. This statement is somewhat at variance with some of those contained in the text-books on anatomy, the diagrams being all made from male cadavers. It is of importance not merely in locating the organs, but in fastening them in place, as all methods thus far devised leave much to be desired in complete replacement. A kidney prolapsed only to the waist-line can scarcely be sutured to the loin without displacing it even farther backward. On the other hand, the kidney which lies near the brim of the pelvis rarely causes acute symptoms, because, supported from below, it enjoys accommodation of its ureter to its abnormal relations, so that hydronephrosis rarely occurs. The truth is that in most aggravated cases of nephroptosis nearly all the viscera have been displaced downward, and Ingall’s suggestion to fasten in place at one and the same time the kidney, the liver, the spleen, the stomach, and the transverse colon is well founded, although difficult to carry into effect.
—Fixation of an abnormally mobile kidney is indicated in every case where its displacement causes unpleasant symptoms, yet simple as it is in theory it is neither easy nor always successful in practice. To completely restore the kidney to place is to fasten it higher than the natural routes easily permit, and requires either resection of a rib or fixation of the kidney to one of the lower ribs, a method which has been recommended and practised by some operators. Because of the disappointment so often resulting from these operations conservative practitioners have felt that by pressure from below, as by an abdominal binder with a suitably placed pad, the kidney could be so pushed upward and held as to be made comfortable. This may at least be tried in the[968] milder cases. The supports should never be put in place until the patient is on her back and completely undressed. This method of external support failing or proving unsatisfactory, the surgeon may choose from many different methods the peculiar plan for nephropexy or kidney fixation which he will adopt.
Fig. 636
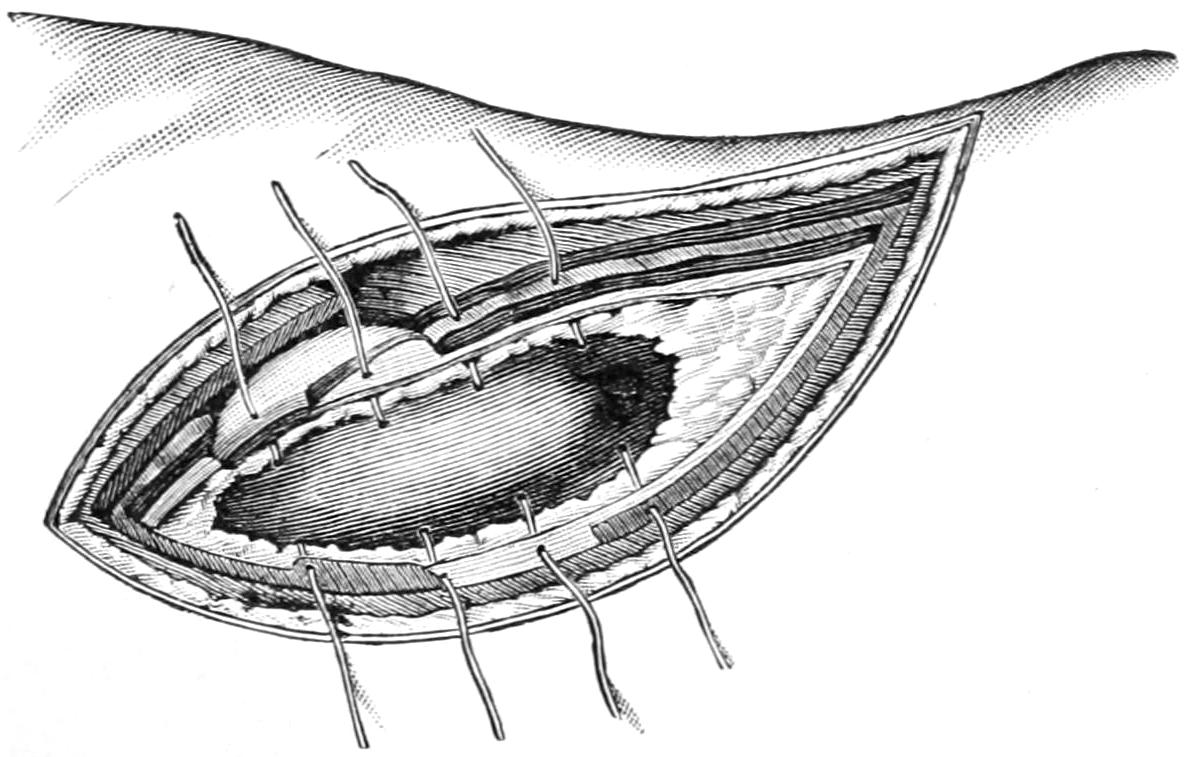
Nephropexy. Method by sutures passed through both kidney and capsule. (Hartmann.)
—These methods all have in common the intent to produce adhesions between the kidney and its normal environment, by which it shall be held in or near its proper place and prevented from dropping. The kidney more than any other organ is held in a cushion of fat, and it becomes a question to what extent this mass of surrounding fat shall be removed. To take it all away considerably complicates the procedure; to leave it is to not furnish the firmest possible surroundings for the purpose. The patient should be placed either flat upon the abdomen or turned well over on the side opposite that to be operated, a cushion or bolster being usually placed beneath the abdomen and loin in such a way as to push upward and into prominence the side to be attacked. The incision employed may be parallel to the spine, about three inches away from it, and carried down to the tissues outside the quadratus lumborum and other spinal muscles. Most operators prefer an oblique incision, made between the lower rib and the upper margin of the pelvis, its centre about four inches from the spine, extending in either direction two inches or more, in order to afford sufficient access. It is carried down until the abdominal aponeurosis and muscles are exposed. These are then divided and the perirenal fat, which is sometimes excessive in amount, is exposed. The deep opening should now be stretched to a size to permit the introduction of a hand, and exploration made for the identification and retraction of the kidney. Much aid may be afforded in this effort by the use of the other hand upon the outside of the patient’s abdomen, which should all have been protected and sterilized to permit such free manipulation. Sometimes it is easy to find such a kidney, at other times and in persons of certain build it is a difficult matter. It lies behind the peritoneum, and this should never be opened during the effort. More or less of the perirenal fat may be cleared away. The more or less elusive kidney being identified, it should be seized with tenaculum forceps, which should secure only its capsule and not injure its substance. With these it is drawn up at least to the wound, or in some methods, it is withdrawn through it and delivered upon the surface of the body. If sutures alone are to be depended upon they may be placed after any one of a number of different methods. The older method was to place the kidney as nearly as possible in its normal relations and then unite the deep margins of the wound to the capsule, and perhaps the cortex of the kidney, by a series of two or three sutures on either side, either of chromic gut or of silk. The theoretical objections which prevail against passing sutures through the renal cortex are hardly well founded, and stitches may be so placed, if desired, but they should not be drawn too tightly (Fig. 636).
Senn and others have endeavored to induce the formation of dense adhesions by packing around the kidney with gauze, left in situ for several days, whose presence should provoke the formation of granulation tissue. In theory this works well, but in practise the presence of the gauze is painful, its removal especially so, and the wound must be left more or less open for the purpose. Since I have learned of the harmlessness and the advantages of decortication I have made a practise of decapsulating almost every kidney thus exposed, and of endeavoring to utilize a portion of the capsule for the purpose of support, as by cutting it into strips, which are threaded into a needle, and then passed through the tissues, thus utilizing the capsule for suture material, or by fastening it with sutures which are not passed through the kidney substance. All in all I have had best results from a combination of some such method as this with one of suspension, for[969] which purpose tapes or gauze are used and passed beneath the kidney—one above the hilum and one below it—after it has been delivered well into the wound, by which it is, first of all, lowered into the position in which it is intended to hold it and then maintained there, the ends being left hanging out of the wound, where they are tied over a roll of gauze or something similar. This provides the smallest amount of gauze, whose presence may provoke granulation tissue, at the same time proving an efficient means of support, and leaving trifling strips to remove when the time for their removal has come. I have usually left them in place for nine or ten days, by which time they are comfortably loosened by the presence of granulations around them, and consequent moisture, so that they are easily withdrawn, with a minimum of discomfort to the patient. Da Costa has suggested an improvement on this by sewing the ends of strips of gauze with chromic gut and letting these sewed ends be placed beneath the kidney. In the course of time, as the catgut softens, the union is separated, and the strips are easily withdrawn. If there be a tendency in these tapes to slip from their desired position, they may be attached to the capsule by a single suture of catgut, which will have softened and disappeared before the time for their withdrawal has arrived. Again in many of these instances the capsule which has been stripped off, or more or less detached, may be utilized for the purpose of fixation by suture with its own tissue.
Nearly all of these operations are without mortality, although they are not yet as satisfactory as could be desired, the trouble inhering partly in the fact that the kidney is not fastened as high up as it should be, or else not in quite the same relative position, so that there is some strain upon its vessels or upon its ureter. Every effort should be made to imitate the original position as accurately as possible. Methods theoretically more perfect, yet more complicated and but little more advantageous, include fixation of the kidney to the twelfth rib, by suture passing through the capsule and then around the rib. No matter what method be adopted, it is necessary to keep the patient in bed for several weeks after these operations, in order that adhesions may not only form but may not be stretched by too early change of posture.
The kidney is the site of an occasionally benign and frequently of a malignant tumor of some of the known varieties. The simplest forms, like the fatty and the fibrous, are uncommon and deserve no special consideration here. There is a so-called adenoma of the kidney, which does not deserve this expression any more than does the so-called adenoma of the thyroid, in that it is not built up of the normal type of secreting gland, but represents something more or less similar to it, perhaps only undergoing multicystic degeneration, its commonest expressions being of congenital origin. The consequence is the production of the so-called congenital adenoma or cystic or multicystic or polycystic kidney, in which may be seen a conversion of original renal tissue into a mass of cysts, surrounded by degenerated kidney tissue, all semblance to the original being lost, and the whole constituting a partial or complete invasion of the organ, by which sometimes its proportions are enormously increased. The condition is essentially of congenital origin, although its serious clinical expressions may not occur for years. The result is to destroy the renal function, to produce a growing mass, and to constitute an essentially surgical condition to be relieved only by nephrectomy. (See Fig. 637.) I recall one child of twenty-three months with a tumor of this character, of such size and extent that it could only stand erect when wearing from its neck a sort of suspensory in which the lower part of the abdomen was contained. I removed this kidney by abdominal section, the child recovering, and being at that time the youngest case that had ever survived a nephrectomy. A number of years later a similar condition developed in the other kidney, of which the child finally died, it having passed during the last thirteen days of its life not more than an ounce or two of urine.
Of the solid tumors of the kidney both carcinoma and sarcoma occur, the former usually as a secondary growth, the latter usually as primary, although any form may be met. The sarcomas are more frequent in early life and in general more common. On account of the kidney having a well-marked capsule metastasis is not so common, in the early stages, as from some other organs. These malignant tumors may attain great[970] size; some grow regularly in shape, others constitute most irregular masses. The entire organ may be involved or only a part.
There are no indicative symptoms of renal cancer that may not be met in other conditions; the development of tumor, perhaps its displacement, pain, and hematuria, though late, and, in proportion to the rapidity of growth, enlargement of superficial veins and general cachexia. When the tumor is large enough to press upon the vena cava or upon one of the common iliacs there will be edema of one or both lower extremities. The veins of the external genitals are more likely to suffer early rather than late (Figs. 638, 639).
Fig. 637
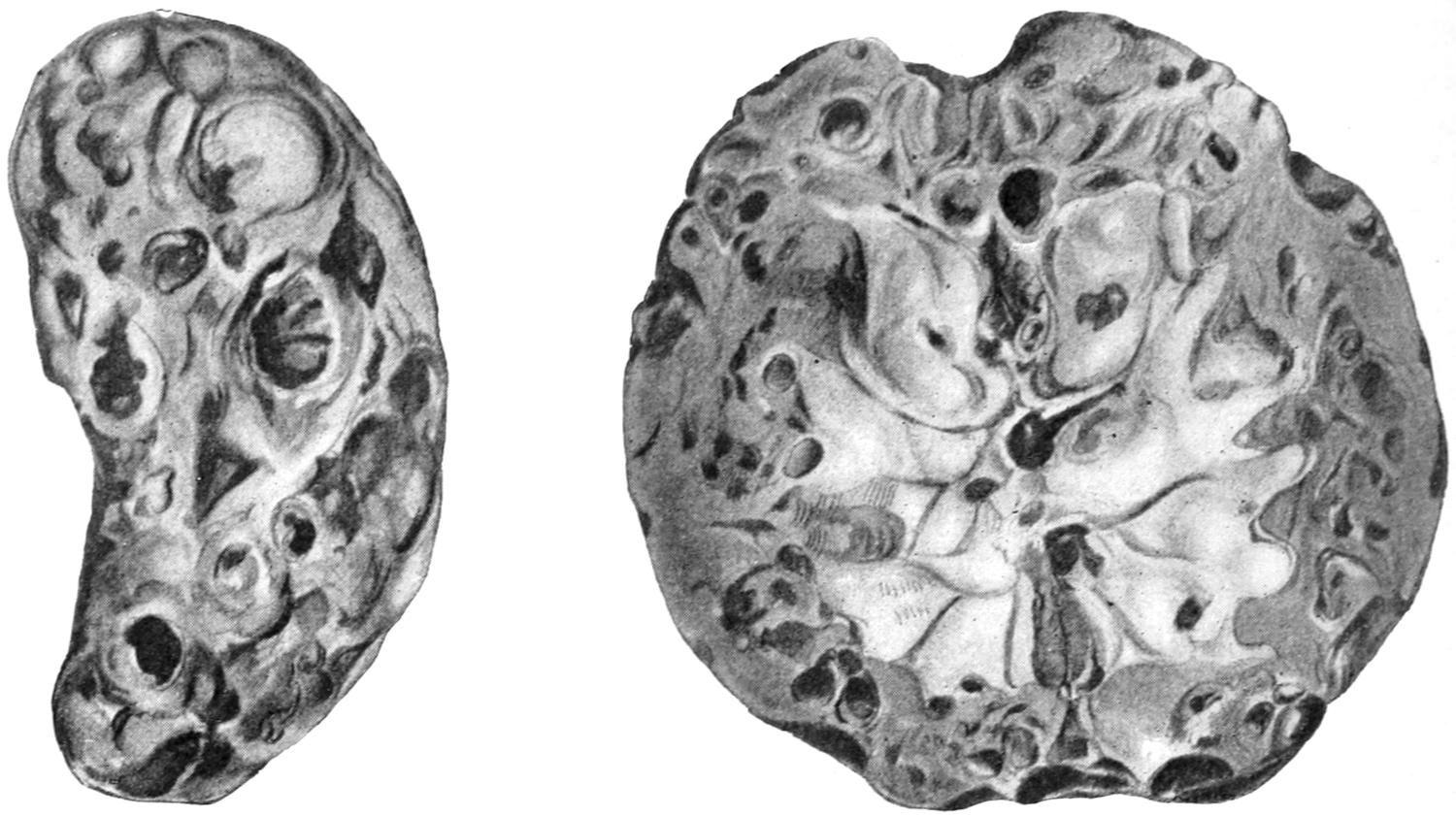
Congenital cystic kidney; exterior and internal appearance; patient forty-two years of age. (Schmidt.)
Fig. 638
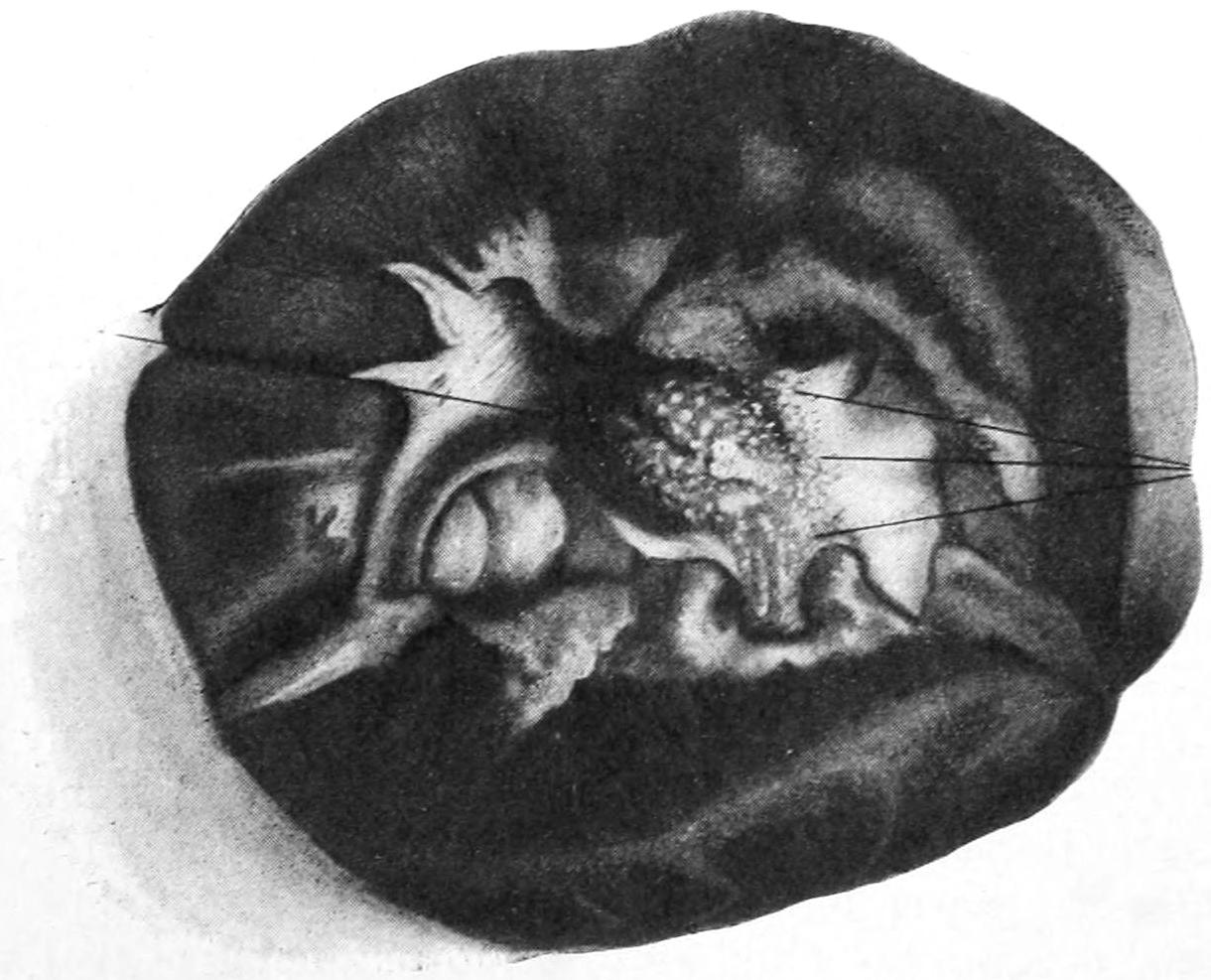
Cancer of kidney, intramural, as seen after dividing the organ. (Israel.)
—There is one peculiar variety of solid tumor of the kidney which deserves special mention, the so-called hypernephroma. These tumors consist essentially of adrenal tissue, although when they develop within the kidney their occurrence there is due to the presence of aberrant rests of the original suprarenal tissue. Gravitz, in 1883, was the first to recognize their real character. Supernumerary adrenal rests have been met with in many parts of the body, not alone in the kidney and perinephric[971] tissue, but in the broad ligament, along the spermatic vessels, in the sexual glands of both sexes, in the liver, the mesentery, and even the solar and renal plexuses. Their occurrence in these localities may be explained by the close relationship between the mesonephros and the origins of these various organs. Hypernephroma has no pathognomonic signs or symptoms. It is usually a single tumor, although both kidneys have been affected. When the organ is not so involved as to mask all its original features the tumor will be found beneath the capsule, varying in size from that of a pea to that of a child’s head, its outer surface lobulated by depressed bands of capsule, its color lighter than that of the surrounding kidney texture, while projecting portions will be soft and almost cystic. When met with in other parts of the body its gross characteristics are essentially the same. Metastasis is very common, the tumor often extending along the walls of the veins, or even more often partially filling them than the lymphatics. A common method of extension also is by implantation within the peritoneal cavity; for the secondary implantation occurs most often along some portion of the urinary tract—e. g., the bladder.[66]
[66] It may assist in the recognition of hypernephromatous tissue, after removal, to remember that adrenal tissue has the property of decolorizing starch which has been turned blue by the addition of iodine. Crofton has shown how there may be put into a test-tube a 1 per cent. starch solution colored with a drop of weak tincture of iodine. If to this solution hypernephromatous tissue be added the blue color changes gradually to a pink and then fades out.
Fig. 639
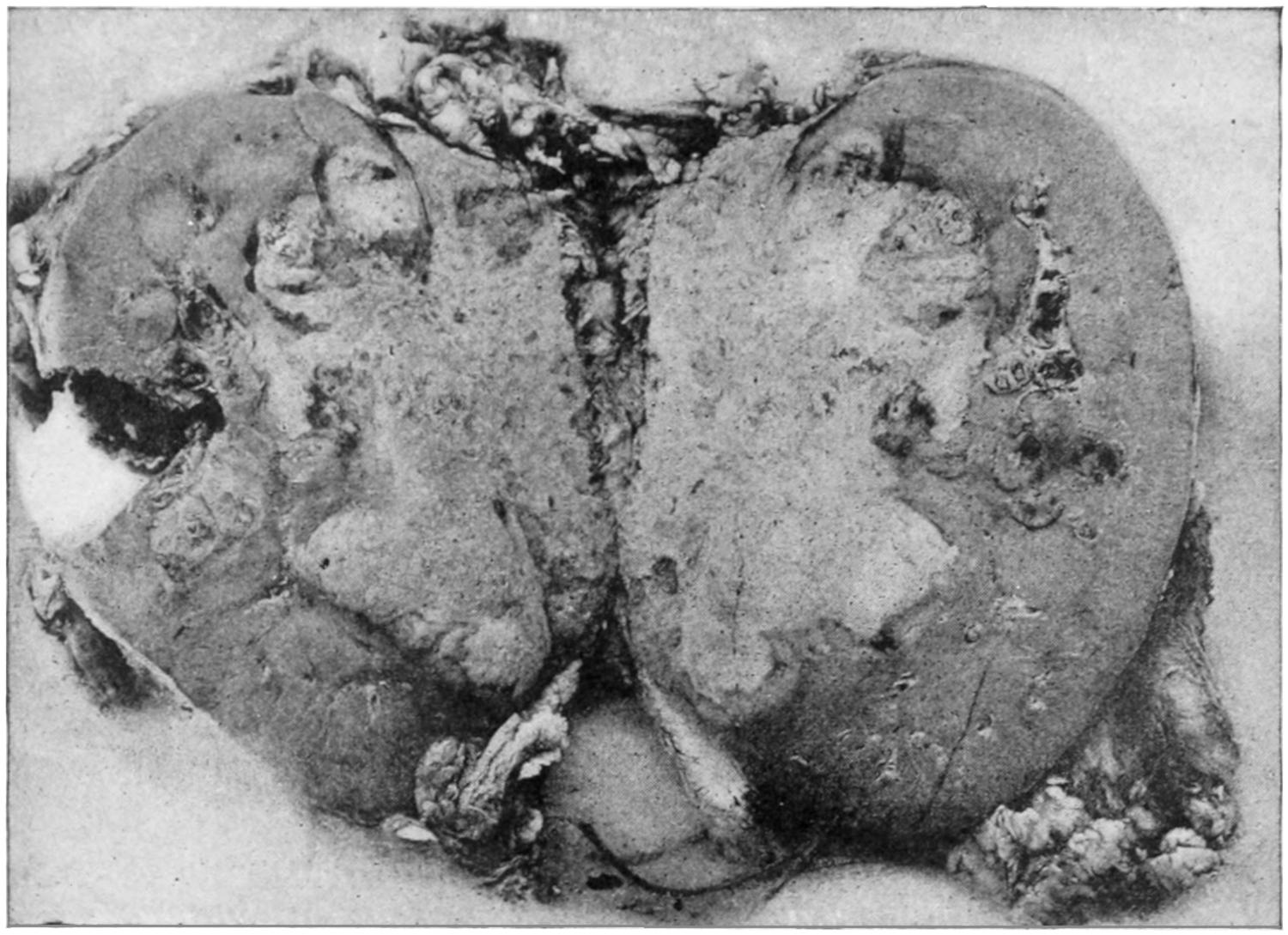
Infiltrating form of cancer of the kidney. (Israel.)
Hematuria and renal colic are the most conspicuous features connected with the growth of these tumors. The former often occurs during sleep, and blood is passed in almost pure form, perhaps for a considerable period of time, after which spontaneous recovery apparently takes place, the trouble recurring at intervals.
There is but one method of treating hypernephromas, like other solid tumors, namely, by complete extirpation, i. e., nephrectomy. Even this may be too late, but should be undertaken, except in the most unpromising instances. If the existence of metastatic involvement can be determined even nephrectomy may be considered useless. (See chapter on Cysts and Tumors.)
This term refers to a more or less permanent distention of the kidney cavity by retention of urine, due to partial or intermittent obstruction to its escape. An intermittent form is common, which, however, at almost any time may lead to some degree[972] of enlargement, while when the obstruction is permanent the resulting tumor becomes practically a thin-walled cyst, which may contain an enormous amount of fluid, more or less altered urine, which will contain, in addition to the ordinary urinary elements, cholesterin crystals and other adventitious products. Hydronephrosis, then, may be congenital or acquired in origin, intermittent or permanent in character, and unilateral or bilateral in location. Among the acquired causes are strictures of any portion of the urinary tract below, either in the ureter, the prostate, or the urethra; tumors of any kind making pressure; movable kidney which permits of kinking; tuberculous diseases which lead to chemosis of the mucosa and consequent obstruction; renal calculi which plug the ureter; foreign bodies, blood clot, and the like (Figs. 640 and 641).
Fig. 640
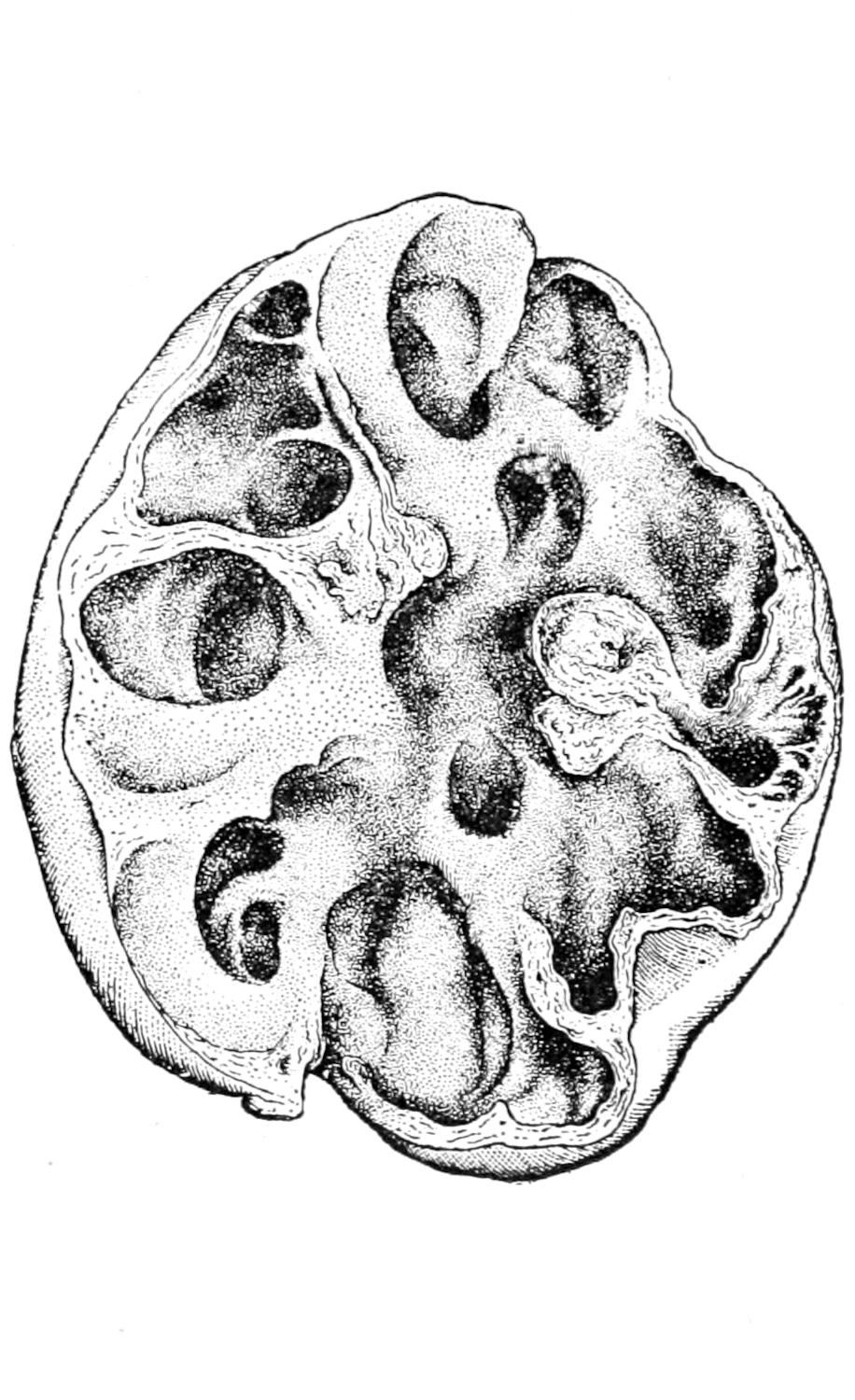
Hydronephrosis from obliteration of ureter by tuberculous disease. (Tuffier.)
Fig. 641
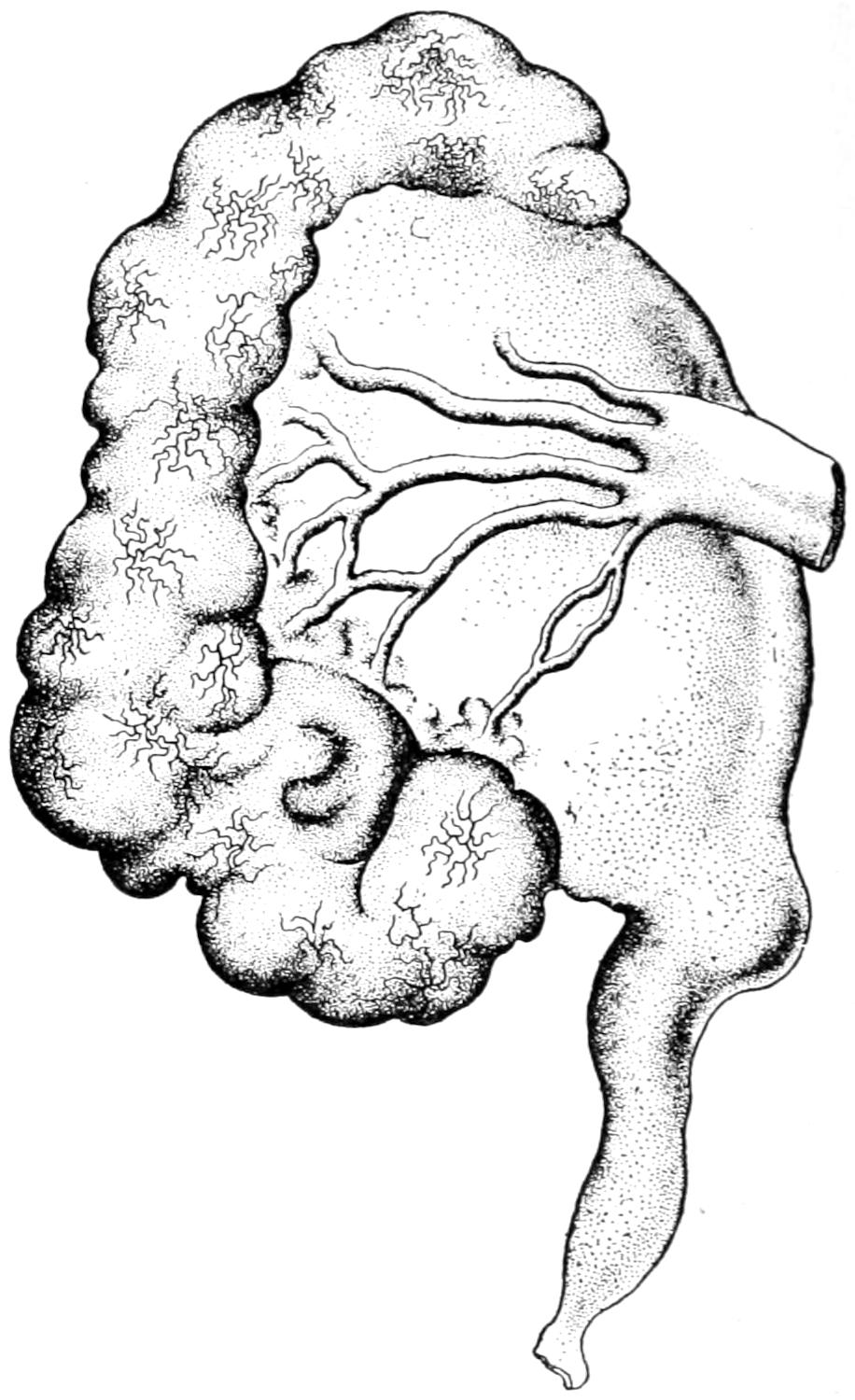
Hydronephrosis in first stage of development. (Rayer.)
Fig. 642
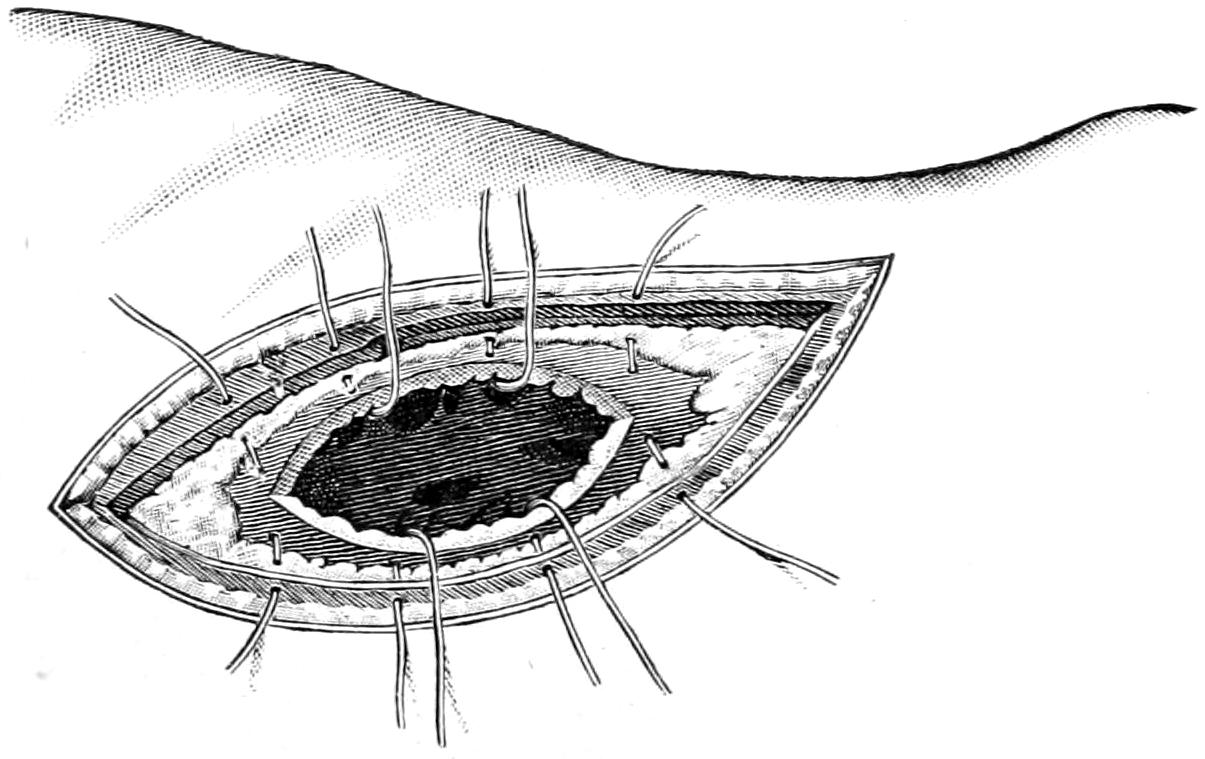
Operative treatment of hydronephrosis or pyonephrosis. (Hartmann.)
Until the infectious or suppurative element be added the urine is in these cases but little changed. When infection is added the case becomes one of pyohydronephrosis, and perhaps finally one of distinct pyonephrosis. The symptoms produced at first are not very pronounced and will vary with the exciting cause. If the result of acute obstruction, renal colic is perhaps the most significant. When this is accompanied by tumor in the region of the kidney the interpretation of the phenomenon is easy. Sudden decrease in[973] size of such tumor, with unusually great escape of urine, is also pathognomonic of intermittent hydronephrosis. The discovery and the history of a gradually increasing tumor in which, when large, fluctuation can be determined, and in which fluid is easily found with the aspirating needle, will permit a differentiation of these pseudocysts from solid tumors of the kidney. They are to be distinguished from ovarian cysts, from general ascitic accumulations within the abdomen, and from perinephritic and spinal abscesses. Their location, which corresponds so closely with that of the kidney, especially while they are small, their gradual growth, the displacement of the abdominal viscera forward and to their inner side, their enlargement downward and their fluctuating character will usually provide features by which they may be accurately recognized.
—The treatment of intermittent hydronephrosis in its earlier stage may be accomplished by some measure less radical than nephrectomy or nephrotomy, particularly when due simply to abnormal movability or to pressure of some extrinsic growth. Hydronephrosis due to obstruction by renal calculus may be relieved by removal of the obstructing stone, but a hydronephritic cyst, which has attained large size, in which practically all semblance to secreting kidney structure has disappeared, should be extirpated, unless this should entail too formidable an operation, in which case it should be freely opened and drained until such time as it has contracted to a size justifying enucleation (Fig. 642).
There are a few morbid surgical conditions of the ureters, so distinct from those of the bladder below or the kidneys above as to require separate consideration here. They are frequently involved in the pyogenic and tuberculous infections, which spread along them in either direction, but the chief surgical diseases deserving mention here are stricture and calculus.
Stricture of the ureter may result from intrinsic or extrinsic lesions. Thus it has been injured in operations upon the pelvic viscera, as in parturition, and it is not infrequently pressed upon by neoplasms; but the majority of its contractions are cicatricial, and are consequences of ulceration or injuries done by calculi. Stricture of the ureter is to be recognized rather by its consequences—i. e., hydronephrosis—than by more direct symptoms. Its accurate location is now possible by the use of the cystoscope and the ureteral bougie or catheter. When by the cystoscope no urine is seen escaping from the ureter one naturally infers its complete obstruction—in fact, the degree of the latter is fairly estimable with this instrument. However, with the passage of a bougie the trouble may be found. This is particularly of value when the lesion is an impacted calculus, for it indicates to the surgeon the level at which he should direct his operative relief, a matter which may also be decided by a skiagram.
While in the hands of experts dilatation of the ureters may be accomplished from below, it is usually beyond the ability of the average surgeon. He has to decide, then, as to whether the ureter should be exposed along its course, from the loin, extraperitoneally along the groin, or by abdominal section. A ureter hopelessly entangled in a mass of cancer may be turned into the other ureter or into the bowel. A ureter fixed in a narrow, cicatricial band may be divided and its upper end turned into the tube below the stricture by a process of transplantation or anastomosis, which is one of the feats of modern surgery; but a ureter hopelessly involved for a considerable portion, or hopelessly diseased, will require nephrectomy, as the kidney above it may be compromised and can probably be well spared.
Calculi impacted in the ureter are most commonly arrested at those points where its caliber is normally smallest, just below its origin, at the pelvic brim, and just above its orifice. The symptoms of impaction are those of renal colic, already considered. It should be sufficient that extreme pain and the escape of pus and blood in the urine, accompanied by more or less distention of the kidney above, are noted. If there be a history of previous attacks of this kind, with the passage of small calculi, the diagnosis may be regarded as positive. This may or may not be confirmed by the x-rays, or by the catheterization of the ureter from below.
[974]
Gibbon has suggested intra-abdominal exploration and palpation of the ureter for the discovery and location of impacted calculi, and recommends that when discovered they may be removed by extraperitoneal incision, which may be lumbar, iliac, inguinal, vaginal, or even sacral or rectal; while with the advantage of combined manipulation, the operator having one hand in the abdominal cavity, the actual work is more rapid and certain.
This procedure is not to be advised in every case by any means, but may prove of advantage in doubtful cases, and especially in those where, when the abdomen has been already opened, a stone is accidentally found in the ureter, since when the latter is opened extraperitoneally it is rarely necessary to suture it.
The non-operative treatment of ureteral calculi has been considered when speaking of renal calculi. The operative treatment, inversion of the patient having failed, may consist of exposure of the upper two inches of the tube, by an incision parallel to the twelfth rib, and carried well forward and downward toward the middle of Poupart’s ligament. Through such an incision the whole length of the ureter may be reached. The opening is made down to the peritoneum, which is then pushed toward the median line. On its posterior surface, adherent to it, will be found the ureter. At the point where the stone is impacted the ureter is to be divided and the stone removed. In theory sutures should be inserted; in practice, they are rarely needed, as these incisions usually heal kindly without them.
A stone impacted at the vesical orifice of the ureter may, in the female, be removed after such dilatation of the urethra as shall permit access, or it may be removed through the vault of the vagina. In the male only the most expert manipulators within the bladder will attempt its removal in this way without at least a perineal section.
In addition to the operative procedures already described the principal operation upon the kidney is nephrectomy. While this may be partial, under rare circumstances, the procedure is so essentially similar to the complete operation that it is only necessary to say that if a portion of the kidney be removed, bleeding from spurting vessels should be arrested by ligature, while the oozing, at first pronounced, will soon subside under the application of hot water, after which absorbable sutures may be used in sufficient number to approximate the parts.
Fig. 643
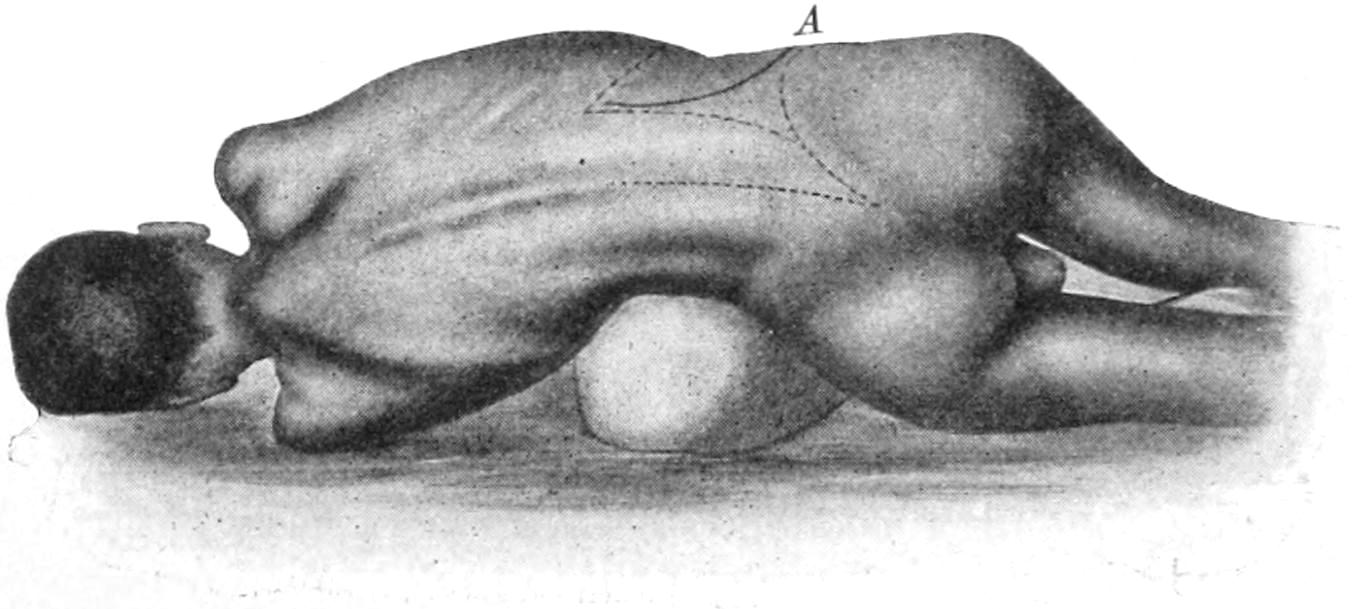
Position of patient and various lines of incision for nephrectomy and other operations upon the kidneys. A, the favorite method of approach for most purposes. (Hartmann.)
Total nephrectomy is usually done by the lumbar route, the kidney being exposed by an oblique incision extending obliquely downward from near the spine, parallel to the lower rib, between it and the crest of the pelvis, and as far forward as may be required for the purpose. For removal of a large solid tumor a large opening should be made, and the above incision may be extended in any required direction, or an additional cut may be made wherever required. In fact, in attacking some of the very largest growths it becomes necessary to apparently almost bisect the patient in order to furnish sufficient space. As the mass to be attacked lies behind the peritoneum it is rarely necessary to open the peritoneal cavity. This is usually done only by inadvertence or because of density of adhesions, and the effort should then be made to at once close it temporarily[975] or permanently. Especially should every attempt be made to prevent contamination when dealing with tuberculous or suppurative renal disease. Ordinarily the abdominal opening does not extend nearer to the spine than the border of the spinal muscles. These may, however, be divided if necessary. So also may the deep fascia be divided in any direction, and, in fact, the last rib may be removed in toto if required. The kidney or the tumor, having now been reached, should be isolated. If the condition be cancerous as much of the surrounding tissue should be removed as the case will permit; if otherwise, an enucleation of the kidney from its more or less infiltrated bed will be sufficient. It is usually removed with its capsule, but sometimes the latter is so adherent that it is easier to enucleate the kidney itself from within it. Adventitious vessels may enter the kidney, more especially from below. The surgeon must be prepared, then, at any time to clamp and secure them if found. Sometimes enucleation of the kidney is exceedingly easy; at other times old adhesions or surrounding infiltration make it a matter of great mechanical difficulty. The intent is to not only isolate it, but to make such exposure of its pedicle that one may be securely protected against hemorrhage. Incidentally the ureter should be examined from above, by passage of a probe, or by injecting a colored solution, in order to know later if it passes freely into the bladder. It is the accurate securement of the renal vessels which is perhaps the most necessary feature of the operation and upon which most depends. When this is made impossible by extraordinary circumstances expedients must be adopted, as, for instance, the use of an elastic ligature—i. e., a piece of small rubber tubing, drawn tightly around the base of the mass and secured by clamp, ligature, or suture, the intent being to leave it for at least two or three days until it shall have accomplished its work, and then either to remove it or to allow it to loosen itself in time and come away.
Fig. 644
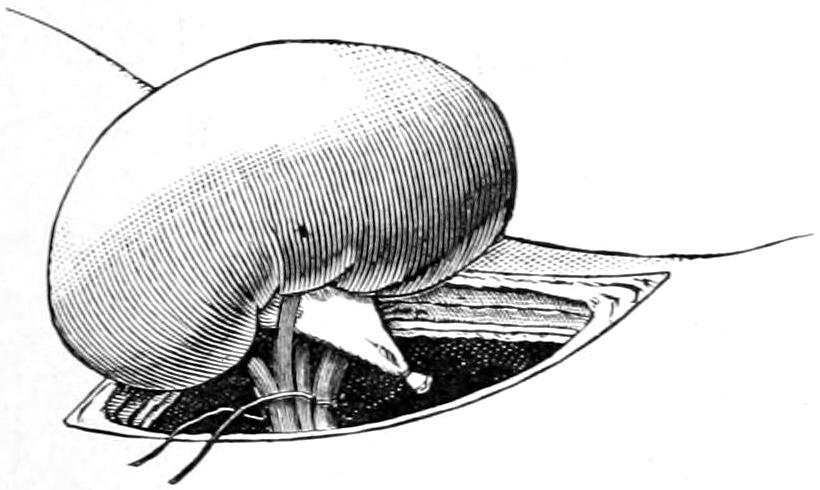
Nephrectomy. Complete delivery of kidney and ligation of its vessels and ureter. (Hartmann.)
Under some circumstances the surgeon may so complete the nephrectomy that the external wound may be closed without drainage; but when there has been contamination, as by escape of contents, either purulent or urinary, or when a considerable mass of tissue has to be left enclosed within an elastic ligature surrounding the stump, then an opening should be left in order that slough may easily escape and ample drainage be afforded. A reliable ligation of the renal vessels should be made, which is best done with at least two ligatures, taking the pedicle in parts, or else carefully isolating the vessels when sufficiently exposed, and tying each one of them separately, after which the whole group may also be enclosed in a single ligature. A few operators have reported such accidents as tearing the renal vein from the vena cava, and such a wound has been successfully sutured, the patient recovering; this requires, however, both coolness and resourcefulness in the presence of serious difficulty and danger. Certain dense tumors can be removed by process of morcellation, i. e., removal of a portion at a time, the separate pieces being cut away with scissors or knife, as may be the more convenient, and hemorrhage being controlled by clamps.
The anterior or Trendelenburg route is rarely selected for nephrectomy, but may be adopted when this procedure is made a part of other abdominal work, or may be necessitated by the presence of a large tumor in a small abdomen, as, for instance, in children. The abdomen will be opened as for any abdominal tumor, either in the middle or to one side, as may seem best. The tumor itself will so far displace the viscera as to perhaps present at once beneath the knife. It may be necessary to go through the peritoneum twice. After being thus exposed, and the abdominal cavity protected, the balance of the operation is again a process of enucleation, with securing access to the pedicle of the[976] tumor, where its vessels and the ureters may be found. These again are ligated and the mass removed as though it were from the peritoneal cavity. Posterior drainage may be added, although rarely necessary.
Other operations have been suggested to meet the needs of individual cases. Thus pyelectomy, or removal of a portion of the dilated pelvis of the kidney, has been performed by Murphy and others, the process being essentially an excision of a portion of the sac wall and its retrenchment by sutures. Plastic attachment of the dilated upper end of a ureter to the floor of the renal pelvis has also been effected in much the same way, as in a case reported by Murphy, where, after opening the sac of the pelvis, the ureter was slit for a considerable distance, while at the lower angle a V-shaped piece of the sac was fastened into the ureteral opening, thus making a funnel-like communication.
Again, as illustrative of some of the radical suggestions of recent years, Watson has proposed that in instances of hopeless bladder conditions, where the patient is made miserable, there should be a turning out of both ureters on the loin, and the formation of two ureteral fistulas, after which the patient may wear a drainage receptacle, and in this way enjoy a comfort otherwise unattainable. He has reported the case of such a patient, who has thus passed all the urine for four years, and urine from one side for eleven years, who was otherwise in comfortable health.
Fig. 645
Fig. 646
Fig. 647
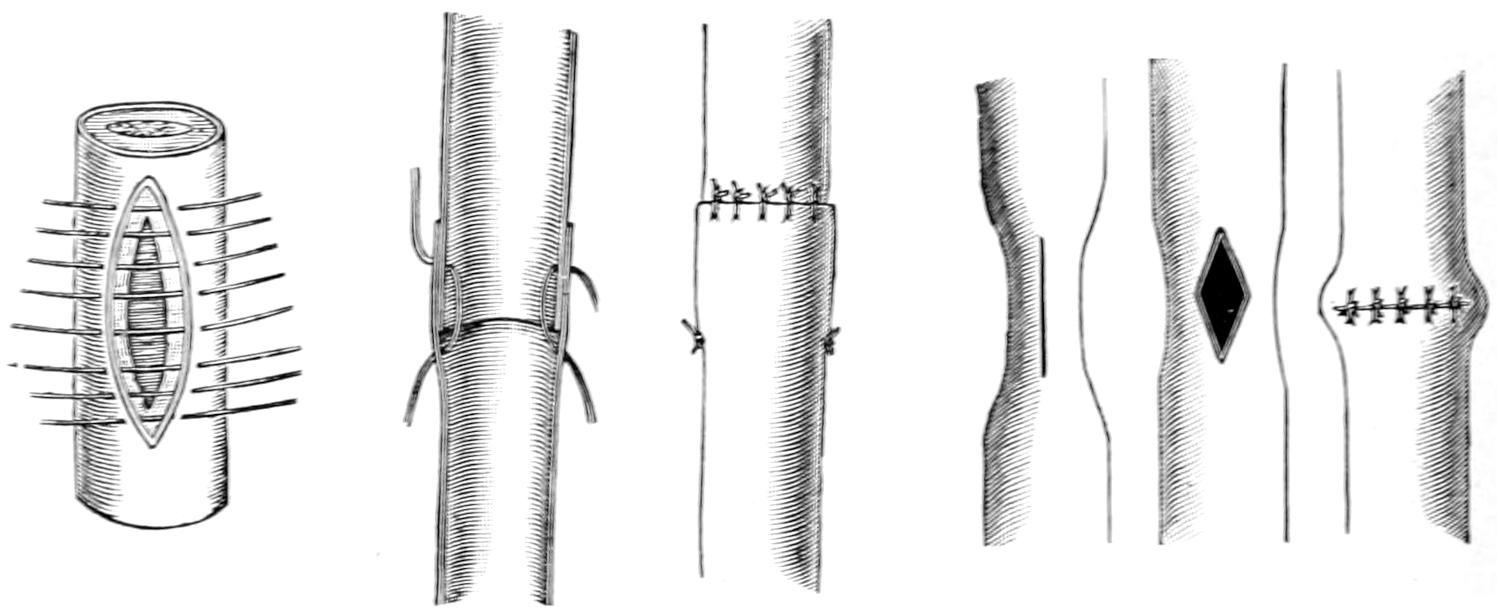
Longitudinal suture of ureter. (Hartmann.)
Implantation or invagination of ureter with fixation and then with circular sutures. (Hartmann.)
Longitudinal incision and transverse suture of ureter for stricture, similar to the pyloroplastic method of dealing with pyloric stenosis. (Hartmann.)
—The surgery of the ureters is also quite modern, and has been worked out in the experimental laboratory. That ureteral tissue will heal has been proved by Murphy, who has remarked that “The peritoneum is the only tissue that unites as kindly as does the ureter.” After accidental injuries during other operations the ureter may be sutured almost as though nothing had happened. These sutures should be made with fine round needles, and be placed closely together. They should be made of fine silk or thread.
Not only end-to-end union but lateral anastomosis and even more ingenious methods of transplantation and implantation are now in vogue. Figs. 645, 646 and 647 illustrate some work in this direction, and show what may be done by work quite similar to that done upon the small intestines or the bloodvessels. More complete instances of transplantation have been effected in connection with exstrophy and carcinoma of the bladder, where, for instance, the ureters individually, or the base of the bladder containing the ureteral orifice, have been dissected out and implanted in the colon or the rectum.[67]
[67] In one case I carried out the following procedure, necessitated by cancer involving the urethra, the base of the bladder, the rectum, and the whole floor of the pelvis, in a female patient, the disease having attained a degree making urination or even catheterization impossible. I opened the abdomen, dissected out the right ureter from the bladder, implanted it into the appendix, and then dissecting the left ureter in the same way implanted it in the right, the intent being to direct the whole urinary stream into the colon and thus spare the bladder. The operation was not finally successful. I afterward found that this method had been tried experimentally by Jacobson, of Toledo, but without success.
[977]
Methods of recognition of surgical diseases of the bladder have been vastly improved, as well as complicated, within the past few years. The bladder has now been made accessible not alone to touch, as through the rectum or vagina, or by incisions above or below the pubis, but to sight, through the use of the cystoscope. It is furthermore possible to detect foreign bodies within it by the Röntgen rays. Palpation is chiefly of value in thin persons, or when the bladder is greatly distended; still, infiltration of the base of the bladder can be detected through the vagina or through the rectum, as can also certain foreign bodies. Much of value is learned by both chemical and microscopic examination of the urine. This may be passed by the patient or withdrawn by the catheter. It has already been indicated how much of value can be learned by separating the urine drawn from each kidney. The difficulties of this procedure are greater in the male than in the female, owing to the complications in the requisite manipulation of the instruments. Nevertheless there is no accurate method of such estimation save by ureteral catheterization. The method of Harris, by the use of the so-called segregator, is of occasional assistance, but is never accurate nor always satisfactory. If the catheter alone be used it should be of metal, if it be desired to have it serve the purpose of a probe, as in the search for a foreign body (calculus and the like) or as a means of estimating the size and shape of the bladder. For the latter purpose an ordinary sound will serve as well, preferably one with a short beak, ordinarily known as a stone searcher. In cases of prostatic enlargement it is of great advantage to estimate the amount of residuary urine after the patient has apparently emptied his bladder. This may be withdrawn by a sterile catheter under aseptic precautions. The use of the catheter is also necessary for lavage of the bladder, a measure of great value in many cases.
The attempt will not be made here to picture nor go into a minute description of the various forms of the cystoscope. Their use, like that of the ophthalmoscope, requires special aptitude and training. With the latter they are of great value; without them they confuse and complicate. The cystoscope may be used for ordinary purposes of inspection, for aid in introducing the ureteral catheter, or even for photographic purposes, for it is now possible with the latest instruments to photograph the image thus obtained of the bladder interior. To one not accustomed to viewing the field seen in such an instrument these revelations are of little interest. To the expert, however, they may be made of the greatest value. Without further description, then, allusions made below to the use of the instrument must presuppose some familiarity with it, and the advantages and even necessity of securing special training in its use.
The lesser malformations of the bladder include mainly irregularity in shape or the formation of diverticula, which are not extremely rare. These are especially likely to be met during hernia operations. I have repeatedly in operating for inguinal, and once in operating for femoral hernia, found a diverticulum of the bladder complicating the situation. Its possibility, then, should be borne in mind. It may be thin and lie in such close relation to the hernial sac as to be mistaken for the latter. When opened urine will escape and contaminate the wound. It would probably be best to close the bladder opening and discontinue the operation rather than run the risk of contamination of the peritoneal cavity, postponing further work for a few days. As the result of allantoic defects a double bladder may be met, each perhaps having one ureter opening into it. More or less complete partitions in the bladder are more frequently met. These conditions could not be appreciated previous to opening the viscus or the use of the cystoscope.
[978]
More complete forms of acquired vesical hernia may be found in such conditions as cystocele, common in women after perineal lacerations, and frequently constituting a most serious condition.
—By far the most serious and extensive of the congenital malformations are those constituted by more or less complete defects of the anterior portions not alone of the bladder, but of the abdominal wall which should cover it, and which are known as ectopia, exstrophy, or extroversion of the bladder. Of this condition there are different degrees, from a small cleft just behind the symphysis pubis, to that which is complicated by prolapse of the remaining posterior wall, the umbilicus being situated just above it, while the pubic arch itself is defective or rudimentary. Thus in the male there is usually epispadias of a more or less rudimentary penis, while in the female the clitoris is cleft and the vulva more or less opened, the urethra being defective or entirely wanting, the vagina often small, and the uterus generally infantile. Extreme cases of this condition constitute one of the most serious and deplorable congenital defects which are not inherently fatal. Obviously, with these conditions, there is constant escape of urine, usually with complete mechanical impotence, although in the female the ovaries are usually present, and practically always the testicles in the male. In the latter the opening of the seminal ducts may be frequently seen on the floor of the urethra, more or less concealed by folds of cystic mucous membrane. The condition is much more frequent in males than in females. The prostate is usually at least rudimentary and may be wholly wanting. Occasionally the testicles are undescended. Double uterus has also been seen in these conditions.
Regarding its causes there is but little known. Doubtless these have to do with allantoic defects, but the allantois is such a temporary organ that there would seem to be some other contributing cause not yet recognized.
Among its most distressing features are not only the lack of control of urine, but the irritation of the exposed mucous surfaces consequent upon friction with clothing, or decomposition of urine and consequent uncleanliness. There is, therefore, nearly always ulceration, with extreme irritability and more or less constant suffering. It is not strange, then, that for its relief surgeons have taxed their ingenuity, or that adult patients, finding the conditions unbearable, are willing to submit to even extreme measures.
—So many operative measures have been devised that it is impossible to include them all. First of all the procedure should be adapted to the particular case. Much will depend, for instance, upon the extent of the defect in the abdominal wall, or in the pubic arch, and in the male upon the rudimentary condition of the penis or the extent of the urinary canal.
Operations for this condition may be divided into palliative and radical—i. e., those which are intended to make it more tolerable and those which are really entitled to the latter term. Thus if only the exposed mucous surface can be covered with a skin covering, the condition may be mitigated since a urinal or some device may be worn by which its worst features may be controlled. Trendelenburg has recently called attention to the fact that a wide separation of the pubic arch not only weakens the pelvis, but constitutes a serious difficulty in closing the defect. He has, therefore, combined direct operation with separation of the pelvic bones at the sacro-iliac joints, afterward enclosing the pelvis in a comprehensive bandage, or suspending the patient in an apparatus in such fashion that the bony defect in front shall be narrowed, if indeed it be not completely obviated. This, of course, is a measure to be carried out in the early years of childhood; in connection with it the bones may even be wired at the symphysis. In fact immediately after the birth of such an infant the attempt should be made to narrow the pelvis, by surrounding that part of the body with a wide rubber band, which shall influence growth without too much interfering with nutrition. Later subcutaneous osteotomy may be done if necessary. At all events, the growing pelvis should be surrounded with an enclosure by which a constant influence may be maintained.
The various plastic operations for this defect have the common purpose of affording a covering, which must unfortunately be without a sphincter to guard the outlet of the cavity. The best that can be accomplished, then, by plastic methods is the formation of a more perfect cavity without affording sphincteric control. A theoretically ideal method would be one which should permit raising of skin flaps around the margin of the defect, and so turning them in that the skin should vicariate as mucous membrane.[979] These flaps when united, and the anterior wall when thus formed, could be covered by other flaps or by skin grafts; but from these flaps hairs will grow into the bladder. These will become encrusted with urinary salts and an amount of irritation be produced which may become not only intolerable but locally destructive.
In the selection of any plastic method much will depend on the size of the defect and its completeness, the condition of the surrounding wall, and varying complications in the surrounding structures. The general method above suggested will answer especially for the smaller exstrophies. Beck has suggested an excellent device, namely, the dissection from the pubes of the recti muscles, their insertions being severed, and the partial division of the transversalis fascia until the muscles are so mobilized that they can be reflected and united, thus forming an anterior bladder covering. By a second operation these partially formed flaps may be again dissected off from the wall and a complete osteoplastic covering afforded. Practically no operation for extroversion can be completed in one sitting. Frequently repeated efforts have to be made, a little being accomplished at a time. One of the greatest difficulties met with is securing primary union along surfaces more or less bathed or in contact with escaping urine. These flaps, even if united, may separate in a few days as a result of this urinary maceration. Against this there is but little possible provision, save perhaps by catheterizing both ureters, and emptying them into a distinct receptacle.
Fig. 648
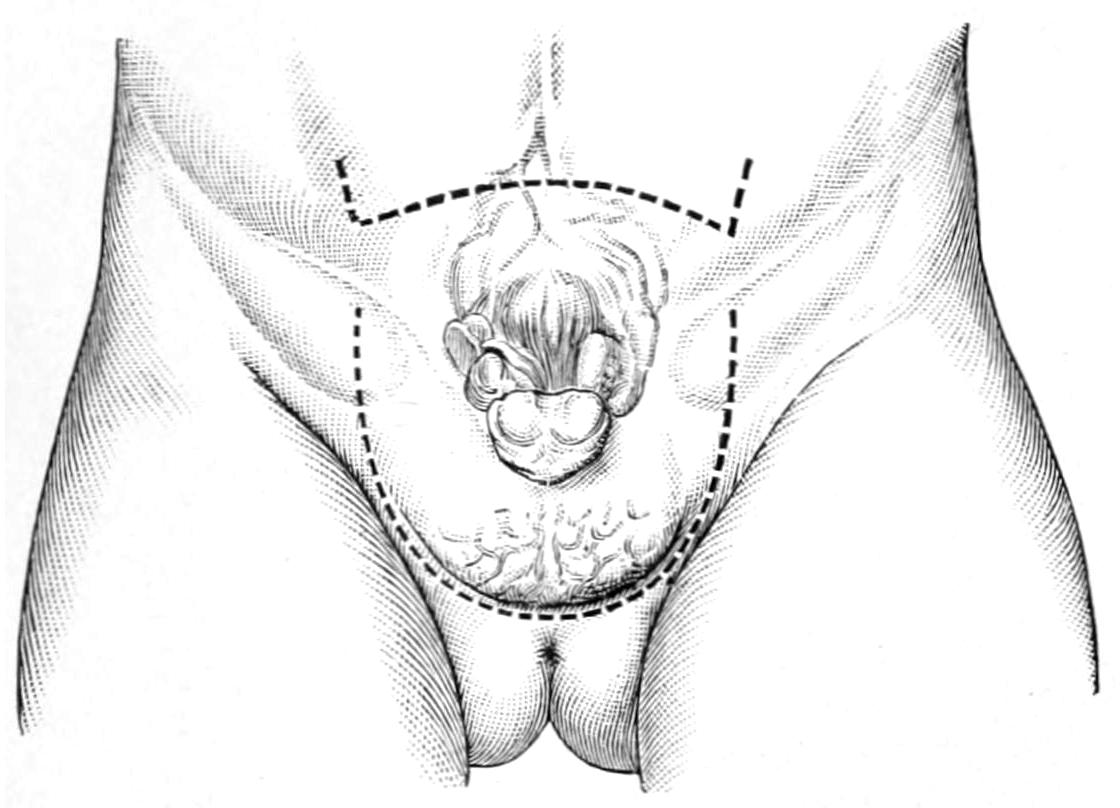
Roux’s autoplastic method of raising a perineoscrotal flap with which to cover the defect. Lines of incision. (Hartmann.)
Fig. 649
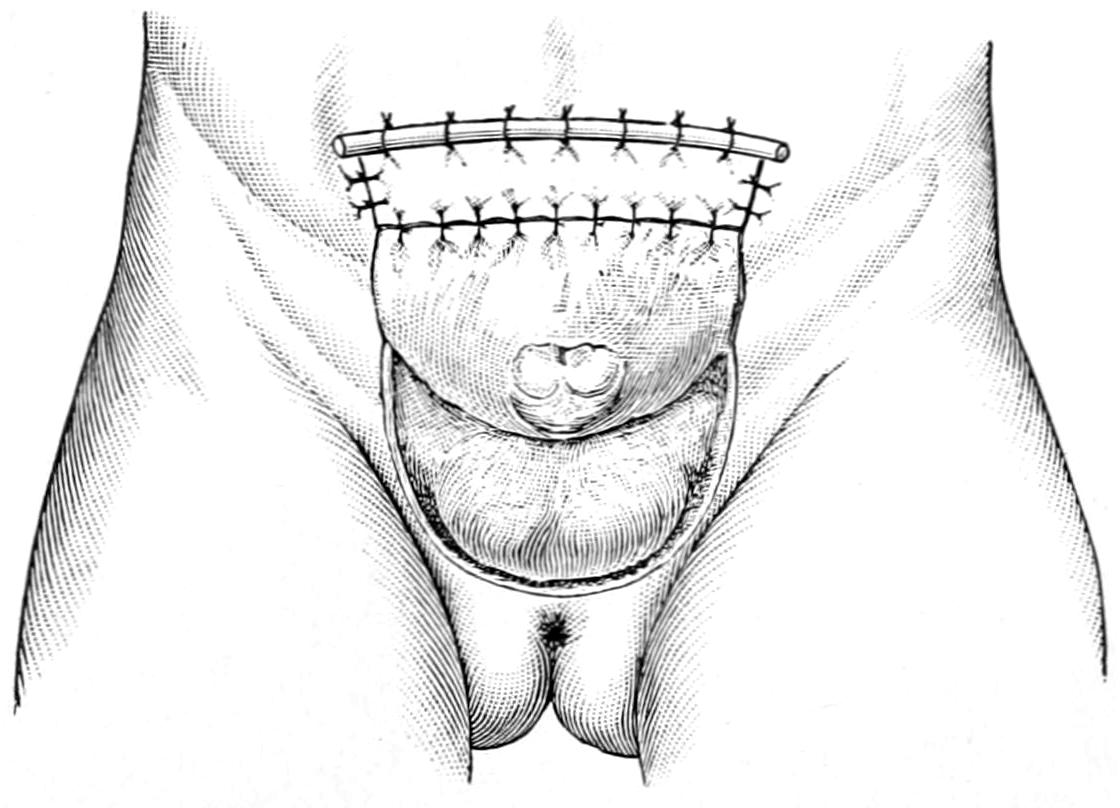
Roux’s autoplastic method of raising a perineoscrotal flap and its fixation. (Hartmann.)
More complicated methods of furnishing a complete cavity have been devised by Rutkowski and Mikulicz, both of whom have suggested to use a small loop of small intestine wherewith to complete the bladder cavity. In each of these methods the abdomen is opened, a loop of bowel brought down, a small portion completely separated by double division, end-to-end anastomosis of the main part being then made, while the separated part is in one method closed at one end, while the other end is fitted over the exposed bladder surfaces as a sort of cap. The method is exceedingly complicated and hazardous, and depends for local success upon a sufficient blood supply to the intestinal loop, which should be carefully ensured by caring for its vessels and mesentery. It has, nevertheless, been successful.
A far simpler method, perhaps the simplest of all, is that of Sonnenburg, which consists in extirpation of the bladder proper, with plastic closure of the opening, while the ureters are carefully separated and sutured into the upper portion of the urethral gutter. This removes all urinary cavity and provides only for continuous escape; but this latter is now provided in an accessible and convenient place, while the wearing of a urinal permits the achievement of the main purpose of the operation. Sterson operates upon young girls by suturing the loosened ureters to the labia minora, which are then sewed together in the median line, after which a urinal can be worn.[68]
[68] Cantwell has suggested the following method for bladder exstrophy, namely, to pass catheters through a perineal fistula up into the ureters, then to dissect off the bladder wall, bringing it over a small rubber balloon, pushing the whole into position, and uniting the abdominal wall in front.
[980]
It has occurred to many operators to more completely divert the urinary stream by displacing the ureters and turning them into the rectum or the sigmoid. Operations for this purpose have been described especially by Maydl (Fig. 650), and by Moynihan, while modifications have been suggested by many others. In practically all of these procedures catheters are first passed into the ureters for their identification and control. Some would dissect out the trigone with both ureters, and, making a sufficiently large opening in the rectum, would transplant it in its entirety within that cavity, closing the opening. Moynihan improved on this by making a vertical incision and entirely dissecting away the bladder, separating it also from the prostate, thus completely isolating it. Then the portion containing the ureters is held upward, while at the bottom of the wound the rectum can either be seen or made visible. The peritoneal reflection is then lifted upward from the front of the rectum, which is opened along its anterior surface by an incision perhaps three inches in length. Into this opening the bladder is placed, being so reflected that its former anterior surface now looks posteriorly. The ureters, instead of passing forward, now pass backward and the catheters contained within them are passed into the rectum and out of the anus. The edge of the bladder and the cut edges of the rectum are carefully sutured, after which the abdominal wound is closed. The sphincter is then stretched, while the catheters remain in the ureters for four or five days.
Fig. 650
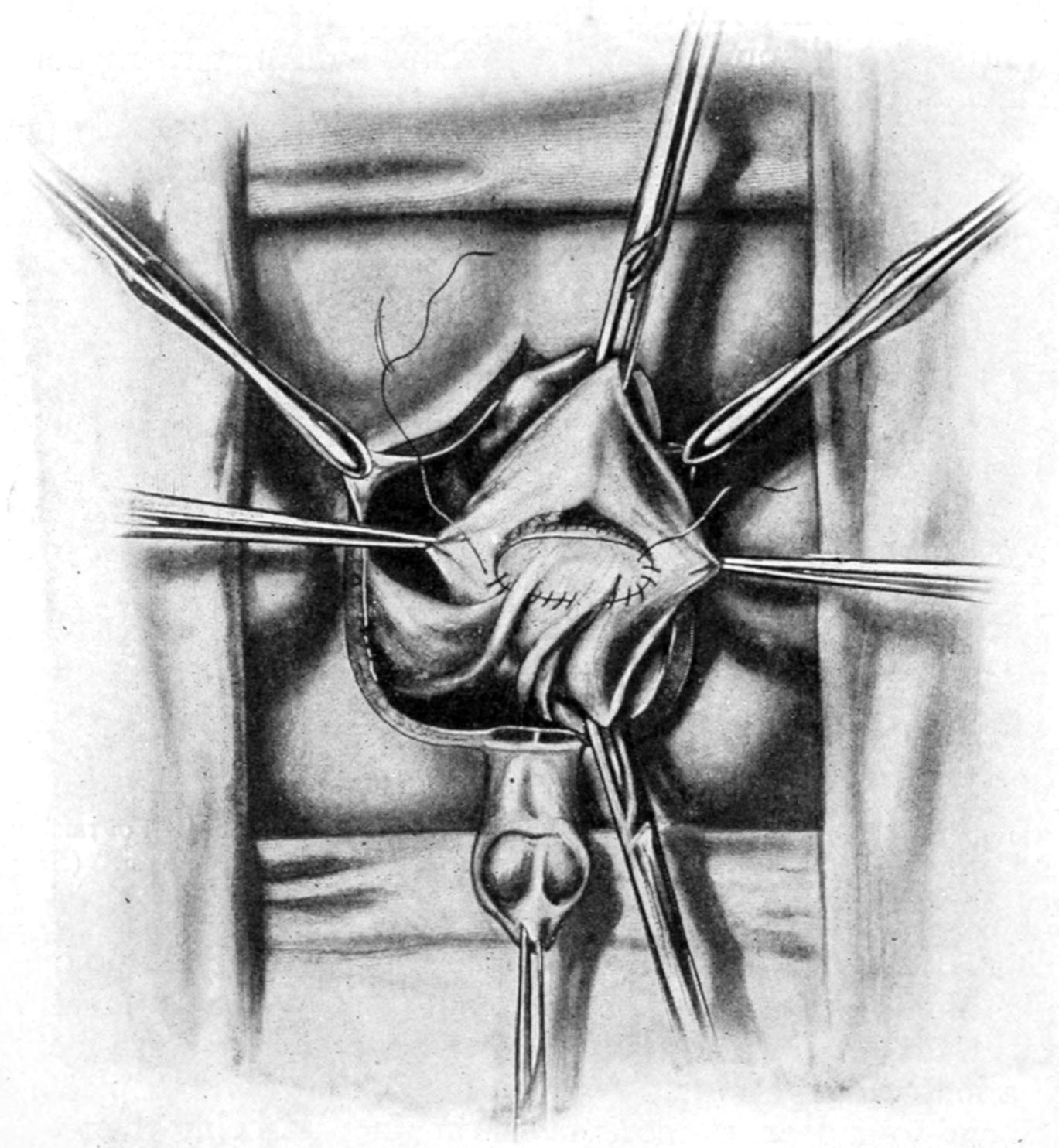
Maydl’s operation; diversion of ureters into rectum. (Hartmann.)
A choice may be made, then, between some such method as that last described or that of Peters, who dissects out the ureters, retaining only a small circular patch of bladder wall, which is folded around the orifice of each, the rest of the bladder being extirpated. Each ureter, with its button of bladder wall, is then drawn through a small slip in the rectal wall, made large enough to admit it, and the end of the ureter is then left hanging for 1 or 2 Cm. into the rectum. It would probably be better to hold the ureters in place by a stitch rather than run the risk of their retraction; but care must be taken that these stitches make no unnecessary constriction. Others have substituted[981] the sigmoid for the rectum, the procedure being otherwise the same, all of these rectal implantations having for their purpose the utilization of the rectum as a cavity, which may not only contain urine, but retain it reasonably under control. In many respects they would be ideal were it not for the attendant dangers. These are (1) those immediately connected with an operation which is serious, and (2) those connected with secondary infection of the kidneys, which seems to occur in almost all cases, no matter how apparently successful at first.
Injuries to the bladder proper may be accompanied by those of the parts without, or may be isolated. They divide themselves mainly into ruptures and lacerations, or penetrations directly connecting with the exterior. Among the causes which predispose to rupture and other injuries may be mentioned intoxication, partly because it is often accompanied by overdistention, and partly because of the partial or incomplete insensibility of the patient. Distention, no matter how permitted, is an important predisposing cause. The injuries usually include blows, falls, and crushes, and gunshot or other perforations.
The location of the rent is more commonly in the upper and posterior portion of the bladder—i. e., in its weakest part. Such tears may vary from one-half to four inches in length. When accompanying fracture of the pelvis the peritoneum is more likely to be injured.
The most significant symptoms are a desire to urinate and inability to do more than perhaps expel a few drops of bloody fluid. Of course the passage of any blood or bloody urine will suggest the occurrence of such an injury. Patients are usually unable to stand upright, and also show a strong tendency to flexion of the thighs. The introduction of a catheter and the withdrawal of bloody urine do not necessarily settle the question as to whether there has been any possible laceration. Some surgeons have taught that normal urine is comparatively harmless and that it is no more likely to produce infection than the catheter used for diagnostic purposes; but this is not safe teaching today. A clean metal instrument is of no more danger than a clean probe under other circumstances. Weir has suggested a valuable test, consisting of removal of all the urine possible, after which a measured quantity of sterile fluid is injected. If on using a catheter again this be all recovered it may be assumed that the bladder is not ruptured, otherwise the contrary. If hours after the injury a catheter be used and no urine secured, this fact will be most suggestive. The cystoscope is usually disappointing, since a bladder so injured cannot often be satisfactorily examined.
Another class of serious injury to the bladder includes the perforations, such as may be effected by gunshot or stab wounds, or, as in one case of my own, where a lad sat down upon an iron spike, about three-quarters of an inch square and nearly six inches in length. The point of the spike entered the anus, and the consequence of the injury was a perforation of the anterior wall of the rectum and the posterior wall of the bladder, with injury to its anterior wall without complete perforation. Prompt operation saved this case, as it will most such instances, although it was shown that a piece of his trousers had been carried into and left in the bladder. I opened the abdomen above the pubis, to be sure that the peritoneum was not injured, and then drained by a tube passed into the anus and out just above the pubis, after removing the piece of cloth. Prompt recovery followed.
The bladder may also be injured by rude manipulation of instruments, especially the metal catheter, by one unaccustomed to using it, or when serious difficulties are offered by prostatic enlargement.
—Diagnosis or even serious suspicion of such injuries to the bladder as above described require either perineal or abdominal section, the choice of the procedure being based upon circumstances. If there be reason to suspect intraperitoneal extravasation, then the abdomen should be opened, carefully cleaned, the bladder rent sought and sutured, the mucosa being first closed with hardened gut, while the peritoneal aspect may be sutured with silk or thread. The bladder should be drained, at least by retention of a catheter, passed if necessary by perineal section, and the abdomen drained. In the female drainage may be made through the cul-de-sac. If there be urinary extravasation[982] behind the perineum, then perineal section should be made, and the bladder, thus freely opened, should be drained with a sufficiently large tube; while in the female it will probably be sufficient to dilate the urethra and insert a tube of sufficient size. It is not always easy to discover an opening placed posteriorly in the bladder wall, and after a wide exposure, with emptying and cleansing of the pelvis, it may be of great assistance to place the patient in the Trendelenburg position. Under rare circumstances the rent may be so placed as to justify a suprapubic drainage of the bladder.
Foreign bodies other than calculi occur in the bladder in consequence of both accident and of design. The former are, e. g., represented by pieces of broken catheter, while the latter are materials introduced from without in consequence of sexual perversion, during intoxication, or from some other vicious tendency. The latter occur more often in girls and women, the former more often in men. In such a collection of cases as was made by Poulet (Foreign Bodies in Surgery) almost every imaginable object that could be introduced into the bladder is mentioned. Some of these have slipped in accidentally after external manipulation, as in masturbation, and some have been deliberately introduced. Perhaps as common an object as any is the ordinary hairpin. It is the short urethra of women which is made the much more frequent resort for such practices than the long urethra of men, in which latter foreign bodies are often entangled or arrested before they reach the bladder.
Any object allowed to remain in the bladder will serve as a nidus for the formation of a calculus, which will form in time, and it may result that not until the removal of the calculus and examination of its interior structure will the original foreign body be found.
All objects of this kind should be removed as early as possible after their introduction. Such removal may be easy and accomplished by dilatation of the female urethra, with or without the use of the cystoscope; or the bladder may require to be opened, either above the pubis, through the perineum, or through the vagina, in order that the object in question may be extracted.
Students often confuse not only terms but conditions, and it is necessary to be accurate in teaching regarding these subjects. Suppression of urine is purely a matter of cessation of renal function, and has nothing to do with the bladder. Retention of urine, on the other hand, has nothing to do with the kidneys, but is purely a bladder affair. It may be due to spasm of the bladder outlet, or to its obstruction by calculi, other foreign body, or by prostatic enlargement, or it may be a consequence of paralysis of bladder muscle. Such retention is the inevitable consequence of fracture of the spine, since paraplegia is to be expected in such cases, and the condition is to be atoned for by careful and regular catheterization. Retention, again, is occasionally seen in hysterical patients. It furnishes the distressing and sometimes permanent or even fatal consequences of prostatic enlargement in old men. No matter how produced, it must be relieved, for urine tends to accumulate and to distend the bladder, which will finally burst unless the difficulty be sufficiently overcome so that urine may in some way escape. Distention of the bladder under these circumstances is recognized by the formation of a rapidly increasing tumor, which finally rises to the level of the umbilicus, fluctuates, and is accompanied or not by pain according to the nature of the cause of retention. In paralytic cases there will be little or no pain. In obstructive cases it will be agonizing.
By natural efforts final rupture of the bladder is usually prevented, as after a certain degree of distention has been attained urine begins to escape drop by drop. This is simply an expression of an overflow, and is not to be confused with incontinence in the proper sense of the term. It may be spoken of as stillicidium, due to retention. The young and indifferent practitioner may mistake this escape of urine for incontinence, which would be a most serious error. Under any circumstances, when such a condition may possibly occur, the lower abdomen should be palpated, when the presence of a distended bladder should be instantly recognized. The first indication is for its prompt[983] relief by the use of the catheter, while the necessary catheterization should be done with the usual precautions. When the passage of an ordinary instrument is made difficult or impossible the cause of the retention is usually thereby revealed, and may be shown to be so serious as to necessitate further operative procedures.
When the bladder is distended and no catheter can be introduced it is advisable to aspirate, the aspirating needle being introduced through the sterilized skin just above the pubis, its point directed toward the centre of the mass formed by the distended bladder. Repeated aspiration may be necessary, and it has been suggested to make more or less permanent use of such a tube or hollow needle. At present no surgeon would continue this as a permanent measure, but simply as a temporary relief, even if repetition be necessary, until more radical procedure can be carried out. Whether this be the removal of a foreign body or calculus, or of an enlarged prostate, it is indicated just the same, the only exception to this statement being those cases already too seriously involved to justify more than perineal section (cystotomy for drainage). Retention of urine, then, is always a preventable condition, and its continuance is inexcusable.
Incontinence implies a paralytic condition, usually of the expulsive muscles, but sometimes of the sphincter apparatus in either sex, by which urinary control is lost and urine escapes involuntarily. It may be a temporary and occasional phenomenon, occurring under the influence of strong excitement or during sleep, especially in children, or it may be due to spinal disease or traumatisms, with paralysis of the lower segments of the cord and nerves given off from them. When originating in the latter way it is usually a hopeless condition, but nocturnal incontinence of children, or even of adults, or that due to hysterical or other neurotic conditions, may usually be benefited. For this purpose the surgeon should search for the cause from which the reflex proceeds. This may be extreme acidity of urine, the irritation of a tight prepuce in either sex, the presence of worms, intestinal disturbances, or any one of a great number of possible causes of disturbance of nerve control. Some of them permit of surgical relief; others require simpler measures. Children thus suffering should be given no fluid late in the evening, but should be made to empty the bladder before retiring, and perhaps be aroused once or twice through the night for the same purpose. In all cases the urine should be examined and hyperacidity overcome. All forms of genital excitement should be obviated. In the adolescent and in adults thus annoyed, and in the insane, it has been shown to be of great benefit to make a few intraspinal injections of sterile salt solution, as for local anesthetic purposes, a little cerebrospinal fluid being first withdrawn, and then from 2 to 10 or 15 Cc. of the solution being introduced. This seems to have been empirically suggested by a French surgeon, but has been found of value by Valentine and others, including the writer.
The above forms of incontinence are to be distinguished from intense irritability of the bladder, with frequent calls to empty it, which accompany many such conditions as cystitis, tuberculosis, tumors, calculi, and the like. This is the extreme irritability of local disease rather than true incontinence. But there is also a form, in women, characterized by falling away of the urethra and neck of the bladder from the pubis, due usually to injuries received during parturition, with consequent sacculation or dilatation of the urethra and formation of a cystocele. (Dudley.) This may also be associated with other results of perineal laceration. Here loss of urine is not constant, but occasional or frequent. For its treatment the following methods have been suggested: the injection of paraffin; partial torsion of the urethra (Gersuny), i. e., a partial dissection of the urethra and revolution upon its own axis, with subsequent suture, by which incontinence may be overcome, but at the possible risk of sloughing. Finally, Dudley has proposed the method of advancement of the urethra. He makes a horseshoe denudation, between the meatus and the clitoris, down on either side of the urethra, and nearly its entire length. Its anterior end is then loosened sufficiently so that the meatus can be drawn forward and secured below the clitoris by two sutures. The balance of the wound is then closed, the effect of the operation being to replace and retain the urethra and prevent its sagging. Other surgical treatment, as for cystocele, laceration, etc., may be added as needed.
[984]
The condition of true cystitis arises invariably either from the irritation of a foreign body or the presence of bacteria; the former need not necessarily be large, and minute and irritating crystals are often sufficient to produce at least some of its features. Sooner or later, however, the germ element enters, and from that time on cystitis is a bacterial infection. Furthermore this infection is usually secondary, rarely if ever primary, and may come from without or within. Thus it may be the consequence of the introduction of unclean instruments; is a very frequent consequence of gonorrhea, including all forms of urethritis; or may be the result of local tuberculous processes or those travelling downward from the kidneys; or, again, of more general toxic or septic conditions, such as typhoid and other infectious fevers. Certain conditions predispose, such as the presence of calculi or the occurrence of traumatism. Again, a bladder weakened by overdistention or paralysis, as in cases of spinal injury, loses its natural resisting power and succumbs to infection abnormally easily. It should be emphasized that the absolutely healthy bladder wall is resistant to all germ activity, but this resistance is easily lost or modified in the presence of disease, either close by or distant. A bladder whose normal shape has been greatly changed by enlargement of the prostate is again rendered not only unhealthy, but incapable of acting normally. It becomes, therefore, easily infected, and cystitis is a frequent accompaniment of prostatic hypertrophy.
Fig. 651
Internal appearance of bladder in some cases of inveterate cystitis; mucosa sacculated by columns of hypertrophied tissue. (Launois.)
—The cardinal symptoms of cystitis are three in number, i. e., pain, frequency of micturition, and pyuria, the latter being the consequence of changes in the urine, as well as in the bladder wall, while the pain and the thamuria are expressions of irritation, especially of the base of the bladder and the posterior urethra. In fact, all the more violent expressions of cystitis are found at the lower part of the bladder rather than in its upper portion. Obviously, then, irritation of adjoining organs is more easily accounted for, e. g., of the urethra, the seminal vesicles, the prostate, and the lower ends of the ureters.
The pain may be severe, and is especially complained of with each act of urination. It is referred not only to the region of the bladder proper, but along the urethra to the end of the penis in the male, and down the thighs in both sexes. With frequency of urination there is also distressing urgency, so that once the necessity be felt nothing can restrain the promptness of the act. In fact so powerful is the expulsive tendency that the tenesmus affects not only the bladder but often the rectum, while the feeling or desire to urinate continues after the bladder has been emptied of its last drop, even for several minutes, and may cause the patient to sit in agony for some time. The distress[985] produced in acute cases of cystitis is excessive, and sedatives and anodynes constitute no small part of the treatment.
The amount of pus contained in the urine will vary with the degree of acuteness and the stage of the disease. At first it is but slight, but rapidly increases, until the urine may contain thick mucus and pus up to one-third or more of its volume. Finally blood may appear, by whose appearance a serious degree of inflammation is betokened.
Later, at a variable date, the putrefactive element is introduced; and when the urine begins to smell of ammonia—i. e., when ammoniacal decomposition has once begun—the bladder is thereby the more irritated and the case made still worse.
No vesical mucosa left suffering from such acute inflammation will remain unaffected in its tissue elements, but will rapidly become more or less thickened. In fact the entire bladder wall undergoes a process of thickening, from hypertrophy of its inner and its muscular or middle coats, the latter due to extra activity in consequence of the constant tenesmus. There results in time a marked eccentric hypertrophy, whose result is really a contraction of the bladder cavity and a distortion of its lining. Under these circumstances, also, the mucosa becomes sacculated, and numerous little pockets, which may contain decomposing urine, serve to complicate the situation; while, finally, more or less incrustation or calculous degeneration and implantation modify the character of the mucous coat. For all these changes to occur requires time, but their combined effect is such thickening and contraction of the bladder as to permanently alter it and lead to a final concentric hypertrophy.
—The picture presented by tuberculous disease of the vesical mucosa is, in the beginning, one of miliary or disseminated involvement; but later, when ulcerative changes have taken place, the end results are scarcely different from those rehearsed above, save that the ulcerative element is more predominant, and there is great probability of involvement of the ureters or of any of the adjoining organs. As conditions do not essentially vary, neither do symptoms, and a diagnosis of tuberculous cystitis often must, in the early stages, be reached by a process of exclusion, corroborated perhaps by the cystoscope.
—A different clinical type of irritation, or mildly infective cystitis, is known to be a sequel of certain operations, not alone those upon the pelvis. In the majority of cases it occurs when catheterization has been required, the first event being urinary retention, by which the bladder mucosa must be more or less disturbed. It may be perhaps accounted for by the fact that the urethra is practically never free from germs, which, in that canal, seem to be innocent, but which, carried upward into an irritated bladder may excite serious inflammation. These cases are perhaps more frequent after pelvic operations for cancer. There seems, however, no doubt but that repeated catheterization for several days lowers bladder resistance.
—When the occurrence of cystitis is imminent prophylactic or preventive treatment is recommended. This should consist in administration of large quantities of fluid, with urinary antiseptics, in lavage of the bladder itself, and in reliable antiseptic precautions in catheterization. Thus to operate upon a bladder which has long held seriously infected or decomposed urine, without previously cleansing it as much as possible, is simply to invite further trouble.
The medicinal treatment of cystitis, on which we mainly rely, consists in dilution of the urine by large amounts of fluid ingested, in overcoming hyperacidity by the administration of alkalies, and in combating putrefactive conditions, so far as possible, by antiseptics which are eliminated through the kidneys. Balsams have been long held in great repute; but remedies like urotropin and other synthetic compounds have taken their place. Of them all, and especially in the presence of ammoniacal urine, urotropin and the alkaline salts of benzoic acid seem most reliable. Excessive irritability may be overcome by local measures, such as frequent hot rectal douches, hot sitz baths; by quieting irritation of the genitospinal centres by administration, e. g., of cannabis indica, in doses pushed to the physiological limit; by local anodynes, as by opium suppositories, or in extreme cases by general anodynes like morphine.
Theoretically a seriously infected bladder should be washed out and cleansed as any other pus cavity, but when so inflamed the bladder becomes so intolerant and exquisitely irritable that the mere act of washing can only with difficulty be borne by the patient. Retention of a catheter, which might be advisable under most circumstances, may also be impossible for the same reason. The condition of a patient under extremes[986] of this kind is pitiable, and resort to general anodynes unavoidable. Still it is possible with patience and the use of selected drugs to gradually allay even a most acute cystitis. Confinement in bed and an almost fluid diet are also necessary features of treatment.
If the introduction of an instrument can be borne it may be possible to leave in the bladder some soothing solution after it has been washed, such as a mild cocaine solution containing a little morphine, or olive oil containing orthoform, or a mild preparation of ichthyol. Even if these be retained but for a short time they will usually afford relief.
Finally in severe forms of cystitis the bladder may be opened for the purpose of giving it physiological rest, selecting either the suprapubic or the median perineal route. The relief thus afforded is usually gratifying, while drainage may be maintained until the local treatment has been sufficiently effective to permit either spontaneous closure of the drainage opening or its repair by suture. This measure is known as cystostomy for the relief of cystitis.
Obviously if cystitis be due to the presence of any foreign body its treatment becomes necessarily surgical, the same being true of those forms due to or connected with hypertrophy of the prostate. It is impossible to accomplish a cure here until the mechanical difficulty is first overcome.
In the urinary bladder as well as in the gall-bladder mineral elements held in solution by the contained fluids are precipitated, the consequence being the formation of calculi or stones in the bladder, which vary in size from the smallest concretions to those weighing many ounces, and in number from one to scores, a large proportion of these representing original concretions passed down from the kidneys, i. e., minute renal calculi. Every calculus has a nucleus, and in many instances this may be a clot, or clump of cells encrusted with salts, which have formed within the bladder and not come down from above. Such foreign bodies will become the nidus for a calculus, while in vesical calculi are frequently found pieces of catheter, of straw, chewing-gum, hairpins, and the like, which have been introduced from without. These stones are constituted mainly of the ordinary urinary salts, i. e., phosphates, urates, or oxalates, deposited as described above. Much more rarely cystin and xanthin are found. Instead of urates crystallized uric acid will be occasionally seen. The oxalates are mostly those of calcium, while the phosphates are those of calcium, magnesium, or ammonium, more or less combined. The first requisite for a calculus is a nidus, the second the deposition of one or more of these salts. Calculi are sometimes composite in structure, some having a uric or urate nucleus becoming later encrusted with phosphates. The oxalic calculi are exceedingly hard and usually rough, being often spoken of as mulberry. They rarely attain large size. The rapidly forming phosphatic calculi are often so small as to disintegrate or break in the process of removal. Thus there may be great differences in density of these stones. Their formation is particularly favored by retention of alkaline urine, as in many cases of prostatic enlargement.
—Discomforts and symptoms produced by bladder stone depend upon their size, number, roughness, movability, and location. The larger and rougher stones, which are more or less easily moved inside a tender and irritable bladder, will cause a large amount of discomfort and actual pain, while a small calculus, which may be formed within a pocket or become encysted at some distance from the urethral opening may remain unnoticed. The indications of calculi are essentially those of cystitis, pain, frequency of urination, and pyuria, sometimes with hematuria. The pain is local and referred, especially along the urethra, to the glans in the male, and is often aggravated by the final expulsive movements of the bladder at the termination of urination. Local discomfort is aggravated by active exercise. Reflex pains have been known in distant parts of the body. The frequency of urination is increased by exposure to cold or by activity. Pyuria and hematuria do not differ from those of non-calculous cystitis. A most significant feature is sudden stoppage of the urinary stream, with more or less pain. Statements to this effect, especially if accompanied by a history of renal calculi in time past, are most suggestive.
Unless, however, particles of calcareous material have been passed the positive diagnosis of calculus rests upon its detection by examination, either with a stone searcher or with the cystoscope. The former is essentially a short-beaked, light sound, which may be[987] more easily manipulated after introduction within the bladder. In using it the same precautions are taken as for catheterization or sounding, while the deep urethra may be made less sensitive by a cocaine solution. The instrument is introduced exactly as is a sound, and its beak is carried completely into the bladder. Sometimes even before this has been accomplished will be noted the rough, grating sensation which indicates contact with a stone. At other times it is only after considerable search that a small stone is “touched.” A stone easily found is within the possibilities of unskilled manipulation, but to accurately examine a bladder, especially behind a large prostate, is a fine art. For this purpose the bladder should be partially distended with fluid, the patient should be in the horizontal position, and the stone searcher so manipulated that its beak may be made to traverse every portion of the lower part of the bladder and to come into contact with its wall, for only in this way can an encysted calculus be discovered. The beak must, moreover, be rotated so as to be carried down into the pocket behind an enlarged prostate, as in such pockets many calculi nestle. Some stones are felt even in introducing a soft catheter; others are discovered only after such manipulation as the above. Nothing but necrosed bone or a foreign body can convey to the metal instrument, and through it to the finger, the peculiar sensation produced by contact with a stone. By attaching an auscultatory tube to the instrument a characteristic sound may also be heard.
With the cystoscope in the hands of an expert it is possible to orient one’s self definitely concerning the size and location of a calculus, but much information can also be obtained by the use of the ordinary searcher.
It has occasionally happened that calculi have been discovered by accident, either during a suprapubic or some other pelvic operation.
—The presence of vesical calculus being established, there is but one rational treatment, i. e., its removal. It remains, then, only to select the method of operation and to perform it. Vesical calculi are removed by two general kinds of operations: by crushing and evacuation of fragments through the natural passages, or by a cutting operation and extraction entire. The former is known as lithotrity, or, as now performed in one sitting, litholapaxy, and the other as lithotomy, which may be performed either above the pubis, through the perineum, through the vagina, or through the rectum. Each method has certain obvious advantages. Thus in favor of crushing there is freedom from an open wound, with its dangers of infection and of hemorrhage, while it appeals to the sentiment of those patients who “dread the knife.” One objection to it is that even when performed with skill assurance cannot be given that the bladder shall be freed from all calcareous particles, one of which may, by remaining, serve as a nidus for another calculus. In favor of the cutting operations are their brevity, i. e., the celerity with which they may be performed, the relief afforded by drainage, which can be carried out through the lithotomy wound, and which is often indicated in bladders that have been long tortured by the presence of calculi; while, finally, their simplicity, at least in most instances, makes lithotomy attractive to the operator of limited ability. It may be added that certain calculi, especially of the oxalic type, are so dense and resistant that even when secured in the grasp of an instrument they can scarcely be crushed. It may be urged also that septic urine is just as harmful in a bladder whose mucous membrane has been slightly injured here and there in the process of crushing as in one which has been more or less opened by a lithotomy.
Between cutting methods choice varies also according to the taste and views of various operators, as well as the nature of the case. When the prostate is large a suprapubic operation was held the simpler for the removal of calculus, and this earlier teaching is not abandoned. In the young the urethra is small and the bladder lies high in the pelvis, and both these conditions favor the suprapubic method. Again it enjoys repute because there is no danger of injury to the prostatic urethra or the seminal ducts or vesicles, and because it leaves the genital apparatus absolutely untouched. It is also free of possibility of harm to the rectum, which was by no means unknown in the hands of the older operators who resorted to the perineal route. But the removal of a large stone by the suprapubic route entails an opening of considerable size, and it is not unlikely that a large calculus may need to be fragmented and removed in pieces rather than leave a large opening at a point where urinary fistulas would likely ensue. It will be seen, then, that even lithotomy is not always to be performed without crushing of the calculus.
[988]
Of the perineal routes only two are in vogue today, the median and the lateral. The median is resorted to for stones of moderate dimensions, while the lateral will be required for large calculi. The vaginal route is often selected in women, although, rather than make an extensive opening between the bladder and the vagina, it will probably be easier and better to dilate the urethra, and, through it, crush a calculus which, in the female, could thus be made more accessible than in the male. Therefore in the female the suprapubic route or a litholapaxy is usually adopted. The operation through the rectum has been long since abandoned.
After a calculus has been removed by crushing a self-retaining catheter should be inserted, for at least a day or two, and the bladder washed, while at the same time treatment for the cystitis, which is still present, should not be discontinued. After opening the bladder the wound is drained for at least a day or two. Drainage has this disadvantage, that if long continued it leaves a urinary fistula, often slow to close, but a metal, glass, or hard or soft rubber tube may be placed in a median perineal opening, around which should be packed gauze to check oozing, and left in this condition for two or three days. Usually within a week after its removal the deep sphincters have recovered their retentive power, and the patient can retain urine for some time, while generally within two weeks the entire wound is closed. In all these cases a sound or bougie should be passed at suitable intervals for the purpose of preventing stricture formation in the deep urethra at the site of the operation.
Litholapaxy is performed by first crushing the stone between the beaks of an instrument known as the lithotrite, which is constructed in various forms, yet all conforming to one type, which is introduced into the bladder through the urethra, after which its blades are separated and manipulated until the stone is felt to be entangled or secured between them. By a device at the handle the blades are then locked, and screw power exerted, also from the handle, by which the blades are forced together and the stone between them more or less broken (Figs. 652 and 653). By repetition of this process each fragment is seized separately and crushed until the bladder contains more or less debris resulting from the manipulation. The lithotrite is then removed and a washing tube or catheter of large dimension inserted, and connected with a so-called washing bottle, which is compressible and permits a stream of water to be violently thrown into the bladder, thus stirring up the fragments and particles, and which is an instant later withdrawn by suction in such a way as to carry them with it. Escaping into the washing bottle they drop by gravity into a glass receptacle at its base, where they become at once visible. This process is repeated until everything has been washed out of the bladder which will come. The lithotrite is then substituted and the maneuver repeated, and as many times as may seem desirable. In this way calculi, especially soft ones of large size, may be disintegrated and removed in small fragments. The final test of success is failure to aspirate any more particles or to discover them with the cystoscope (Fig. 654). The time consumed in the operation will depend on the operator’s skill and the size or hardness of the stone. It is frequently performed under local anesthesia, the bladder being injected with a weak cocaine solution, or under spinal anesthesia.
Lithotomy, by either of the above methods, is performed by utilizing a grooved sound known as a staff, which is first inserted into the bladder, and serves not merely the purpose of a grooved director, but to indicate the course of the urethra.
For the suprapubic operation the staff is passed deeply, and its handle depressed between the thighs, so that the end of the instrument rises behind the pubis and carries the bladder up toward the surface. A median incision above the pubis permits access between the recti muscles to the prevesical space (space of Retzius), which is more or less filled with fatty and connective tissue. If the bladder has been previously distended with fluid and elevated on the point of the staff, there is but little danger of wounding the peritoneum, although its reflection may be sought and carried out of harm’s way. It is a convenience to pass a silk suture with a stout, full-curved needle through the bladder wall after it has been exposed, on either side of the point of the staff which elevates it, and to pass this through in such a way as to have thus a double loop, or two retractors, by which it may be more conveniently manipulated after it has been opened and would otherwise collapse. The bladder should be opened upon the point of the staff, whose groove may then serve as a guide in still further nicking or incising it, the silk sutures on each side preventing it from collapsing as it otherwise would after the gush of escaping[989] fluid. The surgeon should now endeavor so far as possible to dilate rather than to merely cut this opening, and thus give it a size sufficient to permit the introduction of the finger,[990] by which intravesical exploration and orientation are effected. Calculi having been identified and located, suitable forceps are then introduced, and with them the stone or stones seized and withdrawn through the opening, which may be stretched still farther for the purpose unless their size make it advisable to crush them and remove them in fragments.
Fig. 652
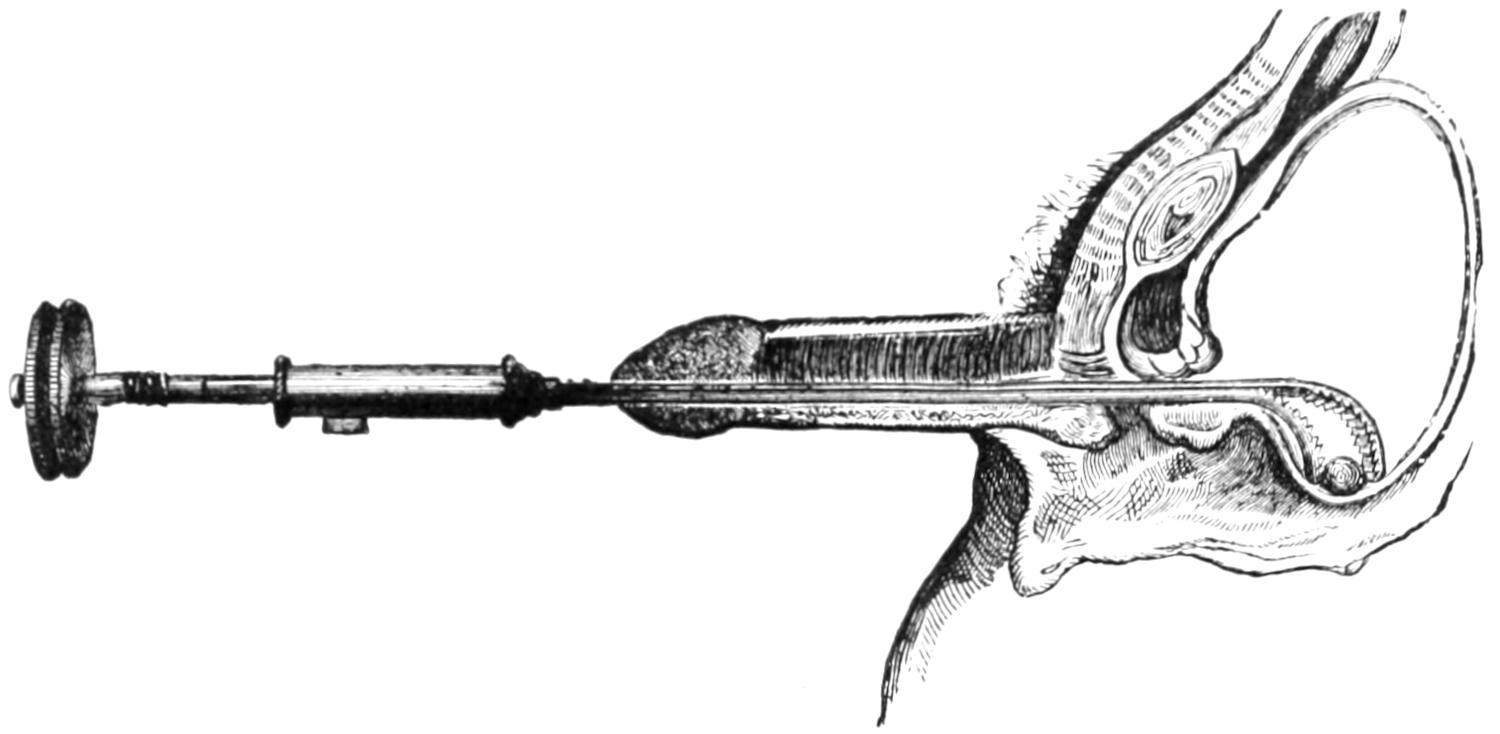
Method of seizing the stone behind the prostate.
Fig. 653
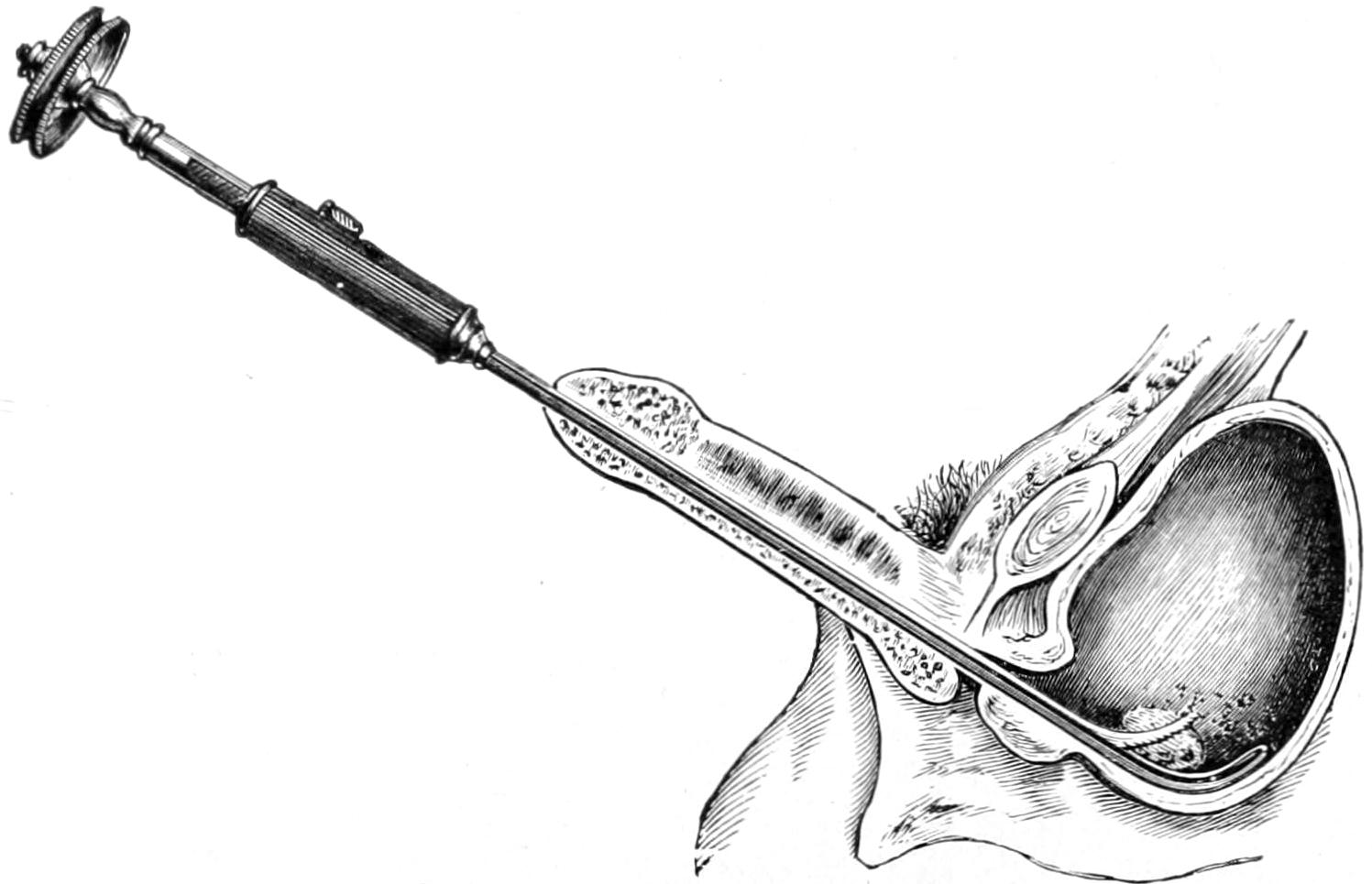
Ordinary position in seizing the stone.
Fig. 654
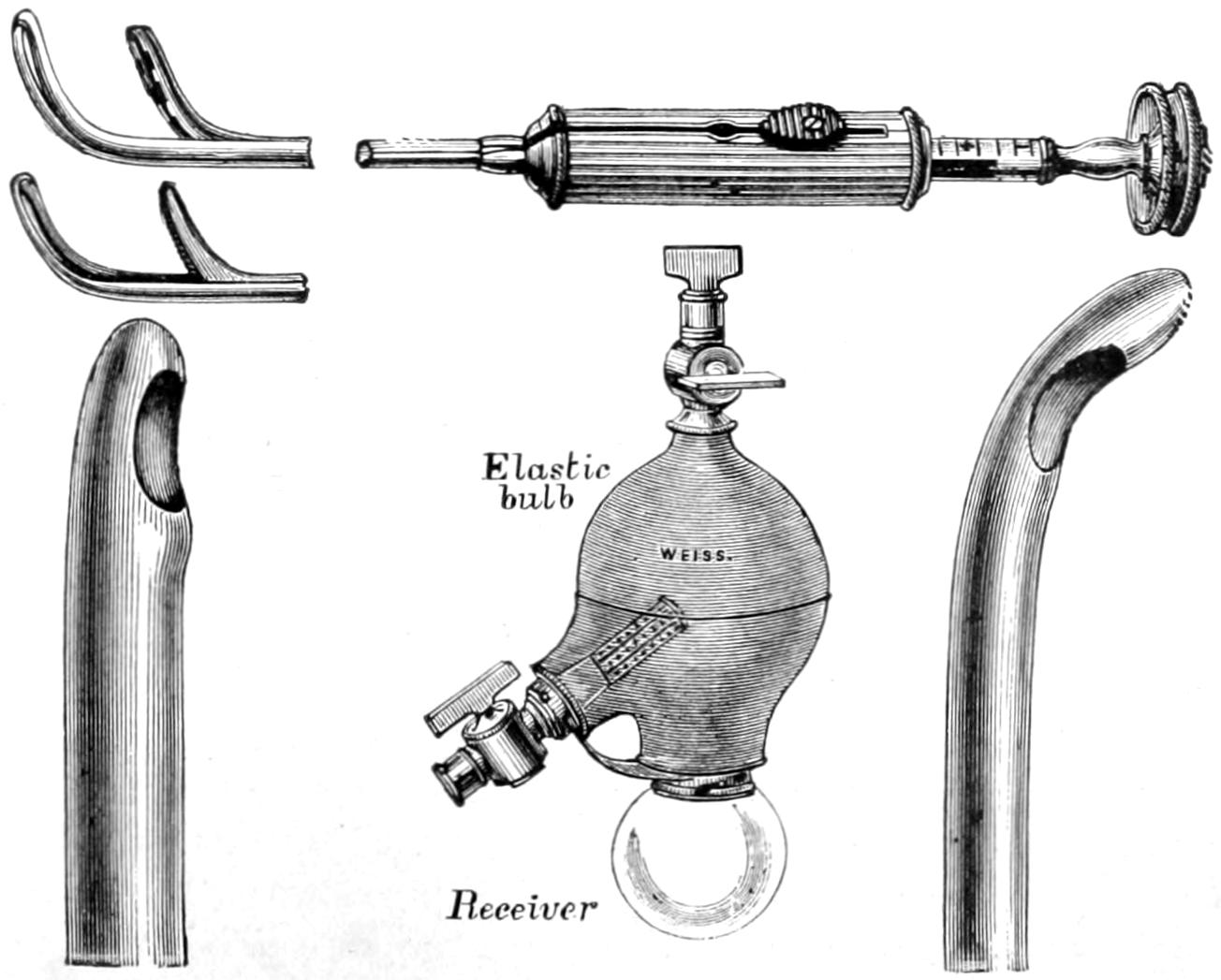
Bigelow’s lithotrites, catheters, and evacuator.
This is suprapubic cystotomy or epicystostomy, according to the purpose for which it is intended. It serves not only for removal of calculi but for extirpation of tumors, or enlarged prostates, and perhaps for permanent drainage. By the silk loops at first introduced the bladder wall may be attached to the abdominal wound, while other stitches may be added to any desired extent. In most instances it is desirable to reduce the opening, for which purpose buried and superficial sutures may be used. As leakage, however, may produce infection it is customary either to provide for drainage by insertion of a catheter through the urethra, or by the implacement of a small tube, whose lower extremity shall reach the base of the bladder and serve for drainage, which latter may be made more effective by siphonage.
Perineal section for exploration, drainage, or stricture is practically accomplished as follows: The patient is first placed in the so-called lithotomy position, i. e., upon the back with the limbs flexed and knees parted, the feet or legs being held either by assistants or in suitable leg holders upon the operating table. This is the position in which nearly all perineal operations in both sexes are made.
A grooved staff, with large curve and long beak, is introduced into the bladder, and not only held in the vertical position by an assistant, but in such a manner as to make its curve bulge the perineum as much as possible toward the operator. The rectum, which should have been previously thoroughly cleaned, may be utilized for identification or for necessary assistance during the operation. The scrotum is held up out of the way by the assistant who holds the staff. The perineum being thus put upon the stretch may be most quickly opened by a straight, sharp-pointed bistoury, which is inserted a little posteriorly to the scrotal junction, its point driven through the tissues and made to engage in the groove of the staff, from which it should not escape until finally withdrawn. As the instrument is pushed backward the handle is depressed; a triangular-shaped opening is thereby effected, whose apex is in the membranous urethra and whose base occupies the raphé of the perineum, to the extent of perhaps one and a half inches. The entire incision may be made with one effort. Its effect is to open the membranous urethra. Into the groove of the staff, the knife being withdrawn, may be introduced either a species of grooved director or the finger-nail of the index finger, which may be passed backward and made to enter the prostatic urethra, while at the same time the staff is withdrawn. If the prostatic urethra be constricted it will be difficult to enter the bladder with the finger, otherwise it will readily yield to pressure, and it is thus possible to enter the bladder within a few seconds after the first incision is begun (Fig. 655).
It is preferable in all these cases to have first washed out the bladder, and then to have filled it with a mild antiseptic solution. This will escape instantly an outlet is made from below. If there is a small calculus within the bladder the effect of the stream will be to carry it toward this outlet, where it is identified by the finger.
The prostatic urethra will bear a considerable amount of gradual dilatation, which will make it more than easily accommodate an ordinary finger. In this way a sufficient channel is made, through which forceps may be introduced and calculi of small or medium size withdrawn. They should be seized as carefully as possible within the proper grasp of these instruments, so that a minimum of laceration may be effected as they are extracted. A small calculus will be easily removed; a large and soft one may crumble in consequence of the pressure made upon it during its extraction. In this event the fragments should be separately removed, the bladder then repeatedly washed out, and the finger finally used to make sure that no particles remain.
Whether one stone or several be present the opportunities for the purpose of their extraction afforded by this median operation are the same. The bladder having been emptied and washed out a self-retaining drainage tube, or a hard rubber or metal perineal tube should be inserted, with such gauze packing around it as may be necessary for[991] its retention and for the checking of hemorrhage. The intent of the tube is a double one, it being intended to serve for easy drainage and for gentle pressure. Sometimes the prostate is more or less torn in the process of dilatation, and in this case will bleed more freely than is comfortable. Such oozing may be checked by plugging gauze around the drainage tube.
Lateral lithotomy may be combined with median section, by deliberately passing a blunt bistoury into the prostatic urethra, and making with it an incision in the prostatic substance, the cut being directed toward a point midway between the anus and the ischiatic tuberosity, and carried to a depth of one-half or three-quarters of an inch. This affords a much larger opening through which to remove larger calculi. Obviously it will bleed more freely and will usually require packing. The old lateral method was to begin the external incision at a point, in the middle line, a little behind the scrotum, and direct it for one and a half or two inches backward and outward to a point between the tuberosity and the anus. The incision was then deepened through the perineal fascia until the index finger-nail of the left hand could identify the staff within the urethra, after which the urethra was opened at this point (i. e., just behind the bulb), when the knife was again introduced and made to divide the prostate obliquely as above. In this way the membranous urethra and lateral aspect of the prostate were divided to the requisite depth. If such incision be extended too far backward and outward the internal pudic artery might be divided, which would at least be awkward and necessitate ligature, and this would be somewhat difficult because it would require further division of tissues.
Fig. 655
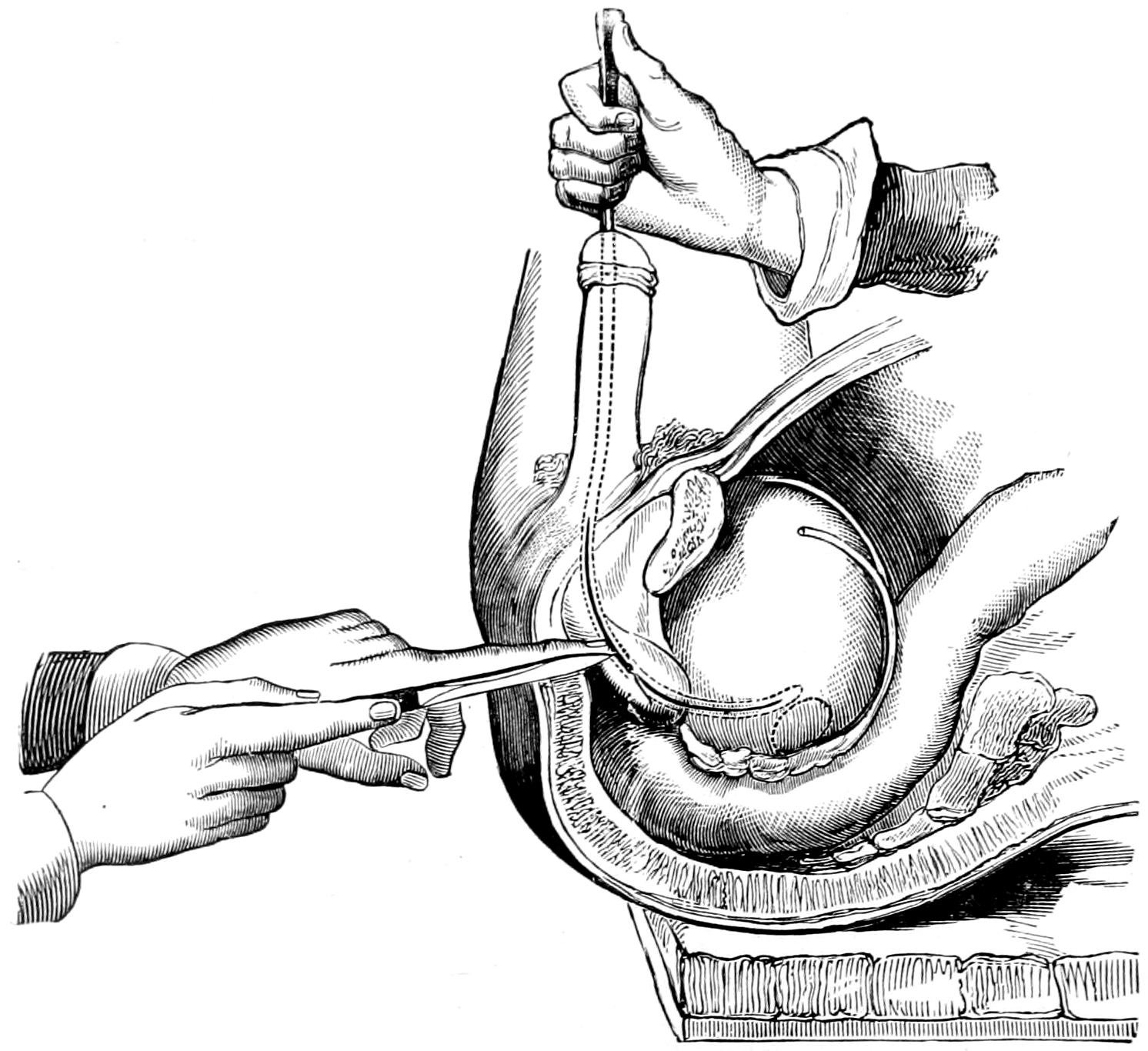
Second stage of lithotomy. (Erichsen.)
The same management is required after lateral as after median operation. Except only when a long and seriously inflamed bladder requires almost permanent drainage the perineal tube should be removed within forty-eight hours, and the external opening allowed to close as rapidly as possible.
[992]
The most common benign tumor of the bladder is papilloma, which here assumes almost invariably the villous form and grows even luxuriantly. It may be solitary or multiple. In the beginning it is usually more or less pedunculated, but may grow in great numbers, as in the mouth. A class of denser tumors are the fibromas, which are covered by a more or less thickened mucous membrane. Myxomas grow mainly in children. Adenomas have been described, but are rare. Dermoid cysts in or about the walls of the bladder have also been described. The malignant tumors of the bladder are mainly of the epithelial type, usually adenocarcinoma, of a somewhat peculiar type, due to malignant degeneration of an original papilloma, an unfortunately common event (Fig. 656).
Fig. 656
Fig. 657
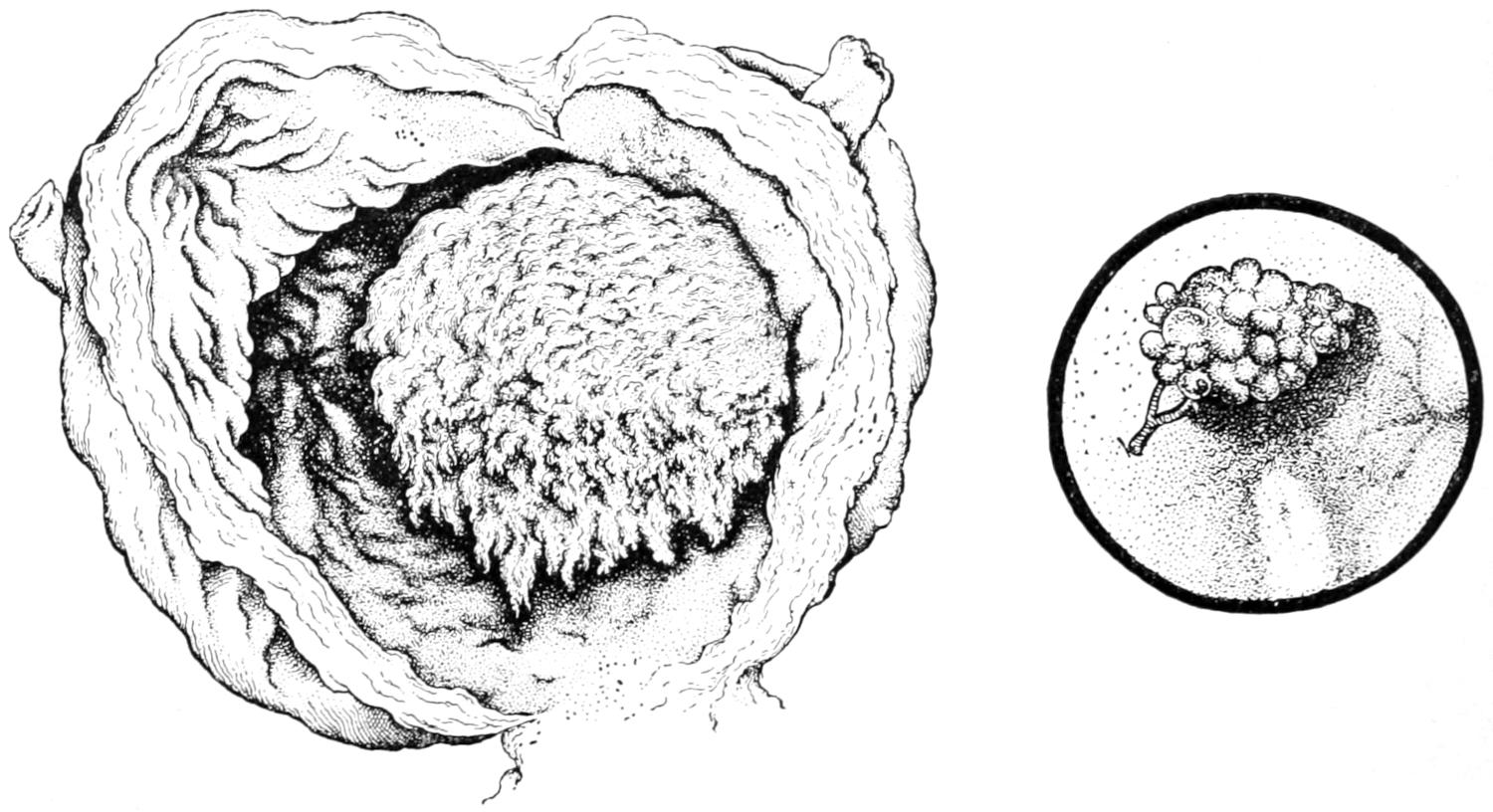
Villous tumor (papilloma) of bladder. (Musée Dupuytren.)
Tumor of bladder as seen with cystoscope. (Nitze.)
—The symptoms due to tumor in the bladder do not differ much from those of calculus, except that there is at first less pain. In nearly all cases there will be hemorrhage, occurring independently of exciting causes, as during sleep, not only abundant but often frequent. In the early stages pain is rarely severe. In cancer it is largely proportionate to involvement of the bladder wall and the adjacent organs, and is more common in cases of basal tumors. It is both local and referred. With a bladder filled or filling up with a tumor mass there will be reduction of capacity and frequency of urination, while in nearly all instances the essential features of cystitis are superadded. The actual evidences of tumor are its detection by the cystoscope, its discovery by vaginal or rectal palpation, or its recognition by fragments discovered in the urine.
When the cystoscope is used in these cases it usually reveals the location, size, vascularity, arrangement, and character of the tumor. Its use, however, is often difficult or impossible, because the manipulation by which the bladder is so distended as to permit its use causes hemorrhage and obscurement of the field of vision (Figs. 657 and 658).
With the cystoscope has been recognized also an early condition of leukoplakia, corresponding to that seen in the mouth and on the tongue, which may be regarded as a precancerous condition.
—The only treatment which can be made effective is complete operative removal. There is no reason why any benign tumor of the bladder should not be attacked, the most unpromising cases being those of general papillomatous involvement, where only small areas of the bladder mucosa are left uninvolved. Such a villous condition as this is serious, and may later justify an effort at extirpation of the bladder. Palliative treatment will include the arrest of hemorrhage (for which a few drops of[993] turpentine oil are often effective), with gentle lavage of the bladder and removal of clots, securing their disintegration by injecting an emulsion of pepsin or of papain; while tenesmus, irritability, and pain are to be controlled by cannabis, suppositories, morphine, or whatever may be needed. In inoperable cases cystotomy for drainage purposes may be the final measure for relief purposes.
Radical measures include opening of the bladder, either above or below the pubis, as the cystoscope may indicate; or the former, when the cystoscope cannot be used, as it affords better means for exploration. Through this opening, which may be made larger than for mere exploratory or lithotomy purposes, and aided by artificial light (small electric lights introduced by suitable mechanism, as within a test-tube), there may be removed with scissors or curette, or even with the finger-nail, by enucleation, such growths as are met, while in nearly every instance it will be an advisable precaution to cauterize their bases with the actual cautery. Through more extensive incisions, with the patient in the Trendelenburg position and the prevesical space widely opened, the bladder mucosa may be excised, and ample drainage provided both by retention of a catheter and insertion of a siphon tube through the lower part of the opening. The suprapubic route affords better opportunities for thorough work than does the perineal, the latter being suitable only for a limited class of cases.
Fig. 658
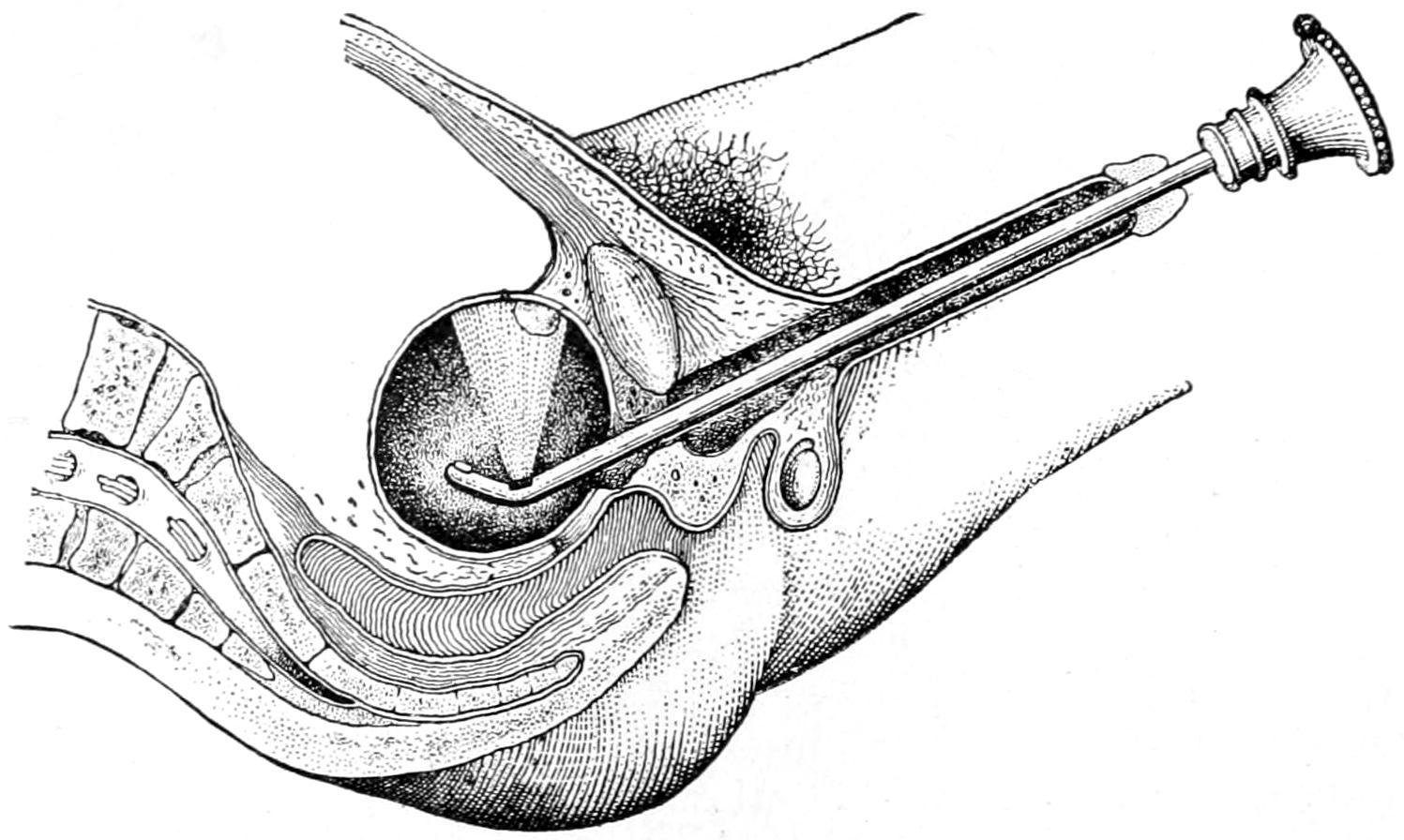
Illumination of anterior vesical wall by Nitze’s cystoscope.
Finally comes the question of extirpation or a complete cystectomy. This radical and difficult measure has been added to the list of possible surgical procedures. In a case of general papillomatous disease it might be successful, but it is questionable whether any case of cancer which would call for such a measure can be cured by it. The operation has been done much oftener in women than in men, and usually by a combined procedure of suprapubic opening, which may be vertical or transverse, with attack from the vagina. If the vaginal wall be involved it may also be cut away. The ureters should be isolated and preserved, when, the affected tissues being removed, it becomes a question of what to do with them. They may either be left to drain into the vagina, which is thus utilized simply as a conduit, and which may be closed later and the urethra thus utilized, a urinal being worn, or they may be immediately or by a secondary operation turned into the rectum. The latter procedure introduces fresh complications, though, if successful, it would minimize the unpleasant features of such a case.[69]
[69] Symphysiotomy may, when required, be combined with suprapubic operation as in the case of young children, for removal of very large stones or tumors, as has been recently demonstrated by Palmer, of Persia.
It is thus possible to successfully extirpate the entire bladder proper, conserving the ureteral orifices or not, as well as the urethra, although the resultant condition can hardly be considered brilliantly satisfactory.[70]
[70] In a recent case I have been able to more easily effect this procedure by raising a flap, including the tissues of the mons, exsecting a portion of the symphysis containing the insertion of the recti, by oblique division, in such a way that when replaced the bone could not be easily displaced, and in this way uncovering the space of Retzius so that, by combined manipulation, it was easier to detach the bladder wall from its surroundings.
[994]
The prostate, with the duct extremities of the seminal vesicles, are enclosed in a fibrous sheath or capsule, of more or less density, which has been called by Belfield the broad ligament of the male. In structure this body is composed of a mixture of adenomatous and muscular (involuntary) fibers, with considerable connective tissue, so that in many respects it is the homologue of the uterus. It not only serves as the portal of the bladder, but through it pass the prostatic urethra and the seminal ducts. Infection proceeding from either direction may, therefore, travel along either one of several paths, spreading disaster and causing a variety of troubles. Such infection may be tuberculous, gonorrheal, or of the ordinary septic type. There will ensue in consequence various forms of prostatitis: the acute, which may lead to abscess, and the chronic, which will always lead to hypertrophy.
Acute prostatitis is generally the result of gonorrheal infection, the consequence of extension from the urethra into the mucous follicles and the prostatic structure. Primary tuberculous disease in this location is rare. Septic infection comes either from the use of unclean instruments, from the presence of infected urine, or from the extension of cellulitis from some adjacent structure. It is not infrequently seen in connection with deep and tight strictures and accompanying cystitis, or in connection with the presence of small concretions, i. e., prostatic calculi.
Acute prostatitis is an exceedingly painful affection, made so particularly by inelasticity of the capsule, which affords no accommodation for the swelling due to the inflammation. In addition to the inevitable pain and tenderness the swelling will sometimes practically close the urethra in such a manner that urination becomes almost impossible. To nearly every case will be added some of the symptoms of acute cystitis, which may have preceded the prostatitis. Prostatic inflammation can be made known by the exquisite tenderness of the organ, discoverable by digital examination through the rectum. This feature, with tenderness in the deep perineum, and the above symptoms make diagnosis easy.
According to the intensity of the lesion will be the liability to suppuration. Prostatic abscess is a frequent result, and its presence is evidenced by accentuated pain and tenderness, with perhaps considerable febrile disturbance. In some cases fluctuation can be detected through the rectum. Such cases sometimes evacuate themselves spontaneously, although often in an undesirable way, when left untreated, or unrecognized, discharge taking place usually into the rectum, but perhaps into the bladder or into the urethra. Should pus burrow into the pelvis there will arise a deep pelvic cellulitis, with probable disastrous consequences.
When a prostatic abscess is suspected the patient should be anesthetized, the sphincter dilated, the exploring needle used if necessary, and any collection of pus, no matter how detected, should be either completely emptied with the aspirator or by free incision.
Chronic prostatitis may be the residue of an acute lesion or the gradual production of a mild but more or less constant septic infection. It leads always to more or less enlargement, is often the basis for the classic prostatic hypertrophy, and causes dull pain, referred in various directions, often to the sacrum and the back, with frequency of urination and escape of a viscid mucus, the natural prostatic mucus in excess, which the patient will usually consider semen, but which is really the product of the overworked prostatic glands.
This last phenomenon is spoken of as prostatorrhea, and deserves consideration not alone from the alarm with which patients often regard it, but because it indicates a significant condition. A prostate whose glandular structures have been unduly active will, in consequence, enlarge; such a prostate is compressed with the passage of every hard stool, the consequence being the expulsion of some of this fluid with each act of[995] defecation, a feature interpreted by too many patients as spermatorrhea. The two conditions are to be differentiated in clinical study, the former being common, the latter quite rare. Acute prostatorrhea is also frequently the consequence of more or less prolonged sexual excitement. It corresponds essentially to a chronic nasal catarrh, which is accentuated by exposure to cold or to irritation of any kind, and is only the overflow of a natural fluid under morbid conditions. With chronic prostatitis, furthermore, the sexual appetite is often decreased, while sensations are more or less disturbed, ejaculation being perhaps premature; the patient is often made thereby despondent, and the case regarded by himself, or by the quack whom he is led to consult, as at least incipient, perhaps hopeless, impotence.
The physical evidences of chronic prostatitis are enlargement, with tenderness not only of the prostate itself, but of the seminal vesicles above it, and often the appearance of a few drops of prostatic mucus at the meatus after pressure or stroking of the prostate itself has expelled them.
—Removal of the cause is the secret of success; if this be a stricture it may be divided and dilated; if cystitis, it must be combated; if chronic constipation, it should be overcome; while excesses, either alcoholic or sexual, should be controlled. Some one or nearly all of these conditions will be seen in nearly every case of this character. To other manipulative features may be advantageously added a certain massage or “milking” of the prostate, at intervals of five or six days, by which it is emptied of its accumulated secretion. Equally beneficial is the occasional passage of a large sound through the prostatic urethra and into the bladder. Its effect also is to make pressure, while at the same time it stimulates and does good in a way perhaps difficult of explanation. Irritation in the prostatic urethra should also be controlled by occasional injections, with a deep urethral syringe, of a drop or two of a ¹⁄₂ per cent. solution of silver nitrate. Improvement in other respects may be expected from constitutional, dietetic, and hygienic measures.
Many theories have been advanced as to the etiology of prostatic enlargement. Those worthy of any consideration may be summarized as follows:
Inasmuch as the prostate is to be regarded as essentially a sexual gland, many cases of hypertrophy are the result of bad sexual habits which produce continued congestion. Nevertheless the importance of previous infections, e. g., gonorrheal, by which hypertrophy of glandular and cell elements may be produced, cannot be overlooked.
Prostatic enlargement assumes one of three principal types:
In consequence the ensuing enlargement assumes one of the three following clinical types:
These types do not necessarily merge into each other, but may remain distinct. There may be atrophy of glandular elements as a result of hypertrophy of the muscle and fibrous elements, or vice versa.
Much confusion has arisen regarding the so-called third lobe, in spite of the fact that[996] the prostate is essentially a bilobed organ. Whence has arisen the tendency to speak of the “third lobe,” or is there such a thing? The explanation is that median enlargement is a common expression of prostatic hypertrophy, occurring toward the interior of the bladder at a point where the prostate has no capsule, and where growth occurs in the direction of least resistance. That morbid specimens show an apparent “third lobe” is true, but that such a condition exists normally is a mistake. It should, therefore, be spoken of as a median enlargement (Fig. 659).
Fig. 659
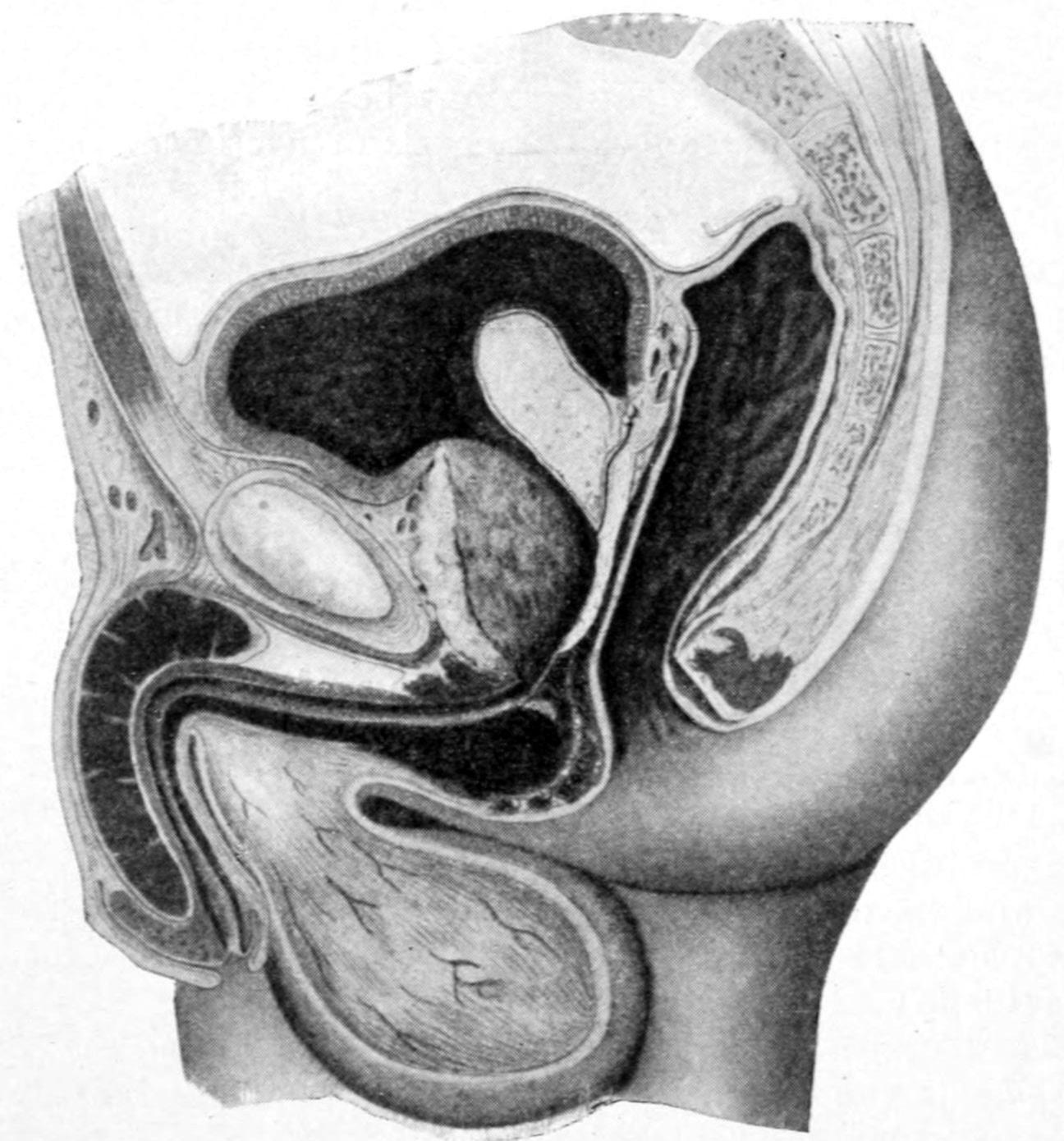
General prostatic enlargement, with formation of a median overgrowth and posterior pocket or sac. Illustrating how residual urine may be retained, as well as the difficulties of all kinds of instrumentation, i. e., an argument, therefore, for radical treatment. (Socin and Burckhardt.)
In addition to the more innocent and purely hypertrophic forms of prostatic enlargement, it has been recently shown, especially by Young, that the element of cancer is present in a proportion of cases hitherto quite unsuspected. It may begin as a small indurated nodule, in one or both lobes, and while developing remains confined for a relatively long period by the strong prostatic capsule. When it extends, its line of invasion is upward toward the vesicles rather than into the bladder. When the latter has become involved, if a radical operation is to be practised, extirpation must include not only the entire prostate, with its capsule, the urethra, the vesicles, but the adjacent portion of the base of the bladder. Early diagnosis in these cases is difficult, since it may occur at any age after fifty years, and, being connected with hypertrophy, produces symptoms masked by it, only the element of pain being more prominent. As the condition develops pain becomes rather disproportionate, spreads to the suprapubic region, and is intensified as the bladder fills. When pain is referred also to the rectum and lower extremities it is a suspicious symptom. The condition does not necessarily, at least at first, cause enormous enlargement. Therefore the obstructive features vary. If the portions involved can be left they will be found more dense and hard than the surrounding tissue. One peculiarity of prostatic cancer is that metastases occur more often in the bones than in the lymphatics. Consequently the pelvic nodes are not so often affected. Ulceration and intravesical tumor are rare.
—Early diagnosis is based on rapidity of growth, disproportionate pain, indurated contraction of the prostatic urethra near its apex, and absence of intravesical enlargement, as shown by the cystoscope. When there is much residual urine, without enlargement of intravesical lobes, suspicion is strengthened. If after removal[997] of such prostate it should be shown to be more or loss dotted with “seed calculi,” as is possible, instead of with cancer, the benefit and relief to the patient would be none the less marked, while the prognosis would be all the better.
Prostatic hypertrophy leads to a collection of phenomena spoken of as prostatism. These include mechanical impediment to urination, with consequent obstruction, sometimes with complete retention, and to the consequences of the same in the direction of infection and cystitis, with added features of pain, tenesmus, and pyuria. Prostatism is a matter of gradual development. Its earliest symptoms are frequent urination with occasionally some difficulty or slowness in the act. From this as a beginning cases become gradually aggravated, until death finally ensues from retention, rupture of the bladder, pyelonephritis, or exhaustion in consequence of the pain and suffering entailed.
Prostatism may be imitated in persons whose prostates are not perceptibly enlarged, in whom the difficulty and obstruction are due to sclerosis and contracture of the vesical neck. This condition is especially common in elderly men, subjects of arterial sclerosis. This will account for instances of prostates which, on removal, are found hard and sclerosed, and yet not enlarged enough to be obstructive. If such a prostate could be divided by the cautery, benefit, even permanent relief, might ensue. Therefore, such a condition might be well attacked when diagnosticated (either by suprapubic operation or by perineal section), with the use of the Bottini galvanocaustic instrument, especially through a perineal opening.
Prostatic enlargement produces distortion of the prostatic urethra, which becomes longer, smaller, and sometimes deviated, with elevation of the level of the vesico-urethral orifice, and causes, by pressure on veins, more or less disturbance of the return circulation. Enlargement with impediment produces dilatation of the bladder, with possible involvement of the ureters or the kidneys, and thickening of the vesical walls, often with sacculation of its mucosa between its disturbed muscle fibers.
Finally come the consequences of septic infection with ammoniacal putrefaction of urine, pyuria, and perhaps pyelonephritis with uremia, which will be terminal. While the condition is generally regarded as belonging to the late years of life it may begin by natural processes at the forty-fifth year, although uncommon before the fifty-fifth.
Fig. 660
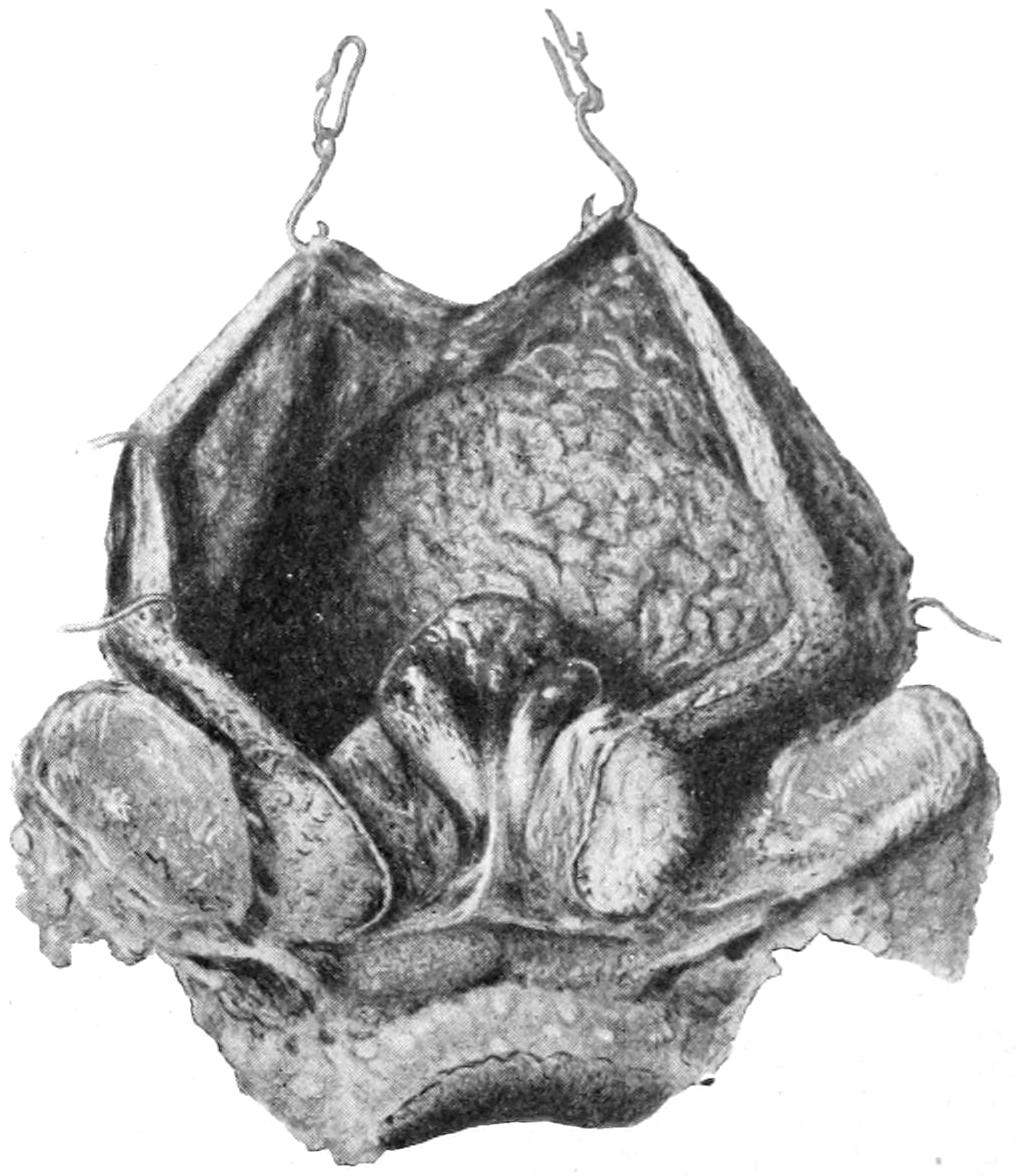
Enormous prostatic hypertrophy, necessitating suprapubic cystotomy because of impossibility of catheterization from below. (Socin and Burckhardt.)
—When a man past the middle years of life, previously free from urinary difficulties, is aroused to urinate more frequently than usual, especially at night, while the desire to urinate and the natural feeling of relief at the conclusion of the act are more or less perverted, the beginning of prostatism may be suspected. If in addition to these features the urine shows fermentative changes, or the presence of mucus or pus, the more or less disastrous consequences of obstruction have begun. Symptoms similar to these may be caused by the presence of calculus. It is therefore necessary to differentiate between this and prostatic enlargement. This is first done by a careful digital examination of the empty rectum, the index finger being gently introduced and made to so completely palpate the prostate, through the anterior wall of the rectum, that an accurate estimate of its relative size, as well as of any marked irregularity, may be made. If the prostate be enlarged the explanation is at once afforded. If there be but little apparent change noted by this method the surgeon should introduce a stone searcher. Manipulation with this, in a bladder distended with fluid, should reveal the presence of a calculus, or should indicate a lengthening of the prostatic urethra, with such distortion,[998] as might make the introduction of the instrument difficult, while by further manipulation, its beak being gently revolved, he learns whether behind the prostate there is a pocket in which residual urine may be retained. The question of calculus being settled the patient should now empty the bladder naturally and as usual, after which a catheter should be introduced, in order to withdraw such residual urine as may be retained, whose amount should then be noted. This is a measure of the size of the postprostatic pocket which the patient fails to empty, and in which decomposition and pathological changes are especially likely to occur. Should such a pocket be found in a case without noticeable other enlargement (as detected through the rectum) it will indicate intravesical growth and the formation of the so-called “third lobe” or “median bar,” as it was formerly called (i. e., an outgrowth at the posterior end of the prostatic urethra, projecting upward into the bladder, impeding alike the exit of urine and the introduction of an ordinary instrument). Those expert with its use may gain still further information of value by use of the cystoscope.
—The diagnosis thus established, the question of treatment is raised. Views concerning what is best have been largely modified by the operative methods recently introduced, and the advice given a few years ago is now frequently modified. So long as surgical treatment was unsatisfactory and incomplete it was to be postponed as long as possible. Under those circumstances patients were taught to use the catheter and established the “catheter habit.” Almost invariably they became careless, and the catheter habit led invariably to cystitis. Nevertheless circumstances may arise which make this good advice even today, as in the presence of other and serious disease, or of anything which makes radical operation inexpedient. Under such circumstances the patient must be impressed as profoundly as possible with the necessity for care and caution. If such a case has progressed to the stage of almost complete retention then the catheter should be used at regular intervals. If it be simply necessary to draw off residual urine once a day, then it may be used at night, at which time it would be well also to gently and carefully wash the bladder. It is possible in this way to temporize for a variable length of time, and until more serious conditions supervene.
When, however, the prostate has enlarged so conspicuously as to be not only a constant impediment but a constant menace to the comfort and even life of the patient, one is brought to seriously consider which of the various mechanical methods for relief should be instituted. The choice must now be governed by the physical condition and the surroundings of the patient, as age, degree and character of the obstruction, and the extent of septic infection. One has again to choose between the most radical and usually the most satisfactory method of extirpation (prostatectomy), or one of the less radical and palliative operations, such as the Bottini operation with the galvanocautery.
A few years ago White and others laid great stress on the fact that after removal of the testicles there was notable atrophy of the prostate, and suggested the expedient of double castration or orchidectomy for this purpose. The method proved disappointing, although doubtless more or less effective in some cases, and so objectionable to many patients, for obvious reasons, that it has been practically abandoned. The less mutilating substitute of division and exsection of a portion of each vas deferens (vasectomy) has for the same reason been discarded.
When radical measures become necessary the choice should be made between the galvanocautery (i. e., canalization of the base of the prostate and its median bar by means of the instrument devised by Bottini) and the bolder and more radical method of extirpation (prostatectomy). This prostatectomy is done by either the suprapubic or the perineal route. As between them there is often room for choice, for reasons mentioned below. Each method has its advocates and its opponents.[71]
[71] The question of credit and priority for these operations has been of late much discussed. To McGill, of Leeds, and Goodfellow, of San Francisco, should be given most of the credit for the earliest perineal operations, while Fuller, of New York, who first performed the suprapubic operation in 1894, should probably be given credit for the latter, although it has been evidently unjustly claimed for Freyer, of London. Belfield, of Chicago, was also one of the earliest advocates of extirpation of the enlarged prostate.
Suprapubic Prostatectomy.
—It is of assistance in this method to have the empty rectum somewhat distended, and held up by the introduction of a rubber bag, which may be later distended with water or with air. By this means the prostate and floor of the bladder are pushed upward toward the operator’s finger. This is, however, by no means necessary, but simply advantageous. The first part of the operation is essentially that[999] described as suprapubic cystotomy. The bladder being thus opened and the prostate carried upward by a sound, which should have been inserted in the urethra, the finger first accurately notes its dimensions and the direction of its enlargement. Blunt scissors are now used, or the sharp finger-nail, for making an opening through the mucosa and prostatic covering, through the capsule of the latter, down upon that body. This opening is preferably made near the urethral entrance. The balance of the operation consists in blunt dissection by the end of the finger, i. e., enucleation of the prostate from within its enclosing capsule and surrounding tissues (Fig. 661). More or less disturbance of the basal structures is necessitated, but as the surgeon becomes expert the amount of this disturbance becomes relatively surprisingly small. In most instances it is possible also to practically strip off the prostatic tissue from the urethra, so that it is rarely necessary to tear or to cut across it in order to lift the prostate out of its bed. In the average case it is possible in this way to enucleate the prostate in a single piece, and to remove it as an entire organ. If, however, it should prove too large for the bladder opening which has permitted the procedure it would be better to morcellate it, or so far divide it with scissors as to permit its extraction piecemeal. Its removal leaves a bleeding cavity at the base of the bladder, with torn and separated tissues, and a pocket where the prostate used to lie, into which urine will be poured from above, while it cannot ordinarily be at first easily emptied from the more or less injured urethra connected with it. From this surface there will be at first considerable oozing, mostly venous. Should this be serious and prolonged a quantity of gauze may be packed into it through the opening, and pressure thus made. Such packing should only be retained for a few hours. Ordinarily it is sufficient to provide at once for drainage. My own preference is to make double provision for this by the passage of a catheter through the urethra, and by the insertion of a drainage tube from above, whose lower end rests within the pocket. It is a great desideratum to drain the urine as fast as it accumulates, and, at the same time, to keep the patient dry. This is best effected by a method described later, of complete bladder siphonage, which can be resorted to in either form of operation. It is again advisable to get the patient into the sitting posture, which should be done within a day or two, or as soon as his strength will permit, in order that gravity may assist in drainage. (See p. 1003.)
Fig. 661
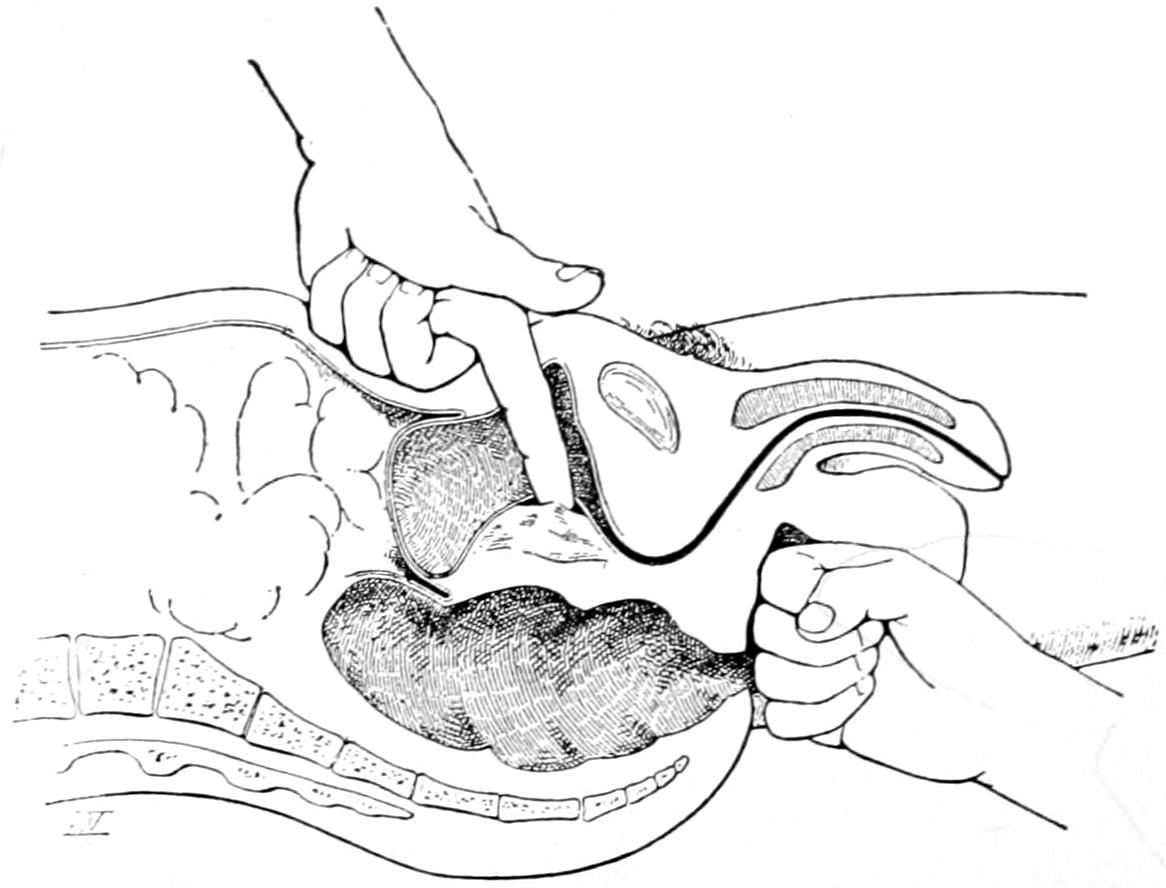
Suprapubic prostatectomy. Process of enucleation by finger-tip of one hand in the bladder, the other hand making pressure in the perineum. (Hartmann.)
When difficulty is met in enucleation assistance is derived by the introduction of one or two fingers of the disengaged hand into the rectum, by which certain manipulation can be effected from below that will be of material help. Pressure in the perineum or manipulation of a sound may also be of assistance.
So soon as satisfactory drainage through the urethra can be effected the suprapubic tube should be removed, and the wound thus encouraged to close.
Perineal Prostatectomy.
—Perineal prostatectomy constitutes a similar attempt at enucleation, effected from a different direction. The patient now being in the lithotomy position, with the rectum not only emptied but sterilized, the perineum is widely opened. While the removal may be accomplished through a median incision it is better to have ample room, therefore by a semilunar flap a sort of trap-door should be raised, its apex downward, through which easy access to the deep perineum is afforded. It is only necessary to divide the central tendon of the recto-urethral muscles before the operator arrives at the apex of the prostate and the membranous urethra. The latter, being exposed at this point, is usually divided upon a grooved staff. Here, at its junction, the capsule is usually divided by a free opening, through which the finger-tip is insinuated and made to strip the capsule from the prostate itself. By different operators instruments[1000] have been devised which facilitate much of the subsequent work. Perhaps the best of these is the double-blade retractor of Young, which, shaped like a sound, can be opened after introduction, and made to serve excellent purpose by traction upon its handles. If, now, the perineal route have been large enough, and retracted sufficiently, the prostate can be so pulled down into the wound as to be exposed to sight as well as to touch. The effort is sometimes made to enucleate the prostate entire and withdraw it whole, but usually to separate each lateral mass by itself. It is advisable to seize with strong tenaculum forceps and pull down the loosened portions of the organ, in order that it may be more easily separated at its upper part; but it has now been found unnecessary to either open the bladder above the pubis, or even to expose it by an opening through the skin so that it may be pressed down, traction from below taking the place of suprapubic pressure, whatever is needed in the latter direction being effected through the uninjured abdominal wall (Figs. 662, 663 and 664).
Fig. 662
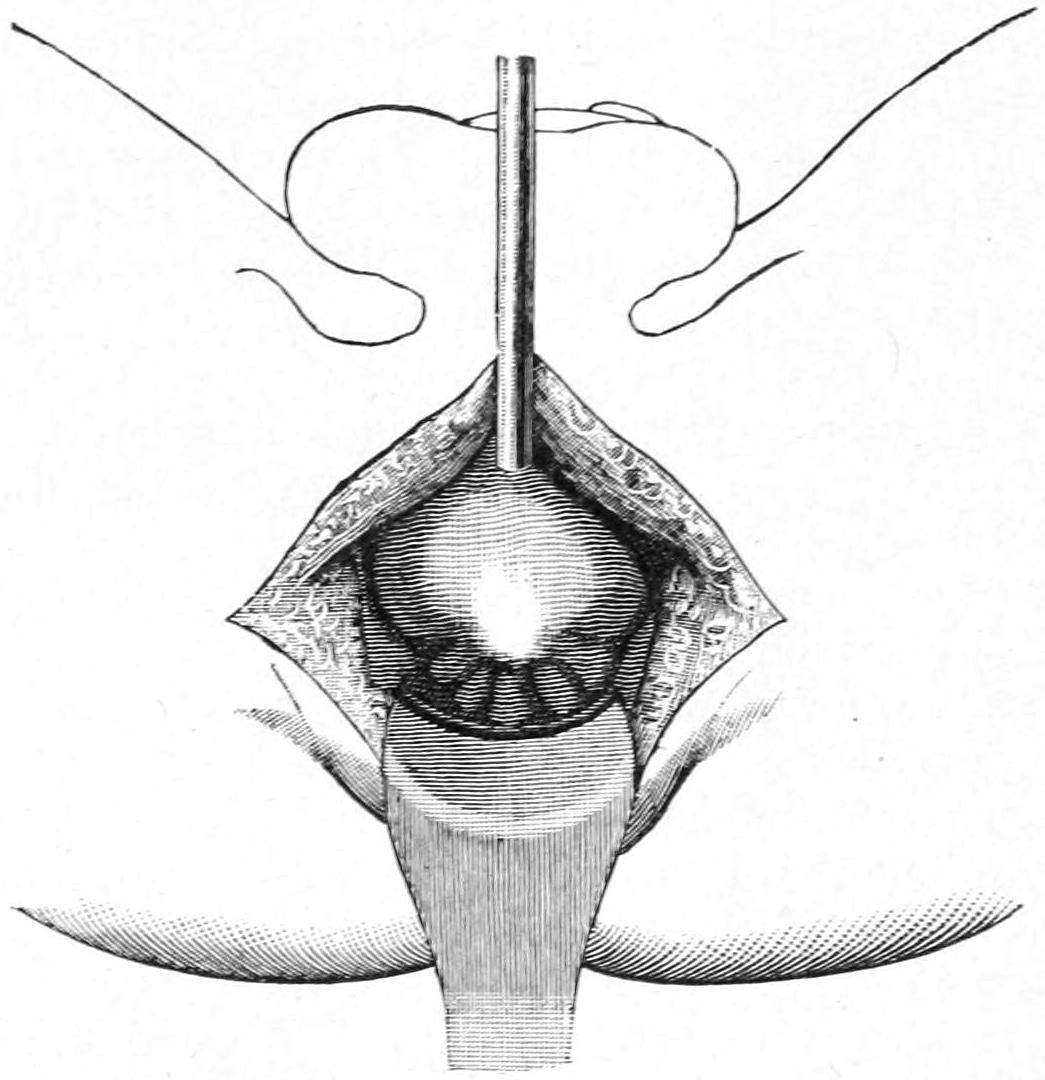
First exposure of prostate after introduction of sound through opening just in front of it. (Proust.)
Fig. 663

Enucleation of a portion or all of the prostate by use of the index finger. (Proust.)
Fig. 664
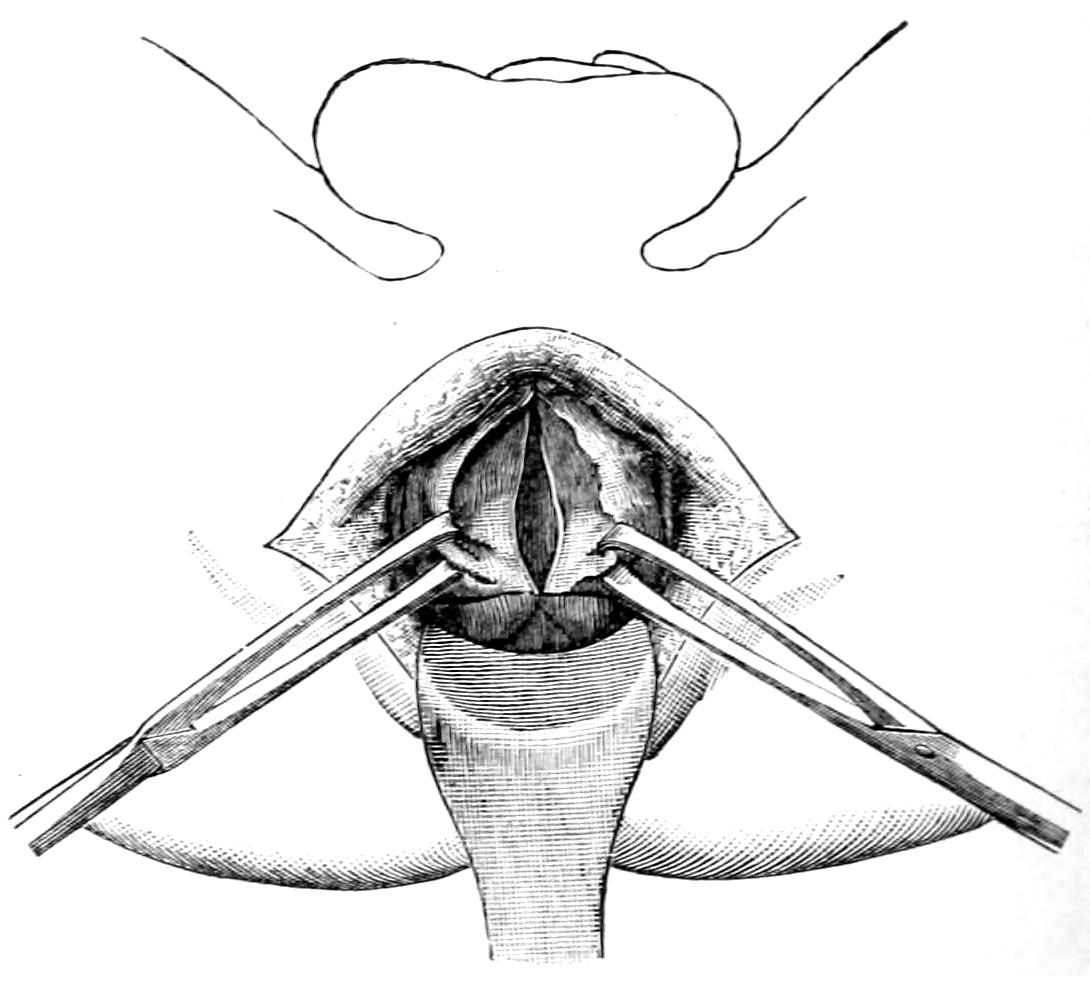
Hemisection of prostate, each half being secured within the bite of vulsellum forceps. (Proust.)
The balance of the procedure must depend on the size and character of the growth.[1001] To strip off a naturally adherent capsule is quite easy, but to detach one which has become firmly adherent through old inflammation or cancerous infiltration is sometimes extremely difficult. Thus enucleation may sometimes be effected in two or three minutes. The stripping and enucleating process should be carried around the prostatic enlargement and into the bladder, and the effort should be to make the smallest possible rent in the vesical mucosa, as well as to separate prostatic tissue from around the urethra rather than to tear or mutilate the latter. Experience and patience will permit the accomplishment of this to a surprising degree. Morcellation may be an aid in removing large masses, and no hesitation should be felt in dividing a mass of tissue which does not come out easily through the wound (Fig. 665).
Fig. 665
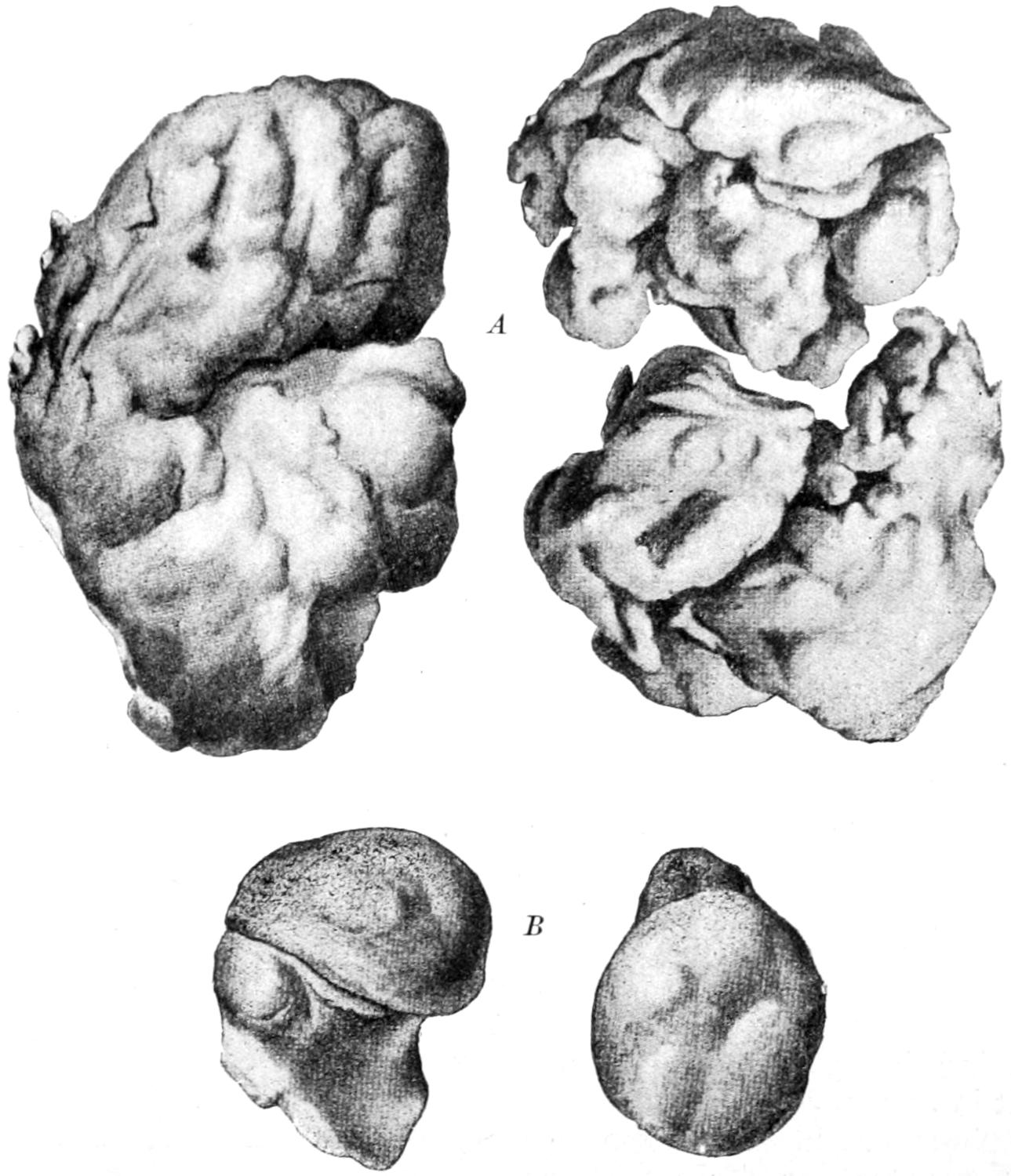
Prostate removed by the perineal route: A, lateral lobes; B, intravesical growth particularly obstructing urethral entrance. (Proust.)
The organ once enucleated, there results a bleeding cavity, at the base of the bladder, which, however, is now opened below and should drain itself easily. If the surgeon’s finger and his instruments have been kept, as they should have been constantly, within the prostatic capsule there is no possibility of harm to the rectum, which, however, may be utilized for assistance in the manipulation should it be required. There remain, therefore, after enucleation the checking of hemorrhage, provision for drainage, and suitable narrowing of the wound. The first and second of these are usually combined by the insertion of a tube, of sufficient rigidity to permit a gauze packing to be placed around it. This should be connected exteriorly with a suitable drainage tube, and bladder siphonage be provided. The wound around the tube is closed by two or three deep sutures, usually of silkworm-gut, since it tends naturally to close by pressure and requires but little further attention.
The greatest harm likely to be done in this operation is injury to the seminal vesicles, above the prostate, between which and the prostate itself the surgeon may not distinguish, with unnecessary mutilation of the posterior urethra. Occasionally, in spite of great care,[1002] the rectum will be slightly lacerated. Injury or destruction of the vesicles might lead to impotence, while mutilation of the urethra would be followed by delay in repair, with uncertainty of subsequent bladder action and control.
Subsequent treatment consists in removing both gauze and tube at the earliest possible date, which should not be later than the fourth day; after this irrigation may be given once or twice a day, with the least possible use of instruments.
In either of these methods of prostatectomy the greatest reliance is to be placed upon natural processes of repair. In some way, which seems almost inscrutable, torn bladder and more or less mutilated urethra come naturally together and connection is reëstablished.
After this brief description of operative methods there remains only to contrast them. The especial advantages of the suprapubic method are the total avoidance of perineal fistula, of disturbance of the deep urethra, of the perineal structures, of the seminal vesicles, and a minimum of disturbance of the entire basal portion of the bladder, with a greater theoretical possibility of speedy restoration of its function. It is the method of choice with certain operators of large experience. It seems especially indicated in cases of pronounced intravesical enlargement, but may be made difficult in obese individuals.
In behalf of the perineal route must be alleged the advantage of seeing much of what one is doing, of being really nearer to the field of activity, and of more perfect control of the mass which is to be removed, as well as the fact that the prostate is not an intravesical organ.
Whichever method be adopted the patient should be encouraged to be up and about as soon as possible. Subsequent bladder control comes with varying rapidity to different patients. Urinary fistulas are not likely to persist in patients who have not worn drainage tubes too long. After two or three weeks it is advisable to pass a sound occasionally, in order to maintain proper direction of the urethral canal and prevent formation of stricture. Bladders in which there has been a serious complication of cystitis should be irrigated through the openings so long as they are maintained.
The operation of itself is not a very serious nor difficult measure. It is too often performed on feeble or septic patients, as a last resort, when it is too late.
The galvanocaustic operation is done with an instrument devised by Bottini, shaped like a lithotrite, with a movable platinum blade, which can be heated to the desired degree by the electric current. This instrument is introduced into the deep urethra until its beak enters the bladder, after which the latter is turned half around; then the electric current is turned on, the movable caustic blade gradually withdrawn by a screw mechanism in the handle, and made to traverse a distance of one inch to one inch and a half, previously measured, and in such a way as to burn a channel through the floor of the prostatic urethra, and through any median bar or obstruction which may exist. This is the principle of its use. At one time it was popular, although of late prostatectomy seems to have supplanted nearly every other method. Nevertheless in certain cases it will be found of advantage. I have preferred to combine it, in most cases, with a small perineal opening, introducing the instrument after opening the membranous urethra, and having it in this way much more completely under control. Through the opening thus made subsequent bladder drainage can be effected if desired. It permits also of more perfect exploration of the bladder with the finger.
Extensive cancerous involvement of the prostate puts a case beyond the pale of operative surgery, except for palliative purposes, though either perineal or suprapubic drainage may be made for final and temporary relief, the case admitting of nothing else. As mentioned above many apparently ordinarily enlarged prostates prove to contain cancerous elements. It has been found that, when not too extensively involved, prostatectomy in these cases gives as good results as in the absolutely non-malignant.
[1003]
Fig. 666
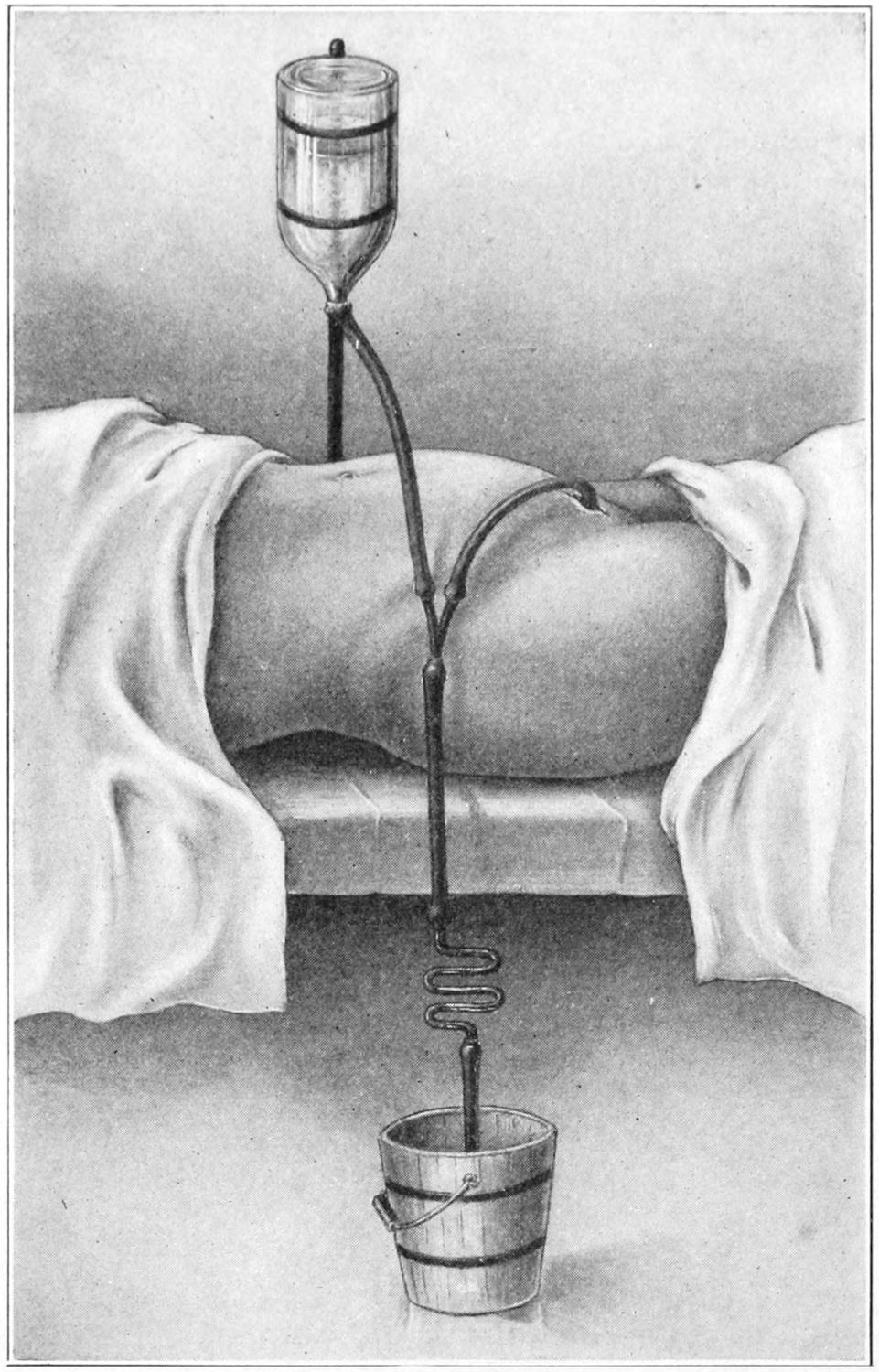
Siphon drainage of bladder, with Cathcart’s S-tube (its essential feature). May be applied equally well to perineal or urethral tubes, or to drainage of other cavities.
A matter of great importance and comfort for the patient is an effective siphonage of the bladder after it has been opened. This has usually been accomplished by the use of a Y-shaped tube, one of the branches connecting with a suitable reservoir for water, hung above the level of the body, the other with a tube connecting with the bladder, while from the lower end another tube connects with a suitable reservoir on the floor. This is rarely effective, and can only be made so by inserting the S-shaped tube devised by Cathcart in the lower drainage tube. With this, and a suitable regulation of the flow, the water can be made to escape, drop by drop, and make an effective suction that completely fails without the use of Cathcart’s tube. The device is illustrated in Fig. 666.
[1004]
The most common congenital defects of the penis are connected with elongation of the prepuce or with abnormality in the construction of the urethra. Aside from these, however, rare congenital abnormalities have been met with, as, for instance, a double or bifid penis, or its almost complete absence. The former is perhaps to be regarded as an atavistic condition, having its prototype in the kangaroo. Misplacement of the organ is usually apparent rather than real.
Except as produced in consequence of disease, i. e., by edema or inflammation with swelling, phimosis indicates a congenital condition, either of elongation or constriction of the prepuce, usually with adhesions to the glans. A considerable proportion of male children are born with more or less complete conditions of this kind. These are not so abnormal anatomically, but they lead to serious complications later in life. An extremely tight prepuce is often complicated with stenosis of the meatus, the combined result being a practical stricture at the end of the urethra, through which the infant has to strain with each act of urination. This is a common predisposing cause of hernia. Whether the prepuce be adherent, or so constricted as to make it a retentive sac, there will accumulate between it and the sensitive mucous surface of the glans more or less smegma which, as it decomposes in the course of time, becomes excessively irritating, and a fertile source of reflex disorders, involving even distant parts of the body. Thus in young boys especially, convulsions, chorea, epilepsy, and various other neuroses are produced, while, in addition, its perpetuation produces a condition of unnatural excitability which leads again to habits of masturbation or to sexual irritability and unnatural excitability.
Every newborn male infant should be carefully examined in order that the above condition, if present, may be remedied. This remedy will consist, in mild cases, of forcible retraction of the elongated prepuce, with separation of any adhesions uniting it to the glans. Preputial stenosis may be overcome in some cases by simply slitting up the dorsum, which, if not too long, may be thus released and not require circumcision. On the other hand a much elongated and contracted prepuce should be sufficient justification for prompt circumcision. At the same time any unnatural contraction of the meatus may be overcome by trifling incision. If every boy baby were thus carefully inspected and relieved, if necessary, there would be fewer reflex disorders in young children.
Incidentally it may be said that, in lesser degree, the same thing may apply to girl infants, in whom the clitoris, although small, should nevertheless be freely uncovered by retraction of its miniature hood or prepuce. When this is not easily possible it should be made so. Disorders of the same general character as easily arise in girls, from this same general cause, as in boys, nocturnal incontinence being a frequent expression thereof. In my opinion the teaching of obstetrics should not be considered complete without unmistakable reference to these matters.
Phimosis in the adult may be brought about by disease, especially in connection with a prepuce already retentive, or elongated and difficult of retraction. Retained secretion beneath such a prepuce is a fertile source of danger of all kinds, as well of venereal infection as of cancerous growth. Surgeons in the Orient have described calculi, even of considerable size, found in this location as the result of retention of matter which should not have been at all retained, this condition being noted most often among the Chinese.
[1005]
Infection, usually gonorrheal, of the concealed surface of the prepuce, which has a distinctly mucous character, is known as posthitis; that of the covering of the glans as balanitis; while, in effect, whatever appears in this location will essentially be a balanoposthitis. If such a condition do not easily subside by irrigation, with a small nozzle introduced beneath the margin of the prepuce, it will then be necessary to slit up the dorsum, or make a complete circumcision, in order that the affected surfaces may be made accessible. The same is true in cases of chancroid and even in cases of chancre; incision or circumcision being justifiable whenever indicated.
Paraphimosis implies an opposite condition, where the prepuce, having been retracted, is caught behind the margin of the glans and cannot be released nor brought forward. This may be the result of undue effort to retract a very tight but otherwise normal prepuce, or is frequently the result of an acute inflammation, where edema and solid exudate so solidify the tissues as to make them inflexible and almost immovable. In mild cases of paraphimosis cold applications, or pressure with patient manipulation, may be sufficient to restore the proper condition. An extreme degree of such constriction would threaten the nutrition of the glans, to the extent even of possible gangrene, and sloughing of some portion of the end of the penis is not an infrequent result of a neglected condition of this kind. Under these circumstances constriction must be released, it being usually sufficient to apply or inject cocaine, and then with scissors or blunt bistoury nick or incise the constricting ring, to a degree sufficient to release it and permit the desired result; in one way or another this must be attained, else more or less sloughing is sure to follow.
Other rare malformations of the urethra include its more or less complete obliteration, in some portion at least, or, more often, its sacculation or dilatation in certain areas, the result being the formation of pockets or pouches. Such abnormality may persist to adult life, and finally contain a considerable amount of retained urine.
Epispadias and hypospadias constitute defects in the urethral construction, so that urine escapes at some point much nearer the body than normally intended. A complete degree of epispadias nearly always accompanies extroversion of the bladder, already described. Milder conditions may be met in any degree. In these cases the urethra becomes a canal open above, and the glans is more or less defective. Cases of epispadias may be divided into the balanic, where the urethra terminates on the upper portion of the glans, and the penile, where it terminates between the glans and the pubis; while cases of hypospadias may be divided into balanic and penile, similar to the above, the penoscrotal, where the urethra opens at the junction, and the perineoscrotal, where both the perineum and scrotum are involved. While all of these defects are more or less mutilating and unphysiological, none of them menace life. The physiological requirements of either case demand conditions permitting normal urination, and coitus to a degree permitting fecundation. (See Fig. 667.)
Fig. 667
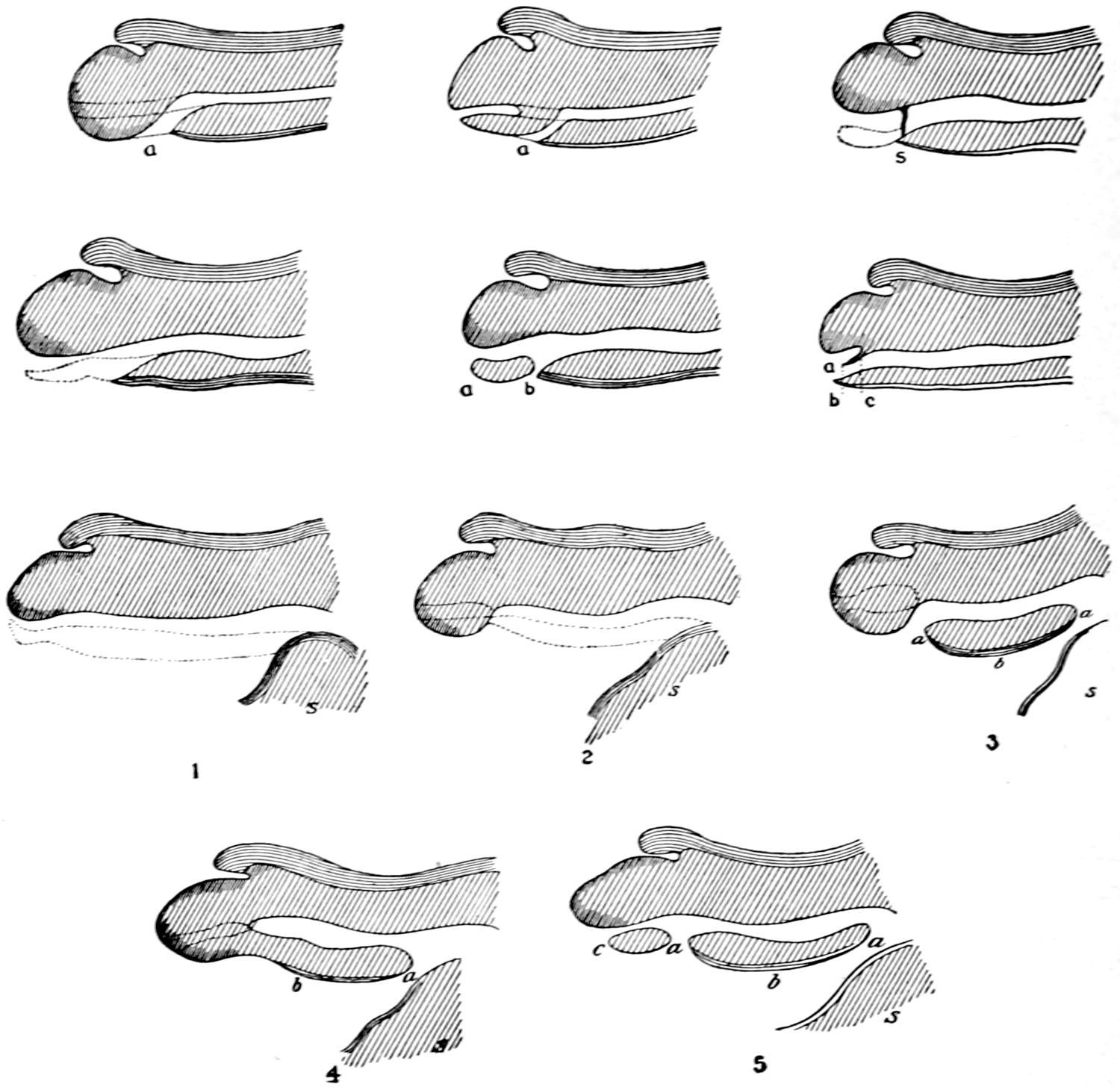
Diagrammatic sections showing different varieties of hypospadias: 1, hypospadias with imperforate glans; 2, hypospadias with blind canal in glans; 3, with barrier placed between penile urethra and balanitic groove; 4, typical case of hypospadias; 5, hypospadias with normal meatus; 6, penile urethra opening below glans; 7, absence of the whole inferior part of the penile urethra; 8, hypospadias with absence of urethra through glans; 9, case of d’Arnaud; 10, case of Lacroix; 11, case of Lippert with normal meatus. (Kauffmann.)
Fig. 668
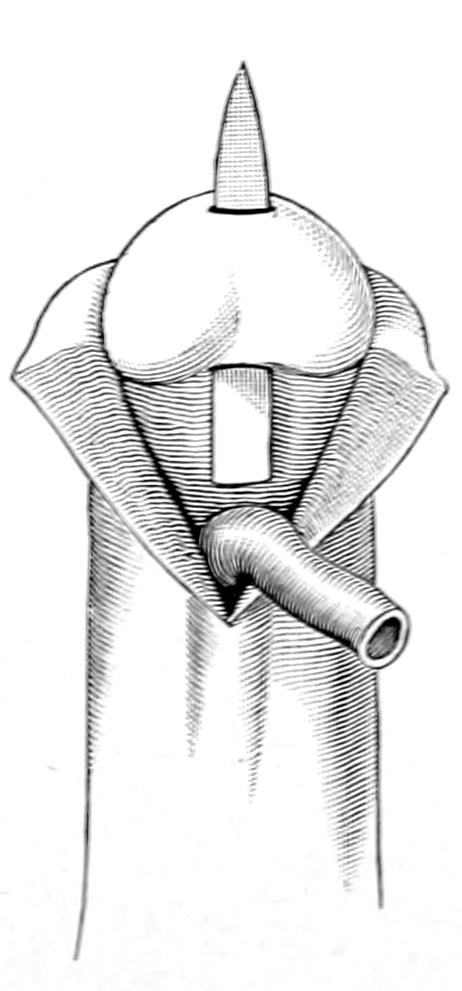
Hypospadias. Liberation of anterior urethra and tunnelling the glans. (Hartmann.)
Fig. 669
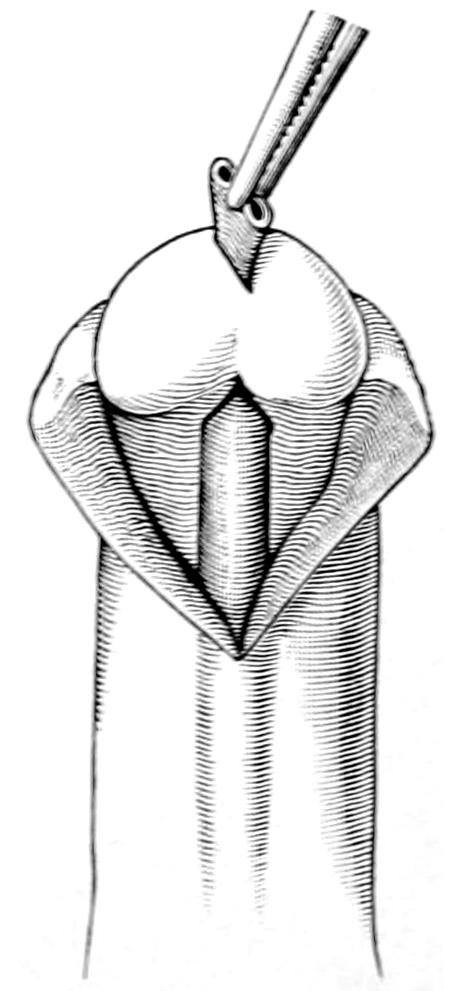
Hypospadias. Drawing the liberated urethra through the tunnel in the glans. (Hartmann.)
Most cases of hypospadias are accompanied by other defects on the inferior surface of the penis and the scrotum, which, more or less, bind them down and interfere with the normal method of urination as well as of insemination. The indications, then, in such cases are to straighten the penis and to restore the continuity of the urethra. The former may be accomplished by transverse incisions through the bands which cause the curvature, or, if necessary, division of the intracavernous septum, or even of the sheaths of or the cavernous bodies themselves. Wedge-shaped pieces of cavernosa have often been successfully excised. The restoration of the urethra is a much more difficult matter, especially in an extensive case, to make it sufficient for insemination. The methods may be grouped under simple canalization or approximation and the construction of flaps. Nearly all of these methods are more or less simple in theory but difficult in practice, and frequently unpromising because of the difficulties in securing final union of tissues, no matter how neatly united, where the same may be interfered with by the[1006] presence of urine or the occurrence of erections. The former may be prevented by a perineal section, with drainage of the bladder, and this is probably the best method to[1007] adopt in nearly all of these cases. The latter is to some extent overcome by drugs, but is sometimes produced by the local irritation of the operation and the dressings. To describe all these methods would require a long chapter. They have included efforts at tunnelling the glans, by the passage of a trocar, maintaining the channel by keeping within it some bougie or foreign body until its interior has healed, then connecting this up with the balance of the urethra (Figs. 668 and 669). The urethral passage-way is rarely sufficiently wide to permit of approximation of freshened edges by stitches, and these will almost surely pull out. Therefore some more plastic method of formation of flaps must be devised. Many ingenious expedients have been suggested, among them the utilization of a strip of skin, dissected up on one side, whose external surface is turned in and made to vicariate as mucous membrane, while its raw surface, now faced outward, is covered with another flap, raised either from the penis itself or from the scrotum. It is the operations based on this general plan which have given the best results in well-marked cases, and yet they have to be conducted with great care. American surgeons, among them particularly Beck, of New York, have done a great deal to advance the plastic surgery of these parts and for these purposes. He, for instance, has especially exploited the movability of the urethra, and shown how by dissecting it out it may be drawn forward and made much more available. Beck has suggested a similar method of displacement and reëmployment of the urethra for epispadias.
Epispadias is far more uncommon than hypospadias, occurring in proportion of 1 to 150 cases of the latter, and is rarely seen except in connection with vesical extroversion, except in minor degree, in which the defect is simply a little grooving of the upper surface of the glans. The best method of dealing with the urethra, in epispadias, is to displace it, as suggested by Beck, separating the cavernous bodies and dropping it down to its normal situation beneath them, and uniting with this procedure more or less of the transplantation suggested by him. It is surprising how much can be accomplished by this method, even in extreme cases. The glans, if necessary, may be tunnelled, and the anterior end of the urethra may even be given a hypospadiac termination.
Hermaphrodism, spurious and actual, implies the existence of sexual organs of both sexes in the same individual. It is a condition actually existent in many of the lower forms of life, but its occurrence in the human being is a matter of extreme rarity. There are numerous malformations which, by the laity, are often mistaken for indications of this condition, but the actual co-existence of both testicle and ovary—e. g., which may perhaps be assumed as the true test—is one of the rarest of all phenomena in human anatomy. External malformations which more or less simulate the appearance of the organs of one sex in those of the other include such conditions in the male, for instance, as atrophy of the penis, hypospadias, a more or less complete division of the scrotum into halves, retained testicles with atrophy of the external organs, and similar conditions by which the external genitalia are made to appear divided or relatively too small. In the female, on the contrary, may be seen occasionally an hypertrophy of the clitoris, which causes it to assume almost the proportions and even the erectibility of the male organ, while other deformities of the vulva simulate more or less the scrotum. Again in the female one meets occasional congenital absence of the uterus or of the ovaries, or congenital atresia, or almost complete absence of the vagina, or vulvas which are almost impassable by virtue of exceedingly dense hymens, where the natural appearances are so perverted as to mislead the ignorant. These are, however, cases of pseudohermaphrodism, although in many of them there are certain general changes in appearance, as of the breast, the figure, speech, and even in manner, which are regarded as evidences of effeminacy in a male individual, or of masculinity in a female.
Strange mistakes and errors have thus arisen, and children about whose sex ignorant parents have been in doubt have been mistakenly brought up, even to a point in life when it was sociologically almost too late to remedy the error. Such cases require careful study for the actual determination of sex, especially in young infants.
True hermaphrodism is not to be denied, as certain historical cases have proved, and as has been demonstrated in certain individuals who travel from city to city, exposing[1008] themselves for a consideration for scientific examination. In general it is sufficient to say here that true hermaphrodism is a rare possibility, while spurious or pseudohermaphrodism is a condition not uncommonly met.
The great vascularity of the penis makes it peculiarly liable to obstinate hemorrhage in cases of incision or laceration. For the same reason when strangulated, as may occur in some drunken orgy or otherwise, it may swell enormously and quickly become gangrenous. An actual fracture of the cavernosa has occurred, through violence in the erected condition. Subcutaneous lacerations or contusions may lead to extensive hemorrhages, possibly with gangrene as the result. Any injury by which the urethra is lacerated, especially torn across, will be followed by much hemorrhage, probably with urinary extravasation, and perhaps great difficulty in establishing the continuity of the channel. Under any circumstances urinary infiltration of any part, deep or superficial, is likely to be followed by abscess and sloughing. An absolute dislocation of the penis is not unknown, it having been displaced beneath the integument of the perineum, abdomen, or thigh, especially in extremely obese individuals.
Urethral injuries are not all accidental. Some of them are the result of design, or of the introduction of foreign bodies which cannot be removed by the patient himself. Such articles may also be introduced, during a drunken orgy, by another individual, or under conditions of sexual perversion by the man himself; and such bodies as pencils, slate-pencils, twigs, and almost every imaginable small object have been found within the urethra. Again it has been seriously injured and even punctured by the careless use of sounds, or by the wire stillette of the old-fashioned linen catheter. Both the anterior and deep urethra may be seriously injured by such accidents as falls upon the external genitals, or upon the perineum, and serious deep lacerations, with complete severance of the membranous urethra, and the infliction of even greater damage, are by no means unknown in such cases.
Fig. 670
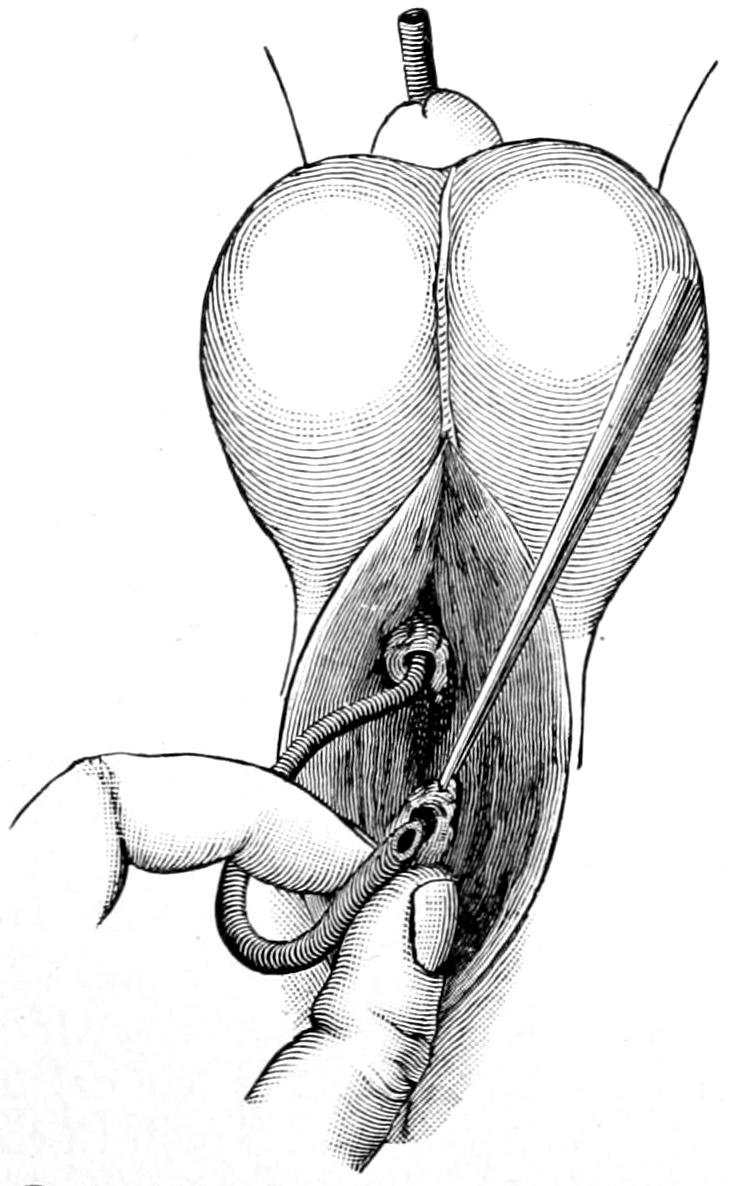
Perineal section for deep rupture of urethra. Posterior opening is identified and catheter, which has been introduced from the meatus, is guided through it into the bladder. (Lejars.)
The first determination should be as to the presence of any foreign body. This being eliminated an effort should be made to check the hemorrhage, and to make sure that there is no such obstruction of the urethra as to interfere with the freedom of the urinary stream. The constant discharge of blood from the meatus, or the admixture of blood with the urine, is always suggestive and should lead to careful investigation. This should include not merely the gentle passage of a sound or catheter, or at least attempt thereat, but perhaps an inspection of the site of injury through the endoscope. When the injury is compound, in the sense of being an external laceration, the deep conditions are more easily ascertained. If with gentleness and yet with difficulty a catheter can be passed through the injured portion of the urethra it would be well to leave it in situ, at least for several hours, perhaps for three or four days, in order that it may act as a splint and the parts more kindly heal around it. If the urethra be so lacerated as to not permit the passage of an instrument, the safer course is an external perineal section, for the purpose of temporary bladder drainage, or to find a deep tear, while a retrograde catheterization may perhaps be practised, and an instrument introduced and carried through in the reverse of the ordinary direction; this may be possible even when ordinary methods fail. Extravasation of blood may be extensive and serious, but extravasation of urine is always followed by disastrous consequences, which should be prevented by external urethrotomy and bladder drainage.
[1009]
These cases may not be seen until the dangers have already occurred. If it should so happen, an effort should be made, by deep incision and free dissection, to open up all pockets containing urine or blood and to afford free outlet from the bladder. Under some of these circumstances, especially when attempted at night with poor light, the performance of an external perineal urethrotomy is by no means an easy matter, since the torn urethra may be lost in ragged and infiltrated tissues, and may sometimes be found only after long and tedious search.
What to do with a torn urethra, under these circumstances, is sometimes a problem. If it be ragged and more or less torn away it may sometimes be resected, and the ends re-united by sutures, if necessary with a certain amount of dislocation of the urethra by dissecting around it. Pringle and others have resorted to the fresh urethra of the ox, for grafting into cases of recent or old defect, as in instances of extensive deep rupture; as well as in cases of hypospadias, with defect in the floor of the urethra throughout its entire penile portion.
The removal of foreign bodies from the urethra is not easy when these have passed into its deeper portion. With special instruments it is sometimes possible to grasp and extract them, although a pointed extremity may interfere with the ease of removal. More harm will come from leaving them than from removing them. Therefore when their extraction is impracticable there need be no hesitation in button-holing the membranous or the deep urethra, and by pushing the object down toward the opening, there effecting its removal.
The urethral walls will take fine sutures, with every prospect of repair, providing their vascular supply be not too seriously disturbed. Therefore lateral or end-to-end suture may be attempted whenever it appears promising, but in such cases it would be well either to leave a catheter for a few days or to make bladder drainage back of the injury.
Cavernitis refers to an acute or chronic inflammation of the corpus cavernosum on one or both sides. It may be the result of the exudate connected with an injury or with the process of repair. It may ensue in consequence of a local gonorrheal inflammation, or it may be an induration due to chronic syphilis. The condition is one which causes local tenderness rather than pain, while the induration causes a perceptible lump or tumor, and infiltration of vascular tissue interferes with symmetry during erection. Again pressure may cause some ureteral obstruction. Cases of syphilitic origin are to be treated by local inunctions of mercurial ointment, perhaps with ichthyol, which are of benefit in any instance, while the internal administration of the iodides is of more or less assistance. The non-specific cases yield only to time and to massage.
Gummas of the penis may assume the above type, but usually occur in more distinct form, either in the cavernous bodies or between them. An abruptly limited nodule in any such locality will always naturally arouse suspicion of specific disease and lead to its appropriate treatment.
Upon the glans and the prepuce, especially, herpetic vesicles frequently appear, constituting an annoying local lesion, corresponding minutely to the ordinary “cold-sore” upon the lip. This is known as herpes preputialis. It is the result usually of uncleanly habits or local irritation. It is of no consequence, save that in some individuals it occurs frequently, with considerable local irritation. The broken surface thus produced is liable to chancroidal or septic infection, which constitutes its greatest danger, while such a sore, irritated by caustics or injudicious applications, is sometimes mistaken for a specific lesion. A chronic herpes may frequently prove a precancerous lesion.
The papillomas, or warty growths, are frequently noted about the glans and prepuce, being expressions of local irritation, while, under the conditions of local warmth and moisture which prevail, they luxuriate and may develop into condylomatous masses, known as “strawberry” or “mulberry” growths, which may attain large size. In the female they occur on all parts of the vulva and anal region; in the male they rarely appear except as above.
All that such papillomatous growths require is complete excision or extirpation (i. e. destruction), with cauterization of their bases and subsequent local cleanliness. They are not infrequently referred to as venereal warts, which, in effect, they usually are. The other benign tumors of the penis are rare. Occasionally some dermoid cyst or small fatty or fibrous growth may be seen. Sarcoma of the penis is also rare, while epithelioma is not uncommon, constituting the ordinary cancer of the penis.
[1010]
Epithelioma in this region has its origin around some portion of the mucous surface of the glans, spreading in time to the prepuce, more or less involving the entire organ, while by its rich lymphatic supply involvement of the inguinal and other nodes happens early, whereby the situation is sadly complicated. Epithelial cancer here evinces the same local tendencies toward extension and destructive ulceration as elsewhere, made more rapid by exposure to surface irritation. Its base is indurated, even if sometimes everted; it grows irregularly, but destroys everything with which it comes in contact.
Epithelioma of the penis should be recognized and extirpated early to offer any prospect of success. It is usually as unpromising a condition as epithelioma of the tongue, because of the early lymphatic involvement. A lesion of limited area may justify local excision, but a distinctly marked lesion can only be successfully treated by amputation, at least of the anterior portion of the organ, perhaps of the entire structure of the penis, and thus ensure complete eradication.
Amputation of the penis is easily effected with a circular sweep of the knife, or by an abrupt cross-section, there being but little choice of method, the intent being only to save sufficient of the organ so that cleanliness during and after the act of urination may be maintained. When any portion of the pendulous organ is preserved the margin of the divided skin should be attached to that of the urethra by a series, say, of four sutures, placed at equal intervals, after hemorrhage, which will be somewhat difficult of control, both from the larger vessels and from the cavernosa, has been subdued. It may require buried sutures through the divided cavernosa in order to permit of such control.
If, however, it seem necessary to remove the organ close to the pubis it will probably be found more desirable to make a more complete dissection, taking out the corpora cavernosa entirely, and then making a median incision in the perineum, dissecting out the urethra, bringing it out through the wound, shortening it to the proper extent, and fastening its termination to the skin margin, thus making, as it were, a vulvar outlet, which will not interfere with urinary control, but will permit urination to be satisfactorily accomplished, though only in the sitting posture. This is usually known as Demarquay’s operation.
In children this requires a general anesthetic; in adults it can almost always be satisfactorily performed under local cocaine anesthesia; the intent being to remove the redundant foreskin. A circular incision is necessary, which may be made with knife or scissors. The parts being prepared for operation, the prepuce is drawn forward, being caught either with forceps or fingers of an assistant, and the little circular amputation is made just in front of the corona of the glans. The first incision extends through the skin, after which there remains a cuff of mucous membrane, which is sometimes adherent to the glans, as in children, or may be infiltrated with exudate, as by a concealed chancroid or chancre beneath. Ordinarily this cuff is split in the middle line of the dorsum and removed in halves, in order to avoid any possible injury to the glans itself. The cut is made somewhat obliquely from above downward and forward, the intent being to divide it at the frenum, sufficiently far from the meatus in order to not distort the latter by subsequent cicatricial contraction. These tissues are sometimes inordinately vascular, and bleeding points need to be quite carefully secured. In one case known to me an infant bled to death from an unsecured vessel near the frenum, the operator having neglected it at the time and having left the patient. In a clean case, the vessels having been secured, a running suture of fine catgut should unite the cut edges of the mucosa and of the skin. It is not necessary to apply sutures in a venereally infected case, for raw surfaces will also become infected, and would be best protected by immediate cauterization, in which case primary union would be prevented.
The little procedure may be modified in various ways to meet individual needs. After its performance there will occur considerable local swelling and edema, which can be best kept under subjection by a dressing moistened with cold saturated boric acid solution or its equivalent. If the sutures have been too tightly applied there may be a species of paraphimosis, with too much constriction, which would require their division.
[1011]
In Chapter XII, on Gonorrhea, were described the usual specific forms of urethritis, with their complications and results. To this chapter the reader is referred for all data regarding gonorrhea as it involves this passage-way, with its complications. Such lesions as ulcers may persist for some time, while the papillomatous outgrowths, polypi, etc., connected with gonorrhea and gleet, which are not discoverable from without, are now easily examined and estimated with the endoscope. Specific ulcers of the syphilitic type, and virulent ulcers even of the chancroidal type, also occur, usually within the first inch of the urethra, causing more or less discharge, with local soreness, and leading, unless promptly recognized, to cicatricial stricture formation.
Strictures of the urethra may be of traumatic origin, as when produced by external accident, with or without laceration, or by the introduction of foreign bodies, or the minor injuries inflicted during their extraction. Deep traumatic stricture is the result of serious injuries to the perineum. The common type of urethral stricture is the consequence of one or more attacks of gonorrhea, which, not having been promptly cured, has merged into so-called gleet, and this into these inevitable consequences, with more or less infiltration of the peri-urethral tissues, and subsequent encroachment upon the caliber of the urethra, either by irregular new tissue formations or well-marked annular constriction. In addition to the above conditions there is also known a spasmodic stricture, due to involuntary contraction of the muscular fibers encircling the urethra, and of the deeper perineal muscles which concern it. Otis held that such urethral spasm is a frequent accompaniment of a contracted meatus, and taught that the best method to deal with it is by first enlarging the meatus, as may be easily done with a simple bistoury, under local cocaine anesthesia (meatotomy), and the subsequent passage of instruments of proper size.
To persistent and well-marked contraction of the urethra is given the term organic stricture, and such a stricture is generally the consequence of injury or disease, whereas purely spasmodic stricture, mentioned above, is a not infrequent occurrence in perfectly chaste individuals.
Organic stricture may be single or multiple, of large or small caliber, or even impassable and impermeable—that is, from before backward—so that even while urine may leak through, drop by drop, from behind it seems impossible to introduce an instrument from the front. In aggravated cases three or four inches of the urethral canal may be involved in lesions of this kind, which constitute a formidable condition for satisfactory treatment. The ordinary non-traumatic organic strictures are all in front of the prostate and more common near the meatus. The size of a stricture is determined either by the urethrometer devised by Otis, or, more simply, by determining the diameter of the bulbous bougie which may be made to easily slip through it, the latter being the common method. These instruments are indicated by numbers, which refer to the millimeters in circumference of the bulb; thus No. 27 implies that the bulb has a circumference of 27 Mm. The bulbous instrument is far better for examination than the sound, since it indicates the exact depth as well as the length of the strictured passage, and gives a better idea of its density or resilience. (See Figs. 671 and 672.)
The indications of stricture are difficulty in micturition, even to the degree of impossibility, persistence of gleety discharge, and slowness or impossibility of ejaculation, while sometimes cicatricial tissue can be felt from the outside.
The strictured urethral canal should be restored to normal dimensions at the earliest practicable moment. This may be effected through gradual dilatation with a conical steel sound, passed at intervals of two or three days, or rapidly, by the improved instrument of Otis known as the dilating urethrotome, which, being passed through the stricture, has its blades expanded by a mechanism at the handle, while the stricture when it is stretched is divided by the working of a concealed blade. The Otis instrument is illustrated in Fig. 673.
[1012]
A meatus too small to admit a suitable instrument should be incised to the necessary degree.
Gradual dilatation may be employed in the milder cases, and has been combined with a method of electrolysis, in which I have little faith. No matter which method be adopted, the patient should be impressed with the force of the old adage, “Once a stricture always a stricture,” and should be warned that the occasional passage of an instrument is necessary for a long period, and that while he may be taught the procedure he should not neglect it. This is true alike of every method of treatment.
Fig. 671

Bulbous sound.
Divulsion was a method employed during the past generation of rupturing a stricture by forcible separation of the blades of a divided instrument, tearing it instead of neatly cutting it, thus inflicting a maximum instead of a minimum of local damage. Every divulsion thus led to a subsequent stricture formation. The procedure has been abandoned. Now by the employment of the Otis instrument, or one of its substitutes, the stricture is first found, then penetrated with the instrument, and divided to an extent easily regulated, thus permitting exact work, which is preferable to the older methods of drawing a large blade along the urethral tract.
Fig. 672

Otis’ urethrometer.
In tight strictures the operator proceeds at first with small filiform bougies made of whalebone, with which, sometimes after considerable effort with a bundle of them in the urethra, trying one after another, he may succeed in passing one and causing it to enter the bladder. The others are then withdrawn. It may now be possible to thread over the whalebone a perforated tip made for the urethrotome, and thus to slip the latter down into the depths over the fine bougie as a guide, and then to push it farther, using now more force because it must necessarily follow the urethral canal. When, however, what seems to be judicious manipulation by this method is unsuccessful the metal instrument should be withdrawn, the whalebone bougie remaining in situ, and thus serving as a guide for that which is now made necessary, namely, external urethrotomy.[72]
[72] Van Hook has recommended the following excellent expedient for the discovery of the urethral canal when apparently lost in the depths of a dense, deep stricture: He gives a dose of potassium iodide two or three hours before the operation. During the latter, and when seeking the proximal end of the urethra, he drops a little acetate of lead solution at the point where the urine is expected to appear. The formation of the bright-yellow lead iodide will mark the actual appearance of the urine and indicate its source.
Fig. 673
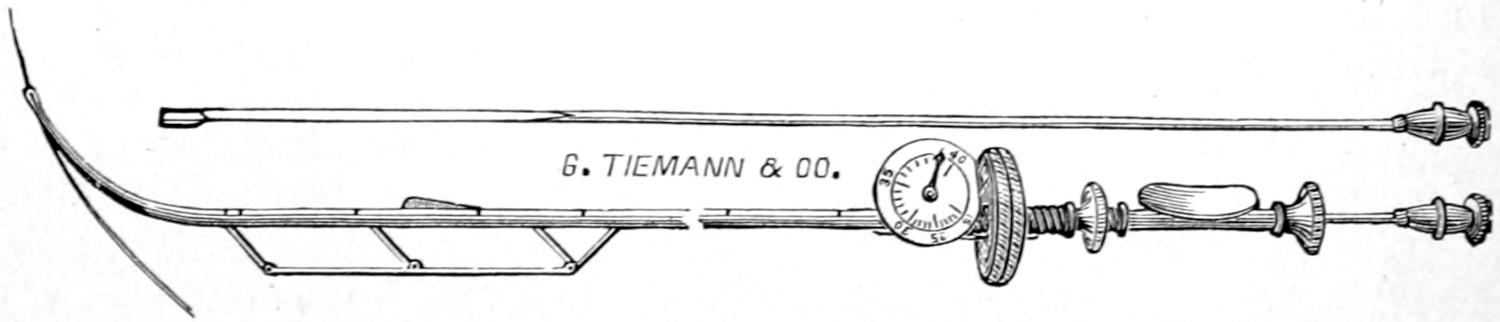
Otis’ dilating urethrotome.
External urethrotomy is essentially a median perineal section, carried down at least to the urethra. It is done preferably with a guide, usually a fine bougie. With it the urethral channel may be easily identified; without a guide, in aggravated cases, it is often a difficult matter to identify and dissect out the urethra, and then to find its tortuous passage-way and follow it into the bladder. Patience and a knowledge of the anatomy of the perineum will lead to success. Sometimes extensive dissections are necessary, and the perineal wound needs to be widely retracted in order to better expose the deep[1013] tissue. Once the urethra is identified it may be followed in each direction, and the case should not be left until the entire canal has been restored to its normal caliber. In these cases it is best to leave a self-retaining catheter in the perineal wound for at least a day, after which it is sometimes of benefit to introduce a catheter through the meatus, and leave it in the urethra for two or three days. Such a urethra is an infected channel, and must be so cared for that no retention or infection of fresh wounds occurs.
Perineal abscess is the not infrequent consequence of a very tight and deep stricture, having its beginnings as a folliculitis, with subsequent extension and perforation, with escape of urine, and sometimes with the formation of acute, diffuse phlegmon, which may even extend into the scrotum or to the abdominal wall. Ordinarily it constitutes a circumscribed collection of pus. Such a phlegmon when neglected may be followed by extensive burrowing of pus, or local sloughing, with gangrene, and partial or complete destruction of the external genitals. When such a phlegmon occurs above the triangular ligament there will be swelling about the prostate, with edema of the anterior rectal wall, while the prostate itself may become later involved. Such a collection may terminate as an ischiorectal abscess, associated with perineal fistulas.
The inevitable results of such conditions have two or three disastrous tendencies, such as burrowing of pus and the formation of urinary fistulas, sometimes at considerable distance from the urinary channels. The same is true in traumatic cases, for in such cases there may be the expression of an old and neglected stricture. To the chronic condition may be added that of tuberculous infection.
—The treatment of such abscesses and fistulas is based upon the principles of evacuation of pus and restoration of the urinary canal to its proper size. This may be an easy or a difficult task, but it should be accomplished by whatever method will permit it with the least damage to tissues. When urinary infiltration threatens gangrene extensive incisions should be made. When the scrotum is swollen, as it may be to enormous dimensions, free opening should be made into it to permit escape of serum and pus if present. Even the surrounding tissues, including the penis, may be enormously edematous. This swelling will rapidly subside when pressure upon the deep veins has been relieved, but pus, no matter where present, must be evacuated.
Instrumentation of any kind within the urethra may, in some individuals, be followed by what has been called urethral or urinary fever, including chill, pyrexia, with sometimes the development of an acute inflammatory affection, either of the urethra or even of the kidney, with not only retention but actual suppression of urine. These manifestations are ordinarily regarded as due to toxemia, but are sometimes difficult to explain, because their violence seems so disproportionate to the amount of intervention. Thus I have known an individual to die, of apparently acute uremia, within four days after the painless passage of a sound for dilatation of an old stricture, the same not being followed by any blood or local disturbance.
These accidents were more prone to occur before the introduction of antiseptic methods in all urethral instrumentation. At present they are much rarer than in former days. Nevertheless the passage of any instrument, even for legitimate examination, as for stone, may be followed by unpleasant consequences. These are preventable to some degree as well as curable, by antiseptic local measures, as well as by the administration of quinine or urotropin, especially the latter, with sitz baths and perhaps general antifebrile measures, while any local disturbance thus set up is to be treated on general principles.
The testicle is originally formed by differentiation from the Wolffian bodies, at a level above the pelvis. Its migration from its original location into the pouch where it normally belongs is known as the descent of the testicle. When it fails to appear at[1014] the external ring it is spoken of as retained testicle, and when detained outside the ring above its proper level the condition is referred to as incomplete descent, these being purely arbitrary terms. The reasons for incompleteness of the descent are as little understood as those for its completion, and have but little reference to clinical surgery.
The surgical anatomy of the testicle may be only briefly considered here. Each is essentially a double organ, consisting of the testis proper, the secreting portion, with its more or less complete double peritoneal covering (originally peritoneum), and the epididymis, or conducting portion, variable in size, and corresponding to the parovarium in the ovary in respect that it is subject to cystic degeneration. The pathway made by the testicle as it passes from the abdominal wall should be completely obliterated. When unobliterated it facilitates the occurrence of hernia, while when partially obliterated cystic dilatations of the enclosed portions (hydroceles of the cord) occur. The lowermost portion of the accompanying peritoneal pouch is normally left as a closed sac, which constitutes the cavity of the tunica vaginalis testis. In the ordinary standing posture the epididymis occupies toward the testis proper the same relative position that the heel does toward the anterior part of the foot, i. e., it lies to its posterior and inner sides. While both portions of the organ may be involved in acute or chronic diseases, each of them may be by itself involved with a minimum of disturbance of the other.
As above indicated failure in descent varies in degree from complete absence from sight and touch to a presentation of the testicle at a point where it can be both seen and felt but still at too high a level. Ordinarily the condition is symptomless, its only signs being those above rehearsed. Strange to say the condition sometimes passes unrecognized until adult life is reached. Commonly it is early discovered. Pain is felt only when friction or traumatism lead to the same unpleasant sensations which would be produced by pressure upon a normal organ. Thus a testicle retained at the external ring may be irritated by the clothing, and has been many a time mistaken for an incomplete hernia, upon which a truss pad has been applied with inevitably resulting suffering. While accompanying malformations in other parts of the body may be found it does not follow that the individual may not be otherwise perfectly developed.
It is usually held that an incompletely descended testicle is more or less functionless; often it is at least more or less atrophied. Its functional capacity varies. It is usually more or less surrounded by a cavity formed from the peritoneum. While the condition is ordinarily one of minor importance, it has been established by numerous observations that retained testicles are relatively prone to undergo malignant degeneration.[73]
[73] In the pathological museum of the University of Buffalo I deposited specimens illustrating this fact, one testicle forming a tumor as large as the patient’s head, the other as large as a cocoanut. These were both successfully removed from an adult, and without the patient developing any subsequent evidence of malignant infection. It is thus important in every case of intrapelvic tumor in the male to examine the scrotum and be sure that both testicles are in their proper position.
—The proper early treatment of cryptorchidism has been a matter of dispute, some advising to leave the condition entirely untouched so long as it be not troublesome; others that early intervention should be practised. If the organ be simply displaced and not otherwise diseased, whatever be done may be limited to freeing it from its abnormal surroundings and restoring it as nearly as possible to the position where it belongs. If it be actually diseased it should be removed. What may be accomplished will depend much upon its movability and its blood supply.
Thus Keetley would liberate the testicle, when retained within the inguinal canal, by division of the latter and lengthening of the cord by blunt dissection, with division also of the lateral portions of the gubernaculum near the pillars of the external ring and as far as possible from the testicle. By traction upon this it is then often practicable to bring the testicle down, without undue tension, to the lower part of a new scrotal pouch, which is formed by making for it a nest, as it were, with the finger, with an opening at its lower extremity, through which forceps are thrust, passed upward and made to seize the end of the gubernaculum, or through which a suture may be passed for the same purpose. By means of this device the testicle is now drawn downward into the scrotal pouch, where, being once present, it is held by sutures, both direct and those[1015] which close the pouch above it. It is then advisable to close the inguinal canal, as after a hernia operation. In order to prevent upward traction on the scrotum it is necessary to attach its lower end to the skin of the thigh, by a suture which should remain for several days. If this be done on both sides the limbs should be snugly bandaged together and movement of all kinds prevented. Complete separation of the scrotum from the thighs should not be permitted for several weeks, unless unavoidable.
Beck recommends an incision from the external ring three inches downward along the cord, after which he opens the pouch of the testicle, lifts it from its bed, pulls it down, carefully dividing all bands of connective tissue or peritoneum which tend to immobilize it. It is then deposited in a scrotal pocket, in which it is held by a flap dissected from the outer margin of the inguinal ring, and turned downward in such a way that it can be attached to the opposite layer in semilunar shape. Thus a band of aponeurotic tissue is made to surround the testicle “like a necktie,” the organ being retained as in a buttonhole, the length of the flap being determined by the extensibility of the cord. The inguinal canal is then closed as after any other procedure.
Other abnormalities of the testicle include congenital atrophy or absence, while in a few cases a third testicle has been found, it lying in contact with one or the other of the naturally separated normal pair.
Injuries to the testicle are of common occurrence, on account of their exposed position, yet less common than would otherwise occur were it not for their extreme movability. Aside from the lacerated, incised, or punctured wounds which may be inflicted the testicle suffers most often from contusions, always with resulting swelling, and sometimes with considerable effusion, of which a large amount may be accommodated in a distended tunica vaginalis.
Hematomas of the testicle are also thus frequently produced. When of a limited degree of severity spontaneous absorption of blood may be expected, and should be favored by physiological rest, i. e., confinement in bed, with elevation of the scrotum and the application of water dressings. Large extravasations of blood, when fresh, may be withdrawn by the trocar, but when clotted will require incision and evacuation of clots, which should always be practised, as it leads to great saving of time. Extravasation is usually followed by induration, and more or less permanent enlargement, which will be slow to disappear; absorption may be encouraged by the use of a weak mercurial ointment.
Tuberculosis of the testicle simulates very closely that occurring in the lungs, in that one may see a disseminated miliary process, with subsequent coalescence and formation of caseous nodules, subsequently breaking down into abscess cavities, while at the same time the surrounding membranes, i. e., the tunica vaginalis, are involved, and effusion (hydrocele) occurs just as in the pleural cavity. In other words every appearance of pulmonary consumption may be imitated within the small extent of the testicles and the epididymis. Of these two parts the latter suffers much more frequently. Here are caused irregular nodules, which may later unite, giving to the entire epididymis a much enlarged, irregular shape, with induration, frequently extending upward along the cord, and always tending so to extend unless the disease be early seen and recognized. Too often adhesions to the skin occur, with ulceration and formation of fistulas, and perhaps more or less extensive ulcers, while in many instances the entire length of the vas becomes infected, and frequently even the prostate and corresponding vesicle become involved. By this time there will be more or less involvement of the inguinal lymphatics, and the patient may be already showing evidences of general tuberculous infection, at least those of some serious constitutional impression made by the local disease. One has to differentiate as between tuberculosis, syphilis, and cancer, which may be difficult in[1016] the early stages; but when the disease has extended beyond the epididymis itself it is rarely difficult to recognize, unless entirely masked by distention of the tunica vaginalis with fluid.
—The treatment for tuberculosis of the testicle is extirpation, i. e., castration, which includes the removal not only of the diseased organ, but of all the tissues, including the skin, to which it may be abnormally adherent, and of the spermatic cord, which, if necessary, should be followed into the pelvis by a long incision extending up along the inguinal canal. To remove a tuberculous testis and leave a tuberculous cord is to accomplish very little, while the latter, being an extraperitoneal tissue, may be followed with relative safety, even to the depths of the pelvis. Local applications in these cases give little relief. This teaching is at variance with that of some writers, but is justified by experience.
Syphilis occurs in secondary and tertiary manifestations, usually first in the testis, sometimes in the epididymis, but always in the testicle before the cord. It produces nodules which may be mistaken for those of tuberculous trouble, but which often attain much larger size. They are usually painless. Nevertheless a syphilitic testicle is sometimes tender, and constantly so, to a degree causing no little annoyance. The occurrence of nodules in the epididymis, in connection with other evidences of syphilis, is regarded by some as pathognomonic. In this location the condition yields readily to properly directed treatment.
Cysts are frequently found along the course of the epididymis. Some of them are expansions of the natural tubes of the paradidymis, while others are distinctly new. Dermoids are occasionally met, and either of these may attain considerable size. Cyst of the epididymis proper is to be distinguished from encysted hydrocele of the cord. All of these purely cystic conditions are essentially innocent, and need similar treatment. They may be evacuated and injected with an irritant like pure carbolic acid, which is sometimes an effective way, or they are better treated by open incision with extirpation of the cyst, which is, in the end, far the more satisfactory course to pursue.
Each of the separate portions of the testis may have its own nearly self-limited inflammations and infections, or both may participate in a common lesion. The most frequent cause of an acute epididymitis is gonorrhea, the infection travelling from the urethra along the vas, and causing acute and well-marked swelling of the epididymis, which becomes tender and painful in proportion to the amount of exudate. It may come on early or late, during the course of the urethritis. The condition is known to the laity as “swelled testicle.” It has been frequently called orchitis, which is an error, since however much the testis may later participate the primary trouble is in the epididymis. It may be easily distinguished by palpation, the enlarged and hardened epididymis, often very tender, being prominent behind the testis proper. The condition may, however, be masked by the acute effusion likely to occur in the tunica vaginalis, constituting a mild degree of acute hydrocele. This may be expected in nearly all severe cases, and serves to increase the size of the entire mass. A testicle thus affected may assume much more than normal dimensions, and, becoming thereby much heavier, drag upon the cord, which is its normal support. More or less fever and malaise accompany the condition, part of which may be due to the toxemia of gonorrheal infection. Usually but one side is involved. Both are rarely affected simultaneously, but one may follow the other.
The acute stage of gonorrheal epididymitis persists for a week or ten days, even under the best of treatment, and is followed by gradual subsidence, characterized by amelioration of symptoms and decrease in size.
[1017]
—This improvement is to be induced, first, by rest in bed, with elevation of the scrotum, and the ordinary eliminative treatment suitable for any febrile condition. Local relief may come from the application either of heat or of ice-bags, the latter being preferable, but will be made more effective by the application over the scrotum of a mixture of two parts of olive oil with one part of methyl salicylate, or of guaiacol reduced with equal parts of oil or glycerin. The anointed surface should be covered with some impervious material, and the dressing be changed every few hours. Later, as the acute merges into the chronic condition, absorption may be stimulated by the ordinary mercurial ichthyol ointment.
In some exceedingly acute cases suppuration ensues, the consequences being a collection of pus in the epididymis, which will give the ordinary signs and call for the usual evacuation which every collection of pus demands. Epididymitis, more or less acute, has been known to follow the introduction of the catheter or sound, even in cases so far as known not previously infected. It is difficult to explain, but requires the same treatment as above.
—This condition is rare except as an occasional complication of mumps, or, much more rarely, of one of the other exanthems. Why after acute parotiditis there should be a tendency to inflammation of the testis or the ovary has never been fully explained. Nevertheless it is sufficiently frequent to be well known to the laity, and is occasionally so pronounced as to lead to actual atrophy, with loss of function of the testis involved. In any true orchitis there will be considerable pain and tenderness, because the testis proper is so tightly confined within its tunica albuginea, i. e., a firm, inelastic membrane. By proximity there will also be set up more or less involvement of the tunica vaginalis, with effusion, so that some degree of acute hydrocele may be looked for in every such instance.
Treatment.
—The treatment of the condition above described consists essentially in rest, with local soothing applications, of which perhaps nothing will be more satisfactory than guaiacol, which, however, should always be used with caution.
Dermoid cysts and tumors and teratomas, i. e., those of mixed type, are frequently met in this region. Their explanation is doubtless afforded by the extreme complexity of the elements which help to make up the part, while in the embryonic condition, and the confusion of tissue elements which may then and there arise. These growths of embryonic origin vary from single cysts to a mass of cystic tumors, which may replace the organ, or constitute neoplasms of large size, while some of the teratomas have features causing them to resemble the mixed growths occasionally found within or about the ovary. In this way is to be explained the occurrence in such masses of hair, teeth, and other epiblastic elements, as well as of cartilage or bone or other mesoblastic elements. Taken together these growths constitute an interesting group for the pathologist to study. For the surgeon, however, they require essentially the same class of treatment, namely, extirpation, or, if this be impossible, complete removal of the organ, i. e., castration. There should be no hesitation in performing this upon any such growth, as no testicle thus affected is likely to be functionable, and the individual suffers no possible deprivation of potency by its removal.
The other benign and simple tumors, especially fibromas and chondromas, are occasionally met, and I have described one rare case of large lipoma within the limits of the testicle proper.
—This includes, usually, sarcoma, developing from the mesoblastic elements, although adenocarcinoma may be met here, but as an extension from some growth occurring first in the skin or in the immediate neighborhood. Deep cancer in this region is difficult to at first distinguish from the induration produced by tuberculosis or syphilis. In doubtful cases the therapeutic test may be tried in order to differentiate it from the latter. From the former it is usually separated by its more consistent and regular (i. e., its less nodular) character. In all three cases the lymphatics of the groin may be early involved, or perhaps not until late. As a rule cancer is met in the later years of life, while the other conditions are more frequently seen in the first half. In the more rapid cases there will be considerable pain, with dilatation of the[1018] scrotal veins, and evidences of constitutional involvement. Sarcoma may grow rapidly and metastasis is almost invariably to the lungs.
Of tumors in the testicle, as of those in the breast, it may be said that any new-growth which tends to enlarge, become more dense or adherent, to spread, or to be accompanied by lymphatic involvement should be removed; no mistake will be made in applying this rule in these cases, especially if by the therapeutic test or otherwise syphilis can be excluded. Malignant disease sometimes travels rapidly up the cord, and the main fear is not so much of local recurrence as of deep involvement within the pelvis. Cases of cancerous growth of the testicle should be not only thoroughly extirpated from the scrotum, but the inguinal canal should be opened, and the cord followed as far as possible and completely removed.
Cases may arise where amputation of the scrotum may be justifiable for the purpose of temporary relief, in order to avoid discomfort, hemorrhage, or offensive ulceration.
Strictly speaking the term hydrocele means accumulation of watery fluid in any pre-existing cavity. By universal consent, unless some other cavity be specified, the tunica vaginalis is understood. The consequence is a more or less distended sac of serous fluid, which first occupies a position in front, but finally is spread around the lateral portion of the testicle, and may form a tumor the size even of the individual’s head. It is an innocent collection of serum, but the walls of such a sac will be thickened in proportion to its age and size, and may in the course of time undergo such degenerations as the calcareous, for instance, by which it becomes more or less infiltrated or encrusted with calcareous material. Thus I have in my possession a tumor of this kind, nearly the size and almost as hard as an ostrich egg, the old tunic being converted practically into a shell.
Acute hydrocele occurs, as above mentioned, in connection with the acute infections, but is then ordinarily a matter of but a few days or weeks.
Hydrocele, as usually implied by the term, is an exceedingly chronic and almost painless affection, which may follow injury, but which comes often without any known cause. Many theories have been advanced to account for it, but none are generally satisfactory. These cases, however, occur usually after the fortieth year of life, but may be seen in the young. Their greatest unpleasantness is that produced by the weight of the mass as it drags upon the cord and the scrotum.
The tumor is pear-shaped, and abruptly circumscribed at its upper limit, below the external ring (unless there be also involvement of the cord), and gives no impulse when the individual coughs. By these features it is distinguished from hernia, for which it is often inexcusably mistaken. A hernia is a distinct prolongation from above, whereas a hydrocele terminates below the hernial outlet, and by its smaller extremity. The distended sac will fluctuate, and will return clear fluid upon puncture with a hypodermic needle, and is so translucent that light may be transmitted through it when it is interposed between a candle-flame and the surgeon’s eye. (Serious thickening of the sac may interfere with the value of this test.) A congenital form of hydrocele is also known, due to failure of obliteration of the canal of Nuck, and it might be possible in some such cases to get a slight impulse on coughing, as when the sac connects with the abdominal cavity, in which case it should be possible to gently press its contained fluid back into the abdomen above. In most congenital cases there is a tendency to spontaneous cure, at least to obliteration of the canal.
Occasionally both sides are involved, or the sacculation may be multilocular, or accompanied by cystic extensions along the cord.
—In regard to methods of treatment, but two will be considered here, aspiration with injection of carbolic acid, and extirpation. The former consists in the insertion of an ordinary (small) trocar, which is thrust in from below upward, care being taken that its point avoid the testicle, which is always found to the posterior and inner side of the sac. Through this trocar the contained fluid should be completely evacuated, so that the sac is practically dry. Into it is now injected with some force from 2 to 6 Cc. of absolutely pure carbolic acid, after which the trocar is instantly withdrawn, pressure made upon the opening, and massage made upon the scrotum and the contained testicle,[1019] in order to distribute the acid freely over the serous surface. Its effect is to completely sear the entire surface so that the mouths of all the absorbents are closed. In this way danger of carbolic poisoning is quite avoided, a danger which would be imminent were the acid reduced in strength. But little pain is caused by the procedure. Its immediate effect is to produce exudate, with some recurrence of swelling, which ordinarily rapidly absorbs, while the exudate, coagulating, serves to produce obliteration of the cavity of the sac. This is the carbolic method of Levis, who introduced the acid as a substitute for the iodine formerly employed, upon which it was a great improvement. For cases of moderate age, whose sacs are not too thick, it often proves satisfactory. Having failed, or the case being considered not adapted to it, the other method is that by open incision and extirpation.
This open method consists in making an incision through the skin, down upon and into the sac, which, being thus instantly evacuated, will collapse. It is now possible to make a more or less complete enucleation of the sac wall, stripping it from the external tissues to which it adheres, as it is not necessary to separate it from the testicle itself. It has been found that when the major portion is thus removed the condition is effectually combated. The cavity may be drained with silkworm strands or with a small tube, but only for a short time, if the technique have been correct.
The cord participates essentially by its contained vas deferens and lymphatics in the consequences of acute and chronic infections, travelling in either direction, and thus it may be involved in tuberculous, syphilitic, or malignant disease. These expressions, however, are secondary and the conditions have been described above. Encysted hydrocele of the cord implies simple dilatation of an incompletely obliterated canal of Nuck, by which there may be formed along the cord one or more cystic expansions, causing tumors rarely attaining a size greater than a pigeon’s egg, which are innocent collections of fluid, corresponding to the ordinary hydroceles that may occur below. They are ordinarily not difficult of recognition, and are the most common form of neoplasms occurring in this region. They are amenable to the same treatment as that described for hydrocele.
Fig. 674
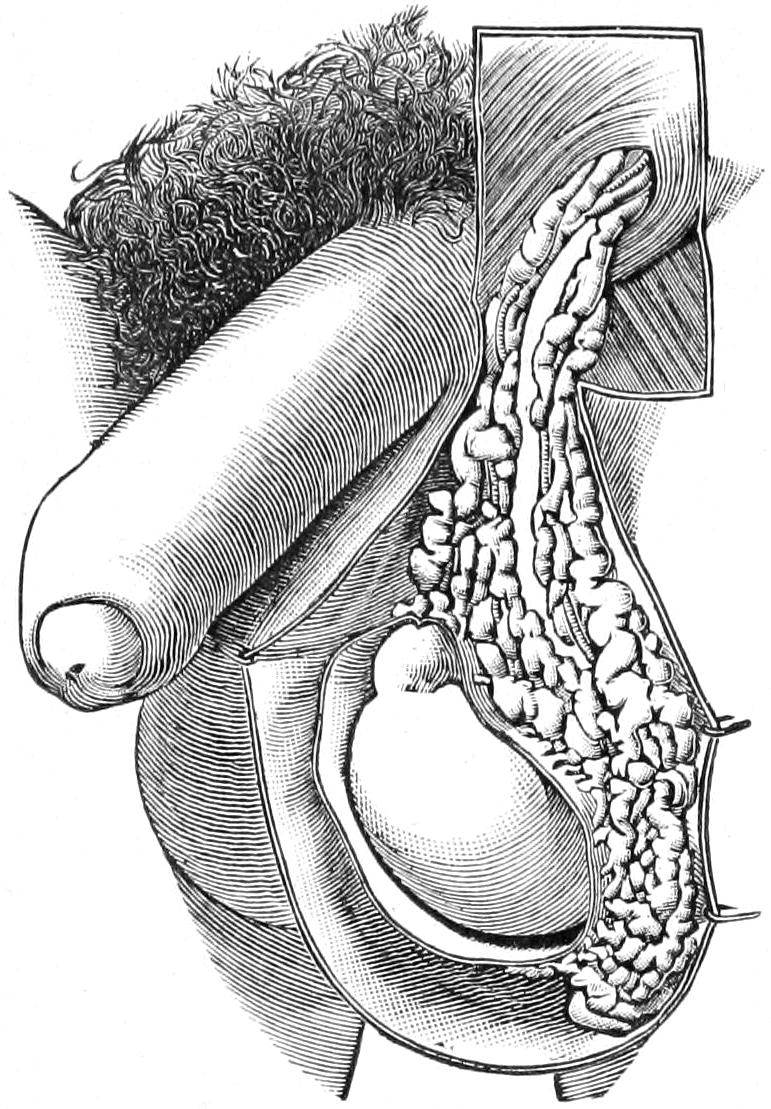
Varicocele. (Hartmann.)
Spermatocele implies a cystic tumor in whose contained fluid, no matter what its source, are found spermatozoa, which may be seen alive under the microscope if examined immediately after removal. Spermatoceles are usually found at the lower end of the cord and in close connection with the testicle. Their occurrence is not uncommon, but somewhat difficult to explain, for it implies connection, at least at some time, between the structures of the cord and a more or less displaced seminiferous tubule. Spermatoceles are rarely diagnosticated as such until aspiration or evacuation and examination of their fluid contents, which usually are of a milky appearance. In general they are to be treated like any other cysts, and by the same methods.
This exceedingly prevalent affection is the result of a varicose condition of the pampiniform plexuses and of the spermatic veins. It occurs in perhaps 10 or 12 per cent. of adult males, rarely before puberty, and almost invariably upon the left side, varicocele upon the right side being as rare as 1 in 500 cases. Its confinement to the left side is explained partly by compression of the left spermatic veins beneath an overloaded and distended sigmoid, and by the disadvantage at which the blood current from the left spermatic vein empties into the vena cava, this being on the left side at a right angle, while on the right the angle is oblique. It has occasionally to do with accident or injury, as well as with occupation or habit. It occurs more frequently in those who are long in the saddle and in those who ride the bicycle to excess. (See Fig. 674.)
Varicocele is usually of slow development, and discovered finally by accident or by[1020] attention being drawn to these parts through quack advertisements or misleading statements. The effect is to produce an elongated mass of varicose veins, often described as feeling like a “bag of angle worms,” occupying the lower portion of the cord and extending down upon the back of the testicle. In the more advanced cases the condition can be traced almost to the external ring, but is always more marked low down than higher up. Sometimes it is so extreme that the entire group of veins corresponds in bulk to a hen’s egg; ordinarily it is but a fraction of this size. The consequence is increase of weight and production of dragging sensation upon the cord, often referred to the back, and displacement downward of the testicle, with consequent elongation of the scrotum, which may so greatly relax that it appears to be twice its normal length and contains this varicose mass at its lower extremity. Such a condition will naturally produce a certain degree of discomfort and annoyance, but beyond this it is innocent, save that it is made to cause much mental anxiety, mainly through ignorance, and has led thousands of victims to quacks, for treatment for conditions dishonestly represented and treated as both distressing and extreme. It is true that a large mass of enlarged veins may in time produce some atrophy of the testicle; it is likewise true, also, that virility or masculine potency may be to a trifling extent limited in this way. It is not true, however, that impotence can be so produced, because the affection is limited to but one organ, so that the impotency of which many men complain is mainly of psychical origin. Such individuals need explanations and advice as much as treatment, although it is difficult to elevate many of them from the condition of sexual hypochondria into which they gradually fall.
Fig. 675
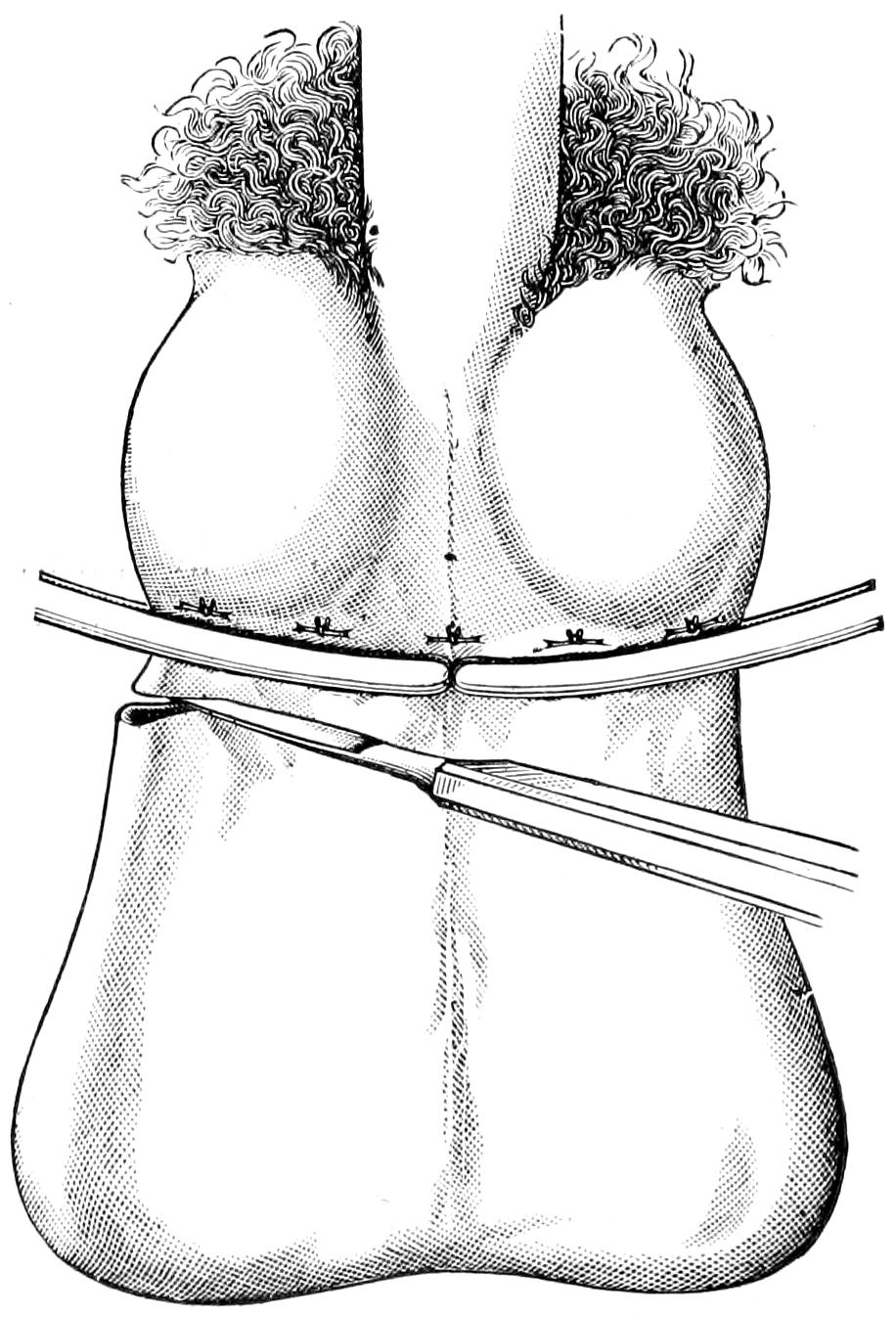
Fig. 676
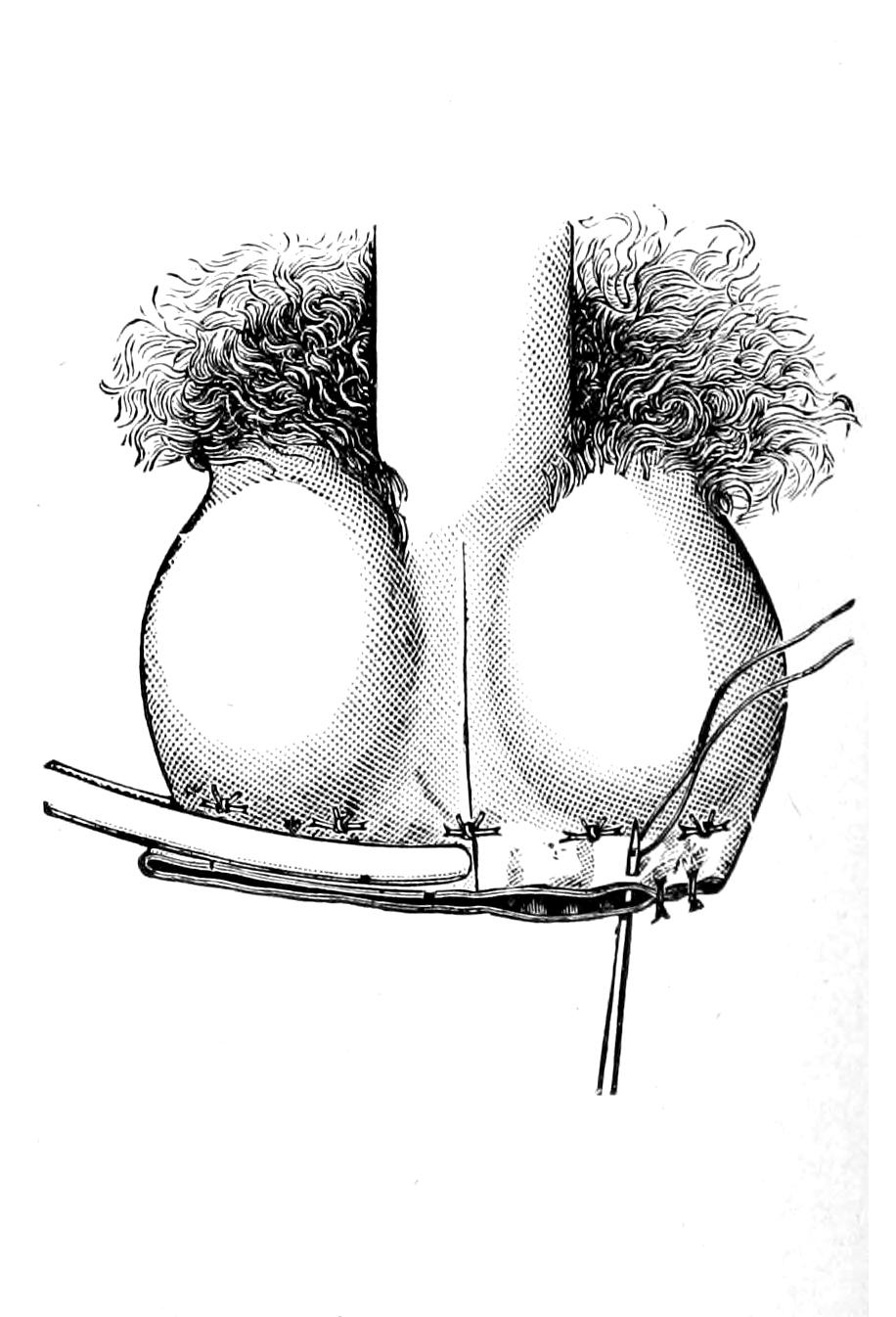
Resection of scrotum for varicocele. (Hartmann.)
[1021]
—Treatment of varicocele may be palliative, i. e., it may consist of suspension of the overloaded testicle and somewhat relaxed scrotum within a well-fitting suspensory bandage, and this suffices for most mild cases in normally minded individuals. When, however, the condition preys deeply upon the mind or upon the body, or when it is actually and anatomically advanced, then radical operation is legitimate and humane. Of the many operations recommended in time past only two will be described here, for it seems to me that all subcutaneous and blind methods are bad in theory as in practise.
Excision of the varicose veins is easily performed under local cocaine anesthesia. It is done by incision below the external ring, over the course of the cord, the cord itself being exposed for two to three inches. Here the enlarged veins appear usually in a group (the pampiniform plexus), and as such can be isolated and separated from the balance of the cord, it being essential to carefully exclude the vas, as injury to or division of this canal would naturally be followed by impotence of that testicle. The veins involved being isolated to an extent of two inches, are ligated above and below, the intervening portion being then exsected, after which it is my custom to utilize the catgut with which this ligation is effected, threading it on each side into a needle, using each as a suture, thus providing two sutures, by which the divided ends are approximated and tied together, the effect being to bring the testicle up and make a more effective suspensory of the cord itself.
Shortening of the Scrotum.
—To the above procedure, when the scrotum is much elongated and relaxed, may be added its shortening by a species of amputation. The entire procedure may be practised as follows: The scrotum being stretched downward is shortened by removing one and a half to three inches from the lower end of the scrotal pouch of skin and the contained connective tissue, including the septum. In this way the tunical sacs and lower ends of the testicle will be immediately exposed. The left testicle can now be drawn down, and the operation, described above, of exsection of a portion of its veins, may then be practised. This being completed the scrotal wound is closed with sutures, with or without catgut drainage. The effect is to not only remove the varicose veins, but to reduce the size of the scrotum, and to make it, as it were, a suspensory of living tissue (Figs. 675 and 676).
The lower ends of the vasa and the seminal vesicles themselves suffer most commonly from the consequences of tuberculous or of gonorrheal infection, travelling in either direction, they being easily invaded from the prostatic urethra along the seminal ducts. The consequence is seminal vesiculitis, which produces a more or less tender swelling, with discomfort referred to the lower end of the rectum, and discoverable by digital examination above the prostate. When the vesicles are distended or infiltrated they may be felt with the finger in the rectum. In addition there may be on pressure more or less discharge of fluid into the prostatic urethra, while the semen when emitted may be more or less mixed with blood.
It is necessary usually to differentiate between prostatitis or prostatic hypertrophy and vesiculitis.
Chronic involvement of the seminal vesicles may be best treated by a species of massage or “milking,” by which retained contents are coaxed along the ducts and into the urethra. Its local treatment is almost impossible. When the conditions resulting from infection of either type have become chronic and intractable we may take advantage of recent advances and decide upon removal of the vesicles by operation. Fuller suggested that this be done by putting the patient in the knee-chest position or a modified Sims position. While it is not difficult to reach the vesicles through the rectum, the method has its disadvantages and the perineal route is much the better. The operation is then effected, much as is prostatectomy, by perineal opening and blunt dissection between the rectum and the prostate, carried upward until the vesicles themselves are reached, after which they may be curetted or extirpated by a process of enucleation.[74]
[74] In the treatment of infections of the seminal vesicles, particularly those of gonorrheal origin, Belfield has advised irrigation and drainage of the same through the vas deferens. He brings this up against the skin of the scrotum, where it is easily identified, and then, through a one to two-inch incision, made under local anesthesia, exposes the vas, into which the blunted end of a hypodermic-syringe needle may be introduced, by means of which a solution of any desired agent may be injected. This being thrown in the direction of the seminal current passes up through the vas and into the vesicle. He has even recommended in certain cases to attach the vas to the skin by a fine silkworm suture, and in this way to make a minute fistula, which can be used for the purpose as long as may be necessary. He considers the method invaluable in the treatment of chronic gonorrheal vesiculitis or the chronic infections of the seminal canal in the elderly, which are often mistaken for enlarged prostate, as well as in cases of recurrent epididymitis resulting from repeated invasion from behind. Thus he has seen benefit follow, in tuberculosis of the epididymis, from irrigation with carbolic solution. The amount injected into the vesicle should never exceed 2 Cc.
[1022]
Accurately defined this term refers to the escape of semen under abnormal and involuntary conditions, an occurrence which is of great rarity. Most cases of so-called spermatorrhea are, in effect, but the escape of excessive or superfluous amounts of prostatic mucus (prostatorrhea), the fluid, whether it appear drop by drop or in considerable quantity, being mistaken by the patient for semen. Thus with the extrusion of a hard fecal mass there may be sufficient pressure upon the prostate to express from it 1 Cc. or more of this fluid. True spermatorrhea, on the other hand, rarely occurs except in connection with disease of the vesicles or prostate, and will then be recognized rather by the detection of spermatozoa in the urine than from any phenomenon noticeable by the patient. All statements, therefore, made by patients to the effect that they suffer from involuntary escape of semen should be taken with the greatest allowance, and will usually be found to be misleading.
All of this might lead up to a considerable discussion of matters included within the domain of sexual physiology and hygiene, topics which, however, cannot be afforded space in the present work; all that can be said being that many patients are in need of accurate information who suffer acutely in mind, and sometimes slightly in body, for lack of it, and who are tempted by motives of delicacy to consult quacks and charlatans rather than their family physician.
The only operation of importance upon the external genitals not yet described is that of castration, i. e., removal of the testicle. This is ordinarily a simple procedure, requiring, first, incision of sufficient length. If the disease condition include the slightest infiltration or involvement of the overlying skin a little or the greater portion of it, as required, should be included in an oval incision, in order that it may be totally removed. The testicle and its coverings, being now exposed, are to be loosened from all their surroundings, the organ pulled down, and the cord brought into sight. If there be no reason for following up the spermatic cord it is sufficient to surround it with a ligature (chromic gut), at a convenient height above the testicle, after which the cord is divided below it and the mass removed. In most instances, however, the disease which calls for so much operating will require to be followed up along the cord, and perhaps through the inguinal canal down into the pelvis. This is done by continuing the incision in the proper direction, isolating the cord, ligating bleeding vessels, and finally dividing the cord itself at a point of election decided to be above the disease. Previous generations were hesitant about including the entire cord in a ligature, for fear of tetanus, but we now know that if the technique be carefully carried out there need be no fear on this score. The diseased mass being removed the wound is closed, with or without catgut drainage at one or more points, as may be indicated.
[1023]
Amputations are performed for (a) the results of injury, (b) the results of disease, and (c) removal of deformity or mutilation, or the possible results of congenital defects. While generally they are measures of necessity, made such by traumatism or by actively advancing disease, there are occasional instances where an individual decides that an artificial limb will be more useful or that he will be freed from an intolerable annoyance by the sacrifice. The principal diseases which may require such mutilation are the exceedingly acute, e. g., osteomyelitis, the slower destructive forms of ulcer, tuberculosis or of sepsis, the gangrene caused by vascular or diabetic conditions, or the slow involvement of tumors, usually malignant, but sometimes benign.
When a serious and mutilating injury has been received, if there have been complete crushing of a limb or avulsion, of course no doubt exists as to the necessity. Amputation is not now made for compound fractures nearly as often as in former times, for if only the vascular supply be good much may be done by resection of bone ends, wiring, or other expedients; and the attempt should always be made to save a limb unless it appear that even should the effort succeed the limb itself would be too useless to justify the attempt. With the possibilities of modern asepsis, and with immediate attention to the injury, the question of what should be done with an injured limb is largely a question of its blood supply. Extensive contusions with lacerations do not of themselves necessitate amputation, neither does injury to the skin unless it be most extensive.
It is unfortunate when vacillation or any misguided effort at conservatism call for great delay. While this may sometimes be advantageous, at other times the favorable moment has passed before permission to amputate may be obtained. Should delay seem advisable the surgeon should use his best endeavor to effect suitable antisepsis, to provide physiological rest, and to preserve the circulation, all of which require a thorough antiseptic technique, which will include the removal of blood clot, of fragments, and of all tissue which evidently cannot live, and suitable splinting or its equivalent, and of everything that can be done by local warmth and general stimulation to maintain the vigor of the circulation. When once infection has occurred, and especially been allowed to spread, the possibility of recovery inheres only in immediate amputation.
Such mutilations as necessitate immediate amputation are usually accompanied by profound degrees of shock, as well as perhaps by other complicating injuries, whose existence may change the whole complexion of the case. For example, with a patient suffering from probably fatal fracture of the skull one would hardly seriously discuss the matter of immediate amputation of a foot; nevertheless he should take such care of the local lower injury as to permit operation to be done under still favorable circumstances should the head condition justify it. Wide discretion is therefore called for in all these cases. Furthermore the condition of lowered blood pressure or shock may be so extreme that the operator is compelled to delay, for at least a certain time, in order that by the employment of those measures already considered in the chapter on this subject the circulation may be sufficiently restored to make it adequate for the purpose, remembering that scarcely anything predisposes to infection more than such lowered vitality. While resorting to general stimulation, hypodermoclysis, or infusion, with or without adrenalin, the use of such antiseptics should not be omitted, as the local condition may require in order to combat what otherwise may be actively occurring.
Amputations are sometimes referred to as typical, when done according to long-established methods, or atypical, when the entire procedure is planned to fit the necessities of the case. Amputation at a joint is usually spoken of as disarticulation. Amputations, again, are classified as (a) immediate, i. e., before complete reaction from shock or within the first few hours; (b) primary, when done after reaction has occurred, but before visible[1024] occurrence of inflammatory changes, (c) intermediate, as done when suppuration is threatening, but before its actual occurrence; (d) secondary, i. e., after the occurrence of suppuration.
The control of hemorrhage is one of the most conspicuous and necessary features of any amputation method. Below the shoulder and at the hip this may be effected by the old-fashioned tourniquet, or the modern elastic bandage, which may or may not be combined with the more complete bloodless method with which Esmarch’s name will always be connected. The pure rubber gum bandage, I believe, was introduced by Martin, of Boston, but the method of its use for bloodless operations upon the extremities is to be credited to Esmarch. The surgeon may avail himself of this method in all suitable cases, but should never resort to it in septic or malignant disease. It includes the application of a Martin elastic bandage from the tip of the extremity to the necessary height, by turns which shall make gentle and equable pressure, gradually forcing the blood from the compressed tissues and out of the limb, and up to a height where another elastic, or, at all events, suitable constricting band is placed with a sufficient degree of tightness to completely shut off access of blood. To so apply a bandage in septic and malignant cases would be to coax septic and malignant material into the veins, and would evince the worst possible judgment. A sufficiently strong rubber tubing forms an effective tourniquet, which, however, should be applied over a folded towel, or in some manner so that it does not too deeply constrict and compress the soft tissues of the limb. Instead of tying a knot it may be secured with an ordinary clamp forceps.
The tourniquet should never be applied over the leg or forearm, for it can here make no impression upon the interosseous vessels. Its application should be begun by pressure upon the vascular, i. e., the adductor side of the limb, so that venous choking may be avoided. After it is once in place the limb should not be completely flexed nor extended, lest the tissues firmly enclosed by the constriction be more or less spontaneously torn; nor should the tourniquet be too long left in place, as injury to the vessels is the possible result.
The bloodless method of Esmarch is furthermore subject to the following disadvantages. It is sometimes followed by serious and permanent paralysis of the limb, the result of prolonged or excessive constriction and compression of the motor nerve trunks. Similar results (in the arms) follow the use of crutches as well as of pressure of the side of the operating table when the limbs are allowed to hang over it. Again after removal of the bandage there is sometimes most pronounced capillary oozing due to vasomotor paresis. This may be controlled by the stimulation of hot irrigation or applications, and by more or less massage of the limb. The dangers of forcing undesirable material into the circulation have been mentioned, in addition to which should be recorded the increased absorption of toxic substances.
When there is good reason for not using the elastic bandage, save as a tourniquet, much of the desired effect may be obtained by holding the limb for a few minutes in a vertical position, so that its contained blood is drained out of it by gravity, after which the tourniquet may be applied as before.
The cocainization of nerve trunks, as they are exposed and divided, is one of the new measures for the prevention of shock for which we are largely indebted to Crile. It has proved to be a most valuable expedient which should not be neglected. (See Chapter XVIII.)
Under modern methods more is expected of an amputation stump than in days gone by, and the first demand is that it shall be useful, to which end it is necessary that it be both movable and that its end be not too irritable, nor the scar too sensitive to stand at least a certain amount of pressure. It is expected that suitable prosthetic apparatus, i. e. artificial limbs, shall take the place of severed lower extremities and of most arms or hands removed. The skill and the mechanical ingenuity of the maker of artificial limbs have now reached a point where most acceptable substitutes are thus provided, but for them suitable stumps should be afforded by the surgeon, and there should be coöperation from each direction. Thus it used to be held that the bone end in every stump should be covered with periosteum, yet it has been recently shown, especially by Hirsch, that such bone ends are as acceptable, and perhaps more so, when stripped of rather than covered with this membrane, the latter being sensitive, and there being no advantage in the presence of such new bone as may be formed by its preservation.
Many a good stump may be molded in various ways, but always provided that the end[1025] of the bone be smoothly divided, and have no corners or osteophytic outgrowths to make pressure upon the sensitive scar. For this reason it should be manipulated as early as possible, and should not be allowed to undergo the atrophy noticeable in stumps left after old operations. If primary union be gained, so long as the cicatrix and the nerve ends be kept out of the way, one may expect a stump which is serviceable in every respect. The ideal method is that the skin and the periosteum should retain their normal relationship, an ideal best attained in the supracondyloid operation after Gritti’s method. Various osteoplastic methods have been devised, first by Walther, in 1813, and since him especially by Ollier, Pirogoff, Gritti, and Bier. The latter would cover every bone end not merely with periosteum, but with a bone flap so arranged that its lower surface is one normally covered by periosteum. The introduction of the x-rays has permitted a more thorough study of bone ends in stumps which are, on one hand, extremely tender, or, on the other, extremely serviceable, and the osteoplastic methods seem to conduce to the latter condition. Another matter of great importance is to so place the scar that it shall be neither subject to pressure nor to traction. If, therefore, the sawed surfaces be covered with a periosteum which shall retain its normal relation to its coverings, a minimum of disturbance in the scar is the result.
The value of early use of the stump and of accustoming it to pressure is considerable, as atrophic stumps are tender, like other disused parts, and there is, therefore, every reason for resorting to prosthetic apparatus as early as possible. As Kocher puts it, the following is the best procedure for the normal operation: “An oblique incision, combined if necessary with a longitudinal one, in the form of a racket or lanceolate incision through skin and fascia. After retracting the elastic skin the muscles are divided obliquely down to the bone. The periosteum is also to be divided obliquely. Periosteum is then separated along with the superficial layer of the cortex of the bone, by means of a sharp raspatory or chisel, or, when possible, a flap of bone having a movable periosteal hinge is made by means of the saw. Lastly, if only a thin shell of the cortex have been raised up along with the periosteum, the end of the bone is simply rounded off, while if a distinct flap of bone, by any osteoplastic method, have been divided, the end of the bone must be sawed in a curved direction so as to fit it. The periosteal or bony flap is sutured over the sawed surface of the bone to its periosteum, and the stumps of the muscles or tendons are sutured to each other, or to the surface of the bone at a distance from the sawed surface. Finally the skin and fascia are sutured; but in case where a periosteal flap or flap of bone and periosteum cannot be obtained in normal relation to other soft parts it is better to remove the periosteum entirely from the end of the stump, to scrape out the medullary cavity, and to round off edges of the bone as dentists do.”
While these methods give better results than those formerly in vogue, they also consume more time; but the days of brilliancy and rapidity in amputation are past, as time should be devoted to careful work, except only in those cases where emergency demands the most rapid and dexterous removal of a limb in the shortest possible time, and where every other consideration is sacrificed to the principal interest of preserving life.[75]
[75] The following is taken from the article of Professor Matas in the third edition of “Surgery by American Authors.” It furnishes a brief but admirable introduction to the general study of amputation methods:
“From Hippocrates to the time of Celsus the surgeon simply followed in the wake of Nature, never venturing to apply the knife for the removal of a limb except within the limits of the mortified tissues; and this seems to have prevailed for at least four hundred years. Celsus, the prince of Roman physicians, who lived shortly after the time of Christ, introduced the first innovation by cutting down to the bone between the living and the dead tissues. It is probable, according to the evidence furnished by his writings, that he was aware of the value of the ligature and that he applied it to control bleeding vessels. Archigenes, following closely after Celsus, was the first to attempt prophylactic hemostasis by applying a cord or band around the limb to control the hemorrhage during the amputation. With the fall of the Roman empire and the advent of the long night of the middle ages the Celsian method was lost in the general darkness and the old Hippocratic doctrines survived, and were maintained by the all-potent influence of Galen and his Arabian commentators. As late as the middle of the seventeenth century the only hemostatic was the actual cautery and boiling oil, though Guy de Chauliac had revived the teaching of Archigenes by constricting the limb, on a level with a joint, with a cord which was allowed to remain in situ, to ensure not only hemostasis, but a certain mortification of the stump. In cutting limbs huge chisels and mallets were used. At this period Botalli invented his guillotine, consisting of a sharp, heavy, axe, which, being allowed to fall from a height upon the limb, severed it instantaneously at a single blow. The revived or independent rediscovery of the ligature by Ambrose Paré in 1579, and the discovery of the circulation of the blood by Harvey, in 1628, led to the invention of Morel’s tourniquet (1674), more commonly known as the Spanish windlass, and to the familiar instrument, Pettit’s tourniquet, which (introduced in 1718) perfected the means of securing prophylactic and direct hemostasis. From this time onward the treatment of the stump began to receive more systematic attention. Instead of merely chopping off a limb, the soft parts were detached from the bone, so that this could be sawed off at a higher level, in order to avoid the conical projection of the stump which invariably resulted when the primitive methods were adopted. All the methods of amputation that followed—and these were numerous—aimed chiefly at celerity, to reduce the pain of the operation to a minimum; hence the rapid, circular section of the soft parts or the rapid transfixion methods which were so much popularized by the brilliant work of Liston, Lisfranc, Desault, Dupuytren, Langenbeck, and others. These finally yielded, in this modern period, to less rapid but more conservative and perfected methods, which aim chiefly at the preservation of useful tissue and at securing the very best functional prosthetic stump for the patient. Such methods could only be perfected after the advent of anesthesia and antisepsis.”
[1026]
With a view to simplifying this subject as much as possible the following methods alone will be considered: (1) The circular with its modifications, the oblique, the elliptical, the ovoid, etc.; (2) the flap method; (3) the mixed or skin flap and deep circular.
Choice of method sometimes leaves much, sometimes nothing, to the tastes or wishes of the operator. It should be based solely on the primary consideration of saving life and the secondary consideration of furnishing the most useful possible stump. To obtain the latter it is necessary that the bone be amply covered, except that its coverings be not adherent, that there be a minimum of disturbance of blood supply, that nerves be drawn down and divided as far from the stump end as possible, in order that they may not be entangled in the scar, and that the scar be so planned for and arranged that it shall be at one side, at all events in such position that no pressure shall be made upon it, and, if possible, also no tension by muscle action.
Elasticity of skin and contractility of the muscles vary much in different individuals, and it is not always easy to estimate either of them previous to their division. Consequently it is much better to make cuffs or flaps too long at first rather than too short. The existence of previous disease will always modify these local conditions, but, in general, the rule is laid down that the external flaps should be longer than the bone by from one-third to one-half the diameter of the limb.
—The simple circular method is the simplest and easiest of all. It may be so performed as to furnish a solid musculotegumentary division, or skin cuffs may be made, which being turned up, permit a further circular division of the muscles and other tissues directly down to the bone. The former is preferable when possible. With an ordinarily long amputating knife the skin, down to and including the superficial fascia, is divided by one clean circular incision, made in one stroke; then by further circular cuts the muscles are divided in sections, the outer group being allowed to retract and expose the deeper layers, which are then divided at a higher plane. In this way the periosteum is reached. If sufficient time be afforded it may be circularly divided at the level of the last incision through the muscles, and then separated with a strong elevator or, as done by Kocher, with a chisel, in order that some portion of the exterior of the bone be raised with it. In this way a cuff of periosteum, or enough of it to cover the bone end, is detached upward, to the level where the bone itself is finally divided. The bone division is done with the ordinary amputating saw, or with the wire or chain saw.
The skin-cuff (Manchette) method differs in that the exterior flap is made wholly of skin, which is dissected as a cuff nearly up to the level of bone section, at which point the muscles are divided directly down to the bone. In this method the skin, fat, and superficial fascia should be raised together, and at no points separated from each other.
Modification of the cuff method, by which it is more easy to evert the circular flap, is made by one or two vertical incisions, by which the cuff is split some distance on one or both sides, thus transforming the cuff proper into two nearly square skin flaps. At other times the first method may be similarly modified, in which case we have to deal with two square flaps, including not only the skin, but all the tissues down to the bone.
Neudörfer still further modified the circular method for certain purposes by first making an incision along the outer or least vascular part of the limb, carrying the knife directly down to the bone, retracting the wound edges, and thus exposing the bone, which is then divided with a chain or Gigli saw. After the bone is divided the soft coverings are lifted to a sufficient distance below the saw line to ensure ample covering,[1027] then divided as above. The method is a slow one and is especially serviceable for amputation of the thigh, at its middle, for diabetic or senile gangrene, where it is so desirable to protect vascular supply from injury (Fig. 677).
The so-called elliptical method is practically a circular incision carried obliquely around the limb, the upper and lower ends of the ellipse being indicated by previous small incisions at the proper height. The skin and superficial fascia are retracted from the lower portion of the ellipse by turning them up to the level of the highest point, at which level the muscles are divided transversely by a plain circular incision. A modification of this method is the so-called ovoid or racket, which is simply an oval division with a pointed end, the margins of the flap being united in the long axis of the bone. This method is frequently applied in amputation of the fingers. (See Fig. 683.)
—Flaps are either cutaneous or musculocutaneous. In every case the skin surface must be larger than the muscular. They are objectionable in that the skin flap is apt to slough, although least so about joints. The flap method is advantageous in that one flap may usually be made much longer than the other, and the longer one so doubled over at its end as to place the scar out of harm’s way. In certain injuries where the skin is much more injured on one side of the limb than on the other the operator is compelled to resort to flaps, unless he divide the limb much higher than might otherwise be demanded. Double flaps may be anteroposterior or lateral. A double flap practically results from a circular incision, carried through to the bone, with lateral division on either side, while a double flap with one long member may be similarly furnished by an oblique circular incision with the lateral prolongations.
Fig. 677
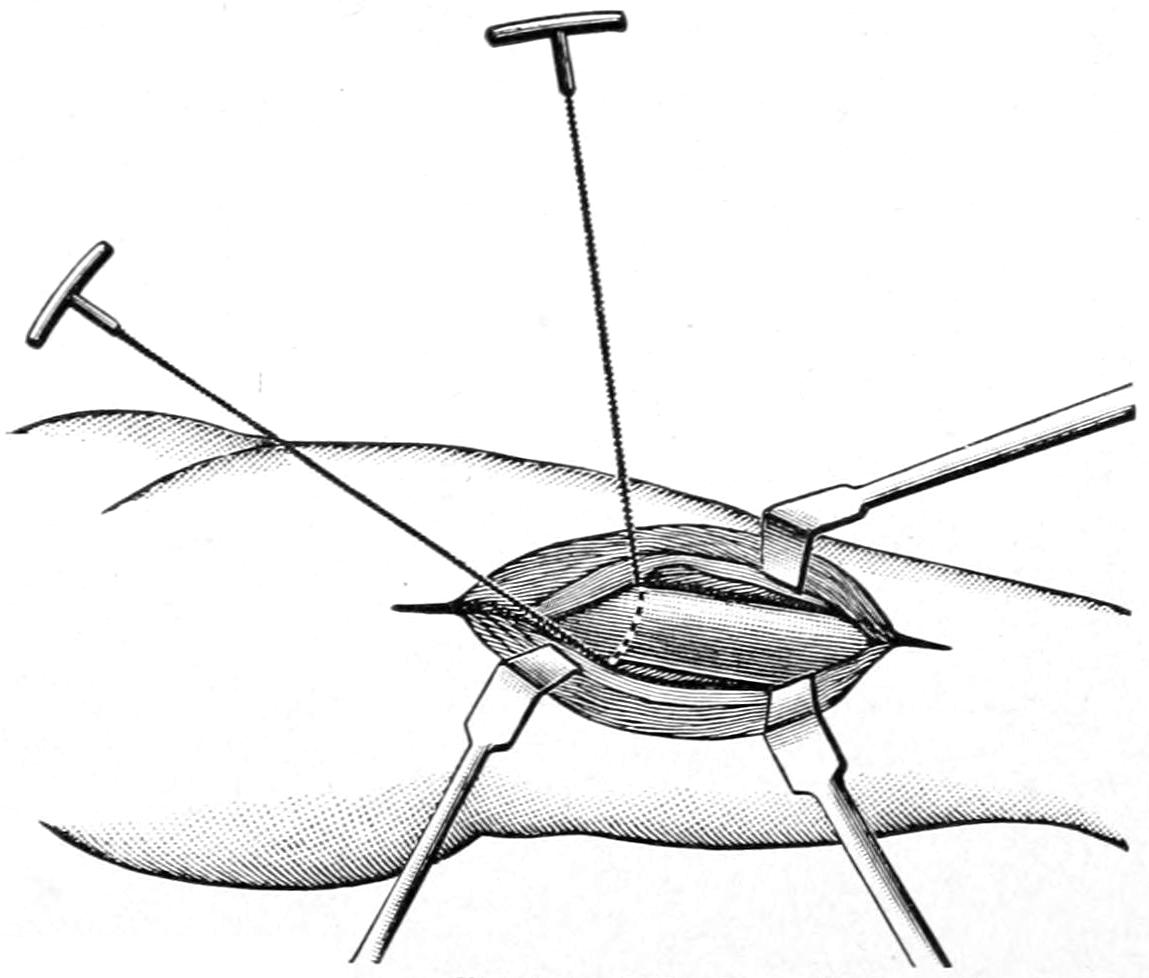
Neudörfer’s method of amputation by primary division of the bone, before shaping the flaps. Neudörfer used the chisel, but one may use the Gigli saw with special advantage in performing this operation. The method is applicable to any portion of the upper or lower extremity, especially in the continuity of the long bones. (Matas.)
Flaps may be formed by transfixion, for which purpose a long, sharp, amputating knife is required. Inasmuch as it makes an oblique and irregular division of the principal vessels, which are in consequence more difficult to secure, and by which nutrition of flaps is endangered, it is not to be commended, save perhaps in certain amputations about the wrist. A better method of making the flap is to divide the skin and fascia with an ordinary stout scalpel, and then, permitting them to retract, to divide the muscles obliquely toward the bone in such a way as to leave a flap wedge-shaped at its base. The anteroposterior amputations of the foot, thigh, and arm are better performed in this way, each flap being in length preferably three-fourths the diameter of the limb. (Matas.) An extension of this method furnishes the possibility for various subperiosteal amputations to be described below.
The osteoplastic methods of today furnish desirable operative procedures. One of the earliest of the good ones was Teale’s method, as applied to the leg, of double quadrangular flaps, the anterior being much the longer. A minor degree of this work includes[1028] simply the preservation of a cuff of periosteum, which is supposed to afford protection to the marrow cavity and a smoothly rounded bone end, without adhesions to the overlying soft parts; but much more complete operations are afforded by Pirogoff’s amputation at the heel, and by Wladimiroff and Mikulicz’s amputation of the foot (practically an exsection of the heel), or by Gritti’s and the other methods of supracondyloid knee amputation, with preservation of the patella. Bier and other foreign and domestic surgeons have also devised methods of reflecting or raising bone flaps from the continuity of bone shafts, which, being still connected by periosteal bridges, are so turned and fastened in place as to furnish a complete bone end over the stump (Figs. 678 and 679).
The choice of method must depend, to a large extent, on the character of the case. Some injuries will leave parts so exposed that a portion of a limb can still be utilized if only flaps be cut in an atypical way. One need never hesitate to resort to these, especially about the hand and upper extremity, where it is so desirable to save every inch of tissue. It is not necessary to preserve every possible inch of tissue in the foot and leg, as the makers of artificial limbs can adapt an artificial leg to any kind of a stump. The intent in making these statements is that while it is best to follow conventional methods under ordinary circumstances, there need be no hesitation in departing from them when occasion demands it.
Fig. 678
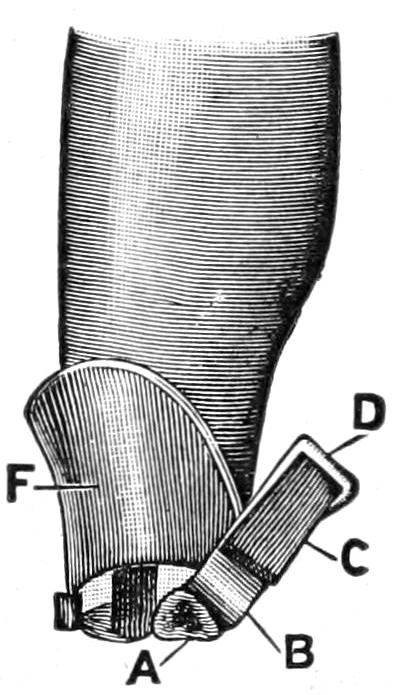
Bier’s osteoplastic amputation of the leg (procedure advocated by Bier in 1897 and 1899): F, long anterior flap reflected on the tibia; A, cross-section of tibia; B, periosteal flap after excision of intervening section of bone; C, osteoperiosteal flap; D, projecting border of periosteum to be sutured to tibial periosteum.
Fig. 679
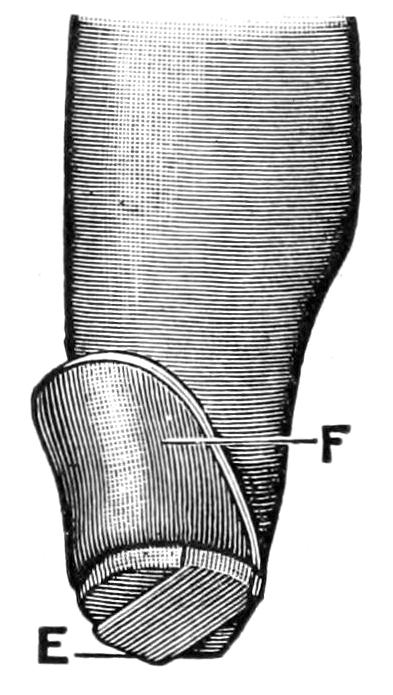
Bier’s osteoplastic amputation of the leg, with osteoperiosteal flap in position.
It is essential in caring for every stump, after the actual amputation has been performed, (1) that bleeding be absolutely controlled; (2) that nerve ends be placed out of the way of cicatricial entanglement; (3) that proper drainage be provided; (4) that the soft parts be so brought together as to unite in the promptest and most perfect fashion. The possibility of the latter will depend very much on the occasion for the operation and the condition of the tissues. Operating in the presence of previous disease, as when the parts are inflamed or edematous, or as when one amputates at a point where more or less sloughing and separation of tissues have already occurred, the surgeon cannot look for such primary repair as furnishes an ideal termination, nor should he endeavor to make such close suturing or approximation as he would otherwise attempt. In fact, under these circumstances, it is often desirable to leave the wound widely open, perhaps packing it with yeast, in order to hasten sloughing and secure healthy granulating surfaces, which may be then brought together by secondary suture or by suitable strapping and bandaging. Nothing worse can happen than imprisonment of the debris resulting from the sloughing process.
But an amputation wound made with faultless technique, and in tissues previously healthy, may be closed with a minimum of drainage, or often without any, providing it be so closed as to leave no dead spaces in which blood clot may accumulate. This requires careful suturing, by numerous buried sutures, of muscle to muscle, tendon to tendon or to periosteum, and the like, the wound being gradually closed from its depth, and finally so bandaged that equable pressure shall be made, with comfortable support,[1029] but without undue pressure at any point. In aseptic cases animal ligatures and sutures (chromic gut) will prove reliable and efficient. In septic cases it would probably be better to trust to (secondary) silk, especially if parts are to be long exposed, so that it can be later removed. For the superficial wound silkworm sutures answer admirably.
For drainage a gauze packing for the worst cases, one or two tubes for ordinary cases, and for those which scarcely need it strands of catgut or of silkworm-gut, or two or three little rolls of oiled silk, will be sufficient.
In this country Link and in Germany Credé have practised the method of bringing parts together merely by equable pressure and bandaging. This has been of late modified by the use of strips of sterile adhesive plaster; and in certain instances, everything else favoring, it has given good results. It might be advantageously adopted in cases where it is feared that it may be necessary to reopen the wound, as it would permit an easy method of so doing.
Dressings should be copious and snugly applied, and the limb involved should be immobilized. Thus after a leg amputation it is well to bind the leg and thigh upon a suitably arranged splint, physiological rest, which is so essential to success, being in this way attained. The same is also true of the arm.
—It is desirable in the upper extremity to save every portion which can be preserved and still made useful. This is particularly true of the fingers, where every half-inch adds to their usefulness. When it is possible the palmar surface should be saved and made to cover the stump end, as it is not only more sensitive but denser and stands wear better. This is equally true of disarticulations or of divisions between the joint ends of the phalanges, which are best exposed by bending the finger, cutting the dorsal flap in this position, then stretching it and cutting the palmar flap (Fig. 680).
The vessels and nerves lying on the lateral aspect should be secured against hemorrhage, and cocaine solution introduced if local anesthesia is being practised. It is important also to remember the arrangement of the common palmar synovial bursa, with the digital prolongations to the thumb and the little finger, and that the three middle fingers are ordinarily shut off from it. Nevertheless if tendons be divided near the hand, and short finger stumps be made, it is easy to infect this common palmar bursa through retraction of the tendon and the consequent opening up of a tunnel directly into that cavity.
Fig. 680
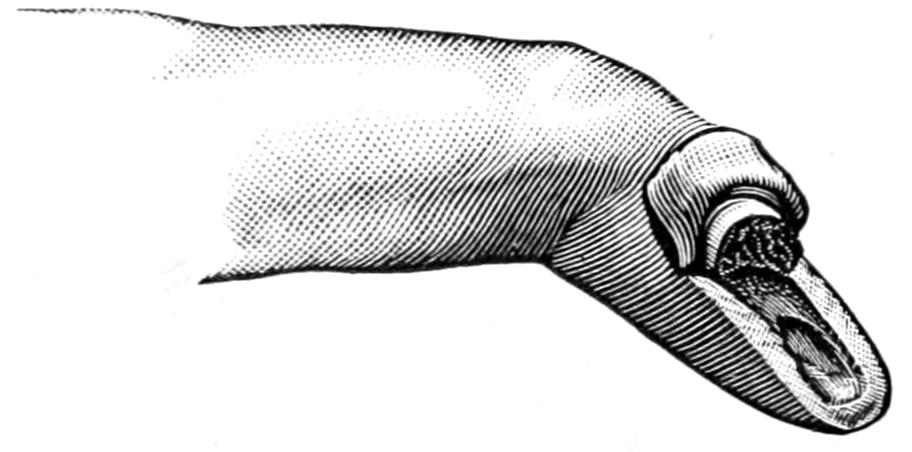
Typical amputation of finger in continuity (through a phalanx); long palmar and short dorsal flaps. (Farabeuf.)
Fig. 681
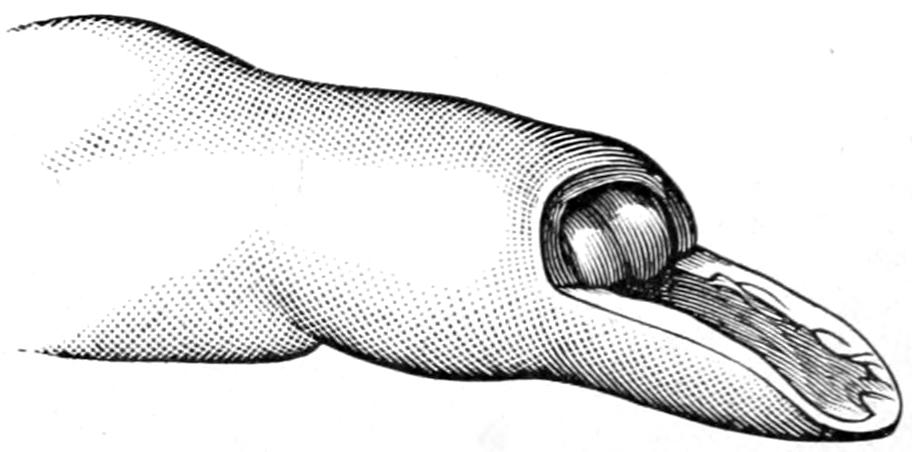
Typical or preferred method of disarticulating a finger by long single palmar flap. (Farabeuf.)
Figs. 680 and 681 illustrate the best methods of amputating fingers through a phalanx or at the joints, while Fig. 682 shows the best method of closing the wound. In this way a serviceable finger-tip is preserved which will stand every irritation to which it will probably be subjected.
When the finger is to be disarticulated from the hand a modified oval flap is preferable, with its long flap on the radial side and the scar on the dorsum rather than in the palm. The thumb is perhaps best separated at an articulation by a single palmar flap, without the preservation of the sesamoids which belong to its short flexor. Fig. 683 illustrates the various flaps and methods preferable at the bases of the different fingers.
When two or more fingers have to be removed the incision should be planned to meet[1030] the indications. When the first three fingers have to be removed, with or without that portion of the hand to which they are attached, leaving only the thumb and little finger, I have repeatedly followed to advantage the suggestion of Lauenstein, and through a small incision properly placed have, with cutting forceps, divided the first and fifth metacarpal bones at about their middle, and have then given to each of the remaining digits a quarter of a revolution toward each other, in such a way that when their tips are flexed there was better prehensile power, the hand acting similarly to a more perfect claw. If they are to be maintained in this position during healing they must be suitably held upon the splint to which the entire hand and forearm should be attached.
Fig. 683
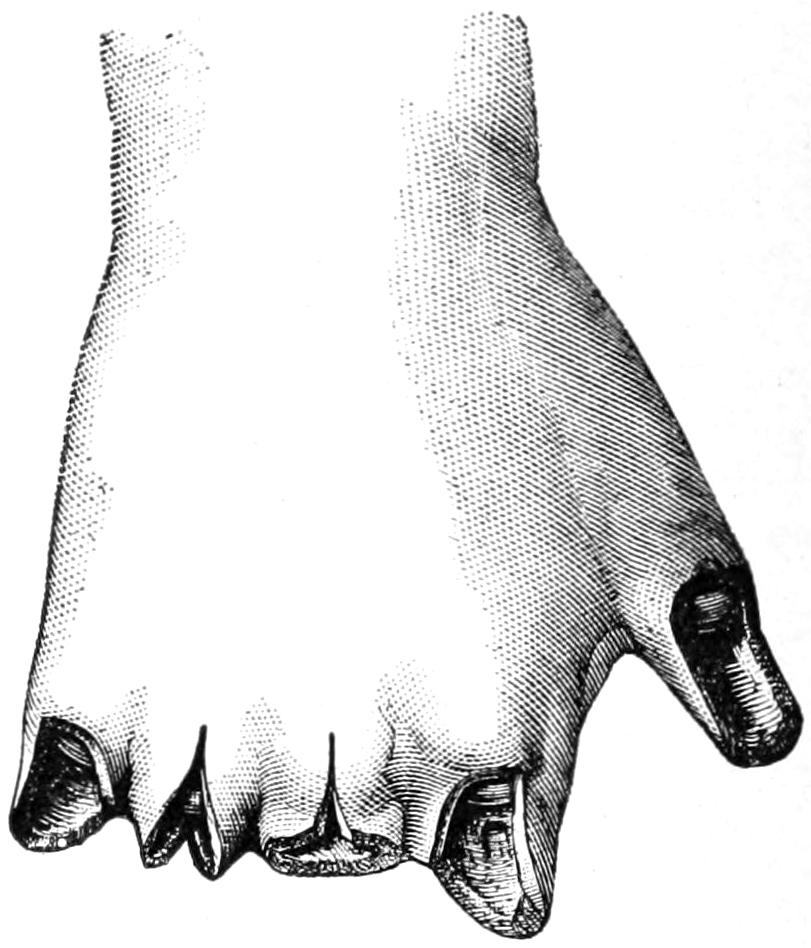
Illustrating various finger amputation. (Farabeuf.)
Fig. 684
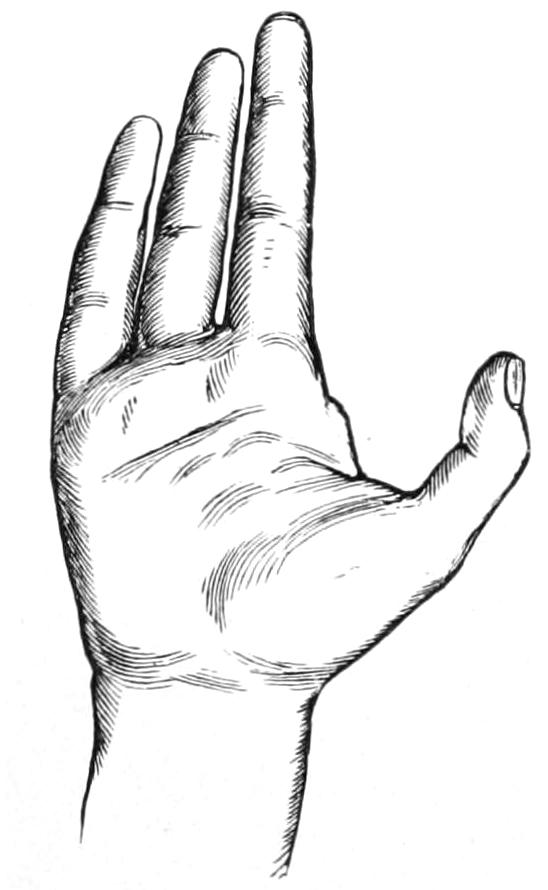
Removal of index finger. (Erichsen.)
Fig. 685

Removal of little finger. (Erichsen.)
Fig. 686

Results of amputation above metacarpo-phalangeal articulation in middle, index, and ring fingers. (Erichsen.)
Fig. 687
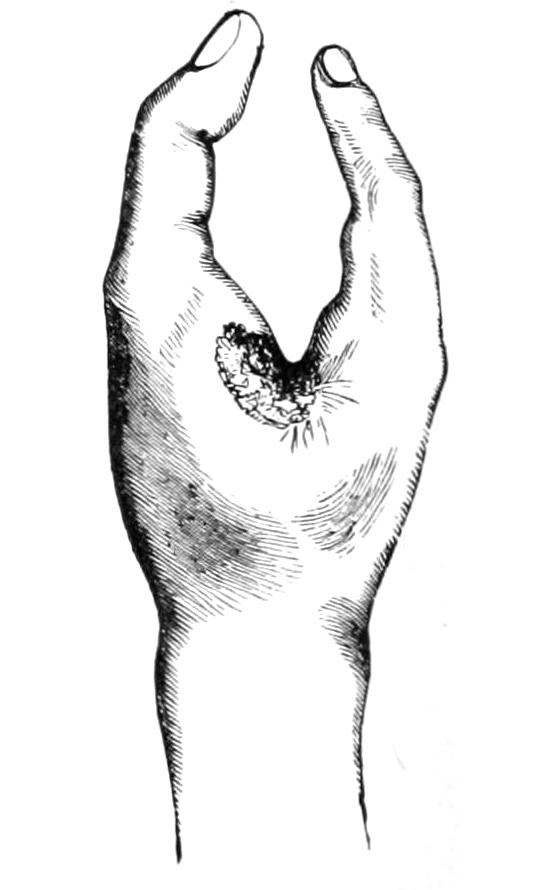
Hand after removal of metacarpal bones and three fingers, leaving thumb and little finger. (Erichsen.)
When an entire finger is to be removed it is a question whether the metacarpal belonging thereto should also be sacrificed for cosmetic purposes. In general this is undesirable except in the case of the fifth metacarpal with the little finger. This is easily exposed by lateral incision along the ulnar border of the hand, sufficient to disclose the bone and permit its disarticulation from the carpus. The same is also true, in at least some instances, of the thumb, but it is unwise to expose the carpal joints to the possibility of infection when this can be avoided; moreover, the deep palmar arch crosses just in[1031] front of the bases of the second to the fourth metacarpals, where it must be carefully avoided. If, then, the metacarpal is to be sacrificed this should be done rather from the dorsal side, while for cosmetic purposes alone it is usually sufficient to disarticulate the finger at its base and then simply remove the head end of the corresponding metacarpal. Figs. 688 to 692 furnish illustrations of how the incisions may be best planned to effect either of these purposes.
—While it makes but little difference whether the metacarpals be disarticulated from the carpus or the latter from the radial end, it is advisable to adopt whichever line of separation will best meet the indications. For a removal of the hand at or near the wrist two flaps usually afford the most serviceable method, the palmar tissues being preserved, if possible, in order that they may cover the stump. This operation is usually done for injury, and it is more than likely that one will have to plan his flap according to the tissues which still are serviceable.
Fig. 688
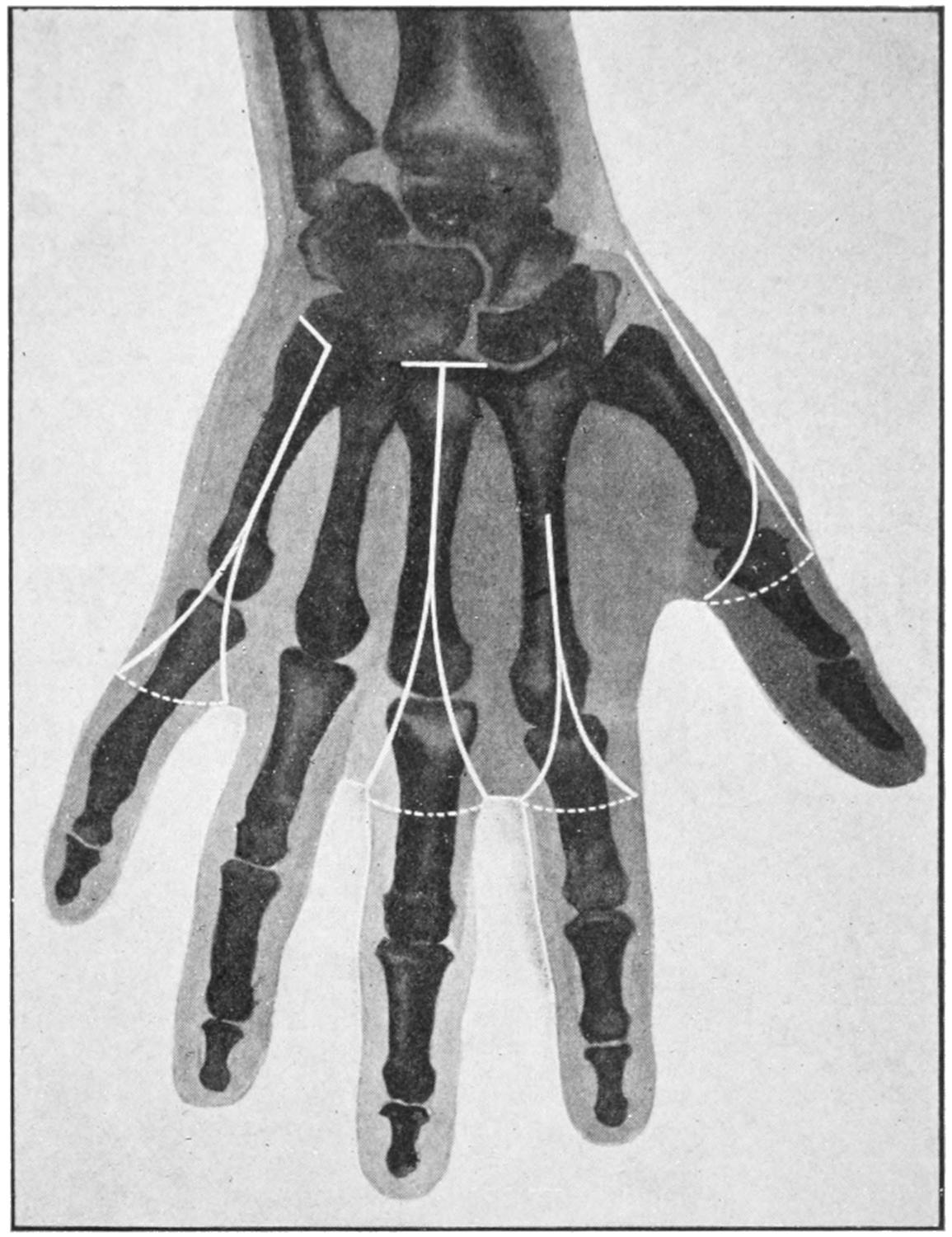
Outline of amputation of fingers, with their metacarpals. (Modified by Matas from Mignon.)
In the lower part of the forearm the flap method furnishes a serviceable stump. As the elbow is approached the circular or elliptical methods are preferable, as illustrated in Fig. 690.
—With elbow disarticulations caution should be observed to have flaps of sufficient length. The joint is opened more readily from its radial side. The integument of the back of the elbow region lies closely upon the bone, is thin, and retracts but slightly. Anteriorly there is more muscular covering and consequently a tendency to retraction. Therefore the anterior flap should be made longer than might otherwise seem to be required. Here the ideal scar will be behind the end of the humerus, but it is difficult to obtain because of the tendency to drag it around beneath the end of the bone. An elliptical incision, directed obliquely downward and forward, is the easiest method and furnishes the best stump. The lower end of the posterior part of the flap should be at a distance below the articulation, at least equal to the transverse diameter[1032] of the joint itself, i. e., in an adult nearly one hand-breadth from the line of the joint to the point of dissection. (Matas.) (Fig. 690.)
—The arm furnishes that nearly cylindrical outline best adapted for circular amputations. Here, as at the elbow, the greatest retraction is on the flexor side. With the arm should be saved all that is possible even up to its upper extremity.
Remembering the greater tendency of the flexors to contraction the truly circular method should be modified to a somewhat elliptical incision, in order to compensate for this difficulty, while an external liberating incision is often of assistance. Abrupt transverse division of the muscle down to the bone should be made after the oblique incision of the skin.
Fig. 689
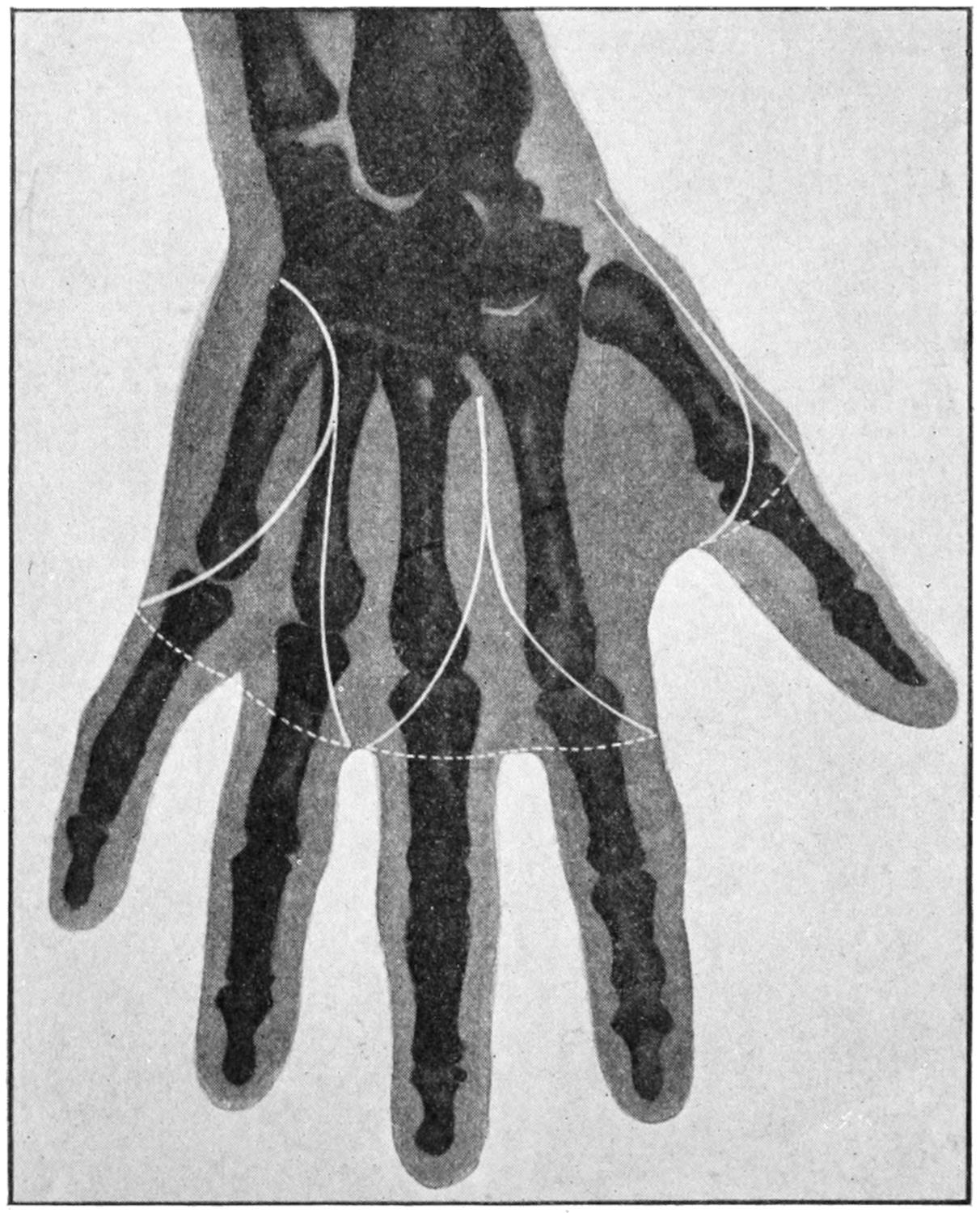
Outline of amputation of two fingers simultaneously with their metacarpals; also thumb with its metacarpal. (Modified from Mignon.)
—Until accurate methods of blood control were introduced this was an amputation viewed usually with disfavor, in spite of the fact that compression of the axillary artery in theory is easy. The older methods comprised this compression, either above the clavicle, or by exposure of the vessel and its proximal ligation, or by opening and separating the joint and then seizing the vessels within the inner flap, and controlling them by digital pressure until their division. Now with the use of Wyeth’s pins and the elastic bandage, effectual control may be secured without resorting to any of the former expedients. If the removal is to be a high amputation, just below the neck of the humerus, the method shown in Fig. 691, of application of the tourniquet and its control by a constricting strap, may be adopted.
If the surgeon expect to disarticulate he should resort to the pins of Wyeth (i. e., to the use of long mattress needles), which are passed through from above downward, or from the axilla upward, one of them being passed anteriorly and the other posteriorly, and brought out at corresponding points on the upper aspect of the shoulder, where, their points being protected by sterilized corks, they serve to prevent sliding of the elastic bandage or tourniquet, which is now placed proximally to them, and is thus held more securely than is possible in any other way.
PLATE LVII
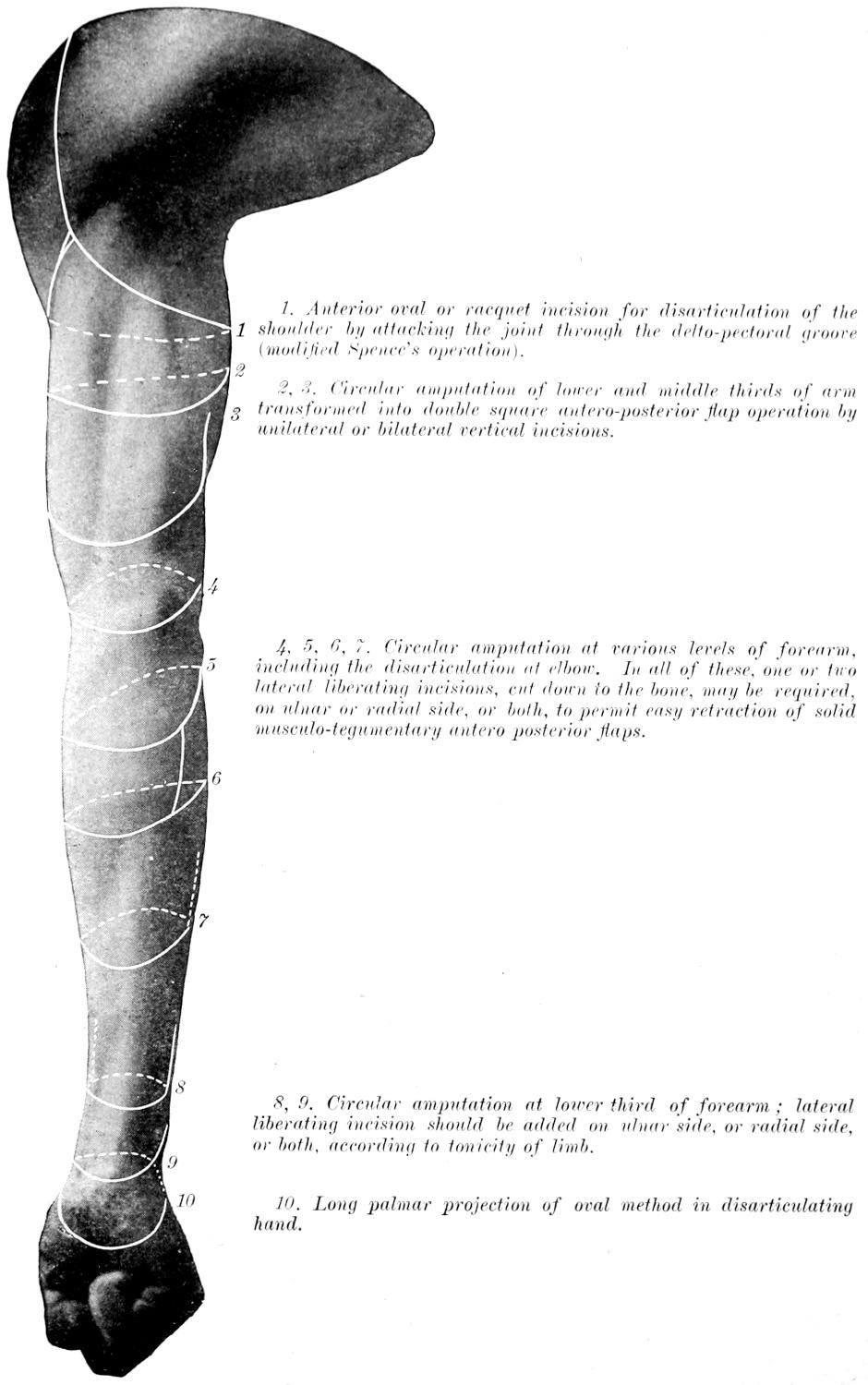
Cutaneous Incisions in Amputations of the Upper Extremity (Ventral or Flexor Side).
1. Anterior oval or racquet incision for disarticulation of the shoulder by attacking the joint through the delto-pectoral groove (modified Spence’s operation).
2, 3. Circular amputation of lower and middle thirds of arm transformed into double square, antero-posterior flap operation by unilateral or bilateral vertical incisions.
4, 5, 6, 7. Circular amputation at various levels of forearm, including the disarticulation at elbow. In all of these, one or two lateral liberating incisions, cut down to the bone, may be required, on ulnar or radial side, or both, to permit easy retraction of solid musculo-tegumentary antero posterior flaps.
8, 9. Circular amputation at lower third of forearm; lateral liberating incision should be added on ulnar side, or radial side, or both, according to tonicity of limb.
10. Long palmar projection of oval method in disarticulating hand.
PLATE LVIII
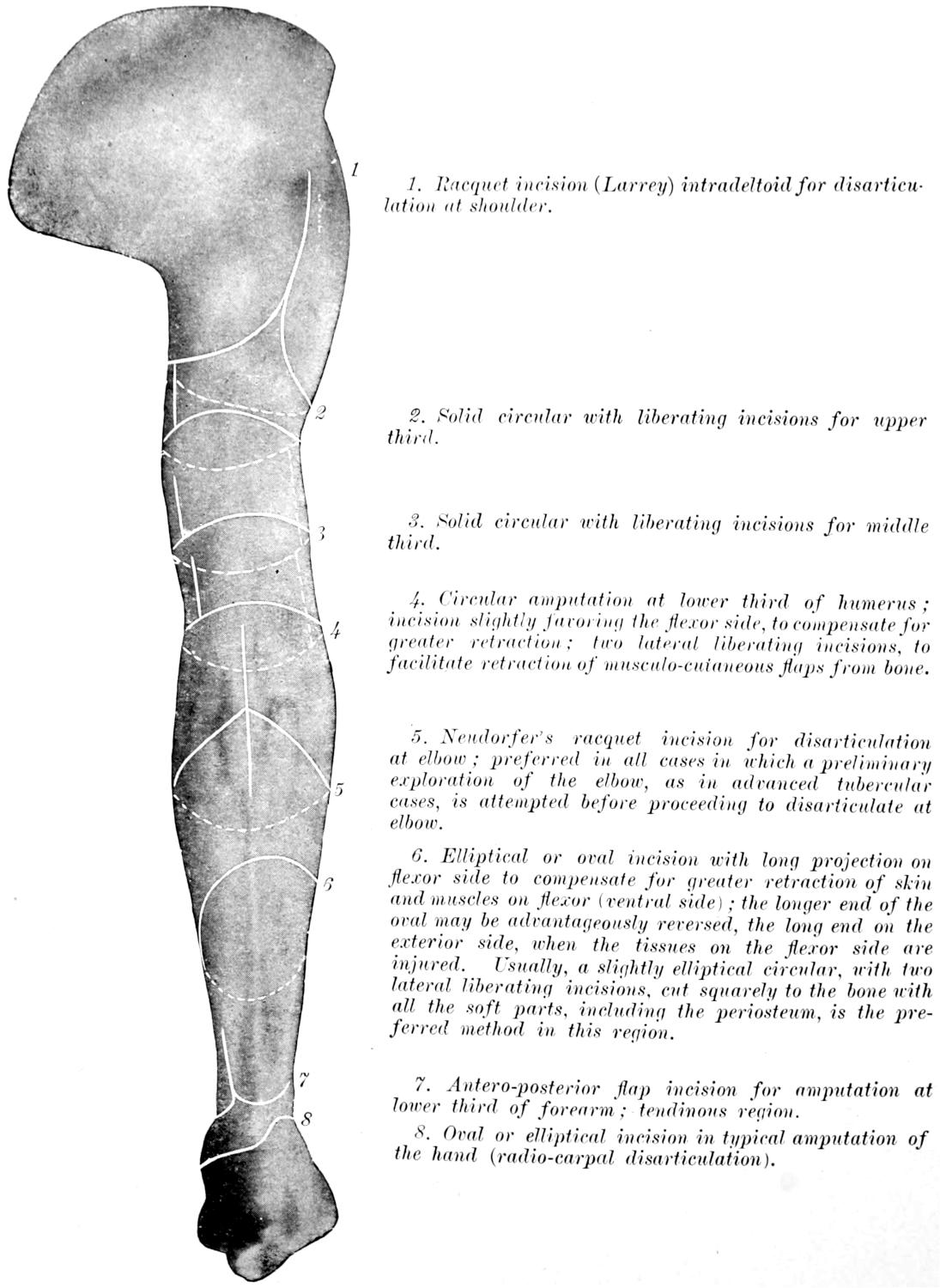
Surface Tracings showing Some of the More Useful Lines of Skin Incision in Amputations of the Upper Extremity (Dorsal or Extensor Surface).
1. Racquet incision (Larrey) intradeltoid for disarticulation at shoulder.
2. Solid circular with liberating incisions for upper third.
3. Solid circular with liberating incisions for middle third.
4. Circular amputation at lower third of humerus; incision slightly favoring the flexor side, to compensate for greater retraction; two lateral liberating incisions, to facilitate retraction of musculo-cutaneous flaps from bone.
5. Neudörfer’s racquet incision for disarticulation at elbow; preferred in all cases in which a preliminary exploration of the elbow, as in advanced tubercular cases, is attempted before proceeding to disarticulate at elbow.
6. Elliptical or oval incision with long projection on flexor side to compensate for greater retraction of skin and muscles on flexor (ventral side); the longer end of the oval may be advantageously reversed, the long end on the exterior side, when the tissues on the flexor side are injured. Usually, a slightly elliptical circular, with two lateral liberating incisions, cut squarely to the bone with all the soft parts, including the periosteum, is the preferred method in this region.
7. Antero-posterior flap incision for amputation at lower third of forearm; tendinous region.
8. Oval or elliptical incision in typical amputation of the hand (radio-carpal disarticulation).
[1033]
Fig. 690
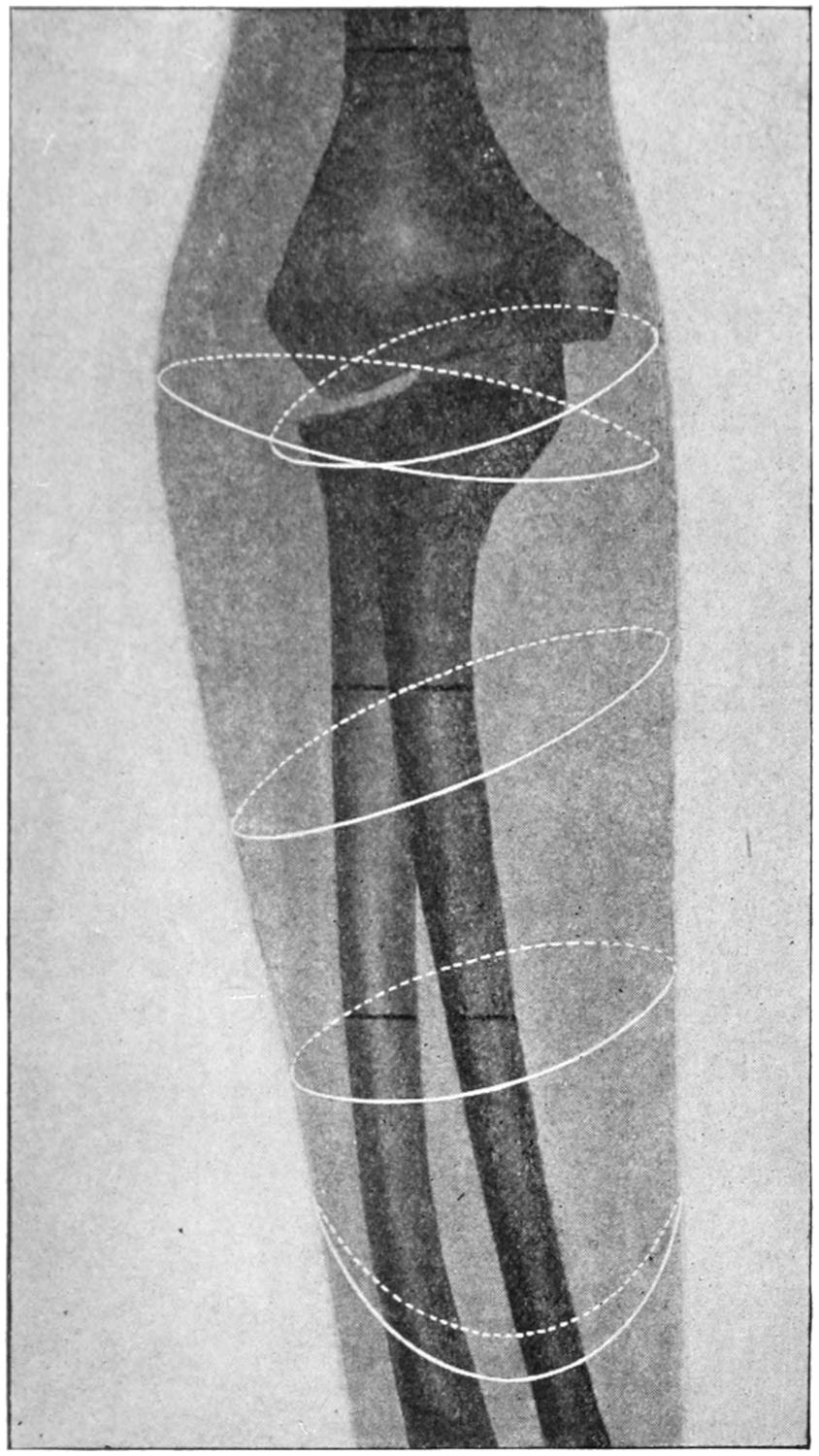
Lines of amputation in lower third of forearm, of elbow, and lower third of arm. (Modified from Mignon.)
Circulation being thus controlled, a modified circular operation may be made or a long external and superior flap cut, matching it with another one dissected from the axillary aspect. In the former case the circular incision is made on a level a little below the anatomical axillary border. Then a cuff of skin being raised while the arm is held in adduction, all the soft parts are divided to the bone and separated from it. Now a liberating incision may be made from the anterior border of the acromion to the coracoid process, then over to the deltoid groove, and along it to the first circular incision. Through this all the soft tissues surrounding the glenoid margin are separated, and then the bone is enucleated by opening the capsular ligament, reserving perhaps the detachment of the group of scapular tendons until the last. If one have any fear as to the efficiency of his hemostatic precautions he may secure the axillary vessels so soon as they are divided and then proceed with the disarticulation as above. In some cases it may be preferable to cut a wide flap from the deltoid region, preserving that muscle or not as may be desired, and, after having thus exposed the joint, make the disarticulation, separating the head of the bone sufficiently to allow the passage of an amputating knife behind it and down along the shaft to a distance sufficient to justify turning it abruptly and toward the surface, and then cutting out the axillary flap. The attempt should be to cut all the vessels at right angles rather than obliquely.
Plates LVII and LVIII, prepared by Professor Matas, afford a synoptic view of the more useful lines of skin incision in the principal amputations of the arm and shoulder.
—This includes removal not only of the arm, but of the scapula and clavicle as well, or at least its outer portion. It is not often required, and inasmuch as the circumstances which justify it are seldom duplicated, a suitable method for each individual case should be planned, rather than try to make one set of directions cover them all. Much will depend upon whether sufficient skin can be saved in order to cover the large defect thus made. In general, however, an incision should first be made along the clavicle, exposing it and dividing it near its middle. It is convenient to take out the middle portion at this time, and in this way to afford ample room through which a proximal ligation of the subclavian vessels may be made, they being here carefully dissected out, secured by double ligation, and divided. From the outer part of the above incision[1034] another is carried downward and outward toward the deltoid groove and then beneath the axilla to its posterior margin. The posterior flap is then furnished by an incision continuous with the last one, which terminates below about opposite the lower angle of the scapula, and is then continued upward along the inner scapular border and over the shoulder until it reaches the outer end of the incision first made. In this manner will be furnished a sufficient covering. The balance of the operation consists in the gradual separation of the entire mass from the outer wall of the thorax. With a preliminary ligation of the subclavian vessels there will be no hemorrhage which cannot be easily checked by pressure and forceps.
The above, however, is only a general description, which may need to be modified in most cases. If the amputation be done for injury all the skin which is still viable should be utilized, no matter how shaped, while if done for disease the incisions may have to be modified materially, taking more skin from one side and less from the other, in order to avoid that involved in the disease process.
In the majority of cases the result is satisfactory, in spite of the mutilation thus afforded.
Fig. 691
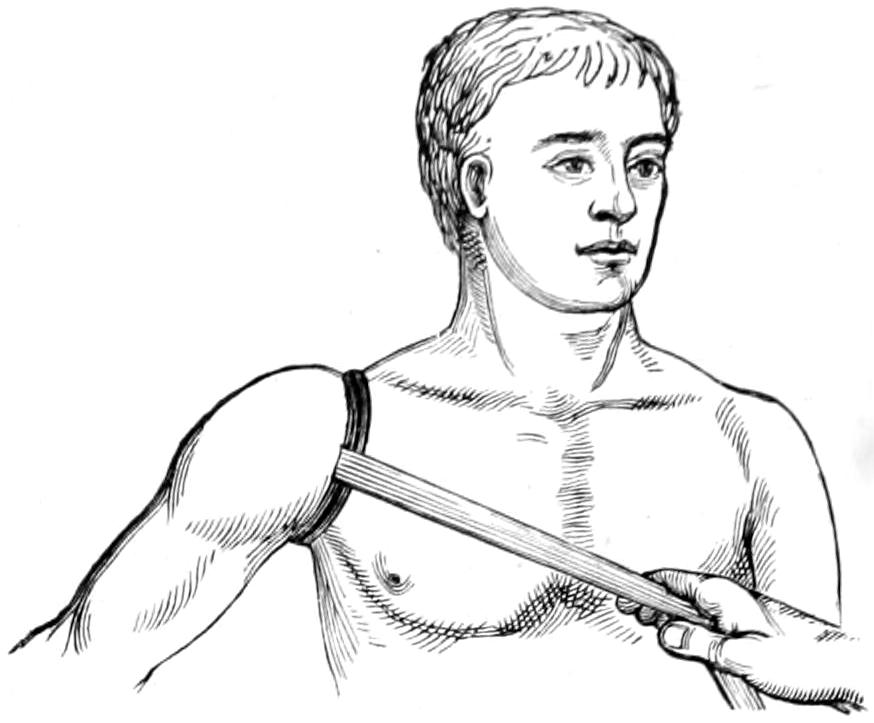
Esmarch’s elastic constrictor applied and held in place by a bandage or a strap (Wyeth’s pins may also be used to hold the constrictor in place) in high amputation of the arm. (S. Smith.)
The most important physiological purposes of the foot are those of support and locomotion, not mere tactile sensibility nor prehension. Its purposes being different from those of the upper extremity, the tenets previously held regarding the advantage of conservatism may be changed to some degree, for a tender foot or leg-stump is sometimes extremely annoying, even disabling, and it is in the end far better to so plan an amputation of this extremity as to make the stump most serviceable, without primary reference to its exact length. As in the hand, foot-stumps should be covered with dense plantar (instead of palmar) tissues, and the long flap should, therefore, be made from the sole. When this is impossible it would be wiser to shorten the stump. Moreover, as there will be constant friction upon the resulting cicatrix, this should be placed in the most protected location, on the dorsum of the foot.
The most important indication, then, in all foot amputations is to furnish a complete plantar flap and to place the scar on top of the foot.
—Amputations of the toes are, by virtue of their shortness, nearly always disarticulations. The basal row of phalanges should be preserved when possible, and even here the covering of the stump should be as far as possible fashioned from the sole.
The big toe may be removed by either internal or oval plantar flaps, which should be long enough to cover the metatarsal head, otherwise the latter must be decapitated. These same principles also apply to the little toe. When all or most of the toes have to be severed it may as well be done by a single dorsal incision, as seen in Fig. 692, which will permit either their disarticulation or their removal along with that of the ends of the metatarsals. These methods are shown in Figs. 692 and 693.
Amputation of a toe with its metatarsal is best effected by a racket incision. This may extend up to the posterior tarsal joint. Some have recommended to enucleate the metatarsals subperiosteally, through dorsal incisions, all the soft parts being scrupulously left behind. With the first and fifth toes the scar should be so placed as to be removed from the edge of the foot (Fig. 693).
Partial amputations of the foot have been suggested and devised in great numbers, and the subject has been greatly complicated by the number of methods that were taught. Modern ideas of conservative surgery have caused a complete departure from the anatomist’s standard, and it has been shown that with aseptic technique there is no advantage in disarticulating when it leaves irregular lines. As Matas says: “As Agnew taught long ago in this country, and others elsewhere, the skeleton of the foot must be considered a surgical unity, to be treated by the knife and saw just as the femur and humerus would be, at the exact point which will yield the longest and most useful stump to the patient. What is essential in every case is the application of the principle of plantar flaps—preservation and scar protection.”
Concerning the utility of many of these methods and the usefulness of the resulting stumps we may learn more from the makers of artificial limbs than from almost any other source. Thus, Truax, for instance, who has had large experience as a mechanic, has given this advice, as quoted by Matas: “Avoid amputation within three inches of the ankle-joint; do not amputate between the metatarsal bones and the junction of the lower and middle thirds of the tibia. At other points save all you can, and you will in every case have done the best for your patient.” Should one be rationally governed by this advice a large number of amputation methods which cumber most text-books would be discarded.
[1035]
Fig. 692
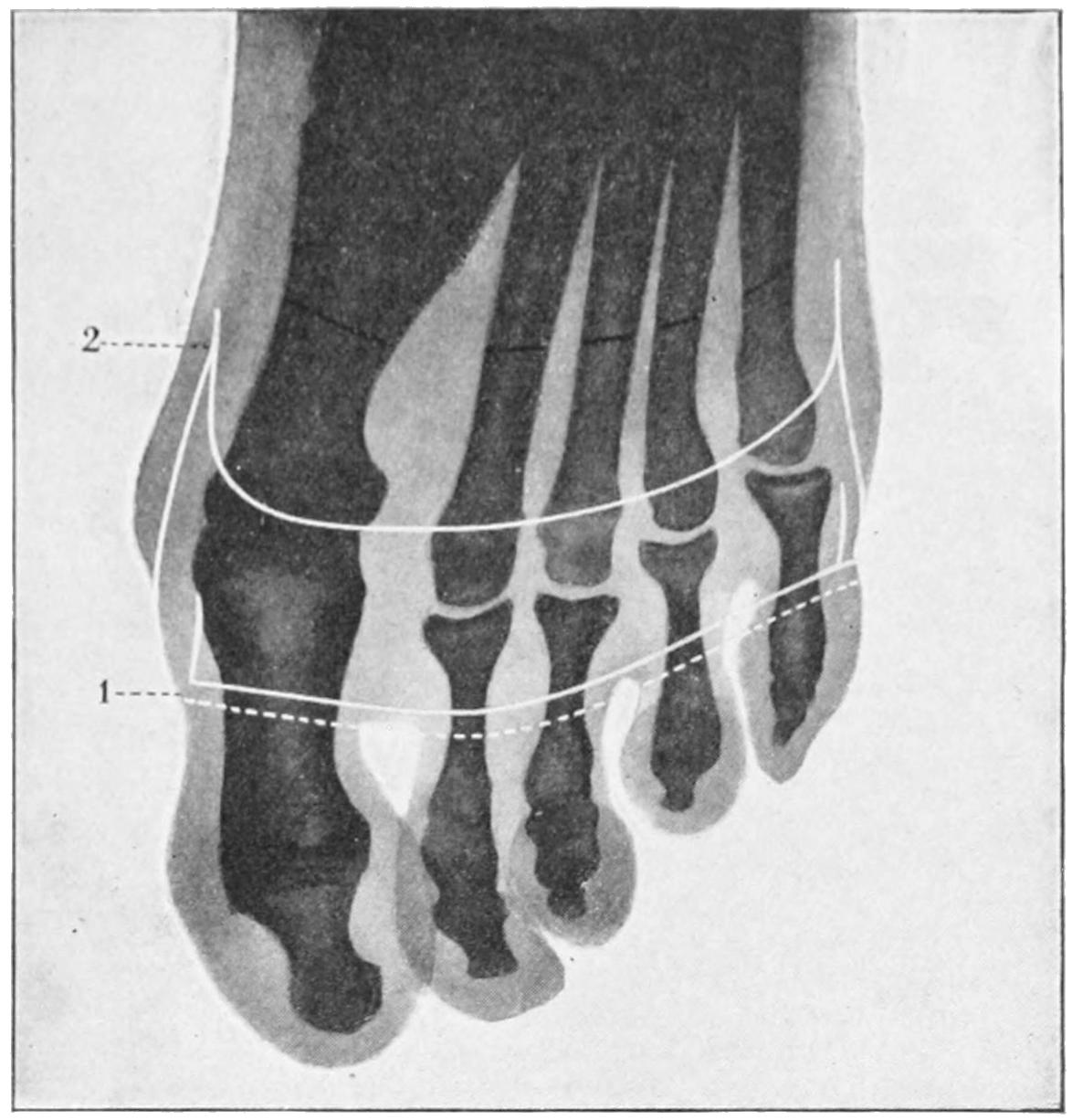
1, simultaneous disarticulation of all the toes; 2, amputation of the toes in their continuity. (Mignon.)
Fig. 693
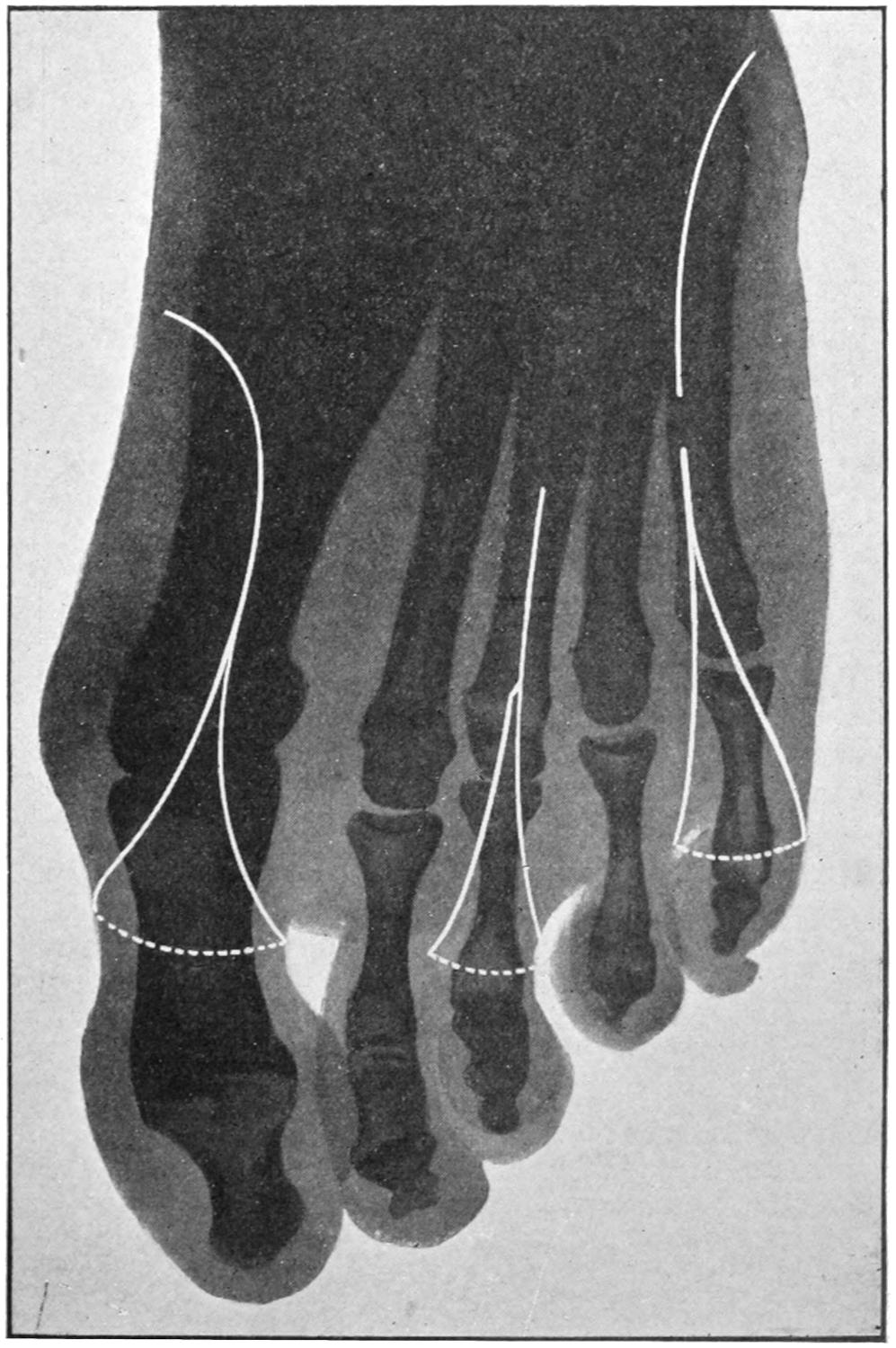
1, partial amputations of the third and fifth metatarsals; 2, disarticulation of the first and fifth metatarsals. (Mignon and Matas.)
[1036]
Fig. 694
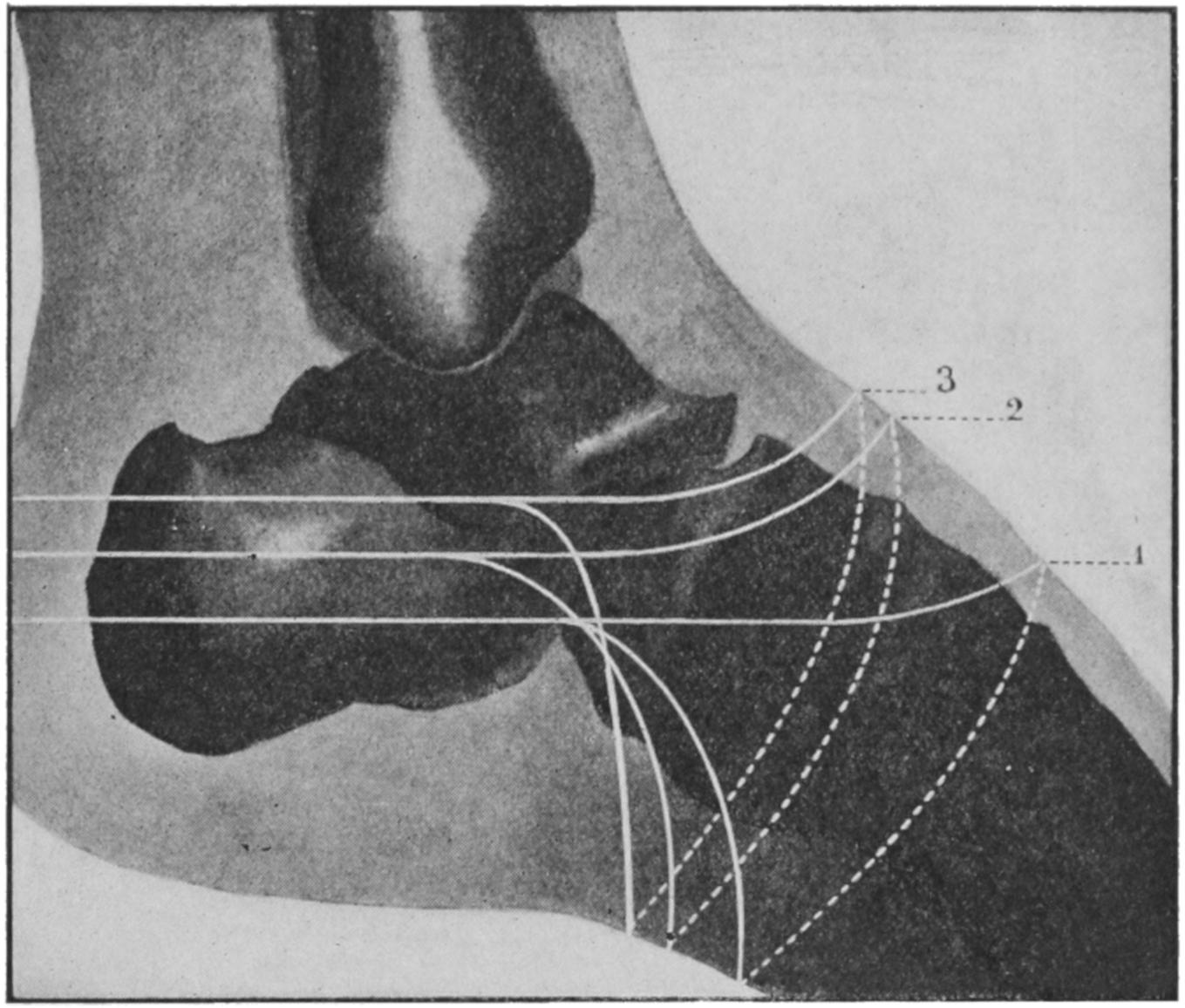
Tracings of intratarsal amputations at various levels (outer side): 1, subastragaloid; 2, tibiotarsal; 3, tibiocalcaneal; the different lengths of flaps shown in relation to skeleton.
Fig. 695
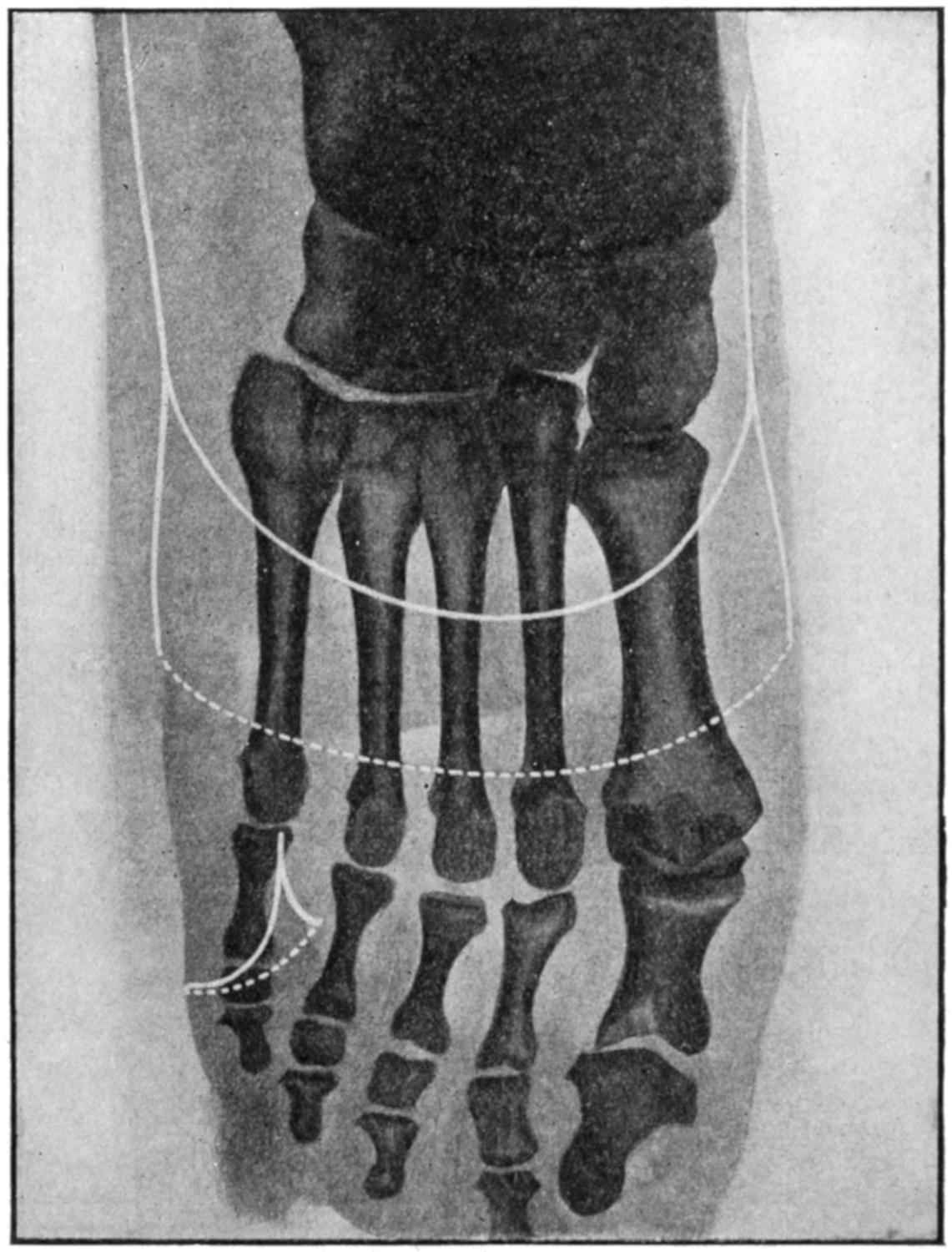
Tracings of incisions in mediotarsal amputations and total amputation of fifth toe. (Mignon and Matas.)
[1037]
For my own part I would advise to save all of a foot that can be saved, providing a sufficiently long plantar or heel flap can be retained; but if these are not available, then I would advise amputation, at least three inches above the ankle.
I would advise, moreover, to discard the complicated rules and technique of stilted methods and to use the saw whenever it can be made useful, rather than to go farther back to a row of joints simply because they are joints (Fig. 694).
Figs. 695 and 696 illustrate conservative modern methods, which are perfectly available for most purposes, and from which departure need be made only when peculiar circumstances obtain, which so complicate the case that none of the ordinary rules would apply. A surgeon of judgment and experience is competent to devise a flap for a given case, whether it complies with standard methods or not. It seems to me, therefore, worth while to describe only the so-called mediotarsal disarticulation of Chopart, in which but the astragalus and calcis remain of the proper bones of the foot. The joint line extends from just behind the tuberosity of the scaphoid to the outer side of the body of the calcis, where a tubercle can be usually felt. Across this line an incision is carried obliquely over the dorsum of the foot. The plantar flap is the long one, and the line of division is just behind the balls of the toes. Two lateral incisions can be made to facilitate disarticulation if desirable.
Fig. 696
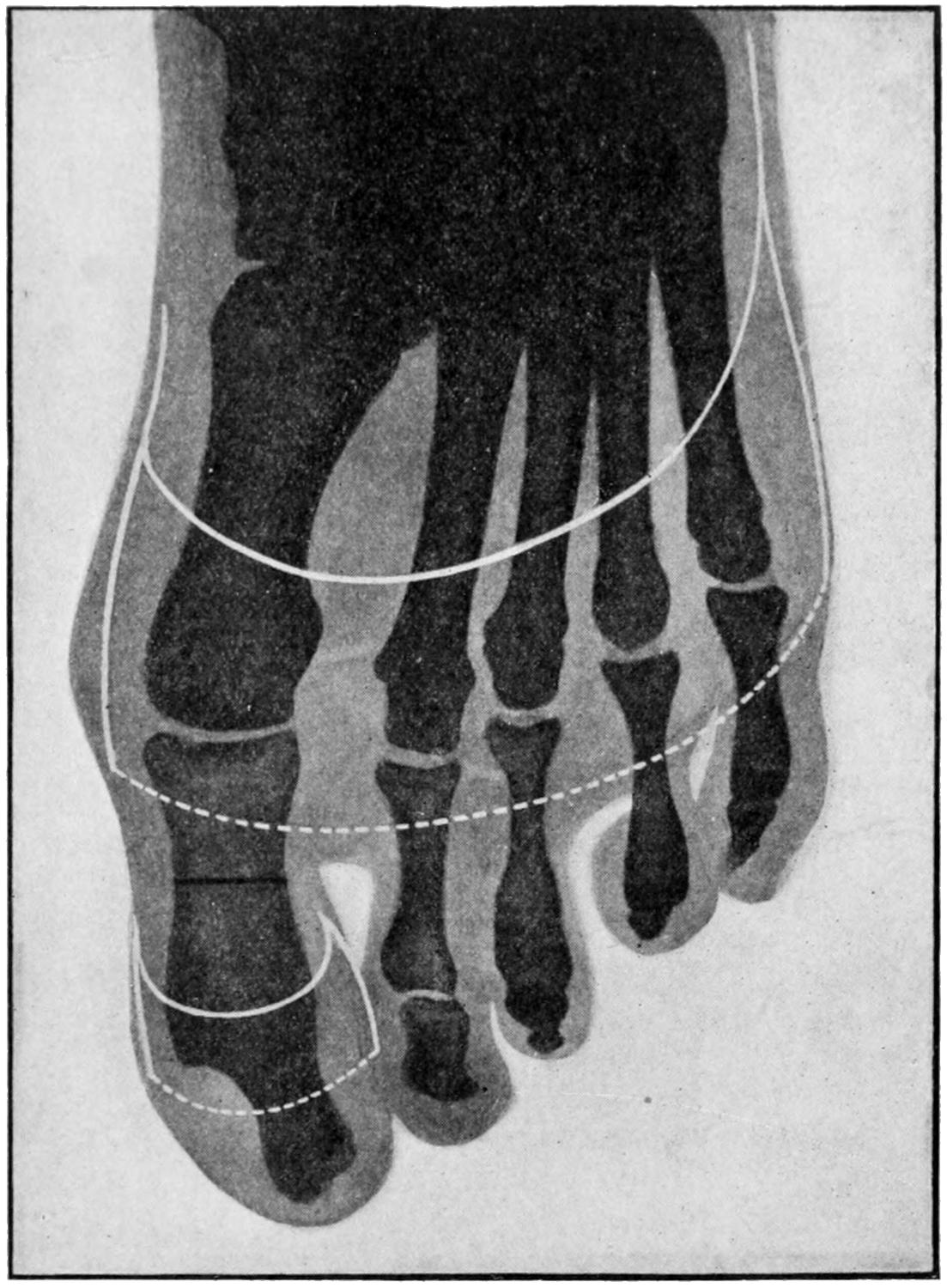
1, disarticulation at the tarsometatarsal joint, showing length of flaps; 2, disarticulation of the big toe in continuity. (Mignon.)
This operation sometimes leaves the foot in a bad equinus position; accordingly it is wise to make tenotomy of the tendo Achillis, as well as to attach the dorsal or extensor tendons to the stump end. (See Figs. 699 and 700.)
—The former favorite method of amputating the foot proper was that of Syme, illustrated in Fig. 701. This preserved[1038] the plantar surface and tip of the heel, thus forming a cutaneous hood, which was made to cover the lower ends of the tibia and fibula, whose malleoli were usually removed close to their terminations. The incision is made directly down to the bone, from the apex of one malleolus across the sole and up to the other. Then the foot is forced into extreme flexion and another incision carried directly across the dorsum, by which the upper ends of the first are joined. This permits opening the ankle-joint in front, after which the lateral ligaments are divided and the astragalus dislocated forward. The heel hood is next carefully separated from the calcis with the knife, and it and all the parts retracted from the ends of the leg bones, which are divided just above the articular surfaces, or the latter may be left and the malleoli alone removed. Now the heel hood is raised, made to cover the end of the leg, and united to the anterior incision, drainage being made by a small opening on the outer side of the tendo Achillis, as the plantar surface of the flap should not be opened (Fig. 703).
Fig. 697
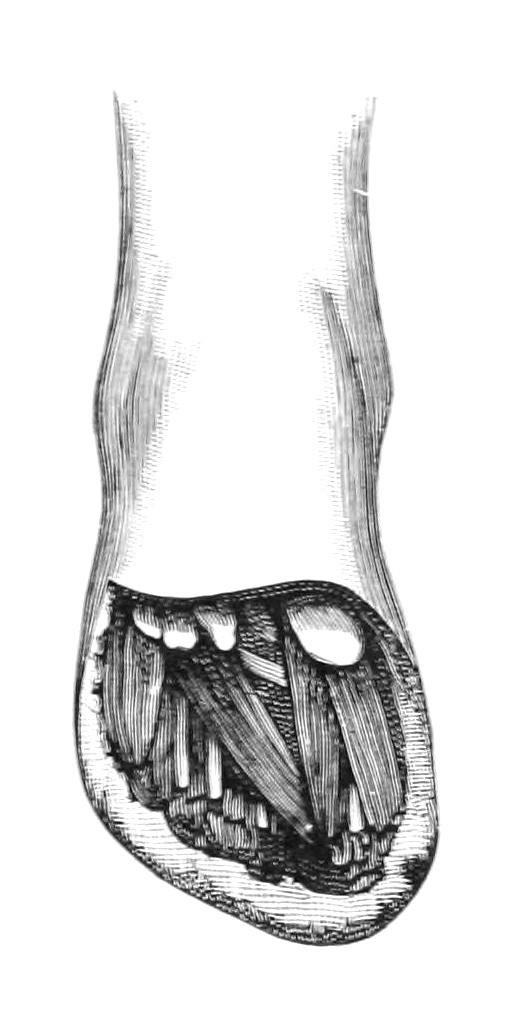
Lisfranc’s tarsometatarsal disarticulation. (Farabeuf.)
Fig. 698
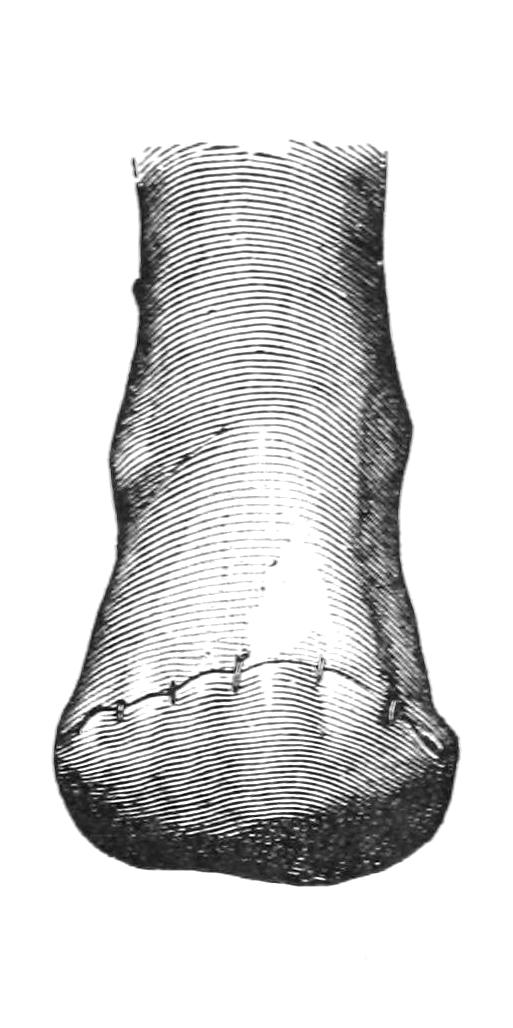
Stump after same.
Fig. 699
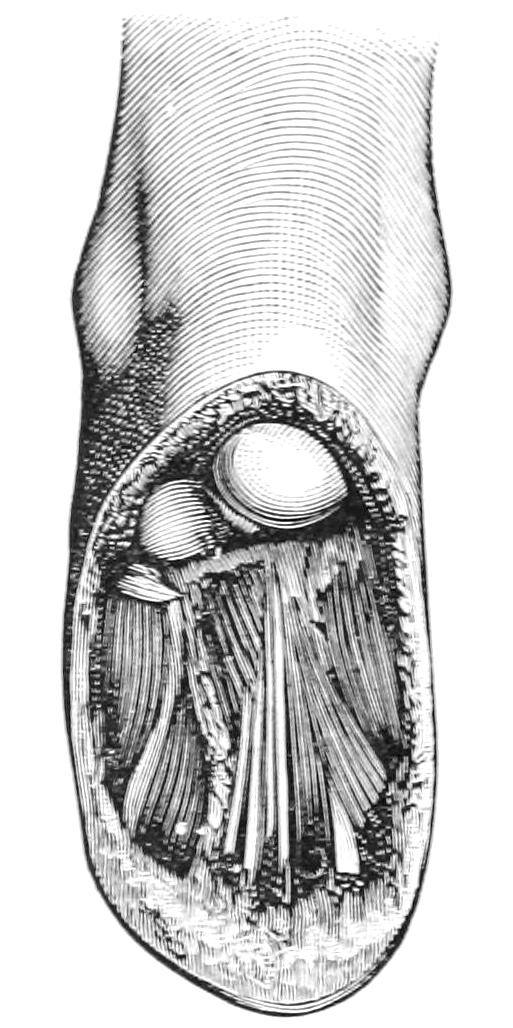
Classical mediotarsal amputation (Chopart), showing length of plantar flap. (Farabeuf.)
Fig. 700
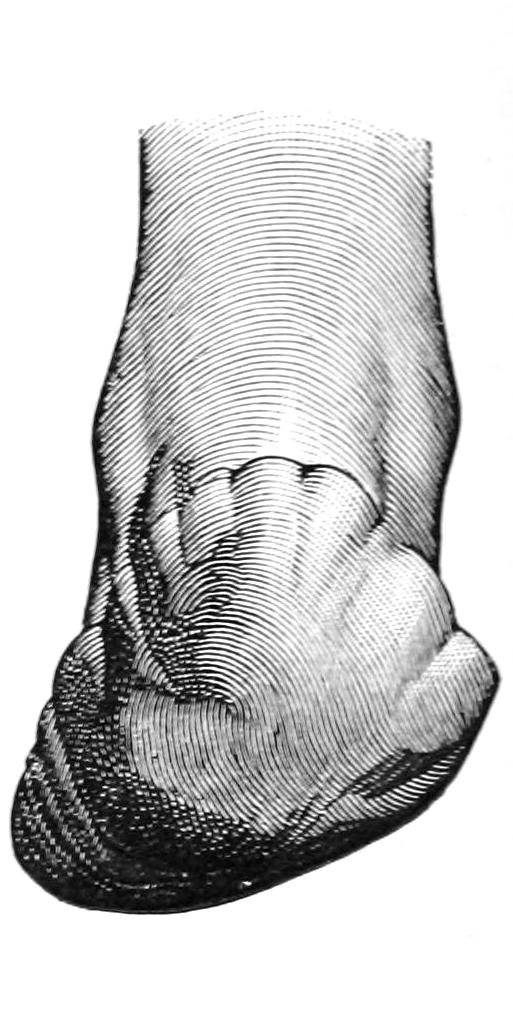
Stump after Chopart’s amputation. (Farabeuf.)
Fig. 701
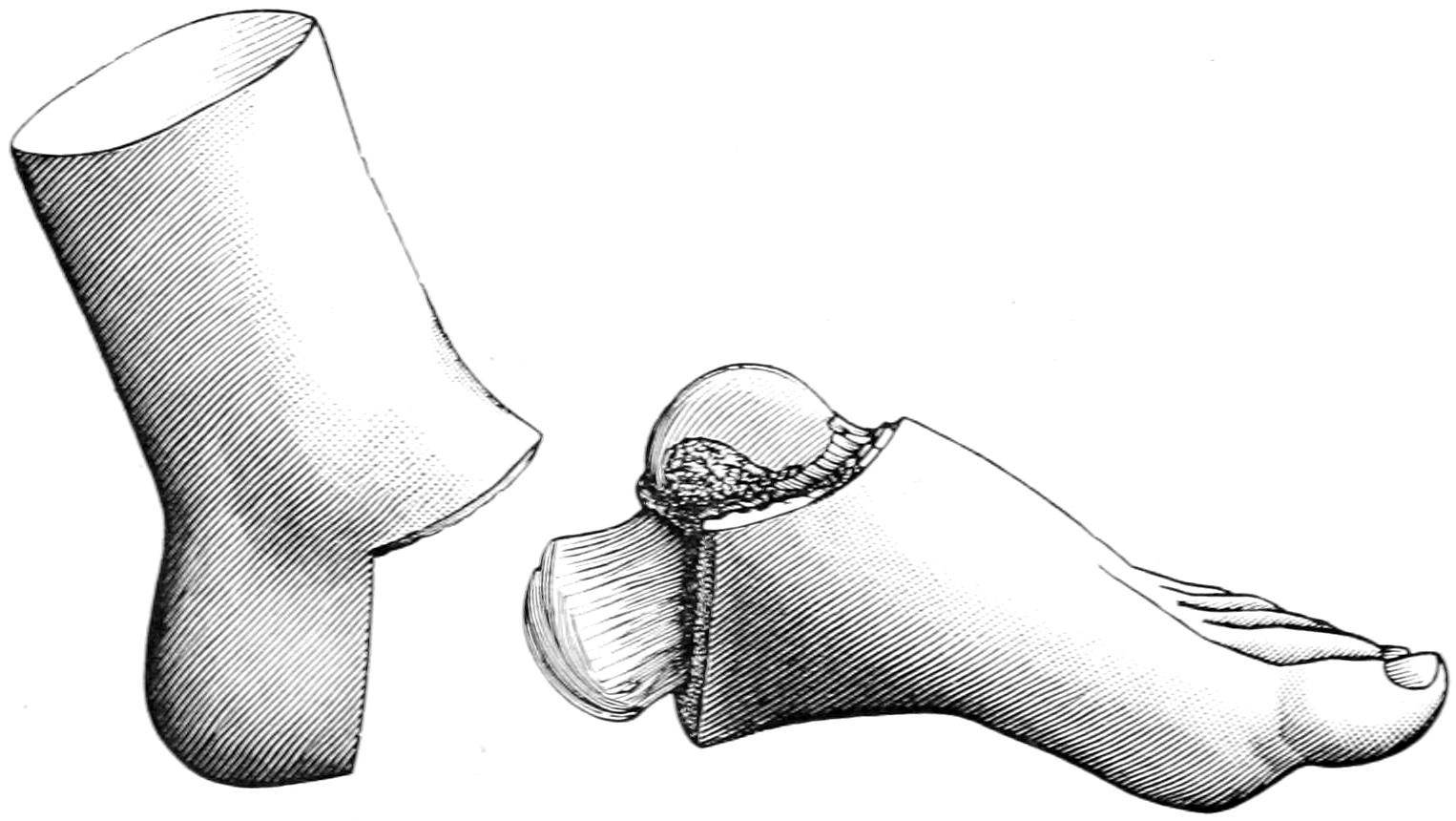
Syme’s tibiotarsal operation, showing part removed and lines of section, before division of malleoli. (Farabeuf.)
Fig. 702, the complement of Fig. 701, illustrates the appearance of the stump after the completion of the disarticulation and before the removal of the malleoli.
Pirogoff introduced a serviceable modification by obliquely dividing the os calcis in[1039] front of the heel, turning up its sawed surfaces without any dissection of the hood from the heel, and uniting its fresh bone aspect with that made by removal of the articular ends of the leg bones. This would seem to be preferable to Syme’s disarticulation, affording a better walking stump. (See Figs. 704 and 705.)
A reverse of this operation was suggested by Mikulicz and Wladimiroff, independently, and at about the same time, the heel being excised by an incision across the sole and then behind the ankle, the calcis being divided and its posterior end removed, while the articular surfaces of the leg bones are also removed. The foot is then brought down so that these surfaces can be brought in contact, it being expected that after their reunion the individual will walk in the exaggerated equinus position and upon the ends of the metatarsal bones. The operation is, in effect, an exsection rather than an amputation, and is applicable to but a very small number of cases, in which, however, it sometimes gives excellent results. (See Fig. 707).
Fig. 702
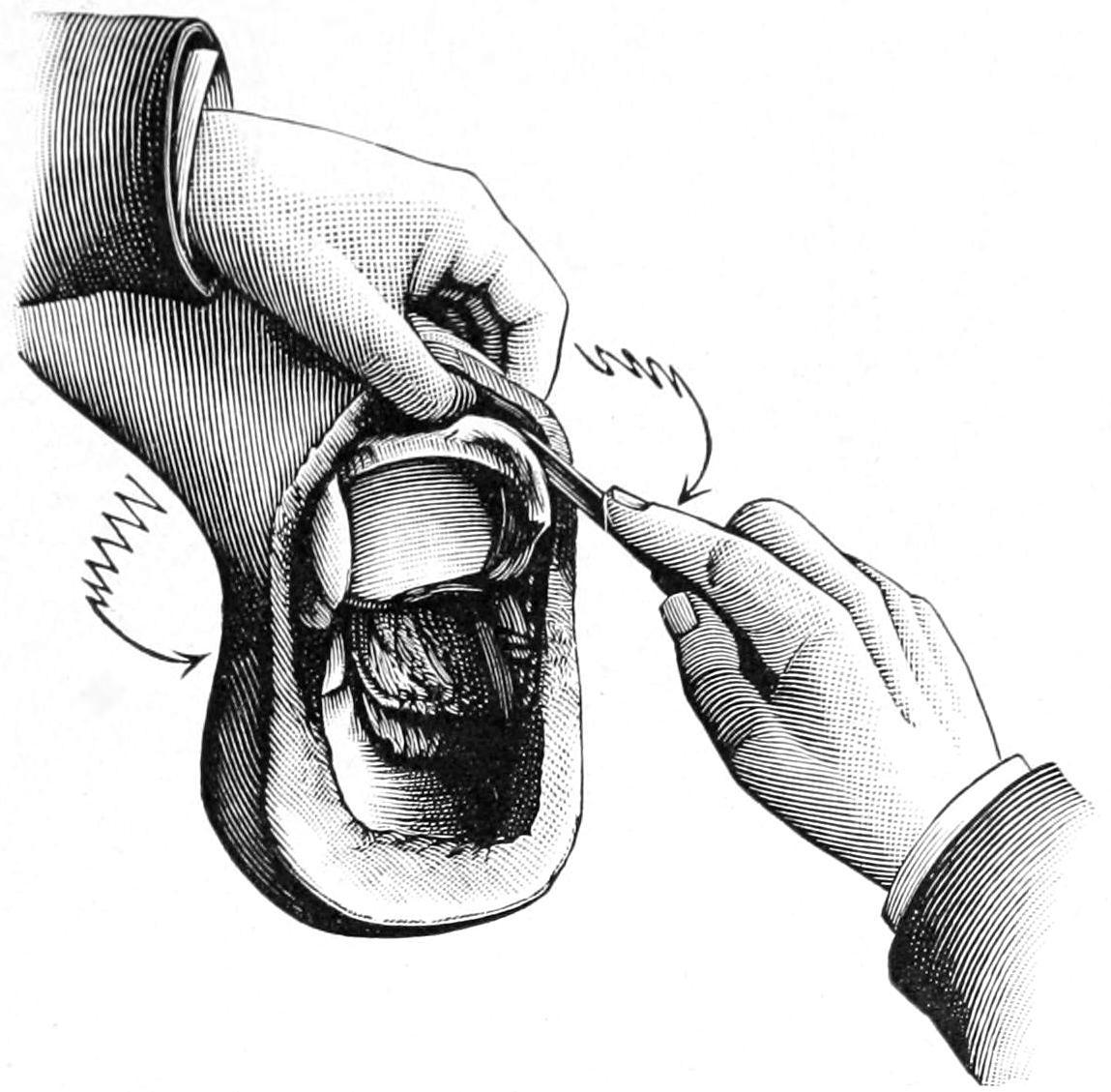
Syme’s amputation after disarticulation of the foot at the ankle-joint. The soft parts are being cleared from the malleoli preparatory to sawing the malleoli and lower articular surface of tibia. (Farabeuf.)
Fig. 703
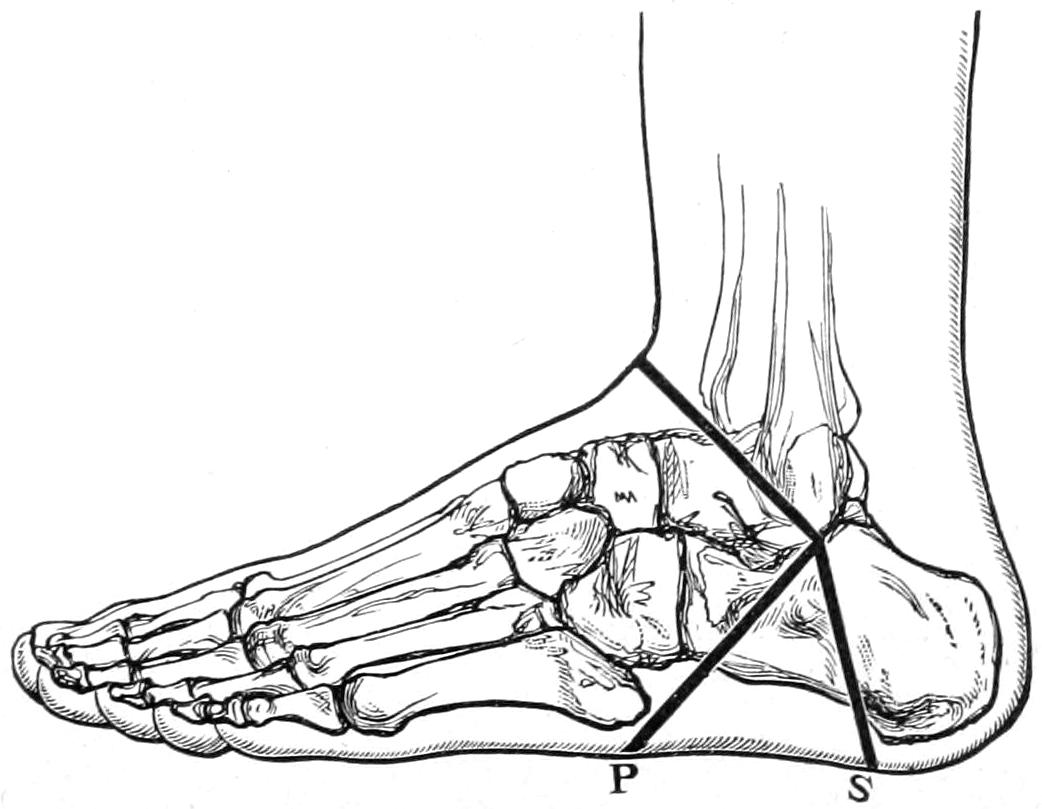
S, line of incision for Syme’s operation; P, line of incision for Pirogoff’s operation. (Erichsen.)
—Modern prosthetic methods have materially changed the indications in amputating the leg. The pressure in artificial limbs is not borne upon the end of the stump, but is rather circumferential and borne by a conical socket. It is now, therefore, an object to preserve as much of the limb as practicable, in order to[1040] have better leverage or control of the artificial member. Consequently the point of election is now the middle of the leg, unless the amputation may be made even below this point. The objection to a short leg stump is the inevitable flexion which the hamstring flexors will produce; in such cases the pressure will be borne upon the knee, while the appearance of the stump is by no means ideal. If, therefore, one is forced to make a high amputation of the leg it would be far preferable to make a good knee disarticulation, or, better still, a supracondyloid amputation, with preservation of the patella, thus furnishing a stump which affords perhaps the only exception to the general rule, i. e., that weight cannot be borne upon the stump end.
Fig. 704
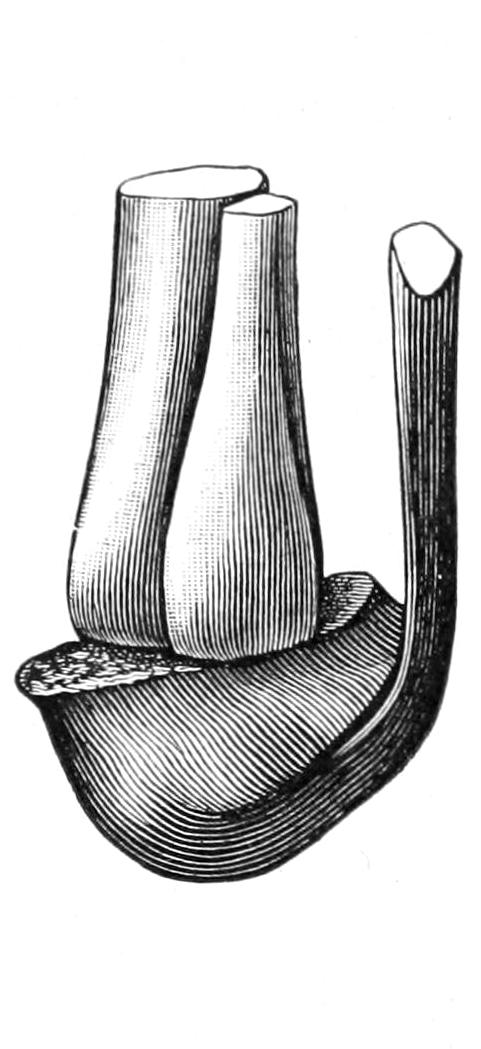
Skeleton of stump after Pirogoff’s osteoplastic amputation. The sawed surface of the calcaneum in apposition with divided surface of tibia. (Farabeuf.)
Fig. 705
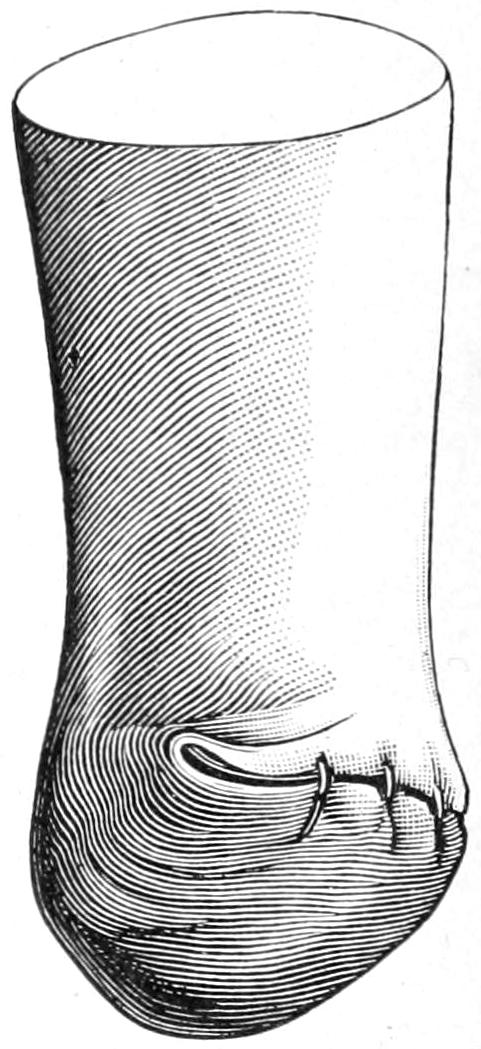
Stump after Pirogoff’s operation. The weight of the body must rest upon the thick plantar skin of the heel and never on the thin skin of the retrocalcaneal surface. (Farabeuf.)
Fig. 706
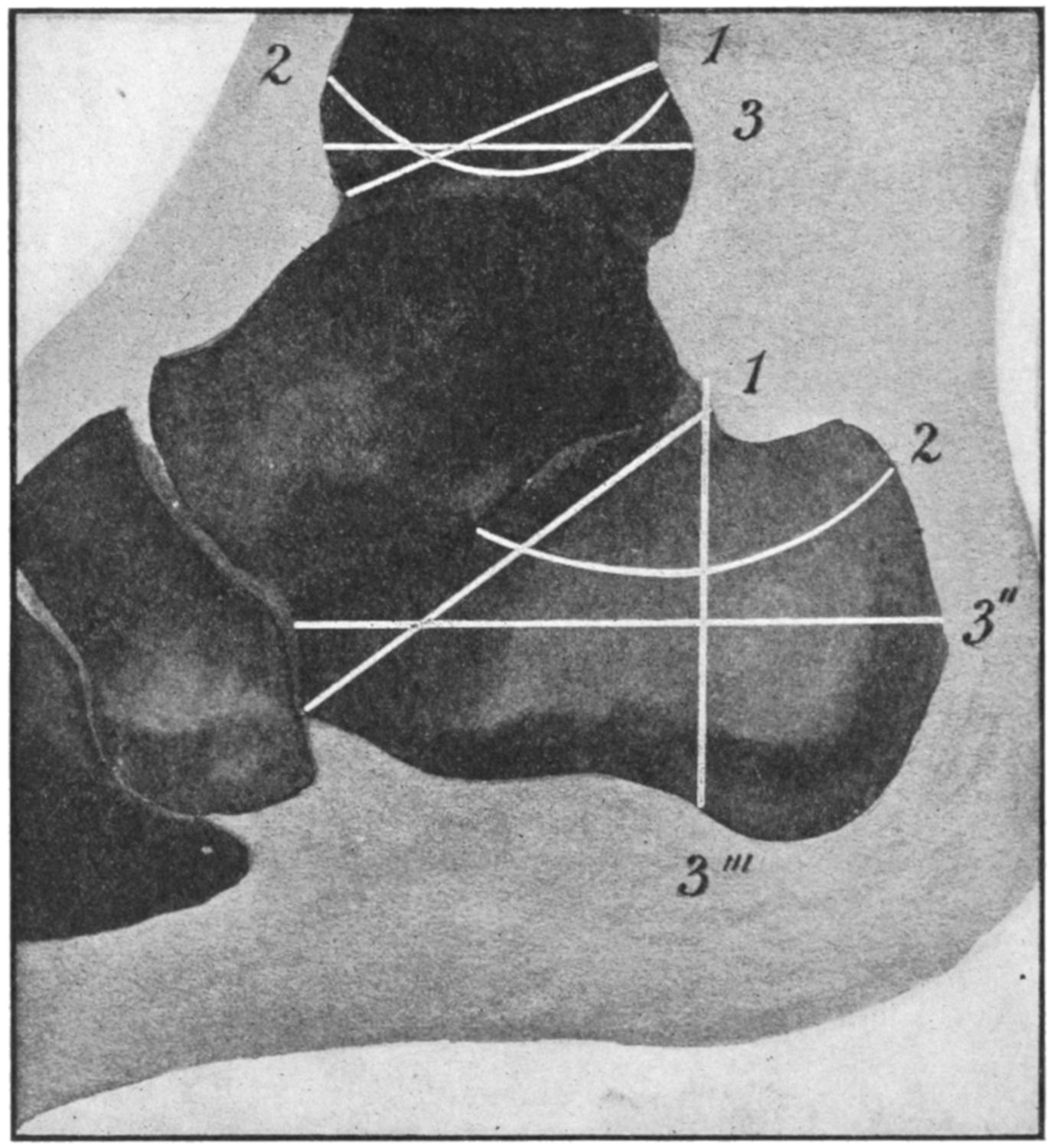
Sections of bone in Pirogoff’s amputation and its modifications: 1, oblique section of calcaneum to correspond with (1) oblique section of tibia. (Gunther.) 2, curvilinear or concave section of calcaneum to correspond with (2) convex section of tibia. (v. Bruns.) 3″, horizontal section of calcaneum to correspond with (3) similar section of tibia. (Pasquier Le Fort.) 3‴, vertical section of calcaneum to correspond with (3) horizontal section of tibia. (Typical Pirogoff.) (Modified by Matas from Mignon.)
[1041]
Fig. 707
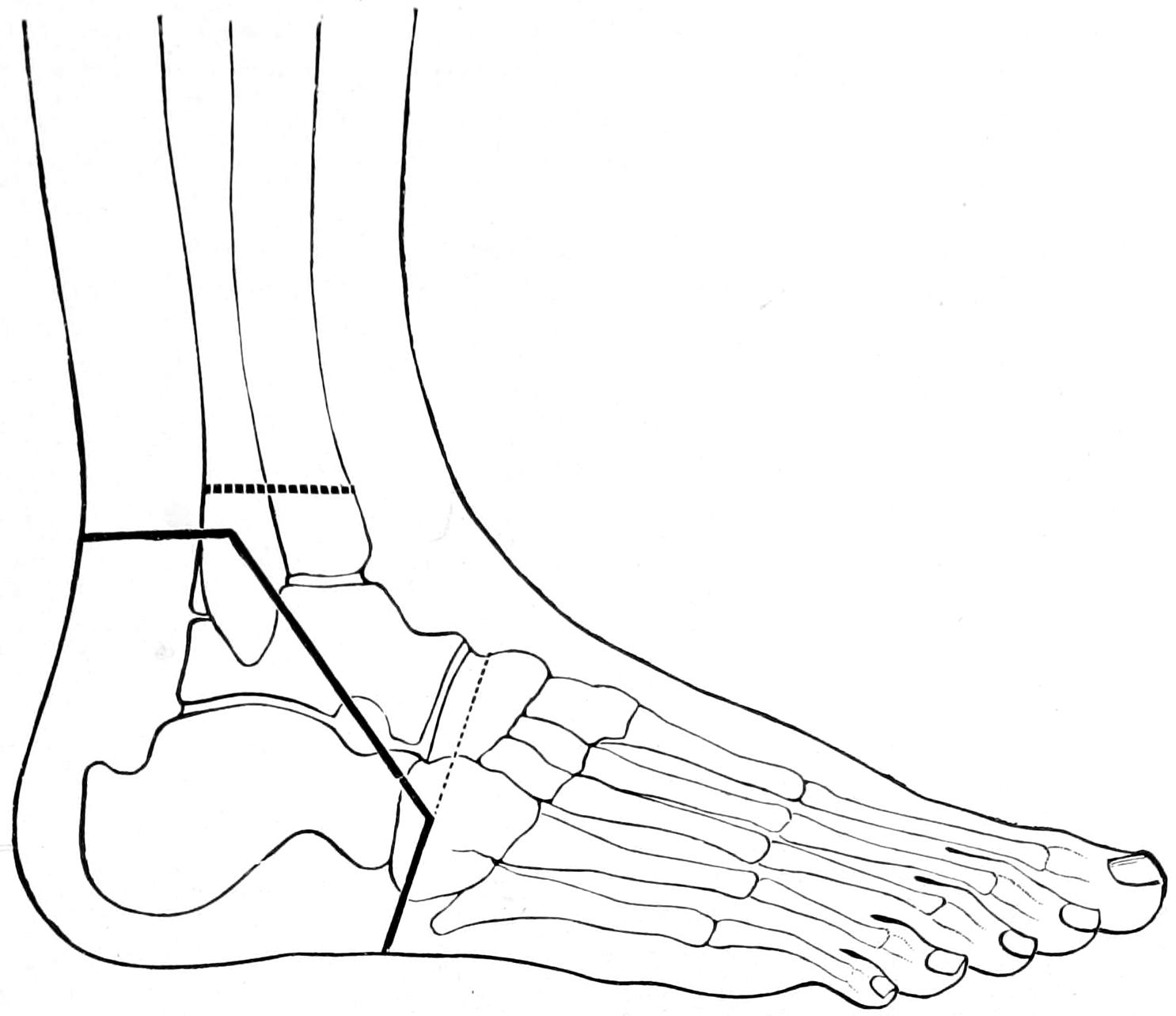
Osteoplastic excision of foot. (Mikulicz.)
Let us, then, consider but one or two amputations of the leg—that low down or near the middle and that at the knee. Whatever the method it is most desirable that the scar be kept off to the side, and especially away from the front of the shin. This can be best accomplished by a modified circular (Fig. 708) or a bilateral flap method (Fig. 711), or by the oblique method with lateral incisions, which practically convert it into an anteroposterior operation, while for certain instances the method of Teale may be preferred, i. e., that with a long anterior and short posterior flap, or its modification by which the flaps are made more lateral, or the even long flap method of Bell.
Fig. 708
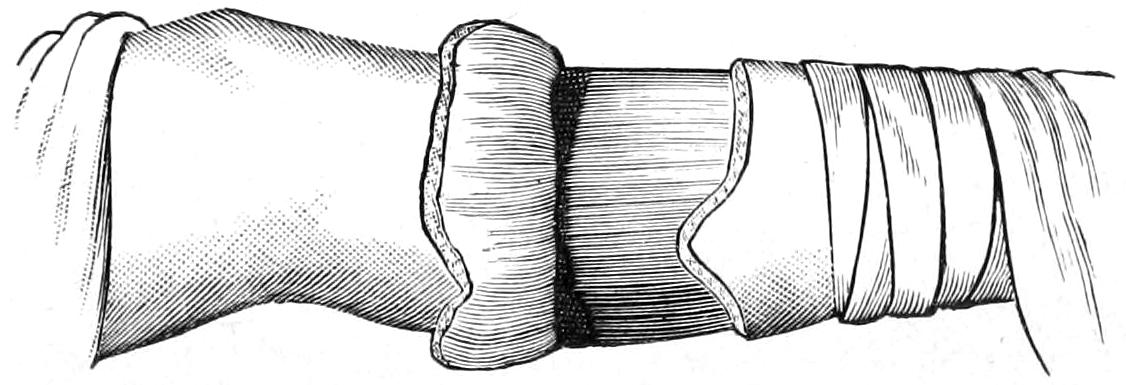
Modified circular amputation of upper third of leg. (Erichsen.)
Whichever of these be selected, after division of the muscles and exposure of the bone, it is usually helpful to retract the flaps, whatever their shape, by a cloth retractor made of a piece of sterile bandage torn into three strips, the middle of which should be inserted between the bones of the leg, the interosseous membrane being divided for this purpose; by this they are held more perfectly out of the way during the act of dividing the bones. The anterior border of the tibia, which is practically a sharp ridge, should be divided obliquely (bevelled), either by a small oblique section before the transverse division is made, or by effecting this later, in order that there shall not remain a sharp point to[1042] project through the skin or be subject to constant irritation. The tibia is usually divided transversely, with the above exception. The fibula may be divided slightly obliquely. It is customary, however, to make the division simultaneously, and to so conduct the sawing process as to divide the fibula completely before the last strokes of the saw cut through the tibia.
There is greater difficulty in the recognition and securing of vessels in leg amputations than in any other, especially if they have been divided obliquely. The principal vessels may be found from their known anatomical location. They nevertheless sometimes tend to retract and they must be followed up in order to properly secure them. The accompanying nerve trunks should also be seized firmly, drawn down, and divided two or three inches above the line of division of the other tissues, in order that they may retract out of harm’s way. Every nerve which can be recognized, even in the skin, should be thus treated. Before closing the wound it is well, unless one is absolutely sure of his work, to release the tourniquet and ascertain if any vessel which would otherwise bleed be not yet secured. Oozing may be checked with hot water, while muscle surfaces which leak too much blood may be lightly enclosed within catgut sutures inserted with a curved needle.
Providing that these stumps have well-nourished flaps, and that no sharp or angular bone ends interfere with subsequent comfort, and that the scars be kept away from their lower surfaces, they serve their purpose admirably.
Supposing, then, that amputation is to be about the middle, the first incision, made with a stout scalpel, is begun at the anterior border of the tibia and carried downward along it until it is turned abruptly backward to the posterior aspect, and then upward until a point is reached opposite that of commencement. The skin is dissected up for perhaps an inch. Then the flap on the other side is cut after the same fashion, after which, with a short or long knife, the muscles are divided transversely or circularly down to the bone. Much will depend now upon whether the desire is to resort to the more modern osteoplastic methods or adhere to the old. In the latter case it is well to separate the flaps for the necessary distance from the bone, with or without the periosteum, dividing the bones after suitable retraction, as above suggested. If preference be for an osteoplastic flap it is planned and made at this time, the bone being divided at the same level as the muscles, and the amputation being thus practically completed, after which the osteoplastic flap is arranged, it being now necessary to carefully preserve the periosteal bridge and to again divide the bone at the base of this periosteal flap, this being the true end of the bone stump. In this case the fibula is divided at a higher level.
It is perhaps less desirable to preserve periosteum in young children than in adults, for if bone be permitted to grow too rapidly conical stumps result, sometimes even with protrusion of bone ends. Ollier and his pupil Mondan have shown that this so-called atrophic elongation of bone is a consequence of abnormally rapid growth from the upper epiphyseal direction, permitted by lack of pressure from below, and that conical stumps will often happen in children in spite of every precaution. Nevertheless it should not be encouraged, and for this reason periosteum should not be preserved.
The method of Teale was to cut a long anterior flap, raising the coverings from the bone with the least possible disturbance, to divide the bone at the high level, then to double the flap upon itself in such a way as to bring the scar at a level one inch or more above the stump end. Heine modified this slightly by raising the periosteum with the rest of the anterior flap. In cases which permit such a long flap to be formed from one aspect of the leg the method gives excellent results (Fig. 709).
Fig. 709
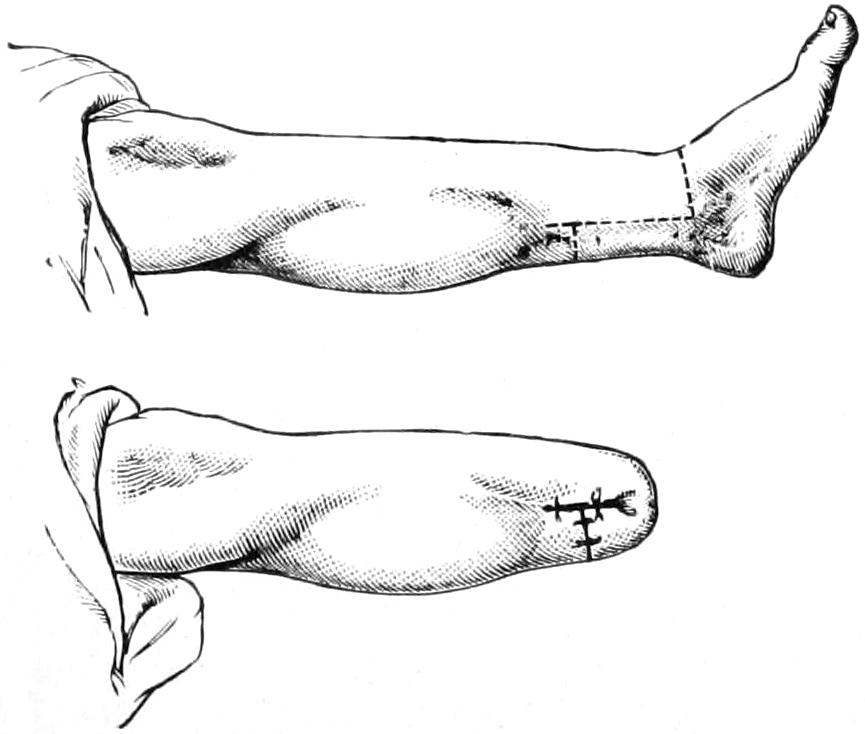
Teale’s method of amputation.
Bruns devised a method which is begun almost as an exsection, by an oblique circular incision, with liberating lateral incisions, and division of all the tissues over the inner border of the tibia and the outer side of the fibula; after which, without disturbing skin attachments in front, the periosteum is separated from the bones as high as the liberating[1043] lateral incisions permit, and then the fibula first and later the tibia divided. It is practically a subperiosteal excision of the leg bones and affords a well-protected stump. In effect it is an anteroposterior flap method.
Fig. 710
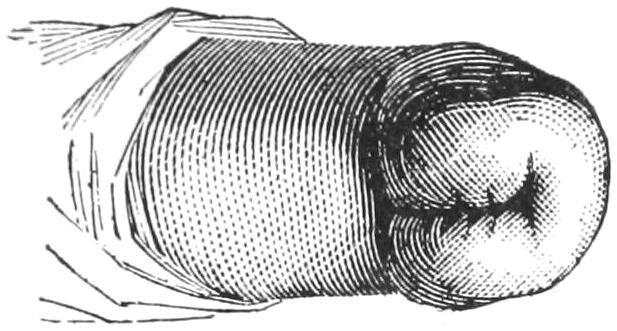
Stump after Stephen Smith’s amputation at knee.
—It was Brinton who, in 1872, suggested the preservation of the semilunar cartilages in all knee disarticulations, as in this way all the normal relations are preserved and retraction is prevented. But the makers of prosthetic apparatus have urged to abandon all true disarticulations, and to substitute for them the supracondyloid method, which affords ideal stumps. Disarticulations are supposed to produce less shock, less loss of blood, and less danger of sepsis from opening up the bone-marrow, while muscle insertions are less disturbed and the stump covering usually is mobile and not very sensitive. No disarticulation should be thought of unless the joint involved be free from disease and unless about it there be met sufficient healthy integument to furnish a satisfactory flap.
For a true disarticulation Stephen Smith’s bilateral method is now almost universally adopted. Here the incision is begun one inch below the tubercle of the tibia and is carried directly down to the bone, downward and forward around the side of the leg, and then inward and upward toward the middle of the popliteal space, the lateral flaps thus made being nearly duplicates. The flaps thus cut out are completely separated from the bone up to the joint level, where the ligaments are divided, the joint being manipulated as may be necessary to best expose them and facilitate division. In this operation the patella is usually removed, the joint being opened by separating its ligament at its insertion into this bone. One should remember that the internal condyle is lower and longer than the external, and that the internal flap should be perhaps made on this account a little the longer of the two. Fig. 710 illustrates the stump resulting from this operation and shows the cicatrix drawn up out of harm’s way and resting in the fossa between the condyles. Fig. 711 illustrates the simple method by lateral flaps.
Fig. 711
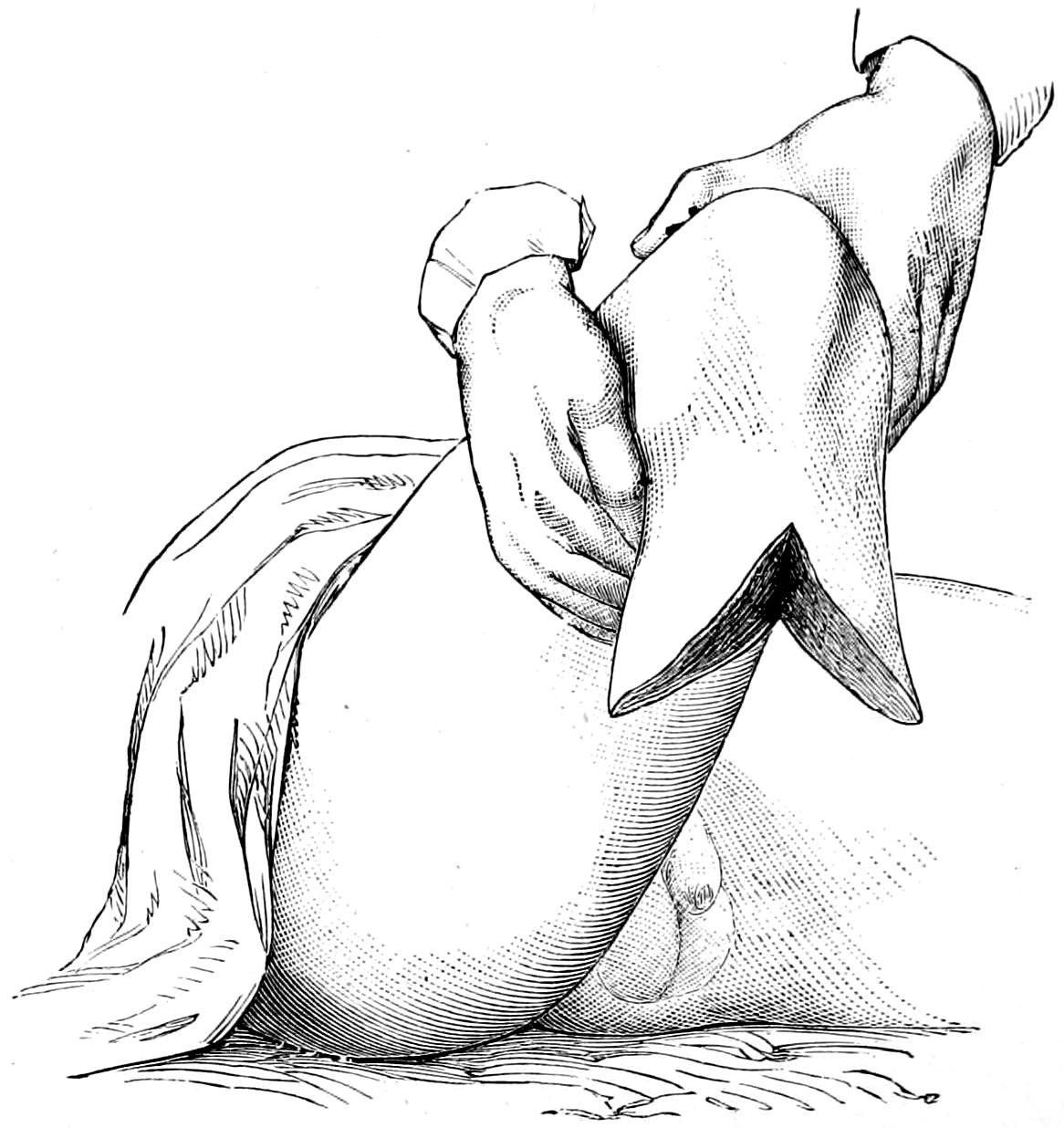
Amputation at knee by lateral flap. (Erichsen.)
—Under this head, rather than that of amputation at the knee, should be described the supracondyloid amputations which give decidedly the best results of all, and which are preferable to any others for the middle of the lower extremity. Of these the best is that suggested by Gritti, which consists in not only removing the condyles but sawing off the articular surface of the patella, which is then drawn upward and applied to the end of the femur, the division of the latter being made at a point above the condyles, where the diameter of both bones will nearly correspond, this latter perhaps being a suggestion of Stokes rather than of Gritti, who did not divide the bone quite so high. (See Fig. 712.)
Fig. 712
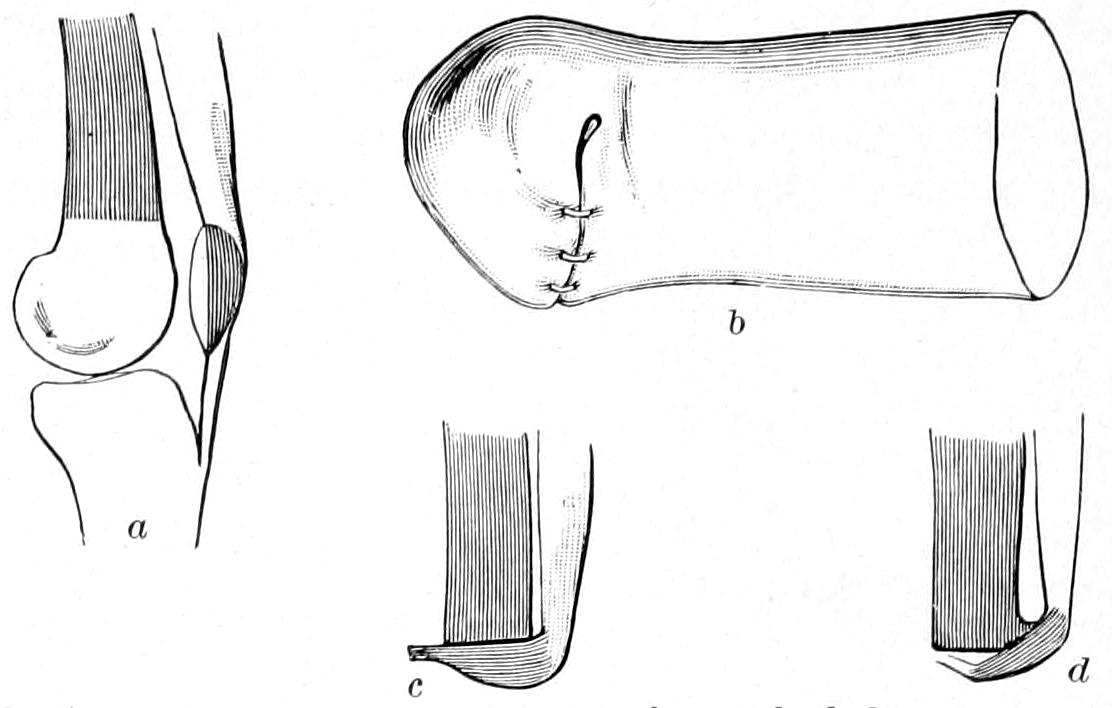
Gritti’s osteoplastic supracondyloid knee amputation, patella utilized: a, shaded parts are those brought in apposition; b, appearance of Gritti stump after suture; c, correct apposition of patella to femur; d, defective apposition. (Farabeuf.)
Fig. 712 will best illustrate the intent of the method as well as its performance. The incisions are planned much as in the Stephen Smith disarticulation method, only they are placed higher, and the patellar tendon is divided as low down as possible, or even separated from the tibia, in order that it may be made of use in attaching the divided[1044] patellar surface to the femoral end. The rest of the operation is performed as by other methods, the attachment of the patella being effected by tendon sutures, or, if necessary, by an ivory peg, or even a metal tack or nail which may be left in place.
The beauty of this method is that the anterior surface of the patella is preserved with its natural weight-bearing facilities and the bursa between it and the skin, while the latter is undisturbed. On the end of this stump as much weight can be steadily borne as when one ordinarily kneels, and to it a most serviceable kind of artificial limb can be attached, with which one may walk as though nothing had ever happened.
Another osteoplastic method, namely, that of Sabanejeff, is illustrated in Figs. 713 and 714. In this instance the bone covering over the end of the femur is taken from the upper end of the tibia, the patella not being disturbed. It permits a lower division of the femur and the formation of a stump which is of practically the same length as the original thigh.
—For removal of the thigh it is well to preserve as much of its length as possible, and yet not at the expense of all other considerations. A thigh stump too short is likely to be pulled awkwardly upward by the psoas muscle, and upon such a stump it is difficult to secure an artificial limb tolerable of control against such action of this muscle. On this account, then, thigh stumps should be long. So far as the method is concerned the circular, or some modification thereof, gives the best results in the majority of instances. It may easily be modified into one of the oblique methods, or liberating incisions may be used whenever they will be of service. If it be absolutely necessary to make the amputation high hemostasis[1045] can be secured by the same methods that are used in hip-joint amputations. The dense and strong fascia lata, which lies beneath the superficial fascia, should be divided at the same level with the skin, since it serves admirably, when secured by a separate set of sutures, to make a good covering for the ends of the muscles, after these have been themselves carefully united by buried sutures. The sciatic nerve should be especially sought, thoroughly stretched, and divided high up. The vessels often evince a tendency to retract within Hunter’s canal; it is not, however, difficult to separate the vastus internus from the adductor longus, between which they lie, and in this way gain access to them. Even for high work on the thigh one may, if necessary, do as some have done at the hip, make a preliminary ligation of the femoral artery. This may be especially serviceable as an emergency measure, or in special cases of tumors which have attained large size, are placed high up and call for somewhat atypical methods.
—Amputation here is essentially a disarticulation and constitutes one of the usually formidable and serious operations of major surgery. Although the joint itself is generally easily reached there are many things to be considered in the performance of this operation, of which the mere arthrotomy is by no means the most important.
Preparations being all made, the first consideration is the control of hemorrhage, for which several methods have been suggested, but of which but two or three are in general use. Such procedures as compression of the abdominal aorta, either with the hand or by tourniquet, or of the common aorta through the rectum, with a lever, as suggested by Davey, or with the hand, as suggested by Woodbury, or the exposure of the common iliac, either within the peritoneum as practised by McBurney, or externally, or exposing the common femoral above Poupart’s ligament, are now adopted by very few surgeons. Langenbeck used to be fond of preliminary ligation of the femoral where it is most accessible in the groin, and this is probably the best of all of these methods. But they have been all practically discarded since Wyeth introduced the simple method of transfixing the limb with his pins (i. e., long mattress needles or skewers made for the purpose), these serving to hold in place an elastic cord or tourniquet (Fig. 715). This has been found to be a great improvement on the suggestion of Senn, who excised the femoral head and then compressed each half of the limb with a separate elastic band.
Fig. 715
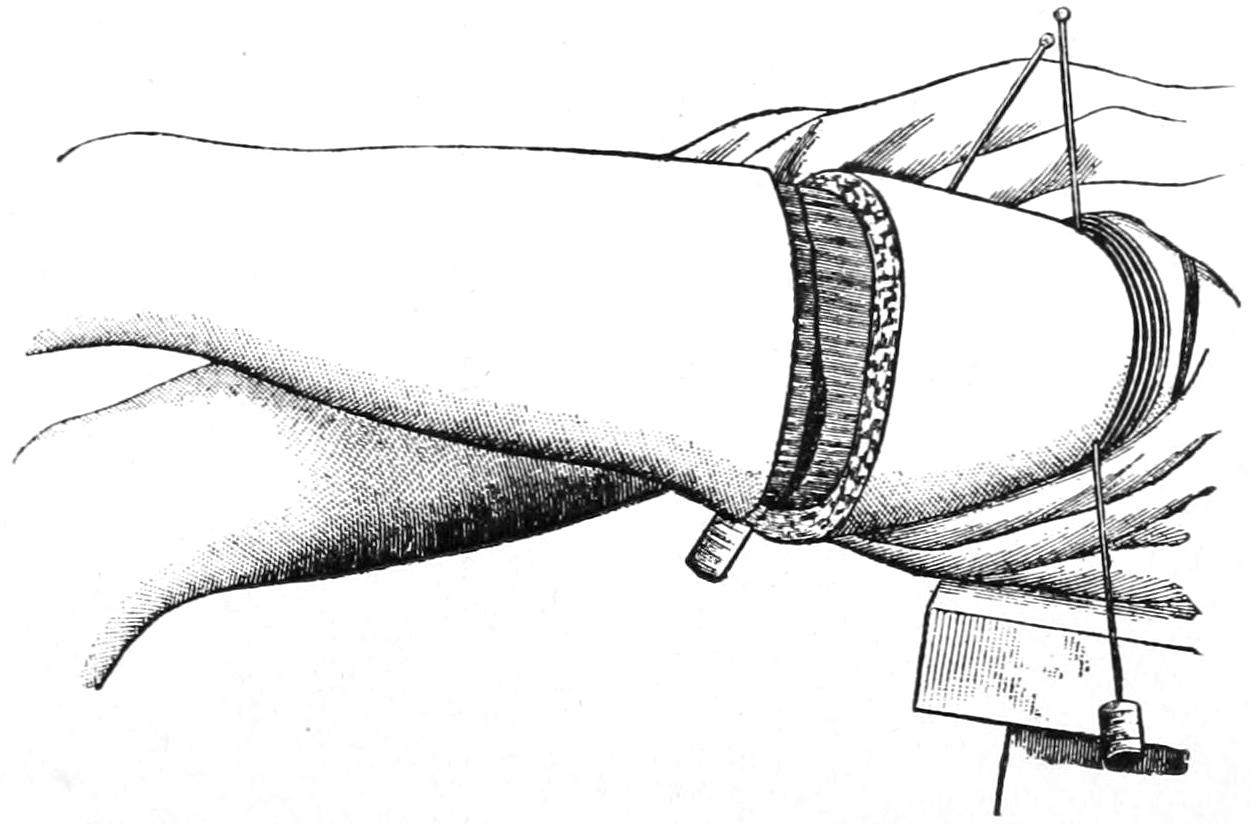
Wyeth’s bloodless method: pins inserted and tube applied.
The directions for the use of Wyeth’s pins are simple. Here, as in other cases, it may not be practicable to use the elastic bandage from the lower end of the limb, but one may at least elevate the limb and thus coax the blood out of it by gravity or by gentle manipulation. While it is still in this position one of the long pins is introduced just below the anterosuperior spine and a trifle to its inner side, and made to emerge on a level with and about three inches from the point of its entrance. The other needle is inserted just to the inner side of the saphenous opening, and below the level of the crotch, and brought out about one inch below the tuberosity of the ischium. Corks should then be placed upon them so as to protect the needle points. Next a piece of elastic tubing or band is placed around the limb above these pins and tightened, each turn being made a little tighter, so as to absolutely control the circulation. The effect of[1046] this is felt upon practically every vessel in that part of the body, and if the method be properly practised it affords absolute security.
The surgeon now has his choice of various methods of disarticulation, either that by anteroposterior flaps or lateral flaps, or by the circular, with the free liberating lateral incision; or he may devise any method of his own which will best meet the indication in a given case. Fig. 715 illustrates the employment of Wyeth’s pins and the first circular incision made as for the circular method. Of these all the latter seems preferable when circumstances permit. It should be combined with a sufficient lateral incision, which should be made to pass well over the great trochanter. The cuff raised through this incision should extend down to the deep fascia and up to the level of the lesser trochanter, at which level the deeper tissues are divided transversely or by a circular cut.
It is well next to lay down the knife and secure the large vessels, after which the deep muscles are separated from the upper end of the shaft and the proximity of the joint, while the entire limb may be still used as a lever in so stretching the joint capsule as to better expose and divide it. So soon as the capsule has been opened, and the entrance of air thus permitted, it will be easy to expose and divide the teres ligament, after which the balance of the disarticulation is easily effected. The large nerve trunks are now sought, retracted, and divided high up, all visible vessels are secured firmly, after which the elastic constriction may be gradually released and any vessels that spurt may still be secured. There will nearly always be troublesome oozing from the cut ends of the large muscles, and here, if hot water prove insufficient to check it, with large curved needles and catgut sutures the muscle ends may be secured by ligature en masse, before they are brought together for the purpose of closing the stump.
Whatever the method selected as perfect a closure of the wound as possible should be made, with ample provision for drainage. By careful deep suturing, with tiers of buried sutures, it is possible to avoid leaving dead spaces at any point except perhaps the acetabulum. Through retaining sutures may also be used to advantage. It is most desirable to so plan the incisions and the closure of the wound as to keep them, so far as possible, away from the region of the perineum. Therefore the longer the inner flap or inside of the stump the better. As conditions which necessitate removal of the limb at the hip-joint are always serious, and have each their own peculiarities, any method which will best serve the purpose should be used.
Plates LIX and LX, designed by Prof. Matas, afford the best and briefest epitome of the choicest amputation methods which can be furnished.
An amputation having been effected, and the stump closed, there is still occasion to consider how it may best be treated to fit it for its future purposes. When entire chapters, or even small monographs, can be written on the subject of “diseases of stumps” it would appear that the consideration is not one of merely trifling import.
A good stump has a regular outline, with a protected scar, and should be firm, yet mobile, and without tender or sensitive surfaces. It should constitute the lower end of a truncated cone, and needs to be of sufficient length to permit leverage within the socket of the artificial limb which will be fitted about it.
A stump failing in these characteristics is a bad stump, the features which especially tend to make it bad being undue conicity (Fig. 716) or sensitiveness of surfaces, ulceration from friction, or, worse yet, occurring without it, and neuralgia from inclusion of nerve ends, or from bone ends which present osteophytic outgrowths and thus distort and displace tissues (Fig. 717). Acute osteomyelitis occurs in stumps, as do slower carious processes which may call for re-amputation, perhaps even at a distance. The stump is for a long time more or less tender and troublesome, and its owner may be a sufferer from hyperesthesia or perverted sensations.
The possibility of the production of a conical stump in children as the result of atrophic elongation was mentioned early in this chapter. While this cannot always be prevented it may sometimes be foreseen, and one should be prepared at any time in such cases to circumcise the bone, forcibly retract the tissues, and then divide the bone ends on a higher level.
PLATE LIX
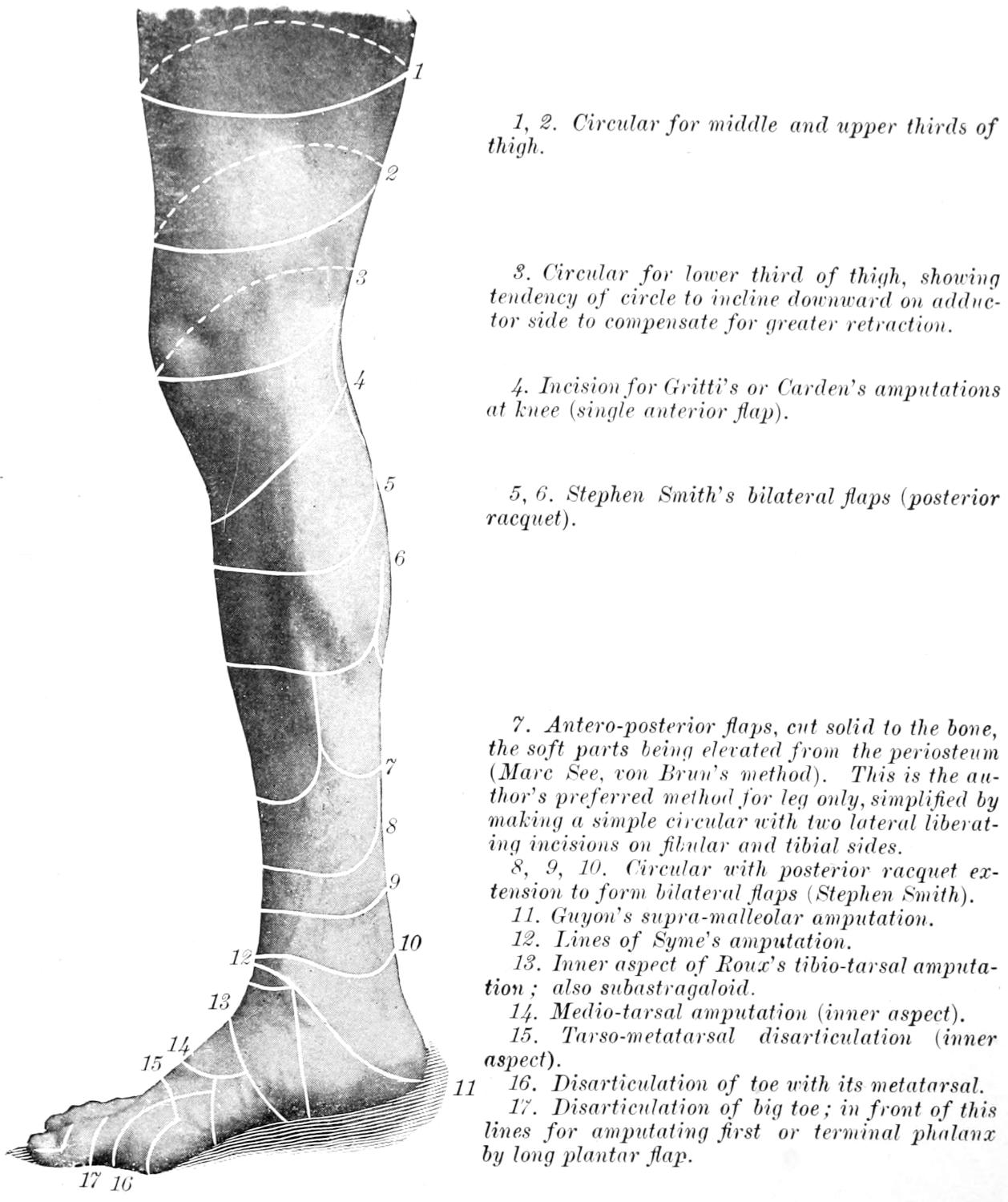
The Right Lower Limb, Internal Lateral View (Surface Incisions).
1, 2. Circular for middle and upper thirds of thigh.
3. Circular for lower third of thigh, showing tendency of circle to incline downward on adductor side to compensate for greater retraction.
4. Incision for Gritti’s or Carden’s amputations at knee (single anterior flap).
5, 6. Stephen Smith’s bilateral flaps (posterior racquet).
7. Antero-posterior flaps, cut solid to the bone, the soft parts being elevated from the periosteum (Marc See, von Brun’s method). This is the author’s preferred method for leg only, simplified by making a simple circular with two lateral liberating incisions on fibular and tibial sides.
8, 9, 10. Circular with posterior racquet extension to form bilateral flaps (Stephen Smith).
11. Guyon’s supra-malleolar amputation.
12. Lines of Syme’s amputation.
13. Inner aspect of Roux’s tibio-tarsal amputation; also subastragaloid.
14. Medio-tarsal amputation (inner aspect).
15. Tarso-metatarsal disarticulation (inner aspect).
16. Disarticulation of toe with its metatarsal.
17. Disarticulation of big toe; in front of this lines for amputating first or terminal phalanx by long plantar flap.
PLATE LX
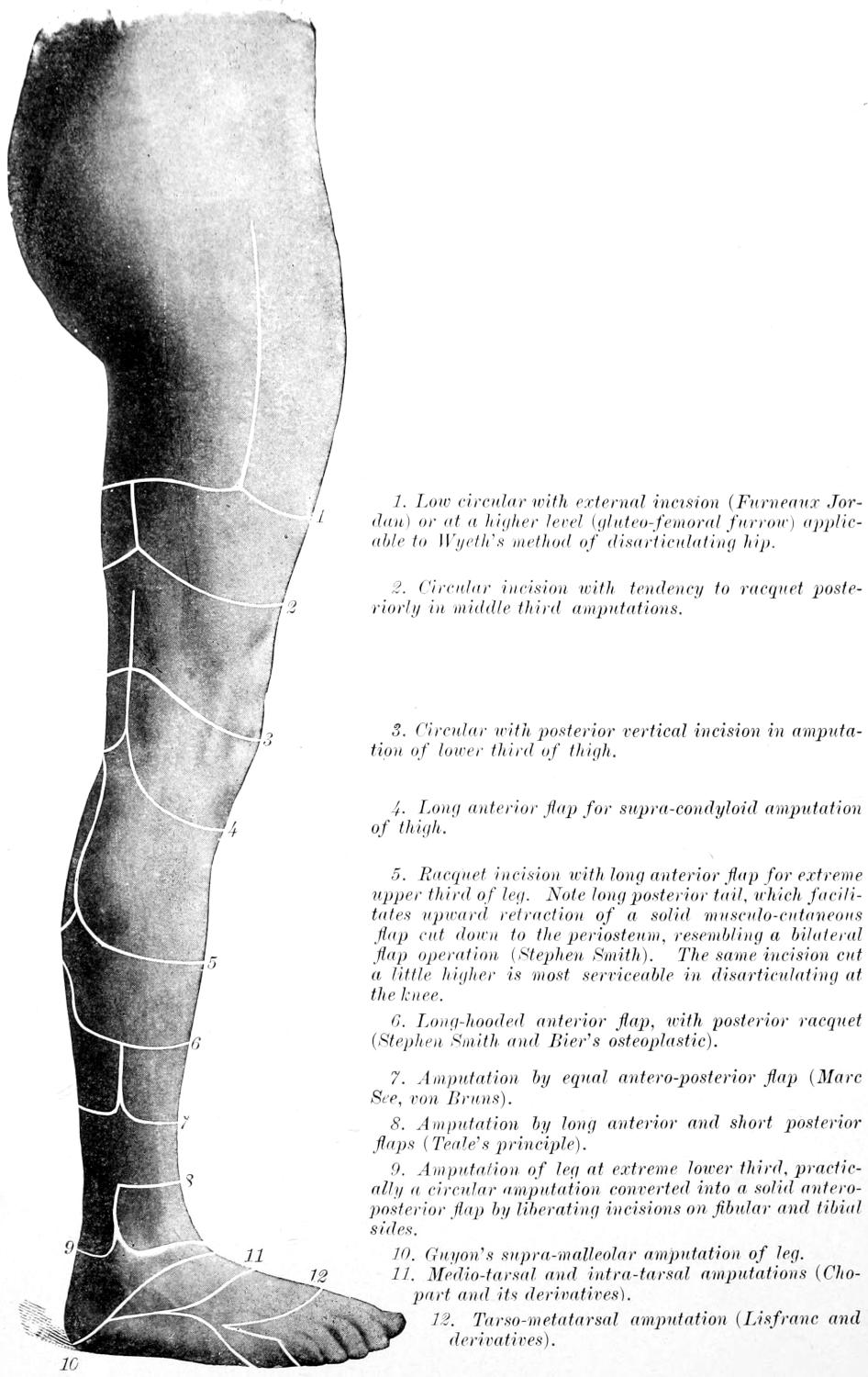
Surface Outlines of Amputations Practised in the Lower Extremity.
1. Low circular with external incision (Furneaux Jordan) or at a higher level (gluteo-femoral furrow) applicable to Wyeth’s method of disarticulating hip.
2. Circular incision with tendency to racquet posteriorly in middle third amputations.
3. Circular with posterior vertical incision in amputation of lower third of thigh.
4. Long anterior flap for supra-condyloid amputation of thigh.
5. Racquet incision with long anterior flap for extreme upper third of leg. Note long posterior tail, which facilitates upward retraction of a solid musculo-cutaneous flap cut down to the periosteum, resembling a bilateral flap operation (Stephen Smith). The same incision cut a little higher is most serviceable in disarticulating at the knee.
6. Long-hooded anterior flap, with posterior racquet (Stephen Smith and Bier’s osteoplastic).
7. Amputation by equal antero-posterior flap (Marc See, von Bruns).
8. Amputation by long anterior and short posterior flaps (Teale’s principle).
9. Amputation of leg at extreme lower third, practically a circular amputation converted into a solid antero-posterior flap by liberating incisions on fibular and tibial sides.
10. Guyon’s supra-malleolar amputation of leg.
11. Medio-tarsal and intra-tarsal amputations (Chopart and its derivatives).
12. Tarso-metatarsal amputation (Lisfranc and derivatives).
[1047]
An exquisitely neuralgic stump is usually made so by the entanglement of nerve ends and their subsequent enlargement into so-called amputation stump neuromas (which are histologically fibromas), from pressure upon nerve terminals. Under these circumstances their excision through incisions planned for the purpose, or the exsection of a portion of the nerve trunk at a higher level, may be necessitated (Fig. 717).
Fig. 716

Extreme case of conical stump.
Fig. 717
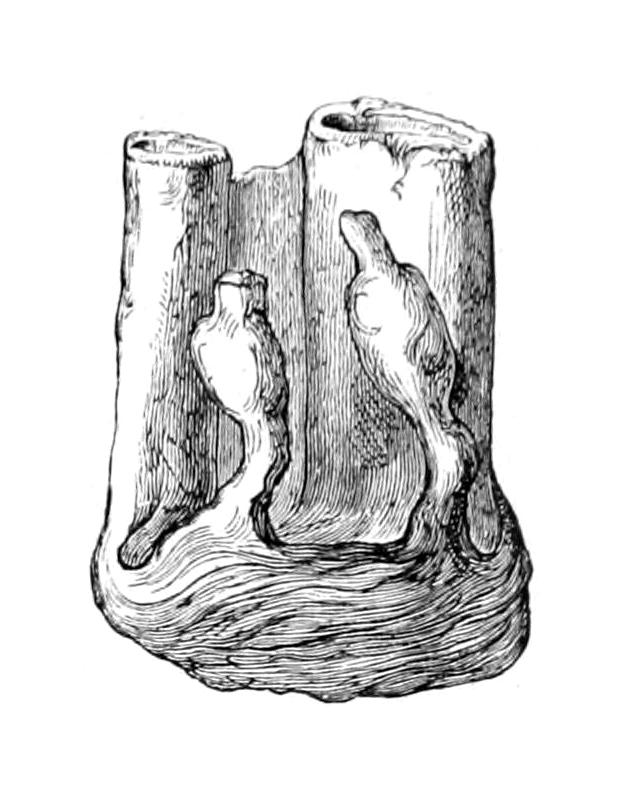
Neuromatous endings of nerves in a stump.
Fig. 718
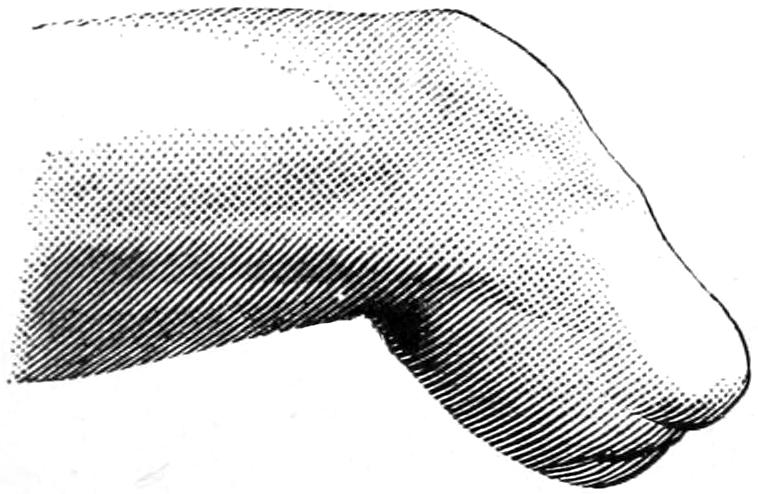
Ideal stump.
Fig. 719
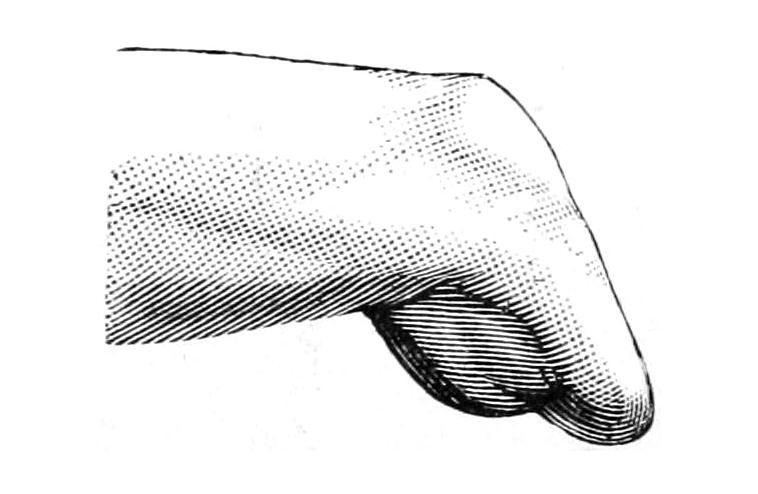
Bad stump, because posterior flap was cut too short, and there has been great retraction of all soft tissues. (Farabeuf.)
While patients may prefer disuse of a stump for as long a time as possible the judicious surgeon will prepare it as rapidly as he may for early application of the expected artificial limb. Inasmuch as leg stumps allowed to hang downward become cyanotic and edematous it is well to keep them bandaged, and the makers of artificial limbs prefer to have the bandages kept wet. When the stump is healed, passive motion of the remainder of the limb should be begun, in order that there may be a minimum of stiffening of joints. If, then, such a stump be bathed, massaged, moved, and then bandaged with comfortable snugness with cold, wet bandages, over which oiled silk may be fastened, and if this be done at least once each day, the stump will be prepared for the artificial limb, on the average, in two to three months. One should not wait for this expiration of time if it be thoroughly healed; or, on the other hand, he may have to wait much longer under unfortunate circumstances; but the above general principles of treatment and general statements will be found to prevail. Figs. 718 and 719 illustrate the difference between good and bad stumps, while Plates LIX and LX (reproduced from Matas) furnish the surface outlines for selection of the various amputations of the lower limb.
[1048]
The most pronounced and illustrative of recent methods is perhaps the “cinematic” or “cineplastic” procedure of Vanghetti. This Italian surgeon proposed a prosthetic method, in 1898, which is illustrated in Figs. 720, 721 and 722. He has shown that tendon terminations may be left exposed in stumps, under favorable conditions, and so utilized as to serve remarkably useful purposes—though under exceptional conditions. For a description of these methods the reader is referred to his monograph. (G. Vanghetti, Plastica e Protesi Cinematiche, Empoli, 1906.)
Fig. 720
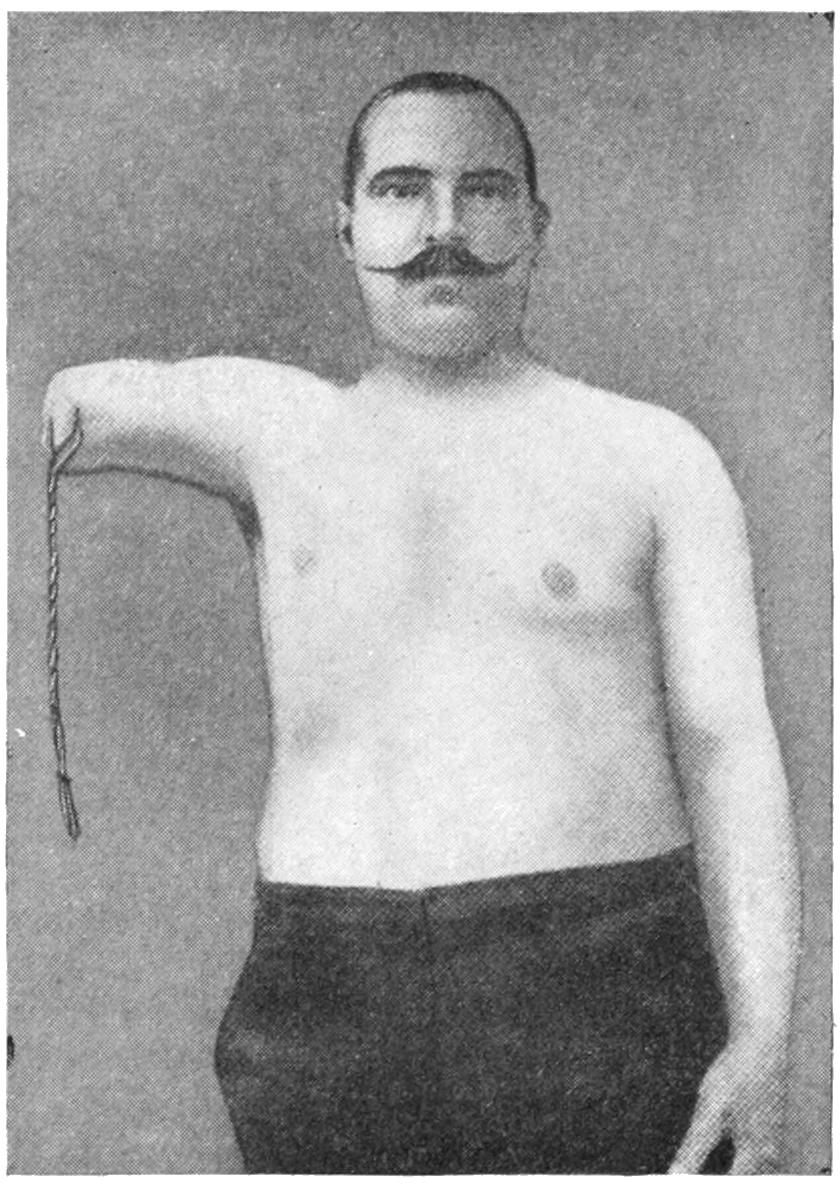
Fig. 721
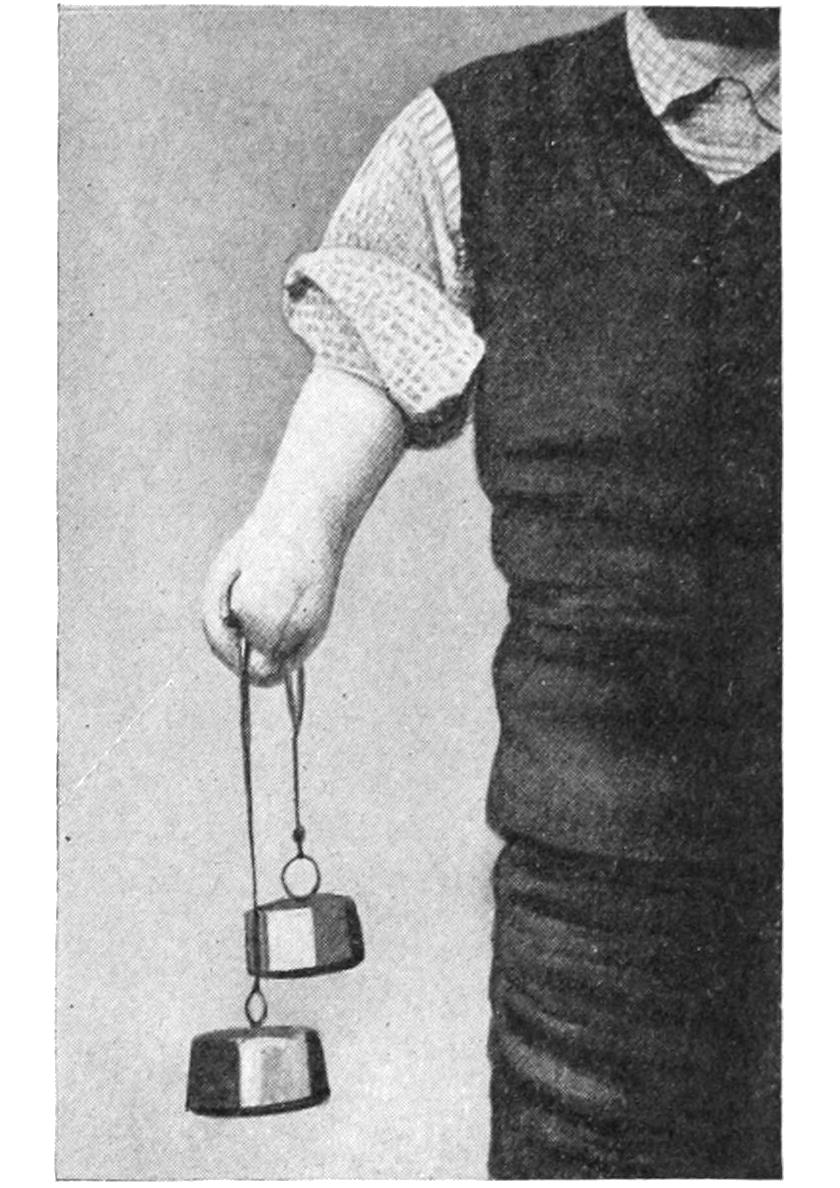
Fig. 722
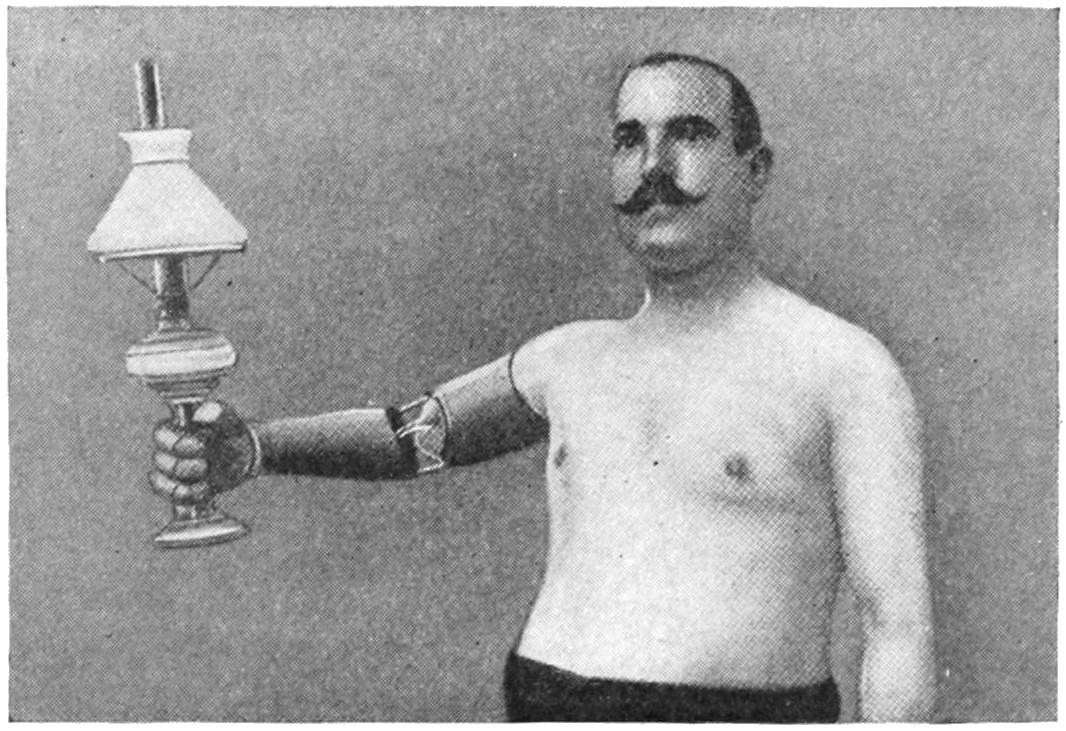
Results of Vanghetti’s “cinematic” method, with preservation and utilization of tendons.
[1049]
Inconsistent and archaic spelling, hyphenation and capitalisation have been retained, also in anatomical and medical terminology and in proper names, except as mentioned under Changes made below.
Depending on the hard- and software used to read this text, not all elements may display as intended.
Texts in a dashed box under illustrations have been copied from the accompanying illustration for better legibility.
Most illustrations may be enlarged by opening them in a new tab or window. This may not be available in all formats.
The page numbering is as in the source document, where page numbering jumps from page ix to page 17.
Due to the lack of detail in the Table of Contents, the structure of the book ((sub-)sections, chapters, parts) as used in this e-text is based mainly on the typography used in the source document; this has lead to some inconsistencies that may appear in auto-generated tables of contents.
Page 195, ... that 5 per cent. is more than adequate ...: appears to be contradicted by the remainder of the sentence; possibly 5 per cent. is an error for .5 per cent.
Page 275, Fig. 80: There is no line in the source document to indicate item a.
Page 411, ... two lateral incisions, with through drainage ...: possibly an error for ... thorough drainage.
Page 425, ... absorbents are eared or closed ...: as printed in the source document; possibly erroneously.
Page 534, ... the section on fractures of the elbow-joint ...: there is no such section in the book; these fractures are discussed under fractures of the arm and the forearm.
Page 1037, Fig. 696: reference numbers 1 and 2 are not present in the illustration.
Changes made
Some obvious minor typographical, lay-out and punctuation errors and inconsistencies have been corrected silently.
Footnotes, tables and illustrations have been moved out of text paragraphs.
Plate I: the heading PLATE I has been inserted as in other plates.
Page 25: ... their lumen marrowed ... changed to ... their lumen narrowed ....
Page 229: (See Chapter XXXV.) changed to (See Chapter XXXVI.)
Page 234: (See Chapter LVI.) changed to (See Chapter LVII.)
Page 266, 267: Numbers 2 and 3 inserted before subsection headings Tubulodermoids and Ovarian Dermoids and Teratomas.
Page 278: (See Aneurysm, Chapter XXVIII.) changed to (See Aneurysm, Chapter XXIX.)
Page 293: ... will be found in Chapter IX. changed to ... will be found in Chapter X.
Page 332, caption Plate XXX: Chapter XXVII changed to Chapter XXVIII.
Page 352, ... the diagastric upward, or divided ... changed to ... the digastric upward, or divided ....
Page 552: Splintered or Comminuted Fractures. changed to Splintered or Comminuted Fractures.
Page 599: ... the site of tumors either nor-malignant ... changed to ... the site of tumors either non-malignant ....
Page 650: Mukulicz has described ... changed to Mikulicz has described ....
Page 767: ... as it were as a punishment for forgetfulness or intention ... changed to ... as it were as a punishment for forgetfulness or inattention ....
Page 824: Blood may occear in the vomitus ... changed to Page 824, Blood may occur in the vomitus ... (possibly the phrase was intended to read Blood may appear in the vomitus ...).
Index: Some page numbers and (spelling of) some entries changed to conform to the main body of the text.